User login
Official Newspaper of the American College of Surgeons
Laparoscopic colectomy cost savings linked to surgeon experience
Laparoscopic colectomy is less expensive than open colectomy only when it is performed by surgeons experienced with the laparoscopic approach, according to a study published in the Annals of Surgery.
Many studies have demonstrated that compared with the open surgery, the laparoscopic approach reduces the cost of major abdominal operations including colectomy by as much as 50%. These savings are attributed to the shorter length of stay and lower complication rate associated with laparoscopic surgery.

“The present study underscores and clarifies the complex relationship between surgeon experience, postoperative complications, and healthcare payments. It builds on prior analyses of surgical cohorts that demonstrate an association of higher complication rates with significantly increased total episode payments,” the investigators wrote.
To assess payments for laparoscopic vs. open colectomy, they performed a population-based analysis of information in a national Medicare database regarding 182,852 procedures done in 2010-2012. They included payments for complications, readmissions, and postacute care as well as for the surgery and hospital stay.
To examine any possible effects of the surgeons’ experience on the resulting costs, the data were divided into quartiles of experience with laparoscopy. The investigators then compared surgeons with the least experience (the lowest quartile), the most experience (the highest quartile), and intermediate experience (the two middle quartiles).
Among the surgeons with the least experience in laparoscopy, Medicare payments were actually higher for laparoscopic ($26,915) than for open colectomy ($23,312). In contrast, among surgeons with the most experience, payments were substantially lower for laparoscopic ($20,476) than for open colectomy ($23,793).
This difference was attributed to the less experienced surgeons’ higher complication rates; higher readmission rates; and greater need for postacute care services, such as discharging the patient to a skilled nursing facility rather than home, the investigators said (Ann Surg. 2017 May 25. doi: 10.1097/SLA.0000000000002312).
These findings demonstrate that “the financial benefits of laparoscopy are only realized when the surgeon has appropriate experience or proficiency.” They have important implications, highlighting the need for more rigorous credentialing standards for individual surgeons and for improving continuing medical education through more extensive proctoring or coaching to enhance surgical skills, Dr. Sheetz and his associates said.
The study results also “make a business case for investing in the training and retraining of surgeons in practice,” they added
“New procedures are continually introduced into practice, and surgeons need to take the time to learn them safely. Taking time to learn new procedures is expensive. Increasing the number of surgeons at a given hospital who are, however, proficient with complex laparoscopy has an important beneficial impact on the financial bottom line for hospitals and health care payers,” the investigators noted.
This study was supported by The National Institutes of Health. Dr. Sheetz and his associates reported having no relevant financial disclosures.
Laparoscopic colectomy is less expensive than open colectomy only when it is performed by surgeons experienced with the laparoscopic approach, according to a study published in the Annals of Surgery.
Many studies have demonstrated that compared with the open surgery, the laparoscopic approach reduces the cost of major abdominal operations including colectomy by as much as 50%. These savings are attributed to the shorter length of stay and lower complication rate associated with laparoscopic surgery.
“The present study underscores and clarifies the complex relationship between surgeon experience, postoperative complications, and healthcare payments. It builds on prior analyses of surgical cohorts that demonstrate an association of higher complication rates with significantly increased total episode payments,” the investigators wrote.
To assess payments for laparoscopic vs. open colectomy, they performed a population-based analysis of information in a national Medicare database regarding 182,852 procedures done in 2010-2012. They included payments for complications, readmissions, and postacute care as well as for the surgery and hospital stay.
To examine any possible effects of the surgeons’ experience on the resulting costs, the data were divided into quartiles of experience with laparoscopy. The investigators then compared surgeons with the least experience (the lowest quartile), the most experience (the highest quartile), and intermediate experience (the two middle quartiles).
Among the surgeons with the least experience in laparoscopy, Medicare payments were actually higher for laparoscopic ($26,915) than for open colectomy ($23,312). In contrast, among surgeons with the most experience, payments were substantially lower for laparoscopic ($20,476) than for open colectomy ($23,793).
This difference was attributed to the less experienced surgeons’ higher complication rates; higher readmission rates; and greater need for postacute care services, such as discharging the patient to a skilled nursing facility rather than home, the investigators said (Ann Surg. 2017 May 25. doi: 10.1097/SLA.0000000000002312).
These findings demonstrate that “the financial benefits of laparoscopy are only realized when the surgeon has appropriate experience or proficiency.” They have important implications, highlighting the need for more rigorous credentialing standards for individual surgeons and for improving continuing medical education through more extensive proctoring or coaching to enhance surgical skills, Dr. Sheetz and his associates said.
The study results also “make a business case for investing in the training and retraining of surgeons in practice,” they added
“New procedures are continually introduced into practice, and surgeons need to take the time to learn them safely. Taking time to learn new procedures is expensive. Increasing the number of surgeons at a given hospital who are, however, proficient with complex laparoscopy has an important beneficial impact on the financial bottom line for hospitals and health care payers,” the investigators noted.
This study was supported by The National Institutes of Health. Dr. Sheetz and his associates reported having no relevant financial disclosures.
Laparoscopic colectomy is less expensive than open colectomy only when it is performed by surgeons experienced with the laparoscopic approach, according to a study published in the Annals of Surgery.
Many studies have demonstrated that compared with the open surgery, the laparoscopic approach reduces the cost of major abdominal operations including colectomy by as much as 50%. These savings are attributed to the shorter length of stay and lower complication rate associated with laparoscopic surgery.
“The present study underscores and clarifies the complex relationship between surgeon experience, postoperative complications, and healthcare payments. It builds on prior analyses of surgical cohorts that demonstrate an association of higher complication rates with significantly increased total episode payments,” the investigators wrote.
To assess payments for laparoscopic vs. open colectomy, they performed a population-based analysis of information in a national Medicare database regarding 182,852 procedures done in 2010-2012. They included payments for complications, readmissions, and postacute care as well as for the surgery and hospital stay.
To examine any possible effects of the surgeons’ experience on the resulting costs, the data were divided into quartiles of experience with laparoscopy. The investigators then compared surgeons with the least experience (the lowest quartile), the most experience (the highest quartile), and intermediate experience (the two middle quartiles).
Among the surgeons with the least experience in laparoscopy, Medicare payments were actually higher for laparoscopic ($26,915) than for open colectomy ($23,312). In contrast, among surgeons with the most experience, payments were substantially lower for laparoscopic ($20,476) than for open colectomy ($23,793).
This difference was attributed to the less experienced surgeons’ higher complication rates; higher readmission rates; and greater need for postacute care services, such as discharging the patient to a skilled nursing facility rather than home, the investigators said (Ann Surg. 2017 May 25. doi: 10.1097/SLA.0000000000002312).
These findings demonstrate that “the financial benefits of laparoscopy are only realized when the surgeon has appropriate experience or proficiency.” They have important implications, highlighting the need for more rigorous credentialing standards for individual surgeons and for improving continuing medical education through more extensive proctoring or coaching to enhance surgical skills, Dr. Sheetz and his associates said.
The study results also “make a business case for investing in the training and retraining of surgeons in practice,” they added
“New procedures are continually introduced into practice, and surgeons need to take the time to learn them safely. Taking time to learn new procedures is expensive. Increasing the number of surgeons at a given hospital who are, however, proficient with complex laparoscopy has an important beneficial impact on the financial bottom line for hospitals and health care payers,” the investigators noted.
This study was supported by The National Institutes of Health. Dr. Sheetz and his associates reported having no relevant financial disclosures.
FROM THE ANNALS OF SURGERY
Key clinical point: Laparoscopic colectomy is less expensive than open colectomy only when it is performed by surgeons experienced with the laparoscopic approach.
Major finding: Among the surgeons with the least experience in laparoscopy, Medicare payments were actually higher for laparoscopic ($26,915) than for open colectomy ($23,312).
Data source: An analysis of Medicare payment data for 182,852 patients who had laparoscopic or open colectomy in 2010-2012.
Disclosures: This study was supported by The National Institutes of Health. Dr. Sheetz and his associates reported having no relevant financial disclosures.
Rural patients less likely to have bariatric surgery
Obese patients living in rural areas of West Virginia were substantially less likely than were their urban and suburban counterparts to have bariatric surgery, according to findings from a study comparing outcomes in two patient groups.
This discrepancy is attributed to a difference between rural and nonrural patients in type of insurance coverage. In this 2-year study, rural patients were nearly five times more likely to be covered by West Virginia Medicaid than were patients living in nonrural areas of the state, said Kristie L. Bergmann, PhD, of the department of behavioral medicine and psychiatry, West Virginia University, Morgantown, and her associates. The findings were published in Surgery for Obesity and Related Diseases (2017;13[4]:632-6), the journal of the American Society for Metabolic and Bariatric Surgery.
Previous research has identified rural patients’ lack of insurance as a barrier to health care. “Our results suggest that insurance denial represents a successive barrier. Despite being insured, rural individuals may be barred from surgery if insurance carriers do not offer it as a covered benefit, deny approval, or require indomitable prerequisites for surgery,” Dr. Bergmann and her associates said.
They examined the associations among rural status, access to bariatric surgery, and surgical outcomes in West Virginia in part because the state’s residents “have been consistently ranked as the most obese population in the United States, with approximately 35.1% of residents meeting criteria for obesity.” West Virginia also has the highest rates of diabetes (13%) and hypertension (41%) in the United States.
At the same time, rural populations are known to have decreased access to all forms of health care and specifically to bariatric surgery. This makes rural West Virginians “a particularly vulnerable population of interest,” the investigators said.
They performed a retrospective cohort study involving 122 obese patients seeking bariatric surgery at their university’s medical center during 2012-2014. A total of 97% of these patients were white, 83% were women, and the mean age was 47 years. Only 82 of the 122 study participants underwent bariatric surgery: 77 had Roux-en-Y gastric bypass and 5 had sleeve gastrectomy.
Rural residents were significantly less likely to undergo bariatric surgery than were nonrural patients, but coverage by West Virginia Medicaid explained 83.6% of this difference. When Medicaid patients were excluded from the analysis, nonrural status no longer predicted the use of bariatric surgery.
Moreover, when Medicaid coverage was controlled for, rural status had no effect on the effectiveness of bariatric surgery. Patients residing in rural areas had the same attendance at follow-up visits and the same reduction in body mass index at 6 months and at 12 months as did nonrural patients.
In addition, patients who had higher levels of education and who worked full-time were more likely to undergo bariatric surgery, but overall, rural patients were more likely to have comorbidities, disability, and lower rates of full-time work. “An argument can be made that rural individuals may have a greater medical need for bariatric surgery, as obesity and associated health conditions may contribute to lower rates of employment. Unfortunately, barring these patients from receiving care may reinforce a cycle of disability and declining health status,” Dr. Bergmann and her associates noted.
This study was limited in that it had a relatively small sample size, particularly in analyses that excluded Medicaid recipients. It also had a follow-up of only 1 year, so longer-term outcomes of bariatric surgery could not be assessed. “Our sample is also predominantly Caucasian and may have unique culturally-based characteristics” that limit the generalizability of the study findings, they added.
No specific sponsor was cited for this study. Dr. Bergmann and her associates reported having no relevant financial disclosures.
Obese patients living in rural areas of West Virginia were substantially less likely than were their urban and suburban counterparts to have bariatric surgery, according to findings from a study comparing outcomes in two patient groups.
This discrepancy is attributed to a difference between rural and nonrural patients in type of insurance coverage. In this 2-year study, rural patients were nearly five times more likely to be covered by West Virginia Medicaid than were patients living in nonrural areas of the state, said Kristie L. Bergmann, PhD, of the department of behavioral medicine and psychiatry, West Virginia University, Morgantown, and her associates. The findings were published in Surgery for Obesity and Related Diseases (2017;13[4]:632-6), the journal of the American Society for Metabolic and Bariatric Surgery.
Previous research has identified rural patients’ lack of insurance as a barrier to health care. “Our results suggest that insurance denial represents a successive barrier. Despite being insured, rural individuals may be barred from surgery if insurance carriers do not offer it as a covered benefit, deny approval, or require indomitable prerequisites for surgery,” Dr. Bergmann and her associates said.
They examined the associations among rural status, access to bariatric surgery, and surgical outcomes in West Virginia in part because the state’s residents “have been consistently ranked as the most obese population in the United States, with approximately 35.1% of residents meeting criteria for obesity.” West Virginia also has the highest rates of diabetes (13%) and hypertension (41%) in the United States.
At the same time, rural populations are known to have decreased access to all forms of health care and specifically to bariatric surgery. This makes rural West Virginians “a particularly vulnerable population of interest,” the investigators said.
They performed a retrospective cohort study involving 122 obese patients seeking bariatric surgery at their university’s medical center during 2012-2014. A total of 97% of these patients were white, 83% were women, and the mean age was 47 years. Only 82 of the 122 study participants underwent bariatric surgery: 77 had Roux-en-Y gastric bypass and 5 had sleeve gastrectomy.
Rural residents were significantly less likely to undergo bariatric surgery than were nonrural patients, but coverage by West Virginia Medicaid explained 83.6% of this difference. When Medicaid patients were excluded from the analysis, nonrural status no longer predicted the use of bariatric surgery.
Moreover, when Medicaid coverage was controlled for, rural status had no effect on the effectiveness of bariatric surgery. Patients residing in rural areas had the same attendance at follow-up visits and the same reduction in body mass index at 6 months and at 12 months as did nonrural patients.
In addition, patients who had higher levels of education and who worked full-time were more likely to undergo bariatric surgery, but overall, rural patients were more likely to have comorbidities, disability, and lower rates of full-time work. “An argument can be made that rural individuals may have a greater medical need for bariatric surgery, as obesity and associated health conditions may contribute to lower rates of employment. Unfortunately, barring these patients from receiving care may reinforce a cycle of disability and declining health status,” Dr. Bergmann and her associates noted.
This study was limited in that it had a relatively small sample size, particularly in analyses that excluded Medicaid recipients. It also had a follow-up of only 1 year, so longer-term outcomes of bariatric surgery could not be assessed. “Our sample is also predominantly Caucasian and may have unique culturally-based characteristics” that limit the generalizability of the study findings, they added.
No specific sponsor was cited for this study. Dr. Bergmann and her associates reported having no relevant financial disclosures.
Obese patients living in rural areas of West Virginia were substantially less likely than were their urban and suburban counterparts to have bariatric surgery, according to findings from a study comparing outcomes in two patient groups.
This discrepancy is attributed to a difference between rural and nonrural patients in type of insurance coverage. In this 2-year study, rural patients were nearly five times more likely to be covered by West Virginia Medicaid than were patients living in nonrural areas of the state, said Kristie L. Bergmann, PhD, of the department of behavioral medicine and psychiatry, West Virginia University, Morgantown, and her associates. The findings were published in Surgery for Obesity and Related Diseases (2017;13[4]:632-6), the journal of the American Society for Metabolic and Bariatric Surgery.
Previous research has identified rural patients’ lack of insurance as a barrier to health care. “Our results suggest that insurance denial represents a successive barrier. Despite being insured, rural individuals may be barred from surgery if insurance carriers do not offer it as a covered benefit, deny approval, or require indomitable prerequisites for surgery,” Dr. Bergmann and her associates said.
They examined the associations among rural status, access to bariatric surgery, and surgical outcomes in West Virginia in part because the state’s residents “have been consistently ranked as the most obese population in the United States, with approximately 35.1% of residents meeting criteria for obesity.” West Virginia also has the highest rates of diabetes (13%) and hypertension (41%) in the United States.
At the same time, rural populations are known to have decreased access to all forms of health care and specifically to bariatric surgery. This makes rural West Virginians “a particularly vulnerable population of interest,” the investigators said.
They performed a retrospective cohort study involving 122 obese patients seeking bariatric surgery at their university’s medical center during 2012-2014. A total of 97% of these patients were white, 83% were women, and the mean age was 47 years. Only 82 of the 122 study participants underwent bariatric surgery: 77 had Roux-en-Y gastric bypass and 5 had sleeve gastrectomy.
Rural residents were significantly less likely to undergo bariatric surgery than were nonrural patients, but coverage by West Virginia Medicaid explained 83.6% of this difference. When Medicaid patients were excluded from the analysis, nonrural status no longer predicted the use of bariatric surgery.
Moreover, when Medicaid coverage was controlled for, rural status had no effect on the effectiveness of bariatric surgery. Patients residing in rural areas had the same attendance at follow-up visits and the same reduction in body mass index at 6 months and at 12 months as did nonrural patients.
In addition, patients who had higher levels of education and who worked full-time were more likely to undergo bariatric surgery, but overall, rural patients were more likely to have comorbidities, disability, and lower rates of full-time work. “An argument can be made that rural individuals may have a greater medical need for bariatric surgery, as obesity and associated health conditions may contribute to lower rates of employment. Unfortunately, barring these patients from receiving care may reinforce a cycle of disability and declining health status,” Dr. Bergmann and her associates noted.
This study was limited in that it had a relatively small sample size, particularly in analyses that excluded Medicaid recipients. It also had a follow-up of only 1 year, so longer-term outcomes of bariatric surgery could not be assessed. “Our sample is also predominantly Caucasian and may have unique culturally-based characteristics” that limit the generalizability of the study findings, they added.
No specific sponsor was cited for this study. Dr. Bergmann and her associates reported having no relevant financial disclosures.
FROM SURGERY FOR OBESITY AND RELATED DISEASES
Key clinical point: Obese patients living in rural areas of West Virginia are substantially less likely than are their urban and suburban counterparts to have bariatric surgery.
Major finding: Rural residents were significantly less likely to undergo bariatric surgery than were nonrural patients, but coverage by West Virginia Medicaid explained 83.6% of this difference.
Data source: A retrospective single-center cohort study involving 122 obese West Virginians seeking bariatric surgery in 2012-2014.
Disclosures: No specific sponsor was cited for this study. Dr. Bergmann and her associates reported having no relevant financial disclosures.
The perils of the National Practitioner Data Bank
Question: With reference to the National Practitioner Data Bank (NPDB), which of the following statements is incorrect?
A. Both court judgments and out-of-court settlements are reportable to the NPDB.
B. Adverse actions by a hospital against a physician are reportable within 15 days.
C. In states with “Disclosure, Apology, and Offer” laws, a prompt settlement through mediation need not be reported.
D. Hospitals, state licensing boards, medical organizations, and the physician himself/herself can access the NPDB.
E. A plaintiff’s attorney cannot access the NPDB for information regarding a defendant.
Answer: C. Congress implemented the NPDB to collect information about an individual doctor’s malpractice and disciplinary histories, with the objective of restricting errant doctors from moving from one state to another.1
Federal law requires medical liability payments stemming from either a court judgment or an out-of-court settlement be reported to the NPDB. An institution’s disciplinary actions against a medical staff member must also be reported. In turn, the NPDB is obligated to make its information available to hospitals, state licensure boards, and legitimate medical organizations charged with granting privileges or membership. A physician also can ask to see his or her own records, but a plaintiff’s attorney cannot access the NPDB unless there is evidence that a hospital failed to query the NPDB as part of its credentialing process.

Some observers have claimed that the NPDB’s existence has hindered settlement negotiations, because many doctors fear being listed in the NPDB, thus significantly diminishing the likelihood of payments to satisfy a claim. It has been stated that within 6 years of NPDB’s inception, the probability that an injured patient’s claim would receive payment had fallen to 59% of the pre-NPDB level.
Many states have enacted so-called “apology laws” that promote full disclosure of medical errors and prompt out-of-court settlements, if warranted. However, the federal Department of Health and Human Services has ruled that all written demands for payment must be reported, even if the cases are resolved under state programs designed for early out-of-court resolution.
For example, a provision in the Oregon law asserts that a payment under the measure’s mediation mechanism “is not a payment resulting from a written claim or demand for payment.” The HHS has rejected this as “explicitly designed to avoid medical malpractice reporting to the NPDB for any claims that are part of the new process that do not proceed to litigation.”
Massachusetts’ 2012 apology law had proposed reporting only those cases where it was determined that a practitioner failed to meet the standard of care. The HHS responded by indicating that all cases had to be reported, regardless of whether care was determined to be up to standards, and that the state’s prelitigation notice to initiate the meditation process qualified as a reportable “written claim.”
Physicians can be impacted greatly by the NPDB. How much of an impact depends in large part on the underlying events and the wording of the report.
An NPDB account of a medical malpractice payment doesn’t necessarily affect a physician’s ability to practice, while those – especially when “severely-worded” – involving denial or restriction of privileges are taken more seriously by state licensing boards and employers. Physicians should therefore play an active role whenever a report to the NPDB appears likely.
The dispute review process is highly technical and requires the knowledge and skill of an experienced health law attorney. To start out, consider making a request to the reporting entity to correct or vacate the report due to error. If the reporting entity declines, the physician may request a review by the HHS and file an accompanying statement seeking to explain the report.
Yet, out of more than 800,000 total reports for all practitioner types captured in the system, apparently only 44,273 included accompanying clarifying statements by the physician. Risk managers have urged vigilance.
For example, it may be that multiple reports involved a single incident, leading to a “piling on” effect. If an adverse decision at one hospital caused a physician’s clinical privileges to be terminated, this might lead the state medical board to restrict the physician’s license. It is necessary to explain that both of these NPDB-reportable events involved the same incident, and that the state board did not have any independent knowledge of anything that was wrong.
Others have advised that one should always clarify one’s involvement, e.g., “I was not the main doctor in the case.” And if dismissed in a malpractice lawsuit, be sure your name or identifying information isn’t included in the judgment or settlement agreement.
Hospital disciplinary actions being far more serious, physicians would do well to familiarize themselves with medical staff bylaws dealing with peer review and investigations. To avoid being reported to the NPDB, physicians must resist adverse actions that would be in effect for more than 30 days and fight attempts to place restrictions or sanctions on their licenses by the hospital or professional societies. Don’t withdraw applications for privileges during an investigation.
The 2015 NPDB Guidebook, the first update in more than 10 years, contains important changes pertaining to hospital adverse actions.2 The regulations now require any “surrender” of privileges while the physician is a subject of an investigation to be a reportable event. Previously, physicians sought to avoid being reported by simply giving up their privileges when an adverse decision appeared imminent.
Surrender includes not renewing one’s hospital privileges or the taking of a leave of absence, and “investigation” is widely defined to include any formal inquiry into a physician’s competence or conduct. And there need not be any “nexus,” i.e., connection, between what is being investigated and the privileges surrendered, in order to be reportable.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Health Care Quality Improvement Act of 1986, 42 U.S.C. 11101 et seq.
2. 2015 NPDB e-Guidebook, available at www.npdb.hrsa.gov/resources/aboutGuidebooks.jsp.
Question: With reference to the National Practitioner Data Bank (NPDB), which of the following statements is incorrect?
A. Both court judgments and out-of-court settlements are reportable to the NPDB.
B. Adverse actions by a hospital against a physician are reportable within 15 days.
C. In states with “Disclosure, Apology, and Offer” laws, a prompt settlement through mediation need not be reported.
D. Hospitals, state licensing boards, medical organizations, and the physician himself/herself can access the NPDB.
E. A plaintiff’s attorney cannot access the NPDB for information regarding a defendant.
Answer: C. Congress implemented the NPDB to collect information about an individual doctor’s malpractice and disciplinary histories, with the objective of restricting errant doctors from moving from one state to another.1
Federal law requires medical liability payments stemming from either a court judgment or an out-of-court settlement be reported to the NPDB. An institution’s disciplinary actions against a medical staff member must also be reported. In turn, the NPDB is obligated to make its information available to hospitals, state licensure boards, and legitimate medical organizations charged with granting privileges or membership. A physician also can ask to see his or her own records, but a plaintiff’s attorney cannot access the NPDB unless there is evidence that a hospital failed to query the NPDB as part of its credentialing process.
Some observers have claimed that the NPDB’s existence has hindered settlement negotiations, because many doctors fear being listed in the NPDB, thus significantly diminishing the likelihood of payments to satisfy a claim. It has been stated that within 6 years of NPDB’s inception, the probability that an injured patient’s claim would receive payment had fallen to 59% of the pre-NPDB level.
Many states have enacted so-called “apology laws” that promote full disclosure of medical errors and prompt out-of-court settlements, if warranted. However, the federal Department of Health and Human Services has ruled that all written demands for payment must be reported, even if the cases are resolved under state programs designed for early out-of-court resolution.
For example, a provision in the Oregon law asserts that a payment under the measure’s mediation mechanism “is not a payment resulting from a written claim or demand for payment.” The HHS has rejected this as “explicitly designed to avoid medical malpractice reporting to the NPDB for any claims that are part of the new process that do not proceed to litigation.”
Massachusetts’ 2012 apology law had proposed reporting only those cases where it was determined that a practitioner failed to meet the standard of care. The HHS responded by indicating that all cases had to be reported, regardless of whether care was determined to be up to standards, and that the state’s prelitigation notice to initiate the meditation process qualified as a reportable “written claim.”
Physicians can be impacted greatly by the NPDB. How much of an impact depends in large part on the underlying events and the wording of the report.
An NPDB account of a medical malpractice payment doesn’t necessarily affect a physician’s ability to practice, while those – especially when “severely-worded” – involving denial or restriction of privileges are taken more seriously by state licensing boards and employers. Physicians should therefore play an active role whenever a report to the NPDB appears likely.
The dispute review process is highly technical and requires the knowledge and skill of an experienced health law attorney. To start out, consider making a request to the reporting entity to correct or vacate the report due to error. If the reporting entity declines, the physician may request a review by the HHS and file an accompanying statement seeking to explain the report.
Yet, out of more than 800,000 total reports for all practitioner types captured in the system, apparently only 44,273 included accompanying clarifying statements by the physician. Risk managers have urged vigilance.
For example, it may be that multiple reports involved a single incident, leading to a “piling on” effect. If an adverse decision at one hospital caused a physician’s clinical privileges to be terminated, this might lead the state medical board to restrict the physician’s license. It is necessary to explain that both of these NPDB-reportable events involved the same incident, and that the state board did not have any independent knowledge of anything that was wrong.
Others have advised that one should always clarify one’s involvement, e.g., “I was not the main doctor in the case.” And if dismissed in a malpractice lawsuit, be sure your name or identifying information isn’t included in the judgment or settlement agreement.
Hospital disciplinary actions being far more serious, physicians would do well to familiarize themselves with medical staff bylaws dealing with peer review and investigations. To avoid being reported to the NPDB, physicians must resist adverse actions that would be in effect for more than 30 days and fight attempts to place restrictions or sanctions on their licenses by the hospital or professional societies. Don’t withdraw applications for privileges during an investigation.
The 2015 NPDB Guidebook, the first update in more than 10 years, contains important changes pertaining to hospital adverse actions.2 The regulations now require any “surrender” of privileges while the physician is a subject of an investigation to be a reportable event. Previously, physicians sought to avoid being reported by simply giving up their privileges when an adverse decision appeared imminent.
Surrender includes not renewing one’s hospital privileges or the taking of a leave of absence, and “investigation” is widely defined to include any formal inquiry into a physician’s competence or conduct. And there need not be any “nexus,” i.e., connection, between what is being investigated and the privileges surrendered, in order to be reportable.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Health Care Quality Improvement Act of 1986, 42 U.S.C. 11101 et seq.
2. 2015 NPDB e-Guidebook, available at www.npdb.hrsa.gov/resources/aboutGuidebooks.jsp.
Question: With reference to the National Practitioner Data Bank (NPDB), which of the following statements is incorrect?
A. Both court judgments and out-of-court settlements are reportable to the NPDB.
B. Adverse actions by a hospital against a physician are reportable within 15 days.
C. In states with “Disclosure, Apology, and Offer” laws, a prompt settlement through mediation need not be reported.
D. Hospitals, state licensing boards, medical organizations, and the physician himself/herself can access the NPDB.
E. A plaintiff’s attorney cannot access the NPDB for information regarding a defendant.
Answer: C. Congress implemented the NPDB to collect information about an individual doctor’s malpractice and disciplinary histories, with the objective of restricting errant doctors from moving from one state to another.1
Federal law requires medical liability payments stemming from either a court judgment or an out-of-court settlement be reported to the NPDB. An institution’s disciplinary actions against a medical staff member must also be reported. In turn, the NPDB is obligated to make its information available to hospitals, state licensure boards, and legitimate medical organizations charged with granting privileges or membership. A physician also can ask to see his or her own records, but a plaintiff’s attorney cannot access the NPDB unless there is evidence that a hospital failed to query the NPDB as part of its credentialing process.
Some observers have claimed that the NPDB’s existence has hindered settlement negotiations, because many doctors fear being listed in the NPDB, thus significantly diminishing the likelihood of payments to satisfy a claim. It has been stated that within 6 years of NPDB’s inception, the probability that an injured patient’s claim would receive payment had fallen to 59% of the pre-NPDB level.
Many states have enacted so-called “apology laws” that promote full disclosure of medical errors and prompt out-of-court settlements, if warranted. However, the federal Department of Health and Human Services has ruled that all written demands for payment must be reported, even if the cases are resolved under state programs designed for early out-of-court resolution.
For example, a provision in the Oregon law asserts that a payment under the measure’s mediation mechanism “is not a payment resulting from a written claim or demand for payment.” The HHS has rejected this as “explicitly designed to avoid medical malpractice reporting to the NPDB for any claims that are part of the new process that do not proceed to litigation.”
Massachusetts’ 2012 apology law had proposed reporting only those cases where it was determined that a practitioner failed to meet the standard of care. The HHS responded by indicating that all cases had to be reported, regardless of whether care was determined to be up to standards, and that the state’s prelitigation notice to initiate the meditation process qualified as a reportable “written claim.”
Physicians can be impacted greatly by the NPDB. How much of an impact depends in large part on the underlying events and the wording of the report.
An NPDB account of a medical malpractice payment doesn’t necessarily affect a physician’s ability to practice, while those – especially when “severely-worded” – involving denial or restriction of privileges are taken more seriously by state licensing boards and employers. Physicians should therefore play an active role whenever a report to the NPDB appears likely.
The dispute review process is highly technical and requires the knowledge and skill of an experienced health law attorney. To start out, consider making a request to the reporting entity to correct or vacate the report due to error. If the reporting entity declines, the physician may request a review by the HHS and file an accompanying statement seeking to explain the report.
Yet, out of more than 800,000 total reports for all practitioner types captured in the system, apparently only 44,273 included accompanying clarifying statements by the physician. Risk managers have urged vigilance.
For example, it may be that multiple reports involved a single incident, leading to a “piling on” effect. If an adverse decision at one hospital caused a physician’s clinical privileges to be terminated, this might lead the state medical board to restrict the physician’s license. It is necessary to explain that both of these NPDB-reportable events involved the same incident, and that the state board did not have any independent knowledge of anything that was wrong.
Others have advised that one should always clarify one’s involvement, e.g., “I was not the main doctor in the case.” And if dismissed in a malpractice lawsuit, be sure your name or identifying information isn’t included in the judgment or settlement agreement.
Hospital disciplinary actions being far more serious, physicians would do well to familiarize themselves with medical staff bylaws dealing with peer review and investigations. To avoid being reported to the NPDB, physicians must resist adverse actions that would be in effect for more than 30 days and fight attempts to place restrictions or sanctions on their licenses by the hospital or professional societies. Don’t withdraw applications for privileges during an investigation.
The 2015 NPDB Guidebook, the first update in more than 10 years, contains important changes pertaining to hospital adverse actions.2 The regulations now require any “surrender” of privileges while the physician is a subject of an investigation to be a reportable event. Previously, physicians sought to avoid being reported by simply giving up their privileges when an adverse decision appeared imminent.
Surrender includes not renewing one’s hospital privileges or the taking of a leave of absence, and “investigation” is widely defined to include any formal inquiry into a physician’s competence or conduct. And there need not be any “nexus,” i.e., connection, between what is being investigated and the privileges surrendered, in order to be reportable.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Health Care Quality Improvement Act of 1986, 42 U.S.C. 11101 et seq.
2. 2015 NPDB e-Guidebook, available at www.npdb.hrsa.gov/resources/aboutGuidebooks.jsp.
Maryland passes generic drug anti–price gouging law
Maryland has become the first state to prohibit unreasonable price increases on essential off-patent or generic drugs.
The anti–price gouging law authorizes Maryland’s Attorney General to take legal action against manufacturers or distributors that raise drug prices in noncompetitive drug markets if the firms can’t prove the legitimacy of their price increases. Companies could face a civil penalty of up to $10,000 for each violation, according to the law, which goes into effect in October.
Stephen Rockower, MD, president of MedChi, the Maryland State Medical Society, said the medical society has long supported the bill and hailed its passage as beneficial for doctors and their patients.
“It’s been a long time coming,” Dr. Rockower said in an interview. “There have been lots of problems with the huge rising costs of drugs. Manufacturers and pharmacy benefit managers are completely uncontrolled in terms of their pricing. [With this law], we’ll be able to take care of our patients better. It’s hard to prescribe things if it’s going to cost patients $700 a day [for] a drug that used to cost $5 a day. Patients have to be able to afford their medicine, or they don’t take it.”

Chester “Chip” Davis, Jr. president and CEO of the Association for Accessible Medicines, a trade association for manufacturers and distributors of generic drugs, criticized the law.
“By giving the Attorney General unbounded and unprecedented authority to control pricing in a competitive free market, generic companies will be exposed to a level of risk in Maryland that will require them to evaluate whether they want to continue to market affordable medicines within the state,” Mr. Davis said in a statement. “One day, in the not too distant future, [Maryland lawmakers] should be prepared to defend why Maryland was the first state to lead the nation in creating less market-based competition, higher overall prescription drug costs, while also simultaneously increasing the risk of future drug shortages for Maryland’s patients.”
The law has two provisions. It prevents a generic drug manufacturer or wholesale distributor from engaging in price gouging in the sale of an essential off-patent or generic drug, defined as a prescription drug that no longer has market exclusivity and has been designated as essential for treating a life-threatening or chronic health condition by the Maryland Secretary of Health and Mental Hygiene, is actively marketed in the United States by three or fewer manufacturers, and is available for sale in Maryland.
The law also authorizes the Maryland Medical Assistance Program to notify the Attorney General of a price increase when the wholesale acquisition cost of a prescription drug increases by at least 50% in a given year for medications that cost more than $80 per 30-day course.
This first-of-its-kind law is a way to deter manufacturers from exploiting noncompetitive drug markets for short-term profit through unconscionable behavior that “imperils public health and individual welfare,” according to Jeremy A. Greene, MD, PhD, and William V. Padula, PhD.
“Perhaps, [the law will] help reestablish public trust in U.S. policy’s balancing of innovation and access, by reaffirming that older drugs of proven value should be accessible and subject to competition so that they are priced as the commodities they’ve become,” the authors wrote in a perspective published in the New England Journal of Medicine (doi: 10.1056/NEJMp1704907).
Maryland’s law is part of a growing movement among states to address unreasonable pricing spikes in prescription drugs, noted Dr. Greene and Dr. Padula, both of Johns Hopkins University in Baltimore. In April, Louisiana health officials requested feedback about the possibility of invoking an obscure U.S. patent and copyright law to ensure better affordability of hepatitis drugs. In May, the Nevada Senate passed a bill that would force drug makers to publish the list prices they set and the profits they make on insulin, as well as the amount of insulin discounts they give third parties. Additional pharmaceutical price-transparency laws have been proposed in 16 states and Puerto Rico.
“My first concern relates to the provisions of the legislation which directly regulate interstate commerce and pricing by prohibiting and penalizing manufacturer pricing which may occur outside of Maryland,” Gov. Hogan wrote. “These provisions would likely violate the dormant commerce clause of the Constitution. I am also concerned that the definition of ‘unconscionable increase’ and ‘excessive’ are vague, and would likely not stand a ‘vagueness challenge’ under the procedural due process concepts of the 14th Amendment.”
Gov. Hogan added that he is not convinced that the legislation is a solution to Marylanders having better access to medications and that the law may even have the unintended consequences of harming patients by restricting drug access.
[email protected]
On Twitter @legal_med
Maryland has become the first state to prohibit unreasonable price increases on essential off-patent or generic drugs.
The anti–price gouging law authorizes Maryland’s Attorney General to take legal action against manufacturers or distributors that raise drug prices in noncompetitive drug markets if the firms can’t prove the legitimacy of their price increases. Companies could face a civil penalty of up to $10,000 for each violation, according to the law, which goes into effect in October.
Stephen Rockower, MD, president of MedChi, the Maryland State Medical Society, said the medical society has long supported the bill and hailed its passage as beneficial for doctors and their patients.
“It’s been a long time coming,” Dr. Rockower said in an interview. “There have been lots of problems with the huge rising costs of drugs. Manufacturers and pharmacy benefit managers are completely uncontrolled in terms of their pricing. [With this law], we’ll be able to take care of our patients better. It’s hard to prescribe things if it’s going to cost patients $700 a day [for] a drug that used to cost $5 a day. Patients have to be able to afford their medicine, or they don’t take it.”
Chester “Chip” Davis, Jr. president and CEO of the Association for Accessible Medicines, a trade association for manufacturers and distributors of generic drugs, criticized the law.
“By giving the Attorney General unbounded and unprecedented authority to control pricing in a competitive free market, generic companies will be exposed to a level of risk in Maryland that will require them to evaluate whether they want to continue to market affordable medicines within the state,” Mr. Davis said in a statement. “One day, in the not too distant future, [Maryland lawmakers] should be prepared to defend why Maryland was the first state to lead the nation in creating less market-based competition, higher overall prescription drug costs, while also simultaneously increasing the risk of future drug shortages for Maryland’s patients.”
The law has two provisions. It prevents a generic drug manufacturer or wholesale distributor from engaging in price gouging in the sale of an essential off-patent or generic drug, defined as a prescription drug that no longer has market exclusivity and has been designated as essential for treating a life-threatening or chronic health condition by the Maryland Secretary of Health and Mental Hygiene, is actively marketed in the United States by three or fewer manufacturers, and is available for sale in Maryland.
The law also authorizes the Maryland Medical Assistance Program to notify the Attorney General of a price increase when the wholesale acquisition cost of a prescription drug increases by at least 50% in a given year for medications that cost more than $80 per 30-day course.
This first-of-its-kind law is a way to deter manufacturers from exploiting noncompetitive drug markets for short-term profit through unconscionable behavior that “imperils public health and individual welfare,” according to Jeremy A. Greene, MD, PhD, and William V. Padula, PhD.
“Perhaps, [the law will] help reestablish public trust in U.S. policy’s balancing of innovation and access, by reaffirming that older drugs of proven value should be accessible and subject to competition so that they are priced as the commodities they’ve become,” the authors wrote in a perspective published in the New England Journal of Medicine (doi: 10.1056/NEJMp1704907).
Maryland’s law is part of a growing movement among states to address unreasonable pricing spikes in prescription drugs, noted Dr. Greene and Dr. Padula, both of Johns Hopkins University in Baltimore. In April, Louisiana health officials requested feedback about the possibility of invoking an obscure U.S. patent and copyright law to ensure better affordability of hepatitis drugs. In May, the Nevada Senate passed a bill that would force drug makers to publish the list prices they set and the profits they make on insulin, as well as the amount of insulin discounts they give third parties. Additional pharmaceutical price-transparency laws have been proposed in 16 states and Puerto Rico.
“My first concern relates to the provisions of the legislation which directly regulate interstate commerce and pricing by prohibiting and penalizing manufacturer pricing which may occur outside of Maryland,” Gov. Hogan wrote. “These provisions would likely violate the dormant commerce clause of the Constitution. I am also concerned that the definition of ‘unconscionable increase’ and ‘excessive’ are vague, and would likely not stand a ‘vagueness challenge’ under the procedural due process concepts of the 14th Amendment.”
Gov. Hogan added that he is not convinced that the legislation is a solution to Marylanders having better access to medications and that the law may even have the unintended consequences of harming patients by restricting drug access.
[email protected]
On Twitter @legal_med
Maryland has become the first state to prohibit unreasonable price increases on essential off-patent or generic drugs.
The anti–price gouging law authorizes Maryland’s Attorney General to take legal action against manufacturers or distributors that raise drug prices in noncompetitive drug markets if the firms can’t prove the legitimacy of their price increases. Companies could face a civil penalty of up to $10,000 for each violation, according to the law, which goes into effect in October.
Stephen Rockower, MD, president of MedChi, the Maryland State Medical Society, said the medical society has long supported the bill and hailed its passage as beneficial for doctors and their patients.
“It’s been a long time coming,” Dr. Rockower said in an interview. “There have been lots of problems with the huge rising costs of drugs. Manufacturers and pharmacy benefit managers are completely uncontrolled in terms of their pricing. [With this law], we’ll be able to take care of our patients better. It’s hard to prescribe things if it’s going to cost patients $700 a day [for] a drug that used to cost $5 a day. Patients have to be able to afford their medicine, or they don’t take it.”
Chester “Chip” Davis, Jr. president and CEO of the Association for Accessible Medicines, a trade association for manufacturers and distributors of generic drugs, criticized the law.
“By giving the Attorney General unbounded and unprecedented authority to control pricing in a competitive free market, generic companies will be exposed to a level of risk in Maryland that will require them to evaluate whether they want to continue to market affordable medicines within the state,” Mr. Davis said in a statement. “One day, in the not too distant future, [Maryland lawmakers] should be prepared to defend why Maryland was the first state to lead the nation in creating less market-based competition, higher overall prescription drug costs, while also simultaneously increasing the risk of future drug shortages for Maryland’s patients.”
The law has two provisions. It prevents a generic drug manufacturer or wholesale distributor from engaging in price gouging in the sale of an essential off-patent or generic drug, defined as a prescription drug that no longer has market exclusivity and has been designated as essential for treating a life-threatening or chronic health condition by the Maryland Secretary of Health and Mental Hygiene, is actively marketed in the United States by three or fewer manufacturers, and is available for sale in Maryland.
The law also authorizes the Maryland Medical Assistance Program to notify the Attorney General of a price increase when the wholesale acquisition cost of a prescription drug increases by at least 50% in a given year for medications that cost more than $80 per 30-day course.
This first-of-its-kind law is a way to deter manufacturers from exploiting noncompetitive drug markets for short-term profit through unconscionable behavior that “imperils public health and individual welfare,” according to Jeremy A. Greene, MD, PhD, and William V. Padula, PhD.
“Perhaps, [the law will] help reestablish public trust in U.S. policy’s balancing of innovation and access, by reaffirming that older drugs of proven value should be accessible and subject to competition so that they are priced as the commodities they’ve become,” the authors wrote in a perspective published in the New England Journal of Medicine (doi: 10.1056/NEJMp1704907).
Maryland’s law is part of a growing movement among states to address unreasonable pricing spikes in prescription drugs, noted Dr. Greene and Dr. Padula, both of Johns Hopkins University in Baltimore. In April, Louisiana health officials requested feedback about the possibility of invoking an obscure U.S. patent and copyright law to ensure better affordability of hepatitis drugs. In May, the Nevada Senate passed a bill that would force drug makers to publish the list prices they set and the profits they make on insulin, as well as the amount of insulin discounts they give third parties. Additional pharmaceutical price-transparency laws have been proposed in 16 states and Puerto Rico.
“My first concern relates to the provisions of the legislation which directly regulate interstate commerce and pricing by prohibiting and penalizing manufacturer pricing which may occur outside of Maryland,” Gov. Hogan wrote. “These provisions would likely violate the dormant commerce clause of the Constitution. I am also concerned that the definition of ‘unconscionable increase’ and ‘excessive’ are vague, and would likely not stand a ‘vagueness challenge’ under the procedural due process concepts of the 14th Amendment.”
Gov. Hogan added that he is not convinced that the legislation is a solution to Marylanders having better access to medications and that the law may even have the unintended consequences of harming patients by restricting drug access.
[email protected]
On Twitter @legal_med
Outpatient appendectomy success depends on patient selection, communication
Outpatient laparoscopic surgery for uncomplicated appendicitis can be safely implemented in a large county hospital that serves a poor, underserved population, findings from a prospective, observational trial have shown.
Outpatient appendectomy has gradually gained acceptance in the United States, and numerous studies support the practice. David R. Rosen, MD, of the University of Southern California, Los Angeles, and his colleagues considered the possible advantages of outpatient laparoscopic appendectomy for their institution, such as decreased length of stay, decreased costs, and fewer admissions.

The research team hypothesized that with a “well-defined protocol consisting of strict inclusion and exclusion criteria, clear patient instructions, and close observation to identify patients who would not succeed with the outpatient appendectomy treatment strategy, outpatient appendectomy would be feasible without worsening patient outcomes or satisfaction.”
The findings were published in the Journal of the American College of Surgeons (2017 May;224[5]:862-7).
The investigators conducted a study of patients presenting at a safety-net county hospital and diagnosed with acute appendicitis. A year-long observation period produced a control group of 178 admitted patients.
The outpatient protocol was then introduced. Patients were counseled on the possibility of their being discharged from the postanesthesia care unit (PACU), depending on intraoperative findings and their capacity to arrange a ride home and willingness to participate in postoperative follow-up. Patient education was a key element of the protocol. In all, 173 patients were identified for the outpatient program.
The intraoperative criteria for discharge from the PACU included no evidence of perforation or gangrene, and no surgical complications or adverse events. Patients were cleared for discharge if they met the following criteria: heart rate less than 100 beats/min; systolic blood pressure greater than 110 mm Hg; pain well controlled (less than 4 on a 1-10 scale); ambulatory; urinated since surgery; oral intake; and dressings dry without evidence of bleeding.
The patients had been thoroughly briefed on what to expect and problems that would necessitate a return to the emergency department. The physician assessed each patient’s readiness to be discharged, wrote a discharge order, and confirmed the pain medication prescription and follow-up appointment.
Of the 173 patients selected for the outpatient program, 113 (65%) ended up being discharged from the PACU. The reasons for these admissions included interoperative findings, failure to pass the discharge criteria, homelessness, and no transportation to get home.
The control and outpatient groups were similar demographically, except that the latter were on average significantly older (mean age 32.4 years vs. 36.6 years, respectively). The outpatient group had a significantly shorter operative time (69 minutes vs. 83 minutes), a significantly longer stay in the PACU (242 minutes vs.141 minutes), and a significantly shorter total postoperative length of stay (9 hours vs.19 hours).
There were no differences between the groups in terms of complications, postdischarge ED visits, or readmissions. Those who were discharged from the PACU had no postoperative complications and no readmissions.
The length of stay in the PACU gradually decreased for the outpatient group. “This can be attributed to the adoption of a new protocol,” the researchers noted. However, “we purposely did not want to rush the discharge process to ensure our patients and families had all questions answered and were comfortable leaving the hospital.”
A key component of the protocol was the follow-up appointment for all appendectomy patients; about one-third of both groups did not return for their follow-up appointments. Those missed follow-ups could mean some patients returned to another hospital, but the investigators suggested that this was unlikely.
“Because our hospital serves a patient population of low socioeconomic status and often without health insurance, our public hospital is often the only hospital to which they would present,” the investigators wrote.
Most of those who did return completed a questionnaire on their level of satisfaction. Survey results showed no differences in satisfaction between the groups and a generally positive view of the protocol among the outpatient group.
The study did not account for actual cost savings, but reduced hospital admissions and readmissions were achieved. Investigators assert that other studies have shown that each day of hospitalization avoided saves about $1,900.
“It is challenging to deliver high-quality, efficient care to an underserved population in a public hospital,” Dr. Rosen said in an interview. “In this setting, communication and patient education are vital components for success. By setting clear expectations and empowering patients to participate in their care, we can maximize our patients’ outcomes.”
The investigators had no disclosures.
Outpatient laparoscopic surgery for uncomplicated appendicitis can be safely implemented in a large county hospital that serves a poor, underserved population, findings from a prospective, observational trial have shown.
Outpatient appendectomy has gradually gained acceptance in the United States, and numerous studies support the practice. David R. Rosen, MD, of the University of Southern California, Los Angeles, and his colleagues considered the possible advantages of outpatient laparoscopic appendectomy for their institution, such as decreased length of stay, decreased costs, and fewer admissions.
The research team hypothesized that with a “well-defined protocol consisting of strict inclusion and exclusion criteria, clear patient instructions, and close observation to identify patients who would not succeed with the outpatient appendectomy treatment strategy, outpatient appendectomy would be feasible without worsening patient outcomes or satisfaction.”
The findings were published in the Journal of the American College of Surgeons (2017 May;224[5]:862-7).
The investigators conducted a study of patients presenting at a safety-net county hospital and diagnosed with acute appendicitis. A year-long observation period produced a control group of 178 admitted patients.
The outpatient protocol was then introduced. Patients were counseled on the possibility of their being discharged from the postanesthesia care unit (PACU), depending on intraoperative findings and their capacity to arrange a ride home and willingness to participate in postoperative follow-up. Patient education was a key element of the protocol. In all, 173 patients were identified for the outpatient program.
The intraoperative criteria for discharge from the PACU included no evidence of perforation or gangrene, and no surgical complications or adverse events. Patients were cleared for discharge if they met the following criteria: heart rate less than 100 beats/min; systolic blood pressure greater than 110 mm Hg; pain well controlled (less than 4 on a 1-10 scale); ambulatory; urinated since surgery; oral intake; and dressings dry without evidence of bleeding.
The patients had been thoroughly briefed on what to expect and problems that would necessitate a return to the emergency department. The physician assessed each patient’s readiness to be discharged, wrote a discharge order, and confirmed the pain medication prescription and follow-up appointment.
Of the 173 patients selected for the outpatient program, 113 (65%) ended up being discharged from the PACU. The reasons for these admissions included interoperative findings, failure to pass the discharge criteria, homelessness, and no transportation to get home.
The control and outpatient groups were similar demographically, except that the latter were on average significantly older (mean age 32.4 years vs. 36.6 years, respectively). The outpatient group had a significantly shorter operative time (69 minutes vs. 83 minutes), a significantly longer stay in the PACU (242 minutes vs.141 minutes), and a significantly shorter total postoperative length of stay (9 hours vs.19 hours).
There were no differences between the groups in terms of complications, postdischarge ED visits, or readmissions. Those who were discharged from the PACU had no postoperative complications and no readmissions.
The length of stay in the PACU gradually decreased for the outpatient group. “This can be attributed to the adoption of a new protocol,” the researchers noted. However, “we purposely did not want to rush the discharge process to ensure our patients and families had all questions answered and were comfortable leaving the hospital.”
A key component of the protocol was the follow-up appointment for all appendectomy patients; about one-third of both groups did not return for their follow-up appointments. Those missed follow-ups could mean some patients returned to another hospital, but the investigators suggested that this was unlikely.
“Because our hospital serves a patient population of low socioeconomic status and often without health insurance, our public hospital is often the only hospital to which they would present,” the investigators wrote.
Most of those who did return completed a questionnaire on their level of satisfaction. Survey results showed no differences in satisfaction between the groups and a generally positive view of the protocol among the outpatient group.
The study did not account for actual cost savings, but reduced hospital admissions and readmissions were achieved. Investigators assert that other studies have shown that each day of hospitalization avoided saves about $1,900.
“It is challenging to deliver high-quality, efficient care to an underserved population in a public hospital,” Dr. Rosen said in an interview. “In this setting, communication and patient education are vital components for success. By setting clear expectations and empowering patients to participate in their care, we can maximize our patients’ outcomes.”
The investigators had no disclosures.
Outpatient laparoscopic surgery for uncomplicated appendicitis can be safely implemented in a large county hospital that serves a poor, underserved population, findings from a prospective, observational trial have shown.
Outpatient appendectomy has gradually gained acceptance in the United States, and numerous studies support the practice. David R. Rosen, MD, of the University of Southern California, Los Angeles, and his colleagues considered the possible advantages of outpatient laparoscopic appendectomy for their institution, such as decreased length of stay, decreased costs, and fewer admissions.
The research team hypothesized that with a “well-defined protocol consisting of strict inclusion and exclusion criteria, clear patient instructions, and close observation to identify patients who would not succeed with the outpatient appendectomy treatment strategy, outpatient appendectomy would be feasible without worsening patient outcomes or satisfaction.”
The findings were published in the Journal of the American College of Surgeons (2017 May;224[5]:862-7).
The investigators conducted a study of patients presenting at a safety-net county hospital and diagnosed with acute appendicitis. A year-long observation period produced a control group of 178 admitted patients.
The outpatient protocol was then introduced. Patients were counseled on the possibility of their being discharged from the postanesthesia care unit (PACU), depending on intraoperative findings and their capacity to arrange a ride home and willingness to participate in postoperative follow-up. Patient education was a key element of the protocol. In all, 173 patients were identified for the outpatient program.
The intraoperative criteria for discharge from the PACU included no evidence of perforation or gangrene, and no surgical complications or adverse events. Patients were cleared for discharge if they met the following criteria: heart rate less than 100 beats/min; systolic blood pressure greater than 110 mm Hg; pain well controlled (less than 4 on a 1-10 scale); ambulatory; urinated since surgery; oral intake; and dressings dry without evidence of bleeding.
The patients had been thoroughly briefed on what to expect and problems that would necessitate a return to the emergency department. The physician assessed each patient’s readiness to be discharged, wrote a discharge order, and confirmed the pain medication prescription and follow-up appointment.
Of the 173 patients selected for the outpatient program, 113 (65%) ended up being discharged from the PACU. The reasons for these admissions included interoperative findings, failure to pass the discharge criteria, homelessness, and no transportation to get home.
The control and outpatient groups were similar demographically, except that the latter were on average significantly older (mean age 32.4 years vs. 36.6 years, respectively). The outpatient group had a significantly shorter operative time (69 minutes vs. 83 minutes), a significantly longer stay in the PACU (242 minutes vs.141 minutes), and a significantly shorter total postoperative length of stay (9 hours vs.19 hours).
There were no differences between the groups in terms of complications, postdischarge ED visits, or readmissions. Those who were discharged from the PACU had no postoperative complications and no readmissions.
The length of stay in the PACU gradually decreased for the outpatient group. “This can be attributed to the adoption of a new protocol,” the researchers noted. However, “we purposely did not want to rush the discharge process to ensure our patients and families had all questions answered and were comfortable leaving the hospital.”
A key component of the protocol was the follow-up appointment for all appendectomy patients; about one-third of both groups did not return for their follow-up appointments. Those missed follow-ups could mean some patients returned to another hospital, but the investigators suggested that this was unlikely.
“Because our hospital serves a patient population of low socioeconomic status and often without health insurance, our public hospital is often the only hospital to which they would present,” the investigators wrote.
Most of those who did return completed a questionnaire on their level of satisfaction. Survey results showed no differences in satisfaction between the groups and a generally positive view of the protocol among the outpatient group.
The study did not account for actual cost savings, but reduced hospital admissions and readmissions were achieved. Investigators assert that other studies have shown that each day of hospitalization avoided saves about $1,900.
“It is challenging to deliver high-quality, efficient care to an underserved population in a public hospital,” Dr. Rosen said in an interview. “In this setting, communication and patient education are vital components for success. By setting clear expectations and empowering patients to participate in their care, we can maximize our patients’ outcomes.”
The investigators had no disclosures.
FROM JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: .
Major finding: The outpatient group had a shorter postoperative hospital length of stay (9 hours vs. 19 hours).
Data source: A prospective, observational study of 351 patients with a diagnosis of acute appendicitis at a public safety-net hospital that serves poor and mostly uninsured patients.
Disclosures: The authors had no disclosures.
Mesh use for lap paraesophageal hernia repair held steady
Utilization of mesh in laparoscopic paraesophageal hernia repair (PEHR) remained steady from 2011 to 2014, despite a lack of evidence supporting its use, according to Francisco Schlottmann, MD, and his associates.
In an analysis of 9,590 laparoscopic PEHR performed from 2011 to 2014, 60.6% procedures were done without mesh and 39.4% were done with mesh. Over the 3-year study period, mesh utilization fell only 1.2% overall, with laparoscopic PEHR with mesh accounting for 39.4% of procedures in 2011 and 38.2% in 2014.
Patients who received mesh were slightly older and significantly more likely to be an inpatient admission. Postoperative urinary tract infection was less common in patients with mesh, occurring in 1% of patients, compared with 1.5% of patients without mesh. No significant difference in demographics was seen, and 30-day risk of comorbidity and mortality was the same. Mean length of stay was 2.7 days for PEHR with mesh and 2.5 days for PEHR without mesh.
“The use of mesh is associated with high expenses, and biomedical technology continues to offer newer and more expensive mesh products on the market. Given the progressive aging of the U.S. population, PEHR are expected to increase in the future. The indiscriminate and not supported by evidence use of mesh may determine unnecessary costs for the health care system,” the investigators noted.
Find the full study in the Journal of Gastrointestinal Surgery (2017 May 26. doi: 10.1007/s11605-017-3452-8).
Utilization of mesh in laparoscopic paraesophageal hernia repair (PEHR) remained steady from 2011 to 2014, despite a lack of evidence supporting its use, according to Francisco Schlottmann, MD, and his associates.
In an analysis of 9,590 laparoscopic PEHR performed from 2011 to 2014, 60.6% procedures were done without mesh and 39.4% were done with mesh. Over the 3-year study period, mesh utilization fell only 1.2% overall, with laparoscopic PEHR with mesh accounting for 39.4% of procedures in 2011 and 38.2% in 2014.
Patients who received mesh were slightly older and significantly more likely to be an inpatient admission. Postoperative urinary tract infection was less common in patients with mesh, occurring in 1% of patients, compared with 1.5% of patients without mesh. No significant difference in demographics was seen, and 30-day risk of comorbidity and mortality was the same. Mean length of stay was 2.7 days for PEHR with mesh and 2.5 days for PEHR without mesh.
“The use of mesh is associated with high expenses, and biomedical technology continues to offer newer and more expensive mesh products on the market. Given the progressive aging of the U.S. population, PEHR are expected to increase in the future. The indiscriminate and not supported by evidence use of mesh may determine unnecessary costs for the health care system,” the investigators noted.
Find the full study in the Journal of Gastrointestinal Surgery (2017 May 26. doi: 10.1007/s11605-017-3452-8).
Utilization of mesh in laparoscopic paraesophageal hernia repair (PEHR) remained steady from 2011 to 2014, despite a lack of evidence supporting its use, according to Francisco Schlottmann, MD, and his associates.
In an analysis of 9,590 laparoscopic PEHR performed from 2011 to 2014, 60.6% procedures were done without mesh and 39.4% were done with mesh. Over the 3-year study period, mesh utilization fell only 1.2% overall, with laparoscopic PEHR with mesh accounting for 39.4% of procedures in 2011 and 38.2% in 2014.
Patients who received mesh were slightly older and significantly more likely to be an inpatient admission. Postoperative urinary tract infection was less common in patients with mesh, occurring in 1% of patients, compared with 1.5% of patients without mesh. No significant difference in demographics was seen, and 30-day risk of comorbidity and mortality was the same. Mean length of stay was 2.7 days for PEHR with mesh and 2.5 days for PEHR without mesh.
“The use of mesh is associated with high expenses, and biomedical technology continues to offer newer and more expensive mesh products on the market. Given the progressive aging of the U.S. population, PEHR are expected to increase in the future. The indiscriminate and not supported by evidence use of mesh may determine unnecessary costs for the health care system,” the investigators noted.
Find the full study in the Journal of Gastrointestinal Surgery (2017 May 26. doi: 10.1007/s11605-017-3452-8).
FROM THE JOURNAL OF GASTROINTESTINAL SURGERY
Should convicted sex offender get penile prosthetic implant?
SAN DIEGO – Should a man with a distant history of pedophilia be allowed to get a penile prosthetic implant to treat his erectile dysfunction? Mental health professionals at a Veterans Affairs medical center in San Diego recently faced this question and decided the risk was too great. They denied his request.
“This kind of dilemma occurs throughout all health systems, and it’s very challenging. It obviously puts the physician in a very ethically challenging situation,” said Kristin Beizai, MD, a psychiatrist and coauthor of a case report presented at the annual meeting of the American Psychiatric Association.
Yash B. Joshi, MD, PhD, and Dr. Beizai, both psychiatrists at the University of California, San Diego, and the VA San Diego Healthcare System, reported the penile prosthetic implant case in a poster at APA.
According to them, a married veteran sought treatment for erectile dysfunction (ED) from VA hospital urologists after oral treatment had failed. The elderly man, who had been imprisoned for 3 years some 25-30 years previously, sought a penile prosthetic implant – an alternative to treatments for ED when drugs have failed. Other options include self-injections and vacuum devices.
Men with the implants trigger erections by squeezing a pump in the scrotum that allows fluid to flow from a reservoir into the cylinder.
The man had been imprisoned in his 40s for 3 years because of a single incident of sexually abusing a toddler. According to the case report, his primary care doctors previously had offered him ED treatments “without acknowledging this history in their clinical-decision making process.”
A psychologist determined the man to be at low risk of committing a sexual offense again and cleared him for an implant. But his urologists requested an ethics consultation, which was provided by a team that included representatives from the fields of psychiatry, internal medicine, nursing, and social work.
“The ethics team determined that the most appropriate course of action hinged on a thorough and individualized risk-benefit assessment to determine if providing the treatment was ethically justifiable,” Dr. Beizai said in an interview.
An on-site psychologist and an outside expert evaluated the patient using a tool known as the Violence Risk Assessment Instrument–Sexual and determined the man was at moderate to severe risk of committing a sexual offense again.
“It was also discovered that the patient never completed treatment for pedophilia in the community as previously recommended,” the psychiatrists reported. “He was offered a plan for reevaluation and rehabilitation by subspecialists but declined this option.”
The man subsequently died of natural causes.
Dr. Beizai said those kinds of cases present numerous challenges. “This case involves surgery/urology, but this is an issue with primary care as well, and they likely do not have the time, resources, or protocol to address fully, particularly when legal information may be withheld and there are confidentiality issues.”
In regard to a risk-benefit analysis, she said, “a general mental health practitioner may not be comfortable completing this kind of assessment, and there may be an indication to refer to a forensic psychiatrist or psychologist. But this can be an expensive and scarce resource.”
There’s also the potential for political storms if the news gets out that a convicted sex offender received ED treatment. News reports in the mid-2000s about this kind of care persuaded several states to ban government payments for ED treatment for convicted sex offenders, and Medicaid funding was eliminated.
Two researchers who study pedophilia said in an interview that these decisions are far from simple and must take several factors into account.
Fred S. Berlin, MD, PhD, director of the Sexual Behavior Consultation Unit, and associate professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore, said a sexual offense background isn’t necessarily enough of a reason to deny ED treatment to a patient. Important factors for decision making, he said, include the nature of the previous offenses (such as whether they involved penile penetration, or the use of drugs or alcohol) and the state of an offender’s current relationship.
He added that it’s important to understand that the lack of functioning genitals isn’t a barrier to sexual abuse. “There shouldn’t be a narrow focus on the capacity of the penis to have an erection,” he said.
Treatment for ED in convicted sex offenders can be helpful in some cases, said Richard B. Krueger, MD, an associate clinical professor of psychiatry at Columbia University, New York, and medical director of the Sexual Behavior Clinic at New York State Psychiatric Institute. “The general sense is that it would be a benefit to enable an appropriate, peer-related relationship with a spouse, significant other, or adults,” Dr. Krueger said.
Red flags regarding ED treatment in sex offenders, he said, include high scores on predictive tests, a history of extreme sadism or sociopathy, and challenges regarding monitoring of the offender.
Dr. Beizai, Dr. Joshi, Dr. Krueger, and Dr. Berlin reported no relevant disclosures.
[polldaddy:9767052]
SAN DIEGO – Should a man with a distant history of pedophilia be allowed to get a penile prosthetic implant to treat his erectile dysfunction? Mental health professionals at a Veterans Affairs medical center in San Diego recently faced this question and decided the risk was too great. They denied his request.
“This kind of dilemma occurs throughout all health systems, and it’s very challenging. It obviously puts the physician in a very ethically challenging situation,” said Kristin Beizai, MD, a psychiatrist and coauthor of a case report presented at the annual meeting of the American Psychiatric Association.
Yash B. Joshi, MD, PhD, and Dr. Beizai, both psychiatrists at the University of California, San Diego, and the VA San Diego Healthcare System, reported the penile prosthetic implant case in a poster at APA.
According to them, a married veteran sought treatment for erectile dysfunction (ED) from VA hospital urologists after oral treatment had failed. The elderly man, who had been imprisoned for 3 years some 25-30 years previously, sought a penile prosthetic implant – an alternative to treatments for ED when drugs have failed. Other options include self-injections and vacuum devices.
Men with the implants trigger erections by squeezing a pump in the scrotum that allows fluid to flow from a reservoir into the cylinder.
The man had been imprisoned in his 40s for 3 years because of a single incident of sexually abusing a toddler. According to the case report, his primary care doctors previously had offered him ED treatments “without acknowledging this history in their clinical-decision making process.”
A psychologist determined the man to be at low risk of committing a sexual offense again and cleared him for an implant. But his urologists requested an ethics consultation, which was provided by a team that included representatives from the fields of psychiatry, internal medicine, nursing, and social work.
“The ethics team determined that the most appropriate course of action hinged on a thorough and individualized risk-benefit assessment to determine if providing the treatment was ethically justifiable,” Dr. Beizai said in an interview.
An on-site psychologist and an outside expert evaluated the patient using a tool known as the Violence Risk Assessment Instrument–Sexual and determined the man was at moderate to severe risk of committing a sexual offense again.
“It was also discovered that the patient never completed treatment for pedophilia in the community as previously recommended,” the psychiatrists reported. “He was offered a plan for reevaluation and rehabilitation by subspecialists but declined this option.”
The man subsequently died of natural causes.
Dr. Beizai said those kinds of cases present numerous challenges. “This case involves surgery/urology, but this is an issue with primary care as well, and they likely do not have the time, resources, or protocol to address fully, particularly when legal information may be withheld and there are confidentiality issues.”
In regard to a risk-benefit analysis, she said, “a general mental health practitioner may not be comfortable completing this kind of assessment, and there may be an indication to refer to a forensic psychiatrist or psychologist. But this can be an expensive and scarce resource.”
There’s also the potential for political storms if the news gets out that a convicted sex offender received ED treatment. News reports in the mid-2000s about this kind of care persuaded several states to ban government payments for ED treatment for convicted sex offenders, and Medicaid funding was eliminated.
Two researchers who study pedophilia said in an interview that these decisions are far from simple and must take several factors into account.
Fred S. Berlin, MD, PhD, director of the Sexual Behavior Consultation Unit, and associate professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore, said a sexual offense background isn’t necessarily enough of a reason to deny ED treatment to a patient. Important factors for decision making, he said, include the nature of the previous offenses (such as whether they involved penile penetration, or the use of drugs or alcohol) and the state of an offender’s current relationship.
He added that it’s important to understand that the lack of functioning genitals isn’t a barrier to sexual abuse. “There shouldn’t be a narrow focus on the capacity of the penis to have an erection,” he said.
Treatment for ED in convicted sex offenders can be helpful in some cases, said Richard B. Krueger, MD, an associate clinical professor of psychiatry at Columbia University, New York, and medical director of the Sexual Behavior Clinic at New York State Psychiatric Institute. “The general sense is that it would be a benefit to enable an appropriate, peer-related relationship with a spouse, significant other, or adults,” Dr. Krueger said.
Red flags regarding ED treatment in sex offenders, he said, include high scores on predictive tests, a history of extreme sadism or sociopathy, and challenges regarding monitoring of the offender.
Dr. Beizai, Dr. Joshi, Dr. Krueger, and Dr. Berlin reported no relevant disclosures.
[polldaddy:9767052]
SAN DIEGO – Should a man with a distant history of pedophilia be allowed to get a penile prosthetic implant to treat his erectile dysfunction? Mental health professionals at a Veterans Affairs medical center in San Diego recently faced this question and decided the risk was too great. They denied his request.
“This kind of dilemma occurs throughout all health systems, and it’s very challenging. It obviously puts the physician in a very ethically challenging situation,” said Kristin Beizai, MD, a psychiatrist and coauthor of a case report presented at the annual meeting of the American Psychiatric Association.
Yash B. Joshi, MD, PhD, and Dr. Beizai, both psychiatrists at the University of California, San Diego, and the VA San Diego Healthcare System, reported the penile prosthetic implant case in a poster at APA.
According to them, a married veteran sought treatment for erectile dysfunction (ED) from VA hospital urologists after oral treatment had failed. The elderly man, who had been imprisoned for 3 years some 25-30 years previously, sought a penile prosthetic implant – an alternative to treatments for ED when drugs have failed. Other options include self-injections and vacuum devices.
Men with the implants trigger erections by squeezing a pump in the scrotum that allows fluid to flow from a reservoir into the cylinder.
The man had been imprisoned in his 40s for 3 years because of a single incident of sexually abusing a toddler. According to the case report, his primary care doctors previously had offered him ED treatments “without acknowledging this history in their clinical-decision making process.”
A psychologist determined the man to be at low risk of committing a sexual offense again and cleared him for an implant. But his urologists requested an ethics consultation, which was provided by a team that included representatives from the fields of psychiatry, internal medicine, nursing, and social work.
“The ethics team determined that the most appropriate course of action hinged on a thorough and individualized risk-benefit assessment to determine if providing the treatment was ethically justifiable,” Dr. Beizai said in an interview.
An on-site psychologist and an outside expert evaluated the patient using a tool known as the Violence Risk Assessment Instrument–Sexual and determined the man was at moderate to severe risk of committing a sexual offense again.
“It was also discovered that the patient never completed treatment for pedophilia in the community as previously recommended,” the psychiatrists reported. “He was offered a plan for reevaluation and rehabilitation by subspecialists but declined this option.”
The man subsequently died of natural causes.
Dr. Beizai said those kinds of cases present numerous challenges. “This case involves surgery/urology, but this is an issue with primary care as well, and they likely do not have the time, resources, or protocol to address fully, particularly when legal information may be withheld and there are confidentiality issues.”
In regard to a risk-benefit analysis, she said, “a general mental health practitioner may not be comfortable completing this kind of assessment, and there may be an indication to refer to a forensic psychiatrist or psychologist. But this can be an expensive and scarce resource.”
There’s also the potential for political storms if the news gets out that a convicted sex offender received ED treatment. News reports in the mid-2000s about this kind of care persuaded several states to ban government payments for ED treatment for convicted sex offenders, and Medicaid funding was eliminated.
Two researchers who study pedophilia said in an interview that these decisions are far from simple and must take several factors into account.
Fred S. Berlin, MD, PhD, director of the Sexual Behavior Consultation Unit, and associate professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore, said a sexual offense background isn’t necessarily enough of a reason to deny ED treatment to a patient. Important factors for decision making, he said, include the nature of the previous offenses (such as whether they involved penile penetration, or the use of drugs or alcohol) and the state of an offender’s current relationship.
He added that it’s important to understand that the lack of functioning genitals isn’t a barrier to sexual abuse. “There shouldn’t be a narrow focus on the capacity of the penis to have an erection,” he said.
Treatment for ED in convicted sex offenders can be helpful in some cases, said Richard B. Krueger, MD, an associate clinical professor of psychiatry at Columbia University, New York, and medical director of the Sexual Behavior Clinic at New York State Psychiatric Institute. “The general sense is that it would be a benefit to enable an appropriate, peer-related relationship with a spouse, significant other, or adults,” Dr. Krueger said.
Red flags regarding ED treatment in sex offenders, he said, include high scores on predictive tests, a history of extreme sadism or sociopathy, and challenges regarding monitoring of the offender.
Dr. Beizai, Dr. Joshi, Dr. Krueger, and Dr. Berlin reported no relevant disclosures.
[polldaddy:9767052]
AT APA
FDA asks drug maker to shelve Opana ER
The Food and Drug Administration has asked Endo Pharmaceuticals to voluntarily remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market in the United States, citing the potential for its abuse as a concern.
“We are facing an opioid epidemic – a public health crisis, and we must take all necessary steps to reduce the scope of opioid misuse and abuse,” FDA Commissioner Scott Gottlieb, MD, said in a June 8 press release . “We will continue to take regulatory steps when we see situations where an opioid product’s risks outweigh its benefits, not only for its intended patient population but also in regard to its potential for misuse and abuse.”
Opana ER was first approved in 2006 for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time. It was reformulated in 2012, with the intent of making it “resistant to physical and chemical manipulation for abuse by snorting or injecting,” according to the FDA release.
The Food and Drug Administration has asked Endo Pharmaceuticals to voluntarily remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market in the United States, citing the potential for its abuse as a concern.
“We are facing an opioid epidemic – a public health crisis, and we must take all necessary steps to reduce the scope of opioid misuse and abuse,” FDA Commissioner Scott Gottlieb, MD, said in a June 8 press release . “We will continue to take regulatory steps when we see situations where an opioid product’s risks outweigh its benefits, not only for its intended patient population but also in regard to its potential for misuse and abuse.”
Opana ER was first approved in 2006 for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time. It was reformulated in 2012, with the intent of making it “resistant to physical and chemical manipulation for abuse by snorting or injecting,” according to the FDA release.
The Food and Drug Administration has asked Endo Pharmaceuticals to voluntarily remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market in the United States, citing the potential for its abuse as a concern.
“We are facing an opioid epidemic – a public health crisis, and we must take all necessary steps to reduce the scope of opioid misuse and abuse,” FDA Commissioner Scott Gottlieb, MD, said in a June 8 press release . “We will continue to take regulatory steps when we see situations where an opioid product’s risks outweigh its benefits, not only for its intended patient population but also in regard to its potential for misuse and abuse.”
Opana ER was first approved in 2006 for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time. It was reformulated in 2012, with the intent of making it “resistant to physical and chemical manipulation for abuse by snorting or injecting,” according to the FDA release.
Supreme Court: Faith-based hospitals are exempt from federal pension requirements
The U.S. Supreme Court has ruled that faith-based hospitals are exempt from federal pension requirements, holding that employees of religious-affiliated entities are not protected under the Employee Retirement Income Security Act (ERISA). The unanimous decision overturns rulings in the three circuit courts of appeals.
The opinion preserves the status quo, so it should not have an immediate effect on the affected employers and employees, said Ronald J. Mann, a law professor at Columbia University in New York who has written about one case, Advocate Health Care Network v. Stapleton, for Scotusblog.com.
The high court’s opinion centers on logic and the plain language of the ERISA statute, which is sensible, said Paul Secunda, a law professor and director of the labor and employment law program at Marquette University in Milwaukee. However, the decision does not address the larger question that matters to physicians and hospitals, he said.
“Some of these church-affiliated hospitals look an awful lot like their secular competitors,” he said. “They have thousands of employees. They make billions of dollars in revenue.”
Associate Justice Sonia Sotomayor raised similar concerns in a concurring opinion to the decision. While she agreed with her fellow justices on the ruling, she said the case outcome was still troubling.
“Despite their relationship to churches, organizations such as petitioners operate for-profit subsidiaries ... and compete in the secular market with companies that must bear the cost of complying with ERISA,” Justice Sotomayor wrote.
The Supreme Court ruling comes after current and former employees of three hospital chains – Dignity Health, Advocate Health Care, and Saint Peter’s Healthcare System – sued their employers in an effort to make them comply with ERISA. The employees argued that pension plans established by the large health care providers should not fall under ERISA’s “church plan” exception because the plans were not established by churches. ERISA requires that all private employers offering pension plans adhere to federal requirements designed to ensure plan solvency and protect plan participants.
The hospitals argued that pension plans do not have to be established by a church for the ERISA exemption to apply because the plans are maintained by qualifying church-affiliated organizations. The defendants based their position on a 1980 ERISA amendment that included the “maintained” exception. Since the amendment, the federal agencies charged with interpreting ERISA – the IRS, the Department of Labor, and the Pension Benefit Guaranty Corporation – have issued opinion after opinion reaffirming that view, the defendants noted.
Courts of appeals for the Third, Seventh, and Ninth circuits agreed with the employees, concluding that ERISA’s “plain text” requires that a pension plan be established by a church to qualify for the church-plan exemption.
The Supreme Court disagreed, however, ruling that a defined-benefit pension plan maintained by a principal-purpose organization – one controlled by or associate

However, the hospital sector has changed dramatically since the 1980 ERISA amendment, Mr. Secunda pointed out. “If you think back to when this reform was passed ... almost 40 years ago, we have a whole different animal [today] with regard to these large church-oriented hospital organizations.”
Justice Sotomayor raised similar concerns. “These organizations thus bear little resemblance to those Congress considered when enacting the 1980 amendment to the church plan definition. This current reality might prompt Congress to take a different path,” she wrote.
The legal battle over whether faith-based hospitals should comply with ERISA is not likely over, according to Mr. Secunda.
“This is not the end of the story,” he said. “This is just the beginning, and now the next big issue to be decided will be, okay, principal purpose organizations come under the church plan exemption, but do these large billion-dollar hospitals qualify? Are they principal purpose organizations? I think that’s a very open question.”
[email protected]
On Twitter @legal_med
The U.S. Supreme Court has ruled that faith-based hospitals are exempt from federal pension requirements, holding that employees of religious-affiliated entities are not protected under the Employee Retirement Income Security Act (ERISA). The unanimous decision overturns rulings in the three circuit courts of appeals.
The opinion preserves the status quo, so it should not have an immediate effect on the affected employers and employees, said Ronald J. Mann, a law professor at Columbia University in New York who has written about one case, Advocate Health Care Network v. Stapleton, for Scotusblog.com.
The high court’s opinion centers on logic and the plain language of the ERISA statute, which is sensible, said Paul Secunda, a law professor and director of the labor and employment law program at Marquette University in Milwaukee. However, the decision does not address the larger question that matters to physicians and hospitals, he said.
“Some of these church-affiliated hospitals look an awful lot like their secular competitors,” he said. “They have thousands of employees. They make billions of dollars in revenue.”
Associate Justice Sonia Sotomayor raised similar concerns in a concurring opinion to the decision. While she agreed with her fellow justices on the ruling, she said the case outcome was still troubling.
“Despite their relationship to churches, organizations such as petitioners operate for-profit subsidiaries ... and compete in the secular market with companies that must bear the cost of complying with ERISA,” Justice Sotomayor wrote.
The Supreme Court ruling comes after current and former employees of three hospital chains – Dignity Health, Advocate Health Care, and Saint Peter’s Healthcare System – sued their employers in an effort to make them comply with ERISA. The employees argued that pension plans established by the large health care providers should not fall under ERISA’s “church plan” exception because the plans were not established by churches. ERISA requires that all private employers offering pension plans adhere to federal requirements designed to ensure plan solvency and protect plan participants.
The hospitals argued that pension plans do not have to be established by a church for the ERISA exemption to apply because the plans are maintained by qualifying church-affiliated organizations. The defendants based their position on a 1980 ERISA amendment that included the “maintained” exception. Since the amendment, the federal agencies charged with interpreting ERISA – the IRS, the Department of Labor, and the Pension Benefit Guaranty Corporation – have issued opinion after opinion reaffirming that view, the defendants noted.
Courts of appeals for the Third, Seventh, and Ninth circuits agreed with the employees, concluding that ERISA’s “plain text” requires that a pension plan be established by a church to qualify for the church-plan exemption.
The Supreme Court disagreed, however, ruling that a defined-benefit pension plan maintained by a principal-purpose organization – one controlled by or associate
However, the hospital sector has changed dramatically since the 1980 ERISA amendment, Mr. Secunda pointed out. “If you think back to when this reform was passed ... almost 40 years ago, we have a whole different animal [today] with regard to these large church-oriented hospital organizations.”
Justice Sotomayor raised similar concerns. “These organizations thus bear little resemblance to those Congress considered when enacting the 1980 amendment to the church plan definition. This current reality might prompt Congress to take a different path,” she wrote.
The legal battle over whether faith-based hospitals should comply with ERISA is not likely over, according to Mr. Secunda.
“This is not the end of the story,” he said. “This is just the beginning, and now the next big issue to be decided will be, okay, principal purpose organizations come under the church plan exemption, but do these large billion-dollar hospitals qualify? Are they principal purpose organizations? I think that’s a very open question.”
[email protected]
On Twitter @legal_med
The U.S. Supreme Court has ruled that faith-based hospitals are exempt from federal pension requirements, holding that employees of religious-affiliated entities are not protected under the Employee Retirement Income Security Act (ERISA). The unanimous decision overturns rulings in the three circuit courts of appeals.
The opinion preserves the status quo, so it should not have an immediate effect on the affected employers and employees, said Ronald J. Mann, a law professor at Columbia University in New York who has written about one case, Advocate Health Care Network v. Stapleton, for Scotusblog.com.
The high court’s opinion centers on logic and the plain language of the ERISA statute, which is sensible, said Paul Secunda, a law professor and director of the labor and employment law program at Marquette University in Milwaukee. However, the decision does not address the larger question that matters to physicians and hospitals, he said.
“Some of these church-affiliated hospitals look an awful lot like their secular competitors,” he said. “They have thousands of employees. They make billions of dollars in revenue.”
Associate Justice Sonia Sotomayor raised similar concerns in a concurring opinion to the decision. While she agreed with her fellow justices on the ruling, she said the case outcome was still troubling.
“Despite their relationship to churches, organizations such as petitioners operate for-profit subsidiaries ... and compete in the secular market with companies that must bear the cost of complying with ERISA,” Justice Sotomayor wrote.
The Supreme Court ruling comes after current and former employees of three hospital chains – Dignity Health, Advocate Health Care, and Saint Peter’s Healthcare System – sued their employers in an effort to make them comply with ERISA. The employees argued that pension plans established by the large health care providers should not fall under ERISA’s “church plan” exception because the plans were not established by churches. ERISA requires that all private employers offering pension plans adhere to federal requirements designed to ensure plan solvency and protect plan participants.
The hospitals argued that pension plans do not have to be established by a church for the ERISA exemption to apply because the plans are maintained by qualifying church-affiliated organizations. The defendants based their position on a 1980 ERISA amendment that included the “maintained” exception. Since the amendment, the federal agencies charged with interpreting ERISA – the IRS, the Department of Labor, and the Pension Benefit Guaranty Corporation – have issued opinion after opinion reaffirming that view, the defendants noted.
Courts of appeals for the Third, Seventh, and Ninth circuits agreed with the employees, concluding that ERISA’s “plain text” requires that a pension plan be established by a church to qualify for the church-plan exemption.
The Supreme Court disagreed, however, ruling that a defined-benefit pension plan maintained by a principal-purpose organization – one controlled by or associate
However, the hospital sector has changed dramatically since the 1980 ERISA amendment, Mr. Secunda pointed out. “If you think back to when this reform was passed ... almost 40 years ago, we have a whole different animal [today] with regard to these large church-oriented hospital organizations.”
Justice Sotomayor raised similar concerns. “These organizations thus bear little resemblance to those Congress considered when enacting the 1980 amendment to the church plan definition. This current reality might prompt Congress to take a different path,” she wrote.
The legal battle over whether faith-based hospitals should comply with ERISA is not likely over, according to Mr. Secunda.
“This is not the end of the story,” he said. “This is just the beginning, and now the next big issue to be decided will be, okay, principal purpose organizations come under the church plan exemption, but do these large billion-dollar hospitals qualify? Are they principal purpose organizations? I think that’s a very open question.”
[email protected]
On Twitter @legal_med
Low-dose aspirin bests dual-antiplatelet therapy in TAVR
PARIS – Single-antiplatelet therapy with low-dose aspirin following transcatheter aortic valve replacement (TAVR) reduced the occurrence of major adverse events, compared with guideline-recommended dual-antiplatelet therapy (DAPT), in the randomized ARTE trial.
The TAVR guideline recommendation for DAPT with low-dose aspirin plus clopidogrel is not based on evidence. It relies on expert opinion. ARTE (Aspirin Versus Aspirin + Clopidogrel Following TAVR) is the first sizable randomized trial to address the safety and efficacy of aspirin alone versus DAPT in the setting of TAVR, Josep Rodés-Cabau, MD, noted in presenting the ARTE results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

ARTE was a multicenter, prospective, international open-label study of 222 TAVR patients who were randomized to 3 months of single-antiplatelet therapy (SAPT) with aspirin at 80-100 mg/day or to DAPT with aspirin at 80-100 mg/day plus clopidogrel at 75 mg/day after a single 300-mg loading dose. Participants had a mean Society of Thoracic Surgery Predicted Risk of Mortality score of 6.3%. The vast majority of participants received the balloon-expandable Edwards Lifesciences Sapien XT valve. The remainder got the Sapien 3 valve.
The primary outcome was the 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack. It occurred in 15.3% of the DAPT group and 7.2% on SAPT, a difference that didn’t reach statistical significance (P = .065) because of small patient numbers.
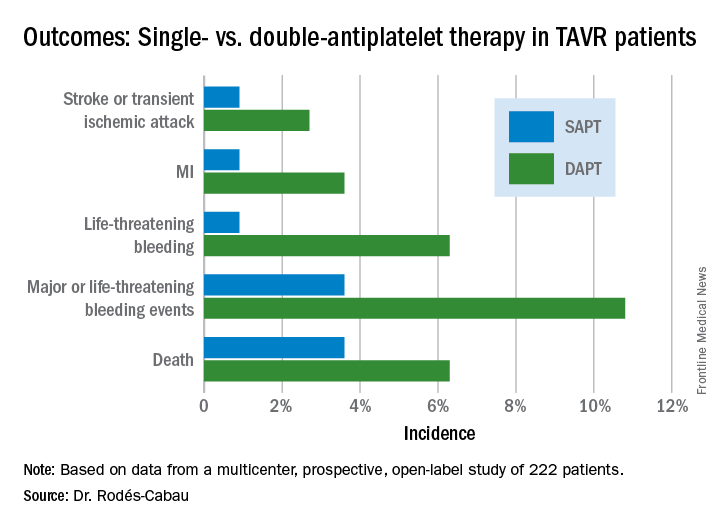
All subjects were on a proton pump inhibitor. The type, timing, and severity of bleeding events differed between the two study arms. All 4 bleeding events in the SAPT group were vascular in nature, while 5 of the 12 in the DAPT group were gastrointestinal. All the bleeding events in the SAPT group occurred within 72 hours after TAVR, whereas 5 of 12 in the DAPT recipients occurred later. Only one patient on SAPT experienced life-threatening bleeding, compared with seven DAPT patients who did.
“There were two prior smaller studies before ours,” according to Dr. Rodés-Cabau of Laval University in Quebec City. “One showed no differences, and an Italian one showed a tendency toward more bleeding with DAPT. So, I think there has been no sign to date that adding clopidogrel protects this group of patients from anything.”
Discussant Luis Nombela-Franco, MD, an interventional cardiologist at San Carlos Hospital in Madrid, pronounced the ARTE trial guideline-changing despite its limitations.
ARTE was supported by grants from Edwards Lifesciences and the Quebec Heart and Lung Institute.
Simultaneous with Dr. Rodés-Cabau’s presentation in Paris, the ARTE trial was published online (JACC Cardiovasc Interv. 2017 May 11. pii: S1936-8798[17]30812-9).

PARIS – Single-antiplatelet therapy with low-dose aspirin following transcatheter aortic valve replacement (TAVR) reduced the occurrence of major adverse events, compared with guideline-recommended dual-antiplatelet therapy (DAPT), in the randomized ARTE trial.
The TAVR guideline recommendation for DAPT with low-dose aspirin plus clopidogrel is not based on evidence. It relies on expert opinion. ARTE (Aspirin Versus Aspirin + Clopidogrel Following TAVR) is the first sizable randomized trial to address the safety and efficacy of aspirin alone versus DAPT in the setting of TAVR, Josep Rodés-Cabau, MD, noted in presenting the ARTE results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
ARTE was a multicenter, prospective, international open-label study of 222 TAVR patients who were randomized to 3 months of single-antiplatelet therapy (SAPT) with aspirin at 80-100 mg/day or to DAPT with aspirin at 80-100 mg/day plus clopidogrel at 75 mg/day after a single 300-mg loading dose. Participants had a mean Society of Thoracic Surgery Predicted Risk of Mortality score of 6.3%. The vast majority of participants received the balloon-expandable Edwards Lifesciences Sapien XT valve. The remainder got the Sapien 3 valve.
The primary outcome was the 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack. It occurred in 15.3% of the DAPT group and 7.2% on SAPT, a difference that didn’t reach statistical significance (P = .065) because of small patient numbers.
All subjects were on a proton pump inhibitor. The type, timing, and severity of bleeding events differed between the two study arms. All 4 bleeding events in the SAPT group were vascular in nature, while 5 of the 12 in the DAPT group were gastrointestinal. All the bleeding events in the SAPT group occurred within 72 hours after TAVR, whereas 5 of 12 in the DAPT recipients occurred later. Only one patient on SAPT experienced life-threatening bleeding, compared with seven DAPT patients who did.
“There were two prior smaller studies before ours,” according to Dr. Rodés-Cabau of Laval University in Quebec City. “One showed no differences, and an Italian one showed a tendency toward more bleeding with DAPT. So, I think there has been no sign to date that adding clopidogrel protects this group of patients from anything.”
Discussant Luis Nombela-Franco, MD, an interventional cardiologist at San Carlos Hospital in Madrid, pronounced the ARTE trial guideline-changing despite its limitations.
ARTE was supported by grants from Edwards Lifesciences and the Quebec Heart and Lung Institute.
Simultaneous with Dr. Rodés-Cabau’s presentation in Paris, the ARTE trial was published online (JACC Cardiovasc Interv. 2017 May 11. pii: S1936-8798[17]30812-9).
PARIS – Single-antiplatelet therapy with low-dose aspirin following transcatheter aortic valve replacement (TAVR) reduced the occurrence of major adverse events, compared with guideline-recommended dual-antiplatelet therapy (DAPT), in the randomized ARTE trial.
The TAVR guideline recommendation for DAPT with low-dose aspirin plus clopidogrel is not based on evidence. It relies on expert opinion. ARTE (Aspirin Versus Aspirin + Clopidogrel Following TAVR) is the first sizable randomized trial to address the safety and efficacy of aspirin alone versus DAPT in the setting of TAVR, Josep Rodés-Cabau, MD, noted in presenting the ARTE results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
ARTE was a multicenter, prospective, international open-label study of 222 TAVR patients who were randomized to 3 months of single-antiplatelet therapy (SAPT) with aspirin at 80-100 mg/day or to DAPT with aspirin at 80-100 mg/day plus clopidogrel at 75 mg/day after a single 300-mg loading dose. Participants had a mean Society of Thoracic Surgery Predicted Risk of Mortality score of 6.3%. The vast majority of participants received the balloon-expandable Edwards Lifesciences Sapien XT valve. The remainder got the Sapien 3 valve.
The primary outcome was the 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack. It occurred in 15.3% of the DAPT group and 7.2% on SAPT, a difference that didn’t reach statistical significance (P = .065) because of small patient numbers.
All subjects were on a proton pump inhibitor. The type, timing, and severity of bleeding events differed between the two study arms. All 4 bleeding events in the SAPT group were vascular in nature, while 5 of the 12 in the DAPT group were gastrointestinal. All the bleeding events in the SAPT group occurred within 72 hours after TAVR, whereas 5 of 12 in the DAPT recipients occurred later. Only one patient on SAPT experienced life-threatening bleeding, compared with seven DAPT patients who did.
“There were two prior smaller studies before ours,” according to Dr. Rodés-Cabau of Laval University in Quebec City. “One showed no differences, and an Italian one showed a tendency toward more bleeding with DAPT. So, I think there has been no sign to date that adding clopidogrel protects this group of patients from anything.”
Discussant Luis Nombela-Franco, MD, an interventional cardiologist at San Carlos Hospital in Madrid, pronounced the ARTE trial guideline-changing despite its limitations.
ARTE was supported by grants from Edwards Lifesciences and the Quebec Heart and Lung Institute.
Simultaneous with Dr. Rodés-Cabau’s presentation in Paris, the ARTE trial was published online (JACC Cardiovasc Interv. 2017 May 11. pii: S1936-8798[17]30812-9).
AT EUROPCR
Key clinical point:
Major finding: The 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack occurred in 15.3% of TAVR patients randomized to DAPT with low-dose aspirin plus clopidogrel, compared with 7.2% on aspirin only.
Data source: A randomized, multicenter, international, prospective open-label trial in 222 TAVR patients.
Disclosures: The presenter reported receiving research grants from Edwards Lifesciences and the Quebec Heart and Lung Institute, which supported the ARTE trial.