User login
ED visits for life-threatening conditions declined early in COVID-19 pandemic
ED visits for myocardial infarction, stroke, and hyperglycemic crisis dropped substantially in the 10 weeks after COVID-19 was declared a national emergency on March 13, according to the Centers for Disease Control and Prevention.
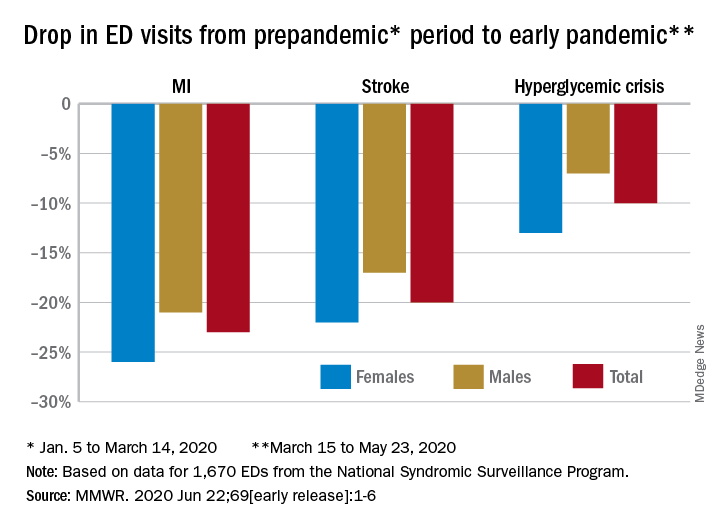
Compared with the 10-week period from Jan. 5 to March 14, ED visits were down by 23% for MI, 20% for stroke, and 10% for hyperglycemic crisis from March 15 to May 23, Samantha J. Lange, MPH, and associates at the CDC reported June 22 in the Morbidity and Mortality Weekly Report.
“A short-term decline of this magnitude … is biologically implausible for MI and stroke, especially for older adults, and unlikely for hyperglycemic crisis, and the finding suggests that patients with these conditions either could not access care or were delaying or avoiding seeking care during the early pandemic period,” they wrote.
The largest decreases in the actual number of visits for MI occurred among both men (down by 2,114, –24%) and women (down by 1,459, –25%) aged 65-74 years. For stroke, men aged 65-74 years had 1,406 (–19%) fewer visits to the ED and women 75-84 years had 1,642 (–23%) fewer visits, the CDC researchers said.
For hypoglycemic crisis, the largest declines during the early pandemic period occurred among younger adults: ED visits for men and women aged 18-44 years were down, respectively, by 419 (–8%) and 775 (–16%), they reported based on data from the National Syndromic Surveillance Program.
“Decreases in ED visits for hyperglycemic crisis might be less striking because patient recognition of this crisis is typically augmented by home glucose monitoring and not reliant upon symptoms alone, as is the case for MI and stroke,” Ms. Lange and her associates noted.
Charting weekly visit numbers showed that the drop for all three conditions actually started the week before the emergency was declared and reached its nadir the week after (March 22) for MI and 2 weeks later (March 29) for stroke and hypoglycemic crisis.
Visits for hypoglycemic crisis have largely returned to normal since those low points, but MI and stroke visits “remain below prepandemic levels” despite gradual increases through April and May, they said.
It has been reported that “deaths not associated with confirmed or probable COVID-19 might have been directly or indirectly attributed to the pandemic. The striking decline in ED visits for acute life-threatening conditions might partially explain observed excess mortality not associated with COVID-19,” the investigators wrote.
ED visits for myocardial infarction, stroke, and hyperglycemic crisis dropped substantially in the 10 weeks after COVID-19 was declared a national emergency on March 13, according to the Centers for Disease Control and Prevention.
Compared with the 10-week period from Jan. 5 to March 14, ED visits were down by 23% for MI, 20% for stroke, and 10% for hyperglycemic crisis from March 15 to May 23, Samantha J. Lange, MPH, and associates at the CDC reported June 22 in the Morbidity and Mortality Weekly Report.
“A short-term decline of this magnitude … is biologically implausible for MI and stroke, especially for older adults, and unlikely for hyperglycemic crisis, and the finding suggests that patients with these conditions either could not access care or were delaying or avoiding seeking care during the early pandemic period,” they wrote.
The largest decreases in the actual number of visits for MI occurred among both men (down by 2,114, –24%) and women (down by 1,459, –25%) aged 65-74 years. For stroke, men aged 65-74 years had 1,406 (–19%) fewer visits to the ED and women 75-84 years had 1,642 (–23%) fewer visits, the CDC researchers said.
For hypoglycemic crisis, the largest declines during the early pandemic period occurred among younger adults: ED visits for men and women aged 18-44 years were down, respectively, by 419 (–8%) and 775 (–16%), they reported based on data from the National Syndromic Surveillance Program.
“Decreases in ED visits for hyperglycemic crisis might be less striking because patient recognition of this crisis is typically augmented by home glucose monitoring and not reliant upon symptoms alone, as is the case for MI and stroke,” Ms. Lange and her associates noted.
Charting weekly visit numbers showed that the drop for all three conditions actually started the week before the emergency was declared and reached its nadir the week after (March 22) for MI and 2 weeks later (March 29) for stroke and hypoglycemic crisis.
Visits for hypoglycemic crisis have largely returned to normal since those low points, but MI and stroke visits “remain below prepandemic levels” despite gradual increases through April and May, they said.
It has been reported that “deaths not associated with confirmed or probable COVID-19 might have been directly or indirectly attributed to the pandemic. The striking decline in ED visits for acute life-threatening conditions might partially explain observed excess mortality not associated with COVID-19,” the investigators wrote.
ED visits for myocardial infarction, stroke, and hyperglycemic crisis dropped substantially in the 10 weeks after COVID-19 was declared a national emergency on March 13, according to the Centers for Disease Control and Prevention.
Compared with the 10-week period from Jan. 5 to March 14, ED visits were down by 23% for MI, 20% for stroke, and 10% for hyperglycemic crisis from March 15 to May 23, Samantha J. Lange, MPH, and associates at the CDC reported June 22 in the Morbidity and Mortality Weekly Report.
“A short-term decline of this magnitude … is biologically implausible for MI and stroke, especially for older adults, and unlikely for hyperglycemic crisis, and the finding suggests that patients with these conditions either could not access care or were delaying or avoiding seeking care during the early pandemic period,” they wrote.
The largest decreases in the actual number of visits for MI occurred among both men (down by 2,114, –24%) and women (down by 1,459, –25%) aged 65-74 years. For stroke, men aged 65-74 years had 1,406 (–19%) fewer visits to the ED and women 75-84 years had 1,642 (–23%) fewer visits, the CDC researchers said.
For hypoglycemic crisis, the largest declines during the early pandemic period occurred among younger adults: ED visits for men and women aged 18-44 years were down, respectively, by 419 (–8%) and 775 (–16%), they reported based on data from the National Syndromic Surveillance Program.
“Decreases in ED visits for hyperglycemic crisis might be less striking because patient recognition of this crisis is typically augmented by home glucose monitoring and not reliant upon symptoms alone, as is the case for MI and stroke,” Ms. Lange and her associates noted.
Charting weekly visit numbers showed that the drop for all three conditions actually started the week before the emergency was declared and reached its nadir the week after (March 22) for MI and 2 weeks later (March 29) for stroke and hypoglycemic crisis.
Visits for hypoglycemic crisis have largely returned to normal since those low points, but MI and stroke visits “remain below prepandemic levels” despite gradual increases through April and May, they said.
It has been reported that “deaths not associated with confirmed or probable COVID-19 might have been directly or indirectly attributed to the pandemic. The striking decline in ED visits for acute life-threatening conditions might partially explain observed excess mortality not associated with COVID-19,” the investigators wrote.
FROM MMWR
Social isolation tied to higher risk of cardiovascular events, death
“These results are especially important in the current times of social isolation during the coronavirus crisis,” Janine Gronewold, PhD, University Hospital in Essen, Germany, told a press briefing.
The mechanism by which social isolation may boost risk for stroke, MI, or death is not clear, but other research has shown that loneliness or lack of contact with close friends and family can affect physical health, said Dr. Gronewold.
The findings were presented at the sixth Congress of the European Academy of Neurology (EAN) 2020, which transitioned to a virtual/online meeting because of the COVID-19 pandemic.
For this new study, researchers analyzed data from 4,139 participants, ranging in age from 45 to 75 years (mean 59.1 years), who were recruited into the large community-based Heinz Nixdorf Recall study. The randomly selected study group was representative of an industrial rural area of Germany, said Dr. Gronewold.
Study participants entered the study with no known cardiovascular disease and were followed for a mean of 13.4 years.
Social supports
Investigators collected information on three types of social support: instrumental (getting help with everyday activities such as buying food), emotional (provided with comfort), and financial (receiving monetary assistance when needed). They also looked at social integration (or social isolation) using an index with scores for marital status, number of contacts with family and friends, and membership in political, religious, community, sports, or professional associations.
Of the total, 501 participants reported a lack of instrumental support, 659 a lack of emotional support, and 907 a lack of financial support. A total of 309 lacked social integration, defined by the lowest level on the social integration index.
Participants were asked annually about new cardiovascular events, including stroke and MI. Over the follow-up period, there were 339 such events and 530 deaths.
After adjustment for age, sex, and social support, the analysis showed that social isolation was significantly associated with an increased risk of cardiovascular events (hazard ratio, 1.44; 95% confidence interval, 0.97-2.14) and all-cause mortality (HR, 1.47; 95% CI, 1.09-1.97).
The new research also showed that lack of financial support was significantly associated with increased risk for a cardiovascular event (HR, 1.30; 95% CI, 1.01-1.67).
Direct effect
Additional models that also adjusted for cardiovascular risk factors, health behaviors, depression, and socioeconomic factors, did not significantly change effect estimates.
“Social relationships protect us from cardiovascular events and mortality, not only via good mood, healthy behavior, and lower cardiovascular risk profile,” Dr. Gronewold said. “They seem to have a direct effect on these outcomes.”
Having strong social relationships is as important to cardiovascular health as classic protective factors such as controlling blood pressure and cholesterol levels, and maintaining a normal weight, said Dr. Gronewold.
The new results are worrying and are particularly important during the current COVID-19 pandemic, as social contact has been restricted in many areas, said Dr. Gronewold.
It is not yet clear why people who are socially isolated have such poor health outcomes, she added.
Dr. Gronewold has reported no relevant financial relationships.
This article first appeared on Medscape.com.
“These results are especially important in the current times of social isolation during the coronavirus crisis,” Janine Gronewold, PhD, University Hospital in Essen, Germany, told a press briefing.
The mechanism by which social isolation may boost risk for stroke, MI, or death is not clear, but other research has shown that loneliness or lack of contact with close friends and family can affect physical health, said Dr. Gronewold.
The findings were presented at the sixth Congress of the European Academy of Neurology (EAN) 2020, which transitioned to a virtual/online meeting because of the COVID-19 pandemic.
For this new study, researchers analyzed data from 4,139 participants, ranging in age from 45 to 75 years (mean 59.1 years), who were recruited into the large community-based Heinz Nixdorf Recall study. The randomly selected study group was representative of an industrial rural area of Germany, said Dr. Gronewold.
Study participants entered the study with no known cardiovascular disease and were followed for a mean of 13.4 years.
Social supports
Investigators collected information on three types of social support: instrumental (getting help with everyday activities such as buying food), emotional (provided with comfort), and financial (receiving monetary assistance when needed). They also looked at social integration (or social isolation) using an index with scores for marital status, number of contacts with family and friends, and membership in political, religious, community, sports, or professional associations.
Of the total, 501 participants reported a lack of instrumental support, 659 a lack of emotional support, and 907 a lack of financial support. A total of 309 lacked social integration, defined by the lowest level on the social integration index.
Participants were asked annually about new cardiovascular events, including stroke and MI. Over the follow-up period, there were 339 such events and 530 deaths.
After adjustment for age, sex, and social support, the analysis showed that social isolation was significantly associated with an increased risk of cardiovascular events (hazard ratio, 1.44; 95% confidence interval, 0.97-2.14) and all-cause mortality (HR, 1.47; 95% CI, 1.09-1.97).
The new research also showed that lack of financial support was significantly associated with increased risk for a cardiovascular event (HR, 1.30; 95% CI, 1.01-1.67).
Direct effect
Additional models that also adjusted for cardiovascular risk factors, health behaviors, depression, and socioeconomic factors, did not significantly change effect estimates.
“Social relationships protect us from cardiovascular events and mortality, not only via good mood, healthy behavior, and lower cardiovascular risk profile,” Dr. Gronewold said. “They seem to have a direct effect on these outcomes.”
Having strong social relationships is as important to cardiovascular health as classic protective factors such as controlling blood pressure and cholesterol levels, and maintaining a normal weight, said Dr. Gronewold.
The new results are worrying and are particularly important during the current COVID-19 pandemic, as social contact has been restricted in many areas, said Dr. Gronewold.
It is not yet clear why people who are socially isolated have such poor health outcomes, she added.
Dr. Gronewold has reported no relevant financial relationships.
This article first appeared on Medscape.com.
“These results are especially important in the current times of social isolation during the coronavirus crisis,” Janine Gronewold, PhD, University Hospital in Essen, Germany, told a press briefing.
The mechanism by which social isolation may boost risk for stroke, MI, or death is not clear, but other research has shown that loneliness or lack of contact with close friends and family can affect physical health, said Dr. Gronewold.
The findings were presented at the sixth Congress of the European Academy of Neurology (EAN) 2020, which transitioned to a virtual/online meeting because of the COVID-19 pandemic.
For this new study, researchers analyzed data from 4,139 participants, ranging in age from 45 to 75 years (mean 59.1 years), who were recruited into the large community-based Heinz Nixdorf Recall study. The randomly selected study group was representative of an industrial rural area of Germany, said Dr. Gronewold.
Study participants entered the study with no known cardiovascular disease and were followed for a mean of 13.4 years.
Social supports
Investigators collected information on three types of social support: instrumental (getting help with everyday activities such as buying food), emotional (provided with comfort), and financial (receiving monetary assistance when needed). They also looked at social integration (or social isolation) using an index with scores for marital status, number of contacts with family and friends, and membership in political, religious, community, sports, or professional associations.
Of the total, 501 participants reported a lack of instrumental support, 659 a lack of emotional support, and 907 a lack of financial support. A total of 309 lacked social integration, defined by the lowest level on the social integration index.
Participants were asked annually about new cardiovascular events, including stroke and MI. Over the follow-up period, there were 339 such events and 530 deaths.
After adjustment for age, sex, and social support, the analysis showed that social isolation was significantly associated with an increased risk of cardiovascular events (hazard ratio, 1.44; 95% confidence interval, 0.97-2.14) and all-cause mortality (HR, 1.47; 95% CI, 1.09-1.97).
The new research also showed that lack of financial support was significantly associated with increased risk for a cardiovascular event (HR, 1.30; 95% CI, 1.01-1.67).
Direct effect
Additional models that also adjusted for cardiovascular risk factors, health behaviors, depression, and socioeconomic factors, did not significantly change effect estimates.
“Social relationships protect us from cardiovascular events and mortality, not only via good mood, healthy behavior, and lower cardiovascular risk profile,” Dr. Gronewold said. “They seem to have a direct effect on these outcomes.”
Having strong social relationships is as important to cardiovascular health as classic protective factors such as controlling blood pressure and cholesterol levels, and maintaining a normal weight, said Dr. Gronewold.
The new results are worrying and are particularly important during the current COVID-19 pandemic, as social contact has been restricted in many areas, said Dr. Gronewold.
It is not yet clear why people who are socially isolated have such poor health outcomes, she added.
Dr. Gronewold has reported no relevant financial relationships.
This article first appeared on Medscape.com.
FROM EAN 2020
AHA offers advice on prehospital acute stroke triage amid COVID-19
A key goal is to ensure timely transfer of patients while minimizing the risk of infectious exposure for EMS personnel, coworkers, and other patients, the writing group says.
“Acute ischemic stroke is still a highly devastating disease and the Time Is Brain paradigm remains true during the COVID-19 pandemic as well,” said writing group chair Mayank Goyal, MD, of the University of Calgary (Alta.)
“We have highly effective and proven treatments available. As such, treatment delays due to additional screening requirements and personal protection equipment (PPE) should be kept at a minimum,” Dr. Goyal said.
“Practicing COVID-19 stroke work flows, through simulation training, can help to reduce treatment delays, minimize the risk of infectious exposure for patients and staff, and help alleviate stress,” he added.
A new layer of complexity
The guidance statement, Prehospital Triage of Acute Stroke Patients During the COVID-19 Pandemic, was published online May 13 in the journal Stroke.
“The need to limit infectious spread during the COVID-19 pandemic has added a new layer of complexity to prehospital stroke triage and transfer,” the writing group noted. “Timely and enhanced” communication between EMS, hospitals, and local coordinating authorities are critical, especially ambulance-and facility-based telestroke networks, they wrote.
The main factors to guide the triage decision are the likelihood of a large vessel occlusion; the magnitude of additional delays because of interhospital transfer and work flow efficiency at the primary stroke center or acute stroke ready hospital; the need for advanced critical care resources; and the available bed, staff, and PPE resources at the hospitals.
The group said it “seems reasonable” to lower the threshold to bypass hospitals that can’t provide acute stroke treatment in favor of transporting to a hospital that is “stroke ready,” particularly in patients likely to require advanced care. They cautioned, however, that taking all acute stroke patients to a comprehensive stroke center could overwhelm these centers and lead to clustering of COVID-19 patients.
They said it is equally important to ensure “necessary transfers” of stroke patients who would benefit from endovascular therapy or neurocritical care and avoid unnecessary patient transfers. “Doing so will likely require local hospital boards and health care authorities to collaborate and establish local guidelines and protocols,” the writing group said.
“During the COVID-19 pandemic, it is more important than ever to ensure that stroke patients are taken to the right hospital that can meet their urgent needs at the outset,” Dr. Goyal commented in an AHA news release.
The writing group emphasized that the principles put forth in the document are intended as suggestions rather than strict rules and will be adapted and updated to meet the evolving needs during the COVID-19 crisis and future pandemics.
“The process of improving stroke work flow and getting the correct patient to the correct hospital fast is dependent on training, protocols, simulation, technology, and – probably most importantly – teamwork. These principles are extremely important during the current pandemic but will be useful in improving stroke care afterwards as well,” Dr. Goyal said.
This research had no commercial funding. Members of the writing committee are on several AHA/ASA Council Science Subcommittees, including the Emergency Neurovascular Care, the Telestroke, and the Neurovascular Intervention committees. Goyal is a consultant for Medtronic, Stryker, Microvention, GE Healthcare, and Mentice. A complete list of author disclosures is available with the original article.
This article first appeared on Medscape.com.
A key goal is to ensure timely transfer of patients while minimizing the risk of infectious exposure for EMS personnel, coworkers, and other patients, the writing group says.
“Acute ischemic stroke is still a highly devastating disease and the Time Is Brain paradigm remains true during the COVID-19 pandemic as well,” said writing group chair Mayank Goyal, MD, of the University of Calgary (Alta.)
“We have highly effective and proven treatments available. As such, treatment delays due to additional screening requirements and personal protection equipment (PPE) should be kept at a minimum,” Dr. Goyal said.
“Practicing COVID-19 stroke work flows, through simulation training, can help to reduce treatment delays, minimize the risk of infectious exposure for patients and staff, and help alleviate stress,” he added.
A new layer of complexity
The guidance statement, Prehospital Triage of Acute Stroke Patients During the COVID-19 Pandemic, was published online May 13 in the journal Stroke.
“The need to limit infectious spread during the COVID-19 pandemic has added a new layer of complexity to prehospital stroke triage and transfer,” the writing group noted. “Timely and enhanced” communication between EMS, hospitals, and local coordinating authorities are critical, especially ambulance-and facility-based telestroke networks, they wrote.
The main factors to guide the triage decision are the likelihood of a large vessel occlusion; the magnitude of additional delays because of interhospital transfer and work flow efficiency at the primary stroke center or acute stroke ready hospital; the need for advanced critical care resources; and the available bed, staff, and PPE resources at the hospitals.
The group said it “seems reasonable” to lower the threshold to bypass hospitals that can’t provide acute stroke treatment in favor of transporting to a hospital that is “stroke ready,” particularly in patients likely to require advanced care. They cautioned, however, that taking all acute stroke patients to a comprehensive stroke center could overwhelm these centers and lead to clustering of COVID-19 patients.
They said it is equally important to ensure “necessary transfers” of stroke patients who would benefit from endovascular therapy or neurocritical care and avoid unnecessary patient transfers. “Doing so will likely require local hospital boards and health care authorities to collaborate and establish local guidelines and protocols,” the writing group said.
“During the COVID-19 pandemic, it is more important than ever to ensure that stroke patients are taken to the right hospital that can meet their urgent needs at the outset,” Dr. Goyal commented in an AHA news release.
The writing group emphasized that the principles put forth in the document are intended as suggestions rather than strict rules and will be adapted and updated to meet the evolving needs during the COVID-19 crisis and future pandemics.
“The process of improving stroke work flow and getting the correct patient to the correct hospital fast is dependent on training, protocols, simulation, technology, and – probably most importantly – teamwork. These principles are extremely important during the current pandemic but will be useful in improving stroke care afterwards as well,” Dr. Goyal said.
This research had no commercial funding. Members of the writing committee are on several AHA/ASA Council Science Subcommittees, including the Emergency Neurovascular Care, the Telestroke, and the Neurovascular Intervention committees. Goyal is a consultant for Medtronic, Stryker, Microvention, GE Healthcare, and Mentice. A complete list of author disclosures is available with the original article.
This article first appeared on Medscape.com.
A key goal is to ensure timely transfer of patients while minimizing the risk of infectious exposure for EMS personnel, coworkers, and other patients, the writing group says.
“Acute ischemic stroke is still a highly devastating disease and the Time Is Brain paradigm remains true during the COVID-19 pandemic as well,” said writing group chair Mayank Goyal, MD, of the University of Calgary (Alta.)
“We have highly effective and proven treatments available. As such, treatment delays due to additional screening requirements and personal protection equipment (PPE) should be kept at a minimum,” Dr. Goyal said.
“Practicing COVID-19 stroke work flows, through simulation training, can help to reduce treatment delays, minimize the risk of infectious exposure for patients and staff, and help alleviate stress,” he added.
A new layer of complexity
The guidance statement, Prehospital Triage of Acute Stroke Patients During the COVID-19 Pandemic, was published online May 13 in the journal Stroke.
“The need to limit infectious spread during the COVID-19 pandemic has added a new layer of complexity to prehospital stroke triage and transfer,” the writing group noted. “Timely and enhanced” communication between EMS, hospitals, and local coordinating authorities are critical, especially ambulance-and facility-based telestroke networks, they wrote.
The main factors to guide the triage decision are the likelihood of a large vessel occlusion; the magnitude of additional delays because of interhospital transfer and work flow efficiency at the primary stroke center or acute stroke ready hospital; the need for advanced critical care resources; and the available bed, staff, and PPE resources at the hospitals.
The group said it “seems reasonable” to lower the threshold to bypass hospitals that can’t provide acute stroke treatment in favor of transporting to a hospital that is “stroke ready,” particularly in patients likely to require advanced care. They cautioned, however, that taking all acute stroke patients to a comprehensive stroke center could overwhelm these centers and lead to clustering of COVID-19 patients.
They said it is equally important to ensure “necessary transfers” of stroke patients who would benefit from endovascular therapy or neurocritical care and avoid unnecessary patient transfers. “Doing so will likely require local hospital boards and health care authorities to collaborate and establish local guidelines and protocols,” the writing group said.
“During the COVID-19 pandemic, it is more important than ever to ensure that stroke patients are taken to the right hospital that can meet their urgent needs at the outset,” Dr. Goyal commented in an AHA news release.
The writing group emphasized that the principles put forth in the document are intended as suggestions rather than strict rules and will be adapted and updated to meet the evolving needs during the COVID-19 crisis and future pandemics.
“The process of improving stroke work flow and getting the correct patient to the correct hospital fast is dependent on training, protocols, simulation, technology, and – probably most importantly – teamwork. These principles are extremely important during the current pandemic but will be useful in improving stroke care afterwards as well,” Dr. Goyal said.
This research had no commercial funding. Members of the writing committee are on several AHA/ASA Council Science Subcommittees, including the Emergency Neurovascular Care, the Telestroke, and the Neurovascular Intervention committees. Goyal is a consultant for Medtronic, Stryker, Microvention, GE Healthcare, and Mentice. A complete list of author disclosures is available with the original article.
This article first appeared on Medscape.com.
New ‘atlas’ maps links between mental disorders, physical illnesses
Mental illnesses are associated with a significantly increased risk of subsequent physical diseases, new research shows.
An international team of researchers has created an “atlas” that maps the relationship between specific mental disorders and the risk of subsequent physical illnesses.
The researchers found that, following the diagnosis of a mental disorder, psychiatric patients are significantly more likely than the general population to develop potentially life-threatening conditions, including heart disease and stroke.
These findings, the investigators noted, highlight the need for better medical care in this vulnerable population. They have created a website with detailed information about the risks of specific physical ailments and the link to particular mental disorders.
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke – over 15 years, one in three women with anxiety disorders will develop these medical disorders,” lead investigator John McGrath, MD, PhD, University of Queensland’s Brain Institute, Brisbane, Australia, and Aarhus (Denmark) University, said in a statement.
“We also looked at men with substance use disorders such as alcohol-related disorders and found they have a 400% increased risk of gut or liver disorders, while over 15 years, one in five of them will develop gut or liver conditions,” he added.
The study was published in the New England Journal of Medicine.
New ‘atlas’
It’s well known that patients with mental disorders have decreased quality of life, increased health care utilization, and a shorter life expectancy than individuals in the general population – about 10 years for men and 7 years for women.
However, the investigators noted, previous research examining the relationship between mental disorders and medical conditions only focused on “particular pairs or a small set of mental disorders and medical conditions.”
“We needed a comprehensive study to map the links between different types of mental disorders versus different types of general medical conditions. Our study has provided this atlas,” Dr. McGrath said in an interview.
The clinical utility of such a map could provide comprehensive data on relative and absolute risks of various medical conditions after a diagnosis of a mental disorder. This information, the researchers noted, would “help clinicians and health care planners identify the primary prevention needs of their patients.”
The study included 5.9 million people born in Denmark between 1900 and 2015 and followed them from 2000 to 2016, a total of 83.9 million person-years. The researchers followed patients for up to 17 years (2000-2016) for medical diagnoses and up to 48 years (1969-2016) for diagnoses of mental disorders.
The study’s large sample size allowed investigators to assess 10 broad types of mental disorders and 9 broad categories of medical conditions that encompassed 31 specific conditions.
Categories of medical conditions included circulatory, endocrine, pulmonary, gastrointestinal, urogenital, musculoskeletal, hematologic, neurologic, and cancer. Mental disorder categories included organic disorders such as Alzheimer’s, substance abuse disorders, schizophrenia, mood disorders, neurotic disorders, eating disorders, personality disorders, developmental disorders, behavioral/emotional disorders, and intellectual disabilities.
The researchers estimated associations between 90 pairs of mental disorders and broad-category medical conditions, as well as 310 pairs of mental disorders and specific medical conditions.
‘Curious’ finding
Individuals with mental disorders showed a higher risk of medical conditions in 76 out of 90 specific mental disorder–medical condition pairs.
After adjusting for sex, age, calendar time, and previous coexisting mental disorders, the median hazard ratio for a subsequent medical condition was 1.37 in patients with a mental disorder.
The lowest HR was 0.82 for organic mental disorders and the broad category of cancer (95% confidence interval, 0.80-0.84), and the highest was 3.62 for eating disorders and urogenital conditions (95% CI, 3.11-4.22). On the other hand, schizophrenia was associated with a reduced risk of developing musculoskeletal conditions (HR, 0.87; 95% CI, 0.84-0.91).
Dr. McGrath described this finding as “curious” and speculated it “may be related to underlying genetic risk factors.”
compared with the matched reference group without a mood disorder (40.9% vs. 32.6%, respectively).
The risk of developing subsequent medical conditions after a mental disorder diagnosis did not remain steady over time. For instance, although mood disorders were associated with an increased risk of developing circulatory problems (HR, 1.32; 95% CI, 1.31-1.34), the highest risk occurred during the first 6 months following diagnosis and gradually decreased over the next 15 years (HR, 2.39; 95% CI, 2.29-2.48 and HR, 1.18; 95% CI, 1.17-1.20, respectively).
“Many people with mental disorders have unhealthy lifestyle, including low exercise, poor diet, smoking, and alcohol, which may account for the increased risk of physical illness, and also they may not seek and/or may not get quick treatment for their health conditions,” said Dr. McGrath.
Additionally, “perhaps some genetic and early life exposures, such as trauma, may increase the risk of both medical conditions and mental disorders,” he added. “We need better treatments for mental disorders, so that they do not slip into unemployment or poverty.”
A strong case
In a comment, Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto and head of the mood disorders psychopharmacology unit, University Health Network, said that the research “really makes a strong case for the fact that persons who have mental disorders are at higher risk of chronic diseases, and it’s the chronic diseases that decrease their lifespan.”
Dr. McIntyre, who is also director of the Depression and Bipolar Support Alliance, said that the “takeaway message is that mental disorders are not just brain disorders but are multisystem disorders.”
For this reason, “the most appropriate way to provide care would be to provide a holistic approach to treat and prevent the chronic diseases that lead to increase in mortality,” recommended Dr. McIntyre, who was not involved with the current study.
The study was supported by grants from the Danish National Research Foundation, the National Health and Medical Research Council, the Novo Nordisk Foundation , the European Union’s Horizon 2020 Research and Innovation Program, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the European Commission, Helsefonden, the Danish Council for Independent Research, the Independent Research Fund Denmark, the National Health and Medical Research Council of Australia, and the National Institute on Drug Abuse.
Dr. McGrath has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. McIntyre reports receiving grants from Stanley Medical Research Institute; the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation; and receiving speaking/consultation fees from Lundbeck, Janssen, Shire, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, and Minerva.
A version of this article originally appeared on Medscape.com.
Mental illnesses are associated with a significantly increased risk of subsequent physical diseases, new research shows.
An international team of researchers has created an “atlas” that maps the relationship between specific mental disorders and the risk of subsequent physical illnesses.
The researchers found that, following the diagnosis of a mental disorder, psychiatric patients are significantly more likely than the general population to develop potentially life-threatening conditions, including heart disease and stroke.
These findings, the investigators noted, highlight the need for better medical care in this vulnerable population. They have created a website with detailed information about the risks of specific physical ailments and the link to particular mental disorders.
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke – over 15 years, one in three women with anxiety disorders will develop these medical disorders,” lead investigator John McGrath, MD, PhD, University of Queensland’s Brain Institute, Brisbane, Australia, and Aarhus (Denmark) University, said in a statement.
“We also looked at men with substance use disorders such as alcohol-related disorders and found they have a 400% increased risk of gut or liver disorders, while over 15 years, one in five of them will develop gut or liver conditions,” he added.
The study was published in the New England Journal of Medicine.
New ‘atlas’
It’s well known that patients with mental disorders have decreased quality of life, increased health care utilization, and a shorter life expectancy than individuals in the general population – about 10 years for men and 7 years for women.
However, the investigators noted, previous research examining the relationship between mental disorders and medical conditions only focused on “particular pairs or a small set of mental disorders and medical conditions.”
“We needed a comprehensive study to map the links between different types of mental disorders versus different types of general medical conditions. Our study has provided this atlas,” Dr. McGrath said in an interview.
The clinical utility of such a map could provide comprehensive data on relative and absolute risks of various medical conditions after a diagnosis of a mental disorder. This information, the researchers noted, would “help clinicians and health care planners identify the primary prevention needs of their patients.”
The study included 5.9 million people born in Denmark between 1900 and 2015 and followed them from 2000 to 2016, a total of 83.9 million person-years. The researchers followed patients for up to 17 years (2000-2016) for medical diagnoses and up to 48 years (1969-2016) for diagnoses of mental disorders.
The study’s large sample size allowed investigators to assess 10 broad types of mental disorders and 9 broad categories of medical conditions that encompassed 31 specific conditions.
Categories of medical conditions included circulatory, endocrine, pulmonary, gastrointestinal, urogenital, musculoskeletal, hematologic, neurologic, and cancer. Mental disorder categories included organic disorders such as Alzheimer’s, substance abuse disorders, schizophrenia, mood disorders, neurotic disorders, eating disorders, personality disorders, developmental disorders, behavioral/emotional disorders, and intellectual disabilities.
The researchers estimated associations between 90 pairs of mental disorders and broad-category medical conditions, as well as 310 pairs of mental disorders and specific medical conditions.
‘Curious’ finding
Individuals with mental disorders showed a higher risk of medical conditions in 76 out of 90 specific mental disorder–medical condition pairs.
After adjusting for sex, age, calendar time, and previous coexisting mental disorders, the median hazard ratio for a subsequent medical condition was 1.37 in patients with a mental disorder.
The lowest HR was 0.82 for organic mental disorders and the broad category of cancer (95% confidence interval, 0.80-0.84), and the highest was 3.62 for eating disorders and urogenital conditions (95% CI, 3.11-4.22). On the other hand, schizophrenia was associated with a reduced risk of developing musculoskeletal conditions (HR, 0.87; 95% CI, 0.84-0.91).
Dr. McGrath described this finding as “curious” and speculated it “may be related to underlying genetic risk factors.”
compared with the matched reference group without a mood disorder (40.9% vs. 32.6%, respectively).
The risk of developing subsequent medical conditions after a mental disorder diagnosis did not remain steady over time. For instance, although mood disorders were associated with an increased risk of developing circulatory problems (HR, 1.32; 95% CI, 1.31-1.34), the highest risk occurred during the first 6 months following diagnosis and gradually decreased over the next 15 years (HR, 2.39; 95% CI, 2.29-2.48 and HR, 1.18; 95% CI, 1.17-1.20, respectively).
“Many people with mental disorders have unhealthy lifestyle, including low exercise, poor diet, smoking, and alcohol, which may account for the increased risk of physical illness, and also they may not seek and/or may not get quick treatment for their health conditions,” said Dr. McGrath.
Additionally, “perhaps some genetic and early life exposures, such as trauma, may increase the risk of both medical conditions and mental disorders,” he added. “We need better treatments for mental disorders, so that they do not slip into unemployment or poverty.”
A strong case
In a comment, Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto and head of the mood disorders psychopharmacology unit, University Health Network, said that the research “really makes a strong case for the fact that persons who have mental disorders are at higher risk of chronic diseases, and it’s the chronic diseases that decrease their lifespan.”
Dr. McIntyre, who is also director of the Depression and Bipolar Support Alliance, said that the “takeaway message is that mental disorders are not just brain disorders but are multisystem disorders.”
For this reason, “the most appropriate way to provide care would be to provide a holistic approach to treat and prevent the chronic diseases that lead to increase in mortality,” recommended Dr. McIntyre, who was not involved with the current study.
The study was supported by grants from the Danish National Research Foundation, the National Health and Medical Research Council, the Novo Nordisk Foundation , the European Union’s Horizon 2020 Research and Innovation Program, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the European Commission, Helsefonden, the Danish Council for Independent Research, the Independent Research Fund Denmark, the National Health and Medical Research Council of Australia, and the National Institute on Drug Abuse.
Dr. McGrath has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. McIntyre reports receiving grants from Stanley Medical Research Institute; the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation; and receiving speaking/consultation fees from Lundbeck, Janssen, Shire, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, and Minerva.
A version of this article originally appeared on Medscape.com.
Mental illnesses are associated with a significantly increased risk of subsequent physical diseases, new research shows.
An international team of researchers has created an “atlas” that maps the relationship between specific mental disorders and the risk of subsequent physical illnesses.
The researchers found that, following the diagnosis of a mental disorder, psychiatric patients are significantly more likely than the general population to develop potentially life-threatening conditions, including heart disease and stroke.
These findings, the investigators noted, highlight the need for better medical care in this vulnerable population. They have created a website with detailed information about the risks of specific physical ailments and the link to particular mental disorders.
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke – over 15 years, one in three women with anxiety disorders will develop these medical disorders,” lead investigator John McGrath, MD, PhD, University of Queensland’s Brain Institute, Brisbane, Australia, and Aarhus (Denmark) University, said in a statement.
“We also looked at men with substance use disorders such as alcohol-related disorders and found they have a 400% increased risk of gut or liver disorders, while over 15 years, one in five of them will develop gut or liver conditions,” he added.
The study was published in the New England Journal of Medicine.
New ‘atlas’
It’s well known that patients with mental disorders have decreased quality of life, increased health care utilization, and a shorter life expectancy than individuals in the general population – about 10 years for men and 7 years for women.
However, the investigators noted, previous research examining the relationship between mental disorders and medical conditions only focused on “particular pairs or a small set of mental disorders and medical conditions.”
“We needed a comprehensive study to map the links between different types of mental disorders versus different types of general medical conditions. Our study has provided this atlas,” Dr. McGrath said in an interview.
The clinical utility of such a map could provide comprehensive data on relative and absolute risks of various medical conditions after a diagnosis of a mental disorder. This information, the researchers noted, would “help clinicians and health care planners identify the primary prevention needs of their patients.”
The study included 5.9 million people born in Denmark between 1900 and 2015 and followed them from 2000 to 2016, a total of 83.9 million person-years. The researchers followed patients for up to 17 years (2000-2016) for medical diagnoses and up to 48 years (1969-2016) for diagnoses of mental disorders.
The study’s large sample size allowed investigators to assess 10 broad types of mental disorders and 9 broad categories of medical conditions that encompassed 31 specific conditions.
Categories of medical conditions included circulatory, endocrine, pulmonary, gastrointestinal, urogenital, musculoskeletal, hematologic, neurologic, and cancer. Mental disorder categories included organic disorders such as Alzheimer’s, substance abuse disorders, schizophrenia, mood disorders, neurotic disorders, eating disorders, personality disorders, developmental disorders, behavioral/emotional disorders, and intellectual disabilities.
The researchers estimated associations between 90 pairs of mental disorders and broad-category medical conditions, as well as 310 pairs of mental disorders and specific medical conditions.
‘Curious’ finding
Individuals with mental disorders showed a higher risk of medical conditions in 76 out of 90 specific mental disorder–medical condition pairs.
After adjusting for sex, age, calendar time, and previous coexisting mental disorders, the median hazard ratio for a subsequent medical condition was 1.37 in patients with a mental disorder.
The lowest HR was 0.82 for organic mental disorders and the broad category of cancer (95% confidence interval, 0.80-0.84), and the highest was 3.62 for eating disorders and urogenital conditions (95% CI, 3.11-4.22). On the other hand, schizophrenia was associated with a reduced risk of developing musculoskeletal conditions (HR, 0.87; 95% CI, 0.84-0.91).
Dr. McGrath described this finding as “curious” and speculated it “may be related to underlying genetic risk factors.”
compared with the matched reference group without a mood disorder (40.9% vs. 32.6%, respectively).
The risk of developing subsequent medical conditions after a mental disorder diagnosis did not remain steady over time. For instance, although mood disorders were associated with an increased risk of developing circulatory problems (HR, 1.32; 95% CI, 1.31-1.34), the highest risk occurred during the first 6 months following diagnosis and gradually decreased over the next 15 years (HR, 2.39; 95% CI, 2.29-2.48 and HR, 1.18; 95% CI, 1.17-1.20, respectively).
“Many people with mental disorders have unhealthy lifestyle, including low exercise, poor diet, smoking, and alcohol, which may account for the increased risk of physical illness, and also they may not seek and/or may not get quick treatment for their health conditions,” said Dr. McGrath.
Additionally, “perhaps some genetic and early life exposures, such as trauma, may increase the risk of both medical conditions and mental disorders,” he added. “We need better treatments for mental disorders, so that they do not slip into unemployment or poverty.”
A strong case
In a comment, Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto and head of the mood disorders psychopharmacology unit, University Health Network, said that the research “really makes a strong case for the fact that persons who have mental disorders are at higher risk of chronic diseases, and it’s the chronic diseases that decrease their lifespan.”
Dr. McIntyre, who is also director of the Depression and Bipolar Support Alliance, said that the “takeaway message is that mental disorders are not just brain disorders but are multisystem disorders.”
For this reason, “the most appropriate way to provide care would be to provide a holistic approach to treat and prevent the chronic diseases that lead to increase in mortality,” recommended Dr. McIntyre, who was not involved with the current study.
The study was supported by grants from the Danish National Research Foundation, the National Health and Medical Research Council, the Novo Nordisk Foundation , the European Union’s Horizon 2020 Research and Innovation Program, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the European Commission, Helsefonden, the Danish Council for Independent Research, the Independent Research Fund Denmark, the National Health and Medical Research Council of Australia, and the National Institute on Drug Abuse.
Dr. McGrath has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. McIntyre reports receiving grants from Stanley Medical Research Institute; the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation; and receiving speaking/consultation fees from Lundbeck, Janssen, Shire, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, and Minerva.
A version of this article originally appeared on Medscape.com.
Updated AAN advisory outlines when PFO closure may be option for patients with stroke
Patients with an embolic-appearing infarct who are younger than 60 years, have undergone a thorough evaluation to rule out other stroke mechanisms, and have discussed with doctors the potential risks and benefits may be candidates for the procedure.
“For patients with cryptogenic stroke and PFO, percutaneous PFO closure probably reduces the risk of stroke recurrence with [a hazard ratio] of 0.41 and an absolute risk reduction of 3.4% at 5 years; probably is associated with a periprocedural complication rate of 3.9%; and probably is associated with the development of serious nonperiprocedural atrial fibrillation, with a relative risk of 2.72,” according to the advisory authors’ meta-analysis.
Most procedural complications and instances of atrial fibrillation were “self-limited and are of uncertain long-term clinical consequence, given the lower rate of stroke in patients whose PFOs were closed,” the authors said. “Subgroup analysis suggests that the overall benefit seen across trials may not extend to those patients with small shunts and small, deep infarcts.” The authors estimated that the number of patients who need to be treated to prevent one stroke at 5 years is 29.
The advisory updates 2016 guidance that said clinicians should not routinely offer PFO closure outside of a research setting. Since then, three trials published in 2017 the New England Journal of Medicine (RESPECT, CLOSE, and REDUCE) and one trial published in 2018 in the Journal of the American College of Cardiology (DEFENSE-PFO) found that PFO closure reduces the risk of recurrent stroke in patients with a PFO who have had a cryptogenic stroke, compared with medical therapy alone. In addition, the Food and Drug Administration approved the Amplatzer PFO Occluder and Gore Cardioform Septal Occluder. These developments necessitated the practice advisory, the authors said. The advisory was published online April 29 in Neurology. It is endorsed by the American Heart Association/American Stroke Association, the Society for Cardiovascular Angiography and Interventions, and the European Academy of Neurology.
Systematic review
For the update, Steven R. Messé, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and a panel of neurologists, internists, and cardiologists with expertise in stroke and PFO systematically reviewed relevant randomized studies published through August 2019 and conducted meta-analyses to make their recommendations. The literature search identified eight articles that met inclusion criteria, including one article that provided follow-up from a trial that had been included in the previous practice advisory.
“The risk of a second stroke in people with PFO and no other possible causes of stroke is very low, approximately 1% per year while being treated with just medication alone,” Dr. Messé said in a news release. “Also, it is difficult to determine with absolute certainty that the PFO is the cause of a person’s stroke. So it is important that people with PFO are educated about the benefits and risks of PFO closure.” For patients who opt to take medication only, doctors may consider prescribing antiplatelet or anticoagulant drugs, according to the advisory. “All patients with previous stroke should be treated with an antithrombotic medication indefinitely if there is no bleeding contraindication, regardless of whether a PFO is present or if it is closed,” Dr. Messé and colleagues wrote. “However, specific antithrombotic management for patients with stroke thought to be caused by PFO remains uncertain.”
Calls for thorough work-up
“If an alternative plausible higher-risk mechanism of stroke is identified, it is likely that the PFO was an innocent bystander,” the authors said. “Secondary stroke prevention is optimized by targeting the most likely etiology of the preceding event. ... The randomized PFO closure trials all mandated thorough evaluations for participants before enrollment ... to rule out other stroke mechanisms; moreover, all studies required TEE [transesophageal echocardiography] to characterize the PFO and ensure that it was the most likely etiology for the initial event.”
In patients being considered for PFO closure, clinicians should obtain brain imaging to confirm stroke size and distribution (level B); obtain vascular imaging of the cervical and intracranial vessels to look for dissection, vasculopathy, and atherosclerosis (level B); and perform hypercoagulable studies (level B), according to the advisory. Clinicians must perform a baseline ECG to look for atrial fibrillation (level A), and patients thought to be at risk of atrial fibrillation should receive prolonged cardiac monitoring for at least 28 days (level B).
Before PFO closure, a clinician with expertise in stroke should assess the patient to ensure that the PFO is the most plausible mechanism of stroke (level B). “If a higher-risk alternative mechanism of stroke is identified, clinicians should not routinely recommend PFO closure (level B),” the authors said. Patients also should be assessed by a clinician with expertise in assessing the anatomic features of a PFO and performing PFO closure (level B).
The randomized trials focused on patients whose PFOs were closed within 6 months of a stroke, and registry studies are needed to assess long-term outcomes, noted Dr. Messé and colleagues. “It remains unclear whether closure provides a similar benefit in these patients who otherwise still fit the studies’ inclusion criteria,” the authors said. “Long-term and large-scale safety registries for patients who have received PFO closure are needed to assess the risk of device erosion, fracture, embolization, and thrombotic and endocarditis risks, and the effect of residual shunts and incidence of atrial fibrillation.”
About 25% of the general adult population has a PFO. “It’s important to note that having a PFO is common, and that most people with PFO will never know they have it because it usually does not cause any problems,” Dr. Messé said. “However, while there is generally a very low risk of stroke in patients with PFO, in younger people who have had a stroke without any other possible causes identified, closing the PFO may reduce the risk of having another stroke better than medication alone.”
The practice advisory was developed with financial support from the AAN. Dr. Messé and most of the authors had no relevant conflicts of interest. Several authors disclosed ties to medical device and pharmaceutical companies.
SOURCE: Messé SR et al. Neurology. 2020 Apr 29. doi: 10.1212/WNL.0000000000009443.
Patients with an embolic-appearing infarct who are younger than 60 years, have undergone a thorough evaluation to rule out other stroke mechanisms, and have discussed with doctors the potential risks and benefits may be candidates for the procedure.
“For patients with cryptogenic stroke and PFO, percutaneous PFO closure probably reduces the risk of stroke recurrence with [a hazard ratio] of 0.41 and an absolute risk reduction of 3.4% at 5 years; probably is associated with a periprocedural complication rate of 3.9%; and probably is associated with the development of serious nonperiprocedural atrial fibrillation, with a relative risk of 2.72,” according to the advisory authors’ meta-analysis.
Most procedural complications and instances of atrial fibrillation were “self-limited and are of uncertain long-term clinical consequence, given the lower rate of stroke in patients whose PFOs were closed,” the authors said. “Subgroup analysis suggests that the overall benefit seen across trials may not extend to those patients with small shunts and small, deep infarcts.” The authors estimated that the number of patients who need to be treated to prevent one stroke at 5 years is 29.
The advisory updates 2016 guidance that said clinicians should not routinely offer PFO closure outside of a research setting. Since then, three trials published in 2017 the New England Journal of Medicine (RESPECT, CLOSE, and REDUCE) and one trial published in 2018 in the Journal of the American College of Cardiology (DEFENSE-PFO) found that PFO closure reduces the risk of recurrent stroke in patients with a PFO who have had a cryptogenic stroke, compared with medical therapy alone. In addition, the Food and Drug Administration approved the Amplatzer PFO Occluder and Gore Cardioform Septal Occluder. These developments necessitated the practice advisory, the authors said. The advisory was published online April 29 in Neurology. It is endorsed by the American Heart Association/American Stroke Association, the Society for Cardiovascular Angiography and Interventions, and the European Academy of Neurology.
Systematic review
For the update, Steven R. Messé, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and a panel of neurologists, internists, and cardiologists with expertise in stroke and PFO systematically reviewed relevant randomized studies published through August 2019 and conducted meta-analyses to make their recommendations. The literature search identified eight articles that met inclusion criteria, including one article that provided follow-up from a trial that had been included in the previous practice advisory.
“The risk of a second stroke in people with PFO and no other possible causes of stroke is very low, approximately 1% per year while being treated with just medication alone,” Dr. Messé said in a news release. “Also, it is difficult to determine with absolute certainty that the PFO is the cause of a person’s stroke. So it is important that people with PFO are educated about the benefits and risks of PFO closure.” For patients who opt to take medication only, doctors may consider prescribing antiplatelet or anticoagulant drugs, according to the advisory. “All patients with previous stroke should be treated with an antithrombotic medication indefinitely if there is no bleeding contraindication, regardless of whether a PFO is present or if it is closed,” Dr. Messé and colleagues wrote. “However, specific antithrombotic management for patients with stroke thought to be caused by PFO remains uncertain.”
Calls for thorough work-up
“If an alternative plausible higher-risk mechanism of stroke is identified, it is likely that the PFO was an innocent bystander,” the authors said. “Secondary stroke prevention is optimized by targeting the most likely etiology of the preceding event. ... The randomized PFO closure trials all mandated thorough evaluations for participants before enrollment ... to rule out other stroke mechanisms; moreover, all studies required TEE [transesophageal echocardiography] to characterize the PFO and ensure that it was the most likely etiology for the initial event.”
In patients being considered for PFO closure, clinicians should obtain brain imaging to confirm stroke size and distribution (level B); obtain vascular imaging of the cervical and intracranial vessels to look for dissection, vasculopathy, and atherosclerosis (level B); and perform hypercoagulable studies (level B), according to the advisory. Clinicians must perform a baseline ECG to look for atrial fibrillation (level A), and patients thought to be at risk of atrial fibrillation should receive prolonged cardiac monitoring for at least 28 days (level B).
Before PFO closure, a clinician with expertise in stroke should assess the patient to ensure that the PFO is the most plausible mechanism of stroke (level B). “If a higher-risk alternative mechanism of stroke is identified, clinicians should not routinely recommend PFO closure (level B),” the authors said. Patients also should be assessed by a clinician with expertise in assessing the anatomic features of a PFO and performing PFO closure (level B).
The randomized trials focused on patients whose PFOs were closed within 6 months of a stroke, and registry studies are needed to assess long-term outcomes, noted Dr. Messé and colleagues. “It remains unclear whether closure provides a similar benefit in these patients who otherwise still fit the studies’ inclusion criteria,” the authors said. “Long-term and large-scale safety registries for patients who have received PFO closure are needed to assess the risk of device erosion, fracture, embolization, and thrombotic and endocarditis risks, and the effect of residual shunts and incidence of atrial fibrillation.”
About 25% of the general adult population has a PFO. “It’s important to note that having a PFO is common, and that most people with PFO will never know they have it because it usually does not cause any problems,” Dr. Messé said. “However, while there is generally a very low risk of stroke in patients with PFO, in younger people who have had a stroke without any other possible causes identified, closing the PFO may reduce the risk of having another stroke better than medication alone.”
The practice advisory was developed with financial support from the AAN. Dr. Messé and most of the authors had no relevant conflicts of interest. Several authors disclosed ties to medical device and pharmaceutical companies.
SOURCE: Messé SR et al. Neurology. 2020 Apr 29. doi: 10.1212/WNL.0000000000009443.
Patients with an embolic-appearing infarct who are younger than 60 years, have undergone a thorough evaluation to rule out other stroke mechanisms, and have discussed with doctors the potential risks and benefits may be candidates for the procedure.
“For patients with cryptogenic stroke and PFO, percutaneous PFO closure probably reduces the risk of stroke recurrence with [a hazard ratio] of 0.41 and an absolute risk reduction of 3.4% at 5 years; probably is associated with a periprocedural complication rate of 3.9%; and probably is associated with the development of serious nonperiprocedural atrial fibrillation, with a relative risk of 2.72,” according to the advisory authors’ meta-analysis.
Most procedural complications and instances of atrial fibrillation were “self-limited and are of uncertain long-term clinical consequence, given the lower rate of stroke in patients whose PFOs were closed,” the authors said. “Subgroup analysis suggests that the overall benefit seen across trials may not extend to those patients with small shunts and small, deep infarcts.” The authors estimated that the number of patients who need to be treated to prevent one stroke at 5 years is 29.
The advisory updates 2016 guidance that said clinicians should not routinely offer PFO closure outside of a research setting. Since then, three trials published in 2017 the New England Journal of Medicine (RESPECT, CLOSE, and REDUCE) and one trial published in 2018 in the Journal of the American College of Cardiology (DEFENSE-PFO) found that PFO closure reduces the risk of recurrent stroke in patients with a PFO who have had a cryptogenic stroke, compared with medical therapy alone. In addition, the Food and Drug Administration approved the Amplatzer PFO Occluder and Gore Cardioform Septal Occluder. These developments necessitated the practice advisory, the authors said. The advisory was published online April 29 in Neurology. It is endorsed by the American Heart Association/American Stroke Association, the Society for Cardiovascular Angiography and Interventions, and the European Academy of Neurology.
Systematic review
For the update, Steven R. Messé, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and a panel of neurologists, internists, and cardiologists with expertise in stroke and PFO systematically reviewed relevant randomized studies published through August 2019 and conducted meta-analyses to make their recommendations. The literature search identified eight articles that met inclusion criteria, including one article that provided follow-up from a trial that had been included in the previous practice advisory.
“The risk of a second stroke in people with PFO and no other possible causes of stroke is very low, approximately 1% per year while being treated with just medication alone,” Dr. Messé said in a news release. “Also, it is difficult to determine with absolute certainty that the PFO is the cause of a person’s stroke. So it is important that people with PFO are educated about the benefits and risks of PFO closure.” For patients who opt to take medication only, doctors may consider prescribing antiplatelet or anticoagulant drugs, according to the advisory. “All patients with previous stroke should be treated with an antithrombotic medication indefinitely if there is no bleeding contraindication, regardless of whether a PFO is present or if it is closed,” Dr. Messé and colleagues wrote. “However, specific antithrombotic management for patients with stroke thought to be caused by PFO remains uncertain.”
Calls for thorough work-up
“If an alternative plausible higher-risk mechanism of stroke is identified, it is likely that the PFO was an innocent bystander,” the authors said. “Secondary stroke prevention is optimized by targeting the most likely etiology of the preceding event. ... The randomized PFO closure trials all mandated thorough evaluations for participants before enrollment ... to rule out other stroke mechanisms; moreover, all studies required TEE [transesophageal echocardiography] to characterize the PFO and ensure that it was the most likely etiology for the initial event.”
In patients being considered for PFO closure, clinicians should obtain brain imaging to confirm stroke size and distribution (level B); obtain vascular imaging of the cervical and intracranial vessels to look for dissection, vasculopathy, and atherosclerosis (level B); and perform hypercoagulable studies (level B), according to the advisory. Clinicians must perform a baseline ECG to look for atrial fibrillation (level A), and patients thought to be at risk of atrial fibrillation should receive prolonged cardiac monitoring for at least 28 days (level B).
Before PFO closure, a clinician with expertise in stroke should assess the patient to ensure that the PFO is the most plausible mechanism of stroke (level B). “If a higher-risk alternative mechanism of stroke is identified, clinicians should not routinely recommend PFO closure (level B),” the authors said. Patients also should be assessed by a clinician with expertise in assessing the anatomic features of a PFO and performing PFO closure (level B).
The randomized trials focused on patients whose PFOs were closed within 6 months of a stroke, and registry studies are needed to assess long-term outcomes, noted Dr. Messé and colleagues. “It remains unclear whether closure provides a similar benefit in these patients who otherwise still fit the studies’ inclusion criteria,” the authors said. “Long-term and large-scale safety registries for patients who have received PFO closure are needed to assess the risk of device erosion, fracture, embolization, and thrombotic and endocarditis risks, and the effect of residual shunts and incidence of atrial fibrillation.”
About 25% of the general adult population has a PFO. “It’s important to note that having a PFO is common, and that most people with PFO will never know they have it because it usually does not cause any problems,” Dr. Messé said. “However, while there is generally a very low risk of stroke in patients with PFO, in younger people who have had a stroke without any other possible causes identified, closing the PFO may reduce the risk of having another stroke better than medication alone.”
The practice advisory was developed with financial support from the AAN. Dr. Messé and most of the authors had no relevant conflicts of interest. Several authors disclosed ties to medical device and pharmaceutical companies.
SOURCE: Messé SR et al. Neurology. 2020 Apr 29. doi: 10.1212/WNL.0000000000009443.
FROM NEUROLOGY
Silent brain infarcts found in 3% of AFib patients, tied to cognitive decline
Patients with atrial fibrillation, even those on oral anticoagulant therapy, developed clinically silent brain infarctions at a striking rate of close to 3% per year, according to results from SWISS-AF, a prospective of study of 1,227 Swiss patients followed with serial MR brain scans over a 2 year period.

The results also showed that these brain infarctions – which occurred in 68 (5.5%) of the atrial fibrillation (AFib) patients, including 58 (85%) who did not have any strokes or transient ischemic attacks during follow-up – appeared to represent enough pathology to link with a small but statistically significant decline in three separate cognitive measures, compared with patients who did not develop brain infarctions during follow-up.
“Cognitive decline may go unrecognized for a long time in clinical practice because usually no one tests for it,” plus “the absolute declines were small and probably not appreciable” in the everyday behavior of affected patients, David Conen, MD, said at the annual scientific sessions of the Heart Rhythm Society, held online because of COVID-19. But “we were surprised to see a significant change after just 2 years. We expect much larger effects to develop over time,” he said during a press briefing.
Another key finding was that roughly half the patients had large cortical or noncortical infarcts, which usually have a thromboembolic cause, but the other half had small noncortical infarcts that likely have a different etiology involving the microvasculature. Causes for those small infarcts might include localized atherosclerotic disease or amyloidosis, proposed Dr. Conen, a cardiologist at McMaster University, Hamilton, Ont.
This finding also suggests that, as a consequence, anticoagulation alone may not be enough to prevent this brain damage in Afib patients. “It calls for a more comprehensive approach to prevention,” with attention to atherosclerotic cardiovascular disease risk factors in AFib patients, including interventions that address hypertension, diabetes, hyperlipidemia, and smoking cessation. “Anticoagulation in AFib patients is critical, but it also is not enough,” Dr. Conen said.

These data “are very important. The two pillars for taking care of AFib patients have traditionally been to manage the patient’s stroke risk and to treat symptoms. Dr. Conen’s data suggest that simply starting anticoagulation is not sufficient, and it stresses the importance of continued management of hypertension, diabetes, and other medical and social issues,” commented Fred Kusumoto, MD, director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla.
“The risk factors associated with the development of cardiovascular disease are similar to those associated with the development of AFib and heart failure. It is important to understand the importance of managing hypertension, diabetes, and obesity; encouraging exercise and a healthy diet; and stopping smoking in all AFib patients as well as in the general population. Many clinicians have not emphasized the importance of continually addressing these behaviors,” Dr. Kusumoto said in an interview.
The SWISS-AF (Swiss Atrial Fibrillation Cohort) study enrolled 2,415 AFib patients at 14 Swiss centers during 2014-2017, and obtained both a baseline brain MR scan and baseline cognitive-test results for 1,737 patients (J Am Coll Cardiol. 2019 Mar;73[9]:989-99). Patients retook the cognitive tests annually, and 1,227 had a second MR brain scan after 2 years in the study, the cohort that supplied the data Dr. Conen presented. At baseline, these patients averaged 71 years of age, just over a quarter were women, and 90% were on an oral anticoagulant, with 84% on an oral anticoagulant at 2-year follow-up. Treatment split roughly equally between direct-acting oral anticoagulants and vitamin K antagonists like warfarin.
Among the 68 patients with evidence for an incident brain infarct after 2 years, 59 (87%) were on treatment with an OAC, and 51 (75%) who were both on treatment with a direct-acting oral anticoagulant and developed their brain infarct without also having a stroke or transient ischemic attack, which Dr. Conen called a “silent event.” The cognitive tests that showed statistically significant declines after 2 years in the patients with silent brain infarcts compared with those without a new infarct were the Trail Making Test parts A and B, and the animal-naming verbal fluency test. The two other tests applied were the Montreal Cognitive Assessment and the Digital Symbol Substitution Test.

Results from several prior studies also indicated a relationship between AFib and cognitive decline, but SWISS-AF is “the largest study to rigorously examine the incidence of silent brain infarcts in AFib patients,” commented Christine M. Albert, MD, chair of cardiology at the Smidt Heart Institute of Cedars-Sinai Medical Center in Los Angeles. “Silent infarcts could be the cause, at least in part, for the cognitive decline and dementia associated with AFib,” she noted. But divining the therapeutic implications of the finding will require further investigation that looks at factors such as the impact of anticoagulant type, other treatment that addresses AFib such as ablation and rate control, the duration and type of AFib, and the prevalence of hypertension and other stroke risk factors, she said as a designated discussant for Dr. Conen’s report.
SWISS-AF received no commercial funding. Dr. Conen has been a speaker on behalf of Servier. Dr. Kusumoto had no disclosures. Dr. Albert has been a consultant to Roche Diagnostics and has received research funding from Abbott, Roche Diagnostics, and St. Jude Medical.
Patients with atrial fibrillation, even those on oral anticoagulant therapy, developed clinically silent brain infarctions at a striking rate of close to 3% per year, according to results from SWISS-AF, a prospective of study of 1,227 Swiss patients followed with serial MR brain scans over a 2 year period.
The results also showed that these brain infarctions – which occurred in 68 (5.5%) of the atrial fibrillation (AFib) patients, including 58 (85%) who did not have any strokes or transient ischemic attacks during follow-up – appeared to represent enough pathology to link with a small but statistically significant decline in three separate cognitive measures, compared with patients who did not develop brain infarctions during follow-up.
“Cognitive decline may go unrecognized for a long time in clinical practice because usually no one tests for it,” plus “the absolute declines were small and probably not appreciable” in the everyday behavior of affected patients, David Conen, MD, said at the annual scientific sessions of the Heart Rhythm Society, held online because of COVID-19. But “we were surprised to see a significant change after just 2 years. We expect much larger effects to develop over time,” he said during a press briefing.
Another key finding was that roughly half the patients had large cortical or noncortical infarcts, which usually have a thromboembolic cause, but the other half had small noncortical infarcts that likely have a different etiology involving the microvasculature. Causes for those small infarcts might include localized atherosclerotic disease or amyloidosis, proposed Dr. Conen, a cardiologist at McMaster University, Hamilton, Ont.
This finding also suggests that, as a consequence, anticoagulation alone may not be enough to prevent this brain damage in Afib patients. “It calls for a more comprehensive approach to prevention,” with attention to atherosclerotic cardiovascular disease risk factors in AFib patients, including interventions that address hypertension, diabetes, hyperlipidemia, and smoking cessation. “Anticoagulation in AFib patients is critical, but it also is not enough,” Dr. Conen said.
These data “are very important. The two pillars for taking care of AFib patients have traditionally been to manage the patient’s stroke risk and to treat symptoms. Dr. Conen’s data suggest that simply starting anticoagulation is not sufficient, and it stresses the importance of continued management of hypertension, diabetes, and other medical and social issues,” commented Fred Kusumoto, MD, director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla.
“The risk factors associated with the development of cardiovascular disease are similar to those associated with the development of AFib and heart failure. It is important to understand the importance of managing hypertension, diabetes, and obesity; encouraging exercise and a healthy diet; and stopping smoking in all AFib patients as well as in the general population. Many clinicians have not emphasized the importance of continually addressing these behaviors,” Dr. Kusumoto said in an interview.
The SWISS-AF (Swiss Atrial Fibrillation Cohort) study enrolled 2,415 AFib patients at 14 Swiss centers during 2014-2017, and obtained both a baseline brain MR scan and baseline cognitive-test results for 1,737 patients (J Am Coll Cardiol. 2019 Mar;73[9]:989-99). Patients retook the cognitive tests annually, and 1,227 had a second MR brain scan after 2 years in the study, the cohort that supplied the data Dr. Conen presented. At baseline, these patients averaged 71 years of age, just over a quarter were women, and 90% were on an oral anticoagulant, with 84% on an oral anticoagulant at 2-year follow-up. Treatment split roughly equally between direct-acting oral anticoagulants and vitamin K antagonists like warfarin.
Among the 68 patients with evidence for an incident brain infarct after 2 years, 59 (87%) were on treatment with an OAC, and 51 (75%) who were both on treatment with a direct-acting oral anticoagulant and developed their brain infarct without also having a stroke or transient ischemic attack, which Dr. Conen called a “silent event.” The cognitive tests that showed statistically significant declines after 2 years in the patients with silent brain infarcts compared with those without a new infarct were the Trail Making Test parts A and B, and the animal-naming verbal fluency test. The two other tests applied were the Montreal Cognitive Assessment and the Digital Symbol Substitution Test.
Results from several prior studies also indicated a relationship between AFib and cognitive decline, but SWISS-AF is “the largest study to rigorously examine the incidence of silent brain infarcts in AFib patients,” commented Christine M. Albert, MD, chair of cardiology at the Smidt Heart Institute of Cedars-Sinai Medical Center in Los Angeles. “Silent infarcts could be the cause, at least in part, for the cognitive decline and dementia associated with AFib,” she noted. But divining the therapeutic implications of the finding will require further investigation that looks at factors such as the impact of anticoagulant type, other treatment that addresses AFib such as ablation and rate control, the duration and type of AFib, and the prevalence of hypertension and other stroke risk factors, she said as a designated discussant for Dr. Conen’s report.
SWISS-AF received no commercial funding. Dr. Conen has been a speaker on behalf of Servier. Dr. Kusumoto had no disclosures. Dr. Albert has been a consultant to Roche Diagnostics and has received research funding from Abbott, Roche Diagnostics, and St. Jude Medical.
Patients with atrial fibrillation, even those on oral anticoagulant therapy, developed clinically silent brain infarctions at a striking rate of close to 3% per year, according to results from SWISS-AF, a prospective of study of 1,227 Swiss patients followed with serial MR brain scans over a 2 year period.
The results also showed that these brain infarctions – which occurred in 68 (5.5%) of the atrial fibrillation (AFib) patients, including 58 (85%) who did not have any strokes or transient ischemic attacks during follow-up – appeared to represent enough pathology to link with a small but statistically significant decline in three separate cognitive measures, compared with patients who did not develop brain infarctions during follow-up.
“Cognitive decline may go unrecognized for a long time in clinical practice because usually no one tests for it,” plus “the absolute declines were small and probably not appreciable” in the everyday behavior of affected patients, David Conen, MD, said at the annual scientific sessions of the Heart Rhythm Society, held online because of COVID-19. But “we were surprised to see a significant change after just 2 years. We expect much larger effects to develop over time,” he said during a press briefing.
Another key finding was that roughly half the patients had large cortical or noncortical infarcts, which usually have a thromboembolic cause, but the other half had small noncortical infarcts that likely have a different etiology involving the microvasculature. Causes for those small infarcts might include localized atherosclerotic disease or amyloidosis, proposed Dr. Conen, a cardiologist at McMaster University, Hamilton, Ont.
This finding also suggests that, as a consequence, anticoagulation alone may not be enough to prevent this brain damage in Afib patients. “It calls for a more comprehensive approach to prevention,” with attention to atherosclerotic cardiovascular disease risk factors in AFib patients, including interventions that address hypertension, diabetes, hyperlipidemia, and smoking cessation. “Anticoagulation in AFib patients is critical, but it also is not enough,” Dr. Conen said.
These data “are very important. The two pillars for taking care of AFib patients have traditionally been to manage the patient’s stroke risk and to treat symptoms. Dr. Conen’s data suggest that simply starting anticoagulation is not sufficient, and it stresses the importance of continued management of hypertension, diabetes, and other medical and social issues,” commented Fred Kusumoto, MD, director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla.
“The risk factors associated with the development of cardiovascular disease are similar to those associated with the development of AFib and heart failure. It is important to understand the importance of managing hypertension, diabetes, and obesity; encouraging exercise and a healthy diet; and stopping smoking in all AFib patients as well as in the general population. Many clinicians have not emphasized the importance of continually addressing these behaviors,” Dr. Kusumoto said in an interview.
The SWISS-AF (Swiss Atrial Fibrillation Cohort) study enrolled 2,415 AFib patients at 14 Swiss centers during 2014-2017, and obtained both a baseline brain MR scan and baseline cognitive-test results for 1,737 patients (J Am Coll Cardiol. 2019 Mar;73[9]:989-99). Patients retook the cognitive tests annually, and 1,227 had a second MR brain scan after 2 years in the study, the cohort that supplied the data Dr. Conen presented. At baseline, these patients averaged 71 years of age, just over a quarter were women, and 90% were on an oral anticoagulant, with 84% on an oral anticoagulant at 2-year follow-up. Treatment split roughly equally between direct-acting oral anticoagulants and vitamin K antagonists like warfarin.
Among the 68 patients with evidence for an incident brain infarct after 2 years, 59 (87%) were on treatment with an OAC, and 51 (75%) who were both on treatment with a direct-acting oral anticoagulant and developed their brain infarct without also having a stroke or transient ischemic attack, which Dr. Conen called a “silent event.” The cognitive tests that showed statistically significant declines after 2 years in the patients with silent brain infarcts compared with those without a new infarct were the Trail Making Test parts A and B, and the animal-naming verbal fluency test. The two other tests applied were the Montreal Cognitive Assessment and the Digital Symbol Substitution Test.
Results from several prior studies also indicated a relationship between AFib and cognitive decline, but SWISS-AF is “the largest study to rigorously examine the incidence of silent brain infarcts in AFib patients,” commented Christine M. Albert, MD, chair of cardiology at the Smidt Heart Institute of Cedars-Sinai Medical Center in Los Angeles. “Silent infarcts could be the cause, at least in part, for the cognitive decline and dementia associated with AFib,” she noted. But divining the therapeutic implications of the finding will require further investigation that looks at factors such as the impact of anticoagulant type, other treatment that addresses AFib such as ablation and rate control, the duration and type of AFib, and the prevalence of hypertension and other stroke risk factors, she said as a designated discussant for Dr. Conen’s report.
SWISS-AF received no commercial funding. Dr. Conen has been a speaker on behalf of Servier. Dr. Kusumoto had no disclosures. Dr. Albert has been a consultant to Roche Diagnostics and has received research funding from Abbott, Roche Diagnostics, and St. Jude Medical.
FROM HEART RHYTHM 2020
Statins and ICH: new meta-analysis
The meta-analysis was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Coauthor Abhi Pandhi, MD, the University of Tennessee Health Science Center, Memphis, explained that some previous studies have suggested that statin therapy may be associated with an increased risk for ICH, especially at higher doses. Other studies, however, have failed to confirm this and have shown an increase in cardiovascular events if statins are stopped.
To look further into this issue, Dr. Pandhi and colleagues conducted a meta-analysis of 19 clinical studies involving patients who had a history of cardiovascular or cerebrovascular events and who had been treated with statins. A total of 35,842 patients were included.
Results showed that statin use was not significantly associated with the risk for combined primary and secondary ICH (relative risk, 1.03; 95% confidence interval, 0.85–1.08). But the risk for cerebral ischemia (stroke and transient ischemic attack) was significantly lower in those who received statins (RR, 0.79; 95% CI, 0.61–0.87).
“Overall, we found no effect of statins on the risk of ICH, and benefits on reducing ischemic events are clear,” Dr. Pandhi said.
Increased secondary ICH?
However, a sensitivity analysis showed a trend toward a higher risk for secondary ICH among those who were assigned to statin treatment (odds ratio, 1.87; 95% CI, 0.91–3.86).
“While this may suggest an increased risk of secondary ICH, when we look at the big picture, putting all the data together, and given that ischemic events are far more common than ICH, the risk of stopping statins and losing the protection against ischemic events is probably greater than any harm even in patients with underlying risk factors for ICH,” Dr. Pandhi concluded.
Commenting on the study, Michael Szarek, PhD, who has also conducted research in this field, said: “The results of this meta-analysis appear to be consistent with individual randomized trials of statins in patients with cerebrovascular disease that have shown clear benefit in terms of ischemic stroke or TIA and potential harm in terms of hemorrhagic stroke.”
Dr. Szarek is chair and professor in the Department of Epidemiology and Biostatistics at the SUNY Downstate Health Sciences University, New York City.
“However, the much greater frequency of ischemic events, coupled with benefits in coronary and peripheral vascular territories, suggest the risk/benefit of statin treatment remains favorable in this patient population, with the possible exception of patients with a history of hemorrhagic stroke,” he added.
Also commenting on this latest meta-analysis, Pamela Rist, ScD, associate epidemiologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston, who has also authored studies in this area, said the results of this study seem similar to prior results from meta-analyses of clinical trials.
“It will be interesting to see the full manuscript to learn more about the sensitivity analyses they conducted and why they may have observed a nonsignificant increased risk of secondary ICH among some individuals using statins,” Dr. Rist added.
“Based on prior published meta-analyses of statin use and ICH, any potential increase in risk of hemorrhagic stroke is probably outweighed by the reduction in ischemic stroke and other cardiovascular events,” she concluded.
Dr. Pandhi has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Ishfaq A et al. AAN 2020. Abstract S9.010.
The meta-analysis was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Coauthor Abhi Pandhi, MD, the University of Tennessee Health Science Center, Memphis, explained that some previous studies have suggested that statin therapy may be associated with an increased risk for ICH, especially at higher doses. Other studies, however, have failed to confirm this and have shown an increase in cardiovascular events if statins are stopped.
To look further into this issue, Dr. Pandhi and colleagues conducted a meta-analysis of 19 clinical studies involving patients who had a history of cardiovascular or cerebrovascular events and who had been treated with statins. A total of 35,842 patients were included.
Results showed that statin use was not significantly associated with the risk for combined primary and secondary ICH (relative risk, 1.03; 95% confidence interval, 0.85–1.08). But the risk for cerebral ischemia (stroke and transient ischemic attack) was significantly lower in those who received statins (RR, 0.79; 95% CI, 0.61–0.87).
“Overall, we found no effect of statins on the risk of ICH, and benefits on reducing ischemic events are clear,” Dr. Pandhi said.
Increased secondary ICH?
However, a sensitivity analysis showed a trend toward a higher risk for secondary ICH among those who were assigned to statin treatment (odds ratio, 1.87; 95% CI, 0.91–3.86).
“While this may suggest an increased risk of secondary ICH, when we look at the big picture, putting all the data together, and given that ischemic events are far more common than ICH, the risk of stopping statins and losing the protection against ischemic events is probably greater than any harm even in patients with underlying risk factors for ICH,” Dr. Pandhi concluded.
Commenting on the study, Michael Szarek, PhD, who has also conducted research in this field, said: “The results of this meta-analysis appear to be consistent with individual randomized trials of statins in patients with cerebrovascular disease that have shown clear benefit in terms of ischemic stroke or TIA and potential harm in terms of hemorrhagic stroke.”
Dr. Szarek is chair and professor in the Department of Epidemiology and Biostatistics at the SUNY Downstate Health Sciences University, New York City.
“However, the much greater frequency of ischemic events, coupled with benefits in coronary and peripheral vascular territories, suggest the risk/benefit of statin treatment remains favorable in this patient population, with the possible exception of patients with a history of hemorrhagic stroke,” he added.
Also commenting on this latest meta-analysis, Pamela Rist, ScD, associate epidemiologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston, who has also authored studies in this area, said the results of this study seem similar to prior results from meta-analyses of clinical trials.
“It will be interesting to see the full manuscript to learn more about the sensitivity analyses they conducted and why they may have observed a nonsignificant increased risk of secondary ICH among some individuals using statins,” Dr. Rist added.
“Based on prior published meta-analyses of statin use and ICH, any potential increase in risk of hemorrhagic stroke is probably outweighed by the reduction in ischemic stroke and other cardiovascular events,” she concluded.
Dr. Pandhi has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Ishfaq A et al. AAN 2020. Abstract S9.010.
The meta-analysis was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Coauthor Abhi Pandhi, MD, the University of Tennessee Health Science Center, Memphis, explained that some previous studies have suggested that statin therapy may be associated with an increased risk for ICH, especially at higher doses. Other studies, however, have failed to confirm this and have shown an increase in cardiovascular events if statins are stopped.
To look further into this issue, Dr. Pandhi and colleagues conducted a meta-analysis of 19 clinical studies involving patients who had a history of cardiovascular or cerebrovascular events and who had been treated with statins. A total of 35,842 patients were included.
Results showed that statin use was not significantly associated with the risk for combined primary and secondary ICH (relative risk, 1.03; 95% confidence interval, 0.85–1.08). But the risk for cerebral ischemia (stroke and transient ischemic attack) was significantly lower in those who received statins (RR, 0.79; 95% CI, 0.61–0.87).
“Overall, we found no effect of statins on the risk of ICH, and benefits on reducing ischemic events are clear,” Dr. Pandhi said.
Increased secondary ICH?
However, a sensitivity analysis showed a trend toward a higher risk for secondary ICH among those who were assigned to statin treatment (odds ratio, 1.87; 95% CI, 0.91–3.86).
“While this may suggest an increased risk of secondary ICH, when we look at the big picture, putting all the data together, and given that ischemic events are far more common than ICH, the risk of stopping statins and losing the protection against ischemic events is probably greater than any harm even in patients with underlying risk factors for ICH,” Dr. Pandhi concluded.
Commenting on the study, Michael Szarek, PhD, who has also conducted research in this field, said: “The results of this meta-analysis appear to be consistent with individual randomized trials of statins in patients with cerebrovascular disease that have shown clear benefit in terms of ischemic stroke or TIA and potential harm in terms of hemorrhagic stroke.”
Dr. Szarek is chair and professor in the Department of Epidemiology and Biostatistics at the SUNY Downstate Health Sciences University, New York City.
“However, the much greater frequency of ischemic events, coupled with benefits in coronary and peripheral vascular territories, suggest the risk/benefit of statin treatment remains favorable in this patient population, with the possible exception of patients with a history of hemorrhagic stroke,” he added.
Also commenting on this latest meta-analysis, Pamela Rist, ScD, associate epidemiologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston, who has also authored studies in this area, said the results of this study seem similar to prior results from meta-analyses of clinical trials.
“It will be interesting to see the full manuscript to learn more about the sensitivity analyses they conducted and why they may have observed a nonsignificant increased risk of secondary ICH among some individuals using statins,” Dr. Rist added.
“Based on prior published meta-analyses of statin use and ICH, any potential increase in risk of hemorrhagic stroke is probably outweighed by the reduction in ischemic stroke and other cardiovascular events,” she concluded.
Dr. Pandhi has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Ishfaq A et al. AAN 2020. Abstract S9.010.
AAN 2020
FOURIER: Evolocumab follow-up shows no cognitive adverse effects
Treatment with a PCSK9 inhibitor, as well as achieving dramatically lowered cholesterol levels, did not mess with patients’ minds. Results from a cognition self-assessment completed by more than 22,000 patients when they finished participation in the FOURIER pivotal outcomes trial for evolocumab showed no signal of mental harm from either treatment with this PCSK9 inhibitor or from reaching a serum level of low-density lipoprotein cholesterol (LDL-C) of less than 20 mg/dL.

“We observed that patients treated with evolocumab, as well as those who achieved progressively very low LDL-C at 4 weeks in the FOURIER trial, had similar self-reported cognition in comparison with those receiving placebo and those with higher achieved LDL-C levels,” wrote a team of researchers from the trial in an article published online on May 4 (J Am Coll Cardiol. 2020 May 12;75[18]: 2283-93). “These data confirm the neurocognitive safety of intensive LDL-C reduction with evolocumab while reducing recurrent CV [cardiovascular] events in high-risk patients, and suggest that very low achieved LDL-C levels may be safely targeted for high-risk patients.”
The findings added to prior results documenting the cognitive safety of evolocumab (Repatha) from a much smaller FOURIER substudy that involved more intensive testing, the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study with 1,204 patients drawn from the broader study and tested after a median 19 months on treatment (N Engl J Med. 2017 Aug 17;377[17]: 633-43), as well as reports of neurocognitive safety for the other U.S. approved PCSK9 (proprotein convertase subtilisin kexin 9) inhibitor, alirocumab (Praluent) (N Engl J Med. 2015 Apr 16;372[16]:1489-99), various statins (J Gen Intern Med. 2015 Mar;30[3]: 348-58), and a third type of LDL-C–lowering agent, ezetimibe (JAMA Cardiol. 2017 May;2[5]:547-55).
Despite this evidence from across several drug classes that all cut LDL-C a long-standing but unsubstantiated belief persists among some that lipid lowering, especially by statins, blunts mental function, misinformation that’s easy to find on the Internet. “I estimate that about 20% of patients prescribed a statin won’t take it because of something they’ve heard” including that statins make you stupid. “It’s hard to undo that,” said Robert P. Giugliano, MD, a cardiologist at Brigham and Women’s Hospital in Boston and senior author for the new FOURIER study as well as for EBBINGHAUS. The same stigma has not gained nearly as much traction for PCSK9 inhibitors, however, and Dr. Giugliano said he has also recently sensed what may be a downtrend in statin apprehension.
“The information added by this study is very important,” commented Massimo R. Mannarino, MD, an atherosclerotic disease researcher at the University of Perugia (Italy). “The prejudice and misinformation regarding possible side effects of statins among patients and also some physicians unfortunately remains very strong today,” he said in an interview. “My impression is that PCSK9 inhibitors are less affected by this negative bias and are seen as a safer alternative to statins.” Concerns about PCSK9 inhibitors have especially focused on “the possible risks from very low cholesterol levels on the brain.” The evidence from both studies and clinical experience “allows for a very positive opinion about the efficacy and safety of PCSK9 inhibitors, although the long-term effects still require a few more years of observation,” said Dr. Mannarino, who led a review of the evidence that clears this class from links to neurocognitive loss (J Clin Lipid. 2018 Sep 1;12[5]:1123-32).
FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) randomized 27,564 patients with atherosclerotic cardiovascular disease and elevated LDL cholesterol despite maximally tolerated standard treatment. Treatment with evolocumab for a median of 2.2 years resulted in a statistically significant 15% reduction in the study’s primary efficacy endpoint, compared with placebo (N Engl J Med. 2017 May 4;376[18]:1713-22), and led to the drug receiving an indication for lowering rates of MI, stroke, and symptom-driven coronary revascularization.
The prespecified substudy reported by Dr. Giugliano and his associates focused on a 23-question, validated, self-assessment survey of cognitive function completed by 22,655 of the FOURIER patients (82%). The more than 4,900 other patients in the study who did not complete the survey had modestly higher prevalence rates of various comorbidities at baseline, and also higher rates of adverse outcomes during follow-up, and in many cases these adverse outcome may have contributed to these patients not being able to complete their end-of-study cognitive assessment. For example, almost a quarter of the patients who did not complete their end-of-study cognitive assessment failed to do so because they had already died.
Overall, the prevalence of patients indicating a cognitive decline was virtually identical among 11,363 patients who had been maintained on evolocumab, with a 3.7% rate, and the 11,292 patients in the placebo group, with a 3.6% rate. When analyzed by achieved level of LDL-C after 4 weeks on treatment, the 2,338 patients with a level below 20 mg/dL had a 3.8% rate of self-reported cognitive loss, compared with a 4.5% rate among 3,613 patients who had an LDL-C level of at least 100 mg/dL when measured 4 weeks into the study.
One of the strengths of the new cognitive analysis is that, although it did not use the more sophisticated assessment tests employed on fewer patients in the EBBINGHAUS substudy, it used the Everyday Cognition scale (Neuropsychiatry. 2008 Jul;22[4]: 531-44). “We asked patients what they have experienced, and in the end that is what’s important, so this adds to the neurocognitive testing,” run in EBBINGHAUS, Dr. Giugliano said in an interview.
“The neurocognitive results in the present study were self-reported, and that might be a limitation, as it is less specific and objective, but it is also a strength, as it could be more sensitive” especially for a “nocebo effect common to all lipid-lowering drugs linked to the bad reputation historically attributed to statins,” Dr. Mannarino said.

Should the new FOURIER data “be interpreted as definitive evidence that intensive LDL-C lowering with PCSK9 monoclonal antibodies has no major harmful cognitive effects, at least over a period of 3 years? The answer appears to be a qualified yes, but with three important caveats,” Jennifer G. Robinson, MD, a professor of epidemiology at the University of Iowa College of Public Health in Iowa City, said in an editorial that accompanied the new report (J Am Coll Cardiol. 2020 May 12;75[18]:2294-6). Her three caveats are the missing 18% of patients who never took the end-of-study assessment, the relative paucity of patients at very advanced age in FOURIER, in which patients averaged 62.5 years old, and the exclusion from FOURIER of patients with a history of hemorrhagic stroke. Dr. Robinson also cited the 2.2 year median follow-up as leaving unsettled the potential cognitive impact of longer treatment.
In response, Dr. Giugliano noted that the very large size of FOURIER and the 22,655 patients who completed their survey provided substantial numbers of patients to address some of these concerns in robust subgroup analyses. For example, the new report showed no signal of excess cognitive complaints with evolocumab treatment among 1,999 patients who were at least 75 years old when entering the study, or in more than 5,000 patients with a history of cerebrovascular disease at baseline, or in 1,990 patients with a history of a nonstroke neurologic disease. In addition, while he conceded that the 18% of patients not accounted for in the new study placed some limits on generalizability of the findings, he also maintained that this unavoidable failure to collect data from a modest percentage of patients doesn’t scuttle the overarching signal of cognitive safety for most patients. And regarding the duration of treatment monitored, he noted that 5-year follow-up cognitive assessments are planned.
FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Giugliano has received personal fees and research support from Amgen and from several other companies. Dr. Mannarino had no disclosures. Dr. Robinson has been a consultant to The Medicines Company, Novartis, and Pfizer, and she has received research funding to her institution from Amgen and several other companies.
SOURCE: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Correction: Dr. Giugliano's name was misspelled in an earlier version of this article.
Treatment with a PCSK9 inhibitor, as well as achieving dramatically lowered cholesterol levels, did not mess with patients’ minds. Results from a cognition self-assessment completed by more than 22,000 patients when they finished participation in the FOURIER pivotal outcomes trial for evolocumab showed no signal of mental harm from either treatment with this PCSK9 inhibitor or from reaching a serum level of low-density lipoprotein cholesterol (LDL-C) of less than 20 mg/dL.
“We observed that patients treated with evolocumab, as well as those who achieved progressively very low LDL-C at 4 weeks in the FOURIER trial, had similar self-reported cognition in comparison with those receiving placebo and those with higher achieved LDL-C levels,” wrote a team of researchers from the trial in an article published online on May 4 (J Am Coll Cardiol. 2020 May 12;75[18]: 2283-93). “These data confirm the neurocognitive safety of intensive LDL-C reduction with evolocumab while reducing recurrent CV [cardiovascular] events in high-risk patients, and suggest that very low achieved LDL-C levels may be safely targeted for high-risk patients.”
The findings added to prior results documenting the cognitive safety of evolocumab (Repatha) from a much smaller FOURIER substudy that involved more intensive testing, the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study with 1,204 patients drawn from the broader study and tested after a median 19 months on treatment (N Engl J Med. 2017 Aug 17;377[17]: 633-43), as well as reports of neurocognitive safety for the other U.S. approved PCSK9 (proprotein convertase subtilisin kexin 9) inhibitor, alirocumab (Praluent) (N Engl J Med. 2015 Apr 16;372[16]:1489-99), various statins (J Gen Intern Med. 2015 Mar;30[3]: 348-58), and a third type of LDL-C–lowering agent, ezetimibe (JAMA Cardiol. 2017 May;2[5]:547-55).
Despite this evidence from across several drug classes that all cut LDL-C a long-standing but unsubstantiated belief persists among some that lipid lowering, especially by statins, blunts mental function, misinformation that’s easy to find on the Internet. “I estimate that about 20% of patients prescribed a statin won’t take it because of something they’ve heard” including that statins make you stupid. “It’s hard to undo that,” said Robert P. Giugliano, MD, a cardiologist at Brigham and Women’s Hospital in Boston and senior author for the new FOURIER study as well as for EBBINGHAUS. The same stigma has not gained nearly as much traction for PCSK9 inhibitors, however, and Dr. Giugliano said he has also recently sensed what may be a downtrend in statin apprehension.
“The information added by this study is very important,” commented Massimo R. Mannarino, MD, an atherosclerotic disease researcher at the University of Perugia (Italy). “The prejudice and misinformation regarding possible side effects of statins among patients and also some physicians unfortunately remains very strong today,” he said in an interview. “My impression is that PCSK9 inhibitors are less affected by this negative bias and are seen as a safer alternative to statins.” Concerns about PCSK9 inhibitors have especially focused on “the possible risks from very low cholesterol levels on the brain.” The evidence from both studies and clinical experience “allows for a very positive opinion about the efficacy and safety of PCSK9 inhibitors, although the long-term effects still require a few more years of observation,” said Dr. Mannarino, who led a review of the evidence that clears this class from links to neurocognitive loss (J Clin Lipid. 2018 Sep 1;12[5]:1123-32).
FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) randomized 27,564 patients with atherosclerotic cardiovascular disease and elevated LDL cholesterol despite maximally tolerated standard treatment. Treatment with evolocumab for a median of 2.2 years resulted in a statistically significant 15% reduction in the study’s primary efficacy endpoint, compared with placebo (N Engl J Med. 2017 May 4;376[18]:1713-22), and led to the drug receiving an indication for lowering rates of MI, stroke, and symptom-driven coronary revascularization.
The prespecified substudy reported by Dr. Giugliano and his associates focused on a 23-question, validated, self-assessment survey of cognitive function completed by 22,655 of the FOURIER patients (82%). The more than 4,900 other patients in the study who did not complete the survey had modestly higher prevalence rates of various comorbidities at baseline, and also higher rates of adverse outcomes during follow-up, and in many cases these adverse outcome may have contributed to these patients not being able to complete their end-of-study cognitive assessment. For example, almost a quarter of the patients who did not complete their end-of-study cognitive assessment failed to do so because they had already died.
Overall, the prevalence of patients indicating a cognitive decline was virtually identical among 11,363 patients who had been maintained on evolocumab, with a 3.7% rate, and the 11,292 patients in the placebo group, with a 3.6% rate. When analyzed by achieved level of LDL-C after 4 weeks on treatment, the 2,338 patients with a level below 20 mg/dL had a 3.8% rate of self-reported cognitive loss, compared with a 4.5% rate among 3,613 patients who had an LDL-C level of at least 100 mg/dL when measured 4 weeks into the study.
One of the strengths of the new cognitive analysis is that, although it did not use the more sophisticated assessment tests employed on fewer patients in the EBBINGHAUS substudy, it used the Everyday Cognition scale (Neuropsychiatry. 2008 Jul;22[4]: 531-44). “We asked patients what they have experienced, and in the end that is what’s important, so this adds to the neurocognitive testing,” run in EBBINGHAUS, Dr. Giugliano said in an interview.
“The neurocognitive results in the present study were self-reported, and that might be a limitation, as it is less specific and objective, but it is also a strength, as it could be more sensitive” especially for a “nocebo effect common to all lipid-lowering drugs linked to the bad reputation historically attributed to statins,” Dr. Mannarino said.
Should the new FOURIER data “be interpreted as definitive evidence that intensive LDL-C lowering with PCSK9 monoclonal antibodies has no major harmful cognitive effects, at least over a period of 3 years? The answer appears to be a qualified yes, but with three important caveats,” Jennifer G. Robinson, MD, a professor of epidemiology at the University of Iowa College of Public Health in Iowa City, said in an editorial that accompanied the new report (J Am Coll Cardiol. 2020 May 12;75[18]:2294-6). Her three caveats are the missing 18% of patients who never took the end-of-study assessment, the relative paucity of patients at very advanced age in FOURIER, in which patients averaged 62.5 years old, and the exclusion from FOURIER of patients with a history of hemorrhagic stroke. Dr. Robinson also cited the 2.2 year median follow-up as leaving unsettled the potential cognitive impact of longer treatment.
In response, Dr. Giugliano noted that the very large size of FOURIER and the 22,655 patients who completed their survey provided substantial numbers of patients to address some of these concerns in robust subgroup analyses. For example, the new report showed no signal of excess cognitive complaints with evolocumab treatment among 1,999 patients who were at least 75 years old when entering the study, or in more than 5,000 patients with a history of cerebrovascular disease at baseline, or in 1,990 patients with a history of a nonstroke neurologic disease. In addition, while he conceded that the 18% of patients not accounted for in the new study placed some limits on generalizability of the findings, he also maintained that this unavoidable failure to collect data from a modest percentage of patients doesn’t scuttle the overarching signal of cognitive safety for most patients. And regarding the duration of treatment monitored, he noted that 5-year follow-up cognitive assessments are planned.
FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Giugliano has received personal fees and research support from Amgen and from several other companies. Dr. Mannarino had no disclosures. Dr. Robinson has been a consultant to The Medicines Company, Novartis, and Pfizer, and she has received research funding to her institution from Amgen and several other companies.
SOURCE: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Correction: Dr. Giugliano's name was misspelled in an earlier version of this article.
Treatment with a PCSK9 inhibitor, as well as achieving dramatically lowered cholesterol levels, did not mess with patients’ minds. Results from a cognition self-assessment completed by more than 22,000 patients when they finished participation in the FOURIER pivotal outcomes trial for evolocumab showed no signal of mental harm from either treatment with this PCSK9 inhibitor or from reaching a serum level of low-density lipoprotein cholesterol (LDL-C) of less than 20 mg/dL.
“We observed that patients treated with evolocumab, as well as those who achieved progressively very low LDL-C at 4 weeks in the FOURIER trial, had similar self-reported cognition in comparison with those receiving placebo and those with higher achieved LDL-C levels,” wrote a team of researchers from the trial in an article published online on May 4 (J Am Coll Cardiol. 2020 May 12;75[18]: 2283-93). “These data confirm the neurocognitive safety of intensive LDL-C reduction with evolocumab while reducing recurrent CV [cardiovascular] events in high-risk patients, and suggest that very low achieved LDL-C levels may be safely targeted for high-risk patients.”
The findings added to prior results documenting the cognitive safety of evolocumab (Repatha) from a much smaller FOURIER substudy that involved more intensive testing, the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study with 1,204 patients drawn from the broader study and tested after a median 19 months on treatment (N Engl J Med. 2017 Aug 17;377[17]: 633-43), as well as reports of neurocognitive safety for the other U.S. approved PCSK9 (proprotein convertase subtilisin kexin 9) inhibitor, alirocumab (Praluent) (N Engl J Med. 2015 Apr 16;372[16]:1489-99), various statins (J Gen Intern Med. 2015 Mar;30[3]: 348-58), and a third type of LDL-C–lowering agent, ezetimibe (JAMA Cardiol. 2017 May;2[5]:547-55).
Despite this evidence from across several drug classes that all cut LDL-C a long-standing but unsubstantiated belief persists among some that lipid lowering, especially by statins, blunts mental function, misinformation that’s easy to find on the Internet. “I estimate that about 20% of patients prescribed a statin won’t take it because of something they’ve heard” including that statins make you stupid. “It’s hard to undo that,” said Robert P. Giugliano, MD, a cardiologist at Brigham and Women’s Hospital in Boston and senior author for the new FOURIER study as well as for EBBINGHAUS. The same stigma has not gained nearly as much traction for PCSK9 inhibitors, however, and Dr. Giugliano said he has also recently sensed what may be a downtrend in statin apprehension.
“The information added by this study is very important,” commented Massimo R. Mannarino, MD, an atherosclerotic disease researcher at the University of Perugia (Italy). “The prejudice and misinformation regarding possible side effects of statins among patients and also some physicians unfortunately remains very strong today,” he said in an interview. “My impression is that PCSK9 inhibitors are less affected by this negative bias and are seen as a safer alternative to statins.” Concerns about PCSK9 inhibitors have especially focused on “the possible risks from very low cholesterol levels on the brain.” The evidence from both studies and clinical experience “allows for a very positive opinion about the efficacy and safety of PCSK9 inhibitors, although the long-term effects still require a few more years of observation,” said Dr. Mannarino, who led a review of the evidence that clears this class from links to neurocognitive loss (J Clin Lipid. 2018 Sep 1;12[5]:1123-32).
FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) randomized 27,564 patients with atherosclerotic cardiovascular disease and elevated LDL cholesterol despite maximally tolerated standard treatment. Treatment with evolocumab for a median of 2.2 years resulted in a statistically significant 15% reduction in the study’s primary efficacy endpoint, compared with placebo (N Engl J Med. 2017 May 4;376[18]:1713-22), and led to the drug receiving an indication for lowering rates of MI, stroke, and symptom-driven coronary revascularization.
The prespecified substudy reported by Dr. Giugliano and his associates focused on a 23-question, validated, self-assessment survey of cognitive function completed by 22,655 of the FOURIER patients (82%). The more than 4,900 other patients in the study who did not complete the survey had modestly higher prevalence rates of various comorbidities at baseline, and also higher rates of adverse outcomes during follow-up, and in many cases these adverse outcome may have contributed to these patients not being able to complete their end-of-study cognitive assessment. For example, almost a quarter of the patients who did not complete their end-of-study cognitive assessment failed to do so because they had already died.
Overall, the prevalence of patients indicating a cognitive decline was virtually identical among 11,363 patients who had been maintained on evolocumab, with a 3.7% rate, and the 11,292 patients in the placebo group, with a 3.6% rate. When analyzed by achieved level of LDL-C after 4 weeks on treatment, the 2,338 patients with a level below 20 mg/dL had a 3.8% rate of self-reported cognitive loss, compared with a 4.5% rate among 3,613 patients who had an LDL-C level of at least 100 mg/dL when measured 4 weeks into the study.
One of the strengths of the new cognitive analysis is that, although it did not use the more sophisticated assessment tests employed on fewer patients in the EBBINGHAUS substudy, it used the Everyday Cognition scale (Neuropsychiatry. 2008 Jul;22[4]: 531-44). “We asked patients what they have experienced, and in the end that is what’s important, so this adds to the neurocognitive testing,” run in EBBINGHAUS, Dr. Giugliano said in an interview.
“The neurocognitive results in the present study were self-reported, and that might be a limitation, as it is less specific and objective, but it is also a strength, as it could be more sensitive” especially for a “nocebo effect common to all lipid-lowering drugs linked to the bad reputation historically attributed to statins,” Dr. Mannarino said.
Should the new FOURIER data “be interpreted as definitive evidence that intensive LDL-C lowering with PCSK9 monoclonal antibodies has no major harmful cognitive effects, at least over a period of 3 years? The answer appears to be a qualified yes, but with three important caveats,” Jennifer G. Robinson, MD, a professor of epidemiology at the University of Iowa College of Public Health in Iowa City, said in an editorial that accompanied the new report (J Am Coll Cardiol. 2020 May 12;75[18]:2294-6). Her three caveats are the missing 18% of patients who never took the end-of-study assessment, the relative paucity of patients at very advanced age in FOURIER, in which patients averaged 62.5 years old, and the exclusion from FOURIER of patients with a history of hemorrhagic stroke. Dr. Robinson also cited the 2.2 year median follow-up as leaving unsettled the potential cognitive impact of longer treatment.
In response, Dr. Giugliano noted that the very large size of FOURIER and the 22,655 patients who completed their survey provided substantial numbers of patients to address some of these concerns in robust subgroup analyses. For example, the new report showed no signal of excess cognitive complaints with evolocumab treatment among 1,999 patients who were at least 75 years old when entering the study, or in more than 5,000 patients with a history of cerebrovascular disease at baseline, or in 1,990 patients with a history of a nonstroke neurologic disease. In addition, while he conceded that the 18% of patients not accounted for in the new study placed some limits on generalizability of the findings, he also maintained that this unavoidable failure to collect data from a modest percentage of patients doesn’t scuttle the overarching signal of cognitive safety for most patients. And regarding the duration of treatment monitored, he noted that 5-year follow-up cognitive assessments are planned.
FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Giugliano has received personal fees and research support from Amgen and from several other companies. Dr. Mannarino had no disclosures. Dr. Robinson has been a consultant to The Medicines Company, Novartis, and Pfizer, and she has received research funding to her institution from Amgen and several other companies.
SOURCE: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Correction: Dr. Giugliano's name was misspelled in an earlier version of this article.
FROM JACC
Key clinical point: A cognition survey of a large number of trial participants showed no signal of adverse effects from evolocumab treatment.
Major finding: Survey results showed cognitive compromise in 3.7% of patients on evolocumab and in 3.6% control patients on placebo.
Study details:
Disclosures: FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Guigliano has received personal fees and research support from Amgen and from several other companies.
Source: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Predictors of ICH after thrombectomy identified
(ICH), new research suggests. In a study of nearly 600 patients undergoing thrombectomy, investigators combined a modified Thrombolysis in Cerebral Ischemia (TICI) score, an Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and glucose levels (the “TAG score”) to predict risk. Results showed that each unit increase in the combination score was associated with a significant, nearly twofold greater likelihood of symptomatic ICH.

“It is very easy” to calculate the new score in a clinical setting, lead author Mayra Johana Montalvo Perero, MD, Department of Neurology, Brown University and Rhode Island Hospital, Providence, said. “You just need three variables.”
The findings were presented online as part of the 2020 American Academy of Neurology Science Highlights.
Limited data
High TAG scores are associated with symptomatic ICH in patients receiving mechanical thrombectomy, Dr. Montalvo Perero and colleagues said.
Although clinical predictors of symptomatic ICH are well established, “there is limited data in patients who underwent mechanical thrombectomy,” the researchers noted.
To learn more, they assessed 578 patients (52% women; mean age, 73 years) who had mechanical thrombectomy for acute ischemic stroke at a comprehensive stroke center. Within this cohort, 19 patients (3.3%) developed symptomatic ICH.
The investigators compared clinical and radiographic findings between patients who experienced symptomatic ICH and those who did not.
The TICI score emerged as a predictor when each unit decrease in this score was associated with greater risk for symptomatic ICH (odds ratio, 5.13; 95% confidence interval, 1.84-14.29; P = .002).
Each one-point decrease in the ASPECTS score also predicted increased risk (OR, 1.52; 95% CI, 1.1-2.0; P = .003).
“The main driver is the size of the stroke core, which is correlated with the ASPECTS score,” Dr. Montalvo Perero said.
Each 10 mg/dL increase in glucose level also correlated with increased risk (OR, 1.07; 95% CI, 1.01-1.13; P = .018).
Twice the risk
The investigators then combined these three independent variables into a weighted TAG score based on a multivariate analysis. Each unit increase in this composite score was associated with increased risk of symptomatic ICH (OR, 1.98; 95% CI, 1.48-2.66; P < .001).
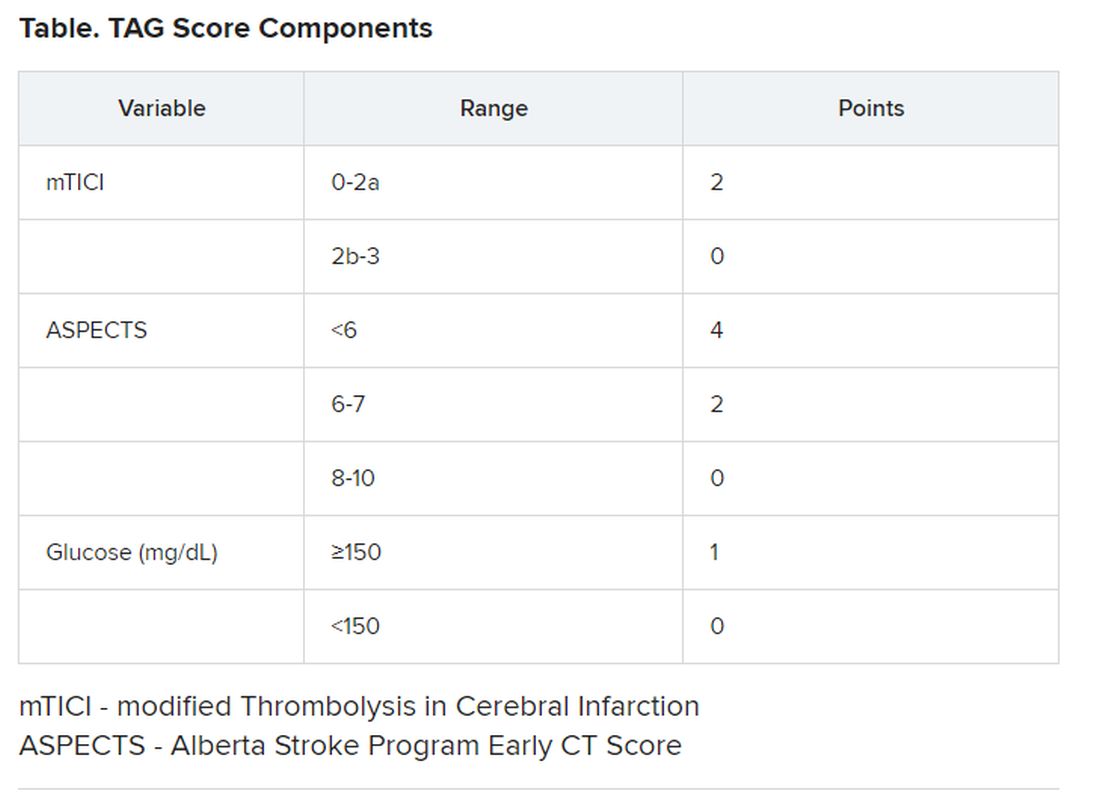
There was no association between patients who received tissue plasminogen activator (tPA) and risk of symptomatic ICH, which Dr. Montalvo Perero said was surprising.
However, “that may be due to a small number” of patients with symptomatic ICH included in the study, she said. “Therefore, that would be an interesting question to ask in future studies with bigger cohorts.”
Larger studies are also needed to validate this scoring system and to test strategies to reduce risk of symptomatic ICH and make thrombectomy safer in patients with elevated TAG scores, Dr. Montalvo Perero said.
A step in the right direction?
Commenting on the study, Jeremy Payne, MD, PhD, director of the Stroke Center at Banner Health’s University Medicine Neuroscience Institute in Phoenix, Arizona, noted the importance of predicting which patients might have secondary bleeding after interventional treatment of a large vessel occlusion stroke
“In aggregate, the role of endovascular thrombectomy is quite clear, but we still struggle to predict at the individual patient level who will benefit,” said Dr. Payne, who was not involved with the research.
Transfer and treatment of these patients also carries an economic cost. “Just getting patients to our center, where about 80% of the complex stroke patients come by helicopter, costs upwards of $30,000,” Dr. Payne said. “The financial argument isn’t one we like to talk much about, but we’re committing to spending probably $100,000-$200,000 on each person’s care.”
This study “attempts to address an important issue,” he said.
Predicting who is more likely to benefit leads to the assumption that if that were to happen, “we could skip all the rigamarole of helicopters and procedures, avoid the extra expense and particularly not make things worse than they already are,” explained Dr. Payne.
Potential limitations include that this is a single-center study and is based on an analysis of 19 patients out of 578. As a result, it is not clear that these findings will necessarily be generalizable to other centers, said Dr. Payne.
The TICI and ASPECTS “are pretty obvious markers of risk,” he noted. “The glucose levels, however, are more subtly interesting.”
He also pointed out that an association between diabetes and worse stroke outcomes is well established.
“The mechanisms are poorly understood, but the role of glucose keeps popping up as a potential marker of risk, and so it’s interesting that it bubbles up in their work too,” Dr. Payne said.
Furthermore, unlike TICI and ASPECTS, glucose levels are modifiable.
“Overall, then, we will continue to study this,” Dr. Payne said. “It’s very important to refine our ability to predict which patients may receive benefit versus harm from such procedures, and this is a step in the right direction.”
Some findings were also published December 2019 in the Journal of Neurology, Neurosurgery & Psychiatry.
Montalvo Perero and Payne have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Motalvo Perero MJ et al. AAN 2020, Abstract S20.001.
(ICH), new research suggests. In a study of nearly 600 patients undergoing thrombectomy, investigators combined a modified Thrombolysis in Cerebral Ischemia (TICI) score, an Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and glucose levels (the “TAG score”) to predict risk. Results showed that each unit increase in the combination score was associated with a significant, nearly twofold greater likelihood of symptomatic ICH.
“It is very easy” to calculate the new score in a clinical setting, lead author Mayra Johana Montalvo Perero, MD, Department of Neurology, Brown University and Rhode Island Hospital, Providence, said. “You just need three variables.”
The findings were presented online as part of the 2020 American Academy of Neurology Science Highlights.
Limited data
High TAG scores are associated with symptomatic ICH in patients receiving mechanical thrombectomy, Dr. Montalvo Perero and colleagues said.
Although clinical predictors of symptomatic ICH are well established, “there is limited data in patients who underwent mechanical thrombectomy,” the researchers noted.
To learn more, they assessed 578 patients (52% women; mean age, 73 years) who had mechanical thrombectomy for acute ischemic stroke at a comprehensive stroke center. Within this cohort, 19 patients (3.3%) developed symptomatic ICH.
The investigators compared clinical and radiographic findings between patients who experienced symptomatic ICH and those who did not.
The TICI score emerged as a predictor when each unit decrease in this score was associated with greater risk for symptomatic ICH (odds ratio, 5.13; 95% confidence interval, 1.84-14.29; P = .002).
Each one-point decrease in the ASPECTS score also predicted increased risk (OR, 1.52; 95% CI, 1.1-2.0; P = .003).
“The main driver is the size of the stroke core, which is correlated with the ASPECTS score,” Dr. Montalvo Perero said.
Each 10 mg/dL increase in glucose level also correlated with increased risk (OR, 1.07; 95% CI, 1.01-1.13; P = .018).
Twice the risk
The investigators then combined these three independent variables into a weighted TAG score based on a multivariate analysis. Each unit increase in this composite score was associated with increased risk of symptomatic ICH (OR, 1.98; 95% CI, 1.48-2.66; P < .001).
There was no association between patients who received tissue plasminogen activator (tPA) and risk of symptomatic ICH, which Dr. Montalvo Perero said was surprising.
However, “that may be due to a small number” of patients with symptomatic ICH included in the study, she said. “Therefore, that would be an interesting question to ask in future studies with bigger cohorts.”
Larger studies are also needed to validate this scoring system and to test strategies to reduce risk of symptomatic ICH and make thrombectomy safer in patients with elevated TAG scores, Dr. Montalvo Perero said.
A step in the right direction?
Commenting on the study, Jeremy Payne, MD, PhD, director of the Stroke Center at Banner Health’s University Medicine Neuroscience Institute in Phoenix, Arizona, noted the importance of predicting which patients might have secondary bleeding after interventional treatment of a large vessel occlusion stroke
“In aggregate, the role of endovascular thrombectomy is quite clear, but we still struggle to predict at the individual patient level who will benefit,” said Dr. Payne, who was not involved with the research.
Transfer and treatment of these patients also carries an economic cost. “Just getting patients to our center, where about 80% of the complex stroke patients come by helicopter, costs upwards of $30,000,” Dr. Payne said. “The financial argument isn’t one we like to talk much about, but we’re committing to spending probably $100,000-$200,000 on each person’s care.”
This study “attempts to address an important issue,” he said.
Predicting who is more likely to benefit leads to the assumption that if that were to happen, “we could skip all the rigamarole of helicopters and procedures, avoid the extra expense and particularly not make things worse than they already are,” explained Dr. Payne.
Potential limitations include that this is a single-center study and is based on an analysis of 19 patients out of 578. As a result, it is not clear that these findings will necessarily be generalizable to other centers, said Dr. Payne.
The TICI and ASPECTS “are pretty obvious markers of risk,” he noted. “The glucose levels, however, are more subtly interesting.”
He also pointed out that an association between diabetes and worse stroke outcomes is well established.
“The mechanisms are poorly understood, but the role of glucose keeps popping up as a potential marker of risk, and so it’s interesting that it bubbles up in their work too,” Dr. Payne said.
Furthermore, unlike TICI and ASPECTS, glucose levels are modifiable.
“Overall, then, we will continue to study this,” Dr. Payne said. “It’s very important to refine our ability to predict which patients may receive benefit versus harm from such procedures, and this is a step in the right direction.”
Some findings were also published December 2019 in the Journal of Neurology, Neurosurgery & Psychiatry.
Montalvo Perero and Payne have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Motalvo Perero MJ et al. AAN 2020, Abstract S20.001.
(ICH), new research suggests. In a study of nearly 600 patients undergoing thrombectomy, investigators combined a modified Thrombolysis in Cerebral Ischemia (TICI) score, an Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and glucose levels (the “TAG score”) to predict risk. Results showed that each unit increase in the combination score was associated with a significant, nearly twofold greater likelihood of symptomatic ICH.
“It is very easy” to calculate the new score in a clinical setting, lead author Mayra Johana Montalvo Perero, MD, Department of Neurology, Brown University and Rhode Island Hospital, Providence, said. “You just need three variables.”
The findings were presented online as part of the 2020 American Academy of Neurology Science Highlights.
Limited data
High TAG scores are associated with symptomatic ICH in patients receiving mechanical thrombectomy, Dr. Montalvo Perero and colleagues said.
Although clinical predictors of symptomatic ICH are well established, “there is limited data in patients who underwent mechanical thrombectomy,” the researchers noted.
To learn more, they assessed 578 patients (52% women; mean age, 73 years) who had mechanical thrombectomy for acute ischemic stroke at a comprehensive stroke center. Within this cohort, 19 patients (3.3%) developed symptomatic ICH.
The investigators compared clinical and radiographic findings between patients who experienced symptomatic ICH and those who did not.
The TICI score emerged as a predictor when each unit decrease in this score was associated with greater risk for symptomatic ICH (odds ratio, 5.13; 95% confidence interval, 1.84-14.29; P = .002).
Each one-point decrease in the ASPECTS score also predicted increased risk (OR, 1.52; 95% CI, 1.1-2.0; P = .003).
“The main driver is the size of the stroke core, which is correlated with the ASPECTS score,” Dr. Montalvo Perero said.
Each 10 mg/dL increase in glucose level also correlated with increased risk (OR, 1.07; 95% CI, 1.01-1.13; P = .018).
Twice the risk
The investigators then combined these three independent variables into a weighted TAG score based on a multivariate analysis. Each unit increase in this composite score was associated with increased risk of symptomatic ICH (OR, 1.98; 95% CI, 1.48-2.66; P < .001).
There was no association between patients who received tissue plasminogen activator (tPA) and risk of symptomatic ICH, which Dr. Montalvo Perero said was surprising.
However, “that may be due to a small number” of patients with symptomatic ICH included in the study, she said. “Therefore, that would be an interesting question to ask in future studies with bigger cohorts.”
Larger studies are also needed to validate this scoring system and to test strategies to reduce risk of symptomatic ICH and make thrombectomy safer in patients with elevated TAG scores, Dr. Montalvo Perero said.
A step in the right direction?
Commenting on the study, Jeremy Payne, MD, PhD, director of the Stroke Center at Banner Health’s University Medicine Neuroscience Institute in Phoenix, Arizona, noted the importance of predicting which patients might have secondary bleeding after interventional treatment of a large vessel occlusion stroke
“In aggregate, the role of endovascular thrombectomy is quite clear, but we still struggle to predict at the individual patient level who will benefit,” said Dr. Payne, who was not involved with the research.
Transfer and treatment of these patients also carries an economic cost. “Just getting patients to our center, where about 80% of the complex stroke patients come by helicopter, costs upwards of $30,000,” Dr. Payne said. “The financial argument isn’t one we like to talk much about, but we’re committing to spending probably $100,000-$200,000 on each person’s care.”
This study “attempts to address an important issue,” he said.
Predicting who is more likely to benefit leads to the assumption that if that were to happen, “we could skip all the rigamarole of helicopters and procedures, avoid the extra expense and particularly not make things worse than they already are,” explained Dr. Payne.
Potential limitations include that this is a single-center study and is based on an analysis of 19 patients out of 578. As a result, it is not clear that these findings will necessarily be generalizable to other centers, said Dr. Payne.
The TICI and ASPECTS “are pretty obvious markers of risk,” he noted. “The glucose levels, however, are more subtly interesting.”
He also pointed out that an association between diabetes and worse stroke outcomes is well established.
“The mechanisms are poorly understood, but the role of glucose keeps popping up as a potential marker of risk, and so it’s interesting that it bubbles up in their work too,” Dr. Payne said.
Furthermore, unlike TICI and ASPECTS, glucose levels are modifiable.
“Overall, then, we will continue to study this,” Dr. Payne said. “It’s very important to refine our ability to predict which patients may receive benefit versus harm from such procedures, and this is a step in the right direction.”
Some findings were also published December 2019 in the Journal of Neurology, Neurosurgery & Psychiatry.
Montalvo Perero and Payne have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Motalvo Perero MJ et al. AAN 2020, Abstract S20.001.
AAN 2020
COVID-19: Are acute stroke patients avoiding emergency care?
(EDs).
Stroke specialists in New Orleans, Chicago, Seattle, and elsewhere told Medscape Medical News they are seeing a precipitous drop in the number of acute strokes at their institutions – and not just in the number of milder cases. Doctors on Twitter are sharing similar reports and are using social media to highlight this issue.
Gabriel Vidal, MD, a vascular and interventional neurologist at the Ochsner Medical Center, New Orleans, Louisiana, said there are “definitely” fewer patients with stroke and transient ischemic attack (TIA) seeking care at his facility and others throughout the New Orleans area, which has been hard hit by COVID-19.
“Even in Louisiana, we have a very large 53-hospital telestroke network, and the number of consults has diminished greatly,” Vidal added.
In Chicago, emergency medical service activations for patients with suspected strokes are down about 30%, Shyam Prabhakaran, MD, professor and chair of neurology at the University of Chicago Biological Sciences, Illinois, told Medscape Medical News.
“It appears to be that mild stroke and TIA patients may be more likely to stay at home and seek alternative care rather than come to the ED,” Prabhakaran said. However, “the severe strokes may be less affected and continue to come to emergency departments.”
“Getting the Word Out”
That may not be the whole story in Seattle, Washington, where a stroke specialist at Harborview Medical Center reported a drop in patients across the stroke-severity spectrum.
Some patients with milder strokes no longer come to Harborview for a comprehensive evaluation and workup, but that is only “a partial explanation,” said David Tirschwell, MD, medical director of comprehensive stroke care at the University of Washington (UW) Medicine Stroke Center at Harborview and a professor of neurology at UW.
“The thrombectomies are down also,” he added. “It’s hard to have great numbers in real time, but it’s probably safe to say it’s at least a 50% reduction in the number of admissions.”
As a stroke referral center, his institution is seeing fewer local cases and referrals from outside hospitals. “I think both of those sources for admissions of stroke cases are down,” Tirschwell said.
Recognizing the seriousness of forgoing essential care for acute stroke, neurologists, institutions, and medical groups are taking to social media to potentially save lives.
“Across our @FLStrokeReg we are seeing less patients with #stroke symptoms coming to our hospitals. We need to get the word out that our teams are working hard to safely provide care when needed during #COVID19,” tweeted Ralph Sacco, MD, chief and professor of neurology, University of Miami Miller School of Medicine in South Florida.
Although Florida Stroke Registry data are not publicly available, anecdotal reports suggest that stroke admissions are down among many hospitals, Sacco told Medscape Medical News.
Furthermore, this is not a phenomenon only in the United States. “This has also been reported in other nations hit by COVID-19,” he said.
China is a prime example. There, many stroke centers have shown reduced functioning “because of fear of in-hospital cross infection and lack of experienced stroke care experts,” Jing Zhao, MD, PhD, and colleagues write in an editorial published online March 31 in Stroke.
Preliminary data show that “thrombectomies in Shanghai decreased by 50% in the first month after the Spring Festival compared with the same period in 2019,” write the editorialists, who are from Kings College London and the University of Pennsylvania in Philadelphia.
“Although the control of the COVID-19 is very important, at the same time, the management of stroke must not be neglected,” they add.
“Over 9000 new stroke cases occur each day in China alone. It cannot be right that treatment for one potentially curable disease is euthanized at the expense of another.”
Fear Factor?
The reasons individuals who may have experienced a stroke are avoiding emergency care is unclear at the moment. “I’m not really sure anyone really understands why, quite honestly,” Tirschwell said.
Until survey data or other data emerge, many experts are assuming that fear of COVID-19 is trumping other medical concerns, including emergency treatment of stroke.
“We believe this could represent patients being fearful to come to medical facilities with stroke-like symptoms, given the COVID-19 pandemic,” said Sacco, who is also incoming editor-in-chief of Stroke.
The BBC has been getting the word out in the United Kingdom via social media, with a tweet to “Dial 999 for stroke emergencies despite coronavirus.”
The World Stroke Campaign is also using Twitter to emphasize the need for urgent stroke care when appropriate:
“Don’t let concerns about COVID19 prevent you from seeking emergency treatment for stroke. If you spot the signs of stroke act FAST. Get emergency medical assistance,” the group urged in a tweet.
Don’t Hesitate
The American Heart Association (AHA) has addressed this troubling trend as well.
“People with serious symptoms shouldn’t ignore them,” Sarah Perlman, MD, associate professor of emergency medicine at the University of Colorado School of Medicine, Denver, states in an article on the AHA website.
Perlman added that some individuals who have signs of stroke and heart disease may hesitate to seek care because of fear that they are adding to an overburdened healthcare staff and system. However, she dismissed those concerns outright.
“If you’re experiencing warning signs of a heart attack or stroke, call 911,” she said. “Clearly, if there’s an emergency, we are available and capable and eager to take care of you.”
This article first appeared on Medscape.com.
(EDs).
Stroke specialists in New Orleans, Chicago, Seattle, and elsewhere told Medscape Medical News they are seeing a precipitous drop in the number of acute strokes at their institutions – and not just in the number of milder cases. Doctors on Twitter are sharing similar reports and are using social media to highlight this issue.
Gabriel Vidal, MD, a vascular and interventional neurologist at the Ochsner Medical Center, New Orleans, Louisiana, said there are “definitely” fewer patients with stroke and transient ischemic attack (TIA) seeking care at his facility and others throughout the New Orleans area, which has been hard hit by COVID-19.
“Even in Louisiana, we have a very large 53-hospital telestroke network, and the number of consults has diminished greatly,” Vidal added.
In Chicago, emergency medical service activations for patients with suspected strokes are down about 30%, Shyam Prabhakaran, MD, professor and chair of neurology at the University of Chicago Biological Sciences, Illinois, told Medscape Medical News.
“It appears to be that mild stroke and TIA patients may be more likely to stay at home and seek alternative care rather than come to the ED,” Prabhakaran said. However, “the severe strokes may be less affected and continue to come to emergency departments.”
“Getting the Word Out”
That may not be the whole story in Seattle, Washington, where a stroke specialist at Harborview Medical Center reported a drop in patients across the stroke-severity spectrum.
Some patients with milder strokes no longer come to Harborview for a comprehensive evaluation and workup, but that is only “a partial explanation,” said David Tirschwell, MD, medical director of comprehensive stroke care at the University of Washington (UW) Medicine Stroke Center at Harborview and a professor of neurology at UW.
“The thrombectomies are down also,” he added. “It’s hard to have great numbers in real time, but it’s probably safe to say it’s at least a 50% reduction in the number of admissions.”
As a stroke referral center, his institution is seeing fewer local cases and referrals from outside hospitals. “I think both of those sources for admissions of stroke cases are down,” Tirschwell said.
Recognizing the seriousness of forgoing essential care for acute stroke, neurologists, institutions, and medical groups are taking to social media to potentially save lives.
“Across our @FLStrokeReg we are seeing less patients with #stroke symptoms coming to our hospitals. We need to get the word out that our teams are working hard to safely provide care when needed during #COVID19,” tweeted Ralph Sacco, MD, chief and professor of neurology, University of Miami Miller School of Medicine in South Florida.
Although Florida Stroke Registry data are not publicly available, anecdotal reports suggest that stroke admissions are down among many hospitals, Sacco told Medscape Medical News.
Furthermore, this is not a phenomenon only in the United States. “This has also been reported in other nations hit by COVID-19,” he said.
China is a prime example. There, many stroke centers have shown reduced functioning “because of fear of in-hospital cross infection and lack of experienced stroke care experts,” Jing Zhao, MD, PhD, and colleagues write in an editorial published online March 31 in Stroke.
Preliminary data show that “thrombectomies in Shanghai decreased by 50% in the first month after the Spring Festival compared with the same period in 2019,” write the editorialists, who are from Kings College London and the University of Pennsylvania in Philadelphia.
“Although the control of the COVID-19 is very important, at the same time, the management of stroke must not be neglected,” they add.
“Over 9000 new stroke cases occur each day in China alone. It cannot be right that treatment for one potentially curable disease is euthanized at the expense of another.”
Fear Factor?
The reasons individuals who may have experienced a stroke are avoiding emergency care is unclear at the moment. “I’m not really sure anyone really understands why, quite honestly,” Tirschwell said.
Until survey data or other data emerge, many experts are assuming that fear of COVID-19 is trumping other medical concerns, including emergency treatment of stroke.
“We believe this could represent patients being fearful to come to medical facilities with stroke-like symptoms, given the COVID-19 pandemic,” said Sacco, who is also incoming editor-in-chief of Stroke.
The BBC has been getting the word out in the United Kingdom via social media, with a tweet to “Dial 999 for stroke emergencies despite coronavirus.”
The World Stroke Campaign is also using Twitter to emphasize the need for urgent stroke care when appropriate:
“Don’t let concerns about COVID19 prevent you from seeking emergency treatment for stroke. If you spot the signs of stroke act FAST. Get emergency medical assistance,” the group urged in a tweet.
Don’t Hesitate
The American Heart Association (AHA) has addressed this troubling trend as well.
“People with serious symptoms shouldn’t ignore them,” Sarah Perlman, MD, associate professor of emergency medicine at the University of Colorado School of Medicine, Denver, states in an article on the AHA website.
Perlman added that some individuals who have signs of stroke and heart disease may hesitate to seek care because of fear that they are adding to an overburdened healthcare staff and system. However, she dismissed those concerns outright.
“If you’re experiencing warning signs of a heart attack or stroke, call 911,” she said. “Clearly, if there’s an emergency, we are available and capable and eager to take care of you.”
This article first appeared on Medscape.com.
(EDs).
Stroke specialists in New Orleans, Chicago, Seattle, and elsewhere told Medscape Medical News they are seeing a precipitous drop in the number of acute strokes at their institutions – and not just in the number of milder cases. Doctors on Twitter are sharing similar reports and are using social media to highlight this issue.
Gabriel Vidal, MD, a vascular and interventional neurologist at the Ochsner Medical Center, New Orleans, Louisiana, said there are “definitely” fewer patients with stroke and transient ischemic attack (TIA) seeking care at his facility and others throughout the New Orleans area, which has been hard hit by COVID-19.
“Even in Louisiana, we have a very large 53-hospital telestroke network, and the number of consults has diminished greatly,” Vidal added.
In Chicago, emergency medical service activations for patients with suspected strokes are down about 30%, Shyam Prabhakaran, MD, professor and chair of neurology at the University of Chicago Biological Sciences, Illinois, told Medscape Medical News.
“It appears to be that mild stroke and TIA patients may be more likely to stay at home and seek alternative care rather than come to the ED,” Prabhakaran said. However, “the severe strokes may be less affected and continue to come to emergency departments.”
“Getting the Word Out”
That may not be the whole story in Seattle, Washington, where a stroke specialist at Harborview Medical Center reported a drop in patients across the stroke-severity spectrum.
Some patients with milder strokes no longer come to Harborview for a comprehensive evaluation and workup, but that is only “a partial explanation,” said David Tirschwell, MD, medical director of comprehensive stroke care at the University of Washington (UW) Medicine Stroke Center at Harborview and a professor of neurology at UW.
“The thrombectomies are down also,” he added. “It’s hard to have great numbers in real time, but it’s probably safe to say it’s at least a 50% reduction in the number of admissions.”
As a stroke referral center, his institution is seeing fewer local cases and referrals from outside hospitals. “I think both of those sources for admissions of stroke cases are down,” Tirschwell said.
Recognizing the seriousness of forgoing essential care for acute stroke, neurologists, institutions, and medical groups are taking to social media to potentially save lives.
“Across our @FLStrokeReg we are seeing less patients with #stroke symptoms coming to our hospitals. We need to get the word out that our teams are working hard to safely provide care when needed during #COVID19,” tweeted Ralph Sacco, MD, chief and professor of neurology, University of Miami Miller School of Medicine in South Florida.
Although Florida Stroke Registry data are not publicly available, anecdotal reports suggest that stroke admissions are down among many hospitals, Sacco told Medscape Medical News.
Furthermore, this is not a phenomenon only in the United States. “This has also been reported in other nations hit by COVID-19,” he said.
China is a prime example. There, many stroke centers have shown reduced functioning “because of fear of in-hospital cross infection and lack of experienced stroke care experts,” Jing Zhao, MD, PhD, and colleagues write in an editorial published online March 31 in Stroke.
Preliminary data show that “thrombectomies in Shanghai decreased by 50% in the first month after the Spring Festival compared with the same period in 2019,” write the editorialists, who are from Kings College London and the University of Pennsylvania in Philadelphia.
“Although the control of the COVID-19 is very important, at the same time, the management of stroke must not be neglected,” they add.
“Over 9000 new stroke cases occur each day in China alone. It cannot be right that treatment for one potentially curable disease is euthanized at the expense of another.”
Fear Factor?
The reasons individuals who may have experienced a stroke are avoiding emergency care is unclear at the moment. “I’m not really sure anyone really understands why, quite honestly,” Tirschwell said.
Until survey data or other data emerge, many experts are assuming that fear of COVID-19 is trumping other medical concerns, including emergency treatment of stroke.
“We believe this could represent patients being fearful to come to medical facilities with stroke-like symptoms, given the COVID-19 pandemic,” said Sacco, who is also incoming editor-in-chief of Stroke.
The BBC has been getting the word out in the United Kingdom via social media, with a tweet to “Dial 999 for stroke emergencies despite coronavirus.”
The World Stroke Campaign is also using Twitter to emphasize the need for urgent stroke care when appropriate:
“Don’t let concerns about COVID19 prevent you from seeking emergency treatment for stroke. If you spot the signs of stroke act FAST. Get emergency medical assistance,” the group urged in a tweet.
Don’t Hesitate
The American Heart Association (AHA) has addressed this troubling trend as well.
“People with serious symptoms shouldn’t ignore them,” Sarah Perlman, MD, associate professor of emergency medicine at the University of Colorado School of Medicine, Denver, states in an article on the AHA website.
Perlman added that some individuals who have signs of stroke and heart disease may hesitate to seek care because of fear that they are adding to an overburdened healthcare staff and system. However, she dismissed those concerns outright.
“If you’re experiencing warning signs of a heart attack or stroke, call 911,” she said. “Clearly, if there’s an emergency, we are available and capable and eager to take care of you.”
This article first appeared on Medscape.com.