User login
Official Newspaper of the American College of Surgeons
Register for ACS TQIP Conference November 11−13 in Chicago
The eighth annual Trauma Quality Improvement Program (TQIP®) Scientific Meeting and Training will take place November 11−13 at the Hilton Chicago. Register online for the meeting at facs.org/tqipmeeting.
This meeting will bring together trauma medical directors, program managers, coordinators, and registrars from participating and prospective TQIP hospitals. The conference will have multiple presentations from TQIP participants highlighting how they are using the program to improve care in their hospitals. Breakout sessions focused on registrar and abstractor concerns, matters that relate to the trauma medical director, and trauma program manager-focused issues will enhance the learning experience and instruct participants about their role on the TQIP team. In addition, dedicated sessions for staff who are new to the TQIP program will take place and may be invaluable to medical centers joining TQIP in the near future.
Conference topics of note for 2017 will include TQIP Collaboratives, Pediatric TQIP, management of bleeding pelvic fractures, and the continued integration of verification, TQIP, and performance improvement and patient safety. The TQIP Best Practices project team will present on adult and pediatric imaging, followed by a discussion by a panel of experts. The keynote address will be given by Lenworth M. Jacobs, Jr., MD, MPH, FACS, Chair, Hartford Consensus Joint Committee to Enhance Survivability from Active Shooter and Intentional Mass Casualty Events.
Visit the TQIP annual meeting website at facs.org/tqipmeeting to view the conference schedule and to obtain information about lodging and transportation options.
The eighth annual Trauma Quality Improvement Program (TQIP®) Scientific Meeting and Training will take place November 11−13 at the Hilton Chicago. Register online for the meeting at facs.org/tqipmeeting.
This meeting will bring together trauma medical directors, program managers, coordinators, and registrars from participating and prospective TQIP hospitals. The conference will have multiple presentations from TQIP participants highlighting how they are using the program to improve care in their hospitals. Breakout sessions focused on registrar and abstractor concerns, matters that relate to the trauma medical director, and trauma program manager-focused issues will enhance the learning experience and instruct participants about their role on the TQIP team. In addition, dedicated sessions for staff who are new to the TQIP program will take place and may be invaluable to medical centers joining TQIP in the near future.
Conference topics of note for 2017 will include TQIP Collaboratives, Pediatric TQIP, management of bleeding pelvic fractures, and the continued integration of verification, TQIP, and performance improvement and patient safety. The TQIP Best Practices project team will present on adult and pediatric imaging, followed by a discussion by a panel of experts. The keynote address will be given by Lenworth M. Jacobs, Jr., MD, MPH, FACS, Chair, Hartford Consensus Joint Committee to Enhance Survivability from Active Shooter and Intentional Mass Casualty Events.
Visit the TQIP annual meeting website at facs.org/tqipmeeting to view the conference schedule and to obtain information about lodging and transportation options.
The eighth annual Trauma Quality Improvement Program (TQIP®) Scientific Meeting and Training will take place November 11−13 at the Hilton Chicago. Register online for the meeting at facs.org/tqipmeeting.
This meeting will bring together trauma medical directors, program managers, coordinators, and registrars from participating and prospective TQIP hospitals. The conference will have multiple presentations from TQIP participants highlighting how they are using the program to improve care in their hospitals. Breakout sessions focused on registrar and abstractor concerns, matters that relate to the trauma medical director, and trauma program manager-focused issues will enhance the learning experience and instruct participants about their role on the TQIP team. In addition, dedicated sessions for staff who are new to the TQIP program will take place and may be invaluable to medical centers joining TQIP in the near future.
Conference topics of note for 2017 will include TQIP Collaboratives, Pediatric TQIP, management of bleeding pelvic fractures, and the continued integration of verification, TQIP, and performance improvement and patient safety. The TQIP Best Practices project team will present on adult and pediatric imaging, followed by a discussion by a panel of experts. The keynote address will be given by Lenworth M. Jacobs, Jr., MD, MPH, FACS, Chair, Hartford Consensus Joint Committee to Enhance Survivability from Active Shooter and Intentional Mass Casualty Events.
Visit the TQIP annual meeting website at facs.org/tqipmeeting to view the conference schedule and to obtain information about lodging and transportation options.
Dr. Ronald Maier Awarded Prize of the “Société Internationale de Chirurgie”
Ronald V. Maier, MD, FACS, FRCSEd(Hon), Past-First Vice-President of the American College of Surgeons (ACS), received the prestigious Prize of the “Société Internationale de Chirurgie” at the 47th Annual World Congress of Surgery in Basel, Switzerland. The prize is awarded to “the surgeon who has published work which has made the most notable and useful contributions to surgical science.” Read more about the Prize of the “Société Internationale de Chirurgie” on the International Society of Surgery/Société Internationale de Chirurgie website.

Throughout his career, Dr. Maier has been interested in the critically ill surgical patient, focusing on the underlying pathophysiology driving the aberrant host immuno-inflammatory response, and subsequent clinical syndrome of multiple organ failure with its attendant high morbidity and mortality. He has received funding continuously from the National Institutes of Health (NIH) since 1981 and has been a member and Chair of the NIH Surgery, Anesthesiology and Trauma Study Section. His interest in trauma has also involved extensive clinical studies of the acute management of the severely injured and critically ill patient. Dr. Maier has presented his work worldwide, and has delivered more than 400 lectures on trauma, critical care, and surgical immunology. He has published more than 400 peer-reviewed articles, and contributed to or co-authored more than 60 book chapters.
Ronald V. Maier, MD, FACS, FRCSEd(Hon), Past-First Vice-President of the American College of Surgeons (ACS), received the prestigious Prize of the “Société Internationale de Chirurgie” at the 47th Annual World Congress of Surgery in Basel, Switzerland. The prize is awarded to “the surgeon who has published work which has made the most notable and useful contributions to surgical science.” Read more about the Prize of the “Société Internationale de Chirurgie” on the International Society of Surgery/Société Internationale de Chirurgie website.
Throughout his career, Dr. Maier has been interested in the critically ill surgical patient, focusing on the underlying pathophysiology driving the aberrant host immuno-inflammatory response, and subsequent clinical syndrome of multiple organ failure with its attendant high morbidity and mortality. He has received funding continuously from the National Institutes of Health (NIH) since 1981 and has been a member and Chair of the NIH Surgery, Anesthesiology and Trauma Study Section. His interest in trauma has also involved extensive clinical studies of the acute management of the severely injured and critically ill patient. Dr. Maier has presented his work worldwide, and has delivered more than 400 lectures on trauma, critical care, and surgical immunology. He has published more than 400 peer-reviewed articles, and contributed to or co-authored more than 60 book chapters.
Ronald V. Maier, MD, FACS, FRCSEd(Hon), Past-First Vice-President of the American College of Surgeons (ACS), received the prestigious Prize of the “Société Internationale de Chirurgie” at the 47th Annual World Congress of Surgery in Basel, Switzerland. The prize is awarded to “the surgeon who has published work which has made the most notable and useful contributions to surgical science.” Read more about the Prize of the “Société Internationale de Chirurgie” on the International Society of Surgery/Société Internationale de Chirurgie website.
Throughout his career, Dr. Maier has been interested in the critically ill surgical patient, focusing on the underlying pathophysiology driving the aberrant host immuno-inflammatory response, and subsequent clinical syndrome of multiple organ failure with its attendant high morbidity and mortality. He has received funding continuously from the National Institutes of Health (NIH) since 1981 and has been a member and Chair of the NIH Surgery, Anesthesiology and Trauma Study Section. His interest in trauma has also involved extensive clinical studies of the acute management of the severely injured and critically ill patient. Dr. Maier has presented his work worldwide, and has delivered more than 400 lectures on trauma, critical care, and surgical immunology. He has published more than 400 peer-reviewed articles, and contributed to or co-authored more than 60 book chapters.
From the Editors: Hanging up the scalpel
The decision to stop practicing surgery is a monumental one when you have been a surgeon for almost 40 years, have loved operating, and have defined yourself by the word “surgeon.”
The decision to cease operating should at best be a personal one that the surgeon makes, rather than one imposed by others. The “others” could be an institutional policy mandating retirement at a given age, the results of a series of psychomotor examinations, or even a kind department chair’s suggestion that you should stop operating because your complications have increased and it is in your patients’ best interests. As we approach “a certain age,” I suspect that most surgeons would prefer to decide their own fate and, especially, to avoid the last of the three above options.

Literature is emerging about the aging physician and how best the decisions should be made about ceasing practice. A recent such article published online by some dear and respected colleagues (JAMA Surg. 2017 July 19;doi:10.1001/jamasurg.2017.2342) proposes that institutions and professional organizations develop policies to address the aging physician that leave “flexibility to customize the approach” lest regulators and legislators impose “more draconian measures.” Their suggestions include mandatory cognitive evaluation, voluntary annual physical examinations, and confidential peer evaluations of wellness and competence as physicians reach a certain (unspecified) age.
I most certainly concur with the authors’ well-reasoned arguments. As they relate, only a handful of institutions to date have developed policies that require assessments of physician wellness and competence at a given age. Most institutions still rely on physicians’ voluntary submission to physical examinations, cognitive testing, or peer referral of a colleague if declining function is observed. Yet we all know that individuals tend to overlook signs of declining physical and cognitive function both in themselves and in colleagues. Moreover, we all know that even the most carefully designed and implemented tests have shortcomings and may fail to identify the exact nature of an individual’s malady or fail to identify a remediable issue early. And just as individuals’ physical and cognitive abilities decline at different chronological ages, problems with burnout, mental illness, and substance abuse have no reliable age threshold and may be difficult to diagnose accurately.
Whatever the age of the individual, it is critical that a decline in function of a practitioner be addressed promptly and effectively, for the benefit of the affected individual, his or her patients, and the institution. It is therefore most appropriate for every institution to develop a firm policy to deal with concerns of competency of all staff members, regardless of age.
It is also appropriate for peers to pay attention to a colleague’s stumbles and have the courage to first initiate a dialogue directly with that person, referring the issue to an individual in authority if the direct approach fails. A culture that promotes responsible self-policing protects patients and the reputations of both the affected individual and the institution.
Most of us with “seniority” will recall situations during our training when surgeons with diminished physical or cognitive capacity continued operating well beyond their prime. In those days, it was not unusual for a chief resident to be told, “Your job is to scrub with Dr. X and keep him out of trouble.” As inappropriate as that was, we complied, all the while vowing that we would never let ourselves be in the same position when we aged.
It therefore became my habit as I aged to “listen to my body” and pay attention to evidence that my skills might be declining and perhaps it was time to hang up the scalpel. As an almost lifelong runner, I marked my athletic decline by noting an increase in minutes per mile from 7 to 14 over 40 years and wondered whether my cognitive decline might be comparable, if not so obvious. I had to admit to a bit of lost hand dexterity, less sharpness of eyesight, and slowed memory for the names of people and even of surgical instruments. Although I believed that my diagnostic acumen and decisions were unaffected, I weathered a sleepless night on call less well, requiring two or more full nights of eight hours’ sleep to recover my energy completely.
Part of the reluctance to cease surgical practice that I share with many colleagues my age is the fear of becoming irrelevant and unproductive. It was therefore critical to prepare for retirement from practice by identifying activities that I considered both meaningful and also challenging: writing and editing, teaching students and residents in surgical skills labs, teaching residents “open” surgical techniques on cadavers, advising younger colleagues when they have a challenging case in my area of expertise, and filling a myriad of needs in our department that match my skill set but that my younger counterparts are too busy to attend to.
I now also have the freedom to pursue activities for which I had little time during the years of intense practice, including service on nonprofit boards and other community activities. There may even come a day when my definition of self has fully accepted the word “retired,” even though I hope that day is many years in the future.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The decision to stop practicing surgery is a monumental one when you have been a surgeon for almost 40 years, have loved operating, and have defined yourself by the word “surgeon.”
The decision to cease operating should at best be a personal one that the surgeon makes, rather than one imposed by others. The “others” could be an institutional policy mandating retirement at a given age, the results of a series of psychomotor examinations, or even a kind department chair’s suggestion that you should stop operating because your complications have increased and it is in your patients’ best interests. As we approach “a certain age,” I suspect that most surgeons would prefer to decide their own fate and, especially, to avoid the last of the three above options.
Literature is emerging about the aging physician and how best the decisions should be made about ceasing practice. A recent such article published online by some dear and respected colleagues (JAMA Surg. 2017 July 19;doi:10.1001/jamasurg.2017.2342) proposes that institutions and professional organizations develop policies to address the aging physician that leave “flexibility to customize the approach” lest regulators and legislators impose “more draconian measures.” Their suggestions include mandatory cognitive evaluation, voluntary annual physical examinations, and confidential peer evaluations of wellness and competence as physicians reach a certain (unspecified) age.
I most certainly concur with the authors’ well-reasoned arguments. As they relate, only a handful of institutions to date have developed policies that require assessments of physician wellness and competence at a given age. Most institutions still rely on physicians’ voluntary submission to physical examinations, cognitive testing, or peer referral of a colleague if declining function is observed. Yet we all know that individuals tend to overlook signs of declining physical and cognitive function both in themselves and in colleagues. Moreover, we all know that even the most carefully designed and implemented tests have shortcomings and may fail to identify the exact nature of an individual’s malady or fail to identify a remediable issue early. And just as individuals’ physical and cognitive abilities decline at different chronological ages, problems with burnout, mental illness, and substance abuse have no reliable age threshold and may be difficult to diagnose accurately.
Whatever the age of the individual, it is critical that a decline in function of a practitioner be addressed promptly and effectively, for the benefit of the affected individual, his or her patients, and the institution. It is therefore most appropriate for every institution to develop a firm policy to deal with concerns of competency of all staff members, regardless of age.
It is also appropriate for peers to pay attention to a colleague’s stumbles and have the courage to first initiate a dialogue directly with that person, referring the issue to an individual in authority if the direct approach fails. A culture that promotes responsible self-policing protects patients and the reputations of both the affected individual and the institution.
Most of us with “seniority” will recall situations during our training when surgeons with diminished physical or cognitive capacity continued operating well beyond their prime. In those days, it was not unusual for a chief resident to be told, “Your job is to scrub with Dr. X and keep him out of trouble.” As inappropriate as that was, we complied, all the while vowing that we would never let ourselves be in the same position when we aged.
It therefore became my habit as I aged to “listen to my body” and pay attention to evidence that my skills might be declining and perhaps it was time to hang up the scalpel. As an almost lifelong runner, I marked my athletic decline by noting an increase in minutes per mile from 7 to 14 over 40 years and wondered whether my cognitive decline might be comparable, if not so obvious. I had to admit to a bit of lost hand dexterity, less sharpness of eyesight, and slowed memory for the names of people and even of surgical instruments. Although I believed that my diagnostic acumen and decisions were unaffected, I weathered a sleepless night on call less well, requiring two or more full nights of eight hours’ sleep to recover my energy completely.
Part of the reluctance to cease surgical practice that I share with many colleagues my age is the fear of becoming irrelevant and unproductive. It was therefore critical to prepare for retirement from practice by identifying activities that I considered both meaningful and also challenging: writing and editing, teaching students and residents in surgical skills labs, teaching residents “open” surgical techniques on cadavers, advising younger colleagues when they have a challenging case in my area of expertise, and filling a myriad of needs in our department that match my skill set but that my younger counterparts are too busy to attend to.
I now also have the freedom to pursue activities for which I had little time during the years of intense practice, including service on nonprofit boards and other community activities. There may even come a day when my definition of self has fully accepted the word “retired,” even though I hope that day is many years in the future.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The decision to stop practicing surgery is a monumental one when you have been a surgeon for almost 40 years, have loved operating, and have defined yourself by the word “surgeon.”
The decision to cease operating should at best be a personal one that the surgeon makes, rather than one imposed by others. The “others” could be an institutional policy mandating retirement at a given age, the results of a series of psychomotor examinations, or even a kind department chair’s suggestion that you should stop operating because your complications have increased and it is in your patients’ best interests. As we approach “a certain age,” I suspect that most surgeons would prefer to decide their own fate and, especially, to avoid the last of the three above options.
Literature is emerging about the aging physician and how best the decisions should be made about ceasing practice. A recent such article published online by some dear and respected colleagues (JAMA Surg. 2017 July 19;doi:10.1001/jamasurg.2017.2342) proposes that institutions and professional organizations develop policies to address the aging physician that leave “flexibility to customize the approach” lest regulators and legislators impose “more draconian measures.” Their suggestions include mandatory cognitive evaluation, voluntary annual physical examinations, and confidential peer evaluations of wellness and competence as physicians reach a certain (unspecified) age.
I most certainly concur with the authors’ well-reasoned arguments. As they relate, only a handful of institutions to date have developed policies that require assessments of physician wellness and competence at a given age. Most institutions still rely on physicians’ voluntary submission to physical examinations, cognitive testing, or peer referral of a colleague if declining function is observed. Yet we all know that individuals tend to overlook signs of declining physical and cognitive function both in themselves and in colleagues. Moreover, we all know that even the most carefully designed and implemented tests have shortcomings and may fail to identify the exact nature of an individual’s malady or fail to identify a remediable issue early. And just as individuals’ physical and cognitive abilities decline at different chronological ages, problems with burnout, mental illness, and substance abuse have no reliable age threshold and may be difficult to diagnose accurately.
Whatever the age of the individual, it is critical that a decline in function of a practitioner be addressed promptly and effectively, for the benefit of the affected individual, his or her patients, and the institution. It is therefore most appropriate for every institution to develop a firm policy to deal with concerns of competency of all staff members, regardless of age.
It is also appropriate for peers to pay attention to a colleague’s stumbles and have the courage to first initiate a dialogue directly with that person, referring the issue to an individual in authority if the direct approach fails. A culture that promotes responsible self-policing protects patients and the reputations of both the affected individual and the institution.
Most of us with “seniority” will recall situations during our training when surgeons with diminished physical or cognitive capacity continued operating well beyond their prime. In those days, it was not unusual for a chief resident to be told, “Your job is to scrub with Dr. X and keep him out of trouble.” As inappropriate as that was, we complied, all the while vowing that we would never let ourselves be in the same position when we aged.
It therefore became my habit as I aged to “listen to my body” and pay attention to evidence that my skills might be declining and perhaps it was time to hang up the scalpel. As an almost lifelong runner, I marked my athletic decline by noting an increase in minutes per mile from 7 to 14 over 40 years and wondered whether my cognitive decline might be comparable, if not so obvious. I had to admit to a bit of lost hand dexterity, less sharpness of eyesight, and slowed memory for the names of people and even of surgical instruments. Although I believed that my diagnostic acumen and decisions were unaffected, I weathered a sleepless night on call less well, requiring two or more full nights of eight hours’ sleep to recover my energy completely.
Part of the reluctance to cease surgical practice that I share with many colleagues my age is the fear of becoming irrelevant and unproductive. It was therefore critical to prepare for retirement from practice by identifying activities that I considered both meaningful and also challenging: writing and editing, teaching students and residents in surgical skills labs, teaching residents “open” surgical techniques on cadavers, advising younger colleagues when they have a challenging case in my area of expertise, and filling a myriad of needs in our department that match my skill set but that my younger counterparts are too busy to attend to.
I now also have the freedom to pursue activities for which I had little time during the years of intense practice, including service on nonprofit boards and other community activities. There may even come a day when my definition of self has fully accepted the word “retired,” even though I hope that day is many years in the future.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
From the Washington Office: Receiving an increase in Medicare payment and avoiding a penalty
We are now well over halfway through 2017, the initial year of the new Quality Payment Program (QPP) mandated by MACRA. Accordingly, I thought it might be useful to revisit the topic of the QPP and MIPS (Merit-based Incentive Payment System) for purposes of emphasizing the key steps surgeons should take if they want to potentially see an increase in their Medicare physician payment in 2019 based on their performance in 2017. At the same time, I also want to make sure that all surgeons understand the ease with which they can avoid a payment penalty.
First, I want to assure all who have yet to take any action that there is still more than adequate time to do so. You absolutely can still compete for a positive update, or at a minimum, avoid a penalty. Further, it is so easy to avoid a penalty that no surgeon should be resigned to accepting a penalty without having a look at the minimal reporting requirements necessary to avoid it.

One of the resources available on the ACS’ QPP website is an algorhythm intended to simplify surgeons’ decision making at their initial starting point. It is reproduced below:
1. Determine if all of your MIPS data will be reported by your institution or group via a Group Reporting option (GPRO).
a. If “YES,” you are done.
b. If “NO,” move to number 2.
2. Has CMS notified you that you are exempt from participating in MIPS due to the low-volume threshold?
a. If “YES,” you are done.
b. If “NO,” move to number 3.
3. If you want to compete for positive updates in your Medicare payment rates in 2019 (based on 2017 reporting), read the ACS Quality Payment Program Manual, watch the videos, and develop your plan.
4. If your goal is simply to avoid a penalty, CMS only requires data be reported for one of the following:
a. Required Base Score measures for your EHR (now known as Advancing Care Information) OR
b. One Improvement Activity for 90 days (report by attestation) OR
c. One Quality Measure on one patient (report by registry, QCDR, EHR, or claims)
Note: One is NOT required to have a certified EHR to avoid a penalty for 2017
5. If you did not report PQRS data and did not participate in the electronic health record meaningful use program in 2016 and have no intention of participating in MIPS in 2017:
a. Your lack of participation in 2016 programs will lead to a 10% negative payment adjustment in 2018.
b. Your lack of participation in MIPS in 2017 will lead to a 4% negative payment adjustment in 2019.
Note: This option is not recommended, as in future years the annual cuts will gradually increase to 9%.
MIPS is set up as a tournament model. In other words, “Losers” pay for “Winners.” Please do not put your money in someone else’s pocket. The ACS strongly encourages all Fellows to, at the minimum, participate at the level sufficient to avoid a penalty in 2017 and, thus, not serve as the “pay for” for another provider.
If you are not exempt from MIPS and therefore, one whose performance will be assessed in 2017, you still have plenty of time to start the process of reporting enough data to compete for a positive update. On the other hand, if your goal is simply to avoid a penalty in 2019, (based on your performance in 2017), you should take the few simple steps necessary to preclude such as outlined above.
We believe the QPP website, (www.facs.org/qpp), is an excellent resource for surgeons. It was designed to facilitate participation by those surgeons who must report for MIPS. As always, ACS staff are also available to answer your questions by phone or via e-mail: [email protected].
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
We are now well over halfway through 2017, the initial year of the new Quality Payment Program (QPP) mandated by MACRA. Accordingly, I thought it might be useful to revisit the topic of the QPP and MIPS (Merit-based Incentive Payment System) for purposes of emphasizing the key steps surgeons should take if they want to potentially see an increase in their Medicare physician payment in 2019 based on their performance in 2017. At the same time, I also want to make sure that all surgeons understand the ease with which they can avoid a payment penalty.
First, I want to assure all who have yet to take any action that there is still more than adequate time to do so. You absolutely can still compete for a positive update, or at a minimum, avoid a penalty. Further, it is so easy to avoid a penalty that no surgeon should be resigned to accepting a penalty without having a look at the minimal reporting requirements necessary to avoid it.
One of the resources available on the ACS’ QPP website is an algorhythm intended to simplify surgeons’ decision making at their initial starting point. It is reproduced below:
1. Determine if all of your MIPS data will be reported by your institution or group via a Group Reporting option (GPRO).
a. If “YES,” you are done.
b. If “NO,” move to number 2.
2. Has CMS notified you that you are exempt from participating in MIPS due to the low-volume threshold?
a. If “YES,” you are done.
b. If “NO,” move to number 3.
3. If you want to compete for positive updates in your Medicare payment rates in 2019 (based on 2017 reporting), read the ACS Quality Payment Program Manual, watch the videos, and develop your plan.
4. If your goal is simply to avoid a penalty, CMS only requires data be reported for one of the following:
a. Required Base Score measures for your EHR (now known as Advancing Care Information) OR
b. One Improvement Activity for 90 days (report by attestation) OR
c. One Quality Measure on one patient (report by registry, QCDR, EHR, or claims)
Note: One is NOT required to have a certified EHR to avoid a penalty for 2017
5. If you did not report PQRS data and did not participate in the electronic health record meaningful use program in 2016 and have no intention of participating in MIPS in 2017:
a. Your lack of participation in 2016 programs will lead to a 10% negative payment adjustment in 2018.
b. Your lack of participation in MIPS in 2017 will lead to a 4% negative payment adjustment in 2019.
Note: This option is not recommended, as in future years the annual cuts will gradually increase to 9%.
MIPS is set up as a tournament model. In other words, “Losers” pay for “Winners.” Please do not put your money in someone else’s pocket. The ACS strongly encourages all Fellows to, at the minimum, participate at the level sufficient to avoid a penalty in 2017 and, thus, not serve as the “pay for” for another provider.
If you are not exempt from MIPS and therefore, one whose performance will be assessed in 2017, you still have plenty of time to start the process of reporting enough data to compete for a positive update. On the other hand, if your goal is simply to avoid a penalty in 2019, (based on your performance in 2017), you should take the few simple steps necessary to preclude such as outlined above.
We believe the QPP website, (www.facs.org/qpp), is an excellent resource for surgeons. It was designed to facilitate participation by those surgeons who must report for MIPS. As always, ACS staff are also available to answer your questions by phone or via e-mail: [email protected].
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
We are now well over halfway through 2017, the initial year of the new Quality Payment Program (QPP) mandated by MACRA. Accordingly, I thought it might be useful to revisit the topic of the QPP and MIPS (Merit-based Incentive Payment System) for purposes of emphasizing the key steps surgeons should take if they want to potentially see an increase in their Medicare physician payment in 2019 based on their performance in 2017. At the same time, I also want to make sure that all surgeons understand the ease with which they can avoid a payment penalty.
First, I want to assure all who have yet to take any action that there is still more than adequate time to do so. You absolutely can still compete for a positive update, or at a minimum, avoid a penalty. Further, it is so easy to avoid a penalty that no surgeon should be resigned to accepting a penalty without having a look at the minimal reporting requirements necessary to avoid it.
One of the resources available on the ACS’ QPP website is an algorhythm intended to simplify surgeons’ decision making at their initial starting point. It is reproduced below:
1. Determine if all of your MIPS data will be reported by your institution or group via a Group Reporting option (GPRO).
a. If “YES,” you are done.
b. If “NO,” move to number 2.
2. Has CMS notified you that you are exempt from participating in MIPS due to the low-volume threshold?
a. If “YES,” you are done.
b. If “NO,” move to number 3.
3. If you want to compete for positive updates in your Medicare payment rates in 2019 (based on 2017 reporting), read the ACS Quality Payment Program Manual, watch the videos, and develop your plan.
4. If your goal is simply to avoid a penalty, CMS only requires data be reported for one of the following:
a. Required Base Score measures for your EHR (now known as Advancing Care Information) OR
b. One Improvement Activity for 90 days (report by attestation) OR
c. One Quality Measure on one patient (report by registry, QCDR, EHR, or claims)
Note: One is NOT required to have a certified EHR to avoid a penalty for 2017
5. If you did not report PQRS data and did not participate in the electronic health record meaningful use program in 2016 and have no intention of participating in MIPS in 2017:
a. Your lack of participation in 2016 programs will lead to a 10% negative payment adjustment in 2018.
b. Your lack of participation in MIPS in 2017 will lead to a 4% negative payment adjustment in 2019.
Note: This option is not recommended, as in future years the annual cuts will gradually increase to 9%.
MIPS is set up as a tournament model. In other words, “Losers” pay for “Winners.” Please do not put your money in someone else’s pocket. The ACS strongly encourages all Fellows to, at the minimum, participate at the level sufficient to avoid a penalty in 2017 and, thus, not serve as the “pay for” for another provider.
If you are not exempt from MIPS and therefore, one whose performance will be assessed in 2017, you still have plenty of time to start the process of reporting enough data to compete for a positive update. On the other hand, if your goal is simply to avoid a penalty in 2019, (based on your performance in 2017), you should take the few simple steps necessary to preclude such as outlined above.
We believe the QPP website, (www.facs.org/qpp), is an excellent resource for surgeons. It was designed to facilitate participation by those surgeons who must report for MIPS. As always, ACS staff are also available to answer your questions by phone or via e-mail: [email protected].
Until next month ….
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Richard J. Finley, MD, FACS, FRCSC, to receive Distinguished Service Award
The Board of Regents of the American College of Surgeons (ACS) has chosen Richard J. Finley, MD, FACS, FRCSC, a general thoracic surgeon, Vancouver General and Surrey Memorial Hospitals, BC, and emeritus professor, department of surgery, University of British Columbia (UBC), Vancouver, to receive the 2017 Distinguished Service Award (DSA). The Regents will present the award—the College’s highest honor—Sunday, October 22, during the Convocation preceding Clinical Congress 2017 at the San Diego Convention Center, CA.
The Board of Regents is presenting the DSA to Dr. Finley in appreciation for his longstanding and devoted service as an ACS Fellow, the Chair (1993−1995) and Vice-Chair (1992−1993) of the Board of Governors (B/G), a member of the Board of Regents (2000−2009), and as ACS First Vice-President (2010). The award citation recognizes his “long-term commitment to improving graduate education for future generations” and his pioneering contributions in the area of health information technology, including his service as Chair of the ACS Web Portal Editorial Board (2005−2012) and Chair of the ACS Education Task Force on Practice-Based Learning and Improvement (2002−2009).

Commitment to education
Dr. Finley has devoted much of his career to surgical education. The many residents and fellows he has trained describe Dr. Finley as an outstanding teacher and mentor, enthusiastic and innovative, and an asset to residency education. Dr. Finley has participated in the training of 14 general thoracic surgeons who now practice in academic hospitals across Canada. He is the recipient of several teaching and scholarship awards, including the UBC department of surgery Master Teaching Award (1991) and Best Teacher, Interns and Residents, University of Western Ontario, London.
Prior to assuming the position of emeritus professor at UBC, he was professor of surgery (1989−2016); head, department of surgery (1989−2001); and head, division of thoracic surgery (1994−2014) at UBC. In addition, Dr. Finley was surgeon-in-chief at Vancouver Hospital (1997–2001); head (1989–2001), department of surgery, and medical director (1992), clinical practice unit, Vancouver Hospital & Health Sciences Center, BC; and consultant staff at British Columbia Cancer Agency, Vancouver (1989–2015). Previously, Dr. Finley was chief of surgery (1985–1988) and attending surgeon, Victoria Hospital, London, ON, and a consulting surgeon, University Hospital & Ontario Cancer Foundation (1979–1988).
After graduating with honors from the University of Western Ontario Medical School, he did an internship at Vancouver General Hospital, followed by residency in surgery and cardiothoracic surgery at the University of Western Ontario. He then completed a medical research fellowship at Harvard Medical School, Boston, MA, and another year of postgraduate training at the University of Toronto, department of surgery, division of thoracic surgery. Dr. Finley then returned to the University of Western Ontario, working his way up from assistant professor (1979–1983) to associate professor (1983–1989), department of surgery.
He has chaired multiple committees at the institutions where he has practiced and taught, including the faculty executive committee and surgical advisory committee at UBC and the surgical advisory committee, minimally invasive surgery, operating room council, and operating room executive team at Vancouver Hospital & Health Sciences Centre.
Dr. Finley’s areas of special interest and accomplishment include pulmonary and esophageal surgery; metabolic and cardiopulmonary responses to sepsis, trauma, and cancer; computed tomography-guided video-assisted thoracoscopic resection of small peripheral lung cancers; quality improvement of perioperative processes; and regionalization of thoracic surgery services in British Columbia. He has been awarded 12 competitive research or equivalent grants from the Canadian Institute of Health Research, the National Cancer Institute, and a number of health care organizations.
Dedicated leader
Dr. Finley has been a Fellow of the ACS since 1983. In addition to his many achievements within the organization described earlier, he served as an ACS Governor (1989–1995), working on the B/G Ambulatory Surgery (1991), Surgical Infection (1993), Surgical Practice (1993), Communications (1991–1995), and Executive (1990–1995) Committees. As an ACS Regent, he served on the Advisory Council for General Surgery (2000–2009), the Research and Optimal Patient Care Committee (Chair, 2009), the Nominating Committee (2005–2007, Chair 2008), and the Finance Committee (2002–2004).
Dr. Finley has served as president of the International James IV Surgical Association (1998–2001), the British Columbia Surgical Association (2006), and the Canadian Association of Thoracic Surgeons (2004–2006). He also served as a Vice-President of the American Surgical Association and Chair of the Canadian Association of Surgical Chairs. He has been a member of the editorial boards for the Journal of the American College of Surgeons (1999–2006), Annals of Surgery (2002–2015), and Canadian Journal of Surgery (2004–2009). He has authored or co-authored 103 journal articles and 23 book chapters and has delivered 117 invited lectureships.
The Board of Regents of the American College of Surgeons (ACS) has chosen Richard J. Finley, MD, FACS, FRCSC, a general thoracic surgeon, Vancouver General and Surrey Memorial Hospitals, BC, and emeritus professor, department of surgery, University of British Columbia (UBC), Vancouver, to receive the 2017 Distinguished Service Award (DSA). The Regents will present the award—the College’s highest honor—Sunday, October 22, during the Convocation preceding Clinical Congress 2017 at the San Diego Convention Center, CA.
The Board of Regents is presenting the DSA to Dr. Finley in appreciation for his longstanding and devoted service as an ACS Fellow, the Chair (1993−1995) and Vice-Chair (1992−1993) of the Board of Governors (B/G), a member of the Board of Regents (2000−2009), and as ACS First Vice-President (2010). The award citation recognizes his “long-term commitment to improving graduate education for future generations” and his pioneering contributions in the area of health information technology, including his service as Chair of the ACS Web Portal Editorial Board (2005−2012) and Chair of the ACS Education Task Force on Practice-Based Learning and Improvement (2002−2009).
Commitment to education
Dr. Finley has devoted much of his career to surgical education. The many residents and fellows he has trained describe Dr. Finley as an outstanding teacher and mentor, enthusiastic and innovative, and an asset to residency education. Dr. Finley has participated in the training of 14 general thoracic surgeons who now practice in academic hospitals across Canada. He is the recipient of several teaching and scholarship awards, including the UBC department of surgery Master Teaching Award (1991) and Best Teacher, Interns and Residents, University of Western Ontario, London.
Prior to assuming the position of emeritus professor at UBC, he was professor of surgery (1989−2016); head, department of surgery (1989−2001); and head, division of thoracic surgery (1994−2014) at UBC. In addition, Dr. Finley was surgeon-in-chief at Vancouver Hospital (1997–2001); head (1989–2001), department of surgery, and medical director (1992), clinical practice unit, Vancouver Hospital & Health Sciences Center, BC; and consultant staff at British Columbia Cancer Agency, Vancouver (1989–2015). Previously, Dr. Finley was chief of surgery (1985–1988) and attending surgeon, Victoria Hospital, London, ON, and a consulting surgeon, University Hospital & Ontario Cancer Foundation (1979–1988).
After graduating with honors from the University of Western Ontario Medical School, he did an internship at Vancouver General Hospital, followed by residency in surgery and cardiothoracic surgery at the University of Western Ontario. He then completed a medical research fellowship at Harvard Medical School, Boston, MA, and another year of postgraduate training at the University of Toronto, department of surgery, division of thoracic surgery. Dr. Finley then returned to the University of Western Ontario, working his way up from assistant professor (1979–1983) to associate professor (1983–1989), department of surgery.
He has chaired multiple committees at the institutions where he has practiced and taught, including the faculty executive committee and surgical advisory committee at UBC and the surgical advisory committee, minimally invasive surgery, operating room council, and operating room executive team at Vancouver Hospital & Health Sciences Centre.
Dr. Finley’s areas of special interest and accomplishment include pulmonary and esophageal surgery; metabolic and cardiopulmonary responses to sepsis, trauma, and cancer; computed tomography-guided video-assisted thoracoscopic resection of small peripheral lung cancers; quality improvement of perioperative processes; and regionalization of thoracic surgery services in British Columbia. He has been awarded 12 competitive research or equivalent grants from the Canadian Institute of Health Research, the National Cancer Institute, and a number of health care organizations.
Dedicated leader
Dr. Finley has been a Fellow of the ACS since 1983. In addition to his many achievements within the organization described earlier, he served as an ACS Governor (1989–1995), working on the B/G Ambulatory Surgery (1991), Surgical Infection (1993), Surgical Practice (1993), Communications (1991–1995), and Executive (1990–1995) Committees. As an ACS Regent, he served on the Advisory Council for General Surgery (2000–2009), the Research and Optimal Patient Care Committee (Chair, 2009), the Nominating Committee (2005–2007, Chair 2008), and the Finance Committee (2002–2004).
Dr. Finley has served as president of the International James IV Surgical Association (1998–2001), the British Columbia Surgical Association (2006), and the Canadian Association of Thoracic Surgeons (2004–2006). He also served as a Vice-President of the American Surgical Association and Chair of the Canadian Association of Surgical Chairs. He has been a member of the editorial boards for the Journal of the American College of Surgeons (1999–2006), Annals of Surgery (2002–2015), and Canadian Journal of Surgery (2004–2009). He has authored or co-authored 103 journal articles and 23 book chapters and has delivered 117 invited lectureships.
The Board of Regents of the American College of Surgeons (ACS) has chosen Richard J. Finley, MD, FACS, FRCSC, a general thoracic surgeon, Vancouver General and Surrey Memorial Hospitals, BC, and emeritus professor, department of surgery, University of British Columbia (UBC), Vancouver, to receive the 2017 Distinguished Service Award (DSA). The Regents will present the award—the College’s highest honor—Sunday, October 22, during the Convocation preceding Clinical Congress 2017 at the San Diego Convention Center, CA.
The Board of Regents is presenting the DSA to Dr. Finley in appreciation for his longstanding and devoted service as an ACS Fellow, the Chair (1993−1995) and Vice-Chair (1992−1993) of the Board of Governors (B/G), a member of the Board of Regents (2000−2009), and as ACS First Vice-President (2010). The award citation recognizes his “long-term commitment to improving graduate education for future generations” and his pioneering contributions in the area of health information technology, including his service as Chair of the ACS Web Portal Editorial Board (2005−2012) and Chair of the ACS Education Task Force on Practice-Based Learning and Improvement (2002−2009).
Commitment to education
Dr. Finley has devoted much of his career to surgical education. The many residents and fellows he has trained describe Dr. Finley as an outstanding teacher and mentor, enthusiastic and innovative, and an asset to residency education. Dr. Finley has participated in the training of 14 general thoracic surgeons who now practice in academic hospitals across Canada. He is the recipient of several teaching and scholarship awards, including the UBC department of surgery Master Teaching Award (1991) and Best Teacher, Interns and Residents, University of Western Ontario, London.
Prior to assuming the position of emeritus professor at UBC, he was professor of surgery (1989−2016); head, department of surgery (1989−2001); and head, division of thoracic surgery (1994−2014) at UBC. In addition, Dr. Finley was surgeon-in-chief at Vancouver Hospital (1997–2001); head (1989–2001), department of surgery, and medical director (1992), clinical practice unit, Vancouver Hospital & Health Sciences Center, BC; and consultant staff at British Columbia Cancer Agency, Vancouver (1989–2015). Previously, Dr. Finley was chief of surgery (1985–1988) and attending surgeon, Victoria Hospital, London, ON, and a consulting surgeon, University Hospital & Ontario Cancer Foundation (1979–1988).
After graduating with honors from the University of Western Ontario Medical School, he did an internship at Vancouver General Hospital, followed by residency in surgery and cardiothoracic surgery at the University of Western Ontario. He then completed a medical research fellowship at Harvard Medical School, Boston, MA, and another year of postgraduate training at the University of Toronto, department of surgery, division of thoracic surgery. Dr. Finley then returned to the University of Western Ontario, working his way up from assistant professor (1979–1983) to associate professor (1983–1989), department of surgery.
He has chaired multiple committees at the institutions where he has practiced and taught, including the faculty executive committee and surgical advisory committee at UBC and the surgical advisory committee, minimally invasive surgery, operating room council, and operating room executive team at Vancouver Hospital & Health Sciences Centre.
Dr. Finley’s areas of special interest and accomplishment include pulmonary and esophageal surgery; metabolic and cardiopulmonary responses to sepsis, trauma, and cancer; computed tomography-guided video-assisted thoracoscopic resection of small peripheral lung cancers; quality improvement of perioperative processes; and regionalization of thoracic surgery services in British Columbia. He has been awarded 12 competitive research or equivalent grants from the Canadian Institute of Health Research, the National Cancer Institute, and a number of health care organizations.
Dedicated leader
Dr. Finley has been a Fellow of the ACS since 1983. In addition to his many achievements within the organization described earlier, he served as an ACS Governor (1989–1995), working on the B/G Ambulatory Surgery (1991), Surgical Infection (1993), Surgical Practice (1993), Communications (1991–1995), and Executive (1990–1995) Committees. As an ACS Regent, he served on the Advisory Council for General Surgery (2000–2009), the Research and Optimal Patient Care Committee (Chair, 2009), the Nominating Committee (2005–2007, Chair 2008), and the Finance Committee (2002–2004).
Dr. Finley has served as president of the International James IV Surgical Association (1998–2001), the British Columbia Surgical Association (2006), and the Canadian Association of Thoracic Surgeons (2004–2006). He also served as a Vice-President of the American Surgical Association and Chair of the Canadian Association of Surgical Chairs. He has been a member of the editorial boards for the Journal of the American College of Surgeons (1999–2006), Annals of Surgery (2002–2015), and Canadian Journal of Surgery (2004–2009). He has authored or co-authored 103 journal articles and 23 book chapters and has delivered 117 invited lectureships.
Winds of change at the American Board of Surgery: An interview with Executive Director Jo Buyske, MD, FACS
Just as surgeons must maintain currency in their profession, the American Board of Surgery is doing the same: revising and reinventing the recertification process to better fulfill its mission. The ABS aims to make the recertification a lifelong learning activity that is more relevant to the way surgeons actually practice. The high-stakes exam taken every decade will be supplemented with other options for demonstrating competence and currency in various surgical specialties.

Dr. Buyske will be the first woman to assume the role of Executive Director of the ABS, and she will take the lead in implementing the overhaul of recertification.
We asked Dr. Buyske to share with us some of her insights on the new direction of the ABS, the challenges ahead, and her plans to carry out the mission.
Surgery News: The recent ABS announcement regarding a new direction for the program of recertification has come at a time when many medical specialties are facing challenges in the means by which practitioners are required to demonstrate currency in their fields. Is this initiative a response to complaints from surgeons about the Maintenance of Certification (MOC)?
Dr. Buyske: The ABS has been looking at options for the initiation and maintenance of certification for over 10 years. This effort isn’t really reactive but an ongoing process in the works for some time. This initial statement is a first swing at an attempt to better serve the profession. We all understand that it is necessary to stay up to date and demonstrate mastery.
SN: What has been the response from the Diplomates to the announcement?
Dr. Buyske: We haven’t gotten formal feedback yet, but all the response has been quite positive and, rightfully, conservative. People say, “That sounds good, but what does it really mean?” This is an entirely legitimate question, because all we really said is that we are going to change the process, make it more practice focused and less onerous. That sounds good to many. Diplomates want to know the practical implications of this approach.
SN: What happens now in this process of overhauling the recertification process?
Dr. Buyske: We have a hardworking, fast-moving task force that is taking up all the information we have gathered over the past months and years. We did a survey at this time last year that gave us a lot of information about what the Diplomates want. The concerns were on a more practice-focused recertification process, and also one that is less onerous in terms of cost and time away from practice for study and travel.
Right now, the task force is fanning out across the country to talk to state and local societies, regional representatives, and nominating societies to ask for time on their programs to meet with their members and leadership. The objective is feedback and input to help us get a handle on what people’s practices are really about.
Mary Klingensmith, MD, FACS, the Mary Culver Distinguished Professor and the vice chair of education in the department of surgery at Washington University in St. Louis, has been elected as the chair of the ABS. She will be leading a town hall at the American College of Surgeons Clinical Congress in October to discuss the process and get input.
The communications division will be recruiting additional staff and will be undertaking another survey. We will be asking ABS directors to be a presence in their regional societies and to listen to their members on behalf of the ABS. We also hope the directors will participate in the ACS Communities and be a part of a discussion on recertification.
The task force timeline will be to have a basic structure for 2018, but this will not be a final project set in granite. We will have more options available in 2018, and we will continue to roll out ever more options. This is a moving target and needs to be continually reassessed as technology improves and practice needs change. And we will get better as time goes on at understanding what practices are about and what the needs of recertification are.
SN: Many of our readers are general surgeons. What do you think the new approach to recertification will mean to general surgeons?
Dr. Buyske: General surgery is a large umbrella. I have thought for years that the MOC is a general surgery exam. It covers the entire waterfront of surgery, but it doesn’t represent how people actually practice. But the new approach will apply to the many ways that people practice general surgery.
We know from our research that most general surgeons perform about 10 different operations, depending on where they live and what their interests are. And each general surgeon has a different list of operations. We want the recertification process to reflect and be relevant to each surgeon’s list of around 10, although it may be too high an expectation to have this ready by 2018. But we will begin, and we will roll out more options as time goes on.
SN: Anti-MOC legislation has been initiated in several states recently, some of which involved laws that prevent hospitals, licensing boards, insurance companies, and health systems from requiring MOC. How is the ABS responding to this trend?
Dr. Buyske: When ABS becomes aware of a particular legislative movement along these lines, we reach out to directors and senior directors and ask them to write to their state legislators and to testify. What we really want is to be allowed to continue to self-regulate our profession. We don’t want the government to intervene with the process that hospitals and insurance companies use to hire staff and compensate surgeons. For legislation to dictate how hospitals hire is a slippery slope. I feel strongly that it is incumbent that we police our own standards.
It is a fair expectation of our patients that physicians in our field keep up to date and demonstrate this. I have to dispute the argument that patients should “just trust us.” The whole argument that being up to date is unnecessary and insulting is just off base. People from all lines of work are required to demonstrate that they are up to date on their profession. You can argue that the methods used in the surgical profession are currently not the best, but not that the principle of maintenance of currency in our field is invalid. I continue to believe in the value of certification.
SN: What would you like to tell us about ABS that surgeons may be unaware of or may not have a the complete picture of?
Dr. Buyske: I would like your readers to get a sense of how much volunteer effort goes into the certification process. We have 30+ volunteer directors that give 30 days per year of time – an amazing commitment. We invite local surgeons to give examinations with us. We also have a 200+ pool of surgeons who write questions for the exams and another pool of 600 surgeons who help out in a variety of ways. We work to make sure there is a great diversity of people who take part – from all over the country, from different points in the surgical career, specialists, fellowship and nonfellowship surgeons, etc. We have people from rural practices, from the military, and some just 1 year out of training. We also have a “standard setting” meeting where we revisit and review questions to make sure they are pertinent and to evaluate their difficulty. We invite surgeons who have never done any work for the board to help us review our examinations. These can be daylong events or 4-day–long events, and most of the work is done by volunteer surgeons as a contribution to their profession.
SN: How would you describe your leadership style, and how do you think it will play out in the reinvention of the certification process?Dr. Buyske: My leadership mode is collaborative. When it comes to the new look of recertification, I have my opinions about what I want it to look like, and I think they are in line with ideas of other ABS leaders, but I don’t want to hamstring the task force in advance, before it has had a chance to do its work. I have ideas, but I consider it my job to be convincing and persuasive and listen to other very smart and committed people on the board, and they have the opportunity to try to convince me. I am grateful every day for the quality of the people I work with, both here in the office and the volunteer directors, the leaders in surgical societies, and ABS leaders.
SN: Is there something in particular you would like to say to Diplomates who are reading this?Dr. Buyske: I would say to them that I feel in my heart that we are all on the same side: We all want to take good care of the patients. The charge of the board is to protect the public and enhance the profession, and both of those things are of great importance to me. I still take care of patients, I go to the hospital, I put on scrubs, I train with residents, and I deal with the electronic medical record. I really honor the hard work required to take care of patients. And I understand the gravity of the charge of the board, which is to protect the public and enhance the profession. We all want that and we are all on the same side.
Just as surgeons must maintain currency in their profession, the American Board of Surgery is doing the same: revising and reinventing the recertification process to better fulfill its mission. The ABS aims to make the recertification a lifelong learning activity that is more relevant to the way surgeons actually practice. The high-stakes exam taken every decade will be supplemented with other options for demonstrating competence and currency in various surgical specialties.
Dr. Buyske will be the first woman to assume the role of Executive Director of the ABS, and she will take the lead in implementing the overhaul of recertification.
We asked Dr. Buyske to share with us some of her insights on the new direction of the ABS, the challenges ahead, and her plans to carry out the mission.
Surgery News: The recent ABS announcement regarding a new direction for the program of recertification has come at a time when many medical specialties are facing challenges in the means by which practitioners are required to demonstrate currency in their fields. Is this initiative a response to complaints from surgeons about the Maintenance of Certification (MOC)?
Dr. Buyske: The ABS has been looking at options for the initiation and maintenance of certification for over 10 years. This effort isn’t really reactive but an ongoing process in the works for some time. This initial statement is a first swing at an attempt to better serve the profession. We all understand that it is necessary to stay up to date and demonstrate mastery.
SN: What has been the response from the Diplomates to the announcement?
Dr. Buyske: We haven’t gotten formal feedback yet, but all the response has been quite positive and, rightfully, conservative. People say, “That sounds good, but what does it really mean?” This is an entirely legitimate question, because all we really said is that we are going to change the process, make it more practice focused and less onerous. That sounds good to many. Diplomates want to know the practical implications of this approach.
SN: What happens now in this process of overhauling the recertification process?
Dr. Buyske: We have a hardworking, fast-moving task force that is taking up all the information we have gathered over the past months and years. We did a survey at this time last year that gave us a lot of information about what the Diplomates want. The concerns were on a more practice-focused recertification process, and also one that is less onerous in terms of cost and time away from practice for study and travel.
Right now, the task force is fanning out across the country to talk to state and local societies, regional representatives, and nominating societies to ask for time on their programs to meet with their members and leadership. The objective is feedback and input to help us get a handle on what people’s practices are really about.
Mary Klingensmith, MD, FACS, the Mary Culver Distinguished Professor and the vice chair of education in the department of surgery at Washington University in St. Louis, has been elected as the chair of the ABS. She will be leading a town hall at the American College of Surgeons Clinical Congress in October to discuss the process and get input.
The communications division will be recruiting additional staff and will be undertaking another survey. We will be asking ABS directors to be a presence in their regional societies and to listen to their members on behalf of the ABS. We also hope the directors will participate in the ACS Communities and be a part of a discussion on recertification.
The task force timeline will be to have a basic structure for 2018, but this will not be a final project set in granite. We will have more options available in 2018, and we will continue to roll out ever more options. This is a moving target and needs to be continually reassessed as technology improves and practice needs change. And we will get better as time goes on at understanding what practices are about and what the needs of recertification are.
SN: Many of our readers are general surgeons. What do you think the new approach to recertification will mean to general surgeons?
Dr. Buyske: General surgery is a large umbrella. I have thought for years that the MOC is a general surgery exam. It covers the entire waterfront of surgery, but it doesn’t represent how people actually practice. But the new approach will apply to the many ways that people practice general surgery.
We know from our research that most general surgeons perform about 10 different operations, depending on where they live and what their interests are. And each general surgeon has a different list of operations. We want the recertification process to reflect and be relevant to each surgeon’s list of around 10, although it may be too high an expectation to have this ready by 2018. But we will begin, and we will roll out more options as time goes on.
SN: Anti-MOC legislation has been initiated in several states recently, some of which involved laws that prevent hospitals, licensing boards, insurance companies, and health systems from requiring MOC. How is the ABS responding to this trend?
Dr. Buyske: When ABS becomes aware of a particular legislative movement along these lines, we reach out to directors and senior directors and ask them to write to their state legislators and to testify. What we really want is to be allowed to continue to self-regulate our profession. We don’t want the government to intervene with the process that hospitals and insurance companies use to hire staff and compensate surgeons. For legislation to dictate how hospitals hire is a slippery slope. I feel strongly that it is incumbent that we police our own standards.
It is a fair expectation of our patients that physicians in our field keep up to date and demonstrate this. I have to dispute the argument that patients should “just trust us.” The whole argument that being up to date is unnecessary and insulting is just off base. People from all lines of work are required to demonstrate that they are up to date on their profession. You can argue that the methods used in the surgical profession are currently not the best, but not that the principle of maintenance of currency in our field is invalid. I continue to believe in the value of certification.
SN: What would you like to tell us about ABS that surgeons may be unaware of or may not have a the complete picture of?
Dr. Buyske: I would like your readers to get a sense of how much volunteer effort goes into the certification process. We have 30+ volunteer directors that give 30 days per year of time – an amazing commitment. We invite local surgeons to give examinations with us. We also have a 200+ pool of surgeons who write questions for the exams and another pool of 600 surgeons who help out in a variety of ways. We work to make sure there is a great diversity of people who take part – from all over the country, from different points in the surgical career, specialists, fellowship and nonfellowship surgeons, etc. We have people from rural practices, from the military, and some just 1 year out of training. We also have a “standard setting” meeting where we revisit and review questions to make sure they are pertinent and to evaluate their difficulty. We invite surgeons who have never done any work for the board to help us review our examinations. These can be daylong events or 4-day–long events, and most of the work is done by volunteer surgeons as a contribution to their profession.
SN: How would you describe your leadership style, and how do you think it will play out in the reinvention of the certification process?Dr. Buyske: My leadership mode is collaborative. When it comes to the new look of recertification, I have my opinions about what I want it to look like, and I think they are in line with ideas of other ABS leaders, but I don’t want to hamstring the task force in advance, before it has had a chance to do its work. I have ideas, but I consider it my job to be convincing and persuasive and listen to other very smart and committed people on the board, and they have the opportunity to try to convince me. I am grateful every day for the quality of the people I work with, both here in the office and the volunteer directors, the leaders in surgical societies, and ABS leaders.
SN: Is there something in particular you would like to say to Diplomates who are reading this?Dr. Buyske: I would say to them that I feel in my heart that we are all on the same side: We all want to take good care of the patients. The charge of the board is to protect the public and enhance the profession, and both of those things are of great importance to me. I still take care of patients, I go to the hospital, I put on scrubs, I train with residents, and I deal with the electronic medical record. I really honor the hard work required to take care of patients. And I understand the gravity of the charge of the board, which is to protect the public and enhance the profession. We all want that and we are all on the same side.
Just as surgeons must maintain currency in their profession, the American Board of Surgery is doing the same: revising and reinventing the recertification process to better fulfill its mission. The ABS aims to make the recertification a lifelong learning activity that is more relevant to the way surgeons actually practice. The high-stakes exam taken every decade will be supplemented with other options for demonstrating competence and currency in various surgical specialties.
Dr. Buyske will be the first woman to assume the role of Executive Director of the ABS, and she will take the lead in implementing the overhaul of recertification.
We asked Dr. Buyske to share with us some of her insights on the new direction of the ABS, the challenges ahead, and her plans to carry out the mission.
Surgery News: The recent ABS announcement regarding a new direction for the program of recertification has come at a time when many medical specialties are facing challenges in the means by which practitioners are required to demonstrate currency in their fields. Is this initiative a response to complaints from surgeons about the Maintenance of Certification (MOC)?
Dr. Buyske: The ABS has been looking at options for the initiation and maintenance of certification for over 10 years. This effort isn’t really reactive but an ongoing process in the works for some time. This initial statement is a first swing at an attempt to better serve the profession. We all understand that it is necessary to stay up to date and demonstrate mastery.
SN: What has been the response from the Diplomates to the announcement?
Dr. Buyske: We haven’t gotten formal feedback yet, but all the response has been quite positive and, rightfully, conservative. People say, “That sounds good, but what does it really mean?” This is an entirely legitimate question, because all we really said is that we are going to change the process, make it more practice focused and less onerous. That sounds good to many. Diplomates want to know the practical implications of this approach.
SN: What happens now in this process of overhauling the recertification process?
Dr. Buyske: We have a hardworking, fast-moving task force that is taking up all the information we have gathered over the past months and years. We did a survey at this time last year that gave us a lot of information about what the Diplomates want. The concerns were on a more practice-focused recertification process, and also one that is less onerous in terms of cost and time away from practice for study and travel.
Right now, the task force is fanning out across the country to talk to state and local societies, regional representatives, and nominating societies to ask for time on their programs to meet with their members and leadership. The objective is feedback and input to help us get a handle on what people’s practices are really about.
Mary Klingensmith, MD, FACS, the Mary Culver Distinguished Professor and the vice chair of education in the department of surgery at Washington University in St. Louis, has been elected as the chair of the ABS. She will be leading a town hall at the American College of Surgeons Clinical Congress in October to discuss the process and get input.
The communications division will be recruiting additional staff and will be undertaking another survey. We will be asking ABS directors to be a presence in their regional societies and to listen to their members on behalf of the ABS. We also hope the directors will participate in the ACS Communities and be a part of a discussion on recertification.
The task force timeline will be to have a basic structure for 2018, but this will not be a final project set in granite. We will have more options available in 2018, and we will continue to roll out ever more options. This is a moving target and needs to be continually reassessed as technology improves and practice needs change. And we will get better as time goes on at understanding what practices are about and what the needs of recertification are.
SN: Many of our readers are general surgeons. What do you think the new approach to recertification will mean to general surgeons?
Dr. Buyske: General surgery is a large umbrella. I have thought for years that the MOC is a general surgery exam. It covers the entire waterfront of surgery, but it doesn’t represent how people actually practice. But the new approach will apply to the many ways that people practice general surgery.
We know from our research that most general surgeons perform about 10 different operations, depending on where they live and what their interests are. And each general surgeon has a different list of operations. We want the recertification process to reflect and be relevant to each surgeon’s list of around 10, although it may be too high an expectation to have this ready by 2018. But we will begin, and we will roll out more options as time goes on.
SN: Anti-MOC legislation has been initiated in several states recently, some of which involved laws that prevent hospitals, licensing boards, insurance companies, and health systems from requiring MOC. How is the ABS responding to this trend?
Dr. Buyske: When ABS becomes aware of a particular legislative movement along these lines, we reach out to directors and senior directors and ask them to write to their state legislators and to testify. What we really want is to be allowed to continue to self-regulate our profession. We don’t want the government to intervene with the process that hospitals and insurance companies use to hire staff and compensate surgeons. For legislation to dictate how hospitals hire is a slippery slope. I feel strongly that it is incumbent that we police our own standards.
It is a fair expectation of our patients that physicians in our field keep up to date and demonstrate this. I have to dispute the argument that patients should “just trust us.” The whole argument that being up to date is unnecessary and insulting is just off base. People from all lines of work are required to demonstrate that they are up to date on their profession. You can argue that the methods used in the surgical profession are currently not the best, but not that the principle of maintenance of currency in our field is invalid. I continue to believe in the value of certification.
SN: What would you like to tell us about ABS that surgeons may be unaware of or may not have a the complete picture of?
Dr. Buyske: I would like your readers to get a sense of how much volunteer effort goes into the certification process. We have 30+ volunteer directors that give 30 days per year of time – an amazing commitment. We invite local surgeons to give examinations with us. We also have a 200+ pool of surgeons who write questions for the exams and another pool of 600 surgeons who help out in a variety of ways. We work to make sure there is a great diversity of people who take part – from all over the country, from different points in the surgical career, specialists, fellowship and nonfellowship surgeons, etc. We have people from rural practices, from the military, and some just 1 year out of training. We also have a “standard setting” meeting where we revisit and review questions to make sure they are pertinent and to evaluate their difficulty. We invite surgeons who have never done any work for the board to help us review our examinations. These can be daylong events or 4-day–long events, and most of the work is done by volunteer surgeons as a contribution to their profession.
SN: How would you describe your leadership style, and how do you think it will play out in the reinvention of the certification process?Dr. Buyske: My leadership mode is collaborative. When it comes to the new look of recertification, I have my opinions about what I want it to look like, and I think they are in line with ideas of other ABS leaders, but I don’t want to hamstring the task force in advance, before it has had a chance to do its work. I have ideas, but I consider it my job to be convincing and persuasive and listen to other very smart and committed people on the board, and they have the opportunity to try to convince me. I am grateful every day for the quality of the people I work with, both here in the office and the volunteer directors, the leaders in surgical societies, and ABS leaders.
SN: Is there something in particular you would like to say to Diplomates who are reading this?Dr. Buyske: I would say to them that I feel in my heart that we are all on the same side: We all want to take good care of the patients. The charge of the board is to protect the public and enhance the profession, and both of those things are of great importance to me. I still take care of patients, I go to the hospital, I put on scrubs, I train with residents, and I deal with the electronic medical record. I really honor the hard work required to take care of patients. And I understand the gravity of the charge of the board, which is to protect the public and enhance the profession. We all want that and we are all on the same side.
Docs, insurers condemn latest ‘repeal and replace’ plan
Medical societies and insurers are voicing their opposition to legislation that would alter provisions of the Affordable Care Act and fundamentally change how Medicaid is funded.
The bill, introduced by Sen. Lindsey Graham (R-S.C.), Sen. Bill Cassidy (R-La.), Sen. Dean Heller (R-Nev.), and Sen. Ron Johnson (R-Wis.), features a number of provisions long sought by the GOP, including the repeal of the individual and employer mandates, repeal of individual tax credits as of 2020, and repeal of the medical device tax. The bill also would promote the use of health savings accounts and turn Medicaid funding into a block grant program, allowing states to implement policies such as work requirements.
James L. Madara, MD, CEO of the American Medical Association, told congressional leaders in a Sept. 19 letter that the bill would violate the precept of “first do no harm” and results in millions of Americans losing their health coverage. Additionally, it would destabilize health insurance markets and decrease access to affordable coverage.
“We are also concerned that the proposal would convert the Medicaid program into a system that limits federal support to care for needy patients to an insufficient predetermined formula based on per capita caps,” Dr. Madara continued. “Per capita caps fail to take into account unanticipated costs of new medical innovations or the fiscal impact of public health epidemics, such as the crisis of opioid abuse currently ravaging our nation. In addition, the amendment does not take steps toward coverage and access for all Americans, and while insurers are still required to offer coverage to patients with preexisting conditions, allowing states to get waivers to vary premiums based on health status would allow insurers to charge unaffordable premiums based on those preexisting conditions. Also, waivers of essential health benefits will mean patients may not have access to coverage for services pertinent to treating their conditions.”
The American Congress of Obstetricians and Gynecologists called the bill an “assault on women’s health.” The bill would end guaranteed insurance coverage of maternity care and women’s health preventive services, including cancer screenings and contraception, ACOG president Haywood Brown, MD, said in a statement.
Dr. Brown added that the bill “jeopardizes access to care for women with high-risk and expensive pregnancies, such as those with Zika virus, opioid use disorder, and preeclampsia. It further obstructs safety net patients’ access to care by forbidding Planned Parenthood’s participation in the Medicaid program.”
Doctors aren’t the only ones objecting to the GOP legislation. America’s Health Insurance Plans president and CEO Marilyn Tavenner said in a Sept. 20 letter to Congress that the bill would further destabilize the individual health insurance market.
The bill’s road to passage is far from certain. Once again, the GOP is aiming to use the budget reconciliation process to pass this legislation, which means it needs only a simple majority to pass (a minimum of 50 votes with Vice President Mike Pence offering the tiebreaker if the bill cannot get 51 votes). But even getting to 50 votes is going to be a challenge as the last attempt to pass similar repeal and replace language failed when Sen. Susan Collins (R-Maine), Sen. Lisa Murkowski (R-Alaska), and Sen. John McCain (R-Ariz.) voted that package down. Given the similar features, Sen. Collins and Sen. Murkowski may still oppose the bill, while Sen. Rand Paul (R-Ky.) has been vocal about his displeasure with the bill and other GOP senators are getting pressure from their state governors to oppose the bill.
The Senate Finance Committee has scheduled a Sept. 25 hearing to consider the bill, but as of press time, no witnesses have been announced, and the bill likely will not follow the regular order of allowing for amendments by committee members prior to its introduction on the Senate floor later that week.
Based on current budget rules, the bill must be passed by Sept. 30 in order for the budget reconciliation process to be used and to allow for passage with a simple majority. If the Senate is able to pass the bill, House Speaker Paul Ryan (R-Wisc.) has said he will bring it up in the House. President Trump has indicated he will sign it into law if it reaches his desk.
Medical societies and insurers are voicing their opposition to legislation that would alter provisions of the Affordable Care Act and fundamentally change how Medicaid is funded.
The bill, introduced by Sen. Lindsey Graham (R-S.C.), Sen. Bill Cassidy (R-La.), Sen. Dean Heller (R-Nev.), and Sen. Ron Johnson (R-Wis.), features a number of provisions long sought by the GOP, including the repeal of the individual and employer mandates, repeal of individual tax credits as of 2020, and repeal of the medical device tax. The bill also would promote the use of health savings accounts and turn Medicaid funding into a block grant program, allowing states to implement policies such as work requirements.
James L. Madara, MD, CEO of the American Medical Association, told congressional leaders in a Sept. 19 letter that the bill would violate the precept of “first do no harm” and results in millions of Americans losing their health coverage. Additionally, it would destabilize health insurance markets and decrease access to affordable coverage.
“We are also concerned that the proposal would convert the Medicaid program into a system that limits federal support to care for needy patients to an insufficient predetermined formula based on per capita caps,” Dr. Madara continued. “Per capita caps fail to take into account unanticipated costs of new medical innovations or the fiscal impact of public health epidemics, such as the crisis of opioid abuse currently ravaging our nation. In addition, the amendment does not take steps toward coverage and access for all Americans, and while insurers are still required to offer coverage to patients with preexisting conditions, allowing states to get waivers to vary premiums based on health status would allow insurers to charge unaffordable premiums based on those preexisting conditions. Also, waivers of essential health benefits will mean patients may not have access to coverage for services pertinent to treating their conditions.”
The American Congress of Obstetricians and Gynecologists called the bill an “assault on women’s health.” The bill would end guaranteed insurance coverage of maternity care and women’s health preventive services, including cancer screenings and contraception, ACOG president Haywood Brown, MD, said in a statement.
Dr. Brown added that the bill “jeopardizes access to care for women with high-risk and expensive pregnancies, such as those with Zika virus, opioid use disorder, and preeclampsia. It further obstructs safety net patients’ access to care by forbidding Planned Parenthood’s participation in the Medicaid program.”
Doctors aren’t the only ones objecting to the GOP legislation. America’s Health Insurance Plans president and CEO Marilyn Tavenner said in a Sept. 20 letter to Congress that the bill would further destabilize the individual health insurance market.
The bill’s road to passage is far from certain. Once again, the GOP is aiming to use the budget reconciliation process to pass this legislation, which means it needs only a simple majority to pass (a minimum of 50 votes with Vice President Mike Pence offering the tiebreaker if the bill cannot get 51 votes). But even getting to 50 votes is going to be a challenge as the last attempt to pass similar repeal and replace language failed when Sen. Susan Collins (R-Maine), Sen. Lisa Murkowski (R-Alaska), and Sen. John McCain (R-Ariz.) voted that package down. Given the similar features, Sen. Collins and Sen. Murkowski may still oppose the bill, while Sen. Rand Paul (R-Ky.) has been vocal about his displeasure with the bill and other GOP senators are getting pressure from their state governors to oppose the bill.
The Senate Finance Committee has scheduled a Sept. 25 hearing to consider the bill, but as of press time, no witnesses have been announced, and the bill likely will not follow the regular order of allowing for amendments by committee members prior to its introduction on the Senate floor later that week.
Based on current budget rules, the bill must be passed by Sept. 30 in order for the budget reconciliation process to be used and to allow for passage with a simple majority. If the Senate is able to pass the bill, House Speaker Paul Ryan (R-Wisc.) has said he will bring it up in the House. President Trump has indicated he will sign it into law if it reaches his desk.
Medical societies and insurers are voicing their opposition to legislation that would alter provisions of the Affordable Care Act and fundamentally change how Medicaid is funded.
The bill, introduced by Sen. Lindsey Graham (R-S.C.), Sen. Bill Cassidy (R-La.), Sen. Dean Heller (R-Nev.), and Sen. Ron Johnson (R-Wis.), features a number of provisions long sought by the GOP, including the repeal of the individual and employer mandates, repeal of individual tax credits as of 2020, and repeal of the medical device tax. The bill also would promote the use of health savings accounts and turn Medicaid funding into a block grant program, allowing states to implement policies such as work requirements.
James L. Madara, MD, CEO of the American Medical Association, told congressional leaders in a Sept. 19 letter that the bill would violate the precept of “first do no harm” and results in millions of Americans losing their health coverage. Additionally, it would destabilize health insurance markets and decrease access to affordable coverage.
“We are also concerned that the proposal would convert the Medicaid program into a system that limits federal support to care for needy patients to an insufficient predetermined formula based on per capita caps,” Dr. Madara continued. “Per capita caps fail to take into account unanticipated costs of new medical innovations or the fiscal impact of public health epidemics, such as the crisis of opioid abuse currently ravaging our nation. In addition, the amendment does not take steps toward coverage and access for all Americans, and while insurers are still required to offer coverage to patients with preexisting conditions, allowing states to get waivers to vary premiums based on health status would allow insurers to charge unaffordable premiums based on those preexisting conditions. Also, waivers of essential health benefits will mean patients may not have access to coverage for services pertinent to treating their conditions.”
The American Congress of Obstetricians and Gynecologists called the bill an “assault on women’s health.” The bill would end guaranteed insurance coverage of maternity care and women’s health preventive services, including cancer screenings and contraception, ACOG president Haywood Brown, MD, said in a statement.
Dr. Brown added that the bill “jeopardizes access to care for women with high-risk and expensive pregnancies, such as those with Zika virus, opioid use disorder, and preeclampsia. It further obstructs safety net patients’ access to care by forbidding Planned Parenthood’s participation in the Medicaid program.”
Doctors aren’t the only ones objecting to the GOP legislation. America’s Health Insurance Plans president and CEO Marilyn Tavenner said in a Sept. 20 letter to Congress that the bill would further destabilize the individual health insurance market.
The bill’s road to passage is far from certain. Once again, the GOP is aiming to use the budget reconciliation process to pass this legislation, which means it needs only a simple majority to pass (a minimum of 50 votes with Vice President Mike Pence offering the tiebreaker if the bill cannot get 51 votes). But even getting to 50 votes is going to be a challenge as the last attempt to pass similar repeal and replace language failed when Sen. Susan Collins (R-Maine), Sen. Lisa Murkowski (R-Alaska), and Sen. John McCain (R-Ariz.) voted that package down. Given the similar features, Sen. Collins and Sen. Murkowski may still oppose the bill, while Sen. Rand Paul (R-Ky.) has been vocal about his displeasure with the bill and other GOP senators are getting pressure from their state governors to oppose the bill.
The Senate Finance Committee has scheduled a Sept. 25 hearing to consider the bill, but as of press time, no witnesses have been announced, and the bill likely will not follow the regular order of allowing for amendments by committee members prior to its introduction on the Senate floor later that week.
Based on current budget rules, the bill must be passed by Sept. 30 in order for the budget reconciliation process to be used and to allow for passage with a simple majority. If the Senate is able to pass the bill, House Speaker Paul Ryan (R-Wisc.) has said he will bring it up in the House. President Trump has indicated he will sign it into law if it reaches his desk.
Roux-en-Y gastric bypass produced durable clinical improvements at 12 years
Severely obese individuals in the United States who underwent Roux-en-Y gastric bypass (RYGB) averaged a 27% weight loss 12 years later, with only a 3% incidence of type 2 diabetes mellitus and a 51% rate of diabetes remission, according to the results of a large multicenter observational prospective study.
In striking contrast, patients who did not undergo bariatric surgery averaged a 1%-2% weight loss at 12 years, a 26% incidence of diabetes, and only a 5%-10% rate of diabetes remission, said Ted D. Adams, PhD, of the University of Utah, Salt Lake City, and his associates. RYGB surgery also conferred substantial and statistically significant improvements long-term improvements in systolic hypertension and lipid levels, the researchers reported in the New England Journal of Medicine (2017 Sep 20. doi: 10.1056/NEJMoa1700459).

“The follow-up rate exceeded 90% at 12 years,” the researchers wrote. Two years after undergoing Roux-en-Y gastric bypass, patients had lost an average of 45 kg (95% confidence interval, 43-47 kg). By postoperative year 6, they had regained an average of 9 kg (average loss from baseline, 36 kg; 95% CI, 34-39 kg). But they typically gained only about 1.3 kg more between years 6 and 12, and they had about a 92% lower odds of developing diabetes mellitus, compared with individuals who did not undergo bariatric surgery (odds ratio, 0.08; P less than .001). “Remission of type 2 diabetes was much more likely if the Roux-en-Y gastric bypass occurred before [patients began] treatment with insulin, presumably owing to the ability of partially viable beta cells to improve their function,” the researchers noted.
Funders included the National Institute of Diabetes and Digestive and Kidney Diseases, the National Center for Research Resources, Weill Cornell Medicine, and Intermountain Healthcare. Dr. Adams reported having no relevant conflicts of interest. One coinvestigator disclosed royalties from licensing a questionnaire on weight loss and quality of life, and another coinvestigator disclosed fees for services rendered during a trial of an intragastric balloon. The remaining researchers had no relevant disclosures.
Severely obese individuals in the United States who underwent Roux-en-Y gastric bypass (RYGB) averaged a 27% weight loss 12 years later, with only a 3% incidence of type 2 diabetes mellitus and a 51% rate of diabetes remission, according to the results of a large multicenter observational prospective study.
In striking contrast, patients who did not undergo bariatric surgery averaged a 1%-2% weight loss at 12 years, a 26% incidence of diabetes, and only a 5%-10% rate of diabetes remission, said Ted D. Adams, PhD, of the University of Utah, Salt Lake City, and his associates. RYGB surgery also conferred substantial and statistically significant improvements long-term improvements in systolic hypertension and lipid levels, the researchers reported in the New England Journal of Medicine (2017 Sep 20. doi: 10.1056/NEJMoa1700459).
“The follow-up rate exceeded 90% at 12 years,” the researchers wrote. Two years after undergoing Roux-en-Y gastric bypass, patients had lost an average of 45 kg (95% confidence interval, 43-47 kg). By postoperative year 6, they had regained an average of 9 kg (average loss from baseline, 36 kg; 95% CI, 34-39 kg). But they typically gained only about 1.3 kg more between years 6 and 12, and they had about a 92% lower odds of developing diabetes mellitus, compared with individuals who did not undergo bariatric surgery (odds ratio, 0.08; P less than .001). “Remission of type 2 diabetes was much more likely if the Roux-en-Y gastric bypass occurred before [patients began] treatment with insulin, presumably owing to the ability of partially viable beta cells to improve their function,” the researchers noted.
Funders included the National Institute of Diabetes and Digestive and Kidney Diseases, the National Center for Research Resources, Weill Cornell Medicine, and Intermountain Healthcare. Dr. Adams reported having no relevant conflicts of interest. One coinvestigator disclosed royalties from licensing a questionnaire on weight loss and quality of life, and another coinvestigator disclosed fees for services rendered during a trial of an intragastric balloon. The remaining researchers had no relevant disclosures.
Severely obese individuals in the United States who underwent Roux-en-Y gastric bypass (RYGB) averaged a 27% weight loss 12 years later, with only a 3% incidence of type 2 diabetes mellitus and a 51% rate of diabetes remission, according to the results of a large multicenter observational prospective study.
In striking contrast, patients who did not undergo bariatric surgery averaged a 1%-2% weight loss at 12 years, a 26% incidence of diabetes, and only a 5%-10% rate of diabetes remission, said Ted D. Adams, PhD, of the University of Utah, Salt Lake City, and his associates. RYGB surgery also conferred substantial and statistically significant improvements long-term improvements in systolic hypertension and lipid levels, the researchers reported in the New England Journal of Medicine (2017 Sep 20. doi: 10.1056/NEJMoa1700459).
“The follow-up rate exceeded 90% at 12 years,” the researchers wrote. Two years after undergoing Roux-en-Y gastric bypass, patients had lost an average of 45 kg (95% confidence interval, 43-47 kg). By postoperative year 6, they had regained an average of 9 kg (average loss from baseline, 36 kg; 95% CI, 34-39 kg). But they typically gained only about 1.3 kg more between years 6 and 12, and they had about a 92% lower odds of developing diabetes mellitus, compared with individuals who did not undergo bariatric surgery (odds ratio, 0.08; P less than .001). “Remission of type 2 diabetes was much more likely if the Roux-en-Y gastric bypass occurred before [patients began] treatment with insulin, presumably owing to the ability of partially viable beta cells to improve their function,” the researchers noted.
Funders included the National Institute of Diabetes and Digestive and Kidney Diseases, the National Center for Research Resources, Weill Cornell Medicine, and Intermountain Healthcare. Dr. Adams reported having no relevant conflicts of interest. One coinvestigator disclosed royalties from licensing a questionnaire on weight loss and quality of life, and another coinvestigator disclosed fees for services rendered during a trial of an intragastric balloon. The remaining researchers had no relevant disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Roux-en-Y gastric bypass produced durable results on numerous clinical outcome measures.
Major finding: Twelve years after surgery, RYGB patients averaged a 27% weight loss from baseline, with a 51% rate of remission and a 3% incidence of type 2 diabetes mellitus.
Data source: A prospective study of 1,156 severely obese individuals, of whom 418 underwent Roux-en-Y gastric bypass.
Disclosures: Funders included the National Institute of Diabetes and Digestive and Kidney Diseases, the National Center for Research Resources, Weill Cornell Medicine, and Intermountain Healthcare. Dr. Adams reported having no relevant conflicts of interest. One coinvestigator disclosed royalties from licensing a questionnaire on weight loss and the quality of life, and another coinvestigator disclosed fees for services rendered during a trial of an intragastric balloon. The remaining researchers had no relevant disclosures.
Readmission rates linked to hospital quality measures
Poorer-performing hospitals have higher readmission rates than better-performing hospitals for patients with similar diagnoses, a study shows.
Lead author Harlan M. Krumholz, MD, of Yale University, New Haven, Conn., and his colleagues analyzed Centers for Medicare and Medicaid Services hospital-wide readmission data and divided data from July 2014 through June 2015 into two random samples. Researchers used the first sample to calculate the risk-standardized readmission rate within 30 days for each hospital and classified hospitals into performance quartiles, with a lower readmission rate indicating better performance. The second study sample included patients who had two admissions for similar diagnoses at different hospitals that occurred more than 1 month and less than 1 year apart. Researchers compared the observed readmission rates among patients who had been admitted to hospitals in different performance quartiles. The analysis included all discharges occurring from July 1, 2014, through June 30, 2015, from short-term acute care or critical access hospitals in the United States involving Medicare patients who were aged 65 years or older.
Results found that among the patients hospitalized more than once for similar diagnoses at different hospitals, the readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points; 95% confidence interval, 0.4-3.5; P = .001) (N Engl J Med. 2017. doi: 10.1056/NEJMsa1702321). The differences in the comparisons of the other quartiles were smaller and not significant, according to the study. 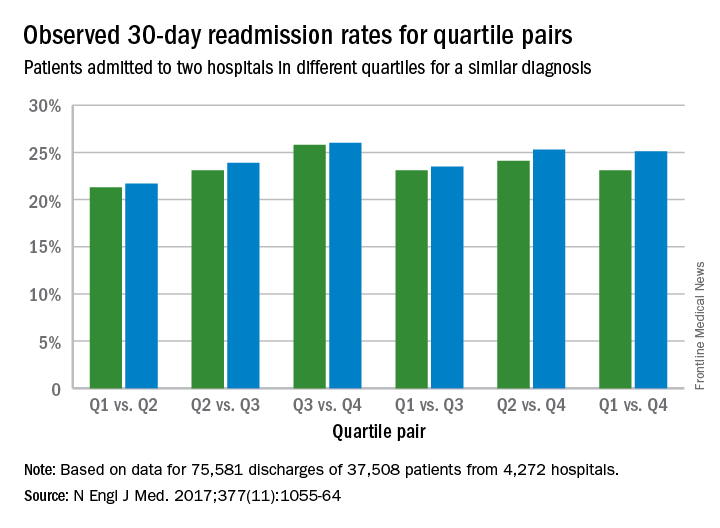
The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors, study authors concluded.
“This study addresses a persistent concern that national readmission measures may reflect differences in unmeasured factors rather than in hospital performance,” study authors noted in the study. “The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors. By studying patients who were admitted twice within 1 year with similar diagnoses to different hospitals, this study design was able to isolate hospital signals of performance while minimizing differences among the patients. In these cases, because the same patients had similar admissions at two hospitals, the characteristics of the patients, including their level of social disadvantage, level of education, or degree of underlying illness, were broadly the same. The alignment of the differences that we observed with the results of the CMS hospital-wide readmission measure also adds to evidence that the readmission measure classifies true differences in performance.”
Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
[email protected]
On Twitter @legal_med
Poorer-performing hospitals have higher readmission rates than better-performing hospitals for patients with similar diagnoses, a study shows.
Lead author Harlan M. Krumholz, MD, of Yale University, New Haven, Conn., and his colleagues analyzed Centers for Medicare and Medicaid Services hospital-wide readmission data and divided data from July 2014 through June 2015 into two random samples. Researchers used the first sample to calculate the risk-standardized readmission rate within 30 days for each hospital and classified hospitals into performance quartiles, with a lower readmission rate indicating better performance. The second study sample included patients who had two admissions for similar diagnoses at different hospitals that occurred more than 1 month and less than 1 year apart. Researchers compared the observed readmission rates among patients who had been admitted to hospitals in different performance quartiles. The analysis included all discharges occurring from July 1, 2014, through June 30, 2015, from short-term acute care or critical access hospitals in the United States involving Medicare patients who were aged 65 years or older.
Results found that among the patients hospitalized more than once for similar diagnoses at different hospitals, the readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points; 95% confidence interval, 0.4-3.5; P = .001) (N Engl J Med. 2017. doi: 10.1056/NEJMsa1702321). The differences in the comparisons of the other quartiles were smaller and not significant, according to the study.
The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors, study authors concluded.
“This study addresses a persistent concern that national readmission measures may reflect differences in unmeasured factors rather than in hospital performance,” study authors noted in the study. “The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors. By studying patients who were admitted twice within 1 year with similar diagnoses to different hospitals, this study design was able to isolate hospital signals of performance while minimizing differences among the patients. In these cases, because the same patients had similar admissions at two hospitals, the characteristics of the patients, including their level of social disadvantage, level of education, or degree of underlying illness, were broadly the same. The alignment of the differences that we observed with the results of the CMS hospital-wide readmission measure also adds to evidence that the readmission measure classifies true differences in performance.”
Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
[email protected]
On Twitter @legal_med
Poorer-performing hospitals have higher readmission rates than better-performing hospitals for patients with similar diagnoses, a study shows.
Lead author Harlan M. Krumholz, MD, of Yale University, New Haven, Conn., and his colleagues analyzed Centers for Medicare and Medicaid Services hospital-wide readmission data and divided data from July 2014 through June 2015 into two random samples. Researchers used the first sample to calculate the risk-standardized readmission rate within 30 days for each hospital and classified hospitals into performance quartiles, with a lower readmission rate indicating better performance. The second study sample included patients who had two admissions for similar diagnoses at different hospitals that occurred more than 1 month and less than 1 year apart. Researchers compared the observed readmission rates among patients who had been admitted to hospitals in different performance quartiles. The analysis included all discharges occurring from July 1, 2014, through June 30, 2015, from short-term acute care or critical access hospitals in the United States involving Medicare patients who were aged 65 years or older.
Results found that among the patients hospitalized more than once for similar diagnoses at different hospitals, the readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points; 95% confidence interval, 0.4-3.5; P = .001) (N Engl J Med. 2017. doi: 10.1056/NEJMsa1702321). The differences in the comparisons of the other quartiles were smaller and not significant, according to the study.
The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors, study authors concluded.
“This study addresses a persistent concern that national readmission measures may reflect differences in unmeasured factors rather than in hospital performance,” study authors noted in the study. “The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors. By studying patients who were admitted twice within 1 year with similar diagnoses to different hospitals, this study design was able to isolate hospital signals of performance while minimizing differences among the patients. In these cases, because the same patients had similar admissions at two hospitals, the characteristics of the patients, including their level of social disadvantage, level of education, or degree of underlying illness, were broadly the same. The alignment of the differences that we observed with the results of the CMS hospital-wide readmission measure also adds to evidence that the readmission measure classifies true differences in performance.”
Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
[email protected]
On Twitter @legal_med
FROM NEJM
Key clinical point:
Major finding: The readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points).
Data source: Analysis of Centers for Medicare and Medicaid Services hospital-wide readmission data from July 2014 through June 2015.
Disclosures: Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
Postsurgical antibiotics cut infection in obese women after C-section
A 48-hour course of postoperative cephalexin and metronidazole, plus typical preoperative antibiotics, cut surgical site infections by 59% in obese women who had a cesarean delivery.
The benefit of the additional postoperative treatment was driven by a significant, 69% risk reduction among women who had ruptured membranes, Amy M. Valent, DO, and her colleagues reported (JAMA. 2017;318[11]:1026-34). However, the authors noted, “tests for interaction between the intact membranes and [ruptured] subgroups and postpartum cephalexin-metronidazole were not statistically different and should not be interpreted as showing a difference in significance or effect size among the subgroups with and without [rupture].”
The trial comprised 403 obese women who had a cesarean delivery. They were a mean of 28 years old. The mean body mass index was 40 kg/m2, and the mean subcutaneous adipose tissue thickness was about 3.4 cm. About a third of each treatment group was positive for Group B streptococcus; 31% had ruptured membranes at the onset of labor. More than 60% of women in both groups had a scheduled cesarean delivery.
All women had standard preoperative care, including skin prep with a chlorhexidine or povidone-iodine cleansing and an intravenous infusion of 2 g cefazolin. After delivery, they were randomized to placebo or to oral cephalexin 500 mg plus metronidazole 500 mg every 8 hours for 48 hours. The primary outcome was surgical site infection incidence within 30 days.
The overall rate of surgical site infection was 10.9% (44 women). Infections developed in 13 women in the active group and 31 in the placebo group (6.4% vs. 15.4%) – a significant difference, translating to a 59% risk reduction (relative risk, 0.41). Cellulitis was the only secondary outcome that was significantly reduced by prophylactic antibiotics, with infections occurring in 5.9% of the metronidazole-cephalexin group vs. 13.4% of the placebo group (RR, 0.44). The antibiotic regimen didn’t affect the other secondary endpoints, which included rates of incisional morbidity, endometritis, fever of unknown etiology, and wound separation.
The authors conducted a post-hoc analysis to examine the antibiotics’ effects on women who had ruptured and intact membranes at the time of delivery. The benefit was greatest among those with ruptured membranes. There were six infections among the active group and 19 among the placebo group (9.5% vs. 30.2%). This difference translated to a relative risk of 0.31 – a 69% risk reduction.
Among women with intact membranes, there were seven infections in the active group and 12 in the placebo group (5% vs. 8.7%). This translated to a 0.58 relative risk, which was not statistically significant.
“Interaction testing was performed between study groups (cephalexin-metronidazole vs. placebo) and by membrane status (intact vs. ruptured),” the authors noted. “The rate of surgical site infection was highest in those with [ruptured membranes] who received placebo (30.2%) and lowest in those with intact membranes who received antibiotics (5.0%), but the test for interaction did not show statistical significance at P = .30.”
There were no serious adverse events or allergic reactions reported for cephalexin or metronidazole. The authors noted that both drugs are excreted into breast milk in small amounts, but that no study has ever linked them with neonatal harm through breast milk exposure. However, they added, “Long-term childhood or adverse neonatal outcomes specific to cephalexin-metronidazole exposure cannot be determined, as outcome measures were not evaluated for this study protocol. Recognizing the maternal and neonatal benefit of breastfeeding, the lack of known neonatal adverse effects, and maternal reduction in [surgical site infection], the benefit of this antibiotic regimen likely outweighs the theoretical risks of breast milk exposure in the obese population.”
The University of Cincinnati Department of Obstetrics and Gynecology sponsored the trial. None of the authors reported any financial conflicts.
Despite the positive outcomes of this trial, it’s not yet time to tack on yet more antibiotics for every obese woman who undergoes a cesarean delivery, David P. Calfee, MD, and Amos Grünebaum, MD, wrote in an accompanying editorial (JAMA. 2017;318[11]:1012-3).
“When determining if and how the results of this study should alter current clinical practice, it is important to recognize that the results of this study are quite different from those of several previous studies conducted in other surgical patient populations in which no benefit from postoperative antimicrobial prophylaxis was found and on which current clinical guidelines for antimicrobial prophylaxis are based,” they wrote. “The explanation for this difference may be as simple as the identification in the current study of a very specific, high-risk group of patients for which the intervention is effective. However, several questions are worthy of additional consideration and study.”
For instance, the study was conducted over 5 years and may not reflect current practices for managing these patients, such as glycemic control and maintaining normothermia. Additionally, there may be additional risks to women that were not identified in the study, such as infection from antimicrobial-resistant pathogens.
Dr. Calfee and Dr. Grünebaum are at Weill Cornell Medical Center in New York. Dr. Calfee reported receiving grants from Merck, Sharp, and Dohme.
Despite the positive outcomes of this trial, it’s not yet time to tack on yet more antibiotics for every obese woman who undergoes a cesarean delivery, David P. Calfee, MD, and Amos Grünebaum, MD, wrote in an accompanying editorial (JAMA. 2017;318[11]:1012-3).
“When determining if and how the results of this study should alter current clinical practice, it is important to recognize that the results of this study are quite different from those of several previous studies conducted in other surgical patient populations in which no benefit from postoperative antimicrobial prophylaxis was found and on which current clinical guidelines for antimicrobial prophylaxis are based,” they wrote. “The explanation for this difference may be as simple as the identification in the current study of a very specific, high-risk group of patients for which the intervention is effective. However, several questions are worthy of additional consideration and study.”
For instance, the study was conducted over 5 years and may not reflect current practices for managing these patients, such as glycemic control and maintaining normothermia. Additionally, there may be additional risks to women that were not identified in the study, such as infection from antimicrobial-resistant pathogens.
Dr. Calfee and Dr. Grünebaum are at Weill Cornell Medical Center in New York. Dr. Calfee reported receiving grants from Merck, Sharp, and Dohme.
Despite the positive outcomes of this trial, it’s not yet time to tack on yet more antibiotics for every obese woman who undergoes a cesarean delivery, David P. Calfee, MD, and Amos Grünebaum, MD, wrote in an accompanying editorial (JAMA. 2017;318[11]:1012-3).
“When determining if and how the results of this study should alter current clinical practice, it is important to recognize that the results of this study are quite different from those of several previous studies conducted in other surgical patient populations in which no benefit from postoperative antimicrobial prophylaxis was found and on which current clinical guidelines for antimicrobial prophylaxis are based,” they wrote. “The explanation for this difference may be as simple as the identification in the current study of a very specific, high-risk group of patients for which the intervention is effective. However, several questions are worthy of additional consideration and study.”
For instance, the study was conducted over 5 years and may not reflect current practices for managing these patients, such as glycemic control and maintaining normothermia. Additionally, there may be additional risks to women that were not identified in the study, such as infection from antimicrobial-resistant pathogens.
Dr. Calfee and Dr. Grünebaum are at Weill Cornell Medical Center in New York. Dr. Calfee reported receiving grants from Merck, Sharp, and Dohme.
A 48-hour course of postoperative cephalexin and metronidazole, plus typical preoperative antibiotics, cut surgical site infections by 59% in obese women who had a cesarean delivery.
The benefit of the additional postoperative treatment was driven by a significant, 69% risk reduction among women who had ruptured membranes, Amy M. Valent, DO, and her colleagues reported (JAMA. 2017;318[11]:1026-34). However, the authors noted, “tests for interaction between the intact membranes and [ruptured] subgroups and postpartum cephalexin-metronidazole were not statistically different and should not be interpreted as showing a difference in significance or effect size among the subgroups with and without [rupture].”
The trial comprised 403 obese women who had a cesarean delivery. They were a mean of 28 years old. The mean body mass index was 40 kg/m2, and the mean subcutaneous adipose tissue thickness was about 3.4 cm. About a third of each treatment group was positive for Group B streptococcus; 31% had ruptured membranes at the onset of labor. More than 60% of women in both groups had a scheduled cesarean delivery.
All women had standard preoperative care, including skin prep with a chlorhexidine or povidone-iodine cleansing and an intravenous infusion of 2 g cefazolin. After delivery, they were randomized to placebo or to oral cephalexin 500 mg plus metronidazole 500 mg every 8 hours for 48 hours. The primary outcome was surgical site infection incidence within 30 days.
The overall rate of surgical site infection was 10.9% (44 women). Infections developed in 13 women in the active group and 31 in the placebo group (6.4% vs. 15.4%) – a significant difference, translating to a 59% risk reduction (relative risk, 0.41). Cellulitis was the only secondary outcome that was significantly reduced by prophylactic antibiotics, with infections occurring in 5.9% of the metronidazole-cephalexin group vs. 13.4% of the placebo group (RR, 0.44). The antibiotic regimen didn’t affect the other secondary endpoints, which included rates of incisional morbidity, endometritis, fever of unknown etiology, and wound separation.
The authors conducted a post-hoc analysis to examine the antibiotics’ effects on women who had ruptured and intact membranes at the time of delivery. The benefit was greatest among those with ruptured membranes. There were six infections among the active group and 19 among the placebo group (9.5% vs. 30.2%). This difference translated to a relative risk of 0.31 – a 69% risk reduction.
Among women with intact membranes, there were seven infections in the active group and 12 in the placebo group (5% vs. 8.7%). This translated to a 0.58 relative risk, which was not statistically significant.
“Interaction testing was performed between study groups (cephalexin-metronidazole vs. placebo) and by membrane status (intact vs. ruptured),” the authors noted. “The rate of surgical site infection was highest in those with [ruptured membranes] who received placebo (30.2%) and lowest in those with intact membranes who received antibiotics (5.0%), but the test for interaction did not show statistical significance at P = .30.”
There were no serious adverse events or allergic reactions reported for cephalexin or metronidazole. The authors noted that both drugs are excreted into breast milk in small amounts, but that no study has ever linked them with neonatal harm through breast milk exposure. However, they added, “Long-term childhood or adverse neonatal outcomes specific to cephalexin-metronidazole exposure cannot be determined, as outcome measures were not evaluated for this study protocol. Recognizing the maternal and neonatal benefit of breastfeeding, the lack of known neonatal adverse effects, and maternal reduction in [surgical site infection], the benefit of this antibiotic regimen likely outweighs the theoretical risks of breast milk exposure in the obese population.”
The University of Cincinnati Department of Obstetrics and Gynecology sponsored the trial. None of the authors reported any financial conflicts.
A 48-hour course of postoperative cephalexin and metronidazole, plus typical preoperative antibiotics, cut surgical site infections by 59% in obese women who had a cesarean delivery.
The benefit of the additional postoperative treatment was driven by a significant, 69% risk reduction among women who had ruptured membranes, Amy M. Valent, DO, and her colleagues reported (JAMA. 2017;318[11]:1026-34). However, the authors noted, “tests for interaction between the intact membranes and [ruptured] subgroups and postpartum cephalexin-metronidazole were not statistically different and should not be interpreted as showing a difference in significance or effect size among the subgroups with and without [rupture].”
The trial comprised 403 obese women who had a cesarean delivery. They were a mean of 28 years old. The mean body mass index was 40 kg/m2, and the mean subcutaneous adipose tissue thickness was about 3.4 cm. About a third of each treatment group was positive for Group B streptococcus; 31% had ruptured membranes at the onset of labor. More than 60% of women in both groups had a scheduled cesarean delivery.
All women had standard preoperative care, including skin prep with a chlorhexidine or povidone-iodine cleansing and an intravenous infusion of 2 g cefazolin. After delivery, they were randomized to placebo or to oral cephalexin 500 mg plus metronidazole 500 mg every 8 hours for 48 hours. The primary outcome was surgical site infection incidence within 30 days.
The overall rate of surgical site infection was 10.9% (44 women). Infections developed in 13 women in the active group and 31 in the placebo group (6.4% vs. 15.4%) – a significant difference, translating to a 59% risk reduction (relative risk, 0.41). Cellulitis was the only secondary outcome that was significantly reduced by prophylactic antibiotics, with infections occurring in 5.9% of the metronidazole-cephalexin group vs. 13.4% of the placebo group (RR, 0.44). The antibiotic regimen didn’t affect the other secondary endpoints, which included rates of incisional morbidity, endometritis, fever of unknown etiology, and wound separation.
The authors conducted a post-hoc analysis to examine the antibiotics’ effects on women who had ruptured and intact membranes at the time of delivery. The benefit was greatest among those with ruptured membranes. There were six infections among the active group and 19 among the placebo group (9.5% vs. 30.2%). This difference translated to a relative risk of 0.31 – a 69% risk reduction.
Among women with intact membranes, there were seven infections in the active group and 12 in the placebo group (5% vs. 8.7%). This translated to a 0.58 relative risk, which was not statistically significant.
“Interaction testing was performed between study groups (cephalexin-metronidazole vs. placebo) and by membrane status (intact vs. ruptured),” the authors noted. “The rate of surgical site infection was highest in those with [ruptured membranes] who received placebo (30.2%) and lowest in those with intact membranes who received antibiotics (5.0%), but the test for interaction did not show statistical significance at P = .30.”
There were no serious adverse events or allergic reactions reported for cephalexin or metronidazole. The authors noted that both drugs are excreted into breast milk in small amounts, but that no study has ever linked them with neonatal harm through breast milk exposure. However, they added, “Long-term childhood or adverse neonatal outcomes specific to cephalexin-metronidazole exposure cannot be determined, as outcome measures were not evaluated for this study protocol. Recognizing the maternal and neonatal benefit of breastfeeding, the lack of known neonatal adverse effects, and maternal reduction in [surgical site infection], the benefit of this antibiotic regimen likely outweighs the theoretical risks of breast milk exposure in the obese population.”
The University of Cincinnati Department of Obstetrics and Gynecology sponsored the trial. None of the authors reported any financial conflicts.
FROM JAMA
Key clinical point:
Major finding: Infections developed in 13 women in the active group and 31 in the placebo group (6.4% vs. 15.4%) – a significant difference, translating to a 59% risk reduction (relative risk, 0.41).
Data source: The randomized, placebo-controlled study comprised 403 women.
Disclosures: The University of Cincinnati Department of Obstetrics and Gynecology sponsored the study. None of the authors reported any financial conflicts.