User login
Priorities and Gender Pay Gap
Hospitalists are a growing workforce numbering over 40,000 physicians, one‐third of whom are women.[1] Flexibility of work schedules and control over personal time have been the traditional selling points of the specialty.[2] Multiple studies of physician work life reveal growing physician dissatisfaction and a high prevalence of burnout.[3] To mitigate burnout risk, leaders in hospital medicine recognize the importance of creating a sustainable profession that offers both job and career satisfaction as well as work‐life balance and, importantly, fairness within the work environment.[4] Although success in some of these endeavors has been realized sporadically, sustaining work‐life balance and fairness in the specialty remains a work in progress, whereas evidence of high job attrition and pay inequities remain.[5, 6]
Pay inequity for women relative to men continues to be pervasive in medicine, including among early‐career physicians, researchers, and various specialists.[6, 7, 8, 9, 10, 11, 12, 13] The earnings gap seems to persist for physicians, even as federal efforts such as the Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aim to end wage discrimination.[11, 14] Differences in specialty, part‐time status, and practice type do not mitigate the disparity.[8, 10, 15] Additional explanations have been proposed to explain the variability, including gender differences in negotiating skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.[12, 16, 17, 18, 19, 20]
The earnings gap is also a consequence of what is commonly called the glass ceiling.[18, 19] Most agree that obstacles to fair advancement of women include absence of collaborative environments and role models who have successfully achieved work‐life balance.[17, 20, 21, 22] Somewhat surprisingly, women leaders in medicine seem to suffer greater income disparity than nonleaders; this income gap is prevalent among leaders in other elite professions as well.[7, 23] It is unknown whether women physicians' emphasis on work‐life balance, seen repeatedly in surveys, explains any of the pay disparity.[24] Little research to date has examined whether work‐life priorities of women in hospital medicine differ from men.
In this study, we sought to examine differences in job priorities between men and women hospitalists. In particular, we examine the relative prioritization of substantial pay to job satisfaction. We also examined gender differences in work patterns and earnings to explore potential sources of the persistent gender earnings gap.
METHODS
We analyzed data from the 20092010 Hospital Medicine Physician Worklife Survey, the design of which is detailed elsewhere.[4] Briefly, a 118‐item survey was administered by mail to a stratified sample of hospitalists from the Society of Hospital Medicine database and 3 large multisite hospitalist groups. A single survey item asked respondents to identify up to 4 out of 12 most important domains to their satisfaction with a hospitalist job. The domains were distilled from focus groups of nationally representative hospitalists as described previously,[4] and the survey item allowed up to one‐third of these domains to be identified as respondents' personal priorities. The list included: optimal variety of tasks, optimal workload, substantial pay, collegiality with other physicians, recognition by leaders, rewarding relationships with patients, satisfaction with nurses, optimal autonomy, control over personal time, fairness within organization, ample availability of resources to do job, and organizational climate of trust and belonging. We tabulated and ranked the frequency with which respondents selected each satisfaction domain by gender. Due to the nonstandard format of the survey item, we a priori decided to analyze only responses that were completed as instructed.
We also used demographic data including detailed work characteristics, clinical and nonclinical workload, total pretax earnings in 2009 as a hospitalist, and self‐identification as leader of their hospital medicine group. Respondent characteristics were tabulated and gender differences were tested using the t test, rank sum test, and the Fischer exact test as appropriate. We also listed the number of nonrespondents for each item. In estimating gender differences in earnings, we opted to use multiple‐imputation techniques to more conservatively account for greater variance inherent in the presence of missing data. Consistent with existing guidelines,[25] we demonstrated that item responses were not missing monotonically by visually inspecting patterns of nonresponse. We further demonstrated that data were missing at random by showing that response patterns of completed survey items did not predict whether or not a given variable response was missing using logistic regression models. We found no significant differences between respondents with complete and missing data. We verified that appropriate regression models for each variable on every other variable converged. We used Stata 13.1 (StataCorp, College Station, TX) to perform multiple imputations using chain equations (mi impute chain) to create 10 imputed tables for 7 normally distributed continuous variables using the ordinary least squares method, 3 non‐normally distributed variables using the predictive mean matching method, 2 nonordinal categorical variables using the multinomial logit method, and 1 binary variable using the logit method.[26, 27] Gender, pediatric specialty status, region of practice, and whether or not respondents prioritized substantial pay for job satisfaction were used as regular variables without missing data points.
Differences in earnings were assessed using a multivariate ordinary linear regression model applied to the imputed datasets fitted by forward selection of explanatory variables using P < 0.20 in bivariate analysis for inclusion and manual backward elimination of all statistically nonsignificant variables. We tested the significance of the women leader interaction term in the final parsimonious model. We used the usual significance threshold of P < 0.05 for inferences. Our analysis of publicly available anonymous data was exempt from IRB review.
RESULTS
Of the 816 survey respondents (response rate 25.6%), 40 either omitted the item soliciting work priorities or completed it incorrectly. Data from the remaining 776 respondents were used for the present analysis. Respondent characteristics are tabulated in Table 1. The characteristics of hospitalists by age, gender, specialty, practice model, and practice region were representative of US hospitalists from other surveys.[28]
| Women | Men | P Value | No. of Missing Responses | |
|---|---|---|---|---|
| ||||
| No. | 263 | 513 | 0 | |
| Role, n (%) | <0.01 | 0 | ||
| Frontline hospitalist | 201 (76) | 337 (66) | ||
| Hospitalist leader | 53 (24) | 176 (34) | ||
| Age, y, mean (SD) | 42 (8) | 45 (9) | <0.01 | 67 |
| Years in current job, mean (SD) | 5 (4) | 6 (5) | 0.07 | 14 |
| Specialty, n (%) | <0.01 | 0 | ||
| Internal medicine | 160 (61) | 369 (72) | ||
| Pediatrics | 56 (21) | 57 (11) | ||
| Other | 39 (15) | 47 (9) | ||
| Family medicine | 8 (3) | 40 (8) | ||
| Practice model, n (%) | 0.02 | 19 | ||
| Hospital employed | 110 (43) | 227 (46) | ||
| Multispecialty group | 44 (17) | 68 (14) | ||
| University/medical school | 47 (18) | 58 (12) | ||
| Multistate group | 27 (11) | 73 (15) | ||
| Local hospitalist group | 22 (8) | 65 (13) | ||
| Other | 7 (3) | 9 (2) | ||
| Practice region, n (%) | 0.14 | 0 | ||
| Southeast | 56 (21) | 151 (29) | ||
| Midwest | 58 (22) | 106 (21) | ||
| Northeast | 54 (21) | 96 (19) | ||
| Southwest | 44 (17) | 83 (16) | ||
| West | 51 (19) | 77 (15) | ||
| Full‐time equivalents, n (%) | <0.01 | 42 | ||
| <100% | 46 (18) | 60 (12) | ||
| 100% | 202 (81) | 402 (83) | ||
| >100% | 2 (1) | 22 (5) | ||
| Days per month doing clinical work if FTE 100%, median (IQR) | 15 (1418) | 16 (1420) | 0.12 | 11 |
| Hours per day doing clinical work, median (IQR) | 11 (912) | 11 (912) | 0.67 | 30 |
| Consecutive days doing clinical work, median (IQR) | 7 (57) | 7 (57) | 0.94 | 17 |
| Percentage of work at night, median (IQR) | 15 (530) | 15 (525) | 0.45 | 16 |
| Percentage of night work in hospital if working nights, median (IQR) | 100 (5100) | 100 (10100) | 0.12 | 8 |
| Hours per month doing nonclinical work, median (IQR) | 12 (540) | 15 (540) | 0.77 | 26 |
| Estimated daily billable encounters, mean (IQR) | 14 (1116) | 15 (1218) | 0.01 | 54 |
| Total earnings in fiscal year 2009, median US$1,000 (IQR) | 185 (150210) | 202 (180240) | <0.01 | 56 |
| Marriage/domestic partnership status, n (%) | 0.15 | 43 | ||
| Married/currently in DP | 197 (80) | 421 (86) | ||
| Never married/never in DP | 26 (11) | 42 (9) | ||
| Divorced or separated | 18 (7) | 20 (4) | ||
| Other | 4 (2) | 5 (1) | ||
| Dependent children under 7 years old living in home, n (%) | 0.22 | 42 | ||
| 0 | 136 (55) | 265 (54) | ||
| 1 | 47 (19) | 92 (19) | ||
| 2 | 52 (21) | 87 (18) | ||
| 3 | 12 (5) | 43 (9) | ||
Several gender differences were seen in the characteristics of hospitalists and their work (Table 1). Women compared to men hospitalists were less likely to be leaders, more likely to be pediatricians, work in university settings, and practice in Western states. Women compared to men, on average, were younger by 3 years, worked fewer full‐time equivalents (FTEs), worked a greater percentage of nights, and reported fewer billable encounters per shift. They were also more likely to be divorced or separated.
Job satisfaction priorities differed for women and men hospitalists. Table 2 lists job satisfaction domains in descending order of the frequency prioritized by men. The largest proportion of women and men prioritized optimal workload. However, although substantial pay was prioritized next most frequently by men, more women prioritized collegiality and control over personal time than substantial pay.
| Women, % | Rank | Men, % | Rank | |
|---|---|---|---|---|
| Optimal workload | 59 | 1 | 59 | 1 |
| Substantial pay | 41 | 4 | 50 | 2 |
| Control over personal time | 44 | 3 | 41 | 3 |
| Collegiality with physicians | 47 | 2 | 38 | 4 |
| Rewarding relationships with patients | 35 | 5 | 34 | 5 |
| Organizational climate of trust and belonging | 27 | 7 | 33 | 6 |
| Ample availability of resources to do job | 24 | 9 | 27 | 7 |
| Optimal autonomy | 26 | 8 | 24 | 8 |
| Fairness within organization | 15 | 10 | 23 | 9 |
| Optimal variety of tasks | 29 | 6 | 22 | 10 |
| Recognition by leaders | 11 | 12 | 10 | 11 |
| Satisfaction with nurses | 12 | 11 | 7 | 12 |
Key differences in individual characteristics, work patterns, and indicating substantial pay as a priority were associated with self‐reported total earnings in 2009 from respondents' work as a hospitalist. As shown in Table 3, the inclusion of detailed productivity measures such as FTE, days of monthly clinical work, and estimated number of daily billable encounters yielded a model that explained 33% of variance in earnings. After adjusting for significant covariates including pediatric specialty, practice model, geography, and amount and type of clinical work, the estimated underpayment of women compared to men was $14,581. Hospitalists who prioritized substantial pay earned $10,771 more than those who did not. The female x leader interaction term testing the hypothesis that gender disparity is greater among leaders than frontline hospitalists was not statistically significant ($16,720, P = 0.087) and excluded from the final model.
| Differences in Salary, 2009 US$ (95% CI) | P Value | |
|---|---|---|
| ||
| Women | 14,581 (23,074 to 6,089) | <0.01 |
| Leader | 21,997 (13,313 to 30,682) | <0.01 |
| Prioritized substantial pay | 10,771 (2,651 to 18,891) | <0.01 |
| Pediatric specialty | 31,126 (43,007 to 19,244) | <0.01 |
| Practice model | ||
| Hospital employed | REF | |
| Multispecialty group | 1,922 (13,891 to 10,047) | 0.75 |
| University/medical school | 33,503 (46,336 to 20,671) | <0.01 |
| Multistate group | 6,505 (72,69 to 20,279) | 0.35 |
| Local hospitalist group | 9,330 (4,352 to 23,012) | 0.18 |
| Other | 17,364 (45,741 to 11,012) | 0.23 |
| Practice region | ||
| Southeast | REF | |
| Midwest | 1,225 (10,595 to 13,044) | 0.84 |
| Northeast | 15,712 (28,182 to 3,242) | 0.01 |
| Southwest | 722 (13,545 to 12,101) | 0.91 |
| West | 5,251 (7,383 to 17,885) | 0.41 |
| FTE | 1,021 (762 to 1,279) | <0.01 |
| Days per month doing clinical work | 1,209 (443 to 1,975) | <0.01 |
| Estimated daily billable encounters | 608 (20 to 1,196) | 0.04 |
DISCUSSION
In a national stratified sample of US hospitalists, we found gender differences in job satisfaction priorities and hospitalist work characteristics. We also confirmed the persistence of a substantial gender earnings disparity. Lower earnings among women compared to men hospitalists were present in our data after controlling for age, pediatric specialty, practice model, geography, type of clinical work, and productivity measures. The gender earnings disparity noted in 1999[6] persists, although it appears to have decreased, possibly indicating progress toward equity. We showed that women hospitalists' relative tendency not to prioritize pay explains a significant portion of the residual income gap.
Hoff examined hospitalist earnings in a large national survey of hospitalists in 1999. Our cohorts differed in age and experience (both lower in the Hoff study). An estimated $24,000 ($124,266 vs. $148,132) earnings gap between women and men was greater than our estimate of $14,581 following an interval of 10 years. Although survey items differed, both studies found that women were less interested in pay than men when considering a hospitalist job. Hoff also found that work setting and attitudes about pay and lifestyle were significantly related to earnings. We extended the previous analyses of gender differences in job satisfaction priorities, work, and demographic characteristics to explain the earnings gap and understand how it may be remedied.
When considering job satisfaction, we found that more men than women prioritized substantial pay and that prioritization of substantial pay was directly related to higher earnings. Therefore, fewer women prioritizing pay partly explains women's lower earnings. Reasons for why fewer women prioritize pay were not assessed in this study but may include factors like being part of 2‐income households and competing commitments.[29] Priorities may even be influenced by empirically observed gender differences in discussions of financial matters, governed by cultural norms. Such norms may implicitly sanction employers to offer women less pay than men for the same or similar work. Women may disadvantage themselves by negotiating less or less well than men for higher starting and promotion salaries. They may be perceived more negatively than men when they do negotiate pay, leading to unintended negative consequences such as loss of social networks, decreased likability, and even loss of job offers.[29, 30, 31, 32]
More women prioritized optimal variety of tasks (6th most prevalent among women and 10th among men). Women who highly rate optimal variety of tasks as a job satisfier may choose positions in which they teach, perform research, and participate in hospital committees and quality‐improvement work, but offer lower pay. Yet hours per month doing nonclinical work was not significantly different between men and women, nor associated with earnings differences in our earnings models. Understanding whether women self‐select into hospitalist jobs with like‐minded colleagues to achieve complementary fit or end up supplementing their skills with hospitalists with different priorities may inform strategies to reduce the gender income disparity.[5] Unlike disparities between various hospital medicine groups, systematic disparities within practices risk generating low levels of organizational fairness and burnout among employees.
Not surprisingly, productivity was positively associated with earnings but did not fully account for the gender earnings gap. Our data demonstrated that women, on average, were associated with work characteristics that expectedly generate less compensation. For example, women were younger, more often part time, academic, pediatric, less often leaders, and reported fewer billable encounters compared to men. These differences account for some of the earnings gap between men and women, but these factors were controlled for in the earnings model. In addition, our analysis may have underestimated the gap by not incorporating loss of fringe benefits from part‐time status and not comprehensively counting incentive pay associated with high productivity. Other work patterns more commonly associated with women suggest an imbalance in reimbursement. More women than men work nights that are often compensated at higher rates than daytime work, yet their average pay was less, suggesting that compensation for night work may need to be adjusted to reflect its unique burdens and responsibilities.[33]
Although the gender pay gap was not more extreme among leaders compared to frontline hospitalists in our data, the trend, nonetheless, underscores an important consideration. Whereas clinical work is paid for in mostly measurable ways, pay for leadership may be influenced by intangible factors such as reputation, negotiation, and confidence that may disadvantage women relative to men.[7, 19, 23, 34, 35, 36] Efforts to overcome implicit gender bias should be most effective when we consciously couple fair promotion of women to leadership with fair compensation commensurate with their male peers.[21]
Our data are vulnerable to nonresponse bias.[1, 4, 5] Post hoc analyses demonstrated that distributions of age, gender, practice model and region of our respondents were similar to other nationally representative cohorts of hospitalists. Consequently, we believe our data can make valid estimates about a nationally representative sample of hospitalists. However, we acknowledge several additional weaknesses of self‐reported data, including recall bias and accuracy of productivity figures, which were rounded to variable significant digits by respondents. Earnings analysis using this data was intended to be exploratory, but the findings echoed analyses using more authoritative data sources.[11] Still, we made inferences conservatively by adopting multiple imputation techniques for dealing with nonresponse surveys in adherence to established reporting guidelines.[25] We also note several limitations relevant to multiple imputations. The greater prevalence of missing data for survey items soliciting earnings and the number of billable encounters suggest they were not truly missing at random as assumed. However, we showed that missingness is unrelated to the variables under study, justifying use of the technique. The wider measures of variance derived from multiple imputations make us vulnerable to not detecting associations that may exist.
The gender earnings gap found in hospital medicine echoes the gap found in multiple medical specialties, including but not limited to pediatrics, academic medicine, gastroenterology, and plastic surgery.[7, 8, 9, 11, 12, 13, 37] Hospital medicine employment models and practice patterns have important structural differences compared to previously studied populations that could mitigate factors contributing to women physicians' lower earnings. However, despite well‐defined working hours, lack of control over the number of patient encounters per day and high prevalence of hospital‐employed practice models, the gender earnings gap persists. We showed that lower prioritization for pay may reflect the self‐selection of women into lower paying jobs. Unmeasured factors, including implicit bias and differences in negotiations, social networks and mentoring opportunities[38, 39] may also contribute to pay differences between men and women hospitalists. As hospital medicine tackles gender inequities and other disparities, strategies to assess and address fair physician compensation must be on the table.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task F. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO study. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation. Vol. 1. Research Findings. Rockville, MD; Agency for Healthcare Research and Quality; 2005.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , . Person‐job fit: an exploratory cross‐sectional analysis of hospitalists. J Hosp Med. 2013;8(2):96–101.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- , , , . Compensation and advancement of women in academic medicine: Is there equity? Ann Intern Med. 2004;141(3):205–212.
- . Differences in earnings between male and female physicians. N Engl J Med. 1996;334(15):960–964.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , , , . The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J Gen Intern Med. 2000;15(6):372–380.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30(2):193–201.
- , , , . Assessing gender equity in a large academic department of pediatrics. Acad Med. 2012;87(1):98–104.
- , , , , , . Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005;100(2):259–264.
- H.R. 438, Fair Pay Act of 2013. 113th Congress (2013‐2014).
- , , , , . Topics to ponder: part‐time practice and pay parity. Gend Med. 2010;7(4):350–356.
- , . Understanding and finding mentorship: a review for junior faculty. J Palliat Med. 2010;13(11):1373–1379.
- , , , et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA. 1996;276(11):898–905.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335(17):1282–1289.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–1025.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86(6):752–758.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , . Why aren't there more women leaders in academic medicine? tHe views of clinical department chairs. Acad Med. 2001;76(5):453–465.
- . The gender gap in executive compensation: the role of female directors and chief executive officers. Ann Am Acad Pol Soc Sci. 2012(639):258–278.
- , , . Keys to career satisfaction: insights from a survey of women pediatric surgeons. J Pediatr Surg. 2004;39(6):984–990.
- , , , et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
- Imputation and Variance Estimation Software [computer program]. Ann Arbor, MI: Universtiy of Michigan; 2007.
- , , . Multiple Imputation using chained equations: issues and guidance for practice. Stat Med. 2010;30(4):377–399.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2010.
- , . The Changing Face of Medicine: Women Doctors and the Evolution Of Health Care in America. Ithaca, NY: ILR Press/Cornell University Press; 2008.
- , . Women Don't Ask: Negotiation and the Gender Divide. Princeton, NJ: Princeton University Press; 2003.
- , , , et al. Negotiation in academic medicine: a necessary career skill. J Womens Health (Larchmt). 2007;16(2):235–244.
- . Women and salary negotiation: the costs of self‐advocacy. Psychol Women Q. 2001;25:65–76.
- State of Hospital Medicine: 2014 Report Based on 2013 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2014.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , . Sociology. The gender gap in NIH grant applications. Science. 2008;322(5907):1472–1474.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , . Gender differences in the professional and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775–779.
- . Gender and supportive co‐worker relations in the medical profession. Gend Work Organ. 2014;21(1):1–17.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
Hospitalists are a growing workforce numbering over 40,000 physicians, one‐third of whom are women.[1] Flexibility of work schedules and control over personal time have been the traditional selling points of the specialty.[2] Multiple studies of physician work life reveal growing physician dissatisfaction and a high prevalence of burnout.[3] To mitigate burnout risk, leaders in hospital medicine recognize the importance of creating a sustainable profession that offers both job and career satisfaction as well as work‐life balance and, importantly, fairness within the work environment.[4] Although success in some of these endeavors has been realized sporadically, sustaining work‐life balance and fairness in the specialty remains a work in progress, whereas evidence of high job attrition and pay inequities remain.[5, 6]
Pay inequity for women relative to men continues to be pervasive in medicine, including among early‐career physicians, researchers, and various specialists.[6, 7, 8, 9, 10, 11, 12, 13] The earnings gap seems to persist for physicians, even as federal efforts such as the Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aim to end wage discrimination.[11, 14] Differences in specialty, part‐time status, and practice type do not mitigate the disparity.[8, 10, 15] Additional explanations have been proposed to explain the variability, including gender differences in negotiating skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.[12, 16, 17, 18, 19, 20]
The earnings gap is also a consequence of what is commonly called the glass ceiling.[18, 19] Most agree that obstacles to fair advancement of women include absence of collaborative environments and role models who have successfully achieved work‐life balance.[17, 20, 21, 22] Somewhat surprisingly, women leaders in medicine seem to suffer greater income disparity than nonleaders; this income gap is prevalent among leaders in other elite professions as well.[7, 23] It is unknown whether women physicians' emphasis on work‐life balance, seen repeatedly in surveys, explains any of the pay disparity.[24] Little research to date has examined whether work‐life priorities of women in hospital medicine differ from men.
In this study, we sought to examine differences in job priorities between men and women hospitalists. In particular, we examine the relative prioritization of substantial pay to job satisfaction. We also examined gender differences in work patterns and earnings to explore potential sources of the persistent gender earnings gap.
METHODS
We analyzed data from the 20092010 Hospital Medicine Physician Worklife Survey, the design of which is detailed elsewhere.[4] Briefly, a 118‐item survey was administered by mail to a stratified sample of hospitalists from the Society of Hospital Medicine database and 3 large multisite hospitalist groups. A single survey item asked respondents to identify up to 4 out of 12 most important domains to their satisfaction with a hospitalist job. The domains were distilled from focus groups of nationally representative hospitalists as described previously,[4] and the survey item allowed up to one‐third of these domains to be identified as respondents' personal priorities. The list included: optimal variety of tasks, optimal workload, substantial pay, collegiality with other physicians, recognition by leaders, rewarding relationships with patients, satisfaction with nurses, optimal autonomy, control over personal time, fairness within organization, ample availability of resources to do job, and organizational climate of trust and belonging. We tabulated and ranked the frequency with which respondents selected each satisfaction domain by gender. Due to the nonstandard format of the survey item, we a priori decided to analyze only responses that were completed as instructed.
We also used demographic data including detailed work characteristics, clinical and nonclinical workload, total pretax earnings in 2009 as a hospitalist, and self‐identification as leader of their hospital medicine group. Respondent characteristics were tabulated and gender differences were tested using the t test, rank sum test, and the Fischer exact test as appropriate. We also listed the number of nonrespondents for each item. In estimating gender differences in earnings, we opted to use multiple‐imputation techniques to more conservatively account for greater variance inherent in the presence of missing data. Consistent with existing guidelines,[25] we demonstrated that item responses were not missing monotonically by visually inspecting patterns of nonresponse. We further demonstrated that data were missing at random by showing that response patterns of completed survey items did not predict whether or not a given variable response was missing using logistic regression models. We found no significant differences between respondents with complete and missing data. We verified that appropriate regression models for each variable on every other variable converged. We used Stata 13.1 (StataCorp, College Station, TX) to perform multiple imputations using chain equations (mi impute chain) to create 10 imputed tables for 7 normally distributed continuous variables using the ordinary least squares method, 3 non‐normally distributed variables using the predictive mean matching method, 2 nonordinal categorical variables using the multinomial logit method, and 1 binary variable using the logit method.[26, 27] Gender, pediatric specialty status, region of practice, and whether or not respondents prioritized substantial pay for job satisfaction were used as regular variables without missing data points.
Differences in earnings were assessed using a multivariate ordinary linear regression model applied to the imputed datasets fitted by forward selection of explanatory variables using P < 0.20 in bivariate analysis for inclusion and manual backward elimination of all statistically nonsignificant variables. We tested the significance of the women leader interaction term in the final parsimonious model. We used the usual significance threshold of P < 0.05 for inferences. Our analysis of publicly available anonymous data was exempt from IRB review.
RESULTS
Of the 816 survey respondents (response rate 25.6%), 40 either omitted the item soliciting work priorities or completed it incorrectly. Data from the remaining 776 respondents were used for the present analysis. Respondent characteristics are tabulated in Table 1. The characteristics of hospitalists by age, gender, specialty, practice model, and practice region were representative of US hospitalists from other surveys.[28]
| Women | Men | P Value | No. of Missing Responses | |
|---|---|---|---|---|
| ||||
| No. | 263 | 513 | 0 | |
| Role, n (%) | <0.01 | 0 | ||
| Frontline hospitalist | 201 (76) | 337 (66) | ||
| Hospitalist leader | 53 (24) | 176 (34) | ||
| Age, y, mean (SD) | 42 (8) | 45 (9) | <0.01 | 67 |
| Years in current job, mean (SD) | 5 (4) | 6 (5) | 0.07 | 14 |
| Specialty, n (%) | <0.01 | 0 | ||
| Internal medicine | 160 (61) | 369 (72) | ||
| Pediatrics | 56 (21) | 57 (11) | ||
| Other | 39 (15) | 47 (9) | ||
| Family medicine | 8 (3) | 40 (8) | ||
| Practice model, n (%) | 0.02 | 19 | ||
| Hospital employed | 110 (43) | 227 (46) | ||
| Multispecialty group | 44 (17) | 68 (14) | ||
| University/medical school | 47 (18) | 58 (12) | ||
| Multistate group | 27 (11) | 73 (15) | ||
| Local hospitalist group | 22 (8) | 65 (13) | ||
| Other | 7 (3) | 9 (2) | ||
| Practice region, n (%) | 0.14 | 0 | ||
| Southeast | 56 (21) | 151 (29) | ||
| Midwest | 58 (22) | 106 (21) | ||
| Northeast | 54 (21) | 96 (19) | ||
| Southwest | 44 (17) | 83 (16) | ||
| West | 51 (19) | 77 (15) | ||
| Full‐time equivalents, n (%) | <0.01 | 42 | ||
| <100% | 46 (18) | 60 (12) | ||
| 100% | 202 (81) | 402 (83) | ||
| >100% | 2 (1) | 22 (5) | ||
| Days per month doing clinical work if FTE 100%, median (IQR) | 15 (1418) | 16 (1420) | 0.12 | 11 |
| Hours per day doing clinical work, median (IQR) | 11 (912) | 11 (912) | 0.67 | 30 |
| Consecutive days doing clinical work, median (IQR) | 7 (57) | 7 (57) | 0.94 | 17 |
| Percentage of work at night, median (IQR) | 15 (530) | 15 (525) | 0.45 | 16 |
| Percentage of night work in hospital if working nights, median (IQR) | 100 (5100) | 100 (10100) | 0.12 | 8 |
| Hours per month doing nonclinical work, median (IQR) | 12 (540) | 15 (540) | 0.77 | 26 |
| Estimated daily billable encounters, mean (IQR) | 14 (1116) | 15 (1218) | 0.01 | 54 |
| Total earnings in fiscal year 2009, median US$1,000 (IQR) | 185 (150210) | 202 (180240) | <0.01 | 56 |
| Marriage/domestic partnership status, n (%) | 0.15 | 43 | ||
| Married/currently in DP | 197 (80) | 421 (86) | ||
| Never married/never in DP | 26 (11) | 42 (9) | ||
| Divorced or separated | 18 (7) | 20 (4) | ||
| Other | 4 (2) | 5 (1) | ||
| Dependent children under 7 years old living in home, n (%) | 0.22 | 42 | ||
| 0 | 136 (55) | 265 (54) | ||
| 1 | 47 (19) | 92 (19) | ||
| 2 | 52 (21) | 87 (18) | ||
| 3 | 12 (5) | 43 (9) | ||
Several gender differences were seen in the characteristics of hospitalists and their work (Table 1). Women compared to men hospitalists were less likely to be leaders, more likely to be pediatricians, work in university settings, and practice in Western states. Women compared to men, on average, were younger by 3 years, worked fewer full‐time equivalents (FTEs), worked a greater percentage of nights, and reported fewer billable encounters per shift. They were also more likely to be divorced or separated.
Job satisfaction priorities differed for women and men hospitalists. Table 2 lists job satisfaction domains in descending order of the frequency prioritized by men. The largest proportion of women and men prioritized optimal workload. However, although substantial pay was prioritized next most frequently by men, more women prioritized collegiality and control over personal time than substantial pay.
| Women, % | Rank | Men, % | Rank | |
|---|---|---|---|---|
| Optimal workload | 59 | 1 | 59 | 1 |
| Substantial pay | 41 | 4 | 50 | 2 |
| Control over personal time | 44 | 3 | 41 | 3 |
| Collegiality with physicians | 47 | 2 | 38 | 4 |
| Rewarding relationships with patients | 35 | 5 | 34 | 5 |
| Organizational climate of trust and belonging | 27 | 7 | 33 | 6 |
| Ample availability of resources to do job | 24 | 9 | 27 | 7 |
| Optimal autonomy | 26 | 8 | 24 | 8 |
| Fairness within organization | 15 | 10 | 23 | 9 |
| Optimal variety of tasks | 29 | 6 | 22 | 10 |
| Recognition by leaders | 11 | 12 | 10 | 11 |
| Satisfaction with nurses | 12 | 11 | 7 | 12 |
Key differences in individual characteristics, work patterns, and indicating substantial pay as a priority were associated with self‐reported total earnings in 2009 from respondents' work as a hospitalist. As shown in Table 3, the inclusion of detailed productivity measures such as FTE, days of monthly clinical work, and estimated number of daily billable encounters yielded a model that explained 33% of variance in earnings. After adjusting for significant covariates including pediatric specialty, practice model, geography, and amount and type of clinical work, the estimated underpayment of women compared to men was $14,581. Hospitalists who prioritized substantial pay earned $10,771 more than those who did not. The female x leader interaction term testing the hypothesis that gender disparity is greater among leaders than frontline hospitalists was not statistically significant ($16,720, P = 0.087) and excluded from the final model.
| Differences in Salary, 2009 US$ (95% CI) | P Value | |
|---|---|---|
| ||
| Women | 14,581 (23,074 to 6,089) | <0.01 |
| Leader | 21,997 (13,313 to 30,682) | <0.01 |
| Prioritized substantial pay | 10,771 (2,651 to 18,891) | <0.01 |
| Pediatric specialty | 31,126 (43,007 to 19,244) | <0.01 |
| Practice model | ||
| Hospital employed | REF | |
| Multispecialty group | 1,922 (13,891 to 10,047) | 0.75 |
| University/medical school | 33,503 (46,336 to 20,671) | <0.01 |
| Multistate group | 6,505 (72,69 to 20,279) | 0.35 |
| Local hospitalist group | 9,330 (4,352 to 23,012) | 0.18 |
| Other | 17,364 (45,741 to 11,012) | 0.23 |
| Practice region | ||
| Southeast | REF | |
| Midwest | 1,225 (10,595 to 13,044) | 0.84 |
| Northeast | 15,712 (28,182 to 3,242) | 0.01 |
| Southwest | 722 (13,545 to 12,101) | 0.91 |
| West | 5,251 (7,383 to 17,885) | 0.41 |
| FTE | 1,021 (762 to 1,279) | <0.01 |
| Days per month doing clinical work | 1,209 (443 to 1,975) | <0.01 |
| Estimated daily billable encounters | 608 (20 to 1,196) | 0.04 |
DISCUSSION
In a national stratified sample of US hospitalists, we found gender differences in job satisfaction priorities and hospitalist work characteristics. We also confirmed the persistence of a substantial gender earnings disparity. Lower earnings among women compared to men hospitalists were present in our data after controlling for age, pediatric specialty, practice model, geography, type of clinical work, and productivity measures. The gender earnings disparity noted in 1999[6] persists, although it appears to have decreased, possibly indicating progress toward equity. We showed that women hospitalists' relative tendency not to prioritize pay explains a significant portion of the residual income gap.
Hoff examined hospitalist earnings in a large national survey of hospitalists in 1999. Our cohorts differed in age and experience (both lower in the Hoff study). An estimated $24,000 ($124,266 vs. $148,132) earnings gap between women and men was greater than our estimate of $14,581 following an interval of 10 years. Although survey items differed, both studies found that women were less interested in pay than men when considering a hospitalist job. Hoff also found that work setting and attitudes about pay and lifestyle were significantly related to earnings. We extended the previous analyses of gender differences in job satisfaction priorities, work, and demographic characteristics to explain the earnings gap and understand how it may be remedied.
When considering job satisfaction, we found that more men than women prioritized substantial pay and that prioritization of substantial pay was directly related to higher earnings. Therefore, fewer women prioritizing pay partly explains women's lower earnings. Reasons for why fewer women prioritize pay were not assessed in this study but may include factors like being part of 2‐income households and competing commitments.[29] Priorities may even be influenced by empirically observed gender differences in discussions of financial matters, governed by cultural norms. Such norms may implicitly sanction employers to offer women less pay than men for the same or similar work. Women may disadvantage themselves by negotiating less or less well than men for higher starting and promotion salaries. They may be perceived more negatively than men when they do negotiate pay, leading to unintended negative consequences such as loss of social networks, decreased likability, and even loss of job offers.[29, 30, 31, 32]
More women prioritized optimal variety of tasks (6th most prevalent among women and 10th among men). Women who highly rate optimal variety of tasks as a job satisfier may choose positions in which they teach, perform research, and participate in hospital committees and quality‐improvement work, but offer lower pay. Yet hours per month doing nonclinical work was not significantly different between men and women, nor associated with earnings differences in our earnings models. Understanding whether women self‐select into hospitalist jobs with like‐minded colleagues to achieve complementary fit or end up supplementing their skills with hospitalists with different priorities may inform strategies to reduce the gender income disparity.[5] Unlike disparities between various hospital medicine groups, systematic disparities within practices risk generating low levels of organizational fairness and burnout among employees.
Not surprisingly, productivity was positively associated with earnings but did not fully account for the gender earnings gap. Our data demonstrated that women, on average, were associated with work characteristics that expectedly generate less compensation. For example, women were younger, more often part time, academic, pediatric, less often leaders, and reported fewer billable encounters compared to men. These differences account for some of the earnings gap between men and women, but these factors were controlled for in the earnings model. In addition, our analysis may have underestimated the gap by not incorporating loss of fringe benefits from part‐time status and not comprehensively counting incentive pay associated with high productivity. Other work patterns more commonly associated with women suggest an imbalance in reimbursement. More women than men work nights that are often compensated at higher rates than daytime work, yet their average pay was less, suggesting that compensation for night work may need to be adjusted to reflect its unique burdens and responsibilities.[33]
Although the gender pay gap was not more extreme among leaders compared to frontline hospitalists in our data, the trend, nonetheless, underscores an important consideration. Whereas clinical work is paid for in mostly measurable ways, pay for leadership may be influenced by intangible factors such as reputation, negotiation, and confidence that may disadvantage women relative to men.[7, 19, 23, 34, 35, 36] Efforts to overcome implicit gender bias should be most effective when we consciously couple fair promotion of women to leadership with fair compensation commensurate with their male peers.[21]
Our data are vulnerable to nonresponse bias.[1, 4, 5] Post hoc analyses demonstrated that distributions of age, gender, practice model and region of our respondents were similar to other nationally representative cohorts of hospitalists. Consequently, we believe our data can make valid estimates about a nationally representative sample of hospitalists. However, we acknowledge several additional weaknesses of self‐reported data, including recall bias and accuracy of productivity figures, which were rounded to variable significant digits by respondents. Earnings analysis using this data was intended to be exploratory, but the findings echoed analyses using more authoritative data sources.[11] Still, we made inferences conservatively by adopting multiple imputation techniques for dealing with nonresponse surveys in adherence to established reporting guidelines.[25] We also note several limitations relevant to multiple imputations. The greater prevalence of missing data for survey items soliciting earnings and the number of billable encounters suggest they were not truly missing at random as assumed. However, we showed that missingness is unrelated to the variables under study, justifying use of the technique. The wider measures of variance derived from multiple imputations make us vulnerable to not detecting associations that may exist.
The gender earnings gap found in hospital medicine echoes the gap found in multiple medical specialties, including but not limited to pediatrics, academic medicine, gastroenterology, and plastic surgery.[7, 8, 9, 11, 12, 13, 37] Hospital medicine employment models and practice patterns have important structural differences compared to previously studied populations that could mitigate factors contributing to women physicians' lower earnings. However, despite well‐defined working hours, lack of control over the number of patient encounters per day and high prevalence of hospital‐employed practice models, the gender earnings gap persists. We showed that lower prioritization for pay may reflect the self‐selection of women into lower paying jobs. Unmeasured factors, including implicit bias and differences in negotiations, social networks and mentoring opportunities[38, 39] may also contribute to pay differences between men and women hospitalists. As hospital medicine tackles gender inequities and other disparities, strategies to assess and address fair physician compensation must be on the table.
Hospitalists are a growing workforce numbering over 40,000 physicians, one‐third of whom are women.[1] Flexibility of work schedules and control over personal time have been the traditional selling points of the specialty.[2] Multiple studies of physician work life reveal growing physician dissatisfaction and a high prevalence of burnout.[3] To mitigate burnout risk, leaders in hospital medicine recognize the importance of creating a sustainable profession that offers both job and career satisfaction as well as work‐life balance and, importantly, fairness within the work environment.[4] Although success in some of these endeavors has been realized sporadically, sustaining work‐life balance and fairness in the specialty remains a work in progress, whereas evidence of high job attrition and pay inequities remain.[5, 6]
Pay inequity for women relative to men continues to be pervasive in medicine, including among early‐career physicians, researchers, and various specialists.[6, 7, 8, 9, 10, 11, 12, 13] The earnings gap seems to persist for physicians, even as federal efforts such as the Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aim to end wage discrimination.[11, 14] Differences in specialty, part‐time status, and practice type do not mitigate the disparity.[8, 10, 15] Additional explanations have been proposed to explain the variability, including gender differences in negotiating skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.[12, 16, 17, 18, 19, 20]
The earnings gap is also a consequence of what is commonly called the glass ceiling.[18, 19] Most agree that obstacles to fair advancement of women include absence of collaborative environments and role models who have successfully achieved work‐life balance.[17, 20, 21, 22] Somewhat surprisingly, women leaders in medicine seem to suffer greater income disparity than nonleaders; this income gap is prevalent among leaders in other elite professions as well.[7, 23] It is unknown whether women physicians' emphasis on work‐life balance, seen repeatedly in surveys, explains any of the pay disparity.[24] Little research to date has examined whether work‐life priorities of women in hospital medicine differ from men.
In this study, we sought to examine differences in job priorities between men and women hospitalists. In particular, we examine the relative prioritization of substantial pay to job satisfaction. We also examined gender differences in work patterns and earnings to explore potential sources of the persistent gender earnings gap.
METHODS
We analyzed data from the 20092010 Hospital Medicine Physician Worklife Survey, the design of which is detailed elsewhere.[4] Briefly, a 118‐item survey was administered by mail to a stratified sample of hospitalists from the Society of Hospital Medicine database and 3 large multisite hospitalist groups. A single survey item asked respondents to identify up to 4 out of 12 most important domains to their satisfaction with a hospitalist job. The domains were distilled from focus groups of nationally representative hospitalists as described previously,[4] and the survey item allowed up to one‐third of these domains to be identified as respondents' personal priorities. The list included: optimal variety of tasks, optimal workload, substantial pay, collegiality with other physicians, recognition by leaders, rewarding relationships with patients, satisfaction with nurses, optimal autonomy, control over personal time, fairness within organization, ample availability of resources to do job, and organizational climate of trust and belonging. We tabulated and ranked the frequency with which respondents selected each satisfaction domain by gender. Due to the nonstandard format of the survey item, we a priori decided to analyze only responses that were completed as instructed.
We also used demographic data including detailed work characteristics, clinical and nonclinical workload, total pretax earnings in 2009 as a hospitalist, and self‐identification as leader of their hospital medicine group. Respondent characteristics were tabulated and gender differences were tested using the t test, rank sum test, and the Fischer exact test as appropriate. We also listed the number of nonrespondents for each item. In estimating gender differences in earnings, we opted to use multiple‐imputation techniques to more conservatively account for greater variance inherent in the presence of missing data. Consistent with existing guidelines,[25] we demonstrated that item responses were not missing monotonically by visually inspecting patterns of nonresponse. We further demonstrated that data were missing at random by showing that response patterns of completed survey items did not predict whether or not a given variable response was missing using logistic regression models. We found no significant differences between respondents with complete and missing data. We verified that appropriate regression models for each variable on every other variable converged. We used Stata 13.1 (StataCorp, College Station, TX) to perform multiple imputations using chain equations (mi impute chain) to create 10 imputed tables for 7 normally distributed continuous variables using the ordinary least squares method, 3 non‐normally distributed variables using the predictive mean matching method, 2 nonordinal categorical variables using the multinomial logit method, and 1 binary variable using the logit method.[26, 27] Gender, pediatric specialty status, region of practice, and whether or not respondents prioritized substantial pay for job satisfaction were used as regular variables without missing data points.
Differences in earnings were assessed using a multivariate ordinary linear regression model applied to the imputed datasets fitted by forward selection of explanatory variables using P < 0.20 in bivariate analysis for inclusion and manual backward elimination of all statistically nonsignificant variables. We tested the significance of the women leader interaction term in the final parsimonious model. We used the usual significance threshold of P < 0.05 for inferences. Our analysis of publicly available anonymous data was exempt from IRB review.
RESULTS
Of the 816 survey respondents (response rate 25.6%), 40 either omitted the item soliciting work priorities or completed it incorrectly. Data from the remaining 776 respondents were used for the present analysis. Respondent characteristics are tabulated in Table 1. The characteristics of hospitalists by age, gender, specialty, practice model, and practice region were representative of US hospitalists from other surveys.[28]
| Women | Men | P Value | No. of Missing Responses | |
|---|---|---|---|---|
| ||||
| No. | 263 | 513 | 0 | |
| Role, n (%) | <0.01 | 0 | ||
| Frontline hospitalist | 201 (76) | 337 (66) | ||
| Hospitalist leader | 53 (24) | 176 (34) | ||
| Age, y, mean (SD) | 42 (8) | 45 (9) | <0.01 | 67 |
| Years in current job, mean (SD) | 5 (4) | 6 (5) | 0.07 | 14 |
| Specialty, n (%) | <0.01 | 0 | ||
| Internal medicine | 160 (61) | 369 (72) | ||
| Pediatrics | 56 (21) | 57 (11) | ||
| Other | 39 (15) | 47 (9) | ||
| Family medicine | 8 (3) | 40 (8) | ||
| Practice model, n (%) | 0.02 | 19 | ||
| Hospital employed | 110 (43) | 227 (46) | ||
| Multispecialty group | 44 (17) | 68 (14) | ||
| University/medical school | 47 (18) | 58 (12) | ||
| Multistate group | 27 (11) | 73 (15) | ||
| Local hospitalist group | 22 (8) | 65 (13) | ||
| Other | 7 (3) | 9 (2) | ||
| Practice region, n (%) | 0.14 | 0 | ||
| Southeast | 56 (21) | 151 (29) | ||
| Midwest | 58 (22) | 106 (21) | ||
| Northeast | 54 (21) | 96 (19) | ||
| Southwest | 44 (17) | 83 (16) | ||
| West | 51 (19) | 77 (15) | ||
| Full‐time equivalents, n (%) | <0.01 | 42 | ||
| <100% | 46 (18) | 60 (12) | ||
| 100% | 202 (81) | 402 (83) | ||
| >100% | 2 (1) | 22 (5) | ||
| Days per month doing clinical work if FTE 100%, median (IQR) | 15 (1418) | 16 (1420) | 0.12 | 11 |
| Hours per day doing clinical work, median (IQR) | 11 (912) | 11 (912) | 0.67 | 30 |
| Consecutive days doing clinical work, median (IQR) | 7 (57) | 7 (57) | 0.94 | 17 |
| Percentage of work at night, median (IQR) | 15 (530) | 15 (525) | 0.45 | 16 |
| Percentage of night work in hospital if working nights, median (IQR) | 100 (5100) | 100 (10100) | 0.12 | 8 |
| Hours per month doing nonclinical work, median (IQR) | 12 (540) | 15 (540) | 0.77 | 26 |
| Estimated daily billable encounters, mean (IQR) | 14 (1116) | 15 (1218) | 0.01 | 54 |
| Total earnings in fiscal year 2009, median US$1,000 (IQR) | 185 (150210) | 202 (180240) | <0.01 | 56 |
| Marriage/domestic partnership status, n (%) | 0.15 | 43 | ||
| Married/currently in DP | 197 (80) | 421 (86) | ||
| Never married/never in DP | 26 (11) | 42 (9) | ||
| Divorced or separated | 18 (7) | 20 (4) | ||
| Other | 4 (2) | 5 (1) | ||
| Dependent children under 7 years old living in home, n (%) | 0.22 | 42 | ||
| 0 | 136 (55) | 265 (54) | ||
| 1 | 47 (19) | 92 (19) | ||
| 2 | 52 (21) | 87 (18) | ||
| 3 | 12 (5) | 43 (9) | ||
Several gender differences were seen in the characteristics of hospitalists and their work (Table 1). Women compared to men hospitalists were less likely to be leaders, more likely to be pediatricians, work in university settings, and practice in Western states. Women compared to men, on average, were younger by 3 years, worked fewer full‐time equivalents (FTEs), worked a greater percentage of nights, and reported fewer billable encounters per shift. They were also more likely to be divorced or separated.
Job satisfaction priorities differed for women and men hospitalists. Table 2 lists job satisfaction domains in descending order of the frequency prioritized by men. The largest proportion of women and men prioritized optimal workload. However, although substantial pay was prioritized next most frequently by men, more women prioritized collegiality and control over personal time than substantial pay.
| Women, % | Rank | Men, % | Rank | |
|---|---|---|---|---|
| Optimal workload | 59 | 1 | 59 | 1 |
| Substantial pay | 41 | 4 | 50 | 2 |
| Control over personal time | 44 | 3 | 41 | 3 |
| Collegiality with physicians | 47 | 2 | 38 | 4 |
| Rewarding relationships with patients | 35 | 5 | 34 | 5 |
| Organizational climate of trust and belonging | 27 | 7 | 33 | 6 |
| Ample availability of resources to do job | 24 | 9 | 27 | 7 |
| Optimal autonomy | 26 | 8 | 24 | 8 |
| Fairness within organization | 15 | 10 | 23 | 9 |
| Optimal variety of tasks | 29 | 6 | 22 | 10 |
| Recognition by leaders | 11 | 12 | 10 | 11 |
| Satisfaction with nurses | 12 | 11 | 7 | 12 |
Key differences in individual characteristics, work patterns, and indicating substantial pay as a priority were associated with self‐reported total earnings in 2009 from respondents' work as a hospitalist. As shown in Table 3, the inclusion of detailed productivity measures such as FTE, days of monthly clinical work, and estimated number of daily billable encounters yielded a model that explained 33% of variance in earnings. After adjusting for significant covariates including pediatric specialty, practice model, geography, and amount and type of clinical work, the estimated underpayment of women compared to men was $14,581. Hospitalists who prioritized substantial pay earned $10,771 more than those who did not. The female x leader interaction term testing the hypothesis that gender disparity is greater among leaders than frontline hospitalists was not statistically significant ($16,720, P = 0.087) and excluded from the final model.
| Differences in Salary, 2009 US$ (95% CI) | P Value | |
|---|---|---|
| ||
| Women | 14,581 (23,074 to 6,089) | <0.01 |
| Leader | 21,997 (13,313 to 30,682) | <0.01 |
| Prioritized substantial pay | 10,771 (2,651 to 18,891) | <0.01 |
| Pediatric specialty | 31,126 (43,007 to 19,244) | <0.01 |
| Practice model | ||
| Hospital employed | REF | |
| Multispecialty group | 1,922 (13,891 to 10,047) | 0.75 |
| University/medical school | 33,503 (46,336 to 20,671) | <0.01 |
| Multistate group | 6,505 (72,69 to 20,279) | 0.35 |
| Local hospitalist group | 9,330 (4,352 to 23,012) | 0.18 |
| Other | 17,364 (45,741 to 11,012) | 0.23 |
| Practice region | ||
| Southeast | REF | |
| Midwest | 1,225 (10,595 to 13,044) | 0.84 |
| Northeast | 15,712 (28,182 to 3,242) | 0.01 |
| Southwest | 722 (13,545 to 12,101) | 0.91 |
| West | 5,251 (7,383 to 17,885) | 0.41 |
| FTE | 1,021 (762 to 1,279) | <0.01 |
| Days per month doing clinical work | 1,209 (443 to 1,975) | <0.01 |
| Estimated daily billable encounters | 608 (20 to 1,196) | 0.04 |
DISCUSSION
In a national stratified sample of US hospitalists, we found gender differences in job satisfaction priorities and hospitalist work characteristics. We also confirmed the persistence of a substantial gender earnings disparity. Lower earnings among women compared to men hospitalists were present in our data after controlling for age, pediatric specialty, practice model, geography, type of clinical work, and productivity measures. The gender earnings disparity noted in 1999[6] persists, although it appears to have decreased, possibly indicating progress toward equity. We showed that women hospitalists' relative tendency not to prioritize pay explains a significant portion of the residual income gap.
Hoff examined hospitalist earnings in a large national survey of hospitalists in 1999. Our cohorts differed in age and experience (both lower in the Hoff study). An estimated $24,000 ($124,266 vs. $148,132) earnings gap between women and men was greater than our estimate of $14,581 following an interval of 10 years. Although survey items differed, both studies found that women were less interested in pay than men when considering a hospitalist job. Hoff also found that work setting and attitudes about pay and lifestyle were significantly related to earnings. We extended the previous analyses of gender differences in job satisfaction priorities, work, and demographic characteristics to explain the earnings gap and understand how it may be remedied.
When considering job satisfaction, we found that more men than women prioritized substantial pay and that prioritization of substantial pay was directly related to higher earnings. Therefore, fewer women prioritizing pay partly explains women's lower earnings. Reasons for why fewer women prioritize pay were not assessed in this study but may include factors like being part of 2‐income households and competing commitments.[29] Priorities may even be influenced by empirically observed gender differences in discussions of financial matters, governed by cultural norms. Such norms may implicitly sanction employers to offer women less pay than men for the same or similar work. Women may disadvantage themselves by negotiating less or less well than men for higher starting and promotion salaries. They may be perceived more negatively than men when they do negotiate pay, leading to unintended negative consequences such as loss of social networks, decreased likability, and even loss of job offers.[29, 30, 31, 32]
More women prioritized optimal variety of tasks (6th most prevalent among women and 10th among men). Women who highly rate optimal variety of tasks as a job satisfier may choose positions in which they teach, perform research, and participate in hospital committees and quality‐improvement work, but offer lower pay. Yet hours per month doing nonclinical work was not significantly different between men and women, nor associated with earnings differences in our earnings models. Understanding whether women self‐select into hospitalist jobs with like‐minded colleagues to achieve complementary fit or end up supplementing their skills with hospitalists with different priorities may inform strategies to reduce the gender income disparity.[5] Unlike disparities between various hospital medicine groups, systematic disparities within practices risk generating low levels of organizational fairness and burnout among employees.
Not surprisingly, productivity was positively associated with earnings but did not fully account for the gender earnings gap. Our data demonstrated that women, on average, were associated with work characteristics that expectedly generate less compensation. For example, women were younger, more often part time, academic, pediatric, less often leaders, and reported fewer billable encounters compared to men. These differences account for some of the earnings gap between men and women, but these factors were controlled for in the earnings model. In addition, our analysis may have underestimated the gap by not incorporating loss of fringe benefits from part‐time status and not comprehensively counting incentive pay associated with high productivity. Other work patterns more commonly associated with women suggest an imbalance in reimbursement. More women than men work nights that are often compensated at higher rates than daytime work, yet their average pay was less, suggesting that compensation for night work may need to be adjusted to reflect its unique burdens and responsibilities.[33]
Although the gender pay gap was not more extreme among leaders compared to frontline hospitalists in our data, the trend, nonetheless, underscores an important consideration. Whereas clinical work is paid for in mostly measurable ways, pay for leadership may be influenced by intangible factors such as reputation, negotiation, and confidence that may disadvantage women relative to men.[7, 19, 23, 34, 35, 36] Efforts to overcome implicit gender bias should be most effective when we consciously couple fair promotion of women to leadership with fair compensation commensurate with their male peers.[21]
Our data are vulnerable to nonresponse bias.[1, 4, 5] Post hoc analyses demonstrated that distributions of age, gender, practice model and region of our respondents were similar to other nationally representative cohorts of hospitalists. Consequently, we believe our data can make valid estimates about a nationally representative sample of hospitalists. However, we acknowledge several additional weaknesses of self‐reported data, including recall bias and accuracy of productivity figures, which were rounded to variable significant digits by respondents. Earnings analysis using this data was intended to be exploratory, but the findings echoed analyses using more authoritative data sources.[11] Still, we made inferences conservatively by adopting multiple imputation techniques for dealing with nonresponse surveys in adherence to established reporting guidelines.[25] We also note several limitations relevant to multiple imputations. The greater prevalence of missing data for survey items soliciting earnings and the number of billable encounters suggest they were not truly missing at random as assumed. However, we showed that missingness is unrelated to the variables under study, justifying use of the technique. The wider measures of variance derived from multiple imputations make us vulnerable to not detecting associations that may exist.
The gender earnings gap found in hospital medicine echoes the gap found in multiple medical specialties, including but not limited to pediatrics, academic medicine, gastroenterology, and plastic surgery.[7, 8, 9, 11, 12, 13, 37] Hospital medicine employment models and practice patterns have important structural differences compared to previously studied populations that could mitigate factors contributing to women physicians' lower earnings. However, despite well‐defined working hours, lack of control over the number of patient encounters per day and high prevalence of hospital‐employed practice models, the gender earnings gap persists. We showed that lower prioritization for pay may reflect the self‐selection of women into lower paying jobs. Unmeasured factors, including implicit bias and differences in negotiations, social networks and mentoring opportunities[38, 39] may also contribute to pay differences between men and women hospitalists. As hospital medicine tackles gender inequities and other disparities, strategies to assess and address fair physician compensation must be on the table.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task F. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO study. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation. Vol. 1. Research Findings. Rockville, MD; Agency for Healthcare Research and Quality; 2005.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , . Person‐job fit: an exploratory cross‐sectional analysis of hospitalists. J Hosp Med. 2013;8(2):96–101.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- , , , . Compensation and advancement of women in academic medicine: Is there equity? Ann Intern Med. 2004;141(3):205–212.
- . Differences in earnings between male and female physicians. N Engl J Med. 1996;334(15):960–964.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , , , . The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J Gen Intern Med. 2000;15(6):372–380.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30(2):193–201.
- , , , . Assessing gender equity in a large academic department of pediatrics. Acad Med. 2012;87(1):98–104.
- , , , , , . Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005;100(2):259–264.
- H.R. 438, Fair Pay Act of 2013. 113th Congress (2013‐2014).
- , , , , . Topics to ponder: part‐time practice and pay parity. Gend Med. 2010;7(4):350–356.
- , . Understanding and finding mentorship: a review for junior faculty. J Palliat Med. 2010;13(11):1373–1379.
- , , , et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA. 1996;276(11):898–905.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335(17):1282–1289.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–1025.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86(6):752–758.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , . Why aren't there more women leaders in academic medicine? tHe views of clinical department chairs. Acad Med. 2001;76(5):453–465.
- . The gender gap in executive compensation: the role of female directors and chief executive officers. Ann Am Acad Pol Soc Sci. 2012(639):258–278.
- , , . Keys to career satisfaction: insights from a survey of women pediatric surgeons. J Pediatr Surg. 2004;39(6):984–990.
- , , , et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
- Imputation and Variance Estimation Software [computer program]. Ann Arbor, MI: Universtiy of Michigan; 2007.
- , , . Multiple Imputation using chained equations: issues and guidance for practice. Stat Med. 2010;30(4):377–399.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2010.
- , . The Changing Face of Medicine: Women Doctors and the Evolution Of Health Care in America. Ithaca, NY: ILR Press/Cornell University Press; 2008.
- , . Women Don't Ask: Negotiation and the Gender Divide. Princeton, NJ: Princeton University Press; 2003.
- , , , et al. Negotiation in academic medicine: a necessary career skill. J Womens Health (Larchmt). 2007;16(2):235–244.
- . Women and salary negotiation: the costs of self‐advocacy. Psychol Women Q. 2001;25:65–76.
- State of Hospital Medicine: 2014 Report Based on 2013 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2014.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , . Sociology. The gender gap in NIH grant applications. Science. 2008;322(5907):1472–1474.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , . Gender differences in the professional and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775–779.
- . Gender and supportive co‐worker relations in the medical profession. Gend Work Organ. 2014;21(1):1–17.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task F. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO study. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation. Vol. 1. Research Findings. Rockville, MD; Agency for Healthcare Research and Quality; 2005.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , . Person‐job fit: an exploratory cross‐sectional analysis of hospitalists. J Hosp Med. 2013;8(2):96–101.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- , , , . Compensation and advancement of women in academic medicine: Is there equity? Ann Intern Med. 2004;141(3):205–212.
- . Differences in earnings between male and female physicians. N Engl J Med. 1996;334(15):960–964.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , , , . The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J Gen Intern Med. 2000;15(6):372–380.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30(2):193–201.
- , , , . Assessing gender equity in a large academic department of pediatrics. Acad Med. 2012;87(1):98–104.
- , , , , , . Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005;100(2):259–264.
- H.R. 438, Fair Pay Act of 2013. 113th Congress (2013‐2014).
- , , , , . Topics to ponder: part‐time practice and pay parity. Gend Med. 2010;7(4):350–356.
- , . Understanding and finding mentorship: a review for junior faculty. J Palliat Med. 2010;13(11):1373–1379.
- , , , et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA. 1996;276(11):898–905.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335(17):1282–1289.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–1025.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86(6):752–758.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , . Why aren't there more women leaders in academic medicine? tHe views of clinical department chairs. Acad Med. 2001;76(5):453–465.
- . The gender gap in executive compensation: the role of female directors and chief executive officers. Ann Am Acad Pol Soc Sci. 2012(639):258–278.
- , , . Keys to career satisfaction: insights from a survey of women pediatric surgeons. J Pediatr Surg. 2004;39(6):984–990.
- , , , et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
- Imputation and Variance Estimation Software [computer program]. Ann Arbor, MI: Universtiy of Michigan; 2007.
- , , . Multiple Imputation using chained equations: issues and guidance for practice. Stat Med. 2010;30(4):377–399.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2010.
- , . The Changing Face of Medicine: Women Doctors and the Evolution Of Health Care in America. Ithaca, NY: ILR Press/Cornell University Press; 2008.
- , . Women Don't Ask: Negotiation and the Gender Divide. Princeton, NJ: Princeton University Press; 2003.
- , , , et al. Negotiation in academic medicine: a necessary career skill. J Womens Health (Larchmt). 2007;16(2):235–244.
- . Women and salary negotiation: the costs of self‐advocacy. Psychol Women Q. 2001;25:65–76.
- State of Hospital Medicine: 2014 Report Based on 2013 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2014.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , . Sociology. The gender gap in NIH grant applications. Science. 2008;322(5907):1472–1474.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , . Gender differences in the professional and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775–779.
- . Gender and supportive co‐worker relations in the medical profession. Gend Work Organ. 2014;21(1):1–17.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
© 2015 Society of Hospital Medicine
What Is the Appropriate Treatment of Cancer-Associated Venous Thromboembolic Disease?
Case
A 70-year-old woman with recently diagnosed pancreatic cancer is admitted with worsening abdominal pain and new right-lower-extremity edema. A CT scan of the abdomen and pelvis reveals occlusive IVC and common iliac thromboses. A right-common-femoral DVT appears on Doppler ultrasound. A CT angiogram of her chest is negative for pulmonary emboli. What is the appropriate treatment for this patient’s thromboembolic disease?
Overview
VTE in the setting of malignancy is common, and the incidence of VTE among cancer patients is increasing for unclear reasons.1,2,3 VTE occurs in an estimated 4% to 20% of all malignancy patients. Overall, cancer patients are at a sixfold increased risk of developing VTE compared with the general population, and these patients represent approximately 20% of all VTE cases.4,5
VTE is a leading cause of mortality among hospitalized cancer patients; evidence of VTE exists in up to 50% of cancer patients at autopsy.3,4 VTE complications lead to significant morbidity, including recurrent VTE, pulmonary hypertension, post-thrombophlebitic syndrome, bleeding, and decreased quality of life.6,7
The risk is greatest for hospitalized cancer patients and those receiving active chemotherapy, particularly with such antiangiogenic agents as thalidomide and bevacizumab.4,6 Certain malignancies are more frequently associated with VTE; these include gastrointestinal, gynecologic, brain, lung, renal, and hematologic cancers.4 Table 1 (p. 50) summarizes risk factors associated with VTE in cancer patients.4
Patients with malignancy are hypercoagulable, primarily because of tumor-related alterations in the coagulation cascade.8 Tumors contain cell-surface proteins (e.g., tissue factor and cancer procoagulant) that lead to activation of the clotting cascade via interactions with factors IX and/or X. In addition, tumor-released cytokines cause prothrombotic changes in the vascular endothelium.8
This hypercoagulability is exacerbated by cancer-associated treatment events, including immobility, central venous catheters, erythropoiesis-stimulating agents, and packed red-blood-cell and platelet transfusions.5,9
Cancer-related therapy complications further confound VTE management. Drug interactions, chemotherapy-induced thrombocytopenia, malnutrition, bleeding risk from surgery or tumor location, and liver dysfunction make safe management of cancer-associated VTE a challenge.
Review of the Data
Low-molecular-weight heparin (LMWH) vs. vitamin K antagonists (VKA): There is significant evidence that LMWH is the preferred pharmacologic therapy for the initial and long-term treatment of cancer-related VTE. The most convincing data were published as the CLOT trial, and is supported by several smaller studies.10 Recommendations for the preferred use of LMWH are consistent among several national and international guidelines.6,7
In the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin Versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, six months of treatment with an oral VKA preceded by five to seven days of LMWH was compared with six months of treatment with LMWH (dalteparin). Patients with the diagnosis of acute symptomatic VTE were evaluated. After six months of treatment, 53 of 336 patients in the oral anticoagulant group had recurrent VTE, compared with 27 of 336 patients in the LMWH group—a relative risk reduction of 52% and an absolute risk reduction of 8% (P=0.002). Complication rates (major and minor bleeding) and overall mortality were similar between the two groups.7,10

Two smaller trials compared LMWHs with warfarin in the treatment of VTE in the setting of cancer. In one trial, seven of 67 enoxaparin-treated patients developed bleeding or recurrent VTE, compared with 15 of 71 warfarin-treated subjects; however, this reduction was not statistically significant (P=0.09).11 In another trial, seven of 100 tinzaparin-treated patients developed recurrent VTE, compared with 16 of 100 warfarin-treated patients (P=0.044).12
Thus, LMWH is the preferred therapeutic agent for both DVT and PE in the setting of malignancy.5 Even so, although the clinical evidence supports LMWH use in the treatment of cancer-associated VTE, it’s worth noting that many of the authors of the cited papers received compensation from large pharmaceutical companies. In addition, the CLOT trial was funded by Pharmacia, which supplied the study drug.
Initial treatment (5-10 days): The American Society of Clinical Oncology (ASCO) guidelines advocate the use of LMWH during the initial five to 10 days following VTE diagnosis. Four other cancer research organization guidelines, National Comprehensive Cancer Network (NCCN), the Italian Association of Medical Oncology (AIOM), the European Society of Medical Oncology (ESMO), and the French National Federation of the League of Centers Against Cancer (FNCLCC), echo this approach, with unfractionated heparin (UFH) or fondaparinux as additional initial treatment depending on the clinical situation—i.e., renal failure, heparin-induced thrombocytopenia (HIT), or bleeding risk.6
Table 2 (below) summarizes recommendations for VTE treatment in cancer patients from all five guideline panels.6
Long-term treatment and duration (3-6 months): All of the panels agree LMWH is the preferred agent for long-term therapy of cancer-related VTE. ASCO supports treatment with LMWH for at least six months; oral VKAs with a targeted INR of 2 to 3 are acceptable when LMWH is not feasible. NCCN, AIOM, ESMO, and FNCLCC recommend an LMWH treatment duration from three to six months (ASCO recommends at least six months).
All of the panels, however, advocate indefinite duration of anticoagulation in patients with such continuing risk factors as active (metastatic, recurrent, or persistent) cancer or chemotherapy treatment.6 AIOM and ESMO specify indefinite LMWH, whereas ASCO does not specify oral VKA or LMWH use. Given the difficulties of managing VKA in the setting of advanced malignancy or chemotherapy, LMWH is the most practical choice, if it’s available and isn’t cost-prohibitive.
LMWH availability: Dalteparin, tinzaparin, and enoxaparin are LMWHs currently available in the U.S. for VTE treatment. Dalteparin is the only FDA-approved LMWH drug for long-term use to treat cancer-associated VTE, although enoxaparin and tinzaparin are used in practice. All three are supplied in prefilled syringes, which make self-administration easier and significantly reduce the risk of dosage error.6
LMWH vs. UFH: LMWH is safer and more efficacious than UFH. A summary of 22 clinical trials (including cancer patients and noncancer patients) by a Cochrane systematic review showed that treatment with LMWH in comparison with UFH results in decreased recurrent VTE, bleeding, mortality, HIT, and osteoporosis.7,13
Other agents: Fondaparinux is a factor Xa inhibitor rarely associated with heparin-induced thrombocytopenia (HIT), which makes it an attractive alternate anticoagulant for HIT patients. Its use in comparison with other parenteral anticoagulants has not been established in patients with malignancy.
Fondaparinux is FDA-approved for initial VTE treatment, and is used in practice as an alternative prophylactic anticoagulant for patients with HIT history or heparin allergy.7 However, no randomized clinical trials have evaluated its efficacy in patients with HIT.
Several new oral anticoagulants, including direct thrombin and factor Xa inhibitors, are being investigated; efficacy has not been established in cancer patients.7
Inferior vena cava (IVC) filters: Limited data surround the use of IVC filters, and most consensus guidelines recommend their use only in specific settings. One randomized controlled study (not limited to patients with cancer) showed no difference in overall short-term or long-term survival among patients receiving IVC filters for VTE treatment. However, there was a decrease in symptomatic PE in the filter group 12 days after placement. The tradeoff was significantly more recurrent DVTs at two years’ followup. The authors concluded that systematic use of IVC filters is not recommended.14
Because all of the study participants in this trial were receiving concomitant anticoagulation, it is difficult to generalize results to patients who have contraindications to anticoagulation. Nonetheless, ASCO, NCCN, and several other guideline panels recommend IVC filters only for patients with contraindications to anticoagulation or failure of long-term anticoagulation. NCCN broadens these recommendations for IVC filter placement to include patients with severe cardiac or pulmonary dysfunction.6 However, this recommendation is controversial, given the lack of supporting data, cost, and invasiveness of the procedure.7
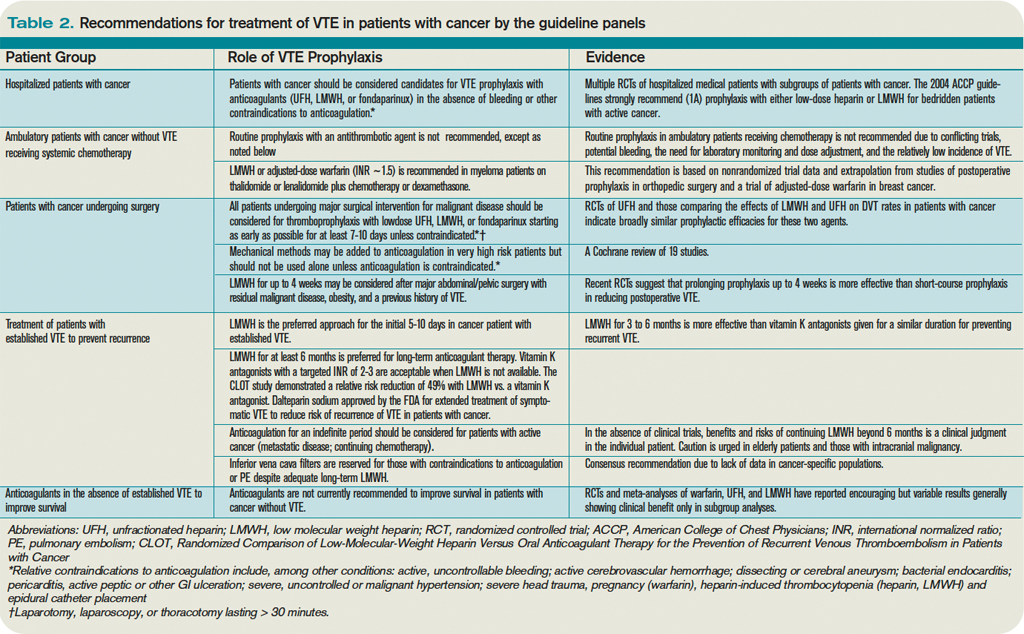
All patients with IVC filters without contraindication to anticoagulation should be anticoagulated.9
Prophylaxis: The importance of VTE prophylaxis in all hospitalized patients, including patients with cancer, is under close scrutiny in an attempt to improve patient safety and quality. The Centers for Medicare & Medicaid Services (CMS), in conjunction with the Joint Commission, has added VTE to its list of conditions that are reasonably preventable, and hospitals will no longer be reimbursed for the cost of treatment if acquired during a hospital stay. This rule currently is in effect for knee and hip replacements.15
The need for improvement in aggressive and appropriate prophylaxis of hospitalized patients was demonstrated by a single study in which just one-third of hospitalized patients received appropriate prophylaxis, according to American College of Chest Physicians (ACCP) guidelines.16
Despite a lack of robust data regarding VTE prophylaxis in patients with malignancy, strong data exist for VTE prophylaxis in hospitalized patients. All patients with cancer, and without contraindications to anticoagulation, should receive pharmacologic VTE prophylaxis while hospitalized. In the absence of supporting data, guidelines do not suggest VTE prophylaxis for ambulatory patients with cancer, except in certain multiple myeloma patients.6
Intracranial malignancies: Patients with intracranial malignancies are at risk for VTE, and the presence of intracranial tumors or metastases are not absolute contraindications to anticoagulation. However, data are sparse regarding VTE therapy in this subgroup. Active intracranial bleeding is an absolute contraindication to anticoagulation, and it should be avoided in patients with recent intracranial surgery or thrombocytopenia (e.g., platelet count < 50 x 109).4 In general, the presence of intracranial lesions without high-risk features should not deter the use of prophylactic anticoagulation.
Thrombocytopenia: Cancer patients frequently have chemotherapy-induced cytopenias, including thrombocytopenia. There is a paucity of data regarding anticoagulation in the setting of thrombocytopenia. In a recent review of VTE in the setting of cancer, Lee suggests dose reduction of LMWH by half in patients with platelet counts between 20 and 50 x 109/L.7 At our institution, hematologists suggest halving treatment-dose LMWH at platelet counts between 30 and 50 x 109/L, and discontinuing pharmacologic prophylaxis at platelet counts of less than 50 x 109/L—although there are little data to support these recommendations. Anticoagulation should be discontinued in patients with platelet counts below 20-30 x 109/L, as the risk of bleeding becomes too high.7
Thrombolytic therapy: Catheter-directed thrombolysis or systemic thrombolytic therapy might be appropriate treatment options for acute VTE. Presence of extensive proximal DVT, symptom duration of less than two weeks, life expectancy of greater than one year, good functional status, and low bleeding risk are prerequisites. Anticoagulation recommendations do not change following thrombolytic therapy.17
In the setting of PE, hemodynamic instability is the primary indication for thrombolysis. ACCP does not recommend thrombolytic therapy for the majority of VTE patients.17
Back to the Case
Our patient’s lower-extremity ultrasound and CT of the abdomen and pelvis both revealed extensive clot burden, which likely is related to her underlying pancreatic cancer. She should be started on an LMWH. Given the low likelihood of cure from her cancer, anticoagulation should be continued indefinitely, and an LMWH should be given for at least the first six months. Whether she should be switched to an oral VKA after six months depends on several factors: cost considerations, nutritional status, chemotherapy, presence of cytopenias, and bleeding risk.
IVC filter placement is not indicated at this time, as the patient does not have any contraindications to anticoagulation, has not failed anticoagulation, and does not have impending cardiac or pulmonary compromise. She is not a candidate for thrombolytic therapy due to her poor functional status and limited life expectancy.
Bottom Line
Cancer-associated VTE is increasingly common, and optimally is treated with LMWH for at least six months—indefinitely in the setting of active cancer or treatment. IVC filters have limited and specific indications in the setting of cancer-associated VTE, and should be reserved for situations when anticoagulation is contraindicated. TH
Dr. Weaver is an instructor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. Dr. Barsuk is an assistant professor in the division of hospital medicine at Feinberg.
References
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10): 2339-2346.
- Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olsen RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006(1);119:60-68.
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-634.
- Lyman GA, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34):5490-5505.
- Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821-4826.
- Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009;27(29):4919-4926.
- Lee, AY. Anticoagulation in the treatment of established venous thromboembolism in patients with cancer. J Clin Oncol. 2009;27(29):4895-4901.
- Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902-4911.
- Prandoni, P. How I treat venous thromboembolism in patients with cancer. Blood. 2005;106(13):4027-4033.
- Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146-153.
- Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
- Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062-1072.
- Van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004:18(4);CD001100.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7): 409-415.
- Amin AN, Deitelzweig SB. Optimizing the prevention of venous thromboembolism: recent quality initiatives and strategies to drive improvement. Jt Comm J Qual Patient Saf. 2009;35(11):558-564.
- Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
- Hirsch J, Guyatt G, Albers W, et al. Executive summary: American College of Chest Physicians evidence-based clinical practice guidelines (8th ed.). Chest. 2008:133(6 Suppl);71S-105S.
Case
A 70-year-old woman with recently diagnosed pancreatic cancer is admitted with worsening abdominal pain and new right-lower-extremity edema. A CT scan of the abdomen and pelvis reveals occlusive IVC and common iliac thromboses. A right-common-femoral DVT appears on Doppler ultrasound. A CT angiogram of her chest is negative for pulmonary emboli. What is the appropriate treatment for this patient’s thromboembolic disease?
Overview
VTE in the setting of malignancy is common, and the incidence of VTE among cancer patients is increasing for unclear reasons.1,2,3 VTE occurs in an estimated 4% to 20% of all malignancy patients. Overall, cancer patients are at a sixfold increased risk of developing VTE compared with the general population, and these patients represent approximately 20% of all VTE cases.4,5
VTE is a leading cause of mortality among hospitalized cancer patients; evidence of VTE exists in up to 50% of cancer patients at autopsy.3,4 VTE complications lead to significant morbidity, including recurrent VTE, pulmonary hypertension, post-thrombophlebitic syndrome, bleeding, and decreased quality of life.6,7
The risk is greatest for hospitalized cancer patients and those receiving active chemotherapy, particularly with such antiangiogenic agents as thalidomide and bevacizumab.4,6 Certain malignancies are more frequently associated with VTE; these include gastrointestinal, gynecologic, brain, lung, renal, and hematologic cancers.4 Table 1 (p. 50) summarizes risk factors associated with VTE in cancer patients.4
Patients with malignancy are hypercoagulable, primarily because of tumor-related alterations in the coagulation cascade.8 Tumors contain cell-surface proteins (e.g., tissue factor and cancer procoagulant) that lead to activation of the clotting cascade via interactions with factors IX and/or X. In addition, tumor-released cytokines cause prothrombotic changes in the vascular endothelium.8
This hypercoagulability is exacerbated by cancer-associated treatment events, including immobility, central venous catheters, erythropoiesis-stimulating agents, and packed red-blood-cell and platelet transfusions.5,9
Cancer-related therapy complications further confound VTE management. Drug interactions, chemotherapy-induced thrombocytopenia, malnutrition, bleeding risk from surgery or tumor location, and liver dysfunction make safe management of cancer-associated VTE a challenge.
Review of the Data
Low-molecular-weight heparin (LMWH) vs. vitamin K antagonists (VKA): There is significant evidence that LMWH is the preferred pharmacologic therapy for the initial and long-term treatment of cancer-related VTE. The most convincing data were published as the CLOT trial, and is supported by several smaller studies.10 Recommendations for the preferred use of LMWH are consistent among several national and international guidelines.6,7
In the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin Versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, six months of treatment with an oral VKA preceded by five to seven days of LMWH was compared with six months of treatment with LMWH (dalteparin). Patients with the diagnosis of acute symptomatic VTE were evaluated. After six months of treatment, 53 of 336 patients in the oral anticoagulant group had recurrent VTE, compared with 27 of 336 patients in the LMWH group—a relative risk reduction of 52% and an absolute risk reduction of 8% (P=0.002). Complication rates (major and minor bleeding) and overall mortality were similar between the two groups.7,10
Two smaller trials compared LMWHs with warfarin in the treatment of VTE in the setting of cancer. In one trial, seven of 67 enoxaparin-treated patients developed bleeding or recurrent VTE, compared with 15 of 71 warfarin-treated subjects; however, this reduction was not statistically significant (P=0.09).11 In another trial, seven of 100 tinzaparin-treated patients developed recurrent VTE, compared with 16 of 100 warfarin-treated patients (P=0.044).12
Thus, LMWH is the preferred therapeutic agent for both DVT and PE in the setting of malignancy.5 Even so, although the clinical evidence supports LMWH use in the treatment of cancer-associated VTE, it’s worth noting that many of the authors of the cited papers received compensation from large pharmaceutical companies. In addition, the CLOT trial was funded by Pharmacia, which supplied the study drug.
Initial treatment (5-10 days): The American Society of Clinical Oncology (ASCO) guidelines advocate the use of LMWH during the initial five to 10 days following VTE diagnosis. Four other cancer research organization guidelines, National Comprehensive Cancer Network (NCCN), the Italian Association of Medical Oncology (AIOM), the European Society of Medical Oncology (ESMO), and the French National Federation of the League of Centers Against Cancer (FNCLCC), echo this approach, with unfractionated heparin (UFH) or fondaparinux as additional initial treatment depending on the clinical situation—i.e., renal failure, heparin-induced thrombocytopenia (HIT), or bleeding risk.6
Table 2 (below) summarizes recommendations for VTE treatment in cancer patients from all five guideline panels.6
Long-term treatment and duration (3-6 months): All of the panels agree LMWH is the preferred agent for long-term therapy of cancer-related VTE. ASCO supports treatment with LMWH for at least six months; oral VKAs with a targeted INR of 2 to 3 are acceptable when LMWH is not feasible. NCCN, AIOM, ESMO, and FNCLCC recommend an LMWH treatment duration from three to six months (ASCO recommends at least six months).
All of the panels, however, advocate indefinite duration of anticoagulation in patients with such continuing risk factors as active (metastatic, recurrent, or persistent) cancer or chemotherapy treatment.6 AIOM and ESMO specify indefinite LMWH, whereas ASCO does not specify oral VKA or LMWH use. Given the difficulties of managing VKA in the setting of advanced malignancy or chemotherapy, LMWH is the most practical choice, if it’s available and isn’t cost-prohibitive.
LMWH availability: Dalteparin, tinzaparin, and enoxaparin are LMWHs currently available in the U.S. for VTE treatment. Dalteparin is the only FDA-approved LMWH drug for long-term use to treat cancer-associated VTE, although enoxaparin and tinzaparin are used in practice. All three are supplied in prefilled syringes, which make self-administration easier and significantly reduce the risk of dosage error.6
LMWH vs. UFH: LMWH is safer and more efficacious than UFH. A summary of 22 clinical trials (including cancer patients and noncancer patients) by a Cochrane systematic review showed that treatment with LMWH in comparison with UFH results in decreased recurrent VTE, bleeding, mortality, HIT, and osteoporosis.7,13
Other agents: Fondaparinux is a factor Xa inhibitor rarely associated with heparin-induced thrombocytopenia (HIT), which makes it an attractive alternate anticoagulant for HIT patients. Its use in comparison with other parenteral anticoagulants has not been established in patients with malignancy.
Fondaparinux is FDA-approved for initial VTE treatment, and is used in practice as an alternative prophylactic anticoagulant for patients with HIT history or heparin allergy.7 However, no randomized clinical trials have evaluated its efficacy in patients with HIT.
Several new oral anticoagulants, including direct thrombin and factor Xa inhibitors, are being investigated; efficacy has not been established in cancer patients.7
Inferior vena cava (IVC) filters: Limited data surround the use of IVC filters, and most consensus guidelines recommend their use only in specific settings. One randomized controlled study (not limited to patients with cancer) showed no difference in overall short-term or long-term survival among patients receiving IVC filters for VTE treatment. However, there was a decrease in symptomatic PE in the filter group 12 days after placement. The tradeoff was significantly more recurrent DVTs at two years’ followup. The authors concluded that systematic use of IVC filters is not recommended.14
Because all of the study participants in this trial were receiving concomitant anticoagulation, it is difficult to generalize results to patients who have contraindications to anticoagulation. Nonetheless, ASCO, NCCN, and several other guideline panels recommend IVC filters only for patients with contraindications to anticoagulation or failure of long-term anticoagulation. NCCN broadens these recommendations for IVC filter placement to include patients with severe cardiac or pulmonary dysfunction.6 However, this recommendation is controversial, given the lack of supporting data, cost, and invasiveness of the procedure.7
All patients with IVC filters without contraindication to anticoagulation should be anticoagulated.9
Prophylaxis: The importance of VTE prophylaxis in all hospitalized patients, including patients with cancer, is under close scrutiny in an attempt to improve patient safety and quality. The Centers for Medicare & Medicaid Services (CMS), in conjunction with the Joint Commission, has added VTE to its list of conditions that are reasonably preventable, and hospitals will no longer be reimbursed for the cost of treatment if acquired during a hospital stay. This rule currently is in effect for knee and hip replacements.15
The need for improvement in aggressive and appropriate prophylaxis of hospitalized patients was demonstrated by a single study in which just one-third of hospitalized patients received appropriate prophylaxis, according to American College of Chest Physicians (ACCP) guidelines.16
Despite a lack of robust data regarding VTE prophylaxis in patients with malignancy, strong data exist for VTE prophylaxis in hospitalized patients. All patients with cancer, and without contraindications to anticoagulation, should receive pharmacologic VTE prophylaxis while hospitalized. In the absence of supporting data, guidelines do not suggest VTE prophylaxis for ambulatory patients with cancer, except in certain multiple myeloma patients.6
Intracranial malignancies: Patients with intracranial malignancies are at risk for VTE, and the presence of intracranial tumors or metastases are not absolute contraindications to anticoagulation. However, data are sparse regarding VTE therapy in this subgroup. Active intracranial bleeding is an absolute contraindication to anticoagulation, and it should be avoided in patients with recent intracranial surgery or thrombocytopenia (e.g., platelet count < 50 x 109).4 In general, the presence of intracranial lesions without high-risk features should not deter the use of prophylactic anticoagulation.
Thrombocytopenia: Cancer patients frequently have chemotherapy-induced cytopenias, including thrombocytopenia. There is a paucity of data regarding anticoagulation in the setting of thrombocytopenia. In a recent review of VTE in the setting of cancer, Lee suggests dose reduction of LMWH by half in patients with platelet counts between 20 and 50 x 109/L.7 At our institution, hematologists suggest halving treatment-dose LMWH at platelet counts between 30 and 50 x 109/L, and discontinuing pharmacologic prophylaxis at platelet counts of less than 50 x 109/L—although there are little data to support these recommendations. Anticoagulation should be discontinued in patients with platelet counts below 20-30 x 109/L, as the risk of bleeding becomes too high.7
Thrombolytic therapy: Catheter-directed thrombolysis or systemic thrombolytic therapy might be appropriate treatment options for acute VTE. Presence of extensive proximal DVT, symptom duration of less than two weeks, life expectancy of greater than one year, good functional status, and low bleeding risk are prerequisites. Anticoagulation recommendations do not change following thrombolytic therapy.17
In the setting of PE, hemodynamic instability is the primary indication for thrombolysis. ACCP does not recommend thrombolytic therapy for the majority of VTE patients.17
Back to the Case
Our patient’s lower-extremity ultrasound and CT of the abdomen and pelvis both revealed extensive clot burden, which likely is related to her underlying pancreatic cancer. She should be started on an LMWH. Given the low likelihood of cure from her cancer, anticoagulation should be continued indefinitely, and an LMWH should be given for at least the first six months. Whether she should be switched to an oral VKA after six months depends on several factors: cost considerations, nutritional status, chemotherapy, presence of cytopenias, and bleeding risk.
IVC filter placement is not indicated at this time, as the patient does not have any contraindications to anticoagulation, has not failed anticoagulation, and does not have impending cardiac or pulmonary compromise. She is not a candidate for thrombolytic therapy due to her poor functional status and limited life expectancy.
Bottom Line
Cancer-associated VTE is increasingly common, and optimally is treated with LMWH for at least six months—indefinitely in the setting of active cancer or treatment. IVC filters have limited and specific indications in the setting of cancer-associated VTE, and should be reserved for situations when anticoagulation is contraindicated. TH
Dr. Weaver is an instructor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. Dr. Barsuk is an assistant professor in the division of hospital medicine at Feinberg.
References
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10): 2339-2346.
- Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olsen RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006(1);119:60-68.
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-634.
- Lyman GA, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34):5490-5505.
- Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821-4826.
- Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009;27(29):4919-4926.
- Lee, AY. Anticoagulation in the treatment of established venous thromboembolism in patients with cancer. J Clin Oncol. 2009;27(29):4895-4901.
- Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902-4911.
- Prandoni, P. How I treat venous thromboembolism in patients with cancer. Blood. 2005;106(13):4027-4033.
- Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146-153.
- Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
- Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062-1072.
- Van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004:18(4);CD001100.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7): 409-415.
- Amin AN, Deitelzweig SB. Optimizing the prevention of venous thromboembolism: recent quality initiatives and strategies to drive improvement. Jt Comm J Qual Patient Saf. 2009;35(11):558-564.
- Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
- Hirsch J, Guyatt G, Albers W, et al. Executive summary: American College of Chest Physicians evidence-based clinical practice guidelines (8th ed.). Chest. 2008:133(6 Suppl);71S-105S.
Case
A 70-year-old woman with recently diagnosed pancreatic cancer is admitted with worsening abdominal pain and new right-lower-extremity edema. A CT scan of the abdomen and pelvis reveals occlusive IVC and common iliac thromboses. A right-common-femoral DVT appears on Doppler ultrasound. A CT angiogram of her chest is negative for pulmonary emboli. What is the appropriate treatment for this patient’s thromboembolic disease?
Overview
VTE in the setting of malignancy is common, and the incidence of VTE among cancer patients is increasing for unclear reasons.1,2,3 VTE occurs in an estimated 4% to 20% of all malignancy patients. Overall, cancer patients are at a sixfold increased risk of developing VTE compared with the general population, and these patients represent approximately 20% of all VTE cases.4,5
VTE is a leading cause of mortality among hospitalized cancer patients; evidence of VTE exists in up to 50% of cancer patients at autopsy.3,4 VTE complications lead to significant morbidity, including recurrent VTE, pulmonary hypertension, post-thrombophlebitic syndrome, bleeding, and decreased quality of life.6,7
The risk is greatest for hospitalized cancer patients and those receiving active chemotherapy, particularly with such antiangiogenic agents as thalidomide and bevacizumab.4,6 Certain malignancies are more frequently associated with VTE; these include gastrointestinal, gynecologic, brain, lung, renal, and hematologic cancers.4 Table 1 (p. 50) summarizes risk factors associated with VTE in cancer patients.4
Patients with malignancy are hypercoagulable, primarily because of tumor-related alterations in the coagulation cascade.8 Tumors contain cell-surface proteins (e.g., tissue factor and cancer procoagulant) that lead to activation of the clotting cascade via interactions with factors IX and/or X. In addition, tumor-released cytokines cause prothrombotic changes in the vascular endothelium.8
This hypercoagulability is exacerbated by cancer-associated treatment events, including immobility, central venous catheters, erythropoiesis-stimulating agents, and packed red-blood-cell and platelet transfusions.5,9
Cancer-related therapy complications further confound VTE management. Drug interactions, chemotherapy-induced thrombocytopenia, malnutrition, bleeding risk from surgery or tumor location, and liver dysfunction make safe management of cancer-associated VTE a challenge.
Review of the Data
Low-molecular-weight heparin (LMWH) vs. vitamin K antagonists (VKA): There is significant evidence that LMWH is the preferred pharmacologic therapy for the initial and long-term treatment of cancer-related VTE. The most convincing data were published as the CLOT trial, and is supported by several smaller studies.10 Recommendations for the preferred use of LMWH are consistent among several national and international guidelines.6,7
In the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin Versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, six months of treatment with an oral VKA preceded by five to seven days of LMWH was compared with six months of treatment with LMWH (dalteparin). Patients with the diagnosis of acute symptomatic VTE were evaluated. After six months of treatment, 53 of 336 patients in the oral anticoagulant group had recurrent VTE, compared with 27 of 336 patients in the LMWH group—a relative risk reduction of 52% and an absolute risk reduction of 8% (P=0.002). Complication rates (major and minor bleeding) and overall mortality were similar between the two groups.7,10
Two smaller trials compared LMWHs with warfarin in the treatment of VTE in the setting of cancer. In one trial, seven of 67 enoxaparin-treated patients developed bleeding or recurrent VTE, compared with 15 of 71 warfarin-treated subjects; however, this reduction was not statistically significant (P=0.09).11 In another trial, seven of 100 tinzaparin-treated patients developed recurrent VTE, compared with 16 of 100 warfarin-treated patients (P=0.044).12
Thus, LMWH is the preferred therapeutic agent for both DVT and PE in the setting of malignancy.5 Even so, although the clinical evidence supports LMWH use in the treatment of cancer-associated VTE, it’s worth noting that many of the authors of the cited papers received compensation from large pharmaceutical companies. In addition, the CLOT trial was funded by Pharmacia, which supplied the study drug.
Initial treatment (5-10 days): The American Society of Clinical Oncology (ASCO) guidelines advocate the use of LMWH during the initial five to 10 days following VTE diagnosis. Four other cancer research organization guidelines, National Comprehensive Cancer Network (NCCN), the Italian Association of Medical Oncology (AIOM), the European Society of Medical Oncology (ESMO), and the French National Federation of the League of Centers Against Cancer (FNCLCC), echo this approach, with unfractionated heparin (UFH) or fondaparinux as additional initial treatment depending on the clinical situation—i.e., renal failure, heparin-induced thrombocytopenia (HIT), or bleeding risk.6
Table 2 (below) summarizes recommendations for VTE treatment in cancer patients from all five guideline panels.6
Long-term treatment and duration (3-6 months): All of the panels agree LMWH is the preferred agent for long-term therapy of cancer-related VTE. ASCO supports treatment with LMWH for at least six months; oral VKAs with a targeted INR of 2 to 3 are acceptable when LMWH is not feasible. NCCN, AIOM, ESMO, and FNCLCC recommend an LMWH treatment duration from three to six months (ASCO recommends at least six months).
All of the panels, however, advocate indefinite duration of anticoagulation in patients with such continuing risk factors as active (metastatic, recurrent, or persistent) cancer or chemotherapy treatment.6 AIOM and ESMO specify indefinite LMWH, whereas ASCO does not specify oral VKA or LMWH use. Given the difficulties of managing VKA in the setting of advanced malignancy or chemotherapy, LMWH is the most practical choice, if it’s available and isn’t cost-prohibitive.
LMWH availability: Dalteparin, tinzaparin, and enoxaparin are LMWHs currently available in the U.S. for VTE treatment. Dalteparin is the only FDA-approved LMWH drug for long-term use to treat cancer-associated VTE, although enoxaparin and tinzaparin are used in practice. All three are supplied in prefilled syringes, which make self-administration easier and significantly reduce the risk of dosage error.6
LMWH vs. UFH: LMWH is safer and more efficacious than UFH. A summary of 22 clinical trials (including cancer patients and noncancer patients) by a Cochrane systematic review showed that treatment with LMWH in comparison with UFH results in decreased recurrent VTE, bleeding, mortality, HIT, and osteoporosis.7,13
Other agents: Fondaparinux is a factor Xa inhibitor rarely associated with heparin-induced thrombocytopenia (HIT), which makes it an attractive alternate anticoagulant for HIT patients. Its use in comparison with other parenteral anticoagulants has not been established in patients with malignancy.
Fondaparinux is FDA-approved for initial VTE treatment, and is used in practice as an alternative prophylactic anticoagulant for patients with HIT history or heparin allergy.7 However, no randomized clinical trials have evaluated its efficacy in patients with HIT.
Several new oral anticoagulants, including direct thrombin and factor Xa inhibitors, are being investigated; efficacy has not been established in cancer patients.7
Inferior vena cava (IVC) filters: Limited data surround the use of IVC filters, and most consensus guidelines recommend their use only in specific settings. One randomized controlled study (not limited to patients with cancer) showed no difference in overall short-term or long-term survival among patients receiving IVC filters for VTE treatment. However, there was a decrease in symptomatic PE in the filter group 12 days after placement. The tradeoff was significantly more recurrent DVTs at two years’ followup. The authors concluded that systematic use of IVC filters is not recommended.14
Because all of the study participants in this trial were receiving concomitant anticoagulation, it is difficult to generalize results to patients who have contraindications to anticoagulation. Nonetheless, ASCO, NCCN, and several other guideline panels recommend IVC filters only for patients with contraindications to anticoagulation or failure of long-term anticoagulation. NCCN broadens these recommendations for IVC filter placement to include patients with severe cardiac or pulmonary dysfunction.6 However, this recommendation is controversial, given the lack of supporting data, cost, and invasiveness of the procedure.7
All patients with IVC filters without contraindication to anticoagulation should be anticoagulated.9
Prophylaxis: The importance of VTE prophylaxis in all hospitalized patients, including patients with cancer, is under close scrutiny in an attempt to improve patient safety and quality. The Centers for Medicare & Medicaid Services (CMS), in conjunction with the Joint Commission, has added VTE to its list of conditions that are reasonably preventable, and hospitals will no longer be reimbursed for the cost of treatment if acquired during a hospital stay. This rule currently is in effect for knee and hip replacements.15
The need for improvement in aggressive and appropriate prophylaxis of hospitalized patients was demonstrated by a single study in which just one-third of hospitalized patients received appropriate prophylaxis, according to American College of Chest Physicians (ACCP) guidelines.16
Despite a lack of robust data regarding VTE prophylaxis in patients with malignancy, strong data exist for VTE prophylaxis in hospitalized patients. All patients with cancer, and without contraindications to anticoagulation, should receive pharmacologic VTE prophylaxis while hospitalized. In the absence of supporting data, guidelines do not suggest VTE prophylaxis for ambulatory patients with cancer, except in certain multiple myeloma patients.6
Intracranial malignancies: Patients with intracranial malignancies are at risk for VTE, and the presence of intracranial tumors or metastases are not absolute contraindications to anticoagulation. However, data are sparse regarding VTE therapy in this subgroup. Active intracranial bleeding is an absolute contraindication to anticoagulation, and it should be avoided in patients with recent intracranial surgery or thrombocytopenia (e.g., platelet count < 50 x 109).4 In general, the presence of intracranial lesions without high-risk features should not deter the use of prophylactic anticoagulation.
Thrombocytopenia: Cancer patients frequently have chemotherapy-induced cytopenias, including thrombocytopenia. There is a paucity of data regarding anticoagulation in the setting of thrombocytopenia. In a recent review of VTE in the setting of cancer, Lee suggests dose reduction of LMWH by half in patients with platelet counts between 20 and 50 x 109/L.7 At our institution, hematologists suggest halving treatment-dose LMWH at platelet counts between 30 and 50 x 109/L, and discontinuing pharmacologic prophylaxis at platelet counts of less than 50 x 109/L—although there are little data to support these recommendations. Anticoagulation should be discontinued in patients with platelet counts below 20-30 x 109/L, as the risk of bleeding becomes too high.7
Thrombolytic therapy: Catheter-directed thrombolysis or systemic thrombolytic therapy might be appropriate treatment options for acute VTE. Presence of extensive proximal DVT, symptom duration of less than two weeks, life expectancy of greater than one year, good functional status, and low bleeding risk are prerequisites. Anticoagulation recommendations do not change following thrombolytic therapy.17
In the setting of PE, hemodynamic instability is the primary indication for thrombolysis. ACCP does not recommend thrombolytic therapy for the majority of VTE patients.17
Back to the Case
Our patient’s lower-extremity ultrasound and CT of the abdomen and pelvis both revealed extensive clot burden, which likely is related to her underlying pancreatic cancer. She should be started on an LMWH. Given the low likelihood of cure from her cancer, anticoagulation should be continued indefinitely, and an LMWH should be given for at least the first six months. Whether she should be switched to an oral VKA after six months depends on several factors: cost considerations, nutritional status, chemotherapy, presence of cytopenias, and bleeding risk.
IVC filter placement is not indicated at this time, as the patient does not have any contraindications to anticoagulation, has not failed anticoagulation, and does not have impending cardiac or pulmonary compromise. She is not a candidate for thrombolytic therapy due to her poor functional status and limited life expectancy.
Bottom Line
Cancer-associated VTE is increasingly common, and optimally is treated with LMWH for at least six months—indefinitely in the setting of active cancer or treatment. IVC filters have limited and specific indications in the setting of cancer-associated VTE, and should be reserved for situations when anticoagulation is contraindicated. TH
Dr. Weaver is an instructor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. Dr. Barsuk is an assistant professor in the division of hospital medicine at Feinberg.
References
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10): 2339-2346.
- Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olsen RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006(1);119:60-68.
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-634.
- Lyman GA, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34):5490-5505.
- Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821-4826.
- Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009;27(29):4919-4926.
- Lee, AY. Anticoagulation in the treatment of established venous thromboembolism in patients with cancer. J Clin Oncol. 2009;27(29):4895-4901.
- Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902-4911.
- Prandoni, P. How I treat venous thromboembolism in patients with cancer. Blood. 2005;106(13):4027-4033.
- Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146-153.
- Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
- Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062-1072.
- Van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004:18(4);CD001100.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7): 409-415.
- Amin AN, Deitelzweig SB. Optimizing the prevention of venous thromboembolism: recent quality initiatives and strategies to drive improvement. Jt Comm J Qual Patient Saf. 2009;35(11):558-564.
- Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
- Hirsch J, Guyatt G, Albers W, et al. Executive summary: American College of Chest Physicians evidence-based clinical practice guidelines (8th ed.). Chest. 2008:133(6 Suppl);71S-105S.