User login
The Hospitalist only
A Time to Be Recognized
Like so many things in HM, the story of how hospitalists first learned about the focused practice program is a modern one.
It started with a text message, which led to a blog post, which reached thousands of readers, many of them hospitalists interested in how to bolster their bona fides in a specialty known for its explosive growth in recent years.
Now, hospitalists certified in internal medicine have the opportunity to reinforce their commitment to the specialty by maintaining their certification through the Focused Practice in Hospital Medicine pathway offered by the American Board of Internal Medicine (ABIM). The Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program enables hospitalists to distinguish their practice within the larger specialty of internal medicine.
The Evolution of FPHM
The new pathway has been years in the making, and it reflects the growing influence of HM in healthcare, according to ABIM Chief Medical Officer Eric Holmboe, MD. He sees the FPHM as the result of a combination of factors, including the fact that the specialty now has more than 30,000 hospitalists practicing nationwide. “If you look at the past years, this has been a viable and vibrant practice,” he says. “If you look at the number of people doing hospital medicine, it’s a factor.”
For Holmboe, it also is a shift in how individuals are recognized based on their practice areas. “This is an acknowledgement by ABIM and the American Board of Medical Specialties to look at Maintenance of Certification in terms of what the individual actually does,” he explains. “Hospitalists play a very important role in the hospital.”
He also credits the leadership of the HM movement—especially pioneers like Robert Wachter, MD, FHM. One of HM’s most ardent champions, Dr. Wachter, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, worked with ABIM to find a way to recognize hospitalists’ specialized skill sets and their commitment to inpatient medicine. After more than a decade of advocating for a board-certified process to recognize the field, Dr. Wachter, an ABIM board member, began receiving multiple text messages from colleagues announcing that ABIM had approved the focused-practice program. He wrote a post on his blog, Wachter’s World (www.wachtersworld.com), that outlined the need for the FPHM and the significance for aspiring hospitalists.
“In any case, this is an important milestone for the field,” Dr. Wachter wrote in his Sept. 23, 2009, blog entry, “Board Certification for Hospitalists: It’s Heeeere!” “In fact, when I first began speaking to groups of hospitalists nearly 15 years ago, I often showed a slide listing the elements of a true specialty, and one by one we’ve ticked them off,” wrote Dr. Wachter, a former SHM president. “The only unchecked box was recognition of the field as a legitimate ‘specialty,’ as codified by the ABMS board certification process.”
Unchecked, that is, until now.
In early 2011, the medical world will be introduced to the first internists recognized for their focus in HM. For Holmboe, the FPHM is the beginning of an even larger movement.
“The goal is continued interest: getting people involved in quality in their hospital and encouraging people to change behaviors and be recognized by patients and credentialists as valuable,” he says. “That’s the primary mission of ABIM: using certification to improve care.”
Fellow in Hospital Medicine Spotlight
O’Neil Pyke, MD, FHM

Dr. Pyke is a clinical instructor at Commonwealth Medical College and a medical director at the Wyoming Valley Health Care System in Wilkes-Barre, Pa. He also serves as a consultant for various hospitalist programs, most actively for his own private consulting company, AMP Hospitalist Consulting, which partners with Salem, N.H.-based physician staffing company Medicus Healthcare Solutions.
Undergraduate Education: Queens College, City University of New York, Flushing, N.Y.
Medical School: Ohio State University College of Medicine and Public Health, Columbus
Notable: Dr. Pyke was born in Jamaica and moved to New York during high school. He says he owes everything to his parents. His parents, who had no education beyond high school, pushed Dr. Pyke and his siblings to achieve more than they did. His sister is an OB-GYN and his brother is pursuing a medical degree.
FYI: Dr. Pyke enjoys playing golf, cheering for his beloved Ohio State Buckeyes, and spends every Friday night with his wife and two daughters—he even admits to watching “chick flicks” on family night.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
Requirements and Process
Shortly after the program’s approval, ABIM, which administers the FPHM program, went to work in defining the process for the FPHM application and building infrastructure to support the tests. Holmboe expects ABIM will be ready to process pre-applications by April or May. While some details may change, the FPHM application will dovetail with ABIM’s MOC process.
Although hospitalists’ MOC must be current in order to apply for FPHM, hospitalists can begin the FPHM application process at any time. Hospitalists do not need to wait until their next MOC renewal.
Before beginning the application process, hospitalists should ensure that they are eligible. ABIM requires FPHM candidates to have:
- A current or previous ABIM certification in internal medicine;
- A valid, unrestricted medical license and confirmation of good standing in the local practice community;
- ACLS certification; and
- At least three years of hospital medicine practice experience.
Candidates who meet the requirements can then begin the enrollment process by:
- Submitting attestations. Both the hospitalist and a senior officer at the hospital must provide attestations that demonstrate the hospitalist’s experience in HM and his or her commitment to the principles of the specialty.
- Performing a self-assessment. Hospitalists must quantify their experience in HM through an MOC self-assessment. Candidates must achieve at least 100 MOC points. Successful applicants must submit a new self-assessment every three years. The self-assessment can be conducted before or after the exam.
- Taking the MOC examination in Hospital Medicine. Registration for the first HM examination will begin in May. The exam will be conducted in October, and diplomates can take the exam at any time in the process.
Passing the exam and completing the other requirements will earn ABIM diplomats recognition as “Board Certified in Internal Medicine with a Focused Practice in Hospital Medicine.” ABIM will notify successful applicants in late 2010 and ship personalized certificates in early 2011. TH
Brendon Shank is a freelance writer based in Philadelphia.
Like so many things in HM, the story of how hospitalists first learned about the focused practice program is a modern one.
It started with a text message, which led to a blog post, which reached thousands of readers, many of them hospitalists interested in how to bolster their bona fides in a specialty known for its explosive growth in recent years.
Now, hospitalists certified in internal medicine have the opportunity to reinforce their commitment to the specialty by maintaining their certification through the Focused Practice in Hospital Medicine pathway offered by the American Board of Internal Medicine (ABIM). The Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program enables hospitalists to distinguish their practice within the larger specialty of internal medicine.
The Evolution of FPHM
The new pathway has been years in the making, and it reflects the growing influence of HM in healthcare, according to ABIM Chief Medical Officer Eric Holmboe, MD. He sees the FPHM as the result of a combination of factors, including the fact that the specialty now has more than 30,000 hospitalists practicing nationwide. “If you look at the past years, this has been a viable and vibrant practice,” he says. “If you look at the number of people doing hospital medicine, it’s a factor.”
For Holmboe, it also is a shift in how individuals are recognized based on their practice areas. “This is an acknowledgement by ABIM and the American Board of Medical Specialties to look at Maintenance of Certification in terms of what the individual actually does,” he explains. “Hospitalists play a very important role in the hospital.”
He also credits the leadership of the HM movement—especially pioneers like Robert Wachter, MD, FHM. One of HM’s most ardent champions, Dr. Wachter, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, worked with ABIM to find a way to recognize hospitalists’ specialized skill sets and their commitment to inpatient medicine. After more than a decade of advocating for a board-certified process to recognize the field, Dr. Wachter, an ABIM board member, began receiving multiple text messages from colleagues announcing that ABIM had approved the focused-practice program. He wrote a post on his blog, Wachter’s World (www.wachtersworld.com), that outlined the need for the FPHM and the significance for aspiring hospitalists.
“In any case, this is an important milestone for the field,” Dr. Wachter wrote in his Sept. 23, 2009, blog entry, “Board Certification for Hospitalists: It’s Heeeere!” “In fact, when I first began speaking to groups of hospitalists nearly 15 years ago, I often showed a slide listing the elements of a true specialty, and one by one we’ve ticked them off,” wrote Dr. Wachter, a former SHM president. “The only unchecked box was recognition of the field as a legitimate ‘specialty,’ as codified by the ABMS board certification process.”
Unchecked, that is, until now.
In early 2011, the medical world will be introduced to the first internists recognized for their focus in HM. For Holmboe, the FPHM is the beginning of an even larger movement.
“The goal is continued interest: getting people involved in quality in their hospital and encouraging people to change behaviors and be recognized by patients and credentialists as valuable,” he says. “That’s the primary mission of ABIM: using certification to improve care.”
Fellow in Hospital Medicine Spotlight
O’Neil Pyke, MD, FHM
Dr. Pyke is a clinical instructor at Commonwealth Medical College and a medical director at the Wyoming Valley Health Care System in Wilkes-Barre, Pa. He also serves as a consultant for various hospitalist programs, most actively for his own private consulting company, AMP Hospitalist Consulting, which partners with Salem, N.H.-based physician staffing company Medicus Healthcare Solutions.
Undergraduate Education: Queens College, City University of New York, Flushing, N.Y.
Medical School: Ohio State University College of Medicine and Public Health, Columbus
Notable: Dr. Pyke was born in Jamaica and moved to New York during high school. He says he owes everything to his parents. His parents, who had no education beyond high school, pushed Dr. Pyke and his siblings to achieve more than they did. His sister is an OB-GYN and his brother is pursuing a medical degree.
FYI: Dr. Pyke enjoys playing golf, cheering for his beloved Ohio State Buckeyes, and spends every Friday night with his wife and two daughters—he even admits to watching “chick flicks” on family night.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
Requirements and Process
Shortly after the program’s approval, ABIM, which administers the FPHM program, went to work in defining the process for the FPHM application and building infrastructure to support the tests. Holmboe expects ABIM will be ready to process pre-applications by April or May. While some details may change, the FPHM application will dovetail with ABIM’s MOC process.
Although hospitalists’ MOC must be current in order to apply for FPHM, hospitalists can begin the FPHM application process at any time. Hospitalists do not need to wait until their next MOC renewal.
Before beginning the application process, hospitalists should ensure that they are eligible. ABIM requires FPHM candidates to have:
- A current or previous ABIM certification in internal medicine;
- A valid, unrestricted medical license and confirmation of good standing in the local practice community;
- ACLS certification; and
- At least three years of hospital medicine practice experience.
Candidates who meet the requirements can then begin the enrollment process by:
- Submitting attestations. Both the hospitalist and a senior officer at the hospital must provide attestations that demonstrate the hospitalist’s experience in HM and his or her commitment to the principles of the specialty.
- Performing a self-assessment. Hospitalists must quantify their experience in HM through an MOC self-assessment. Candidates must achieve at least 100 MOC points. Successful applicants must submit a new self-assessment every three years. The self-assessment can be conducted before or after the exam.
- Taking the MOC examination in Hospital Medicine. Registration for the first HM examination will begin in May. The exam will be conducted in October, and diplomates can take the exam at any time in the process.
Passing the exam and completing the other requirements will earn ABIM diplomats recognition as “Board Certified in Internal Medicine with a Focused Practice in Hospital Medicine.” ABIM will notify successful applicants in late 2010 and ship personalized certificates in early 2011. TH
Brendon Shank is a freelance writer based in Philadelphia.
Like so many things in HM, the story of how hospitalists first learned about the focused practice program is a modern one.
It started with a text message, which led to a blog post, which reached thousands of readers, many of them hospitalists interested in how to bolster their bona fides in a specialty known for its explosive growth in recent years.
Now, hospitalists certified in internal medicine have the opportunity to reinforce their commitment to the specialty by maintaining their certification through the Focused Practice in Hospital Medicine pathway offered by the American Board of Internal Medicine (ABIM). The Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program enables hospitalists to distinguish their practice within the larger specialty of internal medicine.
The Evolution of FPHM
The new pathway has been years in the making, and it reflects the growing influence of HM in healthcare, according to ABIM Chief Medical Officer Eric Holmboe, MD. He sees the FPHM as the result of a combination of factors, including the fact that the specialty now has more than 30,000 hospitalists practicing nationwide. “If you look at the past years, this has been a viable and vibrant practice,” he says. “If you look at the number of people doing hospital medicine, it’s a factor.”
For Holmboe, it also is a shift in how individuals are recognized based on their practice areas. “This is an acknowledgement by ABIM and the American Board of Medical Specialties to look at Maintenance of Certification in terms of what the individual actually does,” he explains. “Hospitalists play a very important role in the hospital.”
He also credits the leadership of the HM movement—especially pioneers like Robert Wachter, MD, FHM. One of HM’s most ardent champions, Dr. Wachter, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, worked with ABIM to find a way to recognize hospitalists’ specialized skill sets and their commitment to inpatient medicine. After more than a decade of advocating for a board-certified process to recognize the field, Dr. Wachter, an ABIM board member, began receiving multiple text messages from colleagues announcing that ABIM had approved the focused-practice program. He wrote a post on his blog, Wachter’s World (www.wachtersworld.com), that outlined the need for the FPHM and the significance for aspiring hospitalists.
“In any case, this is an important milestone for the field,” Dr. Wachter wrote in his Sept. 23, 2009, blog entry, “Board Certification for Hospitalists: It’s Heeeere!” “In fact, when I first began speaking to groups of hospitalists nearly 15 years ago, I often showed a slide listing the elements of a true specialty, and one by one we’ve ticked them off,” wrote Dr. Wachter, a former SHM president. “The only unchecked box was recognition of the field as a legitimate ‘specialty,’ as codified by the ABMS board certification process.”
Unchecked, that is, until now.
In early 2011, the medical world will be introduced to the first internists recognized for their focus in HM. For Holmboe, the FPHM is the beginning of an even larger movement.
“The goal is continued interest: getting people involved in quality in their hospital and encouraging people to change behaviors and be recognized by patients and credentialists as valuable,” he says. “That’s the primary mission of ABIM: using certification to improve care.”
Fellow in Hospital Medicine Spotlight
O’Neil Pyke, MD, FHM
Dr. Pyke is a clinical instructor at Commonwealth Medical College and a medical director at the Wyoming Valley Health Care System in Wilkes-Barre, Pa. He also serves as a consultant for various hospitalist programs, most actively for his own private consulting company, AMP Hospitalist Consulting, which partners with Salem, N.H.-based physician staffing company Medicus Healthcare Solutions.
Undergraduate Education: Queens College, City University of New York, Flushing, N.Y.
Medical School: Ohio State University College of Medicine and Public Health, Columbus
Notable: Dr. Pyke was born in Jamaica and moved to New York during high school. He says he owes everything to his parents. His parents, who had no education beyond high school, pushed Dr. Pyke and his siblings to achieve more than they did. His sister is an OB-GYN and his brother is pursuing a medical degree.
FYI: Dr. Pyke enjoys playing golf, cheering for his beloved Ohio State Buckeyes, and spends every Friday night with his wife and two daughters—he even admits to watching “chick flicks” on family night.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
Requirements and Process
Shortly after the program’s approval, ABIM, which administers the FPHM program, went to work in defining the process for the FPHM application and building infrastructure to support the tests. Holmboe expects ABIM will be ready to process pre-applications by April or May. While some details may change, the FPHM application will dovetail with ABIM’s MOC process.
Although hospitalists’ MOC must be current in order to apply for FPHM, hospitalists can begin the FPHM application process at any time. Hospitalists do not need to wait until their next MOC renewal.
Before beginning the application process, hospitalists should ensure that they are eligible. ABIM requires FPHM candidates to have:
- A current or previous ABIM certification in internal medicine;
- A valid, unrestricted medical license and confirmation of good standing in the local practice community;
- ACLS certification; and
- At least three years of hospital medicine practice experience.
Candidates who meet the requirements can then begin the enrollment process by:
- Submitting attestations. Both the hospitalist and a senior officer at the hospital must provide attestations that demonstrate the hospitalist’s experience in HM and his or her commitment to the principles of the specialty.
- Performing a self-assessment. Hospitalists must quantify their experience in HM through an MOC self-assessment. Candidates must achieve at least 100 MOC points. Successful applicants must submit a new self-assessment every three years. The self-assessment can be conducted before or after the exam.
- Taking the MOC examination in Hospital Medicine. Registration for the first HM examination will begin in May. The exam will be conducted in October, and diplomates can take the exam at any time in the process.
Passing the exam and completing the other requirements will earn ABIM diplomats recognition as “Board Certified in Internal Medicine with a Focused Practice in Hospital Medicine.” ABIM will notify successful applicants in late 2010 and ship personalized certificates in early 2011. TH
Brendon Shank is a freelance writer based in Philadelphia.
Group Leaders Can Shift the HM Negotiation Paradigm
Whether hospitalists like it or not, the art of negotiation has a significant impact on their daily activities. Negotiations take place with consultants over what the perceived optimal plan of care should be. Discussions are held with patients on how best to overcome the social, financial, and psychological barriers that may impede their health. Hospitalists negotiate with administrators over schedules, benefits, and responsibilities.
Quite frequently, negotiation is viewed as a process where one party wins and the other loses, a zero-sum game, like chess. The spoils may be financial (e.g., better reimbursements) or they may be cognitive (e.g., success in convincing someone of your particular viewpoint). Significant value that could potentially benefit both parties may be lost if the negotiation is approached with a win-loss mentality. However, with proper preparation and insight, a hospitalist can create value in a negotiation that otherwise may be lost by shifting their negotiation paradigm to a collaborative strategy.
A collaborative strategy is when the relationship—and not just the outcome—is important. This would apply to most negotiations that hospitalists take part in.
A significant part of this strategy involves listening and allowing the other side to divulge their interests and positions. Information must flow freely. Once the problem is identified, it must then be detailed further, ensuring both parties understand each other.
Only once both party’s issues are presented can an alternative solution be contemplated that will be win-win in nature. The parties then must both agree to choose that solution and move forward.
The optimal result is that the chosen solution appeases both parties and has a greater total value than if both sides were solely vying for their own interests.
Riyad Fares, MD,
hospitalist,
Adventist Hospital, Portland, Ore.
Whether hospitalists like it or not, the art of negotiation has a significant impact on their daily activities. Negotiations take place with consultants over what the perceived optimal plan of care should be. Discussions are held with patients on how best to overcome the social, financial, and psychological barriers that may impede their health. Hospitalists negotiate with administrators over schedules, benefits, and responsibilities.
Quite frequently, negotiation is viewed as a process where one party wins and the other loses, a zero-sum game, like chess. The spoils may be financial (e.g., better reimbursements) or they may be cognitive (e.g., success in convincing someone of your particular viewpoint). Significant value that could potentially benefit both parties may be lost if the negotiation is approached with a win-loss mentality. However, with proper preparation and insight, a hospitalist can create value in a negotiation that otherwise may be lost by shifting their negotiation paradigm to a collaborative strategy.
A collaborative strategy is when the relationship—and not just the outcome—is important. This would apply to most negotiations that hospitalists take part in.
A significant part of this strategy involves listening and allowing the other side to divulge their interests and positions. Information must flow freely. Once the problem is identified, it must then be detailed further, ensuring both parties understand each other.
Only once both party’s issues are presented can an alternative solution be contemplated that will be win-win in nature. The parties then must both agree to choose that solution and move forward.
The optimal result is that the chosen solution appeases both parties and has a greater total value than if both sides were solely vying for their own interests.
Riyad Fares, MD,
hospitalist,
Adventist Hospital, Portland, Ore.
Whether hospitalists like it or not, the art of negotiation has a significant impact on their daily activities. Negotiations take place with consultants over what the perceived optimal plan of care should be. Discussions are held with patients on how best to overcome the social, financial, and psychological barriers that may impede their health. Hospitalists negotiate with administrators over schedules, benefits, and responsibilities.
Quite frequently, negotiation is viewed as a process where one party wins and the other loses, a zero-sum game, like chess. The spoils may be financial (e.g., better reimbursements) or they may be cognitive (e.g., success in convincing someone of your particular viewpoint). Significant value that could potentially benefit both parties may be lost if the negotiation is approached with a win-loss mentality. However, with proper preparation and insight, a hospitalist can create value in a negotiation that otherwise may be lost by shifting their negotiation paradigm to a collaborative strategy.
A collaborative strategy is when the relationship—and not just the outcome—is important. This would apply to most negotiations that hospitalists take part in.
A significant part of this strategy involves listening and allowing the other side to divulge their interests and positions. Information must flow freely. Once the problem is identified, it must then be detailed further, ensuring both parties understand each other.
Only once both party’s issues are presented can an alternative solution be contemplated that will be win-win in nature. The parties then must both agree to choose that solution and move forward.
The optimal result is that the chosen solution appeases both parties and has a greater total value than if both sides were solely vying for their own interests.
Riyad Fares, MD,
hospitalist,
Adventist Hospital, Portland, Ore.
Patient Distribution

Editor’s note: This is the first of a three-part series.
My experience is that some, maybe even most, hospitalists tend to assume there is a standard or “right” way to organize things like work schedules, compensation, or even the assignment of patients among the group’s providers. Some will say things like “SHM says the best hospitalist schedule is …” or “The best way to compensate hospitalists is …”
But there really isn’t a “best” way to manage any particular attribute of a practice. Don’t make the mistake of assuming your method is best, or that it’s the way “everybody else does it.” Although scheduling and compensation are marquee issues for hospitalists, approaches to distributing new patients is much less visible. Many groups tend to assume their method is the only reasonable approach. The best approach, however, varies from one practice to the next. You should be open to hearing approaches to scheduling that are different from your own.
Assign Patients by “Load Leveling”
I’ve come across a lot—and I mean a lot—of different approaches to distributing new patients in HM groups around the country, but it seems pretty clear that the most common method is to undertake “load leveling” on a daily or ongoing basis.
For example, groups that have a separate night shift (the night doctor performs no daytime work the day before or the day after a night shift) typically distribute the night’s new patients with the intent of having each daytime doctor start with the same number of patients. The group might more heavily weight some patients, such as those in the ICU (e.g., each ICU patient counts as 1.5 or two non-ICU patients), but most groups don’t. Over the course of the day shift, new referrals will be distributed evenly among the doctors one at a time, sort of like dealing a deck of cards.
This approach aims to avoid significant imbalances in patient loads and has the potential cultural benefit of everyone sharing equally in busy and slow days. Groups that use it tend to see it as the best option because it is the fairest way to divide up the workload.
Practices that use load-leveling almost always use a schedule built on shifts of a predetermined and fixed duration. For example, say the day shift always works from 7 a.m. to 7 p.m. This schedule usually has the majority of compensation paid via a fixed annual salary or fixed shift rate. One potential problem with this approach is that the doctor who is efficient and discharges a lot of patients today is “rewarded” with more new patients tomorrow. Hospitalists who are allergic to work might have an incentive to have a patient wait until tomorrow to discharge to avoid having to assume the care of yet another patient tomorrow morning. Hospital executives who are focused on length-of-stay management might be concerned if they knew this was a potential issue. Of course, the reverse is true as well. In a practice that doesn’t aggressively undertake load-leveling, a less-than-admirable hospitalist could push patients to discharge earlier than optimal just to have one less patient the next day.
Another cost of this approach is that the distribution of patients can be time-consuming each morning. It also offers the opportunity for some in the group to decide they’re treated unfairly. For instance, you might hear the occasional “just last Tuesday, I started with 16 patients, compared with 15 for everyone else. Now you want me to do it again? You’re being unfair to me; it’s someone else’s turn to take the extra patient.”
Assignment by Location
Groups that use “unit-based” hospitalists distribute patients according to the unit the patient is admitted to—and the hospitalist covering that unit. The pros and cons of unit-based hospitalists are many (see “A Unit-Based Approach,” September 2007), but there is an obvious tension between keeping patient loads even among hospitalists and ensuring that all of a hospitalist’s patients are on “their” unit. Practicality usually requires a compromise between pure unit-based assignment and load-leveling.
Uneven Assignments
Some groups assign patients according to a predetermined algorithm and employ load-leveling only when patient loads become extremely unbalanced. For example, Dr. Jones gets all the new referrals today, and Dr. James gets them tomorrow. The idea is that patient loads end up close to even over time, even if they’re unbalanced on any given day.
A system like this allows everyone, including the hospitalists themselves, ED staff, etc., to know who will take the next patient. It decreases the need to communicate the “who’s next” information time after time during the course of the day. In small- to medium-sized practices, it could mean no one needs to function as the triage doctor (i.e., the person who inefficiently answers the service calls, scribbles down clinical information, then calls the hospitalist who is due to take the next patient and relays all the pertinent patient info). This system allows the
hospitalists to know which days will be harder (e.g., taking on the care of new patients) and which days will be easier (e.g., rounding but not assuming care of new patients). Allowing uneven loads also eliminates the need to spend energy working to even the loads and risking that some in the group feel as if they aren’t being treated fairly.
Uncommon yet Intriguing Approaches
Pair referring primary-care physicians (PCPs) with specific hospitalists. I’ve encountered two groups that had hospitalists always admit patients from the same PCPs. In other words, hospitalist Dr. Hancock always serves as attending for patients referred by the same nine PCPs, and hospitalist Dr. Franklin always attends to patients from a different set of PCPs. It seems to me that there could be tremendous benefit in working closely with the same PCPs, most notably getting to know the PCPs’ office staff. But this system raises the risk of creating out-of-balance patient loads, among other problems. It is really attractive to me, but most groups will decide its costs outweigh its benefits.
Hospitalist and patient stay connected during admission. I’m not aware of any group that uses this method (let me know if you do!), but there could be benefits to having each patient see the same hospitalist during each hospital stay. Of course, that is assuming the hospitalist is on duty. Hospitalist and patient could be paired upon the patient’s first admission. The hospitalist could form an excellent relationship with the patient and family; the time spent by the hospitalist getting to know patients on admission would be reduced, and I suspect there might be some benefit in the quality of care.
This method, however, likely results in the most uneven patient loads, and load-leveling would be difficult, if not impossible. Even if hospitalist and patient did form a tight bond, there is a high probability that the hospitalist would be off for the duration of the patient’s next admission. So despite what I suspect are tremendous benefits, this approach may not be feasible for any group.
In next month’s column, I will discuss issues related to the way patients are distributed. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: This is the first of a three-part series.
My experience is that some, maybe even most, hospitalists tend to assume there is a standard or “right” way to organize things like work schedules, compensation, or even the assignment of patients among the group’s providers. Some will say things like “SHM says the best hospitalist schedule is …” or “The best way to compensate hospitalists is …”
But there really isn’t a “best” way to manage any particular attribute of a practice. Don’t make the mistake of assuming your method is best, or that it’s the way “everybody else does it.” Although scheduling and compensation are marquee issues for hospitalists, approaches to distributing new patients is much less visible. Many groups tend to assume their method is the only reasonable approach. The best approach, however, varies from one practice to the next. You should be open to hearing approaches to scheduling that are different from your own.
Assign Patients by “Load Leveling”
I’ve come across a lot—and I mean a lot—of different approaches to distributing new patients in HM groups around the country, but it seems pretty clear that the most common method is to undertake “load leveling” on a daily or ongoing basis.
For example, groups that have a separate night shift (the night doctor performs no daytime work the day before or the day after a night shift) typically distribute the night’s new patients with the intent of having each daytime doctor start with the same number of patients. The group might more heavily weight some patients, such as those in the ICU (e.g., each ICU patient counts as 1.5 or two non-ICU patients), but most groups don’t. Over the course of the day shift, new referrals will be distributed evenly among the doctors one at a time, sort of like dealing a deck of cards.
This approach aims to avoid significant imbalances in patient loads and has the potential cultural benefit of everyone sharing equally in busy and slow days. Groups that use it tend to see it as the best option because it is the fairest way to divide up the workload.
Practices that use load-leveling almost always use a schedule built on shifts of a predetermined and fixed duration. For example, say the day shift always works from 7 a.m. to 7 p.m. This schedule usually has the majority of compensation paid via a fixed annual salary or fixed shift rate. One potential problem with this approach is that the doctor who is efficient and discharges a lot of patients today is “rewarded” with more new patients tomorrow. Hospitalists who are allergic to work might have an incentive to have a patient wait until tomorrow to discharge to avoid having to assume the care of yet another patient tomorrow morning. Hospital executives who are focused on length-of-stay management might be concerned if they knew this was a potential issue. Of course, the reverse is true as well. In a practice that doesn’t aggressively undertake load-leveling, a less-than-admirable hospitalist could push patients to discharge earlier than optimal just to have one less patient the next day.
Another cost of this approach is that the distribution of patients can be time-consuming each morning. It also offers the opportunity for some in the group to decide they’re treated unfairly. For instance, you might hear the occasional “just last Tuesday, I started with 16 patients, compared with 15 for everyone else. Now you want me to do it again? You’re being unfair to me; it’s someone else’s turn to take the extra patient.”
Assignment by Location
Groups that use “unit-based” hospitalists distribute patients according to the unit the patient is admitted to—and the hospitalist covering that unit. The pros and cons of unit-based hospitalists are many (see “A Unit-Based Approach,” September 2007), but there is an obvious tension between keeping patient loads even among hospitalists and ensuring that all of a hospitalist’s patients are on “their” unit. Practicality usually requires a compromise between pure unit-based assignment and load-leveling.
Uneven Assignments
Some groups assign patients according to a predetermined algorithm and employ load-leveling only when patient loads become extremely unbalanced. For example, Dr. Jones gets all the new referrals today, and Dr. James gets them tomorrow. The idea is that patient loads end up close to even over time, even if they’re unbalanced on any given day.
A system like this allows everyone, including the hospitalists themselves, ED staff, etc., to know who will take the next patient. It decreases the need to communicate the “who’s next” information time after time during the course of the day. In small- to medium-sized practices, it could mean no one needs to function as the triage doctor (i.e., the person who inefficiently answers the service calls, scribbles down clinical information, then calls the hospitalist who is due to take the next patient and relays all the pertinent patient info). This system allows the
hospitalists to know which days will be harder (e.g., taking on the care of new patients) and which days will be easier (e.g., rounding but not assuming care of new patients). Allowing uneven loads also eliminates the need to spend energy working to even the loads and risking that some in the group feel as if they aren’t being treated fairly.
Uncommon yet Intriguing Approaches
Pair referring primary-care physicians (PCPs) with specific hospitalists. I’ve encountered two groups that had hospitalists always admit patients from the same PCPs. In other words, hospitalist Dr. Hancock always serves as attending for patients referred by the same nine PCPs, and hospitalist Dr. Franklin always attends to patients from a different set of PCPs. It seems to me that there could be tremendous benefit in working closely with the same PCPs, most notably getting to know the PCPs’ office staff. But this system raises the risk of creating out-of-balance patient loads, among other problems. It is really attractive to me, but most groups will decide its costs outweigh its benefits.
Hospitalist and patient stay connected during admission. I’m not aware of any group that uses this method (let me know if you do!), but there could be benefits to having each patient see the same hospitalist during each hospital stay. Of course, that is assuming the hospitalist is on duty. Hospitalist and patient could be paired upon the patient’s first admission. The hospitalist could form an excellent relationship with the patient and family; the time spent by the hospitalist getting to know patients on admission would be reduced, and I suspect there might be some benefit in the quality of care.
This method, however, likely results in the most uneven patient loads, and load-leveling would be difficult, if not impossible. Even if hospitalist and patient did form a tight bond, there is a high probability that the hospitalist would be off for the duration of the patient’s next admission. So despite what I suspect are tremendous benefits, this approach may not be feasible for any group.
In next month’s column, I will discuss issues related to the way patients are distributed. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: This is the first of a three-part series.
My experience is that some, maybe even most, hospitalists tend to assume there is a standard or “right” way to organize things like work schedules, compensation, or even the assignment of patients among the group’s providers. Some will say things like “SHM says the best hospitalist schedule is …” or “The best way to compensate hospitalists is …”
But there really isn’t a “best” way to manage any particular attribute of a practice. Don’t make the mistake of assuming your method is best, or that it’s the way “everybody else does it.” Although scheduling and compensation are marquee issues for hospitalists, approaches to distributing new patients is much less visible. Many groups tend to assume their method is the only reasonable approach. The best approach, however, varies from one practice to the next. You should be open to hearing approaches to scheduling that are different from your own.
Assign Patients by “Load Leveling”
I’ve come across a lot—and I mean a lot—of different approaches to distributing new patients in HM groups around the country, but it seems pretty clear that the most common method is to undertake “load leveling” on a daily or ongoing basis.
For example, groups that have a separate night shift (the night doctor performs no daytime work the day before or the day after a night shift) typically distribute the night’s new patients with the intent of having each daytime doctor start with the same number of patients. The group might more heavily weight some patients, such as those in the ICU (e.g., each ICU patient counts as 1.5 or two non-ICU patients), but most groups don’t. Over the course of the day shift, new referrals will be distributed evenly among the doctors one at a time, sort of like dealing a deck of cards.
This approach aims to avoid significant imbalances in patient loads and has the potential cultural benefit of everyone sharing equally in busy and slow days. Groups that use it tend to see it as the best option because it is the fairest way to divide up the workload.
Practices that use load-leveling almost always use a schedule built on shifts of a predetermined and fixed duration. For example, say the day shift always works from 7 a.m. to 7 p.m. This schedule usually has the majority of compensation paid via a fixed annual salary or fixed shift rate. One potential problem with this approach is that the doctor who is efficient and discharges a lot of patients today is “rewarded” with more new patients tomorrow. Hospitalists who are allergic to work might have an incentive to have a patient wait until tomorrow to discharge to avoid having to assume the care of yet another patient tomorrow morning. Hospital executives who are focused on length-of-stay management might be concerned if they knew this was a potential issue. Of course, the reverse is true as well. In a practice that doesn’t aggressively undertake load-leveling, a less-than-admirable hospitalist could push patients to discharge earlier than optimal just to have one less patient the next day.
Another cost of this approach is that the distribution of patients can be time-consuming each morning. It also offers the opportunity for some in the group to decide they’re treated unfairly. For instance, you might hear the occasional “just last Tuesday, I started with 16 patients, compared with 15 for everyone else. Now you want me to do it again? You’re being unfair to me; it’s someone else’s turn to take the extra patient.”
Assignment by Location
Groups that use “unit-based” hospitalists distribute patients according to the unit the patient is admitted to—and the hospitalist covering that unit. The pros and cons of unit-based hospitalists are many (see “A Unit-Based Approach,” September 2007), but there is an obvious tension between keeping patient loads even among hospitalists and ensuring that all of a hospitalist’s patients are on “their” unit. Practicality usually requires a compromise between pure unit-based assignment and load-leveling.
Uneven Assignments
Some groups assign patients according to a predetermined algorithm and employ load-leveling only when patient loads become extremely unbalanced. For example, Dr. Jones gets all the new referrals today, and Dr. James gets them tomorrow. The idea is that patient loads end up close to even over time, even if they’re unbalanced on any given day.
A system like this allows everyone, including the hospitalists themselves, ED staff, etc., to know who will take the next patient. It decreases the need to communicate the “who’s next” information time after time during the course of the day. In small- to medium-sized practices, it could mean no one needs to function as the triage doctor (i.e., the person who inefficiently answers the service calls, scribbles down clinical information, then calls the hospitalist who is due to take the next patient and relays all the pertinent patient info). This system allows the
hospitalists to know which days will be harder (e.g., taking on the care of new patients) and which days will be easier (e.g., rounding but not assuming care of new patients). Allowing uneven loads also eliminates the need to spend energy working to even the loads and risking that some in the group feel as if they aren’t being treated fairly.
Uncommon yet Intriguing Approaches
Pair referring primary-care physicians (PCPs) with specific hospitalists. I’ve encountered two groups that had hospitalists always admit patients from the same PCPs. In other words, hospitalist Dr. Hancock always serves as attending for patients referred by the same nine PCPs, and hospitalist Dr. Franklin always attends to patients from a different set of PCPs. It seems to me that there could be tremendous benefit in working closely with the same PCPs, most notably getting to know the PCPs’ office staff. But this system raises the risk of creating out-of-balance patient loads, among other problems. It is really attractive to me, but most groups will decide its costs outweigh its benefits.
Hospitalist and patient stay connected during admission. I’m not aware of any group that uses this method (let me know if you do!), but there could be benefits to having each patient see the same hospitalist during each hospital stay. Of course, that is assuming the hospitalist is on duty. Hospitalist and patient could be paired upon the patient’s first admission. The hospitalist could form an excellent relationship with the patient and family; the time spent by the hospitalist getting to know patients on admission would be reduced, and I suspect there might be some benefit in the quality of care.
This method, however, likely results in the most uneven patient loads, and load-leveling would be difficult, if not impossible. Even if hospitalist and patient did form a tight bond, there is a high probability that the hospitalist would be off for the duration of the patient’s next admission. So despite what I suspect are tremendous benefits, this approach may not be feasible for any group.
In next month’s column, I will discuss issues related to the way patients are distributed. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Should Hospitalists Report for Service during a Life-Threatening Event?
PRO
When the community is in need, physicians must honor call to duty

As the American Medical Association (AMA) states in its inaugural Code of Ethics from 1847: “When pestilence prevails, it is their duty to face the danger and to continue their labors for the alleviation of the suffering, even at the jeopardy of their own lives.”1 It meant doctors have taken on a calling and social duty to treat sick patients, even at personal expense.
Today, the AMA’s Code of Ethics puts it this way: “Physicians should balance immediate benefits to individual patients with ability to care for patients in future.”2 Over two centuries, the focus remains on the physician’s duty to patient and society.
As a former Air Force physician, I believe in this deontological stance. In the Air Force, we often spoke of our sense of duty, of “service before self, and integrity in everything we do.” This code of conduct applies to combat as well as the peacetime challenges of pandemic flu. If the medical corps’ mantra is to “preserve the fighting force,” the mission of the civilian physician is the community’s survival. This implicit contract with society extends from moments of tranquillity to when the peace is disrupted by either manmade disasters (e.g., war) or biological threats (e.g., pandemic disease).
Having made this assertion, a physician’s obligation is not without its limitations. Doctors have a responsibility to protect themselves and their families from undue harm. We have to stay alive for utilitarian reasons in order to serve others. A society without its physician workforce is imperiled and at enhanced risk, so a physician’s self-preservation is also in the interest of the collective.3
All of this compels doctors to stay alive and remain healthy. Our duty can only be achieved by careful action and avoiding forays into Hollywood heroism. No one asked us to be heroes, only dutiful physicians.4
We have to prepare doctors to meet this challenge. Alexander and Wynia surveyed senior physicians: While 80% were willing to treat high-risk patients, as in bioterrorism or a pandemic, only 21% felt logistically prepared to meet such a challenge in practice.5
If we expect physicians to answer the call, we need to equip them with the knowledge, skills, and equipment necessary to safely and effectively meet their professional responsibilities.
That responsibility is one that society owes its physicians. TH
References
- Code of Medical Ethics of the American Medical Association. American Medical Association Web site. Available at: www.ama-assn.org. Accessed Nov. 30, 2009.
- American Medical Association. Physician Obligation in Disaster Preparedness and Response. Chicago: American Medical Association; 2004.
- Simonds AK, Sokol DK. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur Respir J. 2009;34(2):303-309.
- Sokol D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg Infect Dis. 2006;12(8):1238-1241.
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
CON
Some healthcare providers should be considered exceptions to rule

Infectious illnesses frequently affect healthcare providers disproportionately. Whether physicians are obligated to put themselves at risk is not clear. Many sources argue that participation in infectious epidemic or pandemic events is obligatory, but there is another side to the discussion. Healthcare providers might have risk factors that mitigate this obligation. Two such subgroups are providers with pre-existing health concerns and providers who are caregivers for others.
Studies show that not all providers will report to work in the face of an epidemic. One self-reporting study found that 20% of physicians would report to work.1 Every hospital effected by the SARS epidemic had difficulty with employee attrition.2 Thus, the concern is more than hypothetical.
There is a difference in putting oneself at risk for an illness and putting oneself at risk of death. Providers might be immunosuppressed or have, say, an underlying lung disease. Should higher-risk providers with direct patient contact responsibilities have the same obligation as providers who are not?
Providers who care for others will face different challenges. First, if social distancing becomes widespread and schools and daycare centers are closed, providers will face a dilemma over how to care for their dependents. A second issue for providers with responsibilities to care for others is that those dependent populations are likely to be at higher risk of bad outcomes if they are affected. A provider who is infectious puts their family at risk. Children may be disproportionately affected, and people who require assistance are more likely to have comorbid conditions. Should providers with other responsibilities have the same obligation as providers who do not?
Given that risk is not the same among providers, it is unfair to say that responsibility is the same. Parents simply cannot abandon their children. Risk of death is a serious concern for providers at higher risk. Hospitals should have an explicit plan in place for a pandemic; most do have a plan. The plan needs to consider these issues and have explicit provisions.
Another approach would be to ask providers to state their availability. If the hospital knows that a certain group of providers has specific concerns, the plan can take into account what impact those concerns will have. Transparency in the plan, expectations, and resources will better prepare hospitals.
There is a fundamental duty to provide care to patients who need it, and failure to do so is a violation of a societal and professional trust. However, this duty is not absolute. Giving providers that benefit of the doubt—that they will honor their duty to ill or injured patients—means that providers can be trusted to opt out only for valid reasons. The system must be designed to accommodate special needs. A one-size-fits-all approach is bound to fail. TH
References
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
- Wynia MK. Ethics and public health emergencies: encouraging responsibility. Am J Bioeth. 2007;7(4):1-4.
The opinions expressed herein are those of the authors and do not represent those of the Society of Hospital Medicine or The Hospitalist.
PRO
When the community is in need, physicians must honor call to duty
As the American Medical Association (AMA) states in its inaugural Code of Ethics from 1847: “When pestilence prevails, it is their duty to face the danger and to continue their labors for the alleviation of the suffering, even at the jeopardy of their own lives.”1 It meant doctors have taken on a calling and social duty to treat sick patients, even at personal expense.
Today, the AMA’s Code of Ethics puts it this way: “Physicians should balance immediate benefits to individual patients with ability to care for patients in future.”2 Over two centuries, the focus remains on the physician’s duty to patient and society.
As a former Air Force physician, I believe in this deontological stance. In the Air Force, we often spoke of our sense of duty, of “service before self, and integrity in everything we do.” This code of conduct applies to combat as well as the peacetime challenges of pandemic flu. If the medical corps’ mantra is to “preserve the fighting force,” the mission of the civilian physician is the community’s survival. This implicit contract with society extends from moments of tranquillity to when the peace is disrupted by either manmade disasters (e.g., war) or biological threats (e.g., pandemic disease).
Having made this assertion, a physician’s obligation is not without its limitations. Doctors have a responsibility to protect themselves and their families from undue harm. We have to stay alive for utilitarian reasons in order to serve others. A society without its physician workforce is imperiled and at enhanced risk, so a physician’s self-preservation is also in the interest of the collective.3
All of this compels doctors to stay alive and remain healthy. Our duty can only be achieved by careful action and avoiding forays into Hollywood heroism. No one asked us to be heroes, only dutiful physicians.4
We have to prepare doctors to meet this challenge. Alexander and Wynia surveyed senior physicians: While 80% were willing to treat high-risk patients, as in bioterrorism or a pandemic, only 21% felt logistically prepared to meet such a challenge in practice.5
If we expect physicians to answer the call, we need to equip them with the knowledge, skills, and equipment necessary to safely and effectively meet their professional responsibilities.
That responsibility is one that society owes its physicians. TH
References
- Code of Medical Ethics of the American Medical Association. American Medical Association Web site. Available at: www.ama-assn.org. Accessed Nov. 30, 2009.
- American Medical Association. Physician Obligation in Disaster Preparedness and Response. Chicago: American Medical Association; 2004.
- Simonds AK, Sokol DK. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur Respir J. 2009;34(2):303-309.
- Sokol D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg Infect Dis. 2006;12(8):1238-1241.
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
CON
Some healthcare providers should be considered exceptions to rule
Infectious illnesses frequently affect healthcare providers disproportionately. Whether physicians are obligated to put themselves at risk is not clear. Many sources argue that participation in infectious epidemic or pandemic events is obligatory, but there is another side to the discussion. Healthcare providers might have risk factors that mitigate this obligation. Two such subgroups are providers with pre-existing health concerns and providers who are caregivers for others.
Studies show that not all providers will report to work in the face of an epidemic. One self-reporting study found that 20% of physicians would report to work.1 Every hospital effected by the SARS epidemic had difficulty with employee attrition.2 Thus, the concern is more than hypothetical.
There is a difference in putting oneself at risk for an illness and putting oneself at risk of death. Providers might be immunosuppressed or have, say, an underlying lung disease. Should higher-risk providers with direct patient contact responsibilities have the same obligation as providers who are not?
Providers who care for others will face different challenges. First, if social distancing becomes widespread and schools and daycare centers are closed, providers will face a dilemma over how to care for their dependents. A second issue for providers with responsibilities to care for others is that those dependent populations are likely to be at higher risk of bad outcomes if they are affected. A provider who is infectious puts their family at risk. Children may be disproportionately affected, and people who require assistance are more likely to have comorbid conditions. Should providers with other responsibilities have the same obligation as providers who do not?
Given that risk is not the same among providers, it is unfair to say that responsibility is the same. Parents simply cannot abandon their children. Risk of death is a serious concern for providers at higher risk. Hospitals should have an explicit plan in place for a pandemic; most do have a plan. The plan needs to consider these issues and have explicit provisions.
Another approach would be to ask providers to state their availability. If the hospital knows that a certain group of providers has specific concerns, the plan can take into account what impact those concerns will have. Transparency in the plan, expectations, and resources will better prepare hospitals.
There is a fundamental duty to provide care to patients who need it, and failure to do so is a violation of a societal and professional trust. However, this duty is not absolute. Giving providers that benefit of the doubt—that they will honor their duty to ill or injured patients—means that providers can be trusted to opt out only for valid reasons. The system must be designed to accommodate special needs. A one-size-fits-all approach is bound to fail. TH
References
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
- Wynia MK. Ethics and public health emergencies: encouraging responsibility. Am J Bioeth. 2007;7(4):1-4.
The opinions expressed herein are those of the authors and do not represent those of the Society of Hospital Medicine or The Hospitalist.
PRO
When the community is in need, physicians must honor call to duty
As the American Medical Association (AMA) states in its inaugural Code of Ethics from 1847: “When pestilence prevails, it is their duty to face the danger and to continue their labors for the alleviation of the suffering, even at the jeopardy of their own lives.”1 It meant doctors have taken on a calling and social duty to treat sick patients, even at personal expense.
Today, the AMA’s Code of Ethics puts it this way: “Physicians should balance immediate benefits to individual patients with ability to care for patients in future.”2 Over two centuries, the focus remains on the physician’s duty to patient and society.
As a former Air Force physician, I believe in this deontological stance. In the Air Force, we often spoke of our sense of duty, of “service before self, and integrity in everything we do.” This code of conduct applies to combat as well as the peacetime challenges of pandemic flu. If the medical corps’ mantra is to “preserve the fighting force,” the mission of the civilian physician is the community’s survival. This implicit contract with society extends from moments of tranquillity to when the peace is disrupted by either manmade disasters (e.g., war) or biological threats (e.g., pandemic disease).
Having made this assertion, a physician’s obligation is not without its limitations. Doctors have a responsibility to protect themselves and their families from undue harm. We have to stay alive for utilitarian reasons in order to serve others. A society without its physician workforce is imperiled and at enhanced risk, so a physician’s self-preservation is also in the interest of the collective.3
All of this compels doctors to stay alive and remain healthy. Our duty can only be achieved by careful action and avoiding forays into Hollywood heroism. No one asked us to be heroes, only dutiful physicians.4
We have to prepare doctors to meet this challenge. Alexander and Wynia surveyed senior physicians: While 80% were willing to treat high-risk patients, as in bioterrorism or a pandemic, only 21% felt logistically prepared to meet such a challenge in practice.5
If we expect physicians to answer the call, we need to equip them with the knowledge, skills, and equipment necessary to safely and effectively meet their professional responsibilities.
That responsibility is one that society owes its physicians. TH
References
- Code of Medical Ethics of the American Medical Association. American Medical Association Web site. Available at: www.ama-assn.org. Accessed Nov. 30, 2009.
- American Medical Association. Physician Obligation in Disaster Preparedness and Response. Chicago: American Medical Association; 2004.
- Simonds AK, Sokol DK. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur Respir J. 2009;34(2):303-309.
- Sokol D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg Infect Dis. 2006;12(8):1238-1241.
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
CON
Some healthcare providers should be considered exceptions to rule
Infectious illnesses frequently affect healthcare providers disproportionately. Whether physicians are obligated to put themselves at risk is not clear. Many sources argue that participation in infectious epidemic or pandemic events is obligatory, but there is another side to the discussion. Healthcare providers might have risk factors that mitigate this obligation. Two such subgroups are providers with pre-existing health concerns and providers who are caregivers for others.
Studies show that not all providers will report to work in the face of an epidemic. One self-reporting study found that 20% of physicians would report to work.1 Every hospital effected by the SARS epidemic had difficulty with employee attrition.2 Thus, the concern is more than hypothetical.
There is a difference in putting oneself at risk for an illness and putting oneself at risk of death. Providers might be immunosuppressed or have, say, an underlying lung disease. Should higher-risk providers with direct patient contact responsibilities have the same obligation as providers who are not?
Providers who care for others will face different challenges. First, if social distancing becomes widespread and schools and daycare centers are closed, providers will face a dilemma over how to care for their dependents. A second issue for providers with responsibilities to care for others is that those dependent populations are likely to be at higher risk of bad outcomes if they are affected. A provider who is infectious puts their family at risk. Children may be disproportionately affected, and people who require assistance are more likely to have comorbid conditions. Should providers with other responsibilities have the same obligation as providers who do not?
Given that risk is not the same among providers, it is unfair to say that responsibility is the same. Parents simply cannot abandon their children. Risk of death is a serious concern for providers at higher risk. Hospitals should have an explicit plan in place for a pandemic; most do have a plan. The plan needs to consider these issues and have explicit provisions.
Another approach would be to ask providers to state their availability. If the hospital knows that a certain group of providers has specific concerns, the plan can take into account what impact those concerns will have. Transparency in the plan, expectations, and resources will better prepare hospitals.
There is a fundamental duty to provide care to patients who need it, and failure to do so is a violation of a societal and professional trust. However, this duty is not absolute. Giving providers that benefit of the doubt—that they will honor their duty to ill or injured patients—means that providers can be trusted to opt out only for valid reasons. The system must be designed to accommodate special needs. A one-size-fits-all approach is bound to fail. TH
References
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
- Wynia MK. Ethics and public health emergencies: encouraging responsibility. Am J Bioeth. 2007;7(4):1-4.
The opinions expressed herein are those of the authors and do not represent those of the Society of Hospital Medicine or The Hospitalist.
The Year Ahead
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Effective Communication Ensures Patient Safety

Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Necessary Evil: Change

The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Consultation Elimination
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
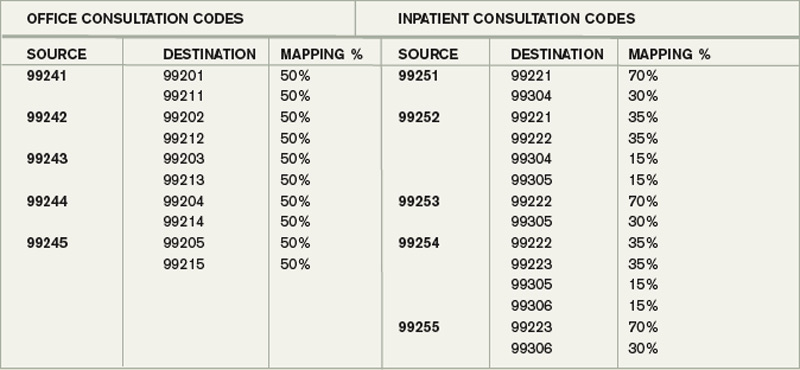
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
Quality over Quantity
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
Submission Support
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.