User login
Official Newspaper of the American College of Surgeons
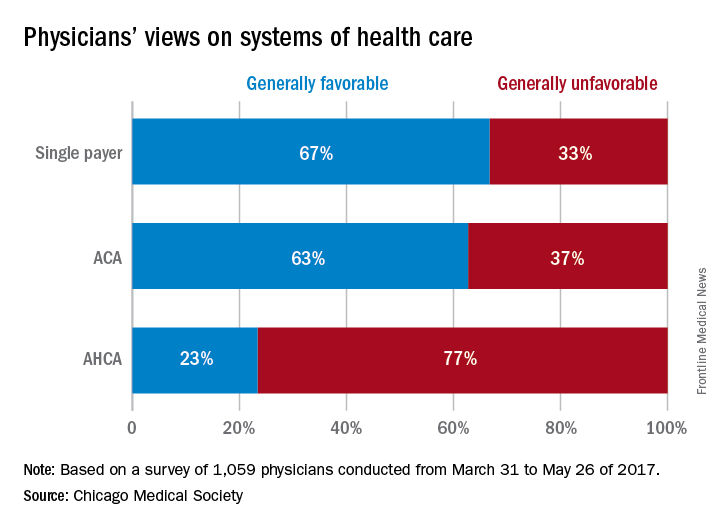
Survey: Most doctors would pick single payer over ACA, ACHA
CHICAGO – If given the option, the majority of physicians would scrap both the Affordable Care Act and the proposed American Health Care Act (AHCA) and opt for a single payer health care system, according to a survey of 1,059 doctors by the Chicago Medical Society (CMS).
When asked their preferred health care structure, 53% of physician said they would prefer a single payer health system, while 26% preferred the Affordable Care Act, and 13% said they would like to see the ACA repealed and replaced with the AHCA. Another 8% of doctors stated they would prefer repeal of the ACA but did not offer a replacement option.
The high percentage of physicians who favored a single payer system was surprising, said A. Jay Chauhan, DO, secretary and chair of public health for the Chicago Medical Society.
“That is a shift from past surveys,” Dr. Chauhan said during an interview at a conference held by the American Bar Association. “It certainly speaks to the frustration that physicians are [feeling] and how difficult it is to practice. I think they’re trying to reach out for other alternatives because the current manner in which we’re practicing doesn’t seem to fulfill our desires to better take care of patients.”
Respondents also choose a single payer system as their top preference when asked which health care system they believed would provide “the best care to the greatest number of people for a given amount of funding.”
A primary takeaway from the survey is that physicians want to see better access to health care for their patients and more affordable insurance coverage, said Katherine M. Tynus, MD, immediate past president of the Chicago Medical Society and president-elect of the Illinois State Medical Society.
“I think what the Affordable Care Act did was raise expectations as far as access to care and people being able to afford their health care,” Dr. Tynus said in an interview at the meeting. “Since that system seems to be failing, the expectation remains. Now, we need to find an alternative solution to achieve that.”
The online survey, released at the Physicians Legal Issues Conference held by the American Bar Association, was conducted between March 2017 and May 2017 and featured questions about health reform. Survey participants were physicians primarily based in the Chicago area or within Illinois and the majority practiced in an urban area. Respondents represented a variety of political affiliations and medical specialties. The majority said they identifying as independent (43%), and the most common specialty was general medicine (19%).
[email protected]
On Twitter @legal_med
CHICAGO – If given the option, the majority of physicians would scrap both the Affordable Care Act and the proposed American Health Care Act (AHCA) and opt for a single payer health care system, according to a survey of 1,059 doctors by the Chicago Medical Society (CMS).
When asked their preferred health care structure, 53% of physician said they would prefer a single payer health system, while 26% preferred the Affordable Care Act, and 13% said they would like to see the ACA repealed and replaced with the AHCA. Another 8% of doctors stated they would prefer repeal of the ACA but did not offer a replacement option.
The high percentage of physicians who favored a single payer system was surprising, said A. Jay Chauhan, DO, secretary and chair of public health for the Chicago Medical Society.
“That is a shift from past surveys,” Dr. Chauhan said during an interview at a conference held by the American Bar Association. “It certainly speaks to the frustration that physicians are [feeling] and how difficult it is to practice. I think they’re trying to reach out for other alternatives because the current manner in which we’re practicing doesn’t seem to fulfill our desires to better take care of patients.”
Respondents also choose a single payer system as their top preference when asked which health care system they believed would provide “the best care to the greatest number of people for a given amount of funding.”
A primary takeaway from the survey is that physicians want to see better access to health care for their patients and more affordable insurance coverage, said Katherine M. Tynus, MD, immediate past president of the Chicago Medical Society and president-elect of the Illinois State Medical Society.
“I think what the Affordable Care Act did was raise expectations as far as access to care and people being able to afford their health care,” Dr. Tynus said in an interview at the meeting. “Since that system seems to be failing, the expectation remains. Now, we need to find an alternative solution to achieve that.”
The online survey, released at the Physicians Legal Issues Conference held by the American Bar Association, was conducted between March 2017 and May 2017 and featured questions about health reform. Survey participants were physicians primarily based in the Chicago area or within Illinois and the majority practiced in an urban area. Respondents represented a variety of political affiliations and medical specialties. The majority said they identifying as independent (43%), and the most common specialty was general medicine (19%).
[email protected]
On Twitter @legal_med
CHICAGO – If given the option, the majority of physicians would scrap both the Affordable Care Act and the proposed American Health Care Act (AHCA) and opt for a single payer health care system, according to a survey of 1,059 doctors by the Chicago Medical Society (CMS).
When asked their preferred health care structure, 53% of physician said they would prefer a single payer health system, while 26% preferred the Affordable Care Act, and 13% said they would like to see the ACA repealed and replaced with the AHCA. Another 8% of doctors stated they would prefer repeal of the ACA but did not offer a replacement option.
The high percentage of physicians who favored a single payer system was surprising, said A. Jay Chauhan, DO, secretary and chair of public health for the Chicago Medical Society.
“That is a shift from past surveys,” Dr. Chauhan said during an interview at a conference held by the American Bar Association. “It certainly speaks to the frustration that physicians are [feeling] and how difficult it is to practice. I think they’re trying to reach out for other alternatives because the current manner in which we’re practicing doesn’t seem to fulfill our desires to better take care of patients.”
Respondents also choose a single payer system as their top preference when asked which health care system they believed would provide “the best care to the greatest number of people for a given amount of funding.”
A primary takeaway from the survey is that physicians want to see better access to health care for their patients and more affordable insurance coverage, said Katherine M. Tynus, MD, immediate past president of the Chicago Medical Society and president-elect of the Illinois State Medical Society.
“I think what the Affordable Care Act did was raise expectations as far as access to care and people being able to afford their health care,” Dr. Tynus said in an interview at the meeting. “Since that system seems to be failing, the expectation remains. Now, we need to find an alternative solution to achieve that.”
The online survey, released at the Physicians Legal Issues Conference held by the American Bar Association, was conducted between March 2017 and May 2017 and featured questions about health reform. Survey participants were physicians primarily based in the Chicago area or within Illinois and the majority practiced in an urban area. Respondents represented a variety of political affiliations and medical specialties. The majority said they identifying as independent (43%), and the most common specialty was general medicine (19%).
[email protected]
On Twitter @legal_med
AT THE PHYSICIANS LEGAL ISSUES CONFERENCE
KHN Exclusive: White House task force echoes Pharma proposals
President Donald Trump repeatedly talks tough about reining in the pharmaceutical industry, but his administration’s efforts to lower drug prices are shrouded in secrecy.
Senior administrative officials met Friday to discuss an executive order on the cost of pharmaceuticals, a roundtable informed by Trump’s “Drug Pricing and Innovation Working Group.” Kaiser Health News examined documents that shed light on the workings of this working group.
The documents reveal behind-the-scenes discussions that are influenced by the pharmaceutical industry. Joe Grogan, associate director of health programs for the Office of Management and Budget (OMB), has led the group. Until March, Grogan served as a lobbyist for Gilead Sciences, the pharmaceutical company that priced its hepatitis C drugs at $1,000 per pill.
To solve the crisis of high drug prices, the group discussed strengthening the monopoly rights of pharmaceuticals overseas, ending discounts for low-income hospitals and accelerating drug approvals by the Food and Drug Administration. The White House declined to comment on the working group.
The group initially met May 4 in the Eisenhower Executive Office Building and has since met every two weeks. In addition to OMB, the working group includes officials from the White House National Economic Council, the Domestic Policy Council, Health and Human Services, the FDA, the Federal Trade Commission, the Department of Commerce, the Office of the U.S. Trade Representative and the Department of Justice.
According to the documents – the latest of which is dated June 1– the working group focused on the following “principles” and “talking points”:
1. Extending the patent life of drugs in foreign markets to “provide for protection and enforcement of intellectual property rights.” This will ensure “that American consumers do not unfairly subsidize research and development for people throughout the globe.” Extending monopoly protections for drugs overseas has been one of the pharmaceutical industry’s top priorities since the Trans-Pacific Partnership was defeated last year. That policy would push up global drug prices, according to Médecins Sans Frontières.
2. Promoting competition in the U.S. drug market – both by “modernizing our regulatory and reimbursement systems” and limiting “barrier to entry, including the cost of research and development,” according to the documents. The working group also discussed two broad policy ideas that have been championed by the pharmaceutical industry, according to sources familiar with the process:
3. Value-based pricing, under which pharmaceutical companies keep the list prices of drugs unchanged but offer rebates if patients don’t improve, is one option. It’s unclear who would audit the effectiveness of the drugs, what criteria they would use to evaluate them, and who would receive the rebates. Grogan invited Robert Shapiro – an adviser for Gilead and former secretary of Commerce under President Bill Clinton – to brief the working group on value-based pricing on May 18. Shapiro is the chairman and cofounder of Sonecon, a Washington, D.C., firm that consulted with Gilead, Amgen, and PhRMA, according to his curriculum vitae.
4. Grogan and Shapiro also discussed issuing 10-year U.S. Treasury bonds to drug manufacturers to pay for expensive hepatitis C drugs like Sovaldi and Harvoni under Medicare and Medicaid, to avoid rationing drugs to the sickest patients. The 2015 Senate investigation, for example, found that, though Medicaid spent more than $1 billion on Sovaldi, just 2.4% of Medicaid patients with hepatitis C were treated.
After the working group’s first meeting on May 4, Grogan distributed detailed policy recommendations on options for expediting generic drug approvals, creating a new tax credit “of up to 50%” for investments in generic drug manufacturing, distribution, and research and development. The documents also propose scaling back the 340B program, which requires drug manufacturers to provide some medicines at a discount to hospitals that treat low-income patients.
Most of these policies would not ease patient costs, and at least one would increase prices, said experts who reviewed the documents at the request of Kaiser Health News.
“This six-page document contains the kinds of solutions to the cost-of-drugs problem that you would get if you gathered together all the executives of pharma and asked them ‘What sort of token gestures can we do?’ ” said Vinay Prasad, MD, a professor of medicine at Oregon Health and Sciences University who studies the costs of cancer drugs.
The pharma-friendly recommendations appear to clash with earlier press reports indicating that OMB Director Mick Mulvaney was considering requiring drug makers to pay rebates to Medicare patients, a measure the pharmaceutical lobby fiercely opposes.
Brand-name drug prices – which account for 72% of drug spending – go untouched in the handouts, said Fiona Scott Morton, PhD, a Yale economics professor and former attorney with the Justice Department’s antitrust division.
“The changes to generic markets to promote competition look helpful, but there need to be some more ideas to create more competition for branded drugs or consumers aren’t really going to notice this,” Scott Morton said.
Some of the text in the document is cribbed directly from policy papers published by the pharmaceutical industry’s powerful lobby – Pharmaceutical Research and Manufacturers Association (PhRMA).
Under the subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval,” one handout proposes the FDA use less rigorous clinical trial standards to speed drug approvals.
The handout cites a PhRMA paper from March 2016 that includes an identical subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval” and recommends the FDA implement less rigorous clinical trial standards.
These recommendations would not lower drug prices, experts say. Such measures “would be like a firefighter spraying gasoline on your burning garage,” Prasad said.
Another section – which recommends giving the FDA more discretion to evaluate generic copies of complex drugs – closely resembles a National Law Review article written by two lobbyists in the pharmaceutical division of Foley & Lardner, whose clients include generic drug makers.
The handouts further recommend allowing drug makers to supply data and off-label information to insurers and pharmacy benefit managers during the clinical trial period, before they secure FDA approval.
That’s a “terrible idea,” said Jerry Avorn, MD, a professor at Harvard Medical School and the chief of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. “That’s why we have the whole approval process, to determine what’s actually true,” he said.
KHN’s coverage of prescription drug development, costs and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump repeatedly talks tough about reining in the pharmaceutical industry, but his administration’s efforts to lower drug prices are shrouded in secrecy.
Senior administrative officials met Friday to discuss an executive order on the cost of pharmaceuticals, a roundtable informed by Trump’s “Drug Pricing and Innovation Working Group.” Kaiser Health News examined documents that shed light on the workings of this working group.
The documents reveal behind-the-scenes discussions that are influenced by the pharmaceutical industry. Joe Grogan, associate director of health programs for the Office of Management and Budget (OMB), has led the group. Until March, Grogan served as a lobbyist for Gilead Sciences, the pharmaceutical company that priced its hepatitis C drugs at $1,000 per pill.
To solve the crisis of high drug prices, the group discussed strengthening the monopoly rights of pharmaceuticals overseas, ending discounts for low-income hospitals and accelerating drug approvals by the Food and Drug Administration. The White House declined to comment on the working group.
The group initially met May 4 in the Eisenhower Executive Office Building and has since met every two weeks. In addition to OMB, the working group includes officials from the White House National Economic Council, the Domestic Policy Council, Health and Human Services, the FDA, the Federal Trade Commission, the Department of Commerce, the Office of the U.S. Trade Representative and the Department of Justice.
According to the documents – the latest of which is dated June 1– the working group focused on the following “principles” and “talking points”:
1. Extending the patent life of drugs in foreign markets to “provide for protection and enforcement of intellectual property rights.” This will ensure “that American consumers do not unfairly subsidize research and development for people throughout the globe.” Extending monopoly protections for drugs overseas has been one of the pharmaceutical industry’s top priorities since the Trans-Pacific Partnership was defeated last year. That policy would push up global drug prices, according to Médecins Sans Frontières.
2. Promoting competition in the U.S. drug market – both by “modernizing our regulatory and reimbursement systems” and limiting “barrier to entry, including the cost of research and development,” according to the documents. The working group also discussed two broad policy ideas that have been championed by the pharmaceutical industry, according to sources familiar with the process:
3. Value-based pricing, under which pharmaceutical companies keep the list prices of drugs unchanged but offer rebates if patients don’t improve, is one option. It’s unclear who would audit the effectiveness of the drugs, what criteria they would use to evaluate them, and who would receive the rebates. Grogan invited Robert Shapiro – an adviser for Gilead and former secretary of Commerce under President Bill Clinton – to brief the working group on value-based pricing on May 18. Shapiro is the chairman and cofounder of Sonecon, a Washington, D.C., firm that consulted with Gilead, Amgen, and PhRMA, according to his curriculum vitae.
4. Grogan and Shapiro also discussed issuing 10-year U.S. Treasury bonds to drug manufacturers to pay for expensive hepatitis C drugs like Sovaldi and Harvoni under Medicare and Medicaid, to avoid rationing drugs to the sickest patients. The 2015 Senate investigation, for example, found that, though Medicaid spent more than $1 billion on Sovaldi, just 2.4% of Medicaid patients with hepatitis C were treated.
After the working group’s first meeting on May 4, Grogan distributed detailed policy recommendations on options for expediting generic drug approvals, creating a new tax credit “of up to 50%” for investments in generic drug manufacturing, distribution, and research and development. The documents also propose scaling back the 340B program, which requires drug manufacturers to provide some medicines at a discount to hospitals that treat low-income patients.
Most of these policies would not ease patient costs, and at least one would increase prices, said experts who reviewed the documents at the request of Kaiser Health News.
“This six-page document contains the kinds of solutions to the cost-of-drugs problem that you would get if you gathered together all the executives of pharma and asked them ‘What sort of token gestures can we do?’ ” said Vinay Prasad, MD, a professor of medicine at Oregon Health and Sciences University who studies the costs of cancer drugs.
The pharma-friendly recommendations appear to clash with earlier press reports indicating that OMB Director Mick Mulvaney was considering requiring drug makers to pay rebates to Medicare patients, a measure the pharmaceutical lobby fiercely opposes.
Brand-name drug prices – which account for 72% of drug spending – go untouched in the handouts, said Fiona Scott Morton, PhD, a Yale economics professor and former attorney with the Justice Department’s antitrust division.
“The changes to generic markets to promote competition look helpful, but there need to be some more ideas to create more competition for branded drugs or consumers aren’t really going to notice this,” Scott Morton said.
Some of the text in the document is cribbed directly from policy papers published by the pharmaceutical industry’s powerful lobby – Pharmaceutical Research and Manufacturers Association (PhRMA).
Under the subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval,” one handout proposes the FDA use less rigorous clinical trial standards to speed drug approvals.
The handout cites a PhRMA paper from March 2016 that includes an identical subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval” and recommends the FDA implement less rigorous clinical trial standards.
These recommendations would not lower drug prices, experts say. Such measures “would be like a firefighter spraying gasoline on your burning garage,” Prasad said.
Another section – which recommends giving the FDA more discretion to evaluate generic copies of complex drugs – closely resembles a National Law Review article written by two lobbyists in the pharmaceutical division of Foley & Lardner, whose clients include generic drug makers.
The handouts further recommend allowing drug makers to supply data and off-label information to insurers and pharmacy benefit managers during the clinical trial period, before they secure FDA approval.
That’s a “terrible idea,” said Jerry Avorn, MD, a professor at Harvard Medical School and the chief of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. “That’s why we have the whole approval process, to determine what’s actually true,” he said.
KHN’s coverage of prescription drug development, costs and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump repeatedly talks tough about reining in the pharmaceutical industry, but his administration’s efforts to lower drug prices are shrouded in secrecy.
Senior administrative officials met Friday to discuss an executive order on the cost of pharmaceuticals, a roundtable informed by Trump’s “Drug Pricing and Innovation Working Group.” Kaiser Health News examined documents that shed light on the workings of this working group.
The documents reveal behind-the-scenes discussions that are influenced by the pharmaceutical industry. Joe Grogan, associate director of health programs for the Office of Management and Budget (OMB), has led the group. Until March, Grogan served as a lobbyist for Gilead Sciences, the pharmaceutical company that priced its hepatitis C drugs at $1,000 per pill.
To solve the crisis of high drug prices, the group discussed strengthening the monopoly rights of pharmaceuticals overseas, ending discounts for low-income hospitals and accelerating drug approvals by the Food and Drug Administration. The White House declined to comment on the working group.
The group initially met May 4 in the Eisenhower Executive Office Building and has since met every two weeks. In addition to OMB, the working group includes officials from the White House National Economic Council, the Domestic Policy Council, Health and Human Services, the FDA, the Federal Trade Commission, the Department of Commerce, the Office of the U.S. Trade Representative and the Department of Justice.
According to the documents – the latest of which is dated June 1– the working group focused on the following “principles” and “talking points”:
1. Extending the patent life of drugs in foreign markets to “provide for protection and enforcement of intellectual property rights.” This will ensure “that American consumers do not unfairly subsidize research and development for people throughout the globe.” Extending monopoly protections for drugs overseas has been one of the pharmaceutical industry’s top priorities since the Trans-Pacific Partnership was defeated last year. That policy would push up global drug prices, according to Médecins Sans Frontières.
2. Promoting competition in the U.S. drug market – both by “modernizing our regulatory and reimbursement systems” and limiting “barrier to entry, including the cost of research and development,” according to the documents. The working group also discussed two broad policy ideas that have been championed by the pharmaceutical industry, according to sources familiar with the process:
3. Value-based pricing, under which pharmaceutical companies keep the list prices of drugs unchanged but offer rebates if patients don’t improve, is one option. It’s unclear who would audit the effectiveness of the drugs, what criteria they would use to evaluate them, and who would receive the rebates. Grogan invited Robert Shapiro – an adviser for Gilead and former secretary of Commerce under President Bill Clinton – to brief the working group on value-based pricing on May 18. Shapiro is the chairman and cofounder of Sonecon, a Washington, D.C., firm that consulted with Gilead, Amgen, and PhRMA, according to his curriculum vitae.
4. Grogan and Shapiro also discussed issuing 10-year U.S. Treasury bonds to drug manufacturers to pay for expensive hepatitis C drugs like Sovaldi and Harvoni under Medicare and Medicaid, to avoid rationing drugs to the sickest patients. The 2015 Senate investigation, for example, found that, though Medicaid spent more than $1 billion on Sovaldi, just 2.4% of Medicaid patients with hepatitis C were treated.
After the working group’s first meeting on May 4, Grogan distributed detailed policy recommendations on options for expediting generic drug approvals, creating a new tax credit “of up to 50%” for investments in generic drug manufacturing, distribution, and research and development. The documents also propose scaling back the 340B program, which requires drug manufacturers to provide some medicines at a discount to hospitals that treat low-income patients.
Most of these policies would not ease patient costs, and at least one would increase prices, said experts who reviewed the documents at the request of Kaiser Health News.
“This six-page document contains the kinds of solutions to the cost-of-drugs problem that you would get if you gathered together all the executives of pharma and asked them ‘What sort of token gestures can we do?’ ” said Vinay Prasad, MD, a professor of medicine at Oregon Health and Sciences University who studies the costs of cancer drugs.
The pharma-friendly recommendations appear to clash with earlier press reports indicating that OMB Director Mick Mulvaney was considering requiring drug makers to pay rebates to Medicare patients, a measure the pharmaceutical lobby fiercely opposes.
Brand-name drug prices – which account for 72% of drug spending – go untouched in the handouts, said Fiona Scott Morton, PhD, a Yale economics professor and former attorney with the Justice Department’s antitrust division.
“The changes to generic markets to promote competition look helpful, but there need to be some more ideas to create more competition for branded drugs or consumers aren’t really going to notice this,” Scott Morton said.
Some of the text in the document is cribbed directly from policy papers published by the pharmaceutical industry’s powerful lobby – Pharmaceutical Research and Manufacturers Association (PhRMA).
Under the subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval,” one handout proposes the FDA use less rigorous clinical trial standards to speed drug approvals.
The handout cites a PhRMA paper from March 2016 that includes an identical subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval” and recommends the FDA implement less rigorous clinical trial standards.
These recommendations would not lower drug prices, experts say. Such measures “would be like a firefighter spraying gasoline on your burning garage,” Prasad said.
Another section – which recommends giving the FDA more discretion to evaluate generic copies of complex drugs – closely resembles a National Law Review article written by two lobbyists in the pharmaceutical division of Foley & Lardner, whose clients include generic drug makers.
The handouts further recommend allowing drug makers to supply data and off-label information to insurers and pharmacy benefit managers during the clinical trial period, before they secure FDA approval.
That’s a “terrible idea,” said Jerry Avorn, MD, a professor at Harvard Medical School and the chief of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. “That’s why we have the whole approval process, to determine what’s actually true,” he said.
KHN’s coverage of prescription drug development, costs and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Ear to the door: Five things being weighed in secret health bill also weigh it down
Anyone following the debate over the “repeal and replace” of the Affordable Care Act knows that the 13 Republican senators writing the bill are meeting behind closed doors.
While Senate Majority Leader Mitch McConnell (R-Ky.) continues to push for a vote before the July 4 Senate recess, Washington’s favorite parlor game has become guessing what is, or will be, in the Senate bill.
Spoiler: No one knows what the final Senate bill will look like – not even those writing it.
“It’s an iterative process,” Senate Majority Whip John Cornyn (R-Texas) told Politico, adding that senators in the room are sending options to the Congressional Budget Office to try to figure out, in general, how much they would cost. Those conversations between senators and the CBO – common for lawmakers working on major, complex pieces of legislation – sometimes prompt members to press through and other times to change course.
Although specifics, to the extent there are any, have largely stayed secret, some of the policies under consideration have slipped out, and pressure points of the debate are fairly clear. Anything can happen, but here’s what we know so far:
1. Medicaid expansion
The Republicans are determined to roll back the expansion of Medicaid under the Affordable Care Act. The question is, How to do it? The ACA called for an expansion of the Medicaid program for those with low incomes to everyone who earns less than 133% of poverty (around $16,000 a year for an individual), with the federal government footing much of the bill. The Supreme Court ruled in 2012 that the expansion was optional for states, but 31 have done so, providing new coverage to an estimated 14 million people.
The Republican bill passed by the House on May 4 would phase out the federal funding for those made eligible by the ACA over 2 years, beginning in 2020. But, Republican moderates in the Senate want a much slower end to the additional federal aid. Several have suggested that they could accept a 7-year phaseout.
Keeping the federal expansion money flowing that long, however, would cut into the bill’s budget savings. That matters: In order to protect the Senate’s ability to pass the bill under budget rules that require only a simple majority rather than 60 votes, the bill’s savings must at least match those of the House version. Any extra money spent on Medicaid expansion would have to be cut elsewhere.
2. Medicaid caps
A related issue is whether and at what level to cap federal Medicaid spending. Medicaid currently covers more than 70 million low-income people. Medicaid covers half of all births and half of the nation’s bill for long-term care, including nursing home stays. Right now, the federal government matches whatever states spend at least 50-50 and provides more matching funds for less wealthy states.
The House bill would, for the first time, cap the amount the federal government provides to states for their Medicaid programs. The CBO estimated that the caps would put more of the financial burden for the program on states, which would respond by a combination of cutting payments to health care providers like doctors and hospitals, eliminating benefits for patients, and restricting eligibility.
The Medicaid cap may or may not be included in the Senate bill, depending on whom you ask. However, sources with direct knowledge of the negotiations say the real sticking point is not whether or not to impose a cap – they want to do that. The hurdles are how to be fair to states that get less federal money and how fast the caps should rise.
Again, if the Senate proposal is more generous than the House’s version, it will be harder to meet the bill’s required budget targets.
3. Restrictions on abortion coverage
The senators are actively considering two measures that would limit funding for abortions, though it is not clear if either would be allowed to remain in the bill according to the Senate’s rules. The Senate Parliamentarian, who must review the bill after the senators complete it but before it comes to the floor, will decide.
The House-passed bill would ban the use of federal tax credits to purchase private coverage that includes abortion as a benefit. This is a key demand for a large portion of the Republican base. However, the Senate version of the bill must abide by strict rules that limit its content to provisions that directly impact the federal budget. In the past, abortion language in budget bills has been ruled out of order.
4. Reading between the lines
A related issue is whether House language to temporarily bar Planned Parenthood from participating in the Medicaid program will be allowed in the Senate.
While the Parliamentarian allowed identical language defunding Planned Parenthood to remain in a similar budget bill in 2015, it was not clear at the time that Planned Parenthood would have been the only provider affected by the language. Planned Parenthood backers say they will argue to the Parliamentarian that the budget impact of the language is “merely incidental” to the policy aim and, therefore, should not be allowed in the Senate bill.
5. Insurance market reforms
Senators are also struggling with provisions of the House-passed bill that would allow states to waive certain insurance requirements in the Affordable Care Act, including those laying out “essential” benefits that policies must cover and those banning insurers from charging sicker people higher premiums. That language, as well as an amendment seeking to ensure more funding to help people with preexisting conditions, was instrumental in gaining enough votes for the bill to pass the House.
Eliminating insurance regulations imposed by the ACA is a top priority for conservatives. “Conservatives would like to clear the books of Obamacare’s most costly regulations and free the states to regulate their markets how they wish,” wrote Sen. Mike Lee (R-Utah), who is one of the 13 senators negotiating the details of the bill, in an op-ed in May.
However, budget experts suggest that none of the insurance market provisions is likely to clear the Parliamentarian hurdle as being primarily budget-related.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Anyone following the debate over the “repeal and replace” of the Affordable Care Act knows that the 13 Republican senators writing the bill are meeting behind closed doors.
While Senate Majority Leader Mitch McConnell (R-Ky.) continues to push for a vote before the July 4 Senate recess, Washington’s favorite parlor game has become guessing what is, or will be, in the Senate bill.
Spoiler: No one knows what the final Senate bill will look like – not even those writing it.
“It’s an iterative process,” Senate Majority Whip John Cornyn (R-Texas) told Politico, adding that senators in the room are sending options to the Congressional Budget Office to try to figure out, in general, how much they would cost. Those conversations between senators and the CBO – common for lawmakers working on major, complex pieces of legislation – sometimes prompt members to press through and other times to change course.
Although specifics, to the extent there are any, have largely stayed secret, some of the policies under consideration have slipped out, and pressure points of the debate are fairly clear. Anything can happen, but here’s what we know so far:
1. Medicaid expansion
The Republicans are determined to roll back the expansion of Medicaid under the Affordable Care Act. The question is, How to do it? The ACA called for an expansion of the Medicaid program for those with low incomes to everyone who earns less than 133% of poverty (around $16,000 a year for an individual), with the federal government footing much of the bill. The Supreme Court ruled in 2012 that the expansion was optional for states, but 31 have done so, providing new coverage to an estimated 14 million people.
The Republican bill passed by the House on May 4 would phase out the federal funding for those made eligible by the ACA over 2 years, beginning in 2020. But, Republican moderates in the Senate want a much slower end to the additional federal aid. Several have suggested that they could accept a 7-year phaseout.
Keeping the federal expansion money flowing that long, however, would cut into the bill’s budget savings. That matters: In order to protect the Senate’s ability to pass the bill under budget rules that require only a simple majority rather than 60 votes, the bill’s savings must at least match those of the House version. Any extra money spent on Medicaid expansion would have to be cut elsewhere.
2. Medicaid caps
A related issue is whether and at what level to cap federal Medicaid spending. Medicaid currently covers more than 70 million low-income people. Medicaid covers half of all births and half of the nation’s bill for long-term care, including nursing home stays. Right now, the federal government matches whatever states spend at least 50-50 and provides more matching funds for less wealthy states.
The House bill would, for the first time, cap the amount the federal government provides to states for their Medicaid programs. The CBO estimated that the caps would put more of the financial burden for the program on states, which would respond by a combination of cutting payments to health care providers like doctors and hospitals, eliminating benefits for patients, and restricting eligibility.
The Medicaid cap may or may not be included in the Senate bill, depending on whom you ask. However, sources with direct knowledge of the negotiations say the real sticking point is not whether or not to impose a cap – they want to do that. The hurdles are how to be fair to states that get less federal money and how fast the caps should rise.
Again, if the Senate proposal is more generous than the House’s version, it will be harder to meet the bill’s required budget targets.
3. Restrictions on abortion coverage
The senators are actively considering two measures that would limit funding for abortions, though it is not clear if either would be allowed to remain in the bill according to the Senate’s rules. The Senate Parliamentarian, who must review the bill after the senators complete it but before it comes to the floor, will decide.
The House-passed bill would ban the use of federal tax credits to purchase private coverage that includes abortion as a benefit. This is a key demand for a large portion of the Republican base. However, the Senate version of the bill must abide by strict rules that limit its content to provisions that directly impact the federal budget. In the past, abortion language in budget bills has been ruled out of order.
4. Reading between the lines
A related issue is whether House language to temporarily bar Planned Parenthood from participating in the Medicaid program will be allowed in the Senate.
While the Parliamentarian allowed identical language defunding Planned Parenthood to remain in a similar budget bill in 2015, it was not clear at the time that Planned Parenthood would have been the only provider affected by the language. Planned Parenthood backers say they will argue to the Parliamentarian that the budget impact of the language is “merely incidental” to the policy aim and, therefore, should not be allowed in the Senate bill.
5. Insurance market reforms
Senators are also struggling with provisions of the House-passed bill that would allow states to waive certain insurance requirements in the Affordable Care Act, including those laying out “essential” benefits that policies must cover and those banning insurers from charging sicker people higher premiums. That language, as well as an amendment seeking to ensure more funding to help people with preexisting conditions, was instrumental in gaining enough votes for the bill to pass the House.
Eliminating insurance regulations imposed by the ACA is a top priority for conservatives. “Conservatives would like to clear the books of Obamacare’s most costly regulations and free the states to regulate their markets how they wish,” wrote Sen. Mike Lee (R-Utah), who is one of the 13 senators negotiating the details of the bill, in an op-ed in May.
However, budget experts suggest that none of the insurance market provisions is likely to clear the Parliamentarian hurdle as being primarily budget-related.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Anyone following the debate over the “repeal and replace” of the Affordable Care Act knows that the 13 Republican senators writing the bill are meeting behind closed doors.
While Senate Majority Leader Mitch McConnell (R-Ky.) continues to push for a vote before the July 4 Senate recess, Washington’s favorite parlor game has become guessing what is, or will be, in the Senate bill.
Spoiler: No one knows what the final Senate bill will look like – not even those writing it.
“It’s an iterative process,” Senate Majority Whip John Cornyn (R-Texas) told Politico, adding that senators in the room are sending options to the Congressional Budget Office to try to figure out, in general, how much they would cost. Those conversations between senators and the CBO – common for lawmakers working on major, complex pieces of legislation – sometimes prompt members to press through and other times to change course.
Although specifics, to the extent there are any, have largely stayed secret, some of the policies under consideration have slipped out, and pressure points of the debate are fairly clear. Anything can happen, but here’s what we know so far:
1. Medicaid expansion
The Republicans are determined to roll back the expansion of Medicaid under the Affordable Care Act. The question is, How to do it? The ACA called for an expansion of the Medicaid program for those with low incomes to everyone who earns less than 133% of poverty (around $16,000 a year for an individual), with the federal government footing much of the bill. The Supreme Court ruled in 2012 that the expansion was optional for states, but 31 have done so, providing new coverage to an estimated 14 million people.
The Republican bill passed by the House on May 4 would phase out the federal funding for those made eligible by the ACA over 2 years, beginning in 2020. But, Republican moderates in the Senate want a much slower end to the additional federal aid. Several have suggested that they could accept a 7-year phaseout.
Keeping the federal expansion money flowing that long, however, would cut into the bill’s budget savings. That matters: In order to protect the Senate’s ability to pass the bill under budget rules that require only a simple majority rather than 60 votes, the bill’s savings must at least match those of the House version. Any extra money spent on Medicaid expansion would have to be cut elsewhere.
2. Medicaid caps
A related issue is whether and at what level to cap federal Medicaid spending. Medicaid currently covers more than 70 million low-income people. Medicaid covers half of all births and half of the nation’s bill for long-term care, including nursing home stays. Right now, the federal government matches whatever states spend at least 50-50 and provides more matching funds for less wealthy states.
The House bill would, for the first time, cap the amount the federal government provides to states for their Medicaid programs. The CBO estimated that the caps would put more of the financial burden for the program on states, which would respond by a combination of cutting payments to health care providers like doctors and hospitals, eliminating benefits for patients, and restricting eligibility.
The Medicaid cap may or may not be included in the Senate bill, depending on whom you ask. However, sources with direct knowledge of the negotiations say the real sticking point is not whether or not to impose a cap – they want to do that. The hurdles are how to be fair to states that get less federal money and how fast the caps should rise.
Again, if the Senate proposal is more generous than the House’s version, it will be harder to meet the bill’s required budget targets.
3. Restrictions on abortion coverage
The senators are actively considering two measures that would limit funding for abortions, though it is not clear if either would be allowed to remain in the bill according to the Senate’s rules. The Senate Parliamentarian, who must review the bill after the senators complete it but before it comes to the floor, will decide.
The House-passed bill would ban the use of federal tax credits to purchase private coverage that includes abortion as a benefit. This is a key demand for a large portion of the Republican base. However, the Senate version of the bill must abide by strict rules that limit its content to provisions that directly impact the federal budget. In the past, abortion language in budget bills has been ruled out of order.
4. Reading between the lines
A related issue is whether House language to temporarily bar Planned Parenthood from participating in the Medicaid program will be allowed in the Senate.
While the Parliamentarian allowed identical language defunding Planned Parenthood to remain in a similar budget bill in 2015, it was not clear at the time that Planned Parenthood would have been the only provider affected by the language. Planned Parenthood backers say they will argue to the Parliamentarian that the budget impact of the language is “merely incidental” to the policy aim and, therefore, should not be allowed in the Senate bill.
5. Insurance market reforms
Senators are also struggling with provisions of the House-passed bill that would allow states to waive certain insurance requirements in the Affordable Care Act, including those laying out “essential” benefits that policies must cover and those banning insurers from charging sicker people higher premiums. That language, as well as an amendment seeking to ensure more funding to help people with preexisting conditions, was instrumental in gaining enough votes for the bill to pass the House.
Eliminating insurance regulations imposed by the ACA is a top priority for conservatives. “Conservatives would like to clear the books of Obamacare’s most costly regulations and free the states to regulate their markets how they wish,” wrote Sen. Mike Lee (R-Utah), who is one of the 13 senators negotiating the details of the bill, in an op-ed in May.
However, budget experts suggest that none of the insurance market provisions is likely to clear the Parliamentarian hurdle as being primarily budget-related.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Shift to minimally invasive MV surgery picks up
NEW YORK – An analysis of a Society of Thoracic Surgeons database has identified a significant increase in volumes for isolated mitral valve surgery and leaflet prolapse this decade, with a shift toward minimally invasive approaches, according to a study of trends in mitral valve surgery in the United States presented here at the American Association for Thoracic Surgery Mitral Conclave 2017.
James Gammie, MD, of the University of Maryland School of Medicine, Baltimore, reported on the analysis of the STS Adult Cardiac Surgery Database in which more than 90% of the adult cardiac surgery centers in North America participate.

“Degenerative disease remains the most common reason patients are referred for surgery,” Dr. Gammie said, noting that 60.7% of patients with an identified etiology had degenerative leaflet prolapse (etiology was unknown in 31% of the patients in the dataset).
“The operative approach has changed and continues to shift toward a less invasive approach,” Dr. Gammie said. Overall, 74.1% of operations involved sternotomy, but only 67.5% of those in the leaflet prolapse subgroup, with less invasive operations comprising 23% of all operations and 29.1% of those in the leaflet prolapse subgroup. From 2011 to 2016, total mitral surgical volume grew at a rate of 1.1% annually, but the volume for isolated MV operations grew 4.4% annually while leaflet prolapse procedures increased 7.6% annually, Dr. Gammie said.
Dr. Gammie described surgeons’ decision to perform ablation for preoperative AF during MV surgery a “coin toss.” One-third (34%) had AF, but only 51.2% of patients with AF in the total cohort and 54.4% of those in the leaflet prolapse subgroup got ablation. The overall MV repair rate was 65% for the total cohort but 83% for those with leaflet prolapse. For those who had MV replacement, the share of bioprosthetic devices increased steadily through the study period, from around 65% to 75.8%, Dr. Gammie said.
In the leaflet prolapse subgroup, 96.1% had annuloplasty and 29.2% had artificial chords implanted, with an average of two chords per operation. “There’s an increasing use of artificial ePTFE chords,” Dr. Gammie said. He noted the leaflet prolapse subgroup was composed of low-risk healthy patients. The mean ejection fraction (EF) for the cohort was 57%, and 47% of patients had EF of less than 60%. The overwhelming majority of patients (88%) had Class I indications for surgery with the remainder having Class IIa indications.
Dr. Gammie noted a few other emerging trends of MV surgery during the study period. “Patients with functional mitral regurgitation are rarely referred for operation: these patients made up fewer than 5% of patients undergoing mitral valve operations during the study period,” he said.;
With regard to outcomes, Dr. Gammie said, “There remain substantial differences between repair and replacement.” Replacement had almost twice the rate of reoperation for bleeding than repair (4.1% vs. 2.1%) and renal failure (3.4% vs. 1.4%).
“We observed that a substantial number of patients have an unsuccessful attempt at mitral valve repair before undergoing replacement – 16 % of the overall replacement group and 27% of patients having replacement for degenerative leaflet prolapse,” he said. “This does not appear to penalize patients in terms of outcome.”
The rate of permanent pacemaker was also significantly higher in the replacement cohort, 9.8% vs. 3.8% for repair operations, as was operative mortality, 3.7% vs. 1.1%. Said Dr. Gammie.
“This is something to think about as we move to less invasive approaches and overall operative mortality remains over threefold higher for replacement than repair.”
The leaflet prolapse subgroup showed similar disparities between replacement and repair groups. “The increased application of repair when feasible will be of value to improve outcomes, as will referral of patients earlier in the disease process ,” Dr. Gammie said.
“In our own STS database, about one-third of patients who were coded as having AF had no evidence of it, and that’s why in our institution they don’t get treated.” He added, “I’m not that surprised at the low repair rate when the average surgeon in the United States does five mitral repairs a year.”
Dr. Gammie disclosed that he is a consultant to Edwards Lifesciences and has an ownership interest in Harpoon Medical. Dr. Damiano disclosed that he is a speaker for LivaNova and a consultant to and a research grant recipient of Atricure.
NEW YORK – An analysis of a Society of Thoracic Surgeons database has identified a significant increase in volumes for isolated mitral valve surgery and leaflet prolapse this decade, with a shift toward minimally invasive approaches, according to a study of trends in mitral valve surgery in the United States presented here at the American Association for Thoracic Surgery Mitral Conclave 2017.
James Gammie, MD, of the University of Maryland School of Medicine, Baltimore, reported on the analysis of the STS Adult Cardiac Surgery Database in which more than 90% of the adult cardiac surgery centers in North America participate.
“Degenerative disease remains the most common reason patients are referred for surgery,” Dr. Gammie said, noting that 60.7% of patients with an identified etiology had degenerative leaflet prolapse (etiology was unknown in 31% of the patients in the dataset).
“The operative approach has changed and continues to shift toward a less invasive approach,” Dr. Gammie said. Overall, 74.1% of operations involved sternotomy, but only 67.5% of those in the leaflet prolapse subgroup, with less invasive operations comprising 23% of all operations and 29.1% of those in the leaflet prolapse subgroup. From 2011 to 2016, total mitral surgical volume grew at a rate of 1.1% annually, but the volume for isolated MV operations grew 4.4% annually while leaflet prolapse procedures increased 7.6% annually, Dr. Gammie said.
Dr. Gammie described surgeons’ decision to perform ablation for preoperative AF during MV surgery a “coin toss.” One-third (34%) had AF, but only 51.2% of patients with AF in the total cohort and 54.4% of those in the leaflet prolapse subgroup got ablation. The overall MV repair rate was 65% for the total cohort but 83% for those with leaflet prolapse. For those who had MV replacement, the share of bioprosthetic devices increased steadily through the study period, from around 65% to 75.8%, Dr. Gammie said.
In the leaflet prolapse subgroup, 96.1% had annuloplasty and 29.2% had artificial chords implanted, with an average of two chords per operation. “There’s an increasing use of artificial ePTFE chords,” Dr. Gammie said. He noted the leaflet prolapse subgroup was composed of low-risk healthy patients. The mean ejection fraction (EF) for the cohort was 57%, and 47% of patients had EF of less than 60%. The overwhelming majority of patients (88%) had Class I indications for surgery with the remainder having Class IIa indications.
Dr. Gammie noted a few other emerging trends of MV surgery during the study period. “Patients with functional mitral regurgitation are rarely referred for operation: these patients made up fewer than 5% of patients undergoing mitral valve operations during the study period,” he said.;
With regard to outcomes, Dr. Gammie said, “There remain substantial differences between repair and replacement.” Replacement had almost twice the rate of reoperation for bleeding than repair (4.1% vs. 2.1%) and renal failure (3.4% vs. 1.4%).
“We observed that a substantial number of patients have an unsuccessful attempt at mitral valve repair before undergoing replacement – 16 % of the overall replacement group and 27% of patients having replacement for degenerative leaflet prolapse,” he said. “This does not appear to penalize patients in terms of outcome.”
The rate of permanent pacemaker was also significantly higher in the replacement cohort, 9.8% vs. 3.8% for repair operations, as was operative mortality, 3.7% vs. 1.1%. Said Dr. Gammie.
“This is something to think about as we move to less invasive approaches and overall operative mortality remains over threefold higher for replacement than repair.”
The leaflet prolapse subgroup showed similar disparities between replacement and repair groups. “The increased application of repair when feasible will be of value to improve outcomes, as will referral of patients earlier in the disease process ,” Dr. Gammie said.
“In our own STS database, about one-third of patients who were coded as having AF had no evidence of it, and that’s why in our institution they don’t get treated.” He added, “I’m not that surprised at the low repair rate when the average surgeon in the United States does five mitral repairs a year.”
Dr. Gammie disclosed that he is a consultant to Edwards Lifesciences and has an ownership interest in Harpoon Medical. Dr. Damiano disclosed that he is a speaker for LivaNova and a consultant to and a research grant recipient of Atricure.
NEW YORK – An analysis of a Society of Thoracic Surgeons database has identified a significant increase in volumes for isolated mitral valve surgery and leaflet prolapse this decade, with a shift toward minimally invasive approaches, according to a study of trends in mitral valve surgery in the United States presented here at the American Association for Thoracic Surgery Mitral Conclave 2017.
James Gammie, MD, of the University of Maryland School of Medicine, Baltimore, reported on the analysis of the STS Adult Cardiac Surgery Database in which more than 90% of the adult cardiac surgery centers in North America participate.
“Degenerative disease remains the most common reason patients are referred for surgery,” Dr. Gammie said, noting that 60.7% of patients with an identified etiology had degenerative leaflet prolapse (etiology was unknown in 31% of the patients in the dataset).
“The operative approach has changed and continues to shift toward a less invasive approach,” Dr. Gammie said. Overall, 74.1% of operations involved sternotomy, but only 67.5% of those in the leaflet prolapse subgroup, with less invasive operations comprising 23% of all operations and 29.1% of those in the leaflet prolapse subgroup. From 2011 to 2016, total mitral surgical volume grew at a rate of 1.1% annually, but the volume for isolated MV operations grew 4.4% annually while leaflet prolapse procedures increased 7.6% annually, Dr. Gammie said.
Dr. Gammie described surgeons’ decision to perform ablation for preoperative AF during MV surgery a “coin toss.” One-third (34%) had AF, but only 51.2% of patients with AF in the total cohort and 54.4% of those in the leaflet prolapse subgroup got ablation. The overall MV repair rate was 65% for the total cohort but 83% for those with leaflet prolapse. For those who had MV replacement, the share of bioprosthetic devices increased steadily through the study period, from around 65% to 75.8%, Dr. Gammie said.
In the leaflet prolapse subgroup, 96.1% had annuloplasty and 29.2% had artificial chords implanted, with an average of two chords per operation. “There’s an increasing use of artificial ePTFE chords,” Dr. Gammie said. He noted the leaflet prolapse subgroup was composed of low-risk healthy patients. The mean ejection fraction (EF) for the cohort was 57%, and 47% of patients had EF of less than 60%. The overwhelming majority of patients (88%) had Class I indications for surgery with the remainder having Class IIa indications.
Dr. Gammie noted a few other emerging trends of MV surgery during the study period. “Patients with functional mitral regurgitation are rarely referred for operation: these patients made up fewer than 5% of patients undergoing mitral valve operations during the study period,” he said.;
With regard to outcomes, Dr. Gammie said, “There remain substantial differences between repair and replacement.” Replacement had almost twice the rate of reoperation for bleeding than repair (4.1% vs. 2.1%) and renal failure (3.4% vs. 1.4%).
“We observed that a substantial number of patients have an unsuccessful attempt at mitral valve repair before undergoing replacement – 16 % of the overall replacement group and 27% of patients having replacement for degenerative leaflet prolapse,” he said. “This does not appear to penalize patients in terms of outcome.”
The rate of permanent pacemaker was also significantly higher in the replacement cohort, 9.8% vs. 3.8% for repair operations, as was operative mortality, 3.7% vs. 1.1%. Said Dr. Gammie.
“This is something to think about as we move to less invasive approaches and overall operative mortality remains over threefold higher for replacement than repair.”
The leaflet prolapse subgroup showed similar disparities between replacement and repair groups. “The increased application of repair when feasible will be of value to improve outcomes, as will referral of patients earlier in the disease process ,” Dr. Gammie said.
“In our own STS database, about one-third of patients who were coded as having AF had no evidence of it, and that’s why in our institution they don’t get treated.” He added, “I’m not that surprised at the low repair rate when the average surgeon in the United States does five mitral repairs a year.”
Dr. Gammie disclosed that he is a consultant to Edwards Lifesciences and has an ownership interest in Harpoon Medical. Dr. Damiano disclosed that he is a speaker for LivaNova and a consultant to and a research grant recipient of Atricure.
AT THE AATS MITRAL CONCLAVE 2017
Key clinical point: The volume of mitral valve surgery has increased substantially, according to an analysis of the Society for Thoracic Surgery database, and an increasing percentage of procedures are minimally invasive in nature.
Major finding: Sternotomy continues to be the most widely used approach for mitral valve surgery, but less invasive options most recently comprised 23% of the overall group and 29.1% of those with isolated leaflet prolapse.
Data source: Retrospective study of 15,360 isolated mitral valve operations performed from July 2011 to September 2016 in the Society of Thoracic Surgeons database.
Disclosures: Dr. Gammie reported being a consultant to Edwards Lifesciences and having an ownership interest in Harpoon Medical.
Urgent surgery said to deserve separate classification
Urgent surgery deserves a separate classification from elective surgery and emergency surgery for assessments of healthcare quality and performance, because the three types of surgery have distinct morbidity and mortality profiles, according to a report published in JAMA Surgery.
Current methods of assessing pay-for-performance reimbursement, surgical outcomes, and value-based care programs all classify surgeries as either elective or emergent procedures. They do not account for the many surgeries that are instead urgent – performed after a trial of nonoperative conservative management or after patients with acute disease processes undergo a brief period of medical optimization.
Common examples of surgeries that occupy this middle ‘urgent’ ground between elective and emergent procedures are those done for cholecystitis, adhesive small-bowel obstruction, and acute diverticulitis, said Matthew G. Mullen, MD, and his associates at the University of Virginia Health System, Charlottesville.
Such urgent surgeries should not be lumped together with elective surgeries, as they usually are at present, because they carry substantially higher complication rates and mortality. “At a time when reimbursement is contingent on value-based outcomes reporting and performance, it is imperative to ensure that appropriate risk adjustment is performed,” the researchers stated.
“Surgeons who commonly operate on an urgent basis, including many acute-care and emergency general surgeons, are at risk of being penalized” in Medicare’s value-based reimbursement for their services.
“These surgeons may even unfairly be labeled as poor performers by current outcome reporting guidelines,” the investigators noted.
Morbidity and mortality rates associated with the “substantial” population of patients undergoing urgent surgery have not been well-studied until now. Dr. Mullen and his associates examined the issue using information from a national database, the American College of Surgeons’ National Quality Improvement Program Participant Use File. They focused on 173,643 general surgeries performed at 435 hospitals during a 1-year period: 130,235 (75%) were categorized as elective, 20,816 (12%) as urgent (nonelective and nonemergency), and 22,592 (13%) as emergency procedures.
Urgent general surgeries carried a 12.3% rate of morbidity and a 2.3% rate of mortality. These rates are much greater than those of elective surgeries (6.7% and 0.4%, respectively), even though urgent surgeries typically fall into the category of “elective.” In fact, the morbidity and mortality rates for urgent surgeries closely approached those of emergency surgeries (13.8% and 3.7%, respectively), the investigators said (JAMA Surg. 2017 May 10 [doi:10.1001/jamasurg.2017.0918]).
In this cohort, patients in the “urgent” surgery category had the highest preoperative rates of congestive heart failure, chronic obstructive pulmonary disease, diabetes, hemodialysis, corticosteroid use, and disseminated cancer – all factors that markedly elevate mortality and morbidity risks.
“We have identified operative urgency as a key consideration for patient risk stratification. If this issue is not recognized, quality outcome reporting and value-based reimbursement will continue to incentivize operating on an elective basis and will make surgeons more reluctant to operate on patients who urgently require care,” Dr. Mullen and his associates said. And such delays in surgical intervention could further increase patient morbidity and mortality.
This study was supported by the National Institutes of Health. Dr. Mullen and his associates reported having no relevant financial disclosures.
Urgent surgery deserves a separate classification from elective surgery and emergency surgery for assessments of healthcare quality and performance, because the three types of surgery have distinct morbidity and mortality profiles, according to a report published in JAMA Surgery.
Current methods of assessing pay-for-performance reimbursement, surgical outcomes, and value-based care programs all classify surgeries as either elective or emergent procedures. They do not account for the many surgeries that are instead urgent – performed after a trial of nonoperative conservative management or after patients with acute disease processes undergo a brief period of medical optimization.
Common examples of surgeries that occupy this middle ‘urgent’ ground between elective and emergent procedures are those done for cholecystitis, adhesive small-bowel obstruction, and acute diverticulitis, said Matthew G. Mullen, MD, and his associates at the University of Virginia Health System, Charlottesville.
Such urgent surgeries should not be lumped together with elective surgeries, as they usually are at present, because they carry substantially higher complication rates and mortality. “At a time when reimbursement is contingent on value-based outcomes reporting and performance, it is imperative to ensure that appropriate risk adjustment is performed,” the researchers stated.
“Surgeons who commonly operate on an urgent basis, including many acute-care and emergency general surgeons, are at risk of being penalized” in Medicare’s value-based reimbursement for their services.
“These surgeons may even unfairly be labeled as poor performers by current outcome reporting guidelines,” the investigators noted.
Morbidity and mortality rates associated with the “substantial” population of patients undergoing urgent surgery have not been well-studied until now. Dr. Mullen and his associates examined the issue using information from a national database, the American College of Surgeons’ National Quality Improvement Program Participant Use File. They focused on 173,643 general surgeries performed at 435 hospitals during a 1-year period: 130,235 (75%) were categorized as elective, 20,816 (12%) as urgent (nonelective and nonemergency), and 22,592 (13%) as emergency procedures.
Urgent general surgeries carried a 12.3% rate of morbidity and a 2.3% rate of mortality. These rates are much greater than those of elective surgeries (6.7% and 0.4%, respectively), even though urgent surgeries typically fall into the category of “elective.” In fact, the morbidity and mortality rates for urgent surgeries closely approached those of emergency surgeries (13.8% and 3.7%, respectively), the investigators said (JAMA Surg. 2017 May 10 [doi:10.1001/jamasurg.2017.0918]).
In this cohort, patients in the “urgent” surgery category had the highest preoperative rates of congestive heart failure, chronic obstructive pulmonary disease, diabetes, hemodialysis, corticosteroid use, and disseminated cancer – all factors that markedly elevate mortality and morbidity risks.
“We have identified operative urgency as a key consideration for patient risk stratification. If this issue is not recognized, quality outcome reporting and value-based reimbursement will continue to incentivize operating on an elective basis and will make surgeons more reluctant to operate on patients who urgently require care,” Dr. Mullen and his associates said. And such delays in surgical intervention could further increase patient morbidity and mortality.
This study was supported by the National Institutes of Health. Dr. Mullen and his associates reported having no relevant financial disclosures.
Urgent surgery deserves a separate classification from elective surgery and emergency surgery for assessments of healthcare quality and performance, because the three types of surgery have distinct morbidity and mortality profiles, according to a report published in JAMA Surgery.
Current methods of assessing pay-for-performance reimbursement, surgical outcomes, and value-based care programs all classify surgeries as either elective or emergent procedures. They do not account for the many surgeries that are instead urgent – performed after a trial of nonoperative conservative management or after patients with acute disease processes undergo a brief period of medical optimization.
Common examples of surgeries that occupy this middle ‘urgent’ ground between elective and emergent procedures are those done for cholecystitis, adhesive small-bowel obstruction, and acute diverticulitis, said Matthew G. Mullen, MD, and his associates at the University of Virginia Health System, Charlottesville.
Such urgent surgeries should not be lumped together with elective surgeries, as they usually are at present, because they carry substantially higher complication rates and mortality. “At a time when reimbursement is contingent on value-based outcomes reporting and performance, it is imperative to ensure that appropriate risk adjustment is performed,” the researchers stated.
“Surgeons who commonly operate on an urgent basis, including many acute-care and emergency general surgeons, are at risk of being penalized” in Medicare’s value-based reimbursement for their services.
“These surgeons may even unfairly be labeled as poor performers by current outcome reporting guidelines,” the investigators noted.
Morbidity and mortality rates associated with the “substantial” population of patients undergoing urgent surgery have not been well-studied until now. Dr. Mullen and his associates examined the issue using information from a national database, the American College of Surgeons’ National Quality Improvement Program Participant Use File. They focused on 173,643 general surgeries performed at 435 hospitals during a 1-year period: 130,235 (75%) were categorized as elective, 20,816 (12%) as urgent (nonelective and nonemergency), and 22,592 (13%) as emergency procedures.
Urgent general surgeries carried a 12.3% rate of morbidity and a 2.3% rate of mortality. These rates are much greater than those of elective surgeries (6.7% and 0.4%, respectively), even though urgent surgeries typically fall into the category of “elective.” In fact, the morbidity and mortality rates for urgent surgeries closely approached those of emergency surgeries (13.8% and 3.7%, respectively), the investigators said (JAMA Surg. 2017 May 10 [doi:10.1001/jamasurg.2017.0918]).
In this cohort, patients in the “urgent” surgery category had the highest preoperative rates of congestive heart failure, chronic obstructive pulmonary disease, diabetes, hemodialysis, corticosteroid use, and disseminated cancer – all factors that markedly elevate mortality and morbidity risks.
“We have identified operative urgency as a key consideration for patient risk stratification. If this issue is not recognized, quality outcome reporting and value-based reimbursement will continue to incentivize operating on an elective basis and will make surgeons more reluctant to operate on patients who urgently require care,” Dr. Mullen and his associates said. And such delays in surgical intervention could further increase patient morbidity and mortality.
This study was supported by the National Institutes of Health. Dr. Mullen and his associates reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point: Urgent surgery deserves a separate classification from elective and emergency surgeries for assessments of healthcare quality and performance.
Major finding: Urgent general surgeries carried a 12.3% rate of morbidity and a 2.3% rate of mortality, approximately double the morbidity rate and 6 times the mortality rate of elective surgeries (6.7% and 0.4%, respectively).
Data source: A retrospective analysis of outcomes for 173,643 general surgeries performed during a 1-year period at 435 hospitals across U.S.
Disclosures: This study was supported by the National Institutes of Health. Dr. Mullen and his associates reported having no relevant financial disclosures.
Sooner is better than later for acute UC surgery
SEATTLE – Postponing surgery for acute ulcerative colitis more than a day increases postoperative complications, lengths of stay, and hospital costs, according to a review by Johns Hopkins University, Baltimore, of almost 2,000 patients.
It’s not uncommon to wait 5 or even 10 days to give biologics a chance to work when patients are admitted for acute ulcerative colitis (UC). Based on the review, however, “we believe that the need for prolonged medical therapy and resuscitation in this patient population prior to colectomy may be overstated,” and that “the lasting effects of persistent inflammation cascade are underestimated.”

The team reviewed 1,953 index UC admissions with emergent non-elective abdominal surgery in the National Inpatient Sample (NIS) database from 2008-13; 546 patients (28%) had early operations - within 24 hours of admission – and the other 1,407 had operations after that time.
Although it’s impossible to say for sure given the limits of administrative data in the NIS, patients who had surgery soon after admission were probably sicker. Even so, they were less likely to have complications than patients in the delayed surgery group (55% versus 43%), and they had shorter hospital stays, with just 8% in the hospital past 21 days, versus 29% of patients who had delayed operations. The findings were similar for both overall length of stay and post-op length of stay.
Renal complications (8% versus 14%), pulmonary complications (20% versus 25%), and thromboembolic events (4% versus 6%) were also less common in the early surgery group. On multivariable analysis, delayed surgery increased the complication rate by 64%.
With fewer complications and shorter hospital stays, early operations were also less expensive, with a mean total hospitalization cost of $19,985 versus $34,258. The findings were all statistically significant.
Dr. Leeds noted the limits of the study; medical management regimes and the reasons for variations in surgical timing are unknown, among other things. “This is not the final answer on what to do with patients like this, but it opens the door to prospective studies that could control” for such variables, he said.
Early surgery patients were more likely to be male (57% versus 51%) and from households with incomes higher than the national median. There were no difference in age, race, comorbidities, region, or hospital type between the two groups.
Dr. Leeds said he had no disclosures.
SEATTLE – Postponing surgery for acute ulcerative colitis more than a day increases postoperative complications, lengths of stay, and hospital costs, according to a review by Johns Hopkins University, Baltimore, of almost 2,000 patients.
It’s not uncommon to wait 5 or even 10 days to give biologics a chance to work when patients are admitted for acute ulcerative colitis (UC). Based on the review, however, “we believe that the need for prolonged medical therapy and resuscitation in this patient population prior to colectomy may be overstated,” and that “the lasting effects of persistent inflammation cascade are underestimated.”
The team reviewed 1,953 index UC admissions with emergent non-elective abdominal surgery in the National Inpatient Sample (NIS) database from 2008-13; 546 patients (28%) had early operations - within 24 hours of admission – and the other 1,407 had operations after that time.
Although it’s impossible to say for sure given the limits of administrative data in the NIS, patients who had surgery soon after admission were probably sicker. Even so, they were less likely to have complications than patients in the delayed surgery group (55% versus 43%), and they had shorter hospital stays, with just 8% in the hospital past 21 days, versus 29% of patients who had delayed operations. The findings were similar for both overall length of stay and post-op length of stay.
Renal complications (8% versus 14%), pulmonary complications (20% versus 25%), and thromboembolic events (4% versus 6%) were also less common in the early surgery group. On multivariable analysis, delayed surgery increased the complication rate by 64%.
With fewer complications and shorter hospital stays, early operations were also less expensive, with a mean total hospitalization cost of $19,985 versus $34,258. The findings were all statistically significant.
Dr. Leeds noted the limits of the study; medical management regimes and the reasons for variations in surgical timing are unknown, among other things. “This is not the final answer on what to do with patients like this, but it opens the door to prospective studies that could control” for such variables, he said.
Early surgery patients were more likely to be male (57% versus 51%) and from households with incomes higher than the national median. There were no difference in age, race, comorbidities, region, or hospital type between the two groups.
Dr. Leeds said he had no disclosures.
SEATTLE – Postponing surgery for acute ulcerative colitis more than a day increases postoperative complications, lengths of stay, and hospital costs, according to a review by Johns Hopkins University, Baltimore, of almost 2,000 patients.
It’s not uncommon to wait 5 or even 10 days to give biologics a chance to work when patients are admitted for acute ulcerative colitis (UC). Based on the review, however, “we believe that the need for prolonged medical therapy and resuscitation in this patient population prior to colectomy may be overstated,” and that “the lasting effects of persistent inflammation cascade are underestimated.”
The team reviewed 1,953 index UC admissions with emergent non-elective abdominal surgery in the National Inpatient Sample (NIS) database from 2008-13; 546 patients (28%) had early operations - within 24 hours of admission – and the other 1,407 had operations after that time.
Although it’s impossible to say for sure given the limits of administrative data in the NIS, patients who had surgery soon after admission were probably sicker. Even so, they were less likely to have complications than patients in the delayed surgery group (55% versus 43%), and they had shorter hospital stays, with just 8% in the hospital past 21 days, versus 29% of patients who had delayed operations. The findings were similar for both overall length of stay and post-op length of stay.
Renal complications (8% versus 14%), pulmonary complications (20% versus 25%), and thromboembolic events (4% versus 6%) were also less common in the early surgery group. On multivariable analysis, delayed surgery increased the complication rate by 64%.
With fewer complications and shorter hospital stays, early operations were also less expensive, with a mean total hospitalization cost of $19,985 versus $34,258. The findings were all statistically significant.
Dr. Leeds noted the limits of the study; medical management regimes and the reasons for variations in surgical timing are unknown, among other things. “This is not the final answer on what to do with patients like this, but it opens the door to prospective studies that could control” for such variables, he said.
Early surgery patients were more likely to be male (57% versus 51%) and from households with incomes higher than the national median. There were no difference in age, race, comorbidities, region, or hospital type between the two groups.
Dr. Leeds said he had no disclosures.
AT ASCRS 2017
Key clinical point:
Major finding: Patients who had surgery soon after admission were probably sicker. Even so, they were less likely to have complications than patients in the delayed surgery group (55% versus 43%), and they had shorter hospital stays, with just 8% in the hospital past 21 days, versus 29% of patients who had delayed operations.
Data source: Review of almost 2,000 patients in the National Inpatient Sample
Disclosures: The lead investigator had no disclosures.
Anal dysplasia surveillance called into question
SEATTLE – Aggressive screening and treatment of HPV anal dysplasia probably doesn’t decrease the incidence of anal cancer, even in high-risk groups, according to investigators from Kaiser Permanente of Southern California.
The increase in anal squamous cell carcinoma (SCC) over the past 20 years has led to surveillance programs for anal dysplasia in many institutions, based on the assumption that finding and destroying the lesions will prevent anal cancer, similar to the reason why polyps are removed during colonoscopy to prevent colon cancer, said lead investigator Marco Tomassi, MD, a general surgeon with Kaiser in San Diego.

Kaiser in Southern California doesn’t have an intensive surveillance program for anal HPV. Instead, high risk patients – those with HIV, past cervical cancer, anogenital warts, among others – are screened with digital rectal exams and anoscopy every 3-12 months, and only anal warts and other grossly abnormal growths are removed.
Physicians there do not routinely use high resolution anoscopy (HRA), Pap smears, and other techniques to identify and destroy microscopic foci of dysplasia, as in more intensive programs.
To see how the approach has worked, Dr. Tomassi and his colleagues reviewed the incidence of anal SCC among almost 6 million Kaiser patients from 2005 through 2015.
The cumulative incidence in all groups of patients, even those at risk for the disease, was less than 1%; 425 of the 460 anal cancers (92%) were in the general population, among patients who would not have been part of a high risk surveillance program.
Even without an aggressive surveillance program, high grade anal dysplasia was identified in 377 patients; their incidence of anal SCC was 0.8%, the highest found in the study.
There were no incident cases of SCC among the 133 HIV patients with anal dysplasia. Among over 5,000 HIV patients in the study, the anal SCC incidence was 0.09%. In the general population of 5.86 million, it was 0.01%.
“The cumulative incidence in our group, despite not performing ablative techniques for dysplasia, was comparable to those institutions that routinely perform high resolution anoscopy and destruction of dysplasia. The low rate of malignant conversion suggests that aggressive surveillance regimens, such as HRA, may lead to unnecessary procedures even in high risk patients,” Dr. Tomassi said.
Intensive surveillance doesn’t seem to make much difference because “the incidence of anal cancer is very low even in very high risk populations,” and “most SCC cases develop in the general population,” so “regimens dedicated to identifying cancer in high risk groups will ultimate miss the majority of patients who will succumb to this disease,” he said.
“It’s rare that I come to a meeting and hear a paper that’s going to change my practice. Thank you for that,” an audience member said after Dr. Tomassi presented his findings at the American Society of Colon and Rectal Surgeons annual meeting.
Dr. Tomassi did not have any disclosures.
SEATTLE – Aggressive screening and treatment of HPV anal dysplasia probably doesn’t decrease the incidence of anal cancer, even in high-risk groups, according to investigators from Kaiser Permanente of Southern California.
The increase in anal squamous cell carcinoma (SCC) over the past 20 years has led to surveillance programs for anal dysplasia in many institutions, based on the assumption that finding and destroying the lesions will prevent anal cancer, similar to the reason why polyps are removed during colonoscopy to prevent colon cancer, said lead investigator Marco Tomassi, MD, a general surgeon with Kaiser in San Diego.
Kaiser in Southern California doesn’t have an intensive surveillance program for anal HPV. Instead, high risk patients – those with HIV, past cervical cancer, anogenital warts, among others – are screened with digital rectal exams and anoscopy every 3-12 months, and only anal warts and other grossly abnormal growths are removed.
Physicians there do not routinely use high resolution anoscopy (HRA), Pap smears, and other techniques to identify and destroy microscopic foci of dysplasia, as in more intensive programs.
To see how the approach has worked, Dr. Tomassi and his colleagues reviewed the incidence of anal SCC among almost 6 million Kaiser patients from 2005 through 2015.
The cumulative incidence in all groups of patients, even those at risk for the disease, was less than 1%; 425 of the 460 anal cancers (92%) were in the general population, among patients who would not have been part of a high risk surveillance program.
Even without an aggressive surveillance program, high grade anal dysplasia was identified in 377 patients; their incidence of anal SCC was 0.8%, the highest found in the study.
There were no incident cases of SCC among the 133 HIV patients with anal dysplasia. Among over 5,000 HIV patients in the study, the anal SCC incidence was 0.09%. In the general population of 5.86 million, it was 0.01%.
“The cumulative incidence in our group, despite not performing ablative techniques for dysplasia, was comparable to those institutions that routinely perform high resolution anoscopy and destruction of dysplasia. The low rate of malignant conversion suggests that aggressive surveillance regimens, such as HRA, may lead to unnecessary procedures even in high risk patients,” Dr. Tomassi said.
Intensive surveillance doesn’t seem to make much difference because “the incidence of anal cancer is very low even in very high risk populations,” and “most SCC cases develop in the general population,” so “regimens dedicated to identifying cancer in high risk groups will ultimate miss the majority of patients who will succumb to this disease,” he said.
“It’s rare that I come to a meeting and hear a paper that’s going to change my practice. Thank you for that,” an audience member said after Dr. Tomassi presented his findings at the American Society of Colon and Rectal Surgeons annual meeting.
Dr. Tomassi did not have any disclosures.
SEATTLE – Aggressive screening and treatment of HPV anal dysplasia probably doesn’t decrease the incidence of anal cancer, even in high-risk groups, according to investigators from Kaiser Permanente of Southern California.
The increase in anal squamous cell carcinoma (SCC) over the past 20 years has led to surveillance programs for anal dysplasia in many institutions, based on the assumption that finding and destroying the lesions will prevent anal cancer, similar to the reason why polyps are removed during colonoscopy to prevent colon cancer, said lead investigator Marco Tomassi, MD, a general surgeon with Kaiser in San Diego.
Kaiser in Southern California doesn’t have an intensive surveillance program for anal HPV. Instead, high risk patients – those with HIV, past cervical cancer, anogenital warts, among others – are screened with digital rectal exams and anoscopy every 3-12 months, and only anal warts and other grossly abnormal growths are removed.
Physicians there do not routinely use high resolution anoscopy (HRA), Pap smears, and other techniques to identify and destroy microscopic foci of dysplasia, as in more intensive programs.
To see how the approach has worked, Dr. Tomassi and his colleagues reviewed the incidence of anal SCC among almost 6 million Kaiser patients from 2005 through 2015.
The cumulative incidence in all groups of patients, even those at risk for the disease, was less than 1%; 425 of the 460 anal cancers (92%) were in the general population, among patients who would not have been part of a high risk surveillance program.
Even without an aggressive surveillance program, high grade anal dysplasia was identified in 377 patients; their incidence of anal SCC was 0.8%, the highest found in the study.
There were no incident cases of SCC among the 133 HIV patients with anal dysplasia. Among over 5,000 HIV patients in the study, the anal SCC incidence was 0.09%. In the general population of 5.86 million, it was 0.01%.
“The cumulative incidence in our group, despite not performing ablative techniques for dysplasia, was comparable to those institutions that routinely perform high resolution anoscopy and destruction of dysplasia. The low rate of malignant conversion suggests that aggressive surveillance regimens, such as HRA, may lead to unnecessary procedures even in high risk patients,” Dr. Tomassi said.
Intensive surveillance doesn’t seem to make much difference because “the incidence of anal cancer is very low even in very high risk populations,” and “most SCC cases develop in the general population,” so “regimens dedicated to identifying cancer in high risk groups will ultimate miss the majority of patients who will succumb to this disease,” he said.
“It’s rare that I come to a meeting and hear a paper that’s going to change my practice. Thank you for that,” an audience member said after Dr. Tomassi presented his findings at the American Society of Colon and Rectal Surgeons annual meeting.
Dr. Tomassi did not have any disclosures.
AT ASCRS 2017
Key clinical point:
Major finding: When high risk patients were not screened and treated for anal dysplasia, the cumulative incidence of anal squamous cell carcinoma was 0.8% or less, similar to programs that target and treat the lesions.
Data source: Review of almost 6 million patients at Kaiser Permanente of Southern California
Disclosures: The lead investigator had no disclosures.
Fewer early neurologic complications with TAVR than SAVR
PARIS – Patients with severe aortic stenosis at intermediate operative risk have a significantly lower 30-day risk of stroke and other neurologic complications with transcatheter aortic valve replacement than with surgical replacement, according to new results from the landmark SURTAVI trial.
“This is the first time the stroke rate has been shown to be lower with TAVR than with surgery,” A. Pieter Kappetein, MD, noted in presenting the results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
It’s a finding that adds to the momentum for studying TAVR in low-surgical-risk patients, he added.
“As we move toward lower-risk patients it will become even more important to see whether there is a difference in stroke. Suppose the stroke rate in SURTAVI had been a little higher with TAVR than SAVR? It would really make us more cautious about moving toward lower-risk patients. Now that we see that in intermediate-risk patients the stroke rate is actually a little bit lower than with surgery, I think we’ll feel more comfortable moving toward lower-risk patients,” according to Dr. Kappetein, professor of cardiothoracic surgery at Erasmus University Medical Center in Rotterdam.
SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) involved randomization of 1,660 patients with severe symptomatic aortic stenosis to TAVR or SAVR. All participants were deemed to be at intermediate operative risk based upon a predicted surgical mortality of 3%-15%. The primary outcome -- a composite of all-cause mortality and disabling stroke at 2 years -- was presented at the 2017 meeting of the American College of Cardiology and simultaneously published (N Engl J Med. 2017 Apr 6;376(14):1321-1331). The rate was 12.6% with TAVR using the self-expanding CoreValve or Evolut R bioprosthesis and noninferior at 14% with SAVR.
Dr. Kappetein presented a prespecified secondary analysis of the 30-day rate of all neurologic complications, including nondisabling strokes and encephalopathy. He and the other SURTAVI organizers felt this was an important outcome because these early neurologic events have a major impact upon quality of life, including whether a patient will be discharged home or to a rehabilitation clinic or skilled nursing facility following aortic valve replacement.
The 30-day incidence of all stroke was 3.3% in the TAVR patients, significantly lower than the 5.4% rate in the SAVR group. By the 2-year mark, however, the difference was no longer statistically significant, with a rate of 6.3% in the TAVR group compared with 8.0% with SAVR.
Ninety-five percent of the early strokes were ischemic.
The 30-day incidence of disabling stroke was 1.2% with TAVR and 2.4% with SAVR, a difference that was not significant (P=0.057). The 2-year rate was 2.4% in the TAVR arm and 4.5% with SAVR, again not significantly different.
Half of the strokes in the TAVR group had a modified Rankin score of 0-1 at 30 days, meaning no or only minimal signs of stroke. In contrast, most of the strokes in the SAVR group were disabling, with a modified Rankin score of 2-6.
Only 36% of patients who had an early stroke were discharged home, compared with 87% of patients without a stroke. Not surprisingly, quality of life as assessed using the SF-36 physical summary was significantly worse in the early-stroke group. However, with or without stroke, TAVR patients recovered quality of life faster than SAVR patients.
He noted that the timing of the early strokes differed between the two groups. The great majority of both disabling and nondisabling strokes in the TAVR patients were periprocedural, occurring on the day of TAVR or the next day. Strokes in the SAVR group occurred then as well, but also on days 2-6.
One reason why SURTAVI is the first study to show a lower stroke risk with TAVR is that it was the first TAVR-versus-SAVR study to feature comprehensive neurologic testing pre- and post-procedure, along with evaluation of all suspected events by a neurologist or stroke specialist, according to Dr. Kappetein.
“As surgeons we all have said the stroke rate after SAVR is 1%-1.5%, but only when the patient wasn’t waving to us the next morning would we say, ‘Oh, that patient may have a stroke.’ Then we would call a neurologist. So there were many more subtle strokes that we never actually detected. If you do a proper examination of the patient before and after the procedure you’ll find many more strokes,” he said.
He and his coinvestigators systematically searched in vain for predictors of increased stroke risk among the TAVR and SAVR patients.
“Actually, the stroke risk is present for every patient we treat with TAVR or SAVR,” the surgeon continued.
However, discussant Adnan Kastrati, MD, chief physician at the German Heart Center in Munich, thought he spied in the SURTAVI data a potential opportunity to reduce early strokes in SAVR patients. He noted that new-onset atrial fibrillation is consistently more common in SAVR than TAVR patients, and that many of the strokes in the SAVR group occurred on days 2-6. When do heart surgeons typically start oral anticoagulation in their patients with postsurgical atrial fibrillation? he asked.
Not until after 48 hours, Dr. Kappetein replied.
“Those strokes on days 4, 5, and 6 might have to do with atrial fibrillation, and we may need to be more aggressive as surgeons in anticoagulating patients with atrial fibrillation after surgery,” he said.
Dr. Kappetein reported receiving research grant support from Medtronic, sponsor of SURTAVI.
This article was updated July 28, 2107.
PARIS – Patients with severe aortic stenosis at intermediate operative risk have a significantly lower 30-day risk of stroke and other neurologic complications with transcatheter aortic valve replacement than with surgical replacement, according to new results from the landmark SURTAVI trial.
“This is the first time the stroke rate has been shown to be lower with TAVR than with surgery,” A. Pieter Kappetein, MD, noted in presenting the results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
It’s a finding that adds to the momentum for studying TAVR in low-surgical-risk patients, he added.
“As we move toward lower-risk patients it will become even more important to see whether there is a difference in stroke. Suppose the stroke rate in SURTAVI had been a little higher with TAVR than SAVR? It would really make us more cautious about moving toward lower-risk patients. Now that we see that in intermediate-risk patients the stroke rate is actually a little bit lower than with surgery, I think we’ll feel more comfortable moving toward lower-risk patients,” according to Dr. Kappetein, professor of cardiothoracic surgery at Erasmus University Medical Center in Rotterdam.
SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) involved randomization of 1,660 patients with severe symptomatic aortic stenosis to TAVR or SAVR. All participants were deemed to be at intermediate operative risk based upon a predicted surgical mortality of 3%-15%. The primary outcome -- a composite of all-cause mortality and disabling stroke at 2 years -- was presented at the 2017 meeting of the American College of Cardiology and simultaneously published (N Engl J Med. 2017 Apr 6;376(14):1321-1331). The rate was 12.6% with TAVR using the self-expanding CoreValve or Evolut R bioprosthesis and noninferior at 14% with SAVR.
Dr. Kappetein presented a prespecified secondary analysis of the 30-day rate of all neurologic complications, including nondisabling strokes and encephalopathy. He and the other SURTAVI organizers felt this was an important outcome because these early neurologic events have a major impact upon quality of life, including whether a patient will be discharged home or to a rehabilitation clinic or skilled nursing facility following aortic valve replacement.
The 30-day incidence of all stroke was 3.3% in the TAVR patients, significantly lower than the 5.4% rate in the SAVR group. By the 2-year mark, however, the difference was no longer statistically significant, with a rate of 6.3% in the TAVR group compared with 8.0% with SAVR.
Ninety-five percent of the early strokes were ischemic.
The 30-day incidence of disabling stroke was 1.2% with TAVR and 2.4% with SAVR, a difference that was not significant (P=0.057). The 2-year rate was 2.4% in the TAVR arm and 4.5% with SAVR, again not significantly different.
Half of the strokes in the TAVR group had a modified Rankin score of 0-1 at 30 days, meaning no or only minimal signs of stroke. In contrast, most of the strokes in the SAVR group were disabling, with a modified Rankin score of 2-6.
Only 36% of patients who had an early stroke were discharged home, compared with 87% of patients without a stroke. Not surprisingly, quality of life as assessed using the SF-36 physical summary was significantly worse in the early-stroke group. However, with or without stroke, TAVR patients recovered quality of life faster than SAVR patients.
He noted that the timing of the early strokes differed between the two groups. The great majority of both disabling and nondisabling strokes in the TAVR patients were periprocedural, occurring on the day of TAVR or the next day. Strokes in the SAVR group occurred then as well, but also on days 2-6.
One reason why SURTAVI is the first study to show a lower stroke risk with TAVR is that it was the first TAVR-versus-SAVR study to feature comprehensive neurologic testing pre- and post-procedure, along with evaluation of all suspected events by a neurologist or stroke specialist, according to Dr. Kappetein.
“As surgeons we all have said the stroke rate after SAVR is 1%-1.5%, but only when the patient wasn’t waving to us the next morning would we say, ‘Oh, that patient may have a stroke.’ Then we would call a neurologist. So there were many more subtle strokes that we never actually detected. If you do a proper examination of the patient before and after the procedure you’ll find many more strokes,” he said.
He and his coinvestigators systematically searched in vain for predictors of increased stroke risk among the TAVR and SAVR patients.
“Actually, the stroke risk is present for every patient we treat with TAVR or SAVR,” the surgeon continued.
However, discussant Adnan Kastrati, MD, chief physician at the German Heart Center in Munich, thought he spied in the SURTAVI data a potential opportunity to reduce early strokes in SAVR patients. He noted that new-onset atrial fibrillation is consistently more common in SAVR than TAVR patients, and that many of the strokes in the SAVR group occurred on days 2-6. When do heart surgeons typically start oral anticoagulation in their patients with postsurgical atrial fibrillation? he asked.
Not until after 48 hours, Dr. Kappetein replied.
“Those strokes on days 4, 5, and 6 might have to do with atrial fibrillation, and we may need to be more aggressive as surgeons in anticoagulating patients with atrial fibrillation after surgery,” he said.
Dr. Kappetein reported receiving research grant support from Medtronic, sponsor of SURTAVI.
This article was updated July 28, 2107.
PARIS – Patients with severe aortic stenosis at intermediate operative risk have a significantly lower 30-day risk of stroke and other neurologic complications with transcatheter aortic valve replacement than with surgical replacement, according to new results from the landmark SURTAVI trial.
“This is the first time the stroke rate has been shown to be lower with TAVR than with surgery,” A. Pieter Kappetein, MD, noted in presenting the results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
It’s a finding that adds to the momentum for studying TAVR in low-surgical-risk patients, he added.
“As we move toward lower-risk patients it will become even more important to see whether there is a difference in stroke. Suppose the stroke rate in SURTAVI had been a little higher with TAVR than SAVR? It would really make us more cautious about moving toward lower-risk patients. Now that we see that in intermediate-risk patients the stroke rate is actually a little bit lower than with surgery, I think we’ll feel more comfortable moving toward lower-risk patients,” according to Dr. Kappetein, professor of cardiothoracic surgery at Erasmus University Medical Center in Rotterdam.
SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) involved randomization of 1,660 patients with severe symptomatic aortic stenosis to TAVR or SAVR. All participants were deemed to be at intermediate operative risk based upon a predicted surgical mortality of 3%-15%. The primary outcome -- a composite of all-cause mortality and disabling stroke at 2 years -- was presented at the 2017 meeting of the American College of Cardiology and simultaneously published (N Engl J Med. 2017 Apr 6;376(14):1321-1331). The rate was 12.6% with TAVR using the self-expanding CoreValve or Evolut R bioprosthesis and noninferior at 14% with SAVR.
Dr. Kappetein presented a prespecified secondary analysis of the 30-day rate of all neurologic complications, including nondisabling strokes and encephalopathy. He and the other SURTAVI organizers felt this was an important outcome because these early neurologic events have a major impact upon quality of life, including whether a patient will be discharged home or to a rehabilitation clinic or skilled nursing facility following aortic valve replacement.
The 30-day incidence of all stroke was 3.3% in the TAVR patients, significantly lower than the 5.4% rate in the SAVR group. By the 2-year mark, however, the difference was no longer statistically significant, with a rate of 6.3% in the TAVR group compared with 8.0% with SAVR.
Ninety-five percent of the early strokes were ischemic.
The 30-day incidence of disabling stroke was 1.2% with TAVR and 2.4% with SAVR, a difference that was not significant (P=0.057). The 2-year rate was 2.4% in the TAVR arm and 4.5% with SAVR, again not significantly different.
Half of the strokes in the TAVR group had a modified Rankin score of 0-1 at 30 days, meaning no or only minimal signs of stroke. In contrast, most of the strokes in the SAVR group were disabling, with a modified Rankin score of 2-6.
Only 36% of patients who had an early stroke were discharged home, compared with 87% of patients without a stroke. Not surprisingly, quality of life as assessed using the SF-36 physical summary was significantly worse in the early-stroke group. However, with or without stroke, TAVR patients recovered quality of life faster than SAVR patients.
He noted that the timing of the early strokes differed between the two groups. The great majority of both disabling and nondisabling strokes in the TAVR patients were periprocedural, occurring on the day of TAVR or the next day. Strokes in the SAVR group occurred then as well, but also on days 2-6.
One reason why SURTAVI is the first study to show a lower stroke risk with TAVR is that it was the first TAVR-versus-SAVR study to feature comprehensive neurologic testing pre- and post-procedure, along with evaluation of all suspected events by a neurologist or stroke specialist, according to Dr. Kappetein.
“As surgeons we all have said the stroke rate after SAVR is 1%-1.5%, but only when the patient wasn’t waving to us the next morning would we say, ‘Oh, that patient may have a stroke.’ Then we would call a neurologist. So there were many more subtle strokes that we never actually detected. If you do a proper examination of the patient before and after the procedure you’ll find many more strokes,” he said.
He and his coinvestigators systematically searched in vain for predictors of increased stroke risk among the TAVR and SAVR patients.
“Actually, the stroke risk is present for every patient we treat with TAVR or SAVR,” the surgeon continued.
However, discussant Adnan Kastrati, MD, chief physician at the German Heart Center in Munich, thought he spied in the SURTAVI data a potential opportunity to reduce early strokes in SAVR patients. He noted that new-onset atrial fibrillation is consistently more common in SAVR than TAVR patients, and that many of the strokes in the SAVR group occurred on days 2-6. When do heart surgeons typically start oral anticoagulation in their patients with postsurgical atrial fibrillation? he asked.
Not until after 48 hours, Dr. Kappetein replied.
“Those strokes on days 4, 5, and 6 might have to do with atrial fibrillation, and we may need to be more aggressive as surgeons in anticoagulating patients with atrial fibrillation after surgery,” he said.
Dr. Kappetein reported receiving research grant support from Medtronic, sponsor of SURTAVI.
This article was updated July 28, 2107.
AT EUROPCR
Key clinical point:
Major finding: The combined incidence of disabling and nondisabling stroke within 30 days of TAVR was 3.3%, significantly better than the 5.4% rate in patients who underwent SAVR.
Data source: SURTAVI was a multicenter trial which included 1,660 patients with severe aortic stenosis who were at intermediate operative risk and were randomized to TAVR or SAVR.
Disclosures: The study presenter reported receiving research grant support from Medtronic, sponsor of the SURTAVI trial.
In 8 years, TMVR means more procedures
NEW YORK – Since the commercialization of transcatheter mitral valve repair, the share of these procedures among all mitral operations has grown exponentially and has also contributed to an increase in the number of overall mitral procedures, including surgical repair, according to an analysis of a national German database reported at the American Association for Thoracic Surgery Mitral Conclave here.
Transcatheter mitral valve repair (TMVR) using the MitraClip device (Abbott Vascular) was first commercialized in Germany in 2008, and in the years since the share of TMVR procedures among all mitral operations increased from 0.3% to 18.1% in 2015 throughout Germany, said Lenard Conradi, MD, surgical director of minimally-invasive and transcatheter heart valve procedures at the University Heart Center Hamburg.
The goal of the study was to gain insights into how cardiothoracic surgeons in Germany and at Dr. Conradi’s center in particular were approaching TMVR and what types of patients were having the procedure, Dr. Conradi said.
“While the EuroSCORE I of patients we operated on didn’t change at all between these two time frames, there were subtle changes in the patients that we operated on,” he said. “Before the commercialization of TMVR, we tended to have a ratio of organic vs. functional MR [mitral regurgitation] of 50-50; after commercialization of TMVR, many of the functional MR patients were allocated to TMVR.”
Dr. Conradi noted the profile of patients who had mitral valve repair also changed once the transcatheter approach became available. “Ischemic disease with coronary artery disease, previous infarction, or previous cardiac surgery – mostly coronary artery bypass grafting – were much less prevalent in this surgery population after TMVR became available,” he said.
The study also found that 30-day mortality declined from 7% to 4% during the study period. “That was probably due to more adequate patient selection because we had a more appropriate treatment that we could offer these high-risk patients as an alternative to high-risk surgical approaches,” Dr. Conradi said.
The analysis stratified procedure volumes and growth by four age groups: younger than 65 years; 65-74; 75-84; and greater than ore equal to 85. Older patients were more likely to have TMVR. Surgical procedure volumes increased most in the less than 65 group and least in the greater than or equal to 85 group.
In Germany, transcatheter mitral valve procedures are reimbursed at a higher rate than surgical procedures, but that doesn’t fully explain the uptake in TMVR, Dr. Conradi said. “The patients receiving the transcatheter approach vs. surgery still differ fundamentally, but the addition of an interventional program decreases the surgical patient’s mean risk profile and thus optimizes surgical results,” he said. “I think this can only happen if surgeons are closely involved. The indications will broaden for these therapies. There’s no doubt about that.”
Dr. Conradi disclosed receiving travel support and lecture fees from Abbott Vascular.
NEW YORK – Since the commercialization of transcatheter mitral valve repair, the share of these procedures among all mitral operations has grown exponentially and has also contributed to an increase in the number of overall mitral procedures, including surgical repair, according to an analysis of a national German database reported at the American Association for Thoracic Surgery Mitral Conclave here.
Transcatheter mitral valve repair (TMVR) using the MitraClip device (Abbott Vascular) was first commercialized in Germany in 2008, and in the years since the share of TMVR procedures among all mitral operations increased from 0.3% to 18.1% in 2015 throughout Germany, said Lenard Conradi, MD, surgical director of minimally-invasive and transcatheter heart valve procedures at the University Heart Center Hamburg.
The goal of the study was to gain insights into how cardiothoracic surgeons in Germany and at Dr. Conradi’s center in particular were approaching TMVR and what types of patients were having the procedure, Dr. Conradi said.
“While the EuroSCORE I of patients we operated on didn’t change at all between these two time frames, there were subtle changes in the patients that we operated on,” he said. “Before the commercialization of TMVR, we tended to have a ratio of organic vs. functional MR [mitral regurgitation] of 50-50; after commercialization of TMVR, many of the functional MR patients were allocated to TMVR.”
Dr. Conradi noted the profile of patients who had mitral valve repair also changed once the transcatheter approach became available. “Ischemic disease with coronary artery disease, previous infarction, or previous cardiac surgery – mostly coronary artery bypass grafting – were much less prevalent in this surgery population after TMVR became available,” he said.
The study also found that 30-day mortality declined from 7% to 4% during the study period. “That was probably due to more adequate patient selection because we had a more appropriate treatment that we could offer these high-risk patients as an alternative to high-risk surgical approaches,” Dr. Conradi said.
The analysis stratified procedure volumes and growth by four age groups: younger than 65 years; 65-74; 75-84; and greater than ore equal to 85. Older patients were more likely to have TMVR. Surgical procedure volumes increased most in the less than 65 group and least in the greater than or equal to 85 group.
In Germany, transcatheter mitral valve procedures are reimbursed at a higher rate than surgical procedures, but that doesn’t fully explain the uptake in TMVR, Dr. Conradi said. “The patients receiving the transcatheter approach vs. surgery still differ fundamentally, but the addition of an interventional program decreases the surgical patient’s mean risk profile and thus optimizes surgical results,” he said. “I think this can only happen if surgeons are closely involved. The indications will broaden for these therapies. There’s no doubt about that.”
Dr. Conradi disclosed receiving travel support and lecture fees from Abbott Vascular.
NEW YORK – Since the commercialization of transcatheter mitral valve repair, the share of these procedures among all mitral operations has grown exponentially and has also contributed to an increase in the number of overall mitral procedures, including surgical repair, according to an analysis of a national German database reported at the American Association for Thoracic Surgery Mitral Conclave here.
Transcatheter mitral valve repair (TMVR) using the MitraClip device (Abbott Vascular) was first commercialized in Germany in 2008, and in the years since the share of TMVR procedures among all mitral operations increased from 0.3% to 18.1% in 2015 throughout Germany, said Lenard Conradi, MD, surgical director of minimally-invasive and transcatheter heart valve procedures at the University Heart Center Hamburg.
The goal of the study was to gain insights into how cardiothoracic surgeons in Germany and at Dr. Conradi’s center in particular were approaching TMVR and what types of patients were having the procedure, Dr. Conradi said.
“While the EuroSCORE I of patients we operated on didn’t change at all between these two time frames, there were subtle changes in the patients that we operated on,” he said. “Before the commercialization of TMVR, we tended to have a ratio of organic vs. functional MR [mitral regurgitation] of 50-50; after commercialization of TMVR, many of the functional MR patients were allocated to TMVR.”
Dr. Conradi noted the profile of patients who had mitral valve repair also changed once the transcatheter approach became available. “Ischemic disease with coronary artery disease, previous infarction, or previous cardiac surgery – mostly coronary artery bypass grafting – were much less prevalent in this surgery population after TMVR became available,” he said.
The study also found that 30-day mortality declined from 7% to 4% during the study period. “That was probably due to more adequate patient selection because we had a more appropriate treatment that we could offer these high-risk patients as an alternative to high-risk surgical approaches,” Dr. Conradi said.
The analysis stratified procedure volumes and growth by four age groups: younger than 65 years; 65-74; 75-84; and greater than ore equal to 85. Older patients were more likely to have TMVR. Surgical procedure volumes increased most in the less than 65 group and least in the greater than or equal to 85 group.
In Germany, transcatheter mitral valve procedures are reimbursed at a higher rate than surgical procedures, but that doesn’t fully explain the uptake in TMVR, Dr. Conradi said. “The patients receiving the transcatheter approach vs. surgery still differ fundamentally, but the addition of an interventional program decreases the surgical patient’s mean risk profile and thus optimizes surgical results,” he said. “I think this can only happen if surgeons are closely involved. The indications will broaden for these therapies. There’s no doubt about that.”
Dr. Conradi disclosed receiving travel support and lecture fees from Abbott Vascular.
AT THE AATS MITRAL CONCLAVE 2017
Key clinical point: Since its commercialization, transcatheter mitral valve repair (TMVR) has accounted for an increasing share of all mitral surgeries in Germany and driven greater mitral surgery volume overall.
Major finding: Volume of surgical mitral valve procedures increased 70% overall and TMVR procedures 57% in Germany since 2008.
Data source: Analysis of data from German Federal statistics office.
Disclosures: Dr. Conradi reported receiving travel support and lecture fees from Abbott Vascular.
What’s driving the ‘failure’ of the ACA marketplaces?
Two reports from the Centers for Medicare & Medicaid Services show declines in the number of consumers who are activating the health insurance purchased via an Affordable Care Act exchange, a development Trump administration officials say underlines the failure of the ACA.

As of March 15, 10.3 million people paid premiums to activate coverage they purchased on the exchanges out of 12.2 million who enrolled in plans as of the Jan. 31 deadline for 2017, according to a June 12 report from CMS.
Further, some consumers who began paying premiums stopped.
Two key factors are behind the drop off, according to a second CMS report.
According to a voluntary online survey of consumers who left the exchanges between August 2016 and April 2017, 46% who canceled coverage prior to paying premiums cited cost as the main reason, including 20% who cited increased premiums over the previous year and 17% who claimed ineligibility for financial assistance.
Of those who activated their coverage by paying premiums, half (49%) said they stopped because they became eligible and received coverage elsewhere, mostly through an employer or Medicare. About a quarter (27%) cited affordability as the reason why they dropped coverage.
According to the Commonwealth Fund, CMS officials missed a few big reasons why people did not consistently pay for their coverage: Many were reacting to uncertainty around the Trump administration’s ACA repeal and replace efforts. Others were missed because of policy changes undertaken by the administration.
“One of the things that we know affected enrollment this year was the pullback of outreach efforts in the last weekend of the open enrollment period by the Trump administration,” Sara Collins, PhD, vice president of health care access and coverage at the Commonwealth Fund, said in an interview. “It did have an affect on enrollment and might be part of the reason why we are seeing – compared to last year – a lower effectuate enrollment.”
Other administration actions are taking a toll, Dr. Collins said.
There is a “general uncertainty that the administration is generating with respect to the enforcement of the individual mandate and also the uncertainty that is affecting insurers’ commitment to the marketplaces for 2018 [cost sharing reduction payments],” she said, noting both insurers and consumers are affected by this uncertainty.
While acknowledging that the main reason consumers dropped exchange policies was gaining coverage from source, Dr. Collins noted that “we are in such a strange environment, where it’s not clear what Congress is going to do or what the administration is going to do. It probably has confused the public somewhat about what their options are and maybe a concern even if they stay in a plan whether or not they will continue to get their tax credits. There has just been a general sense of uncertainty that has been created by the Trump administration and Congress in terms of the future of marketplace plans.”
Two reports from the Centers for Medicare & Medicaid Services show declines in the number of consumers who are activating the health insurance purchased via an Affordable Care Act exchange, a development Trump administration officials say underlines the failure of the ACA.
As of March 15, 10.3 million people paid premiums to activate coverage they purchased on the exchanges out of 12.2 million who enrolled in plans as of the Jan. 31 deadline for 2017, according to a June 12 report from CMS.
Further, some consumers who began paying premiums stopped.
Two key factors are behind the drop off, according to a second CMS report.
According to a voluntary online survey of consumers who left the exchanges between August 2016 and April 2017, 46% who canceled coverage prior to paying premiums cited cost as the main reason, including 20% who cited increased premiums over the previous year and 17% who claimed ineligibility for financial assistance.
Of those who activated their coverage by paying premiums, half (49%) said they stopped because they became eligible and received coverage elsewhere, mostly through an employer or Medicare. About a quarter (27%) cited affordability as the reason why they dropped coverage.
According to the Commonwealth Fund, CMS officials missed a few big reasons why people did not consistently pay for their coverage: Many were reacting to uncertainty around the Trump administration’s ACA repeal and replace efforts. Others were missed because of policy changes undertaken by the administration.
“One of the things that we know affected enrollment this year was the pullback of outreach efforts in the last weekend of the open enrollment period by the Trump administration,” Sara Collins, PhD, vice president of health care access and coverage at the Commonwealth Fund, said in an interview. “It did have an affect on enrollment and might be part of the reason why we are seeing – compared to last year – a lower effectuate enrollment.”
Other administration actions are taking a toll, Dr. Collins said.
There is a “general uncertainty that the administration is generating with respect to the enforcement of the individual mandate and also the uncertainty that is affecting insurers’ commitment to the marketplaces for 2018 [cost sharing reduction payments],” she said, noting both insurers and consumers are affected by this uncertainty.
While acknowledging that the main reason consumers dropped exchange policies was gaining coverage from source, Dr. Collins noted that “we are in such a strange environment, where it’s not clear what Congress is going to do or what the administration is going to do. It probably has confused the public somewhat about what their options are and maybe a concern even if they stay in a plan whether or not they will continue to get their tax credits. There has just been a general sense of uncertainty that has been created by the Trump administration and Congress in terms of the future of marketplace plans.”
Two reports from the Centers for Medicare & Medicaid Services show declines in the number of consumers who are activating the health insurance purchased via an Affordable Care Act exchange, a development Trump administration officials say underlines the failure of the ACA.
As of March 15, 10.3 million people paid premiums to activate coverage they purchased on the exchanges out of 12.2 million who enrolled in plans as of the Jan. 31 deadline for 2017, according to a June 12 report from CMS.
Further, some consumers who began paying premiums stopped.
Two key factors are behind the drop off, according to a second CMS report.
According to a voluntary online survey of consumers who left the exchanges between August 2016 and April 2017, 46% who canceled coverage prior to paying premiums cited cost as the main reason, including 20% who cited increased premiums over the previous year and 17% who claimed ineligibility for financial assistance.
Of those who activated their coverage by paying premiums, half (49%) said they stopped because they became eligible and received coverage elsewhere, mostly through an employer or Medicare. About a quarter (27%) cited affordability as the reason why they dropped coverage.
According to the Commonwealth Fund, CMS officials missed a few big reasons why people did not consistently pay for their coverage: Many were reacting to uncertainty around the Trump administration’s ACA repeal and replace efforts. Others were missed because of policy changes undertaken by the administration.
“One of the things that we know affected enrollment this year was the pullback of outreach efforts in the last weekend of the open enrollment period by the Trump administration,” Sara Collins, PhD, vice president of health care access and coverage at the Commonwealth Fund, said in an interview. “It did have an affect on enrollment and might be part of the reason why we are seeing – compared to last year – a lower effectuate enrollment.”
Other administration actions are taking a toll, Dr. Collins said.
There is a “general uncertainty that the administration is generating with respect to the enforcement of the individual mandate and also the uncertainty that is affecting insurers’ commitment to the marketplaces for 2018 [cost sharing reduction payments],” she said, noting both insurers and consumers are affected by this uncertainty.
While acknowledging that the main reason consumers dropped exchange policies was gaining coverage from source, Dr. Collins noted that “we are in such a strange environment, where it’s not clear what Congress is going to do or what the administration is going to do. It probably has confused the public somewhat about what their options are and maybe a concern even if they stay in a plan whether or not they will continue to get their tax credits. There has just been a general sense of uncertainty that has been created by the Trump administration and Congress in terms of the future of marketplace plans.”