User login
Treating patients during COVID-19: What I observed
I am a psychiatrist at a community mental health center located close to a large city. I want to report on our experience treating 100 consecutive, non-duplicative patients during the coronavirus disease 2019 (COVID-19) pandemic. Most of these patients had medical assistance or Medicare. Fifty-one were white, 46 were black, and 3 were Asian; 50 were men, and their ages ranged from 16 to 83 (mean: 54; median: 56). Using each patient as his/her own control (pre- and post–COVID-19), here I report 6 observations I made while treating these patients.
1. Telehealth worked for most patients. Of the 100 patients, 18 were seen in-person. Of the 18 seen in person, 14 received long-acting IM injections, and 2 patients presented with urgent matters that I felt required in-person evaluations. One patient needed to fill out several forms and provide consents, and 1 patient with chronic illness was treated at the clinic because he mistakenly arrived in person for his appointment.
The remaining 82 patients had telehealth sessions. Only 9 patients said they were able to use video conferencing, so the remaining 73 patients were treated by phone. These patients were mostly poor and/or older and had no access to smartphones or computers. This is especially important because the current emergency telehealth rules allow phone-only sessions, while regular telehealth rules do not. Our clinic strongly advocates for the extension of emergency telehealth rules. I have e-mailed many elected officials about this, but I have received few replies and no substantive responses. Our clinic also needs to help our patients obtain increased audiovisual capabilities.
2. Female patients fared better in their treatment than males.
3. Older patients did better than younger patients. Older patients’ experiences of living through past crises were helpful because they were able to compare how they persevered in the past with the current pandemic.
4. White patients showed more improvements compared with black patients. White patients generally had greater access to resources and support.
5. Patients with psychotic diagnoses/symptoms improved more than those with neurotic/anxiety/depressive diagnoses or symptoms. Most of our patients with psychotic diagnoses were already in a supportive, structured living environment, so the new “COVID-19 world” may be less disruptive for them. Additionally, it was more difficult for our patients to get substances of abuse because they had less mobility and access during the pandemic.
Continue to: Support
6. Support, especially from family but also institutional support, trumped other factors. The more support and structure our patients had, the better they did.
My observations may not be generalizable because I am reporting on a relatively small population size, most patients were older, and most were established patients who were likely more stable. I plan to follow up with these patients to see how the new COVID-19 world continues to affect them, and us.
Daniel D. Storch, MD
Key Point Health Services
Catonsville, Maryland
Disclosure: The author reports no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
I am a psychiatrist at a community mental health center located close to a large city. I want to report on our experience treating 100 consecutive, non-duplicative patients during the coronavirus disease 2019 (COVID-19) pandemic. Most of these patients had medical assistance or Medicare. Fifty-one were white, 46 were black, and 3 were Asian; 50 were men, and their ages ranged from 16 to 83 (mean: 54; median: 56). Using each patient as his/her own control (pre- and post–COVID-19), here I report 6 observations I made while treating these patients.
1. Telehealth worked for most patients. Of the 100 patients, 18 were seen in-person. Of the 18 seen in person, 14 received long-acting IM injections, and 2 patients presented with urgent matters that I felt required in-person evaluations. One patient needed to fill out several forms and provide consents, and 1 patient with chronic illness was treated at the clinic because he mistakenly arrived in person for his appointment.
The remaining 82 patients had telehealth sessions. Only 9 patients said they were able to use video conferencing, so the remaining 73 patients were treated by phone. These patients were mostly poor and/or older and had no access to smartphones or computers. This is especially important because the current emergency telehealth rules allow phone-only sessions, while regular telehealth rules do not. Our clinic strongly advocates for the extension of emergency telehealth rules. I have e-mailed many elected officials about this, but I have received few replies and no substantive responses. Our clinic also needs to help our patients obtain increased audiovisual capabilities.
2. Female patients fared better in their treatment than males.
3. Older patients did better than younger patients. Older patients’ experiences of living through past crises were helpful because they were able to compare how they persevered in the past with the current pandemic.
4. White patients showed more improvements compared with black patients. White patients generally had greater access to resources and support.
5. Patients with psychotic diagnoses/symptoms improved more than those with neurotic/anxiety/depressive diagnoses or symptoms. Most of our patients with psychotic diagnoses were already in a supportive, structured living environment, so the new “COVID-19 world” may be less disruptive for them. Additionally, it was more difficult for our patients to get substances of abuse because they had less mobility and access during the pandemic.
Continue to: Support
6. Support, especially from family but also institutional support, trumped other factors. The more support and structure our patients had, the better they did.
My observations may not be generalizable because I am reporting on a relatively small population size, most patients were older, and most were established patients who were likely more stable. I plan to follow up with these patients to see how the new COVID-19 world continues to affect them, and us.
Daniel D. Storch, MD
Key Point Health Services
Catonsville, Maryland
Disclosure: The author reports no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
I am a psychiatrist at a community mental health center located close to a large city. I want to report on our experience treating 100 consecutive, non-duplicative patients during the coronavirus disease 2019 (COVID-19) pandemic. Most of these patients had medical assistance or Medicare. Fifty-one were white, 46 were black, and 3 were Asian; 50 were men, and their ages ranged from 16 to 83 (mean: 54; median: 56). Using each patient as his/her own control (pre- and post–COVID-19), here I report 6 observations I made while treating these patients.
1. Telehealth worked for most patients. Of the 100 patients, 18 were seen in-person. Of the 18 seen in person, 14 received long-acting IM injections, and 2 patients presented with urgent matters that I felt required in-person evaluations. One patient needed to fill out several forms and provide consents, and 1 patient with chronic illness was treated at the clinic because he mistakenly arrived in person for his appointment.
The remaining 82 patients had telehealth sessions. Only 9 patients said they were able to use video conferencing, so the remaining 73 patients were treated by phone. These patients were mostly poor and/or older and had no access to smartphones or computers. This is especially important because the current emergency telehealth rules allow phone-only sessions, while regular telehealth rules do not. Our clinic strongly advocates for the extension of emergency telehealth rules. I have e-mailed many elected officials about this, but I have received few replies and no substantive responses. Our clinic also needs to help our patients obtain increased audiovisual capabilities.
2. Female patients fared better in their treatment than males.
3. Older patients did better than younger patients. Older patients’ experiences of living through past crises were helpful because they were able to compare how they persevered in the past with the current pandemic.
4. White patients showed more improvements compared with black patients. White patients generally had greater access to resources and support.
5. Patients with psychotic diagnoses/symptoms improved more than those with neurotic/anxiety/depressive diagnoses or symptoms. Most of our patients with psychotic diagnoses were already in a supportive, structured living environment, so the new “COVID-19 world” may be less disruptive for them. Additionally, it was more difficult for our patients to get substances of abuse because they had less mobility and access during the pandemic.
Continue to: Support
6. Support, especially from family but also institutional support, trumped other factors. The more support and structure our patients had, the better they did.
My observations may not be generalizable because I am reporting on a relatively small population size, most patients were older, and most were established patients who were likely more stable. I plan to follow up with these patients to see how the new COVID-19 world continues to affect them, and us.
Daniel D. Storch, MD
Key Point Health Services
Catonsville, Maryland
Disclosure: The author reports no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
Cannabis-derived compounds: What you need to know
Cannabis-derived compounds, such as cannabidiol (CBD), are popping up like weeds (so to speak) in retail and online stores, and are being marketed for a wide range of purported health benefits, most of which are unsubstantiated. Cannabidiol—a chemical component of the Cannabis sativa plant (marijuana)—does not produce intoxication or euphoria (ie, the “high”) that comes from delta-9-tetrahydrocannabinol (THC), which is the psychoactive component of marijuana.1 Cannabidiol has become popular partly due to increased cultural acceptance of marijuana. In a 2019 Pew Research Center survey, 67% of Americans supported marijuana legalization.2
In addition, changing laws have increased the interest in and availability of CBD. The Agricultural Improvement Act of 2018 legalized hemp, which is defined as cannabis and cannabis-derived compounds with significantly low concentrations of THC (<0.3% on a dry weight basis).1,3 However, this act also preserved the FDA’s authority to regulate products containing cannabis and cannabis-derived compounds.1
With the recent emphasis on CBD, it is easy to forget that the FDA has approved a few medications that are derived from or related to cannabis. In this article, I review the current FDA-approved cannabis-related treatments and their indications, and concerns regarding CBD products.
FDA-approved treatments
To date, the FDA has not approved cannabis for the treatment of any medical or psychiatric condition. However, the FDA has approved 1 cannabis-derived medication (CBD) and 2 cannabis-related medications (dronabinol and nabilone) for specific indications (these medications are available by prescription only):
Cannabidiol (brand name: Epidiolex) is approved for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients age ≥2, and for the treatment of seizures associated with tuberous sclerosis complex in patients age ≥1.1,4 There are no other FDA-approved medications that contain CBD.
Dronabinol (brand names: Marinol and Syndros) is an antiemetic agent that contains synthetic THC. It is approved for treating or preventing nausea and vomiting caused by cancer medications and for increasing the appetite of individuals with AIDS.1
Nabilone (brand name: Cesamet) is a synthetic compound that is structurally similar to THC. It is approved for treating or preventing nausea and vomiting caused by cancer medications.1
Continue to: Questionable claims about CBD
Questionable claims about CBD
Some manufacturers market CBD products as having a variety of health benefits for both humans and pets, but most of these claims are unsubstantiated.1 The FDA has issued warning letters to several manufacturers who have marketed CBD products as producing therapeutic effects.5
Under the Federal Food, Drug, and Cosmetic Act, any products intended to have a therapeutic effect are considered drugs, and unapproved drugs cannot be distributed or sold in interstate commerce.1 Cannabidiol products cannot be sold as dietary supplements.1 In addition, food products containing CBD cannot be introduced or delivered for introduction into interstate commerce.1 Many CBD products do not contain the amount of CBD advertised, and some contain contaminants such as pesticides and heavy metals.1 Also, CBD products can affect the therapeutic effectiveness of prescription medications.
Discuss CBD with your patients
Ask your patients if they use CBD and, if so, find out which product(s), the quantity and frequency of use, and any effects they have experienced from using them. Patients can report any adverse effects from CBD products to the FDA’s MedWatch program (www.accessdata.fda.gov/scripts/medwatch/). Tell your patients that there is limited or inconclusive evidence regarding the therapeutic efficacy of over-the-counter CBD products for any medical or psychiatric condition. Encourage your patients to be open with you about using these products, so you can make appropriate treatment decisions.
1. US Food and Drug Administration. FDA regulation of cannabis and cannabis-derived products, including cannabidiol (CBD). https://www.fda.gov/news-events/public-health-focus/fda-regulation-cannabis-and-cannabis-derived-products-questions-and-answers. Updated August 3, 2020. Accessed September 1, 2020.
2. Daniller A. Two-thirds of Americans support marijuana legalization. Pew Research Center. https://www.pewresearch.org/fact-tank/2018/10/08/americans-support-marijuana-legalization/. Updated November 14, 2019. Accessed September 1, 2020.
3. Agricultural Improvement Act of 2018, HR 2—115th Cong, Public L No. 115-334 (2018). https://www.congress.gov/bill/115th-congress/house-bill/2/text?overview=closed. Accessed September 1, 2020.
4. US Food and Drug Administration. FDA approves new indication for drug containing an active ingredient derived from cannabis to treat seizures in rare genetic disease. https://www.fda.gov/news-events/press-announcements/fda-approves-new-indication-drug-containing-active-ingredient-derived-cannabis-treat-seizures-rare. Published July 31, 2020. Accessed September 1, 2020.
5. US Food and Drug Administration. Warning letters and test results for cannabidiol-related products. https://www.fda.gov/news-events/public-health-focus/warning-letters-and-test-results-cannabidiol-related-products. Updated August 20, 2020. Accessed September 1, 2020.
Cannabis-derived compounds, such as cannabidiol (CBD), are popping up like weeds (so to speak) in retail and online stores, and are being marketed for a wide range of purported health benefits, most of which are unsubstantiated. Cannabidiol—a chemical component of the Cannabis sativa plant (marijuana)—does not produce intoxication or euphoria (ie, the “high”) that comes from delta-9-tetrahydrocannabinol (THC), which is the psychoactive component of marijuana.1 Cannabidiol has become popular partly due to increased cultural acceptance of marijuana. In a 2019 Pew Research Center survey, 67% of Americans supported marijuana legalization.2
In addition, changing laws have increased the interest in and availability of CBD. The Agricultural Improvement Act of 2018 legalized hemp, which is defined as cannabis and cannabis-derived compounds with significantly low concentrations of THC (<0.3% on a dry weight basis).1,3 However, this act also preserved the FDA’s authority to regulate products containing cannabis and cannabis-derived compounds.1
With the recent emphasis on CBD, it is easy to forget that the FDA has approved a few medications that are derived from or related to cannabis. In this article, I review the current FDA-approved cannabis-related treatments and their indications, and concerns regarding CBD products.
FDA-approved treatments
To date, the FDA has not approved cannabis for the treatment of any medical or psychiatric condition. However, the FDA has approved 1 cannabis-derived medication (CBD) and 2 cannabis-related medications (dronabinol and nabilone) for specific indications (these medications are available by prescription only):
Cannabidiol (brand name: Epidiolex) is approved for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients age ≥2, and for the treatment of seizures associated with tuberous sclerosis complex in patients age ≥1.1,4 There are no other FDA-approved medications that contain CBD.
Dronabinol (brand names: Marinol and Syndros) is an antiemetic agent that contains synthetic THC. It is approved for treating or preventing nausea and vomiting caused by cancer medications and for increasing the appetite of individuals with AIDS.1
Nabilone (brand name: Cesamet) is a synthetic compound that is structurally similar to THC. It is approved for treating or preventing nausea and vomiting caused by cancer medications.1
Continue to: Questionable claims about CBD
Questionable claims about CBD
Some manufacturers market CBD products as having a variety of health benefits for both humans and pets, but most of these claims are unsubstantiated.1 The FDA has issued warning letters to several manufacturers who have marketed CBD products as producing therapeutic effects.5
Under the Federal Food, Drug, and Cosmetic Act, any products intended to have a therapeutic effect are considered drugs, and unapproved drugs cannot be distributed or sold in interstate commerce.1 Cannabidiol products cannot be sold as dietary supplements.1 In addition, food products containing CBD cannot be introduced or delivered for introduction into interstate commerce.1 Many CBD products do not contain the amount of CBD advertised, and some contain contaminants such as pesticides and heavy metals.1 Also, CBD products can affect the therapeutic effectiveness of prescription medications.
Discuss CBD with your patients
Ask your patients if they use CBD and, if so, find out which product(s), the quantity and frequency of use, and any effects they have experienced from using them. Patients can report any adverse effects from CBD products to the FDA’s MedWatch program (www.accessdata.fda.gov/scripts/medwatch/). Tell your patients that there is limited or inconclusive evidence regarding the therapeutic efficacy of over-the-counter CBD products for any medical or psychiatric condition. Encourage your patients to be open with you about using these products, so you can make appropriate treatment decisions.
Cannabis-derived compounds, such as cannabidiol (CBD), are popping up like weeds (so to speak) in retail and online stores, and are being marketed for a wide range of purported health benefits, most of which are unsubstantiated. Cannabidiol—a chemical component of the Cannabis sativa plant (marijuana)—does not produce intoxication or euphoria (ie, the “high”) that comes from delta-9-tetrahydrocannabinol (THC), which is the psychoactive component of marijuana.1 Cannabidiol has become popular partly due to increased cultural acceptance of marijuana. In a 2019 Pew Research Center survey, 67% of Americans supported marijuana legalization.2
In addition, changing laws have increased the interest in and availability of CBD. The Agricultural Improvement Act of 2018 legalized hemp, which is defined as cannabis and cannabis-derived compounds with significantly low concentrations of THC (<0.3% on a dry weight basis).1,3 However, this act also preserved the FDA’s authority to regulate products containing cannabis and cannabis-derived compounds.1
With the recent emphasis on CBD, it is easy to forget that the FDA has approved a few medications that are derived from or related to cannabis. In this article, I review the current FDA-approved cannabis-related treatments and their indications, and concerns regarding CBD products.
FDA-approved treatments
To date, the FDA has not approved cannabis for the treatment of any medical or psychiatric condition. However, the FDA has approved 1 cannabis-derived medication (CBD) and 2 cannabis-related medications (dronabinol and nabilone) for specific indications (these medications are available by prescription only):
Cannabidiol (brand name: Epidiolex) is approved for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients age ≥2, and for the treatment of seizures associated with tuberous sclerosis complex in patients age ≥1.1,4 There are no other FDA-approved medications that contain CBD.
Dronabinol (brand names: Marinol and Syndros) is an antiemetic agent that contains synthetic THC. It is approved for treating or preventing nausea and vomiting caused by cancer medications and for increasing the appetite of individuals with AIDS.1
Nabilone (brand name: Cesamet) is a synthetic compound that is structurally similar to THC. It is approved for treating or preventing nausea and vomiting caused by cancer medications.1
Continue to: Questionable claims about CBD
Questionable claims about CBD
Some manufacturers market CBD products as having a variety of health benefits for both humans and pets, but most of these claims are unsubstantiated.1 The FDA has issued warning letters to several manufacturers who have marketed CBD products as producing therapeutic effects.5
Under the Federal Food, Drug, and Cosmetic Act, any products intended to have a therapeutic effect are considered drugs, and unapproved drugs cannot be distributed or sold in interstate commerce.1 Cannabidiol products cannot be sold as dietary supplements.1 In addition, food products containing CBD cannot be introduced or delivered for introduction into interstate commerce.1 Many CBD products do not contain the amount of CBD advertised, and some contain contaminants such as pesticides and heavy metals.1 Also, CBD products can affect the therapeutic effectiveness of prescription medications.
Discuss CBD with your patients
Ask your patients if they use CBD and, if so, find out which product(s), the quantity and frequency of use, and any effects they have experienced from using them. Patients can report any adverse effects from CBD products to the FDA’s MedWatch program (www.accessdata.fda.gov/scripts/medwatch/). Tell your patients that there is limited or inconclusive evidence regarding the therapeutic efficacy of over-the-counter CBD products for any medical or psychiatric condition. Encourage your patients to be open with you about using these products, so you can make appropriate treatment decisions.
1. US Food and Drug Administration. FDA regulation of cannabis and cannabis-derived products, including cannabidiol (CBD). https://www.fda.gov/news-events/public-health-focus/fda-regulation-cannabis-and-cannabis-derived-products-questions-and-answers. Updated August 3, 2020. Accessed September 1, 2020.
2. Daniller A. Two-thirds of Americans support marijuana legalization. Pew Research Center. https://www.pewresearch.org/fact-tank/2018/10/08/americans-support-marijuana-legalization/. Updated November 14, 2019. Accessed September 1, 2020.
3. Agricultural Improvement Act of 2018, HR 2—115th Cong, Public L No. 115-334 (2018). https://www.congress.gov/bill/115th-congress/house-bill/2/text?overview=closed. Accessed September 1, 2020.
4. US Food and Drug Administration. FDA approves new indication for drug containing an active ingredient derived from cannabis to treat seizures in rare genetic disease. https://www.fda.gov/news-events/press-announcements/fda-approves-new-indication-drug-containing-active-ingredient-derived-cannabis-treat-seizures-rare. Published July 31, 2020. Accessed September 1, 2020.
5. US Food and Drug Administration. Warning letters and test results for cannabidiol-related products. https://www.fda.gov/news-events/public-health-focus/warning-letters-and-test-results-cannabidiol-related-products. Updated August 20, 2020. Accessed September 1, 2020.
1. US Food and Drug Administration. FDA regulation of cannabis and cannabis-derived products, including cannabidiol (CBD). https://www.fda.gov/news-events/public-health-focus/fda-regulation-cannabis-and-cannabis-derived-products-questions-and-answers. Updated August 3, 2020. Accessed September 1, 2020.
2. Daniller A. Two-thirds of Americans support marijuana legalization. Pew Research Center. https://www.pewresearch.org/fact-tank/2018/10/08/americans-support-marijuana-legalization/. Updated November 14, 2019. Accessed September 1, 2020.
3. Agricultural Improvement Act of 2018, HR 2—115th Cong, Public L No. 115-334 (2018). https://www.congress.gov/bill/115th-congress/house-bill/2/text?overview=closed. Accessed September 1, 2020.
4. US Food and Drug Administration. FDA approves new indication for drug containing an active ingredient derived from cannabis to treat seizures in rare genetic disease. https://www.fda.gov/news-events/press-announcements/fda-approves-new-indication-drug-containing-active-ingredient-derived-cannabis-treat-seizures-rare. Published July 31, 2020. Accessed September 1, 2020.
5. US Food and Drug Administration. Warning letters and test results for cannabidiol-related products. https://www.fda.gov/news-events/public-health-focus/warning-letters-and-test-results-cannabidiol-related-products. Updated August 20, 2020. Accessed September 1, 2020.

COVID-19 shutdown fuels sharp rise in alcohol use
Americans sharply increased their alcohol intake last spring as many areas of the country shutdown because of the coronavirus pandemic, results of a national survey show.

The overall frequency of alcohol consumption increased by 14% among adults over age 30 in the spring of 2020 versus the same period a year earlier.
The increase was most evident in adults aged 30-59, women, and non-Hispanic Whites.
“Alcohol consumption can have significant negative health consequences, so this information suggests another way that the pandemic may be affecting the physical and mental health of Americans,” Michael Pollard, PhD, lead investigator and sociologist at Rand, said in a news release.
The results were published online as a research letter Sept. 29 in JAMA Network Open.
Booming business
After some U.S. states issued stay-at-home orders to fight the spread of SARS-CoV-2, one study noted a 54% increase in national sales of alcohol for the week ending March 21, 2020, relative to 1 year earlier and a 262% increase in online alcohol sales.
“We’ve had anecdotal information about people buying and consuming more alcohol,” Dr. Pollard said, but the Rand study provides the first survey-based information that shows how much alcohol consumption has increased during the pandemic.
The findings are based on 1,540 adults (mean age, 56.6 years; 57% women) from the Rand American Life Panel, a nationally representative sample of Americans who were surveyed about their alcohol consumption before the pandemic in the spring of 2019, and again in the spring of 2020 during the early months of the shutdown.
Overall, in spring 2020, respondents reported drinking alcohol 6.22 days in the prior month on average, a 14% increase from the monthly average of 5.48 days reported in spring 2019.
Among adults aged 30 to 59 years, the frequency of alcohol consumption increased from 4.98 days prepandemic to 5.91 days during the pandemic, a 19% increase.
Women reported drinking an average of 5.36 days in the prior month in the early pandemic period, a 17% increase from 4.58 monthly drinking days before the pandemic.
In addition, compared with spring 2019, in spring 2020 women reported a 41% increase in heavy drinking days – four or more drinks in a couple of hours.
Independent of consumption level, nearly 1 in 10 women had an increase in alcohol-related problems in the pandemic period, based on responses to the Short Inventory of Problems scale.
For non-Hispanic White individuals, the overall frequency of alcohol intake rose 10% during the early pandemic period.
“The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19,” write Dr. Pollard and colleagues.
The authors note , and whether psychological and physical well-being are subsequently affected.
The study was supported by the National Institute of Alcohol Abuse and Alcoholism. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Americans sharply increased their alcohol intake last spring as many areas of the country shutdown because of the coronavirus pandemic, results of a national survey show.
The overall frequency of alcohol consumption increased by 14% among adults over age 30 in the spring of 2020 versus the same period a year earlier.
The increase was most evident in adults aged 30-59, women, and non-Hispanic Whites.
“Alcohol consumption can have significant negative health consequences, so this information suggests another way that the pandemic may be affecting the physical and mental health of Americans,” Michael Pollard, PhD, lead investigator and sociologist at Rand, said in a news release.
The results were published online as a research letter Sept. 29 in JAMA Network Open.
Booming business
After some U.S. states issued stay-at-home orders to fight the spread of SARS-CoV-2, one study noted a 54% increase in national sales of alcohol for the week ending March 21, 2020, relative to 1 year earlier and a 262% increase in online alcohol sales.
“We’ve had anecdotal information about people buying and consuming more alcohol,” Dr. Pollard said, but the Rand study provides the first survey-based information that shows how much alcohol consumption has increased during the pandemic.
The findings are based on 1,540 adults (mean age, 56.6 years; 57% women) from the Rand American Life Panel, a nationally representative sample of Americans who were surveyed about their alcohol consumption before the pandemic in the spring of 2019, and again in the spring of 2020 during the early months of the shutdown.
Overall, in spring 2020, respondents reported drinking alcohol 6.22 days in the prior month on average, a 14% increase from the monthly average of 5.48 days reported in spring 2019.
Among adults aged 30 to 59 years, the frequency of alcohol consumption increased from 4.98 days prepandemic to 5.91 days during the pandemic, a 19% increase.
Women reported drinking an average of 5.36 days in the prior month in the early pandemic period, a 17% increase from 4.58 monthly drinking days before the pandemic.
In addition, compared with spring 2019, in spring 2020 women reported a 41% increase in heavy drinking days – four or more drinks in a couple of hours.
Independent of consumption level, nearly 1 in 10 women had an increase in alcohol-related problems in the pandemic period, based on responses to the Short Inventory of Problems scale.
For non-Hispanic White individuals, the overall frequency of alcohol intake rose 10% during the early pandemic period.
“The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19,” write Dr. Pollard and colleagues.
The authors note , and whether psychological and physical well-being are subsequently affected.
The study was supported by the National Institute of Alcohol Abuse and Alcoholism. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Americans sharply increased their alcohol intake last spring as many areas of the country shutdown because of the coronavirus pandemic, results of a national survey show.
The overall frequency of alcohol consumption increased by 14% among adults over age 30 in the spring of 2020 versus the same period a year earlier.
The increase was most evident in adults aged 30-59, women, and non-Hispanic Whites.
“Alcohol consumption can have significant negative health consequences, so this information suggests another way that the pandemic may be affecting the physical and mental health of Americans,” Michael Pollard, PhD, lead investigator and sociologist at Rand, said in a news release.
The results were published online as a research letter Sept. 29 in JAMA Network Open.
Booming business
After some U.S. states issued stay-at-home orders to fight the spread of SARS-CoV-2, one study noted a 54% increase in national sales of alcohol for the week ending March 21, 2020, relative to 1 year earlier and a 262% increase in online alcohol sales.
“We’ve had anecdotal information about people buying and consuming more alcohol,” Dr. Pollard said, but the Rand study provides the first survey-based information that shows how much alcohol consumption has increased during the pandemic.
The findings are based on 1,540 adults (mean age, 56.6 years; 57% women) from the Rand American Life Panel, a nationally representative sample of Americans who were surveyed about their alcohol consumption before the pandemic in the spring of 2019, and again in the spring of 2020 during the early months of the shutdown.
Overall, in spring 2020, respondents reported drinking alcohol 6.22 days in the prior month on average, a 14% increase from the monthly average of 5.48 days reported in spring 2019.
Among adults aged 30 to 59 years, the frequency of alcohol consumption increased from 4.98 days prepandemic to 5.91 days during the pandemic, a 19% increase.
Women reported drinking an average of 5.36 days in the prior month in the early pandemic period, a 17% increase from 4.58 monthly drinking days before the pandemic.
In addition, compared with spring 2019, in spring 2020 women reported a 41% increase in heavy drinking days – four or more drinks in a couple of hours.
Independent of consumption level, nearly 1 in 10 women had an increase in alcohol-related problems in the pandemic period, based on responses to the Short Inventory of Problems scale.
For non-Hispanic White individuals, the overall frequency of alcohol intake rose 10% during the early pandemic period.
“The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19,” write Dr. Pollard and colleagues.
The authors note , and whether psychological and physical well-being are subsequently affected.
The study was supported by the National Institute of Alcohol Abuse and Alcoholism. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
What to do when a patient is not ready to stop smoking
Recommendations from the American Thoracic Society
Below is a case involving a patient who is not yet ready to quit smoking. We later provide treatment recommendations for this patient based on a new guideline from the American Thoracic Society.
Case

A 58-year-old female comes into the office for a physical exam. She has been smoking two packs a day since she was 23 years of age. You have tried at previous visits to get her to quit, but she hasn’t been interested. The patient says she has a lot of stress, and that it is still not the right time for her to stop smoking. You tell her she needs to quit and, though the patient understands that quitting would be beneficial for her health, she just isn’t ready to try to kick the habit. How do you proceed?
The Guideline in context
Even though this patient stated that she is not ready to stop smoking, she is still a candidate for pharmacological treatment for her tobacco dependence and can be offered varenicline, according to the ATS guideline.1
In a previously published column, we have discussed the ATS’ recommended approaches for treating patients who are ready to stop smoking cigarettes. The reality is that many patients, if not most, are not ready to quit when we speak to them during any given office visit. The ATS guideline addresses this critical issue by recommending treatment with varenicline in patients who are not ready to stop smoking. It also states that this is a better strategy than waiting to start treatment until patients say they are ready for it.
This recommendation – to prescribe varenicline to smokers even when they are not ready to quit smoking – is based on solid clinical trial evidence. Research has shown that behavior change is dynamic and that the decision to stop smoking is not always a planned one.1 Patients often make quit attempts between office visits, and are often successful in those attempts. Because the decision to try to stop smoking is influenced by the satisfaction and physical addiction that comes from smoking, a medication such as varenicline that is a partial agonist/antagonist at the alpha4-beta2 nicotinic receptor might increase the likelihood that a patient would decide to try to stop smoking. This is because taking this type of a drug would lead the patient to no longer experience the reinforcing effects of nicotine.2 This hypothesis was examined in five randomized trials.1
In these studies, regular smokers who were not ready to make a quit attempt were randomized to varenicline versus placebo. Twice as many individuals who took varenicline stopped smoking 6 months after starting treatment.1
Suggested treatment
This patient should be offered varenicline. This individual meets the criteria for this treatment according to the ATS guideline in that the patient is a regular smoker who doesn’t think she is ready to stop smoking but understands she needs to stop and is open to taking medication to assist her with quitting.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Sprogell is a third-year resident in the family medicine residency program at Abington Jefferson Health. They have no conflicts related to the content of this piece. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Leone F T et al. Initiating pharmacologic treatment in tobacco-dependent adults: An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Jul 15;202(2):e5–e31.
2. Ebbert JO et al. Varenicline for smoking cessation: Efficacy, safety, and treatment recommendations. Patient Prefer Adherence. 2010;4:355-62.
Recommendations from the American Thoracic Society
Recommendations from the American Thoracic Society
Below is a case involving a patient who is not yet ready to quit smoking. We later provide treatment recommendations for this patient based on a new guideline from the American Thoracic Society.
Case
A 58-year-old female comes into the office for a physical exam. She has been smoking two packs a day since she was 23 years of age. You have tried at previous visits to get her to quit, but she hasn’t been interested. The patient says she has a lot of stress, and that it is still not the right time for her to stop smoking. You tell her she needs to quit and, though the patient understands that quitting would be beneficial for her health, she just isn’t ready to try to kick the habit. How do you proceed?
The Guideline in context
Even though this patient stated that she is not ready to stop smoking, she is still a candidate for pharmacological treatment for her tobacco dependence and can be offered varenicline, according to the ATS guideline.1
In a previously published column, we have discussed the ATS’ recommended approaches for treating patients who are ready to stop smoking cigarettes. The reality is that many patients, if not most, are not ready to quit when we speak to them during any given office visit. The ATS guideline addresses this critical issue by recommending treatment with varenicline in patients who are not ready to stop smoking. It also states that this is a better strategy than waiting to start treatment until patients say they are ready for it.
This recommendation – to prescribe varenicline to smokers even when they are not ready to quit smoking – is based on solid clinical trial evidence. Research has shown that behavior change is dynamic and that the decision to stop smoking is not always a planned one.1 Patients often make quit attempts between office visits, and are often successful in those attempts. Because the decision to try to stop smoking is influenced by the satisfaction and physical addiction that comes from smoking, a medication such as varenicline that is a partial agonist/antagonist at the alpha4-beta2 nicotinic receptor might increase the likelihood that a patient would decide to try to stop smoking. This is because taking this type of a drug would lead the patient to no longer experience the reinforcing effects of nicotine.2 This hypothesis was examined in five randomized trials.1
In these studies, regular smokers who were not ready to make a quit attempt were randomized to varenicline versus placebo. Twice as many individuals who took varenicline stopped smoking 6 months after starting treatment.1
Suggested treatment
This patient should be offered varenicline. This individual meets the criteria for this treatment according to the ATS guideline in that the patient is a regular smoker who doesn’t think she is ready to stop smoking but understands she needs to stop and is open to taking medication to assist her with quitting.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Sprogell is a third-year resident in the family medicine residency program at Abington Jefferson Health. They have no conflicts related to the content of this piece. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Leone F T et al. Initiating pharmacologic treatment in tobacco-dependent adults: An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Jul 15;202(2):e5–e31.
2. Ebbert JO et al. Varenicline for smoking cessation: Efficacy, safety, and treatment recommendations. Patient Prefer Adherence. 2010;4:355-62.
Below is a case involving a patient who is not yet ready to quit smoking. We later provide treatment recommendations for this patient based on a new guideline from the American Thoracic Society.
Case
A 58-year-old female comes into the office for a physical exam. She has been smoking two packs a day since she was 23 years of age. You have tried at previous visits to get her to quit, but she hasn’t been interested. The patient says she has a lot of stress, and that it is still not the right time for her to stop smoking. You tell her she needs to quit and, though the patient understands that quitting would be beneficial for her health, she just isn’t ready to try to kick the habit. How do you proceed?
The Guideline in context
Even though this patient stated that she is not ready to stop smoking, she is still a candidate for pharmacological treatment for her tobacco dependence and can be offered varenicline, according to the ATS guideline.1
In a previously published column, we have discussed the ATS’ recommended approaches for treating patients who are ready to stop smoking cigarettes. The reality is that many patients, if not most, are not ready to quit when we speak to them during any given office visit. The ATS guideline addresses this critical issue by recommending treatment with varenicline in patients who are not ready to stop smoking. It also states that this is a better strategy than waiting to start treatment until patients say they are ready for it.
This recommendation – to prescribe varenicline to smokers even when they are not ready to quit smoking – is based on solid clinical trial evidence. Research has shown that behavior change is dynamic and that the decision to stop smoking is not always a planned one.1 Patients often make quit attempts between office visits, and are often successful in those attempts. Because the decision to try to stop smoking is influenced by the satisfaction and physical addiction that comes from smoking, a medication such as varenicline that is a partial agonist/antagonist at the alpha4-beta2 nicotinic receptor might increase the likelihood that a patient would decide to try to stop smoking. This is because taking this type of a drug would lead the patient to no longer experience the reinforcing effects of nicotine.2 This hypothesis was examined in five randomized trials.1
In these studies, regular smokers who were not ready to make a quit attempt were randomized to varenicline versus placebo. Twice as many individuals who took varenicline stopped smoking 6 months after starting treatment.1
Suggested treatment
This patient should be offered varenicline. This individual meets the criteria for this treatment according to the ATS guideline in that the patient is a regular smoker who doesn’t think she is ready to stop smoking but understands she needs to stop and is open to taking medication to assist her with quitting.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Sprogell is a third-year resident in the family medicine residency program at Abington Jefferson Health. They have no conflicts related to the content of this piece. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Leone F T et al. Initiating pharmacologic treatment in tobacco-dependent adults: An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Jul 15;202(2):e5–e31.
2. Ebbert JO et al. Varenicline for smoking cessation: Efficacy, safety, and treatment recommendations. Patient Prefer Adherence. 2010;4:355-62.
Is psychiatry coddling the American mind?
A trainee recently observed that psychiatrists frequently seem motivated to protect patients from emotional and internal disruption. He suggested that we often did so by validating their maladaptive perspectives regarding their impaired relationships to society and close attachments. These maneuvers were justified by referring to the need to establish a therapeutic alliance and reduce patients’ suffering.

As an example, he mentioned a patient with alcohol use disorder. The patient came in with complaints that he could not stay sober with his current level of depression. The patient also complained of a family member who was setting limits. To the trainee’s surprise, the patient was not challenged on his perceived victimhood and his fantasy that a sober life should mean a life without negative effect. Instead, the patient was validated in his anger toward the family member. In addition, his medications were adjusted, seemingly confirming to the patient that one could only ask for sobriety once life is empty of pain.
The observation of the trainee reminded us of the three great “untruths” mentioned by Greg Lukianoff and Jonathan Haidt, PhD, in their famous book, “The Coddling of the American Mind.”1 In the book they warn against the idea of fragility – what doesn’t kill you makes you weaker; emotional reasoning – always trust your feelings; and us-versus-them thinking – life is a battle between good people and evil people. The authors compare these three great untruths with the cognitive distortions of cognitive-behavioral therapy.
We ponder the trainee’s observation that psychiatrists appear to encourage the untruths rather than challenge them. Part of psychiatric and all medical training involves learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition generates a desire to protect patients from a moralistic shaming position. However, we wonder if, at times, psychiatry takes this approach too far.
Reconceptualizing shame
Shame can be a toxic presence in the overwhelmed superego of a patient, but it can serve an important role in psychic development and should not be avoided out of hand. We suggest that it can be appropriate for a patient with an alcohol use disorder to feel some shame for the harm caused by their drinking, and we question the limit of psychiatry’s current pursuit of incessant validation. As an extreme example, would modern psychiatry discourage a patient who killed someone while driving in an intoxicated state from feeling remorse and shame?
Modern psychiatry appears to have other examples of the three great untruths on display. In our work, we are often faced with patients who are prematurely placed on disability, an example of fragility. Instead of encouraging patients to return to the workforce, they are “protected” from the emotional difficulty of work. In many patients this results in a decline in functioning and worsening of psychiatric symptoms. We are also confronted with patients who define themselves by how they feel, an example of emotional reasoning. Instead of using our clinical judgments to define and assess symptoms, patients are left to decide for themselves through self-rated scales with questionable validity.2 This can result in patients having their emotional experiences not only validated when inappropriate but can also give emotional reasoning a false sense of medical legitimacy.
Finally, we commonly see patients who endlessly blame family members and others for any life difficulties, a form of us-versus-them thinking. Instead of acknowledging and then integrating life challenges to achieve recovery, patients are affirmed despite clinicians having little evidence on the veracity of the patients’ perspective. As a consequence, patients can be further isolated from their greatest source of support.

In some ways, a mindlessly validating approach in psychiatry is unexpected since the practice of psychiatry would seem to promote the development of strong attachments and resilience. After all, connections to family, employment, social institutions, and even religious worship are associated with vastly better outcomes. Those who have become alienated to these pillars of social cohesion fare much worse. One may deplore the static and at times oppressive nature of these institutions but the empirical experience of practicing psychiatry leads one to a healthy respect for the stabilizing influence they accord for individuals struggling with life’s vicissitudes, unpredictability, and loneliness. Overcoming the fear of responsibility, living up to the demands and expectations of society, and having the strength to overcome difficult emotions should be the standard goals of psychiatric treatment.
From the knowledge gained from working with patients struggling from psychic pain, we wonder how to encourage patients to pursue those adaptive approaches to life. We argue that a stoic emphasis on learning to manage one’s affective and mental response to the inevitable changes of life is key to achieving wisdom and stability in our humble lives. This perspective is a common denominator of multiple different psychotherapies. The goal is to provide patients with the ability to be in a place where they are engaged with the world in a meaningful way that is not overwhelmed by distorted, self-absorbed psychic anguish. This perspective discourages externalization as a relatively low-yield way to understand and overcome one’s problems. One identifies childhood experiences with one’s mother as a source of adult distress not for the purpose of blaming her, but for the purpose of recognizing one’s own childish motivations for making maladaptive decisions as an adult.
For many patients, the goal should be to emphasize an internal locus of control and responsibility. We should also avoid constantly relying on society and government’s role in helping the individual achieve a satisfactory life. We wonder if this endless pursuit of nonjudgment and validation corrupts the doctor-patient interaction. In other words, and individual responsibility for their own psychic development. Psychotherapy that ends with the patient being able to identify all the traumas that led to their sorrow has simply left the patient in the role of helpless and sorrowful victim. Instead, we should allow patients to proceed to the next step, which is empowerment and transformation. From this angle, the field of psychiatry should be cautious of encouraging movements that promote victimhood and grievance as a meaningful psychic position to take in society.
Mr. Lukianoff and Dr. Haidt use cognitive therapy as an analogy throughout their books for how to confront the great untruths. They perceive those modern forms of thinking as cognitive distortions, which can be remedied using the techniques of cognitive restructuring found in cognitive-behavioral therapy. They encourage us to recognize those maladaptive thoughts, and create more accurate and adaptive ways of viewing the world – a view that would be able to grow from challenges not just survive them; a view referred to as antifragile.3 We believe that those techniques and others would certainly be of assistance in our current times. However, the first step is to recognize our problem – a problem that is not rooted in the DSM, research, or biology but in an exaggerated intention to be patient centered. We should, however, remember that, when a patient has negative schemas, being too patient centered can be encouraging to maladaptive behaviors.
In conclusion, we wonder what modern psychiatry could look like if it made a concerted effort at also treating mental illness by reinforcing the importance of individual agency and responsibility. Modern psychiatry has been so focused on describing biological symptoms needing biological treatments that we sometimes forget that having no symptom (being asymptomatic) is not the only goal. Having a fulfilling and meaningful life, which is resilient to future symptoms is just as important to patients. We seem to have entrenched ourselves so deeply in an overly basic approach of problem-solution and diagnosis-treatment paradigm. However, we don’t need to renege on modern advances to promote the patient’s strength, adaptability, and antifragility. An emphasis on patient growth can complement the medical model. We wonder what effect such an approach would have if the trainee’s patient with alcohol use disorder was instead told: “Given the suffering you have and have caused because of your alcohol use disorder, how do you plan to make changes in your life to help the treatment plan we create together?”
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
References
1. Lukianoff G, Haidt J. The Coddling of the American Mind: How Good Intentions and Bad Ideas are Setting Up a Generation for Failure. New York: Penguin Books, 2019.
2. Levis B et al. J Clin Epidemiol. 2020 Jun;122:115-128.e1.,
3. Taleb NN. Antifragile: Things That Gain from Disorder. Vol. 3. New York: Random House, 2012.
A trainee recently observed that psychiatrists frequently seem motivated to protect patients from emotional and internal disruption. He suggested that we often did so by validating their maladaptive perspectives regarding their impaired relationships to society and close attachments. These maneuvers were justified by referring to the need to establish a therapeutic alliance and reduce patients’ suffering.
As an example, he mentioned a patient with alcohol use disorder. The patient came in with complaints that he could not stay sober with his current level of depression. The patient also complained of a family member who was setting limits. To the trainee’s surprise, the patient was not challenged on his perceived victimhood and his fantasy that a sober life should mean a life without negative effect. Instead, the patient was validated in his anger toward the family member. In addition, his medications were adjusted, seemingly confirming to the patient that one could only ask for sobriety once life is empty of pain.
The observation of the trainee reminded us of the three great “untruths” mentioned by Greg Lukianoff and Jonathan Haidt, PhD, in their famous book, “The Coddling of the American Mind.”1 In the book they warn against the idea of fragility – what doesn’t kill you makes you weaker; emotional reasoning – always trust your feelings; and us-versus-them thinking – life is a battle between good people and evil people. The authors compare these three great untruths with the cognitive distortions of cognitive-behavioral therapy.
We ponder the trainee’s observation that psychiatrists appear to encourage the untruths rather than challenge them. Part of psychiatric and all medical training involves learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition generates a desire to protect patients from a moralistic shaming position. However, we wonder if, at times, psychiatry takes this approach too far.
Reconceptualizing shame
Shame can be a toxic presence in the overwhelmed superego of a patient, but it can serve an important role in psychic development and should not be avoided out of hand. We suggest that it can be appropriate for a patient with an alcohol use disorder to feel some shame for the harm caused by their drinking, and we question the limit of psychiatry’s current pursuit of incessant validation. As an extreme example, would modern psychiatry discourage a patient who killed someone while driving in an intoxicated state from feeling remorse and shame?
Modern psychiatry appears to have other examples of the three great untruths on display. In our work, we are often faced with patients who are prematurely placed on disability, an example of fragility. Instead of encouraging patients to return to the workforce, they are “protected” from the emotional difficulty of work. In many patients this results in a decline in functioning and worsening of psychiatric symptoms. We are also confronted with patients who define themselves by how they feel, an example of emotional reasoning. Instead of using our clinical judgments to define and assess symptoms, patients are left to decide for themselves through self-rated scales with questionable validity.2 This can result in patients having their emotional experiences not only validated when inappropriate but can also give emotional reasoning a false sense of medical legitimacy.
Finally, we commonly see patients who endlessly blame family members and others for any life difficulties, a form of us-versus-them thinking. Instead of acknowledging and then integrating life challenges to achieve recovery, patients are affirmed despite clinicians having little evidence on the veracity of the patients’ perspective. As a consequence, patients can be further isolated from their greatest source of support.
In some ways, a mindlessly validating approach in psychiatry is unexpected since the practice of psychiatry would seem to promote the development of strong attachments and resilience. After all, connections to family, employment, social institutions, and even religious worship are associated with vastly better outcomes. Those who have become alienated to these pillars of social cohesion fare much worse. One may deplore the static and at times oppressive nature of these institutions but the empirical experience of practicing psychiatry leads one to a healthy respect for the stabilizing influence they accord for individuals struggling with life’s vicissitudes, unpredictability, and loneliness. Overcoming the fear of responsibility, living up to the demands and expectations of society, and having the strength to overcome difficult emotions should be the standard goals of psychiatric treatment.
From the knowledge gained from working with patients struggling from psychic pain, we wonder how to encourage patients to pursue those adaptive approaches to life. We argue that a stoic emphasis on learning to manage one’s affective and mental response to the inevitable changes of life is key to achieving wisdom and stability in our humble lives. This perspective is a common denominator of multiple different psychotherapies. The goal is to provide patients with the ability to be in a place where they are engaged with the world in a meaningful way that is not overwhelmed by distorted, self-absorbed psychic anguish. This perspective discourages externalization as a relatively low-yield way to understand and overcome one’s problems. One identifies childhood experiences with one’s mother as a source of adult distress not for the purpose of blaming her, but for the purpose of recognizing one’s own childish motivations for making maladaptive decisions as an adult.
For many patients, the goal should be to emphasize an internal locus of control and responsibility. We should also avoid constantly relying on society and government’s role in helping the individual achieve a satisfactory life. We wonder if this endless pursuit of nonjudgment and validation corrupts the doctor-patient interaction. In other words, and individual responsibility for their own psychic development. Psychotherapy that ends with the patient being able to identify all the traumas that led to their sorrow has simply left the patient in the role of helpless and sorrowful victim. Instead, we should allow patients to proceed to the next step, which is empowerment and transformation. From this angle, the field of psychiatry should be cautious of encouraging movements that promote victimhood and grievance as a meaningful psychic position to take in society.
Mr. Lukianoff and Dr. Haidt use cognitive therapy as an analogy throughout their books for how to confront the great untruths. They perceive those modern forms of thinking as cognitive distortions, which can be remedied using the techniques of cognitive restructuring found in cognitive-behavioral therapy. They encourage us to recognize those maladaptive thoughts, and create more accurate and adaptive ways of viewing the world – a view that would be able to grow from challenges not just survive them; a view referred to as antifragile.3 We believe that those techniques and others would certainly be of assistance in our current times. However, the first step is to recognize our problem – a problem that is not rooted in the DSM, research, or biology but in an exaggerated intention to be patient centered. We should, however, remember that, when a patient has negative schemas, being too patient centered can be encouraging to maladaptive behaviors.
In conclusion, we wonder what modern psychiatry could look like if it made a concerted effort at also treating mental illness by reinforcing the importance of individual agency and responsibility. Modern psychiatry has been so focused on describing biological symptoms needing biological treatments that we sometimes forget that having no symptom (being asymptomatic) is not the only goal. Having a fulfilling and meaningful life, which is resilient to future symptoms is just as important to patients. We seem to have entrenched ourselves so deeply in an overly basic approach of problem-solution and diagnosis-treatment paradigm. However, we don’t need to renege on modern advances to promote the patient’s strength, adaptability, and antifragility. An emphasis on patient growth can complement the medical model. We wonder what effect such an approach would have if the trainee’s patient with alcohol use disorder was instead told: “Given the suffering you have and have caused because of your alcohol use disorder, how do you plan to make changes in your life to help the treatment plan we create together?”
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
References
1. Lukianoff G, Haidt J. The Coddling of the American Mind: How Good Intentions and Bad Ideas are Setting Up a Generation for Failure. New York: Penguin Books, 2019.
2. Levis B et al. J Clin Epidemiol. 2020 Jun;122:115-128.e1.,
3. Taleb NN. Antifragile: Things That Gain from Disorder. Vol. 3. New York: Random House, 2012.
A trainee recently observed that psychiatrists frequently seem motivated to protect patients from emotional and internal disruption. He suggested that we often did so by validating their maladaptive perspectives regarding their impaired relationships to society and close attachments. These maneuvers were justified by referring to the need to establish a therapeutic alliance and reduce patients’ suffering.
As an example, he mentioned a patient with alcohol use disorder. The patient came in with complaints that he could not stay sober with his current level of depression. The patient also complained of a family member who was setting limits. To the trainee’s surprise, the patient was not challenged on his perceived victimhood and his fantasy that a sober life should mean a life without negative effect. Instead, the patient was validated in his anger toward the family member. In addition, his medications were adjusted, seemingly confirming to the patient that one could only ask for sobriety once life is empty of pain.
The observation of the trainee reminded us of the three great “untruths” mentioned by Greg Lukianoff and Jonathan Haidt, PhD, in their famous book, “The Coddling of the American Mind.”1 In the book they warn against the idea of fragility – what doesn’t kill you makes you weaker; emotional reasoning – always trust your feelings; and us-versus-them thinking – life is a battle between good people and evil people. The authors compare these three great untruths with the cognitive distortions of cognitive-behavioral therapy.
We ponder the trainee’s observation that psychiatrists appear to encourage the untruths rather than challenge them. Part of psychiatric and all medical training involves learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition generates a desire to protect patients from a moralistic shaming position. However, we wonder if, at times, psychiatry takes this approach too far.
Reconceptualizing shame
Shame can be a toxic presence in the overwhelmed superego of a patient, but it can serve an important role in psychic development and should not be avoided out of hand. We suggest that it can be appropriate for a patient with an alcohol use disorder to feel some shame for the harm caused by their drinking, and we question the limit of psychiatry’s current pursuit of incessant validation. As an extreme example, would modern psychiatry discourage a patient who killed someone while driving in an intoxicated state from feeling remorse and shame?
Modern psychiatry appears to have other examples of the three great untruths on display. In our work, we are often faced with patients who are prematurely placed on disability, an example of fragility. Instead of encouraging patients to return to the workforce, they are “protected” from the emotional difficulty of work. In many patients this results in a decline in functioning and worsening of psychiatric symptoms. We are also confronted with patients who define themselves by how they feel, an example of emotional reasoning. Instead of using our clinical judgments to define and assess symptoms, patients are left to decide for themselves through self-rated scales with questionable validity.2 This can result in patients having their emotional experiences not only validated when inappropriate but can also give emotional reasoning a false sense of medical legitimacy.
Finally, we commonly see patients who endlessly blame family members and others for any life difficulties, a form of us-versus-them thinking. Instead of acknowledging and then integrating life challenges to achieve recovery, patients are affirmed despite clinicians having little evidence on the veracity of the patients’ perspective. As a consequence, patients can be further isolated from their greatest source of support.
In some ways, a mindlessly validating approach in psychiatry is unexpected since the practice of psychiatry would seem to promote the development of strong attachments and resilience. After all, connections to family, employment, social institutions, and even religious worship are associated with vastly better outcomes. Those who have become alienated to these pillars of social cohesion fare much worse. One may deplore the static and at times oppressive nature of these institutions but the empirical experience of practicing psychiatry leads one to a healthy respect for the stabilizing influence they accord for individuals struggling with life’s vicissitudes, unpredictability, and loneliness. Overcoming the fear of responsibility, living up to the demands and expectations of society, and having the strength to overcome difficult emotions should be the standard goals of psychiatric treatment.
From the knowledge gained from working with patients struggling from psychic pain, we wonder how to encourage patients to pursue those adaptive approaches to life. We argue that a stoic emphasis on learning to manage one’s affective and mental response to the inevitable changes of life is key to achieving wisdom and stability in our humble lives. This perspective is a common denominator of multiple different psychotherapies. The goal is to provide patients with the ability to be in a place where they are engaged with the world in a meaningful way that is not overwhelmed by distorted, self-absorbed psychic anguish. This perspective discourages externalization as a relatively low-yield way to understand and overcome one’s problems. One identifies childhood experiences with one’s mother as a source of adult distress not for the purpose of blaming her, but for the purpose of recognizing one’s own childish motivations for making maladaptive decisions as an adult.
For many patients, the goal should be to emphasize an internal locus of control and responsibility. We should also avoid constantly relying on society and government’s role in helping the individual achieve a satisfactory life. We wonder if this endless pursuit of nonjudgment and validation corrupts the doctor-patient interaction. In other words, and individual responsibility for their own psychic development. Psychotherapy that ends with the patient being able to identify all the traumas that led to their sorrow has simply left the patient in the role of helpless and sorrowful victim. Instead, we should allow patients to proceed to the next step, which is empowerment and transformation. From this angle, the field of psychiatry should be cautious of encouraging movements that promote victimhood and grievance as a meaningful psychic position to take in society.
Mr. Lukianoff and Dr. Haidt use cognitive therapy as an analogy throughout their books for how to confront the great untruths. They perceive those modern forms of thinking as cognitive distortions, which can be remedied using the techniques of cognitive restructuring found in cognitive-behavioral therapy. They encourage us to recognize those maladaptive thoughts, and create more accurate and adaptive ways of viewing the world – a view that would be able to grow from challenges not just survive them; a view referred to as antifragile.3 We believe that those techniques and others would certainly be of assistance in our current times. However, the first step is to recognize our problem – a problem that is not rooted in the DSM, research, or biology but in an exaggerated intention to be patient centered. We should, however, remember that, when a patient has negative schemas, being too patient centered can be encouraging to maladaptive behaviors.
In conclusion, we wonder what modern psychiatry could look like if it made a concerted effort at also treating mental illness by reinforcing the importance of individual agency and responsibility. Modern psychiatry has been so focused on describing biological symptoms needing biological treatments that we sometimes forget that having no symptom (being asymptomatic) is not the only goal. Having a fulfilling and meaningful life, which is resilient to future symptoms is just as important to patients. We seem to have entrenched ourselves so deeply in an overly basic approach of problem-solution and diagnosis-treatment paradigm. However, we don’t need to renege on modern advances to promote the patient’s strength, adaptability, and antifragility. An emphasis on patient growth can complement the medical model. We wonder what effect such an approach would have if the trainee’s patient with alcohol use disorder was instead told: “Given the suffering you have and have caused because of your alcohol use disorder, how do you plan to make changes in your life to help the treatment plan we create together?”
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
References
1. Lukianoff G, Haidt J. The Coddling of the American Mind: How Good Intentions and Bad Ideas are Setting Up a Generation for Failure. New York: Penguin Books, 2019.
2. Levis B et al. J Clin Epidemiol. 2020 Jun;122:115-128.e1.,
3. Taleb NN. Antifragile: Things That Gain from Disorder. Vol. 3. New York: Random House, 2012.
New acute pain guidelines from the ACP and AAFP have limitations
The American College of Physicians and the American Academy of Family Physicians recently authored a guideline regarding the treatment of acute, non–low back, musculoskeletal injuries in adults in the outpatient setting.

According to the authors, musculoskeletal injuries result in more than 65 million medical visits a year with an annual estimated cost of $176.1 billion in 2010.
In summary, the guideline, which was published in the Annals of Internal Medicine, is based on a review of the best available evidence. The research reviewed by the guideline authors showed favorable results with topical NSAIDs, oral NSAIDs, oral acetaminophen, acupressure, and transcutaneous electrical nerve stimulation in reducing pain and/or improving function. The guideline authors “recommend that clinicians treat patients with acute pain from non–low back, musculoskeletal injuries with topical [NSAIDs] with or without gel as first-line therapy to reduce or relieve symptoms, including pain; improve physical function; and improve the patient’s treatment satisfaction (Grade: strong recommendation; moderate-certainty evidence).” Additionally, the guideline recommends against treating acute pain from non–low back, musculoskeletal injuries with opioids, including tramadol (Grade: conditional recommendation; low-certainty evidence).
The guideline also mentions improving function in relation to decreasing pain, which can be multifactorial.
Treating pain requires a multipronged approach. Many patients require more than one therapy to treat their pain, such as NSAIDs plus physical therapy. The ACP and AAFP did not make any recommendations for combination therapies in this guideline.
When physical therapy is needed
Nonopioid pain medications can do a great job of reducing a patient’s physical discomfort, which the evidence for these guideline demonstrates. However, much of the dysfunction caused by musculoskeletal injuries will not improve by reducing the pain alone. Physical therapy, exercise, and mobilization did not show a significant benefit in reducing symptoms in the systematic review and meta-analysis of randomized trials that appeared alongside the guideline. The type of pain, however, was not evaluated in relation to the effectiveness of these treatments. A fractured bone, for example, may heal just fine with casting and pain management, without the need for additional therapies. However, the muscles surrounding that bone can atrophy and become weak from not being used. Physical therapy may be needed to restrengthen those muscles. Therefore, a multifaceted approach is often needed, even for uncomplicated conditions.
Mental pain often comes with physical pain, and this is an aspect of care that is often neglected. It can be quite devastating for patients to not be able to do the things they were previously able to do. While this is easily recognized in professional athletes when they can no longer play, it is not so readily apparent with a mother who is just trying to take care of her kids. As doctors, especially those of us in family medicine, we should be addressing more than just physical pain.
Patients can also do activities that exacerbate their pain. As doctors, we need to be asking questions that help us determine whether a patient’s pain is caused by a particular action. Maybe that increase in shoulder pain is due to nothing more than lifting something heavy rather than a failure in a prescribed medication. Pain diaries are helpful, and clinicians don’t use them often enough.
How pain affects mental health
Acute injuries can also lead to disability. Many patients become quite distressed about being unable to work. They often need Famiy & Medical Leave Act forms filled out, and this task usually falls to the primary care doctor. In addition to assessing the pain, we need to be evaluating, at each visit, a patient’s level of functioning and their ability to do their job.
Every patient responds to pain differently, and it is important to evaluate patients’ mindsets regarding theirs. A patient may be in severe pain and may try to ignore it for a variety of reasons. A patient may “catastrophize” their pain, believing only the worst outcome will happen to them. Helping patients set appropriate expectations and having a positive mindset can help.
Overall, the new recommendations are a great tool as a guideline, but they are not complete enough to be the only ones used in managing acute, non–low back, musculoskeletal pain in adults.
They are very important for clinicians who may be prescribing opioid medications for patients with this type of pain. Amid an opioid crisis, it is the responsibility of every doctor to prescribe these medications appropriately. The evidence clearly shows they provide little benefit and place patients at risk of addiction.
We should all be following these recommendations as the baseline of care for acute pain. However, we need to delve deeper and manage all the components involved. We would be ignoring very real suffering in our patients if we limited our focus to only the physical discomfort.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Rutgers RWJ Medical School.
SOURCE: Ann Intern Med. 2020 Aug 18. doi: 10.7326/M19-3602.
The American College of Physicians and the American Academy of Family Physicians recently authored a guideline regarding the treatment of acute, non–low back, musculoskeletal injuries in adults in the outpatient setting.
According to the authors, musculoskeletal injuries result in more than 65 million medical visits a year with an annual estimated cost of $176.1 billion in 2010.
In summary, the guideline, which was published in the Annals of Internal Medicine, is based on a review of the best available evidence. The research reviewed by the guideline authors showed favorable results with topical NSAIDs, oral NSAIDs, oral acetaminophen, acupressure, and transcutaneous electrical nerve stimulation in reducing pain and/or improving function. The guideline authors “recommend that clinicians treat patients with acute pain from non–low back, musculoskeletal injuries with topical [NSAIDs] with or without gel as first-line therapy to reduce or relieve symptoms, including pain; improve physical function; and improve the patient’s treatment satisfaction (Grade: strong recommendation; moderate-certainty evidence).” Additionally, the guideline recommends against treating acute pain from non–low back, musculoskeletal injuries with opioids, including tramadol (Grade: conditional recommendation; low-certainty evidence).
The guideline also mentions improving function in relation to decreasing pain, which can be multifactorial.
Treating pain requires a multipronged approach. Many patients require more than one therapy to treat their pain, such as NSAIDs plus physical therapy. The ACP and AAFP did not make any recommendations for combination therapies in this guideline.
When physical therapy is needed
Nonopioid pain medications can do a great job of reducing a patient’s physical discomfort, which the evidence for these guideline demonstrates. However, much of the dysfunction caused by musculoskeletal injuries will not improve by reducing the pain alone. Physical therapy, exercise, and mobilization did not show a significant benefit in reducing symptoms in the systematic review and meta-analysis of randomized trials that appeared alongside the guideline. The type of pain, however, was not evaluated in relation to the effectiveness of these treatments. A fractured bone, for example, may heal just fine with casting and pain management, without the need for additional therapies. However, the muscles surrounding that bone can atrophy and become weak from not being used. Physical therapy may be needed to restrengthen those muscles. Therefore, a multifaceted approach is often needed, even for uncomplicated conditions.
Mental pain often comes with physical pain, and this is an aspect of care that is often neglected. It can be quite devastating for patients to not be able to do the things they were previously able to do. While this is easily recognized in professional athletes when they can no longer play, it is not so readily apparent with a mother who is just trying to take care of her kids. As doctors, especially those of us in family medicine, we should be addressing more than just physical pain.
Patients can also do activities that exacerbate their pain. As doctors, we need to be asking questions that help us determine whether a patient’s pain is caused by a particular action. Maybe that increase in shoulder pain is due to nothing more than lifting something heavy rather than a failure in a prescribed medication. Pain diaries are helpful, and clinicians don’t use them often enough.
How pain affects mental health
Acute injuries can also lead to disability. Many patients become quite distressed about being unable to work. They often need Famiy & Medical Leave Act forms filled out, and this task usually falls to the primary care doctor. In addition to assessing the pain, we need to be evaluating, at each visit, a patient’s level of functioning and their ability to do their job.
Every patient responds to pain differently, and it is important to evaluate patients’ mindsets regarding theirs. A patient may be in severe pain and may try to ignore it for a variety of reasons. A patient may “catastrophize” their pain, believing only the worst outcome will happen to them. Helping patients set appropriate expectations and having a positive mindset can help.
Overall, the new recommendations are a great tool as a guideline, but they are not complete enough to be the only ones used in managing acute, non–low back, musculoskeletal pain in adults.
They are very important for clinicians who may be prescribing opioid medications for patients with this type of pain. Amid an opioid crisis, it is the responsibility of every doctor to prescribe these medications appropriately. The evidence clearly shows they provide little benefit and place patients at risk of addiction.
We should all be following these recommendations as the baseline of care for acute pain. However, we need to delve deeper and manage all the components involved. We would be ignoring very real suffering in our patients if we limited our focus to only the physical discomfort.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Rutgers RWJ Medical School.
SOURCE: Ann Intern Med. 2020 Aug 18. doi: 10.7326/M19-3602.
The American College of Physicians and the American Academy of Family Physicians recently authored a guideline regarding the treatment of acute, non–low back, musculoskeletal injuries in adults in the outpatient setting.
According to the authors, musculoskeletal injuries result in more than 65 million medical visits a year with an annual estimated cost of $176.1 billion in 2010.
In summary, the guideline, which was published in the Annals of Internal Medicine, is based on a review of the best available evidence. The research reviewed by the guideline authors showed favorable results with topical NSAIDs, oral NSAIDs, oral acetaminophen, acupressure, and transcutaneous electrical nerve stimulation in reducing pain and/or improving function. The guideline authors “recommend that clinicians treat patients with acute pain from non–low back, musculoskeletal injuries with topical [NSAIDs] with or without gel as first-line therapy to reduce or relieve symptoms, including pain; improve physical function; and improve the patient’s treatment satisfaction (Grade: strong recommendation; moderate-certainty evidence).” Additionally, the guideline recommends against treating acute pain from non–low back, musculoskeletal injuries with opioids, including tramadol (Grade: conditional recommendation; low-certainty evidence).
The guideline also mentions improving function in relation to decreasing pain, which can be multifactorial.
Treating pain requires a multipronged approach. Many patients require more than one therapy to treat their pain, such as NSAIDs plus physical therapy. The ACP and AAFP did not make any recommendations for combination therapies in this guideline.
When physical therapy is needed
Nonopioid pain medications can do a great job of reducing a patient’s physical discomfort, which the evidence for these guideline demonstrates. However, much of the dysfunction caused by musculoskeletal injuries will not improve by reducing the pain alone. Physical therapy, exercise, and mobilization did not show a significant benefit in reducing symptoms in the systematic review and meta-analysis of randomized trials that appeared alongside the guideline. The type of pain, however, was not evaluated in relation to the effectiveness of these treatments. A fractured bone, for example, may heal just fine with casting and pain management, without the need for additional therapies. However, the muscles surrounding that bone can atrophy and become weak from not being used. Physical therapy may be needed to restrengthen those muscles. Therefore, a multifaceted approach is often needed, even for uncomplicated conditions.
Mental pain often comes with physical pain, and this is an aspect of care that is often neglected. It can be quite devastating for patients to not be able to do the things they were previously able to do. While this is easily recognized in professional athletes when they can no longer play, it is not so readily apparent with a mother who is just trying to take care of her kids. As doctors, especially those of us in family medicine, we should be addressing more than just physical pain.
Patients can also do activities that exacerbate their pain. As doctors, we need to be asking questions that help us determine whether a patient’s pain is caused by a particular action. Maybe that increase in shoulder pain is due to nothing more than lifting something heavy rather than a failure in a prescribed medication. Pain diaries are helpful, and clinicians don’t use them often enough.
How pain affects mental health
Acute injuries can also lead to disability. Many patients become quite distressed about being unable to work. They often need Famiy & Medical Leave Act forms filled out, and this task usually falls to the primary care doctor. In addition to assessing the pain, we need to be evaluating, at each visit, a patient’s level of functioning and their ability to do their job.
Every patient responds to pain differently, and it is important to evaluate patients’ mindsets regarding theirs. A patient may be in severe pain and may try to ignore it for a variety of reasons. A patient may “catastrophize” their pain, believing only the worst outcome will happen to them. Helping patients set appropriate expectations and having a positive mindset can help.
Overall, the new recommendations are a great tool as a guideline, but they are not complete enough to be the only ones used in managing acute, non–low back, musculoskeletal pain in adults.
They are very important for clinicians who may be prescribing opioid medications for patients with this type of pain. Amid an opioid crisis, it is the responsibility of every doctor to prescribe these medications appropriately. The evidence clearly shows they provide little benefit and place patients at risk of addiction.
We should all be following these recommendations as the baseline of care for acute pain. However, we need to delve deeper and manage all the components involved. We would be ignoring very real suffering in our patients if we limited our focus to only the physical discomfort.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Rutgers RWJ Medical School.
SOURCE: Ann Intern Med. 2020 Aug 18. doi: 10.7326/M19-3602.
Reworked OxyContin fails to cut overall opioid abuse, FDA panel says
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.

After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.

During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.

There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.
After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.
During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.
There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.
After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.
During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.
There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
High schoolers prefer tobacco as vapor, not smoke
according to the Centers for Disease Control and Prevention.
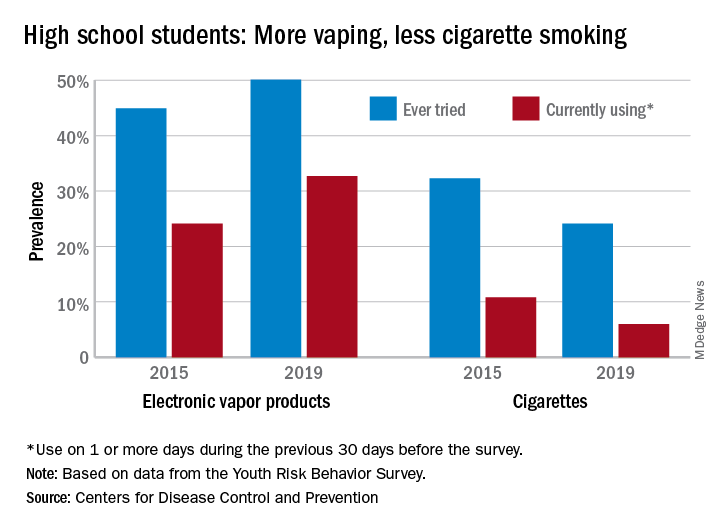
From 2015 to 2019, current use of electronic vapor products among students in grades 9-12 rose from 24.1% to 32.7%, while the same level of cigarette use – on 1 or more days in the previous 30 – dropped from 10.8% to 6.0%, based on data from the Youth Risk Behavior Survey.
Among the survey respondents, 50.1% had at least tried an electronic vapor product by 2019, up from 44.9% in 2015. Cigarettes again showed a decline, as ever use fell from 32.3% to 24.1%, or less than half of the e-product prevalence. Everyday use of vaping products was 7.2% in 2019 (up from 2.0% in 2015), compared with 1.1% for cigarettes (down from 2.3%), the YRBS data show.
“The dramatic increase in electronic vapor product use among high school students has led to increases in overall tobacco product use among U.S. youths, erasing gains made in previous years and leading the U.S. Surgeon General to declare youth e-cigarette use an epidemic in the United States,” MeLisa R. Creamer, PhD, and associates at the CDC wrote in the MMWR.
Electronic vapor products, as defined by the survey, “include e-cigarettes, vapes, vape pens, e-cigars, e-hookahs, hookah pens, and mods.”
Current use of cigarettes among high school students, as measured by the YRBS, has been declining since reaching a high of 36.4% in 1997; the prevalence of everyday use peaked at 12.8% in 1999. Current use of cigars declined as well, falling from 17.7% in 1999 to 5.7% in 2019, according to YRBS data.
“In 2019, a total of 36.5% of high school students currently used any tobacco product, with electronic vapor products being the most commonly used product,” Dr. Creamer and associates wrote in their recent analysis of the YRBS data (MMWR Supp. 2020 Aug 21;69[1]:56-63).
For the first time since the use of electronic vapor products was included in the every-other-year survey in 2015, females were more likely than males to be current users of vaping products last year, 33.5% to 32.0%. Males were heavier users of cigarettes by a margin of 6.9% to 4.9%, the CDC reported.
Geographically speaking, use of both electronic vapor products and cigarettes varied considerably among the 43 states with available data. Current use of electronic products ranged from a low of 9.7% in Utah to a high of 35.7% in West Virginia, with the two states in the same positions regarding current cigarette use: Utah (2.2%) lowest and West Virginia (13.5%) highest, based on the 2019 YRBS data.
“Tobacco product usage has evolved, and the increasing prevalence of electronic vapor product use among youths during recent years is concerning,” Dr. Creamer and associates wrote.
according to the Centers for Disease Control and Prevention.
From 2015 to 2019, current use of electronic vapor products among students in grades 9-12 rose from 24.1% to 32.7%, while the same level of cigarette use – on 1 or more days in the previous 30 – dropped from 10.8% to 6.0%, based on data from the Youth Risk Behavior Survey.
Among the survey respondents, 50.1% had at least tried an electronic vapor product by 2019, up from 44.9% in 2015. Cigarettes again showed a decline, as ever use fell from 32.3% to 24.1%, or less than half of the e-product prevalence. Everyday use of vaping products was 7.2% in 2019 (up from 2.0% in 2015), compared with 1.1% for cigarettes (down from 2.3%), the YRBS data show.
“The dramatic increase in electronic vapor product use among high school students has led to increases in overall tobacco product use among U.S. youths, erasing gains made in previous years and leading the U.S. Surgeon General to declare youth e-cigarette use an epidemic in the United States,” MeLisa R. Creamer, PhD, and associates at the CDC wrote in the MMWR.
Electronic vapor products, as defined by the survey, “include e-cigarettes, vapes, vape pens, e-cigars, e-hookahs, hookah pens, and mods.”
Current use of cigarettes among high school students, as measured by the YRBS, has been declining since reaching a high of 36.4% in 1997; the prevalence of everyday use peaked at 12.8% in 1999. Current use of cigars declined as well, falling from 17.7% in 1999 to 5.7% in 2019, according to YRBS data.
“In 2019, a total of 36.5% of high school students currently used any tobacco product, with electronic vapor products being the most commonly used product,” Dr. Creamer and associates wrote in their recent analysis of the YRBS data (MMWR Supp. 2020 Aug 21;69[1]:56-63).
For the first time since the use of electronic vapor products was included in the every-other-year survey in 2015, females were more likely than males to be current users of vaping products last year, 33.5% to 32.0%. Males were heavier users of cigarettes by a margin of 6.9% to 4.9%, the CDC reported.
Geographically speaking, use of both electronic vapor products and cigarettes varied considerably among the 43 states with available data. Current use of electronic products ranged from a low of 9.7% in Utah to a high of 35.7% in West Virginia, with the two states in the same positions regarding current cigarette use: Utah (2.2%) lowest and West Virginia (13.5%) highest, based on the 2019 YRBS data.
“Tobacco product usage has evolved, and the increasing prevalence of electronic vapor product use among youths during recent years is concerning,” Dr. Creamer and associates wrote.
according to the Centers for Disease Control and Prevention.
From 2015 to 2019, current use of electronic vapor products among students in grades 9-12 rose from 24.1% to 32.7%, while the same level of cigarette use – on 1 or more days in the previous 30 – dropped from 10.8% to 6.0%, based on data from the Youth Risk Behavior Survey.
Among the survey respondents, 50.1% had at least tried an electronic vapor product by 2019, up from 44.9% in 2015. Cigarettes again showed a decline, as ever use fell from 32.3% to 24.1%, or less than half of the e-product prevalence. Everyday use of vaping products was 7.2% in 2019 (up from 2.0% in 2015), compared with 1.1% for cigarettes (down from 2.3%), the YRBS data show.
“The dramatic increase in electronic vapor product use among high school students has led to increases in overall tobacco product use among U.S. youths, erasing gains made in previous years and leading the U.S. Surgeon General to declare youth e-cigarette use an epidemic in the United States,” MeLisa R. Creamer, PhD, and associates at the CDC wrote in the MMWR.
Electronic vapor products, as defined by the survey, “include e-cigarettes, vapes, vape pens, e-cigars, e-hookahs, hookah pens, and mods.”
Current use of cigarettes among high school students, as measured by the YRBS, has been declining since reaching a high of 36.4% in 1997; the prevalence of everyday use peaked at 12.8% in 1999. Current use of cigars declined as well, falling from 17.7% in 1999 to 5.7% in 2019, according to YRBS data.
“In 2019, a total of 36.5% of high school students currently used any tobacco product, with electronic vapor products being the most commonly used product,” Dr. Creamer and associates wrote in their recent analysis of the YRBS data (MMWR Supp. 2020 Aug 21;69[1]:56-63).
For the first time since the use of electronic vapor products was included in the every-other-year survey in 2015, females were more likely than males to be current users of vaping products last year, 33.5% to 32.0%. Males were heavier users of cigarettes by a margin of 6.9% to 4.9%, the CDC reported.
Geographically speaking, use of both electronic vapor products and cigarettes varied considerably among the 43 states with available data. Current use of electronic products ranged from a low of 9.7% in Utah to a high of 35.7% in West Virginia, with the two states in the same positions regarding current cigarette use: Utah (2.2%) lowest and West Virginia (13.5%) highest, based on the 2019 YRBS data.
“Tobacco product usage has evolved, and the increasing prevalence of electronic vapor product use among youths during recent years is concerning,” Dr. Creamer and associates wrote.
Fecal transplant shows promise in reducing alcohol craving
Fecal microbiota transplantation results in a short-term reduction in alcohol craving in patients with alcohol-induced cirrhosis who can’t stop drinking, results from a new study show.
And that reduction could lead to a better psychosocial quality of life for patients with cirrhosis and alcohol use disorder, said investigator Jasmohan Bajaj, MD, from Virginia Commonwealth University, Richmond.
“This is the most common addiction disorder worldwide, but we have nothing to treat these patients with,” he said.
Cirrhosis is associated with an altered gut-brain axis. It leads to organ damage in several parts of the body, including the brain, gut, pancreas, and liver. This makes changing the gut microbes “an attractive target,” Dr. Bajaj said at the Digital International Liver Congress 2020.
For their phase 1, double-blind study, he and his colleagues assessed 20 men from a Virginia veteran’s hospital with untreatable alcohol use disorder who were not eligible for liver transplantation.
All had failed behavioral or pharmacologic therapy and were unwilling to try again. “That’s what made them good candidates to try something new,” Dr. Bajaj said during a press briefing.
Mean age in the study cohort was 65 years, mean Model for End-Stage Liver disease score was 8.9, and demographic characteristics were similar between the 10 men randomly assigned to fecal transplantation and the 10 assigned to placebo. One man in each group dropped out of the study.
The investigators evaluated cravings, microbiota, and quality of life during the 30-day study period.
At day 15, significantly more men in the transplant group than in the placebo group experienced a reduction in alcohol cravings (90% vs. 30%).
At 30 days, levels of creatinine, serum interleukin-6, and lipopolysaccharide-binding protein were lower in the transplant group than in the placebo group. In addition, levels of butyrate and isobutyrate increased, as did cognition and quality of life scores.
There was also a decrease in urinary ethyl glucuronide in the transplant group, which “is the objective criteria for alcohol intake,” Dr. Bajaj reported, noting that there was no change in ethyl glucuronide in the placebo group.
The increase in microbiota diversity was significant in the transplant group but not in the placebo group. Alistipes, Odoribacter, and Roseburia were more abundant in the transplant group than in the placebo group.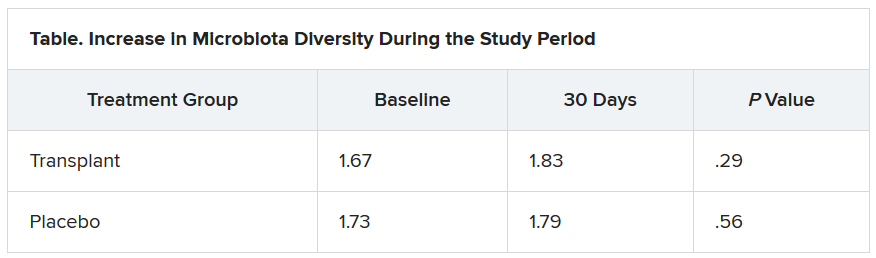
During the 30-day study period, two men in the placebo group required medical attention, one for hyponatremia and the other for atrial fibrillation. However, no adverse events were seen in any men in the transplant group. “This was the No. 1 result,” Dr. Bajaj said.
Liver disease and the microbiome
“Understanding of interactions between the human and microbiome genome [metagenome] in health and disease has represented one of the major areas of progress in the last few years,” said Luca Valenti, MD, from the University of Milan, who is a member of the scientific committee of the European Association the Study of the Liver, which organized the congress.
“These studies lay the groundwork for the exploitation of this new knowledge for the treatment of liver disease,” he said.
“We are [now] diagnosing liver disease and the stages of liver disease based on microbiome changes,” said Jonel Trebicka, MD, PhD, from University Hospital Frankfurt (Germany), who chaired a session at the congress on the role of the microbiome in liver disease.
“This and other studies have shown us that the microbiome itself may influence liver disease,” he added.
Dr. Bajaj is considered one of the world’s experts on cirrhosis and the microbiome, Dr. Trebicka explained. Last year, Dr. Bajaj and his team demonstrated that fecal microbiota transplantation can reduce the incidence of recurrent hepatic encephalopathy, as reported by Medscape Medical News.
The current study also “shows clearly that the microbiome plays a role in craving. FMT reduces the desire for alcohol,” said Dr. Trebicka.
“The way to the brain is through the gut,” Dr. Bajaj said.
Dr. Bajaj, Dr. Trebicka, and Dr. Valenti disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Fecal microbiota transplantation results in a short-term reduction in alcohol craving in patients with alcohol-induced cirrhosis who can’t stop drinking, results from a new study show.
And that reduction could lead to a better psychosocial quality of life for patients with cirrhosis and alcohol use disorder, said investigator Jasmohan Bajaj, MD, from Virginia Commonwealth University, Richmond.
“This is the most common addiction disorder worldwide, but we have nothing to treat these patients with,” he said.
Cirrhosis is associated with an altered gut-brain axis. It leads to organ damage in several parts of the body, including the brain, gut, pancreas, and liver. This makes changing the gut microbes “an attractive target,” Dr. Bajaj said at the Digital International Liver Congress 2020.
For their phase 1, double-blind study, he and his colleagues assessed 20 men from a Virginia veteran’s hospital with untreatable alcohol use disorder who were not eligible for liver transplantation.
All had failed behavioral or pharmacologic therapy and were unwilling to try again. “That’s what made them good candidates to try something new,” Dr. Bajaj said during a press briefing.
Mean age in the study cohort was 65 years, mean Model for End-Stage Liver disease score was 8.9, and demographic characteristics were similar between the 10 men randomly assigned to fecal transplantation and the 10 assigned to placebo. One man in each group dropped out of the study.
The investigators evaluated cravings, microbiota, and quality of life during the 30-day study period.
At day 15, significantly more men in the transplant group than in the placebo group experienced a reduction in alcohol cravings (90% vs. 30%).
At 30 days, levels of creatinine, serum interleukin-6, and lipopolysaccharide-binding protein were lower in the transplant group than in the placebo group. In addition, levels of butyrate and isobutyrate increased, as did cognition and quality of life scores.
There was also a decrease in urinary ethyl glucuronide in the transplant group, which “is the objective criteria for alcohol intake,” Dr. Bajaj reported, noting that there was no change in ethyl glucuronide in the placebo group.
The increase in microbiota diversity was significant in the transplant group but not in the placebo group. Alistipes, Odoribacter, and Roseburia were more abundant in the transplant group than in the placebo group.
During the 30-day study period, two men in the placebo group required medical attention, one for hyponatremia and the other for atrial fibrillation. However, no adverse events were seen in any men in the transplant group. “This was the No. 1 result,” Dr. Bajaj said.
Liver disease and the microbiome
“Understanding of interactions between the human and microbiome genome [metagenome] in health and disease has represented one of the major areas of progress in the last few years,” said Luca Valenti, MD, from the University of Milan, who is a member of the scientific committee of the European Association the Study of the Liver, which organized the congress.
“These studies lay the groundwork for the exploitation of this new knowledge for the treatment of liver disease,” he said.
“We are [now] diagnosing liver disease and the stages of liver disease based on microbiome changes,” said Jonel Trebicka, MD, PhD, from University Hospital Frankfurt (Germany), who chaired a session at the congress on the role of the microbiome in liver disease.
“This and other studies have shown us that the microbiome itself may influence liver disease,” he added.
Dr. Bajaj is considered one of the world’s experts on cirrhosis and the microbiome, Dr. Trebicka explained. Last year, Dr. Bajaj and his team demonstrated that fecal microbiota transplantation can reduce the incidence of recurrent hepatic encephalopathy, as reported by Medscape Medical News.
The current study also “shows clearly that the microbiome plays a role in craving. FMT reduces the desire for alcohol,” said Dr. Trebicka.
“The way to the brain is through the gut,” Dr. Bajaj said.
Dr. Bajaj, Dr. Trebicka, and Dr. Valenti disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Fecal microbiota transplantation results in a short-term reduction in alcohol craving in patients with alcohol-induced cirrhosis who can’t stop drinking, results from a new study show.
And that reduction could lead to a better psychosocial quality of life for patients with cirrhosis and alcohol use disorder, said investigator Jasmohan Bajaj, MD, from Virginia Commonwealth University, Richmond.
“This is the most common addiction disorder worldwide, but we have nothing to treat these patients with,” he said.
Cirrhosis is associated with an altered gut-brain axis. It leads to organ damage in several parts of the body, including the brain, gut, pancreas, and liver. This makes changing the gut microbes “an attractive target,” Dr. Bajaj said at the Digital International Liver Congress 2020.
For their phase 1, double-blind study, he and his colleagues assessed 20 men from a Virginia veteran’s hospital with untreatable alcohol use disorder who were not eligible for liver transplantation.
All had failed behavioral or pharmacologic therapy and were unwilling to try again. “That’s what made them good candidates to try something new,” Dr. Bajaj said during a press briefing.
Mean age in the study cohort was 65 years, mean Model for End-Stage Liver disease score was 8.9, and demographic characteristics were similar between the 10 men randomly assigned to fecal transplantation and the 10 assigned to placebo. One man in each group dropped out of the study.
The investigators evaluated cravings, microbiota, and quality of life during the 30-day study period.
At day 15, significantly more men in the transplant group than in the placebo group experienced a reduction in alcohol cravings (90% vs. 30%).
At 30 days, levels of creatinine, serum interleukin-6, and lipopolysaccharide-binding protein were lower in the transplant group than in the placebo group. In addition, levels of butyrate and isobutyrate increased, as did cognition and quality of life scores.
There was also a decrease in urinary ethyl glucuronide in the transplant group, which “is the objective criteria for alcohol intake,” Dr. Bajaj reported, noting that there was no change in ethyl glucuronide in the placebo group.
The increase in microbiota diversity was significant in the transplant group but not in the placebo group. Alistipes, Odoribacter, and Roseburia were more abundant in the transplant group than in the placebo group.
During the 30-day study period, two men in the placebo group required medical attention, one for hyponatremia and the other for atrial fibrillation. However, no adverse events were seen in any men in the transplant group. “This was the No. 1 result,” Dr. Bajaj said.
Liver disease and the microbiome
“Understanding of interactions between the human and microbiome genome [metagenome] in health and disease has represented one of the major areas of progress in the last few years,” said Luca Valenti, MD, from the University of Milan, who is a member of the scientific committee of the European Association the Study of the Liver, which organized the congress.
“These studies lay the groundwork for the exploitation of this new knowledge for the treatment of liver disease,” he said.
“We are [now] diagnosing liver disease and the stages of liver disease based on microbiome changes,” said Jonel Trebicka, MD, PhD, from University Hospital Frankfurt (Germany), who chaired a session at the congress on the role of the microbiome in liver disease.
“This and other studies have shown us that the microbiome itself may influence liver disease,” he added.
Dr. Bajaj is considered one of the world’s experts on cirrhosis and the microbiome, Dr. Trebicka explained. Last year, Dr. Bajaj and his team demonstrated that fecal microbiota transplantation can reduce the incidence of recurrent hepatic encephalopathy, as reported by Medscape Medical News.
The current study also “shows clearly that the microbiome plays a role in craving. FMT reduces the desire for alcohol,” said Dr. Trebicka.
“The way to the brain is through the gut,” Dr. Bajaj said.
Dr. Bajaj, Dr. Trebicka, and Dr. Valenti disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Adolescent e-cigarette use: A public health crisis
The use of electronic cigarettes (e-cigarettes) in teenagers has been increasing rapidly in the United States, leading Surgeon General Jerome Adams, MD, MPH, to label it a public health concern.1 Easy accessibility and extensive marketing for e-cigarettes counteract public education campaigns and policies aimed at decreasing e-cigarette use in teenagers.
E-cigarettes are marketed to teenagers as small, easy-to-use pens or USB flash drive–like devices that can be hidden easily. Some devices can be used to smoke nicotine, delta-9-tetrahydrocannabinol (THC), cannabidiol, and butane hash oil. Some are sold with different nicotine flavors to increase their appeal. E-cigarette ads appear in retail stores, movies, magazines, newspapers, and on the internet.
According to the CDC, the number of middle and high school students using e-cigarettes increased from 3.6 million in 2018 to 5.4 million in 2019.2 Nicotine dependence from e-cigarette use can increase the risk of starting to smoke cigarettes. A 2015-2016 National Institute on Drug Abuse survey found a higher prevalence of e-cigarette use among 9th-, 10th-, and 12th-grade students compared with cigarette smoking (9.5%, 14%, 16.2% vs 3.6%, 6.2%, 11.4%, respectively).3 Due to the growing popularity of vaping among adolescents in the United States, Congress recently raised the legal age to purchase tobacco and vaping products to 21 years.
Evidence of adverse health effects associated with e-cigarette use continues to grow. In 2020, the Department of Health and Services in Wisconsin and the Department of Public Health in Illinois looked at e-cigarette use and pulmonary disease.4 Of 98 participants who reported e-cigarette use, 97% presented with respiratory symptoms, 77% had gastrointestinal symptoms, and 100% had constitutional symptoms. Chest imaging showed bilateral infiltrates in all patients. In addition, 95% were hospitalized, 26% underwent intubation and mechanical ventilation, and 1 patient died. Most participants (89%) reported using THC in their e-cigarette devices.4 Blount et al5 recently found a link between e-cigarette- or vaping-associated lung injury and vitamin E acetate, a toxicant found in bronchoalveolar lavage fluid of some patients who reported using e-cigarettes. Also, nicotine dependency from e-cigarettes may adversely affect brain development in children and adolescents.2
The first step in fighting this crisis is to educate children, parents, teachers, and health care professionals about e-cigarette use, including its prevalence, use compared with cigarette smoking, trends among teenagers, marketing techniques, and adverse effects. Fortunately, the US government and medical professionals and organizations have made ongoing efforts to discourage e-cigarette use. For example, the American Academy of Child and Adolescent Psychiatry supports the FDA’s regulation of e-cigarette use; encourages using evidence-based treatments for tobacco cessation; advocates for vigorous education regarding adolescent e-cigarette use; and endorses restrictions on e-cigarette advertisement.6 We strongly urge clinicians to be vigilant about e-cigarette use in their adolescent patients and to intervene in this public health crisis.
Immad A. Kiani, MD
PGY-3 Psychiatry Resident
Christiana Care Health Services
Department of Psychiatry
Wilmington, Delaware
Narpinder K. Malhi, MD
Child and Adolescent Psychiatrist
Christiana Care Health Services
Wilmington, Delaware
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
1. Adams J. Surgeon General’s advisory on e-cigarette use among youth. US Department of Health & Human Services. https://e-cigarettes.surgeongeneral.gov/documents/surgeon-generals-advisory-on-e-cigarette-use-among-youth-2018.pdf. Published 2018. Accessed August 7, 2020.
2. US Federal Drug and Drug Administration. Results from 2018 National Youth Tobacco Survey show dramatic increase in e-cigarette use among youth over past year. https://www.fda.gov/news-events/press-announcements/results-2018-national-youth-tobacco-survey-show-dramatic-increase-e-cigarette-use-among-youth-over. Published November 15, 2018. Accessed August 7, 2020.
3. Johnston LD, O’Malley PM, Miech RA, et al. Monitoring the future national survey results on drug use, 1975-2016: overview, key findings on adolescent drug use. The University of Michigan Institute for Social Research. https://files.eric.ed.gov/fulltext/ED578534.pdf. Published January 2017. Accessed August 7, 2020.
4. Layden JE, Ghinai I, Pray I, et al. Pulmonary illness related to e-cigarette use in Illinois and Wisconsin—final report. N Engl J Med. 2020;382(10):903-916.
5. Blount BC, Karwowski MP, Shields PG, et al; Lung Injury Response Laboratory Working Group. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med. 2020;382(8):697-705.
6. Electronic cigarettes. The American Academy of Child and Adolescent Psychiatry. https://www.aacap.org/AACAP/Policy_Statements/2015/Policy_Statement_on_Electronic_Cigarettes.aspx. Published June 2015. Accessed August 7, 2020.
The use of electronic cigarettes (e-cigarettes) in teenagers has been increasing rapidly in the United States, leading Surgeon General Jerome Adams, MD, MPH, to label it a public health concern.1 Easy accessibility and extensive marketing for e-cigarettes counteract public education campaigns and policies aimed at decreasing e-cigarette use in teenagers.
E-cigarettes are marketed to teenagers as small, easy-to-use pens or USB flash drive–like devices that can be hidden easily. Some devices can be used to smoke nicotine, delta-9-tetrahydrocannabinol (THC), cannabidiol, and butane hash oil. Some are sold with different nicotine flavors to increase their appeal. E-cigarette ads appear in retail stores, movies, magazines, newspapers, and on the internet.
According to the CDC, the number of middle and high school students using e-cigarettes increased from 3.6 million in 2018 to 5.4 million in 2019.2 Nicotine dependence from e-cigarette use can increase the risk of starting to smoke cigarettes. A 2015-2016 National Institute on Drug Abuse survey found a higher prevalence of e-cigarette use among 9th-, 10th-, and 12th-grade students compared with cigarette smoking (9.5%, 14%, 16.2% vs 3.6%, 6.2%, 11.4%, respectively).3 Due to the growing popularity of vaping among adolescents in the United States, Congress recently raised the legal age to purchase tobacco and vaping products to 21 years.
Evidence of adverse health effects associated with e-cigarette use continues to grow. In 2020, the Department of Health and Services in Wisconsin and the Department of Public Health in Illinois looked at e-cigarette use and pulmonary disease.4 Of 98 participants who reported e-cigarette use, 97% presented with respiratory symptoms, 77% had gastrointestinal symptoms, and 100% had constitutional symptoms. Chest imaging showed bilateral infiltrates in all patients. In addition, 95% were hospitalized, 26% underwent intubation and mechanical ventilation, and 1 patient died. Most participants (89%) reported using THC in their e-cigarette devices.4 Blount et al5 recently found a link between e-cigarette- or vaping-associated lung injury and vitamin E acetate, a toxicant found in bronchoalveolar lavage fluid of some patients who reported using e-cigarettes. Also, nicotine dependency from e-cigarettes may adversely affect brain development in children and adolescents.2
The first step in fighting this crisis is to educate children, parents, teachers, and health care professionals about e-cigarette use, including its prevalence, use compared with cigarette smoking, trends among teenagers, marketing techniques, and adverse effects. Fortunately, the US government and medical professionals and organizations have made ongoing efforts to discourage e-cigarette use. For example, the American Academy of Child and Adolescent Psychiatry supports the FDA’s regulation of e-cigarette use; encourages using evidence-based treatments for tobacco cessation; advocates for vigorous education regarding adolescent e-cigarette use; and endorses restrictions on e-cigarette advertisement.6 We strongly urge clinicians to be vigilant about e-cigarette use in their adolescent patients and to intervene in this public health crisis.
Immad A. Kiani, MD
PGY-3 Psychiatry Resident
Christiana Care Health Services
Department of Psychiatry
Wilmington, Delaware
Narpinder K. Malhi, MD
Child and Adolescent Psychiatrist
Christiana Care Health Services
Wilmington, Delaware
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
The use of electronic cigarettes (e-cigarettes) in teenagers has been increasing rapidly in the United States, leading Surgeon General Jerome Adams, MD, MPH, to label it a public health concern.1 Easy accessibility and extensive marketing for e-cigarettes counteract public education campaigns and policies aimed at decreasing e-cigarette use in teenagers.
E-cigarettes are marketed to teenagers as small, easy-to-use pens or USB flash drive–like devices that can be hidden easily. Some devices can be used to smoke nicotine, delta-9-tetrahydrocannabinol (THC), cannabidiol, and butane hash oil. Some are sold with different nicotine flavors to increase their appeal. E-cigarette ads appear in retail stores, movies, magazines, newspapers, and on the internet.
According to the CDC, the number of middle and high school students using e-cigarettes increased from 3.6 million in 2018 to 5.4 million in 2019.2 Nicotine dependence from e-cigarette use can increase the risk of starting to smoke cigarettes. A 2015-2016 National Institute on Drug Abuse survey found a higher prevalence of e-cigarette use among 9th-, 10th-, and 12th-grade students compared with cigarette smoking (9.5%, 14%, 16.2% vs 3.6%, 6.2%, 11.4%, respectively).3 Due to the growing popularity of vaping among adolescents in the United States, Congress recently raised the legal age to purchase tobacco and vaping products to 21 years.
Evidence of adverse health effects associated with e-cigarette use continues to grow. In 2020, the Department of Health and Services in Wisconsin and the Department of Public Health in Illinois looked at e-cigarette use and pulmonary disease.4 Of 98 participants who reported e-cigarette use, 97% presented with respiratory symptoms, 77% had gastrointestinal symptoms, and 100% had constitutional symptoms. Chest imaging showed bilateral infiltrates in all patients. In addition, 95% were hospitalized, 26% underwent intubation and mechanical ventilation, and 1 patient died. Most participants (89%) reported using THC in their e-cigarette devices.4 Blount et al5 recently found a link between e-cigarette- or vaping-associated lung injury and vitamin E acetate, a toxicant found in bronchoalveolar lavage fluid of some patients who reported using e-cigarettes. Also, nicotine dependency from e-cigarettes may adversely affect brain development in children and adolescents.2
The first step in fighting this crisis is to educate children, parents, teachers, and health care professionals about e-cigarette use, including its prevalence, use compared with cigarette smoking, trends among teenagers, marketing techniques, and adverse effects. Fortunately, the US government and medical professionals and organizations have made ongoing efforts to discourage e-cigarette use. For example, the American Academy of Child and Adolescent Psychiatry supports the FDA’s regulation of e-cigarette use; encourages using evidence-based treatments for tobacco cessation; advocates for vigorous education regarding adolescent e-cigarette use; and endorses restrictions on e-cigarette advertisement.6 We strongly urge clinicians to be vigilant about e-cigarette use in their adolescent patients and to intervene in this public health crisis.
Immad A. Kiani, MD
PGY-3 Psychiatry Resident
Christiana Care Health Services
Department of Psychiatry
Wilmington, Delaware
Narpinder K. Malhi, MD
Child and Adolescent Psychiatrist
Christiana Care Health Services
Wilmington, Delaware
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
1. Adams J. Surgeon General’s advisory on e-cigarette use among youth. US Department of Health & Human Services. https://e-cigarettes.surgeongeneral.gov/documents/surgeon-generals-advisory-on-e-cigarette-use-among-youth-2018.pdf. Published 2018. Accessed August 7, 2020.
2. US Federal Drug and Drug Administration. Results from 2018 National Youth Tobacco Survey show dramatic increase in e-cigarette use among youth over past year. https://www.fda.gov/news-events/press-announcements/results-2018-national-youth-tobacco-survey-show-dramatic-increase-e-cigarette-use-among-youth-over. Published November 15, 2018. Accessed August 7, 2020.
3. Johnston LD, O’Malley PM, Miech RA, et al. Monitoring the future national survey results on drug use, 1975-2016: overview, key findings on adolescent drug use. The University of Michigan Institute for Social Research. https://files.eric.ed.gov/fulltext/ED578534.pdf. Published January 2017. Accessed August 7, 2020.
4. Layden JE, Ghinai I, Pray I, et al. Pulmonary illness related to e-cigarette use in Illinois and Wisconsin—final report. N Engl J Med. 2020;382(10):903-916.
5. Blount BC, Karwowski MP, Shields PG, et al; Lung Injury Response Laboratory Working Group. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med. 2020;382(8):697-705.
6. Electronic cigarettes. The American Academy of Child and Adolescent Psychiatry. https://www.aacap.org/AACAP/Policy_Statements/2015/Policy_Statement_on_Electronic_Cigarettes.aspx. Published June 2015. Accessed August 7, 2020.
1. Adams J. Surgeon General’s advisory on e-cigarette use among youth. US Department of Health & Human Services. https://e-cigarettes.surgeongeneral.gov/documents/surgeon-generals-advisory-on-e-cigarette-use-among-youth-2018.pdf. Published 2018. Accessed August 7, 2020.
2. US Federal Drug and Drug Administration. Results from 2018 National Youth Tobacco Survey show dramatic increase in e-cigarette use among youth over past year. https://www.fda.gov/news-events/press-announcements/results-2018-national-youth-tobacco-survey-show-dramatic-increase-e-cigarette-use-among-youth-over. Published November 15, 2018. Accessed August 7, 2020.
3. Johnston LD, O’Malley PM, Miech RA, et al. Monitoring the future national survey results on drug use, 1975-2016: overview, key findings on adolescent drug use. The University of Michigan Institute for Social Research. https://files.eric.ed.gov/fulltext/ED578534.pdf. Published January 2017. Accessed August 7, 2020.
4. Layden JE, Ghinai I, Pray I, et al. Pulmonary illness related to e-cigarette use in Illinois and Wisconsin—final report. N Engl J Med. 2020;382(10):903-916.
5. Blount BC, Karwowski MP, Shields PG, et al; Lung Injury Response Laboratory Working Group. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med. 2020;382(8):697-705.
6. Electronic cigarettes. The American Academy of Child and Adolescent Psychiatry. https://www.aacap.org/AACAP/Policy_Statements/2015/Policy_Statement_on_Electronic_Cigarettes.aspx. Published June 2015. Accessed August 7, 2020.