User login
Superficial and Deep/Organ-Space Surgical Site Infections Should Not Be Combined for Quality Measurement
Clinical question: What patient-risk factors predict superficial and deep/organ-space surgical site infections (SSIs) following colectomy procedures?
Background: SSIs are often targeted by policymakers for quality improvement and cost saving. Superficial and deep/organ-specific SSIs are traditionally considered a single entity for quality measurement, although they vary by anatomic location and clinical severity.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement program (ACS-NSQIP).
Synopsis: Researchers used the ACS-NSQIP registry to identify all patients who underwent colectomy procedures across 305 hospitals. Various patient variables, such as demographics, pre-operative risk factors, comorbidities, and operative information, were collected on all patients. The primary outcome was 30-day post-operative superficial SSI and deep/organ-space SSI.
Overall, 27,011 patients underwent colectomy procedures, of which 6.2% developed a superficial SSI and 4.7% developed deep/organ-space SSI. Open surgical approach (vs. laparoscopic) and current smoking were the only risk factors that predicted the occurrence of both superficial and deep/organ-space SSI. Other risk factors (e.g., post-operative diagnoses, disseminated cancer, and irradiation therapy) had a differential effect and only predicted the occurrence of deep/organ-space SSI. Elevated body mass index was strongly correlated with the occurrence of superficial SSI.
Key limitations of the study included unavailability of infection rates beyond 30 days and grouping of deep and organ-space SSIs, as the latter might vary in magnitude and significance.
Bottom Line: Risk factors that predict superficial and deep/organ-space SSI differ significantly, suggesting that future quality initiatives and reporting should evaluate different types of SSIs independently.
Citation: Lawson EH, Hall BL, Ko CY. Risk factors for superficial vs. deep/organ-space surgical site infections: implications for quality improvement initiatives [published online ahead of print July 17, 2013]. JAMA Surg.
Clinical question: What patient-risk factors predict superficial and deep/organ-space surgical site infections (SSIs) following colectomy procedures?
Background: SSIs are often targeted by policymakers for quality improvement and cost saving. Superficial and deep/organ-specific SSIs are traditionally considered a single entity for quality measurement, although they vary by anatomic location and clinical severity.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement program (ACS-NSQIP).
Synopsis: Researchers used the ACS-NSQIP registry to identify all patients who underwent colectomy procedures across 305 hospitals. Various patient variables, such as demographics, pre-operative risk factors, comorbidities, and operative information, were collected on all patients. The primary outcome was 30-day post-operative superficial SSI and deep/organ-space SSI.
Overall, 27,011 patients underwent colectomy procedures, of which 6.2% developed a superficial SSI and 4.7% developed deep/organ-space SSI. Open surgical approach (vs. laparoscopic) and current smoking were the only risk factors that predicted the occurrence of both superficial and deep/organ-space SSI. Other risk factors (e.g., post-operative diagnoses, disseminated cancer, and irradiation therapy) had a differential effect and only predicted the occurrence of deep/organ-space SSI. Elevated body mass index was strongly correlated with the occurrence of superficial SSI.
Key limitations of the study included unavailability of infection rates beyond 30 days and grouping of deep and organ-space SSIs, as the latter might vary in magnitude and significance.
Bottom Line: Risk factors that predict superficial and deep/organ-space SSI differ significantly, suggesting that future quality initiatives and reporting should evaluate different types of SSIs independently.
Citation: Lawson EH, Hall BL, Ko CY. Risk factors for superficial vs. deep/organ-space surgical site infections: implications for quality improvement initiatives [published online ahead of print July 17, 2013]. JAMA Surg.
Clinical question: What patient-risk factors predict superficial and deep/organ-space surgical site infections (SSIs) following colectomy procedures?
Background: SSIs are often targeted by policymakers for quality improvement and cost saving. Superficial and deep/organ-specific SSIs are traditionally considered a single entity for quality measurement, although they vary by anatomic location and clinical severity.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement program (ACS-NSQIP).
Synopsis: Researchers used the ACS-NSQIP registry to identify all patients who underwent colectomy procedures across 305 hospitals. Various patient variables, such as demographics, pre-operative risk factors, comorbidities, and operative information, were collected on all patients. The primary outcome was 30-day post-operative superficial SSI and deep/organ-space SSI.
Overall, 27,011 patients underwent colectomy procedures, of which 6.2% developed a superficial SSI and 4.7% developed deep/organ-space SSI. Open surgical approach (vs. laparoscopic) and current smoking were the only risk factors that predicted the occurrence of both superficial and deep/organ-space SSI. Other risk factors (e.g., post-operative diagnoses, disseminated cancer, and irradiation therapy) had a differential effect and only predicted the occurrence of deep/organ-space SSI. Elevated body mass index was strongly correlated with the occurrence of superficial SSI.
Key limitations of the study included unavailability of infection rates beyond 30 days and grouping of deep and organ-space SSIs, as the latter might vary in magnitude and significance.
Bottom Line: Risk factors that predict superficial and deep/organ-space SSI differ significantly, suggesting that future quality initiatives and reporting should evaluate different types of SSIs independently.
Citation: Lawson EH, Hall BL, Ko CY. Risk factors for superficial vs. deep/organ-space surgical site infections: implications for quality improvement initiatives [published online ahead of print July 17, 2013]. JAMA Surg.
Report on England’s Health System Mirrors Need for Improvement in U.S.

Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Hospitalists Have Opportunity to Transform Healthcare

“I’m going to the sun,” my TWO-and-a-half-year-old daughter confidently declared. She said it so casually, as if she was letting me know that she was going to the playground.
Thinking I could use this as a great parenting opportunity and push my toddler to think through her decisions, I replied in a concerned tone: “Sweetie, the sun is really, really hot. What are you going to do about that?”
She replied effortlessly, as if the solution had always been right there in front of me, and somehow I had failed to see it, “I’m going to wear a really, really big hat!”
Later that night, I was reflecting on the little exchange with my daughter. Why had I been so determined to point out to her that it was impossible to travel to the sun? After all, two is the age to dream and imagine. As we grow up, why do we stop believing that we can do anything, absolutely anything, we imagine?
Since I started working as a hospitalist in 2007, the state of healthcare has been in constant turmoil and distress. Everyone, from providers to policymakers to patients, has been critical about the current state of our healthcare system. Many are concerned with the future, too. In fact, headlines regularly describe healthcare as “deficient,” “error-prone,” “deadly,” “bankrupt,” or “wasteful.”
This is not the vision of the medical profession that I had when I was an idealistic medical student. I was filled with aspirations of curing the sick, alleviating suffering, and helping to make the world a better place.
Don’t get me wrong...I get it. Hospitals, hospitalists, and all forms of care providers have a long way to go before we provide the highest quality of care at a cost our nation and our patients can afford. But in the critical evaluation of the current state of healthcare, where is the positive beacon of hope?
When did we, providers of care, stop believing that we could do anything, absolutely anything, to improve the state of healthcare?
Over the past decade, numerous innovations have been introduced to address the deficiencies in our system. However, efforts to come together as a medical profession and address these issues systematically have been lacking. And new initiatives, such as the ABIM Foundation’s Choosing Wisely campaign, are still in the early stages of widespread acceptance and adoption.
We have come a long way from the witchcraft of early healers and the barber-surgeons of medieval times. Modern medicine comes from a tradition of discovering the germ theory, eradicating polio, sequencing the entire genome, and performing simultaneous multiple organ transplantation. Providers are more than healers of the individual patient; they are healers of populations. By advancing health, they have enabled societies to thrive, grow, discover, and innovate. We shoulder significant responsibility, and our impact has shaped the course of human history.
Despite the stated challenges in healthcare, I’d like to think this is our finest hour, our time to shine. We have a rare and unique opportunity to completely reinvent the system and redefine the practice of medicine—to transform it from how it is practiced to how it should be delivered: high quality, high value, patient-centered, yet population-focused. This goes beyond ensuring that every patient with acute myocardial infarction receives an aspirin or working to prevent surgical site infections. This opportunity affords us the possibility to deliver extraordinary care.
Can hospitalists bridge this gap and change the world? Absolutely!
Inherent in our work is continuous improvement, not solely the improvement of our specialty, but also of the services we help co-manage, the hospital-wide committees we sit on, and the C-suite conversations we partake in. And, unlike most of healthcare, we manage to do this, not in isolation, but in multidisciplinary teams of physicians, nurses, staff, and, most importantly, patients and families.
If we unleash the potential of our specialty, the possibilities are endless. Here are some examples from our own hospitalists and society:
- Imagine the future of care with mentored implementation.
SHM’s award-winning mentored implementation model has helped transform care in more than 300 hospitals through best practices in venous thromboembolism, readmissions, and care of diabetic patients.
- Lead with the academy.
The future of healthcare will belong to clinicians who can lead teams and make the case for real change. That’s one of the reasons that SHM’s Leadership Academy has been so successful: It is creating a cadre of more than 2,000 hospitalists who are armed with the confidence and know-how to envision the hospital of the future and manage hospital-based teams toward that vision.
- Collaborate with HMX.
If you’ve ever been to SHM’s annual meeting, you know that hospitalists are a collaborative bunch. In fact, it’s that tendency toward collaboration and problem solving that has led more than 2,300 hospitalists to participate in SHM’s new online community, Hospital Medicine Exchange (www.hmxchange.org). It’s unlike any other platform for hospital-based clinicians, and the conversations on HMX are helping hospitalists everywhere benefit from the experience of colleagues nationally.
- Learn through the portal.
Hospitalists can’t shape the future of healthcare without staying up to date, but the days of getting continuing medical education (CME) credit exclusively from conferences is over. SHM is helping hospitalists with its brand new eLearning Portal (www.shmlearningportal.org), which can be accessed on PCs, tablets, or mobile devices.
Expectation High
So, be bold! The sky is the limit. Continue to learn, collaborate, and lead. Most of all, never stop believing that you can create the future you imagine. After all, it was Albert Einstein who cleverly said, “Imagination is more important than knowledge.”
As for my daughter and I, well, I guess I’m going to start investing in really big hats.
Dr. Afsar is associate chief medical officer at UCLA Hospitals in Los Angeles. She is also assistant clinical professor and executive director of quality and safety in the Department of Medicine and Neurosurgery at UCLA Hospitals. She is an SHM board member. Contact her at [email protected].
“I’m going to the sun,” my TWO-and-a-half-year-old daughter confidently declared. She said it so casually, as if she was letting me know that she was going to the playground.
Thinking I could use this as a great parenting opportunity and push my toddler to think through her decisions, I replied in a concerned tone: “Sweetie, the sun is really, really hot. What are you going to do about that?”
She replied effortlessly, as if the solution had always been right there in front of me, and somehow I had failed to see it, “I’m going to wear a really, really big hat!”
Later that night, I was reflecting on the little exchange with my daughter. Why had I been so determined to point out to her that it was impossible to travel to the sun? After all, two is the age to dream and imagine. As we grow up, why do we stop believing that we can do anything, absolutely anything, we imagine?
Since I started working as a hospitalist in 2007, the state of healthcare has been in constant turmoil and distress. Everyone, from providers to policymakers to patients, has been critical about the current state of our healthcare system. Many are concerned with the future, too. In fact, headlines regularly describe healthcare as “deficient,” “error-prone,” “deadly,” “bankrupt,” or “wasteful.”
This is not the vision of the medical profession that I had when I was an idealistic medical student. I was filled with aspirations of curing the sick, alleviating suffering, and helping to make the world a better place.
Don’t get me wrong...I get it. Hospitals, hospitalists, and all forms of care providers have a long way to go before we provide the highest quality of care at a cost our nation and our patients can afford. But in the critical evaluation of the current state of healthcare, where is the positive beacon of hope?
When did we, providers of care, stop believing that we could do anything, absolutely anything, to improve the state of healthcare?
Over the past decade, numerous innovations have been introduced to address the deficiencies in our system. However, efforts to come together as a medical profession and address these issues systematically have been lacking. And new initiatives, such as the ABIM Foundation’s Choosing Wisely campaign, are still in the early stages of widespread acceptance and adoption.
We have come a long way from the witchcraft of early healers and the barber-surgeons of medieval times. Modern medicine comes from a tradition of discovering the germ theory, eradicating polio, sequencing the entire genome, and performing simultaneous multiple organ transplantation. Providers are more than healers of the individual patient; they are healers of populations. By advancing health, they have enabled societies to thrive, grow, discover, and innovate. We shoulder significant responsibility, and our impact has shaped the course of human history.
Despite the stated challenges in healthcare, I’d like to think this is our finest hour, our time to shine. We have a rare and unique opportunity to completely reinvent the system and redefine the practice of medicine—to transform it from how it is practiced to how it should be delivered: high quality, high value, patient-centered, yet population-focused. This goes beyond ensuring that every patient with acute myocardial infarction receives an aspirin or working to prevent surgical site infections. This opportunity affords us the possibility to deliver extraordinary care.
Can hospitalists bridge this gap and change the world? Absolutely!
Inherent in our work is continuous improvement, not solely the improvement of our specialty, but also of the services we help co-manage, the hospital-wide committees we sit on, and the C-suite conversations we partake in. And, unlike most of healthcare, we manage to do this, not in isolation, but in multidisciplinary teams of physicians, nurses, staff, and, most importantly, patients and families.
If we unleash the potential of our specialty, the possibilities are endless. Here are some examples from our own hospitalists and society:
- Imagine the future of care with mentored implementation.
SHM’s award-winning mentored implementation model has helped transform care in more than 300 hospitals through best practices in venous thromboembolism, readmissions, and care of diabetic patients.
- Lead with the academy.
The future of healthcare will belong to clinicians who can lead teams and make the case for real change. That’s one of the reasons that SHM’s Leadership Academy has been so successful: It is creating a cadre of more than 2,000 hospitalists who are armed with the confidence and know-how to envision the hospital of the future and manage hospital-based teams toward that vision.
- Collaborate with HMX.
If you’ve ever been to SHM’s annual meeting, you know that hospitalists are a collaborative bunch. In fact, it’s that tendency toward collaboration and problem solving that has led more than 2,300 hospitalists to participate in SHM’s new online community, Hospital Medicine Exchange (www.hmxchange.org). It’s unlike any other platform for hospital-based clinicians, and the conversations on HMX are helping hospitalists everywhere benefit from the experience of colleagues nationally.
- Learn through the portal.
Hospitalists can’t shape the future of healthcare without staying up to date, but the days of getting continuing medical education (CME) credit exclusively from conferences is over. SHM is helping hospitalists with its brand new eLearning Portal (www.shmlearningportal.org), which can be accessed on PCs, tablets, or mobile devices.
Expectation High
So, be bold! The sky is the limit. Continue to learn, collaborate, and lead. Most of all, never stop believing that you can create the future you imagine. After all, it was Albert Einstein who cleverly said, “Imagination is more important than knowledge.”
As for my daughter and I, well, I guess I’m going to start investing in really big hats.
Dr. Afsar is associate chief medical officer at UCLA Hospitals in Los Angeles. She is also assistant clinical professor and executive director of quality and safety in the Department of Medicine and Neurosurgery at UCLA Hospitals. She is an SHM board member. Contact her at [email protected].
“I’m going to the sun,” my TWO-and-a-half-year-old daughter confidently declared. She said it so casually, as if she was letting me know that she was going to the playground.
Thinking I could use this as a great parenting opportunity and push my toddler to think through her decisions, I replied in a concerned tone: “Sweetie, the sun is really, really hot. What are you going to do about that?”
She replied effortlessly, as if the solution had always been right there in front of me, and somehow I had failed to see it, “I’m going to wear a really, really big hat!”
Later that night, I was reflecting on the little exchange with my daughter. Why had I been so determined to point out to her that it was impossible to travel to the sun? After all, two is the age to dream and imagine. As we grow up, why do we stop believing that we can do anything, absolutely anything, we imagine?
Since I started working as a hospitalist in 2007, the state of healthcare has been in constant turmoil and distress. Everyone, from providers to policymakers to patients, has been critical about the current state of our healthcare system. Many are concerned with the future, too. In fact, headlines regularly describe healthcare as “deficient,” “error-prone,” “deadly,” “bankrupt,” or “wasteful.”
This is not the vision of the medical profession that I had when I was an idealistic medical student. I was filled with aspirations of curing the sick, alleviating suffering, and helping to make the world a better place.
Don’t get me wrong...I get it. Hospitals, hospitalists, and all forms of care providers have a long way to go before we provide the highest quality of care at a cost our nation and our patients can afford. But in the critical evaluation of the current state of healthcare, where is the positive beacon of hope?
When did we, providers of care, stop believing that we could do anything, absolutely anything, to improve the state of healthcare?
Over the past decade, numerous innovations have been introduced to address the deficiencies in our system. However, efforts to come together as a medical profession and address these issues systematically have been lacking. And new initiatives, such as the ABIM Foundation’s Choosing Wisely campaign, are still in the early stages of widespread acceptance and adoption.
We have come a long way from the witchcraft of early healers and the barber-surgeons of medieval times. Modern medicine comes from a tradition of discovering the germ theory, eradicating polio, sequencing the entire genome, and performing simultaneous multiple organ transplantation. Providers are more than healers of the individual patient; they are healers of populations. By advancing health, they have enabled societies to thrive, grow, discover, and innovate. We shoulder significant responsibility, and our impact has shaped the course of human history.
Despite the stated challenges in healthcare, I’d like to think this is our finest hour, our time to shine. We have a rare and unique opportunity to completely reinvent the system and redefine the practice of medicine—to transform it from how it is practiced to how it should be delivered: high quality, high value, patient-centered, yet population-focused. This goes beyond ensuring that every patient with acute myocardial infarction receives an aspirin or working to prevent surgical site infections. This opportunity affords us the possibility to deliver extraordinary care.
Can hospitalists bridge this gap and change the world? Absolutely!
Inherent in our work is continuous improvement, not solely the improvement of our specialty, but also of the services we help co-manage, the hospital-wide committees we sit on, and the C-suite conversations we partake in. And, unlike most of healthcare, we manage to do this, not in isolation, but in multidisciplinary teams of physicians, nurses, staff, and, most importantly, patients and families.
If we unleash the potential of our specialty, the possibilities are endless. Here are some examples from our own hospitalists and society:
- Imagine the future of care with mentored implementation.
SHM’s award-winning mentored implementation model has helped transform care in more than 300 hospitals through best practices in venous thromboembolism, readmissions, and care of diabetic patients.
- Lead with the academy.
The future of healthcare will belong to clinicians who can lead teams and make the case for real change. That’s one of the reasons that SHM’s Leadership Academy has been so successful: It is creating a cadre of more than 2,000 hospitalists who are armed with the confidence and know-how to envision the hospital of the future and manage hospital-based teams toward that vision.
- Collaborate with HMX.
If you’ve ever been to SHM’s annual meeting, you know that hospitalists are a collaborative bunch. In fact, it’s that tendency toward collaboration and problem solving that has led more than 2,300 hospitalists to participate in SHM’s new online community, Hospital Medicine Exchange (www.hmxchange.org). It’s unlike any other platform for hospital-based clinicians, and the conversations on HMX are helping hospitalists everywhere benefit from the experience of colleagues nationally.
- Learn through the portal.
Hospitalists can’t shape the future of healthcare without staying up to date, but the days of getting continuing medical education (CME) credit exclusively from conferences is over. SHM is helping hospitalists with its brand new eLearning Portal (www.shmlearningportal.org), which can be accessed on PCs, tablets, or mobile devices.
Expectation High
So, be bold! The sky is the limit. Continue to learn, collaborate, and lead. Most of all, never stop believing that you can create the future you imagine. After all, it was Albert Einstein who cleverly said, “Imagination is more important than knowledge.”
As for my daughter and I, well, I guess I’m going to start investing in really big hats.
Dr. Afsar is associate chief medical officer at UCLA Hospitals in Los Angeles. She is also assistant clinical professor and executive director of quality and safety in the Department of Medicine and Neurosurgery at UCLA Hospitals. She is an SHM board member. Contact her at [email protected].
How to Handle Medicare Documentation Audits

The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
Hospitalists' Role in PQRS, Pay for Performance Gets Boost
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
SHM Report Provides New Insights About Physician Practice Leaders
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
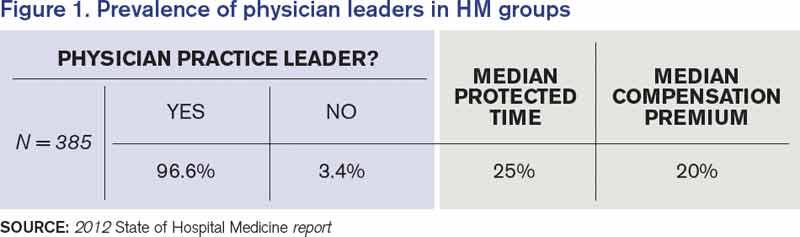
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.

Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
Two Hospitalist Groups Join SHM's Hospital Medicine Exchange

HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
Hospitalists Poised to Prevent, Combat Antibiotic-Resistant Pathogens
Describing formally for the first time the enormity of the problem of antibiotic resistance and warning of the “potentially catastrophic consequences of inaction,” the Centers for Disease Control and Prevention (CDC) announced in September that more than two million people a year are sickened by infections that are resistant to treatment with antibiotics.
Moreover, the CDC says 23,000 people die as a result.
And because those numbers are based only on the data available—and the agency assumes that many infections are not captured—the CDC says its estimate is a conservative one and the real number is probably higher.
The report is a call to action for hospitalists, who are in an almost ideal position to participate in efforts to prevent infections and control their spread once they’re discovered, says Jean Patel, PhD, deputy director of the office of antimicrobial resistance at the CDC.
“I think it’s a sobering number, and it indicates how far we have to go in combating this problem of antimicrobial resistance,” Dr. Patel says.
The medical community, she adds, cannot expect that new treatments will become available to fight all of these new infections.
“All of the drugs also are going to have some gaps in their range of activity, so there’s no drug coming that’s going to be effective against all the antimicrobial-resistant drugs that we face today,” Dr. Patel explains. “For that reason, we’re sounding the alarm that it’s important to pay attention to infection control and antibiotic stewardship practices.”
The report, “Antibiotic Resistance Threats to the United States, 2013,” creates three categories of antibiotic-resistant pathogens. In the “urgent” tier are Clostridium difficile, which the CDC estimates is responsible for 250,000 infections a year and 14,000 deaths; carbapenem-resistant Enterobacteriaceae, estimated to be responsible for 9,000 drug-resistant infections a year and 600 deaths; and drug-resistant Neisseria gonorrhoeae, at 246,000 drug-resistant infections.
These bacteria are considered an “immediate public health threat that requires urgent and aggressive action.”
There are 12 pathogens in the second category, described as “a serious concern” requiring “prompt and sustained action to ensure the problem does not grow.”
Of particular interest to hospitalists in this group, Dr. Patel says, is methicillin-resistant Staphylococcus aureus (MRSA). The CDC estimates that more than 80,000 severe MRSA infections and more than 11,000 deaths occur in the U.S. every year.
MRSA was not ranked as an “urgent” threat only because the number of infections is actually decreasing, especially in healthcare institutions, and because there are antibiotics that still work on MRSA.
“If either of those things were to change—for example, if the rate of infections were to increase, or if these isolates were to become more resistant—then we would have to think about changing this from a serious threat to an urgent threat,” Dr. Patel says.
Another infection in the serious category that should be on hospitalists’ radar is drug-resistant Streptococcus pneumoniae. A new vaccine is helping to decrease the number of these infections, but hospitalists should be vigilant about infections that could escape the vaccine and become resistant, Dr. Patel says.
The report estimates as much as $20 billion in excess healthcare costs due to antimicrobial-resistant infections, with $35 billion in lost productivity in 2008 dollars.1
Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine in Atlanta and a member of the antimicrobial stewardship and infectious disease control committees at Emory University Hospital Midtown, says the sheer numbers are sure to get people to take notice.
“Two million is lots of patients,” she says. “It’s eye-opening, really, for many doctors and patients and society.”
The silver lining, she says, is that the field is moving toward diagnostic tools that will provide quick feedback on the type of infection at work.
It may be that hospitalists have no choice but to give an antibiotic to a patient because of the risk involved in not giving one; however, providers should quickly tailor that treatment to target the specific pathogen when more information is available.
—Ketino Kobaidze, MD, assistant professor, Emory University School of Medicine, Atlanta, member, antimicrobial stewardship and infectious disease control committees, Emory University Hospital Midtown
“The most important thing, I think, for hospital medicine and medicine anywhere, is to follow up with whatever you’re ordering and notice right away what happens with these tests. If it’s positive or negative, redirect your care,” Dr. Kobaidze says. “Time is really an important issue here.
“As hospitalists, we need to be extremely cautious not to give them something they don’t need.”
Dr. Kobaidze was particularly struck by gonorrhea being listed in the “urgent” threat category.
“It was so easy to treat before,” she says. “It was nothing, piece of cake. This makes me a little bit concerned.”
Robert Orenstein, DO, an infectious disease expert at Mayo Clinic, praises the report and says hospitalists have a key role to play.
“I think this has a clear impact on hospitalists, who are the primary caregivers of many of these ill patients,” he says. “We need to educate them and build systems that target antimicrobials to the infecting agents and limit their use. Hospitalists are also the people who can help protect patients from the spread of these in the hospital by following appropriate infection prevention guidelines and educating their colleagues of the importance of this.”
He also stresses the importance of being aware of threats within your specific region.
“Many of these MDROs [multi-drug resistant organisms] have regional prevalence,” he says. “And it’s important to know which bugs are in your region so you can work with your institution and public health to tackle these.”
Tom Collins is a freelance writer in South Florida.
Reference
Describing formally for the first time the enormity of the problem of antibiotic resistance and warning of the “potentially catastrophic consequences of inaction,” the Centers for Disease Control and Prevention (CDC) announced in September that more than two million people a year are sickened by infections that are resistant to treatment with antibiotics.
Moreover, the CDC says 23,000 people die as a result.
And because those numbers are based only on the data available—and the agency assumes that many infections are not captured—the CDC says its estimate is a conservative one and the real number is probably higher.
The report is a call to action for hospitalists, who are in an almost ideal position to participate in efforts to prevent infections and control their spread once they’re discovered, says Jean Patel, PhD, deputy director of the office of antimicrobial resistance at the CDC.
“I think it’s a sobering number, and it indicates how far we have to go in combating this problem of antimicrobial resistance,” Dr. Patel says.
The medical community, she adds, cannot expect that new treatments will become available to fight all of these new infections.
“All of the drugs also are going to have some gaps in their range of activity, so there’s no drug coming that’s going to be effective against all the antimicrobial-resistant drugs that we face today,” Dr. Patel explains. “For that reason, we’re sounding the alarm that it’s important to pay attention to infection control and antibiotic stewardship practices.”
The report, “Antibiotic Resistance Threats to the United States, 2013,” creates three categories of antibiotic-resistant pathogens. In the “urgent” tier are Clostridium difficile, which the CDC estimates is responsible for 250,000 infections a year and 14,000 deaths; carbapenem-resistant Enterobacteriaceae, estimated to be responsible for 9,000 drug-resistant infections a year and 600 deaths; and drug-resistant Neisseria gonorrhoeae, at 246,000 drug-resistant infections.
These bacteria are considered an “immediate public health threat that requires urgent and aggressive action.”
There are 12 pathogens in the second category, described as “a serious concern” requiring “prompt and sustained action to ensure the problem does not grow.”
Of particular interest to hospitalists in this group, Dr. Patel says, is methicillin-resistant Staphylococcus aureus (MRSA). The CDC estimates that more than 80,000 severe MRSA infections and more than 11,000 deaths occur in the U.S. every year.
MRSA was not ranked as an “urgent” threat only because the number of infections is actually decreasing, especially in healthcare institutions, and because there are antibiotics that still work on MRSA.
“If either of those things were to change—for example, if the rate of infections were to increase, or if these isolates were to become more resistant—then we would have to think about changing this from a serious threat to an urgent threat,” Dr. Patel says.
Another infection in the serious category that should be on hospitalists’ radar is drug-resistant Streptococcus pneumoniae. A new vaccine is helping to decrease the number of these infections, but hospitalists should be vigilant about infections that could escape the vaccine and become resistant, Dr. Patel says.
The report estimates as much as $20 billion in excess healthcare costs due to antimicrobial-resistant infections, with $35 billion in lost productivity in 2008 dollars.1
Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine in Atlanta and a member of the antimicrobial stewardship and infectious disease control committees at Emory University Hospital Midtown, says the sheer numbers are sure to get people to take notice.
“Two million is lots of patients,” she says. “It’s eye-opening, really, for many doctors and patients and society.”
The silver lining, she says, is that the field is moving toward diagnostic tools that will provide quick feedback on the type of infection at work.
It may be that hospitalists have no choice but to give an antibiotic to a patient because of the risk involved in not giving one; however, providers should quickly tailor that treatment to target the specific pathogen when more information is available.
—Ketino Kobaidze, MD, assistant professor, Emory University School of Medicine, Atlanta, member, antimicrobial stewardship and infectious disease control committees, Emory University Hospital Midtown
“The most important thing, I think, for hospital medicine and medicine anywhere, is to follow up with whatever you’re ordering and notice right away what happens with these tests. If it’s positive or negative, redirect your care,” Dr. Kobaidze says. “Time is really an important issue here.
“As hospitalists, we need to be extremely cautious not to give them something they don’t need.”
Dr. Kobaidze was particularly struck by gonorrhea being listed in the “urgent” threat category.
“It was so easy to treat before,” she says. “It was nothing, piece of cake. This makes me a little bit concerned.”
Robert Orenstein, DO, an infectious disease expert at Mayo Clinic, praises the report and says hospitalists have a key role to play.
“I think this has a clear impact on hospitalists, who are the primary caregivers of many of these ill patients,” he says. “We need to educate them and build systems that target antimicrobials to the infecting agents and limit their use. Hospitalists are also the people who can help protect patients from the spread of these in the hospital by following appropriate infection prevention guidelines and educating their colleagues of the importance of this.”
He also stresses the importance of being aware of threats within your specific region.
“Many of these MDROs [multi-drug resistant organisms] have regional prevalence,” he says. “And it’s important to know which bugs are in your region so you can work with your institution and public health to tackle these.”
Tom Collins is a freelance writer in South Florida.
Reference
Describing formally for the first time the enormity of the problem of antibiotic resistance and warning of the “potentially catastrophic consequences of inaction,” the Centers for Disease Control and Prevention (CDC) announced in September that more than two million people a year are sickened by infections that are resistant to treatment with antibiotics.
Moreover, the CDC says 23,000 people die as a result.
And because those numbers are based only on the data available—and the agency assumes that many infections are not captured—the CDC says its estimate is a conservative one and the real number is probably higher.
The report is a call to action for hospitalists, who are in an almost ideal position to participate in efforts to prevent infections and control their spread once they’re discovered, says Jean Patel, PhD, deputy director of the office of antimicrobial resistance at the CDC.
“I think it’s a sobering number, and it indicates how far we have to go in combating this problem of antimicrobial resistance,” Dr. Patel says.
The medical community, she adds, cannot expect that new treatments will become available to fight all of these new infections.
“All of the drugs also are going to have some gaps in their range of activity, so there’s no drug coming that’s going to be effective against all the antimicrobial-resistant drugs that we face today,” Dr. Patel explains. “For that reason, we’re sounding the alarm that it’s important to pay attention to infection control and antibiotic stewardship practices.”
The report, “Antibiotic Resistance Threats to the United States, 2013,” creates three categories of antibiotic-resistant pathogens. In the “urgent” tier are Clostridium difficile, which the CDC estimates is responsible for 250,000 infections a year and 14,000 deaths; carbapenem-resistant Enterobacteriaceae, estimated to be responsible for 9,000 drug-resistant infections a year and 600 deaths; and drug-resistant Neisseria gonorrhoeae, at 246,000 drug-resistant infections.
These bacteria are considered an “immediate public health threat that requires urgent and aggressive action.”
There are 12 pathogens in the second category, described as “a serious concern” requiring “prompt and sustained action to ensure the problem does not grow.”
Of particular interest to hospitalists in this group, Dr. Patel says, is methicillin-resistant Staphylococcus aureus (MRSA). The CDC estimates that more than 80,000 severe MRSA infections and more than 11,000 deaths occur in the U.S. every year.
MRSA was not ranked as an “urgent” threat only because the number of infections is actually decreasing, especially in healthcare institutions, and because there are antibiotics that still work on MRSA.
“If either of those things were to change—for example, if the rate of infections were to increase, or if these isolates were to become more resistant—then we would have to think about changing this from a serious threat to an urgent threat,” Dr. Patel says.
Another infection in the serious category that should be on hospitalists’ radar is drug-resistant Streptococcus pneumoniae. A new vaccine is helping to decrease the number of these infections, but hospitalists should be vigilant about infections that could escape the vaccine and become resistant, Dr. Patel says.
The report estimates as much as $20 billion in excess healthcare costs due to antimicrobial-resistant infections, with $35 billion in lost productivity in 2008 dollars.1
Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine in Atlanta and a member of the antimicrobial stewardship and infectious disease control committees at Emory University Hospital Midtown, says the sheer numbers are sure to get people to take notice.
“Two million is lots of patients,” she says. “It’s eye-opening, really, for many doctors and patients and society.”
The silver lining, she says, is that the field is moving toward diagnostic tools that will provide quick feedback on the type of infection at work.
It may be that hospitalists have no choice but to give an antibiotic to a patient because of the risk involved in not giving one; however, providers should quickly tailor that treatment to target the specific pathogen when more information is available.
—Ketino Kobaidze, MD, assistant professor, Emory University School of Medicine, Atlanta, member, antimicrobial stewardship and infectious disease control committees, Emory University Hospital Midtown
“The most important thing, I think, for hospital medicine and medicine anywhere, is to follow up with whatever you’re ordering and notice right away what happens with these tests. If it’s positive or negative, redirect your care,” Dr. Kobaidze says. “Time is really an important issue here.
“As hospitalists, we need to be extremely cautious not to give them something they don’t need.”
Dr. Kobaidze was particularly struck by gonorrhea being listed in the “urgent” threat category.
“It was so easy to treat before,” she says. “It was nothing, piece of cake. This makes me a little bit concerned.”
Robert Orenstein, DO, an infectious disease expert at Mayo Clinic, praises the report and says hospitalists have a key role to play.
“I think this has a clear impact on hospitalists, who are the primary caregivers of many of these ill patients,” he says. “We need to educate them and build systems that target antimicrobials to the infecting agents and limit their use. Hospitalists are also the people who can help protect patients from the spread of these in the hospital by following appropriate infection prevention guidelines and educating their colleagues of the importance of this.”
He also stresses the importance of being aware of threats within your specific region.
“Many of these MDROs [multi-drug resistant organisms] have regional prevalence,” he says. “And it’s important to know which bugs are in your region so you can work with your institution and public health to tackle these.”
Tom Collins is a freelance writer in South Florida.
Reference
Why Hospitalists Should Focus on Patient-Care Basics


We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
New Rules for Value-Based Purchasing, Readmission Penalties, Admissions


The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].