User login
CML: Preventing chemo-induced vascular toxicity
PARIS –
Cardiologist Gabrielle Sarlon, MD, PhD, a professor at Marseille (France) University Hospital, offered her recommendations at the European Days of the French Society of Cardiology Conference 2023.
In the literature, we find many hypotheses that seek to explain why these drugs bring about the formation of atheromatous plaque. The findings of one French study led Dr. Sarlon to state, “I firmly believe that, in some patients, these treatments make LDL cholesterol go up.” This would be the main cause of the coronary and peripheral arterial diseases that are being seen.
Therefore, “LDL-C should start being monitored when the therapy starts, and a statin may have to be prescribed,” she said.
Arterial diseases
By bringing about a marked improvement in patients’ chances of survival, TKIs “have revolutionized the management of chronic myeloid leukemia,” Dr. Sarlon added. But these treatments have side effects. The most common is high blood pressure, “an effect that attests to the efficacy of targeted therapies and that must be quickly treated” with antihypertensives.
It is well known that the targeted therapies cause the rise in blood pressure. What was unexpected, though, was the vascular toxicity seen with the latest generation of TKIs. “This is a real toxicity that we need to know about, detect, and manage,” said Dr. Sarlon.
The prevalence of arterial diseases induced by nilotinib, a second-generation TKI, can be as high as 10%. Single-center studies have indicated much higher numbers. In a small study that Dr. Sarlon and her team conducted at Marseille University Hospital, atherosclerotic-type arterial injuries were observed in more than 30% of patients treated with nilotinib.
Dr. Sarlon noted that the signs of arterial toxicity occurring with this treatment have not appeared in clinical trials. Observations of the real-life use of nilotinib led French and German teams to sound the alarm. They noticed that some patients treated for CML had developed claudication and progression to critical limb ischemia of the lower extremities.
Risk factors uncovered
The first retrospective analysis to explore this risk was carried out by a German team. They included 179 patients who received nilotinib and found that 11 (6.2%) developed severe and previously unrecognized lower-extremity peripheral arterial disease (PAD) that required invasive therapy. The mean time from initiation of nilotinib to the first PAD event was 105.1 weeks (range = 16-212 weeks).
The following have emerged as major risk factors for nilotinib-induced PAD: the presence of cardiovascular risk factors, age older than 60 years, and long duration of exposure to nilotinib. Some of these factors were confirmed in the more recent study conducted at Marseille University Hospital involving patients treated with nilotinib. According to other research, there seems to be a correlation between this risk and the dose administered.
In the case of ponatinib, the side effects are even more common – so much so that, a few months after this third-generation TKI was authorized, a warning was issued about its use. A long-term follow-up study reported a 28% prevalence of cardiovascular events, while arterial diseases were observed in 20% of cases after 1-2 years on the treatment.
In terms of pathophysiology, the Marseilles University Hospital study found that arterial injuries were associated with stenosis greater than 50% in almost half of cases. “The atheromatous plaques were found where they typically are,” with the carotid bulb being the most involved territory, according to the researchers. But they’re also found in other arteries – femoral, vertebral, even renal – “sometimes in patients without cardiovascular risk factors.”
One distinctive characteristic to keep in mind is that “lipid-rich atheromatous plaques appear very dark on imaging” and thus can go unnoticed during a Doppler ultrasound. And, Dr. Sarlon added, “surprisingly, the thickening can extend to the external carotid artery.”
Ankle-brachial index
Published last year, the first European Society of Cardiology Guidelines on Cardio-Oncology present specific baseline risk-assessment and monitoring recommendations regarding patients treated with nilotinib and ponatinib. One suggests that a cardiovascular risk assessment be done every 3 months during the first year and every 6-12 months thereafter. This assessment would include such items as ECGs, blood pressure measurements, and lipid profile tests.
In addition, it is advised that every 6 months an ankle-brachial index test be performed to check for PAD. At Marseille University Hospital, a Doppler ultrasound is also done at each follow-up appointment to look for arterial plaques, “even for patients at low risk for cardiovascular disease,” said Dr. Sarlon. “It seems, above all, absolutely necessary that hematologists order an LDL-C test and, if needed, consider statin therapy,” all the while keeping in mind that “the target LDL-C level is 1 gram per liter.”
This article was translated from the Medscape French edition. A version of this article first appeared on Medscape.com.
PARIS –
Cardiologist Gabrielle Sarlon, MD, PhD, a professor at Marseille (France) University Hospital, offered her recommendations at the European Days of the French Society of Cardiology Conference 2023.
In the literature, we find many hypotheses that seek to explain why these drugs bring about the formation of atheromatous plaque. The findings of one French study led Dr. Sarlon to state, “I firmly believe that, in some patients, these treatments make LDL cholesterol go up.” This would be the main cause of the coronary and peripheral arterial diseases that are being seen.
Therefore, “LDL-C should start being monitored when the therapy starts, and a statin may have to be prescribed,” she said.
Arterial diseases
By bringing about a marked improvement in patients’ chances of survival, TKIs “have revolutionized the management of chronic myeloid leukemia,” Dr. Sarlon added. But these treatments have side effects. The most common is high blood pressure, “an effect that attests to the efficacy of targeted therapies and that must be quickly treated” with antihypertensives.
It is well known that the targeted therapies cause the rise in blood pressure. What was unexpected, though, was the vascular toxicity seen with the latest generation of TKIs. “This is a real toxicity that we need to know about, detect, and manage,” said Dr. Sarlon.
The prevalence of arterial diseases induced by nilotinib, a second-generation TKI, can be as high as 10%. Single-center studies have indicated much higher numbers. In a small study that Dr. Sarlon and her team conducted at Marseille University Hospital, atherosclerotic-type arterial injuries were observed in more than 30% of patients treated with nilotinib.
Dr. Sarlon noted that the signs of arterial toxicity occurring with this treatment have not appeared in clinical trials. Observations of the real-life use of nilotinib led French and German teams to sound the alarm. They noticed that some patients treated for CML had developed claudication and progression to critical limb ischemia of the lower extremities.
Risk factors uncovered
The first retrospective analysis to explore this risk was carried out by a German team. They included 179 patients who received nilotinib and found that 11 (6.2%) developed severe and previously unrecognized lower-extremity peripheral arterial disease (PAD) that required invasive therapy. The mean time from initiation of nilotinib to the first PAD event was 105.1 weeks (range = 16-212 weeks).
The following have emerged as major risk factors for nilotinib-induced PAD: the presence of cardiovascular risk factors, age older than 60 years, and long duration of exposure to nilotinib. Some of these factors were confirmed in the more recent study conducted at Marseille University Hospital involving patients treated with nilotinib. According to other research, there seems to be a correlation between this risk and the dose administered.
In the case of ponatinib, the side effects are even more common – so much so that, a few months after this third-generation TKI was authorized, a warning was issued about its use. A long-term follow-up study reported a 28% prevalence of cardiovascular events, while arterial diseases were observed in 20% of cases after 1-2 years on the treatment.
In terms of pathophysiology, the Marseilles University Hospital study found that arterial injuries were associated with stenosis greater than 50% in almost half of cases. “The atheromatous plaques were found where they typically are,” with the carotid bulb being the most involved territory, according to the researchers. But they’re also found in other arteries – femoral, vertebral, even renal – “sometimes in patients without cardiovascular risk factors.”
One distinctive characteristic to keep in mind is that “lipid-rich atheromatous plaques appear very dark on imaging” and thus can go unnoticed during a Doppler ultrasound. And, Dr. Sarlon added, “surprisingly, the thickening can extend to the external carotid artery.”
Ankle-brachial index
Published last year, the first European Society of Cardiology Guidelines on Cardio-Oncology present specific baseline risk-assessment and monitoring recommendations regarding patients treated with nilotinib and ponatinib. One suggests that a cardiovascular risk assessment be done every 3 months during the first year and every 6-12 months thereafter. This assessment would include such items as ECGs, blood pressure measurements, and lipid profile tests.
In addition, it is advised that every 6 months an ankle-brachial index test be performed to check for PAD. At Marseille University Hospital, a Doppler ultrasound is also done at each follow-up appointment to look for arterial plaques, “even for patients at low risk for cardiovascular disease,” said Dr. Sarlon. “It seems, above all, absolutely necessary that hematologists order an LDL-C test and, if needed, consider statin therapy,” all the while keeping in mind that “the target LDL-C level is 1 gram per liter.”
This article was translated from the Medscape French edition. A version of this article first appeared on Medscape.com.
PARIS –
Cardiologist Gabrielle Sarlon, MD, PhD, a professor at Marseille (France) University Hospital, offered her recommendations at the European Days of the French Society of Cardiology Conference 2023.
In the literature, we find many hypotheses that seek to explain why these drugs bring about the formation of atheromatous plaque. The findings of one French study led Dr. Sarlon to state, “I firmly believe that, in some patients, these treatments make LDL cholesterol go up.” This would be the main cause of the coronary and peripheral arterial diseases that are being seen.
Therefore, “LDL-C should start being monitored when the therapy starts, and a statin may have to be prescribed,” she said.
Arterial diseases
By bringing about a marked improvement in patients’ chances of survival, TKIs “have revolutionized the management of chronic myeloid leukemia,” Dr. Sarlon added. But these treatments have side effects. The most common is high blood pressure, “an effect that attests to the efficacy of targeted therapies and that must be quickly treated” with antihypertensives.
It is well known that the targeted therapies cause the rise in blood pressure. What was unexpected, though, was the vascular toxicity seen with the latest generation of TKIs. “This is a real toxicity that we need to know about, detect, and manage,” said Dr. Sarlon.
The prevalence of arterial diseases induced by nilotinib, a second-generation TKI, can be as high as 10%. Single-center studies have indicated much higher numbers. In a small study that Dr. Sarlon and her team conducted at Marseille University Hospital, atherosclerotic-type arterial injuries were observed in more than 30% of patients treated with nilotinib.
Dr. Sarlon noted that the signs of arterial toxicity occurring with this treatment have not appeared in clinical trials. Observations of the real-life use of nilotinib led French and German teams to sound the alarm. They noticed that some patients treated for CML had developed claudication and progression to critical limb ischemia of the lower extremities.
Risk factors uncovered
The first retrospective analysis to explore this risk was carried out by a German team. They included 179 patients who received nilotinib and found that 11 (6.2%) developed severe and previously unrecognized lower-extremity peripheral arterial disease (PAD) that required invasive therapy. The mean time from initiation of nilotinib to the first PAD event was 105.1 weeks (range = 16-212 weeks).
The following have emerged as major risk factors for nilotinib-induced PAD: the presence of cardiovascular risk factors, age older than 60 years, and long duration of exposure to nilotinib. Some of these factors were confirmed in the more recent study conducted at Marseille University Hospital involving patients treated with nilotinib. According to other research, there seems to be a correlation between this risk and the dose administered.
In the case of ponatinib, the side effects are even more common – so much so that, a few months after this third-generation TKI was authorized, a warning was issued about its use. A long-term follow-up study reported a 28% prevalence of cardiovascular events, while arterial diseases were observed in 20% of cases after 1-2 years on the treatment.
In terms of pathophysiology, the Marseilles University Hospital study found that arterial injuries were associated with stenosis greater than 50% in almost half of cases. “The atheromatous plaques were found where they typically are,” with the carotid bulb being the most involved territory, according to the researchers. But they’re also found in other arteries – femoral, vertebral, even renal – “sometimes in patients without cardiovascular risk factors.”
One distinctive characteristic to keep in mind is that “lipid-rich atheromatous plaques appear very dark on imaging” and thus can go unnoticed during a Doppler ultrasound. And, Dr. Sarlon added, “surprisingly, the thickening can extend to the external carotid artery.”
Ankle-brachial index
Published last year, the first European Society of Cardiology Guidelines on Cardio-Oncology present specific baseline risk-assessment and monitoring recommendations regarding patients treated with nilotinib and ponatinib. One suggests that a cardiovascular risk assessment be done every 3 months during the first year and every 6-12 months thereafter. This assessment would include such items as ECGs, blood pressure measurements, and lipid profile tests.
In addition, it is advised that every 6 months an ankle-brachial index test be performed to check for PAD. At Marseille University Hospital, a Doppler ultrasound is also done at each follow-up appointment to look for arterial plaques, “even for patients at low risk for cardiovascular disease,” said Dr. Sarlon. “It seems, above all, absolutely necessary that hematologists order an LDL-C test and, if needed, consider statin therapy,” all the while keeping in mind that “the target LDL-C level is 1 gram per liter.”
This article was translated from the Medscape French edition. A version of this article first appeared on Medscape.com.
Off their pricey CML meds, many thrive
When imatinib (Gleevec) appeared on the market just over 2 decades ago, it revolutionized the treatment of chronic myelogenous leukemia (CML) and transformed it from a grim diagnosis into a largely treatable form of blood cancer. New generations of tyrosine kinase inhibitors (TKIs) have continued to expand options for patients, and many can look forward to normal lifespans.
But these medications cause side effects and can be expensive. Long-term data doesn’t exist for the newer therapies, so no one knows whether they can harm patients over time. None of this is particularly unusual for medications to treat chronic illness, but now there’s a twist:
“Our focus has changed because the results of treatment are so good,” hematologist-oncologist Ehab L. Atallah, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview. “We’re trying to get people off their medication.”
Still, research estimates that only 20% of patients with CML will be eligible for treatment discontinuation and benefit from it in the long term. As a result, the wide majority of patients will need to be on drugs indefinitely.
Gleevec: A new age dawns
In the early 1990s, before the era of TKIs, the 5-year relative survival rate from CML was just 27%, and the 10-year rate was only 9.5%, according to a 2008 report. “If someone showed up with CML, their only option was to go to a bone marrow transplant. About half survived the transplant, and half of those had significant complications from it,” Dr. Atallah said. According to him, just about everyone who didn’t get transplantation would go on to die.
Then came Gleevec, which received Food and Drug Administration approval in 2001. It ushered in the era of “targeted” cancer treatment by specifically killing CML cells, instead of relying on traditional chemotherapy’s carpet-bombing approach.
“Gleevec and other TKIs have revolutionized how CML is treated, and patients are now living normal lives,” hematologist-oncologist Catherine Lai, MD, MPH, of the University of Pennsylvania, Philadelphia, said in an interview.
Alan Fahnestock, a 68-year-old retired telecommunications specialist in north-central Washington state, is one of the fortunate patients.
He was diagnosed with CML in 2004 after he underwent a thoracic CT scan in light of his tobacco use. “My GP found something odd in my lungs and referred me to a pulmonologist, who couldn’t figure it out either. He transmitted blood samples to my eventual hematologist/oncologist,” Mr. Fahnestock said in an interview. “It’s not clear to me that anybody ever figured out what the ‘oddity’ was. It has since apparently gone away. But the oncologist ran all the tests and came up with CML.”
Mr. Fahnestock hadn’t noticed any symptoms, although “this is, perhaps, because I tend not to pay a lot of attention to such things, having abused my body fairly severely over the years and having been borderline anemic since I was a kid. I don’t really expect to feel great and am a bit of a fatalist: I just get on with things until I no longer can.”
His physician prescribed Gleevec. “I had no particularly notable side effects, and carried on with my life pretty much as if nothing had happened,” Mr. Fahnestock said. He stayed on the drug for almost 20 years.
CML rooted in chromosome swap
It’s not clear exactly what causes CML, although the Mayo Clinic says most cases are linked to an abnormal, extra-short “Philadelphia chromosome,” created when two chromosomes swap material. This happens after birth.
Mr. Fahnestock thinks he happened to develop a random mutation. He also wonders if his work stints in the former Soviet Union in Vladivostok, “where the Soviet nuclear submarine fleet was decomposing,” and in Kiev, Ukraine, “which is not all that far from Chernobyl,” may be responsible.
Most patients, like Mr. Fahnestock, are men. Males will account for about 5,190 of the cases diagnosed in 2023, according to the American Cancer Society, compared to 3,740 in females.
Mr. Fahnestock’s CML diagnosis came at a fairly young age, when he was in his 40s. The average patient is diagnosed at 64. But it’s not unusual that he experienced no apparent symptoms when the cancer was found. In fact, that’s the norm.
Most patients with the disease – which is diagnosed in about 8,900 patients in the United States each year – are asymptomatic or have mild symptoms, Dr. Lai said. Their disease is discovered when “an elevated white count is found on routine blood work,” she said.
“The other group of patients typically present with very elevated white blood cell counts and splenomegaly with symptoms of fatigue and other constitutional symptoms. When the WBC count is very high, it is important to rule out transformation to accelerated or blast phase and also rule out an acute leukemia.”
Polymerase chain reaction is an especially important test during diagnosis, Dr. Atallah said, since it provides baseline data about the cancer that can be tracked.
TKIs: Mainstay of treatment
Four drugs are FDA approved for initial treatment of CML: imatinib (Gleevec), the second-generation TKIs dasatinib (Sprycel) and the third-generation TKI nilotinib (Tasigna). The third-generation TKIs bosutinib (Bosulif) and ponatinib (Iclusig) are approved for use as first-line treatments for patients who cannot tolerate the other drugs or are resistant to them.
The first-in-class drug asciminib (Scemblix), approved by the FDA in 2021, is a third-line drug for patients who failed treatment with two other TKIs and certain patients with the T315I mutation.
Dr. Lai said that it’s crucial to avoid side effects as much as possible “since the goal is for patients to be compliant and take the pill every day and not miss doses.” In younger patients, “I typically choose a second-generation TKI as my first choice, since there is a higher likelihood of getting into a deep molecular remission more quickly. If treatment-free remission is something a patient is interested in, a second-generation TKI is more likely to make this happen.”
According to Dr. Atallah, about half of patients end up using more than one drug because their initial choices either don’t work or cause intolerable side effects. Nevertheless, Dr. Lai noted: “Overall, patients do extremely well if compliant with their medication.”
Exceptions include the noncompliant and patients with more aggressive disease, like an accelerated or a blast phase, she said. For the latter patients, “allogenic bone marrow transplant should be considered once the patient is in remission.”
In remission, consider drug omission
How should patients be monitored if they are doing well?
“In general, I tend to follow patients monthly for the first six months after starting therapy, to make sure they are tolerating it well and to help manage side effects,” Dr. Lai said. “After that, I follow once every three months, and then often space out visits depending on whether they hit their molecular milestones and how long they’re in remission.”
In certain cases, patients may be taken off medication. The most recent National Comprehensive Cancer Network guidelines for treatment of CML, published in 2021, say that “discontinuation of TKI therapy (with close monitoring) is feasible in carefully selected, consenting patients” with early stage CML who’ve reached remission, defined as deep molecular response (DMR) of at least MR 4.0 for at least 2 years.
The guidelines caution that disease recurrence appears in “approximately 40%-60% of patients who discontinue TKI therapy after achieving DMR experience recurrence within 12 months of treatment cessation, in some cases as early as one month after discontinuation of TKI therapy.”
Still, the guidelines add that “resumption of TKI therapy immediately after recurrence results in the achievement of DMR in almost all patients.”
Dr. Atallah said stopping medication can be especially helpful for patients who grapple with side effects such as fatigue, diarrhea, and muscle aches. Some patients who take the drugs fear losing their health insurance and facing sky-high drug expenses. In 2018, average daily TKI costs for patients with CML were over $350, a 2020 report found.
Many patients were prescribed hugely expensive second-line treatments rather than inexpensive generic imatinib, the report said, despite “no evidence that later-generation TKIs provide superior progression free or overall survival.”
Many patients, however, refuse to consider stopping their medication, Dr. Atallah said. More data about treatment-free remission is needed, and the 21 U.S. academic medical centers in the H. Jean Khoury Cure CML Consortium are gathering information about patient outcomes.
Mr. Fahnestock is a fan of treatment-free remission. He stopped taking Gleevec about 2 years ago on the advice of his physician after he reached undetectable levels of disease.
“It was sort of a nonevent, really, with no discernible physical effects beyond exacerbation of the osteoarthritis in my hands,” he said. According to him, it’s not clear if this effect is linked to his eliminating the medication.
“I also vaguely hoped I’d feel better, even though I’d never been able to nail down any deleterious side effects,” he said. “No such luck, as it happens.”
Blood work has indicated no resurgence of the disease, and Mr. Fahnestock continues to volunteer as a rural firefighter.
“In general, I’m apparently reasonably healthy for my age, despite my folly [in younger years], and firefighting requires me to stay in reasonable shape,” he said. “I’ve recently been made aware of minor kidney issues and prediabetes. But, hell, I’m genetically scheduled to croak within 5 years or so, so why worry?”
National survival statistics in CML vary by factors such as gender and age, as a 2021 study revealed, and men have worse outcomes. Still, there’s a good chance Mr. Fahnestock won’t need to worry about CML ever again.
Dr. Atallah disclosed research support from Novartis and Takeda and has served both of those firms and Bristol-Myers Squibb as a consultant advisor. Dr. Lai discloses tied with Bristol-Myers Squibb, Jazz, Genentech, Novartis, Abbvie, Daiichi Sankyo, Astellas, MacroGenics, Servier, and Taiho. Mr. Fahnestock has no disclosures.
When imatinib (Gleevec) appeared on the market just over 2 decades ago, it revolutionized the treatment of chronic myelogenous leukemia (CML) and transformed it from a grim diagnosis into a largely treatable form of blood cancer. New generations of tyrosine kinase inhibitors (TKIs) have continued to expand options for patients, and many can look forward to normal lifespans.
But these medications cause side effects and can be expensive. Long-term data doesn’t exist for the newer therapies, so no one knows whether they can harm patients over time. None of this is particularly unusual for medications to treat chronic illness, but now there’s a twist:
“Our focus has changed because the results of treatment are so good,” hematologist-oncologist Ehab L. Atallah, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview. “We’re trying to get people off their medication.”
Still, research estimates that only 20% of patients with CML will be eligible for treatment discontinuation and benefit from it in the long term. As a result, the wide majority of patients will need to be on drugs indefinitely.
Gleevec: A new age dawns
In the early 1990s, before the era of TKIs, the 5-year relative survival rate from CML was just 27%, and the 10-year rate was only 9.5%, according to a 2008 report. “If someone showed up with CML, their only option was to go to a bone marrow transplant. About half survived the transplant, and half of those had significant complications from it,” Dr. Atallah said. According to him, just about everyone who didn’t get transplantation would go on to die.
Then came Gleevec, which received Food and Drug Administration approval in 2001. It ushered in the era of “targeted” cancer treatment by specifically killing CML cells, instead of relying on traditional chemotherapy’s carpet-bombing approach.
“Gleevec and other TKIs have revolutionized how CML is treated, and patients are now living normal lives,” hematologist-oncologist Catherine Lai, MD, MPH, of the University of Pennsylvania, Philadelphia, said in an interview.
Alan Fahnestock, a 68-year-old retired telecommunications specialist in north-central Washington state, is one of the fortunate patients.
He was diagnosed with CML in 2004 after he underwent a thoracic CT scan in light of his tobacco use. “My GP found something odd in my lungs and referred me to a pulmonologist, who couldn’t figure it out either. He transmitted blood samples to my eventual hematologist/oncologist,” Mr. Fahnestock said in an interview. “It’s not clear to me that anybody ever figured out what the ‘oddity’ was. It has since apparently gone away. But the oncologist ran all the tests and came up with CML.”
Mr. Fahnestock hadn’t noticed any symptoms, although “this is, perhaps, because I tend not to pay a lot of attention to such things, having abused my body fairly severely over the years and having been borderline anemic since I was a kid. I don’t really expect to feel great and am a bit of a fatalist: I just get on with things until I no longer can.”
His physician prescribed Gleevec. “I had no particularly notable side effects, and carried on with my life pretty much as if nothing had happened,” Mr. Fahnestock said. He stayed on the drug for almost 20 years.
CML rooted in chromosome swap
It’s not clear exactly what causes CML, although the Mayo Clinic says most cases are linked to an abnormal, extra-short “Philadelphia chromosome,” created when two chromosomes swap material. This happens after birth.
Mr. Fahnestock thinks he happened to develop a random mutation. He also wonders if his work stints in the former Soviet Union in Vladivostok, “where the Soviet nuclear submarine fleet was decomposing,” and in Kiev, Ukraine, “which is not all that far from Chernobyl,” may be responsible.
Most patients, like Mr. Fahnestock, are men. Males will account for about 5,190 of the cases diagnosed in 2023, according to the American Cancer Society, compared to 3,740 in females.
Mr. Fahnestock’s CML diagnosis came at a fairly young age, when he was in his 40s. The average patient is diagnosed at 64. But it’s not unusual that he experienced no apparent symptoms when the cancer was found. In fact, that’s the norm.
Most patients with the disease – which is diagnosed in about 8,900 patients in the United States each year – are asymptomatic or have mild symptoms, Dr. Lai said. Their disease is discovered when “an elevated white count is found on routine blood work,” she said.
“The other group of patients typically present with very elevated white blood cell counts and splenomegaly with symptoms of fatigue and other constitutional symptoms. When the WBC count is very high, it is important to rule out transformation to accelerated or blast phase and also rule out an acute leukemia.”
Polymerase chain reaction is an especially important test during diagnosis, Dr. Atallah said, since it provides baseline data about the cancer that can be tracked.
TKIs: Mainstay of treatment
Four drugs are FDA approved for initial treatment of CML: imatinib (Gleevec), the second-generation TKIs dasatinib (Sprycel) and the third-generation TKI nilotinib (Tasigna). The third-generation TKIs bosutinib (Bosulif) and ponatinib (Iclusig) are approved for use as first-line treatments for patients who cannot tolerate the other drugs or are resistant to them.
The first-in-class drug asciminib (Scemblix), approved by the FDA in 2021, is a third-line drug for patients who failed treatment with two other TKIs and certain patients with the T315I mutation.
Dr. Lai said that it’s crucial to avoid side effects as much as possible “since the goal is for patients to be compliant and take the pill every day and not miss doses.” In younger patients, “I typically choose a second-generation TKI as my first choice, since there is a higher likelihood of getting into a deep molecular remission more quickly. If treatment-free remission is something a patient is interested in, a second-generation TKI is more likely to make this happen.”
According to Dr. Atallah, about half of patients end up using more than one drug because their initial choices either don’t work or cause intolerable side effects. Nevertheless, Dr. Lai noted: “Overall, patients do extremely well if compliant with their medication.”
Exceptions include the noncompliant and patients with more aggressive disease, like an accelerated or a blast phase, she said. For the latter patients, “allogenic bone marrow transplant should be considered once the patient is in remission.”
In remission, consider drug omission
How should patients be monitored if they are doing well?
“In general, I tend to follow patients monthly for the first six months after starting therapy, to make sure they are tolerating it well and to help manage side effects,” Dr. Lai said. “After that, I follow once every three months, and then often space out visits depending on whether they hit their molecular milestones and how long they’re in remission.”
In certain cases, patients may be taken off medication. The most recent National Comprehensive Cancer Network guidelines for treatment of CML, published in 2021, say that “discontinuation of TKI therapy (with close monitoring) is feasible in carefully selected, consenting patients” with early stage CML who’ve reached remission, defined as deep molecular response (DMR) of at least MR 4.0 for at least 2 years.
The guidelines caution that disease recurrence appears in “approximately 40%-60% of patients who discontinue TKI therapy after achieving DMR experience recurrence within 12 months of treatment cessation, in some cases as early as one month after discontinuation of TKI therapy.”
Still, the guidelines add that “resumption of TKI therapy immediately after recurrence results in the achievement of DMR in almost all patients.”
Dr. Atallah said stopping medication can be especially helpful for patients who grapple with side effects such as fatigue, diarrhea, and muscle aches. Some patients who take the drugs fear losing their health insurance and facing sky-high drug expenses. In 2018, average daily TKI costs for patients with CML were over $350, a 2020 report found.
Many patients were prescribed hugely expensive second-line treatments rather than inexpensive generic imatinib, the report said, despite “no evidence that later-generation TKIs provide superior progression free or overall survival.”
Many patients, however, refuse to consider stopping their medication, Dr. Atallah said. More data about treatment-free remission is needed, and the 21 U.S. academic medical centers in the H. Jean Khoury Cure CML Consortium are gathering information about patient outcomes.
Mr. Fahnestock is a fan of treatment-free remission. He stopped taking Gleevec about 2 years ago on the advice of his physician after he reached undetectable levels of disease.
“It was sort of a nonevent, really, with no discernible physical effects beyond exacerbation of the osteoarthritis in my hands,” he said. According to him, it’s not clear if this effect is linked to his eliminating the medication.
“I also vaguely hoped I’d feel better, even though I’d never been able to nail down any deleterious side effects,” he said. “No such luck, as it happens.”
Blood work has indicated no resurgence of the disease, and Mr. Fahnestock continues to volunteer as a rural firefighter.
“In general, I’m apparently reasonably healthy for my age, despite my folly [in younger years], and firefighting requires me to stay in reasonable shape,” he said. “I’ve recently been made aware of minor kidney issues and prediabetes. But, hell, I’m genetically scheduled to croak within 5 years or so, so why worry?”
National survival statistics in CML vary by factors such as gender and age, as a 2021 study revealed, and men have worse outcomes. Still, there’s a good chance Mr. Fahnestock won’t need to worry about CML ever again.
Dr. Atallah disclosed research support from Novartis and Takeda and has served both of those firms and Bristol-Myers Squibb as a consultant advisor. Dr. Lai discloses tied with Bristol-Myers Squibb, Jazz, Genentech, Novartis, Abbvie, Daiichi Sankyo, Astellas, MacroGenics, Servier, and Taiho. Mr. Fahnestock has no disclosures.
When imatinib (Gleevec) appeared on the market just over 2 decades ago, it revolutionized the treatment of chronic myelogenous leukemia (CML) and transformed it from a grim diagnosis into a largely treatable form of blood cancer. New generations of tyrosine kinase inhibitors (TKIs) have continued to expand options for patients, and many can look forward to normal lifespans.
But these medications cause side effects and can be expensive. Long-term data doesn’t exist for the newer therapies, so no one knows whether they can harm patients over time. None of this is particularly unusual for medications to treat chronic illness, but now there’s a twist:
“Our focus has changed because the results of treatment are so good,” hematologist-oncologist Ehab L. Atallah, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview. “We’re trying to get people off their medication.”
Still, research estimates that only 20% of patients with CML will be eligible for treatment discontinuation and benefit from it in the long term. As a result, the wide majority of patients will need to be on drugs indefinitely.
Gleevec: A new age dawns
In the early 1990s, before the era of TKIs, the 5-year relative survival rate from CML was just 27%, and the 10-year rate was only 9.5%, according to a 2008 report. “If someone showed up with CML, their only option was to go to a bone marrow transplant. About half survived the transplant, and half of those had significant complications from it,” Dr. Atallah said. According to him, just about everyone who didn’t get transplantation would go on to die.
Then came Gleevec, which received Food and Drug Administration approval in 2001. It ushered in the era of “targeted” cancer treatment by specifically killing CML cells, instead of relying on traditional chemotherapy’s carpet-bombing approach.
“Gleevec and other TKIs have revolutionized how CML is treated, and patients are now living normal lives,” hematologist-oncologist Catherine Lai, MD, MPH, of the University of Pennsylvania, Philadelphia, said in an interview.
Alan Fahnestock, a 68-year-old retired telecommunications specialist in north-central Washington state, is one of the fortunate patients.
He was diagnosed with CML in 2004 after he underwent a thoracic CT scan in light of his tobacco use. “My GP found something odd in my lungs and referred me to a pulmonologist, who couldn’t figure it out either. He transmitted blood samples to my eventual hematologist/oncologist,” Mr. Fahnestock said in an interview. “It’s not clear to me that anybody ever figured out what the ‘oddity’ was. It has since apparently gone away. But the oncologist ran all the tests and came up with CML.”
Mr. Fahnestock hadn’t noticed any symptoms, although “this is, perhaps, because I tend not to pay a lot of attention to such things, having abused my body fairly severely over the years and having been borderline anemic since I was a kid. I don’t really expect to feel great and am a bit of a fatalist: I just get on with things until I no longer can.”
His physician prescribed Gleevec. “I had no particularly notable side effects, and carried on with my life pretty much as if nothing had happened,” Mr. Fahnestock said. He stayed on the drug for almost 20 years.
CML rooted in chromosome swap
It’s not clear exactly what causes CML, although the Mayo Clinic says most cases are linked to an abnormal, extra-short “Philadelphia chromosome,” created when two chromosomes swap material. This happens after birth.
Mr. Fahnestock thinks he happened to develop a random mutation. He also wonders if his work stints in the former Soviet Union in Vladivostok, “where the Soviet nuclear submarine fleet was decomposing,” and in Kiev, Ukraine, “which is not all that far from Chernobyl,” may be responsible.
Most patients, like Mr. Fahnestock, are men. Males will account for about 5,190 of the cases diagnosed in 2023, according to the American Cancer Society, compared to 3,740 in females.
Mr. Fahnestock’s CML diagnosis came at a fairly young age, when he was in his 40s. The average patient is diagnosed at 64. But it’s not unusual that he experienced no apparent symptoms when the cancer was found. In fact, that’s the norm.
Most patients with the disease – which is diagnosed in about 8,900 patients in the United States each year – are asymptomatic or have mild symptoms, Dr. Lai said. Their disease is discovered when “an elevated white count is found on routine blood work,” she said.
“The other group of patients typically present with very elevated white blood cell counts and splenomegaly with symptoms of fatigue and other constitutional symptoms. When the WBC count is very high, it is important to rule out transformation to accelerated or blast phase and also rule out an acute leukemia.”
Polymerase chain reaction is an especially important test during diagnosis, Dr. Atallah said, since it provides baseline data about the cancer that can be tracked.
TKIs: Mainstay of treatment
Four drugs are FDA approved for initial treatment of CML: imatinib (Gleevec), the second-generation TKIs dasatinib (Sprycel) and the third-generation TKI nilotinib (Tasigna). The third-generation TKIs bosutinib (Bosulif) and ponatinib (Iclusig) are approved for use as first-line treatments for patients who cannot tolerate the other drugs or are resistant to them.
The first-in-class drug asciminib (Scemblix), approved by the FDA in 2021, is a third-line drug for patients who failed treatment with two other TKIs and certain patients with the T315I mutation.
Dr. Lai said that it’s crucial to avoid side effects as much as possible “since the goal is for patients to be compliant and take the pill every day and not miss doses.” In younger patients, “I typically choose a second-generation TKI as my first choice, since there is a higher likelihood of getting into a deep molecular remission more quickly. If treatment-free remission is something a patient is interested in, a second-generation TKI is more likely to make this happen.”
According to Dr. Atallah, about half of patients end up using more than one drug because their initial choices either don’t work or cause intolerable side effects. Nevertheless, Dr. Lai noted: “Overall, patients do extremely well if compliant with their medication.”
Exceptions include the noncompliant and patients with more aggressive disease, like an accelerated or a blast phase, she said. For the latter patients, “allogenic bone marrow transplant should be considered once the patient is in remission.”
In remission, consider drug omission
How should patients be monitored if they are doing well?
“In general, I tend to follow patients monthly for the first six months after starting therapy, to make sure they are tolerating it well and to help manage side effects,” Dr. Lai said. “After that, I follow once every three months, and then often space out visits depending on whether they hit their molecular milestones and how long they’re in remission.”
In certain cases, patients may be taken off medication. The most recent National Comprehensive Cancer Network guidelines for treatment of CML, published in 2021, say that “discontinuation of TKI therapy (with close monitoring) is feasible in carefully selected, consenting patients” with early stage CML who’ve reached remission, defined as deep molecular response (DMR) of at least MR 4.0 for at least 2 years.
The guidelines caution that disease recurrence appears in “approximately 40%-60% of patients who discontinue TKI therapy after achieving DMR experience recurrence within 12 months of treatment cessation, in some cases as early as one month after discontinuation of TKI therapy.”
Still, the guidelines add that “resumption of TKI therapy immediately after recurrence results in the achievement of DMR in almost all patients.”
Dr. Atallah said stopping medication can be especially helpful for patients who grapple with side effects such as fatigue, diarrhea, and muscle aches. Some patients who take the drugs fear losing their health insurance and facing sky-high drug expenses. In 2018, average daily TKI costs for patients with CML were over $350, a 2020 report found.
Many patients were prescribed hugely expensive second-line treatments rather than inexpensive generic imatinib, the report said, despite “no evidence that later-generation TKIs provide superior progression free or overall survival.”
Many patients, however, refuse to consider stopping their medication, Dr. Atallah said. More data about treatment-free remission is needed, and the 21 U.S. academic medical centers in the H. Jean Khoury Cure CML Consortium are gathering information about patient outcomes.
Mr. Fahnestock is a fan of treatment-free remission. He stopped taking Gleevec about 2 years ago on the advice of his physician after he reached undetectable levels of disease.
“It was sort of a nonevent, really, with no discernible physical effects beyond exacerbation of the osteoarthritis in my hands,” he said. According to him, it’s not clear if this effect is linked to his eliminating the medication.
“I also vaguely hoped I’d feel better, even though I’d never been able to nail down any deleterious side effects,” he said. “No such luck, as it happens.”
Blood work has indicated no resurgence of the disease, and Mr. Fahnestock continues to volunteer as a rural firefighter.
“In general, I’m apparently reasonably healthy for my age, despite my folly [in younger years], and firefighting requires me to stay in reasonable shape,” he said. “I’ve recently been made aware of minor kidney issues and prediabetes. But, hell, I’m genetically scheduled to croak within 5 years or so, so why worry?”
National survival statistics in CML vary by factors such as gender and age, as a 2021 study revealed, and men have worse outcomes. Still, there’s a good chance Mr. Fahnestock won’t need to worry about CML ever again.
Dr. Atallah disclosed research support from Novartis and Takeda and has served both of those firms and Bristol-Myers Squibb as a consultant advisor. Dr. Lai discloses tied with Bristol-Myers Squibb, Jazz, Genentech, Novartis, Abbvie, Daiichi Sankyo, Astellas, MacroGenics, Servier, and Taiho. Mr. Fahnestock has no disclosures.
Momelotinib hits the mark for deadly bone marrow cancer
“The current state for the treatment of myelofibrosis relies on JAK2,” said Ruben Mesa, MD, of the Mays Cancer Center at the UT Health San Antonio MD Anderson Cancer Center.
“Momelotinib is a JAK1 and JAK2 inhibitor.” However, in the early days of studying momelotinib,“it became clear that there was also potentially an improvement in anemia,” which may be related to the additional inhibition of ACVR1, he explained.
Data suggest that the ability to curb anemia in anemic myelofibrosis patients prolongs their lives for up to 8 years, Dr. Mesa added.
Previous studies, notably the phase 3 SIMPLIFY study, showed that momelotinib was associated with comparable effects on spleen volume, transfusion, and total symptom scores from baseline that were similar to ruxolitinib.
In the current study, known as MOMENTUM, a daily dose of momelotinib was compared to danazol for treatment of symptomatic and anemic myelofibrosis (MF) patients who had previously received standard JAK-inhibitor therapy.
In the study, the researchers randomized 130 patients to momelotinib and 65 to danazol. After 24 weeks, those in the danazol group were allowed to cross over to momelotinib. The primary endpoint of the study was total symptom score (TSS) response after 24 weeks. Secondary endpoints included transfusion independence and splenic response at 24 weeks. The median age of the patients in the momelotinib group was 71 years, 60.8% were male, and 82% were white. The baseline demographics were not significantly different in the danazol group.
Overall, 24.6% of momelotinib patients responded with improved total symptom scores at 24 weeks vs. 9.2% of the danazol group. Spleen response also was significantly higher in the momelotinib group; 40% of patients showed a 25% reduction and 23% showed a 35% reduction, compared with 6.2% and 3.1%, respectively, of patients in the danazol group. Transfusion independence at week 24 also was higher for momelotinib patients, compared with danazol patients (31% vs. 20%, respectively, P = 0064).
Adverse events of grade 3 or higher occurred in 53.8% of momelotinib patients and 64.6% of danazol patients, and serious adverse events occurred in 34.6% and 40.0%, respectively. Nearly all patients had anemia, but only 27.7% and 26.2% of the momelotinib and danazol groups, respectively, had thrombocytopenia of grade 3 or higher. The most common nonhematologic adverse events were diarrhea, nausea, and increased blood creatinine. A total of 27.7% of the patients in the momelotinib group discontinued treatment; 16 of whom did so because of an adverse event.
Also, at 24 weeks, patients in the momelotinib group showed a trend towards increased overall survival, compared with danazol (HR, 0.506, P = 0.719).
With momelotinib, there is a consistent thrombocytopenic profile across subgroups, the data on which were presented separately at ASCO (poster 7061), Dr. Mesa added.
“We feel that these findings support the future use of momelotinib as an effective treatment in MF patients, especially those with anemia,” he concluded.
Cytopenia data are exciting
The key finding in the current study is that “momelotinib leads to important endpoints including significant improvement in symptoms and spleen reduction,” said Dr. Gabriela Hobbs of Harvard Medical School, Boston, who served as the discussant for the study.
“I think a novel finding of momelotinib that is definitely exciting from the treatment perspective is that momelotinib can also lead to improvement in cytopenias,” she said. “We often have to decide between treating the symptoms of the spleen at the expense of blood counts,” in MF patients, she noted.
The study was sponsored by Sierra Oncology. Dr. Mesa disclosed relationships with companies including Constellation Pharmaceutical, La Jolla Pharma, and study sponsor Sierra Oncology, as well as funding from AbbVie, Celgene, Constellation Pharmaceuticals, CTI, Genentech, Incyte, Mays Cancer Center, NCI, Promedior, and Samus. Dr. Hobbs had no financial conflicts to disclose.
This article was updated 06/14/2022.
“The current state for the treatment of myelofibrosis relies on JAK2,” said Ruben Mesa, MD, of the Mays Cancer Center at the UT Health San Antonio MD Anderson Cancer Center.
“Momelotinib is a JAK1 and JAK2 inhibitor.” However, in the early days of studying momelotinib,“it became clear that there was also potentially an improvement in anemia,” which may be related to the additional inhibition of ACVR1, he explained.
Data suggest that the ability to curb anemia in anemic myelofibrosis patients prolongs their lives for up to 8 years, Dr. Mesa added.
Previous studies, notably the phase 3 SIMPLIFY study, showed that momelotinib was associated with comparable effects on spleen volume, transfusion, and total symptom scores from baseline that were similar to ruxolitinib.
In the current study, known as MOMENTUM, a daily dose of momelotinib was compared to danazol for treatment of symptomatic and anemic myelofibrosis (MF) patients who had previously received standard JAK-inhibitor therapy.
In the study, the researchers randomized 130 patients to momelotinib and 65 to danazol. After 24 weeks, those in the danazol group were allowed to cross over to momelotinib. The primary endpoint of the study was total symptom score (TSS) response after 24 weeks. Secondary endpoints included transfusion independence and splenic response at 24 weeks. The median age of the patients in the momelotinib group was 71 years, 60.8% were male, and 82% were white. The baseline demographics were not significantly different in the danazol group.
Overall, 24.6% of momelotinib patients responded with improved total symptom scores at 24 weeks vs. 9.2% of the danazol group. Spleen response also was significantly higher in the momelotinib group; 40% of patients showed a 25% reduction and 23% showed a 35% reduction, compared with 6.2% and 3.1%, respectively, of patients in the danazol group. Transfusion independence at week 24 also was higher for momelotinib patients, compared with danazol patients (31% vs. 20%, respectively, P = 0064).
Adverse events of grade 3 or higher occurred in 53.8% of momelotinib patients and 64.6% of danazol patients, and serious adverse events occurred in 34.6% and 40.0%, respectively. Nearly all patients had anemia, but only 27.7% and 26.2% of the momelotinib and danazol groups, respectively, had thrombocytopenia of grade 3 or higher. The most common nonhematologic adverse events were diarrhea, nausea, and increased blood creatinine. A total of 27.7% of the patients in the momelotinib group discontinued treatment; 16 of whom did so because of an adverse event.
Also, at 24 weeks, patients in the momelotinib group showed a trend towards increased overall survival, compared with danazol (HR, 0.506, P = 0.719).
With momelotinib, there is a consistent thrombocytopenic profile across subgroups, the data on which were presented separately at ASCO (poster 7061), Dr. Mesa added.
“We feel that these findings support the future use of momelotinib as an effective treatment in MF patients, especially those with anemia,” he concluded.
Cytopenia data are exciting
The key finding in the current study is that “momelotinib leads to important endpoints including significant improvement in symptoms and spleen reduction,” said Dr. Gabriela Hobbs of Harvard Medical School, Boston, who served as the discussant for the study.
“I think a novel finding of momelotinib that is definitely exciting from the treatment perspective is that momelotinib can also lead to improvement in cytopenias,” she said. “We often have to decide between treating the symptoms of the spleen at the expense of blood counts,” in MF patients, she noted.
The study was sponsored by Sierra Oncology. Dr. Mesa disclosed relationships with companies including Constellation Pharmaceutical, La Jolla Pharma, and study sponsor Sierra Oncology, as well as funding from AbbVie, Celgene, Constellation Pharmaceuticals, CTI, Genentech, Incyte, Mays Cancer Center, NCI, Promedior, and Samus. Dr. Hobbs had no financial conflicts to disclose.
This article was updated 06/14/2022.
“The current state for the treatment of myelofibrosis relies on JAK2,” said Ruben Mesa, MD, of the Mays Cancer Center at the UT Health San Antonio MD Anderson Cancer Center.
“Momelotinib is a JAK1 and JAK2 inhibitor.” However, in the early days of studying momelotinib,“it became clear that there was also potentially an improvement in anemia,” which may be related to the additional inhibition of ACVR1, he explained.
Data suggest that the ability to curb anemia in anemic myelofibrosis patients prolongs their lives for up to 8 years, Dr. Mesa added.
Previous studies, notably the phase 3 SIMPLIFY study, showed that momelotinib was associated with comparable effects on spleen volume, transfusion, and total symptom scores from baseline that were similar to ruxolitinib.
In the current study, known as MOMENTUM, a daily dose of momelotinib was compared to danazol for treatment of symptomatic and anemic myelofibrosis (MF) patients who had previously received standard JAK-inhibitor therapy.
In the study, the researchers randomized 130 patients to momelotinib and 65 to danazol. After 24 weeks, those in the danazol group were allowed to cross over to momelotinib. The primary endpoint of the study was total symptom score (TSS) response after 24 weeks. Secondary endpoints included transfusion independence and splenic response at 24 weeks. The median age of the patients in the momelotinib group was 71 years, 60.8% were male, and 82% were white. The baseline demographics were not significantly different in the danazol group.
Overall, 24.6% of momelotinib patients responded with improved total symptom scores at 24 weeks vs. 9.2% of the danazol group. Spleen response also was significantly higher in the momelotinib group; 40% of patients showed a 25% reduction and 23% showed a 35% reduction, compared with 6.2% and 3.1%, respectively, of patients in the danazol group. Transfusion independence at week 24 also was higher for momelotinib patients, compared with danazol patients (31% vs. 20%, respectively, P = 0064).
Adverse events of grade 3 or higher occurred in 53.8% of momelotinib patients and 64.6% of danazol patients, and serious adverse events occurred in 34.6% and 40.0%, respectively. Nearly all patients had anemia, but only 27.7% and 26.2% of the momelotinib and danazol groups, respectively, had thrombocytopenia of grade 3 or higher. The most common nonhematologic adverse events were diarrhea, nausea, and increased blood creatinine. A total of 27.7% of the patients in the momelotinib group discontinued treatment; 16 of whom did so because of an adverse event.
Also, at 24 weeks, patients in the momelotinib group showed a trend towards increased overall survival, compared with danazol (HR, 0.506, P = 0.719).
With momelotinib, there is a consistent thrombocytopenic profile across subgroups, the data on which were presented separately at ASCO (poster 7061), Dr. Mesa added.
“We feel that these findings support the future use of momelotinib as an effective treatment in MF patients, especially those with anemia,” he concluded.
Cytopenia data are exciting
The key finding in the current study is that “momelotinib leads to important endpoints including significant improvement in symptoms and spleen reduction,” said Dr. Gabriela Hobbs of Harvard Medical School, Boston, who served as the discussant for the study.
“I think a novel finding of momelotinib that is definitely exciting from the treatment perspective is that momelotinib can also lead to improvement in cytopenias,” she said. “We often have to decide between treating the symptoms of the spleen at the expense of blood counts,” in MF patients, she noted.
The study was sponsored by Sierra Oncology. Dr. Mesa disclosed relationships with companies including Constellation Pharmaceutical, La Jolla Pharma, and study sponsor Sierra Oncology, as well as funding from AbbVie, Celgene, Constellation Pharmaceuticals, CTI, Genentech, Incyte, Mays Cancer Center, NCI, Promedior, and Samus. Dr. Hobbs had no financial conflicts to disclose.
This article was updated 06/14/2022.
FROM ASCO 2022
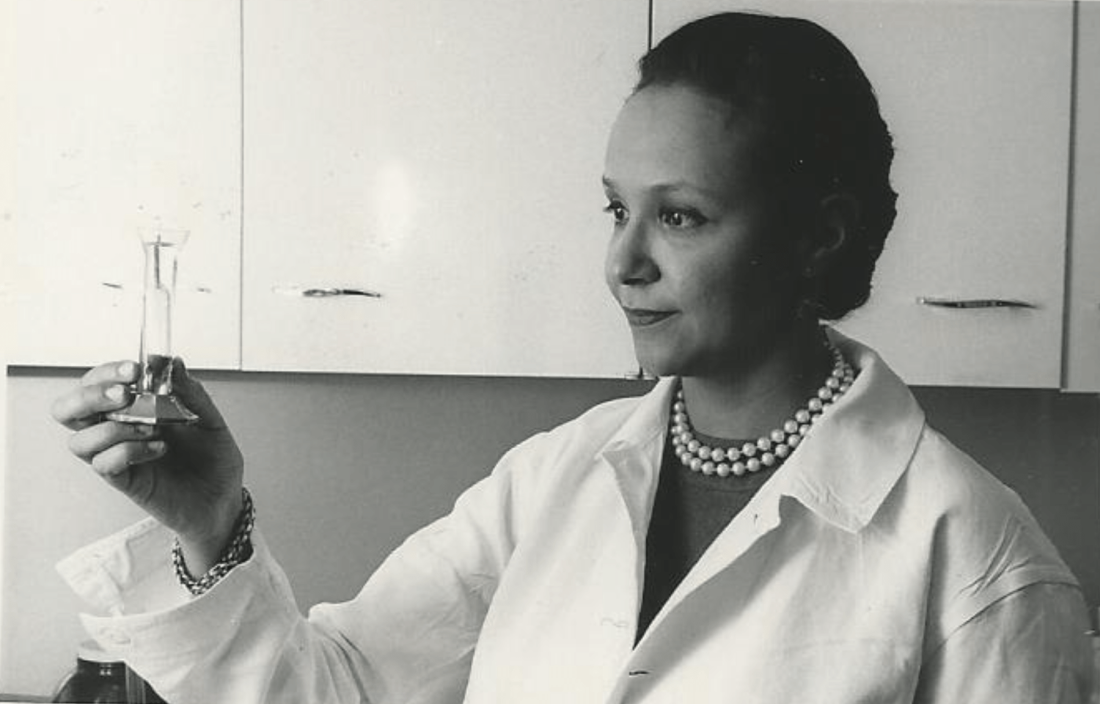
Third-generation Black woman physician makes cancer research history
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
9/11 first responders show mutations linked to blood cancers
. These results add to concerns about the long-term health effects of that exposure and further underscore a need for screening of those exposed.
“These data demonstrate that environmental exposure to the WTC disaster site is associated with a higher burden of clonal hematopoiesis, exceeding that expected in normal aging, and establish a rationale for mutational testing of the larger WTC-exposed population,” report the authors in the study, published March 7 in Nature Medicine.
The findings come from a study of blood samples from WTC first responders, including 429 firefighters and 52 emergency medical service workers, collected between December 2013 and October 2015.
For comparisons, the authors collected blood samples from 255 firefighters from in and around Nashville, Tenn., none of whom had been exposed to the 9/11 disaster.
Genetic analysis of the samples showed that 10% of those in the WTC-exposed cohort (n = 48) had unique somatic mutations considered to likely be pathogenic, and six of those individuals carried one or more of the mutations.
After a multivariate adjustment controlling for age, sex and race/ethnicity, those among the WTC-exposed first responders had a significantly increased odds of clonal hematopoiesis versus nonexposed workers (odds ratio [OR] = 3.14; P = .0006).
The higher risk was further observed in a comparison limited only to the WTC-exposed firefighters versus nonexposed firefighters (OR = 2.93; P = .0014) after the multivariate adjustment. The greater association between WTC exposure and clonal hematopoiesis remained after the researchers controlled for smoking as well as other risk factors among the WTC-exposed group overall (OR = 3.05; P = .0015) and the firefighters-only comparison (OR = 2.78; P = .004).
A history of smoking was not significantly associated with an increased risk of clonal hematopoiesis in either model.
As a risk factor for hematologic malignancy, cardiovascular events, and mortality, “clonal hematopoiesis is a concerning acquired risk not only for diseases that are already associated with WTC exposure but also as the population ages, this may exacerbate their risk profile,” Dr. Anna Nolan, coauthor of the study, and professor of medicine and environmental medicine in the division of pulmonary and critical care, New York University, said in an interview.
The most common gene mutations observed in the WTC-exposed group were those associated with myeloid malignancies, such as chronic myeloid leukemia; however, blood counts in the exposed group showed no association between exposure and mutations linked to cytopenias.
A further analysis on mice, investigating how WTC particulate matter uniquely affects DNA, surprisingly showed that just one exposure to the material was associated with clonal hematopoietic changes.

“Exposure to particulates, even at a single time point, can yield clonal mutations that may be risk for multisystem end-organ changes,” Dr. Nolan said.
While the serious health effects of WTC exposure on humans, have been extensively documented, including a study published in February showing increases in skin, prostate and thyroid cancers, clonal hematopoiesis suggests further heightened risks as the exposed population grows older, Dr. Nolan noted.
“[Clonal hematopoiesis] is a concerning acquired risk not only for diseases that are already associated with WTC exposure, but also, as the population ages, this may exacerbate their risk profile,” she said.
Due to the risk, “clinicians should be aware that WTC-exposed first responders have had a significant exposure and that they are at risk for developing several conditions.”
Commenting on this study, William K. Oh, MD, whose team at the Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, has reported in a previous study on the increased risk of prostate cancer among WTC first responders, noted that more time may be necessary to better understand the full effects of the increases in clonal hematopoiesis.
“Though these findings are of concern, there were still no differences in the cohorts in actual hematologic cancers or even cytopenias, suggesting that more time and additional DNA damaging events were needed to transform the clonal hematopoiesis findings to clinically relevant diseases,” Dr. Oh, clinical professor of medicine, said in an interview.
Nevertheless, “if a patient is found on testing to have clonal hematopoiesis, they should be screened more closely for blood disorders and cardiovascular issues than they might otherwise be, though this remains an area of active investigation,” Dr. Oh said.
Dr. Nolan had no disclosures to report. Dr. Oh is the chief medical science officer at Sema4, a genomic testing and data company.
. These results add to concerns about the long-term health effects of that exposure and further underscore a need for screening of those exposed.
“These data demonstrate that environmental exposure to the WTC disaster site is associated with a higher burden of clonal hematopoiesis, exceeding that expected in normal aging, and establish a rationale for mutational testing of the larger WTC-exposed population,” report the authors in the study, published March 7 in Nature Medicine.
The findings come from a study of blood samples from WTC first responders, including 429 firefighters and 52 emergency medical service workers, collected between December 2013 and October 2015.
For comparisons, the authors collected blood samples from 255 firefighters from in and around Nashville, Tenn., none of whom had been exposed to the 9/11 disaster.
Genetic analysis of the samples showed that 10% of those in the WTC-exposed cohort (n = 48) had unique somatic mutations considered to likely be pathogenic, and six of those individuals carried one or more of the mutations.
After a multivariate adjustment controlling for age, sex and race/ethnicity, those among the WTC-exposed first responders had a significantly increased odds of clonal hematopoiesis versus nonexposed workers (odds ratio [OR] = 3.14; P = .0006).
The higher risk was further observed in a comparison limited only to the WTC-exposed firefighters versus nonexposed firefighters (OR = 2.93; P = .0014) after the multivariate adjustment. The greater association between WTC exposure and clonal hematopoiesis remained after the researchers controlled for smoking as well as other risk factors among the WTC-exposed group overall (OR = 3.05; P = .0015) and the firefighters-only comparison (OR = 2.78; P = .004).
A history of smoking was not significantly associated with an increased risk of clonal hematopoiesis in either model.
As a risk factor for hematologic malignancy, cardiovascular events, and mortality, “clonal hematopoiesis is a concerning acquired risk not only for diseases that are already associated with WTC exposure but also as the population ages, this may exacerbate their risk profile,” Dr. Anna Nolan, coauthor of the study, and professor of medicine and environmental medicine in the division of pulmonary and critical care, New York University, said in an interview.
The most common gene mutations observed in the WTC-exposed group were those associated with myeloid malignancies, such as chronic myeloid leukemia; however, blood counts in the exposed group showed no association between exposure and mutations linked to cytopenias.
A further analysis on mice, investigating how WTC particulate matter uniquely affects DNA, surprisingly showed that just one exposure to the material was associated with clonal hematopoietic changes.
“Exposure to particulates, even at a single time point, can yield clonal mutations that may be risk for multisystem end-organ changes,” Dr. Nolan said.
While the serious health effects of WTC exposure on humans, have been extensively documented, including a study published in February showing increases in skin, prostate and thyroid cancers, clonal hematopoiesis suggests further heightened risks as the exposed population grows older, Dr. Nolan noted.
“[Clonal hematopoiesis] is a concerning acquired risk not only for diseases that are already associated with WTC exposure, but also, as the population ages, this may exacerbate their risk profile,” she said.
Due to the risk, “clinicians should be aware that WTC-exposed first responders have had a significant exposure and that they are at risk for developing several conditions.”
Commenting on this study, William K. Oh, MD, whose team at the Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, has reported in a previous study on the increased risk of prostate cancer among WTC first responders, noted that more time may be necessary to better understand the full effects of the increases in clonal hematopoiesis.
“Though these findings are of concern, there were still no differences in the cohorts in actual hematologic cancers or even cytopenias, suggesting that more time and additional DNA damaging events were needed to transform the clonal hematopoiesis findings to clinically relevant diseases,” Dr. Oh, clinical professor of medicine, said in an interview.
Nevertheless, “if a patient is found on testing to have clonal hematopoiesis, they should be screened more closely for blood disorders and cardiovascular issues than they might otherwise be, though this remains an area of active investigation,” Dr. Oh said.
Dr. Nolan had no disclosures to report. Dr. Oh is the chief medical science officer at Sema4, a genomic testing and data company.
. These results add to concerns about the long-term health effects of that exposure and further underscore a need for screening of those exposed.
“These data demonstrate that environmental exposure to the WTC disaster site is associated with a higher burden of clonal hematopoiesis, exceeding that expected in normal aging, and establish a rationale for mutational testing of the larger WTC-exposed population,” report the authors in the study, published March 7 in Nature Medicine.
The findings come from a study of blood samples from WTC first responders, including 429 firefighters and 52 emergency medical service workers, collected between December 2013 and October 2015.
For comparisons, the authors collected blood samples from 255 firefighters from in and around Nashville, Tenn., none of whom had been exposed to the 9/11 disaster.
Genetic analysis of the samples showed that 10% of those in the WTC-exposed cohort (n = 48) had unique somatic mutations considered to likely be pathogenic, and six of those individuals carried one or more of the mutations.
After a multivariate adjustment controlling for age, sex and race/ethnicity, those among the WTC-exposed first responders had a significantly increased odds of clonal hematopoiesis versus nonexposed workers (odds ratio [OR] = 3.14; P = .0006).
The higher risk was further observed in a comparison limited only to the WTC-exposed firefighters versus nonexposed firefighters (OR = 2.93; P = .0014) after the multivariate adjustment. The greater association between WTC exposure and clonal hematopoiesis remained after the researchers controlled for smoking as well as other risk factors among the WTC-exposed group overall (OR = 3.05; P = .0015) and the firefighters-only comparison (OR = 2.78; P = .004).
A history of smoking was not significantly associated with an increased risk of clonal hematopoiesis in either model.
As a risk factor for hematologic malignancy, cardiovascular events, and mortality, “clonal hematopoiesis is a concerning acquired risk not only for diseases that are already associated with WTC exposure but also as the population ages, this may exacerbate their risk profile,” Dr. Anna Nolan, coauthor of the study, and professor of medicine and environmental medicine in the division of pulmonary and critical care, New York University, said in an interview.
The most common gene mutations observed in the WTC-exposed group were those associated with myeloid malignancies, such as chronic myeloid leukemia; however, blood counts in the exposed group showed no association between exposure and mutations linked to cytopenias.
A further analysis on mice, investigating how WTC particulate matter uniquely affects DNA, surprisingly showed that just one exposure to the material was associated with clonal hematopoietic changes.
“Exposure to particulates, even at a single time point, can yield clonal mutations that may be risk for multisystem end-organ changes,” Dr. Nolan said.
While the serious health effects of WTC exposure on humans, have been extensively documented, including a study published in February showing increases in skin, prostate and thyroid cancers, clonal hematopoiesis suggests further heightened risks as the exposed population grows older, Dr. Nolan noted.
“[Clonal hematopoiesis] is a concerning acquired risk not only for diseases that are already associated with WTC exposure, but also, as the population ages, this may exacerbate their risk profile,” she said.
Due to the risk, “clinicians should be aware that WTC-exposed first responders have had a significant exposure and that they are at risk for developing several conditions.”
Commenting on this study, William K. Oh, MD, whose team at the Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, has reported in a previous study on the increased risk of prostate cancer among WTC first responders, noted that more time may be necessary to better understand the full effects of the increases in clonal hematopoiesis.
“Though these findings are of concern, there were still no differences in the cohorts in actual hematologic cancers or even cytopenias, suggesting that more time and additional DNA damaging events were needed to transform the clonal hematopoiesis findings to clinically relevant diseases,” Dr. Oh, clinical professor of medicine, said in an interview.
Nevertheless, “if a patient is found on testing to have clonal hematopoiesis, they should be screened more closely for blood disorders and cardiovascular issues than they might otherwise be, though this remains an area of active investigation,” Dr. Oh said.
Dr. Nolan had no disclosures to report. Dr. Oh is the chief medical science officer at Sema4, a genomic testing and data company.
FROM NATURE MEDICINE
U.S. cancer deaths continue to fall, especially lung cancer
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
FROM CA: A CANCER JOURNAL FOR CLINICIANS
Clinical Edge Journal Scan Commentary: CML December 2021
Patients who adhere to their tyrosine kinase inhibitor (TKI) medication regimen will achieve CML survival goals that would be expected for their age group. Imatinib is a first generation TKI inhibitor. In a recent post hoc analysis of the ADAGIO study patients, Obeng-Kusi M et al1 showed that compared with 90% adherence, a 100% adherence to imatinib was associated with a 2-fold increase in achieving or maintaining treatment response in patients with chronic myeloid leukemia (CML), highlighting the urgent need to assess and promote patient adherence. There is virtually no margin for nonadherence, if the objective is to optimize the likelihood of treatment response, and a minimal margin to avoid impaired treatment response.
On the same topic, Davis TC et al.2also recently reported a study of suboptimal adherence to TKI. From the 86 patients with CML studied, almost 17.9% of participants reported nonadherence, i.e., missing at least 1 dose of CML medication in the previous week. The main reason that patients reported nonadherence were side effects, a busy schedule, and the difficulty of complying daily with the TKI regimen.
Cardiovascular adverse events (AE) have been described with TKI treatment at different rates, but cardiovascular risk stratification was not included in the design of many trials. Baggio D et al3 in a retrospective study included 88 patients with CML treated with any TKI and a median follow up of 3.8 months. They described the rates of major cardiovascular AEs by combining age, history of prior cardiovascular diseases, and Framingham risk score, along with additional insights from coronary artery calcium scoring (CACS). The authors found cardiovascular AEs in 0%, 10%, and 19%, of the low-, intermediate-, and high-risk groups respectively. By using CACS score they were able to reclassify patients from intermediate to low risk and none of those patients experienced a major adverse cardiovascular event.
The use of kinase domain mutation analysis at diagnosis is not a recommended practice by the National Comprehensive Cancer Network (NCCN) or the European Leukemia Net (ELN), but is reserved for use in patents who failed first or subsequent lines of therapies. Furthermore, previous publications in the topic have showed discordant results. More recently, the use of ultra-deep sequencing has detected low-frequency genetic mutations with high sensitivity. Park H et al.4 recently described the most common mutations found in a population of 50 CML patients treated with nilotinib. V299 L mutation associated with dasatinib resistance and nilotinib sensitivity were observed in 98% of patients. Two uncommon mutations S417Y and the V371A were associated with reduced molecular response.
References
- Obeng-Kusi M et al. No margin for non-adherence: Probabilistic Kaplan-Meier modeling of imatinib non-adherence and treatment response in CML (ADAGIO study). Leuk Res. 2021;111:106734 (Oct 21).
- Davis TC et al. Assessment of oral chemotherapy nonadherence in chronic myeloid leukemia patients using brief measures in community cancer clinics: a pilot study. Int J Environ Res Public Health. 2021;18(21):11045 (Oct 21).
- Baggio D et al. Prediction of cardiovascular events in patients with chronic myeloid leukaemia using baseline risk factors and coronary artery calcium scoring. Intern Med J. 2021;51(10):1736-40 (Oct 18).
- Park H et al. Ultra-deep sequencing mutation analysis of the BCR/ABL1 kinase domain in newly diagnosed chronic myeloid leukemia patients. Leuk Res. 2021;111:106728 (Oct 15).
Patients who adhere to their tyrosine kinase inhibitor (TKI) medication regimen will achieve CML survival goals that would be expected for their age group. Imatinib is a first generation TKI inhibitor. In a recent post hoc analysis of the ADAGIO study patients, Obeng-Kusi M et al1 showed that compared with 90% adherence, a 100% adherence to imatinib was associated with a 2-fold increase in achieving or maintaining treatment response in patients with chronic myeloid leukemia (CML), highlighting the urgent need to assess and promote patient adherence. There is virtually no margin for nonadherence, if the objective is to optimize the likelihood of treatment response, and a minimal margin to avoid impaired treatment response.
On the same topic, Davis TC et al.2also recently reported a study of suboptimal adherence to TKI. From the 86 patients with CML studied, almost 17.9% of participants reported nonadherence, i.e., missing at least 1 dose of CML medication in the previous week. The main reason that patients reported nonadherence were side effects, a busy schedule, and the difficulty of complying daily with the TKI regimen.
Cardiovascular adverse events (AE) have been described with TKI treatment at different rates, but cardiovascular risk stratification was not included in the design of many trials. Baggio D et al3 in a retrospective study included 88 patients with CML treated with any TKI and a median follow up of 3.8 months. They described the rates of major cardiovascular AEs by combining age, history of prior cardiovascular diseases, and Framingham risk score, along with additional insights from coronary artery calcium scoring (CACS). The authors found cardiovascular AEs in 0%, 10%, and 19%, of the low-, intermediate-, and high-risk groups respectively. By using CACS score they were able to reclassify patients from intermediate to low risk and none of those patients experienced a major adverse cardiovascular event.
The use of kinase domain mutation analysis at diagnosis is not a recommended practice by the National Comprehensive Cancer Network (NCCN) or the European Leukemia Net (ELN), but is reserved for use in patents who failed first or subsequent lines of therapies. Furthermore, previous publications in the topic have showed discordant results. More recently, the use of ultra-deep sequencing has detected low-frequency genetic mutations with high sensitivity. Park H et al.4 recently described the most common mutations found in a population of 50 CML patients treated with nilotinib. V299 L mutation associated with dasatinib resistance and nilotinib sensitivity were observed in 98% of patients. Two uncommon mutations S417Y and the V371A were associated with reduced molecular response.
References
- Obeng-Kusi M et al. No margin for non-adherence: Probabilistic Kaplan-Meier modeling of imatinib non-adherence and treatment response in CML (ADAGIO study). Leuk Res. 2021;111:106734 (Oct 21).
- Davis TC et al. Assessment of oral chemotherapy nonadherence in chronic myeloid leukemia patients using brief measures in community cancer clinics: a pilot study. Int J Environ Res Public Health. 2021;18(21):11045 (Oct 21).
- Baggio D et al. Prediction of cardiovascular events in patients with chronic myeloid leukaemia using baseline risk factors and coronary artery calcium scoring. Intern Med J. 2021;51(10):1736-40 (Oct 18).
- Park H et al. Ultra-deep sequencing mutation analysis of the BCR/ABL1 kinase domain in newly diagnosed chronic myeloid leukemia patients. Leuk Res. 2021;111:106728 (Oct 15).
Patients who adhere to their tyrosine kinase inhibitor (TKI) medication regimen will achieve CML survival goals that would be expected for their age group. Imatinib is a first generation TKI inhibitor. In a recent post hoc analysis of the ADAGIO study patients, Obeng-Kusi M et al1 showed that compared with 90% adherence, a 100% adherence to imatinib was associated with a 2-fold increase in achieving or maintaining treatment response in patients with chronic myeloid leukemia (CML), highlighting the urgent need to assess and promote patient adherence. There is virtually no margin for nonadherence, if the objective is to optimize the likelihood of treatment response, and a minimal margin to avoid impaired treatment response.
On the same topic, Davis TC et al.2also recently reported a study of suboptimal adherence to TKI. From the 86 patients with CML studied, almost 17.9% of participants reported nonadherence, i.e., missing at least 1 dose of CML medication in the previous week. The main reason that patients reported nonadherence were side effects, a busy schedule, and the difficulty of complying daily with the TKI regimen.
Cardiovascular adverse events (AE) have been described with TKI treatment at different rates, but cardiovascular risk stratification was not included in the design of many trials. Baggio D et al3 in a retrospective study included 88 patients with CML treated with any TKI and a median follow up of 3.8 months. They described the rates of major cardiovascular AEs by combining age, history of prior cardiovascular diseases, and Framingham risk score, along with additional insights from coronary artery calcium scoring (CACS). The authors found cardiovascular AEs in 0%, 10%, and 19%, of the low-, intermediate-, and high-risk groups respectively. By using CACS score they were able to reclassify patients from intermediate to low risk and none of those patients experienced a major adverse cardiovascular event.
The use of kinase domain mutation analysis at diagnosis is not a recommended practice by the National Comprehensive Cancer Network (NCCN) or the European Leukemia Net (ELN), but is reserved for use in patents who failed first or subsequent lines of therapies. Furthermore, previous publications in the topic have showed discordant results. More recently, the use of ultra-deep sequencing has detected low-frequency genetic mutations with high sensitivity. Park H et al.4 recently described the most common mutations found in a population of 50 CML patients treated with nilotinib. V299 L mutation associated with dasatinib resistance and nilotinib sensitivity were observed in 98% of patients. Two uncommon mutations S417Y and the V371A were associated with reduced molecular response.
References
- Obeng-Kusi M et al. No margin for non-adherence: Probabilistic Kaplan-Meier modeling of imatinib non-adherence and treatment response in CML (ADAGIO study). Leuk Res. 2021;111:106734 (Oct 21).
- Davis TC et al. Assessment of oral chemotherapy nonadherence in chronic myeloid leukemia patients using brief measures in community cancer clinics: a pilot study. Int J Environ Res Public Health. 2021;18(21):11045 (Oct 21).
- Baggio D et al. Prediction of cardiovascular events in patients with chronic myeloid leukaemia using baseline risk factors and coronary artery calcium scoring. Intern Med J. 2021;51(10):1736-40 (Oct 18).
- Park H et al. Ultra-deep sequencing mutation analysis of the BCR/ABL1 kinase domain in newly diagnosed chronic myeloid leukemia patients. Leuk Res. 2021;111:106728 (Oct 15).
ANKRD36: A novel biomarker of CML disease progression
Key clinical point: Mutations in a novel gene ANKRD36 were associated with disease progression in chronic myeloid leukemia (CML) and may help identify patients at risk of disease progression.
Major finding: Mutations in the ANKRD36 gene (c.1183_1184 delGC and c.1187_1188 dupTT) were exclusively found in all patients with CML in blast crisis (CML-BC) and accelerated phase (CML-AP) but not in those with chronic-phase CML (CML-CP) and healthy controls.
Study details: This study included 141 patients with either CML-CP (n = 123), CML-AP (n = 6), or CML-BC (n = 12) and 10 age- and gender-matched healthy controls.
Disclosures: This study was funded by the National Plan for Science, Technology and Innovation, King Abdul-Aziz City for Science and Technology, Kingdom of Saudi Arabia. The authors declared no conflict of interests.
Source: Iqbal Z et al. Biology. 2021;10(11):1182 (Nov 15). Doi: 10.3390/biology10111182.
Key clinical point: Mutations in a novel gene ANKRD36 were associated with disease progression in chronic myeloid leukemia (CML) and may help identify patients at risk of disease progression.
Major finding: Mutations in the ANKRD36 gene (c.1183_1184 delGC and c.1187_1188 dupTT) were exclusively found in all patients with CML in blast crisis (CML-BC) and accelerated phase (CML-AP) but not in those with chronic-phase CML (CML-CP) and healthy controls.
Study details: This study included 141 patients with either CML-CP (n = 123), CML-AP (n = 6), or CML-BC (n = 12) and 10 age- and gender-matched healthy controls.
Disclosures: This study was funded by the National Plan for Science, Technology and Innovation, King Abdul-Aziz City for Science and Technology, Kingdom of Saudi Arabia. The authors declared no conflict of interests.
Source: Iqbal Z et al. Biology. 2021;10(11):1182 (Nov 15). Doi: 10.3390/biology10111182.
Key clinical point: Mutations in a novel gene ANKRD36 were associated with disease progression in chronic myeloid leukemia (CML) and may help identify patients at risk of disease progression.
Major finding: Mutations in the ANKRD36 gene (c.1183_1184 delGC and c.1187_1188 dupTT) were exclusively found in all patients with CML in blast crisis (CML-BC) and accelerated phase (CML-AP) but not in those with chronic-phase CML (CML-CP) and healthy controls.
Study details: This study included 141 patients with either CML-CP (n = 123), CML-AP (n = 6), or CML-BC (n = 12) and 10 age- and gender-matched healthy controls.
Disclosures: This study was funded by the National Plan for Science, Technology and Innovation, King Abdul-Aziz City for Science and Technology, Kingdom of Saudi Arabia. The authors declared no conflict of interests.
Source: Iqbal Z et al. Biology. 2021;10(11):1182 (Nov 15). Doi: 10.3390/biology10111182.
Factors affecting HRQoL in children with CML-CP on TKI therapy
Key clinical point: Female sex, tyrosine kinase inhibitor (TKI) therapy-related symptoms, older age at diagnosis, younger age at the time of the study, and low maternal education were associated with worse health-related quality of life (HRQoL) in children with chronic-phase chronic myeloid leukemia (CML-CP) receiving TKI therapy.
Major finding: Worse HRQoL was observed in children with symptoms (P < .001), children with mothers having low educational qualifications (P = .005), children at a younger age at the time of the study (P = .008), children with older age at the time of diagnosis (P = .007), and female children (P = .038).
Study details: Findings are from a cross-sectional study of 240 respondents including children with CML-CP (age < 18 years at diagnosis) receiving TKI therapy and whose parents responded to a cross-sectional questionnaire.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflict of interests.
Source: Zheng F et al. J Cancer Res Clin Oncol. 2021(Oct 29). Doi: 10.1007/s00432-021-03832-y.
Key clinical point: Female sex, tyrosine kinase inhibitor (TKI) therapy-related symptoms, older age at diagnosis, younger age at the time of the study, and low maternal education were associated with worse health-related quality of life (HRQoL) in children with chronic-phase chronic myeloid leukemia (CML-CP) receiving TKI therapy.
Major finding: Worse HRQoL was observed in children with symptoms (P < .001), children with mothers having low educational qualifications (P = .005), children at a younger age at the time of the study (P = .008), children with older age at the time of diagnosis (P = .007), and female children (P = .038).
Study details: Findings are from a cross-sectional study of 240 respondents including children with CML-CP (age < 18 years at diagnosis) receiving TKI therapy and whose parents responded to a cross-sectional questionnaire.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflict of interests.
Source: Zheng F et al. J Cancer Res Clin Oncol. 2021(Oct 29). Doi: 10.1007/s00432-021-03832-y.
Key clinical point: Female sex, tyrosine kinase inhibitor (TKI) therapy-related symptoms, older age at diagnosis, younger age at the time of the study, and low maternal education were associated with worse health-related quality of life (HRQoL) in children with chronic-phase chronic myeloid leukemia (CML-CP) receiving TKI therapy.
Major finding: Worse HRQoL was observed in children with symptoms (P < .001), children with mothers having low educational qualifications (P = .005), children at a younger age at the time of the study (P = .008), children with older age at the time of diagnosis (P = .007), and female children (P = .038).
Study details: Findings are from a cross-sectional study of 240 respondents including children with CML-CP (age < 18 years at diagnosis) receiving TKI therapy and whose parents responded to a cross-sectional questionnaire.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflict of interests.
Source: Zheng F et al. J Cancer Res Clin Oncol. 2021(Oct 29). Doi: 10.1007/s00432-021-03832-y.
Better clinical outcomes with adjuvant IFN therapy vs. adjuvant vaccine in TKI-treated patients with CML-CP
Key clinical point: Adjuvant therapy with interferon-a+sargramostim (IFN) vs. K562/granulocyte macrophage-colony stimulating factor (GM-CSF) vaccine led to better molecular responses with sustained treatment-free remission (TFR) in tyrosine kinase inhibitor (TKI)-treated patients with chronic-phase chronic myeloid leukemia (CML-CP).
Major finding: Patients receiving IFN vs. K562/GM-CSF vaccine had a higher rate of undetectable minimal residual disease at 1 year (47.4%; 95% CI 16.7%-66.7% vs. 25%; 95% CI 0.5%-43.5%). TFR was maintained by 36.6% vs. 0.0% of patients receiving IFN vs. K562/GM-CSF vaccine. Treatment discontinuation because of side effects was higher in IFN-treated patients.
Study details: Findings are from a phase 2 trial including 34 adult patients with CML-CP receiving stable dosing of frontline TKI therapy for ≥1 year with a complete cytogenic response who were randomly assigned to IFN or K562/GM-CSF vaccine.
Disclosures: This study was supported by grants from US National Institute of Health. The authors declared no conflict of interests.
Source: Webster JA et al. Leuk Res. 2021;111:106737 (Nov 2). Doi: 10.1016/j.leukres.2021.106737.
Key clinical point: Adjuvant therapy with interferon-a+sargramostim (IFN) vs. K562/granulocyte macrophage-colony stimulating factor (GM-CSF) vaccine led to better molecular responses with sustained treatment-free remission (TFR) in tyrosine kinase inhibitor (TKI)-treated patients with chronic-phase chronic myeloid leukemia (CML-CP).
Major finding: Patients receiving IFN vs. K562/GM-CSF vaccine had a higher rate of undetectable minimal residual disease at 1 year (47.4%; 95% CI 16.7%-66.7% vs. 25%; 95% CI 0.5%-43.5%). TFR was maintained by 36.6% vs. 0.0% of patients receiving IFN vs. K562/GM-CSF vaccine. Treatment discontinuation because of side effects was higher in IFN-treated patients.
Study details: Findings are from a phase 2 trial including 34 adult patients with CML-CP receiving stable dosing of frontline TKI therapy for ≥1 year with a complete cytogenic response who were randomly assigned to IFN or K562/GM-CSF vaccine.
Disclosures: This study was supported by grants from US National Institute of Health. The authors declared no conflict of interests.
Source: Webster JA et al. Leuk Res. 2021;111:106737 (Nov 2). Doi: 10.1016/j.leukres.2021.106737.
Key clinical point: Adjuvant therapy with interferon-a+sargramostim (IFN) vs. K562/granulocyte macrophage-colony stimulating factor (GM-CSF) vaccine led to better molecular responses with sustained treatment-free remission (TFR) in tyrosine kinase inhibitor (TKI)-treated patients with chronic-phase chronic myeloid leukemia (CML-CP).
Major finding: Patients receiving IFN vs. K562/GM-CSF vaccine had a higher rate of undetectable minimal residual disease at 1 year (47.4%; 95% CI 16.7%-66.7% vs. 25%; 95% CI 0.5%-43.5%). TFR was maintained by 36.6% vs. 0.0% of patients receiving IFN vs. K562/GM-CSF vaccine. Treatment discontinuation because of side effects was higher in IFN-treated patients.
Study details: Findings are from a phase 2 trial including 34 adult patients with CML-CP receiving stable dosing of frontline TKI therapy for ≥1 year with a complete cytogenic response who were randomly assigned to IFN or K562/GM-CSF vaccine.
Disclosures: This study was supported by grants from US National Institute of Health. The authors declared no conflict of interests.
Source: Webster JA et al. Leuk Res. 2021;111:106737 (Nov 2). Doi: 10.1016/j.leukres.2021.106737.