User login
A Midwest Partnership
Quite likely things are different in Minnesota than they are on either coast. People are polite, know how to work together, and are respectful about consuming resources. Or as Tom Anderson, MD, a HealthPartners Medical Group (HPMG) hospitalist says: “In Minnesota affable usually beats good.” Fortunately, the 25 physician members of the hospitalist team who belong to the 580-member HPMG, are beyond affable and good. By many measures they are excellent, and they are shaping the field of hospital medicine.
At the heart of the HPMG hospitalist program’s quality are its people. Burke Kealey, MD, HPMG’s assistant medical director, helped start the program in 1997, recruiting young, energetic, and personable physicians who liked practicing big city hospital medicine, Midwestern style. “Our hospitalist program was one of the early ones operating before the term ‘hospitalist’ was well-known,” says Dr. Kealey.
The hospitalists are employed neither by an academic medical nor a community hospital. Instead, they are members of a 580-multispecialty physician group that anchors HealthPartners Network, an organization that consistently ranks among The National Committee for Quality Assurance’s (NCQA) top five health plans regionally and top 10 nationally. Yet excellence has its price, as the perverse incentives of the U.S. healthcare system reveal. Mary Brainerd, HealthPartner’s CEO, comments that although the company consistently ranks high, it gets paid thousands of dollars less per patient by Medicare than poor performing plans.
“The way Medicare is set up, it actually punishes you for being good,” says Brainerd, referring to Medicare’s rules that qualify hospitals to receive additional payments each time a patient returns for more treatment—even if their return was caused by sub-par diagnosis and treatment. Under Medicare’s incentives, hospitals and doctors who order unnecessary tests, provide poor care, or even make patients worse often receive higher payments than those who provide efficient, high-quality care. That doesn’t stop HPMG from doing things correctly.
With the physician group employing both clinic and inpatient physicians, it’s more straightforward getting metrics and incentives aligned than in a healthcare environment where the outpatient physician’s loss may be the hospitalist’s gain—or vice versa. “Working closely with clinic and ER doctors decreases length of stay, improves clinical outcomes, and decreases costs,” says Dr. Kealey. “That helps the whole medical group.”
Another major contributor to clinical excellence goes beyond HPMG. Using the Minnesota mindset, HPMG’s physicians work with the area’s other medical heavyweights, the Mayo Clinic (Rochester, Minn.) and the Allina Medical Group (Minneapolis), forging a consensus on best practices and evidence-based guidelines (www.icsi.org). An example of HPMG’s outpatient and inpatient physician collaboration is their approach to CHF. After both groups tackled the job of operationalizing “perfect” CHF care in a one-day Rapid Design Workshop, “perfect treatment” outcomes rose from 22% in January 2005 to 50% in March 2005.
Nuts and Bolts
Scheduling logistics is among the challenges a hospitalist program’s manager faces, and Dr. Kealey and his colleagues have—through experience—done well. Each hospitalist selects a block schedule (either one week on, one week off or 14 days straight for 24 weeks). They also serve two night shift weeks (6 p.m.—8 a.m.), although residents run things at night. Hospitalists reconfigure their schedules every six months, helping to avoid burnout. Geographic deployment is another energy saver. Each hospitalist works in one or two units, allowing them to know patients, family, and the nursing staff well. It also cuts the nine-story hospital down to a size.
To communicate effectively, physicians use electronic technology. Voice pagers connect all HPMG physicians. Other devices sound alerts, allow for co-management of patients with chronic diseases, quick referrals to specialists within the group, in-box messaging, and a discharge summary to the primary physician in six to eight hours.
As for compensation, physicians receive a base salary, set at 80% of SHM’s annual average for the Midwest, accounting for 65% of pay. Of the balance, productivity as measured by relative value units (RVUs) accounts for 40%, with 20% each for high marks on patient and provider satisfaction surveys, and the medical director’s discretion.
Myriad Opportunities
The HPMG hospitalist program offers opportunities to pursue many professional paths, as its SHM award roster shows. SHM’s Award for Outstanding Service in Clinical Medicine to HPMG Hospitalists have included:
- 2002 Rusty Holman, Outstanding Service in Hospital Medicine;
- 2003 Burke Kealey, Clinical Excellence; and
- 2005 Shaun Frost, Clinical Excellence.
Adding depth to the program involves embracing physicians on unusual career paths, such as Tom Anderson, MD, one of HPMG’s family practice hospitalists. After finishing training at Ramsey County Hospital of St. Paul, Minn., which became Regions Hospital in 1997 (and where Dr. Kealey also trained), Dr. Anderson joined a seven-doctor rural practice in Iron Range, Wis.
“It was in a hard-working blue collar town, and we were throwbacks,” says Dr. Anderson, “doing all our own obstetrics, covering the ER, helping surgeons. I was a real person in that community. Everyone knew each other from the church or hardware store.” If the doctors wanted to change anything, they talked over doughnuts and coffee, deciding how it would affect them and their patients. Dr. Anderson loved the work, but wanted more family time than the all-consuming rural practice allowed.
A recruiting call from Dr. Kealey changed everything. Dr. Kealey calls Dr. Anderson “a bright and shining star, someone who sits in the front row and asks all the questions.”
Dr. Anderson joined HPMG’s hospitalist team in 2004, enjoying the one-week-on/one-week-off schedule and the continuity of care afforded by a large team. “This is a big busy hospital,” he says. “The patients are really sick, and we plan our 12-hour shift around them.” He starts with a 7 a.m. huddle of nurses and physicians to plan the day by prioritizing patient needs, reviewing orders, arranging time to talk to specialists, and visiting all patients. “By 9 a.m. we’ve planned the day, including 3 p.m. patient discharges. I like prioritizing what has to be done, and defining what has to be fixed.”
Rick Hilger, MD, board certified in internal medicine and pediatrics, is on another mission. After residency at the University of Minnesota Medical School (Duluth), he became Regions Hospital’s chief resident and then stayed on. He wanted a pediatrics hospitalist practice, which proved impractical because 95% of Regions’ pediatric cases now go to another hospital. “Down the line I’d like a 50/50 adult/peds mix, but that’s hard to accomplish in a hospitalist program,” he says.
Still looking for a challenge, Dr. Hilger chose the Institute for Healthcare Improvement’s “100K Lives” initiative, becoming the lead physician for Region’s rapid response team to prevent unnecessary code-blue calls. With the hospitalists’ geographic deployment to specific units that meant planning who would respond to codes and how that would be communicated. Dr. Hilger encouraged administration to hire full-time employees to field a rapid response team and created a pre-code team.
“At least 30%-40% of patients code outside the ICU,” he says. “We’ve observed that they often have unstable vital signs six to eight hours before coding. We’ve cut through administrative minutiae and red tape so that patients don’t sit there with unstable vitals for long.”
The pre-code team—an ICU trained nurse and respiratory therapist—are alerted to those signs and respond in five minutes or less, 24/7. The rest of the team is alerted via pagers, with hospitalists fielding an average of three calls per day.
Other hospitalists find their special niches. Shaun Frost, MD, is breaking ground in peri-surgical care in orthopedics, urology and neurology, and is active in process improvement teams. Howard Epstein, MD, leads the palliative care team, while John Degelau, MD, chief of hospital medical at North Memorial, pursues his interest in geriatrics. Rich Mahr, MD, is the physician champion for electronic health records.
So being an HPMG hospitalist allows physicians to pursue many avenues of clinical and process improvement, including national initiatives and teaching. Dr. Anderson sums up what HPMG is about: “I joined this group because of its passion for medicine. When we get older we’ll look back and say that we had our moment, our time to give it 100%.”
Dr. Kealey calls them “an energized creative group. Everyone wants to go to national meetings and to keep ahead of the pack, to ask what’s next to learn?” TH
Writer Marlene Piturro regularly writes practice profiles for The Hospitalist.
Quite likely things are different in Minnesota than they are on either coast. People are polite, know how to work together, and are respectful about consuming resources. Or as Tom Anderson, MD, a HealthPartners Medical Group (HPMG) hospitalist says: “In Minnesota affable usually beats good.” Fortunately, the 25 physician members of the hospitalist team who belong to the 580-member HPMG, are beyond affable and good. By many measures they are excellent, and they are shaping the field of hospital medicine.
At the heart of the HPMG hospitalist program’s quality are its people. Burke Kealey, MD, HPMG’s assistant medical director, helped start the program in 1997, recruiting young, energetic, and personable physicians who liked practicing big city hospital medicine, Midwestern style. “Our hospitalist program was one of the early ones operating before the term ‘hospitalist’ was well-known,” says Dr. Kealey.
The hospitalists are employed neither by an academic medical nor a community hospital. Instead, they are members of a 580-multispecialty physician group that anchors HealthPartners Network, an organization that consistently ranks among The National Committee for Quality Assurance’s (NCQA) top five health plans regionally and top 10 nationally. Yet excellence has its price, as the perverse incentives of the U.S. healthcare system reveal. Mary Brainerd, HealthPartner’s CEO, comments that although the company consistently ranks high, it gets paid thousands of dollars less per patient by Medicare than poor performing plans.
“The way Medicare is set up, it actually punishes you for being good,” says Brainerd, referring to Medicare’s rules that qualify hospitals to receive additional payments each time a patient returns for more treatment—even if their return was caused by sub-par diagnosis and treatment. Under Medicare’s incentives, hospitals and doctors who order unnecessary tests, provide poor care, or even make patients worse often receive higher payments than those who provide efficient, high-quality care. That doesn’t stop HPMG from doing things correctly.
With the physician group employing both clinic and inpatient physicians, it’s more straightforward getting metrics and incentives aligned than in a healthcare environment where the outpatient physician’s loss may be the hospitalist’s gain—or vice versa. “Working closely with clinic and ER doctors decreases length of stay, improves clinical outcomes, and decreases costs,” says Dr. Kealey. “That helps the whole medical group.”
Another major contributor to clinical excellence goes beyond HPMG. Using the Minnesota mindset, HPMG’s physicians work with the area’s other medical heavyweights, the Mayo Clinic (Rochester, Minn.) and the Allina Medical Group (Minneapolis), forging a consensus on best practices and evidence-based guidelines (www.icsi.org). An example of HPMG’s outpatient and inpatient physician collaboration is their approach to CHF. After both groups tackled the job of operationalizing “perfect” CHF care in a one-day Rapid Design Workshop, “perfect treatment” outcomes rose from 22% in January 2005 to 50% in March 2005.
Nuts and Bolts
Scheduling logistics is among the challenges a hospitalist program’s manager faces, and Dr. Kealey and his colleagues have—through experience—done well. Each hospitalist selects a block schedule (either one week on, one week off or 14 days straight for 24 weeks). They also serve two night shift weeks (6 p.m.—8 a.m.), although residents run things at night. Hospitalists reconfigure their schedules every six months, helping to avoid burnout. Geographic deployment is another energy saver. Each hospitalist works in one or two units, allowing them to know patients, family, and the nursing staff well. It also cuts the nine-story hospital down to a size.
To communicate effectively, physicians use electronic technology. Voice pagers connect all HPMG physicians. Other devices sound alerts, allow for co-management of patients with chronic diseases, quick referrals to specialists within the group, in-box messaging, and a discharge summary to the primary physician in six to eight hours.
As for compensation, physicians receive a base salary, set at 80% of SHM’s annual average for the Midwest, accounting for 65% of pay. Of the balance, productivity as measured by relative value units (RVUs) accounts for 40%, with 20% each for high marks on patient and provider satisfaction surveys, and the medical director’s discretion.
Myriad Opportunities
The HPMG hospitalist program offers opportunities to pursue many professional paths, as its SHM award roster shows. SHM’s Award for Outstanding Service in Clinical Medicine to HPMG Hospitalists have included:
- 2002 Rusty Holman, Outstanding Service in Hospital Medicine;
- 2003 Burke Kealey, Clinical Excellence; and
- 2005 Shaun Frost, Clinical Excellence.
Adding depth to the program involves embracing physicians on unusual career paths, such as Tom Anderson, MD, one of HPMG’s family practice hospitalists. After finishing training at Ramsey County Hospital of St. Paul, Minn., which became Regions Hospital in 1997 (and where Dr. Kealey also trained), Dr. Anderson joined a seven-doctor rural practice in Iron Range, Wis.
“It was in a hard-working blue collar town, and we were throwbacks,” says Dr. Anderson, “doing all our own obstetrics, covering the ER, helping surgeons. I was a real person in that community. Everyone knew each other from the church or hardware store.” If the doctors wanted to change anything, they talked over doughnuts and coffee, deciding how it would affect them and their patients. Dr. Anderson loved the work, but wanted more family time than the all-consuming rural practice allowed.
A recruiting call from Dr. Kealey changed everything. Dr. Kealey calls Dr. Anderson “a bright and shining star, someone who sits in the front row and asks all the questions.”
Dr. Anderson joined HPMG’s hospitalist team in 2004, enjoying the one-week-on/one-week-off schedule and the continuity of care afforded by a large team. “This is a big busy hospital,” he says. “The patients are really sick, and we plan our 12-hour shift around them.” He starts with a 7 a.m. huddle of nurses and physicians to plan the day by prioritizing patient needs, reviewing orders, arranging time to talk to specialists, and visiting all patients. “By 9 a.m. we’ve planned the day, including 3 p.m. patient discharges. I like prioritizing what has to be done, and defining what has to be fixed.”
Rick Hilger, MD, board certified in internal medicine and pediatrics, is on another mission. After residency at the University of Minnesota Medical School (Duluth), he became Regions Hospital’s chief resident and then stayed on. He wanted a pediatrics hospitalist practice, which proved impractical because 95% of Regions’ pediatric cases now go to another hospital. “Down the line I’d like a 50/50 adult/peds mix, but that’s hard to accomplish in a hospitalist program,” he says.
Still looking for a challenge, Dr. Hilger chose the Institute for Healthcare Improvement’s “100K Lives” initiative, becoming the lead physician for Region’s rapid response team to prevent unnecessary code-blue calls. With the hospitalists’ geographic deployment to specific units that meant planning who would respond to codes and how that would be communicated. Dr. Hilger encouraged administration to hire full-time employees to field a rapid response team and created a pre-code team.
“At least 30%-40% of patients code outside the ICU,” he says. “We’ve observed that they often have unstable vital signs six to eight hours before coding. We’ve cut through administrative minutiae and red tape so that patients don’t sit there with unstable vitals for long.”
The pre-code team—an ICU trained nurse and respiratory therapist—are alerted to those signs and respond in five minutes or less, 24/7. The rest of the team is alerted via pagers, with hospitalists fielding an average of three calls per day.
Other hospitalists find their special niches. Shaun Frost, MD, is breaking ground in peri-surgical care in orthopedics, urology and neurology, and is active in process improvement teams. Howard Epstein, MD, leads the palliative care team, while John Degelau, MD, chief of hospital medical at North Memorial, pursues his interest in geriatrics. Rich Mahr, MD, is the physician champion for electronic health records.
So being an HPMG hospitalist allows physicians to pursue many avenues of clinical and process improvement, including national initiatives and teaching. Dr. Anderson sums up what HPMG is about: “I joined this group because of its passion for medicine. When we get older we’ll look back and say that we had our moment, our time to give it 100%.”
Dr. Kealey calls them “an energized creative group. Everyone wants to go to national meetings and to keep ahead of the pack, to ask what’s next to learn?” TH
Writer Marlene Piturro regularly writes practice profiles for The Hospitalist.
Quite likely things are different in Minnesota than they are on either coast. People are polite, know how to work together, and are respectful about consuming resources. Or as Tom Anderson, MD, a HealthPartners Medical Group (HPMG) hospitalist says: “In Minnesota affable usually beats good.” Fortunately, the 25 physician members of the hospitalist team who belong to the 580-member HPMG, are beyond affable and good. By many measures they are excellent, and they are shaping the field of hospital medicine.
At the heart of the HPMG hospitalist program’s quality are its people. Burke Kealey, MD, HPMG’s assistant medical director, helped start the program in 1997, recruiting young, energetic, and personable physicians who liked practicing big city hospital medicine, Midwestern style. “Our hospitalist program was one of the early ones operating before the term ‘hospitalist’ was well-known,” says Dr. Kealey.
The hospitalists are employed neither by an academic medical nor a community hospital. Instead, they are members of a 580-multispecialty physician group that anchors HealthPartners Network, an organization that consistently ranks among The National Committee for Quality Assurance’s (NCQA) top five health plans regionally and top 10 nationally. Yet excellence has its price, as the perverse incentives of the U.S. healthcare system reveal. Mary Brainerd, HealthPartner’s CEO, comments that although the company consistently ranks high, it gets paid thousands of dollars less per patient by Medicare than poor performing plans.
“The way Medicare is set up, it actually punishes you for being good,” says Brainerd, referring to Medicare’s rules that qualify hospitals to receive additional payments each time a patient returns for more treatment—even if their return was caused by sub-par diagnosis and treatment. Under Medicare’s incentives, hospitals and doctors who order unnecessary tests, provide poor care, or even make patients worse often receive higher payments than those who provide efficient, high-quality care. That doesn’t stop HPMG from doing things correctly.
With the physician group employing both clinic and inpatient physicians, it’s more straightforward getting metrics and incentives aligned than in a healthcare environment where the outpatient physician’s loss may be the hospitalist’s gain—or vice versa. “Working closely with clinic and ER doctors decreases length of stay, improves clinical outcomes, and decreases costs,” says Dr. Kealey. “That helps the whole medical group.”
Another major contributor to clinical excellence goes beyond HPMG. Using the Minnesota mindset, HPMG’s physicians work with the area’s other medical heavyweights, the Mayo Clinic (Rochester, Minn.) and the Allina Medical Group (Minneapolis), forging a consensus on best practices and evidence-based guidelines (www.icsi.org). An example of HPMG’s outpatient and inpatient physician collaboration is their approach to CHF. After both groups tackled the job of operationalizing “perfect” CHF care in a one-day Rapid Design Workshop, “perfect treatment” outcomes rose from 22% in January 2005 to 50% in March 2005.
Nuts and Bolts
Scheduling logistics is among the challenges a hospitalist program’s manager faces, and Dr. Kealey and his colleagues have—through experience—done well. Each hospitalist selects a block schedule (either one week on, one week off or 14 days straight for 24 weeks). They also serve two night shift weeks (6 p.m.—8 a.m.), although residents run things at night. Hospitalists reconfigure their schedules every six months, helping to avoid burnout. Geographic deployment is another energy saver. Each hospitalist works in one or two units, allowing them to know patients, family, and the nursing staff well. It also cuts the nine-story hospital down to a size.
To communicate effectively, physicians use electronic technology. Voice pagers connect all HPMG physicians. Other devices sound alerts, allow for co-management of patients with chronic diseases, quick referrals to specialists within the group, in-box messaging, and a discharge summary to the primary physician in six to eight hours.
As for compensation, physicians receive a base salary, set at 80% of SHM’s annual average for the Midwest, accounting for 65% of pay. Of the balance, productivity as measured by relative value units (RVUs) accounts for 40%, with 20% each for high marks on patient and provider satisfaction surveys, and the medical director’s discretion.
Myriad Opportunities
The HPMG hospitalist program offers opportunities to pursue many professional paths, as its SHM award roster shows. SHM’s Award for Outstanding Service in Clinical Medicine to HPMG Hospitalists have included:
- 2002 Rusty Holman, Outstanding Service in Hospital Medicine;
- 2003 Burke Kealey, Clinical Excellence; and
- 2005 Shaun Frost, Clinical Excellence.
Adding depth to the program involves embracing physicians on unusual career paths, such as Tom Anderson, MD, one of HPMG’s family practice hospitalists. After finishing training at Ramsey County Hospital of St. Paul, Minn., which became Regions Hospital in 1997 (and where Dr. Kealey also trained), Dr. Anderson joined a seven-doctor rural practice in Iron Range, Wis.
“It was in a hard-working blue collar town, and we were throwbacks,” says Dr. Anderson, “doing all our own obstetrics, covering the ER, helping surgeons. I was a real person in that community. Everyone knew each other from the church or hardware store.” If the doctors wanted to change anything, they talked over doughnuts and coffee, deciding how it would affect them and their patients. Dr. Anderson loved the work, but wanted more family time than the all-consuming rural practice allowed.
A recruiting call from Dr. Kealey changed everything. Dr. Kealey calls Dr. Anderson “a bright and shining star, someone who sits in the front row and asks all the questions.”
Dr. Anderson joined HPMG’s hospitalist team in 2004, enjoying the one-week-on/one-week-off schedule and the continuity of care afforded by a large team. “This is a big busy hospital,” he says. “The patients are really sick, and we plan our 12-hour shift around them.” He starts with a 7 a.m. huddle of nurses and physicians to plan the day by prioritizing patient needs, reviewing orders, arranging time to talk to specialists, and visiting all patients. “By 9 a.m. we’ve planned the day, including 3 p.m. patient discharges. I like prioritizing what has to be done, and defining what has to be fixed.”
Rick Hilger, MD, board certified in internal medicine and pediatrics, is on another mission. After residency at the University of Minnesota Medical School (Duluth), he became Regions Hospital’s chief resident and then stayed on. He wanted a pediatrics hospitalist practice, which proved impractical because 95% of Regions’ pediatric cases now go to another hospital. “Down the line I’d like a 50/50 adult/peds mix, but that’s hard to accomplish in a hospitalist program,” he says.
Still looking for a challenge, Dr. Hilger chose the Institute for Healthcare Improvement’s “100K Lives” initiative, becoming the lead physician for Region’s rapid response team to prevent unnecessary code-blue calls. With the hospitalists’ geographic deployment to specific units that meant planning who would respond to codes and how that would be communicated. Dr. Hilger encouraged administration to hire full-time employees to field a rapid response team and created a pre-code team.
“At least 30%-40% of patients code outside the ICU,” he says. “We’ve observed that they often have unstable vital signs six to eight hours before coding. We’ve cut through administrative minutiae and red tape so that patients don’t sit there with unstable vitals for long.”
The pre-code team—an ICU trained nurse and respiratory therapist—are alerted to those signs and respond in five minutes or less, 24/7. The rest of the team is alerted via pagers, with hospitalists fielding an average of three calls per day.
Other hospitalists find their special niches. Shaun Frost, MD, is breaking ground in peri-surgical care in orthopedics, urology and neurology, and is active in process improvement teams. Howard Epstein, MD, leads the palliative care team, while John Degelau, MD, chief of hospital medical at North Memorial, pursues his interest in geriatrics. Rich Mahr, MD, is the physician champion for electronic health records.
So being an HPMG hospitalist allows physicians to pursue many avenues of clinical and process improvement, including national initiatives and teaching. Dr. Anderson sums up what HPMG is about: “I joined this group because of its passion for medicine. When we get older we’ll look back and say that we had our moment, our time to give it 100%.”
Dr. Kealey calls them “an energized creative group. Everyone wants to go to national meetings and to keep ahead of the pack, to ask what’s next to learn?” TH
Writer Marlene Piturro regularly writes practice profiles for The Hospitalist.
Like Mortar and Pestle

Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. Each installment of “Alliances” provides valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
At the bedside or in committee, hospitalists are earning high marks from their pharmacist colleagues for their flexibility, approachability, and availability. By most accounts, hospitalists make the job of hospital pharmacists much easier, say the clinical pharmacists whom The Hospitalist recently interviewed—two from large university teaching hospitals and one from a community-based for-profit facility. In fact, attempts to extricate even constructive recommendations for hospitalists from these PharmDs proved fruitless.
“I think they do just about everything right,” says Tom Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California San Francisco Medical Center and a clinical professor of pharmacy at the UCSF School of Medicine. “I don’t find any fault with them.”
On the unit and in policy and procedure committee meetings, say the sources interviewed for this article, hospitalists develop good rapport with other staff members, address problems promptly, and are committed to improving processes for staff and patients alike.
Strengths of Hospitalists
As a clinical pharmacy specialist in general medicine on floor 15 at Brigham and Women’s Hospital (BWH) (Boston), Stephanie A. Wahlstrom, PharmD BCPS, begins rounds with the clinical team at 8 a.m. The group—typically consisting of Dr. Wahlstrom, a pharmacy student under her supervision, two or three physician assistants, a hospitalist, a nurse and a care coordinator—“runs the list” of patients to be seen until about 10:30 a.m. On floor 15, a general medicine unit, Dr. Wahlstrom and the clinical team usually care for 15 patients.
Most of Dr.Wahlstrom’s dealings with attending physicians in her four years at BWH have involved hospitalists. “Our team does accept other patients from Harvard Vanguard Medical Associates, so I do see those attending physicians, but I always round with the hospitalist from BWH.
“One of their major strengths is that they get to know the system so well, and they are committed to improving the hospital system,” she explains. “They know its efficiencies—and its inefficiencies—and they are familiar with processes and how long they take.”
For instance, a physician unfamiliar with the workings of the hospital laboratory timing might not know how long it would take to obtain lab results. A patient on enoxaparin who is being monitored would have an anti-Xa level drawn, and an attending physician from outside the hospital system would have to call the lab to find out when results would appear.
A hospitalist, on the other hand, “has an intuition about how long that lab [result] would take to come back,” says Dr. Wahlstrom, and times his or her return visit to the unit to review results with the pharmacist.
Robert Quinn, PharmD, is director of pharmacy services at Sierra Vista Regional Hospital, a 182-bed acute care facility owned by Tenet Healthcare Corporation and located in California. He is especially appreciative of hospitalists’ availability to staff.
“In ‘the old days,’ before hospitalists, one could feel disconnected from the medical staff. They didn’t always know or understand procedures,” says Dr. Quinn. In addition, “reaching community-based attending physicians was much more difficult. Now, [the hospitalists] know the ins and outs of the hospital system, and they know who to speak with in certain departments.
“Another physician not familiar with our system may call and ask for a pharmacist, but our hospitalists will know when they need to speak with the director of pharmacy services or when they should talk with a clinical pharmacist,” he continues. “They really do know the inner workings of the hospital on a much more intimate level.”
For instance, says Dr. Quinn, when hospitalists want a certain medication to be added to the hospital’s medication formulary, they know that their request should be routed to the director of pharmacy services. Direct patient care, including monitoring for blood levels of medications, drug information, and the like are the bailiwick of the clinical pharmacists.
“In my experience here at UCSF,” says Dr. Bookwalter, “[hospitalists] are very concerned about making the hospital work, which is one of their major missions. They’re also very collaborative. We really do work together—not just pharmacy and hospitalists—but with everybody.”
As an example of that collaborative approach, Dr. Bookwalter points to a palliative care program developed under the leadership of Hospitalist and SHM President Steve Pantilat, MD. The program has garnered Palliative Care Leadership Center status for the UCSF Medical Center.

—Robert Quinn, PharmD
Collaboration Is Primary
Dr. Bookwalter does have comparisons to his current situation on the General Medicine Service because he previously worked in the Intensive Care Nursery and with the General Surgery Service at UCSF. The latter, he says, “was very hierarchical. The team I was on included some very famous surgeons. They were all very personable and certainly knew what they were doing—they were really great. But, if you made a suggestion to them, chances were it would be rejected, since they insisted on ‘caring for their patients themselves.’”
At BWH Dr. Wahlstrom has also observed that hospitalists are very inclusive.
“When we do rounds, they ask the nurse to join us, so that we can have all points of care in our meetings,” she says. “If I recommend a change in a patient’s medication regimen, such as adding basal insulin for a patient, the hospitalist generally includes that in the patient’s plan immediately, and an order is written when we are on rounds. Then I approve it, and the patient can be started on medication promptly. We discuss what is going to happen and the care plan is made right there on the spot.”
Hospitalists with whom Dr. Wahlstrom works are comfortable with collaboration and open to ideas. “You’re not worried about suggesting ideas, or that your ideas might be rejected,” she explains. For instance, suggesting a change from IV to PO antibiotics would be welcomely discussed. “The hospitalists make the environment for presenting ideas regarding patient care open and encouraging.”
Communication a Plus
Availability of hospitalists is enhanced by their communication skills, says Dr. Quinn. “Once hospitalists get to know us, and we get to know them, the communication is just absolutely great,” he says. “Although I don’t get out as much as my clinicians do, if I have an issue I can go to the unit anytime and discuss it.”
The hospitalists with whom Dr. Quinn deals are interested in process issues as well as patient issues. For instance, if medication-administration records are not being placed in patients’ charts in a timely manner, hospital staff have the ability to quickly set up meetings with department managers and hospitalists to devise ways to improve procedures.
Meeting with other attending physicians is not as easy, says Dr. Quinn because they usually have very little time after making rounds and may have to be contacted at their practice office. “That’s one of the main advantages of having hospitalists,” he says. “They’re available. If anything happens, they’re there.”
During orientation at the UCSF Medical Center with new hospitalists, the General Medicine Service hospitalist residents take their teams on a tour of the pharmacy guided by Dr. Bookwalter. He explains the configuration of his department, which includes clinical pharmacists, pharmacy students, and a pharmacy practice resident. During the tour, he demonstrates how a medication order is processed, following it from the time the physician writes the prescription until the patient receives it. This contributes to both the residents’ and medical students’ understanding of how the hospital works.
If hospitalists have a concern about hospital policies, Dr. Bookwalter is there to aid them. “We promote rational drug therapy while the patient is in the hospital, smooth transitions in care, with the admit and discharge interviews, and we also follow up after patients leave to make sure they had no problems getting the medications they needed,” says Dr. Bookwalter.
During these contacts with patients, pharmacists also perform triage by asking patients how they feel at home. If they uncover problems during these interviews, “we first go to the team that took care of them in the hospital, and then to their primary physician,” he says.
A Boon for Patients, Staff
Are patients less comfortable with a new physician taking over their care? Dr. Quinn does not think this is a drawback. While the primary care physician may have a long-standing relationship with his or her patients, Dr. Quinn believes the availability of hospitalists can be very comforting to the patient.
“When a physician makes rounds and then leaves, patients may have a little bit of anxiety about whether they asked all their questions,” he speculates. It can be very comforting, he says, for the patient to know that the hospitalist is still on site.
Dr. Wahlstrom admits that sometimes she observes that patients may initially be uncomfortable meeting a physician other than their primary care physician. Again, building patient rapport seems to be no problem with the hospitalists with whom she works. “Patients seem to warm up to them right away,” she enthuses.
Dr. Quinn appreciates the fact that hospitalists are able and willing to participate in committees. “As a director of pharmacy services, I notice that their participation really helps—they understand the inner workings of the hospital and are able to look at situations in a different way.”
The hospital’s monthly hospitalist meeting is very well attended, Dr. Quinn reports: “[Our pharmacists] show up because we know that this is a tremendous forum for us to interact with physicians.”
Dr. Bookwalter also praises hospitalists’ interest in hospital safety and continuity of care. An innovative training program begun at UCSF Medical Center last year to address these issues entails sending pairs of pharmacy and medical students to patients’ homes after their hospital release.
“This has been very well received by both the pharmacy and medical students,” says Dr. Bookwalter. While at the patient’s home, the pharmacy student checks whether the patient has everything he or she needs, whether the patient understands how to take the medication, and whether it is being stored properly. If there are problems, the students can call the patient’s pharmacy, obtain special authorizations for third-party insurance coverage if needed, and help the patients obtain the care they need.
The program is designed to help students understand the change between hospital and home. “It’s a huge transition,” emphasizes Dr. Bookwalter. “Here in the hospital, the nurse is giving them their medicine every day, and then when they get home—and most of our patients are elderly—they get confused. Ultimately, we don’t want any discontinuities in care.”
High Ratings
It is their attention to innovation and collaboration among members of the multidisciplinary that our sources repeatedly praised about their hospitalist colleagues. Dr. Bookwalter doesn’t think there are any areas where hospitalists needed improvement.
“They all take it seriously, and they all perform well. You can really tell when you have someone on rotation who is not a hospitalist,” he says. “There are MDs who do research, are very well known, and are very familiar with the hospital, but it’s not the same collaborative experience. It’s like day and night.”
When pressed for recommendations he would give to hospitalists for improvement, Dr. Quinn admits he has one complaint: “I wish we had more. I’d like to see dozens of them!” TH
Writer Gretchen Henkel regularly writes “Alliances” for The Hospitalist.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. Each installment of “Alliances” provides valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
At the bedside or in committee, hospitalists are earning high marks from their pharmacist colleagues for their flexibility, approachability, and availability. By most accounts, hospitalists make the job of hospital pharmacists much easier, say the clinical pharmacists whom The Hospitalist recently interviewed—two from large university teaching hospitals and one from a community-based for-profit facility. In fact, attempts to extricate even constructive recommendations for hospitalists from these PharmDs proved fruitless.
“I think they do just about everything right,” says Tom Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California San Francisco Medical Center and a clinical professor of pharmacy at the UCSF School of Medicine. “I don’t find any fault with them.”
On the unit and in policy and procedure committee meetings, say the sources interviewed for this article, hospitalists develop good rapport with other staff members, address problems promptly, and are committed to improving processes for staff and patients alike.
Strengths of Hospitalists
As a clinical pharmacy specialist in general medicine on floor 15 at Brigham and Women’s Hospital (BWH) (Boston), Stephanie A. Wahlstrom, PharmD BCPS, begins rounds with the clinical team at 8 a.m. The group—typically consisting of Dr. Wahlstrom, a pharmacy student under her supervision, two or three physician assistants, a hospitalist, a nurse and a care coordinator—“runs the list” of patients to be seen until about 10:30 a.m. On floor 15, a general medicine unit, Dr. Wahlstrom and the clinical team usually care for 15 patients.
Most of Dr.Wahlstrom’s dealings with attending physicians in her four years at BWH have involved hospitalists. “Our team does accept other patients from Harvard Vanguard Medical Associates, so I do see those attending physicians, but I always round with the hospitalist from BWH.
“One of their major strengths is that they get to know the system so well, and they are committed to improving the hospital system,” she explains. “They know its efficiencies—and its inefficiencies—and they are familiar with processes and how long they take.”
For instance, a physician unfamiliar with the workings of the hospital laboratory timing might not know how long it would take to obtain lab results. A patient on enoxaparin who is being monitored would have an anti-Xa level drawn, and an attending physician from outside the hospital system would have to call the lab to find out when results would appear.
A hospitalist, on the other hand, “has an intuition about how long that lab [result] would take to come back,” says Dr. Wahlstrom, and times his or her return visit to the unit to review results with the pharmacist.
Robert Quinn, PharmD, is director of pharmacy services at Sierra Vista Regional Hospital, a 182-bed acute care facility owned by Tenet Healthcare Corporation and located in California. He is especially appreciative of hospitalists’ availability to staff.
“In ‘the old days,’ before hospitalists, one could feel disconnected from the medical staff. They didn’t always know or understand procedures,” says Dr. Quinn. In addition, “reaching community-based attending physicians was much more difficult. Now, [the hospitalists] know the ins and outs of the hospital system, and they know who to speak with in certain departments.
“Another physician not familiar with our system may call and ask for a pharmacist, but our hospitalists will know when they need to speak with the director of pharmacy services or when they should talk with a clinical pharmacist,” he continues. “They really do know the inner workings of the hospital on a much more intimate level.”
For instance, says Dr. Quinn, when hospitalists want a certain medication to be added to the hospital’s medication formulary, they know that their request should be routed to the director of pharmacy services. Direct patient care, including monitoring for blood levels of medications, drug information, and the like are the bailiwick of the clinical pharmacists.
“In my experience here at UCSF,” says Dr. Bookwalter, “[hospitalists] are very concerned about making the hospital work, which is one of their major missions. They’re also very collaborative. We really do work together—not just pharmacy and hospitalists—but with everybody.”
As an example of that collaborative approach, Dr. Bookwalter points to a palliative care program developed under the leadership of Hospitalist and SHM President Steve Pantilat, MD. The program has garnered Palliative Care Leadership Center status for the UCSF Medical Center.
—Robert Quinn, PharmD
Collaboration Is Primary
Dr. Bookwalter does have comparisons to his current situation on the General Medicine Service because he previously worked in the Intensive Care Nursery and with the General Surgery Service at UCSF. The latter, he says, “was very hierarchical. The team I was on included some very famous surgeons. They were all very personable and certainly knew what they were doing—they were really great. But, if you made a suggestion to them, chances were it would be rejected, since they insisted on ‘caring for their patients themselves.’”
At BWH Dr. Wahlstrom has also observed that hospitalists are very inclusive.
“When we do rounds, they ask the nurse to join us, so that we can have all points of care in our meetings,” she says. “If I recommend a change in a patient’s medication regimen, such as adding basal insulin for a patient, the hospitalist generally includes that in the patient’s plan immediately, and an order is written when we are on rounds. Then I approve it, and the patient can be started on medication promptly. We discuss what is going to happen and the care plan is made right there on the spot.”
Hospitalists with whom Dr. Wahlstrom works are comfortable with collaboration and open to ideas. “You’re not worried about suggesting ideas, or that your ideas might be rejected,” she explains. For instance, suggesting a change from IV to PO antibiotics would be welcomely discussed. “The hospitalists make the environment for presenting ideas regarding patient care open and encouraging.”
Communication a Plus
Availability of hospitalists is enhanced by their communication skills, says Dr. Quinn. “Once hospitalists get to know us, and we get to know them, the communication is just absolutely great,” he says. “Although I don’t get out as much as my clinicians do, if I have an issue I can go to the unit anytime and discuss it.”
The hospitalists with whom Dr. Quinn deals are interested in process issues as well as patient issues. For instance, if medication-administration records are not being placed in patients’ charts in a timely manner, hospital staff have the ability to quickly set up meetings with department managers and hospitalists to devise ways to improve procedures.
Meeting with other attending physicians is not as easy, says Dr. Quinn because they usually have very little time after making rounds and may have to be contacted at their practice office. “That’s one of the main advantages of having hospitalists,” he says. “They’re available. If anything happens, they’re there.”
During orientation at the UCSF Medical Center with new hospitalists, the General Medicine Service hospitalist residents take their teams on a tour of the pharmacy guided by Dr. Bookwalter. He explains the configuration of his department, which includes clinical pharmacists, pharmacy students, and a pharmacy practice resident. During the tour, he demonstrates how a medication order is processed, following it from the time the physician writes the prescription until the patient receives it. This contributes to both the residents’ and medical students’ understanding of how the hospital works.
If hospitalists have a concern about hospital policies, Dr. Bookwalter is there to aid them. “We promote rational drug therapy while the patient is in the hospital, smooth transitions in care, with the admit and discharge interviews, and we also follow up after patients leave to make sure they had no problems getting the medications they needed,” says Dr. Bookwalter.
During these contacts with patients, pharmacists also perform triage by asking patients how they feel at home. If they uncover problems during these interviews, “we first go to the team that took care of them in the hospital, and then to their primary physician,” he says.
A Boon for Patients, Staff
Are patients less comfortable with a new physician taking over their care? Dr. Quinn does not think this is a drawback. While the primary care physician may have a long-standing relationship with his or her patients, Dr. Quinn believes the availability of hospitalists can be very comforting to the patient.
“When a physician makes rounds and then leaves, patients may have a little bit of anxiety about whether they asked all their questions,” he speculates. It can be very comforting, he says, for the patient to know that the hospitalist is still on site.
Dr. Wahlstrom admits that sometimes she observes that patients may initially be uncomfortable meeting a physician other than their primary care physician. Again, building patient rapport seems to be no problem with the hospitalists with whom she works. “Patients seem to warm up to them right away,” she enthuses.
Dr. Quinn appreciates the fact that hospitalists are able and willing to participate in committees. “As a director of pharmacy services, I notice that their participation really helps—they understand the inner workings of the hospital and are able to look at situations in a different way.”
The hospital’s monthly hospitalist meeting is very well attended, Dr. Quinn reports: “[Our pharmacists] show up because we know that this is a tremendous forum for us to interact with physicians.”
Dr. Bookwalter also praises hospitalists’ interest in hospital safety and continuity of care. An innovative training program begun at UCSF Medical Center last year to address these issues entails sending pairs of pharmacy and medical students to patients’ homes after their hospital release.
“This has been very well received by both the pharmacy and medical students,” says Dr. Bookwalter. While at the patient’s home, the pharmacy student checks whether the patient has everything he or she needs, whether the patient understands how to take the medication, and whether it is being stored properly. If there are problems, the students can call the patient’s pharmacy, obtain special authorizations for third-party insurance coverage if needed, and help the patients obtain the care they need.
The program is designed to help students understand the change between hospital and home. “It’s a huge transition,” emphasizes Dr. Bookwalter. “Here in the hospital, the nurse is giving them their medicine every day, and then when they get home—and most of our patients are elderly—they get confused. Ultimately, we don’t want any discontinuities in care.”
High Ratings
It is their attention to innovation and collaboration among members of the multidisciplinary that our sources repeatedly praised about their hospitalist colleagues. Dr. Bookwalter doesn’t think there are any areas where hospitalists needed improvement.
“They all take it seriously, and they all perform well. You can really tell when you have someone on rotation who is not a hospitalist,” he says. “There are MDs who do research, are very well known, and are very familiar with the hospital, but it’s not the same collaborative experience. It’s like day and night.”
When pressed for recommendations he would give to hospitalists for improvement, Dr. Quinn admits he has one complaint: “I wish we had more. I’d like to see dozens of them!” TH
Writer Gretchen Henkel regularly writes “Alliances” for The Hospitalist.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. Each installment of “Alliances” provides valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
At the bedside or in committee, hospitalists are earning high marks from their pharmacist colleagues for their flexibility, approachability, and availability. By most accounts, hospitalists make the job of hospital pharmacists much easier, say the clinical pharmacists whom The Hospitalist recently interviewed—two from large university teaching hospitals and one from a community-based for-profit facility. In fact, attempts to extricate even constructive recommendations for hospitalists from these PharmDs proved fruitless.
“I think they do just about everything right,” says Tom Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California San Francisco Medical Center and a clinical professor of pharmacy at the UCSF School of Medicine. “I don’t find any fault with them.”
On the unit and in policy and procedure committee meetings, say the sources interviewed for this article, hospitalists develop good rapport with other staff members, address problems promptly, and are committed to improving processes for staff and patients alike.
Strengths of Hospitalists
As a clinical pharmacy specialist in general medicine on floor 15 at Brigham and Women’s Hospital (BWH) (Boston), Stephanie A. Wahlstrom, PharmD BCPS, begins rounds with the clinical team at 8 a.m. The group—typically consisting of Dr. Wahlstrom, a pharmacy student under her supervision, two or three physician assistants, a hospitalist, a nurse and a care coordinator—“runs the list” of patients to be seen until about 10:30 a.m. On floor 15, a general medicine unit, Dr. Wahlstrom and the clinical team usually care for 15 patients.
Most of Dr.Wahlstrom’s dealings with attending physicians in her four years at BWH have involved hospitalists. “Our team does accept other patients from Harvard Vanguard Medical Associates, so I do see those attending physicians, but I always round with the hospitalist from BWH.
“One of their major strengths is that they get to know the system so well, and they are committed to improving the hospital system,” she explains. “They know its efficiencies—and its inefficiencies—and they are familiar with processes and how long they take.”
For instance, a physician unfamiliar with the workings of the hospital laboratory timing might not know how long it would take to obtain lab results. A patient on enoxaparin who is being monitored would have an anti-Xa level drawn, and an attending physician from outside the hospital system would have to call the lab to find out when results would appear.
A hospitalist, on the other hand, “has an intuition about how long that lab [result] would take to come back,” says Dr. Wahlstrom, and times his or her return visit to the unit to review results with the pharmacist.
Robert Quinn, PharmD, is director of pharmacy services at Sierra Vista Regional Hospital, a 182-bed acute care facility owned by Tenet Healthcare Corporation and located in California. He is especially appreciative of hospitalists’ availability to staff.
“In ‘the old days,’ before hospitalists, one could feel disconnected from the medical staff. They didn’t always know or understand procedures,” says Dr. Quinn. In addition, “reaching community-based attending physicians was much more difficult. Now, [the hospitalists] know the ins and outs of the hospital system, and they know who to speak with in certain departments.
“Another physician not familiar with our system may call and ask for a pharmacist, but our hospitalists will know when they need to speak with the director of pharmacy services or when they should talk with a clinical pharmacist,” he continues. “They really do know the inner workings of the hospital on a much more intimate level.”
For instance, says Dr. Quinn, when hospitalists want a certain medication to be added to the hospital’s medication formulary, they know that their request should be routed to the director of pharmacy services. Direct patient care, including monitoring for blood levels of medications, drug information, and the like are the bailiwick of the clinical pharmacists.
“In my experience here at UCSF,” says Dr. Bookwalter, “[hospitalists] are very concerned about making the hospital work, which is one of their major missions. They’re also very collaborative. We really do work together—not just pharmacy and hospitalists—but with everybody.”
As an example of that collaborative approach, Dr. Bookwalter points to a palliative care program developed under the leadership of Hospitalist and SHM President Steve Pantilat, MD. The program has garnered Palliative Care Leadership Center status for the UCSF Medical Center.
—Robert Quinn, PharmD
Collaboration Is Primary
Dr. Bookwalter does have comparisons to his current situation on the General Medicine Service because he previously worked in the Intensive Care Nursery and with the General Surgery Service at UCSF. The latter, he says, “was very hierarchical. The team I was on included some very famous surgeons. They were all very personable and certainly knew what they were doing—they were really great. But, if you made a suggestion to them, chances were it would be rejected, since they insisted on ‘caring for their patients themselves.’”
At BWH Dr. Wahlstrom has also observed that hospitalists are very inclusive.
“When we do rounds, they ask the nurse to join us, so that we can have all points of care in our meetings,” she says. “If I recommend a change in a patient’s medication regimen, such as adding basal insulin for a patient, the hospitalist generally includes that in the patient’s plan immediately, and an order is written when we are on rounds. Then I approve it, and the patient can be started on medication promptly. We discuss what is going to happen and the care plan is made right there on the spot.”
Hospitalists with whom Dr. Wahlstrom works are comfortable with collaboration and open to ideas. “You’re not worried about suggesting ideas, or that your ideas might be rejected,” she explains. For instance, suggesting a change from IV to PO antibiotics would be welcomely discussed. “The hospitalists make the environment for presenting ideas regarding patient care open and encouraging.”
Communication a Plus
Availability of hospitalists is enhanced by their communication skills, says Dr. Quinn. “Once hospitalists get to know us, and we get to know them, the communication is just absolutely great,” he says. “Although I don’t get out as much as my clinicians do, if I have an issue I can go to the unit anytime and discuss it.”
The hospitalists with whom Dr. Quinn deals are interested in process issues as well as patient issues. For instance, if medication-administration records are not being placed in patients’ charts in a timely manner, hospital staff have the ability to quickly set up meetings with department managers and hospitalists to devise ways to improve procedures.
Meeting with other attending physicians is not as easy, says Dr. Quinn because they usually have very little time after making rounds and may have to be contacted at their practice office. “That’s one of the main advantages of having hospitalists,” he says. “They’re available. If anything happens, they’re there.”
During orientation at the UCSF Medical Center with new hospitalists, the General Medicine Service hospitalist residents take their teams on a tour of the pharmacy guided by Dr. Bookwalter. He explains the configuration of his department, which includes clinical pharmacists, pharmacy students, and a pharmacy practice resident. During the tour, he demonstrates how a medication order is processed, following it from the time the physician writes the prescription until the patient receives it. This contributes to both the residents’ and medical students’ understanding of how the hospital works.
If hospitalists have a concern about hospital policies, Dr. Bookwalter is there to aid them. “We promote rational drug therapy while the patient is in the hospital, smooth transitions in care, with the admit and discharge interviews, and we also follow up after patients leave to make sure they had no problems getting the medications they needed,” says Dr. Bookwalter.
During these contacts with patients, pharmacists also perform triage by asking patients how they feel at home. If they uncover problems during these interviews, “we first go to the team that took care of them in the hospital, and then to their primary physician,” he says.
A Boon for Patients, Staff
Are patients less comfortable with a new physician taking over their care? Dr. Quinn does not think this is a drawback. While the primary care physician may have a long-standing relationship with his or her patients, Dr. Quinn believes the availability of hospitalists can be very comforting to the patient.
“When a physician makes rounds and then leaves, patients may have a little bit of anxiety about whether they asked all their questions,” he speculates. It can be very comforting, he says, for the patient to know that the hospitalist is still on site.
Dr. Wahlstrom admits that sometimes she observes that patients may initially be uncomfortable meeting a physician other than their primary care physician. Again, building patient rapport seems to be no problem with the hospitalists with whom she works. “Patients seem to warm up to them right away,” she enthuses.
Dr. Quinn appreciates the fact that hospitalists are able and willing to participate in committees. “As a director of pharmacy services, I notice that their participation really helps—they understand the inner workings of the hospital and are able to look at situations in a different way.”
The hospital’s monthly hospitalist meeting is very well attended, Dr. Quinn reports: “[Our pharmacists] show up because we know that this is a tremendous forum for us to interact with physicians.”
Dr. Bookwalter also praises hospitalists’ interest in hospital safety and continuity of care. An innovative training program begun at UCSF Medical Center last year to address these issues entails sending pairs of pharmacy and medical students to patients’ homes after their hospital release.
“This has been very well received by both the pharmacy and medical students,” says Dr. Bookwalter. While at the patient’s home, the pharmacy student checks whether the patient has everything he or she needs, whether the patient understands how to take the medication, and whether it is being stored properly. If there are problems, the students can call the patient’s pharmacy, obtain special authorizations for third-party insurance coverage if needed, and help the patients obtain the care they need.
The program is designed to help students understand the change between hospital and home. “It’s a huge transition,” emphasizes Dr. Bookwalter. “Here in the hospital, the nurse is giving them their medicine every day, and then when they get home—and most of our patients are elderly—they get confused. Ultimately, we don’t want any discontinuities in care.”
High Ratings
It is their attention to innovation and collaboration among members of the multidisciplinary that our sources repeatedly praised about their hospitalist colleagues. Dr. Bookwalter doesn’t think there are any areas where hospitalists needed improvement.
“They all take it seriously, and they all perform well. You can really tell when you have someone on rotation who is not a hospitalist,” he says. “There are MDs who do research, are very well known, and are very familiar with the hospital, but it’s not the same collaborative experience. It’s like day and night.”
When pressed for recommendations he would give to hospitalists for improvement, Dr. Quinn admits he has one complaint: “I wish we had more. I’d like to see dozens of them!” TH
Writer Gretchen Henkel regularly writes “Alliances” for The Hospitalist.
11 Steps to a Successful Transition
A65-lb., 25-year-old, male cerebral palsy (CP) patient with pneumonia arrives at your Children’s Hospital via ambulance. Although chronologically this patient is an adult, in many ways he’s still a child, and the parents told the paramedics that they’ve always taken their son to Children’s. You’ve been the treating physician during the patient’s frequent hospital stays. Is Children’s Hospital still the best destination for this patient? Will the family’s insurance still cover an admission at Children’s?
During the hospital stay, the patient has complications. He has to be intubated. IV antibiotics need to be continued for a course after hospital discharge. A long recovery is expected. Is it time for the family to consider discharge to a long-term care facility rather than home? Are there any long-term care facilities in the area that accept young adult CP patients?
As the treating pediatric hospitalist, what is your role in helping this patient and his family transition from pediatric care to an adult-care medical home?
Introduction
Approximately 8.6 million children in the United States age 10–17 have a disability, according to the Adolescent Health Transition Project, which is housed at the Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Of these, 16% (or 1.4 million) experience limitations in their activities and will likely have difficulty making the transition to adult healthcare.1
Given enough time in the profession, every pediatric hospitalist will face the challenge of transitioning patients from child-centered to adult-oriented healthcare systems. The good news: Medical advances have made it increasingly possible for children who once would have died in childhood to survive into adulthood.
Example: One in 2,500 children is born with cystic fibrosis (CF); however, with the recent, unprecedented increase in the success of diagnosis and treatment modalities for the pulmonary component of CF, the estimated median survival age for those born in the 1990s is now 40.2 As of the year 2004, 41.8% of the 22,301 patients with CF were 18 or older.3 In fact, each year nearly 500,000 children with special healthcare needs reach adulthood, and 90% of children with a chronic illness and/or disability now survive to adulthood.4,5
The bad news: Many physicians whose practices focus on adults aren’t familiar with disease processes, such as CF, that have historically been considered pediatric illnesses.
For patients with chronic physical and medical conditions—particularly for those who are medically fragile and/or technology-dependent—the transition can prove especially difficult. And pediatric hospitalists in children’s hospitals face different challenges than those in facilities that admit patients of all ages. One thing remains the same, though, the goal: to provide uninterrupted, coordinated, developmentally appropriate healthcare.
Why Transition?
There are several good reasons for patients to be transitioned from pediatric care to adult care. First, as patients age medical issues develop that are beyond the sphere of pediatricians. In CF, for example, diabetes and biliary tract problems occur with greater frequency in adults. However, because so few CF patients historically survived to adulthood, few physicians who care for adults learned about the disease. Thus, the pediatricians who cared for CF patients continued to do so, leading to situations in which 30- and 40-year-olds have been hospitalized with children. But is that truly appropriate?
Adult patients may have high blood pressure, gynecologic issues, osteoporosis, or other problems the pediatrician may not be prepared to deal with. Example: A primary care pediatrician has been the “medical home” for a small, cerebral palsy patient since she was 10. She’s now 25. If she presents with a breast mass, will the pediatrician pick up on the condition adequately? Will they know where to send the patient?
“Adult providers know those systems better,” says Brett Pickering, MD, director of the Special Needs Clinic at San Diego’s UCSD Medical Center, Department of Pediatrics.
The adult patient has different emotional needs than the pediatric patient, and the pediatric hospitalist may not be in tune with adult needs. “Pediatricians do a lot of handholding,” says Dr. Pickering. “Adult providers are more matter of fact.”
Age restrictions on admissions, insurance, and funding issues also affect transition. For example, funding under the Social Security Act’s Title V Children with Special Health Care Needs typically ends at 21 despite a patient’s education or employment status.
Given these factors, what is the appropriate age to transition care from a pediatric floor or facility to an adult-oriented unit? According to the American Academy of Pediatrics, the responsibility of pediatrics continues through age 21, but there’s no hard-and-fast rule.
Challenges
The transition to adult-care facilities is typically a lengthy process involving multiple specialties and possibly joint care during a transition period—and a process that should ideally be coordinated by the patient’s primary care pediatrician. But hospitalists know that circumstances are typically far from ideal.
First, during a transition, the patient may feel abandoned by the medical team they’ve known for most of their lives. It takes time to develop trust and confidence in a new doctor. In this respect, pediatric hospitalists in facilities that care for patients of all ages have an advantage over hospitalists in children’s hospitals. They can call on their adult-care colleagues in other areas of the hospital for consultations and transfer care over time.
“The pediatric hospitalist must make bridges with their adult colleagues who are comfortable [with the issues] and willing to take on this patient population,” says Dr. Pickering.
Second, parents may feel an emotional dependency on the pediatric team and can feel threatened by the adult environment as they lose some control. To the parents, the patient will always be their child, Dr. Pickering notes.
Third, pediatric hospitalists may be reluctant to let go, particularly if they feel adult services are inferior to those they have provided, which brings us to the fourth major challenge: To whom do you transition care?
Many adult healthcare providers receive only limited training in disorders associated with pediatrics (e.g., CF, spina bifida). The Cystic Fibrosis Foundation is leading the way in educating physicians in what have historically been considered pediatric problems. In the 1980s, the foundation launched an educational program to train physicians already involved in adult pulmonary care in CF. Unfortunately, education in other areas has lagged. And finding a physician with both an interest in and knowledge of such disorders can prove challenging.
“It’s incumbent on our adult colleagues to take these patients on, but they need training,” says Dr. Pickering. “Long-term issues require long-term solutions.
How do you jazz people up to take care of this population?” she asks. Physicians must have at least a little bit of desire to learn about these special patient populations, but academic institutions also need to identify core knowledge and skills and make them part of training and certification requirements for primary care residents and physicians in practice. Continuing medical education for physicians, nurses, and allied healthcare professionals should include drug dosing, medical complications seen in transition populations, and related developmental, psychosocial, and behavioral issues.
Steps to a Successful Transition
So what should hospitalists do? In an April 2005 presentation at the SHM Annual Meeting, Joseph M. Geskey, DO, assistant professor of pediatrics and medicine, and director of inpatient pediatrics at Penn State College of Medicine, Hershey, Penn., recommended that pediatric hospitalists take the following steps:
- Identify the key aspects of transition;
- Bring stakeholders together;
- Identify transitional needs;
- Identify and provide resources;
- Create an audit and evaluation process;
- Decide who will hand off care of these patients when they are admitted to the hospital (the hospitalist or the disease-specific specialist);
- Create an up-to-date medical summary that is portable and accessible. It should include important historic information, such as diagnostic data, procedures, operations, and medications;
- Upon patient discharge, include specific instructions on who to call if the patient develops a problem after leaving the hospital;
- Create a working group in your area that represents pediatric and adult hospitalists to examine transition issues in the hospitalized patient; and
- Facilitate effective communication between patients and their families, primary care physicians and specialists; and
- Know when to transfer care to a center with more expertise in caring for specific conditions.
Conclusion
Just as every patient is different and every patient’s circumstances are unique, every transition needs to be individualized. “It’s hard to set policy,” says Dr. Pickering. Open, direct communication, specific discharge instructions, an up-to-date medical summary and knowledge of the adult resources in your area can make any transition a success. TH
Keri Losavio regularly writes for “Pediatric Special Section.”
References
- Adolescent Health Transition Project, Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Available at http://depts.washington.edu/healthtr/Providers/intro.htm. Last accessed January 16, 2006.
- Bufi PL. Cystic fibrosis: therapeutic options for co-management. Available at www.thorne.com/altmedrev/fulltext/cystic.html. Last accessed January 16, 2006.
- Cystic Fibrosis Foundation: 2004 Patient Registry Report. Available at www.cff.org/living_with_cf/. Last accessed Jan. 26, 2006
- Newacheck PW, Taylor WR. Childhood chronic illness: prevalence, severity, and impact. Am J Pub Health. 1992;82(3):364-371.
- Committee on Children with Disabilities and Committee on Adolescence, American Academy of Pediatrics. Transition of care provided for adolescents with special health care needs. Pediatrics. 1996;98(6):1203–1206.
Pediatric Special Section
In the Literature
By Mary Ann Queen, MD, and Amita Amonker, MD
Utilization of a Clinical Pathway Improves Care for Bronchiolitis
Cheney J, Barber S, Altamirano L, et al. A Clinical Pathway for Bronchiolitis is Effective in Reducing Readmission Rates. J Pediatr. 2005;147(5):622-626.
Bronchiolitis is the most common respiratory illness in infants that results in hospitalization. Many hospitals have developed clinical pathways to assist clinicians in managing this common infection; however, the effectiveness of such pathways has not been fully studied. Of those clinical practice guidelines analyzed, varying results have been identified.
To determine the effectiveness of a bronchiolitis pathway, this study compared infants managed prospectively using a pathway protocol with a retrospective analysis of infants managed without a pathway. Infants from a tertiary care children’s hospital and three regional hospitals were enrolled prospectively from May 2000 to August 2001. (One must note this study was completed in Australia, hence the difference from the typical Northern Hemisphere winter months.) The historical control group was admitted between May 1998 and August 1999 at the same four institutions. Two-hundred-twenty-nine patients admitted with bronchiolitis were treated using the pathway protocol. These patients were compared with 207 randomly selected control patients who were admitted prior to the institution of the bronchiolitis pathway. All patients were less than 12 months of age with their first episode of wheezing necessitating hospitalization.
These particular guidelines were developed and used to promote consistency of nursing management during a separate study on bronchiolitis. The pathway included an initial admission assessment. It also stated parameters for initiating and stopping both oxygen therapy and intravenous fluid therapy along with discharge guidelines.
The authors found no significant difference in length of stay or time in oxygen. Fifteen infants (7.2%) in the control group required readmission within two weeks of discharge compared with two infants (0.9%) in the pathway group (p=.001). Of the control group 33.8% received intravenous fluids (IVFs) compared with 19.2% of the pathway infants (p=.001). There was also greater steroid use in the control group but no difference in antibiotic usage. Specific data regarding steroids and antibiotics is not included.
The clinical pathway appears a useful tool for discharge planning with a decreased incidence of hospital readmission when specific discharge goals are utilized. The authors also reported a decreased use of IVFs in the pathway group. This was attributed to having specific parameters (O2 required, RR>60/min or inadequate oral feeding) for when to initiate them. It is unclear from the article whether meeting a single parameter or all three parameters triggered the initiation of IVFs.
The authors also point out the limitation of using a historical control given annual variations in severity sometimes seen with bronchiolitis. They attempted to minimize this by collecting data for each group over two consecutive winters.
Preprinted Paper Orders Reduce Medication Errors
Kozer E, Scolnik D, MacPherson A, et al. Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: A randomized, controlled trial. Pediatrics. 2005(116):1299-1302.
Medical errors, including medication errors, are common and are written about with increasing frequency in the lay press. Accreditation bodies and individual hospitals are striving for ways to decrease these errors. In some instances potential solutions include purchasing new computer systems for electronic physician order entry. This study looks at whether implementing a preprinted paper order sheet can decrease the incidence of medication errors in a pediatric ED.
This randomized, prospective study occurred during 18 days in July 2001 with nine days randomly assigned into each arm. The first arm used the hospital’s regular blank order sheets for all medication orders. The second arm used the experimental preprinted order sheet. This sheet required the staff to specify the dose, weight-adjusted dose, total daily dose, route of administration, and frequency for each medication ordered. Two medical students entered the data into a database that included information about patients’ demographics, diagnosis, acuity, details on the prescribing physician, the form used, and all medications prescribed and given to the patient. This information was subsequently reviewed by two blinded pediatric emergency physicians who determined if an error occurred and, if so, the degree of the error.
During the study period there were 2,157 visits to the ED with 95.4% charts available for review. Seven-hundred-ninety-five medications were prescribed with 376 ordered on the new form. Drug errors were identified in 68 (16.6%) orders when the regular form was used and in 37 (9.8%) orders on the new form. There was one severe error and 13 significant errors using the new form and 36 significant errors on the regular form. The new form was associated with a twofold decrease in the risk for a medication error even after accounting for the level of training of the ordering practitioner. There was an even greater reduction in the risk for a severe or significant error.
The literature has shown that computerized physician order entry can reduce the number of medication errors in the inpatient setting; however, it is not available in many hospitals and its effectiveness has not been shown in EDs. The authors point out that most medications ordered in the ED are prepared and given by nurses. The benefits of a computerized system in this setting is unclear.
This study occurred over an 18-day period with the new form only used for nine days outside of an earlier pilot period. One could speculate that the novelty of the form encouraged the physicians to examine orders more carefully, leading to decreased errors. It is unknown if the decrease in errors would be sustained over time.
Also important to note is that the definition of an error was limited to a mistake in dose, interval between doses, dose unit, and/or route. Errors such as legibility, medication allergy, or drug interactions are not discussed. However, as hospitals strive to implement technologies aimed at reducing errors this simple, economical solution may be of benefit.
No Association between Kawasaki Disease and Adenovirus
Shike H, Shimizu C, Kanegaye J, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005;24:1011-1014.
Kawasaki disease is a self-limited acute vasculitis of children with a suspected infectious etiology and defined seasonality. In an attempt to find a clue for a possible infectious cause of Kawasaki disease this study examined the seasonality of different viruses. The study recognized a similar bimodal seasonality for some serotypes of adenovirus. Adenovirus accounts for 5%-10% of respiratory tract infections in children and can mimic the clinical manifestations and laboratory abnormalities seen in Kawasaki disease.
This study postulated that infection with a non-cultivatable adenovirus or antecedent adenovirus infection might be a trigger for Kawasaki disease. The study analyzed patient samples using polymerase chain reaction primers for all 51 adenovirus serotypes, viral culture, and neutralization assay for the most common adenovirus serotypes. This study also investigated possible involvement of adeno-associated viruses (AAVs), because AAVs depend on helper viruses, such as adenovirus.
Kawasaki disease patients were enrolled during a 25-month period from February 2002 to February 2004 at Children’s Hospital and Health Center in San Diego. Illness day one was defined as the first day of fever. Clinical samples used in this study were collected within the first 14 days of fever onset and before intravenous immunoglobulin (IVIG) therapy.
Nasopharyngeal swabs were cultured for adenovirus. Standard adenoviral neutralization assays for the five most common serotypes were performed with the use of patient sera. Sera with a titer of 1/10 or greater were scored as positive. At least two clinical samples from each patient, including throat swabs, sera or urine, were tested by quantitative polymerase chain reaction (PCR) for adenovirus and AAV.
Nasopharyngeal viral cultures were collected before IVIG administration on illness day three—14 from 70 Kawasaki disease patients. Of the 70 patients, 52 patients fulfilled four of the five classic criteria or three of the five criteria with abnormal coronary arteries by echocardiogram. Of the remaining 18 patients with atypical Kawasaki disease, six had coronary artery abnormalities. Overall, seven patients had coronary artery aneurysms and 22 patients had coronary artery dilatation. Viral cultures were negative in 66 of the 70 Kawasaki disease patients. The viral isolates in four patients were respiratory syncytial (one), parainfluenza virus 3 (one) and adenovirus (two). Therefore adenovirus culture was negative in 97% of patients.
Fifteen Kawasaki disease patients with negative adenovirus cultures were evaluated by PCR assay on at least two clinical samples. Fourteen patients had a negative PCR result. The throat swab from one patient collected on illness day seven contained 800 adenovirus genome copies.
Results of the adenovirus neutralization assays from 26 Kawasaki disease patients revealed that neutralization titers against any of the five most common adenovirus serotypes were undetectable in four of 26 patients.
None of the 36 samples from the same 15 acute Kawasaki disease patients described for the PCR assay was positive for AAV.
This study concluded that despite the striking similarities between Kawasaki disease and adenovirus infection there is no evidence to suggest a link between the two.
Epidemiology and Clinical Description of Severe, Multifocal Staphylococcus aureus Infection
Miles F, Voss L, Segedin E, et al. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child. 2005;90(12):1274-1278.
Staphylococcus aureus is a recognized cause of multifocal infection with a high mortality rate. Children with community acquired S. aureus bacteremia (SAB) have higher frequencies of unknown foci compared with hospital-acquired SAB. Those children with S. aureus sepsis (SAS) presenting to the pediatric intensive care unit tend to have multisystemic disease—either by direct invasion or toxin production—before the diagnosis is made and treatment is initiated.
This study evaluates the clinical features and mortality from SAS in those children who required intensive care management. A retrospective review of clinical notes from all children with SAS admitted from October 1993 to April 2004 to the PICU in Auckland Children’s Hospital in New Zealand was undertaken. Children coded for SAS were identified from the PICU database.
All clinical notes were reviewed by one investigator using a standardized questionnaire that sought information on patient demographics, clinical findings, investigations, microbiology, and management in the PICU. Cases were included if blood or an isolate from a site that is normally sterile was positive for S. aureus. Hospital-acquired infection was defined by an isolate obtained at least 48 hours after hospital admission; community acquired infection was defined by an isolate obtained within 48 hours of admission.
Fifty-eight patients were identified with SAS over the 10-year study period; 55 were community acquired. Children with staphylococcal illness comprised 1% of all admission to the PICU. Musculoskeletal symptoms (79%) dominated presentation rather than isolated pneumonia (10%). An aggressive search for foci and surgical drainage of infective foci was required in 50% of children.
Most children (67%) either presented with multiple site involvement or secondary sites developed during their hospital stay. These pathologies included pneumonia, septic arthritis, osteomyelitis, and soft tissue involvement (cellulitis, fasciitis, abscess). A transthoracic echocardiogram detected valve abnormalities in only 5% of children, and these children were known to have pre-existing cardiac lesions. Few children (12%) presenting with methicillin-resistant S. aureus (MRSA) had community-acquired infection. The median length of stay in the PICU was three (mean 5.8, range one-44) days. Mortality due to SAS was 8.6%. Ten children had significant morbidity after discharge; these morbidities included renal failure requiring dialysis (three), an ongoing oxygen requirement at three months follow-up (two), and problems relating to limb movement and function (eight). Two children with epidural abscesses were paraplegic.
Community-acquired SAS affects healthy children, is multifocal, and has a high morbidity and mortality. It is imperative to look for sites of dissemination and to drain and debride foci. Routine echocardiography had a low yield in the absence of pre-existing cardiac lesions, persisting fever, or persisting bacteremia.
Long-Term Outcomes for Childhood Headache
Brna P, Dooley J, Gordon K Dewan T. The prognosis of childhood headache. Arch Pediatr Adolesc Med. 2005;159(12):1157-1160.
Headaches affect most children and rank third among illness-related causes of school absenteeism. Although the short-term outcome for most children appears favorable, few studies have reported long-term outcome. The objective of this study was to evaluate the long-term prognosis of childhood headaches 20 years after initial diagnosis in a cohort of Atlantic Canadian children who had headaches diagnosed in 1983.
Ninety-five patients with headaches who consulted one of the authors in 1983 were subsequently studied in 1993. The 77 patients contacted in 1993 were followed up in 2003. A standard telephone interview was used. Data were collected regarding headache symptoms, severity, frequency, treatment, and precipitants. Headache severity was simply classified as mild, moderate, or severe.
Sixty (78%) of 77 patients responded (60 of the 95 in the original cohort). At 20 years 16 (27%) were headache free, 20 (33%) had tension-type headaches, 10 (17%) had migraine, 14 (23%) had migraine and tension-type headaches. Having more than one headache type was more than at diagnosis or initial follow-up, and headache type varied across time. Of those who had headaches at follow-up, 80% (35/44) described their headaches as moderate or severe, although improvement in headaches was reported by 29 (66%). Tension-type headaches were more likely than migraine to resolve. During the month before follow-up, non-prescription medications were used by six (14%). However, 20 (45%) felt that non-pharmacological methods were most effective. Medication use increased during the 10 years since the last follow-up. No patient used selective serotonin receptor agonists.
This study concluded that 20 years after the diagnosis of pediatric headache, most patients continue to have headache, although the headache classification often changed across time. Most patients report moderate or severe headache and increasingly choose to care for their headaches pharmacologically. TH
A65-lb., 25-year-old, male cerebral palsy (CP) patient with pneumonia arrives at your Children’s Hospital via ambulance. Although chronologically this patient is an adult, in many ways he’s still a child, and the parents told the paramedics that they’ve always taken their son to Children’s. You’ve been the treating physician during the patient’s frequent hospital stays. Is Children’s Hospital still the best destination for this patient? Will the family’s insurance still cover an admission at Children’s?
During the hospital stay, the patient has complications. He has to be intubated. IV antibiotics need to be continued for a course after hospital discharge. A long recovery is expected. Is it time for the family to consider discharge to a long-term care facility rather than home? Are there any long-term care facilities in the area that accept young adult CP patients?
As the treating pediatric hospitalist, what is your role in helping this patient and his family transition from pediatric care to an adult-care medical home?
Introduction
Approximately 8.6 million children in the United States age 10–17 have a disability, according to the Adolescent Health Transition Project, which is housed at the Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Of these, 16% (or 1.4 million) experience limitations in their activities and will likely have difficulty making the transition to adult healthcare.1
Given enough time in the profession, every pediatric hospitalist will face the challenge of transitioning patients from child-centered to adult-oriented healthcare systems. The good news: Medical advances have made it increasingly possible for children who once would have died in childhood to survive into adulthood.
Example: One in 2,500 children is born with cystic fibrosis (CF); however, with the recent, unprecedented increase in the success of diagnosis and treatment modalities for the pulmonary component of CF, the estimated median survival age for those born in the 1990s is now 40.2 As of the year 2004, 41.8% of the 22,301 patients with CF were 18 or older.3 In fact, each year nearly 500,000 children with special healthcare needs reach adulthood, and 90% of children with a chronic illness and/or disability now survive to adulthood.4,5
The bad news: Many physicians whose practices focus on adults aren’t familiar with disease processes, such as CF, that have historically been considered pediatric illnesses.
For patients with chronic physical and medical conditions—particularly for those who are medically fragile and/or technology-dependent—the transition can prove especially difficult. And pediatric hospitalists in children’s hospitals face different challenges than those in facilities that admit patients of all ages. One thing remains the same, though, the goal: to provide uninterrupted, coordinated, developmentally appropriate healthcare.
Why Transition?
There are several good reasons for patients to be transitioned from pediatric care to adult care. First, as patients age medical issues develop that are beyond the sphere of pediatricians. In CF, for example, diabetes and biliary tract problems occur with greater frequency in adults. However, because so few CF patients historically survived to adulthood, few physicians who care for adults learned about the disease. Thus, the pediatricians who cared for CF patients continued to do so, leading to situations in which 30- and 40-year-olds have been hospitalized with children. But is that truly appropriate?
Adult patients may have high blood pressure, gynecologic issues, osteoporosis, or other problems the pediatrician may not be prepared to deal with. Example: A primary care pediatrician has been the “medical home” for a small, cerebral palsy patient since she was 10. She’s now 25. If she presents with a breast mass, will the pediatrician pick up on the condition adequately? Will they know where to send the patient?
“Adult providers know those systems better,” says Brett Pickering, MD, director of the Special Needs Clinic at San Diego’s UCSD Medical Center, Department of Pediatrics.
The adult patient has different emotional needs than the pediatric patient, and the pediatric hospitalist may not be in tune with adult needs. “Pediatricians do a lot of handholding,” says Dr. Pickering. “Adult providers are more matter of fact.”
Age restrictions on admissions, insurance, and funding issues also affect transition. For example, funding under the Social Security Act’s Title V Children with Special Health Care Needs typically ends at 21 despite a patient’s education or employment status.
Given these factors, what is the appropriate age to transition care from a pediatric floor or facility to an adult-oriented unit? According to the American Academy of Pediatrics, the responsibility of pediatrics continues through age 21, but there’s no hard-and-fast rule.
Challenges
The transition to adult-care facilities is typically a lengthy process involving multiple specialties and possibly joint care during a transition period—and a process that should ideally be coordinated by the patient’s primary care pediatrician. But hospitalists know that circumstances are typically far from ideal.
First, during a transition, the patient may feel abandoned by the medical team they’ve known for most of their lives. It takes time to develop trust and confidence in a new doctor. In this respect, pediatric hospitalists in facilities that care for patients of all ages have an advantage over hospitalists in children’s hospitals. They can call on their adult-care colleagues in other areas of the hospital for consultations and transfer care over time.
“The pediatric hospitalist must make bridges with their adult colleagues who are comfortable [with the issues] and willing to take on this patient population,” says Dr. Pickering.
Second, parents may feel an emotional dependency on the pediatric team and can feel threatened by the adult environment as they lose some control. To the parents, the patient will always be their child, Dr. Pickering notes.
Third, pediatric hospitalists may be reluctant to let go, particularly if they feel adult services are inferior to those they have provided, which brings us to the fourth major challenge: To whom do you transition care?
Many adult healthcare providers receive only limited training in disorders associated with pediatrics (e.g., CF, spina bifida). The Cystic Fibrosis Foundation is leading the way in educating physicians in what have historically been considered pediatric problems. In the 1980s, the foundation launched an educational program to train physicians already involved in adult pulmonary care in CF. Unfortunately, education in other areas has lagged. And finding a physician with both an interest in and knowledge of such disorders can prove challenging.
“It’s incumbent on our adult colleagues to take these patients on, but they need training,” says Dr. Pickering. “Long-term issues require long-term solutions.
How do you jazz people up to take care of this population?” she asks. Physicians must have at least a little bit of desire to learn about these special patient populations, but academic institutions also need to identify core knowledge and skills and make them part of training and certification requirements for primary care residents and physicians in practice. Continuing medical education for physicians, nurses, and allied healthcare professionals should include drug dosing, medical complications seen in transition populations, and related developmental, psychosocial, and behavioral issues.
Steps to a Successful Transition
So what should hospitalists do? In an April 2005 presentation at the SHM Annual Meeting, Joseph M. Geskey, DO, assistant professor of pediatrics and medicine, and director of inpatient pediatrics at Penn State College of Medicine, Hershey, Penn., recommended that pediatric hospitalists take the following steps:
- Identify the key aspects of transition;
- Bring stakeholders together;
- Identify transitional needs;
- Identify and provide resources;
- Create an audit and evaluation process;
- Decide who will hand off care of these patients when they are admitted to the hospital (the hospitalist or the disease-specific specialist);
- Create an up-to-date medical summary that is portable and accessible. It should include important historic information, such as diagnostic data, procedures, operations, and medications;
- Upon patient discharge, include specific instructions on who to call if the patient develops a problem after leaving the hospital;
- Create a working group in your area that represents pediatric and adult hospitalists to examine transition issues in the hospitalized patient; and
- Facilitate effective communication between patients and their families, primary care physicians and specialists; and
- Know when to transfer care to a center with more expertise in caring for specific conditions.
Conclusion
Just as every patient is different and every patient’s circumstances are unique, every transition needs to be individualized. “It’s hard to set policy,” says Dr. Pickering. Open, direct communication, specific discharge instructions, an up-to-date medical summary and knowledge of the adult resources in your area can make any transition a success. TH
Keri Losavio regularly writes for “Pediatric Special Section.”
References
- Adolescent Health Transition Project, Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Available at http://depts.washington.edu/healthtr/Providers/intro.htm. Last accessed January 16, 2006.
- Bufi PL. Cystic fibrosis: therapeutic options for co-management. Available at www.thorne.com/altmedrev/fulltext/cystic.html. Last accessed January 16, 2006.
- Cystic Fibrosis Foundation: 2004 Patient Registry Report. Available at www.cff.org/living_with_cf/. Last accessed Jan. 26, 2006
- Newacheck PW, Taylor WR. Childhood chronic illness: prevalence, severity, and impact. Am J Pub Health. 1992;82(3):364-371.
- Committee on Children with Disabilities and Committee on Adolescence, American Academy of Pediatrics. Transition of care provided for adolescents with special health care needs. Pediatrics. 1996;98(6):1203–1206.
Pediatric Special Section
In the Literature
By Mary Ann Queen, MD, and Amita Amonker, MD
Utilization of a Clinical Pathway Improves Care for Bronchiolitis
Cheney J, Barber S, Altamirano L, et al. A Clinical Pathway for Bronchiolitis is Effective in Reducing Readmission Rates. J Pediatr. 2005;147(5):622-626.
Bronchiolitis is the most common respiratory illness in infants that results in hospitalization. Many hospitals have developed clinical pathways to assist clinicians in managing this common infection; however, the effectiveness of such pathways has not been fully studied. Of those clinical practice guidelines analyzed, varying results have been identified.
To determine the effectiveness of a bronchiolitis pathway, this study compared infants managed prospectively using a pathway protocol with a retrospective analysis of infants managed without a pathway. Infants from a tertiary care children’s hospital and three regional hospitals were enrolled prospectively from May 2000 to August 2001. (One must note this study was completed in Australia, hence the difference from the typical Northern Hemisphere winter months.) The historical control group was admitted between May 1998 and August 1999 at the same four institutions. Two-hundred-twenty-nine patients admitted with bronchiolitis were treated using the pathway protocol. These patients were compared with 207 randomly selected control patients who were admitted prior to the institution of the bronchiolitis pathway. All patients were less than 12 months of age with their first episode of wheezing necessitating hospitalization.
These particular guidelines were developed and used to promote consistency of nursing management during a separate study on bronchiolitis. The pathway included an initial admission assessment. It also stated parameters for initiating and stopping both oxygen therapy and intravenous fluid therapy along with discharge guidelines.
The authors found no significant difference in length of stay or time in oxygen. Fifteen infants (7.2%) in the control group required readmission within two weeks of discharge compared with two infants (0.9%) in the pathway group (p=.001). Of the control group 33.8% received intravenous fluids (IVFs) compared with 19.2% of the pathway infants (p=.001). There was also greater steroid use in the control group but no difference in antibiotic usage. Specific data regarding steroids and antibiotics is not included.
The clinical pathway appears a useful tool for discharge planning with a decreased incidence of hospital readmission when specific discharge goals are utilized. The authors also reported a decreased use of IVFs in the pathway group. This was attributed to having specific parameters (O2 required, RR>60/min or inadequate oral feeding) for when to initiate them. It is unclear from the article whether meeting a single parameter or all three parameters triggered the initiation of IVFs.
The authors also point out the limitation of using a historical control given annual variations in severity sometimes seen with bronchiolitis. They attempted to minimize this by collecting data for each group over two consecutive winters.
Preprinted Paper Orders Reduce Medication Errors
Kozer E, Scolnik D, MacPherson A, et al. Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: A randomized, controlled trial. Pediatrics. 2005(116):1299-1302.
Medical errors, including medication errors, are common and are written about with increasing frequency in the lay press. Accreditation bodies and individual hospitals are striving for ways to decrease these errors. In some instances potential solutions include purchasing new computer systems for electronic physician order entry. This study looks at whether implementing a preprinted paper order sheet can decrease the incidence of medication errors in a pediatric ED.
This randomized, prospective study occurred during 18 days in July 2001 with nine days randomly assigned into each arm. The first arm used the hospital’s regular blank order sheets for all medication orders. The second arm used the experimental preprinted order sheet. This sheet required the staff to specify the dose, weight-adjusted dose, total daily dose, route of administration, and frequency for each medication ordered. Two medical students entered the data into a database that included information about patients’ demographics, diagnosis, acuity, details on the prescribing physician, the form used, and all medications prescribed and given to the patient. This information was subsequently reviewed by two blinded pediatric emergency physicians who determined if an error occurred and, if so, the degree of the error.
During the study period there were 2,157 visits to the ED with 95.4% charts available for review. Seven-hundred-ninety-five medications were prescribed with 376 ordered on the new form. Drug errors were identified in 68 (16.6%) orders when the regular form was used and in 37 (9.8%) orders on the new form. There was one severe error and 13 significant errors using the new form and 36 significant errors on the regular form. The new form was associated with a twofold decrease in the risk for a medication error even after accounting for the level of training of the ordering practitioner. There was an even greater reduction in the risk for a severe or significant error.
The literature has shown that computerized physician order entry can reduce the number of medication errors in the inpatient setting; however, it is not available in many hospitals and its effectiveness has not been shown in EDs. The authors point out that most medications ordered in the ED are prepared and given by nurses. The benefits of a computerized system in this setting is unclear.
This study occurred over an 18-day period with the new form only used for nine days outside of an earlier pilot period. One could speculate that the novelty of the form encouraged the physicians to examine orders more carefully, leading to decreased errors. It is unknown if the decrease in errors would be sustained over time.
Also important to note is that the definition of an error was limited to a mistake in dose, interval between doses, dose unit, and/or route. Errors such as legibility, medication allergy, or drug interactions are not discussed. However, as hospitals strive to implement technologies aimed at reducing errors this simple, economical solution may be of benefit.
No Association between Kawasaki Disease and Adenovirus
Shike H, Shimizu C, Kanegaye J, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005;24:1011-1014.
Kawasaki disease is a self-limited acute vasculitis of children with a suspected infectious etiology and defined seasonality. In an attempt to find a clue for a possible infectious cause of Kawasaki disease this study examined the seasonality of different viruses. The study recognized a similar bimodal seasonality for some serotypes of adenovirus. Adenovirus accounts for 5%-10% of respiratory tract infections in children and can mimic the clinical manifestations and laboratory abnormalities seen in Kawasaki disease.
This study postulated that infection with a non-cultivatable adenovirus or antecedent adenovirus infection might be a trigger for Kawasaki disease. The study analyzed patient samples using polymerase chain reaction primers for all 51 adenovirus serotypes, viral culture, and neutralization assay for the most common adenovirus serotypes. This study also investigated possible involvement of adeno-associated viruses (AAVs), because AAVs depend on helper viruses, such as adenovirus.
Kawasaki disease patients were enrolled during a 25-month period from February 2002 to February 2004 at Children’s Hospital and Health Center in San Diego. Illness day one was defined as the first day of fever. Clinical samples used in this study were collected within the first 14 days of fever onset and before intravenous immunoglobulin (IVIG) therapy.
Nasopharyngeal swabs were cultured for adenovirus. Standard adenoviral neutralization assays for the five most common serotypes were performed with the use of patient sera. Sera with a titer of 1/10 or greater were scored as positive. At least two clinical samples from each patient, including throat swabs, sera or urine, were tested by quantitative polymerase chain reaction (PCR) for adenovirus and AAV.
Nasopharyngeal viral cultures were collected before IVIG administration on illness day three—14 from 70 Kawasaki disease patients. Of the 70 patients, 52 patients fulfilled four of the five classic criteria or three of the five criteria with abnormal coronary arteries by echocardiogram. Of the remaining 18 patients with atypical Kawasaki disease, six had coronary artery abnormalities. Overall, seven patients had coronary artery aneurysms and 22 patients had coronary artery dilatation. Viral cultures were negative in 66 of the 70 Kawasaki disease patients. The viral isolates in four patients were respiratory syncytial (one), parainfluenza virus 3 (one) and adenovirus (two). Therefore adenovirus culture was negative in 97% of patients.
Fifteen Kawasaki disease patients with negative adenovirus cultures were evaluated by PCR assay on at least two clinical samples. Fourteen patients had a negative PCR result. The throat swab from one patient collected on illness day seven contained 800 adenovirus genome copies.
Results of the adenovirus neutralization assays from 26 Kawasaki disease patients revealed that neutralization titers against any of the five most common adenovirus serotypes were undetectable in four of 26 patients.
None of the 36 samples from the same 15 acute Kawasaki disease patients described for the PCR assay was positive for AAV.
This study concluded that despite the striking similarities between Kawasaki disease and adenovirus infection there is no evidence to suggest a link between the two.
Epidemiology and Clinical Description of Severe, Multifocal Staphylococcus aureus Infection
Miles F, Voss L, Segedin E, et al. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child. 2005;90(12):1274-1278.
Staphylococcus aureus is a recognized cause of multifocal infection with a high mortality rate. Children with community acquired S. aureus bacteremia (SAB) have higher frequencies of unknown foci compared with hospital-acquired SAB. Those children with S. aureus sepsis (SAS) presenting to the pediatric intensive care unit tend to have multisystemic disease—either by direct invasion or toxin production—before the diagnosis is made and treatment is initiated.
This study evaluates the clinical features and mortality from SAS in those children who required intensive care management. A retrospective review of clinical notes from all children with SAS admitted from October 1993 to April 2004 to the PICU in Auckland Children’s Hospital in New Zealand was undertaken. Children coded for SAS were identified from the PICU database.
All clinical notes were reviewed by one investigator using a standardized questionnaire that sought information on patient demographics, clinical findings, investigations, microbiology, and management in the PICU. Cases were included if blood or an isolate from a site that is normally sterile was positive for S. aureus. Hospital-acquired infection was defined by an isolate obtained at least 48 hours after hospital admission; community acquired infection was defined by an isolate obtained within 48 hours of admission.
Fifty-eight patients were identified with SAS over the 10-year study period; 55 were community acquired. Children with staphylococcal illness comprised 1% of all admission to the PICU. Musculoskeletal symptoms (79%) dominated presentation rather than isolated pneumonia (10%). An aggressive search for foci and surgical drainage of infective foci was required in 50% of children.
Most children (67%) either presented with multiple site involvement or secondary sites developed during their hospital stay. These pathologies included pneumonia, septic arthritis, osteomyelitis, and soft tissue involvement (cellulitis, fasciitis, abscess). A transthoracic echocardiogram detected valve abnormalities in only 5% of children, and these children were known to have pre-existing cardiac lesions. Few children (12%) presenting with methicillin-resistant S. aureus (MRSA) had community-acquired infection. The median length of stay in the PICU was three (mean 5.8, range one-44) days. Mortality due to SAS was 8.6%. Ten children had significant morbidity after discharge; these morbidities included renal failure requiring dialysis (three), an ongoing oxygen requirement at three months follow-up (two), and problems relating to limb movement and function (eight). Two children with epidural abscesses were paraplegic.
Community-acquired SAS affects healthy children, is multifocal, and has a high morbidity and mortality. It is imperative to look for sites of dissemination and to drain and debride foci. Routine echocardiography had a low yield in the absence of pre-existing cardiac lesions, persisting fever, or persisting bacteremia.
Long-Term Outcomes for Childhood Headache
Brna P, Dooley J, Gordon K Dewan T. The prognosis of childhood headache. Arch Pediatr Adolesc Med. 2005;159(12):1157-1160.
Headaches affect most children and rank third among illness-related causes of school absenteeism. Although the short-term outcome for most children appears favorable, few studies have reported long-term outcome. The objective of this study was to evaluate the long-term prognosis of childhood headaches 20 years after initial diagnosis in a cohort of Atlantic Canadian children who had headaches diagnosed in 1983.
Ninety-five patients with headaches who consulted one of the authors in 1983 were subsequently studied in 1993. The 77 patients contacted in 1993 were followed up in 2003. A standard telephone interview was used. Data were collected regarding headache symptoms, severity, frequency, treatment, and precipitants. Headache severity was simply classified as mild, moderate, or severe.
Sixty (78%) of 77 patients responded (60 of the 95 in the original cohort). At 20 years 16 (27%) were headache free, 20 (33%) had tension-type headaches, 10 (17%) had migraine, 14 (23%) had migraine and tension-type headaches. Having more than one headache type was more than at diagnosis or initial follow-up, and headache type varied across time. Of those who had headaches at follow-up, 80% (35/44) described their headaches as moderate or severe, although improvement in headaches was reported by 29 (66%). Tension-type headaches were more likely than migraine to resolve. During the month before follow-up, non-prescription medications were used by six (14%). However, 20 (45%) felt that non-pharmacological methods were most effective. Medication use increased during the 10 years since the last follow-up. No patient used selective serotonin receptor agonists.
This study concluded that 20 years after the diagnosis of pediatric headache, most patients continue to have headache, although the headache classification often changed across time. Most patients report moderate or severe headache and increasingly choose to care for their headaches pharmacologically. TH
A65-lb., 25-year-old, male cerebral palsy (CP) patient with pneumonia arrives at your Children’s Hospital via ambulance. Although chronologically this patient is an adult, in many ways he’s still a child, and the parents told the paramedics that they’ve always taken their son to Children’s. You’ve been the treating physician during the patient’s frequent hospital stays. Is Children’s Hospital still the best destination for this patient? Will the family’s insurance still cover an admission at Children’s?
During the hospital stay, the patient has complications. He has to be intubated. IV antibiotics need to be continued for a course after hospital discharge. A long recovery is expected. Is it time for the family to consider discharge to a long-term care facility rather than home? Are there any long-term care facilities in the area that accept young adult CP patients?
As the treating pediatric hospitalist, what is your role in helping this patient and his family transition from pediatric care to an adult-care medical home?
Introduction
Approximately 8.6 million children in the United States age 10–17 have a disability, according to the Adolescent Health Transition Project, which is housed at the Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Of these, 16% (or 1.4 million) experience limitations in their activities and will likely have difficulty making the transition to adult healthcare.1
Given enough time in the profession, every pediatric hospitalist will face the challenge of transitioning patients from child-centered to adult-oriented healthcare systems. The good news: Medical advances have made it increasingly possible for children who once would have died in childhood to survive into adulthood.
Example: One in 2,500 children is born with cystic fibrosis (CF); however, with the recent, unprecedented increase in the success of diagnosis and treatment modalities for the pulmonary component of CF, the estimated median survival age for those born in the 1990s is now 40.2 As of the year 2004, 41.8% of the 22,301 patients with CF were 18 or older.3 In fact, each year nearly 500,000 children with special healthcare needs reach adulthood, and 90% of children with a chronic illness and/or disability now survive to adulthood.4,5
The bad news: Many physicians whose practices focus on adults aren’t familiar with disease processes, such as CF, that have historically been considered pediatric illnesses.
For patients with chronic physical and medical conditions—particularly for those who are medically fragile and/or technology-dependent—the transition can prove especially difficult. And pediatric hospitalists in children’s hospitals face different challenges than those in facilities that admit patients of all ages. One thing remains the same, though, the goal: to provide uninterrupted, coordinated, developmentally appropriate healthcare.
Why Transition?
There are several good reasons for patients to be transitioned from pediatric care to adult care. First, as patients age medical issues develop that are beyond the sphere of pediatricians. In CF, for example, diabetes and biliary tract problems occur with greater frequency in adults. However, because so few CF patients historically survived to adulthood, few physicians who care for adults learned about the disease. Thus, the pediatricians who cared for CF patients continued to do so, leading to situations in which 30- and 40-year-olds have been hospitalized with children. But is that truly appropriate?
Adult patients may have high blood pressure, gynecologic issues, osteoporosis, or other problems the pediatrician may not be prepared to deal with. Example: A primary care pediatrician has been the “medical home” for a small, cerebral palsy patient since she was 10. She’s now 25. If she presents with a breast mass, will the pediatrician pick up on the condition adequately? Will they know where to send the patient?
“Adult providers know those systems better,” says Brett Pickering, MD, director of the Special Needs Clinic at San Diego’s UCSD Medical Center, Department of Pediatrics.
The adult patient has different emotional needs than the pediatric patient, and the pediatric hospitalist may not be in tune with adult needs. “Pediatricians do a lot of handholding,” says Dr. Pickering. “Adult providers are more matter of fact.”
Age restrictions on admissions, insurance, and funding issues also affect transition. For example, funding under the Social Security Act’s Title V Children with Special Health Care Needs typically ends at 21 despite a patient’s education or employment status.
Given these factors, what is the appropriate age to transition care from a pediatric floor or facility to an adult-oriented unit? According to the American Academy of Pediatrics, the responsibility of pediatrics continues through age 21, but there’s no hard-and-fast rule.
Challenges
The transition to adult-care facilities is typically a lengthy process involving multiple specialties and possibly joint care during a transition period—and a process that should ideally be coordinated by the patient’s primary care pediatrician. But hospitalists know that circumstances are typically far from ideal.
First, during a transition, the patient may feel abandoned by the medical team they’ve known for most of their lives. It takes time to develop trust and confidence in a new doctor. In this respect, pediatric hospitalists in facilities that care for patients of all ages have an advantage over hospitalists in children’s hospitals. They can call on their adult-care colleagues in other areas of the hospital for consultations and transfer care over time.
“The pediatric hospitalist must make bridges with their adult colleagues who are comfortable [with the issues] and willing to take on this patient population,” says Dr. Pickering.
Second, parents may feel an emotional dependency on the pediatric team and can feel threatened by the adult environment as they lose some control. To the parents, the patient will always be their child, Dr. Pickering notes.
Third, pediatric hospitalists may be reluctant to let go, particularly if they feel adult services are inferior to those they have provided, which brings us to the fourth major challenge: To whom do you transition care?
Many adult healthcare providers receive only limited training in disorders associated with pediatrics (e.g., CF, spina bifida). The Cystic Fibrosis Foundation is leading the way in educating physicians in what have historically been considered pediatric problems. In the 1980s, the foundation launched an educational program to train physicians already involved in adult pulmonary care in CF. Unfortunately, education in other areas has lagged. And finding a physician with both an interest in and knowledge of such disorders can prove challenging.
“It’s incumbent on our adult colleagues to take these patients on, but they need training,” says Dr. Pickering. “Long-term issues require long-term solutions.
How do you jazz people up to take care of this population?” she asks. Physicians must have at least a little bit of desire to learn about these special patient populations, but academic institutions also need to identify core knowledge and skills and make them part of training and certification requirements for primary care residents and physicians in practice. Continuing medical education for physicians, nurses, and allied healthcare professionals should include drug dosing, medical complications seen in transition populations, and related developmental, psychosocial, and behavioral issues.
Steps to a Successful Transition
So what should hospitalists do? In an April 2005 presentation at the SHM Annual Meeting, Joseph M. Geskey, DO, assistant professor of pediatrics and medicine, and director of inpatient pediatrics at Penn State College of Medicine, Hershey, Penn., recommended that pediatric hospitalists take the following steps:
- Identify the key aspects of transition;
- Bring stakeholders together;
- Identify transitional needs;
- Identify and provide resources;
- Create an audit and evaluation process;
- Decide who will hand off care of these patients when they are admitted to the hospital (the hospitalist or the disease-specific specialist);
- Create an up-to-date medical summary that is portable and accessible. It should include important historic information, such as diagnostic data, procedures, operations, and medications;
- Upon patient discharge, include specific instructions on who to call if the patient develops a problem after leaving the hospital;
- Create a working group in your area that represents pediatric and adult hospitalists to examine transition issues in the hospitalized patient; and
- Facilitate effective communication between patients and their families, primary care physicians and specialists; and
- Know when to transfer care to a center with more expertise in caring for specific conditions.
Conclusion
Just as every patient is different and every patient’s circumstances are unique, every transition needs to be individualized. “It’s hard to set policy,” says Dr. Pickering. Open, direct communication, specific discharge instructions, an up-to-date medical summary and knowledge of the adult resources in your area can make any transition a success. TH
Keri Losavio regularly writes for “Pediatric Special Section.”
References
- Adolescent Health Transition Project, Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Available at http://depts.washington.edu/healthtr/Providers/intro.htm. Last accessed January 16, 2006.
- Bufi PL. Cystic fibrosis: therapeutic options for co-management. Available at www.thorne.com/altmedrev/fulltext/cystic.html. Last accessed January 16, 2006.
- Cystic Fibrosis Foundation: 2004 Patient Registry Report. Available at www.cff.org/living_with_cf/. Last accessed Jan. 26, 2006
- Newacheck PW, Taylor WR. Childhood chronic illness: prevalence, severity, and impact. Am J Pub Health. 1992;82(3):364-371.
- Committee on Children with Disabilities and Committee on Adolescence, American Academy of Pediatrics. Transition of care provided for adolescents with special health care needs. Pediatrics. 1996;98(6):1203–1206.
Pediatric Special Section
In the Literature
By Mary Ann Queen, MD, and Amita Amonker, MD
Utilization of a Clinical Pathway Improves Care for Bronchiolitis
Cheney J, Barber S, Altamirano L, et al. A Clinical Pathway for Bronchiolitis is Effective in Reducing Readmission Rates. J Pediatr. 2005;147(5):622-626.
Bronchiolitis is the most common respiratory illness in infants that results in hospitalization. Many hospitals have developed clinical pathways to assist clinicians in managing this common infection; however, the effectiveness of such pathways has not been fully studied. Of those clinical practice guidelines analyzed, varying results have been identified.
To determine the effectiveness of a bronchiolitis pathway, this study compared infants managed prospectively using a pathway protocol with a retrospective analysis of infants managed without a pathway. Infants from a tertiary care children’s hospital and three regional hospitals were enrolled prospectively from May 2000 to August 2001. (One must note this study was completed in Australia, hence the difference from the typical Northern Hemisphere winter months.) The historical control group was admitted between May 1998 and August 1999 at the same four institutions. Two-hundred-twenty-nine patients admitted with bronchiolitis were treated using the pathway protocol. These patients were compared with 207 randomly selected control patients who were admitted prior to the institution of the bronchiolitis pathway. All patients were less than 12 months of age with their first episode of wheezing necessitating hospitalization.
These particular guidelines were developed and used to promote consistency of nursing management during a separate study on bronchiolitis. The pathway included an initial admission assessment. It also stated parameters for initiating and stopping both oxygen therapy and intravenous fluid therapy along with discharge guidelines.
The authors found no significant difference in length of stay or time in oxygen. Fifteen infants (7.2%) in the control group required readmission within two weeks of discharge compared with two infants (0.9%) in the pathway group (p=.001). Of the control group 33.8% received intravenous fluids (IVFs) compared with 19.2% of the pathway infants (p=.001). There was also greater steroid use in the control group but no difference in antibiotic usage. Specific data regarding steroids and antibiotics is not included.
The clinical pathway appears a useful tool for discharge planning with a decreased incidence of hospital readmission when specific discharge goals are utilized. The authors also reported a decreased use of IVFs in the pathway group. This was attributed to having specific parameters (O2 required, RR>60/min or inadequate oral feeding) for when to initiate them. It is unclear from the article whether meeting a single parameter or all three parameters triggered the initiation of IVFs.
The authors also point out the limitation of using a historical control given annual variations in severity sometimes seen with bronchiolitis. They attempted to minimize this by collecting data for each group over two consecutive winters.
Preprinted Paper Orders Reduce Medication Errors
Kozer E, Scolnik D, MacPherson A, et al. Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: A randomized, controlled trial. Pediatrics. 2005(116):1299-1302.
Medical errors, including medication errors, are common and are written about with increasing frequency in the lay press. Accreditation bodies and individual hospitals are striving for ways to decrease these errors. In some instances potential solutions include purchasing new computer systems for electronic physician order entry. This study looks at whether implementing a preprinted paper order sheet can decrease the incidence of medication errors in a pediatric ED.
This randomized, prospective study occurred during 18 days in July 2001 with nine days randomly assigned into each arm. The first arm used the hospital’s regular blank order sheets for all medication orders. The second arm used the experimental preprinted order sheet. This sheet required the staff to specify the dose, weight-adjusted dose, total daily dose, route of administration, and frequency for each medication ordered. Two medical students entered the data into a database that included information about patients’ demographics, diagnosis, acuity, details on the prescribing physician, the form used, and all medications prescribed and given to the patient. This information was subsequently reviewed by two blinded pediatric emergency physicians who determined if an error occurred and, if so, the degree of the error.
During the study period there were 2,157 visits to the ED with 95.4% charts available for review. Seven-hundred-ninety-five medications were prescribed with 376 ordered on the new form. Drug errors were identified in 68 (16.6%) orders when the regular form was used and in 37 (9.8%) orders on the new form. There was one severe error and 13 significant errors using the new form and 36 significant errors on the regular form. The new form was associated with a twofold decrease in the risk for a medication error even after accounting for the level of training of the ordering practitioner. There was an even greater reduction in the risk for a severe or significant error.
The literature has shown that computerized physician order entry can reduce the number of medication errors in the inpatient setting; however, it is not available in many hospitals and its effectiveness has not been shown in EDs. The authors point out that most medications ordered in the ED are prepared and given by nurses. The benefits of a computerized system in this setting is unclear.
This study occurred over an 18-day period with the new form only used for nine days outside of an earlier pilot period. One could speculate that the novelty of the form encouraged the physicians to examine orders more carefully, leading to decreased errors. It is unknown if the decrease in errors would be sustained over time.
Also important to note is that the definition of an error was limited to a mistake in dose, interval between doses, dose unit, and/or route. Errors such as legibility, medication allergy, or drug interactions are not discussed. However, as hospitals strive to implement technologies aimed at reducing errors this simple, economical solution may be of benefit.
No Association between Kawasaki Disease and Adenovirus
Shike H, Shimizu C, Kanegaye J, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005;24:1011-1014.
Kawasaki disease is a self-limited acute vasculitis of children with a suspected infectious etiology and defined seasonality. In an attempt to find a clue for a possible infectious cause of Kawasaki disease this study examined the seasonality of different viruses. The study recognized a similar bimodal seasonality for some serotypes of adenovirus. Adenovirus accounts for 5%-10% of respiratory tract infections in children and can mimic the clinical manifestations and laboratory abnormalities seen in Kawasaki disease.
This study postulated that infection with a non-cultivatable adenovirus or antecedent adenovirus infection might be a trigger for Kawasaki disease. The study analyzed patient samples using polymerase chain reaction primers for all 51 adenovirus serotypes, viral culture, and neutralization assay for the most common adenovirus serotypes. This study also investigated possible involvement of adeno-associated viruses (AAVs), because AAVs depend on helper viruses, such as adenovirus.
Kawasaki disease patients were enrolled during a 25-month period from February 2002 to February 2004 at Children’s Hospital and Health Center in San Diego. Illness day one was defined as the first day of fever. Clinical samples used in this study were collected within the first 14 days of fever onset and before intravenous immunoglobulin (IVIG) therapy.
Nasopharyngeal swabs were cultured for adenovirus. Standard adenoviral neutralization assays for the five most common serotypes were performed with the use of patient sera. Sera with a titer of 1/10 or greater were scored as positive. At least two clinical samples from each patient, including throat swabs, sera or urine, were tested by quantitative polymerase chain reaction (PCR) for adenovirus and AAV.
Nasopharyngeal viral cultures were collected before IVIG administration on illness day three—14 from 70 Kawasaki disease patients. Of the 70 patients, 52 patients fulfilled four of the five classic criteria or three of the five criteria with abnormal coronary arteries by echocardiogram. Of the remaining 18 patients with atypical Kawasaki disease, six had coronary artery abnormalities. Overall, seven patients had coronary artery aneurysms and 22 patients had coronary artery dilatation. Viral cultures were negative in 66 of the 70 Kawasaki disease patients. The viral isolates in four patients were respiratory syncytial (one), parainfluenza virus 3 (one) and adenovirus (two). Therefore adenovirus culture was negative in 97% of patients.
Fifteen Kawasaki disease patients with negative adenovirus cultures were evaluated by PCR assay on at least two clinical samples. Fourteen patients had a negative PCR result. The throat swab from one patient collected on illness day seven contained 800 adenovirus genome copies.
Results of the adenovirus neutralization assays from 26 Kawasaki disease patients revealed that neutralization titers against any of the five most common adenovirus serotypes were undetectable in four of 26 patients.
None of the 36 samples from the same 15 acute Kawasaki disease patients described for the PCR assay was positive for AAV.
This study concluded that despite the striking similarities between Kawasaki disease and adenovirus infection there is no evidence to suggest a link between the two.
Epidemiology and Clinical Description of Severe, Multifocal Staphylococcus aureus Infection
Miles F, Voss L, Segedin E, et al. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child. 2005;90(12):1274-1278.
Staphylococcus aureus is a recognized cause of multifocal infection with a high mortality rate. Children with community acquired S. aureus bacteremia (SAB) have higher frequencies of unknown foci compared with hospital-acquired SAB. Those children with S. aureus sepsis (SAS) presenting to the pediatric intensive care unit tend to have multisystemic disease—either by direct invasion or toxin production—before the diagnosis is made and treatment is initiated.
This study evaluates the clinical features and mortality from SAS in those children who required intensive care management. A retrospective review of clinical notes from all children with SAS admitted from October 1993 to April 2004 to the PICU in Auckland Children’s Hospital in New Zealand was undertaken. Children coded for SAS were identified from the PICU database.
All clinical notes were reviewed by one investigator using a standardized questionnaire that sought information on patient demographics, clinical findings, investigations, microbiology, and management in the PICU. Cases were included if blood or an isolate from a site that is normally sterile was positive for S. aureus. Hospital-acquired infection was defined by an isolate obtained at least 48 hours after hospital admission; community acquired infection was defined by an isolate obtained within 48 hours of admission.
Fifty-eight patients were identified with SAS over the 10-year study period; 55 were community acquired. Children with staphylococcal illness comprised 1% of all admission to the PICU. Musculoskeletal symptoms (79%) dominated presentation rather than isolated pneumonia (10%). An aggressive search for foci and surgical drainage of infective foci was required in 50% of children.
Most children (67%) either presented with multiple site involvement or secondary sites developed during their hospital stay. These pathologies included pneumonia, septic arthritis, osteomyelitis, and soft tissue involvement (cellulitis, fasciitis, abscess). A transthoracic echocardiogram detected valve abnormalities in only 5% of children, and these children were known to have pre-existing cardiac lesions. Few children (12%) presenting with methicillin-resistant S. aureus (MRSA) had community-acquired infection. The median length of stay in the PICU was three (mean 5.8, range one-44) days. Mortality due to SAS was 8.6%. Ten children had significant morbidity after discharge; these morbidities included renal failure requiring dialysis (three), an ongoing oxygen requirement at three months follow-up (two), and problems relating to limb movement and function (eight). Two children with epidural abscesses were paraplegic.
Community-acquired SAS affects healthy children, is multifocal, and has a high morbidity and mortality. It is imperative to look for sites of dissemination and to drain and debride foci. Routine echocardiography had a low yield in the absence of pre-existing cardiac lesions, persisting fever, or persisting bacteremia.
Long-Term Outcomes for Childhood Headache
Brna P, Dooley J, Gordon K Dewan T. The prognosis of childhood headache. Arch Pediatr Adolesc Med. 2005;159(12):1157-1160.
Headaches affect most children and rank third among illness-related causes of school absenteeism. Although the short-term outcome for most children appears favorable, few studies have reported long-term outcome. The objective of this study was to evaluate the long-term prognosis of childhood headaches 20 years after initial diagnosis in a cohort of Atlantic Canadian children who had headaches diagnosed in 1983.
Ninety-five patients with headaches who consulted one of the authors in 1983 were subsequently studied in 1993. The 77 patients contacted in 1993 were followed up in 2003. A standard telephone interview was used. Data were collected regarding headache symptoms, severity, frequency, treatment, and precipitants. Headache severity was simply classified as mild, moderate, or severe.
Sixty (78%) of 77 patients responded (60 of the 95 in the original cohort). At 20 years 16 (27%) were headache free, 20 (33%) had tension-type headaches, 10 (17%) had migraine, 14 (23%) had migraine and tension-type headaches. Having more than one headache type was more than at diagnosis or initial follow-up, and headache type varied across time. Of those who had headaches at follow-up, 80% (35/44) described their headaches as moderate or severe, although improvement in headaches was reported by 29 (66%). Tension-type headaches were more likely than migraine to resolve. During the month before follow-up, non-prescription medications were used by six (14%). However, 20 (45%) felt that non-pharmacological methods were most effective. Medication use increased during the 10 years since the last follow-up. No patient used selective serotonin receptor agonists.
This study concluded that 20 years after the diagnosis of pediatric headache, most patients continue to have headache, although the headache classification often changed across time. Most patients report moderate or severe headache and increasingly choose to care for their headaches pharmacologically. TH
Survey Responses Exceed Goal
The Benchmarks Committee has completed the data accumulation portion of the SHM 2005-2006 Productivity and Compensation Survey. As you might recall, we set a goal of 400 group respondents. With a final push for responses in early December, we exceeded our target. The responses were invaluable in making this survey a worthwhile effort and a credible reflection of the national hospitalist movement.
The Benchmarks Committee would like to specially thank those who attempted to complete the survey online and gave us feedback on this process. We had a few glitches with the online survey, and thanks to these folks and their communication we learned a few valuable lessons regarding this electronic process. We were able to intervene immediately and re-direct folks to the written survey. We’ll apply these lessons to the electronic component of future surveys as well.
Over the next few months we will be analyzing the data in preparation for presentation of the results to be offered up initially at the SHM Annual Meeting in Washington, D.C., the first week in May. (Visit www.hospitalmedicine.org under “Upcoming Events” to register.) Additionally, results will be available to survey participants online later in the year following the national presentation.
On a different note, the committee continues to work on the Hospitalist Dashboard Project. We are creating a dashboard that deals with metrics in the categories of resource utilization, clinical quality, productivity, and satisfaction.
Subsequently, we have worked through a Delphi process to whittle a long list of possible metrics down to 10 key metrics. These have been divided among the committee members, who will use an agreed-upon outline to write a brief description of the metric, how it is measured, and how it can be utilized to manage a hospitalist practice. The final product will be a white paper made available to the SHM membership.
How to Develop a Hospital-Based Palliative Care Program
Why your hospital needs such a program and how to create it
By Eva H. Chittenden, MD, and the SHM Palliative Care Task Force
Palliative care consists of medical care focused on the relief of suffering for patients living with chronic, advanced illness and it also helps their families. It is offered at any stage of disease, concurrently with all other appropriate medical treatment.
Palliative care providers treat the many physical symptoms that patients experience, including pain, dyspnea, nausea, and delirium. In addition, providers assist patients and families with complex medical decision-making, and attend to patients’ and families’ spiritual and psychosocial needs. Physicians work closely with an interdisciplinary team of nurses, chaplains, social workers, and pharmacists. Care continues beyond the point of death, with phone calls and consolation letters, as well as bereavement services.
Arguments for inpatient Palliative Care
The clinical imperative: We need better quality of care for people with serious and complex illness. The multicenter SUPPORT study, published in JAMA in 1995, looked at more than 9,000 hospitalized patients with life-threatening illness and demonstrated significant problems with pain and symptom control and with patient-doctor communication.1 Of the patients who died, more than 50% had moderate to severe pain more than half the time during the last three days of their lives. Of patients preferring do-not-resuscitate status, less than 50% of their physicians were aware of their wishes.
In another study, Nelson, et al. documented that more than half of cancer patients receiving intensive care had moderate to severe pain, anxiety, thirst, and hunger, and that 75% had moderate to severe discomfort of some kind.2 These studies have been a wake-up call to clinicians and hospitals across the country.
Patient and Family Preferences
Family members—especially women—shoulder most of the care of patients with serious illness. A minority of caregivers are over age 65 themselves and in ill health. When asked what they want from the medical system, family caregivers ask for help with transportation and personal care of their loved one at home, and for better home nursing support. They want 24/7 access to providers, better communication with their doctors, and to be remembered and contacted after the death of their family member.3-5 Caregiving itself has been shown to increase likelihood of premature mortality and lead to financial crisis.6
In the SUPPORT study, one-third of families lost most of their savings due to illness.7 Patients want pain and symptom control, avoidance of inappropriate prolongation of the dying process, and relief of burdens on family.8 Palliative care programs, both inpatient and ambulatory, can help provide families with needed services and improve communication at all levels.
The Demographic Argument
Hospitals need palliative care to effectively treat the growing numbers of people with serious, advanced, and complex illness. By 2030, the number of people over age 85 will double to almost 10 million.9 Many of these patients will have multiple chronic conditions, making their care complicated and expensive. And for many chronic conditions, including heart and lung disease, diabetes, and hypertension, death is not predictable.
Therefore, people need better care throughout the multiyear course of advanced illness. And while the Medicare Hospice Benefit is helpful for care of the dying (defined as people with six months or less to live) we need additional approaches for the much larger number of patients with chronic, progressive illness, years to live, continued benefit from disease-modifying therapy, and obvious palliative care needs.
The Educational Imperative
Hospitals are the site of training for most clinicians. Researchers have documented significant deficits in palliative care knowledge, skills, and attitudes among medical students, residents, and practicing physicians. Medical school and residency curricula, although improving, offer relatively little teaching in palliative care principles and practice.10,11
In 2000 the Liaison Committee on Medical Education mandated that medical school curricula include “important aspects of … end-of-life-care.” That same year the Accreditation Council for Graduate Medical Education encouraged internal medicine training programs to provide instruction in the principles of palliative care. Inpatient palliative care programs could provide much of this teaching through medical student and resident rotations, informal teaching during the consultation process, and through workshops and grand rounds.
The Financial Argument
Medical costs are rising exponentially due to multiple factors, including effective yet expensive new technologies and an expanding elderly population with more chronic conditions. Under the current Diagnosis Related Group (DRG) system, long, high-intensity hospital stays are causing a fiscal crisis for hospitals. The hospital and insurer of the future will have to work together to learn how to treat serious and complex illness efficiently and in the most cost-effective manner possible. Palliative care programs have the potential to ease this looming crisis through decreasing length of stay, both in the ICU and on the floors, and decreasing direct costs, including radiology, pharmacy, and laboratory costs. Researchers are beginning to document the positive fiscal impacts in rigorous studies.
Palliative Care: The Bottom Line
Palliative care teams have demonstrated improvement in pain and other symptom scores, in patient and family satisfaction with care, and in patient-provider communication. In addition, they have improved compliance with Joint Commission on Accreditation of Healthcare Organizations (JCAHO) quality measures. They have had these positive effects while simultaneously showing decreases in length of stay and costs. As a result, many programs have gained significant financial and administrative support from their hospitals.
Hospitalists and Palliative Care
Many hospitalist groups have found that building and staffing a palliative care consultation team is an important addition to their portfolio of services, further solidifying their value in the eyes of their hospital administration. The professional fee revenues are one more funding source, and palliative care is a critical service the group can provide the institution to improve the quality of care, improve patient satisfaction, and decrease costs.
The work involved in starting a program, including needs assessment, internal marketing, building a financial case, and developing a staffing model, is similar to that done when starting a hospitalist program. Hospitalists are ideally positioned to start palliative care services because they have already built relationships with key administrators and opinion leaders, and they understand the institution’s method for evaluating financial data, and how to access outcome and satisfaction data.
What Hospitalists Gain
By leading and staffing palliative care programs, hospitalists gain visibility and respect from colleagues, and improve their patients’ quality of care and their hospital’s financial bottom line. Clinically palliative care adds variety and depth to the work life of hospitalists and allows them to work with a rich interdisciplinary team. Although hospitalists should obtain additional training, they already possess the building blocks to provide excellent palliative care, such as skillfully leading family conferences and treating complex symptoms. When wearing the palliative care “hat,” providers have the luxury of spending more time at a patient’s bedside discussing what is truly important to the patient and his or her loved ones. The work is meaningful and rewarding.
Obtaining the Tools to Start a Program
The Center to Advance Palliative Care (CAPC), funded by the Robert Wood Johnson Foundation, is dedicated to advancing inpatient palliative care programs through their Web site (www.capc.org) and through their manual, “A Guide to Building a Hospital-Based Palliative Care Program,” available for purchase on its Web site.
In addition, CAPC sponsors the six national Palliative Care Leadership Centers (PCLCs) that each hold two-day, hands-on workshops on the nuts and bolts of starting inpatient palliative care programs, followed by a year of personalized mentoring by phone. The University of California, San Francisco’s PCLC, which is tailored specifically to hospitalists, will hold its last workshop in April 2006. For more information, visit www.capc.org/palliative-care-leadership-initiative.
At the upcoming SHM Annual Meeting in May, the Palliative Care Taskforce will present a workshop, “The Basic Why and How to Develop a Hospital-Based Palliative Care Program.”
Obtaining the Clinical Expertise
There are numerous opportunities for hospitalists to gain clinical expertise in palliative care, including Web-based and written materials and CME courses. Highlights include the Education in Palliative and End of Life Care programs; courses and study guides through the American Association of Hospice and Palliative Medicine, as well as Fast Facts (one-page synopses of relevant palliative care concepts that can be made into handouts or downloaded to one’s PDA). For more information on these resources and others, visit www.capc.org/palliative-care-professional-development/Education_Material_for _Professionals.
In addition, on Thursday, May 4, at 1:20, there will be a breakout session on pain management at the SHM Annual Meeting.
Hospitalists and other physicians can get certified in Hospice and Palliative Medicine by documenting relevant clinical experience and sitting for a qualifying exam. The American Board of Hospice and Palliative Medicine will administer its last exam in November 2006 (final application deadline is May 31, 2006). In September 2006 the field of Hospice and Palliative Medicine is expected to win American Board of Medical Specialties’ (ABMS) recognition as a subspecialty. After that the ABMS will take over administration of the exams. There will likely be a grandfathering period with the ABMS in which relevant clinical experience can substitute for completion of an ACGME-approved palliative care fellowship. For more information, visit the AAHPM Web site at www.abhpm.org/gfxc_100.aspx.
Summary/Conclusions
Inpatient palliative care programs benefit patients, hospitalists, and hospitals alike. Hospitalists are in the perfect position to lead the next generation of inpatient palliative care programs. Currently, about 20% of hospitals in the United States have programs. With the help of hospitalists, the percentage can increase significantly.
Special thanks to Diane Meier, MD, whose work inspired and informed this article.
References
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatment. The SUPPORT Principal Investigators. JAMA. 1995;274:1591-1598.
- Nelson JE, Meier DE, Oei EJ, et al. Self-reported
- symptom experience of critically ill cancer patients receiving intensive care. Crit Care Med. 2001;29 (2):277-282.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999;341 (13):956-963.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Understanding economic and other burdens of terminal Illness: the experience of patients and their caregivers. Ann Intern Med. 2000;132(6):451-459.
- Tolle et al. The Oregon report card: Improving care of the dying. 1999. Available at www.ohsu.edu/ethics/barriers2.pdf. Last accessed Feb. 3, 2006.
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282 (23):2215-2219.
- Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients’ families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994;272:1839-1844.
- Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA. 1999;281(2):163-168.
- U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Table 2a. US Census Bureau/CDC. 2002. Available at www.census.gov/ipc/www/usinterimproj/. Last accessed Feb. 3, 2006.
- Meier DE, Morrison RS, Cassel CK. Improving palliative care. Ann Intern Med. 1997;127:225-230.
- Billings JA, Block S. Palliative care in undergraduate medical education. Status report and future directions. JAMA. 1997;278:733-738.
Update:
New Hospitalist Productivity & Compensation Data
Survey results to be presented at 2006 SHM Annual Meeting
By the end of the data collection period in December 2005 approximately 400 hospital medicine programs had submitted responses for SHM’s 2005-2006 Hospitalist Productivity and Compensation Survey—a 35% increase from 2003. In addition to salary and production trends, this year’s survey should provide new insights into hospitalist responsibilities, the concerns of hospitalist program leaders, night coverage arrangements, and the use of nurse practitioners and physician assistants.
SHM thanks the program leaders who completed the comprehensive survey questionnaire. The following participants were randomly selected to receive awards:
- Danny Moore, MD, of Gilmore Memorial Hospital (Amory, Miss.) received a complimentary registration at the SHM Leadership Academy; and
- Four hospitalists received complimentary registration to the SHM Annual Meeting: Adrienne L. Bennett, MD, PhD, Ohio State University College of Medicine (Columbus, Ohio); Jasvinder S. Dhillon, St. Mary’s Hospital PICU Pediatric Hospitalist Program (Richmond, Va.); Howard Dubin, MD, Inpatient Medical Services of Bristol Hospital (Cheshire, Conn.); and Sujith Sundararaj MD, Signature Healthcare Solutions (Chicago).
The results of the 2005-2006 Hospitalist Productivity and Compensation Survey will be presented for the first time on Thursday, May 4 at 8:10 a.m. at the SHM Annual Meeting. A panel representing different perspectives within hospital medicine will react to the data. The panelists—SHM co-founder John Nelson, MD, President-Elect Mary Jo Gorman, MD, and Past-President Bob Wachter, MD—will represent hospital-employed practices, private groups, and academic programs, respectively. A report of the survey results will be available to survey participants for free. SHM members will be able to purchase the report at a discounted price. TH
The Benchmarks Committee has completed the data accumulation portion of the SHM 2005-2006 Productivity and Compensation Survey. As you might recall, we set a goal of 400 group respondents. With a final push for responses in early December, we exceeded our target. The responses were invaluable in making this survey a worthwhile effort and a credible reflection of the national hospitalist movement.
The Benchmarks Committee would like to specially thank those who attempted to complete the survey online and gave us feedback on this process. We had a few glitches with the online survey, and thanks to these folks and their communication we learned a few valuable lessons regarding this electronic process. We were able to intervene immediately and re-direct folks to the written survey. We’ll apply these lessons to the electronic component of future surveys as well.
Over the next few months we will be analyzing the data in preparation for presentation of the results to be offered up initially at the SHM Annual Meeting in Washington, D.C., the first week in May. (Visit www.hospitalmedicine.org under “Upcoming Events” to register.) Additionally, results will be available to survey participants online later in the year following the national presentation.
On a different note, the committee continues to work on the Hospitalist Dashboard Project. We are creating a dashboard that deals with metrics in the categories of resource utilization, clinical quality, productivity, and satisfaction.
Subsequently, we have worked through a Delphi process to whittle a long list of possible metrics down to 10 key metrics. These have been divided among the committee members, who will use an agreed-upon outline to write a brief description of the metric, how it is measured, and how it can be utilized to manage a hospitalist practice. The final product will be a white paper made available to the SHM membership.
How to Develop a Hospital-Based Palliative Care Program
Why your hospital needs such a program and how to create it
By Eva H. Chittenden, MD, and the SHM Palliative Care Task Force
Palliative care consists of medical care focused on the relief of suffering for patients living with chronic, advanced illness and it also helps their families. It is offered at any stage of disease, concurrently with all other appropriate medical treatment.
Palliative care providers treat the many physical symptoms that patients experience, including pain, dyspnea, nausea, and delirium. In addition, providers assist patients and families with complex medical decision-making, and attend to patients’ and families’ spiritual and psychosocial needs. Physicians work closely with an interdisciplinary team of nurses, chaplains, social workers, and pharmacists. Care continues beyond the point of death, with phone calls and consolation letters, as well as bereavement services.
Arguments for inpatient Palliative Care
The clinical imperative: We need better quality of care for people with serious and complex illness. The multicenter SUPPORT study, published in JAMA in 1995, looked at more than 9,000 hospitalized patients with life-threatening illness and demonstrated significant problems with pain and symptom control and with patient-doctor communication.1 Of the patients who died, more than 50% had moderate to severe pain more than half the time during the last three days of their lives. Of patients preferring do-not-resuscitate status, less than 50% of their physicians were aware of their wishes.
In another study, Nelson, et al. documented that more than half of cancer patients receiving intensive care had moderate to severe pain, anxiety, thirst, and hunger, and that 75% had moderate to severe discomfort of some kind.2 These studies have been a wake-up call to clinicians and hospitals across the country.
Patient and Family Preferences
Family members—especially women—shoulder most of the care of patients with serious illness. A minority of caregivers are over age 65 themselves and in ill health. When asked what they want from the medical system, family caregivers ask for help with transportation and personal care of their loved one at home, and for better home nursing support. They want 24/7 access to providers, better communication with their doctors, and to be remembered and contacted after the death of their family member.3-5 Caregiving itself has been shown to increase likelihood of premature mortality and lead to financial crisis.6
In the SUPPORT study, one-third of families lost most of their savings due to illness.7 Patients want pain and symptom control, avoidance of inappropriate prolongation of the dying process, and relief of burdens on family.8 Palliative care programs, both inpatient and ambulatory, can help provide families with needed services and improve communication at all levels.
The Demographic Argument
Hospitals need palliative care to effectively treat the growing numbers of people with serious, advanced, and complex illness. By 2030, the number of people over age 85 will double to almost 10 million.9 Many of these patients will have multiple chronic conditions, making their care complicated and expensive. And for many chronic conditions, including heart and lung disease, diabetes, and hypertension, death is not predictable.
Therefore, people need better care throughout the multiyear course of advanced illness. And while the Medicare Hospice Benefit is helpful for care of the dying (defined as people with six months or less to live) we need additional approaches for the much larger number of patients with chronic, progressive illness, years to live, continued benefit from disease-modifying therapy, and obvious palliative care needs.
The Educational Imperative
Hospitals are the site of training for most clinicians. Researchers have documented significant deficits in palliative care knowledge, skills, and attitudes among medical students, residents, and practicing physicians. Medical school and residency curricula, although improving, offer relatively little teaching in palliative care principles and practice.10,11
In 2000 the Liaison Committee on Medical Education mandated that medical school curricula include “important aspects of … end-of-life-care.” That same year the Accreditation Council for Graduate Medical Education encouraged internal medicine training programs to provide instruction in the principles of palliative care. Inpatient palliative care programs could provide much of this teaching through medical student and resident rotations, informal teaching during the consultation process, and through workshops and grand rounds.
The Financial Argument
Medical costs are rising exponentially due to multiple factors, including effective yet expensive new technologies and an expanding elderly population with more chronic conditions. Under the current Diagnosis Related Group (DRG) system, long, high-intensity hospital stays are causing a fiscal crisis for hospitals. The hospital and insurer of the future will have to work together to learn how to treat serious and complex illness efficiently and in the most cost-effective manner possible. Palliative care programs have the potential to ease this looming crisis through decreasing length of stay, both in the ICU and on the floors, and decreasing direct costs, including radiology, pharmacy, and laboratory costs. Researchers are beginning to document the positive fiscal impacts in rigorous studies.
Palliative Care: The Bottom Line
Palliative care teams have demonstrated improvement in pain and other symptom scores, in patient and family satisfaction with care, and in patient-provider communication. In addition, they have improved compliance with Joint Commission on Accreditation of Healthcare Organizations (JCAHO) quality measures. They have had these positive effects while simultaneously showing decreases in length of stay and costs. As a result, many programs have gained significant financial and administrative support from their hospitals.
Hospitalists and Palliative Care
Many hospitalist groups have found that building and staffing a palliative care consultation team is an important addition to their portfolio of services, further solidifying their value in the eyes of their hospital administration. The professional fee revenues are one more funding source, and palliative care is a critical service the group can provide the institution to improve the quality of care, improve patient satisfaction, and decrease costs.
The work involved in starting a program, including needs assessment, internal marketing, building a financial case, and developing a staffing model, is similar to that done when starting a hospitalist program. Hospitalists are ideally positioned to start palliative care services because they have already built relationships with key administrators and opinion leaders, and they understand the institution’s method for evaluating financial data, and how to access outcome and satisfaction data.
What Hospitalists Gain
By leading and staffing palliative care programs, hospitalists gain visibility and respect from colleagues, and improve their patients’ quality of care and their hospital’s financial bottom line. Clinically palliative care adds variety and depth to the work life of hospitalists and allows them to work with a rich interdisciplinary team. Although hospitalists should obtain additional training, they already possess the building blocks to provide excellent palliative care, such as skillfully leading family conferences and treating complex symptoms. When wearing the palliative care “hat,” providers have the luxury of spending more time at a patient’s bedside discussing what is truly important to the patient and his or her loved ones. The work is meaningful and rewarding.
Obtaining the Tools to Start a Program
The Center to Advance Palliative Care (CAPC), funded by the Robert Wood Johnson Foundation, is dedicated to advancing inpatient palliative care programs through their Web site (www.capc.org) and through their manual, “A Guide to Building a Hospital-Based Palliative Care Program,” available for purchase on its Web site.
In addition, CAPC sponsors the six national Palliative Care Leadership Centers (PCLCs) that each hold two-day, hands-on workshops on the nuts and bolts of starting inpatient palliative care programs, followed by a year of personalized mentoring by phone. The University of California, San Francisco’s PCLC, which is tailored specifically to hospitalists, will hold its last workshop in April 2006. For more information, visit www.capc.org/palliative-care-leadership-initiative.
At the upcoming SHM Annual Meeting in May, the Palliative Care Taskforce will present a workshop, “The Basic Why and How to Develop a Hospital-Based Palliative Care Program.”
Obtaining the Clinical Expertise
There are numerous opportunities for hospitalists to gain clinical expertise in palliative care, including Web-based and written materials and CME courses. Highlights include the Education in Palliative and End of Life Care programs; courses and study guides through the American Association of Hospice and Palliative Medicine, as well as Fast Facts (one-page synopses of relevant palliative care concepts that can be made into handouts or downloaded to one’s PDA). For more information on these resources and others, visit www.capc.org/palliative-care-professional-development/Education_Material_for _Professionals.
In addition, on Thursday, May 4, at 1:20, there will be a breakout session on pain management at the SHM Annual Meeting.
Hospitalists and other physicians can get certified in Hospice and Palliative Medicine by documenting relevant clinical experience and sitting for a qualifying exam. The American Board of Hospice and Palliative Medicine will administer its last exam in November 2006 (final application deadline is May 31, 2006). In September 2006 the field of Hospice and Palliative Medicine is expected to win American Board of Medical Specialties’ (ABMS) recognition as a subspecialty. After that the ABMS will take over administration of the exams. There will likely be a grandfathering period with the ABMS in which relevant clinical experience can substitute for completion of an ACGME-approved palliative care fellowship. For more information, visit the AAHPM Web site at www.abhpm.org/gfxc_100.aspx.
Summary/Conclusions
Inpatient palliative care programs benefit patients, hospitalists, and hospitals alike. Hospitalists are in the perfect position to lead the next generation of inpatient palliative care programs. Currently, about 20% of hospitals in the United States have programs. With the help of hospitalists, the percentage can increase significantly.
Special thanks to Diane Meier, MD, whose work inspired and informed this article.
References
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatment. The SUPPORT Principal Investigators. JAMA. 1995;274:1591-1598.
- Nelson JE, Meier DE, Oei EJ, et al. Self-reported
- symptom experience of critically ill cancer patients receiving intensive care. Crit Care Med. 2001;29 (2):277-282.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999;341 (13):956-963.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Understanding economic and other burdens of terminal Illness: the experience of patients and their caregivers. Ann Intern Med. 2000;132(6):451-459.
- Tolle et al. The Oregon report card: Improving care of the dying. 1999. Available at www.ohsu.edu/ethics/barriers2.pdf. Last accessed Feb. 3, 2006.
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282 (23):2215-2219.
- Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients’ families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994;272:1839-1844.
- Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA. 1999;281(2):163-168.
- U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Table 2a. US Census Bureau/CDC. 2002. Available at www.census.gov/ipc/www/usinterimproj/. Last accessed Feb. 3, 2006.
- Meier DE, Morrison RS, Cassel CK. Improving palliative care. Ann Intern Med. 1997;127:225-230.
- Billings JA, Block S. Palliative care in undergraduate medical education. Status report and future directions. JAMA. 1997;278:733-738.
Update:
New Hospitalist Productivity & Compensation Data
Survey results to be presented at 2006 SHM Annual Meeting
By the end of the data collection period in December 2005 approximately 400 hospital medicine programs had submitted responses for SHM’s 2005-2006 Hospitalist Productivity and Compensation Survey—a 35% increase from 2003. In addition to salary and production trends, this year’s survey should provide new insights into hospitalist responsibilities, the concerns of hospitalist program leaders, night coverage arrangements, and the use of nurse practitioners and physician assistants.
SHM thanks the program leaders who completed the comprehensive survey questionnaire. The following participants were randomly selected to receive awards:
- Danny Moore, MD, of Gilmore Memorial Hospital (Amory, Miss.) received a complimentary registration at the SHM Leadership Academy; and
- Four hospitalists received complimentary registration to the SHM Annual Meeting: Adrienne L. Bennett, MD, PhD, Ohio State University College of Medicine (Columbus, Ohio); Jasvinder S. Dhillon, St. Mary’s Hospital PICU Pediatric Hospitalist Program (Richmond, Va.); Howard Dubin, MD, Inpatient Medical Services of Bristol Hospital (Cheshire, Conn.); and Sujith Sundararaj MD, Signature Healthcare Solutions (Chicago).
The results of the 2005-2006 Hospitalist Productivity and Compensation Survey will be presented for the first time on Thursday, May 4 at 8:10 a.m. at the SHM Annual Meeting. A panel representing different perspectives within hospital medicine will react to the data. The panelists—SHM co-founder John Nelson, MD, President-Elect Mary Jo Gorman, MD, and Past-President Bob Wachter, MD—will represent hospital-employed practices, private groups, and academic programs, respectively. A report of the survey results will be available to survey participants for free. SHM members will be able to purchase the report at a discounted price. TH
The Benchmarks Committee has completed the data accumulation portion of the SHM 2005-2006 Productivity and Compensation Survey. As you might recall, we set a goal of 400 group respondents. With a final push for responses in early December, we exceeded our target. The responses were invaluable in making this survey a worthwhile effort and a credible reflection of the national hospitalist movement.
The Benchmarks Committee would like to specially thank those who attempted to complete the survey online and gave us feedback on this process. We had a few glitches with the online survey, and thanks to these folks and their communication we learned a few valuable lessons regarding this electronic process. We were able to intervene immediately and re-direct folks to the written survey. We’ll apply these lessons to the electronic component of future surveys as well.
Over the next few months we will be analyzing the data in preparation for presentation of the results to be offered up initially at the SHM Annual Meeting in Washington, D.C., the first week in May. (Visit www.hospitalmedicine.org under “Upcoming Events” to register.) Additionally, results will be available to survey participants online later in the year following the national presentation.
On a different note, the committee continues to work on the Hospitalist Dashboard Project. We are creating a dashboard that deals with metrics in the categories of resource utilization, clinical quality, productivity, and satisfaction.
Subsequently, we have worked through a Delphi process to whittle a long list of possible metrics down to 10 key metrics. These have been divided among the committee members, who will use an agreed-upon outline to write a brief description of the metric, how it is measured, and how it can be utilized to manage a hospitalist practice. The final product will be a white paper made available to the SHM membership.
How to Develop a Hospital-Based Palliative Care Program
Why your hospital needs such a program and how to create it
By Eva H. Chittenden, MD, and the SHM Palliative Care Task Force
Palliative care consists of medical care focused on the relief of suffering for patients living with chronic, advanced illness and it also helps their families. It is offered at any stage of disease, concurrently with all other appropriate medical treatment.
Palliative care providers treat the many physical symptoms that patients experience, including pain, dyspnea, nausea, and delirium. In addition, providers assist patients and families with complex medical decision-making, and attend to patients’ and families’ spiritual and psychosocial needs. Physicians work closely with an interdisciplinary team of nurses, chaplains, social workers, and pharmacists. Care continues beyond the point of death, with phone calls and consolation letters, as well as bereavement services.
Arguments for inpatient Palliative Care
The clinical imperative: We need better quality of care for people with serious and complex illness. The multicenter SUPPORT study, published in JAMA in 1995, looked at more than 9,000 hospitalized patients with life-threatening illness and demonstrated significant problems with pain and symptom control and with patient-doctor communication.1 Of the patients who died, more than 50% had moderate to severe pain more than half the time during the last three days of their lives. Of patients preferring do-not-resuscitate status, less than 50% of their physicians were aware of their wishes.
In another study, Nelson, et al. documented that more than half of cancer patients receiving intensive care had moderate to severe pain, anxiety, thirst, and hunger, and that 75% had moderate to severe discomfort of some kind.2 These studies have been a wake-up call to clinicians and hospitals across the country.
Patient and Family Preferences
Family members—especially women—shoulder most of the care of patients with serious illness. A minority of caregivers are over age 65 themselves and in ill health. When asked what they want from the medical system, family caregivers ask for help with transportation and personal care of their loved one at home, and for better home nursing support. They want 24/7 access to providers, better communication with their doctors, and to be remembered and contacted after the death of their family member.3-5 Caregiving itself has been shown to increase likelihood of premature mortality and lead to financial crisis.6
In the SUPPORT study, one-third of families lost most of their savings due to illness.7 Patients want pain and symptom control, avoidance of inappropriate prolongation of the dying process, and relief of burdens on family.8 Palliative care programs, both inpatient and ambulatory, can help provide families with needed services and improve communication at all levels.
The Demographic Argument
Hospitals need palliative care to effectively treat the growing numbers of people with serious, advanced, and complex illness. By 2030, the number of people over age 85 will double to almost 10 million.9 Many of these patients will have multiple chronic conditions, making their care complicated and expensive. And for many chronic conditions, including heart and lung disease, diabetes, and hypertension, death is not predictable.
Therefore, people need better care throughout the multiyear course of advanced illness. And while the Medicare Hospice Benefit is helpful for care of the dying (defined as people with six months or less to live) we need additional approaches for the much larger number of patients with chronic, progressive illness, years to live, continued benefit from disease-modifying therapy, and obvious palliative care needs.
The Educational Imperative
Hospitals are the site of training for most clinicians. Researchers have documented significant deficits in palliative care knowledge, skills, and attitudes among medical students, residents, and practicing physicians. Medical school and residency curricula, although improving, offer relatively little teaching in palliative care principles and practice.10,11
In 2000 the Liaison Committee on Medical Education mandated that medical school curricula include “important aspects of … end-of-life-care.” That same year the Accreditation Council for Graduate Medical Education encouraged internal medicine training programs to provide instruction in the principles of palliative care. Inpatient palliative care programs could provide much of this teaching through medical student and resident rotations, informal teaching during the consultation process, and through workshops and grand rounds.
The Financial Argument
Medical costs are rising exponentially due to multiple factors, including effective yet expensive new technologies and an expanding elderly population with more chronic conditions. Under the current Diagnosis Related Group (DRG) system, long, high-intensity hospital stays are causing a fiscal crisis for hospitals. The hospital and insurer of the future will have to work together to learn how to treat serious and complex illness efficiently and in the most cost-effective manner possible. Palliative care programs have the potential to ease this looming crisis through decreasing length of stay, both in the ICU and on the floors, and decreasing direct costs, including radiology, pharmacy, and laboratory costs. Researchers are beginning to document the positive fiscal impacts in rigorous studies.
Palliative Care: The Bottom Line
Palliative care teams have demonstrated improvement in pain and other symptom scores, in patient and family satisfaction with care, and in patient-provider communication. In addition, they have improved compliance with Joint Commission on Accreditation of Healthcare Organizations (JCAHO) quality measures. They have had these positive effects while simultaneously showing decreases in length of stay and costs. As a result, many programs have gained significant financial and administrative support from their hospitals.
Hospitalists and Palliative Care
Many hospitalist groups have found that building and staffing a palliative care consultation team is an important addition to their portfolio of services, further solidifying their value in the eyes of their hospital administration. The professional fee revenues are one more funding source, and palliative care is a critical service the group can provide the institution to improve the quality of care, improve patient satisfaction, and decrease costs.
The work involved in starting a program, including needs assessment, internal marketing, building a financial case, and developing a staffing model, is similar to that done when starting a hospitalist program. Hospitalists are ideally positioned to start palliative care services because they have already built relationships with key administrators and opinion leaders, and they understand the institution’s method for evaluating financial data, and how to access outcome and satisfaction data.
What Hospitalists Gain
By leading and staffing palliative care programs, hospitalists gain visibility and respect from colleagues, and improve their patients’ quality of care and their hospital’s financial bottom line. Clinically palliative care adds variety and depth to the work life of hospitalists and allows them to work with a rich interdisciplinary team. Although hospitalists should obtain additional training, they already possess the building blocks to provide excellent palliative care, such as skillfully leading family conferences and treating complex symptoms. When wearing the palliative care “hat,” providers have the luxury of spending more time at a patient’s bedside discussing what is truly important to the patient and his or her loved ones. The work is meaningful and rewarding.
Obtaining the Tools to Start a Program
The Center to Advance Palliative Care (CAPC), funded by the Robert Wood Johnson Foundation, is dedicated to advancing inpatient palliative care programs through their Web site (www.capc.org) and through their manual, “A Guide to Building a Hospital-Based Palliative Care Program,” available for purchase on its Web site.
In addition, CAPC sponsors the six national Palliative Care Leadership Centers (PCLCs) that each hold two-day, hands-on workshops on the nuts and bolts of starting inpatient palliative care programs, followed by a year of personalized mentoring by phone. The University of California, San Francisco’s PCLC, which is tailored specifically to hospitalists, will hold its last workshop in April 2006. For more information, visit www.capc.org/palliative-care-leadership-initiative.
At the upcoming SHM Annual Meeting in May, the Palliative Care Taskforce will present a workshop, “The Basic Why and How to Develop a Hospital-Based Palliative Care Program.”
Obtaining the Clinical Expertise
There are numerous opportunities for hospitalists to gain clinical expertise in palliative care, including Web-based and written materials and CME courses. Highlights include the Education in Palliative and End of Life Care programs; courses and study guides through the American Association of Hospice and Palliative Medicine, as well as Fast Facts (one-page synopses of relevant palliative care concepts that can be made into handouts or downloaded to one’s PDA). For more information on these resources and others, visit www.capc.org/palliative-care-professional-development/Education_Material_for _Professionals.
In addition, on Thursday, May 4, at 1:20, there will be a breakout session on pain management at the SHM Annual Meeting.
Hospitalists and other physicians can get certified in Hospice and Palliative Medicine by documenting relevant clinical experience and sitting for a qualifying exam. The American Board of Hospice and Palliative Medicine will administer its last exam in November 2006 (final application deadline is May 31, 2006). In September 2006 the field of Hospice and Palliative Medicine is expected to win American Board of Medical Specialties’ (ABMS) recognition as a subspecialty. After that the ABMS will take over administration of the exams. There will likely be a grandfathering period with the ABMS in which relevant clinical experience can substitute for completion of an ACGME-approved palliative care fellowship. For more information, visit the AAHPM Web site at www.abhpm.org/gfxc_100.aspx.
Summary/Conclusions
Inpatient palliative care programs benefit patients, hospitalists, and hospitals alike. Hospitalists are in the perfect position to lead the next generation of inpatient palliative care programs. Currently, about 20% of hospitals in the United States have programs. With the help of hospitalists, the percentage can increase significantly.
Special thanks to Diane Meier, MD, whose work inspired and informed this article.
References
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatment. The SUPPORT Principal Investigators. JAMA. 1995;274:1591-1598.
- Nelson JE, Meier DE, Oei EJ, et al. Self-reported
- symptom experience of critically ill cancer patients receiving intensive care. Crit Care Med. 2001;29 (2):277-282.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999;341 (13):956-963.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Understanding economic and other burdens of terminal Illness: the experience of patients and their caregivers. Ann Intern Med. 2000;132(6):451-459.
- Tolle et al. The Oregon report card: Improving care of the dying. 1999. Available at www.ohsu.edu/ethics/barriers2.pdf. Last accessed Feb. 3, 2006.
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282 (23):2215-2219.
- Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients’ families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994;272:1839-1844.
- Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA. 1999;281(2):163-168.
- U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Table 2a. US Census Bureau/CDC. 2002. Available at www.census.gov/ipc/www/usinterimproj/. Last accessed Feb. 3, 2006.
- Meier DE, Morrison RS, Cassel CK. Improving palliative care. Ann Intern Med. 1997;127:225-230.
- Billings JA, Block S. Palliative care in undergraduate medical education. Status report and future directions. JAMA. 1997;278:733-738.
Update:
New Hospitalist Productivity & Compensation Data
Survey results to be presented at 2006 SHM Annual Meeting
By the end of the data collection period in December 2005 approximately 400 hospital medicine programs had submitted responses for SHM’s 2005-2006 Hospitalist Productivity and Compensation Survey—a 35% increase from 2003. In addition to salary and production trends, this year’s survey should provide new insights into hospitalist responsibilities, the concerns of hospitalist program leaders, night coverage arrangements, and the use of nurse practitioners and physician assistants.
SHM thanks the program leaders who completed the comprehensive survey questionnaire. The following participants were randomly selected to receive awards:
- Danny Moore, MD, of Gilmore Memorial Hospital (Amory, Miss.) received a complimentary registration at the SHM Leadership Academy; and
- Four hospitalists received complimentary registration to the SHM Annual Meeting: Adrienne L. Bennett, MD, PhD, Ohio State University College of Medicine (Columbus, Ohio); Jasvinder S. Dhillon, St. Mary’s Hospital PICU Pediatric Hospitalist Program (Richmond, Va.); Howard Dubin, MD, Inpatient Medical Services of Bristol Hospital (Cheshire, Conn.); and Sujith Sundararaj MD, Signature Healthcare Solutions (Chicago).
The results of the 2005-2006 Hospitalist Productivity and Compensation Survey will be presented for the first time on Thursday, May 4 at 8:10 a.m. at the SHM Annual Meeting. A panel representing different perspectives within hospital medicine will react to the data. The panelists—SHM co-founder John Nelson, MD, President-Elect Mary Jo Gorman, MD, and Past-President Bob Wachter, MD—will represent hospital-employed practices, private groups, and academic programs, respectively. A report of the survey results will be available to survey participants for free. SHM members will be able to purchase the report at a discounted price. TH
A Case of Shortness of Breath, Abdominal Pain, and Hematuria
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
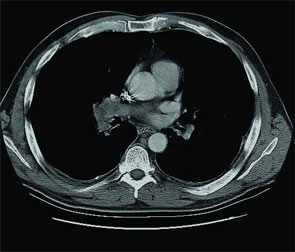
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5

Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
The Colonial Formulary
Pharmacies have plotted a dynamic course through history, arriving late to North America in relation to other nations. Before the origin of the first true hospital pharmacy, medicinal therapies were often distributed by public officials, heads of households, and religious leaders or sold in drug stores and other free-standing apothecaries. Colonists followed books on self-treatment and methods of cultivating herbs. With the introduction of hospitals came the hospital pharmacy.
Great Britain had long been a glowing example of how pharmacists could prepare, compound, and administer prescriptions ordered by physicians in an organized manner. In contrast, the role of physicians, surgeons, and apothecaries in the British colonies were blurred, each with overlapping responsibilities of caring for patients and treating ailments.
It was not until 1751 after Benjamin Franklin and Dr. Thomas Bond founded the first hospital in the British Colonies—Pennsylvania Hospital in Philadelphia—that the idea for a hospital pharmacy was cultivated in North America. Because the first hospital’s mission was to provide charity for the poor, there initially was resistance to Dr. Bond’s idea of creating an apothecary in the same institution. Colonists feared that it would become costly to those in Philadelphia being served by the hospital. However, with Franklin’s persuading, enough funds were eventually solicited to purchase more than 112 pounds worth of drugs from London. In 1752, these drugs filled shelves in the hospital president’s office in the Pine Building of Pennsylvania Hospital instituting the first “Apothecary’s Shop in the Hospital” in the British colonies.
The first salaried hospital pharmacist, making 15 pounds per year, was Jonathon Roberts who worked until 1755 fulfilling the role of preparing medications requested by physicians. Medical and surgical students were often hired for short tenures in the apothecary to obtain experience in pharmacy or to simply cover their room and board expenses. John Morgan replaced Roberts in May 1755, and he worked for only one year before using that experience as a springboard for stirring up great influence in the future direction of American pharmacy. Morgan went on to become a physician and a vocal advocate for a more distinct separation of professions among physicians, surgeons, and pharmacists in America.
Most of the drugs available in the first American hospital pharmacy could be found in the London Pharmacopoeia of 1650, whereas very few drugs were of North American origin. Contributions from the colonies came primarily from the American Indian traditions that involved the extraction of botanical drugs such as cascara, bloodroot, and jalap. Nearly 170 of these particular preparations used by Indians north of the Rio Grande or their derivatives are still used today.
Other drugs used at the time of the first hospital pharmacy included emetic ipecac, an expectorant made of benzoin known as “Jesuit’s Drops,” antimony in “Plummer’s Pills,” and tincture of lavender (originally referred to as “Palsy Drops” and used to treat muscle spasms and headaches).
The advent of the American Revolution made importing drugs nearly impossible, requiring an increase in the number of patented drugs from North America. The first colonial hospital pharmacy, thanks to the ingenuity and persistence of Benjamin Franklin and Dr. Bond, set the stage for the development and transformation of pharmacies as we know them to today. TH
Nordman is a senior medical student at Penn State University.
Resources
- Bender GA. The First Hospital Pharmacy in Colonial America. In: Great Moments in Pharmacy. Detroit: Northwood Institute Press; 1966:84-87.
- Franklin B. Some Account of the Pennsylvania Hospital. Baltimore: The Johns Hopkins Press; 1954.
- Harris MR, Paracandola J. Images of Hospital Pharmacy in America. Am J Hosp Pharm. Reprint. June 1992.
- Lawall CH. Four Thousand Years of Pharmacy: An Outline History of Pharmacy and the Allied Sciences. Philadelphia: Lippincott; 1927.
- Massengill SE. American Pharmacy. In: A Sketch of Medicine and Pharmacy. Bristol, Tenn.: The S.E. Massengill Company. Chapter XV.
- Osborne GE. Pharmacy in British Colonial America. In: Bender GA, Parascandolam J, eds. American Pharmacy in the Colonial and Revolutionary Periods: A Bicentential Symposium held April 5, 1976. Madison, Wis.: American Institute of Pharmacy; 1977.
- Williams WH. Pharmacists at America’s First Hospital, 1752–1841 [abstract]. Am J Health Sys Pharm. 1976;33:804-804.
Pharmacies have plotted a dynamic course through history, arriving late to North America in relation to other nations. Before the origin of the first true hospital pharmacy, medicinal therapies were often distributed by public officials, heads of households, and religious leaders or sold in drug stores and other free-standing apothecaries. Colonists followed books on self-treatment and methods of cultivating herbs. With the introduction of hospitals came the hospital pharmacy.
Great Britain had long been a glowing example of how pharmacists could prepare, compound, and administer prescriptions ordered by physicians in an organized manner. In contrast, the role of physicians, surgeons, and apothecaries in the British colonies were blurred, each with overlapping responsibilities of caring for patients and treating ailments.
It was not until 1751 after Benjamin Franklin and Dr. Thomas Bond founded the first hospital in the British Colonies—Pennsylvania Hospital in Philadelphia—that the idea for a hospital pharmacy was cultivated in North America. Because the first hospital’s mission was to provide charity for the poor, there initially was resistance to Dr. Bond’s idea of creating an apothecary in the same institution. Colonists feared that it would become costly to those in Philadelphia being served by the hospital. However, with Franklin’s persuading, enough funds were eventually solicited to purchase more than 112 pounds worth of drugs from London. In 1752, these drugs filled shelves in the hospital president’s office in the Pine Building of Pennsylvania Hospital instituting the first “Apothecary’s Shop in the Hospital” in the British colonies.
The first salaried hospital pharmacist, making 15 pounds per year, was Jonathon Roberts who worked until 1755 fulfilling the role of preparing medications requested by physicians. Medical and surgical students were often hired for short tenures in the apothecary to obtain experience in pharmacy or to simply cover their room and board expenses. John Morgan replaced Roberts in May 1755, and he worked for only one year before using that experience as a springboard for stirring up great influence in the future direction of American pharmacy. Morgan went on to become a physician and a vocal advocate for a more distinct separation of professions among physicians, surgeons, and pharmacists in America.
Most of the drugs available in the first American hospital pharmacy could be found in the London Pharmacopoeia of 1650, whereas very few drugs were of North American origin. Contributions from the colonies came primarily from the American Indian traditions that involved the extraction of botanical drugs such as cascara, bloodroot, and jalap. Nearly 170 of these particular preparations used by Indians north of the Rio Grande or their derivatives are still used today.
Other drugs used at the time of the first hospital pharmacy included emetic ipecac, an expectorant made of benzoin known as “Jesuit’s Drops,” antimony in “Plummer’s Pills,” and tincture of lavender (originally referred to as “Palsy Drops” and used to treat muscle spasms and headaches).
The advent of the American Revolution made importing drugs nearly impossible, requiring an increase in the number of patented drugs from North America. The first colonial hospital pharmacy, thanks to the ingenuity and persistence of Benjamin Franklin and Dr. Bond, set the stage for the development and transformation of pharmacies as we know them to today. TH
Nordman is a senior medical student at Penn State University.
Resources
- Bender GA. The First Hospital Pharmacy in Colonial America. In: Great Moments in Pharmacy. Detroit: Northwood Institute Press; 1966:84-87.
- Franklin B. Some Account of the Pennsylvania Hospital. Baltimore: The Johns Hopkins Press; 1954.
- Harris MR, Paracandola J. Images of Hospital Pharmacy in America. Am J Hosp Pharm. Reprint. June 1992.
- Lawall CH. Four Thousand Years of Pharmacy: An Outline History of Pharmacy and the Allied Sciences. Philadelphia: Lippincott; 1927.
- Massengill SE. American Pharmacy. In: A Sketch of Medicine and Pharmacy. Bristol, Tenn.: The S.E. Massengill Company. Chapter XV.
- Osborne GE. Pharmacy in British Colonial America. In: Bender GA, Parascandolam J, eds. American Pharmacy in the Colonial and Revolutionary Periods: A Bicentential Symposium held April 5, 1976. Madison, Wis.: American Institute of Pharmacy; 1977.
- Williams WH. Pharmacists at America’s First Hospital, 1752–1841 [abstract]. Am J Health Sys Pharm. 1976;33:804-804.
Pharmacies have plotted a dynamic course through history, arriving late to North America in relation to other nations. Before the origin of the first true hospital pharmacy, medicinal therapies were often distributed by public officials, heads of households, and religious leaders or sold in drug stores and other free-standing apothecaries. Colonists followed books on self-treatment and methods of cultivating herbs. With the introduction of hospitals came the hospital pharmacy.
Great Britain had long been a glowing example of how pharmacists could prepare, compound, and administer prescriptions ordered by physicians in an organized manner. In contrast, the role of physicians, surgeons, and apothecaries in the British colonies were blurred, each with overlapping responsibilities of caring for patients and treating ailments.
It was not until 1751 after Benjamin Franklin and Dr. Thomas Bond founded the first hospital in the British Colonies—Pennsylvania Hospital in Philadelphia—that the idea for a hospital pharmacy was cultivated in North America. Because the first hospital’s mission was to provide charity for the poor, there initially was resistance to Dr. Bond’s idea of creating an apothecary in the same institution. Colonists feared that it would become costly to those in Philadelphia being served by the hospital. However, with Franklin’s persuading, enough funds were eventually solicited to purchase more than 112 pounds worth of drugs from London. In 1752, these drugs filled shelves in the hospital president’s office in the Pine Building of Pennsylvania Hospital instituting the first “Apothecary’s Shop in the Hospital” in the British colonies.
The first salaried hospital pharmacist, making 15 pounds per year, was Jonathon Roberts who worked until 1755 fulfilling the role of preparing medications requested by physicians. Medical and surgical students were often hired for short tenures in the apothecary to obtain experience in pharmacy or to simply cover their room and board expenses. John Morgan replaced Roberts in May 1755, and he worked for only one year before using that experience as a springboard for stirring up great influence in the future direction of American pharmacy. Morgan went on to become a physician and a vocal advocate for a more distinct separation of professions among physicians, surgeons, and pharmacists in America.
Most of the drugs available in the first American hospital pharmacy could be found in the London Pharmacopoeia of 1650, whereas very few drugs were of North American origin. Contributions from the colonies came primarily from the American Indian traditions that involved the extraction of botanical drugs such as cascara, bloodroot, and jalap. Nearly 170 of these particular preparations used by Indians north of the Rio Grande or their derivatives are still used today.
Other drugs used at the time of the first hospital pharmacy included emetic ipecac, an expectorant made of benzoin known as “Jesuit’s Drops,” antimony in “Plummer’s Pills,” and tincture of lavender (originally referred to as “Palsy Drops” and used to treat muscle spasms and headaches).
The advent of the American Revolution made importing drugs nearly impossible, requiring an increase in the number of patented drugs from North America. The first colonial hospital pharmacy, thanks to the ingenuity and persistence of Benjamin Franklin and Dr. Bond, set the stage for the development and transformation of pharmacies as we know them to today. TH
Nordman is a senior medical student at Penn State University.
Resources
- Bender GA. The First Hospital Pharmacy in Colonial America. In: Great Moments in Pharmacy. Detroit: Northwood Institute Press; 1966:84-87.
- Franklin B. Some Account of the Pennsylvania Hospital. Baltimore: The Johns Hopkins Press; 1954.
- Harris MR, Paracandola J. Images of Hospital Pharmacy in America. Am J Hosp Pharm. Reprint. June 1992.
- Lawall CH. Four Thousand Years of Pharmacy: An Outline History of Pharmacy and the Allied Sciences. Philadelphia: Lippincott; 1927.
- Massengill SE. American Pharmacy. In: A Sketch of Medicine and Pharmacy. Bristol, Tenn.: The S.E. Massengill Company. Chapter XV.
- Osborne GE. Pharmacy in British Colonial America. In: Bender GA, Parascandolam J, eds. American Pharmacy in the Colonial and Revolutionary Periods: A Bicentential Symposium held April 5, 1976. Madison, Wis.: American Institute of Pharmacy; 1977.
- Williams WH. Pharmacists at America’s First Hospital, 1752–1841 [abstract]. Am J Health Sys Pharm. 1976;33:804-804.
Medication Compliance, the New C. Diff
The Tricky Nature of Medication Compliance
Review by Osterberg L, Blaschke T. Adherence to Medication. N Engl J Med. 2005;353:487-497.
Adherence to (or compliance with) a medication regimen is generally defined as the extent to which patients take medications as prescribed by their healthcare providers. Adherence rates are typically higher among patients with acute conditions, as compared with those with chronic conditions; persistence among patients with chronic conditions is disappointingly low, dropping most drastically after the first six months of therapy. Of all medication-related hospital admissions in the United States, 33% to 69% are because of poor medication adherence, with a resultant cost of approximately $100 billion a year.
Electronic medication-monitoring devices have provided very detailed information about the patterns of medication-taking behavior. Studies using these monitors have shown six general patterns of taking medication among patients treated for chronic illnesses who continue to take their medications. Approximately one-sixth come close to perfect adherence to a regimen; one-sixth take nearly all doses, but with some timing irregularity; one-sixth miss an occasional single day’s dose and have some timing inconsistency; one-sixth take drug holidays three to four times a year, with occasional omissions of doses; one-sixth have a drug holiday monthly or more often, with frequent omissions of doses; and one-sixth take few or no doses while giving the impression of good adherence.
Poor adherence to medication regimens is common, contributing to substantial worsening of disease, death, and increased healthcare costs. Practitioners should always look for poor adherence and can enhance adherence by emphasizing the value of a patient’s regimen, making the regimen simple, and customizing the regimen to the patient’s lifestyle. Asking patients nonjudgmentally about medication-taking behavior is a practical strategy for identifying poor adherence. A collaborative approach to care augments adherence. Patients who have difficulty maintaining adequate adherence need more intensive strategies than do patients who have less difficulty with adherence, a more forgiving medication regimen, or both. Innovative methods of managing chronic diseases have had some success in improving adherence when a regimen has been difficult to follow.
The New Clostridium Difficile—What Does It Mean?
McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxic gene-variant of Clostridium difficile. N Eng J Med. 2005;353;2433-2441.
Clostridium difficile is the only anaerobe that causes nosocomial infections. It colonizes the colon in 3% of the healthy population and about 20% to 40% of hospitalized patients.
This study was done in response to reports of increasing rate and severity of this infection. This study looked at healthcare facilities in Pennsylvania, Maine, Georgia, Oregon, Illinois, and New Jersey and did indeed find a new strain of Clostridium difficile isolate which showed 100% resistance to gatifloxacin and moxifloxacin, compared with no resistance in the historic strain.
Resistance to clindamycin was similar in both the groups, which was measured at 79%. This particular strain secretes 16 to 23 times more toxins A and B in vitro than other strains. And in this study the new strain accounted for 51% of the infections compared with 17% in the historic control isolates. Fluoroquinolones were implicated alone or in combination with other antibiotics in 52% of the cases. Those infected with the new strain were more likely to have higher rates of toxic megacolon, need for colectomy, leukemoid reaction, shock, and death. Like any disease, the interaction between host and pathogen is key to severity, thereby making patients who are chronically ill and elderly more susceptible.
For hospitalists the implications for this study are certainly important. We need to be aware of whether this strain is prevalent in our work environment. Close collaboration with our colleagues from infectious disease services along with monitoring clinical outcomes of patients with Clostridium difficile infection is the need of the hour. Also recommended is investigation of any increases in caseload of this infection. Simple measures such as judicious use of antibiotics, early diagnosis, and appropriate treatment of Clostridium difficile infection and strict isolation of the patients infected or colonized with Clostridium difficile would go a long way in controlling the spread of the new more virulent strain. It must be pointed out that alcohol-based waterless hand-sanitizing agents do not kill the Clostridium difficile spores; washing hands with soap and water is a prudent option after coming in contact with a patient with Clostridium difficile. TH
Nasal MRSA Carriage: A Study of Current Prevalence with Commentary
Creech CB, Kernodle DS, Alsectzer M, et al. Increasing rates of nasal carriage of methicillin-resistant Staphylococcus aureus in healthy children. Pediatr Infect Dis J. 2005;24:617-621.
Review by Laura Ortman, MD
The incidence of methicillin-resistant Staphylococcus aureus (MRSA) infections seen in outpatient clinics and emergency rooms appears to be on the rise. In 2001 a study done at Vanderbilt University Medical Center found the prevalence of MRSA in its pediatric community to be 0.8%1. Creech, et al., devised a study to describe the current prevalence of MRSA colonization in the same population.
The study population was children between the ages of two weeks and 21 years of age presenting for a health maintenance visit at two outpatient clinics. Nasal swabs were obtained and cultures preformed on plates with and without oxacillin containing media. Possible MRSA isolates were confirmed with PCR for the mecA gene, which codes for the protein responsible for beta-lactam resistance.
Of the 500 children enrolled 182 (36.4%) were found to be colonized with S. aureus. 46 (9.2%) isolates were positive for the mecA gene and considered MRSA. The only risk factor found to increase risk for MRSA colonization was having a family member who works in a hospital (odds ratio, 2.0; 95% confidence interval, 1.03-4.1). Fifty-four percent of MRSA isolates were resistant to erythromycin, and 32% of these had inducible clindamycin resistance.
Commentary: This study shows a greater than tenfold increase in MRSA colonization in a three-year time period in a healthy outpatient population. This finding is consistent with other studies that have shown increasing rates of colonization.2-3 This increase has led some institutions to attempt decolonization of MRSA, most often using nasal mupirocin. To determine if current evidence supports attempts to eradicate MRSA nasal colonization, the following literature search was performed: Cochrane DSR, ACP Journal Club, PubMed, and PubMed Clinical Queries were searched using the search terms “MRSA,” “colonization,” and “staphylococcus.”
One Cochrane review summarizes the evidence for use of antimicrobial agents on MRSA colonized patients4. Of six randomized controlled trials, only one compares rates of infection during follow-up between the study and control groups. The difference in infections was not statistically significant. Five other studies of inconsistent quality followed eradication rates of MRSA and varied widely in their results. The Cochrane review concluded that there was insufficient evidence to recommend nasal decolonization of MRSA.
One article reviewed the evidence for intranasal mupirocin for S. aureus.5 This review did not differentiate between MRSA and MSSA. The authors appraised clinical trials that evaluated the effect of mupirocin on MRSA colonization and infection. In a trial of patients undergoing dialysis there was no overall difference in the rate of infection between groups. In trials using mupirocin for preoperative prophylaxis there was no difference in number of surgical site infections. The authors concluded that mupirocin did not result in long-term clearance of S. aureus and that the available evidence does not support its use for prevention of infection. With the current evidence routine decolonization of patients colonized with MRSA cannot be recommended.
References
- Nakamura MM, Rohling KL, Shashaty M, et al. Prevalence of methicillin-resistant Staphylococcus aureus nasal carriage in the community pediatric population. Pediatr Infect Dis J. 2002;21:917-922.
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593-598.
- Fergie JE, Purcell K. Community-acquired methicillin-resistant Staphylococcus aureus infections in south Texas children. Pediatr Infect Dis J. 2001;20:860-863.
- Loeb M, Main C, Walker-Dilks C. Antimicrobial drugs for treating methicillin-resistant Staphylococcus aureus colonization. Cochrane Database Syst Rev. 2003;(4):CD003340.
- Laupland KB, Conly JM. Treatment of Staphylococcus aureus colonization and prophylaxis for infection with topical intranasal mupirocin: an evidence-based review. Clin Infect Dis. 2003;37:933-938.
Is Ultrasound Sufficient for Diagnosing Urolithiasis in the Pediatric Patient?
Palmer JS, Donaher ER, O’Riordan MA, et al. Diagnosis of Pediatric Urolithiasis: Role of ultrasound and computerized tomography. J Urol. 2005;174:1413-1416.
Review by Ann Mattison, RN, CPNP
Pediatric urolithiasis is uncommon and may present without the classic symptoms of renal colic, making diagnosis of pediatric urolithiasis problematic. Previously published data has revealed that unenhanced spiral CT is the gold standard in diagnosing urinary tract calculi in adults. However, CT carries the risk of exposure to ionizing radiation, which can be a significant issue in children.
Due to the low prevalence of urolithiasis in addition to concerns about radiation exposure, many primary care providers choose ultrasound as the initial radiographic study for children with symptoms that can be associated with urolithiasis, such as flank pain, abdominal pain, and gross hematuria. But the accuracy of ultrasound in detecting pediatric urolithiasis has not been well studied.
A retrospective chart review was performed in all patients 0-18 evaluated as outpatients and inpatients at the study institution. Subjects were identified by ICD-9 codes and billing records. The study showed the accuracy of ultrasounds performed was variable and dependent on the location of the calculi. In contrast, CT was highly accurate regardless of calculi location.
The study concluded that ultrasound may still be the appropriate initial study for the majority of children presenting with symptoms suggestive of urolithiasis; however, a negative ultrasound should not be considered sufficient to rule out the diagnosis of urolithiasis in pediatric patients. The authors recommended the patient with persistent symptoms and negative ultrasound undergo unenhanced CT. The retrospective design of this study limits application of these results; however, the study does highlight the need for a heightened index of suspicion for the diagnosis as well as the need for further prospective studies describing the most safe and efficient method for confirming the diagnosis. TH
The Tricky Nature of Medication Compliance
Review by Osterberg L, Blaschke T. Adherence to Medication. N Engl J Med. 2005;353:487-497.
Adherence to (or compliance with) a medication regimen is generally defined as the extent to which patients take medications as prescribed by their healthcare providers. Adherence rates are typically higher among patients with acute conditions, as compared with those with chronic conditions; persistence among patients with chronic conditions is disappointingly low, dropping most drastically after the first six months of therapy. Of all medication-related hospital admissions in the United States, 33% to 69% are because of poor medication adherence, with a resultant cost of approximately $100 billion a year.
Electronic medication-monitoring devices have provided very detailed information about the patterns of medication-taking behavior. Studies using these monitors have shown six general patterns of taking medication among patients treated for chronic illnesses who continue to take their medications. Approximately one-sixth come close to perfect adherence to a regimen; one-sixth take nearly all doses, but with some timing irregularity; one-sixth miss an occasional single day’s dose and have some timing inconsistency; one-sixth take drug holidays three to four times a year, with occasional omissions of doses; one-sixth have a drug holiday monthly or more often, with frequent omissions of doses; and one-sixth take few or no doses while giving the impression of good adherence.
Poor adherence to medication regimens is common, contributing to substantial worsening of disease, death, and increased healthcare costs. Practitioners should always look for poor adherence and can enhance adherence by emphasizing the value of a patient’s regimen, making the regimen simple, and customizing the regimen to the patient’s lifestyle. Asking patients nonjudgmentally about medication-taking behavior is a practical strategy for identifying poor adherence. A collaborative approach to care augments adherence. Patients who have difficulty maintaining adequate adherence need more intensive strategies than do patients who have less difficulty with adherence, a more forgiving medication regimen, or both. Innovative methods of managing chronic diseases have had some success in improving adherence when a regimen has been difficult to follow.
The New Clostridium Difficile—What Does It Mean?
McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxic gene-variant of Clostridium difficile. N Eng J Med. 2005;353;2433-2441.
Clostridium difficile is the only anaerobe that causes nosocomial infections. It colonizes the colon in 3% of the healthy population and about 20% to 40% of hospitalized patients.
This study was done in response to reports of increasing rate and severity of this infection. This study looked at healthcare facilities in Pennsylvania, Maine, Georgia, Oregon, Illinois, and New Jersey and did indeed find a new strain of Clostridium difficile isolate which showed 100% resistance to gatifloxacin and moxifloxacin, compared with no resistance in the historic strain.
Resistance to clindamycin was similar in both the groups, which was measured at 79%. This particular strain secretes 16 to 23 times more toxins A and B in vitro than other strains. And in this study the new strain accounted for 51% of the infections compared with 17% in the historic control isolates. Fluoroquinolones were implicated alone or in combination with other antibiotics in 52% of the cases. Those infected with the new strain were more likely to have higher rates of toxic megacolon, need for colectomy, leukemoid reaction, shock, and death. Like any disease, the interaction between host and pathogen is key to severity, thereby making patients who are chronically ill and elderly more susceptible.
For hospitalists the implications for this study are certainly important. We need to be aware of whether this strain is prevalent in our work environment. Close collaboration with our colleagues from infectious disease services along with monitoring clinical outcomes of patients with Clostridium difficile infection is the need of the hour. Also recommended is investigation of any increases in caseload of this infection. Simple measures such as judicious use of antibiotics, early diagnosis, and appropriate treatment of Clostridium difficile infection and strict isolation of the patients infected or colonized with Clostridium difficile would go a long way in controlling the spread of the new more virulent strain. It must be pointed out that alcohol-based waterless hand-sanitizing agents do not kill the Clostridium difficile spores; washing hands with soap and water is a prudent option after coming in contact with a patient with Clostridium difficile. TH
Nasal MRSA Carriage: A Study of Current Prevalence with Commentary
Creech CB, Kernodle DS, Alsectzer M, et al. Increasing rates of nasal carriage of methicillin-resistant Staphylococcus aureus in healthy children. Pediatr Infect Dis J. 2005;24:617-621.
Review by Laura Ortman, MD
The incidence of methicillin-resistant Staphylococcus aureus (MRSA) infections seen in outpatient clinics and emergency rooms appears to be on the rise. In 2001 a study done at Vanderbilt University Medical Center found the prevalence of MRSA in its pediatric community to be 0.8%1. Creech, et al., devised a study to describe the current prevalence of MRSA colonization in the same population.
The study population was children between the ages of two weeks and 21 years of age presenting for a health maintenance visit at two outpatient clinics. Nasal swabs were obtained and cultures preformed on plates with and without oxacillin containing media. Possible MRSA isolates were confirmed with PCR for the mecA gene, which codes for the protein responsible for beta-lactam resistance.
Of the 500 children enrolled 182 (36.4%) were found to be colonized with S. aureus. 46 (9.2%) isolates were positive for the mecA gene and considered MRSA. The only risk factor found to increase risk for MRSA colonization was having a family member who works in a hospital (odds ratio, 2.0; 95% confidence interval, 1.03-4.1). Fifty-four percent of MRSA isolates were resistant to erythromycin, and 32% of these had inducible clindamycin resistance.
Commentary: This study shows a greater than tenfold increase in MRSA colonization in a three-year time period in a healthy outpatient population. This finding is consistent with other studies that have shown increasing rates of colonization.2-3 This increase has led some institutions to attempt decolonization of MRSA, most often using nasal mupirocin. To determine if current evidence supports attempts to eradicate MRSA nasal colonization, the following literature search was performed: Cochrane DSR, ACP Journal Club, PubMed, and PubMed Clinical Queries were searched using the search terms “MRSA,” “colonization,” and “staphylococcus.”
One Cochrane review summarizes the evidence for use of antimicrobial agents on MRSA colonized patients4. Of six randomized controlled trials, only one compares rates of infection during follow-up between the study and control groups. The difference in infections was not statistically significant. Five other studies of inconsistent quality followed eradication rates of MRSA and varied widely in their results. The Cochrane review concluded that there was insufficient evidence to recommend nasal decolonization of MRSA.
One article reviewed the evidence for intranasal mupirocin for S. aureus.5 This review did not differentiate between MRSA and MSSA. The authors appraised clinical trials that evaluated the effect of mupirocin on MRSA colonization and infection. In a trial of patients undergoing dialysis there was no overall difference in the rate of infection between groups. In trials using mupirocin for preoperative prophylaxis there was no difference in number of surgical site infections. The authors concluded that mupirocin did not result in long-term clearance of S. aureus and that the available evidence does not support its use for prevention of infection. With the current evidence routine decolonization of patients colonized with MRSA cannot be recommended.
References
- Nakamura MM, Rohling KL, Shashaty M, et al. Prevalence of methicillin-resistant Staphylococcus aureus nasal carriage in the community pediatric population. Pediatr Infect Dis J. 2002;21:917-922.
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593-598.
- Fergie JE, Purcell K. Community-acquired methicillin-resistant Staphylococcus aureus infections in south Texas children. Pediatr Infect Dis J. 2001;20:860-863.
- Loeb M, Main C, Walker-Dilks C. Antimicrobial drugs for treating methicillin-resistant Staphylococcus aureus colonization. Cochrane Database Syst Rev. 2003;(4):CD003340.
- Laupland KB, Conly JM. Treatment of Staphylococcus aureus colonization and prophylaxis for infection with topical intranasal mupirocin: an evidence-based review. Clin Infect Dis. 2003;37:933-938.
Is Ultrasound Sufficient for Diagnosing Urolithiasis in the Pediatric Patient?
Palmer JS, Donaher ER, O’Riordan MA, et al. Diagnosis of Pediatric Urolithiasis: Role of ultrasound and computerized tomography. J Urol. 2005;174:1413-1416.
Review by Ann Mattison, RN, CPNP
Pediatric urolithiasis is uncommon and may present without the classic symptoms of renal colic, making diagnosis of pediatric urolithiasis problematic. Previously published data has revealed that unenhanced spiral CT is the gold standard in diagnosing urinary tract calculi in adults. However, CT carries the risk of exposure to ionizing radiation, which can be a significant issue in children.
Due to the low prevalence of urolithiasis in addition to concerns about radiation exposure, many primary care providers choose ultrasound as the initial radiographic study for children with symptoms that can be associated with urolithiasis, such as flank pain, abdominal pain, and gross hematuria. But the accuracy of ultrasound in detecting pediatric urolithiasis has not been well studied.
A retrospective chart review was performed in all patients 0-18 evaluated as outpatients and inpatients at the study institution. Subjects were identified by ICD-9 codes and billing records. The study showed the accuracy of ultrasounds performed was variable and dependent on the location of the calculi. In contrast, CT was highly accurate regardless of calculi location.
The study concluded that ultrasound may still be the appropriate initial study for the majority of children presenting with symptoms suggestive of urolithiasis; however, a negative ultrasound should not be considered sufficient to rule out the diagnosis of urolithiasis in pediatric patients. The authors recommended the patient with persistent symptoms and negative ultrasound undergo unenhanced CT. The retrospective design of this study limits application of these results; however, the study does highlight the need for a heightened index of suspicion for the diagnosis as well as the need for further prospective studies describing the most safe and efficient method for confirming the diagnosis. TH
The Tricky Nature of Medication Compliance
Review by Osterberg L, Blaschke T. Adherence to Medication. N Engl J Med. 2005;353:487-497.
Adherence to (or compliance with) a medication regimen is generally defined as the extent to which patients take medications as prescribed by their healthcare providers. Adherence rates are typically higher among patients with acute conditions, as compared with those with chronic conditions; persistence among patients with chronic conditions is disappointingly low, dropping most drastically after the first six months of therapy. Of all medication-related hospital admissions in the United States, 33% to 69% are because of poor medication adherence, with a resultant cost of approximately $100 billion a year.
Electronic medication-monitoring devices have provided very detailed information about the patterns of medication-taking behavior. Studies using these monitors have shown six general patterns of taking medication among patients treated for chronic illnesses who continue to take their medications. Approximately one-sixth come close to perfect adherence to a regimen; one-sixth take nearly all doses, but with some timing irregularity; one-sixth miss an occasional single day’s dose and have some timing inconsistency; one-sixth take drug holidays three to four times a year, with occasional omissions of doses; one-sixth have a drug holiday monthly or more often, with frequent omissions of doses; and one-sixth take few or no doses while giving the impression of good adherence.
Poor adherence to medication regimens is common, contributing to substantial worsening of disease, death, and increased healthcare costs. Practitioners should always look for poor adherence and can enhance adherence by emphasizing the value of a patient’s regimen, making the regimen simple, and customizing the regimen to the patient’s lifestyle. Asking patients nonjudgmentally about medication-taking behavior is a practical strategy for identifying poor adherence. A collaborative approach to care augments adherence. Patients who have difficulty maintaining adequate adherence need more intensive strategies than do patients who have less difficulty with adherence, a more forgiving medication regimen, or both. Innovative methods of managing chronic diseases have had some success in improving adherence when a regimen has been difficult to follow.
The New Clostridium Difficile—What Does It Mean?
McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxic gene-variant of Clostridium difficile. N Eng J Med. 2005;353;2433-2441.
Clostridium difficile is the only anaerobe that causes nosocomial infections. It colonizes the colon in 3% of the healthy population and about 20% to 40% of hospitalized patients.
This study was done in response to reports of increasing rate and severity of this infection. This study looked at healthcare facilities in Pennsylvania, Maine, Georgia, Oregon, Illinois, and New Jersey and did indeed find a new strain of Clostridium difficile isolate which showed 100% resistance to gatifloxacin and moxifloxacin, compared with no resistance in the historic strain.
Resistance to clindamycin was similar in both the groups, which was measured at 79%. This particular strain secretes 16 to 23 times more toxins A and B in vitro than other strains. And in this study the new strain accounted for 51% of the infections compared with 17% in the historic control isolates. Fluoroquinolones were implicated alone or in combination with other antibiotics in 52% of the cases. Those infected with the new strain were more likely to have higher rates of toxic megacolon, need for colectomy, leukemoid reaction, shock, and death. Like any disease, the interaction between host and pathogen is key to severity, thereby making patients who are chronically ill and elderly more susceptible.
For hospitalists the implications for this study are certainly important. We need to be aware of whether this strain is prevalent in our work environment. Close collaboration with our colleagues from infectious disease services along with monitoring clinical outcomes of patients with Clostridium difficile infection is the need of the hour. Also recommended is investigation of any increases in caseload of this infection. Simple measures such as judicious use of antibiotics, early diagnosis, and appropriate treatment of Clostridium difficile infection and strict isolation of the patients infected or colonized with Clostridium difficile would go a long way in controlling the spread of the new more virulent strain. It must be pointed out that alcohol-based waterless hand-sanitizing agents do not kill the Clostridium difficile spores; washing hands with soap and water is a prudent option after coming in contact with a patient with Clostridium difficile. TH
Nasal MRSA Carriage: A Study of Current Prevalence with Commentary
Creech CB, Kernodle DS, Alsectzer M, et al. Increasing rates of nasal carriage of methicillin-resistant Staphylococcus aureus in healthy children. Pediatr Infect Dis J. 2005;24:617-621.
Review by Laura Ortman, MD
The incidence of methicillin-resistant Staphylococcus aureus (MRSA) infections seen in outpatient clinics and emergency rooms appears to be on the rise. In 2001 a study done at Vanderbilt University Medical Center found the prevalence of MRSA in its pediatric community to be 0.8%1. Creech, et al., devised a study to describe the current prevalence of MRSA colonization in the same population.
The study population was children between the ages of two weeks and 21 years of age presenting for a health maintenance visit at two outpatient clinics. Nasal swabs were obtained and cultures preformed on plates with and without oxacillin containing media. Possible MRSA isolates were confirmed with PCR for the mecA gene, which codes for the protein responsible for beta-lactam resistance.
Of the 500 children enrolled 182 (36.4%) were found to be colonized with S. aureus. 46 (9.2%) isolates were positive for the mecA gene and considered MRSA. The only risk factor found to increase risk for MRSA colonization was having a family member who works in a hospital (odds ratio, 2.0; 95% confidence interval, 1.03-4.1). Fifty-four percent of MRSA isolates were resistant to erythromycin, and 32% of these had inducible clindamycin resistance.
Commentary: This study shows a greater than tenfold increase in MRSA colonization in a three-year time period in a healthy outpatient population. This finding is consistent with other studies that have shown increasing rates of colonization.2-3 This increase has led some institutions to attempt decolonization of MRSA, most often using nasal mupirocin. To determine if current evidence supports attempts to eradicate MRSA nasal colonization, the following literature search was performed: Cochrane DSR, ACP Journal Club, PubMed, and PubMed Clinical Queries were searched using the search terms “MRSA,” “colonization,” and “staphylococcus.”
One Cochrane review summarizes the evidence for use of antimicrobial agents on MRSA colonized patients4. Of six randomized controlled trials, only one compares rates of infection during follow-up between the study and control groups. The difference in infections was not statistically significant. Five other studies of inconsistent quality followed eradication rates of MRSA and varied widely in their results. The Cochrane review concluded that there was insufficient evidence to recommend nasal decolonization of MRSA.
One article reviewed the evidence for intranasal mupirocin for S. aureus.5 This review did not differentiate between MRSA and MSSA. The authors appraised clinical trials that evaluated the effect of mupirocin on MRSA colonization and infection. In a trial of patients undergoing dialysis there was no overall difference in the rate of infection between groups. In trials using mupirocin for preoperative prophylaxis there was no difference in number of surgical site infections. The authors concluded that mupirocin did not result in long-term clearance of S. aureus and that the available evidence does not support its use for prevention of infection. With the current evidence routine decolonization of patients colonized with MRSA cannot be recommended.
References
- Nakamura MM, Rohling KL, Shashaty M, et al. Prevalence of methicillin-resistant Staphylococcus aureus nasal carriage in the community pediatric population. Pediatr Infect Dis J. 2002;21:917-922.
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593-598.
- Fergie JE, Purcell K. Community-acquired methicillin-resistant Staphylococcus aureus infections in south Texas children. Pediatr Infect Dis J. 2001;20:860-863.
- Loeb M, Main C, Walker-Dilks C. Antimicrobial drugs for treating methicillin-resistant Staphylococcus aureus colonization. Cochrane Database Syst Rev. 2003;(4):CD003340.
- Laupland KB, Conly JM. Treatment of Staphylococcus aureus colonization and prophylaxis for infection with topical intranasal mupirocin: an evidence-based review. Clin Infect Dis. 2003;37:933-938.
Is Ultrasound Sufficient for Diagnosing Urolithiasis in the Pediatric Patient?
Palmer JS, Donaher ER, O’Riordan MA, et al. Diagnosis of Pediatric Urolithiasis: Role of ultrasound and computerized tomography. J Urol. 2005;174:1413-1416.
Review by Ann Mattison, RN, CPNP
Pediatric urolithiasis is uncommon and may present without the classic symptoms of renal colic, making diagnosis of pediatric urolithiasis problematic. Previously published data has revealed that unenhanced spiral CT is the gold standard in diagnosing urinary tract calculi in adults. However, CT carries the risk of exposure to ionizing radiation, which can be a significant issue in children.
Due to the low prevalence of urolithiasis in addition to concerns about radiation exposure, many primary care providers choose ultrasound as the initial radiographic study for children with symptoms that can be associated with urolithiasis, such as flank pain, abdominal pain, and gross hematuria. But the accuracy of ultrasound in detecting pediatric urolithiasis has not been well studied.
A retrospective chart review was performed in all patients 0-18 evaluated as outpatients and inpatients at the study institution. Subjects were identified by ICD-9 codes and billing records. The study showed the accuracy of ultrasounds performed was variable and dependent on the location of the calculi. In contrast, CT was highly accurate regardless of calculi location.
The study concluded that ultrasound may still be the appropriate initial study for the majority of children presenting with symptoms suggestive of urolithiasis; however, a negative ultrasound should not be considered sufficient to rule out the diagnosis of urolithiasis in pediatric patients. The authors recommended the patient with persistent symptoms and negative ultrasound undergo unenhanced CT. The retrospective design of this study limits application of these results; however, the study does highlight the need for a heightened index of suspicion for the diagnosis as well as the need for further prospective studies describing the most safe and efficient method for confirming the diagnosis. TH
There Was a Farmer Had a Rash ...
A61-year-old farmer from Iowa with a medical history significant for non-Hodgkin’s lymphoma in remission presented for evaluation and treatment of two ulcerating lesions, located on his left forearm and left thigh of two months’ duration. He denied a history of pulmonary symptoms, fever, or unintentional weight loss. Physical examination was negative for lymphadenopathy or splenomegaly. Two large, beefy hyperkeratotic plaques with an underlying border with pustules were noted. The lesion shown is on the left lateral leg and is 5.3 x 4.0 cm.
What is your diagnosis:
- Cutaneous sarcoidosis;
- Recurrent lymphoma with skin metastasis;
- Blastomycosis;
- Pyoderma gangrenosum; or
- Anthrax.

Discussion
The answer is C: blastomycosis. A pathology specimen from a left arm skin punch biopsy was read as pseudoepitheliomatous hyperplasia, dermal abscess, and broad-based yeast organisms suggestive of blastomycosis. Fungal cultures grew a white-like colony of hyphae suggestive of blastomycosis. DNA probe was positive for blastomycosis dermatitidis. Interestingly, his fungal serologies were negative. The patient was started on itraconazole 200 mg twice daily.
Blastomycosis typically presents in one of two ways:
- Pulmonary infection and/or
- Cutaneous infection.
Typically, the spores of Blastomyces dermatitidis are inhaled from the soil, decomposed vegetation, or rotting wood, and the respiratory system is the first site of infection. Occupations with frequent outdoor exposure in highly endemic areas (including the southeastern states of the United States) connote increased risk. Case series have documented inoculation arising after outdoor activities in the woods near water sources.
Although pulmonary infection is subclinical in 50% of inhalational cases, one study found that pulmonary manifestations were present in 154 of 170 cases (91%) with cough (90%), fever (75%), night sweats (68%), weight loss (66%), chest pain (63%), dyspnea (54%), and aches (50%). Therefore, respiratory symptoms may signal the disease.
According to another review of 100 cases in an endemic area, pulmonary blastomycosis should be considered for any pulmonary infiltrate, especially in the upper lobes. For this patient, because there were no pulmonary symptoms or cutaneous trauma, the most likely etiology is via hematogenous spread. However, whereas the chest radiograph did not show classic signs of blastomycosis (one or more densely consolidated areas of pneumonia or nodular infiltrates), it did show slight fibrosis and pleural thickenings in the apices that is occasionally associated with blastomycosis infection.
As in this case, a presenting cutaneous lesion may be the first sign of disease. The cutaneous findings are usually the result of hematogenous spread; however, uncommon primary cutaneous blastomycosis can occur after direct inoculation from trauma to the skin. Classically, they are described as well-demarcated papulopustules and verrucous plaques with central scarring and black crusting. But the skin lesions can present in many forms and often confound the differential diagnosis. Other cutaneous infectious etiologies include verrucae, nocardiosis, cutaneous tuberculosis, and other dimorphic fungi. However, other dimorphic fungi are less likely to infect the skin. Inflammatory conditions, such as pyoderma gangrenosum and sarcoidosis, must be considered. Ulcerating squamous cell carcinoma is also a consideration.
Blastomycosis is recognized histologically by its broad-based budding and thick, double-contoured walls of the yeast forms found at body temperature (37º C) while it grows as tan or white mold at room temperature. Cultures can be drawn from sputum, pus, or urine. Severe disease often requires systemic antifungal treatment, whereas more moderate to mild disease can be treated topically. TH
References
- Baumgardner DJ, Halsmer SE, Eagan G. Symptoms of pulmonary blastomycosis: northern Wisconsin, United States. Wilderness Environ Med. 2004;15:250-256.
- Patel RG, Patel B, Petrini MF, et al. Clinical presentation, radiographic findings, and diagnostic methods of pulmonary blastomycosis: a review of 100 consecutive cases. South Med J. 1999;92:289-295.
- Bolognia J, ed. Dermatology. Barcelona, Spain: Mosby; 2003.
- Kasper DL, ed. Harrison’s Online Principles of Internal Medicine. 16th ed. New York: McGraw-Hill; 2005.
A61-year-old farmer from Iowa with a medical history significant for non-Hodgkin’s lymphoma in remission presented for evaluation and treatment of two ulcerating lesions, located on his left forearm and left thigh of two months’ duration. He denied a history of pulmonary symptoms, fever, or unintentional weight loss. Physical examination was negative for lymphadenopathy or splenomegaly. Two large, beefy hyperkeratotic plaques with an underlying border with pustules were noted. The lesion shown is on the left lateral leg and is 5.3 x 4.0 cm.
What is your diagnosis:
- Cutaneous sarcoidosis;
- Recurrent lymphoma with skin metastasis;
- Blastomycosis;
- Pyoderma gangrenosum; or
- Anthrax.
Discussion
The answer is C: blastomycosis. A pathology specimen from a left arm skin punch biopsy was read as pseudoepitheliomatous hyperplasia, dermal abscess, and broad-based yeast organisms suggestive of blastomycosis. Fungal cultures grew a white-like colony of hyphae suggestive of blastomycosis. DNA probe was positive for blastomycosis dermatitidis. Interestingly, his fungal serologies were negative. The patient was started on itraconazole 200 mg twice daily.
Blastomycosis typically presents in one of two ways:
- Pulmonary infection and/or
- Cutaneous infection.
Typically, the spores of Blastomyces dermatitidis are inhaled from the soil, decomposed vegetation, or rotting wood, and the respiratory system is the first site of infection. Occupations with frequent outdoor exposure in highly endemic areas (including the southeastern states of the United States) connote increased risk. Case series have documented inoculation arising after outdoor activities in the woods near water sources.
Although pulmonary infection is subclinical in 50% of inhalational cases, one study found that pulmonary manifestations were present in 154 of 170 cases (91%) with cough (90%), fever (75%), night sweats (68%), weight loss (66%), chest pain (63%), dyspnea (54%), and aches (50%). Therefore, respiratory symptoms may signal the disease.
According to another review of 100 cases in an endemic area, pulmonary blastomycosis should be considered for any pulmonary infiltrate, especially in the upper lobes. For this patient, because there were no pulmonary symptoms or cutaneous trauma, the most likely etiology is via hematogenous spread. However, whereas the chest radiograph did not show classic signs of blastomycosis (one or more densely consolidated areas of pneumonia or nodular infiltrates), it did show slight fibrosis and pleural thickenings in the apices that is occasionally associated with blastomycosis infection.
As in this case, a presenting cutaneous lesion may be the first sign of disease. The cutaneous findings are usually the result of hematogenous spread; however, uncommon primary cutaneous blastomycosis can occur after direct inoculation from trauma to the skin. Classically, they are described as well-demarcated papulopustules and verrucous plaques with central scarring and black crusting. But the skin lesions can present in many forms and often confound the differential diagnosis. Other cutaneous infectious etiologies include verrucae, nocardiosis, cutaneous tuberculosis, and other dimorphic fungi. However, other dimorphic fungi are less likely to infect the skin. Inflammatory conditions, such as pyoderma gangrenosum and sarcoidosis, must be considered. Ulcerating squamous cell carcinoma is also a consideration.
Blastomycosis is recognized histologically by its broad-based budding and thick, double-contoured walls of the yeast forms found at body temperature (37º C) while it grows as tan or white mold at room temperature. Cultures can be drawn from sputum, pus, or urine. Severe disease often requires systemic antifungal treatment, whereas more moderate to mild disease can be treated topically. TH
References
- Baumgardner DJ, Halsmer SE, Eagan G. Symptoms of pulmonary blastomycosis: northern Wisconsin, United States. Wilderness Environ Med. 2004;15:250-256.
- Patel RG, Patel B, Petrini MF, et al. Clinical presentation, radiographic findings, and diagnostic methods of pulmonary blastomycosis: a review of 100 consecutive cases. South Med J. 1999;92:289-295.
- Bolognia J, ed. Dermatology. Barcelona, Spain: Mosby; 2003.
- Kasper DL, ed. Harrison’s Online Principles of Internal Medicine. 16th ed. New York: McGraw-Hill; 2005.
A61-year-old farmer from Iowa with a medical history significant for non-Hodgkin’s lymphoma in remission presented for evaluation and treatment of two ulcerating lesions, located on his left forearm and left thigh of two months’ duration. He denied a history of pulmonary symptoms, fever, or unintentional weight loss. Physical examination was negative for lymphadenopathy or splenomegaly. Two large, beefy hyperkeratotic plaques with an underlying border with pustules were noted. The lesion shown is on the left lateral leg and is 5.3 x 4.0 cm.
What is your diagnosis:
- Cutaneous sarcoidosis;
- Recurrent lymphoma with skin metastasis;
- Blastomycosis;
- Pyoderma gangrenosum; or
- Anthrax.
Discussion
The answer is C: blastomycosis. A pathology specimen from a left arm skin punch biopsy was read as pseudoepitheliomatous hyperplasia, dermal abscess, and broad-based yeast organisms suggestive of blastomycosis. Fungal cultures grew a white-like colony of hyphae suggestive of blastomycosis. DNA probe was positive for blastomycosis dermatitidis. Interestingly, his fungal serologies were negative. The patient was started on itraconazole 200 mg twice daily.
Blastomycosis typically presents in one of two ways:
- Pulmonary infection and/or
- Cutaneous infection.
Typically, the spores of Blastomyces dermatitidis are inhaled from the soil, decomposed vegetation, or rotting wood, and the respiratory system is the first site of infection. Occupations with frequent outdoor exposure in highly endemic areas (including the southeastern states of the United States) connote increased risk. Case series have documented inoculation arising after outdoor activities in the woods near water sources.
Although pulmonary infection is subclinical in 50% of inhalational cases, one study found that pulmonary manifestations were present in 154 of 170 cases (91%) with cough (90%), fever (75%), night sweats (68%), weight loss (66%), chest pain (63%), dyspnea (54%), and aches (50%). Therefore, respiratory symptoms may signal the disease.
According to another review of 100 cases in an endemic area, pulmonary blastomycosis should be considered for any pulmonary infiltrate, especially in the upper lobes. For this patient, because there were no pulmonary symptoms or cutaneous trauma, the most likely etiology is via hematogenous spread. However, whereas the chest radiograph did not show classic signs of blastomycosis (one or more densely consolidated areas of pneumonia or nodular infiltrates), it did show slight fibrosis and pleural thickenings in the apices that is occasionally associated with blastomycosis infection.
As in this case, a presenting cutaneous lesion may be the first sign of disease. The cutaneous findings are usually the result of hematogenous spread; however, uncommon primary cutaneous blastomycosis can occur after direct inoculation from trauma to the skin. Classically, they are described as well-demarcated papulopustules and verrucous plaques with central scarring and black crusting. But the skin lesions can present in many forms and often confound the differential diagnosis. Other cutaneous infectious etiologies include verrucae, nocardiosis, cutaneous tuberculosis, and other dimorphic fungi. However, other dimorphic fungi are less likely to infect the skin. Inflammatory conditions, such as pyoderma gangrenosum and sarcoidosis, must be considered. Ulcerating squamous cell carcinoma is also a consideration.
Blastomycosis is recognized histologically by its broad-based budding and thick, double-contoured walls of the yeast forms found at body temperature (37º C) while it grows as tan or white mold at room temperature. Cultures can be drawn from sputum, pus, or urine. Severe disease often requires systemic antifungal treatment, whereas more moderate to mild disease can be treated topically. TH
References
- Baumgardner DJ, Halsmer SE, Eagan G. Symptoms of pulmonary blastomycosis: northern Wisconsin, United States. Wilderness Environ Med. 2004;15:250-256.
- Patel RG, Patel B, Petrini MF, et al. Clinical presentation, radiographic findings, and diagnostic methods of pulmonary blastomycosis: a review of 100 consecutive cases. South Med J. 1999;92:289-295.
- Bolognia J, ed. Dermatology. Barcelona, Spain: Mosby; 2003.
- Kasper DL, ed. Harrison’s Online Principles of Internal Medicine. 16th ed. New York: McGraw-Hill; 2005.
Improve Glycemic Control in Inpatients
For most of recent history, it has been standard practice to tolerate hyperglycemia and expect some hypoglycemia when caring for diabetic patients in the hospital. This attitude stems from the many barriers to controlling glucose levels in hospitalized patients (e.g., the stress of acute illness and the changes in diet and medications that occur on admission to the hospital). In addition, most diabetic patients are hospitalized for illness other than their diabetes. In these situations, glycemic control may not be a priority, and fear of hypoglycemia may be prominent.
However, in recent years, there has been a change in attitude regarding glycemic control in the hospitalized patient. Recently, clinical studies have shown that hyperglycemia leads to poor outcomes in some hospitalized patients, prompting the American College of Endocrinology and the American Association of Clinical Endocrinologists to publish a position statement on inpatient diabetes and metabolic control.1 In addition, best practice strategies for controlling glucose levels in hospitalized patients have been recently reviewed.2
At the same time, hospitalists have emerged on the scene, bringing with them a new awareness of the gaps between the best practice and real practice. In real practice, both hyperglycemia and hypoglycemia are common, and insulin use in the hospital is often guided by strategies that are based on simplicity, instead of strategies that are based on established principles of diabetes management. There has been remarkably little attention given to the management of diabetes and hyperglycemia in noncritically ill hospitalized patients, and glucose levels are often far outside of the recommended range in this group.
SHM’s Glycemic Control Task Force
The Glycemic Control Task Force was assembled with the intent of improving glycemic control in hospitals nationally by providing hospitalists with an understanding of the best practice of glycemic control in the hospital, and by providing them with the tools and skills to make real changes in their own systems. With the assistance of a grant from Sanofi-Aventis, the Glycemic Control Summit was held on Oct. 20, 2005, in Chicago. A distinguished panel of experts attended, including hospitalists, endocrinologists, nurses, case managers, diabetes educators, and pharmacists. The goals of the meeting were as follows:
- To identify the currently available resources pertinent to glycemic control in the hospital (e.g., resources related to best practice, education, quality improvement, awareness, clinical tools, research, metrics/quality parameters);
- To identify the gaps in those resources; and
- To assemble several focused work groups to address the major gaps in the existing resources, and to determine specific interventions or products that could fill those gaps.
The meeting spawned several smaller work groups that will address the major barriers to improving glycemic control in hospitalized patients. These groups were formed in direct response to the gaps that were identified during the meeting. A description of each of the work groups is provided below, highlighting the major gaps that were identified and the strategies being considered to overcome them.
Education: This group will focus on creating case-based, educational materials that will provide physicians, nurses, and other providers with pragmatic examples illustrating the best practice of glycemic control and insulin management in the hospital and at the transition of care. In addition, this group will address patient education issues, educational metrics, and other issues.
Potential deliverables from this group include Web-based, case-based educational modules applicable to CME or to support quality improvement efforts at individual institutions and patient education materials.
Quality improvement process: This group will focus on formulating a how-to resource for performing quality improvement projects related to glycemic control. This group will attempt to provide hospitalists with a practical guideline to help them successfully implement changes in their own institutions. Topics will include forming and leading a multidisciplinary team, setting goals, defining metrics, and identifying process analysis and evaluation methods.
Deliverables from this group will likely include a glycemic control quality improvement workbook that will guide individuals through the complex process of performing robust quality improvement projects in their own hospitals. This workbook will be similar in format to one that is currently available in the “VTE Quality Improvement Resource Room” on the SHM Web site.
Clinical tools: This group will focus on compiling and appraising already existing clinical tools (e.g., standardized order sets, protocols) and identifying the key features of these tools and the differences among them. The emphasis will be on either compiling or creating ready-to-use clinical tools.
Potential deliverables from this group include a collection of tools that will have substantial built-in decision support and will be useful in a range of settings. These might include standardized order sets, protocols, and charting tools.
Metrics: This group will focus on defining useful metrics for performing glycemic control research and quality improvement projects. This group intends to define the best ways to measure glycemic control, balancing measures, process measures, and other specific outcomes. These metrics will allow hospitals to examine their current performance and to develop quality standards for inpatient glycemic control.
Care transitions: This group is charged with beginning to identify and address the many challenges that are faced when diabetic and/or hyperglycemic patients move from one care setting to another (e.g., ICU to general ward, hospital to outpatient setting). The work done by this group is likely to have an impact on all of the other groups.
Potential deliverables from this group include a set of standards that can be applied to care transitions. There may also be specific clinical tools developed to improve the process of these care transitions, such as checklists, order sets, and protocols.
Promotional: This group will focus on creating national awareness of the importance of glycemic control in hospitals, particularly at the administrative level. This may include efforts to partner with relevant medical societies, regulatory agencies, and other professional organizations focused on improving glycemic control.
Goals and Timelines
The three-month goal is for each of the focus groups is to further delineate the gaps in the existing resources, and to further refine the specific deliverables that they will produce. Each group will need to determine specific goals and timelines.
An intermediate-term goal is the formation of a white paper that will describe, in detail, the existing glycemic control resources, the gaps in these resources, and the need for additional work in these areas.
In addition, work on the glycemic control quality improvement workbook is under way, and this resource will be used in the “Quality Improvement Precourse” that will take place May 3, 2006, at the SHM Annual Meeting.
The work being done by this task force will lead to a collection of high-quality, user-friendly resources that will enhance awareness of the issue of inpatient glycemic control and facilitate the implementation of effective inpatient diabetes quality improvement across the nation. The longer term goal will be to bring about demonstration projects in the area of inpatient glycemic control and advance the science of diabetes care in the hospital.
References
- American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Prac. 2004;10:77-82.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
Non-Physician Provider Task Force Progress
Annual meeting workshop plans, plus continued Web development
Shm’s Non-Physician Provider Task Force has continued to meet via conference calls on a regular basis. The task force now has representation from the ranks of nurse practitioners, physician assistants, hospitalist clinical care coordinators, health systems pharmacists, and hospitalist physicians. We realize that there are many other professionals vital to hospital medicine and plan to recruit more representatives from the SHM member ranks as qualified individuals are brought to our attention.
Task force members will provide important contributions to the annual meeting. The special interest forum on non-physician providers in hospital medicine has been growing each year. This forum is an important venue for exchanging ideas and meeting fellow professionals. It also gives the task force members a chance to make contact with individuals who want to get involved in Non-Physician Provider Task Force activities.
This year task force members Scarlett Blue, RNC, MSN, CNA, and Ryan Genzink, PAC, will lead the forum. Mitchell Wilson, MD, will lead a workshop, “Integrating Non-Physician Providers into Hospital Medicine Services.” National trends that include decreasing availability of generalist physicians, decreasing workloads for resident physicians, and the rapid growth in hospital medicine as a specialty will make this workshop vital to SHM members faced with these pressures.
The task force remains interested in developing a network for communication within the community of professionals in hospital medicine who have an interest in non-physician provider issues and practice. The Hub-and-Spoke initiative is intended to provide a network to allow more individuals to provide input to the task force. The forum at the annual meeting will be an opportunity to meet task force members, exchange e-mail addresses, and discuss how to become involved.
SHM’s Web site has a link for “Non-Physician Provider Resources,” and the task force has continued to work on the content of this site. The priorities for expansion include adding staffing models, billing and documentation resources, value added by non-physician providers, and FAQs. The task force welcomes SHM members to submit documents for posting to the resource center.
For most of recent history, it has been standard practice to tolerate hyperglycemia and expect some hypoglycemia when caring for diabetic patients in the hospital. This attitude stems from the many barriers to controlling glucose levels in hospitalized patients (e.g., the stress of acute illness and the changes in diet and medications that occur on admission to the hospital). In addition, most diabetic patients are hospitalized for illness other than their diabetes. In these situations, glycemic control may not be a priority, and fear of hypoglycemia may be prominent.
However, in recent years, there has been a change in attitude regarding glycemic control in the hospitalized patient. Recently, clinical studies have shown that hyperglycemia leads to poor outcomes in some hospitalized patients, prompting the American College of Endocrinology and the American Association of Clinical Endocrinologists to publish a position statement on inpatient diabetes and metabolic control.1 In addition, best practice strategies for controlling glucose levels in hospitalized patients have been recently reviewed.2
At the same time, hospitalists have emerged on the scene, bringing with them a new awareness of the gaps between the best practice and real practice. In real practice, both hyperglycemia and hypoglycemia are common, and insulin use in the hospital is often guided by strategies that are based on simplicity, instead of strategies that are based on established principles of diabetes management. There has been remarkably little attention given to the management of diabetes and hyperglycemia in noncritically ill hospitalized patients, and glucose levels are often far outside of the recommended range in this group.
SHM’s Glycemic Control Task Force
The Glycemic Control Task Force was assembled with the intent of improving glycemic control in hospitals nationally by providing hospitalists with an understanding of the best practice of glycemic control in the hospital, and by providing them with the tools and skills to make real changes in their own systems. With the assistance of a grant from Sanofi-Aventis, the Glycemic Control Summit was held on Oct. 20, 2005, in Chicago. A distinguished panel of experts attended, including hospitalists, endocrinologists, nurses, case managers, diabetes educators, and pharmacists. The goals of the meeting were as follows:
- To identify the currently available resources pertinent to glycemic control in the hospital (e.g., resources related to best practice, education, quality improvement, awareness, clinical tools, research, metrics/quality parameters);
- To identify the gaps in those resources; and
- To assemble several focused work groups to address the major gaps in the existing resources, and to determine specific interventions or products that could fill those gaps.
The meeting spawned several smaller work groups that will address the major barriers to improving glycemic control in hospitalized patients. These groups were formed in direct response to the gaps that were identified during the meeting. A description of each of the work groups is provided below, highlighting the major gaps that were identified and the strategies being considered to overcome them.
Education: This group will focus on creating case-based, educational materials that will provide physicians, nurses, and other providers with pragmatic examples illustrating the best practice of glycemic control and insulin management in the hospital and at the transition of care. In addition, this group will address patient education issues, educational metrics, and other issues.
Potential deliverables from this group include Web-based, case-based educational modules applicable to CME or to support quality improvement efforts at individual institutions and patient education materials.
Quality improvement process: This group will focus on formulating a how-to resource for performing quality improvement projects related to glycemic control. This group will attempt to provide hospitalists with a practical guideline to help them successfully implement changes in their own institutions. Topics will include forming and leading a multidisciplinary team, setting goals, defining metrics, and identifying process analysis and evaluation methods.
Deliverables from this group will likely include a glycemic control quality improvement workbook that will guide individuals through the complex process of performing robust quality improvement projects in their own hospitals. This workbook will be similar in format to one that is currently available in the “VTE Quality Improvement Resource Room” on the SHM Web site.
Clinical tools: This group will focus on compiling and appraising already existing clinical tools (e.g., standardized order sets, protocols) and identifying the key features of these tools and the differences among them. The emphasis will be on either compiling or creating ready-to-use clinical tools.
Potential deliverables from this group include a collection of tools that will have substantial built-in decision support and will be useful in a range of settings. These might include standardized order sets, protocols, and charting tools.
Metrics: This group will focus on defining useful metrics for performing glycemic control research and quality improvement projects. This group intends to define the best ways to measure glycemic control, balancing measures, process measures, and other specific outcomes. These metrics will allow hospitals to examine their current performance and to develop quality standards for inpatient glycemic control.
Care transitions: This group is charged with beginning to identify and address the many challenges that are faced when diabetic and/or hyperglycemic patients move from one care setting to another (e.g., ICU to general ward, hospital to outpatient setting). The work done by this group is likely to have an impact on all of the other groups.
Potential deliverables from this group include a set of standards that can be applied to care transitions. There may also be specific clinical tools developed to improve the process of these care transitions, such as checklists, order sets, and protocols.
Promotional: This group will focus on creating national awareness of the importance of glycemic control in hospitals, particularly at the administrative level. This may include efforts to partner with relevant medical societies, regulatory agencies, and other professional organizations focused on improving glycemic control.
Goals and Timelines
The three-month goal is for each of the focus groups is to further delineate the gaps in the existing resources, and to further refine the specific deliverables that they will produce. Each group will need to determine specific goals and timelines.
An intermediate-term goal is the formation of a white paper that will describe, in detail, the existing glycemic control resources, the gaps in these resources, and the need for additional work in these areas.
In addition, work on the glycemic control quality improvement workbook is under way, and this resource will be used in the “Quality Improvement Precourse” that will take place May 3, 2006, at the SHM Annual Meeting.
The work being done by this task force will lead to a collection of high-quality, user-friendly resources that will enhance awareness of the issue of inpatient glycemic control and facilitate the implementation of effective inpatient diabetes quality improvement across the nation. The longer term goal will be to bring about demonstration projects in the area of inpatient glycemic control and advance the science of diabetes care in the hospital.
References
- American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Prac. 2004;10:77-82.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
Non-Physician Provider Task Force Progress
Annual meeting workshop plans, plus continued Web development
Shm’s Non-Physician Provider Task Force has continued to meet via conference calls on a regular basis. The task force now has representation from the ranks of nurse practitioners, physician assistants, hospitalist clinical care coordinators, health systems pharmacists, and hospitalist physicians. We realize that there are many other professionals vital to hospital medicine and plan to recruit more representatives from the SHM member ranks as qualified individuals are brought to our attention.
Task force members will provide important contributions to the annual meeting. The special interest forum on non-physician providers in hospital medicine has been growing each year. This forum is an important venue for exchanging ideas and meeting fellow professionals. It also gives the task force members a chance to make contact with individuals who want to get involved in Non-Physician Provider Task Force activities.
This year task force members Scarlett Blue, RNC, MSN, CNA, and Ryan Genzink, PAC, will lead the forum. Mitchell Wilson, MD, will lead a workshop, “Integrating Non-Physician Providers into Hospital Medicine Services.” National trends that include decreasing availability of generalist physicians, decreasing workloads for resident physicians, and the rapid growth in hospital medicine as a specialty will make this workshop vital to SHM members faced with these pressures.
The task force remains interested in developing a network for communication within the community of professionals in hospital medicine who have an interest in non-physician provider issues and practice. The Hub-and-Spoke initiative is intended to provide a network to allow more individuals to provide input to the task force. The forum at the annual meeting will be an opportunity to meet task force members, exchange e-mail addresses, and discuss how to become involved.
SHM’s Web site has a link for “Non-Physician Provider Resources,” and the task force has continued to work on the content of this site. The priorities for expansion include adding staffing models, billing and documentation resources, value added by non-physician providers, and FAQs. The task force welcomes SHM members to submit documents for posting to the resource center.
For most of recent history, it has been standard practice to tolerate hyperglycemia and expect some hypoglycemia when caring for diabetic patients in the hospital. This attitude stems from the many barriers to controlling glucose levels in hospitalized patients (e.g., the stress of acute illness and the changes in diet and medications that occur on admission to the hospital). In addition, most diabetic patients are hospitalized for illness other than their diabetes. In these situations, glycemic control may not be a priority, and fear of hypoglycemia may be prominent.
However, in recent years, there has been a change in attitude regarding glycemic control in the hospitalized patient. Recently, clinical studies have shown that hyperglycemia leads to poor outcomes in some hospitalized patients, prompting the American College of Endocrinology and the American Association of Clinical Endocrinologists to publish a position statement on inpatient diabetes and metabolic control.1 In addition, best practice strategies for controlling glucose levels in hospitalized patients have been recently reviewed.2
At the same time, hospitalists have emerged on the scene, bringing with them a new awareness of the gaps between the best practice and real practice. In real practice, both hyperglycemia and hypoglycemia are common, and insulin use in the hospital is often guided by strategies that are based on simplicity, instead of strategies that are based on established principles of diabetes management. There has been remarkably little attention given to the management of diabetes and hyperglycemia in noncritically ill hospitalized patients, and glucose levels are often far outside of the recommended range in this group.
SHM’s Glycemic Control Task Force
The Glycemic Control Task Force was assembled with the intent of improving glycemic control in hospitals nationally by providing hospitalists with an understanding of the best practice of glycemic control in the hospital, and by providing them with the tools and skills to make real changes in their own systems. With the assistance of a grant from Sanofi-Aventis, the Glycemic Control Summit was held on Oct. 20, 2005, in Chicago. A distinguished panel of experts attended, including hospitalists, endocrinologists, nurses, case managers, diabetes educators, and pharmacists. The goals of the meeting were as follows:
- To identify the currently available resources pertinent to glycemic control in the hospital (e.g., resources related to best practice, education, quality improvement, awareness, clinical tools, research, metrics/quality parameters);
- To identify the gaps in those resources; and
- To assemble several focused work groups to address the major gaps in the existing resources, and to determine specific interventions or products that could fill those gaps.
The meeting spawned several smaller work groups that will address the major barriers to improving glycemic control in hospitalized patients. These groups were formed in direct response to the gaps that were identified during the meeting. A description of each of the work groups is provided below, highlighting the major gaps that were identified and the strategies being considered to overcome them.
Education: This group will focus on creating case-based, educational materials that will provide physicians, nurses, and other providers with pragmatic examples illustrating the best practice of glycemic control and insulin management in the hospital and at the transition of care. In addition, this group will address patient education issues, educational metrics, and other issues.
Potential deliverables from this group include Web-based, case-based educational modules applicable to CME or to support quality improvement efforts at individual institutions and patient education materials.
Quality improvement process: This group will focus on formulating a how-to resource for performing quality improvement projects related to glycemic control. This group will attempt to provide hospitalists with a practical guideline to help them successfully implement changes in their own institutions. Topics will include forming and leading a multidisciplinary team, setting goals, defining metrics, and identifying process analysis and evaluation methods.
Deliverables from this group will likely include a glycemic control quality improvement workbook that will guide individuals through the complex process of performing robust quality improvement projects in their own hospitals. This workbook will be similar in format to one that is currently available in the “VTE Quality Improvement Resource Room” on the SHM Web site.
Clinical tools: This group will focus on compiling and appraising already existing clinical tools (e.g., standardized order sets, protocols) and identifying the key features of these tools and the differences among them. The emphasis will be on either compiling or creating ready-to-use clinical tools.
Potential deliverables from this group include a collection of tools that will have substantial built-in decision support and will be useful in a range of settings. These might include standardized order sets, protocols, and charting tools.
Metrics: This group will focus on defining useful metrics for performing glycemic control research and quality improvement projects. This group intends to define the best ways to measure glycemic control, balancing measures, process measures, and other specific outcomes. These metrics will allow hospitals to examine their current performance and to develop quality standards for inpatient glycemic control.
Care transitions: This group is charged with beginning to identify and address the many challenges that are faced when diabetic and/or hyperglycemic patients move from one care setting to another (e.g., ICU to general ward, hospital to outpatient setting). The work done by this group is likely to have an impact on all of the other groups.
Potential deliverables from this group include a set of standards that can be applied to care transitions. There may also be specific clinical tools developed to improve the process of these care transitions, such as checklists, order sets, and protocols.
Promotional: This group will focus on creating national awareness of the importance of glycemic control in hospitals, particularly at the administrative level. This may include efforts to partner with relevant medical societies, regulatory agencies, and other professional organizations focused on improving glycemic control.
Goals and Timelines
The three-month goal is for each of the focus groups is to further delineate the gaps in the existing resources, and to further refine the specific deliverables that they will produce. Each group will need to determine specific goals and timelines.
An intermediate-term goal is the formation of a white paper that will describe, in detail, the existing glycemic control resources, the gaps in these resources, and the need for additional work in these areas.
In addition, work on the glycemic control quality improvement workbook is under way, and this resource will be used in the “Quality Improvement Precourse” that will take place May 3, 2006, at the SHM Annual Meeting.
The work being done by this task force will lead to a collection of high-quality, user-friendly resources that will enhance awareness of the issue of inpatient glycemic control and facilitate the implementation of effective inpatient diabetes quality improvement across the nation. The longer term goal will be to bring about demonstration projects in the area of inpatient glycemic control and advance the science of diabetes care in the hospital.
References
- American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Prac. 2004;10:77-82.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
Non-Physician Provider Task Force Progress
Annual meeting workshop plans, plus continued Web development
Shm’s Non-Physician Provider Task Force has continued to meet via conference calls on a regular basis. The task force now has representation from the ranks of nurse practitioners, physician assistants, hospitalist clinical care coordinators, health systems pharmacists, and hospitalist physicians. We realize that there are many other professionals vital to hospital medicine and plan to recruit more representatives from the SHM member ranks as qualified individuals are brought to our attention.
Task force members will provide important contributions to the annual meeting. The special interest forum on non-physician providers in hospital medicine has been growing each year. This forum is an important venue for exchanging ideas and meeting fellow professionals. It also gives the task force members a chance to make contact with individuals who want to get involved in Non-Physician Provider Task Force activities.
This year task force members Scarlett Blue, RNC, MSN, CNA, and Ryan Genzink, PAC, will lead the forum. Mitchell Wilson, MD, will lead a workshop, “Integrating Non-Physician Providers into Hospital Medicine Services.” National trends that include decreasing availability of generalist physicians, decreasing workloads for resident physicians, and the rapid growth in hospital medicine as a specialty will make this workshop vital to SHM members faced with these pressures.
The task force remains interested in developing a network for communication within the community of professionals in hospital medicine who have an interest in non-physician provider issues and practice. The Hub-and-Spoke initiative is intended to provide a network to allow more individuals to provide input to the task force. The forum at the annual meeting will be an opportunity to meet task force members, exchange e-mail addresses, and discuss how to become involved.
SHM’s Web site has a link for “Non-Physician Provider Resources,” and the task force has continued to work on the content of this site. The priorities for expansion include adding staffing models, billing and documentation resources, value added by non-physician providers, and FAQs. The task force welcomes SHM members to submit documents for posting to the resource center.
What to tell patients about side effects
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.