User login
Regular Physical Activity Linked to Larger Brain Volume
TOPLINE:
, new data suggest.
METHODOLOGY:
- The potential neuroprotective effects of regular physical activity on brain structure are unclear despite reported links between physical activity and reduced dementia risk.
- To investigate, researchers analyzed MRI brain scans from 10,125 healthy adults (mean age, 53 years; 52% male) who self-reported their level of physical activity.
- Moderate to vigorous physical activities, defined as those increasing respiration and pulse rate for at least 10 continuous minutes, was modeled with brain volumes, adjusting for covariates.
- The threshold for defining physically active (vs nonactive) adults was intentionally set at 2.5 days per week, a level far lower than current guidelines.
TAKEAWAY:
- Three quarters of the cohort reported engaging in moderate to vigorous physical activity approximately 4 days per week.
- Physically active adults tended to be younger, with a higher proportion of White individuals, and with lower rates of hypertension and type 2 diabetes.
- After adjusting for multiple factors, increased days of moderate to vigorous activity correlated with larger normalized brain volume in multiple regions including total gray matter; white matter; hippocampus; and frontal, parietal, and occipital lobes.
IN PRACTICE:
“We found that even moderate levels of physical activity, such as taking fewer than 4,000 steps a day, can have a positive effect on brain health. This is much less than the often-suggested 10,000 steps, making it a more achievable goal for many people,” co-author David Merrill, MD, with Pacific Brain Health Center, Santa Monica, California, said in a statement.
SOURCE:
The study, with first author Cyrus A. Raji, MD, PhD, Washington University School of Medicine, St. Louis, was published online in the Journal of Alzheimer’s Disease.
LIMITATIONS:
Participants self-reported physical activity in the past 2 weeks, which does not reflect a lifetime of activity levels. The correlation identified between physical activity and brain volumes may not be solely attributable to physical activity alone.
DISCLOSURES:
The study received funding from several health centers and foundations. Dr. Raji consults for Brainreader ApS, Neurevolution LLC, Apollo Health, Voxelwise Imaging Technology, and Pacific Neuroscience Foundation and is an editorial board member of the Journal of Alzheimer’s Disease but was not involved in the peer-review process.
A version of this article appeared on Medscape.com.
TOPLINE:
, new data suggest.
METHODOLOGY:
- The potential neuroprotective effects of regular physical activity on brain structure are unclear despite reported links between physical activity and reduced dementia risk.
- To investigate, researchers analyzed MRI brain scans from 10,125 healthy adults (mean age, 53 years; 52% male) who self-reported their level of physical activity.
- Moderate to vigorous physical activities, defined as those increasing respiration and pulse rate for at least 10 continuous minutes, was modeled with brain volumes, adjusting for covariates.
- The threshold for defining physically active (vs nonactive) adults was intentionally set at 2.5 days per week, a level far lower than current guidelines.
TAKEAWAY:
- Three quarters of the cohort reported engaging in moderate to vigorous physical activity approximately 4 days per week.
- Physically active adults tended to be younger, with a higher proportion of White individuals, and with lower rates of hypertension and type 2 diabetes.
- After adjusting for multiple factors, increased days of moderate to vigorous activity correlated with larger normalized brain volume in multiple regions including total gray matter; white matter; hippocampus; and frontal, parietal, and occipital lobes.
IN PRACTICE:
“We found that even moderate levels of physical activity, such as taking fewer than 4,000 steps a day, can have a positive effect on brain health. This is much less than the often-suggested 10,000 steps, making it a more achievable goal for many people,” co-author David Merrill, MD, with Pacific Brain Health Center, Santa Monica, California, said in a statement.
SOURCE:
The study, with first author Cyrus A. Raji, MD, PhD, Washington University School of Medicine, St. Louis, was published online in the Journal of Alzheimer’s Disease.
LIMITATIONS:
Participants self-reported physical activity in the past 2 weeks, which does not reflect a lifetime of activity levels. The correlation identified between physical activity and brain volumes may not be solely attributable to physical activity alone.
DISCLOSURES:
The study received funding from several health centers and foundations. Dr. Raji consults for Brainreader ApS, Neurevolution LLC, Apollo Health, Voxelwise Imaging Technology, and Pacific Neuroscience Foundation and is an editorial board member of the Journal of Alzheimer’s Disease but was not involved in the peer-review process.
A version of this article appeared on Medscape.com.
TOPLINE:
, new data suggest.
METHODOLOGY:
- The potential neuroprotective effects of regular physical activity on brain structure are unclear despite reported links between physical activity and reduced dementia risk.
- To investigate, researchers analyzed MRI brain scans from 10,125 healthy adults (mean age, 53 years; 52% male) who self-reported their level of physical activity.
- Moderate to vigorous physical activities, defined as those increasing respiration and pulse rate for at least 10 continuous minutes, was modeled with brain volumes, adjusting for covariates.
- The threshold for defining physically active (vs nonactive) adults was intentionally set at 2.5 days per week, a level far lower than current guidelines.
TAKEAWAY:
- Three quarters of the cohort reported engaging in moderate to vigorous physical activity approximately 4 days per week.
- Physically active adults tended to be younger, with a higher proportion of White individuals, and with lower rates of hypertension and type 2 diabetes.
- After adjusting for multiple factors, increased days of moderate to vigorous activity correlated with larger normalized brain volume in multiple regions including total gray matter; white matter; hippocampus; and frontal, parietal, and occipital lobes.
IN PRACTICE:
“We found that even moderate levels of physical activity, such as taking fewer than 4,000 steps a day, can have a positive effect on brain health. This is much less than the often-suggested 10,000 steps, making it a more achievable goal for many people,” co-author David Merrill, MD, with Pacific Brain Health Center, Santa Monica, California, said in a statement.
SOURCE:
The study, with first author Cyrus A. Raji, MD, PhD, Washington University School of Medicine, St. Louis, was published online in the Journal of Alzheimer’s Disease.
LIMITATIONS:
Participants self-reported physical activity in the past 2 weeks, which does not reflect a lifetime of activity levels. The correlation identified between physical activity and brain volumes may not be solely attributable to physical activity alone.
DISCLOSURES:
The study received funding from several health centers and foundations. Dr. Raji consults for Brainreader ApS, Neurevolution LLC, Apollo Health, Voxelwise Imaging Technology, and Pacific Neuroscience Foundation and is an editorial board member of the Journal of Alzheimer’s Disease but was not involved in the peer-review process.
A version of this article appeared on Medscape.com.
Building a Toolkit for the Treatment of Acute Migraine
Selecting a treatment plan to deal with acute migraine attacks can be like putting together a toolkit of possible therapies, individualized for each patient, one expert said.
The toolkit should comprise reliable treatments that patients know are going to work and that act quickly, allowing them to get back to functioning normally in their daily lives, said Jessica Ailani, MD, during a talk at the 17th European Headache Congress held recently in Barcelona, Spain.
“Everyone with migraine needs acute treatment,” Dr. Ailani, who is a clinical professor of neurology at MedStar Georgetown University Hospital and director of the Georgetown Headache Center, Washington, DC, noted. “Sometimes we can reduce acute treatment with preventative agents, but some disability will remain, so we have to focus on good acute treatment, and this becomes more complex if a person has a lot of comorbidities, which is common in older patients.”
In selecting suitable treatments for migraine, consideration has to be given to the patient profile, any other conditions they have, speed of onset of the migraine attack, length of the attack, associated symptoms, and side effects of the medications, she said.
A Complex Case
As an example, Dr. Ailani described the process she used to treat one of her patients who had frequent severe migraines and other issues causing difficult decisions when selecting medications — a woman in her late 60s with several other comorbidities.
“This is the kind of case I see on a daily basis and which keeps me up at night,” she said. “Many times in clinical practice, we see complex cases like this, and through the course of a year, we may try every treatment option we have in a patient like this.”
On the first presentation, the patient had a chronic migraine with severe headaches every day. She had a history of previous cervical discectomy with fusion surgery; uncontrolled hypertension, for which she was taking an angiotensin blocker; high cholesterol, for which she was taking a statin; and diabetes with an A1c of 8. She did not smoke or drink alcohol, exercised moderately, and her body mass index was in a good range.
“Before a patient ever sees a doctor for their migraine, they will have already tried a lot of different things. Most people are already using NSAIDs and acetaminophen, the most commonly used treatments for acute migraine,” Dr. Ailani explains.
Her patient was taking a triptan and the barbiturate, butalbital. Dr. Ailani notes that the triptan is very effective, but in the United States, they are not available over the counter, and the patient is only allowed nine doses per month on her insurance, so she was supplementing with butalbital.
Over the course of a year, Dr. Ailani got her off the butalbital and started her on onabotulinum toxin A for migraine prevention, which reduced her headache days to about 15 per month (8 severe). She then added the anti-calcitonin gene-related peptide (CGRP) monoclonal antibody, galcanezumab, as another preventative, which further reduced the headache days down to 8-10 days per month (all migraine).
The attacks are rapid onset and can last multiple days. They come with photophobia and phonophobia and cause her to be bedridden, she noted.
“I was still worried about this frequency of headache and the fact she was using a triptan for acute treatment when she had uncontrolled hypertension and other cardiovascular risk factors, Dr. Ailani commented.
She explained that triptans are generally not used in individuals aged over 65 years because of a lack of data in this age group. They are also contraindicated in patients with cardiovascular (CV) disease, and caution is advised in patients with CV risk factors. Noting that migraine is an independent risk factor for stroke in healthy individuals, and this patient already had three other major risk factors for stroke, Dr. Ailani said she did not think a triptan was the best option.
When triptans do not work, Dr. Ailani said she thinks about dihydroergotamine, which she describes as “a great drug for long-lasting migraine” as it tends to have a sustained response. But it also has vasoconstrictive effects and can increase blood pressure, so it was not suitable for this patient.
CV risk is also an issue with nonsteroidal anti-inflammatory drugs (NSAIDs), one of the staple treatments for acute migraine.
“NSAIDs are available over the counter, inexpensive, quite effective, and have minimal immediate side effects,” Dr. Ailani said. But long-term adverse events include CV events, particularly in those who already have CV risk factors, and it is now thought that NSAIDs actually carry more CV risk than triptans.
She noted that out of all the NSAIDs, celecoxib carries the lowest CV risk, and in the United States, it is available as a liquid formulation. There is also a study of ketorolac nasal spray showing it to be as effective as sumatriptan nasal spray for acute migraine.
As her patient was still going to the emergency room (ER) quite frequently at this point, Dr. Ailani prescribed ketorolac nasal spray as an emergency rescue medication, which did help to reduce ER visits but did not solve the acute treatment problem.
The next option she tried was the CGRP antagonists or “gepants” because of their good tolerability.
Because her patient had long attacks, Dr. Ailani said her first choice gepant was rimegepant as it has a long half-life.
She noted that in patients who have frequent migraine attacks (> 6 migraine days per month), using rimegepant as needed has been shown to lead to migraine frequency declining over time. “This shows that if we treat acute attacks properly, we can minimize the risk of chronic migraine.”
She pointed out that if a patient has prodrome that is easy to identify or has short attacks, ubrogepant may be a good option, having shown effectiveness in preventing or reducing the onset of the headache in the recently reported PRODROME trial when given the day before migraine starts.
Then there is also zavegepant, which is available as a nasal spray, so it is a good option for patients with nausea and vomiting. Dr. Ailani suggested that zavegepant as a third-generation gepant may be worth trying in patients who have tried the other gepants, as it is a different type of molecule.
For this patient, neither rimegepant nor ubrogepant worked. “We tried treating in the prodrome, when the pain was starting, adding to other treatments, but she is not a ‘gepant’ responder. We have yet to try zavegepant,” she said.
The next consideration was lasmiditan. “This patient is a triptan responder and lasmiditan is a 5HT1 agonist, so it makes sense to try this. Also, it doesn’t have a vasoconstrictor effect as it doesn’t work on the blood vessels, so it is safe for patients with high blood pressure,” Dr. Ailani noted.
She pointed out, however, that lasmiditan has become a rescue medication in her practice because of side effect issues such as dizziness and sleepiness.
But Dr. Ailani said she has learned how to use the medication to minimize the side effects, by increasing the dose slowly and advising patients to take it later in the day.
“We start with 50 mg for a few doses then increase to 100 mg. This seems to build tolerability.”
Her patient has found good relief from lasmiditan 100 mg, but she can’t take it during the day as it makes her sleepy.
As a last resort, Dr. Ailani went back to metoclopramide, which she described as “a tried and tested old-time drug.”
While this does not make the patient sleepy, it has other adverse effects limiting the frequency of its use, she noted. “I ask her to try to limit it to twice a week, and this has been pretty effective. She can function when she uses it.”
Dr. Ailani also points out that neuromodulation should be in everyone’s tool kit. “So, we added an external combined occipital and trigeminal (eCOT device) neurostimulation device.”
The patient’s tool kit now looks like this:
- Neuromodulation device and meditation at first sign of an attack.
- Add metoclopramide 10 mg and acetaminophen 1000 mg.
- If the attack lasts into the second day, add lasmiditan 100 mg in the evening of the second day (limit 8 days a month).
- If the patient has a sudden onset severe migraine with nausea and vomiting that might make her go to the ER, add in ketorolac nasal spray (not > 5 days per month).
Dr. Ailani noted that other patients will need different toolkits, and in most cases, it is recommended to think about “situational prevention” for times when migraine attacks are predictable, which may include air travel, high-stress times (holidays, etc.), occasions when alcohol will be consumed, and at times of certain weather triggers.
Dr. Ailani disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Selecting a treatment plan to deal with acute migraine attacks can be like putting together a toolkit of possible therapies, individualized for each patient, one expert said.
The toolkit should comprise reliable treatments that patients know are going to work and that act quickly, allowing them to get back to functioning normally in their daily lives, said Jessica Ailani, MD, during a talk at the 17th European Headache Congress held recently in Barcelona, Spain.
“Everyone with migraine needs acute treatment,” Dr. Ailani, who is a clinical professor of neurology at MedStar Georgetown University Hospital and director of the Georgetown Headache Center, Washington, DC, noted. “Sometimes we can reduce acute treatment with preventative agents, but some disability will remain, so we have to focus on good acute treatment, and this becomes more complex if a person has a lot of comorbidities, which is common in older patients.”
In selecting suitable treatments for migraine, consideration has to be given to the patient profile, any other conditions they have, speed of onset of the migraine attack, length of the attack, associated symptoms, and side effects of the medications, she said.
A Complex Case
As an example, Dr. Ailani described the process she used to treat one of her patients who had frequent severe migraines and other issues causing difficult decisions when selecting medications — a woman in her late 60s with several other comorbidities.
“This is the kind of case I see on a daily basis and which keeps me up at night,” she said. “Many times in clinical practice, we see complex cases like this, and through the course of a year, we may try every treatment option we have in a patient like this.”
On the first presentation, the patient had a chronic migraine with severe headaches every day. She had a history of previous cervical discectomy with fusion surgery; uncontrolled hypertension, for which she was taking an angiotensin blocker; high cholesterol, for which she was taking a statin; and diabetes with an A1c of 8. She did not smoke or drink alcohol, exercised moderately, and her body mass index was in a good range.
“Before a patient ever sees a doctor for their migraine, they will have already tried a lot of different things. Most people are already using NSAIDs and acetaminophen, the most commonly used treatments for acute migraine,” Dr. Ailani explains.
Her patient was taking a triptan and the barbiturate, butalbital. Dr. Ailani notes that the triptan is very effective, but in the United States, they are not available over the counter, and the patient is only allowed nine doses per month on her insurance, so she was supplementing with butalbital.
Over the course of a year, Dr. Ailani got her off the butalbital and started her on onabotulinum toxin A for migraine prevention, which reduced her headache days to about 15 per month (8 severe). She then added the anti-calcitonin gene-related peptide (CGRP) monoclonal antibody, galcanezumab, as another preventative, which further reduced the headache days down to 8-10 days per month (all migraine).
The attacks are rapid onset and can last multiple days. They come with photophobia and phonophobia and cause her to be bedridden, she noted.
“I was still worried about this frequency of headache and the fact she was using a triptan for acute treatment when she had uncontrolled hypertension and other cardiovascular risk factors, Dr. Ailani commented.
She explained that triptans are generally not used in individuals aged over 65 years because of a lack of data in this age group. They are also contraindicated in patients with cardiovascular (CV) disease, and caution is advised in patients with CV risk factors. Noting that migraine is an independent risk factor for stroke in healthy individuals, and this patient already had three other major risk factors for stroke, Dr. Ailani said she did not think a triptan was the best option.
When triptans do not work, Dr. Ailani said she thinks about dihydroergotamine, which she describes as “a great drug for long-lasting migraine” as it tends to have a sustained response. But it also has vasoconstrictive effects and can increase blood pressure, so it was not suitable for this patient.
CV risk is also an issue with nonsteroidal anti-inflammatory drugs (NSAIDs), one of the staple treatments for acute migraine.
“NSAIDs are available over the counter, inexpensive, quite effective, and have minimal immediate side effects,” Dr. Ailani said. But long-term adverse events include CV events, particularly in those who already have CV risk factors, and it is now thought that NSAIDs actually carry more CV risk than triptans.
She noted that out of all the NSAIDs, celecoxib carries the lowest CV risk, and in the United States, it is available as a liquid formulation. There is also a study of ketorolac nasal spray showing it to be as effective as sumatriptan nasal spray for acute migraine.
As her patient was still going to the emergency room (ER) quite frequently at this point, Dr. Ailani prescribed ketorolac nasal spray as an emergency rescue medication, which did help to reduce ER visits but did not solve the acute treatment problem.
The next option she tried was the CGRP antagonists or “gepants” because of their good tolerability.
Because her patient had long attacks, Dr. Ailani said her first choice gepant was rimegepant as it has a long half-life.
She noted that in patients who have frequent migraine attacks (> 6 migraine days per month), using rimegepant as needed has been shown to lead to migraine frequency declining over time. “This shows that if we treat acute attacks properly, we can minimize the risk of chronic migraine.”
She pointed out that if a patient has prodrome that is easy to identify or has short attacks, ubrogepant may be a good option, having shown effectiveness in preventing or reducing the onset of the headache in the recently reported PRODROME trial when given the day before migraine starts.
Then there is also zavegepant, which is available as a nasal spray, so it is a good option for patients with nausea and vomiting. Dr. Ailani suggested that zavegepant as a third-generation gepant may be worth trying in patients who have tried the other gepants, as it is a different type of molecule.
For this patient, neither rimegepant nor ubrogepant worked. “We tried treating in the prodrome, when the pain was starting, adding to other treatments, but she is not a ‘gepant’ responder. We have yet to try zavegepant,” she said.
The next consideration was lasmiditan. “This patient is a triptan responder and lasmiditan is a 5HT1 agonist, so it makes sense to try this. Also, it doesn’t have a vasoconstrictor effect as it doesn’t work on the blood vessels, so it is safe for patients with high blood pressure,” Dr. Ailani noted.
She pointed out, however, that lasmiditan has become a rescue medication in her practice because of side effect issues such as dizziness and sleepiness.
But Dr. Ailani said she has learned how to use the medication to minimize the side effects, by increasing the dose slowly and advising patients to take it later in the day.
“We start with 50 mg for a few doses then increase to 100 mg. This seems to build tolerability.”
Her patient has found good relief from lasmiditan 100 mg, but she can’t take it during the day as it makes her sleepy.
As a last resort, Dr. Ailani went back to metoclopramide, which she described as “a tried and tested old-time drug.”
While this does not make the patient sleepy, it has other adverse effects limiting the frequency of its use, she noted. “I ask her to try to limit it to twice a week, and this has been pretty effective. She can function when she uses it.”
Dr. Ailani also points out that neuromodulation should be in everyone’s tool kit. “So, we added an external combined occipital and trigeminal (eCOT device) neurostimulation device.”
The patient’s tool kit now looks like this:
- Neuromodulation device and meditation at first sign of an attack.
- Add metoclopramide 10 mg and acetaminophen 1000 mg.
- If the attack lasts into the second day, add lasmiditan 100 mg in the evening of the second day (limit 8 days a month).
- If the patient has a sudden onset severe migraine with nausea and vomiting that might make her go to the ER, add in ketorolac nasal spray (not > 5 days per month).
Dr. Ailani noted that other patients will need different toolkits, and in most cases, it is recommended to think about “situational prevention” for times when migraine attacks are predictable, which may include air travel, high-stress times (holidays, etc.), occasions when alcohol will be consumed, and at times of certain weather triggers.
Dr. Ailani disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Selecting a treatment plan to deal with acute migraine attacks can be like putting together a toolkit of possible therapies, individualized for each patient, one expert said.
The toolkit should comprise reliable treatments that patients know are going to work and that act quickly, allowing them to get back to functioning normally in their daily lives, said Jessica Ailani, MD, during a talk at the 17th European Headache Congress held recently in Barcelona, Spain.
“Everyone with migraine needs acute treatment,” Dr. Ailani, who is a clinical professor of neurology at MedStar Georgetown University Hospital and director of the Georgetown Headache Center, Washington, DC, noted. “Sometimes we can reduce acute treatment with preventative agents, but some disability will remain, so we have to focus on good acute treatment, and this becomes more complex if a person has a lot of comorbidities, which is common in older patients.”
In selecting suitable treatments for migraine, consideration has to be given to the patient profile, any other conditions they have, speed of onset of the migraine attack, length of the attack, associated symptoms, and side effects of the medications, she said.
A Complex Case
As an example, Dr. Ailani described the process she used to treat one of her patients who had frequent severe migraines and other issues causing difficult decisions when selecting medications — a woman in her late 60s with several other comorbidities.
“This is the kind of case I see on a daily basis and which keeps me up at night,” she said. “Many times in clinical practice, we see complex cases like this, and through the course of a year, we may try every treatment option we have in a patient like this.”
On the first presentation, the patient had a chronic migraine with severe headaches every day. She had a history of previous cervical discectomy with fusion surgery; uncontrolled hypertension, for which she was taking an angiotensin blocker; high cholesterol, for which she was taking a statin; and diabetes with an A1c of 8. She did not smoke or drink alcohol, exercised moderately, and her body mass index was in a good range.
“Before a patient ever sees a doctor for their migraine, they will have already tried a lot of different things. Most people are already using NSAIDs and acetaminophen, the most commonly used treatments for acute migraine,” Dr. Ailani explains.
Her patient was taking a triptan and the barbiturate, butalbital. Dr. Ailani notes that the triptan is very effective, but in the United States, they are not available over the counter, and the patient is only allowed nine doses per month on her insurance, so she was supplementing with butalbital.
Over the course of a year, Dr. Ailani got her off the butalbital and started her on onabotulinum toxin A for migraine prevention, which reduced her headache days to about 15 per month (8 severe). She then added the anti-calcitonin gene-related peptide (CGRP) monoclonal antibody, galcanezumab, as another preventative, which further reduced the headache days down to 8-10 days per month (all migraine).
The attacks are rapid onset and can last multiple days. They come with photophobia and phonophobia and cause her to be bedridden, she noted.
“I was still worried about this frequency of headache and the fact she was using a triptan for acute treatment when she had uncontrolled hypertension and other cardiovascular risk factors, Dr. Ailani commented.
She explained that triptans are generally not used in individuals aged over 65 years because of a lack of data in this age group. They are also contraindicated in patients with cardiovascular (CV) disease, and caution is advised in patients with CV risk factors. Noting that migraine is an independent risk factor for stroke in healthy individuals, and this patient already had three other major risk factors for stroke, Dr. Ailani said she did not think a triptan was the best option.
When triptans do not work, Dr. Ailani said she thinks about dihydroergotamine, which she describes as “a great drug for long-lasting migraine” as it tends to have a sustained response. But it also has vasoconstrictive effects and can increase blood pressure, so it was not suitable for this patient.
CV risk is also an issue with nonsteroidal anti-inflammatory drugs (NSAIDs), one of the staple treatments for acute migraine.
“NSAIDs are available over the counter, inexpensive, quite effective, and have minimal immediate side effects,” Dr. Ailani said. But long-term adverse events include CV events, particularly in those who already have CV risk factors, and it is now thought that NSAIDs actually carry more CV risk than triptans.
She noted that out of all the NSAIDs, celecoxib carries the lowest CV risk, and in the United States, it is available as a liquid formulation. There is also a study of ketorolac nasal spray showing it to be as effective as sumatriptan nasal spray for acute migraine.
As her patient was still going to the emergency room (ER) quite frequently at this point, Dr. Ailani prescribed ketorolac nasal spray as an emergency rescue medication, which did help to reduce ER visits but did not solve the acute treatment problem.
The next option she tried was the CGRP antagonists or “gepants” because of their good tolerability.
Because her patient had long attacks, Dr. Ailani said her first choice gepant was rimegepant as it has a long half-life.
She noted that in patients who have frequent migraine attacks (> 6 migraine days per month), using rimegepant as needed has been shown to lead to migraine frequency declining over time. “This shows that if we treat acute attacks properly, we can minimize the risk of chronic migraine.”
She pointed out that if a patient has prodrome that is easy to identify or has short attacks, ubrogepant may be a good option, having shown effectiveness in preventing or reducing the onset of the headache in the recently reported PRODROME trial when given the day before migraine starts.
Then there is also zavegepant, which is available as a nasal spray, so it is a good option for patients with nausea and vomiting. Dr. Ailani suggested that zavegepant as a third-generation gepant may be worth trying in patients who have tried the other gepants, as it is a different type of molecule.
For this patient, neither rimegepant nor ubrogepant worked. “We tried treating in the prodrome, when the pain was starting, adding to other treatments, but she is not a ‘gepant’ responder. We have yet to try zavegepant,” she said.
The next consideration was lasmiditan. “This patient is a triptan responder and lasmiditan is a 5HT1 agonist, so it makes sense to try this. Also, it doesn’t have a vasoconstrictor effect as it doesn’t work on the blood vessels, so it is safe for patients with high blood pressure,” Dr. Ailani noted.
She pointed out, however, that lasmiditan has become a rescue medication in her practice because of side effect issues such as dizziness and sleepiness.
But Dr. Ailani said she has learned how to use the medication to minimize the side effects, by increasing the dose slowly and advising patients to take it later in the day.
“We start with 50 mg for a few doses then increase to 100 mg. This seems to build tolerability.”
Her patient has found good relief from lasmiditan 100 mg, but she can’t take it during the day as it makes her sleepy.
As a last resort, Dr. Ailani went back to metoclopramide, which she described as “a tried and tested old-time drug.”
While this does not make the patient sleepy, it has other adverse effects limiting the frequency of its use, she noted. “I ask her to try to limit it to twice a week, and this has been pretty effective. She can function when she uses it.”
Dr. Ailani also points out that neuromodulation should be in everyone’s tool kit. “So, we added an external combined occipital and trigeminal (eCOT device) neurostimulation device.”
The patient’s tool kit now looks like this:
- Neuromodulation device and meditation at first sign of an attack.
- Add metoclopramide 10 mg and acetaminophen 1000 mg.
- If the attack lasts into the second day, add lasmiditan 100 mg in the evening of the second day (limit 8 days a month).
- If the patient has a sudden onset severe migraine with nausea and vomiting that might make her go to the ER, add in ketorolac nasal spray (not > 5 days per month).
Dr. Ailani noted that other patients will need different toolkits, and in most cases, it is recommended to think about “situational prevention” for times when migraine attacks are predictable, which may include air travel, high-stress times (holidays, etc.), occasions when alcohol will be consumed, and at times of certain weather triggers.
Dr. Ailani disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM THE EUROPEAN HEADACHE CONGRESS
Hearing Aids and Dementia Risk Study Retracted
The study was published April 13 in The Lancet Public Health and reported at that time. It was retracted by the journal on December 12.
According to the retraction notice, the journal editors in late November were informed by the authors of the paper that an error was introduced in the output format setting of their SAS codes, which led to data for people with hearing loss using hearing aids and those with hearing loss without using hearing aids being switched.
This led to errors in their analysis, “which render their findings and conclusions false and misleading,” the retraction notice states.
These errors were identified by the researchers following an exchange with scientists seeking to reproduce the authors’ findings.In a statement, The Lancet Group said it “takes issues relating to research integrity extremely seriously” and follows best-practice guidance from the Committee on Publication Ethics (COPE) and the International Committee of Medical Journal Editors (ICMJE).
“Retractions are a rare but important part of the publishing process, and we are grateful to the scientists who prompted the re-examination of the data,” the statement reads.
Despite the retraction, other studies have suggested a link between hearing and dementia.
One study of US Medicare beneficiaries found a 61% higher dementia prevalence in those with moderate to severe hearing loss compared to those with normal hearing.
In this research, even mild hearing loss was associated with increased dementia risk, although it was not statistically significant, and use of hearing aids was tied to a 32% decrease in dementia prevalence.
In addition, a large meta-analysis showed that hearing aids significantly reduce the risk for cognitive decline and dementia and even improve short-term cognitive function in individuals with hearing loss.
A version of this article appeared on Medscape.com.
The study was published April 13 in The Lancet Public Health and reported at that time. It was retracted by the journal on December 12.
According to the retraction notice, the journal editors in late November were informed by the authors of the paper that an error was introduced in the output format setting of their SAS codes, which led to data for people with hearing loss using hearing aids and those with hearing loss without using hearing aids being switched.
This led to errors in their analysis, “which render their findings and conclusions false and misleading,” the retraction notice states.
These errors were identified by the researchers following an exchange with scientists seeking to reproduce the authors’ findings.In a statement, The Lancet Group said it “takes issues relating to research integrity extremely seriously” and follows best-practice guidance from the Committee on Publication Ethics (COPE) and the International Committee of Medical Journal Editors (ICMJE).
“Retractions are a rare but important part of the publishing process, and we are grateful to the scientists who prompted the re-examination of the data,” the statement reads.
Despite the retraction, other studies have suggested a link between hearing and dementia.
One study of US Medicare beneficiaries found a 61% higher dementia prevalence in those with moderate to severe hearing loss compared to those with normal hearing.
In this research, even mild hearing loss was associated with increased dementia risk, although it was not statistically significant, and use of hearing aids was tied to a 32% decrease in dementia prevalence.
In addition, a large meta-analysis showed that hearing aids significantly reduce the risk for cognitive decline and dementia and even improve short-term cognitive function in individuals with hearing loss.
A version of this article appeared on Medscape.com.
The study was published April 13 in The Lancet Public Health and reported at that time. It was retracted by the journal on December 12.
According to the retraction notice, the journal editors in late November were informed by the authors of the paper that an error was introduced in the output format setting of their SAS codes, which led to data for people with hearing loss using hearing aids and those with hearing loss without using hearing aids being switched.
This led to errors in their analysis, “which render their findings and conclusions false and misleading,” the retraction notice states.
These errors were identified by the researchers following an exchange with scientists seeking to reproduce the authors’ findings.In a statement, The Lancet Group said it “takes issues relating to research integrity extremely seriously” and follows best-practice guidance from the Committee on Publication Ethics (COPE) and the International Committee of Medical Journal Editors (ICMJE).
“Retractions are a rare but important part of the publishing process, and we are grateful to the scientists who prompted the re-examination of the data,” the statement reads.
Despite the retraction, other studies have suggested a link between hearing and dementia.
One study of US Medicare beneficiaries found a 61% higher dementia prevalence in those with moderate to severe hearing loss compared to those with normal hearing.
In this research, even mild hearing loss was associated with increased dementia risk, although it was not statistically significant, and use of hearing aids was tied to a 32% decrease in dementia prevalence.
In addition, a large meta-analysis showed that hearing aids significantly reduce the risk for cognitive decline and dementia and even improve short-term cognitive function in individuals with hearing loss.
A version of this article appeared on Medscape.com.
FROM THE LANCET PUBLIC HEALTH
Light therapy a beacon of hope for Alzheimer’s?
TOPLINE:
Light therapy leads to significant improvement in several sleep measures and helps alleviate depression and agitation in patients with Alzheimer’s disease (AD), a meta-analysis of 15 high-quality trials shows.
METHODOLOGY:
- This meta-analysis included 15 randomized controlled trials involving 598 patients with mild to moderate AD.
- The included trials were written in English, published between 2005 and 2022, and performed in seven countries. A fixed-effects model was used for data analysis.
TAKEAWAY:
- Light therapy significantly improved sleep efficiency (mean difference [MD], −2.42; P < .00001), increased interdaily stability (MD, −0.04; P < .00001), and reduced intradaily variability (MD, −0.04; P < .00001), indicating better sleep quality.
- Light therapy reduced agitation (MD, −3.97; P < .00001), depression (MD, −2.55; P < .00001), and caregiver burden (MD, −3.57; P < .00001).
- Light therapy also had a significant advantage over usual care in reducing the severity of psychobehavioral symptoms as assessed by the Neuropsychiatric Inventory (MD, −3.07; P < .00001).
- Light therapy had no statistically significant effect on improving cognitive function as measured by the Mini-Mental State Examination.
IN PRACTICE:
“These findings, combined with its low side-effects, suggest the role of light therapy as a promising treatment for AD. Although light therapy has fewer side effects than pharmacological treatment, adverse behavioral outcomes in patients due to bright light exposure should be considered,” the authors wrote.
SOURCE:
The study by Lili Zang and colleagues from Weifang Medical University School of Nursing, Shandong Province, China, was published online on December 6, 2023, in PLOS One.
LIMITATIONS:
The types and degrees of dementia in the included studies were inconsistent, potentially affecting the outcome indicators. Some articles did not clearly describe their randomization and allocation concealment methods, indicating possible bias in these studies.
DISCLOSURES:
The study was supported by the Natural Science Foundation of Shandong Province, China. The authors declared no competing interests.
Megan Brooks has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
Light therapy leads to significant improvement in several sleep measures and helps alleviate depression and agitation in patients with Alzheimer’s disease (AD), a meta-analysis of 15 high-quality trials shows.
METHODOLOGY:
- This meta-analysis included 15 randomized controlled trials involving 598 patients with mild to moderate AD.
- The included trials were written in English, published between 2005 and 2022, and performed in seven countries. A fixed-effects model was used for data analysis.
TAKEAWAY:
- Light therapy significantly improved sleep efficiency (mean difference [MD], −2.42; P < .00001), increased interdaily stability (MD, −0.04; P < .00001), and reduced intradaily variability (MD, −0.04; P < .00001), indicating better sleep quality.
- Light therapy reduced agitation (MD, −3.97; P < .00001), depression (MD, −2.55; P < .00001), and caregiver burden (MD, −3.57; P < .00001).
- Light therapy also had a significant advantage over usual care in reducing the severity of psychobehavioral symptoms as assessed by the Neuropsychiatric Inventory (MD, −3.07; P < .00001).
- Light therapy had no statistically significant effect on improving cognitive function as measured by the Mini-Mental State Examination.
IN PRACTICE:
“These findings, combined with its low side-effects, suggest the role of light therapy as a promising treatment for AD. Although light therapy has fewer side effects than pharmacological treatment, adverse behavioral outcomes in patients due to bright light exposure should be considered,” the authors wrote.
SOURCE:
The study by Lili Zang and colleagues from Weifang Medical University School of Nursing, Shandong Province, China, was published online on December 6, 2023, in PLOS One.
LIMITATIONS:
The types and degrees of dementia in the included studies were inconsistent, potentially affecting the outcome indicators. Some articles did not clearly describe their randomization and allocation concealment methods, indicating possible bias in these studies.
DISCLOSURES:
The study was supported by the Natural Science Foundation of Shandong Province, China. The authors declared no competing interests.
Megan Brooks has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
Light therapy leads to significant improvement in several sleep measures and helps alleviate depression and agitation in patients with Alzheimer’s disease (AD), a meta-analysis of 15 high-quality trials shows.
METHODOLOGY:
- This meta-analysis included 15 randomized controlled trials involving 598 patients with mild to moderate AD.
- The included trials were written in English, published between 2005 and 2022, and performed in seven countries. A fixed-effects model was used for data analysis.
TAKEAWAY:
- Light therapy significantly improved sleep efficiency (mean difference [MD], −2.42; P < .00001), increased interdaily stability (MD, −0.04; P < .00001), and reduced intradaily variability (MD, −0.04; P < .00001), indicating better sleep quality.
- Light therapy reduced agitation (MD, −3.97; P < .00001), depression (MD, −2.55; P < .00001), and caregiver burden (MD, −3.57; P < .00001).
- Light therapy also had a significant advantage over usual care in reducing the severity of psychobehavioral symptoms as assessed by the Neuropsychiatric Inventory (MD, −3.07; P < .00001).
- Light therapy had no statistically significant effect on improving cognitive function as measured by the Mini-Mental State Examination.
IN PRACTICE:
“These findings, combined with its low side-effects, suggest the role of light therapy as a promising treatment for AD. Although light therapy has fewer side effects than pharmacological treatment, adverse behavioral outcomes in patients due to bright light exposure should be considered,” the authors wrote.
SOURCE:
The study by Lili Zang and colleagues from Weifang Medical University School of Nursing, Shandong Province, China, was published online on December 6, 2023, in PLOS One.
LIMITATIONS:
The types and degrees of dementia in the included studies were inconsistent, potentially affecting the outcome indicators. Some articles did not clearly describe their randomization and allocation concealment methods, indicating possible bias in these studies.
DISCLOSURES:
The study was supported by the Natural Science Foundation of Shandong Province, China. The authors declared no competing interests.
Megan Brooks has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Depression, constipation, UTIs early signs of MS?
However, these prodromal symptoms are also more likely to occur in people with two other autoimmune diseases — lupus and Crohn’s disease — and therefore, will not help earlier diagnosis, study investigator, Céline Louapre, professor of neurology, Sorbonne University and Paris Brain Institute, Paris, France, said in an interview.
“On the other hand, in certain patients who may be at particular risk of developing MS, such as in certain familial forms or in patients with incidental inflammatory lesions discovered on MRI, the presence of these symptoms could suggest an already active process, prior to the first typical symptoms of the disease,” she noted.
Retracing MS Origins
The case-control study, published online in Neurology, included 20,174 people with newly diagnosed MS who were matched to 54,790 without MS, as well as 30,477 with Crohn’s disease and 7337 with lupus.
Using International Classification of Diseases, 10th revision (ICD-10) codes in electronic health records, the researchers assessed the associations between 113 diseases and symptoms in the 5 years before and after an MS diagnosis.
Twelve ICD-10 codes were significantly positively associated with the risk for MS compared with controls without MS.
After considering ICD-10 codes suggestive of neurologic symptoms as the first diagnosis of MS, the following five ICD-10 codes remained significantly associated with MS:
- Depression (odds ratio [OR], 1.22; 95% CI, 1.11-1.34)
- Sexual dysfunction (OR, 1.47; 95% CI, 1.11-1.95)
- Constipation (OR, 1.5; 95% CI, 1.27-1.78)
- Cystitis (OR, 1.21; 95% CI, 1.05-1.39)
- UTIs of unspecified site (OR, 1.38; 95% CI, 1.18-1.61)
However, none of these conditions was selectively associated with MS in comparison with both lupus and Crohn’s disease. All five ICD-10 codes identified were still associated with MS during the 5 years after diagnosis.
“The importance of investigating prodromal signs in MS is that it allows us to retrace the origins of the disease,” said Dr. Louapre.
“The main contribution of the data on prodromes in MS is to clarify that the disease and its mechanisms are frequently underway well before the first typical neurological symptoms, and that the causes of MS are probably present many years before diagnosis,” she added.
A limitation of the study was that data were not available for other factors that could influence people’s risk of developing MS, such as education level, ethnicity, body mass index, socioeconomic status, or genetic information.
It also remains unclear whether the conditions linked to MS are risk factors for the disease or nonspecific early MS symptoms.
Preventing Disease Evolution
In a linked editorial, Ruth Ann Marrie, MD, PhD, with the University of Manitoba, Manitoba, Canada, and Raffaele Palladino, MD, PhD, with the University of Naples Federico II, Naples, Italy, note these findings highlight the challenges of accurately identifying the prodromal stage of a specific disease.
“Commonalities of prodromal features are recognized across neurodegenerative diseases; this is also true for immune-mediated diseases, and it is not surprising, given shared etiologic factors and pathobiological mechanisms,” they point out.
“This suggests that we should be trying to link prodromal features to specific underlying pathobiological changes rather than specific diseases. This approach would require use of different study designs, including broad, deeply phenotyped cohorts, but would allow us to develop and test interventions targeted at those mechanisms, and could ultimately achieve the goal of preventing disease evolution,” they add.
The study was supported by the French National Research Agency. Dr. Louapre has received consulting or travel fees from Biogen, Novartis, Roche, Sanofi, Teva, and Merck Serono, unrelated to this study. Dr. Marrie is a coinvestigator on studies receiving funding from Biogen Idec and Roche Canada; receives research funding from CIHR, Research Manitoba, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the Arthritis Society and the US Department of Defense; and serves on the editorial board of Neurology. Dr. Palladino has taken part in advisory boards/consultancy for MSD and Sanofi and has received support from the UK MS Society.
A version of this article appeared on Medscape.com.
However, these prodromal symptoms are also more likely to occur in people with two other autoimmune diseases — lupus and Crohn’s disease — and therefore, will not help earlier diagnosis, study investigator, Céline Louapre, professor of neurology, Sorbonne University and Paris Brain Institute, Paris, France, said in an interview.
“On the other hand, in certain patients who may be at particular risk of developing MS, such as in certain familial forms or in patients with incidental inflammatory lesions discovered on MRI, the presence of these symptoms could suggest an already active process, prior to the first typical symptoms of the disease,” she noted.
Retracing MS Origins
The case-control study, published online in Neurology, included 20,174 people with newly diagnosed MS who were matched to 54,790 without MS, as well as 30,477 with Crohn’s disease and 7337 with lupus.
Using International Classification of Diseases, 10th revision (ICD-10) codes in electronic health records, the researchers assessed the associations between 113 diseases and symptoms in the 5 years before and after an MS diagnosis.
Twelve ICD-10 codes were significantly positively associated with the risk for MS compared with controls without MS.
After considering ICD-10 codes suggestive of neurologic symptoms as the first diagnosis of MS, the following five ICD-10 codes remained significantly associated with MS:
- Depression (odds ratio [OR], 1.22; 95% CI, 1.11-1.34)
- Sexual dysfunction (OR, 1.47; 95% CI, 1.11-1.95)
- Constipation (OR, 1.5; 95% CI, 1.27-1.78)
- Cystitis (OR, 1.21; 95% CI, 1.05-1.39)
- UTIs of unspecified site (OR, 1.38; 95% CI, 1.18-1.61)
However, none of these conditions was selectively associated with MS in comparison with both lupus and Crohn’s disease. All five ICD-10 codes identified were still associated with MS during the 5 years after diagnosis.
“The importance of investigating prodromal signs in MS is that it allows us to retrace the origins of the disease,” said Dr. Louapre.
“The main contribution of the data on prodromes in MS is to clarify that the disease and its mechanisms are frequently underway well before the first typical neurological symptoms, and that the causes of MS are probably present many years before diagnosis,” she added.
A limitation of the study was that data were not available for other factors that could influence people’s risk of developing MS, such as education level, ethnicity, body mass index, socioeconomic status, or genetic information.
It also remains unclear whether the conditions linked to MS are risk factors for the disease or nonspecific early MS symptoms.
Preventing Disease Evolution
In a linked editorial, Ruth Ann Marrie, MD, PhD, with the University of Manitoba, Manitoba, Canada, and Raffaele Palladino, MD, PhD, with the University of Naples Federico II, Naples, Italy, note these findings highlight the challenges of accurately identifying the prodromal stage of a specific disease.
“Commonalities of prodromal features are recognized across neurodegenerative diseases; this is also true for immune-mediated diseases, and it is not surprising, given shared etiologic factors and pathobiological mechanisms,” they point out.
“This suggests that we should be trying to link prodromal features to specific underlying pathobiological changes rather than specific diseases. This approach would require use of different study designs, including broad, deeply phenotyped cohorts, but would allow us to develop and test interventions targeted at those mechanisms, and could ultimately achieve the goal of preventing disease evolution,” they add.
The study was supported by the French National Research Agency. Dr. Louapre has received consulting or travel fees from Biogen, Novartis, Roche, Sanofi, Teva, and Merck Serono, unrelated to this study. Dr. Marrie is a coinvestigator on studies receiving funding from Biogen Idec and Roche Canada; receives research funding from CIHR, Research Manitoba, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the Arthritis Society and the US Department of Defense; and serves on the editorial board of Neurology. Dr. Palladino has taken part in advisory boards/consultancy for MSD and Sanofi and has received support from the UK MS Society.
A version of this article appeared on Medscape.com.
However, these prodromal symptoms are also more likely to occur in people with two other autoimmune diseases — lupus and Crohn’s disease — and therefore, will not help earlier diagnosis, study investigator, Céline Louapre, professor of neurology, Sorbonne University and Paris Brain Institute, Paris, France, said in an interview.
“On the other hand, in certain patients who may be at particular risk of developing MS, such as in certain familial forms or in patients with incidental inflammatory lesions discovered on MRI, the presence of these symptoms could suggest an already active process, prior to the first typical symptoms of the disease,” she noted.
Retracing MS Origins
The case-control study, published online in Neurology, included 20,174 people with newly diagnosed MS who were matched to 54,790 without MS, as well as 30,477 with Crohn’s disease and 7337 with lupus.
Using International Classification of Diseases, 10th revision (ICD-10) codes in electronic health records, the researchers assessed the associations between 113 diseases and symptoms in the 5 years before and after an MS diagnosis.
Twelve ICD-10 codes were significantly positively associated with the risk for MS compared with controls without MS.
After considering ICD-10 codes suggestive of neurologic symptoms as the first diagnosis of MS, the following five ICD-10 codes remained significantly associated with MS:
- Depression (odds ratio [OR], 1.22; 95% CI, 1.11-1.34)
- Sexual dysfunction (OR, 1.47; 95% CI, 1.11-1.95)
- Constipation (OR, 1.5; 95% CI, 1.27-1.78)
- Cystitis (OR, 1.21; 95% CI, 1.05-1.39)
- UTIs of unspecified site (OR, 1.38; 95% CI, 1.18-1.61)
However, none of these conditions was selectively associated with MS in comparison with both lupus and Crohn’s disease. All five ICD-10 codes identified were still associated with MS during the 5 years after diagnosis.
“The importance of investigating prodromal signs in MS is that it allows us to retrace the origins of the disease,” said Dr. Louapre.
“The main contribution of the data on prodromes in MS is to clarify that the disease and its mechanisms are frequently underway well before the first typical neurological symptoms, and that the causes of MS are probably present many years before diagnosis,” she added.
A limitation of the study was that data were not available for other factors that could influence people’s risk of developing MS, such as education level, ethnicity, body mass index, socioeconomic status, or genetic information.
It also remains unclear whether the conditions linked to MS are risk factors for the disease or nonspecific early MS symptoms.
Preventing Disease Evolution
In a linked editorial, Ruth Ann Marrie, MD, PhD, with the University of Manitoba, Manitoba, Canada, and Raffaele Palladino, MD, PhD, with the University of Naples Federico II, Naples, Italy, note these findings highlight the challenges of accurately identifying the prodromal stage of a specific disease.
“Commonalities of prodromal features are recognized across neurodegenerative diseases; this is also true for immune-mediated diseases, and it is not surprising, given shared etiologic factors and pathobiological mechanisms,” they point out.
“This suggests that we should be trying to link prodromal features to specific underlying pathobiological changes rather than specific diseases. This approach would require use of different study designs, including broad, deeply phenotyped cohorts, but would allow us to develop and test interventions targeted at those mechanisms, and could ultimately achieve the goal of preventing disease evolution,” they add.
The study was supported by the French National Research Agency. Dr. Louapre has received consulting or travel fees from Biogen, Novartis, Roche, Sanofi, Teva, and Merck Serono, unrelated to this study. Dr. Marrie is a coinvestigator on studies receiving funding from Biogen Idec and Roche Canada; receives research funding from CIHR, Research Manitoba, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the Arthritis Society and the US Department of Defense; and serves on the editorial board of Neurology. Dr. Palladino has taken part in advisory boards/consultancy for MSD and Sanofi and has received support from the UK MS Society.
A version of this article appeared on Medscape.com.
FROM NEUROLOGY
Neighborhood Disadvantage Tied to Higher Risk for ASD
TOPLINE
, a population-based prospective cohort study shows.
METHODOLOGY
- Investigators analyzed data from a large cohort of singleton children with insurance born in Kaiser Permanente Southern California hospitals between 2001 and 2014.
- They ascertained ASD diagnosis, maternal race and ethnicity, and maternal address at time of birth.
- Neighborhood disadvantage was determined by the percentage of families in the mother’s neighborhood considered to be living in poverty, unemployed, have female-headed households with children, using public assistance, less than a high school education, among other variables.
TAKEAWAY
- Among 318,300 mothers who delivered babies during the study period, 6350 children were diagnosed with ASD during follow-up, and median age at diagnosis was 3.5 years.
- Greater neighborhood disadvantage at birth was associated with a higher likelihood of ASD diagnosis (adjusted hazard ratio [aHR], 1.07; 95% CI, 1.02-1.11)
- ASD diagnoses were more likely among children of mothers who were Black (aHR, 1.13; 95% CI, 1.02-1.25), Asian/Pacific Islander (aHR, 1.11; 95% CI, 1.02-1.20), or Hispanic (aHR, 1.07; 95% CI, 1.00-1.15), even after the researchers controlled for neighborhood.
- While odds of an ASD diagnosis were higher among children from minority racial and ethnic groups, neighborhood disadvantage was significantly associated with ASD diagnosis only for children of White mothers (aHR, 1.17; 95% CI, 1.09-1.26).
IN PRACTICE
Investigators noted that they could only speculate about the factors driving the association between neighborhood disadvantage and a stronger risk for ASD diagnosis in children of White mothers. “They may be due to systemic racism, discrimination, and their impact on maternal health during pregnancy,” they wrote.
SOURCE
Xin Yu, MS, and Daniel Hackman, PhD, of the University of Southern California Los Angeles, led the study, which was published online November 15 in JAMA Psychiatry.
LIMITATIONS
The research was limited by a lack of information on fathers and variables such as incomes, which may have confounded the findings. The authors also acknowledged that the study should be replicated in other health service settings.
DISCLOSURES
The study was funded by the National Institutes on Environmental Health Sciences, the National Institutes of Health (NIH), and the Environmental Protection Agency. Dr. Hackman reported receiving grant funding from NIH during the conduct of the study. Other disclosures are available in the original study.
A version of this article appeared on Medscape.com.
TOPLINE
, a population-based prospective cohort study shows.
METHODOLOGY
- Investigators analyzed data from a large cohort of singleton children with insurance born in Kaiser Permanente Southern California hospitals between 2001 and 2014.
- They ascertained ASD diagnosis, maternal race and ethnicity, and maternal address at time of birth.
- Neighborhood disadvantage was determined by the percentage of families in the mother’s neighborhood considered to be living in poverty, unemployed, have female-headed households with children, using public assistance, less than a high school education, among other variables.
TAKEAWAY
- Among 318,300 mothers who delivered babies during the study period, 6350 children were diagnosed with ASD during follow-up, and median age at diagnosis was 3.5 years.
- Greater neighborhood disadvantage at birth was associated with a higher likelihood of ASD diagnosis (adjusted hazard ratio [aHR], 1.07; 95% CI, 1.02-1.11)
- ASD diagnoses were more likely among children of mothers who were Black (aHR, 1.13; 95% CI, 1.02-1.25), Asian/Pacific Islander (aHR, 1.11; 95% CI, 1.02-1.20), or Hispanic (aHR, 1.07; 95% CI, 1.00-1.15), even after the researchers controlled for neighborhood.
- While odds of an ASD diagnosis were higher among children from minority racial and ethnic groups, neighborhood disadvantage was significantly associated with ASD diagnosis only for children of White mothers (aHR, 1.17; 95% CI, 1.09-1.26).
IN PRACTICE
Investigators noted that they could only speculate about the factors driving the association between neighborhood disadvantage and a stronger risk for ASD diagnosis in children of White mothers. “They may be due to systemic racism, discrimination, and their impact on maternal health during pregnancy,” they wrote.
SOURCE
Xin Yu, MS, and Daniel Hackman, PhD, of the University of Southern California Los Angeles, led the study, which was published online November 15 in JAMA Psychiatry.
LIMITATIONS
The research was limited by a lack of information on fathers and variables such as incomes, which may have confounded the findings. The authors also acknowledged that the study should be replicated in other health service settings.
DISCLOSURES
The study was funded by the National Institutes on Environmental Health Sciences, the National Institutes of Health (NIH), and the Environmental Protection Agency. Dr. Hackman reported receiving grant funding from NIH during the conduct of the study. Other disclosures are available in the original study.
A version of this article appeared on Medscape.com.
TOPLINE
, a population-based prospective cohort study shows.
METHODOLOGY
- Investigators analyzed data from a large cohort of singleton children with insurance born in Kaiser Permanente Southern California hospitals between 2001 and 2014.
- They ascertained ASD diagnosis, maternal race and ethnicity, and maternal address at time of birth.
- Neighborhood disadvantage was determined by the percentage of families in the mother’s neighborhood considered to be living in poverty, unemployed, have female-headed households with children, using public assistance, less than a high school education, among other variables.
TAKEAWAY
- Among 318,300 mothers who delivered babies during the study period, 6350 children were diagnosed with ASD during follow-up, and median age at diagnosis was 3.5 years.
- Greater neighborhood disadvantage at birth was associated with a higher likelihood of ASD diagnosis (adjusted hazard ratio [aHR], 1.07; 95% CI, 1.02-1.11)
- ASD diagnoses were more likely among children of mothers who were Black (aHR, 1.13; 95% CI, 1.02-1.25), Asian/Pacific Islander (aHR, 1.11; 95% CI, 1.02-1.20), or Hispanic (aHR, 1.07; 95% CI, 1.00-1.15), even after the researchers controlled for neighborhood.
- While odds of an ASD diagnosis were higher among children from minority racial and ethnic groups, neighborhood disadvantage was significantly associated with ASD diagnosis only for children of White mothers (aHR, 1.17; 95% CI, 1.09-1.26).
IN PRACTICE
Investigators noted that they could only speculate about the factors driving the association between neighborhood disadvantage and a stronger risk for ASD diagnosis in children of White mothers. “They may be due to systemic racism, discrimination, and their impact on maternal health during pregnancy,” they wrote.
SOURCE
Xin Yu, MS, and Daniel Hackman, PhD, of the University of Southern California Los Angeles, led the study, which was published online November 15 in JAMA Psychiatry.
LIMITATIONS
The research was limited by a lack of information on fathers and variables such as incomes, which may have confounded the findings. The authors also acknowledged that the study should be replicated in other health service settings.
DISCLOSURES
The study was funded by the National Institutes on Environmental Health Sciences, the National Institutes of Health (NIH), and the Environmental Protection Agency. Dr. Hackman reported receiving grant funding from NIH during the conduct of the study. Other disclosures are available in the original study.
A version of this article appeared on Medscape.com.
Exercise plan cost-effective in post-stroke cognitive rehab
A multicomponent exercise program that includes strength, aerobic, agility, and balance training exercises is cost-effective and results in improved cognition among stroke survivors, compared with a balance and tone control group, according to a new analysis.
On the other hand, a program consisting of cognitive and social enrichment activities that includes memory, brain training, and group social games entailed higher costs, compared with the balance and tone group, which included stretches, deep breathing and relaxation techniques, posture education, and core control exercises.
“Cognitive impairment is experienced in approximately one-third of stroke survivors,” study author Jennifer Davis, PhD, a Canada research chair in applied health economics and assistant professor of management at the University of British Columbia in Kelowna, said in an interview.
“The economic evaluation of the exercise intervention demonstrated that the multicomponent exercise program provided good value for the money when comparing costs and cognitive outcomes,” she said. However, “impacts on health-related quality of life were not observed.”
The study was published online November 30 in JAMA Network Open.
Comparing Three Approaches
Despite improved care, patients with stroke often face challenges with physical function, cognitive abilities, and quality of life, the authors wrote. Among older adults, in particular, cognitive deficits remain prevalent and are associated with increased risks for dementia, mortality, and increased burdens for patients, caregivers, and health systems.
Numerous interventions have shown promise for post-stroke cognitive rehabilitation, including exercise and cognitive training, the authors wrote. Research hasn’t indicated which programs offer the most efficient or cost-effective options, however.
Dr. Davis and colleagues conducted an economic evaluation alongside the Vitality study, a three-group randomized clinical trial that examined the efficacy of improving cognitive function among patients with chronic stroke through a multicomponent exercise program, cognitive and social enrichment activities, or a control group with balance and tone activities.
The economic evaluation team included a cost-effectiveness analysis (based on incremental cost per cognitive function change) and a cost-utility analysis (incremental cost per quality-adjusted life-year [QALY] gained). The researchers used a cost-effectiveness threshold of CAD $50,000 (Canadian dollars) per QALY for the cost-utility analysis, which was based on precedent treatment in Canada.
The clinical trial included 120 community-dwelling adults aged 55 years and older who had a stroke at least 12 months before the study. Based in the Vancouver metropolitan area, participants were randomly assigned to twice-weekly, 60-minute classes led by trained instructors for 26 weeks. The mean age was 71 years, and 62% of participants were men.
Exercise Effective
Overall, the balance and tone control group had the lowest delivery cost at CAD $777 per person, followed by CAD $1090 per person for the exercise group and CAD $1492 per person for the cognitive and social enrichment group.
After the 6-month intervention, the mean cognitive scores were –0.192 for the exercise group, –0.184 for the cognitive and social enrichment group, and –0.171 for the balance and tone group, indicating better cognitive function across all three groups.
In the cost-effectiveness analysis, the exercise intervention was costlier but more effective than the control group, with an incremental cost-effectiveness ratio (ICER) of CAD –$8823.
In the cost-utility analysis, the exercise intervention was cost saving (less costly and more effective), compared with the control group, with an ICER of CAD –$3381 per QALY gained at the end of the intervention and an ICER of CAD –$154,198 per QALY gained at the end of the 12-month follow-up period. The cognitive and social enrichment program was more costly and more effective than the control group, with an ICER of CAD $101,687 per QALY gained at the end of the intervention and an ICER of CAD $331,306 per QALY gained at the end of the follow-up period.
In additional analyses, the exercise group had the lowest healthcare resource utilization due to lower healthcare costs for physician visits and lab tests.
“This study provides initial data that suggests multicomponent exercise may be a cost-effective solution for combating cognitive decline among stroke survivors,” said Dr. Davis.
Overall, exercise was cost-effective for improving cognitive function but not quality of life among participants. The clinical trial was powered to detect changes in cognitive function rather than quality of life, so it lacked statistical power to detect differences in quality of life, said Dr. Davis.
Exercise programs and cognitive and social enrichment programs show promise for improving cognitive function after stroke, the authors wrote, though future research should focus on optimizing cost-effectiveness and enhancing health-related quality of life.
Considering Additional Benefits
Commenting on the study, Alan Tam, MD, a physiatrist at the Toronto Rehabilitation Institute’s Brain Rehabilitation Program, said, “The authors show that within the timeframe of their analysis, there is a trend to cost-effectiveness for the cognitive intervention being offered.” Dr. Tam did not participate in the research.
“However, the finding is not robust, as less than 50% of their simulations would meet their acceptability level they have defined,” he said. “Given that most of the cost of the intervention is up front, but the benefits are likely lifelong, potentially taking the 12-month analysis to a lifetime analysis would show more significant findings.”
Dr. Tam researches factors associated with brain injury rehabilitation and has explored the cost-effectiveness of a high-intensity outpatient stroke rehabilitation program.
“Presenting this type of work is important,” he said. “While there are interventions that do not meet our definition of statistical significance, especially in the rehabilitation world, there can still be a benefit for patients and health systems.”
The primary study was funded by the Canadian Institutes of Health Research (CIHR) and the Jack Brown and Family Alzheimer Research Foundation Society. Dr. Davis reported receiving grants from the CIHR and Michael Smith Health Research BC during the conduct of the study. Dr. Tam reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
A multicomponent exercise program that includes strength, aerobic, agility, and balance training exercises is cost-effective and results in improved cognition among stroke survivors, compared with a balance and tone control group, according to a new analysis.
On the other hand, a program consisting of cognitive and social enrichment activities that includes memory, brain training, and group social games entailed higher costs, compared with the balance and tone group, which included stretches, deep breathing and relaxation techniques, posture education, and core control exercises.
“Cognitive impairment is experienced in approximately one-third of stroke survivors,” study author Jennifer Davis, PhD, a Canada research chair in applied health economics and assistant professor of management at the University of British Columbia in Kelowna, said in an interview.
“The economic evaluation of the exercise intervention demonstrated that the multicomponent exercise program provided good value for the money when comparing costs and cognitive outcomes,” she said. However, “impacts on health-related quality of life were not observed.”
The study was published online November 30 in JAMA Network Open.
Comparing Three Approaches
Despite improved care, patients with stroke often face challenges with physical function, cognitive abilities, and quality of life, the authors wrote. Among older adults, in particular, cognitive deficits remain prevalent and are associated with increased risks for dementia, mortality, and increased burdens for patients, caregivers, and health systems.
Numerous interventions have shown promise for post-stroke cognitive rehabilitation, including exercise and cognitive training, the authors wrote. Research hasn’t indicated which programs offer the most efficient or cost-effective options, however.
Dr. Davis and colleagues conducted an economic evaluation alongside the Vitality study, a three-group randomized clinical trial that examined the efficacy of improving cognitive function among patients with chronic stroke through a multicomponent exercise program, cognitive and social enrichment activities, or a control group with balance and tone activities.
The economic evaluation team included a cost-effectiveness analysis (based on incremental cost per cognitive function change) and a cost-utility analysis (incremental cost per quality-adjusted life-year [QALY] gained). The researchers used a cost-effectiveness threshold of CAD $50,000 (Canadian dollars) per QALY for the cost-utility analysis, which was based on precedent treatment in Canada.
The clinical trial included 120 community-dwelling adults aged 55 years and older who had a stroke at least 12 months before the study. Based in the Vancouver metropolitan area, participants were randomly assigned to twice-weekly, 60-minute classes led by trained instructors for 26 weeks. The mean age was 71 years, and 62% of participants were men.
Exercise Effective
Overall, the balance and tone control group had the lowest delivery cost at CAD $777 per person, followed by CAD $1090 per person for the exercise group and CAD $1492 per person for the cognitive and social enrichment group.
After the 6-month intervention, the mean cognitive scores were –0.192 for the exercise group, –0.184 for the cognitive and social enrichment group, and –0.171 for the balance and tone group, indicating better cognitive function across all three groups.
In the cost-effectiveness analysis, the exercise intervention was costlier but more effective than the control group, with an incremental cost-effectiveness ratio (ICER) of CAD –$8823.
In the cost-utility analysis, the exercise intervention was cost saving (less costly and more effective), compared with the control group, with an ICER of CAD –$3381 per QALY gained at the end of the intervention and an ICER of CAD –$154,198 per QALY gained at the end of the 12-month follow-up period. The cognitive and social enrichment program was more costly and more effective than the control group, with an ICER of CAD $101,687 per QALY gained at the end of the intervention and an ICER of CAD $331,306 per QALY gained at the end of the follow-up period.
In additional analyses, the exercise group had the lowest healthcare resource utilization due to lower healthcare costs for physician visits and lab tests.
“This study provides initial data that suggests multicomponent exercise may be a cost-effective solution for combating cognitive decline among stroke survivors,” said Dr. Davis.
Overall, exercise was cost-effective for improving cognitive function but not quality of life among participants. The clinical trial was powered to detect changes in cognitive function rather than quality of life, so it lacked statistical power to detect differences in quality of life, said Dr. Davis.
Exercise programs and cognitive and social enrichment programs show promise for improving cognitive function after stroke, the authors wrote, though future research should focus on optimizing cost-effectiveness and enhancing health-related quality of life.
Considering Additional Benefits
Commenting on the study, Alan Tam, MD, a physiatrist at the Toronto Rehabilitation Institute’s Brain Rehabilitation Program, said, “The authors show that within the timeframe of their analysis, there is a trend to cost-effectiveness for the cognitive intervention being offered.” Dr. Tam did not participate in the research.
“However, the finding is not robust, as less than 50% of their simulations would meet their acceptability level they have defined,” he said. “Given that most of the cost of the intervention is up front, but the benefits are likely lifelong, potentially taking the 12-month analysis to a lifetime analysis would show more significant findings.”
Dr. Tam researches factors associated with brain injury rehabilitation and has explored the cost-effectiveness of a high-intensity outpatient stroke rehabilitation program.
“Presenting this type of work is important,” he said. “While there are interventions that do not meet our definition of statistical significance, especially in the rehabilitation world, there can still be a benefit for patients and health systems.”
The primary study was funded by the Canadian Institutes of Health Research (CIHR) and the Jack Brown and Family Alzheimer Research Foundation Society. Dr. Davis reported receiving grants from the CIHR and Michael Smith Health Research BC during the conduct of the study. Dr. Tam reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
A multicomponent exercise program that includes strength, aerobic, agility, and balance training exercises is cost-effective and results in improved cognition among stroke survivors, compared with a balance and tone control group, according to a new analysis.
On the other hand, a program consisting of cognitive and social enrichment activities that includes memory, brain training, and group social games entailed higher costs, compared with the balance and tone group, which included stretches, deep breathing and relaxation techniques, posture education, and core control exercises.
“Cognitive impairment is experienced in approximately one-third of stroke survivors,” study author Jennifer Davis, PhD, a Canada research chair in applied health economics and assistant professor of management at the University of British Columbia in Kelowna, said in an interview.
“The economic evaluation of the exercise intervention demonstrated that the multicomponent exercise program provided good value for the money when comparing costs and cognitive outcomes,” she said. However, “impacts on health-related quality of life were not observed.”
The study was published online November 30 in JAMA Network Open.
Comparing Three Approaches
Despite improved care, patients with stroke often face challenges with physical function, cognitive abilities, and quality of life, the authors wrote. Among older adults, in particular, cognitive deficits remain prevalent and are associated with increased risks for dementia, mortality, and increased burdens for patients, caregivers, and health systems.
Numerous interventions have shown promise for post-stroke cognitive rehabilitation, including exercise and cognitive training, the authors wrote. Research hasn’t indicated which programs offer the most efficient or cost-effective options, however.
Dr. Davis and colleagues conducted an economic evaluation alongside the Vitality study, a three-group randomized clinical trial that examined the efficacy of improving cognitive function among patients with chronic stroke through a multicomponent exercise program, cognitive and social enrichment activities, or a control group with balance and tone activities.
The economic evaluation team included a cost-effectiveness analysis (based on incremental cost per cognitive function change) and a cost-utility analysis (incremental cost per quality-adjusted life-year [QALY] gained). The researchers used a cost-effectiveness threshold of CAD $50,000 (Canadian dollars) per QALY for the cost-utility analysis, which was based on precedent treatment in Canada.
The clinical trial included 120 community-dwelling adults aged 55 years and older who had a stroke at least 12 months before the study. Based in the Vancouver metropolitan area, participants were randomly assigned to twice-weekly, 60-minute classes led by trained instructors for 26 weeks. The mean age was 71 years, and 62% of participants were men.
Exercise Effective
Overall, the balance and tone control group had the lowest delivery cost at CAD $777 per person, followed by CAD $1090 per person for the exercise group and CAD $1492 per person for the cognitive and social enrichment group.
After the 6-month intervention, the mean cognitive scores were –0.192 for the exercise group, –0.184 for the cognitive and social enrichment group, and –0.171 for the balance and tone group, indicating better cognitive function across all three groups.
In the cost-effectiveness analysis, the exercise intervention was costlier but more effective than the control group, with an incremental cost-effectiveness ratio (ICER) of CAD –$8823.
In the cost-utility analysis, the exercise intervention was cost saving (less costly and more effective), compared with the control group, with an ICER of CAD –$3381 per QALY gained at the end of the intervention and an ICER of CAD –$154,198 per QALY gained at the end of the 12-month follow-up period. The cognitive and social enrichment program was more costly and more effective than the control group, with an ICER of CAD $101,687 per QALY gained at the end of the intervention and an ICER of CAD $331,306 per QALY gained at the end of the follow-up period.
In additional analyses, the exercise group had the lowest healthcare resource utilization due to lower healthcare costs for physician visits and lab tests.
“This study provides initial data that suggests multicomponent exercise may be a cost-effective solution for combating cognitive decline among stroke survivors,” said Dr. Davis.
Overall, exercise was cost-effective for improving cognitive function but not quality of life among participants. The clinical trial was powered to detect changes in cognitive function rather than quality of life, so it lacked statistical power to detect differences in quality of life, said Dr. Davis.
Exercise programs and cognitive and social enrichment programs show promise for improving cognitive function after stroke, the authors wrote, though future research should focus on optimizing cost-effectiveness and enhancing health-related quality of life.
Considering Additional Benefits
Commenting on the study, Alan Tam, MD, a physiatrist at the Toronto Rehabilitation Institute’s Brain Rehabilitation Program, said, “The authors show that within the timeframe of their analysis, there is a trend to cost-effectiveness for the cognitive intervention being offered.” Dr. Tam did not participate in the research.
“However, the finding is not robust, as less than 50% of their simulations would meet their acceptability level they have defined,” he said. “Given that most of the cost of the intervention is up front, but the benefits are likely lifelong, potentially taking the 12-month analysis to a lifetime analysis would show more significant findings.”
Dr. Tam researches factors associated with brain injury rehabilitation and has explored the cost-effectiveness of a high-intensity outpatient stroke rehabilitation program.
“Presenting this type of work is important,” he said. “While there are interventions that do not meet our definition of statistical significance, especially in the rehabilitation world, there can still be a benefit for patients and health systems.”
The primary study was funded by the Canadian Institutes of Health Research (CIHR) and the Jack Brown and Family Alzheimer Research Foundation Society. Dr. Davis reported receiving grants from the CIHR and Michael Smith Health Research BC during the conduct of the study. Dr. Tam reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
More evidence that modified Atkins diet lowers seizures in adults
ORLANDO —
The results of the small new review and meta-analysis suggest that “the MAD may be an effective adjuvant therapy for older patients who have failed anti-seizure medications,” study investigator Aiswarya Raj, MBBS, Aster Malabar Institute of Medical Sciences, Kerala, India, said in an interview.
The findings were presented at the annual meeting of the American Epilepsy Society.
Paucity of Adult Data
The MAD is a less restrictive hybrid of the ketogenic diet that limits carbohydrate intake and encourages fat consumption. It does not restrict fluids, calories, or proteins and does not require fats to be weighed or measured.
The diet includes fewer carbohydrates than the traditional Atkins diet and places more emphasis on fat intake. Dr. Raj said that the research suggests that the MAD “is a promising therapy in pediatric populations, but there’s not a lot of data in adults.”
Dr. Raj noted that this diet type has not been that popular in patients who clinicians believe might be better treated with drug therapy, possibly because of concern about the cardiac impact of consuming high-fat foods.
After conducting a systematic literature review assessing the efficacy of MAD in adults, the researchers included three randomized controlled trials and four observational studies published from January 2000 to May 2023 in the analysis.
The randomized controlled trials in the review assessed the primary outcome, a greater than 50% seizure reduction, at the end of 2 months, 3 months, and 6 months. In the MAD group, 32.5% of participants had more than a 50% seizure reduction vs 3% in the control group (odds ratio [OR], 12.62; 95% CI, 4.05-39.29; P < .0001).
Four participants who followed the diet achieved complete seizure-freedom compared with no participants in the control group (OR, 16.20; 95% CI, 0.82-318.82; P = .07).
The prospective studies examined this outcome at the end of 1 month or 3 months. In these studies, 41.9% of individuals experienced more than a 50% seizure reduction after 1 month of following the MAD, and 34.2% experienced this reduction after 3 months (OR, 1.41; 95% CI, 0.79-2.52; P = .24), with zero heterogeneity across studies.
It’s difficult to interpret the difference in seizure reduction between 1 and 3 months of therapy, Dr. Raj noted, because “there’s always the issue of compliance when you put a patient on a long-term diet.”
Positive results for MAD in adults were shown in another recent systematic review and meta-analysis published in Seizure: European Journal of Epilepsy.
That analysis included six studies with 575 patients who were randomly assigned to MAD or usual diet (UD) plus standard drug therapy. After an average follow-up of 12 weeks, MAD was associated with a higher rate of 50% or greater reduction in seizure frequency (relative risk [RR], 6.28; 95% CI, 3.52-10.50; P < .001), both in adults with drug-resistant epilepsy (RR, 6.14; 95% CI, 1.15-32.66; P = .033) and children (RR, 6.28; 95% CI, 3.43-11.49; P < .001).
MAD was also associated with a higher seizure freedom rate compared with UD (RR, 5.94; 95% CI, 1.93-18.31; P = .002).
Cholesterol Concern
In Dr. Raj’s analysis, there was an increment in blood total cholesterol level after 3 months of MAD (standard mean difference, -0.82; 95% CI, -1.23 to -0.40; P = .0001).
Concern about elevated blood cholesterol affecting coronary artery disease risk may explain why doctors sometimes shy away from recommending the MAD to their adult patients. “Some may not want to take that risk; you don’t want patients to succumb to coronary artery disease,” said Dr. Raj.
She noted that 3 months “is a very short time period,” and studies looking at cholesterol levels at the end of at least 1 year are needed to determine whether levels return to normal.
“We’re seeing a lot of literature now that suggests dietary intake does not really have a link with cholesterol levels,” she said. If this can be proven, “then this is definitely a great therapy.”
The evidence of cardiovascular safety of the MAD includes a study of 37 patients who showed that although total cholesterol and low-density lipoprotein (LDL) cholesterol increased over the first 3 months of MAD treatment, these values normalized within 1 year of treatment, including in patients treated with MAD for more than 3 years.
Primary Diet Recommendation
This news organization asked one of the authors of that study, Mackenzie C. Cervenka, MD, professor of neurology and medical director of the Adult Epilepsy Diet Center, Johns Hopkins Hospital, Baltimore, Maryland, to comment on the new research.
She said that she was “thrilled” to see more evidence showing that this diet therapy can be as effective for adults as for children. “This is a really important message to get out there.”
At her adult epilepsy diet center, the MAD is the “primary” diet recommended for patients who are resistant to seizure medication, not tube fed, and are keen to try diet therapy, said Dr. Cervenka.
In her experience, the likelihood of having a 50% or greater seizure reduction is about 40% among medication-resistant patients, “so very similar to what they reported in that review,” she said.
However, she noted that she emphasizes to patients that “diet therapy is not meant to be monotherapy.”
Dr. Cervenka’s team is examining LDL cholesterol levels as well as LDL particle size in adults who have been on the MAD for 2 years. LDL particle size, she noted, is a better predictor of long-term cardiovascular health.
No conflicts of interest were reported.
A version of this article appeared on Medscape.com.
ORLANDO —
The results of the small new review and meta-analysis suggest that “the MAD may be an effective adjuvant therapy for older patients who have failed anti-seizure medications,” study investigator Aiswarya Raj, MBBS, Aster Malabar Institute of Medical Sciences, Kerala, India, said in an interview.
The findings were presented at the annual meeting of the American Epilepsy Society.
Paucity of Adult Data
The MAD is a less restrictive hybrid of the ketogenic diet that limits carbohydrate intake and encourages fat consumption. It does not restrict fluids, calories, or proteins and does not require fats to be weighed or measured.
The diet includes fewer carbohydrates than the traditional Atkins diet and places more emphasis on fat intake. Dr. Raj said that the research suggests that the MAD “is a promising therapy in pediatric populations, but there’s not a lot of data in adults.”
Dr. Raj noted that this diet type has not been that popular in patients who clinicians believe might be better treated with drug therapy, possibly because of concern about the cardiac impact of consuming high-fat foods.
After conducting a systematic literature review assessing the efficacy of MAD in adults, the researchers included three randomized controlled trials and four observational studies published from January 2000 to May 2023 in the analysis.
The randomized controlled trials in the review assessed the primary outcome, a greater than 50% seizure reduction, at the end of 2 months, 3 months, and 6 months. In the MAD group, 32.5% of participants had more than a 50% seizure reduction vs 3% in the control group (odds ratio [OR], 12.62; 95% CI, 4.05-39.29; P < .0001).
Four participants who followed the diet achieved complete seizure-freedom compared with no participants in the control group (OR, 16.20; 95% CI, 0.82-318.82; P = .07).
The prospective studies examined this outcome at the end of 1 month or 3 months. In these studies, 41.9% of individuals experienced more than a 50% seizure reduction after 1 month of following the MAD, and 34.2% experienced this reduction after 3 months (OR, 1.41; 95% CI, 0.79-2.52; P = .24), with zero heterogeneity across studies.
It’s difficult to interpret the difference in seizure reduction between 1 and 3 months of therapy, Dr. Raj noted, because “there’s always the issue of compliance when you put a patient on a long-term diet.”
Positive results for MAD in adults were shown in another recent systematic review and meta-analysis published in Seizure: European Journal of Epilepsy.
That analysis included six studies with 575 patients who were randomly assigned to MAD or usual diet (UD) plus standard drug therapy. After an average follow-up of 12 weeks, MAD was associated with a higher rate of 50% or greater reduction in seizure frequency (relative risk [RR], 6.28; 95% CI, 3.52-10.50; P < .001), both in adults with drug-resistant epilepsy (RR, 6.14; 95% CI, 1.15-32.66; P = .033) and children (RR, 6.28; 95% CI, 3.43-11.49; P < .001).
MAD was also associated with a higher seizure freedom rate compared with UD (RR, 5.94; 95% CI, 1.93-18.31; P = .002).
Cholesterol Concern
In Dr. Raj’s analysis, there was an increment in blood total cholesterol level after 3 months of MAD (standard mean difference, -0.82; 95% CI, -1.23 to -0.40; P = .0001).
Concern about elevated blood cholesterol affecting coronary artery disease risk may explain why doctors sometimes shy away from recommending the MAD to their adult patients. “Some may not want to take that risk; you don’t want patients to succumb to coronary artery disease,” said Dr. Raj.
She noted that 3 months “is a very short time period,” and studies looking at cholesterol levels at the end of at least 1 year are needed to determine whether levels return to normal.
“We’re seeing a lot of literature now that suggests dietary intake does not really have a link with cholesterol levels,” she said. If this can be proven, “then this is definitely a great therapy.”
The evidence of cardiovascular safety of the MAD includes a study of 37 patients who showed that although total cholesterol and low-density lipoprotein (LDL) cholesterol increased over the first 3 months of MAD treatment, these values normalized within 1 year of treatment, including in patients treated with MAD for more than 3 years.
Primary Diet Recommendation
This news organization asked one of the authors of that study, Mackenzie C. Cervenka, MD, professor of neurology and medical director of the Adult Epilepsy Diet Center, Johns Hopkins Hospital, Baltimore, Maryland, to comment on the new research.
She said that she was “thrilled” to see more evidence showing that this diet therapy can be as effective for adults as for children. “This is a really important message to get out there.”
At her adult epilepsy diet center, the MAD is the “primary” diet recommended for patients who are resistant to seizure medication, not tube fed, and are keen to try diet therapy, said Dr. Cervenka.
In her experience, the likelihood of having a 50% or greater seizure reduction is about 40% among medication-resistant patients, “so very similar to what they reported in that review,” she said.
However, she noted that she emphasizes to patients that “diet therapy is not meant to be monotherapy.”
Dr. Cervenka’s team is examining LDL cholesterol levels as well as LDL particle size in adults who have been on the MAD for 2 years. LDL particle size, she noted, is a better predictor of long-term cardiovascular health.
No conflicts of interest were reported.
A version of this article appeared on Medscape.com.
ORLANDO —
The results of the small new review and meta-analysis suggest that “the MAD may be an effective adjuvant therapy for older patients who have failed anti-seizure medications,” study investigator Aiswarya Raj, MBBS, Aster Malabar Institute of Medical Sciences, Kerala, India, said in an interview.
The findings were presented at the annual meeting of the American Epilepsy Society.
Paucity of Adult Data
The MAD is a less restrictive hybrid of the ketogenic diet that limits carbohydrate intake and encourages fat consumption. It does not restrict fluids, calories, or proteins and does not require fats to be weighed or measured.
The diet includes fewer carbohydrates than the traditional Atkins diet and places more emphasis on fat intake. Dr. Raj said that the research suggests that the MAD “is a promising therapy in pediatric populations, but there’s not a lot of data in adults.”
Dr. Raj noted that this diet type has not been that popular in patients who clinicians believe might be better treated with drug therapy, possibly because of concern about the cardiac impact of consuming high-fat foods.
After conducting a systematic literature review assessing the efficacy of MAD in adults, the researchers included three randomized controlled trials and four observational studies published from January 2000 to May 2023 in the analysis.
The randomized controlled trials in the review assessed the primary outcome, a greater than 50% seizure reduction, at the end of 2 months, 3 months, and 6 months. In the MAD group, 32.5% of participants had more than a 50% seizure reduction vs 3% in the control group (odds ratio [OR], 12.62; 95% CI, 4.05-39.29; P < .0001).
Four participants who followed the diet achieved complete seizure-freedom compared with no participants in the control group (OR, 16.20; 95% CI, 0.82-318.82; P = .07).
The prospective studies examined this outcome at the end of 1 month or 3 months. In these studies, 41.9% of individuals experienced more than a 50% seizure reduction after 1 month of following the MAD, and 34.2% experienced this reduction after 3 months (OR, 1.41; 95% CI, 0.79-2.52; P = .24), with zero heterogeneity across studies.
It’s difficult to interpret the difference in seizure reduction between 1 and 3 months of therapy, Dr. Raj noted, because “there’s always the issue of compliance when you put a patient on a long-term diet.”
Positive results for MAD in adults were shown in another recent systematic review and meta-analysis published in Seizure: European Journal of Epilepsy.
That analysis included six studies with 575 patients who were randomly assigned to MAD or usual diet (UD) plus standard drug therapy. After an average follow-up of 12 weeks, MAD was associated with a higher rate of 50% or greater reduction in seizure frequency (relative risk [RR], 6.28; 95% CI, 3.52-10.50; P < .001), both in adults with drug-resistant epilepsy (RR, 6.14; 95% CI, 1.15-32.66; P = .033) and children (RR, 6.28; 95% CI, 3.43-11.49; P < .001).
MAD was also associated with a higher seizure freedom rate compared with UD (RR, 5.94; 95% CI, 1.93-18.31; P = .002).
Cholesterol Concern
In Dr. Raj’s analysis, there was an increment in blood total cholesterol level after 3 months of MAD (standard mean difference, -0.82; 95% CI, -1.23 to -0.40; P = .0001).
Concern about elevated blood cholesterol affecting coronary artery disease risk may explain why doctors sometimes shy away from recommending the MAD to their adult patients. “Some may not want to take that risk; you don’t want patients to succumb to coronary artery disease,” said Dr. Raj.
She noted that 3 months “is a very short time period,” and studies looking at cholesterol levels at the end of at least 1 year are needed to determine whether levels return to normal.
“We’re seeing a lot of literature now that suggests dietary intake does not really have a link with cholesterol levels,” she said. If this can be proven, “then this is definitely a great therapy.”
The evidence of cardiovascular safety of the MAD includes a study of 37 patients who showed that although total cholesterol and low-density lipoprotein (LDL) cholesterol increased over the first 3 months of MAD treatment, these values normalized within 1 year of treatment, including in patients treated with MAD for more than 3 years.
Primary Diet Recommendation
This news organization asked one of the authors of that study, Mackenzie C. Cervenka, MD, professor of neurology and medical director of the Adult Epilepsy Diet Center, Johns Hopkins Hospital, Baltimore, Maryland, to comment on the new research.
She said that she was “thrilled” to see more evidence showing that this diet therapy can be as effective for adults as for children. “This is a really important message to get out there.”
At her adult epilepsy diet center, the MAD is the “primary” diet recommended for patients who are resistant to seizure medication, not tube fed, and are keen to try diet therapy, said Dr. Cervenka.
In her experience, the likelihood of having a 50% or greater seizure reduction is about 40% among medication-resistant patients, “so very similar to what they reported in that review,” she said.
However, she noted that she emphasizes to patients that “diet therapy is not meant to be monotherapy.”
Dr. Cervenka’s team is examining LDL cholesterol levels as well as LDL particle size in adults who have been on the MAD for 2 years. LDL particle size, she noted, is a better predictor of long-term cardiovascular health.
No conflicts of interest were reported.
A version of this article appeared on Medscape.com.
FROM AES 2023
CGRP in migraine prodrome can stop headache, reduce severity
BARCELONA, SPAIN — In the randomized, placebo-controlled crossover PRODROME trial, treatment with ubrogepant (Ubrelvy) 100 mg, one of the new CGRP receptor antagonists, during the prodrome prevented the development of moderate/severe headache at both 24 hours and 48 hours post-dose. The medication also reduced headache of any intensity within 24 hours and functional disability compared with placebo.
“This represents a totally different way of treating a migraine attack – to treat it before the headache starts. This is a paradigm shift in the way we approach the acute treatment of migraine,” study investigator Peter Goadsby, MBBS, MD, PhD, professor of neurology at Kings College London, UK, said in an interview.
The findings were presented at 17th European Headache Congress (EHC) and were also recently published online in The Lancet.
A New Way to Manage Migraine?
The prodrome is usually the earliest phase of a migraine attack and is believed to be experienced by the vast majority of patients with migraine. It consists of various symptoms, including sensitivity to light, fatigue, mood changes, cognitive dysfunction, craving certain foods, and neck pain, which can occur several hours or days before onset.
Dr. Goadsby notes that, at present, there isn’t very much a patient can do about the prodrome.
“We advise patients if they feel an attack is coming not to do anything that might make it worse and make sure they have their acute treatment available for when the headache phase starts. So, we just advise people to prepare for the attack rather than doing anything specific to stop it. But with new data from this study, we now have something that can be done. Patients have an option,” he said.
Dr. Goadsby explained that currently patients are not encouraged to use acute migraine medications such as triptans in the prodrome phase.
“There is actually no evidence that taking a triptan during the prodromal phase works. The advice is to take a triptan as soon as the headache starts, but not before the headache starts.”
He noted that there is also the problem of medication overuse that is seen with triptans, and most other medications used to treat acute migraine, which leads to medication overuse headache, “so we don’t like to encourage patients to increase the frequency of taking triptans for this reason.”
But ubrogepant and other members of the “gepant” class do not seem to have the propensity for medication overuse problems. “Rather, the more a patient takes the less likely they are to get a headache as these drugs also have a preventative effect,” Dr. Goadsby said.
Major Reduction in Severity
The PRODROME trial was conducted at 75 sites in the United States in 518 patients who had at least a 1-year history of migraine with or without aura and a history of two to eight migraine attacks per month with moderate to severe headache in each of the 3 months before study entry.
Participants underwent a rigorous screening period during which they were required to show that they could identify prodromal symptoms that were reliably followed by migraine headache within 1-6 hours.
They were randomly assigned to receive either placebo to treat the first qualifying prodrome event and ubrogepant 100 mg to treat the second qualifying prodrome event or vice versa, with instructions to take the study drug at the onset of the prodrome event.
Efficacy assessments during the double-blind treatment period were recorded by the participant in an electronic diary. On identifying a qualifying prodrome, the patient recorded prodromal symptoms, and was then required to report the absence or presence of a headache at regular intervals up to 48 hours after the study drug dose. If a headache was reported, participants rated the intensity as mild, moderate, or severe and reported whether rescue medication was taken to treat it.
The primary endpoint was absence of moderate or severe intensity headache within 24 hours after study-drug dose. This occurred after 46% of 418 qualifying prodrome events that had been treated with ubrogepant and after 29% of 423 qualifying prodrome events that had been treated with placebo (odds ratio, 2.09; 95% CI, 1.63 - 2.69; P < .0001).
“The incidence of moderate to severe headache was almost halved when ubrogepant was taken in the prodrome,” Dr. Goadsby reported.
Ubrogepant also showed similar impressive results for the secondary endpoints in the absence of moderate to severe headache within 48 hours post-dose and the absence of any headache of any intensity at 24 hours.
Little to No Disability
The researchers also evaluated functional ability, and more participants reported “no disability or able to function normally” during the 24 hours after treatment with ubrogepant than after placebo (OR, 1.66; P < .0001).
Other findings showed that the prodromal symptoms themselves, such as light sensitivity and cognitive dysfunction, were also reduced with ubrogepant.
Dr. Goadsby said he was pleased but not surprised by the results, as the “gepant” class of drugs are used in both the acute treatment of migraine and as preventive agents, although different agents have been approved for different indications in this regard.
“The ‘gepants’ are a class of medication that can be used in almost any way in migraine — to treat an acute migraine headache, to prevent migraine if taken chronically, and now we see that they can also stop a migraine from developing if taken during the initial prodromal phase. That’s unique for a migraine medication,” he said.
While the current study was conducted with ubrogepant, Dr. Goadsby suspects that any of the “gepants” would probably have a similar effect.
He noted that the prodromal phase of migraine has only just started to be explored, with functional imaging studies showing that structural brain changes occur during this phase.
Dr. Goadsby said the current study opens up a whole new area of interest, emphasizing the clinical value of identifying the prodrome in individuals with migraine, better characterizing the symptomology of the prodrome and understanding more about how to treat it.
“It’s the ultimate way of treating migraine early, and by taking this type of medication in the prodromal phase, patients may be able to stop having pain. That’s quite an implication,” he concluded.
The PRODROME study was funded by AbbVie. Dr. Goadsby reports personal fees from AbbVie.
A version of this article appeared on Medscape.com.
BARCELONA, SPAIN — In the randomized, placebo-controlled crossover PRODROME trial, treatment with ubrogepant (Ubrelvy) 100 mg, one of the new CGRP receptor antagonists, during the prodrome prevented the development of moderate/severe headache at both 24 hours and 48 hours post-dose. The medication also reduced headache of any intensity within 24 hours and functional disability compared with placebo.
“This represents a totally different way of treating a migraine attack – to treat it before the headache starts. This is a paradigm shift in the way we approach the acute treatment of migraine,” study investigator Peter Goadsby, MBBS, MD, PhD, professor of neurology at Kings College London, UK, said in an interview.
The findings were presented at 17th European Headache Congress (EHC) and were also recently published online in The Lancet.
A New Way to Manage Migraine?
The prodrome is usually the earliest phase of a migraine attack and is believed to be experienced by the vast majority of patients with migraine. It consists of various symptoms, including sensitivity to light, fatigue, mood changes, cognitive dysfunction, craving certain foods, and neck pain, which can occur several hours or days before onset.
Dr. Goadsby notes that, at present, there isn’t very much a patient can do about the prodrome.
“We advise patients if they feel an attack is coming not to do anything that might make it worse and make sure they have their acute treatment available for when the headache phase starts. So, we just advise people to prepare for the attack rather than doing anything specific to stop it. But with new data from this study, we now have something that can be done. Patients have an option,” he said.
Dr. Goadsby explained that currently patients are not encouraged to use acute migraine medications such as triptans in the prodrome phase.
“There is actually no evidence that taking a triptan during the prodromal phase works. The advice is to take a triptan as soon as the headache starts, but not before the headache starts.”
He noted that there is also the problem of medication overuse that is seen with triptans, and most other medications used to treat acute migraine, which leads to medication overuse headache, “so we don’t like to encourage patients to increase the frequency of taking triptans for this reason.”
But ubrogepant and other members of the “gepant” class do not seem to have the propensity for medication overuse problems. “Rather, the more a patient takes the less likely they are to get a headache as these drugs also have a preventative effect,” Dr. Goadsby said.
Major Reduction in Severity
The PRODROME trial was conducted at 75 sites in the United States in 518 patients who had at least a 1-year history of migraine with or without aura and a history of two to eight migraine attacks per month with moderate to severe headache in each of the 3 months before study entry.
Participants underwent a rigorous screening period during which they were required to show that they could identify prodromal symptoms that were reliably followed by migraine headache within 1-6 hours.
They were randomly assigned to receive either placebo to treat the first qualifying prodrome event and ubrogepant 100 mg to treat the second qualifying prodrome event or vice versa, with instructions to take the study drug at the onset of the prodrome event.
Efficacy assessments during the double-blind treatment period were recorded by the participant in an electronic diary. On identifying a qualifying prodrome, the patient recorded prodromal symptoms, and was then required to report the absence or presence of a headache at regular intervals up to 48 hours after the study drug dose. If a headache was reported, participants rated the intensity as mild, moderate, or severe and reported whether rescue medication was taken to treat it.
The primary endpoint was absence of moderate or severe intensity headache within 24 hours after study-drug dose. This occurred after 46% of 418 qualifying prodrome events that had been treated with ubrogepant and after 29% of 423 qualifying prodrome events that had been treated with placebo (odds ratio, 2.09; 95% CI, 1.63 - 2.69; P < .0001).
“The incidence of moderate to severe headache was almost halved when ubrogepant was taken in the prodrome,” Dr. Goadsby reported.
Ubrogepant also showed similar impressive results for the secondary endpoints in the absence of moderate to severe headache within 48 hours post-dose and the absence of any headache of any intensity at 24 hours.
Little to No Disability
The researchers also evaluated functional ability, and more participants reported “no disability or able to function normally” during the 24 hours after treatment with ubrogepant than after placebo (OR, 1.66; P < .0001).
Other findings showed that the prodromal symptoms themselves, such as light sensitivity and cognitive dysfunction, were also reduced with ubrogepant.
Dr. Goadsby said he was pleased but not surprised by the results, as the “gepant” class of drugs are used in both the acute treatment of migraine and as preventive agents, although different agents have been approved for different indications in this regard.
“The ‘gepants’ are a class of medication that can be used in almost any way in migraine — to treat an acute migraine headache, to prevent migraine if taken chronically, and now we see that they can also stop a migraine from developing if taken during the initial prodromal phase. That’s unique for a migraine medication,” he said.
While the current study was conducted with ubrogepant, Dr. Goadsby suspects that any of the “gepants” would probably have a similar effect.
He noted that the prodromal phase of migraine has only just started to be explored, with functional imaging studies showing that structural brain changes occur during this phase.
Dr. Goadsby said the current study opens up a whole new area of interest, emphasizing the clinical value of identifying the prodrome in individuals with migraine, better characterizing the symptomology of the prodrome and understanding more about how to treat it.
“It’s the ultimate way of treating migraine early, and by taking this type of medication in the prodromal phase, patients may be able to stop having pain. That’s quite an implication,” he concluded.
The PRODROME study was funded by AbbVie. Dr. Goadsby reports personal fees from AbbVie.
A version of this article appeared on Medscape.com.
BARCELONA, SPAIN — In the randomized, placebo-controlled crossover PRODROME trial, treatment with ubrogepant (Ubrelvy) 100 mg, one of the new CGRP receptor antagonists, during the prodrome prevented the development of moderate/severe headache at both 24 hours and 48 hours post-dose. The medication also reduced headache of any intensity within 24 hours and functional disability compared with placebo.
“This represents a totally different way of treating a migraine attack – to treat it before the headache starts. This is a paradigm shift in the way we approach the acute treatment of migraine,” study investigator Peter Goadsby, MBBS, MD, PhD, professor of neurology at Kings College London, UK, said in an interview.
The findings were presented at 17th European Headache Congress (EHC) and were also recently published online in The Lancet.
A New Way to Manage Migraine?
The prodrome is usually the earliest phase of a migraine attack and is believed to be experienced by the vast majority of patients with migraine. It consists of various symptoms, including sensitivity to light, fatigue, mood changes, cognitive dysfunction, craving certain foods, and neck pain, which can occur several hours or days before onset.
Dr. Goadsby notes that, at present, there isn’t very much a patient can do about the prodrome.
“We advise patients if they feel an attack is coming not to do anything that might make it worse and make sure they have their acute treatment available for when the headache phase starts. So, we just advise people to prepare for the attack rather than doing anything specific to stop it. But with new data from this study, we now have something that can be done. Patients have an option,” he said.
Dr. Goadsby explained that currently patients are not encouraged to use acute migraine medications such as triptans in the prodrome phase.
“There is actually no evidence that taking a triptan during the prodromal phase works. The advice is to take a triptan as soon as the headache starts, but not before the headache starts.”
He noted that there is also the problem of medication overuse that is seen with triptans, and most other medications used to treat acute migraine, which leads to medication overuse headache, “so we don’t like to encourage patients to increase the frequency of taking triptans for this reason.”
But ubrogepant and other members of the “gepant” class do not seem to have the propensity for medication overuse problems. “Rather, the more a patient takes the less likely they are to get a headache as these drugs also have a preventative effect,” Dr. Goadsby said.
Major Reduction in Severity
The PRODROME trial was conducted at 75 sites in the United States in 518 patients who had at least a 1-year history of migraine with or without aura and a history of two to eight migraine attacks per month with moderate to severe headache in each of the 3 months before study entry.
Participants underwent a rigorous screening period during which they were required to show that they could identify prodromal symptoms that were reliably followed by migraine headache within 1-6 hours.
They were randomly assigned to receive either placebo to treat the first qualifying prodrome event and ubrogepant 100 mg to treat the second qualifying prodrome event or vice versa, with instructions to take the study drug at the onset of the prodrome event.
Efficacy assessments during the double-blind treatment period were recorded by the participant in an electronic diary. On identifying a qualifying prodrome, the patient recorded prodromal symptoms, and was then required to report the absence or presence of a headache at regular intervals up to 48 hours after the study drug dose. If a headache was reported, participants rated the intensity as mild, moderate, or severe and reported whether rescue medication was taken to treat it.
The primary endpoint was absence of moderate or severe intensity headache within 24 hours after study-drug dose. This occurred after 46% of 418 qualifying prodrome events that had been treated with ubrogepant and after 29% of 423 qualifying prodrome events that had been treated with placebo (odds ratio, 2.09; 95% CI, 1.63 - 2.69; P < .0001).
“The incidence of moderate to severe headache was almost halved when ubrogepant was taken in the prodrome,” Dr. Goadsby reported.
Ubrogepant also showed similar impressive results for the secondary endpoints in the absence of moderate to severe headache within 48 hours post-dose and the absence of any headache of any intensity at 24 hours.
Little to No Disability
The researchers also evaluated functional ability, and more participants reported “no disability or able to function normally” during the 24 hours after treatment with ubrogepant than after placebo (OR, 1.66; P < .0001).
Other findings showed that the prodromal symptoms themselves, such as light sensitivity and cognitive dysfunction, were also reduced with ubrogepant.
Dr. Goadsby said he was pleased but not surprised by the results, as the “gepant” class of drugs are used in both the acute treatment of migraine and as preventive agents, although different agents have been approved for different indications in this regard.
“The ‘gepants’ are a class of medication that can be used in almost any way in migraine — to treat an acute migraine headache, to prevent migraine if taken chronically, and now we see that they can also stop a migraine from developing if taken during the initial prodromal phase. That’s unique for a migraine medication,” he said.
While the current study was conducted with ubrogepant, Dr. Goadsby suspects that any of the “gepants” would probably have a similar effect.
He noted that the prodromal phase of migraine has only just started to be explored, with functional imaging studies showing that structural brain changes occur during this phase.
Dr. Goadsby said the current study opens up a whole new area of interest, emphasizing the clinical value of identifying the prodrome in individuals with migraine, better characterizing the symptomology of the prodrome and understanding more about how to treat it.
“It’s the ultimate way of treating migraine early, and by taking this type of medication in the prodromal phase, patients may be able to stop having pain. That’s quite an implication,” he concluded.
The PRODROME study was funded by AbbVie. Dr. Goadsby reports personal fees from AbbVie.
A version of this article appeared on Medscape.com.
FROM EHC 2023
Why Are Prion Diseases on the Rise?
This transcript has been edited for clarity.
In 1986, in Britain, cattle started dying.
The condition, quickly nicknamed “mad cow disease,” was clearly infectious, but the particular pathogen was difficult to identify. By 1993, 120,000 cattle in Britain were identified as being infected. As yet, no human cases had occurred and the UK government insisted that cattle were a dead-end host for the pathogen. By the mid-1990s, however, multiple human cases, attributable to ingestion of meat and organs from infected cattle, were discovered. In humans, variant Creutzfeldt-Jakob disease (CJD) was a media sensation — a nearly uniformly fatal, untreatable condition with a rapid onset of dementia, mobility issues characterized by jerky movements, and autopsy reports finding that the brain itself had turned into a spongy mess.
The United States banned UK beef imports in 1996 and only lifted the ban in 2020.
The disease was made all the more mysterious because the pathogen involved was not a bacterium, parasite, or virus, but a protein — or a proteinaceous infectious particle, shortened to “prion.”
Prions are misfolded proteins that aggregate in cells — in this case, in nerve cells. But what makes prions different from other misfolded proteins is that the misfolded protein catalyzes the conversion of its non-misfolded counterpart into the misfolded configuration. It creates a chain reaction, leading to rapid accumulation of misfolded proteins and cell death.
And, like a time bomb, we all have prion protein inside us. In its normally folded state, the function of prion protein remains unclear — knockout mice do okay without it — but it is also highly conserved across mammalian species, so it probably does something worthwhile, perhaps protecting nerve fibers.
Far more common than humans contracting mad cow disease is the condition known as sporadic CJD, responsible for 85% of all cases of prion-induced brain disease. The cause of sporadic CJD is unknown.
But one thing is known: Cases are increasing.
I don’t want you to freak out; we are not in the midst of a CJD epidemic. But it’s been a while since I’ve seen people discussing the condition — which remains as horrible as it was in the 1990s — and a new research letter appearing in JAMA Neurology brought it back to the top of my mind.
Researchers, led by Matthew Crane at Hopkins, used the CDC’s WONDER cause-of-death database, which pulls diagnoses from death certificates. Normally, I’m not a fan of using death certificates for cause-of-death analyses, but in this case I’ll give it a pass. Assuming that the diagnosis of CJD is made, it would be really unlikely for it not to appear on a death certificate.
The main findings are seen here. 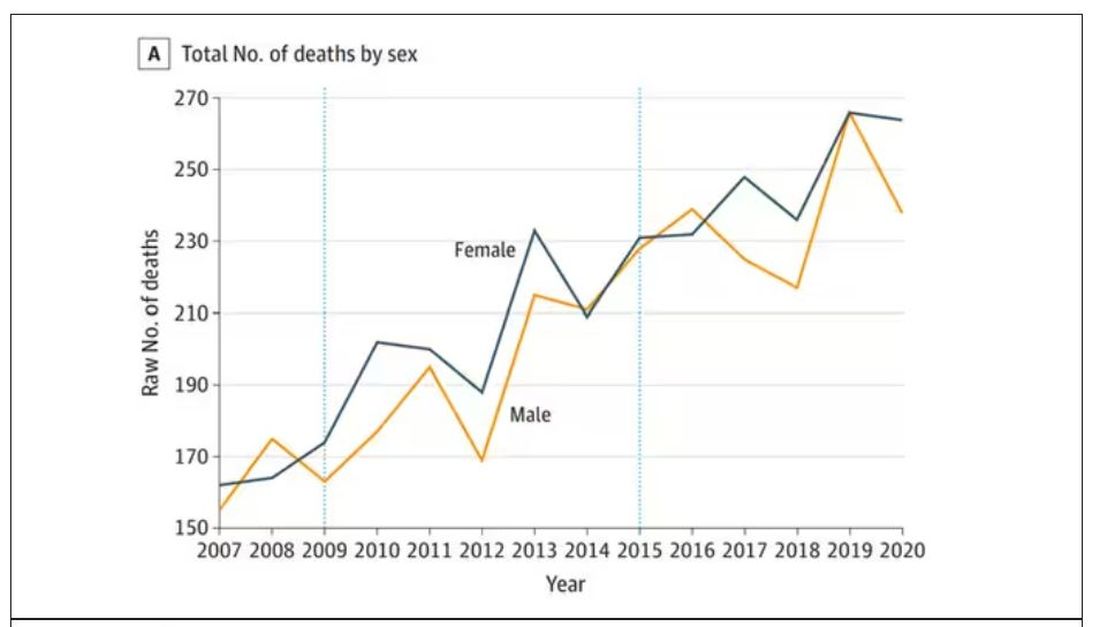
Note that we can’t tell whether these are sporadic CJD cases or variant CJD cases or even familial CJD cases; however, unless there has been a dramatic change in epidemiology, the vast majority of these will be sporadic.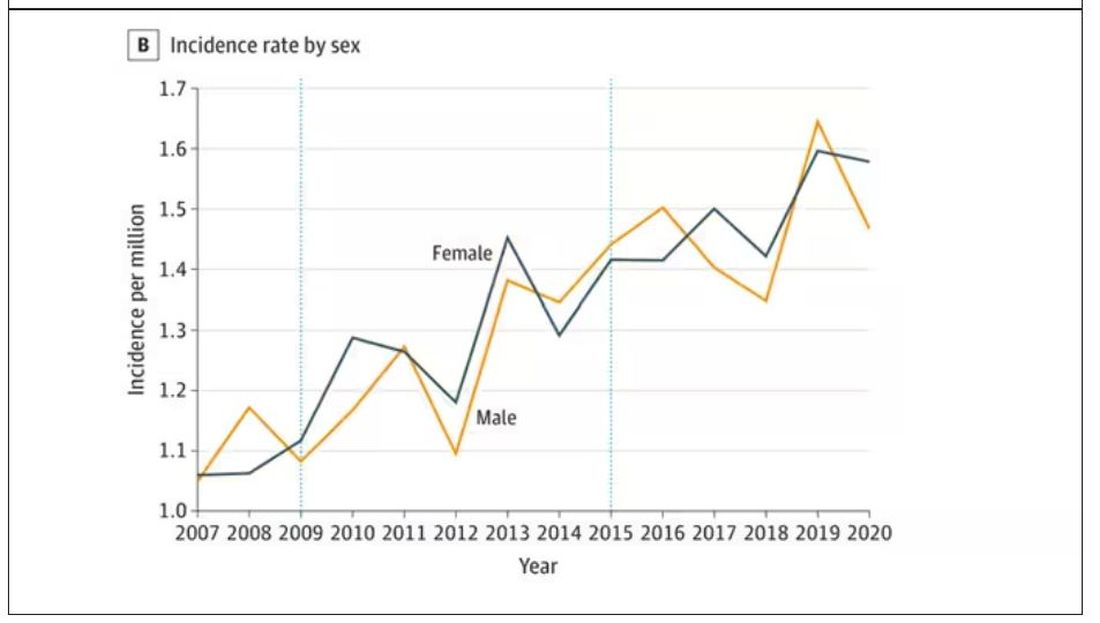
The question is, why are there more cases?
Whenever this type of question comes up with any disease, there are basically three possibilities:
First, there may be an increase in the susceptible, or at-risk, population. In this case, we know that older people are at higher risk of developing sporadic CJD, and over time, the population has aged. To be fair, the authors adjusted for this and still saw an increase, though it was attenuated.
Second, we might be better at diagnosing the condition. A lot has happened since the mid-1990s, when the diagnosis was based more or less on symptoms. The advent of more sophisticated MRI protocols as well as a new diagnostic test called “real-time quaking-induced conversion testing” may mean we are just better at detecting people with this disease.
Third (and most concerning), a new exposure has occurred. What that exposure might be, where it might come from, is anyone’s guess. It’s hard to do broad-scale epidemiology on very rare diseases.
But given these findings, it seems that a bit more surveillance for this rare but devastating condition is well merited.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now.
F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
In 1986, in Britain, cattle started dying.
The condition, quickly nicknamed “mad cow disease,” was clearly infectious, but the particular pathogen was difficult to identify. By 1993, 120,000 cattle in Britain were identified as being infected. As yet, no human cases had occurred and the UK government insisted that cattle were a dead-end host for the pathogen. By the mid-1990s, however, multiple human cases, attributable to ingestion of meat and organs from infected cattle, were discovered. In humans, variant Creutzfeldt-Jakob disease (CJD) was a media sensation — a nearly uniformly fatal, untreatable condition with a rapid onset of dementia, mobility issues characterized by jerky movements, and autopsy reports finding that the brain itself had turned into a spongy mess.
The United States banned UK beef imports in 1996 and only lifted the ban in 2020.
The disease was made all the more mysterious because the pathogen involved was not a bacterium, parasite, or virus, but a protein — or a proteinaceous infectious particle, shortened to “prion.”
Prions are misfolded proteins that aggregate in cells — in this case, in nerve cells. But what makes prions different from other misfolded proteins is that the misfolded protein catalyzes the conversion of its non-misfolded counterpart into the misfolded configuration. It creates a chain reaction, leading to rapid accumulation of misfolded proteins and cell death.
And, like a time bomb, we all have prion protein inside us. In its normally folded state, the function of prion protein remains unclear — knockout mice do okay without it — but it is also highly conserved across mammalian species, so it probably does something worthwhile, perhaps protecting nerve fibers.
Far more common than humans contracting mad cow disease is the condition known as sporadic CJD, responsible for 85% of all cases of prion-induced brain disease. The cause of sporadic CJD is unknown.
But one thing is known: Cases are increasing.
I don’t want you to freak out; we are not in the midst of a CJD epidemic. But it’s been a while since I’ve seen people discussing the condition — which remains as horrible as it was in the 1990s — and a new research letter appearing in JAMA Neurology brought it back to the top of my mind.
Researchers, led by Matthew Crane at Hopkins, used the CDC’s WONDER cause-of-death database, which pulls diagnoses from death certificates. Normally, I’m not a fan of using death certificates for cause-of-death analyses, but in this case I’ll give it a pass. Assuming that the diagnosis of CJD is made, it would be really unlikely for it not to appear on a death certificate.
The main findings are seen here.
Note that we can’t tell whether these are sporadic CJD cases or variant CJD cases or even familial CJD cases; however, unless there has been a dramatic change in epidemiology, the vast majority of these will be sporadic.
The question is, why are there more cases?
Whenever this type of question comes up with any disease, there are basically three possibilities:
First, there may be an increase in the susceptible, or at-risk, population. In this case, we know that older people are at higher risk of developing sporadic CJD, and over time, the population has aged. To be fair, the authors adjusted for this and still saw an increase, though it was attenuated.
Second, we might be better at diagnosing the condition. A lot has happened since the mid-1990s, when the diagnosis was based more or less on symptoms. The advent of more sophisticated MRI protocols as well as a new diagnostic test called “real-time quaking-induced conversion testing” may mean we are just better at detecting people with this disease.
Third (and most concerning), a new exposure has occurred. What that exposure might be, where it might come from, is anyone’s guess. It’s hard to do broad-scale epidemiology on very rare diseases.
But given these findings, it seems that a bit more surveillance for this rare but devastating condition is well merited.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now.
F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
In 1986, in Britain, cattle started dying.
The condition, quickly nicknamed “mad cow disease,” was clearly infectious, but the particular pathogen was difficult to identify. By 1993, 120,000 cattle in Britain were identified as being infected. As yet, no human cases had occurred and the UK government insisted that cattle were a dead-end host for the pathogen. By the mid-1990s, however, multiple human cases, attributable to ingestion of meat and organs from infected cattle, were discovered. In humans, variant Creutzfeldt-Jakob disease (CJD) was a media sensation — a nearly uniformly fatal, untreatable condition with a rapid onset of dementia, mobility issues characterized by jerky movements, and autopsy reports finding that the brain itself had turned into a spongy mess.
The United States banned UK beef imports in 1996 and only lifted the ban in 2020.
The disease was made all the more mysterious because the pathogen involved was not a bacterium, parasite, or virus, but a protein — or a proteinaceous infectious particle, shortened to “prion.”
Prions are misfolded proteins that aggregate in cells — in this case, in nerve cells. But what makes prions different from other misfolded proteins is that the misfolded protein catalyzes the conversion of its non-misfolded counterpart into the misfolded configuration. It creates a chain reaction, leading to rapid accumulation of misfolded proteins and cell death.
And, like a time bomb, we all have prion protein inside us. In its normally folded state, the function of prion protein remains unclear — knockout mice do okay without it — but it is also highly conserved across mammalian species, so it probably does something worthwhile, perhaps protecting nerve fibers.
Far more common than humans contracting mad cow disease is the condition known as sporadic CJD, responsible for 85% of all cases of prion-induced brain disease. The cause of sporadic CJD is unknown.
But one thing is known: Cases are increasing.
I don’t want you to freak out; we are not in the midst of a CJD epidemic. But it’s been a while since I’ve seen people discussing the condition — which remains as horrible as it was in the 1990s — and a new research letter appearing in JAMA Neurology brought it back to the top of my mind.
Researchers, led by Matthew Crane at Hopkins, used the CDC’s WONDER cause-of-death database, which pulls diagnoses from death certificates. Normally, I’m not a fan of using death certificates for cause-of-death analyses, but in this case I’ll give it a pass. Assuming that the diagnosis of CJD is made, it would be really unlikely for it not to appear on a death certificate.
The main findings are seen here.
Note that we can’t tell whether these are sporadic CJD cases or variant CJD cases or even familial CJD cases; however, unless there has been a dramatic change in epidemiology, the vast majority of these will be sporadic.
The question is, why are there more cases?
Whenever this type of question comes up with any disease, there are basically three possibilities:
First, there may be an increase in the susceptible, or at-risk, population. In this case, we know that older people are at higher risk of developing sporadic CJD, and over time, the population has aged. To be fair, the authors adjusted for this and still saw an increase, though it was attenuated.
Second, we might be better at diagnosing the condition. A lot has happened since the mid-1990s, when the diagnosis was based more or less on symptoms. The advent of more sophisticated MRI protocols as well as a new diagnostic test called “real-time quaking-induced conversion testing” may mean we are just better at detecting people with this disease.
Third (and most concerning), a new exposure has occurred. What that exposure might be, where it might come from, is anyone’s guess. It’s hard to do broad-scale epidemiology on very rare diseases.
But given these findings, it seems that a bit more surveillance for this rare but devastating condition is well merited.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now.
F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.