User login
Neurosurgery at the End of Life
The juxtaposition between my first 2 days of neurosurgery could not have been more profound. On my first day as a third-year medical student, the attending and chief resident let me take the lead on the first case: a straightforward brain biopsy. I got to make the incision, drill the burr hole, and perform the needle biopsy. I still remember the thrill of the technical challenge, the controlled violence of drilling into the skull, and the finesse of accessing the tumor core.
The buzz was so strong that I barely registered the diagnosis that was called back from the pathologist: glioblastoma. It was not until I saw the face of the disease the next morning that I understood the reality of a GBM diagnosis. That face belonged to a 47-year-old man who hadn’t slept all night, wide eyed with apprehension at what news I might bring. He beseeched me with questions, and though his aphasia left him stammering to get the words out, I knew exactly what he was asking: Would he live or die? It was a question I was in no position to answer. Instead, I reassured him that we were waiting on the final pathology, all the while trying to forget the fact that the frozen section suggested an aggressive subtype, surely heralding a poor prognosis.
In his poignant memoir, “Do No Harm: Stories of Life, Death and Brain Surgery” (New York: Thomas Dunne Book, 2015), Dr. Henry Marsh writes beautifully about how difficult it can be to find the balance between optimism and realism. In one memorable passage, Dr. Marsh shows a house officer a scan of a highly malignant brain tumor and asks him what he would say to the patient. The trainee reflexively hides behind jargon, skirting around what he knew to be the truth: This tumor would kill her. Marsh presses him to admit that he’s lying, before lamenting at how hard it is to improve these critical communication skills: “When I have had to break bad news I never know whether I have done it well or not. The patients aren’t going to ring me up afterward and say, ‘Mr. Marsh, I really liked the way you told me that I was going to die,’ or ‘Mr. Marsh, you were crap.’ You can only hope that you haven’t made too much of a mess of it.”
I could certainly relate to Dr. Marsh’s house officer as I walked away from my own patient. I felt almost deceitful withholding diagnostic information from him, even if I did the “right” thing. It made me wonder, why did I want to become a neurosurgeon? Surely to help people through some of the most difficult moments of their lives. But is it possible to be a source of comfort when you are required so often to be a harbinger of death? The answer depends on whether one can envision a role for the neurosurgeon beyond the mandate of “life at all costs.”
While the field has become known for its life-saving procedures, neurosurgeons are called just as often to preside over the end of their patient’s lives – work that requires just as much skill as any technical procedure. Dr. Marsh recognized the tremendous human cost of neglecting that work. For cases that appear “hopeless,” he writes, “We often end up operating because it’s easier than being honest, and it means that we can avoid a painful conversation.”
We are only beginning to understand the many issues that neurosurgical patients face at the end of life, but so far it is clear that neurosurgical trainees require substantive training in prognostication, communication, and palliation (Crit Care Med. 2015 Sep;43[9]:1964-77 1,2; J Neurooncol. 2009 Jan;91[1]:39-43). Is there room in the current training paradigm for more formal education in these domains? As we move further into the 21st century, we must embrace the need for masterful clinicians outside of the operating room if we are to ever challenge the axiom set forth by the renowned French surgeon, René Leriche, some 65 years ago: “Every surgeon carries within himself a small cemetery, where from time to time he goes to pray – a place of bitterness and regret, where he must look for an explanation for his failures.” Let us look forward to the day when this is no longer the case.
Stephen Miranda is a medical student from the University of Rochester, who is now working as a research fellow at Ariadne Labs, a joint center for health systems innovation at Brigham & Women’s Hospital and Harvard T.H. Chan School of Public Health, both in Boston.
The juxtaposition between my first 2 days of neurosurgery could not have been more profound. On my first day as a third-year medical student, the attending and chief resident let me take the lead on the first case: a straightforward brain biopsy. I got to make the incision, drill the burr hole, and perform the needle biopsy. I still remember the thrill of the technical challenge, the controlled violence of drilling into the skull, and the finesse of accessing the tumor core.
The buzz was so strong that I barely registered the diagnosis that was called back from the pathologist: glioblastoma. It was not until I saw the face of the disease the next morning that I understood the reality of a GBM diagnosis. That face belonged to a 47-year-old man who hadn’t slept all night, wide eyed with apprehension at what news I might bring. He beseeched me with questions, and though his aphasia left him stammering to get the words out, I knew exactly what he was asking: Would he live or die? It was a question I was in no position to answer. Instead, I reassured him that we were waiting on the final pathology, all the while trying to forget the fact that the frozen section suggested an aggressive subtype, surely heralding a poor prognosis.
In his poignant memoir, “Do No Harm: Stories of Life, Death and Brain Surgery” (New York: Thomas Dunne Book, 2015), Dr. Henry Marsh writes beautifully about how difficult it can be to find the balance between optimism and realism. In one memorable passage, Dr. Marsh shows a house officer a scan of a highly malignant brain tumor and asks him what he would say to the patient. The trainee reflexively hides behind jargon, skirting around what he knew to be the truth: This tumor would kill her. Marsh presses him to admit that he’s lying, before lamenting at how hard it is to improve these critical communication skills: “When I have had to break bad news I never know whether I have done it well or not. The patients aren’t going to ring me up afterward and say, ‘Mr. Marsh, I really liked the way you told me that I was going to die,’ or ‘Mr. Marsh, you were crap.’ You can only hope that you haven’t made too much of a mess of it.”
I could certainly relate to Dr. Marsh’s house officer as I walked away from my own patient. I felt almost deceitful withholding diagnostic information from him, even if I did the “right” thing. It made me wonder, why did I want to become a neurosurgeon? Surely to help people through some of the most difficult moments of their lives. But is it possible to be a source of comfort when you are required so often to be a harbinger of death? The answer depends on whether one can envision a role for the neurosurgeon beyond the mandate of “life at all costs.”
While the field has become known for its life-saving procedures, neurosurgeons are called just as often to preside over the end of their patient’s lives – work that requires just as much skill as any technical procedure. Dr. Marsh recognized the tremendous human cost of neglecting that work. For cases that appear “hopeless,” he writes, “We often end up operating because it’s easier than being honest, and it means that we can avoid a painful conversation.”
We are only beginning to understand the many issues that neurosurgical patients face at the end of life, but so far it is clear that neurosurgical trainees require substantive training in prognostication, communication, and palliation (Crit Care Med. 2015 Sep;43[9]:1964-77 1,2; J Neurooncol. 2009 Jan;91[1]:39-43). Is there room in the current training paradigm for more formal education in these domains? As we move further into the 21st century, we must embrace the need for masterful clinicians outside of the operating room if we are to ever challenge the axiom set forth by the renowned French surgeon, René Leriche, some 65 years ago: “Every surgeon carries within himself a small cemetery, where from time to time he goes to pray – a place of bitterness and regret, where he must look for an explanation for his failures.” Let us look forward to the day when this is no longer the case.
Stephen Miranda is a medical student from the University of Rochester, who is now working as a research fellow at Ariadne Labs, a joint center for health systems innovation at Brigham & Women’s Hospital and Harvard T.H. Chan School of Public Health, both in Boston.
The juxtaposition between my first 2 days of neurosurgery could not have been more profound. On my first day as a third-year medical student, the attending and chief resident let me take the lead on the first case: a straightforward brain biopsy. I got to make the incision, drill the burr hole, and perform the needle biopsy. I still remember the thrill of the technical challenge, the controlled violence of drilling into the skull, and the finesse of accessing the tumor core.
The buzz was so strong that I barely registered the diagnosis that was called back from the pathologist: glioblastoma. It was not until I saw the face of the disease the next morning that I understood the reality of a GBM diagnosis. That face belonged to a 47-year-old man who hadn’t slept all night, wide eyed with apprehension at what news I might bring. He beseeched me with questions, and though his aphasia left him stammering to get the words out, I knew exactly what he was asking: Would he live or die? It was a question I was in no position to answer. Instead, I reassured him that we were waiting on the final pathology, all the while trying to forget the fact that the frozen section suggested an aggressive subtype, surely heralding a poor prognosis.
In his poignant memoir, “Do No Harm: Stories of Life, Death and Brain Surgery” (New York: Thomas Dunne Book, 2015), Dr. Henry Marsh writes beautifully about how difficult it can be to find the balance between optimism and realism. In one memorable passage, Dr. Marsh shows a house officer a scan of a highly malignant brain tumor and asks him what he would say to the patient. The trainee reflexively hides behind jargon, skirting around what he knew to be the truth: This tumor would kill her. Marsh presses him to admit that he’s lying, before lamenting at how hard it is to improve these critical communication skills: “When I have had to break bad news I never know whether I have done it well or not. The patients aren’t going to ring me up afterward and say, ‘Mr. Marsh, I really liked the way you told me that I was going to die,’ or ‘Mr. Marsh, you were crap.’ You can only hope that you haven’t made too much of a mess of it.”
I could certainly relate to Dr. Marsh’s house officer as I walked away from my own patient. I felt almost deceitful withholding diagnostic information from him, even if I did the “right” thing. It made me wonder, why did I want to become a neurosurgeon? Surely to help people through some of the most difficult moments of their lives. But is it possible to be a source of comfort when you are required so often to be a harbinger of death? The answer depends on whether one can envision a role for the neurosurgeon beyond the mandate of “life at all costs.”
While the field has become known for its life-saving procedures, neurosurgeons are called just as often to preside over the end of their patient’s lives – work that requires just as much skill as any technical procedure. Dr. Marsh recognized the tremendous human cost of neglecting that work. For cases that appear “hopeless,” he writes, “We often end up operating because it’s easier than being honest, and it means that we can avoid a painful conversation.”
We are only beginning to understand the many issues that neurosurgical patients face at the end of life, but so far it is clear that neurosurgical trainees require substantive training in prognostication, communication, and palliation (Crit Care Med. 2015 Sep;43[9]:1964-77 1,2; J Neurooncol. 2009 Jan;91[1]:39-43). Is there room in the current training paradigm for more formal education in these domains? As we move further into the 21st century, we must embrace the need for masterful clinicians outside of the operating room if we are to ever challenge the axiom set forth by the renowned French surgeon, René Leriche, some 65 years ago: “Every surgeon carries within himself a small cemetery, where from time to time he goes to pray – a place of bitterness and regret, where he must look for an explanation for his failures.” Let us look forward to the day when this is no longer the case.
Stephen Miranda is a medical student from the University of Rochester, who is now working as a research fellow at Ariadne Labs, a joint center for health systems innovation at Brigham & Women’s Hospital and Harvard T.H. Chan School of Public Health, both in Boston.

The palliative path: Talking with elderly patients facing emergency surgery
An expert panel has developed a communication framework to improve treatment of older, seriously ill patients who have surgical emergencies, which has been published online in Annals of Surgery.
A substantial portion of older patients who undergo emergency surgeries already have serious life-limiting illnesses such as cardiopulmonary disease, renal failure, liver failure, dementia, severe neurological impairment, or malignancy. The advisory panel based its work on the premise that surgery in these circumstances can lead to significant further morbidity, health care utilization, functional decline, prolonged hospital stay or institutionalization, and death, with attendant physical discomfort and psychological distress at the end of these patients’ lives.
Surgeons consulted in the emergency setting for these patients are hampered by patients unable to communicate well because they are in extremis, by surrogates who are unprepared for their role, and by time constraints, lack of familiarity with the patient, poor understanding of the illness by patients and families, prognostic uncertainty, and inadequate advance care planning. In addition, “many surgeons lack skills to engage in conversations about end-of-life care, or are too unfamiliar with palliative options to discuss them well,” or feel obligated to maintain postoperative life support despite the patient’s wishes, said Dr. Zara Cooper, of Ariadne Labs and the Center for Surgery and Public Health at Brigham and Women’s Hospital, both in Boston, and her associates.
To address these issues and assist surgeons in caring for such patients, an expert panel of 23 national leaders in acute care surgery, general surgery, surgical oncology, palliative medicine, critical care, emergency medicine, anesthesia, and health care innovation was convened at Harvard Medical School, Boston.
The focus of the panel’s recommendations was a structured communications framework prototype to facilitate shared decision-making in these difficult circumstances.
Among the panel’s recommendations for surgeons were the following priorities:
• Review the medical record and consult the treatment team to fully understand the patient’s current condition, comorbidities, expected illness trajectory, and preferences for end-of-life care.
• Assess functional performance as part of the routine history and physical to fully understand the patient’s fitness for surgery.
• Formulate a prognosis regarding the patient’s overall health both with and without surgery.
The panel offered a set of principles and specific elements for the meeting with the patient and family:
• The surgeon should begin by introducing himself or herself; according to reports in the literature, physicians fail to do this approximately half of the time.
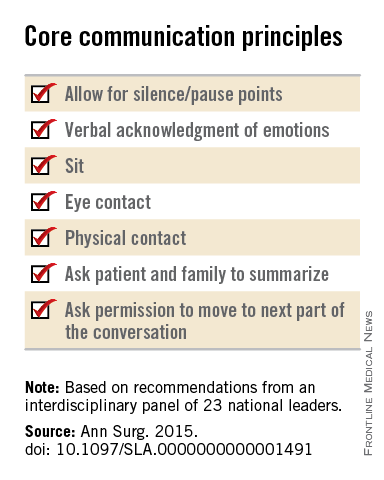
• Pay attention to nonverbal communication, such as eye contact and physical contact, as this is critical to building rapport. Immediately address pain, anxiety, and other indicators of distress, to maximize the patients’ and the families’ engagement in subsequent medical discussions. “Although adequate analgesia may render a patient unable to make their own decisions, surrogates are more likely to make appropriate decisions when they feel their loved one is comfortable,” the panel noted.
• Allow pauses and silences to occur. Let the patient and the family process information and their own emotions.
• Elicit the patients’ or the surrogates’ understanding of the illness and their views of the patients’ likely trajectory, correcting any inaccuracies. This substantially influences their decisions regarding the aggressiveness of subsequent treatments.
• Inform the patient and family of the life-threatening nature of the patient’s acute condition and its potential impact on the rest of his or her life, including the possibility of prolonged life support, ICU stay, burdensome treatment, and loss of independence. Use accepted techniques for breaking bad news, and check to be sure the patient understands what was conveyed.
• At this point, the surgeon should synthesize and summarize the information from the patient, the family, and the medical record, then pause to give them time to process the information and to assess their emotional state. It is helpful to label and respond to the patient’s emotions at this juncture, and to build empathy with statements such as “I know this is difficult news, and I wish it were different.”
• Describe the benefits, burdens, and range of likely outcomes if surgery is undertaken and if it is not. The surgeon should use nonmedical language to describe symptoms, and should convey his or her expectations regarding length of hospitalization, need for and duration of life support, burdensome symptoms, discharge to an institution, and functional recovery.
• Surgeons should be able to communicate palliative options possible either in combination with surgery or instead of surgery. Palliative care can aid in managing advanced symptoms, providing psychosocial support for patients and caregivers, facilitating interdisciplinary communication, and facilitating medical decisions and care transitions.
• Avoid describing surgical procedures as “doing everything” and palliative care as “doing nothing.” This can make patients and families “feel abandoned, fearful, isolated, and angry, and fails to encompass palliative care’s practices of proactive communication, aggressive symptom management, and timely emotional support to alleviate suffering and affirm quality of life,” the panel said.
• Surgeons should explicitly support the patients’ medical decisions, whether or not they choose surgery.
The panel also cited a few factors that would assist surgeons in following these recommendations. First, surgeons must recognize the importance of communicating well with seriously ill older patients and acknowledge that this is a crucial clinical skill for them to cultivate. They must also recognize that palliative care is vital to delivering high-quality surgical care. Surgeons should consider discharging patients to hospice, which can improve pain and symptom management, improve patient and family satisfaction with care, and avoid unwanted hospitalization or cardiopulmonary resuscitation.
“There are a number of major barriers to introducing palliative care in these situations. One is an education problem - the perception on the part of patients and clinicians, and surgeons in particular, that palliative care is only limited to end-of-life care, which it is not. It is a misperception of what palliative care means in this equation - that palliative care and hospice are the same thing, which they absolutely are not,”said Dr. Cooper in an interview.
”The definition of palliative care has evolved over the past decade and the focus of palliative care is on quality of life and alleviating symptoms. End-of-life palliative care is part of that, and as patients get closer to the end of life, symptom management and quality of life become more focal than life-prolonging treatment... But for patients with chronic and serious illness, there has to be a role for palliative care because we know that when patients feel better, they tend to live longer. And when patients feel their emotional concerns and physical needs are being addressed, they tend to do better. Patients families have improved satisfaction when their loved one receives palliative care,” she noted.”
However, the number of palliative providers is completely inadequate to meet the needs of the number of seriously ill patients, she said. And a lot of hospital-based palliative care is by necessity limited to end-of-life care because of a lack of palliative resources.
Dr. Atul Gawande, a coauthor of the panel recommendations, wrote a best-selling book, Being Mortal (New York: Metropolitan Books, 2014) addressing the shortcomings and potential remaking of medical care in the context of age-related frailty, grave illness, and death. Dr. Cooper noted that there is a growing sentiment among the general public that they want to have their quality of life addressed in the type of medical care they receive. She said that Dr. Gawande’s book tapped into the perception of a lack of recognition of personhood of seriously ill patients.
“We often focus on diagnosis and we don’t have the ‘bandwidth’ to focus on the person carrying that diagnosis, and our patients and focus on the person carrying that diagnosis, but our patients and their families are demanding different types of care. So, ultimately, the patients will be the ones to push us to do better for them.”
The next steps to further developing a widely used and validated communication framework would be to create educational opportunities for clinicians to develop clinical skills in communication with seriously ill patients and palliative care, and to study the impact of these initiatives on improving outcomes most relevant to older patient. This work was supported by the Ariadne Labs, a Joint Center for Health System Innovation at Brigham and Women’s Hospital. Dr. Cooper and her associates reported having no relevant financial disclosures.
An expert panel has developed a communication framework to improve treatment of older, seriously ill patients who have surgical emergencies, which has been published online in Annals of Surgery.
A substantial portion of older patients who undergo emergency surgeries already have serious life-limiting illnesses such as cardiopulmonary disease, renal failure, liver failure, dementia, severe neurological impairment, or malignancy. The advisory panel based its work on the premise that surgery in these circumstances can lead to significant further morbidity, health care utilization, functional decline, prolonged hospital stay or institutionalization, and death, with attendant physical discomfort and psychological distress at the end of these patients’ lives.
Surgeons consulted in the emergency setting for these patients are hampered by patients unable to communicate well because they are in extremis, by surrogates who are unprepared for their role, and by time constraints, lack of familiarity with the patient, poor understanding of the illness by patients and families, prognostic uncertainty, and inadequate advance care planning. In addition, “many surgeons lack skills to engage in conversations about end-of-life care, or are too unfamiliar with palliative options to discuss them well,” or feel obligated to maintain postoperative life support despite the patient’s wishes, said Dr. Zara Cooper, of Ariadne Labs and the Center for Surgery and Public Health at Brigham and Women’s Hospital, both in Boston, and her associates.
To address these issues and assist surgeons in caring for such patients, an expert panel of 23 national leaders in acute care surgery, general surgery, surgical oncology, palliative medicine, critical care, emergency medicine, anesthesia, and health care innovation was convened at Harvard Medical School, Boston.
The focus of the panel’s recommendations was a structured communications framework prototype to facilitate shared decision-making in these difficult circumstances.
Among the panel’s recommendations for surgeons were the following priorities:
• Review the medical record and consult the treatment team to fully understand the patient’s current condition, comorbidities, expected illness trajectory, and preferences for end-of-life care.
• Assess functional performance as part of the routine history and physical to fully understand the patient’s fitness for surgery.
• Formulate a prognosis regarding the patient’s overall health both with and without surgery.
The panel offered a set of principles and specific elements for the meeting with the patient and family:
• The surgeon should begin by introducing himself or herself; according to reports in the literature, physicians fail to do this approximately half of the time.
• Pay attention to nonverbal communication, such as eye contact and physical contact, as this is critical to building rapport. Immediately address pain, anxiety, and other indicators of distress, to maximize the patients’ and the families’ engagement in subsequent medical discussions. “Although adequate analgesia may render a patient unable to make their own decisions, surrogates are more likely to make appropriate decisions when they feel their loved one is comfortable,” the panel noted.
• Allow pauses and silences to occur. Let the patient and the family process information and their own emotions.
• Elicit the patients’ or the surrogates’ understanding of the illness and their views of the patients’ likely trajectory, correcting any inaccuracies. This substantially influences their decisions regarding the aggressiveness of subsequent treatments.
• Inform the patient and family of the life-threatening nature of the patient’s acute condition and its potential impact on the rest of his or her life, including the possibility of prolonged life support, ICU stay, burdensome treatment, and loss of independence. Use accepted techniques for breaking bad news, and check to be sure the patient understands what was conveyed.
• At this point, the surgeon should synthesize and summarize the information from the patient, the family, and the medical record, then pause to give them time to process the information and to assess their emotional state. It is helpful to label and respond to the patient’s emotions at this juncture, and to build empathy with statements such as “I know this is difficult news, and I wish it were different.”
• Describe the benefits, burdens, and range of likely outcomes if surgery is undertaken and if it is not. The surgeon should use nonmedical language to describe symptoms, and should convey his or her expectations regarding length of hospitalization, need for and duration of life support, burdensome symptoms, discharge to an institution, and functional recovery.
• Surgeons should be able to communicate palliative options possible either in combination with surgery or instead of surgery. Palliative care can aid in managing advanced symptoms, providing psychosocial support for patients and caregivers, facilitating interdisciplinary communication, and facilitating medical decisions and care transitions.
• Avoid describing surgical procedures as “doing everything” and palliative care as “doing nothing.” This can make patients and families “feel abandoned, fearful, isolated, and angry, and fails to encompass palliative care’s practices of proactive communication, aggressive symptom management, and timely emotional support to alleviate suffering and affirm quality of life,” the panel said.
• Surgeons should explicitly support the patients’ medical decisions, whether or not they choose surgery.
The panel also cited a few factors that would assist surgeons in following these recommendations. First, surgeons must recognize the importance of communicating well with seriously ill older patients and acknowledge that this is a crucial clinical skill for them to cultivate. They must also recognize that palliative care is vital to delivering high-quality surgical care. Surgeons should consider discharging patients to hospice, which can improve pain and symptom management, improve patient and family satisfaction with care, and avoid unwanted hospitalization or cardiopulmonary resuscitation.
“There are a number of major barriers to introducing palliative care in these situations. One is an education problem - the perception on the part of patients and clinicians, and surgeons in particular, that palliative care is only limited to end-of-life care, which it is not. It is a misperception of what palliative care means in this equation - that palliative care and hospice are the same thing, which they absolutely are not,”said Dr. Cooper in an interview.
”The definition of palliative care has evolved over the past decade and the focus of palliative care is on quality of life and alleviating symptoms. End-of-life palliative care is part of that, and as patients get closer to the end of life, symptom management and quality of life become more focal than life-prolonging treatment... But for patients with chronic and serious illness, there has to be a role for palliative care because we know that when patients feel better, they tend to live longer. And when patients feel their emotional concerns and physical needs are being addressed, they tend to do better. Patients families have improved satisfaction when their loved one receives palliative care,” she noted.”
However, the number of palliative providers is completely inadequate to meet the needs of the number of seriously ill patients, she said. And a lot of hospital-based palliative care is by necessity limited to end-of-life care because of a lack of palliative resources.
Dr. Atul Gawande, a coauthor of the panel recommendations, wrote a best-selling book, Being Mortal (New York: Metropolitan Books, 2014) addressing the shortcomings and potential remaking of medical care in the context of age-related frailty, grave illness, and death. Dr. Cooper noted that there is a growing sentiment among the general public that they want to have their quality of life addressed in the type of medical care they receive. She said that Dr. Gawande’s book tapped into the perception of a lack of recognition of personhood of seriously ill patients.
“We often focus on diagnosis and we don’t have the ‘bandwidth’ to focus on the person carrying that diagnosis, and our patients and focus on the person carrying that diagnosis, but our patients and their families are demanding different types of care. So, ultimately, the patients will be the ones to push us to do better for them.”
The next steps to further developing a widely used and validated communication framework would be to create educational opportunities for clinicians to develop clinical skills in communication with seriously ill patients and palliative care, and to study the impact of these initiatives on improving outcomes most relevant to older patient. This work was supported by the Ariadne Labs, a Joint Center for Health System Innovation at Brigham and Women’s Hospital. Dr. Cooper and her associates reported having no relevant financial disclosures.
An expert panel has developed a communication framework to improve treatment of older, seriously ill patients who have surgical emergencies, which has been published online in Annals of Surgery.
A substantial portion of older patients who undergo emergency surgeries already have serious life-limiting illnesses such as cardiopulmonary disease, renal failure, liver failure, dementia, severe neurological impairment, or malignancy. The advisory panel based its work on the premise that surgery in these circumstances can lead to significant further morbidity, health care utilization, functional decline, prolonged hospital stay or institutionalization, and death, with attendant physical discomfort and psychological distress at the end of these patients’ lives.
Surgeons consulted in the emergency setting for these patients are hampered by patients unable to communicate well because they are in extremis, by surrogates who are unprepared for their role, and by time constraints, lack of familiarity with the patient, poor understanding of the illness by patients and families, prognostic uncertainty, and inadequate advance care planning. In addition, “many surgeons lack skills to engage in conversations about end-of-life care, or are too unfamiliar with palliative options to discuss them well,” or feel obligated to maintain postoperative life support despite the patient’s wishes, said Dr. Zara Cooper, of Ariadne Labs and the Center for Surgery and Public Health at Brigham and Women’s Hospital, both in Boston, and her associates.
To address these issues and assist surgeons in caring for such patients, an expert panel of 23 national leaders in acute care surgery, general surgery, surgical oncology, palliative medicine, critical care, emergency medicine, anesthesia, and health care innovation was convened at Harvard Medical School, Boston.
The focus of the panel’s recommendations was a structured communications framework prototype to facilitate shared decision-making in these difficult circumstances.
Among the panel’s recommendations for surgeons were the following priorities:
• Review the medical record and consult the treatment team to fully understand the patient’s current condition, comorbidities, expected illness trajectory, and preferences for end-of-life care.
• Assess functional performance as part of the routine history and physical to fully understand the patient’s fitness for surgery.
• Formulate a prognosis regarding the patient’s overall health both with and without surgery.
The panel offered a set of principles and specific elements for the meeting with the patient and family:
• The surgeon should begin by introducing himself or herself; according to reports in the literature, physicians fail to do this approximately half of the time.
• Pay attention to nonverbal communication, such as eye contact and physical contact, as this is critical to building rapport. Immediately address pain, anxiety, and other indicators of distress, to maximize the patients’ and the families’ engagement in subsequent medical discussions. “Although adequate analgesia may render a patient unable to make their own decisions, surrogates are more likely to make appropriate decisions when they feel their loved one is comfortable,” the panel noted.
• Allow pauses and silences to occur. Let the patient and the family process information and their own emotions.
• Elicit the patients’ or the surrogates’ understanding of the illness and their views of the patients’ likely trajectory, correcting any inaccuracies. This substantially influences their decisions regarding the aggressiveness of subsequent treatments.
• Inform the patient and family of the life-threatening nature of the patient’s acute condition and its potential impact on the rest of his or her life, including the possibility of prolonged life support, ICU stay, burdensome treatment, and loss of independence. Use accepted techniques for breaking bad news, and check to be sure the patient understands what was conveyed.
• At this point, the surgeon should synthesize and summarize the information from the patient, the family, and the medical record, then pause to give them time to process the information and to assess their emotional state. It is helpful to label and respond to the patient’s emotions at this juncture, and to build empathy with statements such as “I know this is difficult news, and I wish it were different.”
• Describe the benefits, burdens, and range of likely outcomes if surgery is undertaken and if it is not. The surgeon should use nonmedical language to describe symptoms, and should convey his or her expectations regarding length of hospitalization, need for and duration of life support, burdensome symptoms, discharge to an institution, and functional recovery.
• Surgeons should be able to communicate palliative options possible either in combination with surgery or instead of surgery. Palliative care can aid in managing advanced symptoms, providing psychosocial support for patients and caregivers, facilitating interdisciplinary communication, and facilitating medical decisions and care transitions.
• Avoid describing surgical procedures as “doing everything” and palliative care as “doing nothing.” This can make patients and families “feel abandoned, fearful, isolated, and angry, and fails to encompass palliative care’s practices of proactive communication, aggressive symptom management, and timely emotional support to alleviate suffering and affirm quality of life,” the panel said.
• Surgeons should explicitly support the patients’ medical decisions, whether or not they choose surgery.
The panel also cited a few factors that would assist surgeons in following these recommendations. First, surgeons must recognize the importance of communicating well with seriously ill older patients and acknowledge that this is a crucial clinical skill for them to cultivate. They must also recognize that palliative care is vital to delivering high-quality surgical care. Surgeons should consider discharging patients to hospice, which can improve pain and symptom management, improve patient and family satisfaction with care, and avoid unwanted hospitalization or cardiopulmonary resuscitation.
“There are a number of major barriers to introducing palliative care in these situations. One is an education problem - the perception on the part of patients and clinicians, and surgeons in particular, that palliative care is only limited to end-of-life care, which it is not. It is a misperception of what palliative care means in this equation - that palliative care and hospice are the same thing, which they absolutely are not,”said Dr. Cooper in an interview.
”The definition of palliative care has evolved over the past decade and the focus of palliative care is on quality of life and alleviating symptoms. End-of-life palliative care is part of that, and as patients get closer to the end of life, symptom management and quality of life become more focal than life-prolonging treatment... But for patients with chronic and serious illness, there has to be a role for palliative care because we know that when patients feel better, they tend to live longer. And when patients feel their emotional concerns and physical needs are being addressed, they tend to do better. Patients families have improved satisfaction when their loved one receives palliative care,” she noted.”
However, the number of palliative providers is completely inadequate to meet the needs of the number of seriously ill patients, she said. And a lot of hospital-based palliative care is by necessity limited to end-of-life care because of a lack of palliative resources.
Dr. Atul Gawande, a coauthor of the panel recommendations, wrote a best-selling book, Being Mortal (New York: Metropolitan Books, 2014) addressing the shortcomings and potential remaking of medical care in the context of age-related frailty, grave illness, and death. Dr. Cooper noted that there is a growing sentiment among the general public that they want to have their quality of life addressed in the type of medical care they receive. She said that Dr. Gawande’s book tapped into the perception of a lack of recognition of personhood of seriously ill patients.
“We often focus on diagnosis and we don’t have the ‘bandwidth’ to focus on the person carrying that diagnosis, and our patients and focus on the person carrying that diagnosis, but our patients and their families are demanding different types of care. So, ultimately, the patients will be the ones to push us to do better for them.”
The next steps to further developing a widely used and validated communication framework would be to create educational opportunities for clinicians to develop clinical skills in communication with seriously ill patients and palliative care, and to study the impact of these initiatives on improving outcomes most relevant to older patient. This work was supported by the Ariadne Labs, a Joint Center for Health System Innovation at Brigham and Women’s Hospital. Dr. Cooper and her associates reported having no relevant financial disclosures.
FROM ANNALS OF SURGERY

Early Palliative Care Can Save Money
Clinical question: Does time to consult after admission change the effect palliative care consultation has on cost of care?
Background: Studies have shown that early palliative care involvement improves quality of life and survival among cancer patients while reducing the cost of care. Little is known about the optimal timing of palliative care consultation and its effect on cost.

Study design: Prospective, observational study.
Setting: Multi-site, high-volume, tertiary care hospitals with established palliative care teams.
Synopsis: Clinical and cost data were collected for 969 adult patients with advanced cancer admitted to the five participating hospitals. Among those, 256 patients received palliative care consultation and 713 received usual care. Subsamples were created based on time to consultation after admission.
The study found that earlier consultation yielded larger effects on cost savings. There was a 24% reduction in total cost if consultation occurred within two days (95% CI, -$3,438 to -$1,122; P<0.001), with estimated savings of $2,280. For consultation within six days of admission, there was a $1,312 savings (95% CI, -$2,568 to -$ 1,122; P<0.04), consistent with a 14% reduction in total cost.
There are notable limitations to this study. Half of eligible patients were excluded due to incomplete data collection, resulting in a small sample size. Further, these results can be generalized only to inpatients with advanced cancer.
Bottom line: Reducing the time to consultation with palliative care increases cost savings. In advanced cancer patients, a 24% reduction in total costs was realized for consultation within two days following admission.
Citation: May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33(25):2745-2752.
Clinical question: Does time to consult after admission change the effect palliative care consultation has on cost of care?
Background: Studies have shown that early palliative care involvement improves quality of life and survival among cancer patients while reducing the cost of care. Little is known about the optimal timing of palliative care consultation and its effect on cost.
Study design: Prospective, observational study.
Setting: Multi-site, high-volume, tertiary care hospitals with established palliative care teams.
Synopsis: Clinical and cost data were collected for 969 adult patients with advanced cancer admitted to the five participating hospitals. Among those, 256 patients received palliative care consultation and 713 received usual care. Subsamples were created based on time to consultation after admission.
The study found that earlier consultation yielded larger effects on cost savings. There was a 24% reduction in total cost if consultation occurred within two days (95% CI, -$3,438 to -$1,122; P<0.001), with estimated savings of $2,280. For consultation within six days of admission, there was a $1,312 savings (95% CI, -$2,568 to -$ 1,122; P<0.04), consistent with a 14% reduction in total cost.
There are notable limitations to this study. Half of eligible patients were excluded due to incomplete data collection, resulting in a small sample size. Further, these results can be generalized only to inpatients with advanced cancer.
Bottom line: Reducing the time to consultation with palliative care increases cost savings. In advanced cancer patients, a 24% reduction in total costs was realized for consultation within two days following admission.
Citation: May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33(25):2745-2752.
Clinical question: Does time to consult after admission change the effect palliative care consultation has on cost of care?
Background: Studies have shown that early palliative care involvement improves quality of life and survival among cancer patients while reducing the cost of care. Little is known about the optimal timing of palliative care consultation and its effect on cost.
Study design: Prospective, observational study.
Setting: Multi-site, high-volume, tertiary care hospitals with established palliative care teams.
Synopsis: Clinical and cost data were collected for 969 adult patients with advanced cancer admitted to the five participating hospitals. Among those, 256 patients received palliative care consultation and 713 received usual care. Subsamples were created based on time to consultation after admission.
The study found that earlier consultation yielded larger effects on cost savings. There was a 24% reduction in total cost if consultation occurred within two days (95% CI, -$3,438 to -$1,122; P<0.001), with estimated savings of $2,280. For consultation within six days of admission, there was a $1,312 savings (95% CI, -$2,568 to -$ 1,122; P<0.04), consistent with a 14% reduction in total cost.
There are notable limitations to this study. Half of eligible patients were excluded due to incomplete data collection, resulting in a small sample size. Further, these results can be generalized only to inpatients with advanced cancer.
Bottom line: Reducing the time to consultation with palliative care increases cost savings. In advanced cancer patients, a 24% reduction in total costs was realized for consultation within two days following admission.
Citation: May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33(25):2745-2752.

Review: Opioid prescriptions are the work of many physicians
A “broad swath” of Medicare providers wrote scripts for opioids in 2013, contradicting the idea that the overdose epidemic is mainly the work of “small groups of prolific prescribers and corrupt pill mills,” investigators wrote online in JAMA Internal Medicine.
“Contrary to the California workers’ compensation data showing a small subset of prescribers accounting for a disproportionately large percentage of opioid prescribing, Medicare opioid prescribing is distributed across many prescribers and is, if anything, less skewed than all drug prescribing,” said Dr. Jonathan H. Chen of the Veterans Affairs Palo Alto (Calif.) Health Care System, and his associates.
Their study included 808,020 prescribers and almost 1.2 billion Medicare Part D claims worth nearly $81 billion dollars. They focused on schedule II opioid prescriptions containing oxycodone, fentanyl, hydrocodone, morphine, methadone, hydromorphone, oxymorphone, meperidine, codeine, opium, or levorphanol (JAMA Intern Med. 2015 Dec 14. doi: 10.1001/jamainternmed.2015.6662).
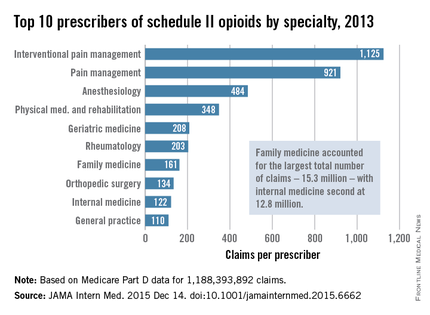
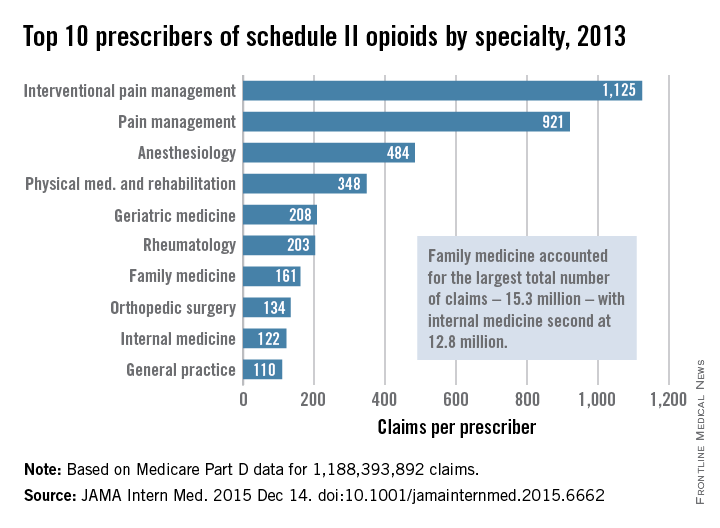
Not surprisingly, specialists in pain management, anesthesia, and physical medicine wrote the most prescriptions per provider. But family practitioners, internists, nurse practitioners, and physician assistants wrote 35,268,234 prescriptions – more than all other specialties combined. “The trends hold up across state lines, with negligible geographic variability,” the researchers said.
The findings contradict an analysis of California workers’ compensation data, in which 1% of prescribers accounted for a third of schedule II opioid prescriptions, and 10% of prescribers accounted for 80% of prescriptions, the investigators noted. Nonetheless, 10% of Medicare prescribers in Dr. Chen’s study accounted for 78% of the total cost of opioids, possibly because they were prescribing pricier formulations or higher doses.
Overall, the findings suggest that opioid prescribing is “widespread” and “relatively indifferent to individual physicians, specialty, or region” – and that efforts to stem the tide must be equally broad, the researchers concluded.
Their study was supported by the VA Office of Academic Affiliations, the VA Health Services Research and Development Service, the National Institute of General Medical Sciences, and the Peter F. McManus Charitable Trust. The researchers had no disclosures.
A “broad swath” of Medicare providers wrote scripts for opioids in 2013, contradicting the idea that the overdose epidemic is mainly the work of “small groups of prolific prescribers and corrupt pill mills,” investigators wrote online in JAMA Internal Medicine.
“Contrary to the California workers’ compensation data showing a small subset of prescribers accounting for a disproportionately large percentage of opioid prescribing, Medicare opioid prescribing is distributed across many prescribers and is, if anything, less skewed than all drug prescribing,” said Dr. Jonathan H. Chen of the Veterans Affairs Palo Alto (Calif.) Health Care System, and his associates.
Their study included 808,020 prescribers and almost 1.2 billion Medicare Part D claims worth nearly $81 billion dollars. They focused on schedule II opioid prescriptions containing oxycodone, fentanyl, hydrocodone, morphine, methadone, hydromorphone, oxymorphone, meperidine, codeine, opium, or levorphanol (JAMA Intern Med. 2015 Dec 14. doi: 10.1001/jamainternmed.2015.6662).
Not surprisingly, specialists in pain management, anesthesia, and physical medicine wrote the most prescriptions per provider. But family practitioners, internists, nurse practitioners, and physician assistants wrote 35,268,234 prescriptions – more than all other specialties combined. “The trends hold up across state lines, with negligible geographic variability,” the researchers said.
The findings contradict an analysis of California workers’ compensation data, in which 1% of prescribers accounted for a third of schedule II opioid prescriptions, and 10% of prescribers accounted for 80% of prescriptions, the investigators noted. Nonetheless, 10% of Medicare prescribers in Dr. Chen’s study accounted for 78% of the total cost of opioids, possibly because they were prescribing pricier formulations or higher doses.
Overall, the findings suggest that opioid prescribing is “widespread” and “relatively indifferent to individual physicians, specialty, or region” – and that efforts to stem the tide must be equally broad, the researchers concluded.
Their study was supported by the VA Office of Academic Affiliations, the VA Health Services Research and Development Service, the National Institute of General Medical Sciences, and the Peter F. McManus Charitable Trust. The researchers had no disclosures.
A “broad swath” of Medicare providers wrote scripts for opioids in 2013, contradicting the idea that the overdose epidemic is mainly the work of “small groups of prolific prescribers and corrupt pill mills,” investigators wrote online in JAMA Internal Medicine.
“Contrary to the California workers’ compensation data showing a small subset of prescribers accounting for a disproportionately large percentage of opioid prescribing, Medicare opioid prescribing is distributed across many prescribers and is, if anything, less skewed than all drug prescribing,” said Dr. Jonathan H. Chen of the Veterans Affairs Palo Alto (Calif.) Health Care System, and his associates.
Their study included 808,020 prescribers and almost 1.2 billion Medicare Part D claims worth nearly $81 billion dollars. They focused on schedule II opioid prescriptions containing oxycodone, fentanyl, hydrocodone, morphine, methadone, hydromorphone, oxymorphone, meperidine, codeine, opium, or levorphanol (JAMA Intern Med. 2015 Dec 14. doi: 10.1001/jamainternmed.2015.6662).
Not surprisingly, specialists in pain management, anesthesia, and physical medicine wrote the most prescriptions per provider. But family practitioners, internists, nurse practitioners, and physician assistants wrote 35,268,234 prescriptions – more than all other specialties combined. “The trends hold up across state lines, with negligible geographic variability,” the researchers said.
The findings contradict an analysis of California workers’ compensation data, in which 1% of prescribers accounted for a third of schedule II opioid prescriptions, and 10% of prescribers accounted for 80% of prescriptions, the investigators noted. Nonetheless, 10% of Medicare prescribers in Dr. Chen’s study accounted for 78% of the total cost of opioids, possibly because they were prescribing pricier formulations or higher doses.
Overall, the findings suggest that opioid prescribing is “widespread” and “relatively indifferent to individual physicians, specialty, or region” – and that efforts to stem the tide must be equally broad, the researchers concluded.
Their study was supported by the VA Office of Academic Affiliations, the VA Health Services Research and Development Service, the National Institute of General Medical Sciences, and the Peter F. McManus Charitable Trust. The researchers had no disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Many different types of general practitioners and specialists often prescribe opioids to Medicare beneficiaries.
Major finding: Family practitioners, internists, nurse practitioners, and physician assistants wrote 35,268,234 prescriptions – more than all other specialties combined.
Data source: An analysis of nearly 1.2 billion Medicare part D claims from 2013.
Disclosures: The study was supported by the VA Office of Academic Affiliations, the VA Health Services Research and Development Service, the National Institute of General Medical Sciences, and the Peter F. McManus Charitable Trust. The researchers had no disclosures.
Putting the Focus on Quality of Life in Cancer Care
Patient-centered care increasingly means focusing on quality of life. For the past 26 years, Betty Ferrell, PhD, MA, FAAN, FPCN, director and professor, nursing research and education at City of Hope has focused on quality of life research.
Dr. Ferrell recently sat down Federal Practitioner to discuss the components of quality cancer care, the role of family caregivers, and the importance of patient communication.
According to Dr. Ferrell, quality cancer care starts a comprehensive assessment so that care providers understand not only comorbidities, but also family help and psychosocial concerns. Interdisciplinary collaboration is also an essential element of quality care, bringing together an entire team to focus on the patient. Finally, Dr. Ferrell noted, care must include patient and family education.
0:15 Quality of life research
1:35 Quality of life interventions
2:52 Family care givers
3:30 Three components of quality cancer care
4:38 Communication
5:20 VA cancer care
Patient-centered care increasingly means focusing on quality of life. For the past 26 years, Betty Ferrell, PhD, MA, FAAN, FPCN, director and professor, nursing research and education at City of Hope has focused on quality of life research.
Dr. Ferrell recently sat down Federal Practitioner to discuss the components of quality cancer care, the role of family caregivers, and the importance of patient communication.
According to Dr. Ferrell, quality cancer care starts a comprehensive assessment so that care providers understand not only comorbidities, but also family help and psychosocial concerns. Interdisciplinary collaboration is also an essential element of quality care, bringing together an entire team to focus on the patient. Finally, Dr. Ferrell noted, care must include patient and family education.
0:15 Quality of life research
1:35 Quality of life interventions
2:52 Family care givers
3:30 Three components of quality cancer care
4:38 Communication
5:20 VA cancer care
Patient-centered care increasingly means focusing on quality of life. For the past 26 years, Betty Ferrell, PhD, MA, FAAN, FPCN, director and professor, nursing research and education at City of Hope has focused on quality of life research.
Dr. Ferrell recently sat down Federal Practitioner to discuss the components of quality cancer care, the role of family caregivers, and the importance of patient communication.
According to Dr. Ferrell, quality cancer care starts a comprehensive assessment so that care providers understand not only comorbidities, but also family help and psychosocial concerns. Interdisciplinary collaboration is also an essential element of quality care, bringing together an entire team to focus on the patient. Finally, Dr. Ferrell noted, care must include patient and family education.
0:15 Quality of life research
1:35 Quality of life interventions
2:52 Family care givers
3:30 Three components of quality cancer care
4:38 Communication
5:20 VA cancer care

Myth of the Month: Does Colace work?
Myth: Docusate is a stool softener and helps with constipation.
A 60-year-old man is injured in a fall and breaks four ribs. He is in severe pain and is prescribed oxycodone and naproxen for pain. What treatment would you prescribe to help decrease problems with constipation?
A. Docusate.
B. Docusate and polyethylene glycol.
C. Psyllium.
D. Polyethylene glycol.
Constipation is extremely common, occurring in up to 20%-25% of the elderly population and 90% of patients treated with opioids. The formal definition of constipation is fewer than three bowel movements per week. Patients are concerned with other symptoms as well, including hard stool consistency and the feeling of incomplete evacuation.
An extremely commonly prescribed medication for patients with symptoms of constipation/hard stool passage is docusate (Colace). This medication is often a part of bowel programs for institutionalized/hospitalized patients, as well as being frequently prescribed when patients are treated with opiates.
Does it work?

Docusate is frequently prescribed as a “stool softener,” but does it increase water content in stool? In a randomized, controlled trial of docusate vs. psyllium, 170 adult patients with chronic constipation received either 5.1 g twice a day of psyllium or 100 mg twice a day of docusate (Aliment Pharmacol Ther. 1998 May;12[5]:491-7).
Psyllium was superior in its effect on stool frequency, stool water content, total stool output, and the combination of several objective measures of constipation. Compared with baseline, psyllium increased stool water content by 2.33%, vs .01% for docusate (P =. 007), and stool weight was increased in the group treated with psyllium, compared with docusate-treated patients (359.9 g/week vs. 271.9 g/week, respectively; P = .005). Docusate does not appear to have any effect on stool water content or amount of stool.
In a study of constipation treatment in patients receiving opioids, Dr. Yoko Tarumi and her colleagues studied 74 patients admitted to hospice units (J Pain Symptom Manage. 2013 Jan;45[1]:2-13). A total of 74 patients were randomized to receive docusate 100 mg twice a day plus senna, or placebo plus senna. Once the study was started, inclusion criteria were broadened to include hospice patients with nonmalignant disease and patients who were not on opioids.
Almost all patients in the study did receive opioids (94% of the docusate patients and 100% of placebo-treated patients). There were no significant between the groups in stool volume, frequency, consistency, or in perceived completeness of evacuation.
In a randomized, controlled study of elderly patients on a medicine ward, 34 patients were randomized to docusate or control (no laxatives)(J Chronic Dis. 1976 Jan;29[1]:59-63). There was no difference in frequency or quality of stools between groups.
A systematic review of the usefulness of docusate in chronically ill patients concluded that the widespread use of docusate for the treatment of constipation in palliative-care patients is based on inadequate experimental evidence (J Pain Symptom Manage. 2000 Feb;19[2]:130-6).
The Canadian Agency for Drugs and Technologies in Health concluded “the available evidence suggests that docusate is no more effective than placebo in the prevention or management of constipation” (Dioctyl sulfosuccinate or docusate [calcium or sodium] for the prevention or management of constipation: a review of the clinical effectiveness. Canadian Agency for Drugs and Technologies in Health; 2014 Jun 26).
Dr. Davendra Ramkumar and his colleagues published a systematic review of drug trials for the treatment of constipation in 2005 (Am J Gastroenterol. 2005 Apr;100[4]:936-71). Only polyethylene glycol and tegaserod received grade A evidence for published trials. Psyllium and lactulose received grade B evidence. Docusate received a level 3, grade C for evidence (poor quality evidence, poor evidence to support a recommendation for or against the use of the modality).
I have been surprised at how docusate has been the most commonly prescribed laxative agent. Polyethylene glycol or psyllium are better evidence-based options. Docusate is often prescribed as a stool softener, and it has even less evidence that it softens stool than its poor evidence as a laxative.
Acknowledgments
My thanks to the late Dr. David Saunders for teaching me 30 years ago that docusate was not a helpful option for the management of constipation, and to Sarah Steinkruger for doing much of the research that was used in this column.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
Myth: Docusate is a stool softener and helps with constipation.
A 60-year-old man is injured in a fall and breaks four ribs. He is in severe pain and is prescribed oxycodone and naproxen for pain. What treatment would you prescribe to help decrease problems with constipation?
A. Docusate.
B. Docusate and polyethylene glycol.
C. Psyllium.
D. Polyethylene glycol.
Constipation is extremely common, occurring in up to 20%-25% of the elderly population and 90% of patients treated with opioids. The formal definition of constipation is fewer than three bowel movements per week. Patients are concerned with other symptoms as well, including hard stool consistency and the feeling of incomplete evacuation.
An extremely commonly prescribed medication for patients with symptoms of constipation/hard stool passage is docusate (Colace). This medication is often a part of bowel programs for institutionalized/hospitalized patients, as well as being frequently prescribed when patients are treated with opiates.
Does it work?
Docusate is frequently prescribed as a “stool softener,” but does it increase water content in stool? In a randomized, controlled trial of docusate vs. psyllium, 170 adult patients with chronic constipation received either 5.1 g twice a day of psyllium or 100 mg twice a day of docusate (Aliment Pharmacol Ther. 1998 May;12[5]:491-7).
Psyllium was superior in its effect on stool frequency, stool water content, total stool output, and the combination of several objective measures of constipation. Compared with baseline, psyllium increased stool water content by 2.33%, vs .01% for docusate (P =. 007), and stool weight was increased in the group treated with psyllium, compared with docusate-treated patients (359.9 g/week vs. 271.9 g/week, respectively; P = .005). Docusate does not appear to have any effect on stool water content or amount of stool.
In a study of constipation treatment in patients receiving opioids, Dr. Yoko Tarumi and her colleagues studied 74 patients admitted to hospice units (J Pain Symptom Manage. 2013 Jan;45[1]:2-13). A total of 74 patients were randomized to receive docusate 100 mg twice a day plus senna, or placebo plus senna. Once the study was started, inclusion criteria were broadened to include hospice patients with nonmalignant disease and patients who were not on opioids.
Almost all patients in the study did receive opioids (94% of the docusate patients and 100% of placebo-treated patients). There were no significant between the groups in stool volume, frequency, consistency, or in perceived completeness of evacuation.
In a randomized, controlled study of elderly patients on a medicine ward, 34 patients were randomized to docusate or control (no laxatives)(J Chronic Dis. 1976 Jan;29[1]:59-63). There was no difference in frequency or quality of stools between groups.
A systematic review of the usefulness of docusate in chronically ill patients concluded that the widespread use of docusate for the treatment of constipation in palliative-care patients is based on inadequate experimental evidence (J Pain Symptom Manage. 2000 Feb;19[2]:130-6).
The Canadian Agency for Drugs and Technologies in Health concluded “the available evidence suggests that docusate is no more effective than placebo in the prevention or management of constipation” (Dioctyl sulfosuccinate or docusate [calcium or sodium] for the prevention or management of constipation: a review of the clinical effectiveness. Canadian Agency for Drugs and Technologies in Health; 2014 Jun 26).
Dr. Davendra Ramkumar and his colleagues published a systematic review of drug trials for the treatment of constipation in 2005 (Am J Gastroenterol. 2005 Apr;100[4]:936-71). Only polyethylene glycol and tegaserod received grade A evidence for published trials. Psyllium and lactulose received grade B evidence. Docusate received a level 3, grade C for evidence (poor quality evidence, poor evidence to support a recommendation for or against the use of the modality).
I have been surprised at how docusate has been the most commonly prescribed laxative agent. Polyethylene glycol or psyllium are better evidence-based options. Docusate is often prescribed as a stool softener, and it has even less evidence that it softens stool than its poor evidence as a laxative.
Acknowledgments
My thanks to the late Dr. David Saunders for teaching me 30 years ago that docusate was not a helpful option for the management of constipation, and to Sarah Steinkruger for doing much of the research that was used in this column.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
Myth: Docusate is a stool softener and helps with constipation.
A 60-year-old man is injured in a fall and breaks four ribs. He is in severe pain and is prescribed oxycodone and naproxen for pain. What treatment would you prescribe to help decrease problems with constipation?
A. Docusate.
B. Docusate and polyethylene glycol.
C. Psyllium.
D. Polyethylene glycol.
Constipation is extremely common, occurring in up to 20%-25% of the elderly population and 90% of patients treated with opioids. The formal definition of constipation is fewer than three bowel movements per week. Patients are concerned with other symptoms as well, including hard stool consistency and the feeling of incomplete evacuation.
An extremely commonly prescribed medication for patients with symptoms of constipation/hard stool passage is docusate (Colace). This medication is often a part of bowel programs for institutionalized/hospitalized patients, as well as being frequently prescribed when patients are treated with opiates.
Does it work?
Docusate is frequently prescribed as a “stool softener,” but does it increase water content in stool? In a randomized, controlled trial of docusate vs. psyllium, 170 adult patients with chronic constipation received either 5.1 g twice a day of psyllium or 100 mg twice a day of docusate (Aliment Pharmacol Ther. 1998 May;12[5]:491-7).
Psyllium was superior in its effect on stool frequency, stool water content, total stool output, and the combination of several objective measures of constipation. Compared with baseline, psyllium increased stool water content by 2.33%, vs .01% for docusate (P =. 007), and stool weight was increased in the group treated with psyllium, compared with docusate-treated patients (359.9 g/week vs. 271.9 g/week, respectively; P = .005). Docusate does not appear to have any effect on stool water content or amount of stool.
In a study of constipation treatment in patients receiving opioids, Dr. Yoko Tarumi and her colleagues studied 74 patients admitted to hospice units (J Pain Symptom Manage. 2013 Jan;45[1]:2-13). A total of 74 patients were randomized to receive docusate 100 mg twice a day plus senna, or placebo plus senna. Once the study was started, inclusion criteria were broadened to include hospice patients with nonmalignant disease and patients who were not on opioids.
Almost all patients in the study did receive opioids (94% of the docusate patients and 100% of placebo-treated patients). There were no significant between the groups in stool volume, frequency, consistency, or in perceived completeness of evacuation.
In a randomized, controlled study of elderly patients on a medicine ward, 34 patients were randomized to docusate or control (no laxatives)(J Chronic Dis. 1976 Jan;29[1]:59-63). There was no difference in frequency or quality of stools between groups.
A systematic review of the usefulness of docusate in chronically ill patients concluded that the widespread use of docusate for the treatment of constipation in palliative-care patients is based on inadequate experimental evidence (J Pain Symptom Manage. 2000 Feb;19[2]:130-6).
The Canadian Agency for Drugs and Technologies in Health concluded “the available evidence suggests that docusate is no more effective than placebo in the prevention or management of constipation” (Dioctyl sulfosuccinate or docusate [calcium or sodium] for the prevention or management of constipation: a review of the clinical effectiveness. Canadian Agency for Drugs and Technologies in Health; 2014 Jun 26).
Dr. Davendra Ramkumar and his colleagues published a systematic review of drug trials for the treatment of constipation in 2005 (Am J Gastroenterol. 2005 Apr;100[4]:936-71). Only polyethylene glycol and tegaserod received grade A evidence for published trials. Psyllium and lactulose received grade B evidence. Docusate received a level 3, grade C for evidence (poor quality evidence, poor evidence to support a recommendation for or against the use of the modality).
I have been surprised at how docusate has been the most commonly prescribed laxative agent. Polyethylene glycol or psyllium are better evidence-based options. Docusate is often prescribed as a stool softener, and it has even less evidence that it softens stool than its poor evidence as a laxative.
Acknowledgments
My thanks to the late Dr. David Saunders for teaching me 30 years ago that docusate was not a helpful option for the management of constipation, and to Sarah Steinkruger for doing much of the research that was used in this column.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].

PTSD in Patients With Cancer
Patients with PTSD already face difficulties, but the diagnosis of a serious illness, such as cancer, can have an effect on their symptoms in a treatment-hindering way. Matthew Cordova, PhD, a staff psychologist at the VA Northern California Martinez Outpatient Clinic, explained how PTSD can create difficulties for patients when they are diagnosed with a life-threating illness like cancer.
“Clinically what we see is that these patients are triggered to experience anxiety and avoidance specifically because of their cancer experience,” explained Dr. Cordova. Patients’ symptoms also worsen with “button pushers” such as the uncertainties of a treatment setting, diagnosis, and of people who will be around them.
Dr. Cordova also spoke about the challenge in creating trust between the patient and practitioner, which requires extra effort by the practitioner. Some best practices, he suggested, were focusing on the emotional safety of the patient, being emotionally and physically present during their time together, and creating a sense of predictability.
Another important way to make treatment transitions easier for patients is having a mental health team always present at the oncology and hematology clinics. In the video below Dr. Cordova elaborated on other best practices caregivers should be aware of when treating a patient with cancer and preexisting PTSD.
Patients with PTSD already face difficulties, but the diagnosis of a serious illness, such as cancer, can have an effect on their symptoms in a treatment-hindering way. Matthew Cordova, PhD, a staff psychologist at the VA Northern California Martinez Outpatient Clinic, explained how PTSD can create difficulties for patients when they are diagnosed with a life-threating illness like cancer.
“Clinically what we see is that these patients are triggered to experience anxiety and avoidance specifically because of their cancer experience,” explained Dr. Cordova. Patients’ symptoms also worsen with “button pushers” such as the uncertainties of a treatment setting, diagnosis, and of people who will be around them.
Dr. Cordova also spoke about the challenge in creating trust between the patient and practitioner, which requires extra effort by the practitioner. Some best practices, he suggested, were focusing on the emotional safety of the patient, being emotionally and physically present during their time together, and creating a sense of predictability.
Another important way to make treatment transitions easier for patients is having a mental health team always present at the oncology and hematology clinics. In the video below Dr. Cordova elaborated on other best practices caregivers should be aware of when treating a patient with cancer and preexisting PTSD.
Patients with PTSD already face difficulties, but the diagnosis of a serious illness, such as cancer, can have an effect on their symptoms in a treatment-hindering way. Matthew Cordova, PhD, a staff psychologist at the VA Northern California Martinez Outpatient Clinic, explained how PTSD can create difficulties for patients when they are diagnosed with a life-threating illness like cancer.
“Clinically what we see is that these patients are triggered to experience anxiety and avoidance specifically because of their cancer experience,” explained Dr. Cordova. Patients’ symptoms also worsen with “button pushers” such as the uncertainties of a treatment setting, diagnosis, and of people who will be around them.
Dr. Cordova also spoke about the challenge in creating trust between the patient and practitioner, which requires extra effort by the practitioner. Some best practices, he suggested, were focusing on the emotional safety of the patient, being emotionally and physically present during their time together, and creating a sense of predictability.
Another important way to make treatment transitions easier for patients is having a mental health team always present at the oncology and hematology clinics. In the video below Dr. Cordova elaborated on other best practices caregivers should be aware of when treating a patient with cancer and preexisting PTSD.

Million Veteran Program Sees Significant Research, Enrollment Progress
The Million Veterans Program (MVP) has reached 40% of its goal, registering more than 400,000 participants. Veterans who participate in the program donate blood for DNA extraction, which is linked to their health records. Created in 2012, MVP was expected to take 5 to 7 years to reach 1 million participants. Recently started research studies associated with MVP include cardiovascular risk factors, multisubstance use, pharmacogenomics of kidney disease, and metabolic conditions, among others.
“We are proud to see the progress being made in MVP, and we are confident the knowledge gained through this research will have a very tangible and positive impact on the health care that Veterans and all Americans receive,” said Secretary of Veterans Affairs Robert A. McDonald. “We applaud our Veterans participating in the program. The selfless sacrifice they are making will allow researchers to gain valuable, important information.”
Genomic programs such as MVP received a significant boost earlier this year with the announcement of President Obama’s Precision Medicine Initiative. Both the Precision Medicine Initiative and MVP are part of a larger effort to better tailor treatment to individual patients based in part on their genetics. “VA is thrilled to be working closely with the White House and other federal partners on the president’s Precision Medicine Initiative,” said VA Chief Research and Development Officer Timothy O’Leary, MD, PhD. “We are committed to making precision medicine a reality for veterans and the nation."
Federal Practitioner recently spoke with Robert Nussbaum, MD, of the University of California—San Francisco on the potential impact of MVP on genomics research. Watch the video below for more on the importance of MVP and its role in genomics.
The Million Veterans Program (MVP) has reached 40% of its goal, registering more than 400,000 participants. Veterans who participate in the program donate blood for DNA extraction, which is linked to their health records. Created in 2012, MVP was expected to take 5 to 7 years to reach 1 million participants. Recently started research studies associated with MVP include cardiovascular risk factors, multisubstance use, pharmacogenomics of kidney disease, and metabolic conditions, among others.
“We are proud to see the progress being made in MVP, and we are confident the knowledge gained through this research will have a very tangible and positive impact on the health care that Veterans and all Americans receive,” said Secretary of Veterans Affairs Robert A. McDonald. “We applaud our Veterans participating in the program. The selfless sacrifice they are making will allow researchers to gain valuable, important information.”
Genomic programs such as MVP received a significant boost earlier this year with the announcement of President Obama’s Precision Medicine Initiative. Both the Precision Medicine Initiative and MVP are part of a larger effort to better tailor treatment to individual patients based in part on their genetics. “VA is thrilled to be working closely with the White House and other federal partners on the president’s Precision Medicine Initiative,” said VA Chief Research and Development Officer Timothy O’Leary, MD, PhD. “We are committed to making precision medicine a reality for veterans and the nation."
Federal Practitioner recently spoke with Robert Nussbaum, MD, of the University of California—San Francisco on the potential impact of MVP on genomics research. Watch the video below for more on the importance of MVP and its role in genomics.
The Million Veterans Program (MVP) has reached 40% of its goal, registering more than 400,000 participants. Veterans who participate in the program donate blood for DNA extraction, which is linked to their health records. Created in 2012, MVP was expected to take 5 to 7 years to reach 1 million participants. Recently started research studies associated with MVP include cardiovascular risk factors, multisubstance use, pharmacogenomics of kidney disease, and metabolic conditions, among others.
“We are proud to see the progress being made in MVP, and we are confident the knowledge gained through this research will have a very tangible and positive impact on the health care that Veterans and all Americans receive,” said Secretary of Veterans Affairs Robert A. McDonald. “We applaud our Veterans participating in the program. The selfless sacrifice they are making will allow researchers to gain valuable, important information.”
Genomic programs such as MVP received a significant boost earlier this year with the announcement of President Obama’s Precision Medicine Initiative. Both the Precision Medicine Initiative and MVP are part of a larger effort to better tailor treatment to individual patients based in part on their genetics. “VA is thrilled to be working closely with the White House and other federal partners on the president’s Precision Medicine Initiative,” said VA Chief Research and Development Officer Timothy O’Leary, MD, PhD. “We are committed to making precision medicine a reality for veterans and the nation."
Federal Practitioner recently spoke with Robert Nussbaum, MD, of the University of California—San Francisco on the potential impact of MVP on genomics research. Watch the video below for more on the importance of MVP and its role in genomics.
We hold the pen, but who writes the story?
Mrs. J, a physically frail but mentally sharp 75-year-old with known metastatic gastric cancer was admitted to the hospital 2 days ago with a small bowel obstruction. Despite appropriate conservative management, her symptoms are worsening. Her prior cancer treatment consisted of gastric resection with reconstruction and chemo and radiation therapy. The probability of identifying a treatable cause for her bowel obstruction during exploratory laparotomy is believed to be small.
Mr. S, a debilitated 58-year-old previously treated with primary chemotherapy and radiation for cancer at the base of his tongue, presents to your office with severe pain due to recurrent disease. The cancer is potentially resectable, but it will require an extensive resection necessitating complex free flap reconstruction in this previously irradiated field.
Is an operation indicated in either/both of these patients? The risk of causing harm with these operations may outweigh the potential benefits, so how do you decide?
Surgery residents have a lot to learn during their residency training. Not only must they gain a mastery of the pathophysiology of surgical disease, they must learn a multitude of operations while they hone their manual dexterity skills. And they must learn how to take care of a multitude of patients.

Less understood and explicitly taught is how to determine whether an operation is appropriate for this specific patient. Understanding the pathophysiology of the patient’s illness is not enough; it requires an ability to effectively communicate with the patient, to understand that person’s hopes and goals, and then honestly determine whether an operation is in fact indicated. It may sound like the antithesis of surgical training, but learning when not to operate is as important as learning when to do so.
Sometimes it’s easy. When the underlying condition is easily treatable by an operation and without it the previously healthy patient will likely die, operation is usually warranted and accepted. For the critically ill patient who will not survive transfer to the operating room and induction of anesthesia, an operation would be impossible.
As illustrated by the patients described at the beginning of this piece, the decision making can be a bit more complicated.
These are the type of patients the surgeon intuitively believes will not do well, but they are referred for an operation and what surgeons do, is ... operate. “To cut is to cure,” is the old adage, not “To cut is to care.”
These are some of the toughest decisions a surgeon can make and are the ones surgeons seem to remember. The enormous responsibility that accompanies the decision to take someone to the operating room and through a potentially difficult postoperative period can be burdensome for the surgeon and potentially fraught with suffering for all.
Understanding how to address goals of care with patients and families can make these decisions easier. Yet these communication skills are not necessarily emphasized during surgical training, and in fact, they are not the forte of many physicians in general, which has led to the growth of the specialty of palliative medicine. Palliative medicine specialists are trained experts in these communication techniques.
One of the cardinal goals of palliative medicine is to help patients and families think about and clarify their treatment goals. Asking questions about “code status” is not the same as exploring someone’s overall treatment goals. Goals can range from wanting to stay alive no matter in what condition to wanting to be kept comfortable at home surrounded by loved ones even if it means a potentially shorter lifespan. By having patients clarify their ultimate goals it may become apparent that a high-risk operation is not the best way to proceed. Perhaps aggressive pain management and arranging effective home support better meets the patient’s overall goals.
You don’t have to be a palliative medicine specialist to have these conversations with patients, but it does require specific communication skills, which can be taught.
For example, many clinicians start their patient encounters by giving a brief overview of the current situation or skip straight to discussions concerning the various treatment options. But are you sure you and your patient are really starting from the same place? You can’t assume that the patient/family truly understands the medical condition, no matter what may be implied in the medical record or the referring physician’s notes. And you can’t assume a patient wants an operation just because he or she shows up in your office.
A more effective way to start the conversation is to begin by asking patients what they understand about their conditions. This will ensure your subsequent discussion corrects any misinformation and better clarifies their understanding of the situation. Starting your encounter in this fashion is critical and can avoid misunderstandings that can lead to treatments the patients do not actually want, and mistrust should complications arise.
An elective rotation with palliative medicine providers to learn these skills can be a great addition to surgical residency training. These conversations can be some of the most meaningful patient interactions a physician can experience. Incorporating an elective rotation with a palliative medicine team into surgical residency training can add value to residency training and have long-lasting benefit for future surgeons, and ultimately, for their patients, as they venture on in their surgical careers.
Nadine B. Semer, M.D., MPH, FACS, is board certified in general surgery, plastic surgery, and palliative medicine. As a reconstructive plastic surgeon, she has worked not only in the United States, but has had the privilege of taking her skills to underserved and resource-poor areas throughout the world. She currently is practicing palliative medicine full time, and is an assistant professor at UT Southwestern Medical School, in Dallas, based at Parkland Hospital.
Mrs. J, a physically frail but mentally sharp 75-year-old with known metastatic gastric cancer was admitted to the hospital 2 days ago with a small bowel obstruction. Despite appropriate conservative management, her symptoms are worsening. Her prior cancer treatment consisted of gastric resection with reconstruction and chemo and radiation therapy. The probability of identifying a treatable cause for her bowel obstruction during exploratory laparotomy is believed to be small.
Mr. S, a debilitated 58-year-old previously treated with primary chemotherapy and radiation for cancer at the base of his tongue, presents to your office with severe pain due to recurrent disease. The cancer is potentially resectable, but it will require an extensive resection necessitating complex free flap reconstruction in this previously irradiated field.
Is an operation indicated in either/both of these patients? The risk of causing harm with these operations may outweigh the potential benefits, so how do you decide?
Surgery residents have a lot to learn during their residency training. Not only must they gain a mastery of the pathophysiology of surgical disease, they must learn a multitude of operations while they hone their manual dexterity skills. And they must learn how to take care of a multitude of patients.
Less understood and explicitly taught is how to determine whether an operation is appropriate for this specific patient. Understanding the pathophysiology of the patient’s illness is not enough; it requires an ability to effectively communicate with the patient, to understand that person’s hopes and goals, and then honestly determine whether an operation is in fact indicated. It may sound like the antithesis of surgical training, but learning when not to operate is as important as learning when to do so.
Sometimes it’s easy. When the underlying condition is easily treatable by an operation and without it the previously healthy patient will likely die, operation is usually warranted and accepted. For the critically ill patient who will not survive transfer to the operating room and induction of anesthesia, an operation would be impossible.
As illustrated by the patients described at the beginning of this piece, the decision making can be a bit more complicated.
These are the type of patients the surgeon intuitively believes will not do well, but they are referred for an operation and what surgeons do, is ... operate. “To cut is to cure,” is the old adage, not “To cut is to care.”
These are some of the toughest decisions a surgeon can make and are the ones surgeons seem to remember. The enormous responsibility that accompanies the decision to take someone to the operating room and through a potentially difficult postoperative period can be burdensome for the surgeon and potentially fraught with suffering for all.
Understanding how to address goals of care with patients and families can make these decisions easier. Yet these communication skills are not necessarily emphasized during surgical training, and in fact, they are not the forte of many physicians in general, which has led to the growth of the specialty of palliative medicine. Palliative medicine specialists are trained experts in these communication techniques.
One of the cardinal goals of palliative medicine is to help patients and families think about and clarify their treatment goals. Asking questions about “code status” is not the same as exploring someone’s overall treatment goals. Goals can range from wanting to stay alive no matter in what condition to wanting to be kept comfortable at home surrounded by loved ones even if it means a potentially shorter lifespan. By having patients clarify their ultimate goals it may become apparent that a high-risk operation is not the best way to proceed. Perhaps aggressive pain management and arranging effective home support better meets the patient’s overall goals.
You don’t have to be a palliative medicine specialist to have these conversations with patients, but it does require specific communication skills, which can be taught.
For example, many clinicians start their patient encounters by giving a brief overview of the current situation or skip straight to discussions concerning the various treatment options. But are you sure you and your patient are really starting from the same place? You can’t assume that the patient/family truly understands the medical condition, no matter what may be implied in the medical record or the referring physician’s notes. And you can’t assume a patient wants an operation just because he or she shows up in your office.
A more effective way to start the conversation is to begin by asking patients what they understand about their conditions. This will ensure your subsequent discussion corrects any misinformation and better clarifies their understanding of the situation. Starting your encounter in this fashion is critical and can avoid misunderstandings that can lead to treatments the patients do not actually want, and mistrust should complications arise.
An elective rotation with palliative medicine providers to learn these skills can be a great addition to surgical residency training. These conversations can be some of the most meaningful patient interactions a physician can experience. Incorporating an elective rotation with a palliative medicine team into surgical residency training can add value to residency training and have long-lasting benefit for future surgeons, and ultimately, for their patients, as they venture on in their surgical careers.
Nadine B. Semer, M.D., MPH, FACS, is board certified in general surgery, plastic surgery, and palliative medicine. As a reconstructive plastic surgeon, she has worked not only in the United States, but has had the privilege of taking her skills to underserved and resource-poor areas throughout the world. She currently is practicing palliative medicine full time, and is an assistant professor at UT Southwestern Medical School, in Dallas, based at Parkland Hospital.
Mrs. J, a physically frail but mentally sharp 75-year-old with known metastatic gastric cancer was admitted to the hospital 2 days ago with a small bowel obstruction. Despite appropriate conservative management, her symptoms are worsening. Her prior cancer treatment consisted of gastric resection with reconstruction and chemo and radiation therapy. The probability of identifying a treatable cause for her bowel obstruction during exploratory laparotomy is believed to be small.
Mr. S, a debilitated 58-year-old previously treated with primary chemotherapy and radiation for cancer at the base of his tongue, presents to your office with severe pain due to recurrent disease. The cancer is potentially resectable, but it will require an extensive resection necessitating complex free flap reconstruction in this previously irradiated field.
Is an operation indicated in either/both of these patients? The risk of causing harm with these operations may outweigh the potential benefits, so how do you decide?
Surgery residents have a lot to learn during their residency training. Not only must they gain a mastery of the pathophysiology of surgical disease, they must learn a multitude of operations while they hone their manual dexterity skills. And they must learn how to take care of a multitude of patients.
Less understood and explicitly taught is how to determine whether an operation is appropriate for this specific patient. Understanding the pathophysiology of the patient’s illness is not enough; it requires an ability to effectively communicate with the patient, to understand that person’s hopes and goals, and then honestly determine whether an operation is in fact indicated. It may sound like the antithesis of surgical training, but learning when not to operate is as important as learning when to do so.
Sometimes it’s easy. When the underlying condition is easily treatable by an operation and without it the previously healthy patient will likely die, operation is usually warranted and accepted. For the critically ill patient who will not survive transfer to the operating room and induction of anesthesia, an operation would be impossible.
As illustrated by the patients described at the beginning of this piece, the decision making can be a bit more complicated.
These are the type of patients the surgeon intuitively believes will not do well, but they are referred for an operation and what surgeons do, is ... operate. “To cut is to cure,” is the old adage, not “To cut is to care.”
These are some of the toughest decisions a surgeon can make and are the ones surgeons seem to remember. The enormous responsibility that accompanies the decision to take someone to the operating room and through a potentially difficult postoperative period can be burdensome for the surgeon and potentially fraught with suffering for all.
Understanding how to address goals of care with patients and families can make these decisions easier. Yet these communication skills are not necessarily emphasized during surgical training, and in fact, they are not the forte of many physicians in general, which has led to the growth of the specialty of palliative medicine. Palliative medicine specialists are trained experts in these communication techniques.
One of the cardinal goals of palliative medicine is to help patients and families think about and clarify their treatment goals. Asking questions about “code status” is not the same as exploring someone’s overall treatment goals. Goals can range from wanting to stay alive no matter in what condition to wanting to be kept comfortable at home surrounded by loved ones even if it means a potentially shorter lifespan. By having patients clarify their ultimate goals it may become apparent that a high-risk operation is not the best way to proceed. Perhaps aggressive pain management and arranging effective home support better meets the patient’s overall goals.
You don’t have to be a palliative medicine specialist to have these conversations with patients, but it does require specific communication skills, which can be taught.
For example, many clinicians start their patient encounters by giving a brief overview of the current situation or skip straight to discussions concerning the various treatment options. But are you sure you and your patient are really starting from the same place? You can’t assume that the patient/family truly understands the medical condition, no matter what may be implied in the medical record or the referring physician’s notes. And you can’t assume a patient wants an operation just because he or she shows up in your office.
A more effective way to start the conversation is to begin by asking patients what they understand about their conditions. This will ensure your subsequent discussion corrects any misinformation and better clarifies their understanding of the situation. Starting your encounter in this fashion is critical and can avoid misunderstandings that can lead to treatments the patients do not actually want, and mistrust should complications arise.
An elective rotation with palliative medicine providers to learn these skills can be a great addition to surgical residency training. These conversations can be some of the most meaningful patient interactions a physician can experience. Incorporating an elective rotation with a palliative medicine team into surgical residency training can add value to residency training and have long-lasting benefit for future surgeons, and ultimately, for their patients, as they venture on in their surgical careers.
Nadine B. Semer, M.D., MPH, FACS, is board certified in general surgery, plastic surgery, and palliative medicine. As a reconstructive plastic surgeon, she has worked not only in the United States, but has had the privilege of taking her skills to underserved and resource-poor areas throughout the world. She currently is practicing palliative medicine full time, and is an assistant professor at UT Southwestern Medical School, in Dallas, based at Parkland Hospital.

California governor signs physician-assisted suicide bill into law
California Gov. Jerry Brown (D) has signed into law a controversial measure that allows physicians to help terminally ill patients legally end their lives, making California the fourth state to permit doctor-assisted suicide through its legislature.
Gov. Brown, a former seminary student, approved the End of Life Option Act Oct. 5, after state lawmakers passed the bill Sept. 11.

In a signing message, Gov. Brown said that he had considered all sides of the issue and carefully weighed religious and theological perspectives that shortening a patient’s life is sinful.
“In the end, I was left to reflect on what I would want in the face of my own death,” Gov. Brown said in the message. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Modeled after Oregon’s statute, California’s law requires two doctors to determine that a patient has 6 months or less to live before doctors could prescribe life-ending medication. Patients must have the mental capacity to make medical decisions and would physically have to be able to swallow the drugs.
In addition, patients seeking physician aid in dying must submit two oral requests, a minimum of 15 days apart, and a written request to their physician. The attending physician must receive all three requests directly from the patient and not through a designee. Before prescribing end-of-life drugs, the attending physician must refer the patient to a consulting physician for confirmation of the diagnosis and prognosis and of the patient’s capacity to make the decision.
Oregon, Vermont, and Washington each have laws permitting physician-assisted death. Court rulings in New Mexico and Montana have allowed for the practice, but litigation in those states is ongoing and the decisions have yet to be enforced.
The signing ends nearly a year of passionate debate in California that divided physicians, religious groups, lawmakers, and community members. In May, the California Medical Association (CMA) became the first state medical society to change its stance against physician-assisted suicide to that of being neutral.
“The decision to participate in the End of Life Option Act is a very personal one between a doctor and their patient, which is why CMA has removed policy that outright objects to physicians aiding terminally ill patients in end of life options,” Dr. Luther F. Cobb, CMA president, said in a statement. “We believe it is up to the individual physician and their patient to decide voluntarily whether the End of Life Option Act is something in which they want to engage. Protecting that physician-patient relationship is essential.”
The California law will take effect 90 days after the state legislature adjourns its special session on health care, which may not be until early next year. The earliest likely enactment would be spring 2016.
On Twitter @legal_med
California Gov. Jerry Brown (D) has signed into law a controversial measure that allows physicians to help terminally ill patients legally end their lives, making California the fourth state to permit doctor-assisted suicide through its legislature.
Gov. Brown, a former seminary student, approved the End of Life Option Act Oct. 5, after state lawmakers passed the bill Sept. 11.
In a signing message, Gov. Brown said that he had considered all sides of the issue and carefully weighed religious and theological perspectives that shortening a patient’s life is sinful.
“In the end, I was left to reflect on what I would want in the face of my own death,” Gov. Brown said in the message. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Modeled after Oregon’s statute, California’s law requires two doctors to determine that a patient has 6 months or less to live before doctors could prescribe life-ending medication. Patients must have the mental capacity to make medical decisions and would physically have to be able to swallow the drugs.
In addition, patients seeking physician aid in dying must submit two oral requests, a minimum of 15 days apart, and a written request to their physician. The attending physician must receive all three requests directly from the patient and not through a designee. Before prescribing end-of-life drugs, the attending physician must refer the patient to a consulting physician for confirmation of the diagnosis and prognosis and of the patient’s capacity to make the decision.
Oregon, Vermont, and Washington each have laws permitting physician-assisted death. Court rulings in New Mexico and Montana have allowed for the practice, but litigation in those states is ongoing and the decisions have yet to be enforced.
The signing ends nearly a year of passionate debate in California that divided physicians, religious groups, lawmakers, and community members. In May, the California Medical Association (CMA) became the first state medical society to change its stance against physician-assisted suicide to that of being neutral.
“The decision to participate in the End of Life Option Act is a very personal one between a doctor and their patient, which is why CMA has removed policy that outright objects to physicians aiding terminally ill patients in end of life options,” Dr. Luther F. Cobb, CMA president, said in a statement. “We believe it is up to the individual physician and their patient to decide voluntarily whether the End of Life Option Act is something in which they want to engage. Protecting that physician-patient relationship is essential.”
The California law will take effect 90 days after the state legislature adjourns its special session on health care, which may not be until early next year. The earliest likely enactment would be spring 2016.
On Twitter @legal_med
California Gov. Jerry Brown (D) has signed into law a controversial measure that allows physicians to help terminally ill patients legally end their lives, making California the fourth state to permit doctor-assisted suicide through its legislature.
Gov. Brown, a former seminary student, approved the End of Life Option Act Oct. 5, after state lawmakers passed the bill Sept. 11.
In a signing message, Gov. Brown said that he had considered all sides of the issue and carefully weighed religious and theological perspectives that shortening a patient’s life is sinful.
“In the end, I was left to reflect on what I would want in the face of my own death,” Gov. Brown said in the message. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Modeled after Oregon’s statute, California’s law requires two doctors to determine that a patient has 6 months or less to live before doctors could prescribe life-ending medication. Patients must have the mental capacity to make medical decisions and would physically have to be able to swallow the drugs.
In addition, patients seeking physician aid in dying must submit two oral requests, a minimum of 15 days apart, and a written request to their physician. The attending physician must receive all three requests directly from the patient and not through a designee. Before prescribing end-of-life drugs, the attending physician must refer the patient to a consulting physician for confirmation of the diagnosis and prognosis and of the patient’s capacity to make the decision.
Oregon, Vermont, and Washington each have laws permitting physician-assisted death. Court rulings in New Mexico and Montana have allowed for the practice, but litigation in those states is ongoing and the decisions have yet to be enforced.
The signing ends nearly a year of passionate debate in California that divided physicians, religious groups, lawmakers, and community members. In May, the California Medical Association (CMA) became the first state medical society to change its stance against physician-assisted suicide to that of being neutral.
“The decision to participate in the End of Life Option Act is a very personal one between a doctor and their patient, which is why CMA has removed policy that outright objects to physicians aiding terminally ill patients in end of life options,” Dr. Luther F. Cobb, CMA president, said in a statement. “We believe it is up to the individual physician and their patient to decide voluntarily whether the End of Life Option Act is something in which they want to engage. Protecting that physician-patient relationship is essential.”
The California law will take effect 90 days after the state legislature adjourns its special session on health care, which may not be until early next year. The earliest likely enactment would be spring 2016.
On Twitter @legal_med
