User login
For MD-IQ use only
Physical fitness guidelines from HHS
Also today, hydroxychloroquine treatment of SLE is hobbled by fears of blindness, antiepileptic drugs are strongly linked to rare serious skin reactions, and the FDA aims to squash vaping and smoking among youth.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, hydroxychloroquine treatment of SLE is hobbled by fears of blindness, antiepileptic drugs are strongly linked to rare serious skin reactions, and the FDA aims to squash vaping and smoking among youth.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, hydroxychloroquine treatment of SLE is hobbled by fears of blindness, antiepileptic drugs are strongly linked to rare serious skin reactions, and the FDA aims to squash vaping and smoking among youth.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

How do hospital medicine groups deal with staffing shortages?
Persistent demand for hospitalists nationally
During the last two decades, the United States health care labor market had an almost insatiable appetite for hospitalists, driving the specialty from nothing to over 50,000 members. Evidence of persistent demand for hospitalists abounds in the freshly released 2018 State of Hospital Medicine (SoHM) report: rising salaries, growing responsibility for the overall hospital census, and a diversifying scope of services.

The SoHM offers fascinating and detailed insights into these trends, as well as hundreds of other aspects of the field’s growth. Unfortunately, this expanding and dynamic labor market has a challenging side for hospitals, management companies, and hospitalist group leaders – we are constantly recruiting and dealing with open positions!
As a multisite leader at an academic health system, I’m looking toward the next season of recruitment with excitement. In the fall and winter we’re fortunate to receive applications from the best and brightest graduating residents and hospitalists. I realize this is a blessing, particularly compared with programs in rural areas that may not hear from many applicants. However, even when we succeed at filling the openings, there is an inevitable trickle of talent out of our clinical labor pool during the spring and summer. One person is invited to spend 20% of their time leading a teaching program, another secures a highly coveted grant, and yet another has to move because their spouse is relocated. By then, we don’t have a packed roster of applicants and have to solve the challenge in other ways. What does the typical hospital medicine program do when faced with this circumstance?
The 2018 SoHM survey first asked program leaders whether they had open and unfilled physician positions during the last year because of turnover, growth, or other factors. On average, 66% of groups serving adults and 48% of groups serving children said “yes.” For the job seekers out there, take note of some important regional differences: The regions with the highest percentage of programs dealing with unfilled positions were the East and West Coasts at 79% and 73%, respectively.
Next, the survey asked respondents to describe the percentage of total approved physician staffing that was open or unfilled during the year. On average, 12% of positions went unfilled, with important variation between different types of employers. For a typical HM group with 15 full-time equivalents, that means constantly working short two physicians!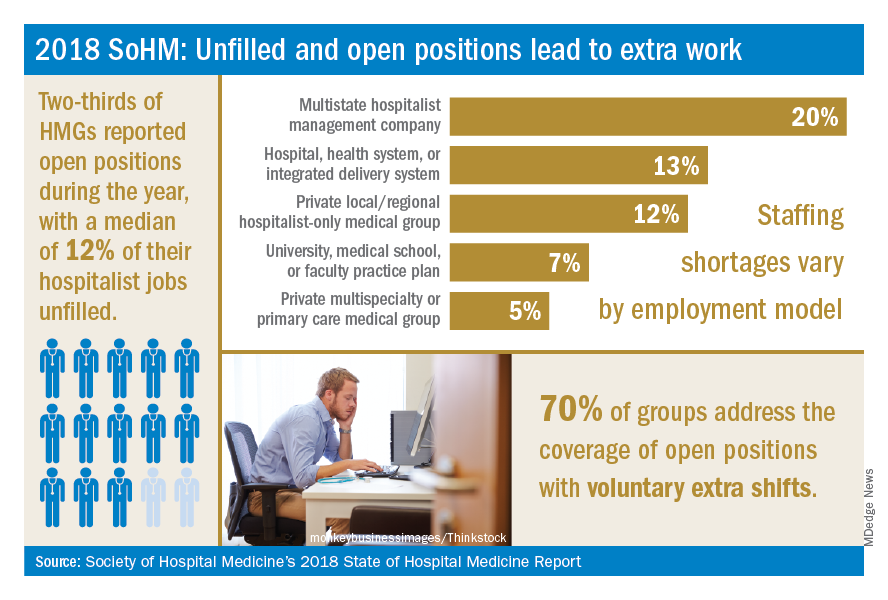
Not only is it hard for group leaders to manage chronic understaffing, it definitely takes a toll on the group. We asked leaders to describe all of the ways their groups address coverage of the open positions. The most common tactics were for existing hospitalists to perform voluntary extra shifts (70%) and the use of moonlighters (57%). Also important were the use of locum tenens physicians (44%) and just leaving some shifts uncovered (31%).
The last option might work in a large group, where everyone can pick up an extra couple of patients, but it nonetheless degrades continuity and care progression. In a small group, leaving shifts uncovered sounds like a recipe for burnout and unsafe care – hopefully subsequent surveys will find that we can avoid that approach! Obviously, the solutions must be tailored to the group, their resources, and the alternative sources of labor available in that locality.
The SoHM report provides insight into how this is commonly handled by different employers and in different regions – we encourage anyone who is interested to purchase the report (www.hospitalmedicine.org/sohm) to dig deeper. For better or worse, the issue of unfilled positions looks likely to persist for the intermediate future. The exciting rise of hospital medicine against the backdrop of an aging population means job security, rising income, and opportunities for many to live where they choose. Until the job market saturates, though, we’ll all find ourselves looking at email inboxes with a request or two to pick up an extra shift!
Dr. White is associate professor of medicine at the University of Washington, Seattle. He is the chair of SHM’s Practice Analysis Committee.
Reference
Society of Hospital Medicine. 2018 State of Hospital Medicine Report. pp. 89, 90, 181, 152.
Persistent demand for hospitalists nationally
Persistent demand for hospitalists nationally
During the last two decades, the United States health care labor market had an almost insatiable appetite for hospitalists, driving the specialty from nothing to over 50,000 members. Evidence of persistent demand for hospitalists abounds in the freshly released 2018 State of Hospital Medicine (SoHM) report: rising salaries, growing responsibility for the overall hospital census, and a diversifying scope of services.
The SoHM offers fascinating and detailed insights into these trends, as well as hundreds of other aspects of the field’s growth. Unfortunately, this expanding and dynamic labor market has a challenging side for hospitals, management companies, and hospitalist group leaders – we are constantly recruiting and dealing with open positions!
As a multisite leader at an academic health system, I’m looking toward the next season of recruitment with excitement. In the fall and winter we’re fortunate to receive applications from the best and brightest graduating residents and hospitalists. I realize this is a blessing, particularly compared with programs in rural areas that may not hear from many applicants. However, even when we succeed at filling the openings, there is an inevitable trickle of talent out of our clinical labor pool during the spring and summer. One person is invited to spend 20% of their time leading a teaching program, another secures a highly coveted grant, and yet another has to move because their spouse is relocated. By then, we don’t have a packed roster of applicants and have to solve the challenge in other ways. What does the typical hospital medicine program do when faced with this circumstance?
The 2018 SoHM survey first asked program leaders whether they had open and unfilled physician positions during the last year because of turnover, growth, or other factors. On average, 66% of groups serving adults and 48% of groups serving children said “yes.” For the job seekers out there, take note of some important regional differences: The regions with the highest percentage of programs dealing with unfilled positions were the East and West Coasts at 79% and 73%, respectively.
Next, the survey asked respondents to describe the percentage of total approved physician staffing that was open or unfilled during the year. On average, 12% of positions went unfilled, with important variation between different types of employers. For a typical HM group with 15 full-time equivalents, that means constantly working short two physicians!
Not only is it hard for group leaders to manage chronic understaffing, it definitely takes a toll on the group. We asked leaders to describe all of the ways their groups address coverage of the open positions. The most common tactics were for existing hospitalists to perform voluntary extra shifts (70%) and the use of moonlighters (57%). Also important were the use of locum tenens physicians (44%) and just leaving some shifts uncovered (31%).
The last option might work in a large group, where everyone can pick up an extra couple of patients, but it nonetheless degrades continuity and care progression. In a small group, leaving shifts uncovered sounds like a recipe for burnout and unsafe care – hopefully subsequent surveys will find that we can avoid that approach! Obviously, the solutions must be tailored to the group, their resources, and the alternative sources of labor available in that locality.
The SoHM report provides insight into how this is commonly handled by different employers and in different regions – we encourage anyone who is interested to purchase the report (www.hospitalmedicine.org/sohm) to dig deeper. For better or worse, the issue of unfilled positions looks likely to persist for the intermediate future. The exciting rise of hospital medicine against the backdrop of an aging population means job security, rising income, and opportunities for many to live where they choose. Until the job market saturates, though, we’ll all find ourselves looking at email inboxes with a request or two to pick up an extra shift!
Dr. White is associate professor of medicine at the University of Washington, Seattle. He is the chair of SHM’s Practice Analysis Committee.
Reference
Society of Hospital Medicine. 2018 State of Hospital Medicine Report. pp. 89, 90, 181, 152.
During the last two decades, the United States health care labor market had an almost insatiable appetite for hospitalists, driving the specialty from nothing to over 50,000 members. Evidence of persistent demand for hospitalists abounds in the freshly released 2018 State of Hospital Medicine (SoHM) report: rising salaries, growing responsibility for the overall hospital census, and a diversifying scope of services.
The SoHM offers fascinating and detailed insights into these trends, as well as hundreds of other aspects of the field’s growth. Unfortunately, this expanding and dynamic labor market has a challenging side for hospitals, management companies, and hospitalist group leaders – we are constantly recruiting and dealing with open positions!
As a multisite leader at an academic health system, I’m looking toward the next season of recruitment with excitement. In the fall and winter we’re fortunate to receive applications from the best and brightest graduating residents and hospitalists. I realize this is a blessing, particularly compared with programs in rural areas that may not hear from many applicants. However, even when we succeed at filling the openings, there is an inevitable trickle of talent out of our clinical labor pool during the spring and summer. One person is invited to spend 20% of their time leading a teaching program, another secures a highly coveted grant, and yet another has to move because their spouse is relocated. By then, we don’t have a packed roster of applicants and have to solve the challenge in other ways. What does the typical hospital medicine program do when faced with this circumstance?
The 2018 SoHM survey first asked program leaders whether they had open and unfilled physician positions during the last year because of turnover, growth, or other factors. On average, 66% of groups serving adults and 48% of groups serving children said “yes.” For the job seekers out there, take note of some important regional differences: The regions with the highest percentage of programs dealing with unfilled positions were the East and West Coasts at 79% and 73%, respectively.
Next, the survey asked respondents to describe the percentage of total approved physician staffing that was open or unfilled during the year. On average, 12% of positions went unfilled, with important variation between different types of employers. For a typical HM group with 15 full-time equivalents, that means constantly working short two physicians!
Not only is it hard for group leaders to manage chronic understaffing, it definitely takes a toll on the group. We asked leaders to describe all of the ways their groups address coverage of the open positions. The most common tactics were for existing hospitalists to perform voluntary extra shifts (70%) and the use of moonlighters (57%). Also important were the use of locum tenens physicians (44%) and just leaving some shifts uncovered (31%).
The last option might work in a large group, where everyone can pick up an extra couple of patients, but it nonetheless degrades continuity and care progression. In a small group, leaving shifts uncovered sounds like a recipe for burnout and unsafe care – hopefully subsequent surveys will find that we can avoid that approach! Obviously, the solutions must be tailored to the group, their resources, and the alternative sources of labor available in that locality.
The SoHM report provides insight into how this is commonly handled by different employers and in different regions – we encourage anyone who is interested to purchase the report (www.hospitalmedicine.org/sohm) to dig deeper. For better or worse, the issue of unfilled positions looks likely to persist for the intermediate future. The exciting rise of hospital medicine against the backdrop of an aging population means job security, rising income, and opportunities for many to live where they choose. Until the job market saturates, though, we’ll all find ourselves looking at email inboxes with a request or two to pick up an extra shift!
Dr. White is associate professor of medicine at the University of Washington, Seattle. He is the chair of SHM’s Practice Analysis Committee.
Reference
Society of Hospital Medicine. 2018 State of Hospital Medicine Report. pp. 89, 90, 181, 152.
Will AI or robotics steal your job?
NEW YORK – Artificial intelligence is currently linked to specific problem solving and is not some form of Terminator model capable of handling multiple tasks with autonomy. In other words, each time you hear the term “AI,” it is a computer solving a specific problem or task using algorithms “and not ‘thinking’ like you and me,” said Ido Weinberg, MD, assistant professor, Harvard Medical School, Boston.
AI is present in daily life – everything from cellphones to the Alexa voice interface on a smart speaker. That AI system, however, is amassing data, learning about you, and using that data intelligently, Dr. Weinberg said at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
AI in health care make sense, he said, because the health sector is a vast consumer market with potential for financial gain. Repetition, which is common in the health sector, is one of the foundations required for using AI and robotics. If a task can be repeated, then it means a machine can do it, said Dr. Weinberg.
The spread of AI and robotics one day may improve health care accessibility in remote areas where physicians with the appropriate training may not be available.
AI is already at work in the health care industry. “Pulmonary nodule detection can be done better with machines than by people, pathological identification and scanning of various slides can be done better by a machine than by a humans,” he said.
Artificial intelligence also can be designed to detect emotion by assessing various cues in phrasing, key words, and tone. These AI functions already are being used by sales reps on the phone to defuse and control interactions with customers and complainants. AI also can be implemented in interactions with people, which is an important part of dealing with patients, Dr. Weinberg said. Drug discovery is a key area where AI is flourishing, as well.
Luckily, in terms of physicians keeping their jobs, there are barriers to the use of AI to replace clinicians, Dr. Weinberg pointed out. Health care is not a monolith, and every specialty is different, meaning AI would have to be tailored to each task and specialty for each unique field. Quick proliferation of AI across the board is unlikely, especially when the varying roles of nurses and physician assistants are included.
Although robots in science fiction stories and films often are capable of multitasking a variety of needs, robots at present are much more limited in real life. In surgical situations, for example, they can perform specifically tailored tasks but cannot extend beyond those defined parameters as a real surgeon can, according to Dr. Weinberg, and this lack of flexibility is a severe limitation on the expansion of AI into health care.
Despite these limitations, Dr. Weinberg urged attendees to consider how AI can be used to facilitate their work.
“Believe in the roadblocks, but be a fast adopter – an early adopter – and understand where AI can currently augment you and make you better and more productive,” he said. “And keep doing procedures; AI and robotics currently have a problem with most of those,” Dr. Weinberg concluded.
Dr. Weinberg reported no conflicts relevant to his talk.
NEW YORK – Artificial intelligence is currently linked to specific problem solving and is not some form of Terminator model capable of handling multiple tasks with autonomy. In other words, each time you hear the term “AI,” it is a computer solving a specific problem or task using algorithms “and not ‘thinking’ like you and me,” said Ido Weinberg, MD, assistant professor, Harvard Medical School, Boston.
AI is present in daily life – everything from cellphones to the Alexa voice interface on a smart speaker. That AI system, however, is amassing data, learning about you, and using that data intelligently, Dr. Weinberg said at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
AI in health care make sense, he said, because the health sector is a vast consumer market with potential for financial gain. Repetition, which is common in the health sector, is one of the foundations required for using AI and robotics. If a task can be repeated, then it means a machine can do it, said Dr. Weinberg.
The spread of AI and robotics one day may improve health care accessibility in remote areas where physicians with the appropriate training may not be available.
AI is already at work in the health care industry. “Pulmonary nodule detection can be done better with machines than by people, pathological identification and scanning of various slides can be done better by a machine than by a humans,” he said.
Artificial intelligence also can be designed to detect emotion by assessing various cues in phrasing, key words, and tone. These AI functions already are being used by sales reps on the phone to defuse and control interactions with customers and complainants. AI also can be implemented in interactions with people, which is an important part of dealing with patients, Dr. Weinberg said. Drug discovery is a key area where AI is flourishing, as well.
Luckily, in terms of physicians keeping their jobs, there are barriers to the use of AI to replace clinicians, Dr. Weinberg pointed out. Health care is not a monolith, and every specialty is different, meaning AI would have to be tailored to each task and specialty for each unique field. Quick proliferation of AI across the board is unlikely, especially when the varying roles of nurses and physician assistants are included.
Although robots in science fiction stories and films often are capable of multitasking a variety of needs, robots at present are much more limited in real life. In surgical situations, for example, they can perform specifically tailored tasks but cannot extend beyond those defined parameters as a real surgeon can, according to Dr. Weinberg, and this lack of flexibility is a severe limitation on the expansion of AI into health care.
Despite these limitations, Dr. Weinberg urged attendees to consider how AI can be used to facilitate their work.
“Believe in the roadblocks, but be a fast adopter – an early adopter – and understand where AI can currently augment you and make you better and more productive,” he said. “And keep doing procedures; AI and robotics currently have a problem with most of those,” Dr. Weinberg concluded.
Dr. Weinberg reported no conflicts relevant to his talk.
NEW YORK – Artificial intelligence is currently linked to specific problem solving and is not some form of Terminator model capable of handling multiple tasks with autonomy. In other words, each time you hear the term “AI,” it is a computer solving a specific problem or task using algorithms “and not ‘thinking’ like you and me,” said Ido Weinberg, MD, assistant professor, Harvard Medical School, Boston.
AI is present in daily life – everything from cellphones to the Alexa voice interface on a smart speaker. That AI system, however, is amassing data, learning about you, and using that data intelligently, Dr. Weinberg said at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
AI in health care make sense, he said, because the health sector is a vast consumer market with potential for financial gain. Repetition, which is common in the health sector, is one of the foundations required for using AI and robotics. If a task can be repeated, then it means a machine can do it, said Dr. Weinberg.
The spread of AI and robotics one day may improve health care accessibility in remote areas where physicians with the appropriate training may not be available.
AI is already at work in the health care industry. “Pulmonary nodule detection can be done better with machines than by people, pathological identification and scanning of various slides can be done better by a machine than by a humans,” he said.
Artificial intelligence also can be designed to detect emotion by assessing various cues in phrasing, key words, and tone. These AI functions already are being used by sales reps on the phone to defuse and control interactions with customers and complainants. AI also can be implemented in interactions with people, which is an important part of dealing with patients, Dr. Weinberg said. Drug discovery is a key area where AI is flourishing, as well.
Luckily, in terms of physicians keeping their jobs, there are barriers to the use of AI to replace clinicians, Dr. Weinberg pointed out. Health care is not a monolith, and every specialty is different, meaning AI would have to be tailored to each task and specialty for each unique field. Quick proliferation of AI across the board is unlikely, especially when the varying roles of nurses and physician assistants are included.
Although robots in science fiction stories and films often are capable of multitasking a variety of needs, robots at present are much more limited in real life. In surgical situations, for example, they can perform specifically tailored tasks but cannot extend beyond those defined parameters as a real surgeon can, according to Dr. Weinberg, and this lack of flexibility is a severe limitation on the expansion of AI into health care.
Despite these limitations, Dr. Weinberg urged attendees to consider how AI can be used to facilitate their work.
“Believe in the roadblocks, but be a fast adopter – an early adopter – and understand where AI can currently augment you and make you better and more productive,” he said. “And keep doing procedures; AI and robotics currently have a problem with most of those,” Dr. Weinberg concluded.
Dr. Weinberg reported no conflicts relevant to his talk.
REPORTING FROM THE VEITHSYMPOSIUM
Congenital Syphilis Is on the Rise
Diagnoses of primary and secondary syphilis, the most infectious stages of the disease, jumped 76% from 2013 to 2017. And reported cases of congenital syphilis—passed from mother to infant during pregnancy—rose 44% between 2016 and 2017, from 16 cases to 23 cases per 100,000 live births, according to the CDC’s annual Sexually Transmitted Disease Surveillance Report. Those data highlight the need for better prenatal care that includes syphilis testing at the first visit and follow-up testing for women at high risk of the infection, the CDC says. Syphilis can cause miscarriage, newborn death, and severe lifelong physical and mental health problems.
The 918 cases reported in 2017 represent the highest number of recorded cases in 20 years. Cases were reported in 37 states, primarily western and southern states. The report notes that the surge in cases parallels similar increases in syphilis among women of reproductive age and outpaces national increases in sexually transmitted dieseases (STDs) overall.
Syphilis during pregnancy is easily cured with the right antibiotics. Left untreated, a pregnant woman with syphilis has as much as an 80% chance of passing it to the baby.
Early testing, prompt treatment, and follow-up are key. Recent CDC research found that 1 in 3 women who gave birth to a baby with syphilis in 2016 had in fact been tested during pregnancy but either acquired syphilis after that test or was not treated in time to cure the infection in the fetus.
“Too many women are falling through the cracks of the system,” said Gail Bolan, MD, director of the CDC’s Division of STD Prevention. The CDC recommends that all pregnant women be treated for syphilis at the first prenatal visit. But for many women, 1 test may not be enough. Woman at high risk, or those who live in high-prevalence areas, should be tested again early in the third trimester and at delivery.
“To protect every baby,” Bolan says, “we have to start by protecting every mother.”
Diagnoses of primary and secondary syphilis, the most infectious stages of the disease, jumped 76% from 2013 to 2017. And reported cases of congenital syphilis—passed from mother to infant during pregnancy—rose 44% between 2016 and 2017, from 16 cases to 23 cases per 100,000 live births, according to the CDC’s annual Sexually Transmitted Disease Surveillance Report. Those data highlight the need for better prenatal care that includes syphilis testing at the first visit and follow-up testing for women at high risk of the infection, the CDC says. Syphilis can cause miscarriage, newborn death, and severe lifelong physical and mental health problems.
The 918 cases reported in 2017 represent the highest number of recorded cases in 20 years. Cases were reported in 37 states, primarily western and southern states. The report notes that the surge in cases parallels similar increases in syphilis among women of reproductive age and outpaces national increases in sexually transmitted dieseases (STDs) overall.
Syphilis during pregnancy is easily cured with the right antibiotics. Left untreated, a pregnant woman with syphilis has as much as an 80% chance of passing it to the baby.
Early testing, prompt treatment, and follow-up are key. Recent CDC research found that 1 in 3 women who gave birth to a baby with syphilis in 2016 had in fact been tested during pregnancy but either acquired syphilis after that test or was not treated in time to cure the infection in the fetus.
“Too many women are falling through the cracks of the system,” said Gail Bolan, MD, director of the CDC’s Division of STD Prevention. The CDC recommends that all pregnant women be treated for syphilis at the first prenatal visit. But for many women, 1 test may not be enough. Woman at high risk, or those who live in high-prevalence areas, should be tested again early in the third trimester and at delivery.
“To protect every baby,” Bolan says, “we have to start by protecting every mother.”
Diagnoses of primary and secondary syphilis, the most infectious stages of the disease, jumped 76% from 2013 to 2017. And reported cases of congenital syphilis—passed from mother to infant during pregnancy—rose 44% between 2016 and 2017, from 16 cases to 23 cases per 100,000 live births, according to the CDC’s annual Sexually Transmitted Disease Surveillance Report. Those data highlight the need for better prenatal care that includes syphilis testing at the first visit and follow-up testing for women at high risk of the infection, the CDC says. Syphilis can cause miscarriage, newborn death, and severe lifelong physical and mental health problems.
The 918 cases reported in 2017 represent the highest number of recorded cases in 20 years. Cases were reported in 37 states, primarily western and southern states. The report notes that the surge in cases parallels similar increases in syphilis among women of reproductive age and outpaces national increases in sexually transmitted dieseases (STDs) overall.
Syphilis during pregnancy is easily cured with the right antibiotics. Left untreated, a pregnant woman with syphilis has as much as an 80% chance of passing it to the baby.
Early testing, prompt treatment, and follow-up are key. Recent CDC research found that 1 in 3 women who gave birth to a baby with syphilis in 2016 had in fact been tested during pregnancy but either acquired syphilis after that test or was not treated in time to cure the infection in the fetus.
“Too many women are falling through the cracks of the system,” said Gail Bolan, MD, director of the CDC’s Division of STD Prevention. The CDC recommends that all pregnant women be treated for syphilis at the first prenatal visit. But for many women, 1 test may not be enough. Woman at high risk, or those who live in high-prevalence areas, should be tested again early in the third trimester and at delivery.
“To protect every baby,” Bolan says, “we have to start by protecting every mother.”
Obesity curbs decades of CVD progress
Also today, there is an increased risk of atrial fibrillation with migraine aura, adjunctive testosterone may reduce depressive symptoms in men, and the American Academy of Pediatrics advises moderate physical and cognitive activity after sports concussions.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, there is an increased risk of atrial fibrillation with migraine aura, adjunctive testosterone may reduce depressive symptoms in men, and the American Academy of Pediatrics advises moderate physical and cognitive activity after sports concussions.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, there is an increased risk of atrial fibrillation with migraine aura, adjunctive testosterone may reduce depressive symptoms in men, and the American Academy of Pediatrics advises moderate physical and cognitive activity after sports concussions.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Don’t just work hard; work hard at living
NEW YORK – “A physician falls overboard on a large cruise ship and passengers gather at the guard rail. The first passenger at the guardrail shakes his finger down at the drowning physician and says, ‘You need to learn how to swim!’ Another passenger says, ‘No, man, throw him a life preserver.’ ... Finally, a passenger says, ‘We need better guard rails.’ ”

That’s the analogy Cynthia K. Shortell, MD used to kick off her presentation on physician burnout and the need for resilience at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
“Which of these is right? Well, of course, the answer is they all are,” said Dr. Shortell, who is a professor of surgery at Duke University Durham, N.C. But certainly, only the life preserver answer was appropriate at that time for the drowning physician, she added.
Continuing the analogy, Dr. Shortell pointed out that surely there is a man overboard, with 1 in 20 surgeons reporting suicidal ideation. That rate jumps threefold if the surgeon has had a recent medical error. In addition, vascular surgeons in particular are within the top tier of specialties at risk for burnout.
“We do need better guardrails,” she said, and described the need to actively engage with the health care system to help solve these issues, including those involving electronic medical records and operating room inefficiency and use. In addition, there is a great need for additional services that are provided to other high-end professionals, including food, concierge service, gym access, and other services that help with tasks of daily life when physicians need to spend most of their time at the hospital.
But, in the end, Dr. Shortell said, “We do need to learn to swim. Ultimately, we do need to take a role in having responsibility to solve this problem on our own. We need to change the way we think about our work, and the way we think about our health, and the way our culture values working hard instead of working hard at living.”
Dr. Shortell also highlighted the need to deal with musculoskeletal issues arising from the way that surgeons operate. This, along with good leadership, are key factors in preventing and remediating burnout.
Dr. Shortell had no disclosures relevant to her talk.
NEW YORK – “A physician falls overboard on a large cruise ship and passengers gather at the guard rail. The first passenger at the guardrail shakes his finger down at the drowning physician and says, ‘You need to learn how to swim!’ Another passenger says, ‘No, man, throw him a life preserver.’ ... Finally, a passenger says, ‘We need better guard rails.’ ”
That’s the analogy Cynthia K. Shortell, MD used to kick off her presentation on physician burnout and the need for resilience at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
“Which of these is right? Well, of course, the answer is they all are,” said Dr. Shortell, who is a professor of surgery at Duke University Durham, N.C. But certainly, only the life preserver answer was appropriate at that time for the drowning physician, she added.
Continuing the analogy, Dr. Shortell pointed out that surely there is a man overboard, with 1 in 20 surgeons reporting suicidal ideation. That rate jumps threefold if the surgeon has had a recent medical error. In addition, vascular surgeons in particular are within the top tier of specialties at risk for burnout.
“We do need better guardrails,” she said, and described the need to actively engage with the health care system to help solve these issues, including those involving electronic medical records and operating room inefficiency and use. In addition, there is a great need for additional services that are provided to other high-end professionals, including food, concierge service, gym access, and other services that help with tasks of daily life when physicians need to spend most of their time at the hospital.
But, in the end, Dr. Shortell said, “We do need to learn to swim. Ultimately, we do need to take a role in having responsibility to solve this problem on our own. We need to change the way we think about our work, and the way we think about our health, and the way our culture values working hard instead of working hard at living.”
Dr. Shortell also highlighted the need to deal with musculoskeletal issues arising from the way that surgeons operate. This, along with good leadership, are key factors in preventing and remediating burnout.
Dr. Shortell had no disclosures relevant to her talk.
NEW YORK – “A physician falls overboard on a large cruise ship and passengers gather at the guard rail. The first passenger at the guardrail shakes his finger down at the drowning physician and says, ‘You need to learn how to swim!’ Another passenger says, ‘No, man, throw him a life preserver.’ ... Finally, a passenger says, ‘We need better guard rails.’ ”
That’s the analogy Cynthia K. Shortell, MD used to kick off her presentation on physician burnout and the need for resilience at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
“Which of these is right? Well, of course, the answer is they all are,” said Dr. Shortell, who is a professor of surgery at Duke University Durham, N.C. But certainly, only the life preserver answer was appropriate at that time for the drowning physician, she added.
Continuing the analogy, Dr. Shortell pointed out that surely there is a man overboard, with 1 in 20 surgeons reporting suicidal ideation. That rate jumps threefold if the surgeon has had a recent medical error. In addition, vascular surgeons in particular are within the top tier of specialties at risk for burnout.
“We do need better guardrails,” she said, and described the need to actively engage with the health care system to help solve these issues, including those involving electronic medical records and operating room inefficiency and use. In addition, there is a great need for additional services that are provided to other high-end professionals, including food, concierge service, gym access, and other services that help with tasks of daily life when physicians need to spend most of their time at the hospital.
But, in the end, Dr. Shortell said, “We do need to learn to swim. Ultimately, we do need to take a role in having responsibility to solve this problem on our own. We need to change the way we think about our work, and the way we think about our health, and the way our culture values working hard instead of working hard at living.”
Dr. Shortell also highlighted the need to deal with musculoskeletal issues arising from the way that surgeons operate. This, along with good leadership, are key factors in preventing and remediating burnout.
Dr. Shortell had no disclosures relevant to her talk.
REPORTING FROM THE VEITHSYMPOSIUM
What’s new with the SVS VQI?
NEW YORK – The Vascular Quality Initiative (VQI) is designed to improve the quality, safety, and effectiveness of vascular health care, but also reduce costs through the collection and exchange of information, according to Larry W. Kraiss, MD, professor of surgery, University of Utah, Salt Lake City.

The VQI consists of three major components: a federally accredited patient safety organization (PSO), a registry, and a distributed network of quality groups, which can also serve as a platform for internal quality improvement efforts.
Even though registries are considered less reliable than the venerated randomized clinical trial models are, registries have some unique advantages, according to Dr. Kraiss, who spoke at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation. Randomized clinical trials (RCTs) are very expensive to conduct and are criticized for potentially not being generalizable because of their rigidly defined inclusion/exclusion criteria. Despite inherent problems with registry data, especially bias, there are now statistical methods to help account for the biases. Registry-controlled trials are going to be important to answer many questions that cannot be answered by RCTs. Such trials can be too costly or actually unethical to randomize under certain circumstances. Registries, however, provide real-world patient populations in greater numbers than RCTs can manage, including access to rare events that would otherwise not be detected.
The VQI holds an important place in this second tier and is an important source of information for clinical care.
The VQI has grown steadily since its inception, and there are more than 500 centers now participating, including 6 international centers, and 18 regional groups, according to Dr. Kraiss. There are more than 530,000 procedures contained within the VQI’s 12 registries, with more than half of them involving peripheral vascular interventions and carotid endarterectomies. “But there [are] a healthy number of cases in all of the other registries, which provide a very rich resource and evidence base,” he added.
The VQI is becoming very important in the regulatory framework, with the Food and Drug Administration embracing “real-world evidence” as a way to justify some of its decisions, and the VQI has been involved in this process. The VQI has coordinated several post-market surveillance programs, the two most important being in the areas of thoracic endovascular aortic repair (TEVAR) and transcarotid artery revascularization (TCAR), said Dr. Kraiss.
One of the important values of the VQI is the ability to examine benchmarks and to compare performance across centers. For example, looking at aortic abdominal aneurysm (AAA) repair data, the results showed that a number of centers were not following established Society for Vascular Society guidelines and that there were a substantial number of AAAs reported in the VQI that were treated when they were below the threshold for intervention and should have received routine observation only.
So, ultimately two of the greatest values of the VQI are the ability to use it as a means of local quality improvement, and to provide an avenue for important clinical research, Dr. Kraiss concluded.
Dr. Kraiss reported that they had no disclosures.
NEW YORK – The Vascular Quality Initiative (VQI) is designed to improve the quality, safety, and effectiveness of vascular health care, but also reduce costs through the collection and exchange of information, according to Larry W. Kraiss, MD, professor of surgery, University of Utah, Salt Lake City.
The VQI consists of three major components: a federally accredited patient safety organization (PSO), a registry, and a distributed network of quality groups, which can also serve as a platform for internal quality improvement efforts.
Even though registries are considered less reliable than the venerated randomized clinical trial models are, registries have some unique advantages, according to Dr. Kraiss, who spoke at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation. Randomized clinical trials (RCTs) are very expensive to conduct and are criticized for potentially not being generalizable because of their rigidly defined inclusion/exclusion criteria. Despite inherent problems with registry data, especially bias, there are now statistical methods to help account for the biases. Registry-controlled trials are going to be important to answer many questions that cannot be answered by RCTs. Such trials can be too costly or actually unethical to randomize under certain circumstances. Registries, however, provide real-world patient populations in greater numbers than RCTs can manage, including access to rare events that would otherwise not be detected.
The VQI holds an important place in this second tier and is an important source of information for clinical care.
The VQI has grown steadily since its inception, and there are more than 500 centers now participating, including 6 international centers, and 18 regional groups, according to Dr. Kraiss. There are more than 530,000 procedures contained within the VQI’s 12 registries, with more than half of them involving peripheral vascular interventions and carotid endarterectomies. “But there [are] a healthy number of cases in all of the other registries, which provide a very rich resource and evidence base,” he added.
The VQI is becoming very important in the regulatory framework, with the Food and Drug Administration embracing “real-world evidence” as a way to justify some of its decisions, and the VQI has been involved in this process. The VQI has coordinated several post-market surveillance programs, the two most important being in the areas of thoracic endovascular aortic repair (TEVAR) and transcarotid artery revascularization (TCAR), said Dr. Kraiss.
One of the important values of the VQI is the ability to examine benchmarks and to compare performance across centers. For example, looking at aortic abdominal aneurysm (AAA) repair data, the results showed that a number of centers were not following established Society for Vascular Society guidelines and that there were a substantial number of AAAs reported in the VQI that were treated when they were below the threshold for intervention and should have received routine observation only.
So, ultimately two of the greatest values of the VQI are the ability to use it as a means of local quality improvement, and to provide an avenue for important clinical research, Dr. Kraiss concluded.
Dr. Kraiss reported that they had no disclosures.
NEW YORK – The Vascular Quality Initiative (VQI) is designed to improve the quality, safety, and effectiveness of vascular health care, but also reduce costs through the collection and exchange of information, according to Larry W. Kraiss, MD, professor of surgery, University of Utah, Salt Lake City.
The VQI consists of three major components: a federally accredited patient safety organization (PSO), a registry, and a distributed network of quality groups, which can also serve as a platform for internal quality improvement efforts.
Even though registries are considered less reliable than the venerated randomized clinical trial models are, registries have some unique advantages, according to Dr. Kraiss, who spoke at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation. Randomized clinical trials (RCTs) are very expensive to conduct and are criticized for potentially not being generalizable because of their rigidly defined inclusion/exclusion criteria. Despite inherent problems with registry data, especially bias, there are now statistical methods to help account for the biases. Registry-controlled trials are going to be important to answer many questions that cannot be answered by RCTs. Such trials can be too costly or actually unethical to randomize under certain circumstances. Registries, however, provide real-world patient populations in greater numbers than RCTs can manage, including access to rare events that would otherwise not be detected.
The VQI holds an important place in this second tier and is an important source of information for clinical care.
The VQI has grown steadily since its inception, and there are more than 500 centers now participating, including 6 international centers, and 18 regional groups, according to Dr. Kraiss. There are more than 530,000 procedures contained within the VQI’s 12 registries, with more than half of them involving peripheral vascular interventions and carotid endarterectomies. “But there [are] a healthy number of cases in all of the other registries, which provide a very rich resource and evidence base,” he added.
The VQI is becoming very important in the regulatory framework, with the Food and Drug Administration embracing “real-world evidence” as a way to justify some of its decisions, and the VQI has been involved in this process. The VQI has coordinated several post-market surveillance programs, the two most important being in the areas of thoracic endovascular aortic repair (TEVAR) and transcarotid artery revascularization (TCAR), said Dr. Kraiss.
One of the important values of the VQI is the ability to examine benchmarks and to compare performance across centers. For example, looking at aortic abdominal aneurysm (AAA) repair data, the results showed that a number of centers were not following established Society for Vascular Society guidelines and that there were a substantial number of AAAs reported in the VQI that were treated when they were below the threshold for intervention and should have received routine observation only.
So, ultimately two of the greatest values of the VQI are the ability to use it as a means of local quality improvement, and to provide an avenue for important clinical research, Dr. Kraiss concluded.
Dr. Kraiss reported that they had no disclosures.
REPORTING FROM THE VEITHSYMPOSIUM
AHA 2018: Part I

USPSTF: screen for ‘unhealthy’ alcohol use
Also today, dialysis decisions in elderly patients need to account for comorbidities, chronic liver disease is independently linked to increased risk of falls, and barriers to naloxone remain, despite new access laws.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, dialysis decisions in elderly patients need to account for comorbidities, chronic liver disease is independently linked to increased risk of falls, and barriers to naloxone remain, despite new access laws.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, dialysis decisions in elderly patients need to account for comorbidities, chronic liver disease is independently linked to increased risk of falls, and barriers to naloxone remain, despite new access laws.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Update on integrated vascular surgery residencies
NEW YORK – In March 2005, the Accreditation Council for Graduate Medical Education approved the primary certificate in vascular surgery, and the first integrated vascular surgery residencies (0+5) were approved shortly thereafter. By 2015, there was more than a 900% increase in both the number of programs and positions, which were offered for matriculation in July 2016, according to Murray L. Shames, MD, professor of surgery and radiology at the University of South Florida, Tampa, and chief of the division of vascular surgery at Tampa General Hospital.
In 2009, Dr. Shames and his colleagues first looked at the issue to try to better understand the applicant pool, and they found that there was a 900% increase in demand for the 0+5 residency positions, compared with the traditional 5+2 vascular fellowships, and that there was a 0+5 applicant-to-position ratio of 8:1 that year. “Despite initial concerns regarding the shortened training, studies have demonstrated equivalent case volumes and job opportunities for integrated vascular residents and vascular fellows,” Dr. Shames stated at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
His current presentation was an update of that assessment done for the 2015 data, as integrated vascular surgery residents have begun to enter the workforce. They looked at the current supply and demand for 0+5 training programs (as well as the traditional 5+2 programs), and the quality and attributes of the 0+5 residency applicants. They obtained data for applicants for both types of programs: 2008-2015 for 0+2 and 2007-2016 for 5+2) and comparable match data were queried for 2008-2016. They looked at the number of programs, the number of positions, the total number of applicants, sex of the applicants, applications/program and applications/position, and the U.S. versus international applicant ratios.
They found that the number of integrated programs increased from 4 to 48, with an increase from 4 to 56 positions, during the study period, said Dr. Shames. Demand for integrated vascular residencies has increased nearly 300%, from 112 applicants in 2008 to 434 in 2015. The total number of U.S. medical school graduate applicants to these programs has increased from 40 in 2008 to 2,030 in 2015, with the increase in program applicants driven primarily by these U.S. medical school graduates; the number of international applicants per program decrease over this time period from 57 to 37. The percentage of women applicants has steadily increased, from 16% to 27%, and currently women constitute 41% of all integrated vascular surgery residents.
“Overall, the supply for integrated vascular surgery residency positions continues to be outnumbered by the number of applicants, with increasing applicant to position ratios at 7.8:1 in 2015, while the total number for vascular surgery fellowships has remained stable at about 1:1,” Dr. Shames concluded.
Dr. Shames reported having no relevant disclosures for his presentation.
NEW YORK – In March 2005, the Accreditation Council for Graduate Medical Education approved the primary certificate in vascular surgery, and the first integrated vascular surgery residencies (0+5) were approved shortly thereafter. By 2015, there was more than a 900% increase in both the number of programs and positions, which were offered for matriculation in July 2016, according to Murray L. Shames, MD, professor of surgery and radiology at the University of South Florida, Tampa, and chief of the division of vascular surgery at Tampa General Hospital.
In 2009, Dr. Shames and his colleagues first looked at the issue to try to better understand the applicant pool, and they found that there was a 900% increase in demand for the 0+5 residency positions, compared with the traditional 5+2 vascular fellowships, and that there was a 0+5 applicant-to-position ratio of 8:1 that year. “Despite initial concerns regarding the shortened training, studies have demonstrated equivalent case volumes and job opportunities for integrated vascular residents and vascular fellows,” Dr. Shames stated at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
His current presentation was an update of that assessment done for the 2015 data, as integrated vascular surgery residents have begun to enter the workforce. They looked at the current supply and demand for 0+5 training programs (as well as the traditional 5+2 programs), and the quality and attributes of the 0+5 residency applicants. They obtained data for applicants for both types of programs: 2008-2015 for 0+2 and 2007-2016 for 5+2) and comparable match data were queried for 2008-2016. They looked at the number of programs, the number of positions, the total number of applicants, sex of the applicants, applications/program and applications/position, and the U.S. versus international applicant ratios.
They found that the number of integrated programs increased from 4 to 48, with an increase from 4 to 56 positions, during the study period, said Dr. Shames. Demand for integrated vascular residencies has increased nearly 300%, from 112 applicants in 2008 to 434 in 2015. The total number of U.S. medical school graduate applicants to these programs has increased from 40 in 2008 to 2,030 in 2015, with the increase in program applicants driven primarily by these U.S. medical school graduates; the number of international applicants per program decrease over this time period from 57 to 37. The percentage of women applicants has steadily increased, from 16% to 27%, and currently women constitute 41% of all integrated vascular surgery residents.
“Overall, the supply for integrated vascular surgery residency positions continues to be outnumbered by the number of applicants, with increasing applicant to position ratios at 7.8:1 in 2015, while the total number for vascular surgery fellowships has remained stable at about 1:1,” Dr. Shames concluded.
Dr. Shames reported having no relevant disclosures for his presentation.
NEW YORK – In March 2005, the Accreditation Council for Graduate Medical Education approved the primary certificate in vascular surgery, and the first integrated vascular surgery residencies (0+5) were approved shortly thereafter. By 2015, there was more than a 900% increase in both the number of programs and positions, which were offered for matriculation in July 2016, according to Murray L. Shames, MD, professor of surgery and radiology at the University of South Florida, Tampa, and chief of the division of vascular surgery at Tampa General Hospital.
In 2009, Dr. Shames and his colleagues first looked at the issue to try to better understand the applicant pool, and they found that there was a 900% increase in demand for the 0+5 residency positions, compared with the traditional 5+2 vascular fellowships, and that there was a 0+5 applicant-to-position ratio of 8:1 that year. “Despite initial concerns regarding the shortened training, studies have demonstrated equivalent case volumes and job opportunities for integrated vascular residents and vascular fellows,” Dr. Shames stated at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
His current presentation was an update of that assessment done for the 2015 data, as integrated vascular surgery residents have begun to enter the workforce. They looked at the current supply and demand for 0+5 training programs (as well as the traditional 5+2 programs), and the quality and attributes of the 0+5 residency applicants. They obtained data for applicants for both types of programs: 2008-2015 for 0+2 and 2007-2016 for 5+2) and comparable match data were queried for 2008-2016. They looked at the number of programs, the number of positions, the total number of applicants, sex of the applicants, applications/program and applications/position, and the U.S. versus international applicant ratios.
They found that the number of integrated programs increased from 4 to 48, with an increase from 4 to 56 positions, during the study period, said Dr. Shames. Demand for integrated vascular residencies has increased nearly 300%, from 112 applicants in 2008 to 434 in 2015. The total number of U.S. medical school graduate applicants to these programs has increased from 40 in 2008 to 2,030 in 2015, with the increase in program applicants driven primarily by these U.S. medical school graduates; the number of international applicants per program decrease over this time period from 57 to 37. The percentage of women applicants has steadily increased, from 16% to 27%, and currently women constitute 41% of all integrated vascular surgery residents.
“Overall, the supply for integrated vascular surgery residency positions continues to be outnumbered by the number of applicants, with increasing applicant to position ratios at 7.8:1 in 2015, while the total number for vascular surgery fellowships has remained stable at about 1:1,” Dr. Shames concluded.
Dr. Shames reported having no relevant disclosures for his presentation.
REPORTING FROM THE VEITHSYMPOSIUM