User login
Genetic testing for best antidepressant accurate, cost effective
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EPA 2022
Schizophrenia patients in long-term facilities benefit from lower-dose antipsychotics
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.

The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.

Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.
The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.
Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.
The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.
Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
FROM APA 2022
Novel drug ‘promising’ for concomitant depression, insomnia
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.

“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”

“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.
“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”
“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized, placebo-controlled, adaptive dose–finding study conducted in more than 200 patients with MDD, those with more severe insomnia at baseline had a greater improvement in depressive symptoms versus those with less severe insomnia.
“As seltorexant is an orexin receptor antagonist, it is related to other medications that are marketed as sleeping pills, so it was important to show that its antidepressant efficacy was actually caused by improved sleep,” coinvestigator Michael E. Thase, MD, professor of psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, told this news organization.
“This novel antidepressant may well turn out to be a treatment of choice for depressed patients with insomnia,” said Dr. Thase, who is also a member of the medical and research staff of the Corporal Michael J. Crescenz Department of Veterans Affairs Medical Center.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Clinically meaningful?
In an earlier exploratory study, seltorexant showed antidepressant and sleep-promoting effects in patients with MDD. In a phase 2b study, a 20-mg dose of the drug showed clinically meaningful improvement in the Montgomery-Åsberg Depression Rating Scale (MADRS) total score after 6 weeks of treatment.
In the current analysis, the investigators evaluated the effect of seltorexant in improving depressive symptoms beyond sleep-related improvement in patients with MDD, using the MADRS-WOSI (MADRS without the sleep item).
They also used the six-item core MADRS subscale, which excludes sleep, anxiety, and appetite items.
The 283 participants were randomly assigned 3:3:1 to receive seltorexant 10 mg or 20 mg or placebo once daily. They were also stratified into two groups according to the severity of their insomnia: those with a baseline Insomnia Severity Index [ISI] score of 15 or higher (58%) and those with a baseline ISI score of less than 15 (42%).
Results showed that the group receiving the 20-mg/day dose of seltorexant (n = 61 patients) obtained a statistically and clinically meaningful response, compared with the placebo group (n = 137 patients) after removing the insomnia and other “not core items” of the MADRS. The effect was clearest among those with high insomnia ratings.
Improvement in the MADRS-WOSI score was also observed in the seltorexant 20-mg group at week 3 and week 6, compared with the placebo group.
The LSM average distance
The least squares mean (LSM) average difference between the treatment and placebo groups in the MADRS-WOSI score at week 3 was −3.8 (90% confidence interval, −5.98 to −1.57; P = .005).
At week 6, the LSM between the groups in the MADRS-WOSI score was −2.5 (90% CI, −5.24 to 0.15; P = .12).
The results were consistent with improvement in the MADRS total score. At week 3, the LSM in the MADRS total score was -4.5 (90% CI, -6.96 to -2.07; P = .003) and, at week 6, it was -3.1 (90% CI, -6.13 to -0.16; P = .083).
Seltorexant 20 mg was especially effective in patients who had more severe insomnia.
Commenting on the study, Nagy Youssef, MD, PhD, professor of psychiatry, The Ohio State University Wexner Medical Center, Columbus, said this was “a well-designed study examining a promising compound.”
“Especially if replicated, this study shows the promise of this molecule for this patient population,” said Dr. Youssef, who was not involved with the research.
The study was funded by Janssen Pharmaceutical of Johnson & Johnson. Dr. Thase reports financial relationships with numerous companies. Dr. Youssef reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
Social activities may offset psychosis risk in poor communities
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.

The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
Antipsychotic tied to dose-related weight gain, higher cholesterol
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.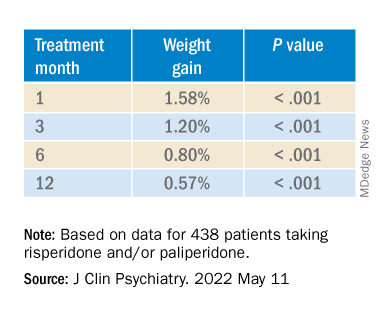
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.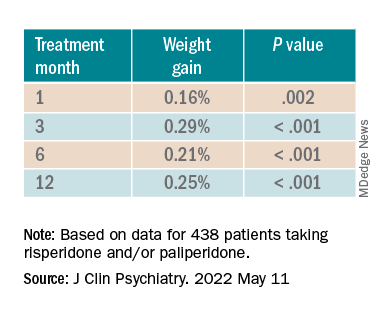
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.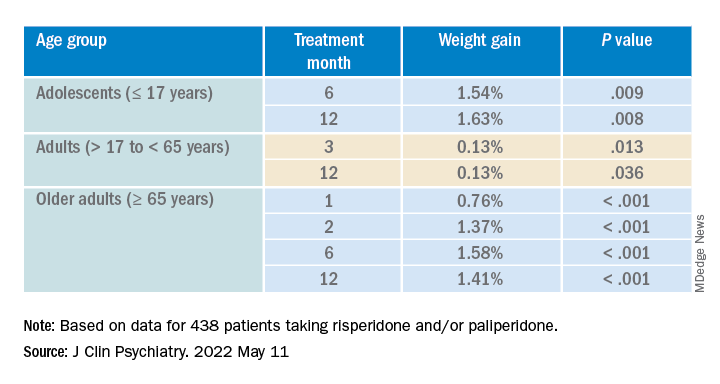
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”

It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Trans teens less likely to commit acts of sexual violence, says new study
Transgender and nonbinary adolescents are twice as likely to experience sexual violence as their cisgendered peers but are less likely to attempt rape or commit sexual assault, researchers have found.
The study, which was published online in JAMA Network Open, is among the first on the sexual violence that trans, nonbinary, and other gender nonconforming adolescents experience. Previous studies have focused on adults.
“In the busy world of clinical care, it is essential that clinicians be aware of potential disparities their patients are navigating,” said Michele Ybarra, PhD, MPH, president and research director of the Center for Innovative Public Health Research, San Clemente, California, who led the study. “This includes sexual violence victimization for gender minority youth and the need to talk about consent and boundaries for youth of all genders.”
Dr. Ybarra said that while clinicians may be aware that transgender young people face stigma, discrimination, and bullying, they may not be aware that trans youth are also the targets of sexual violence.
Studies indicate that health care providers and communities have significant misconceptions about sexually explicit behavior among trans and nonbinary teens. Misconceptions can lead to discrimination, resulting in higher rates of drug abuse, dropping out of school, suicide, and homelessness.
Dr. Ybarra and her colleagues surveyed 911 trans, nonbinary, or questioning youth on Instagram and Facebook through a collaboration with Growing Up With Media, a national longitudinal survey designed to investigate sexual violence during adolescence.
They also surveyed 3,282 cisgender persons aged 14-16 years who were recruited to the study between June 2018 and March 2020. The term “cisgender” refers to youth who identify with their gender at birth.
The questionnaires asked teens about gender identity, race, economic status, and support systems at home. Factors associated with not experiencing sexual violence included having a strong network of friends, family, and educators; involvement in the community; and having people close who affirm their gender identity.
More than three-fourths (78%) of youth surveyed identified as cisgender, 13.9% identified as questioning, and 7.9% identified as transgender.
Roughly two-thirds (67%) of transgender adolescents said they had experienced serious sexual violence, 73% reported experiencing violence in their communities, and 63% said they had been exposed to aggressive behavior. In contrast, 6.7% of trans youth said they had ever committed sexual violence, while 7.4% of cisgender teens surveyed, or 243 students, said they had done so.
“The relative lack of visibility of gender minority youth in sexual violence research is unacceptable,” Dr. Ybarra told this news organization. “To be counted, one needs to be seen. We aimed to start addressing this exclusion with the current study.”
The findings provide a lens into the levels of sexual violence that LGBTQIA+ youth experience and an opportunity to provide more inclusive care, according to Elizabeth Miller, MD, PhD, FSAHM, Distinguished Professor of Pediatrics, director of the Division of Adolescent and Young Adult Medicine, and medical director of community and population health at UPMC Children’s Hospital of Pittsburgh, who was not involved in the study.
“There are unfortunately pervasive and harmful stereotypes in our society about the ‘sexual deviancy’ attributed to LGBTQIA+ individuals,” Dr. Miller told this news organization. “This study adds to the research literature that counters and challenges these harmful – and inaccurate – perceptions.”
Dr. Miller said clinicians can help this population by offering youth accurate information about relevant support and services, including how to help a friend.
Programs that providers could incorporate include gender transformative approaches, which guide youth to examine gender norms and inequities and that develop leadership skills.
Such programs are more common outside the United States and have been shown to decrease LGBTQIA+ youth exposure to sexual violence, she said.
Dr. Miller said more research is needed to understand the contexts in which gender minority youth experience sexual violence to guide prevention efforts: “We need to move beyond individual-focused interventions to considering community-level interventions to create safer and more inclusive spaces for all youth.”
Dr. Miller has received royalties for writing content for UptoDate Wolters Kluwer outside of the current study. Dr. Ybarra has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Transgender and nonbinary adolescents are twice as likely to experience sexual violence as their cisgendered peers but are less likely to attempt rape or commit sexual assault, researchers have found.
The study, which was published online in JAMA Network Open, is among the first on the sexual violence that trans, nonbinary, and other gender nonconforming adolescents experience. Previous studies have focused on adults.
“In the busy world of clinical care, it is essential that clinicians be aware of potential disparities their patients are navigating,” said Michele Ybarra, PhD, MPH, president and research director of the Center for Innovative Public Health Research, San Clemente, California, who led the study. “This includes sexual violence victimization for gender minority youth and the need to talk about consent and boundaries for youth of all genders.”
Dr. Ybarra said that while clinicians may be aware that transgender young people face stigma, discrimination, and bullying, they may not be aware that trans youth are also the targets of sexual violence.
Studies indicate that health care providers and communities have significant misconceptions about sexually explicit behavior among trans and nonbinary teens. Misconceptions can lead to discrimination, resulting in higher rates of drug abuse, dropping out of school, suicide, and homelessness.
Dr. Ybarra and her colleagues surveyed 911 trans, nonbinary, or questioning youth on Instagram and Facebook through a collaboration with Growing Up With Media, a national longitudinal survey designed to investigate sexual violence during adolescence.
They also surveyed 3,282 cisgender persons aged 14-16 years who were recruited to the study between June 2018 and March 2020. The term “cisgender” refers to youth who identify with their gender at birth.
The questionnaires asked teens about gender identity, race, economic status, and support systems at home. Factors associated with not experiencing sexual violence included having a strong network of friends, family, and educators; involvement in the community; and having people close who affirm their gender identity.
More than three-fourths (78%) of youth surveyed identified as cisgender, 13.9% identified as questioning, and 7.9% identified as transgender.
Roughly two-thirds (67%) of transgender adolescents said they had experienced serious sexual violence, 73% reported experiencing violence in their communities, and 63% said they had been exposed to aggressive behavior. In contrast, 6.7% of trans youth said they had ever committed sexual violence, while 7.4% of cisgender teens surveyed, or 243 students, said they had done so.
“The relative lack of visibility of gender minority youth in sexual violence research is unacceptable,” Dr. Ybarra told this news organization. “To be counted, one needs to be seen. We aimed to start addressing this exclusion with the current study.”
The findings provide a lens into the levels of sexual violence that LGBTQIA+ youth experience and an opportunity to provide more inclusive care, according to Elizabeth Miller, MD, PhD, FSAHM, Distinguished Professor of Pediatrics, director of the Division of Adolescent and Young Adult Medicine, and medical director of community and population health at UPMC Children’s Hospital of Pittsburgh, who was not involved in the study.
“There are unfortunately pervasive and harmful stereotypes in our society about the ‘sexual deviancy’ attributed to LGBTQIA+ individuals,” Dr. Miller told this news organization. “This study adds to the research literature that counters and challenges these harmful – and inaccurate – perceptions.”
Dr. Miller said clinicians can help this population by offering youth accurate information about relevant support and services, including how to help a friend.
Programs that providers could incorporate include gender transformative approaches, which guide youth to examine gender norms and inequities and that develop leadership skills.
Such programs are more common outside the United States and have been shown to decrease LGBTQIA+ youth exposure to sexual violence, she said.
Dr. Miller said more research is needed to understand the contexts in which gender minority youth experience sexual violence to guide prevention efforts: “We need to move beyond individual-focused interventions to considering community-level interventions to create safer and more inclusive spaces for all youth.”
Dr. Miller has received royalties for writing content for UptoDate Wolters Kluwer outside of the current study. Dr. Ybarra has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Transgender and nonbinary adolescents are twice as likely to experience sexual violence as their cisgendered peers but are less likely to attempt rape or commit sexual assault, researchers have found.
The study, which was published online in JAMA Network Open, is among the first on the sexual violence that trans, nonbinary, and other gender nonconforming adolescents experience. Previous studies have focused on adults.
“In the busy world of clinical care, it is essential that clinicians be aware of potential disparities their patients are navigating,” said Michele Ybarra, PhD, MPH, president and research director of the Center for Innovative Public Health Research, San Clemente, California, who led the study. “This includes sexual violence victimization for gender minority youth and the need to talk about consent and boundaries for youth of all genders.”
Dr. Ybarra said that while clinicians may be aware that transgender young people face stigma, discrimination, and bullying, they may not be aware that trans youth are also the targets of sexual violence.
Studies indicate that health care providers and communities have significant misconceptions about sexually explicit behavior among trans and nonbinary teens. Misconceptions can lead to discrimination, resulting in higher rates of drug abuse, dropping out of school, suicide, and homelessness.
Dr. Ybarra and her colleagues surveyed 911 trans, nonbinary, or questioning youth on Instagram and Facebook through a collaboration with Growing Up With Media, a national longitudinal survey designed to investigate sexual violence during adolescence.
They also surveyed 3,282 cisgender persons aged 14-16 years who were recruited to the study between June 2018 and March 2020. The term “cisgender” refers to youth who identify with their gender at birth.
The questionnaires asked teens about gender identity, race, economic status, and support systems at home. Factors associated with not experiencing sexual violence included having a strong network of friends, family, and educators; involvement in the community; and having people close who affirm their gender identity.
More than three-fourths (78%) of youth surveyed identified as cisgender, 13.9% identified as questioning, and 7.9% identified as transgender.
Roughly two-thirds (67%) of transgender adolescents said they had experienced serious sexual violence, 73% reported experiencing violence in their communities, and 63% said they had been exposed to aggressive behavior. In contrast, 6.7% of trans youth said they had ever committed sexual violence, while 7.4% of cisgender teens surveyed, or 243 students, said they had done so.
“The relative lack of visibility of gender minority youth in sexual violence research is unacceptable,” Dr. Ybarra told this news organization. “To be counted, one needs to be seen. We aimed to start addressing this exclusion with the current study.”
The findings provide a lens into the levels of sexual violence that LGBTQIA+ youth experience and an opportunity to provide more inclusive care, according to Elizabeth Miller, MD, PhD, FSAHM, Distinguished Professor of Pediatrics, director of the Division of Adolescent and Young Adult Medicine, and medical director of community and population health at UPMC Children’s Hospital of Pittsburgh, who was not involved in the study.
“There are unfortunately pervasive and harmful stereotypes in our society about the ‘sexual deviancy’ attributed to LGBTQIA+ individuals,” Dr. Miller told this news organization. “This study adds to the research literature that counters and challenges these harmful – and inaccurate – perceptions.”
Dr. Miller said clinicians can help this population by offering youth accurate information about relevant support and services, including how to help a friend.
Programs that providers could incorporate include gender transformative approaches, which guide youth to examine gender norms and inequities and that develop leadership skills.
Such programs are more common outside the United States and have been shown to decrease LGBTQIA+ youth exposure to sexual violence, she said.
Dr. Miller said more research is needed to understand the contexts in which gender minority youth experience sexual violence to guide prevention efforts: “We need to move beyond individual-focused interventions to considering community-level interventions to create safer and more inclusive spaces for all youth.”
Dr. Miller has received royalties for writing content for UptoDate Wolters Kluwer outside of the current study. Dr. Ybarra has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
High rates of med student burnout during COVID
NEW ORLEANS –
Researchers surveyed 613 medical students representing all years of a medical program during the last week of the Spring semester of 2021.
Based on the Maslach Burnout Inventory-Student Survey (MBI-SS), more than half (54%) of the students had symptoms of burnout.
Eighty percent of students scored high on emotional exhaustion, 57% scored high on cynicism, and 36% scored low on academic effectiveness.
Compared with male medical students, female medical students were more apt to exhibit signs of burnout (60% vs. 44%), emotional exhaustion (80% vs. 73%), and cynicism (62% vs. 49%).
After adjusting for associated factors, female medical students were significantly more likely to suffer from burnout than male students (odds ratio, 1.90; 95% confidence interval, 1.34-2.70; P < .001).
Smoking was also linked to higher likelihood of burnout among medical students (OR, 2.12; 95% CI, 1.18-3.81; P < .05). The death of a family member from COVID-19 also put medical students at heightened risk for burnout (OR, 1.60; 95% CI, 1.08-2.36; P < .05).
The survey results were presented at the American Psychiatric Association (APA) Annual Meeting.
The findings point to the need to study burnout prevalence in universities and develop strategies to promote the mental health of future physicians, presenter Sofia Jezzini-Martínez, fourth-year medical student, Autonomous University of Nuevo Leon, Monterrey, Mexico, wrote in her conference abstract.
In related research presented at the APA meeting, researchers surveyed second-, third-, and fourth-year medical students from California during the pandemic.
Roughly 80% exhibited symptoms of anxiety and 68% exhibited depressive symptoms, of whom about 18% also reported having thoughts of suicide.
Yet only about half of the medical students exhibiting anxiety or depressive symptoms sought help from a mental health professional, and 20% reported using substances to cope with stress.
“Given that the pandemic is ongoing, we hope to draw attention to mental health needs of medical students and influence medical schools to direct appropriate and timely resources to this group,” presenter Sarthak Angal, MD, psychiatry resident, Kaiser Permanente San Jose Medical Center, California, wrote in his conference abstract.
Managing expectations
Weighing in on medical student burnout, Ihuoma Njoku, MD, department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville, noted that, “particularly for women in multiple fields, including medicine, there’s a lot of burden placed on them.”
“Women are pulled in a lot of different directions and have increased demands, which may help explain their higher rate of burnout,” Dr. Njoku commented.
She noted that these surveys were conducted during the COVID-19 pandemic, “a period when students’ education experience was a lot different than what they expected and maybe what they wanted.”
Dr. Njoku noted that the challenges of the pandemic are particularly hard on fourth-year medical students.
“A big part of fourth year is applying to residency, and many were doing virtual interviews for residency. That makes it hard to really get an appreciation of the place you will spend the next three to eight years of your life,” she told this news organization.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
Researchers surveyed 613 medical students representing all years of a medical program during the last week of the Spring semester of 2021.
Based on the Maslach Burnout Inventory-Student Survey (MBI-SS), more than half (54%) of the students had symptoms of burnout.
Eighty percent of students scored high on emotional exhaustion, 57% scored high on cynicism, and 36% scored low on academic effectiveness.
Compared with male medical students, female medical students were more apt to exhibit signs of burnout (60% vs. 44%), emotional exhaustion (80% vs. 73%), and cynicism (62% vs. 49%).
After adjusting for associated factors, female medical students were significantly more likely to suffer from burnout than male students (odds ratio, 1.90; 95% confidence interval, 1.34-2.70; P < .001).
Smoking was also linked to higher likelihood of burnout among medical students (OR, 2.12; 95% CI, 1.18-3.81; P < .05). The death of a family member from COVID-19 also put medical students at heightened risk for burnout (OR, 1.60; 95% CI, 1.08-2.36; P < .05).
The survey results were presented at the American Psychiatric Association (APA) Annual Meeting.
The findings point to the need to study burnout prevalence in universities and develop strategies to promote the mental health of future physicians, presenter Sofia Jezzini-Martínez, fourth-year medical student, Autonomous University of Nuevo Leon, Monterrey, Mexico, wrote in her conference abstract.
In related research presented at the APA meeting, researchers surveyed second-, third-, and fourth-year medical students from California during the pandemic.
Roughly 80% exhibited symptoms of anxiety and 68% exhibited depressive symptoms, of whom about 18% also reported having thoughts of suicide.
Yet only about half of the medical students exhibiting anxiety or depressive symptoms sought help from a mental health professional, and 20% reported using substances to cope with stress.
“Given that the pandemic is ongoing, we hope to draw attention to mental health needs of medical students and influence medical schools to direct appropriate and timely resources to this group,” presenter Sarthak Angal, MD, psychiatry resident, Kaiser Permanente San Jose Medical Center, California, wrote in his conference abstract.
Managing expectations
Weighing in on medical student burnout, Ihuoma Njoku, MD, department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville, noted that, “particularly for women in multiple fields, including medicine, there’s a lot of burden placed on them.”
“Women are pulled in a lot of different directions and have increased demands, which may help explain their higher rate of burnout,” Dr. Njoku commented.
She noted that these surveys were conducted during the COVID-19 pandemic, “a period when students’ education experience was a lot different than what they expected and maybe what they wanted.”
Dr. Njoku noted that the challenges of the pandemic are particularly hard on fourth-year medical students.
“A big part of fourth year is applying to residency, and many were doing virtual interviews for residency. That makes it hard to really get an appreciation of the place you will spend the next three to eight years of your life,” she told this news organization.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
Researchers surveyed 613 medical students representing all years of a medical program during the last week of the Spring semester of 2021.
Based on the Maslach Burnout Inventory-Student Survey (MBI-SS), more than half (54%) of the students had symptoms of burnout.
Eighty percent of students scored high on emotional exhaustion, 57% scored high on cynicism, and 36% scored low on academic effectiveness.
Compared with male medical students, female medical students were more apt to exhibit signs of burnout (60% vs. 44%), emotional exhaustion (80% vs. 73%), and cynicism (62% vs. 49%).
After adjusting for associated factors, female medical students were significantly more likely to suffer from burnout than male students (odds ratio, 1.90; 95% confidence interval, 1.34-2.70; P < .001).
Smoking was also linked to higher likelihood of burnout among medical students (OR, 2.12; 95% CI, 1.18-3.81; P < .05). The death of a family member from COVID-19 also put medical students at heightened risk for burnout (OR, 1.60; 95% CI, 1.08-2.36; P < .05).
The survey results were presented at the American Psychiatric Association (APA) Annual Meeting.
The findings point to the need to study burnout prevalence in universities and develop strategies to promote the mental health of future physicians, presenter Sofia Jezzini-Martínez, fourth-year medical student, Autonomous University of Nuevo Leon, Monterrey, Mexico, wrote in her conference abstract.
In related research presented at the APA meeting, researchers surveyed second-, third-, and fourth-year medical students from California during the pandemic.
Roughly 80% exhibited symptoms of anxiety and 68% exhibited depressive symptoms, of whom about 18% also reported having thoughts of suicide.
Yet only about half of the medical students exhibiting anxiety or depressive symptoms sought help from a mental health professional, and 20% reported using substances to cope with stress.
“Given that the pandemic is ongoing, we hope to draw attention to mental health needs of medical students and influence medical schools to direct appropriate and timely resources to this group,” presenter Sarthak Angal, MD, psychiatry resident, Kaiser Permanente San Jose Medical Center, California, wrote in his conference abstract.
Managing expectations
Weighing in on medical student burnout, Ihuoma Njoku, MD, department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville, noted that, “particularly for women in multiple fields, including medicine, there’s a lot of burden placed on them.”
“Women are pulled in a lot of different directions and have increased demands, which may help explain their higher rate of burnout,” Dr. Njoku commented.
She noted that these surveys were conducted during the COVID-19 pandemic, “a period when students’ education experience was a lot different than what they expected and maybe what they wanted.”
Dr. Njoku noted that the challenges of the pandemic are particularly hard on fourth-year medical students.
“A big part of fourth year is applying to residency, and many were doing virtual interviews for residency. That makes it hard to really get an appreciation of the place you will spend the next three to eight years of your life,” she told this news organization.
A version of this article first appeared on Medscape.com.
FROM APA 2022
At-home vagus nerve stimulation promising for postpartum depression
At-home, noninvasive auricular vagus nerve stimulation (aVNS) therapy is well-tolerated and associated with a significant reduction in postpartum depressive and anxiety symptoms, new research suggests.
In a small proof-of-concept pilot study of 25 women with postpartum depression receiving 6 weeks of daily aVNS treatment, results showed that 74% achieved response and 61% achieved remission, as shown in reduced scores on the Hamilton Rating Scale for Depression (HAM-D17).
Although invasive electrical stimulation of the vagus nerve was approved by the U.S. Food and Drug Administration for treatment-resistant depression in 2005, it involves risk for implantation, infection, and significant side effects, coinvestigator Kristina M. Deligiannidis, MD, director, Women’s Behavioral Health, Zucker Hillside Hospital, Northwell Health, Glen Oaks, New York, told this news organization.

“This newer approach, transcutaneous auricular VNS, is non-invasive, is well tolerated, and has shown initial efficacy in major depression in men and women,” she said.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) Annual Meeting.
Potential alternative to meds
“Given that aVNS is a non-invasive treatment which can be administered at home, we wanted to test if this approach was safe, feasible, and could reduce depressive symptoms in women with postpartum depression, as many of these women have barriers to accessing current treatments,” Dr. Deligiannidis said.
Auricular VNS uses surface skin electrodes to stimulate nerve endings of a branch of the vagus nerve, located on the surface of the outer ear. Those nerve endings travel to the brain where they have been shown to modulate brain communication in areas important for mood and anxiety regulation, she said.
Dr. Deligiannidis noted that evidence-based treatments for postpartum depression include psychotherapies and antidepressants. However, some women have difficulty accessing weekly psychotherapy, and, when antidepressants are indicated, many are reluctant to take them if they are breastfeeding because of concerns about the medications getting into their breast milk, she said.
Although most antidepressants are safe in lactation, many women postpone antidepressant treatment until they have finished breastfeeding, which can postpone their postpartum depression treatment, Dr. Deligiannidis added.
“At home treatments reduce many barriers women have to current treatments, and this intervention [of aVNS] does not impact breastfeeding, as it is not a medication approach,” she said.
The researchers enrolled 25 women (mean age, 33.7 years) diagnosed with postpartum depression. Ten of the women (40%) were on a stable dose of antidepressant medication.
The participants self-administered 6 weeks of open-label aVNS for 15 minutes daily at home. They were then observed without intervention for an additional 2 weeks. The women also completed medical, psychiatric, and safety interviews throughout the study period.
Promising findings
At baseline, the mean HAM-D17 was 18.4 and was similar for those on (17.8) and off (18.9) antidepressants.
By week 6, the mean HAM-D17 total score decreased by 9.7 points overall, compared with baseline score. For participants on antidepressants, the HAM-D17 decreased by 8.7 points; for women off antidepressants, it decreased by 10.3 points.
In addition, 74% of the women achieved a response to the therapy, and 61% achieved remission of their depressive symptoms.
The most common adverse effects were discomfort (n = 5 patients), headache (n = 3), and dizziness (n = 2). All resolved without intervention.
Commenting on the findings, Anita Clayton, MD, professor and chair, department of psychiatry and neurobehavioral sciences, University of Virginia School of Medicine, Charlottesville, said the study was “quite interesting.”

Dr. Clayton, who was not involved with the research, also noted the “pretty high” response and remission rates.
“So, I think this does have promise, and it would be worth doing a study where you look at placebo versus this treatment,” she said.
“Many women are fearful of taking medicines postpartum, even peripartum, unless they have had pre-existing severe depression. This is not a medicine, and it sounds like it could be useful even in people who are pregnant, although it’s harder to do studies in pregnant women,” Dr. Clayton added.
The study was funded by Nesos Corporation. Dr. Deligiannidis received contracted research funds from Nesos Corporation to conduct this study. She also serves as a consultant to Sage Therapeutics, Brii Biosciences, and GH Research. Dr. Clayton reports financial relationships with Dare Bioscience, Janssen, Praxis Precision Medicines, Relmada Therapeutics, Sage Therapeutics, AbbVie, Brii Biosciences, Fabre-Kramer, Field Trip Health, Mind Cure Health, Ovoca Bio, PureTech Health, S1 Biopharma, Takeda/Lundbeck, Vella Bioscience, WCG MedAvante-ProPhase, Ballantine Books/Random House, Changes in Sexual Functioning Questionnaire, Guilford Publications, Euthymics Bioscience, and Mediflix.
A version of this article first appeared on Medscape.com.
At-home, noninvasive auricular vagus nerve stimulation (aVNS) therapy is well-tolerated and associated with a significant reduction in postpartum depressive and anxiety symptoms, new research suggests.
In a small proof-of-concept pilot study of 25 women with postpartum depression receiving 6 weeks of daily aVNS treatment, results showed that 74% achieved response and 61% achieved remission, as shown in reduced scores on the Hamilton Rating Scale for Depression (HAM-D17).
Although invasive electrical stimulation of the vagus nerve was approved by the U.S. Food and Drug Administration for treatment-resistant depression in 2005, it involves risk for implantation, infection, and significant side effects, coinvestigator Kristina M. Deligiannidis, MD, director, Women’s Behavioral Health, Zucker Hillside Hospital, Northwell Health, Glen Oaks, New York, told this news organization.
“This newer approach, transcutaneous auricular VNS, is non-invasive, is well tolerated, and has shown initial efficacy in major depression in men and women,” she said.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) Annual Meeting.
Potential alternative to meds
“Given that aVNS is a non-invasive treatment which can be administered at home, we wanted to test if this approach was safe, feasible, and could reduce depressive symptoms in women with postpartum depression, as many of these women have barriers to accessing current treatments,” Dr. Deligiannidis said.
Auricular VNS uses surface skin electrodes to stimulate nerve endings of a branch of the vagus nerve, located on the surface of the outer ear. Those nerve endings travel to the brain where they have been shown to modulate brain communication in areas important for mood and anxiety regulation, she said.
Dr. Deligiannidis noted that evidence-based treatments for postpartum depression include psychotherapies and antidepressants. However, some women have difficulty accessing weekly psychotherapy, and, when antidepressants are indicated, many are reluctant to take them if they are breastfeeding because of concerns about the medications getting into their breast milk, she said.
Although most antidepressants are safe in lactation, many women postpone antidepressant treatment until they have finished breastfeeding, which can postpone their postpartum depression treatment, Dr. Deligiannidis added.
“At home treatments reduce many barriers women have to current treatments, and this intervention [of aVNS] does not impact breastfeeding, as it is not a medication approach,” she said.
The researchers enrolled 25 women (mean age, 33.7 years) diagnosed with postpartum depression. Ten of the women (40%) were on a stable dose of antidepressant medication.
The participants self-administered 6 weeks of open-label aVNS for 15 minutes daily at home. They were then observed without intervention for an additional 2 weeks. The women also completed medical, psychiatric, and safety interviews throughout the study period.
Promising findings
At baseline, the mean HAM-D17 was 18.4 and was similar for those on (17.8) and off (18.9) antidepressants.
By week 6, the mean HAM-D17 total score decreased by 9.7 points overall, compared with baseline score. For participants on antidepressants, the HAM-D17 decreased by 8.7 points; for women off antidepressants, it decreased by 10.3 points.
In addition, 74% of the women achieved a response to the therapy, and 61% achieved remission of their depressive symptoms.
The most common adverse effects were discomfort (n = 5 patients), headache (n = 3), and dizziness (n = 2). All resolved without intervention.
Commenting on the findings, Anita Clayton, MD, professor and chair, department of psychiatry and neurobehavioral sciences, University of Virginia School of Medicine, Charlottesville, said the study was “quite interesting.”
Dr. Clayton, who was not involved with the research, also noted the “pretty high” response and remission rates.
“So, I think this does have promise, and it would be worth doing a study where you look at placebo versus this treatment,” she said.
“Many women are fearful of taking medicines postpartum, even peripartum, unless they have had pre-existing severe depression. This is not a medicine, and it sounds like it could be useful even in people who are pregnant, although it’s harder to do studies in pregnant women,” Dr. Clayton added.
The study was funded by Nesos Corporation. Dr. Deligiannidis received contracted research funds from Nesos Corporation to conduct this study. She also serves as a consultant to Sage Therapeutics, Brii Biosciences, and GH Research. Dr. Clayton reports financial relationships with Dare Bioscience, Janssen, Praxis Precision Medicines, Relmada Therapeutics, Sage Therapeutics, AbbVie, Brii Biosciences, Fabre-Kramer, Field Trip Health, Mind Cure Health, Ovoca Bio, PureTech Health, S1 Biopharma, Takeda/Lundbeck, Vella Bioscience, WCG MedAvante-ProPhase, Ballantine Books/Random House, Changes in Sexual Functioning Questionnaire, Guilford Publications, Euthymics Bioscience, and Mediflix.
A version of this article first appeared on Medscape.com.
At-home, noninvasive auricular vagus nerve stimulation (aVNS) therapy is well-tolerated and associated with a significant reduction in postpartum depressive and anxiety symptoms, new research suggests.
In a small proof-of-concept pilot study of 25 women with postpartum depression receiving 6 weeks of daily aVNS treatment, results showed that 74% achieved response and 61% achieved remission, as shown in reduced scores on the Hamilton Rating Scale for Depression (HAM-D17).
Although invasive electrical stimulation of the vagus nerve was approved by the U.S. Food and Drug Administration for treatment-resistant depression in 2005, it involves risk for implantation, infection, and significant side effects, coinvestigator Kristina M. Deligiannidis, MD, director, Women’s Behavioral Health, Zucker Hillside Hospital, Northwell Health, Glen Oaks, New York, told this news organization.
“This newer approach, transcutaneous auricular VNS, is non-invasive, is well tolerated, and has shown initial efficacy in major depression in men and women,” she said.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) Annual Meeting.
Potential alternative to meds
“Given that aVNS is a non-invasive treatment which can be administered at home, we wanted to test if this approach was safe, feasible, and could reduce depressive symptoms in women with postpartum depression, as many of these women have barriers to accessing current treatments,” Dr. Deligiannidis said.
Auricular VNS uses surface skin electrodes to stimulate nerve endings of a branch of the vagus nerve, located on the surface of the outer ear. Those nerve endings travel to the brain where they have been shown to modulate brain communication in areas important for mood and anxiety regulation, she said.
Dr. Deligiannidis noted that evidence-based treatments for postpartum depression include psychotherapies and antidepressants. However, some women have difficulty accessing weekly psychotherapy, and, when antidepressants are indicated, many are reluctant to take them if they are breastfeeding because of concerns about the medications getting into their breast milk, she said.
Although most antidepressants are safe in lactation, many women postpone antidepressant treatment until they have finished breastfeeding, which can postpone their postpartum depression treatment, Dr. Deligiannidis added.
“At home treatments reduce many barriers women have to current treatments, and this intervention [of aVNS] does not impact breastfeeding, as it is not a medication approach,” she said.
The researchers enrolled 25 women (mean age, 33.7 years) diagnosed with postpartum depression. Ten of the women (40%) were on a stable dose of antidepressant medication.
The participants self-administered 6 weeks of open-label aVNS for 15 minutes daily at home. They were then observed without intervention for an additional 2 weeks. The women also completed medical, psychiatric, and safety interviews throughout the study period.
Promising findings
At baseline, the mean HAM-D17 was 18.4 and was similar for those on (17.8) and off (18.9) antidepressants.
By week 6, the mean HAM-D17 total score decreased by 9.7 points overall, compared with baseline score. For participants on antidepressants, the HAM-D17 decreased by 8.7 points; for women off antidepressants, it decreased by 10.3 points.
In addition, 74% of the women achieved a response to the therapy, and 61% achieved remission of their depressive symptoms.
The most common adverse effects were discomfort (n = 5 patients), headache (n = 3), and dizziness (n = 2). All resolved without intervention.
Commenting on the findings, Anita Clayton, MD, professor and chair, department of psychiatry and neurobehavioral sciences, University of Virginia School of Medicine, Charlottesville, said the study was “quite interesting.”
Dr. Clayton, who was not involved with the research, also noted the “pretty high” response and remission rates.
“So, I think this does have promise, and it would be worth doing a study where you look at placebo versus this treatment,” she said.
“Many women are fearful of taking medicines postpartum, even peripartum, unless they have had pre-existing severe depression. This is not a medicine, and it sounds like it could be useful even in people who are pregnant, although it’s harder to do studies in pregnant women,” Dr. Clayton added.
The study was funded by Nesos Corporation. Dr. Deligiannidis received contracted research funds from Nesos Corporation to conduct this study. She also serves as a consultant to Sage Therapeutics, Brii Biosciences, and GH Research. Dr. Clayton reports financial relationships with Dare Bioscience, Janssen, Praxis Precision Medicines, Relmada Therapeutics, Sage Therapeutics, AbbVie, Brii Biosciences, Fabre-Kramer, Field Trip Health, Mind Cure Health, Ovoca Bio, PureTech Health, S1 Biopharma, Takeda/Lundbeck, Vella Bioscience, WCG MedAvante-ProPhase, Ballantine Books/Random House, Changes in Sexual Functioning Questionnaire, Guilford Publications, Euthymics Bioscience, and Mediflix.
A version of this article first appeared on Medscape.com.
Intensive outpatient PTSD treatment linked to fewer emergency encounters
NEW ORLEANS – , according to a new study released at the annual meeting of the American Psychiatric Association.
In an analysis of 256 individuals, over the 12 months before they joined the IOP, 28.7% and 24.8% had inpatient and emergency department encounters, respectively, according to the researchers. Afterward, those numbers fell to 15.9% (P < .01) and 18.2% (P = .04), respectively.
“Engagement in IOP for patients with PTSD may help avoid the need for higher levels of care such as residential or inpatient treatment,” Nathan Lingafelter, MD, a psychiatrist and researcher at Kaiser Permanente in Oakland, Calif., said in an interview.
Dr. Lingafelter described IOP programs as typically “offering patients a combination of individual therapy, group therapy, and medication management all at an increased frequency of about 3 half-days per week. IOPs are thought to be helpful in helping patients with severe symptoms while they are still in the community – i.e., living in their homes, with their families, occasionally still working at reduced time.”
While other studies have examined the effects of IOP, “the existing literature focuses on how IOP reduces symptoms, rather than looking at how IOP involvement might be associated with patients utilizing different acute care resources,” he said. “Prior studies have also been conducted mostly in veteran populations and in populations with less diversity than our population in Oakland.”
For the new study, researchers tracked 256 IOP participants (83% female; mean age = 39; 44% White, 27% Black, 14% Hispanic, and 7% Asian). The wide majority – 85% – had comorbid depressive disorders.
“Patients are assigned a case manager when they enter the program who they can meet with individually, and they spend time attending group therapy sessions. Patients are also able to meet with a psychiatrist to discuss medications,” Dr. Lingafelter said. “A major component in both the group and individual therapy is helping patients identify which kind of interventions work for them and what we can do now that will help. IOP can really help clarify for patients what their trauma responses are and how to start treatments that actually fit their symptoms.”
The subjects had a mean 0.3 psychiatric encounters in the year before joining the program and 0.2 in the year after (P < .01). Their mean emergency department visits related to mental health fell from 0.5 to 0.3 (P = .03).
The study has limitations. Participants took part in IOP therapy from 2017 to 2018, before the pandemic disrupted mental health treatment. It does not examine whether medication use changed after IOP treatment. It is retrospective and doesn’t confirm that IOP had any positive effect.
Multiple benefits of IOP
In an interview, Deborah C. Beidel, PhD, director of UCF RESTORES at the University of Central Florida, Orlando, said IOP has several advantages as a treatment for PTSD. Her clinic, which focuses on PTSD treatment for military veterans, has used the approach to treat hundreds of people.

“First, IOPs can address the stigma that surrounds mental health treatment. If you have a physical injury, you take time off from work to go to physical therapy, which is time-limited. If you have a stress injury, why not do the same? Take a few weeks, get it treated, and get back to work,” she said. “The second reason is that the most effective treatment for PTSD is exposure therapy, which is more effective when treatment sessions occur in a daily as opposed to a weekly or monthly time frame. Third, from a cost and feasibility perspective, an intensive program could reduce overall medical costs and get people back to work sooner.”
The new study is “definitely useful” since it examines the impact of IOP over a longer term, Dr. Beidel said. This kind of data “can influence policy, particularly with insurance companies. If we can build the evidence that short, intensive treatment produces better long-term outcomes, insurance companies will be more likely to pay for the IOP.”
The University of Central Florida program is funded by federal research grants and state funding, she said. “When we calculate the cost, it comes to about $10,000 in therapy time plus an average of about $3,000 in travel related costs – transportation, lodging, meals – for those who travel from out of state for our program.”
What’s next? “Further study is needed to characterize whether these findings are applicable to other practice settings, including virtual treatment programs; the long-term durability of these findings; and whether similar patterns of reduced resource use extend to non–mental health–specific care utilization,” said Dr. Lingafelter, the study’s lead author.
No study funding and no author disclosures were reported. Dr. Beidel disclosed IOP-related research support from the U.S. Army Medical Research and Development Command–Military Operational Medicine Research Program.
NEW ORLEANS – , according to a new study released at the annual meeting of the American Psychiatric Association.
In an analysis of 256 individuals, over the 12 months before they joined the IOP, 28.7% and 24.8% had inpatient and emergency department encounters, respectively, according to the researchers. Afterward, those numbers fell to 15.9% (P < .01) and 18.2% (P = .04), respectively.
“Engagement in IOP for patients with PTSD may help avoid the need for higher levels of care such as residential or inpatient treatment,” Nathan Lingafelter, MD, a psychiatrist and researcher at Kaiser Permanente in Oakland, Calif., said in an interview.
Dr. Lingafelter described IOP programs as typically “offering patients a combination of individual therapy, group therapy, and medication management all at an increased frequency of about 3 half-days per week. IOPs are thought to be helpful in helping patients with severe symptoms while they are still in the community – i.e., living in their homes, with their families, occasionally still working at reduced time.”
While other studies have examined the effects of IOP, “the existing literature focuses on how IOP reduces symptoms, rather than looking at how IOP involvement might be associated with patients utilizing different acute care resources,” he said. “Prior studies have also been conducted mostly in veteran populations and in populations with less diversity than our population in Oakland.”
For the new study, researchers tracked 256 IOP participants (83% female; mean age = 39; 44% White, 27% Black, 14% Hispanic, and 7% Asian). The wide majority – 85% – had comorbid depressive disorders.
“Patients are assigned a case manager when they enter the program who they can meet with individually, and they spend time attending group therapy sessions. Patients are also able to meet with a psychiatrist to discuss medications,” Dr. Lingafelter said. “A major component in both the group and individual therapy is helping patients identify which kind of interventions work for them and what we can do now that will help. IOP can really help clarify for patients what their trauma responses are and how to start treatments that actually fit their symptoms.”
The subjects had a mean 0.3 psychiatric encounters in the year before joining the program and 0.2 in the year after (P < .01). Their mean emergency department visits related to mental health fell from 0.5 to 0.3 (P = .03).
The study has limitations. Participants took part in IOP therapy from 2017 to 2018, before the pandemic disrupted mental health treatment. It does not examine whether medication use changed after IOP treatment. It is retrospective and doesn’t confirm that IOP had any positive effect.
Multiple benefits of IOP
In an interview, Deborah C. Beidel, PhD, director of UCF RESTORES at the University of Central Florida, Orlando, said IOP has several advantages as a treatment for PTSD. Her clinic, which focuses on PTSD treatment for military veterans, has used the approach to treat hundreds of people.
“First, IOPs can address the stigma that surrounds mental health treatment. If you have a physical injury, you take time off from work to go to physical therapy, which is time-limited. If you have a stress injury, why not do the same? Take a few weeks, get it treated, and get back to work,” she said. “The second reason is that the most effective treatment for PTSD is exposure therapy, which is more effective when treatment sessions occur in a daily as opposed to a weekly or monthly time frame. Third, from a cost and feasibility perspective, an intensive program could reduce overall medical costs and get people back to work sooner.”
The new study is “definitely useful” since it examines the impact of IOP over a longer term, Dr. Beidel said. This kind of data “can influence policy, particularly with insurance companies. If we can build the evidence that short, intensive treatment produces better long-term outcomes, insurance companies will be more likely to pay for the IOP.”
The University of Central Florida program is funded by federal research grants and state funding, she said. “When we calculate the cost, it comes to about $10,000 in therapy time plus an average of about $3,000 in travel related costs – transportation, lodging, meals – for those who travel from out of state for our program.”
What’s next? “Further study is needed to characterize whether these findings are applicable to other practice settings, including virtual treatment programs; the long-term durability of these findings; and whether similar patterns of reduced resource use extend to non–mental health–specific care utilization,” said Dr. Lingafelter, the study’s lead author.
No study funding and no author disclosures were reported. Dr. Beidel disclosed IOP-related research support from the U.S. Army Medical Research and Development Command–Military Operational Medicine Research Program.
NEW ORLEANS – , according to a new study released at the annual meeting of the American Psychiatric Association.
In an analysis of 256 individuals, over the 12 months before they joined the IOP, 28.7% and 24.8% had inpatient and emergency department encounters, respectively, according to the researchers. Afterward, those numbers fell to 15.9% (P < .01) and 18.2% (P = .04), respectively.
“Engagement in IOP for patients with PTSD may help avoid the need for higher levels of care such as residential or inpatient treatment,” Nathan Lingafelter, MD, a psychiatrist and researcher at Kaiser Permanente in Oakland, Calif., said in an interview.
Dr. Lingafelter described IOP programs as typically “offering patients a combination of individual therapy, group therapy, and medication management all at an increased frequency of about 3 half-days per week. IOPs are thought to be helpful in helping patients with severe symptoms while they are still in the community – i.e., living in their homes, with their families, occasionally still working at reduced time.”
While other studies have examined the effects of IOP, “the existing literature focuses on how IOP reduces symptoms, rather than looking at how IOP involvement might be associated with patients utilizing different acute care resources,” he said. “Prior studies have also been conducted mostly in veteran populations and in populations with less diversity than our population in Oakland.”
For the new study, researchers tracked 256 IOP participants (83% female; mean age = 39; 44% White, 27% Black, 14% Hispanic, and 7% Asian). The wide majority – 85% – had comorbid depressive disorders.
“Patients are assigned a case manager when they enter the program who they can meet with individually, and they spend time attending group therapy sessions. Patients are also able to meet with a psychiatrist to discuss medications,” Dr. Lingafelter said. “A major component in both the group and individual therapy is helping patients identify which kind of interventions work for them and what we can do now that will help. IOP can really help clarify for patients what their trauma responses are and how to start treatments that actually fit their symptoms.”
The subjects had a mean 0.3 psychiatric encounters in the year before joining the program and 0.2 in the year after (P < .01). Their mean emergency department visits related to mental health fell from 0.5 to 0.3 (P = .03).
The study has limitations. Participants took part in IOP therapy from 2017 to 2018, before the pandemic disrupted mental health treatment. It does not examine whether medication use changed after IOP treatment. It is retrospective and doesn’t confirm that IOP had any positive effect.
Multiple benefits of IOP
In an interview, Deborah C. Beidel, PhD, director of UCF RESTORES at the University of Central Florida, Orlando, said IOP has several advantages as a treatment for PTSD. Her clinic, which focuses on PTSD treatment for military veterans, has used the approach to treat hundreds of people.
“First, IOPs can address the stigma that surrounds mental health treatment. If you have a physical injury, you take time off from work to go to physical therapy, which is time-limited. If you have a stress injury, why not do the same? Take a few weeks, get it treated, and get back to work,” she said. “The second reason is that the most effective treatment for PTSD is exposure therapy, which is more effective when treatment sessions occur in a daily as opposed to a weekly or monthly time frame. Third, from a cost and feasibility perspective, an intensive program could reduce overall medical costs and get people back to work sooner.”
The new study is “definitely useful” since it examines the impact of IOP over a longer term, Dr. Beidel said. This kind of data “can influence policy, particularly with insurance companies. If we can build the evidence that short, intensive treatment produces better long-term outcomes, insurance companies will be more likely to pay for the IOP.”
The University of Central Florida program is funded by federal research grants and state funding, she said. “When we calculate the cost, it comes to about $10,000 in therapy time plus an average of about $3,000 in travel related costs – transportation, lodging, meals – for those who travel from out of state for our program.”
What’s next? “Further study is needed to characterize whether these findings are applicable to other practice settings, including virtual treatment programs; the long-term durability of these findings; and whether similar patterns of reduced resource use extend to non–mental health–specific care utilization,” said Dr. Lingafelter, the study’s lead author.
No study funding and no author disclosures were reported. Dr. Beidel disclosed IOP-related research support from the U.S. Army Medical Research and Development Command–Military Operational Medicine Research Program.
AT APA 2022
Early metformin minimizes antipsychotic-induced weight gain
MAR DEL PLATA, ARGENTINA – , according to a new evidence-based Irish guideline for the management of this common complication in adults with psychoses who are taking medications.
The document was discussed during one of the sessions of the XXXV Argentine Congress of Psychiatry of the Association of Argentine Psychiatrists. The document also was presented by one of its authors at the European Congress on Obesity 2022.
The guideline encourages psychiatrists not to underestimate the adverse metabolic effects of their treatments and encourages them to contemplate and carry out this prevention and management strategy, commented María Delia Michat, PhD, professor of clinical psychiatry and psychopharmacology at the APSA Postgraduate Training Institute, Buenos Aires.
“Although it is always good to work as a team, it is usually we psychiatrists who coordinate the pharmacological treatment of our patients, and we have to know how to manage drugs that can prevent cardiovascular disease,” Dr. Michat said in an interview.
“The new guideline is helpful because it protocolizes the use of metformin, which is the cheapest drug and has the most evidence for antipsychotic-induced weight gain,” she added.
Avoiding metabolic syndrome
In patients with schizophrenia, obesity rates are 40% higher than in the general population, and 80% of patients develop weight gain after their first treatment, noted Dr. Michat. “Right away, weight gain is seen in the first month. And it is a serious problem, because patients with schizophrenia, major depression, or bipolar disorder already have an increased risk of premature mortality, especially from cardiovascular diseases, and they have an increased risk of metabolic syndrome. And we sometimes give drugs that further increase that risk,” she said.
Being overweight is a major criterion for defining metabolic syndrome. Dr. Michat noted that, among the antipsychotic drugs that increase weight the most are clozapine, olanzapine, chlorpromazine, quetiapine, and risperidone, in addition to other psychoactive drugs, such as valproic acid, lithium, mirtazapine, and tricyclic antidepressants.
Several clinical trials, such as a pioneering Chinese study from 2008, have shown the potential of metformin to mitigate the weight gain induced by this type of drug.
However, Dr. Michat noted that so far the major guidelines (for example, the Canadian Network for Mood and Anxiety Treatments [CANMAT]/International Society for Bipolar Disorders [ISBD] for bipolar disorder and the American Psychiatric Association [APA] for schizophrenia) “say very little” on how to address this complication. They propose what she defined as a “problematic” order of action in which the initial emphasis is on promoting lifestyle changes, which are difficult for these patients to carry out, as well as general proposals for changing medication (which is not simple to implement when the patient’s condition is stabilized) and eventual consultation with a clinician to start therapy with metformin or other drugs, such as liraglutide, semaglutide, and topiramate.
The new clinical practice guideline, which was published in Evidence-Based Mental Health (of the BMJ journal group), was written by a multidisciplinary team of pharmacists, psychiatrists, and mental health nurses from Ireland. It aims to fill that gap. The investigators reviewed 1,270 scientific articles and analyzed 26 of them in depth, including seven randomized clinical trials and a 2016 systematic review and meta-analysis. The authors made a “strong” recommendation, for which there was moderate-quality evidence, that for patients for whom a lifestyle intervention is unacceptable or inappropriate the use of metformin is an “alternative first-line intervention” for antipsychotic drug–induced weight gain.
Likewise, as a strong recommendation with moderate-quality evidence, the guidance encourages the use of metformin when nonpharmacologic intervention does not seem to be effective.
The guideline also says it is preferable to start metformin early for patients who gain more than 7% of their baseline weight within the first month of antipsychotic treatment. It also endorses metformin when weight gain is established.
Other recommendations include evaluating baseline kidney function before starting metformin treatment and suggest a dose adjustment when the estimated glomerular filtration rate (eGFR) is < 60 mL/min/1.73 m2. The guidance says the use of metformin is contraindicated for patients in whom eGFR is <30 mL/min per 1.73 m2. The proposed starting dosage is 500 mg twice per day with meals, with increments of 500 mg every 1-2 weeks until reaching a target dose of 2,000 mg/day. The guidance recommends that consideration always be given to individual tolerability and efficacy.
Treatment goals should be personalized and agreed upon with patients. In the case of early intervention, the guideline proposes initially stabilizing the weight gained or, if possible, reverse excess weight. When weight gain is established, the goal would be to lose at least 5% of the weight within the next 6 months.
The authors also recommend monitoring kidney function annually, as well as vitamin B12 levels and individual tolerability and compliance. Gastrointestinal adverse effects can be managed by dose reduction or slower dose titration. The risk of lactic acidosis, which affects 4.3 per 100,000 person-years among those taking metformin, can be attenuated by adjusting the dose according to kidney function or avoiding prescribing it to patients who have a history of alcohol abuse or who are receiving treatment that may interact with the drug.
Validating pharmacologic management
The lead author of the new guideline, Ita Fitzgerald, a teacher in clinical pharmacy and senior pharmacist at St. Patrick’s Mental Health Services in Dublin, pointed out that there is a bias toward not using drugs for weight management and shifting the responsibility onto the patients themselves, something that is very often out of their control.
“The purpose of the guideline was to decide on a range of criteria to maximize the use of metformin, to recognize that for many people, pharmacological management is a valid and important option that could and should be more widely used and to provide precise and practical guidance to physicians to facilitate a more widespread use,” Ms. Fitzgerald said in an interview.
According to Fitzgerald, who is pursuing her doctorate at University College Cork (Ireland), one of the most outstanding results of the work is that it highlights that the main benefit of metformin is to flatten rather than reverse antipsychotic-induced weight gain and that indicating it late can nullify that effect.
“In all the recommendations, we try very hard to shift the focus from metformin’s role as a weight reversal agent to one as a weight management agent that should be used early in treatment, which is when most weight gain occurs. If metformin succeeds in flattening that increase, that’s a huge potential benefit for an inexpensive and easily accessible drug. When people have already established weight gain, metformin may not be enough and alternative treatments should be used,” she said.
In addition to its effects on weight, metformin has many other potential health benefits. Of particular importance is that it reduces hyperphagia-mediated antipsychotic-induced weight gain, Ms. Fitzgerald pointed out.
“This is subjectively very important for patients and provides a more positive experience when taking antipsychotics. Antipsychotic-induced weight gain is one of the main reasons for premature discontinuation or incomplete adherence to these drugs and therefore needs to be addressed proactively,” she concluded.
Ms. Fitzgerald and Dr. Michat have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com. This article was translated from the Medscape Spanish edition.
MAR DEL PLATA, ARGENTINA – , according to a new evidence-based Irish guideline for the management of this common complication in adults with psychoses who are taking medications.
The document was discussed during one of the sessions of the XXXV Argentine Congress of Psychiatry of the Association of Argentine Psychiatrists. The document also was presented by one of its authors at the European Congress on Obesity 2022.
The guideline encourages psychiatrists not to underestimate the adverse metabolic effects of their treatments and encourages them to contemplate and carry out this prevention and management strategy, commented María Delia Michat, PhD, professor of clinical psychiatry and psychopharmacology at the APSA Postgraduate Training Institute, Buenos Aires.
“Although it is always good to work as a team, it is usually we psychiatrists who coordinate the pharmacological treatment of our patients, and we have to know how to manage drugs that can prevent cardiovascular disease,” Dr. Michat said in an interview.
“The new guideline is helpful because it protocolizes the use of metformin, which is the cheapest drug and has the most evidence for antipsychotic-induced weight gain,” she added.
Avoiding metabolic syndrome
In patients with schizophrenia, obesity rates are 40% higher than in the general population, and 80% of patients develop weight gain after their first treatment, noted Dr. Michat. “Right away, weight gain is seen in the first month. And it is a serious problem, because patients with schizophrenia, major depression, or bipolar disorder already have an increased risk of premature mortality, especially from cardiovascular diseases, and they have an increased risk of metabolic syndrome. And we sometimes give drugs that further increase that risk,” she said.
Being overweight is a major criterion for defining metabolic syndrome. Dr. Michat noted that, among the antipsychotic drugs that increase weight the most are clozapine, olanzapine, chlorpromazine, quetiapine, and risperidone, in addition to other psychoactive drugs, such as valproic acid, lithium, mirtazapine, and tricyclic antidepressants.
Several clinical trials, such as a pioneering Chinese study from 2008, have shown the potential of metformin to mitigate the weight gain induced by this type of drug.
However, Dr. Michat noted that so far the major guidelines (for example, the Canadian Network for Mood and Anxiety Treatments [CANMAT]/International Society for Bipolar Disorders [ISBD] for bipolar disorder and the American Psychiatric Association [APA] for schizophrenia) “say very little” on how to address this complication. They propose what she defined as a “problematic” order of action in which the initial emphasis is on promoting lifestyle changes, which are difficult for these patients to carry out, as well as general proposals for changing medication (which is not simple to implement when the patient’s condition is stabilized) and eventual consultation with a clinician to start therapy with metformin or other drugs, such as liraglutide, semaglutide, and topiramate.
The new clinical practice guideline, which was published in Evidence-Based Mental Health (of the BMJ journal group), was written by a multidisciplinary team of pharmacists, psychiatrists, and mental health nurses from Ireland. It aims to fill that gap. The investigators reviewed 1,270 scientific articles and analyzed 26 of them in depth, including seven randomized clinical trials and a 2016 systematic review and meta-analysis. The authors made a “strong” recommendation, for which there was moderate-quality evidence, that for patients for whom a lifestyle intervention is unacceptable or inappropriate the use of metformin is an “alternative first-line intervention” for antipsychotic drug–induced weight gain.
Likewise, as a strong recommendation with moderate-quality evidence, the guidance encourages the use of metformin when nonpharmacologic intervention does not seem to be effective.
The guideline also says it is preferable to start metformin early for patients who gain more than 7% of their baseline weight within the first month of antipsychotic treatment. It also endorses metformin when weight gain is established.
Other recommendations include evaluating baseline kidney function before starting metformin treatment and suggest a dose adjustment when the estimated glomerular filtration rate (eGFR) is < 60 mL/min/1.73 m2. The guidance says the use of metformin is contraindicated for patients in whom eGFR is <30 mL/min per 1.73 m2. The proposed starting dosage is 500 mg twice per day with meals, with increments of 500 mg every 1-2 weeks until reaching a target dose of 2,000 mg/day. The guidance recommends that consideration always be given to individual tolerability and efficacy.
Treatment goals should be personalized and agreed upon with patients. In the case of early intervention, the guideline proposes initially stabilizing the weight gained or, if possible, reverse excess weight. When weight gain is established, the goal would be to lose at least 5% of the weight within the next 6 months.
The authors also recommend monitoring kidney function annually, as well as vitamin B12 levels and individual tolerability and compliance. Gastrointestinal adverse effects can be managed by dose reduction or slower dose titration. The risk of lactic acidosis, which affects 4.3 per 100,000 person-years among those taking metformin, can be attenuated by adjusting the dose according to kidney function or avoiding prescribing it to patients who have a history of alcohol abuse or who are receiving treatment that may interact with the drug.
Validating pharmacologic management
The lead author of the new guideline, Ita Fitzgerald, a teacher in clinical pharmacy and senior pharmacist at St. Patrick’s Mental Health Services in Dublin, pointed out that there is a bias toward not using drugs for weight management and shifting the responsibility onto the patients themselves, something that is very often out of their control.
“The purpose of the guideline was to decide on a range of criteria to maximize the use of metformin, to recognize that for many people, pharmacological management is a valid and important option that could and should be more widely used and to provide precise and practical guidance to physicians to facilitate a more widespread use,” Ms. Fitzgerald said in an interview.
According to Fitzgerald, who is pursuing her doctorate at University College Cork (Ireland), one of the most outstanding results of the work is that it highlights that the main benefit of metformin is to flatten rather than reverse antipsychotic-induced weight gain and that indicating it late can nullify that effect.
“In all the recommendations, we try very hard to shift the focus from metformin’s role as a weight reversal agent to one as a weight management agent that should be used early in treatment, which is when most weight gain occurs. If metformin succeeds in flattening that increase, that’s a huge potential benefit for an inexpensive and easily accessible drug. When people have already established weight gain, metformin may not be enough and alternative treatments should be used,” she said.
In addition to its effects on weight, metformin has many other potential health benefits. Of particular importance is that it reduces hyperphagia-mediated antipsychotic-induced weight gain, Ms. Fitzgerald pointed out.
“This is subjectively very important for patients and provides a more positive experience when taking antipsychotics. Antipsychotic-induced weight gain is one of the main reasons for premature discontinuation or incomplete adherence to these drugs and therefore needs to be addressed proactively,” she concluded.
Ms. Fitzgerald and Dr. Michat have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com. This article was translated from the Medscape Spanish edition.
MAR DEL PLATA, ARGENTINA – , according to a new evidence-based Irish guideline for the management of this common complication in adults with psychoses who are taking medications.
The document was discussed during one of the sessions of the XXXV Argentine Congress of Psychiatry of the Association of Argentine Psychiatrists. The document also was presented by one of its authors at the European Congress on Obesity 2022.
The guideline encourages psychiatrists not to underestimate the adverse metabolic effects of their treatments and encourages them to contemplate and carry out this prevention and management strategy, commented María Delia Michat, PhD, professor of clinical psychiatry and psychopharmacology at the APSA Postgraduate Training Institute, Buenos Aires.
“Although it is always good to work as a team, it is usually we psychiatrists who coordinate the pharmacological treatment of our patients, and we have to know how to manage drugs that can prevent cardiovascular disease,” Dr. Michat said in an interview.
“The new guideline is helpful because it protocolizes the use of metformin, which is the cheapest drug and has the most evidence for antipsychotic-induced weight gain,” she added.
Avoiding metabolic syndrome
In patients with schizophrenia, obesity rates are 40% higher than in the general population, and 80% of patients develop weight gain after their first treatment, noted Dr. Michat. “Right away, weight gain is seen in the first month. And it is a serious problem, because patients with schizophrenia, major depression, or bipolar disorder already have an increased risk of premature mortality, especially from cardiovascular diseases, and they have an increased risk of metabolic syndrome. And we sometimes give drugs that further increase that risk,” she said.
Being overweight is a major criterion for defining metabolic syndrome. Dr. Michat noted that, among the antipsychotic drugs that increase weight the most are clozapine, olanzapine, chlorpromazine, quetiapine, and risperidone, in addition to other psychoactive drugs, such as valproic acid, lithium, mirtazapine, and tricyclic antidepressants.
Several clinical trials, such as a pioneering Chinese study from 2008, have shown the potential of metformin to mitigate the weight gain induced by this type of drug.
However, Dr. Michat noted that so far the major guidelines (for example, the Canadian Network for Mood and Anxiety Treatments [CANMAT]/International Society for Bipolar Disorders [ISBD] for bipolar disorder and the American Psychiatric Association [APA] for schizophrenia) “say very little” on how to address this complication. They propose what she defined as a “problematic” order of action in which the initial emphasis is on promoting lifestyle changes, which are difficult for these patients to carry out, as well as general proposals for changing medication (which is not simple to implement when the patient’s condition is stabilized) and eventual consultation with a clinician to start therapy with metformin or other drugs, such as liraglutide, semaglutide, and topiramate.
The new clinical practice guideline, which was published in Evidence-Based Mental Health (of the BMJ journal group), was written by a multidisciplinary team of pharmacists, psychiatrists, and mental health nurses from Ireland. It aims to fill that gap. The investigators reviewed 1,270 scientific articles and analyzed 26 of them in depth, including seven randomized clinical trials and a 2016 systematic review and meta-analysis. The authors made a “strong” recommendation, for which there was moderate-quality evidence, that for patients for whom a lifestyle intervention is unacceptable or inappropriate the use of metformin is an “alternative first-line intervention” for antipsychotic drug–induced weight gain.
Likewise, as a strong recommendation with moderate-quality evidence, the guidance encourages the use of metformin when nonpharmacologic intervention does not seem to be effective.
The guideline also says it is preferable to start metformin early for patients who gain more than 7% of their baseline weight within the first month of antipsychotic treatment. It also endorses metformin when weight gain is established.
Other recommendations include evaluating baseline kidney function before starting metformin treatment and suggest a dose adjustment when the estimated glomerular filtration rate (eGFR) is < 60 mL/min/1.73 m2. The guidance says the use of metformin is contraindicated for patients in whom eGFR is <30 mL/min per 1.73 m2. The proposed starting dosage is 500 mg twice per day with meals, with increments of 500 mg every 1-2 weeks until reaching a target dose of 2,000 mg/day. The guidance recommends that consideration always be given to individual tolerability and efficacy.
Treatment goals should be personalized and agreed upon with patients. In the case of early intervention, the guideline proposes initially stabilizing the weight gained or, if possible, reverse excess weight. When weight gain is established, the goal would be to lose at least 5% of the weight within the next 6 months.
The authors also recommend monitoring kidney function annually, as well as vitamin B12 levels and individual tolerability and compliance. Gastrointestinal adverse effects can be managed by dose reduction or slower dose titration. The risk of lactic acidosis, which affects 4.3 per 100,000 person-years among those taking metformin, can be attenuated by adjusting the dose according to kidney function or avoiding prescribing it to patients who have a history of alcohol abuse or who are receiving treatment that may interact with the drug.
Validating pharmacologic management
The lead author of the new guideline, Ita Fitzgerald, a teacher in clinical pharmacy and senior pharmacist at St. Patrick’s Mental Health Services in Dublin, pointed out that there is a bias toward not using drugs for weight management and shifting the responsibility onto the patients themselves, something that is very often out of their control.
“The purpose of the guideline was to decide on a range of criteria to maximize the use of metformin, to recognize that for many people, pharmacological management is a valid and important option that could and should be more widely used and to provide precise and practical guidance to physicians to facilitate a more widespread use,” Ms. Fitzgerald said in an interview.
According to Fitzgerald, who is pursuing her doctorate at University College Cork (Ireland), one of the most outstanding results of the work is that it highlights that the main benefit of metformin is to flatten rather than reverse antipsychotic-induced weight gain and that indicating it late can nullify that effect.
“In all the recommendations, we try very hard to shift the focus from metformin’s role as a weight reversal agent to one as a weight management agent that should be used early in treatment, which is when most weight gain occurs. If metformin succeeds in flattening that increase, that’s a huge potential benefit for an inexpensive and easily accessible drug. When people have already established weight gain, metformin may not be enough and alternative treatments should be used,” she said.
In addition to its effects on weight, metformin has many other potential health benefits. Of particular importance is that it reduces hyperphagia-mediated antipsychotic-induced weight gain, Ms. Fitzgerald pointed out.
“This is subjectively very important for patients and provides a more positive experience when taking antipsychotics. Antipsychotic-induced weight gain is one of the main reasons for premature discontinuation or incomplete adherence to these drugs and therefore needs to be addressed proactively,” she concluded.
Ms. Fitzgerald and Dr. Michat have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com. This article was translated from the Medscape Spanish edition.