User login
Should your practice be acquired by private equity?
Dear colleagues and friends,

The Perspectives series continues! Few current issues in Gastroenterology practice are as passionately debated as those associated with private equity. In this edition, our own Dr. John Allen and Dr. Marc Sonenshine explain private equity’s evolution in the GI field, dispel misconceptions, and dissect the central question of whether it is right for your practice. Thank you for your support, and I hope you will find the discussions enlightening and relevant to your practices. As always, I welcome your comments and suggestions for future topics at [email protected].
Charles Kahi, MD, MS, AGAF, is a professor of medicine, Indiana University School of Medicine, Indianapolis. He is also an Associate Editor for GI & Hepatology News.
Yes
But, at a minimum, you should absolutely lean-in, listen, and learn.
The physician leadership team at Atlanta Gastroenterology Associates has been focused on developing strategies and partnerships that strengthen our ability to thrive in our marketplace while also fending off threats to our mission. The path to forming the managed services organization (MSO) United Digestive (UD) through our agreement with the private equity firm Frazier Healthcare Partners was arduous and required a significant investment of resources and time. Like at Atlanta Gastroenterology Associates, many influential leaders within our field, also supported by their physician partners, have concluded that the investment of a private equity firm to build an MSO led by professional business executives will reduce the administrative stresses looming over the traditional independent gastroenterologist business model. Now, and after almost 2 years as a member of UD, I unequivocally believe my ability to provide timely, high-quality, and affordable care to my community is currently more stable and in a stronger position for the future.
Like we did in deciding whether to establish a formal relationship with a private equity–backed platform group, here are some critical questions you should explore and answer:
-What advantages and disadvantages will being a part of a private equity–backed MSO group bring to our patients, our practice, our team, and our providers?
-What forces threaten our practice’s ability to remain viable and pertinent in both the near and long term? And, how can our group ward off these threats?
-There are many private equity firms interested in our practice as well as already established platform groups. How do we decide which is best?
-If remaining completely independent is not a sustainable long-term option, why not just become employed by a hospital, join a strategic partner, or form/join a multi-specialty group or accountable care organization (ACO)?
In the first 2 years, UD has answered many of the questions and executed on desired priorities. Our management team helped us to navigate the chaos of COVID, and UD still remains on target to meet many annual budget goals as well as end of the year financial targets. Processes and enhanced technologies like real-time dashboards provide immediate insight into all aspects of our business, allowing for more analytical decision-making. Our payor and vendor negotiations yielded stronger returns than anticipated leading to material earnings. The revamped patient services center improved clinic utilization rates, reduced patient call wait times, deployed an online patient scheduling option, and employed medical assistants for handling clinical phone matters.
Most importantly, not one change at UD has negatively affected our clinical autonomy and decision-making. The MSO and its management team has steered all medical-related issues to our chief medical officer and physician executive committee. Moreover, there was much less consternation amongst partners when the time arose for significant capital expenditures (i.e., upgrading our endoscopic equipment, instituting a new electronic health record and practice management system, or surviving the cash-flow crunch during the beginning of COVID), as our annual compensation was not affected.
A few broader points to consider that pertain to private equity activity in physician services (i.e., not specific to gastroenterology or UD):
- Private equity firms invest money in private companies with the expectation of superior financial returns. Their principals are searching for opportunities with significant upside and potential to generate the necessary earnings for such returns. In fragmented fields, there is potential to use MSO relationships to consolidate providers into a larger organization. Then, economies of scale will create benefits through sharing and saving costs, increased leverage in contract negotiations, and augmenting organic, de-novo growth through the addition of new lines of services. Make sure you understand the overall business strategy, how your addition impacts the overall MSO, and how you may personally benefit.
- It appears that many groups are overly-focused on the deal multiple, yet understanding the comprehensive value of a deal goes far beyond the multiple. A complete evaluation must also explore the principles of the compensation model, rollover equity, compounding interest, tax deferral strategies, utilization of debt, and potential earn-out terms. Experienced legal counsel can shed light on these issues.
- The timing in one’s professional career may cloud the perspective of whether partnering with a private equity group through an MSO is wise. However, I would argue the more important perspective is the judgement of the trajectory of your current practice versus adopting a new business model. If a practice can skillfully withstand the headwinds of the regulatory challenges, fierce competition for patient referrals from hospitals plus new provider entrants, and continued downward pressure from payors, then remaining independent may be reasonable. On the other hand, there is great value, security and protection of being within an organization with sizeable financial and experiential capital with like-minded colleagues.
- Many independent practices are also often approached by local and national hospitals. Relationships with hospitals are popular as they too offer professional management teams lessening administrative burdens, often secure referral networks and higher contractual rates for services rendered. Unlike with a PE deal, these partnerships may limit patient choice, almost inevitably increase patient cost, and do not include equity for the provider.
While there are many questions that need to be answered for each practice considering joining a PE backed MSO, what is clear from my experience is that there are enough benefits to such a partnership that it should be explored to understand how it might improve your ability to serve your patients and secure a long term “home” for your practice, providers, and employees.
Marc Sonenshine, MD, is a partner in United Digestive and the chairman of medicine at Northside Hospital, Atlanta.
A note of caution
Is private equity good for gastroenterology? The answer is not a definitive “yes” or “no”; it is “depends”. That said, private equity is here so you must understand the implications.

Private equity is an alternative investment strategy focused on assets not listed on a public exchange. Capital usually is derived from investors who can tolerate risk with the hope of a high return such as pension funds, university endowments, and high net-worth individuals. Capital is collected within a fund (or funds) managed by a professional team who invests in, or buys private companies using internal capital leveraged with debt (leveraged buy-out or LBO). Assets and governance both are sold to fund managers, who restructure operations, centralize or standardize workflows, acquire similar companies to achieve economies of scale, and eventually resell the new company to another entity (usually a larger private equity fund). Typically, the resale (second bite) occurs 5-7 years after initial acquisition and during that 5-7-year period, Private equity funds expect a substantial (10%-20%) annual return on investment resulting from revenue enhancement, new service lines, and overhead reduction.
Since 2016, private equity has actively courted GI practices and there now have been over 20 closed deals. Private equity fund managers have specific expertise in valuing GI practices, enhancing revenue, reducing overhead, collecting other regional (and sometimes distant) practices, centralizing operations, converting all practices to a single EMR, payer negotiations, and other practice functions, while leaving clinical care decisions to providers. Although this postacquisition scenario sounds attractive, there are downsides.
First, let’s review the upsides. As a mature partner in a highly valued practice, you could expect an acquisition payment in the range of $1 million (subject to capital gains tax). You receive a gross distribution based on a purchase multiple (9-12 times EBITA – a measure of your annual profit), minus investment in the new company, and annual payments to the Management Services Organization or MSO. Your income going forward will be reduced by annual obligations to the private equity fund, about 10%-40% of your production. Typically, a second sale occurs between 5 and 7 years after acquisition (yet to occur in GI), where the new company sells for another EBITA multiple (so it is in your financial interest to keep increasing practice value). Even with a modest EBITA multiple, you might net an amount that is double the initial acquisition payout. A senior partner could benefit financially in ways not readily available through other avenues of retirement.
Another benefit is access to capital to acquire more practices, bring new technology, improve facilities, integrate clinical and practice information, and weather reduced demand (like occurred with COVID-19). Independent practices are struggling to incorporate digital technologies that patients now expect, enhanced (and more expensive) endoscopes, new service lines, and the demand for real patient outcomes data during payer or health system negotiations.
So, what takes private equity from a clear “yes” to a “depends”? During COVID-19, physician incomes dropped substantially, since any revenue went first to pay bank debt, then fund fees, payment of overhead (leases, vendor commitments, residual staff), and finally to the doctors. A recent Medscape survey of 5,000 US physicians, revealed that 62% of MDs saw their income drop (23% by more than 50%). Physicians employed by health systems did not see nearly that income drop.
Once a practice is sold, physicians lose autonomy. When you are acquired by a private equity fund, the primary goal of the fund is a financial target. Long-term staff may be downsized, you may be asked to use equipment or supplies that are not to your standard, relationships with regional payers or health systems may become adversarial, productivity targets may alter your patient care decisions (more procedures, less external referrals), and relations with your partners may be strained (younger versus older).
A young physician who enters a private equity–acquired practice may work for decades at an income level discounted from preacquisition levels. They face a substantial buy-in if they hope to benefit from the second sale. Of course, one might argue that future salaries for all gastroenterologists will be reduced by increasing technology costs (endoscope companies are adding AI – can’t wait to see their pricing), reduced reimbursements, and increasing labor and supply costs. Serious threats to colonoscopy-based cancer screening are here, a development that makes future values of GI practices more tenuous. Finally, our payer mix will be worse than before COVID-19 because of long-term financial strains on the US economy.
We have to reflect on a similar practice acquisition trend that occurred in the 1990s, where practice management companies bought independent practices. While times are different now (for many reasons), all but one of those companies went bankrupt and the acquired practices had to rebuild from the ground up. Private equity funds that are heavily leveraged are especially vulnerable, as can be seen by current bankruptcies of large established companies (Hertz, Neiman-Marcus, and others).
Finally, we have to ask ourselves how patients will view your practice as more of us become acquired by financially driven partners. No matter how we paint private equity acquisitions, people understand that these funds are financially driven and practice sales are an income enhancement play for physicians. In 1986, Arnold Relman (Editor of the New England Journal of Medicine) gave two Tanner Lectures on human values at the University of Utah. He asked the following question:
“Is medical care a consumer good like any other, a commercial service provided by skilled vendors for consumers willing to pay the market price, or is there something fundamentally different about the relation between doctor and patient?”
I am not a Luddite, nor am I Don Quixote jousting at windmills. I do, however, want you to consider carefully before giving up on the traditional practice models that made our specialty what it is.
John I. Allen, MD, MBA, AGAF, is clinical professor of medicine, department of internal medicine, division of gastroenterology and hepatology, Institute for Healthcare Policy and Innovation, University School of Medicine, Chief Clinical Officer, University of Michigan Medical Group, Ann Arbor. He has no disclosures and takes full responsibility for the content.
Dear colleagues and friends,
The Perspectives series continues! Few current issues in Gastroenterology practice are as passionately debated as those associated with private equity. In this edition, our own Dr. John Allen and Dr. Marc Sonenshine explain private equity’s evolution in the GI field, dispel misconceptions, and dissect the central question of whether it is right for your practice. Thank you for your support, and I hope you will find the discussions enlightening and relevant to your practices. As always, I welcome your comments and suggestions for future topics at [email protected].
Charles Kahi, MD, MS, AGAF, is a professor of medicine, Indiana University School of Medicine, Indianapolis. He is also an Associate Editor for GI & Hepatology News.
Yes
But, at a minimum, you should absolutely lean-in, listen, and learn.
The physician leadership team at Atlanta Gastroenterology Associates has been focused on developing strategies and partnerships that strengthen our ability to thrive in our marketplace while also fending off threats to our mission. The path to forming the managed services organization (MSO) United Digestive (UD) through our agreement with the private equity firm Frazier Healthcare Partners was arduous and required a significant investment of resources and time. Like at Atlanta Gastroenterology Associates, many influential leaders within our field, also supported by their physician partners, have concluded that the investment of a private equity firm to build an MSO led by professional business executives will reduce the administrative stresses looming over the traditional independent gastroenterologist business model. Now, and after almost 2 years as a member of UD, I unequivocally believe my ability to provide timely, high-quality, and affordable care to my community is currently more stable and in a stronger position for the future.
Like we did in deciding whether to establish a formal relationship with a private equity–backed platform group, here are some critical questions you should explore and answer:
-What advantages and disadvantages will being a part of a private equity–backed MSO group bring to our patients, our practice, our team, and our providers?
-What forces threaten our practice’s ability to remain viable and pertinent in both the near and long term? And, how can our group ward off these threats?
-There are many private equity firms interested in our practice as well as already established platform groups. How do we decide which is best?
-If remaining completely independent is not a sustainable long-term option, why not just become employed by a hospital, join a strategic partner, or form/join a multi-specialty group or accountable care organization (ACO)?
In the first 2 years, UD has answered many of the questions and executed on desired priorities. Our management team helped us to navigate the chaos of COVID, and UD still remains on target to meet many annual budget goals as well as end of the year financial targets. Processes and enhanced technologies like real-time dashboards provide immediate insight into all aspects of our business, allowing for more analytical decision-making. Our payor and vendor negotiations yielded stronger returns than anticipated leading to material earnings. The revamped patient services center improved clinic utilization rates, reduced patient call wait times, deployed an online patient scheduling option, and employed medical assistants for handling clinical phone matters.
Most importantly, not one change at UD has negatively affected our clinical autonomy and decision-making. The MSO and its management team has steered all medical-related issues to our chief medical officer and physician executive committee. Moreover, there was much less consternation amongst partners when the time arose for significant capital expenditures (i.e., upgrading our endoscopic equipment, instituting a new electronic health record and practice management system, or surviving the cash-flow crunch during the beginning of COVID), as our annual compensation was not affected.
A few broader points to consider that pertain to private equity activity in physician services (i.e., not specific to gastroenterology or UD):
- Private equity firms invest money in private companies with the expectation of superior financial returns. Their principals are searching for opportunities with significant upside and potential to generate the necessary earnings for such returns. In fragmented fields, there is potential to use MSO relationships to consolidate providers into a larger organization. Then, economies of scale will create benefits through sharing and saving costs, increased leverage in contract negotiations, and augmenting organic, de-novo growth through the addition of new lines of services. Make sure you understand the overall business strategy, how your addition impacts the overall MSO, and how you may personally benefit.
- It appears that many groups are overly-focused on the deal multiple, yet understanding the comprehensive value of a deal goes far beyond the multiple. A complete evaluation must also explore the principles of the compensation model, rollover equity, compounding interest, tax deferral strategies, utilization of debt, and potential earn-out terms. Experienced legal counsel can shed light on these issues.
- The timing in one’s professional career may cloud the perspective of whether partnering with a private equity group through an MSO is wise. However, I would argue the more important perspective is the judgement of the trajectory of your current practice versus adopting a new business model. If a practice can skillfully withstand the headwinds of the regulatory challenges, fierce competition for patient referrals from hospitals plus new provider entrants, and continued downward pressure from payors, then remaining independent may be reasonable. On the other hand, there is great value, security and protection of being within an organization with sizeable financial and experiential capital with like-minded colleagues.
- Many independent practices are also often approached by local and national hospitals. Relationships with hospitals are popular as they too offer professional management teams lessening administrative burdens, often secure referral networks and higher contractual rates for services rendered. Unlike with a PE deal, these partnerships may limit patient choice, almost inevitably increase patient cost, and do not include equity for the provider.
While there are many questions that need to be answered for each practice considering joining a PE backed MSO, what is clear from my experience is that there are enough benefits to such a partnership that it should be explored to understand how it might improve your ability to serve your patients and secure a long term “home” for your practice, providers, and employees.
Marc Sonenshine, MD, is a partner in United Digestive and the chairman of medicine at Northside Hospital, Atlanta.
A note of caution
Is private equity good for gastroenterology? The answer is not a definitive “yes” or “no”; it is “depends”. That said, private equity is here so you must understand the implications.
Private equity is an alternative investment strategy focused on assets not listed on a public exchange. Capital usually is derived from investors who can tolerate risk with the hope of a high return such as pension funds, university endowments, and high net-worth individuals. Capital is collected within a fund (or funds) managed by a professional team who invests in, or buys private companies using internal capital leveraged with debt (leveraged buy-out or LBO). Assets and governance both are sold to fund managers, who restructure operations, centralize or standardize workflows, acquire similar companies to achieve economies of scale, and eventually resell the new company to another entity (usually a larger private equity fund). Typically, the resale (second bite) occurs 5-7 years after initial acquisition and during that 5-7-year period, Private equity funds expect a substantial (10%-20%) annual return on investment resulting from revenue enhancement, new service lines, and overhead reduction.
Since 2016, private equity has actively courted GI practices and there now have been over 20 closed deals. Private equity fund managers have specific expertise in valuing GI practices, enhancing revenue, reducing overhead, collecting other regional (and sometimes distant) practices, centralizing operations, converting all practices to a single EMR, payer negotiations, and other practice functions, while leaving clinical care decisions to providers. Although this postacquisition scenario sounds attractive, there are downsides.
First, let’s review the upsides. As a mature partner in a highly valued practice, you could expect an acquisition payment in the range of $1 million (subject to capital gains tax). You receive a gross distribution based on a purchase multiple (9-12 times EBITA – a measure of your annual profit), minus investment in the new company, and annual payments to the Management Services Organization or MSO. Your income going forward will be reduced by annual obligations to the private equity fund, about 10%-40% of your production. Typically, a second sale occurs between 5 and 7 years after acquisition (yet to occur in GI), where the new company sells for another EBITA multiple (so it is in your financial interest to keep increasing practice value). Even with a modest EBITA multiple, you might net an amount that is double the initial acquisition payout. A senior partner could benefit financially in ways not readily available through other avenues of retirement.
Another benefit is access to capital to acquire more practices, bring new technology, improve facilities, integrate clinical and practice information, and weather reduced demand (like occurred with COVID-19). Independent practices are struggling to incorporate digital technologies that patients now expect, enhanced (and more expensive) endoscopes, new service lines, and the demand for real patient outcomes data during payer or health system negotiations.
So, what takes private equity from a clear “yes” to a “depends”? During COVID-19, physician incomes dropped substantially, since any revenue went first to pay bank debt, then fund fees, payment of overhead (leases, vendor commitments, residual staff), and finally to the doctors. A recent Medscape survey of 5,000 US physicians, revealed that 62% of MDs saw their income drop (23% by more than 50%). Physicians employed by health systems did not see nearly that income drop.
Once a practice is sold, physicians lose autonomy. When you are acquired by a private equity fund, the primary goal of the fund is a financial target. Long-term staff may be downsized, you may be asked to use equipment or supplies that are not to your standard, relationships with regional payers or health systems may become adversarial, productivity targets may alter your patient care decisions (more procedures, less external referrals), and relations with your partners may be strained (younger versus older).
A young physician who enters a private equity–acquired practice may work for decades at an income level discounted from preacquisition levels. They face a substantial buy-in if they hope to benefit from the second sale. Of course, one might argue that future salaries for all gastroenterologists will be reduced by increasing technology costs (endoscope companies are adding AI – can’t wait to see their pricing), reduced reimbursements, and increasing labor and supply costs. Serious threats to colonoscopy-based cancer screening are here, a development that makes future values of GI practices more tenuous. Finally, our payer mix will be worse than before COVID-19 because of long-term financial strains on the US economy.
We have to reflect on a similar practice acquisition trend that occurred in the 1990s, where practice management companies bought independent practices. While times are different now (for many reasons), all but one of those companies went bankrupt and the acquired practices had to rebuild from the ground up. Private equity funds that are heavily leveraged are especially vulnerable, as can be seen by current bankruptcies of large established companies (Hertz, Neiman-Marcus, and others).
Finally, we have to ask ourselves how patients will view your practice as more of us become acquired by financially driven partners. No matter how we paint private equity acquisitions, people understand that these funds are financially driven and practice sales are an income enhancement play for physicians. In 1986, Arnold Relman (Editor of the New England Journal of Medicine) gave two Tanner Lectures on human values at the University of Utah. He asked the following question:
“Is medical care a consumer good like any other, a commercial service provided by skilled vendors for consumers willing to pay the market price, or is there something fundamentally different about the relation between doctor and patient?”
I am not a Luddite, nor am I Don Quixote jousting at windmills. I do, however, want you to consider carefully before giving up on the traditional practice models that made our specialty what it is.
John I. Allen, MD, MBA, AGAF, is clinical professor of medicine, department of internal medicine, division of gastroenterology and hepatology, Institute for Healthcare Policy and Innovation, University School of Medicine, Chief Clinical Officer, University of Michigan Medical Group, Ann Arbor. He has no disclosures and takes full responsibility for the content.
Dear colleagues and friends,
The Perspectives series continues! Few current issues in Gastroenterology practice are as passionately debated as those associated with private equity. In this edition, our own Dr. John Allen and Dr. Marc Sonenshine explain private equity’s evolution in the GI field, dispel misconceptions, and dissect the central question of whether it is right for your practice. Thank you for your support, and I hope you will find the discussions enlightening and relevant to your practices. As always, I welcome your comments and suggestions for future topics at [email protected].
Charles Kahi, MD, MS, AGAF, is a professor of medicine, Indiana University School of Medicine, Indianapolis. He is also an Associate Editor for GI & Hepatology News.
Yes
But, at a minimum, you should absolutely lean-in, listen, and learn.
The physician leadership team at Atlanta Gastroenterology Associates has been focused on developing strategies and partnerships that strengthen our ability to thrive in our marketplace while also fending off threats to our mission. The path to forming the managed services organization (MSO) United Digestive (UD) through our agreement with the private equity firm Frazier Healthcare Partners was arduous and required a significant investment of resources and time. Like at Atlanta Gastroenterology Associates, many influential leaders within our field, also supported by their physician partners, have concluded that the investment of a private equity firm to build an MSO led by professional business executives will reduce the administrative stresses looming over the traditional independent gastroenterologist business model. Now, and after almost 2 years as a member of UD, I unequivocally believe my ability to provide timely, high-quality, and affordable care to my community is currently more stable and in a stronger position for the future.
Like we did in deciding whether to establish a formal relationship with a private equity–backed platform group, here are some critical questions you should explore and answer:
-What advantages and disadvantages will being a part of a private equity–backed MSO group bring to our patients, our practice, our team, and our providers?
-What forces threaten our practice’s ability to remain viable and pertinent in both the near and long term? And, how can our group ward off these threats?
-There are many private equity firms interested in our practice as well as already established platform groups. How do we decide which is best?
-If remaining completely independent is not a sustainable long-term option, why not just become employed by a hospital, join a strategic partner, or form/join a multi-specialty group or accountable care organization (ACO)?
In the first 2 years, UD has answered many of the questions and executed on desired priorities. Our management team helped us to navigate the chaos of COVID, and UD still remains on target to meet many annual budget goals as well as end of the year financial targets. Processes and enhanced technologies like real-time dashboards provide immediate insight into all aspects of our business, allowing for more analytical decision-making. Our payor and vendor negotiations yielded stronger returns than anticipated leading to material earnings. The revamped patient services center improved clinic utilization rates, reduced patient call wait times, deployed an online patient scheduling option, and employed medical assistants for handling clinical phone matters.
Most importantly, not one change at UD has negatively affected our clinical autonomy and decision-making. The MSO and its management team has steered all medical-related issues to our chief medical officer and physician executive committee. Moreover, there was much less consternation amongst partners when the time arose for significant capital expenditures (i.e., upgrading our endoscopic equipment, instituting a new electronic health record and practice management system, or surviving the cash-flow crunch during the beginning of COVID), as our annual compensation was not affected.
A few broader points to consider that pertain to private equity activity in physician services (i.e., not specific to gastroenterology or UD):
- Private equity firms invest money in private companies with the expectation of superior financial returns. Their principals are searching for opportunities with significant upside and potential to generate the necessary earnings for such returns. In fragmented fields, there is potential to use MSO relationships to consolidate providers into a larger organization. Then, economies of scale will create benefits through sharing and saving costs, increased leverage in contract negotiations, and augmenting organic, de-novo growth through the addition of new lines of services. Make sure you understand the overall business strategy, how your addition impacts the overall MSO, and how you may personally benefit.
- It appears that many groups are overly-focused on the deal multiple, yet understanding the comprehensive value of a deal goes far beyond the multiple. A complete evaluation must also explore the principles of the compensation model, rollover equity, compounding interest, tax deferral strategies, utilization of debt, and potential earn-out terms. Experienced legal counsel can shed light on these issues.
- The timing in one’s professional career may cloud the perspective of whether partnering with a private equity group through an MSO is wise. However, I would argue the more important perspective is the judgement of the trajectory of your current practice versus adopting a new business model. If a practice can skillfully withstand the headwinds of the regulatory challenges, fierce competition for patient referrals from hospitals plus new provider entrants, and continued downward pressure from payors, then remaining independent may be reasonable. On the other hand, there is great value, security and protection of being within an organization with sizeable financial and experiential capital with like-minded colleagues.
- Many independent practices are also often approached by local and national hospitals. Relationships with hospitals are popular as they too offer professional management teams lessening administrative burdens, often secure referral networks and higher contractual rates for services rendered. Unlike with a PE deal, these partnerships may limit patient choice, almost inevitably increase patient cost, and do not include equity for the provider.
While there are many questions that need to be answered for each practice considering joining a PE backed MSO, what is clear from my experience is that there are enough benefits to such a partnership that it should be explored to understand how it might improve your ability to serve your patients and secure a long term “home” for your practice, providers, and employees.
Marc Sonenshine, MD, is a partner in United Digestive and the chairman of medicine at Northside Hospital, Atlanta.
A note of caution
Is private equity good for gastroenterology? The answer is not a definitive “yes” or “no”; it is “depends”. That said, private equity is here so you must understand the implications.
Private equity is an alternative investment strategy focused on assets not listed on a public exchange. Capital usually is derived from investors who can tolerate risk with the hope of a high return such as pension funds, university endowments, and high net-worth individuals. Capital is collected within a fund (or funds) managed by a professional team who invests in, or buys private companies using internal capital leveraged with debt (leveraged buy-out or LBO). Assets and governance both are sold to fund managers, who restructure operations, centralize or standardize workflows, acquire similar companies to achieve economies of scale, and eventually resell the new company to another entity (usually a larger private equity fund). Typically, the resale (second bite) occurs 5-7 years after initial acquisition and during that 5-7-year period, Private equity funds expect a substantial (10%-20%) annual return on investment resulting from revenue enhancement, new service lines, and overhead reduction.
Since 2016, private equity has actively courted GI practices and there now have been over 20 closed deals. Private equity fund managers have specific expertise in valuing GI practices, enhancing revenue, reducing overhead, collecting other regional (and sometimes distant) practices, centralizing operations, converting all practices to a single EMR, payer negotiations, and other practice functions, while leaving clinical care decisions to providers. Although this postacquisition scenario sounds attractive, there are downsides.
First, let’s review the upsides. As a mature partner in a highly valued practice, you could expect an acquisition payment in the range of $1 million (subject to capital gains tax). You receive a gross distribution based on a purchase multiple (9-12 times EBITA – a measure of your annual profit), minus investment in the new company, and annual payments to the Management Services Organization or MSO. Your income going forward will be reduced by annual obligations to the private equity fund, about 10%-40% of your production. Typically, a second sale occurs between 5 and 7 years after acquisition (yet to occur in GI), where the new company sells for another EBITA multiple (so it is in your financial interest to keep increasing practice value). Even with a modest EBITA multiple, you might net an amount that is double the initial acquisition payout. A senior partner could benefit financially in ways not readily available through other avenues of retirement.
Another benefit is access to capital to acquire more practices, bring new technology, improve facilities, integrate clinical and practice information, and weather reduced demand (like occurred with COVID-19). Independent practices are struggling to incorporate digital technologies that patients now expect, enhanced (and more expensive) endoscopes, new service lines, and the demand for real patient outcomes data during payer or health system negotiations.
So, what takes private equity from a clear “yes” to a “depends”? During COVID-19, physician incomes dropped substantially, since any revenue went first to pay bank debt, then fund fees, payment of overhead (leases, vendor commitments, residual staff), and finally to the doctors. A recent Medscape survey of 5,000 US physicians, revealed that 62% of MDs saw their income drop (23% by more than 50%). Physicians employed by health systems did not see nearly that income drop.
Once a practice is sold, physicians lose autonomy. When you are acquired by a private equity fund, the primary goal of the fund is a financial target. Long-term staff may be downsized, you may be asked to use equipment or supplies that are not to your standard, relationships with regional payers or health systems may become adversarial, productivity targets may alter your patient care decisions (more procedures, less external referrals), and relations with your partners may be strained (younger versus older).
A young physician who enters a private equity–acquired practice may work for decades at an income level discounted from preacquisition levels. They face a substantial buy-in if they hope to benefit from the second sale. Of course, one might argue that future salaries for all gastroenterologists will be reduced by increasing technology costs (endoscope companies are adding AI – can’t wait to see their pricing), reduced reimbursements, and increasing labor and supply costs. Serious threats to colonoscopy-based cancer screening are here, a development that makes future values of GI practices more tenuous. Finally, our payer mix will be worse than before COVID-19 because of long-term financial strains on the US economy.
We have to reflect on a similar practice acquisition trend that occurred in the 1990s, where practice management companies bought independent practices. While times are different now (for many reasons), all but one of those companies went bankrupt and the acquired practices had to rebuild from the ground up. Private equity funds that are heavily leveraged are especially vulnerable, as can be seen by current bankruptcies of large established companies (Hertz, Neiman-Marcus, and others).
Finally, we have to ask ourselves how patients will view your practice as more of us become acquired by financially driven partners. No matter how we paint private equity acquisitions, people understand that these funds are financially driven and practice sales are an income enhancement play for physicians. In 1986, Arnold Relman (Editor of the New England Journal of Medicine) gave two Tanner Lectures on human values at the University of Utah. He asked the following question:
“Is medical care a consumer good like any other, a commercial service provided by skilled vendors for consumers willing to pay the market price, or is there something fundamentally different about the relation between doctor and patient?”
I am not a Luddite, nor am I Don Quixote jousting at windmills. I do, however, want you to consider carefully before giving up on the traditional practice models that made our specialty what it is.
John I. Allen, MD, MBA, AGAF, is clinical professor of medicine, department of internal medicine, division of gastroenterology and hepatology, Institute for Healthcare Policy and Innovation, University School of Medicine, Chief Clinical Officer, University of Michigan Medical Group, Ann Arbor. He has no disclosures and takes full responsibility for the content.
What to keep in mind as 2021 begins
As 2020 comes to a close, most of us are looking forward to a (hopefully) brighter 2021. This year has been full of challenges and new experiences, but we have learned a lot. Pandemic or not, there are some things that you and your practice can do to ensure that you are prepared to make 2021 a success.
Tips for your practice

Assess staff morale: It seems simple but checking in with your staff can go a long way. Everyone is dealing with challenges both in and out of the workplace. Check in, show them you care, and think of ways that you can make their work a positive experience in the new year. During our May 2020 GI division chief townhall, John Inadomi, MD, gave a great presentation on the importance of staff morale during the pandemic.
Listen to colleagues: Find out about their experiences, challenges, and solutions. In October, the American Gastroenterological Association held a town hall with some great information and resources called “Adapting to Changing Practice Paradigms.” The agenda covered topics from telehealth to private equity and planning for the next potential wave of COVID-19.
Celebrate the wins: It can often feel like not much went right in 2020, but we did accomplish significant wins for GIs, including achieving payment parity for telephone evaluation and management (E/M) visits with video visits, increases in digestive disease and GI cancer research funding, and inclusion/expansion of GI cancers research opportunities. We couldn’t have done it without you, though, and we will continue to need your help to move important issues forward in 2021. Get involved today! Visit “Get Involved” under Advocacy and Policy on www.gastro.org.
Prepare for E/M changes: The Current Procedural Terminology (CPT) E/M for new and established patient office/outpatient codes (99201-99205, 99211-99215), guidelines, and Medicare payments will undergo major changes beginning Jan. 1, 2021. See the AGA’s coding and reimbursement experts’ article from the March 2020 issue of GI & Hepatology News, “Prepare for major changes to E/M coding starting in 2021,” to learn about the changes and get resources to help practices prepare.
Keep up with new Medicare payment rules: The release of the 2021 physician payments and rules for the Medicare program was delayed this year because of the COVID-19 public health emergency. We were dismayed to learn that Medicare did not make any changes that substantively mitigated the expected cuts to most specialties. Instead of a 5% cut for GI, the Centers for Medicare & Medicaid Services now projects GI will experience a 4% payment cut for 2021. AGA is calling on Congress to pass legislation to stop the cuts. This situation is evolving quickly. Watch for AGA member alerts for breaking news and resources, including the AGA’s “Medicare plans significant payment cuts for 2021.”
Stay current on telehealth and telephone E/M coverage: The commercial payer community came together to cover telehealth (video visits) and telephone E/M at the beginning of the COVID-19 pandemic but have since regularly teased the end of coverage only to extend it just before it expires. It’s impossible to predict what each payer will do, but you can use the following resources to keep current on most payers’ policies and correct coding/reporting for telehealth and telephone E/M:
- “Current State Laws & Reimbursement Policies ” from the Center for Connected Health.
- “Coding for Telehealth & Virtual Visits During COVID-19” from the AGA University.
Check to see if you can report on additional quality measures: AGA has expanded the Merit-Based Incentive Payment System (MIPS) measure portfolio by assuming ownership and stewardship of two hepatitis C virus (HCV) measures from PCPI, including annually checking for HCV in active injection drug users (measure 387) and performing a one-time screening for HCV among patients at risk (measure 400). As a result, gastroenterologists can now report on even more GI-specific measures. There have been the following two changes to GI-specific measures in 2021:
- Measure 275: “Inflammatory Bowel Disease (IBD): Assessment of Hepatitis B Virus (HBV) Status Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy” now includes coding to allow reporting for all age groups, including pediatric populations.
- Measure 439: “Age Appropriate Screening Colonoscopy” now includes all colonoscopies for patients 50 years and older; however, there’s an exclusion for those patients between the ages of 50 and 85 years.
These changes will help more gastroenterologists qualify for these measures.
Dates and deadlines to remember
January 2021
- Jan. 1 – MIPS Performance Year 2021 begins.
- Jan. 4 – Submission window opens for MIPS Performance Year 2020.
- Changes to Improvement Activity category go into effect (if approved in final rule).
March 2021
- March 31 – First snapshot for Qualifying Participant (QP) determinations and MIPS APM participation.
April 2021
- April 1 – Registration begins for CMS web interface and Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey.
June 2021
- June 30 – Second snapshot for QP determinations and MIPS APM participation.
- June 30 – Registration ends for CMS web interface and CAHPS for MIPS survey.
July 2021
- CMS publishes proposed reimbursement values for 2022 in the Medicare Physician Fee Schedule proposed rule.
- CMS “Targeted Review” opens once CMS makes your MIPS payment adjustment available.
- July 1 - MIPS Performance Feedback Available. CMS will provide you with performance feedback based on the data you submitted for Performance Year 2020. You can use this feedback to improve your care and optimize the payments you receive from CMS in the future.
August 2021
- Aug. 31 - Targeted Review period closes (appeals process).
September 2021
- AMA releases CPT 2022 book, including a new CPT code for Peroral Endoscopic Myotomy (POEM).
October 2021
- Oct. 3 - Last day to start a 90-day performance period for promoting Interoperability and Improvement Activities.
November 2021
- CMS finalizes reimbursement values for 2022 in the MPFS final rule. New payment rates take effect Jan. 1, 2022.
December 2021
- Dec. 31 – Quality Payment Program Exception Applications window closes.
- Dec. 31 – MIPS Performance year 2020 ends.
- Dec. 31 – Fourth snapshot for full TIN APMs (Medicare Shared Savings Program).
G. Anton Decker, MD, is chair of the AGA Practice Management and Economics Committee, Mayo Clinic International; Dawn Francis, MD, is chair-elect of the AGA Practice Management and Economics Committee, Mayo Clinic, Jacksonville, Fla.
They have no conflicts of interest.
As 2020 comes to a close, most of us are looking forward to a (hopefully) brighter 2021. This year has been full of challenges and new experiences, but we have learned a lot. Pandemic or not, there are some things that you and your practice can do to ensure that you are prepared to make 2021 a success.
Tips for your practice
Assess staff morale: It seems simple but checking in with your staff can go a long way. Everyone is dealing with challenges both in and out of the workplace. Check in, show them you care, and think of ways that you can make their work a positive experience in the new year. During our May 2020 GI division chief townhall, John Inadomi, MD, gave a great presentation on the importance of staff morale during the pandemic.
Listen to colleagues: Find out about their experiences, challenges, and solutions. In October, the American Gastroenterological Association held a town hall with some great information and resources called “Adapting to Changing Practice Paradigms.” The agenda covered topics from telehealth to private equity and planning for the next potential wave of COVID-19.
Celebrate the wins: It can often feel like not much went right in 2020, but we did accomplish significant wins for GIs, including achieving payment parity for telephone evaluation and management (E/M) visits with video visits, increases in digestive disease and GI cancer research funding, and inclusion/expansion of GI cancers research opportunities. We couldn’t have done it without you, though, and we will continue to need your help to move important issues forward in 2021. Get involved today! Visit “Get Involved” under Advocacy and Policy on www.gastro.org.
Prepare for E/M changes: The Current Procedural Terminology (CPT) E/M for new and established patient office/outpatient codes (99201-99205, 99211-99215), guidelines, and Medicare payments will undergo major changes beginning Jan. 1, 2021. See the AGA’s coding and reimbursement experts’ article from the March 2020 issue of GI & Hepatology News, “Prepare for major changes to E/M coding starting in 2021,” to learn about the changes and get resources to help practices prepare.
Keep up with new Medicare payment rules: The release of the 2021 physician payments and rules for the Medicare program was delayed this year because of the COVID-19 public health emergency. We were dismayed to learn that Medicare did not make any changes that substantively mitigated the expected cuts to most specialties. Instead of a 5% cut for GI, the Centers for Medicare & Medicaid Services now projects GI will experience a 4% payment cut for 2021. AGA is calling on Congress to pass legislation to stop the cuts. This situation is evolving quickly. Watch for AGA member alerts for breaking news and resources, including the AGA’s “Medicare plans significant payment cuts for 2021.”
Stay current on telehealth and telephone E/M coverage: The commercial payer community came together to cover telehealth (video visits) and telephone E/M at the beginning of the COVID-19 pandemic but have since regularly teased the end of coverage only to extend it just before it expires. It’s impossible to predict what each payer will do, but you can use the following resources to keep current on most payers’ policies and correct coding/reporting for telehealth and telephone E/M:
- “Current State Laws & Reimbursement Policies ” from the Center for Connected Health.
- “Coding for Telehealth & Virtual Visits During COVID-19” from the AGA University.
Check to see if you can report on additional quality measures: AGA has expanded the Merit-Based Incentive Payment System (MIPS) measure portfolio by assuming ownership and stewardship of two hepatitis C virus (HCV) measures from PCPI, including annually checking for HCV in active injection drug users (measure 387) and performing a one-time screening for HCV among patients at risk (measure 400). As a result, gastroenterologists can now report on even more GI-specific measures. There have been the following two changes to GI-specific measures in 2021:
- Measure 275: “Inflammatory Bowel Disease (IBD): Assessment of Hepatitis B Virus (HBV) Status Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy” now includes coding to allow reporting for all age groups, including pediatric populations.
- Measure 439: “Age Appropriate Screening Colonoscopy” now includes all colonoscopies for patients 50 years and older; however, there’s an exclusion for those patients between the ages of 50 and 85 years.
These changes will help more gastroenterologists qualify for these measures.
Dates and deadlines to remember
January 2021
- Jan. 1 – MIPS Performance Year 2021 begins.
- Jan. 4 – Submission window opens for MIPS Performance Year 2020.
- Changes to Improvement Activity category go into effect (if approved in final rule).
March 2021
- March 31 – First snapshot for Qualifying Participant (QP) determinations and MIPS APM participation.
April 2021
- April 1 – Registration begins for CMS web interface and Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey.
June 2021
- June 30 – Second snapshot for QP determinations and MIPS APM participation.
- June 30 – Registration ends for CMS web interface and CAHPS for MIPS survey.
July 2021
- CMS publishes proposed reimbursement values for 2022 in the Medicare Physician Fee Schedule proposed rule.
- CMS “Targeted Review” opens once CMS makes your MIPS payment adjustment available.
- July 1 - MIPS Performance Feedback Available. CMS will provide you with performance feedback based on the data you submitted for Performance Year 2020. You can use this feedback to improve your care and optimize the payments you receive from CMS in the future.
August 2021
- Aug. 31 - Targeted Review period closes (appeals process).
September 2021
- AMA releases CPT 2022 book, including a new CPT code for Peroral Endoscopic Myotomy (POEM).
October 2021
- Oct. 3 - Last day to start a 90-day performance period for promoting Interoperability and Improvement Activities.
November 2021
- CMS finalizes reimbursement values for 2022 in the MPFS final rule. New payment rates take effect Jan. 1, 2022.
December 2021
- Dec. 31 – Quality Payment Program Exception Applications window closes.
- Dec. 31 – MIPS Performance year 2020 ends.
- Dec. 31 – Fourth snapshot for full TIN APMs (Medicare Shared Savings Program).
G. Anton Decker, MD, is chair of the AGA Practice Management and Economics Committee, Mayo Clinic International; Dawn Francis, MD, is chair-elect of the AGA Practice Management and Economics Committee, Mayo Clinic, Jacksonville, Fla.
They have no conflicts of interest.
As 2020 comes to a close, most of us are looking forward to a (hopefully) brighter 2021. This year has been full of challenges and new experiences, but we have learned a lot. Pandemic or not, there are some things that you and your practice can do to ensure that you are prepared to make 2021 a success.
Tips for your practice
Assess staff morale: It seems simple but checking in with your staff can go a long way. Everyone is dealing with challenges both in and out of the workplace. Check in, show them you care, and think of ways that you can make their work a positive experience in the new year. During our May 2020 GI division chief townhall, John Inadomi, MD, gave a great presentation on the importance of staff morale during the pandemic.
Listen to colleagues: Find out about their experiences, challenges, and solutions. In October, the American Gastroenterological Association held a town hall with some great information and resources called “Adapting to Changing Practice Paradigms.” The agenda covered topics from telehealth to private equity and planning for the next potential wave of COVID-19.
Celebrate the wins: It can often feel like not much went right in 2020, but we did accomplish significant wins for GIs, including achieving payment parity for telephone evaluation and management (E/M) visits with video visits, increases in digestive disease and GI cancer research funding, and inclusion/expansion of GI cancers research opportunities. We couldn’t have done it without you, though, and we will continue to need your help to move important issues forward in 2021. Get involved today! Visit “Get Involved” under Advocacy and Policy on www.gastro.org.
Prepare for E/M changes: The Current Procedural Terminology (CPT) E/M for new and established patient office/outpatient codes (99201-99205, 99211-99215), guidelines, and Medicare payments will undergo major changes beginning Jan. 1, 2021. See the AGA’s coding and reimbursement experts’ article from the March 2020 issue of GI & Hepatology News, “Prepare for major changes to E/M coding starting in 2021,” to learn about the changes and get resources to help practices prepare.
Keep up with new Medicare payment rules: The release of the 2021 physician payments and rules for the Medicare program was delayed this year because of the COVID-19 public health emergency. We were dismayed to learn that Medicare did not make any changes that substantively mitigated the expected cuts to most specialties. Instead of a 5% cut for GI, the Centers for Medicare & Medicaid Services now projects GI will experience a 4% payment cut for 2021. AGA is calling on Congress to pass legislation to stop the cuts. This situation is evolving quickly. Watch for AGA member alerts for breaking news and resources, including the AGA’s “Medicare plans significant payment cuts for 2021.”
Stay current on telehealth and telephone E/M coverage: The commercial payer community came together to cover telehealth (video visits) and telephone E/M at the beginning of the COVID-19 pandemic but have since regularly teased the end of coverage only to extend it just before it expires. It’s impossible to predict what each payer will do, but you can use the following resources to keep current on most payers’ policies and correct coding/reporting for telehealth and telephone E/M:
- “Current State Laws & Reimbursement Policies ” from the Center for Connected Health.
- “Coding for Telehealth & Virtual Visits During COVID-19” from the AGA University.
Check to see if you can report on additional quality measures: AGA has expanded the Merit-Based Incentive Payment System (MIPS) measure portfolio by assuming ownership and stewardship of two hepatitis C virus (HCV) measures from PCPI, including annually checking for HCV in active injection drug users (measure 387) and performing a one-time screening for HCV among patients at risk (measure 400). As a result, gastroenterologists can now report on even more GI-specific measures. There have been the following two changes to GI-specific measures in 2021:
- Measure 275: “Inflammatory Bowel Disease (IBD): Assessment of Hepatitis B Virus (HBV) Status Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy” now includes coding to allow reporting for all age groups, including pediatric populations.
- Measure 439: “Age Appropriate Screening Colonoscopy” now includes all colonoscopies for patients 50 years and older; however, there’s an exclusion for those patients between the ages of 50 and 85 years.
These changes will help more gastroenterologists qualify for these measures.
Dates and deadlines to remember
January 2021
- Jan. 1 – MIPS Performance Year 2021 begins.
- Jan. 4 – Submission window opens for MIPS Performance Year 2020.
- Changes to Improvement Activity category go into effect (if approved in final rule).
March 2021
- March 31 – First snapshot for Qualifying Participant (QP) determinations and MIPS APM participation.
April 2021
- April 1 – Registration begins for CMS web interface and Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey.
June 2021
- June 30 – Second snapshot for QP determinations and MIPS APM participation.
- June 30 – Registration ends for CMS web interface and CAHPS for MIPS survey.
July 2021
- CMS publishes proposed reimbursement values for 2022 in the Medicare Physician Fee Schedule proposed rule.
- CMS “Targeted Review” opens once CMS makes your MIPS payment adjustment available.
- July 1 - MIPS Performance Feedback Available. CMS will provide you with performance feedback based on the data you submitted for Performance Year 2020. You can use this feedback to improve your care and optimize the payments you receive from CMS in the future.
August 2021
- Aug. 31 - Targeted Review period closes (appeals process).
September 2021
- AMA releases CPT 2022 book, including a new CPT code for Peroral Endoscopic Myotomy (POEM).
October 2021
- Oct. 3 - Last day to start a 90-day performance period for promoting Interoperability and Improvement Activities.
November 2021
- CMS finalizes reimbursement values for 2022 in the MPFS final rule. New payment rates take effect Jan. 1, 2022.
December 2021
- Dec. 31 – Quality Payment Program Exception Applications window closes.
- Dec. 31 – MIPS Performance year 2020 ends.
- Dec. 31 – Fourth snapshot for full TIN APMs (Medicare Shared Savings Program).
G. Anton Decker, MD, is chair of the AGA Practice Management and Economics Committee, Mayo Clinic International; Dawn Francis, MD, is chair-elect of the AGA Practice Management and Economics Committee, Mayo Clinic, Jacksonville, Fla.
They have no conflicts of interest.
CMS finalizes 2021 physician pay rule with E/M changes
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests. While gastroenterology is estimated to experience a 4% cut, other fields are expecting cuts up to 10%.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule takes effect on Jan. 1, 2021, within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%). The changes also would lead to an expected 4% decrease for gastroenterology. The GI societies are among the groups pressing Congress to intercede.
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’s planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Dr. Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Dr. Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on Jan. 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020. AGA has been advocating for passage of this bill before the end of the 116th Congress and urges GIs to contact their lawmakers to prevent these cuts to specialty care. While the GI societies are in support of the bill, they have expressed concerns regarding the financial cliff H.R. 8702 would create. With the payment cuts pushed to 2023, this financial cliff would require physicians to return to Congress to prevent future cuts once the 2-year delay is up.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a Nov. 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last-minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
Based on reporting from Medscape.com.
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests. While gastroenterology is estimated to experience a 4% cut, other fields are expecting cuts up to 10%.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule takes effect on Jan. 1, 2021, within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%). The changes also would lead to an expected 4% decrease for gastroenterology. The GI societies are among the groups pressing Congress to intercede.
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’s planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Dr. Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Dr. Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on Jan. 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020. AGA has been advocating for passage of this bill before the end of the 116th Congress and urges GIs to contact their lawmakers to prevent these cuts to specialty care. While the GI societies are in support of the bill, they have expressed concerns regarding the financial cliff H.R. 8702 would create. With the payment cuts pushed to 2023, this financial cliff would require physicians to return to Congress to prevent future cuts once the 2-year delay is up.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a Nov. 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last-minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
Based on reporting from Medscape.com.
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests. While gastroenterology is estimated to experience a 4% cut, other fields are expecting cuts up to 10%.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule takes effect on Jan. 1, 2021, within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%). The changes also would lead to an expected 4% decrease for gastroenterology. The GI societies are among the groups pressing Congress to intercede.
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’s planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Dr. Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Dr. Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on Jan. 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020. AGA has been advocating for passage of this bill before the end of the 116th Congress and urges GIs to contact their lawmakers to prevent these cuts to specialty care. While the GI societies are in support of the bill, they have expressed concerns regarding the financial cliff H.R. 8702 would create. With the payment cuts pushed to 2023, this financial cliff would require physicians to return to Congress to prevent future cuts once the 2-year delay is up.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a Nov. 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last-minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
Based on reporting from Medscape.com.
Prospects dim for Medicare drug reimbursement cuts
A proposal to lower Medicare Part B reimbursements for 50 physician-administered drugs and biologics to what drug manufacturers receive for them in other wealthy nations seems unlikely to take effect as planned on January 1, 2021. The proposal has been strongly opposed by the pharmaceutical industry as well as oncologists and other physicians who use the products most often.
At least four lawsuits have been filed in US district courts to block the move, including from Regeneron, manufacturer of the ophthalmic biologic aflibercept, the first agent on the list; the Community Oncology Alliance; the Biotechnology Innovation Organization, California Life Sciences Association, and Biocom; and Pharmaceutical Research and Manufacturers of America, the Association of Community Cancer Centers, the Global Colon Cancer Association, and National Infusion Center Association.
The proposal could hit oncologists/hematologists particularly hard because they are the primary prescribers of about 30 of the 50 agents on the list, including mainstay breast, lung, and prostate cancer treatments and newer immunotherapies. In its filing for injunctive relieve, the Community Oncology Alliance, a trade group for community oncologists, said the proposal exposes “the health and safety of cancer patients and other patients with potentially life-threatening diseases to real danger.”
Hearings are imminent
Hearings on the proposal, which was published by the Centers for Medicare & Medicaid Services (CMS) on November 27 following an executive order September 13, are scheduled for coming days. The first hearing is scheduled for December 18.
Given the looming implementation date, judges are likely to rule quickly on the motions for injunctive relief, said attorney Rachel Sachs, a health law expert and associate professor at the Washington University School of Law, St. Louis, Missouri. The odds are in plaintiffs’ favor based on procedural and Constitutional grounds. “It’s extremely unlikely to survive” the legal onslaught, she told Medscape Medical News.
Among the many issues raised in court filings, the proposal was released as an interim final rule (IFR), meaning it would take effect outside of the usual process of proposed rule, comment period, revision, then implementation. The law allows for bypassing normal rule-making requirements with an IFR, but they are meant for emergency situations — several have been issued in response to the COVID-19 pandemic — and the government must be able to show that delay would be “impracticable, unnecessary, or contrary to the public interest,” Sachs explained.
In contrast, some form of CMS’s new proposal, dubbed the “Most Favored Nation” (MFN) model for drug reimbursements, has been under consideration by the Trump administration since 2018.
“The way the [Trump] administration rolled this rule out at pretty much the last minute opens them up to greater legal challenges than if they pursued more normal regulatory pathways, which they had the opportunity to do. They are attempting to implement this on a time frame that is unprecedented for as large a change as this is,” said Juliette Cubanski, PhD, deputy director of Medicare policy at the Kaiser Family Foundation, San Francisco, California.
Reimbursement less than acquisition costs
In the proposal, CMS sought to offset the higher prices that pharmaceutical companies charge in the United States when compared with other developed nations — the prices are about double on average.
“One of the largest drivers of increasing Medicare spending is the growing prices for physician-administered separately payable Medicare Part B drugs, which have risen an average of 11.5% annually since 2015, with total spending of approximately $30 billion in 2019,” the agency said in a fact sheet. This is due in large part to “lack of competitive market forces on Medicare Part B drug costs,” it added.
The 50 agents covered by the new proposal are the ones Part B spends the most on, almost $3 billion in 2019 for aflibercept alone, followed closely by pembrolizumab, an immunotherapy used in many different cancer types.
A full list of the drugs and biologicals included in the proposal is on page 50 of the IFR.
CMS estimated that its move would cut reimbursements by approximately 65% once fully implemented in 4 years and save $87.8 billion over the 7 years of the proposed model, as well as reduce cost sharing for beneficiaries.
This model puts the onus on providers to negotiate down drug prices with companies to meet proposed reimbursement limits. However, if companies do not lower their prices, acquisition costs could be substantially lower than reimbursements.
Prescribers and their practices would either have to take the financial hit or stop offering the pharmaceuticals, in which case patients would have to do without, try a different option, or seek care elsewhere, including facilities excluded from the proposal: children’s hospitals, critical access hospitals, cancer hospitals, federally qualified health centers, rural health clinics, and extended neoplastic disease care hospitals.
CMS estimates that in the first year of MFN reimbursements, 9% of beneficiaries would forgo MFN therapies, growing to 19% by year 3, figures that were included in cost savings estimates.
The reimbursement cuts are meant to motivate manufactures to lower prices, but “we have not seen this occur with similar efforts in the past, and drug prices have continued to rise,” said American College of Rheumatology President David Karp, MD, PhD, in a press release. Many of the agents on the list are used by rheumatologists.
Under current policy, Medicare Part B prescribers are reimbursed manufactures’ average sales price plus a 6% add-on. Under the new proposal, reimbursements would be pegged to the lowest price charged among nations of the Organization for Economic Co-operation and Development with a gross domestic product per capita of at least 60% of the US price. In addition to the United States, there are 36 other member countries, including Canada, the United Kingdom, Japan, and Germany.
To remove incentives to prescribe more expensive drugs, the 6% add-on would be replaced with a flat add-on payment per dose, pegged at $148.73 for the first quarter of 2021. There is a hardship exemption for providers if the reimbursement cuts are too drastic, but that involves a lot of paperwork.
This article first appeared on Medscape.com.
A proposal to lower Medicare Part B reimbursements for 50 physician-administered drugs and biologics to what drug manufacturers receive for them in other wealthy nations seems unlikely to take effect as planned on January 1, 2021. The proposal has been strongly opposed by the pharmaceutical industry as well as oncologists and other physicians who use the products most often.
At least four lawsuits have been filed in US district courts to block the move, including from Regeneron, manufacturer of the ophthalmic biologic aflibercept, the first agent on the list; the Community Oncology Alliance; the Biotechnology Innovation Organization, California Life Sciences Association, and Biocom; and Pharmaceutical Research and Manufacturers of America, the Association of Community Cancer Centers, the Global Colon Cancer Association, and National Infusion Center Association.
The proposal could hit oncologists/hematologists particularly hard because they are the primary prescribers of about 30 of the 50 agents on the list, including mainstay breast, lung, and prostate cancer treatments and newer immunotherapies. In its filing for injunctive relieve, the Community Oncology Alliance, a trade group for community oncologists, said the proposal exposes “the health and safety of cancer patients and other patients with potentially life-threatening diseases to real danger.”
Hearings are imminent
Hearings on the proposal, which was published by the Centers for Medicare & Medicaid Services (CMS) on November 27 following an executive order September 13, are scheduled for coming days. The first hearing is scheduled for December 18.
Given the looming implementation date, judges are likely to rule quickly on the motions for injunctive relief, said attorney Rachel Sachs, a health law expert and associate professor at the Washington University School of Law, St. Louis, Missouri. The odds are in plaintiffs’ favor based on procedural and Constitutional grounds. “It’s extremely unlikely to survive” the legal onslaught, she told Medscape Medical News.
Among the many issues raised in court filings, the proposal was released as an interim final rule (IFR), meaning it would take effect outside of the usual process of proposed rule, comment period, revision, then implementation. The law allows for bypassing normal rule-making requirements with an IFR, but they are meant for emergency situations — several have been issued in response to the COVID-19 pandemic — and the government must be able to show that delay would be “impracticable, unnecessary, or contrary to the public interest,” Sachs explained.
In contrast, some form of CMS’s new proposal, dubbed the “Most Favored Nation” (MFN) model for drug reimbursements, has been under consideration by the Trump administration since 2018.
“The way the [Trump] administration rolled this rule out at pretty much the last minute opens them up to greater legal challenges than if they pursued more normal regulatory pathways, which they had the opportunity to do. They are attempting to implement this on a time frame that is unprecedented for as large a change as this is,” said Juliette Cubanski, PhD, deputy director of Medicare policy at the Kaiser Family Foundation, San Francisco, California.
Reimbursement less than acquisition costs
In the proposal, CMS sought to offset the higher prices that pharmaceutical companies charge in the United States when compared with other developed nations — the prices are about double on average.
“One of the largest drivers of increasing Medicare spending is the growing prices for physician-administered separately payable Medicare Part B drugs, which have risen an average of 11.5% annually since 2015, with total spending of approximately $30 billion in 2019,” the agency said in a fact sheet. This is due in large part to “lack of competitive market forces on Medicare Part B drug costs,” it added.
The 50 agents covered by the new proposal are the ones Part B spends the most on, almost $3 billion in 2019 for aflibercept alone, followed closely by pembrolizumab, an immunotherapy used in many different cancer types.
A full list of the drugs and biologicals included in the proposal is on page 50 of the IFR.
CMS estimated that its move would cut reimbursements by approximately 65% once fully implemented in 4 years and save $87.8 billion over the 7 years of the proposed model, as well as reduce cost sharing for beneficiaries.
This model puts the onus on providers to negotiate down drug prices with companies to meet proposed reimbursement limits. However, if companies do not lower their prices, acquisition costs could be substantially lower than reimbursements.
Prescribers and their practices would either have to take the financial hit or stop offering the pharmaceuticals, in which case patients would have to do without, try a different option, or seek care elsewhere, including facilities excluded from the proposal: children’s hospitals, critical access hospitals, cancer hospitals, federally qualified health centers, rural health clinics, and extended neoplastic disease care hospitals.
CMS estimates that in the first year of MFN reimbursements, 9% of beneficiaries would forgo MFN therapies, growing to 19% by year 3, figures that were included in cost savings estimates.
The reimbursement cuts are meant to motivate manufactures to lower prices, but “we have not seen this occur with similar efforts in the past, and drug prices have continued to rise,” said American College of Rheumatology President David Karp, MD, PhD, in a press release. Many of the agents on the list are used by rheumatologists.
Under current policy, Medicare Part B prescribers are reimbursed manufactures’ average sales price plus a 6% add-on. Under the new proposal, reimbursements would be pegged to the lowest price charged among nations of the Organization for Economic Co-operation and Development with a gross domestic product per capita of at least 60% of the US price. In addition to the United States, there are 36 other member countries, including Canada, the United Kingdom, Japan, and Germany.
To remove incentives to prescribe more expensive drugs, the 6% add-on would be replaced with a flat add-on payment per dose, pegged at $148.73 for the first quarter of 2021. There is a hardship exemption for providers if the reimbursement cuts are too drastic, but that involves a lot of paperwork.
This article first appeared on Medscape.com.
A proposal to lower Medicare Part B reimbursements for 50 physician-administered drugs and biologics to what drug manufacturers receive for them in other wealthy nations seems unlikely to take effect as planned on January 1, 2021. The proposal has been strongly opposed by the pharmaceutical industry as well as oncologists and other physicians who use the products most often.
At least four lawsuits have been filed in US district courts to block the move, including from Regeneron, manufacturer of the ophthalmic biologic aflibercept, the first agent on the list; the Community Oncology Alliance; the Biotechnology Innovation Organization, California Life Sciences Association, and Biocom; and Pharmaceutical Research and Manufacturers of America, the Association of Community Cancer Centers, the Global Colon Cancer Association, and National Infusion Center Association.
The proposal could hit oncologists/hematologists particularly hard because they are the primary prescribers of about 30 of the 50 agents on the list, including mainstay breast, lung, and prostate cancer treatments and newer immunotherapies. In its filing for injunctive relieve, the Community Oncology Alliance, a trade group for community oncologists, said the proposal exposes “the health and safety of cancer patients and other patients with potentially life-threatening diseases to real danger.”
Hearings are imminent
Hearings on the proposal, which was published by the Centers for Medicare & Medicaid Services (CMS) on November 27 following an executive order September 13, are scheduled for coming days. The first hearing is scheduled for December 18.
Given the looming implementation date, judges are likely to rule quickly on the motions for injunctive relief, said attorney Rachel Sachs, a health law expert and associate professor at the Washington University School of Law, St. Louis, Missouri. The odds are in plaintiffs’ favor based on procedural and Constitutional grounds. “It’s extremely unlikely to survive” the legal onslaught, she told Medscape Medical News.
Among the many issues raised in court filings, the proposal was released as an interim final rule (IFR), meaning it would take effect outside of the usual process of proposed rule, comment period, revision, then implementation. The law allows for bypassing normal rule-making requirements with an IFR, but they are meant for emergency situations — several have been issued in response to the COVID-19 pandemic — and the government must be able to show that delay would be “impracticable, unnecessary, or contrary to the public interest,” Sachs explained.
In contrast, some form of CMS’s new proposal, dubbed the “Most Favored Nation” (MFN) model for drug reimbursements, has been under consideration by the Trump administration since 2018.
“The way the [Trump] administration rolled this rule out at pretty much the last minute opens them up to greater legal challenges than if they pursued more normal regulatory pathways, which they had the opportunity to do. They are attempting to implement this on a time frame that is unprecedented for as large a change as this is,” said Juliette Cubanski, PhD, deputy director of Medicare policy at the Kaiser Family Foundation, San Francisco, California.
Reimbursement less than acquisition costs
In the proposal, CMS sought to offset the higher prices that pharmaceutical companies charge in the United States when compared with other developed nations — the prices are about double on average.
“One of the largest drivers of increasing Medicare spending is the growing prices for physician-administered separately payable Medicare Part B drugs, which have risen an average of 11.5% annually since 2015, with total spending of approximately $30 billion in 2019,” the agency said in a fact sheet. This is due in large part to “lack of competitive market forces on Medicare Part B drug costs,” it added.
The 50 agents covered by the new proposal are the ones Part B spends the most on, almost $3 billion in 2019 for aflibercept alone, followed closely by pembrolizumab, an immunotherapy used in many different cancer types.
A full list of the drugs and biologicals included in the proposal is on page 50 of the IFR.
CMS estimated that its move would cut reimbursements by approximately 65% once fully implemented in 4 years and save $87.8 billion over the 7 years of the proposed model, as well as reduce cost sharing for beneficiaries.
This model puts the onus on providers to negotiate down drug prices with companies to meet proposed reimbursement limits. However, if companies do not lower their prices, acquisition costs could be substantially lower than reimbursements.
Prescribers and their practices would either have to take the financial hit or stop offering the pharmaceuticals, in which case patients would have to do without, try a different option, or seek care elsewhere, including facilities excluded from the proposal: children’s hospitals, critical access hospitals, cancer hospitals, federally qualified health centers, rural health clinics, and extended neoplastic disease care hospitals.
CMS estimates that in the first year of MFN reimbursements, 9% of beneficiaries would forgo MFN therapies, growing to 19% by year 3, figures that were included in cost savings estimates.
The reimbursement cuts are meant to motivate manufactures to lower prices, but “we have not seen this occur with similar efforts in the past, and drug prices have continued to rise,” said American College of Rheumatology President David Karp, MD, PhD, in a press release. Many of the agents on the list are used by rheumatologists.
Under current policy, Medicare Part B prescribers are reimbursed manufactures’ average sales price plus a 6% add-on. Under the new proposal, reimbursements would be pegged to the lowest price charged among nations of the Organization for Economic Co-operation and Development with a gross domestic product per capita of at least 60% of the US price. In addition to the United States, there are 36 other member countries, including Canada, the United Kingdom, Japan, and Germany.
To remove incentives to prescribe more expensive drugs, the 6% add-on would be replaced with a flat add-on payment per dose, pegged at $148.73 for the first quarter of 2021. There is a hardship exemption for providers if the reimbursement cuts are too drastic, but that involves a lot of paperwork.
This article first appeared on Medscape.com.
Six big changes coming for office-visit coding
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to [email protected].
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
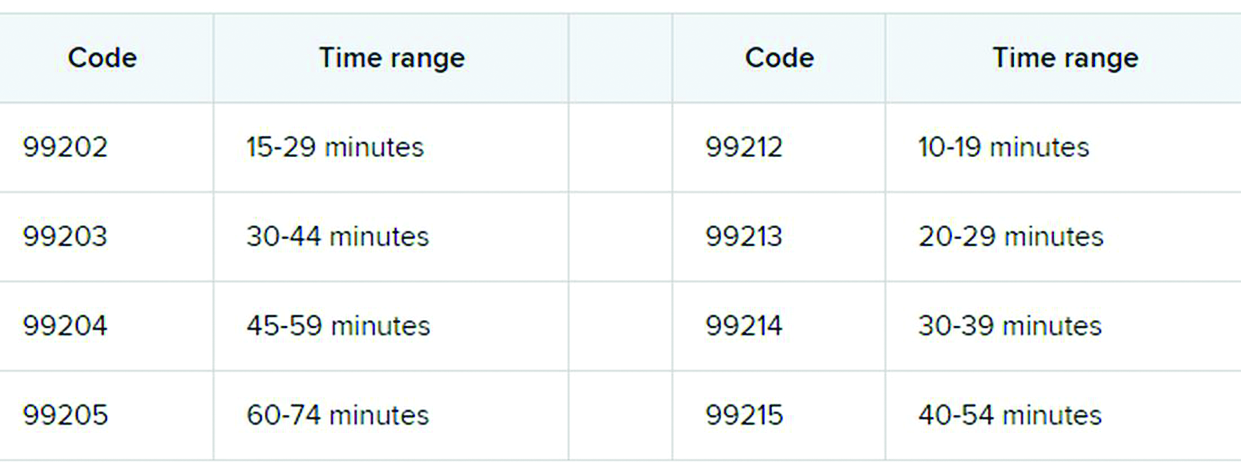
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to [email protected].
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to [email protected].
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Proposed HIPAA overhaul to ease access to patient health info
The Department of Health & Human Services is proposing an overhaul of HIPAA that will make it easier to access patients’ personal health information, including the health records of patients with mental illness. The proposal would also do away with the requirement that all patients sign a notice of privacy practices.
The changes are contained in a 357-page proposed rule, which was unveiled by federal officials Dec. 10. Roger Severino, director of HHS’ Office for Civil Rights, said in a briefing that the sweeping proposal would empower patients, reduce the administrative burden for health care providers, and pave the way to better-coordinated care.
HHS estimated that the rule could save $3.2 billion over 5 years, but it’s not clear how much of that would accrue to clinical practices.
The most obvious cost-saving aspect for medical and dental practices is the proposal that practitioners would no longer have to provide and collect signed notifications of privacy practices.
“This has been a tremendous waste of time and effort and has caused massive confusion,” said Mr. Severino. He said some patients thought they were waiving privacy rights and that, in some cases, physicians refused to administer care unless patients signed the notices. “That was never the intent.”
Requiring that patients sign the form and that practices keep copies for 6 years is an “unnecessary burden,” said Mr. Severino. “We’ve lost whole forests from this regulation.”
Under the new proposal, health care providers would merely have to let patients know where to find their privacy policies.
Sharing mental health info
The rule would also ease the standard for sharing information about a patient who is in a mental health crisis, such as an exacerbation of a serious mental illness or a crisis related to a substance use disorder, including an overdose.
Currently, clinicians can choose to disclose protected health information – to a family member, a caregiver, a law enforcement official, a doctor, or an insurer – if they believe that doing so is advisable in their “professional judgment.” The rule proposes to ease that to a “good faith” belief that a disclosure would be in the best interest of the patient. In both instances, the patient can still object and block the disclosure.
As an example, HHS said that, in the case of a young adult who had experienced an overdose of opioids, a licensed health care professional could make the determination to “disclose relevant information to a parent who is involved in the patient’s treatment and who the young adult would expect, based on their relationship, to participate in or be involved with the patient’s recovery from the overdose.”
HHS is also proposing to let clinicians disclose information in cases in which an individual might be a threat to himself or others, provided the harm is “serious and reasonably foreseeable.”
Currently, information can only be disclosed if it appears there is a “serious and imminent” threat to health or safety. If an individual experienced suicidal ideation, for instance, a health care professional could notify family that the individual is at risk.
Fast, no-cost access
The rule also aims to make it easier for patients to get access to their own health care information quickly – within 15 days of a request – instead of the 30 days currently allowed, and sometimes at no cost.
The 30-day time frame is “a relic of a pre-Internet age that should be dispensed with,” said Mr. Severino.
Patients can also request that a treating physician get his or her records from a clinician who had previously treated the individual. The request would be fulfilled within 15 days, although extensions might be possible.
“That takes away the burden of coordination from the patient and puts it on those parties that are responsible for the actual provision of care and that are better positioned to do that coordination,” Mr. Severino said.
Health care professionals will also have to share with patients a fee schedule for records requests. However, if records are shared through a patient portal with view, download, and transmit capabilities, the provider can’t charge the patient for the time it took to upload the information into the system.
“We do not believe a patient’s personal medical record should be profit centers for providers,” Mr. Severino said.
Patients will be allowed to take photos with a smartphone of personal health information – such as an x-ray or sonogram – while receiving care.
The rule is open for public comment until mid-February. After that, it will become final in 180 days. The agency said it would not begin enforcement until 240 days after the final rule was published.
A version of this article originally appeared on Medscape.com.
The Department of Health & Human Services is proposing an overhaul of HIPAA that will make it easier to access patients’ personal health information, including the health records of patients with mental illness. The proposal would also do away with the requirement that all patients sign a notice of privacy practices.
The changes are contained in a 357-page proposed rule, which was unveiled by federal officials Dec. 10. Roger Severino, director of HHS’ Office for Civil Rights, said in a briefing that the sweeping proposal would empower patients, reduce the administrative burden for health care providers, and pave the way to better-coordinated care.
HHS estimated that the rule could save $3.2 billion over 5 years, but it’s not clear how much of that would accrue to clinical practices.
The most obvious cost-saving aspect for medical and dental practices is the proposal that practitioners would no longer have to provide and collect signed notifications of privacy practices.
“This has been a tremendous waste of time and effort and has caused massive confusion,” said Mr. Severino. He said some patients thought they were waiving privacy rights and that, in some cases, physicians refused to administer care unless patients signed the notices. “That was never the intent.”
Requiring that patients sign the form and that practices keep copies for 6 years is an “unnecessary burden,” said Mr. Severino. “We’ve lost whole forests from this regulation.”
Under the new proposal, health care providers would merely have to let patients know where to find their privacy policies.
Sharing mental health info
The rule would also ease the standard for sharing information about a patient who is in a mental health crisis, such as an exacerbation of a serious mental illness or a crisis related to a substance use disorder, including an overdose.
Currently, clinicians can choose to disclose protected health information – to a family member, a caregiver, a law enforcement official, a doctor, or an insurer – if they believe that doing so is advisable in their “professional judgment.” The rule proposes to ease that to a “good faith” belief that a disclosure would be in the best interest of the patient. In both instances, the patient can still object and block the disclosure.
As an example, HHS said that, in the case of a young adult who had experienced an overdose of opioids, a licensed health care professional could make the determination to “disclose relevant information to a parent who is involved in the patient’s treatment and who the young adult would expect, based on their relationship, to participate in or be involved with the patient’s recovery from the overdose.”
HHS is also proposing to let clinicians disclose information in cases in which an individual might be a threat to himself or others, provided the harm is “serious and reasonably foreseeable.”
Currently, information can only be disclosed if it appears there is a “serious and imminent” threat to health or safety. If an individual experienced suicidal ideation, for instance, a health care professional could notify family that the individual is at risk.
Fast, no-cost access
The rule also aims to make it easier for patients to get access to their own health care information quickly – within 15 days of a request – instead of the 30 days currently allowed, and sometimes at no cost.
The 30-day time frame is “a relic of a pre-Internet age that should be dispensed with,” said Mr. Severino.
Patients can also request that a treating physician get his or her records from a clinician who had previously treated the individual. The request would be fulfilled within 15 days, although extensions might be possible.
“That takes away the burden of coordination from the patient and puts it on those parties that are responsible for the actual provision of care and that are better positioned to do that coordination,” Mr. Severino said.
Health care professionals will also have to share with patients a fee schedule for records requests. However, if records are shared through a patient portal with view, download, and transmit capabilities, the provider can’t charge the patient for the time it took to upload the information into the system.
“We do not believe a patient’s personal medical record should be profit centers for providers,” Mr. Severino said.
Patients will be allowed to take photos with a smartphone of personal health information – such as an x-ray or sonogram – while receiving care.
The rule is open for public comment until mid-February. After that, it will become final in 180 days. The agency said it would not begin enforcement until 240 days after the final rule was published.
A version of this article originally appeared on Medscape.com.
The Department of Health & Human Services is proposing an overhaul of HIPAA that will make it easier to access patients’ personal health information, including the health records of patients with mental illness. The proposal would also do away with the requirement that all patients sign a notice of privacy practices.
The changes are contained in a 357-page proposed rule, which was unveiled by federal officials Dec. 10. Roger Severino, director of HHS’ Office for Civil Rights, said in a briefing that the sweeping proposal would empower patients, reduce the administrative burden for health care providers, and pave the way to better-coordinated care.
HHS estimated that the rule could save $3.2 billion over 5 years, but it’s not clear how much of that would accrue to clinical practices.
The most obvious cost-saving aspect for medical and dental practices is the proposal that practitioners would no longer have to provide and collect signed notifications of privacy practices.
“This has been a tremendous waste of time and effort and has caused massive confusion,” said Mr. Severino. He said some patients thought they were waiving privacy rights and that, in some cases, physicians refused to administer care unless patients signed the notices. “That was never the intent.”
Requiring that patients sign the form and that practices keep copies for 6 years is an “unnecessary burden,” said Mr. Severino. “We’ve lost whole forests from this regulation.”
Under the new proposal, health care providers would merely have to let patients know where to find their privacy policies.
Sharing mental health info
The rule would also ease the standard for sharing information about a patient who is in a mental health crisis, such as an exacerbation of a serious mental illness or a crisis related to a substance use disorder, including an overdose.
Currently, clinicians can choose to disclose protected health information – to a family member, a caregiver, a law enforcement official, a doctor, or an insurer – if they believe that doing so is advisable in their “professional judgment.” The rule proposes to ease that to a “good faith” belief that a disclosure would be in the best interest of the patient. In both instances, the patient can still object and block the disclosure.
As an example, HHS said that, in the case of a young adult who had experienced an overdose of opioids, a licensed health care professional could make the determination to “disclose relevant information to a parent who is involved in the patient’s treatment and who the young adult would expect, based on their relationship, to participate in or be involved with the patient’s recovery from the overdose.”
HHS is also proposing to let clinicians disclose information in cases in which an individual might be a threat to himself or others, provided the harm is “serious and reasonably foreseeable.”
Currently, information can only be disclosed if it appears there is a “serious and imminent” threat to health or safety. If an individual experienced suicidal ideation, for instance, a health care professional could notify family that the individual is at risk.
Fast, no-cost access
The rule also aims to make it easier for patients to get access to their own health care information quickly – within 15 days of a request – instead of the 30 days currently allowed, and sometimes at no cost.
The 30-day time frame is “a relic of a pre-Internet age that should be dispensed with,” said Mr. Severino.
Patients can also request that a treating physician get his or her records from a clinician who had previously treated the individual. The request would be fulfilled within 15 days, although extensions might be possible.
“That takes away the burden of coordination from the patient and puts it on those parties that are responsible for the actual provision of care and that are better positioned to do that coordination,” Mr. Severino said.
Health care professionals will also have to share with patients a fee schedule for records requests. However, if records are shared through a patient portal with view, download, and transmit capabilities, the provider can’t charge the patient for the time it took to upload the information into the system.
“We do not believe a patient’s personal medical record should be profit centers for providers,” Mr. Severino said.
Patients will be allowed to take photos with a smartphone of personal health information – such as an x-ray or sonogram – while receiving care.
The rule is open for public comment until mid-February. After that, it will become final in 180 days. The agency said it would not begin enforcement until 240 days after the final rule was published.
A version of this article originally appeared on Medscape.com.
Medicare payments could get tougher for docs
More than 40 value-based payment models – from direct contracting to bundled payments – have been introduced into the Medicare program in the past 10 years, with the goal of improving care while lowering costs. Hopes were high that they would be successful.
Physicians could suffer a huge blow to their income.
Many of the value-based care models simply did not work as expected, said Seema Verma, head of the Centers for Medicare & Medicaid Services, at a recent HLTH Conference. “They are not producing the types of savings the taxpayers deserve,” Ms. Verma said.
The Medicare Payment Advisory Commission (MedPac) concluded that, while dozens of payment models were tested, most failed to generate net savings for Medicare. Even the most successful of the models produced only modest savings. MedPac elaborated: “The track record raises the question of whether changes to particular models or CMMI’s [Center for Medicare & Medicaid Innovation’s] broader strategies might be warranted.”
What will happen now, as government officials admit that their value-based programs haven’t worked? The value-based programs could become more stringent. Here’s what physicians will have to contend with.
More risk. Experts agree that risk – financial risk – will be a component of future programs. Two-sided risk is likely to be the norm. This means that both parties – the provider and the insurer – are at financial risk for the patients covered by the program.
For example, a plan with 50,000 beneficiary patients would estimate the cost of caring for those patients on the basis of multiple variables. If the actual cost is lower than anticipated, both parties share in the savings. However, both share in the loss if the cost of caring for their patient population exceeds expectations.
This may compel physicians to enhance efficiency and potentially limit the services provided to patients. Typically, however, the strategy is to make efforts to prevent services like ED visits and admissions by focusing on health maintenance.
In contrast to most current value-based models, which feature little to no downside risk for physicians, double-sided risk means physicians could lose money. The loss may incorporate a cap – 5%, for example – but programs may differ. Experts concur that double-sided risk will be a hallmark of future programs.
Better data. The majority of health care services are rendered via fee-for-service: Patients receive services and physicians are paid, yet little or no information about outcomes is exchanged between insurers and physicians.
Penny Noyes, president of Health Business Navigators and contract negotiator for physicians, is not a fan of the current crop of value-based programs and feels that data transparency is positive. Sound metrics can lead to improvement, she said, adding: “It’s not money that drives physicians to make decisions; it’s what’s in the best interest of their patients and their patients’ long-term care.”
Value-based programs can work but only if applicable data are developed and given to physicians so that they can better understand their current performance and how to improve.
Mandated participation. Participation in value-based programs has been voluntary, but that may have skewed the results, which were better than what typical practice would have shown. Acknowledging this may lead CMS to call for mandated participation as a component of future programs. Physicians may be brought into programs, if only to determine whether the models really work. To date, participation in the programs has been voluntary, but that may change in the future.
Innovation. The private insurance market may end up as a key player. Over the past 6 months, health insurers have either consolidated partnerships with telemedicine companies to provide no-cost care to beneficiaries or have launched their own initiatives.
Others are focused on bringing together patients and providers operating outside of the traditional health care system, such as Aetna’s merger with CVS which now offers retail-based acute care (MinuteClinic) and chronic care (HealthHUB). Still other payers are gambling with physician practice ownership, as in the case of United Healthcare’s OptumHealth, which now boasts around 50,000 physicians throughout the country.
New practice models are emerging in private practices as well. Physicians are embracing remote care, proactively managing care transitions, and seeking out more methods to keep patients healthy and at home.
Not much was expected from value-based plans
Many are not surprised that the value-based models did not produce impressive results. Ms. Noyes doubted that positive outcomes will be achieved for physicians in comparison with what could have been attained under fee-for-service arrangements with lower administrative costs.
While the Affordable Care Act attempted to encourage alternative reimbursement, it limits the maximum medical loss ratio (MLR) a payer could achieve. For many plans, that maximum was 85%. Simply put, at least $0.85 of each premium collected had to be paid in claims; the remaining $0.15 went to margin, claims, and other administrative costs. A payer with an 82% MLR then would have to rebate the 3% difference to enrollees.
But that’s not what occurred, according to Ms. Noyes. Because value-based payments to providers are considered a claims expense, an MLR ratio of 82% allowed the payer to distribute the 3% difference to providers as value-based payments. Ms. Noyes said: “That may sound good for the provider, but the result was essentially a freeze on the provider’s fee-for-service reimbursement with the prospect of getting value-based payments like ‘shared savings.’
“When the providers tried to increase their base fee-for-service rates just to match inflation, payers often advised that any future raises had to be earned through value-based programs,” Ms. Noyes added. The value-based formulas confuse providers because payments are often made for periods as far back as 18 months, and providers do not have data systems to reconcile their payer report cards retrospectively. The result is that providers tended to accept whatever amount the payer distributed.
Executives at Lumeris, a company that helps health systems participate successfully in value-based care, see potential in a newer approach to alternative payments, such as CMS’ Direct Contracting initiative. This voluntary payment model offers options tailored to several types of organizations that aim to reduce costs while preserving or enhancing the quality of care for Medicare fee-for-service beneficiaries.
Jeff Smith, chief commercial officer for population health at Lumeris, explained that the Direct Contracting initiative can provide physicians with a more attractive option than prior value-based models because it adjusts for the complexity and fragility of patients with complex and chronic conditions. By allowing providers to participate in the savings generated, the initiative stands in stark contrast to what Mr. Smith described as the “shared savings to nothingness” experienced by providers in earlier-stage alternative payment models.
Physicians engaged with value-based programs like Direct Contracting are investing in nurses to aid with initiatives regarding health promotion and transitions of care. When a patient is discharged, for example, the nurse contacts the patient to discuss medications, schedule follow-up appointments, and so forth – tasks typically left to the patient (or caregiver) to navigate in the traditional system.
The initiative recognizes the importance of managing high-risk patients, those whom physicians identify as having an extraordinary number of ED visits and admissions. These patients, as well as so-called “rising-risk” patients, are targeted by nurses who proactively communicate with patients (and caregivers) to address patient’s needs, including social determinants of health.
Physicians who have a large load of patients in value-based programs are hiring social workers, pharmacists, and behavioral health experts to help. Of course, these personnel are costly, but that’s what the value-based programs aim to reimburse.
Still, the road ahead to value based is rocky and may not gain momentum for some time. Johns Hopkins University’s Doug Hough, PhD, an economist, recounts a government research study that sought to assess the university’s health system participation in a value-based payment program. While there were positive impacts on the program’s target population, Hough and his team discovered that the returns achieved by the optional model didn’t justify the health system’s financial support for it. The increasingly indebted health system ultimately decided to drop the optional program.
Dr. Hough indicated that the health system – Johns Hopkins Medicine – likely would have continued its support for the program had the government at least allowed it to break even. Although the payment program under study was a 3-year project, the bigger challenge, declared Dr. Hough, is that “we can’t turn an aircraft carrier that quickly.”
“Three years won’t show whether value-based care is really working,” Dr. Hough said.
Robert Zipper, MD, a hospitalist and senior policy advisor for Sound Physicians, a company that works to improve outcomes in acute care, agreed with Dr. Hough that performance tends to improve with time. Yet, Dr. Zipper doesn’t see much change in the near term, because “after all, there is nothing to replace them [the programs].”
The problem gets even stickier for private payers because patients may be on an insurance panel for as little as a year or 2. Thanks to this rapid churn of beneficiaries, even the best-designed value-based program will have little time to prove its worth.
Dr. Zipper is among the many who don’t expect significant changes in the near term, asserting that “President Biden will want to get a few policy wins first, and health care is not the easiest place to start.”
But it’s likely that payers and others will want to see more emphasis on value-based programs despite these programs’ possible value to patients, physicians, and health systems alike.
A version of this article originally appeared on Medscape.com.
More than 40 value-based payment models – from direct contracting to bundled payments – have been introduced into the Medicare program in the past 10 years, with the goal of improving care while lowering costs. Hopes were high that they would be successful.
Physicians could suffer a huge blow to their income.
Many of the value-based care models simply did not work as expected, said Seema Verma, head of the Centers for Medicare & Medicaid Services, at a recent HLTH Conference. “They are not producing the types of savings the taxpayers deserve,” Ms. Verma said.
The Medicare Payment Advisory Commission (MedPac) concluded that, while dozens of payment models were tested, most failed to generate net savings for Medicare. Even the most successful of the models produced only modest savings. MedPac elaborated: “The track record raises the question of whether changes to particular models or CMMI’s [Center for Medicare & Medicaid Innovation’s] broader strategies might be warranted.”
What will happen now, as government officials admit that their value-based programs haven’t worked? The value-based programs could become more stringent. Here’s what physicians will have to contend with.
More risk. Experts agree that risk – financial risk – will be a component of future programs. Two-sided risk is likely to be the norm. This means that both parties – the provider and the insurer – are at financial risk for the patients covered by the program.
For example, a plan with 50,000 beneficiary patients would estimate the cost of caring for those patients on the basis of multiple variables. If the actual cost is lower than anticipated, both parties share in the savings. However, both share in the loss if the cost of caring for their patient population exceeds expectations.
This may compel physicians to enhance efficiency and potentially limit the services provided to patients. Typically, however, the strategy is to make efforts to prevent services like ED visits and admissions by focusing on health maintenance.
In contrast to most current value-based models, which feature little to no downside risk for physicians, double-sided risk means physicians could lose money. The loss may incorporate a cap – 5%, for example – but programs may differ. Experts concur that double-sided risk will be a hallmark of future programs.
Better data. The majority of health care services are rendered via fee-for-service: Patients receive services and physicians are paid, yet little or no information about outcomes is exchanged between insurers and physicians.
Penny Noyes, president of Health Business Navigators and contract negotiator for physicians, is not a fan of the current crop of value-based programs and feels that data transparency is positive. Sound metrics can lead to improvement, she said, adding: “It’s not money that drives physicians to make decisions; it’s what’s in the best interest of their patients and their patients’ long-term care.”
Value-based programs can work but only if applicable data are developed and given to physicians so that they can better understand their current performance and how to improve.
Mandated participation. Participation in value-based programs has been voluntary, but that may have skewed the results, which were better than what typical practice would have shown. Acknowledging this may lead CMS to call for mandated participation as a component of future programs. Physicians may be brought into programs, if only to determine whether the models really work. To date, participation in the programs has been voluntary, but that may change in the future.
Innovation. The private insurance market may end up as a key player. Over the past 6 months, health insurers have either consolidated partnerships with telemedicine companies to provide no-cost care to beneficiaries or have launched their own initiatives.
Others are focused on bringing together patients and providers operating outside of the traditional health care system, such as Aetna’s merger with CVS which now offers retail-based acute care (MinuteClinic) and chronic care (HealthHUB). Still other payers are gambling with physician practice ownership, as in the case of United Healthcare’s OptumHealth, which now boasts around 50,000 physicians throughout the country.
New practice models are emerging in private practices as well. Physicians are embracing remote care, proactively managing care transitions, and seeking out more methods to keep patients healthy and at home.
Not much was expected from value-based plans
Many are not surprised that the value-based models did not produce impressive results. Ms. Noyes doubted that positive outcomes will be achieved for physicians in comparison with what could have been attained under fee-for-service arrangements with lower administrative costs.
While the Affordable Care Act attempted to encourage alternative reimbursement, it limits the maximum medical loss ratio (MLR) a payer could achieve. For many plans, that maximum was 85%. Simply put, at least $0.85 of each premium collected had to be paid in claims; the remaining $0.15 went to margin, claims, and other administrative costs. A payer with an 82% MLR then would have to rebate the 3% difference to enrollees.
But that’s not what occurred, according to Ms. Noyes. Because value-based payments to providers are considered a claims expense, an MLR ratio of 82% allowed the payer to distribute the 3% difference to providers as value-based payments. Ms. Noyes said: “That may sound good for the provider, but the result was essentially a freeze on the provider’s fee-for-service reimbursement with the prospect of getting value-based payments like ‘shared savings.’
“When the providers tried to increase their base fee-for-service rates just to match inflation, payers often advised that any future raises had to be earned through value-based programs,” Ms. Noyes added. The value-based formulas confuse providers because payments are often made for periods as far back as 18 months, and providers do not have data systems to reconcile their payer report cards retrospectively. The result is that providers tended to accept whatever amount the payer distributed.
Executives at Lumeris, a company that helps health systems participate successfully in value-based care, see potential in a newer approach to alternative payments, such as CMS’ Direct Contracting initiative. This voluntary payment model offers options tailored to several types of organizations that aim to reduce costs while preserving or enhancing the quality of care for Medicare fee-for-service beneficiaries.
Jeff Smith, chief commercial officer for population health at Lumeris, explained that the Direct Contracting initiative can provide physicians with a more attractive option than prior value-based models because it adjusts for the complexity and fragility of patients with complex and chronic conditions. By allowing providers to participate in the savings generated, the initiative stands in stark contrast to what Mr. Smith described as the “shared savings to nothingness” experienced by providers in earlier-stage alternative payment models.
Physicians engaged with value-based programs like Direct Contracting are investing in nurses to aid with initiatives regarding health promotion and transitions of care. When a patient is discharged, for example, the nurse contacts the patient to discuss medications, schedule follow-up appointments, and so forth – tasks typically left to the patient (or caregiver) to navigate in the traditional system.
The initiative recognizes the importance of managing high-risk patients, those whom physicians identify as having an extraordinary number of ED visits and admissions. These patients, as well as so-called “rising-risk” patients, are targeted by nurses who proactively communicate with patients (and caregivers) to address patient’s needs, including social determinants of health.
Physicians who have a large load of patients in value-based programs are hiring social workers, pharmacists, and behavioral health experts to help. Of course, these personnel are costly, but that’s what the value-based programs aim to reimburse.
Still, the road ahead to value based is rocky and may not gain momentum for some time. Johns Hopkins University’s Doug Hough, PhD, an economist, recounts a government research study that sought to assess the university’s health system participation in a value-based payment program. While there were positive impacts on the program’s target population, Hough and his team discovered that the returns achieved by the optional model didn’t justify the health system’s financial support for it. The increasingly indebted health system ultimately decided to drop the optional program.
Dr. Hough indicated that the health system – Johns Hopkins Medicine – likely would have continued its support for the program had the government at least allowed it to break even. Although the payment program under study was a 3-year project, the bigger challenge, declared Dr. Hough, is that “we can’t turn an aircraft carrier that quickly.”
“Three years won’t show whether value-based care is really working,” Dr. Hough said.
Robert Zipper, MD, a hospitalist and senior policy advisor for Sound Physicians, a company that works to improve outcomes in acute care, agreed with Dr. Hough that performance tends to improve with time. Yet, Dr. Zipper doesn’t see much change in the near term, because “after all, there is nothing to replace them [the programs].”
The problem gets even stickier for private payers because patients may be on an insurance panel for as little as a year or 2. Thanks to this rapid churn of beneficiaries, even the best-designed value-based program will have little time to prove its worth.
Dr. Zipper is among the many who don’t expect significant changes in the near term, asserting that “President Biden will want to get a few policy wins first, and health care is not the easiest place to start.”
But it’s likely that payers and others will want to see more emphasis on value-based programs despite these programs’ possible value to patients, physicians, and health systems alike.
A version of this article originally appeared on Medscape.com.
More than 40 value-based payment models – from direct contracting to bundled payments – have been introduced into the Medicare program in the past 10 years, with the goal of improving care while lowering costs. Hopes were high that they would be successful.
Physicians could suffer a huge blow to their income.
Many of the value-based care models simply did not work as expected, said Seema Verma, head of the Centers for Medicare & Medicaid Services, at a recent HLTH Conference. “They are not producing the types of savings the taxpayers deserve,” Ms. Verma said.
The Medicare Payment Advisory Commission (MedPac) concluded that, while dozens of payment models were tested, most failed to generate net savings for Medicare. Even the most successful of the models produced only modest savings. MedPac elaborated: “The track record raises the question of whether changes to particular models or CMMI’s [Center for Medicare & Medicaid Innovation’s] broader strategies might be warranted.”
What will happen now, as government officials admit that their value-based programs haven’t worked? The value-based programs could become more stringent. Here’s what physicians will have to contend with.
More risk. Experts agree that risk – financial risk – will be a component of future programs. Two-sided risk is likely to be the norm. This means that both parties – the provider and the insurer – are at financial risk for the patients covered by the program.
For example, a plan with 50,000 beneficiary patients would estimate the cost of caring for those patients on the basis of multiple variables. If the actual cost is lower than anticipated, both parties share in the savings. However, both share in the loss if the cost of caring for their patient population exceeds expectations.
This may compel physicians to enhance efficiency and potentially limit the services provided to patients. Typically, however, the strategy is to make efforts to prevent services like ED visits and admissions by focusing on health maintenance.
In contrast to most current value-based models, which feature little to no downside risk for physicians, double-sided risk means physicians could lose money. The loss may incorporate a cap – 5%, for example – but programs may differ. Experts concur that double-sided risk will be a hallmark of future programs.
Better data. The majority of health care services are rendered via fee-for-service: Patients receive services and physicians are paid, yet little or no information about outcomes is exchanged between insurers and physicians.
Penny Noyes, president of Health Business Navigators and contract negotiator for physicians, is not a fan of the current crop of value-based programs and feels that data transparency is positive. Sound metrics can lead to improvement, she said, adding: “It’s not money that drives physicians to make decisions; it’s what’s in the best interest of their patients and their patients’ long-term care.”
Value-based programs can work but only if applicable data are developed and given to physicians so that they can better understand their current performance and how to improve.
Mandated participation. Participation in value-based programs has been voluntary, but that may have skewed the results, which were better than what typical practice would have shown. Acknowledging this may lead CMS to call for mandated participation as a component of future programs. Physicians may be brought into programs, if only to determine whether the models really work. To date, participation in the programs has been voluntary, but that may change in the future.
Innovation. The private insurance market may end up as a key player. Over the past 6 months, health insurers have either consolidated partnerships with telemedicine companies to provide no-cost care to beneficiaries or have launched their own initiatives.
Others are focused on bringing together patients and providers operating outside of the traditional health care system, such as Aetna’s merger with CVS which now offers retail-based acute care (MinuteClinic) and chronic care (HealthHUB). Still other payers are gambling with physician practice ownership, as in the case of United Healthcare’s OptumHealth, which now boasts around 50,000 physicians throughout the country.
New practice models are emerging in private practices as well. Physicians are embracing remote care, proactively managing care transitions, and seeking out more methods to keep patients healthy and at home.
Not much was expected from value-based plans
Many are not surprised that the value-based models did not produce impressive results. Ms. Noyes doubted that positive outcomes will be achieved for physicians in comparison with what could have been attained under fee-for-service arrangements with lower administrative costs.
While the Affordable Care Act attempted to encourage alternative reimbursement, it limits the maximum medical loss ratio (MLR) a payer could achieve. For many plans, that maximum was 85%. Simply put, at least $0.85 of each premium collected had to be paid in claims; the remaining $0.15 went to margin, claims, and other administrative costs. A payer with an 82% MLR then would have to rebate the 3% difference to enrollees.
But that’s not what occurred, according to Ms. Noyes. Because value-based payments to providers are considered a claims expense, an MLR ratio of 82% allowed the payer to distribute the 3% difference to providers as value-based payments. Ms. Noyes said: “That may sound good for the provider, but the result was essentially a freeze on the provider’s fee-for-service reimbursement with the prospect of getting value-based payments like ‘shared savings.’
“When the providers tried to increase their base fee-for-service rates just to match inflation, payers often advised that any future raises had to be earned through value-based programs,” Ms. Noyes added. The value-based formulas confuse providers because payments are often made for periods as far back as 18 months, and providers do not have data systems to reconcile their payer report cards retrospectively. The result is that providers tended to accept whatever amount the payer distributed.
Executives at Lumeris, a company that helps health systems participate successfully in value-based care, see potential in a newer approach to alternative payments, such as CMS’ Direct Contracting initiative. This voluntary payment model offers options tailored to several types of organizations that aim to reduce costs while preserving or enhancing the quality of care for Medicare fee-for-service beneficiaries.
Jeff Smith, chief commercial officer for population health at Lumeris, explained that the Direct Contracting initiative can provide physicians with a more attractive option than prior value-based models because it adjusts for the complexity and fragility of patients with complex and chronic conditions. By allowing providers to participate in the savings generated, the initiative stands in stark contrast to what Mr. Smith described as the “shared savings to nothingness” experienced by providers in earlier-stage alternative payment models.
Physicians engaged with value-based programs like Direct Contracting are investing in nurses to aid with initiatives regarding health promotion and transitions of care. When a patient is discharged, for example, the nurse contacts the patient to discuss medications, schedule follow-up appointments, and so forth – tasks typically left to the patient (or caregiver) to navigate in the traditional system.
The initiative recognizes the importance of managing high-risk patients, those whom physicians identify as having an extraordinary number of ED visits and admissions. These patients, as well as so-called “rising-risk” patients, are targeted by nurses who proactively communicate with patients (and caregivers) to address patient’s needs, including social determinants of health.
Physicians who have a large load of patients in value-based programs are hiring social workers, pharmacists, and behavioral health experts to help. Of course, these personnel are costly, but that’s what the value-based programs aim to reimburse.
Still, the road ahead to value based is rocky and may not gain momentum for some time. Johns Hopkins University’s Doug Hough, PhD, an economist, recounts a government research study that sought to assess the university’s health system participation in a value-based payment program. While there were positive impacts on the program’s target population, Hough and his team discovered that the returns achieved by the optional model didn’t justify the health system’s financial support for it. The increasingly indebted health system ultimately decided to drop the optional program.
Dr. Hough indicated that the health system – Johns Hopkins Medicine – likely would have continued its support for the program had the government at least allowed it to break even. Although the payment program under study was a 3-year project, the bigger challenge, declared Dr. Hough, is that “we can’t turn an aircraft carrier that quickly.”
“Three years won’t show whether value-based care is really working,” Dr. Hough said.
Robert Zipper, MD, a hospitalist and senior policy advisor for Sound Physicians, a company that works to improve outcomes in acute care, agreed with Dr. Hough that performance tends to improve with time. Yet, Dr. Zipper doesn’t see much change in the near term, because “after all, there is nothing to replace them [the programs].”
The problem gets even stickier for private payers because patients may be on an insurance panel for as little as a year or 2. Thanks to this rapid churn of beneficiaries, even the best-designed value-based program will have little time to prove its worth.
Dr. Zipper is among the many who don’t expect significant changes in the near term, asserting that “President Biden will want to get a few policy wins first, and health care is not the easiest place to start.”
But it’s likely that payers and others will want to see more emphasis on value-based programs despite these programs’ possible value to patients, physicians, and health systems alike.
A version of this article originally appeared on Medscape.com.
A new model of care to return holism to family medicine
Here is our problem: Family medicine has allowed itself, and its patients, to be picked apart by the forces of reductionism and a system that profits from the sick and suffering. We have lost sight of our purpose and our vision to care for the whole person. We have lost our way as healers.
The result is not only a decline in the specialty of family medicine as a leader in primary care but declining value and worsening outcomes in health care overall. We need to get our mojo back. We can do this by focusing less on trying to be all things to all people at all times, and more on creating better models for preventing, managing, and reversing chronic disease. This means providing health care that is person centered, relationship based, recovery focused, and paid for comprehensively.
I call this model Advanced Primary Care, or APC (FIGURE). In this article, I describe exemplars of APC from across the United States. I also provide tools to help you recover its central feature, holism—care of the whole person in mind, body, community, and spirit—in your practice, thus returning us to the core purpose of family medicine.

Holism is central to family medicine
More than 40 years ago, psychiatrist George Engel, MD, published a seminal article in Science that inspired a radical vision of how health care should be practiced.1 Called the biopsychosocial model, it stated what, in some ways, is obvious: Human beings are complex organisms embedded in complex environments made up of distinct, yet interacting, dimensions. These dimensions included physical, psychological, and social components. Engel’s radical proposition was that these dimensions are definable and measurable and that good medicine cannot afford to ignore any of them.
Engel’s assertion that good medicine requires holism was a clarion call during a time of rapidly expanding knowledge and subspecialization. That call was the inspiration for a new medical specialty called family medicine, which dared to proclaim that the best way to heal was to care for the whole person within the context of that person’s emotional and social environment. Family medicine reinvigorated primary care and grew rapidly, becoming a preeminent primary care specialty in the United States.
Continue to : Reductionism is relentless
Reductionism is relentless
But the forces of medicine were—and still are—driving relentlessly the other way. The science of the small and particular (reductionism), with dazzling technology and exploding subspecialty knowledge, and backed by powerful economic drivers, rewards health care for pulling the patient and the medical profession apart. We pay more to those who treat small parts of a person over a short period than to those who attend to the whole person over the lifetime.
Today, family medicine—for all of its common sense, scientific soundness, connectedness to patients, and demonstrated value—struggles to survive.2-6 The holistic vision of Engel is declining. The struggle in primary care is that its holistic vision gets co-opted by specialized medical science—and then it desperately attempts to apply those small and specialized tools to the care of patients in their wholeness. Holism is largely dead in health care, and everyone pays the consequences.7
Health care is losing its value
The damage from this decline in holism is not just to primary care but to the value of health care in general. Most medical care being delivered today—comprising diagnosis, treatment, and payment (the innermost circle of the FIGURE)—is not producing good health.8 Only 15% to 20% of the healing of an individual or a population comes from health care.9 The rest—nearly 80%—comes from other factors rarely addressed in the health care system: behavioral and lifestyle choices that people make in their daily life, including those related to food, movement, sleep, stress, and substance use.10 Increasingly, it is the economic and social determinants of health that influence this behavior and have a greater impact on health and lifespan than physiology or genes.11 The same social determinants of health also influence patients’ ability to obtain medical care and pursue a meaningful life.12
The result of this decline in holism and in the value of health care in general has been a relentless rise in the cost of medical care13-15 and the need for social services; declining life expectancy16,17 and quality of life18; growing patient dissatisfaction; and burnout in providers.19,20 Health care has become, as investor and business leader Warren Buffet remarked, the “tapeworm” of the economy and a major contributor to growing disparities in health and well-being between the haves and have-nots.21 Engel’s prediction that good medicine cannot afford to ignore holism has come to pass.
3-step solution:Return to whole-person care
Family medicine needs to return to whole-person care, but it can do so only if it attends to, and effectively delivers on, the prevention, treatment, and reversal of chronic disease and the enhancement of health and well-being. This can happen only if family medicine stops trying to be all things to all people at all times and, instead, focuses on what matters to the patient as a person.
Continue to: This means that the core...
This means that the core interaction in family medicine must be to assess the whole person—mind, body, social, spirit—and help that person make changes that improve his/her/their health and well-being based on his/her/their individualized needs and social context. In other words, family medicine needs to deliver a holistic model of APC that is person centered, relationship based, recovery focused, and paid for comprehensively.
How does one get from “standard” primary care of today (the innermost circle of the FIGURE) to a framework that truly delivers on the promise of healing? I propose 3 steps to return holism to family medicine.
STEP 1: Start with comprehensive, coordinated primary care. We know that this works. Starfield and others demonstrated this 2 decades ago, defining and devising what we know as quality primary care—characterized by first-contact care, comprehensive primary care (CPC), continuous care, and coordinated care.22 This type of primary care improves outcomes, lowers costs, and is satisfying to patients and providers.23 The physician cares for the patient throughout that person’s entire life cycle and provides all evidence-based services needed to prevent and treat common conditions. Comprehensive primary care is positioned in the first circle outward from the innermost circle of the FIGURE.
As medicine has become increasingly complex and subspecialized, however, the ability to coordinate care is often frayed, adding cost and reducing quality.24-26 Today, comprehensive primary care needs enhanced coordination. At a minimum, this means coordinating services for:
- chronic disease management (outpatient and inpatient transitions and emergency department use)
- referral (specialists and tests)
- pharmacy services (including delivery and patient education support).
An example of a primary care system that meets these requirements is the Catalyst Health Network in central Texas, which supplies coordination services to more than 1000 comprehensive primary care practices and 1.5 million patients.27 The Catalyst Network makes money for those practices, saves money in the system, enhances patient and provider satisfaction, and improves population health in the community.27 I call this enhanced primary care (EPC), shown in the second circle out from the innermost circle of the FIGURE.
STEP 2: Add integrative medicine and mental health. EPC improves fragmented care but does not necessarily address a patient’s underlying determinants of healing. We know that health behaviors such as smoking cessation, avoidance of alcohol and drug abuse, improved diet, physical activity, sleep, and stress management contribute 40% to 60% of a person’s and a population’s health.10 In addition, evidence shows that behavioral health services, along with lifestyle change support, can even reverse many chronic diseases seen in primary care, such as obesity, diabetes, hypertension, cardiovascular disease, depression, and substance abuse.28,29
Continue to: Therefore, we need to add...
Therefore, we need to add routine mental health services and nonpharmacotherapeutic approaches (eg, complementary and alternative medicine) to primary care.30 Doing so requires that behavioral change and self-care become a central feature of the doctor–patient dialogue and team skills31 and be added to primary care.30,31 I call this integrative primary care (IPC), shown on the left side in the third circle out from the innermost circle of the FIGURE.
An example of IPC is Whole Health, an initiative of the US Veteran’s Health Administration. Whole Health empowers and informs a person-centered approach and integrates it into the delivery of routine care.32 Evaluation of Whole Health implementation, which involved more than 130,000 veterans followed for 2 years, found a net overall reduction in the total cost of care of 20%—saving nearly $650 million or, on average, more than $4500 per veteran.33
STEP 3: Address social determinants of health. Primary care will not fully be part of the solution for producing health and well-being unless it becomes instrumental in addressing the social determinants of health (SDH), defined as “… conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.”34 These determinants include not only basic needs, such as housing, food, safety, and transportation (ie, social needs), but also what are known as structural determinants, such as income, education, language, and racial and ethnic bias. Health care cannot solve all of these social ills,but it is increasingly being called on to be the nexus of coordination for services that address these needs when they affect health outcomes.35,36
Examples of health systems that provide for social needs include the free “food prescription” program of Pennsylvania’s Geisinger Health System, for patients with diabetes who do not have the resources to pay for food.37 This approach improves blood glucose control by patients and saves money on medications and other interventions. Similarly, Kaiser Permanente has experimented with housing vouchers for homeless patients,and most Federally Qualified Health Centers provide bus or other transportation tickets to patients for their appointments and free or discounted tests and specialty care.38
Implementing whole-person care for all
I propose that we make APC the central focus of family medicine. This model would comprise CPC, plus EPC, IPC, and community coordination to address SDH. This is expressed as:
CPC + EPC + IPC + SDH = APC
Continue to: APC would mean...
APC would mean health for the whole person and for all people. Again, the FIGURE shows how this model, encompassing the entire third circle out from the center circle, could be created from current models of care.
How do we pay for this? We already do—and way too much. The problem is not lack of money in the health care system but how it is organized and distributed. The Centers for Medicare and Medicaid Services and other payers are developing value-based payment models to help cover this type of care,39 but payers cannot pay for something if it is unavailable.
Can family physicians deliver APC? I believe they can, and have given a few examples here to show how this is already happening. To help primary care providers start to deliver APC in their system, my team and I have built the HOPE (Healing Oriented Practices & Environments) Note Toolkit to use in daily practice.40 These and other tools are being used by a number of large hospital systems and health care networks around the country. (You can download the HOPE Note Toolkit, at no cost, at https://drwaynejonas.com/resources/hope-note/.)
Whatever we call this new type of primary care, it needs to care for the whole person and to be available to all. It finds expression in these assertions:
- We cannot ignore an essential part of what a human being is and expect them to heal or become whole.
- We cannot ignore essential people in our communities and expect our costs to go down or our compassion to go up.
- We need to stop allowing family medicine to be co-opted by reductionism and its profits.
In sum, we need a new vision of primary care—like Engel’s holistic vision in the 1970s—to motivate us, and we need to return to fundamental concepts of how healing works in medicine.41
CORRESPONDENCE
Wayne B. Jonas, MD, Samueli Integrative Health Programs, 1800 Diagonal Road, Suite 617, Alexandria, VA 22314; [email protected].
1. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-136.
2. Schwartz MD, Durning S, Linzer M, et al. Changes in medical students’ views of internal medicine careers from 1990 to 2007. Arch Intern Med. 2011;171:744-749.
3. Bronchetti ET, Christensen GS, Hoynes HW. Local food prices, SNAP purchasing power, and child health. Cambridge, MA: National Bureau of Economic Research. June 2018. www.nber.org/papers/w24762?mc_cid=8c7211d34b&mc_eid=fbbc7df813. Accessed November 24, 2020.
4. Federal Student Aid, US Department of Education. Public Service Loan Forgiveness (PSLF). 2018. https://studentaid.ed.gov/sa/repay-loans/forgiveness-cancellation/public-service. Accessed November 24, 2020.
5. Aten B, Figueroa E, Martin T. Notes on estimating the multi-year regional price parities by 16 expenditure categories: 2005-2009. WP2011-03. Washington, DC: Bureau of Economic Analysis, US Department of Commerce; April 2011. www.bea.gov/system/files/papers/WP2011-3.pdf. Accessed November 24, 2020.
6. Aten BH, Figueroa EB, Martin TM. Regional price parities for states and metropolitan areas, 2006-2010. Washington, DC: Bureau of Economic Analysis, US Department of Commerce; August 2012. https://apps.bea.gov/scb/pdf/2012/08%20August/0812_regional_price_parities.pdf. Accessed November 24, 2020.
7. Stange KC, Ferrer RL. The paradox of primary care. Ann Fam Med. 2009;7:293-299.
8. Panel on Understanding Cross-national Health Differences Among High-income Countries, Committee on Population, Division of Behavioral and Social Sciences and Education, and Board on Population Health and Public Health Practice, National Research Council and Institute of Medicine of the National Academies. US Health in International Perspective: Shorter Lives, Poorer Health. Woolf SH, Aron L, eds. The National Academies Press; 2013.
9. Hood CM, Gennuso KP, Swain GR, et al. County health rankings: relationships between determinant factors and health outcomes. Am J Prev Med. 2016;50:129-135.
10. McGinnis JM, Williams-Russo P, Knickman JR. The case for more active policy attention to health promotion. Health Aff (Millwood). 2002;21:78-93.
11. Roeder A. Zip code better predictor of health than genetic code. Harvard T. H. Chan School of Public Health Web site. News release. August 4, 2014. www.hsph.harvard.edu/news/features/zip-code-better-predictor-of-health-than-genetic-code/. Accessed November 24, 2020.

12. US health map. Seattle, WA: University of Washington Institute for Health Metrics and Evaluation; March 13, 2018. www.healthdata.org/data-visualization/us-health-map. Accessed November 24, 2020.
13. Highfill T. Comparing estimates of U.S. health care expenditures by medical condition, 2000-2012. Survey of Current Business. 2016;1-5. https://apps.bea.gov/scb/pdf/2016/3%20March/0316_comparing_u.s._health_care_expenditures_by_medical_condition.pdf. Accessed November 24, 2020.
14. Waters H, Graf M. The Costs of Chronic Disease in the US. Washington, DC: Milken Institute; August 2018. https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf. Accessed November 24, 2020.
15. Meyer H. Health care spending will hit 19.4% of GDP in the next decade, CMS projects. Modern Health care. February 20, 2019. www.modernhealthcare.com/article/20190220/NEWS/190229989/healthcare-spending-will-hit-19-4-of-gdp-in-the-next-decade-cms-projects. Accessed November 24, 2020.
16. Woolf SH, Schoomaker H. Life expectancy and mortality rates in the United States, 1959-2017. JAMA. 2019;322:1996-2016.
17. Basu S, Berkowitz SA, Phillips RL, et al. Association of primary care physician supply with population mortality in the United States, 2005-2015. JAMA Intern Med. 2019;179:506-514.
18. Zack MM, Moriarty DG, Stroup DF, et al. Worsening trends in adult health-related quality of life and self-rated health—United States, 1993–2001. Public Health Rep. 2004;119:493-505.
19. Windover AK, Martinez K, Mercer, MB, et al. Correlates and outcomes of physician burnout within a large academic medical center. Research letter. JAMA Intern Med. 2018;178:856-858.
20. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283:516-529.
21. Buffett: Health care is a tapeworm on the economic system. CNBC Squawk Box. February 26, 2018. www.cnbc.com/video/2018/02/26/buffett-health-care-is-a-tapeworm-on-the-economic-system.html. Accessed November 24, 2020.
22. Starfield B. Primary Care: Concept, Evaluation, and Policy. Oxford University Press; 1992.
23. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457-502.
24. Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press (US); 2001.
25. Burton R. Health policy brief: improving care transitions. Health Affairs. September 13, 2012. www.healthaffairs.org/do/10.1377/hpb20120913.327236/full/healthpolicybrief_76.pdf. Accessed November 24, 2020.
26. Toulany A, Stukel TA, Kurdyak P, et al. Association of primary care continuity with outcomes following transition to adult care for adolescents with severe mental illness. JAMA Netw Open. 2019;2:e198415.
27. Helping communities thrive. Catalyst Health Network Web site. www.catalysthealthnetwork.com/. Accessed November 24, 2020.
28. Diabetes Prevention Program (DPP) Research Group. The Diabetes Prevention Program (DPP): description of lifestyle intervention. Diabetes Care. 2002;25:2165-2171.
29. Scherger JE. Lean and Fit: A Doctor’s Journey to Healthy Nutrition and Greater Wellness. 2nd ed. Scotts Valley, CA: CreateSpace Publishing; 2016.
30. Qaseem A, Wilt TJ, McLean RM, et al; . Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166:514-530.
31. Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013;32:207-214.
32. What is whole health? Washington, DC: US Department of Veterans Affairs. October 13, 2020. www.va.gov/patientcenteredcare/explore/about-whole-health.asp. Accessed November 25, 2020.
33. COVER Commission. Creating options for veterans’ expedited recovery. Final report. Washington, DC: US Veterans Administration. January 24, 2020. www.va.gov/COVER/docs/COVER-Commission-Final-Report-2020-01-24.pdf. Accessed November 24, 2020.
34. Social determinants of health. Washington, DC: Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. HealthyPeople.gov Web site. www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health. Accessed November 24, 2020.
35. Breslin E, Lambertino A. Medicaid and social determinants of health: adjusting payment and measuring health outcomes. Princeton University Woodrow Wilson School of Public and International Affairs, State Health and Value Strategies Program Web site. July 2017. www.shvs.org/wp-content/uploads/2017/07/SHVS_SocialDeterminants_HMA_July2017.pdf. Accessed November 24, 2020.
36. James CV. Actively addressing social determinants of health will help us achieve health equity. US Centers for Medicare & Medicaid Services Web site. April 26, 2019. www.cms.gov/blog/actively-addressing-social-determinants-health-will-help-us-achieve-health-equity. Accessed November 24, 2020.
37. Geisinger receives “Innovation in Advancing Health Equity” award. Geisinger Health Web site. April 24, 2018. www.geisinger.org/health-plan/news-releases/2018/04/23/19/28/geisinger-receives-innovation-in-advancing-health-equity-award. Accessed November 24, 2020.
38. Bresnick J. Kaiser Permanente launches full-network social determinants program. HealthITAnalytics Web site. May 6, 2019. https://healthitanalytics.com/news/kaiser-permanente-launches-full-network-social-determinants-program. Accessed November 25, 2020.
39. Medicare Payment Advisory Commission (MEDPAC). Physician and other health Professional services. In: Report to the Congress: Medicare Payment Policy. March 2016: 115-117. http://medpac.gov/docs/default-source/reports/chapter-4-physician-and-other-health-professional-services-march-2016-report-.pdf. Accessed November 24, 2020.
40. Jonas W. Helping patients with chronic diseases and conditions heal with the HOPE Note: integrative primary care case study. https://drwaynejonas.com/wp-content/uploads/2018/09/CS_HOPE-Note_FINAL.pdf. Accessed November 24, 2020.
41. Jonas W. How Healing Works. Berkley, CA: Lorena Jones Books; 2018.
Here is our problem: Family medicine has allowed itself, and its patients, to be picked apart by the forces of reductionism and a system that profits from the sick and suffering. We have lost sight of our purpose and our vision to care for the whole person. We have lost our way as healers.
The result is not only a decline in the specialty of family medicine as a leader in primary care but declining value and worsening outcomes in health care overall. We need to get our mojo back. We can do this by focusing less on trying to be all things to all people at all times, and more on creating better models for preventing, managing, and reversing chronic disease. This means providing health care that is person centered, relationship based, recovery focused, and paid for comprehensively.
I call this model Advanced Primary Care, or APC (FIGURE). In this article, I describe exemplars of APC from across the United States. I also provide tools to help you recover its central feature, holism—care of the whole person in mind, body, community, and spirit—in your practice, thus returning us to the core purpose of family medicine.
Holism is central to family medicine
More than 40 years ago, psychiatrist George Engel, MD, published a seminal article in Science that inspired a radical vision of how health care should be practiced.1 Called the biopsychosocial model, it stated what, in some ways, is obvious: Human beings are complex organisms embedded in complex environments made up of distinct, yet interacting, dimensions. These dimensions included physical, psychological, and social components. Engel’s radical proposition was that these dimensions are definable and measurable and that good medicine cannot afford to ignore any of them.
Engel’s assertion that good medicine requires holism was a clarion call during a time of rapidly expanding knowledge and subspecialization. That call was the inspiration for a new medical specialty called family medicine, which dared to proclaim that the best way to heal was to care for the whole person within the context of that person’s emotional and social environment. Family medicine reinvigorated primary care and grew rapidly, becoming a preeminent primary care specialty in the United States.
Continue to : Reductionism is relentless
Reductionism is relentless
But the forces of medicine were—and still are—driving relentlessly the other way. The science of the small and particular (reductionism), with dazzling technology and exploding subspecialty knowledge, and backed by powerful economic drivers, rewards health care for pulling the patient and the medical profession apart. We pay more to those who treat small parts of a person over a short period than to those who attend to the whole person over the lifetime.
Today, family medicine—for all of its common sense, scientific soundness, connectedness to patients, and demonstrated value—struggles to survive.2-6 The holistic vision of Engel is declining. The struggle in primary care is that its holistic vision gets co-opted by specialized medical science—and then it desperately attempts to apply those small and specialized tools to the care of patients in their wholeness. Holism is largely dead in health care, and everyone pays the consequences.7
Health care is losing its value
The damage from this decline in holism is not just to primary care but to the value of health care in general. Most medical care being delivered today—comprising diagnosis, treatment, and payment (the innermost circle of the FIGURE)—is not producing good health.8 Only 15% to 20% of the healing of an individual or a population comes from health care.9 The rest—nearly 80%—comes from other factors rarely addressed in the health care system: behavioral and lifestyle choices that people make in their daily life, including those related to food, movement, sleep, stress, and substance use.10 Increasingly, it is the economic and social determinants of health that influence this behavior and have a greater impact on health and lifespan than physiology or genes.11 The same social determinants of health also influence patients’ ability to obtain medical care and pursue a meaningful life.12
The result of this decline in holism and in the value of health care in general has been a relentless rise in the cost of medical care13-15 and the need for social services; declining life expectancy16,17 and quality of life18; growing patient dissatisfaction; and burnout in providers.19,20 Health care has become, as investor and business leader Warren Buffet remarked, the “tapeworm” of the economy and a major contributor to growing disparities in health and well-being between the haves and have-nots.21 Engel’s prediction that good medicine cannot afford to ignore holism has come to pass.
3-step solution:Return to whole-person care
Family medicine needs to return to whole-person care, but it can do so only if it attends to, and effectively delivers on, the prevention, treatment, and reversal of chronic disease and the enhancement of health and well-being. This can happen only if family medicine stops trying to be all things to all people at all times and, instead, focuses on what matters to the patient as a person.
Continue to: This means that the core...
This means that the core interaction in family medicine must be to assess the whole person—mind, body, social, spirit—and help that person make changes that improve his/her/their health and well-being based on his/her/their individualized needs and social context. In other words, family medicine needs to deliver a holistic model of APC that is person centered, relationship based, recovery focused, and paid for comprehensively.
How does one get from “standard” primary care of today (the innermost circle of the FIGURE) to a framework that truly delivers on the promise of healing? I propose 3 steps to return holism to family medicine.
STEP 1: Start with comprehensive, coordinated primary care. We know that this works. Starfield and others demonstrated this 2 decades ago, defining and devising what we know as quality primary care—characterized by first-contact care, comprehensive primary care (CPC), continuous care, and coordinated care.22 This type of primary care improves outcomes, lowers costs, and is satisfying to patients and providers.23 The physician cares for the patient throughout that person’s entire life cycle and provides all evidence-based services needed to prevent and treat common conditions. Comprehensive primary care is positioned in the first circle outward from the innermost circle of the FIGURE.
As medicine has become increasingly complex and subspecialized, however, the ability to coordinate care is often frayed, adding cost and reducing quality.24-26 Today, comprehensive primary care needs enhanced coordination. At a minimum, this means coordinating services for:
- chronic disease management (outpatient and inpatient transitions and emergency department use)
- referral (specialists and tests)
- pharmacy services (including delivery and patient education support).
An example of a primary care system that meets these requirements is the Catalyst Health Network in central Texas, which supplies coordination services to more than 1000 comprehensive primary care practices and 1.5 million patients.27 The Catalyst Network makes money for those practices, saves money in the system, enhances patient and provider satisfaction, and improves population health in the community.27 I call this enhanced primary care (EPC), shown in the second circle out from the innermost circle of the FIGURE.
STEP 2: Add integrative medicine and mental health. EPC improves fragmented care but does not necessarily address a patient’s underlying determinants of healing. We know that health behaviors such as smoking cessation, avoidance of alcohol and drug abuse, improved diet, physical activity, sleep, and stress management contribute 40% to 60% of a person’s and a population’s health.10 In addition, evidence shows that behavioral health services, along with lifestyle change support, can even reverse many chronic diseases seen in primary care, such as obesity, diabetes, hypertension, cardiovascular disease, depression, and substance abuse.28,29
Continue to: Therefore, we need to add...
Therefore, we need to add routine mental health services and nonpharmacotherapeutic approaches (eg, complementary and alternative medicine) to primary care.30 Doing so requires that behavioral change and self-care become a central feature of the doctor–patient dialogue and team skills31 and be added to primary care.30,31 I call this integrative primary care (IPC), shown on the left side in the third circle out from the innermost circle of the FIGURE.
An example of IPC is Whole Health, an initiative of the US Veteran’s Health Administration. Whole Health empowers and informs a person-centered approach and integrates it into the delivery of routine care.32 Evaluation of Whole Health implementation, which involved more than 130,000 veterans followed for 2 years, found a net overall reduction in the total cost of care of 20%—saving nearly $650 million or, on average, more than $4500 per veteran.33
STEP 3: Address social determinants of health. Primary care will not fully be part of the solution for producing health and well-being unless it becomes instrumental in addressing the social determinants of health (SDH), defined as “… conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.”34 These determinants include not only basic needs, such as housing, food, safety, and transportation (ie, social needs), but also what are known as structural determinants, such as income, education, language, and racial and ethnic bias. Health care cannot solve all of these social ills,but it is increasingly being called on to be the nexus of coordination for services that address these needs when they affect health outcomes.35,36
Examples of health systems that provide for social needs include the free “food prescription” program of Pennsylvania’s Geisinger Health System, for patients with diabetes who do not have the resources to pay for food.37 This approach improves blood glucose control by patients and saves money on medications and other interventions. Similarly, Kaiser Permanente has experimented with housing vouchers for homeless patients,and most Federally Qualified Health Centers provide bus or other transportation tickets to patients for their appointments and free or discounted tests and specialty care.38
Implementing whole-person care for all
I propose that we make APC the central focus of family medicine. This model would comprise CPC, plus EPC, IPC, and community coordination to address SDH. This is expressed as:
CPC + EPC + IPC + SDH = APC
Continue to: APC would mean...
APC would mean health for the whole person and for all people. Again, the FIGURE shows how this model, encompassing the entire third circle out from the center circle, could be created from current models of care.
How do we pay for this? We already do—and way too much. The problem is not lack of money in the health care system but how it is organized and distributed. The Centers for Medicare and Medicaid Services and other payers are developing value-based payment models to help cover this type of care,39 but payers cannot pay for something if it is unavailable.
Can family physicians deliver APC? I believe they can, and have given a few examples here to show how this is already happening. To help primary care providers start to deliver APC in their system, my team and I have built the HOPE (Healing Oriented Practices & Environments) Note Toolkit to use in daily practice.40 These and other tools are being used by a number of large hospital systems and health care networks around the country. (You can download the HOPE Note Toolkit, at no cost, at https://drwaynejonas.com/resources/hope-note/.)
Whatever we call this new type of primary care, it needs to care for the whole person and to be available to all. It finds expression in these assertions:
- We cannot ignore an essential part of what a human being is and expect them to heal or become whole.
- We cannot ignore essential people in our communities and expect our costs to go down or our compassion to go up.
- We need to stop allowing family medicine to be co-opted by reductionism and its profits.
In sum, we need a new vision of primary care—like Engel’s holistic vision in the 1970s—to motivate us, and we need to return to fundamental concepts of how healing works in medicine.41
CORRESPONDENCE
Wayne B. Jonas, MD, Samueli Integrative Health Programs, 1800 Diagonal Road, Suite 617, Alexandria, VA 22314; [email protected].
Here is our problem: Family medicine has allowed itself, and its patients, to be picked apart by the forces of reductionism and a system that profits from the sick and suffering. We have lost sight of our purpose and our vision to care for the whole person. We have lost our way as healers.
The result is not only a decline in the specialty of family medicine as a leader in primary care but declining value and worsening outcomes in health care overall. We need to get our mojo back. We can do this by focusing less on trying to be all things to all people at all times, and more on creating better models for preventing, managing, and reversing chronic disease. This means providing health care that is person centered, relationship based, recovery focused, and paid for comprehensively.
I call this model Advanced Primary Care, or APC (FIGURE). In this article, I describe exemplars of APC from across the United States. I also provide tools to help you recover its central feature, holism—care of the whole person in mind, body, community, and spirit—in your practice, thus returning us to the core purpose of family medicine.
Holism is central to family medicine
More than 40 years ago, psychiatrist George Engel, MD, published a seminal article in Science that inspired a radical vision of how health care should be practiced.1 Called the biopsychosocial model, it stated what, in some ways, is obvious: Human beings are complex organisms embedded in complex environments made up of distinct, yet interacting, dimensions. These dimensions included physical, psychological, and social components. Engel’s radical proposition was that these dimensions are definable and measurable and that good medicine cannot afford to ignore any of them.
Engel’s assertion that good medicine requires holism was a clarion call during a time of rapidly expanding knowledge and subspecialization. That call was the inspiration for a new medical specialty called family medicine, which dared to proclaim that the best way to heal was to care for the whole person within the context of that person’s emotional and social environment. Family medicine reinvigorated primary care and grew rapidly, becoming a preeminent primary care specialty in the United States.
Continue to : Reductionism is relentless
Reductionism is relentless
But the forces of medicine were—and still are—driving relentlessly the other way. The science of the small and particular (reductionism), with dazzling technology and exploding subspecialty knowledge, and backed by powerful economic drivers, rewards health care for pulling the patient and the medical profession apart. We pay more to those who treat small parts of a person over a short period than to those who attend to the whole person over the lifetime.
Today, family medicine—for all of its common sense, scientific soundness, connectedness to patients, and demonstrated value—struggles to survive.2-6 The holistic vision of Engel is declining. The struggle in primary care is that its holistic vision gets co-opted by specialized medical science—and then it desperately attempts to apply those small and specialized tools to the care of patients in their wholeness. Holism is largely dead in health care, and everyone pays the consequences.7
Health care is losing its value
The damage from this decline in holism is not just to primary care but to the value of health care in general. Most medical care being delivered today—comprising diagnosis, treatment, and payment (the innermost circle of the FIGURE)—is not producing good health.8 Only 15% to 20% of the healing of an individual or a population comes from health care.9 The rest—nearly 80%—comes from other factors rarely addressed in the health care system: behavioral and lifestyle choices that people make in their daily life, including those related to food, movement, sleep, stress, and substance use.10 Increasingly, it is the economic and social determinants of health that influence this behavior and have a greater impact on health and lifespan than physiology or genes.11 The same social determinants of health also influence patients’ ability to obtain medical care and pursue a meaningful life.12
The result of this decline in holism and in the value of health care in general has been a relentless rise in the cost of medical care13-15 and the need for social services; declining life expectancy16,17 and quality of life18; growing patient dissatisfaction; and burnout in providers.19,20 Health care has become, as investor and business leader Warren Buffet remarked, the “tapeworm” of the economy and a major contributor to growing disparities in health and well-being between the haves and have-nots.21 Engel’s prediction that good medicine cannot afford to ignore holism has come to pass.
3-step solution:Return to whole-person care
Family medicine needs to return to whole-person care, but it can do so only if it attends to, and effectively delivers on, the prevention, treatment, and reversal of chronic disease and the enhancement of health and well-being. This can happen only if family medicine stops trying to be all things to all people at all times and, instead, focuses on what matters to the patient as a person.
Continue to: This means that the core...
This means that the core interaction in family medicine must be to assess the whole person—mind, body, social, spirit—and help that person make changes that improve his/her/their health and well-being based on his/her/their individualized needs and social context. In other words, family medicine needs to deliver a holistic model of APC that is person centered, relationship based, recovery focused, and paid for comprehensively.
How does one get from “standard” primary care of today (the innermost circle of the FIGURE) to a framework that truly delivers on the promise of healing? I propose 3 steps to return holism to family medicine.
STEP 1: Start with comprehensive, coordinated primary care. We know that this works. Starfield and others demonstrated this 2 decades ago, defining and devising what we know as quality primary care—characterized by first-contact care, comprehensive primary care (CPC), continuous care, and coordinated care.22 This type of primary care improves outcomes, lowers costs, and is satisfying to patients and providers.23 The physician cares for the patient throughout that person’s entire life cycle and provides all evidence-based services needed to prevent and treat common conditions. Comprehensive primary care is positioned in the first circle outward from the innermost circle of the FIGURE.
As medicine has become increasingly complex and subspecialized, however, the ability to coordinate care is often frayed, adding cost and reducing quality.24-26 Today, comprehensive primary care needs enhanced coordination. At a minimum, this means coordinating services for:
- chronic disease management (outpatient and inpatient transitions and emergency department use)
- referral (specialists and tests)
- pharmacy services (including delivery and patient education support).
An example of a primary care system that meets these requirements is the Catalyst Health Network in central Texas, which supplies coordination services to more than 1000 comprehensive primary care practices and 1.5 million patients.27 The Catalyst Network makes money for those practices, saves money in the system, enhances patient and provider satisfaction, and improves population health in the community.27 I call this enhanced primary care (EPC), shown in the second circle out from the innermost circle of the FIGURE.
STEP 2: Add integrative medicine and mental health. EPC improves fragmented care but does not necessarily address a patient’s underlying determinants of healing. We know that health behaviors such as smoking cessation, avoidance of alcohol and drug abuse, improved diet, physical activity, sleep, and stress management contribute 40% to 60% of a person’s and a population’s health.10 In addition, evidence shows that behavioral health services, along with lifestyle change support, can even reverse many chronic diseases seen in primary care, such as obesity, diabetes, hypertension, cardiovascular disease, depression, and substance abuse.28,29
Continue to: Therefore, we need to add...
Therefore, we need to add routine mental health services and nonpharmacotherapeutic approaches (eg, complementary and alternative medicine) to primary care.30 Doing so requires that behavioral change and self-care become a central feature of the doctor–patient dialogue and team skills31 and be added to primary care.30,31 I call this integrative primary care (IPC), shown on the left side in the third circle out from the innermost circle of the FIGURE.
An example of IPC is Whole Health, an initiative of the US Veteran’s Health Administration. Whole Health empowers and informs a person-centered approach and integrates it into the delivery of routine care.32 Evaluation of Whole Health implementation, which involved more than 130,000 veterans followed for 2 years, found a net overall reduction in the total cost of care of 20%—saving nearly $650 million or, on average, more than $4500 per veteran.33
STEP 3: Address social determinants of health. Primary care will not fully be part of the solution for producing health and well-being unless it becomes instrumental in addressing the social determinants of health (SDH), defined as “… conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.”34 These determinants include not only basic needs, such as housing, food, safety, and transportation (ie, social needs), but also what are known as structural determinants, such as income, education, language, and racial and ethnic bias. Health care cannot solve all of these social ills,but it is increasingly being called on to be the nexus of coordination for services that address these needs when they affect health outcomes.35,36
Examples of health systems that provide for social needs include the free “food prescription” program of Pennsylvania’s Geisinger Health System, for patients with diabetes who do not have the resources to pay for food.37 This approach improves blood glucose control by patients and saves money on medications and other interventions. Similarly, Kaiser Permanente has experimented with housing vouchers for homeless patients,and most Federally Qualified Health Centers provide bus or other transportation tickets to patients for their appointments and free or discounted tests and specialty care.38
Implementing whole-person care for all
I propose that we make APC the central focus of family medicine. This model would comprise CPC, plus EPC, IPC, and community coordination to address SDH. This is expressed as:
CPC + EPC + IPC + SDH = APC
Continue to: APC would mean...
APC would mean health for the whole person and for all people. Again, the FIGURE shows how this model, encompassing the entire third circle out from the center circle, could be created from current models of care.
How do we pay for this? We already do—and way too much. The problem is not lack of money in the health care system but how it is organized and distributed. The Centers for Medicare and Medicaid Services and other payers are developing value-based payment models to help cover this type of care,39 but payers cannot pay for something if it is unavailable.
Can family physicians deliver APC? I believe they can, and have given a few examples here to show how this is already happening. To help primary care providers start to deliver APC in their system, my team and I have built the HOPE (Healing Oriented Practices & Environments) Note Toolkit to use in daily practice.40 These and other tools are being used by a number of large hospital systems and health care networks around the country. (You can download the HOPE Note Toolkit, at no cost, at https://drwaynejonas.com/resources/hope-note/.)
Whatever we call this new type of primary care, it needs to care for the whole person and to be available to all. It finds expression in these assertions:
- We cannot ignore an essential part of what a human being is and expect them to heal or become whole.
- We cannot ignore essential people in our communities and expect our costs to go down or our compassion to go up.
- We need to stop allowing family medicine to be co-opted by reductionism and its profits.
In sum, we need a new vision of primary care—like Engel’s holistic vision in the 1970s—to motivate us, and we need to return to fundamental concepts of how healing works in medicine.41
CORRESPONDENCE
Wayne B. Jonas, MD, Samueli Integrative Health Programs, 1800 Diagonal Road, Suite 617, Alexandria, VA 22314; [email protected].
1. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-136.
2. Schwartz MD, Durning S, Linzer M, et al. Changes in medical students’ views of internal medicine careers from 1990 to 2007. Arch Intern Med. 2011;171:744-749.
3. Bronchetti ET, Christensen GS, Hoynes HW. Local food prices, SNAP purchasing power, and child health. Cambridge, MA: National Bureau of Economic Research. June 2018. www.nber.org/papers/w24762?mc_cid=8c7211d34b&mc_eid=fbbc7df813. Accessed November 24, 2020.
4. Federal Student Aid, US Department of Education. Public Service Loan Forgiveness (PSLF). 2018. https://studentaid.ed.gov/sa/repay-loans/forgiveness-cancellation/public-service. Accessed November 24, 2020.
5. Aten B, Figueroa E, Martin T. Notes on estimating the multi-year regional price parities by 16 expenditure categories: 2005-2009. WP2011-03. Washington, DC: Bureau of Economic Analysis, US Department of Commerce; April 2011. www.bea.gov/system/files/papers/WP2011-3.pdf. Accessed November 24, 2020.
6. Aten BH, Figueroa EB, Martin TM. Regional price parities for states and metropolitan areas, 2006-2010. Washington, DC: Bureau of Economic Analysis, US Department of Commerce; August 2012. https://apps.bea.gov/scb/pdf/2012/08%20August/0812_regional_price_parities.pdf. Accessed November 24, 2020.
7. Stange KC, Ferrer RL. The paradox of primary care. Ann Fam Med. 2009;7:293-299.
8. Panel on Understanding Cross-national Health Differences Among High-income Countries, Committee on Population, Division of Behavioral and Social Sciences and Education, and Board on Population Health and Public Health Practice, National Research Council and Institute of Medicine of the National Academies. US Health in International Perspective: Shorter Lives, Poorer Health. Woolf SH, Aron L, eds. The National Academies Press; 2013.
9. Hood CM, Gennuso KP, Swain GR, et al. County health rankings: relationships between determinant factors and health outcomes. Am J Prev Med. 2016;50:129-135.
10. McGinnis JM, Williams-Russo P, Knickman JR. The case for more active policy attention to health promotion. Health Aff (Millwood). 2002;21:78-93.
11. Roeder A. Zip code better predictor of health than genetic code. Harvard T. H. Chan School of Public Health Web site. News release. August 4, 2014. www.hsph.harvard.edu/news/features/zip-code-better-predictor-of-health-than-genetic-code/. Accessed November 24, 2020.
12. US health map. Seattle, WA: University of Washington Institute for Health Metrics and Evaluation; March 13, 2018. www.healthdata.org/data-visualization/us-health-map. Accessed November 24, 2020.
13. Highfill T. Comparing estimates of U.S. health care expenditures by medical condition, 2000-2012. Survey of Current Business. 2016;1-5. https://apps.bea.gov/scb/pdf/2016/3%20March/0316_comparing_u.s._health_care_expenditures_by_medical_condition.pdf. Accessed November 24, 2020.
14. Waters H, Graf M. The Costs of Chronic Disease in the US. Washington, DC: Milken Institute; August 2018. https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf. Accessed November 24, 2020.
15. Meyer H. Health care spending will hit 19.4% of GDP in the next decade, CMS projects. Modern Health care. February 20, 2019. www.modernhealthcare.com/article/20190220/NEWS/190229989/healthcare-spending-will-hit-19-4-of-gdp-in-the-next-decade-cms-projects. Accessed November 24, 2020.
16. Woolf SH, Schoomaker H. Life expectancy and mortality rates in the United States, 1959-2017. JAMA. 2019;322:1996-2016.
17. Basu S, Berkowitz SA, Phillips RL, et al. Association of primary care physician supply with population mortality in the United States, 2005-2015. JAMA Intern Med. 2019;179:506-514.
18. Zack MM, Moriarty DG, Stroup DF, et al. Worsening trends in adult health-related quality of life and self-rated health—United States, 1993–2001. Public Health Rep. 2004;119:493-505.
19. Windover AK, Martinez K, Mercer, MB, et al. Correlates and outcomes of physician burnout within a large academic medical center. Research letter. JAMA Intern Med. 2018;178:856-858.
20. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283:516-529.
21. Buffett: Health care is a tapeworm on the economic system. CNBC Squawk Box. February 26, 2018. www.cnbc.com/video/2018/02/26/buffett-health-care-is-a-tapeworm-on-the-economic-system.html. Accessed November 24, 2020.
22. Starfield B. Primary Care: Concept, Evaluation, and Policy. Oxford University Press; 1992.
23. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457-502.
24. Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press (US); 2001.
25. Burton R. Health policy brief: improving care transitions. Health Affairs. September 13, 2012. www.healthaffairs.org/do/10.1377/hpb20120913.327236/full/healthpolicybrief_76.pdf. Accessed November 24, 2020.
26. Toulany A, Stukel TA, Kurdyak P, et al. Association of primary care continuity with outcomes following transition to adult care for adolescents with severe mental illness. JAMA Netw Open. 2019;2:e198415.
27. Helping communities thrive. Catalyst Health Network Web site. www.catalysthealthnetwork.com/. Accessed November 24, 2020.
28. Diabetes Prevention Program (DPP) Research Group. The Diabetes Prevention Program (DPP): description of lifestyle intervention. Diabetes Care. 2002;25:2165-2171.
29. Scherger JE. Lean and Fit: A Doctor’s Journey to Healthy Nutrition and Greater Wellness. 2nd ed. Scotts Valley, CA: CreateSpace Publishing; 2016.
30. Qaseem A, Wilt TJ, McLean RM, et al; . Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166:514-530.
31. Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013;32:207-214.
32. What is whole health? Washington, DC: US Department of Veterans Affairs. October 13, 2020. www.va.gov/patientcenteredcare/explore/about-whole-health.asp. Accessed November 25, 2020.
33. COVER Commission. Creating options for veterans’ expedited recovery. Final report. Washington, DC: US Veterans Administration. January 24, 2020. www.va.gov/COVER/docs/COVER-Commission-Final-Report-2020-01-24.pdf. Accessed November 24, 2020.
34. Social determinants of health. Washington, DC: Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. HealthyPeople.gov Web site. www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health. Accessed November 24, 2020.
35. Breslin E, Lambertino A. Medicaid and social determinants of health: adjusting payment and measuring health outcomes. Princeton University Woodrow Wilson School of Public and International Affairs, State Health and Value Strategies Program Web site. July 2017. www.shvs.org/wp-content/uploads/2017/07/SHVS_SocialDeterminants_HMA_July2017.pdf. Accessed November 24, 2020.
36. James CV. Actively addressing social determinants of health will help us achieve health equity. US Centers for Medicare & Medicaid Services Web site. April 26, 2019. www.cms.gov/blog/actively-addressing-social-determinants-health-will-help-us-achieve-health-equity. Accessed November 24, 2020.
37. Geisinger receives “Innovation in Advancing Health Equity” award. Geisinger Health Web site. April 24, 2018. www.geisinger.org/health-plan/news-releases/2018/04/23/19/28/geisinger-receives-innovation-in-advancing-health-equity-award. Accessed November 24, 2020.
38. Bresnick J. Kaiser Permanente launches full-network social determinants program. HealthITAnalytics Web site. May 6, 2019. https://healthitanalytics.com/news/kaiser-permanente-launches-full-network-social-determinants-program. Accessed November 25, 2020.
39. Medicare Payment Advisory Commission (MEDPAC). Physician and other health Professional services. In: Report to the Congress: Medicare Payment Policy. March 2016: 115-117. http://medpac.gov/docs/default-source/reports/chapter-4-physician-and-other-health-professional-services-march-2016-report-.pdf. Accessed November 24, 2020.
40. Jonas W. Helping patients with chronic diseases and conditions heal with the HOPE Note: integrative primary care case study. https://drwaynejonas.com/wp-content/uploads/2018/09/CS_HOPE-Note_FINAL.pdf. Accessed November 24, 2020.
41. Jonas W. How Healing Works. Berkley, CA: Lorena Jones Books; 2018.
1. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-136.
2. Schwartz MD, Durning S, Linzer M, et al. Changes in medical students’ views of internal medicine careers from 1990 to 2007. Arch Intern Med. 2011;171:744-749.
3. Bronchetti ET, Christensen GS, Hoynes HW. Local food prices, SNAP purchasing power, and child health. Cambridge, MA: National Bureau of Economic Research. June 2018. www.nber.org/papers/w24762?mc_cid=8c7211d34b&mc_eid=fbbc7df813. Accessed November 24, 2020.
4. Federal Student Aid, US Department of Education. Public Service Loan Forgiveness (PSLF). 2018. https://studentaid.ed.gov/sa/repay-loans/forgiveness-cancellation/public-service. Accessed November 24, 2020.
5. Aten B, Figueroa E, Martin T. Notes on estimating the multi-year regional price parities by 16 expenditure categories: 2005-2009. WP2011-03. Washington, DC: Bureau of Economic Analysis, US Department of Commerce; April 2011. www.bea.gov/system/files/papers/WP2011-3.pdf. Accessed November 24, 2020.
6. Aten BH, Figueroa EB, Martin TM. Regional price parities for states and metropolitan areas, 2006-2010. Washington, DC: Bureau of Economic Analysis, US Department of Commerce; August 2012. https://apps.bea.gov/scb/pdf/2012/08%20August/0812_regional_price_parities.pdf. Accessed November 24, 2020.
7. Stange KC, Ferrer RL. The paradox of primary care. Ann Fam Med. 2009;7:293-299.
8. Panel on Understanding Cross-national Health Differences Among High-income Countries, Committee on Population, Division of Behavioral and Social Sciences and Education, and Board on Population Health and Public Health Practice, National Research Council and Institute of Medicine of the National Academies. US Health in International Perspective: Shorter Lives, Poorer Health. Woolf SH, Aron L, eds. The National Academies Press; 2013.
9. Hood CM, Gennuso KP, Swain GR, et al. County health rankings: relationships between determinant factors and health outcomes. Am J Prev Med. 2016;50:129-135.
10. McGinnis JM, Williams-Russo P, Knickman JR. The case for more active policy attention to health promotion. Health Aff (Millwood). 2002;21:78-93.
11. Roeder A. Zip code better predictor of health than genetic code. Harvard T. H. Chan School of Public Health Web site. News release. August 4, 2014. www.hsph.harvard.edu/news/features/zip-code-better-predictor-of-health-than-genetic-code/. Accessed November 24, 2020.
12. US health map. Seattle, WA: University of Washington Institute for Health Metrics and Evaluation; March 13, 2018. www.healthdata.org/data-visualization/us-health-map. Accessed November 24, 2020.
13. Highfill T. Comparing estimates of U.S. health care expenditures by medical condition, 2000-2012. Survey of Current Business. 2016;1-5. https://apps.bea.gov/scb/pdf/2016/3%20March/0316_comparing_u.s._health_care_expenditures_by_medical_condition.pdf. Accessed November 24, 2020.
14. Waters H, Graf M. The Costs of Chronic Disease in the US. Washington, DC: Milken Institute; August 2018. https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf. Accessed November 24, 2020.
15. Meyer H. Health care spending will hit 19.4% of GDP in the next decade, CMS projects. Modern Health care. February 20, 2019. www.modernhealthcare.com/article/20190220/NEWS/190229989/healthcare-spending-will-hit-19-4-of-gdp-in-the-next-decade-cms-projects. Accessed November 24, 2020.
16. Woolf SH, Schoomaker H. Life expectancy and mortality rates in the United States, 1959-2017. JAMA. 2019;322:1996-2016.
17. Basu S, Berkowitz SA, Phillips RL, et al. Association of primary care physician supply with population mortality in the United States, 2005-2015. JAMA Intern Med. 2019;179:506-514.
18. Zack MM, Moriarty DG, Stroup DF, et al. Worsening trends in adult health-related quality of life and self-rated health—United States, 1993–2001. Public Health Rep. 2004;119:493-505.
19. Windover AK, Martinez K, Mercer, MB, et al. Correlates and outcomes of physician burnout within a large academic medical center. Research letter. JAMA Intern Med. 2018;178:856-858.
20. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283:516-529.
21. Buffett: Health care is a tapeworm on the economic system. CNBC Squawk Box. February 26, 2018. www.cnbc.com/video/2018/02/26/buffett-health-care-is-a-tapeworm-on-the-economic-system.html. Accessed November 24, 2020.
22. Starfield B. Primary Care: Concept, Evaluation, and Policy. Oxford University Press; 1992.
23. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457-502.
24. Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press (US); 2001.
25. Burton R. Health policy brief: improving care transitions. Health Affairs. September 13, 2012. www.healthaffairs.org/do/10.1377/hpb20120913.327236/full/healthpolicybrief_76.pdf. Accessed November 24, 2020.
26. Toulany A, Stukel TA, Kurdyak P, et al. Association of primary care continuity with outcomes following transition to adult care for adolescents with severe mental illness. JAMA Netw Open. 2019;2:e198415.
27. Helping communities thrive. Catalyst Health Network Web site. www.catalysthealthnetwork.com/. Accessed November 24, 2020.
28. Diabetes Prevention Program (DPP) Research Group. The Diabetes Prevention Program (DPP): description of lifestyle intervention. Diabetes Care. 2002;25:2165-2171.
29. Scherger JE. Lean and Fit: A Doctor’s Journey to Healthy Nutrition and Greater Wellness. 2nd ed. Scotts Valley, CA: CreateSpace Publishing; 2016.
30. Qaseem A, Wilt TJ, McLean RM, et al; . Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166:514-530.
31. Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013;32:207-214.
32. What is whole health? Washington, DC: US Department of Veterans Affairs. October 13, 2020. www.va.gov/patientcenteredcare/explore/about-whole-health.asp. Accessed November 25, 2020.
33. COVER Commission. Creating options for veterans’ expedited recovery. Final report. Washington, DC: US Veterans Administration. January 24, 2020. www.va.gov/COVER/docs/COVER-Commission-Final-Report-2020-01-24.pdf. Accessed November 24, 2020.
34. Social determinants of health. Washington, DC: Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. HealthyPeople.gov Web site. www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health. Accessed November 24, 2020.
35. Breslin E, Lambertino A. Medicaid and social determinants of health: adjusting payment and measuring health outcomes. Princeton University Woodrow Wilson School of Public and International Affairs, State Health and Value Strategies Program Web site. July 2017. www.shvs.org/wp-content/uploads/2017/07/SHVS_SocialDeterminants_HMA_July2017.pdf. Accessed November 24, 2020.
36. James CV. Actively addressing social determinants of health will help us achieve health equity. US Centers for Medicare & Medicaid Services Web site. April 26, 2019. www.cms.gov/blog/actively-addressing-social-determinants-health-will-help-us-achieve-health-equity. Accessed November 24, 2020.
37. Geisinger receives “Innovation in Advancing Health Equity” award. Geisinger Health Web site. April 24, 2018. www.geisinger.org/health-plan/news-releases/2018/04/23/19/28/geisinger-receives-innovation-in-advancing-health-equity-award. Accessed November 24, 2020.
38. Bresnick J. Kaiser Permanente launches full-network social determinants program. HealthITAnalytics Web site. May 6, 2019. https://healthitanalytics.com/news/kaiser-permanente-launches-full-network-social-determinants-program. Accessed November 25, 2020.
39. Medicare Payment Advisory Commission (MEDPAC). Physician and other health Professional services. In: Report to the Congress: Medicare Payment Policy. March 2016: 115-117. http://medpac.gov/docs/default-source/reports/chapter-4-physician-and-other-health-professional-services-march-2016-report-.pdf. Accessed November 24, 2020.
40. Jonas W. Helping patients with chronic diseases and conditions heal with the HOPE Note: integrative primary care case study. https://drwaynejonas.com/wp-content/uploads/2018/09/CS_HOPE-Note_FINAL.pdf. Accessed November 24, 2020.
41. Jonas W. How Healing Works. Berkley, CA: Lorena Jones Books; 2018.
PRACTICE RECOMMENDATIONS
❯ Build care teams into your practice so that you integrate “what matters” into the center of the clinical encounter. C
❯ Add practice approaches that help patients engage in healthy lifestyles and that remove social and economic barriers for improving health and well-being. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series

Whole-person care: Our foundation, our future
In this issue of The Journal of Family Practice, Dr. Wayne Jonas explains his model for Advanced Primary Care (see page 493). The figure he uses to illustrate Advanced Primary Care is compelling, and the effectiveness of this model of health care is supported by a great deal of research and evaluation over the past 20 years. Let me provide some historical context.
The idea that healing requires more than curative, biology-based medical care dates back to Greek mythology. Asclepius, the god of medicine, had 5 daughters, Hygeia (the goddess of good health and hygiene), Iaso (cures and remedies), Aceso (healing wounds), Aegle (radiant good health), and Panacea (cures).1 Clearly, the Greeks believed that integrative care is essential for maintaining good health!
Modern, scientific medicine is a relatively recent development in human history. Other traditions of healing such as acupuncture and herbal medicines are actually much older than mainstream Western medicine. But they come together in family medicine—a specialty founded on the principles of whole person, whole family, and whole community care.
The first modern model of comprehensive care, the patient-centered medical home (PCMH), was introduced by the American Academy of Pediatrics in 1967. This idea caught on widely and was institutionalized by the National Committee for Quality Assurance in 2008 with PCMH certification.
Advanced Primary Care is the latest and best rendition of comprehensive primary health care. Funding this model through our current payment mechanisms, however, has been difficult because of the need to support social and behavioral interventions in addition to medical care—areas of care not traditionally paid for by medical premiums. In 2011, CMS collaborated with private insurers in a national demonstration project to test the financial feasibility of implementing Advanced Primary Care. Some organizations have been highly successful; others not as much.
We can no longer go “halfway” into whole-person care. The COVID-19 pandemic has put a spotlight on our need to transform payment models away from fee-for-service to reimbursement for whole person primary care. Our nation’s health and the viability of our health care system depend on it.
PS: I recommend reading Dr. Jonas’ book, How Healing Works, which provides a scientific rationale for the application of whole-person care to healing.
1. Theoi Greek Mythology Web site. https://www.theoi.com/Ouranios/Asklepios.html. Accessed November 30, 2020.
Editor-in-Chief

Editor-in-Chief
Editor-in-Chief
In this issue of The Journal of Family Practice, Dr. Wayne Jonas explains his model for Advanced Primary Care (see page 493). The figure he uses to illustrate Advanced Primary Care is compelling, and the effectiveness of this model of health care is supported by a great deal of research and evaluation over the past 20 years. Let me provide some historical context.
The idea that healing requires more than curative, biology-based medical care dates back to Greek mythology. Asclepius, the god of medicine, had 5 daughters, Hygeia (the goddess of good health and hygiene), Iaso (cures and remedies), Aceso (healing wounds), Aegle (radiant good health), and Panacea (cures).1 Clearly, the Greeks believed that integrative care is essential for maintaining good health!
Modern, scientific medicine is a relatively recent development in human history. Other traditions of healing such as acupuncture and herbal medicines are actually much older than mainstream Western medicine. But they come together in family medicine—a specialty founded on the principles of whole person, whole family, and whole community care.
The first modern model of comprehensive care, the patient-centered medical home (PCMH), was introduced by the American Academy of Pediatrics in 1967. This idea caught on widely and was institutionalized by the National Committee for Quality Assurance in 2008 with PCMH certification.
Advanced Primary Care is the latest and best rendition of comprehensive primary health care. Funding this model through our current payment mechanisms, however, has been difficult because of the need to support social and behavioral interventions in addition to medical care—areas of care not traditionally paid for by medical premiums. In 2011, CMS collaborated with private insurers in a national demonstration project to test the financial feasibility of implementing Advanced Primary Care. Some organizations have been highly successful; others not as much.
We can no longer go “halfway” into whole-person care. The COVID-19 pandemic has put a spotlight on our need to transform payment models away from fee-for-service to reimbursement for whole person primary care. Our nation’s health and the viability of our health care system depend on it.
PS: I recommend reading Dr. Jonas’ book, How Healing Works, which provides a scientific rationale for the application of whole-person care to healing.
In this issue of The Journal of Family Practice, Dr. Wayne Jonas explains his model for Advanced Primary Care (see page 493). The figure he uses to illustrate Advanced Primary Care is compelling, and the effectiveness of this model of health care is supported by a great deal of research and evaluation over the past 20 years. Let me provide some historical context.
The idea that healing requires more than curative, biology-based medical care dates back to Greek mythology. Asclepius, the god of medicine, had 5 daughters, Hygeia (the goddess of good health and hygiene), Iaso (cures and remedies), Aceso (healing wounds), Aegle (radiant good health), and Panacea (cures).1 Clearly, the Greeks believed that integrative care is essential for maintaining good health!
Modern, scientific medicine is a relatively recent development in human history. Other traditions of healing such as acupuncture and herbal medicines are actually much older than mainstream Western medicine. But they come together in family medicine—a specialty founded on the principles of whole person, whole family, and whole community care.
The first modern model of comprehensive care, the patient-centered medical home (PCMH), was introduced by the American Academy of Pediatrics in 1967. This idea caught on widely and was institutionalized by the National Committee for Quality Assurance in 2008 with PCMH certification.
Advanced Primary Care is the latest and best rendition of comprehensive primary health care. Funding this model through our current payment mechanisms, however, has been difficult because of the need to support social and behavioral interventions in addition to medical care—areas of care not traditionally paid for by medical premiums. In 2011, CMS collaborated with private insurers in a national demonstration project to test the financial feasibility of implementing Advanced Primary Care. Some organizations have been highly successful; others not as much.
We can no longer go “halfway” into whole-person care. The COVID-19 pandemic has put a spotlight on our need to transform payment models away from fee-for-service to reimbursement for whole person primary care. Our nation’s health and the viability of our health care system depend on it.
PS: I recommend reading Dr. Jonas’ book, How Healing Works, which provides a scientific rationale for the application of whole-person care to healing.
1. Theoi Greek Mythology Web site. https://www.theoi.com/Ouranios/Asklepios.html. Accessed November 30, 2020.
1. Theoi Greek Mythology Web site. https://www.theoi.com/Ouranios/Asklepios.html. Accessed November 30, 2020.
New residency matching sets record, says NRMP
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.
beginning in 2021, the NRMP reported.
“Specifically, the 2020 MSMP included 6,847 applicants submitting certified rank order lists (an 8.9% increase), 2042 programs submitting certified rank order lists (a 4.3% increase), 5,734 positions (a 2.8% increase), and 5,208 positions filled (a 6.1% increase),” according to a news release.
The MSMP now includes 14 internal medicine subspecialties and four sub-subspecialties. The MSMP offered 5,734 positions this year, and 5,208 (90.8%) were successfully filled. That represents an increase of almost 3 percentage points, compared with last year’s results.
Among those subspecialties that offered 30 positions or more, the most competitive were allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, gastroenterology, hematology and oncology, and pulmonary/critical care. Each of those filled at least 95% of available slots. More than half of the positions were filled by U.S. MDs.
By contrast, the least competitive subspecialties were geriatric medicine and nephrology. Programs in these two fields filled less than 75% of positions offered. Less than 45% were filled by U.S. MDs.
More than 76% of the 6,847 applicants who submitted rank order lists (5,208) matched into residency programs.
The number of U.S. MDs in this category increased nearly 7% over last year, with a total of 2,935. The number of DO graduates increased as well, with a total of 855, which was 9.6% more than the previous year.
More U.S. citizens who graduated from international medical schools matched this year as well; 1,087 placed into subspecialty residency, a 9% increase, compared with last year.
A version of this article originally appeared on Medscape.com.