Mature cystic teratoma of the ovary invading the rectum
The patient was diagnosed with an ovarian dermoid cyst that was fistulating into the rectum. In view of these findings, a decision was made for surgical intervention to remove this lesion. A diagnostic laparoscopy, robotic-assisted left salpingo-oopherectomy, excision of cystorectal fistula, proctotomy, and primary repair of the rectal defect was performed. Intraoperative findings include a large left ovarian dermoid cyst with sebaceous content and hair fistulating into the upper rectum just above the rectovaginal pouch, and was adherent to surrounding structures. After excision of the fistula, the anterior rectal wall defect measured 1.5 cm and was closed primarily. Histology revealed a mature cystic teratoma and a fistula tract in the rectum; no malignant features were found. The patient had an uneventful recovery and was well at follow-up.
Mature cystic teratomas of the ovary, also referred to as ovarian dermoid cysts, are benign germ cell tumors of the ovary. These account for 10%-20% of all ovarian neoplasms.1 These are commonly asymptomatic and are found incidentally on imaging studies performed for other indications.2 Complications of these tumors include torsion (16%), rupture (0.5%), and malignant degeneration (2%-6%).3 Rectal invasion via fistulation by these lesions are rare; to date, six cases of colorectal involvement by mature cystic teratomas of the ovary are reported in the literature. These fistulas are a result of rupture of the cyst into the pouch of Douglas, which leads to an intense inflammatory response that results in fistulation, rather than freely into the peritoneum.3 These are therefore undetected until symptoms such as diarrhea or passage of cystic contents (mucus, hair, teeth) develop. The management of mature cystic teratomas of the ovary with symptoms or complications commonly involves surgical intervention to resect the involved ovary and address other pathology.
References
1. Rajaganeshan R., Wang H., Abouleid A., et al. Conservative surgery in the management of a benign ovarian cystic teratoma presenting as a rectal mass: a case report. Ann R Coll Surg Engl. 2001;93 e46-8.
2. Wichremasinghe D., Samarasekera D. A benign teratoma of the ovary fistulating into the rectum. Ceylon Med J. 2010;55:133.
3. Stern J.L., Buscema J., Rosenshein N.B., et al. Spontaneous rupture of benign cystic teratomas. Obstet Gynecol. 1981;57:363-6.
Mature cystic teratoma of the ovary invading the rectum
The patient was diagnosed with an ovarian dermoid cyst that was fistulating into the rectum. In view of these findings, a decision was made for surgical intervention to remove this lesion. A diagnostic laparoscopy, robotic-assisted left salpingo-oopherectomy, excision of cystorectal fistula, proctotomy, and primary repair of the rectal defect was performed. Intraoperative findings include a large left ovarian dermoid cyst with sebaceous content and hair fistulating into the upper rectum just above the rectovaginal pouch, and was adherent to surrounding structures. After excision of the fistula, the anterior rectal wall defect measured 1.5 cm and was closed primarily. Histology revealed a mature cystic teratoma and a fistula tract in the rectum; no malignant features were found. The patient had an uneventful recovery and was well at follow-up.
Mature cystic teratomas of the ovary, also referred to as ovarian dermoid cysts, are benign germ cell tumors of the ovary. These account for 10%-20% of all ovarian neoplasms.1 These are commonly asymptomatic and are found incidentally on imaging studies performed for other indications.2 Complications of these tumors include torsion (16%), rupture (0.5%), and malignant degeneration (2%-6%).3 Rectal invasion via fistulation by these lesions are rare; to date, six cases of colorectal involvement by mature cystic teratomas of the ovary are reported in the literature. These fistulas are a result of rupture of the cyst into the pouch of Douglas, which leads to an intense inflammatory response that results in fistulation, rather than freely into the peritoneum.3 These are therefore undetected until symptoms such as diarrhea or passage of cystic contents (mucus, hair, teeth) develop. The management of mature cystic teratomas of the ovary with symptoms or complications commonly involves surgical intervention to resect the involved ovary and address other pathology.
References
1. Rajaganeshan R., Wang H., Abouleid A., et al. Conservative surgery in the management of a benign ovarian cystic teratoma presenting as a rectal mass: a case report. Ann R Coll Surg Engl. 2001;93 e46-8.
2. Wichremasinghe D., Samarasekera D. A benign teratoma of the ovary fistulating into the rectum. Ceylon Med J. 2010;55:133.
3. Stern J.L., Buscema J., Rosenshein N.B., et al. Spontaneous rupture of benign cystic teratomas. Obstet Gynecol. 1981;57:363-6.
Mature cystic teratoma of the ovary invading the rectum
The patient was diagnosed with an ovarian dermoid cyst that was fistulating into the rectum. In view of these findings, a decision was made for surgical intervention to remove this lesion. A diagnostic laparoscopy, robotic-assisted left salpingo-oopherectomy, excision of cystorectal fistula, proctotomy, and primary repair of the rectal defect was performed. Intraoperative findings include a large left ovarian dermoid cyst with sebaceous content and hair fistulating into the upper rectum just above the rectovaginal pouch, and was adherent to surrounding structures. After excision of the fistula, the anterior rectal wall defect measured 1.5 cm and was closed primarily. Histology revealed a mature cystic teratoma and a fistula tract in the rectum; no malignant features were found. The patient had an uneventful recovery and was well at follow-up.
Mature cystic teratomas of the ovary, also referred to as ovarian dermoid cysts, are benign germ cell tumors of the ovary. These account for 10%-20% of all ovarian neoplasms.1 These are commonly asymptomatic and are found incidentally on imaging studies performed for other indications.2 Complications of these tumors include torsion (16%), rupture (0.5%), and malignant degeneration (2%-6%).3 Rectal invasion via fistulation by these lesions are rare; to date, six cases of colorectal involvement by mature cystic teratomas of the ovary are reported in the literature. These fistulas are a result of rupture of the cyst into the pouch of Douglas, which leads to an intense inflammatory response that results in fistulation, rather than freely into the peritoneum.3 These are therefore undetected until symptoms such as diarrhea or passage of cystic contents (mucus, hair, teeth) develop. The management of mature cystic teratomas of the ovary with symptoms or complications commonly involves surgical intervention to resect the involved ovary and address other pathology.
References
1. Rajaganeshan R., Wang H., Abouleid A., et al. Conservative surgery in the management of a benign ovarian cystic teratoma presenting as a rectal mass: a case report. Ann R Coll Surg Engl. 2001;93 e46-8.
2. Wichremasinghe D., Samarasekera D. A benign teratoma of the ovary fistulating into the rectum. Ceylon Med J. 2010;55:133.
3. Stern J.L., Buscema J., Rosenshein N.B., et al. Spontaneous rupture of benign cystic teratomas. Obstet Gynecol. 1981;57:363-6.
A 37-year-old woman with no significant past medical history presented with an 8-month history of hemoserous anal discharge. A rectal mass was palpable on digital rectal examination.
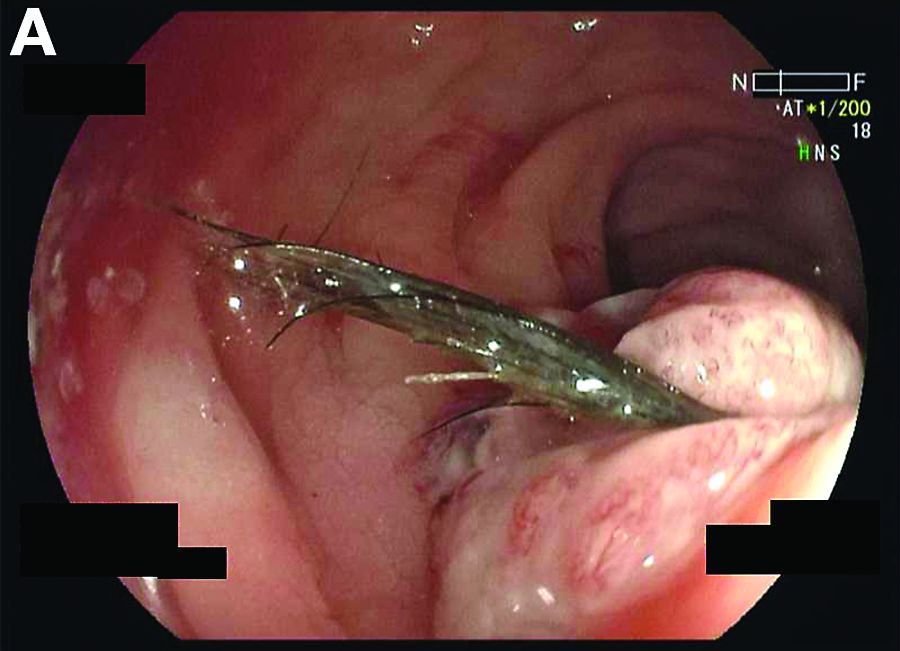
Colonoscopy revealed an upper rectal tumor approximately 9 cm from the anal verge that seemed to contain hair (Figure A). Multiple biopsies from this tumor were inconclusive and tumor markers alpha-fetoprotein, carcinoembryonic antigen, and CA 19-9 were unremarkable.
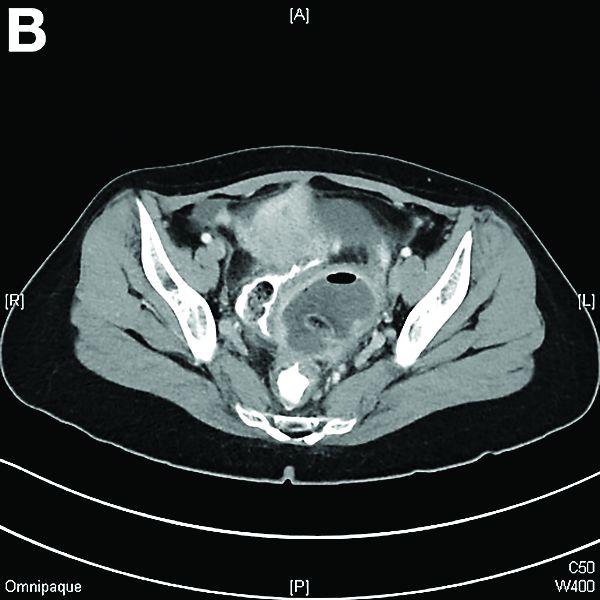
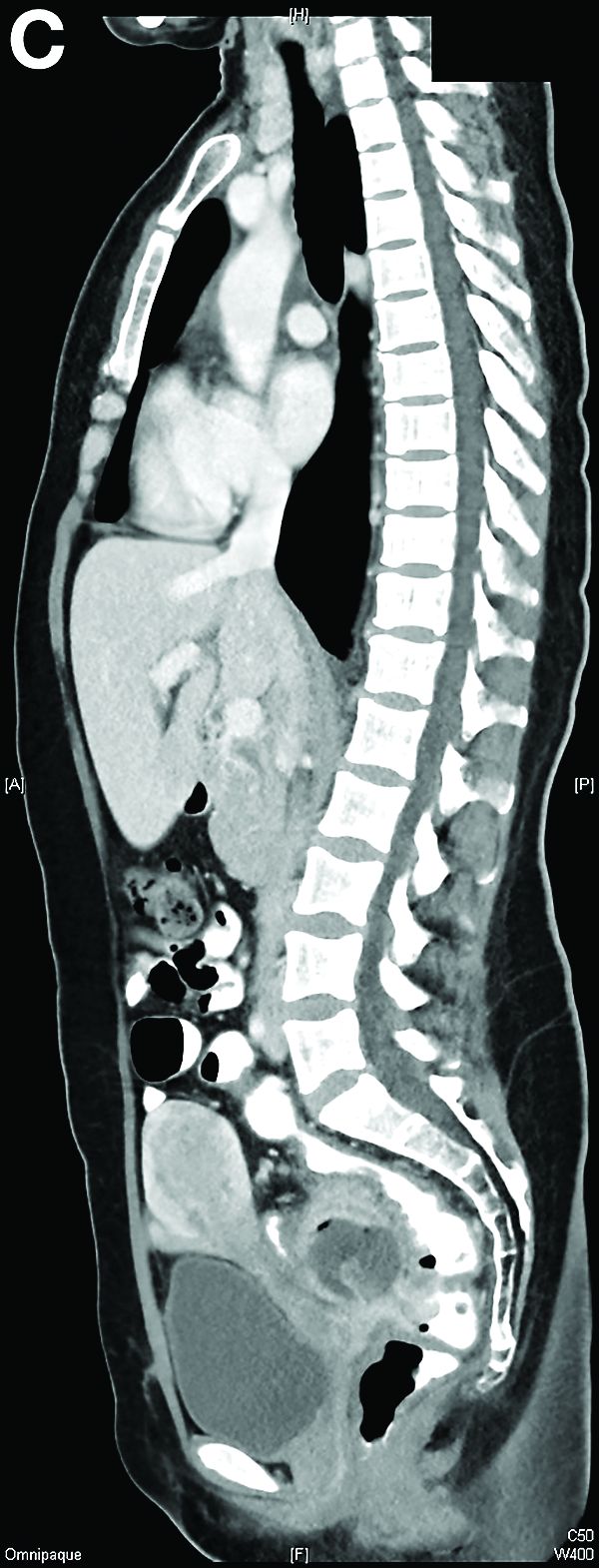
Subsequently, a computed tomography scan of the abdomen and pelvis revealed a left pelvic mass with anterior rectal wall infiltration (Figure B, C).
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
The horrors faced by migrant families forced to separate under the new U.S. “zero tolerance” policy continue to unfold. Tragic emblems of this policy include tapes of crying children and the reported suicide of a father who had been separated from his children.
A federal judge had issued an injunction requiring the reunification of thousands of families by July 26. Despite that deadline, hundreds of adults are no longer in the United States, and hundreds of children are scattered in shelters across the country.
In response to those events, mental health and medical organizations have released powerful statements. The American Psychological Association stated: “The administration’s policy ... is not only needless and cruel, it threatens the mental and physical health of both the children and their caregivers.” The American Medical Association issued a call asserting that separating children from their parents “will do great harm” and “create negative health impacts that will last an individual’s entire lifespan.” Meanwhile, the American Psychiatric Association’s president, Altha J. Stewart, MD, released a statement affirming that “any forced separation is highly stressful for children and can cause lifelong trauma, as well as an increased risk of other mental illnesses, such as depression, anxiety, and posttraumatic stress disorder.”
As forensic experts who testify about the mental well-being of immigration detainees, we applaud those powerful and unambiguous messages from the leaders in our fields. Yet, their statements also underscore the limitations of our diagnostic models: Our field is caught in the difficult position of either applying ill-fitting diagnostic labels or overpathologizing a normal reaction to horrific circumstances. While not applying diagnoses potentially minimizes the enormous psychological burden of separation, diagnosing depression or PTSD as catchalls for suffering incorrectly defines the experience of many survivors of ongoing trauma.
Dr. Francesca Lehman
Currently, most providers, in trying to communicate the effects of ongoing trauma, rely on the diagnoses of depression or PTSD. Both of these diagnoses, however, are problematic. The diagnosis of major depressive disorder, for example, is useful in communicating a loss of hope, and the inability to enjoy pleasurable things. However, depression is an episodic illness, often part of a larger chronic disorder.1 Depression often has a genetic-hereditary component. On the other hand, children suffering from childhood traumas often present lifelong and wide-ranging problems, which may be triggered by reminders but are not episodic. For example, children experiencing parental separation have difficulty forming attachments, which, in turn, leads to subsequent difficulty forming meaningful interpersonal relationships.
The diagnosis of PTSD is useful in communicating a myriad of possible symptoms, which may accompany the trauma. However, PTSD implies a traumatic event as described in criteria A of the DSM-5: “exposure to actual or threatened death, serious injury, or sexual violence.” As such, PTSD poorly encompasses the wide array of smaller yet repetitive traumas experienced by victims of ongoing trauma, such as those youth separated from their parents at the U.S. border. Furthermore, PTSD is a disorder with specific symptoms that, based on a vast body of research,2,3 inadequately describes the multitude of interpersonal, psychological, and physical consequences associated with the type of trauma caused by family separations.
Our understanding of the long-term sequelae of childhood trauma has been greatly influenced by the adverse childhood experiences (ACE) study. The ACE study, one of the largest investigations ever conducted to assess associations between childhood maltreatment and later-life health and well-being, collected the life histories of more than 17,000 patients in a collaborative effort between the Centers for Disease Control and Prevention and Kaiser Permanente’s Health Appraisal Clinic.
The ACE study identified 10 forms of childhood trauma, including: abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes such as depression, suicide attempts, and engagement in high-risk behaviors, as well as significant medical consequences, including higher incidence of heart disease, diabetes, and stroke. Ultimately, having four or more ACEs was associated with early death.
In response to the emerging body of research on childhood trauma, various terms, including complex trauma, type-II trauma, and complex PTSD, have entered our professional lexicon as a means of communicating the wide-ranging consequences of developmental trauma. On the one hand, the less defined and rigid nature of these terms permits mental health providers to develop a rich narrative of a patient’s background, encompassing the patient’s behavior, character, and symptoms. However, the absence of formal terminology also has its drawbacks: Courts and juries have grown accustomed to diagnoses, labels, and syndromes. Most forensic mental health providers who testify about developmental trauma in court can predict the question: “So doctor, you are saying that the individual’s presentation is not severe enough to be considered PTSD, am I correct?” Disorders justify treatment, can explain disability, and warrant empathy; concomitantly, “complex trauma” runs the risk of being considered an academic explanation for trauma victims’ lifelong problems, rather than a societal failure that merits care.
Dr. Nicolas Badre
Recognizing the limitations of our current diagnoses, the forthcoming update to the International Classification of Diseases (ICD-11) will add a new category: complex PTSD. The ICD-11 will attempt to widen the concept of trauma to include “conditions of prolonged adversity, in the form of sustained, repeated, or multiple forms of traumatic exposure.” Trauma exposure examples include genocide campaigns, childhood sexual abuse, child soldiering, severe domestic violence, torture, or slavery. The ICD-11 also expands our understanding of the consequences of trauma to include “affective dysregulation,” “negative self-concept,” and “disturbances in relationships” as part of a concept called “disturbances in self-organization.” Those are important steps in acknowledging the consequences of different forms of trauma as well as noticing a richer array of damages from those incidents.4
While the World Health Organization’s latest iteration of the ICD takes an important step in widening the scope of our diagnostic tools, we are cognizant that our field’s obsessional search for diagnoses, labels, and nomenclature reinforces a detrimental focus on symptoms over stories. However, as forensic mental health providers, we also are keenly aware that a failure to adopt common definitions impedes forensic evaluations, patient advocacy, public policy, and most importantly, patient care.
In the end, we have trained society to understand pathology through narrow lenses, and therefore, in the face of tragic events such as family separations, we need the appropriate language to clearly define and communicate the experiences of our patients. So, despite the limitations of labels, let’s be encouraged by the World Health Organization’s efforts and continue in that direction.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Lehman is a licensed clinical and forensic psychologist in San Diego. Her practice consists of conducting forensic psychological evaluations for the courts with children, adolescents, and adults. Dr. Lehman has been qualified as an expert witness in California as well as in the federal courts. She previously was a supervisor at Sharper Future, a forensic rehabilitation program, and previously served as an adjunct faculty member at Alliant International University, San Diego. Dr. Lehman can be reached at [email protected].
The horrors faced by migrant families forced to separate under the new U.S. “zero tolerance” policy continue to unfold. Tragic emblems of this policy include tapes of crying children and the reported suicide of a father who had been separated from his children.
A federal judge had issued an injunction requiring the reunification of thousands of families by July 26. Despite that deadline, hundreds of adults are no longer in the United States, and hundreds of children are scattered in shelters across the country.
In response to those events, mental health and medical organizations have released powerful statements. The American Psychological Association stated: “The administration’s policy ... is not only needless and cruel, it threatens the mental and physical health of both the children and their caregivers.” The American Medical Association issued a call asserting that separating children from their parents “will do great harm” and “create negative health impacts that will last an individual’s entire lifespan.” Meanwhile, the American Psychiatric Association’s president, Altha J. Stewart, MD, released a statement affirming that “any forced separation is highly stressful for children and can cause lifelong trauma, as well as an increased risk of other mental illnesses, such as depression, anxiety, and posttraumatic stress disorder.”
As forensic experts who testify about the mental well-being of immigration detainees, we applaud those powerful and unambiguous messages from the leaders in our fields. Yet, their statements also underscore the limitations of our diagnostic models: Our field is caught in the difficult position of either applying ill-fitting diagnostic labels or overpathologizing a normal reaction to horrific circumstances. While not applying diagnoses potentially minimizes the enormous psychological burden of separation, diagnosing depression or PTSD as catchalls for suffering incorrectly defines the experience of many survivors of ongoing trauma.
Dr. Francesca Lehman
Currently, most providers, in trying to communicate the effects of ongoing trauma, rely on the diagnoses of depression or PTSD. Both of these diagnoses, however, are problematic. The diagnosis of major depressive disorder, for example, is useful in communicating a loss of hope, and the inability to enjoy pleasurable things. However, depression is an episodic illness, often part of a larger chronic disorder.1 Depression often has a genetic-hereditary component. On the other hand, children suffering from childhood traumas often present lifelong and wide-ranging problems, which may be triggered by reminders but are not episodic. For example, children experiencing parental separation have difficulty forming attachments, which, in turn, leads to subsequent difficulty forming meaningful interpersonal relationships.
The diagnosis of PTSD is useful in communicating a myriad of possible symptoms, which may accompany the trauma. However, PTSD implies a traumatic event as described in criteria A of the DSM-5: “exposure to actual or threatened death, serious injury, or sexual violence.” As such, PTSD poorly encompasses the wide array of smaller yet repetitive traumas experienced by victims of ongoing trauma, such as those youth separated from their parents at the U.S. border. Furthermore, PTSD is a disorder with specific symptoms that, based on a vast body of research,2,3 inadequately describes the multitude of interpersonal, psychological, and physical consequences associated with the type of trauma caused by family separations.
Our understanding of the long-term sequelae of childhood trauma has been greatly influenced by the adverse childhood experiences (ACE) study. The ACE study, one of the largest investigations ever conducted to assess associations between childhood maltreatment and later-life health and well-being, collected the life histories of more than 17,000 patients in a collaborative effort between the Centers for Disease Control and Prevention and Kaiser Permanente’s Health Appraisal Clinic.
The ACE study identified 10 forms of childhood trauma, including: abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes such as depression, suicide attempts, and engagement in high-risk behaviors, as well as significant medical consequences, including higher incidence of heart disease, diabetes, and stroke. Ultimately, having four or more ACEs was associated with early death.
In response to the emerging body of research on childhood trauma, various terms, including complex trauma, type-II trauma, and complex PTSD, have entered our professional lexicon as a means of communicating the wide-ranging consequences of developmental trauma. On the one hand, the less defined and rigid nature of these terms permits mental health providers to develop a rich narrative of a patient’s background, encompassing the patient’s behavior, character, and symptoms. However, the absence of formal terminology also has its drawbacks: Courts and juries have grown accustomed to diagnoses, labels, and syndromes. Most forensic mental health providers who testify about developmental trauma in court can predict the question: “So doctor, you are saying that the individual’s presentation is not severe enough to be considered PTSD, am I correct?” Disorders justify treatment, can explain disability, and warrant empathy; concomitantly, “complex trauma” runs the risk of being considered an academic explanation for trauma victims’ lifelong problems, rather than a societal failure that merits care.
Dr. Nicolas Badre
Recognizing the limitations of our current diagnoses, the forthcoming update to the International Classification of Diseases (ICD-11) will add a new category: complex PTSD. The ICD-11 will attempt to widen the concept of trauma to include “conditions of prolonged adversity, in the form of sustained, repeated, or multiple forms of traumatic exposure.” Trauma exposure examples include genocide campaigns, childhood sexual abuse, child soldiering, severe domestic violence, torture, or slavery. The ICD-11 also expands our understanding of the consequences of trauma to include “affective dysregulation,” “negative self-concept,” and “disturbances in relationships” as part of a concept called “disturbances in self-organization.” Those are important steps in acknowledging the consequences of different forms of trauma as well as noticing a richer array of damages from those incidents.4
While the World Health Organization’s latest iteration of the ICD takes an important step in widening the scope of our diagnostic tools, we are cognizant that our field’s obsessional search for diagnoses, labels, and nomenclature reinforces a detrimental focus on symptoms over stories. However, as forensic mental health providers, we also are keenly aware that a failure to adopt common definitions impedes forensic evaluations, patient advocacy, public policy, and most importantly, patient care.
In the end, we have trained society to understand pathology through narrow lenses, and therefore, in the face of tragic events such as family separations, we need the appropriate language to clearly define and communicate the experiences of our patients. So, despite the limitations of labels, let’s be encouraged by the World Health Organization’s efforts and continue in that direction.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Lehman is a licensed clinical and forensic psychologist in San Diego. Her practice consists of conducting forensic psychological evaluations for the courts with children, adolescents, and adults. Dr. Lehman has been qualified as an expert witness in California as well as in the federal courts. She previously was a supervisor at Sharper Future, a forensic rehabilitation program, and previously served as an adjunct faculty member at Alliant International University, San Diego. Dr. Lehman can be reached at [email protected].
The horrors faced by migrant families forced to separate under the new U.S. “zero tolerance” policy continue to unfold. Tragic emblems of this policy include tapes of crying children and the reported suicide of a father who had been separated from his children.
A federal judge had issued an injunction requiring the reunification of thousands of families by July 26. Despite that deadline, hundreds of adults are no longer in the United States, and hundreds of children are scattered in shelters across the country.
In response to those events, mental health and medical organizations have released powerful statements. The American Psychological Association stated: “The administration’s policy ... is not only needless and cruel, it threatens the mental and physical health of both the children and their caregivers.” The American Medical Association issued a call asserting that separating children from their parents “will do great harm” and “create negative health impacts that will last an individual’s entire lifespan.” Meanwhile, the American Psychiatric Association’s president, Altha J. Stewart, MD, released a statement affirming that “any forced separation is highly stressful for children and can cause lifelong trauma, as well as an increased risk of other mental illnesses, such as depression, anxiety, and posttraumatic stress disorder.”
As forensic experts who testify about the mental well-being of immigration detainees, we applaud those powerful and unambiguous messages from the leaders in our fields. Yet, their statements also underscore the limitations of our diagnostic models: Our field is caught in the difficult position of either applying ill-fitting diagnostic labels or overpathologizing a normal reaction to horrific circumstances. While not applying diagnoses potentially minimizes the enormous psychological burden of separation, diagnosing depression or PTSD as catchalls for suffering incorrectly defines the experience of many survivors of ongoing trauma.
Dr. Francesca Lehman
Currently, most providers, in trying to communicate the effects of ongoing trauma, rely on the diagnoses of depression or PTSD. Both of these diagnoses, however, are problematic. The diagnosis of major depressive disorder, for example, is useful in communicating a loss of hope, and the inability to enjoy pleasurable things. However, depression is an episodic illness, often part of a larger chronic disorder.1 Depression often has a genetic-hereditary component. On the other hand, children suffering from childhood traumas often present lifelong and wide-ranging problems, which may be triggered by reminders but are not episodic. For example, children experiencing parental separation have difficulty forming attachments, which, in turn, leads to subsequent difficulty forming meaningful interpersonal relationships.
The diagnosis of PTSD is useful in communicating a myriad of possible symptoms, which may accompany the trauma. However, PTSD implies a traumatic event as described in criteria A of the DSM-5: “exposure to actual or threatened death, serious injury, or sexual violence.” As such, PTSD poorly encompasses the wide array of smaller yet repetitive traumas experienced by victims of ongoing trauma, such as those youth separated from their parents at the U.S. border. Furthermore, PTSD is a disorder with specific symptoms that, based on a vast body of research,2,3 inadequately describes the multitude of interpersonal, psychological, and physical consequences associated with the type of trauma caused by family separations.
Our understanding of the long-term sequelae of childhood trauma has been greatly influenced by the adverse childhood experiences (ACE) study. The ACE study, one of the largest investigations ever conducted to assess associations between childhood maltreatment and later-life health and well-being, collected the life histories of more than 17,000 patients in a collaborative effort between the Centers for Disease Control and Prevention and Kaiser Permanente’s Health Appraisal Clinic.
The ACE study identified 10 forms of childhood trauma, including: abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes such as depression, suicide attempts, and engagement in high-risk behaviors, as well as significant medical consequences, including higher incidence of heart disease, diabetes, and stroke. Ultimately, having four or more ACEs was associated with early death.
In response to the emerging body of research on childhood trauma, various terms, including complex trauma, type-II trauma, and complex PTSD, have entered our professional lexicon as a means of communicating the wide-ranging consequences of developmental trauma. On the one hand, the less defined and rigid nature of these terms permits mental health providers to develop a rich narrative of a patient’s background, encompassing the patient’s behavior, character, and symptoms. However, the absence of formal terminology also has its drawbacks: Courts and juries have grown accustomed to diagnoses, labels, and syndromes. Most forensic mental health providers who testify about developmental trauma in court can predict the question: “So doctor, you are saying that the individual’s presentation is not severe enough to be considered PTSD, am I correct?” Disorders justify treatment, can explain disability, and warrant empathy; concomitantly, “complex trauma” runs the risk of being considered an academic explanation for trauma victims’ lifelong problems, rather than a societal failure that merits care.
Dr. Nicolas Badre
Recognizing the limitations of our current diagnoses, the forthcoming update to the International Classification of Diseases (ICD-11) will add a new category: complex PTSD. The ICD-11 will attempt to widen the concept of trauma to include “conditions of prolonged adversity, in the form of sustained, repeated, or multiple forms of traumatic exposure.” Trauma exposure examples include genocide campaigns, childhood sexual abuse, child soldiering, severe domestic violence, torture, or slavery. The ICD-11 also expands our understanding of the consequences of trauma to include “affective dysregulation,” “negative self-concept,” and “disturbances in relationships” as part of a concept called “disturbances in self-organization.” Those are important steps in acknowledging the consequences of different forms of trauma as well as noticing a richer array of damages from those incidents.4
While the World Health Organization’s latest iteration of the ICD takes an important step in widening the scope of our diagnostic tools, we are cognizant that our field’s obsessional search for diagnoses, labels, and nomenclature reinforces a detrimental focus on symptoms over stories. However, as forensic mental health providers, we also are keenly aware that a failure to adopt common definitions impedes forensic evaluations, patient advocacy, public policy, and most importantly, patient care.
In the end, we have trained society to understand pathology through narrow lenses, and therefore, in the face of tragic events such as family separations, we need the appropriate language to clearly define and communicate the experiences of our patients. So, despite the limitations of labels, let’s be encouraged by the World Health Organization’s efforts and continue in that direction.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Lehman is a licensed clinical and forensic psychologist in San Diego. Her practice consists of conducting forensic psychological evaluations for the courts with children, adolescents, and adults. Dr. Lehman has been qualified as an expert witness in California as well as in the federal courts. She previously was a supervisor at Sharper Future, a forensic rehabilitation program, and previously served as an adjunct faculty member at Alliant International University, San Diego. Dr. Lehman can be reached at [email protected].
Pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension are all terms to describe a syndrome of increased intracranial pressure, headaches, vision loss, or changes without an associated mass lesion.1 The condition was considered relatively rare, presenting most commonly in obese women in childbearing years. Surprisingly, with the obesity rates increasing among children and adolescents, rates of pseudotumor cerebri also are rising sharply in these populations.2
Dr. Francine Pearce
Obesity is the fastest growing morbidity among adolescents. The Centers for Disease Control and Prevention reported 32% of children 2-19 years were obese.1 This reality is impacting many areas of an adolescent’s health, but it also is changing the landscape of diseases that present in this age group. Although pediatric and adult pseudotumor cerebri always have had slightly varied features, many features were similar such as the papilledema, vision loss, headaches, and sixth nerve palsy. Obesity and female predominance tended to present more in the adult population, as many pediatric patients were not obese,2 and had fewer associated symptoms at the time of diagnosis, and the cause was thought to idiopathic.
Now, with the increase in obesity, more adolescents and more male patients are presenting with pseudotumor cerebri as a cause for their headache, and 57%-100% are obese, making it a compounding factor.3
Pediatric populations also are at risk of secondary pseudotumor cerebri, which is an increase in intracranial pressure from the use of medication, or other disease states such as anemia, kidney disease, or Down syndrome. Minocycline use is the most common medication cause and usually presents 1-2 months after normal use.4 Discontinuing the drug does lead to resolution. Retinoids, vitamin A products, growth hormone, and steroids also have been implicated. Given that acne is a common complaint amongst teens, knowledge of these side effects is important.4
In 2013, the criteria for diagnosis of pseudotumor cerebri was revised. Currently, the presence of papilledema, normal neurologic exam except for abnormal sixth cranial nerve, normal cerebral spinal fluid, elevated lumbar opening pressure, and normal imaging are needed for a definitive diagnosis. A probable diagnosis can be made if papilledema is not present but there abducens nerve palsy.2
In a routine physical exam, when I questioned a patient on any medication that was used daily, she replied she took ibuprofen daily for headaches and that she had been doing this for several months. Headaches were not in her chief complaints as she had learned to live with and ignore this symptom. Upon further evaluation, she was slightly overweight and has a questionable fundoscopic exam. After further evaluation by an ophthalmologist and a neurologist, pseudotumor cerebri was diagnosed.
Index of suspicion is key in correctly diagnosing patients, and understanding the changing landscape of medicine will lead to more thoughtful questioning during routine health exams and better outcomes for your patients.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at [email protected].
Pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension are all terms to describe a syndrome of increased intracranial pressure, headaches, vision loss, or changes without an associated mass lesion.1 The condition was considered relatively rare, presenting most commonly in obese women in childbearing years. Surprisingly, with the obesity rates increasing among children and adolescents, rates of pseudotumor cerebri also are rising sharply in these populations.2
Dr. Francine Pearce
Obesity is the fastest growing morbidity among adolescents. The Centers for Disease Control and Prevention reported 32% of children 2-19 years were obese.1 This reality is impacting many areas of an adolescent’s health, but it also is changing the landscape of diseases that present in this age group. Although pediatric and adult pseudotumor cerebri always have had slightly varied features, many features were similar such as the papilledema, vision loss, headaches, and sixth nerve palsy. Obesity and female predominance tended to present more in the adult population, as many pediatric patients were not obese,2 and had fewer associated symptoms at the time of diagnosis, and the cause was thought to idiopathic.
Now, with the increase in obesity, more adolescents and more male patients are presenting with pseudotumor cerebri as a cause for their headache, and 57%-100% are obese, making it a compounding factor.3
Pediatric populations also are at risk of secondary pseudotumor cerebri, which is an increase in intracranial pressure from the use of medication, or other disease states such as anemia, kidney disease, or Down syndrome. Minocycline use is the most common medication cause and usually presents 1-2 months after normal use.4 Discontinuing the drug does lead to resolution. Retinoids, vitamin A products, growth hormone, and steroids also have been implicated. Given that acne is a common complaint amongst teens, knowledge of these side effects is important.4
In 2013, the criteria for diagnosis of pseudotumor cerebri was revised. Currently, the presence of papilledema, normal neurologic exam except for abnormal sixth cranial nerve, normal cerebral spinal fluid, elevated lumbar opening pressure, and normal imaging are needed for a definitive diagnosis. A probable diagnosis can be made if papilledema is not present but there abducens nerve palsy.2
In a routine physical exam, when I questioned a patient on any medication that was used daily, she replied she took ibuprofen daily for headaches and that she had been doing this for several months. Headaches were not in her chief complaints as she had learned to live with and ignore this symptom. Upon further evaluation, she was slightly overweight and has a questionable fundoscopic exam. After further evaluation by an ophthalmologist and a neurologist, pseudotumor cerebri was diagnosed.
Index of suspicion is key in correctly diagnosing patients, and understanding the changing landscape of medicine will lead to more thoughtful questioning during routine health exams and better outcomes for your patients.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at [email protected].
Pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension are all terms to describe a syndrome of increased intracranial pressure, headaches, vision loss, or changes without an associated mass lesion.1 The condition was considered relatively rare, presenting most commonly in obese women in childbearing years. Surprisingly, with the obesity rates increasing among children and adolescents, rates of pseudotumor cerebri also are rising sharply in these populations.2
Dr. Francine Pearce
Obesity is the fastest growing morbidity among adolescents. The Centers for Disease Control and Prevention reported 32% of children 2-19 years were obese.1 This reality is impacting many areas of an adolescent’s health, but it also is changing the landscape of diseases that present in this age group. Although pediatric and adult pseudotumor cerebri always have had slightly varied features, many features were similar such as the papilledema, vision loss, headaches, and sixth nerve palsy. Obesity and female predominance tended to present more in the adult population, as many pediatric patients were not obese,2 and had fewer associated symptoms at the time of diagnosis, and the cause was thought to idiopathic.
Now, with the increase in obesity, more adolescents and more male patients are presenting with pseudotumor cerebri as a cause for their headache, and 57%-100% are obese, making it a compounding factor.3
Pediatric populations also are at risk of secondary pseudotumor cerebri, which is an increase in intracranial pressure from the use of medication, or other disease states such as anemia, kidney disease, or Down syndrome. Minocycline use is the most common medication cause and usually presents 1-2 months after normal use.4 Discontinuing the drug does lead to resolution. Retinoids, vitamin A products, growth hormone, and steroids also have been implicated. Given that acne is a common complaint amongst teens, knowledge of these side effects is important.4
In 2013, the criteria for diagnosis of pseudotumor cerebri was revised. Currently, the presence of papilledema, normal neurologic exam except for abnormal sixth cranial nerve, normal cerebral spinal fluid, elevated lumbar opening pressure, and normal imaging are needed for a definitive diagnosis. A probable diagnosis can be made if papilledema is not present but there abducens nerve palsy.2
In a routine physical exam, when I questioned a patient on any medication that was used daily, she replied she took ibuprofen daily for headaches and that she had been doing this for several months. Headaches were not in her chief complaints as she had learned to live with and ignore this symptom. Upon further evaluation, she was slightly overweight and has a questionable fundoscopic exam. After further evaluation by an ophthalmologist and a neurologist, pseudotumor cerebri was diagnosed.
Index of suspicion is key in correctly diagnosing patients, and understanding the changing landscape of medicine will lead to more thoughtful questioning during routine health exams and better outcomes for your patients.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at [email protected].
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting. The dream of tomorrow’s integrated behavioral health care should not preclude the possibility of coordinated or better colocated behavioral health care today.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
KatarzynaBialasiewicz/Thinkstock
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
Dr. Michael S. Jellinek
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Susan D. Swick
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting. The dream of tomorrow’s integrated behavioral health care should not preclude the possibility of coordinated or better colocated behavioral health care today.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
KatarzynaBialasiewicz/Thinkstock
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
Dr. Michael S. Jellinek
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Susan D. Swick
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting. The dream of tomorrow’s integrated behavioral health care should not preclude the possibility of coordinated or better colocated behavioral health care today.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
KatarzynaBialasiewicz/Thinkstock
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
Dr. Michael S. Jellinek
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Susan D. Swick
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at [email protected].
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
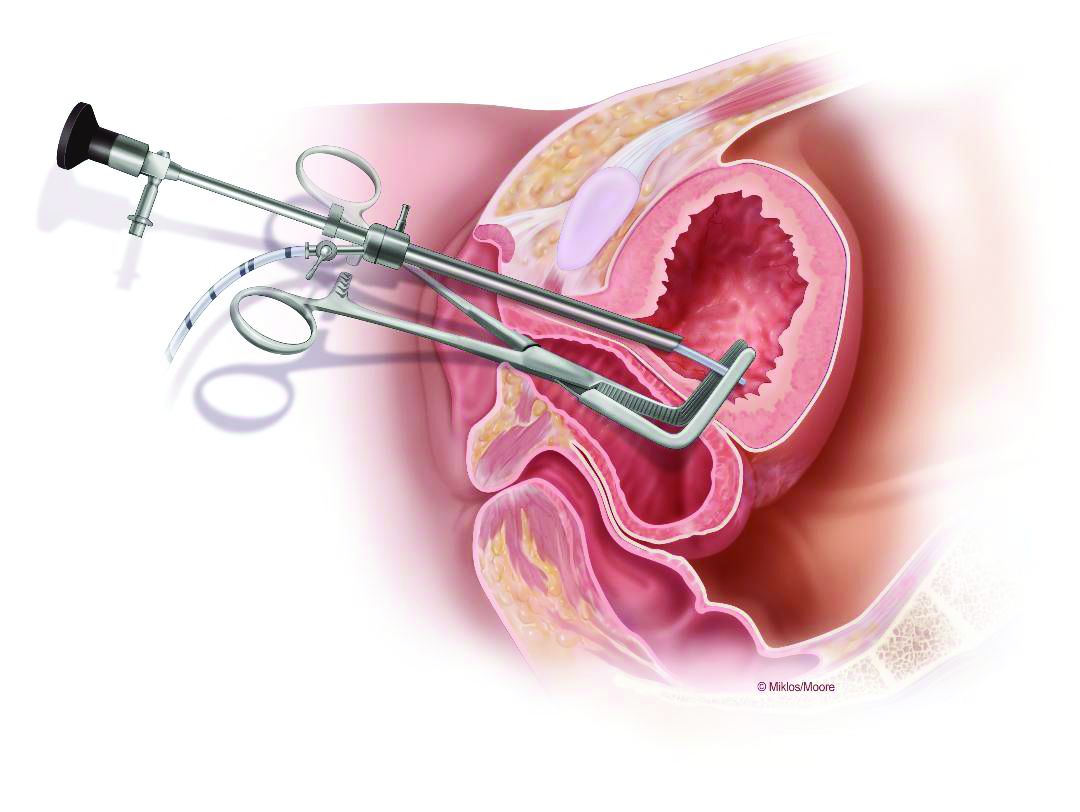
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
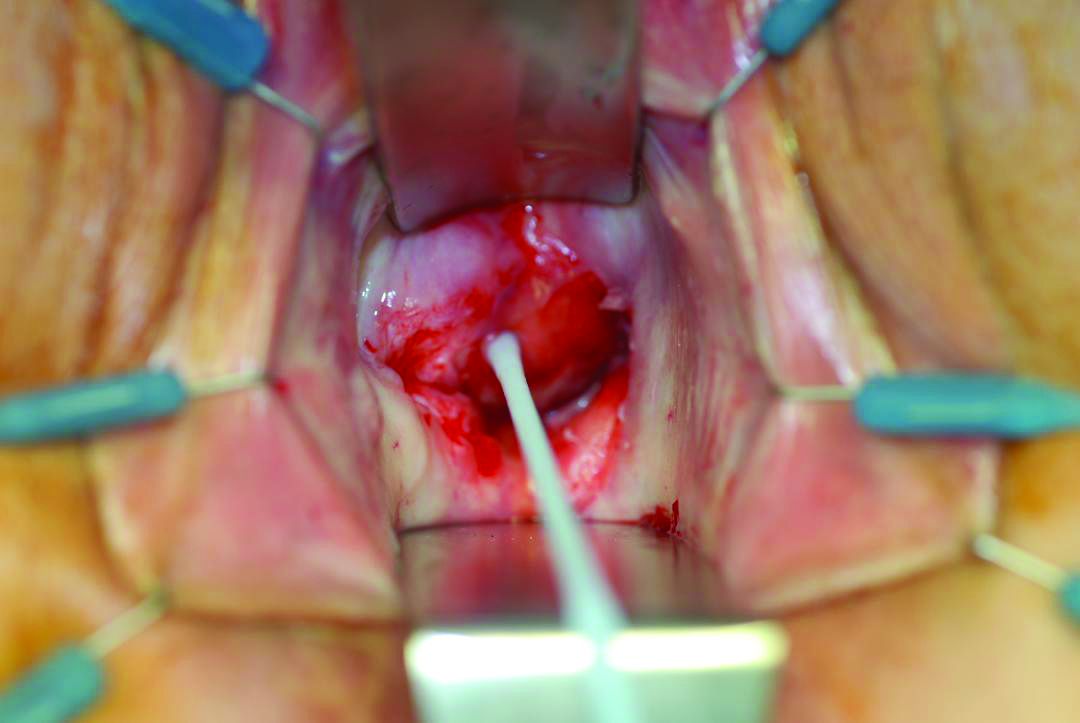
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
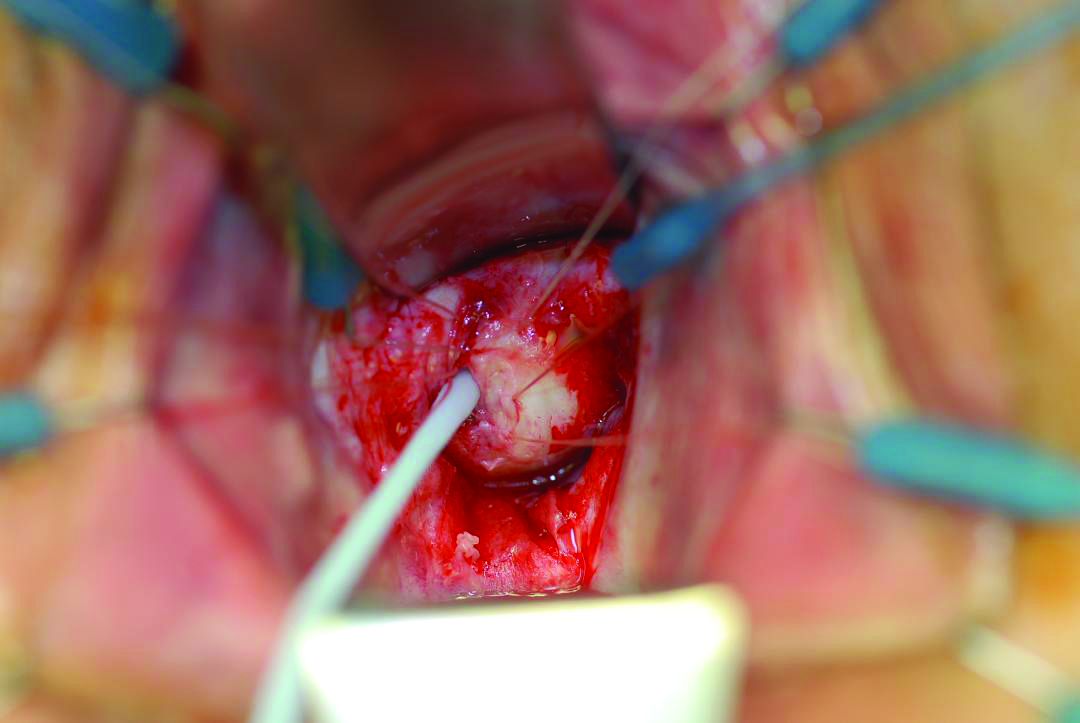
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Ten months after Hurricane Maria pummeled into the island of Puerto Rico, things have begun to get better.
Dr. Judith R. Milner
Leaves are appearing on defoliated trees; the devastated rain forest is slowly improving. Wildlife is returning. Homeless dogs are reappearing on the streets. But how are residents faring in the wake of Maria’s devastation?
Despite some signs of recovery, mental – and physical – health problems are ongoing. The official death toll was recorded at 64, but a recent study by the Harvard School of Public Health estimates that it is closer to 5,000 (N Engl J Med. 2018 May 28. doi: 10.1056/NEJMsa1803972). Some reports show that the suicide rate on the island has soared by nearly 30%. Other reports show that unemployment has increased as has crime, and some estimates show that up to 200,000 people have left the island. As of this writing, thousands of people still are without power. And the hurricane season has begun yet again.
Week-long training gets underway
A few weeks ago, I joined a team of mental health professionals affiliated with the International Center for Psychosocial Trauma at the University of Missouri–Columbia (UMICPT) that went to Puerto Rico for a week. Under the leadership of UMICPT founder Syed Arshad Husain, MD, our goals were train our colleagues and teachers how to help children suffering from posttraumatic stress disorder after Maria. Several months earlier, our team had traveled to the island to train doctors, psychologists, social workers, and other mental health workers in San Juan and Ponce, and we were eager to return to continue our work.
Courtesy Dr. Judith R. Milner
Dr. Syed Arshad Husain shares his expertise about how to help children with PTSD and other mental health problems.
Upon our arrival in late May, we heard anecdotal reports of children manifesting ongoing and escalating symptoms of PTSD. In 2014, the U.S. Census Bureau reported that 58% of the children in Puerto Rico lived below the federal poverty level, and there is reason to believe that this percentage is even higher after Maria. The reasons are many, including transportation challenges, impassable roads, gasoline shortages, and the difficulty of tracking appointments without cell phone service. Other explanations include a shortage of clinicians, and challenges of parents who are preoccupied with the daily struggle of mere survival. Another deterrent is the stigma of mental illness.
Carlos Sellas, PsyD, a faculty member and supervisor of child and adolescent mental health clinics at Ponce Health Sciences University, attended the training. Dr. Sellas reported that somatic symptoms among the children had escalated after the hurricane. One child, whose grandfather suffered a myocardial infarction after Maria, repeatedly complains of chest pain. Pseudoseizures also have been observed.
Dr. Sellas said he also is seeing increased suicidal ideation and behavior in children and adolescents. In addition, some children are reporting auditory and visual hallucinations, and phobic reaction to rainstorms and lightening – in addition to fears of the dark.
Regressive behaviors cited
Laura Deliz, PsyD, director of the Autism Center at Ponce Health Sciences University, also attended the training. She reported that some of the autistic children under her care are manifesting regressive behaviors and are losing learned skills. They are more insecure, cling to transitional objects, and complain of pains, sleep problems, and show signs of having eating disorders. “Little things bother them more,” Dr. Deliz said. They cry more frequently, display more problems with concentration and attention, and are having more tantrums.
Comorbid with PTSD, symptoms of depression, anxiety disorders, conduct disorders, attention deficit disorders, and substance use disorders also are being encountered. Substance abuse more often is a comorbid condition in adolescents, but clinicians also are seeing this in children. Impulsive behaviors, self-destructive behaviors, and feelings of guilt also are being observed.
Compassion fatigue
Many trainees also are reporting symptoms of secondary traumatization and compassion fatigue. One trainee who lives in a mountain area had no electricity until 3 weeks before the training. Access to clean water has been sporadic, because power is required to pump the water.
Efforts to obtain gasoline has entailed waiting in line for 5 hours, sometimes only to have the supply run out upon reaching the pump. Puerto Rico continues to experience rolling blackouts. The island’s power company has lacked the proper materials to fix the problems. The elderly seem to be the main victims of this failing. Many of the elderly in the mountain areas, for example, still have no clean drinking water or electricity. Many of them live alone, and the churches are trying to help them.
Another trainee from the north coast, where the primary source of work is the dairy industry, reported that, when the power went off, the electric fences failed – and the cows wandered. Many became ill and died. An entire herd perished when an electric wire fell into nearby water.
Meanwhile, another trainee reported seeing a lot of anxiety and fear in the faces of the people waiting in long lines in the supermarkets trying to buy water, food that did not require refrigeration or cooking, and among people waiting in long lines at gas stations. Some people were sociable and supportive to one another; others were encouraging and telling stories. But there also were reports of fights breaking out. People were feeling frustrated because they could not get their basic needs met.
Among the adults, according to one observer, a sense of hopelessness and sadness prevailed. In the first weeks after the hurricane, just trying to communicate with other family members was a struggle because of the absence of cell phone service. In some ways, the children seemed more resilient, because they still managed to find ways to engage in play.
Compassion fatigue also is being experienced by many of the teachers on the island, our team learned. Many of them do not know whether they will have jobs at the beginning of the new school year. The public education system, already hit hard by a decade-long recession that preceded Maria, remains challenged. Of the 1,113 public schools, only 828 will remain operational, according to the Orlando Sentinel. Meanwhile, the psychosocial environment in many of the schools is not healthy, “not when you have students who are hungry and emotionally hurting,” according to one of our students.
UMICPT curriculum
When our team travels to a traumatized area, we use the model of “training the trainers.” We teach local mental health professionals and teachers how to recognize some of the negative sequelae of trauma in children, including PTSD, complex traumatic grief, depression, and phobias. It is our aim to train them, so they can train others to recognize these conditions, and provide evidence-based interventions, which in turn can help to alleviate symptoms and promote healing. Interventions focus on efforts to build resiliency in children, and the model is collaborative, interactive, and experiential.
Our students already have some training in mental health. We seek to use their training and their experiences in our exercises. They learn from us, and we also learn much from them. When they share their experiences with us, we learn about their cultural values, which in turn enables us to provide culturally sensitive training. Skills for recovering from trauma include psychoeducation, relaxation and visualization training, dialectical behavioral therapy strategies for stress reduction, art therapy, narrative therapy, mindfulness training, and group therapy.
Future plans
UMICPT plans to make two more trips to Puerto Rico. A group of trainees will be further trained to serve as trainers to others in some of the techniques they have been taught. There is a plan to conduct a needs assessment in the schools and train teachers during the visit. Trained teachers would then have the option of introducing a weekly mental hygiene hour into the schools, with the aim of providing some relief to the children suffering from PTSD and other psychiatric problems.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee, the Committee on Diversity and Culture, and the Membership Committee for the American Academy of Child and Adolescent Psychiatry.
Ten months after Hurricane Maria pummeled into the island of Puerto Rico, things have begun to get better.
Dr. Judith R. Milner
Leaves are appearing on defoliated trees; the devastated rain forest is slowly improving. Wildlife is returning. Homeless dogs are reappearing on the streets. But how are residents faring in the wake of Maria’s devastation?
Despite some signs of recovery, mental – and physical – health problems are ongoing. The official death toll was recorded at 64, but a recent study by the Harvard School of Public Health estimates that it is closer to 5,000 (N Engl J Med. 2018 May 28. doi: 10.1056/NEJMsa1803972). Some reports show that the suicide rate on the island has soared by nearly 30%. Other reports show that unemployment has increased as has crime, and some estimates show that up to 200,000 people have left the island. As of this writing, thousands of people still are without power. And the hurricane season has begun yet again.
Week-long training gets underway
A few weeks ago, I joined a team of mental health professionals affiliated with the International Center for Psychosocial Trauma at the University of Missouri–Columbia (UMICPT) that went to Puerto Rico for a week. Under the leadership of UMICPT founder Syed Arshad Husain, MD, our goals were train our colleagues and teachers how to help children suffering from posttraumatic stress disorder after Maria. Several months earlier, our team had traveled to the island to train doctors, psychologists, social workers, and other mental health workers in San Juan and Ponce, and we were eager to return to continue our work.
Courtesy Dr. Judith R. Milner
Dr. Syed Arshad Husain shares his expertise about how to help children with PTSD and other mental health problems.
Upon our arrival in late May, we heard anecdotal reports of children manifesting ongoing and escalating symptoms of PTSD. In 2014, the U.S. Census Bureau reported that 58% of the children in Puerto Rico lived below the federal poverty level, and there is reason to believe that this percentage is even higher after Maria. The reasons are many, including transportation challenges, impassable roads, gasoline shortages, and the difficulty of tracking appointments without cell phone service. Other explanations include a shortage of clinicians, and challenges of parents who are preoccupied with the daily struggle of mere survival. Another deterrent is the stigma of mental illness.
Carlos Sellas, PsyD, a faculty member and supervisor of child and adolescent mental health clinics at Ponce Health Sciences University, attended the training. Dr. Sellas reported that somatic symptoms among the children had escalated after the hurricane. One child, whose grandfather suffered a myocardial infarction after Maria, repeatedly complains of chest pain. Pseudoseizures also have been observed.
Dr. Sellas said he also is seeing increased suicidal ideation and behavior in children and adolescents. In addition, some children are reporting auditory and visual hallucinations, and phobic reaction to rainstorms and lightening – in addition to fears of the dark.
Regressive behaviors cited
Laura Deliz, PsyD, director of the Autism Center at Ponce Health Sciences University, also attended the training. She reported that some of the autistic children under her care are manifesting regressive behaviors and are losing learned skills. They are more insecure, cling to transitional objects, and complain of pains, sleep problems, and show signs of having eating disorders. “Little things bother them more,” Dr. Deliz said. They cry more frequently, display more problems with concentration and attention, and are having more tantrums.
Comorbid with PTSD, symptoms of depression, anxiety disorders, conduct disorders, attention deficit disorders, and substance use disorders also are being encountered. Substance abuse more often is a comorbid condition in adolescents, but clinicians also are seeing this in children. Impulsive behaviors, self-destructive behaviors, and feelings of guilt also are being observed.
Compassion fatigue
Many trainees also are reporting symptoms of secondary traumatization and compassion fatigue. One trainee who lives in a mountain area had no electricity until 3 weeks before the training. Access to clean water has been sporadic, because power is required to pump the water.
Efforts to obtain gasoline has entailed waiting in line for 5 hours, sometimes only to have the supply run out upon reaching the pump. Puerto Rico continues to experience rolling blackouts. The island’s power company has lacked the proper materials to fix the problems. The elderly seem to be the main victims of this failing. Many of the elderly in the mountain areas, for example, still have no clean drinking water or electricity. Many of them live alone, and the churches are trying to help them.
Another trainee from the north coast, where the primary source of work is the dairy industry, reported that, when the power went off, the electric fences failed – and the cows wandered. Many became ill and died. An entire herd perished when an electric wire fell into nearby water.
Meanwhile, another trainee reported seeing a lot of anxiety and fear in the faces of the people waiting in long lines in the supermarkets trying to buy water, food that did not require refrigeration or cooking, and among people waiting in long lines at gas stations. Some people were sociable and supportive to one another; others were encouraging and telling stories. But there also were reports of fights breaking out. People were feeling frustrated because they could not get their basic needs met.
Among the adults, according to one observer, a sense of hopelessness and sadness prevailed. In the first weeks after the hurricane, just trying to communicate with other family members was a struggle because of the absence of cell phone service. In some ways, the children seemed more resilient, because they still managed to find ways to engage in play.
Compassion fatigue also is being experienced by many of the teachers on the island, our team learned. Many of them do not know whether they will have jobs at the beginning of the new school year. The public education system, already hit hard by a decade-long recession that preceded Maria, remains challenged. Of the 1,113 public schools, only 828 will remain operational, according to the Orlando Sentinel. Meanwhile, the psychosocial environment in many of the schools is not healthy, “not when you have students who are hungry and emotionally hurting,” according to one of our students.
UMICPT curriculum
When our team travels to a traumatized area, we use the model of “training the trainers.” We teach local mental health professionals and teachers how to recognize some of the negative sequelae of trauma in children, including PTSD, complex traumatic grief, depression, and phobias. It is our aim to train them, so they can train others to recognize these conditions, and provide evidence-based interventions, which in turn can help to alleviate symptoms and promote healing. Interventions focus on efforts to build resiliency in children, and the model is collaborative, interactive, and experiential.
Our students already have some training in mental health. We seek to use their training and their experiences in our exercises. They learn from us, and we also learn much from them. When they share their experiences with us, we learn about their cultural values, which in turn enables us to provide culturally sensitive training. Skills for recovering from trauma include psychoeducation, relaxation and visualization training, dialectical behavioral therapy strategies for stress reduction, art therapy, narrative therapy, mindfulness training, and group therapy.
Future plans
UMICPT plans to make two more trips to Puerto Rico. A group of trainees will be further trained to serve as trainers to others in some of the techniques they have been taught. There is a plan to conduct a needs assessment in the schools and train teachers during the visit. Trained teachers would then have the option of introducing a weekly mental hygiene hour into the schools, with the aim of providing some relief to the children suffering from PTSD and other psychiatric problems.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee, the Committee on Diversity and Culture, and the Membership Committee for the American Academy of Child and Adolescent Psychiatry.
Ten months after Hurricane Maria pummeled into the island of Puerto Rico, things have begun to get better.
Dr. Judith R. Milner
Leaves are appearing on defoliated trees; the devastated rain forest is slowly improving. Wildlife is returning. Homeless dogs are reappearing on the streets. But how are residents faring in the wake of Maria’s devastation?
Despite some signs of recovery, mental – and physical – health problems are ongoing. The official death toll was recorded at 64, but a recent study by the Harvard School of Public Health estimates that it is closer to 5,000 (N Engl J Med. 2018 May 28. doi: 10.1056/NEJMsa1803972). Some reports show that the suicide rate on the island has soared by nearly 30%. Other reports show that unemployment has increased as has crime, and some estimates show that up to 200,000 people have left the island. As of this writing, thousands of people still are without power. And the hurricane season has begun yet again.
Week-long training gets underway
A few weeks ago, I joined a team of mental health professionals affiliated with the International Center for Psychosocial Trauma at the University of Missouri–Columbia (UMICPT) that went to Puerto Rico for a week. Under the leadership of UMICPT founder Syed Arshad Husain, MD, our goals were train our colleagues and teachers how to help children suffering from posttraumatic stress disorder after Maria. Several months earlier, our team had traveled to the island to train doctors, psychologists, social workers, and other mental health workers in San Juan and Ponce, and we were eager to return to continue our work.
Courtesy Dr. Judith R. Milner
Dr. Syed Arshad Husain shares his expertise about how to help children with PTSD and other mental health problems.
Upon our arrival in late May, we heard anecdotal reports of children manifesting ongoing and escalating symptoms of PTSD. In 2014, the U.S. Census Bureau reported that 58% of the children in Puerto Rico lived below the federal poverty level, and there is reason to believe that this percentage is even higher after Maria. The reasons are many, including transportation challenges, impassable roads, gasoline shortages, and the difficulty of tracking appointments without cell phone service. Other explanations include a shortage of clinicians, and challenges of parents who are preoccupied with the daily struggle of mere survival. Another deterrent is the stigma of mental illness.
Carlos Sellas, PsyD, a faculty member and supervisor of child and adolescent mental health clinics at Ponce Health Sciences University, attended the training. Dr. Sellas reported that somatic symptoms among the children had escalated after the hurricane. One child, whose grandfather suffered a myocardial infarction after Maria, repeatedly complains of chest pain. Pseudoseizures also have been observed.
Dr. Sellas said he also is seeing increased suicidal ideation and behavior in children and adolescents. In addition, some children are reporting auditory and visual hallucinations, and phobic reaction to rainstorms and lightening – in addition to fears of the dark.
Regressive behaviors cited
Laura Deliz, PsyD, director of the Autism Center at Ponce Health Sciences University, also attended the training. She reported that some of the autistic children under her care are manifesting regressive behaviors and are losing learned skills. They are more insecure, cling to transitional objects, and complain of pains, sleep problems, and show signs of having eating disorders. “Little things bother them more,” Dr. Deliz said. They cry more frequently, display more problems with concentration and attention, and are having more tantrums.
Comorbid with PTSD, symptoms of depression, anxiety disorders, conduct disorders, attention deficit disorders, and substance use disorders also are being encountered. Substance abuse more often is a comorbid condition in adolescents, but clinicians also are seeing this in children. Impulsive behaviors, self-destructive behaviors, and feelings of guilt also are being observed.
Compassion fatigue
Many trainees also are reporting symptoms of secondary traumatization and compassion fatigue. One trainee who lives in a mountain area had no electricity until 3 weeks before the training. Access to clean water has been sporadic, because power is required to pump the water.
Efforts to obtain gasoline has entailed waiting in line for 5 hours, sometimes only to have the supply run out upon reaching the pump. Puerto Rico continues to experience rolling blackouts. The island’s power company has lacked the proper materials to fix the problems. The elderly seem to be the main victims of this failing. Many of the elderly in the mountain areas, for example, still have no clean drinking water or electricity. Many of them live alone, and the churches are trying to help them.
Another trainee from the north coast, where the primary source of work is the dairy industry, reported that, when the power went off, the electric fences failed – and the cows wandered. Many became ill and died. An entire herd perished when an electric wire fell into nearby water.
Meanwhile, another trainee reported seeing a lot of anxiety and fear in the faces of the people waiting in long lines in the supermarkets trying to buy water, food that did not require refrigeration or cooking, and among people waiting in long lines at gas stations. Some people were sociable and supportive to one another; others were encouraging and telling stories. But there also were reports of fights breaking out. People were feeling frustrated because they could not get their basic needs met.
Among the adults, according to one observer, a sense of hopelessness and sadness prevailed. In the first weeks after the hurricane, just trying to communicate with other family members was a struggle because of the absence of cell phone service. In some ways, the children seemed more resilient, because they still managed to find ways to engage in play.
Compassion fatigue also is being experienced by many of the teachers on the island, our team learned. Many of them do not know whether they will have jobs at the beginning of the new school year. The public education system, already hit hard by a decade-long recession that preceded Maria, remains challenged. Of the 1,113 public schools, only 828 will remain operational, according to the Orlando Sentinel. Meanwhile, the psychosocial environment in many of the schools is not healthy, “not when you have students who are hungry and emotionally hurting,” according to one of our students.
UMICPT curriculum
When our team travels to a traumatized area, we use the model of “training the trainers.” We teach local mental health professionals and teachers how to recognize some of the negative sequelae of trauma in children, including PTSD, complex traumatic grief, depression, and phobias. It is our aim to train them, so they can train others to recognize these conditions, and provide evidence-based interventions, which in turn can help to alleviate symptoms and promote healing. Interventions focus on efforts to build resiliency in children, and the model is collaborative, interactive, and experiential.
Our students already have some training in mental health. We seek to use their training and their experiences in our exercises. They learn from us, and we also learn much from them. When they share their experiences with us, we learn about their cultural values, which in turn enables us to provide culturally sensitive training. Skills for recovering from trauma include psychoeducation, relaxation and visualization training, dialectical behavioral therapy strategies for stress reduction, art therapy, narrative therapy, mindfulness training, and group therapy.
Future plans
UMICPT plans to make two more trips to Puerto Rico. A group of trainees will be further trained to serve as trainers to others in some of the techniques they have been taught. There is a plan to conduct a needs assessment in the schools and train teachers during the visit. Trained teachers would then have the option of introducing a weekly mental hygiene hour into the schools, with the aim of providing some relief to the children suffering from PTSD and other psychiatric problems.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee, the Committee on Diversity and Culture, and the Membership Committee for the American Academy of Child and Adolescent Psychiatry.
Fish pedicures have recently received attention in the media because of a case report potentially linking a fish pedicure to onychomadesis. A letter published in JAMA Dermatology describes an otherwise healthy woman in her 20s who experienced nail abnormalities some months after having a fish pedicure. Onychomadesis, or transverse splitting of the nail plate, occurs when the nail matrix has arrested in producing the nail plate. It can be thought of as more severe form of Beau’s lines, in which the nail itself actually breaks and separates from the proximal nail plate and eventually sheds.
RomoloTavani/iStock/Getty Images Plus
Fish pedicures have a long-standing history in Mediterranean and Middle Eastern cultures for aiding such skin conditions as psoriasis and helping to remove scaly skin. The Garra rufa fish are nonmigratory freshwater fish native to the Persian Gulf and Eastern Mediterranean. Suction allows them to attach to rocks and eat plankton. These “doctor fish,” as they are nicknamed, when placed in a warm bath of 25°C to 30°C, will also eat human skin when starved of their natural food source. As the JAMA Dermatology letter mentions, this was demonstrated in a study in Kangal, Turkey, where Garra rufa fish were used to improve psoriasis by feeding on psoriasis plaques but not normal skin. After 3 weeks of therapy with Garra rufa in 67 patients, there was a 72% reduction in the Psoriasis Area and Severity Index (PASI) score from baseline (Evid Based Complement Alternat Med. 2006 Dec;3[4]:483-8).
Popular in the United States and Europe about a decade ago, fish pedicures have now been banned in 10 U.S. states and in some parts of Europe. While the trend in the United States has waned, fish pedicures have recently become more popular in vacation destinations, such as the Caribbean. The inherent concern of fish pedicures is risk of infection as the same fish are used successively and cannot be adequately sanitized between people.
Two cases of staphylococcus infections and one of Mycobacterium marinum have been reported after fish pedicures. Whether these infections were caused by the fish or the water source, however, remains to be determined. If the fish were transmitting infections, it seems that more infections would likely have been reported, considering the widespread popularity in the past. I, like Antonella Tosti, MD, who commented in a CNN report on the JAMA Dermatology case, also doubt that the fish pedicure alone caused onychomadesis in this woman. In order for onychomadesis to occur, there would have had to have been significant trauma to all 10 nails at the matrix. Would the fish been able to have caused the same amount of trauma to all 10 nails in one setting? While it is possible, I believe a more likely explanation would be an alternate endogenous or exogenous source.
Dr. Naissan O. Wesley
Traditional medicine has been used to enhance beauty and cure ailments for thousands of years before the advent of modern medicine as demonstrated by the Kangal study. Before discounting fish pedicures completely, perhaps some thought should also be given to how this practice affects wildlife and the fish. The CNN report refers to a 2011 investigation by the U.K.’s Fish Health Inspectorate, which “found a bacterial outbreak among thousands of these fish, which had been transported from Indonesia to the United Kingdom pedicure spas. Fish were found with bulging eyes, many hemorrhaging around the gills and mouth. The culprit was found to be a streptococcal bacteria, a strain that is associated with fish like tilapia, according to David Verner-Jeffreys, a senior microbiologist at the Centre for Environment, Fisheries and Aquaculture Science in the U.K.”
Whether or not these fish would pose any risk to humans is unknown, but certainly, this practice adversely affects the welfare of the fish and their environment. The overharvesting of these fish has led the Turkish government to introduce legal protections for the country’s Garra rufa in an attempt to combat overfishing and exploitation.
Perhaps fish pedicures solely for aesthetic reasons should not be practiced because of the potential infection risk – as well as the harm (to both humans and fish) and overharvesting of the fish. If used properly, these fish, however, could be an aid in treating certain skin pathologies.
Dr. Lily Talakoub
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Fish pedicures have recently received attention in the media because of a case report potentially linking a fish pedicure to onychomadesis. A letter published in JAMA Dermatology describes an otherwise healthy woman in her 20s who experienced nail abnormalities some months after having a fish pedicure. Onychomadesis, or transverse splitting of the nail plate, occurs when the nail matrix has arrested in producing the nail plate. It can be thought of as more severe form of Beau’s lines, in which the nail itself actually breaks and separates from the proximal nail plate and eventually sheds.
RomoloTavani/iStock/Getty Images Plus
Fish pedicures have a long-standing history in Mediterranean and Middle Eastern cultures for aiding such skin conditions as psoriasis and helping to remove scaly skin. The Garra rufa fish are nonmigratory freshwater fish native to the Persian Gulf and Eastern Mediterranean. Suction allows them to attach to rocks and eat plankton. These “doctor fish,” as they are nicknamed, when placed in a warm bath of 25°C to 30°C, will also eat human skin when starved of their natural food source. As the JAMA Dermatology letter mentions, this was demonstrated in a study in Kangal, Turkey, where Garra rufa fish were used to improve psoriasis by feeding on psoriasis plaques but not normal skin. After 3 weeks of therapy with Garra rufa in 67 patients, there was a 72% reduction in the Psoriasis Area and Severity Index (PASI) score from baseline (Evid Based Complement Alternat Med. 2006 Dec;3[4]:483-8).
Popular in the United States and Europe about a decade ago, fish pedicures have now been banned in 10 U.S. states and in some parts of Europe. While the trend in the United States has waned, fish pedicures have recently become more popular in vacation destinations, such as the Caribbean. The inherent concern of fish pedicures is risk of infection as the same fish are used successively and cannot be adequately sanitized between people.
Two cases of staphylococcus infections and one of Mycobacterium marinum have been reported after fish pedicures. Whether these infections were caused by the fish or the water source, however, remains to be determined. If the fish were transmitting infections, it seems that more infections would likely have been reported, considering the widespread popularity in the past. I, like Antonella Tosti, MD, who commented in a CNN report on the JAMA Dermatology case, also doubt that the fish pedicure alone caused onychomadesis in this woman. In order for onychomadesis to occur, there would have had to have been significant trauma to all 10 nails at the matrix. Would the fish been able to have caused the same amount of trauma to all 10 nails in one setting? While it is possible, I believe a more likely explanation would be an alternate endogenous or exogenous source.
Dr. Naissan O. Wesley
Traditional medicine has been used to enhance beauty and cure ailments for thousands of years before the advent of modern medicine as demonstrated by the Kangal study. Before discounting fish pedicures completely, perhaps some thought should also be given to how this practice affects wildlife and the fish. The CNN report refers to a 2011 investigation by the U.K.’s Fish Health Inspectorate, which “found a bacterial outbreak among thousands of these fish, which had been transported from Indonesia to the United Kingdom pedicure spas. Fish were found with bulging eyes, many hemorrhaging around the gills and mouth. The culprit was found to be a streptococcal bacteria, a strain that is associated with fish like tilapia, according to David Verner-Jeffreys, a senior microbiologist at the Centre for Environment, Fisheries and Aquaculture Science in the U.K.”
Whether or not these fish would pose any risk to humans is unknown, but certainly, this practice adversely affects the welfare of the fish and their environment. The overharvesting of these fish has led the Turkish government to introduce legal protections for the country’s Garra rufa in an attempt to combat overfishing and exploitation.
Perhaps fish pedicures solely for aesthetic reasons should not be practiced because of the potential infection risk – as well as the harm (to both humans and fish) and overharvesting of the fish. If used properly, these fish, however, could be an aid in treating certain skin pathologies.
Dr. Lily Talakoub
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Fish pedicures have recently received attention in the media because of a case report potentially linking a fish pedicure to onychomadesis. A letter published in JAMA Dermatology describes an otherwise healthy woman in her 20s who experienced nail abnormalities some months after having a fish pedicure. Onychomadesis, or transverse splitting of the nail plate, occurs when the nail matrix has arrested in producing the nail plate. It can be thought of as more severe form of Beau’s lines, in which the nail itself actually breaks and separates from the proximal nail plate and eventually sheds.
RomoloTavani/iStock/Getty Images Plus
Fish pedicures have a long-standing history in Mediterranean and Middle Eastern cultures for aiding such skin conditions as psoriasis and helping to remove scaly skin. The Garra rufa fish are nonmigratory freshwater fish native to the Persian Gulf and Eastern Mediterranean. Suction allows them to attach to rocks and eat plankton. These “doctor fish,” as they are nicknamed, when placed in a warm bath of 25°C to 30°C, will also eat human skin when starved of their natural food source. As the JAMA Dermatology letter mentions, this was demonstrated in a study in Kangal, Turkey, where Garra rufa fish were used to improve psoriasis by feeding on psoriasis plaques but not normal skin. After 3 weeks of therapy with Garra rufa in 67 patients, there was a 72% reduction in the Psoriasis Area and Severity Index (PASI) score from baseline (Evid Based Complement Alternat Med. 2006 Dec;3[4]:483-8).
Popular in the United States and Europe about a decade ago, fish pedicures have now been banned in 10 U.S. states and in some parts of Europe. While the trend in the United States has waned, fish pedicures have recently become more popular in vacation destinations, such as the Caribbean. The inherent concern of fish pedicures is risk of infection as the same fish are used successively and cannot be adequately sanitized between people.
Two cases of staphylococcus infections and one of Mycobacterium marinum have been reported after fish pedicures. Whether these infections were caused by the fish or the water source, however, remains to be determined. If the fish were transmitting infections, it seems that more infections would likely have been reported, considering the widespread popularity in the past. I, like Antonella Tosti, MD, who commented in a CNN report on the JAMA Dermatology case, also doubt that the fish pedicure alone caused onychomadesis in this woman. In order for onychomadesis to occur, there would have had to have been significant trauma to all 10 nails at the matrix. Would the fish been able to have caused the same amount of trauma to all 10 nails in one setting? While it is possible, I believe a more likely explanation would be an alternate endogenous or exogenous source.
Dr. Naissan O. Wesley
Traditional medicine has been used to enhance beauty and cure ailments for thousands of years before the advent of modern medicine as demonstrated by the Kangal study. Before discounting fish pedicures completely, perhaps some thought should also be given to how this practice affects wildlife and the fish. The CNN report refers to a 2011 investigation by the U.K.’s Fish Health Inspectorate, which “found a bacterial outbreak among thousands of these fish, which had been transported from Indonesia to the United Kingdom pedicure spas. Fish were found with bulging eyes, many hemorrhaging around the gills and mouth. The culprit was found to be a streptococcal bacteria, a strain that is associated with fish like tilapia, according to David Verner-Jeffreys, a senior microbiologist at the Centre for Environment, Fisheries and Aquaculture Science in the U.K.”
Whether or not these fish would pose any risk to humans is unknown, but certainly, this practice adversely affects the welfare of the fish and their environment. The overharvesting of these fish has led the Turkish government to introduce legal protections for the country’s Garra rufa in an attempt to combat overfishing and exploitation.
Perhaps fish pedicures solely for aesthetic reasons should not be practiced because of the potential infection risk – as well as the harm (to both humans and fish) and overharvesting of the fish. If used properly, these fish, however, could be an aid in treating certain skin pathologies.
Dr. Lily Talakoub
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Mentorship is a hot topic. Mentors are generally perceived as knowledgeable, kind, generous souls who will guide mentees through tough challenges and be your pal. I suggest to you that while such encounters are marvelous, and to be sought out, some of the most important lessons are taught by members of the opposite cast.
erhui1979/Getty Images
The presiding secretary of the Ohio state medical board was a brigadier general, still active reserve, tall with a bristling countenance. I was president of the Ohio Dermatological Association and was accompanied by Mark Bechtel, MD, who was our chair of state legislation. We had been invited to discuss possible office surgery regulations with the medical board. We were secure in our personal knowledge that local anesthesia was very safe, and that there had not been any deaths related to local anesthesia administered by dermatologists in Ohio (or anywhere else). We expected to tell the medical board there was nothing to worry about, and we could all go home. This was 17 years ago.
It quickly became apparent that there had been an extensive prior dialogue between the medical board and representatives of the American College of Surgeons and the American Society of Anesthesiologists. They sat at the head table with the secretary of the medical board.
“In our experience, there are really some dangerous procedures going on in the office setting under local anesthesia, and this area desperately needs regulation,” the anesthesiologist’s representative said. The surgeon’s representative chimed in: “From what I’ve heard, office surgery is a ticking time bomb and needs regulation, and as soon as possible.” This prattle went on and on, with the medical board secretary sympathetically nodding his head. I raised my hand and was ignored – and ignored. It became apparent that this was a show trial, and our opinion was not really wanted, just our attendance noted in the minutes. Finally, I stood up and protested, and pointed out that all of this “testimony” was conjecture and personal opinion, and that there was no factual basis for their claims. The president stiffened, stood up, and started barking orders.He told me to “sit down and not speak unless I was called on.” I sat down and shut up. And I was never called on. Mark Bechtel put a calming hand on my arm. Goodness, I had not been treated like that since junior high.
I soon realized that dermatologists were not at all important to the medical board, and that the medical board had no idea about our safety and efficiency and really did not care.
Following the meeting,I was told by Larry Lanier (the American Academy of Dermatology state legislative liaison at the time) that Ohio was to be the test state to restrict local anesthesia and tumescent anesthesia nationwide. He explained that some widely reported liposuction-related deaths in Florida had given the medical board the “justification” to act. He went on to explain that yes, there were no data either way, but we had better hire a lobbyist and hope for the best.
Dr. Brett M. Coldiron
I was stunned by what I now call (in this case, rough) “mentorship”by the medical board secretary.I understood I could meekly go along – or get angry. I chose the latter, and it has greatly changed my career.
Now, this was not a hot, red, foam-at-the-mouth mad, but a slow burn, the kind that sustains, not consumes.
I went home and did a literature review and was disheartened to find absolutely nothing in the literature on the safety record of dermatologists in the office setting or on the safety of office surgery in general under local anesthesia. We had nothing to back us up.
I looked up the liposuction deaths in Florida and discovered the procedures were all done under general anesthesia or deep sedation by surgeons of one type or another. I also discovered that Florida had enacted mandatory reporting, and the reports could be had for copying costs. I ordered all available, 9 months of data.
We dermatologists passed a special assessment and hired a lobbyist who told us we were too late to have any impact on the impending restrictions. We took a resolution opposing the medical board rules – which would have eliminated using any sedation in the office, even haloperidol and tumescent anesthesia – to the state medical society and got it passed despite the medical board secretary (who was a former president of the society) testifying against us. The Florida data showed no deaths or injuries from using local anesthesia in the office by anyone, and I succeeded in getting a letter addressing that data published expeditiously in the Journal of the American Medical Association (JAMA 2001;285[20]:2582).
The president of the American Society for Dermatologic Surgery at that time, Stephen Mandy, MD, came to town and testified against the proposed restrictions along with about 60 physicians, including dermatologists, plastic surgeons, and other physicians who perform office-based surgery who we had rallied to join us from across the state. So many colleagues joined us, in fact, that some of us had to sit on the floor during the proceedings.
The proposed restrictions evaporated. I and many others have since devoted our research efforts to solidifying dermatology’s safety and quality record. Dr. Bechtel, professor of dermatology at Ohio State University, Columbus, is now secretary of the state medical board. At the last annual state meeting, I thanked the brigadier general, the former secretary of themedical board, for his unlikely mentorship. He smiled and we got our picture taken together.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
Mentorship is a hot topic. Mentors are generally perceived as knowledgeable, kind, generous souls who will guide mentees through tough challenges and be your pal. I suggest to you that while such encounters are marvelous, and to be sought out, some of the most important lessons are taught by members of the opposite cast.
erhui1979/Getty Images
The presiding secretary of the Ohio state medical board was a brigadier general, still active reserve, tall with a bristling countenance. I was president of the Ohio Dermatological Association and was accompanied by Mark Bechtel, MD, who was our chair of state legislation. We had been invited to discuss possible office surgery regulations with the medical board. We were secure in our personal knowledge that local anesthesia was very safe, and that there had not been any deaths related to local anesthesia administered by dermatologists in Ohio (or anywhere else). We expected to tell the medical board there was nothing to worry about, and we could all go home. This was 17 years ago.
It quickly became apparent that there had been an extensive prior dialogue between the medical board and representatives of the American College of Surgeons and the American Society of Anesthesiologists. They sat at the head table with the secretary of the medical board.
“In our experience, there are really some dangerous procedures going on in the office setting under local anesthesia, and this area desperately needs regulation,” the anesthesiologist’s representative said. The surgeon’s representative chimed in: “From what I’ve heard, office surgery is a ticking time bomb and needs regulation, and as soon as possible.” This prattle went on and on, with the medical board secretary sympathetically nodding his head. I raised my hand and was ignored – and ignored. It became apparent that this was a show trial, and our opinion was not really wanted, just our attendance noted in the minutes. Finally, I stood up and protested, and pointed out that all of this “testimony” was conjecture and personal opinion, and that there was no factual basis for their claims. The president stiffened, stood up, and started barking orders.He told me to “sit down and not speak unless I was called on.” I sat down and shut up. And I was never called on. Mark Bechtel put a calming hand on my arm. Goodness, I had not been treated like that since junior high.
I soon realized that dermatologists were not at all important to the medical board, and that the medical board had no idea about our safety and efficiency and really did not care.
Following the meeting,I was told by Larry Lanier (the American Academy of Dermatology state legislative liaison at the time) that Ohio was to be the test state to restrict local anesthesia and tumescent anesthesia nationwide. He explained that some widely reported liposuction-related deaths in Florida had given the medical board the “justification” to act. He went on to explain that yes, there were no data either way, but we had better hire a lobbyist and hope for the best.
Dr. Brett M. Coldiron
I was stunned by what I now call (in this case, rough) “mentorship”by the medical board secretary.I understood I could meekly go along – or get angry. I chose the latter, and it has greatly changed my career.
Now, this was not a hot, red, foam-at-the-mouth mad, but a slow burn, the kind that sustains, not consumes.
I went home and did a literature review and was disheartened to find absolutely nothing in the literature on the safety record of dermatologists in the office setting or on the safety of office surgery in general under local anesthesia. We had nothing to back us up.
I looked up the liposuction deaths in Florida and discovered the procedures were all done under general anesthesia or deep sedation by surgeons of one type or another. I also discovered that Florida had enacted mandatory reporting, and the reports could be had for copying costs. I ordered all available, 9 months of data.
We dermatologists passed a special assessment and hired a lobbyist who told us we were too late to have any impact on the impending restrictions. We took a resolution opposing the medical board rules – which would have eliminated using any sedation in the office, even haloperidol and tumescent anesthesia – to the state medical society and got it passed despite the medical board secretary (who was a former president of the society) testifying against us. The Florida data showed no deaths or injuries from using local anesthesia in the office by anyone, and I succeeded in getting a letter addressing that data published expeditiously in the Journal of the American Medical Association (JAMA 2001;285[20]:2582).
The president of the American Society for Dermatologic Surgery at that time, Stephen Mandy, MD, came to town and testified against the proposed restrictions along with about 60 physicians, including dermatologists, plastic surgeons, and other physicians who perform office-based surgery who we had rallied to join us from across the state. So many colleagues joined us, in fact, that some of us had to sit on the floor during the proceedings.
The proposed restrictions evaporated. I and many others have since devoted our research efforts to solidifying dermatology’s safety and quality record. Dr. Bechtel, professor of dermatology at Ohio State University, Columbus, is now secretary of the state medical board. At the last annual state meeting, I thanked the brigadier general, the former secretary of themedical board, for his unlikely mentorship. He smiled and we got our picture taken together.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
Mentorship is a hot topic. Mentors are generally perceived as knowledgeable, kind, generous souls who will guide mentees through tough challenges and be your pal. I suggest to you that while such encounters are marvelous, and to be sought out, some of the most important lessons are taught by members of the opposite cast.
erhui1979/Getty Images
The presiding secretary of the Ohio state medical board was a brigadier general, still active reserve, tall with a bristling countenance. I was president of the Ohio Dermatological Association and was accompanied by Mark Bechtel, MD, who was our chair of state legislation. We had been invited to discuss possible office surgery regulations with the medical board. We were secure in our personal knowledge that local anesthesia was very safe, and that there had not been any deaths related to local anesthesia administered by dermatologists in Ohio (or anywhere else). We expected to tell the medical board there was nothing to worry about, and we could all go home. This was 17 years ago.
It quickly became apparent that there had been an extensive prior dialogue between the medical board and representatives of the American College of Surgeons and the American Society of Anesthesiologists. They sat at the head table with the secretary of the medical board.
“In our experience, there are really some dangerous procedures going on in the office setting under local anesthesia, and this area desperately needs regulation,” the anesthesiologist’s representative said. The surgeon’s representative chimed in: “From what I’ve heard, office surgery is a ticking time bomb and needs regulation, and as soon as possible.” This prattle went on and on, with the medical board secretary sympathetically nodding his head. I raised my hand and was ignored – and ignored. It became apparent that this was a show trial, and our opinion was not really wanted, just our attendance noted in the minutes. Finally, I stood up and protested, and pointed out that all of this “testimony” was conjecture and personal opinion, and that there was no factual basis for their claims. The president stiffened, stood up, and started barking orders.He told me to “sit down and not speak unless I was called on.” I sat down and shut up. And I was never called on. Mark Bechtel put a calming hand on my arm. Goodness, I had not been treated like that since junior high.
I soon realized that dermatologists were not at all important to the medical board, and that the medical board had no idea about our safety and efficiency and really did not care.
Following the meeting,I was told by Larry Lanier (the American Academy of Dermatology state legislative liaison at the time) that Ohio was to be the test state to restrict local anesthesia and tumescent anesthesia nationwide. He explained that some widely reported liposuction-related deaths in Florida had given the medical board the “justification” to act. He went on to explain that yes, there were no data either way, but we had better hire a lobbyist and hope for the best.
Dr. Brett M. Coldiron
I was stunned by what I now call (in this case, rough) “mentorship”by the medical board secretary.I understood I could meekly go along – or get angry. I chose the latter, and it has greatly changed my career.
Now, this was not a hot, red, foam-at-the-mouth mad, but a slow burn, the kind that sustains, not consumes.
I went home and did a literature review and was disheartened to find absolutely nothing in the literature on the safety record of dermatologists in the office setting or on the safety of office surgery in general under local anesthesia. We had nothing to back us up.
I looked up the liposuction deaths in Florida and discovered the procedures were all done under general anesthesia or deep sedation by surgeons of one type or another. I also discovered that Florida had enacted mandatory reporting, and the reports could be had for copying costs. I ordered all available, 9 months of data.
We dermatologists passed a special assessment and hired a lobbyist who told us we were too late to have any impact on the impending restrictions. We took a resolution opposing the medical board rules – which would have eliminated using any sedation in the office, even haloperidol and tumescent anesthesia – to the state medical society and got it passed despite the medical board secretary (who was a former president of the society) testifying against us. The Florida data showed no deaths or injuries from using local anesthesia in the office by anyone, and I succeeded in getting a letter addressing that data published expeditiously in the Journal of the American Medical Association (JAMA 2001;285[20]:2582).
The president of the American Society for Dermatologic Surgery at that time, Stephen Mandy, MD, came to town and testified against the proposed restrictions along with about 60 physicians, including dermatologists, plastic surgeons, and other physicians who perform office-based surgery who we had rallied to join us from across the state. So many colleagues joined us, in fact, that some of us had to sit on the floor during the proceedings.
The proposed restrictions evaporated. I and many others have since devoted our research efforts to solidifying dermatology’s safety and quality record. Dr. Bechtel, professor of dermatology at Ohio State University, Columbus, is now secretary of the state medical board. At the last annual state meeting, I thanked the brigadier general, the former secretary of themedical board, for his unlikely mentorship. He smiled and we got our picture taken together.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].