User login
Mortality, outcomes good in AAA repair in octogenarians
SCOTTSDALE, ARIZ.– Abdominal aortic aneurysm repair in patients 80 years and older can be performed safely and with good medium-term survival rates, a prospective single-site study has shown.
Perioperative mortality in elective and emergent AAA repair for octogenarians was 2% and 35%, respectively, with a median survival rate of 19 months in both groups.

According to these data, “Patients shouldn’t be turned down for aneurysm repair on the basis of their age alone,” Dr. Christopher M. Lamb, a vascular surgery fellow at the University of California Davis Medical Center in Sacramento, said during a presentation at this year’s Southern Association for Vascular Surgery annual meeting.
“However, whether we should be doing these procedures is a different question, and I don’t think these data allow us to answer that question properly.”Dr. Lamb and his colleagues reviewed the records of 847 consecutive patients aged 80 years or older, seen between April 2005 and February 2014 for any type of AAA repair. Cases were sorted according to whether they were elective, ruptured, or urgent but unruptured. A total of 226 patients met the study’s age criteria; there were nearly seven men for every woman, all with a median age of 83 years. Of the elective AAA repair arm of the study, 131 patients (116 men) with a median age of 82 years had an endovascular repair, while the rest underwent open surgical repair. The combined 30-day mortality rate for these patients was 2.3%, with no significant difference between either the endovascular aneurysm repair (EVAR) or the open surgical repair (OSR) patients (1.9% vs. 4.2%; P = .458). The median survival of all elective repair patients was 19 months (interquartile range, 10-35), with no difference seen between the two groups (P = .113)Of the 65 patients (53 men) with ruptured AAA, the median age was 83 years. A third had open repair (32.3%), while the rest had EVAR. The combined 30-day mortality rate was 35.4% but was significantly higher after OSR (52.4% vs. 27.3%; P = .048). The median survival rate was 6 months (IQR, 6-42) when 30-day mortality rates were excluded. The median survival rates in patients who lived longer than 30 days was significantly higher in OSR patients (42.5 months vs. 11 months; P = .019).
Of the 23 men and 7 women with symptomatic but unruptured AAA, all but 1 had EVAR. At 30 days, there was one diverticular perforation–related postoperative death in the EVAR group, which had a median survival rate of 29 months. There being only a single patient in the OSR group obviated a comparative median survival rate analysis.
A subanalysis of the final 20 months of the study showed that 41% of octogenarians seeking any type of AAA repair at the site were rejected (48 rejections vs. 69 repairs). Those who were rejected for repair tended to be older, with a median age of 86 years vs. 83 years for patients who underwent repair (P = .0004).
Dr. Lamb noted that although the findings demonstrate acceptable overall safety rates for the entire cohort, without a control group of patients that did not have AAA repair, it would be hard to draw a definite conclusion about the utility of the findings, and that more data were warranted; however, the potential for limited long-term survival with what previous reports have suggested may include “a reduced quality of life for a good part of it, possibly raises the question that these patients should be treated conservatively, more often.”
The rejection rate data prompted the presentation’s discussant, Dr. William D. Jordan Jr., section chief of vascular surgery at the University of Alabama at Birmingham and the presentation’s discussant, to challenge the findings and asked whether a single surgeon selected the patients.

“You said there is not a selection bias in your study, but I beg to differ. Perhaps all these kinds of studies have a selection bias, and I believe they should. We should select the appropriate patients for the appropriate procedure at the appropriate time, with the appropriate expectation of outcome. Bias in this setting may be seen as good,” Dr. Jordan said.Dr. Lamb responded that the treatment algorithm at the site for all patients with a confirmed AAA of 5.5 cm or greater included CT imaging that is reviewed by a multidisciplinary team comprising vascular surgeons and interventional radiologists, who then evaluated the patients according to their physiology and anatomy, as well as their comorbidities, with the intention that whenever possible, EVAR rather than open repair would be performed.
As to whether there was a bias toward not repairing AAA in older patients, Dr. Lamb said it was incumbent on any health system to evaluate a procedure’s cost-effectiveness, but that, “the life expectancy of a vascular patient is often more limited than I think we’d like to believe ... we don’t know what the natural history of these patients’ life expectancy is. We don’t know from these data what the cause of death was, but anecdotally, we didn’t see hundreds of patients return with ruptured aneurysms after an EVAR.”
“I would truly like to see how many [of these patients] who make it out of the hospital return to normal living within 6 months,” Dr. Samuel R. Money, chair of surgery at the Mayo Clinic in Scottsdale, Ariz., said in an interview following the presentation. “At some point, the question becomes ‘Can we afford to spend $100,000 dollars to keep a 90-year-old patient alive for 6 more months?’ Can this society sustain the cost of that?”
On Twitter @whitneymcknight
This discussion is provocative and raises some interesting points. Obviously cost-effectiveness considerations are important, and our country does not have unlimited funds to spend on medical care. And perhaps there are some elderly and frail individuals who should not have their AAAs repaired electively because the risk of rupture during the patients’ remaining months or years of life is small.
This is particularly true if the patient’s AAA is less than 7 cm and his or her anatomy and condition are unsuitable for an easy repair. However, if the AAA is large and threatening, and the patient has the possibility of living several years, elective repair is justified and reasonable – especially if it can be accomplished endovascularly. As someone who is near 80 [years old], I could not feel more strongly about this, and I would maintain this view if I were near 90 and healthy.

|
Dr. Frank J. Veith |
I hold the same view even more strongly regarding a ruptured AAA. In this setting, the alternative management is nontreatment, which is uniformly fatal. The common term “palliative treatment” for such nontreatment is a misleading misnomer. No sane, reasonably healthy elderly patient would knowingly choose such nontreatment when a good alternative with well over an even chance of living a lot longer is offered. That good alternative – again especially if it can be performed endovascularly – should be offered, and our health system should pay for it and compensate by saving money on unnecessary SFA [superficial femoral artery] stents and carotid procedures.
Dr. Frank J. Veith is professor of surgery at New York University Medical Center and the Cleveland Clinic and is an associate medical editor for Vascular Specialist.
This discussion is provocative and raises some interesting points. Obviously cost-effectiveness considerations are important, and our country does not have unlimited funds to spend on medical care. And perhaps there are some elderly and frail individuals who should not have their AAAs repaired electively because the risk of rupture during the patients’ remaining months or years of life is small.
This is particularly true if the patient’s AAA is less than 7 cm and his or her anatomy and condition are unsuitable for an easy repair. However, if the AAA is large and threatening, and the patient has the possibility of living several years, elective repair is justified and reasonable – especially if it can be accomplished endovascularly. As someone who is near 80 [years old], I could not feel more strongly about this, and I would maintain this view if I were near 90 and healthy.
|
|
Dr. Frank J. Veith |
I hold the same view even more strongly regarding a ruptured AAA. In this setting, the alternative management is nontreatment, which is uniformly fatal. The common term “palliative treatment” for such nontreatment is a misleading misnomer. No sane, reasonably healthy elderly patient would knowingly choose such nontreatment when a good alternative with well over an even chance of living a lot longer is offered. That good alternative – again especially if it can be performed endovascularly – should be offered, and our health system should pay for it and compensate by saving money on unnecessary SFA [superficial femoral artery] stents and carotid procedures.
Dr. Frank J. Veith is professor of surgery at New York University Medical Center and the Cleveland Clinic and is an associate medical editor for Vascular Specialist.
This discussion is provocative and raises some interesting points. Obviously cost-effectiveness considerations are important, and our country does not have unlimited funds to spend on medical care. And perhaps there are some elderly and frail individuals who should not have their AAAs repaired electively because the risk of rupture during the patients’ remaining months or years of life is small.
This is particularly true if the patient’s AAA is less than 7 cm and his or her anatomy and condition are unsuitable for an easy repair. However, if the AAA is large and threatening, and the patient has the possibility of living several years, elective repair is justified and reasonable – especially if it can be accomplished endovascularly. As someone who is near 80 [years old], I could not feel more strongly about this, and I would maintain this view if I were near 90 and healthy.
|
|
Dr. Frank J. Veith |
I hold the same view even more strongly regarding a ruptured AAA. In this setting, the alternative management is nontreatment, which is uniformly fatal. The common term “palliative treatment” for such nontreatment is a misleading misnomer. No sane, reasonably healthy elderly patient would knowingly choose such nontreatment when a good alternative with well over an even chance of living a lot longer is offered. That good alternative – again especially if it can be performed endovascularly – should be offered, and our health system should pay for it and compensate by saving money on unnecessary SFA [superficial femoral artery] stents and carotid procedures.
Dr. Frank J. Veith is professor of surgery at New York University Medical Center and the Cleveland Clinic and is an associate medical editor for Vascular Specialist.
SCOTTSDALE, ARIZ.– Abdominal aortic aneurysm repair in patients 80 years and older can be performed safely and with good medium-term survival rates, a prospective single-site study has shown.
Perioperative mortality in elective and emergent AAA repair for octogenarians was 2% and 35%, respectively, with a median survival rate of 19 months in both groups.
According to these data, “Patients shouldn’t be turned down for aneurysm repair on the basis of their age alone,” Dr. Christopher M. Lamb, a vascular surgery fellow at the University of California Davis Medical Center in Sacramento, said during a presentation at this year’s Southern Association for Vascular Surgery annual meeting.
“However, whether we should be doing these procedures is a different question, and I don’t think these data allow us to answer that question properly.”Dr. Lamb and his colleagues reviewed the records of 847 consecutive patients aged 80 years or older, seen between April 2005 and February 2014 for any type of AAA repair. Cases were sorted according to whether they were elective, ruptured, or urgent but unruptured. A total of 226 patients met the study’s age criteria; there were nearly seven men for every woman, all with a median age of 83 years. Of the elective AAA repair arm of the study, 131 patients (116 men) with a median age of 82 years had an endovascular repair, while the rest underwent open surgical repair. The combined 30-day mortality rate for these patients was 2.3%, with no significant difference between either the endovascular aneurysm repair (EVAR) or the open surgical repair (OSR) patients (1.9% vs. 4.2%; P = .458). The median survival of all elective repair patients was 19 months (interquartile range, 10-35), with no difference seen between the two groups (P = .113)Of the 65 patients (53 men) with ruptured AAA, the median age was 83 years. A third had open repair (32.3%), while the rest had EVAR. The combined 30-day mortality rate was 35.4% but was significantly higher after OSR (52.4% vs. 27.3%; P = .048). The median survival rate was 6 months (IQR, 6-42) when 30-day mortality rates were excluded. The median survival rates in patients who lived longer than 30 days was significantly higher in OSR patients (42.5 months vs. 11 months; P = .019).
Of the 23 men and 7 women with symptomatic but unruptured AAA, all but 1 had EVAR. At 30 days, there was one diverticular perforation–related postoperative death in the EVAR group, which had a median survival rate of 29 months. There being only a single patient in the OSR group obviated a comparative median survival rate analysis.
A subanalysis of the final 20 months of the study showed that 41% of octogenarians seeking any type of AAA repair at the site were rejected (48 rejections vs. 69 repairs). Those who were rejected for repair tended to be older, with a median age of 86 years vs. 83 years for patients who underwent repair (P = .0004).
Dr. Lamb noted that although the findings demonstrate acceptable overall safety rates for the entire cohort, without a control group of patients that did not have AAA repair, it would be hard to draw a definite conclusion about the utility of the findings, and that more data were warranted; however, the potential for limited long-term survival with what previous reports have suggested may include “a reduced quality of life for a good part of it, possibly raises the question that these patients should be treated conservatively, more often.”
The rejection rate data prompted the presentation’s discussant, Dr. William D. Jordan Jr., section chief of vascular surgery at the University of Alabama at Birmingham and the presentation’s discussant, to challenge the findings and asked whether a single surgeon selected the patients.
“You said there is not a selection bias in your study, but I beg to differ. Perhaps all these kinds of studies have a selection bias, and I believe they should. We should select the appropriate patients for the appropriate procedure at the appropriate time, with the appropriate expectation of outcome. Bias in this setting may be seen as good,” Dr. Jordan said.Dr. Lamb responded that the treatment algorithm at the site for all patients with a confirmed AAA of 5.5 cm or greater included CT imaging that is reviewed by a multidisciplinary team comprising vascular surgeons and interventional radiologists, who then evaluated the patients according to their physiology and anatomy, as well as their comorbidities, with the intention that whenever possible, EVAR rather than open repair would be performed.
As to whether there was a bias toward not repairing AAA in older patients, Dr. Lamb said it was incumbent on any health system to evaluate a procedure’s cost-effectiveness, but that, “the life expectancy of a vascular patient is often more limited than I think we’d like to believe ... we don’t know what the natural history of these patients’ life expectancy is. We don’t know from these data what the cause of death was, but anecdotally, we didn’t see hundreds of patients return with ruptured aneurysms after an EVAR.”
“I would truly like to see how many [of these patients] who make it out of the hospital return to normal living within 6 months,” Dr. Samuel R. Money, chair of surgery at the Mayo Clinic in Scottsdale, Ariz., said in an interview following the presentation. “At some point, the question becomes ‘Can we afford to spend $100,000 dollars to keep a 90-year-old patient alive for 6 more months?’ Can this society sustain the cost of that?”
On Twitter @whitneymcknight
SCOTTSDALE, ARIZ.– Abdominal aortic aneurysm repair in patients 80 years and older can be performed safely and with good medium-term survival rates, a prospective single-site study has shown.
Perioperative mortality in elective and emergent AAA repair for octogenarians was 2% and 35%, respectively, with a median survival rate of 19 months in both groups.
According to these data, “Patients shouldn’t be turned down for aneurysm repair on the basis of their age alone,” Dr. Christopher M. Lamb, a vascular surgery fellow at the University of California Davis Medical Center in Sacramento, said during a presentation at this year’s Southern Association for Vascular Surgery annual meeting.
“However, whether we should be doing these procedures is a different question, and I don’t think these data allow us to answer that question properly.”Dr. Lamb and his colleagues reviewed the records of 847 consecutive patients aged 80 years or older, seen between April 2005 and February 2014 for any type of AAA repair. Cases were sorted according to whether they were elective, ruptured, or urgent but unruptured. A total of 226 patients met the study’s age criteria; there were nearly seven men for every woman, all with a median age of 83 years. Of the elective AAA repair arm of the study, 131 patients (116 men) with a median age of 82 years had an endovascular repair, while the rest underwent open surgical repair. The combined 30-day mortality rate for these patients was 2.3%, with no significant difference between either the endovascular aneurysm repair (EVAR) or the open surgical repair (OSR) patients (1.9% vs. 4.2%; P = .458). The median survival of all elective repair patients was 19 months (interquartile range, 10-35), with no difference seen between the two groups (P = .113)Of the 65 patients (53 men) with ruptured AAA, the median age was 83 years. A third had open repair (32.3%), while the rest had EVAR. The combined 30-day mortality rate was 35.4% but was significantly higher after OSR (52.4% vs. 27.3%; P = .048). The median survival rate was 6 months (IQR, 6-42) when 30-day mortality rates were excluded. The median survival rates in patients who lived longer than 30 days was significantly higher in OSR patients (42.5 months vs. 11 months; P = .019).
Of the 23 men and 7 women with symptomatic but unruptured AAA, all but 1 had EVAR. At 30 days, there was one diverticular perforation–related postoperative death in the EVAR group, which had a median survival rate of 29 months. There being only a single patient in the OSR group obviated a comparative median survival rate analysis.
A subanalysis of the final 20 months of the study showed that 41% of octogenarians seeking any type of AAA repair at the site were rejected (48 rejections vs. 69 repairs). Those who were rejected for repair tended to be older, with a median age of 86 years vs. 83 years for patients who underwent repair (P = .0004).
Dr. Lamb noted that although the findings demonstrate acceptable overall safety rates for the entire cohort, without a control group of patients that did not have AAA repair, it would be hard to draw a definite conclusion about the utility of the findings, and that more data were warranted; however, the potential for limited long-term survival with what previous reports have suggested may include “a reduced quality of life for a good part of it, possibly raises the question that these patients should be treated conservatively, more often.”
The rejection rate data prompted the presentation’s discussant, Dr. William D. Jordan Jr., section chief of vascular surgery at the University of Alabama at Birmingham and the presentation’s discussant, to challenge the findings and asked whether a single surgeon selected the patients.
“You said there is not a selection bias in your study, but I beg to differ. Perhaps all these kinds of studies have a selection bias, and I believe they should. We should select the appropriate patients for the appropriate procedure at the appropriate time, with the appropriate expectation of outcome. Bias in this setting may be seen as good,” Dr. Jordan said.Dr. Lamb responded that the treatment algorithm at the site for all patients with a confirmed AAA of 5.5 cm or greater included CT imaging that is reviewed by a multidisciplinary team comprising vascular surgeons and interventional radiologists, who then evaluated the patients according to their physiology and anatomy, as well as their comorbidities, with the intention that whenever possible, EVAR rather than open repair would be performed.
As to whether there was a bias toward not repairing AAA in older patients, Dr. Lamb said it was incumbent on any health system to evaluate a procedure’s cost-effectiveness, but that, “the life expectancy of a vascular patient is often more limited than I think we’d like to believe ... we don’t know what the natural history of these patients’ life expectancy is. We don’t know from these data what the cause of death was, but anecdotally, we didn’t see hundreds of patients return with ruptured aneurysms after an EVAR.”
“I would truly like to see how many [of these patients] who make it out of the hospital return to normal living within 6 months,” Dr. Samuel R. Money, chair of surgery at the Mayo Clinic in Scottsdale, Ariz., said in an interview following the presentation. “At some point, the question becomes ‘Can we afford to spend $100,000 dollars to keep a 90-year-old patient alive for 6 more months?’ Can this society sustain the cost of that?”
On Twitter @whitneymcknight

If you find your bliss in research....
There’s no place like San Francisco. And it’s even better when you’re surrounded by your fellow researchers at the Vascular Research Initiatives Conference. This year’s translational session will be “Biomarkers for Vascular Disease Prediction and Therapeutic Screen.”
Don’t miss this special day, May 6, 2015, which is right before the AHA ATVB meeting in the same location. Learn more and register at vsweb.org/VRIC.
There’s no place like San Francisco. And it’s even better when you’re surrounded by your fellow researchers at the Vascular Research Initiatives Conference. This year’s translational session will be “Biomarkers for Vascular Disease Prediction and Therapeutic Screen.”
Don’t miss this special day, May 6, 2015, which is right before the AHA ATVB meeting in the same location. Learn more and register at vsweb.org/VRIC.
There’s no place like San Francisco. And it’s even better when you’re surrounded by your fellow researchers at the Vascular Research Initiatives Conference. This year’s translational session will be “Biomarkers for Vascular Disease Prediction and Therapeutic Screen.”
Don’t miss this special day, May 6, 2015, which is right before the AHA ATVB meeting in the same location. Learn more and register at vsweb.org/VRIC.
Still time to register for Coding Class
Hotel reservations are closed, but you can still sign up for the 2015 Coding Class, titled, “Challenges in Vascular Surgery 2015: Coding and Reimbursement for Vascular Surgeons.”
The course is designed for surgeons and office staff, including practice managers, nurse practitioners, physician assistants, coders and schedulers.
The two-day, intensive course is slated for April 17-18 near Chicago’s O’Hare International Airport. An additional workshop, “E&M Coding for Vascular Surgeons,” is also offered Friday morning.
Learn more and register for the class by clicking here.
Hotel reservations are closed, but you can still sign up for the 2015 Coding Class, titled, “Challenges in Vascular Surgery 2015: Coding and Reimbursement for Vascular Surgeons.”
The course is designed for surgeons and office staff, including practice managers, nurse practitioners, physician assistants, coders and schedulers.
The two-day, intensive course is slated for April 17-18 near Chicago’s O’Hare International Airport. An additional workshop, “E&M Coding for Vascular Surgeons,” is also offered Friday morning.
Learn more and register for the class by clicking here.
Hotel reservations are closed, but you can still sign up for the 2015 Coding Class, titled, “Challenges in Vascular Surgery 2015: Coding and Reimbursement for Vascular Surgeons.”
The course is designed for surgeons and office staff, including practice managers, nurse practitioners, physician assistants, coders and schedulers.
The two-day, intensive course is slated for April 17-18 near Chicago’s O’Hare International Airport. An additional workshop, “E&M Coding for Vascular Surgeons,” is also offered Friday morning.
Learn more and register for the class by clicking here.
We’re expecting a crowd at VAM - Sign up today
Based on the pace of early sign ups, we’re expecting an excellent turnout for the Vascular Annual Meeting, set for June 17-20 in Chicago. Our session speakers, presenters and exhibitors are working hard to bring you the latest information and products. A record 705 abstract and video submissions were received, which should ensure invigorating sessions and debates.
This year you will find more hands-on training, more interdisciplinary topics, more presentations and speakers, and more for international guests. Our revised program guide, together with an updated meeting app, will make it easy to plan your day. Be sure to make time to visit the exhibit hall and catch Vascular Live.
To ensure that you get the best prices on hotel reservations, get registered soon.
Based on the pace of early sign ups, we’re expecting an excellent turnout for the Vascular Annual Meeting, set for June 17-20 in Chicago. Our session speakers, presenters and exhibitors are working hard to bring you the latest information and products. A record 705 abstract and video submissions were received, which should ensure invigorating sessions and debates.
This year you will find more hands-on training, more interdisciplinary topics, more presentations and speakers, and more for international guests. Our revised program guide, together with an updated meeting app, will make it easy to plan your day. Be sure to make time to visit the exhibit hall and catch Vascular Live.
To ensure that you get the best prices on hotel reservations, get registered soon.
Based on the pace of early sign ups, we’re expecting an excellent turnout for the Vascular Annual Meeting, set for June 17-20 in Chicago. Our session speakers, presenters and exhibitors are working hard to bring you the latest information and products. A record 705 abstract and video submissions were received, which should ensure invigorating sessions and debates.
This year you will find more hands-on training, more interdisciplinary topics, more presentations and speakers, and more for international guests. Our revised program guide, together with an updated meeting app, will make it easy to plan your day. Be sure to make time to visit the exhibit hall and catch Vascular Live.
To ensure that you get the best prices on hotel reservations, get registered soon.
April 6 - Deadline to apply for Women’s Leadership Training Grant
A host of learning and training opportunities are open to the winners of this year’s Women’s Leadership Training Grant. The deadline to apply is Monday, April 6. Sponsored by the SVS Diversity and Inclusion Committee, the grant program is designed to develop strong women leaders in vascular surgery who will demonstrate the outstanding accomplishments and personal qualities of surgeons recognized by SVS for lifetime achievements. Applicants should have demonstrated leadership in SVS or other vascular societies, contributed to vascular education, science or research, and have made other contributions to the field.
Awards of $5,000 are given annually to recipients in three categories: 0-5 years out of training; 6-10 years and more than 10 years out of training. Learn more here.
A host of learning and training opportunities are open to the winners of this year’s Women’s Leadership Training Grant. The deadline to apply is Monday, April 6. Sponsored by the SVS Diversity and Inclusion Committee, the grant program is designed to develop strong women leaders in vascular surgery who will demonstrate the outstanding accomplishments and personal qualities of surgeons recognized by SVS for lifetime achievements. Applicants should have demonstrated leadership in SVS or other vascular societies, contributed to vascular education, science or research, and have made other contributions to the field.
Awards of $5,000 are given annually to recipients in three categories: 0-5 years out of training; 6-10 years and more than 10 years out of training. Learn more here.
A host of learning and training opportunities are open to the winners of this year’s Women’s Leadership Training Grant. The deadline to apply is Monday, April 6. Sponsored by the SVS Diversity and Inclusion Committee, the grant program is designed to develop strong women leaders in vascular surgery who will demonstrate the outstanding accomplishments and personal qualities of surgeons recognized by SVS for lifetime achievements. Applicants should have demonstrated leadership in SVS or other vascular societies, contributed to vascular education, science or research, and have made other contributions to the field.
Awards of $5,000 are given annually to recipients in three categories: 0-5 years out of training; 6-10 years and more than 10 years out of training. Learn more here.
ACA – What it takes for surgeons to survive and succeed
Each year, one of the highlights of the Vascular Annual Meeting is the lively Crawford Critical Issues Symposium, headed this year by Dr. Bruce Perler of Johns Hopkins Hospital Division of Vascular Surgery. His topic, “How You Can Succeed Under the Affordable Care Act,” will be addressed by stakeholders from all sides of the issue.
Speakers will be –
• Dr. Stephen Ondra,senior vice president and CMO of Health Care Service Corporation, offering the viewpoint of the insurance industry
• Larry Boress, president and CEO, Midwest Business Group on Health, an agency that helps employers choose and manage health care benefits for employees
• Dr. Bruce Landon, professor of health care policy, Harvard Medical School, discussing how ACA may impact vascular surgeons
• Dr. Dan Clair, chair, Department of Vascular Surgery, the Cleveland Clinic, discussing how vascular surgeons can succeed as hospital employees
Vascular Specialist asked Dr. Perler to tell us more about this event, scheduled for 10:30 a.m. to noon on Thursday, June 18.
VS:Why did you pick this topic? Dr. Perler: There is no more important and overarching issue for all vascular surgeons today than the rapidly changing contemporary health care environment related to the Affordable Care Act. Quite honestly, for a number of reasons and in large part due to these changes, I believe the lines of demarcation between private and academic practice are increasingly blurring. The pressures, external threats, and challenges to achieving a satisfying and economically viable practice are quite similar today irrespective of practice type or location.
The increasing movement to full-time hospital employment, the increasing emphasis on quality outcomes, impending changes in reimbursement models, and the emergence of Accountable Care Organizations (ACOs) are factors affecting the practices of all vascular surgeons. I therefore believed that this was a most appropriate topic to address at the 2015 Crawford Critical Issues Symposium. “How You Can Succeed Under the Affordable Care Act” will provide strategies that our members can follow to not only survive but thrive in this new health care order.
VS: What takeaways do you hope attendees will have at the end of the session? Dr. Perler: We will be bringing together in one forum a world class group of nationally recognized experts and stakeholders in health care to share their knowledge about, and expectations for, the immediate and mid-term future of health care economics. The panel includes individuals with diverse backgrounds and interests including the perspectives of the employer, the payor, public health policy-makers, and the practicing institution-employed vascular surgeon. We believe these presentations and the opportunity for our attendees to engage these leaders in a question-and-answer session will provide education about the expectations these stakeholders have of clinicians and therefore allow our members to develop strategies that they might incorporate in their own practices to continue professionally satisfying and economically productive practices.
While all medical practitioners are affected by these changes inherent in the Affordable Care Act, because of our relatively small numbers and the increasing multispecialty completion that vascular surgeons face, including for many participation in multispecialty cardiovascular centers as well as increasing hospital employment, I believe that these issues are particularly relevant to our specialty.
VS: You have an interesting line-up of panelists, what were your reasons for selecting each?Dr. Perler: There are clearly multiple stakeholders or components in our health care system with unique backgrounds, interests, and agendas. Each of them will bring to the Crawford Symposium a perspective from his specific component of the system, the insurer, the employer, the hospital-employed surgeon, and someone with specific expertise in Accountable Care Organizations and knowledge of vascular surgical practice.
It was my expectation to bring these experts together in one setting to not only provide useful information for our attendees, but to allow them to engage in a collective discourse that should provide an unparalleled educational experience for our attendees.
VS: Where do you think their biggest areas of agreement, and of disagreement, will be during the discussion?
Dr. Perler: That’s a great question and the short answer is I can’t precisely predict. In general, I would assume that there will be a consensus that rising health care costs must come under control and physician reimbursement in the future will be increasingly linked to quality outcomes rather than pure case volume. There also may be a consensus on the importance of longitudinal patient care.
Beyond the obvious, however, the key question is whether or how the health care system will align reimbursement to the distinctive competencies of vascular surgeons as the only truly comprehensive vascular specialists who provide the totality of care including diagnosis as well as medical, surgical, and endovascular therapy. Will employers and insurers recognize the value of the comprehensive care that only vascular surgeons provide? Will ACOs factor that competency into specialty referral patterns? Further, will payors and hospitals recognize the unique leadership that vascular surgeons can provide in the care of cardiovascular patients in the hospital environment?
Each year, one of the highlights of the Vascular Annual Meeting is the lively Crawford Critical Issues Symposium, headed this year by Dr. Bruce Perler of Johns Hopkins Hospital Division of Vascular Surgery. His topic, “How You Can Succeed Under the Affordable Care Act,” will be addressed by stakeholders from all sides of the issue.
Speakers will be –
• Dr. Stephen Ondra,senior vice president and CMO of Health Care Service Corporation, offering the viewpoint of the insurance industry
• Larry Boress, president and CEO, Midwest Business Group on Health, an agency that helps employers choose and manage health care benefits for employees
• Dr. Bruce Landon, professor of health care policy, Harvard Medical School, discussing how ACA may impact vascular surgeons
• Dr. Dan Clair, chair, Department of Vascular Surgery, the Cleveland Clinic, discussing how vascular surgeons can succeed as hospital employees
Vascular Specialist asked Dr. Perler to tell us more about this event, scheduled for 10:30 a.m. to noon on Thursday, June 18.
VS:Why did you pick this topic? Dr. Perler: There is no more important and overarching issue for all vascular surgeons today than the rapidly changing contemporary health care environment related to the Affordable Care Act. Quite honestly, for a number of reasons and in large part due to these changes, I believe the lines of demarcation between private and academic practice are increasingly blurring. The pressures, external threats, and challenges to achieving a satisfying and economically viable practice are quite similar today irrespective of practice type or location.
The increasing movement to full-time hospital employment, the increasing emphasis on quality outcomes, impending changes in reimbursement models, and the emergence of Accountable Care Organizations (ACOs) are factors affecting the practices of all vascular surgeons. I therefore believed that this was a most appropriate topic to address at the 2015 Crawford Critical Issues Symposium. “How You Can Succeed Under the Affordable Care Act” will provide strategies that our members can follow to not only survive but thrive in this new health care order.
VS: What takeaways do you hope attendees will have at the end of the session? Dr. Perler: We will be bringing together in one forum a world class group of nationally recognized experts and stakeholders in health care to share their knowledge about, and expectations for, the immediate and mid-term future of health care economics. The panel includes individuals with diverse backgrounds and interests including the perspectives of the employer, the payor, public health policy-makers, and the practicing institution-employed vascular surgeon. We believe these presentations and the opportunity for our attendees to engage these leaders in a question-and-answer session will provide education about the expectations these stakeholders have of clinicians and therefore allow our members to develop strategies that they might incorporate in their own practices to continue professionally satisfying and economically productive practices.
While all medical practitioners are affected by these changes inherent in the Affordable Care Act, because of our relatively small numbers and the increasing multispecialty completion that vascular surgeons face, including for many participation in multispecialty cardiovascular centers as well as increasing hospital employment, I believe that these issues are particularly relevant to our specialty.
VS: You have an interesting line-up of panelists, what were your reasons for selecting each?Dr. Perler: There are clearly multiple stakeholders or components in our health care system with unique backgrounds, interests, and agendas. Each of them will bring to the Crawford Symposium a perspective from his specific component of the system, the insurer, the employer, the hospital-employed surgeon, and someone with specific expertise in Accountable Care Organizations and knowledge of vascular surgical practice.
It was my expectation to bring these experts together in one setting to not only provide useful information for our attendees, but to allow them to engage in a collective discourse that should provide an unparalleled educational experience for our attendees.
VS: Where do you think their biggest areas of agreement, and of disagreement, will be during the discussion?
Dr. Perler: That’s a great question and the short answer is I can’t precisely predict. In general, I would assume that there will be a consensus that rising health care costs must come under control and physician reimbursement in the future will be increasingly linked to quality outcomes rather than pure case volume. There also may be a consensus on the importance of longitudinal patient care.
Beyond the obvious, however, the key question is whether or how the health care system will align reimbursement to the distinctive competencies of vascular surgeons as the only truly comprehensive vascular specialists who provide the totality of care including diagnosis as well as medical, surgical, and endovascular therapy. Will employers and insurers recognize the value of the comprehensive care that only vascular surgeons provide? Will ACOs factor that competency into specialty referral patterns? Further, will payors and hospitals recognize the unique leadership that vascular surgeons can provide in the care of cardiovascular patients in the hospital environment?
Each year, one of the highlights of the Vascular Annual Meeting is the lively Crawford Critical Issues Symposium, headed this year by Dr. Bruce Perler of Johns Hopkins Hospital Division of Vascular Surgery. His topic, “How You Can Succeed Under the Affordable Care Act,” will be addressed by stakeholders from all sides of the issue.
Speakers will be –
• Dr. Stephen Ondra,senior vice president and CMO of Health Care Service Corporation, offering the viewpoint of the insurance industry
• Larry Boress, president and CEO, Midwest Business Group on Health, an agency that helps employers choose and manage health care benefits for employees
• Dr. Bruce Landon, professor of health care policy, Harvard Medical School, discussing how ACA may impact vascular surgeons
• Dr. Dan Clair, chair, Department of Vascular Surgery, the Cleveland Clinic, discussing how vascular surgeons can succeed as hospital employees
Vascular Specialist asked Dr. Perler to tell us more about this event, scheduled for 10:30 a.m. to noon on Thursday, June 18.
VS:Why did you pick this topic? Dr. Perler: There is no more important and overarching issue for all vascular surgeons today than the rapidly changing contemporary health care environment related to the Affordable Care Act. Quite honestly, for a number of reasons and in large part due to these changes, I believe the lines of demarcation between private and academic practice are increasingly blurring. The pressures, external threats, and challenges to achieving a satisfying and economically viable practice are quite similar today irrespective of practice type or location.
The increasing movement to full-time hospital employment, the increasing emphasis on quality outcomes, impending changes in reimbursement models, and the emergence of Accountable Care Organizations (ACOs) are factors affecting the practices of all vascular surgeons. I therefore believed that this was a most appropriate topic to address at the 2015 Crawford Critical Issues Symposium. “How You Can Succeed Under the Affordable Care Act” will provide strategies that our members can follow to not only survive but thrive in this new health care order.
VS: What takeaways do you hope attendees will have at the end of the session? Dr. Perler: We will be bringing together in one forum a world class group of nationally recognized experts and stakeholders in health care to share their knowledge about, and expectations for, the immediate and mid-term future of health care economics. The panel includes individuals with diverse backgrounds and interests including the perspectives of the employer, the payor, public health policy-makers, and the practicing institution-employed vascular surgeon. We believe these presentations and the opportunity for our attendees to engage these leaders in a question-and-answer session will provide education about the expectations these stakeholders have of clinicians and therefore allow our members to develop strategies that they might incorporate in their own practices to continue professionally satisfying and economically productive practices.
While all medical practitioners are affected by these changes inherent in the Affordable Care Act, because of our relatively small numbers and the increasing multispecialty completion that vascular surgeons face, including for many participation in multispecialty cardiovascular centers as well as increasing hospital employment, I believe that these issues are particularly relevant to our specialty.
VS: You have an interesting line-up of panelists, what were your reasons for selecting each?Dr. Perler: There are clearly multiple stakeholders or components in our health care system with unique backgrounds, interests, and agendas. Each of them will bring to the Crawford Symposium a perspective from his specific component of the system, the insurer, the employer, the hospital-employed surgeon, and someone with specific expertise in Accountable Care Organizations and knowledge of vascular surgical practice.
It was my expectation to bring these experts together in one setting to not only provide useful information for our attendees, but to allow them to engage in a collective discourse that should provide an unparalleled educational experience for our attendees.
VS: Where do you think their biggest areas of agreement, and of disagreement, will be during the discussion?
Dr. Perler: That’s a great question and the short answer is I can’t precisely predict. In general, I would assume that there will be a consensus that rising health care costs must come under control and physician reimbursement in the future will be increasingly linked to quality outcomes rather than pure case volume. There also may be a consensus on the importance of longitudinal patient care.
Beyond the obvious, however, the key question is whether or how the health care system will align reimbursement to the distinctive competencies of vascular surgeons as the only truly comprehensive vascular specialists who provide the totality of care including diagnosis as well as medical, surgical, and endovascular therapy. Will employers and insurers recognize the value of the comprehensive care that only vascular surgeons provide? Will ACOs factor that competency into specialty referral patterns? Further, will payors and hospitals recognize the unique leadership that vascular surgeons can provide in the care of cardiovascular patients in the hospital environment?
Study: Surgery offers chance to adjust vascular medications
Patients who are treated at sites with longer participation in the VQI had better medical management and this was associated with higher survival rates, according to a new study reported in the April 2015 issue of The Journal of Vascular Surgery. Further, surgery at a VQI site may relate to optimized medications with the goal to improve survival rates.
Led by Dr. Randall R. De Martino, a team of researchers studied medical management for vascular surgery patients at sites participating in the Vascular Quality Initiative and associated patient survival rates.
Two key outcomes were noted: Site participation in VQI is associated with improved use of antiplatelets and statin medication for that site’s patients undergoing vascular procedures; and, treatment with AP and statins is associated with a 14 percent survival advantage for patients at five years postsurgery.
“Medical therapy for patients with vascular disease remains important for their long-term prevention of cardiovascular events,” noted Dr. De Martino. “The surgical encounter provides an excellent opportunity to ensure that appropriate medications are prescribed. As our data demonstrate, many patients remain medically undertreated and this is associated with worse long-term survival. Importantly, participating in a quality improvement initiative, like the VQI, is associated with improvements in medical management. This highlights how we can use a quality improvement collaborative to improve care for our patients.”
Since up to 75 percent of patients with peripheral arterial disease will ultimately die of cardiovascular causes, it seems that medical management is a strong tool to ensure patient survival.
Additional authors are Drs. Andrew W. Hoel, Adam W. Beck, Jens Eldrup-Jorgensen, John W. Hallett, Gilbert R. Upchurch, Jack L. Cronenwett, and Philip P. Goodney.
Patients who are treated at sites with longer participation in the VQI had better medical management and this was associated with higher survival rates, according to a new study reported in the April 2015 issue of The Journal of Vascular Surgery. Further, surgery at a VQI site may relate to optimized medications with the goal to improve survival rates.
Led by Dr. Randall R. De Martino, a team of researchers studied medical management for vascular surgery patients at sites participating in the Vascular Quality Initiative and associated patient survival rates.
Two key outcomes were noted: Site participation in VQI is associated with improved use of antiplatelets and statin medication for that site’s patients undergoing vascular procedures; and, treatment with AP and statins is associated with a 14 percent survival advantage for patients at five years postsurgery.
“Medical therapy for patients with vascular disease remains important for their long-term prevention of cardiovascular events,” noted Dr. De Martino. “The surgical encounter provides an excellent opportunity to ensure that appropriate medications are prescribed. As our data demonstrate, many patients remain medically undertreated and this is associated with worse long-term survival. Importantly, participating in a quality improvement initiative, like the VQI, is associated with improvements in medical management. This highlights how we can use a quality improvement collaborative to improve care for our patients.”
Since up to 75 percent of patients with peripheral arterial disease will ultimately die of cardiovascular causes, it seems that medical management is a strong tool to ensure patient survival.
Additional authors are Drs. Andrew W. Hoel, Adam W. Beck, Jens Eldrup-Jorgensen, John W. Hallett, Gilbert R. Upchurch, Jack L. Cronenwett, and Philip P. Goodney.
Patients who are treated at sites with longer participation in the VQI had better medical management and this was associated with higher survival rates, according to a new study reported in the April 2015 issue of The Journal of Vascular Surgery. Further, surgery at a VQI site may relate to optimized medications with the goal to improve survival rates.
Led by Dr. Randall R. De Martino, a team of researchers studied medical management for vascular surgery patients at sites participating in the Vascular Quality Initiative and associated patient survival rates.
Two key outcomes were noted: Site participation in VQI is associated with improved use of antiplatelets and statin medication for that site’s patients undergoing vascular procedures; and, treatment with AP and statins is associated with a 14 percent survival advantage for patients at five years postsurgery.
“Medical therapy for patients with vascular disease remains important for their long-term prevention of cardiovascular events,” noted Dr. De Martino. “The surgical encounter provides an excellent opportunity to ensure that appropriate medications are prescribed. As our data demonstrate, many patients remain medically undertreated and this is associated with worse long-term survival. Importantly, participating in a quality improvement initiative, like the VQI, is associated with improvements in medical management. This highlights how we can use a quality improvement collaborative to improve care for our patients.”
Since up to 75 percent of patients with peripheral arterial disease will ultimately die of cardiovascular causes, it seems that medical management is a strong tool to ensure patient survival.
Additional authors are Drs. Andrew W. Hoel, Adam W. Beck, Jens Eldrup-Jorgensen, John W. Hallett, Gilbert R. Upchurch, Jack L. Cronenwett, and Philip P. Goodney.
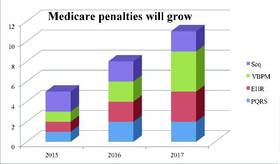
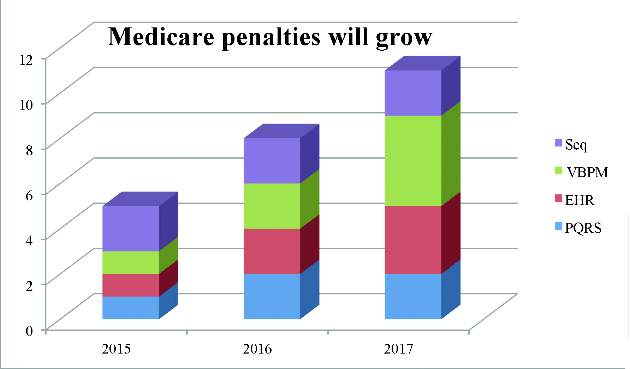
Growing Medicare penalties start this year
Along with the usual threat of cuts to physician payment using the Sustainable Growth Rate (SGR) formula, which sets payment rates through a formula based on economic growth, physicians are also facing other potential cuts.
Physician Quality Report System (PQRS) – for eligible professionals (EPs), which include vascular surgeons, who do not successfully report nine quality measures:
1. 2015 – 1 percent payment adjustment
2. 2016 and beyond – 2 percent payment adjustment
3. According to the American Medical Association, only 35 percent of EPs are participating in PQRS
Meaningful Use of Electronic Health Record Incentive Program – for EPs who fail to participate:
1. 2015 – 1 percent payment adjustment
2. 2016 – 2 percent payment adjustment
3. 2017 – 3 percent payment adjustment
4. Hardship exemptions – insufficient Internet access, new physician, natural disaster or other unforeseeable barrier, lack of face-to-face or telemedicine interaction or lack of follow-up needed with patients and lack of control over availability of certified EHR technology
5. According to a 2014 Medscape Report, 22 percent of physicians are opting out of Meaningful Use
Value-Based Payment Modifier – for physicians who do not meet the benchmark for both cost and quality data:
1. 2015 – 1 percent payment adjustment for physicians in group practices of 100 or more EPs under a single tax identification number based on 2013 data
2. 2016 – 2 percent payment adjustment for physicians in group practices of 10 or more EPs based on 2014 data
3. 2017 – 4 percent for physicians in group practices of 10 or more EPs/2 percent for physicians in group practices under 10 EPs based on 2015 data
Sequestration – 2 percent across-the-board cut on Medicare to reduce the deficit
The result – penalties go as high as 11 percent in 2017 for these programs
According to the Medical Group Management Association survey conducted in October 2014 with 1,000 physician group practices in which 48,000 physicians practice:
1. 84 percent do not believe that Medicare’s quality reporting programs enhance physicians’ ability to provide high quality patient care
2. 71 percent rated the regulatory complexity of the quality reporting programs as very or extremely complex
3. 74 percent are concerned with their practices’ ability to successfully participate in Medicare quality reporting programs in 2015
SVS supports replacing the three programs with a Merit-Based Incentive Payment System, which was included in last year’s SGR repeal and reform bill. Even though there is bipartisan, bicameral support for this legislation, Congress will likely enact another SGR “patch” for six months before the current patch expires on March 31; otherwise, there will be a 22 percent cut that would take effect on April 1.
Along with the usual threat of cuts to physician payment using the Sustainable Growth Rate (SGR) formula, which sets payment rates through a formula based on economic growth, physicians are also facing other potential cuts.
Physician Quality Report System (PQRS) – for eligible professionals (EPs), which include vascular surgeons, who do not successfully report nine quality measures:
1. 2015 – 1 percent payment adjustment
2. 2016 and beyond – 2 percent payment adjustment
3. According to the American Medical Association, only 35 percent of EPs are participating in PQRS
Meaningful Use of Electronic Health Record Incentive Program – for EPs who fail to participate:
1. 2015 – 1 percent payment adjustment
2. 2016 – 2 percent payment adjustment
3. 2017 – 3 percent payment adjustment
4. Hardship exemptions – insufficient Internet access, new physician, natural disaster or other unforeseeable barrier, lack of face-to-face or telemedicine interaction or lack of follow-up needed with patients and lack of control over availability of certified EHR technology
5. According to a 2014 Medscape Report, 22 percent of physicians are opting out of Meaningful Use
Value-Based Payment Modifier – for physicians who do not meet the benchmark for both cost and quality data:
1. 2015 – 1 percent payment adjustment for physicians in group practices of 100 or more EPs under a single tax identification number based on 2013 data
2. 2016 – 2 percent payment adjustment for physicians in group practices of 10 or more EPs based on 2014 data
3. 2017 – 4 percent for physicians in group practices of 10 or more EPs/2 percent for physicians in group practices under 10 EPs based on 2015 data
Sequestration – 2 percent across-the-board cut on Medicare to reduce the deficit
The result – penalties go as high as 11 percent in 2017 for these programs
According to the Medical Group Management Association survey conducted in October 2014 with 1,000 physician group practices in which 48,000 physicians practice:
1. 84 percent do not believe that Medicare’s quality reporting programs enhance physicians’ ability to provide high quality patient care
2. 71 percent rated the regulatory complexity of the quality reporting programs as very or extremely complex
3. 74 percent are concerned with their practices’ ability to successfully participate in Medicare quality reporting programs in 2015
SVS supports replacing the three programs with a Merit-Based Incentive Payment System, which was included in last year’s SGR repeal and reform bill. Even though there is bipartisan, bicameral support for this legislation, Congress will likely enact another SGR “patch” for six months before the current patch expires on March 31; otherwise, there will be a 22 percent cut that would take effect on April 1.
Along with the usual threat of cuts to physician payment using the Sustainable Growth Rate (SGR) formula, which sets payment rates through a formula based on economic growth, physicians are also facing other potential cuts.
Physician Quality Report System (PQRS) – for eligible professionals (EPs), which include vascular surgeons, who do not successfully report nine quality measures:
1. 2015 – 1 percent payment adjustment
2. 2016 and beyond – 2 percent payment adjustment
3. According to the American Medical Association, only 35 percent of EPs are participating in PQRS
Meaningful Use of Electronic Health Record Incentive Program – for EPs who fail to participate:
1. 2015 – 1 percent payment adjustment
2. 2016 – 2 percent payment adjustment
3. 2017 – 3 percent payment adjustment
4. Hardship exemptions – insufficient Internet access, new physician, natural disaster or other unforeseeable barrier, lack of face-to-face or telemedicine interaction or lack of follow-up needed with patients and lack of control over availability of certified EHR technology
5. According to a 2014 Medscape Report, 22 percent of physicians are opting out of Meaningful Use
Value-Based Payment Modifier – for physicians who do not meet the benchmark for both cost and quality data:
1. 2015 – 1 percent payment adjustment for physicians in group practices of 100 or more EPs under a single tax identification number based on 2013 data
2. 2016 – 2 percent payment adjustment for physicians in group practices of 10 or more EPs based on 2014 data
3. 2017 – 4 percent for physicians in group practices of 10 or more EPs/2 percent for physicians in group practices under 10 EPs based on 2015 data
Sequestration – 2 percent across-the-board cut on Medicare to reduce the deficit
The result – penalties go as high as 11 percent in 2017 for these programs
According to the Medical Group Management Association survey conducted in October 2014 with 1,000 physician group practices in which 48,000 physicians practice:
1. 84 percent do not believe that Medicare’s quality reporting programs enhance physicians’ ability to provide high quality patient care
2. 71 percent rated the regulatory complexity of the quality reporting programs as very or extremely complex
3. 74 percent are concerned with their practices’ ability to successfully participate in Medicare quality reporting programs in 2015
SVS supports replacing the three programs with a Merit-Based Incentive Payment System, which was included in last year’s SGR repeal and reform bill. Even though there is bipartisan, bicameral support for this legislation, Congress will likely enact another SGR “patch” for six months before the current patch expires on March 31; otherwise, there will be a 22 percent cut that would take effect on April 1.
The March issue of Vascular Specialist is now online
This issue features a special section of editorial opinion from our associate medical editors and letters from the SVS membership addressing the issue of excessive peripheral artery disease stenting, which was reported in the New York Times and then discussed by SVS President Dr. Peter Lawrence in our February issue.
Also featured in our online PDF is a clinical story on EVAR infection care, a discussion of the private/academic surgeon salary gap, and a point/counterpoint on renal artery stenting.
The News from SVS section outlines the Crawford Critical Issues Symposium at the upcoming Vascular Annual Meeting in Chicago and raises the issue of the Medicare penalties that are starting this year.
Be sure to check out the online PDF of the March issue here.
This issue features a special section of editorial opinion from our associate medical editors and letters from the SVS membership addressing the issue of excessive peripheral artery disease stenting, which was reported in the New York Times and then discussed by SVS President Dr. Peter Lawrence in our February issue.
Also featured in our online PDF is a clinical story on EVAR infection care, a discussion of the private/academic surgeon salary gap, and a point/counterpoint on renal artery stenting.
The News from SVS section outlines the Crawford Critical Issues Symposium at the upcoming Vascular Annual Meeting in Chicago and raises the issue of the Medicare penalties that are starting this year.
Be sure to check out the online PDF of the March issue here.
This issue features a special section of editorial opinion from our associate medical editors and letters from the SVS membership addressing the issue of excessive peripheral artery disease stenting, which was reported in the New York Times and then discussed by SVS President Dr. Peter Lawrence in our February issue.
Also featured in our online PDF is a clinical story on EVAR infection care, a discussion of the private/academic surgeon salary gap, and a point/counterpoint on renal artery stenting.
The News from SVS section outlines the Crawford Critical Issues Symposium at the upcoming Vascular Annual Meeting in Chicago and raises the issue of the Medicare penalties that are starting this year.
Be sure to check out the online PDF of the March issue here.

SVS member quoted in New York Times
Dr. Gretchen Schwarze of the University of Wisconsin-Madison was quoted in, “A surgery standard under fire,” in the New York Times March 2, 2015. The article examines the 30-day mortality standard and its unintended consequences. “Thirty days is a game-able number,” Dr. Schwarze said. Last fall she led a session about 30-day mortality at a conference sponsored by the American College of Surgeons.
Read the whole story here.
And learn more about Dr. Schwarze’s research in this article in the January issue of Vascular Specialist.
Dr. Gretchen Schwarze of the University of Wisconsin-Madison was quoted in, “A surgery standard under fire,” in the New York Times March 2, 2015. The article examines the 30-day mortality standard and its unintended consequences. “Thirty days is a game-able number,” Dr. Schwarze said. Last fall she led a session about 30-day mortality at a conference sponsored by the American College of Surgeons.
Read the whole story here.
And learn more about Dr. Schwarze’s research in this article in the January issue of Vascular Specialist.
Dr. Gretchen Schwarze of the University of Wisconsin-Madison was quoted in, “A surgery standard under fire,” in the New York Times March 2, 2015. The article examines the 30-day mortality standard and its unintended consequences. “Thirty days is a game-able number,” Dr. Schwarze said. Last fall she led a session about 30-day mortality at a conference sponsored by the American College of Surgeons.
Read the whole story here.
And learn more about Dr. Schwarze’s research in this article in the January issue of Vascular Specialist.