User login
See for yourself
About 800 million radiology exams were performed in this country in the past year, and they generated approximately 60 billion images, according to an article published in 2017 in the Wall Street Journal (“No need for radiologists to be negative on AI,” by Greg Ip, Nov. 24, 2017). How many of those millions of radiology studies did you order? And how many of the scores of images you requested did you see with your own two eyes? In fact, how many of the radiologists’ reports that were sent to you did you read in their entirety? How often did you just skip over the radiologist’s CYA disclaimers and simply read the final summary, “exam negative”?

I enjoy the challenge of interpreting x-ray images. In fact, I toyed with becoming a pediatric radiologist, but that career path would have meant settling in or near a large city, a compromise my wife and I were unwilling to make. I hoped to continue my habit of looking at all my patients’ x-rays, but because my practice was not in or near the hospital, I reluctantly had to bend my rules and admit I didn’t see every image I had ordered. But, I did read every report in its entirety. In one case, an offhand comment buried in the middle of the radiologist’s report referring to the “residual barium from a previous study” caught my eye, because I knew the patient hadn’t had a previous contrast study. Unfortunately, the neuroblastoma that the radiologist had missed initially, and I had seen the next day, never responded to treatment.
Toward the end of my career, digital imagery allowed me to view my patients’ x-rays without having to leave my desk, which got me closer to my goal of seeing all my patients’ studies. However, the advent of computerized axial tomography and magnetic resonance imaging meant that an increasing number of studies pushed my anatomic knowledge beyond its limits.
I suspect that many of you benefited from the if-you-order-it-look-at-it mantra during your training. How many of you have continued to follow the dictum? With the advent of digitized imagery, there is really little excuse for not taking a minute or 2 to pull up your patients’ images on your desktop. One could argue that looking inside your patient is part of a complete exam. Forcing yourself to take that extra step and look at the study may nudge you into thinking twice about whether you really needed the information the imaging study might add to the diagnostic process. Was your click to order the study just a reflex subliminally related to the fear of a lawsuit? Was it important enough to deserve a firsthand look?
At the very least, being able to say, “I’ve looked at your x-rays myself, and they look fine” may be more comforting to your patient than a third-hand relay of a “negative reading” performed by someone whom they have likely never met.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
About 800 million radiology exams were performed in this country in the past year, and they generated approximately 60 billion images, according to an article published in 2017 in the Wall Street Journal (“No need for radiologists to be negative on AI,” by Greg Ip, Nov. 24, 2017). How many of those millions of radiology studies did you order? And how many of the scores of images you requested did you see with your own two eyes? In fact, how many of the radiologists’ reports that were sent to you did you read in their entirety? How often did you just skip over the radiologist’s CYA disclaimers and simply read the final summary, “exam negative”?
I enjoy the challenge of interpreting x-ray images. In fact, I toyed with becoming a pediatric radiologist, but that career path would have meant settling in or near a large city, a compromise my wife and I were unwilling to make. I hoped to continue my habit of looking at all my patients’ x-rays, but because my practice was not in or near the hospital, I reluctantly had to bend my rules and admit I didn’t see every image I had ordered. But, I did read every report in its entirety. In one case, an offhand comment buried in the middle of the radiologist’s report referring to the “residual barium from a previous study” caught my eye, because I knew the patient hadn’t had a previous contrast study. Unfortunately, the neuroblastoma that the radiologist had missed initially, and I had seen the next day, never responded to treatment.
Toward the end of my career, digital imagery allowed me to view my patients’ x-rays without having to leave my desk, which got me closer to my goal of seeing all my patients’ studies. However, the advent of computerized axial tomography and magnetic resonance imaging meant that an increasing number of studies pushed my anatomic knowledge beyond its limits.
I suspect that many of you benefited from the if-you-order-it-look-at-it mantra during your training. How many of you have continued to follow the dictum? With the advent of digitized imagery, there is really little excuse for not taking a minute or 2 to pull up your patients’ images on your desktop. One could argue that looking inside your patient is part of a complete exam. Forcing yourself to take that extra step and look at the study may nudge you into thinking twice about whether you really needed the information the imaging study might add to the diagnostic process. Was your click to order the study just a reflex subliminally related to the fear of a lawsuit? Was it important enough to deserve a firsthand look?
At the very least, being able to say, “I’ve looked at your x-rays myself, and they look fine” may be more comforting to your patient than a third-hand relay of a “negative reading” performed by someone whom they have likely never met.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
About 800 million radiology exams were performed in this country in the past year, and they generated approximately 60 billion images, according to an article published in 2017 in the Wall Street Journal (“No need for radiologists to be negative on AI,” by Greg Ip, Nov. 24, 2017). How many of those millions of radiology studies did you order? And how many of the scores of images you requested did you see with your own two eyes? In fact, how many of the radiologists’ reports that were sent to you did you read in their entirety? How often did you just skip over the radiologist’s CYA disclaimers and simply read the final summary, “exam negative”?
I enjoy the challenge of interpreting x-ray images. In fact, I toyed with becoming a pediatric radiologist, but that career path would have meant settling in or near a large city, a compromise my wife and I were unwilling to make. I hoped to continue my habit of looking at all my patients’ x-rays, but because my practice was not in or near the hospital, I reluctantly had to bend my rules and admit I didn’t see every image I had ordered. But, I did read every report in its entirety. In one case, an offhand comment buried in the middle of the radiologist’s report referring to the “residual barium from a previous study” caught my eye, because I knew the patient hadn’t had a previous contrast study. Unfortunately, the neuroblastoma that the radiologist had missed initially, and I had seen the next day, never responded to treatment.
Toward the end of my career, digital imagery allowed me to view my patients’ x-rays without having to leave my desk, which got me closer to my goal of seeing all my patients’ studies. However, the advent of computerized axial tomography and magnetic resonance imaging meant that an increasing number of studies pushed my anatomic knowledge beyond its limits.
I suspect that many of you benefited from the if-you-order-it-look-at-it mantra during your training. How many of you have continued to follow the dictum? With the advent of digitized imagery, there is really little excuse for not taking a minute or 2 to pull up your patients’ images on your desktop. One could argue that looking inside your patient is part of a complete exam. Forcing yourself to take that extra step and look at the study may nudge you into thinking twice about whether you really needed the information the imaging study might add to the diagnostic process. Was your click to order the study just a reflex subliminally related to the fear of a lawsuit? Was it important enough to deserve a firsthand look?
At the very least, being able to say, “I’ve looked at your x-rays myself, and they look fine” may be more comforting to your patient than a third-hand relay of a “negative reading” performed by someone whom they have likely never met.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
ISSOP’s Budapest Declaration: A call to action for children on the move
In late October 2017, pediatricians from over 25 countries gathered at the annual meeting of the International Society of Social Pediatrics and Child Health in Budapest to develop strategies to address the health and well-being of children on the move. With the staggering global increase in the displacement of children – due to conflict, climate change, natural disasters, and economic deprivation – there is a critical need for action.
An international slate of experts, including pediatricians who are responding to the needs of these children, provided an evidence base for intervention and action. These discussions informed the development of a consensus statement, the Budapest Declaration, that establishes a framework for a global response to the exigencies confronting these children and families.

The Budapest Declaration is grounded in children’s rights as guaranteed in the United Nation’s Convention on the Rights of the Child (CRC). All countries in the world have signed onto the CRC, with a notable exception being the United States. But leading American pediatric groups, including the American Academy of Pediatrics, have endorsed the CRC, making it a basis of organizational advocacy. The CRC entitles all children to optimal survival and development (Article 6) and optimal health and health care (Article 24).
As prescribed by these accepted legal rights for children, children and youth on the move are entitled to the same services, including health care, as resident populations of children, regardless of their legal status. Countries can be held accountable to ensure they receive the full rights due them as articulated in the CRC. Furthermore, efforts to do so should be assessed in national periodic reports to the Committee on the Rights of the Child to ensure accountability.
The relevance of the Budapest Declaration to the United States cannot be overstated. National and regional public policy throughout our country, and in particular along our Southern border, is having a devastating effect on the physical and mental health of children and youth on the move – and will continue to do so throughout their life course.
The involvement of pediatricians and other child health providers is essential to the planning and implementation of clinical and public health programs for children on the move. Child health professionals, in conjunction with their professional organizations, must be engaged in all aspects of local, national, and global responses. Leadership and contributions by pediatricians and pediatric societies and academic institutions are integral to the success of key partners, such as UNICEF, the World Health Organization, the International Organization for Migration, and the UN High Commissioner for Refugees.

Systems of care should be provided that address the physical, mental, and social health care needs of these children without bias and prejudice. Pregnant mothers on the move also should receive services to ensure the delivery of healthy newborns. Every nation should develop approaches and commitments to advance equity in the health and well-being for these children and families.

For much of the world, working within the realm of children’s rights provides a strategy and moral and legal basis for our efforts. Pediatricians need to work with colleagues in a transdisciplinary approach to ensure all children live in nurturing, rights-respecting environments. Our ongoing efforts should include encouraging academic institutions to assist with professional education, research, and evaluation in this regard. We need evaluations that contribute to continuous quality improvement in our efforts and integrate the metrics of child rights, social justice, and health equity into our care of children on the move.
We call on other national and international public, private, and academic sector organizations to advance the health and well-being of children and youth on the move. These children and families are depending on us to do so.
For the complete text of the Budapest Declaration, see www.issop.org/2017/11/10/budapest-declaration-rights-health-well-children-youth-move/.
Dr. Rushton is medical director of the South Carolina Quality Through Innovation in Pediatrics (SCQTIP) network. Dr. Goldhagen is president-elect, International Society for Social Pediatrics and Child Health, and professor of pediatrics, University of Florida, Jacksonville. Email them at [email protected].
In late October 2017, pediatricians from over 25 countries gathered at the annual meeting of the International Society of Social Pediatrics and Child Health in Budapest to develop strategies to address the health and well-being of children on the move. With the staggering global increase in the displacement of children – due to conflict, climate change, natural disasters, and economic deprivation – there is a critical need for action.
An international slate of experts, including pediatricians who are responding to the needs of these children, provided an evidence base for intervention and action. These discussions informed the development of a consensus statement, the Budapest Declaration, that establishes a framework for a global response to the exigencies confronting these children and families.
The Budapest Declaration is grounded in children’s rights as guaranteed in the United Nation’s Convention on the Rights of the Child (CRC). All countries in the world have signed onto the CRC, with a notable exception being the United States. But leading American pediatric groups, including the American Academy of Pediatrics, have endorsed the CRC, making it a basis of organizational advocacy. The CRC entitles all children to optimal survival and development (Article 6) and optimal health and health care (Article 24).
As prescribed by these accepted legal rights for children, children and youth on the move are entitled to the same services, including health care, as resident populations of children, regardless of their legal status. Countries can be held accountable to ensure they receive the full rights due them as articulated in the CRC. Furthermore, efforts to do so should be assessed in national periodic reports to the Committee on the Rights of the Child to ensure accountability.
The relevance of the Budapest Declaration to the United States cannot be overstated. National and regional public policy throughout our country, and in particular along our Southern border, is having a devastating effect on the physical and mental health of children and youth on the move – and will continue to do so throughout their life course.
The involvement of pediatricians and other child health providers is essential to the planning and implementation of clinical and public health programs for children on the move. Child health professionals, in conjunction with their professional organizations, must be engaged in all aspects of local, national, and global responses. Leadership and contributions by pediatricians and pediatric societies and academic institutions are integral to the success of key partners, such as UNICEF, the World Health Organization, the International Organization for Migration, and the UN High Commissioner for Refugees.
Systems of care should be provided that address the physical, mental, and social health care needs of these children without bias and prejudice. Pregnant mothers on the move also should receive services to ensure the delivery of healthy newborns. Every nation should develop approaches and commitments to advance equity in the health and well-being for these children and families.
For much of the world, working within the realm of children’s rights provides a strategy and moral and legal basis for our efforts. Pediatricians need to work with colleagues in a transdisciplinary approach to ensure all children live in nurturing, rights-respecting environments. Our ongoing efforts should include encouraging academic institutions to assist with professional education, research, and evaluation in this regard. We need evaluations that contribute to continuous quality improvement in our efforts and integrate the metrics of child rights, social justice, and health equity into our care of children on the move.
We call on other national and international public, private, and academic sector organizations to advance the health and well-being of children and youth on the move. These children and families are depending on us to do so.
For the complete text of the Budapest Declaration, see www.issop.org/2017/11/10/budapest-declaration-rights-health-well-children-youth-move/.
Dr. Rushton is medical director of the South Carolina Quality Through Innovation in Pediatrics (SCQTIP) network. Dr. Goldhagen is president-elect, International Society for Social Pediatrics and Child Health, and professor of pediatrics, University of Florida, Jacksonville. Email them at [email protected].
In late October 2017, pediatricians from over 25 countries gathered at the annual meeting of the International Society of Social Pediatrics and Child Health in Budapest to develop strategies to address the health and well-being of children on the move. With the staggering global increase in the displacement of children – due to conflict, climate change, natural disasters, and economic deprivation – there is a critical need for action.
An international slate of experts, including pediatricians who are responding to the needs of these children, provided an evidence base for intervention and action. These discussions informed the development of a consensus statement, the Budapest Declaration, that establishes a framework for a global response to the exigencies confronting these children and families.
The Budapest Declaration is grounded in children’s rights as guaranteed in the United Nation’s Convention on the Rights of the Child (CRC). All countries in the world have signed onto the CRC, with a notable exception being the United States. But leading American pediatric groups, including the American Academy of Pediatrics, have endorsed the CRC, making it a basis of organizational advocacy. The CRC entitles all children to optimal survival and development (Article 6) and optimal health and health care (Article 24).
As prescribed by these accepted legal rights for children, children and youth on the move are entitled to the same services, including health care, as resident populations of children, regardless of their legal status. Countries can be held accountable to ensure they receive the full rights due them as articulated in the CRC. Furthermore, efforts to do so should be assessed in national periodic reports to the Committee on the Rights of the Child to ensure accountability.
The relevance of the Budapest Declaration to the United States cannot be overstated. National and regional public policy throughout our country, and in particular along our Southern border, is having a devastating effect on the physical and mental health of children and youth on the move – and will continue to do so throughout their life course.
The involvement of pediatricians and other child health providers is essential to the planning and implementation of clinical and public health programs for children on the move. Child health professionals, in conjunction with their professional organizations, must be engaged in all aspects of local, national, and global responses. Leadership and contributions by pediatricians and pediatric societies and academic institutions are integral to the success of key partners, such as UNICEF, the World Health Organization, the International Organization for Migration, and the UN High Commissioner for Refugees.
Systems of care should be provided that address the physical, mental, and social health care needs of these children without bias and prejudice. Pregnant mothers on the move also should receive services to ensure the delivery of healthy newborns. Every nation should develop approaches and commitments to advance equity in the health and well-being for these children and families.
For much of the world, working within the realm of children’s rights provides a strategy and moral and legal basis for our efforts. Pediatricians need to work with colleagues in a transdisciplinary approach to ensure all children live in nurturing, rights-respecting environments. Our ongoing efforts should include encouraging academic institutions to assist with professional education, research, and evaluation in this regard. We need evaluations that contribute to continuous quality improvement in our efforts and integrate the metrics of child rights, social justice, and health equity into our care of children on the move.
We call on other national and international public, private, and academic sector organizations to advance the health and well-being of children and youth on the move. These children and families are depending on us to do so.
For the complete text of the Budapest Declaration, see www.issop.org/2017/11/10/budapest-declaration-rights-health-well-children-youth-move/.
Dr. Rushton is medical director of the South Carolina Quality Through Innovation in Pediatrics (SCQTIP) network. Dr. Goldhagen is president-elect, International Society for Social Pediatrics and Child Health, and professor of pediatrics, University of Florida, Jacksonville. Email them at [email protected].
More thoughts about hospitalist burnout
I wrote about physician burnout and well-being in the July 2017 version of this column, and am still thinking a great deal about those issues. In the past 6 months, I can’t identify anything that strikes me as a real breakthrough in addressing these issues. However, the ever-increasing attention and resources directed at physician burnout and wellness, on both a local and national level, strike me as reason for cautious optimism.
A chief wellness officer
In summer 2017, Stanford University created a new physician executive role called chief wellness officer (CWO). As far as I am aware, this is the first such position connected with a hospital or medical school. It will be interesting to see if other organizations create similar positions, although I suspect that in places where it is explicitly recognized as a priority, responsibility for this work will be one of the many duties of a chief medical officer or other such executive, and not a position devoted solely to wellness. Interestingly, an Internet search revealed that some non–health care businesses have executive positions with that title, though the role seems focused more on physical health – as in exercise and smoking cessation – than emotional well-being and burnout.
According to a statement on the Stanford Medicine website, the new CWO will work with colleagues to continue “building on its innovative WellMD Center , which was established in 2016. The center has engaged more than 200 physicians through programs focusing on peer support, stress reduction, and ways to cultivate compassion and resilience, as well as a literature and a dinner series in which physicians explore the challenges and rewards of being a doctor. The center also aims to relieve some of the burden on physicians by improving efficiency and simplifying workplace systems, such as electronic medical records.”
A national conference
Over the last 2 or 3 years many, if not most, physician conferences, including the SHM annual conference, have added some content around physician burnout and well-being. But for the first time I’m aware of, an entire conference, the American Conference on Physician Health, addressed these topics in San Francisco in October 2017, and attracted 425 attendees along with an all-star faculty. I couldn’t attend myself, but found a reporter’s summary informative and I recommend it.
While the summary didn’t suggest the conference provided a cure or simple path to improvement, I’m encouraged that the topic has attracted the attention of some pretty smart people. If there is a second edition of this conference, I’ll try hard to attend.
Worthwhile web resources
The home page of Stanford’s WellMD Center provides a continuously updated list of recent research publications on physician health and links to many other resources, and is worth bookmarking.
Another great educational resource for physician wellness is the AMA’s STEPS Forward, a site devoted to practice improvement that provides guidance on patient care, work flow and process, leading change, technology and finance, as well as professional well-being. Of the five separate education modules in the latter category, I found the one on “Preventing Physician Burnout” especially informative. The site is free, doesn’t require an AMA membership, and can provide CME credit.
Making a difference locally: Individuals
Surveys, research, and the experience of experts available via the above resources and others are very valuable, but may be hard to translate into action for you and your fellow local caregivers. My sense is that many hospitalists address their own work-related distress by simply working less in total – reducing their full-time equivalents. That may be the most tangible and accessible intervention, and undeniably the right thing to do in some cases. But it isn’t an ideal approach for our field, which faces chronic staffing shortages. And it doesn’t do anything to change the average level of distress of a day of work. I worry that many people will find disappointment if working fewer shifts is their only burnout mitigation strategy.

Ensuring that you have some work-related interest outside of direct patient care, such as being the local electronic health record expert, or even the person leading formation of a support committee, can be really valuable. I first addressed this topic in the June 2011 issue of The Hospitalist, and there is a long list of things to consider: mindfulness, practicing “ self-compassion ,” cultivating deeper social connections in and out of the workplace, etc. Ultimately, each of us will have to choose our own path, and for some that should include professional help, e.g., from a mental health care provider.
But as a colleague once put it, a focus on changing ourselves is akin to just learning to take a punch better. A worthwhile endeavor, but it’s also necessary to try to decrease the number of punches thrown our way.
Making a difference locally: Medical staff
I’m part of the Provider Support Committee at my hospital, and I have concluded that nearly every hospital should have a group like this. Our own committee was modeled after the support committee at a hospital five miles away, and both groups see value in collaborating in our efforts. In fact, a person from each hospital’s committee serves on the committee at the other hospital.
These committees have popped up in other institutions, and many have been at it longer than at my hospital. But they all seem to share a mission of developing and implementing programs to position caregivers to thrive in their work, increase resilience, and reduce their risk of burnout. Some interventions are focused on making changes to an EHR, work schedules, work flows, or even staffing levels (i.e., reducing the “number of punches”). Other efforts are directed toward establishing groups that support personal reflection and/or social connections among providers.
A review of activities undertaken by seven different organizations is available at the AMA STEPS forward Preventing Physician Burnout website (click on “STEPS in practice.”)
Dr. Nelson has had a career in clinical practice as a hospitalist starting in 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice management courses. Contact him at [email protected]
I wrote about physician burnout and well-being in the July 2017 version of this column, and am still thinking a great deal about those issues. In the past 6 months, I can’t identify anything that strikes me as a real breakthrough in addressing these issues. However, the ever-increasing attention and resources directed at physician burnout and wellness, on both a local and national level, strike me as reason for cautious optimism.
A chief wellness officer
In summer 2017, Stanford University created a new physician executive role called chief wellness officer (CWO). As far as I am aware, this is the first such position connected with a hospital or medical school. It will be interesting to see if other organizations create similar positions, although I suspect that in places where it is explicitly recognized as a priority, responsibility for this work will be one of the many duties of a chief medical officer or other such executive, and not a position devoted solely to wellness. Interestingly, an Internet search revealed that some non–health care businesses have executive positions with that title, though the role seems focused more on physical health – as in exercise and smoking cessation – than emotional well-being and burnout.
According to a statement on the Stanford Medicine website, the new CWO will work with colleagues to continue “building on its innovative WellMD Center , which was established in 2016. The center has engaged more than 200 physicians through programs focusing on peer support, stress reduction, and ways to cultivate compassion and resilience, as well as a literature and a dinner series in which physicians explore the challenges and rewards of being a doctor. The center also aims to relieve some of the burden on physicians by improving efficiency and simplifying workplace systems, such as electronic medical records.”
A national conference
Over the last 2 or 3 years many, if not most, physician conferences, including the SHM annual conference, have added some content around physician burnout and well-being. But for the first time I’m aware of, an entire conference, the American Conference on Physician Health, addressed these topics in San Francisco in October 2017, and attracted 425 attendees along with an all-star faculty. I couldn’t attend myself, but found a reporter’s summary informative and I recommend it.
While the summary didn’t suggest the conference provided a cure or simple path to improvement, I’m encouraged that the topic has attracted the attention of some pretty smart people. If there is a second edition of this conference, I’ll try hard to attend.
Worthwhile web resources
The home page of Stanford’s WellMD Center provides a continuously updated list of recent research publications on physician health and links to many other resources, and is worth bookmarking.
Another great educational resource for physician wellness is the AMA’s STEPS Forward, a site devoted to practice improvement that provides guidance on patient care, work flow and process, leading change, technology and finance, as well as professional well-being. Of the five separate education modules in the latter category, I found the one on “Preventing Physician Burnout” especially informative. The site is free, doesn’t require an AMA membership, and can provide CME credit.
Making a difference locally: Individuals
Surveys, research, and the experience of experts available via the above resources and others are very valuable, but may be hard to translate into action for you and your fellow local caregivers. My sense is that many hospitalists address their own work-related distress by simply working less in total – reducing their full-time equivalents. That may be the most tangible and accessible intervention, and undeniably the right thing to do in some cases. But it isn’t an ideal approach for our field, which faces chronic staffing shortages. And it doesn’t do anything to change the average level of distress of a day of work. I worry that many people will find disappointment if working fewer shifts is their only burnout mitigation strategy.
Ensuring that you have some work-related interest outside of direct patient care, such as being the local electronic health record expert, or even the person leading formation of a support committee, can be really valuable. I first addressed this topic in the June 2011 issue of The Hospitalist, and there is a long list of things to consider: mindfulness, practicing “ self-compassion ,” cultivating deeper social connections in and out of the workplace, etc. Ultimately, each of us will have to choose our own path, and for some that should include professional help, e.g., from a mental health care provider.
But as a colleague once put it, a focus on changing ourselves is akin to just learning to take a punch better. A worthwhile endeavor, but it’s also necessary to try to decrease the number of punches thrown our way.
Making a difference locally: Medical staff
I’m part of the Provider Support Committee at my hospital, and I have concluded that nearly every hospital should have a group like this. Our own committee was modeled after the support committee at a hospital five miles away, and both groups see value in collaborating in our efforts. In fact, a person from each hospital’s committee serves on the committee at the other hospital.
These committees have popped up in other institutions, and many have been at it longer than at my hospital. But they all seem to share a mission of developing and implementing programs to position caregivers to thrive in their work, increase resilience, and reduce their risk of burnout. Some interventions are focused on making changes to an EHR, work schedules, work flows, or even staffing levels (i.e., reducing the “number of punches”). Other efforts are directed toward establishing groups that support personal reflection and/or social connections among providers.
A review of activities undertaken by seven different organizations is available at the AMA STEPS forward Preventing Physician Burnout website (click on “STEPS in practice.”)
Dr. Nelson has had a career in clinical practice as a hospitalist starting in 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice management courses. Contact him at [email protected]
I wrote about physician burnout and well-being in the July 2017 version of this column, and am still thinking a great deal about those issues. In the past 6 months, I can’t identify anything that strikes me as a real breakthrough in addressing these issues. However, the ever-increasing attention and resources directed at physician burnout and wellness, on both a local and national level, strike me as reason for cautious optimism.
A chief wellness officer
In summer 2017, Stanford University created a new physician executive role called chief wellness officer (CWO). As far as I am aware, this is the first such position connected with a hospital or medical school. It will be interesting to see if other organizations create similar positions, although I suspect that in places where it is explicitly recognized as a priority, responsibility for this work will be one of the many duties of a chief medical officer or other such executive, and not a position devoted solely to wellness. Interestingly, an Internet search revealed that some non–health care businesses have executive positions with that title, though the role seems focused more on physical health – as in exercise and smoking cessation – than emotional well-being and burnout.
According to a statement on the Stanford Medicine website, the new CWO will work with colleagues to continue “building on its innovative WellMD Center , which was established in 2016. The center has engaged more than 200 physicians through programs focusing on peer support, stress reduction, and ways to cultivate compassion and resilience, as well as a literature and a dinner series in which physicians explore the challenges and rewards of being a doctor. The center also aims to relieve some of the burden on physicians by improving efficiency and simplifying workplace systems, such as electronic medical records.”
A national conference
Over the last 2 or 3 years many, if not most, physician conferences, including the SHM annual conference, have added some content around physician burnout and well-being. But for the first time I’m aware of, an entire conference, the American Conference on Physician Health, addressed these topics in San Francisco in October 2017, and attracted 425 attendees along with an all-star faculty. I couldn’t attend myself, but found a reporter’s summary informative and I recommend it.
While the summary didn’t suggest the conference provided a cure or simple path to improvement, I’m encouraged that the topic has attracted the attention of some pretty smart people. If there is a second edition of this conference, I’ll try hard to attend.
Worthwhile web resources
The home page of Stanford’s WellMD Center provides a continuously updated list of recent research publications on physician health and links to many other resources, and is worth bookmarking.
Another great educational resource for physician wellness is the AMA’s STEPS Forward, a site devoted to practice improvement that provides guidance on patient care, work flow and process, leading change, technology and finance, as well as professional well-being. Of the five separate education modules in the latter category, I found the one on “Preventing Physician Burnout” especially informative. The site is free, doesn’t require an AMA membership, and can provide CME credit.
Making a difference locally: Individuals
Surveys, research, and the experience of experts available via the above resources and others are very valuable, but may be hard to translate into action for you and your fellow local caregivers. My sense is that many hospitalists address their own work-related distress by simply working less in total – reducing their full-time equivalents. That may be the most tangible and accessible intervention, and undeniably the right thing to do in some cases. But it isn’t an ideal approach for our field, which faces chronic staffing shortages. And it doesn’t do anything to change the average level of distress of a day of work. I worry that many people will find disappointment if working fewer shifts is their only burnout mitigation strategy.
Ensuring that you have some work-related interest outside of direct patient care, such as being the local electronic health record expert, or even the person leading formation of a support committee, can be really valuable. I first addressed this topic in the June 2011 issue of The Hospitalist, and there is a long list of things to consider: mindfulness, practicing “ self-compassion ,” cultivating deeper social connections in and out of the workplace, etc. Ultimately, each of us will have to choose our own path, and for some that should include professional help, e.g., from a mental health care provider.
But as a colleague once put it, a focus on changing ourselves is akin to just learning to take a punch better. A worthwhile endeavor, but it’s also necessary to try to decrease the number of punches thrown our way.
Making a difference locally: Medical staff
I’m part of the Provider Support Committee at my hospital, and I have concluded that nearly every hospital should have a group like this. Our own committee was modeled after the support committee at a hospital five miles away, and both groups see value in collaborating in our efforts. In fact, a person from each hospital’s committee serves on the committee at the other hospital.
These committees have popped up in other institutions, and many have been at it longer than at my hospital. But they all seem to share a mission of developing and implementing programs to position caregivers to thrive in their work, increase resilience, and reduce their risk of burnout. Some interventions are focused on making changes to an EHR, work schedules, work flows, or even staffing levels (i.e., reducing the “number of punches”). Other efforts are directed toward establishing groups that support personal reflection and/or social connections among providers.
A review of activities undertaken by seven different organizations is available at the AMA STEPS forward Preventing Physician Burnout website (click on “STEPS in practice.”)
Dr. Nelson has had a career in clinical practice as a hospitalist starting in 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice management courses. Contact him at [email protected]
Snake in the grass
Most accomplished public speakers will tell you that critical to their success is the ability to understand and adapt to their audiences. It turns out that even chimpanzees accept and use this cornerstone of effective communication.
In a study published in Science Advances (2017 Nov 15;3[11]:e1701742), three scientists working in Uganda reported that chimpanzees who encounter a potential threat in the form of a realistic snake model will vocalize significantly fewer alert hoots if they hear other alert calls coming from the jungle in the vicinity. In other words, the chimp is saying to himself, “Why should I bother wasting my time and lung power hooting to warn my troop mates? Those guys already know about the snake.”
To select which anticipatory guidance topics to include and still be effective communicators, we have to know the families we are trying to help. Gaining this more nuanced picture of a family takes time and is fostered by continuity. Seeing a different provider at each visit doesn’t work very well here. What are this unique family’s concerns, regardless of what some committee thinks we should be asking?
How much can we rely on the media and groups such as the American Academy of Pediatrics and the Centers for Disease Control and Prevention to get out the messages that we have decided to skip over to address this family’s special concerns? Is the message about the benefits of breastfeeding so widely known that we will be wasting our limited office time repeating it? Is the same true for gun safety and seat belts? This is where research can help us decide where to target messages on a national level. But large population studies don’t always apply to our communities and the families we serve.
Where does our role as primary care physicians fit into the bigger picture of health education? The warning messages issued on a national level may have little relevance for our individual patients’ concerns. Is it our role to echo the message, or are we the ones who must do the fine-tuning?
And then there are the recent depressing and counterintuitive findings that for hot-button topics like immunization, education has little if any value. Those families with firmly held beliefs might acknowledge the rationale of our reasoning, but then quickly slide to another argument to tighten their grips on their original position.
Finally, we must be careful to avoid being labeled as the folks whose message is all about what parents should be afraid of. There are plenty of snakes out there in the jungle, but the chimpanzees have realized that when enough of the population is aware of the threat, then it is time to adjust their message. Certainly enough health problems exist on a national level to warrant continued messaging from the large groups in organized medicine. However, it is up to us out in the jungle to learn enough about our patients to know when we should echo those alerts and when it’s time to save our breath. We can’t hoot about every snake in the grass.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Most accomplished public speakers will tell you that critical to their success is the ability to understand and adapt to their audiences. It turns out that even chimpanzees accept and use this cornerstone of effective communication.
In a study published in Science Advances (2017 Nov 15;3[11]:e1701742), three scientists working in Uganda reported that chimpanzees who encounter a potential threat in the form of a realistic snake model will vocalize significantly fewer alert hoots if they hear other alert calls coming from the jungle in the vicinity. In other words, the chimp is saying to himself, “Why should I bother wasting my time and lung power hooting to warn my troop mates? Those guys already know about the snake.”
To select which anticipatory guidance topics to include and still be effective communicators, we have to know the families we are trying to help. Gaining this more nuanced picture of a family takes time and is fostered by continuity. Seeing a different provider at each visit doesn’t work very well here. What are this unique family’s concerns, regardless of what some committee thinks we should be asking?
How much can we rely on the media and groups such as the American Academy of Pediatrics and the Centers for Disease Control and Prevention to get out the messages that we have decided to skip over to address this family’s special concerns? Is the message about the benefits of breastfeeding so widely known that we will be wasting our limited office time repeating it? Is the same true for gun safety and seat belts? This is where research can help us decide where to target messages on a national level. But large population studies don’t always apply to our communities and the families we serve.
Where does our role as primary care physicians fit into the bigger picture of health education? The warning messages issued on a national level may have little relevance for our individual patients’ concerns. Is it our role to echo the message, or are we the ones who must do the fine-tuning?
And then there are the recent depressing and counterintuitive findings that for hot-button topics like immunization, education has little if any value. Those families with firmly held beliefs might acknowledge the rationale of our reasoning, but then quickly slide to another argument to tighten their grips on their original position.
Finally, we must be careful to avoid being labeled as the folks whose message is all about what parents should be afraid of. There are plenty of snakes out there in the jungle, but the chimpanzees have realized that when enough of the population is aware of the threat, then it is time to adjust their message. Certainly enough health problems exist on a national level to warrant continued messaging from the large groups in organized medicine. However, it is up to us out in the jungle to learn enough about our patients to know when we should echo those alerts and when it’s time to save our breath. We can’t hoot about every snake in the grass.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Most accomplished public speakers will tell you that critical to their success is the ability to understand and adapt to their audiences. It turns out that even chimpanzees accept and use this cornerstone of effective communication.
In a study published in Science Advances (2017 Nov 15;3[11]:e1701742), three scientists working in Uganda reported that chimpanzees who encounter a potential threat in the form of a realistic snake model will vocalize significantly fewer alert hoots if they hear other alert calls coming from the jungle in the vicinity. In other words, the chimp is saying to himself, “Why should I bother wasting my time and lung power hooting to warn my troop mates? Those guys already know about the snake.”
To select which anticipatory guidance topics to include and still be effective communicators, we have to know the families we are trying to help. Gaining this more nuanced picture of a family takes time and is fostered by continuity. Seeing a different provider at each visit doesn’t work very well here. What are this unique family’s concerns, regardless of what some committee thinks we should be asking?
How much can we rely on the media and groups such as the American Academy of Pediatrics and the Centers for Disease Control and Prevention to get out the messages that we have decided to skip over to address this family’s special concerns? Is the message about the benefits of breastfeeding so widely known that we will be wasting our limited office time repeating it? Is the same true for gun safety and seat belts? This is where research can help us decide where to target messages on a national level. But large population studies don’t always apply to our communities and the families we serve.
Where does our role as primary care physicians fit into the bigger picture of health education? The warning messages issued on a national level may have little relevance for our individual patients’ concerns. Is it our role to echo the message, or are we the ones who must do the fine-tuning?
And then there are the recent depressing and counterintuitive findings that for hot-button topics like immunization, education has little if any value. Those families with firmly held beliefs might acknowledge the rationale of our reasoning, but then quickly slide to another argument to tighten their grips on their original position.
Finally, we must be careful to avoid being labeled as the folks whose message is all about what parents should be afraid of. There are plenty of snakes out there in the jungle, but the chimpanzees have realized that when enough of the population is aware of the threat, then it is time to adjust their message. Certainly enough health problems exist on a national level to warrant continued messaging from the large groups in organized medicine. However, it is up to us out in the jungle to learn enough about our patients to know when we should echo those alerts and when it’s time to save our breath. We can’t hoot about every snake in the grass.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
CMS clinical trials raise cardiac mortality
Nearly 2 years ago I speculated in this column that health planners or health economists would attempt to manipulate the patterns of patient care to influence the cost and/or quality of clinical care. At that time I suggested that, in that event, the intervention should be managed as we have with drug or device trials to ensure the authenticity and accuracy and most of all assuring the safety of the patient. Furthermore, the design should be incorporated in the intervention, that equipoise be present in the arms of the trial and that a safety monitoring board be in place to alert investigators when and if patient safety is threatened. Patient consent should also be obtained.

Beginning in 2012, CMS, using claims data from 2008 to 2012, penalized hospitals if they did not achieve acceptable readmission rates. At the same time, the agency established the Hospital Admission Reduction Program to monitor 30-day mortality and standardize readmission data. The recent data indicate that the incentives did achieve some decrease in rehospitalization but this was associated with a 16.5% relative increase in 30-day mortality. It was of particular concern that in the previous decade there had been a progressive decrease in 30-day mortality (Circulation 2014;130:966-75). The increase in 30-day mortality observed in the 4-year observational period appears to have interrupted the progressive decrease in 30-day mortality, which would have decreased to 30% if not impacted by the plan.
My previous concerns with this type of social experimentation and manipulation of health care was carried out, and as far as I can tell, continues without any oversight and little insight into the possible risks of this process. A better designed study would have provided better understanding of these results and might have mitigated the adverse effects and mortality events. It is suggested that some hospitals actually gamed the system to their economic advantage. In addition, no oversight board was or is in place as we have with drug trials to allow monitors to become aware of adverse events before there any further loss of life occurs.
I would agree that a randomized trial in this environment would be difficult to achieve. Obtaining consent from thousands of patients would also be difficult. Nevertheless, .
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Nearly 2 years ago I speculated in this column that health planners or health economists would attempt to manipulate the patterns of patient care to influence the cost and/or quality of clinical care. At that time I suggested that, in that event, the intervention should be managed as we have with drug or device trials to ensure the authenticity and accuracy and most of all assuring the safety of the patient. Furthermore, the design should be incorporated in the intervention, that equipoise be present in the arms of the trial and that a safety monitoring board be in place to alert investigators when and if patient safety is threatened. Patient consent should also be obtained.
Beginning in 2012, CMS, using claims data from 2008 to 2012, penalized hospitals if they did not achieve acceptable readmission rates. At the same time, the agency established the Hospital Admission Reduction Program to monitor 30-day mortality and standardize readmission data. The recent data indicate that the incentives did achieve some decrease in rehospitalization but this was associated with a 16.5% relative increase in 30-day mortality. It was of particular concern that in the previous decade there had been a progressive decrease in 30-day mortality (Circulation 2014;130:966-75). The increase in 30-day mortality observed in the 4-year observational period appears to have interrupted the progressive decrease in 30-day mortality, which would have decreased to 30% if not impacted by the plan.
My previous concerns with this type of social experimentation and manipulation of health care was carried out, and as far as I can tell, continues without any oversight and little insight into the possible risks of this process. A better designed study would have provided better understanding of these results and might have mitigated the adverse effects and mortality events. It is suggested that some hospitals actually gamed the system to their economic advantage. In addition, no oversight board was or is in place as we have with drug trials to allow monitors to become aware of adverse events before there any further loss of life occurs.
I would agree that a randomized trial in this environment would be difficult to achieve. Obtaining consent from thousands of patients would also be difficult. Nevertheless, .
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Nearly 2 years ago I speculated in this column that health planners or health economists would attempt to manipulate the patterns of patient care to influence the cost and/or quality of clinical care. At that time I suggested that, in that event, the intervention should be managed as we have with drug or device trials to ensure the authenticity and accuracy and most of all assuring the safety of the patient. Furthermore, the design should be incorporated in the intervention, that equipoise be present in the arms of the trial and that a safety monitoring board be in place to alert investigators when and if patient safety is threatened. Patient consent should also be obtained.
Beginning in 2012, CMS, using claims data from 2008 to 2012, penalized hospitals if they did not achieve acceptable readmission rates. At the same time, the agency established the Hospital Admission Reduction Program to monitor 30-day mortality and standardize readmission data. The recent data indicate that the incentives did achieve some decrease in rehospitalization but this was associated with a 16.5% relative increase in 30-day mortality. It was of particular concern that in the previous decade there had been a progressive decrease in 30-day mortality (Circulation 2014;130:966-75). The increase in 30-day mortality observed in the 4-year observational period appears to have interrupted the progressive decrease in 30-day mortality, which would have decreased to 30% if not impacted by the plan.
My previous concerns with this type of social experimentation and manipulation of health care was carried out, and as far as I can tell, continues without any oversight and little insight into the possible risks of this process. A better designed study would have provided better understanding of these results and might have mitigated the adverse effects and mortality events. It is suggested that some hospitals actually gamed the system to their economic advantage. In addition, no oversight board was or is in place as we have with drug trials to allow monitors to become aware of adverse events before there any further loss of life occurs.
I would agree that a randomized trial in this environment would be difficult to achieve. Obtaining consent from thousands of patients would also be difficult. Nevertheless, .
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Sneak Peek: The Hospital Leader blog – Dec. 2017
Cultivating women leaders in health care #WIMmonth #ThisIsWhatADoctorLooksLike
On my flight home from Scotland, I had a moment to watch a movie while my daughter was caught up in the encore adventures of Moana. I stumbled upon “Hidden Figures,” the story of the African American women at NASA who helped launch John Glenn into space, reviving the nation’s space program.

Turns out I wasn’t the only one who stumbled upon this. Harvard researcher Julie Silver, MD, raised the question about invisible women leaders when reviewing quotes in magazines like Modern Healthcare or Forbes. Moreover, her research demonstrates that, for many professional society awards, 0% are given to women! This is happening in specialties that had nearly even proportions of women and men in practice, such as dermatology and rehab medicine. Last month, I was dumbfounded when I saw a full-page New York Times ad of Top Surgeons by Castle Connolly featuring 16 surgeons, all male.
While Castle Connolly does name female top doctors and market ad opportunities to women and men, I learned that only men sign up for the ads. While this raises more questions, the optics remain problematic – women doctors are hidden. Regardless of the venue, we must do a better job profiling our female leaders. In addition, it is important to recognize that female leaders face well-documented and somewhat controversial challenges that require careful thought:
- Stereotype threat: Some of the original research on stereotype threat done in college students showed that, if women who are about to take a math test are told that the test will expose gender differences, such as men do better at math, women will perform worse AND men will do better. The threat of stereotypes is that women can internalize them and this may hamper their progress. The good news is that education on stereotype threat apparently helps.
- Impostor syndrome: Even highly successful people apparently suffer from impostor syndrome, the fear that they do not deserve their success, but it is much worse in women than in men. You are always trying to conquer the little voice in your head that tells you that you are not good enough.
Read the full post at hospitalleader.org.
Also on The Hospital Leader …
- If I were you, I would not be bullish on long-term care by Brad Flansbaum, DO, MPH, MHM
- Da Vinci wuz here by Jordan Messler, MD, SFHM
- Making the implicit explicit by Leslie Flores, MHA, SFHM
- Should we really focus on “patient-centered care”? by Tracy Cardin, ACNP-BC, SFHM
Cultivating women leaders in health care #WIMmonth #ThisIsWhatADoctorLooksLike
On my flight home from Scotland, I had a moment to watch a movie while my daughter was caught up in the encore adventures of Moana. I stumbled upon “Hidden Figures,” the story of the African American women at NASA who helped launch John Glenn into space, reviving the nation’s space program.
Turns out I wasn’t the only one who stumbled upon this. Harvard researcher Julie Silver, MD, raised the question about invisible women leaders when reviewing quotes in magazines like Modern Healthcare or Forbes. Moreover, her research demonstrates that, for many professional society awards, 0% are given to women! This is happening in specialties that had nearly even proportions of women and men in practice, such as dermatology and rehab medicine. Last month, I was dumbfounded when I saw a full-page New York Times ad of Top Surgeons by Castle Connolly featuring 16 surgeons, all male.
While Castle Connolly does name female top doctors and market ad opportunities to women and men, I learned that only men sign up for the ads. While this raises more questions, the optics remain problematic – women doctors are hidden. Regardless of the venue, we must do a better job profiling our female leaders. In addition, it is important to recognize that female leaders face well-documented and somewhat controversial challenges that require careful thought:
- Stereotype threat: Some of the original research on stereotype threat done in college students showed that, if women who are about to take a math test are told that the test will expose gender differences, such as men do better at math, women will perform worse AND men will do better. The threat of stereotypes is that women can internalize them and this may hamper their progress. The good news is that education on stereotype threat apparently helps.
- Impostor syndrome: Even highly successful people apparently suffer from impostor syndrome, the fear that they do not deserve their success, but it is much worse in women than in men. You are always trying to conquer the little voice in your head that tells you that you are not good enough.
Read the full post at hospitalleader.org.
Also on The Hospital Leader …
- If I were you, I would not be bullish on long-term care by Brad Flansbaum, DO, MPH, MHM
- Da Vinci wuz here by Jordan Messler, MD, SFHM
- Making the implicit explicit by Leslie Flores, MHA, SFHM
- Should we really focus on “patient-centered care”? by Tracy Cardin, ACNP-BC, SFHM
Cultivating women leaders in health care #WIMmonth #ThisIsWhatADoctorLooksLike
On my flight home from Scotland, I had a moment to watch a movie while my daughter was caught up in the encore adventures of Moana. I stumbled upon “Hidden Figures,” the story of the African American women at NASA who helped launch John Glenn into space, reviving the nation’s space program.
Turns out I wasn’t the only one who stumbled upon this. Harvard researcher Julie Silver, MD, raised the question about invisible women leaders when reviewing quotes in magazines like Modern Healthcare or Forbes. Moreover, her research demonstrates that, for many professional society awards, 0% are given to women! This is happening in specialties that had nearly even proportions of women and men in practice, such as dermatology and rehab medicine. Last month, I was dumbfounded when I saw a full-page New York Times ad of Top Surgeons by Castle Connolly featuring 16 surgeons, all male.
While Castle Connolly does name female top doctors and market ad opportunities to women and men, I learned that only men sign up for the ads. While this raises more questions, the optics remain problematic – women doctors are hidden. Regardless of the venue, we must do a better job profiling our female leaders. In addition, it is important to recognize that female leaders face well-documented and somewhat controversial challenges that require careful thought:
- Stereotype threat: Some of the original research on stereotype threat done in college students showed that, if women who are about to take a math test are told that the test will expose gender differences, such as men do better at math, women will perform worse AND men will do better. The threat of stereotypes is that women can internalize them and this may hamper their progress. The good news is that education on stereotype threat apparently helps.
- Impostor syndrome: Even highly successful people apparently suffer from impostor syndrome, the fear that they do not deserve their success, but it is much worse in women than in men. You are always trying to conquer the little voice in your head that tells you that you are not good enough.
Read the full post at hospitalleader.org.
Also on The Hospital Leader …
- If I were you, I would not be bullish on long-term care by Brad Flansbaum, DO, MPH, MHM
- Da Vinci wuz here by Jordan Messler, MD, SFHM
- Making the implicit explicit by Leslie Flores, MHA, SFHM
- Should we really focus on “patient-centered care”? by Tracy Cardin, ACNP-BC, SFHM
Massachusetts and the opioid crisis: Can involuntary holds work?
My son played on a neighborhood little league team for several years. I have such sweet memories of little boys in baseball uniforms lined up on the bench singing cheers while they waited their turns to go to bat. The two devoted dads who worked together coaching the team were a gentle presence in the background of my family’s life every spring for years. One might hope that the love and attention those fathers invested in their sons and their teammates might confer some special protection from life’s tragedies, but the opioid epidemic spares no hostages, and last year, one of those singing little boys from so many years ago – the son of one of the coaches – died of a drug overdose.
President Trump has punted on how to stop the epidemic, one he finally deemed a national public health emergency in October, with no clear addition of federal resources. States have varied in their responses, and Massachusetts, in particular, has been aggressive with new legislation and funding. The laws in Massachusetts allow for involuntary rehab for substance abusers if a family member petitions the court under the state’s decades-old section 35. The irony is that much of this “involuntary” treatment is voluntary: People will ask family members to apply for them as a way of getting into treatment and as a way of bypassing the cost. Section 35 admissions are funded by the state, not by the individual or by health insurance.

As a Boston Globe article (“Mass. governor aims to expand battle against opioid addiction,” Nov. 15, 2017) explains, “Two years ago, Baker stirred controversy with a proposal to hold addicted patients for 72 hours against their will in emergency departments. That idea was rejected by the Legislature. The new bill takes a different approach to the 72-hour hold, enabling doctors to transfer patients with addiction to a treatment facility, much as they would with a person deemed a danger because of mental illness.”
The issues with involuntary care are complicated and nuanced in psychiatric disorders, and perhaps even more so with substance abuse. The time frame of 72 hours for mental health conditions allows for assessment and sometimes for the start of treatment. In some states, a hearing must be held for continued involuntary detention; in other states, a decision must be made as to whether further inpatient care will be pursued, and the actual hearing takes place days to weeks later, depending on the state. For the purposes of allowing someone to clear from an opioid intoxication, then persuading them to engage in voluntary substance abuse treatment, it seems that 72 hours could be the exact wrong time period.
Ideally, a patient would be placed in a comfortable inpatient unit, begun on medication-assisted withdrawal, and offered a high quality of care for those 72 hours so that continuing with treatment might be a palatable option. But would that actually happen? Does Massachusetts have the means and facilities for all its overdose patients? Massachusetts has, in fact, been aggressive with funding. Since 2015, the state has added 1,100 new treatment beds. The efforts to fund and offer novel treatments are commendable. My concern remains that without adequate treatment or a positive experience – a difficult target in the best of circumstances for a patient who is 72 hours into opioid withdrawal – patients would leave only to resume their substance abuse. In a disastrous scenario, patients who have overdosed and fear being detained might not call for help, and the death rate could actually rise.
John A. Renner Jr., MD, is the past president of the American Academy of Addiction Psychiatry and coeditor of Office-Based Buprenorphine Treatment of Opioid Use Disorder (American Psychiatric Association Publishing, 2018). Dr. Renner, who is a professor at Boston University, said, “I would like to see some evidence and research to be sure there were not unintended harms before we go this route.”
Eric C. Strain, MD, director of the Johns Hopkins Center for Substance Abuse Treatment and Research, Baltimore, noted: “Simply holding someone for 3 days, especially against their will, doesn’t make a lot of sense. They are certainly not going to be all better either from a physiological or psychological standpoint. It might, however, be possible to get a person who was not interested in treatment engaged in treatment, and that would be a success.”
Despite the increased numbers of beds and aggressive, thoughtful interventions, Massachusetts still had 1,450 overdose deaths in the first 9 months of 2017, a decrease of only 10% from the year before, according to the Globe article. For the sake of the former Little League players in Maryland, and all the other victims of this lethal nationwide epidemic, it is imperative that any untested treatments be the source of new research. If these measures are implemented, it is essential that Massachusetts follow the people who are the beneficiaries of interventions and create the data that allow other states to either follow suit if these efforts are successful, or allocate resources to other treatments if they are not.
Dr. Miller is coauthor with Annette Hanson, MD, of Committed: The Battle Over Involuntary Psychiatry Care (Baltimore: Johns Hopkins University Press, 2016).
My son played on a neighborhood little league team for several years. I have such sweet memories of little boys in baseball uniforms lined up on the bench singing cheers while they waited their turns to go to bat. The two devoted dads who worked together coaching the team were a gentle presence in the background of my family’s life every spring for years. One might hope that the love and attention those fathers invested in their sons and their teammates might confer some special protection from life’s tragedies, but the opioid epidemic spares no hostages, and last year, one of those singing little boys from so many years ago – the son of one of the coaches – died of a drug overdose.
President Trump has punted on how to stop the epidemic, one he finally deemed a national public health emergency in October, with no clear addition of federal resources. States have varied in their responses, and Massachusetts, in particular, has been aggressive with new legislation and funding. The laws in Massachusetts allow for involuntary rehab for substance abusers if a family member petitions the court under the state’s decades-old section 35. The irony is that much of this “involuntary” treatment is voluntary: People will ask family members to apply for them as a way of getting into treatment and as a way of bypassing the cost. Section 35 admissions are funded by the state, not by the individual or by health insurance.
As a Boston Globe article (“Mass. governor aims to expand battle against opioid addiction,” Nov. 15, 2017) explains, “Two years ago, Baker stirred controversy with a proposal to hold addicted patients for 72 hours against their will in emergency departments. That idea was rejected by the Legislature. The new bill takes a different approach to the 72-hour hold, enabling doctors to transfer patients with addiction to a treatment facility, much as they would with a person deemed a danger because of mental illness.”
The issues with involuntary care are complicated and nuanced in psychiatric disorders, and perhaps even more so with substance abuse. The time frame of 72 hours for mental health conditions allows for assessment and sometimes for the start of treatment. In some states, a hearing must be held for continued involuntary detention; in other states, a decision must be made as to whether further inpatient care will be pursued, and the actual hearing takes place days to weeks later, depending on the state. For the purposes of allowing someone to clear from an opioid intoxication, then persuading them to engage in voluntary substance abuse treatment, it seems that 72 hours could be the exact wrong time period.
Ideally, a patient would be placed in a comfortable inpatient unit, begun on medication-assisted withdrawal, and offered a high quality of care for those 72 hours so that continuing with treatment might be a palatable option. But would that actually happen? Does Massachusetts have the means and facilities for all its overdose patients? Massachusetts has, in fact, been aggressive with funding. Since 2015, the state has added 1,100 new treatment beds. The efforts to fund and offer novel treatments are commendable. My concern remains that without adequate treatment or a positive experience – a difficult target in the best of circumstances for a patient who is 72 hours into opioid withdrawal – patients would leave only to resume their substance abuse. In a disastrous scenario, patients who have overdosed and fear being detained might not call for help, and the death rate could actually rise.
John A. Renner Jr., MD, is the past president of the American Academy of Addiction Psychiatry and coeditor of Office-Based Buprenorphine Treatment of Opioid Use Disorder (American Psychiatric Association Publishing, 2018). Dr. Renner, who is a professor at Boston University, said, “I would like to see some evidence and research to be sure there were not unintended harms before we go this route.”
Eric C. Strain, MD, director of the Johns Hopkins Center for Substance Abuse Treatment and Research, Baltimore, noted: “Simply holding someone for 3 days, especially against their will, doesn’t make a lot of sense. They are certainly not going to be all better either from a physiological or psychological standpoint. It might, however, be possible to get a person who was not interested in treatment engaged in treatment, and that would be a success.”
Despite the increased numbers of beds and aggressive, thoughtful interventions, Massachusetts still had 1,450 overdose deaths in the first 9 months of 2017, a decrease of only 10% from the year before, according to the Globe article. For the sake of the former Little League players in Maryland, and all the other victims of this lethal nationwide epidemic, it is imperative that any untested treatments be the source of new research. If these measures are implemented, it is essential that Massachusetts follow the people who are the beneficiaries of interventions and create the data that allow other states to either follow suit if these efforts are successful, or allocate resources to other treatments if they are not.
Dr. Miller is coauthor with Annette Hanson, MD, of Committed: The Battle Over Involuntary Psychiatry Care (Baltimore: Johns Hopkins University Press, 2016).
My son played on a neighborhood little league team for several years. I have such sweet memories of little boys in baseball uniforms lined up on the bench singing cheers while they waited their turns to go to bat. The two devoted dads who worked together coaching the team were a gentle presence in the background of my family’s life every spring for years. One might hope that the love and attention those fathers invested in their sons and their teammates might confer some special protection from life’s tragedies, but the opioid epidemic spares no hostages, and last year, one of those singing little boys from so many years ago – the son of one of the coaches – died of a drug overdose.
President Trump has punted on how to stop the epidemic, one he finally deemed a national public health emergency in October, with no clear addition of federal resources. States have varied in their responses, and Massachusetts, in particular, has been aggressive with new legislation and funding. The laws in Massachusetts allow for involuntary rehab for substance abusers if a family member petitions the court under the state’s decades-old section 35. The irony is that much of this “involuntary” treatment is voluntary: People will ask family members to apply for them as a way of getting into treatment and as a way of bypassing the cost. Section 35 admissions are funded by the state, not by the individual or by health insurance.
As a Boston Globe article (“Mass. governor aims to expand battle against opioid addiction,” Nov. 15, 2017) explains, “Two years ago, Baker stirred controversy with a proposal to hold addicted patients for 72 hours against their will in emergency departments. That idea was rejected by the Legislature. The new bill takes a different approach to the 72-hour hold, enabling doctors to transfer patients with addiction to a treatment facility, much as they would with a person deemed a danger because of mental illness.”
The issues with involuntary care are complicated and nuanced in psychiatric disorders, and perhaps even more so with substance abuse. The time frame of 72 hours for mental health conditions allows for assessment and sometimes for the start of treatment. In some states, a hearing must be held for continued involuntary detention; in other states, a decision must be made as to whether further inpatient care will be pursued, and the actual hearing takes place days to weeks later, depending on the state. For the purposes of allowing someone to clear from an opioid intoxication, then persuading them to engage in voluntary substance abuse treatment, it seems that 72 hours could be the exact wrong time period.
Ideally, a patient would be placed in a comfortable inpatient unit, begun on medication-assisted withdrawal, and offered a high quality of care for those 72 hours so that continuing with treatment might be a palatable option. But would that actually happen? Does Massachusetts have the means and facilities for all its overdose patients? Massachusetts has, in fact, been aggressive with funding. Since 2015, the state has added 1,100 new treatment beds. The efforts to fund and offer novel treatments are commendable. My concern remains that without adequate treatment or a positive experience – a difficult target in the best of circumstances for a patient who is 72 hours into opioid withdrawal – patients would leave only to resume their substance abuse. In a disastrous scenario, patients who have overdosed and fear being detained might not call for help, and the death rate could actually rise.
John A. Renner Jr., MD, is the past president of the American Academy of Addiction Psychiatry and coeditor of Office-Based Buprenorphine Treatment of Opioid Use Disorder (American Psychiatric Association Publishing, 2018). Dr. Renner, who is a professor at Boston University, said, “I would like to see some evidence and research to be sure there were not unintended harms before we go this route.”
Eric C. Strain, MD, director of the Johns Hopkins Center for Substance Abuse Treatment and Research, Baltimore, noted: “Simply holding someone for 3 days, especially against their will, doesn’t make a lot of sense. They are certainly not going to be all better either from a physiological or psychological standpoint. It might, however, be possible to get a person who was not interested in treatment engaged in treatment, and that would be a success.”
Despite the increased numbers of beds and aggressive, thoughtful interventions, Massachusetts still had 1,450 overdose deaths in the first 9 months of 2017, a decrease of only 10% from the year before, according to the Globe article. For the sake of the former Little League players in Maryland, and all the other victims of this lethal nationwide epidemic, it is imperative that any untested treatments be the source of new research. If these measures are implemented, it is essential that Massachusetts follow the people who are the beneficiaries of interventions and create the data that allow other states to either follow suit if these efforts are successful, or allocate resources to other treatments if they are not.
Dr. Miller is coauthor with Annette Hanson, MD, of Committed: The Battle Over Involuntary Psychiatry Care (Baltimore: Johns Hopkins University Press, 2016).
The enemy of good
“But no perfection is so absolute,
That some impurity doth not pollute.”
– William Shakespeare
While lounging in the ivory tower of academia, we frequently find ourselves condemning the peasantry who fail to grasp limitations of clinical trials. We deride the ignorant masses who insist on flaunting the inclusion criteria of the latest study and extrapolate the results to the ineligible patient sitting in front of them. The disrespect heaped on the “referring doctor” for treating their patients in the absence of evidence from prospective, randomized, multi-institutional trials is routine in conference rooms across the National Cancer Institute’s designated cancer centers.

The introduction of third-party insurers decades ago warped the economics of health care to the point that modern patients generally expect to pay little or nothing for pretty much any medical intervention. As a result, physicians tend to prescribe treatments without regard to cost. Predictably, this results in a steady increase in costs, which have now become unsustainable for our nation. Those rising costs have resulted in many proposals for control, including the Affordable Care Act and the efforts to reverse it. Many see a single payer, government administered system as the only viable way forward.
No matter the final system our society settles on, it will have to account for the almost miraculous results from modern therapeutics, which seem to be announced more and more frequently.
As I write this column, the annual meeting of the American Society of Hematology is being held in Atlanta. The presentations recount studies of new agents alone, or in combination, that report unprecedented response and survival rates. In particular, cellular immunotherapy with chimeric antigen receptor T cells (CAR T cells) has captured the attention of physicians, patients, and investors. Simultaneously – and recognizing this revolution in oncologic therapeutics – the New England Journal of Medicine prepublished two papers presenting the results of CAR T-cell therapy for diffuse large B-cell lymphoma (DLBCL). The results are impressive, and earlier this year, the Food and Drug Administration approved axicabtagene ciloleucel for the treatment of relapsed or refractory DLBCL based on these data. An approval for tisagenlecleucel exists for the treatment of B-cell acute lymphoblastic leukemia, but approval for DLBCL is likely forthcoming, too.
These are wonderful developments. Patients with incurable lymphoma may now be offered potentially curative treatment. Hematology News has covered the development of these treatments closely.
Yet, there is a glaring problem that has also attracted attention: CAR T-cell therapy is incredibly expensive. The potentially mitigating effect of competing products on cost will be canceled by the demand, as well as by geographic scarcity, because only certain large centers will provide this treatment. Remember that the price of imatinib went up over time even though competitors entered the market.
Entering CAR T-cell treatments into the nation’s formulary for some patients will lead to rising premiums for all patients. Disturbingly, CAR T cells are just a treatment for hematology patients at present. What about the equally impressive new – and expensive – technologies in cardiology, neurology, surgery, and every other medical subspecialty? Our system is already struggling to accommodate rapidly rising costs as our population ages and demands more and more medical care.
Many believe that our society will ultimately require strict controls on access to these expensive treatments. While the idea of rationing care is abhorrent to clinicians, “evidence-based” restrictions to access appear not to be. For example, rituximab is effective for immune thrombocytopenic purpura (ITP), but is not FDA approved for it. Despite the restriction, rituximab is frequently used for ITP and generally reimbursed. Venetoclax is a useful agent for patients in relapse of chronic lymphocytic leukemia, but the FDA only approved it for those harboring a deletion of 17p. While insurers seem willing to reimburse the use of rituximab for ITP, they balk at covering venetoclax for off-label indications. More recently, and more ominously for the implications, the FDA approval for tisagenlecleucel in the treatment of B-cell acute lymphoblastic leukemia only extends to those up to age 25. That could mean a 26-year-old in relapse after an allogeneic transplant would be denied coverage for potentially curative CAR T-cell therapy.
The federal government is not the only bureaucracy with a financial interest in limiting access to expensive treatments. Commercial insurers have a fiduciary duty to their shareholders, not to the patients who consume their services. They employ thousands, among them physicians, tasked with reviewing our treatment recommendations to determine whether treatments will be paid for, often citing FDA approvals. Preauthorization for coverage results in innumerable treatment delays and added administrative costs that frustrate us and anger our patients. The insurers defend this incessant obstructionism by claiming they are protecting patients from unnecessary or unhelpful care. Like the FDA, they invoke our own penchant for evidence-based medicine or declare that some care pathway is the ultimate arbiter of truth in coverage determination. Therein lies the danger.
Where do you suppose the evidence and care pathways the FDA and insurers rely on come from? They come from academics like many of this publication’s readers. We gladly provide them with the data needed to restrict care. Through published studies in “major” journals, consensus guidelines promulgated through national organizations, and care pathways generated by our own institutions, we provide the fodder that feeds the regulatory apparatus that decides whose care is approved and paid for. As Walt Kelly’s Pogo stated in 1970, “We have met the enemy and he is us.”
In the interest of science and in the interest of safety – but mostly in the interest of ensuring regulatory approval – clinical trials of new agents often restrict eligibility. Our group recently found that randomized trials routinely exclude patients for rather arbitrary organ dysfunction (Leukemia. 2017 Aug;31[8]:1808-15).
Another recent study concluded, “Current oncology clinical trials stipulate many inclusion and exclusion criteria that specifically define the patient population under study. Although eligibility criteria are needed to define the study population and improve safety, overly restrictive eligibility criteria limit participation in clinical trials, cause the study population to be unrepresentative of the general population of patients with cancer, and limit patient access to new treatments.” (J Clin Oncol. 2017 Nov 20;35[33]:3745-52).
Federal and private agencies will necessarily become stricter in their interpretations of studies and policies in order to control costs. They will happily cite the data we produce in order to do so. For the vast majority of patients who do not meet stringent inclusion criteria, access to new treatments may well be denied. To ensure that patients are provided with the best and most economical care, I am an advocate for evidence-based medicine and care pathways to standardize practice. However, I am progressively more wary of their potential to restrict the availability of innovative remedies to our patients who are not fortunate enough to meet exacting inclusion criteria. Faced with complex patients for whom no study applies, our colleagues in the fields who feed us need flexibility to provide the best care for their patients. Those of us in the ivory tower who determine such inclusion criteria should not let perfect be the enemy of good and must do everything we can to help them and our patients.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at [email protected].
“But no perfection is so absolute,
That some impurity doth not pollute.”
– William Shakespeare
While lounging in the ivory tower of academia, we frequently find ourselves condemning the peasantry who fail to grasp limitations of clinical trials. We deride the ignorant masses who insist on flaunting the inclusion criteria of the latest study and extrapolate the results to the ineligible patient sitting in front of them. The disrespect heaped on the “referring doctor” for treating their patients in the absence of evidence from prospective, randomized, multi-institutional trials is routine in conference rooms across the National Cancer Institute’s designated cancer centers.
The introduction of third-party insurers decades ago warped the economics of health care to the point that modern patients generally expect to pay little or nothing for pretty much any medical intervention. As a result, physicians tend to prescribe treatments without regard to cost. Predictably, this results in a steady increase in costs, which have now become unsustainable for our nation. Those rising costs have resulted in many proposals for control, including the Affordable Care Act and the efforts to reverse it. Many see a single payer, government administered system as the only viable way forward.
No matter the final system our society settles on, it will have to account for the almost miraculous results from modern therapeutics, which seem to be announced more and more frequently.
As I write this column, the annual meeting of the American Society of Hematology is being held in Atlanta. The presentations recount studies of new agents alone, or in combination, that report unprecedented response and survival rates. In particular, cellular immunotherapy with chimeric antigen receptor T cells (CAR T cells) has captured the attention of physicians, patients, and investors. Simultaneously – and recognizing this revolution in oncologic therapeutics – the New England Journal of Medicine prepublished two papers presenting the results of CAR T-cell therapy for diffuse large B-cell lymphoma (DLBCL). The results are impressive, and earlier this year, the Food and Drug Administration approved axicabtagene ciloleucel for the treatment of relapsed or refractory DLBCL based on these data. An approval for tisagenlecleucel exists for the treatment of B-cell acute lymphoblastic leukemia, but approval for DLBCL is likely forthcoming, too.
These are wonderful developments. Patients with incurable lymphoma may now be offered potentially curative treatment. Hematology News has covered the development of these treatments closely.
Yet, there is a glaring problem that has also attracted attention: CAR T-cell therapy is incredibly expensive. The potentially mitigating effect of competing products on cost will be canceled by the demand, as well as by geographic scarcity, because only certain large centers will provide this treatment. Remember that the price of imatinib went up over time even though competitors entered the market.
Entering CAR T-cell treatments into the nation’s formulary for some patients will lead to rising premiums for all patients. Disturbingly, CAR T cells are just a treatment for hematology patients at present. What about the equally impressive new – and expensive – technologies in cardiology, neurology, surgery, and every other medical subspecialty? Our system is already struggling to accommodate rapidly rising costs as our population ages and demands more and more medical care.
Many believe that our society will ultimately require strict controls on access to these expensive treatments. While the idea of rationing care is abhorrent to clinicians, “evidence-based” restrictions to access appear not to be. For example, rituximab is effective for immune thrombocytopenic purpura (ITP), but is not FDA approved for it. Despite the restriction, rituximab is frequently used for ITP and generally reimbursed. Venetoclax is a useful agent for patients in relapse of chronic lymphocytic leukemia, but the FDA only approved it for those harboring a deletion of 17p. While insurers seem willing to reimburse the use of rituximab for ITP, they balk at covering venetoclax for off-label indications. More recently, and more ominously for the implications, the FDA approval for tisagenlecleucel in the treatment of B-cell acute lymphoblastic leukemia only extends to those up to age 25. That could mean a 26-year-old in relapse after an allogeneic transplant would be denied coverage for potentially curative CAR T-cell therapy.
The federal government is not the only bureaucracy with a financial interest in limiting access to expensive treatments. Commercial insurers have a fiduciary duty to their shareholders, not to the patients who consume their services. They employ thousands, among them physicians, tasked with reviewing our treatment recommendations to determine whether treatments will be paid for, often citing FDA approvals. Preauthorization for coverage results in innumerable treatment delays and added administrative costs that frustrate us and anger our patients. The insurers defend this incessant obstructionism by claiming they are protecting patients from unnecessary or unhelpful care. Like the FDA, they invoke our own penchant for evidence-based medicine or declare that some care pathway is the ultimate arbiter of truth in coverage determination. Therein lies the danger.
Where do you suppose the evidence and care pathways the FDA and insurers rely on come from? They come from academics like many of this publication’s readers. We gladly provide them with the data needed to restrict care. Through published studies in “major” journals, consensus guidelines promulgated through national organizations, and care pathways generated by our own institutions, we provide the fodder that feeds the regulatory apparatus that decides whose care is approved and paid for. As Walt Kelly’s Pogo stated in 1970, “We have met the enemy and he is us.”
In the interest of science and in the interest of safety – but mostly in the interest of ensuring regulatory approval – clinical trials of new agents often restrict eligibility. Our group recently found that randomized trials routinely exclude patients for rather arbitrary organ dysfunction (Leukemia. 2017 Aug;31[8]:1808-15).
Another recent study concluded, “Current oncology clinical trials stipulate many inclusion and exclusion criteria that specifically define the patient population under study. Although eligibility criteria are needed to define the study population and improve safety, overly restrictive eligibility criteria limit participation in clinical trials, cause the study population to be unrepresentative of the general population of patients with cancer, and limit patient access to new treatments.” (J Clin Oncol. 2017 Nov 20;35[33]:3745-52).
Federal and private agencies will necessarily become stricter in their interpretations of studies and policies in order to control costs. They will happily cite the data we produce in order to do so. For the vast majority of patients who do not meet stringent inclusion criteria, access to new treatments may well be denied. To ensure that patients are provided with the best and most economical care, I am an advocate for evidence-based medicine and care pathways to standardize practice. However, I am progressively more wary of their potential to restrict the availability of innovative remedies to our patients who are not fortunate enough to meet exacting inclusion criteria. Faced with complex patients for whom no study applies, our colleagues in the fields who feed us need flexibility to provide the best care for their patients. Those of us in the ivory tower who determine such inclusion criteria should not let perfect be the enemy of good and must do everything we can to help them and our patients.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at [email protected].
“But no perfection is so absolute,
That some impurity doth not pollute.”
– William Shakespeare
While lounging in the ivory tower of academia, we frequently find ourselves condemning the peasantry who fail to grasp limitations of clinical trials. We deride the ignorant masses who insist on flaunting the inclusion criteria of the latest study and extrapolate the results to the ineligible patient sitting in front of them. The disrespect heaped on the “referring doctor” for treating their patients in the absence of evidence from prospective, randomized, multi-institutional trials is routine in conference rooms across the National Cancer Institute’s designated cancer centers.
The introduction of third-party insurers decades ago warped the economics of health care to the point that modern patients generally expect to pay little or nothing for pretty much any medical intervention. As a result, physicians tend to prescribe treatments without regard to cost. Predictably, this results in a steady increase in costs, which have now become unsustainable for our nation. Those rising costs have resulted in many proposals for control, including the Affordable Care Act and the efforts to reverse it. Many see a single payer, government administered system as the only viable way forward.
No matter the final system our society settles on, it will have to account for the almost miraculous results from modern therapeutics, which seem to be announced more and more frequently.
As I write this column, the annual meeting of the American Society of Hematology is being held in Atlanta. The presentations recount studies of new agents alone, or in combination, that report unprecedented response and survival rates. In particular, cellular immunotherapy with chimeric antigen receptor T cells (CAR T cells) has captured the attention of physicians, patients, and investors. Simultaneously – and recognizing this revolution in oncologic therapeutics – the New England Journal of Medicine prepublished two papers presenting the results of CAR T-cell therapy for diffuse large B-cell lymphoma (DLBCL). The results are impressive, and earlier this year, the Food and Drug Administration approved axicabtagene ciloleucel for the treatment of relapsed or refractory DLBCL based on these data. An approval for tisagenlecleucel exists for the treatment of B-cell acute lymphoblastic leukemia, but approval for DLBCL is likely forthcoming, too.
These are wonderful developments. Patients with incurable lymphoma may now be offered potentially curative treatment. Hematology News has covered the development of these treatments closely.
Yet, there is a glaring problem that has also attracted attention: CAR T-cell therapy is incredibly expensive. The potentially mitigating effect of competing products on cost will be canceled by the demand, as well as by geographic scarcity, because only certain large centers will provide this treatment. Remember that the price of imatinib went up over time even though competitors entered the market.
Entering CAR T-cell treatments into the nation’s formulary for some patients will lead to rising premiums for all patients. Disturbingly, CAR T cells are just a treatment for hematology patients at present. What about the equally impressive new – and expensive – technologies in cardiology, neurology, surgery, and every other medical subspecialty? Our system is already struggling to accommodate rapidly rising costs as our population ages and demands more and more medical care.
Many believe that our society will ultimately require strict controls on access to these expensive treatments. While the idea of rationing care is abhorrent to clinicians, “evidence-based” restrictions to access appear not to be. For example, rituximab is effective for immune thrombocytopenic purpura (ITP), but is not FDA approved for it. Despite the restriction, rituximab is frequently used for ITP and generally reimbursed. Venetoclax is a useful agent for patients in relapse of chronic lymphocytic leukemia, but the FDA only approved it for those harboring a deletion of 17p. While insurers seem willing to reimburse the use of rituximab for ITP, they balk at covering venetoclax for off-label indications. More recently, and more ominously for the implications, the FDA approval for tisagenlecleucel in the treatment of B-cell acute lymphoblastic leukemia only extends to those up to age 25. That could mean a 26-year-old in relapse after an allogeneic transplant would be denied coverage for potentially curative CAR T-cell therapy.
The federal government is not the only bureaucracy with a financial interest in limiting access to expensive treatments. Commercial insurers have a fiduciary duty to their shareholders, not to the patients who consume their services. They employ thousands, among them physicians, tasked with reviewing our treatment recommendations to determine whether treatments will be paid for, often citing FDA approvals. Preauthorization for coverage results in innumerable treatment delays and added administrative costs that frustrate us and anger our patients. The insurers defend this incessant obstructionism by claiming they are protecting patients from unnecessary or unhelpful care. Like the FDA, they invoke our own penchant for evidence-based medicine or declare that some care pathway is the ultimate arbiter of truth in coverage determination. Therein lies the danger.
Where do you suppose the evidence and care pathways the FDA and insurers rely on come from? They come from academics like many of this publication’s readers. We gladly provide them with the data needed to restrict care. Through published studies in “major” journals, consensus guidelines promulgated through national organizations, and care pathways generated by our own institutions, we provide the fodder that feeds the regulatory apparatus that decides whose care is approved and paid for. As Walt Kelly’s Pogo stated in 1970, “We have met the enemy and he is us.”
In the interest of science and in the interest of safety – but mostly in the interest of ensuring regulatory approval – clinical trials of new agents often restrict eligibility. Our group recently found that randomized trials routinely exclude patients for rather arbitrary organ dysfunction (Leukemia. 2017 Aug;31[8]:1808-15).
Another recent study concluded, “Current oncology clinical trials stipulate many inclusion and exclusion criteria that specifically define the patient population under study. Although eligibility criteria are needed to define the study population and improve safety, overly restrictive eligibility criteria limit participation in clinical trials, cause the study population to be unrepresentative of the general population of patients with cancer, and limit patient access to new treatments.” (J Clin Oncol. 2017 Nov 20;35[33]:3745-52).
Federal and private agencies will necessarily become stricter in their interpretations of studies and policies in order to control costs. They will happily cite the data we produce in order to do so. For the vast majority of patients who do not meet stringent inclusion criteria, access to new treatments may well be denied. To ensure that patients are provided with the best and most economical care, I am an advocate for evidence-based medicine and care pathways to standardize practice. However, I am progressively more wary of their potential to restrict the availability of innovative remedies to our patients who are not fortunate enough to meet exacting inclusion criteria. Faced with complex patients for whom no study applies, our colleagues in the fields who feed us need flexibility to provide the best care for their patients. Those of us in the ivory tower who determine such inclusion criteria should not let perfect be the enemy of good and must do everything we can to help them and our patients.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at [email protected].

Project improves noninvasive IUC alternatives
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
It truly has been a rewarding experience participating in a quality improvement project and I am excited to see what the future holds. Our project, “Reducing CAUTI with Noninvasive UC Alternatives and Measure-vention,” aimed to combat catheter associated urinary tract infections, with a three-pronged approach: by reducing UC placement, performing proper maintenance of IUC, and ensuring prompt removal of unnecessary UC.
To date, our project has demonstrated qualitative success. Specifically, we have implemented a pipeline to perform “measure-vention,” or real-time monitoring and correction of defects. The surgical care intensive unit (SICU) was identified as an appropriate candidate for a pilot partnership due to its high utilization of UC. A daily report of patients with UC is generated and then checked against the EMR for UC necessity. Subsequently, we contact the unit RN for details and physicians for removal orders, when possible. Simultaneously, this enables us to reinforce our management bundle in real time. This protocol is being effectively implemented in the SICU and we are hoping to expand to other units as well. Quantitative data collection is still ongoing and hopefully forthcoming.
Previous CAUTI reduction efforts have had variable and partial success. We are very excited to have improved noninvasive IUC alternatives that address staff concerns about incontinence workload, urine output monitoring, and patient comfort. We hope to protect our patients from harm and eventually publicize our experience to help other health care facilities reduce IUC use and CAUTI.
It has been a rewarding experience to participate in a quality improvement project and I am enjoying the challenges of collaborating with a diverse team of medical professionals to improve the patient experience.
Victor Ekuta is a third-year medical student at UC San Diego.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
It truly has been a rewarding experience participating in a quality improvement project and I am excited to see what the future holds. Our project, “Reducing CAUTI with Noninvasive UC Alternatives and Measure-vention,” aimed to combat catheter associated urinary tract infections, with a three-pronged approach: by reducing UC placement, performing proper maintenance of IUC, and ensuring prompt removal of unnecessary UC.
To date, our project has demonstrated qualitative success. Specifically, we have implemented a pipeline to perform “measure-vention,” or real-time monitoring and correction of defects. The surgical care intensive unit (SICU) was identified as an appropriate candidate for a pilot partnership due to its high utilization of UC. A daily report of patients with UC is generated and then checked against the EMR for UC necessity. Subsequently, we contact the unit RN for details and physicians for removal orders, when possible. Simultaneously, this enables us to reinforce our management bundle in real time. This protocol is being effectively implemented in the SICU and we are hoping to expand to other units as well. Quantitative data collection is still ongoing and hopefully forthcoming.
Previous CAUTI reduction efforts have had variable and partial success. We are very excited to have improved noninvasive IUC alternatives that address staff concerns about incontinence workload, urine output monitoring, and patient comfort. We hope to protect our patients from harm and eventually publicize our experience to help other health care facilities reduce IUC use and CAUTI.
It has been a rewarding experience to participate in a quality improvement project and I am enjoying the challenges of collaborating with a diverse team of medical professionals to improve the patient experience.
Victor Ekuta is a third-year medical student at UC San Diego.
Editor’s note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the longitudinal (18-month) program, recipients are required to write about their experience on a monthly basis.
It truly has been a rewarding experience participating in a quality improvement project and I am excited to see what the future holds. Our project, “Reducing CAUTI with Noninvasive UC Alternatives and Measure-vention,” aimed to combat catheter associated urinary tract infections, with a three-pronged approach: by reducing UC placement, performing proper maintenance of IUC, and ensuring prompt removal of unnecessary UC.
To date, our project has demonstrated qualitative success. Specifically, we have implemented a pipeline to perform “measure-vention,” or real-time monitoring and correction of defects. The surgical care intensive unit (SICU) was identified as an appropriate candidate for a pilot partnership due to its high utilization of UC. A daily report of patients with UC is generated and then checked against the EMR for UC necessity. Subsequently, we contact the unit RN for details and physicians for removal orders, when possible. Simultaneously, this enables us to reinforce our management bundle in real time. This protocol is being effectively implemented in the SICU and we are hoping to expand to other units as well. Quantitative data collection is still ongoing and hopefully forthcoming.
Previous CAUTI reduction efforts have had variable and partial success. We are very excited to have improved noninvasive IUC alternatives that address staff concerns about incontinence workload, urine output monitoring, and patient comfort. We hope to protect our patients from harm and eventually publicize our experience to help other health care facilities reduce IUC use and CAUTI.
It has been a rewarding experience to participate in a quality improvement project and I am enjoying the challenges of collaborating with a diverse team of medical professionals to improve the patient experience.
Victor Ekuta is a third-year medical student at UC San Diego.
Fetal alcohol spectrum disorders and suicidality
As psychiatrists, we understand that behavior is complex and determined by multiple factors. However, despite our understanding that behavior is cultural, sociological, psychological, and biological, we often lose sight of the biological perspective because the brain is such a complex organ and because we are inundated with psychological theories of behavior. As I have said before, we cannot abdicate our role of being biologists in the reflection of mental health and wellness.
Accordingly, I feel it is my duty to bring our attention to a biologic etiology of suicidal behavior. I came across an article on the life expectancy of individuals afflicted with fetal alcohol syndrome in the Journal of Population Therapeutics and Clinical Pharmacology (2016;23[1]:e53-9). The findings were astonishing. As it turns out, the life expectancy of people with fetal alcohol syndrome is 34 years of age on average, and the leading causes of death were “external causes,” which accounted for 44% of the deaths. Suicide was responsible for 15% of those deaths, accidents for 14%, poisoning by illegal drugs or alcohol for 7%, and other external causes for another 7%, according to the article.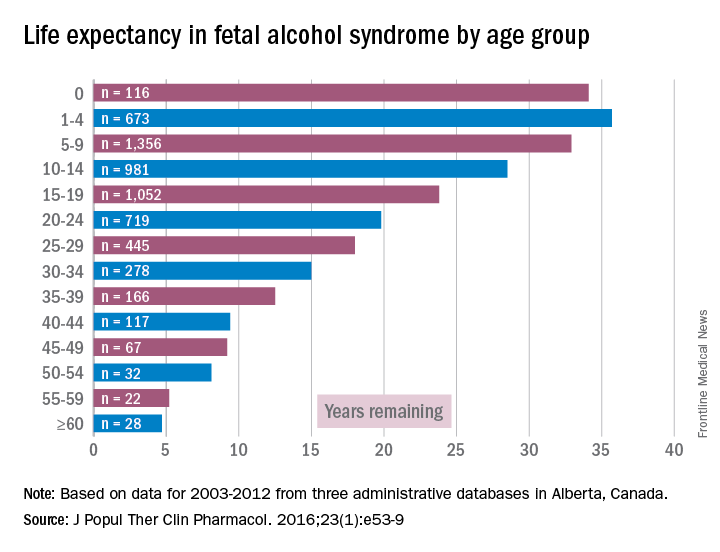
While working in a general hospital in a low-income African American environment where there are high rates of fetal alcohol exposure, I see at least 3-4 suicide attempts a week on the medical-surgical/psychiatric inpatient units where I serve. I am always looking for patients who have ND-PAE because determining such a diagnosis is critical to those patients’ medical-surgical care. For example, there was one woman with ND-PAE who had operable breast carcinoma but did not come in for a return visit until after her carcinoma had become inoperable (she forgot how important it was to get timely treatment). There was a patient who always had out-of-control diabetes because he did not know how to use his glucometer. There was a patient who was taking his antipsychotic medication during the day instead of as prescribed – at bedtime – because he could not read the instructions on his medication bottle. (I have altered several key aspects of my patients’ stories to protect their confidentiality.)
However, until I read that suicide was responsible for 15% of deaths with external causes among patients with fetal alcohol syndrome – patients whose life expectancy averages only 34 years – it did not occur to me that affect dysregulation also was likely to lead to suicide attempts among patients with ND-PAE.

When several of us who were working on the issue of suicide prevention while part of the Committee on Psychopathology & Prevention of Adolescent & Adult Suicide produced our report called “Reducing Suicide: A National Perspective” in 2002, the idea that paying attention to fetal environments and birth outcomes could inform the area of suicide prevention was an alien one. Now, it is a serious consideration because this dynamic just might explain part of the complex phenomena of some suicidal behaviors.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital Family Medicine Clinic in Chicago; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago.
As psychiatrists, we understand that behavior is complex and determined by multiple factors. However, despite our understanding that behavior is cultural, sociological, psychological, and biological, we often lose sight of the biological perspective because the brain is such a complex organ and because we are inundated with psychological theories of behavior. As I have said before, we cannot abdicate our role of being biologists in the reflection of mental health and wellness.
Accordingly, I feel it is my duty to bring our attention to a biologic etiology of suicidal behavior. I came across an article on the life expectancy of individuals afflicted with fetal alcohol syndrome in the Journal of Population Therapeutics and Clinical Pharmacology (2016;23[1]:e53-9). The findings were astonishing. As it turns out, the life expectancy of people with fetal alcohol syndrome is 34 years of age on average, and the leading causes of death were “external causes,” which accounted for 44% of the deaths. Suicide was responsible for 15% of those deaths, accidents for 14%, poisoning by illegal drugs or alcohol for 7%, and other external causes for another 7%, according to the article.
While working in a general hospital in a low-income African American environment where there are high rates of fetal alcohol exposure, I see at least 3-4 suicide attempts a week on the medical-surgical/psychiatric inpatient units where I serve. I am always looking for patients who have ND-PAE because determining such a diagnosis is critical to those patients’ medical-surgical care. For example, there was one woman with ND-PAE who had operable breast carcinoma but did not come in for a return visit until after her carcinoma had become inoperable (she forgot how important it was to get timely treatment). There was a patient who always had out-of-control diabetes because he did not know how to use his glucometer. There was a patient who was taking his antipsychotic medication during the day instead of as prescribed – at bedtime – because he could not read the instructions on his medication bottle. (I have altered several key aspects of my patients’ stories to protect their confidentiality.)
However, until I read that suicide was responsible for 15% of deaths with external causes among patients with fetal alcohol syndrome – patients whose life expectancy averages only 34 years – it did not occur to me that affect dysregulation also was likely to lead to suicide attempts among patients with ND-PAE.
When several of us who were working on the issue of suicide prevention while part of the Committee on Psychopathology & Prevention of Adolescent & Adult Suicide produced our report called “Reducing Suicide: A National Perspective” in 2002, the idea that paying attention to fetal environments and birth outcomes could inform the area of suicide prevention was an alien one. Now, it is a serious consideration because this dynamic just might explain part of the complex phenomena of some suicidal behaviors.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital Family Medicine Clinic in Chicago; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago.
As psychiatrists, we understand that behavior is complex and determined by multiple factors. However, despite our understanding that behavior is cultural, sociological, psychological, and biological, we often lose sight of the biological perspective because the brain is such a complex organ and because we are inundated with psychological theories of behavior. As I have said before, we cannot abdicate our role of being biologists in the reflection of mental health and wellness.
Accordingly, I feel it is my duty to bring our attention to a biologic etiology of suicidal behavior. I came across an article on the life expectancy of individuals afflicted with fetal alcohol syndrome in the Journal of Population Therapeutics and Clinical Pharmacology (2016;23[1]:e53-9). The findings were astonishing. As it turns out, the life expectancy of people with fetal alcohol syndrome is 34 years of age on average, and the leading causes of death were “external causes,” which accounted for 44% of the deaths. Suicide was responsible for 15% of those deaths, accidents for 14%, poisoning by illegal drugs or alcohol for 7%, and other external causes for another 7%, according to the article.
While working in a general hospital in a low-income African American environment where there are high rates of fetal alcohol exposure, I see at least 3-4 suicide attempts a week on the medical-surgical/psychiatric inpatient units where I serve. I am always looking for patients who have ND-PAE because determining such a diagnosis is critical to those patients’ medical-surgical care. For example, there was one woman with ND-PAE who had operable breast carcinoma but did not come in for a return visit until after her carcinoma had become inoperable (she forgot how important it was to get timely treatment). There was a patient who always had out-of-control diabetes because he did not know how to use his glucometer. There was a patient who was taking his antipsychotic medication during the day instead of as prescribed – at bedtime – because he could not read the instructions on his medication bottle. (I have altered several key aspects of my patients’ stories to protect their confidentiality.)
However, until I read that suicide was responsible for 15% of deaths with external causes among patients with fetal alcohol syndrome – patients whose life expectancy averages only 34 years – it did not occur to me that affect dysregulation also was likely to lead to suicide attempts among patients with ND-PAE.
When several of us who were working on the issue of suicide prevention while part of the Committee on Psychopathology & Prevention of Adolescent & Adult Suicide produced our report called “Reducing Suicide: A National Perspective” in 2002, the idea that paying attention to fetal environments and birth outcomes could inform the area of suicide prevention was an alien one. Now, it is a serious consideration because this dynamic just might explain part of the complex phenomena of some suicidal behaviors.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital Family Medicine Clinic in Chicago; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago.