User login
What is the diagnosis?
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4

HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.

Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.


Physician as trusted counselor
Pediatricians play many roles as they fulfill their duties and responsibilities. Among these is the role of trusted counselor.
A pediatrician is a risk manager. Not the risk manager at a brokerage firm assessing financial risks. Not the hospital lawyer providing legal advice to minimize lawsuits against the hospital. The pediatrician, as risk manager, is a fiduciary, confidant, partner, and guide for parents seeking to protect and maximize the health of their children.

The practice of pediatrics deals with many low-probability, high-impact threats. This begins before birth. The obstetrician has already ordered a litany of prenatal screens, blood tests, and ultrasounds. Many of these have a positive predictive value of less than 20%. That means the alarming positive results are wrong more than 80% of the time. Tests done purportedly to reassure the parents are likely to falsely terrify them. This devilish process continues immediately after birth. The newborns are subjected to a wide variety of screening tests that they must pass before being stamped USDA Prime baby. Early in my career, a thorough newborn physical exam was the key means of identifying problems. Modern medicine employs a wide variety of blood tests, a hearing screen, a pulse ox check, and a transcutaneous bilirubin test before discharge. It is a gauntlet that few escape unscathed. Even the totally normal infant is going to flunk a handful of these screens. Then the nursery doctor is ready to erect additional hoops to jump through. Too big or too small? You need glucose checks. Breech presentation? A hip ultrasound. Too long in labor? Blood tests. Too pale or too ruddy? Blood tests. Not acting quite right? Temperature too high? Temperature too low? Too irritable? Too lethargic? Baby, you’ve hit the jackpot for extra blood tests, an app to estimate the risk of early-onset sepsis, and maybe a trip to the NICU.
Many of these protocols have poor positive predictive value results that are not easy to explain to lay people. The ideas are not easily taught to medical students. Those results can be even harder to communicate to new parents with health care careers. A little knowledge goes a long ways toward long, sleepless nights of worrying even though the baby is just fine. Even cute. Snuggly. A good baby! Parents, hug your baby! Feed the baby! Let the professional do most of the worrying.
What does a professional worrier offer? First, a comprehension of the science. The professional understands sensitivity and specificity, false-positive rates, prevalence, and positive predictive value. Second, particular knowledge of the various tests involved, including the confirmatory tests and the risk-benefit of treatment. Third, experienced clinical judgment that knows that lotteries are bad investments even though two people are splitting a $600 million lottery win this week. Most people don’t emotionally cope with small risks. Fourth, the ability to do values clarification. There is not a one-size-fits-all bedside approach in pediatrics. Parents have differing expectations, differing levels of risk aversion, and different methods for handling anxiety. First-time parents may be very risk intolerant with their baby. Some people deal with fear by seeking more information. Others are looking for evidence that the expert physician is committed to compassionately providing whatever is best for their child.
How has medicine evolved recently? I will highlight four items. First, as described earlier, there has been a large increase in the number of these screens that will be failed. Typical office practice continues the methodology with well child exams and developmental screening. Second, many screens have been introduced that have very low positive predictive value. This leads to many anxious parents who will benefit from pediatricians with the bedside manner to guide the parents and their precious baby through this maze of scientific interventions. The science is difficult enough to master during training. It takes more time to learn the art of counseling parents, listening to their concerns, and earning their trust. That art is practiced in face-to-face encounters with the parents. The classic approach to residency training limits the opportunity to observe and mentor the knowledge, skills, and empathy of a good bedside manner.
A third evolution, more recent, has been the widespread pollution of scientific knowledge with misinformation and disinformation through social media. I addressed that issue in my columns in January and March 2019.
Fourth, most recently, I believe the pandemic has emphasized to the public that nothing in life is totally risk free. Extreme efforts to reduce risk produce unwanted consequences. There is a window of opportunity here to work with parents and patients to build relationships that help people to assess risks and make more rational and beneficial choices. For example, when is the risk of meningitis in a febrile young infant low enough to manage at home? The risk will never be zero. But admission to the hospital “just in case” is not risk free either. People are acutely aware of that right now.
Health care professionals can position themselves as the trusted source of health information specific to a particular person’s situation. Health care professionals can be competent, committed, and compassionate listeners to what really worries people. In this way, we manage risk. This role also involves addressing the mental health crisis causing so much suicide and addiction. Severe problems should be referred to specialists, but I anticipate in the near future that most pediatricians will require more skills dealing with risk and anxiety rather than microbes.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Pediatricians play many roles as they fulfill their duties and responsibilities. Among these is the role of trusted counselor.
A pediatrician is a risk manager. Not the risk manager at a brokerage firm assessing financial risks. Not the hospital lawyer providing legal advice to minimize lawsuits against the hospital. The pediatrician, as risk manager, is a fiduciary, confidant, partner, and guide for parents seeking to protect and maximize the health of their children.
The practice of pediatrics deals with many low-probability, high-impact threats. This begins before birth. The obstetrician has already ordered a litany of prenatal screens, blood tests, and ultrasounds. Many of these have a positive predictive value of less than 20%. That means the alarming positive results are wrong more than 80% of the time. Tests done purportedly to reassure the parents are likely to falsely terrify them. This devilish process continues immediately after birth. The newborns are subjected to a wide variety of screening tests that they must pass before being stamped USDA Prime baby. Early in my career, a thorough newborn physical exam was the key means of identifying problems. Modern medicine employs a wide variety of blood tests, a hearing screen, a pulse ox check, and a transcutaneous bilirubin test before discharge. It is a gauntlet that few escape unscathed. Even the totally normal infant is going to flunk a handful of these screens. Then the nursery doctor is ready to erect additional hoops to jump through. Too big or too small? You need glucose checks. Breech presentation? A hip ultrasound. Too long in labor? Blood tests. Too pale or too ruddy? Blood tests. Not acting quite right? Temperature too high? Temperature too low? Too irritable? Too lethargic? Baby, you’ve hit the jackpot for extra blood tests, an app to estimate the risk of early-onset sepsis, and maybe a trip to the NICU.
Many of these protocols have poor positive predictive value results that are not easy to explain to lay people. The ideas are not easily taught to medical students. Those results can be even harder to communicate to new parents with health care careers. A little knowledge goes a long ways toward long, sleepless nights of worrying even though the baby is just fine. Even cute. Snuggly. A good baby! Parents, hug your baby! Feed the baby! Let the professional do most of the worrying.
What does a professional worrier offer? First, a comprehension of the science. The professional understands sensitivity and specificity, false-positive rates, prevalence, and positive predictive value. Second, particular knowledge of the various tests involved, including the confirmatory tests and the risk-benefit of treatment. Third, experienced clinical judgment that knows that lotteries are bad investments even though two people are splitting a $600 million lottery win this week. Most people don’t emotionally cope with small risks. Fourth, the ability to do values clarification. There is not a one-size-fits-all bedside approach in pediatrics. Parents have differing expectations, differing levels of risk aversion, and different methods for handling anxiety. First-time parents may be very risk intolerant with their baby. Some people deal with fear by seeking more information. Others are looking for evidence that the expert physician is committed to compassionately providing whatever is best for their child.
How has medicine evolved recently? I will highlight four items. First, as described earlier, there has been a large increase in the number of these screens that will be failed. Typical office practice continues the methodology with well child exams and developmental screening. Second, many screens have been introduced that have very low positive predictive value. This leads to many anxious parents who will benefit from pediatricians with the bedside manner to guide the parents and their precious baby through this maze of scientific interventions. The science is difficult enough to master during training. It takes more time to learn the art of counseling parents, listening to their concerns, and earning their trust. That art is practiced in face-to-face encounters with the parents. The classic approach to residency training limits the opportunity to observe and mentor the knowledge, skills, and empathy of a good bedside manner.
A third evolution, more recent, has been the widespread pollution of scientific knowledge with misinformation and disinformation through social media. I addressed that issue in my columns in January and March 2019.
Fourth, most recently, I believe the pandemic has emphasized to the public that nothing in life is totally risk free. Extreme efforts to reduce risk produce unwanted consequences. There is a window of opportunity here to work with parents and patients to build relationships that help people to assess risks and make more rational and beneficial choices. For example, when is the risk of meningitis in a febrile young infant low enough to manage at home? The risk will never be zero. But admission to the hospital “just in case” is not risk free either. People are acutely aware of that right now.
Health care professionals can position themselves as the trusted source of health information specific to a particular person’s situation. Health care professionals can be competent, committed, and compassionate listeners to what really worries people. In this way, we manage risk. This role also involves addressing the mental health crisis causing so much suicide and addiction. Severe problems should be referred to specialists, but I anticipate in the near future that most pediatricians will require more skills dealing with risk and anxiety rather than microbes.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Pediatricians play many roles as they fulfill their duties and responsibilities. Among these is the role of trusted counselor.
A pediatrician is a risk manager. Not the risk manager at a brokerage firm assessing financial risks. Not the hospital lawyer providing legal advice to minimize lawsuits against the hospital. The pediatrician, as risk manager, is a fiduciary, confidant, partner, and guide for parents seeking to protect and maximize the health of their children.
The practice of pediatrics deals with many low-probability, high-impact threats. This begins before birth. The obstetrician has already ordered a litany of prenatal screens, blood tests, and ultrasounds. Many of these have a positive predictive value of less than 20%. That means the alarming positive results are wrong more than 80% of the time. Tests done purportedly to reassure the parents are likely to falsely terrify them. This devilish process continues immediately after birth. The newborns are subjected to a wide variety of screening tests that they must pass before being stamped USDA Prime baby. Early in my career, a thorough newborn physical exam was the key means of identifying problems. Modern medicine employs a wide variety of blood tests, a hearing screen, a pulse ox check, and a transcutaneous bilirubin test before discharge. It is a gauntlet that few escape unscathed. Even the totally normal infant is going to flunk a handful of these screens. Then the nursery doctor is ready to erect additional hoops to jump through. Too big or too small? You need glucose checks. Breech presentation? A hip ultrasound. Too long in labor? Blood tests. Too pale or too ruddy? Blood tests. Not acting quite right? Temperature too high? Temperature too low? Too irritable? Too lethargic? Baby, you’ve hit the jackpot for extra blood tests, an app to estimate the risk of early-onset sepsis, and maybe a trip to the NICU.
Many of these protocols have poor positive predictive value results that are not easy to explain to lay people. The ideas are not easily taught to medical students. Those results can be even harder to communicate to new parents with health care careers. A little knowledge goes a long ways toward long, sleepless nights of worrying even though the baby is just fine. Even cute. Snuggly. A good baby! Parents, hug your baby! Feed the baby! Let the professional do most of the worrying.
What does a professional worrier offer? First, a comprehension of the science. The professional understands sensitivity and specificity, false-positive rates, prevalence, and positive predictive value. Second, particular knowledge of the various tests involved, including the confirmatory tests and the risk-benefit of treatment. Third, experienced clinical judgment that knows that lotteries are bad investments even though two people are splitting a $600 million lottery win this week. Most people don’t emotionally cope with small risks. Fourth, the ability to do values clarification. There is not a one-size-fits-all bedside approach in pediatrics. Parents have differing expectations, differing levels of risk aversion, and different methods for handling anxiety. First-time parents may be very risk intolerant with their baby. Some people deal with fear by seeking more information. Others are looking for evidence that the expert physician is committed to compassionately providing whatever is best for their child.
How has medicine evolved recently? I will highlight four items. First, as described earlier, there has been a large increase in the number of these screens that will be failed. Typical office practice continues the methodology with well child exams and developmental screening. Second, many screens have been introduced that have very low positive predictive value. This leads to many anxious parents who will benefit from pediatricians with the bedside manner to guide the parents and their precious baby through this maze of scientific interventions. The science is difficult enough to master during training. It takes more time to learn the art of counseling parents, listening to their concerns, and earning their trust. That art is practiced in face-to-face encounters with the parents. The classic approach to residency training limits the opportunity to observe and mentor the knowledge, skills, and empathy of a good bedside manner.
A third evolution, more recent, has been the widespread pollution of scientific knowledge with misinformation and disinformation through social media. I addressed that issue in my columns in January and March 2019.
Fourth, most recently, I believe the pandemic has emphasized to the public that nothing in life is totally risk free. Extreme efforts to reduce risk produce unwanted consequences. There is a window of opportunity here to work with parents and patients to build relationships that help people to assess risks and make more rational and beneficial choices. For example, when is the risk of meningitis in a febrile young infant low enough to manage at home? The risk will never be zero. But admission to the hospital “just in case” is not risk free either. People are acutely aware of that right now.
Health care professionals can position themselves as the trusted source of health information specific to a particular person’s situation. Health care professionals can be competent, committed, and compassionate listeners to what really worries people. In this way, we manage risk. This role also involves addressing the mental health crisis causing so much suicide and addiction. Severe problems should be referred to specialists, but I anticipate in the near future that most pediatricians will require more skills dealing with risk and anxiety rather than microbes.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
The death of expertise
Unless your social circle is packed with medical professionals, I suspect you are the go-to gal/guy when there is a question about the pandemic. Seated around the fire pit trying to stay warm and socially distanced, inevitably the discussion will turn to COVID. Someone will report something they have read about vaccine side effects or the appropriate timing of isolation or quarantine and then turn to me assuming that I have inside information and ask: “But Will you know all about that. Tell us what have you heard.”
By now, well into our second year of the pandemic, my friends and neighbors should have come to expect my usual answer. “I don’t really know any more about this than you have read on the Internet or seen on television.” I am flattered that folks keep asking for my observations. I guess old habits die slowly. Although I usually introduce myself as an ex-pediatrician, the “doctor” descriptor still seems to command some respect, whether it is deserved or not.

It is not just my waning ability to speak authoritatively about the pandemic that has put expertise at death’s door. Although my formal medical education is more than a half-century old, like most physicians I have tried to stay abreast of what’s happening in health care. Keeping up to date with the new developments in pathophysiology and pharmacology does take some work, but the pandemic has shone a spotlight on how quickly these changes can occur.
With the pandemic, a sense of urgency has thrust onto the world stage opinions that in the past might have been quietly held theories based on preliminary studies. However, even the most careful scientists who might otherwise have been content to patiently wait for peer review are sharing their findings prematurely with international news sources and on social media. Not surprisingly, this rush to share has generated confusion and concern and in many cases resulted in retractions or corrections. Even more importantly, it has made us all skeptical about who these “experts” are, making often disproven pronouncements.
While my friends still persist in politely asking my opinion based on the same reports we are all reading on the Internet, I sense the nation as a whole has become wary of claimed expertise. I haven’t done a Google search but I wouldn’t be surprised if “expert” gets far fewer hits than the term “so-called expert.”
Even before we were engulfed by the pandemic, there has been an unfortunate phenomenon in which health care providers and other scientists are parlaying their degrees to promote products with little if any proven efficacy. Of course, this country has a long history of snake oil salesmen making their rounds. However, the electronic media and the Internet have increased the power to persuade so that we are awash in so-called experts. Many good scientists, in an attempt to be helpful, have succumbed to the sin of impatience. And there are a few who had never earned the moniker “expert.”
I hope that expertise returns to the landscape when the pandemic abates. But, I fear it may be a while.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Unless your social circle is packed with medical professionals, I suspect you are the go-to gal/guy when there is a question about the pandemic. Seated around the fire pit trying to stay warm and socially distanced, inevitably the discussion will turn to COVID. Someone will report something they have read about vaccine side effects or the appropriate timing of isolation or quarantine and then turn to me assuming that I have inside information and ask: “But Will you know all about that. Tell us what have you heard.”
By now, well into our second year of the pandemic, my friends and neighbors should have come to expect my usual answer. “I don’t really know any more about this than you have read on the Internet or seen on television.” I am flattered that folks keep asking for my observations. I guess old habits die slowly. Although I usually introduce myself as an ex-pediatrician, the “doctor” descriptor still seems to command some respect, whether it is deserved or not.
It is not just my waning ability to speak authoritatively about the pandemic that has put expertise at death’s door. Although my formal medical education is more than a half-century old, like most physicians I have tried to stay abreast of what’s happening in health care. Keeping up to date with the new developments in pathophysiology and pharmacology does take some work, but the pandemic has shone a spotlight on how quickly these changes can occur.
With the pandemic, a sense of urgency has thrust onto the world stage opinions that in the past might have been quietly held theories based on preliminary studies. However, even the most careful scientists who might otherwise have been content to patiently wait for peer review are sharing their findings prematurely with international news sources and on social media. Not surprisingly, this rush to share has generated confusion and concern and in many cases resulted in retractions or corrections. Even more importantly, it has made us all skeptical about who these “experts” are, making often disproven pronouncements.
While my friends still persist in politely asking my opinion based on the same reports we are all reading on the Internet, I sense the nation as a whole has become wary of claimed expertise. I haven’t done a Google search but I wouldn’t be surprised if “expert” gets far fewer hits than the term “so-called expert.”
Even before we were engulfed by the pandemic, there has been an unfortunate phenomenon in which health care providers and other scientists are parlaying their degrees to promote products with little if any proven efficacy. Of course, this country has a long history of snake oil salesmen making their rounds. However, the electronic media and the Internet have increased the power to persuade so that we are awash in so-called experts. Many good scientists, in an attempt to be helpful, have succumbed to the sin of impatience. And there are a few who had never earned the moniker “expert.”
I hope that expertise returns to the landscape when the pandemic abates. But, I fear it may be a while.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Unless your social circle is packed with medical professionals, I suspect you are the go-to gal/guy when there is a question about the pandemic. Seated around the fire pit trying to stay warm and socially distanced, inevitably the discussion will turn to COVID. Someone will report something they have read about vaccine side effects or the appropriate timing of isolation or quarantine and then turn to me assuming that I have inside information and ask: “But Will you know all about that. Tell us what have you heard.”
By now, well into our second year of the pandemic, my friends and neighbors should have come to expect my usual answer. “I don’t really know any more about this than you have read on the Internet or seen on television.” I am flattered that folks keep asking for my observations. I guess old habits die slowly. Although I usually introduce myself as an ex-pediatrician, the “doctor” descriptor still seems to command some respect, whether it is deserved or not.
It is not just my waning ability to speak authoritatively about the pandemic that has put expertise at death’s door. Although my formal medical education is more than a half-century old, like most physicians I have tried to stay abreast of what’s happening in health care. Keeping up to date with the new developments in pathophysiology and pharmacology does take some work, but the pandemic has shone a spotlight on how quickly these changes can occur.
With the pandemic, a sense of urgency has thrust onto the world stage opinions that in the past might have been quietly held theories based on preliminary studies. However, even the most careful scientists who might otherwise have been content to patiently wait for peer review are sharing their findings prematurely with international news sources and on social media. Not surprisingly, this rush to share has generated confusion and concern and in many cases resulted in retractions or corrections. Even more importantly, it has made us all skeptical about who these “experts” are, making often disproven pronouncements.
While my friends still persist in politely asking my opinion based on the same reports we are all reading on the Internet, I sense the nation as a whole has become wary of claimed expertise. I haven’t done a Google search but I wouldn’t be surprised if “expert” gets far fewer hits than the term “so-called expert.”
Even before we were engulfed by the pandemic, there has been an unfortunate phenomenon in which health care providers and other scientists are parlaying their degrees to promote products with little if any proven efficacy. Of course, this country has a long history of snake oil salesmen making their rounds. However, the electronic media and the Internet have increased the power to persuade so that we are awash in so-called experts. Many good scientists, in an attempt to be helpful, have succumbed to the sin of impatience. And there are a few who had never earned the moniker “expert.”
I hope that expertise returns to the landscape when the pandemic abates. But, I fear it may be a while.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Pediatric depression and parents
In October of 2021, the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the Children’s Hospital Association jointly declared a National State of Emergency in Children’s Mental Health and called on policy makers to address a host of challenges that have impeded access to effective mental health care for youth.
In November, we wrote about how pediatricians may increase their use of screening for adolescent depression and initiate treatment when appropriate.

Now we complement that piece with guidance you may offer the parents of your depressed adolescent patients. Adolescent depression is a common pediatric disorder, especially in the COVID-19 era when so many relationships and activities have been limited or cut off. With treatment, most adolescents recover. Accepting that it may be taking longer to find a therapist, you can make treatment recommendations, support the teenager and parents, address safety concerns and, if the depression is of moderate or more serious severity, start medications. Parents are your natural partners as they are concerned about their children’s health and safety and eager for guidance on how to best support their recovery.

Adolescence is a time in which parents transition to more of a consulting than a controlling posture with their children, but illness calls for a shift toward setting rules and routines that will support health and healing. Prepare both the teenager (in a 1:1 discussion) and parents for this temporary shift, and for some teenagers, expect resistance. Depression will make the teenager more unhappy and irritable. It also causes withdrawal, by sapping energy and making one feel unwelcome at activities, believing his or her presence will be a burden to others. Treatment includes something called “behavioral activation,” or continuous nudging, to keep the patient involved in social, intellectual, and physical activities. Parents (and siblings) are the keys to this behavioral activation, whether nudging to participate in a board game or a walk. Reassure parents they should not take it personally when their teen resists, and not be discouraged if they fail sometimes. Their focus is on calmly, warmly, and repeatedly prompting their children with nudges toward these routines and activities. They should be ready to remind them why they are “nagging,” framing these efforts explicitly as supporting recovery from depression. If possible, applying these rules to everyone at home will help. They need to avoid being drawn into conflict, focusing instead on staying connected to their teens. Their task is to keep planning and cajoling, giving their children multiple opportunities to participate, pushing back against depression’s gravitational pull for total withdrawal.
Sleep
One of the most important thing parents can do for their depressed adolescents is to support their healthy restful sleep. During adolescence, the timing of sleep naturally shifts later, and the need for restful sleep increases. Working against the demands of homework, extracurricular activities, and social connections, sleep often suffers during adolescence. Further sleep disruptions, including difficulty falling asleep and frequent awakening during sleep or in the early morning, are typical of depression. Restful sleep is instrumental to recovery, and parents need to help their depressed teens set good sleep habits. This includes setting a time for bed that is realistic and consistent and turning off screens 30 minutes before lights out. A soothing, consistent bedtime routine, including a hot shower and reading in bed, is a powerful cue for sleep. Getting daily exercise and avoiding a heavy meal and caffeine in the hours before bed supports both falling and staying asleep. Having light reading near bed (magazines or comics) instead of screens can provide a way to pass 30 minutes if they wake up during the night (ideally reading out of bed), one that will not make it harder for them to go back to sleep. Finally, teens should not be allowed to spend all day in bed or nap in the afternoon. This may be the hardest task for parents, as adolescents naturally treat their beds like their center of operations and depression lowers their energy and initiative. If parents set these rules and routines for all members of the family, it can improve the chances that their depressed adolescents may begin to return to healthy sleep.
Exercise
Vigorous exercise (for 20 minutes three times weekly) is as effective as SSRIs in treating mild to moderate depression. Even in severe depression, exercise may accelerate recovery and certainly contributes to returning to restful sleep and a feeling of improved energy. Inviting their depressed teens to join them on a trip to the gym may seem like a fool’s errand to parents, but they should prioritize getting their children moving. Don’t offer choices or ask what activity they would like to do. Most invitations will be met with “no, thanks” (or probably something less polite). Instead, initiate simple activities and then cajole the children with “let’s go!” They should use loving persistence to get them out the door. Parents are the experts on their children and will know if there is an activity that they are more likely to enjoy. Make any activities group ones, easy to start and not too long. They could initiate family walks or bike rides in their neighborhood. If it helps, they can blame you, “these are doctor’s orders!” This approach of warm persistence should be applied across the board, helping their depressed teens participate in mealtimes and other activities. Prepare parents that this can feel unnatural, if they have been letting their healthy teenagers have more space and independence and less time in family activities.
Social connections
Behavioral activation includes keeping a depressed teen engaged in social activities. Friendships are a potent motivator in the lives of healthy adolescents. If depressed teens can stay connected to close friends, it is a powerful force for recovery. Find out if their friends know about their depression, whom do they trust to tell about it? Help them find comfortable language to speak about their depression with trusted friends. Parents can use their behavioral activation strategies to prompt their teenagers to participate in social activities. If texting, video chatting, or social media platforms are how they stay connected with close friends, support their use of these platforms. But be mindful that social media promotes social comparison over connection, and depression sets them up to feel less than others even without assistance. Parents should support real time with their friends in small groups, for short periods during the time of day when they have the most energy.
Safety
Suicide is the second leading cause of death for adolescents in the United States, and the rate of attempted and completed suicide in adolescents has been steadily climbing over the past decade according to the CDC. The rate is higher in older adolescents, though thankfully relatively uncommon (about 1 in 10,000 a year), and, although we know risk factors, no one has been able to predict reliably the risk for an individual teenager at a point in time. In a clinically referred sample, 85% of depressed adolescents will have suicidal ideation and 32% will make a suicide attempt. The risk is higher in those adolescents with more than one psychiatric diagnosis and with a history of impulsive behaviors, substance abuse, prior suicide attempts, and a family history of suicide. It is important that parents hear that asking about suicidal thoughts will not cause them. On the contrary, preserving open communication and a warm relationship is very protective. Adolescent suicide attempts are likely to be impulsive, so helping the family to consider ways to “put up obstacles” that would slow down any possible attempt is an effective way to improve safety. Ask your patients about suicidal thoughts, plans, and what keeps them safe. Find out if they worry about sharing these thoughts with their parents and why. Ask if there are ways their parents can check on them that “aren’t too annoying.” Determine if there are guns in the home, and if so, are they safely stored (locked, separate from ammunition)? More than 50% of completed adolescent suicides involve firearms, so this question is critical. What about access to medications that could be dangerous in overdose in your home or a relative’s home they may visit? Discussing these facts with your patients and their parents together will make it easier for them to continue the conversation outside of your office and can make an enormous difference in their recovery.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Kovacs M et al. J Am Acad Child Adolesc Psychiatry. 1993 Jan;32(1):8-20.
In October of 2021, the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the Children’s Hospital Association jointly declared a National State of Emergency in Children’s Mental Health and called on policy makers to address a host of challenges that have impeded access to effective mental health care for youth.
In November, we wrote about how pediatricians may increase their use of screening for adolescent depression and initiate treatment when appropriate.
Now we complement that piece with guidance you may offer the parents of your depressed adolescent patients. Adolescent depression is a common pediatric disorder, especially in the COVID-19 era when so many relationships and activities have been limited or cut off. With treatment, most adolescents recover. Accepting that it may be taking longer to find a therapist, you can make treatment recommendations, support the teenager and parents, address safety concerns and, if the depression is of moderate or more serious severity, start medications. Parents are your natural partners as they are concerned about their children’s health and safety and eager for guidance on how to best support their recovery.
Adolescence is a time in which parents transition to more of a consulting than a controlling posture with their children, but illness calls for a shift toward setting rules and routines that will support health and healing. Prepare both the teenager (in a 1:1 discussion) and parents for this temporary shift, and for some teenagers, expect resistance. Depression will make the teenager more unhappy and irritable. It also causes withdrawal, by sapping energy and making one feel unwelcome at activities, believing his or her presence will be a burden to others. Treatment includes something called “behavioral activation,” or continuous nudging, to keep the patient involved in social, intellectual, and physical activities. Parents (and siblings) are the keys to this behavioral activation, whether nudging to participate in a board game or a walk. Reassure parents they should not take it personally when their teen resists, and not be discouraged if they fail sometimes. Their focus is on calmly, warmly, and repeatedly prompting their children with nudges toward these routines and activities. They should be ready to remind them why they are “nagging,” framing these efforts explicitly as supporting recovery from depression. If possible, applying these rules to everyone at home will help. They need to avoid being drawn into conflict, focusing instead on staying connected to their teens. Their task is to keep planning and cajoling, giving their children multiple opportunities to participate, pushing back against depression’s gravitational pull for total withdrawal.
Sleep
One of the most important thing parents can do for their depressed adolescents is to support their healthy restful sleep. During adolescence, the timing of sleep naturally shifts later, and the need for restful sleep increases. Working against the demands of homework, extracurricular activities, and social connections, sleep often suffers during adolescence. Further sleep disruptions, including difficulty falling asleep and frequent awakening during sleep or in the early morning, are typical of depression. Restful sleep is instrumental to recovery, and parents need to help their depressed teens set good sleep habits. This includes setting a time for bed that is realistic and consistent and turning off screens 30 minutes before lights out. A soothing, consistent bedtime routine, including a hot shower and reading in bed, is a powerful cue for sleep. Getting daily exercise and avoiding a heavy meal and caffeine in the hours before bed supports both falling and staying asleep. Having light reading near bed (magazines or comics) instead of screens can provide a way to pass 30 minutes if they wake up during the night (ideally reading out of bed), one that will not make it harder for them to go back to sleep. Finally, teens should not be allowed to spend all day in bed or nap in the afternoon. This may be the hardest task for parents, as adolescents naturally treat their beds like their center of operations and depression lowers their energy and initiative. If parents set these rules and routines for all members of the family, it can improve the chances that their depressed adolescents may begin to return to healthy sleep.
Exercise
Vigorous exercise (for 20 minutes three times weekly) is as effective as SSRIs in treating mild to moderate depression. Even in severe depression, exercise may accelerate recovery and certainly contributes to returning to restful sleep and a feeling of improved energy. Inviting their depressed teens to join them on a trip to the gym may seem like a fool’s errand to parents, but they should prioritize getting their children moving. Don’t offer choices or ask what activity they would like to do. Most invitations will be met with “no, thanks” (or probably something less polite). Instead, initiate simple activities and then cajole the children with “let’s go!” They should use loving persistence to get them out the door. Parents are the experts on their children and will know if there is an activity that they are more likely to enjoy. Make any activities group ones, easy to start and not too long. They could initiate family walks or bike rides in their neighborhood. If it helps, they can blame you, “these are doctor’s orders!” This approach of warm persistence should be applied across the board, helping their depressed teens participate in mealtimes and other activities. Prepare parents that this can feel unnatural, if they have been letting their healthy teenagers have more space and independence and less time in family activities.
Social connections
Behavioral activation includes keeping a depressed teen engaged in social activities. Friendships are a potent motivator in the lives of healthy adolescents. If depressed teens can stay connected to close friends, it is a powerful force for recovery. Find out if their friends know about their depression, whom do they trust to tell about it? Help them find comfortable language to speak about their depression with trusted friends. Parents can use their behavioral activation strategies to prompt their teenagers to participate in social activities. If texting, video chatting, or social media platforms are how they stay connected with close friends, support their use of these platforms. But be mindful that social media promotes social comparison over connection, and depression sets them up to feel less than others even without assistance. Parents should support real time with their friends in small groups, for short periods during the time of day when they have the most energy.
Safety
Suicide is the second leading cause of death for adolescents in the United States, and the rate of attempted and completed suicide in adolescents has been steadily climbing over the past decade according to the CDC. The rate is higher in older adolescents, though thankfully relatively uncommon (about 1 in 10,000 a year), and, although we know risk factors, no one has been able to predict reliably the risk for an individual teenager at a point in time. In a clinically referred sample, 85% of depressed adolescents will have suicidal ideation and 32% will make a suicide attempt. The risk is higher in those adolescents with more than one psychiatric diagnosis and with a history of impulsive behaviors, substance abuse, prior suicide attempts, and a family history of suicide. It is important that parents hear that asking about suicidal thoughts will not cause them. On the contrary, preserving open communication and a warm relationship is very protective. Adolescent suicide attempts are likely to be impulsive, so helping the family to consider ways to “put up obstacles” that would slow down any possible attempt is an effective way to improve safety. Ask your patients about suicidal thoughts, plans, and what keeps them safe. Find out if they worry about sharing these thoughts with their parents and why. Ask if there are ways their parents can check on them that “aren’t too annoying.” Determine if there are guns in the home, and if so, are they safely stored (locked, separate from ammunition)? More than 50% of completed adolescent suicides involve firearms, so this question is critical. What about access to medications that could be dangerous in overdose in your home or a relative’s home they may visit? Discussing these facts with your patients and their parents together will make it easier for them to continue the conversation outside of your office and can make an enormous difference in their recovery.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Kovacs M et al. J Am Acad Child Adolesc Psychiatry. 1993 Jan;32(1):8-20.
In October of 2021, the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the Children’s Hospital Association jointly declared a National State of Emergency in Children’s Mental Health and called on policy makers to address a host of challenges that have impeded access to effective mental health care for youth.
In November, we wrote about how pediatricians may increase their use of screening for adolescent depression and initiate treatment when appropriate.
Now we complement that piece with guidance you may offer the parents of your depressed adolescent patients. Adolescent depression is a common pediatric disorder, especially in the COVID-19 era when so many relationships and activities have been limited or cut off. With treatment, most adolescents recover. Accepting that it may be taking longer to find a therapist, you can make treatment recommendations, support the teenager and parents, address safety concerns and, if the depression is of moderate or more serious severity, start medications. Parents are your natural partners as they are concerned about their children’s health and safety and eager for guidance on how to best support their recovery.
Adolescence is a time in which parents transition to more of a consulting than a controlling posture with their children, but illness calls for a shift toward setting rules and routines that will support health and healing. Prepare both the teenager (in a 1:1 discussion) and parents for this temporary shift, and for some teenagers, expect resistance. Depression will make the teenager more unhappy and irritable. It also causes withdrawal, by sapping energy and making one feel unwelcome at activities, believing his or her presence will be a burden to others. Treatment includes something called “behavioral activation,” or continuous nudging, to keep the patient involved in social, intellectual, and physical activities. Parents (and siblings) are the keys to this behavioral activation, whether nudging to participate in a board game or a walk. Reassure parents they should not take it personally when their teen resists, and not be discouraged if they fail sometimes. Their focus is on calmly, warmly, and repeatedly prompting their children with nudges toward these routines and activities. They should be ready to remind them why they are “nagging,” framing these efforts explicitly as supporting recovery from depression. If possible, applying these rules to everyone at home will help. They need to avoid being drawn into conflict, focusing instead on staying connected to their teens. Their task is to keep planning and cajoling, giving their children multiple opportunities to participate, pushing back against depression’s gravitational pull for total withdrawal.
Sleep
One of the most important thing parents can do for their depressed adolescents is to support their healthy restful sleep. During adolescence, the timing of sleep naturally shifts later, and the need for restful sleep increases. Working against the demands of homework, extracurricular activities, and social connections, sleep often suffers during adolescence. Further sleep disruptions, including difficulty falling asleep and frequent awakening during sleep or in the early morning, are typical of depression. Restful sleep is instrumental to recovery, and parents need to help their depressed teens set good sleep habits. This includes setting a time for bed that is realistic and consistent and turning off screens 30 minutes before lights out. A soothing, consistent bedtime routine, including a hot shower and reading in bed, is a powerful cue for sleep. Getting daily exercise and avoiding a heavy meal and caffeine in the hours before bed supports both falling and staying asleep. Having light reading near bed (magazines or comics) instead of screens can provide a way to pass 30 minutes if they wake up during the night (ideally reading out of bed), one that will not make it harder for them to go back to sleep. Finally, teens should not be allowed to spend all day in bed or nap in the afternoon. This may be the hardest task for parents, as adolescents naturally treat their beds like their center of operations and depression lowers their energy and initiative. If parents set these rules and routines for all members of the family, it can improve the chances that their depressed adolescents may begin to return to healthy sleep.
Exercise
Vigorous exercise (for 20 minutes three times weekly) is as effective as SSRIs in treating mild to moderate depression. Even in severe depression, exercise may accelerate recovery and certainly contributes to returning to restful sleep and a feeling of improved energy. Inviting their depressed teens to join them on a trip to the gym may seem like a fool’s errand to parents, but they should prioritize getting their children moving. Don’t offer choices or ask what activity they would like to do. Most invitations will be met with “no, thanks” (or probably something less polite). Instead, initiate simple activities and then cajole the children with “let’s go!” They should use loving persistence to get them out the door. Parents are the experts on their children and will know if there is an activity that they are more likely to enjoy. Make any activities group ones, easy to start and not too long. They could initiate family walks or bike rides in their neighborhood. If it helps, they can blame you, “these are doctor’s orders!” This approach of warm persistence should be applied across the board, helping their depressed teens participate in mealtimes and other activities. Prepare parents that this can feel unnatural, if they have been letting their healthy teenagers have more space and independence and less time in family activities.
Social connections
Behavioral activation includes keeping a depressed teen engaged in social activities. Friendships are a potent motivator in the lives of healthy adolescents. If depressed teens can stay connected to close friends, it is a powerful force for recovery. Find out if their friends know about their depression, whom do they trust to tell about it? Help them find comfortable language to speak about their depression with trusted friends. Parents can use their behavioral activation strategies to prompt their teenagers to participate in social activities. If texting, video chatting, or social media platforms are how they stay connected with close friends, support their use of these platforms. But be mindful that social media promotes social comparison over connection, and depression sets them up to feel less than others even without assistance. Parents should support real time with their friends in small groups, for short periods during the time of day when they have the most energy.
Safety
Suicide is the second leading cause of death for adolescents in the United States, and the rate of attempted and completed suicide in adolescents has been steadily climbing over the past decade according to the CDC. The rate is higher in older adolescents, though thankfully relatively uncommon (about 1 in 10,000 a year), and, although we know risk factors, no one has been able to predict reliably the risk for an individual teenager at a point in time. In a clinically referred sample, 85% of depressed adolescents will have suicidal ideation and 32% will make a suicide attempt. The risk is higher in those adolescents with more than one psychiatric diagnosis and with a history of impulsive behaviors, substance abuse, prior suicide attempts, and a family history of suicide. It is important that parents hear that asking about suicidal thoughts will not cause them. On the contrary, preserving open communication and a warm relationship is very protective. Adolescent suicide attempts are likely to be impulsive, so helping the family to consider ways to “put up obstacles” that would slow down any possible attempt is an effective way to improve safety. Ask your patients about suicidal thoughts, plans, and what keeps them safe. Find out if they worry about sharing these thoughts with their parents and why. Ask if there are ways their parents can check on them that “aren’t too annoying.” Determine if there are guns in the home, and if so, are they safely stored (locked, separate from ammunition)? More than 50% of completed adolescent suicides involve firearms, so this question is critical. What about access to medications that could be dangerous in overdose in your home or a relative’s home they may visit? Discussing these facts with your patients and their parents together will make it easier for them to continue the conversation outside of your office and can make an enormous difference in their recovery.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
Reference
Kovacs M et al. J Am Acad Child Adolesc Psychiatry. 1993 Jan;32(1):8-20.
The etiology of acute otitis media in young children in recent years
Since the COVID-19 pandemic began, pediatricians have been seeing fewer cases of all respiratory illnesses, including acute otitis media (AOM). However, as I prepare this column, an uptick has commenced and likely will continue in an upward trajectory as we emerge from the pandemic into an endemic coronavirus era. Our group in Rochester, N.Y., has continued prospective studies of AOM throughout the pandemic. We found that nasopharyngeal colonization by Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, and Moraxella catarrhalis remained prevalent in our study cohort of children aged 6-36 months. However, with all the precautions of masking, social distancing, hand washing, and quick exclusion from day care when illness occurred, the frequency of detecting these common otopathogens decreased, as one might expect.1
Leading up to the pandemic, we had an abundance of data to characterize AOM etiology and found that the cause of AOM continues to change following the introduction of the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13). Our most recent report on otopathogen distribution and antibiotic susceptibility covered the years 2015-2019.2 A total of 589 children were enrolled prospectively and we collected 495 middle ear fluid samples (MEF) from 319 AOM cases using tympanocentesis. The frequency of isolates was H. influenzae (34%), pneumococcus (24%), and M. catarrhalis (15%). Beta-lactamase–positive H. influenzae strains were identified among 49% of the isolates, rendering them resistant to amoxicillin. PCV13 serotypes were infrequently isolated. However, we did isolate vaccine types (VTs) in some children from MEF, notably serotypes 19F, 19A, and 3. Non-PCV13 pneumococcus serotypes 35B, 23B, and 15B/C emerged as the most common serotypes. Amoxicillin resistance was identified among 25% of pneumococcal strains. Out of 16 antibiotics tested, 9 (56%) showed a significant increase in nonsusceptibility among pneumococcal isolates. 100% of M. catarrhalis isolates were beta-lactamase producers and therefore resistant to amoxicillin.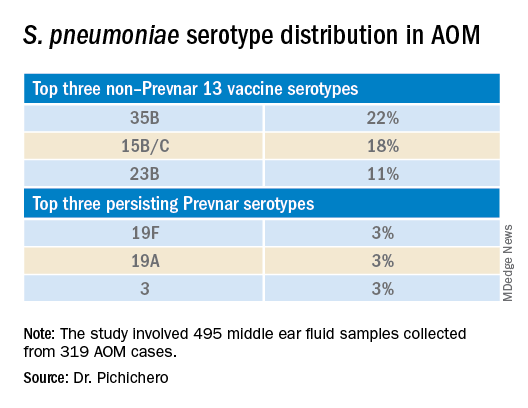
PCV13 has resulted in a decline in both invasive and noninvasive pneumococcal infections caused by strains expressing the 13 capsular serotypes included in the vaccine. However, the emergence of replacement serotypes occurred after introduction of PCV73,4 and continues to occur during the PCV13 era, as shown from the results presented here. Non-PCV13 serotypes accounted for more than 90% of MEF isolates during 2015-2019, with 35B, 21 and 23B being the most commonly isolated. Other emergent serotypes of potential importance were nonvaccine serotypes 15A, 15B, 15C, 23A and 11A. This is highly relevant because forthcoming higher-valency PCVs – PCV15 (manufactured by Merck) and PCV20 (manufactured by Pfizer) will not include many of the dominant capsular serotypes of pneumococcus strains causing AOM. Consequently, the impact of higher-valency PCVs on AOM will not be as great as was observed with the introduction of PCV7 or PCV13.
Of special interest, 22% of pneumococcus isolates from MEF were serotype 35B, making it the most prevalent. Recently we reported a significant rise in antibiotic nonsusceptibility in Spn isolates, contributed mainly by serotype 35B5 and we have been studying how 35B strains transitioned from commensal to otopathogen in children.6 Because serotype 35B strains are increasingly prevalent and often antibiotic resistant, absence of this serotype from PCV15 and PCV20 is cause for concern.

The frequency of isolation of H. influenzae and M. catarrhalis has remained stable across the PCV13 era as the No. 1 and No. 3 pathogens. Similarly, the production of beta-lactamase among strains causing AOM has remained stable at close to 50% and 100%, respectively. Use of amoxicillin, either high dose or standard dose, would not be expected to kill these bacteria.
Our study design has limitations. The population is derived from a predominantly middle-class, suburban population of children in upstate New York and may not be representative of other types of populations in the United States. The children are 6-36 months old, the age when most AOM occurs. MEF samples that were culture negative for bacteria were not further tested by polymerase chain reaction methods.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Front Pediatr. 2021;9:722483.
2. Kaur R et al. Euro J Clin Microbiol Infect Dis. 2021;41:37-44
3. Pelton SI et al. Pediatr Infect Disease J. 2004;23:1015-22.
4. Farrell DJ et al. Pediatr Infect Disease J. 2007;26:123-8..
5. Kaur R et al. Clin Infect Dis 2021;72(5):797-805.
6. Fuji N et al. Front Cell Infect Microbiol. 2021;11:744742.
Since the COVID-19 pandemic began, pediatricians have been seeing fewer cases of all respiratory illnesses, including acute otitis media (AOM). However, as I prepare this column, an uptick has commenced and likely will continue in an upward trajectory as we emerge from the pandemic into an endemic coronavirus era. Our group in Rochester, N.Y., has continued prospective studies of AOM throughout the pandemic. We found that nasopharyngeal colonization by Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, and Moraxella catarrhalis remained prevalent in our study cohort of children aged 6-36 months. However, with all the precautions of masking, social distancing, hand washing, and quick exclusion from day care when illness occurred, the frequency of detecting these common otopathogens decreased, as one might expect.1
Leading up to the pandemic, we had an abundance of data to characterize AOM etiology and found that the cause of AOM continues to change following the introduction of the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13). Our most recent report on otopathogen distribution and antibiotic susceptibility covered the years 2015-2019.2 A total of 589 children were enrolled prospectively and we collected 495 middle ear fluid samples (MEF) from 319 AOM cases using tympanocentesis. The frequency of isolates was H. influenzae (34%), pneumococcus (24%), and M. catarrhalis (15%). Beta-lactamase–positive H. influenzae strains were identified among 49% of the isolates, rendering them resistant to amoxicillin. PCV13 serotypes were infrequently isolated. However, we did isolate vaccine types (VTs) in some children from MEF, notably serotypes 19F, 19A, and 3. Non-PCV13 pneumococcus serotypes 35B, 23B, and 15B/C emerged as the most common serotypes. Amoxicillin resistance was identified among 25% of pneumococcal strains. Out of 16 antibiotics tested, 9 (56%) showed a significant increase in nonsusceptibility among pneumococcal isolates. 100% of M. catarrhalis isolates were beta-lactamase producers and therefore resistant to amoxicillin.
PCV13 has resulted in a decline in both invasive and noninvasive pneumococcal infections caused by strains expressing the 13 capsular serotypes included in the vaccine. However, the emergence of replacement serotypes occurred after introduction of PCV73,4 and continues to occur during the PCV13 era, as shown from the results presented here. Non-PCV13 serotypes accounted for more than 90% of MEF isolates during 2015-2019, with 35B, 21 and 23B being the most commonly isolated. Other emergent serotypes of potential importance were nonvaccine serotypes 15A, 15B, 15C, 23A and 11A. This is highly relevant because forthcoming higher-valency PCVs – PCV15 (manufactured by Merck) and PCV20 (manufactured by Pfizer) will not include many of the dominant capsular serotypes of pneumococcus strains causing AOM. Consequently, the impact of higher-valency PCVs on AOM will not be as great as was observed with the introduction of PCV7 or PCV13.
Of special interest, 22% of pneumococcus isolates from MEF were serotype 35B, making it the most prevalent. Recently we reported a significant rise in antibiotic nonsusceptibility in Spn isolates, contributed mainly by serotype 35B5 and we have been studying how 35B strains transitioned from commensal to otopathogen in children.6 Because serotype 35B strains are increasingly prevalent and often antibiotic resistant, absence of this serotype from PCV15 and PCV20 is cause for concern.
The frequency of isolation of H. influenzae and M. catarrhalis has remained stable across the PCV13 era as the No. 1 and No. 3 pathogens. Similarly, the production of beta-lactamase among strains causing AOM has remained stable at close to 50% and 100%, respectively. Use of amoxicillin, either high dose or standard dose, would not be expected to kill these bacteria.
Our study design has limitations. The population is derived from a predominantly middle-class, suburban population of children in upstate New York and may not be representative of other types of populations in the United States. The children are 6-36 months old, the age when most AOM occurs. MEF samples that were culture negative for bacteria were not further tested by polymerase chain reaction methods.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Front Pediatr. 2021;9:722483.
2. Kaur R et al. Euro J Clin Microbiol Infect Dis. 2021;41:37-44
3. Pelton SI et al. Pediatr Infect Disease J. 2004;23:1015-22.
4. Farrell DJ et al. Pediatr Infect Disease J. 2007;26:123-8..
5. Kaur R et al. Clin Infect Dis 2021;72(5):797-805.
6. Fuji N et al. Front Cell Infect Microbiol. 2021;11:744742.
Since the COVID-19 pandemic began, pediatricians have been seeing fewer cases of all respiratory illnesses, including acute otitis media (AOM). However, as I prepare this column, an uptick has commenced and likely will continue in an upward trajectory as we emerge from the pandemic into an endemic coronavirus era. Our group in Rochester, N.Y., has continued prospective studies of AOM throughout the pandemic. We found that nasopharyngeal colonization by Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, and Moraxella catarrhalis remained prevalent in our study cohort of children aged 6-36 months. However, with all the precautions of masking, social distancing, hand washing, and quick exclusion from day care when illness occurred, the frequency of detecting these common otopathogens decreased, as one might expect.1
Leading up to the pandemic, we had an abundance of data to characterize AOM etiology and found that the cause of AOM continues to change following the introduction of the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13). Our most recent report on otopathogen distribution and antibiotic susceptibility covered the years 2015-2019.2 A total of 589 children were enrolled prospectively and we collected 495 middle ear fluid samples (MEF) from 319 AOM cases using tympanocentesis. The frequency of isolates was H. influenzae (34%), pneumococcus (24%), and M. catarrhalis (15%). Beta-lactamase–positive H. influenzae strains were identified among 49% of the isolates, rendering them resistant to amoxicillin. PCV13 serotypes were infrequently isolated. However, we did isolate vaccine types (VTs) in some children from MEF, notably serotypes 19F, 19A, and 3. Non-PCV13 pneumococcus serotypes 35B, 23B, and 15B/C emerged as the most common serotypes. Amoxicillin resistance was identified among 25% of pneumococcal strains. Out of 16 antibiotics tested, 9 (56%) showed a significant increase in nonsusceptibility among pneumococcal isolates. 100% of M. catarrhalis isolates were beta-lactamase producers and therefore resistant to amoxicillin.
PCV13 has resulted in a decline in both invasive and noninvasive pneumococcal infections caused by strains expressing the 13 capsular serotypes included in the vaccine. However, the emergence of replacement serotypes occurred after introduction of PCV73,4 and continues to occur during the PCV13 era, as shown from the results presented here. Non-PCV13 serotypes accounted for more than 90% of MEF isolates during 2015-2019, with 35B, 21 and 23B being the most commonly isolated. Other emergent serotypes of potential importance were nonvaccine serotypes 15A, 15B, 15C, 23A and 11A. This is highly relevant because forthcoming higher-valency PCVs – PCV15 (manufactured by Merck) and PCV20 (manufactured by Pfizer) will not include many of the dominant capsular serotypes of pneumococcus strains causing AOM. Consequently, the impact of higher-valency PCVs on AOM will not be as great as was observed with the introduction of PCV7 or PCV13.
Of special interest, 22% of pneumococcus isolates from MEF were serotype 35B, making it the most prevalent. Recently we reported a significant rise in antibiotic nonsusceptibility in Spn isolates, contributed mainly by serotype 35B5 and we have been studying how 35B strains transitioned from commensal to otopathogen in children.6 Because serotype 35B strains are increasingly prevalent and often antibiotic resistant, absence of this serotype from PCV15 and PCV20 is cause for concern.
The frequency of isolation of H. influenzae and M. catarrhalis has remained stable across the PCV13 era as the No. 1 and No. 3 pathogens. Similarly, the production of beta-lactamase among strains causing AOM has remained stable at close to 50% and 100%, respectively. Use of amoxicillin, either high dose or standard dose, would not be expected to kill these bacteria.
Our study design has limitations. The population is derived from a predominantly middle-class, suburban population of children in upstate New York and may not be representative of other types of populations in the United States. The children are 6-36 months old, the age when most AOM occurs. MEF samples that were culture negative for bacteria were not further tested by polymerase chain reaction methods.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Front Pediatr. 2021;9:722483.
2. Kaur R et al. Euro J Clin Microbiol Infect Dis. 2021;41:37-44
3. Pelton SI et al. Pediatr Infect Disease J. 2004;23:1015-22.
4. Farrell DJ et al. Pediatr Infect Disease J. 2007;26:123-8..
5. Kaur R et al. Clin Infect Dis 2021;72(5):797-805.
6. Fuji N et al. Front Cell Infect Microbiol. 2021;11:744742.
Increased electronic media use and youth suicidality: What can clinicians do?
Pediatric suicide was an emerging public health crisis prior to COVID-19, and recent data indicate that pediatric suicide attempts continued to increase during the pandemic.1 In October 2021, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association declared a national state of emergency for pediatric mental health because of a surge in youth suicide attempts.2 Isolation mediated by the degradation of community and exacerbated by the pandemic, has been identified as a contributor to increasing pediatric suicidality.
It is impossible to understand this current public health crisis and to seek solutions without recognizing the ways in which the degradation of community and consequent social isolation play a central role. While the degradation of community and the isolation epidemic that preceded COVID-19 have been mediated by multiple factors, one factor associated with mental health problems in youth is electronic media use.3 During COVID-19, when physical distancing and virtual learning have been necessary to curb the spread, electronic media use has increased exponentially in the pediatric demographic. Some of this increase in screen time has been attributable to virtual schooling, but electronic devices also have become the only means by which kids can stay in contact with one another. While electronic communication has been viewed as an antidote to isolation, disturbing consequences associated with electronic media use have also been noted in our pediatric population.

In the health care system where I (P.L.L.) work as a pediatrician and a child and adolescent psychiatrist, electronic media use has been implicated in more than 90% of our inpatient admissions for suicidal ideation. Use of electronic devices has contributed to suicidal thoughts and attempts in most patients admitted to our acute crisis stabilization unit over the past year. During the pandemic, and in the absence of meaningful interpersonal interactions, many in our pediatric population have become even more dependent on electronic devices to cope with isolation. This has created an often-devastating irony, where the very devices already associated with mental health problems in youth are now being endorsed as “necessary” by mental health professionals.
So how does electronic media use relate to isolation and the continued degradation of community, and why might electronic media use be exacerbating pediatric suicide? One way we have coped with the deterioration of our communities has been the creation of the synthetic community-substitutes found on electronic devices. Unfortunately, our electronic devices create only an illusion of community, where interpersonal interaction occurs by way of inanimate objects, and by electronic text and ideograms. These become substitutes for genuine intimacy, personal contact, and reciprocity. Instead of engaging with one another, our youth are spending hours daily in isolation engaging with a piece of plastic. The mirage generated by pixels on a plastic screen creates an illusion of connectivity, but in reality, this only increases the isolation of our youth.
Human evolution and connection
Intimate social connectivity, woven together in our communities, was a fundamental mechanism for human survival. Historically, for our hunter-gatherer ancestors, the community provided access to our fundamental needs, such as safety from predators and access to substantive nutrition.4 Community allowed our ancestors to survive and procreate, and facilitated their triumph over predation and disease.5 Our distinction as the dominant species on Earth has been afforded by our social connectivity. Unfortunately, in the virtual worlds of our electronic devices the intimate social connectivity of community is absent. Our children wander in isolation, left to navigate age-old evolutionary pressures in the absence of the fundamental advantage for our survival as a species.

Unlike the living, breathing bears and wolves that threatened our ancestors, in the virtual world of the electronic device children are stalked by invisible predators seeking sexual or monetary exploitation. Children are being consumed by digital advertising and social media platforms that perpetually reinforce the requirement of perfection, and they fall prey to cyberbullies who mercilessly disparage their imperfections. In their virtual worlds, where their value is predicated upon anonymous others’ opinions, they succumb to the idea that they will never be enough.6 Their fundamental needs of competence and relatedness go unmet, and they lose their sense of purpose, belonging, and often their will to live. More importantly, absent from their children’s virtual worlds, and preoccupied within their own, parents cannot protect their children from online predators, deflect the vicious attacks of cyberbullies, or reframe their children’s imperfections as distinctive or empowering. They are unable to provide their children with the substantive interpersonal contact necessary for resilience and that bolsters their self-worth.
Human beings are inherently social creatures, who regardless of era require community to meet their fundamental needs. As the duration of daily screen time steadily increases, our youth are spending more and more of their waking hours living in isolation in an electronic world. Without the protective social connectivity of community, they are hunted by online predators, and they are consumed by the predatory culture of perfectionism that is contradictory to the reciprocal caretaking necessary to support their healthy development. Evolutionary biology informs us that, when children are isolated, they are susceptible to predation and disease. And in the socialized isolation of their electronic worlds, they are succumbing to predation and to the depressive diseases that are exacerbating the pediatric mental health crisis.
Creating and building community amid a pandemic has been challenging at best. However, now that we have better tools to fight COVID, it is important to encourage our young patients to reduce their nonacademic screen time, and to get outside and engage with others. Their mental health depends on it.
Dr. Loper is a pediatrician and child and adolescent psychiatrist at Prisma Health–Midlands in Columbia, S.C. He is an assistant professor in the department of neuropsychiatry and behavioral science at the University of South Carolina, Columbia. Dr. Loper has no conflicts of interest. Dr. Kaminstein is an adjunct assistant professor at the graduate school of education and affiliated faculty in the organizational dynamics program, School of Arts and Sciences, at the University of Pennsylvania, Philadelphia. He is a social psychologist who has been studying groups and organizations for more than 40 years. He has no conflicts of interest.
References
1. MMWR. 2021 Jun 18;70(24):888-94.
2. Ray G. “Pediatricians, Child and Adolescent Psychiatrists and Children’s Hospitals Declare National Emergency in Children’s Mental Health.” Childrenshospitals.org. 2021 Oct 19.
3. JAMA Netw Open. 2020(8):e2011381.
4. Am J Phys Anthropol. 2018 April:165(4):777-800.
5. The influence of predation on primate and early human evolution: Impetus for cooperation, in “Origins of Altruism and Cooperation. Developments in Primatology: Progress and Prospects.” (Basingstoke, England: Springer Nature, 2011, pp. 19-40).
6. Media Psychology. 2020;23(1):52-78.
Pediatric suicide was an emerging public health crisis prior to COVID-19, and recent data indicate that pediatric suicide attempts continued to increase during the pandemic.1 In October 2021, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association declared a national state of emergency for pediatric mental health because of a surge in youth suicide attempts.2 Isolation mediated by the degradation of community and exacerbated by the pandemic, has been identified as a contributor to increasing pediatric suicidality.
It is impossible to understand this current public health crisis and to seek solutions without recognizing the ways in which the degradation of community and consequent social isolation play a central role. While the degradation of community and the isolation epidemic that preceded COVID-19 have been mediated by multiple factors, one factor associated with mental health problems in youth is electronic media use.3 During COVID-19, when physical distancing and virtual learning have been necessary to curb the spread, electronic media use has increased exponentially in the pediatric demographic. Some of this increase in screen time has been attributable to virtual schooling, but electronic devices also have become the only means by which kids can stay in contact with one another. While electronic communication has been viewed as an antidote to isolation, disturbing consequences associated with electronic media use have also been noted in our pediatric population.
In the health care system where I (P.L.L.) work as a pediatrician and a child and adolescent psychiatrist, electronic media use has been implicated in more than 90% of our inpatient admissions for suicidal ideation. Use of electronic devices has contributed to suicidal thoughts and attempts in most patients admitted to our acute crisis stabilization unit over the past year. During the pandemic, and in the absence of meaningful interpersonal interactions, many in our pediatric population have become even more dependent on electronic devices to cope with isolation. This has created an often-devastating irony, where the very devices already associated with mental health problems in youth are now being endorsed as “necessary” by mental health professionals.
So how does electronic media use relate to isolation and the continued degradation of community, and why might electronic media use be exacerbating pediatric suicide? One way we have coped with the deterioration of our communities has been the creation of the synthetic community-substitutes found on electronic devices. Unfortunately, our electronic devices create only an illusion of community, where interpersonal interaction occurs by way of inanimate objects, and by electronic text and ideograms. These become substitutes for genuine intimacy, personal contact, and reciprocity. Instead of engaging with one another, our youth are spending hours daily in isolation engaging with a piece of plastic. The mirage generated by pixels on a plastic screen creates an illusion of connectivity, but in reality, this only increases the isolation of our youth.
Human evolution and connection
Intimate social connectivity, woven together in our communities, was a fundamental mechanism for human survival. Historically, for our hunter-gatherer ancestors, the community provided access to our fundamental needs, such as safety from predators and access to substantive nutrition.4 Community allowed our ancestors to survive and procreate, and facilitated their triumph over predation and disease.5 Our distinction as the dominant species on Earth has been afforded by our social connectivity. Unfortunately, in the virtual worlds of our electronic devices the intimate social connectivity of community is absent. Our children wander in isolation, left to navigate age-old evolutionary pressures in the absence of the fundamental advantage for our survival as a species.
Unlike the living, breathing bears and wolves that threatened our ancestors, in the virtual world of the electronic device children are stalked by invisible predators seeking sexual or monetary exploitation. Children are being consumed by digital advertising and social media platforms that perpetually reinforce the requirement of perfection, and they fall prey to cyberbullies who mercilessly disparage their imperfections. In their virtual worlds, where their value is predicated upon anonymous others’ opinions, they succumb to the idea that they will never be enough.6 Their fundamental needs of competence and relatedness go unmet, and they lose their sense of purpose, belonging, and often their will to live. More importantly, absent from their children’s virtual worlds, and preoccupied within their own, parents cannot protect their children from online predators, deflect the vicious attacks of cyberbullies, or reframe their children’s imperfections as distinctive or empowering. They are unable to provide their children with the substantive interpersonal contact necessary for resilience and that bolsters their self-worth.
Human beings are inherently social creatures, who regardless of era require community to meet their fundamental needs. As the duration of daily screen time steadily increases, our youth are spending more and more of their waking hours living in isolation in an electronic world. Without the protective social connectivity of community, they are hunted by online predators, and they are consumed by the predatory culture of perfectionism that is contradictory to the reciprocal caretaking necessary to support their healthy development. Evolutionary biology informs us that, when children are isolated, they are susceptible to predation and disease. And in the socialized isolation of their electronic worlds, they are succumbing to predation and to the depressive diseases that are exacerbating the pediatric mental health crisis.
Creating and building community amid a pandemic has been challenging at best. However, now that we have better tools to fight COVID, it is important to encourage our young patients to reduce their nonacademic screen time, and to get outside and engage with others. Their mental health depends on it.
Dr. Loper is a pediatrician and child and adolescent psychiatrist at Prisma Health–Midlands in Columbia, S.C. He is an assistant professor in the department of neuropsychiatry and behavioral science at the University of South Carolina, Columbia. Dr. Loper has no conflicts of interest. Dr. Kaminstein is an adjunct assistant professor at the graduate school of education and affiliated faculty in the organizational dynamics program, School of Arts and Sciences, at the University of Pennsylvania, Philadelphia. He is a social psychologist who has been studying groups and organizations for more than 40 years. He has no conflicts of interest.
References
1. MMWR. 2021 Jun 18;70(24):888-94.
2. Ray G. “Pediatricians, Child and Adolescent Psychiatrists and Children’s Hospitals Declare National Emergency in Children’s Mental Health.” Childrenshospitals.org. 2021 Oct 19.
3. JAMA Netw Open. 2020(8):e2011381.
4. Am J Phys Anthropol. 2018 April:165(4):777-800.
5. The influence of predation on primate and early human evolution: Impetus for cooperation, in “Origins of Altruism and Cooperation. Developments in Primatology: Progress and Prospects.” (Basingstoke, England: Springer Nature, 2011, pp. 19-40).
6. Media Psychology. 2020;23(1):52-78.
Pediatric suicide was an emerging public health crisis prior to COVID-19, and recent data indicate that pediatric suicide attempts continued to increase during the pandemic.1 In October 2021, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association declared a national state of emergency for pediatric mental health because of a surge in youth suicide attempts.2 Isolation mediated by the degradation of community and exacerbated by the pandemic, has been identified as a contributor to increasing pediatric suicidality.
It is impossible to understand this current public health crisis and to seek solutions without recognizing the ways in which the degradation of community and consequent social isolation play a central role. While the degradation of community and the isolation epidemic that preceded COVID-19 have been mediated by multiple factors, one factor associated with mental health problems in youth is electronic media use.3 During COVID-19, when physical distancing and virtual learning have been necessary to curb the spread, electronic media use has increased exponentially in the pediatric demographic. Some of this increase in screen time has been attributable to virtual schooling, but electronic devices also have become the only means by which kids can stay in contact with one another. While electronic communication has been viewed as an antidote to isolation, disturbing consequences associated with electronic media use have also been noted in our pediatric population.
In the health care system where I (P.L.L.) work as a pediatrician and a child and adolescent psychiatrist, electronic media use has been implicated in more than 90% of our inpatient admissions for suicidal ideation. Use of electronic devices has contributed to suicidal thoughts and attempts in most patients admitted to our acute crisis stabilization unit over the past year. During the pandemic, and in the absence of meaningful interpersonal interactions, many in our pediatric population have become even more dependent on electronic devices to cope with isolation. This has created an often-devastating irony, where the very devices already associated with mental health problems in youth are now being endorsed as “necessary” by mental health professionals.
So how does electronic media use relate to isolation and the continued degradation of community, and why might electronic media use be exacerbating pediatric suicide? One way we have coped with the deterioration of our communities has been the creation of the synthetic community-substitutes found on electronic devices. Unfortunately, our electronic devices create only an illusion of community, where interpersonal interaction occurs by way of inanimate objects, and by electronic text and ideograms. These become substitutes for genuine intimacy, personal contact, and reciprocity. Instead of engaging with one another, our youth are spending hours daily in isolation engaging with a piece of plastic. The mirage generated by pixels on a plastic screen creates an illusion of connectivity, but in reality, this only increases the isolation of our youth.
Human evolution and connection
Intimate social connectivity, woven together in our communities, was a fundamental mechanism for human survival. Historically, for our hunter-gatherer ancestors, the community provided access to our fundamental needs, such as safety from predators and access to substantive nutrition.4 Community allowed our ancestors to survive and procreate, and facilitated their triumph over predation and disease.5 Our distinction as the dominant species on Earth has been afforded by our social connectivity. Unfortunately, in the virtual worlds of our electronic devices the intimate social connectivity of community is absent. Our children wander in isolation, left to navigate age-old evolutionary pressures in the absence of the fundamental advantage for our survival as a species.
Unlike the living, breathing bears and wolves that threatened our ancestors, in the virtual world of the electronic device children are stalked by invisible predators seeking sexual or monetary exploitation. Children are being consumed by digital advertising and social media platforms that perpetually reinforce the requirement of perfection, and they fall prey to cyberbullies who mercilessly disparage their imperfections. In their virtual worlds, where their value is predicated upon anonymous others’ opinions, they succumb to the idea that they will never be enough.6 Their fundamental needs of competence and relatedness go unmet, and they lose their sense of purpose, belonging, and often their will to live. More importantly, absent from their children’s virtual worlds, and preoccupied within their own, parents cannot protect their children from online predators, deflect the vicious attacks of cyberbullies, or reframe their children’s imperfections as distinctive or empowering. They are unable to provide their children with the substantive interpersonal contact necessary for resilience and that bolsters their self-worth.
Human beings are inherently social creatures, who regardless of era require community to meet their fundamental needs. As the duration of daily screen time steadily increases, our youth are spending more and more of their waking hours living in isolation in an electronic world. Without the protective social connectivity of community, they are hunted by online predators, and they are consumed by the predatory culture of perfectionism that is contradictory to the reciprocal caretaking necessary to support their healthy development. Evolutionary biology informs us that, when children are isolated, they are susceptible to predation and disease. And in the socialized isolation of their electronic worlds, they are succumbing to predation and to the depressive diseases that are exacerbating the pediatric mental health crisis.
Creating and building community amid a pandemic has been challenging at best. However, now that we have better tools to fight COVID, it is important to encourage our young patients to reduce their nonacademic screen time, and to get outside and engage with others. Their mental health depends on it.
Dr. Loper is a pediatrician and child and adolescent psychiatrist at Prisma Health–Midlands in Columbia, S.C. He is an assistant professor in the department of neuropsychiatry and behavioral science at the University of South Carolina, Columbia. Dr. Loper has no conflicts of interest. Dr. Kaminstein is an adjunct assistant professor at the graduate school of education and affiliated faculty in the organizational dynamics program, School of Arts and Sciences, at the University of Pennsylvania, Philadelphia. He is a social psychologist who has been studying groups and organizations for more than 40 years. He has no conflicts of interest.
References
1. MMWR. 2021 Jun 18;70(24):888-94.
2. Ray G. “Pediatricians, Child and Adolescent Psychiatrists and Children’s Hospitals Declare National Emergency in Children’s Mental Health.” Childrenshospitals.org. 2021 Oct 19.
3. JAMA Netw Open. 2020(8):e2011381.
4. Am J Phys Anthropol. 2018 April:165(4):777-800.
5. The influence of predation on primate and early human evolution: Impetus for cooperation, in “Origins of Altruism and Cooperation. Developments in Primatology: Progress and Prospects.” (Basingstoke, England: Springer Nature, 2011, pp. 19-40).
6. Media Psychology. 2020;23(1):52-78.
Note to self: Relax!
During my usual 2 weeks off over the holidays I did my usual stuff – taxes, read journals, do CME, review legal cases that have come in, hang out with my family, nap with my dogs.
Somewhere in that stretch of time off. I run out of things to do, and that’s when I have to confront an odd truth: I’ve forgotten how to relax.

In medical school and residency I certainly could enjoy the rare weekend time off. I’d watch sports, go running, do things with friends.
But now it’s a different world. My friends, while still people I enjoy, are on the other end of a computer, far away. My interest in sports and movies waned years ago, and I avoid televisions as part of my aversion to the news. Even the books I used to enjoy, such as the late Clive Cussler’s, don’t hold my attention anymore. If I’m going to read anything it’s going to be humor, because the medical field is serious enough as it is.
The bottom line is that it’s hard for me to relax and “do nothing” anymore. I don’t know if that’s just me, or if it’s part of the personality of being a doctor, or both.
If I’m not at my desk working, I feel like I’m not doing anything. Do other doctors feel that way?
Is this a bad thing?
It probably is, and I should look to the beginning of a new year to make some changes. Maybe I should go back to running (or, at this point in my life, walking) or finding some humor books I enjoy and reading them. The old standby of going on a vacation is kind of limited right now.
I’ve been an attending physician for 24 years now, which is still hard to believe. My retirement isn’t (hopefully) anytime soon, but is coming up faster than it seems. If I don’t relearn to relax by then, when will I?
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
During my usual 2 weeks off over the holidays I did my usual stuff – taxes, read journals, do CME, review legal cases that have come in, hang out with my family, nap with my dogs.
Somewhere in that stretch of time off. I run out of things to do, and that’s when I have to confront an odd truth: I’ve forgotten how to relax.
In medical school and residency I certainly could enjoy the rare weekend time off. I’d watch sports, go running, do things with friends.
But now it’s a different world. My friends, while still people I enjoy, are on the other end of a computer, far away. My interest in sports and movies waned years ago, and I avoid televisions as part of my aversion to the news. Even the books I used to enjoy, such as the late Clive Cussler’s, don’t hold my attention anymore. If I’m going to read anything it’s going to be humor, because the medical field is serious enough as it is.
The bottom line is that it’s hard for me to relax and “do nothing” anymore. I don’t know if that’s just me, or if it’s part of the personality of being a doctor, or both.
If I’m not at my desk working, I feel like I’m not doing anything. Do other doctors feel that way?
Is this a bad thing?
It probably is, and I should look to the beginning of a new year to make some changes. Maybe I should go back to running (or, at this point in my life, walking) or finding some humor books I enjoy and reading them. The old standby of going on a vacation is kind of limited right now.
I’ve been an attending physician for 24 years now, which is still hard to believe. My retirement isn’t (hopefully) anytime soon, but is coming up faster than it seems. If I don’t relearn to relax by then, when will I?
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
During my usual 2 weeks off over the holidays I did my usual stuff – taxes, read journals, do CME, review legal cases that have come in, hang out with my family, nap with my dogs.
Somewhere in that stretch of time off. I run out of things to do, and that’s when I have to confront an odd truth: I’ve forgotten how to relax.
In medical school and residency I certainly could enjoy the rare weekend time off. I’d watch sports, go running, do things with friends.
But now it’s a different world. My friends, while still people I enjoy, are on the other end of a computer, far away. My interest in sports and movies waned years ago, and I avoid televisions as part of my aversion to the news. Even the books I used to enjoy, such as the late Clive Cussler’s, don’t hold my attention anymore. If I’m going to read anything it’s going to be humor, because the medical field is serious enough as it is.
The bottom line is that it’s hard for me to relax and “do nothing” anymore. I don’t know if that’s just me, or if it’s part of the personality of being a doctor, or both.
If I’m not at my desk working, I feel like I’m not doing anything. Do other doctors feel that way?
Is this a bad thing?
It probably is, and I should look to the beginning of a new year to make some changes. Maybe I should go back to running (or, at this point in my life, walking) or finding some humor books I enjoy and reading them. The old standby of going on a vacation is kind of limited right now.
I’ve been an attending physician for 24 years now, which is still hard to believe. My retirement isn’t (hopefully) anytime soon, but is coming up faster than it seems. If I don’t relearn to relax by then, when will I?
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
PA name change bad for patients and the profession
Physician assistants (PAs) are angry with me, and with good reason. I had the audacity to lump them together with nurse practitioners (NPs) in my book “Patients at Risk,” an act which one highly placed PA leader called “distasteful” in a private conversation with me.
I will admit that PAs have reason to be upset. With competitive acceptance rates including a requirement for extensive health care experience before PA school, standardized training, and at least 2,000 hours of clinical experience before graduation, the profession is a stark contrast to the haphazard training and 500 clinical hours required of NPs today. Further, unlike NPs, who have sought independent practice since the 1980s, PAs have traditionally been close allies with physicians, generally working in a 1:1 supervision model.
The truth is that it hurt to include PAs with NPs in my book. I’ve had my own close relationships with PAs over the years and found the PAs I worked with to be outstanding clinicians. Unfortunately, the profession has given me no choice. Following a model set by the NP profession,
Their efforts began with a change in terminology. “Optimal team practice” (OTP) was supposed to give PAs more flexibility, allowing them to work for hospitals or physician groups rather than under the responsibility of one physician. Not surprisingly, corporations and even academic centers have been quick to take advantage, hiring PAs and placing them in positions without adequate physician support. OTP paved the way for independent practice, as PAs sought and gained independence from any physician supervision in North Dakota, the first state to grant them that right.
Most recently, PAs have determined to change their name entirely, calling themselves physician associates. This move by the American Academy of Physician Assistants is the culmination of a years-long marketing study on how to increase the relevance and improve patient perception of the PA profession. The AAPA decision is expected to galvanize state and local PA organizations to lobby legislators for legal and regulatory changes that allow the use of the “physician associate” title, which is not currently a legal representation of PA licensure.
PAs’ latest attempt at title and branding reform follows years of advocacy to not be referred to as physician extenders or midlevel providers. For example, to gain more public acceptance of the PA model, the profession launched the public relations campaign “Your PA Can,” closely mirroring the “We Choose NPs” media blitz. PAs have also followed other dangerous precedents set by NPs, including 100% online training and a new “Doctor of Medical Science” degree, allowing PAs, as well as NPs, to now be called “doctors.”
I can understand PA reasoning even if I don’t agree with it. PAs are frustrated to be treated as second-class citizens compared with NPs, who have been granted independent practice in half the states in the union despite having a fraction of PA training. Frankly, it’s unfair that NPs are being hired preferentially over PAs simply because of looser legal requirements for physician oversight. The bottom line is that NPs have been more successful at persuading legislators to allow them independence – but that doesn’t make it right for either group.
While PAs have more clinical training upon graduation than NPs, they still have far less than physicians. PAs generally attend a 2-year master’s degree program after college which includes 2,000 hours of hands-on clinical work. By comparison, the average medical student spends 4 years and receives 5,000-6,000 hours of supervised clinical training upon graduation. But this isn’t considered enough for a graduate medical student to practice medicine independently.
Physicians must complete at least 3 years of postgraduate residency training in most states to receive a medical license, and by the time a physician is permitted to practice medicine unsupervised, they will have attained no fewer than 15,000-20,000 hours of supervised clinical practice, with years of specialty-specific training.
Patients want and deserve access to truly physician-led care, but in many parts of the country, physicians are being replaced by nonphysician practitioners to boost corporate profits. In many cases, patients are kept in the dark about the differences in training between the medical professionals now in charge of their care. The American Medical Association and other critics have expressed concern that the proposed title of “physician associate” is likely to further obscure the training and roles of medical professionals, already a source of confusion to patients.
One specific criticism is that a physician associate has historically referred to a physician (MD or DO) in a private practice group who has not yet achieved the status of partner. These physician associates are fully licensed medical doctors who have completed medical school and residency training and are in the process of completing a partnership track with their group to participate fully in financial and administrative processes. This nomenclature is similar to that of attorneys on a partnership track. Thus, the use of the term “physician associate” for someone other than a medical doctor is seen as misleading, particularly to patients who cannot be expected to have familiarity with the differences in training.
Efforts to separate the PA profession from a close-working relationship with a physician are bad not only for patients but for PAs as well. Many PAs who desire physician involvement may find themselves hung out to dry, hired by companies and expected to perform outside of their comfort level. The profession also risks ostracizing physician allies, many of whom have preferentially sought to work with PAs.
My sincere hope is that the PA profession will return to its traditional roots of a physician-PA relationship, a model that has been demonstrated to result in high-quality patient care. When that day comes, I will happily re-title my book. But as long as the AAPA continues to work to remove physicians from the equation, patients are indeed at risk.
Rebekah Bernard, MD, is a family physician in Fort Myers, Florida, and president of Physicians for Patient Protection. She is the coauthor of Patients at Risk: The Rise of the Nurse Practitioner and Physician Assistant in Healthcare (Irvine, Calif.: Universal Publishers, 2020). She had no relevant financial disclosures. A version of this article first appeared on Medscape.com.
Physician assistants (PAs) are angry with me, and with good reason. I had the audacity to lump them together with nurse practitioners (NPs) in my book “Patients at Risk,” an act which one highly placed PA leader called “distasteful” in a private conversation with me.
I will admit that PAs have reason to be upset. With competitive acceptance rates including a requirement for extensive health care experience before PA school, standardized training, and at least 2,000 hours of clinical experience before graduation, the profession is a stark contrast to the haphazard training and 500 clinical hours required of NPs today. Further, unlike NPs, who have sought independent practice since the 1980s, PAs have traditionally been close allies with physicians, generally working in a 1:1 supervision model.
The truth is that it hurt to include PAs with NPs in my book. I’ve had my own close relationships with PAs over the years and found the PAs I worked with to be outstanding clinicians. Unfortunately, the profession has given me no choice. Following a model set by the NP profession,
Their efforts began with a change in terminology. “Optimal team practice” (OTP) was supposed to give PAs more flexibility, allowing them to work for hospitals or physician groups rather than under the responsibility of one physician. Not surprisingly, corporations and even academic centers have been quick to take advantage, hiring PAs and placing them in positions without adequate physician support. OTP paved the way for independent practice, as PAs sought and gained independence from any physician supervision in North Dakota, the first state to grant them that right.
Most recently, PAs have determined to change their name entirely, calling themselves physician associates. This move by the American Academy of Physician Assistants is the culmination of a years-long marketing study on how to increase the relevance and improve patient perception of the PA profession. The AAPA decision is expected to galvanize state and local PA organizations to lobby legislators for legal and regulatory changes that allow the use of the “physician associate” title, which is not currently a legal representation of PA licensure.
PAs’ latest attempt at title and branding reform follows years of advocacy to not be referred to as physician extenders or midlevel providers. For example, to gain more public acceptance of the PA model, the profession launched the public relations campaign “Your PA Can,” closely mirroring the “We Choose NPs” media blitz. PAs have also followed other dangerous precedents set by NPs, including 100% online training and a new “Doctor of Medical Science” degree, allowing PAs, as well as NPs, to now be called “doctors.”
I can understand PA reasoning even if I don’t agree with it. PAs are frustrated to be treated as second-class citizens compared with NPs, who have been granted independent practice in half the states in the union despite having a fraction of PA training. Frankly, it’s unfair that NPs are being hired preferentially over PAs simply because of looser legal requirements for physician oversight. The bottom line is that NPs have been more successful at persuading legislators to allow them independence – but that doesn’t make it right for either group.
While PAs have more clinical training upon graduation than NPs, they still have far less than physicians. PAs generally attend a 2-year master’s degree program after college which includes 2,000 hours of hands-on clinical work. By comparison, the average medical student spends 4 years and receives 5,000-6,000 hours of supervised clinical training upon graduation. But this isn’t considered enough for a graduate medical student to practice medicine independently.
Physicians must complete at least 3 years of postgraduate residency training in most states to receive a medical license, and by the time a physician is permitted to practice medicine unsupervised, they will have attained no fewer than 15,000-20,000 hours of supervised clinical practice, with years of specialty-specific training.
Patients want and deserve access to truly physician-led care, but in many parts of the country, physicians are being replaced by nonphysician practitioners to boost corporate profits. In many cases, patients are kept in the dark about the differences in training between the medical professionals now in charge of their care. The American Medical Association and other critics have expressed concern that the proposed title of “physician associate” is likely to further obscure the training and roles of medical professionals, already a source of confusion to patients.
One specific criticism is that a physician associate has historically referred to a physician (MD or DO) in a private practice group who has not yet achieved the status of partner. These physician associates are fully licensed medical doctors who have completed medical school and residency training and are in the process of completing a partnership track with their group to participate fully in financial and administrative processes. This nomenclature is similar to that of attorneys on a partnership track. Thus, the use of the term “physician associate” for someone other than a medical doctor is seen as misleading, particularly to patients who cannot be expected to have familiarity with the differences in training.
Efforts to separate the PA profession from a close-working relationship with a physician are bad not only for patients but for PAs as well. Many PAs who desire physician involvement may find themselves hung out to dry, hired by companies and expected to perform outside of their comfort level. The profession also risks ostracizing physician allies, many of whom have preferentially sought to work with PAs.
My sincere hope is that the PA profession will return to its traditional roots of a physician-PA relationship, a model that has been demonstrated to result in high-quality patient care. When that day comes, I will happily re-title my book. But as long as the AAPA continues to work to remove physicians from the equation, patients are indeed at risk.
Rebekah Bernard, MD, is a family physician in Fort Myers, Florida, and president of Physicians for Patient Protection. She is the coauthor of Patients at Risk: The Rise of the Nurse Practitioner and Physician Assistant in Healthcare (Irvine, Calif.: Universal Publishers, 2020). She had no relevant financial disclosures. A version of this article first appeared on Medscape.com.
Physician assistants (PAs) are angry with me, and with good reason. I had the audacity to lump them together with nurse practitioners (NPs) in my book “Patients at Risk,” an act which one highly placed PA leader called “distasteful” in a private conversation with me.
I will admit that PAs have reason to be upset. With competitive acceptance rates including a requirement for extensive health care experience before PA school, standardized training, and at least 2,000 hours of clinical experience before graduation, the profession is a stark contrast to the haphazard training and 500 clinical hours required of NPs today. Further, unlike NPs, who have sought independent practice since the 1980s, PAs have traditionally been close allies with physicians, generally working in a 1:1 supervision model.
The truth is that it hurt to include PAs with NPs in my book. I’ve had my own close relationships with PAs over the years and found the PAs I worked with to be outstanding clinicians. Unfortunately, the profession has given me no choice. Following a model set by the NP profession,
Their efforts began with a change in terminology. “Optimal team practice” (OTP) was supposed to give PAs more flexibility, allowing them to work for hospitals or physician groups rather than under the responsibility of one physician. Not surprisingly, corporations and even academic centers have been quick to take advantage, hiring PAs and placing them in positions without adequate physician support. OTP paved the way for independent practice, as PAs sought and gained independence from any physician supervision in North Dakota, the first state to grant them that right.
Most recently, PAs have determined to change their name entirely, calling themselves physician associates. This move by the American Academy of Physician Assistants is the culmination of a years-long marketing study on how to increase the relevance and improve patient perception of the PA profession. The AAPA decision is expected to galvanize state and local PA organizations to lobby legislators for legal and regulatory changes that allow the use of the “physician associate” title, which is not currently a legal representation of PA licensure.
PAs’ latest attempt at title and branding reform follows years of advocacy to not be referred to as physician extenders or midlevel providers. For example, to gain more public acceptance of the PA model, the profession launched the public relations campaign “Your PA Can,” closely mirroring the “We Choose NPs” media blitz. PAs have also followed other dangerous precedents set by NPs, including 100% online training and a new “Doctor of Medical Science” degree, allowing PAs, as well as NPs, to now be called “doctors.”
I can understand PA reasoning even if I don’t agree with it. PAs are frustrated to be treated as second-class citizens compared with NPs, who have been granted independent practice in half the states in the union despite having a fraction of PA training. Frankly, it’s unfair that NPs are being hired preferentially over PAs simply because of looser legal requirements for physician oversight. The bottom line is that NPs have been more successful at persuading legislators to allow them independence – but that doesn’t make it right for either group.
While PAs have more clinical training upon graduation than NPs, they still have far less than physicians. PAs generally attend a 2-year master’s degree program after college which includes 2,000 hours of hands-on clinical work. By comparison, the average medical student spends 4 years and receives 5,000-6,000 hours of supervised clinical training upon graduation. But this isn’t considered enough for a graduate medical student to practice medicine independently.
Physicians must complete at least 3 years of postgraduate residency training in most states to receive a medical license, and by the time a physician is permitted to practice medicine unsupervised, they will have attained no fewer than 15,000-20,000 hours of supervised clinical practice, with years of specialty-specific training.
Patients want and deserve access to truly physician-led care, but in many parts of the country, physicians are being replaced by nonphysician practitioners to boost corporate profits. In many cases, patients are kept in the dark about the differences in training between the medical professionals now in charge of their care. The American Medical Association and other critics have expressed concern that the proposed title of “physician associate” is likely to further obscure the training and roles of medical professionals, already a source of confusion to patients.
One specific criticism is that a physician associate has historically referred to a physician (MD or DO) in a private practice group who has not yet achieved the status of partner. These physician associates are fully licensed medical doctors who have completed medical school and residency training and are in the process of completing a partnership track with their group to participate fully in financial and administrative processes. This nomenclature is similar to that of attorneys on a partnership track. Thus, the use of the term “physician associate” for someone other than a medical doctor is seen as misleading, particularly to patients who cannot be expected to have familiarity with the differences in training.
Efforts to separate the PA profession from a close-working relationship with a physician are bad not only for patients but for PAs as well. Many PAs who desire physician involvement may find themselves hung out to dry, hired by companies and expected to perform outside of their comfort level. The profession also risks ostracizing physician allies, many of whom have preferentially sought to work with PAs.
My sincere hope is that the PA profession will return to its traditional roots of a physician-PA relationship, a model that has been demonstrated to result in high-quality patient care. When that day comes, I will happily re-title my book. But as long as the AAPA continues to work to remove physicians from the equation, patients are indeed at risk.
Rebekah Bernard, MD, is a family physician in Fort Myers, Florida, and president of Physicians for Patient Protection. She is the coauthor of Patients at Risk: The Rise of the Nurse Practitioner and Physician Assistant in Healthcare (Irvine, Calif.: Universal Publishers, 2020). She had no relevant financial disclosures. A version of this article first appeared on Medscape.com.
Should psychiatry categorize ‘substance-induced paraphilia?’
‘substance-induced paraphilia?’
The dopamine receptors of the brain get their fair share amid the didactics we receive in residency. From discussions of antipsychotics and schizophrenia to stimulants and ADHD, dopamine plays a key role. Depending on the program and interest of faculty, methamphetamine may get its own lecture or be mixed in with other stimulants of abuse. During that discussion, a comment might be made in passing on the impact of methamphetamine on sexual desire and activity.
Experiences in the emergency department caring for patients who are intoxicated from methamphetamine then effectively make up for any gaps in trainees’ knowledge base. From patients engaging in self-pleasing pursuits in the emergency room to unfiltered reports of sexual exploits and desires, the impact of methamphetamine on sexual behavior quickly becomes apparent. Those experiences are later reinforced when residents are exposed to more long-term rehabilitation programs and have more in-depth conversations with patients about the sex-culture surrounding methamphetamine.

It is common to hear that, under the influence of methamphetamine, any available body will become an acceptable sexual partner – at times resulting in significant regrets, dangerous sexual activity, and complicated questions surrounding consent. Some early studies have found up to 72% increase in risky sexual behavior in methamphetamine users.1 This is particularly problematic as society has recently taken on the difficult and important work to re-examine the role and nature of consent in sexual activities. This falls within the larger #MeToo movement and has led to advocating for harsher sentencing of sexual offenders.
Yet simultaneously, society has also reconsidered its approach to apportioning blame on drug users.2 This shift to a more compassionate stance has resulted in a desire to treat and care for a disorder, rather than punish and condemn a poor choice. As forensic psychiatrists, we have noted this significant change. Where substance use disorders were once considered a risk factor for recidivism, they are now considered a disability that not only warrants treatment but can also diminish the share of blame one may be responsible for.
The convergence of those two societal movements often plays out in the courtroom, and in our experience when faced with those two opposing viewpoints, triers of fact (judges and juries) often favor punishing sexual offense over empathizing with an addictive disorder. While certainly not implying methamphetamine use condones sexual offense, we do posit the particular relationship between methamphetamine use and sexual activity should be explained to those entrusted with deciding guilt.
Examples of such problems are extremely common. A routine case involves IK,3 a 48-year-old male without significant history of legal problems, arrested for indecent exposure. His history of mental illness is closely intertwined with a history of substance use, leading to many psychiatric hospitalizations for methamphetamine-induced psychosis. After many hospitalizations he was placed in an assertive community treatment (ACT) team.
One day, IK is approached by an industrious drug dealer who frequents multiple board-and-cares in search for customers interested in relapsing. IK uses methamphetamine and within hours finds himself having walked miles away, naked, in the middle of an RV park. He subsequently describes the experience of unrelenting sexual desire, accompanied by ideas of reference involving billboards encouraging him to demonstrate his sexual prowess, as well as auditory hallucinations of women cheering him on. This leads to him pleasing himself publicly and his subsequent arrest.
Interviewing IK, 3 months later, he is embarrassed and apologetic. He is cognizant of the inappropriate nature of the incident and the foolishness of his actions. However, when asked whether he considers himself a sexual offender, he protests that he would never act in such a manner if not under the influence of methamphetamine. He points to his lack of significant sexual urges when sober, his lack of prior sexual offense, his lack of sexually violent offense, and his lack of unusual sexual interests.
It is unclear to us how society will or should adjudicate on such a case. It is not under the purview of forensic psychiatry to become a trier of fact. However, psychiatry should have a better working framework of how to discuss and conceptualize such situations, especially considering the dire consequences for those involved.
While any criminal conviction already has the potential to destroy a person’s life, sexual crimes bring particularly serious consequences. Entry into the national sex offender registry, in addition to carrying an unshakable stigma, comes with additional degrees of lost freedom. These individuals are prohibited from living or working in areas that have children in proximity, subjecting them to the outskirts of society and greatly restricting any chance of economic escape from poverty. Parks, libraries, and shopping malls can become off limits. Privacy for these individuals is nonexistent; from websites they visit to where they travel physically can be monitored. Even where they live and a detailed physical description are often easily accessible by members of their community.

When should it be permissible to consider sex offender status for someone on the grounds of a mental illness? A patient with obsessive-compulsive disorder might have sadistic obsessions and compulsions to commit violent sexual acts, which, along with being repugnant to society, are entirely ego-dystonic to the suffering patient. Psychosis is often characterized as involving a loss of insight and impaired reality testing. If society accepts insanity as grounds to mitigate sentencing, then why not permit it for grounds to wave the designation of sex offender to those with certain disorders, including substance use disorder? Wherever we come down on this issue,
Should IK have to register as a sex offender? Regardless of the circumstances, he did publicly masturbate. Society has determined that public sexual displays are a crime worth carrying the pariah status of sex offender – why should an exception be made for methamphetamine use? On the other hand, it is difficult to claim that IK’s behavior was entirely of his own free will. Most triers of fact will have never experienced that amount of dopamine reward. They can’t attest to the remaining free will after experiencing more pleasurable salience and positive reinforcement than ever naturally possible.
How we deal with the behavioral consequences, and other sequelae, of methamphetamine use is a growing problem. Access to and use of methamphetamine is no longer reserved for soldiers patrolling the jungles of Vietnam. Once thought to be a scourge of the West Coast, methamphetamine is now widely available throughout the United States.4 The use of methamphetamine is likely to continue to expand as society keeps pursuing the decriminalizing of drug use. Psychiatrists practicing in areas heavily affected by methamphetamine see firsthand the burden it places on community resources in the form of increased psychosis, emergency room utilization, medical resource strain, and encounters with police.5
The presence of mental illness is tied to a small but statistically significant risk of violence. However, substance use is a well-established risk factor for violence.6 What is often missed is that many sexual offenders have not committed a violent offense. However, like IK, they have been charged with indecent exposure or other nonviolent sexual offenses, such as prostitution and solicitation. Those nonviolent offenses are driven by poor judgment and impulsivity, the trademarks of substance use. The answer cannot be to incarcerate, and eventually add to the sex offender registry, the growing number of these individuals.
Yet, as psychiatrists, we seem at a loss for how to treat these patients. The prescription of allowing them to spend a night in the ED with a complementary sandwich garnished with olanzapine often feels like enabling. Substance use treatment programs are too limited, and the wait list is rarely shorter than the time it takes our patient to purchase their next hit.
There are no effective pharmacologic treatments for methamphetamine use disorder.7 The recommendations of cognitive-behavioral therapy, family and group therapy, contingency management, and a 12-step program may be sufficient for the most motivated and well-supported patients but are inadequate for the vast majority.8 As much as we want to laud the merits of community psychiatry and the ACT [assertive community treatment] model of care, it is hard to carry that banner while confronted with the reality these patients face on a day-to-day basis during any shift in the emergency room. Eventually the countless encounters with homeless, helplessly meth-addicted patients ending in discharge back to the streets begins to tarnish the bright rhetoric surrounding community care, which starts to sound more and more like abandonment of patients to suffer in futility.9
It is not up to forensic psychiatrists, or even psychiatry as a whole, to fix the myriad of inadequacies surrounding how society handles those suffering from methamphetamine addiction. However, it is essential for psychiatry to study and educate society on the interaction of methamphetamine use and sexual behavior. There has been some exploration into other risk factors for paraphilic behavior while under the influence of substances, but there is a dearth of information on this topic. Establishing a nomenclature called “substance-induced paraphilia” might be a way to bring clarity to such instances in both a forensic and general psychiatric setting.
Dr. Compton is a psychiatry resident at University of California, San Diego. His background includes medical education, mental health advocacy, work with underserved populations, and brain cancer research. Dr. Compton has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Psychol Addict Behav. 2016;30(2)147-57.
2. Monitor Psychol. 2019;50(6).
3. IK’s case has been modified in certain ways to maintain confidentiality.
4. J Psychoactive Drugs. 2000;(2):137-41.
5. Acad Emerg Med. 2020 Nov;27(11):1116-25.
6. Swanson JW. Mental disorder, substance abuse, and community violence: An epidemiological approach, in: Monahan J and Steadman HJ, eds. “Violence and Mental Disorder: Developments in Risk Assessment” (Chicago: University of Chicago Press, 1994, pp. 101-36).
7. Addiction. 2004 Jun;99(6)708-17.
8. Am Fam Physician. 2007 Oct 15;76(8):1169-74.
9. Perspect Biol Med. 2021;64(1)70-81.
The dopamine receptors of the brain get their fair share amid the didactics we receive in residency. From discussions of antipsychotics and schizophrenia to stimulants and ADHD, dopamine plays a key role. Depending on the program and interest of faculty, methamphetamine may get its own lecture or be mixed in with other stimulants of abuse. During that discussion, a comment might be made in passing on the impact of methamphetamine on sexual desire and activity.
Experiences in the emergency department caring for patients who are intoxicated from methamphetamine then effectively make up for any gaps in trainees’ knowledge base. From patients engaging in self-pleasing pursuits in the emergency room to unfiltered reports of sexual exploits and desires, the impact of methamphetamine on sexual behavior quickly becomes apparent. Those experiences are later reinforced when residents are exposed to more long-term rehabilitation programs and have more in-depth conversations with patients about the sex-culture surrounding methamphetamine.
It is common to hear that, under the influence of methamphetamine, any available body will become an acceptable sexual partner – at times resulting in significant regrets, dangerous sexual activity, and complicated questions surrounding consent. Some early studies have found up to 72% increase in risky sexual behavior in methamphetamine users.1 This is particularly problematic as society has recently taken on the difficult and important work to re-examine the role and nature of consent in sexual activities. This falls within the larger #MeToo movement and has led to advocating for harsher sentencing of sexual offenders.
Yet simultaneously, society has also reconsidered its approach to apportioning blame on drug users.2 This shift to a more compassionate stance has resulted in a desire to treat and care for a disorder, rather than punish and condemn a poor choice. As forensic psychiatrists, we have noted this significant change. Where substance use disorders were once considered a risk factor for recidivism, they are now considered a disability that not only warrants treatment but can also diminish the share of blame one may be responsible for.
The convergence of those two societal movements often plays out in the courtroom, and in our experience when faced with those two opposing viewpoints, triers of fact (judges and juries) often favor punishing sexual offense over empathizing with an addictive disorder. While certainly not implying methamphetamine use condones sexual offense, we do posit the particular relationship between methamphetamine use and sexual activity should be explained to those entrusted with deciding guilt.
Examples of such problems are extremely common. A routine case involves IK,3 a 48-year-old male without significant history of legal problems, arrested for indecent exposure. His history of mental illness is closely intertwined with a history of substance use, leading to many psychiatric hospitalizations for methamphetamine-induced psychosis. After many hospitalizations he was placed in an assertive community treatment (ACT) team.
One day, IK is approached by an industrious drug dealer who frequents multiple board-and-cares in search for customers interested in relapsing. IK uses methamphetamine and within hours finds himself having walked miles away, naked, in the middle of an RV park. He subsequently describes the experience of unrelenting sexual desire, accompanied by ideas of reference involving billboards encouraging him to demonstrate his sexual prowess, as well as auditory hallucinations of women cheering him on. This leads to him pleasing himself publicly and his subsequent arrest.
Interviewing IK, 3 months later, he is embarrassed and apologetic. He is cognizant of the inappropriate nature of the incident and the foolishness of his actions. However, when asked whether he considers himself a sexual offender, he protests that he would never act in such a manner if not under the influence of methamphetamine. He points to his lack of significant sexual urges when sober, his lack of prior sexual offense, his lack of sexually violent offense, and his lack of unusual sexual interests.
It is unclear to us how society will or should adjudicate on such a case. It is not under the purview of forensic psychiatry to become a trier of fact. However, psychiatry should have a better working framework of how to discuss and conceptualize such situations, especially considering the dire consequences for those involved.
While any criminal conviction already has the potential to destroy a person’s life, sexual crimes bring particularly serious consequences. Entry into the national sex offender registry, in addition to carrying an unshakable stigma, comes with additional degrees of lost freedom. These individuals are prohibited from living or working in areas that have children in proximity, subjecting them to the outskirts of society and greatly restricting any chance of economic escape from poverty. Parks, libraries, and shopping malls can become off limits. Privacy for these individuals is nonexistent; from websites they visit to where they travel physically can be monitored. Even where they live and a detailed physical description are often easily accessible by members of their community.
When should it be permissible to consider sex offender status for someone on the grounds of a mental illness? A patient with obsessive-compulsive disorder might have sadistic obsessions and compulsions to commit violent sexual acts, which, along with being repugnant to society, are entirely ego-dystonic to the suffering patient. Psychosis is often characterized as involving a loss of insight and impaired reality testing. If society accepts insanity as grounds to mitigate sentencing, then why not permit it for grounds to wave the designation of sex offender to those with certain disorders, including substance use disorder? Wherever we come down on this issue,
Should IK have to register as a sex offender? Regardless of the circumstances, he did publicly masturbate. Society has determined that public sexual displays are a crime worth carrying the pariah status of sex offender – why should an exception be made for methamphetamine use? On the other hand, it is difficult to claim that IK’s behavior was entirely of his own free will. Most triers of fact will have never experienced that amount of dopamine reward. They can’t attest to the remaining free will after experiencing more pleasurable salience and positive reinforcement than ever naturally possible.
How we deal with the behavioral consequences, and other sequelae, of methamphetamine use is a growing problem. Access to and use of methamphetamine is no longer reserved for soldiers patrolling the jungles of Vietnam. Once thought to be a scourge of the West Coast, methamphetamine is now widely available throughout the United States.4 The use of methamphetamine is likely to continue to expand as society keeps pursuing the decriminalizing of drug use. Psychiatrists practicing in areas heavily affected by methamphetamine see firsthand the burden it places on community resources in the form of increased psychosis, emergency room utilization, medical resource strain, and encounters with police.5
The presence of mental illness is tied to a small but statistically significant risk of violence. However, substance use is a well-established risk factor for violence.6 What is often missed is that many sexual offenders have not committed a violent offense. However, like IK, they have been charged with indecent exposure or other nonviolent sexual offenses, such as prostitution and solicitation. Those nonviolent offenses are driven by poor judgment and impulsivity, the trademarks of substance use. The answer cannot be to incarcerate, and eventually add to the sex offender registry, the growing number of these individuals.
Yet, as psychiatrists, we seem at a loss for how to treat these patients. The prescription of allowing them to spend a night in the ED with a complementary sandwich garnished with olanzapine often feels like enabling. Substance use treatment programs are too limited, and the wait list is rarely shorter than the time it takes our patient to purchase their next hit.
There are no effective pharmacologic treatments for methamphetamine use disorder.7 The recommendations of cognitive-behavioral therapy, family and group therapy, contingency management, and a 12-step program may be sufficient for the most motivated and well-supported patients but are inadequate for the vast majority.8 As much as we want to laud the merits of community psychiatry and the ACT [assertive community treatment] model of care, it is hard to carry that banner while confronted with the reality these patients face on a day-to-day basis during any shift in the emergency room. Eventually the countless encounters with homeless, helplessly meth-addicted patients ending in discharge back to the streets begins to tarnish the bright rhetoric surrounding community care, which starts to sound more and more like abandonment of patients to suffer in futility.9
It is not up to forensic psychiatrists, or even psychiatry as a whole, to fix the myriad of inadequacies surrounding how society handles those suffering from methamphetamine addiction. However, it is essential for psychiatry to study and educate society on the interaction of methamphetamine use and sexual behavior. There has been some exploration into other risk factors for paraphilic behavior while under the influence of substances, but there is a dearth of information on this topic. Establishing a nomenclature called “substance-induced paraphilia” might be a way to bring clarity to such instances in both a forensic and general psychiatric setting.
Dr. Compton is a psychiatry resident at University of California, San Diego. His background includes medical education, mental health advocacy, work with underserved populations, and brain cancer research. Dr. Compton has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Psychol Addict Behav. 2016;30(2)147-57.
2. Monitor Psychol. 2019;50(6).
3. IK’s case has been modified in certain ways to maintain confidentiality.
4. J Psychoactive Drugs. 2000;(2):137-41.
5. Acad Emerg Med. 2020 Nov;27(11):1116-25.
6. Swanson JW. Mental disorder, substance abuse, and community violence: An epidemiological approach, in: Monahan J and Steadman HJ, eds. “Violence and Mental Disorder: Developments in Risk Assessment” (Chicago: University of Chicago Press, 1994, pp. 101-36).
7. Addiction. 2004 Jun;99(6)708-17.
8. Am Fam Physician. 2007 Oct 15;76(8):1169-74.
9. Perspect Biol Med. 2021;64(1)70-81.
The dopamine receptors of the brain get their fair share amid the didactics we receive in residency. From discussions of antipsychotics and schizophrenia to stimulants and ADHD, dopamine plays a key role. Depending on the program and interest of faculty, methamphetamine may get its own lecture or be mixed in with other stimulants of abuse. During that discussion, a comment might be made in passing on the impact of methamphetamine on sexual desire and activity.
Experiences in the emergency department caring for patients who are intoxicated from methamphetamine then effectively make up for any gaps in trainees’ knowledge base. From patients engaging in self-pleasing pursuits in the emergency room to unfiltered reports of sexual exploits and desires, the impact of methamphetamine on sexual behavior quickly becomes apparent. Those experiences are later reinforced when residents are exposed to more long-term rehabilitation programs and have more in-depth conversations with patients about the sex-culture surrounding methamphetamine.
It is common to hear that, under the influence of methamphetamine, any available body will become an acceptable sexual partner – at times resulting in significant regrets, dangerous sexual activity, and complicated questions surrounding consent. Some early studies have found up to 72% increase in risky sexual behavior in methamphetamine users.1 This is particularly problematic as society has recently taken on the difficult and important work to re-examine the role and nature of consent in sexual activities. This falls within the larger #MeToo movement and has led to advocating for harsher sentencing of sexual offenders.
Yet simultaneously, society has also reconsidered its approach to apportioning blame on drug users.2 This shift to a more compassionate stance has resulted in a desire to treat and care for a disorder, rather than punish and condemn a poor choice. As forensic psychiatrists, we have noted this significant change. Where substance use disorders were once considered a risk factor for recidivism, they are now considered a disability that not only warrants treatment but can also diminish the share of blame one may be responsible for.
The convergence of those two societal movements often plays out in the courtroom, and in our experience when faced with those two opposing viewpoints, triers of fact (judges and juries) often favor punishing sexual offense over empathizing with an addictive disorder. While certainly not implying methamphetamine use condones sexual offense, we do posit the particular relationship between methamphetamine use and sexual activity should be explained to those entrusted with deciding guilt.
Examples of such problems are extremely common. A routine case involves IK,3 a 48-year-old male without significant history of legal problems, arrested for indecent exposure. His history of mental illness is closely intertwined with a history of substance use, leading to many psychiatric hospitalizations for methamphetamine-induced psychosis. After many hospitalizations he was placed in an assertive community treatment (ACT) team.
One day, IK is approached by an industrious drug dealer who frequents multiple board-and-cares in search for customers interested in relapsing. IK uses methamphetamine and within hours finds himself having walked miles away, naked, in the middle of an RV park. He subsequently describes the experience of unrelenting sexual desire, accompanied by ideas of reference involving billboards encouraging him to demonstrate his sexual prowess, as well as auditory hallucinations of women cheering him on. This leads to him pleasing himself publicly and his subsequent arrest.
Interviewing IK, 3 months later, he is embarrassed and apologetic. He is cognizant of the inappropriate nature of the incident and the foolishness of his actions. However, when asked whether he considers himself a sexual offender, he protests that he would never act in such a manner if not under the influence of methamphetamine. He points to his lack of significant sexual urges when sober, his lack of prior sexual offense, his lack of sexually violent offense, and his lack of unusual sexual interests.
It is unclear to us how society will or should adjudicate on such a case. It is not under the purview of forensic psychiatry to become a trier of fact. However, psychiatry should have a better working framework of how to discuss and conceptualize such situations, especially considering the dire consequences for those involved.
While any criminal conviction already has the potential to destroy a person’s life, sexual crimes bring particularly serious consequences. Entry into the national sex offender registry, in addition to carrying an unshakable stigma, comes with additional degrees of lost freedom. These individuals are prohibited from living or working in areas that have children in proximity, subjecting them to the outskirts of society and greatly restricting any chance of economic escape from poverty. Parks, libraries, and shopping malls can become off limits. Privacy for these individuals is nonexistent; from websites they visit to where they travel physically can be monitored. Even where they live and a detailed physical description are often easily accessible by members of their community.
When should it be permissible to consider sex offender status for someone on the grounds of a mental illness? A patient with obsessive-compulsive disorder might have sadistic obsessions and compulsions to commit violent sexual acts, which, along with being repugnant to society, are entirely ego-dystonic to the suffering patient. Psychosis is often characterized as involving a loss of insight and impaired reality testing. If society accepts insanity as grounds to mitigate sentencing, then why not permit it for grounds to wave the designation of sex offender to those with certain disorders, including substance use disorder? Wherever we come down on this issue,
Should IK have to register as a sex offender? Regardless of the circumstances, he did publicly masturbate. Society has determined that public sexual displays are a crime worth carrying the pariah status of sex offender – why should an exception be made for methamphetamine use? On the other hand, it is difficult to claim that IK’s behavior was entirely of his own free will. Most triers of fact will have never experienced that amount of dopamine reward. They can’t attest to the remaining free will after experiencing more pleasurable salience and positive reinforcement than ever naturally possible.
How we deal with the behavioral consequences, and other sequelae, of methamphetamine use is a growing problem. Access to and use of methamphetamine is no longer reserved for soldiers patrolling the jungles of Vietnam. Once thought to be a scourge of the West Coast, methamphetamine is now widely available throughout the United States.4 The use of methamphetamine is likely to continue to expand as society keeps pursuing the decriminalizing of drug use. Psychiatrists practicing in areas heavily affected by methamphetamine see firsthand the burden it places on community resources in the form of increased psychosis, emergency room utilization, medical resource strain, and encounters with police.5
The presence of mental illness is tied to a small but statistically significant risk of violence. However, substance use is a well-established risk factor for violence.6 What is often missed is that many sexual offenders have not committed a violent offense. However, like IK, they have been charged with indecent exposure or other nonviolent sexual offenses, such as prostitution and solicitation. Those nonviolent offenses are driven by poor judgment and impulsivity, the trademarks of substance use. The answer cannot be to incarcerate, and eventually add to the sex offender registry, the growing number of these individuals.
Yet, as psychiatrists, we seem at a loss for how to treat these patients. The prescription of allowing them to spend a night in the ED with a complementary sandwich garnished with olanzapine often feels like enabling. Substance use treatment programs are too limited, and the wait list is rarely shorter than the time it takes our patient to purchase their next hit.
There are no effective pharmacologic treatments for methamphetamine use disorder.7 The recommendations of cognitive-behavioral therapy, family and group therapy, contingency management, and a 12-step program may be sufficient for the most motivated and well-supported patients but are inadequate for the vast majority.8 As much as we want to laud the merits of community psychiatry and the ACT [assertive community treatment] model of care, it is hard to carry that banner while confronted with the reality these patients face on a day-to-day basis during any shift in the emergency room. Eventually the countless encounters with homeless, helplessly meth-addicted patients ending in discharge back to the streets begins to tarnish the bright rhetoric surrounding community care, which starts to sound more and more like abandonment of patients to suffer in futility.9
It is not up to forensic psychiatrists, or even psychiatry as a whole, to fix the myriad of inadequacies surrounding how society handles those suffering from methamphetamine addiction. However, it is essential for psychiatry to study and educate society on the interaction of methamphetamine use and sexual behavior. There has been some exploration into other risk factors for paraphilic behavior while under the influence of substances, but there is a dearth of information on this topic. Establishing a nomenclature called “substance-induced paraphilia” might be a way to bring clarity to such instances in both a forensic and general psychiatric setting.
Dr. Compton is a psychiatry resident at University of California, San Diego. His background includes medical education, mental health advocacy, work with underserved populations, and brain cancer research. Dr. Compton has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Psychol Addict Behav. 2016;30(2)147-57.
2. Monitor Psychol. 2019;50(6).
3. IK’s case has been modified in certain ways to maintain confidentiality.
4. J Psychoactive Drugs. 2000;(2):137-41.
5. Acad Emerg Med. 2020 Nov;27(11):1116-25.
6. Swanson JW. Mental disorder, substance abuse, and community violence: An epidemiological approach, in: Monahan J and Steadman HJ, eds. “Violence and Mental Disorder: Developments in Risk Assessment” (Chicago: University of Chicago Press, 1994, pp. 101-36).
7. Addiction. 2004 Jun;99(6)708-17.
8. Am Fam Physician. 2007 Oct 15;76(8):1169-74.
9. Perspect Biol Med. 2021;64(1)70-81.
‘substance-induced paraphilia?’
‘substance-induced paraphilia?’
Changing terminology in LGBTQ+ spaces: How to keep up with the lingo
For those of us who see adolescent patients on a regular basis, it seems that they use new vocabulary almost every day. While you may not need to know what “lit” means, you probably do need to understand terms used to describe your patients’ identities. At times it feels like we, as providers, have to be on TikTok to keep up with our patients, and while this may be an amusing way to educate ourselves, a judicious Google search can be much more helpful. The interesting part about LGBTQ+ terminology is that it stems from the community and thus is frequently updated to reflect our evolving understanding of gender, sexuality, and identity. That being said, it can make it difficult for those who are not plugged in to the community to keep up to date. While we have learned in medicine to use accurate terminology and appropriate three-letter acronyms (or “TLAs” as one of my residents referenced them when I was a medical student) to describe medical conditions, the LGBTQ+ community has its own set of terms and acronyms. These new words may seem daunting, but they are often based in Latin roots or prefixes such as a-, demi-, poly-, and pan-, which may be familiar to those of us who use plenty of other Latin-based terms in medicine and our everyday lives. By paying attention to how people define and use terminology, we can better recognize their true identities and become better providers.
The first, and perhaps most important, piece of advice is to maintain cultural humility. Know when to admit you don’t recognize a term and politely ask the definition. For example, the first time I heard the term “demiboy” I said “I’m not familiar with that word. Can you explain what it means to you?” Phrasing the question as such is also helpful in that it gives the individuals a chance to really define their identity. In addition, some words may be used differently by various individuals and by asking what the word means to them, you can have a better understanding of how they are using the terminology. In this particular instance, the patient felt more masculine, but not 100%, partway between agender (meaning having no gender identity) and being “all male.” By embracing cultural humility, we place the patients in the role of expert on their own identity and orientation. According to Maria Ruud, DNP, of the University of Minnesota, Minneapolis, cultural humility is the “ongoing self-reflection and education …[seeking] to gain an awareness of their own assumptions and biases that may contribute to health disparities.”1

Another reason it is important to keep up on the language is that some adolescents, particularly younger adolescents, may not be using the terminology correctly. It can be very helpful to know the difference between polyamorous and pansexual when a 12-year-old describes themselves as polyamorous (having consenting, nonmonogamous relationships) but provides the definition for pansexual (being attracted to all gender identities). Yes, this has happened to me, and yes, my resident was appropriately confused. Correcting someone else’s vocabulary can be tricky and even inappropriate or condescending; therefore, tread cautiously. It may be appropriate, however, to correct colleagues’ or even patients’ family members’ language if they are using terms that may be hurtful to your patients. I do not allow slurs in my clinic, and when parents are using incorrect pronouns on purpose, I will often let them know that it is my job to respect their child’s identity where it is in the moment and that they have asked me to use specific pronouns, so I will continue to refer to their child with those pronouns. Reflecting the language of the patient can be a powerful statement providing them with the autonomy that they deserve as burgeoning adults navigating the complicated journey of identity.
As providers who often have to defend ourselves against “Dr. Google,” we may be leery of just searching randomly for the definition of a new word and hoping a site is credible. One site that I have used repeatedly is www.itspronouncedmetrosexual.com by Sam Killermann,2 a gender and sexuality educator.
Mr. Killermann has also produced an E-book that is regularly updated to reflect changing terminology, which can be obtained for a small donation. As Mr. Killermann explains, “New language can be intimidating, and the language of gender and sexuality is often that.”3 In reality, the definitions aren’t scary and often the words can describe something you already know exists but didn’t recognize had a specific term. Not everyone can know every term and its definition; in fact, many members of the LGBTQ+ community don’t know or even understand every term. Below is a shortened list with some of the more common terms you may encounter; however, individuals may use them differently so it is never out of place to clarify your understanding of the term’s definition.
With these resources, along with cultural humility and reflection of others’ language, we can all start to have more meaningful conversations with our patients around their identity and relationships with others.
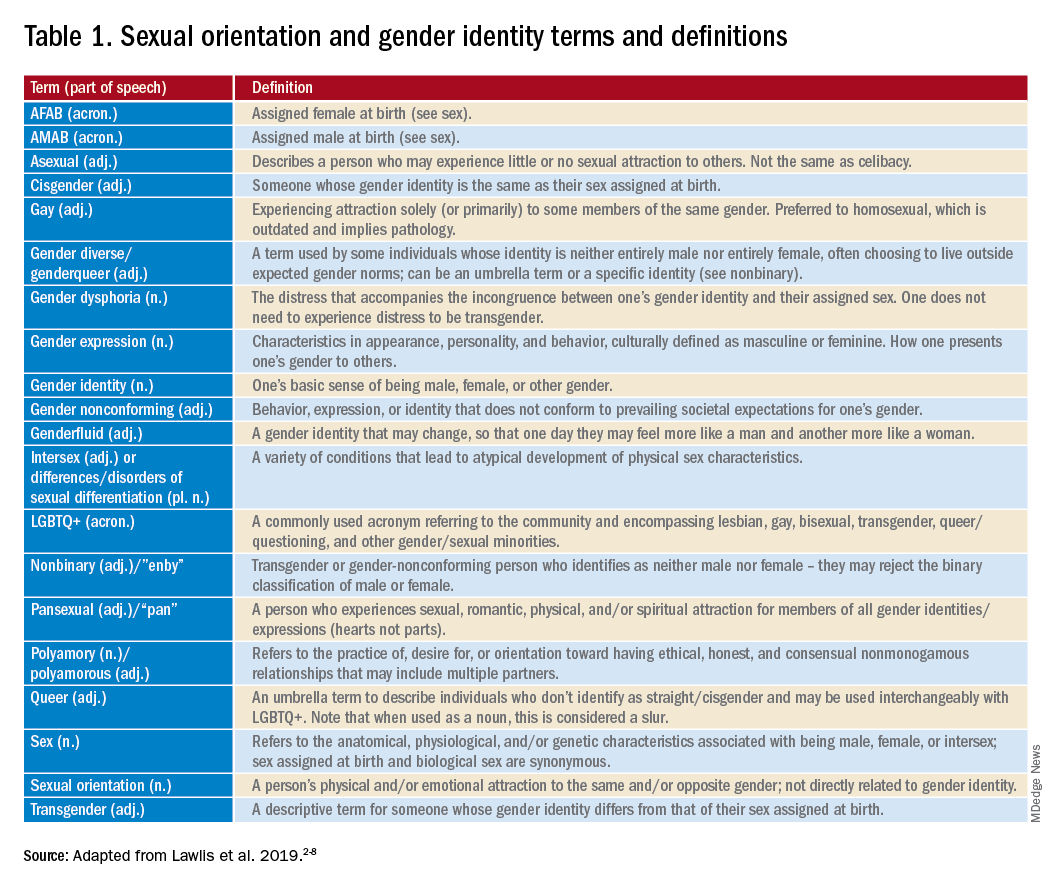
Dr. Lawlis is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures. Email her at [email protected].
References
1. Ruud M. Nursing for women’s health. 2018;22(3):255-63.
2. Killermann S. It’s Pronounced Metrosexual. 2020.
3. Killermann S. Defining LGBTQ+: A guide to gender and sexuality terminology. 2019, Feb 25.
4. The Joint Commission. Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Oak Brook, Ill. 2011.
5. LGBT health disparities. American Psychiatric Association Public Interest Government Relations Office. 2013 May.
6. Lawlis S et al. Health services for LGBTQ+ patients. Psychiatr Ann. 2019;49(10):426-35.
7. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
8. Center of Excellence for Transgender Health, department of family and community medicine, UCSF. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2016 Jun 17.
For those of us who see adolescent patients on a regular basis, it seems that they use new vocabulary almost every day. While you may not need to know what “lit” means, you probably do need to understand terms used to describe your patients’ identities. At times it feels like we, as providers, have to be on TikTok to keep up with our patients, and while this may be an amusing way to educate ourselves, a judicious Google search can be much more helpful. The interesting part about LGBTQ+ terminology is that it stems from the community and thus is frequently updated to reflect our evolving understanding of gender, sexuality, and identity. That being said, it can make it difficult for those who are not plugged in to the community to keep up to date. While we have learned in medicine to use accurate terminology and appropriate three-letter acronyms (or “TLAs” as one of my residents referenced them when I was a medical student) to describe medical conditions, the LGBTQ+ community has its own set of terms and acronyms. These new words may seem daunting, but they are often based in Latin roots or prefixes such as a-, demi-, poly-, and pan-, which may be familiar to those of us who use plenty of other Latin-based terms in medicine and our everyday lives. By paying attention to how people define and use terminology, we can better recognize their true identities and become better providers.
The first, and perhaps most important, piece of advice is to maintain cultural humility. Know when to admit you don’t recognize a term and politely ask the definition. For example, the first time I heard the term “demiboy” I said “I’m not familiar with that word. Can you explain what it means to you?” Phrasing the question as such is also helpful in that it gives the individuals a chance to really define their identity. In addition, some words may be used differently by various individuals and by asking what the word means to them, you can have a better understanding of how they are using the terminology. In this particular instance, the patient felt more masculine, but not 100%, partway between agender (meaning having no gender identity) and being “all male.” By embracing cultural humility, we place the patients in the role of expert on their own identity and orientation. According to Maria Ruud, DNP, of the University of Minnesota, Minneapolis, cultural humility is the “ongoing self-reflection and education …[seeking] to gain an awareness of their own assumptions and biases that may contribute to health disparities.”1
Another reason it is important to keep up on the language is that some adolescents, particularly younger adolescents, may not be using the terminology correctly. It can be very helpful to know the difference between polyamorous and pansexual when a 12-year-old describes themselves as polyamorous (having consenting, nonmonogamous relationships) but provides the definition for pansexual (being attracted to all gender identities). Yes, this has happened to me, and yes, my resident was appropriately confused. Correcting someone else’s vocabulary can be tricky and even inappropriate or condescending; therefore, tread cautiously. It may be appropriate, however, to correct colleagues’ or even patients’ family members’ language if they are using terms that may be hurtful to your patients. I do not allow slurs in my clinic, and when parents are using incorrect pronouns on purpose, I will often let them know that it is my job to respect their child’s identity where it is in the moment and that they have asked me to use specific pronouns, so I will continue to refer to their child with those pronouns. Reflecting the language of the patient can be a powerful statement providing them with the autonomy that they deserve as burgeoning adults navigating the complicated journey of identity.
As providers who often have to defend ourselves against “Dr. Google,” we may be leery of just searching randomly for the definition of a new word and hoping a site is credible. One site that I have used repeatedly is www.itspronouncedmetrosexual.com by Sam Killermann,2 a gender and sexuality educator.
Mr. Killermann has also produced an E-book that is regularly updated to reflect changing terminology, which can be obtained for a small donation. As Mr. Killermann explains, “New language can be intimidating, and the language of gender and sexuality is often that.”3 In reality, the definitions aren’t scary and often the words can describe something you already know exists but didn’t recognize had a specific term. Not everyone can know every term and its definition; in fact, many members of the LGBTQ+ community don’t know or even understand every term. Below is a shortened list with some of the more common terms you may encounter; however, individuals may use them differently so it is never out of place to clarify your understanding of the term’s definition.
With these resources, along with cultural humility and reflection of others’ language, we can all start to have more meaningful conversations with our patients around their identity and relationships with others.
Dr. Lawlis is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures. Email her at [email protected].
References
1. Ruud M. Nursing for women’s health. 2018;22(3):255-63.
2. Killermann S. It’s Pronounced Metrosexual. 2020.
3. Killermann S. Defining LGBTQ+: A guide to gender and sexuality terminology. 2019, Feb 25.
4. The Joint Commission. Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Oak Brook, Ill. 2011.
5. LGBT health disparities. American Psychiatric Association Public Interest Government Relations Office. 2013 May.
6. Lawlis S et al. Health services for LGBTQ+ patients. Psychiatr Ann. 2019;49(10):426-35.
7. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
8. Center of Excellence for Transgender Health, department of family and community medicine, UCSF. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2016 Jun 17.
For those of us who see adolescent patients on a regular basis, it seems that they use new vocabulary almost every day. While you may not need to know what “lit” means, you probably do need to understand terms used to describe your patients’ identities. At times it feels like we, as providers, have to be on TikTok to keep up with our patients, and while this may be an amusing way to educate ourselves, a judicious Google search can be much more helpful. The interesting part about LGBTQ+ terminology is that it stems from the community and thus is frequently updated to reflect our evolving understanding of gender, sexuality, and identity. That being said, it can make it difficult for those who are not plugged in to the community to keep up to date. While we have learned in medicine to use accurate terminology and appropriate three-letter acronyms (or “TLAs” as one of my residents referenced them when I was a medical student) to describe medical conditions, the LGBTQ+ community has its own set of terms and acronyms. These new words may seem daunting, but they are often based in Latin roots or prefixes such as a-, demi-, poly-, and pan-, which may be familiar to those of us who use plenty of other Latin-based terms in medicine and our everyday lives. By paying attention to how people define and use terminology, we can better recognize their true identities and become better providers.
The first, and perhaps most important, piece of advice is to maintain cultural humility. Know when to admit you don’t recognize a term and politely ask the definition. For example, the first time I heard the term “demiboy” I said “I’m not familiar with that word. Can you explain what it means to you?” Phrasing the question as such is also helpful in that it gives the individuals a chance to really define their identity. In addition, some words may be used differently by various individuals and by asking what the word means to them, you can have a better understanding of how they are using the terminology. In this particular instance, the patient felt more masculine, but not 100%, partway between agender (meaning having no gender identity) and being “all male.” By embracing cultural humility, we place the patients in the role of expert on their own identity and orientation. According to Maria Ruud, DNP, of the University of Minnesota, Minneapolis, cultural humility is the “ongoing self-reflection and education …[seeking] to gain an awareness of their own assumptions and biases that may contribute to health disparities.”1
Another reason it is important to keep up on the language is that some adolescents, particularly younger adolescents, may not be using the terminology correctly. It can be very helpful to know the difference between polyamorous and pansexual when a 12-year-old describes themselves as polyamorous (having consenting, nonmonogamous relationships) but provides the definition for pansexual (being attracted to all gender identities). Yes, this has happened to me, and yes, my resident was appropriately confused. Correcting someone else’s vocabulary can be tricky and even inappropriate or condescending; therefore, tread cautiously. It may be appropriate, however, to correct colleagues’ or even patients’ family members’ language if they are using terms that may be hurtful to your patients. I do not allow slurs in my clinic, and when parents are using incorrect pronouns on purpose, I will often let them know that it is my job to respect their child’s identity where it is in the moment and that they have asked me to use specific pronouns, so I will continue to refer to their child with those pronouns. Reflecting the language of the patient can be a powerful statement providing them with the autonomy that they deserve as burgeoning adults navigating the complicated journey of identity.
As providers who often have to defend ourselves against “Dr. Google,” we may be leery of just searching randomly for the definition of a new word and hoping a site is credible. One site that I have used repeatedly is www.itspronouncedmetrosexual.com by Sam Killermann,2 a gender and sexuality educator.
Mr. Killermann has also produced an E-book that is regularly updated to reflect changing terminology, which can be obtained for a small donation. As Mr. Killermann explains, “New language can be intimidating, and the language of gender and sexuality is often that.”3 In reality, the definitions aren’t scary and often the words can describe something you already know exists but didn’t recognize had a specific term. Not everyone can know every term and its definition; in fact, many members of the LGBTQ+ community don’t know or even understand every term. Below is a shortened list with some of the more common terms you may encounter; however, individuals may use them differently so it is never out of place to clarify your understanding of the term’s definition.
With these resources, along with cultural humility and reflection of others’ language, we can all start to have more meaningful conversations with our patients around their identity and relationships with others.
Dr. Lawlis is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures. Email her at [email protected].
References
1. Ruud M. Nursing for women’s health. 2018;22(3):255-63.
2. Killermann S. It’s Pronounced Metrosexual. 2020.
3. Killermann S. Defining LGBTQ+: A guide to gender and sexuality terminology. 2019, Feb 25.
4. The Joint Commission. Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Oak Brook, Ill. 2011.
5. LGBT health disparities. American Psychiatric Association Public Interest Government Relations Office. 2013 May.
6. Lawlis S et al. Health services for LGBTQ+ patients. Psychiatr Ann. 2019;49(10):426-35.
7. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
8. Center of Excellence for Transgender Health, department of family and community medicine, UCSF. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people. 2016 Jun 17.