User login
Malpractice Chronicle
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Ethmoid Roof Penetrated During Sinus Surgery
The plaintiff, a 14-year-old boy, was evaluated by his pediatrician, then by a family physician, for pain in his left cheek and significant postnasal drip. He was given several courses of antibiotics, which did not relieve his symptoms. He was then referred to the defendant otolaryngologist, who recommended endoscopic sinus surgery.
The procedure, performed one month after the boy’s initial presentation, included four endoscopic bilateral procedures (total ethmoidectomy, maxillary sinus antrostomy, frontal sinusotomy, and reduction of inferior turbinates), in addition to partial resection of the left middle turbinate. The surgery left the patient with persistent bitemporal headaches, photophobia, and phonophobia.
The plaintiff claimed that during surgery, the right ethmoid roof was penetrated, causing a bone shard to become dislodged. A review of the materials sent to pathology after surgery, the plaintiff said, revealed the presence of brain matter. The plaintiff claimed negligence in the performance of the procedures and lack of informed consent.
According to a published report, a defense verdict was returned. Posttrial motions were pending.
”He Said, She Said” Over Obstetrics Patient
A 24-year-old woman expecting her second child went to the defendant hospital in labor. The defendant anesthesiologist, Dr. R., administered an epidural anesthetic block.
About 15 minutes later, the patient complained of difficulty breathing, and a nurse responded by raising the head of the bed, administering oxygen by mask, and calling Dr. R. to return to the room. The plaintiff soon complained of not being able to feel her legs and said she felt nauseous. She vomited and again complained of having trouble breathing.
The nurse made an emergency call for Dr. R. to return and began to administer oxygen using a manual ventilator. The anesthesiologist arrived, ordered the ventilation to be stopped, and pronounced the patient fine. The nurse, contesting this determination, placed a pulse oximetry clip on the patient; her oxygen saturation was measured at 62%.
The nurse urged intubation, but when Dr. R. attempted the intervention, he placed the tube into the esophagus rather than the trachea. The nurse then called a “code 99” emergency.
Responding members of the code team testified that Dr. R. had misplaced the intubation tube and that when the team leader attempted to reintubate the patient, Dr. R. shouted an expletive and shoved him away (which Dr. R. denied). Dr. R. then intubated the woman but did not secure the intubation tube. The code team leader also claimed that Dr. R. called for defibrillation, although the patient had a nonshockable rhythm.
An emergency cesarean delivery was performed, after which the code team defibrillated the patient. This maneuver apparently dislodged the intubation tube, necessitating a third intubation. The patient then began spontaneous respirations.
The plaintiff suffered anoxic brain injury. Despite three months of inpatient rehabilitation, she has the mental acuity of a five- to six-year-old and requires constant supervision.
Dr. R. denied that he was called the first time the nurse claimed to have called him. Dr. R. claimed that when he arrived, the plaintiff was turning blue; he argued that he, not the nurse, began to administer supplementary oxygen. He claimed that when he then attempted intubation, the plaintiff became agitated and broke the laryngoscope blade, necessitating reintubation. He also claimed that he, not the nurse, called the code.
The plaintiff claimed that the nurse had been negligent and that numerous late chart entries showed that she had ignored the plaintiff while she was decompensating. The hospital claimed that Dr. R. had placed a high epidural block, leading to the patient’s respiratory distress; this, along with Dr. R.’s failure to properly intubate the patient, resulted in her injuries.
According to a published report, a defense verdict was returned.
Anticoagulation Therapy Times Two
A 45-year-old woman who was taking warfarin underwent a cholecystectomy, with preoperative and postoperative medication adjustment based on her international normalized ratio (INR). IV heparin was administered after the surgery to raise her INR. At the time of the woman’s discharge, the primary surgeon prescribed her usual dose of warfarin. Unknown to the surgeon, a second-year resident also prescribed warfarin, as well as heparin injections.
The patient was instructed to follow up in the anticoagulation therapy clinic every three days. On the way home from her first visit there, she experienced a massive abdominal hemorrhage. Emergency laparotomy was required at a different hospital, where doctors were unable to identify the source of the bleeding.
Two weeks later, the patient was transferred to the original hospital. Shortly thereafter, she died of complications of a massive abdominal hemorrhage, including acute respiratory distress syndrome, sepsis, and multiorgan failure.
The plaintiffs claimed that the defendants were negligent in monitoring the decedent’s INR levels, which should have been done daily. The hemorrhage, the plaintiffs claimed, was caused by the heparin. The order was for heparin to be administered “per pharmacy protocol,” but the hospital pharmacy had no such protocol in place at the time. As a result, too much heparin was given.
The defendants contended that the decedent’s treatment was proper and that abdominal hemorrhaging is a known complication of anticoagulation therapy. Her hemorrhage, they claimed, was triggered by the restriction of her seatbelt when she drove over the railroad tracks on the way home from the anticoagulation therapy clinic. The defendants maintained that the decedent’s INR level was properly monitored and that the use of heparin was within the standard of care.
The matter was arbitrated, resulting in an award of $385,376.
Loss of Vision After Screening Colonoscopy
A 54-year-old man was referred to the defendant gastroenterologist for a screening colonoscopy. The patient had a family history of colon cancer and a long history of multiple medical problems, including four heart attacks, organic heart disease, diabetes, dyslipidemia, and hypertension.
The previous month, when testing revealed the presence of a kidney stone, the man’s blood pressure was 160/88 mm Hg. Before the colonoscopy, his blood pressure measured 93/50 mm Hg. He had no lightheadedness, dizziness, or chest pain.
An IV was started, and the patient was given meperidine and midazolam. After the scope was inserted, his blood pressure declined. The endoscopy nurse reported this to the gastroenterologist, who ordered an increase in IV fluids. The plaintiff’s blood pressure rose, and the procedure was completed.
In recovery, the patient was noted to be alert and oriented. He received a perfect score on discharge criteria and was released from the recovery area with a blood pressure reading of 90/60 mm Hg.
The man went straight to a donut shop, where he ate two donuts. He then experienced nausea that lasted throughout the afternoon, after attempts to eat and drink a number of items.
At about 4 PM, a call was made to the gastroenterologist’s office. The defendant returned the call, instructing the patient to report to the emergency department; the plaintiff later claimed that this was stated only as an option. Instead, the man elected to take an OTC antinausea medication and remain at home. The nausea subsided, and he went to bed and slept through the night.
When the man awoke at 5 AM, he was totally blind. He was taken to the hospital, where he was evaluated by a neuro-ophthalmologist and diagnosed with a posterior ischemic optic neuropathy.
The plaintiff charged that the rare form of blindness he experienced was the result of hypotension during the colonoscopy. He claimed that he was not given sufficient IV fluids to elevate his blood pressure and that he should not have been discharged home.
The defendant claimed that the plaintiff’s blindness was unrelated to the colonoscopy but resulted from hypotension that developed while he was sleeping.
An initial trial ended with a hung jury. At a second trial, a defense verdict was returned.
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Ethmoid Roof Penetrated During Sinus Surgery
The plaintiff, a 14-year-old boy, was evaluated by his pediatrician, then by a family physician, for pain in his left cheek and significant postnasal drip. He was given several courses of antibiotics, which did not relieve his symptoms. He was then referred to the defendant otolaryngologist, who recommended endoscopic sinus surgery.
The procedure, performed one month after the boy’s initial presentation, included four endoscopic bilateral procedures (total ethmoidectomy, maxillary sinus antrostomy, frontal sinusotomy, and reduction of inferior turbinates), in addition to partial resection of the left middle turbinate. The surgery left the patient with persistent bitemporal headaches, photophobia, and phonophobia.
The plaintiff claimed that during surgery, the right ethmoid roof was penetrated, causing a bone shard to become dislodged. A review of the materials sent to pathology after surgery, the plaintiff said, revealed the presence of brain matter. The plaintiff claimed negligence in the performance of the procedures and lack of informed consent.
According to a published report, a defense verdict was returned. Posttrial motions were pending.
”He Said, She Said” Over Obstetrics Patient
A 24-year-old woman expecting her second child went to the defendant hospital in labor. The defendant anesthesiologist, Dr. R., administered an epidural anesthetic block.
About 15 minutes later, the patient complained of difficulty breathing, and a nurse responded by raising the head of the bed, administering oxygen by mask, and calling Dr. R. to return to the room. The plaintiff soon complained of not being able to feel her legs and said she felt nauseous. She vomited and again complained of having trouble breathing.
The nurse made an emergency call for Dr. R. to return and began to administer oxygen using a manual ventilator. The anesthesiologist arrived, ordered the ventilation to be stopped, and pronounced the patient fine. The nurse, contesting this determination, placed a pulse oximetry clip on the patient; her oxygen saturation was measured at 62%.
The nurse urged intubation, but when Dr. R. attempted the intervention, he placed the tube into the esophagus rather than the trachea. The nurse then called a “code 99” emergency.
Responding members of the code team testified that Dr. R. had misplaced the intubation tube and that when the team leader attempted to reintubate the patient, Dr. R. shouted an expletive and shoved him away (which Dr. R. denied). Dr. R. then intubated the woman but did not secure the intubation tube. The code team leader also claimed that Dr. R. called for defibrillation, although the patient had a nonshockable rhythm.
An emergency cesarean delivery was performed, after which the code team defibrillated the patient. This maneuver apparently dislodged the intubation tube, necessitating a third intubation. The patient then began spontaneous respirations.
The plaintiff suffered anoxic brain injury. Despite three months of inpatient rehabilitation, she has the mental acuity of a five- to six-year-old and requires constant supervision.
Dr. R. denied that he was called the first time the nurse claimed to have called him. Dr. R. claimed that when he arrived, the plaintiff was turning blue; he argued that he, not the nurse, began to administer supplementary oxygen. He claimed that when he then attempted intubation, the plaintiff became agitated and broke the laryngoscope blade, necessitating reintubation. He also claimed that he, not the nurse, called the code.
The plaintiff claimed that the nurse had been negligent and that numerous late chart entries showed that she had ignored the plaintiff while she was decompensating. The hospital claimed that Dr. R. had placed a high epidural block, leading to the patient’s respiratory distress; this, along with Dr. R.’s failure to properly intubate the patient, resulted in her injuries.
According to a published report, a defense verdict was returned.
Anticoagulation Therapy Times Two
A 45-year-old woman who was taking warfarin underwent a cholecystectomy, with preoperative and postoperative medication adjustment based on her international normalized ratio (INR). IV heparin was administered after the surgery to raise her INR. At the time of the woman’s discharge, the primary surgeon prescribed her usual dose of warfarin. Unknown to the surgeon, a second-year resident also prescribed warfarin, as well as heparin injections.
The patient was instructed to follow up in the anticoagulation therapy clinic every three days. On the way home from her first visit there, she experienced a massive abdominal hemorrhage. Emergency laparotomy was required at a different hospital, where doctors were unable to identify the source of the bleeding.
Two weeks later, the patient was transferred to the original hospital. Shortly thereafter, she died of complications of a massive abdominal hemorrhage, including acute respiratory distress syndrome, sepsis, and multiorgan failure.
The plaintiffs claimed that the defendants were negligent in monitoring the decedent’s INR levels, which should have been done daily. The hemorrhage, the plaintiffs claimed, was caused by the heparin. The order was for heparin to be administered “per pharmacy protocol,” but the hospital pharmacy had no such protocol in place at the time. As a result, too much heparin was given.
The defendants contended that the decedent’s treatment was proper and that abdominal hemorrhaging is a known complication of anticoagulation therapy. Her hemorrhage, they claimed, was triggered by the restriction of her seatbelt when she drove over the railroad tracks on the way home from the anticoagulation therapy clinic. The defendants maintained that the decedent’s INR level was properly monitored and that the use of heparin was within the standard of care.
The matter was arbitrated, resulting in an award of $385,376.
Loss of Vision After Screening Colonoscopy
A 54-year-old man was referred to the defendant gastroenterologist for a screening colonoscopy. The patient had a family history of colon cancer and a long history of multiple medical problems, including four heart attacks, organic heart disease, diabetes, dyslipidemia, and hypertension.
The previous month, when testing revealed the presence of a kidney stone, the man’s blood pressure was 160/88 mm Hg. Before the colonoscopy, his blood pressure measured 93/50 mm Hg. He had no lightheadedness, dizziness, or chest pain.
An IV was started, and the patient was given meperidine and midazolam. After the scope was inserted, his blood pressure declined. The endoscopy nurse reported this to the gastroenterologist, who ordered an increase in IV fluids. The plaintiff’s blood pressure rose, and the procedure was completed.
In recovery, the patient was noted to be alert and oriented. He received a perfect score on discharge criteria and was released from the recovery area with a blood pressure reading of 90/60 mm Hg.
The man went straight to a donut shop, where he ate two donuts. He then experienced nausea that lasted throughout the afternoon, after attempts to eat and drink a number of items.
At about 4 PM, a call was made to the gastroenterologist’s office. The defendant returned the call, instructing the patient to report to the emergency department; the plaintiff later claimed that this was stated only as an option. Instead, the man elected to take an OTC antinausea medication and remain at home. The nausea subsided, and he went to bed and slept through the night.
When the man awoke at 5 AM, he was totally blind. He was taken to the hospital, where he was evaluated by a neuro-ophthalmologist and diagnosed with a posterior ischemic optic neuropathy.
The plaintiff charged that the rare form of blindness he experienced was the result of hypotension during the colonoscopy. He claimed that he was not given sufficient IV fluids to elevate his blood pressure and that he should not have been discharged home.
The defendant claimed that the plaintiff’s blindness was unrelated to the colonoscopy but resulted from hypotension that developed while he was sleeping.
An initial trial ended with a hung jury. At a second trial, a defense verdict was returned.
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Ethmoid Roof Penetrated During Sinus Surgery
The plaintiff, a 14-year-old boy, was evaluated by his pediatrician, then by a family physician, for pain in his left cheek and significant postnasal drip. He was given several courses of antibiotics, which did not relieve his symptoms. He was then referred to the defendant otolaryngologist, who recommended endoscopic sinus surgery.
The procedure, performed one month after the boy’s initial presentation, included four endoscopic bilateral procedures (total ethmoidectomy, maxillary sinus antrostomy, frontal sinusotomy, and reduction of inferior turbinates), in addition to partial resection of the left middle turbinate. The surgery left the patient with persistent bitemporal headaches, photophobia, and phonophobia.
The plaintiff claimed that during surgery, the right ethmoid roof was penetrated, causing a bone shard to become dislodged. A review of the materials sent to pathology after surgery, the plaintiff said, revealed the presence of brain matter. The plaintiff claimed negligence in the performance of the procedures and lack of informed consent.
According to a published report, a defense verdict was returned. Posttrial motions were pending.
”He Said, She Said” Over Obstetrics Patient
A 24-year-old woman expecting her second child went to the defendant hospital in labor. The defendant anesthesiologist, Dr. R., administered an epidural anesthetic block.
About 15 minutes later, the patient complained of difficulty breathing, and a nurse responded by raising the head of the bed, administering oxygen by mask, and calling Dr. R. to return to the room. The plaintiff soon complained of not being able to feel her legs and said she felt nauseous. She vomited and again complained of having trouble breathing.
The nurse made an emergency call for Dr. R. to return and began to administer oxygen using a manual ventilator. The anesthesiologist arrived, ordered the ventilation to be stopped, and pronounced the patient fine. The nurse, contesting this determination, placed a pulse oximetry clip on the patient; her oxygen saturation was measured at 62%.
The nurse urged intubation, but when Dr. R. attempted the intervention, he placed the tube into the esophagus rather than the trachea. The nurse then called a “code 99” emergency.
Responding members of the code team testified that Dr. R. had misplaced the intubation tube and that when the team leader attempted to reintubate the patient, Dr. R. shouted an expletive and shoved him away (which Dr. R. denied). Dr. R. then intubated the woman but did not secure the intubation tube. The code team leader also claimed that Dr. R. called for defibrillation, although the patient had a nonshockable rhythm.
An emergency cesarean delivery was performed, after which the code team defibrillated the patient. This maneuver apparently dislodged the intubation tube, necessitating a third intubation. The patient then began spontaneous respirations.
The plaintiff suffered anoxic brain injury. Despite three months of inpatient rehabilitation, she has the mental acuity of a five- to six-year-old and requires constant supervision.
Dr. R. denied that he was called the first time the nurse claimed to have called him. Dr. R. claimed that when he arrived, the plaintiff was turning blue; he argued that he, not the nurse, began to administer supplementary oxygen. He claimed that when he then attempted intubation, the plaintiff became agitated and broke the laryngoscope blade, necessitating reintubation. He also claimed that he, not the nurse, called the code.
The plaintiff claimed that the nurse had been negligent and that numerous late chart entries showed that she had ignored the plaintiff while she was decompensating. The hospital claimed that Dr. R. had placed a high epidural block, leading to the patient’s respiratory distress; this, along with Dr. R.’s failure to properly intubate the patient, resulted in her injuries.
According to a published report, a defense verdict was returned.
Anticoagulation Therapy Times Two
A 45-year-old woman who was taking warfarin underwent a cholecystectomy, with preoperative and postoperative medication adjustment based on her international normalized ratio (INR). IV heparin was administered after the surgery to raise her INR. At the time of the woman’s discharge, the primary surgeon prescribed her usual dose of warfarin. Unknown to the surgeon, a second-year resident also prescribed warfarin, as well as heparin injections.
The patient was instructed to follow up in the anticoagulation therapy clinic every three days. On the way home from her first visit there, she experienced a massive abdominal hemorrhage. Emergency laparotomy was required at a different hospital, where doctors were unable to identify the source of the bleeding.
Two weeks later, the patient was transferred to the original hospital. Shortly thereafter, she died of complications of a massive abdominal hemorrhage, including acute respiratory distress syndrome, sepsis, and multiorgan failure.
The plaintiffs claimed that the defendants were negligent in monitoring the decedent’s INR levels, which should have been done daily. The hemorrhage, the plaintiffs claimed, was caused by the heparin. The order was for heparin to be administered “per pharmacy protocol,” but the hospital pharmacy had no such protocol in place at the time. As a result, too much heparin was given.
The defendants contended that the decedent’s treatment was proper and that abdominal hemorrhaging is a known complication of anticoagulation therapy. Her hemorrhage, they claimed, was triggered by the restriction of her seatbelt when she drove over the railroad tracks on the way home from the anticoagulation therapy clinic. The defendants maintained that the decedent’s INR level was properly monitored and that the use of heparin was within the standard of care.
The matter was arbitrated, resulting in an award of $385,376.
Loss of Vision After Screening Colonoscopy
A 54-year-old man was referred to the defendant gastroenterologist for a screening colonoscopy. The patient had a family history of colon cancer and a long history of multiple medical problems, including four heart attacks, organic heart disease, diabetes, dyslipidemia, and hypertension.
The previous month, when testing revealed the presence of a kidney stone, the man’s blood pressure was 160/88 mm Hg. Before the colonoscopy, his blood pressure measured 93/50 mm Hg. He had no lightheadedness, dizziness, or chest pain.
An IV was started, and the patient was given meperidine and midazolam. After the scope was inserted, his blood pressure declined. The endoscopy nurse reported this to the gastroenterologist, who ordered an increase in IV fluids. The plaintiff’s blood pressure rose, and the procedure was completed.
In recovery, the patient was noted to be alert and oriented. He received a perfect score on discharge criteria and was released from the recovery area with a blood pressure reading of 90/60 mm Hg.
The man went straight to a donut shop, where he ate two donuts. He then experienced nausea that lasted throughout the afternoon, after attempts to eat and drink a number of items.
At about 4 PM, a call was made to the gastroenterologist’s office. The defendant returned the call, instructing the patient to report to the emergency department; the plaintiff later claimed that this was stated only as an option. Instead, the man elected to take an OTC antinausea medication and remain at home. The nausea subsided, and he went to bed and slept through the night.
When the man awoke at 5 AM, he was totally blind. He was taken to the hospital, where he was evaluated by a neuro-ophthalmologist and diagnosed with a posterior ischemic optic neuropathy.
The plaintiff charged that the rare form of blindness he experienced was the result of hypotension during the colonoscopy. He claimed that he was not given sufficient IV fluids to elevate his blood pressure and that he should not have been discharged home.
The defendant claimed that the plaintiff’s blindness was unrelated to the colonoscopy but resulted from hypotension that developed while he was sleeping.
An initial trial ended with a hung jury. At a second trial, a defense verdict was returned.
Got malpractice distress? You can help yourself survive
The author reports no financial relationships relevant to this article.
“Immediately after the event I was a wreck. I vaguely remember talking to the family; I don’t know if I was much use to them.… That night I got drunk. It was the only way I could sleep. A sensitive colleague came and sat with me.”1
As an ObGyn, it is almost certain that you will be sued sometime during your career. Specific actions that I’ll describe in this article can help you deal with the stress associated with the adverse event that precipitates the lawsuit and the lawsuit itself. To begin, remember:
- Anticipation is the best defense
- Knowledge is power
- Action counters passivity
- A supportive environment is essential.
How can you anticipate litigation?
What is the risk? No nationwide reporting system tracks the incidence of medical malpractice claims. A recent survey by the American College of Obstetricians and Gynecologists, however, found that 89% of practicing ObGyns had been sued at least once in their career, with an average of 2.62 claims for every ObGyn.2 Because a claim usually takes years to resolve, a substantial number of ObGyns are involved in litigation at any one time.

You can successfully anticipate litigation by maintaining familiarity with your state’s statute of limitations—usually, this period is 2 to 3 years after discovery of the incident, with exceptions for children, the disabled, and designated special circumstances. If a plaintiff’s case is not filed within this time, a disputed outcome can never be the subject of a malpractice claim.
ObGyns are keenly aware of the exception that extends the time period during which a case may be filed on behalf of a child after discovery of the alleged injury. Many states set 8 years as the cutoff for filing a claim; others, such as Illinois, extend the period for as long as 2 years after a child’s 18th birthday. This long tail of vulnerability creates unpredictability for insurers, who must estimate the relationship between current premiums and potential payouts (often in the distant future), resulting in high premiums for ObGyns’ insurance. More importantly, it creates an undercurrent of anxiety and uncertainty for those ObGyns who must contemplate defending themselves in court for incidents that occurred in the distant past.
Listen to your feelings whenever you suspect that a patient is dissatisfied or that a bad outcome may lead to a claim, and take appropriate action. Reexamine your risk management procedures and discuss your concerns with your risk manager. Because it may take years for a case to be filed and many more for it to be adjudicated, possibly by trial, your best defense is clear, accurate, comprehensive, and contemporaneous documentation of the situation. Any later review of the case will be based on records that, if clearly kept, will be easily and unambiguously interpreted despite the passage of time.
Responding to an adverse event
The severity of the outcome, the nature of your relationship with the patient, and the degree of your responsibility for an adverse event contribute to the intensity of your initial emotional response. If a mistake caused the event, your reaction may be even more severe.3-6 Whatever the specifics of the event, you may ruminate about your role and degree of responsibility (TABLE 1).
TABLE 1
Questions that might nag you after a “bad” outcome
|
|
|
|
|
|
|
|
|
TABLE 2
The 3 “must-do” actions after an adverse event
Medical steps
|
Notifications
|
Disclosures
|
Expect that your view of the circumstances will generate a complex array of feelings: shock, anxiety, depression, shame, guilt, self-blame, disbelief, self-doubt and inadequacy, anger, and, even, relief from not having to work with a difficult patient anymore.
Most physicians feel a personal sense of failure and inadequacy when they are unable to prevent a patient’s death or serious injury. Although serious events evoke greater distress, any event that may eventually be judged an error or become the subject of a lawsuit can give rise to anxiety, decreased confidence, sleep disturbances, and decreased job satisfaction.6 In the midst of such feelings, you must:
- deal with the event’s medical complications, relevant notifications, and disclosures (TABLE 2)
- address the emotional pain of the injured patient or family
- participate in mandated reviews
- recognize and manage the emotional disruption to you (TABLE 3).
Self-evaluation. To cope with distress when a patient dies, you could attend the funeral. You also might:
- make changes in your practice that alert you to problem patients
- introduce a more structured approach to patients with particular clinical conditions, using practice guidelines as a resource7
- become more alert to patients who may benefit from consultation or referral.
Balance the time you devote to work and personal life. Schedule regular time for recreation and active sports, which can help you prepare for the prolonged stress that follows being sued. Engage a personal physician to monitor your physical and emotional health and to recommend appropriate referrals, when indicated.
TABLE 3
Get a grip on your emotions, before and during litigation
| Anticipate having repeated thoughts and preoccupations about the event; work toward a realistic view of it |
| Recognize your feelings and work to understand their source |
| Talk with a trusted confidant (spouse, colleague) about your feelings |
| Monitor your emotional and physical status; if indicated, seek appropriate consultation |
| Avoid situations that generate anxiety and increase stress |
| Monitor and address changes in your relationships with family, patients, colleagues, and staff |
| Be understanding of yourself and others; develop a realistic view of yourself as a “good doctor” |
| Engage in active sports and take regular vacations unrelated to professional activities |
| Control what can be controlled |
Knowledge is power
What can I expect? A lawsuit generates a mixture of common emotions and exacerbates those felt at the time of the bad outcome: shock, outrage, anxiety, anguish, dread, depression, helplessness, hopelessness, feelings of being misunderstood, and the anger and vulnerability associated with a narcissistic injury. Ordinarily we possess a healthy narcissism—that is, good feelings of self-esteem and a set of ideals that motivate and gratify us. When we suffer a tragic outcome or are sued, our self-esteem and ideals are directly challenged, resulting in feelings of failure, criticism, and public humiliation. These feelings can damage our sense of self and generate further feelings of shame, depression, and rage—all signs of a so-called narcissistic injury. As one ObGyn stated, learning that a lawsuit was filed “just prolonged my misery.”8
Each of us reacts in our own way to a lawsuit—and differently to each lawsuit if we are sued more than once—because of:
- our personality traits and personal circumstances
- the specifics of a case
- our relationship with the patient
- the public nature of a lawsuit
- a range of other variables that makes each case unique.
Suddenly, you who perceive yourself as caring, beneficent, well-meaning, and devoted to your patients are publicly accused of being careless and incompetent, of harming the patient by failing to meet your minimal obligations. Psychiatrists Ferrell and Price9 capture the impact of these allegations:
Here are the sense of assault and violation, the feelings of outrage and fear. Most painfully, here is the narcissistic injury, the astonishing wound to our understanding of ourselves as admirable, well-meaning people.
Litigation is a lengthy process with defined stages (TABLE 4). You have little control over a slow-paced process that involves an array of participants (lawyers, judges, jury, experts) whose behavior is unpredictable. This can make you feel dependent, vulnerable, and impotent.
TABLE 4
Pocket guide to what happens in court
| STAGE OF ACTION | WHAT IT MEANS FOR DEFENDANT AND PLAINTIFF |
|---|---|
| Summons | Notification that a suit has been filed |
| Complaint | The nature of the allegation in legal terms |
| Pleadings | The attorney begins to communicate with the court by filing motions; a request that the court do something |
| Discovery | A process designed to obtain information about the case:
|
| Summary judgment | A motion asking the court, after the facts have been established by discovery, to decide the validity of the case; if granted, the case is resolved without a trial by jury |
| Settlement | An agreement between parties that resolves their legal dispute |
| Trial | Case is presented to the judge or a judge and jury to determine culpability |
| Verdict | Decision reached by the deciding body |
| Posttrial | If the defendant receives an unfavorable verdict, motions may be offered to the court to void or appeal the verdict |
Be active, not passive
What you can do. Contact your insurer and risk manager immediately. Inquire about the average length of litigation in your jurisdiction (it might be 1 to 5, or more, years, depending on locality, type of case, and severity of injury). Ask your attorney to describe the steps in the process and your role as the case proceeds.
Take whatever steps are necessary to cover your clinical duties. If your initial emotional reaction is disruptive, obtain coverage or rearrange your schedule. Expect to change or limit your schedule before depositions and during trial to allow adequate time for preparation.
Accept the fact that you must play by rules far different from those of medical care. Litigation is time-consuming and frustrating. Delays and so-called continuances are common in legal proceedings, so expect them. Consider adapting to your situation the strategies that other sued physicians have found useful in regaining control over their life and work (TABLE 5).
TABLE 5
Regain control and manage your practice during litigation
| Learn as much as you can about the legal process |
| Introduce good risk-management strategies, such as efficient record-keeping, into your practice |
| Clarify the responsibilities of office personnel and coverage responsibilities with associates |
| Rearrange office schedules during periods of increased stress |
| Reevaluate your time commitments to work and family |
| Participate in relevant continuing education |
| Make sure your financial and estate planning is current |
| Cooperate with legal counsel |
| Devote sufficient time to deposition preparation and other demands of the case |
| Carefully evaluate the advice of legal and insurance counsel regarding a settlement |
| Don’t try to “fit patients in” while on trial; a trial is a full-time job |
Get needed support
Talking about the case. Sharing, with responsible confidants, your emotional reactions to being sued is healthy for you and others affected. Lawyers, however, may caution you not to “talk to anybody” about the case. They don’t want you to say anything that would suggest liability or jeopardize their defense of the case.
This may be good legal advice, but it is not good psychological advice. The support of others is a natural help during major life events that cause enormous stress and disruption.10 You can resolve this dilemma by accepting the discipline of talking about your feelings regarding the case without discussing the specifics of the case.
In addition to lawyers and claims representatives, you may talk with your spouse or another trusted person or colleague about your feelings. When you choose to talk with a psychiatrist or other mental health professional about your litigation experiences, you are protected by the confidentiality inherent in the doctor–patient relationship.
Trust issues. At the core of all medical work lies trust. As a well-trained and competent professional, you do not expect to be sued by patients with whom you have trusting and often long-term relationships. Most physicians acknowledge that after being sued their relationships with patients change.11,12 You may find it difficult to reestablish trusting and comfortable relationships with other patients, especially those who have conditions similar, often high-risk, to that of the suing patient.
A charge of negligence exposes our vulnerabilities and leaves us feeling hurt and betrayed, feelings that are not easily overcome. As one psychiatrist ruefully observed: “I lost my innocence.”8
Conflicted feelings may emerge. The distress associated with a lawsuit often exacerbates the many outside stressors associated with practice. Many solo practitioners find themselves already overextended, working longer hours, covering more hospitals, and rarely taking vacations. Younger physicians who prize “time off” and lifestyle above other incentives remain stressed by the unpredictable schedules associated with ObGyn practice. Women physicians increasingly constitute a greater percentage of the ObGyn specialty. Although some work part-time or, at least, fewer hours than their male counterparts, they must nonetheless keep current and continually hone their skills.
The stress associated with all of these conditions can increase an ObGyn’s vulnerability to the occurrence of an adverse event and, eventually, to a lawsuit. It is also known that physicians involved in a claim-producing event are twice as likely as their non–claim-producing counterparts to have another such event within the ensuing 12 months.13
When you are sued, you may feel overwhelmed and out of control. Because physicians’ ability to control their schedule and work hours is a known major predictor of their overall health (as evidenced by a balance between their work and personal life),14 regaining control over those aspects of your life that are “controllable” (TABLE 5) is an essential strategy in dealing with a lawsuit.
As a result of your lawsuit, you may contemplate changing practice circumstances or retiring early. Feelings that you must change the way you practice and chronic anxiety about your work are barriers to good practice. Personal therapy may help if you remain uneasy or cannot resolve life choices that overshadow your work with patients.
Seek medical or psychiatric care?
Be alert to the point at which you or others involved in litigation need a referral for medical or psychiatric consultation. Sued physicians, their families, and colleagues often experience psychiatric conditions or other problems, such as:
- major depression
- adjustment disorder
- posttraumatic stress disorder
- worsening of a previously diagnosed psychiatric illness
- physical symptoms that require diagnosis and treatment
- alcohol and drug misuse or abuse
- anxiety and distress that interfere with work
- self-medication, especially for insomnia
- disturbances and dysfunctional behaviors that affect marital and family life.15,16
Take stock—then, it’s “steady as you go”
Most of us have stable and supportive relationships and are, for the most part, psychologically healthy and professionally competent. It is normal, however, to experience distress in response to the trauma of a bad outcome (whatever its origin) and the lawsuit that may follow. Most physicians are resilient—that is, able to manage the stress without developing major symptoms—but some benefit from professional support.
Whatever your reaction to being sued, become familiar with the climate of litigation in the jurisdiction where the case was filed, including the incidence and outcome of cases. For example, does a similar case to yours usually result in settlement or—if it goes to trial—does it take 2 to 5, or more, years to resolve?
Last, it’s a comfort to know that approximately 70% of complaints filed result in no payment (no settlement) for the plaintiff. When a case does go to trial, physicians win 80% of the time.
The challenge, then, for you when you are sued? Take an active role in managing your distress in ways that contribute to your vindication and to the continuity of care for your patients.
- American College of Obstetricians and Gynecologists. From exam room to court room: navigating litigation and coping with stress (CD-ROM). http://sales.acog.com/acb/stores/1/product1.cfm?SID=1&Product_ID=589).
- Charles SC, Frisch PR. Adverse Events, Stress and Litigation: A Physician’s Guide. New York: Oxford University Press; 2005.
- Physician Litigation Stress Resource Center. htttp://www.physicianlitigationstress.org.
1. Looking back. BMJ. 2000;320(7237):812.-
2. American College of Obstetricians and Gynecologists. ACOG 2006 Survey on Professional Liability Results. Washington, DC; 2006. Available at: http://www.acog.org/departments/dept_notice.cfm?recno=4&bulletin=3963. Accessed January 7, 2008.
3. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med. 1992;7:424-431.
4. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ. 2000;320(7237):726-727.
5. Aasland OG, Forde R. Impact of feeling responsible for adverse events on doctors’ personal and professional lives: the importance of being open to criticism from colleagues. Qual Saf Health Care. 2005;14:13-17.
6. Waterman AD, Garbutt J, Hazel E, et al. The emotional impact of medical errors on practicing physicians in the United States and Canada. Jt Comm J Qual Patient Saf. 2007;33:467-475.
7. National Guideline Clearinghouse. http://guideline.gov/. Accessed January 7, 2008.
8. Charles SC, Frisch PR. Adverse Events, Stress and Litigation: A Physician’s Guide. New York: Oxford University Press; 2005;94,120.-
9. Ferrell RB, Price TRP. Effects of malpractice suits on physicians. In: Gold JH, Nemiah JC, eds. Beyond Transference. Washington, DC: American Psychiatric Press; 1993;141-158.
10. Watson PJ, Friedman MJ, Gibson LE, et al. Early intervention in trauma-related problems. In: Ursano R, Norwood AE, eds. Trauma and Disaster: Responses and Management. Review of Psychiatry. Vol. 22. Washington, DC: American Psychiatric Press; 2003;100-101.
11. Charles SC, Psykoty CE, Nelson A. Physicians on trial—self-reported reactions to malpractice trials. West J Med. 1988;148;358-360.
12. Charles SC. The doctor–patient relationship and medical malpractice litigation. Bull Menninger Clin. 1993;57:195-207.
13. Frisch PR, Charles SC, Gibbons RD, Hedeker D. Role of previous claims and specialty on the effectiveness of risk-management education for office-based physicians. West J Med. 1995;163:346-350.
14. Keeton K, Fenner DE, Johnson TRB, Hayward RA. Predictors of physician career satisfaction, work-life balance, and burnout. Obstet Gynecol. 2007;109;949-955.
15. Charles SC, Wilbert JR, Franke KJ. Sued and non-sued physicians’ self-reported reactions to malpractice litigation. Am J Psychiatry. 1985;142:437-440.
16. Martin CA, Wilson JA, Fiebelman ND, 3rd, Gurley DN, Miller TW. Physicians’ psychologic reactions to malpractice litigation. South Med J. 1991;84:1300-1304.
The author reports no financial relationships relevant to this article.
“Immediately after the event I was a wreck. I vaguely remember talking to the family; I don’t know if I was much use to them.… That night I got drunk. It was the only way I could sleep. A sensitive colleague came and sat with me.”1
As an ObGyn, it is almost certain that you will be sued sometime during your career. Specific actions that I’ll describe in this article can help you deal with the stress associated with the adverse event that precipitates the lawsuit and the lawsuit itself. To begin, remember:
- Anticipation is the best defense
- Knowledge is power
- Action counters passivity
- A supportive environment is essential.
How can you anticipate litigation?
What is the risk? No nationwide reporting system tracks the incidence of medical malpractice claims. A recent survey by the American College of Obstetricians and Gynecologists, however, found that 89% of practicing ObGyns had been sued at least once in their career, with an average of 2.62 claims for every ObGyn.2 Because a claim usually takes years to resolve, a substantial number of ObGyns are involved in litigation at any one time.
You can successfully anticipate litigation by maintaining familiarity with your state’s statute of limitations—usually, this period is 2 to 3 years after discovery of the incident, with exceptions for children, the disabled, and designated special circumstances. If a plaintiff’s case is not filed within this time, a disputed outcome can never be the subject of a malpractice claim.
ObGyns are keenly aware of the exception that extends the time period during which a case may be filed on behalf of a child after discovery of the alleged injury. Many states set 8 years as the cutoff for filing a claim; others, such as Illinois, extend the period for as long as 2 years after a child’s 18th birthday. This long tail of vulnerability creates unpredictability for insurers, who must estimate the relationship between current premiums and potential payouts (often in the distant future), resulting in high premiums for ObGyns’ insurance. More importantly, it creates an undercurrent of anxiety and uncertainty for those ObGyns who must contemplate defending themselves in court for incidents that occurred in the distant past.
Listen to your feelings whenever you suspect that a patient is dissatisfied or that a bad outcome may lead to a claim, and take appropriate action. Reexamine your risk management procedures and discuss your concerns with your risk manager. Because it may take years for a case to be filed and many more for it to be adjudicated, possibly by trial, your best defense is clear, accurate, comprehensive, and contemporaneous documentation of the situation. Any later review of the case will be based on records that, if clearly kept, will be easily and unambiguously interpreted despite the passage of time.
Responding to an adverse event
The severity of the outcome, the nature of your relationship with the patient, and the degree of your responsibility for an adverse event contribute to the intensity of your initial emotional response. If a mistake caused the event, your reaction may be even more severe.3-6 Whatever the specifics of the event, you may ruminate about your role and degree of responsibility (TABLE 1).
TABLE 1
Questions that might nag you after a “bad” outcome
|
|
|
|
|
|
|
|
|
TABLE 2
The 3 “must-do” actions after an adverse event
Medical steps
|
Notifications
|
Disclosures
|
Expect that your view of the circumstances will generate a complex array of feelings: shock, anxiety, depression, shame, guilt, self-blame, disbelief, self-doubt and inadequacy, anger, and, even, relief from not having to work with a difficult patient anymore.
Most physicians feel a personal sense of failure and inadequacy when they are unable to prevent a patient’s death or serious injury. Although serious events evoke greater distress, any event that may eventually be judged an error or become the subject of a lawsuit can give rise to anxiety, decreased confidence, sleep disturbances, and decreased job satisfaction.6 In the midst of such feelings, you must:
- deal with the event’s medical complications, relevant notifications, and disclosures (TABLE 2)
- address the emotional pain of the injured patient or family
- participate in mandated reviews
- recognize and manage the emotional disruption to you (TABLE 3).
Self-evaluation. To cope with distress when a patient dies, you could attend the funeral. You also might:
- make changes in your practice that alert you to problem patients
- introduce a more structured approach to patients with particular clinical conditions, using practice guidelines as a resource7
- become more alert to patients who may benefit from consultation or referral.
Balance the time you devote to work and personal life. Schedule regular time for recreation and active sports, which can help you prepare for the prolonged stress that follows being sued. Engage a personal physician to monitor your physical and emotional health and to recommend appropriate referrals, when indicated.
TABLE 3
Get a grip on your emotions, before and during litigation
| Anticipate having repeated thoughts and preoccupations about the event; work toward a realistic view of it |
| Recognize your feelings and work to understand their source |
| Talk with a trusted confidant (spouse, colleague) about your feelings |
| Monitor your emotional and physical status; if indicated, seek appropriate consultation |
| Avoid situations that generate anxiety and increase stress |
| Monitor and address changes in your relationships with family, patients, colleagues, and staff |
| Be understanding of yourself and others; develop a realistic view of yourself as a “good doctor” |
| Engage in active sports and take regular vacations unrelated to professional activities |
| Control what can be controlled |
Knowledge is power
What can I expect? A lawsuit generates a mixture of common emotions and exacerbates those felt at the time of the bad outcome: shock, outrage, anxiety, anguish, dread, depression, helplessness, hopelessness, feelings of being misunderstood, and the anger and vulnerability associated with a narcissistic injury. Ordinarily we possess a healthy narcissism—that is, good feelings of self-esteem and a set of ideals that motivate and gratify us. When we suffer a tragic outcome or are sued, our self-esteem and ideals are directly challenged, resulting in feelings of failure, criticism, and public humiliation. These feelings can damage our sense of self and generate further feelings of shame, depression, and rage—all signs of a so-called narcissistic injury. As one ObGyn stated, learning that a lawsuit was filed “just prolonged my misery.”8
Each of us reacts in our own way to a lawsuit—and differently to each lawsuit if we are sued more than once—because of:
- our personality traits and personal circumstances
- the specifics of a case
- our relationship with the patient
- the public nature of a lawsuit
- a range of other variables that makes each case unique.
Suddenly, you who perceive yourself as caring, beneficent, well-meaning, and devoted to your patients are publicly accused of being careless and incompetent, of harming the patient by failing to meet your minimal obligations. Psychiatrists Ferrell and Price9 capture the impact of these allegations:
Here are the sense of assault and violation, the feelings of outrage and fear. Most painfully, here is the narcissistic injury, the astonishing wound to our understanding of ourselves as admirable, well-meaning people.
Litigation is a lengthy process with defined stages (TABLE 4). You have little control over a slow-paced process that involves an array of participants (lawyers, judges, jury, experts) whose behavior is unpredictable. This can make you feel dependent, vulnerable, and impotent.
TABLE 4
Pocket guide to what happens in court
| STAGE OF ACTION | WHAT IT MEANS FOR DEFENDANT AND PLAINTIFF |
|---|---|
| Summons | Notification that a suit has been filed |
| Complaint | The nature of the allegation in legal terms |
| Pleadings | The attorney begins to communicate with the court by filing motions; a request that the court do something |
| Discovery | A process designed to obtain information about the case:
|
| Summary judgment | A motion asking the court, after the facts have been established by discovery, to decide the validity of the case; if granted, the case is resolved without a trial by jury |
| Settlement | An agreement between parties that resolves their legal dispute |
| Trial | Case is presented to the judge or a judge and jury to determine culpability |
| Verdict | Decision reached by the deciding body |
| Posttrial | If the defendant receives an unfavorable verdict, motions may be offered to the court to void or appeal the verdict |
Be active, not passive
What you can do. Contact your insurer and risk manager immediately. Inquire about the average length of litigation in your jurisdiction (it might be 1 to 5, or more, years, depending on locality, type of case, and severity of injury). Ask your attorney to describe the steps in the process and your role as the case proceeds.
Take whatever steps are necessary to cover your clinical duties. If your initial emotional reaction is disruptive, obtain coverage or rearrange your schedule. Expect to change or limit your schedule before depositions and during trial to allow adequate time for preparation.
Accept the fact that you must play by rules far different from those of medical care. Litigation is time-consuming and frustrating. Delays and so-called continuances are common in legal proceedings, so expect them. Consider adapting to your situation the strategies that other sued physicians have found useful in regaining control over their life and work (TABLE 5).
TABLE 5
Regain control and manage your practice during litigation
| Learn as much as you can about the legal process |
| Introduce good risk-management strategies, such as efficient record-keeping, into your practice |
| Clarify the responsibilities of office personnel and coverage responsibilities with associates |
| Rearrange office schedules during periods of increased stress |
| Reevaluate your time commitments to work and family |
| Participate in relevant continuing education |
| Make sure your financial and estate planning is current |
| Cooperate with legal counsel |
| Devote sufficient time to deposition preparation and other demands of the case |
| Carefully evaluate the advice of legal and insurance counsel regarding a settlement |
| Don’t try to “fit patients in” while on trial; a trial is a full-time job |
Get needed support
Talking about the case. Sharing, with responsible confidants, your emotional reactions to being sued is healthy for you and others affected. Lawyers, however, may caution you not to “talk to anybody” about the case. They don’t want you to say anything that would suggest liability or jeopardize their defense of the case.
This may be good legal advice, but it is not good psychological advice. The support of others is a natural help during major life events that cause enormous stress and disruption.10 You can resolve this dilemma by accepting the discipline of talking about your feelings regarding the case without discussing the specifics of the case.
In addition to lawyers and claims representatives, you may talk with your spouse or another trusted person or colleague about your feelings. When you choose to talk with a psychiatrist or other mental health professional about your litigation experiences, you are protected by the confidentiality inherent in the doctor–patient relationship.
Trust issues. At the core of all medical work lies trust. As a well-trained and competent professional, you do not expect to be sued by patients with whom you have trusting and often long-term relationships. Most physicians acknowledge that after being sued their relationships with patients change.11,12 You may find it difficult to reestablish trusting and comfortable relationships with other patients, especially those who have conditions similar, often high-risk, to that of the suing patient.
A charge of negligence exposes our vulnerabilities and leaves us feeling hurt and betrayed, feelings that are not easily overcome. As one psychiatrist ruefully observed: “I lost my innocence.”8
Conflicted feelings may emerge. The distress associated with a lawsuit often exacerbates the many outside stressors associated with practice. Many solo practitioners find themselves already overextended, working longer hours, covering more hospitals, and rarely taking vacations. Younger physicians who prize “time off” and lifestyle above other incentives remain stressed by the unpredictable schedules associated with ObGyn practice. Women physicians increasingly constitute a greater percentage of the ObGyn specialty. Although some work part-time or, at least, fewer hours than their male counterparts, they must nonetheless keep current and continually hone their skills.
The stress associated with all of these conditions can increase an ObGyn’s vulnerability to the occurrence of an adverse event and, eventually, to a lawsuit. It is also known that physicians involved in a claim-producing event are twice as likely as their non–claim-producing counterparts to have another such event within the ensuing 12 months.13
When you are sued, you may feel overwhelmed and out of control. Because physicians’ ability to control their schedule and work hours is a known major predictor of their overall health (as evidenced by a balance between their work and personal life),14 regaining control over those aspects of your life that are “controllable” (TABLE 5) is an essential strategy in dealing with a lawsuit.
As a result of your lawsuit, you may contemplate changing practice circumstances or retiring early. Feelings that you must change the way you practice and chronic anxiety about your work are barriers to good practice. Personal therapy may help if you remain uneasy or cannot resolve life choices that overshadow your work with patients.
Seek medical or psychiatric care?
Be alert to the point at which you or others involved in litigation need a referral for medical or psychiatric consultation. Sued physicians, their families, and colleagues often experience psychiatric conditions or other problems, such as:
- major depression
- adjustment disorder
- posttraumatic stress disorder
- worsening of a previously diagnosed psychiatric illness
- physical symptoms that require diagnosis and treatment
- alcohol and drug misuse or abuse
- anxiety and distress that interfere with work
- self-medication, especially for insomnia
- disturbances and dysfunctional behaviors that affect marital and family life.15,16
Take stock—then, it’s “steady as you go”
Most of us have stable and supportive relationships and are, for the most part, psychologically healthy and professionally competent. It is normal, however, to experience distress in response to the trauma of a bad outcome (whatever its origin) and the lawsuit that may follow. Most physicians are resilient—that is, able to manage the stress without developing major symptoms—but some benefit from professional support.
Whatever your reaction to being sued, become familiar with the climate of litigation in the jurisdiction where the case was filed, including the incidence and outcome of cases. For example, does a similar case to yours usually result in settlement or—if it goes to trial—does it take 2 to 5, or more, years to resolve?
Last, it’s a comfort to know that approximately 70% of complaints filed result in no payment (no settlement) for the plaintiff. When a case does go to trial, physicians win 80% of the time.
The challenge, then, for you when you are sued? Take an active role in managing your distress in ways that contribute to your vindication and to the continuity of care for your patients.
- American College of Obstetricians and Gynecologists. From exam room to court room: navigating litigation and coping with stress (CD-ROM). http://sales.acog.com/acb/stores/1/product1.cfm?SID=1&Product_ID=589).
- Charles SC, Frisch PR. Adverse Events, Stress and Litigation: A Physician’s Guide. New York: Oxford University Press; 2005.
- Physician Litigation Stress Resource Center. htttp://www.physicianlitigationstress.org.
The author reports no financial relationships relevant to this article.
“Immediately after the event I was a wreck. I vaguely remember talking to the family; I don’t know if I was much use to them.… That night I got drunk. It was the only way I could sleep. A sensitive colleague came and sat with me.”1
As an ObGyn, it is almost certain that you will be sued sometime during your career. Specific actions that I’ll describe in this article can help you deal with the stress associated with the adverse event that precipitates the lawsuit and the lawsuit itself. To begin, remember:
- Anticipation is the best defense
- Knowledge is power
- Action counters passivity
- A supportive environment is essential.
How can you anticipate litigation?
What is the risk? No nationwide reporting system tracks the incidence of medical malpractice claims. A recent survey by the American College of Obstetricians and Gynecologists, however, found that 89% of practicing ObGyns had been sued at least once in their career, with an average of 2.62 claims for every ObGyn.2 Because a claim usually takes years to resolve, a substantial number of ObGyns are involved in litigation at any one time.
You can successfully anticipate litigation by maintaining familiarity with your state’s statute of limitations—usually, this period is 2 to 3 years after discovery of the incident, with exceptions for children, the disabled, and designated special circumstances. If a plaintiff’s case is not filed within this time, a disputed outcome can never be the subject of a malpractice claim.
ObGyns are keenly aware of the exception that extends the time period during which a case may be filed on behalf of a child after discovery of the alleged injury. Many states set 8 years as the cutoff for filing a claim; others, such as Illinois, extend the period for as long as 2 years after a child’s 18th birthday. This long tail of vulnerability creates unpredictability for insurers, who must estimate the relationship between current premiums and potential payouts (often in the distant future), resulting in high premiums for ObGyns’ insurance. More importantly, it creates an undercurrent of anxiety and uncertainty for those ObGyns who must contemplate defending themselves in court for incidents that occurred in the distant past.
Listen to your feelings whenever you suspect that a patient is dissatisfied or that a bad outcome may lead to a claim, and take appropriate action. Reexamine your risk management procedures and discuss your concerns with your risk manager. Because it may take years for a case to be filed and many more for it to be adjudicated, possibly by trial, your best defense is clear, accurate, comprehensive, and contemporaneous documentation of the situation. Any later review of the case will be based on records that, if clearly kept, will be easily and unambiguously interpreted despite the passage of time.
Responding to an adverse event
The severity of the outcome, the nature of your relationship with the patient, and the degree of your responsibility for an adverse event contribute to the intensity of your initial emotional response. If a mistake caused the event, your reaction may be even more severe.3-6 Whatever the specifics of the event, you may ruminate about your role and degree of responsibility (TABLE 1).
TABLE 1
Questions that might nag you after a “bad” outcome
|
|
|
|
|
|
|
|
|
TABLE 2
The 3 “must-do” actions after an adverse event
Medical steps
|
Notifications
|
Disclosures
|
Expect that your view of the circumstances will generate a complex array of feelings: shock, anxiety, depression, shame, guilt, self-blame, disbelief, self-doubt and inadequacy, anger, and, even, relief from not having to work with a difficult patient anymore.
Most physicians feel a personal sense of failure and inadequacy when they are unable to prevent a patient’s death or serious injury. Although serious events evoke greater distress, any event that may eventually be judged an error or become the subject of a lawsuit can give rise to anxiety, decreased confidence, sleep disturbances, and decreased job satisfaction.6 In the midst of such feelings, you must:
- deal with the event’s medical complications, relevant notifications, and disclosures (TABLE 2)
- address the emotional pain of the injured patient or family
- participate in mandated reviews
- recognize and manage the emotional disruption to you (TABLE 3).
Self-evaluation. To cope with distress when a patient dies, you could attend the funeral. You also might:
- make changes in your practice that alert you to problem patients
- introduce a more structured approach to patients with particular clinical conditions, using practice guidelines as a resource7
- become more alert to patients who may benefit from consultation or referral.
Balance the time you devote to work and personal life. Schedule regular time for recreation and active sports, which can help you prepare for the prolonged stress that follows being sued. Engage a personal physician to monitor your physical and emotional health and to recommend appropriate referrals, when indicated.
TABLE 3
Get a grip on your emotions, before and during litigation
| Anticipate having repeated thoughts and preoccupations about the event; work toward a realistic view of it |
| Recognize your feelings and work to understand their source |
| Talk with a trusted confidant (spouse, colleague) about your feelings |
| Monitor your emotional and physical status; if indicated, seek appropriate consultation |
| Avoid situations that generate anxiety and increase stress |
| Monitor and address changes in your relationships with family, patients, colleagues, and staff |
| Be understanding of yourself and others; develop a realistic view of yourself as a “good doctor” |
| Engage in active sports and take regular vacations unrelated to professional activities |
| Control what can be controlled |
Knowledge is power
What can I expect? A lawsuit generates a mixture of common emotions and exacerbates those felt at the time of the bad outcome: shock, outrage, anxiety, anguish, dread, depression, helplessness, hopelessness, feelings of being misunderstood, and the anger and vulnerability associated with a narcissistic injury. Ordinarily we possess a healthy narcissism—that is, good feelings of self-esteem and a set of ideals that motivate and gratify us. When we suffer a tragic outcome or are sued, our self-esteem and ideals are directly challenged, resulting in feelings of failure, criticism, and public humiliation. These feelings can damage our sense of self and generate further feelings of shame, depression, and rage—all signs of a so-called narcissistic injury. As one ObGyn stated, learning that a lawsuit was filed “just prolonged my misery.”8
Each of us reacts in our own way to a lawsuit—and differently to each lawsuit if we are sued more than once—because of:
- our personality traits and personal circumstances
- the specifics of a case
- our relationship with the patient
- the public nature of a lawsuit
- a range of other variables that makes each case unique.
Suddenly, you who perceive yourself as caring, beneficent, well-meaning, and devoted to your patients are publicly accused of being careless and incompetent, of harming the patient by failing to meet your minimal obligations. Psychiatrists Ferrell and Price9 capture the impact of these allegations:
Here are the sense of assault and violation, the feelings of outrage and fear. Most painfully, here is the narcissistic injury, the astonishing wound to our understanding of ourselves as admirable, well-meaning people.
Litigation is a lengthy process with defined stages (TABLE 4). You have little control over a slow-paced process that involves an array of participants (lawyers, judges, jury, experts) whose behavior is unpredictable. This can make you feel dependent, vulnerable, and impotent.
TABLE 4
Pocket guide to what happens in court
| STAGE OF ACTION | WHAT IT MEANS FOR DEFENDANT AND PLAINTIFF |
|---|---|
| Summons | Notification that a suit has been filed |
| Complaint | The nature of the allegation in legal terms |
| Pleadings | The attorney begins to communicate with the court by filing motions; a request that the court do something |
| Discovery | A process designed to obtain information about the case:
|
| Summary judgment | A motion asking the court, after the facts have been established by discovery, to decide the validity of the case; if granted, the case is resolved without a trial by jury |
| Settlement | An agreement between parties that resolves their legal dispute |
| Trial | Case is presented to the judge or a judge and jury to determine culpability |
| Verdict | Decision reached by the deciding body |
| Posttrial | If the defendant receives an unfavorable verdict, motions may be offered to the court to void or appeal the verdict |
Be active, not passive
What you can do. Contact your insurer and risk manager immediately. Inquire about the average length of litigation in your jurisdiction (it might be 1 to 5, or more, years, depending on locality, type of case, and severity of injury). Ask your attorney to describe the steps in the process and your role as the case proceeds.
Take whatever steps are necessary to cover your clinical duties. If your initial emotional reaction is disruptive, obtain coverage or rearrange your schedule. Expect to change or limit your schedule before depositions and during trial to allow adequate time for preparation.
Accept the fact that you must play by rules far different from those of medical care. Litigation is time-consuming and frustrating. Delays and so-called continuances are common in legal proceedings, so expect them. Consider adapting to your situation the strategies that other sued physicians have found useful in regaining control over their life and work (TABLE 5).
TABLE 5
Regain control and manage your practice during litigation
| Learn as much as you can about the legal process |
| Introduce good risk-management strategies, such as efficient record-keeping, into your practice |
| Clarify the responsibilities of office personnel and coverage responsibilities with associates |
| Rearrange office schedules during periods of increased stress |
| Reevaluate your time commitments to work and family |
| Participate in relevant continuing education |
| Make sure your financial and estate planning is current |
| Cooperate with legal counsel |
| Devote sufficient time to deposition preparation and other demands of the case |
| Carefully evaluate the advice of legal and insurance counsel regarding a settlement |
| Don’t try to “fit patients in” while on trial; a trial is a full-time job |
Get needed support
Talking about the case. Sharing, with responsible confidants, your emotional reactions to being sued is healthy for you and others affected. Lawyers, however, may caution you not to “talk to anybody” about the case. They don’t want you to say anything that would suggest liability or jeopardize their defense of the case.
This may be good legal advice, but it is not good psychological advice. The support of others is a natural help during major life events that cause enormous stress and disruption.10 You can resolve this dilemma by accepting the discipline of talking about your feelings regarding the case without discussing the specifics of the case.
In addition to lawyers and claims representatives, you may talk with your spouse or another trusted person or colleague about your feelings. When you choose to talk with a psychiatrist or other mental health professional about your litigation experiences, you are protected by the confidentiality inherent in the doctor–patient relationship.
Trust issues. At the core of all medical work lies trust. As a well-trained and competent professional, you do not expect to be sued by patients with whom you have trusting and often long-term relationships. Most physicians acknowledge that after being sued their relationships with patients change.11,12 You may find it difficult to reestablish trusting and comfortable relationships with other patients, especially those who have conditions similar, often high-risk, to that of the suing patient.
A charge of negligence exposes our vulnerabilities and leaves us feeling hurt and betrayed, feelings that are not easily overcome. As one psychiatrist ruefully observed: “I lost my innocence.”8
Conflicted feelings may emerge. The distress associated with a lawsuit often exacerbates the many outside stressors associated with practice. Many solo practitioners find themselves already overextended, working longer hours, covering more hospitals, and rarely taking vacations. Younger physicians who prize “time off” and lifestyle above other incentives remain stressed by the unpredictable schedules associated with ObGyn practice. Women physicians increasingly constitute a greater percentage of the ObGyn specialty. Although some work part-time or, at least, fewer hours than their male counterparts, they must nonetheless keep current and continually hone their skills.
The stress associated with all of these conditions can increase an ObGyn’s vulnerability to the occurrence of an adverse event and, eventually, to a lawsuit. It is also known that physicians involved in a claim-producing event are twice as likely as their non–claim-producing counterparts to have another such event within the ensuing 12 months.13
When you are sued, you may feel overwhelmed and out of control. Because physicians’ ability to control their schedule and work hours is a known major predictor of their overall health (as evidenced by a balance between their work and personal life),14 regaining control over those aspects of your life that are “controllable” (TABLE 5) is an essential strategy in dealing with a lawsuit.
As a result of your lawsuit, you may contemplate changing practice circumstances or retiring early. Feelings that you must change the way you practice and chronic anxiety about your work are barriers to good practice. Personal therapy may help if you remain uneasy or cannot resolve life choices that overshadow your work with patients.
Seek medical or psychiatric care?
Be alert to the point at which you or others involved in litigation need a referral for medical or psychiatric consultation. Sued physicians, their families, and colleagues often experience psychiatric conditions or other problems, such as:
- major depression
- adjustment disorder
- posttraumatic stress disorder
- worsening of a previously diagnosed psychiatric illness
- physical symptoms that require diagnosis and treatment
- alcohol and drug misuse or abuse
- anxiety and distress that interfere with work
- self-medication, especially for insomnia
- disturbances and dysfunctional behaviors that affect marital and family life.15,16
Take stock—then, it’s “steady as you go”
Most of us have stable and supportive relationships and are, for the most part, psychologically healthy and professionally competent. It is normal, however, to experience distress in response to the trauma of a bad outcome (whatever its origin) and the lawsuit that may follow. Most physicians are resilient—that is, able to manage the stress without developing major symptoms—but some benefit from professional support.
Whatever your reaction to being sued, become familiar with the climate of litigation in the jurisdiction where the case was filed, including the incidence and outcome of cases. For example, does a similar case to yours usually result in settlement or—if it goes to trial—does it take 2 to 5, or more, years to resolve?
Last, it’s a comfort to know that approximately 70% of complaints filed result in no payment (no settlement) for the plaintiff. When a case does go to trial, physicians win 80% of the time.
The challenge, then, for you when you are sued? Take an active role in managing your distress in ways that contribute to your vindication and to the continuity of care for your patients.
- American College of Obstetricians and Gynecologists. From exam room to court room: navigating litigation and coping with stress (CD-ROM). http://sales.acog.com/acb/stores/1/product1.cfm?SID=1&Product_ID=589).
- Charles SC, Frisch PR. Adverse Events, Stress and Litigation: A Physician’s Guide. New York: Oxford University Press; 2005.
- Physician Litigation Stress Resource Center. htttp://www.physicianlitigationstress.org.
1. Looking back. BMJ. 2000;320(7237):812.-
2. American College of Obstetricians and Gynecologists. ACOG 2006 Survey on Professional Liability Results. Washington, DC; 2006. Available at: http://www.acog.org/departments/dept_notice.cfm?recno=4&bulletin=3963. Accessed January 7, 2008.
3. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med. 1992;7:424-431.
4. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ. 2000;320(7237):726-727.
5. Aasland OG, Forde R. Impact of feeling responsible for adverse events on doctors’ personal and professional lives: the importance of being open to criticism from colleagues. Qual Saf Health Care. 2005;14:13-17.
6. Waterman AD, Garbutt J, Hazel E, et al. The emotional impact of medical errors on practicing physicians in the United States and Canada. Jt Comm J Qual Patient Saf. 2007;33:467-475.
7. National Guideline Clearinghouse. http://guideline.gov/. Accessed January 7, 2008.
8. Charles SC, Frisch PR. Adverse Events, Stress and Litigation: A Physician’s Guide. New York: Oxford University Press; 2005;94,120.-
9. Ferrell RB, Price TRP. Effects of malpractice suits on physicians. In: Gold JH, Nemiah JC, eds. Beyond Transference. Washington, DC: American Psychiatric Press; 1993;141-158.
10. Watson PJ, Friedman MJ, Gibson LE, et al. Early intervention in trauma-related problems. In: Ursano R, Norwood AE, eds. Trauma and Disaster: Responses and Management. Review of Psychiatry. Vol. 22. Washington, DC: American Psychiatric Press; 2003;100-101.
11. Charles SC, Psykoty CE, Nelson A. Physicians on trial—self-reported reactions to malpractice trials. West J Med. 1988;148;358-360.
12. Charles SC. The doctor–patient relationship and medical malpractice litigation. Bull Menninger Clin. 1993;57:195-207.
13. Frisch PR, Charles SC, Gibbons RD, Hedeker D. Role of previous claims and specialty on the effectiveness of risk-management education for office-based physicians. West J Med. 1995;163:346-350.
14. Keeton K, Fenner DE, Johnson TRB, Hayward RA. Predictors of physician career satisfaction, work-life balance, and burnout. Obstet Gynecol. 2007;109;949-955.
15. Charles SC, Wilbert JR, Franke KJ. Sued and non-sued physicians’ self-reported reactions to malpractice litigation. Am J Psychiatry. 1985;142:437-440.
16. Martin CA, Wilson JA, Fiebelman ND, 3rd, Gurley DN, Miller TW. Physicians’ psychologic reactions to malpractice litigation. South Med J. 1991;84:1300-1304.
1. Looking back. BMJ. 2000;320(7237):812.-
2. American College of Obstetricians and Gynecologists. ACOG 2006 Survey on Professional Liability Results. Washington, DC; 2006. Available at: http://www.acog.org/departments/dept_notice.cfm?recno=4&bulletin=3963. Accessed January 7, 2008.
3. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med. 1992;7:424-431.
4. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ. 2000;320(7237):726-727.
5. Aasland OG, Forde R. Impact of feeling responsible for adverse events on doctors’ personal and professional lives: the importance of being open to criticism from colleagues. Qual Saf Health Care. 2005;14:13-17.
6. Waterman AD, Garbutt J, Hazel E, et al. The emotional impact of medical errors on practicing physicians in the United States and Canada. Jt Comm J Qual Patient Saf. 2007;33:467-475.
7. National Guideline Clearinghouse. http://guideline.gov/. Accessed January 7, 2008.
8. Charles SC, Frisch PR. Adverse Events, Stress and Litigation: A Physician’s Guide. New York: Oxford University Press; 2005;94,120.-
9. Ferrell RB, Price TRP. Effects of malpractice suits on physicians. In: Gold JH, Nemiah JC, eds. Beyond Transference. Washington, DC: American Psychiatric Press; 1993;141-158.
10. Watson PJ, Friedman MJ, Gibson LE, et al. Early intervention in trauma-related problems. In: Ursano R, Norwood AE, eds. Trauma and Disaster: Responses and Management. Review of Psychiatry. Vol. 22. Washington, DC: American Psychiatric Press; 2003;100-101.
11. Charles SC, Psykoty CE, Nelson A. Physicians on trial—self-reported reactions to malpractice trials. West J Med. 1988;148;358-360.
12. Charles SC. The doctor–patient relationship and medical malpractice litigation. Bull Menninger Clin. 1993;57:195-207.
13. Frisch PR, Charles SC, Gibbons RD, Hedeker D. Role of previous claims and specialty on the effectiveness of risk-management education for office-based physicians. West J Med. 1995;163:346-350.
14. Keeton K, Fenner DE, Johnson TRB, Hayward RA. Predictors of physician career satisfaction, work-life balance, and burnout. Obstet Gynecol. 2007;109;949-955.
15. Charles SC, Wilbert JR, Franke KJ. Sued and non-sued physicians’ self-reported reactions to malpractice litigation. Am J Psychiatry. 1985;142:437-440.
16. Martin CA, Wilson JA, Fiebelman ND, 3rd, Gurley DN, Miller TW. Physicians’ psychologic reactions to malpractice litigation. South Med J. 1991;84:1300-1304.
Was the patient still suicidal?
THE PATIENT. A 30-year-old police officer reports thoughts of suicide. He was under investigation for illegal work-related activities and feared he would have to report his coworkers’ involvement in these activities and lose his job.
CASE FACTS. The patient was voluntarily hospitalized for 4 days and received medication and inpatient psychotherapy. When he was discharged, a psychiatrist prescribed follow-up outpatient psychotherapy and antidepressant and antipsychotic medications. The next day, the officer fatally shot himself.
THE PATIENT’S FAMILY’S CLAIM. The psychiatrist did not adequately weigh the patient’s depression and stressors, including possibly losing his job, and did not properly assess suicidal ideation. Also, the patient’s mother claims she attended the discharge meeting with the psychiatrist and that her son expressed suicidal intentions at that time.
THE DOCTOR’S DEFENSE. The patient believed he could get another job if necessary and was no longer contemplating suicide. Also, he was a voluntary patient and could not be hospitalized any longer without consent.
Submit your verdict and find out how the court ruled at CurrentPsychiatry.com. Click on “Have more to say about this topic?” to comment.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
THE PATIENT. A 30-year-old police officer reports thoughts of suicide. He was under investigation for illegal work-related activities and feared he would have to report his coworkers’ involvement in these activities and lose his job.
CASE FACTS. The patient was voluntarily hospitalized for 4 days and received medication and inpatient psychotherapy. When he was discharged, a psychiatrist prescribed follow-up outpatient psychotherapy and antidepressant and antipsychotic medications. The next day, the officer fatally shot himself.
THE PATIENT’S FAMILY’S CLAIM. The psychiatrist did not adequately weigh the patient’s depression and stressors, including possibly losing his job, and did not properly assess suicidal ideation. Also, the patient’s mother claims she attended the discharge meeting with the psychiatrist and that her son expressed suicidal intentions at that time.
THE DOCTOR’S DEFENSE. The patient believed he could get another job if necessary and was no longer contemplating suicide. Also, he was a voluntary patient and could not be hospitalized any longer without consent.
Submit your verdict and find out how the court ruled at CurrentPsychiatry.com. Click on “Have more to say about this topic?” to comment.
THE PATIENT. A 30-year-old police officer reports thoughts of suicide. He was under investigation for illegal work-related activities and feared he would have to report his coworkers’ involvement in these activities and lose his job.
CASE FACTS. The patient was voluntarily hospitalized for 4 days and received medication and inpatient psychotherapy. When he was discharged, a psychiatrist prescribed follow-up outpatient psychotherapy and antidepressant and antipsychotic medications. The next day, the officer fatally shot himself.
THE PATIENT’S FAMILY’S CLAIM. The psychiatrist did not adequately weigh the patient’s depression and stressors, including possibly losing his job, and did not properly assess suicidal ideation. Also, the patient’s mother claims she attended the discharge meeting with the psychiatrist and that her son expressed suicidal intentions at that time.
THE DOCTOR’S DEFENSE. The patient believed he could get another job if necessary and was no longer contemplating suicide. Also, he was a voluntary patient and could not be hospitalized any longer without consent.
Submit your verdict and find out how the court ruled at CurrentPsychiatry.com. Click on “Have more to say about this topic?” to comment.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Tips to make documentation easier, faster, and more satisfying
Current Psychiatry’s malpractice column is evolving. Previously, “Malpractice Verdicts,” used case decisions to initiate discussions of clinical situations that can generate lawsuits. The verdicts remain as “Malpractice Minute”, but Current Psychiatry has invited me to contribute a new column, “Malpractice Rx,” that will solicit questions and address practicing clinicians’ concerns about malpractice risk.
To start this dialogue, I’ll begin with a question that often comes up in discussions with colleagues, and especially when I teach psychiatry residents: “What should I document?” In this article, we will review why proper documentation is essential. We’ll also look at some ideas that might make documentation easier, more efficient, and more satisfying.
- If so, please submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
When I was in medical school, my professors said the primary reason for accurate charting was to communicate with the rest of the treatment team. This is still true. But in these sadder-but-wiser days, when I ask psychiatry residents “What is the purpose of documentation?” they always answer, “to create a legal record.”
Documentation plays many roles (Table 1). From the standpoint of preventing a malpractice judgment, the clinical record can accomplish 3 important things:
Lawsuit deterrence. Records are a key source—and often the only source—of information an attorney uses when deciding whether to file a lawsuit. An attorney won’t risk time and money on a malpractice case if the clinical record suggests that a psychiatrist was conscientious and met the standard of care.1
Impression management. The patient’s chart is what plaintiffs’ and defendants’ experts use when forming their initial opinions about the quality of care delivered.
Credibility. Clinical records are the most believable source of information about what you observed, what you thought, what you did, why you did it, and when you did it. The adage “if it wasn’t written, it didn’t happen” is not always applicable,2 but if an adverse event occurs, a defendant doctor’s verbal testimony about delivering good care will be more convincing when backed up by documentation created before the event.
Table 1
Purposes of medical record documentation
|
Improving documentation
Because it is impossible to describe everything you see, hear, say, do, and think during clinical encounters with patients, you must make choices about what to include in the record. The components of good documentation depend on the clinical context, but the following general principles may avert some malpractice actions.
1 More is better. Psychiatric practice often requires you to be discreet about patients’ personal information. Within appropriate bounds, however, the more information the record contains about objective findings, patients’ statements, clinical judgments, and your decision making, the better the portrayal of competent care.
2 Record the time and date. When attorneys and experts try to reconstruct what happened before an adverse occurrence, knowing the exact time you saw the patient, recorded findings, wrote orders, followed up on lab tests, or discussed problems with others—including family and treatment team members—can make a big difference.
3 Sooner is better. The most credible charting is done during or just after a service is rendered. Charting completed after an adverse event is vulnerable to accusations of fabrication.
4 Describe your thinking. Most aspects of clinical medicine are far from certain. Documenting the reasoning behind your diagnosis and treatment selection—what you’ve ruled out, what still seems tentative, and what risks and benefits you’ve weighed—helps emphasize this reality.3 After something bad happens, people retrospectively regard the event as more probable than it really was.4 Documenting your uncertainty and ways of addressing it may help counter this “hindsight bias.” It also shows that you were thoughtful and took therapeutic steps prudently.
5
6 Clarify capacity. Jurors may believe that all psychiatric patients are incompetent, and plaintiff’s attorneys sometimes try to create the impression that patients are completely controlled by weird whims and aberrant thoughts. To counter this, when appropriate indicate in the chart that the patient can handle responsibilities such as reporting side effects, seeking emergency attention, or notifying you about changes in thought or mood.3,5
7 Manage appearance and content. Under Health Insurance Portability and Accountability Act (HIPAA) regulations, patients have the right to review their medical records.6 If a lawsuit occurs, the records might be read out loud in court. Documentation will make a better impression if it is clear, legible, and free of gratuitous comments.
8 Include quotations. Documenting verbatim statements from a patient, such as “I’ve never considered suicide,” can quickly convey key information that you considered when making a therapeutic decision.
Technical approaches
Table 27,8 lists several techniques and technologies that might improve documentation. For example, computer users can create templates or customize software to quickly produce thorough documentation for frequently encountered procedures or clinical events. Whether these approaches are useful and appropriate will depend on your work setting, but all aim to improve the speed and quality of clinical documentation.
Think creatively about improving documentation. Even if you’re never sued, better documentation helps you and your patients. For example, several years ago a colleague9 designed an emergency room form that allowed clinicians to complete in a few seconds a Brief Psychiatric Rating Scale on every patient we evaluated. This innovation shortened the time needed to document a systematic, comprehensive assessment and increased the quantity, quality, and reliability of information in patients’ records.
Table 2
Purposes of medical record documentation
| Idea | Comment |
|---|---|
| Use speech recognition | You speak faster than you write. Transcription software |
| Software | accuracy has improved in the last few years. |
| Use handouts and | Patients often do not remember or understand much of what |
| medication instructions | doctors tell them,7,8 so handouts may be more useful than verbal instructions. Good handouts about medications are available on the Internet. Note in the chart that you gave the patient the document. |
| Seek anonymous | Documenting consultations shows you are prudent and |
| consultations with colleagues | a colleague agreed with your treatment. |
| Ask patients to rate their | This practice may improve your information gathering |
| own symptoms and progress | and help document what the patient told you. |
| Use standard rating scales | Rating scales can help you record more information in a scientifically validated format. |
| Use macros and templates | Macros can reduce time needed for documentation. Your memory isn’t perfect, but templates can help you include everything you need to cover. |
1. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract 2004;10:185-9.
2. Zurad EG. Don’t be the target of a malpractice suit. Fam Pract Manag 2006;13(6):57-64.
3. Gutheil TG. Fundamentals of medical record documentation. Psychiatry 2004;1:26-8.
4. Fischhoff B, Beyth R. “I knew it would happen” remembered probabilities of once-future things. Organ Behav Hum Perform 1975;13:1-16.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
6. 45 CFR § 164.524(a)(1).
7. Rogers AE, Addington-Hall JM, Abery AJ, et al. Knowledge and communication difficulties for patients with chronic heart failure: qualitative study. BMJ 2000;321:605-7.
8. Chesanow N. Are you getting through? Med Econ 2006;83(13):41,45-6.
9. Somoza E, Somoza JR. A neural-network approach to predicting admission decisions in a psychiatric emergency room. Med Decis Making 1993;13:273-80.
Current Psychiatry’s malpractice column is evolving. Previously, “Malpractice Verdicts,” used case decisions to initiate discussions of clinical situations that can generate lawsuits. The verdicts remain as “Malpractice Minute”, but Current Psychiatry has invited me to contribute a new column, “Malpractice Rx,” that will solicit questions and address practicing clinicians’ concerns about malpractice risk.
To start this dialogue, I’ll begin with a question that often comes up in discussions with colleagues, and especially when I teach psychiatry residents: “What should I document?” In this article, we will review why proper documentation is essential. We’ll also look at some ideas that might make documentation easier, more efficient, and more satisfying.
- If so, please submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
When I was in medical school, my professors said the primary reason for accurate charting was to communicate with the rest of the treatment team. This is still true. But in these sadder-but-wiser days, when I ask psychiatry residents “What is the purpose of documentation?” they always answer, “to create a legal record.”
Documentation plays many roles (Table 1). From the standpoint of preventing a malpractice judgment, the clinical record can accomplish 3 important things:
Lawsuit deterrence. Records are a key source—and often the only source—of information an attorney uses when deciding whether to file a lawsuit. An attorney won’t risk time and money on a malpractice case if the clinical record suggests that a psychiatrist was conscientious and met the standard of care.1
Impression management. The patient’s chart is what plaintiffs’ and defendants’ experts use when forming their initial opinions about the quality of care delivered.
Credibility. Clinical records are the most believable source of information about what you observed, what you thought, what you did, why you did it, and when you did it. The adage “if it wasn’t written, it didn’t happen” is not always applicable,2 but if an adverse event occurs, a defendant doctor’s verbal testimony about delivering good care will be more convincing when backed up by documentation created before the event.
Table 1
Purposes of medical record documentation
|
Improving documentation
Because it is impossible to describe everything you see, hear, say, do, and think during clinical encounters with patients, you must make choices about what to include in the record. The components of good documentation depend on the clinical context, but the following general principles may avert some malpractice actions.
1 More is better. Psychiatric practice often requires you to be discreet about patients’ personal information. Within appropriate bounds, however, the more information the record contains about objective findings, patients’ statements, clinical judgments, and your decision making, the better the portrayal of competent care.
2 Record the time and date. When attorneys and experts try to reconstruct what happened before an adverse occurrence, knowing the exact time you saw the patient, recorded findings, wrote orders, followed up on lab tests, or discussed problems with others—including family and treatment team members—can make a big difference.
3 Sooner is better. The most credible charting is done during or just after a service is rendered. Charting completed after an adverse event is vulnerable to accusations of fabrication.
4 Describe your thinking. Most aspects of clinical medicine are far from certain. Documenting the reasoning behind your diagnosis and treatment selection—what you’ve ruled out, what still seems tentative, and what risks and benefits you’ve weighed—helps emphasize this reality.3 After something bad happens, people retrospectively regard the event as more probable than it really was.4 Documenting your uncertainty and ways of addressing it may help counter this “hindsight bias.” It also shows that you were thoughtful and took therapeutic steps prudently.
5
6 Clarify capacity. Jurors may believe that all psychiatric patients are incompetent, and plaintiff’s attorneys sometimes try to create the impression that patients are completely controlled by weird whims and aberrant thoughts. To counter this, when appropriate indicate in the chart that the patient can handle responsibilities such as reporting side effects, seeking emergency attention, or notifying you about changes in thought or mood.3,5
7 Manage appearance and content. Under Health Insurance Portability and Accountability Act (HIPAA) regulations, patients have the right to review their medical records.6 If a lawsuit occurs, the records might be read out loud in court. Documentation will make a better impression if it is clear, legible, and free of gratuitous comments.
8 Include quotations. Documenting verbatim statements from a patient, such as “I’ve never considered suicide,” can quickly convey key information that you considered when making a therapeutic decision.
Technical approaches
Table 27,8 lists several techniques and technologies that might improve documentation. For example, computer users can create templates or customize software to quickly produce thorough documentation for frequently encountered procedures or clinical events. Whether these approaches are useful and appropriate will depend on your work setting, but all aim to improve the speed and quality of clinical documentation.
Think creatively about improving documentation. Even if you’re never sued, better documentation helps you and your patients. For example, several years ago a colleague9 designed an emergency room form that allowed clinicians to complete in a few seconds a Brief Psychiatric Rating Scale on every patient we evaluated. This innovation shortened the time needed to document a systematic, comprehensive assessment and increased the quantity, quality, and reliability of information in patients’ records.
Table 2
Purposes of medical record documentation
| Idea | Comment |
|---|---|
| Use speech recognition | You speak faster than you write. Transcription software |
| Software | accuracy has improved in the last few years. |
| Use handouts and | Patients often do not remember or understand much of what |
| medication instructions | doctors tell them,7,8 so handouts may be more useful than verbal instructions. Good handouts about medications are available on the Internet. Note in the chart that you gave the patient the document. |
| Seek anonymous | Documenting consultations shows you are prudent and |
| consultations with colleagues | a colleague agreed with your treatment. |
| Ask patients to rate their | This practice may improve your information gathering |
| own symptoms and progress | and help document what the patient told you. |
| Use standard rating scales | Rating scales can help you record more information in a scientifically validated format. |
| Use macros and templates | Macros can reduce time needed for documentation. Your memory isn’t perfect, but templates can help you include everything you need to cover. |
Current Psychiatry’s malpractice column is evolving. Previously, “Malpractice Verdicts,” used case decisions to initiate discussions of clinical situations that can generate lawsuits. The verdicts remain as “Malpractice Minute”, but Current Psychiatry has invited me to contribute a new column, “Malpractice Rx,” that will solicit questions and address practicing clinicians’ concerns about malpractice risk.
To start this dialogue, I’ll begin with a question that often comes up in discussions with colleagues, and especially when I teach psychiatry residents: “What should I document?” In this article, we will review why proper documentation is essential. We’ll also look at some ideas that might make documentation easier, more efficient, and more satisfying.
- If so, please submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
When I was in medical school, my professors said the primary reason for accurate charting was to communicate with the rest of the treatment team. This is still true. But in these sadder-but-wiser days, when I ask psychiatry residents “What is the purpose of documentation?” they always answer, “to create a legal record.”
Documentation plays many roles (Table 1). From the standpoint of preventing a malpractice judgment, the clinical record can accomplish 3 important things:
Lawsuit deterrence. Records are a key source—and often the only source—of information an attorney uses when deciding whether to file a lawsuit. An attorney won’t risk time and money on a malpractice case if the clinical record suggests that a psychiatrist was conscientious and met the standard of care.1
Impression management. The patient’s chart is what plaintiffs’ and defendants’ experts use when forming their initial opinions about the quality of care delivered.
Credibility. Clinical records are the most believable source of information about what you observed, what you thought, what you did, why you did it, and when you did it. The adage “if it wasn’t written, it didn’t happen” is not always applicable,2 but if an adverse event occurs, a defendant doctor’s verbal testimony about delivering good care will be more convincing when backed up by documentation created before the event.
Table 1
Purposes of medical record documentation
|
Improving documentation
Because it is impossible to describe everything you see, hear, say, do, and think during clinical encounters with patients, you must make choices about what to include in the record. The components of good documentation depend on the clinical context, but the following general principles may avert some malpractice actions.
1 More is better. Psychiatric practice often requires you to be discreet about patients’ personal information. Within appropriate bounds, however, the more information the record contains about objective findings, patients’ statements, clinical judgments, and your decision making, the better the portrayal of competent care.
2 Record the time and date. When attorneys and experts try to reconstruct what happened before an adverse occurrence, knowing the exact time you saw the patient, recorded findings, wrote orders, followed up on lab tests, or discussed problems with others—including family and treatment team members—can make a big difference.
3 Sooner is better. The most credible charting is done during or just after a service is rendered. Charting completed after an adverse event is vulnerable to accusations of fabrication.
4 Describe your thinking. Most aspects of clinical medicine are far from certain. Documenting the reasoning behind your diagnosis and treatment selection—what you’ve ruled out, what still seems tentative, and what risks and benefits you’ve weighed—helps emphasize this reality.3 After something bad happens, people retrospectively regard the event as more probable than it really was.4 Documenting your uncertainty and ways of addressing it may help counter this “hindsight bias.” It also shows that you were thoughtful and took therapeutic steps prudently.
5
6 Clarify capacity. Jurors may believe that all psychiatric patients are incompetent, and plaintiff’s attorneys sometimes try to create the impression that patients are completely controlled by weird whims and aberrant thoughts. To counter this, when appropriate indicate in the chart that the patient can handle responsibilities such as reporting side effects, seeking emergency attention, or notifying you about changes in thought or mood.3,5
7 Manage appearance and content. Under Health Insurance Portability and Accountability Act (HIPAA) regulations, patients have the right to review their medical records.6 If a lawsuit occurs, the records might be read out loud in court. Documentation will make a better impression if it is clear, legible, and free of gratuitous comments.
8 Include quotations. Documenting verbatim statements from a patient, such as “I’ve never considered suicide,” can quickly convey key information that you considered when making a therapeutic decision.
Technical approaches
Table 27,8 lists several techniques and technologies that might improve documentation. For example, computer users can create templates or customize software to quickly produce thorough documentation for frequently encountered procedures or clinical events. Whether these approaches are useful and appropriate will depend on your work setting, but all aim to improve the speed and quality of clinical documentation.
Think creatively about improving documentation. Even if you’re never sued, better documentation helps you and your patients. For example, several years ago a colleague9 designed an emergency room form that allowed clinicians to complete in a few seconds a Brief Psychiatric Rating Scale on every patient we evaluated. This innovation shortened the time needed to document a systematic, comprehensive assessment and increased the quantity, quality, and reliability of information in patients’ records.
Table 2
Purposes of medical record documentation
| Idea | Comment |
|---|---|
| Use speech recognition | You speak faster than you write. Transcription software |
| Software | accuracy has improved in the last few years. |
| Use handouts and | Patients often do not remember or understand much of what |
| medication instructions | doctors tell them,7,8 so handouts may be more useful than verbal instructions. Good handouts about medications are available on the Internet. Note in the chart that you gave the patient the document. |
| Seek anonymous | Documenting consultations shows you are prudent and |
| consultations with colleagues | a colleague agreed with your treatment. |
| Ask patients to rate their | This practice may improve your information gathering |
| own symptoms and progress | and help document what the patient told you. |
| Use standard rating scales | Rating scales can help you record more information in a scientifically validated format. |
| Use macros and templates | Macros can reduce time needed for documentation. Your memory isn’t perfect, but templates can help you include everything you need to cover. |
1. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract 2004;10:185-9.
2. Zurad EG. Don’t be the target of a malpractice suit. Fam Pract Manag 2006;13(6):57-64.
3. Gutheil TG. Fundamentals of medical record documentation. Psychiatry 2004;1:26-8.
4. Fischhoff B, Beyth R. “I knew it would happen” remembered probabilities of once-future things. Organ Behav Hum Perform 1975;13:1-16.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
6. 45 CFR § 164.524(a)(1).
7. Rogers AE, Addington-Hall JM, Abery AJ, et al. Knowledge and communication difficulties for patients with chronic heart failure: qualitative study. BMJ 2000;321:605-7.
8. Chesanow N. Are you getting through? Med Econ 2006;83(13):41,45-6.
9. Somoza E, Somoza JR. A neural-network approach to predicting admission decisions in a psychiatric emergency room. Med Decis Making 1993;13:273-80.
1. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract 2004;10:185-9.
2. Zurad EG. Don’t be the target of a malpractice suit. Fam Pract Manag 2006;13(6):57-64.
3. Gutheil TG. Fundamentals of medical record documentation. Psychiatry 2004;1:26-8.
4. Fischhoff B, Beyth R. “I knew it would happen” remembered probabilities of once-future things. Organ Behav Hum Perform 1975;13:1-16.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
6. 45 CFR § 164.524(a)(1).
7. Rogers AE, Addington-Hall JM, Abery AJ, et al. Knowledge and communication difficulties for patients with chronic heart failure: qualitative study. BMJ 2000;321:605-7.
8. Chesanow N. Are you getting through? Med Econ 2006;83(13):41,45-6.
9. Somoza E, Somoza JR. A neural-network approach to predicting admission decisions in a psychiatric emergency room. Med Decis Making 1993;13:273-80.
Can CT coronary angiography effectively rule out coronary disease in a patient admitted with chest pain?
Case
A 58-year-old male with a past medical history significant for hypertension and hypercholesterolemia presents four hours after acute onset of substernal chest pain that rates eight on a scale of 10. There is no radiation of the pain or associated dyspnea. He describes diaphoresis and nausea. Cardiac enzymes are negative on admission, and the electrocardiogram (ECG) is unchanged. Can computed tomography (CT) coronary angiography effectively rule out coronary disease in this patient admitted with chest pain?
Overview
Approximately 5 million patients presented to U.S. hospitals in 2002 for evaluation of chest pain.1 Less than a third of these patients were ultimately diagnosed with acute coronary syndrome.2 Current strategies to differentiate acute coronary syndrome from non-cardiac causes of chest pain have included electrocardiography, cardiac enzymes, exercise treadmill, echocardiography, and nuclear perfusion.
Unfortunately, each of these modalities has false positive and negative rates that result in a significant number of patients undergoing further evaluation for coronary artery stenosis. Although coronary angiography is the current gold standard to evaluate coronary luminal obstruction, it has many drawbacks. It is costly and inconvenient for patients, invasive, and demonstrates only the later stages of atherosclerosis—not which plaques are prone to rupture. All these limitations necessitate a search for a non-invasive evaluation of the coronary vasculature.
Because 64-slice CT scanners allow for visualization of the cardiac anatomy and coronary vasculature without catheters, there has been increasing interest in this modality to evaluate for coronary artery stenosis in low- to intermediate-risk patients presenting with chest pain. Comparative studies have found it allows for faster, safer evaluation of chest pain with sensitivity and specificity comparable to traditional angiography and a negative predictive value superior to nuclear imaging.3,4
Additional advantages include easy access to CT scanners over cardiac catheterization facilities; 88% of community hospitals with six or more beds had CT scanners in 2004. Further, turnaround is faster (15 to 20 minutes for the CT angiography versus six to eight hours of observation after cardiac catheterization). Also, physicians can simultaneously exclude other life-threatening causes of chest pain including aortic dissection and pulmonary embolus.5 Finally, CT angiography is less expensive (about $800 to $1,000) than invasive coronary angiography (approximately $3,000 to $4,000).6
Review of the Data
Patients undergoing CT angiography require a target heart rate of less than 70 beats per minute. Oral or intravenous beta-blockers are typically given prior to the procedure.
Nitroglycerin 0.4-0.8 mg is also administered sublingually to enhance visualization of the coronary vasculature.
Pulse, ECG, and blood pressure are monitored throughout the imaging process. Initially, a non-contrast scan is performed for coronary artery calcium (CAC) scoring. This is followed by angiography using a bolus of iodinated contrast. At this time, multislice cardiac scanning is synchronized with an ECG (i.e., gating the scan) and images are obtained during diastole.
Two types of CT are capable of obtaining the necessary high-speed images. Electron-beam CT (EBCT) and helical or spiral CT scanning. Multidetector helical CT (MDCT) or multislice CT (MSCT) is an evolution of helical CT. MDCT is available in four-, eight-, 16-, 32-, or 64-slice. Interpretation of the imaging uses the American College of Cardiology nomenclature: no stenosis, insignificant stenosis (less than 50% of coronary luminal diameter), significant stenosis (more than 50%), and total occlusion.
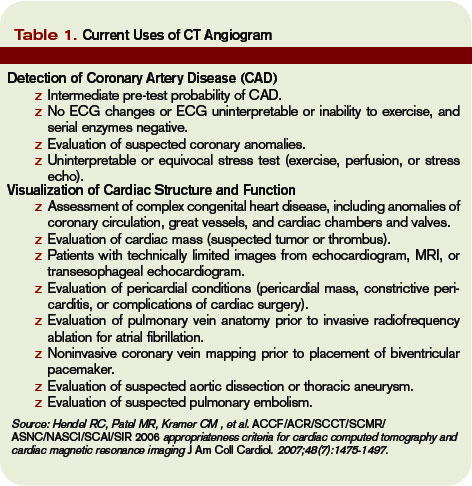
The presence of CAC has been shown in numerous studies to have prognostic significance for cardiac events and death. An elevated CAC score more accurately predicts coronary heart disease (CHD) risk in adults with an initial Framingham risk score between 10% and 19%. In addition, compared with a CAC score of zero, a score of more than 300 was predictive of CHD risk.7
Some studies suggest negative CAC scores alone are enough to risk-stratify patients presenting with chest pain, reporting sensitivities between 96% and 100% for the detection of significant cardiac events.8
Clinical studies of CT angiography typically consist of patients already selected to receive traditional invasive coronary angiography. Initial reports by Leschka, et al., showed sensitivity and specificity of 94% and 97%, respectively, with positive predictive values and negative predictive values of 87% and 99%.9
Additionally, a meta-analysis revealed multislice computed tomography (MSCT) for the diagnosis of CHD was highly sensitive (95% to 100%) for the detection of significant CHD. Specificity was 100% with the 64-slice MSCT and only slightly lower with the four- and 16-slice scanners (87%). A positive predictive value of 66% and negative predictive value of 98% for the presence of significant coronary stenosis have also been reported.10
Gallagher, et al., and previous studies comparing CT angiography with traditional invasive coronary angiography suggest further testing, such as stress nuclear imaging for any patient with stenosis more than 25% or CCS of greater than 100 and further recommends cardiac catheterization of any patient with greater than 70% stenosis by MSCT.

The utility of CT coronary angiography in the evaluation of patients presenting to the ED with chest pain was studied by Goldstein and peers.11 A randomized trial was conducted with patients admitted with chest pain or anginal equivalent, considered to be at low risk for CAD. Patients with negative cardiac enzymes and non-diagnostic ECG were assigned to either MSCCT or myocardial perfusion scan. CT angiography was adequate to diagnose or exclude CAD as the cause of chest pain in 75% of patients. The remaining 25% of patients had additional nuclear stress imaging. Average cost of the MDCT cohort was $1,586 compared with $1,872 for standard diagnostic evaluation. The time required for diagnosis was significantly shorter in the CT cohort: 3.4 hours, compared with 15 hours in the standard group.
An ongoing study at Beaumont Hospital in Royal Oak, Mich., is evaluating the length of stay and cost of care in patients presenting to the ED with chest pain. Patients are randomized to standard evaluation with serial enzymes, ECG, and nuclear perfusion testing or 64-slice CT angiography, plus coronary calcium score. Preliminary results presented at the 2006 American College of Cardiology Annual Scientific Session regarding the initial 200 patients showed a shorter length of stay and lower cost of care with similar patient outcomes in the group that underwent CT angiography.12
A large randomized controlled trial, Coronary Computed Tomography for Systematic Triage of Acute Chest Pain Patients to Treatment (CT-STAT), is planned to definitively study the use of coronary CT angiography in low-risk patients with chest pain. The large-scale study will involve 750 patients in 15 U.S. hospitals.
CT angiography remains limited despite many recent advances. A stable rhythm is a prerequisite, precluding use in patients with atrial fibrillation or frequent extra-systoles. Also, the required dose of 80 cc to 100 cc of iodinated contrast puts patients at risk for contrast-induced nephropathy, especially those with renal insufficiency.
Finally, radiation exposure is higher than that required for cardiac catheterization.13 Coronary calcification interferes with the images obtained by CT. Therefore, patients with heavy coronary calcium burden (CAC more than 400) may have reduced specificity and negative predictive value. Because this calcification increases with age, the diagnostic accuracy of CT angiography may decrease with age.
Morbidly obese patients may also have decreased image quality. Raff. et al., found significant stenosis in patients with normal body-mass index (BMI) (less than 25 kg/m2). Sensitivity, specificity, and positive and negative predictive values were all 100% and remained accurate in overweight patients. When BMI was more than 30, sensitivity and specificity were reduced to 90% and 86%, respectively.
Visualization of the coronary artery within a stent may be less accurate with CT angiography due to beam artifact, but evaluation of native coronary arteries and bypass grafts maintain similar sensitivity and specificity in these patients.14 A final concern is that CT angiography is only diagnostic. Although only 25% to 30% of diagnostic cardiac catheterizations reveal disease that meets criteria for stent placement, the study is redundant in these high-risk patients, who likely will be referred for traditional coronary angiography with stenting.
Back to the Case
The patient underwent nuclear stress testing the morning following admission. He had minimal attenuation in the infero-lateral distribution. A 64-slice CT angiogram was obtained, and images of the coronary anatomy demonstrated no plaque. The patient was reassured, and no further cardiac imaging was pursued. TH
Dr. Jenkins is an associate clinical professor and associate chief of hospital medicine in the Department of Family Medicine and Community Health at the University of Massachusetts medical school, Worcester.
References
- Statistics CNCH, ed. National Hospital Ambulatory Medical Care Survey: 2002 Emergency Department Summary, 2004. Available at www.cdc.gov/nchs/pressroom/04facts/emergencydept.htm. Last accessed Nov. 8, 2007.
- Kohn MA, Kwan E, Gupta M, et al. Prevalence of acute myocardial infarction and other serious diagnoses in patients presenting to an urban emergency department with chest pain. J Emerg Med. 2005;29(4):383-390.
- Stein PD, Beemath A, Kayali F, et al. Multidetector computed tomography for the diagnosis of coronary artery disease: a systematic review. Am J Med. 2006;119(3):203-216.
- Gallagher MJ, Ross MA, Raff G, et al. The diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patients. Ann of Emerg Med. 200;49(2):125-136.
- AHA Hospital Statistics, 2006 Edition. Chicago: American Hospital Association; 2006:158, 161.
- Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, HCUPnet. Available at www.ahrq.gov/data/hcup. Last accessed Nov. 8, 2007.
- Greenland P, LaBree L, Azen SP, et al. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004;291(2):210-215.
- Kondos GT, Hoff JA, Sevrkov A, et al. Electron-beam tomography coronary artery calcium and cardiac events: a 37-month follow-up of 5,635 initially asymptomatic low- to intermediate-risk adults. Circulation. 2003;107(20):2571-2676.
- Leschka S, Alkadhi H, Plass A, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005;177:1482-1487.
- Raff GL, Gallagher MJ, O’Neill WW, et al. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005;46:552-557.
- Goldstein JA, Gallagher MJ, O’Neill WW, et al. A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol. 2007;49(8):863-871.
- Raff GL, Gallagher MJ, O’Neill WW. Immediate coronary artery computed tomographic angiography rapidly and definitively excludes coronary artery disease in low-risk acute chest pain. Abstract 807-8. 55th Annual Scientific Session of the American College of Cardiology, March 11-14, 2006.
- de Feyter PJ, Nieman K. Noninvasive multi-slice computed tomography coronary angiography: an emerging clinical modality. J Am Coll Cardiol. 2004;44(6):1238-1240.
- Garcia MJ. Noninvasive coronary angiography: hype or new paradigm? J Am Med Assoc. 2005; 293:2531-2533.
Case
A 58-year-old male with a past medical history significant for hypertension and hypercholesterolemia presents four hours after acute onset of substernal chest pain that rates eight on a scale of 10. There is no radiation of the pain or associated dyspnea. He describes diaphoresis and nausea. Cardiac enzymes are negative on admission, and the electrocardiogram (ECG) is unchanged. Can computed tomography (CT) coronary angiography effectively rule out coronary disease in this patient admitted with chest pain?
Overview
Approximately 5 million patients presented to U.S. hospitals in 2002 for evaluation of chest pain.1 Less than a third of these patients were ultimately diagnosed with acute coronary syndrome.2 Current strategies to differentiate acute coronary syndrome from non-cardiac causes of chest pain have included electrocardiography, cardiac enzymes, exercise treadmill, echocardiography, and nuclear perfusion.
Unfortunately, each of these modalities has false positive and negative rates that result in a significant number of patients undergoing further evaluation for coronary artery stenosis. Although coronary angiography is the current gold standard to evaluate coronary luminal obstruction, it has many drawbacks. It is costly and inconvenient for patients, invasive, and demonstrates only the later stages of atherosclerosis—not which plaques are prone to rupture. All these limitations necessitate a search for a non-invasive evaluation of the coronary vasculature.
Because 64-slice CT scanners allow for visualization of the cardiac anatomy and coronary vasculature without catheters, there has been increasing interest in this modality to evaluate for coronary artery stenosis in low- to intermediate-risk patients presenting with chest pain. Comparative studies have found it allows for faster, safer evaluation of chest pain with sensitivity and specificity comparable to traditional angiography and a negative predictive value superior to nuclear imaging.3,4
Additional advantages include easy access to CT scanners over cardiac catheterization facilities; 88% of community hospitals with six or more beds had CT scanners in 2004. Further, turnaround is faster (15 to 20 minutes for the CT angiography versus six to eight hours of observation after cardiac catheterization). Also, physicians can simultaneously exclude other life-threatening causes of chest pain including aortic dissection and pulmonary embolus.5 Finally, CT angiography is less expensive (about $800 to $1,000) than invasive coronary angiography (approximately $3,000 to $4,000).6
Review of the Data
Patients undergoing CT angiography require a target heart rate of less than 70 beats per minute. Oral or intravenous beta-blockers are typically given prior to the procedure.
Nitroglycerin 0.4-0.8 mg is also administered sublingually to enhance visualization of the coronary vasculature.
Pulse, ECG, and blood pressure are monitored throughout the imaging process. Initially, a non-contrast scan is performed for coronary artery calcium (CAC) scoring. This is followed by angiography using a bolus of iodinated contrast. At this time, multislice cardiac scanning is synchronized with an ECG (i.e., gating the scan) and images are obtained during diastole.
Two types of CT are capable of obtaining the necessary high-speed images. Electron-beam CT (EBCT) and helical or spiral CT scanning. Multidetector helical CT (MDCT) or multislice CT (MSCT) is an evolution of helical CT. MDCT is available in four-, eight-, 16-, 32-, or 64-slice. Interpretation of the imaging uses the American College of Cardiology nomenclature: no stenosis, insignificant stenosis (less than 50% of coronary luminal diameter), significant stenosis (more than 50%), and total occlusion.
The presence of CAC has been shown in numerous studies to have prognostic significance for cardiac events and death. An elevated CAC score more accurately predicts coronary heart disease (CHD) risk in adults with an initial Framingham risk score between 10% and 19%. In addition, compared with a CAC score of zero, a score of more than 300 was predictive of CHD risk.7
Some studies suggest negative CAC scores alone are enough to risk-stratify patients presenting with chest pain, reporting sensitivities between 96% and 100% for the detection of significant cardiac events.8
Clinical studies of CT angiography typically consist of patients already selected to receive traditional invasive coronary angiography. Initial reports by Leschka, et al., showed sensitivity and specificity of 94% and 97%, respectively, with positive predictive values and negative predictive values of 87% and 99%.9
Additionally, a meta-analysis revealed multislice computed tomography (MSCT) for the diagnosis of CHD was highly sensitive (95% to 100%) for the detection of significant CHD. Specificity was 100% with the 64-slice MSCT and only slightly lower with the four- and 16-slice scanners (87%). A positive predictive value of 66% and negative predictive value of 98% for the presence of significant coronary stenosis have also been reported.10
Gallagher, et al., and previous studies comparing CT angiography with traditional invasive coronary angiography suggest further testing, such as stress nuclear imaging for any patient with stenosis more than 25% or CCS of greater than 100 and further recommends cardiac catheterization of any patient with greater than 70% stenosis by MSCT.
The utility of CT coronary angiography in the evaluation of patients presenting to the ED with chest pain was studied by Goldstein and peers.11 A randomized trial was conducted with patients admitted with chest pain or anginal equivalent, considered to be at low risk for CAD. Patients with negative cardiac enzymes and non-diagnostic ECG were assigned to either MSCCT or myocardial perfusion scan. CT angiography was adequate to diagnose or exclude CAD as the cause of chest pain in 75% of patients. The remaining 25% of patients had additional nuclear stress imaging. Average cost of the MDCT cohort was $1,586 compared with $1,872 for standard diagnostic evaluation. The time required for diagnosis was significantly shorter in the CT cohort: 3.4 hours, compared with 15 hours in the standard group.
An ongoing study at Beaumont Hospital in Royal Oak, Mich., is evaluating the length of stay and cost of care in patients presenting to the ED with chest pain. Patients are randomized to standard evaluation with serial enzymes, ECG, and nuclear perfusion testing or 64-slice CT angiography, plus coronary calcium score. Preliminary results presented at the 2006 American College of Cardiology Annual Scientific Session regarding the initial 200 patients showed a shorter length of stay and lower cost of care with similar patient outcomes in the group that underwent CT angiography.12
A large randomized controlled trial, Coronary Computed Tomography for Systematic Triage of Acute Chest Pain Patients to Treatment (CT-STAT), is planned to definitively study the use of coronary CT angiography in low-risk patients with chest pain. The large-scale study will involve 750 patients in 15 U.S. hospitals.
CT angiography remains limited despite many recent advances. A stable rhythm is a prerequisite, precluding use in patients with atrial fibrillation or frequent extra-systoles. Also, the required dose of 80 cc to 100 cc of iodinated contrast puts patients at risk for contrast-induced nephropathy, especially those with renal insufficiency.
Finally, radiation exposure is higher than that required for cardiac catheterization.13 Coronary calcification interferes with the images obtained by CT. Therefore, patients with heavy coronary calcium burden (CAC more than 400) may have reduced specificity and negative predictive value. Because this calcification increases with age, the diagnostic accuracy of CT angiography may decrease with age.
Morbidly obese patients may also have decreased image quality. Raff. et al., found significant stenosis in patients with normal body-mass index (BMI) (less than 25 kg/m2). Sensitivity, specificity, and positive and negative predictive values were all 100% and remained accurate in overweight patients. When BMI was more than 30, sensitivity and specificity were reduced to 90% and 86%, respectively.
Visualization of the coronary artery within a stent may be less accurate with CT angiography due to beam artifact, but evaluation of native coronary arteries and bypass grafts maintain similar sensitivity and specificity in these patients.14 A final concern is that CT angiography is only diagnostic. Although only 25% to 30% of diagnostic cardiac catheterizations reveal disease that meets criteria for stent placement, the study is redundant in these high-risk patients, who likely will be referred for traditional coronary angiography with stenting.
Back to the Case
The patient underwent nuclear stress testing the morning following admission. He had minimal attenuation in the infero-lateral distribution. A 64-slice CT angiogram was obtained, and images of the coronary anatomy demonstrated no plaque. The patient was reassured, and no further cardiac imaging was pursued. TH
Dr. Jenkins is an associate clinical professor and associate chief of hospital medicine in the Department of Family Medicine and Community Health at the University of Massachusetts medical school, Worcester.
References
- Statistics CNCH, ed. National Hospital Ambulatory Medical Care Survey: 2002 Emergency Department Summary, 2004. Available at www.cdc.gov/nchs/pressroom/04facts/emergencydept.htm. Last accessed Nov. 8, 2007.
- Kohn MA, Kwan E, Gupta M, et al. Prevalence of acute myocardial infarction and other serious diagnoses in patients presenting to an urban emergency department with chest pain. J Emerg Med. 2005;29(4):383-390.
- Stein PD, Beemath A, Kayali F, et al. Multidetector computed tomography for the diagnosis of coronary artery disease: a systematic review. Am J Med. 2006;119(3):203-216.
- Gallagher MJ, Ross MA, Raff G, et al. The diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patients. Ann of Emerg Med. 200;49(2):125-136.
- AHA Hospital Statistics, 2006 Edition. Chicago: American Hospital Association; 2006:158, 161.
- Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, HCUPnet. Available at www.ahrq.gov/data/hcup. Last accessed Nov. 8, 2007.
- Greenland P, LaBree L, Azen SP, et al. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004;291(2):210-215.
- Kondos GT, Hoff JA, Sevrkov A, et al. Electron-beam tomography coronary artery calcium and cardiac events: a 37-month follow-up of 5,635 initially asymptomatic low- to intermediate-risk adults. Circulation. 2003;107(20):2571-2676.
- Leschka S, Alkadhi H, Plass A, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005;177:1482-1487.
- Raff GL, Gallagher MJ, O’Neill WW, et al. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005;46:552-557.
- Goldstein JA, Gallagher MJ, O’Neill WW, et al. A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol. 2007;49(8):863-871.
- Raff GL, Gallagher MJ, O’Neill WW. Immediate coronary artery computed tomographic angiography rapidly and definitively excludes coronary artery disease in low-risk acute chest pain. Abstract 807-8. 55th Annual Scientific Session of the American College of Cardiology, March 11-14, 2006.
- de Feyter PJ, Nieman K. Noninvasive multi-slice computed tomography coronary angiography: an emerging clinical modality. J Am Coll Cardiol. 2004;44(6):1238-1240.
- Garcia MJ. Noninvasive coronary angiography: hype or new paradigm? J Am Med Assoc. 2005; 293:2531-2533.
Case
A 58-year-old male with a past medical history significant for hypertension and hypercholesterolemia presents four hours after acute onset of substernal chest pain that rates eight on a scale of 10. There is no radiation of the pain or associated dyspnea. He describes diaphoresis and nausea. Cardiac enzymes are negative on admission, and the electrocardiogram (ECG) is unchanged. Can computed tomography (CT) coronary angiography effectively rule out coronary disease in this patient admitted with chest pain?
Overview
Approximately 5 million patients presented to U.S. hospitals in 2002 for evaluation of chest pain.1 Less than a third of these patients were ultimately diagnosed with acute coronary syndrome.2 Current strategies to differentiate acute coronary syndrome from non-cardiac causes of chest pain have included electrocardiography, cardiac enzymes, exercise treadmill, echocardiography, and nuclear perfusion.
Unfortunately, each of these modalities has false positive and negative rates that result in a significant number of patients undergoing further evaluation for coronary artery stenosis. Although coronary angiography is the current gold standard to evaluate coronary luminal obstruction, it has many drawbacks. It is costly and inconvenient for patients, invasive, and demonstrates only the later stages of atherosclerosis—not which plaques are prone to rupture. All these limitations necessitate a search for a non-invasive evaluation of the coronary vasculature.
Because 64-slice CT scanners allow for visualization of the cardiac anatomy and coronary vasculature without catheters, there has been increasing interest in this modality to evaluate for coronary artery stenosis in low- to intermediate-risk patients presenting with chest pain. Comparative studies have found it allows for faster, safer evaluation of chest pain with sensitivity and specificity comparable to traditional angiography and a negative predictive value superior to nuclear imaging.3,4
Additional advantages include easy access to CT scanners over cardiac catheterization facilities; 88% of community hospitals with six or more beds had CT scanners in 2004. Further, turnaround is faster (15 to 20 minutes for the CT angiography versus six to eight hours of observation after cardiac catheterization). Also, physicians can simultaneously exclude other life-threatening causes of chest pain including aortic dissection and pulmonary embolus.5 Finally, CT angiography is less expensive (about $800 to $1,000) than invasive coronary angiography (approximately $3,000 to $4,000).6
Review of the Data
Patients undergoing CT angiography require a target heart rate of less than 70 beats per minute. Oral or intravenous beta-blockers are typically given prior to the procedure.
Nitroglycerin 0.4-0.8 mg is also administered sublingually to enhance visualization of the coronary vasculature.
Pulse, ECG, and blood pressure are monitored throughout the imaging process. Initially, a non-contrast scan is performed for coronary artery calcium (CAC) scoring. This is followed by angiography using a bolus of iodinated contrast. At this time, multislice cardiac scanning is synchronized with an ECG (i.e., gating the scan) and images are obtained during diastole.
Two types of CT are capable of obtaining the necessary high-speed images. Electron-beam CT (EBCT) and helical or spiral CT scanning. Multidetector helical CT (MDCT) or multislice CT (MSCT) is an evolution of helical CT. MDCT is available in four-, eight-, 16-, 32-, or 64-slice. Interpretation of the imaging uses the American College of Cardiology nomenclature: no stenosis, insignificant stenosis (less than 50% of coronary luminal diameter), significant stenosis (more than 50%), and total occlusion.
The presence of CAC has been shown in numerous studies to have prognostic significance for cardiac events and death. An elevated CAC score more accurately predicts coronary heart disease (CHD) risk in adults with an initial Framingham risk score between 10% and 19%. In addition, compared with a CAC score of zero, a score of more than 300 was predictive of CHD risk.7
Some studies suggest negative CAC scores alone are enough to risk-stratify patients presenting with chest pain, reporting sensitivities between 96% and 100% for the detection of significant cardiac events.8
Clinical studies of CT angiography typically consist of patients already selected to receive traditional invasive coronary angiography. Initial reports by Leschka, et al., showed sensitivity and specificity of 94% and 97%, respectively, with positive predictive values and negative predictive values of 87% and 99%.9
Additionally, a meta-analysis revealed multislice computed tomography (MSCT) for the diagnosis of CHD was highly sensitive (95% to 100%) for the detection of significant CHD. Specificity was 100% with the 64-slice MSCT and only slightly lower with the four- and 16-slice scanners (87%). A positive predictive value of 66% and negative predictive value of 98% for the presence of significant coronary stenosis have also been reported.10
Gallagher, et al., and previous studies comparing CT angiography with traditional invasive coronary angiography suggest further testing, such as stress nuclear imaging for any patient with stenosis more than 25% or CCS of greater than 100 and further recommends cardiac catheterization of any patient with greater than 70% stenosis by MSCT.
The utility of CT coronary angiography in the evaluation of patients presenting to the ED with chest pain was studied by Goldstein and peers.11 A randomized trial was conducted with patients admitted with chest pain or anginal equivalent, considered to be at low risk for CAD. Patients with negative cardiac enzymes and non-diagnostic ECG were assigned to either MSCCT or myocardial perfusion scan. CT angiography was adequate to diagnose or exclude CAD as the cause of chest pain in 75% of patients. The remaining 25% of patients had additional nuclear stress imaging. Average cost of the MDCT cohort was $1,586 compared with $1,872 for standard diagnostic evaluation. The time required for diagnosis was significantly shorter in the CT cohort: 3.4 hours, compared with 15 hours in the standard group.
An ongoing study at Beaumont Hospital in Royal Oak, Mich., is evaluating the length of stay and cost of care in patients presenting to the ED with chest pain. Patients are randomized to standard evaluation with serial enzymes, ECG, and nuclear perfusion testing or 64-slice CT angiography, plus coronary calcium score. Preliminary results presented at the 2006 American College of Cardiology Annual Scientific Session regarding the initial 200 patients showed a shorter length of stay and lower cost of care with similar patient outcomes in the group that underwent CT angiography.12
A large randomized controlled trial, Coronary Computed Tomography for Systematic Triage of Acute Chest Pain Patients to Treatment (CT-STAT), is planned to definitively study the use of coronary CT angiography in low-risk patients with chest pain. The large-scale study will involve 750 patients in 15 U.S. hospitals.
CT angiography remains limited despite many recent advances. A stable rhythm is a prerequisite, precluding use in patients with atrial fibrillation or frequent extra-systoles. Also, the required dose of 80 cc to 100 cc of iodinated contrast puts patients at risk for contrast-induced nephropathy, especially those with renal insufficiency.
Finally, radiation exposure is higher than that required for cardiac catheterization.13 Coronary calcification interferes with the images obtained by CT. Therefore, patients with heavy coronary calcium burden (CAC more than 400) may have reduced specificity and negative predictive value. Because this calcification increases with age, the diagnostic accuracy of CT angiography may decrease with age.
Morbidly obese patients may also have decreased image quality. Raff. et al., found significant stenosis in patients with normal body-mass index (BMI) (less than 25 kg/m2). Sensitivity, specificity, and positive and negative predictive values were all 100% and remained accurate in overweight patients. When BMI was more than 30, sensitivity and specificity were reduced to 90% and 86%, respectively.
Visualization of the coronary artery within a stent may be less accurate with CT angiography due to beam artifact, but evaluation of native coronary arteries and bypass grafts maintain similar sensitivity and specificity in these patients.14 A final concern is that CT angiography is only diagnostic. Although only 25% to 30% of diagnostic cardiac catheterizations reveal disease that meets criteria for stent placement, the study is redundant in these high-risk patients, who likely will be referred for traditional coronary angiography with stenting.
Back to the Case
The patient underwent nuclear stress testing the morning following admission. He had minimal attenuation in the infero-lateral distribution. A 64-slice CT angiogram was obtained, and images of the coronary anatomy demonstrated no plaque. The patient was reassured, and no further cardiac imaging was pursued. TH
Dr. Jenkins is an associate clinical professor and associate chief of hospital medicine in the Department of Family Medicine and Community Health at the University of Massachusetts medical school, Worcester.
References
- Statistics CNCH, ed. National Hospital Ambulatory Medical Care Survey: 2002 Emergency Department Summary, 2004. Available at www.cdc.gov/nchs/pressroom/04facts/emergencydept.htm. Last accessed Nov. 8, 2007.
- Kohn MA, Kwan E, Gupta M, et al. Prevalence of acute myocardial infarction and other serious diagnoses in patients presenting to an urban emergency department with chest pain. J Emerg Med. 2005;29(4):383-390.
- Stein PD, Beemath A, Kayali F, et al. Multidetector computed tomography for the diagnosis of coronary artery disease: a systematic review. Am J Med. 2006;119(3):203-216.
- Gallagher MJ, Ross MA, Raff G, et al. The diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patients. Ann of Emerg Med. 200;49(2):125-136.
- AHA Hospital Statistics, 2006 Edition. Chicago: American Hospital Association; 2006:158, 161.
- Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, HCUPnet. Available at www.ahrq.gov/data/hcup. Last accessed Nov. 8, 2007.
- Greenland P, LaBree L, Azen SP, et al. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004;291(2):210-215.
- Kondos GT, Hoff JA, Sevrkov A, et al. Electron-beam tomography coronary artery calcium and cardiac events: a 37-month follow-up of 5,635 initially asymptomatic low- to intermediate-risk adults. Circulation. 2003;107(20):2571-2676.
- Leschka S, Alkadhi H, Plass A, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005;177:1482-1487.
- Raff GL, Gallagher MJ, O’Neill WW, et al. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005;46:552-557.
- Goldstein JA, Gallagher MJ, O’Neill WW, et al. A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol. 2007;49(8):863-871.
- Raff GL, Gallagher MJ, O’Neill WW. Immediate coronary artery computed tomographic angiography rapidly and definitively excludes coronary artery disease in low-risk acute chest pain. Abstract 807-8. 55th Annual Scientific Session of the American College of Cardiology, March 11-14, 2006.
- de Feyter PJ, Nieman K. Noninvasive multi-slice computed tomography coronary angiography: an emerging clinical modality. J Am Coll Cardiol. 2004;44(6):1238-1240.
- Garcia MJ. Noninvasive coronary angiography: hype or new paradigm? J Am Med Assoc. 2005; 293:2531-2533.
Your First Job
Within the next few months, many of you will have a new job as an attending hospitalist. As daunting as that may seem, now is the time to think about what you can do to ensure a smooth transition and successful beginning to your career.
Although residency prepared you to face the medical challenges ahead, here are 10 pointers that may help as you move to the next stage of your professional life.
1) Familiarize yourself with the licensing/credentialing process: Do not underestimate the amount of time it takes to get this paperwork approved—up to six months in some cases. Many new hires’ first days on the job are delayed because they didn’t complete this step. Check with state licensing boards for special requirements unique to that state. Also, every hospital has its own gauntlet of infectious disease, HIPAA, and information- technology hoops to jump through. Getting your applications in as early as possible puts you in position to begin on your planned start date and prevent last-minute catastrophes for your new program.
2) Gain valuable insight through observation: Study your current hospitalist group to gain perspective that will help in your new setting. All programs and hospitals operate differently and have room for quality/process improvement. Interview hospitalists, ask questions, and observe the workflow in your current hospital(s) to help in your new job.
3) Contemplate your career direction: Think strategically about your strengths and plans. Although you will learn an incredible amount about hospital medicine careers after you begin, having a sense of direction will help your new group and its leadership get you where you want to be. Making connections and making your goals known within your new program before you start will put your new career on the right path.
4) Seek mentors: Having mentors from your prior program and your new program is a key to a healthy and happy career. Choose people you respect and pick their brains about their careers, how they acquired their skills, and how they would advise you to do the same. Good mentors will help you for many years, and the most valuable may be the ones who have known you throughout your residency. Nurture and maintain these relationships even if you are moving on to new horizons. Inquire whether your new program has a mentorship structure or if your new group leader can recommend someone who shares common interests and goals.
5) Study SHM’s Core Com-petencies: Although you may have trepidation about your medical skills and knowledge as you move into uncharted waters, step back and relax. Know that you are prepared. That said, you can always learn more. One excellent resource is The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (available on SHM’s Web site, www.hospitalmedicine.org). This is a set of standards with which programs can teach hospital medicine and you can learn the scope of expectations and competencies for someone in your position.
6) Understand the nuts and bolts of your new program: Although there are many things you will learn on the job, gain an appreciation for some of the following before your first day:
- Billing: If this is your responsibility, you need to learn a little about this before you start, preferably from one of your future colleagues.
- Reimbursement structure: Find out how your productivity is tracked and rewarded. You’d be amazed how variable this can be.
- Time allotment: How are administrative, research, committee and teaching time balanced against your clinical time?
7) Get to know your new hospital: Before hitting the wards it pays to do a little homework on your new workplace. Do you have access to a medical library, journals, UpToDate, or other online databases? If not, do you need to purchase this access on your own? Many programs have academic funds allotted so you can use those resources. Also, familiarize yourself with the local antibiogram, formularies, guidelines, and order sets. Most facilities have tools specific to their hospital. Know how these affect you in your new role. Prior to starting, you will also want to be sufficiently oriented to any computer systems and understand how they’re used for documentation and order entry, and for viewing lab, radiology, and microbiology results.
8) Shadow a hospitalist: Spending a few hours with someone during a typical hospitalist work day will give you an idea of the pace of the work, the layout of the hospital and floors, the medical and ancillary staff you will work with, and the patient population. This will prompt questions you hadn’t thought of previously.
9) Prepare for each specific role: Hospitalists wear many hats, including teaching attending, non-teaching attending, consultant, researcher, committee member, and hospital medicine leader. Each role carries specific responsibilities and expectations. Prior to each new role, train with someone who leads that service or knows the job intimately.
10) Comprehend your benefits: Does your employer have a retirement program? Do they match retirement contributions? How does the malpractice insurance work? A meeting with human resources will usually help you arrange your health, dental, malpractice, and disability insurance prior to your start date. TH
Dr. Chacko is chair of SHM’s young physician committee and the hospitalist program medical director for Preferred Health Partners in New York City. Dr. Markoff is an assistant professor of medicine and associate director of the hospitalist service at the Mount Sinai Hospital in New York City. Dr. Sliwka is a hospitalist and assistant professor of clinical medicine at the University of California, San Francisco Medical Center.
Within the next few months, many of you will have a new job as an attending hospitalist. As daunting as that may seem, now is the time to think about what you can do to ensure a smooth transition and successful beginning to your career.
Although residency prepared you to face the medical challenges ahead, here are 10 pointers that may help as you move to the next stage of your professional life.
1) Familiarize yourself with the licensing/credentialing process: Do not underestimate the amount of time it takes to get this paperwork approved—up to six months in some cases. Many new hires’ first days on the job are delayed because they didn’t complete this step. Check with state licensing boards for special requirements unique to that state. Also, every hospital has its own gauntlet of infectious disease, HIPAA, and information- technology hoops to jump through. Getting your applications in as early as possible puts you in position to begin on your planned start date and prevent last-minute catastrophes for your new program.
2) Gain valuable insight through observation: Study your current hospitalist group to gain perspective that will help in your new setting. All programs and hospitals operate differently and have room for quality/process improvement. Interview hospitalists, ask questions, and observe the workflow in your current hospital(s) to help in your new job.
3) Contemplate your career direction: Think strategically about your strengths and plans. Although you will learn an incredible amount about hospital medicine careers after you begin, having a sense of direction will help your new group and its leadership get you where you want to be. Making connections and making your goals known within your new program before you start will put your new career on the right path.
4) Seek mentors: Having mentors from your prior program and your new program is a key to a healthy and happy career. Choose people you respect and pick their brains about their careers, how they acquired their skills, and how they would advise you to do the same. Good mentors will help you for many years, and the most valuable may be the ones who have known you throughout your residency. Nurture and maintain these relationships even if you are moving on to new horizons. Inquire whether your new program has a mentorship structure or if your new group leader can recommend someone who shares common interests and goals.
5) Study SHM’s Core Com-petencies: Although you may have trepidation about your medical skills and knowledge as you move into uncharted waters, step back and relax. Know that you are prepared. That said, you can always learn more. One excellent resource is The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (available on SHM’s Web site, www.hospitalmedicine.org). This is a set of standards with which programs can teach hospital medicine and you can learn the scope of expectations and competencies for someone in your position.
6) Understand the nuts and bolts of your new program: Although there are many things you will learn on the job, gain an appreciation for some of the following before your first day:
- Billing: If this is your responsibility, you need to learn a little about this before you start, preferably from one of your future colleagues.
- Reimbursement structure: Find out how your productivity is tracked and rewarded. You’d be amazed how variable this can be.
- Time allotment: How are administrative, research, committee and teaching time balanced against your clinical time?
7) Get to know your new hospital: Before hitting the wards it pays to do a little homework on your new workplace. Do you have access to a medical library, journals, UpToDate, or other online databases? If not, do you need to purchase this access on your own? Many programs have academic funds allotted so you can use those resources. Also, familiarize yourself with the local antibiogram, formularies, guidelines, and order sets. Most facilities have tools specific to their hospital. Know how these affect you in your new role. Prior to starting, you will also want to be sufficiently oriented to any computer systems and understand how they’re used for documentation and order entry, and for viewing lab, radiology, and microbiology results.
8) Shadow a hospitalist: Spending a few hours with someone during a typical hospitalist work day will give you an idea of the pace of the work, the layout of the hospital and floors, the medical and ancillary staff you will work with, and the patient population. This will prompt questions you hadn’t thought of previously.
9) Prepare for each specific role: Hospitalists wear many hats, including teaching attending, non-teaching attending, consultant, researcher, committee member, and hospital medicine leader. Each role carries specific responsibilities and expectations. Prior to each new role, train with someone who leads that service or knows the job intimately.
10) Comprehend your benefits: Does your employer have a retirement program? Do they match retirement contributions? How does the malpractice insurance work? A meeting with human resources will usually help you arrange your health, dental, malpractice, and disability insurance prior to your start date. TH
Dr. Chacko is chair of SHM’s young physician committee and the hospitalist program medical director for Preferred Health Partners in New York City. Dr. Markoff is an assistant professor of medicine and associate director of the hospitalist service at the Mount Sinai Hospital in New York City. Dr. Sliwka is a hospitalist and assistant professor of clinical medicine at the University of California, San Francisco Medical Center.
Within the next few months, many of you will have a new job as an attending hospitalist. As daunting as that may seem, now is the time to think about what you can do to ensure a smooth transition and successful beginning to your career.
Although residency prepared you to face the medical challenges ahead, here are 10 pointers that may help as you move to the next stage of your professional life.
1) Familiarize yourself with the licensing/credentialing process: Do not underestimate the amount of time it takes to get this paperwork approved—up to six months in some cases. Many new hires’ first days on the job are delayed because they didn’t complete this step. Check with state licensing boards for special requirements unique to that state. Also, every hospital has its own gauntlet of infectious disease, HIPAA, and information- technology hoops to jump through. Getting your applications in as early as possible puts you in position to begin on your planned start date and prevent last-minute catastrophes for your new program.
2) Gain valuable insight through observation: Study your current hospitalist group to gain perspective that will help in your new setting. All programs and hospitals operate differently and have room for quality/process improvement. Interview hospitalists, ask questions, and observe the workflow in your current hospital(s) to help in your new job.
3) Contemplate your career direction: Think strategically about your strengths and plans. Although you will learn an incredible amount about hospital medicine careers after you begin, having a sense of direction will help your new group and its leadership get you where you want to be. Making connections and making your goals known within your new program before you start will put your new career on the right path.
4) Seek mentors: Having mentors from your prior program and your new program is a key to a healthy and happy career. Choose people you respect and pick their brains about their careers, how they acquired their skills, and how they would advise you to do the same. Good mentors will help you for many years, and the most valuable may be the ones who have known you throughout your residency. Nurture and maintain these relationships even if you are moving on to new horizons. Inquire whether your new program has a mentorship structure or if your new group leader can recommend someone who shares common interests and goals.
5) Study SHM’s Core Com-petencies: Although you may have trepidation about your medical skills and knowledge as you move into uncharted waters, step back and relax. Know that you are prepared. That said, you can always learn more. One excellent resource is The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (available on SHM’s Web site, www.hospitalmedicine.org). This is a set of standards with which programs can teach hospital medicine and you can learn the scope of expectations and competencies for someone in your position.
6) Understand the nuts and bolts of your new program: Although there are many things you will learn on the job, gain an appreciation for some of the following before your first day:
- Billing: If this is your responsibility, you need to learn a little about this before you start, preferably from one of your future colleagues.
- Reimbursement structure: Find out how your productivity is tracked and rewarded. You’d be amazed how variable this can be.
- Time allotment: How are administrative, research, committee and teaching time balanced against your clinical time?
7) Get to know your new hospital: Before hitting the wards it pays to do a little homework on your new workplace. Do you have access to a medical library, journals, UpToDate, or other online databases? If not, do you need to purchase this access on your own? Many programs have academic funds allotted so you can use those resources. Also, familiarize yourself with the local antibiogram, formularies, guidelines, and order sets. Most facilities have tools specific to their hospital. Know how these affect you in your new role. Prior to starting, you will also want to be sufficiently oriented to any computer systems and understand how they’re used for documentation and order entry, and for viewing lab, radiology, and microbiology results.
8) Shadow a hospitalist: Spending a few hours with someone during a typical hospitalist work day will give you an idea of the pace of the work, the layout of the hospital and floors, the medical and ancillary staff you will work with, and the patient population. This will prompt questions you hadn’t thought of previously.
9) Prepare for each specific role: Hospitalists wear many hats, including teaching attending, non-teaching attending, consultant, researcher, committee member, and hospital medicine leader. Each role carries specific responsibilities and expectations. Prior to each new role, train with someone who leads that service or knows the job intimately.
10) Comprehend your benefits: Does your employer have a retirement program? Do they match retirement contributions? How does the malpractice insurance work? A meeting with human resources will usually help you arrange your health, dental, malpractice, and disability insurance prior to your start date. TH
Dr. Chacko is chair of SHM’s young physician committee and the hospitalist program medical director for Preferred Health Partners in New York City. Dr. Markoff is an assistant professor of medicine and associate director of the hospitalist service at the Mount Sinai Hospital in New York City. Dr. Sliwka is a hospitalist and assistant professor of clinical medicine at the University of California, San Francisco Medical Center.
Daily Care Conundrums
Subsequent hospital care, also known as daily care, presents a variety of daily-care scenarios that cause confusion for billing providers.
Subsequent hospital care codes are reported once per day after the initial patient encounter (e.g., admission or consultation service), but only when a face-to-face visit occurs between provider and patient.
The entire visit need not take place at the bedside. It may include other important elements performed on the patient’s unit/floor such as data review, discussions with other healthcare professionals, coordination of care, and family meetings. In addition, subsequent hospital care codes represent the cumulative evaluation and management service performed on a calendar date, even if the hospitalist evaluates the patient for different reasons or at different times throughout the day.
Concurrent Care
Traditionally, concurrent care occurs when physicians of different specialties and group practices participate in a patient’s care. Each physician manages a particular aspect while considering the patient’s overall condition.
When submitting claims for concurrent care services, each physician should report the appropriate subsequent hospital care code and the corresponding diagnosis each primarily manages. If billed correctly, each hospitalist will have a different primary diagnosis code and be more likely to receive payment.
Some managed-care payers require each hospitalist to append modifier 25 to their evaluation and management (E/M) visit code (99232-25) even though each submits claims under different tax identification numbers. Modifier 25 is a separately identifiable E/M service performed on the same day as a procedure or other E/M service. In this situation, Medicare is likely to reimburse as appropriate.
Payment by managed-care companies is less easily obtained: Payment for the first received claim is likely, and denial of any claim received beyond the first claim is inevitable. Appealing the denied claims with documentation for each hospitalist’s visit on a given date helps the payer understand the need for each service.
Group Practice
When concurrent care is provided by members of the same group practice, claim reporting becomes more complex. Physicians in the same group practice and specialty bill and are paid as though to a single physician. In other words, if two hospitalists evaluate a patient on the same day (e.g., one hospitalist sees the patient in the morning, and another one sees the patient in the afternoon), the efforts of each medically necessary evaluation and management service may be captured.
However, the billing mechanism used in this situation varies from the standard. Instead of reporting each service separately under each corresponding hospitalist’s name, the hospitalists select subsequent hospital care code 99231-99233 representing the combined visits and submit one appropriate code for the collective level of service.
The difficulty is selecting the name that will appear on the claim form. Solutions range from reporting the hospitalist who provided the first encounter of the day to identifying the hospitalist who provided the most extensive or best-documented encounter of the day. For productivity analysis, some practices develop an internal accounting system and credit each hospitalist for their medically necessary joint efforts. The latter option is a labor-intensive task for administrators.
Physicians in the same group practice but different specialties may bill and be paid without regard to their membership in the same group. For example, a hospitalist and an infectious disease specialist may be part of the same multispecialty group practice and bill under a group tax-identification number, yet qualify for separate payment.
This is permitted if each physician has a differing specialty code designation. Specialty codes are self-designated, two-digit representations that describe the kind of medicine physicians, non-physician practitioners, or other healthcare providers/suppliers practice. They are initially selected and registered with each payer during the enrollment process.
A list of qualifying specialty codes can be found at www.cms.hhs.gov/MedicareFeeforSvcPartsAB/Downloads/SpecialtyCodes2207.pdf.
Covering Physicians
Hospital inpatient situations involving physician coverage are complicated. If Dr. Richards sees the patient earlier in the day and Dr. Andrews, covering for Dr. Richards, sees the same patient later that same day, Dr. Andrews cannot be paid for the second visit.
Subsequent hospital care descriptors emphasize “per day” to account for all care provided during the calendar day. Insurers treat the covering physician as if he were the physician being covered. Services provided by each are handled in the same manner described above.
If each hospitalist is responsible for a different aspect of the patient’s care, payment is made for both visits if:
- The hospitalists are in different specialties and different group practices;
- The visits are billed with different diagnoses; and
- The patient is a Medicare beneficiary or a member of an insurance plan that adopts Medicare rules.
There are limited circumstances where concurrent care can be billed to Medicare by hospitalists of the same specialty (e.g., an internist and a hospitalist, one with significant and demonstrated expertise in pain management).
Each hospitalist must belong to a different group practice and submit claims under different tax identification numbers. The patient’s condition must require the expertise possessed by the “sub-specialist.” Payment will be denied in the initial claim determination. But formulating a Medicare appeal with documentation from both encounters can demonstrate the medical necessity and separateness of each service and help earn reimbursement—although it is not guaranteed.
Managed-care payment for two visits on the same day by physicians of the same registered specialty (e.g., internal medicine), regardless of sub-specialization, is highly unlikely. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Subsequent hospital care, also known as daily care, presents a variety of daily-care scenarios that cause confusion for billing providers.
Subsequent hospital care codes are reported once per day after the initial patient encounter (e.g., admission or consultation service), but only when a face-to-face visit occurs between provider and patient.
The entire visit need not take place at the bedside. It may include other important elements performed on the patient’s unit/floor such as data review, discussions with other healthcare professionals, coordination of care, and family meetings. In addition, subsequent hospital care codes represent the cumulative evaluation and management service performed on a calendar date, even if the hospitalist evaluates the patient for different reasons or at different times throughout the day.
Concurrent Care
Traditionally, concurrent care occurs when physicians of different specialties and group practices participate in a patient’s care. Each physician manages a particular aspect while considering the patient’s overall condition.
When submitting claims for concurrent care services, each physician should report the appropriate subsequent hospital care code and the corresponding diagnosis each primarily manages. If billed correctly, each hospitalist will have a different primary diagnosis code and be more likely to receive payment.
Some managed-care payers require each hospitalist to append modifier 25 to their evaluation and management (E/M) visit code (99232-25) even though each submits claims under different tax identification numbers. Modifier 25 is a separately identifiable E/M service performed on the same day as a procedure or other E/M service. In this situation, Medicare is likely to reimburse as appropriate.
Payment by managed-care companies is less easily obtained: Payment for the first received claim is likely, and denial of any claim received beyond the first claim is inevitable. Appealing the denied claims with documentation for each hospitalist’s visit on a given date helps the payer understand the need for each service.
Group Practice
When concurrent care is provided by members of the same group practice, claim reporting becomes more complex. Physicians in the same group practice and specialty bill and are paid as though to a single physician. In other words, if two hospitalists evaluate a patient on the same day (e.g., one hospitalist sees the patient in the morning, and another one sees the patient in the afternoon), the efforts of each medically necessary evaluation and management service may be captured.
However, the billing mechanism used in this situation varies from the standard. Instead of reporting each service separately under each corresponding hospitalist’s name, the hospitalists select subsequent hospital care code 99231-99233 representing the combined visits and submit one appropriate code for the collective level of service.
The difficulty is selecting the name that will appear on the claim form. Solutions range from reporting the hospitalist who provided the first encounter of the day to identifying the hospitalist who provided the most extensive or best-documented encounter of the day. For productivity analysis, some practices develop an internal accounting system and credit each hospitalist for their medically necessary joint efforts. The latter option is a labor-intensive task for administrators.
Physicians in the same group practice but different specialties may bill and be paid without regard to their membership in the same group. For example, a hospitalist and an infectious disease specialist may be part of the same multispecialty group practice and bill under a group tax-identification number, yet qualify for separate payment.
This is permitted if each physician has a differing specialty code designation. Specialty codes are self-designated, two-digit representations that describe the kind of medicine physicians, non-physician practitioners, or other healthcare providers/suppliers practice. They are initially selected and registered with each payer during the enrollment process.
A list of qualifying specialty codes can be found at www.cms.hhs.gov/MedicareFeeforSvcPartsAB/Downloads/SpecialtyCodes2207.pdf.
Covering Physicians
Hospital inpatient situations involving physician coverage are complicated. If Dr. Richards sees the patient earlier in the day and Dr. Andrews, covering for Dr. Richards, sees the same patient later that same day, Dr. Andrews cannot be paid for the second visit.
Subsequent hospital care descriptors emphasize “per day” to account for all care provided during the calendar day. Insurers treat the covering physician as if he were the physician being covered. Services provided by each are handled in the same manner described above.
If each hospitalist is responsible for a different aspect of the patient’s care, payment is made for both visits if:
- The hospitalists are in different specialties and different group practices;
- The visits are billed with different diagnoses; and
- The patient is a Medicare beneficiary or a member of an insurance plan that adopts Medicare rules.
There are limited circumstances where concurrent care can be billed to Medicare by hospitalists of the same specialty (e.g., an internist and a hospitalist, one with significant and demonstrated expertise in pain management).
Each hospitalist must belong to a different group practice and submit claims under different tax identification numbers. The patient’s condition must require the expertise possessed by the “sub-specialist.” Payment will be denied in the initial claim determination. But formulating a Medicare appeal with documentation from both encounters can demonstrate the medical necessity and separateness of each service and help earn reimbursement—although it is not guaranteed.
Managed-care payment for two visits on the same day by physicians of the same registered specialty (e.g., internal medicine), regardless of sub-specialization, is highly unlikely. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Subsequent hospital care, also known as daily care, presents a variety of daily-care scenarios that cause confusion for billing providers.
Subsequent hospital care codes are reported once per day after the initial patient encounter (e.g., admission or consultation service), but only when a face-to-face visit occurs between provider and patient.
The entire visit need not take place at the bedside. It may include other important elements performed on the patient’s unit/floor such as data review, discussions with other healthcare professionals, coordination of care, and family meetings. In addition, subsequent hospital care codes represent the cumulative evaluation and management service performed on a calendar date, even if the hospitalist evaluates the patient for different reasons or at different times throughout the day.
Concurrent Care
Traditionally, concurrent care occurs when physicians of different specialties and group practices participate in a patient’s care. Each physician manages a particular aspect while considering the patient’s overall condition.
When submitting claims for concurrent care services, each physician should report the appropriate subsequent hospital care code and the corresponding diagnosis each primarily manages. If billed correctly, each hospitalist will have a different primary diagnosis code and be more likely to receive payment.
Some managed-care payers require each hospitalist to append modifier 25 to their evaluation and management (E/M) visit code (99232-25) even though each submits claims under different tax identification numbers. Modifier 25 is a separately identifiable E/M service performed on the same day as a procedure or other E/M service. In this situation, Medicare is likely to reimburse as appropriate.
Payment by managed-care companies is less easily obtained: Payment for the first received claim is likely, and denial of any claim received beyond the first claim is inevitable. Appealing the denied claims with documentation for each hospitalist’s visit on a given date helps the payer understand the need for each service.
Group Practice
When concurrent care is provided by members of the same group practice, claim reporting becomes more complex. Physicians in the same group practice and specialty bill and are paid as though to a single physician. In other words, if two hospitalists evaluate a patient on the same day (e.g., one hospitalist sees the patient in the morning, and another one sees the patient in the afternoon), the efforts of each medically necessary evaluation and management service may be captured.
However, the billing mechanism used in this situation varies from the standard. Instead of reporting each service separately under each corresponding hospitalist’s name, the hospitalists select subsequent hospital care code 99231-99233 representing the combined visits and submit one appropriate code for the collective level of service.
The difficulty is selecting the name that will appear on the claim form. Solutions range from reporting the hospitalist who provided the first encounter of the day to identifying the hospitalist who provided the most extensive or best-documented encounter of the day. For productivity analysis, some practices develop an internal accounting system and credit each hospitalist for their medically necessary joint efforts. The latter option is a labor-intensive task for administrators.
Physicians in the same group practice but different specialties may bill and be paid without regard to their membership in the same group. For example, a hospitalist and an infectious disease specialist may be part of the same multispecialty group practice and bill under a group tax-identification number, yet qualify for separate payment.
This is permitted if each physician has a differing specialty code designation. Specialty codes are self-designated, two-digit representations that describe the kind of medicine physicians, non-physician practitioners, or other healthcare providers/suppliers practice. They are initially selected and registered with each payer during the enrollment process.
A list of qualifying specialty codes can be found at www.cms.hhs.gov/MedicareFeeforSvcPartsAB/Downloads/SpecialtyCodes2207.pdf.
Covering Physicians
Hospital inpatient situations involving physician coverage are complicated. If Dr. Richards sees the patient earlier in the day and Dr. Andrews, covering for Dr. Richards, sees the same patient later that same day, Dr. Andrews cannot be paid for the second visit.
Subsequent hospital care descriptors emphasize “per day” to account for all care provided during the calendar day. Insurers treat the covering physician as if he were the physician being covered. Services provided by each are handled in the same manner described above.
If each hospitalist is responsible for a different aspect of the patient’s care, payment is made for both visits if:
- The hospitalists are in different specialties and different group practices;
- The visits are billed with different diagnoses; and
- The patient is a Medicare beneficiary or a member of an insurance plan that adopts Medicare rules.
There are limited circumstances where concurrent care can be billed to Medicare by hospitalists of the same specialty (e.g., an internist and a hospitalist, one with significant and demonstrated expertise in pain management).
Each hospitalist must belong to a different group practice and submit claims under different tax identification numbers. The patient’s condition must require the expertise possessed by the “sub-specialist.” Payment will be denied in the initial claim determination. But formulating a Medicare appeal with documentation from both encounters can demonstrate the medical necessity and separateness of each service and help earn reimbursement—although it is not guaranteed.
Managed-care payment for two visits on the same day by physicians of the same registered specialty (e.g., internal medicine), regardless of sub-specialization, is highly unlikely. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Medicare, Money, More
The new payment system for hospitalized Medicare patients spells big changes for hospitals and hospitalists.
On Aug. 1, 2006, the Centers for Medicare and Medicaid (CMS) issued final regulations for Medicare payments to hospitals in 2008. This update to the hospital inpatient prospective payment system (IPPS) is designed to improve the accuracy of Medicare payments and includes a new reporting system with new incentives for participating hospitals, restructured inpatient diagnosis-related groups (DRGs), and the exclusion of some hospital-acquired conditions.
The IPPS contains a number of provisions that will affect hospital medicine, and the incentives paid will come from many hospitalist-treated patients. “Realistically, the majority of patients that hospitalists admit are Medicare patients,” says Eric Siegal, MD, regional medical director of Cogent Healthcare in Madison, Wis., and chair of SHM’s Public Policy Committee.
27 Quality Measures
Under the IPPS, hospitals must now report on 27 quality measures to receive their full update. These include 30-day mortality measures for acute myocardial infarction and heart failure for Medicare patients, three measures related to surgical care, and the Hospital Consumer Assessment of Healthcare Providers and Systems patient satisfaction survey.
The set of measures will be expanded for 2009 to include a 30-day mortality measure for pneumonia and four additional measures related to surgical care, contingent on their endorsement by the National Quality Forum (NQF).
More Precise DRGs
The new IPPS uses restructured DRGs to better account for the severity of each patient’s condition. Now, 745 severity-adjusted DRGs have replaced the previous 538. This means hospitals that serve more severely ill patients will receive increased payments in an effort to prevent rewards for cherry-picking the healthiest patients.
“At least conceptually, this is a better way of doing things,” says Dr. Siegal. “Hospitals have been effectively penalized for taking care of really sick patients, because the DRGs weren’t really differentiating degrees of serious illness. Now that hospital comparison is becoming a big deal, people look at a statistic like mortality rates,” and the figures don’t specify which patients were mortally ill upon admission.
What’s Not Covered?
One interesting aspect to IPPS is that it specifies that Medicare will not cover additional costs of eight preventable, hospital-acquired conditions. These conditions include an object mistakenly left in a patient during surgery, air embolism, blood incompatibility, falls, mediastinitis, catheter-associated urinary tract infections (UTIs), pressure ulcers, and vascular catheter associated infections. For 2009, CMS will also propose excluding ventilator associated pneumonia, staphylococcus aureus septicemia, and deep-vein thrombosis/pulmonary embolism.
“Some of this stuff will be easy. Some cases, like ‘object left in patient during surgery’ are so obvious as to be laughable,” says Dr. Siegal. “Others are a tougher call, such as a catheter-associated UTI. These are not always as clear-cut as [CMS] says they will be. Philosophically, I think this is the right thing to do—it’s not right to pay a hospital for treating something they caused.”
Hospitalists and hospital staff are likely to see added paperwork as a result of this rule. “I can guarantee that there will be an added checklist for these conditions on admission,” says Dr. Siegal. “We’ll have to check for pressure ulcer, UTI, etc.—and that’s not necessarily a bad thing.”
Key Role for Hospitalists
When hospital payment based on reporting is involved, hospitalists are quickly drawn in. “This puts more money for hospitals at risk,” explains Dr. Siegal. “There’s a clear imperative to document better, and to identify who’s really sick. This will all land squarely on the shoulders of hospitalists—and, in fact, it already [has].”
On average, hospitals that comply with all provisions of the rule will earn an additional 3.5% in Medicare payments. This is really a result of the 3.3% market basket increase.
“The difference between doing this well and doing it poorly can add up to the margin for some hospitals,” stresses Dr. Siegal. “There’s absolutely no question that if I’m a hospital and I’m shelling out for a hospital medicine program, the single thing I want them to do and do well is report properly on these measures.”
Careful documentation includes the DRGs. Dr. Siegal points out that there’s a $4,000 swing between the DRG for low-acuity heart failure (a $3,900 payment) and high-acuity heart failure (a $7,900 payment). “Clearly, there will be a shift in reimbursement to those hospitals with sicker patients—or those that do a better job of documenting those patients,” he says. “You can bet that hospitals will make this a priority. They’re going to get much more finicky about how we document.”
Here’s an example: If presented with a patient with sepsis and a UTI, different physicians will have different diagnoses—or rather, use different terms, whether it’s sepsis, severe sepsis, urosepsis, SIRS, or something else. “Hospitals will try to force all physicians to get more crisp in their definitions,” says Dr. Siegal. “This could be good, because we’ll all be using the same language. But some aspects of this will just be a pain … like any other broadly applied rule. If you admit someone with chest pains, you will no longer be able to note ‘chest pains’; you’ll have to describe the pains.”
Starting now, the new IPPS will force hospitalists to perform more—and more careful—documentation for each patient. “It feels like one more hoop to jump through,” says Dr. Siegal. “But there should be no doubt that this is the future of healthcare, like it or not.” TH
Jane Jerrard has been writing for The Hospitalist since 2005.
The new payment system for hospitalized Medicare patients spells big changes for hospitals and hospitalists.
On Aug. 1, 2006, the Centers for Medicare and Medicaid (CMS) issued final regulations for Medicare payments to hospitals in 2008. This update to the hospital inpatient prospective payment system (IPPS) is designed to improve the accuracy of Medicare payments and includes a new reporting system with new incentives for participating hospitals, restructured inpatient diagnosis-related groups (DRGs), and the exclusion of some hospital-acquired conditions.
The IPPS contains a number of provisions that will affect hospital medicine, and the incentives paid will come from many hospitalist-treated patients. “Realistically, the majority of patients that hospitalists admit are Medicare patients,” says Eric Siegal, MD, regional medical director of Cogent Healthcare in Madison, Wis., and chair of SHM’s Public Policy Committee.
27 Quality Measures
Under the IPPS, hospitals must now report on 27 quality measures to receive their full update. These include 30-day mortality measures for acute myocardial infarction and heart failure for Medicare patients, three measures related to surgical care, and the Hospital Consumer Assessment of Healthcare Providers and Systems patient satisfaction survey.
The set of measures will be expanded for 2009 to include a 30-day mortality measure for pneumonia and four additional measures related to surgical care, contingent on their endorsement by the National Quality Forum (NQF).
More Precise DRGs
The new IPPS uses restructured DRGs to better account for the severity of each patient’s condition. Now, 745 severity-adjusted DRGs have replaced the previous 538. This means hospitals that serve more severely ill patients will receive increased payments in an effort to prevent rewards for cherry-picking the healthiest patients.
“At least conceptually, this is a better way of doing things,” says Dr. Siegal. “Hospitals have been effectively penalized for taking care of really sick patients, because the DRGs weren’t really differentiating degrees of serious illness. Now that hospital comparison is becoming a big deal, people look at a statistic like mortality rates,” and the figures don’t specify which patients were mortally ill upon admission.
What’s Not Covered?
One interesting aspect to IPPS is that it specifies that Medicare will not cover additional costs of eight preventable, hospital-acquired conditions. These conditions include an object mistakenly left in a patient during surgery, air embolism, blood incompatibility, falls, mediastinitis, catheter-associated urinary tract infections (UTIs), pressure ulcers, and vascular catheter associated infections. For 2009, CMS will also propose excluding ventilator associated pneumonia, staphylococcus aureus septicemia, and deep-vein thrombosis/pulmonary embolism.
“Some of this stuff will be easy. Some cases, like ‘object left in patient during surgery’ are so obvious as to be laughable,” says Dr. Siegal. “Others are a tougher call, such as a catheter-associated UTI. These are not always as clear-cut as [CMS] says they will be. Philosophically, I think this is the right thing to do—it’s not right to pay a hospital for treating something they caused.”
Hospitalists and hospital staff are likely to see added paperwork as a result of this rule. “I can guarantee that there will be an added checklist for these conditions on admission,” says Dr. Siegal. “We’ll have to check for pressure ulcer, UTI, etc.—and that’s not necessarily a bad thing.”
Key Role for Hospitalists
When hospital payment based on reporting is involved, hospitalists are quickly drawn in. “This puts more money for hospitals at risk,” explains Dr. Siegal. “There’s a clear imperative to document better, and to identify who’s really sick. This will all land squarely on the shoulders of hospitalists—and, in fact, it already [has].”
On average, hospitals that comply with all provisions of the rule will earn an additional 3.5% in Medicare payments. This is really a result of the 3.3% market basket increase.
“The difference between doing this well and doing it poorly can add up to the margin for some hospitals,” stresses Dr. Siegal. “There’s absolutely no question that if I’m a hospital and I’m shelling out for a hospital medicine program, the single thing I want them to do and do well is report properly on these measures.”
Careful documentation includes the DRGs. Dr. Siegal points out that there’s a $4,000 swing between the DRG for low-acuity heart failure (a $3,900 payment) and high-acuity heart failure (a $7,900 payment). “Clearly, there will be a shift in reimbursement to those hospitals with sicker patients—or those that do a better job of documenting those patients,” he says. “You can bet that hospitals will make this a priority. They’re going to get much more finicky about how we document.”
Here’s an example: If presented with a patient with sepsis and a UTI, different physicians will have different diagnoses—or rather, use different terms, whether it’s sepsis, severe sepsis, urosepsis, SIRS, or something else. “Hospitals will try to force all physicians to get more crisp in their definitions,” says Dr. Siegal. “This could be good, because we’ll all be using the same language. But some aspects of this will just be a pain … like any other broadly applied rule. If you admit someone with chest pains, you will no longer be able to note ‘chest pains’; you’ll have to describe the pains.”
Starting now, the new IPPS will force hospitalists to perform more—and more careful—documentation for each patient. “It feels like one more hoop to jump through,” says Dr. Siegal. “But there should be no doubt that this is the future of healthcare, like it or not.” TH
Jane Jerrard has been writing for The Hospitalist since 2005.
The new payment system for hospitalized Medicare patients spells big changes for hospitals and hospitalists.
On Aug. 1, 2006, the Centers for Medicare and Medicaid (CMS) issued final regulations for Medicare payments to hospitals in 2008. This update to the hospital inpatient prospective payment system (IPPS) is designed to improve the accuracy of Medicare payments and includes a new reporting system with new incentives for participating hospitals, restructured inpatient diagnosis-related groups (DRGs), and the exclusion of some hospital-acquired conditions.
The IPPS contains a number of provisions that will affect hospital medicine, and the incentives paid will come from many hospitalist-treated patients. “Realistically, the majority of patients that hospitalists admit are Medicare patients,” says Eric Siegal, MD, regional medical director of Cogent Healthcare in Madison, Wis., and chair of SHM’s Public Policy Committee.
27 Quality Measures
Under the IPPS, hospitals must now report on 27 quality measures to receive their full update. These include 30-day mortality measures for acute myocardial infarction and heart failure for Medicare patients, three measures related to surgical care, and the Hospital Consumer Assessment of Healthcare Providers and Systems patient satisfaction survey.
The set of measures will be expanded for 2009 to include a 30-day mortality measure for pneumonia and four additional measures related to surgical care, contingent on their endorsement by the National Quality Forum (NQF).
More Precise DRGs
The new IPPS uses restructured DRGs to better account for the severity of each patient’s condition. Now, 745 severity-adjusted DRGs have replaced the previous 538. This means hospitals that serve more severely ill patients will receive increased payments in an effort to prevent rewards for cherry-picking the healthiest patients.
“At least conceptually, this is a better way of doing things,” says Dr. Siegal. “Hospitals have been effectively penalized for taking care of really sick patients, because the DRGs weren’t really differentiating degrees of serious illness. Now that hospital comparison is becoming a big deal, people look at a statistic like mortality rates,” and the figures don’t specify which patients were mortally ill upon admission.
What’s Not Covered?
One interesting aspect to IPPS is that it specifies that Medicare will not cover additional costs of eight preventable, hospital-acquired conditions. These conditions include an object mistakenly left in a patient during surgery, air embolism, blood incompatibility, falls, mediastinitis, catheter-associated urinary tract infections (UTIs), pressure ulcers, and vascular catheter associated infections. For 2009, CMS will also propose excluding ventilator associated pneumonia, staphylococcus aureus septicemia, and deep-vein thrombosis/pulmonary embolism.
“Some of this stuff will be easy. Some cases, like ‘object left in patient during surgery’ are so obvious as to be laughable,” says Dr. Siegal. “Others are a tougher call, such as a catheter-associated UTI. These are not always as clear-cut as [CMS] says they will be. Philosophically, I think this is the right thing to do—it’s not right to pay a hospital for treating something they caused.”
Hospitalists and hospital staff are likely to see added paperwork as a result of this rule. “I can guarantee that there will be an added checklist for these conditions on admission,” says Dr. Siegal. “We’ll have to check for pressure ulcer, UTI, etc.—and that’s not necessarily a bad thing.”
Key Role for Hospitalists
When hospital payment based on reporting is involved, hospitalists are quickly drawn in. “This puts more money for hospitals at risk,” explains Dr. Siegal. “There’s a clear imperative to document better, and to identify who’s really sick. This will all land squarely on the shoulders of hospitalists—and, in fact, it already [has].”
On average, hospitals that comply with all provisions of the rule will earn an additional 3.5% in Medicare payments. This is really a result of the 3.3% market basket increase.
“The difference between doing this well and doing it poorly can add up to the margin for some hospitals,” stresses Dr. Siegal. “There’s absolutely no question that if I’m a hospital and I’m shelling out for a hospital medicine program, the single thing I want them to do and do well is report properly on these measures.”
Careful documentation includes the DRGs. Dr. Siegal points out that there’s a $4,000 swing between the DRG for low-acuity heart failure (a $3,900 payment) and high-acuity heart failure (a $7,900 payment). “Clearly, there will be a shift in reimbursement to those hospitals with sicker patients—or those that do a better job of documenting those patients,” he says. “You can bet that hospitals will make this a priority. They’re going to get much more finicky about how we document.”
Here’s an example: If presented with a patient with sepsis and a UTI, different physicians will have different diagnoses—or rather, use different terms, whether it’s sepsis, severe sepsis, urosepsis, SIRS, or something else. “Hospitals will try to force all physicians to get more crisp in their definitions,” says Dr. Siegal. “This could be good, because we’ll all be using the same language. But some aspects of this will just be a pain … like any other broadly applied rule. If you admit someone with chest pains, you will no longer be able to note ‘chest pains’; you’ll have to describe the pains.”
Starting now, the new IPPS will force hospitalists to perform more—and more careful—documentation for each patient. “It feels like one more hoop to jump through,” says Dr. Siegal. “But there should be no doubt that this is the future of healthcare, like it or not.” TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Tips from the Top
Whether your goal is to build your management skills, stay on top of industry trends, or simply continue your education, self-study should be part of your career plans.
There are many resources for ambitious physicians. How does one choose? Here, four hospitalists who have advanced their careers share their favorite resources—the Web sites, books, and periodicals that have helped them and that they recommend to other hospitalists.
Fred A. McCurdy, MD, PhD, MBA, associate dean for faculty development, Texas Tech University Health Sciences Center at Amarillo
Dr. McCurdy has an extensive list of resources he regularly recommends to colleagues. The following are a sample from his continually growing list:
- “I’m a member of the American College of Physician Executives and find that membership, along with their journal Physician Executive, pretty valuable,” he says.
- Other journals he recommends include Academic Medicine. (www.academicmedicine.org) and Leader to Leader. (www.leadertoleader.org/knowledgecenter/journal.aspx).
- Any booklet published by the Walk The Talk Company (www.walkthetalk.com).
- The Health Leaders Web site: www.healthleadersmedia.com.
- “Jim Clemmer has some really good, practical books that [can be generalized] to almost any context,” says Dr. McCurdy. “And he has free information via a newsletter and e-mail bulletins at www.clemmer.net.”
Dr. McCurdy also recommends these books:
- Leading Others, Managing Yourself by Peter McGunn;
- Leadership in Healthcare by Carson Dye;
- Leading Physicians through Change by Jack Silversin and Mary Jane Kornacki; and
- John P. Kotter’s works on change and change management (e.g., Leading Change and The Heart of Change).
Eric E. Howell MD, director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore
Dr. Howell chairs SHM’s Leadership Committee and says: “I have personal favorites [for reading recommendations]. However, the Leadership Committee is coming up with a list of recommended books.” That list can be found online this month on the SHM Web site (www.hospitalmedicine.org).
Here are Dr. Howell’s top six books for hospitalists:
- Getting to Yes: Negotiating Agreement Without Giving In by Roger Fisher, Bruce M. Patton, and William L. Ury. “This is a first, easier book for hospitalists starting out. It doesn’t matter if you’re working on the wards or running a 50-person department. Everyone needs negotiation skills—they’re crucial to being happy and successful.”
- Good to Great: Why Some Companies Make the Leap ... and Others Don’t by Jim Collins. “This book is important to hospitalists because many of us have small groups that are good and need to be great. This book has actually helped our practice a good deal.”
- 21 Irrefutable Laws of Leadership by John C. Maxwell. “Simple and basic, this is a very good book that gives concrete steps for building leadership skills.”
- 7 Habits of Highly Effective People by Stephen Covey. “This isn’t a great book, but it’s got important information for people who want to get ahead in life.”
- Team of Rivals: The Political Genius of Abraham Lincoln by Doris Kearns Goodwin. “My chairman recommended this to each of us. It’s a really good, higher level leadership book for someone in middle or upper management who wants to get to the next level.”
- Moneyball: The Art of Winning an Unfair Game by Michael Lewis. “This talks about baseball. Lewis compares the Oakland A’s to the New York Yankees. Both teams have been to the World Series … but the Yankees spend loads of cash while Oakland does it by being smarter. They’ve found a way to use little-known statistics to choose players. This book is about measuring your organization—something that hospitalists already do more than any other physician group.”
Bob Wachter, MD professor and associate chairman of the Department of Medicine at the University of California, San Francisco Resources Dr. Wachter recommends or checks regularly include:
- Wachter’s World blog: Dr. Wachter suggests reading his new blog, now available at www.wachtersworld.org, to keep up with relevant issues in the industry and opinions you’re not likely to find anywhere else.
- AHRQ Patient Safety Network (which he edits), at http://psnet.ahrq.gov: “This is a weekly round up of key articles, Web sites, and tools in patient safety. It’s also the world’s most extensive, searchable patient safety library. It’s an essential tool for those trying to keep up on safety, quality, and IT.”
- Modern Healthcare’s Daily Dose: An electronic newsletter delivered daily. Subscriptions are available for $49/year at www.modernhealthcare.com. “An excellent news aggregator that keeps you up to date on the key policy issues affecting hospital care.”
- California Healthline: A free daily e-newsletter, available at www.californiahealthline.org. “Particularly for Californians, this newsletter includes news and policy changes, as well as some interesting blogs and links to California Healthcare Foundation reports, which are usually very well done and helpful.”
- ihealthbeat: The California Healthcare Foundation’s free daily healthcare IT e-newsletter is available at www.ihealthbeat.org.
- HITS: Modern Healthcare’s daily healthcare IT enewsletter is available free at www.modernhealthcare.com. These resources obviously focus on information technology news. “I’m not an informationist, but anyone interested in hospital care, quality, and safety needs to keep a finger on the pulse of the IT movement.”
Mary Jo Gorman, MD, MBA, chief executive officer, Advanced ICU Care, St. Louis, Mo., and former SHM president
“My recommendations are all books,” says Dr. Gorman. “I consider them timeless in their application to leadership growth.” Her reading list includes:
- How to Win Friends & Influence People by Dale Carnegie. “Anyone who has to work with others—all of us, I think—can pick up some gems here.”
- Who Moved My Cheese? by Spencer Johnson and Kenneth Blanchard. “A growing field like hospital medicine calls for constantly changing strategy and being open to new things. Whining that things have changed is not a strategy. This book can be an eye-opener in the midst of upheaval.”
- Books by Deborah Tannen. “She is a linguist, and some of her books are more focused on work or family. Two examples are Talking from 9 to 5: Women and Men at Work and That’s Not What I Meant! All of us are conversing with other those of other genders; these books give good insight into what others might mean and how to overcome misunderstandings.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Whether your goal is to build your management skills, stay on top of industry trends, or simply continue your education, self-study should be part of your career plans.
There are many resources for ambitious physicians. How does one choose? Here, four hospitalists who have advanced their careers share their favorite resources—the Web sites, books, and periodicals that have helped them and that they recommend to other hospitalists.
Fred A. McCurdy, MD, PhD, MBA, associate dean for faculty development, Texas Tech University Health Sciences Center at Amarillo
Dr. McCurdy has an extensive list of resources he regularly recommends to colleagues. The following are a sample from his continually growing list:
- “I’m a member of the American College of Physician Executives and find that membership, along with their journal Physician Executive, pretty valuable,” he says.
- Other journals he recommends include Academic Medicine. (www.academicmedicine.org) and Leader to Leader. (www.leadertoleader.org/knowledgecenter/journal.aspx).
- Any booklet published by the Walk The Talk Company (www.walkthetalk.com).
- The Health Leaders Web site: www.healthleadersmedia.com.
- “Jim Clemmer has some really good, practical books that [can be generalized] to almost any context,” says Dr. McCurdy. “And he has free information via a newsletter and e-mail bulletins at www.clemmer.net.”
Dr. McCurdy also recommends these books:
- Leading Others, Managing Yourself by Peter McGunn;
- Leadership in Healthcare by Carson Dye;
- Leading Physicians through Change by Jack Silversin and Mary Jane Kornacki; and
- John P. Kotter’s works on change and change management (e.g., Leading Change and The Heart of Change).
Eric E. Howell MD, director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore
Dr. Howell chairs SHM’s Leadership Committee and says: “I have personal favorites [for reading recommendations]. However, the Leadership Committee is coming up with a list of recommended books.” That list can be found online this month on the SHM Web site (www.hospitalmedicine.org).
Here are Dr. Howell’s top six books for hospitalists:
- Getting to Yes: Negotiating Agreement Without Giving In by Roger Fisher, Bruce M. Patton, and William L. Ury. “This is a first, easier book for hospitalists starting out. It doesn’t matter if you’re working on the wards or running a 50-person department. Everyone needs negotiation skills—they’re crucial to being happy and successful.”
- Good to Great: Why Some Companies Make the Leap ... and Others Don’t by Jim Collins. “This book is important to hospitalists because many of us have small groups that are good and need to be great. This book has actually helped our practice a good deal.”
- 21 Irrefutable Laws of Leadership by John C. Maxwell. “Simple and basic, this is a very good book that gives concrete steps for building leadership skills.”
- 7 Habits of Highly Effective People by Stephen Covey. “This isn’t a great book, but it’s got important information for people who want to get ahead in life.”
- Team of Rivals: The Political Genius of Abraham Lincoln by Doris Kearns Goodwin. “My chairman recommended this to each of us. It’s a really good, higher level leadership book for someone in middle or upper management who wants to get to the next level.”
- Moneyball: The Art of Winning an Unfair Game by Michael Lewis. “This talks about baseball. Lewis compares the Oakland A’s to the New York Yankees. Both teams have been to the World Series … but the Yankees spend loads of cash while Oakland does it by being smarter. They’ve found a way to use little-known statistics to choose players. This book is about measuring your organization—something that hospitalists already do more than any other physician group.”
Bob Wachter, MD professor and associate chairman of the Department of Medicine at the University of California, San Francisco Resources Dr. Wachter recommends or checks regularly include:
- Wachter’s World blog: Dr. Wachter suggests reading his new blog, now available at www.wachtersworld.org, to keep up with relevant issues in the industry and opinions you’re not likely to find anywhere else.
- AHRQ Patient Safety Network (which he edits), at http://psnet.ahrq.gov: “This is a weekly round up of key articles, Web sites, and tools in patient safety. It’s also the world’s most extensive, searchable patient safety library. It’s an essential tool for those trying to keep up on safety, quality, and IT.”
- Modern Healthcare’s Daily Dose: An electronic newsletter delivered daily. Subscriptions are available for $49/year at www.modernhealthcare.com. “An excellent news aggregator that keeps you up to date on the key policy issues affecting hospital care.”
- California Healthline: A free daily e-newsletter, available at www.californiahealthline.org. “Particularly for Californians, this newsletter includes news and policy changes, as well as some interesting blogs and links to California Healthcare Foundation reports, which are usually very well done and helpful.”
- ihealthbeat: The California Healthcare Foundation’s free daily healthcare IT e-newsletter is available at www.ihealthbeat.org.
- HITS: Modern Healthcare’s daily healthcare IT enewsletter is available free at www.modernhealthcare.com. These resources obviously focus on information technology news. “I’m not an informationist, but anyone interested in hospital care, quality, and safety needs to keep a finger on the pulse of the IT movement.”
Mary Jo Gorman, MD, MBA, chief executive officer, Advanced ICU Care, St. Louis, Mo., and former SHM president
“My recommendations are all books,” says Dr. Gorman. “I consider them timeless in their application to leadership growth.” Her reading list includes:
- How to Win Friends & Influence People by Dale Carnegie. “Anyone who has to work with others—all of us, I think—can pick up some gems here.”
- Who Moved My Cheese? by Spencer Johnson and Kenneth Blanchard. “A growing field like hospital medicine calls for constantly changing strategy and being open to new things. Whining that things have changed is not a strategy. This book can be an eye-opener in the midst of upheaval.”
- Books by Deborah Tannen. “She is a linguist, and some of her books are more focused on work or family. Two examples are Talking from 9 to 5: Women and Men at Work and That’s Not What I Meant! All of us are conversing with other those of other genders; these books give good insight into what others might mean and how to overcome misunderstandings.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Whether your goal is to build your management skills, stay on top of industry trends, or simply continue your education, self-study should be part of your career plans.
There are many resources for ambitious physicians. How does one choose? Here, four hospitalists who have advanced their careers share their favorite resources—the Web sites, books, and periodicals that have helped them and that they recommend to other hospitalists.
Fred A. McCurdy, MD, PhD, MBA, associate dean for faculty development, Texas Tech University Health Sciences Center at Amarillo
Dr. McCurdy has an extensive list of resources he regularly recommends to colleagues. The following are a sample from his continually growing list:
- “I’m a member of the American College of Physician Executives and find that membership, along with their journal Physician Executive, pretty valuable,” he says.
- Other journals he recommends include Academic Medicine. (www.academicmedicine.org) and Leader to Leader. (www.leadertoleader.org/knowledgecenter/journal.aspx).
- Any booklet published by the Walk The Talk Company (www.walkthetalk.com).
- The Health Leaders Web site: www.healthleadersmedia.com.
- “Jim Clemmer has some really good, practical books that [can be generalized] to almost any context,” says Dr. McCurdy. “And he has free information via a newsletter and e-mail bulletins at www.clemmer.net.”
Dr. McCurdy also recommends these books:
- Leading Others, Managing Yourself by Peter McGunn;
- Leadership in Healthcare by Carson Dye;
- Leading Physicians through Change by Jack Silversin and Mary Jane Kornacki; and
- John P. Kotter’s works on change and change management (e.g., Leading Change and The Heart of Change).
Eric E. Howell MD, director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore
Dr. Howell chairs SHM’s Leadership Committee and says: “I have personal favorites [for reading recommendations]. However, the Leadership Committee is coming up with a list of recommended books.” That list can be found online this month on the SHM Web site (www.hospitalmedicine.org).
Here are Dr. Howell’s top six books for hospitalists:
- Getting to Yes: Negotiating Agreement Without Giving In by Roger Fisher, Bruce M. Patton, and William L. Ury. “This is a first, easier book for hospitalists starting out. It doesn’t matter if you’re working on the wards or running a 50-person department. Everyone needs negotiation skills—they’re crucial to being happy and successful.”
- Good to Great: Why Some Companies Make the Leap ... and Others Don’t by Jim Collins. “This book is important to hospitalists because many of us have small groups that are good and need to be great. This book has actually helped our practice a good deal.”
- 21 Irrefutable Laws of Leadership by John C. Maxwell. “Simple and basic, this is a very good book that gives concrete steps for building leadership skills.”
- 7 Habits of Highly Effective People by Stephen Covey. “This isn’t a great book, but it’s got important information for people who want to get ahead in life.”
- Team of Rivals: The Political Genius of Abraham Lincoln by Doris Kearns Goodwin. “My chairman recommended this to each of us. It’s a really good, higher level leadership book for someone in middle or upper management who wants to get to the next level.”
- Moneyball: The Art of Winning an Unfair Game by Michael Lewis. “This talks about baseball. Lewis compares the Oakland A’s to the New York Yankees. Both teams have been to the World Series … but the Yankees spend loads of cash while Oakland does it by being smarter. They’ve found a way to use little-known statistics to choose players. This book is about measuring your organization—something that hospitalists already do more than any other physician group.”
Bob Wachter, MD professor and associate chairman of the Department of Medicine at the University of California, San Francisco Resources Dr. Wachter recommends or checks regularly include:
- Wachter’s World blog: Dr. Wachter suggests reading his new blog, now available at www.wachtersworld.org, to keep up with relevant issues in the industry and opinions you’re not likely to find anywhere else.
- AHRQ Patient Safety Network (which he edits), at http://psnet.ahrq.gov: “This is a weekly round up of key articles, Web sites, and tools in patient safety. It’s also the world’s most extensive, searchable patient safety library. It’s an essential tool for those trying to keep up on safety, quality, and IT.”
- Modern Healthcare’s Daily Dose: An electronic newsletter delivered daily. Subscriptions are available for $49/year at www.modernhealthcare.com. “An excellent news aggregator that keeps you up to date on the key policy issues affecting hospital care.”
- California Healthline: A free daily e-newsletter, available at www.californiahealthline.org. “Particularly for Californians, this newsletter includes news and policy changes, as well as some interesting blogs and links to California Healthcare Foundation reports, which are usually very well done and helpful.”
- ihealthbeat: The California Healthcare Foundation’s free daily healthcare IT e-newsletter is available at www.ihealthbeat.org.
- HITS: Modern Healthcare’s daily healthcare IT enewsletter is available free at www.modernhealthcare.com. These resources obviously focus on information technology news. “I’m not an informationist, but anyone interested in hospital care, quality, and safety needs to keep a finger on the pulse of the IT movement.”
Mary Jo Gorman, MD, MBA, chief executive officer, Advanced ICU Care, St. Louis, Mo., and former SHM president
“My recommendations are all books,” says Dr. Gorman. “I consider them timeless in their application to leadership growth.” Her reading list includes:
- How to Win Friends & Influence People by Dale Carnegie. “Anyone who has to work with others—all of us, I think—can pick up some gems here.”
- Who Moved My Cheese? by Spencer Johnson and Kenneth Blanchard. “A growing field like hospital medicine calls for constantly changing strategy and being open to new things. Whining that things have changed is not a strategy. This book can be an eye-opener in the midst of upheaval.”
- Books by Deborah Tannen. “She is a linguist, and some of her books are more focused on work or family. Two examples are Talking from 9 to 5: Women and Men at Work and That’s Not What I Meant! All of us are conversing with other those of other genders; these books give good insight into what others might mean and how to overcome misunderstandings.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Patients In the Know
Patient autonomy is one of the core principles of medicine in the U.S. All adult patients of sound mind are entitled to know the risks and benefits of the procedures they undergo—especially when surgery or transfusions are involved.
However, sometimes principles collide with practicalities. Hospitals would grind nearly to a halt if clinicians had to stop and inform patients of the remotest risks associated with even the most benign therapies like potassium supplementation or furosemide.
As a result, the vast majority of medical treatments are administered to hospitalized patients with no discussion of risks, benefits, and alternatives. Besides, most patients wouldn’t want to be informed of every single risk associated with those medications if the likelihood of an adverse event were relatively small. Or would they?
A team of investigators at Yale and Bridgeport Hospital in Bridgeport, Conn., led by medical resident Shweta Upadhyay, MD, examined patients’ preferences when it comes to providing informed consent for routine hospital procedures associated with varying degrees of risk.
These researchers submitted questionnaires to 210 patients admitted to the hospital between June and August 2006. The questionnaires described four hypothetical situations of escalating risk:
- Administration of a diuretic to relieve pulmonary congestion resulting from heart failure;
- Supplementation to replace mineral loss associated with diuretic use; and
- Administration of tissue plasminogen activator (TPA) to treat pulmonary emboli, with a 5% or 20% risk of cerebral hemorrhage and stroke.
In each case, patients were asked if they would want their physicians to begin treatment without asking their permission, ask their permission before beginning treatment no matter what, or obtain permission only if time and clinical circumstances permitted.
—Constantine Manthous, MD, associate clinical professor of medicine, Yale and Bridgeport Hospital, Bridgeport, Conn.
“We designed the questionnaire to step up from minimal risk to life-threatening intervention,” says Constantine Manthous, MD, associate clinical professor of medicine at the hospital and senior author of the study.
Surprisingly, the vast majority of patients—85%—wanted to participate in making even the most trivial decisions about their care. Of those answering the question about potassium supplementation, 92% wanted to be informed before receiving a diuretic.
Less surprisingly, 93% and 95% of patients, respectively, wanted their doctors to obtain their permission before administering TPA when the risk of hemorrhage was 5% and 20%. “We did not expect the patients to be interested at all in the mundane things,” Dr. Manthous says.
In general, patients younger than 65 were more likely to want to discuss the risks, but more of the older patients wanted to be informed if time allowed.
“Older patients (>65 years old) were more likely in some questions than younger (<65 years old) patients to allow their physicians to make unilateral decisions regarding their healthcare. This could be explained by the fact that those age 65 and older grew up at a time when physician paternalism was more prevalent in American medicine,” the authors write.
The findings “demonstrate a big change in what it means to be a patient from 30 to 40 years ago,” Dr. Manthous points out. “These data demonstrate that patients’ expectations are high: They want to be fully involved in even the most mundane aspects of their care. I doubt that most physicians realize just how involved their patients want to be.”
Often, the decision to disclose a treatment’s risks boils down to a judgment call, especially when the frequency and severity of those risks are low, John Banja, MD, and Jason Schneider, MD, both of Emory University in Atlanta, wrote in an editorial accompanying the study (“Ethical Challenges in Disclosing Risk”).
The ethical obligation to discuss risks increases when risk severity increases, even if the frequency of those risks remains low. However, hospitals have inconsistent policies for obtaining informed consent.
“Many hospitals, for example, would have staff simply tell patients that they needed diuretics or thrombolytics, even though in certain instances—and especially with thrombolytic agents—the risk of a significant adverse event could well exceed some reasonable disclosure threshold (which is often set at 1%),” Drs. Banja and Schneider write. If a patient is about to undergo a procedure like thrombolysis, in which the risk of cerebral hemorrhage may be as high as 20%, formal informed consent would “most certainly” be required. Failure to get it could be construed as a serious ethical breach.
Like Dr. Manthous, Dr. Schneider, assistant professor of general medicine at Emory University School of Medicine, was startled by the number of patients who took such an interest in even relatively innocuous treatments. “What was most eye-opening for me was the number of people who had so much interest in the intricacies of their medical care,” he says.
Good communication can help doctors strike a balance between fulfilling patients’ wishes for information and working efficiently, Dr. Schneider adds. “Quality can compensate for quantity; with well-tuned communication, you can make up for limited time,” he explains. Unfortunately, although communication has recently been added to the list of core competencies residents should master, “physicians don’t have the interpersonal communication skills they should have. It’s definitely an area where improvement is needed.”
Indeed, doctors could use their newfound expertise in communication to describe to patients the practical implications of listing every risk of every procedure. Right now, “patients probably don’t understand how bothersome and logistically problematic it would be” to make that disclosure, says Dr. Manthous. “I suspect their answers would be different if we explained that care would slow to a crawl.”
Norra MacReady is a medical writer based in California. TH
Norra MacReady is a medical writer based in California.
Patient autonomy is one of the core principles of medicine in the U.S. All adult patients of sound mind are entitled to know the risks and benefits of the procedures they undergo—especially when surgery or transfusions are involved.
However, sometimes principles collide with practicalities. Hospitals would grind nearly to a halt if clinicians had to stop and inform patients of the remotest risks associated with even the most benign therapies like potassium supplementation or furosemide.
As a result, the vast majority of medical treatments are administered to hospitalized patients with no discussion of risks, benefits, and alternatives. Besides, most patients wouldn’t want to be informed of every single risk associated with those medications if the likelihood of an adverse event were relatively small. Or would they?
A team of investigators at Yale and Bridgeport Hospital in Bridgeport, Conn., led by medical resident Shweta Upadhyay, MD, examined patients’ preferences when it comes to providing informed consent for routine hospital procedures associated with varying degrees of risk.
These researchers submitted questionnaires to 210 patients admitted to the hospital between June and August 2006. The questionnaires described four hypothetical situations of escalating risk:
- Administration of a diuretic to relieve pulmonary congestion resulting from heart failure;
- Supplementation to replace mineral loss associated with diuretic use; and
- Administration of tissue plasminogen activator (TPA) to treat pulmonary emboli, with a 5% or 20% risk of cerebral hemorrhage and stroke.
In each case, patients were asked if they would want their physicians to begin treatment without asking their permission, ask their permission before beginning treatment no matter what, or obtain permission only if time and clinical circumstances permitted.
—Constantine Manthous, MD, associate clinical professor of medicine, Yale and Bridgeport Hospital, Bridgeport, Conn.
“We designed the questionnaire to step up from minimal risk to life-threatening intervention,” says Constantine Manthous, MD, associate clinical professor of medicine at the hospital and senior author of the study.
Surprisingly, the vast majority of patients—85%—wanted to participate in making even the most trivial decisions about their care. Of those answering the question about potassium supplementation, 92% wanted to be informed before receiving a diuretic.
Less surprisingly, 93% and 95% of patients, respectively, wanted their doctors to obtain their permission before administering TPA when the risk of hemorrhage was 5% and 20%. “We did not expect the patients to be interested at all in the mundane things,” Dr. Manthous says.
In general, patients younger than 65 were more likely to want to discuss the risks, but more of the older patients wanted to be informed if time allowed.
“Older patients (>65 years old) were more likely in some questions than younger (<65 years old) patients to allow their physicians to make unilateral decisions regarding their healthcare. This could be explained by the fact that those age 65 and older grew up at a time when physician paternalism was more prevalent in American medicine,” the authors write.
The findings “demonstrate a big change in what it means to be a patient from 30 to 40 years ago,” Dr. Manthous points out. “These data demonstrate that patients’ expectations are high: They want to be fully involved in even the most mundane aspects of their care. I doubt that most physicians realize just how involved their patients want to be.”
Often, the decision to disclose a treatment’s risks boils down to a judgment call, especially when the frequency and severity of those risks are low, John Banja, MD, and Jason Schneider, MD, both of Emory University in Atlanta, wrote in an editorial accompanying the study (“Ethical Challenges in Disclosing Risk”).
The ethical obligation to discuss risks increases when risk severity increases, even if the frequency of those risks remains low. However, hospitals have inconsistent policies for obtaining informed consent.
“Many hospitals, for example, would have staff simply tell patients that they needed diuretics or thrombolytics, even though in certain instances—and especially with thrombolytic agents—the risk of a significant adverse event could well exceed some reasonable disclosure threshold (which is often set at 1%),” Drs. Banja and Schneider write. If a patient is about to undergo a procedure like thrombolysis, in which the risk of cerebral hemorrhage may be as high as 20%, formal informed consent would “most certainly” be required. Failure to get it could be construed as a serious ethical breach.
Like Dr. Manthous, Dr. Schneider, assistant professor of general medicine at Emory University School of Medicine, was startled by the number of patients who took such an interest in even relatively innocuous treatments. “What was most eye-opening for me was the number of people who had so much interest in the intricacies of their medical care,” he says.
Good communication can help doctors strike a balance between fulfilling patients’ wishes for information and working efficiently, Dr. Schneider adds. “Quality can compensate for quantity; with well-tuned communication, you can make up for limited time,” he explains. Unfortunately, although communication has recently been added to the list of core competencies residents should master, “physicians don’t have the interpersonal communication skills they should have. It’s definitely an area where improvement is needed.”
Indeed, doctors could use their newfound expertise in communication to describe to patients the practical implications of listing every risk of every procedure. Right now, “patients probably don’t understand how bothersome and logistically problematic it would be” to make that disclosure, says Dr. Manthous. “I suspect their answers would be different if we explained that care would slow to a crawl.”
Norra MacReady is a medical writer based in California. TH
Norra MacReady is a medical writer based in California.
Patient autonomy is one of the core principles of medicine in the U.S. All adult patients of sound mind are entitled to know the risks and benefits of the procedures they undergo—especially when surgery or transfusions are involved.
However, sometimes principles collide with practicalities. Hospitals would grind nearly to a halt if clinicians had to stop and inform patients of the remotest risks associated with even the most benign therapies like potassium supplementation or furosemide.
As a result, the vast majority of medical treatments are administered to hospitalized patients with no discussion of risks, benefits, and alternatives. Besides, most patients wouldn’t want to be informed of every single risk associated with those medications if the likelihood of an adverse event were relatively small. Or would they?
A team of investigators at Yale and Bridgeport Hospital in Bridgeport, Conn., led by medical resident Shweta Upadhyay, MD, examined patients’ preferences when it comes to providing informed consent for routine hospital procedures associated with varying degrees of risk.
These researchers submitted questionnaires to 210 patients admitted to the hospital between June and August 2006. The questionnaires described four hypothetical situations of escalating risk:
- Administration of a diuretic to relieve pulmonary congestion resulting from heart failure;
- Supplementation to replace mineral loss associated with diuretic use; and
- Administration of tissue plasminogen activator (TPA) to treat pulmonary emboli, with a 5% or 20% risk of cerebral hemorrhage and stroke.
In each case, patients were asked if they would want their physicians to begin treatment without asking their permission, ask their permission before beginning treatment no matter what, or obtain permission only if time and clinical circumstances permitted.
—Constantine Manthous, MD, associate clinical professor of medicine, Yale and Bridgeport Hospital, Bridgeport, Conn.
“We designed the questionnaire to step up from minimal risk to life-threatening intervention,” says Constantine Manthous, MD, associate clinical professor of medicine at the hospital and senior author of the study.
Surprisingly, the vast majority of patients—85%—wanted to participate in making even the most trivial decisions about their care. Of those answering the question about potassium supplementation, 92% wanted to be informed before receiving a diuretic.
Less surprisingly, 93% and 95% of patients, respectively, wanted their doctors to obtain their permission before administering TPA when the risk of hemorrhage was 5% and 20%. “We did not expect the patients to be interested at all in the mundane things,” Dr. Manthous says.
In general, patients younger than 65 were more likely to want to discuss the risks, but more of the older patients wanted to be informed if time allowed.
“Older patients (>65 years old) were more likely in some questions than younger (<65 years old) patients to allow their physicians to make unilateral decisions regarding their healthcare. This could be explained by the fact that those age 65 and older grew up at a time when physician paternalism was more prevalent in American medicine,” the authors write.
The findings “demonstrate a big change in what it means to be a patient from 30 to 40 years ago,” Dr. Manthous points out. “These data demonstrate that patients’ expectations are high: They want to be fully involved in even the most mundane aspects of their care. I doubt that most physicians realize just how involved their patients want to be.”
Often, the decision to disclose a treatment’s risks boils down to a judgment call, especially when the frequency and severity of those risks are low, John Banja, MD, and Jason Schneider, MD, both of Emory University in Atlanta, wrote in an editorial accompanying the study (“Ethical Challenges in Disclosing Risk”).
The ethical obligation to discuss risks increases when risk severity increases, even if the frequency of those risks remains low. However, hospitals have inconsistent policies for obtaining informed consent.
“Many hospitals, for example, would have staff simply tell patients that they needed diuretics or thrombolytics, even though in certain instances—and especially with thrombolytic agents—the risk of a significant adverse event could well exceed some reasonable disclosure threshold (which is often set at 1%),” Drs. Banja and Schneider write. If a patient is about to undergo a procedure like thrombolysis, in which the risk of cerebral hemorrhage may be as high as 20%, formal informed consent would “most certainly” be required. Failure to get it could be construed as a serious ethical breach.
Like Dr. Manthous, Dr. Schneider, assistant professor of general medicine at Emory University School of Medicine, was startled by the number of patients who took such an interest in even relatively innocuous treatments. “What was most eye-opening for me was the number of people who had so much interest in the intricacies of their medical care,” he says.
Good communication can help doctors strike a balance between fulfilling patients’ wishes for information and working efficiently, Dr. Schneider adds. “Quality can compensate for quantity; with well-tuned communication, you can make up for limited time,” he explains. Unfortunately, although communication has recently been added to the list of core competencies residents should master, “physicians don’t have the interpersonal communication skills they should have. It’s definitely an area where improvement is needed.”
Indeed, doctors could use their newfound expertise in communication to describe to patients the practical implications of listing every risk of every procedure. Right now, “patients probably don’t understand how bothersome and logistically problematic it would be” to make that disclosure, says Dr. Manthous. “I suspect their answers would be different if we explained that care would slow to a crawl.”
Norra MacReady is a medical writer based in California. TH
Norra MacReady is a medical writer based in California.