User login
Official Newspaper of the American College of Surgeons
Average cost of Healthcare.gov policy up 105% since 2013
The average monthly premium for individuals purchasing a plan from Healthcare.gov increased by 105% from 2013 to 2017, according to the Department of Health & Human Services.
In the 39 states that use Healthcare.gov, the average monthly exchange plan premium went from $232 in 2013 to $476 in 2017, an increase of $244 (105%), the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE) reported.
All 39 states experienced an increase in the cost of an average premium, but there was considerable variation in the size. Alabama had the largest percent increase at 223%, but Alaska had the largest absolute increase – $697 – to go with the second-largest percent increase – 203%. Oklahoma, where the average premium jumped 201%, was third, the ASPE said.
The state with the smallest change, both in terms of dollars and percents, was New Jersey, which had an increase of $51 (12%) over the 4-year period. The only other states with less than a 50% increase were New Hampshire at 32% and North Dakota at 44%, the report showed.
“States with benefit mandates similar to those required in the [Affordable Care Act] in effect before 2014 had smaller premium increases between 2013 and 2017,” the ASPE noted.
One limitation to the analysis is the change among those enrolling from 2013 to 2017. “Older and less healthy people are a larger share of the individual market risk pool now than in 2013. The changing mix of enrollees and adverse selection pressure has likely been a significant cause of the large average premium increases,” the ASPE said.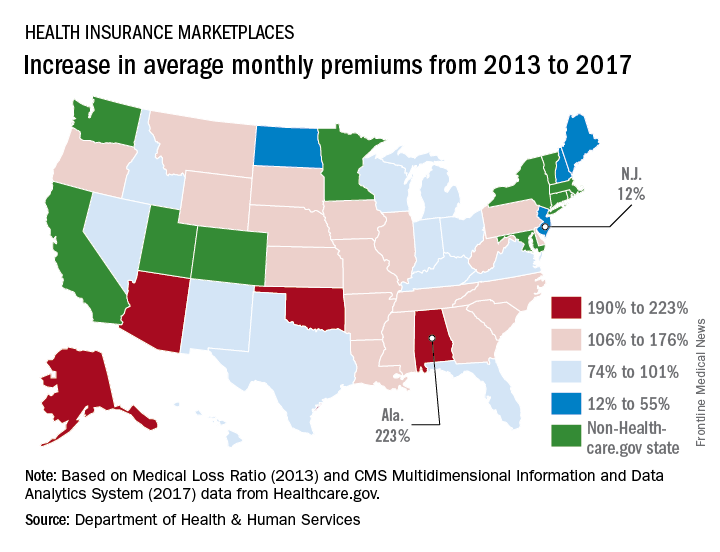
The average monthly premium for individuals purchasing a plan from Healthcare.gov increased by 105% from 2013 to 2017, according to the Department of Health & Human Services.
In the 39 states that use Healthcare.gov, the average monthly exchange plan premium went from $232 in 2013 to $476 in 2017, an increase of $244 (105%), the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE) reported.
All 39 states experienced an increase in the cost of an average premium, but there was considerable variation in the size. Alabama had the largest percent increase at 223%, but Alaska had the largest absolute increase – $697 – to go with the second-largest percent increase – 203%. Oklahoma, where the average premium jumped 201%, was third, the ASPE said.
The state with the smallest change, both in terms of dollars and percents, was New Jersey, which had an increase of $51 (12%) over the 4-year period. The only other states with less than a 50% increase were New Hampshire at 32% and North Dakota at 44%, the report showed.
“States with benefit mandates similar to those required in the [Affordable Care Act] in effect before 2014 had smaller premium increases between 2013 and 2017,” the ASPE noted.
One limitation to the analysis is the change among those enrolling from 2013 to 2017. “Older and less healthy people are a larger share of the individual market risk pool now than in 2013. The changing mix of enrollees and adverse selection pressure has likely been a significant cause of the large average premium increases,” the ASPE said.
The average monthly premium for individuals purchasing a plan from Healthcare.gov increased by 105% from 2013 to 2017, according to the Department of Health & Human Services.
In the 39 states that use Healthcare.gov, the average monthly exchange plan premium went from $232 in 2013 to $476 in 2017, an increase of $244 (105%), the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE) reported.
All 39 states experienced an increase in the cost of an average premium, but there was considerable variation in the size. Alabama had the largest percent increase at 223%, but Alaska had the largest absolute increase – $697 – to go with the second-largest percent increase – 203%. Oklahoma, where the average premium jumped 201%, was third, the ASPE said.
The state with the smallest change, both in terms of dollars and percents, was New Jersey, which had an increase of $51 (12%) over the 4-year period. The only other states with less than a 50% increase were New Hampshire at 32% and North Dakota at 44%, the report showed.
“States with benefit mandates similar to those required in the [Affordable Care Act] in effect before 2014 had smaller premium increases between 2013 and 2017,” the ASPE noted.
One limitation to the analysis is the change among those enrolling from 2013 to 2017. “Older and less healthy people are a larger share of the individual market risk pool now than in 2013. The changing mix of enrollees and adverse selection pressure has likely been a significant cause of the large average premium increases,” the ASPE said.
DESKTOP III: Secondary surgery for recurrent OC improves PFS, TFST
CHICAGO – Secondary cytoreductive surgery resulted in a clinically meaningful increase in progression-free survival and time to first subsequent therapy in a phase III study of carefully selected women with ovarian cancer who experienced their first relapse after a platin-free interval of 6 months.
These interim findings from the randomized international DESKTOP III trial suggest that until final overall survival data are available to more definitively define the role of secondary cytoreductive surgery in this setting, it should at least be considered as an option in patients who are good candidates based on a positive AGO Study Group score, defined as an ECOG performance status score of 0, ascites of 500 mL or less, and complete resection at initial surgery, Andreas du Bois, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The median progression-free survival (PFS) in 204 women who met this criteria and who were randomized to undergo surgery followed by chemotherapy was 19.6 months, compared with 14 months in 203 women who were randomized to receive only second-line chemotherapy (hazard ratio, 0.66), said Dr. du Bois of AGO and Kliniken Essen-Mitte, Essen, Germany.
“Even more important ... only complete resection makes a difference ... and that adds a median 7.2 months PFS with a hazard ratio of 0.56, which is highly significant. Fortunately that translates into time to first subsequent treatment, which is a more patient-oriented outcome,” he said.
The time to third-line therapy was prolonged by a highly statistically significant median of 7.1 month (hazard ratio, 0.6).
“What was the trade-off for these benefits? The patients did not pay for it with excessive mortality,” he said, explaining that no significant differences were seen between the groups in terms of mortality at 30, 60, 90, or 180 days, and that no excessive toxicity or treatment burden was seen in either group.

Median age of the patients was 60 years; they were enrolled at 80 centers in 12 countries between 2010 and 2015. The platin-free interval exceeded 12 months in 75% and 76% of patient in the surgery and control arms, respectively.
Chemotherapy regimens in both the treatment and control arms were selected according to institutional standards, although platinum-based combination therapy was strongly recommended; 87% and 88% in the groups, respectively, received a platinum-containing second-line therapy.
Macroscopic complete resection was achieved in 72.5% of patients in the surgery arm, which was the rate predicted by the AGO scores.
“We know that the surgery and chemotherapy are the cornerstones of ovarian cancer therapy ... however, surgery in recurrent ovarian cancer has not been based on high-level evidence,” Dr. du Bois said. “So far there are only retrospective series suggesting that there might be a benefit or not.”
The German AGO group and the Gynecologic Oncology Group (GOG) in the United States thus initiated clinical trials to evaluate its role in recurrent ovarian cancer, including the DESKTOP series, he explained, noting that the AGO score was developed through these trials as a way to identify good surgical candidates based on preoperative factors.
It was confirmed in a prospective study that the score, which selects about 50% of all patients with platinum-sensitive recurrent ovarian cancer, could predict successful surgery, he added.
In the current study, the data with respect to overall survival – the primary study endpoint – have not reached maturity, but at 2 years it was 83%.
However, the findings of a meaningful benefit in progression-free survival and time to first subsequent treatment (advantages of 5.6 and 7.1 months, respectively) in secondary cytoreductive surgery patients is at least comparable with all phase III trials in second-line therapy for platinum-sensitive recurrent ovarian cancer so far, he said.
“In fact, it’s the most positive trial ever reported in this population,” he added, noted that he was referring to therapy trials, not maintenance trials.
Further, the fact that the surgery benefit was exclusive to patients with complete resection indicates the importance of selecting both the right center with capability of achieving complete resection in most patients, and the right patients, as identified by the AGO score.
“Hopefully, further follow-up will show that this benefit translates into overall survival,” he concluded, noting that overall survival will be evaluated after extended follow-up when 244 overall survival events are observed.
Dr. Du Bois reported serving as a consultant or adviser for AstraZeneca, Mundipharma, Pfizer, Pharmamar, and Roche/Genentech.
The findings from DESKTOP III complement those from prior retrospective studies, but one key difference is the emphasis on the importance of complete resection, abstract discussant Ritu Salani, MD, said at the meeting.
“I no longer believe that optimal resection is good enough in this patient population,” she said.
In fact, given that 67 patients in the study were not completely resected, it is important to look at whether there are any identifying factors that could help prevent surgery in these patients, and whether there are any minimally invasive or less invasive approaches, such as scoping and scoring these patients, to determine who really is completely resectable, she said.
Other studies of cytoreductive surgery, including GOG 213 and the Dutch SOCceR trial, are ongoing, and the primary endpoint of DESKTOP III is overall survival, she noted.
“We look forward to these data maturing.”
Dr. Salani is with the Ohio State University, Columbus. She has received honoraria from Clovis Oncology and Lynparza, and has served in a consulting or advisory role for Genentech/Roche.
The findings from DESKTOP III complement those from prior retrospective studies, but one key difference is the emphasis on the importance of complete resection, abstract discussant Ritu Salani, MD, said at the meeting.
“I no longer believe that optimal resection is good enough in this patient population,” she said.
In fact, given that 67 patients in the study were not completely resected, it is important to look at whether there are any identifying factors that could help prevent surgery in these patients, and whether there are any minimally invasive or less invasive approaches, such as scoping and scoring these patients, to determine who really is completely resectable, she said.
Other studies of cytoreductive surgery, including GOG 213 and the Dutch SOCceR trial, are ongoing, and the primary endpoint of DESKTOP III is overall survival, she noted.
“We look forward to these data maturing.”
Dr. Salani is with the Ohio State University, Columbus. She has received honoraria from Clovis Oncology and Lynparza, and has served in a consulting or advisory role for Genentech/Roche.
The findings from DESKTOP III complement those from prior retrospective studies, but one key difference is the emphasis on the importance of complete resection, abstract discussant Ritu Salani, MD, said at the meeting.
“I no longer believe that optimal resection is good enough in this patient population,” she said.
In fact, given that 67 patients in the study were not completely resected, it is important to look at whether there are any identifying factors that could help prevent surgery in these patients, and whether there are any minimally invasive or less invasive approaches, such as scoping and scoring these patients, to determine who really is completely resectable, she said.
Other studies of cytoreductive surgery, including GOG 213 and the Dutch SOCceR trial, are ongoing, and the primary endpoint of DESKTOP III is overall survival, she noted.
“We look forward to these data maturing.”
Dr. Salani is with the Ohio State University, Columbus. She has received honoraria from Clovis Oncology and Lynparza, and has served in a consulting or advisory role for Genentech/Roche.
CHICAGO – Secondary cytoreductive surgery resulted in a clinically meaningful increase in progression-free survival and time to first subsequent therapy in a phase III study of carefully selected women with ovarian cancer who experienced their first relapse after a platin-free interval of 6 months.
These interim findings from the randomized international DESKTOP III trial suggest that until final overall survival data are available to more definitively define the role of secondary cytoreductive surgery in this setting, it should at least be considered as an option in patients who are good candidates based on a positive AGO Study Group score, defined as an ECOG performance status score of 0, ascites of 500 mL or less, and complete resection at initial surgery, Andreas du Bois, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The median progression-free survival (PFS) in 204 women who met this criteria and who were randomized to undergo surgery followed by chemotherapy was 19.6 months, compared with 14 months in 203 women who were randomized to receive only second-line chemotherapy (hazard ratio, 0.66), said Dr. du Bois of AGO and Kliniken Essen-Mitte, Essen, Germany.
“Even more important ... only complete resection makes a difference ... and that adds a median 7.2 months PFS with a hazard ratio of 0.56, which is highly significant. Fortunately that translates into time to first subsequent treatment, which is a more patient-oriented outcome,” he said.
The time to third-line therapy was prolonged by a highly statistically significant median of 7.1 month (hazard ratio, 0.6).
“What was the trade-off for these benefits? The patients did not pay for it with excessive mortality,” he said, explaining that no significant differences were seen between the groups in terms of mortality at 30, 60, 90, or 180 days, and that no excessive toxicity or treatment burden was seen in either group.
Median age of the patients was 60 years; they were enrolled at 80 centers in 12 countries between 2010 and 2015. The platin-free interval exceeded 12 months in 75% and 76% of patient in the surgery and control arms, respectively.
Chemotherapy regimens in both the treatment and control arms were selected according to institutional standards, although platinum-based combination therapy was strongly recommended; 87% and 88% in the groups, respectively, received a platinum-containing second-line therapy.
Macroscopic complete resection was achieved in 72.5% of patients in the surgery arm, which was the rate predicted by the AGO scores.
“We know that the surgery and chemotherapy are the cornerstones of ovarian cancer therapy ... however, surgery in recurrent ovarian cancer has not been based on high-level evidence,” Dr. du Bois said. “So far there are only retrospective series suggesting that there might be a benefit or not.”
The German AGO group and the Gynecologic Oncology Group (GOG) in the United States thus initiated clinical trials to evaluate its role in recurrent ovarian cancer, including the DESKTOP series, he explained, noting that the AGO score was developed through these trials as a way to identify good surgical candidates based on preoperative factors.
It was confirmed in a prospective study that the score, which selects about 50% of all patients with platinum-sensitive recurrent ovarian cancer, could predict successful surgery, he added.
In the current study, the data with respect to overall survival – the primary study endpoint – have not reached maturity, but at 2 years it was 83%.
However, the findings of a meaningful benefit in progression-free survival and time to first subsequent treatment (advantages of 5.6 and 7.1 months, respectively) in secondary cytoreductive surgery patients is at least comparable with all phase III trials in second-line therapy for platinum-sensitive recurrent ovarian cancer so far, he said.
“In fact, it’s the most positive trial ever reported in this population,” he added, noted that he was referring to therapy trials, not maintenance trials.
Further, the fact that the surgery benefit was exclusive to patients with complete resection indicates the importance of selecting both the right center with capability of achieving complete resection in most patients, and the right patients, as identified by the AGO score.
“Hopefully, further follow-up will show that this benefit translates into overall survival,” he concluded, noting that overall survival will be evaluated after extended follow-up when 244 overall survival events are observed.
Dr. Du Bois reported serving as a consultant or adviser for AstraZeneca, Mundipharma, Pfizer, Pharmamar, and Roche/Genentech.
CHICAGO – Secondary cytoreductive surgery resulted in a clinically meaningful increase in progression-free survival and time to first subsequent therapy in a phase III study of carefully selected women with ovarian cancer who experienced their first relapse after a platin-free interval of 6 months.
These interim findings from the randomized international DESKTOP III trial suggest that until final overall survival data are available to more definitively define the role of secondary cytoreductive surgery in this setting, it should at least be considered as an option in patients who are good candidates based on a positive AGO Study Group score, defined as an ECOG performance status score of 0, ascites of 500 mL or less, and complete resection at initial surgery, Andreas du Bois, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The median progression-free survival (PFS) in 204 women who met this criteria and who were randomized to undergo surgery followed by chemotherapy was 19.6 months, compared with 14 months in 203 women who were randomized to receive only second-line chemotherapy (hazard ratio, 0.66), said Dr. du Bois of AGO and Kliniken Essen-Mitte, Essen, Germany.
“Even more important ... only complete resection makes a difference ... and that adds a median 7.2 months PFS with a hazard ratio of 0.56, which is highly significant. Fortunately that translates into time to first subsequent treatment, which is a more patient-oriented outcome,” he said.
The time to third-line therapy was prolonged by a highly statistically significant median of 7.1 month (hazard ratio, 0.6).
“What was the trade-off for these benefits? The patients did not pay for it with excessive mortality,” he said, explaining that no significant differences were seen between the groups in terms of mortality at 30, 60, 90, or 180 days, and that no excessive toxicity or treatment burden was seen in either group.
Median age of the patients was 60 years; they were enrolled at 80 centers in 12 countries between 2010 and 2015. The platin-free interval exceeded 12 months in 75% and 76% of patient in the surgery and control arms, respectively.
Chemotherapy regimens in both the treatment and control arms were selected according to institutional standards, although platinum-based combination therapy was strongly recommended; 87% and 88% in the groups, respectively, received a platinum-containing second-line therapy.
Macroscopic complete resection was achieved in 72.5% of patients in the surgery arm, which was the rate predicted by the AGO scores.
“We know that the surgery and chemotherapy are the cornerstones of ovarian cancer therapy ... however, surgery in recurrent ovarian cancer has not been based on high-level evidence,” Dr. du Bois said. “So far there are only retrospective series suggesting that there might be a benefit or not.”
The German AGO group and the Gynecologic Oncology Group (GOG) in the United States thus initiated clinical trials to evaluate its role in recurrent ovarian cancer, including the DESKTOP series, he explained, noting that the AGO score was developed through these trials as a way to identify good surgical candidates based on preoperative factors.
It was confirmed in a prospective study that the score, which selects about 50% of all patients with platinum-sensitive recurrent ovarian cancer, could predict successful surgery, he added.
In the current study, the data with respect to overall survival – the primary study endpoint – have not reached maturity, but at 2 years it was 83%.
However, the findings of a meaningful benefit in progression-free survival and time to first subsequent treatment (advantages of 5.6 and 7.1 months, respectively) in secondary cytoreductive surgery patients is at least comparable with all phase III trials in second-line therapy for platinum-sensitive recurrent ovarian cancer so far, he said.
“In fact, it’s the most positive trial ever reported in this population,” he added, noted that he was referring to therapy trials, not maintenance trials.
Further, the fact that the surgery benefit was exclusive to patients with complete resection indicates the importance of selecting both the right center with capability of achieving complete resection in most patients, and the right patients, as identified by the AGO score.
“Hopefully, further follow-up will show that this benefit translates into overall survival,” he concluded, noting that overall survival will be evaluated after extended follow-up when 244 overall survival events are observed.
Dr. Du Bois reported serving as a consultant or adviser for AstraZeneca, Mundipharma, Pfizer, Pharmamar, and Roche/Genentech.
At THE 2017 ASCO ANNUAL MEETING
Key clinical point:
Major finding: Median progression-free survival was 19.6 vs. 14 months in the surgery vs. second-line chemotherapy-only arm.
Data source: The randomized phase III DESKTOP III study of 407 patients.
Disclosures: Dr. du Bois reported serving as a consultant or adviser for AstraZeneca, Mundipharma, Pfizer, Pharmamar, and Roche/Genentech.
ACS Committee on Diversity Issues seeks two new members
The American College of Surgeons (ACS) Committee on Diversity Issues (CODI) is seeking candidates to fill two vacancies on the committee beginning in October 2017.
The mission of the Committee on Diversity Issues is to study the educational and professional needs of underrepresented surgeons and surgical trainees and the impact that its work may have on the elimination of health care disparities among diverse population groups.
Surgeons interested in developing initiatives to expand diversity within the ACS membership and leadership and to developing resources and programming for surgeons related to diversity and cultural competency should apply. Nominations are open to all, and the committee encourages representation by individuals of diverse cultural, racial, and ethnic backgrounds.
Nominees must meet the following criteria:
- Be an active Fellow of the ACS
- Be able to serve an initial three-year term: 2017–2020
- Attend one in-person meeting at the annual ACS Clinical Congress
- Participate in quarterly conference calls
- Contribute to committee initiatives
To apply, go to www.surveymonkey.com/r/CmteDiversityApp to access the application and submit by June 30.
Applicants will need to do the following:
- Upload a summary of your curriculum vitae (five pages or less)
- Upload a letter of interest highlighting your skills and expertise, along with contributions you would like to make to the committee
Eligible candidates will be selected and notified by the committee in July and will be invited to attend the October 23 meeting of the Committee on Diversity Issues as guests. This meeting is held in conjunction with the 2017 Clinical Congress in San Diego. Travel reimbursement will not be provided.
Direct questions to [email protected].
The American College of Surgeons (ACS) Committee on Diversity Issues (CODI) is seeking candidates to fill two vacancies on the committee beginning in October 2017.
The mission of the Committee on Diversity Issues is to study the educational and professional needs of underrepresented surgeons and surgical trainees and the impact that its work may have on the elimination of health care disparities among diverse population groups.
Surgeons interested in developing initiatives to expand diversity within the ACS membership and leadership and to developing resources and programming for surgeons related to diversity and cultural competency should apply. Nominations are open to all, and the committee encourages representation by individuals of diverse cultural, racial, and ethnic backgrounds.
Nominees must meet the following criteria:
- Be an active Fellow of the ACS
- Be able to serve an initial three-year term: 2017–2020
- Attend one in-person meeting at the annual ACS Clinical Congress
- Participate in quarterly conference calls
- Contribute to committee initiatives
To apply, go to www.surveymonkey.com/r/CmteDiversityApp to access the application and submit by June 30.
Applicants will need to do the following:
- Upload a summary of your curriculum vitae (five pages or less)
- Upload a letter of interest highlighting your skills and expertise, along with contributions you would like to make to the committee
Eligible candidates will be selected and notified by the committee in July and will be invited to attend the October 23 meeting of the Committee on Diversity Issues as guests. This meeting is held in conjunction with the 2017 Clinical Congress in San Diego. Travel reimbursement will not be provided.
Direct questions to [email protected].
The American College of Surgeons (ACS) Committee on Diversity Issues (CODI) is seeking candidates to fill two vacancies on the committee beginning in October 2017.
The mission of the Committee on Diversity Issues is to study the educational and professional needs of underrepresented surgeons and surgical trainees and the impact that its work may have on the elimination of health care disparities among diverse population groups.
Surgeons interested in developing initiatives to expand diversity within the ACS membership and leadership and to developing resources and programming for surgeons related to diversity and cultural competency should apply. Nominations are open to all, and the committee encourages representation by individuals of diverse cultural, racial, and ethnic backgrounds.
Nominees must meet the following criteria:
- Be an active Fellow of the ACS
- Be able to serve an initial three-year term: 2017–2020
- Attend one in-person meeting at the annual ACS Clinical Congress
- Participate in quarterly conference calls
- Contribute to committee initiatives
To apply, go to www.surveymonkey.com/r/CmteDiversityApp to access the application and submit by June 30.
Applicants will need to do the following:
- Upload a summary of your curriculum vitae (five pages or less)
- Upload a letter of interest highlighting your skills and expertise, along with contributions you would like to make to the committee
Eligible candidates will be selected and notified by the committee in July and will be invited to attend the October 23 meeting of the Committee on Diversity Issues as guests. This meeting is held in conjunction with the 2017 Clinical Congress in San Diego. Travel reimbursement will not be provided.
Direct questions to [email protected].
Acute cholecystitis: Not always routine
The more we think we know, the less we actually may know. As new techniques develop and their use is closely examined and reported, details about the patient’s disease and the surgeon’s skill and judgment turn out to matter more and more in the decision-making process. So it is with acute cholecystitis.
I have recently been puzzled and intrigued by changing trends in the management of acute cholecystitis that are apparent in the medical literature, discussions in the ACS Communities, and practice in my local community.
When I was a resident, the debate about early cholecystectomy vs antibiotics with interval operation 6 weeks later was just being settled in the literature in favor of early cholecystectomy. The weight of evidence in the surgical literature found that delay made the eventual operation more difficult and costly.

In the following 2 decades, early cholecystectomy became the indicated treatment for acute cholecystitis. In that era, of course, these operations were open, as that was our only option and one which we all learned to perform with confidence during residency. Tube cholecystostomy was a rarity reserved only for the most severely ill and feeble, and done by surgeons, since interventional radiologists had not yet appeared on the scene.
In the rare instance of acute cholecystitis so severe, and anatomic landmarks so obscured, that the gallbladder could not be safely dissected away from the common bile duct, a remnant of the gallbladder might be left behind, the mucosa cauterized, and the right upper quadrant drained.
Fast forward 40 years, and we find a distinctly different landscape. As the Boomer generation reaches geriatric age in expanding numbers, surgeons encounter an increasingly older patient population, often with numerous comorbidities and high surgical risk. Our increased critical care capability to rescue patients from sepsis and organ failure also introduces new challenges in decision-making about whether immediate cholecystectomy or a temporizing option is better for the elderly septic ICU patient before us.
At the same time, our overwhelmingly most common elective biliary procedure has become a laparoscopic cholecystectomy (LC), with which our younger surgeons have become comfortable and facile. Multiple randomized studies also confirm the superiority of early LC for acute cholecystitis, although LC is associated with a higher rate of conversion to open cholecystectomy in acute cholecystitis than in the elective setting. Since it is acknowledged that the mortality and morbidity of an open cholecystectomy is greater than that of its laparoscopic counterpart, especially in the setting of severe inflammation, and the younger surgeons are less confident in performing open cholecystectomy, it is not surprising that they embrace a strategy that allows them to avoid surgical management of acute cholecystitis in the high-risk patient with severe disease.
The ready availability of interventional radiologists in the past 30 years also offers a less invasive option than surgery – the percutaneous tube cholecystostomy (PC). It is no wonder that PC has increasingly become the “go-to” early option when the patient is old and sick or the surgeon lacks confidence in his/her open surgical skills in a potentially hostile, inflamed right upper quadrant. If the increasing number of articles on PC appearing in the literature is any indication, its use has proliferated in the recent past. As yet, no randomized clinical trials or other high-quality evidence have emerged to support its increased use, but a consensus panel of experts has issued the Tokyo Guidelines, recommending PC as primary therapy for stage III acute cholecystitis, the form of disease associated with organ failure, but not citing evidence to support this recommendation (J Hepatobiliary Pancreat Surg. 2007;14[1]:91-7). Although the rate of PC use in Medicare patients with stage III acute cholecystitis has more than doubled in the past 20 years, Tokyo Guidelines have clearly not been uniformly adopted in the U.S., since PC use in patients with stage III acute cholecystitis is only 10% (J Am Coll Surg. 2017;224[4]: 502-14).
Whether the increase in PC use is appropriate or not remains undetermined. Other uncertainties about PC need clarification. When patients have a PC placed for acute cholecystitis, do they always need their gallbladders removed later? The rate of recurrent acute cholecystitis after PC is variable in the literature, although it appears to be more likely in patients with acute calculous than acalculous cholecystitis. The likelihood that the patient will later undergo a cholecystectomy varies from a low of 3% to a high of 57% in various studies.(Surgery. 2014;155[4]:615-22; J Am Coll Surg. 2012; 214[2]:196-201).
The exact rate may not even accurately be known, since some patients may be lost to follow-up or get subsequent care in another facility. The decision to perform cholecystectomy after PC involves assessment of patient risk for surgery and, ultimately, surgeon judgment. Other questions also remain unanswered: What is the role of surgeon experience in the decision to defer surgical therapy for acute cholecystitis? Is the surgeon even the one who is in charge of the decision in all cases, or is that decision being made by an internist, intensivist, or hospitalist, who may judge the patient’s risk differently than a surgeon would? Are we witnessing an evolution in management of severe cholecystitis in the high-risk, septic and elderly patient towards antibiotics and PC unless the patient fails that treatment? This strategy appears to be gaining in popularity, since several studies have shown that the minority of patients who have PC end up having their gallbladders removed. If symptoms recur and nonoperative treatment has clearly failed, should the decision be made to refer to a highly experienced surgeon (by virtue of laparoscopic skills or reputation as a hepatic-pancreatic biliary specialist)? Recent studies show that 46%-86% of elective interval cholecystectomies after successful PC can be performed laparoscopically with low complication rates, although those studies came from institutions with notable laparoscopic expertise (J Am Coll Surg. 2012;214[2]:196-201; J Gastrointest Surg. 2017; 21[5]:761-69).
One of my most revered senior surgical mentors recently opined that the safest strategy for the high-risk patient with severe acute cholecystitis was indeed PC and antibiotics followed by watchful waiting, and reserving cholecystectomy only for those who fail nonoperative therapy. I initially bristled at that concept as being antithetic to the surgical bias in favor of cholecystectomy as the answer to all gallbladder evils. But after reflecting further on the changing landscape of our therapeutic options and our changing surgical training, I’m thinking that his strategy may be reasonable.
After all, it’s about choosing the safest path for the patient. All cholecystectomies are not routine.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The more we think we know, the less we actually may know. As new techniques develop and their use is closely examined and reported, details about the patient’s disease and the surgeon’s skill and judgment turn out to matter more and more in the decision-making process. So it is with acute cholecystitis.
I have recently been puzzled and intrigued by changing trends in the management of acute cholecystitis that are apparent in the medical literature, discussions in the ACS Communities, and practice in my local community.
When I was a resident, the debate about early cholecystectomy vs antibiotics with interval operation 6 weeks later was just being settled in the literature in favor of early cholecystectomy. The weight of evidence in the surgical literature found that delay made the eventual operation more difficult and costly.
In the following 2 decades, early cholecystectomy became the indicated treatment for acute cholecystitis. In that era, of course, these operations were open, as that was our only option and one which we all learned to perform with confidence during residency. Tube cholecystostomy was a rarity reserved only for the most severely ill and feeble, and done by surgeons, since interventional radiologists had not yet appeared on the scene.
In the rare instance of acute cholecystitis so severe, and anatomic landmarks so obscured, that the gallbladder could not be safely dissected away from the common bile duct, a remnant of the gallbladder might be left behind, the mucosa cauterized, and the right upper quadrant drained.
Fast forward 40 years, and we find a distinctly different landscape. As the Boomer generation reaches geriatric age in expanding numbers, surgeons encounter an increasingly older patient population, often with numerous comorbidities and high surgical risk. Our increased critical care capability to rescue patients from sepsis and organ failure also introduces new challenges in decision-making about whether immediate cholecystectomy or a temporizing option is better for the elderly septic ICU patient before us.
At the same time, our overwhelmingly most common elective biliary procedure has become a laparoscopic cholecystectomy (LC), with which our younger surgeons have become comfortable and facile. Multiple randomized studies also confirm the superiority of early LC for acute cholecystitis, although LC is associated with a higher rate of conversion to open cholecystectomy in acute cholecystitis than in the elective setting. Since it is acknowledged that the mortality and morbidity of an open cholecystectomy is greater than that of its laparoscopic counterpart, especially in the setting of severe inflammation, and the younger surgeons are less confident in performing open cholecystectomy, it is not surprising that they embrace a strategy that allows them to avoid surgical management of acute cholecystitis in the high-risk patient with severe disease.
The ready availability of interventional radiologists in the past 30 years also offers a less invasive option than surgery – the percutaneous tube cholecystostomy (PC). It is no wonder that PC has increasingly become the “go-to” early option when the patient is old and sick or the surgeon lacks confidence in his/her open surgical skills in a potentially hostile, inflamed right upper quadrant. If the increasing number of articles on PC appearing in the literature is any indication, its use has proliferated in the recent past. As yet, no randomized clinical trials or other high-quality evidence have emerged to support its increased use, but a consensus panel of experts has issued the Tokyo Guidelines, recommending PC as primary therapy for stage III acute cholecystitis, the form of disease associated with organ failure, but not citing evidence to support this recommendation (J Hepatobiliary Pancreat Surg. 2007;14[1]:91-7). Although the rate of PC use in Medicare patients with stage III acute cholecystitis has more than doubled in the past 20 years, Tokyo Guidelines have clearly not been uniformly adopted in the U.S., since PC use in patients with stage III acute cholecystitis is only 10% (J Am Coll Surg. 2017;224[4]: 502-14).
Whether the increase in PC use is appropriate or not remains undetermined. Other uncertainties about PC need clarification. When patients have a PC placed for acute cholecystitis, do they always need their gallbladders removed later? The rate of recurrent acute cholecystitis after PC is variable in the literature, although it appears to be more likely in patients with acute calculous than acalculous cholecystitis. The likelihood that the patient will later undergo a cholecystectomy varies from a low of 3% to a high of 57% in various studies.(Surgery. 2014;155[4]:615-22; J Am Coll Surg. 2012; 214[2]:196-201).
The exact rate may not even accurately be known, since some patients may be lost to follow-up or get subsequent care in another facility. The decision to perform cholecystectomy after PC involves assessment of patient risk for surgery and, ultimately, surgeon judgment. Other questions also remain unanswered: What is the role of surgeon experience in the decision to defer surgical therapy for acute cholecystitis? Is the surgeon even the one who is in charge of the decision in all cases, or is that decision being made by an internist, intensivist, or hospitalist, who may judge the patient’s risk differently than a surgeon would? Are we witnessing an evolution in management of severe cholecystitis in the high-risk, septic and elderly patient towards antibiotics and PC unless the patient fails that treatment? This strategy appears to be gaining in popularity, since several studies have shown that the minority of patients who have PC end up having their gallbladders removed. If symptoms recur and nonoperative treatment has clearly failed, should the decision be made to refer to a highly experienced surgeon (by virtue of laparoscopic skills or reputation as a hepatic-pancreatic biliary specialist)? Recent studies show that 46%-86% of elective interval cholecystectomies after successful PC can be performed laparoscopically with low complication rates, although those studies came from institutions with notable laparoscopic expertise (J Am Coll Surg. 2012;214[2]:196-201; J Gastrointest Surg. 2017; 21[5]:761-69).
One of my most revered senior surgical mentors recently opined that the safest strategy for the high-risk patient with severe acute cholecystitis was indeed PC and antibiotics followed by watchful waiting, and reserving cholecystectomy only for those who fail nonoperative therapy. I initially bristled at that concept as being antithetic to the surgical bias in favor of cholecystectomy as the answer to all gallbladder evils. But after reflecting further on the changing landscape of our therapeutic options and our changing surgical training, I’m thinking that his strategy may be reasonable.
After all, it’s about choosing the safest path for the patient. All cholecystectomies are not routine.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The more we think we know, the less we actually may know. As new techniques develop and their use is closely examined and reported, details about the patient’s disease and the surgeon’s skill and judgment turn out to matter more and more in the decision-making process. So it is with acute cholecystitis.
I have recently been puzzled and intrigued by changing trends in the management of acute cholecystitis that are apparent in the medical literature, discussions in the ACS Communities, and practice in my local community.
When I was a resident, the debate about early cholecystectomy vs antibiotics with interval operation 6 weeks later was just being settled in the literature in favor of early cholecystectomy. The weight of evidence in the surgical literature found that delay made the eventual operation more difficult and costly.
In the following 2 decades, early cholecystectomy became the indicated treatment for acute cholecystitis. In that era, of course, these operations were open, as that was our only option and one which we all learned to perform with confidence during residency. Tube cholecystostomy was a rarity reserved only for the most severely ill and feeble, and done by surgeons, since interventional radiologists had not yet appeared on the scene.
In the rare instance of acute cholecystitis so severe, and anatomic landmarks so obscured, that the gallbladder could not be safely dissected away from the common bile duct, a remnant of the gallbladder might be left behind, the mucosa cauterized, and the right upper quadrant drained.
Fast forward 40 years, and we find a distinctly different landscape. As the Boomer generation reaches geriatric age in expanding numbers, surgeons encounter an increasingly older patient population, often with numerous comorbidities and high surgical risk. Our increased critical care capability to rescue patients from sepsis and organ failure also introduces new challenges in decision-making about whether immediate cholecystectomy or a temporizing option is better for the elderly septic ICU patient before us.
At the same time, our overwhelmingly most common elective biliary procedure has become a laparoscopic cholecystectomy (LC), with which our younger surgeons have become comfortable and facile. Multiple randomized studies also confirm the superiority of early LC for acute cholecystitis, although LC is associated with a higher rate of conversion to open cholecystectomy in acute cholecystitis than in the elective setting. Since it is acknowledged that the mortality and morbidity of an open cholecystectomy is greater than that of its laparoscopic counterpart, especially in the setting of severe inflammation, and the younger surgeons are less confident in performing open cholecystectomy, it is not surprising that they embrace a strategy that allows them to avoid surgical management of acute cholecystitis in the high-risk patient with severe disease.
The ready availability of interventional radiologists in the past 30 years also offers a less invasive option than surgery – the percutaneous tube cholecystostomy (PC). It is no wonder that PC has increasingly become the “go-to” early option when the patient is old and sick or the surgeon lacks confidence in his/her open surgical skills in a potentially hostile, inflamed right upper quadrant. If the increasing number of articles on PC appearing in the literature is any indication, its use has proliferated in the recent past. As yet, no randomized clinical trials or other high-quality evidence have emerged to support its increased use, but a consensus panel of experts has issued the Tokyo Guidelines, recommending PC as primary therapy for stage III acute cholecystitis, the form of disease associated with organ failure, but not citing evidence to support this recommendation (J Hepatobiliary Pancreat Surg. 2007;14[1]:91-7). Although the rate of PC use in Medicare patients with stage III acute cholecystitis has more than doubled in the past 20 years, Tokyo Guidelines have clearly not been uniformly adopted in the U.S., since PC use in patients with stage III acute cholecystitis is only 10% (J Am Coll Surg. 2017;224[4]: 502-14).
Whether the increase in PC use is appropriate or not remains undetermined. Other uncertainties about PC need clarification. When patients have a PC placed for acute cholecystitis, do they always need their gallbladders removed later? The rate of recurrent acute cholecystitis after PC is variable in the literature, although it appears to be more likely in patients with acute calculous than acalculous cholecystitis. The likelihood that the patient will later undergo a cholecystectomy varies from a low of 3% to a high of 57% in various studies.(Surgery. 2014;155[4]:615-22; J Am Coll Surg. 2012; 214[2]:196-201).
The exact rate may not even accurately be known, since some patients may be lost to follow-up or get subsequent care in another facility. The decision to perform cholecystectomy after PC involves assessment of patient risk for surgery and, ultimately, surgeon judgment. Other questions also remain unanswered: What is the role of surgeon experience in the decision to defer surgical therapy for acute cholecystitis? Is the surgeon even the one who is in charge of the decision in all cases, or is that decision being made by an internist, intensivist, or hospitalist, who may judge the patient’s risk differently than a surgeon would? Are we witnessing an evolution in management of severe cholecystitis in the high-risk, septic and elderly patient towards antibiotics and PC unless the patient fails that treatment? This strategy appears to be gaining in popularity, since several studies have shown that the minority of patients who have PC end up having their gallbladders removed. If symptoms recur and nonoperative treatment has clearly failed, should the decision be made to refer to a highly experienced surgeon (by virtue of laparoscopic skills or reputation as a hepatic-pancreatic biliary specialist)? Recent studies show that 46%-86% of elective interval cholecystectomies after successful PC can be performed laparoscopically with low complication rates, although those studies came from institutions with notable laparoscopic expertise (J Am Coll Surg. 2012;214[2]:196-201; J Gastrointest Surg. 2017; 21[5]:761-69).
One of my most revered senior surgical mentors recently opined that the safest strategy for the high-risk patient with severe acute cholecystitis was indeed PC and antibiotics followed by watchful waiting, and reserving cholecystectomy only for those who fail nonoperative therapy. I initially bristled at that concept as being antithetic to the surgical bias in favor of cholecystectomy as the answer to all gallbladder evils. But after reflecting further on the changing landscape of our therapeutic options and our changing surgical training, I’m thinking that his strategy may be reasonable.
After all, it’s about choosing the safest path for the patient. All cholecystectomies are not routine.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
An Act of Service, an Act of Love
Since its foundation in 1913 as the premier surgical professional organization in the United States, and one of the most influential in the world, the American College of Surgeons has shaped the policies and molded the education of numerous generations of surgeons. All young surgeons should aspire to be invested as Fellows some day as the highest honor in their career.
Service is an important factor in the decision to become a surgeon. As a Fellow of the ACS, the young surgeon will find many opportunities for service. Active participation as a Fellow is an act of service and can be an act of love for our patients, our colleagues, and our profession. And, with it, comes loyalty, a spirit of dedication, and a sense of unity. In addition, by joining the College we contribute to influencing our society in a positive way to protect our patients and our profession.
Becoming an active participant in the College means serving on committees, attending the Clinical Congress as frequently as feasible, and encouraging colleagues to aspire to become a Fellow.
In the end, being a part of our College and contributing to its growth and legacy is an act of service and, for many, an act of love.
Dr. Oviedo is with Capital Regional Surgical Associates, Tallahassee, Fla., and is Assistant Professor of Surgery, Florida State University College of Medicine. He serves as the ACS Young Fellow Association Liaison.
Since its foundation in 1913 as the premier surgical professional organization in the United States, and one of the most influential in the world, the American College of Surgeons has shaped the policies and molded the education of numerous generations of surgeons. All young surgeons should aspire to be invested as Fellows some day as the highest honor in their career.
Service is an important factor in the decision to become a surgeon. As a Fellow of the ACS, the young surgeon will find many opportunities for service. Active participation as a Fellow is an act of service and can be an act of love for our patients, our colleagues, and our profession. And, with it, comes loyalty, a spirit of dedication, and a sense of unity. In addition, by joining the College we contribute to influencing our society in a positive way to protect our patients and our profession.
Becoming an active participant in the College means serving on committees, attending the Clinical Congress as frequently as feasible, and encouraging colleagues to aspire to become a Fellow.
In the end, being a part of our College and contributing to its growth and legacy is an act of service and, for many, an act of love.
Dr. Oviedo is with Capital Regional Surgical Associates, Tallahassee, Fla., and is Assistant Professor of Surgery, Florida State University College of Medicine. He serves as the ACS Young Fellow Association Liaison.
Since its foundation in 1913 as the premier surgical professional organization in the United States, and one of the most influential in the world, the American College of Surgeons has shaped the policies and molded the education of numerous generations of surgeons. All young surgeons should aspire to be invested as Fellows some day as the highest honor in their career.
Service is an important factor in the decision to become a surgeon. As a Fellow of the ACS, the young surgeon will find many opportunities for service. Active participation as a Fellow is an act of service and can be an act of love for our patients, our colleagues, and our profession. And, with it, comes loyalty, a spirit of dedication, and a sense of unity. In addition, by joining the College we contribute to influencing our society in a positive way to protect our patients and our profession.
Becoming an active participant in the College means serving on committees, attending the Clinical Congress as frequently as feasible, and encouraging colleagues to aspire to become a Fellow.
In the end, being a part of our College and contributing to its growth and legacy is an act of service and, for many, an act of love.
Dr. Oviedo is with Capital Regional Surgical Associates, Tallahassee, Fla., and is Assistant Professor of Surgery, Florida State University College of Medicine. He serves as the ACS Young Fellow Association Liaison.
New ACS Resources in Surgical Education Online Now
The American College of Surgeons (ACS) Division of Education’s new Resources in Surgical Education (RISE) recently debuted on the ACS website. RISE is headed by Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education. The RISE web page is available at www.facs.org/education/division-of-education/publications/rise/current.

The inaugural article, “Create a Surgical Faculty Compensation Plan that Supports the Educational Mission,” by David A. Rogers, MD, MHPE, FACS, FAAP, is now available at www.facs.org/education/division-of-education/publications/rise/current. Future articles will be posted every six to eight weeks.
For additional information, contact Krashina Hudson at [email protected] or at 312-202-5335.
The American College of Surgeons (ACS) Division of Education’s new Resources in Surgical Education (RISE) recently debuted on the ACS website. RISE is headed by Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education. The RISE web page is available at www.facs.org/education/division-of-education/publications/rise/current.
The inaugural article, “Create a Surgical Faculty Compensation Plan that Supports the Educational Mission,” by David A. Rogers, MD, MHPE, FACS, FAAP, is now available at www.facs.org/education/division-of-education/publications/rise/current. Future articles will be posted every six to eight weeks.
For additional information, contact Krashina Hudson at [email protected] or at 312-202-5335.
The American College of Surgeons (ACS) Division of Education’s new Resources in Surgical Education (RISE) recently debuted on the ACS website. RISE is headed by Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education. The RISE web page is available at www.facs.org/education/division-of-education/publications/rise/current.
The inaugural article, “Create a Surgical Faculty Compensation Plan that Supports the Educational Mission,” by David A. Rogers, MD, MHPE, FACS, FAAP, is now available at www.facs.org/education/division-of-education/publications/rise/current. Future articles will be posted every six to eight weeks.
For additional information, contact Krashina Hudson at [email protected] or at 312-202-5335.
Surgeons learn about leading, influencing policy at 2017 ACS Leadership & Advocacy Summit
The 2017 American College of Surgeons (ACS) Leadership & Advocacy Summit, May 6–9 in Washington, DC, was a well-attended conference that brought together surgeons from across the U.S. to enhance their leadership skills and to learn about how they can advocate for the advancement of issues important to the field of surgery.
Leadership Summit
More than 450 surgeons and residents participated in the ACS Leadership Summit held May 6–7. The Leadership portion of the Leadership & Advocacy Summit included a series of presentations that provided practical, take-home tips on how to be a better leader. Presentations covered such diverse leadership topics as how to handle difficult conversations, manage difficult people, and lead from behind; how it’s not all about you, and leading by example; volunteering in your own backyard; avoiding burnout and promoting resilience; preparing for leadership positions in medicine; and successfully addressing critical situations in the operating room. PowerPoint presentations shown at the 2017 Leadership Summit are available at facs.org/advocacy/participate/summit/2017-presentations.
In addition, ACS chapter leaders shared success stories. Representatives of the Connecticut Chapter focused on resident engagement, representatives of the North Texas Chapter and South Texas Chapter explained the positive results that can be realized by holding joint chapter meetings, and members of the Georgia Society of the ACS discussed their Stop the Bleed® effort. Participants then convened in state breakout sessions during the lunch hour to identify new strategies and initiatives for implementation at the chapter level. ACS Executive Director David B. Hoyt, MD, FACS, provided an update on ACS activities.
Advocacy Summit
More than 300 surgeons and residents participated in the ACS Advocacy Summit, May 7−9. Participants in the Advocacy Summit portion of the ACS Leadership & Advocacy Summit came to Washington primarily to meet with lawmakers and congressional staff to educate them about key ACS legislative priorities that affect surgical patients, including ensuring an adequate surgical workforce in underserved areas; advancing childhood cancer research and surveillance and providing resources for pediatric cancer survivors; allocating funding for the Children’s Health Insurance Program, which provides health care coverage to uninsured children from low-income families; improving liability protections for trauma care providers; and providing greater flexibility for providers during implementation of the Merit-based Incentive Payment System (MIPS). The issue briefs presented during the Advocacy Summit are available on the ACS Professional Association website at web4.facs.org/eBusiness/login.aspx?ReturnURL=~/SAML/SSOService.aspx?r=1.
In addition, health care reform was discussed during a few panel sessions. Just days before the Advocacy Summit, the House of Representatives had passed the American Health Care Act by a vote of 217-213. Summit attendees were educated about the College’s concerns with the legislation and were advised that the Senate bill likely would be dramatically different. The College continues to work to ensure that ACS health care reform principles—patient safety and quality, patient access to surgical care, reduction of health care costs and medical liability reform—are included in a revised Senate bill. The full ACS 2017 statement on health care reform was published in the May issue of the Bulletin and is available at bulletin.facs.org/2017/05/american-college-of-surgeons-2017-statement-on-health-care-reform/.
The 2017 American College of Surgeons (ACS) Leadership & Advocacy Summit, May 6–9 in Washington, DC, was a well-attended conference that brought together surgeons from across the U.S. to enhance their leadership skills and to learn about how they can advocate for the advancement of issues important to the field of surgery.
Leadership Summit
More than 450 surgeons and residents participated in the ACS Leadership Summit held May 6–7. The Leadership portion of the Leadership & Advocacy Summit included a series of presentations that provided practical, take-home tips on how to be a better leader. Presentations covered such diverse leadership topics as how to handle difficult conversations, manage difficult people, and lead from behind; how it’s not all about you, and leading by example; volunteering in your own backyard; avoiding burnout and promoting resilience; preparing for leadership positions in medicine; and successfully addressing critical situations in the operating room. PowerPoint presentations shown at the 2017 Leadership Summit are available at facs.org/advocacy/participate/summit/2017-presentations.
In addition, ACS chapter leaders shared success stories. Representatives of the Connecticut Chapter focused on resident engagement, representatives of the North Texas Chapter and South Texas Chapter explained the positive results that can be realized by holding joint chapter meetings, and members of the Georgia Society of the ACS discussed their Stop the Bleed® effort. Participants then convened in state breakout sessions during the lunch hour to identify new strategies and initiatives for implementation at the chapter level. ACS Executive Director David B. Hoyt, MD, FACS, provided an update on ACS activities.
Advocacy Summit
More than 300 surgeons and residents participated in the ACS Advocacy Summit, May 7−9. Participants in the Advocacy Summit portion of the ACS Leadership & Advocacy Summit came to Washington primarily to meet with lawmakers and congressional staff to educate them about key ACS legislative priorities that affect surgical patients, including ensuring an adequate surgical workforce in underserved areas; advancing childhood cancer research and surveillance and providing resources for pediatric cancer survivors; allocating funding for the Children’s Health Insurance Program, which provides health care coverage to uninsured children from low-income families; improving liability protections for trauma care providers; and providing greater flexibility for providers during implementation of the Merit-based Incentive Payment System (MIPS). The issue briefs presented during the Advocacy Summit are available on the ACS Professional Association website at web4.facs.org/eBusiness/login.aspx?ReturnURL=~/SAML/SSOService.aspx?r=1.
In addition, health care reform was discussed during a few panel sessions. Just days before the Advocacy Summit, the House of Representatives had passed the American Health Care Act by a vote of 217-213. Summit attendees were educated about the College’s concerns with the legislation and were advised that the Senate bill likely would be dramatically different. The College continues to work to ensure that ACS health care reform principles—patient safety and quality, patient access to surgical care, reduction of health care costs and medical liability reform—are included in a revised Senate bill. The full ACS 2017 statement on health care reform was published in the May issue of the Bulletin and is available at bulletin.facs.org/2017/05/american-college-of-surgeons-2017-statement-on-health-care-reform/.
The 2017 American College of Surgeons (ACS) Leadership & Advocacy Summit, May 6–9 in Washington, DC, was a well-attended conference that brought together surgeons from across the U.S. to enhance their leadership skills and to learn about how they can advocate for the advancement of issues important to the field of surgery.
Leadership Summit
More than 450 surgeons and residents participated in the ACS Leadership Summit held May 6–7. The Leadership portion of the Leadership & Advocacy Summit included a series of presentations that provided practical, take-home tips on how to be a better leader. Presentations covered such diverse leadership topics as how to handle difficult conversations, manage difficult people, and lead from behind; how it’s not all about you, and leading by example; volunteering in your own backyard; avoiding burnout and promoting resilience; preparing for leadership positions in medicine; and successfully addressing critical situations in the operating room. PowerPoint presentations shown at the 2017 Leadership Summit are available at facs.org/advocacy/participate/summit/2017-presentations.
In addition, ACS chapter leaders shared success stories. Representatives of the Connecticut Chapter focused on resident engagement, representatives of the North Texas Chapter and South Texas Chapter explained the positive results that can be realized by holding joint chapter meetings, and members of the Georgia Society of the ACS discussed their Stop the Bleed® effort. Participants then convened in state breakout sessions during the lunch hour to identify new strategies and initiatives for implementation at the chapter level. ACS Executive Director David B. Hoyt, MD, FACS, provided an update on ACS activities.
Advocacy Summit
More than 300 surgeons and residents participated in the ACS Advocacy Summit, May 7−9. Participants in the Advocacy Summit portion of the ACS Leadership & Advocacy Summit came to Washington primarily to meet with lawmakers and congressional staff to educate them about key ACS legislative priorities that affect surgical patients, including ensuring an adequate surgical workforce in underserved areas; advancing childhood cancer research and surveillance and providing resources for pediatric cancer survivors; allocating funding for the Children’s Health Insurance Program, which provides health care coverage to uninsured children from low-income families; improving liability protections for trauma care providers; and providing greater flexibility for providers during implementation of the Merit-based Incentive Payment System (MIPS). The issue briefs presented during the Advocacy Summit are available on the ACS Professional Association website at web4.facs.org/eBusiness/login.aspx?ReturnURL=~/SAML/SSOService.aspx?r=1.
In addition, health care reform was discussed during a few panel sessions. Just days before the Advocacy Summit, the House of Representatives had passed the American Health Care Act by a vote of 217-213. Summit attendees were educated about the College’s concerns with the legislation and were advised that the Senate bill likely would be dramatically different. The College continues to work to ensure that ACS health care reform principles—patient safety and quality, patient access to surgical care, reduction of health care costs and medical liability reform—are included in a revised Senate bill. The full ACS 2017 statement on health care reform was published in the May issue of the Bulletin and is available at bulletin.facs.org/2017/05/american-college-of-surgeons-2017-statement-on-health-care-reform/.
ACS-AEI Forum to Address Early-Career Simulation Training and Assessment
The American College of Surgeons Accredited Education Institutes (ACS-AEI) will host a forum June 12 that seeks to mobilize stakeholders to identify best practices and key considerations in simulation training and to build the case for more standardized implementation of simulation training and assessment in early-career surgical education. The forum, called “Training the Next Generation of Surgeons: Making It Stick, Making It Real, Making It Together,” will take place at the WWAMI (Washington, Wyoming, Alaska, Montana, and Idaho) Institute of Simulation in Healthcare (WISH) at the University of Washington (UW), Seattle. The ultimate goal of the forum will be to begin formulating principles and standards that will maximize the value of simulation and ultimately improve surgeon performance.
Hosting the forum are David B. Hoyt, MD, FACS, ACS Executive Director; Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education; Robert Sweet, MD, FACS, professor of urology, UW, medical director, UW Medicine Kidney Stone Center at Northwest Hospital, and executive director, WISH and Center for Research in Education and Simulation Technologies, UW Medicine; and Carlos A. Pellegrini, MD, FACS, chief medical officer, UW Medicine, vice-president for medical affairs, UW, and Past-President of the ACS.
The forum will include opening remarks from ACS and UW leadership and panel sessions on key topics, including model simulation programs, advances in simulation technologies and tools, and best practices for broadly applying simulation training and assessment. A keynote address centered on the cognitive learning process behind skills acquisition and expert performance, WISH simulation lab tours, and a workshop session on team training will round out the program. To learn more about the forum and to register, visit the ACS-AEI event page at www.facs.org/education/accreditation/aei/next-generation.
The American College of Surgeons Accredited Education Institutes (ACS-AEI) will host a forum June 12 that seeks to mobilize stakeholders to identify best practices and key considerations in simulation training and to build the case for more standardized implementation of simulation training and assessment in early-career surgical education. The forum, called “Training the Next Generation of Surgeons: Making It Stick, Making It Real, Making It Together,” will take place at the WWAMI (Washington, Wyoming, Alaska, Montana, and Idaho) Institute of Simulation in Healthcare (WISH) at the University of Washington (UW), Seattle. The ultimate goal of the forum will be to begin formulating principles and standards that will maximize the value of simulation and ultimately improve surgeon performance.
Hosting the forum are David B. Hoyt, MD, FACS, ACS Executive Director; Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education; Robert Sweet, MD, FACS, professor of urology, UW, medical director, UW Medicine Kidney Stone Center at Northwest Hospital, and executive director, WISH and Center for Research in Education and Simulation Technologies, UW Medicine; and Carlos A. Pellegrini, MD, FACS, chief medical officer, UW Medicine, vice-president for medical affairs, UW, and Past-President of the ACS.
The forum will include opening remarks from ACS and UW leadership and panel sessions on key topics, including model simulation programs, advances in simulation technologies and tools, and best practices for broadly applying simulation training and assessment. A keynote address centered on the cognitive learning process behind skills acquisition and expert performance, WISH simulation lab tours, and a workshop session on team training will round out the program. To learn more about the forum and to register, visit the ACS-AEI event page at www.facs.org/education/accreditation/aei/next-generation.
The American College of Surgeons Accredited Education Institutes (ACS-AEI) will host a forum June 12 that seeks to mobilize stakeholders to identify best practices and key considerations in simulation training and to build the case for more standardized implementation of simulation training and assessment in early-career surgical education. The forum, called “Training the Next Generation of Surgeons: Making It Stick, Making It Real, Making It Together,” will take place at the WWAMI (Washington, Wyoming, Alaska, Montana, and Idaho) Institute of Simulation in Healthcare (WISH) at the University of Washington (UW), Seattle. The ultimate goal of the forum will be to begin formulating principles and standards that will maximize the value of simulation and ultimately improve surgeon performance.
Hosting the forum are David B. Hoyt, MD, FACS, ACS Executive Director; Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education; Robert Sweet, MD, FACS, professor of urology, UW, medical director, UW Medicine Kidney Stone Center at Northwest Hospital, and executive director, WISH and Center for Research in Education and Simulation Technologies, UW Medicine; and Carlos A. Pellegrini, MD, FACS, chief medical officer, UW Medicine, vice-president for medical affairs, UW, and Past-President of the ACS.
The forum will include opening remarks from ACS and UW leadership and panel sessions on key topics, including model simulation programs, advances in simulation technologies and tools, and best practices for broadly applying simulation training and assessment. A keynote address centered on the cognitive learning process behind skills acquisition and expert performance, WISH simulation lab tours, and a workshop session on team training will round out the program. To learn more about the forum and to register, visit the ACS-AEI event page at www.facs.org/education/accreditation/aei/next-generation.
New ACS surgical practice guidelines now include patient education
The American College of Surgeons (ACS) Evidence-Based Decisions in Surgery (EBDS) and Patient Education programs have collaborated to offer established surgical practice guidelines that surgeons can use at the point of care. The modules, which are viewable on all digital platforms, now include relevant patient education information to aid in high-quality care for surgical patients.
The EBDS modules provide peer-reviewed recommendations for surgeons based on clinical practice guidelines promulgated by national and international professional organizations and government agencies. The surgical recommendations are presented along with the strength of the evidence that supports the recommendations. Grading of the evidence is done with the understanding that the contribution of surgical judgment in developing effective and safe treatment strategies is essential for effective care of individual surgical patients. As such, the modules are intended to guide surgical practice but should always take into consideration the needs and preferences of individual patients.
Each EBDS module has a section labeled “Suggested Talking Points for Patient Education,” which covers topics such as who developed the guidelines, recommended actions for patients and physicians, and potential benefits and harms associated with these recommendations. Where applicable, links will now be included in the modules that will lead the user directly to the patient education material that supports the particular topic. For example, the EBDS module for Hemodialysis Access has a link to the Patient Education section of the Central Lines Home Skills Kit. The home page for the Central Lines Home Skills Kit provides a host of information, ranging from a welcome video, to a Central Lines Home Skills booklet, to an evaluation.
At present, 13 EBDS modules have links to patient education material from the ACS. As more modules and patient education materials are developed, more comprehensive offerings will be available to surgeon members. Brochures for patients provide all pre-, peri-, and postoperative information to help patients make informed decisions and fully participate in all aspects of their care for many common surgical procedures. The Home Skills Kit series uses a multimedia approach to explain, demonstrate, and provide directed learning experiences and practice opportunities for patients requiring a lung procedure, an ostomy, feeding tube, central line placement, or complex wound care.
ACS Patient Education resources are based on contemporary principles of evidence-based medicine tailored to the individual patient’s needs, with a focus on health literacy. Patients who are trained to actively participate in their care show improved treatment compliance, decreased complications, and enhanced outcomes and satisfaction.*
With outpatient operations representing a growing share (65 percent, 17.3 million) of all procedures performed in the U.S., patient preparation is essential to the delivery of high-value, safe surgical care.
To learn more and view the modules, go to ebds.facs.org. After logging in with ACS credentials, click on the Topics tab and take note of the modules with a tag labeled “Updated” to find modules that have ACS Patient Education information included. This can be found in the Suggested Talking Points for Patient Education section with links directly to the content available.
Ms. Dalal is Senior Manager, Evidence-Based Decisions in Surgery, ACS Division of Education, Chicago, IL.
Ms. Strand is Manager, ACS Patient Education Program, Division of Education.
The American College of Surgeons (ACS) Evidence-Based Decisions in Surgery (EBDS) and Patient Education programs have collaborated to offer established surgical practice guidelines that surgeons can use at the point of care. The modules, which are viewable on all digital platforms, now include relevant patient education information to aid in high-quality care for surgical patients.
The EBDS modules provide peer-reviewed recommendations for surgeons based on clinical practice guidelines promulgated by national and international professional organizations and government agencies. The surgical recommendations are presented along with the strength of the evidence that supports the recommendations. Grading of the evidence is done with the understanding that the contribution of surgical judgment in developing effective and safe treatment strategies is essential for effective care of individual surgical patients. As such, the modules are intended to guide surgical practice but should always take into consideration the needs and preferences of individual patients.
Each EBDS module has a section labeled “Suggested Talking Points for Patient Education,” which covers topics such as who developed the guidelines, recommended actions for patients and physicians, and potential benefits and harms associated with these recommendations. Where applicable, links will now be included in the modules that will lead the user directly to the patient education material that supports the particular topic. For example, the EBDS module for Hemodialysis Access has a link to the Patient Education section of the Central Lines Home Skills Kit. The home page for the Central Lines Home Skills Kit provides a host of information, ranging from a welcome video, to a Central Lines Home Skills booklet, to an evaluation.
At present, 13 EBDS modules have links to patient education material from the ACS. As more modules and patient education materials are developed, more comprehensive offerings will be available to surgeon members. Brochures for patients provide all pre-, peri-, and postoperative information to help patients make informed decisions and fully participate in all aspects of their care for many common surgical procedures. The Home Skills Kit series uses a multimedia approach to explain, demonstrate, and provide directed learning experiences and practice opportunities for patients requiring a lung procedure, an ostomy, feeding tube, central line placement, or complex wound care.
ACS Patient Education resources are based on contemporary principles of evidence-based medicine tailored to the individual patient’s needs, with a focus on health literacy. Patients who are trained to actively participate in their care show improved treatment compliance, decreased complications, and enhanced outcomes and satisfaction.*
With outpatient operations representing a growing share (65 percent, 17.3 million) of all procedures performed in the U.S., patient preparation is essential to the delivery of high-value, safe surgical care.
To learn more and view the modules, go to ebds.facs.org. After logging in with ACS credentials, click on the Topics tab and take note of the modules with a tag labeled “Updated” to find modules that have ACS Patient Education information included. This can be found in the Suggested Talking Points for Patient Education section with links directly to the content available.
Ms. Dalal is Senior Manager, Evidence-Based Decisions in Surgery, ACS Division of Education, Chicago, IL.
Ms. Strand is Manager, ACS Patient Education Program, Division of Education.
The American College of Surgeons (ACS) Evidence-Based Decisions in Surgery (EBDS) and Patient Education programs have collaborated to offer established surgical practice guidelines that surgeons can use at the point of care. The modules, which are viewable on all digital platforms, now include relevant patient education information to aid in high-quality care for surgical patients.
The EBDS modules provide peer-reviewed recommendations for surgeons based on clinical practice guidelines promulgated by national and international professional organizations and government agencies. The surgical recommendations are presented along with the strength of the evidence that supports the recommendations. Grading of the evidence is done with the understanding that the contribution of surgical judgment in developing effective and safe treatment strategies is essential for effective care of individual surgical patients. As such, the modules are intended to guide surgical practice but should always take into consideration the needs and preferences of individual patients.
Each EBDS module has a section labeled “Suggested Talking Points for Patient Education,” which covers topics such as who developed the guidelines, recommended actions for patients and physicians, and potential benefits and harms associated with these recommendations. Where applicable, links will now be included in the modules that will lead the user directly to the patient education material that supports the particular topic. For example, the EBDS module for Hemodialysis Access has a link to the Patient Education section of the Central Lines Home Skills Kit. The home page for the Central Lines Home Skills Kit provides a host of information, ranging from a welcome video, to a Central Lines Home Skills booklet, to an evaluation.
At present, 13 EBDS modules have links to patient education material from the ACS. As more modules and patient education materials are developed, more comprehensive offerings will be available to surgeon members. Brochures for patients provide all pre-, peri-, and postoperative information to help patients make informed decisions and fully participate in all aspects of their care for many common surgical procedures. The Home Skills Kit series uses a multimedia approach to explain, demonstrate, and provide directed learning experiences and practice opportunities for patients requiring a lung procedure, an ostomy, feeding tube, central line placement, or complex wound care.
ACS Patient Education resources are based on contemporary principles of evidence-based medicine tailored to the individual patient’s needs, with a focus on health literacy. Patients who are trained to actively participate in their care show improved treatment compliance, decreased complications, and enhanced outcomes and satisfaction.*
With outpatient operations representing a growing share (65 percent, 17.3 million) of all procedures performed in the U.S., patient preparation is essential to the delivery of high-value, safe surgical care.
To learn more and view the modules, go to ebds.facs.org. After logging in with ACS credentials, click on the Topics tab and take note of the modules with a tag labeled “Updated” to find modules that have ACS Patient Education information included. This can be found in the Suggested Talking Points for Patient Education section with links directly to the content available.
Ms. Dalal is Senior Manager, Evidence-Based Decisions in Surgery, ACS Division of Education, Chicago, IL.
Ms. Strand is Manager, ACS Patient Education Program, Division of Education.
Dr. Bowyer to Receive Robert Danis Prize from ISS/SIC
Mark W. Bowyer, MD, FACS, Chair of the American College of Surgeons Committee on Trauma’s Surgical Skills Committee, has been named the 2017 recipient of the Robert Danis Prize.
Mark W. Bowyer, MD, FACS, Chair of the American College of Surgeons Committee on Trauma’s Surgical Skills Committee, has been named the 2017 recipient of the Robert Danis Prize awarded by the International Society of Surgery/Société Internationale de Chirurgie (ISS/SIC). This award is presented to a surgeon who has made important contributions to the fields of trauma, burns, or critical care. Dr. Bowyer was selected for his lifelong commitment and broad contributions to the field of trauma and surgical simulation.
Dr. Bowyer, the Ben Eiseman Professor of Surgery and surgical director of simulation, division of trauma and combat surgery, department of surgery, Uniformed Services University of the Health Sciences (USUHS)–Walter Reed National Military Medical Center (WRNMMC), Bethesda, MD, spent more than 22 years as an Air Force trauma and combat surgeon. He has taught trauma skills to thousands of medical students and physicians around the world in the last three decades and is one of the chief architects of the Advanced Surgical Skills for Exposures in Trauma course, which has been presented in more than 100 course sites in 11 countries in the last six years. Dr. Bowyer served as the Air Force’s “trauma czar” while serving Iraq, where he directed and coordinated all care provided to combat trauma patients.
In addition, he is the surgical director of the USUHS Val G. Hemming Simulation Center, where he has been on the forefront of using simulators to teach advanced trauma and acute care surgical skills and where he works to develop and validate augmented and virtual reality, as well as trauma, laparoscopic, acute care surgical, triage, and critical care-based simulators. At present, Dr. Bowyer is working on simulation projects to improve patient safety.
Dr. Bowyer will receive the Danis Prize during the ISS/SIC 2017 World Congress of Surgery, August 13−17 in Basel, Switzerland. (Read more about the World Congress of Surgery at www.wcs2017.org/.) Read more about Dr. Bowyer at bit.ly/2qcpETa.
Mark W. Bowyer, MD, FACS, Chair of the American College of Surgeons Committee on Trauma’s Surgical Skills Committee, has been named the 2017 recipient of the Robert Danis Prize.
Mark W. Bowyer, MD, FACS, Chair of the American College of Surgeons Committee on Trauma’s Surgical Skills Committee, has been named the 2017 recipient of the Robert Danis Prize awarded by the International Society of Surgery/Société Internationale de Chirurgie (ISS/SIC). This award is presented to a surgeon who has made important contributions to the fields of trauma, burns, or critical care. Dr. Bowyer was selected for his lifelong commitment and broad contributions to the field of trauma and surgical simulation.
Dr. Bowyer, the Ben Eiseman Professor of Surgery and surgical director of simulation, division of trauma and combat surgery, department of surgery, Uniformed Services University of the Health Sciences (USUHS)–Walter Reed National Military Medical Center (WRNMMC), Bethesda, MD, spent more than 22 years as an Air Force trauma and combat surgeon. He has taught trauma skills to thousands of medical students and physicians around the world in the last three decades and is one of the chief architects of the Advanced Surgical Skills for Exposures in Trauma course, which has been presented in more than 100 course sites in 11 countries in the last six years. Dr. Bowyer served as the Air Force’s “trauma czar” while serving Iraq, where he directed and coordinated all care provided to combat trauma patients.
In addition, he is the surgical director of the USUHS Val G. Hemming Simulation Center, where he has been on the forefront of using simulators to teach advanced trauma and acute care surgical skills and where he works to develop and validate augmented and virtual reality, as well as trauma, laparoscopic, acute care surgical, triage, and critical care-based simulators. At present, Dr. Bowyer is working on simulation projects to improve patient safety.
Dr. Bowyer will receive the Danis Prize during the ISS/SIC 2017 World Congress of Surgery, August 13−17 in Basel, Switzerland. (Read more about the World Congress of Surgery at www.wcs2017.org/.) Read more about Dr. Bowyer at bit.ly/2qcpETa.
Mark W. Bowyer, MD, FACS, Chair of the American College of Surgeons Committee on Trauma’s Surgical Skills Committee, has been named the 2017 recipient of the Robert Danis Prize.
Mark W. Bowyer, MD, FACS, Chair of the American College of Surgeons Committee on Trauma’s Surgical Skills Committee, has been named the 2017 recipient of the Robert Danis Prize awarded by the International Society of Surgery/Société Internationale de Chirurgie (ISS/SIC). This award is presented to a surgeon who has made important contributions to the fields of trauma, burns, or critical care. Dr. Bowyer was selected for his lifelong commitment and broad contributions to the field of trauma and surgical simulation.
Dr. Bowyer, the Ben Eiseman Professor of Surgery and surgical director of simulation, division of trauma and combat surgery, department of surgery, Uniformed Services University of the Health Sciences (USUHS)–Walter Reed National Military Medical Center (WRNMMC), Bethesda, MD, spent more than 22 years as an Air Force trauma and combat surgeon. He has taught trauma skills to thousands of medical students and physicians around the world in the last three decades and is one of the chief architects of the Advanced Surgical Skills for Exposures in Trauma course, which has been presented in more than 100 course sites in 11 countries in the last six years. Dr. Bowyer served as the Air Force’s “trauma czar” while serving Iraq, where he directed and coordinated all care provided to combat trauma patients.
In addition, he is the surgical director of the USUHS Val G. Hemming Simulation Center, where he has been on the forefront of using simulators to teach advanced trauma and acute care surgical skills and where he works to develop and validate augmented and virtual reality, as well as trauma, laparoscopic, acute care surgical, triage, and critical care-based simulators. At present, Dr. Bowyer is working on simulation projects to improve patient safety.
Dr. Bowyer will receive the Danis Prize during the ISS/SIC 2017 World Congress of Surgery, August 13−17 in Basel, Switzerland. (Read more about the World Congress of Surgery at www.wcs2017.org/.) Read more about Dr. Bowyer at bit.ly/2qcpETa.