User login
Doug Brunk is a San Diego-based award-winning reporter who began covering health care in 1991. Before joining the company, he wrote for the health sciences division of Columbia University and was an associate editor at Contemporary Long Term Care magazine when it won a Jesse H. Neal Award. His work has been syndicated by the Los Angeles Times and he is the author of two books related to the University of Kentucky Wildcats men's basketball program. Doug has a master’s degree in magazine journalism from the S.I. Newhouse School of Public Communications at Syracuse University. Follow him on Twitter @dougbrunk.
Study sheds light on pregnancy outcomes following ocrelizumab treatment
NEW ORLEANS – Data from the ocrelizumab clinical development program gives clinicians a first look at pregnancy outcomes after exposure to the drug, but the small size limits the ability to draw firm conclusions.
In the United States, prescribing information for ocrelizumab states that women of childbearing potential should use contraception while receiving ocrelizumab and for 6 months after the last infusion. At the annual meeting of the Consortium of Multiple Sclerosis Centers, researchers led by Sibyl Wray, MD, set out to assess the pregnancy, fetal, neonatal and infant outcomes in patients who became pregnant during ocrelizumab trials in MS, rheumatoid arthritis (RA), and systemic lupus erythematosus (SLE) through Sept. 15, 2015.

The analysis included ocrelizumab-exposed women in primarily European-based clinical trials in patients with MS, RA, or SLE, in whom doses ranged from 20 mg to 2,000 mg. These included three randomized trials of its use in MS, totaling 1,876 patients with a mean age of 40 years; four trials of its use in RA, totaling 2,759 patients with a mean age of 53 years; and one trial of its use in SLE, totaling 381 patients with a mean age of 31 years. Between 2008 and Sept. 14, 2015, a total of 48 women who were enrolled in the trials reported pregnancies.
MS data
Of the 15 pregnancies in the MS trials, three involved the delivery of full term, healthy newborns. In one case, the last ocrelizumab infusion was given 28 months before conception. In the second case, an infusion was given 20 weeks before conception, and a further infusion was given 17 days after conception. In the third case, the last ocrelizumab infusion was given 26.5 weeks before conception.
One live term birth occurred with an abnormal finding. In this case, the last infusion of ocrelizumab was 23 weeks prior to the last menstrual period or about 6 months prior to conception. The embryo/fetus was not exposed to the drug in utero. The researchers also found that seven elective terminations occurred among MS patients and that four pregnancies were ongoing at the time of this report.
“We have to be cautious because we don’t have enough data yet to know, but it’s encouraging to see that, if you follow the guidelines, the patient population and the newborns seem to be healthy in these exposed individuals,” Dr. Wray said.
RA data
Data from the RA clinical trials revealed 22 pregnancies in 21 patients exposed to ocrelizumab. Of these, eight pregnancies resulted in healthy term babies; four resulted in live births with abnormal findings (structural malformation, growth abnormality) or preterm birth; and eight pregnancies in seven women resulted in spontaneous abortion (one patient experienced a spontaneous abortion on two occasions), missed abortion, or an embryonic pregnancy. One pregnancy was lost to follow-up and another resulted in elective termination.
SLE data
During the SLE trials, 11 pregnancies occurred in 10 patients. Three pregnancies in two women resulted in healthy term babies. Three other pregnancies resulted in live births with an abnormal finding (structural malformation, functional deficit, growth abnormality) and/or preterm birth. Two pregnancies resulted in spontaneous/missed abortion. One pregnancy resulted in fetal death at 7.5 months’ gestation secondary to fatal pulmonary embolism in the mother; one pregnancy resulted in elective termination; and one pregnancy resulted in a healthy baby born at an unknown gestational week.
Dr. Wray emphasized that the small numbers of patients studied make it difficult to draw conclusions about pregnancy outcomes following ocrelizumab in patients with MS and other autoimmune diseases. “We need to pay attention to the half-life of this drug, the time it takes to clear, and how to plan pregnancies around that,” she said. She noted that pregnancy outcomes in ongoing ocrelizumab studies and postmarketing experiences will continue to be collected and assessed.
The study was funded by Roche, Basel, Switzerland. Dr. Wray reported that she has received honoraria and/or research funding from Actelion, Alkermes, Biogen, Celgene, EMD Serono, Genentech/Roche, Genzyme/Sanofi, Novartis, and TG Therapeutics.
NEW ORLEANS – Data from the ocrelizumab clinical development program gives clinicians a first look at pregnancy outcomes after exposure to the drug, but the small size limits the ability to draw firm conclusions.
In the United States, prescribing information for ocrelizumab states that women of childbearing potential should use contraception while receiving ocrelizumab and for 6 months after the last infusion. At the annual meeting of the Consortium of Multiple Sclerosis Centers, researchers led by Sibyl Wray, MD, set out to assess the pregnancy, fetal, neonatal and infant outcomes in patients who became pregnant during ocrelizumab trials in MS, rheumatoid arthritis (RA), and systemic lupus erythematosus (SLE) through Sept. 15, 2015.
The analysis included ocrelizumab-exposed women in primarily European-based clinical trials in patients with MS, RA, or SLE, in whom doses ranged from 20 mg to 2,000 mg. These included three randomized trials of its use in MS, totaling 1,876 patients with a mean age of 40 years; four trials of its use in RA, totaling 2,759 patients with a mean age of 53 years; and one trial of its use in SLE, totaling 381 patients with a mean age of 31 years. Between 2008 and Sept. 14, 2015, a total of 48 women who were enrolled in the trials reported pregnancies.
MS data
Of the 15 pregnancies in the MS trials, three involved the delivery of full term, healthy newborns. In one case, the last ocrelizumab infusion was given 28 months before conception. In the second case, an infusion was given 20 weeks before conception, and a further infusion was given 17 days after conception. In the third case, the last ocrelizumab infusion was given 26.5 weeks before conception.
One live term birth occurred with an abnormal finding. In this case, the last infusion of ocrelizumab was 23 weeks prior to the last menstrual period or about 6 months prior to conception. The embryo/fetus was not exposed to the drug in utero. The researchers also found that seven elective terminations occurred among MS patients and that four pregnancies were ongoing at the time of this report.
“We have to be cautious because we don’t have enough data yet to know, but it’s encouraging to see that, if you follow the guidelines, the patient population and the newborns seem to be healthy in these exposed individuals,” Dr. Wray said.
RA data
Data from the RA clinical trials revealed 22 pregnancies in 21 patients exposed to ocrelizumab. Of these, eight pregnancies resulted in healthy term babies; four resulted in live births with abnormal findings (structural malformation, growth abnormality) or preterm birth; and eight pregnancies in seven women resulted in spontaneous abortion (one patient experienced a spontaneous abortion on two occasions), missed abortion, or an embryonic pregnancy. One pregnancy was lost to follow-up and another resulted in elective termination.
SLE data
During the SLE trials, 11 pregnancies occurred in 10 patients. Three pregnancies in two women resulted in healthy term babies. Three other pregnancies resulted in live births with an abnormal finding (structural malformation, functional deficit, growth abnormality) and/or preterm birth. Two pregnancies resulted in spontaneous/missed abortion. One pregnancy resulted in fetal death at 7.5 months’ gestation secondary to fatal pulmonary embolism in the mother; one pregnancy resulted in elective termination; and one pregnancy resulted in a healthy baby born at an unknown gestational week.
Dr. Wray emphasized that the small numbers of patients studied make it difficult to draw conclusions about pregnancy outcomes following ocrelizumab in patients with MS and other autoimmune diseases. “We need to pay attention to the half-life of this drug, the time it takes to clear, and how to plan pregnancies around that,” she said. She noted that pregnancy outcomes in ongoing ocrelizumab studies and postmarketing experiences will continue to be collected and assessed.
The study was funded by Roche, Basel, Switzerland. Dr. Wray reported that she has received honoraria and/or research funding from Actelion, Alkermes, Biogen, Celgene, EMD Serono, Genentech/Roche, Genzyme/Sanofi, Novartis, and TG Therapeutics.
NEW ORLEANS – Data from the ocrelizumab clinical development program gives clinicians a first look at pregnancy outcomes after exposure to the drug, but the small size limits the ability to draw firm conclusions.
In the United States, prescribing information for ocrelizumab states that women of childbearing potential should use contraception while receiving ocrelizumab and for 6 months after the last infusion. At the annual meeting of the Consortium of Multiple Sclerosis Centers, researchers led by Sibyl Wray, MD, set out to assess the pregnancy, fetal, neonatal and infant outcomes in patients who became pregnant during ocrelizumab trials in MS, rheumatoid arthritis (RA), and systemic lupus erythematosus (SLE) through Sept. 15, 2015.
The analysis included ocrelizumab-exposed women in primarily European-based clinical trials in patients with MS, RA, or SLE, in whom doses ranged from 20 mg to 2,000 mg. These included three randomized trials of its use in MS, totaling 1,876 patients with a mean age of 40 years; four trials of its use in RA, totaling 2,759 patients with a mean age of 53 years; and one trial of its use in SLE, totaling 381 patients with a mean age of 31 years. Between 2008 and Sept. 14, 2015, a total of 48 women who were enrolled in the trials reported pregnancies.
MS data
Of the 15 pregnancies in the MS trials, three involved the delivery of full term, healthy newborns. In one case, the last ocrelizumab infusion was given 28 months before conception. In the second case, an infusion was given 20 weeks before conception, and a further infusion was given 17 days after conception. In the third case, the last ocrelizumab infusion was given 26.5 weeks before conception.
One live term birth occurred with an abnormal finding. In this case, the last infusion of ocrelizumab was 23 weeks prior to the last menstrual period or about 6 months prior to conception. The embryo/fetus was not exposed to the drug in utero. The researchers also found that seven elective terminations occurred among MS patients and that four pregnancies were ongoing at the time of this report.
“We have to be cautious because we don’t have enough data yet to know, but it’s encouraging to see that, if you follow the guidelines, the patient population and the newborns seem to be healthy in these exposed individuals,” Dr. Wray said.
RA data
Data from the RA clinical trials revealed 22 pregnancies in 21 patients exposed to ocrelizumab. Of these, eight pregnancies resulted in healthy term babies; four resulted in live births with abnormal findings (structural malformation, growth abnormality) or preterm birth; and eight pregnancies in seven women resulted in spontaneous abortion (one patient experienced a spontaneous abortion on two occasions), missed abortion, or an embryonic pregnancy. One pregnancy was lost to follow-up and another resulted in elective termination.
SLE data
During the SLE trials, 11 pregnancies occurred in 10 patients. Three pregnancies in two women resulted in healthy term babies. Three other pregnancies resulted in live births with an abnormal finding (structural malformation, functional deficit, growth abnormality) and/or preterm birth. Two pregnancies resulted in spontaneous/missed abortion. One pregnancy resulted in fetal death at 7.5 months’ gestation secondary to fatal pulmonary embolism in the mother; one pregnancy resulted in elective termination; and one pregnancy resulted in a healthy baby born at an unknown gestational week.
Dr. Wray emphasized that the small numbers of patients studied make it difficult to draw conclusions about pregnancy outcomes following ocrelizumab in patients with MS and other autoimmune diseases. “We need to pay attention to the half-life of this drug, the time it takes to clear, and how to plan pregnancies around that,” she said. She noted that pregnancy outcomes in ongoing ocrelizumab studies and postmarketing experiences will continue to be collected and assessed.
The study was funded by Roche, Basel, Switzerland. Dr. Wray reported that she has received honoraria and/or research funding from Actelion, Alkermes, Biogen, Celgene, EMD Serono, Genentech/Roche, Genzyme/Sanofi, Novartis, and TG Therapeutics.
AT THE CMSC ANNUAL MEETING
Key clinical point:
Major finding: Of 15 pregnancies in the MS trials, three involved the delivery of three full term, healthy newborns; one live term birth occurred with an abnormal finding; seven elective terminations occurred; and four pregnancies were ongoing.
Data source: A review of 48 pregnancies among women enrolled in clinical trials for ocrelizumab in MS, rheumatoid arthritis, and systemic lupus erythematosus.
Disclosures: The study was funded by Roche, Basel, Switzerland. Dr. Wray reported that she has received honoraria and/or research funding from Actelion, Alkermes, Biogen, Celgene, EMD Serono, Genentech/Roche, Genzyme/Sanofi, Novartis, and TG Therapeutics.
What’s the evidence for stopping DMTs in MS patients?
NEW ORLEANS – There appear to be four clinical situations “when it might be reasonable to open up conversations with patients about discontinuation of DMTs,” Devyn Parsons said at the annual meeting of the Consortium of Multiple Sclerosis Centers.
While disease-modifying treatments (DMTs) are well established in their ability to decrease relapse rates and slow the progression of disability early in the course of relapsing-remitting MS, it remains unknown whether they maintain their efficacy late in the course of disease after many years of treatment or after progression to secondary progressive MS, said Ms. Parsons, a medical student at the University of British Columbia, Vancouver. Scientific evidence related to when disease-modifying treatments should be discontinued in patients with multiple sclerosis is generally poor, she said.

• Patients with secondary progressive MS who have ongoing progression and no new brain or spinal MRI lesions during the prior 12-24 months.
• Patients with stable relapsing-remitting MS aged 65 or older who have had no new brain or spinal MRI lesions during the prior 12-24 months.
• Patients with stable relapsing-remitting MS aged 55-65 years with no new brain or spinal MRI lesions within the prior 5 years.
• Patients who are pregnant or trying to conceive, or breastfeeding.
“Upon discontinuation of DMTs patients should continue to undergo annual assessments and an annual brain MRI for at least 2-5 years,” Ms. Parsons said. “Reuse of DMTs should be considered if there’s any evidence of relapse or new MRI lesion.”
The investigators conducted a systematic review of medical literature from MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews through June of 2016. They used the keywords “multiple sclerosis” and “disease-modifying treatments” and “treatment withdrawal” or “stopping medication” or “medication withdrawal.” Articles were reviewed in full and classified according to the American Academy of Neurology’s classification of evidence guidelines.
The review yielded what Ms. Parsons described as “a paucity of information” in the existing literature on MS course following discontinuation of DMTs. “There have been no randomized, controlled trials on the subject, and relatively few observational studies,” she said. “Of the observational studies that do exist, several have suggested a return to baseline disease activity following discontinuation of DMTs. In particular these studies examined natalizumab and interferon beta-1a discontinuation. At first glance these studies seem to suggest that discontinuation of DMTs is generally not appropriate, as there is likely to be a return to baseline disease activity. But it’s important to consider that many of these were retrospective, cross-sectional studies with small patient populations and aren’t the best quality data. Furthermore, these studies had relatively short follow-up periods, they didn’t include older patients, and they examined the discontinuation of DMTs after less than 2 years of continuous treatment. These results may not apply to older patients, and they might not apply to patients who have been continuously treated with DMTs for many years. At this point there is sufficient evidence in the literature to allow a randomized, controlled trial in a low-risk patient population of discontinuations of DMTs.”
Ms. Parsons discussed three observational studies from the review. One was a prospective study of 40 patients who discontinued DMTs after a minimum 5 years’ continuous use of a single DMT without new disease activity (Arquivos de Neuro-Psiquiatria 2013;71:516-20). At 46-month follow-up, the investigators found that 90% of patients remained free of clinical attack, and 85% had stable MRIs. “However, this was a really small trial, and the specific DMTs were not reported,” she said.
A larger, separate study evaluated 303 patients aged 40 and older who discontinued DMTs after a minimum of 3 years’ continuous use of a single DMT and who had no clinical relapse in the past 5 years (ECTRIMS Online Library. 2015 Oct 8. 116635). The majority of patients resumed DMT use because of an increase in disease activity following discontinuation. However, for every 10-year increase in patient age, there was a 25% decrease in the rate of resuming DMT. “This might suggest a greater feasibility of discontinuation of DMTs in older patients,” Ms. Parsons said.
The third observational study she discussed included 485 patients, mean age of 45 years, who discontinued DMTs after a minimum of 3 years of treatment with a single DMT and had no clinical relapses in the previous 5 years (J Neurol Neurosurg Psychiatry. 2016 Oct;87[10]:1133-7). These were compared with 854 propensity score–matched individuals who continued DMT. The mean annualized relapse rates and time to first relapse were similar for those who discontinued DMTs and those who continued DMTs. However, survival time to confirmed disability progression was shorter among those who discontinued DMTs (adjusted hazard ratio of 1.47; P = .001). Younger age was found to be a significant predictor of relapse risk among the DMT discontinuation group, with a 25% reduction in relapse risk ratio for every 10-year increase in age.
“DMTs cannot be said with certainty to be effective in older patients, given that patients over the age of 55 have rarely been included in clinical trials of these agents, Ms. Parsons said. Many patients with relapsing-remitting MS are continuously administered DMTs for many years. This long-term use of DMTs is not without cost. It is important to consider things like medication burden of the patient, the potential for adverse effects, as well as the possibility of unnecessary health care costs if these agents are no longer effective in some cases.”
Sanofi Genzyme supported the study. Ms. Parsons reported having no financial disclosures.
NEW ORLEANS – There appear to be four clinical situations “when it might be reasonable to open up conversations with patients about discontinuation of DMTs,” Devyn Parsons said at the annual meeting of the Consortium of Multiple Sclerosis Centers.
While disease-modifying treatments (DMTs) are well established in their ability to decrease relapse rates and slow the progression of disability early in the course of relapsing-remitting MS, it remains unknown whether they maintain their efficacy late in the course of disease after many years of treatment or after progression to secondary progressive MS, said Ms. Parsons, a medical student at the University of British Columbia, Vancouver. Scientific evidence related to when disease-modifying treatments should be discontinued in patients with multiple sclerosis is generally poor, she said.
• Patients with secondary progressive MS who have ongoing progression and no new brain or spinal MRI lesions during the prior 12-24 months.
• Patients with stable relapsing-remitting MS aged 65 or older who have had no new brain or spinal MRI lesions during the prior 12-24 months.
• Patients with stable relapsing-remitting MS aged 55-65 years with no new brain or spinal MRI lesions within the prior 5 years.
• Patients who are pregnant or trying to conceive, or breastfeeding.
“Upon discontinuation of DMTs patients should continue to undergo annual assessments and an annual brain MRI for at least 2-5 years,” Ms. Parsons said. “Reuse of DMTs should be considered if there’s any evidence of relapse or new MRI lesion.”
The investigators conducted a systematic review of medical literature from MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews through June of 2016. They used the keywords “multiple sclerosis” and “disease-modifying treatments” and “treatment withdrawal” or “stopping medication” or “medication withdrawal.” Articles were reviewed in full and classified according to the American Academy of Neurology’s classification of evidence guidelines.
The review yielded what Ms. Parsons described as “a paucity of information” in the existing literature on MS course following discontinuation of DMTs. “There have been no randomized, controlled trials on the subject, and relatively few observational studies,” she said. “Of the observational studies that do exist, several have suggested a return to baseline disease activity following discontinuation of DMTs. In particular these studies examined natalizumab and interferon beta-1a discontinuation. At first glance these studies seem to suggest that discontinuation of DMTs is generally not appropriate, as there is likely to be a return to baseline disease activity. But it’s important to consider that many of these were retrospective, cross-sectional studies with small patient populations and aren’t the best quality data. Furthermore, these studies had relatively short follow-up periods, they didn’t include older patients, and they examined the discontinuation of DMTs after less than 2 years of continuous treatment. These results may not apply to older patients, and they might not apply to patients who have been continuously treated with DMTs for many years. At this point there is sufficient evidence in the literature to allow a randomized, controlled trial in a low-risk patient population of discontinuations of DMTs.”
Ms. Parsons discussed three observational studies from the review. One was a prospective study of 40 patients who discontinued DMTs after a minimum 5 years’ continuous use of a single DMT without new disease activity (Arquivos de Neuro-Psiquiatria 2013;71:516-20). At 46-month follow-up, the investigators found that 90% of patients remained free of clinical attack, and 85% had stable MRIs. “However, this was a really small trial, and the specific DMTs were not reported,” she said.
A larger, separate study evaluated 303 patients aged 40 and older who discontinued DMTs after a minimum of 3 years’ continuous use of a single DMT and who had no clinical relapse in the past 5 years (ECTRIMS Online Library. 2015 Oct 8. 116635). The majority of patients resumed DMT use because of an increase in disease activity following discontinuation. However, for every 10-year increase in patient age, there was a 25% decrease in the rate of resuming DMT. “This might suggest a greater feasibility of discontinuation of DMTs in older patients,” Ms. Parsons said.
The third observational study she discussed included 485 patients, mean age of 45 years, who discontinued DMTs after a minimum of 3 years of treatment with a single DMT and had no clinical relapses in the previous 5 years (J Neurol Neurosurg Psychiatry. 2016 Oct;87[10]:1133-7). These were compared with 854 propensity score–matched individuals who continued DMT. The mean annualized relapse rates and time to first relapse were similar for those who discontinued DMTs and those who continued DMTs. However, survival time to confirmed disability progression was shorter among those who discontinued DMTs (adjusted hazard ratio of 1.47; P = .001). Younger age was found to be a significant predictor of relapse risk among the DMT discontinuation group, with a 25% reduction in relapse risk ratio for every 10-year increase in age.
“DMTs cannot be said with certainty to be effective in older patients, given that patients over the age of 55 have rarely been included in clinical trials of these agents, Ms. Parsons said. Many patients with relapsing-remitting MS are continuously administered DMTs for many years. This long-term use of DMTs is not without cost. It is important to consider things like medication burden of the patient, the potential for adverse effects, as well as the possibility of unnecessary health care costs if these agents are no longer effective in some cases.”
Sanofi Genzyme supported the study. Ms. Parsons reported having no financial disclosures.
NEW ORLEANS – There appear to be four clinical situations “when it might be reasonable to open up conversations with patients about discontinuation of DMTs,” Devyn Parsons said at the annual meeting of the Consortium of Multiple Sclerosis Centers.
While disease-modifying treatments (DMTs) are well established in their ability to decrease relapse rates and slow the progression of disability early in the course of relapsing-remitting MS, it remains unknown whether they maintain their efficacy late in the course of disease after many years of treatment or after progression to secondary progressive MS, said Ms. Parsons, a medical student at the University of British Columbia, Vancouver. Scientific evidence related to when disease-modifying treatments should be discontinued in patients with multiple sclerosis is generally poor, she said.
• Patients with secondary progressive MS who have ongoing progression and no new brain or spinal MRI lesions during the prior 12-24 months.
• Patients with stable relapsing-remitting MS aged 65 or older who have had no new brain or spinal MRI lesions during the prior 12-24 months.
• Patients with stable relapsing-remitting MS aged 55-65 years with no new brain or spinal MRI lesions within the prior 5 years.
• Patients who are pregnant or trying to conceive, or breastfeeding.
“Upon discontinuation of DMTs patients should continue to undergo annual assessments and an annual brain MRI for at least 2-5 years,” Ms. Parsons said. “Reuse of DMTs should be considered if there’s any evidence of relapse or new MRI lesion.”
The investigators conducted a systematic review of medical literature from MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews through June of 2016. They used the keywords “multiple sclerosis” and “disease-modifying treatments” and “treatment withdrawal” or “stopping medication” or “medication withdrawal.” Articles were reviewed in full and classified according to the American Academy of Neurology’s classification of evidence guidelines.
The review yielded what Ms. Parsons described as “a paucity of information” in the existing literature on MS course following discontinuation of DMTs. “There have been no randomized, controlled trials on the subject, and relatively few observational studies,” she said. “Of the observational studies that do exist, several have suggested a return to baseline disease activity following discontinuation of DMTs. In particular these studies examined natalizumab and interferon beta-1a discontinuation. At first glance these studies seem to suggest that discontinuation of DMTs is generally not appropriate, as there is likely to be a return to baseline disease activity. But it’s important to consider that many of these were retrospective, cross-sectional studies with small patient populations and aren’t the best quality data. Furthermore, these studies had relatively short follow-up periods, they didn’t include older patients, and they examined the discontinuation of DMTs after less than 2 years of continuous treatment. These results may not apply to older patients, and they might not apply to patients who have been continuously treated with DMTs for many years. At this point there is sufficient evidence in the literature to allow a randomized, controlled trial in a low-risk patient population of discontinuations of DMTs.”
Ms. Parsons discussed three observational studies from the review. One was a prospective study of 40 patients who discontinued DMTs after a minimum 5 years’ continuous use of a single DMT without new disease activity (Arquivos de Neuro-Psiquiatria 2013;71:516-20). At 46-month follow-up, the investigators found that 90% of patients remained free of clinical attack, and 85% had stable MRIs. “However, this was a really small trial, and the specific DMTs were not reported,” she said.
A larger, separate study evaluated 303 patients aged 40 and older who discontinued DMTs after a minimum of 3 years’ continuous use of a single DMT and who had no clinical relapse in the past 5 years (ECTRIMS Online Library. 2015 Oct 8. 116635). The majority of patients resumed DMT use because of an increase in disease activity following discontinuation. However, for every 10-year increase in patient age, there was a 25% decrease in the rate of resuming DMT. “This might suggest a greater feasibility of discontinuation of DMTs in older patients,” Ms. Parsons said.
The third observational study she discussed included 485 patients, mean age of 45 years, who discontinued DMTs after a minimum of 3 years of treatment with a single DMT and had no clinical relapses in the previous 5 years (J Neurol Neurosurg Psychiatry. 2016 Oct;87[10]:1133-7). These were compared with 854 propensity score–matched individuals who continued DMT. The mean annualized relapse rates and time to first relapse were similar for those who discontinued DMTs and those who continued DMTs. However, survival time to confirmed disability progression was shorter among those who discontinued DMTs (adjusted hazard ratio of 1.47; P = .001). Younger age was found to be a significant predictor of relapse risk among the DMT discontinuation group, with a 25% reduction in relapse risk ratio for every 10-year increase in age.
“DMTs cannot be said with certainty to be effective in older patients, given that patients over the age of 55 have rarely been included in clinical trials of these agents, Ms. Parsons said. Many patients with relapsing-remitting MS are continuously administered DMTs for many years. This long-term use of DMTs is not without cost. It is important to consider things like medication burden of the patient, the potential for adverse effects, as well as the possibility of unnecessary health care costs if these agents are no longer effective in some cases.”
Sanofi Genzyme supported the study. Ms. Parsons reported having no financial disclosures.
AT THE CMSC ANNUAL MEETING
Key clinical point:
Major finding: Meaningful clinical data on discontinuation of DMTs in patients with MS are limited.
Data source: A systematic review of the medical literature using the keywords “multiple sclerosis” and “disease-modifying treatments” and “treatment withdrawal” or “stopping medication” or “medication withdrawal.”
Disclosures: Sanofi Genzyme supported the study. Ms. Parsons reported having no financial disclosures.
DMD use during pregnancy low, study finds
NEW ORLEANS – The proportion of women with multiple sclerosis with a live birth receiving disease-modifying drug therapy was low and declined during the prepregnancy and pregnancy periods, results from a large analysis of national claims data found.
“Multiple sclerosis is up to three times more common in women than in men, and the clinical onset is often during childbearing years,” researchers led by Maria K. Houtchens, MD, wrote in an abstract presented during the annual meeting of the Consortium of Multiple Sclerosis Centers. “A better understanding of the ‘real world’ disease-modifying drug treatment patterns in women with MS and a pregnancy is essential in order to improve available clinical support, health care services, and quality of life for women with MS of childbearing age.”

Dr. Houtchens, a neurologist at Brigham and Women’s Hospital, Boston, and her associates reported results from 2,518 women who were included in the final analysis. Their mean age was 30 years, and 99% had commercial health insurance.
Overall, the proportion of women with MS and a live birth receiving DMD treatment was low, ranging from 1.9% to 25.5%, and the rate of treatment declined during the prepregnancy and pregnancy periods.
During pregnancy, the proportion of women treated with a DMD decreased to 12.05% during the first trimester and to 1.90% during the second trimester, and then increased to 2.97% during the third trimester. At 9-12 months postpartum, the proportion of women treated with a DMD was 25.5%. Most patients were treated with self-injectable DMDs (from 1.7% to 19.6%), while the use of oral and infusion agents was low (0.1%-3.1% and 0%-0.2%, respectively).
The researchers also found that the proportion of women with DMD treatment before and after pregnancy increased significantly with the number of relapses experienced prepregnancy. A greater number of relapses before pregnancy led to more patients treated with DMDs.
They acknowledged certain limitations of the study, including its reliance on information from patients with health insurance administered by regional health plans. “Results may not be generalizable to patients who self-pay or patients without employer-sponsored commercial health insurance.”
The study was supported by EMD Serono. Dr. Houtchens reported that she has received funding support from EMD Serono and that she serves on the scientific advisory boards for Biogen, Novartis, Sanofi Genzyme, and Teva Neuroscience. She also has received research support from Sanofi Genzyme.
NEW ORLEANS – The proportion of women with multiple sclerosis with a live birth receiving disease-modifying drug therapy was low and declined during the prepregnancy and pregnancy periods, results from a large analysis of national claims data found.
“Multiple sclerosis is up to three times more common in women than in men, and the clinical onset is often during childbearing years,” researchers led by Maria K. Houtchens, MD, wrote in an abstract presented during the annual meeting of the Consortium of Multiple Sclerosis Centers. “A better understanding of the ‘real world’ disease-modifying drug treatment patterns in women with MS and a pregnancy is essential in order to improve available clinical support, health care services, and quality of life for women with MS of childbearing age.”
Dr. Houtchens, a neurologist at Brigham and Women’s Hospital, Boston, and her associates reported results from 2,518 women who were included in the final analysis. Their mean age was 30 years, and 99% had commercial health insurance.
Overall, the proportion of women with MS and a live birth receiving DMD treatment was low, ranging from 1.9% to 25.5%, and the rate of treatment declined during the prepregnancy and pregnancy periods.
During pregnancy, the proportion of women treated with a DMD decreased to 12.05% during the first trimester and to 1.90% during the second trimester, and then increased to 2.97% during the third trimester. At 9-12 months postpartum, the proportion of women treated with a DMD was 25.5%. Most patients were treated with self-injectable DMDs (from 1.7% to 19.6%), while the use of oral and infusion agents was low (0.1%-3.1% and 0%-0.2%, respectively).
The researchers also found that the proportion of women with DMD treatment before and after pregnancy increased significantly with the number of relapses experienced prepregnancy. A greater number of relapses before pregnancy led to more patients treated with DMDs.
They acknowledged certain limitations of the study, including its reliance on information from patients with health insurance administered by regional health plans. “Results may not be generalizable to patients who self-pay or patients without employer-sponsored commercial health insurance.”
The study was supported by EMD Serono. Dr. Houtchens reported that she has received funding support from EMD Serono and that she serves on the scientific advisory boards for Biogen, Novartis, Sanofi Genzyme, and Teva Neuroscience. She also has received research support from Sanofi Genzyme.
NEW ORLEANS – The proportion of women with multiple sclerosis with a live birth receiving disease-modifying drug therapy was low and declined during the prepregnancy and pregnancy periods, results from a large analysis of national claims data found.
“Multiple sclerosis is up to three times more common in women than in men, and the clinical onset is often during childbearing years,” researchers led by Maria K. Houtchens, MD, wrote in an abstract presented during the annual meeting of the Consortium of Multiple Sclerosis Centers. “A better understanding of the ‘real world’ disease-modifying drug treatment patterns in women with MS and a pregnancy is essential in order to improve available clinical support, health care services, and quality of life for women with MS of childbearing age.”
Dr. Houtchens, a neurologist at Brigham and Women’s Hospital, Boston, and her associates reported results from 2,518 women who were included in the final analysis. Their mean age was 30 years, and 99% had commercial health insurance.
Overall, the proportion of women with MS and a live birth receiving DMD treatment was low, ranging from 1.9% to 25.5%, and the rate of treatment declined during the prepregnancy and pregnancy periods.
During pregnancy, the proportion of women treated with a DMD decreased to 12.05% during the first trimester and to 1.90% during the second trimester, and then increased to 2.97% during the third trimester. At 9-12 months postpartum, the proportion of women treated with a DMD was 25.5%. Most patients were treated with self-injectable DMDs (from 1.7% to 19.6%), while the use of oral and infusion agents was low (0.1%-3.1% and 0%-0.2%, respectively).
The researchers also found that the proportion of women with DMD treatment before and after pregnancy increased significantly with the number of relapses experienced prepregnancy. A greater number of relapses before pregnancy led to more patients treated with DMDs.
They acknowledged certain limitations of the study, including its reliance on information from patients with health insurance administered by regional health plans. “Results may not be generalizable to patients who self-pay or patients without employer-sponsored commercial health insurance.”
The study was supported by EMD Serono. Dr. Houtchens reported that she has received funding support from EMD Serono and that she serves on the scientific advisory boards for Biogen, Novartis, Sanofi Genzyme, and Teva Neuroscience. She also has received research support from Sanofi Genzyme.
AT THE CMSC ANNUAL MEETING
Key clinical point:
Major finding: Overall, the proportion of women with multiple sclerosis and a live birth receiving DMD treatment was low, ranging from 1.9% to 25.5%.
Data source: A retrospective analysis of claims data from 2,518 women with MS.
Disclosures: The study was supported by EMD Serono. Dr. Houtchens reported that she has received funding support from EMD Serono and that she serves on the scientific advisory boards for Biogen, Novartis, Sanofi Genzyme, and Teva Neuroscience. She also has received research support from Sanofi Genzyme.
Revisions coming to McDonald Criteria for MS
NEW ORLEANS – Changes are coming to the current McDonald Criteria for diagnosing multiple sclerosis, primarily because of advances in the understanding of MS since the criteria were last updated in 2010.
Such advances include the availability of new data regarding the relationship between MS and other spectrum disorders and data concerning the performance of the 2010 McDonald Criteria in several patient populations, according to Jeffrey A. Cohen, MD, who cochaired the effort known as the International Panel on Diagnosis of Multiple Sclerosis. “There also were new data concerning the utility of cerebrospinal fluid evaluation and increasing recognition that the role of cerebrospinal fluid (CSF) examination perhaps needs increased emphasis,” Dr. Cohen said at the annual meeting of the Consortium of Multiple Sclerosis Centers. “It’s been somewhat de-emphasized in previous versions of the criteria. Then, there was identification of subsets of patients that were felt to have a high likelihood of MS but in whom the diagnosis could not be made by the current criteria – patients who fell through the cracks. There was also increasing recognition of the frequency and important consequences of misdiagnosis.”

The panel emphasized that evidence supporting the McDonald criteria is predominately based on patients with a typical clinically isolated syndrome (CIS) at onset. It also acknowledged the difficulty of confirming a diagnosis of MS, the importance of addressing alternative diagnoses and absence of atypical features and red flags, and the rigor necessary for interpreting clinical, imaging, and laboratory studies. “Misdiagnosis is common,” Dr. Cohen told meeting attendees. “In some series, upwards of 50%-60% of patients referred to a specialized MS center turn out to have some other diagnosis. Our panel had discussions related to the tradeoff between sensitivity of the criteria and trying to make the diagnosis earlier and in a broader range of patients but counterbalancing that against the risk of a misdiagnosis. Our conclusion was that, although some of that might be created by the criteria, it’s mostly a problem of misapplying the criteria. One needs to remember that to make the diagnosis of MS does not merely require demonstrating that the patient has a disease process that involves potentially multiple places in the CNS and as recurrent events over time, but one has to apply the diagnostic data with rigor.”
Another emphasis expected to be included in updated McDonald criteria is the use of CSF and spinal cord imaging, as well as the notion that a history, examination, and synthesis of a patient’s overall clinical picture “needs to be made by a clinician with MS-related expertise,” Dr. Cohen said. “One cannot merely use the criteria as a checklist.”
The panelists also discussed modifying the term “possible MS,” which is already in the McDonald criteria, to include patients with CIS who do not (yet) fulfill the diagnostic criteria for MS; radiologically isolated syndrome (RIS); solitary sclerosis; and patients with clinical manifestations, imaging, and other features that are compatible with MS but not typical for those who may or may not be determined to have MS or in the future.
Dr. Cohen noted that additional data concerning the applicability of the McDonald criteria to Asian and Latin populations have been published since 2010 but are modest. “There is no indication the McDonald criteria cannot be used in these populations,” he said. “Care is needed to address alternative diagnoses, particularly neuromyelitis optica spectrum disorder (NMOSD) in both and also infectious diseases in Latin America.” Several studies also support the applicability of the McDonald criteria in children, with certain caveats. “One needs to be careful in diagnosing MS in people younger than 11 years of age,” Dr. Cohen said. “If the initial event is [acute disseminated encephalomyelitis], they also need to have a typical clinically isolated syndrome.”
Panelists also agreed that the McDonald criteria apply to older patients, with caveats that a new diagnosis of MS is rarely considered in older adults. “They are more likely to have a progressive course, either progressive from onset or following previous unrecognized relapses,” Dr. Cohen said. “There needs to be careful consideration of alternative diagnoses and, particularly, comorbidities. This represents an example of a diagnostic scenario for which CSF examination is advised.”
Panel members found that the recognized range of potential clinical manifestations of NMOSD is becoming wider and is still being defined. “Emerging data suggests a substantial proportion of AQP-4 seronegative patients with NMOSD features (about 20%) have anti–myelin oligodendrocyte glycoprotein antibodies,” he said. “Although some features of MS and NMOSD overlap, they are now understood to be distinct disorders.”
Other points under consideration for the 2017 revision of the McDonald Criteria included incorporating the revised phenotype categories (relapse-remitting, secondary progressive, primary progressive, and progressive relapsing), expanding the role of CSF to allow diagnosis of MS with CIS plus DIS plus oligoclonal bands, determining whether to accept 2016 Revised Magnetic Resonance Imaging in Multiple Sclerosis MRI criteria in aggregate or in part, and incorporating optic nerve involvement.
Dr. Cohen disclosed that he has received compensation as a consultant for Adamas, Celgene, Merck, Mallinckrodt, and Novartis.
NEW ORLEANS – Changes are coming to the current McDonald Criteria for diagnosing multiple sclerosis, primarily because of advances in the understanding of MS since the criteria were last updated in 2010.
Such advances include the availability of new data regarding the relationship between MS and other spectrum disorders and data concerning the performance of the 2010 McDonald Criteria in several patient populations, according to Jeffrey A. Cohen, MD, who cochaired the effort known as the International Panel on Diagnosis of Multiple Sclerosis. “There also were new data concerning the utility of cerebrospinal fluid evaluation and increasing recognition that the role of cerebrospinal fluid (CSF) examination perhaps needs increased emphasis,” Dr. Cohen said at the annual meeting of the Consortium of Multiple Sclerosis Centers. “It’s been somewhat de-emphasized in previous versions of the criteria. Then, there was identification of subsets of patients that were felt to have a high likelihood of MS but in whom the diagnosis could not be made by the current criteria – patients who fell through the cracks. There was also increasing recognition of the frequency and important consequences of misdiagnosis.”
The panel emphasized that evidence supporting the McDonald criteria is predominately based on patients with a typical clinically isolated syndrome (CIS) at onset. It also acknowledged the difficulty of confirming a diagnosis of MS, the importance of addressing alternative diagnoses and absence of atypical features and red flags, and the rigor necessary for interpreting clinical, imaging, and laboratory studies. “Misdiagnosis is common,” Dr. Cohen told meeting attendees. “In some series, upwards of 50%-60% of patients referred to a specialized MS center turn out to have some other diagnosis. Our panel had discussions related to the tradeoff between sensitivity of the criteria and trying to make the diagnosis earlier and in a broader range of patients but counterbalancing that against the risk of a misdiagnosis. Our conclusion was that, although some of that might be created by the criteria, it’s mostly a problem of misapplying the criteria. One needs to remember that to make the diagnosis of MS does not merely require demonstrating that the patient has a disease process that involves potentially multiple places in the CNS and as recurrent events over time, but one has to apply the diagnostic data with rigor.”
Another emphasis expected to be included in updated McDonald criteria is the use of CSF and spinal cord imaging, as well as the notion that a history, examination, and synthesis of a patient’s overall clinical picture “needs to be made by a clinician with MS-related expertise,” Dr. Cohen said. “One cannot merely use the criteria as a checklist.”
The panelists also discussed modifying the term “possible MS,” which is already in the McDonald criteria, to include patients with CIS who do not (yet) fulfill the diagnostic criteria for MS; radiologically isolated syndrome (RIS); solitary sclerosis; and patients with clinical manifestations, imaging, and other features that are compatible with MS but not typical for those who may or may not be determined to have MS or in the future.
Dr. Cohen noted that additional data concerning the applicability of the McDonald criteria to Asian and Latin populations have been published since 2010 but are modest. “There is no indication the McDonald criteria cannot be used in these populations,” he said. “Care is needed to address alternative diagnoses, particularly neuromyelitis optica spectrum disorder (NMOSD) in both and also infectious diseases in Latin America.” Several studies also support the applicability of the McDonald criteria in children, with certain caveats. “One needs to be careful in diagnosing MS in people younger than 11 years of age,” Dr. Cohen said. “If the initial event is [acute disseminated encephalomyelitis], they also need to have a typical clinically isolated syndrome.”
Panelists also agreed that the McDonald criteria apply to older patients, with caveats that a new diagnosis of MS is rarely considered in older adults. “They are more likely to have a progressive course, either progressive from onset or following previous unrecognized relapses,” Dr. Cohen said. “There needs to be careful consideration of alternative diagnoses and, particularly, comorbidities. This represents an example of a diagnostic scenario for which CSF examination is advised.”
Panel members found that the recognized range of potential clinical manifestations of NMOSD is becoming wider and is still being defined. “Emerging data suggests a substantial proportion of AQP-4 seronegative patients with NMOSD features (about 20%) have anti–myelin oligodendrocyte glycoprotein antibodies,” he said. “Although some features of MS and NMOSD overlap, they are now understood to be distinct disorders.”
Other points under consideration for the 2017 revision of the McDonald Criteria included incorporating the revised phenotype categories (relapse-remitting, secondary progressive, primary progressive, and progressive relapsing), expanding the role of CSF to allow diagnosis of MS with CIS plus DIS plus oligoclonal bands, determining whether to accept 2016 Revised Magnetic Resonance Imaging in Multiple Sclerosis MRI criteria in aggregate or in part, and incorporating optic nerve involvement.
Dr. Cohen disclosed that he has received compensation as a consultant for Adamas, Celgene, Merck, Mallinckrodt, and Novartis.
NEW ORLEANS – Changes are coming to the current McDonald Criteria for diagnosing multiple sclerosis, primarily because of advances in the understanding of MS since the criteria were last updated in 2010.
Such advances include the availability of new data regarding the relationship between MS and other spectrum disorders and data concerning the performance of the 2010 McDonald Criteria in several patient populations, according to Jeffrey A. Cohen, MD, who cochaired the effort known as the International Panel on Diagnosis of Multiple Sclerosis. “There also were new data concerning the utility of cerebrospinal fluid evaluation and increasing recognition that the role of cerebrospinal fluid (CSF) examination perhaps needs increased emphasis,” Dr. Cohen said at the annual meeting of the Consortium of Multiple Sclerosis Centers. “It’s been somewhat de-emphasized in previous versions of the criteria. Then, there was identification of subsets of patients that were felt to have a high likelihood of MS but in whom the diagnosis could not be made by the current criteria – patients who fell through the cracks. There was also increasing recognition of the frequency and important consequences of misdiagnosis.”
The panel emphasized that evidence supporting the McDonald criteria is predominately based on patients with a typical clinically isolated syndrome (CIS) at onset. It also acknowledged the difficulty of confirming a diagnosis of MS, the importance of addressing alternative diagnoses and absence of atypical features and red flags, and the rigor necessary for interpreting clinical, imaging, and laboratory studies. “Misdiagnosis is common,” Dr. Cohen told meeting attendees. “In some series, upwards of 50%-60% of patients referred to a specialized MS center turn out to have some other diagnosis. Our panel had discussions related to the tradeoff between sensitivity of the criteria and trying to make the diagnosis earlier and in a broader range of patients but counterbalancing that against the risk of a misdiagnosis. Our conclusion was that, although some of that might be created by the criteria, it’s mostly a problem of misapplying the criteria. One needs to remember that to make the diagnosis of MS does not merely require demonstrating that the patient has a disease process that involves potentially multiple places in the CNS and as recurrent events over time, but one has to apply the diagnostic data with rigor.”
Another emphasis expected to be included in updated McDonald criteria is the use of CSF and spinal cord imaging, as well as the notion that a history, examination, and synthesis of a patient’s overall clinical picture “needs to be made by a clinician with MS-related expertise,” Dr. Cohen said. “One cannot merely use the criteria as a checklist.”
The panelists also discussed modifying the term “possible MS,” which is already in the McDonald criteria, to include patients with CIS who do not (yet) fulfill the diagnostic criteria for MS; radiologically isolated syndrome (RIS); solitary sclerosis; and patients with clinical manifestations, imaging, and other features that are compatible with MS but not typical for those who may or may not be determined to have MS or in the future.
Dr. Cohen noted that additional data concerning the applicability of the McDonald criteria to Asian and Latin populations have been published since 2010 but are modest. “There is no indication the McDonald criteria cannot be used in these populations,” he said. “Care is needed to address alternative diagnoses, particularly neuromyelitis optica spectrum disorder (NMOSD) in both and also infectious diseases in Latin America.” Several studies also support the applicability of the McDonald criteria in children, with certain caveats. “One needs to be careful in diagnosing MS in people younger than 11 years of age,” Dr. Cohen said. “If the initial event is [acute disseminated encephalomyelitis], they also need to have a typical clinically isolated syndrome.”
Panelists also agreed that the McDonald criteria apply to older patients, with caveats that a new diagnosis of MS is rarely considered in older adults. “They are more likely to have a progressive course, either progressive from onset or following previous unrecognized relapses,” Dr. Cohen said. “There needs to be careful consideration of alternative diagnoses and, particularly, comorbidities. This represents an example of a diagnostic scenario for which CSF examination is advised.”
Panel members found that the recognized range of potential clinical manifestations of NMOSD is becoming wider and is still being defined. “Emerging data suggests a substantial proportion of AQP-4 seronegative patients with NMOSD features (about 20%) have anti–myelin oligodendrocyte glycoprotein antibodies,” he said. “Although some features of MS and NMOSD overlap, they are now understood to be distinct disorders.”
Other points under consideration for the 2017 revision of the McDonald Criteria included incorporating the revised phenotype categories (relapse-remitting, secondary progressive, primary progressive, and progressive relapsing), expanding the role of CSF to allow diagnosis of MS with CIS plus DIS plus oligoclonal bands, determining whether to accept 2016 Revised Magnetic Resonance Imaging in Multiple Sclerosis MRI criteria in aggregate or in part, and incorporating optic nerve involvement.
Dr. Cohen disclosed that he has received compensation as a consultant for Adamas, Celgene, Merck, Mallinckrodt, and Novartis.
EXPERT ANALYSIS AT THE CMSC ANNUAL MEETING
FDA asks drug maker to shelve Opana ER
The Food and Drug Administration has asked Endo Pharmaceuticals to voluntarily remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market in the United States, citing the potential for its abuse as a concern.
“We are facing an opioid epidemic – a public health crisis, and we must take all necessary steps to reduce the scope of opioid misuse and abuse,” FDA Commissioner Scott Gottlieb, MD, said in a June 8 press release . “We will continue to take regulatory steps when we see situations where an opioid product’s risks outweigh its benefits, not only for its intended patient population but also in regard to its potential for misuse and abuse.”
Opana ER was first approved in 2006 for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time. It was reformulated in 2012, with the intent of making it “resistant to physical and chemical manipulation for abuse by snorting or injecting,” according to the FDA release.
The Food and Drug Administration has asked Endo Pharmaceuticals to voluntarily remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market in the United States, citing the potential for its abuse as a concern.
“We are facing an opioid epidemic – a public health crisis, and we must take all necessary steps to reduce the scope of opioid misuse and abuse,” FDA Commissioner Scott Gottlieb, MD, said in a June 8 press release . “We will continue to take regulatory steps when we see situations where an opioid product’s risks outweigh its benefits, not only for its intended patient population but also in regard to its potential for misuse and abuse.”
Opana ER was first approved in 2006 for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time. It was reformulated in 2012, with the intent of making it “resistant to physical and chemical manipulation for abuse by snorting or injecting,” according to the FDA release.
The Food and Drug Administration has asked Endo Pharmaceuticals to voluntarily remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market in the United States, citing the potential for its abuse as a concern.
“We are facing an opioid epidemic – a public health crisis, and we must take all necessary steps to reduce the scope of opioid misuse and abuse,” FDA Commissioner Scott Gottlieb, MD, said in a June 8 press release . “We will continue to take regulatory steps when we see situations where an opioid product’s risks outweigh its benefits, not only for its intended patient population but also in regard to its potential for misuse and abuse.”
Opana ER was first approved in 2006 for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time. It was reformulated in 2012, with the intent of making it “resistant to physical and chemical manipulation for abuse by snorting or injecting,” according to the FDA release.
Study offers snapshot of common MS comorbidities
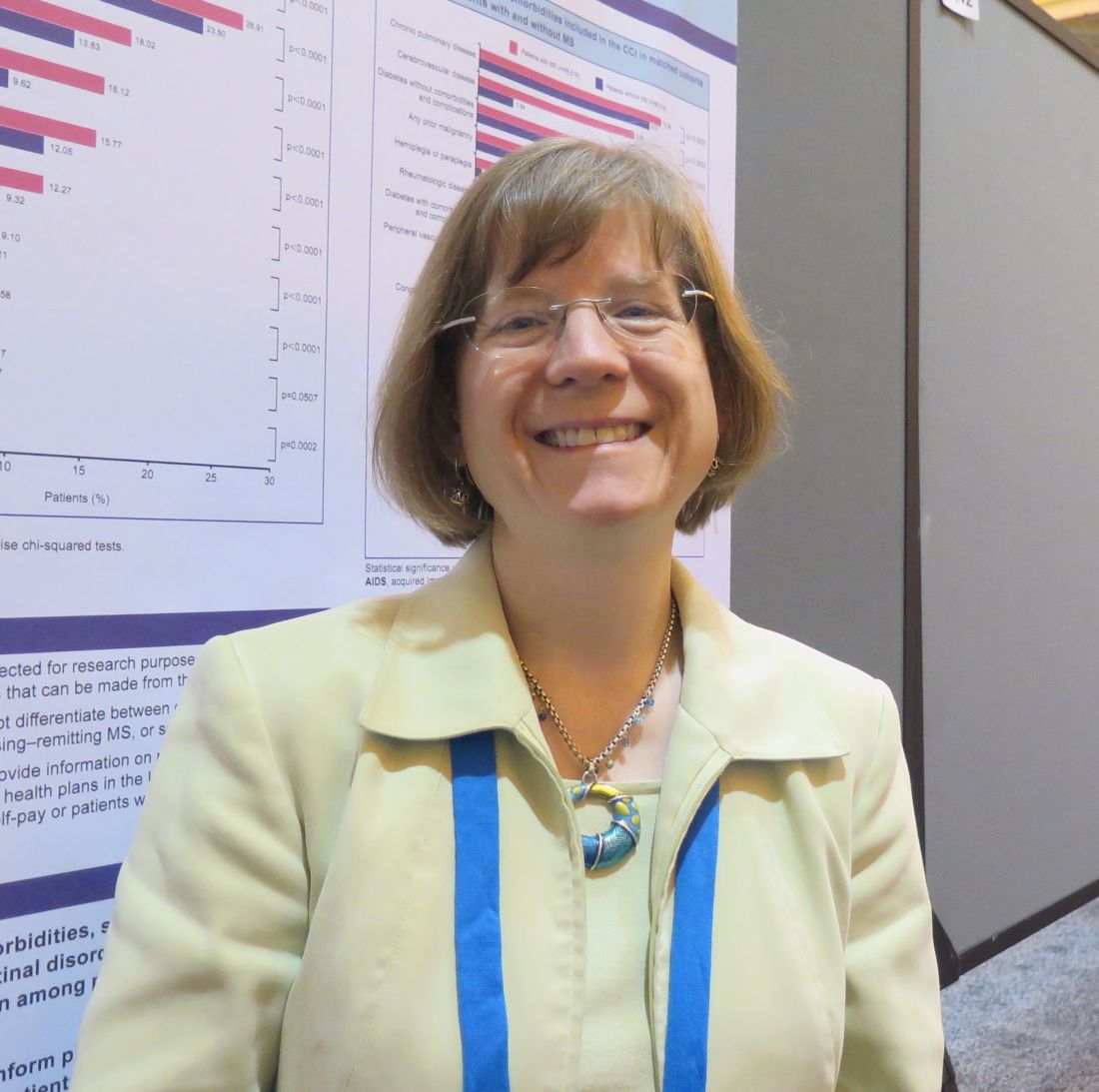
NEW ORLEANS – Comorbidities such as hyperlipidemia, hypertension, gastrointestinal disorders, and depression are significantly more common among patients with multiple sclerosis, compared with patients who do not have the condition.
The findings, based on a large analysis of national claims data that was presented at the annual meeting of the Consortium of Multiple Sclerosis Centers, may better inform physicians and patients about potential comorbidities in patients with MS, lead study author Kiren Kresa-Reahl, MD, said in an interview. “The challenge is, what is the underlying problem?” she asked. “Is it the chicken or the egg? It may be that MS lesions on the brain and microvascular disease look similar, so it’s hard to know. There are also conditions that are caused by MS, such as depression. Is it caused by MS the disease or is it a comorbidity with MS? That’s hard to know.”
In an effort to compare the prevalence of comorbidities in patients with and without MS, Dr. Kresa-Reahl and her associates retrospectively evaluated IMS Health Real World Data Adjudicated Claims-U.S. data between Jan. 1, 2011, and Sept. 30, 2015. The database includes about 150 million patients with a medical benefit and a subset of 95 million patients with both medical and pharmacy benefits. MS patients were required to have at least two claims with an ICD-9 diagnosis of MS 30 days apart and to be between the ages of 18 and 65.
The researchers drew from a systematic review of the 10 most common comorbidities in MS (Mult Scler. 2015;21[3]:263-81) and then matched 69,550 MS patients to a pool of 3,129,573 patients without MS by age group, gender, geographic region, and index quarter year. This left 66,616 patients in each cohort. Their mean age was 46 years, 76% were female, and the majority had commercial health insurance (97% of MS patients and 95% of those without the condition).
Of the 10 common comorbidities, eight occurred significantly more frequently among MS patients, compared with those without the condition (P less than .0001 for all). These included hyperlipidemia (27.76% vs. 24.57%, respectively), hypertension (26.91% vs. 23.50%), GI disorders (18.02% vs. 13.84%), depression (16.12% vs. 9.62%), thyroid disease (15.77% vs. 12.05%), anxiety (12.27% vs. 9.32%), and chronic obstructive pulmonary disease (10.39% vs. 9.52%).
Dr. Kresa-Reahl, a neurologist at the Providence Multiple Sclerosis Center in Portland, Ore., and her associates also found that patients with MS had a significantly lower prevalence of alcohol abuse, AIDS, mild liver disease, and moderate liver disease than did patients without MS (P less than .05 for all). There were no differences between groups in the prevalence of diabetes without complications or in metastatic tumor (P greater than .05).
She acknowledged certain limitations of the study, including the potential for missing information and the inability of the researchers to determine which form of MS the patients had. “It might be that if we looked at just Medicare and Medicaid patients, these diagnoses would be a little bit different,” Dr. Kresa-Reahl added. “Maybe they would have more disability or more depression or more limited mobility. It’s hard to know, but this is a snapshot of people who have commercial insurance, so maybe they would be more likely to be employed.”
The study was sponsored by EMD Serono. Dr. Kresa-Reahl disclosed that she has received consulting fees from Biogen and EMD Serono; speakers fees and honoraria from Biogen, EMD Serono, Genzyme, Mallinckrodt, Novartis, and Teva; and grant/research support from Biogen, Genentech, Genzyme, Mallinckrodt, and Novartis.
NEW ORLEANS – Comorbidities such as hyperlipidemia, hypertension, gastrointestinal disorders, and depression are significantly more common among patients with multiple sclerosis, compared with patients who do not have the condition.
The findings, based on a large analysis of national claims data that was presented at the annual meeting of the Consortium of Multiple Sclerosis Centers, may better inform physicians and patients about potential comorbidities in patients with MS, lead study author Kiren Kresa-Reahl, MD, said in an interview. “The challenge is, what is the underlying problem?” she asked. “Is it the chicken or the egg? It may be that MS lesions on the brain and microvascular disease look similar, so it’s hard to know. There are also conditions that are caused by MS, such as depression. Is it caused by MS the disease or is it a comorbidity with MS? That’s hard to know.”
In an effort to compare the prevalence of comorbidities in patients with and without MS, Dr. Kresa-Reahl and her associates retrospectively evaluated IMS Health Real World Data Adjudicated Claims-U.S. data between Jan. 1, 2011, and Sept. 30, 2015. The database includes about 150 million patients with a medical benefit and a subset of 95 million patients with both medical and pharmacy benefits. MS patients were required to have at least two claims with an ICD-9 diagnosis of MS 30 days apart and to be between the ages of 18 and 65.
The researchers drew from a systematic review of the 10 most common comorbidities in MS (Mult Scler. 2015;21[3]:263-81) and then matched 69,550 MS patients to a pool of 3,129,573 patients without MS by age group, gender, geographic region, and index quarter year. This left 66,616 patients in each cohort. Their mean age was 46 years, 76% were female, and the majority had commercial health insurance (97% of MS patients and 95% of those without the condition).
Of the 10 common comorbidities, eight occurred significantly more frequently among MS patients, compared with those without the condition (P less than .0001 for all). These included hyperlipidemia (27.76% vs. 24.57%, respectively), hypertension (26.91% vs. 23.50%), GI disorders (18.02% vs. 13.84%), depression (16.12% vs. 9.62%), thyroid disease (15.77% vs. 12.05%), anxiety (12.27% vs. 9.32%), and chronic obstructive pulmonary disease (10.39% vs. 9.52%).
Dr. Kresa-Reahl, a neurologist at the Providence Multiple Sclerosis Center in Portland, Ore., and her associates also found that patients with MS had a significantly lower prevalence of alcohol abuse, AIDS, mild liver disease, and moderate liver disease than did patients without MS (P less than .05 for all). There were no differences between groups in the prevalence of diabetes without complications or in metastatic tumor (P greater than .05).
She acknowledged certain limitations of the study, including the potential for missing information and the inability of the researchers to determine which form of MS the patients had. “It might be that if we looked at just Medicare and Medicaid patients, these diagnoses would be a little bit different,” Dr. Kresa-Reahl added. “Maybe they would have more disability or more depression or more limited mobility. It’s hard to know, but this is a snapshot of people who have commercial insurance, so maybe they would be more likely to be employed.”
The study was sponsored by EMD Serono. Dr. Kresa-Reahl disclosed that she has received consulting fees from Biogen and EMD Serono; speakers fees and honoraria from Biogen, EMD Serono, Genzyme, Mallinckrodt, Novartis, and Teva; and grant/research support from Biogen, Genentech, Genzyme, Mallinckrodt, and Novartis.
NEW ORLEANS – Comorbidities such as hyperlipidemia, hypertension, gastrointestinal disorders, and depression are significantly more common among patients with multiple sclerosis, compared with patients who do not have the condition.
The findings, based on a large analysis of national claims data that was presented at the annual meeting of the Consortium of Multiple Sclerosis Centers, may better inform physicians and patients about potential comorbidities in patients with MS, lead study author Kiren Kresa-Reahl, MD, said in an interview. “The challenge is, what is the underlying problem?” she asked. “Is it the chicken or the egg? It may be that MS lesions on the brain and microvascular disease look similar, so it’s hard to know. There are also conditions that are caused by MS, such as depression. Is it caused by MS the disease or is it a comorbidity with MS? That’s hard to know.”
In an effort to compare the prevalence of comorbidities in patients with and without MS, Dr. Kresa-Reahl and her associates retrospectively evaluated IMS Health Real World Data Adjudicated Claims-U.S. data between Jan. 1, 2011, and Sept. 30, 2015. The database includes about 150 million patients with a medical benefit and a subset of 95 million patients with both medical and pharmacy benefits. MS patients were required to have at least two claims with an ICD-9 diagnosis of MS 30 days apart and to be between the ages of 18 and 65.
The researchers drew from a systematic review of the 10 most common comorbidities in MS (Mult Scler. 2015;21[3]:263-81) and then matched 69,550 MS patients to a pool of 3,129,573 patients without MS by age group, gender, geographic region, and index quarter year. This left 66,616 patients in each cohort. Their mean age was 46 years, 76% were female, and the majority had commercial health insurance (97% of MS patients and 95% of those without the condition).
Of the 10 common comorbidities, eight occurred significantly more frequently among MS patients, compared with those without the condition (P less than .0001 for all). These included hyperlipidemia (27.76% vs. 24.57%, respectively), hypertension (26.91% vs. 23.50%), GI disorders (18.02% vs. 13.84%), depression (16.12% vs. 9.62%), thyroid disease (15.77% vs. 12.05%), anxiety (12.27% vs. 9.32%), and chronic obstructive pulmonary disease (10.39% vs. 9.52%).
Dr. Kresa-Reahl, a neurologist at the Providence Multiple Sclerosis Center in Portland, Ore., and her associates also found that patients with MS had a significantly lower prevalence of alcohol abuse, AIDS, mild liver disease, and moderate liver disease than did patients without MS (P less than .05 for all). There were no differences between groups in the prevalence of diabetes without complications or in metastatic tumor (P greater than .05).
She acknowledged certain limitations of the study, including the potential for missing information and the inability of the researchers to determine which form of MS the patients had. “It might be that if we looked at just Medicare and Medicaid patients, these diagnoses would be a little bit different,” Dr. Kresa-Reahl added. “Maybe they would have more disability or more depression or more limited mobility. It’s hard to know, but this is a snapshot of people who have commercial insurance, so maybe they would be more likely to be employed.”
The study was sponsored by EMD Serono. Dr. Kresa-Reahl disclosed that she has received consulting fees from Biogen and EMD Serono; speakers fees and honoraria from Biogen, EMD Serono, Genzyme, Mallinckrodt, Novartis, and Teva; and grant/research support from Biogen, Genentech, Genzyme, Mallinckrodt, and Novartis.
AT THE CMSC ANNUAL MEETING
Key clinical point:
Major finding: Of 10 common comorbidities, eight occurred significantly more frequently among MS patients, compared with those without the condition (P less than .0001 for all).
Data source: A retrospective analysis of claims data from 66,616 MS patients and 66,616 patients without the condition.
Disclosures: The study was sponsored by EMD Serono. Dr. Kresa-Reahl disclosed that she has received consulting fees from Biogen and EMD Serono; speakers fees and honoraria from Biogen, EMD Serono, Genzyme, Mallinckrodt, Novartis, and Teva; and grant/research support from Biogen, Genentech, Genzyme, Mallinckrodt, and Novartis.
Effective monitoring of DMTs for multiple sclerosis can be tricky
NEW ORLEANS – Safety and efficacy laboratory monitoring of adherence to disease-modifying therapies for multiple sclerosis remains challenging, results from a small pilot study showed.
In an effort to determine if select patients on specific DMTs are receiving appropriate and adequate monitoring as outlined by each DMT’s internal guidance document, Felecia Hart, PharmD, and her associates retrospectively reviewed existing patients treated for MS at the Rocky Mountain Multiple Sclerosis Center at the University of Colorado, Denver, between June 1, 2013, and June 1, 2016.
“What we wanted to know was, if patients are getting their infusions or lab work done elsewhere, are we properly documenting it and keeping track of it?” Dr. Hart said in an interview at the meeting. “We’re not looking for core outcomes yet.”
Dr. Hart, a clinical pharmacy neurology fellow at the Skaggs School of Pharmacy and Pharmaceutical Sciences on the University of Colorado Anschutz Medical Campus, reported preliminary results from 50 patients treated with natalizumab and 50 treated with fingolimod. Among those treated with natalizumab, 49 had vitamin D measured within 6 months of drug initiation, 49 had a complete blood count measured within 1 year of drug initiation, and 49 had a comprehensive metabolic panel (CMP) measured within 1 year of drug initiation. “Interestingly, the absent CBC and CMP were from different patients,” she said.
Among patients treated with fingolimod, all had CBC/CMP measured within 1 year of drug initiation, 48 had vitamin D measured within 6 months of drug initiation, and 47 had documented macular optical coherence tomography at baseline, but the proportion of patients who had adequate documentation for other recommended assessments declined significantly. For example, only 19 of 50 had a documented repeat echocardiography within 3 months of drug initiation. Also, several baseline measurements required prior to drug initiation were documented poorly or in an untimely manner. Four patients had their HIV-1 and -2 antibody measured after drug initiation, three had hepatitis B virus surface antigen measured after drug initiation, and three had varicella measured after drug initiation.
Even though the MS center has an electronic medical record system, Dr. Hart and her associates found it difficult to obtain and monitor the parameters of interest. “I’ve been working with our EMR for 6 years, so I know how to navigate it well,” she said. “But I found it difficult to do a simple chart review and find what I wanted to. We have a labs tab in our chart, but the difficulty became including patients who were coming from outside of our center. The lab and the order were referenced in a note but there was never any documentation after that. There are too many holes in getting it documented correctly.”
The findings suggest that having a dedicated clinician such as a clinical pharmacist to oversee pharmacovigilance may improve patient outcomes and ensure that safety and efficacy monitoring doesn’t inadvertently get overlooked because of difficulties with adequate documentation. “That would be ideal,” Dr. Hart said.
She reported having no financial disclosures.
NEW ORLEANS – Safety and efficacy laboratory monitoring of adherence to disease-modifying therapies for multiple sclerosis remains challenging, results from a small pilot study showed.
In an effort to determine if select patients on specific DMTs are receiving appropriate and adequate monitoring as outlined by each DMT’s internal guidance document, Felecia Hart, PharmD, and her associates retrospectively reviewed existing patients treated for MS at the Rocky Mountain Multiple Sclerosis Center at the University of Colorado, Denver, between June 1, 2013, and June 1, 2016.
“What we wanted to know was, if patients are getting their infusions or lab work done elsewhere, are we properly documenting it and keeping track of it?” Dr. Hart said in an interview at the meeting. “We’re not looking for core outcomes yet.”
Dr. Hart, a clinical pharmacy neurology fellow at the Skaggs School of Pharmacy and Pharmaceutical Sciences on the University of Colorado Anschutz Medical Campus, reported preliminary results from 50 patients treated with natalizumab and 50 treated with fingolimod. Among those treated with natalizumab, 49 had vitamin D measured within 6 months of drug initiation, 49 had a complete blood count measured within 1 year of drug initiation, and 49 had a comprehensive metabolic panel (CMP) measured within 1 year of drug initiation. “Interestingly, the absent CBC and CMP were from different patients,” she said.
Among patients treated with fingolimod, all had CBC/CMP measured within 1 year of drug initiation, 48 had vitamin D measured within 6 months of drug initiation, and 47 had documented macular optical coherence tomography at baseline, but the proportion of patients who had adequate documentation for other recommended assessments declined significantly. For example, only 19 of 50 had a documented repeat echocardiography within 3 months of drug initiation. Also, several baseline measurements required prior to drug initiation were documented poorly or in an untimely manner. Four patients had their HIV-1 and -2 antibody measured after drug initiation, three had hepatitis B virus surface antigen measured after drug initiation, and three had varicella measured after drug initiation.
Even though the MS center has an electronic medical record system, Dr. Hart and her associates found it difficult to obtain and monitor the parameters of interest. “I’ve been working with our EMR for 6 years, so I know how to navigate it well,” she said. “But I found it difficult to do a simple chart review and find what I wanted to. We have a labs tab in our chart, but the difficulty became including patients who were coming from outside of our center. The lab and the order were referenced in a note but there was never any documentation after that. There are too many holes in getting it documented correctly.”
The findings suggest that having a dedicated clinician such as a clinical pharmacist to oversee pharmacovigilance may improve patient outcomes and ensure that safety and efficacy monitoring doesn’t inadvertently get overlooked because of difficulties with adequate documentation. “That would be ideal,” Dr. Hart said.
She reported having no financial disclosures.
NEW ORLEANS – Safety and efficacy laboratory monitoring of adherence to disease-modifying therapies for multiple sclerosis remains challenging, results from a small pilot study showed.
In an effort to determine if select patients on specific DMTs are receiving appropriate and adequate monitoring as outlined by each DMT’s internal guidance document, Felecia Hart, PharmD, and her associates retrospectively reviewed existing patients treated for MS at the Rocky Mountain Multiple Sclerosis Center at the University of Colorado, Denver, between June 1, 2013, and June 1, 2016.
“What we wanted to know was, if patients are getting their infusions or lab work done elsewhere, are we properly documenting it and keeping track of it?” Dr. Hart said in an interview at the meeting. “We’re not looking for core outcomes yet.”
Dr. Hart, a clinical pharmacy neurology fellow at the Skaggs School of Pharmacy and Pharmaceutical Sciences on the University of Colorado Anschutz Medical Campus, reported preliminary results from 50 patients treated with natalizumab and 50 treated with fingolimod. Among those treated with natalizumab, 49 had vitamin D measured within 6 months of drug initiation, 49 had a complete blood count measured within 1 year of drug initiation, and 49 had a comprehensive metabolic panel (CMP) measured within 1 year of drug initiation. “Interestingly, the absent CBC and CMP were from different patients,” she said.
Among patients treated with fingolimod, all had CBC/CMP measured within 1 year of drug initiation, 48 had vitamin D measured within 6 months of drug initiation, and 47 had documented macular optical coherence tomography at baseline, but the proportion of patients who had adequate documentation for other recommended assessments declined significantly. For example, only 19 of 50 had a documented repeat echocardiography within 3 months of drug initiation. Also, several baseline measurements required prior to drug initiation were documented poorly or in an untimely manner. Four patients had their HIV-1 and -2 antibody measured after drug initiation, three had hepatitis B virus surface antigen measured after drug initiation, and three had varicella measured after drug initiation.
Even though the MS center has an electronic medical record system, Dr. Hart and her associates found it difficult to obtain and monitor the parameters of interest. “I’ve been working with our EMR for 6 years, so I know how to navigate it well,” she said. “But I found it difficult to do a simple chart review and find what I wanted to. We have a labs tab in our chart, but the difficulty became including patients who were coming from outside of our center. The lab and the order were referenced in a note but there was never any documentation after that. There are too many holes in getting it documented correctly.”
The findings suggest that having a dedicated clinician such as a clinical pharmacist to oversee pharmacovigilance may improve patient outcomes and ensure that safety and efficacy monitoring doesn’t inadvertently get overlooked because of difficulties with adequate documentation. “That would be ideal,” Dr. Hart said.
She reported having no financial disclosures.
AT THE CMSC ANNUAL MEETING
Key clinical point:
Major finding: Among patients treated with fingolimod, only 19 of 50 had a documented repeat ECG within 3 months of drug initiation. Also, several baseline measurements required prior to drug initiation were documented poorly or in an untimely manner.
Data source: Preliminary results from a retrospective review of 50 patients treated with natalizumab and 50 treated with fingolimod.
Disclosures: Dr. Hart reported having no financial disclosures.
Risk tolerance to MS therapies varies widely
NEW ORLEANS – Risk tolerance to current disease modifying therapies by patients with multiple sclerosis varies widely, results from a large national survey demonstrated.
“We have therapies available with a wide range of risks,” study author Sneha Natarajan, PhD, said in an interview at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Some of the risks are relatively minor like injection site reactions or flu-like symptoms and some are as bad as PML [progressive multifocal leukoencephalopathy], which can be fatal. We don’t know what kind of risks people tolerate.”

Dr. Natarajan, research coordinator at the Mellen Center for Multiple Sclerosis at the Cleveland Clinic, reported results from 3,371 survey respondents. Their mean age was 55 years, 93% were white, 61% had the relapsing-remitting form of MS, and 53% were currently taking a DMT. Overall, respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both). Males reported a higher risk tolerance to all six risks (P less than .0001 for all). Females reported a risk tolerance to skin rash that was similar to kidney injury and PML.
“There is a pattern to the risks that our patients accept,” Dr. Natarajan said. “I don’t think a doctor would not recommend a therapy benefit because of a skin rash [risk], but he may need to address the concerns of the patient upfront and have a talk with the patient.”
The researchers also found that current DMT users expressed increased risk tolerance for all outcomes, compared with those not using any DMT (P less than .001). Higher risk tolerance was also expressed by respondents who were older, more disabled, and by those taking infusion therapies.
The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
NEW ORLEANS – Risk tolerance to current disease modifying therapies by patients with multiple sclerosis varies widely, results from a large national survey demonstrated.
“We have therapies available with a wide range of risks,” study author Sneha Natarajan, PhD, said in an interview at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Some of the risks are relatively minor like injection site reactions or flu-like symptoms and some are as bad as PML [progressive multifocal leukoencephalopathy], which can be fatal. We don’t know what kind of risks people tolerate.”
Dr. Natarajan, research coordinator at the Mellen Center for Multiple Sclerosis at the Cleveland Clinic, reported results from 3,371 survey respondents. Their mean age was 55 years, 93% were white, 61% had the relapsing-remitting form of MS, and 53% were currently taking a DMT. Overall, respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both). Males reported a higher risk tolerance to all six risks (P less than .0001 for all). Females reported a risk tolerance to skin rash that was similar to kidney injury and PML.
“There is a pattern to the risks that our patients accept,” Dr. Natarajan said. “I don’t think a doctor would not recommend a therapy benefit because of a skin rash [risk], but he may need to address the concerns of the patient upfront and have a talk with the patient.”
The researchers also found that current DMT users expressed increased risk tolerance for all outcomes, compared with those not using any DMT (P less than .001). Higher risk tolerance was also expressed by respondents who were older, more disabled, and by those taking infusion therapies.
The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
NEW ORLEANS – Risk tolerance to current disease modifying therapies by patients with multiple sclerosis varies widely, results from a large national survey demonstrated.
“We have therapies available with a wide range of risks,” study author Sneha Natarajan, PhD, said in an interview at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Some of the risks are relatively minor like injection site reactions or flu-like symptoms and some are as bad as PML [progressive multifocal leukoencephalopathy], which can be fatal. We don’t know what kind of risks people tolerate.”
Dr. Natarajan, research coordinator at the Mellen Center for Multiple Sclerosis at the Cleveland Clinic, reported results from 3,371 survey respondents. Their mean age was 55 years, 93% were white, 61% had the relapsing-remitting form of MS, and 53% were currently taking a DMT. Overall, respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both). Males reported a higher risk tolerance to all six risks (P less than .0001 for all). Females reported a risk tolerance to skin rash that was similar to kidney injury and PML.
“There is a pattern to the risks that our patients accept,” Dr. Natarajan said. “I don’t think a doctor would not recommend a therapy benefit because of a skin rash [risk], but he may need to address the concerns of the patient upfront and have a talk with the patient.”
The researchers also found that current DMT users expressed increased risk tolerance for all outcomes, compared with those not using any DMT (P less than .001). Higher risk tolerance was also expressed by respondents who were older, more disabled, and by those taking infusion therapies.
The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
AT THE CMSC ANNUAL MEETING
Key clinical point:
Major finding: Survey respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both).
Data source: A survey of 3,371 people who reported having MS.
Disclosures: The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
Inpatient prenatal yoga found feasible for high-risk women
AT ACOG 2017
SAN DIEGO – Inpatient prenatal yoga is a feasible and acceptable intervention for high-risk women admitted to the hospital, results from a single-center study suggested.
“We know that outside of obstetrics, yoga is beneficial to stress relief, musculoskeletal pain, and sleep quality,” Veronica Demtchouk, MD, said in an interview at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Inpatient high-risk obstetrics patients have very limited physical activity that they feel is safe to do.”

In an effort to investigate the feasibility of establishing an inpatient prenatal yoga program, the researchers recruited 40 women with anticipated admission to the antepartum service for at least 72 hours and who received medical clearance from their primary obstetrician. One of the medical center’s nurse practitioners, who is also a certified yoga instructor, taught a 30-minute prenatal yoga session once a week in a waiting room.
“It was a large enough space; we moved away the furniture and did the yoga sessions there,” Dr. Demtchouk said.
Study participants completed a questionnaire after each yoga session and at hospital discharge, while 14 nurses completed questionnaires regarding patient care and patient satisfaction. Of the 40 patients, 16 completed one or more yoga sessions; 24 did not participate because of scheduling conflicts with ultrasound or fetal testing, change in clinical status, lack of interest on the day of the session, and delivery or discharge prior to the yoga session.
Of the 16 study participants, 8 reported a decreased level of stress, 4 reported better sleep, 4 reported applying the yoga techniques outside of class, and 3 reported decreased pain/discomfort.
“Not a single woman complained or was displeased with the yoga sessions,” Dr. Demtchouk said. “The biggest challenge was the timing of the yoga session. It was just once a week, which limited the number of women who could attend.”
Of the 14 nurses who completed questionnaires, all viewed yoga as beneficial to their patients, none found it disruptive to providing patient care, and all indicated they would recommend an inpatient prenatal yoga program to other hospitals with an antepartum service.
“I think having several sessions throughout the week is essential for having adequate patient participation,” Dr. Demtchouk added. “It’s essential to have the nurses on board with it.”
She reported having no relevant financial disclosures.
AT ACOG 2017
SAN DIEGO – Inpatient prenatal yoga is a feasible and acceptable intervention for high-risk women admitted to the hospital, results from a single-center study suggested.
“We know that outside of obstetrics, yoga is beneficial to stress relief, musculoskeletal pain, and sleep quality,” Veronica Demtchouk, MD, said in an interview at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Inpatient high-risk obstetrics patients have very limited physical activity that they feel is safe to do.”
In an effort to investigate the feasibility of establishing an inpatient prenatal yoga program, the researchers recruited 40 women with anticipated admission to the antepartum service for at least 72 hours and who received medical clearance from their primary obstetrician. One of the medical center’s nurse practitioners, who is also a certified yoga instructor, taught a 30-minute prenatal yoga session once a week in a waiting room.
“It was a large enough space; we moved away the furniture and did the yoga sessions there,” Dr. Demtchouk said.
Study participants completed a questionnaire after each yoga session and at hospital discharge, while 14 nurses completed questionnaires regarding patient care and patient satisfaction. Of the 40 patients, 16 completed one or more yoga sessions; 24 did not participate because of scheduling conflicts with ultrasound or fetal testing, change in clinical status, lack of interest on the day of the session, and delivery or discharge prior to the yoga session.
Of the 16 study participants, 8 reported a decreased level of stress, 4 reported better sleep, 4 reported applying the yoga techniques outside of class, and 3 reported decreased pain/discomfort.
“Not a single woman complained or was displeased with the yoga sessions,” Dr. Demtchouk said. “The biggest challenge was the timing of the yoga session. It was just once a week, which limited the number of women who could attend.”
Of the 14 nurses who completed questionnaires, all viewed yoga as beneficial to their patients, none found it disruptive to providing patient care, and all indicated they would recommend an inpatient prenatal yoga program to other hospitals with an antepartum service.
“I think having several sessions throughout the week is essential for having adequate patient participation,” Dr. Demtchouk added. “It’s essential to have the nurses on board with it.”
She reported having no relevant financial disclosures.
AT ACOG 2017
SAN DIEGO – Inpatient prenatal yoga is a feasible and acceptable intervention for high-risk women admitted to the hospital, results from a single-center study suggested.
“We know that outside of obstetrics, yoga is beneficial to stress relief, musculoskeletal pain, and sleep quality,” Veronica Demtchouk, MD, said in an interview at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Inpatient high-risk obstetrics patients have very limited physical activity that they feel is safe to do.”
In an effort to investigate the feasibility of establishing an inpatient prenatal yoga program, the researchers recruited 40 women with anticipated admission to the antepartum service for at least 72 hours and who received medical clearance from their primary obstetrician. One of the medical center’s nurse practitioners, who is also a certified yoga instructor, taught a 30-minute prenatal yoga session once a week in a waiting room.
“It was a large enough space; we moved away the furniture and did the yoga sessions there,” Dr. Demtchouk said.
Study participants completed a questionnaire after each yoga session and at hospital discharge, while 14 nurses completed questionnaires regarding patient care and patient satisfaction. Of the 40 patients, 16 completed one or more yoga sessions; 24 did not participate because of scheduling conflicts with ultrasound or fetal testing, change in clinical status, lack of interest on the day of the session, and delivery or discharge prior to the yoga session.
Of the 16 study participants, 8 reported a decreased level of stress, 4 reported better sleep, 4 reported applying the yoga techniques outside of class, and 3 reported decreased pain/discomfort.
“Not a single woman complained or was displeased with the yoga sessions,” Dr. Demtchouk said. “The biggest challenge was the timing of the yoga session. It was just once a week, which limited the number of women who could attend.”
Of the 14 nurses who completed questionnaires, all viewed yoga as beneficial to their patients, none found it disruptive to providing patient care, and all indicated they would recommend an inpatient prenatal yoga program to other hospitals with an antepartum service.
“I think having several sessions throughout the week is essential for having adequate patient participation,” Dr. Demtchouk added. “It’s essential to have the nurses on board with it.”
She reported having no relevant financial disclosures.
Key clinical point:
Major finding: Of the 16 study participants, 8 reported a decreased level of stress, 4 reported better sleep, 4 reported applying the yoga techniques outside of class, and 3 reported decreased pain/discomfort.
Data source: A feasibility study of 16 hospitalized high-risk pregnant women.
Disclosures: Dr. Demtchouk reported having no relevant financial disclosures.
Experts bust common sports medicine myths
SAN DIEGO – Is it okay for pregnant women to attend CrossFit classes? Are patients who run for fun at increased risk for osteoarthritis? Does stretching before exercise provide any benefits to athletes?
Experts discussed these topics during a session titled “Mythbusters in sports medicine” at the annual meeting of the American Medical Society for Sports Medicine.
Does exercise negatively impact pregnancy?
The idea that strenuous exercise during pregnancy can harm a baby’s health is a myth, according to Elizabeth A. Joy, MD.
“Women having healthy, uncomplicated pregnancies should be encouraged to be physically active throughout pregnancy, with a goal of achieving 150 minutes per week of moderate-intensity activity,” she said. “Fit pregnant women who were habitually performing high-intensity exercise before pregnancy can continue to do so during pregnancy, assuming an otherwise healthy, uncomplicated pregnancy.”
Results from more than 600 studies in the medical literature indicate that exercise during pregnancy is safe for moms and babies, noted Dr. Joy, medical director for community health and food and nutrition at Intermountain Healthcare in Salt Lake City, Utah.
In fact, the 2008 Physical Activity Guidelines for Americans state that pregnant women who habitually engage in vigorous-intensity aerobic activity or who are highly active “can continue physical activity during pregnancy and the postpartum period, provided that they remain healthy and discuss with their health care provider how and when activity should be adjusted over time.”
Such advice wasn’t always supported by the medical profession. In fact, 1985 guidelines from the American College of Obstetricians and Gynecologists recommended that women limit exercise to no more than 15 minutes at a time during pregnancy and keep their maternal heart rate less than 140 beats per minute. ACOG also discouraged previously sedentary women from beginning an exercise program during pregnancy.
“Sadly, women are still getting this advice,” said Dr. Joy, who is also president of the American College of Sports Medicine. According to the 2005-2010 National Ambulatory Medical Care Survey, only 18% of pregnant women reported receiving counseling to be physically active during their pregnancies (Matern Child Health J. 2014 Sep;18[7]:1610-18). “That is just unacceptable,” she said.
In a prospective study of the association between vigorous physical activity during pregnancy and length of gestation and birth weight, researchers evaluated 1,647 births among primiparous women (Matern Child Health J. 2012 Jul;16[5]:1031-44).

They conducted telephone interviews with the women between 7-20 weeks gestation and assigned metabolic equivalent of task values to self-reported levels of physical activity. Of the 1,647 births, 7% were preterm.
Slightly more than one-third of the women (35%) performed first-trimester vigorous physical activity. The average total vigorous activity reported was 76 minutes per week, 38% of which was vigorous recreational activity.
Women who performed first-trimester vigorous recreational physical activity tended to have lower odds of preterm birth. They also tended to have lighter-weight babies, but this did not reach statistical significance (P = .08). The authors concluded that first-trimester vigorous physical activity “does not appear to be detrimental to the timing of birth or birth weight.”
In a separate analysis, researchers evaluated acute fetal responses to individually prescribed exercise according to existing physical activity guidelines in active and inactive pregnant women (Obstet Gynecol. 2012 Mar;119[3]:603-10).
Of the 45 study participants, 15 were classified as nonexercisers, 15 were regularly active, and 15 were highly active. The women underwent treadmill assessment between 28 weeks and 33 weeks, while fetal assessment included umbilical artery Doppler, fetal heart tracing and rate, and biophysical profile at rest and immediately post exercise.
The researchers observed no differences between the groups in mode of delivery, birth weight, and Apgar scores. During vigorous-intensity exercise, all umbilical artery indices showed decreases post exercise.
“Although statistically significant, this decrease is likely not clinically significant,” the researchers wrote. “We did not identify any adverse acute fetal responses to current exercise recommendations.” They went on to conclude that the potential health benefits of exercise “are too great for [physicians] to miss the opportunity to effectively counsel pregnant women about this important heath-enhancing behavior.”
In a more recent randomized study, Swedish researchers evaluated the efficacy of moderate-to-vigorous resistance exercise in 92 pregnant women (Acta Obstet Gynecol Scand. 2015 Jan; 94[1]:35-42).
The intervention group received supervised resistance exercise twice per week at moderate-to-vigorous intensity between 14-25 weeks of their pregnancy, while the control group received a generalized home exercise program. Outcome measures included health-related quality of life, physical strength, pain, weight, blood pressure, functional status, activity level, and perinatal data.
The researchers found no significant differences between the two groups and concluded that “supervised regular, moderate-to-vigorous resistance exercise performed twice per week does not adversely impact childbirth outcome, pain, or blood pressure.”
Despite all that’s known about exercise during pregnancy, a few practice and research gaps remain.
For one, Dr. Joy said, the relationship between performing physically demanding work during pregnancy in combination with moderate-to-vigorous exercise remains largely unknown.
“Even within health care, you have residents, nurses, and others working in hospitals,” she said. “That’s demanding work, but we don’t know whether or not moderate-to-vigorous exercise in combination with that kind of work is safe. Also, although women tend to thermoregulate better during pregnancy, we still don’t fully understand the impact of elevated core body temperature, which may occur with regularly performed vigorous-intensity exercise over the course of pregnancy.”
Does running cause knee OA?
During another talk at the meeting, William O. Roberts, MD, characterized the notion that running causes knee osteoarthritis as largely a myth for recreational runners. However, elite runners and athletes who participate in other sports may face an increased risk of developing the condition.
Well-established risk factors for knee OA include post–joint injury proteases and cytokines and injury load stress on articular cartilage. “Other risk factors include overweight and obesity, a family history of OA, exercise, heavy work that involved squatting and kneeling, and being female,” said Dr. Roberts, professor of family medicine and community health at the University of Minnesota, Minneapolis.
He discussed three articles on the topic drawn from medical literature. One was a retrospective cross-sectional analysis of 2,637 Osteoarthritis Initiative participants, 45-79 years of age, who had knee-specific pain or knee x-ray data 4 years into the 10-year–long study (Arthritis Care Res. 2017 Feb;69[2]:183-91).
More than half of the participants (56%) were female, their mean body mass index was 28.5 kg/m2, only 20% reported more than 2,000 bouts of running during their lifetime, and about 5% had run competitively.
Adjusted odds ratios of pain, radiographic OA, and symptomatic OA for those prior runners and current runners, compared with those who never ran, were 0.82 and 0.76 (P for trend = .02), 0.98 and 0.91 (P for trend = .05), and 0.88 and 0.71 (P for trend = .03), respectively.
The authors concluded that running does not appear to be detrimental to the knees, and the strength of recommendation taxonomy was rated as 2B.
In a separate analysis, researchers performed a systematic review and meta-analysis of 11 cohort (6 retrospective) and 4 case-control studies related to running and knee arthritis (Am J Sports Med. 2016 May;45[6]:1447-57). The mean ages of subjects at outcome assessment ranged from 27 years to 69 years, and the sample size ranged from 15 to 1,279 participants. The four case control studies assessed exposure by mailed questionnaire or by personal interview.
The meta-analysis suggests that runners have a 50% reduced odds of requiring a total knee replacement because of OA.
“It contradicts some previous studies, and there were confounders,” Dr. Roberts said of the analysis. “The one that I noticed is that people would delay surgery to keep running. That’s what I find in my practice.”
The researchers were unable to link running to knee OA development. Moderate- to low-quality evidence suggests a positive association with OA diagnosis but a negative association with requirement for a total knee replacement.
Based on published evidence, they concluded there is no clear advice to give regarding the potential effect of running on musculoskeletal health and rated the strength of evidence as 1A.
A third study Dr. Roberts discussed investigated the association between specific sports participation and knee OA (J Athl Train. 2015 Jan. 9. doi: 10.4085/1062-6050-50.2.08). After locating nearly 18,000 articles on the topic, the researchers limited their meta-analysis to 17 published studies.
They found that the overall risk of knee OA prevalence in sports participants was 7.7%, compared with 7.3% among nonexposed controls (odds ratio, 0.9). However, risks for knee OA were elevated among those who participated in the following sports: soccer (OR, 3.5), elite long-distance running (OR, 3.3), competitive weightlifting (OR, 6.9), and wrestling (OR, 3.8). The researchers concluded that athletes who participate in those sports “should be targeted for risk-reduction strategies.”
“So, does running cause knee OA? It depends,” said Dr. Roberts, who is also medical director of Twin Cities in Motion. “There is a potential risk to high-volume, high-intensity, and long-distance runners, but there does not appear to be a risk in fitness or recreational runners. Of course, you can’t erase your genetics.”
He called for more research on the topic, including prospective longitudinal outcomes studies, those that study the role of genetics/epigenetics in runners and nonrunners who develop knee OA and those focused on the knee joint “chemical environment,” referring to recent work that suggests that running appears to decrease knee intra-articular proinflammatory cytokine concentration (Eur J Appl Physiol. 2016 Dec;116[11-12]:2305-14).
“It’s okay to run for fitness, because the health benefits far outweigh the risk of knee OA,” Dr. Roberts said. “If you run hard and long, it could be a problem. We probably should be screening for neuromuscular control to reduce anterior cruciate ligament disruption.”
Does it help to stretch before exercise?
Stretching before engaging in exercise is a common practice often recommended by coaches and clinicians – but it appears to have no role in preventing injuries during exercise itself.
Several decades ago, investigators subscribed to muscle spasm theory, which held that unaccustomed exercise caused muscle spasms.
“The thought was that muscle spasms impeded blood flow to the muscle, causing ischemic pain and further spasm,” Valerie E. Cothran, MD, said during a presentation at the meeting. “Stretching the muscle was thought to restore blood flow to the muscle and interrupt the pain-spasm-pain cycle. This theory has been discredited for 40 years, but the practice of stretching before exercise persists.”
According to Dr. Cothran, of the department of family and community medicine at the University of Maryland, Baltimore, a limited number of randomized, controlled trials exist on the topic – and many are fraught with limitations, such as the evaluation of multiple stretching methods and variable types of sports activities and the inclusion of multiple cointerventions.
One systematic review evaluated 361 randomized, controlled trials and cohort studies of interventions that included stretching and that appeared in the medical literature from 1966 to 2002 (Med Sci Sports Exerc. 2004 Mar;36[3]:371-8). Studies with no controls were excluded from the analysis, as were those in which stretching could not be assessed independently or those that did not include people engaged in sports or fitness activities.
The researchers determined that stretching was not significantly associated with a reduction in total injuries (OR, 0.93). “There is not sufficient evidence to endorse or discontinue routine stretching before or after exercise to prevent injury among competitive or recreational athletes,” they concluded.

The following year, Lawrence Hart, MBBch, of McMaster University, Hamilton, Ont., assessed the same set of data but eliminated some of the confounding factors of the previous analysis, including studies that had limited statistical power (Clin J Sport Med. 2005 Mar;15[2]:113). The final meta-analysis included six studies.
Dr. Hart found that neither stretching of specific leg-muscle groups or multiple muscle groups led to a reduction in total injuries, such as shin splints, tibial stress reaction, or sprains/strains (OR, 0.93). In addition, reduction in injuries was not significantly greater for stretching of specific muscles or multiple muscle groups (OR, 0.80, and OR, 0.96, respectively). “Limited evidence showed stretching had no effects on injuries,” he concluded.
A more recent systematic review analyzed the efficacy of static stretching as part of a warm-up for the prevention of exercise-related injury (Res Sports Med. 2008;16[3]:213-31). The researchers reviewed 364 studies published after 1990 but before 2008, and they included seven in the final analysis: four randomized, controlled trials and three controlled trials.
All four randomized, controlled trials concluded that static stretching was ineffective in reducing the incidence of exercise-related injury, and only one of the three controlled trials concluded that static stretching reduced the incidence of exercise-related injury. In addition, three of the seven studies reported significant reductions in musculotendinous and ligament injuries following a static stretching protocol.
“There is moderate to strong evidence that routine application of static stretching does not reduce overall injury rates,” the researchers concluded. “There is preliminary evidence, however, that static stretching may reduce musculotendinous injuries.”
The final study Dr. Cothran discussed was a systematic review of two randomized, controlled trials and two prospective cohort studies on the effect of stretching in sports injury prevention that appeared in the literature between 1998 and 2008 (J Comm Health Sci. 2008;3[1]:51-8).
One cohort study found that stretching reduced the incidence of exercise-related injuries, while two randomized, controlled trials and one cohort study found that stretching did not produce a practical reduction on the occurrence of injuries. The researchers concluded that stretching exercises “do not give a practical, useful reduction in the risk of injuries.”
Some studies have demonstrated that explosive athletic performance such as sprinting may be compromised by acute stretching, noted Dr. Cothran, who is also program director of the primary care sports medicine fellowship at the University of Maryland, Baltimore. Current practice and research gaps include few recent randomized, controlled trials; few studies isolating stretching alone; and few that compare the different forms of stretching, such as dynamic and static stretching, she added.
“There is moderate to strong evidence that routine stretching before exercise will not reduce injury rates,” she concluded. “There is evidence that stretching before exercise may negatively affect performance. Flexibility training can be beneficial but should take place at alternative times and not before exercise.”
Dr. Joy disclosed that she receives funding from Savvysherpa and Dexcom for a project on the prevention of gestational diabetes. Dr. Roberts and Dr. Cothran reported having no financial disclosures.
SAN DIEGO – Is it okay for pregnant women to attend CrossFit classes? Are patients who run for fun at increased risk for osteoarthritis? Does stretching before exercise provide any benefits to athletes?
Experts discussed these topics during a session titled “Mythbusters in sports medicine” at the annual meeting of the American Medical Society for Sports Medicine.
Does exercise negatively impact pregnancy?
The idea that strenuous exercise during pregnancy can harm a baby’s health is a myth, according to Elizabeth A. Joy, MD.
“Women having healthy, uncomplicated pregnancies should be encouraged to be physically active throughout pregnancy, with a goal of achieving 150 minutes per week of moderate-intensity activity,” she said. “Fit pregnant women who were habitually performing high-intensity exercise before pregnancy can continue to do so during pregnancy, assuming an otherwise healthy, uncomplicated pregnancy.”
Results from more than 600 studies in the medical literature indicate that exercise during pregnancy is safe for moms and babies, noted Dr. Joy, medical director for community health and food and nutrition at Intermountain Healthcare in Salt Lake City, Utah.
In fact, the 2008 Physical Activity Guidelines for Americans state that pregnant women who habitually engage in vigorous-intensity aerobic activity or who are highly active “can continue physical activity during pregnancy and the postpartum period, provided that they remain healthy and discuss with their health care provider how and when activity should be adjusted over time.”
Such advice wasn’t always supported by the medical profession. In fact, 1985 guidelines from the American College of Obstetricians and Gynecologists recommended that women limit exercise to no more than 15 minutes at a time during pregnancy and keep their maternal heart rate less than 140 beats per minute. ACOG also discouraged previously sedentary women from beginning an exercise program during pregnancy.
“Sadly, women are still getting this advice,” said Dr. Joy, who is also president of the American College of Sports Medicine. According to the 2005-2010 National Ambulatory Medical Care Survey, only 18% of pregnant women reported receiving counseling to be physically active during their pregnancies (Matern Child Health J. 2014 Sep;18[7]:1610-18). “That is just unacceptable,” she said.
In a prospective study of the association between vigorous physical activity during pregnancy and length of gestation and birth weight, researchers evaluated 1,647 births among primiparous women (Matern Child Health J. 2012 Jul;16[5]:1031-44).
They conducted telephone interviews with the women between 7-20 weeks gestation and assigned metabolic equivalent of task values to self-reported levels of physical activity. Of the 1,647 births, 7% were preterm.
Slightly more than one-third of the women (35%) performed first-trimester vigorous physical activity. The average total vigorous activity reported was 76 minutes per week, 38% of which was vigorous recreational activity.
Women who performed first-trimester vigorous recreational physical activity tended to have lower odds of preterm birth. They also tended to have lighter-weight babies, but this did not reach statistical significance (P = .08). The authors concluded that first-trimester vigorous physical activity “does not appear to be detrimental to the timing of birth or birth weight.”
In a separate analysis, researchers evaluated acute fetal responses to individually prescribed exercise according to existing physical activity guidelines in active and inactive pregnant women (Obstet Gynecol. 2012 Mar;119[3]:603-10).
Of the 45 study participants, 15 were classified as nonexercisers, 15 were regularly active, and 15 were highly active. The women underwent treadmill assessment between 28 weeks and 33 weeks, while fetal assessment included umbilical artery Doppler, fetal heart tracing and rate, and biophysical profile at rest and immediately post exercise.
The researchers observed no differences between the groups in mode of delivery, birth weight, and Apgar scores. During vigorous-intensity exercise, all umbilical artery indices showed decreases post exercise.
“Although statistically significant, this decrease is likely not clinically significant,” the researchers wrote. “We did not identify any adverse acute fetal responses to current exercise recommendations.” They went on to conclude that the potential health benefits of exercise “are too great for [physicians] to miss the opportunity to effectively counsel pregnant women about this important heath-enhancing behavior.”
In a more recent randomized study, Swedish researchers evaluated the efficacy of moderate-to-vigorous resistance exercise in 92 pregnant women (Acta Obstet Gynecol Scand. 2015 Jan; 94[1]:35-42).
The intervention group received supervised resistance exercise twice per week at moderate-to-vigorous intensity between 14-25 weeks of their pregnancy, while the control group received a generalized home exercise program. Outcome measures included health-related quality of life, physical strength, pain, weight, blood pressure, functional status, activity level, and perinatal data.
The researchers found no significant differences between the two groups and concluded that “supervised regular, moderate-to-vigorous resistance exercise performed twice per week does not adversely impact childbirth outcome, pain, or blood pressure.”
Despite all that’s known about exercise during pregnancy, a few practice and research gaps remain.
For one, Dr. Joy said, the relationship between performing physically demanding work during pregnancy in combination with moderate-to-vigorous exercise remains largely unknown.
“Even within health care, you have residents, nurses, and others working in hospitals,” she said. “That’s demanding work, but we don’t know whether or not moderate-to-vigorous exercise in combination with that kind of work is safe. Also, although women tend to thermoregulate better during pregnancy, we still don’t fully understand the impact of elevated core body temperature, which may occur with regularly performed vigorous-intensity exercise over the course of pregnancy.”
Does running cause knee OA?
During another talk at the meeting, William O. Roberts, MD, characterized the notion that running causes knee osteoarthritis as largely a myth for recreational runners. However, elite runners and athletes who participate in other sports may face an increased risk of developing the condition.
Well-established risk factors for knee OA include post–joint injury proteases and cytokines and injury load stress on articular cartilage. “Other risk factors include overweight and obesity, a family history of OA, exercise, heavy work that involved squatting and kneeling, and being female,” said Dr. Roberts, professor of family medicine and community health at the University of Minnesota, Minneapolis.
He discussed three articles on the topic drawn from medical literature. One was a retrospective cross-sectional analysis of 2,637 Osteoarthritis Initiative participants, 45-79 years of age, who had knee-specific pain or knee x-ray data 4 years into the 10-year–long study (Arthritis Care Res. 2017 Feb;69[2]:183-91).
More than half of the participants (56%) were female, their mean body mass index was 28.5 kg/m2, only 20% reported more than 2,000 bouts of running during their lifetime, and about 5% had run competitively.
Adjusted odds ratios of pain, radiographic OA, and symptomatic OA for those prior runners and current runners, compared with those who never ran, were 0.82 and 0.76 (P for trend = .02), 0.98 and 0.91 (P for trend = .05), and 0.88 and 0.71 (P for trend = .03), respectively.
The authors concluded that running does not appear to be detrimental to the knees, and the strength of recommendation taxonomy was rated as 2B.
In a separate analysis, researchers performed a systematic review and meta-analysis of 11 cohort (6 retrospective) and 4 case-control studies related to running and knee arthritis (Am J Sports Med. 2016 May;45[6]:1447-57). The mean ages of subjects at outcome assessment ranged from 27 years to 69 years, and the sample size ranged from 15 to 1,279 participants. The four case control studies assessed exposure by mailed questionnaire or by personal interview.
The meta-analysis suggests that runners have a 50% reduced odds of requiring a total knee replacement because of OA.
“It contradicts some previous studies, and there were confounders,” Dr. Roberts said of the analysis. “The one that I noticed is that people would delay surgery to keep running. That’s what I find in my practice.”
The researchers were unable to link running to knee OA development. Moderate- to low-quality evidence suggests a positive association with OA diagnosis but a negative association with requirement for a total knee replacement.
Based on published evidence, they concluded there is no clear advice to give regarding the potential effect of running on musculoskeletal health and rated the strength of evidence as 1A.
A third study Dr. Roberts discussed investigated the association between specific sports participation and knee OA (J Athl Train. 2015 Jan. 9. doi: 10.4085/1062-6050-50.2.08). After locating nearly 18,000 articles on the topic, the researchers limited their meta-analysis to 17 published studies.
They found that the overall risk of knee OA prevalence in sports participants was 7.7%, compared with 7.3% among nonexposed controls (odds ratio, 0.9). However, risks for knee OA were elevated among those who participated in the following sports: soccer (OR, 3.5), elite long-distance running (OR, 3.3), competitive weightlifting (OR, 6.9), and wrestling (OR, 3.8). The researchers concluded that athletes who participate in those sports “should be targeted for risk-reduction strategies.”
“So, does running cause knee OA? It depends,” said Dr. Roberts, who is also medical director of Twin Cities in Motion. “There is a potential risk to high-volume, high-intensity, and long-distance runners, but there does not appear to be a risk in fitness or recreational runners. Of course, you can’t erase your genetics.”
He called for more research on the topic, including prospective longitudinal outcomes studies, those that study the role of genetics/epigenetics in runners and nonrunners who develop knee OA and those focused on the knee joint “chemical environment,” referring to recent work that suggests that running appears to decrease knee intra-articular proinflammatory cytokine concentration (Eur J Appl Physiol. 2016 Dec;116[11-12]:2305-14).
“It’s okay to run for fitness, because the health benefits far outweigh the risk of knee OA,” Dr. Roberts said. “If you run hard and long, it could be a problem. We probably should be screening for neuromuscular control to reduce anterior cruciate ligament disruption.”
Does it help to stretch before exercise?
Stretching before engaging in exercise is a common practice often recommended by coaches and clinicians – but it appears to have no role in preventing injuries during exercise itself.
Several decades ago, investigators subscribed to muscle spasm theory, which held that unaccustomed exercise caused muscle spasms.
“The thought was that muscle spasms impeded blood flow to the muscle, causing ischemic pain and further spasm,” Valerie E. Cothran, MD, said during a presentation at the meeting. “Stretching the muscle was thought to restore blood flow to the muscle and interrupt the pain-spasm-pain cycle. This theory has been discredited for 40 years, but the practice of stretching before exercise persists.”
According to Dr. Cothran, of the department of family and community medicine at the University of Maryland, Baltimore, a limited number of randomized, controlled trials exist on the topic – and many are fraught with limitations, such as the evaluation of multiple stretching methods and variable types of sports activities and the inclusion of multiple cointerventions.
One systematic review evaluated 361 randomized, controlled trials and cohort studies of interventions that included stretching and that appeared in the medical literature from 1966 to 2002 (Med Sci Sports Exerc. 2004 Mar;36[3]:371-8). Studies with no controls were excluded from the analysis, as were those in which stretching could not be assessed independently or those that did not include people engaged in sports or fitness activities.
The researchers determined that stretching was not significantly associated with a reduction in total injuries (OR, 0.93). “There is not sufficient evidence to endorse or discontinue routine stretching before or after exercise to prevent injury among competitive or recreational athletes,” they concluded.
The following year, Lawrence Hart, MBBch, of McMaster University, Hamilton, Ont., assessed the same set of data but eliminated some of the confounding factors of the previous analysis, including studies that had limited statistical power (Clin J Sport Med. 2005 Mar;15[2]:113). The final meta-analysis included six studies.
Dr. Hart found that neither stretching of specific leg-muscle groups or multiple muscle groups led to a reduction in total injuries, such as shin splints, tibial stress reaction, or sprains/strains (OR, 0.93). In addition, reduction in injuries was not significantly greater for stretching of specific muscles or multiple muscle groups (OR, 0.80, and OR, 0.96, respectively). “Limited evidence showed stretching had no effects on injuries,” he concluded.
A more recent systematic review analyzed the efficacy of static stretching as part of a warm-up for the prevention of exercise-related injury (Res Sports Med. 2008;16[3]:213-31). The researchers reviewed 364 studies published after 1990 but before 2008, and they included seven in the final analysis: four randomized, controlled trials and three controlled trials.
All four randomized, controlled trials concluded that static stretching was ineffective in reducing the incidence of exercise-related injury, and only one of the three controlled trials concluded that static stretching reduced the incidence of exercise-related injury. In addition, three of the seven studies reported significant reductions in musculotendinous and ligament injuries following a static stretching protocol.
“There is moderate to strong evidence that routine application of static stretching does not reduce overall injury rates,” the researchers concluded. “There is preliminary evidence, however, that static stretching may reduce musculotendinous injuries.”
The final study Dr. Cothran discussed was a systematic review of two randomized, controlled trials and two prospective cohort studies on the effect of stretching in sports injury prevention that appeared in the literature between 1998 and 2008 (J Comm Health Sci. 2008;3[1]:51-8).
One cohort study found that stretching reduced the incidence of exercise-related injuries, while two randomized, controlled trials and one cohort study found that stretching did not produce a practical reduction on the occurrence of injuries. The researchers concluded that stretching exercises “do not give a practical, useful reduction in the risk of injuries.”
Some studies have demonstrated that explosive athletic performance such as sprinting may be compromised by acute stretching, noted Dr. Cothran, who is also program director of the primary care sports medicine fellowship at the University of Maryland, Baltimore. Current practice and research gaps include few recent randomized, controlled trials; few studies isolating stretching alone; and few that compare the different forms of stretching, such as dynamic and static stretching, she added.
“There is moderate to strong evidence that routine stretching before exercise will not reduce injury rates,” she concluded. “There is evidence that stretching before exercise may negatively affect performance. Flexibility training can be beneficial but should take place at alternative times and not before exercise.”
Dr. Joy disclosed that she receives funding from Savvysherpa and Dexcom for a project on the prevention of gestational diabetes. Dr. Roberts and Dr. Cothran reported having no financial disclosures.
SAN DIEGO – Is it okay for pregnant women to attend CrossFit classes? Are patients who run for fun at increased risk for osteoarthritis? Does stretching before exercise provide any benefits to athletes?
Experts discussed these topics during a session titled “Mythbusters in sports medicine” at the annual meeting of the American Medical Society for Sports Medicine.
Does exercise negatively impact pregnancy?
The idea that strenuous exercise during pregnancy can harm a baby’s health is a myth, according to Elizabeth A. Joy, MD.
“Women having healthy, uncomplicated pregnancies should be encouraged to be physically active throughout pregnancy, with a goal of achieving 150 minutes per week of moderate-intensity activity,” she said. “Fit pregnant women who were habitually performing high-intensity exercise before pregnancy can continue to do so during pregnancy, assuming an otherwise healthy, uncomplicated pregnancy.”
Results from more than 600 studies in the medical literature indicate that exercise during pregnancy is safe for moms and babies, noted Dr. Joy, medical director for community health and food and nutrition at Intermountain Healthcare in Salt Lake City, Utah.
In fact, the 2008 Physical Activity Guidelines for Americans state that pregnant women who habitually engage in vigorous-intensity aerobic activity or who are highly active “can continue physical activity during pregnancy and the postpartum period, provided that they remain healthy and discuss with their health care provider how and when activity should be adjusted over time.”
Such advice wasn’t always supported by the medical profession. In fact, 1985 guidelines from the American College of Obstetricians and Gynecologists recommended that women limit exercise to no more than 15 minutes at a time during pregnancy and keep their maternal heart rate less than 140 beats per minute. ACOG also discouraged previously sedentary women from beginning an exercise program during pregnancy.
“Sadly, women are still getting this advice,” said Dr. Joy, who is also president of the American College of Sports Medicine. According to the 2005-2010 National Ambulatory Medical Care Survey, only 18% of pregnant women reported receiving counseling to be physically active during their pregnancies (Matern Child Health J. 2014 Sep;18[7]:1610-18). “That is just unacceptable,” she said.
In a prospective study of the association between vigorous physical activity during pregnancy and length of gestation and birth weight, researchers evaluated 1,647 births among primiparous women (Matern Child Health J. 2012 Jul;16[5]:1031-44).
They conducted telephone interviews with the women between 7-20 weeks gestation and assigned metabolic equivalent of task values to self-reported levels of physical activity. Of the 1,647 births, 7% were preterm.
Slightly more than one-third of the women (35%) performed first-trimester vigorous physical activity. The average total vigorous activity reported was 76 minutes per week, 38% of which was vigorous recreational activity.
Women who performed first-trimester vigorous recreational physical activity tended to have lower odds of preterm birth. They also tended to have lighter-weight babies, but this did not reach statistical significance (P = .08). The authors concluded that first-trimester vigorous physical activity “does not appear to be detrimental to the timing of birth or birth weight.”
In a separate analysis, researchers evaluated acute fetal responses to individually prescribed exercise according to existing physical activity guidelines in active and inactive pregnant women (Obstet Gynecol. 2012 Mar;119[3]:603-10).
Of the 45 study participants, 15 were classified as nonexercisers, 15 were regularly active, and 15 were highly active. The women underwent treadmill assessment between 28 weeks and 33 weeks, while fetal assessment included umbilical artery Doppler, fetal heart tracing and rate, and biophysical profile at rest and immediately post exercise.
The researchers observed no differences between the groups in mode of delivery, birth weight, and Apgar scores. During vigorous-intensity exercise, all umbilical artery indices showed decreases post exercise.
“Although statistically significant, this decrease is likely not clinically significant,” the researchers wrote. “We did not identify any adverse acute fetal responses to current exercise recommendations.” They went on to conclude that the potential health benefits of exercise “are too great for [physicians] to miss the opportunity to effectively counsel pregnant women about this important heath-enhancing behavior.”
In a more recent randomized study, Swedish researchers evaluated the efficacy of moderate-to-vigorous resistance exercise in 92 pregnant women (Acta Obstet Gynecol Scand. 2015 Jan; 94[1]:35-42).
The intervention group received supervised resistance exercise twice per week at moderate-to-vigorous intensity between 14-25 weeks of their pregnancy, while the control group received a generalized home exercise program. Outcome measures included health-related quality of life, physical strength, pain, weight, blood pressure, functional status, activity level, and perinatal data.
The researchers found no significant differences between the two groups and concluded that “supervised regular, moderate-to-vigorous resistance exercise performed twice per week does not adversely impact childbirth outcome, pain, or blood pressure.”
Despite all that’s known about exercise during pregnancy, a few practice and research gaps remain.
For one, Dr. Joy said, the relationship between performing physically demanding work during pregnancy in combination with moderate-to-vigorous exercise remains largely unknown.
“Even within health care, you have residents, nurses, and others working in hospitals,” she said. “That’s demanding work, but we don’t know whether or not moderate-to-vigorous exercise in combination with that kind of work is safe. Also, although women tend to thermoregulate better during pregnancy, we still don’t fully understand the impact of elevated core body temperature, which may occur with regularly performed vigorous-intensity exercise over the course of pregnancy.”
Does running cause knee OA?
During another talk at the meeting, William O. Roberts, MD, characterized the notion that running causes knee osteoarthritis as largely a myth for recreational runners. However, elite runners and athletes who participate in other sports may face an increased risk of developing the condition.
Well-established risk factors for knee OA include post–joint injury proteases and cytokines and injury load stress on articular cartilage. “Other risk factors include overweight and obesity, a family history of OA, exercise, heavy work that involved squatting and kneeling, and being female,” said Dr. Roberts, professor of family medicine and community health at the University of Minnesota, Minneapolis.
He discussed three articles on the topic drawn from medical literature. One was a retrospective cross-sectional analysis of 2,637 Osteoarthritis Initiative participants, 45-79 years of age, who had knee-specific pain or knee x-ray data 4 years into the 10-year–long study (Arthritis Care Res. 2017 Feb;69[2]:183-91).
More than half of the participants (56%) were female, their mean body mass index was 28.5 kg/m2, only 20% reported more than 2,000 bouts of running during their lifetime, and about 5% had run competitively.
Adjusted odds ratios of pain, radiographic OA, and symptomatic OA for those prior runners and current runners, compared with those who never ran, were 0.82 and 0.76 (P for trend = .02), 0.98 and 0.91 (P for trend = .05), and 0.88 and 0.71 (P for trend = .03), respectively.
The authors concluded that running does not appear to be detrimental to the knees, and the strength of recommendation taxonomy was rated as 2B.
In a separate analysis, researchers performed a systematic review and meta-analysis of 11 cohort (6 retrospective) and 4 case-control studies related to running and knee arthritis (Am J Sports Med. 2016 May;45[6]:1447-57). The mean ages of subjects at outcome assessment ranged from 27 years to 69 years, and the sample size ranged from 15 to 1,279 participants. The four case control studies assessed exposure by mailed questionnaire or by personal interview.
The meta-analysis suggests that runners have a 50% reduced odds of requiring a total knee replacement because of OA.
“It contradicts some previous studies, and there were confounders,” Dr. Roberts said of the analysis. “The one that I noticed is that people would delay surgery to keep running. That’s what I find in my practice.”
The researchers were unable to link running to knee OA development. Moderate- to low-quality evidence suggests a positive association with OA diagnosis but a negative association with requirement for a total knee replacement.
Based on published evidence, they concluded there is no clear advice to give regarding the potential effect of running on musculoskeletal health and rated the strength of evidence as 1A.
A third study Dr. Roberts discussed investigated the association between specific sports participation and knee OA (J Athl Train. 2015 Jan. 9. doi: 10.4085/1062-6050-50.2.08). After locating nearly 18,000 articles on the topic, the researchers limited their meta-analysis to 17 published studies.
They found that the overall risk of knee OA prevalence in sports participants was 7.7%, compared with 7.3% among nonexposed controls (odds ratio, 0.9). However, risks for knee OA were elevated among those who participated in the following sports: soccer (OR, 3.5), elite long-distance running (OR, 3.3), competitive weightlifting (OR, 6.9), and wrestling (OR, 3.8). The researchers concluded that athletes who participate in those sports “should be targeted for risk-reduction strategies.”
“So, does running cause knee OA? It depends,” said Dr. Roberts, who is also medical director of Twin Cities in Motion. “There is a potential risk to high-volume, high-intensity, and long-distance runners, but there does not appear to be a risk in fitness or recreational runners. Of course, you can’t erase your genetics.”
He called for more research on the topic, including prospective longitudinal outcomes studies, those that study the role of genetics/epigenetics in runners and nonrunners who develop knee OA and those focused on the knee joint “chemical environment,” referring to recent work that suggests that running appears to decrease knee intra-articular proinflammatory cytokine concentration (Eur J Appl Physiol. 2016 Dec;116[11-12]:2305-14).
“It’s okay to run for fitness, because the health benefits far outweigh the risk of knee OA,” Dr. Roberts said. “If you run hard and long, it could be a problem. We probably should be screening for neuromuscular control to reduce anterior cruciate ligament disruption.”
Does it help to stretch before exercise?
Stretching before engaging in exercise is a common practice often recommended by coaches and clinicians – but it appears to have no role in preventing injuries during exercise itself.
Several decades ago, investigators subscribed to muscle spasm theory, which held that unaccustomed exercise caused muscle spasms.
“The thought was that muscle spasms impeded blood flow to the muscle, causing ischemic pain and further spasm,” Valerie E. Cothran, MD, said during a presentation at the meeting. “Stretching the muscle was thought to restore blood flow to the muscle and interrupt the pain-spasm-pain cycle. This theory has been discredited for 40 years, but the practice of stretching before exercise persists.”
According to Dr. Cothran, of the department of family and community medicine at the University of Maryland, Baltimore, a limited number of randomized, controlled trials exist on the topic – and many are fraught with limitations, such as the evaluation of multiple stretching methods and variable types of sports activities and the inclusion of multiple cointerventions.
One systematic review evaluated 361 randomized, controlled trials and cohort studies of interventions that included stretching and that appeared in the medical literature from 1966 to 2002 (Med Sci Sports Exerc. 2004 Mar;36[3]:371-8). Studies with no controls were excluded from the analysis, as were those in which stretching could not be assessed independently or those that did not include people engaged in sports or fitness activities.
The researchers determined that stretching was not significantly associated with a reduction in total injuries (OR, 0.93). “There is not sufficient evidence to endorse or discontinue routine stretching before or after exercise to prevent injury among competitive or recreational athletes,” they concluded.
The following year, Lawrence Hart, MBBch, of McMaster University, Hamilton, Ont., assessed the same set of data but eliminated some of the confounding factors of the previous analysis, including studies that had limited statistical power (Clin J Sport Med. 2005 Mar;15[2]:113). The final meta-analysis included six studies.
Dr. Hart found that neither stretching of specific leg-muscle groups or multiple muscle groups led to a reduction in total injuries, such as shin splints, tibial stress reaction, or sprains/strains (OR, 0.93). In addition, reduction in injuries was not significantly greater for stretching of specific muscles or multiple muscle groups (OR, 0.80, and OR, 0.96, respectively). “Limited evidence showed stretching had no effects on injuries,” he concluded.
A more recent systematic review analyzed the efficacy of static stretching as part of a warm-up for the prevention of exercise-related injury (Res Sports Med. 2008;16[3]:213-31). The researchers reviewed 364 studies published after 1990 but before 2008, and they included seven in the final analysis: four randomized, controlled trials and three controlled trials.
All four randomized, controlled trials concluded that static stretching was ineffective in reducing the incidence of exercise-related injury, and only one of the three controlled trials concluded that static stretching reduced the incidence of exercise-related injury. In addition, three of the seven studies reported significant reductions in musculotendinous and ligament injuries following a static stretching protocol.
“There is moderate to strong evidence that routine application of static stretching does not reduce overall injury rates,” the researchers concluded. “There is preliminary evidence, however, that static stretching may reduce musculotendinous injuries.”
The final study Dr. Cothran discussed was a systematic review of two randomized, controlled trials and two prospective cohort studies on the effect of stretching in sports injury prevention that appeared in the literature between 1998 and 2008 (J Comm Health Sci. 2008;3[1]:51-8).
One cohort study found that stretching reduced the incidence of exercise-related injuries, while two randomized, controlled trials and one cohort study found that stretching did not produce a practical reduction on the occurrence of injuries. The researchers concluded that stretching exercises “do not give a practical, useful reduction in the risk of injuries.”
Some studies have demonstrated that explosive athletic performance such as sprinting may be compromised by acute stretching, noted Dr. Cothran, who is also program director of the primary care sports medicine fellowship at the University of Maryland, Baltimore. Current practice and research gaps include few recent randomized, controlled trials; few studies isolating stretching alone; and few that compare the different forms of stretching, such as dynamic and static stretching, she added.
“There is moderate to strong evidence that routine stretching before exercise will not reduce injury rates,” she concluded. “There is evidence that stretching before exercise may negatively affect performance. Flexibility training can be beneficial but should take place at alternative times and not before exercise.”
Dr. Joy disclosed that she receives funding from Savvysherpa and Dexcom for a project on the prevention of gestational diabetes. Dr. Roberts and Dr. Cothran reported having no financial disclosures.