User login
Official Newspaper of the American College of Surgeons
Embolism major cause of stroke after open arch surgery in patients with carotid/intracranial stenosis
Embolization was the major cause of permanent stroke in patients with moderate or severe carotid or intracranial atherosclerosis who underwent elective open aortic arch surgery at a single institution, according to the results of a retrospective study.
Preoperative craniocervical and aortic screening may aid in modifying the operative strategy to reduce the incidence of stroke in these patients, according to a report published in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
Preventing stroke in this patient population is an important consideration, because perioperative stroke is approximately 4 times more common in open aortic arch surgery (OAAS) than in coronary artery bypass grafting or valve surgery, according to Ken-ichi Imasaka, MD, and his colleagues at the National Hospital Organization Kyushu Medical Center, Fukuoka, Japan.
The study population comprised 200 consecutive patients undergoing elective OAAS at the institution between October 2008 and October 2015, including 34% women and with a mean patient age of 71 years (J Thorac Cardiovasc Surg. 2017;153:1045-53).
After preoperative screening, 21% of patients were diagnosed with carotid or intracranial artery disease (CIAD). None of these patients were diagnosed with impaired cerebral perfusion reserve on brain SPECT (single-photon emission computed tomography). A total of 92% of patients underwent ascending aorta or aortic arch replacement through a median sternotomy, while the remaining 8% underwent extended aortic arch replacement via L-incision (15 patients) or combined median sternotomy and left posterior lateral thoracotomy (1 patient). Among the patients, 16% underwent ascending aorta replacement; 8% had partial arch replacement; and the remaining 76% had total arch replacement.
Shaggy aorta was present in 19% of the patients, with 51% of these showing CIAD (P less than .0001). A total of 30% of the patients with shaggy aorta had the total arch replacement through an L-incision or combined median sternotomy and left posterior lateral thoracotomy, a significant difference (P less than .0001).

The overall in-hospital mortality rate was 3.5%. The overall incidence of permanent stroke and paraplegia or paraparesis was 4% (8 patients) and 2% (4 patients), respectively. Three (37.5%) of the 8 permanent stroke patients died during the postoperative hospital stay, compared with 2.1% of the 192 patients without stroke.
Univariate analysis indicated that previous cerebrovascular accident (P = .0002), shaggy aorta (P less than .0001), cardiopulmonary bypass time (P = .003), selective antegrade cerebral perfusion time (P = .004), operation time (P = .02), and extended aortic repair through L-incision or combined median sternotomy and left posterior lateral thoracotomy (P = .0002) were significant risk factors for neurologic morbidity.
“Preoperative intensive screening of carotid and intracranial artery disease is a useful step to identify patients at higher risk of hemodynamic ischemic stroke. Advanced systemic atherosclerosis may be a crucial determinant of perioperative stroke due to atherothrombotic embolization. Antiembolic measures during surgery are essential to prevent perioperative stroke,” the researchers concluded.
The authors reported that they had no disclosures.
During aortic arch surgery, the lack of blood supply as a result of emboli, rather than atherosclerosis itself, kills the cerebral neurons, according to Ourania Preventza, MD, and Joseph S. Coselli, MD, of the Baylor College of Medicine, Houston, in their invited commentary (J Thorac Cardiovasc Surg. 2017;153:1054-5).
Patients with carotid and intracranial disease should indeed have more intensive screening before undergoing major aortic surgery, they agreed, but pointed out that in the absence of carotid disease, large or complex aortic atheromas can be seen in the arch, indicating that, even though atherosclerosis is a systemic disease, using different sites of prediction can be uncertain.
This requires a broader approach to prevent stroke, including careful selection of the cannulation site in patients with diffuse and heavy arch atherosclerosis or currently ulcerated plaque, they added.
“To minimize postoperative neurologic morbidities after aortic arch surgery, an individually tailored perioperative approach should be in the armamentarium of cardiac surgeons,” Dr. Preventza and Dr. Coselli concluded.
Dr. Preventza consults for Medtronic and W. L. Gore & Associates. Dr. Coselli participates in clinical research trials conducted by GlaxoSmithKline, Edwards Lifesciences, and Bolton Medical, and consults for various companies.
During aortic arch surgery, the lack of blood supply as a result of emboli, rather than atherosclerosis itself, kills the cerebral neurons, according to Ourania Preventza, MD, and Joseph S. Coselli, MD, of the Baylor College of Medicine, Houston, in their invited commentary (J Thorac Cardiovasc Surg. 2017;153:1054-5).
Patients with carotid and intracranial disease should indeed have more intensive screening before undergoing major aortic surgery, they agreed, but pointed out that in the absence of carotid disease, large or complex aortic atheromas can be seen in the arch, indicating that, even though atherosclerosis is a systemic disease, using different sites of prediction can be uncertain.
This requires a broader approach to prevent stroke, including careful selection of the cannulation site in patients with diffuse and heavy arch atherosclerosis or currently ulcerated plaque, they added.
“To minimize postoperative neurologic morbidities after aortic arch surgery, an individually tailored perioperative approach should be in the armamentarium of cardiac surgeons,” Dr. Preventza and Dr. Coselli concluded.
Dr. Preventza consults for Medtronic and W. L. Gore & Associates. Dr. Coselli participates in clinical research trials conducted by GlaxoSmithKline, Edwards Lifesciences, and Bolton Medical, and consults for various companies.
During aortic arch surgery, the lack of blood supply as a result of emboli, rather than atherosclerosis itself, kills the cerebral neurons, according to Ourania Preventza, MD, and Joseph S. Coselli, MD, of the Baylor College of Medicine, Houston, in their invited commentary (J Thorac Cardiovasc Surg. 2017;153:1054-5).
Patients with carotid and intracranial disease should indeed have more intensive screening before undergoing major aortic surgery, they agreed, but pointed out that in the absence of carotid disease, large or complex aortic atheromas can be seen in the arch, indicating that, even though atherosclerosis is a systemic disease, using different sites of prediction can be uncertain.
This requires a broader approach to prevent stroke, including careful selection of the cannulation site in patients with diffuse and heavy arch atherosclerosis or currently ulcerated plaque, they added.
“To minimize postoperative neurologic morbidities after aortic arch surgery, an individually tailored perioperative approach should be in the armamentarium of cardiac surgeons,” Dr. Preventza and Dr. Coselli concluded.
Dr. Preventza consults for Medtronic and W. L. Gore & Associates. Dr. Coselli participates in clinical research trials conducted by GlaxoSmithKline, Edwards Lifesciences, and Bolton Medical, and consults for various companies.
Embolization was the major cause of permanent stroke in patients with moderate or severe carotid or intracranial atherosclerosis who underwent elective open aortic arch surgery at a single institution, according to the results of a retrospective study.
Preoperative craniocervical and aortic screening may aid in modifying the operative strategy to reduce the incidence of stroke in these patients, according to a report published in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
Preventing stroke in this patient population is an important consideration, because perioperative stroke is approximately 4 times more common in open aortic arch surgery (OAAS) than in coronary artery bypass grafting or valve surgery, according to Ken-ichi Imasaka, MD, and his colleagues at the National Hospital Organization Kyushu Medical Center, Fukuoka, Japan.
The study population comprised 200 consecutive patients undergoing elective OAAS at the institution between October 2008 and October 2015, including 34% women and with a mean patient age of 71 years (J Thorac Cardiovasc Surg. 2017;153:1045-53).
After preoperative screening, 21% of patients were diagnosed with carotid or intracranial artery disease (CIAD). None of these patients were diagnosed with impaired cerebral perfusion reserve on brain SPECT (single-photon emission computed tomography). A total of 92% of patients underwent ascending aorta or aortic arch replacement through a median sternotomy, while the remaining 8% underwent extended aortic arch replacement via L-incision (15 patients) or combined median sternotomy and left posterior lateral thoracotomy (1 patient). Among the patients, 16% underwent ascending aorta replacement; 8% had partial arch replacement; and the remaining 76% had total arch replacement.
Shaggy aorta was present in 19% of the patients, with 51% of these showing CIAD (P less than .0001). A total of 30% of the patients with shaggy aorta had the total arch replacement through an L-incision or combined median sternotomy and left posterior lateral thoracotomy, a significant difference (P less than .0001).
The overall in-hospital mortality rate was 3.5%. The overall incidence of permanent stroke and paraplegia or paraparesis was 4% (8 patients) and 2% (4 patients), respectively. Three (37.5%) of the 8 permanent stroke patients died during the postoperative hospital stay, compared with 2.1% of the 192 patients without stroke.
Univariate analysis indicated that previous cerebrovascular accident (P = .0002), shaggy aorta (P less than .0001), cardiopulmonary bypass time (P = .003), selective antegrade cerebral perfusion time (P = .004), operation time (P = .02), and extended aortic repair through L-incision or combined median sternotomy and left posterior lateral thoracotomy (P = .0002) were significant risk factors for neurologic morbidity.
“Preoperative intensive screening of carotid and intracranial artery disease is a useful step to identify patients at higher risk of hemodynamic ischemic stroke. Advanced systemic atherosclerosis may be a crucial determinant of perioperative stroke due to atherothrombotic embolization. Antiembolic measures during surgery are essential to prevent perioperative stroke,” the researchers concluded.
The authors reported that they had no disclosures.
Embolization was the major cause of permanent stroke in patients with moderate or severe carotid or intracranial atherosclerosis who underwent elective open aortic arch surgery at a single institution, according to the results of a retrospective study.
Preoperative craniocervical and aortic screening may aid in modifying the operative strategy to reduce the incidence of stroke in these patients, according to a report published in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
Preventing stroke in this patient population is an important consideration, because perioperative stroke is approximately 4 times more common in open aortic arch surgery (OAAS) than in coronary artery bypass grafting or valve surgery, according to Ken-ichi Imasaka, MD, and his colleagues at the National Hospital Organization Kyushu Medical Center, Fukuoka, Japan.
The study population comprised 200 consecutive patients undergoing elective OAAS at the institution between October 2008 and October 2015, including 34% women and with a mean patient age of 71 years (J Thorac Cardiovasc Surg. 2017;153:1045-53).
After preoperative screening, 21% of patients were diagnosed with carotid or intracranial artery disease (CIAD). None of these patients were diagnosed with impaired cerebral perfusion reserve on brain SPECT (single-photon emission computed tomography). A total of 92% of patients underwent ascending aorta or aortic arch replacement through a median sternotomy, while the remaining 8% underwent extended aortic arch replacement via L-incision (15 patients) or combined median sternotomy and left posterior lateral thoracotomy (1 patient). Among the patients, 16% underwent ascending aorta replacement; 8% had partial arch replacement; and the remaining 76% had total arch replacement.
Shaggy aorta was present in 19% of the patients, with 51% of these showing CIAD (P less than .0001). A total of 30% of the patients with shaggy aorta had the total arch replacement through an L-incision or combined median sternotomy and left posterior lateral thoracotomy, a significant difference (P less than .0001).
The overall in-hospital mortality rate was 3.5%. The overall incidence of permanent stroke and paraplegia or paraparesis was 4% (8 patients) and 2% (4 patients), respectively. Three (37.5%) of the 8 permanent stroke patients died during the postoperative hospital stay, compared with 2.1% of the 192 patients without stroke.
Univariate analysis indicated that previous cerebrovascular accident (P = .0002), shaggy aorta (P less than .0001), cardiopulmonary bypass time (P = .003), selective antegrade cerebral perfusion time (P = .004), operation time (P = .02), and extended aortic repair through L-incision or combined median sternotomy and left posterior lateral thoracotomy (P = .0002) were significant risk factors for neurologic morbidity.
“Preoperative intensive screening of carotid and intracranial artery disease is a useful step to identify patients at higher risk of hemodynamic ischemic stroke. Advanced systemic atherosclerosis may be a crucial determinant of perioperative stroke due to atherothrombotic embolization. Antiembolic measures during surgery are essential to prevent perioperative stroke,” the researchers concluded.
The authors reported that they had no disclosures.
Key clinical point:
Major finding: Previous cerebrovascular accident and shaggy aorta were significant determinants of neurologic morbidity.
Data source: Retrospective study of 200 consecutive patients undergoing elective aortic arch surgery at a single institution.
Disclosures: The authors reported having no conflicts of interest.
Do you have to MIPS in 2017? CMS has a tool for that
Want to know if Medicare’s Merit-based Incentive Payment System (MIPS) is in your future?
The Centers for Medicare & Medicaid Services launched a Web tool on May 9. To see if you must participate in MIPS in 2017, just enter your national provider identifier. The agency is also in the process of mailing letters to update physicians on their status. The Web tool can be found at the CMS website.
Physicians who bill Medicare Part B more than $30,000 and see more than 100 Medicare patients must participate in MIPS this year. That threshold will be determined by means of claims submitted Sept. 1, 2015, through Aug. 31, 2016, and Sept. 1, 2016, through Aug. 31, 2017.
Those who don’t meet those criteria but want to participate may do so, but they won’t receive either a bonus or a penalty.
Under the MIPS “pick your pace” option, physicians who meet the threshold but are not ready to participate for either the 90-day period or the full year can report on one measure for 2017. Data on the lone measure need to be submitted to CMS no later than March 31, 2018.
Data need only be submitted for one patient, and, in 2017, all forms of submission – via registry, electronic health record, administrative claims, or attestation – are acceptable, though options may vary based on the performance option selected. Doing this minimum effort will result in no adjustment to Medicare payments in 2019.
Submitting no data at all for 2017, however, will mean a 4% Medicare pay cut in 2019.
To do the bare minimum to avoid any penalty, select a single data measurement from one of three categories: quality measures, improvement activity, or, in the case of Advancing Care Information, four or five base measures, depending on which certified EHR is being used.
There are 271 quality measures from which to choose, as well as 92 improvement activities. Improvement activities focus on care coordination, patient engagement, and patient safety.
For each measure, there is a downloadable spreadsheet that gives detailed information about the measure and how to meet it. The spreadsheet can also be used by physicians to track the data that are collected for submission.
Physicians who are new to Medicare in 2017 do not have to participate in MIPS in 2017.
Another way to be exempt from MIPS is to participate in the Advanced Alternative Payment Model track of the QPP. Doctors participating in APMs will have the opportunity to earn higher payment bonuses but will have to assume more risk and could see payment reductions if quality and value thresholds are not met.
Want to know if Medicare’s Merit-based Incentive Payment System (MIPS) is in your future?
The Centers for Medicare & Medicaid Services launched a Web tool on May 9. To see if you must participate in MIPS in 2017, just enter your national provider identifier. The agency is also in the process of mailing letters to update physicians on their status. The Web tool can be found at the CMS website.
Physicians who bill Medicare Part B more than $30,000 and see more than 100 Medicare patients must participate in MIPS this year. That threshold will be determined by means of claims submitted Sept. 1, 2015, through Aug. 31, 2016, and Sept. 1, 2016, through Aug. 31, 2017.
Those who don’t meet those criteria but want to participate may do so, but they won’t receive either a bonus or a penalty.
Under the MIPS “pick your pace” option, physicians who meet the threshold but are not ready to participate for either the 90-day period or the full year can report on one measure for 2017. Data on the lone measure need to be submitted to CMS no later than March 31, 2018.
Data need only be submitted for one patient, and, in 2017, all forms of submission – via registry, electronic health record, administrative claims, or attestation – are acceptable, though options may vary based on the performance option selected. Doing this minimum effort will result in no adjustment to Medicare payments in 2019.
Submitting no data at all for 2017, however, will mean a 4% Medicare pay cut in 2019.
To do the bare minimum to avoid any penalty, select a single data measurement from one of three categories: quality measures, improvement activity, or, in the case of Advancing Care Information, four or five base measures, depending on which certified EHR is being used.
There are 271 quality measures from which to choose, as well as 92 improvement activities. Improvement activities focus on care coordination, patient engagement, and patient safety.
For each measure, there is a downloadable spreadsheet that gives detailed information about the measure and how to meet it. The spreadsheet can also be used by physicians to track the data that are collected for submission.
Physicians who are new to Medicare in 2017 do not have to participate in MIPS in 2017.
Another way to be exempt from MIPS is to participate in the Advanced Alternative Payment Model track of the QPP. Doctors participating in APMs will have the opportunity to earn higher payment bonuses but will have to assume more risk and could see payment reductions if quality and value thresholds are not met.
Want to know if Medicare’s Merit-based Incentive Payment System (MIPS) is in your future?
The Centers for Medicare & Medicaid Services launched a Web tool on May 9. To see if you must participate in MIPS in 2017, just enter your national provider identifier. The agency is also in the process of mailing letters to update physicians on their status. The Web tool can be found at the CMS website.
Physicians who bill Medicare Part B more than $30,000 and see more than 100 Medicare patients must participate in MIPS this year. That threshold will be determined by means of claims submitted Sept. 1, 2015, through Aug. 31, 2016, and Sept. 1, 2016, through Aug. 31, 2017.
Those who don’t meet those criteria but want to participate may do so, but they won’t receive either a bonus or a penalty.
Under the MIPS “pick your pace” option, physicians who meet the threshold but are not ready to participate for either the 90-day period or the full year can report on one measure for 2017. Data on the lone measure need to be submitted to CMS no later than March 31, 2018.
Data need only be submitted for one patient, and, in 2017, all forms of submission – via registry, electronic health record, administrative claims, or attestation – are acceptable, though options may vary based on the performance option selected. Doing this minimum effort will result in no adjustment to Medicare payments in 2019.
Submitting no data at all for 2017, however, will mean a 4% Medicare pay cut in 2019.
To do the bare minimum to avoid any penalty, select a single data measurement from one of three categories: quality measures, improvement activity, or, in the case of Advancing Care Information, four or five base measures, depending on which certified EHR is being used.
There are 271 quality measures from which to choose, as well as 92 improvement activities. Improvement activities focus on care coordination, patient engagement, and patient safety.
For each measure, there is a downloadable spreadsheet that gives detailed information about the measure and how to meet it. The spreadsheet can also be used by physicians to track the data that are collected for submission.
Physicians who are new to Medicare in 2017 do not have to participate in MIPS in 2017.
Another way to be exempt from MIPS is to participate in the Advanced Alternative Payment Model track of the QPP. Doctors participating in APMs will have the opportunity to earn higher payment bonuses but will have to assume more risk and could see payment reductions if quality and value thresholds are not met.
Determining patients’ decisional capacity
Question: Mrs. Wong, age 80 years, has vascular dementia, and for the last 2 years has lived in a nursing home. She is forgetful and disoriented to time, person, and place, and totally dependent on others for all of her daily living needs. But she remains verbal and recognizes family members.
Recently, her glomerular filtration rate declined to less than 10% normal, and she has developed symptoms of uremia, i.e., nausea, vomiting, and intractable hiccups. The nephrologist has diagnosed end-stage renal failure and recommends hemodialysis, which will improve her renal symptoms and may extend her life by 1-2 years. But it will do nothing for her underlying dementia, which is progressive and irreversible.
Should she undergo hemodialysis? Choose the best single answer:
A. Mrs. Wong definitely lacks the capacity to decide whether to undergo hemodialysis.
B. A court-appointed guardian should make the decision.
C. Hemodialysis is futile and is medically contraindicated, inhumane, and unethical.
D. Hemodialysis is a life-extending form of comfort care, and therefore cannot be withheld.
E. The choice is hers if she understands the procedure and the consequences of her decision.
Answer: E. The terms competence and capacity are often used interchangeably in the health care context, although there are distinctions. Technically, a patient remains competent until a court says otherwise. On the other hand, the determination of medical decision-making capacity can be made by the attending physician and does not ordinarily require a court hearing.
Medical capacity can be determined by the use of the four-point test, which asks whether:
1. The patient understands the nature of the intervention.
2. The patient understands the consequences of the decision (especially refusal of treatment).
3. The patient is able to communicate his/her wishes.
4. Those wishes are compatible with the patient’s known values.

Courts tend to rule in favor of a finding of capacity. In one case, the court found no evidence that the patient’s “forgetfulness and confusion cause, or relate in any way to, impairment of her ability to understand that, in rejecting the amputation, she is, in effect, choosing death over life.”1
In another, the court opined, “However humble the background, sad and deprived the way of life, each individual should have the choice as to what is done to his body, if he is capable of understanding the consequences. This patient, although suffering from an organic brain disease, in the court’s opinion understands the consequences of his refusal. … I find that he has sufficient capacity and competence to consent to or refuse the proposed surgery.”2
Sometimes capacity is truly lacking. In a Tennessee case, Mary Northern, an elderly woman, refused amputation, denying that gangrene had caused her feet to be “dead, black, shriveled, rotting, and stinking.”3 Instead, she believed that they were merely blackened by soot or dust.
The court declared her incompetent, because she was “incapable of recognizing facts which would be obvious to a person of normal perception.” The court said that if she had acknowledged that her legs were gangrenous but refused amputation because she preferred death to the loss of her feet, she would have been considered competent to refuse surgery.
When the patient lacks capacity, a surrogate steps in. This may be a person previously designated by the patient as having durable power of attorney for health care decisions, and he/she is obligated to give voice to what the patient would have wanted. This is called substituted judgment.
Often, no surrogate has been formally mentioned, and a family member assumes the role; rarely, a court-appointed guardian takes over. When there is no knowledge of the patient’s wishes, the decision is then made in the patient’s best interests.
That a surrogate can make life and death decisions was first enunciated in the seminal case of Karen Ann Quinlan, where the New Jersey Supreme Court famously wrote, “The sad truth, however, is that she is grossly incompetent, and we cannot discern her supposed choice based on the testimony of her previous conversations with friends, where such testimony is without sufficient probative weight. Nevertheless, we have concluded that Karen’s right of privacy may be asserted on her behalf by her guardian under the peculiar circumstances here present.”4
The U.S. Supreme Court in Cruzan v. Director Missouri Department of Health has similarly held that an “incompetent person is not able to make an informed and voluntary choice to exercise a hypothetical right to refuse treatment or any other right. Such a ‘right’ must be exercised for her, if at all, by some sort of surrogate.”5 The court also opined that a state – in this case, Missouri – may apply a clear and convincing evidentiary standard in proceedings where a guardian seeks to discontinue nutrition and hydration.
Clear and convincing evidence is said to exist where there is a finding of high probability, based on evidence “so clear as to leave no substantial doubt” and “sufficiently strong to command the unhesitating assent of every reasonable mind.”
However, where a patient’s wishes are not clear and convincing, a court will be reluctant to order cessation of treatment, as in the landmark case of Wendland v. Wendland, where the California Supreme Court unanimously disallowed the discontinuation of a patient’s tube feedings.6
The patient, Robert Wendland, had regained consciousness after 14 months in a coma, but was left hemiparetic and incontinent, and could not feed by mouth or dress, bathe, and communicate consistently. He did not have an advance directive, but had made statements to the effect he would not want to live in a vegetative state.
His wife, Rose, refused to authorize reinsertion of his dislodged feeding tube, believing that Robert would not have wanted it replaced. The patient’s daughter and brother, as well as the hospital’s ethics committee, county ombudsman, and a court-appointed counsel, all agreed with the decision.
But the patient’s mother, Florence, went to court to block the action. The court determined that Robert’s statements were not clear and convincing, because they did not address his current condition, were not sufficiently specific, and were not necessarily intended to direct his medical care. Further, the patient’s spouse had failed to provide sufficient evidence that her decision was in her husband’s best interests.
Issues surrounding treatment at the end of life can be difficult and elusive. Even where there is an advance medical directive, statements made by patients in the document do not always comport with their eventual treatment decisions.
In a telling study, the authors found that only two-thirds of the time were decisions consistent.7 One-third of patients changed their preferences in the face of actual illness, usually in favor of treatments rejected in advance. Surrogate agreement was only 58%, and surrogates tended to overestimate their loved one’s desire for treatment.
The designation of who may be the legitimate alternative decision maker is another contentious issue, with laws varying widely from state to state.8
All of this may have in part prompted Singapore’s newly enacted Mental Capacity Act,9 which permits a surrogate to make wide-ranging decisions on behalf of an incapacitated person, to specifically exclude decisions regarding life-sustaining treatment and any measure that the physician “reasonably believes is necessary to prevent a serious deterioration” in the patient’s condition.
The decisional responsibility resides in the treating physician, who is obligated by law to make an effort to assist the patient to come to a decision, failing which it is made in the patient’s best interests.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Lane v. Candura, 6 Mass. App. 377 (1978).
2. Matter of Roosevelt Hospital, N.Y.L.J. 13 Jan 1977 p. 7 (Sup. Ct., New York Co.).
3. State Dept Human Resources v. Northern, 563 SW 2d 197 (Tenn. Ct. App., 1978).
4. In the matter of Karen Quinlan, 355 A.2d 647 (N.J., 1976).
5. Cruzan v. Director Missouri Department of Health, 110 S. Ct. 2841 (1990).
6. Wendland v. Wendland, 28 P.3d 151 (Cal., 2001).
7. J Clin Ethics. 1998 Fall;9(3):258-62.
8. N Engl J Med. 2017 Apr 13;376(15):1478-82.
9. Singapore’s Mental Capacity Act (Chapter 177A).
Question: Mrs. Wong, age 80 years, has vascular dementia, and for the last 2 years has lived in a nursing home. She is forgetful and disoriented to time, person, and place, and totally dependent on others for all of her daily living needs. But she remains verbal and recognizes family members.
Recently, her glomerular filtration rate declined to less than 10% normal, and she has developed symptoms of uremia, i.e., nausea, vomiting, and intractable hiccups. The nephrologist has diagnosed end-stage renal failure and recommends hemodialysis, which will improve her renal symptoms and may extend her life by 1-2 years. But it will do nothing for her underlying dementia, which is progressive and irreversible.
Should she undergo hemodialysis? Choose the best single answer:
A. Mrs. Wong definitely lacks the capacity to decide whether to undergo hemodialysis.
B. A court-appointed guardian should make the decision.
C. Hemodialysis is futile and is medically contraindicated, inhumane, and unethical.
D. Hemodialysis is a life-extending form of comfort care, and therefore cannot be withheld.
E. The choice is hers if she understands the procedure and the consequences of her decision.
Answer: E. The terms competence and capacity are often used interchangeably in the health care context, although there are distinctions. Technically, a patient remains competent until a court says otherwise. On the other hand, the determination of medical decision-making capacity can be made by the attending physician and does not ordinarily require a court hearing.
Medical capacity can be determined by the use of the four-point test, which asks whether:
1. The patient understands the nature of the intervention.
2. The patient understands the consequences of the decision (especially refusal of treatment).
3. The patient is able to communicate his/her wishes.
4. Those wishes are compatible with the patient’s known values.
Courts tend to rule in favor of a finding of capacity. In one case, the court found no evidence that the patient’s “forgetfulness and confusion cause, or relate in any way to, impairment of her ability to understand that, in rejecting the amputation, she is, in effect, choosing death over life.”1
In another, the court opined, “However humble the background, sad and deprived the way of life, each individual should have the choice as to what is done to his body, if he is capable of understanding the consequences. This patient, although suffering from an organic brain disease, in the court’s opinion understands the consequences of his refusal. … I find that he has sufficient capacity and competence to consent to or refuse the proposed surgery.”2
Sometimes capacity is truly lacking. In a Tennessee case, Mary Northern, an elderly woman, refused amputation, denying that gangrene had caused her feet to be “dead, black, shriveled, rotting, and stinking.”3 Instead, she believed that they were merely blackened by soot or dust.
The court declared her incompetent, because she was “incapable of recognizing facts which would be obvious to a person of normal perception.” The court said that if she had acknowledged that her legs were gangrenous but refused amputation because she preferred death to the loss of her feet, she would have been considered competent to refuse surgery.
When the patient lacks capacity, a surrogate steps in. This may be a person previously designated by the patient as having durable power of attorney for health care decisions, and he/she is obligated to give voice to what the patient would have wanted. This is called substituted judgment.
Often, no surrogate has been formally mentioned, and a family member assumes the role; rarely, a court-appointed guardian takes over. When there is no knowledge of the patient’s wishes, the decision is then made in the patient’s best interests.
That a surrogate can make life and death decisions was first enunciated in the seminal case of Karen Ann Quinlan, where the New Jersey Supreme Court famously wrote, “The sad truth, however, is that she is grossly incompetent, and we cannot discern her supposed choice based on the testimony of her previous conversations with friends, where such testimony is without sufficient probative weight. Nevertheless, we have concluded that Karen’s right of privacy may be asserted on her behalf by her guardian under the peculiar circumstances here present.”4
The U.S. Supreme Court in Cruzan v. Director Missouri Department of Health has similarly held that an “incompetent person is not able to make an informed and voluntary choice to exercise a hypothetical right to refuse treatment or any other right. Such a ‘right’ must be exercised for her, if at all, by some sort of surrogate.”5 The court also opined that a state – in this case, Missouri – may apply a clear and convincing evidentiary standard in proceedings where a guardian seeks to discontinue nutrition and hydration.
Clear and convincing evidence is said to exist where there is a finding of high probability, based on evidence “so clear as to leave no substantial doubt” and “sufficiently strong to command the unhesitating assent of every reasonable mind.”
However, where a patient’s wishes are not clear and convincing, a court will be reluctant to order cessation of treatment, as in the landmark case of Wendland v. Wendland, where the California Supreme Court unanimously disallowed the discontinuation of a patient’s tube feedings.6
The patient, Robert Wendland, had regained consciousness after 14 months in a coma, but was left hemiparetic and incontinent, and could not feed by mouth or dress, bathe, and communicate consistently. He did not have an advance directive, but had made statements to the effect he would not want to live in a vegetative state.
His wife, Rose, refused to authorize reinsertion of his dislodged feeding tube, believing that Robert would not have wanted it replaced. The patient’s daughter and brother, as well as the hospital’s ethics committee, county ombudsman, and a court-appointed counsel, all agreed with the decision.
But the patient’s mother, Florence, went to court to block the action. The court determined that Robert’s statements were not clear and convincing, because they did not address his current condition, were not sufficiently specific, and were not necessarily intended to direct his medical care. Further, the patient’s spouse had failed to provide sufficient evidence that her decision was in her husband’s best interests.
Issues surrounding treatment at the end of life can be difficult and elusive. Even where there is an advance medical directive, statements made by patients in the document do not always comport with their eventual treatment decisions.
In a telling study, the authors found that only two-thirds of the time were decisions consistent.7 One-third of patients changed their preferences in the face of actual illness, usually in favor of treatments rejected in advance. Surrogate agreement was only 58%, and surrogates tended to overestimate their loved one’s desire for treatment.
The designation of who may be the legitimate alternative decision maker is another contentious issue, with laws varying widely from state to state.8
All of this may have in part prompted Singapore’s newly enacted Mental Capacity Act,9 which permits a surrogate to make wide-ranging decisions on behalf of an incapacitated person, to specifically exclude decisions regarding life-sustaining treatment and any measure that the physician “reasonably believes is necessary to prevent a serious deterioration” in the patient’s condition.
The decisional responsibility resides in the treating physician, who is obligated by law to make an effort to assist the patient to come to a decision, failing which it is made in the patient’s best interests.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Lane v. Candura, 6 Mass. App. 377 (1978).
2. Matter of Roosevelt Hospital, N.Y.L.J. 13 Jan 1977 p. 7 (Sup. Ct., New York Co.).
3. State Dept Human Resources v. Northern, 563 SW 2d 197 (Tenn. Ct. App., 1978).
4. In the matter of Karen Quinlan, 355 A.2d 647 (N.J., 1976).
5. Cruzan v. Director Missouri Department of Health, 110 S. Ct. 2841 (1990).
6. Wendland v. Wendland, 28 P.3d 151 (Cal., 2001).
7. J Clin Ethics. 1998 Fall;9(3):258-62.
8. N Engl J Med. 2017 Apr 13;376(15):1478-82.
9. Singapore’s Mental Capacity Act (Chapter 177A).
Question: Mrs. Wong, age 80 years, has vascular dementia, and for the last 2 years has lived in a nursing home. She is forgetful and disoriented to time, person, and place, and totally dependent on others for all of her daily living needs. But she remains verbal and recognizes family members.
Recently, her glomerular filtration rate declined to less than 10% normal, and she has developed symptoms of uremia, i.e., nausea, vomiting, and intractable hiccups. The nephrologist has diagnosed end-stage renal failure and recommends hemodialysis, which will improve her renal symptoms and may extend her life by 1-2 years. But it will do nothing for her underlying dementia, which is progressive and irreversible.
Should she undergo hemodialysis? Choose the best single answer:
A. Mrs. Wong definitely lacks the capacity to decide whether to undergo hemodialysis.
B. A court-appointed guardian should make the decision.
C. Hemodialysis is futile and is medically contraindicated, inhumane, and unethical.
D. Hemodialysis is a life-extending form of comfort care, and therefore cannot be withheld.
E. The choice is hers if she understands the procedure and the consequences of her decision.
Answer: E. The terms competence and capacity are often used interchangeably in the health care context, although there are distinctions. Technically, a patient remains competent until a court says otherwise. On the other hand, the determination of medical decision-making capacity can be made by the attending physician and does not ordinarily require a court hearing.
Medical capacity can be determined by the use of the four-point test, which asks whether:
1. The patient understands the nature of the intervention.
2. The patient understands the consequences of the decision (especially refusal of treatment).
3. The patient is able to communicate his/her wishes.
4. Those wishes are compatible with the patient’s known values.
Courts tend to rule in favor of a finding of capacity. In one case, the court found no evidence that the patient’s “forgetfulness and confusion cause, or relate in any way to, impairment of her ability to understand that, in rejecting the amputation, she is, in effect, choosing death over life.”1
In another, the court opined, “However humble the background, sad and deprived the way of life, each individual should have the choice as to what is done to his body, if he is capable of understanding the consequences. This patient, although suffering from an organic brain disease, in the court’s opinion understands the consequences of his refusal. … I find that he has sufficient capacity and competence to consent to or refuse the proposed surgery.”2
Sometimes capacity is truly lacking. In a Tennessee case, Mary Northern, an elderly woman, refused amputation, denying that gangrene had caused her feet to be “dead, black, shriveled, rotting, and stinking.”3 Instead, she believed that they were merely blackened by soot or dust.
The court declared her incompetent, because she was “incapable of recognizing facts which would be obvious to a person of normal perception.” The court said that if she had acknowledged that her legs were gangrenous but refused amputation because she preferred death to the loss of her feet, she would have been considered competent to refuse surgery.
When the patient lacks capacity, a surrogate steps in. This may be a person previously designated by the patient as having durable power of attorney for health care decisions, and he/she is obligated to give voice to what the patient would have wanted. This is called substituted judgment.
Often, no surrogate has been formally mentioned, and a family member assumes the role; rarely, a court-appointed guardian takes over. When there is no knowledge of the patient’s wishes, the decision is then made in the patient’s best interests.
That a surrogate can make life and death decisions was first enunciated in the seminal case of Karen Ann Quinlan, where the New Jersey Supreme Court famously wrote, “The sad truth, however, is that she is grossly incompetent, and we cannot discern her supposed choice based on the testimony of her previous conversations with friends, where such testimony is without sufficient probative weight. Nevertheless, we have concluded that Karen’s right of privacy may be asserted on her behalf by her guardian under the peculiar circumstances here present.”4
The U.S. Supreme Court in Cruzan v. Director Missouri Department of Health has similarly held that an “incompetent person is not able to make an informed and voluntary choice to exercise a hypothetical right to refuse treatment or any other right. Such a ‘right’ must be exercised for her, if at all, by some sort of surrogate.”5 The court also opined that a state – in this case, Missouri – may apply a clear and convincing evidentiary standard in proceedings where a guardian seeks to discontinue nutrition and hydration.
Clear and convincing evidence is said to exist where there is a finding of high probability, based on evidence “so clear as to leave no substantial doubt” and “sufficiently strong to command the unhesitating assent of every reasonable mind.”
However, where a patient’s wishes are not clear and convincing, a court will be reluctant to order cessation of treatment, as in the landmark case of Wendland v. Wendland, where the California Supreme Court unanimously disallowed the discontinuation of a patient’s tube feedings.6
The patient, Robert Wendland, had regained consciousness after 14 months in a coma, but was left hemiparetic and incontinent, and could not feed by mouth or dress, bathe, and communicate consistently. He did not have an advance directive, but had made statements to the effect he would not want to live in a vegetative state.
His wife, Rose, refused to authorize reinsertion of his dislodged feeding tube, believing that Robert would not have wanted it replaced. The patient’s daughter and brother, as well as the hospital’s ethics committee, county ombudsman, and a court-appointed counsel, all agreed with the decision.
But the patient’s mother, Florence, went to court to block the action. The court determined that Robert’s statements were not clear and convincing, because they did not address his current condition, were not sufficiently specific, and were not necessarily intended to direct his medical care. Further, the patient’s spouse had failed to provide sufficient evidence that her decision was in her husband’s best interests.
Issues surrounding treatment at the end of life can be difficult and elusive. Even where there is an advance medical directive, statements made by patients in the document do not always comport with their eventual treatment decisions.
In a telling study, the authors found that only two-thirds of the time were decisions consistent.7 One-third of patients changed their preferences in the face of actual illness, usually in favor of treatments rejected in advance. Surrogate agreement was only 58%, and surrogates tended to overestimate their loved one’s desire for treatment.
The designation of who may be the legitimate alternative decision maker is another contentious issue, with laws varying widely from state to state.8
All of this may have in part prompted Singapore’s newly enacted Mental Capacity Act,9 which permits a surrogate to make wide-ranging decisions on behalf of an incapacitated person, to specifically exclude decisions regarding life-sustaining treatment and any measure that the physician “reasonably believes is necessary to prevent a serious deterioration” in the patient’s condition.
The decisional responsibility resides in the treating physician, who is obligated by law to make an effort to assist the patient to come to a decision, failing which it is made in the patient’s best interests.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Lane v. Candura, 6 Mass. App. 377 (1978).
2. Matter of Roosevelt Hospital, N.Y.L.J. 13 Jan 1977 p. 7 (Sup. Ct., New York Co.).
3. State Dept Human Resources v. Northern, 563 SW 2d 197 (Tenn. Ct. App., 1978).
4. In the matter of Karen Quinlan, 355 A.2d 647 (N.J., 1976).
5. Cruzan v. Director Missouri Department of Health, 110 S. Ct. 2841 (1990).
6. Wendland v. Wendland, 28 P.3d 151 (Cal., 2001).
7. J Clin Ethics. 1998 Fall;9(3):258-62.
8. N Engl J Med. 2017 Apr 13;376(15):1478-82.
9. Singapore’s Mental Capacity Act (Chapter 177A).
Decision to remove breast cancer metastases depends on location of lesions
LAS VEGAS – Determination of whether excision of persistent breast cancer metastases can benefit the patient and even prolong survival depends on the location of the metastatic lesions, an investigator said at the annual meeting of the American Society of Breast Surgeons.
Before making the decision, it’s important to restage the patient’s disease and to recheck the receptor status if a biopsy is accessible, said Roshni Rao, MD, of the University of Texas Southwestern Medical Center.
Brain

Survival is worse when there are concurrent extracranial metastases or when brain metastases are greater than 5 cm, in patients with triple negative tumors, and in patients with a Karnofsky score of 70 or less, Dr. Rao said.
Surgery has the greatest benefit in patients with a single metastasis, with no extracranial disease, and who are able to undergo adjuvant whole brain radiation. In these cases, surgery improves survival, lowers recurrence rates, and reduces the risk of death neurological causes, she said.
Long-term survival is most common with continuous adjuvant therapy, either trastuzumab or hormonal, and in patients with a longer time interval to development of metastases. One series showed a 20-month survival increase.
Liver
Approximately 15% of patients with synchronous metastases will have liver metastases, and about half of stage IV patients will experience liver metastases at some point during treatment.
There is evidence from colorectal cancer that removing liver metastases is beneficial, and that has prompted interest in a similar approach in breast cancer. Liver resection has also become safer with new advances.
Dr. Rao discussed a single-institution study which took an aggressive approach to liver resection in 85 patients (Ann Surg. 2006;244:897-907). The researchers found that increased survival was associated with a good response to adjuvant chemotherapy, an r0 or r1 resection, and in patients who had a previous liver resection and were healthy enough to undergo another resection.
Overall, existing studies support liver resection if there are one to three lesions, if negative margins can be achieved, if the tumors are hormone receptor positive, and if the cancer is hormone positive and has good response to chemotherapy.
Dr. Rao emphasized that liver resections should be performed with a multidisciplinary team and should only be attempted at centers with low morbidity and where the doctors are experienced with liver resection.
When it’s possible, liver resection is beneficial. “There have been multiple reports of long-term survivors with no evidence of disease. There is likely a survival benefit with careful selection of these patients,” Dr. Rao said.
Lung
Lung surgeries are becoming safer, especially with the availability of video-assisted techniques, and pulmonary metastases are increasingly being spotted using more sensitive techniques such as higher resolution computed tomography.
A lung metastasis registry analysis showed three factors improved survival: prolonged disease-free survival, especially longer than 36 months; a complete resection; and a small number of metastases and success in resecting them all (Eur J Cardiothorac Surg. 2002;22:335-44). A more recent meta-analysis showed the same results (J Thorac Dis. 2015;7:1441-51).
Bone
Bone metastases remain rare choices for surgical treatment. Most of the time, morbidity will be too high, and there are good options for systemic treatment. That leaves surgery reserved mostly for stabilization or the treatment of fractures.
However, there are a couple of exceptions, according to Dr. Rao. One multi-institutional randomized trial looked at metastatic epidural spinal cord compression. Subjects either underwent decompressive surgery with stabilization and radiation or radiation alone. Patients in the surgical group had a longer ambulatory period and had a lower usage rate of steroids and opioids. Morbidity outcomes were similar in both groups. Patients whose primary tumor was in the breast seemed to benefit the most with respect to ambulatory time (Lancet. 2005;9486:643-8; J Neurosurg Spine. 2008;8:271-8).
Sternal metastases represent another special case. 70% of the time, patients with sternal metastases have it as their only metastatic site. A French series of 33 patients who underwent aggressive chest wall and rib resection reported a 36% complication rate, while another study of 28 patients showed a 21% complication rate. Those complications are a problem, “but if you’re able to perform this in a resected tumor, there are long term survivors. As usual, triple negative breast cancers predicted a worse prognosis,” said Dr. Rao.
Dr. Rao concluded that resection of metastatic sites has a role. “I think it’s our responsibility as breast surgeons who are many times continuously following these patients to consider appropriate operations,” said Dr. Rao.
However, she did sound one note of caution. Surgery can interrupt therapy that is helping a patient. “Let’s say you have someone get a big liver resection, and then they have a tough time with recovery. There could be a long period of time they can’t get the therapy that was keeping them alive. That’s the real concern,” she said.
LAS VEGAS – Determination of whether excision of persistent breast cancer metastases can benefit the patient and even prolong survival depends on the location of the metastatic lesions, an investigator said at the annual meeting of the American Society of Breast Surgeons.
Before making the decision, it’s important to restage the patient’s disease and to recheck the receptor status if a biopsy is accessible, said Roshni Rao, MD, of the University of Texas Southwestern Medical Center.
Brain
Survival is worse when there are concurrent extracranial metastases or when brain metastases are greater than 5 cm, in patients with triple negative tumors, and in patients with a Karnofsky score of 70 or less, Dr. Rao said.
Surgery has the greatest benefit in patients with a single metastasis, with no extracranial disease, and who are able to undergo adjuvant whole brain radiation. In these cases, surgery improves survival, lowers recurrence rates, and reduces the risk of death neurological causes, she said.
Long-term survival is most common with continuous adjuvant therapy, either trastuzumab or hormonal, and in patients with a longer time interval to development of metastases. One series showed a 20-month survival increase.
Liver
Approximately 15% of patients with synchronous metastases will have liver metastases, and about half of stage IV patients will experience liver metastases at some point during treatment.
There is evidence from colorectal cancer that removing liver metastases is beneficial, and that has prompted interest in a similar approach in breast cancer. Liver resection has also become safer with new advances.
Dr. Rao discussed a single-institution study which took an aggressive approach to liver resection in 85 patients (Ann Surg. 2006;244:897-907). The researchers found that increased survival was associated with a good response to adjuvant chemotherapy, an r0 or r1 resection, and in patients who had a previous liver resection and were healthy enough to undergo another resection.
Overall, existing studies support liver resection if there are one to three lesions, if negative margins can be achieved, if the tumors are hormone receptor positive, and if the cancer is hormone positive and has good response to chemotherapy.
Dr. Rao emphasized that liver resections should be performed with a multidisciplinary team and should only be attempted at centers with low morbidity and where the doctors are experienced with liver resection.
When it’s possible, liver resection is beneficial. “There have been multiple reports of long-term survivors with no evidence of disease. There is likely a survival benefit with careful selection of these patients,” Dr. Rao said.
Lung
Lung surgeries are becoming safer, especially with the availability of video-assisted techniques, and pulmonary metastases are increasingly being spotted using more sensitive techniques such as higher resolution computed tomography.
A lung metastasis registry analysis showed three factors improved survival: prolonged disease-free survival, especially longer than 36 months; a complete resection; and a small number of metastases and success in resecting them all (Eur J Cardiothorac Surg. 2002;22:335-44). A more recent meta-analysis showed the same results (J Thorac Dis. 2015;7:1441-51).
Bone
Bone metastases remain rare choices for surgical treatment. Most of the time, morbidity will be too high, and there are good options for systemic treatment. That leaves surgery reserved mostly for stabilization or the treatment of fractures.
However, there are a couple of exceptions, according to Dr. Rao. One multi-institutional randomized trial looked at metastatic epidural spinal cord compression. Subjects either underwent decompressive surgery with stabilization and radiation or radiation alone. Patients in the surgical group had a longer ambulatory period and had a lower usage rate of steroids and opioids. Morbidity outcomes were similar in both groups. Patients whose primary tumor was in the breast seemed to benefit the most with respect to ambulatory time (Lancet. 2005;9486:643-8; J Neurosurg Spine. 2008;8:271-8).
Sternal metastases represent another special case. 70% of the time, patients with sternal metastases have it as their only metastatic site. A French series of 33 patients who underwent aggressive chest wall and rib resection reported a 36% complication rate, while another study of 28 patients showed a 21% complication rate. Those complications are a problem, “but if you’re able to perform this in a resected tumor, there are long term survivors. As usual, triple negative breast cancers predicted a worse prognosis,” said Dr. Rao.
Dr. Rao concluded that resection of metastatic sites has a role. “I think it’s our responsibility as breast surgeons who are many times continuously following these patients to consider appropriate operations,” said Dr. Rao.
However, she did sound one note of caution. Surgery can interrupt therapy that is helping a patient. “Let’s say you have someone get a big liver resection, and then they have a tough time with recovery. There could be a long period of time they can’t get the therapy that was keeping them alive. That’s the real concern,” she said.
LAS VEGAS – Determination of whether excision of persistent breast cancer metastases can benefit the patient and even prolong survival depends on the location of the metastatic lesions, an investigator said at the annual meeting of the American Society of Breast Surgeons.
Before making the decision, it’s important to restage the patient’s disease and to recheck the receptor status if a biopsy is accessible, said Roshni Rao, MD, of the University of Texas Southwestern Medical Center.
Brain
Survival is worse when there are concurrent extracranial metastases or when brain metastases are greater than 5 cm, in patients with triple negative tumors, and in patients with a Karnofsky score of 70 or less, Dr. Rao said.
Surgery has the greatest benefit in patients with a single metastasis, with no extracranial disease, and who are able to undergo adjuvant whole brain radiation. In these cases, surgery improves survival, lowers recurrence rates, and reduces the risk of death neurological causes, she said.
Long-term survival is most common with continuous adjuvant therapy, either trastuzumab or hormonal, and in patients with a longer time interval to development of metastases. One series showed a 20-month survival increase.
Liver
Approximately 15% of patients with synchronous metastases will have liver metastases, and about half of stage IV patients will experience liver metastases at some point during treatment.
There is evidence from colorectal cancer that removing liver metastases is beneficial, and that has prompted interest in a similar approach in breast cancer. Liver resection has also become safer with new advances.
Dr. Rao discussed a single-institution study which took an aggressive approach to liver resection in 85 patients (Ann Surg. 2006;244:897-907). The researchers found that increased survival was associated with a good response to adjuvant chemotherapy, an r0 or r1 resection, and in patients who had a previous liver resection and were healthy enough to undergo another resection.
Overall, existing studies support liver resection if there are one to three lesions, if negative margins can be achieved, if the tumors are hormone receptor positive, and if the cancer is hormone positive and has good response to chemotherapy.
Dr. Rao emphasized that liver resections should be performed with a multidisciplinary team and should only be attempted at centers with low morbidity and where the doctors are experienced with liver resection.
When it’s possible, liver resection is beneficial. “There have been multiple reports of long-term survivors with no evidence of disease. There is likely a survival benefit with careful selection of these patients,” Dr. Rao said.
Lung
Lung surgeries are becoming safer, especially with the availability of video-assisted techniques, and pulmonary metastases are increasingly being spotted using more sensitive techniques such as higher resolution computed tomography.
A lung metastasis registry analysis showed three factors improved survival: prolonged disease-free survival, especially longer than 36 months; a complete resection; and a small number of metastases and success in resecting them all (Eur J Cardiothorac Surg. 2002;22:335-44). A more recent meta-analysis showed the same results (J Thorac Dis. 2015;7:1441-51).
Bone
Bone metastases remain rare choices for surgical treatment. Most of the time, morbidity will be too high, and there are good options for systemic treatment. That leaves surgery reserved mostly for stabilization or the treatment of fractures.
However, there are a couple of exceptions, according to Dr. Rao. One multi-institutional randomized trial looked at metastatic epidural spinal cord compression. Subjects either underwent decompressive surgery with stabilization and radiation or radiation alone. Patients in the surgical group had a longer ambulatory period and had a lower usage rate of steroids and opioids. Morbidity outcomes were similar in both groups. Patients whose primary tumor was in the breast seemed to benefit the most with respect to ambulatory time (Lancet. 2005;9486:643-8; J Neurosurg Spine. 2008;8:271-8).
Sternal metastases represent another special case. 70% of the time, patients with sternal metastases have it as their only metastatic site. A French series of 33 patients who underwent aggressive chest wall and rib resection reported a 36% complication rate, while another study of 28 patients showed a 21% complication rate. Those complications are a problem, “but if you’re able to perform this in a resected tumor, there are long term survivors. As usual, triple negative breast cancers predicted a worse prognosis,” said Dr. Rao.
Dr. Rao concluded that resection of metastatic sites has a role. “I think it’s our responsibility as breast surgeons who are many times continuously following these patients to consider appropriate operations,” said Dr. Rao.
However, she did sound one note of caution. Surgery can interrupt therapy that is helping a patient. “Let’s say you have someone get a big liver resection, and then they have a tough time with recovery. There could be a long period of time they can’t get the therapy that was keeping them alive. That’s the real concern,” she said.
EXPERT ANALYSIS FROM ASBS 2017
Think twice before recommending partial meniscectomy
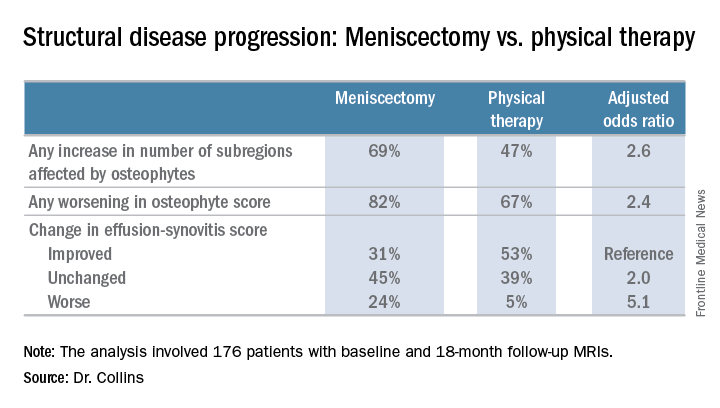
LAS VEGAS – Patients with knee osteoarthritis (OA) and a meniscal tear who underwent arthroscopic partial meniscectomy (APM) subsequently experienced accelerated structural progression of their OA, compared with those randomized to physical therapy alone in the randomized METEOR trial.
“In discussing treatment options for symptomatic meniscal tear, patients and providers must weigh the potential benefits and risks of arthroscopic partial meniscectomy, including this increased risk of structural progression,” Jamie E. Collins, PhD, said at the World Congress on Osteoarthritis.

A thorough physician-patient discussion also needs to mention that several large randomized trials have suggested that patients with meniscal tear and osteoarthritic changes experience similar pain relief with APM plus physical therapy (PT) as compared with PT alone, she added at the congress sponsored by the Osteoarthritis Research Society International.
The METEOR trial was a seven-center U.S. randomized trial of APM plus PT or PT alone in patients with MRI or radiographic evidence of OA changes, a meniscal tear on MRI, and mechanical knee symptoms. Dr. Collins reported on 176 randomized patients with baseline and 18-month follow-up MRIs read by a specialist musculoskeletal radiologist. This analysis excluded the 37 patients in the PT group who crossed over to APM within 6 months after randomization.
There was no significant difference between the two treatment groups in changes in bone marrow lesions or Hoffa-synovitis.
A secondary analysis that incorporated the 37 crossovers from PT to APM within 6 months showed similarly accelerated OA progression after arthroscopic surgery.
“Future work should focus on determining whether this accelerated structural progression is associated with changes in symptoms and ultimately with a higher risk of total knee replacement. In other words, is 2+ structural worsening something that’s noticeable or important for patients?” Dr. Collins concluded.
She reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
LAS VEGAS – Patients with knee osteoarthritis (OA) and a meniscal tear who underwent arthroscopic partial meniscectomy (APM) subsequently experienced accelerated structural progression of their OA, compared with those randomized to physical therapy alone in the randomized METEOR trial.
“In discussing treatment options for symptomatic meniscal tear, patients and providers must weigh the potential benefits and risks of arthroscopic partial meniscectomy, including this increased risk of structural progression,” Jamie E. Collins, PhD, said at the World Congress on Osteoarthritis.
A thorough physician-patient discussion also needs to mention that several large randomized trials have suggested that patients with meniscal tear and osteoarthritic changes experience similar pain relief with APM plus physical therapy (PT) as compared with PT alone, she added at the congress sponsored by the Osteoarthritis Research Society International.
The METEOR trial was a seven-center U.S. randomized trial of APM plus PT or PT alone in patients with MRI or radiographic evidence of OA changes, a meniscal tear on MRI, and mechanical knee symptoms. Dr. Collins reported on 176 randomized patients with baseline and 18-month follow-up MRIs read by a specialist musculoskeletal radiologist. This analysis excluded the 37 patients in the PT group who crossed over to APM within 6 months after randomization.
There was no significant difference between the two treatment groups in changes in bone marrow lesions or Hoffa-synovitis.
A secondary analysis that incorporated the 37 crossovers from PT to APM within 6 months showed similarly accelerated OA progression after arthroscopic surgery.
“Future work should focus on determining whether this accelerated structural progression is associated with changes in symptoms and ultimately with a higher risk of total knee replacement. In other words, is 2+ structural worsening something that’s noticeable or important for patients?” Dr. Collins concluded.
She reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
LAS VEGAS – Patients with knee osteoarthritis (OA) and a meniscal tear who underwent arthroscopic partial meniscectomy (APM) subsequently experienced accelerated structural progression of their OA, compared with those randomized to physical therapy alone in the randomized METEOR trial.
“In discussing treatment options for symptomatic meniscal tear, patients and providers must weigh the potential benefits and risks of arthroscopic partial meniscectomy, including this increased risk of structural progression,” Jamie E. Collins, PhD, said at the World Congress on Osteoarthritis.
A thorough physician-patient discussion also needs to mention that several large randomized trials have suggested that patients with meniscal tear and osteoarthritic changes experience similar pain relief with APM plus physical therapy (PT) as compared with PT alone, she added at the congress sponsored by the Osteoarthritis Research Society International.
The METEOR trial was a seven-center U.S. randomized trial of APM plus PT or PT alone in patients with MRI or radiographic evidence of OA changes, a meniscal tear on MRI, and mechanical knee symptoms. Dr. Collins reported on 176 randomized patients with baseline and 18-month follow-up MRIs read by a specialist musculoskeletal radiologist. This analysis excluded the 37 patients in the PT group who crossed over to APM within 6 months after randomization.
There was no significant difference between the two treatment groups in changes in bone marrow lesions or Hoffa-synovitis.
A secondary analysis that incorporated the 37 crossovers from PT to APM within 6 months showed similarly accelerated OA progression after arthroscopic surgery.
“Future work should focus on determining whether this accelerated structural progression is associated with changes in symptoms and ultimately with a higher risk of total knee replacement. In other words, is 2+ structural worsening something that’s noticeable or important for patients?” Dr. Collins concluded.
She reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
AT OARSI 2017
Key clinical point:
Major finding: Surgically treated patients were 2.6 times more likely to demonstrate MRI evidence of structural disease progression at 18 months than those who received physical therapy alone.
Data source: This analysis from the multicenter METEOR trial included 176 patients with a symptomatic meniscal tear.
Disclosures: The presenter reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
Roux-en-Y bests sleeve gastrectomy for weight loss
AT ENDO 2017
ORLANDO – Roux-en-Y gastric bypass resulted in greater weight loss than sleeve gastrectomy in a study that followed more than 700 patients, an effect that was sustained over time.
However, surgical complications were more common than with sleeve gastrectomy, and patients were more likely to have an extended hospital stay.
The study, conducted by Corey Lager, MD, and his collaborators at the University of Michigan Medical Center, Ann Arbor, looked at 5-year outcomes for 380 patients who had Roux-en-Y gastric bypass (RYGB), compared with those for 336 patients who received sleeve gastrectomy (SG).
Specific outcomes examined included the amount of absolute weight loss and excess body weight loss over the 5-year study period, whether obesity-related comorbidities resolved, and the type and number of complications seen with each procedure.
Sleeve gastrectomy is becoming increasingly popular, even as RYGB and adjustable gastric banding procedures have become more and more rare, Dr. Lager said at the annual meeting of the Endocrine Society. Duodenal switch procedures have continued to represent a very small proportion of surgical weight loss surgeries. Of the four, SG accounted for nearly 80% of the procedures performed in 2013; RYGB, which accounted for about 60% of procedures in 2006, fell to about 30% of procedures by 2013.
The investigators conducted a retrospective analysis of patients undergoing RYGB or SG from January 2008 to November 2013. Patients were seen annually in postoperative follow-up, so the study was able to track body mass index (BMI), weight, excess body weight loss, hemoglobin A1c levels, blood pressure, and serum lipid and vitamin levels over the 5-year period. Additionally, the study captured 30-day postoperative complications for each procedure.
Although about 80% of patients undergoing each procedure were female and baseline lab values and characteristics were similar in many respects, patients undergoing sleeve gastrectomy had higher body weight (mean, 143 kg) and BMI (mean, 50 kg/m2), compared with those who received RYGB (weight, 133 kg; BMI, 47; P less than .001 for both). The average age in both groups was about 45 years.
Sleeve gastrectomy patients were less likely to continue for the full 5 years of follow-up. Of 336 SG patients originally enrolled, 93 had 5-year data. Of the 380 RYGB patients, 188 returned for the 5-year follow-up.
At all time points, the RYGB patients had significantly more total weight loss than the SG patients (P less than .05); the initial weight loss for RYGB patients approached 28% of body weight at year 1, compared with about 23% for the SG patients. By the end of the 5-year period, RYGB patients had maintained about a 24% weight loss, compared with almost 20% for the SG group.
This pattern was mirrored for BMI in each cohort: At year 1, the RYGB patients were down about 14 points, compared with about 12 points for the SG group. By year 5, the difference had narrowed so that each group had lost a mean of between 11 and 12 points from their original BMI, but the difference was still statistically significant (P less than .05).
The final measure of weight loss was excess body weight lost, and again, RYGB patients lost significantly more of their excess body weight at all time points than did the SG patients. At the end of the first year, RYGB had lost more than 65% of their excess body weight, compared with about 48% for the SG patients. By 5 years, the SG patients had regained enough weight that their net excess weight loss was a little less than 40%, while the RYGB patients’ regain put them at about 55% excess weight loss by the end of the study period.
In terms of biomarkers, systolic blood pressure did not differ significantly between the three groups except at study year 3, though the RYGB group had numerically slightly lower systolic blood pressures at all time points. Total cholesterol was lower at 1, 2, 4, and 5 years after surgery for the RYGB group.
Sleeve gastrectomy, as expected, had lower rates of grade I surgical complications, including hemorrhage and infection. Also, the SG patients had fewer postsurgical emergency department visits and a shorter length of stay.
The study results were consistent with those of a 2016 meta-analysis that favored RYGB in terms of excess weight lost, readmission for diabetes-related complications, and resolution of hypertension (Obes Surg. 2016 Feb;26[2]:429-42).
Although this was a large study, it was limited by its retrospective nature and by the lack of randomization, said Dr. Lager. Retaining patients for long-term follow-up was also an issue: Of the original 719 patients, 507 were followed at 3 years and 281 at 5 years, so a significant number weren’t tracked for the full 5 years.
Dr. Lager reported no conflicts of interest, and the study had no outside sources of funding.
[email protected]
On Twitter @karioakes
AT ENDO 2017
ORLANDO – Roux-en-Y gastric bypass resulted in greater weight loss than sleeve gastrectomy in a study that followed more than 700 patients, an effect that was sustained over time.
However, surgical complications were more common than with sleeve gastrectomy, and patients were more likely to have an extended hospital stay.
The study, conducted by Corey Lager, MD, and his collaborators at the University of Michigan Medical Center, Ann Arbor, looked at 5-year outcomes for 380 patients who had Roux-en-Y gastric bypass (RYGB), compared with those for 336 patients who received sleeve gastrectomy (SG).
Specific outcomes examined included the amount of absolute weight loss and excess body weight loss over the 5-year study period, whether obesity-related comorbidities resolved, and the type and number of complications seen with each procedure.
Sleeve gastrectomy is becoming increasingly popular, even as RYGB and adjustable gastric banding procedures have become more and more rare, Dr. Lager said at the annual meeting of the Endocrine Society. Duodenal switch procedures have continued to represent a very small proportion of surgical weight loss surgeries. Of the four, SG accounted for nearly 80% of the procedures performed in 2013; RYGB, which accounted for about 60% of procedures in 2006, fell to about 30% of procedures by 2013.
The investigators conducted a retrospective analysis of patients undergoing RYGB or SG from January 2008 to November 2013. Patients were seen annually in postoperative follow-up, so the study was able to track body mass index (BMI), weight, excess body weight loss, hemoglobin A1c levels, blood pressure, and serum lipid and vitamin levels over the 5-year period. Additionally, the study captured 30-day postoperative complications for each procedure.
Although about 80% of patients undergoing each procedure were female and baseline lab values and characteristics were similar in many respects, patients undergoing sleeve gastrectomy had higher body weight (mean, 143 kg) and BMI (mean, 50 kg/m2), compared with those who received RYGB (weight, 133 kg; BMI, 47; P less than .001 for both). The average age in both groups was about 45 years.
Sleeve gastrectomy patients were less likely to continue for the full 5 years of follow-up. Of 336 SG patients originally enrolled, 93 had 5-year data. Of the 380 RYGB patients, 188 returned for the 5-year follow-up.
At all time points, the RYGB patients had significantly more total weight loss than the SG patients (P less than .05); the initial weight loss for RYGB patients approached 28% of body weight at year 1, compared with about 23% for the SG patients. By the end of the 5-year period, RYGB patients had maintained about a 24% weight loss, compared with almost 20% for the SG group.
This pattern was mirrored for BMI in each cohort: At year 1, the RYGB patients were down about 14 points, compared with about 12 points for the SG group. By year 5, the difference had narrowed so that each group had lost a mean of between 11 and 12 points from their original BMI, but the difference was still statistically significant (P less than .05).
The final measure of weight loss was excess body weight lost, and again, RYGB patients lost significantly more of their excess body weight at all time points than did the SG patients. At the end of the first year, RYGB had lost more than 65% of their excess body weight, compared with about 48% for the SG patients. By 5 years, the SG patients had regained enough weight that their net excess weight loss was a little less than 40%, while the RYGB patients’ regain put them at about 55% excess weight loss by the end of the study period.
In terms of biomarkers, systolic blood pressure did not differ significantly between the three groups except at study year 3, though the RYGB group had numerically slightly lower systolic blood pressures at all time points. Total cholesterol was lower at 1, 2, 4, and 5 years after surgery for the RYGB group.
Sleeve gastrectomy, as expected, had lower rates of grade I surgical complications, including hemorrhage and infection. Also, the SG patients had fewer postsurgical emergency department visits and a shorter length of stay.
The study results were consistent with those of a 2016 meta-analysis that favored RYGB in terms of excess weight lost, readmission for diabetes-related complications, and resolution of hypertension (Obes Surg. 2016 Feb;26[2]:429-42).
Although this was a large study, it was limited by its retrospective nature and by the lack of randomization, said Dr. Lager. Retaining patients for long-term follow-up was also an issue: Of the original 719 patients, 507 were followed at 3 years and 281 at 5 years, so a significant number weren’t tracked for the full 5 years.
Dr. Lager reported no conflicts of interest, and the study had no outside sources of funding.
[email protected]
On Twitter @karioakes
AT ENDO 2017
ORLANDO – Roux-en-Y gastric bypass resulted in greater weight loss than sleeve gastrectomy in a study that followed more than 700 patients, an effect that was sustained over time.
However, surgical complications were more common than with sleeve gastrectomy, and patients were more likely to have an extended hospital stay.
The study, conducted by Corey Lager, MD, and his collaborators at the University of Michigan Medical Center, Ann Arbor, looked at 5-year outcomes for 380 patients who had Roux-en-Y gastric bypass (RYGB), compared with those for 336 patients who received sleeve gastrectomy (SG).
Specific outcomes examined included the amount of absolute weight loss and excess body weight loss over the 5-year study period, whether obesity-related comorbidities resolved, and the type and number of complications seen with each procedure.
Sleeve gastrectomy is becoming increasingly popular, even as RYGB and adjustable gastric banding procedures have become more and more rare, Dr. Lager said at the annual meeting of the Endocrine Society. Duodenal switch procedures have continued to represent a very small proportion of surgical weight loss surgeries. Of the four, SG accounted for nearly 80% of the procedures performed in 2013; RYGB, which accounted for about 60% of procedures in 2006, fell to about 30% of procedures by 2013.
The investigators conducted a retrospective analysis of patients undergoing RYGB or SG from January 2008 to November 2013. Patients were seen annually in postoperative follow-up, so the study was able to track body mass index (BMI), weight, excess body weight loss, hemoglobin A1c levels, blood pressure, and serum lipid and vitamin levels over the 5-year period. Additionally, the study captured 30-day postoperative complications for each procedure.
Although about 80% of patients undergoing each procedure were female and baseline lab values and characteristics were similar in many respects, patients undergoing sleeve gastrectomy had higher body weight (mean, 143 kg) and BMI (mean, 50 kg/m2), compared with those who received RYGB (weight, 133 kg; BMI, 47; P less than .001 for both). The average age in both groups was about 45 years.
Sleeve gastrectomy patients were less likely to continue for the full 5 years of follow-up. Of 336 SG patients originally enrolled, 93 had 5-year data. Of the 380 RYGB patients, 188 returned for the 5-year follow-up.
At all time points, the RYGB patients had significantly more total weight loss than the SG patients (P less than .05); the initial weight loss for RYGB patients approached 28% of body weight at year 1, compared with about 23% for the SG patients. By the end of the 5-year period, RYGB patients had maintained about a 24% weight loss, compared with almost 20% for the SG group.
This pattern was mirrored for BMI in each cohort: At year 1, the RYGB patients were down about 14 points, compared with about 12 points for the SG group. By year 5, the difference had narrowed so that each group had lost a mean of between 11 and 12 points from their original BMI, but the difference was still statistically significant (P less than .05).
The final measure of weight loss was excess body weight lost, and again, RYGB patients lost significantly more of their excess body weight at all time points than did the SG patients. At the end of the first year, RYGB had lost more than 65% of their excess body weight, compared with about 48% for the SG patients. By 5 years, the SG patients had regained enough weight that their net excess weight loss was a little less than 40%, while the RYGB patients’ regain put them at about 55% excess weight loss by the end of the study period.
In terms of biomarkers, systolic blood pressure did not differ significantly between the three groups except at study year 3, though the RYGB group had numerically slightly lower systolic blood pressures at all time points. Total cholesterol was lower at 1, 2, 4, and 5 years after surgery for the RYGB group.
Sleeve gastrectomy, as expected, had lower rates of grade I surgical complications, including hemorrhage and infection. Also, the SG patients had fewer postsurgical emergency department visits and a shorter length of stay.
The study results were consistent with those of a 2016 meta-analysis that favored RYGB in terms of excess weight lost, readmission for diabetes-related complications, and resolution of hypertension (Obes Surg. 2016 Feb;26[2]:429-42).
Although this was a large study, it was limited by its retrospective nature and by the lack of randomization, said Dr. Lager. Retaining patients for long-term follow-up was also an issue: Of the original 719 patients, 507 were followed at 3 years and 281 at 5 years, so a significant number weren’t tracked for the full 5 years.
Dr. Lager reported no conflicts of interest, and the study had no outside sources of funding.
[email protected]
On Twitter @karioakes
Key clinical point:
Major finding: At 5 years post surgery, Roux-en-Y recipients had kept off 25% of their body weight, compared with 20% for sleeve gastrectomy patients (P less than .05).
Data source: Longitudinal follow-up of 716 patients who had one of two surgical procedures for weight loss.
Disclosures: None of the study authors reported relevant disclosures, and no external source of funding was reported.
Nomogram may direct diabetes patients to best operation
PHILADELPHIA – A nomogram that assigns a disease severity score to individuals with type 2 diabetes may provide a tool that helps surgeons, endocrinologists, and primary care physicians determine which weight-loss surgical procedure would be most effective, according to an analysis of 900 patients from Cleveland Clinic and University Hospital Clinic, Barcelona, reported at the annual meeting of the American Surgical Association.
“This is the largest reported cohort with long-term glycemic follow-up data that categorizes diabetes into three validated stages of severity to guide procedure selection,” said Ali Aminian, MD, of Cleveland Clinic. The study also highlighted the importance of surgery in early diabetes. The study involved a modeling cohort of 659 patients who had bariatric procedures at Cleveland Clinic from 2005 to 2011 and a separate data set of 241 patients from Barcelona to validate the findings. Roux-en-Y gastric bypass (RYGB) was performed in 78% of the Cleveland Clinic group and 49% of the Barcelona group, with the remainder having sleeve gastrectomy (SG).

RYGB and SG account for more than 95% of all bariatric procedures in people with type 2 diabetes, Dr. Aminian said, but outcomes of clinical trials have been variable, some reporting up to half of patients having long-term relapses. The Cleveland Clinic study involved all patients with type 2 diabetes who had RYGB or SG from 2005 to 2011 with 5 years or more of glycemic data, with a median follow-up of 7 years. The study used American Diabetes Association targets to define remission and glycemic control.
“Long-term response after bariatric surgery in patients with diabetes significantly differs according to diabetes severity,” Dr. Aminian said. “For example, the outcome of surgery in a patient who has diabetes for 2 years is significantly different than a patient who has diabetes for 15 years taking three medications, including insulin.”
The researchers generated the nomogram based on these four independent preoperative factors:
- Number of preoperative diabetes medications (P less than .0001).
- Insulin use (P = .002).
- Duration of diabetes (P less than .0001).
- Glycemic control (P = .002).
“These factors are readily available in clinical practice and are considered a proxy of functional pancreatic beta-cell reserve,” Dr. Aminian said. The nomogram scores the severity of each factor on a scale of 0 to 100. For example, one preoperative medication scores 12, but five scores 63; duration of diabetes of 1 year scores five points, but 16 years scores 60. The patient’s total points represent the Individualized Metabolic Surgery score.
The researchers assigned three categories: A score of 25 or less represents mild disease, a score of 25-95 represents moderate, and 95 to the maximum 180 is severe disease.
Based on the Cleveland Clinic and Barcelona cohorts, the researchers next developed recommendations for average risk patients in each category.
RYGB is “suggested” in mild disease based on remission rates of 92% in the Cleveland subgroup and 91% in the Barcelona subgroup vs. SG remission rates of 74% and 91%, respectively. On the other end of the spectrum, in patients with severe diabetes, both procedures were less effective in achieving long-term diabetes remission. The disparities were more pronounced for the moderate group: 60% and 70% for RYGB and 25% and 56% for SG in the Cleveland Clinic and Barcelona subgroups, respectively. Hence the nomogram highly “recommends” RYGB. An online calculator to determine Individualized Metabolic Surgery score is available at http://riskcalc.org/Metabolic_Surgery_Score/.
“Obviously, this is the first attempt toward individualized procedure selection and more work needs to be done,” Dr. Aminian said. “Our findings also highlight the importance of surgical intervention in early stages of diabetes in order to achieve sustainable remission.”
In his discussion, Matthew M. Hutter, MD, FACS, of Harvard Medical School, Boston, offered to “quibble” with Dr. Aminian’s conclusions. “I challenge you on your conclusion for the mild and severe categories,” Dr. Hutter said. “My rate-of-cure data makes me want to recommend bypass for any patient with diabetes – mild, moderate or severe.”
Dr. Aminian acknowledged that the number of SG cases in the severe subgroup – 51 – was not great, and long-term diabetes remission was comparable between the two procedures. The key distinguishing measure in the severe category was a net 8% difference between two procedures in glycemic control at last follow-up. “This is the difference that we must decide whether it’s clinically important or not – whether we’re willing to recommend a riskier procedure for an extra 8% achieving glycemic control,” Dr. Aminian said. “If someone thinks it’s worth the risk, then they may suggest gastric bypass. If someone thinks it’s not worth the risk, then they may suggest a sleeve gastrectomy. But, we should remember that patients in the severe group are very high-risk patients.”
Dr. Aminian reported no financial disclosures. Dr. Hutter disclosed receiving conference reimbursement from Olympus.
The complete manuscript of this study and its presentation at the American Surgical Association’s 137th Annual Meeting, April 2017, in Philadelphia, Pennsylvania, is to be published in Annals of Surgery pending editorial review.
PHILADELPHIA – A nomogram that assigns a disease severity score to individuals with type 2 diabetes may provide a tool that helps surgeons, endocrinologists, and primary care physicians determine which weight-loss surgical procedure would be most effective, according to an analysis of 900 patients from Cleveland Clinic and University Hospital Clinic, Barcelona, reported at the annual meeting of the American Surgical Association.
“This is the largest reported cohort with long-term glycemic follow-up data that categorizes diabetes into three validated stages of severity to guide procedure selection,” said Ali Aminian, MD, of Cleveland Clinic. The study also highlighted the importance of surgery in early diabetes. The study involved a modeling cohort of 659 patients who had bariatric procedures at Cleveland Clinic from 2005 to 2011 and a separate data set of 241 patients from Barcelona to validate the findings. Roux-en-Y gastric bypass (RYGB) was performed in 78% of the Cleveland Clinic group and 49% of the Barcelona group, with the remainder having sleeve gastrectomy (SG).
RYGB and SG account for more than 95% of all bariatric procedures in people with type 2 diabetes, Dr. Aminian said, but outcomes of clinical trials have been variable, some reporting up to half of patients having long-term relapses. The Cleveland Clinic study involved all patients with type 2 diabetes who had RYGB or SG from 2005 to 2011 with 5 years or more of glycemic data, with a median follow-up of 7 years. The study used American Diabetes Association targets to define remission and glycemic control.
“Long-term response after bariatric surgery in patients with diabetes significantly differs according to diabetes severity,” Dr. Aminian said. “For example, the outcome of surgery in a patient who has diabetes for 2 years is significantly different than a patient who has diabetes for 15 years taking three medications, including insulin.”
The researchers generated the nomogram based on these four independent preoperative factors:
- Number of preoperative diabetes medications (P less than .0001).
- Insulin use (P = .002).
- Duration of diabetes (P less than .0001).
- Glycemic control (P = .002).
“These factors are readily available in clinical practice and are considered a proxy of functional pancreatic beta-cell reserve,” Dr. Aminian said. The nomogram scores the severity of each factor on a scale of 0 to 100. For example, one preoperative medication scores 12, but five scores 63; duration of diabetes of 1 year scores five points, but 16 years scores 60. The patient’s total points represent the Individualized Metabolic Surgery score.
The researchers assigned three categories: A score of 25 or less represents mild disease, a score of 25-95 represents moderate, and 95 to the maximum 180 is severe disease.
Based on the Cleveland Clinic and Barcelona cohorts, the researchers next developed recommendations for average risk patients in each category.
RYGB is “suggested” in mild disease based on remission rates of 92% in the Cleveland subgroup and 91% in the Barcelona subgroup vs. SG remission rates of 74% and 91%, respectively. On the other end of the spectrum, in patients with severe diabetes, both procedures were less effective in achieving long-term diabetes remission. The disparities were more pronounced for the moderate group: 60% and 70% for RYGB and 25% and 56% for SG in the Cleveland Clinic and Barcelona subgroups, respectively. Hence the nomogram highly “recommends” RYGB. An online calculator to determine Individualized Metabolic Surgery score is available at http://riskcalc.org/Metabolic_Surgery_Score/.
“Obviously, this is the first attempt toward individualized procedure selection and more work needs to be done,” Dr. Aminian said. “Our findings also highlight the importance of surgical intervention in early stages of diabetes in order to achieve sustainable remission.”
In his discussion, Matthew M. Hutter, MD, FACS, of Harvard Medical School, Boston, offered to “quibble” with Dr. Aminian’s conclusions. “I challenge you on your conclusion for the mild and severe categories,” Dr. Hutter said. “My rate-of-cure data makes me want to recommend bypass for any patient with diabetes – mild, moderate or severe.”
Dr. Aminian acknowledged that the number of SG cases in the severe subgroup – 51 – was not great, and long-term diabetes remission was comparable between the two procedures. The key distinguishing measure in the severe category was a net 8% difference between two procedures in glycemic control at last follow-up. “This is the difference that we must decide whether it’s clinically important or not – whether we’re willing to recommend a riskier procedure for an extra 8% achieving glycemic control,” Dr. Aminian said. “If someone thinks it’s worth the risk, then they may suggest gastric bypass. If someone thinks it’s not worth the risk, then they may suggest a sleeve gastrectomy. But, we should remember that patients in the severe group are very high-risk patients.”
Dr. Aminian reported no financial disclosures. Dr. Hutter disclosed receiving conference reimbursement from Olympus.
The complete manuscript of this study and its presentation at the American Surgical Association’s 137th Annual Meeting, April 2017, in Philadelphia, Pennsylvania, is to be published in Annals of Surgery pending editorial review.
PHILADELPHIA – A nomogram that assigns a disease severity score to individuals with type 2 diabetes may provide a tool that helps surgeons, endocrinologists, and primary care physicians determine which weight-loss surgical procedure would be most effective, according to an analysis of 900 patients from Cleveland Clinic and University Hospital Clinic, Barcelona, reported at the annual meeting of the American Surgical Association.
“This is the largest reported cohort with long-term glycemic follow-up data that categorizes diabetes into three validated stages of severity to guide procedure selection,” said Ali Aminian, MD, of Cleveland Clinic. The study also highlighted the importance of surgery in early diabetes. The study involved a modeling cohort of 659 patients who had bariatric procedures at Cleveland Clinic from 2005 to 2011 and a separate data set of 241 patients from Barcelona to validate the findings. Roux-en-Y gastric bypass (RYGB) was performed in 78% of the Cleveland Clinic group and 49% of the Barcelona group, with the remainder having sleeve gastrectomy (SG).
RYGB and SG account for more than 95% of all bariatric procedures in people with type 2 diabetes, Dr. Aminian said, but outcomes of clinical trials have been variable, some reporting up to half of patients having long-term relapses. The Cleveland Clinic study involved all patients with type 2 diabetes who had RYGB or SG from 2005 to 2011 with 5 years or more of glycemic data, with a median follow-up of 7 years. The study used American Diabetes Association targets to define remission and glycemic control.
“Long-term response after bariatric surgery in patients with diabetes significantly differs according to diabetes severity,” Dr. Aminian said. “For example, the outcome of surgery in a patient who has diabetes for 2 years is significantly different than a patient who has diabetes for 15 years taking three medications, including insulin.”
The researchers generated the nomogram based on these four independent preoperative factors:
- Number of preoperative diabetes medications (P less than .0001).
- Insulin use (P = .002).
- Duration of diabetes (P less than .0001).
- Glycemic control (P = .002).
“These factors are readily available in clinical practice and are considered a proxy of functional pancreatic beta-cell reserve,” Dr. Aminian said. The nomogram scores the severity of each factor on a scale of 0 to 100. For example, one preoperative medication scores 12, but five scores 63; duration of diabetes of 1 year scores five points, but 16 years scores 60. The patient’s total points represent the Individualized Metabolic Surgery score.
The researchers assigned three categories: A score of 25 or less represents mild disease, a score of 25-95 represents moderate, and 95 to the maximum 180 is severe disease.
Based on the Cleveland Clinic and Barcelona cohorts, the researchers next developed recommendations for average risk patients in each category.
RYGB is “suggested” in mild disease based on remission rates of 92% in the Cleveland subgroup and 91% in the Barcelona subgroup vs. SG remission rates of 74% and 91%, respectively. On the other end of the spectrum, in patients with severe diabetes, both procedures were less effective in achieving long-term diabetes remission. The disparities were more pronounced for the moderate group: 60% and 70% for RYGB and 25% and 56% for SG in the Cleveland Clinic and Barcelona subgroups, respectively. Hence the nomogram highly “recommends” RYGB. An online calculator to determine Individualized Metabolic Surgery score is available at http://riskcalc.org/Metabolic_Surgery_Score/.
“Obviously, this is the first attempt toward individualized procedure selection and more work needs to be done,” Dr. Aminian said. “Our findings also highlight the importance of surgical intervention in early stages of diabetes in order to achieve sustainable remission.”
In his discussion, Matthew M. Hutter, MD, FACS, of Harvard Medical School, Boston, offered to “quibble” with Dr. Aminian’s conclusions. “I challenge you on your conclusion for the mild and severe categories,” Dr. Hutter said. “My rate-of-cure data makes me want to recommend bypass for any patient with diabetes – mild, moderate or severe.”
Dr. Aminian acknowledged that the number of SG cases in the severe subgroup – 51 – was not great, and long-term diabetes remission was comparable between the two procedures. The key distinguishing measure in the severe category was a net 8% difference between two procedures in glycemic control at last follow-up. “This is the difference that we must decide whether it’s clinically important or not – whether we’re willing to recommend a riskier procedure for an extra 8% achieving glycemic control,” Dr. Aminian said. “If someone thinks it’s worth the risk, then they may suggest gastric bypass. If someone thinks it’s not worth the risk, then they may suggest a sleeve gastrectomy. But, we should remember that patients in the severe group are very high-risk patients.”
Dr. Aminian reported no financial disclosures. Dr. Hutter disclosed receiving conference reimbursement from Olympus.
The complete manuscript of this study and its presentation at the American Surgical Association’s 137th Annual Meeting, April 2017, in Philadelphia, Pennsylvania, is to be published in Annals of Surgery pending editorial review.
AT THE ASA ANNUAL MEETING
Key clinical point: A nomogram has been developed that assigns an Individualized Metabolic Surgery score to individuals with type 2 diabetes to help determine which type of bariatric procedure would provide best outcomes.
Major finding: In mild diabetes (Individualized Metabolic Surgery score less than or equal to 25), Roux-en-Y gastric bypass and sleeve gastrectomy significantly improve diabetes. For patients with severe diabetes (IMS Score greater than 95), both procedures have similarly low efficacy for diabetes remission.
Data source: Analysis of 900 patients with type 2 diabetes who had either Roux-en-Y gastric bypass or sleeve gastrectomy with a minimum 5-year follow-up.
Disclosure: Dr. Aminian reported no financial disclosures. Dr. Hutter disclosed receiving conference reimbursement from Olympus.
How bariatric surgery improves knee osteoarthritis
LAS VEGAS – Most of the improvement in knee pain that occurs following bariatric surgery in obese patients with knee osteoarthritis happens in the first month after surgery, well before the bulk of the weight loss takes place, Jonathan Samuels, MD, reported at the World Congress on Osteoarthritis.
This observation suggests that bariatric surgery’s mechanism of benefit in patients with knee osteoarthritis (OA) isn’t simply a matter of reduced mechanical load on the joints caused by a lessened weight burden, Dr. Samuels observed at the World Congress on Osteoarthritis, sponsored by the Osteoarthritis Research Society International.
Indeed, his prospective study of 150 obese patients with comorbid knee OA points to metabolic factors as likely playing a key role.

His study, featuring 2 years of follow-up to date, showed that bariatric surgery improved knee OA proportionate to the percentage of excess weight loss achieved. The greatest reduction in knee pain as well as the most profound weight loss occurred in the 35 patients who underwent gastric bypass and the 97 who opted for sleeve gastrectomy; patients who underwent laparoscopic adjustable gastric banding had more modest outcomes on both scores.
The disparate timing of the reductions in excess weight and knee pain was particularly eye catching. With all three forms of bariatric surgery, weight loss continued steadily for roughly the first 12 months. It then plateaued and was generally maintained at the new body mass index for the second 12 months.
In contrast, improvement in knee pain according to the validated Knee Injury and Osteoarthritis Outcome Score (KOOS) leveled out after just 1 month post surgery and was then sustained through 23 months. Levels of the inflammatory cytokines and adipokines interleukin-6, interleukin-1 receptor antagonist, and lipopolysaccharides were elevated at baseline but dropped steadily in concert with the reduction in excess body weight during the first 12 months after surgery. In contrast, levels of the anti-inflammatory cytokine sRAGE (soluble receptor for advanced glycation end products) were abnormally low prior to surgery but increased sharply for the first 3 months afterward before leveling off. And levels of serum leptin, which were roughly sevenfold greater than in normal controls at baseline, fell precipitously during the first month after bariatric surgery before plateauing, following the same pattern as the improvement in knee pain.
“This suggests that perhaps leptin is the key mediator in this OA population,” said Dr. Samuels.
Obese patients with knee OA are in a catch-22 situation. Obese individuals are at greatly increased lifetime risk of developing knee OA, and patients with chronic knee pain have a tough time losing weight.
“The treatments that might work with either obesity or knee pain alone often fail when both of these are present,” he observed.
That’s why bariatric surgery is becoming an increasingly popular treatment strategy in these patients. Sleeve gastrectomy, gastric bypass, and laparoscopic adjustable gastric banding are all Food and Drug Administration approved treatments for obesity in the presence of at least one qualifying comorbid condition, and knee OA qualifies.
Dr. Samuels reported having no financial conflicts regarding his study.
LAS VEGAS – Most of the improvement in knee pain that occurs following bariatric surgery in obese patients with knee osteoarthritis happens in the first month after surgery, well before the bulk of the weight loss takes place, Jonathan Samuels, MD, reported at the World Congress on Osteoarthritis.
This observation suggests that bariatric surgery’s mechanism of benefit in patients with knee osteoarthritis (OA) isn’t simply a matter of reduced mechanical load on the joints caused by a lessened weight burden, Dr. Samuels observed at the World Congress on Osteoarthritis, sponsored by the Osteoarthritis Research Society International.
Indeed, his prospective study of 150 obese patients with comorbid knee OA points to metabolic factors as likely playing a key role.
His study, featuring 2 years of follow-up to date, showed that bariatric surgery improved knee OA proportionate to the percentage of excess weight loss achieved. The greatest reduction in knee pain as well as the most profound weight loss occurred in the 35 patients who underwent gastric bypass and the 97 who opted for sleeve gastrectomy; patients who underwent laparoscopic adjustable gastric banding had more modest outcomes on both scores.
The disparate timing of the reductions in excess weight and knee pain was particularly eye catching. With all three forms of bariatric surgery, weight loss continued steadily for roughly the first 12 months. It then plateaued and was generally maintained at the new body mass index for the second 12 months.
In contrast, improvement in knee pain according to the validated Knee Injury and Osteoarthritis Outcome Score (KOOS) leveled out after just 1 month post surgery and was then sustained through 23 months. Levels of the inflammatory cytokines and adipokines interleukin-6, interleukin-1 receptor antagonist, and lipopolysaccharides were elevated at baseline but dropped steadily in concert with the reduction in excess body weight during the first 12 months after surgery. In contrast, levels of the anti-inflammatory cytokine sRAGE (soluble receptor for advanced glycation end products) were abnormally low prior to surgery but increased sharply for the first 3 months afterward before leveling off. And levels of serum leptin, which were roughly sevenfold greater than in normal controls at baseline, fell precipitously during the first month after bariatric surgery before plateauing, following the same pattern as the improvement in knee pain.
“This suggests that perhaps leptin is the key mediator in this OA population,” said Dr. Samuels.
Obese patients with knee OA are in a catch-22 situation. Obese individuals are at greatly increased lifetime risk of developing knee OA, and patients with chronic knee pain have a tough time losing weight.
“The treatments that might work with either obesity or knee pain alone often fail when both of these are present,” he observed.
That’s why bariatric surgery is becoming an increasingly popular treatment strategy in these patients. Sleeve gastrectomy, gastric bypass, and laparoscopic adjustable gastric banding are all Food and Drug Administration approved treatments for obesity in the presence of at least one qualifying comorbid condition, and knee OA qualifies.
Dr. Samuels reported having no financial conflicts regarding his study.
LAS VEGAS – Most of the improvement in knee pain that occurs following bariatric surgery in obese patients with knee osteoarthritis happens in the first month after surgery, well before the bulk of the weight loss takes place, Jonathan Samuels, MD, reported at the World Congress on Osteoarthritis.
This observation suggests that bariatric surgery’s mechanism of benefit in patients with knee osteoarthritis (OA) isn’t simply a matter of reduced mechanical load on the joints caused by a lessened weight burden, Dr. Samuels observed at the World Congress on Osteoarthritis, sponsored by the Osteoarthritis Research Society International.
Indeed, his prospective study of 150 obese patients with comorbid knee OA points to metabolic factors as likely playing a key role.
His study, featuring 2 years of follow-up to date, showed that bariatric surgery improved knee OA proportionate to the percentage of excess weight loss achieved. The greatest reduction in knee pain as well as the most profound weight loss occurred in the 35 patients who underwent gastric bypass and the 97 who opted for sleeve gastrectomy; patients who underwent laparoscopic adjustable gastric banding had more modest outcomes on both scores.
The disparate timing of the reductions in excess weight and knee pain was particularly eye catching. With all three forms of bariatric surgery, weight loss continued steadily for roughly the first 12 months. It then plateaued and was generally maintained at the new body mass index for the second 12 months.
In contrast, improvement in knee pain according to the validated Knee Injury and Osteoarthritis Outcome Score (KOOS) leveled out after just 1 month post surgery and was then sustained through 23 months. Levels of the inflammatory cytokines and adipokines interleukin-6, interleukin-1 receptor antagonist, and lipopolysaccharides were elevated at baseline but dropped steadily in concert with the reduction in excess body weight during the first 12 months after surgery. In contrast, levels of the anti-inflammatory cytokine sRAGE (soluble receptor for advanced glycation end products) were abnormally low prior to surgery but increased sharply for the first 3 months afterward before leveling off. And levels of serum leptin, which were roughly sevenfold greater than in normal controls at baseline, fell precipitously during the first month after bariatric surgery before plateauing, following the same pattern as the improvement in knee pain.
“This suggests that perhaps leptin is the key mediator in this OA population,” said Dr. Samuels.
Obese patients with knee OA are in a catch-22 situation. Obese individuals are at greatly increased lifetime risk of developing knee OA, and patients with chronic knee pain have a tough time losing weight.
“The treatments that might work with either obesity or knee pain alone often fail when both of these are present,” he observed.
That’s why bariatric surgery is becoming an increasingly popular treatment strategy in these patients. Sleeve gastrectomy, gastric bypass, and laparoscopic adjustable gastric banding are all Food and Drug Administration approved treatments for obesity in the presence of at least one qualifying comorbid condition, and knee OA qualifies.
Dr. Samuels reported having no financial conflicts regarding his study.
AT OARSI 2017
Key clinical point:
Major finding: Most of the improvement in knee pain – and most of the accompanying drop in serum leptin – happens in the first month following bariatric surgery, well before most weight loss has occurred.
Data source: A prospective observational study of 150 obese patients with knee osteoarthritis who underwent bariatric surgery.
Disclosures: The study presenter reported having no financial conflicts.
Big data study looks at safety of concurrent surgical procedures
PHILADELPHIA – Overlapping and concurrent surgical procedures operations are not uncommon, but data on their safety and quality are scarce.
An analysis of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data suggests that concurrent operations do not pose any greater risk to patients than do nonconcurrent operations.
“We found that concurrent operations were more often elective inpatient operations at large academic hospitals,” Jason Liu, MD, a clinical scholar-in-residence with the American College of Surgeons, Chicago, said at the annual meeting of the American Surgical Association.
The study evaluated 12,010 concurrent and 521,656 nonconcurrent operations in the ASC NSQIP registry between 2014 and 2015, and propensity-score matched 11,044 operations of each type to evaluate safety. “We then analyzed the three primary outcomes – death or serious morbidity, unplanned reoperation, and unplanned readmission,” Dr. Liu said. “After propensity matching and risk adjustment, we detected no association of concurrent operations with these adverse outcomes.”
Death or serious morbidity had an odds ratio of 1.08, while the odds ratio for reoperation and readmission were 1.16 and 1.14, respectively.
Of the five surgery subspecialty groups presented, ear, nose and throat surgeons performed the highest proportion of concurrent operations, comprising 11.2% of all operations within the subspecialty, followed by neurosurgeons (8.4%) and urological surgeons (5.2%). General surgeons performed more total concurrent cases than did any of the other surgical subspecialties, but these comprised only 1.5% of all general surgery cases.
Among the individual operations presented, the highest percentage of concurrent cases was for spinal operations, comprising 7.1% of all spinal surgeries, followed by total knee and hip replacements, at 2.1% each. Among general surgery procedures, concurrent operations comprised 1.9% of colon surgeries, 1.5% of ventral hernia repairs, and 0.9% of cholecystectomies.
“We found that patients who had concurrent operations tended to have fewer comorbidities,” Dr. Liu said.
Despite the findings suggesting concurrent operations are safe, Dr. Liu added that “failure to detect an effect does not prove its absence. Additional studies and continued vigilance are certainly needed moving forward.”
In her discussion, Valerie W. Rusch, MD, FACS, of Memorial Sloan-Kettering Cancer Center, New York, pointed out that the American College of Surgeons has not revised its statement that considers concurrent surgery “not appropriate,” and that the study itself “reflects both the strengths and weaknesses of ‘big data.’ ” While ACS NSQIP provides a large number of patients, the study authors were still constrained in using time as a proxy for concurrence, she said. “Also, as noted, this analysis reports only a sample of operations rather than all the procedures performed, and the authors were constrained to using simulated statistical methods to avoid misclassification of cases,” Dr. Rusch said.
The death or serious morbidity composite measure the study used may not identify procedure-specific or specialty-specific adverse events that could reflect differences in outcomes between concurrent and nonconcurrent operations, she said. “Nonetheless, this study represents an important step toward bringing science to an extremely important and rightfully contentious aspect of surgical practice,” Dr. Rusch said.
Senior coauthor David Hoyt, MD, FACS, of the ACS, acknowledged the many study limitations Dr. Rusch pointed out. “What this analysis shows is that probably there’s not a huge problem with morbidity and mortality,” Dr. Hoyt said. “It doesn’t really say that we should pursue this without some care of how we do this.”
A key element in planning concurrent surgery is disclosing that to the patient. “Much of what came out of the discussion that led to this was because patients felt that they were not informed,” Dr. Hoyt said. “It really has to do with an ethical issue of patient autonomy.”
Dr. Liu, Dr. Hoyt, and Dr. Rusch had no financial relationships to disclose.
The complete manuscript of this study and its presentation at the American Surgical Association’s 137th Annual Meeting, April 2017, in Philadelphia, Pennsylvania, is anticipated to be published in the Annals of Surgery pending editorial review.
PHILADELPHIA – Overlapping and concurrent surgical procedures operations are not uncommon, but data on their safety and quality are scarce.
An analysis of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data suggests that concurrent operations do not pose any greater risk to patients than do nonconcurrent operations.
“We found that concurrent operations were more often elective inpatient operations at large academic hospitals,” Jason Liu, MD, a clinical scholar-in-residence with the American College of Surgeons, Chicago, said at the annual meeting of the American Surgical Association.
The study evaluated 12,010 concurrent and 521,656 nonconcurrent operations in the ASC NSQIP registry between 2014 and 2015, and propensity-score matched 11,044 operations of each type to evaluate safety. “We then analyzed the three primary outcomes – death or serious morbidity, unplanned reoperation, and unplanned readmission,” Dr. Liu said. “After propensity matching and risk adjustment, we detected no association of concurrent operations with these adverse outcomes.”
Death or serious morbidity had an odds ratio of 1.08, while the odds ratio for reoperation and readmission were 1.16 and 1.14, respectively.
Of the five surgery subspecialty groups presented, ear, nose and throat surgeons performed the highest proportion of concurrent operations, comprising 11.2% of all operations within the subspecialty, followed by neurosurgeons (8.4%) and urological surgeons (5.2%). General surgeons performed more total concurrent cases than did any of the other surgical subspecialties, but these comprised only 1.5% of all general surgery cases.
Among the individual operations presented, the highest percentage of concurrent cases was for spinal operations, comprising 7.1% of all spinal surgeries, followed by total knee and hip replacements, at 2.1% each. Among general surgery procedures, concurrent operations comprised 1.9% of colon surgeries, 1.5% of ventral hernia repairs, and 0.9% of cholecystectomies.
“We found that patients who had concurrent operations tended to have fewer comorbidities,” Dr. Liu said.
Despite the findings suggesting concurrent operations are safe, Dr. Liu added that “failure to detect an effect does not prove its absence. Additional studies and continued vigilance are certainly needed moving forward.”
In her discussion, Valerie W. Rusch, MD, FACS, of Memorial Sloan-Kettering Cancer Center, New York, pointed out that the American College of Surgeons has not revised its statement that considers concurrent surgery “not appropriate,” and that the study itself “reflects both the strengths and weaknesses of ‘big data.’ ” While ACS NSQIP provides a large number of patients, the study authors were still constrained in using time as a proxy for concurrence, she said. “Also, as noted, this analysis reports only a sample of operations rather than all the procedures performed, and the authors were constrained to using simulated statistical methods to avoid misclassification of cases,” Dr. Rusch said.
The death or serious morbidity composite measure the study used may not identify procedure-specific or specialty-specific adverse events that could reflect differences in outcomes between concurrent and nonconcurrent operations, she said. “Nonetheless, this study represents an important step toward bringing science to an extremely important and rightfully contentious aspect of surgical practice,” Dr. Rusch said.
Senior coauthor David Hoyt, MD, FACS, of the ACS, acknowledged the many study limitations Dr. Rusch pointed out. “What this analysis shows is that probably there’s not a huge problem with morbidity and mortality,” Dr. Hoyt said. “It doesn’t really say that we should pursue this without some care of how we do this.”
A key element in planning concurrent surgery is disclosing that to the patient. “Much of what came out of the discussion that led to this was because patients felt that they were not informed,” Dr. Hoyt said. “It really has to do with an ethical issue of patient autonomy.”
Dr. Liu, Dr. Hoyt, and Dr. Rusch had no financial relationships to disclose.
The complete manuscript of this study and its presentation at the American Surgical Association’s 137th Annual Meeting, April 2017, in Philadelphia, Pennsylvania, is anticipated to be published in the Annals of Surgery pending editorial review.
PHILADELPHIA – Overlapping and concurrent surgical procedures operations are not uncommon, but data on their safety and quality are scarce.
An analysis of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data suggests that concurrent operations do not pose any greater risk to patients than do nonconcurrent operations.
“We found that concurrent operations were more often elective inpatient operations at large academic hospitals,” Jason Liu, MD, a clinical scholar-in-residence with the American College of Surgeons, Chicago, said at the annual meeting of the American Surgical Association.
The study evaluated 12,010 concurrent and 521,656 nonconcurrent operations in the ASC NSQIP registry between 2014 and 2015, and propensity-score matched 11,044 operations of each type to evaluate safety. “We then analyzed the three primary outcomes – death or serious morbidity, unplanned reoperation, and unplanned readmission,” Dr. Liu said. “After propensity matching and risk adjustment, we detected no association of concurrent operations with these adverse outcomes.”
Death or serious morbidity had an odds ratio of 1.08, while the odds ratio for reoperation and readmission were 1.16 and 1.14, respectively.
Of the five surgery subspecialty groups presented, ear, nose and throat surgeons performed the highest proportion of concurrent operations, comprising 11.2% of all operations within the subspecialty, followed by neurosurgeons (8.4%) and urological surgeons (5.2%). General surgeons performed more total concurrent cases than did any of the other surgical subspecialties, but these comprised only 1.5% of all general surgery cases.
Among the individual operations presented, the highest percentage of concurrent cases was for spinal operations, comprising 7.1% of all spinal surgeries, followed by total knee and hip replacements, at 2.1% each. Among general surgery procedures, concurrent operations comprised 1.9% of colon surgeries, 1.5% of ventral hernia repairs, and 0.9% of cholecystectomies.
“We found that patients who had concurrent operations tended to have fewer comorbidities,” Dr. Liu said.
Despite the findings suggesting concurrent operations are safe, Dr. Liu added that “failure to detect an effect does not prove its absence. Additional studies and continued vigilance are certainly needed moving forward.”
In her discussion, Valerie W. Rusch, MD, FACS, of Memorial Sloan-Kettering Cancer Center, New York, pointed out that the American College of Surgeons has not revised its statement that considers concurrent surgery “not appropriate,” and that the study itself “reflects both the strengths and weaknesses of ‘big data.’ ” While ACS NSQIP provides a large number of patients, the study authors were still constrained in using time as a proxy for concurrence, she said. “Also, as noted, this analysis reports only a sample of operations rather than all the procedures performed, and the authors were constrained to using simulated statistical methods to avoid misclassification of cases,” Dr. Rusch said.
The death or serious morbidity composite measure the study used may not identify procedure-specific or specialty-specific adverse events that could reflect differences in outcomes between concurrent and nonconcurrent operations, she said. “Nonetheless, this study represents an important step toward bringing science to an extremely important and rightfully contentious aspect of surgical practice,” Dr. Rusch said.
Senior coauthor David Hoyt, MD, FACS, of the ACS, acknowledged the many study limitations Dr. Rusch pointed out. “What this analysis shows is that probably there’s not a huge problem with morbidity and mortality,” Dr. Hoyt said. “It doesn’t really say that we should pursue this without some care of how we do this.”
A key element in planning concurrent surgery is disclosing that to the patient. “Much of what came out of the discussion that led to this was because patients felt that they were not informed,” Dr. Hoyt said. “It really has to do with an ethical issue of patient autonomy.”
Dr. Liu, Dr. Hoyt, and Dr. Rusch had no financial relationships to disclose.
The complete manuscript of this study and its presentation at the American Surgical Association’s 137th Annual Meeting, April 2017, in Philadelphia, Pennsylvania, is anticipated to be published in the Annals of Surgery pending editorial review.
AT THE ASA ANNUAL MEETING
Key clinical point: Concurrent operations were not associated with an increased risk for worse outcomes, compared with nonconcurrent operations.
Major finding: After propensity-score matching and risk adjustment, the adjusted odds ratio for death or serious mortality was 1.08, and for reoperation, 1.16, for concurrent operations vs. nonconcurrent operations.
Data source: Propensity-score-matched concurrent and nonconcurrent operations (n = 11,044 for each) done in 2014 and 2015 in the American College of Surgeons National Surgical Quality Improvement Program registry.
Disclosures: Dr. Liu and coauthors had no financial relationships to disclose.
Novel robotic camera photographs colon
A novel robotically driven capsule successfully navigated a colon in a pig model in 100% of 30 retroflexion maneuvers, setting the stage for further study of robotics in colonoscopy. The data were presented at the annual Digestive Disease Week.
Although capsule technology has expanded exploration of the GI tract, current capsules are limited by passive movement and lack therapeutic capability, said Keith L. Obstein, MD, of Vanderbilt University in Nashville, Tenn.
The researchers developed a capsule with an 18-mm head and interior permanent magnets designed to be automatically controlled by an external robotic arm in difficult areas.
“Retroflexion is a common but mechanically complex maneuver during colonoscopy, and therefore serves as an excellent subject for autonomous control,” the researchers noted.
Logistically, the capsule is soft-tethered after it is introduced through the rectum, which allows the potential for therapeutic procedures such as biopsies and polyp removal. In addition, the use of an external magnet to pull the robot with the tether may reduce the pressure on the colon that typically created when a physician pushes the colonoscope from behind. Therefore, use of a robotic capsule may help reduce patients’ discomfort and make them more amenable to the procedure, Dr. Obstein said.
In the study, an endoscopist performed the first retroflexion with a standard colonoscope at 15 cm from the anal sphincter, and these parameters were used to set the robotic system for autonomous retroflexion at 15 cm from the anal sphincter.
The success rate was 100% for both the standard endoscope and the automatically controlled robot for each of 30 maneuvers. The average time for a robotic maneuver was 12 seconds, and no leaks or histologic abnormalities were noted.
Studies to evaluate additional control algorithms are in progress, and the robot capsule may be ready for human trials in 2018, Dr. Obstein said.
This study was supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health under award number R01EB018992. Dr. Obstein had no relevant financial conflicts to disclose.
Digestive Disease Week® is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE) and the Society for Surgery of the Alimentary Tract (SSAT).
A novel robotically driven capsule successfully navigated a colon in a pig model in 100% of 30 retroflexion maneuvers, setting the stage for further study of robotics in colonoscopy. The data were presented at the annual Digestive Disease Week.
Although capsule technology has expanded exploration of the GI tract, current capsules are limited by passive movement and lack therapeutic capability, said Keith L. Obstein, MD, of Vanderbilt University in Nashville, Tenn.
The researchers developed a capsule with an 18-mm head and interior permanent magnets designed to be automatically controlled by an external robotic arm in difficult areas.
“Retroflexion is a common but mechanically complex maneuver during colonoscopy, and therefore serves as an excellent subject for autonomous control,” the researchers noted.
Logistically, the capsule is soft-tethered after it is introduced through the rectum, which allows the potential for therapeutic procedures such as biopsies and polyp removal. In addition, the use of an external magnet to pull the robot with the tether may reduce the pressure on the colon that typically created when a physician pushes the colonoscope from behind. Therefore, use of a robotic capsule may help reduce patients’ discomfort and make them more amenable to the procedure, Dr. Obstein said.
In the study, an endoscopist performed the first retroflexion with a standard colonoscope at 15 cm from the anal sphincter, and these parameters were used to set the robotic system for autonomous retroflexion at 15 cm from the anal sphincter.
The success rate was 100% for both the standard endoscope and the automatically controlled robot for each of 30 maneuvers. The average time for a robotic maneuver was 12 seconds, and no leaks or histologic abnormalities were noted.
Studies to evaluate additional control algorithms are in progress, and the robot capsule may be ready for human trials in 2018, Dr. Obstein said.
This study was supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health under award number R01EB018992. Dr. Obstein had no relevant financial conflicts to disclose.
Digestive Disease Week® is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE) and the Society for Surgery of the Alimentary Tract (SSAT).
A novel robotically driven capsule successfully navigated a colon in a pig model in 100% of 30 retroflexion maneuvers, setting the stage for further study of robotics in colonoscopy. The data were presented at the annual Digestive Disease Week.
Although capsule technology has expanded exploration of the GI tract, current capsules are limited by passive movement and lack therapeutic capability, said Keith L. Obstein, MD, of Vanderbilt University in Nashville, Tenn.
The researchers developed a capsule with an 18-mm head and interior permanent magnets designed to be automatically controlled by an external robotic arm in difficult areas.
“Retroflexion is a common but mechanically complex maneuver during colonoscopy, and therefore serves as an excellent subject for autonomous control,” the researchers noted.
Logistically, the capsule is soft-tethered after it is introduced through the rectum, which allows the potential for therapeutic procedures such as biopsies and polyp removal. In addition, the use of an external magnet to pull the robot with the tether may reduce the pressure on the colon that typically created when a physician pushes the colonoscope from behind. Therefore, use of a robotic capsule may help reduce patients’ discomfort and make them more amenable to the procedure, Dr. Obstein said.
In the study, an endoscopist performed the first retroflexion with a standard colonoscope at 15 cm from the anal sphincter, and these parameters were used to set the robotic system for autonomous retroflexion at 15 cm from the anal sphincter.
The success rate was 100% for both the standard endoscope and the automatically controlled robot for each of 30 maneuvers. The average time for a robotic maneuver was 12 seconds, and no leaks or histologic abnormalities were noted.
Studies to evaluate additional control algorithms are in progress, and the robot capsule may be ready for human trials in 2018, Dr. Obstein said.
This study was supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health under award number R01EB018992. Dr. Obstein had no relevant financial conflicts to disclose.
Digestive Disease Week® is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE) and the Society for Surgery of the Alimentary Tract (SSAT).
FROM DDW
Key clinical point: An 18-mm magnetized capsule colonoscope successfully navigated a pig colon, and researchers are planning human trials for 2018.
Major finding: An automated robot capsule successfully completed 30 retroflexion maneuvers in a pig colon with an average time of 12 seconds.
Data source: The data come from a test of 30 maneuvers.
Disclosures: This study was supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health under award number R01EB018992. Dr. Obstein had no relevant financial conflicts to disclose.