User login
ED visits for mental health, substance use doubled in 1 decade
ED visits related to mental health conditions increased nearly twofold from 2007-2008 to 2015-2016, new research suggests.

Data from the National Hospital Ambulatory Medical Care Survey (NHAMCS) showed that, over the 10-year study period, the proportion of ED visits for mental health diagnoses increased from 6.6% to 10.9%, with substance use accounting for much of the increase.
Although there have been policy efforts, such as expanding access to mental health care as part of the Affordable Care Act (ACA) of 2011, the senior author Taeho Greg Rhee, PhD, MSW, said in an interview.
“Treating mental health conditions in EDs is often considered suboptimal” because of limited time for full psychiatric assessment, lack of trained providers, and limited privacy in EDs, said Dr. Rhee of Yale University, New Haven, Conn.
The findings were published online July 28 in The Journal of Clinical Psychiatry.
“Outdated” research
Roughly one-fifth of U.S. adults experience some type of mental, behavioral, or emotional disorder annually. Moreover, the suicide rate has been steadily increasing, and there continues to be a “raging opioid epidemic,” the researchers wrote.
Despite these alarming figures, 57.4% of adults with mental illness reported in 2017 that they had not received any mental health treatment in the past year, reported the investigators.
Previous research has suggested that many adults have difficulty seeking outpatient mental health treatment and may turn to EDs instead. However, most studies of mental health ED use “are by now outdated, as they used data from years prior to the full implementation of the ACA,” the researchers noted.
“More Americans are suffering from mental illness, and given the recent policy efforts of expanding access to mental health care, we were questioning if ED visits due to mental health has changed or not,” Dr. Rhee said.
To investigate the question, the researchers conducted a cross-sectional analysis of data from the NHAMCS, a publicly available dataset provided by the National Center for Health Statistics of the Centers for Disease Control and Prevention.
They grouped psychiatric diagnoses into five categories: mood disorders, anxiety disorders, psychosis or schizophrenia, suicide attempt or ideation, or other/unspecified. Substance use diagnoses were grouped into six categories: alcohol, amphetamine, cannabis, cocaine, opioid, or other/unspecified.
These categories were used to determine the type of disorder a patient had, whether the patient had both psychiatric and substance-related diagnoses, and whether the patient received multiple mental health diagnoses at the time of the ED visit.
Sociodemographic covariates included age, sex, race/ethnicity, and insurance coverage.
Twofold and fourfold increases
Of 100.9 million outpatient ED visits that took place between 2007 and 2016, approximately 8.4 million (8.3%) were for psychiatric or substance use–related diagnoses. Also, the visits were more likely from adults who were younger than 45 years, male, non-Hispanic White, and covered by Medicaid or other public insurance types (58.5%, 52.5%, 65.2%, and 58.6%, respectively).
The overall rate of ED visits for any mental health diagnosis nearly doubled between 2007-2008 and 2015-2016. The rate of visits in which both psychiatric and substance use–related diagnoses increased fourfold during that time span. ED visits involving at least two mental health diagnoses increased twofold.
Additional changes in the number of visits are listed below (for each, P < .001).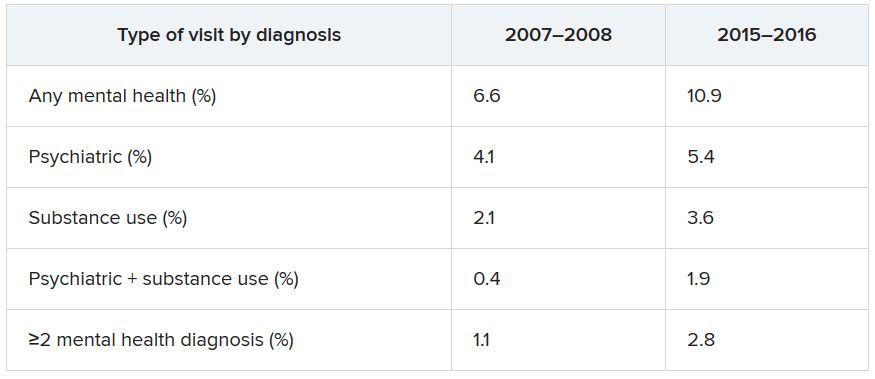
When these comparisons were adjusted for age, sex, and race/ethnicity, “linearly increasing trends of mental health–related ED visits were consistently found in all categories,” the authors reported. No trends were found regarding age, sex, or race/ethnicity. By contrast, mental health–related ED visits in which Medicaid was identified as the primary source of insurance nearly doubled between 2007–2008 and 2015–2016 (from 27.2% to 42.8%).
Other/unspecified psychiatric diagnoses, such as adjustment disorder and personality disorders, almost tripled between 2007-2008 and 2015-2016 (from 1,040 to 2,961 per 100,000 ED visits). ED visits for mood disorders and anxiety disorders also increased over time.
Alcohol-related ED visits were the most common substance use visits, increasing from 1,669 in 2007-2008 to 3,007 per 100,000 visits in 2015-2016. Amphetamine- and opioid-related ED visits more than doubled, and other/unspecified–related ED visits more than tripled during that time.
“One explanation why ED visits for mental health conditions have increased is that substance-related problems, which include overdose/self-injury issues, have increased over time,” Dr. Rhee noted, which “makes sense,” inasmuch as opioid, cannabis, and amphetamine use has increased across the country.
Another explanation is that, although mental health care access has been expanded through the ACA, “people, especially those with lower socioeconomic backgrounds, do not know how to get access to care and are still underserved,” he said.
“If mental health–related ED visits continue to increase in the future, there are several steps to be made. ED providers need to be better equipped with mental health care, and behavioral health should be better integrated as part of the care coordination,” said Dr. Rhee.
He added that reimbursement models across different insurance types, such as Medicare, Medicaid, and private insurance, “should consider expanding their coverage of mental health treatment in ED settings.”
“Canary in the coal mine”

Commenting on the study in an interview, Benjamin Druss, MD, MPH, professor and Rosalynn Carter Chair in Mental Health, Rollins School of Public Health, Emory University, Atlanta, called EDs the “canaries in the coal mine” for the broader health system.
The growing number of ED visits for behavioral problems “could represent both a rise in acute conditions such as substance use and lack of access to outpatient treatment,” said Dr. Druss, who was not involved with the research.
The findings “suggest the importance of strategies to effectively manage patients with behavioral conditions in ED settings and to effectively link them with high-quality outpatient care,” he noted.
Dr. Rhee has received funding from the National Institute on Aging and the American Foundation for Suicide Prevention. The other study authors and Dr. Druss report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
ED visits related to mental health conditions increased nearly twofold from 2007-2008 to 2015-2016, new research suggests.
Data from the National Hospital Ambulatory Medical Care Survey (NHAMCS) showed that, over the 10-year study period, the proportion of ED visits for mental health diagnoses increased from 6.6% to 10.9%, with substance use accounting for much of the increase.
Although there have been policy efforts, such as expanding access to mental health care as part of the Affordable Care Act (ACA) of 2011, the senior author Taeho Greg Rhee, PhD, MSW, said in an interview.
“Treating mental health conditions in EDs is often considered suboptimal” because of limited time for full psychiatric assessment, lack of trained providers, and limited privacy in EDs, said Dr. Rhee of Yale University, New Haven, Conn.
The findings were published online July 28 in The Journal of Clinical Psychiatry.
“Outdated” research
Roughly one-fifth of U.S. adults experience some type of mental, behavioral, or emotional disorder annually. Moreover, the suicide rate has been steadily increasing, and there continues to be a “raging opioid epidemic,” the researchers wrote.
Despite these alarming figures, 57.4% of adults with mental illness reported in 2017 that they had not received any mental health treatment in the past year, reported the investigators.
Previous research has suggested that many adults have difficulty seeking outpatient mental health treatment and may turn to EDs instead. However, most studies of mental health ED use “are by now outdated, as they used data from years prior to the full implementation of the ACA,” the researchers noted.
“More Americans are suffering from mental illness, and given the recent policy efforts of expanding access to mental health care, we were questioning if ED visits due to mental health has changed or not,” Dr. Rhee said.
To investigate the question, the researchers conducted a cross-sectional analysis of data from the NHAMCS, a publicly available dataset provided by the National Center for Health Statistics of the Centers for Disease Control and Prevention.
They grouped psychiatric diagnoses into five categories: mood disorders, anxiety disorders, psychosis or schizophrenia, suicide attempt or ideation, or other/unspecified. Substance use diagnoses were grouped into six categories: alcohol, amphetamine, cannabis, cocaine, opioid, or other/unspecified.
These categories were used to determine the type of disorder a patient had, whether the patient had both psychiatric and substance-related diagnoses, and whether the patient received multiple mental health diagnoses at the time of the ED visit.
Sociodemographic covariates included age, sex, race/ethnicity, and insurance coverage.
Twofold and fourfold increases
Of 100.9 million outpatient ED visits that took place between 2007 and 2016, approximately 8.4 million (8.3%) were for psychiatric or substance use–related diagnoses. Also, the visits were more likely from adults who were younger than 45 years, male, non-Hispanic White, and covered by Medicaid or other public insurance types (58.5%, 52.5%, 65.2%, and 58.6%, respectively).
The overall rate of ED visits for any mental health diagnosis nearly doubled between 2007-2008 and 2015-2016. The rate of visits in which both psychiatric and substance use–related diagnoses increased fourfold during that time span. ED visits involving at least two mental health diagnoses increased twofold.
Additional changes in the number of visits are listed below (for each, P < .001).
When these comparisons were adjusted for age, sex, and race/ethnicity, “linearly increasing trends of mental health–related ED visits were consistently found in all categories,” the authors reported. No trends were found regarding age, sex, or race/ethnicity. By contrast, mental health–related ED visits in which Medicaid was identified as the primary source of insurance nearly doubled between 2007–2008 and 2015–2016 (from 27.2% to 42.8%).
Other/unspecified psychiatric diagnoses, such as adjustment disorder and personality disorders, almost tripled between 2007-2008 and 2015-2016 (from 1,040 to 2,961 per 100,000 ED visits). ED visits for mood disorders and anxiety disorders also increased over time.
Alcohol-related ED visits were the most common substance use visits, increasing from 1,669 in 2007-2008 to 3,007 per 100,000 visits in 2015-2016. Amphetamine- and opioid-related ED visits more than doubled, and other/unspecified–related ED visits more than tripled during that time.
“One explanation why ED visits for mental health conditions have increased is that substance-related problems, which include overdose/self-injury issues, have increased over time,” Dr. Rhee noted, which “makes sense,” inasmuch as opioid, cannabis, and amphetamine use has increased across the country.
Another explanation is that, although mental health care access has been expanded through the ACA, “people, especially those with lower socioeconomic backgrounds, do not know how to get access to care and are still underserved,” he said.
“If mental health–related ED visits continue to increase in the future, there are several steps to be made. ED providers need to be better equipped with mental health care, and behavioral health should be better integrated as part of the care coordination,” said Dr. Rhee.
He added that reimbursement models across different insurance types, such as Medicare, Medicaid, and private insurance, “should consider expanding their coverage of mental health treatment in ED settings.”
“Canary in the coal mine”
Commenting on the study in an interview, Benjamin Druss, MD, MPH, professor and Rosalynn Carter Chair in Mental Health, Rollins School of Public Health, Emory University, Atlanta, called EDs the “canaries in the coal mine” for the broader health system.
The growing number of ED visits for behavioral problems “could represent both a rise in acute conditions such as substance use and lack of access to outpatient treatment,” said Dr. Druss, who was not involved with the research.
The findings “suggest the importance of strategies to effectively manage patients with behavioral conditions in ED settings and to effectively link them with high-quality outpatient care,” he noted.
Dr. Rhee has received funding from the National Institute on Aging and the American Foundation for Suicide Prevention. The other study authors and Dr. Druss report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
ED visits related to mental health conditions increased nearly twofold from 2007-2008 to 2015-2016, new research suggests.
Data from the National Hospital Ambulatory Medical Care Survey (NHAMCS) showed that, over the 10-year study period, the proportion of ED visits for mental health diagnoses increased from 6.6% to 10.9%, with substance use accounting for much of the increase.
Although there have been policy efforts, such as expanding access to mental health care as part of the Affordable Care Act (ACA) of 2011, the senior author Taeho Greg Rhee, PhD, MSW, said in an interview.
“Treating mental health conditions in EDs is often considered suboptimal” because of limited time for full psychiatric assessment, lack of trained providers, and limited privacy in EDs, said Dr. Rhee of Yale University, New Haven, Conn.
The findings were published online July 28 in The Journal of Clinical Psychiatry.
“Outdated” research
Roughly one-fifth of U.S. adults experience some type of mental, behavioral, or emotional disorder annually. Moreover, the suicide rate has been steadily increasing, and there continues to be a “raging opioid epidemic,” the researchers wrote.
Despite these alarming figures, 57.4% of adults with mental illness reported in 2017 that they had not received any mental health treatment in the past year, reported the investigators.
Previous research has suggested that many adults have difficulty seeking outpatient mental health treatment and may turn to EDs instead. However, most studies of mental health ED use “are by now outdated, as they used data from years prior to the full implementation of the ACA,” the researchers noted.
“More Americans are suffering from mental illness, and given the recent policy efforts of expanding access to mental health care, we were questioning if ED visits due to mental health has changed or not,” Dr. Rhee said.
To investigate the question, the researchers conducted a cross-sectional analysis of data from the NHAMCS, a publicly available dataset provided by the National Center for Health Statistics of the Centers for Disease Control and Prevention.
They grouped psychiatric diagnoses into five categories: mood disorders, anxiety disorders, psychosis or schizophrenia, suicide attempt or ideation, or other/unspecified. Substance use diagnoses were grouped into six categories: alcohol, amphetamine, cannabis, cocaine, opioid, or other/unspecified.
These categories were used to determine the type of disorder a patient had, whether the patient had both psychiatric and substance-related diagnoses, and whether the patient received multiple mental health diagnoses at the time of the ED visit.
Sociodemographic covariates included age, sex, race/ethnicity, and insurance coverage.
Twofold and fourfold increases
Of 100.9 million outpatient ED visits that took place between 2007 and 2016, approximately 8.4 million (8.3%) were for psychiatric or substance use–related diagnoses. Also, the visits were more likely from adults who were younger than 45 years, male, non-Hispanic White, and covered by Medicaid or other public insurance types (58.5%, 52.5%, 65.2%, and 58.6%, respectively).
The overall rate of ED visits for any mental health diagnosis nearly doubled between 2007-2008 and 2015-2016. The rate of visits in which both psychiatric and substance use–related diagnoses increased fourfold during that time span. ED visits involving at least two mental health diagnoses increased twofold.
Additional changes in the number of visits are listed below (for each, P < .001).
When these comparisons were adjusted for age, sex, and race/ethnicity, “linearly increasing trends of mental health–related ED visits were consistently found in all categories,” the authors reported. No trends were found regarding age, sex, or race/ethnicity. By contrast, mental health–related ED visits in which Medicaid was identified as the primary source of insurance nearly doubled between 2007–2008 and 2015–2016 (from 27.2% to 42.8%).
Other/unspecified psychiatric diagnoses, such as adjustment disorder and personality disorders, almost tripled between 2007-2008 and 2015-2016 (from 1,040 to 2,961 per 100,000 ED visits). ED visits for mood disorders and anxiety disorders also increased over time.
Alcohol-related ED visits were the most common substance use visits, increasing from 1,669 in 2007-2008 to 3,007 per 100,000 visits in 2015-2016. Amphetamine- and opioid-related ED visits more than doubled, and other/unspecified–related ED visits more than tripled during that time.
“One explanation why ED visits for mental health conditions have increased is that substance-related problems, which include overdose/self-injury issues, have increased over time,” Dr. Rhee noted, which “makes sense,” inasmuch as opioid, cannabis, and amphetamine use has increased across the country.
Another explanation is that, although mental health care access has been expanded through the ACA, “people, especially those with lower socioeconomic backgrounds, do not know how to get access to care and are still underserved,” he said.
“If mental health–related ED visits continue to increase in the future, there are several steps to be made. ED providers need to be better equipped with mental health care, and behavioral health should be better integrated as part of the care coordination,” said Dr. Rhee.
He added that reimbursement models across different insurance types, such as Medicare, Medicaid, and private insurance, “should consider expanding their coverage of mental health treatment in ED settings.”
“Canary in the coal mine”
Commenting on the study in an interview, Benjamin Druss, MD, MPH, professor and Rosalynn Carter Chair in Mental Health, Rollins School of Public Health, Emory University, Atlanta, called EDs the “canaries in the coal mine” for the broader health system.
The growing number of ED visits for behavioral problems “could represent both a rise in acute conditions such as substance use and lack of access to outpatient treatment,” said Dr. Druss, who was not involved with the research.
The findings “suggest the importance of strategies to effectively manage patients with behavioral conditions in ED settings and to effectively link them with high-quality outpatient care,” he noted.
Dr. Rhee has received funding from the National Institute on Aging and the American Foundation for Suicide Prevention. The other study authors and Dr. Druss report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
PANS may be more prevalent than thought
Pediatric acute-onset neuropsychiatric syndrome (PANS), a rare acute onset of psychiatric symptoms, might be more common than initially thought, according to Kiki D. Chang, MD.

PANS is characterized by the National Center for Advancing Translational Sciences Genetic and Rare Diseases Information Center as a “sudden onset of obsessive-compulsive symptoms and/or severe eating restrictions, along with at least two other cognitive, behavioral, or neurological symptoms.” These symptoms can include anxiety, depression, oppositional behavior, difficulty concentrating, abnormalities in motor and sensory skills, and other somatic symptoms. The condition develops as a result of an infection that causes an autoimmune or inflammatory response in the brain, and patients tend to respond well to treatment from antibiotics, anti-inflammatory medication, and immunomodulatory therapy.
Both PANS and a subtype condition, pediatric autoimmune neuropsychiatric disorders associated with Streptococcus infections (PANDAS), are underrecognized, Dr. Chang said in a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists. It is often misdiagnosed as Tourette syndrome or obsessive-compulsive disorder (OCD) because tics are present in about half of cases, he said, but more severe associated symptoms, such as psychosis, can be misdiagnosed as psychotic disorders or mood disorders. Currently, neither PANS nor PANDAS are officially recognized by the American Academy of Pediatrics or the DSM-5.
“We’re hoping that it is soon because it clearly exists,” Dr. Chang said at the meeting, presented by Global Academy for Medical Education. “If you’ve ever treated a child with PANS or PANDAS and you have seen antibiotics totally reverse OCD and tic-like behavior, if you’ve seen prednisone actually treat symptoms of mania or even psychosis and actually make those things better rather than worse, it’s really eye-opening and it makes a believer out of you.”
Anxiety is the most common psychiatric symptom in youth, and anxiety disorders are also common, said Dr. Chang. According to the National Comorbidity Survey: Adolescent Supplement, 2001-2004, 31.9% adolescents overall reported an anxiety disorder, and 8.3% said their anxiety disorder caused severe impairment. The COVID-19 pandemic has increased the level of anxiety for children and adolescents, which can lead to other disorders, such as separation anxiety disorder, panic disorder, specific phobia, social anxiety disorder, acute stress disorder, generalized anxiety disorder, OCD, or posttraumatic stress disorder. Psychiatrists should be suspicious of any sudden onset of symptoms that overlap with PANS, said Dr. Chang, who is now in private practice in Palo Alto, Calif.
“Anxiety disorders are incredibly common. Remember that you’ve got to carefully screen for other anxiety disorders, because they’re highly comorbid,” Dr. Chang said. “You’ve got to do a full workup. If there are other things going on, you’ve got to think PANS. If it’s acute onset, you’ve really got to think [PANS], and you should do that workup or refer to someone who does.”
The prevalence of PANS and PANDAS is not known, but it may be more common than psychiatrists realize, Dr. Chang said. “I’ve been doing this for about 10 years now in the PANS and PANDAS field, and it’s very clear to me that this is something that is prevalent,” he said.
Together with Jennifer Frankovich, MD, Dr. Chang founded a clinic at the Lucile Packard Children’s Hospital Stanford, and also helped to develop treatment guidelines for youth with PANS. At the clinic, patients are approximately 7.7 years old when developing the first symptoms, and are 10.7 years old when presenting for treatment. Most patients at the clinic are male (78%), and 40% are acute onset cases. Nearly all patients have symptoms of anxiety (92%), mood disorder (88%), OCD (86%), sensory/motor abnormalities (88%), irritability/aggression (82%), somatic symptoms, deterioration in school (76%), and behavioral regression (59%). More than one-third present with suicidal ideation (38%) and violence to themselves (29%), others (38%), or objects. About one-fourth have symptoms of psychosis (24%).
“These can be really sick kids,” Dr. Chang said. not able to eat because they’re afraid of things, not able to take care of their body or daily living. These were sometimes highly functional people beforehand, sometimes they weren’t, but it was still an acute change.”
Treatment for PANS
Treatment guidelines released by the PANS/PANDAS Consortium in 2017 recommend a first course of antistreptococcal treatment for new PANS cases. Psychiatrists should look for evidence of strep or other infection and use antibiotics to eradicate any underlying acute or residual infection.
“Very commonly, we’ll use things like azithromycin, or Augmentin, or amoxicillin, and you’ll see suddenly the OCD go away or at least diminish, the sleep return to normal, the mood come back down,” Dr. Chang said. “It’s pretty amazing when you see it.”
In other cases, ongoing treatment is needed for longer than the normal 5-day or 10-day course of antibiotics. “We’re not exactly sure how long: sometimes it’s 3 weeks, sometimes it’s 4 weeks, but you have to give it more than a week. Sometimes it’s the anti-inflammatory properties that are helping.” While concerns about haphazardly prescribing antibiotics are valid, “if you can cure this stuff on antibiotics, it’s low-hanging fruit,” Dr. Chang said.
There is evidence in the literature that prescribing antibiotics for PANS is beneficial. A randomized controlled trial published in 2017 showed that patients with PANS prescribed azithromycin for 4 weeks had greater reductions in severity of OCD, compared with placebo.
“We need more studies, but clearly, antibiotics do have the potential to help with certain kids. And certainly, in my practice, I see sometimes a slam-dunk response,” Dr. Chang said. “Unfortunately, sometimes you don’t see a slam-dunk response or you can’t find an infection. That’s when it might be more of an inflammation from some other reason. It could be a leftover infection, or it could be an anti-inflammatory situation.”
Immunomodulatory treatment for PANS includes use of NSAIDs, such as ibuprofen or naproxen sodium; steroids, such as prednisone or intravenous corticosteroids; intravenous immunoglobulin; or plasma exchange. Other therapies to consider are rituximab, mycophenolate mofetil, and cyclophosphamide.
Some psychiatric treatments may help patients with PANS. While there is no empirical evidence that psychotropics are effective in treating PANS, some SSRIs might help if patients are able to handle any adverse events. Psychotherapy and education of the family are also important for patients with PANS and their caregivers.
“Basically, [PANS] has as high a caregiver burden as having someone in the household with Alzheimer’s disease or cancer. It’s a huge burden, it’s very stressful, and the family needs support for this,” Dr. Chang said.
Global Academy and this news organization are owned by the same parent company. Dr. Chang reports he is a consultant for Allergan, Impel NeuroPharma, and Sunovion. He is also on the speaker’s bureau for Sunovion.
Pediatric acute-onset neuropsychiatric syndrome (PANS), a rare acute onset of psychiatric symptoms, might be more common than initially thought, according to Kiki D. Chang, MD.
PANS is characterized by the National Center for Advancing Translational Sciences Genetic and Rare Diseases Information Center as a “sudden onset of obsessive-compulsive symptoms and/or severe eating restrictions, along with at least two other cognitive, behavioral, or neurological symptoms.” These symptoms can include anxiety, depression, oppositional behavior, difficulty concentrating, abnormalities in motor and sensory skills, and other somatic symptoms. The condition develops as a result of an infection that causes an autoimmune or inflammatory response in the brain, and patients tend to respond well to treatment from antibiotics, anti-inflammatory medication, and immunomodulatory therapy.
Both PANS and a subtype condition, pediatric autoimmune neuropsychiatric disorders associated with Streptococcus infections (PANDAS), are underrecognized, Dr. Chang said in a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists. It is often misdiagnosed as Tourette syndrome or obsessive-compulsive disorder (OCD) because tics are present in about half of cases, he said, but more severe associated symptoms, such as psychosis, can be misdiagnosed as psychotic disorders or mood disorders. Currently, neither PANS nor PANDAS are officially recognized by the American Academy of Pediatrics or the DSM-5.
“We’re hoping that it is soon because it clearly exists,” Dr. Chang said at the meeting, presented by Global Academy for Medical Education. “If you’ve ever treated a child with PANS or PANDAS and you have seen antibiotics totally reverse OCD and tic-like behavior, if you’ve seen prednisone actually treat symptoms of mania or even psychosis and actually make those things better rather than worse, it’s really eye-opening and it makes a believer out of you.”
Anxiety is the most common psychiatric symptom in youth, and anxiety disorders are also common, said Dr. Chang. According to the National Comorbidity Survey: Adolescent Supplement, 2001-2004, 31.9% adolescents overall reported an anxiety disorder, and 8.3% said their anxiety disorder caused severe impairment. The COVID-19 pandemic has increased the level of anxiety for children and adolescents, which can lead to other disorders, such as separation anxiety disorder, panic disorder, specific phobia, social anxiety disorder, acute stress disorder, generalized anxiety disorder, OCD, or posttraumatic stress disorder. Psychiatrists should be suspicious of any sudden onset of symptoms that overlap with PANS, said Dr. Chang, who is now in private practice in Palo Alto, Calif.
“Anxiety disorders are incredibly common. Remember that you’ve got to carefully screen for other anxiety disorders, because they’re highly comorbid,” Dr. Chang said. “You’ve got to do a full workup. If there are other things going on, you’ve got to think PANS. If it’s acute onset, you’ve really got to think [PANS], and you should do that workup or refer to someone who does.”
The prevalence of PANS and PANDAS is not known, but it may be more common than psychiatrists realize, Dr. Chang said. “I’ve been doing this for about 10 years now in the PANS and PANDAS field, and it’s very clear to me that this is something that is prevalent,” he said.
Together with Jennifer Frankovich, MD, Dr. Chang founded a clinic at the Lucile Packard Children’s Hospital Stanford, and also helped to develop treatment guidelines for youth with PANS. At the clinic, patients are approximately 7.7 years old when developing the first symptoms, and are 10.7 years old when presenting for treatment. Most patients at the clinic are male (78%), and 40% are acute onset cases. Nearly all patients have symptoms of anxiety (92%), mood disorder (88%), OCD (86%), sensory/motor abnormalities (88%), irritability/aggression (82%), somatic symptoms, deterioration in school (76%), and behavioral regression (59%). More than one-third present with suicidal ideation (38%) and violence to themselves (29%), others (38%), or objects. About one-fourth have symptoms of psychosis (24%).
“These can be really sick kids,” Dr. Chang said. not able to eat because they’re afraid of things, not able to take care of their body or daily living. These were sometimes highly functional people beforehand, sometimes they weren’t, but it was still an acute change.”
Treatment for PANS
Treatment guidelines released by the PANS/PANDAS Consortium in 2017 recommend a first course of antistreptococcal treatment for new PANS cases. Psychiatrists should look for evidence of strep or other infection and use antibiotics to eradicate any underlying acute or residual infection.
“Very commonly, we’ll use things like azithromycin, or Augmentin, or amoxicillin, and you’ll see suddenly the OCD go away or at least diminish, the sleep return to normal, the mood come back down,” Dr. Chang said. “It’s pretty amazing when you see it.”
In other cases, ongoing treatment is needed for longer than the normal 5-day or 10-day course of antibiotics. “We’re not exactly sure how long: sometimes it’s 3 weeks, sometimes it’s 4 weeks, but you have to give it more than a week. Sometimes it’s the anti-inflammatory properties that are helping.” While concerns about haphazardly prescribing antibiotics are valid, “if you can cure this stuff on antibiotics, it’s low-hanging fruit,” Dr. Chang said.
There is evidence in the literature that prescribing antibiotics for PANS is beneficial. A randomized controlled trial published in 2017 showed that patients with PANS prescribed azithromycin for 4 weeks had greater reductions in severity of OCD, compared with placebo.
“We need more studies, but clearly, antibiotics do have the potential to help with certain kids. And certainly, in my practice, I see sometimes a slam-dunk response,” Dr. Chang said. “Unfortunately, sometimes you don’t see a slam-dunk response or you can’t find an infection. That’s when it might be more of an inflammation from some other reason. It could be a leftover infection, or it could be an anti-inflammatory situation.”
Immunomodulatory treatment for PANS includes use of NSAIDs, such as ibuprofen or naproxen sodium; steroids, such as prednisone or intravenous corticosteroids; intravenous immunoglobulin; or plasma exchange. Other therapies to consider are rituximab, mycophenolate mofetil, and cyclophosphamide.
Some psychiatric treatments may help patients with PANS. While there is no empirical evidence that psychotropics are effective in treating PANS, some SSRIs might help if patients are able to handle any adverse events. Psychotherapy and education of the family are also important for patients with PANS and their caregivers.
“Basically, [PANS] has as high a caregiver burden as having someone in the household with Alzheimer’s disease or cancer. It’s a huge burden, it’s very stressful, and the family needs support for this,” Dr. Chang said.
Global Academy and this news organization are owned by the same parent company. Dr. Chang reports he is a consultant for Allergan, Impel NeuroPharma, and Sunovion. He is also on the speaker’s bureau for Sunovion.
Pediatric acute-onset neuropsychiatric syndrome (PANS), a rare acute onset of psychiatric symptoms, might be more common than initially thought, according to Kiki D. Chang, MD.
PANS is characterized by the National Center for Advancing Translational Sciences Genetic and Rare Diseases Information Center as a “sudden onset of obsessive-compulsive symptoms and/or severe eating restrictions, along with at least two other cognitive, behavioral, or neurological symptoms.” These symptoms can include anxiety, depression, oppositional behavior, difficulty concentrating, abnormalities in motor and sensory skills, and other somatic symptoms. The condition develops as a result of an infection that causes an autoimmune or inflammatory response in the brain, and patients tend to respond well to treatment from antibiotics, anti-inflammatory medication, and immunomodulatory therapy.
Both PANS and a subtype condition, pediatric autoimmune neuropsychiatric disorders associated with Streptococcus infections (PANDAS), are underrecognized, Dr. Chang said in a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists. It is often misdiagnosed as Tourette syndrome or obsessive-compulsive disorder (OCD) because tics are present in about half of cases, he said, but more severe associated symptoms, such as psychosis, can be misdiagnosed as psychotic disorders or mood disorders. Currently, neither PANS nor PANDAS are officially recognized by the American Academy of Pediatrics or the DSM-5.
“We’re hoping that it is soon because it clearly exists,” Dr. Chang said at the meeting, presented by Global Academy for Medical Education. “If you’ve ever treated a child with PANS or PANDAS and you have seen antibiotics totally reverse OCD and tic-like behavior, if you’ve seen prednisone actually treat symptoms of mania or even psychosis and actually make those things better rather than worse, it’s really eye-opening and it makes a believer out of you.”
Anxiety is the most common psychiatric symptom in youth, and anxiety disorders are also common, said Dr. Chang. According to the National Comorbidity Survey: Adolescent Supplement, 2001-2004, 31.9% adolescents overall reported an anxiety disorder, and 8.3% said their anxiety disorder caused severe impairment. The COVID-19 pandemic has increased the level of anxiety for children and adolescents, which can lead to other disorders, such as separation anxiety disorder, panic disorder, specific phobia, social anxiety disorder, acute stress disorder, generalized anxiety disorder, OCD, or posttraumatic stress disorder. Psychiatrists should be suspicious of any sudden onset of symptoms that overlap with PANS, said Dr. Chang, who is now in private practice in Palo Alto, Calif.
“Anxiety disorders are incredibly common. Remember that you’ve got to carefully screen for other anxiety disorders, because they’re highly comorbid,” Dr. Chang said. “You’ve got to do a full workup. If there are other things going on, you’ve got to think PANS. If it’s acute onset, you’ve really got to think [PANS], and you should do that workup or refer to someone who does.”
The prevalence of PANS and PANDAS is not known, but it may be more common than psychiatrists realize, Dr. Chang said. “I’ve been doing this for about 10 years now in the PANS and PANDAS field, and it’s very clear to me that this is something that is prevalent,” he said.
Together with Jennifer Frankovich, MD, Dr. Chang founded a clinic at the Lucile Packard Children’s Hospital Stanford, and also helped to develop treatment guidelines for youth with PANS. At the clinic, patients are approximately 7.7 years old when developing the first symptoms, and are 10.7 years old when presenting for treatment. Most patients at the clinic are male (78%), and 40% are acute onset cases. Nearly all patients have symptoms of anxiety (92%), mood disorder (88%), OCD (86%), sensory/motor abnormalities (88%), irritability/aggression (82%), somatic symptoms, deterioration in school (76%), and behavioral regression (59%). More than one-third present with suicidal ideation (38%) and violence to themselves (29%), others (38%), or objects. About one-fourth have symptoms of psychosis (24%).
“These can be really sick kids,” Dr. Chang said. not able to eat because they’re afraid of things, not able to take care of their body or daily living. These were sometimes highly functional people beforehand, sometimes they weren’t, but it was still an acute change.”
Treatment for PANS
Treatment guidelines released by the PANS/PANDAS Consortium in 2017 recommend a first course of antistreptococcal treatment for new PANS cases. Psychiatrists should look for evidence of strep or other infection and use antibiotics to eradicate any underlying acute or residual infection.
“Very commonly, we’ll use things like azithromycin, or Augmentin, or amoxicillin, and you’ll see suddenly the OCD go away or at least diminish, the sleep return to normal, the mood come back down,” Dr. Chang said. “It’s pretty amazing when you see it.”
In other cases, ongoing treatment is needed for longer than the normal 5-day or 10-day course of antibiotics. “We’re not exactly sure how long: sometimes it’s 3 weeks, sometimes it’s 4 weeks, but you have to give it more than a week. Sometimes it’s the anti-inflammatory properties that are helping.” While concerns about haphazardly prescribing antibiotics are valid, “if you can cure this stuff on antibiotics, it’s low-hanging fruit,” Dr. Chang said.
There is evidence in the literature that prescribing antibiotics for PANS is beneficial. A randomized controlled trial published in 2017 showed that patients with PANS prescribed azithromycin for 4 weeks had greater reductions in severity of OCD, compared with placebo.
“We need more studies, but clearly, antibiotics do have the potential to help with certain kids. And certainly, in my practice, I see sometimes a slam-dunk response,” Dr. Chang said. “Unfortunately, sometimes you don’t see a slam-dunk response or you can’t find an infection. That’s when it might be more of an inflammation from some other reason. It could be a leftover infection, or it could be an anti-inflammatory situation.”
Immunomodulatory treatment for PANS includes use of NSAIDs, such as ibuprofen or naproxen sodium; steroids, such as prednisone or intravenous corticosteroids; intravenous immunoglobulin; or plasma exchange. Other therapies to consider are rituximab, mycophenolate mofetil, and cyclophosphamide.
Some psychiatric treatments may help patients with PANS. While there is no empirical evidence that psychotropics are effective in treating PANS, some SSRIs might help if patients are able to handle any adverse events. Psychotherapy and education of the family are also important for patients with PANS and their caregivers.
“Basically, [PANS] has as high a caregiver burden as having someone in the household with Alzheimer’s disease or cancer. It’s a huge burden, it’s very stressful, and the family needs support for this,” Dr. Chang said.
Global Academy and this news organization are owned by the same parent company. Dr. Chang reports he is a consultant for Allergan, Impel NeuroPharma, and Sunovion. He is also on the speaker’s bureau for Sunovion.
FROM CP/AACP PSYCHIATRY UPDATE
Schizoaffective disorder: A challenging diagnosis
Mr. C, age 34, presented to the emergency department with his wife because of increasingly bizarre behavior. He reported auditory and visual hallucinations, and believed that the “mob had ordered a hit” against him. He had threatened to shoot his wife and children, which led to his arrest and being briefly jailed. In jail, he was agitated, defecated on the floor, and disrobed. His wife reported that Mr. C had a long history of bipolar disorder and had experienced his first manic episode and hospitalization at age 17. Since then, he had been treated with many different antidepressants, antipsychotics, and mood stabilizers.
Mr. C was admitted to the hospital, where he developed a catatonic syndrome that was treated with a course of electroconvulsive therapy. He was eventually stabilized with
Over the next 8 years, Mr. C was often noncompliant with medication and frequently was hospitalized for mania. His symptoms included poor sleep, grandiosity, pressured speech, racing and disorganized thoughts, increased risk-taking behavior (ie, driving at excessive speeds), and hyperreligiosity (ie, speaking with God). Mr. C also occasionally used methamphetamine, cannabis, and cocaine. Although he had responded well to treatment early in the course of his illness, as he entered his late 30s, his response was less complete, and by his 40s, Mr. C was no longer able to function independently. He eventually was prescribed a long-acting injectable antipsychotic, paliperidone palmitate, 156 mg monthly. Eventually, his family was no longer able to care for him at home, so he was admitted to a residential care facility.
In this facility, based on the long-standing nature of Mr. C’s psychotic disorder and frequency with which he presented with mania, his clinicians changed his diagnosis to schizoaffective disorder, bipolar type. It had become clear that mood symptoms comprised >50% of the total duration of his illness.
Schizoaffective disorder (SAD) often has been used as a diagnosis for patients who have an admixture of mood and psychotic symptoms whose diagnosis is uncertain. Its hallmark is the presence of symptoms of a major mood episode (either a depressive or manic episode) concurrent with symptoms characteristic of schizophrenia, such as delusions, hallucinations, or disorganized speech.1
SAD is a controversial diagnosis. There has been inadequate research regarding the epidemiology, course, etiologic factors, and treatment of this disorder. Debate continues to swirl around its conceptualization; some experts view SAD as an independent disorder, while others see SAD as either a form of schizophrenia or a mood disorder.1 In this review, we describe the classification of SAD and its features, diagnosis, and treatment.
An evolving diagnosis
The term schizoaffective was first used by Jacob Kasanin, MD, in 1933.2 He described 9 patients with “acute schizoaffective psychoses,” each of whom had an abrupt onset. The term was used in the first edition of the DSM as a subtype of schizophrenia.3 In DSM-I, the “schizo-affective type” was defined as a diagnosis for patients with a “significant admixture of schizophrenic and affective reactions.”3 Diagnostic criteria for SAD were developed for DSM-III-R, published in 1987.4 These criteria continued to evolve with subsequent editions of the DSM.
Continue to: DSM-5 provides...

DSM-5 provides a clearer separation between schizophrenia with mood symptoms, bipolar disorder, and SAD (Table5). In addition, DSM-5 shifts away from the DSM-IV diagnosis of SAD as an episode, and instead focuses more on the longitudinal course of the illness. It has been suggested that this change will likely lead to reduced rates of diagnosis of SAD.6 Despite improvements in classification, the diagnosis remains controversial (Box7-11).
Box 1
Despite improvements in classification, controversy continues to swirl around the question of whether schizoaffective disorder (SAD) represents an independent disorder that stands apart from schizophrenia and bipolar disorder, whether it is a form of schizophrenia, or whether it is a form of bipolar disorder or a depressive disorder.7,8 Other possibilities are that SAD is heterogeneous or that it represents a middle point on a spectrum that bridges mood and psychotic disorders. While the merits of each possibility are beyond the scope of this review, it is safe to say that each possibility has its proponents. For these reasons, some argue that the concept itself lacks validity and shows the pitfalls of our classification system.7
Poor diagnostic reliability is one reason for concerns about validity. Most recently, a field trial using DSM-5 criteria produced a kappa of 0.50, which is moderate,9 but earlier definitions produced relatively poor results. Wilson et al10 point out that Criterion C, which concerns duration of mood symptoms, produces a particularly low kappa. Another reason is diagnostic switching, whereby patients initially diagnosed with 1 disorder receive a different diagnosis at followup. Diagnostic switching is especially problematic for SAD. In a large meta-analysis by Santelmann et al,11 36% of patients initially diagnosed with SAD had their diagnosis changed when reassessed. This diagnostic shift tended more toward schizophrenia than bipolar disorder. In addition, more than one-half of all patients initially diagnosed with schizophrenia, bipolar disorder, or major depressive disorder were re-diagnosed with SAD when reassessed.
DSM-5 subtypes and specifiers
In DSM-5,SAD has 2 subtypes5:
- Bipolar type. The bipolar type is marked by the presence of a manic episode (major depressive episodes may also occur)
- Depressive type. The depressive type is marked by the presence of only major depressive episodes.
SAD also includes several specifiers, with the express purpose of giving clinicians greater descriptive ability. The course of SAD can be described as either “first episode,” defined as the first manifestation of the disorder, or as having “multiple episodes,” defined as a minimum of 2 episodes with 1 relapse. In addition, SAD can be described as an acute episode, in partial remission, or in full remission. The course can be described as “continuous” if it is clear that symptoms have been present for the majority of the illness with very brief subthreshold periods. The course is designated as “unspecified” when information is unavailable or lacking. The 5-point Clinician-Rated Dimensions of Psychosis Symptoms was introduced to enable clinicians to make a quantitative assessment of the psychotic symptoms, although its use is not required.
Epidemiology and gender ratio
The epidemiology of SAD has not been well studied. DSM-5 estimates that SAD is approximately one-third as common as schizophrenia, which has a lifetime prevalence of 0.5% to 0.8%.5 This is similar to an estimate by Perälä et al12 of a 0.32% lifetime prevalence based on a nationally representative sample of persons in Finland age ≥30. Scully et al13 calculated a prevalence estimate of 1.1% in a representative sample of adults in rural Ireland. Based on pooled clinical data, Keck et al14 estimated the prevalence in clinical settings at 16%, similar to the figure of 19% reported by Levinson et al15 based on data from New York State psychiatric hospitals. In clinical practice, the diagnosis of SAD is used frequently when there is diagnostic uncertainty, which potentially inflates estimates of lifetime prevalence.
The prevalence of SAD is higher in women than men, with a sex ratio of about 2:1, similar to that seen in mood disorders.13,16-19 There are an equal number of men and women with the bipolar subtype, but a female preponderance with the depressive subtype.5 The bipolar subtype is more common in younger patients, while the depressive subtype is more common in older patients. SAD is a rare diagnosis in children.20
Continue to: Course and outcome
Course and outcome
The onset of SAD typically occurs in early adulthood, but can range from childhood to senescence. Approximately one-third of patients are diagnosed before age 25, one-third between age 25 and 35, and one-third after age 35.21-23 Based on a literature review, Cheniaux et al7 concluded that that age at onset for patients with SAD is between those with schizophrenia and those with mood disorders.
The course of SAD is variable but represents a middle ground between that of schizophrenia and the mood disorders. In a 4- to 5-year follow-up,24 patients with SAD had a better overall course than patients with schizophrenia but had poorer functioning than those with bipolar mania, and much poorer than those with unipolar depression. Mood-incongruent psychotic features predict a particularly worse outcome. These findings were reaffirmed at a 10-year follow-up.25 Mood symptoms portend a better outcome than do symptoms of schizophrenia.
The lifetime suicide risk for patients with SAD is estimated at 5%, with a higher risk associated with the presence of depressive symptoms.26 One study found that women with SAD had a 17.5-year reduced life expectancy (64.1 years) compared with a reduction of 8.0 years for men (69.4 years).27
Comorbidity
Patients with SAD are commonly diagnosed with other psychiatric disorders, including anxiety disorders, obsessive-compulsive disorder, posttraumatic stress disorder, and substance use disorders.21,28,29 When compared with the general population, patients with SAD are at higher risk for coronary heart disease, stroke, obesity, and smoking, likely contributing to their decreased life expectancy.27,30 Because second-generation antipsychotics (SGAs) are often used to treat SAD, patients with SAD are at risk for metabolic syndrome and diabetes mellitus.30
Clinical assessment
Because there are no diagnostic, laboratory, or neuroimaging tests for SAD, the most important basis for making the diagnosis is the patient’s history, supplemented by collateral history from family members or friends, and medical records. Determining the percentage of time spent in a mood episode (DSM-5 Criterion C) is especially important.31 This requires the clinician to pay close attention to the temporal relationship of psychotic and mood symptoms.
Continue to: Differential diagnosis
Differential diagnosis
The differential diagnosis for SAD is broad because it includes all of the possibilities usually considered for major mood disorders and for psychotic disorders5:
- schizophrenia
- bipolar disorder with psychotic features
- major depressive disorder with psychotic features
- depressive or bipolar disorders with catatonic features
- personality disorders (especially the schizotypal, paranoid, and borderline types)
- major neurocognitive disorders in which there are mood and psychotic symptoms
- substance/medication-induced psychotic disorder
- disorders induced by medical conditions.
With schizophrenia, the duration of all episodes of a mood syndrome is brief (<50% of the total duration of the illness) relative to the duration of the psychotic symptoms. Although psychotic symptoms may occur in persons with mood disorders, they are generally not present in the absence of depression or mania, helping to set the boundary between SAD and psychotic mania or depression. As for personality disorders, the individual will not have a true psychosis, although some symptoms, such as feelings of unreality, paranoia, or magical thinking, may cause diagnostic confusion.
Medical conditions also can present with psychotic and mood symptoms and need to be ruled out. These include psychotic disorder due to another medical condition, and delirium. A thorough medical workup should be performed to rule out any possible medical causes for the symptoms.
Substance use should also be ruled out as the cause of the symptoms because many substances are associated with mood and psychotic symptoms. It is usually clear from the history, physical examination, or laboratory tests when a medication/illicit substance has initiated and maintained the disorder.
Neurologic conditions. If a neurologic condition is suspected, a neurologic evaluation may be warranted, including laboratory tests, brain imaging to identify specific anatomical abnormalities, lumbar puncture with cerebrospinal fluid analysis, and an electroencephalogram to rule out a convulsive disorder.
Continue to: Clinical symptoms
Clinical symptoms
The signs and symptoms of SAD include those typically seen in schizophrenia and the mood disorders. Thus, the patient may exhibit elated mood and/or grandiosity, or severe depression, combined with mood-incongruent psychotic features such as paranoid delusions. The symptoms may present together or in an alternating fashion, and psychotic symptoms may be mood-congruent or mood-incongruent. Mr. C’s case illustrates some of the symptoms of the disorder.
Brain imaging
Significant changes have been reported to occur in the brain structure and function in persons with SAD. Neuroimaging studies using voxel-based morphometry have shown significant reductions in gray matter volume in several areas of the brain, including the medial prefrontal cortex, insula, Rolandic operculum, parts of the temporal lobe, and the hippocampus.32-35 Amann et al32 found that patients with SAD and schizophrenia had widespread and overlapping areas of significant volume reduction, but patients with bipolar disorder did not. These studies suggest that at least from a neuroimaging standpoint, SAD is more closely related to schizophrenia than bipolar disorder, and could represent a variant of schizophrenia.
Treatment of SAD
The pharmacotherapy of SAD is mostly empirical because of the lack of randomized controlled trials. Clinicians have traditionally prescribed an antipsychotic agent along with either a mood stabilizer (eg,
Since that exhaustive review,
Patients with SAD will require maintenance treatment for ongoing symptom control. Medication that is effective for treatment of an acute episode should be considered for maintenance treatment. Both the extended-release and long-acting injectable (LAI) formulations of paliperidone have been shown to be efficacious in the maintenance treatment of patients with SAD.40 The LAI form of paliperidone significantly delayed psychotic, depressive, and manic relapses, improved clinical rating scale scores, and increased medication adherence.41,42 In an open-label study, olanzapine LAI was effective in long-term maintenance treatment, although approximately 40% of patients experienced significant weight gain.43 One concern with olanzapine is the possible occurrence of a post-injection delirium/sedation syndrome. For that reason, patients receiving olanzapine must be monitored for at least 3 hours post-injection. The paliperidone LAI does not require monitoring after injection.
Continue to: There is a single clinical trial...
There is a single clinical trial showing that patients with SAD can be successfully switched from other antipsychotics to
Other approaches
Electroconvulsive therapy (ECT) should be considered for patients with SAD who are acutely ill and have failed to respond adequately to medication. ECT is especially relevant in the setting of acute mood symptoms (ie, depressive or manic symptoms co-occurring with psychosis or in the absence of psychosis).45
As currently conceptualized, the diagnosis of SAD is made in persons having an admixture of mood and psychotic symptoms, although by definition mood symptoms must take up the majority (≥50%) of the total duration of the illness. Unfortunately, SAD has been inadequately researched due to the unreliability of its definition and concerns about its validity. The long-term course of SAD is midway between mood and psychotic disorders, and the disorder can cause significant disability.
Bottom Line
Schizoaffective disorder (SAD) is characterized by the presence of symptoms of a major mood episode (a depressive or manic episode) concurrent with symptoms of schizophrenia. The most important basis for establishing the diagnosis is the patient’s history. Determining the percentage of time spent in a mood episode is especially important. Treatment usually consists of an antipsychotic plus a mood stabilizer or antidepressant. Electroconvulsive therapy is an option for patients with SAD who do not respond well to medication.
Related Resources
- Wy TJP, Saadabadi A. Schizoaffective disorder. NCBI Bookshelf: StatPearls Publishing. Published January 2020. https://www.ncbi.nlm.nih.gov/books/NBK541012/. Updated April 15, 2020.
- Parker G. How well does the DSM-5 capture schizoaffective disorder? Can J Psychiatry. 2019;64(9):607-610.
Drug Brand Names
Aripiprazole • Abilify
Lithium • Eskalith, Lithobid
Lurasidone • Latuda
Olanzapine • Zyprexa
Olanzapine long-acting injectable • Zyprexa Relprevv
Paliperidone • Invega
Paliperidone palmitate • Invega sustenna
Valproate • Depacon
1. Miller JN, Black DW. Schizoaffective disorder: a review. Ann Clin Psychiatry. 2019;31(1):47-53.
2. Kasanin J. The acute schizoaffective psychoses. Am J Psychiatry. 1933;90:97-126.
3. Diagnostic and statistical manual of mental disorders, 1st ed. Washington, DC: American Psychiatric Association; 1952.
4. Diagnostic and statistical manual of mental disorders, 3rd ed, revision. Washington, DC: American Psychiatric Association; 1987.
5. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013.
6. Malaspina D, Owen M, Heckers S, et al. Schizoaffective disorder in the DSM-5. Schizophr Res. 2013;150:21-25.
7. Cheniaux E, Landeria-Fernandez J, Telles LL, et al. Does schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disorders. J Affect Disord. 2008;106:209-217.
8. Kantrowitz JT, Citrome L. Schizoaffective disorder: a review of current research themes and pharmacologic management. CNS Drugs. 2011;25:317-331.
9. Regier DA, Narrow WE, Clarke DE, et al. DSM-5 field trials in the United States and Canada, Part II: test-retest reliability of selected categorical diagnoses. Am J Psychiatry. 2013;170:59-70.
10. Wilson JE, Nian H, Heckers S. The schizoaffective disorder diagnosis: a conundrum in the clinical setting. Eur Arch Psychiatry Clin Neurosci. 2014;264:29-34.
11. Santelmann H, Franklin J, Bußhoff J, Baethge C. Test-retest reliability of schizoaffective disorder compared with schizophrenia, bipolar disorder, and unipolar depression--a systematic review and meta-analysis. Bipolar Disord. 2015;17:753-768.
12. Perälä J, Suvisaari J, Saarni SI, et al. Lifetime Prevalence of psychotic and bipolar I disorders in a general population. JAMA Psychiatry. 2007;64:19-28.
13. Scully PJ, Owens JM, Kinsella A, et al. Schizophrenia, schizoaffective and bipolar disorder within an epidemiologically complete, homogeneous population in rural Ireland: small area variation in rate. Schizophr Res. 2004;67:143-155.
14. Keck PE Jr, McElroy SE, Strakowski SM, et al. Pharmacologic treatment of schizoaffective disorder. Psychopharmacol. 1994;114:529-538.
15. Levinson DF, Umapathy C, Musthaq M. Treatment of schizoaffective disorder and schizophrenia with mood symptoms. Am J Psychiatry. 1999;156:1138-1148.
16. Angst J, Felder W, Lohmeyer B. Course of schizoaffective psychoses: results of a follow-up study. Schizophr Bull. 1980;6:579-585.
17. Lenz G, Simhandl C, Thau K, et al. Temporal stability of diagnostic criteria for functional psychoses. Psychopathol. 1991;24:328-335.
18. Malhi GS, Green M, Fagiolini A, et al. Schizoaffective disorder: diagnostic issues and future recommendations. Bipolar Disord. 2008;10:215-230.
19. Marneros A, Deister A, Rohde A. Psychopathological and social status of patients with affective, schizophrenic and schizoaffective disorders after long‐term course. Acta Psychiatr Scand. 1990;82:352-358.
20. Werry JS, McClellan JM, Chard L. Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: a clinical and outcome study. J Am Acad Child Adolesc Psychiatry. 1991;30:457-465.
21. Abrams DJ, Rojas DC, Arciniegas DB. Is schizoaffective disorder a distinct categorical diagnosis? A critical review of the literature. Neuropsychiatr Dis Treat. 2008;4:1089-1109.
22. Bromet EJ, Kotov R, Fochtmann LJ, et al. Diagnostic shifts during the decade following first admission for psychosis. Am J Psychiatry. 2011;168:1186-1194.
23. Salvatore P, Baldessarini RJ, Tohen M, et al. The McLean-Harvard First Episode Project: two-year stability of DSM-IV diagnoses in 500 first-episode psychotic disorder patients. J Clin Psychiatry. 2009;70:458-466.
24. Grossman LS, Harrow M, Goldberg JF, et al. Outcome of schizoaffective disorder at two long term follow-ups: comparisons with outcome of schizophrenia and affective disorders. Am J Psychiatry. 1991;148:1359-1365.
25. Harrow M, Grossman L, Herbener E, et al. Ten-year outcome: patients with schizoaffective disorders, schizophrenia, affective disorders and mood-incongruent psychotic symptoms. Br J Psychiatry. 2000;177:421-426.
26. Hor K, Taylor M. Review: suicide and schizophrenia: a systematic review of rates and risk factors. J Psychopharmacol. 2010;24:81-90.
27. Chang CK, Hayes RD, Perera G, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS ONE. 2011;6:e19590.
28. Byerly M, Goodman W, Acholonu W, et al. Obsessive compulsive symptoms in schizophrenia: frequency and clinical features. Schizophr Res. 2005;76:309-316.
29. Strauss JL, Calhoun PS, Marx CE, et al. Comorbid posttraumatic stress disorder is associated with suicidality in male veterans with schizophrenia or schizoaffective disorder. Schizophr Res. 2006;84:165-169.
30. Fagiolini A, Goracci A. The effects of undertreated chronic medical illnesses in patients with severe mental disorders. J Clin Psychiatry. 2009;70:22-29.
31. Black DW, Grant JE. DSM-5 guidebook: the essential companion to the diagnostic and statistical manual of mental disorders, 5th edition. Washington, DC: American Psychiatric Publishing; 2014.
32. Amann BL, Canales-Rodríguez EJ, Madre M, et al. Brain structural changes in schizoaffective disorder compared to schizophrenia and bipolar disorder. Acta Psychiatr Scand. 2016;133:23-33.
33. Ivleva EI, Bidesi AS, Keshavan MS, et al. Gray matter volume as an intermediate phenotype for psychosis: Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP). Am J Psychiatry. 2013;170:1285-1296.
34. Ivleva EI, Bidesi AS, Thomas BP, et al. Brain gray matter phenotypes across the psychosis dimension. Psychiatry Res. 2012;204:13-24.
35. Radonic
36. Jäger M, Becker T, Weinmann S, et al. Treatment of schizoaffective disorder - a challenge for evidence-based psychiatry. Acta Psychiatr Scand. 2010;121:22-32.
37. Glick ID, Mankosli R, Eudicone JM, et al. The efficacy, safety, and tolerability of aripiprazole for the treatment of schizoaffective disorder: results from a pooled analysis of a sub-population of subjects from two randomized, double-blind, placebo controlled, pivotal trials. J Affect Disord. 2009;115:18-26.
38. Canuso CM, Lindenmayer JP, Kosik-Gonzalez C, et al. A randomized, double-blind, placebo controlled study of 2 dose ranges of paliperidone extended-release in the treatment of subjects with schizoaffective disorder. J Clin Psychiatry. 2010;71:587-598.
39. Canuso CM, Schooler NR, Carothers J, et al. Paliperidone extended-release in schizoaffective disorder: a randomized controlled trial comparing a flexible-dose with placebo in patients treated with and without antidepressants and/or mood stabilizers. J Clin Psychopharmacol. 2010;30:487-495.
40. Lindenmayer JP, Kaur A. Antipsychotic management of schizoaffective disorder: a review. Drugs. 2016;76:589-604.
41. Alphs L, Fu DJ, Turkoz I. Paliperidone for the treatment of schizoaffective disorder. Expert Opin Pharmacother. 2016;176:871-883.
42. Bossie CA, Turkoz I, Alphs L, et al. Paliperidone palmitate once-monthly treatment in recent onset and chronic illness patients with schizoaffective disorder. J Nerv Ment Dis. 2017;205:324-328.
43. McDonnell DP, Landry J, Detke HC. Long-term safety and efficacy of olanzapine long-acting injection in patients with schizophrenia or schizoaffective disorder: a 6-year, multinational, single-arm, open-label study. Int Clin Psychopharmacol. 2014;29:322-331.
44. McEvoy JP, Citrome L, Hernandez D, et al. Effectiveness of lurasidone in patients with schizophrenia or schizoaffective disorder switched from other antipsychotics: a randomized, 6-week, open-label study. J Clin Psychiatry. 2013;74:170-179.
45. Mankad MV, Beyer JL, Wiener RD, et al. Manual of electroconvulsive therapy. Washington, DC: American Psychiatric Publishing; 2010.
Mr. C, age 34, presented to the emergency department with his wife because of increasingly bizarre behavior. He reported auditory and visual hallucinations, and believed that the “mob had ordered a hit” against him. He had threatened to shoot his wife and children, which led to his arrest and being briefly jailed. In jail, he was agitated, defecated on the floor, and disrobed. His wife reported that Mr. C had a long history of bipolar disorder and had experienced his first manic episode and hospitalization at age 17. Since then, he had been treated with many different antidepressants, antipsychotics, and mood stabilizers.
Mr. C was admitted to the hospital, where he developed a catatonic syndrome that was treated with a course of electroconvulsive therapy. He was eventually stabilized with
Over the next 8 years, Mr. C was often noncompliant with medication and frequently was hospitalized for mania. His symptoms included poor sleep, grandiosity, pressured speech, racing and disorganized thoughts, increased risk-taking behavior (ie, driving at excessive speeds), and hyperreligiosity (ie, speaking with God). Mr. C also occasionally used methamphetamine, cannabis, and cocaine. Although he had responded well to treatment early in the course of his illness, as he entered his late 30s, his response was less complete, and by his 40s, Mr. C was no longer able to function independently. He eventually was prescribed a long-acting injectable antipsychotic, paliperidone palmitate, 156 mg monthly. Eventually, his family was no longer able to care for him at home, so he was admitted to a residential care facility.
In this facility, based on the long-standing nature of Mr. C’s psychotic disorder and frequency with which he presented with mania, his clinicians changed his diagnosis to schizoaffective disorder, bipolar type. It had become clear that mood symptoms comprised >50% of the total duration of his illness.
Schizoaffective disorder (SAD) often has been used as a diagnosis for patients who have an admixture of mood and psychotic symptoms whose diagnosis is uncertain. Its hallmark is the presence of symptoms of a major mood episode (either a depressive or manic episode) concurrent with symptoms characteristic of schizophrenia, such as delusions, hallucinations, or disorganized speech.1
SAD is a controversial diagnosis. There has been inadequate research regarding the epidemiology, course, etiologic factors, and treatment of this disorder. Debate continues to swirl around its conceptualization; some experts view SAD as an independent disorder, while others see SAD as either a form of schizophrenia or a mood disorder.1 In this review, we describe the classification of SAD and its features, diagnosis, and treatment.
An evolving diagnosis
The term schizoaffective was first used by Jacob Kasanin, MD, in 1933.2 He described 9 patients with “acute schizoaffective psychoses,” each of whom had an abrupt onset. The term was used in the first edition of the DSM as a subtype of schizophrenia.3 In DSM-I, the “schizo-affective type” was defined as a diagnosis for patients with a “significant admixture of schizophrenic and affective reactions.”3 Diagnostic criteria for SAD were developed for DSM-III-R, published in 1987.4 These criteria continued to evolve with subsequent editions of the DSM.
Continue to: DSM-5 provides...
DSM-5 provides a clearer separation between schizophrenia with mood symptoms, bipolar disorder, and SAD (Table5). In addition, DSM-5 shifts away from the DSM-IV diagnosis of SAD as an episode, and instead focuses more on the longitudinal course of the illness. It has been suggested that this change will likely lead to reduced rates of diagnosis of SAD.6 Despite improvements in classification, the diagnosis remains controversial (Box7-11).
Box 1
Despite improvements in classification, controversy continues to swirl around the question of whether schizoaffective disorder (SAD) represents an independent disorder that stands apart from schizophrenia and bipolar disorder, whether it is a form of schizophrenia, or whether it is a form of bipolar disorder or a depressive disorder.7,8 Other possibilities are that SAD is heterogeneous or that it represents a middle point on a spectrum that bridges mood and psychotic disorders. While the merits of each possibility are beyond the scope of this review, it is safe to say that each possibility has its proponents. For these reasons, some argue that the concept itself lacks validity and shows the pitfalls of our classification system.7
Poor diagnostic reliability is one reason for concerns about validity. Most recently, a field trial using DSM-5 criteria produced a kappa of 0.50, which is moderate,9 but earlier definitions produced relatively poor results. Wilson et al10 point out that Criterion C, which concerns duration of mood symptoms, produces a particularly low kappa. Another reason is diagnostic switching, whereby patients initially diagnosed with 1 disorder receive a different diagnosis at followup. Diagnostic switching is especially problematic for SAD. In a large meta-analysis by Santelmann et al,11 36% of patients initially diagnosed with SAD had their diagnosis changed when reassessed. This diagnostic shift tended more toward schizophrenia than bipolar disorder. In addition, more than one-half of all patients initially diagnosed with schizophrenia, bipolar disorder, or major depressive disorder were re-diagnosed with SAD when reassessed.
DSM-5 subtypes and specifiers
In DSM-5,SAD has 2 subtypes5:
- Bipolar type. The bipolar type is marked by the presence of a manic episode (major depressive episodes may also occur)
- Depressive type. The depressive type is marked by the presence of only major depressive episodes.
SAD also includes several specifiers, with the express purpose of giving clinicians greater descriptive ability. The course of SAD can be described as either “first episode,” defined as the first manifestation of the disorder, or as having “multiple episodes,” defined as a minimum of 2 episodes with 1 relapse. In addition, SAD can be described as an acute episode, in partial remission, or in full remission. The course can be described as “continuous” if it is clear that symptoms have been present for the majority of the illness with very brief subthreshold periods. The course is designated as “unspecified” when information is unavailable or lacking. The 5-point Clinician-Rated Dimensions of Psychosis Symptoms was introduced to enable clinicians to make a quantitative assessment of the psychotic symptoms, although its use is not required.
Epidemiology and gender ratio
The epidemiology of SAD has not been well studied. DSM-5 estimates that SAD is approximately one-third as common as schizophrenia, which has a lifetime prevalence of 0.5% to 0.8%.5 This is similar to an estimate by Perälä et al12 of a 0.32% lifetime prevalence based on a nationally representative sample of persons in Finland age ≥30. Scully et al13 calculated a prevalence estimate of 1.1% in a representative sample of adults in rural Ireland. Based on pooled clinical data, Keck et al14 estimated the prevalence in clinical settings at 16%, similar to the figure of 19% reported by Levinson et al15 based on data from New York State psychiatric hospitals. In clinical practice, the diagnosis of SAD is used frequently when there is diagnostic uncertainty, which potentially inflates estimates of lifetime prevalence.
The prevalence of SAD is higher in women than men, with a sex ratio of about 2:1, similar to that seen in mood disorders.13,16-19 There are an equal number of men and women with the bipolar subtype, but a female preponderance with the depressive subtype.5 The bipolar subtype is more common in younger patients, while the depressive subtype is more common in older patients. SAD is a rare diagnosis in children.20
Continue to: Course and outcome
Course and outcome
The onset of SAD typically occurs in early adulthood, but can range from childhood to senescence. Approximately one-third of patients are diagnosed before age 25, one-third between age 25 and 35, and one-third after age 35.21-23 Based on a literature review, Cheniaux et al7 concluded that that age at onset for patients with SAD is between those with schizophrenia and those with mood disorders.
The course of SAD is variable but represents a middle ground between that of schizophrenia and the mood disorders. In a 4- to 5-year follow-up,24 patients with SAD had a better overall course than patients with schizophrenia but had poorer functioning than those with bipolar mania, and much poorer than those with unipolar depression. Mood-incongruent psychotic features predict a particularly worse outcome. These findings were reaffirmed at a 10-year follow-up.25 Mood symptoms portend a better outcome than do symptoms of schizophrenia.
The lifetime suicide risk for patients with SAD is estimated at 5%, with a higher risk associated with the presence of depressive symptoms.26 One study found that women with SAD had a 17.5-year reduced life expectancy (64.1 years) compared with a reduction of 8.0 years for men (69.4 years).27
Comorbidity
Patients with SAD are commonly diagnosed with other psychiatric disorders, including anxiety disorders, obsessive-compulsive disorder, posttraumatic stress disorder, and substance use disorders.21,28,29 When compared with the general population, patients with SAD are at higher risk for coronary heart disease, stroke, obesity, and smoking, likely contributing to their decreased life expectancy.27,30 Because second-generation antipsychotics (SGAs) are often used to treat SAD, patients with SAD are at risk for metabolic syndrome and diabetes mellitus.30
Clinical assessment
Because there are no diagnostic, laboratory, or neuroimaging tests for SAD, the most important basis for making the diagnosis is the patient’s history, supplemented by collateral history from family members or friends, and medical records. Determining the percentage of time spent in a mood episode (DSM-5 Criterion C) is especially important.31 This requires the clinician to pay close attention to the temporal relationship of psychotic and mood symptoms.
Continue to: Differential diagnosis
Differential diagnosis
The differential diagnosis for SAD is broad because it includes all of the possibilities usually considered for major mood disorders and for psychotic disorders5:
- schizophrenia
- bipolar disorder with psychotic features
- major depressive disorder with psychotic features
- depressive or bipolar disorders with catatonic features
- personality disorders (especially the schizotypal, paranoid, and borderline types)
- major neurocognitive disorders in which there are mood and psychotic symptoms
- substance/medication-induced psychotic disorder
- disorders induced by medical conditions.
With schizophrenia, the duration of all episodes of a mood syndrome is brief (<50% of the total duration of the illness) relative to the duration of the psychotic symptoms. Although psychotic symptoms may occur in persons with mood disorders, they are generally not present in the absence of depression or mania, helping to set the boundary between SAD and psychotic mania or depression. As for personality disorders, the individual will not have a true psychosis, although some symptoms, such as feelings of unreality, paranoia, or magical thinking, may cause diagnostic confusion.
Medical conditions also can present with psychotic and mood symptoms and need to be ruled out. These include psychotic disorder due to another medical condition, and delirium. A thorough medical workup should be performed to rule out any possible medical causes for the symptoms.
Substance use should also be ruled out as the cause of the symptoms because many substances are associated with mood and psychotic symptoms. It is usually clear from the history, physical examination, or laboratory tests when a medication/illicit substance has initiated and maintained the disorder.
Neurologic conditions. If a neurologic condition is suspected, a neurologic evaluation may be warranted, including laboratory tests, brain imaging to identify specific anatomical abnormalities, lumbar puncture with cerebrospinal fluid analysis, and an electroencephalogram to rule out a convulsive disorder.
Continue to: Clinical symptoms
Clinical symptoms
The signs and symptoms of SAD include those typically seen in schizophrenia and the mood disorders. Thus, the patient may exhibit elated mood and/or grandiosity, or severe depression, combined with mood-incongruent psychotic features such as paranoid delusions. The symptoms may present together or in an alternating fashion, and psychotic symptoms may be mood-congruent or mood-incongruent. Mr. C’s case illustrates some of the symptoms of the disorder.
Brain imaging
Significant changes have been reported to occur in the brain structure and function in persons with SAD. Neuroimaging studies using voxel-based morphometry have shown significant reductions in gray matter volume in several areas of the brain, including the medial prefrontal cortex, insula, Rolandic operculum, parts of the temporal lobe, and the hippocampus.32-35 Amann et al32 found that patients with SAD and schizophrenia had widespread and overlapping areas of significant volume reduction, but patients with bipolar disorder did not. These studies suggest that at least from a neuroimaging standpoint, SAD is more closely related to schizophrenia than bipolar disorder, and could represent a variant of schizophrenia.
Treatment of SAD
The pharmacotherapy of SAD is mostly empirical because of the lack of randomized controlled trials. Clinicians have traditionally prescribed an antipsychotic agent along with either a mood stabilizer (eg,
Since that exhaustive review,
Patients with SAD will require maintenance treatment for ongoing symptom control. Medication that is effective for treatment of an acute episode should be considered for maintenance treatment. Both the extended-release and long-acting injectable (LAI) formulations of paliperidone have been shown to be efficacious in the maintenance treatment of patients with SAD.40 The LAI form of paliperidone significantly delayed psychotic, depressive, and manic relapses, improved clinical rating scale scores, and increased medication adherence.41,42 In an open-label study, olanzapine LAI was effective in long-term maintenance treatment, although approximately 40% of patients experienced significant weight gain.43 One concern with olanzapine is the possible occurrence of a post-injection delirium/sedation syndrome. For that reason, patients receiving olanzapine must be monitored for at least 3 hours post-injection. The paliperidone LAI does not require monitoring after injection.
Continue to: There is a single clinical trial...
There is a single clinical trial showing that patients with SAD can be successfully switched from other antipsychotics to
Other approaches
Electroconvulsive therapy (ECT) should be considered for patients with SAD who are acutely ill and have failed to respond adequately to medication. ECT is especially relevant in the setting of acute mood symptoms (ie, depressive or manic symptoms co-occurring with psychosis or in the absence of psychosis).45
As currently conceptualized, the diagnosis of SAD is made in persons having an admixture of mood and psychotic symptoms, although by definition mood symptoms must take up the majority (≥50%) of the total duration of the illness. Unfortunately, SAD has been inadequately researched due to the unreliability of its definition and concerns about its validity. The long-term course of SAD is midway between mood and psychotic disorders, and the disorder can cause significant disability.
Bottom Line
Schizoaffective disorder (SAD) is characterized by the presence of symptoms of a major mood episode (a depressive or manic episode) concurrent with symptoms of schizophrenia. The most important basis for establishing the diagnosis is the patient’s history. Determining the percentage of time spent in a mood episode is especially important. Treatment usually consists of an antipsychotic plus a mood stabilizer or antidepressant. Electroconvulsive therapy is an option for patients with SAD who do not respond well to medication.
Related Resources
- Wy TJP, Saadabadi A. Schizoaffective disorder. NCBI Bookshelf: StatPearls Publishing. Published January 2020. https://www.ncbi.nlm.nih.gov/books/NBK541012/. Updated April 15, 2020.
- Parker G. How well does the DSM-5 capture schizoaffective disorder? Can J Psychiatry. 2019;64(9):607-610.
Drug Brand Names
Aripiprazole • Abilify
Lithium • Eskalith, Lithobid
Lurasidone • Latuda
Olanzapine • Zyprexa
Olanzapine long-acting injectable • Zyprexa Relprevv
Paliperidone • Invega
Paliperidone palmitate • Invega sustenna
Valproate • Depacon
Mr. C, age 34, presented to the emergency department with his wife because of increasingly bizarre behavior. He reported auditory and visual hallucinations, and believed that the “mob had ordered a hit” against him. He had threatened to shoot his wife and children, which led to his arrest and being briefly jailed. In jail, he was agitated, defecated on the floor, and disrobed. His wife reported that Mr. C had a long history of bipolar disorder and had experienced his first manic episode and hospitalization at age 17. Since then, he had been treated with many different antidepressants, antipsychotics, and mood stabilizers.
Mr. C was admitted to the hospital, where he developed a catatonic syndrome that was treated with a course of electroconvulsive therapy. He was eventually stabilized with
Over the next 8 years, Mr. C was often noncompliant with medication and frequently was hospitalized for mania. His symptoms included poor sleep, grandiosity, pressured speech, racing and disorganized thoughts, increased risk-taking behavior (ie, driving at excessive speeds), and hyperreligiosity (ie, speaking with God). Mr. C also occasionally used methamphetamine, cannabis, and cocaine. Although he had responded well to treatment early in the course of his illness, as he entered his late 30s, his response was less complete, and by his 40s, Mr. C was no longer able to function independently. He eventually was prescribed a long-acting injectable antipsychotic, paliperidone palmitate, 156 mg monthly. Eventually, his family was no longer able to care for him at home, so he was admitted to a residential care facility.
In this facility, based on the long-standing nature of Mr. C’s psychotic disorder and frequency with which he presented with mania, his clinicians changed his diagnosis to schizoaffective disorder, bipolar type. It had become clear that mood symptoms comprised >50% of the total duration of his illness.
Schizoaffective disorder (SAD) often has been used as a diagnosis for patients who have an admixture of mood and psychotic symptoms whose diagnosis is uncertain. Its hallmark is the presence of symptoms of a major mood episode (either a depressive or manic episode) concurrent with symptoms characteristic of schizophrenia, such as delusions, hallucinations, or disorganized speech.1
SAD is a controversial diagnosis. There has been inadequate research regarding the epidemiology, course, etiologic factors, and treatment of this disorder. Debate continues to swirl around its conceptualization; some experts view SAD as an independent disorder, while others see SAD as either a form of schizophrenia or a mood disorder.1 In this review, we describe the classification of SAD and its features, diagnosis, and treatment.
An evolving diagnosis
The term schizoaffective was first used by Jacob Kasanin, MD, in 1933.2 He described 9 patients with “acute schizoaffective psychoses,” each of whom had an abrupt onset. The term was used in the first edition of the DSM as a subtype of schizophrenia.3 In DSM-I, the “schizo-affective type” was defined as a diagnosis for patients with a “significant admixture of schizophrenic and affective reactions.”3 Diagnostic criteria for SAD were developed for DSM-III-R, published in 1987.4 These criteria continued to evolve with subsequent editions of the DSM.
Continue to: DSM-5 provides...
DSM-5 provides a clearer separation between schizophrenia with mood symptoms, bipolar disorder, and SAD (Table5). In addition, DSM-5 shifts away from the DSM-IV diagnosis of SAD as an episode, and instead focuses more on the longitudinal course of the illness. It has been suggested that this change will likely lead to reduced rates of diagnosis of SAD.6 Despite improvements in classification, the diagnosis remains controversial (Box7-11).
Box 1
Despite improvements in classification, controversy continues to swirl around the question of whether schizoaffective disorder (SAD) represents an independent disorder that stands apart from schizophrenia and bipolar disorder, whether it is a form of schizophrenia, or whether it is a form of bipolar disorder or a depressive disorder.7,8 Other possibilities are that SAD is heterogeneous or that it represents a middle point on a spectrum that bridges mood and psychotic disorders. While the merits of each possibility are beyond the scope of this review, it is safe to say that each possibility has its proponents. For these reasons, some argue that the concept itself lacks validity and shows the pitfalls of our classification system.7
Poor diagnostic reliability is one reason for concerns about validity. Most recently, a field trial using DSM-5 criteria produced a kappa of 0.50, which is moderate,9 but earlier definitions produced relatively poor results. Wilson et al10 point out that Criterion C, which concerns duration of mood symptoms, produces a particularly low kappa. Another reason is diagnostic switching, whereby patients initially diagnosed with 1 disorder receive a different diagnosis at followup. Diagnostic switching is especially problematic for SAD. In a large meta-analysis by Santelmann et al,11 36% of patients initially diagnosed with SAD had their diagnosis changed when reassessed. This diagnostic shift tended more toward schizophrenia than bipolar disorder. In addition, more than one-half of all patients initially diagnosed with schizophrenia, bipolar disorder, or major depressive disorder were re-diagnosed with SAD when reassessed.
DSM-5 subtypes and specifiers
In DSM-5,SAD has 2 subtypes5:
- Bipolar type. The bipolar type is marked by the presence of a manic episode (major depressive episodes may also occur)
- Depressive type. The depressive type is marked by the presence of only major depressive episodes.
SAD also includes several specifiers, with the express purpose of giving clinicians greater descriptive ability. The course of SAD can be described as either “first episode,” defined as the first manifestation of the disorder, or as having “multiple episodes,” defined as a minimum of 2 episodes with 1 relapse. In addition, SAD can be described as an acute episode, in partial remission, or in full remission. The course can be described as “continuous” if it is clear that symptoms have been present for the majority of the illness with very brief subthreshold periods. The course is designated as “unspecified” when information is unavailable or lacking. The 5-point Clinician-Rated Dimensions of Psychosis Symptoms was introduced to enable clinicians to make a quantitative assessment of the psychotic symptoms, although its use is not required.
Epidemiology and gender ratio
The epidemiology of SAD has not been well studied. DSM-5 estimates that SAD is approximately one-third as common as schizophrenia, which has a lifetime prevalence of 0.5% to 0.8%.5 This is similar to an estimate by Perälä et al12 of a 0.32% lifetime prevalence based on a nationally representative sample of persons in Finland age ≥30. Scully et al13 calculated a prevalence estimate of 1.1% in a representative sample of adults in rural Ireland. Based on pooled clinical data, Keck et al14 estimated the prevalence in clinical settings at 16%, similar to the figure of 19% reported by Levinson et al15 based on data from New York State psychiatric hospitals. In clinical practice, the diagnosis of SAD is used frequently when there is diagnostic uncertainty, which potentially inflates estimates of lifetime prevalence.
The prevalence of SAD is higher in women than men, with a sex ratio of about 2:1, similar to that seen in mood disorders.13,16-19 There are an equal number of men and women with the bipolar subtype, but a female preponderance with the depressive subtype.5 The bipolar subtype is more common in younger patients, while the depressive subtype is more common in older patients. SAD is a rare diagnosis in children.20
Continue to: Course and outcome
Course and outcome
The onset of SAD typically occurs in early adulthood, but can range from childhood to senescence. Approximately one-third of patients are diagnosed before age 25, one-third between age 25 and 35, and one-third after age 35.21-23 Based on a literature review, Cheniaux et al7 concluded that that age at onset for patients with SAD is between those with schizophrenia and those with mood disorders.
The course of SAD is variable but represents a middle ground between that of schizophrenia and the mood disorders. In a 4- to 5-year follow-up,24 patients with SAD had a better overall course than patients with schizophrenia but had poorer functioning than those with bipolar mania, and much poorer than those with unipolar depression. Mood-incongruent psychotic features predict a particularly worse outcome. These findings were reaffirmed at a 10-year follow-up.25 Mood symptoms portend a better outcome than do symptoms of schizophrenia.
The lifetime suicide risk for patients with SAD is estimated at 5%, with a higher risk associated with the presence of depressive symptoms.26 One study found that women with SAD had a 17.5-year reduced life expectancy (64.1 years) compared with a reduction of 8.0 years for men (69.4 years).27
Comorbidity
Patients with SAD are commonly diagnosed with other psychiatric disorders, including anxiety disorders, obsessive-compulsive disorder, posttraumatic stress disorder, and substance use disorders.21,28,29 When compared with the general population, patients with SAD are at higher risk for coronary heart disease, stroke, obesity, and smoking, likely contributing to their decreased life expectancy.27,30 Because second-generation antipsychotics (SGAs) are often used to treat SAD, patients with SAD are at risk for metabolic syndrome and diabetes mellitus.30
Clinical assessment
Because there are no diagnostic, laboratory, or neuroimaging tests for SAD, the most important basis for making the diagnosis is the patient’s history, supplemented by collateral history from family members or friends, and medical records. Determining the percentage of time spent in a mood episode (DSM-5 Criterion C) is especially important.31 This requires the clinician to pay close attention to the temporal relationship of psychotic and mood symptoms.
Continue to: Differential diagnosis
Differential diagnosis
The differential diagnosis for SAD is broad because it includes all of the possibilities usually considered for major mood disorders and for psychotic disorders5:
- schizophrenia
- bipolar disorder with psychotic features
- major depressive disorder with psychotic features
- depressive or bipolar disorders with catatonic features
- personality disorders (especially the schizotypal, paranoid, and borderline types)
- major neurocognitive disorders in which there are mood and psychotic symptoms
- substance/medication-induced psychotic disorder
- disorders induced by medical conditions.
With schizophrenia, the duration of all episodes of a mood syndrome is brief (<50% of the total duration of the illness) relative to the duration of the psychotic symptoms. Although psychotic symptoms may occur in persons with mood disorders, they are generally not present in the absence of depression or mania, helping to set the boundary between SAD and psychotic mania or depression. As for personality disorders, the individual will not have a true psychosis, although some symptoms, such as feelings of unreality, paranoia, or magical thinking, may cause diagnostic confusion.
Medical conditions also can present with psychotic and mood symptoms and need to be ruled out. These include psychotic disorder due to another medical condition, and delirium. A thorough medical workup should be performed to rule out any possible medical causes for the symptoms.
Substance use should also be ruled out as the cause of the symptoms because many substances are associated with mood and psychotic symptoms. It is usually clear from the history, physical examination, or laboratory tests when a medication/illicit substance has initiated and maintained the disorder.
Neurologic conditions. If a neurologic condition is suspected, a neurologic evaluation may be warranted, including laboratory tests, brain imaging to identify specific anatomical abnormalities, lumbar puncture with cerebrospinal fluid analysis, and an electroencephalogram to rule out a convulsive disorder.
Continue to: Clinical symptoms
Clinical symptoms
The signs and symptoms of SAD include those typically seen in schizophrenia and the mood disorders. Thus, the patient may exhibit elated mood and/or grandiosity, or severe depression, combined with mood-incongruent psychotic features such as paranoid delusions. The symptoms may present together or in an alternating fashion, and psychotic symptoms may be mood-congruent or mood-incongruent. Mr. C’s case illustrates some of the symptoms of the disorder.
Brain imaging
Significant changes have been reported to occur in the brain structure and function in persons with SAD. Neuroimaging studies using voxel-based morphometry have shown significant reductions in gray matter volume in several areas of the brain, including the medial prefrontal cortex, insula, Rolandic operculum, parts of the temporal lobe, and the hippocampus.32-35 Amann et al32 found that patients with SAD and schizophrenia had widespread and overlapping areas of significant volume reduction, but patients with bipolar disorder did not. These studies suggest that at least from a neuroimaging standpoint, SAD is more closely related to schizophrenia than bipolar disorder, and could represent a variant of schizophrenia.
Treatment of SAD
The pharmacotherapy of SAD is mostly empirical because of the lack of randomized controlled trials. Clinicians have traditionally prescribed an antipsychotic agent along with either a mood stabilizer (eg,
Since that exhaustive review,
Patients with SAD will require maintenance treatment for ongoing symptom control. Medication that is effective for treatment of an acute episode should be considered for maintenance treatment. Both the extended-release and long-acting injectable (LAI) formulations of paliperidone have been shown to be efficacious in the maintenance treatment of patients with SAD.40 The LAI form of paliperidone significantly delayed psychotic, depressive, and manic relapses, improved clinical rating scale scores, and increased medication adherence.41,42 In an open-label study, olanzapine LAI was effective in long-term maintenance treatment, although approximately 40% of patients experienced significant weight gain.43 One concern with olanzapine is the possible occurrence of a post-injection delirium/sedation syndrome. For that reason, patients receiving olanzapine must be monitored for at least 3 hours post-injection. The paliperidone LAI does not require monitoring after injection.
Continue to: There is a single clinical trial...
There is a single clinical trial showing that patients with SAD can be successfully switched from other antipsychotics to
Other approaches
Electroconvulsive therapy (ECT) should be considered for patients with SAD who are acutely ill and have failed to respond adequately to medication. ECT is especially relevant in the setting of acute mood symptoms (ie, depressive or manic symptoms co-occurring with psychosis or in the absence of psychosis).45
As currently conceptualized, the diagnosis of SAD is made in persons having an admixture of mood and psychotic symptoms, although by definition mood symptoms must take up the majority (≥50%) of the total duration of the illness. Unfortunately, SAD has been inadequately researched due to the unreliability of its definition and concerns about its validity. The long-term course of SAD is midway between mood and psychotic disorders, and the disorder can cause significant disability.
Bottom Line
Schizoaffective disorder (SAD) is characterized by the presence of symptoms of a major mood episode (a depressive or manic episode) concurrent with symptoms of schizophrenia. The most important basis for establishing the diagnosis is the patient’s history. Determining the percentage of time spent in a mood episode is especially important. Treatment usually consists of an antipsychotic plus a mood stabilizer or antidepressant. Electroconvulsive therapy is an option for patients with SAD who do not respond well to medication.
Related Resources
- Wy TJP, Saadabadi A. Schizoaffective disorder. NCBI Bookshelf: StatPearls Publishing. Published January 2020. https://www.ncbi.nlm.nih.gov/books/NBK541012/. Updated April 15, 2020.
- Parker G. How well does the DSM-5 capture schizoaffective disorder? Can J Psychiatry. 2019;64(9):607-610.
Drug Brand Names
Aripiprazole • Abilify
Lithium • Eskalith, Lithobid
Lurasidone • Latuda
Olanzapine • Zyprexa
Olanzapine long-acting injectable • Zyprexa Relprevv
Paliperidone • Invega
Paliperidone palmitate • Invega sustenna
Valproate • Depacon
1. Miller JN, Black DW. Schizoaffective disorder: a review. Ann Clin Psychiatry. 2019;31(1):47-53.
2. Kasanin J. The acute schizoaffective psychoses. Am J Psychiatry. 1933;90:97-126.
3. Diagnostic and statistical manual of mental disorders, 1st ed. Washington, DC: American Psychiatric Association; 1952.
4. Diagnostic and statistical manual of mental disorders, 3rd ed, revision. Washington, DC: American Psychiatric Association; 1987.
5. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013.
6. Malaspina D, Owen M, Heckers S, et al. Schizoaffective disorder in the DSM-5. Schizophr Res. 2013;150:21-25.
7. Cheniaux E, Landeria-Fernandez J, Telles LL, et al. Does schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disorders. J Affect Disord. 2008;106:209-217.
8. Kantrowitz JT, Citrome L. Schizoaffective disorder: a review of current research themes and pharmacologic management. CNS Drugs. 2011;25:317-331.
9. Regier DA, Narrow WE, Clarke DE, et al. DSM-5 field trials in the United States and Canada, Part II: test-retest reliability of selected categorical diagnoses. Am J Psychiatry. 2013;170:59-70.
10. Wilson JE, Nian H, Heckers S. The schizoaffective disorder diagnosis: a conundrum in the clinical setting. Eur Arch Psychiatry Clin Neurosci. 2014;264:29-34.
11. Santelmann H, Franklin J, Bußhoff J, Baethge C. Test-retest reliability of schizoaffective disorder compared with schizophrenia, bipolar disorder, and unipolar depression--a systematic review and meta-analysis. Bipolar Disord. 2015;17:753-768.
12. Perälä J, Suvisaari J, Saarni SI, et al. Lifetime Prevalence of psychotic and bipolar I disorders in a general population. JAMA Psychiatry. 2007;64:19-28.
13. Scully PJ, Owens JM, Kinsella A, et al. Schizophrenia, schizoaffective and bipolar disorder within an epidemiologically complete, homogeneous population in rural Ireland: small area variation in rate. Schizophr Res. 2004;67:143-155.
14. Keck PE Jr, McElroy SE, Strakowski SM, et al. Pharmacologic treatment of schizoaffective disorder. Psychopharmacol. 1994;114:529-538.
15. Levinson DF, Umapathy C, Musthaq M. Treatment of schizoaffective disorder and schizophrenia with mood symptoms. Am J Psychiatry. 1999;156:1138-1148.
16. Angst J, Felder W, Lohmeyer B. Course of schizoaffective psychoses: results of a follow-up study. Schizophr Bull. 1980;6:579-585.
17. Lenz G, Simhandl C, Thau K, et al. Temporal stability of diagnostic criteria for functional psychoses. Psychopathol. 1991;24:328-335.
18. Malhi GS, Green M, Fagiolini A, et al. Schizoaffective disorder: diagnostic issues and future recommendations. Bipolar Disord. 2008;10:215-230.
19. Marneros A, Deister A, Rohde A. Psychopathological and social status of patients with affective, schizophrenic and schizoaffective disorders after long‐term course. Acta Psychiatr Scand. 1990;82:352-358.
20. Werry JS, McClellan JM, Chard L. Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: a clinical and outcome study. J Am Acad Child Adolesc Psychiatry. 1991;30:457-465.
21. Abrams DJ, Rojas DC, Arciniegas DB. Is schizoaffective disorder a distinct categorical diagnosis? A critical review of the literature. Neuropsychiatr Dis Treat. 2008;4:1089-1109.
22. Bromet EJ, Kotov R, Fochtmann LJ, et al. Diagnostic shifts during the decade following first admission for psychosis. Am J Psychiatry. 2011;168:1186-1194.
23. Salvatore P, Baldessarini RJ, Tohen M, et al. The McLean-Harvard First Episode Project: two-year stability of DSM-IV diagnoses in 500 first-episode psychotic disorder patients. J Clin Psychiatry. 2009;70:458-466.
24. Grossman LS, Harrow M, Goldberg JF, et al. Outcome of schizoaffective disorder at two long term follow-ups: comparisons with outcome of schizophrenia and affective disorders. Am J Psychiatry. 1991;148:1359-1365.
25. Harrow M, Grossman L, Herbener E, et al. Ten-year outcome: patients with schizoaffective disorders, schizophrenia, affective disorders and mood-incongruent psychotic symptoms. Br J Psychiatry. 2000;177:421-426.
26. Hor K, Taylor M. Review: suicide and schizophrenia: a systematic review of rates and risk factors. J Psychopharmacol. 2010;24:81-90.
27. Chang CK, Hayes RD, Perera G, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS ONE. 2011;6:e19590.
28. Byerly M, Goodman W, Acholonu W, et al. Obsessive compulsive symptoms in schizophrenia: frequency and clinical features. Schizophr Res. 2005;76:309-316.
29. Strauss JL, Calhoun PS, Marx CE, et al. Comorbid posttraumatic stress disorder is associated with suicidality in male veterans with schizophrenia or schizoaffective disorder. Schizophr Res. 2006;84:165-169.
30. Fagiolini A, Goracci A. The effects of undertreated chronic medical illnesses in patients with severe mental disorders. J Clin Psychiatry. 2009;70:22-29.
31. Black DW, Grant JE. DSM-5 guidebook: the essential companion to the diagnostic and statistical manual of mental disorders, 5th edition. Washington, DC: American Psychiatric Publishing; 2014.
32. Amann BL, Canales-Rodríguez EJ, Madre M, et al. Brain structural changes in schizoaffective disorder compared to schizophrenia and bipolar disorder. Acta Psychiatr Scand. 2016;133:23-33.
33. Ivleva EI, Bidesi AS, Keshavan MS, et al. Gray matter volume as an intermediate phenotype for psychosis: Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP). Am J Psychiatry. 2013;170:1285-1296.
34. Ivleva EI, Bidesi AS, Thomas BP, et al. Brain gray matter phenotypes across the psychosis dimension. Psychiatry Res. 2012;204:13-24.
35. Radonic
36. Jäger M, Becker T, Weinmann S, et al. Treatment of schizoaffective disorder - a challenge for evidence-based psychiatry. Acta Psychiatr Scand. 2010;121:22-32.
37. Glick ID, Mankosli R, Eudicone JM, et al. The efficacy, safety, and tolerability of aripiprazole for the treatment of schizoaffective disorder: results from a pooled analysis of a sub-population of subjects from two randomized, double-blind, placebo controlled, pivotal trials. J Affect Disord. 2009;115:18-26.
38. Canuso CM, Lindenmayer JP, Kosik-Gonzalez C, et al. A randomized, double-blind, placebo controlled study of 2 dose ranges of paliperidone extended-release in the treatment of subjects with schizoaffective disorder. J Clin Psychiatry. 2010;71:587-598.
39. Canuso CM, Schooler NR, Carothers J, et al. Paliperidone extended-release in schizoaffective disorder: a randomized controlled trial comparing a flexible-dose with placebo in patients treated with and without antidepressants and/or mood stabilizers. J Clin Psychopharmacol. 2010;30:487-495.
40. Lindenmayer JP, Kaur A. Antipsychotic management of schizoaffective disorder: a review. Drugs. 2016;76:589-604.
41. Alphs L, Fu DJ, Turkoz I. Paliperidone for the treatment of schizoaffective disorder. Expert Opin Pharmacother. 2016;176:871-883.
42. Bossie CA, Turkoz I, Alphs L, et al. Paliperidone palmitate once-monthly treatment in recent onset and chronic illness patients with schizoaffective disorder. J Nerv Ment Dis. 2017;205:324-328.
43. McDonnell DP, Landry J, Detke HC. Long-term safety and efficacy of olanzapine long-acting injection in patients with schizophrenia or schizoaffective disorder: a 6-year, multinational, single-arm, open-label study. Int Clin Psychopharmacol. 2014;29:322-331.
44. McEvoy JP, Citrome L, Hernandez D, et al. Effectiveness of lurasidone in patients with schizophrenia or schizoaffective disorder switched from other antipsychotics: a randomized, 6-week, open-label study. J Clin Psychiatry. 2013;74:170-179.
45. Mankad MV, Beyer JL, Wiener RD, et al. Manual of electroconvulsive therapy. Washington, DC: American Psychiatric Publishing; 2010.
1. Miller JN, Black DW. Schizoaffective disorder: a review. Ann Clin Psychiatry. 2019;31(1):47-53.
2. Kasanin J. The acute schizoaffective psychoses. Am J Psychiatry. 1933;90:97-126.
3. Diagnostic and statistical manual of mental disorders, 1st ed. Washington, DC: American Psychiatric Association; 1952.
4. Diagnostic and statistical manual of mental disorders, 3rd ed, revision. Washington, DC: American Psychiatric Association; 1987.
5. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013.
6. Malaspina D, Owen M, Heckers S, et al. Schizoaffective disorder in the DSM-5. Schizophr Res. 2013;150:21-25.
7. Cheniaux E, Landeria-Fernandez J, Telles LL, et al. Does schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disorders. J Affect Disord. 2008;106:209-217.
8. Kantrowitz JT, Citrome L. Schizoaffective disorder: a review of current research themes and pharmacologic management. CNS Drugs. 2011;25:317-331.
9. Regier DA, Narrow WE, Clarke DE, et al. DSM-5 field trials in the United States and Canada, Part II: test-retest reliability of selected categorical diagnoses. Am J Psychiatry. 2013;170:59-70.
10. Wilson JE, Nian H, Heckers S. The schizoaffective disorder diagnosis: a conundrum in the clinical setting. Eur Arch Psychiatry Clin Neurosci. 2014;264:29-34.
11. Santelmann H, Franklin J, Bußhoff J, Baethge C. Test-retest reliability of schizoaffective disorder compared with schizophrenia, bipolar disorder, and unipolar depression--a systematic review and meta-analysis. Bipolar Disord. 2015;17:753-768.
12. Perälä J, Suvisaari J, Saarni SI, et al. Lifetime Prevalence of psychotic and bipolar I disorders in a general population. JAMA Psychiatry. 2007;64:19-28.
13. Scully PJ, Owens JM, Kinsella A, et al. Schizophrenia, schizoaffective and bipolar disorder within an epidemiologically complete, homogeneous population in rural Ireland: small area variation in rate. Schizophr Res. 2004;67:143-155.
14. Keck PE Jr, McElroy SE, Strakowski SM, et al. Pharmacologic treatment of schizoaffective disorder. Psychopharmacol. 1994;114:529-538.
15. Levinson DF, Umapathy C, Musthaq M. Treatment of schizoaffective disorder and schizophrenia with mood symptoms. Am J Psychiatry. 1999;156:1138-1148.
16. Angst J, Felder W, Lohmeyer B. Course of schizoaffective psychoses: results of a follow-up study. Schizophr Bull. 1980;6:579-585.
17. Lenz G, Simhandl C, Thau K, et al. Temporal stability of diagnostic criteria for functional psychoses. Psychopathol. 1991;24:328-335.
18. Malhi GS, Green M, Fagiolini A, et al. Schizoaffective disorder: diagnostic issues and future recommendations. Bipolar Disord. 2008;10:215-230.
19. Marneros A, Deister A, Rohde A. Psychopathological and social status of patients with affective, schizophrenic and schizoaffective disorders after long‐term course. Acta Psychiatr Scand. 1990;82:352-358.
20. Werry JS, McClellan JM, Chard L. Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: a clinical and outcome study. J Am Acad Child Adolesc Psychiatry. 1991;30:457-465.
21. Abrams DJ, Rojas DC, Arciniegas DB. Is schizoaffective disorder a distinct categorical diagnosis? A critical review of the literature. Neuropsychiatr Dis Treat. 2008;4:1089-1109.
22. Bromet EJ, Kotov R, Fochtmann LJ, et al. Diagnostic shifts during the decade following first admission for psychosis. Am J Psychiatry. 2011;168:1186-1194.
23. Salvatore P, Baldessarini RJ, Tohen M, et al. The McLean-Harvard First Episode Project: two-year stability of DSM-IV diagnoses in 500 first-episode psychotic disorder patients. J Clin Psychiatry. 2009;70:458-466.
24. Grossman LS, Harrow M, Goldberg JF, et al. Outcome of schizoaffective disorder at two long term follow-ups: comparisons with outcome of schizophrenia and affective disorders. Am J Psychiatry. 1991;148:1359-1365.
25. Harrow M, Grossman L, Herbener E, et al. Ten-year outcome: patients with schizoaffective disorders, schizophrenia, affective disorders and mood-incongruent psychotic symptoms. Br J Psychiatry. 2000;177:421-426.
26. Hor K, Taylor M. Review: suicide and schizophrenia: a systematic review of rates and risk factors. J Psychopharmacol. 2010;24:81-90.
27. Chang CK, Hayes RD, Perera G, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS ONE. 2011;6:e19590.
28. Byerly M, Goodman W, Acholonu W, et al. Obsessive compulsive symptoms in schizophrenia: frequency and clinical features. Schizophr Res. 2005;76:309-316.
29. Strauss JL, Calhoun PS, Marx CE, et al. Comorbid posttraumatic stress disorder is associated with suicidality in male veterans with schizophrenia or schizoaffective disorder. Schizophr Res. 2006;84:165-169.
30. Fagiolini A, Goracci A. The effects of undertreated chronic medical illnesses in patients with severe mental disorders. J Clin Psychiatry. 2009;70:22-29.
31. Black DW, Grant JE. DSM-5 guidebook: the essential companion to the diagnostic and statistical manual of mental disorders, 5th edition. Washington, DC: American Psychiatric Publishing; 2014.
32. Amann BL, Canales-Rodríguez EJ, Madre M, et al. Brain structural changes in schizoaffective disorder compared to schizophrenia and bipolar disorder. Acta Psychiatr Scand. 2016;133:23-33.
33. Ivleva EI, Bidesi AS, Keshavan MS, et al. Gray matter volume as an intermediate phenotype for psychosis: Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP). Am J Psychiatry. 2013;170:1285-1296.
34. Ivleva EI, Bidesi AS, Thomas BP, et al. Brain gray matter phenotypes across the psychosis dimension. Psychiatry Res. 2012;204:13-24.
35. Radonic
36. Jäger M, Becker T, Weinmann S, et al. Treatment of schizoaffective disorder - a challenge for evidence-based psychiatry. Acta Psychiatr Scand. 2010;121:22-32.
37. Glick ID, Mankosli R, Eudicone JM, et al. The efficacy, safety, and tolerability of aripiprazole for the treatment of schizoaffective disorder: results from a pooled analysis of a sub-population of subjects from two randomized, double-blind, placebo controlled, pivotal trials. J Affect Disord. 2009;115:18-26.
38. Canuso CM, Lindenmayer JP, Kosik-Gonzalez C, et al. A randomized, double-blind, placebo controlled study of 2 dose ranges of paliperidone extended-release in the treatment of subjects with schizoaffective disorder. J Clin Psychiatry. 2010;71:587-598.
39. Canuso CM, Schooler NR, Carothers J, et al. Paliperidone extended-release in schizoaffective disorder: a randomized controlled trial comparing a flexible-dose with placebo in patients treated with and without antidepressants and/or mood stabilizers. J Clin Psychopharmacol. 2010;30:487-495.
40. Lindenmayer JP, Kaur A. Antipsychotic management of schizoaffective disorder: a review. Drugs. 2016;76:589-604.
41. Alphs L, Fu DJ, Turkoz I. Paliperidone for the treatment of schizoaffective disorder. Expert Opin Pharmacother. 2016;176:871-883.
42. Bossie CA, Turkoz I, Alphs L, et al. Paliperidone palmitate once-monthly treatment in recent onset and chronic illness patients with schizoaffective disorder. J Nerv Ment Dis. 2017;205:324-328.
43. McDonnell DP, Landry J, Detke HC. Long-term safety and efficacy of olanzapine long-acting injection in patients with schizophrenia or schizoaffective disorder: a 6-year, multinational, single-arm, open-label study. Int Clin Psychopharmacol. 2014;29:322-331.
44. McEvoy JP, Citrome L, Hernandez D, et al. Effectiveness of lurasidone in patients with schizophrenia or schizoaffective disorder switched from other antipsychotics: a randomized, 6-week, open-label study. J Clin Psychiatry. 2013;74:170-179.
45. Mankad MV, Beyer JL, Wiener RD, et al. Manual of electroconvulsive therapy. Washington, DC: American Psychiatric Publishing; 2010.

‘Staggering’ increase in COVID-linked depression, anxiety
Since the start of the COVID-19 pandemic, there has been a dramatic increase in depression, anxiety, psychosis, and suicidality, new research shows.
The new data, released by Mental Health America (MHA), came from individuals who completed a voluntary online mental health screen.
As of the end of June, over 169,000 additional participants reported having moderate to severe depression or anxiety, compared with participants who completed the screen prior to the pandemic.
In June alone, 18,000 additional participants were found to be at risk for psychosis, continuing a rising pattern that began in May, when 16,000 reported psychosis risk.
“We continue to see staggering numbers that indicate increased rates in depression and anxiety because of COVID-19,” Paul Gionfriddo, president and CEO of MHA, said in a release.
“In fact, the problem is bigger than anyone imagined, making it clear how the pandemic is affecting people now and will continue to affect people who mourn loved ones and whose serious mental conditions are left untreated. So we need to take this very seriously,” Mr. Gionfriddo said in an interview.
Real-time data
MHA has been conducting online screenings for 6 years. To date, nearly 5.5 million screenings have been completed, making it the largest screening program of its kind in the United States, Mr. Gionfriddo reported.
“At the beginning of the pandemic, we were asked by a member of the media if we could offer any insight about how anxiety in particular was affecting people during the pandemic since we were the only ones with a database that could give quantitative detail,” he said.
The results of their screen could also help find that information “in real time,” he added.
More people are now undergoing mental health screenings, Mr. Gionfriddo noted.
At roughly 7,000 per day in May and June, the number of anxiety and depression screenings that were completed per day were 406% and 457% higher, respectively, than the number completed in January.
The youngest group of participants were those aged 11-17 years; the oldest age group consisted of individuals 65 years and older.
The Patient Health Questionnaire–9 was used to identify those at risk for depression, the General Anxiety Disorder–7 was used to identify those at risk for anxiety, and the Prodromal Questionnaire Brief Version was used to identify those at high risk for psychosis.
Current events
Roughly 90% screened positive for moderate to severe depression, and 80% screened positive for moderate to severe anxiety.
“Kids between the ages of 11 and 17 years have been the most stressed, but it seems to be easier to bear as you get older,” Mr. Gionfriddo said.
Loneliness and isolation were cited as contributors to depression and anxiety by the largest percentage of individuals with these conditions (74% and 65%, respectively).
In June, roughly one quarter of participants also cited grief or loss and financial concerns as contributors to anxiety (25.31% and 24.18%, respectively) and to depression (26.53% and 23.36%).
Current events were cited as an important contributor, leading to more mental health problems in June, compared with May (36.11% vs 29.41 for anxiety; 29.13% vs 21.77% for depression).
The June screen added the category of racism as a potential contributor. Close to 8% reported it as a reason for anxiety, and roughly 5% considered it a reason for depression.
“We will be releasing more data at the end of July, and it will be interesting to see how the racism category compares to data we collected at the end of June,” Mr. Gionfriddo noted.
Dramatic increase
The screen also showed a “dramatic increase” in the number of people who reported being at risk for psychosis, with 18,000 participants screening positive. This represented more than four times the baseline figures recorded through March.
“We were not surprised to see a spike in depression and anxiety, but why were we seeing a spike in psychosis in May/June?” Mr. Gionfriddo asked. He suggested that stress may play a role in driving this increased risk.
“These data, we hope, will get policymakers to pay attention, take it seriously, and intervene to prevent psychosis at an earlier stage before signs and symptoms emerge,” said Mr. Gionfriddo.
One of the most alarming findings was that in June, 25,498 participants who screened positive for depression reported thinking of suicide or self-harm on “more than half of days to nearly every day.” A total of 14,607 participants said they had these thoughts every day.
Overall, the results should reinforce the recommendations of the US Preventive Services Task Force to routinely screen for depression in any clinical setting on a regular basis, Mr. Gionfriddo said.
In addition, policymakers “need to balance reopening vs. quarantining and isolating, and we need to think about what the next 2-4 years look like in terms of balancing physical health risks and mental health risks,” he noted.
“We’ve been treating the pandemic like a sprint and now, 4 or 5 months into it, perhaps as a middle-distance run, when in fact it’s a marathon,” he added.
Advocates needed

The increase in anxiety and depression often centers on the changes and uncertainties in the college experience, such as whether classes will be held in person, online, or a hybrid of the two, said Dr. Ritchie, who was not involved with the research.
Additionally, some college students who have “left the nest” have been forced to “return to the nest,” which compounds stress, she said.
LGBTQ youngsters may be particularly affected because some have “come out of the closet” while away from home and now must negotiate going back to their home of record. They are uncertain whether or not “to go back into the closet,” added Dr. Ritchie, who is also vice chair of psychiatry at Georgetown University, Washington.
Psychiatrists and other mental health professionals should be advocates for “getting services to more people for the greatest good,” she noted.
For example, the MHA data “might be useful in advocating for keeping telehealth accessible and even promoting it,” she said.
The full report is available on MHA’s website.
Mr. Gionfriddo and Dr. Ritchie report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Since the start of the COVID-19 pandemic, there has been a dramatic increase in depression, anxiety, psychosis, and suicidality, new research shows.
The new data, released by Mental Health America (MHA), came from individuals who completed a voluntary online mental health screen.
As of the end of June, over 169,000 additional participants reported having moderate to severe depression or anxiety, compared with participants who completed the screen prior to the pandemic.
In June alone, 18,000 additional participants were found to be at risk for psychosis, continuing a rising pattern that began in May, when 16,000 reported psychosis risk.
“We continue to see staggering numbers that indicate increased rates in depression and anxiety because of COVID-19,” Paul Gionfriddo, president and CEO of MHA, said in a release.
“In fact, the problem is bigger than anyone imagined, making it clear how the pandemic is affecting people now and will continue to affect people who mourn loved ones and whose serious mental conditions are left untreated. So we need to take this very seriously,” Mr. Gionfriddo said in an interview.
Real-time data
MHA has been conducting online screenings for 6 years. To date, nearly 5.5 million screenings have been completed, making it the largest screening program of its kind in the United States, Mr. Gionfriddo reported.
“At the beginning of the pandemic, we were asked by a member of the media if we could offer any insight about how anxiety in particular was affecting people during the pandemic since we were the only ones with a database that could give quantitative detail,” he said.
The results of their screen could also help find that information “in real time,” he added.
More people are now undergoing mental health screenings, Mr. Gionfriddo noted.
At roughly 7,000 per day in May and June, the number of anxiety and depression screenings that were completed per day were 406% and 457% higher, respectively, than the number completed in January.
The youngest group of participants were those aged 11-17 years; the oldest age group consisted of individuals 65 years and older.
The Patient Health Questionnaire–9 was used to identify those at risk for depression, the General Anxiety Disorder–7 was used to identify those at risk for anxiety, and the Prodromal Questionnaire Brief Version was used to identify those at high risk for psychosis.
Current events
Roughly 90% screened positive for moderate to severe depression, and 80% screened positive for moderate to severe anxiety.
“Kids between the ages of 11 and 17 years have been the most stressed, but it seems to be easier to bear as you get older,” Mr. Gionfriddo said.
Loneliness and isolation were cited as contributors to depression and anxiety by the largest percentage of individuals with these conditions (74% and 65%, respectively).
In June, roughly one quarter of participants also cited grief or loss and financial concerns as contributors to anxiety (25.31% and 24.18%, respectively) and to depression (26.53% and 23.36%).
Current events were cited as an important contributor, leading to more mental health problems in June, compared with May (36.11% vs 29.41 for anxiety; 29.13% vs 21.77% for depression).
The June screen added the category of racism as a potential contributor. Close to 8% reported it as a reason for anxiety, and roughly 5% considered it a reason for depression.
“We will be releasing more data at the end of July, and it will be interesting to see how the racism category compares to data we collected at the end of June,” Mr. Gionfriddo noted.
Dramatic increase
The screen also showed a “dramatic increase” in the number of people who reported being at risk for psychosis, with 18,000 participants screening positive. This represented more than four times the baseline figures recorded through March.
“We were not surprised to see a spike in depression and anxiety, but why were we seeing a spike in psychosis in May/June?” Mr. Gionfriddo asked. He suggested that stress may play a role in driving this increased risk.
“These data, we hope, will get policymakers to pay attention, take it seriously, and intervene to prevent psychosis at an earlier stage before signs and symptoms emerge,” said Mr. Gionfriddo.
One of the most alarming findings was that in June, 25,498 participants who screened positive for depression reported thinking of suicide or self-harm on “more than half of days to nearly every day.” A total of 14,607 participants said they had these thoughts every day.
Overall, the results should reinforce the recommendations of the US Preventive Services Task Force to routinely screen for depression in any clinical setting on a regular basis, Mr. Gionfriddo said.
In addition, policymakers “need to balance reopening vs. quarantining and isolating, and we need to think about what the next 2-4 years look like in terms of balancing physical health risks and mental health risks,” he noted.
“We’ve been treating the pandemic like a sprint and now, 4 or 5 months into it, perhaps as a middle-distance run, when in fact it’s a marathon,” he added.
Advocates needed
The increase in anxiety and depression often centers on the changes and uncertainties in the college experience, such as whether classes will be held in person, online, or a hybrid of the two, said Dr. Ritchie, who was not involved with the research.
Additionally, some college students who have “left the nest” have been forced to “return to the nest,” which compounds stress, she said.
LGBTQ youngsters may be particularly affected because some have “come out of the closet” while away from home and now must negotiate going back to their home of record. They are uncertain whether or not “to go back into the closet,” added Dr. Ritchie, who is also vice chair of psychiatry at Georgetown University, Washington.
Psychiatrists and other mental health professionals should be advocates for “getting services to more people for the greatest good,” she noted.
For example, the MHA data “might be useful in advocating for keeping telehealth accessible and even promoting it,” she said.
The full report is available on MHA’s website.
Mr. Gionfriddo and Dr. Ritchie report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Since the start of the COVID-19 pandemic, there has been a dramatic increase in depression, anxiety, psychosis, and suicidality, new research shows.
The new data, released by Mental Health America (MHA), came from individuals who completed a voluntary online mental health screen.
As of the end of June, over 169,000 additional participants reported having moderate to severe depression or anxiety, compared with participants who completed the screen prior to the pandemic.
In June alone, 18,000 additional participants were found to be at risk for psychosis, continuing a rising pattern that began in May, when 16,000 reported psychosis risk.
“We continue to see staggering numbers that indicate increased rates in depression and anxiety because of COVID-19,” Paul Gionfriddo, president and CEO of MHA, said in a release.
“In fact, the problem is bigger than anyone imagined, making it clear how the pandemic is affecting people now and will continue to affect people who mourn loved ones and whose serious mental conditions are left untreated. So we need to take this very seriously,” Mr. Gionfriddo said in an interview.
Real-time data
MHA has been conducting online screenings for 6 years. To date, nearly 5.5 million screenings have been completed, making it the largest screening program of its kind in the United States, Mr. Gionfriddo reported.
“At the beginning of the pandemic, we were asked by a member of the media if we could offer any insight about how anxiety in particular was affecting people during the pandemic since we were the only ones with a database that could give quantitative detail,” he said.
The results of their screen could also help find that information “in real time,” he added.
More people are now undergoing mental health screenings, Mr. Gionfriddo noted.
At roughly 7,000 per day in May and June, the number of anxiety and depression screenings that were completed per day were 406% and 457% higher, respectively, than the number completed in January.
The youngest group of participants were those aged 11-17 years; the oldest age group consisted of individuals 65 years and older.
The Patient Health Questionnaire–9 was used to identify those at risk for depression, the General Anxiety Disorder–7 was used to identify those at risk for anxiety, and the Prodromal Questionnaire Brief Version was used to identify those at high risk for psychosis.
Current events
Roughly 90% screened positive for moderate to severe depression, and 80% screened positive for moderate to severe anxiety.
“Kids between the ages of 11 and 17 years have been the most stressed, but it seems to be easier to bear as you get older,” Mr. Gionfriddo said.
Loneliness and isolation were cited as contributors to depression and anxiety by the largest percentage of individuals with these conditions (74% and 65%, respectively).
In June, roughly one quarter of participants also cited grief or loss and financial concerns as contributors to anxiety (25.31% and 24.18%, respectively) and to depression (26.53% and 23.36%).
Current events were cited as an important contributor, leading to more mental health problems in June, compared with May (36.11% vs 29.41 for anxiety; 29.13% vs 21.77% for depression).
The June screen added the category of racism as a potential contributor. Close to 8% reported it as a reason for anxiety, and roughly 5% considered it a reason for depression.
“We will be releasing more data at the end of July, and it will be interesting to see how the racism category compares to data we collected at the end of June,” Mr. Gionfriddo noted.
Dramatic increase
The screen also showed a “dramatic increase” in the number of people who reported being at risk for psychosis, with 18,000 participants screening positive. This represented more than four times the baseline figures recorded through March.
“We were not surprised to see a spike in depression and anxiety, but why were we seeing a spike in psychosis in May/June?” Mr. Gionfriddo asked. He suggested that stress may play a role in driving this increased risk.
“These data, we hope, will get policymakers to pay attention, take it seriously, and intervene to prevent psychosis at an earlier stage before signs and symptoms emerge,” said Mr. Gionfriddo.
One of the most alarming findings was that in June, 25,498 participants who screened positive for depression reported thinking of suicide or self-harm on “more than half of days to nearly every day.” A total of 14,607 participants said they had these thoughts every day.
Overall, the results should reinforce the recommendations of the US Preventive Services Task Force to routinely screen for depression in any clinical setting on a regular basis, Mr. Gionfriddo said.
In addition, policymakers “need to balance reopening vs. quarantining and isolating, and we need to think about what the next 2-4 years look like in terms of balancing physical health risks and mental health risks,” he noted.
“We’ve been treating the pandemic like a sprint and now, 4 or 5 months into it, perhaps as a middle-distance run, when in fact it’s a marathon,” he added.
Advocates needed
The increase in anxiety and depression often centers on the changes and uncertainties in the college experience, such as whether classes will be held in person, online, or a hybrid of the two, said Dr. Ritchie, who was not involved with the research.
Additionally, some college students who have “left the nest” have been forced to “return to the nest,” which compounds stress, she said.
LGBTQ youngsters may be particularly affected because some have “come out of the closet” while away from home and now must negotiate going back to their home of record. They are uncertain whether or not “to go back into the closet,” added Dr. Ritchie, who is also vice chair of psychiatry at Georgetown University, Washington.
Psychiatrists and other mental health professionals should be advocates for “getting services to more people for the greatest good,” she noted.
For example, the MHA data “might be useful in advocating for keeping telehealth accessible and even promoting it,” she said.
The full report is available on MHA’s website.
Mr. Gionfriddo and Dr. Ritchie report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Psychiatrists report rare case of woman who thinks she’s a chicken
LEUVEN, Belgium — A 54-year-old woman has suffered the delusion of thinking she is a chicken for 24 hours. This very rare condition, known as zoanthropy, in which people think they are an animal is often not recognised, say researchers from the University of Leuven.
Zoanthropy can include people believing they are, or behaving like, any kind of animal: from a dog, to a lion or tiger, crocodile, snake, or bee.
It’s important to recognise this as a potential symptom of something serious, say the researchers in the July issue of the Belgian Journal of Psychiatry, Tijdschrift voor Psychiatrie.
“Additional investigations with brain imaging and electroencephalogram are therefore advised,” say the authors.
Psychiatrists Need to Be Aware That Clinical Zoanthropy Exists
In their paper, they describe the case of the woman who briefly thought she was a chicken, which was followed by her having a generalized epileptic seizure.
“Clinically, we saw a lady who perspired profusely, trembled, blew up her cheeks, and ... seemed to imitate a chicken, [making noises] like clucking, cackling, and crowing like a rooster,” they say.
“After about 10 minutes she seemed to tighten her muscles for a few seconds, her face turned red and for a short time she didn’t react. These symptoms repeated themselves at intervals of a few minutes [and her] consciousness was fluctuating,” with the patient “disoriented in time and space.”
Lead author Dr Athena Beckers of University Psychiatric Centre, KU Leuven, Belgium, said in an interview with MediQuality: “With only 56 case descriptions in the medical literature from 1850 to the present day, the condition is rare. It amounts to about one description every 3 years.
“We suspect, however, that the delusion is not always noticed: the patient shows bizarre behaviour or makes animal sounds, it is probably often catalogued under the general term ‘psychosis’.”
Dr Beckers adds that it is important that the symptoms are recognised, because of the possible underlying causes which can include epilepsy. So this might require a different or complementary treatment “with, for example, antiepileptic drugs”.
“I myself have only seen this type of delusion once, but I ... heard anecdotal stories from other patients whose family member, for example with schizophrenia, sometimes thought he was a cow [during] ... a psychosis.
“After the publication of my article I was also contacted by someone who told me they had experienced the same thing 30 years ago – he thought he was a chicken.
“I think it’s a good thing that we psychiatrists are aware of the fact that clinical zoanthropy exists and may require additional research,” she observed.
Fortunately, this woman’s experience ended well. After about one year of disability, the patient was able to return to work progressively. Her mood remained stable and there were no more psychotic symptoms or any indication of epileptic episodes.
Such Delusions Are Rare
Dr Georges Otte, a recently retired neuropsychiatrist who formerly worked at Ghent University, Belgium, gave his thoughts to Mediquality: “The interface between neurology and psychiatry ... is a fertile meadow on which many crops thrive. But it is in the darkest corners of psychosis that one finds the most bizarre and also rarest excesses.”
There are a number of delusions of identity, said Dr Otte.
These include Cotard’s syndrome, a rare condition marked by the false belief that the person or their body parts are dead, dying, or don’t exist, or Capgras delusion, where the affected person believes that a spouse or close family member has been replaced with an imposter. Delusions can also occur as a result of substance abuse, for example after using psilocybin (magic mushrooms), he added.
“Delusions in which patients are convinced of ‘shape shifting’ (man to animal) are quite rare,” Dr Otte observed.
“In the literature we know that lycanthropy [a person thinks he or she is turning into a werewolf],” has been reported, and has “apparently inspired many authors of horror stories,” he added.
“But it’s not every day that as a psychiatrist, you will encounter such an extreme psychotic depersonalization as someone turning into a chicken.”
This article first appeared on Medscape.com.
LEUVEN, Belgium — A 54-year-old woman has suffered the delusion of thinking she is a chicken for 24 hours. This very rare condition, known as zoanthropy, in which people think they are an animal is often not recognised, say researchers from the University of Leuven.
Zoanthropy can include people believing they are, or behaving like, any kind of animal: from a dog, to a lion or tiger, crocodile, snake, or bee.
It’s important to recognise this as a potential symptom of something serious, say the researchers in the July issue of the Belgian Journal of Psychiatry, Tijdschrift voor Psychiatrie.
“Additional investigations with brain imaging and electroencephalogram are therefore advised,” say the authors.
Psychiatrists Need to Be Aware That Clinical Zoanthropy Exists
In their paper, they describe the case of the woman who briefly thought she was a chicken, which was followed by her having a generalized epileptic seizure.
“Clinically, we saw a lady who perspired profusely, trembled, blew up her cheeks, and ... seemed to imitate a chicken, [making noises] like clucking, cackling, and crowing like a rooster,” they say.
“After about 10 minutes she seemed to tighten her muscles for a few seconds, her face turned red and for a short time she didn’t react. These symptoms repeated themselves at intervals of a few minutes [and her] consciousness was fluctuating,” with the patient “disoriented in time and space.”
Lead author Dr Athena Beckers of University Psychiatric Centre, KU Leuven, Belgium, said in an interview with MediQuality: “With only 56 case descriptions in the medical literature from 1850 to the present day, the condition is rare. It amounts to about one description every 3 years.
“We suspect, however, that the delusion is not always noticed: the patient shows bizarre behaviour or makes animal sounds, it is probably often catalogued under the general term ‘psychosis’.”
Dr Beckers adds that it is important that the symptoms are recognised, because of the possible underlying causes which can include epilepsy. So this might require a different or complementary treatment “with, for example, antiepileptic drugs”.
“I myself have only seen this type of delusion once, but I ... heard anecdotal stories from other patients whose family member, for example with schizophrenia, sometimes thought he was a cow [during] ... a psychosis.
“After the publication of my article I was also contacted by someone who told me they had experienced the same thing 30 years ago – he thought he was a chicken.
“I think it’s a good thing that we psychiatrists are aware of the fact that clinical zoanthropy exists and may require additional research,” she observed.
Fortunately, this woman’s experience ended well. After about one year of disability, the patient was able to return to work progressively. Her mood remained stable and there were no more psychotic symptoms or any indication of epileptic episodes.
Such Delusions Are Rare
Dr Georges Otte, a recently retired neuropsychiatrist who formerly worked at Ghent University, Belgium, gave his thoughts to Mediquality: “The interface between neurology and psychiatry ... is a fertile meadow on which many crops thrive. But it is in the darkest corners of psychosis that one finds the most bizarre and also rarest excesses.”
There are a number of delusions of identity, said Dr Otte.
These include Cotard’s syndrome, a rare condition marked by the false belief that the person or their body parts are dead, dying, or don’t exist, or Capgras delusion, where the affected person believes that a spouse or close family member has been replaced with an imposter. Delusions can also occur as a result of substance abuse, for example after using psilocybin (magic mushrooms), he added.
“Delusions in which patients are convinced of ‘shape shifting’ (man to animal) are quite rare,” Dr Otte observed.
“In the literature we know that lycanthropy [a person thinks he or she is turning into a werewolf],” has been reported, and has “apparently inspired many authors of horror stories,” he added.
“But it’s not every day that as a psychiatrist, you will encounter such an extreme psychotic depersonalization as someone turning into a chicken.”
This article first appeared on Medscape.com.
LEUVEN, Belgium — A 54-year-old woman has suffered the delusion of thinking she is a chicken for 24 hours. This very rare condition, known as zoanthropy, in which people think they are an animal is often not recognised, say researchers from the University of Leuven.
Zoanthropy can include people believing they are, or behaving like, any kind of animal: from a dog, to a lion or tiger, crocodile, snake, or bee.
It’s important to recognise this as a potential symptom of something serious, say the researchers in the July issue of the Belgian Journal of Psychiatry, Tijdschrift voor Psychiatrie.
“Additional investigations with brain imaging and electroencephalogram are therefore advised,” say the authors.
Psychiatrists Need to Be Aware That Clinical Zoanthropy Exists
In their paper, they describe the case of the woman who briefly thought she was a chicken, which was followed by her having a generalized epileptic seizure.
“Clinically, we saw a lady who perspired profusely, trembled, blew up her cheeks, and ... seemed to imitate a chicken, [making noises] like clucking, cackling, and crowing like a rooster,” they say.
“After about 10 minutes she seemed to tighten her muscles for a few seconds, her face turned red and for a short time she didn’t react. These symptoms repeated themselves at intervals of a few minutes [and her] consciousness was fluctuating,” with the patient “disoriented in time and space.”
Lead author Dr Athena Beckers of University Psychiatric Centre, KU Leuven, Belgium, said in an interview with MediQuality: “With only 56 case descriptions in the medical literature from 1850 to the present day, the condition is rare. It amounts to about one description every 3 years.
“We suspect, however, that the delusion is not always noticed: the patient shows bizarre behaviour or makes animal sounds, it is probably often catalogued under the general term ‘psychosis’.”
Dr Beckers adds that it is important that the symptoms are recognised, because of the possible underlying causes which can include epilepsy. So this might require a different or complementary treatment “with, for example, antiepileptic drugs”.
“I myself have only seen this type of delusion once, but I ... heard anecdotal stories from other patients whose family member, for example with schizophrenia, sometimes thought he was a cow [during] ... a psychosis.
“After the publication of my article I was also contacted by someone who told me they had experienced the same thing 30 years ago – he thought he was a chicken.
“I think it’s a good thing that we psychiatrists are aware of the fact that clinical zoanthropy exists and may require additional research,” she observed.
Fortunately, this woman’s experience ended well. After about one year of disability, the patient was able to return to work progressively. Her mood remained stable and there were no more psychotic symptoms or any indication of epileptic episodes.
Such Delusions Are Rare
Dr Georges Otte, a recently retired neuropsychiatrist who formerly worked at Ghent University, Belgium, gave his thoughts to Mediquality: “The interface between neurology and psychiatry ... is a fertile meadow on which many crops thrive. But it is in the darkest corners of psychosis that one finds the most bizarre and also rarest excesses.”
There are a number of delusions of identity, said Dr Otte.
These include Cotard’s syndrome, a rare condition marked by the false belief that the person or their body parts are dead, dying, or don’t exist, or Capgras delusion, where the affected person believes that a spouse or close family member has been replaced with an imposter. Delusions can also occur as a result of substance abuse, for example after using psilocybin (magic mushrooms), he added.
“Delusions in which patients are convinced of ‘shape shifting’ (man to animal) are quite rare,” Dr Otte observed.
“In the literature we know that lycanthropy [a person thinks he or she is turning into a werewolf],” has been reported, and has “apparently inspired many authors of horror stories,” he added.
“But it’s not every day that as a psychiatrist, you will encounter such an extreme psychotic depersonalization as someone turning into a chicken.”
This article first appeared on Medscape.com.
Aerobic exercise may up brain-training benefits in schizophrenia
Recent research has shown that social cognition training can benefit patients with schizophrenia, and a new study suggests that adding regular aerobic exercise sessions substantially increases the improvements in a dose-response manner.

In a randomized controlled trial (RCT) in 47 patients with schizophrenia, improvement in cognition tripled after adding an aerobic exercise program to cognitive training (CT) compared with CT alone.
Investigators, led by Keith H. Nuechterlein, PhD, professor of psychology, University of California, Los Angeles, note that there is “increasing evidence” to support the use of aerobic exercise to improve cognition and functioning in schizophrenia.
However, the “extent to which these gains are dependent on the amount of aerobic exercise completed remains unclear, although variability in adherence to intended exercise regiments is evident,” they write.
They also point out that
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Body Circuit Training
In the study, 47 patients with first-episode schizophrenia were randomly assigned to receive 6 months of CT alone or 6 months of CT plus exercise (CT+E).
All participants underwent 4 hours per week of computerized CT with BrainHQ and SocialVille programs (PositScience).
Patients in the CT+E group also took part in total body circuit training. Two aerobic exercise sessions per week were held at the clinic and two were to be completed at home. The goal was 150 minutes of exercise per week in total.
Exercise intensity was titrated to the individual, at a target of 60% to 80% of heart rate reserve.
Both the CT and CT+E groups showed cognitive gains on the MATRICS Consensus Cognitive Battery (MCCB) test, as well as work/school functioning gains on the Global Assessment Scale: Role.
However, results showed that the improvements in the CT+E group were three times greater than those shown in the CT group (P < .02 for the MCCB overall composite score).
Cognitive Gain Predictors
Because there were also substantial differences in the magnitude of cognitive improvement between the CT+E patients, the investigators sought to identify predictors of cognitive gain.
They found that patients in the CT+E group completed, on average, 85% of their in-clinic exercise sessions but only 39% of their home exercise sessions.
Those who completed a higher overall proportion of the exercise sessions had the largest cognitive gains (P = .03). This relationship was even stronger for patients who completed home exercise sessions (P = .02).
“Thus, aerobic exercise showed a dose-response relationship to cognitive improvement,” the researchers report.
To improve completion rates for home sessions, the investigators tried paying the patients $5 for each session completed, which was “helpful” but did not iron out the variability in adherence.
They also tried assigning points for completing the most exercise sessions in the desired heart rate. They awarded a monthly winner and divided the patients into two completion groups. However, there were “mixed” results.
“Development of systematic incentive strategies to encourage regular aerobic exercise will be critical to successful dissemination of exercise programs as part of the treatment of schizophrenia,” the researchers write.
They add that “pilot work with smartphone reminder systems is underway.”
Effective, but Intensity Is Key
Commenting on the study for Medscape Medical News, David Kimhy, PhD, program leader for New Interventions in Schizophrenia, Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York City, said the results are consistent with previous research.
Aerobic exercise is “highly effective in improving neurocognitive functioning” in patients with schizophrenia, said Kimhy, who was not involved in the research.
“Many individuals with schizophrenia tend to have a highly sedentary lifestyle resulting in poor aerobic fitness,” he said. “Thus, aerobic fitness may represent one of the few modifiable risk factors for ameliorating poor neurocognitive functioning.”
He noted that those benefits are in addition to “the many cardiovascular and health benefits aerobic exercise provide, which are nearly nonexistent for cognitive training and pharmacological interventions.”
However, even if patients do take part in exercise sessions, “an important issue is in-session fidelity with training goals, as individuals may attend scheduled sessions but exercise very lightly,” Kimhy noted.
He pointed out that the proportion of time these patients exercise at their designated target training intensity is highly correlated with neurocognitive improvement. Consequently, “exercising with a trainer may increase both attendance and in-session training fidelity.”
Overall, although the current study suggests that in-clinic exercise sessions can be advantageous, “the recent COVID-19 pandemic made such options very challenging,” Kimhy said.
“To address this issue, our research group and others are currently examining employment of aerobic exercise training at home, connected with trainers via live two-way telehealth video calls,” he added.
Plasticity-Based Training
Two recent studies also indicate that remotely administered training programs can improve social cognition.
In the first study, published online July 2 in Schizophrenia Bulletin, 147 outpatients with schizophrenia were randomly assigned to complete 40 sessions of either SocialVille plasticity-based social cognition training or computer-based games such as crossword puzzles and solitaire.
“To develop these social cognition training exercises, we analyzed a tremendous amount of prior research about how the brain processes social information,” lead author Mor Nahum, PhD, School of Occupational Therapy, Hebrew University, Jerusalem, Israel, said in a press release.
“It turns out that social cognition requires fast and accurate brain information processing, so we developed exercises that trained the brain to process social stimuli, like faces and emotions, quickly and accurately,” Nahum added.
The interventions were conducted at home, with 55 participants completing the cognitive training and 53 completing the computer game sessions. (The remaining 39 either dropped out or withdrew.)
An average of 28 hours of social cognition training over 3 months was associated with a significant improvement on social cognitive composite scores compared with computer games (P < .001), but not on the UCSD Performance-Based Skills Assessment.
Further analysis suggested that more time spent on the cognitive training was associated with greater improvements in social cognition and social functioning, as well as on a motivation subscale.
The results “provide support for the efficacy of a remote, plasticity-based social cognitive training program,” the investigators write.
Such programs “may serve as a cost-effective adjunct to existing psychosocial treatments,” they add.
Auditory vs Visual Training
In the other study, published online May 21 in Schizophrenia Research, investigators led by Rogerio Panizzutti, MD, PhD, Instituto de Ciencias Biomedicas, Federal University of Rio de Janeiro, Brazil, randomly assigned 79 patients with schizophrenia to 40 hours of auditory or visual computerized training.
The exercises were dynamically equivalent between the two types of training, and their difficulty increased as the training progressed.
Both groups showed improvements in reasoning, problem-solving, and reported symptoms. However, the group receiving visual training also had greater improvement in global cognition and attention than the group receiving auditory training.
All studies were supported by Posit Science Corporation. The study authors and Kimhy have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Recent research has shown that social cognition training can benefit patients with schizophrenia, and a new study suggests that adding regular aerobic exercise sessions substantially increases the improvements in a dose-response manner.
In a randomized controlled trial (RCT) in 47 patients with schizophrenia, improvement in cognition tripled after adding an aerobic exercise program to cognitive training (CT) compared with CT alone.
Investigators, led by Keith H. Nuechterlein, PhD, professor of psychology, University of California, Los Angeles, note that there is “increasing evidence” to support the use of aerobic exercise to improve cognition and functioning in schizophrenia.
However, the “extent to which these gains are dependent on the amount of aerobic exercise completed remains unclear, although variability in adherence to intended exercise regiments is evident,” they write.
They also point out that
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Body Circuit Training
In the study, 47 patients with first-episode schizophrenia were randomly assigned to receive 6 months of CT alone or 6 months of CT plus exercise (CT+E).
All participants underwent 4 hours per week of computerized CT with BrainHQ and SocialVille programs (PositScience).
Patients in the CT+E group also took part in total body circuit training. Two aerobic exercise sessions per week were held at the clinic and two were to be completed at home. The goal was 150 minutes of exercise per week in total.
Exercise intensity was titrated to the individual, at a target of 60% to 80% of heart rate reserve.
Both the CT and CT+E groups showed cognitive gains on the MATRICS Consensus Cognitive Battery (MCCB) test, as well as work/school functioning gains on the Global Assessment Scale: Role.
However, results showed that the improvements in the CT+E group were three times greater than those shown in the CT group (P < .02 for the MCCB overall composite score).
Cognitive Gain Predictors
Because there were also substantial differences in the magnitude of cognitive improvement between the CT+E patients, the investigators sought to identify predictors of cognitive gain.
They found that patients in the CT+E group completed, on average, 85% of their in-clinic exercise sessions but only 39% of their home exercise sessions.
Those who completed a higher overall proportion of the exercise sessions had the largest cognitive gains (P = .03). This relationship was even stronger for patients who completed home exercise sessions (P = .02).
“Thus, aerobic exercise showed a dose-response relationship to cognitive improvement,” the researchers report.
To improve completion rates for home sessions, the investigators tried paying the patients $5 for each session completed, which was “helpful” but did not iron out the variability in adherence.
They also tried assigning points for completing the most exercise sessions in the desired heart rate. They awarded a monthly winner and divided the patients into two completion groups. However, there were “mixed” results.
“Development of systematic incentive strategies to encourage regular aerobic exercise will be critical to successful dissemination of exercise programs as part of the treatment of schizophrenia,” the researchers write.
They add that “pilot work with smartphone reminder systems is underway.”
Effective, but Intensity Is Key
Commenting on the study for Medscape Medical News, David Kimhy, PhD, program leader for New Interventions in Schizophrenia, Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York City, said the results are consistent with previous research.
Aerobic exercise is “highly effective in improving neurocognitive functioning” in patients with schizophrenia, said Kimhy, who was not involved in the research.
“Many individuals with schizophrenia tend to have a highly sedentary lifestyle resulting in poor aerobic fitness,” he said. “Thus, aerobic fitness may represent one of the few modifiable risk factors for ameliorating poor neurocognitive functioning.”
He noted that those benefits are in addition to “the many cardiovascular and health benefits aerobic exercise provide, which are nearly nonexistent for cognitive training and pharmacological interventions.”
However, even if patients do take part in exercise sessions, “an important issue is in-session fidelity with training goals, as individuals may attend scheduled sessions but exercise very lightly,” Kimhy noted.
He pointed out that the proportion of time these patients exercise at their designated target training intensity is highly correlated with neurocognitive improvement. Consequently, “exercising with a trainer may increase both attendance and in-session training fidelity.”
Overall, although the current study suggests that in-clinic exercise sessions can be advantageous, “the recent COVID-19 pandemic made such options very challenging,” Kimhy said.
“To address this issue, our research group and others are currently examining employment of aerobic exercise training at home, connected with trainers via live two-way telehealth video calls,” he added.
Plasticity-Based Training
Two recent studies also indicate that remotely administered training programs can improve social cognition.
In the first study, published online July 2 in Schizophrenia Bulletin, 147 outpatients with schizophrenia were randomly assigned to complete 40 sessions of either SocialVille plasticity-based social cognition training or computer-based games such as crossword puzzles and solitaire.
“To develop these social cognition training exercises, we analyzed a tremendous amount of prior research about how the brain processes social information,” lead author Mor Nahum, PhD, School of Occupational Therapy, Hebrew University, Jerusalem, Israel, said in a press release.
“It turns out that social cognition requires fast and accurate brain information processing, so we developed exercises that trained the brain to process social stimuli, like faces and emotions, quickly and accurately,” Nahum added.
The interventions were conducted at home, with 55 participants completing the cognitive training and 53 completing the computer game sessions. (The remaining 39 either dropped out or withdrew.)
An average of 28 hours of social cognition training over 3 months was associated with a significant improvement on social cognitive composite scores compared with computer games (P < .001), but not on the UCSD Performance-Based Skills Assessment.
Further analysis suggested that more time spent on the cognitive training was associated with greater improvements in social cognition and social functioning, as well as on a motivation subscale.
The results “provide support for the efficacy of a remote, plasticity-based social cognitive training program,” the investigators write.
Such programs “may serve as a cost-effective adjunct to existing psychosocial treatments,” they add.
Auditory vs Visual Training
In the other study, published online May 21 in Schizophrenia Research, investigators led by Rogerio Panizzutti, MD, PhD, Instituto de Ciencias Biomedicas, Federal University of Rio de Janeiro, Brazil, randomly assigned 79 patients with schizophrenia to 40 hours of auditory or visual computerized training.
The exercises were dynamically equivalent between the two types of training, and their difficulty increased as the training progressed.
Both groups showed improvements in reasoning, problem-solving, and reported symptoms. However, the group receiving visual training also had greater improvement in global cognition and attention than the group receiving auditory training.
All studies were supported by Posit Science Corporation. The study authors and Kimhy have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Recent research has shown that social cognition training can benefit patients with schizophrenia, and a new study suggests that adding regular aerobic exercise sessions substantially increases the improvements in a dose-response manner.
In a randomized controlled trial (RCT) in 47 patients with schizophrenia, improvement in cognition tripled after adding an aerobic exercise program to cognitive training (CT) compared with CT alone.
Investigators, led by Keith H. Nuechterlein, PhD, professor of psychology, University of California, Los Angeles, note that there is “increasing evidence” to support the use of aerobic exercise to improve cognition and functioning in schizophrenia.
However, the “extent to which these gains are dependent on the amount of aerobic exercise completed remains unclear, although variability in adherence to intended exercise regiments is evident,” they write.
They also point out that
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Body Circuit Training
In the study, 47 patients with first-episode schizophrenia were randomly assigned to receive 6 months of CT alone or 6 months of CT plus exercise (CT+E).
All participants underwent 4 hours per week of computerized CT with BrainHQ and SocialVille programs (PositScience).
Patients in the CT+E group also took part in total body circuit training. Two aerobic exercise sessions per week were held at the clinic and two were to be completed at home. The goal was 150 minutes of exercise per week in total.
Exercise intensity was titrated to the individual, at a target of 60% to 80% of heart rate reserve.
Both the CT and CT+E groups showed cognitive gains on the MATRICS Consensus Cognitive Battery (MCCB) test, as well as work/school functioning gains on the Global Assessment Scale: Role.
However, results showed that the improvements in the CT+E group were three times greater than those shown in the CT group (P < .02 for the MCCB overall composite score).
Cognitive Gain Predictors
Because there were also substantial differences in the magnitude of cognitive improvement between the CT+E patients, the investigators sought to identify predictors of cognitive gain.
They found that patients in the CT+E group completed, on average, 85% of their in-clinic exercise sessions but only 39% of their home exercise sessions.
Those who completed a higher overall proportion of the exercise sessions had the largest cognitive gains (P = .03). This relationship was even stronger for patients who completed home exercise sessions (P = .02).
“Thus, aerobic exercise showed a dose-response relationship to cognitive improvement,” the researchers report.
To improve completion rates for home sessions, the investigators tried paying the patients $5 for each session completed, which was “helpful” but did not iron out the variability in adherence.
They also tried assigning points for completing the most exercise sessions in the desired heart rate. They awarded a monthly winner and divided the patients into two completion groups. However, there were “mixed” results.
“Development of systematic incentive strategies to encourage regular aerobic exercise will be critical to successful dissemination of exercise programs as part of the treatment of schizophrenia,” the researchers write.
They add that “pilot work with smartphone reminder systems is underway.”
Effective, but Intensity Is Key
Commenting on the study for Medscape Medical News, David Kimhy, PhD, program leader for New Interventions in Schizophrenia, Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York City, said the results are consistent with previous research.
Aerobic exercise is “highly effective in improving neurocognitive functioning” in patients with schizophrenia, said Kimhy, who was not involved in the research.
“Many individuals with schizophrenia tend to have a highly sedentary lifestyle resulting in poor aerobic fitness,” he said. “Thus, aerobic fitness may represent one of the few modifiable risk factors for ameliorating poor neurocognitive functioning.”
He noted that those benefits are in addition to “the many cardiovascular and health benefits aerobic exercise provide, which are nearly nonexistent for cognitive training and pharmacological interventions.”
However, even if patients do take part in exercise sessions, “an important issue is in-session fidelity with training goals, as individuals may attend scheduled sessions but exercise very lightly,” Kimhy noted.
He pointed out that the proportion of time these patients exercise at their designated target training intensity is highly correlated with neurocognitive improvement. Consequently, “exercising with a trainer may increase both attendance and in-session training fidelity.”
Overall, although the current study suggests that in-clinic exercise sessions can be advantageous, “the recent COVID-19 pandemic made such options very challenging,” Kimhy said.
“To address this issue, our research group and others are currently examining employment of aerobic exercise training at home, connected with trainers via live two-way telehealth video calls,” he added.
Plasticity-Based Training
Two recent studies also indicate that remotely administered training programs can improve social cognition.
In the first study, published online July 2 in Schizophrenia Bulletin, 147 outpatients with schizophrenia were randomly assigned to complete 40 sessions of either SocialVille plasticity-based social cognition training or computer-based games such as crossword puzzles and solitaire.
“To develop these social cognition training exercises, we analyzed a tremendous amount of prior research about how the brain processes social information,” lead author Mor Nahum, PhD, School of Occupational Therapy, Hebrew University, Jerusalem, Israel, said in a press release.
“It turns out that social cognition requires fast and accurate brain information processing, so we developed exercises that trained the brain to process social stimuli, like faces and emotions, quickly and accurately,” Nahum added.
The interventions were conducted at home, with 55 participants completing the cognitive training and 53 completing the computer game sessions. (The remaining 39 either dropped out or withdrew.)
An average of 28 hours of social cognition training over 3 months was associated with a significant improvement on social cognitive composite scores compared with computer games (P < .001), but not on the UCSD Performance-Based Skills Assessment.
Further analysis suggested that more time spent on the cognitive training was associated with greater improvements in social cognition and social functioning, as well as on a motivation subscale.
The results “provide support for the efficacy of a remote, plasticity-based social cognitive training program,” the investigators write.
Such programs “may serve as a cost-effective adjunct to existing psychosocial treatments,” they add.
Auditory vs Visual Training
In the other study, published online May 21 in Schizophrenia Research, investigators led by Rogerio Panizzutti, MD, PhD, Instituto de Ciencias Biomedicas, Federal University of Rio de Janeiro, Brazil, randomly assigned 79 patients with schizophrenia to 40 hours of auditory or visual computerized training.
The exercises were dynamically equivalent between the two types of training, and their difficulty increased as the training progressed.
Both groups showed improvements in reasoning, problem-solving, and reported symptoms. However, the group receiving visual training also had greater improvement in global cognition and attention than the group receiving auditory training.
All studies were supported by Posit Science Corporation. The study authors and Kimhy have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
‘Defending Jacob’ and defending psychiatry
The 2012 crime fiction novel, “Defending Jacob,” by William Landay was dramatized into a miniseries created by Mark Bomback that premiered on April 24, 2020, on Apple TV+ (and for those resisting a subscription, “The Morning Show” and “Defending Jacob” are both worth it). Both the “Defending Jacob” novel and the miniseries have themes that are of interest to psychiatry, especially to child and forensic psychiatrists, and both the literary and TV versions are excellent, albeit disturbing, diversions from the current pandemic.

(Spoiler alert!) The story is set in the affluent town of Newton, Mass., where crime is generally low and homicides extremely infrequent. Protagonist Andy Barber, a 51-year-old Jewish assistant district attorney, is played by a younger Chris Evans in the miniseries. His wife, Laurie Gold Barber, a 51-year-old Jewish former schoolteacher and stay-at-home mom, is played by a younger Michelle Dockery of Downton Abbey fame. In the miniseries, her character is actively working as a teacher and social activist for children. Other differences between the novel and the miniseries will be pointed out when relevant, but the overall narrative is similar. Both stories are cleverly told through Andy Barber speaking in retrospect as he is being questioned in front of a grand jury for a potential indictment.
When 14-year-old Ben Rifkin is found stabbed to death in Cold Spring Park before school one morning, Andy Barber initially takes the case despite his boss’s reservations that there may be a conflict because Andy’s son Jacob is a student in Ben’s class at school. As the title suggests, it soon becomes clear that Jacob may have had something to do with the murder. At that point, Andy is taken off the case and it is given to a junior colleague, Neal Logiudice, who demonstrates both admiration and contempt for his former mentor, perhaps because of underlying jealousy and insecurity. Neal Logiudice becomes the DA questioning Andy Barber.
Prior to Jacob’s formal accusation of murder, the Barbers appear to be fiercely loyal and unable to fully see and understand their son. The difficulty with objectivity and the reasons why family member physicians should never treat family members – and why family member attorneys should never represent loved ones – is abundantly clear in this story. When Andy receives an anonymous tip that Jacob’s childhood best friend, Derek Yoo, posted on Facebook, “Jake, everyone knows you did it. You have a knife. I’ve seen it,’ ” Andy then looks through Jacob’s drawers and finds a folding knife in one of his T-shirts. In the chapter aptly titled “Denial,” Andy, an experienced prosecutor, does not turn the knife over as evidence, but instead disposes of it – believing Jacob that he did not take the knife to school the day his classmate was stabbed.
After Jacob is indicted, Andy Barber confesses to his wife, Laurie, that his estranged father who left when he was 6 is actually in prison convicted of murdering and raping a woman. In the novel, his grandfather and great-grandfather are also convicted felons. Laurie reveals this family history to Jacob’s attorney, and the attorney subsequently refers the family to a forensic psychologist. In the novel, she is a large Jewish woman; in the miniseries she is played by a very thin Poorna Jagannathan (who incidentally has portrayed a therapist in the television series “Sorry for your Loss,” and a doctor in “The Act,” “Better Call Saul,” “NCIS: Los Angeles,” “House of Cards,” “The Game,” “Law and Order: Criminal Intent,” “Rescue Me,” “Jonny Zero,” “An Actor Prepares,” “The Circle,” “Thanks for Sharing,” and “Montclair.”) Although the goal of the defense was a finding of “not guilty,” a psychiatric defense was going to be used as a last resort if necessary.

Laurie had already googled and learned of “the murder gene,” which was further explained by the forensic psychologist as a mutation called:
“MAOA Knockout. It has been argued in court as a trigger for violence before, but the argument was too simplistic, and it was rejected. Our understanding of the gene-environment interplay has improved since then – the science is getting better and very quickly – and we may have better testimony now. The second mutation is located in what’s called the serotonin transporter gene. The official name for the gene is SLC6A4. It’s located on chromosome 17. It encodes a protein that facilitates the activity of the serotonin transporter system, which is what enables the reuptake of serotonin from the synapse back into the neuron.”1
She further explains that there have been many studies on the “nurture” side of the nature/nurture question and that, with new developments in DNA studies, it is now becoming possible to study the “nature” side.
“Defending Jacob” explores the nature/nurture issue, as well as issues with forensic testimony in court and the criminal justice system in general. The issue of repressing feelings and hiding secrets and then having to confront both in a brutal manner is another theme addressed in the story. Andy tried to hide and forget that his father was in prison and the criminal history in his family, but he was forced to face this and his feelings about it when confronted with his own son being accused of murder. Of note, he does not seek help from a therapist despite these life-altering events. (Humongous spoiler alert:) The story that began with a murder of an unrelated child may end with a family murder, one that would be well described and could be understood by psychiatrists using the categories of motives initially described by Phillip Resnick, MD.2

Once again, and unfortunately, as we have pointed out in other media reviews, the portrayal of psychiatric/psychological themes is problematic. Using a psychologist to explain the science of DNA and not a psychiatrist is an interesting choice. Diagnosing a 14-year-old with personality disorders also contributes to misunderstanding and stigma. In addition, no timely attempt is made to refer the accused Jacob for mental health treatment. The stigmatization of psychiatry in the media was addressed by the World Psychiatric Association task force guidance on how to combat stigmatization of psychiatry and psychiatrists,3 including breaking down negative views of psychiatrists and psychiatry in the general public, among medical students, other health professionals, and patients and relatives. The task force made recommendations for national psychiatric societies and for individual practitioners to help reduce stigma of the profession of psychiatry. We would argue that speaking to the media, including fiction authors, to help educate about mental health is an important role for psychiatrists. It would lead to more realistic portrayals in film and books.
Overall, “Defending Jacob” is a compelling story in both the novel and the miniseries. Despite some problems with how it depicts mental health issues, both are engaging and contain thoughtful, extremely well-written themes of interest to many clinical and forensic psychiatrists.
References
1. Landay W. Defending Jacob, a novel. New York: Delacorte Press, 2012.
2. Friedman SH. Family Murder: Pathologies of Love and Hate. Washington: American Psychiatric Association Publishing, 2019.
3. Sartorius N et al. World Psychiatry. 2010 Oct;9(3):131-44.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and on the faculty at Weill Cornell Medical Center. Dr. Hatters Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Association Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law and was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association.
The 2012 crime fiction novel, “Defending Jacob,” by William Landay was dramatized into a miniseries created by Mark Bomback that premiered on April 24, 2020, on Apple TV+ (and for those resisting a subscription, “The Morning Show” and “Defending Jacob” are both worth it). Both the “Defending Jacob” novel and the miniseries have themes that are of interest to psychiatry, especially to child and forensic psychiatrists, and both the literary and TV versions are excellent, albeit disturbing, diversions from the current pandemic.
(Spoiler alert!) The story is set in the affluent town of Newton, Mass., where crime is generally low and homicides extremely infrequent. Protagonist Andy Barber, a 51-year-old Jewish assistant district attorney, is played by a younger Chris Evans in the miniseries. His wife, Laurie Gold Barber, a 51-year-old Jewish former schoolteacher and stay-at-home mom, is played by a younger Michelle Dockery of Downton Abbey fame. In the miniseries, her character is actively working as a teacher and social activist for children. Other differences between the novel and the miniseries will be pointed out when relevant, but the overall narrative is similar. Both stories are cleverly told through Andy Barber speaking in retrospect as he is being questioned in front of a grand jury for a potential indictment.
When 14-year-old Ben Rifkin is found stabbed to death in Cold Spring Park before school one morning, Andy Barber initially takes the case despite his boss’s reservations that there may be a conflict because Andy’s son Jacob is a student in Ben’s class at school. As the title suggests, it soon becomes clear that Jacob may have had something to do with the murder. At that point, Andy is taken off the case and it is given to a junior colleague, Neal Logiudice, who demonstrates both admiration and contempt for his former mentor, perhaps because of underlying jealousy and insecurity. Neal Logiudice becomes the DA questioning Andy Barber.
Prior to Jacob’s formal accusation of murder, the Barbers appear to be fiercely loyal and unable to fully see and understand their son. The difficulty with objectivity and the reasons why family member physicians should never treat family members – and why family member attorneys should never represent loved ones – is abundantly clear in this story. When Andy receives an anonymous tip that Jacob’s childhood best friend, Derek Yoo, posted on Facebook, “Jake, everyone knows you did it. You have a knife. I’ve seen it,’ ” Andy then looks through Jacob’s drawers and finds a folding knife in one of his T-shirts. In the chapter aptly titled “Denial,” Andy, an experienced prosecutor, does not turn the knife over as evidence, but instead disposes of it – believing Jacob that he did not take the knife to school the day his classmate was stabbed.
After Jacob is indicted, Andy Barber confesses to his wife, Laurie, that his estranged father who left when he was 6 is actually in prison convicted of murdering and raping a woman. In the novel, his grandfather and great-grandfather are also convicted felons. Laurie reveals this family history to Jacob’s attorney, and the attorney subsequently refers the family to a forensic psychologist. In the novel, she is a large Jewish woman; in the miniseries she is played by a very thin Poorna Jagannathan (who incidentally has portrayed a therapist in the television series “Sorry for your Loss,” and a doctor in “The Act,” “Better Call Saul,” “NCIS: Los Angeles,” “House of Cards,” “The Game,” “Law and Order: Criminal Intent,” “Rescue Me,” “Jonny Zero,” “An Actor Prepares,” “The Circle,” “Thanks for Sharing,” and “Montclair.”) Although the goal of the defense was a finding of “not guilty,” a psychiatric defense was going to be used as a last resort if necessary.
Laurie had already googled and learned of “the murder gene,” which was further explained by the forensic psychologist as a mutation called:
“MAOA Knockout. It has been argued in court as a trigger for violence before, but the argument was too simplistic, and it was rejected. Our understanding of the gene-environment interplay has improved since then – the science is getting better and very quickly – and we may have better testimony now. The second mutation is located in what’s called the serotonin transporter gene. The official name for the gene is SLC6A4. It’s located on chromosome 17. It encodes a protein that facilitates the activity of the serotonin transporter system, which is what enables the reuptake of serotonin from the synapse back into the neuron.”1
She further explains that there have been many studies on the “nurture” side of the nature/nurture question and that, with new developments in DNA studies, it is now becoming possible to study the “nature” side.
“Defending Jacob” explores the nature/nurture issue, as well as issues with forensic testimony in court and the criminal justice system in general. The issue of repressing feelings and hiding secrets and then having to confront both in a brutal manner is another theme addressed in the story. Andy tried to hide and forget that his father was in prison and the criminal history in his family, but he was forced to face this and his feelings about it when confronted with his own son being accused of murder. Of note, he does not seek help from a therapist despite these life-altering events. (Humongous spoiler alert:) The story that began with a murder of an unrelated child may end with a family murder, one that would be well described and could be understood by psychiatrists using the categories of motives initially described by Phillip Resnick, MD.2
Once again, and unfortunately, as we have pointed out in other media reviews, the portrayal of psychiatric/psychological themes is problematic. Using a psychologist to explain the science of DNA and not a psychiatrist is an interesting choice. Diagnosing a 14-year-old with personality disorders also contributes to misunderstanding and stigma. In addition, no timely attempt is made to refer the accused Jacob for mental health treatment. The stigmatization of psychiatry in the media was addressed by the World Psychiatric Association task force guidance on how to combat stigmatization of psychiatry and psychiatrists,3 including breaking down negative views of psychiatrists and psychiatry in the general public, among medical students, other health professionals, and patients and relatives. The task force made recommendations for national psychiatric societies and for individual practitioners to help reduce stigma of the profession of psychiatry. We would argue that speaking to the media, including fiction authors, to help educate about mental health is an important role for psychiatrists. It would lead to more realistic portrayals in film and books.
Overall, “Defending Jacob” is a compelling story in both the novel and the miniseries. Despite some problems with how it depicts mental health issues, both are engaging and contain thoughtful, extremely well-written themes of interest to many clinical and forensic psychiatrists.
References
1. Landay W. Defending Jacob, a novel. New York: Delacorte Press, 2012.
2. Friedman SH. Family Murder: Pathologies of Love and Hate. Washington: American Psychiatric Association Publishing, 2019.
3. Sartorius N et al. World Psychiatry. 2010 Oct;9(3):131-44.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and on the faculty at Weill Cornell Medical Center. Dr. Hatters Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Association Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law and was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association.
The 2012 crime fiction novel, “Defending Jacob,” by William Landay was dramatized into a miniseries created by Mark Bomback that premiered on April 24, 2020, on Apple TV+ (and for those resisting a subscription, “The Morning Show” and “Defending Jacob” are both worth it). Both the “Defending Jacob” novel and the miniseries have themes that are of interest to psychiatry, especially to child and forensic psychiatrists, and both the literary and TV versions are excellent, albeit disturbing, diversions from the current pandemic.
(Spoiler alert!) The story is set in the affluent town of Newton, Mass., where crime is generally low and homicides extremely infrequent. Protagonist Andy Barber, a 51-year-old Jewish assistant district attorney, is played by a younger Chris Evans in the miniseries. His wife, Laurie Gold Barber, a 51-year-old Jewish former schoolteacher and stay-at-home mom, is played by a younger Michelle Dockery of Downton Abbey fame. In the miniseries, her character is actively working as a teacher and social activist for children. Other differences between the novel and the miniseries will be pointed out when relevant, but the overall narrative is similar. Both stories are cleverly told through Andy Barber speaking in retrospect as he is being questioned in front of a grand jury for a potential indictment.
When 14-year-old Ben Rifkin is found stabbed to death in Cold Spring Park before school one morning, Andy Barber initially takes the case despite his boss’s reservations that there may be a conflict because Andy’s son Jacob is a student in Ben’s class at school. As the title suggests, it soon becomes clear that Jacob may have had something to do with the murder. At that point, Andy is taken off the case and it is given to a junior colleague, Neal Logiudice, who demonstrates both admiration and contempt for his former mentor, perhaps because of underlying jealousy and insecurity. Neal Logiudice becomes the DA questioning Andy Barber.
Prior to Jacob’s formal accusation of murder, the Barbers appear to be fiercely loyal and unable to fully see and understand their son. The difficulty with objectivity and the reasons why family member physicians should never treat family members – and why family member attorneys should never represent loved ones – is abundantly clear in this story. When Andy receives an anonymous tip that Jacob’s childhood best friend, Derek Yoo, posted on Facebook, “Jake, everyone knows you did it. You have a knife. I’ve seen it,’ ” Andy then looks through Jacob’s drawers and finds a folding knife in one of his T-shirts. In the chapter aptly titled “Denial,” Andy, an experienced prosecutor, does not turn the knife over as evidence, but instead disposes of it – believing Jacob that he did not take the knife to school the day his classmate was stabbed.
After Jacob is indicted, Andy Barber confesses to his wife, Laurie, that his estranged father who left when he was 6 is actually in prison convicted of murdering and raping a woman. In the novel, his grandfather and great-grandfather are also convicted felons. Laurie reveals this family history to Jacob’s attorney, and the attorney subsequently refers the family to a forensic psychologist. In the novel, she is a large Jewish woman; in the miniseries she is played by a very thin Poorna Jagannathan (who incidentally has portrayed a therapist in the television series “Sorry for your Loss,” and a doctor in “The Act,” “Better Call Saul,” “NCIS: Los Angeles,” “House of Cards,” “The Game,” “Law and Order: Criminal Intent,” “Rescue Me,” “Jonny Zero,” “An Actor Prepares,” “The Circle,” “Thanks for Sharing,” and “Montclair.”) Although the goal of the defense was a finding of “not guilty,” a psychiatric defense was going to be used as a last resort if necessary.
Laurie had already googled and learned of “the murder gene,” which was further explained by the forensic psychologist as a mutation called:
“MAOA Knockout. It has been argued in court as a trigger for violence before, but the argument was too simplistic, and it was rejected. Our understanding of the gene-environment interplay has improved since then – the science is getting better and very quickly – and we may have better testimony now. The second mutation is located in what’s called the serotonin transporter gene. The official name for the gene is SLC6A4. It’s located on chromosome 17. It encodes a protein that facilitates the activity of the serotonin transporter system, which is what enables the reuptake of serotonin from the synapse back into the neuron.”1
She further explains that there have been many studies on the “nurture” side of the nature/nurture question and that, with new developments in DNA studies, it is now becoming possible to study the “nature” side.
“Defending Jacob” explores the nature/nurture issue, as well as issues with forensic testimony in court and the criminal justice system in general. The issue of repressing feelings and hiding secrets and then having to confront both in a brutal manner is another theme addressed in the story. Andy tried to hide and forget that his father was in prison and the criminal history in his family, but he was forced to face this and his feelings about it when confronted with his own son being accused of murder. Of note, he does not seek help from a therapist despite these life-altering events. (Humongous spoiler alert:) The story that began with a murder of an unrelated child may end with a family murder, one that would be well described and could be understood by psychiatrists using the categories of motives initially described by Phillip Resnick, MD.2
Once again, and unfortunately, as we have pointed out in other media reviews, the portrayal of psychiatric/psychological themes is problematic. Using a psychologist to explain the science of DNA and not a psychiatrist is an interesting choice. Diagnosing a 14-year-old with personality disorders also contributes to misunderstanding and stigma. In addition, no timely attempt is made to refer the accused Jacob for mental health treatment. The stigmatization of psychiatry in the media was addressed by the World Psychiatric Association task force guidance on how to combat stigmatization of psychiatry and psychiatrists,3 including breaking down negative views of psychiatrists and psychiatry in the general public, among medical students, other health professionals, and patients and relatives. The task force made recommendations for national psychiatric societies and for individual practitioners to help reduce stigma of the profession of psychiatry. We would argue that speaking to the media, including fiction authors, to help educate about mental health is an important role for psychiatrists. It would lead to more realistic portrayals in film and books.
Overall, “Defending Jacob” is a compelling story in both the novel and the miniseries. Despite some problems with how it depicts mental health issues, both are engaging and contain thoughtful, extremely well-written themes of interest to many clinical and forensic psychiatrists.
References
1. Landay W. Defending Jacob, a novel. New York: Delacorte Press, 2012.
2. Friedman SH. Family Murder: Pathologies of Love and Hate. Washington: American Psychiatric Association Publishing, 2019.
3. Sartorius N et al. World Psychiatry. 2010 Oct;9(3):131-44.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and on the faculty at Weill Cornell Medical Center. Dr. Hatters Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Association Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law and was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association.
Some telepsychiatry ‘here to stay’ post COVID
The COVID-19 pandemic has changed life in numerous ways, including use of telehealth services for patients in all specialties. But telepsychiatry is an area not likely to go away even after the pandemic is over, according to Sanjay Gupta, MD.

The use of telepsychiatry has escalated significantly,” said Dr. Gupta, of the DENT Neurologic Institute, in Amherst, N.Y., in a bonus virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
About 90% of clinicians are performing telepsychiatry, Dr. Gupta noted, through methods such as phone consults, email, and video chat. As patients with psychiatric issues grapple with issues related to COVID-19 involving lockdowns, restrictions on travel, and consumption of news, they are presenting with addiction, depression, paranoia, mood lability, and other problems.
One issue immediately facing clinicians is whether to keep patients on long-acting injectables as a way to maintain psychological stability in patients with bipolar disorder, schizophrenia, and alcoholism – something Dr. Gupta and session moderator Henry A. Nasrallah, MD, advocated. “We should never stop the long-acting injectable to switch them to oral medication. Those patients are very likely to relapse,” Dr. Nasrallah said.

During the pandemic, clinicians need to find “safe and novel ways of providing the injection,” and several methods have been pioneered. For example, if a patient with schizophrenia is on lockdown, a nurse can visit monthly or bimonthly to administer an injection, check on the patient’s mental status, and assess whether that patient needs an adjustment to their medication. Other clinics are offering “drive-by” injections to patients who arrive by car, and a nurse wearing a mask and a face shield administers the injection from the car window. Monthly naltrexone also can be administered using one of these methods, and telepsychiatry can be used to monitor patients, Dr. Gupta noted at the meeting, presented by Global Academy for Medical Education.
“In my clinic, what happens is the injection room is set up just next to the door, so they don’t have to walk deep into the clinic,” Dr. Gupta said. “They walk in, go to the left, [and] there’s the injection room. They sit, get an injection, they’re out. It’s kept smooth.”
Choosing the right telehealth option
Clinicians should be aware of important regulatory changes that occurred that made widespread telehealth more appealing during the COVID-19 pandemic. Payment parity with in-office visits makes telehealth a viable consideration, while some states have begun offering telehealth licenses to practice across state lines. There is wide variation with regard to which states provide licensure and prescribing privileges for out-of-state clinicians without seeing those patients in person. “The most important thing: The psychiatry service is provided in the state where the patient is located,” Dr. Gupta said. Clinicians should check with that state’s board to figure out specific requirements. “Preferably if you get it in writing, it’s good for you,” he said.
Deciding who the clinician is seeing – consulting with patients or other physicians/clinicians – and what type of visits a clinician will conduct is an important step in transitioning to telepsychiatry. Visits from evaluation through ongoing care are possible through telepsychiatry, or a clinician can opt to see just second opinion visits, Dr. Gupta said. It is also important to consider the technical ability of the patient to do video conferencing.
As HIPAA requirements for privacy have relaxed, clinicians now have an array of teleconferencing options to choose from; platforms such as FaceTime, Doximity, Vidyo, Doxy.me, Zoom, and video chat through EMR are popular options. However, when regular HIPAA requirements are reinstated after the pandemic, clinicians will need to find a compliant platform and sign a business associate agreement to stay within the law.
“Right now, my preferred use is FaceTime,” Dr. Gupta said. “Quick, simple, easy to use. A lot of people have an iPhone, and they know how to do it. I usually have the patient call me and I don’t use my personal iPhone; my clinic has an iPhone.”
How a clinician looks during a telepsychiatry visit is also important. Lighting, position of the camera, and clothing should all be considered. Keep the camera at eye level, test the lighting in the room where the call will take place, and use artificial lighting sources behind a computer, Dr. Gupta said. Other tips for telepsychiatry visits include silencing devices and microphones before a session begins, wearing solid-colored clothes, and having an identification badge visible to the patient. Sessions should be free of background distractions, such as a dog barking or a child interrupting, with the goal of creating an environment where the patient feels free to answer questions.
Contingency planning is a must for video visits, Dr. Gupta said. “I think the simplest thing is to see the patient. But all the stuff that’s the wraparound is really hard, because issues can arise suddenly, and we need to plan.” If a patient has a medical issue or becomes actively suicidal during a session, it is important to know contact information for the local police and crisis services. Clinicians also must plan for technology failure and provide alternative options for continuing the sessions, such as by phone.
Selecting patients for telepsychiatry
Not all patients will make the transition to telepsychiatry. “You can’t do telepsychiatry with everyone. It is a risk, so pick and choose,” Dr. Gupta said.

“Safety is a big consideration for conducting a telepsychiatry visit, especially when other health care providers are present. For example, when performing telehealth visits in a clinic, nursing home, or correctional facility, “I feel a lot more comfortable if there’s another health care clinician there,” Dr. Gupta said.
Clinicians may want to avoid a telepsychiatry visit for a patient in their own home for reasons of safety, reliability, and privacy. A longitudinal history with collateral information from friends or relatives can be helpful, but some subtle signs and body language may get missed over video, compared with an in-person visit. Sometimes you may not see if the patient is using substances. You have to really reconsider if [there] is violence and self-injurious behavior,” he said.
Discussing the pros and cons of telepsychiatry is important to obtaining patient consent. While consent requirements have relaxed under the COVID-19 pandemic, consent should ideally be obtained in writing, but can also be obtained verbally during a crisis. A plan should be developed for what will happen in the case of technology failure. “The patient should also know you’re maintaining privacy, you’re maintaining confidentiality, but there is a risk of hacking,” Dr. Gupta said. “Those things can happen, [and] there are no guarantees.”
If a patient is uncomfortable after beginning telepsychiatry, moving to in-person visits is also an option. “Many times, I do that if I’m not getting a good handle on things,” Dr. Gupta said. Situations where patients insist on in-patient visits over telepsychiatry are rare in his experience, Dr. Gupta noted, and are usually the result of the patient being unfamiliar with the technology. In cases where a patient cannot be talked through a technology barrier, visits can be done in the clinic while taking proper precautions.
“If it is a first-time visit, then I do it in the clinic,” Dr. Gupta said. “They come in, they have a face mask, and we use our group therapy room. The patients sit in a social-distanced fashion. But then, you document why you did this in-person visit like that.”
Documentation during COVID-19 also includes identifying the patient at the first visit, the nature of the visit (teleconference or other), parties present, referencing the pandemic, writing the location of the patient and the clinician, noting the patient’s satisfaction, evaluating the patient’s mental status, and recording what technology was used and any technical issues that were encountered.
Some populations of patients are better suited to telepsychiatry than others. It is more convenient for chronically psychiatrically ill patients in group homes and their staff to communicate through telepsychiatry, Dr. Gupta said. Consultation liaison in hospitals and emergency departments through telepsychiatry can limit the spread of infection, while increased access and convenience occurs as telepsychiatry is implemented in correctional facilities and nursing homes.
“What we are doing now, some of it is here to stay,” Dr. Gupta said.
In situations where a patient needs to switch providers, clinicians should continue to follow that patient until his first patient visit with that new provider. It is also important to set boundaries and apply some level of formality to the telepsychiatry visit, which means seeing the patient in a secure location where he can speak freely and privately.
“The best practices are [to] maintain faith [and] fidelity of the psychiatric assessment,” Dr. Gupta said. “Keep the trust and do your best to maintain patient privacy, because the privacy is not the same as it may be in a face-to-face session when you use televideo.”
Global Academy and this news organization are owned by the same parent company.
Dr. Gupta reported no relevant financial disclosures. Dr. Nasrallah disclosed serving as a consultant for and on the speakers bureaus of several pharmaceutical companies, including Alkermes, Janssen, and Lundbeck. He also disclosed serving on the speakers bureau of Otsuka.
The COVID-19 pandemic has changed life in numerous ways, including use of telehealth services for patients in all specialties. But telepsychiatry is an area not likely to go away even after the pandemic is over, according to Sanjay Gupta, MD.
The use of telepsychiatry has escalated significantly,” said Dr. Gupta, of the DENT Neurologic Institute, in Amherst, N.Y., in a bonus virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
About 90% of clinicians are performing telepsychiatry, Dr. Gupta noted, through methods such as phone consults, email, and video chat. As patients with psychiatric issues grapple with issues related to COVID-19 involving lockdowns, restrictions on travel, and consumption of news, they are presenting with addiction, depression, paranoia, mood lability, and other problems.
One issue immediately facing clinicians is whether to keep patients on long-acting injectables as a way to maintain psychological stability in patients with bipolar disorder, schizophrenia, and alcoholism – something Dr. Gupta and session moderator Henry A. Nasrallah, MD, advocated. “We should never stop the long-acting injectable to switch them to oral medication. Those patients are very likely to relapse,” Dr. Nasrallah said.
During the pandemic, clinicians need to find “safe and novel ways of providing the injection,” and several methods have been pioneered. For example, if a patient with schizophrenia is on lockdown, a nurse can visit monthly or bimonthly to administer an injection, check on the patient’s mental status, and assess whether that patient needs an adjustment to their medication. Other clinics are offering “drive-by” injections to patients who arrive by car, and a nurse wearing a mask and a face shield administers the injection from the car window. Monthly naltrexone also can be administered using one of these methods, and telepsychiatry can be used to monitor patients, Dr. Gupta noted at the meeting, presented by Global Academy for Medical Education.
“In my clinic, what happens is the injection room is set up just next to the door, so they don’t have to walk deep into the clinic,” Dr. Gupta said. “They walk in, go to the left, [and] there’s the injection room. They sit, get an injection, they’re out. It’s kept smooth.”
Choosing the right telehealth option
Clinicians should be aware of important regulatory changes that occurred that made widespread telehealth more appealing during the COVID-19 pandemic. Payment parity with in-office visits makes telehealth a viable consideration, while some states have begun offering telehealth licenses to practice across state lines. There is wide variation with regard to which states provide licensure and prescribing privileges for out-of-state clinicians without seeing those patients in person. “The most important thing: The psychiatry service is provided in the state where the patient is located,” Dr. Gupta said. Clinicians should check with that state’s board to figure out specific requirements. “Preferably if you get it in writing, it’s good for you,” he said.
Deciding who the clinician is seeing – consulting with patients or other physicians/clinicians – and what type of visits a clinician will conduct is an important step in transitioning to telepsychiatry. Visits from evaluation through ongoing care are possible through telepsychiatry, or a clinician can opt to see just second opinion visits, Dr. Gupta said. It is also important to consider the technical ability of the patient to do video conferencing.
As HIPAA requirements for privacy have relaxed, clinicians now have an array of teleconferencing options to choose from; platforms such as FaceTime, Doximity, Vidyo, Doxy.me, Zoom, and video chat through EMR are popular options. However, when regular HIPAA requirements are reinstated after the pandemic, clinicians will need to find a compliant platform and sign a business associate agreement to stay within the law.
“Right now, my preferred use is FaceTime,” Dr. Gupta said. “Quick, simple, easy to use. A lot of people have an iPhone, and they know how to do it. I usually have the patient call me and I don’t use my personal iPhone; my clinic has an iPhone.”
How a clinician looks during a telepsychiatry visit is also important. Lighting, position of the camera, and clothing should all be considered. Keep the camera at eye level, test the lighting in the room where the call will take place, and use artificial lighting sources behind a computer, Dr. Gupta said. Other tips for telepsychiatry visits include silencing devices and microphones before a session begins, wearing solid-colored clothes, and having an identification badge visible to the patient. Sessions should be free of background distractions, such as a dog barking or a child interrupting, with the goal of creating an environment where the patient feels free to answer questions.
Contingency planning is a must for video visits, Dr. Gupta said. “I think the simplest thing is to see the patient. But all the stuff that’s the wraparound is really hard, because issues can arise suddenly, and we need to plan.” If a patient has a medical issue or becomes actively suicidal during a session, it is important to know contact information for the local police and crisis services. Clinicians also must plan for technology failure and provide alternative options for continuing the sessions, such as by phone.
Selecting patients for telepsychiatry
Not all patients will make the transition to telepsychiatry. “You can’t do telepsychiatry with everyone. It is a risk, so pick and choose,” Dr. Gupta said.
“Safety is a big consideration for conducting a telepsychiatry visit, especially when other health care providers are present. For example, when performing telehealth visits in a clinic, nursing home, or correctional facility, “I feel a lot more comfortable if there’s another health care clinician there,” Dr. Gupta said.
Clinicians may want to avoid a telepsychiatry visit for a patient in their own home for reasons of safety, reliability, and privacy. A longitudinal history with collateral information from friends or relatives can be helpful, but some subtle signs and body language may get missed over video, compared with an in-person visit. Sometimes you may not see if the patient is using substances. You have to really reconsider if [there] is violence and self-injurious behavior,” he said.
Discussing the pros and cons of telepsychiatry is important to obtaining patient consent. While consent requirements have relaxed under the COVID-19 pandemic, consent should ideally be obtained in writing, but can also be obtained verbally during a crisis. A plan should be developed for what will happen in the case of technology failure. “The patient should also know you’re maintaining privacy, you’re maintaining confidentiality, but there is a risk of hacking,” Dr. Gupta said. “Those things can happen, [and] there are no guarantees.”
If a patient is uncomfortable after beginning telepsychiatry, moving to in-person visits is also an option. “Many times, I do that if I’m not getting a good handle on things,” Dr. Gupta said. Situations where patients insist on in-patient visits over telepsychiatry are rare in his experience, Dr. Gupta noted, and are usually the result of the patient being unfamiliar with the technology. In cases where a patient cannot be talked through a technology barrier, visits can be done in the clinic while taking proper precautions.
“If it is a first-time visit, then I do it in the clinic,” Dr. Gupta said. “They come in, they have a face mask, and we use our group therapy room. The patients sit in a social-distanced fashion. But then, you document why you did this in-person visit like that.”
Documentation during COVID-19 also includes identifying the patient at the first visit, the nature of the visit (teleconference or other), parties present, referencing the pandemic, writing the location of the patient and the clinician, noting the patient’s satisfaction, evaluating the patient’s mental status, and recording what technology was used and any technical issues that were encountered.
Some populations of patients are better suited to telepsychiatry than others. It is more convenient for chronically psychiatrically ill patients in group homes and their staff to communicate through telepsychiatry, Dr. Gupta said. Consultation liaison in hospitals and emergency departments through telepsychiatry can limit the spread of infection, while increased access and convenience occurs as telepsychiatry is implemented in correctional facilities and nursing homes.
“What we are doing now, some of it is here to stay,” Dr. Gupta said.
In situations where a patient needs to switch providers, clinicians should continue to follow that patient until his first patient visit with that new provider. It is also important to set boundaries and apply some level of formality to the telepsychiatry visit, which means seeing the patient in a secure location where he can speak freely and privately.
“The best practices are [to] maintain faith [and] fidelity of the psychiatric assessment,” Dr. Gupta said. “Keep the trust and do your best to maintain patient privacy, because the privacy is not the same as it may be in a face-to-face session when you use televideo.”
Global Academy and this news organization are owned by the same parent company.
Dr. Gupta reported no relevant financial disclosures. Dr. Nasrallah disclosed serving as a consultant for and on the speakers bureaus of several pharmaceutical companies, including Alkermes, Janssen, and Lundbeck. He also disclosed serving on the speakers bureau of Otsuka.
The COVID-19 pandemic has changed life in numerous ways, including use of telehealth services for patients in all specialties. But telepsychiatry is an area not likely to go away even after the pandemic is over, according to Sanjay Gupta, MD.
The use of telepsychiatry has escalated significantly,” said Dr. Gupta, of the DENT Neurologic Institute, in Amherst, N.Y., in a bonus virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
About 90% of clinicians are performing telepsychiatry, Dr. Gupta noted, through methods such as phone consults, email, and video chat. As patients with psychiatric issues grapple with issues related to COVID-19 involving lockdowns, restrictions on travel, and consumption of news, they are presenting with addiction, depression, paranoia, mood lability, and other problems.
One issue immediately facing clinicians is whether to keep patients on long-acting injectables as a way to maintain psychological stability in patients with bipolar disorder, schizophrenia, and alcoholism – something Dr. Gupta and session moderator Henry A. Nasrallah, MD, advocated. “We should never stop the long-acting injectable to switch them to oral medication. Those patients are very likely to relapse,” Dr. Nasrallah said.
During the pandemic, clinicians need to find “safe and novel ways of providing the injection,” and several methods have been pioneered. For example, if a patient with schizophrenia is on lockdown, a nurse can visit monthly or bimonthly to administer an injection, check on the patient’s mental status, and assess whether that patient needs an adjustment to their medication. Other clinics are offering “drive-by” injections to patients who arrive by car, and a nurse wearing a mask and a face shield administers the injection from the car window. Monthly naltrexone also can be administered using one of these methods, and telepsychiatry can be used to monitor patients, Dr. Gupta noted at the meeting, presented by Global Academy for Medical Education.
“In my clinic, what happens is the injection room is set up just next to the door, so they don’t have to walk deep into the clinic,” Dr. Gupta said. “They walk in, go to the left, [and] there’s the injection room. They sit, get an injection, they’re out. It’s kept smooth.”
Choosing the right telehealth option
Clinicians should be aware of important regulatory changes that occurred that made widespread telehealth more appealing during the COVID-19 pandemic. Payment parity with in-office visits makes telehealth a viable consideration, while some states have begun offering telehealth licenses to practice across state lines. There is wide variation with regard to which states provide licensure and prescribing privileges for out-of-state clinicians without seeing those patients in person. “The most important thing: The psychiatry service is provided in the state where the patient is located,” Dr. Gupta said. Clinicians should check with that state’s board to figure out specific requirements. “Preferably if you get it in writing, it’s good for you,” he said.
Deciding who the clinician is seeing – consulting with patients or other physicians/clinicians – and what type of visits a clinician will conduct is an important step in transitioning to telepsychiatry. Visits from evaluation through ongoing care are possible through telepsychiatry, or a clinician can opt to see just second opinion visits, Dr. Gupta said. It is also important to consider the technical ability of the patient to do video conferencing.
As HIPAA requirements for privacy have relaxed, clinicians now have an array of teleconferencing options to choose from; platforms such as FaceTime, Doximity, Vidyo, Doxy.me, Zoom, and video chat through EMR are popular options. However, when regular HIPAA requirements are reinstated after the pandemic, clinicians will need to find a compliant platform and sign a business associate agreement to stay within the law.
“Right now, my preferred use is FaceTime,” Dr. Gupta said. “Quick, simple, easy to use. A lot of people have an iPhone, and they know how to do it. I usually have the patient call me and I don’t use my personal iPhone; my clinic has an iPhone.”
How a clinician looks during a telepsychiatry visit is also important. Lighting, position of the camera, and clothing should all be considered. Keep the camera at eye level, test the lighting in the room where the call will take place, and use artificial lighting sources behind a computer, Dr. Gupta said. Other tips for telepsychiatry visits include silencing devices and microphones before a session begins, wearing solid-colored clothes, and having an identification badge visible to the patient. Sessions should be free of background distractions, such as a dog barking or a child interrupting, with the goal of creating an environment where the patient feels free to answer questions.
Contingency planning is a must for video visits, Dr. Gupta said. “I think the simplest thing is to see the patient. But all the stuff that’s the wraparound is really hard, because issues can arise suddenly, and we need to plan.” If a patient has a medical issue or becomes actively suicidal during a session, it is important to know contact information for the local police and crisis services. Clinicians also must plan for technology failure and provide alternative options for continuing the sessions, such as by phone.
Selecting patients for telepsychiatry
Not all patients will make the transition to telepsychiatry. “You can’t do telepsychiatry with everyone. It is a risk, so pick and choose,” Dr. Gupta said.
“Safety is a big consideration for conducting a telepsychiatry visit, especially when other health care providers are present. For example, when performing telehealth visits in a clinic, nursing home, or correctional facility, “I feel a lot more comfortable if there’s another health care clinician there,” Dr. Gupta said.
Clinicians may want to avoid a telepsychiatry visit for a patient in their own home for reasons of safety, reliability, and privacy. A longitudinal history with collateral information from friends or relatives can be helpful, but some subtle signs and body language may get missed over video, compared with an in-person visit. Sometimes you may not see if the patient is using substances. You have to really reconsider if [there] is violence and self-injurious behavior,” he said.
Discussing the pros and cons of telepsychiatry is important to obtaining patient consent. While consent requirements have relaxed under the COVID-19 pandemic, consent should ideally be obtained in writing, but can also be obtained verbally during a crisis. A plan should be developed for what will happen in the case of technology failure. “The patient should also know you’re maintaining privacy, you’re maintaining confidentiality, but there is a risk of hacking,” Dr. Gupta said. “Those things can happen, [and] there are no guarantees.”
If a patient is uncomfortable after beginning telepsychiatry, moving to in-person visits is also an option. “Many times, I do that if I’m not getting a good handle on things,” Dr. Gupta said. Situations where patients insist on in-patient visits over telepsychiatry are rare in his experience, Dr. Gupta noted, and are usually the result of the patient being unfamiliar with the technology. In cases where a patient cannot be talked through a technology barrier, visits can be done in the clinic while taking proper precautions.
“If it is a first-time visit, then I do it in the clinic,” Dr. Gupta said. “They come in, they have a face mask, and we use our group therapy room. The patients sit in a social-distanced fashion. But then, you document why you did this in-person visit like that.”
Documentation during COVID-19 also includes identifying the patient at the first visit, the nature of the visit (teleconference or other), parties present, referencing the pandemic, writing the location of the patient and the clinician, noting the patient’s satisfaction, evaluating the patient’s mental status, and recording what technology was used and any technical issues that were encountered.
Some populations of patients are better suited to telepsychiatry than others. It is more convenient for chronically psychiatrically ill patients in group homes and their staff to communicate through telepsychiatry, Dr. Gupta said. Consultation liaison in hospitals and emergency departments through telepsychiatry can limit the spread of infection, while increased access and convenience occurs as telepsychiatry is implemented in correctional facilities and nursing homes.
“What we are doing now, some of it is here to stay,” Dr. Gupta said.
In situations where a patient needs to switch providers, clinicians should continue to follow that patient until his first patient visit with that new provider. It is also important to set boundaries and apply some level of formality to the telepsychiatry visit, which means seeing the patient in a secure location where he can speak freely and privately.
“The best practices are [to] maintain faith [and] fidelity of the psychiatric assessment,” Dr. Gupta said. “Keep the trust and do your best to maintain patient privacy, because the privacy is not the same as it may be in a face-to-face session when you use televideo.”
Global Academy and this news organization are owned by the same parent company.
Dr. Gupta reported no relevant financial disclosures. Dr. Nasrallah disclosed serving as a consultant for and on the speakers bureaus of several pharmaceutical companies, including Alkermes, Janssen, and Lundbeck. He also disclosed serving on the speakers bureau of Otsuka.
EXPERT ANALYSIS FROM CP/AACP 2020 PSYCHIATRY UPDATE
‘Defund the police’: An important moment for society and psychiatry
Over the past months, society has reflected on the role of law enforcement. The shocking murder of George Floyd has forced Americans to reconsider the place of police officers in maintaining order.

The death of Mr. Floyd is certainly not a lone incident; in 2019, 1,098 people were killed by those tasked with protecting us.1 The United States holds 25% of the world’s incarcerated, though it makes up only 5% of the world’s population.2 Society is demanding a newer and better system.
The phrase “defund the police” can easily be dismissed because, to many, it implies an appeal to lawlessness. While we certainly cannot speak for any one protester, we think that many of the necessary changes are painfully obvious.3 Society wants law enforcement where force is not the default position but the last option. Society wants law enforcement where verbal conflict resolution is the primary focus of training and intervention. Society wants a correctional system that is more rehabilitative than it is punitive.4
Major U.S. cities spend up to 40% of their funds on police budgeting, much more than what is dedicated to community resources and infrastructure. This trend continues to increase between 1986 and 2013, state spending for correctional facilities increased by 141%.5 Yet, as psychiatrists, we are well aware that social determinants are a strong factor in future criminality.6 Increasing police budgets without addressing structural root causes and risk factors for future asocial behavior is not a wise approach to reducing unlawful behavior. Investing more into programs and policies that reduce these risks is essential.
Using the adverse childhood experiences (ACE) questionnaires, researchers have supported the idea that social programs are a key player in an improved criminal system. The ACE study identified 10 forms of childhood trauma in 17,000 patients, including abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes, engagement in high-risk behaviors, significant medical consequences, and even early death.7 More recent research has shown that those ACEs were four times more prevalent in a criminal offender group than in the general population.8 Psychiatry is in a unique position to address and provide education about ACEs as a tool to identify and help at-risk youths.
Many protesters have asked for mental health providers to have a primary role in this societal reflection and in providing a solution.9 This makes particular sense when considering that almost 20% of calls to law enforcement are for persons with impaired judgment from mental illness or intoxication, and one in four patients with mental illness has been arrested.10,11 We are humbled by this public trust and request. We believe psychiatry can provide many answers to this societal angst. After all, psychiatry is a specialty dedicated to addressing behavioral problems in an evidence-based way.
Yet, we should not forget psychiatry’s imperfect past and our own role in the creation of this system. While this article does not attempt to catalog psychiatry’s faults, one can start by recognizing that mass incarceration is partly a response to how poorly human beings were treated in asylums. Psychiatry was at one time a main enforcer of societal disenfranchisement. After most asylums were closed in 1963 with the Community Mental Health Act, correctional facilities became the largest purveyors of mental health care, often with damaging results.12 If psychiatry were to advocate for the reestablishment of asylums as a solution, we fear that psychiatry would have missed the point. We wonder whether the psychiatrists who have railed against deinstitutionalization since the 1970s do not realize that violence, unethical experimentation, and even racism were at times attributes of asylums.13

Psychiatry can and should be much more than what it once was. Instead of indirectly and inaccurately suggesting that our patients commit mass murders, we should improve research in the field of violence risk assessment and management. As many have already pointed out, violence risk assessment is permeated with overestimation of its potential and, more concerningly, tainted by evidence of implicit racism.14 Implicit racism extends to rights-limiting treatments as well. As previously studied, involuntary outpatient programs often referred to as assisted outpatient treatment are disproportionately levied on Black Americans.15 Instead of routinely seeking to expand abilities to involuntary treat and limit the rights of our patients, we should strive to be a violence-free alternative to law enforcement, not the medical version of police.
Psychiatrists should start actively training, practicing, and researching how to address nonviolent emergency calls. Training should include more robust deescalation training, techniques on the evaluation of patients outside of health care facilities (for example, the street), and a broadening of interventions to include proficiency in the treatment of subclinical populations seeking emergency care without the need to be formally labeled with a psychiatric disorder. Ride-alongs with police officers, volunteering at crisis hotlines, and home calls should not be volunteer or elective experiences for psychiatrists but a required part of training.
Thankfully, some local jurisdictions already have started promising practices that merit replication or at least academic review. Austin, Tex., recently implemented the capability of requesting mental health emergency calls when contacting 911.17 Eugene, Ore., has had the CAHOOTS (Crisis Assistance Helping Out On The Streets) program since 1989, where a medical provider and a mental health provider respond to calls without any law enforcement officers.18 Our own San Diego County has an innovative PERT (Psychiatric Emergency Response Team) program, which partners a mental health provider to a police patrol, allowing an ability to quickly provide different types of services.19 Programs like these show us what is possible. At this time, there is little research to evaluate many programs’ effectiveness.20 Psychiatry should seize this moment to be at the forefront of studying, then educating the public on what works and how to reproduce it.
Police officers have a difficult profession. They are tasked with preventing and predicting crime, often to the point of risking their own lives. Historically, police have been the first call to handle issues for which they are not equipped, ranging from fixing homelessness to arresting violent people using nonviolent means. The idea that police should be able to protect us in all situations has been mistakenly ingrained in our minds. Officers themselves do not feel adequately trained to handle mental health crises.21 “Defund the police” also means a recognition by governments, the public, and police themselves that officers should not be on the front lines for every emergency situation. We must diversify our first responders. Psychiatry should hear this call and be ready.

Since the death of Mr. Floyd, mental health professionals have attempted to voice empathy and warmth to those feeling left out and disenfranchised. Mental health professionals have voiced a desire to educate themselves on systemic biases and antiracism. However, we argue that psychiatry is not and has never been a bystander to the societal debate on the management of different and criminal behavior. While it may be enough for many fields to express sympathy from the sidelines, psychiatry has been and continues to be an active player in the disenfranchisement of minority populations in the criminal justice system. Society appears to be offering us a chance at repairing our past and helping the future. Let’s take it with honor and humility.
References
1. Collins S. Police killings can be captured in data. The terror police create cannot. Vox.com. 2020 Jun 19.
2. Lee MYH. Yes, U.S. locks people up at a higher rate than any other country. The Washington Post. 2015 Jul 7.
3. McDowell MG, Fernandez LA. Critical Criminology. 2018;26(3):373-91.
4. Thielo AJ et al. Criminology & Public Policy. 2016;15(1):137-70.
5. The Center for Popular Democracy. Freedom to Thrive.
6. Hipp JR. Criminology. 2007;45(3):665-97.
7. Felitti VJ et al. Am J Prev Med. 1998;14(4):245-58.
8. Reavis JA. Perm J. 2013 Spring;17(2):44-8.
9. McHarris PV, McHarris T. No more money for the police. The New York Times. 2020 May 20.
10. Kaminski RJ et al. Police Quarterly. 2004;7(3):311-38.
11. Livington JD. Psychiatr Serv. 2016 Aug 1;67(8):850-7.
12. Galanek JD. Cult Med Psychiatry. 2013 Mar;37(1):195-225.
13. Raz M. Nature. Book Review. 2020 Apr 21.
14. Dressel J, Farid H. Sci Adv. 2018 J 17;4(1):eaao5580.
15. Swartz MS et al. New York State assisted outpatient treatment program evaluation. 2009 Jun 30.
16. Barnes SS and Badre N. Psychiatr Serv. 2016 Jul 1;67(7):784-6.
17. Fox A. Austin budget adds millions for mental health response in 911 services. efficientgov.com. 2019 Sep 13.
18. Elinson Z. When mental health experts, not police, are the first responders. The Wall Street Journal. 2018 Nov 14.
19. Improved responses in psychiatric crises: The Psychiatric Emergency Response Team.
20. Kane E et al. Crim Behav Ment Health. 2018 Apr;28(2):108-19.
21. Wells W, Schafer JA. Officer perceptions of police responses to persons with a mental illness, in “Policing: An International Journal of Police Strategies & Management,” 2006 Oct;29(4):578-61.
Dr. Malik is a first-year psychiatry resident at the University of California, San Diego. She has a background in policy and grassroots organizing through her time working at the National Coalition for the Homeless and the Women’s Law Project. Dr. Malik has no disclosures.
Dr. Amendolara is a first-year psychiatry resident at University of California, San Diego. He spent years advocating for survivors of rape and domestic violence at the Crime Victims Treatment Center in New York and conducted public health research at Lourdes Center for Public Health in Camden, N.J. Dr. Amendolara has no disclosures.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Among his writings is chapter 7 in the book “Critical Psychiatry: Controversies and Clinical Implications” (Cham, Switzerland: Springer, 2019). He has no disclosures.
Over the past months, society has reflected on the role of law enforcement. The shocking murder of George Floyd has forced Americans to reconsider the place of police officers in maintaining order.
The death of Mr. Floyd is certainly not a lone incident; in 2019, 1,098 people were killed by those tasked with protecting us.1 The United States holds 25% of the world’s incarcerated, though it makes up only 5% of the world’s population.2 Society is demanding a newer and better system.
The phrase “defund the police” can easily be dismissed because, to many, it implies an appeal to lawlessness. While we certainly cannot speak for any one protester, we think that many of the necessary changes are painfully obvious.3 Society wants law enforcement where force is not the default position but the last option. Society wants law enforcement where verbal conflict resolution is the primary focus of training and intervention. Society wants a correctional system that is more rehabilitative than it is punitive.4
Major U.S. cities spend up to 40% of their funds on police budgeting, much more than what is dedicated to community resources and infrastructure. This trend continues to increase between 1986 and 2013, state spending for correctional facilities increased by 141%.5 Yet, as psychiatrists, we are well aware that social determinants are a strong factor in future criminality.6 Increasing police budgets without addressing structural root causes and risk factors for future asocial behavior is not a wise approach to reducing unlawful behavior. Investing more into programs and policies that reduce these risks is essential.
Using the adverse childhood experiences (ACE) questionnaires, researchers have supported the idea that social programs are a key player in an improved criminal system. The ACE study identified 10 forms of childhood trauma in 17,000 patients, including abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes, engagement in high-risk behaviors, significant medical consequences, and even early death.7 More recent research has shown that those ACEs were four times more prevalent in a criminal offender group than in the general population.8 Psychiatry is in a unique position to address and provide education about ACEs as a tool to identify and help at-risk youths.
Many protesters have asked for mental health providers to have a primary role in this societal reflection and in providing a solution.9 This makes particular sense when considering that almost 20% of calls to law enforcement are for persons with impaired judgment from mental illness or intoxication, and one in four patients with mental illness has been arrested.10,11 We are humbled by this public trust and request. We believe psychiatry can provide many answers to this societal angst. After all, psychiatry is a specialty dedicated to addressing behavioral problems in an evidence-based way.
Yet, we should not forget psychiatry’s imperfect past and our own role in the creation of this system. While this article does not attempt to catalog psychiatry’s faults, one can start by recognizing that mass incarceration is partly a response to how poorly human beings were treated in asylums. Psychiatry was at one time a main enforcer of societal disenfranchisement. After most asylums were closed in 1963 with the Community Mental Health Act, correctional facilities became the largest purveyors of mental health care, often with damaging results.12 If psychiatry were to advocate for the reestablishment of asylums as a solution, we fear that psychiatry would have missed the point. We wonder whether the psychiatrists who have railed against deinstitutionalization since the 1970s do not realize that violence, unethical experimentation, and even racism were at times attributes of asylums.13
Psychiatry can and should be much more than what it once was. Instead of indirectly and inaccurately suggesting that our patients commit mass murders, we should improve research in the field of violence risk assessment and management. As many have already pointed out, violence risk assessment is permeated with overestimation of its potential and, more concerningly, tainted by evidence of implicit racism.14 Implicit racism extends to rights-limiting treatments as well. As previously studied, involuntary outpatient programs often referred to as assisted outpatient treatment are disproportionately levied on Black Americans.15 Instead of routinely seeking to expand abilities to involuntary treat and limit the rights of our patients, we should strive to be a violence-free alternative to law enforcement, not the medical version of police.
Psychiatrists should start actively training, practicing, and researching how to address nonviolent emergency calls. Training should include more robust deescalation training, techniques on the evaluation of patients outside of health care facilities (for example, the street), and a broadening of interventions to include proficiency in the treatment of subclinical populations seeking emergency care without the need to be formally labeled with a psychiatric disorder. Ride-alongs with police officers, volunteering at crisis hotlines, and home calls should not be volunteer or elective experiences for psychiatrists but a required part of training.
Thankfully, some local jurisdictions already have started promising practices that merit replication or at least academic review. Austin, Tex., recently implemented the capability of requesting mental health emergency calls when contacting 911.17 Eugene, Ore., has had the CAHOOTS (Crisis Assistance Helping Out On The Streets) program since 1989, where a medical provider and a mental health provider respond to calls without any law enforcement officers.18 Our own San Diego County has an innovative PERT (Psychiatric Emergency Response Team) program, which partners a mental health provider to a police patrol, allowing an ability to quickly provide different types of services.19 Programs like these show us what is possible. At this time, there is little research to evaluate many programs’ effectiveness.20 Psychiatry should seize this moment to be at the forefront of studying, then educating the public on what works and how to reproduce it.
Police officers have a difficult profession. They are tasked with preventing and predicting crime, often to the point of risking their own lives. Historically, police have been the first call to handle issues for which they are not equipped, ranging from fixing homelessness to arresting violent people using nonviolent means. The idea that police should be able to protect us in all situations has been mistakenly ingrained in our minds. Officers themselves do not feel adequately trained to handle mental health crises.21 “Defund the police” also means a recognition by governments, the public, and police themselves that officers should not be on the front lines for every emergency situation. We must diversify our first responders. Psychiatry should hear this call and be ready.
Since the death of Mr. Floyd, mental health professionals have attempted to voice empathy and warmth to those feeling left out and disenfranchised. Mental health professionals have voiced a desire to educate themselves on systemic biases and antiracism. However, we argue that psychiatry is not and has never been a bystander to the societal debate on the management of different and criminal behavior. While it may be enough for many fields to express sympathy from the sidelines, psychiatry has been and continues to be an active player in the disenfranchisement of minority populations in the criminal justice system. Society appears to be offering us a chance at repairing our past and helping the future. Let’s take it with honor and humility.
References
1. Collins S. Police killings can be captured in data. The terror police create cannot. Vox.com. 2020 Jun 19.
2. Lee MYH. Yes, U.S. locks people up at a higher rate than any other country. The Washington Post. 2015 Jul 7.
3. McDowell MG, Fernandez LA. Critical Criminology. 2018;26(3):373-91.
4. Thielo AJ et al. Criminology & Public Policy. 2016;15(1):137-70.
5. The Center for Popular Democracy. Freedom to Thrive.
6. Hipp JR. Criminology. 2007;45(3):665-97.
7. Felitti VJ et al. Am J Prev Med. 1998;14(4):245-58.
8. Reavis JA. Perm J. 2013 Spring;17(2):44-8.
9. McHarris PV, McHarris T. No more money for the police. The New York Times. 2020 May 20.
10. Kaminski RJ et al. Police Quarterly. 2004;7(3):311-38.
11. Livington JD. Psychiatr Serv. 2016 Aug 1;67(8):850-7.
12. Galanek JD. Cult Med Psychiatry. 2013 Mar;37(1):195-225.
13. Raz M. Nature. Book Review. 2020 Apr 21.
14. Dressel J, Farid H. Sci Adv. 2018 J 17;4(1):eaao5580.
15. Swartz MS et al. New York State assisted outpatient treatment program evaluation. 2009 Jun 30.
16. Barnes SS and Badre N. Psychiatr Serv. 2016 Jul 1;67(7):784-6.
17. Fox A. Austin budget adds millions for mental health response in 911 services. efficientgov.com. 2019 Sep 13.
18. Elinson Z. When mental health experts, not police, are the first responders. The Wall Street Journal. 2018 Nov 14.
19. Improved responses in psychiatric crises: The Psychiatric Emergency Response Team.
20. Kane E et al. Crim Behav Ment Health. 2018 Apr;28(2):108-19.
21. Wells W, Schafer JA. Officer perceptions of police responses to persons with a mental illness, in “Policing: An International Journal of Police Strategies & Management,” 2006 Oct;29(4):578-61.
Dr. Malik is a first-year psychiatry resident at the University of California, San Diego. She has a background in policy and grassroots organizing through her time working at the National Coalition for the Homeless and the Women’s Law Project. Dr. Malik has no disclosures.
Dr. Amendolara is a first-year psychiatry resident at University of California, San Diego. He spent years advocating for survivors of rape and domestic violence at the Crime Victims Treatment Center in New York and conducted public health research at Lourdes Center for Public Health in Camden, N.J. Dr. Amendolara has no disclosures.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Among his writings is chapter 7 in the book “Critical Psychiatry: Controversies and Clinical Implications” (Cham, Switzerland: Springer, 2019). He has no disclosures.
Over the past months, society has reflected on the role of law enforcement. The shocking murder of George Floyd has forced Americans to reconsider the place of police officers in maintaining order.
The death of Mr. Floyd is certainly not a lone incident; in 2019, 1,098 people were killed by those tasked with protecting us.1 The United States holds 25% of the world’s incarcerated, though it makes up only 5% of the world’s population.2 Society is demanding a newer and better system.
The phrase “defund the police” can easily be dismissed because, to many, it implies an appeal to lawlessness. While we certainly cannot speak for any one protester, we think that many of the necessary changes are painfully obvious.3 Society wants law enforcement where force is not the default position but the last option. Society wants law enforcement where verbal conflict resolution is the primary focus of training and intervention. Society wants a correctional system that is more rehabilitative than it is punitive.4
Major U.S. cities spend up to 40% of their funds on police budgeting, much more than what is dedicated to community resources and infrastructure. This trend continues to increase between 1986 and 2013, state spending for correctional facilities increased by 141%.5 Yet, as psychiatrists, we are well aware that social determinants are a strong factor in future criminality.6 Increasing police budgets without addressing structural root causes and risk factors for future asocial behavior is not a wise approach to reducing unlawful behavior. Investing more into programs and policies that reduce these risks is essential.
Using the adverse childhood experiences (ACE) questionnaires, researchers have supported the idea that social programs are a key player in an improved criminal system. The ACE study identified 10 forms of childhood trauma in 17,000 patients, including abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes, engagement in high-risk behaviors, significant medical consequences, and even early death.7 More recent research has shown that those ACEs were four times more prevalent in a criminal offender group than in the general population.8 Psychiatry is in a unique position to address and provide education about ACEs as a tool to identify and help at-risk youths.
Many protesters have asked for mental health providers to have a primary role in this societal reflection and in providing a solution.9 This makes particular sense when considering that almost 20% of calls to law enforcement are for persons with impaired judgment from mental illness or intoxication, and one in four patients with mental illness has been arrested.10,11 We are humbled by this public trust and request. We believe psychiatry can provide many answers to this societal angst. After all, psychiatry is a specialty dedicated to addressing behavioral problems in an evidence-based way.
Yet, we should not forget psychiatry’s imperfect past and our own role in the creation of this system. While this article does not attempt to catalog psychiatry’s faults, one can start by recognizing that mass incarceration is partly a response to how poorly human beings were treated in asylums. Psychiatry was at one time a main enforcer of societal disenfranchisement. After most asylums were closed in 1963 with the Community Mental Health Act, correctional facilities became the largest purveyors of mental health care, often with damaging results.12 If psychiatry were to advocate for the reestablishment of asylums as a solution, we fear that psychiatry would have missed the point. We wonder whether the psychiatrists who have railed against deinstitutionalization since the 1970s do not realize that violence, unethical experimentation, and even racism were at times attributes of asylums.13
Psychiatry can and should be much more than what it once was. Instead of indirectly and inaccurately suggesting that our patients commit mass murders, we should improve research in the field of violence risk assessment and management. As many have already pointed out, violence risk assessment is permeated with overestimation of its potential and, more concerningly, tainted by evidence of implicit racism.14 Implicit racism extends to rights-limiting treatments as well. As previously studied, involuntary outpatient programs often referred to as assisted outpatient treatment are disproportionately levied on Black Americans.15 Instead of routinely seeking to expand abilities to involuntary treat and limit the rights of our patients, we should strive to be a violence-free alternative to law enforcement, not the medical version of police.
Psychiatrists should start actively training, practicing, and researching how to address nonviolent emergency calls. Training should include more robust deescalation training, techniques on the evaluation of patients outside of health care facilities (for example, the street), and a broadening of interventions to include proficiency in the treatment of subclinical populations seeking emergency care without the need to be formally labeled with a psychiatric disorder. Ride-alongs with police officers, volunteering at crisis hotlines, and home calls should not be volunteer or elective experiences for psychiatrists but a required part of training.
Thankfully, some local jurisdictions already have started promising practices that merit replication or at least academic review. Austin, Tex., recently implemented the capability of requesting mental health emergency calls when contacting 911.17 Eugene, Ore., has had the CAHOOTS (Crisis Assistance Helping Out On The Streets) program since 1989, where a medical provider and a mental health provider respond to calls without any law enforcement officers.18 Our own San Diego County has an innovative PERT (Psychiatric Emergency Response Team) program, which partners a mental health provider to a police patrol, allowing an ability to quickly provide different types of services.19 Programs like these show us what is possible. At this time, there is little research to evaluate many programs’ effectiveness.20 Psychiatry should seize this moment to be at the forefront of studying, then educating the public on what works and how to reproduce it.
Police officers have a difficult profession. They are tasked with preventing and predicting crime, often to the point of risking their own lives. Historically, police have been the first call to handle issues for which they are not equipped, ranging from fixing homelessness to arresting violent people using nonviolent means. The idea that police should be able to protect us in all situations has been mistakenly ingrained in our minds. Officers themselves do not feel adequately trained to handle mental health crises.21 “Defund the police” also means a recognition by governments, the public, and police themselves that officers should not be on the front lines for every emergency situation. We must diversify our first responders. Psychiatry should hear this call and be ready.
Since the death of Mr. Floyd, mental health professionals have attempted to voice empathy and warmth to those feeling left out and disenfranchised. Mental health professionals have voiced a desire to educate themselves on systemic biases and antiracism. However, we argue that psychiatry is not and has never been a bystander to the societal debate on the management of different and criminal behavior. While it may be enough for many fields to express sympathy from the sidelines, psychiatry has been and continues to be an active player in the disenfranchisement of minority populations in the criminal justice system. Society appears to be offering us a chance at repairing our past and helping the future. Let’s take it with honor and humility.
References
1. Collins S. Police killings can be captured in data. The terror police create cannot. Vox.com. 2020 Jun 19.
2. Lee MYH. Yes, U.S. locks people up at a higher rate than any other country. The Washington Post. 2015 Jul 7.
3. McDowell MG, Fernandez LA. Critical Criminology. 2018;26(3):373-91.
4. Thielo AJ et al. Criminology & Public Policy. 2016;15(1):137-70.
5. The Center for Popular Democracy. Freedom to Thrive.
6. Hipp JR. Criminology. 2007;45(3):665-97.
7. Felitti VJ et al. Am J Prev Med. 1998;14(4):245-58.
8. Reavis JA. Perm J. 2013 Spring;17(2):44-8.
9. McHarris PV, McHarris T. No more money for the police. The New York Times. 2020 May 20.
10. Kaminski RJ et al. Police Quarterly. 2004;7(3):311-38.
11. Livington JD. Psychiatr Serv. 2016 Aug 1;67(8):850-7.
12. Galanek JD. Cult Med Psychiatry. 2013 Mar;37(1):195-225.
13. Raz M. Nature. Book Review. 2020 Apr 21.
14. Dressel J, Farid H. Sci Adv. 2018 J 17;4(1):eaao5580.
15. Swartz MS et al. New York State assisted outpatient treatment program evaluation. 2009 Jun 30.
16. Barnes SS and Badre N. Psychiatr Serv. 2016 Jul 1;67(7):784-6.
17. Fox A. Austin budget adds millions for mental health response in 911 services. efficientgov.com. 2019 Sep 13.
18. Elinson Z. When mental health experts, not police, are the first responders. The Wall Street Journal. 2018 Nov 14.
19. Improved responses in psychiatric crises: The Psychiatric Emergency Response Team.
20. Kane E et al. Crim Behav Ment Health. 2018 Apr;28(2):108-19.
21. Wells W, Schafer JA. Officer perceptions of police responses to persons with a mental illness, in “Policing: An International Journal of Police Strategies & Management,” 2006 Oct;29(4):578-61.
Dr. Malik is a first-year psychiatry resident at the University of California, San Diego. She has a background in policy and grassroots organizing through her time working at the National Coalition for the Homeless and the Women’s Law Project. Dr. Malik has no disclosures.
Dr. Amendolara is a first-year psychiatry resident at University of California, San Diego. He spent years advocating for survivors of rape and domestic violence at the Crime Victims Treatment Center in New York and conducted public health research at Lourdes Center for Public Health in Camden, N.J. Dr. Amendolara has no disclosures.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Among his writings is chapter 7 in the book “Critical Psychiatry: Controversies and Clinical Implications” (Cham, Switzerland: Springer, 2019). He has no disclosures.
Device improves physical exam completion rates in serious mental illness
Using a simple point-of-care (POC) finger prick device to measure blood glucose and lipid levels significantly increases rates of physical health checkups for patients with severe mental illness, new research shows.
In a UK pilot study, use of the Afinion 2 device (Abbott) was associated with a doubling of completed physical health checkups.
However, the effect only occurred in early-intervention services, in which clinicians may feel physical health checkups are most beneficial. This underlines the importance of staff training and payment incentives, the researchers note.
“Clearly, convenience is a great thing about these devices” for both the patient and the mental health clinician, Joseph Butler, MD, a psychiatry trainee at the University of Oxford, United Kingdom, told Medscape Medical News.
He noted that blood test results are rapid, which facilitates immediate discussion of a health management plan.
These tests are “independent from the lab, they’re independent from the general practitioner, and so in terms of convenience, we think it wins on both fronts,” Butler said.
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Poor heart health
Previous research has shown that life expectancy of patients with severe mental illness is 15 to 20 years less than that of the general population, mostly because of complications from poor cardiovascular health.
In the United Kingdom, physical healthcare for patients with serious mental illness is provided by primary care clinicians and community mental health teams (CMHTs). The National Institute for Health and Care Excellence recommends an annual physical examination.
However, a recent audit in the south of England indicated that only 38% of patients with severe mental illness underwent complete physical examinations, primarily because blood glucose and lipid test panels had been omitted.
The researchers note that patients are typically advised to visit their general practitioner for blood tests, “which can be a challenge” for those with severe mental illness.
The Cardiovascular Monitoring in Mental Health (CARMEN) project involved distributing the Afinion 2 device for use in two CMHTs in Oxfordshire, United Kingdom, for 6 months. One CMHT was an early-intervention service, and the other was an adult mental health service.
Care coordinators received training on how to use the device as well as ongoing support to facilitate engagement with the device.
Rates of completion of blood testing and full physical examinations were compared between the intervention CMHTs and two matched control services – an early-intervention group, and an adult metal health services group in Buckinghamshire, a neighboring county.
Better completion rates
The investigators found that .
In contrast, the percentage of physical examinations that were completed remained low in the control CMHT early-intervention service, at just 7.8%.
Direct comparison between the two services showed that use of the POC device was associated with a significant increase in the number of complete physical examinations, at a relative rate of 5.18 (P < .001).
Results were similar when the investigators examined rates at which A1c and lipid panels were completed.
However, there was no difference in completion of physical examinations in the adult mental health service group, for which rates were comparable to those in the control service.
Butler speculated that the way health checkups are funded in the United Kingdom might have contributed to the poor results with the device in the adult mental health service.
In early-intervention services, there is increased awareness of the importance of physical examinations, and funding is contingent on whether clinicians persuade patients to have the examinations.
Overall, the findings show that use of a POC device for physical examinations is acceptable to patients who have severe mental illness as well as to mental health care clinicians, the investigators note.
“In teams where it is well adopted, POC testing can improve physical health check completion...although our qualitative findings highlight important considerations for maximizing clinician engagement,” they add.
The researchers plan to repeat the study across the whole of the south of England, with early-intervention services in the west equipped with POC devices and those in the east serving as controls.
Similar findings
Commenting on the findings for Medscape Medical News, Joe Parks, MD, vice president and practice improvement and medical director at the National Council for Behavioral Health, Washington, DC, noted that he and his colleagues conducted a similar study in the mid-2000s.
Starting in 2004, they distributed a POC finger prick test device for use by community mental health teams to measure blood glucose and lipid levels.
“We required as a condition of payment that the providers get these lab results for everybody they served and report them centrally. Then, we databased them and benchmarked them, and we were able to show significant reductions in HbA1c’s over time,” said Parks, who was not involved with the current research.
Moreover, that program achieved corresponding savings of $23 to $24 million, he noted.
Although his study and the current study show that POC devices work, he emphasized that it’s not enough to make the devices available to clinicians.
“You also have to ensure the providers put it in their clinic workflows and use it with everybody. To do that, it really helps if you have the providers report the results, then give them report cards so they can see who’s doing it and who isn’t,” Parks said.
It wasn’t surprising that in the current study, the introduction of the POC device made less of an impact in the adult community services, he noted.
Although weight reduction is much slower in that setting, “you can still get better control of their lipids and HbA1c›s, and you get at their weight over time. You just have to program for that, too,» said Parks.
He added that it’s hard to achieve weight reduction of more than 5% or 10%, but many of these patients need a 25% to 30% reduction. “The only thing that’s going to get that is bariatric surgery,” he noted.
POC devices are not widely used in the United States.
“The payer paying for the care basically has to insist that [it] be used and then provide the machine and train the staff to use it,” Parks said.
It requires payers “to get actually involved in how providers organize and manage care, which they tend to not like to do. It’s silly because the only way any payer has to make anybody better is through the provider,” he noted.
Parks added that to increase uptake beyond the “motivated few” requires that it be made part of the workflow and not left up to clinician discretion.
The study was funded by the National Institute for Health Research. Butler and Parks have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Using a simple point-of-care (POC) finger prick device to measure blood glucose and lipid levels significantly increases rates of physical health checkups for patients with severe mental illness, new research shows.
In a UK pilot study, use of the Afinion 2 device (Abbott) was associated with a doubling of completed physical health checkups.
However, the effect only occurred in early-intervention services, in which clinicians may feel physical health checkups are most beneficial. This underlines the importance of staff training and payment incentives, the researchers note.
“Clearly, convenience is a great thing about these devices” for both the patient and the mental health clinician, Joseph Butler, MD, a psychiatry trainee at the University of Oxford, United Kingdom, told Medscape Medical News.
He noted that blood test results are rapid, which facilitates immediate discussion of a health management plan.
These tests are “independent from the lab, they’re independent from the general practitioner, and so in terms of convenience, we think it wins on both fronts,” Butler said.
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Poor heart health
Previous research has shown that life expectancy of patients with severe mental illness is 15 to 20 years less than that of the general population, mostly because of complications from poor cardiovascular health.
In the United Kingdom, physical healthcare for patients with serious mental illness is provided by primary care clinicians and community mental health teams (CMHTs). The National Institute for Health and Care Excellence recommends an annual physical examination.
However, a recent audit in the south of England indicated that only 38% of patients with severe mental illness underwent complete physical examinations, primarily because blood glucose and lipid test panels had been omitted.
The researchers note that patients are typically advised to visit their general practitioner for blood tests, “which can be a challenge” for those with severe mental illness.
The Cardiovascular Monitoring in Mental Health (CARMEN) project involved distributing the Afinion 2 device for use in two CMHTs in Oxfordshire, United Kingdom, for 6 months. One CMHT was an early-intervention service, and the other was an adult mental health service.
Care coordinators received training on how to use the device as well as ongoing support to facilitate engagement with the device.
Rates of completion of blood testing and full physical examinations were compared between the intervention CMHTs and two matched control services – an early-intervention group, and an adult metal health services group in Buckinghamshire, a neighboring county.
Better completion rates
The investigators found that .
In contrast, the percentage of physical examinations that were completed remained low in the control CMHT early-intervention service, at just 7.8%.
Direct comparison between the two services showed that use of the POC device was associated with a significant increase in the number of complete physical examinations, at a relative rate of 5.18 (P < .001).
Results were similar when the investigators examined rates at which A1c and lipid panels were completed.
However, there was no difference in completion of physical examinations in the adult mental health service group, for which rates were comparable to those in the control service.
Butler speculated that the way health checkups are funded in the United Kingdom might have contributed to the poor results with the device in the adult mental health service.
In early-intervention services, there is increased awareness of the importance of physical examinations, and funding is contingent on whether clinicians persuade patients to have the examinations.
Overall, the findings show that use of a POC device for physical examinations is acceptable to patients who have severe mental illness as well as to mental health care clinicians, the investigators note.
“In teams where it is well adopted, POC testing can improve physical health check completion...although our qualitative findings highlight important considerations for maximizing clinician engagement,” they add.
The researchers plan to repeat the study across the whole of the south of England, with early-intervention services in the west equipped with POC devices and those in the east serving as controls.
Similar findings
Commenting on the findings for Medscape Medical News, Joe Parks, MD, vice president and practice improvement and medical director at the National Council for Behavioral Health, Washington, DC, noted that he and his colleagues conducted a similar study in the mid-2000s.
Starting in 2004, they distributed a POC finger prick test device for use by community mental health teams to measure blood glucose and lipid levels.
“We required as a condition of payment that the providers get these lab results for everybody they served and report them centrally. Then, we databased them and benchmarked them, and we were able to show significant reductions in HbA1c’s over time,” said Parks, who was not involved with the current research.
Moreover, that program achieved corresponding savings of $23 to $24 million, he noted.
Although his study and the current study show that POC devices work, he emphasized that it’s not enough to make the devices available to clinicians.
“You also have to ensure the providers put it in their clinic workflows and use it with everybody. To do that, it really helps if you have the providers report the results, then give them report cards so they can see who’s doing it and who isn’t,” Parks said.
It wasn’t surprising that in the current study, the introduction of the POC device made less of an impact in the adult community services, he noted.
Although weight reduction is much slower in that setting, “you can still get better control of their lipids and HbA1c›s, and you get at their weight over time. You just have to program for that, too,» said Parks.
He added that it’s hard to achieve weight reduction of more than 5% or 10%, but many of these patients need a 25% to 30% reduction. “The only thing that’s going to get that is bariatric surgery,” he noted.
POC devices are not widely used in the United States.
“The payer paying for the care basically has to insist that [it] be used and then provide the machine and train the staff to use it,” Parks said.
It requires payers “to get actually involved in how providers organize and manage care, which they tend to not like to do. It’s silly because the only way any payer has to make anybody better is through the provider,” he noted.
Parks added that to increase uptake beyond the “motivated few” requires that it be made part of the workflow and not left up to clinician discretion.
The study was funded by the National Institute for Health Research. Butler and Parks have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Using a simple point-of-care (POC) finger prick device to measure blood glucose and lipid levels significantly increases rates of physical health checkups for patients with severe mental illness, new research shows.
In a UK pilot study, use of the Afinion 2 device (Abbott) was associated with a doubling of completed physical health checkups.
However, the effect only occurred in early-intervention services, in which clinicians may feel physical health checkups are most beneficial. This underlines the importance of staff training and payment incentives, the researchers note.
“Clearly, convenience is a great thing about these devices” for both the patient and the mental health clinician, Joseph Butler, MD, a psychiatry trainee at the University of Oxford, United Kingdom, told Medscape Medical News.
He noted that blood test results are rapid, which facilitates immediate discussion of a health management plan.
These tests are “independent from the lab, they’re independent from the general practitioner, and so in terms of convenience, we think it wins on both fronts,” Butler said.
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Poor heart health
Previous research has shown that life expectancy of patients with severe mental illness is 15 to 20 years less than that of the general population, mostly because of complications from poor cardiovascular health.
In the United Kingdom, physical healthcare for patients with serious mental illness is provided by primary care clinicians and community mental health teams (CMHTs). The National Institute for Health and Care Excellence recommends an annual physical examination.
However, a recent audit in the south of England indicated that only 38% of patients with severe mental illness underwent complete physical examinations, primarily because blood glucose and lipid test panels had been omitted.
The researchers note that patients are typically advised to visit their general practitioner for blood tests, “which can be a challenge” for those with severe mental illness.
The Cardiovascular Monitoring in Mental Health (CARMEN) project involved distributing the Afinion 2 device for use in two CMHTs in Oxfordshire, United Kingdom, for 6 months. One CMHT was an early-intervention service, and the other was an adult mental health service.
Care coordinators received training on how to use the device as well as ongoing support to facilitate engagement with the device.
Rates of completion of blood testing and full physical examinations were compared between the intervention CMHTs and two matched control services – an early-intervention group, and an adult metal health services group in Buckinghamshire, a neighboring county.
Better completion rates
The investigators found that .
In contrast, the percentage of physical examinations that were completed remained low in the control CMHT early-intervention service, at just 7.8%.
Direct comparison between the two services showed that use of the POC device was associated with a significant increase in the number of complete physical examinations, at a relative rate of 5.18 (P < .001).
Results were similar when the investigators examined rates at which A1c and lipid panels were completed.
However, there was no difference in completion of physical examinations in the adult mental health service group, for which rates were comparable to those in the control service.
Butler speculated that the way health checkups are funded in the United Kingdom might have contributed to the poor results with the device in the adult mental health service.
In early-intervention services, there is increased awareness of the importance of physical examinations, and funding is contingent on whether clinicians persuade patients to have the examinations.
Overall, the findings show that use of a POC device for physical examinations is acceptable to patients who have severe mental illness as well as to mental health care clinicians, the investigators note.
“In teams where it is well adopted, POC testing can improve physical health check completion...although our qualitative findings highlight important considerations for maximizing clinician engagement,” they add.
The researchers plan to repeat the study across the whole of the south of England, with early-intervention services in the west equipped with POC devices and those in the east serving as controls.
Similar findings
Commenting on the findings for Medscape Medical News, Joe Parks, MD, vice president and practice improvement and medical director at the National Council for Behavioral Health, Washington, DC, noted that he and his colleagues conducted a similar study in the mid-2000s.
Starting in 2004, they distributed a POC finger prick test device for use by community mental health teams to measure blood glucose and lipid levels.
“We required as a condition of payment that the providers get these lab results for everybody they served and report them centrally. Then, we databased them and benchmarked them, and we were able to show significant reductions in HbA1c’s over time,” said Parks, who was not involved with the current research.
Moreover, that program achieved corresponding savings of $23 to $24 million, he noted.
Although his study and the current study show that POC devices work, he emphasized that it’s not enough to make the devices available to clinicians.
“You also have to ensure the providers put it in their clinic workflows and use it with everybody. To do that, it really helps if you have the providers report the results, then give them report cards so they can see who’s doing it and who isn’t,” Parks said.
It wasn’t surprising that in the current study, the introduction of the POC device made less of an impact in the adult community services, he noted.
Although weight reduction is much slower in that setting, “you can still get better control of their lipids and HbA1c›s, and you get at their weight over time. You just have to program for that, too,» said Parks.
He added that it’s hard to achieve weight reduction of more than 5% or 10%, but many of these patients need a 25% to 30% reduction. “The only thing that’s going to get that is bariatric surgery,” he noted.
POC devices are not widely used in the United States.
“The payer paying for the care basically has to insist that [it] be used and then provide the machine and train the staff to use it,” Parks said.
It requires payers “to get actually involved in how providers organize and manage care, which they tend to not like to do. It’s silly because the only way any payer has to make anybody better is through the provider,” he noted.
Parks added that to increase uptake beyond the “motivated few” requires that it be made part of the workflow and not left up to clinician discretion.
The study was funded by the National Institute for Health Research. Butler and Parks have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM SIRS 2020