User login
Top PICS
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.


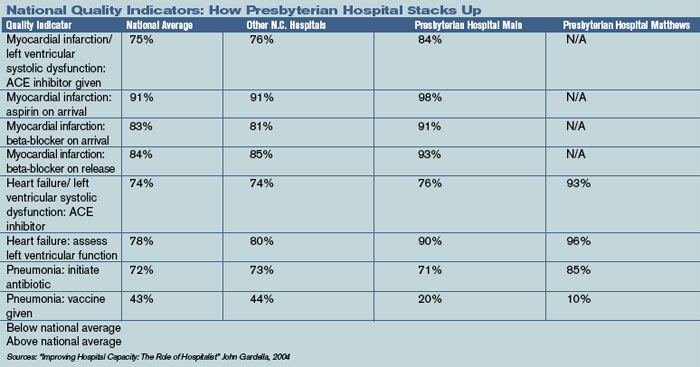
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
A Granary Becomes a Hospital
California gained statehood in 1850. Two months later Navy Secretary William Graham wrote to President Fillmore that “a new empire has, as by magic, sprung into existence. San Francisco promises, at no distant time, to become another New York.” He went on to say that “a Navy yard is very much needed in California, and no time will be lost in accomplishing the work.”
A three-officer commission was soon dispatched to choose a suitable site, and they decided on one protected inside San Francisco Bay at Mare Island. Commander David G. Farragut (of “Damn the torpedoes! Full speed ahead!” fame, a Civil War hero and the first admiral of the U.S. Navy) arrived at the remote place in 1854.
Within two days of his arrival at the California site, Farragut ordered the sloop-of-war over from Sausalito. This ship, soon to be replaced by the much larger USS Independence, served as the first naval medical facility on the West Coast. Ambulatory care was given in the ship’s sick bay, and the “hospitalized” were cared for from wooden bed frames suspended from the sick bay overhead or from their own hammocks. The average inpatient load was 10 sailors or civilian Navy yard workers.

The limitations of care aboard ship are made clear in a note from the yard surgeon in 1863; he wrote, “The frigate Independence, particularly in the winter season, is a very unsuitable place to treat the sick. It is cold, wet, and open to every wind that blows.”
Navy officials, while sympathetic to the plight of men serving in the tiny Pacific squadron, did little to correct the situation—likely because their attentions were focused on prosecuting the Civil War and not on a little Navy yard in far away California. Taking the situation into their own hands, surgeon Bishop and the commandant of the Navy yard submitted plans for a temporary facility—to be fashioned from an unused granary. The plans provided for a 25' x 25' ward on the first floor and a 24' x 40'9" ward space above, and called for a large cistern for year-round water supply, an attached bath approached from outside, and a nearby outdoor privy.
Still, Washington resisted, recommending that sick sailors be sent to the Marine (Public Health) Hospital in San Francisco, 25 miles away. This suggestion was met by stiff resistance both by local Naval authorities who feared desertion by sailors not under their direct observation and by the sailors themselves, who didn’t cotton to being hospitalized with merchant mariners.
Permission from Washington finally came through in July 1863. Work completed, the “Temporary Hospital” at Mare Island Navy Yard opened on Feb. 23, 1864.
The hospital carried an average inpatient load of 30, cared for by a surgeon and a surgeon’s steward, until the first permanent hospital—palatial by comparison—opened in 1871. TH
Dr. Snyder is a retired captain of the U.S. Naval Reserves’ Medical Corps. He writes regularly about naval medicine.
California gained statehood in 1850. Two months later Navy Secretary William Graham wrote to President Fillmore that “a new empire has, as by magic, sprung into existence. San Francisco promises, at no distant time, to become another New York.” He went on to say that “a Navy yard is very much needed in California, and no time will be lost in accomplishing the work.”
A three-officer commission was soon dispatched to choose a suitable site, and they decided on one protected inside San Francisco Bay at Mare Island. Commander David G. Farragut (of “Damn the torpedoes! Full speed ahead!” fame, a Civil War hero and the first admiral of the U.S. Navy) arrived at the remote place in 1854.
Within two days of his arrival at the California site, Farragut ordered the sloop-of-war over from Sausalito. This ship, soon to be replaced by the much larger USS Independence, served as the first naval medical facility on the West Coast. Ambulatory care was given in the ship’s sick bay, and the “hospitalized” were cared for from wooden bed frames suspended from the sick bay overhead or from their own hammocks. The average inpatient load was 10 sailors or civilian Navy yard workers.
The limitations of care aboard ship are made clear in a note from the yard surgeon in 1863; he wrote, “The frigate Independence, particularly in the winter season, is a very unsuitable place to treat the sick. It is cold, wet, and open to every wind that blows.”
Navy officials, while sympathetic to the plight of men serving in the tiny Pacific squadron, did little to correct the situation—likely because their attentions were focused on prosecuting the Civil War and not on a little Navy yard in far away California. Taking the situation into their own hands, surgeon Bishop and the commandant of the Navy yard submitted plans for a temporary facility—to be fashioned from an unused granary. The plans provided for a 25' x 25' ward on the first floor and a 24' x 40'9" ward space above, and called for a large cistern for year-round water supply, an attached bath approached from outside, and a nearby outdoor privy.
Still, Washington resisted, recommending that sick sailors be sent to the Marine (Public Health) Hospital in San Francisco, 25 miles away. This suggestion was met by stiff resistance both by local Naval authorities who feared desertion by sailors not under their direct observation and by the sailors themselves, who didn’t cotton to being hospitalized with merchant mariners.
Permission from Washington finally came through in July 1863. Work completed, the “Temporary Hospital” at Mare Island Navy Yard opened on Feb. 23, 1864.
The hospital carried an average inpatient load of 30, cared for by a surgeon and a surgeon’s steward, until the first permanent hospital—palatial by comparison—opened in 1871. TH
Dr. Snyder is a retired captain of the U.S. Naval Reserves’ Medical Corps. He writes regularly about naval medicine.
California gained statehood in 1850. Two months later Navy Secretary William Graham wrote to President Fillmore that “a new empire has, as by magic, sprung into existence. San Francisco promises, at no distant time, to become another New York.” He went on to say that “a Navy yard is very much needed in California, and no time will be lost in accomplishing the work.”
A three-officer commission was soon dispatched to choose a suitable site, and they decided on one protected inside San Francisco Bay at Mare Island. Commander David G. Farragut (of “Damn the torpedoes! Full speed ahead!” fame, a Civil War hero and the first admiral of the U.S. Navy) arrived at the remote place in 1854.
Within two days of his arrival at the California site, Farragut ordered the sloop-of-war over from Sausalito. This ship, soon to be replaced by the much larger USS Independence, served as the first naval medical facility on the West Coast. Ambulatory care was given in the ship’s sick bay, and the “hospitalized” were cared for from wooden bed frames suspended from the sick bay overhead or from their own hammocks. The average inpatient load was 10 sailors or civilian Navy yard workers.
The limitations of care aboard ship are made clear in a note from the yard surgeon in 1863; he wrote, “The frigate Independence, particularly in the winter season, is a very unsuitable place to treat the sick. It is cold, wet, and open to every wind that blows.”
Navy officials, while sympathetic to the plight of men serving in the tiny Pacific squadron, did little to correct the situation—likely because their attentions were focused on prosecuting the Civil War and not on a little Navy yard in far away California. Taking the situation into their own hands, surgeon Bishop and the commandant of the Navy yard submitted plans for a temporary facility—to be fashioned from an unused granary. The plans provided for a 25' x 25' ward on the first floor and a 24' x 40'9" ward space above, and called for a large cistern for year-round water supply, an attached bath approached from outside, and a nearby outdoor privy.
Still, Washington resisted, recommending that sick sailors be sent to the Marine (Public Health) Hospital in San Francisco, 25 miles away. This suggestion was met by stiff resistance both by local Naval authorities who feared desertion by sailors not under their direct observation and by the sailors themselves, who didn’t cotton to being hospitalized with merchant mariners.
Permission from Washington finally came through in July 1863. Work completed, the “Temporary Hospital” at Mare Island Navy Yard opened on Feb. 23, 1864.
The hospital carried an average inpatient load of 30, cared for by a surgeon and a surgeon’s steward, until the first permanent hospital—palatial by comparison—opened in 1871. TH
Dr. Snyder is a retired captain of the U.S. Naval Reserves’ Medical Corps. He writes regularly about naval medicine.
Limits for Disaster Responders
Most healthcare providers are inexperienced in caring for people in disasters. However, in a national disaster that hinders mobility both into and out of an affected area, available skilled personnel are limited. A disaster response asks more of the scarce manpower: Providers must work longer hours and extend their customary scope of expertise to aid the largest number of victims. While these mandates are designed to maximize the care provided, the emotional and physical burdens on providers and victims in these circumstances are significant, and it is important that we remember the fundamental duty to prevent unnecessary harm in the provision of healthcare.
Should healthcare providers be held to different standards in times of disaster? If so, what are acceptable limits to disaster care, and what ethical dilemmas result during such exceptional times?
Unique Circumstances Call for Unique Standards of Care
Standards in a variety of areas differ in the face of a large-scale disaster, but the fact that standards must change to accommodate the circumstances does not mean that they cease to exist entirely. In the event of a large-scale disaster where populations become isolated and no new resources will arrive in the immediate future, the risks of inaction are magnified and we accept a higher risk resulting from relief action. When only one doctor is available, that doctor is obligated to provide whatever care he or she can to whoever is in need.
When the alternative is that no help will be given, any able doctor should provide whatever help they can. However, there are limits to this responsibility. Greater risks may be justified, and standards may be different, but physicians’ fundamental duties to patients are unchanged and avoidable mistakes causing injuries still need to be prevented. The basic duties of beneficence and non-malfeasance must still guide physician behavior, and the reality of the circumstances in disaster response favors pre-emptive determination on the safety limits that physicians should observe in providing disaster assistance.
Disasters inherently influence doctors to both continue to provide care when they are impaired by sleep or grief and to provide care that under other circumstances they would consider their experience inadequate to undertake. These are realities of disaster response, and all skilled personnel can and should exceed the limits that normally exist in a fully functional system with adequate resources. However, at some point a doctor becomes too impaired or too inexperienced to provide care to patients—even if no one else is available. Doctors are neither trained nor encouraged to weigh the global risks and benefits in this manner; in fact, we are trained to push ourselves beyond our reasonable limits even when absolute scarcity of resources isn’t an issue. People are quite willing to compromise their own comfort and safety in the event of a disaster, but there comes a point at which they may do more harm than good.
There is extensive evidence that sleep deprivation impairs judgment and performance in the medical setting.1-2 Despite the fact that standards change in emergencies and greater risk must be undertaken by both providers and victims, there must still be safety limits. At some point a doctor becomes so sleep deprived that he or she is more dangerous providing care than leaving people entirely without a provider, and further may have impaired judgment on the severity of the various conditions they are facing and the reasonable limits on their expertise. This problem is inherent to the setting. How much risk should doctors subject patients to? In the face of a life-threatening condition should a completely inexperienced physician undertake care? What if the doctor is mistaken as to the severity of the illness or the proper response to it?
In response to Hurricane Katrina, state and national regulatory agencies had to create emergency exceptions to licensing regulations and to HIPAA and EMTALA requirements in order to facilitate patient care.3 Both the Model State Emergency Health Powers Act (legislation designed to serve as template for states to use to create emergency health response mechanisms) and the Louisiana legislation that governed provision of medical care in a state of emergency limit liability of any provider assisting in an emergency.4-5 Providers assisting in an emergency will not be held liable for any injury resulting from action or inaction except for intentional or grossly negligent acts or omissions. Such limitation of liability is essential to ensure that all available resources are utilized in an emergency. However, given that patients will have limited remedies for injuries caused, it is increasingly important to proactively define limitations on provider activity during emergencies. Because other remedies and regulatory structures are relaxed, ethical self-regulation becomes increasingly important.
The first priority in emergency disaster response must be ensuring that providers are available and do not encounter unnecessary barriers to providing care to ill or injured patients. However, a secondary goal must be ensuring that the safest and most effective care is provided under the circumstances. As with many things in disaster response, once the disaster has occurred there is little time for contemplation. Therefore, disaster response plans should include guidelines for providers on how to ensure safety in the care they provide.
Disaster response issues must be dealt with proactively because resources cannot be diverted to these issues in the thick of emergency response. Some organizations and providers have experience with disaster response and can provide guidance. A major goal of medical relief organizations is to provide relief for fatigued providers. When relief is not available and not likely to arrive soon, providers should be encouraged to self-impose sleep periods despite the apparent urgency of the situations they face. Urging providers to ensure that they eat at least twice and sleep for two to four hours in any 24-hour period is a reasonable limit on the physical activity of providers.
Providers and patients need to understand that this is essential to ensure that providers are capable of giving safe care in a sustained fashion. Emergency responders must maintain adequate perspective on their own abilities and patients’ needs to ensure that unnecessary risks are not undertaken nor avoidable injures inflicted. Importantly, these limitations should not be legislated or imposed externally, but should be defined by the profession and self-enforced by providers.
There have been significant discussion of what aspects of the U.S. system of response to large-scale disasters need to be improved. The Katrina disaster has given us the opportunity to enhance essential response mechanisms, whether the cause of the disaster is natural, infectious, or terrorist. A good disaster plan takes steps to ensure availability of care, but also to ensure that the care is as ethical, safe and effective as possible.
References
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294(9):1025-1033.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Eng J Med. 2004;351(18):1838-1848.
- Hyland, et al. Federal, State Regulations Relaxed for Providers Affected by Hurricane. BNA Health Law Reporter. 2005;15(36):1190-1191.
- Gostin, LO, Model State Emergency Health Powers Act, §608 Licensing and Appointment of Health Care Personnel, December 21, 2001. Available at www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Last accessed Dec. 1, 2005.
- La. R.S. 29:656 (2005).
FROM THE PUBLIC POLICY COMMITTEE
Make a Positive Difference in the Politics of Healthcare
SHM to sponsor Legislative Advocacy Day on May 3
By Eric Siegal, MD, committee chair
“The stakes are too high for government to be a spectator sport.”
—Barbara Jordan, former U.S. Congresswoman
SHM is taking advantage of its 2006 annual meeting location in Washington, D.C., and sponsoring its first Legislative Advocacy Day on May 3. The Public Policy Committee is excited about the opportunity this initiative presents for hospitalists to learn more about how government really works and to speak with members of Congress about issues that are vital to patient care and clinical practice.
Are you concerned about continued Medicare cuts? Worried about how pending pay-for-performance legislation will affect hospitalists? SHM members registering for Advocacy Day will meet with their members of Congress and staff to discuss these and other important issues affecting hospital medicine.
I encourage you to register for Advocacy Day. There is no better way to influence how health policy is made in Washington than by meeting directly with your elected officials and their staffs. Lawmakers need constituent input to be effective legislators. Whether your legislator is a newly elected representative or a veteran senator with years of experience, he or she wants—and needs—to hear what you have to say about issues under consideration by the U.S. Congress, particularly in an election year. Input from their constituents always receives attention and consideration and can frequently make the difference in the way a lawmaker votes. Who better to educate members of Congress on changes to Medicare than the physicians directly involved in caring for the program’s beneficiaries?
We will give you the tools and information you need to make the most of your meetings on Capitol Hill. Legislative appointments will be scheduled by SHM as part of the registration process. SHM members will be grouped together by congressional district for House meetings and by state for Senate meetings and each registrant will have a minimum of three Hill appointments. To familiarize you with SHM’s legislative objectives for the second session of the 109th Congress, Laura Allendorf, SHM’s Washington representative, and I will conduct a pre-visit breakfast briefing from 7 a.m. to 8:30 a.m. on May 3. This briefing will cover procedural tips on how to have a successful meeting and update you on the status of the key health issues you will be discussing while on Capitol Hill. These meetings will take place from 9 a.m. to 5 p.m. that day.
Join us on May 3 and help educate members of Congress about the unique role hospitalists play in the delivery of medical care in our nation’s hospitals. We hope Advocacy Day will be the start of regular contact by hospitalists with their elected representatives in Washington.
FROM THE PEDIATRICS COMMITTEE
CME, Pediatric Core Curriculum on the Horizon
Multiple initiatives keep committee active
The Pediatric Committee at SHM is both the center of pediatric activity within SHM and a clearinghouse for SHM committee and task force activity as it relates to pediatrics.
The major pediatric activity in SHM continues to be CME activities and the Pediatric Core Curriculum. The dramatic success of the Pediatric Hospital Medicine Meeting was documented in the October issue of The Hospitalist (p. 33.)
Evaluations of the meeting overwhelmingly favored staging a three- to four-day Pediatric Hospital Medicine meeting on an annual basis during the late summer as a stand-alone meeting, with sponsorship rotating among SHM, the AAP, and the APA. There was insufficient lead time to offer a comprehensive meeting in 2006, but a meeting is scheduled for 2007 sponsored by AAP, with SHM taking the lead in 2008. More information to follow both in the SHM online discussion communities and through these committee reports.
The Pediatric Core Curriculum is nearly complete and should be at the review stage by early 2006. This curriculum is modeled after the adult core curriculum. It will serve as a framework for residency and fellowship directors, as well as a basis for the topics addressed at the Pediatric Hospital Medicine Meetings. Thanks to Tim Cornell, MD, Dan Rauch, MD, and all the authors and editors who have contributed to this work.
We will offer a full pediatric track in May at the SHM Annual Meeting in Washington, D.C., as we have in prior years. Registration is available online. Meetings of both the Pediatric Committee and the Pediatric Forum will be held during the meeting. This year’s meeting immediately precedes the PAS Meetings in San Francisco, and we encourage you to plan early so that at least one member of your program is able to attend the SHM Meeting. Once the Pediatric Hospital Medicine Meetings are held on an annual basis, we will need to decide how to balance SHM meeting offerings between the summer stand-alone Denver meeting and the SHM Annual Meeting.
The second function of Pediatric Committee involves having pediatric representatives on the various SHM committees and task forces report on their individual group’s activities, particularly as it relates to pediatrics. This keeps the broader group of pediatric leadership within SHM informed about the society’s global picture. SHM is committed to having a pediatric representative on each committee. You never know when or where an important issue for pediatricians may arise. Even geriatrics overlaps with pediatrics with regard to both family-centered care and proxy decision-makers.
Major endeavors at this point include the activities of the Benchmark and Career Satisfaction groups. SHM continues to make a strong effort to collect and generate data for workload and compensation, and to provide specific “pediatric only” subsets. Efforts regarding credentialing, sub-specialty designation/certification, and board re-certification are an active focus of SHM for adult hospitalists with ongoing discussions with the Board of Internal Medicine. We pediatricians stand on the sidelines of this battle, with the expectation that once the adults figure out how to do it, we can modify their approach with lower casualties on both sides.
The clinical Resource Rooms on the SHM Web site are clearly targeted toward adult topics. We intend to develop similar resources for pediatrics and are exploring possibilities of doing this collaboratively with the AAP and the APA. Sub-committees on pediatric hospital medicine topics are developing under a loose and shared structure with the AAP’s Section on Hospital Medicine. For example, SHM has taken the lead on a palliative care task force. Maggie Hood is the pediatric representative to this task force and wants to involve other interested pediatric hospitalists in a sub-committee on this topic. The AAP’s Karen Kingry has taken the lead on developing a sub-committee for community (pediatric) hospitalists; membership on her committee is open to SHM members. Expect other topics to develop as well.
If you have any comments, feedback or suggestions for the SHM Pediatric Committee, please contact co-chairs, David Zipes ([email protected]) or Jack Percelay ([email protected]). TH
Most healthcare providers are inexperienced in caring for people in disasters. However, in a national disaster that hinders mobility both into and out of an affected area, available skilled personnel are limited. A disaster response asks more of the scarce manpower: Providers must work longer hours and extend their customary scope of expertise to aid the largest number of victims. While these mandates are designed to maximize the care provided, the emotional and physical burdens on providers and victims in these circumstances are significant, and it is important that we remember the fundamental duty to prevent unnecessary harm in the provision of healthcare.
Should healthcare providers be held to different standards in times of disaster? If so, what are acceptable limits to disaster care, and what ethical dilemmas result during such exceptional times?
Unique Circumstances Call for Unique Standards of Care
Standards in a variety of areas differ in the face of a large-scale disaster, but the fact that standards must change to accommodate the circumstances does not mean that they cease to exist entirely. In the event of a large-scale disaster where populations become isolated and no new resources will arrive in the immediate future, the risks of inaction are magnified and we accept a higher risk resulting from relief action. When only one doctor is available, that doctor is obligated to provide whatever care he or she can to whoever is in need.
When the alternative is that no help will be given, any able doctor should provide whatever help they can. However, there are limits to this responsibility. Greater risks may be justified, and standards may be different, but physicians’ fundamental duties to patients are unchanged and avoidable mistakes causing injuries still need to be prevented. The basic duties of beneficence and non-malfeasance must still guide physician behavior, and the reality of the circumstances in disaster response favors pre-emptive determination on the safety limits that physicians should observe in providing disaster assistance.
Disasters inherently influence doctors to both continue to provide care when they are impaired by sleep or grief and to provide care that under other circumstances they would consider their experience inadequate to undertake. These are realities of disaster response, and all skilled personnel can and should exceed the limits that normally exist in a fully functional system with adequate resources. However, at some point a doctor becomes too impaired or too inexperienced to provide care to patients—even if no one else is available. Doctors are neither trained nor encouraged to weigh the global risks and benefits in this manner; in fact, we are trained to push ourselves beyond our reasonable limits even when absolute scarcity of resources isn’t an issue. People are quite willing to compromise their own comfort and safety in the event of a disaster, but there comes a point at which they may do more harm than good.
There is extensive evidence that sleep deprivation impairs judgment and performance in the medical setting.1-2 Despite the fact that standards change in emergencies and greater risk must be undertaken by both providers and victims, there must still be safety limits. At some point a doctor becomes so sleep deprived that he or she is more dangerous providing care than leaving people entirely without a provider, and further may have impaired judgment on the severity of the various conditions they are facing and the reasonable limits on their expertise. This problem is inherent to the setting. How much risk should doctors subject patients to? In the face of a life-threatening condition should a completely inexperienced physician undertake care? What if the doctor is mistaken as to the severity of the illness or the proper response to it?
In response to Hurricane Katrina, state and national regulatory agencies had to create emergency exceptions to licensing regulations and to HIPAA and EMTALA requirements in order to facilitate patient care.3 Both the Model State Emergency Health Powers Act (legislation designed to serve as template for states to use to create emergency health response mechanisms) and the Louisiana legislation that governed provision of medical care in a state of emergency limit liability of any provider assisting in an emergency.4-5 Providers assisting in an emergency will not be held liable for any injury resulting from action or inaction except for intentional or grossly negligent acts or omissions. Such limitation of liability is essential to ensure that all available resources are utilized in an emergency. However, given that patients will have limited remedies for injuries caused, it is increasingly important to proactively define limitations on provider activity during emergencies. Because other remedies and regulatory structures are relaxed, ethical self-regulation becomes increasingly important.
The first priority in emergency disaster response must be ensuring that providers are available and do not encounter unnecessary barriers to providing care to ill or injured patients. However, a secondary goal must be ensuring that the safest and most effective care is provided under the circumstances. As with many things in disaster response, once the disaster has occurred there is little time for contemplation. Therefore, disaster response plans should include guidelines for providers on how to ensure safety in the care they provide.
Disaster response issues must be dealt with proactively because resources cannot be diverted to these issues in the thick of emergency response. Some organizations and providers have experience with disaster response and can provide guidance. A major goal of medical relief organizations is to provide relief for fatigued providers. When relief is not available and not likely to arrive soon, providers should be encouraged to self-impose sleep periods despite the apparent urgency of the situations they face. Urging providers to ensure that they eat at least twice and sleep for two to four hours in any 24-hour period is a reasonable limit on the physical activity of providers.
Providers and patients need to understand that this is essential to ensure that providers are capable of giving safe care in a sustained fashion. Emergency responders must maintain adequate perspective on their own abilities and patients’ needs to ensure that unnecessary risks are not undertaken nor avoidable injures inflicted. Importantly, these limitations should not be legislated or imposed externally, but should be defined by the profession and self-enforced by providers.
There have been significant discussion of what aspects of the U.S. system of response to large-scale disasters need to be improved. The Katrina disaster has given us the opportunity to enhance essential response mechanisms, whether the cause of the disaster is natural, infectious, or terrorist. A good disaster plan takes steps to ensure availability of care, but also to ensure that the care is as ethical, safe and effective as possible.
References
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294(9):1025-1033.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Eng J Med. 2004;351(18):1838-1848.
- Hyland, et al. Federal, State Regulations Relaxed for Providers Affected by Hurricane. BNA Health Law Reporter. 2005;15(36):1190-1191.
- Gostin, LO, Model State Emergency Health Powers Act, §608 Licensing and Appointment of Health Care Personnel, December 21, 2001. Available at www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Last accessed Dec. 1, 2005.
- La. R.S. 29:656 (2005).
FROM THE PUBLIC POLICY COMMITTEE
Make a Positive Difference in the Politics of Healthcare
SHM to sponsor Legislative Advocacy Day on May 3
By Eric Siegal, MD, committee chair
“The stakes are too high for government to be a spectator sport.”
—Barbara Jordan, former U.S. Congresswoman
SHM is taking advantage of its 2006 annual meeting location in Washington, D.C., and sponsoring its first Legislative Advocacy Day on May 3. The Public Policy Committee is excited about the opportunity this initiative presents for hospitalists to learn more about how government really works and to speak with members of Congress about issues that are vital to patient care and clinical practice.
Are you concerned about continued Medicare cuts? Worried about how pending pay-for-performance legislation will affect hospitalists? SHM members registering for Advocacy Day will meet with their members of Congress and staff to discuss these and other important issues affecting hospital medicine.
I encourage you to register for Advocacy Day. There is no better way to influence how health policy is made in Washington than by meeting directly with your elected officials and their staffs. Lawmakers need constituent input to be effective legislators. Whether your legislator is a newly elected representative or a veteran senator with years of experience, he or she wants—and needs—to hear what you have to say about issues under consideration by the U.S. Congress, particularly in an election year. Input from their constituents always receives attention and consideration and can frequently make the difference in the way a lawmaker votes. Who better to educate members of Congress on changes to Medicare than the physicians directly involved in caring for the program’s beneficiaries?
We will give you the tools and information you need to make the most of your meetings on Capitol Hill. Legislative appointments will be scheduled by SHM as part of the registration process. SHM members will be grouped together by congressional district for House meetings and by state for Senate meetings and each registrant will have a minimum of three Hill appointments. To familiarize you with SHM’s legislative objectives for the second session of the 109th Congress, Laura Allendorf, SHM’s Washington representative, and I will conduct a pre-visit breakfast briefing from 7 a.m. to 8:30 a.m. on May 3. This briefing will cover procedural tips on how to have a successful meeting and update you on the status of the key health issues you will be discussing while on Capitol Hill. These meetings will take place from 9 a.m. to 5 p.m. that day.
Join us on May 3 and help educate members of Congress about the unique role hospitalists play in the delivery of medical care in our nation’s hospitals. We hope Advocacy Day will be the start of regular contact by hospitalists with their elected representatives in Washington.
FROM THE PEDIATRICS COMMITTEE
CME, Pediatric Core Curriculum on the Horizon
Multiple initiatives keep committee active
The Pediatric Committee at SHM is both the center of pediatric activity within SHM and a clearinghouse for SHM committee and task force activity as it relates to pediatrics.
The major pediatric activity in SHM continues to be CME activities and the Pediatric Core Curriculum. The dramatic success of the Pediatric Hospital Medicine Meeting was documented in the October issue of The Hospitalist (p. 33.)
Evaluations of the meeting overwhelmingly favored staging a three- to four-day Pediatric Hospital Medicine meeting on an annual basis during the late summer as a stand-alone meeting, with sponsorship rotating among SHM, the AAP, and the APA. There was insufficient lead time to offer a comprehensive meeting in 2006, but a meeting is scheduled for 2007 sponsored by AAP, with SHM taking the lead in 2008. More information to follow both in the SHM online discussion communities and through these committee reports.
The Pediatric Core Curriculum is nearly complete and should be at the review stage by early 2006. This curriculum is modeled after the adult core curriculum. It will serve as a framework for residency and fellowship directors, as well as a basis for the topics addressed at the Pediatric Hospital Medicine Meetings. Thanks to Tim Cornell, MD, Dan Rauch, MD, and all the authors and editors who have contributed to this work.
We will offer a full pediatric track in May at the SHM Annual Meeting in Washington, D.C., as we have in prior years. Registration is available online. Meetings of both the Pediatric Committee and the Pediatric Forum will be held during the meeting. This year’s meeting immediately precedes the PAS Meetings in San Francisco, and we encourage you to plan early so that at least one member of your program is able to attend the SHM Meeting. Once the Pediatric Hospital Medicine Meetings are held on an annual basis, we will need to decide how to balance SHM meeting offerings between the summer stand-alone Denver meeting and the SHM Annual Meeting.
The second function of Pediatric Committee involves having pediatric representatives on the various SHM committees and task forces report on their individual group’s activities, particularly as it relates to pediatrics. This keeps the broader group of pediatric leadership within SHM informed about the society’s global picture. SHM is committed to having a pediatric representative on each committee. You never know when or where an important issue for pediatricians may arise. Even geriatrics overlaps with pediatrics with regard to both family-centered care and proxy decision-makers.
Major endeavors at this point include the activities of the Benchmark and Career Satisfaction groups. SHM continues to make a strong effort to collect and generate data for workload and compensation, and to provide specific “pediatric only” subsets. Efforts regarding credentialing, sub-specialty designation/certification, and board re-certification are an active focus of SHM for adult hospitalists with ongoing discussions with the Board of Internal Medicine. We pediatricians stand on the sidelines of this battle, with the expectation that once the adults figure out how to do it, we can modify their approach with lower casualties on both sides.
The clinical Resource Rooms on the SHM Web site are clearly targeted toward adult topics. We intend to develop similar resources for pediatrics and are exploring possibilities of doing this collaboratively with the AAP and the APA. Sub-committees on pediatric hospital medicine topics are developing under a loose and shared structure with the AAP’s Section on Hospital Medicine. For example, SHM has taken the lead on a palliative care task force. Maggie Hood is the pediatric representative to this task force and wants to involve other interested pediatric hospitalists in a sub-committee on this topic. The AAP’s Karen Kingry has taken the lead on developing a sub-committee for community (pediatric) hospitalists; membership on her committee is open to SHM members. Expect other topics to develop as well.
If you have any comments, feedback or suggestions for the SHM Pediatric Committee, please contact co-chairs, David Zipes ([email protected]) or Jack Percelay ([email protected]). TH
Most healthcare providers are inexperienced in caring for people in disasters. However, in a national disaster that hinders mobility both into and out of an affected area, available skilled personnel are limited. A disaster response asks more of the scarce manpower: Providers must work longer hours and extend their customary scope of expertise to aid the largest number of victims. While these mandates are designed to maximize the care provided, the emotional and physical burdens on providers and victims in these circumstances are significant, and it is important that we remember the fundamental duty to prevent unnecessary harm in the provision of healthcare.
Should healthcare providers be held to different standards in times of disaster? If so, what are acceptable limits to disaster care, and what ethical dilemmas result during such exceptional times?
Unique Circumstances Call for Unique Standards of Care
Standards in a variety of areas differ in the face of a large-scale disaster, but the fact that standards must change to accommodate the circumstances does not mean that they cease to exist entirely. In the event of a large-scale disaster where populations become isolated and no new resources will arrive in the immediate future, the risks of inaction are magnified and we accept a higher risk resulting from relief action. When only one doctor is available, that doctor is obligated to provide whatever care he or she can to whoever is in need.
When the alternative is that no help will be given, any able doctor should provide whatever help they can. However, there are limits to this responsibility. Greater risks may be justified, and standards may be different, but physicians’ fundamental duties to patients are unchanged and avoidable mistakes causing injuries still need to be prevented. The basic duties of beneficence and non-malfeasance must still guide physician behavior, and the reality of the circumstances in disaster response favors pre-emptive determination on the safety limits that physicians should observe in providing disaster assistance.
Disasters inherently influence doctors to both continue to provide care when they are impaired by sleep or grief and to provide care that under other circumstances they would consider their experience inadequate to undertake. These are realities of disaster response, and all skilled personnel can and should exceed the limits that normally exist in a fully functional system with adequate resources. However, at some point a doctor becomes too impaired or too inexperienced to provide care to patients—even if no one else is available. Doctors are neither trained nor encouraged to weigh the global risks and benefits in this manner; in fact, we are trained to push ourselves beyond our reasonable limits even when absolute scarcity of resources isn’t an issue. People are quite willing to compromise their own comfort and safety in the event of a disaster, but there comes a point at which they may do more harm than good.
There is extensive evidence that sleep deprivation impairs judgment and performance in the medical setting.1-2 Despite the fact that standards change in emergencies and greater risk must be undertaken by both providers and victims, there must still be safety limits. At some point a doctor becomes so sleep deprived that he or she is more dangerous providing care than leaving people entirely without a provider, and further may have impaired judgment on the severity of the various conditions they are facing and the reasonable limits on their expertise. This problem is inherent to the setting. How much risk should doctors subject patients to? In the face of a life-threatening condition should a completely inexperienced physician undertake care? What if the doctor is mistaken as to the severity of the illness or the proper response to it?
In response to Hurricane Katrina, state and national regulatory agencies had to create emergency exceptions to licensing regulations and to HIPAA and EMTALA requirements in order to facilitate patient care.3 Both the Model State Emergency Health Powers Act (legislation designed to serve as template for states to use to create emergency health response mechanisms) and the Louisiana legislation that governed provision of medical care in a state of emergency limit liability of any provider assisting in an emergency.4-5 Providers assisting in an emergency will not be held liable for any injury resulting from action or inaction except for intentional or grossly negligent acts or omissions. Such limitation of liability is essential to ensure that all available resources are utilized in an emergency. However, given that patients will have limited remedies for injuries caused, it is increasingly important to proactively define limitations on provider activity during emergencies. Because other remedies and regulatory structures are relaxed, ethical self-regulation becomes increasingly important.
The first priority in emergency disaster response must be ensuring that providers are available and do not encounter unnecessary barriers to providing care to ill or injured patients. However, a secondary goal must be ensuring that the safest and most effective care is provided under the circumstances. As with many things in disaster response, once the disaster has occurred there is little time for contemplation. Therefore, disaster response plans should include guidelines for providers on how to ensure safety in the care they provide.
Disaster response issues must be dealt with proactively because resources cannot be diverted to these issues in the thick of emergency response. Some organizations and providers have experience with disaster response and can provide guidance. A major goal of medical relief organizations is to provide relief for fatigued providers. When relief is not available and not likely to arrive soon, providers should be encouraged to self-impose sleep periods despite the apparent urgency of the situations they face. Urging providers to ensure that they eat at least twice and sleep for two to four hours in any 24-hour period is a reasonable limit on the physical activity of providers.
Providers and patients need to understand that this is essential to ensure that providers are capable of giving safe care in a sustained fashion. Emergency responders must maintain adequate perspective on their own abilities and patients’ needs to ensure that unnecessary risks are not undertaken nor avoidable injures inflicted. Importantly, these limitations should not be legislated or imposed externally, but should be defined by the profession and self-enforced by providers.
There have been significant discussion of what aspects of the U.S. system of response to large-scale disasters need to be improved. The Katrina disaster has given us the opportunity to enhance essential response mechanisms, whether the cause of the disaster is natural, infectious, or terrorist. A good disaster plan takes steps to ensure availability of care, but also to ensure that the care is as ethical, safe and effective as possible.
References
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294(9):1025-1033.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Eng J Med. 2004;351(18):1838-1848.
- Hyland, et al. Federal, State Regulations Relaxed for Providers Affected by Hurricane. BNA Health Law Reporter. 2005;15(36):1190-1191.
- Gostin, LO, Model State Emergency Health Powers Act, §608 Licensing and Appointment of Health Care Personnel, December 21, 2001. Available at www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Last accessed Dec. 1, 2005.
- La. R.S. 29:656 (2005).
FROM THE PUBLIC POLICY COMMITTEE
Make a Positive Difference in the Politics of Healthcare
SHM to sponsor Legislative Advocacy Day on May 3
By Eric Siegal, MD, committee chair
“The stakes are too high for government to be a spectator sport.”
—Barbara Jordan, former U.S. Congresswoman
SHM is taking advantage of its 2006 annual meeting location in Washington, D.C., and sponsoring its first Legislative Advocacy Day on May 3. The Public Policy Committee is excited about the opportunity this initiative presents for hospitalists to learn more about how government really works and to speak with members of Congress about issues that are vital to patient care and clinical practice.
Are you concerned about continued Medicare cuts? Worried about how pending pay-for-performance legislation will affect hospitalists? SHM members registering for Advocacy Day will meet with their members of Congress and staff to discuss these and other important issues affecting hospital medicine.
I encourage you to register for Advocacy Day. There is no better way to influence how health policy is made in Washington than by meeting directly with your elected officials and their staffs. Lawmakers need constituent input to be effective legislators. Whether your legislator is a newly elected representative or a veteran senator with years of experience, he or she wants—and needs—to hear what you have to say about issues under consideration by the U.S. Congress, particularly in an election year. Input from their constituents always receives attention and consideration and can frequently make the difference in the way a lawmaker votes. Who better to educate members of Congress on changes to Medicare than the physicians directly involved in caring for the program’s beneficiaries?
We will give you the tools and information you need to make the most of your meetings on Capitol Hill. Legislative appointments will be scheduled by SHM as part of the registration process. SHM members will be grouped together by congressional district for House meetings and by state for Senate meetings and each registrant will have a minimum of three Hill appointments. To familiarize you with SHM’s legislative objectives for the second session of the 109th Congress, Laura Allendorf, SHM’s Washington representative, and I will conduct a pre-visit breakfast briefing from 7 a.m. to 8:30 a.m. on May 3. This briefing will cover procedural tips on how to have a successful meeting and update you on the status of the key health issues you will be discussing while on Capitol Hill. These meetings will take place from 9 a.m. to 5 p.m. that day.
Join us on May 3 and help educate members of Congress about the unique role hospitalists play in the delivery of medical care in our nation’s hospitals. We hope Advocacy Day will be the start of regular contact by hospitalists with their elected representatives in Washington.
FROM THE PEDIATRICS COMMITTEE
CME, Pediatric Core Curriculum on the Horizon
Multiple initiatives keep committee active
The Pediatric Committee at SHM is both the center of pediatric activity within SHM and a clearinghouse for SHM committee and task force activity as it relates to pediatrics.
The major pediatric activity in SHM continues to be CME activities and the Pediatric Core Curriculum. The dramatic success of the Pediatric Hospital Medicine Meeting was documented in the October issue of The Hospitalist (p. 33.)
Evaluations of the meeting overwhelmingly favored staging a three- to four-day Pediatric Hospital Medicine meeting on an annual basis during the late summer as a stand-alone meeting, with sponsorship rotating among SHM, the AAP, and the APA. There was insufficient lead time to offer a comprehensive meeting in 2006, but a meeting is scheduled for 2007 sponsored by AAP, with SHM taking the lead in 2008. More information to follow both in the SHM online discussion communities and through these committee reports.
The Pediatric Core Curriculum is nearly complete and should be at the review stage by early 2006. This curriculum is modeled after the adult core curriculum. It will serve as a framework for residency and fellowship directors, as well as a basis for the topics addressed at the Pediatric Hospital Medicine Meetings. Thanks to Tim Cornell, MD, Dan Rauch, MD, and all the authors and editors who have contributed to this work.
We will offer a full pediatric track in May at the SHM Annual Meeting in Washington, D.C., as we have in prior years. Registration is available online. Meetings of both the Pediatric Committee and the Pediatric Forum will be held during the meeting. This year’s meeting immediately precedes the PAS Meetings in San Francisco, and we encourage you to plan early so that at least one member of your program is able to attend the SHM Meeting. Once the Pediatric Hospital Medicine Meetings are held on an annual basis, we will need to decide how to balance SHM meeting offerings between the summer stand-alone Denver meeting and the SHM Annual Meeting.
The second function of Pediatric Committee involves having pediatric representatives on the various SHM committees and task forces report on their individual group’s activities, particularly as it relates to pediatrics. This keeps the broader group of pediatric leadership within SHM informed about the society’s global picture. SHM is committed to having a pediatric representative on each committee. You never know when or where an important issue for pediatricians may arise. Even geriatrics overlaps with pediatrics with regard to both family-centered care and proxy decision-makers.
Major endeavors at this point include the activities of the Benchmark and Career Satisfaction groups. SHM continues to make a strong effort to collect and generate data for workload and compensation, and to provide specific “pediatric only” subsets. Efforts regarding credentialing, sub-specialty designation/certification, and board re-certification are an active focus of SHM for adult hospitalists with ongoing discussions with the Board of Internal Medicine. We pediatricians stand on the sidelines of this battle, with the expectation that once the adults figure out how to do it, we can modify their approach with lower casualties on both sides.
The clinical Resource Rooms on the SHM Web site are clearly targeted toward adult topics. We intend to develop similar resources for pediatrics and are exploring possibilities of doing this collaboratively with the AAP and the APA. Sub-committees on pediatric hospital medicine topics are developing under a loose and shared structure with the AAP’s Section on Hospital Medicine. For example, SHM has taken the lead on a palliative care task force. Maggie Hood is the pediatric representative to this task force and wants to involve other interested pediatric hospitalists in a sub-committee on this topic. The AAP’s Karen Kingry has taken the lead on developing a sub-committee for community (pediatric) hospitalists; membership on her committee is open to SHM members. Expect other topics to develop as well.
If you have any comments, feedback or suggestions for the SHM Pediatric Committee, please contact co-chairs, David Zipes ([email protected]) or Jack Percelay ([email protected]). TH
Make a Difference

Welcome to 2006 and another coming-out party for SHM and hospitalists. In just a few short months more than a thousand hospitalists will come together in our nation’s capitol for the SHM Annual Meeting May 3-5, 2006. In addition to the largest convention of hospitalists, hundreds of other stakeholders in hospital medicine will gather for what has become the centerpiece of their year.
In addition to the opportunity to hear our nation’s experts talk about the up-to-date, state-of-the art medical knowledge for hospitalists, the SHM Annual Meeting is the place to find your next job, reconnect with colleagues from around the country, express your own opinions and vision for hospital medicine at the Special Interest Forums, and so much more.
SHM will be literally in the center of our nation’s capitol. It will be an opportunity for hospitalists to not only see the power center for our country, but with SHM’s help, a time for hospitalists to engage our legislators about issues important to hospitalists and our patients.
Taking advantage of the location of this year’s Annual Meeting, SHM’s Public Policy Committee has organized the first SHM Legislative Day on May 3, 2006. SHM meeting attendees can voluntarily sign up to meet with their congressmen and senators and their staffs.
SHM will make all the appointments for these Congressional visits. In addition, May 3 will kick off with a Washington overview and practical sessions on how best to approach your legislators to get your message across.
In addition, SHM has been working with HPA, a nationally recognized information resource in D.C. to put together a “Hospital Medicine White Paper” to concisely describe the emerging specialty of hospital medicine and how our perspectives and ideas are important to the healthcare debate.
The white paper will be a useful document to leave with your legislator and to use as a reference for your discussions. It will also contain some suggested policy recommendations supported by the SHM Board that can form the basis of what we would like to see move forward in Congress and on the Hill.
I have participated in many of these Legislative Days in my time on the ASIM and ACP Boards. I have found the legislators and their staffs interested in hearing from a passionate, informed part of their constituencies. Often these conversations were informal and personal and led to an ongoing relationship that continued when we were back home. I looked forward to coming back to Washington to renew our discussions.
And there can be real tangible changes as a result of these Congressional visits. I have seen changes in Medicare scope of benefits and reimbursement and methodologies based on messages I carried with the support of my professional medical societies.
Hospitalists are in a unique position to influence the current and future medical debates in Washington. We are young (average age 37) with a long professional career ahead of us. Hospitalists are at the center of many issues and initiatives that affect hospitals and the acutely ill patients they treat. Hospitalists measure and improve inpatient healthcare in an era of decreasing resources and increasing expectations.
Right now there is significant activity in pay for performance and in developing quality performance measures. There is also debate on gain-sharing and discussions of reducing and reshaping reimbursement for physicians. There are discussions on how to fund medical education and how to make sure all Americans get healthcare—even the 45 million without any insurance coverage. There are issues of access and limitations of crowded emergency departments and hospitals running at capacity.
There is no shortage of ideas and proposals, and most of these will affect hospitalists and the patients we treat and the hospitals we work in. In many ways these issues will shape our professional futures and determine how satisfying a career as a physician and specifically as a hospitalist will be.
Hospitalists and SHM must be part of the dialogue. We must clearly state where we stand and be prepared to back this up with data and to propose realistic solutions we are prepared to implement.
So clear your schedules May 3-5, 2006, and come to Washington, D.C., to join more than a thousand of your hospitalist colleagues as we take our first determined steps at the power center of our country. SHM will provide the support and materials for your success. But you must supply the voice and the presence. We owe no less to our profession and our patients now and in the future. TH
Dr. Wellikson has been CEO of SHM since 2000.
Welcome to 2006 and another coming-out party for SHM and hospitalists. In just a few short months more than a thousand hospitalists will come together in our nation’s capitol for the SHM Annual Meeting May 3-5, 2006. In addition to the largest convention of hospitalists, hundreds of other stakeholders in hospital medicine will gather for what has become the centerpiece of their year.
In addition to the opportunity to hear our nation’s experts talk about the up-to-date, state-of-the art medical knowledge for hospitalists, the SHM Annual Meeting is the place to find your next job, reconnect with colleagues from around the country, express your own opinions and vision for hospital medicine at the Special Interest Forums, and so much more.
SHM will be literally in the center of our nation’s capitol. It will be an opportunity for hospitalists to not only see the power center for our country, but with SHM’s help, a time for hospitalists to engage our legislators about issues important to hospitalists and our patients.
Taking advantage of the location of this year’s Annual Meeting, SHM’s Public Policy Committee has organized the first SHM Legislative Day on May 3, 2006. SHM meeting attendees can voluntarily sign up to meet with their congressmen and senators and their staffs.
SHM will make all the appointments for these Congressional visits. In addition, May 3 will kick off with a Washington overview and practical sessions on how best to approach your legislators to get your message across.
In addition, SHM has been working with HPA, a nationally recognized information resource in D.C. to put together a “Hospital Medicine White Paper” to concisely describe the emerging specialty of hospital medicine and how our perspectives and ideas are important to the healthcare debate.
The white paper will be a useful document to leave with your legislator and to use as a reference for your discussions. It will also contain some suggested policy recommendations supported by the SHM Board that can form the basis of what we would like to see move forward in Congress and on the Hill.
I have participated in many of these Legislative Days in my time on the ASIM and ACP Boards. I have found the legislators and their staffs interested in hearing from a passionate, informed part of their constituencies. Often these conversations were informal and personal and led to an ongoing relationship that continued when we were back home. I looked forward to coming back to Washington to renew our discussions.
And there can be real tangible changes as a result of these Congressional visits. I have seen changes in Medicare scope of benefits and reimbursement and methodologies based on messages I carried with the support of my professional medical societies.
Hospitalists are in a unique position to influence the current and future medical debates in Washington. We are young (average age 37) with a long professional career ahead of us. Hospitalists are at the center of many issues and initiatives that affect hospitals and the acutely ill patients they treat. Hospitalists measure and improve inpatient healthcare in an era of decreasing resources and increasing expectations.
Right now there is significant activity in pay for performance and in developing quality performance measures. There is also debate on gain-sharing and discussions of reducing and reshaping reimbursement for physicians. There are discussions on how to fund medical education and how to make sure all Americans get healthcare—even the 45 million without any insurance coverage. There are issues of access and limitations of crowded emergency departments and hospitals running at capacity.
There is no shortage of ideas and proposals, and most of these will affect hospitalists and the patients we treat and the hospitals we work in. In many ways these issues will shape our professional futures and determine how satisfying a career as a physician and specifically as a hospitalist will be.
Hospitalists and SHM must be part of the dialogue. We must clearly state where we stand and be prepared to back this up with data and to propose realistic solutions we are prepared to implement.
So clear your schedules May 3-5, 2006, and come to Washington, D.C., to join more than a thousand of your hospitalist colleagues as we take our first determined steps at the power center of our country. SHM will provide the support and materials for your success. But you must supply the voice and the presence. We owe no less to our profession and our patients now and in the future. TH
Dr. Wellikson has been CEO of SHM since 2000.
Welcome to 2006 and another coming-out party for SHM and hospitalists. In just a few short months more than a thousand hospitalists will come together in our nation’s capitol for the SHM Annual Meeting May 3-5, 2006. In addition to the largest convention of hospitalists, hundreds of other stakeholders in hospital medicine will gather for what has become the centerpiece of their year.
In addition to the opportunity to hear our nation’s experts talk about the up-to-date, state-of-the art medical knowledge for hospitalists, the SHM Annual Meeting is the place to find your next job, reconnect with colleagues from around the country, express your own opinions and vision for hospital medicine at the Special Interest Forums, and so much more.
SHM will be literally in the center of our nation’s capitol. It will be an opportunity for hospitalists to not only see the power center for our country, but with SHM’s help, a time for hospitalists to engage our legislators about issues important to hospitalists and our patients.
Taking advantage of the location of this year’s Annual Meeting, SHM’s Public Policy Committee has organized the first SHM Legislative Day on May 3, 2006. SHM meeting attendees can voluntarily sign up to meet with their congressmen and senators and their staffs.
SHM will make all the appointments for these Congressional visits. In addition, May 3 will kick off with a Washington overview and practical sessions on how best to approach your legislators to get your message across.
In addition, SHM has been working with HPA, a nationally recognized information resource in D.C. to put together a “Hospital Medicine White Paper” to concisely describe the emerging specialty of hospital medicine and how our perspectives and ideas are important to the healthcare debate.
The white paper will be a useful document to leave with your legislator and to use as a reference for your discussions. It will also contain some suggested policy recommendations supported by the SHM Board that can form the basis of what we would like to see move forward in Congress and on the Hill.
I have participated in many of these Legislative Days in my time on the ASIM and ACP Boards. I have found the legislators and their staffs interested in hearing from a passionate, informed part of their constituencies. Often these conversations were informal and personal and led to an ongoing relationship that continued when we were back home. I looked forward to coming back to Washington to renew our discussions.
And there can be real tangible changes as a result of these Congressional visits. I have seen changes in Medicare scope of benefits and reimbursement and methodologies based on messages I carried with the support of my professional medical societies.
Hospitalists are in a unique position to influence the current and future medical debates in Washington. We are young (average age 37) with a long professional career ahead of us. Hospitalists are at the center of many issues and initiatives that affect hospitals and the acutely ill patients they treat. Hospitalists measure and improve inpatient healthcare in an era of decreasing resources and increasing expectations.
Right now there is significant activity in pay for performance and in developing quality performance measures. There is also debate on gain-sharing and discussions of reducing and reshaping reimbursement for physicians. There are discussions on how to fund medical education and how to make sure all Americans get healthcare—even the 45 million without any insurance coverage. There are issues of access and limitations of crowded emergency departments and hospitals running at capacity.
There is no shortage of ideas and proposals, and most of these will affect hospitalists and the patients we treat and the hospitals we work in. In many ways these issues will shape our professional futures and determine how satisfying a career as a physician and specifically as a hospitalist will be.
Hospitalists and SHM must be part of the dialogue. We must clearly state where we stand and be prepared to back this up with data and to propose realistic solutions we are prepared to implement.
So clear your schedules May 3-5, 2006, and come to Washington, D.C., to join more than a thousand of your hospitalist colleagues as we take our first determined steps at the power center of our country. SHM will provide the support and materials for your success. But you must supply the voice and the presence. We owe no less to our profession and our patients now and in the future. TH
Dr. Wellikson has been CEO of SHM since 2000.
I, Intern

Internship is a stressful and life-altering experience. Demands from patients, consulting staff, and paperwork can dehumanize the new physician and make him or her feel like an automaton. The constant exigency of being an intern is further compounded by the increasing use of algorithms and computers. Guidelines for care have existed since the Hermetic books of Thoth in ancient Egypt, but strict “cookbook” medicine limits the intern’s decision-making and individuality. Pressure for electronic record-keeping and redundant documentation further reduce the new physician into not much more than a data entry-and-retrieval terminal. With the intern spending more time with patient records than actual patients, the physician-patient relationship invariably suffers as the intern becomes a small part of the machinery. Consequently, house-staff are constantly searching for a conceptual framework to better understand and cope with their unusual existence.
Isaac Asimov, the visionary science fiction writer and one-time biochemistry professor at Boston University School of Medicine, wrote an entire corpus of work around robots and the three “Laws of Robotics” starting in the 1940s.1 It seems the laws of robotics might also apply to interns as the Three Laws of “Internotics” (original text in parenthesis):
- First Law: An intern (robot) may not injure a patient (human being), or, through inaction, allow a patient (human being) to come to harm.
- Second Law: An intern (robot) must obey orders given it by attendings (human beings) except when such orders would conflict with the First Law.*
- Third Law: An intern (robot) must protect its own existence as long as such protection does not conflict with the First or Second Law.
Ten years after the creation of these laws, Asimov developed a “Zeroth” Law: An intern (robot) may not injure humanity, or through inaction, allow humanity to come to harm.
The First Law
Isolated interpretation of the First Law is the modus operandi of robots and interns. This law is a re-wording of the basic tenet of medicine: First do no harm, or primum non nocere as quoted from Hippocrates in Epidemics. On its surface, the First Law may seem easy for the intern to interpret and follow. However, when the patient’s own perception of benefit and harm deviates from the established norms in medicine, the intern is faced with dilemma of patient autonomy versus beneficence. This may not be a novel phenomenon in the modern consumer-based healthcare system, as Will Mayo, MD, from our own institution once said during a speech at Rush Medical College in 1910: “The best interest of the patient is the only interest to be considered.”
The Second Law
The Second Law explicitly states that the intern must follow the orders of the attending physician, but much rests in the intern’s additional obligation to reconcile obligatory recommendations with their own knowledge and patients’ idiosyncrasy. This may quickly become problematic for the intern, as few orders in modern medicine are considered absolutely risk-free.
The intern must undertake two levels of risk-benefit analysis: They must first determine what type of harm the patient faces in the setting of inaction—as spelled out by the First Law—if the attending’s orders were not carried out; he then must balance such hypothetical harm with the risks associated with the attendings orders of action. If such analysis were to favor inaction, to question the attending’s order is to challenge the attending’s own interpretation of the First Law and to risk the intern’s own existence (Third Law).
Therefore, the best solution for the intern is often to not question whether such order is necessary, but to do whatever possible to protect the patient. An example might be a consultant’s request for a CAT scan in a patient at high risk for contrast-induced nephropathy. In such a case, N-acetylcystein, adequate hydration or urine alkalinization may provide optimal protection against nephropathy. As such, the intern fulfills his or her obligations to the First and Second Laws without testing the limits imposed by the Third.
The Third Law
Much of the practice of—if not the principle of—internship is a violation of the Third Law. Excessive sleepiness and stressors may lead to medical errors, substance abuse, and traffic accidents.2 Work-hour restrictions may alleviate this condition, but can also erode the already limited patient-physician relationship. Further, certain attending physicians may denigrate the performance of the intern, leading to self doubt, lower self esteem, and mental anguish.
Similarly, interaction with certain patients may challenge the intern’s physical or mental well-being. As a result, the intern juxtaposes the new physician’s self-image of competency against the hierarchical stereotype of the rookie. The Third Law allows an opportunity for the intern to be associated with the proud heritage of the caduceus. However, as most interns soon learn, an intern can possibly best ensure his or her well-being and ascent to the next level when the Third Law is not cited as regularly as the first two laws.
The Zeroth Law
The Zeroth Law may be the most challenging law for both robots and interns. While robots and interns are both proficiently trained in serving individual humans, neither positronic programming nor medical education clearly establishes how this leads to the service of humanity.
If humanity is to be defined as the collection of individuals, principles in doctoring of the individual cannot be easily duplicated onto a population. This can be demonstrated through the continuously escalating medical expenditures in the setting of limited resources. For example, if a patient presents with “atypical” chest pain, a diligent medical graduate might order a set of laboratory studies and an electrocardiogram to rule out on-going myocardial infarction despite a low likelihood of abnormality. The slightest normal variation may then involve, by the First or Second Law, observation, stress testing, or cardiac catheterization.
Even though the current economic and legal systems allow for such shotgun approach of affordable technology, such application of the First Law onto humans as a collective will exhaust the population of its limited resources and utterly defy the Zeroth Law.
Alternatively, if humanity is to mean what constitutes each person’s individuality, argument involving maleficence and beneficence must give way to autonomy in the presentation, diagnosis, and treatment of disease, despite what the intern or attending physician perceive as benefits and harm. This obviously violates the First Law in the most fundamental level. However, different from the other laws, the Zeroth Law is not prefaced with the need to comply with the other Three Laws.
Interns can and often do feel dehumanized, whether from loss of decision-making role, from lack of sleep, or as a psychological tool of survival against the rigors of life and death in the hospital. Sometimes even a perfectly beneficent act violates the First Law at a later time and haunts the practitioners. Asimov himself received surgery-related transfusion with the best intention of his treating physicians and surgeons, yet he contracted transfusion-related HIV and died years later of AIDS complications.3
While the Three Laws create a framework of the intern’s existence, it can never create the ideal intern with both the competency of the attending and frailty of the patients. The Laws of Robotics—and Internotics—remind us that just as Asimov’s “Bicentennial man” wanted to transform from robot to human, we want our interns to finish their training more human, not less so.4,** TH
*This makes the assumption that most attendings are humans in the context of this discussion—a hypothesis only. **Dr. Hu was recently a medical intern for Dr. Newman. None of the original Three Laws were violated during the course of their relationship.
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn. Dr. Hu works in the Departments of Internal Medicine and Neurology, Mayo Clinic College of Medicine, Rochester, Minn.
References
- Asimov, I. I, Robot. London: Grafton Books; 1968.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Asimov I, Asimov, JJ. Isaac Asimov: It’s Been a Good Life. New York: Prometheus; 2002.
- Asimov, I. The Bicentennial Man and Other Stories. New York:Doubleday and Co; 1976.
Internship is a stressful and life-altering experience. Demands from patients, consulting staff, and paperwork can dehumanize the new physician and make him or her feel like an automaton. The constant exigency of being an intern is further compounded by the increasing use of algorithms and computers. Guidelines for care have existed since the Hermetic books of Thoth in ancient Egypt, but strict “cookbook” medicine limits the intern’s decision-making and individuality. Pressure for electronic record-keeping and redundant documentation further reduce the new physician into not much more than a data entry-and-retrieval terminal. With the intern spending more time with patient records than actual patients, the physician-patient relationship invariably suffers as the intern becomes a small part of the machinery. Consequently, house-staff are constantly searching for a conceptual framework to better understand and cope with their unusual existence.
Isaac Asimov, the visionary science fiction writer and one-time biochemistry professor at Boston University School of Medicine, wrote an entire corpus of work around robots and the three “Laws of Robotics” starting in the 1940s.1 It seems the laws of robotics might also apply to interns as the Three Laws of “Internotics” (original text in parenthesis):
- First Law: An intern (robot) may not injure a patient (human being), or, through inaction, allow a patient (human being) to come to harm.
- Second Law: An intern (robot) must obey orders given it by attendings (human beings) except when such orders would conflict with the First Law.*
- Third Law: An intern (robot) must protect its own existence as long as such protection does not conflict with the First or Second Law.
Ten years after the creation of these laws, Asimov developed a “Zeroth” Law: An intern (robot) may not injure humanity, or through inaction, allow humanity to come to harm.
The First Law
Isolated interpretation of the First Law is the modus operandi of robots and interns. This law is a re-wording of the basic tenet of medicine: First do no harm, or primum non nocere as quoted from Hippocrates in Epidemics. On its surface, the First Law may seem easy for the intern to interpret and follow. However, when the patient’s own perception of benefit and harm deviates from the established norms in medicine, the intern is faced with dilemma of patient autonomy versus beneficence. This may not be a novel phenomenon in the modern consumer-based healthcare system, as Will Mayo, MD, from our own institution once said during a speech at Rush Medical College in 1910: “The best interest of the patient is the only interest to be considered.”
The Second Law
The Second Law explicitly states that the intern must follow the orders of the attending physician, but much rests in the intern’s additional obligation to reconcile obligatory recommendations with their own knowledge and patients’ idiosyncrasy. This may quickly become problematic for the intern, as few orders in modern medicine are considered absolutely risk-free.
The intern must undertake two levels of risk-benefit analysis: They must first determine what type of harm the patient faces in the setting of inaction—as spelled out by the First Law—if the attending’s orders were not carried out; he then must balance such hypothetical harm with the risks associated with the attendings orders of action. If such analysis were to favor inaction, to question the attending’s order is to challenge the attending’s own interpretation of the First Law and to risk the intern’s own existence (Third Law).
Therefore, the best solution for the intern is often to not question whether such order is necessary, but to do whatever possible to protect the patient. An example might be a consultant’s request for a CAT scan in a patient at high risk for contrast-induced nephropathy. In such a case, N-acetylcystein, adequate hydration or urine alkalinization may provide optimal protection against nephropathy. As such, the intern fulfills his or her obligations to the First and Second Laws without testing the limits imposed by the Third.
The Third Law
Much of the practice of—if not the principle of—internship is a violation of the Third Law. Excessive sleepiness and stressors may lead to medical errors, substance abuse, and traffic accidents.2 Work-hour restrictions may alleviate this condition, but can also erode the already limited patient-physician relationship. Further, certain attending physicians may denigrate the performance of the intern, leading to self doubt, lower self esteem, and mental anguish.
Similarly, interaction with certain patients may challenge the intern’s physical or mental well-being. As a result, the intern juxtaposes the new physician’s self-image of competency against the hierarchical stereotype of the rookie. The Third Law allows an opportunity for the intern to be associated with the proud heritage of the caduceus. However, as most interns soon learn, an intern can possibly best ensure his or her well-being and ascent to the next level when the Third Law is not cited as regularly as the first two laws.
The Zeroth Law
The Zeroth Law may be the most challenging law for both robots and interns. While robots and interns are both proficiently trained in serving individual humans, neither positronic programming nor medical education clearly establishes how this leads to the service of humanity.
If humanity is to be defined as the collection of individuals, principles in doctoring of the individual cannot be easily duplicated onto a population. This can be demonstrated through the continuously escalating medical expenditures in the setting of limited resources. For example, if a patient presents with “atypical” chest pain, a diligent medical graduate might order a set of laboratory studies and an electrocardiogram to rule out on-going myocardial infarction despite a low likelihood of abnormality. The slightest normal variation may then involve, by the First or Second Law, observation, stress testing, or cardiac catheterization.
Even though the current economic and legal systems allow for such shotgun approach of affordable technology, such application of the First Law onto humans as a collective will exhaust the population of its limited resources and utterly defy the Zeroth Law.
Alternatively, if humanity is to mean what constitutes each person’s individuality, argument involving maleficence and beneficence must give way to autonomy in the presentation, diagnosis, and treatment of disease, despite what the intern or attending physician perceive as benefits and harm. This obviously violates the First Law in the most fundamental level. However, different from the other laws, the Zeroth Law is not prefaced with the need to comply with the other Three Laws.
Interns can and often do feel dehumanized, whether from loss of decision-making role, from lack of sleep, or as a psychological tool of survival against the rigors of life and death in the hospital. Sometimes even a perfectly beneficent act violates the First Law at a later time and haunts the practitioners. Asimov himself received surgery-related transfusion with the best intention of his treating physicians and surgeons, yet he contracted transfusion-related HIV and died years later of AIDS complications.3
While the Three Laws create a framework of the intern’s existence, it can never create the ideal intern with both the competency of the attending and frailty of the patients. The Laws of Robotics—and Internotics—remind us that just as Asimov’s “Bicentennial man” wanted to transform from robot to human, we want our interns to finish their training more human, not less so.4,** TH
*This makes the assumption that most attendings are humans in the context of this discussion—a hypothesis only. **Dr. Hu was recently a medical intern for Dr. Newman. None of the original Three Laws were violated during the course of their relationship.
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn. Dr. Hu works in the Departments of Internal Medicine and Neurology, Mayo Clinic College of Medicine, Rochester, Minn.
References
- Asimov, I. I, Robot. London: Grafton Books; 1968.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Asimov I, Asimov, JJ. Isaac Asimov: It’s Been a Good Life. New York: Prometheus; 2002.
- Asimov, I. The Bicentennial Man and Other Stories. New York:Doubleday and Co; 1976.
Internship is a stressful and life-altering experience. Demands from patients, consulting staff, and paperwork can dehumanize the new physician and make him or her feel like an automaton. The constant exigency of being an intern is further compounded by the increasing use of algorithms and computers. Guidelines for care have existed since the Hermetic books of Thoth in ancient Egypt, but strict “cookbook” medicine limits the intern’s decision-making and individuality. Pressure for electronic record-keeping and redundant documentation further reduce the new physician into not much more than a data entry-and-retrieval terminal. With the intern spending more time with patient records than actual patients, the physician-patient relationship invariably suffers as the intern becomes a small part of the machinery. Consequently, house-staff are constantly searching for a conceptual framework to better understand and cope with their unusual existence.
Isaac Asimov, the visionary science fiction writer and one-time biochemistry professor at Boston University School of Medicine, wrote an entire corpus of work around robots and the three “Laws of Robotics” starting in the 1940s.1 It seems the laws of robotics might also apply to interns as the Three Laws of “Internotics” (original text in parenthesis):
- First Law: An intern (robot) may not injure a patient (human being), or, through inaction, allow a patient (human being) to come to harm.
- Second Law: An intern (robot) must obey orders given it by attendings (human beings) except when such orders would conflict with the First Law.*
- Third Law: An intern (robot) must protect its own existence as long as such protection does not conflict with the First or Second Law.
Ten years after the creation of these laws, Asimov developed a “Zeroth” Law: An intern (robot) may not injure humanity, or through inaction, allow humanity to come to harm.
The First Law
Isolated interpretation of the First Law is the modus operandi of robots and interns. This law is a re-wording of the basic tenet of medicine: First do no harm, or primum non nocere as quoted from Hippocrates in Epidemics. On its surface, the First Law may seem easy for the intern to interpret and follow. However, when the patient’s own perception of benefit and harm deviates from the established norms in medicine, the intern is faced with dilemma of patient autonomy versus beneficence. This may not be a novel phenomenon in the modern consumer-based healthcare system, as Will Mayo, MD, from our own institution once said during a speech at Rush Medical College in 1910: “The best interest of the patient is the only interest to be considered.”
The Second Law
The Second Law explicitly states that the intern must follow the orders of the attending physician, but much rests in the intern’s additional obligation to reconcile obligatory recommendations with their own knowledge and patients’ idiosyncrasy. This may quickly become problematic for the intern, as few orders in modern medicine are considered absolutely risk-free.
The intern must undertake two levels of risk-benefit analysis: They must first determine what type of harm the patient faces in the setting of inaction—as spelled out by the First Law—if the attending’s orders were not carried out; he then must balance such hypothetical harm with the risks associated with the attendings orders of action. If such analysis were to favor inaction, to question the attending’s order is to challenge the attending’s own interpretation of the First Law and to risk the intern’s own existence (Third Law).
Therefore, the best solution for the intern is often to not question whether such order is necessary, but to do whatever possible to protect the patient. An example might be a consultant’s request for a CAT scan in a patient at high risk for contrast-induced nephropathy. In such a case, N-acetylcystein, adequate hydration or urine alkalinization may provide optimal protection against nephropathy. As such, the intern fulfills his or her obligations to the First and Second Laws without testing the limits imposed by the Third.
The Third Law
Much of the practice of—if not the principle of—internship is a violation of the Third Law. Excessive sleepiness and stressors may lead to medical errors, substance abuse, and traffic accidents.2 Work-hour restrictions may alleviate this condition, but can also erode the already limited patient-physician relationship. Further, certain attending physicians may denigrate the performance of the intern, leading to self doubt, lower self esteem, and mental anguish.
Similarly, interaction with certain patients may challenge the intern’s physical or mental well-being. As a result, the intern juxtaposes the new physician’s self-image of competency against the hierarchical stereotype of the rookie. The Third Law allows an opportunity for the intern to be associated with the proud heritage of the caduceus. However, as most interns soon learn, an intern can possibly best ensure his or her well-being and ascent to the next level when the Third Law is not cited as regularly as the first two laws.
The Zeroth Law
The Zeroth Law may be the most challenging law for both robots and interns. While robots and interns are both proficiently trained in serving individual humans, neither positronic programming nor medical education clearly establishes how this leads to the service of humanity.
If humanity is to be defined as the collection of individuals, principles in doctoring of the individual cannot be easily duplicated onto a population. This can be demonstrated through the continuously escalating medical expenditures in the setting of limited resources. For example, if a patient presents with “atypical” chest pain, a diligent medical graduate might order a set of laboratory studies and an electrocardiogram to rule out on-going myocardial infarction despite a low likelihood of abnormality. The slightest normal variation may then involve, by the First or Second Law, observation, stress testing, or cardiac catheterization.
Even though the current economic and legal systems allow for such shotgun approach of affordable technology, such application of the First Law onto humans as a collective will exhaust the population of its limited resources and utterly defy the Zeroth Law.
Alternatively, if humanity is to mean what constitutes each person’s individuality, argument involving maleficence and beneficence must give way to autonomy in the presentation, diagnosis, and treatment of disease, despite what the intern or attending physician perceive as benefits and harm. This obviously violates the First Law in the most fundamental level. However, different from the other laws, the Zeroth Law is not prefaced with the need to comply with the other Three Laws.
Interns can and often do feel dehumanized, whether from loss of decision-making role, from lack of sleep, or as a psychological tool of survival against the rigors of life and death in the hospital. Sometimes even a perfectly beneficent act violates the First Law at a later time and haunts the practitioners. Asimov himself received surgery-related transfusion with the best intention of his treating physicians and surgeons, yet he contracted transfusion-related HIV and died years later of AIDS complications.3
While the Three Laws create a framework of the intern’s existence, it can never create the ideal intern with both the competency of the attending and frailty of the patients. The Laws of Robotics—and Internotics—remind us that just as Asimov’s “Bicentennial man” wanted to transform from robot to human, we want our interns to finish their training more human, not less so.4,** TH
*This makes the assumption that most attendings are humans in the context of this discussion—a hypothesis only. **Dr. Hu was recently a medical intern for Dr. Newman. None of the original Three Laws were violated during the course of their relationship.
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn. Dr. Hu works in the Departments of Internal Medicine and Neurology, Mayo Clinic College of Medicine, Rochester, Minn.
References
- Asimov, I. I, Robot. London: Grafton Books; 1968.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Asimov I, Asimov, JJ. Isaac Asimov: It’s Been a Good Life. New York: Prometheus; 2002.
- Asimov, I. The Bicentennial Man and Other Stories. New York:Doubleday and Co; 1976.
Hospitalists Effects on Outcomes, Costs, Point-of-Care HIV Testing, and More
Community Teaching
Halasyamani L, Valenstein P, Friedlander M. et al. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am J Med. 2005;118:536-543.
Background: A growing body of literature has demonstrated the effects of hospitalists on reducing inpatient length of stay and cost of care, with some literature showing a decreased in-hospital and 30-day mortality. However, most prior studies were conducted in academic medical centers or health maintenance organizations where one group of hospitalists, employed by the institution within which they worked, was compared with traditional primary care physicians. Direct comparisons between different hospitalist models practicing within a single institution have not been published. As a result, the impact of different hospitalist characteristics, including employment status and reimbursement incentives, on inpatient resource utilization and patient care outcomes is unknown.
Methods: Halasyamani and colleagues conducted a retrospective cohort study of 10,595 patients in a tertiary care community-based teaching hospital in which private hospitalists, academic hospitalists, and community physicians all practice. They measured risk-adjusted length of stay, variable costs, 30-day readmission rates, and in-hospital and 30-day mortality for patients treated by each of these three groups, controlling for potentially confounding variables. Community physicians belonged to 21 rounding groups, most of which were private or solo. Two of the community physicians groups were hospital-owned practices reimbursed by a relative value unit system. The private hospitalist group was self-employed with no financial relationship to the hospital and worked an average of 40 weeks per year. Community physicians and private hospitalists worked Monday-Friday and covered weekends or holidays about 25% of the time. Academic hospitalists worked with internal medicine residents and students on a teaching service. They were employed by the hospital using a relative value unit system. They worked an average of 14 weeks per year as an inpatient attending in half-month rotations, which included weekend coverage.
Results: There was a 20% reduction (-0.72 days absolute difference) in length of stay on the academic hospitalist service (P<0.0001) and 8% (-0.28 days absolute difference) on the private hospitalist service (P=0.049) compared with community physicians. Case-mix adjusted relative total costs were 10% less ($173 absolute difference) on the academic (P<0.0001) and 6% less ($109 absolute difference) on the private hospitalist services (P=0.02) compared with community physicians. There were no differences in 30-day readmission, in-hospital and 30-day mortality between the three groups.
Discussion: This study is the first to look at the effects of two separate hospitalist models on resource utilization and patient outcomes within the same institution. Although both the academic and private hospitalist groups demonstrated improved resource utilization as compared with the community physicians, the magnitude of benefit was much greater for the academic hospitalist group.
As the authors point out, one major difference between the two groups was employment status, with the academic hospitalists employed directly by the hospital and the private hospitalists receiving all payment directly from payers. Previous studies have also focused on hospitalists, which were employed by the institution at which they worked, raising the question of whether alignment of employee and employer incentives is an important factor affecting resource utilization outcomes.
Results of this study highlight the need for more studies which seek to clarify specific physician-level, group-level, and organization-level characteristics of hospitalists that result in improved resource utilization and patient care outcomes.
The Last Few Hours
Bailey FA, Burgio KL, Woodby LL, et al. Improving the processes of hospital care during the last hours of life. Arch Int Med. 2005;165(15):1722-1727.
Background: End-of-life care in the acute care inpatient setting is often not initiated until very late in the dying process and may be related to inadequate early recognition of dying patients as well as difficulty transitioning from disease-modifying treatments to palliative measures. Additional barriers exist, including lack of familiarity of hospital staff with initiation and implementation of hospice care. Education about end-of-life care and introduction of a physician-led palliative care team available for consultation within acute care hospitals may help promote better recognition of the dying patient by staff and allow for a “good death.”
Methods: A single hospital within the Veterans Affairs (VA) medical system (Birmingham, Ala., VA Medical Center) was chosen as a pilot center for initiation of a physician-led Inpatient Comfort Care Program (ICCP). The study was framed as a “before-after intervention trial” and analyzed all inpatient deaths identified by the Computerized Patient Recognition System during a six-month period before and substantially after the introduction of the ICCP. A structured chart abstraction tool was used and data was obtained from the last seven days of hospitalization analyzing variables associated with recognition of the dying patient and initiation of palliative care. Education of hospital staff on both hospice care and case identification was initiated during the intervention phase of the study. Additionally, a flexible comfort care order set was introduced.
Results: Two hundred and three veterans were identified (98% men, average age 68) and no significant differences in clinical characteristics were noted between the two groups, pre-intervention and post-intervention. Post-intervention, 59.3% of patients had formal palliative care consultation. Significant findings (P<0.01) following implementation of ICCP were increased documentation of end-of-life symptoms, increased documentation of care plans, increased utilization of opioids (57.1% to 87.2%), increased initiation of do-not-resuscitate orders (61.9% to 85.1%) with a concurrent decrease in cardiopulmonary resuscitation at death (34.4% to 15.4%), and a surprising increase in restraint use (6.0% to 22.6%).
Discussion: Data on hospice care patients indicate that 10% to 30% die in an acute care hospital, identifying a need for increased education and training in palliative medicine. This study demonstrates the positive outcomes of implementation of an inpatient palliative care service both for heightened awareness of identifying the dying patient as well as initiation of end-of-life care. The increased use of opioid medications is an important marker given that many patients experience pain and dyspnea at the end of life. This study is limited by its single site and further validation at other centers implementing similar protocols and assessing similar outcomes is needed. While this intervention had important clinical benefits, additional studies examining the cost implications of this system would be helpful.
Education alone has not been shown to be entirely effective in creating change. This single-site implementation of a palliative care consultation service successfully integrated an education program with on-site consultants. Distributing pocket cards with clinical findings identifying the dying patient aided in recognition of those patients and pre-printed order sets facilitated initiation of end-of-life care. The intervention initiated is possible for many medical centers and promotes an environment allowing for a “good death” for dying patients.
Computers, Doctors, and Errors
Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203
For physicians, computerized physician order entry (CPOE) has become an important topic of discussion as many hospitals and health systems embark on the complex and lengthy process of implementing new enterprise clinical systems. Though there are undoubtedly benefits to such systems, practicing clinicians are apt to remain skeptical of the grandiose pictures the more vocal advocates of CPOE may paint. This is not to say that the promises of CPOE are empty; to the contrary, there have been substantial successes, notably in the realm of medication error prevention.
At the same time, CPOE is a mixture of complex technologies that interface in complicated ways with the culture of clinical medicine. The view that medical informatics is a technical problem that has been solved long ago is simplistic and naïve. The article by Koppel, et al, has two important implications: 1) It is critical to look at clinical information systems in the social milieu in which it functions, and 2) there are often unintended consequences that may not beneficial.
This article examines a widely used, commercial CPOE system in use at the University of Pennsylvania (Philadelphia) using both quantitative and qualitative methods. The researchers conducted focus groups and expert interviews in addition to field observations of physicians (house officers and attendings), nurses, and pharmacists in order to identify themes relating to work with the order entry system. This work helped to guide the creation of a survey instrument subsequently used to survey house staff about working conditions and sources of error and stress. There was an 85%-90% response rate that primarily included house staff who ordered more than nine medication orders per month.
Researchers found two broad categories of errors that were fostered in this environment. The first category, which they termed “information errors” were generated by fragmentation of data and the failure to integrate the hospitals various systems both electronic and paper. Examples of this type of error include antibiotic renewal failures. A common way this failure would occur is that renewal reminder stickers would be placed in the patients’ charts, but the house staff would overlook these because medication orders occurred electronically. Another example is assumed dose errors, where house staff would assume that the default dose displayed was the recommended starting dose, when in fact this was the smallest dose unit available. Physicians were assuming decision support was available when it was not.
The second type of error, human-machine interface flaws, occurred when machine rules did not correspond to work behaviors. An example of this is when patients were listed alphabetically rather than by service, making it easy to select the wrong patient. In another instance, many screens (up to 20) were required to view all of a patient’s medications, making it difficult to choose a correct medication for editing.
This study has been criticized by industry advocates for focusing on an older set of technologies or because a number of these issues related to training or “user factors.” At the other extreme, this study has been cited as a cautionary tale about the risks of CPOE. Both types of criticism miss the point. This study demonstrates that CPOE and the social environment in which it sits is a complex entity and that careful design, proper support, and maintenance are critical ingredients to the success of an incredibly complex but vital new component of hospital medicine.
Point-of-Care HIV Testing in Inpatients
Lubelchek R, Kroc K, Hota B, et al. The role of rapid vs conventional human immunodeficiency virus testing for inpatients: effects on quality of care. Arch Intern Med. 2005;165:1956-1960.
Despite advances in treatment, infection with HIV and AIDS remains a public health problem in the United States. According to the CDC the rate of new diagnosis of HIV infection has remained steady from 2000 to 2003 at about 20 per 100,000 people. (Centers for Disease Control and Prevention. Diagnosis of HIV/AIDS–32 states, 2009-2003. MMWR Morb Mortal Wkly Rep. 2004;53:1106-1110). Currently, about 850,000 to 950,000 people are believed to be living with HIV infection, and it is estimated that 180,000 to 280,000 are unaware of their diagnosis. (Fleming P, Byers RH, Sweeney PA, et al., HIV prevalence in the United States, 2000 [Abstract 11]. Presented at the Ninth Conference on Retroviruses and Opportunistic Infections, Seattle; February 24–28, 2002). These patients are not only at risk for disease progression, but can undermine efforts at disease prevention if they continue to engage in unsafe activities. Thus, increasing awareness of HIV status is an important aspect of disease prevention.
HIV testing remains a challenge. Conventional testing with enzyme immunoassay (EIA) and confirmatory Western blot requires patient follow-up for results, which approximately 25% of patients in various outpatient testing sites fail to do. (Centers for Disease Control and Prevention. Update: HIV counseling and testing using rapid tests, United States, 1995. MMWR Morb Mortal Wkly Rep. 1998;47:211-215). Given the difficulties inherent in the transition of care from the inpatient to outpatient setting, conventional testing in the inpatient setting presents additional barriers to appropriate notification. As various point-of-care HIV tests have been developed for commercial use, the possibility of rapid HIV testing presents an opportunity to reduce notification failure and improve patient care. While not replacing traditional testing, the CDC has endorsed rapid HIV testing as a means to initiate therapy and provide counseling with a particular focus on preventing further disease transmission. In this retrospective study, Lubelchek and colleagues present the effects of a rapid HIV test utilized in the emergency department on various inpatient quality of care measures for those patients who received a positive rapid HIV test later confirmed by Western blot as compared with those patients who were diagnosed after admission by traditional diagnostic methods. This study took place in the context of CDC-funded study of the use of OraQuick (OraSure Technologies, Bethlehem, Pa.) rapid HIV testing in the emergency department at Cook County Hospital in Chicago.
The manufacturer claims the product has a sensitivity of 99.6% and a specificity of 100% as compared with conventional testing. (OraQuick rapid HIV-1 antibody test summary of safety and effectiveness. November 7, 2002. Accessed October 1, 2005, at www.fda.gov/cber/pma/P010047.htm). In the initial study, two of the three emergency department’s treatment pods were equipped to provide HIV screening utilizing the point-of-care technology to consenting patients. Patients in the third pod could be referred to rapid testing based on symptoms or risk factors. All patients who received the rapid test also submitted specimens for conventional EIA and confirmatory Western blot testing. All positive rapid HIV tests were confirmed by Western blot.
In this study, patients who were not known to be infected and were subsequently admitted on non-obstetric or surgical services over 17 months from 2003 to 2004 and confirmed to be HIV positive by Western blot were identified utilizing administrative records. Where possible, charts were reviewed to confirm no prior diagnosis of HIV. Patients who received rapid HIV testing were compared with those who only received conventional testing. Endpoints included time to primary inpatient care service awareness of HIV diagnosis, time to admission or transfer to the inpatient HIV service, time to empiric treatment of diagnosis of opportunistic infection, length of stay, discharge with appropriate prophylactic medications, discharge with patient knowledge of HIV diagnosis, and initial engagement in outpatient care. Length of stay was adjusted by multivariate regression on co-morbid diagnoses (congestive heart failure, end-stage renal disease, cirrhosis, chronic obstructive pulmonary disease, and diabetes), opportunistic infections, ICU admission, need for mechanical ventilation, and CD4 count.
A total of 103 patients were identified with complete chart review completed on 86 of them. All patients except one were admitted through the emergency department. Forty-eight patients were diagnosed initially with the rapid HIV test with 58% of these specifically referred for testing by the emergency department physician, and 55 were diagnosed with conventional testing. Overall, 78% were male, 62% African American, and 20% Hispanic. The two groups were comparable in terms of age, sex, ethnicity, history of substance abuse, HIV risk factors, psychiatric diagnoses, homelessness, CD4 count, presence of opportunistic infections, mechanical ventilation, and co-morbidities. However, conventionally tested patients were more likely to require an ICU stay (31% vs. 10%, P=.01).
Patients in the rapid test group were more quickly documented in the chart as having HIV (.8 vs. 6.4 days, p<.001), placed on an HIV service sooner (1.4 versus 6.9 days, P<.001), initiated outpatient follow-up sooner (21.5 versus 49.5 days, p=.05), and had less unawareness of their HIV status (0 vs. 16%, P=.002). There was no significant difference between the two groups in time from admission to empiric treatment or diagnosis of an opportunistic infection. Patients who received the rapid test did have a lower length of stay (6.4 versus 13.2 days, P<.001). Although much of this difference was due to higher number of ICU stays in the conventional group, in multivariate analysis conventional testing still increased length of stay significantly, OR 5.4 days (2.5, 8.3).
This study suggests that patients who are tested with rapid HIV testing can lead to more efficient inpatient treatment of the complications of HIV, improved patient awareness of HIV status, and quicker outpatient follow-up. These findings have ramifications not just to the inpatient management of patients with HIV but to general public health efforts to reduce the spread of HIV infection.
Nevertheless, these results must be interpreted with caution. They reflect the experience of one institution situated in an area with a high prevalence of HIV. Some degree of selection bias is suggested by the higher presence of ICU admissions in the conventional testing group. The multivariate analysis attempted to control for confounding factors, but the possibility remains that other unrecognized factors may have influenced results. The authors do note that an analysis of patients in the rapid test group stratified by whether the test was performed for screening or by referral of the physician did not demonstrate a statistically significant difference in length of stay. This finding provides further support that the sicker patients which triggered the rapid test had shorter lengths of stay on account of the rapid test and not simply because they were sicker.
As recognized by the authors, physicians in routine practice rely on surrogate markers of HIV infection, most notably a patient’s CD4 count, and thus it is not surprising that the rapid test did not affect time to empiric treatment or diagnosis of opportunistic infection. If treatment did not differ, then explaining the longer length of stay remains an unexplained puzzle. The fact that the two groups were equally matched socially and psychiatrically leaves open the possibility that it was actual knowledge of the HIV test result—and not its effect on treatment—that drove the longer length of stay.
One possibility not suggested by the authors is that definitive knowledge of HIV status helped to mobilize patient discharge. If there were legitimate concerns of follow-up, physicians may have delayed discharge in order to receive HIV test results. Alternatively, some patients may have resisted discharge until receiving test results and the development of a more concrete plan. It would be interesting to know if the time to follow-up for the two groups would be the same if the 16% who did not know their HIV status at discharge were excluded. This suggests that knowledge of HIV status drives follow-up time and would lend some support to the notion that patient discharge was delayed for test results and clarification of the follow-up treatment plan.
Even putting aside the difference in length of stay, the difference of rapid testing on improved knowledge of HIV status and quicker follow-up is likely real and meaningful. Although this study was not designed to assess the impact of this knowledge on patient behavior, immediate knowledge of HIV status during hospitalization may translate to decreased transmission as patients alter their behavior and lends further credibility to the utility of rapid HIV testing in conjunction with conventional methods in the management of inpatients. TH
Community Teaching
Halasyamani L, Valenstein P, Friedlander M. et al. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am J Med. 2005;118:536-543.
Background: A growing body of literature has demonstrated the effects of hospitalists on reducing inpatient length of stay and cost of care, with some literature showing a decreased in-hospital and 30-day mortality. However, most prior studies were conducted in academic medical centers or health maintenance organizations where one group of hospitalists, employed by the institution within which they worked, was compared with traditional primary care physicians. Direct comparisons between different hospitalist models practicing within a single institution have not been published. As a result, the impact of different hospitalist characteristics, including employment status and reimbursement incentives, on inpatient resource utilization and patient care outcomes is unknown.
Methods: Halasyamani and colleagues conducted a retrospective cohort study of 10,595 patients in a tertiary care community-based teaching hospital in which private hospitalists, academic hospitalists, and community physicians all practice. They measured risk-adjusted length of stay, variable costs, 30-day readmission rates, and in-hospital and 30-day mortality for patients treated by each of these three groups, controlling for potentially confounding variables. Community physicians belonged to 21 rounding groups, most of which were private or solo. Two of the community physicians groups were hospital-owned practices reimbursed by a relative value unit system. The private hospitalist group was self-employed with no financial relationship to the hospital and worked an average of 40 weeks per year. Community physicians and private hospitalists worked Monday-Friday and covered weekends or holidays about 25% of the time. Academic hospitalists worked with internal medicine residents and students on a teaching service. They were employed by the hospital using a relative value unit system. They worked an average of 14 weeks per year as an inpatient attending in half-month rotations, which included weekend coverage.
Results: There was a 20% reduction (-0.72 days absolute difference) in length of stay on the academic hospitalist service (P<0.0001) and 8% (-0.28 days absolute difference) on the private hospitalist service (P=0.049) compared with community physicians. Case-mix adjusted relative total costs were 10% less ($173 absolute difference) on the academic (P<0.0001) and 6% less ($109 absolute difference) on the private hospitalist services (P=0.02) compared with community physicians. There were no differences in 30-day readmission, in-hospital and 30-day mortality between the three groups.
Discussion: This study is the first to look at the effects of two separate hospitalist models on resource utilization and patient outcomes within the same institution. Although both the academic and private hospitalist groups demonstrated improved resource utilization as compared with the community physicians, the magnitude of benefit was much greater for the academic hospitalist group.
As the authors point out, one major difference between the two groups was employment status, with the academic hospitalists employed directly by the hospital and the private hospitalists receiving all payment directly from payers. Previous studies have also focused on hospitalists, which were employed by the institution at which they worked, raising the question of whether alignment of employee and employer incentives is an important factor affecting resource utilization outcomes.
Results of this study highlight the need for more studies which seek to clarify specific physician-level, group-level, and organization-level characteristics of hospitalists that result in improved resource utilization and patient care outcomes.
The Last Few Hours
Bailey FA, Burgio KL, Woodby LL, et al. Improving the processes of hospital care during the last hours of life. Arch Int Med. 2005;165(15):1722-1727.
Background: End-of-life care in the acute care inpatient setting is often not initiated until very late in the dying process and may be related to inadequate early recognition of dying patients as well as difficulty transitioning from disease-modifying treatments to palliative measures. Additional barriers exist, including lack of familiarity of hospital staff with initiation and implementation of hospice care. Education about end-of-life care and introduction of a physician-led palliative care team available for consultation within acute care hospitals may help promote better recognition of the dying patient by staff and allow for a “good death.”
Methods: A single hospital within the Veterans Affairs (VA) medical system (Birmingham, Ala., VA Medical Center) was chosen as a pilot center for initiation of a physician-led Inpatient Comfort Care Program (ICCP). The study was framed as a “before-after intervention trial” and analyzed all inpatient deaths identified by the Computerized Patient Recognition System during a six-month period before and substantially after the introduction of the ICCP. A structured chart abstraction tool was used and data was obtained from the last seven days of hospitalization analyzing variables associated with recognition of the dying patient and initiation of palliative care. Education of hospital staff on both hospice care and case identification was initiated during the intervention phase of the study. Additionally, a flexible comfort care order set was introduced.
Results: Two hundred and three veterans were identified (98% men, average age 68) and no significant differences in clinical characteristics were noted between the two groups, pre-intervention and post-intervention. Post-intervention, 59.3% of patients had formal palliative care consultation. Significant findings (P<0.01) following implementation of ICCP were increased documentation of end-of-life symptoms, increased documentation of care plans, increased utilization of opioids (57.1% to 87.2%), increased initiation of do-not-resuscitate orders (61.9% to 85.1%) with a concurrent decrease in cardiopulmonary resuscitation at death (34.4% to 15.4%), and a surprising increase in restraint use (6.0% to 22.6%).
Discussion: Data on hospice care patients indicate that 10% to 30% die in an acute care hospital, identifying a need for increased education and training in palliative medicine. This study demonstrates the positive outcomes of implementation of an inpatient palliative care service both for heightened awareness of identifying the dying patient as well as initiation of end-of-life care. The increased use of opioid medications is an important marker given that many patients experience pain and dyspnea at the end of life. This study is limited by its single site and further validation at other centers implementing similar protocols and assessing similar outcomes is needed. While this intervention had important clinical benefits, additional studies examining the cost implications of this system would be helpful.
Education alone has not been shown to be entirely effective in creating change. This single-site implementation of a palliative care consultation service successfully integrated an education program with on-site consultants. Distributing pocket cards with clinical findings identifying the dying patient aided in recognition of those patients and pre-printed order sets facilitated initiation of end-of-life care. The intervention initiated is possible for many medical centers and promotes an environment allowing for a “good death” for dying patients.
Computers, Doctors, and Errors
Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203
For physicians, computerized physician order entry (CPOE) has become an important topic of discussion as many hospitals and health systems embark on the complex and lengthy process of implementing new enterprise clinical systems. Though there are undoubtedly benefits to such systems, practicing clinicians are apt to remain skeptical of the grandiose pictures the more vocal advocates of CPOE may paint. This is not to say that the promises of CPOE are empty; to the contrary, there have been substantial successes, notably in the realm of medication error prevention.
At the same time, CPOE is a mixture of complex technologies that interface in complicated ways with the culture of clinical medicine. The view that medical informatics is a technical problem that has been solved long ago is simplistic and naïve. The article by Koppel, et al, has two important implications: 1) It is critical to look at clinical information systems in the social milieu in which it functions, and 2) there are often unintended consequences that may not beneficial.
This article examines a widely used, commercial CPOE system in use at the University of Pennsylvania (Philadelphia) using both quantitative and qualitative methods. The researchers conducted focus groups and expert interviews in addition to field observations of physicians (house officers and attendings), nurses, and pharmacists in order to identify themes relating to work with the order entry system. This work helped to guide the creation of a survey instrument subsequently used to survey house staff about working conditions and sources of error and stress. There was an 85%-90% response rate that primarily included house staff who ordered more than nine medication orders per month.
Researchers found two broad categories of errors that were fostered in this environment. The first category, which they termed “information errors” were generated by fragmentation of data and the failure to integrate the hospitals various systems both electronic and paper. Examples of this type of error include antibiotic renewal failures. A common way this failure would occur is that renewal reminder stickers would be placed in the patients’ charts, but the house staff would overlook these because medication orders occurred electronically. Another example is assumed dose errors, where house staff would assume that the default dose displayed was the recommended starting dose, when in fact this was the smallest dose unit available. Physicians were assuming decision support was available when it was not.
The second type of error, human-machine interface flaws, occurred when machine rules did not correspond to work behaviors. An example of this is when patients were listed alphabetically rather than by service, making it easy to select the wrong patient. In another instance, many screens (up to 20) were required to view all of a patient’s medications, making it difficult to choose a correct medication for editing.
This study has been criticized by industry advocates for focusing on an older set of technologies or because a number of these issues related to training or “user factors.” At the other extreme, this study has been cited as a cautionary tale about the risks of CPOE. Both types of criticism miss the point. This study demonstrates that CPOE and the social environment in which it sits is a complex entity and that careful design, proper support, and maintenance are critical ingredients to the success of an incredibly complex but vital new component of hospital medicine.
Point-of-Care HIV Testing in Inpatients
Lubelchek R, Kroc K, Hota B, et al. The role of rapid vs conventional human immunodeficiency virus testing for inpatients: effects on quality of care. Arch Intern Med. 2005;165:1956-1960.
Despite advances in treatment, infection with HIV and AIDS remains a public health problem in the United States. According to the CDC the rate of new diagnosis of HIV infection has remained steady from 2000 to 2003 at about 20 per 100,000 people. (Centers for Disease Control and Prevention. Diagnosis of HIV/AIDS–32 states, 2009-2003. MMWR Morb Mortal Wkly Rep. 2004;53:1106-1110). Currently, about 850,000 to 950,000 people are believed to be living with HIV infection, and it is estimated that 180,000 to 280,000 are unaware of their diagnosis. (Fleming P, Byers RH, Sweeney PA, et al., HIV prevalence in the United States, 2000 [Abstract 11]. Presented at the Ninth Conference on Retroviruses and Opportunistic Infections, Seattle; February 24–28, 2002). These patients are not only at risk for disease progression, but can undermine efforts at disease prevention if they continue to engage in unsafe activities. Thus, increasing awareness of HIV status is an important aspect of disease prevention.
HIV testing remains a challenge. Conventional testing with enzyme immunoassay (EIA) and confirmatory Western blot requires patient follow-up for results, which approximately 25% of patients in various outpatient testing sites fail to do. (Centers for Disease Control and Prevention. Update: HIV counseling and testing using rapid tests, United States, 1995. MMWR Morb Mortal Wkly Rep. 1998;47:211-215). Given the difficulties inherent in the transition of care from the inpatient to outpatient setting, conventional testing in the inpatient setting presents additional barriers to appropriate notification. As various point-of-care HIV tests have been developed for commercial use, the possibility of rapid HIV testing presents an opportunity to reduce notification failure and improve patient care. While not replacing traditional testing, the CDC has endorsed rapid HIV testing as a means to initiate therapy and provide counseling with a particular focus on preventing further disease transmission. In this retrospective study, Lubelchek and colleagues present the effects of a rapid HIV test utilized in the emergency department on various inpatient quality of care measures for those patients who received a positive rapid HIV test later confirmed by Western blot as compared with those patients who were diagnosed after admission by traditional diagnostic methods. This study took place in the context of CDC-funded study of the use of OraQuick (OraSure Technologies, Bethlehem, Pa.) rapid HIV testing in the emergency department at Cook County Hospital in Chicago.
The manufacturer claims the product has a sensitivity of 99.6% and a specificity of 100% as compared with conventional testing. (OraQuick rapid HIV-1 antibody test summary of safety and effectiveness. November 7, 2002. Accessed October 1, 2005, at www.fda.gov/cber/pma/P010047.htm). In the initial study, two of the three emergency department’s treatment pods were equipped to provide HIV screening utilizing the point-of-care technology to consenting patients. Patients in the third pod could be referred to rapid testing based on symptoms or risk factors. All patients who received the rapid test also submitted specimens for conventional EIA and confirmatory Western blot testing. All positive rapid HIV tests were confirmed by Western blot.
In this study, patients who were not known to be infected and were subsequently admitted on non-obstetric or surgical services over 17 months from 2003 to 2004 and confirmed to be HIV positive by Western blot were identified utilizing administrative records. Where possible, charts were reviewed to confirm no prior diagnosis of HIV. Patients who received rapid HIV testing were compared with those who only received conventional testing. Endpoints included time to primary inpatient care service awareness of HIV diagnosis, time to admission or transfer to the inpatient HIV service, time to empiric treatment of diagnosis of opportunistic infection, length of stay, discharge with appropriate prophylactic medications, discharge with patient knowledge of HIV diagnosis, and initial engagement in outpatient care. Length of stay was adjusted by multivariate regression on co-morbid diagnoses (congestive heart failure, end-stage renal disease, cirrhosis, chronic obstructive pulmonary disease, and diabetes), opportunistic infections, ICU admission, need for mechanical ventilation, and CD4 count.
A total of 103 patients were identified with complete chart review completed on 86 of them. All patients except one were admitted through the emergency department. Forty-eight patients were diagnosed initially with the rapid HIV test with 58% of these specifically referred for testing by the emergency department physician, and 55 were diagnosed with conventional testing. Overall, 78% were male, 62% African American, and 20% Hispanic. The two groups were comparable in terms of age, sex, ethnicity, history of substance abuse, HIV risk factors, psychiatric diagnoses, homelessness, CD4 count, presence of opportunistic infections, mechanical ventilation, and co-morbidities. However, conventionally tested patients were more likely to require an ICU stay (31% vs. 10%, P=.01).
Patients in the rapid test group were more quickly documented in the chart as having HIV (.8 vs. 6.4 days, p<.001), placed on an HIV service sooner (1.4 versus 6.9 days, P<.001), initiated outpatient follow-up sooner (21.5 versus 49.5 days, p=.05), and had less unawareness of their HIV status (0 vs. 16%, P=.002). There was no significant difference between the two groups in time from admission to empiric treatment or diagnosis of an opportunistic infection. Patients who received the rapid test did have a lower length of stay (6.4 versus 13.2 days, P<.001). Although much of this difference was due to higher number of ICU stays in the conventional group, in multivariate analysis conventional testing still increased length of stay significantly, OR 5.4 days (2.5, 8.3).
This study suggests that patients who are tested with rapid HIV testing can lead to more efficient inpatient treatment of the complications of HIV, improved patient awareness of HIV status, and quicker outpatient follow-up. These findings have ramifications not just to the inpatient management of patients with HIV but to general public health efforts to reduce the spread of HIV infection.
Nevertheless, these results must be interpreted with caution. They reflect the experience of one institution situated in an area with a high prevalence of HIV. Some degree of selection bias is suggested by the higher presence of ICU admissions in the conventional testing group. The multivariate analysis attempted to control for confounding factors, but the possibility remains that other unrecognized factors may have influenced results. The authors do note that an analysis of patients in the rapid test group stratified by whether the test was performed for screening or by referral of the physician did not demonstrate a statistically significant difference in length of stay. This finding provides further support that the sicker patients which triggered the rapid test had shorter lengths of stay on account of the rapid test and not simply because they were sicker.
As recognized by the authors, physicians in routine practice rely on surrogate markers of HIV infection, most notably a patient’s CD4 count, and thus it is not surprising that the rapid test did not affect time to empiric treatment or diagnosis of opportunistic infection. If treatment did not differ, then explaining the longer length of stay remains an unexplained puzzle. The fact that the two groups were equally matched socially and psychiatrically leaves open the possibility that it was actual knowledge of the HIV test result—and not its effect on treatment—that drove the longer length of stay.
One possibility not suggested by the authors is that definitive knowledge of HIV status helped to mobilize patient discharge. If there were legitimate concerns of follow-up, physicians may have delayed discharge in order to receive HIV test results. Alternatively, some patients may have resisted discharge until receiving test results and the development of a more concrete plan. It would be interesting to know if the time to follow-up for the two groups would be the same if the 16% who did not know their HIV status at discharge were excluded. This suggests that knowledge of HIV status drives follow-up time and would lend some support to the notion that patient discharge was delayed for test results and clarification of the follow-up treatment plan.
Even putting aside the difference in length of stay, the difference of rapid testing on improved knowledge of HIV status and quicker follow-up is likely real and meaningful. Although this study was not designed to assess the impact of this knowledge on patient behavior, immediate knowledge of HIV status during hospitalization may translate to decreased transmission as patients alter their behavior and lends further credibility to the utility of rapid HIV testing in conjunction with conventional methods in the management of inpatients. TH
Community Teaching
Halasyamani L, Valenstein P, Friedlander M. et al. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am J Med. 2005;118:536-543.
Background: A growing body of literature has demonstrated the effects of hospitalists on reducing inpatient length of stay and cost of care, with some literature showing a decreased in-hospital and 30-day mortality. However, most prior studies were conducted in academic medical centers or health maintenance organizations where one group of hospitalists, employed by the institution within which they worked, was compared with traditional primary care physicians. Direct comparisons between different hospitalist models practicing within a single institution have not been published. As a result, the impact of different hospitalist characteristics, including employment status and reimbursement incentives, on inpatient resource utilization and patient care outcomes is unknown.
Methods: Halasyamani and colleagues conducted a retrospective cohort study of 10,595 patients in a tertiary care community-based teaching hospital in which private hospitalists, academic hospitalists, and community physicians all practice. They measured risk-adjusted length of stay, variable costs, 30-day readmission rates, and in-hospital and 30-day mortality for patients treated by each of these three groups, controlling for potentially confounding variables. Community physicians belonged to 21 rounding groups, most of which were private or solo. Two of the community physicians groups were hospital-owned practices reimbursed by a relative value unit system. The private hospitalist group was self-employed with no financial relationship to the hospital and worked an average of 40 weeks per year. Community physicians and private hospitalists worked Monday-Friday and covered weekends or holidays about 25% of the time. Academic hospitalists worked with internal medicine residents and students on a teaching service. They were employed by the hospital using a relative value unit system. They worked an average of 14 weeks per year as an inpatient attending in half-month rotations, which included weekend coverage.
Results: There was a 20% reduction (-0.72 days absolute difference) in length of stay on the academic hospitalist service (P<0.0001) and 8% (-0.28 days absolute difference) on the private hospitalist service (P=0.049) compared with community physicians. Case-mix adjusted relative total costs were 10% less ($173 absolute difference) on the academic (P<0.0001) and 6% less ($109 absolute difference) on the private hospitalist services (P=0.02) compared with community physicians. There were no differences in 30-day readmission, in-hospital and 30-day mortality between the three groups.
Discussion: This study is the first to look at the effects of two separate hospitalist models on resource utilization and patient outcomes within the same institution. Although both the academic and private hospitalist groups demonstrated improved resource utilization as compared with the community physicians, the magnitude of benefit was much greater for the academic hospitalist group.
As the authors point out, one major difference between the two groups was employment status, with the academic hospitalists employed directly by the hospital and the private hospitalists receiving all payment directly from payers. Previous studies have also focused on hospitalists, which were employed by the institution at which they worked, raising the question of whether alignment of employee and employer incentives is an important factor affecting resource utilization outcomes.
Results of this study highlight the need for more studies which seek to clarify specific physician-level, group-level, and organization-level characteristics of hospitalists that result in improved resource utilization and patient care outcomes.
The Last Few Hours
Bailey FA, Burgio KL, Woodby LL, et al. Improving the processes of hospital care during the last hours of life. Arch Int Med. 2005;165(15):1722-1727.
Background: End-of-life care in the acute care inpatient setting is often not initiated until very late in the dying process and may be related to inadequate early recognition of dying patients as well as difficulty transitioning from disease-modifying treatments to palliative measures. Additional barriers exist, including lack of familiarity of hospital staff with initiation and implementation of hospice care. Education about end-of-life care and introduction of a physician-led palliative care team available for consultation within acute care hospitals may help promote better recognition of the dying patient by staff and allow for a “good death.”
Methods: A single hospital within the Veterans Affairs (VA) medical system (Birmingham, Ala., VA Medical Center) was chosen as a pilot center for initiation of a physician-led Inpatient Comfort Care Program (ICCP). The study was framed as a “before-after intervention trial” and analyzed all inpatient deaths identified by the Computerized Patient Recognition System during a six-month period before and substantially after the introduction of the ICCP. A structured chart abstraction tool was used and data was obtained from the last seven days of hospitalization analyzing variables associated with recognition of the dying patient and initiation of palliative care. Education of hospital staff on both hospice care and case identification was initiated during the intervention phase of the study. Additionally, a flexible comfort care order set was introduced.
Results: Two hundred and three veterans were identified (98% men, average age 68) and no significant differences in clinical characteristics were noted between the two groups, pre-intervention and post-intervention. Post-intervention, 59.3% of patients had formal palliative care consultation. Significant findings (P<0.01) following implementation of ICCP were increased documentation of end-of-life symptoms, increased documentation of care plans, increased utilization of opioids (57.1% to 87.2%), increased initiation of do-not-resuscitate orders (61.9% to 85.1%) with a concurrent decrease in cardiopulmonary resuscitation at death (34.4% to 15.4%), and a surprising increase in restraint use (6.0% to 22.6%).
Discussion: Data on hospice care patients indicate that 10% to 30% die in an acute care hospital, identifying a need for increased education and training in palliative medicine. This study demonstrates the positive outcomes of implementation of an inpatient palliative care service both for heightened awareness of identifying the dying patient as well as initiation of end-of-life care. The increased use of opioid medications is an important marker given that many patients experience pain and dyspnea at the end of life. This study is limited by its single site and further validation at other centers implementing similar protocols and assessing similar outcomes is needed. While this intervention had important clinical benefits, additional studies examining the cost implications of this system would be helpful.
Education alone has not been shown to be entirely effective in creating change. This single-site implementation of a palliative care consultation service successfully integrated an education program with on-site consultants. Distributing pocket cards with clinical findings identifying the dying patient aided in recognition of those patients and pre-printed order sets facilitated initiation of end-of-life care. The intervention initiated is possible for many medical centers and promotes an environment allowing for a “good death” for dying patients.
Computers, Doctors, and Errors
Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203
For physicians, computerized physician order entry (CPOE) has become an important topic of discussion as many hospitals and health systems embark on the complex and lengthy process of implementing new enterprise clinical systems. Though there are undoubtedly benefits to such systems, practicing clinicians are apt to remain skeptical of the grandiose pictures the more vocal advocates of CPOE may paint. This is not to say that the promises of CPOE are empty; to the contrary, there have been substantial successes, notably in the realm of medication error prevention.
At the same time, CPOE is a mixture of complex technologies that interface in complicated ways with the culture of clinical medicine. The view that medical informatics is a technical problem that has been solved long ago is simplistic and naïve. The article by Koppel, et al, has two important implications: 1) It is critical to look at clinical information systems in the social milieu in which it functions, and 2) there are often unintended consequences that may not beneficial.
This article examines a widely used, commercial CPOE system in use at the University of Pennsylvania (Philadelphia) using both quantitative and qualitative methods. The researchers conducted focus groups and expert interviews in addition to field observations of physicians (house officers and attendings), nurses, and pharmacists in order to identify themes relating to work with the order entry system. This work helped to guide the creation of a survey instrument subsequently used to survey house staff about working conditions and sources of error and stress. There was an 85%-90% response rate that primarily included house staff who ordered more than nine medication orders per month.
Researchers found two broad categories of errors that were fostered in this environment. The first category, which they termed “information errors” were generated by fragmentation of data and the failure to integrate the hospitals various systems both electronic and paper. Examples of this type of error include antibiotic renewal failures. A common way this failure would occur is that renewal reminder stickers would be placed in the patients’ charts, but the house staff would overlook these because medication orders occurred electronically. Another example is assumed dose errors, where house staff would assume that the default dose displayed was the recommended starting dose, when in fact this was the smallest dose unit available. Physicians were assuming decision support was available when it was not.
The second type of error, human-machine interface flaws, occurred when machine rules did not correspond to work behaviors. An example of this is when patients were listed alphabetically rather than by service, making it easy to select the wrong patient. In another instance, many screens (up to 20) were required to view all of a patient’s medications, making it difficult to choose a correct medication for editing.
This study has been criticized by industry advocates for focusing on an older set of technologies or because a number of these issues related to training or “user factors.” At the other extreme, this study has been cited as a cautionary tale about the risks of CPOE. Both types of criticism miss the point. This study demonstrates that CPOE and the social environment in which it sits is a complex entity and that careful design, proper support, and maintenance are critical ingredients to the success of an incredibly complex but vital new component of hospital medicine.
Point-of-Care HIV Testing in Inpatients
Lubelchek R, Kroc K, Hota B, et al. The role of rapid vs conventional human immunodeficiency virus testing for inpatients: effects on quality of care. Arch Intern Med. 2005;165:1956-1960.
Despite advances in treatment, infection with HIV and AIDS remains a public health problem in the United States. According to the CDC the rate of new diagnosis of HIV infection has remained steady from 2000 to 2003 at about 20 per 100,000 people. (Centers for Disease Control and Prevention. Diagnosis of HIV/AIDS–32 states, 2009-2003. MMWR Morb Mortal Wkly Rep. 2004;53:1106-1110). Currently, about 850,000 to 950,000 people are believed to be living with HIV infection, and it is estimated that 180,000 to 280,000 are unaware of their diagnosis. (Fleming P, Byers RH, Sweeney PA, et al., HIV prevalence in the United States, 2000 [Abstract 11]. Presented at the Ninth Conference on Retroviruses and Opportunistic Infections, Seattle; February 24–28, 2002). These patients are not only at risk for disease progression, but can undermine efforts at disease prevention if they continue to engage in unsafe activities. Thus, increasing awareness of HIV status is an important aspect of disease prevention.
HIV testing remains a challenge. Conventional testing with enzyme immunoassay (EIA) and confirmatory Western blot requires patient follow-up for results, which approximately 25% of patients in various outpatient testing sites fail to do. (Centers for Disease Control and Prevention. Update: HIV counseling and testing using rapid tests, United States, 1995. MMWR Morb Mortal Wkly Rep. 1998;47:211-215). Given the difficulties inherent in the transition of care from the inpatient to outpatient setting, conventional testing in the inpatient setting presents additional barriers to appropriate notification. As various point-of-care HIV tests have been developed for commercial use, the possibility of rapid HIV testing presents an opportunity to reduce notification failure and improve patient care. While not replacing traditional testing, the CDC has endorsed rapid HIV testing as a means to initiate therapy and provide counseling with a particular focus on preventing further disease transmission. In this retrospective study, Lubelchek and colleagues present the effects of a rapid HIV test utilized in the emergency department on various inpatient quality of care measures for those patients who received a positive rapid HIV test later confirmed by Western blot as compared with those patients who were diagnosed after admission by traditional diagnostic methods. This study took place in the context of CDC-funded study of the use of OraQuick (OraSure Technologies, Bethlehem, Pa.) rapid HIV testing in the emergency department at Cook County Hospital in Chicago.
The manufacturer claims the product has a sensitivity of 99.6% and a specificity of 100% as compared with conventional testing. (OraQuick rapid HIV-1 antibody test summary of safety and effectiveness. November 7, 2002. Accessed October 1, 2005, at www.fda.gov/cber/pma/P010047.htm). In the initial study, two of the three emergency department’s treatment pods were equipped to provide HIV screening utilizing the point-of-care technology to consenting patients. Patients in the third pod could be referred to rapid testing based on symptoms or risk factors. All patients who received the rapid test also submitted specimens for conventional EIA and confirmatory Western blot testing. All positive rapid HIV tests were confirmed by Western blot.
In this study, patients who were not known to be infected and were subsequently admitted on non-obstetric or surgical services over 17 months from 2003 to 2004 and confirmed to be HIV positive by Western blot were identified utilizing administrative records. Where possible, charts were reviewed to confirm no prior diagnosis of HIV. Patients who received rapid HIV testing were compared with those who only received conventional testing. Endpoints included time to primary inpatient care service awareness of HIV diagnosis, time to admission or transfer to the inpatient HIV service, time to empiric treatment of diagnosis of opportunistic infection, length of stay, discharge with appropriate prophylactic medications, discharge with patient knowledge of HIV diagnosis, and initial engagement in outpatient care. Length of stay was adjusted by multivariate regression on co-morbid diagnoses (congestive heart failure, end-stage renal disease, cirrhosis, chronic obstructive pulmonary disease, and diabetes), opportunistic infections, ICU admission, need for mechanical ventilation, and CD4 count.
A total of 103 patients were identified with complete chart review completed on 86 of them. All patients except one were admitted through the emergency department. Forty-eight patients were diagnosed initially with the rapid HIV test with 58% of these specifically referred for testing by the emergency department physician, and 55 were diagnosed with conventional testing. Overall, 78% were male, 62% African American, and 20% Hispanic. The two groups were comparable in terms of age, sex, ethnicity, history of substance abuse, HIV risk factors, psychiatric diagnoses, homelessness, CD4 count, presence of opportunistic infections, mechanical ventilation, and co-morbidities. However, conventionally tested patients were more likely to require an ICU stay (31% vs. 10%, P=.01).
Patients in the rapid test group were more quickly documented in the chart as having HIV (.8 vs. 6.4 days, p<.001), placed on an HIV service sooner (1.4 versus 6.9 days, P<.001), initiated outpatient follow-up sooner (21.5 versus 49.5 days, p=.05), and had less unawareness of their HIV status (0 vs. 16%, P=.002). There was no significant difference between the two groups in time from admission to empiric treatment or diagnosis of an opportunistic infection. Patients who received the rapid test did have a lower length of stay (6.4 versus 13.2 days, P<.001). Although much of this difference was due to higher number of ICU stays in the conventional group, in multivariate analysis conventional testing still increased length of stay significantly, OR 5.4 days (2.5, 8.3).
This study suggests that patients who are tested with rapid HIV testing can lead to more efficient inpatient treatment of the complications of HIV, improved patient awareness of HIV status, and quicker outpatient follow-up. These findings have ramifications not just to the inpatient management of patients with HIV but to general public health efforts to reduce the spread of HIV infection.
Nevertheless, these results must be interpreted with caution. They reflect the experience of one institution situated in an area with a high prevalence of HIV. Some degree of selection bias is suggested by the higher presence of ICU admissions in the conventional testing group. The multivariate analysis attempted to control for confounding factors, but the possibility remains that other unrecognized factors may have influenced results. The authors do note that an analysis of patients in the rapid test group stratified by whether the test was performed for screening or by referral of the physician did not demonstrate a statistically significant difference in length of stay. This finding provides further support that the sicker patients which triggered the rapid test had shorter lengths of stay on account of the rapid test and not simply because they were sicker.
As recognized by the authors, physicians in routine practice rely on surrogate markers of HIV infection, most notably a patient’s CD4 count, and thus it is not surprising that the rapid test did not affect time to empiric treatment or diagnosis of opportunistic infection. If treatment did not differ, then explaining the longer length of stay remains an unexplained puzzle. The fact that the two groups were equally matched socially and psychiatrically leaves open the possibility that it was actual knowledge of the HIV test result—and not its effect on treatment—that drove the longer length of stay.
One possibility not suggested by the authors is that definitive knowledge of HIV status helped to mobilize patient discharge. If there were legitimate concerns of follow-up, physicians may have delayed discharge in order to receive HIV test results. Alternatively, some patients may have resisted discharge until receiving test results and the development of a more concrete plan. It would be interesting to know if the time to follow-up for the two groups would be the same if the 16% who did not know their HIV status at discharge were excluded. This suggests that knowledge of HIV status drives follow-up time and would lend some support to the notion that patient discharge was delayed for test results and clarification of the follow-up treatment plan.
Even putting aside the difference in length of stay, the difference of rapid testing on improved knowledge of HIV status and quicker follow-up is likely real and meaningful. Although this study was not designed to assess the impact of this knowledge on patient behavior, immediate knowledge of HIV status during hospitalization may translate to decreased transmission as patients alter their behavior and lends further credibility to the utility of rapid HIV testing in conjunction with conventional methods in the management of inpatients. TH
The Constant and Familiar Face
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”

—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”
—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”
—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
An Itchy Neck
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:

- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.

This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
Quality Will Be Job One

One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
Vacationing vs. abandoning
Hospitalized patient hangs himself; estate blames vacationing psychiatrist
Los Angeles County (CA) Superior Court
Police took a 34-year-old man to an inpatient psychiatric facility after they found him walking naked on a city street. The hospital admitted him on a 72-hour involuntary hold because of his suicidal thoughts, although the psychiatrist did not believe he intended to kill himself. The patient had never attempted suicide before. The psychiatrist ordered treatment with risperidone and monitoring every 30 minutes.
Two days later, at the beginning of the psychiatrist’s vacation, the hospital started a 14-day hold process. After 3 days, the on-call psychiatrist documented the patient’s refusal to communicate and take medication, but the patient denied suicidal thinking.
After 3 more days, staff discovered the patient sitting unconscious on the floor next to the toilet, with his pants wrapped around his neck and tied to a grab bar. Staff attempted cardiopulmonary resuscitation and called paramedics, but the patient was dead.
The patient’s estate claimed that the hospital and first treating psychiatrist did not take appropriate measures to prevent the suicide. It charged the hospital with negligence in failing to have a breakaway grab bar and claimed the original psychiatrist did not adequately communicate the patient’s status with the covering psychiatrist before leaving on vacation.
The defense claimed the patient was not at high risk for suicide and that the standard of care is to communicate information regarding high-risk patients to the covering psychiatrist. The original psychiatrist also claimed the patient was doing well when he left for vacation.
- The jury decided for the defense
Dr. Grant’s observations
Patients and their families may feel abandoned in their psychiatrists’ absence. But this absence does not legally constitute abandonment unless:
- a doctor-patient relationship exists
- the doctor terminates the relationship
- there is a need for continuing care
- termination lacks reasonable notice so arrangements for continuing care cannot be made.
- Ensure that a system for getting urgent information to covering psychiatrists is in place.
- Verify that the covering psychiatrist knows he or she is responsible for your patients in emergency distress—including interviewing, reviewing records, and documenting treatment. His or her role is not just to fill space until you return.
- Tell emergency-prone patients the dates you’ll be unavailable and give them the contact information for the covering psychiatrist.
- Inform the covering psychiatrist about patients at high risk for suicide, decompensation, or hospitalization.
While travel is at times necessary, psychiatrists must ensure that emergency-prone patients have access to care in their absence (Box). You can delegate this responsibility to a covering psychiatrist, but choose him or her wisely. Selecting a physician you know is incapable of providing sound treatment is considered negligent. The primary psychiatrist cannot be held responsible for a substitute psychiatrist’s negligence if the choice of substitute is viewed as a competent delegation.
Cases are selected by Current Psychiatry's editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Hospitalized patient hangs himself; estate blames vacationing psychiatrist
Los Angeles County (CA) Superior Court
Police took a 34-year-old man to an inpatient psychiatric facility after they found him walking naked on a city street. The hospital admitted him on a 72-hour involuntary hold because of his suicidal thoughts, although the psychiatrist did not believe he intended to kill himself. The patient had never attempted suicide before. The psychiatrist ordered treatment with risperidone and monitoring every 30 minutes.
Two days later, at the beginning of the psychiatrist’s vacation, the hospital started a 14-day hold process. After 3 days, the on-call psychiatrist documented the patient’s refusal to communicate and take medication, but the patient denied suicidal thinking.
After 3 more days, staff discovered the patient sitting unconscious on the floor next to the toilet, with his pants wrapped around his neck and tied to a grab bar. Staff attempted cardiopulmonary resuscitation and called paramedics, but the patient was dead.
The patient’s estate claimed that the hospital and first treating psychiatrist did not take appropriate measures to prevent the suicide. It charged the hospital with negligence in failing to have a breakaway grab bar and claimed the original psychiatrist did not adequately communicate the patient’s status with the covering psychiatrist before leaving on vacation.
The defense claimed the patient was not at high risk for suicide and that the standard of care is to communicate information regarding high-risk patients to the covering psychiatrist. The original psychiatrist also claimed the patient was doing well when he left for vacation.
- The jury decided for the defense
Dr. Grant’s observations
Patients and their families may feel abandoned in their psychiatrists’ absence. But this absence does not legally constitute abandonment unless:
- a doctor-patient relationship exists
- the doctor terminates the relationship
- there is a need for continuing care
- termination lacks reasonable notice so arrangements for continuing care cannot be made.
- Ensure that a system for getting urgent information to covering psychiatrists is in place.
- Verify that the covering psychiatrist knows he or she is responsible for your patients in emergency distress—including interviewing, reviewing records, and documenting treatment. His or her role is not just to fill space until you return.
- Tell emergency-prone patients the dates you’ll be unavailable and give them the contact information for the covering psychiatrist.
- Inform the covering psychiatrist about patients at high risk for suicide, decompensation, or hospitalization.
While travel is at times necessary, psychiatrists must ensure that emergency-prone patients have access to care in their absence (Box). You can delegate this responsibility to a covering psychiatrist, but choose him or her wisely. Selecting a physician you know is incapable of providing sound treatment is considered negligent. The primary psychiatrist cannot be held responsible for a substitute psychiatrist’s negligence if the choice of substitute is viewed as a competent delegation.
Hospitalized patient hangs himself; estate blames vacationing psychiatrist
Los Angeles County (CA) Superior Court
Police took a 34-year-old man to an inpatient psychiatric facility after they found him walking naked on a city street. The hospital admitted him on a 72-hour involuntary hold because of his suicidal thoughts, although the psychiatrist did not believe he intended to kill himself. The patient had never attempted suicide before. The psychiatrist ordered treatment with risperidone and monitoring every 30 minutes.
Two days later, at the beginning of the psychiatrist’s vacation, the hospital started a 14-day hold process. After 3 days, the on-call psychiatrist documented the patient’s refusal to communicate and take medication, but the patient denied suicidal thinking.
After 3 more days, staff discovered the patient sitting unconscious on the floor next to the toilet, with his pants wrapped around his neck and tied to a grab bar. Staff attempted cardiopulmonary resuscitation and called paramedics, but the patient was dead.
The patient’s estate claimed that the hospital and first treating psychiatrist did not take appropriate measures to prevent the suicide. It charged the hospital with negligence in failing to have a breakaway grab bar and claimed the original psychiatrist did not adequately communicate the patient’s status with the covering psychiatrist before leaving on vacation.
The defense claimed the patient was not at high risk for suicide and that the standard of care is to communicate information regarding high-risk patients to the covering psychiatrist. The original psychiatrist also claimed the patient was doing well when he left for vacation.
- The jury decided for the defense
Dr. Grant’s observations
Patients and their families may feel abandoned in their psychiatrists’ absence. But this absence does not legally constitute abandonment unless:
- a doctor-patient relationship exists
- the doctor terminates the relationship
- there is a need for continuing care
- termination lacks reasonable notice so arrangements for continuing care cannot be made.
- Ensure that a system for getting urgent information to covering psychiatrists is in place.
- Verify that the covering psychiatrist knows he or she is responsible for your patients in emergency distress—including interviewing, reviewing records, and documenting treatment. His or her role is not just to fill space until you return.
- Tell emergency-prone patients the dates you’ll be unavailable and give them the contact information for the covering psychiatrist.
- Inform the covering psychiatrist about patients at high risk for suicide, decompensation, or hospitalization.
While travel is at times necessary, psychiatrists must ensure that emergency-prone patients have access to care in their absence (Box). You can delegate this responsibility to a covering psychiatrist, but choose him or her wisely. Selecting a physician you know is incapable of providing sound treatment is considered negligent. The primary psychiatrist cannot be held responsible for a substitute psychiatrist’s negligence if the choice of substitute is viewed as a competent delegation.
Cases are selected by Current Psychiatry's editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Cases are selected by Current Psychiatry's editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.