User login
Malpractice Chronicle
Echocardiography Not Available on Weekends
One Friday evening in late October, a 58-year-old man presented to the emergency department (ED) of a rural hospital with complaints of jaw pain, chest pain, arm and leg numbness, and difficulty speaking. Within 15 minutes of his arrival, the man’s symptoms resolved spontaneously. Results of testing performed in the ED were consistent with coronary artery disease.
The patient was transferred late that night to another hospital for specialized cardiac care. His condition at the time of admission was stable, and he had no complaints other than the unusual 15-minute episode he had experienced earlier that day. This information was presented to a resident, who examined the patient and ordered an echocardiogram for the next morning (Saturday). The hospital’s echocardiography laboratory was not routinely open on the weekend.
The man was seen by a cardiologist that Saturday morning. It was noted that his heart monitoring had shown abnormalities, and blood work had revealed abnormally elevated cardiac enzyme levels. The cardiologist recommended that the patient remain on high-dose heparin until angiography could be performed on Monday.
The cardiologist also noted that he detected a slight diastolic heart murmur near the left sternal border. He informed the man and his wife that there might be a bacterial infection affecting the aortic valve, which would explain the murmur. The cardiologist ordered an echocardiogram for Monday to rule out the possibility of aortic incompetence due to aneurysm of dissection. The man died that night before testing could be performed.
The cardiologist claimed that the man’s death was the result of a sudden heart attack secondary to coronary artery disease. No autopsy was performed at the time. The body was exhumed 18 months later, however, and a postmortem examination revealed the cause of death to be aortic dissection.
The plaintiff claimed that the ED physician, the resident, and the cardiologist were all negligent in failing to make a diagnosis of aortic dissection and that emergent chest CT should have been performed. The plaintiff also argued that if echocardiography had been performed on Saturday morning as ordered by the resident, the dissection could have been detected in time to perform lifesaving surgery. The plaintiff further claimed that the cardiologist was negligent for recognizing the possibility of a dissection and doing nothing to confirm or rule out the diagnosis, despite the high mortality rate associated with aortic dissection.
The defendants maintained that the decedent’s signs and symptoms were not typical for aortic dissection and were more consistent with coronary artery disease. The defendants also argued that even if the correct diagnosis had been made, the decedent would not have survived surgery.
A settlement of $2 million was reached.
Viral Syndrome—or Lupus?
A 34-year-old woman presented to the defendant hospital ED complaining of chills, fever, and blood in her urine. She underwent laboratory testing and was given IV fluids and antibiotics. She was discharged with a prescription for ciprofloxacin for a urinary tract infection and was given instructions to follow up with her primary care physician or return to the ED if her symptoms worsened.
Two days later, the patient returned to the ED twice and was ultimately admitted with fever, chills, shortness of breath, and a cough. The next day, she suffered a grand mal seizure and was transferred to another hospital, where she died a few days later.
The plaintiff claimed that the decedent had systemic lupus erythematosus and that she should have been transferred to the second hospital immediately.
The defendants claimed that the decedent had a viral syndrome, that her seizure was completely unpredictable, and that nothing could have been done during her ED visits to have changed the outcome.
According to a published report, a defense verdict was returned.
Advanced Heart Disease Recognized, Treated Late
In April 2003, a 47-year-old woman underwent aortic valve repair and mitral valve replacement in an attempt to correct problems with blood flow to and from her heart.
After the surgery, it was discovered that the left ventricle was pumping out a dangerously low amount of blood. She was taken to the ICU in Dr. A.’s care. At midnight, Dr. C. assumed her care.
The following morning, Dr. C. installed an intra-aortic balloon pump (IABP), which required several attempts. The patient was then transferred to another hospital for a possible heart transplant. She experienced cardiac arrest and died the following day.
The plaintiff claimed that Dr. A. and Dr. C. failed to perform appropriate preoperative testing and to administer the proper medication in the hours immediately following surgery. During this time, the decedent suffered multiple myocardial infarctions due to lack of oxygen to the heart. The plaintiff also claimed that the IABP should have been installed earlier.
The defendants argued that the decedent was in extremely poor health before the surgery as a result of advanced heart disease, which they claimed had been misdiagnosed as asthma since 1996.
According to a published account, a jury found no negligence by the hospital or Dr. C. The jury found Dr. A. negligent, but they did not find his negligence to have caused the woman’s death. A defense verdict was entered. Posttrial motions were pending.
Sinus Infection Leads to Brain Abscess
A woman in her 50s presented to a hospital ED complaining of severe headaches for several days. An ED physician made a diagnosis of tension headache and prescribed muscle relaxants and pain medication. Two days later, at her primary care physician’s office, she still had a headache, but it was less severe; she also had nasal discharge, swollen eyes, red sinuses, and nausea. The patient was examined by a PA, who diagnosed an allergic reaction. Steroids were prescribed, and a sinus x-ray and blood work were ordered.
Five days later, the woman developed stroke-like symptoms, including facial drooping and disorientation. She was transported to the same hospital, where CT revealed a brain abscess. She was airlifted to a second hospital for emergency brain surgery, which required part of her skull to be removed and replaced with plastic.
After surgery, the patient experienced respiratory failure and was placed on a ventilator. Following additional brain surgeries, she was left with loss of vision in her left eye and cognitive impairment that could increase her likelihood of developing dementia. She also needed two months of rehabilitation.
The plaintiff alleged negligence by both the ED physician and the PA for their failure to diagnose a sinus infection and to prescribe appropriate antibiotics. She maintained that tests should have been ordered on an urgent basis and that timely diagnosis and treatment would have prevented the abscess. The plaintiff further charged that the PA’s supervising physicians failed to review her chart or consult with the PA regarding her case.
The defendant primary care provider argued that the plaintiff was properly treated. The remaining defendants claimed that the plaintiff was at fault for not undergoing diagnostic testing immediately following the PA’s examination.
According to a published report, a jury found the primary care provider and the PA negligent and awarded the plaintiff $3 million. The ED physician and the first hospital were found not at fault.
Echocardiography Not Available on Weekends
One Friday evening in late October, a 58-year-old man presented to the emergency department (ED) of a rural hospital with complaints of jaw pain, chest pain, arm and leg numbness, and difficulty speaking. Within 15 minutes of his arrival, the man’s symptoms resolved spontaneously. Results of testing performed in the ED were consistent with coronary artery disease.
The patient was transferred late that night to another hospital for specialized cardiac care. His condition at the time of admission was stable, and he had no complaints other than the unusual 15-minute episode he had experienced earlier that day. This information was presented to a resident, who examined the patient and ordered an echocardiogram for the next morning (Saturday). The hospital’s echocardiography laboratory was not routinely open on the weekend.
The man was seen by a cardiologist that Saturday morning. It was noted that his heart monitoring had shown abnormalities, and blood work had revealed abnormally elevated cardiac enzyme levels. The cardiologist recommended that the patient remain on high-dose heparin until angiography could be performed on Monday.
The cardiologist also noted that he detected a slight diastolic heart murmur near the left sternal border. He informed the man and his wife that there might be a bacterial infection affecting the aortic valve, which would explain the murmur. The cardiologist ordered an echocardiogram for Monday to rule out the possibility of aortic incompetence due to aneurysm of dissection. The man died that night before testing could be performed.
The cardiologist claimed that the man’s death was the result of a sudden heart attack secondary to coronary artery disease. No autopsy was performed at the time. The body was exhumed 18 months later, however, and a postmortem examination revealed the cause of death to be aortic dissection.
The plaintiff claimed that the ED physician, the resident, and the cardiologist were all negligent in failing to make a diagnosis of aortic dissection and that emergent chest CT should have been performed. The plaintiff also argued that if echocardiography had been performed on Saturday morning as ordered by the resident, the dissection could have been detected in time to perform lifesaving surgery. The plaintiff further claimed that the cardiologist was negligent for recognizing the possibility of a dissection and doing nothing to confirm or rule out the diagnosis, despite the high mortality rate associated with aortic dissection.
The defendants maintained that the decedent’s signs and symptoms were not typical for aortic dissection and were more consistent with coronary artery disease. The defendants also argued that even if the correct diagnosis had been made, the decedent would not have survived surgery.
A settlement of $2 million was reached.
Viral Syndrome—or Lupus?
A 34-year-old woman presented to the defendant hospital ED complaining of chills, fever, and blood in her urine. She underwent laboratory testing and was given IV fluids and antibiotics. She was discharged with a prescription for ciprofloxacin for a urinary tract infection and was given instructions to follow up with her primary care physician or return to the ED if her symptoms worsened.
Two days later, the patient returned to the ED twice and was ultimately admitted with fever, chills, shortness of breath, and a cough. The next day, she suffered a grand mal seizure and was transferred to another hospital, where she died a few days later.
The plaintiff claimed that the decedent had systemic lupus erythematosus and that she should have been transferred to the second hospital immediately.
The defendants claimed that the decedent had a viral syndrome, that her seizure was completely unpredictable, and that nothing could have been done during her ED visits to have changed the outcome.
According to a published report, a defense verdict was returned.
Advanced Heart Disease Recognized, Treated Late
In April 2003, a 47-year-old woman underwent aortic valve repair and mitral valve replacement in an attempt to correct problems with blood flow to and from her heart.
After the surgery, it was discovered that the left ventricle was pumping out a dangerously low amount of blood. She was taken to the ICU in Dr. A.’s care. At midnight, Dr. C. assumed her care.
The following morning, Dr. C. installed an intra-aortic balloon pump (IABP), which required several attempts. The patient was then transferred to another hospital for a possible heart transplant. She experienced cardiac arrest and died the following day.
The plaintiff claimed that Dr. A. and Dr. C. failed to perform appropriate preoperative testing and to administer the proper medication in the hours immediately following surgery. During this time, the decedent suffered multiple myocardial infarctions due to lack of oxygen to the heart. The plaintiff also claimed that the IABP should have been installed earlier.
The defendants argued that the decedent was in extremely poor health before the surgery as a result of advanced heart disease, which they claimed had been misdiagnosed as asthma since 1996.
According to a published account, a jury found no negligence by the hospital or Dr. C. The jury found Dr. A. negligent, but they did not find his negligence to have caused the woman’s death. A defense verdict was entered. Posttrial motions were pending.
Sinus Infection Leads to Brain Abscess
A woman in her 50s presented to a hospital ED complaining of severe headaches for several days. An ED physician made a diagnosis of tension headache and prescribed muscle relaxants and pain medication. Two days later, at her primary care physician’s office, she still had a headache, but it was less severe; she also had nasal discharge, swollen eyes, red sinuses, and nausea. The patient was examined by a PA, who diagnosed an allergic reaction. Steroids were prescribed, and a sinus x-ray and blood work were ordered.
Five days later, the woman developed stroke-like symptoms, including facial drooping and disorientation. She was transported to the same hospital, where CT revealed a brain abscess. She was airlifted to a second hospital for emergency brain surgery, which required part of her skull to be removed and replaced with plastic.
After surgery, the patient experienced respiratory failure and was placed on a ventilator. Following additional brain surgeries, she was left with loss of vision in her left eye and cognitive impairment that could increase her likelihood of developing dementia. She also needed two months of rehabilitation.
The plaintiff alleged negligence by both the ED physician and the PA for their failure to diagnose a sinus infection and to prescribe appropriate antibiotics. She maintained that tests should have been ordered on an urgent basis and that timely diagnosis and treatment would have prevented the abscess. The plaintiff further charged that the PA’s supervising physicians failed to review her chart or consult with the PA regarding her case.
The defendant primary care provider argued that the plaintiff was properly treated. The remaining defendants claimed that the plaintiff was at fault for not undergoing diagnostic testing immediately following the PA’s examination.
According to a published report, a jury found the primary care provider and the PA negligent and awarded the plaintiff $3 million. The ED physician and the first hospital were found not at fault.
Echocardiography Not Available on Weekends
One Friday evening in late October, a 58-year-old man presented to the emergency department (ED) of a rural hospital with complaints of jaw pain, chest pain, arm and leg numbness, and difficulty speaking. Within 15 minutes of his arrival, the man’s symptoms resolved spontaneously. Results of testing performed in the ED were consistent with coronary artery disease.
The patient was transferred late that night to another hospital for specialized cardiac care. His condition at the time of admission was stable, and he had no complaints other than the unusual 15-minute episode he had experienced earlier that day. This information was presented to a resident, who examined the patient and ordered an echocardiogram for the next morning (Saturday). The hospital’s echocardiography laboratory was not routinely open on the weekend.
The man was seen by a cardiologist that Saturday morning. It was noted that his heart monitoring had shown abnormalities, and blood work had revealed abnormally elevated cardiac enzyme levels. The cardiologist recommended that the patient remain on high-dose heparin until angiography could be performed on Monday.
The cardiologist also noted that he detected a slight diastolic heart murmur near the left sternal border. He informed the man and his wife that there might be a bacterial infection affecting the aortic valve, which would explain the murmur. The cardiologist ordered an echocardiogram for Monday to rule out the possibility of aortic incompetence due to aneurysm of dissection. The man died that night before testing could be performed.
The cardiologist claimed that the man’s death was the result of a sudden heart attack secondary to coronary artery disease. No autopsy was performed at the time. The body was exhumed 18 months later, however, and a postmortem examination revealed the cause of death to be aortic dissection.
The plaintiff claimed that the ED physician, the resident, and the cardiologist were all negligent in failing to make a diagnosis of aortic dissection and that emergent chest CT should have been performed. The plaintiff also argued that if echocardiography had been performed on Saturday morning as ordered by the resident, the dissection could have been detected in time to perform lifesaving surgery. The plaintiff further claimed that the cardiologist was negligent for recognizing the possibility of a dissection and doing nothing to confirm or rule out the diagnosis, despite the high mortality rate associated with aortic dissection.
The defendants maintained that the decedent’s signs and symptoms were not typical for aortic dissection and were more consistent with coronary artery disease. The defendants also argued that even if the correct diagnosis had been made, the decedent would not have survived surgery.
A settlement of $2 million was reached.
Viral Syndrome—or Lupus?
A 34-year-old woman presented to the defendant hospital ED complaining of chills, fever, and blood in her urine. She underwent laboratory testing and was given IV fluids and antibiotics. She was discharged with a prescription for ciprofloxacin for a urinary tract infection and was given instructions to follow up with her primary care physician or return to the ED if her symptoms worsened.
Two days later, the patient returned to the ED twice and was ultimately admitted with fever, chills, shortness of breath, and a cough. The next day, she suffered a grand mal seizure and was transferred to another hospital, where she died a few days later.
The plaintiff claimed that the decedent had systemic lupus erythematosus and that she should have been transferred to the second hospital immediately.
The defendants claimed that the decedent had a viral syndrome, that her seizure was completely unpredictable, and that nothing could have been done during her ED visits to have changed the outcome.
According to a published report, a defense verdict was returned.
Advanced Heart Disease Recognized, Treated Late
In April 2003, a 47-year-old woman underwent aortic valve repair and mitral valve replacement in an attempt to correct problems with blood flow to and from her heart.
After the surgery, it was discovered that the left ventricle was pumping out a dangerously low amount of blood. She was taken to the ICU in Dr. A.’s care. At midnight, Dr. C. assumed her care.
The following morning, Dr. C. installed an intra-aortic balloon pump (IABP), which required several attempts. The patient was then transferred to another hospital for a possible heart transplant. She experienced cardiac arrest and died the following day.
The plaintiff claimed that Dr. A. and Dr. C. failed to perform appropriate preoperative testing and to administer the proper medication in the hours immediately following surgery. During this time, the decedent suffered multiple myocardial infarctions due to lack of oxygen to the heart. The plaintiff also claimed that the IABP should have been installed earlier.
The defendants argued that the decedent was in extremely poor health before the surgery as a result of advanced heart disease, which they claimed had been misdiagnosed as asthma since 1996.
According to a published account, a jury found no negligence by the hospital or Dr. C. The jury found Dr. A. negligent, but they did not find his negligence to have caused the woman’s death. A defense verdict was entered. Posttrial motions were pending.
Sinus Infection Leads to Brain Abscess
A woman in her 50s presented to a hospital ED complaining of severe headaches for several days. An ED physician made a diagnosis of tension headache and prescribed muscle relaxants and pain medication. Two days later, at her primary care physician’s office, she still had a headache, but it was less severe; she also had nasal discharge, swollen eyes, red sinuses, and nausea. The patient was examined by a PA, who diagnosed an allergic reaction. Steroids were prescribed, and a sinus x-ray and blood work were ordered.
Five days later, the woman developed stroke-like symptoms, including facial drooping and disorientation. She was transported to the same hospital, where CT revealed a brain abscess. She was airlifted to a second hospital for emergency brain surgery, which required part of her skull to be removed and replaced with plastic.
After surgery, the patient experienced respiratory failure and was placed on a ventilator. Following additional brain surgeries, she was left with loss of vision in her left eye and cognitive impairment that could increase her likelihood of developing dementia. She also needed two months of rehabilitation.
The plaintiff alleged negligence by both the ED physician and the PA for their failure to diagnose a sinus infection and to prescribe appropriate antibiotics. She maintained that tests should have been ordered on an urgent basis and that timely diagnosis and treatment would have prevented the abscess. The plaintiff further charged that the PA’s supervising physicians failed to review her chart or consult with the PA regarding her case.
The defendant primary care provider argued that the plaintiff was properly treated. The remaining defendants claimed that the plaintiff was at fault for not undergoing diagnostic testing immediately following the PA’s examination.
According to a published report, a jury found the primary care provider and the PA negligent and awarded the plaintiff $3 million. The ED physician and the first hospital were found not at fault.
Why off-label isn’t off base
Dear Dr. Mossman:
When I was a resident, attending physicians occasionally cited journal articles in their consultation notes to substantiate their treatment choices. Since then, I’ve done this at times when I’ve prescribed a drug off-label.
Recently, I mentioned this practice to a physician who is trained as a lawyer. He thought citing articles in a patient’s chart was a bad idea, because by doing so I was automatically making the referred-to article the “expert witness.” If a lawsuit occurred, I might be called upon to justify the article’s validity, statistical details, methodology, etc. My intent is to show that I have a detailed, well-thought-out justification for my treatment choice.
Am I placing myself at greater risk of incurring liability should a lawsuit occur?—Submitted by “Dr. W”
Dr. W wants to know how he can minimize malpractice risk when prescribing a medication off label and wonders if citing an article in a patient’s chart is a good or bad idea. In law school, attorneys-in-training learn to answer very general legal questions with, “It depends.” There’s little certainty about how to avoid successful malpractice litigation, because few if any strategies have been tested systematically. However, this article will explain—and hopefully help you avoid—the medicolegal pitfalls of off-label prescribing.
Off-label: ‘Accepted and necessary’
Off-label prescribing occurs when a physician prescribes a medication or uses a medical device outside the scope of FDA-approved labeling. Most commonly, off-label use involves prescribing a medication for something other than its FDA-approved indication—such as sildenafil for women with antidepressant-induced sexual dysfunction.1
Other examples are prescribing a drug:
- at an unapproved dose
- in an unapproved format, such as mixing capsule contents with applesauce
- outside the approved age group
- for longer than the approved interval
- at a different dose schedule, such as qhs instead of bid or tid.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Typically, it takes years for a new drug to gain FDA approval and additional time for an already-approved drug to gain approval for a new indication. In the mean-time, clinicians treat their patients with available drugs prescribed off-label.
Off-label prescribing is legal. FDA approval means drugs may be sold and marketed in specific ways, but the FDA does not tell physicians how they can use approved drugs. As each edition of the Physicians’ Desk Reference explains, “Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.”2 Federal statutes state that FDA approval does not “limit or interfere with the authority of a health care practitioner to prescribe” approved drugs or devices “for any condition or disease.”3
Courts endorse off-label prescribing. As 1 appellate decision states, “Because the pace of medical discovery runs ahead of the FDA’s regulatory machinery, the off-label use of some drugs is frequently considered to be ‘state-of-the-art’ treatment.”4 The U.S. Supreme Court has concluded that off-label prescribing “is an accepted and necessary corollary of the FDA’s mission to regulate.”5
Limited testing for safety and effectiveness. Experiences such as “Fen-phen” for weight loss11 and estrogens for preventing vascular disease in postmenopausal women12 remind physicians that some untested treatments may do more harm than good.
Commercial influence. Pharmaceutical companies have used advisory boards, consultant meetings, and continuing medical education events to promote unproven off-label indications for drugs.13,14 Many studies ostensibly designed and proposed by researchers show evidence of “ghost authorship” by commercial concerns.15
Study bias. Even published, peer-reviewed, double-blind studies might not sufficiently support off-label prescribing practices, because sponsors of such studies can structure them or use statistical analyses to make results look favorable. Former editors of the British Medical Journal and the Lancet have acknowledged that their publications unwittingly served as “an extension of the marketing arm” or “laundering operations” for drug manufacturers.16,17 Even for FDA-approved indications, a selective, positive-result publication bias and non-reporting of negative results may make drugs seem more effective than the full range of studies would justify.18
Legal use of labeling. Though off-label prescribing is accepted medical practice, doctors “may be found negligent if their decision to use a drug off-label is sufficiently careless, imprudent, or unprofessional.”4 During a malpractice lawsuit, plaintiff’s counsel could try to use FDA-approved labeling or prescribing information to establish a presumptive standard of care. Such evidence usually is admissible if it is supported by expert testimony. It places the burden of proof on the defendant physician to show how an off-label use met the standard of care.19
Is off-label use malpractice?
Off-label use is not only legal, it’s often wise medical practice. Many drug uses that now have FDA approval were off-label just a few years ago. Examples include using selective serotonin reuptake inhibitors (SSRIs) to treat panic disorder and obsessive-compulsive disorder and valproate for bipolar mania. Though fluoxetine is the only FDA-approved drug for treating depression in adolescents, other SSRIs may have a favorable risk-benefit profile.6
Numerous studies have shown that off-label prescribing is common in psychiatry7 and other specialties.8,9 Because the practice is so common, the mere fact that a drug is not FDA-approved for a particular use does not imply that the drug was prescribed negligently.
Are patients human guinea pigs?
Some commentators have suggested that off-label prescribing amounts to human experimentation.10 Without FDA approval, they say physicians lack “hard evidence” that a product is safe and effective, so off-label prescribing is a small-scale clinical trial based on the doctor’s educated guesses. If this reasoning is correct, off-label prescribing would require the same human subject protections used in research, including institution review board approval and special consent forms.
Although this argument sounds plausible, off-label prescribing is not experimentation or research (Box).4,11-19 Researchers investigate hypotheses to obtain generalizable knowledge, whereas medical therapy aims to benefit individual patients. This experimentation/therapy distinction is not perfect because successful off-label treatment of 1 patient might imply beneficial effects for others.10 When courts have looked at this matter, though, they have found that “off-label use…by a physician seeking an optimal treatment for his or her patient is not necessarily…research or an investigational or experimental treatment when the use is customarily followed by physicians.”4
Courts also have said that off-label use does not require special informed consent. Just because a drug is prescribed off-label doesn’t mean it’s risky. FDA approval “is not a material risk inherently involved in a proposed therapy which a physician should have disclosed to a patient prior to the therapy.”20 In other words, a physician is not required to discuss FDA regulatory status—such as off-label uses of a medication—to comply with standards of informed consent. FDA regulatory status has nothing to do with the risks or benefits of a medication and it does not provide information about treatment alternatives.21
What should you do?
Keep abreast of news and scientific evidence concerning drug uses, effects, interactions, and adverse effects, especially when prescribing for uses that are different from the manufacturer’s intended purposes (such as hormone therapy for sex offenders).22
Collect articles on off-label uses, but keep them separate from your patients’ files. Good attorneys are highly skilled at using documents to score legal points, and opposing counsel will prepare questions to focus on the articles’ faults or limitations in isolation.
Know why an article applies to your patient. If you are sued for malpractice, you can use an article to support your treatment choice by explaining how this information contributed to your decision-making.
Tell your patient that the proposed treatment is an off-label use when you obtain consent, even though case law says you don’t have to do this. Telling your patient helps him understand your reasoning and prevents surprises that may give offense. For example, if you prescribe a second-generation antipsychotic for a nonpsychotic patient, you wouldn’t want your patient to think you believe he has schizophrenia when he reads the information his pharmacy attaches to his prescription.
Engage in ongoing informed consent. Uncertainty is part of medical practice and is heightened when doctors prescribe off-label. Ongoing discussions help patients understand, accept, and share that uncertainty.
Document informed consent. This will show—if it becomes necessary—that you and your patient made collaborative, conscientious decisions about treatment.23
Related resources
- Zito JM, Derivan AT, Kratochvil CJ, et al. Off-label psychopharmacologic prescribing for children: history supports close clinical monitoring. Child Adolesc Psychiatry Ment Health. 2008;2:24. www.capmh.com/content/pdf/1753-2000-2-24.pdf.
- Spiesel S. Prozac on the playground. October 15, 2008. Slate. www.slate.com/id/2202338.
Drug brand names
- Fenfluramine and phentermine • Fen-phen
- Fluoxetine • Prozac
- Sildenafil • Viagra
- Valproate • Depakote
1. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404.
2. Physicians’ Desk Reference. 62nd edition. Montvale, NJ: Thomson Healthcare, Inc.; 2007.
3. Food, Drug and Cosmetic Act, 21USC §396.
4. Richardson v Miller, 44 SW3d 1 (Tenn Ct App 2000).
5. Buckman Co. v Plaintiffs’ Legal Comm., 531 US 341 (2001).
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-1696.
7. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Advances in Psychiatric Treatment. 2007;13:414-422.
8. Conroy S, Choonare I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. Br Med J. 2000;320:79-82.
9. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021-1026.
10. Mehlman MJ. Off-label prescribing. Available at: http://www.thedoctorwillseeyounow.com/articles/bioethics/offlabel_11. Accessed October 21, 2008.
11. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
12. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
13. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.
14. Steinman MA, Bero L, Chren M, et al. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
15. Gøtzsche PC, Hrobjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.
16. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.
17. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
18. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
19. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
20. Klein v Biscup, 673 NE2d 225 (Ohio App 1996).
21. Beck JM, Azari ED. FDA, off-label use, and informed consent: debunking myths and misconceptions. Food Drug Law J. 1998;53:71-104.
22. Shajnfeld A, Krueger RB. Reforming (purportedly) non-punitive responses to sexual offending. Developments in Mental Health Law. 2006;25:81-99.
23. Royal College of Psychiatrists CR142. Use of unlicensed medicine for unlicensed applications in psychiatric practice. Available at: http://www.rcpsych.ac.uk/publications/collegereports/cr/cr142.aspx. Accessed October 21, 2008.

Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine.
Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine.
Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine.
Dear Dr. Mossman:
When I was a resident, attending physicians occasionally cited journal articles in their consultation notes to substantiate their treatment choices. Since then, I’ve done this at times when I’ve prescribed a drug off-label.
Recently, I mentioned this practice to a physician who is trained as a lawyer. He thought citing articles in a patient’s chart was a bad idea, because by doing so I was automatically making the referred-to article the “expert witness.” If a lawsuit occurred, I might be called upon to justify the article’s validity, statistical details, methodology, etc. My intent is to show that I have a detailed, well-thought-out justification for my treatment choice.
Am I placing myself at greater risk of incurring liability should a lawsuit occur?—Submitted by “Dr. W”
Dr. W wants to know how he can minimize malpractice risk when prescribing a medication off label and wonders if citing an article in a patient’s chart is a good or bad idea. In law school, attorneys-in-training learn to answer very general legal questions with, “It depends.” There’s little certainty about how to avoid successful malpractice litigation, because few if any strategies have been tested systematically. However, this article will explain—and hopefully help you avoid—the medicolegal pitfalls of off-label prescribing.
Off-label: ‘Accepted and necessary’
Off-label prescribing occurs when a physician prescribes a medication or uses a medical device outside the scope of FDA-approved labeling. Most commonly, off-label use involves prescribing a medication for something other than its FDA-approved indication—such as sildenafil for women with antidepressant-induced sexual dysfunction.1
Other examples are prescribing a drug:
- at an unapproved dose
- in an unapproved format, such as mixing capsule contents with applesauce
- outside the approved age group
- for longer than the approved interval
- at a different dose schedule, such as qhs instead of bid or tid.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Typically, it takes years for a new drug to gain FDA approval and additional time for an already-approved drug to gain approval for a new indication. In the mean-time, clinicians treat their patients with available drugs prescribed off-label.
Off-label prescribing is legal. FDA approval means drugs may be sold and marketed in specific ways, but the FDA does not tell physicians how they can use approved drugs. As each edition of the Physicians’ Desk Reference explains, “Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.”2 Federal statutes state that FDA approval does not “limit or interfere with the authority of a health care practitioner to prescribe” approved drugs or devices “for any condition or disease.”3
Courts endorse off-label prescribing. As 1 appellate decision states, “Because the pace of medical discovery runs ahead of the FDA’s regulatory machinery, the off-label use of some drugs is frequently considered to be ‘state-of-the-art’ treatment.”4 The U.S. Supreme Court has concluded that off-label prescribing “is an accepted and necessary corollary of the FDA’s mission to regulate.”5
Limited testing for safety and effectiveness. Experiences such as “Fen-phen” for weight loss11 and estrogens for preventing vascular disease in postmenopausal women12 remind physicians that some untested treatments may do more harm than good.
Commercial influence. Pharmaceutical companies have used advisory boards, consultant meetings, and continuing medical education events to promote unproven off-label indications for drugs.13,14 Many studies ostensibly designed and proposed by researchers show evidence of “ghost authorship” by commercial concerns.15
Study bias. Even published, peer-reviewed, double-blind studies might not sufficiently support off-label prescribing practices, because sponsors of such studies can structure them or use statistical analyses to make results look favorable. Former editors of the British Medical Journal and the Lancet have acknowledged that their publications unwittingly served as “an extension of the marketing arm” or “laundering operations” for drug manufacturers.16,17 Even for FDA-approved indications, a selective, positive-result publication bias and non-reporting of negative results may make drugs seem more effective than the full range of studies would justify.18
Legal use of labeling. Though off-label prescribing is accepted medical practice, doctors “may be found negligent if their decision to use a drug off-label is sufficiently careless, imprudent, or unprofessional.”4 During a malpractice lawsuit, plaintiff’s counsel could try to use FDA-approved labeling or prescribing information to establish a presumptive standard of care. Such evidence usually is admissible if it is supported by expert testimony. It places the burden of proof on the defendant physician to show how an off-label use met the standard of care.19
Is off-label use malpractice?
Off-label use is not only legal, it’s often wise medical practice. Many drug uses that now have FDA approval were off-label just a few years ago. Examples include using selective serotonin reuptake inhibitors (SSRIs) to treat panic disorder and obsessive-compulsive disorder and valproate for bipolar mania. Though fluoxetine is the only FDA-approved drug for treating depression in adolescents, other SSRIs may have a favorable risk-benefit profile.6
Numerous studies have shown that off-label prescribing is common in psychiatry7 and other specialties.8,9 Because the practice is so common, the mere fact that a drug is not FDA-approved for a particular use does not imply that the drug was prescribed negligently.
Are patients human guinea pigs?
Some commentators have suggested that off-label prescribing amounts to human experimentation.10 Without FDA approval, they say physicians lack “hard evidence” that a product is safe and effective, so off-label prescribing is a small-scale clinical trial based on the doctor’s educated guesses. If this reasoning is correct, off-label prescribing would require the same human subject protections used in research, including institution review board approval and special consent forms.
Although this argument sounds plausible, off-label prescribing is not experimentation or research (Box).4,11-19 Researchers investigate hypotheses to obtain generalizable knowledge, whereas medical therapy aims to benefit individual patients. This experimentation/therapy distinction is not perfect because successful off-label treatment of 1 patient might imply beneficial effects for others.10 When courts have looked at this matter, though, they have found that “off-label use…by a physician seeking an optimal treatment for his or her patient is not necessarily…research or an investigational or experimental treatment when the use is customarily followed by physicians.”4
Courts also have said that off-label use does not require special informed consent. Just because a drug is prescribed off-label doesn’t mean it’s risky. FDA approval “is not a material risk inherently involved in a proposed therapy which a physician should have disclosed to a patient prior to the therapy.”20 In other words, a physician is not required to discuss FDA regulatory status—such as off-label uses of a medication—to comply with standards of informed consent. FDA regulatory status has nothing to do with the risks or benefits of a medication and it does not provide information about treatment alternatives.21
What should you do?
Keep abreast of news and scientific evidence concerning drug uses, effects, interactions, and adverse effects, especially when prescribing for uses that are different from the manufacturer’s intended purposes (such as hormone therapy for sex offenders).22
Collect articles on off-label uses, but keep them separate from your patients’ files. Good attorneys are highly skilled at using documents to score legal points, and opposing counsel will prepare questions to focus on the articles’ faults or limitations in isolation.
Know why an article applies to your patient. If you are sued for malpractice, you can use an article to support your treatment choice by explaining how this information contributed to your decision-making.
Tell your patient that the proposed treatment is an off-label use when you obtain consent, even though case law says you don’t have to do this. Telling your patient helps him understand your reasoning and prevents surprises that may give offense. For example, if you prescribe a second-generation antipsychotic for a nonpsychotic patient, you wouldn’t want your patient to think you believe he has schizophrenia when he reads the information his pharmacy attaches to his prescription.
Engage in ongoing informed consent. Uncertainty is part of medical practice and is heightened when doctors prescribe off-label. Ongoing discussions help patients understand, accept, and share that uncertainty.
Document informed consent. This will show—if it becomes necessary—that you and your patient made collaborative, conscientious decisions about treatment.23
Related resources
- Zito JM, Derivan AT, Kratochvil CJ, et al. Off-label psychopharmacologic prescribing for children: history supports close clinical monitoring. Child Adolesc Psychiatry Ment Health. 2008;2:24. www.capmh.com/content/pdf/1753-2000-2-24.pdf.
- Spiesel S. Prozac on the playground. October 15, 2008. Slate. www.slate.com/id/2202338.
Drug brand names
- Fenfluramine and phentermine • Fen-phen
- Fluoxetine • Prozac
- Sildenafil • Viagra
- Valproate • Depakote
Dear Dr. Mossman:
When I was a resident, attending physicians occasionally cited journal articles in their consultation notes to substantiate their treatment choices. Since then, I’ve done this at times when I’ve prescribed a drug off-label.
Recently, I mentioned this practice to a physician who is trained as a lawyer. He thought citing articles in a patient’s chart was a bad idea, because by doing so I was automatically making the referred-to article the “expert witness.” If a lawsuit occurred, I might be called upon to justify the article’s validity, statistical details, methodology, etc. My intent is to show that I have a detailed, well-thought-out justification for my treatment choice.
Am I placing myself at greater risk of incurring liability should a lawsuit occur?—Submitted by “Dr. W”
Dr. W wants to know how he can minimize malpractice risk when prescribing a medication off label and wonders if citing an article in a patient’s chart is a good or bad idea. In law school, attorneys-in-training learn to answer very general legal questions with, “It depends.” There’s little certainty about how to avoid successful malpractice litigation, because few if any strategies have been tested systematically. However, this article will explain—and hopefully help you avoid—the medicolegal pitfalls of off-label prescribing.
Off-label: ‘Accepted and necessary’
Off-label prescribing occurs when a physician prescribes a medication or uses a medical device outside the scope of FDA-approved labeling. Most commonly, off-label use involves prescribing a medication for something other than its FDA-approved indication—such as sildenafil for women with antidepressant-induced sexual dysfunction.1
Other examples are prescribing a drug:
- at an unapproved dose
- in an unapproved format, such as mixing capsule contents with applesauce
- outside the approved age group
- for longer than the approved interval
- at a different dose schedule, such as qhs instead of bid or tid.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Typically, it takes years for a new drug to gain FDA approval and additional time for an already-approved drug to gain approval for a new indication. In the mean-time, clinicians treat their patients with available drugs prescribed off-label.
Off-label prescribing is legal. FDA approval means drugs may be sold and marketed in specific ways, but the FDA does not tell physicians how they can use approved drugs. As each edition of the Physicians’ Desk Reference explains, “Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.”2 Federal statutes state that FDA approval does not “limit or interfere with the authority of a health care practitioner to prescribe” approved drugs or devices “for any condition or disease.”3
Courts endorse off-label prescribing. As 1 appellate decision states, “Because the pace of medical discovery runs ahead of the FDA’s regulatory machinery, the off-label use of some drugs is frequently considered to be ‘state-of-the-art’ treatment.”4 The U.S. Supreme Court has concluded that off-label prescribing “is an accepted and necessary corollary of the FDA’s mission to regulate.”5
Limited testing for safety and effectiveness. Experiences such as “Fen-phen” for weight loss11 and estrogens for preventing vascular disease in postmenopausal women12 remind physicians that some untested treatments may do more harm than good.
Commercial influence. Pharmaceutical companies have used advisory boards, consultant meetings, and continuing medical education events to promote unproven off-label indications for drugs.13,14 Many studies ostensibly designed and proposed by researchers show evidence of “ghost authorship” by commercial concerns.15
Study bias. Even published, peer-reviewed, double-blind studies might not sufficiently support off-label prescribing practices, because sponsors of such studies can structure them or use statistical analyses to make results look favorable. Former editors of the British Medical Journal and the Lancet have acknowledged that their publications unwittingly served as “an extension of the marketing arm” or “laundering operations” for drug manufacturers.16,17 Even for FDA-approved indications, a selective, positive-result publication bias and non-reporting of negative results may make drugs seem more effective than the full range of studies would justify.18
Legal use of labeling. Though off-label prescribing is accepted medical practice, doctors “may be found negligent if their decision to use a drug off-label is sufficiently careless, imprudent, or unprofessional.”4 During a malpractice lawsuit, plaintiff’s counsel could try to use FDA-approved labeling or prescribing information to establish a presumptive standard of care. Such evidence usually is admissible if it is supported by expert testimony. It places the burden of proof on the defendant physician to show how an off-label use met the standard of care.19
Is off-label use malpractice?
Off-label use is not only legal, it’s often wise medical practice. Many drug uses that now have FDA approval were off-label just a few years ago. Examples include using selective serotonin reuptake inhibitors (SSRIs) to treat panic disorder and obsessive-compulsive disorder and valproate for bipolar mania. Though fluoxetine is the only FDA-approved drug for treating depression in adolescents, other SSRIs may have a favorable risk-benefit profile.6
Numerous studies have shown that off-label prescribing is common in psychiatry7 and other specialties.8,9 Because the practice is so common, the mere fact that a drug is not FDA-approved for a particular use does not imply that the drug was prescribed negligently.
Are patients human guinea pigs?
Some commentators have suggested that off-label prescribing amounts to human experimentation.10 Without FDA approval, they say physicians lack “hard evidence” that a product is safe and effective, so off-label prescribing is a small-scale clinical trial based on the doctor’s educated guesses. If this reasoning is correct, off-label prescribing would require the same human subject protections used in research, including institution review board approval and special consent forms.
Although this argument sounds plausible, off-label prescribing is not experimentation or research (Box).4,11-19 Researchers investigate hypotheses to obtain generalizable knowledge, whereas medical therapy aims to benefit individual patients. This experimentation/therapy distinction is not perfect because successful off-label treatment of 1 patient might imply beneficial effects for others.10 When courts have looked at this matter, though, they have found that “off-label use…by a physician seeking an optimal treatment for his or her patient is not necessarily…research or an investigational or experimental treatment when the use is customarily followed by physicians.”4
Courts also have said that off-label use does not require special informed consent. Just because a drug is prescribed off-label doesn’t mean it’s risky. FDA approval “is not a material risk inherently involved in a proposed therapy which a physician should have disclosed to a patient prior to the therapy.”20 In other words, a physician is not required to discuss FDA regulatory status—such as off-label uses of a medication—to comply with standards of informed consent. FDA regulatory status has nothing to do with the risks or benefits of a medication and it does not provide information about treatment alternatives.21
What should you do?
Keep abreast of news and scientific evidence concerning drug uses, effects, interactions, and adverse effects, especially when prescribing for uses that are different from the manufacturer’s intended purposes (such as hormone therapy for sex offenders).22
Collect articles on off-label uses, but keep them separate from your patients’ files. Good attorneys are highly skilled at using documents to score legal points, and opposing counsel will prepare questions to focus on the articles’ faults or limitations in isolation.
Know why an article applies to your patient. If you are sued for malpractice, you can use an article to support your treatment choice by explaining how this information contributed to your decision-making.
Tell your patient that the proposed treatment is an off-label use when you obtain consent, even though case law says you don’t have to do this. Telling your patient helps him understand your reasoning and prevents surprises that may give offense. For example, if you prescribe a second-generation antipsychotic for a nonpsychotic patient, you wouldn’t want your patient to think you believe he has schizophrenia when he reads the information his pharmacy attaches to his prescription.
Engage in ongoing informed consent. Uncertainty is part of medical practice and is heightened when doctors prescribe off-label. Ongoing discussions help patients understand, accept, and share that uncertainty.
Document informed consent. This will show—if it becomes necessary—that you and your patient made collaborative, conscientious decisions about treatment.23
Related resources
- Zito JM, Derivan AT, Kratochvil CJ, et al. Off-label psychopharmacologic prescribing for children: history supports close clinical monitoring. Child Adolesc Psychiatry Ment Health. 2008;2:24. www.capmh.com/content/pdf/1753-2000-2-24.pdf.
- Spiesel S. Prozac on the playground. October 15, 2008. Slate. www.slate.com/id/2202338.
Drug brand names
- Fenfluramine and phentermine • Fen-phen
- Fluoxetine • Prozac
- Sildenafil • Viagra
- Valproate • Depakote
1. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404.
2. Physicians’ Desk Reference. 62nd edition. Montvale, NJ: Thomson Healthcare, Inc.; 2007.
3. Food, Drug and Cosmetic Act, 21USC §396.
4. Richardson v Miller, 44 SW3d 1 (Tenn Ct App 2000).
5. Buckman Co. v Plaintiffs’ Legal Comm., 531 US 341 (2001).
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-1696.
7. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Advances in Psychiatric Treatment. 2007;13:414-422.
8. Conroy S, Choonare I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. Br Med J. 2000;320:79-82.
9. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021-1026.
10. Mehlman MJ. Off-label prescribing. Available at: http://www.thedoctorwillseeyounow.com/articles/bioethics/offlabel_11. Accessed October 21, 2008.
11. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
12. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
13. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.
14. Steinman MA, Bero L, Chren M, et al. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
15. Gøtzsche PC, Hrobjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.
16. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.
17. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
18. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
19. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
20. Klein v Biscup, 673 NE2d 225 (Ohio App 1996).
21. Beck JM, Azari ED. FDA, off-label use, and informed consent: debunking myths and misconceptions. Food Drug Law J. 1998;53:71-104.
22. Shajnfeld A, Krueger RB. Reforming (purportedly) non-punitive responses to sexual offending. Developments in Mental Health Law. 2006;25:81-99.
23. Royal College of Psychiatrists CR142. Use of unlicensed medicine for unlicensed applications in psychiatric practice. Available at: http://www.rcpsych.ac.uk/publications/collegereports/cr/cr142.aspx. Accessed October 21, 2008.
1. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404.
2. Physicians’ Desk Reference. 62nd edition. Montvale, NJ: Thomson Healthcare, Inc.; 2007.
3. Food, Drug and Cosmetic Act, 21USC §396.
4. Richardson v Miller, 44 SW3d 1 (Tenn Ct App 2000).
5. Buckman Co. v Plaintiffs’ Legal Comm., 531 US 341 (2001).
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-1696.
7. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Advances in Psychiatric Treatment. 2007;13:414-422.
8. Conroy S, Choonare I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. Br Med J. 2000;320:79-82.
9. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021-1026.
10. Mehlman MJ. Off-label prescribing. Available at: http://www.thedoctorwillseeyounow.com/articles/bioethics/offlabel_11. Accessed October 21, 2008.
11. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
12. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
13. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.
14. Steinman MA, Bero L, Chren M, et al. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
15. Gøtzsche PC, Hrobjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.
16. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.
17. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
18. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
19. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
20. Klein v Biscup, 673 NE2d 225 (Ohio App 1996).
21. Beck JM, Azari ED. FDA, off-label use, and informed consent: debunking myths and misconceptions. Food Drug Law J. 1998;53:71-104.
22. Shajnfeld A, Krueger RB. Reforming (purportedly) non-punitive responses to sexual offending. Developments in Mental Health Law. 2006;25:81-99.
23. Royal College of Psychiatrists CR142. Use of unlicensed medicine for unlicensed applications in psychiatric practice. Available at: http://www.rcpsych.ac.uk/publications/collegereports/cr/cr142.aspx. Accessed October 21, 2008.
At Work in Washington

SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at [email protected].
SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at [email protected].
SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at [email protected].
Non-Physician Providers Critical to Hospital Medicine Practices
Non-Physician Providers Critical to Hospital Medicine Practices
In “Maximizing NPPs in Hospitalist Practices” (Practice Management, October 2008, p. 69), John Nelson, MD, implies a financial advantage to hiring nurse practitioners (NPs) rather than physician assistants (PAs):
“A PA’s work will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders. Nurse practitioners, on the other hand, may be able to perform certain patient-care activities independently. Medicare and other payers typically reimburse at 85% of the rate customarily paid to MDs for the same service.”
Dr. Nelson: Do you mean to imply NPs providing hospitalist coverage should function independently, without any physician supervision, oversight, or input? I do not know of any hospitals that allow NPs to admit and manage patients independently, despite their independent practice status. In my opinion, it would be detrimental to patient care to allow non-physician providers to provide completely independent, unsupervised hospital care.
In addition, I know of no hospital practice setting that requires a physician to be physically present during a PA’s exam. In all hospital practice settings that I am aware of, a supervising or attending physician (not necessarily the one on the PA’s license), must see the patient at some time each day, not necessarily at the same time as the PA.
In that scenario, the physician pays a brief visit to the patient to corroborate the PA’s exam and plan. The physician then writes a brief, seen-and-agreed note, and can bill 100% of the Medicare reimbursement, not the 85% for a NP visit. How this compares economically depends, of course, on relative salaries. But it provides physician oversight of the NPP, which assumedly will improve quality of care (though I have no studies to cite to that effect).
Do you have some other reason for your anti-PA, pro-NP bias? Is your personal experience colored by working with more competent NPs, in your opinion, and less competent PAs? Perhaps that would make for a more interesting, better-defined column.
Richard Buckberg, PA-C, Maine Medical Center, Portland, Maine
SHM’s Non-Physician Provider (NPP) Committee was delighted to see the recent article by Dr. Nelson, MD, regarding the use of NPPs in hospital medicine. These columns spotlighted HM’s increasing utilization of NPPs, a role that only is expected to increase in number and breadth, based on the increasing need for competent, comprehensive care of the acutely ill.
Dr. Nelson made many excellent points that may benefit from some clarification or expansion. Dr. Nelson states a PA “will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders.” This is incorrect, and seems to imply PAs are more difficult to assimilate into practice than NPs. Depending upon variability in legal limitations and hospital bylaws, both PAs and NPs may see a patient without a physician present. In order to bill for a shared visit and receive 100% reimbursement, the attending physician needs to have a face-to-face encounter with that patient at some point in the day and document a portion of the evaluation and management (e.g., history, physical exam, or medical decision-making).
Alternatively, in most states, both NPs and PAs can see patients independently and bill for their services at 85% of the physician’s Medicare rate. Obtaining 100% reimbursement for NPP services when using the shared billing model is efficient and simple. Though variability exists, more specifically in hospital culture, utilization of these roles can positively impact the bottom line of reimbursement. Therefore, it is essential to understand all of the regulations before developing a business model incorporating NPPs.
Dr. Nelson also points out that using NPPs in a clerical fashion, such as discharge planning, is not optimizing the NPPs capabilities. This point is well taken. If clerical assistance is needed, hire the appropriate discipline.
He also says in order to integrate and maximize the benefit of the NPP to a particular practice, a careful analysis of the needs of the practice should be performed prior to hiring. This will allow both physicians and the NPP to have clear expectations. An emphasis should be placed on the importance of recognizing the level of experience will likely impact the role. For example, utilizing a new graduate in a short-stay observation unit with limited diagnoses and treatments may make sense, but utilizing an NPP as a nocturnist, cross-covering and independently admitting patients, would require an NPP with years of experience. It is crucial to hire the right NPP with the right qualifications and experience for the job.
Dr. Nelson states patient satisfaction may decline by adding NPPs to the practice. Rather than focusing on possible dilution of a patient experience with the addition of another healthcare provider, one should instead consider the potential of adding another perspective to the team. Two providers with unique educational backgrounds and insight may indeed be better than one. Utilization of NPPs can increase face time with patients, subsequently increasing patient satisfaction. Additionally, research in outpatient settings shows no difference in patient satisfaction between physicians and NPPs; more research in inpatient settings needs to be performed.
We encourage HMG directors to refer to our expanded section on SHM’s Web site, “Practice Resources,” which has a wealth of information regarding NPP utilization. The NPP committee will be hosting two courses at the annual meeting, “The Basics: Can NPs/PAs Meet Our Needs,” and “Advanced Concepts: Three Different Practice Models.”
Jina Saltzman, PA-C, University of Chicago Medical Center
Dear readers: My main goal in writing the column was to indicate that NPs and PAs could be valuable contributors to many hospitalist practices. Yet, many practices fail to create the optimal role for them, one that contributes to patient outcomes, efficiency and economic health, and provides a rewarding role for the NPP.
I do not have an anti-PA, pro-NP bias. My intention was not to take sides regarding whether PAs or NPs are more skilled or better for patients. I think that is a function of the individual, much more than their training certificate (same with MDs). I did not intend to imply “nurse practitioners providing hospitalist coverage should function independently, without any physician supervision, oversight, or input.”
Lastly, I did make a factual error regarding the differences in physician supervision required for NPs and PAs. Saltzman’s letter above addresses the error. TH
Non-Physician Providers Critical to Hospital Medicine Practices
In “Maximizing NPPs in Hospitalist Practices” (Practice Management, October 2008, p. 69), John Nelson, MD, implies a financial advantage to hiring nurse practitioners (NPs) rather than physician assistants (PAs):
“A PA’s work will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders. Nurse practitioners, on the other hand, may be able to perform certain patient-care activities independently. Medicare and other payers typically reimburse at 85% of the rate customarily paid to MDs for the same service.”
Dr. Nelson: Do you mean to imply NPs providing hospitalist coverage should function independently, without any physician supervision, oversight, or input? I do not know of any hospitals that allow NPs to admit and manage patients independently, despite their independent practice status. In my opinion, it would be detrimental to patient care to allow non-physician providers to provide completely independent, unsupervised hospital care.
In addition, I know of no hospital practice setting that requires a physician to be physically present during a PA’s exam. In all hospital practice settings that I am aware of, a supervising or attending physician (not necessarily the one on the PA’s license), must see the patient at some time each day, not necessarily at the same time as the PA.
In that scenario, the physician pays a brief visit to the patient to corroborate the PA’s exam and plan. The physician then writes a brief, seen-and-agreed note, and can bill 100% of the Medicare reimbursement, not the 85% for a NP visit. How this compares economically depends, of course, on relative salaries. But it provides physician oversight of the NPP, which assumedly will improve quality of care (though I have no studies to cite to that effect).
Do you have some other reason for your anti-PA, pro-NP bias? Is your personal experience colored by working with more competent NPs, in your opinion, and less competent PAs? Perhaps that would make for a more interesting, better-defined column.
Richard Buckberg, PA-C, Maine Medical Center, Portland, Maine
SHM’s Non-Physician Provider (NPP) Committee was delighted to see the recent article by Dr. Nelson, MD, regarding the use of NPPs in hospital medicine. These columns spotlighted HM’s increasing utilization of NPPs, a role that only is expected to increase in number and breadth, based on the increasing need for competent, comprehensive care of the acutely ill.
Dr. Nelson made many excellent points that may benefit from some clarification or expansion. Dr. Nelson states a PA “will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders.” This is incorrect, and seems to imply PAs are more difficult to assimilate into practice than NPs. Depending upon variability in legal limitations and hospital bylaws, both PAs and NPs may see a patient without a physician present. In order to bill for a shared visit and receive 100% reimbursement, the attending physician needs to have a face-to-face encounter with that patient at some point in the day and document a portion of the evaluation and management (e.g., history, physical exam, or medical decision-making).
Alternatively, in most states, both NPs and PAs can see patients independently and bill for their services at 85% of the physician’s Medicare rate. Obtaining 100% reimbursement for NPP services when using the shared billing model is efficient and simple. Though variability exists, more specifically in hospital culture, utilization of these roles can positively impact the bottom line of reimbursement. Therefore, it is essential to understand all of the regulations before developing a business model incorporating NPPs.
Dr. Nelson also points out that using NPPs in a clerical fashion, such as discharge planning, is not optimizing the NPPs capabilities. This point is well taken. If clerical assistance is needed, hire the appropriate discipline.
He also says in order to integrate and maximize the benefit of the NPP to a particular practice, a careful analysis of the needs of the practice should be performed prior to hiring. This will allow both physicians and the NPP to have clear expectations. An emphasis should be placed on the importance of recognizing the level of experience will likely impact the role. For example, utilizing a new graduate in a short-stay observation unit with limited diagnoses and treatments may make sense, but utilizing an NPP as a nocturnist, cross-covering and independently admitting patients, would require an NPP with years of experience. It is crucial to hire the right NPP with the right qualifications and experience for the job.
Dr. Nelson states patient satisfaction may decline by adding NPPs to the practice. Rather than focusing on possible dilution of a patient experience with the addition of another healthcare provider, one should instead consider the potential of adding another perspective to the team. Two providers with unique educational backgrounds and insight may indeed be better than one. Utilization of NPPs can increase face time with patients, subsequently increasing patient satisfaction. Additionally, research in outpatient settings shows no difference in patient satisfaction between physicians and NPPs; more research in inpatient settings needs to be performed.
We encourage HMG directors to refer to our expanded section on SHM’s Web site, “Practice Resources,” which has a wealth of information regarding NPP utilization. The NPP committee will be hosting two courses at the annual meeting, “The Basics: Can NPs/PAs Meet Our Needs,” and “Advanced Concepts: Three Different Practice Models.”
Jina Saltzman, PA-C, University of Chicago Medical Center
Dear readers: My main goal in writing the column was to indicate that NPs and PAs could be valuable contributors to many hospitalist practices. Yet, many practices fail to create the optimal role for them, one that contributes to patient outcomes, efficiency and economic health, and provides a rewarding role for the NPP.
I do not have an anti-PA, pro-NP bias. My intention was not to take sides regarding whether PAs or NPs are more skilled or better for patients. I think that is a function of the individual, much more than their training certificate (same with MDs). I did not intend to imply “nurse practitioners providing hospitalist coverage should function independently, without any physician supervision, oversight, or input.”
Lastly, I did make a factual error regarding the differences in physician supervision required for NPs and PAs. Saltzman’s letter above addresses the error. TH
Non-Physician Providers Critical to Hospital Medicine Practices
In “Maximizing NPPs in Hospitalist Practices” (Practice Management, October 2008, p. 69), John Nelson, MD, implies a financial advantage to hiring nurse practitioners (NPs) rather than physician assistants (PAs):
“A PA’s work will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders. Nurse practitioners, on the other hand, may be able to perform certain patient-care activities independently. Medicare and other payers typically reimburse at 85% of the rate customarily paid to MDs for the same service.”
Dr. Nelson: Do you mean to imply NPs providing hospitalist coverage should function independently, without any physician supervision, oversight, or input? I do not know of any hospitals that allow NPs to admit and manage patients independently, despite their independent practice status. In my opinion, it would be detrimental to patient care to allow non-physician providers to provide completely independent, unsupervised hospital care.
In addition, I know of no hospital practice setting that requires a physician to be physically present during a PA’s exam. In all hospital practice settings that I am aware of, a supervising or attending physician (not necessarily the one on the PA’s license), must see the patient at some time each day, not necessarily at the same time as the PA.
In that scenario, the physician pays a brief visit to the patient to corroborate the PA’s exam and plan. The physician then writes a brief, seen-and-agreed note, and can bill 100% of the Medicare reimbursement, not the 85% for a NP visit. How this compares economically depends, of course, on relative salaries. But it provides physician oversight of the NPP, which assumedly will improve quality of care (though I have no studies to cite to that effect).
Do you have some other reason for your anti-PA, pro-NP bias? Is your personal experience colored by working with more competent NPs, in your opinion, and less competent PAs? Perhaps that would make for a more interesting, better-defined column.
Richard Buckberg, PA-C, Maine Medical Center, Portland, Maine
SHM’s Non-Physician Provider (NPP) Committee was delighted to see the recent article by Dr. Nelson, MD, regarding the use of NPPs in hospital medicine. These columns spotlighted HM’s increasing utilization of NPPs, a role that only is expected to increase in number and breadth, based on the increasing need for competent, comprehensive care of the acutely ill.
Dr. Nelson made many excellent points that may benefit from some clarification or expansion. Dr. Nelson states a PA “will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders.” This is incorrect, and seems to imply PAs are more difficult to assimilate into practice than NPs. Depending upon variability in legal limitations and hospital bylaws, both PAs and NPs may see a patient without a physician present. In order to bill for a shared visit and receive 100% reimbursement, the attending physician needs to have a face-to-face encounter with that patient at some point in the day and document a portion of the evaluation and management (e.g., history, physical exam, or medical decision-making).
Alternatively, in most states, both NPs and PAs can see patients independently and bill for their services at 85% of the physician’s Medicare rate. Obtaining 100% reimbursement for NPP services when using the shared billing model is efficient and simple. Though variability exists, more specifically in hospital culture, utilization of these roles can positively impact the bottom line of reimbursement. Therefore, it is essential to understand all of the regulations before developing a business model incorporating NPPs.
Dr. Nelson also points out that using NPPs in a clerical fashion, such as discharge planning, is not optimizing the NPPs capabilities. This point is well taken. If clerical assistance is needed, hire the appropriate discipline.
He also says in order to integrate and maximize the benefit of the NPP to a particular practice, a careful analysis of the needs of the practice should be performed prior to hiring. This will allow both physicians and the NPP to have clear expectations. An emphasis should be placed on the importance of recognizing the level of experience will likely impact the role. For example, utilizing a new graduate in a short-stay observation unit with limited diagnoses and treatments may make sense, but utilizing an NPP as a nocturnist, cross-covering and independently admitting patients, would require an NPP with years of experience. It is crucial to hire the right NPP with the right qualifications and experience for the job.
Dr. Nelson states patient satisfaction may decline by adding NPPs to the practice. Rather than focusing on possible dilution of a patient experience with the addition of another healthcare provider, one should instead consider the potential of adding another perspective to the team. Two providers with unique educational backgrounds and insight may indeed be better than one. Utilization of NPPs can increase face time with patients, subsequently increasing patient satisfaction. Additionally, research in outpatient settings shows no difference in patient satisfaction between physicians and NPPs; more research in inpatient settings needs to be performed.
We encourage HMG directors to refer to our expanded section on SHM’s Web site, “Practice Resources,” which has a wealth of information regarding NPP utilization. The NPP committee will be hosting two courses at the annual meeting, “The Basics: Can NPs/PAs Meet Our Needs,” and “Advanced Concepts: Three Different Practice Models.”
Jina Saltzman, PA-C, University of Chicago Medical Center
Dear readers: My main goal in writing the column was to indicate that NPs and PAs could be valuable contributors to many hospitalist practices. Yet, many practices fail to create the optimal role for them, one that contributes to patient outcomes, efficiency and economic health, and provides a rewarding role for the NPP.
I do not have an anti-PA, pro-NP bias. My intention was not to take sides regarding whether PAs or NPs are more skilled or better for patients. I think that is a function of the individual, much more than their training certificate (same with MDs). I did not intend to imply “nurse practitioners providing hospitalist coverage should function independently, without any physician supervision, oversight, or input.”
Lastly, I did make a factual error regarding the differences in physician supervision required for NPs and PAs. Saltzman’s letter above addresses the error. TH
Staffing Strategies

One of the most difficult challenges in staffing a hospitalist practice is handling the unpredictable daily fluctuations in patient volume. It isn’t difficult to decide how many hospitalists will work each day to handle the average number of daily visits (aka encounters), but the actual number of visits on any given day is almost always significantly different than the average. I think many groups could more effectively handle day-to-day variations in workload by eliminating predetermined lengths of the shifts that the doctors work. It isn’t a perfect strategy, but it is worth some consideration by nearly any practice. Let me explain.

First, think about how the workload for a typical day might be represented. For many or most practices it often looks something like the wavy line in Figure 1. (See Figure 1, p. 52.)
Of course, the line representing a day’s work will be different every day, but I’ve tried to draw it in a way that represents a typical day.
In Figure 2 (see p. 52), I’ve added horizontal bars to represent a common way that groups might schedule four daytime doctors who each work 7 a.m. to 7 p.m., and one night doctor working 7 p.m. to 7 a.m. The four horizontal bars represent the four day doctors, and the one horizontal bar at the bottom right represents the one night doctor. Ideally, the manpower (horizontal bars) should match the workload (wavy line) every hour of the day.
This graph shows that—at least for this particular day—there are many hours in the afternoon when there is excess manpower. The doctors may be sitting around waiting for their shift to end or waiting to see if it will suddenly get busy again. We all know that happens unpredictably. And from about 7 p.m. to about 11:30 p.m., the single night doctor has more work than he/she can reasonably handle.
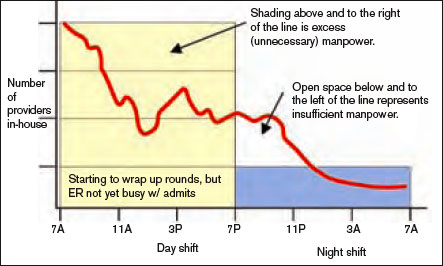
In fact, there probably isn’t ever a day when the work that needs to be done is just the right amount for all four doctors from 7 a.m. to 7 p.m. with a sudden drop at 7 p.m. that is just right for one doctor for the next 12 hours. Because the doctors have scheduled themselves to work 12-hour shifts, they know in advance that their manpower will quite regularly fail to match the workload for that day.
Groups have devised a number of strategies to try to get manpower to more closely match the unpredictable workload for a given day. These include having a member of the group available on standby (often called “jeopardy”) for that day; this physician comes in only if it is unusually busy. Some groups have a patient volume cap to prevent the practice from becoming too busy. I think a cap is a poor strategy that should be used only as a last resort, and I will discuss this in detail in a future column. Other groups have a swing shift from late in the afternoon until around 11 p.m. or so to help with evening admits and cross cover. And an often overlooked but potentially valuable strategy is to eliminate clearly specified start and stop times for the shifts that the doctors work. For an idea of what that might look like, see Figure 3 (p. 52).
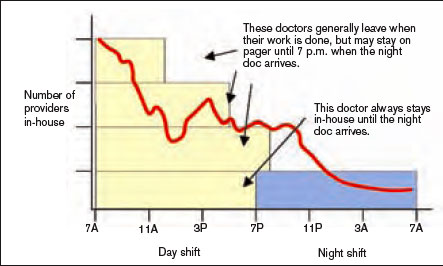
Notice that the right-hand side of each yellow bar in Figures 2 and 3 is indistinct. That is meant to show that the precise time that the doctor leaves varies, depending on the day’s workload. That way the manpower can be adjusted from one day to the next to more closely match the workload than if the doctors work fixed shifts of a specified duration. On some days, all of the doctors may stay 12 hours or more, but on many days at least some of the doctors will end up leaving in less than 12 hours. If all day doctors work a 12-hour shift, they have provided 48 hours—four doctors at 12 hours each—of physician manpower, but if there is some flexibility about when the doctors leave, the same four day doctors could provide between about 34 and 52 hours of manpower, depending on the day’s workload.
If your practice is contracted to keep a doctor in the hospital around the clock, you will probably need the night doctor and at least one day doctor to stay around—even if it is a slow day. But the other doctors might be able to leave when their work is done. And it is also reasonable for some groups to eliminate precise times that the doctors start working in the morning each day, though they might be required to be available by pager by a specified time in the morning.
One common concern about such a system is how to handle issues that arise with the patients cared for by a doctor who has left. I think it is best for the doctor to stay available by pager and handle simple issues by phone. For more complicated issues (e.g., a patient who needs attention at the bedside) the doctor could either come back to the hospital or phone another member of the practice (e.g., the doctor required to stay at least 12 hours that day) and see if he or she can handle the emergency.
All of the specifics of a system that allows doctors to leave when their work is done rather than according to shifts of a predetermined number of hours would be too long for this column. But they aren’t complicated, and given the variability that exists in the number of daily patient visits to any hospitalist practice, the application of this kind of approach is well worth considering. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
One of the most difficult challenges in staffing a hospitalist practice is handling the unpredictable daily fluctuations in patient volume. It isn’t difficult to decide how many hospitalists will work each day to handle the average number of daily visits (aka encounters), but the actual number of visits on any given day is almost always significantly different than the average. I think many groups could more effectively handle day-to-day variations in workload by eliminating predetermined lengths of the shifts that the doctors work. It isn’t a perfect strategy, but it is worth some consideration by nearly any practice. Let me explain.
First, think about how the workload for a typical day might be represented. For many or most practices it often looks something like the wavy line in Figure 1. (See Figure 1, p. 52.)
Of course, the line representing a day’s work will be different every day, but I’ve tried to draw it in a way that represents a typical day.
In Figure 2 (see p. 52), I’ve added horizontal bars to represent a common way that groups might schedule four daytime doctors who each work 7 a.m. to 7 p.m., and one night doctor working 7 p.m. to 7 a.m. The four horizontal bars represent the four day doctors, and the one horizontal bar at the bottom right represents the one night doctor. Ideally, the manpower (horizontal bars) should match the workload (wavy line) every hour of the day.
This graph shows that—at least for this particular day—there are many hours in the afternoon when there is excess manpower. The doctors may be sitting around waiting for their shift to end or waiting to see if it will suddenly get busy again. We all know that happens unpredictably. And from about 7 p.m. to about 11:30 p.m., the single night doctor has more work than he/she can reasonably handle.
In fact, there probably isn’t ever a day when the work that needs to be done is just the right amount for all four doctors from 7 a.m. to 7 p.m. with a sudden drop at 7 p.m. that is just right for one doctor for the next 12 hours. Because the doctors have scheduled themselves to work 12-hour shifts, they know in advance that their manpower will quite regularly fail to match the workload for that day.
Groups have devised a number of strategies to try to get manpower to more closely match the unpredictable workload for a given day. These include having a member of the group available on standby (often called “jeopardy”) for that day; this physician comes in only if it is unusually busy. Some groups have a patient volume cap to prevent the practice from becoming too busy. I think a cap is a poor strategy that should be used only as a last resort, and I will discuss this in detail in a future column. Other groups have a swing shift from late in the afternoon until around 11 p.m. or so to help with evening admits and cross cover. And an often overlooked but potentially valuable strategy is to eliminate clearly specified start and stop times for the shifts that the doctors work. For an idea of what that might look like, see Figure 3 (p. 52).
Notice that the right-hand side of each yellow bar in Figures 2 and 3 is indistinct. That is meant to show that the precise time that the doctor leaves varies, depending on the day’s workload. That way the manpower can be adjusted from one day to the next to more closely match the workload than if the doctors work fixed shifts of a specified duration. On some days, all of the doctors may stay 12 hours or more, but on many days at least some of the doctors will end up leaving in less than 12 hours. If all day doctors work a 12-hour shift, they have provided 48 hours—four doctors at 12 hours each—of physician manpower, but if there is some flexibility about when the doctors leave, the same four day doctors could provide between about 34 and 52 hours of manpower, depending on the day’s workload.
If your practice is contracted to keep a doctor in the hospital around the clock, you will probably need the night doctor and at least one day doctor to stay around—even if it is a slow day. But the other doctors might be able to leave when their work is done. And it is also reasonable for some groups to eliminate precise times that the doctors start working in the morning each day, though they might be required to be available by pager by a specified time in the morning.
One common concern about such a system is how to handle issues that arise with the patients cared for by a doctor who has left. I think it is best for the doctor to stay available by pager and handle simple issues by phone. For more complicated issues (e.g., a patient who needs attention at the bedside) the doctor could either come back to the hospital or phone another member of the practice (e.g., the doctor required to stay at least 12 hours that day) and see if he or she can handle the emergency.
All of the specifics of a system that allows doctors to leave when their work is done rather than according to shifts of a predetermined number of hours would be too long for this column. But they aren’t complicated, and given the variability that exists in the number of daily patient visits to any hospitalist practice, the application of this kind of approach is well worth considering. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
One of the most difficult challenges in staffing a hospitalist practice is handling the unpredictable daily fluctuations in patient volume. It isn’t difficult to decide how many hospitalists will work each day to handle the average number of daily visits (aka encounters), but the actual number of visits on any given day is almost always significantly different than the average. I think many groups could more effectively handle day-to-day variations in workload by eliminating predetermined lengths of the shifts that the doctors work. It isn’t a perfect strategy, but it is worth some consideration by nearly any practice. Let me explain.
First, think about how the workload for a typical day might be represented. For many or most practices it often looks something like the wavy line in Figure 1. (See Figure 1, p. 52.)
Of course, the line representing a day’s work will be different every day, but I’ve tried to draw it in a way that represents a typical day.
In Figure 2 (see p. 52), I’ve added horizontal bars to represent a common way that groups might schedule four daytime doctors who each work 7 a.m. to 7 p.m., and one night doctor working 7 p.m. to 7 a.m. The four horizontal bars represent the four day doctors, and the one horizontal bar at the bottom right represents the one night doctor. Ideally, the manpower (horizontal bars) should match the workload (wavy line) every hour of the day.
This graph shows that—at least for this particular day—there are many hours in the afternoon when there is excess manpower. The doctors may be sitting around waiting for their shift to end or waiting to see if it will suddenly get busy again. We all know that happens unpredictably. And from about 7 p.m. to about 11:30 p.m., the single night doctor has more work than he/she can reasonably handle.
In fact, there probably isn’t ever a day when the work that needs to be done is just the right amount for all four doctors from 7 a.m. to 7 p.m. with a sudden drop at 7 p.m. that is just right for one doctor for the next 12 hours. Because the doctors have scheduled themselves to work 12-hour shifts, they know in advance that their manpower will quite regularly fail to match the workload for that day.
Groups have devised a number of strategies to try to get manpower to more closely match the unpredictable workload for a given day. These include having a member of the group available on standby (often called “jeopardy”) for that day; this physician comes in only if it is unusually busy. Some groups have a patient volume cap to prevent the practice from becoming too busy. I think a cap is a poor strategy that should be used only as a last resort, and I will discuss this in detail in a future column. Other groups have a swing shift from late in the afternoon until around 11 p.m. or so to help with evening admits and cross cover. And an often overlooked but potentially valuable strategy is to eliminate clearly specified start and stop times for the shifts that the doctors work. For an idea of what that might look like, see Figure 3 (p. 52).
Notice that the right-hand side of each yellow bar in Figures 2 and 3 is indistinct. That is meant to show that the precise time that the doctor leaves varies, depending on the day’s workload. That way the manpower can be adjusted from one day to the next to more closely match the workload than if the doctors work fixed shifts of a specified duration. On some days, all of the doctors may stay 12 hours or more, but on many days at least some of the doctors will end up leaving in less than 12 hours. If all day doctors work a 12-hour shift, they have provided 48 hours—four doctors at 12 hours each—of physician manpower, but if there is some flexibility about when the doctors leave, the same four day doctors could provide between about 34 and 52 hours of manpower, depending on the day’s workload.
If your practice is contracted to keep a doctor in the hospital around the clock, you will probably need the night doctor and at least one day doctor to stay around—even if it is a slow day. But the other doctors might be able to leave when their work is done. And it is also reasonable for some groups to eliminate precise times that the doctors start working in the morning each day, though they might be required to be available by pager by a specified time in the morning.
One common concern about such a system is how to handle issues that arise with the patients cared for by a doctor who has left. I think it is best for the doctor to stay available by pager and handle simple issues by phone. For more complicated issues (e.g., a patient who needs attention at the bedside) the doctor could either come back to the hospital or phone another member of the practice (e.g., the doctor required to stay at least 12 hours that day) and see if he or she can handle the emergency.
All of the specifics of a system that allows doctors to leave when their work is done rather than according to shifts of a predetermined number of hours would be too long for this column. But they aren’t complicated, and given the variability that exists in the number of daily patient visits to any hospitalist practice, the application of this kind of approach is well worth considering. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
It’s Good to Be Country

Think a big hospital is where it’s at? Not according to Randy Ferrance, DC, MD, a hospitalist at Riverside Tappahanock Hospital, a 67-bed facility in rural Tappahannock, Va. The community is home to 2,172 residents and located about an hour east of Richmond, just up river from the Chesapeake Bay. Dr. Ferrance, a former chiropractor who has been practicing as a hospitalist at Riverside since 2002, recently spoke with The Hospitalist about why he enjoys the rural setting.
How is Riverside Tappahanock different from other hospitalist groups you’ve worked at?
Answer: The thing I like about it is I get to wear a lot of different hats. We don’t have intensivists; we manage our own ventilators and do our own critical care. And we’re also limited by the number of specialists we have, so of course, anything that is too difficult for us to do we transfer out. I don’t manage consultants, which seems like what hospitalists at a lot of big hospitals do. I’m often wondering what those hospitalists are left doing. Here we have cardiologists available to us, and as far as other specialists go, we have one gastroenterologist and a part-time nephrologist. I like the fact that I’m actually treating and not just stepping back and watching others treat. I especially like the ICU. This way I get to do critical care, and I think do it fairly well.
What are the challenges at a rural hospital?
A: A number of people just assume that, since we are just a small hospital, we can’t be giving good care. They come through the doors and they immediately want us to transfer them to a bigger hospital.
Is there a need for more rural hospitalists?
A: There have been times in the past when we’ve had trouble getting people [recruits] to look at us just because of the location, although I think we’re in a great location. We’re not far from Richmond, not far from good things to do.
Is there a solution to the recruitment problem?
A: The bottom line is we need more primary care physicians. We’re pretty selective and we’ve managed to do well despite that.
How many patients, on average, do you see?
A: We average about five admissions a day. We tend to follow about eight patients at a time. We don’t really do shifts. We take call a quarter of the time, doing admissions for a 24-hour stretch, averaging seven or eight calls in a month. Then we round on our post call days, as well, and the days in between. On average, we take every third day call, with a week off each month. We work 90 hours a week—pretty awful hours. So this is clearly a drawback. There are only four of us here, so if one of us were taken ill, we’d either have to get a [temporary doctor] or pick up the slack.
What are the other drawbacks to a rural hospital?
A: Our denominators are so small that, if we miss aspirin on arrival for one patient, it can pull us from first to the fourth in quality ratings. Everything has to be perfect. We can’t make any omissions. I think it certainly adds to perception. People in small towns talk a lot, and what people talk about are things that did not go well. They don’t talk about things that did go well.
What advice do you have for those considering a position at a rural hospital?
A: You have to be willing to work more than you would at a larger hospital, but I think you get to do more, which is more rewarding from my point of view.
What can rural hospitalists teach other hospitalists?
A: We probably can teach workload management a bit better. I think we can also talk about quality referral patterns. The things we need to do to make sure our quality numbers are good are probably a lot more stringent because our capture needs to be better. TH
Think a big hospital is where it’s at? Not according to Randy Ferrance, DC, MD, a hospitalist at Riverside Tappahanock Hospital, a 67-bed facility in rural Tappahannock, Va. The community is home to 2,172 residents and located about an hour east of Richmond, just up river from the Chesapeake Bay. Dr. Ferrance, a former chiropractor who has been practicing as a hospitalist at Riverside since 2002, recently spoke with The Hospitalist about why he enjoys the rural setting.
How is Riverside Tappahanock different from other hospitalist groups you’ve worked at?
Answer: The thing I like about it is I get to wear a lot of different hats. We don’t have intensivists; we manage our own ventilators and do our own critical care. And we’re also limited by the number of specialists we have, so of course, anything that is too difficult for us to do we transfer out. I don’t manage consultants, which seems like what hospitalists at a lot of big hospitals do. I’m often wondering what those hospitalists are left doing. Here we have cardiologists available to us, and as far as other specialists go, we have one gastroenterologist and a part-time nephrologist. I like the fact that I’m actually treating and not just stepping back and watching others treat. I especially like the ICU. This way I get to do critical care, and I think do it fairly well.
What are the challenges at a rural hospital?
A: A number of people just assume that, since we are just a small hospital, we can’t be giving good care. They come through the doors and they immediately want us to transfer them to a bigger hospital.
Is there a need for more rural hospitalists?
A: There have been times in the past when we’ve had trouble getting people [recruits] to look at us just because of the location, although I think we’re in a great location. We’re not far from Richmond, not far from good things to do.
Is there a solution to the recruitment problem?
A: The bottom line is we need more primary care physicians. We’re pretty selective and we’ve managed to do well despite that.
How many patients, on average, do you see?
A: We average about five admissions a day. We tend to follow about eight patients at a time. We don’t really do shifts. We take call a quarter of the time, doing admissions for a 24-hour stretch, averaging seven or eight calls in a month. Then we round on our post call days, as well, and the days in between. On average, we take every third day call, with a week off each month. We work 90 hours a week—pretty awful hours. So this is clearly a drawback. There are only four of us here, so if one of us were taken ill, we’d either have to get a [temporary doctor] or pick up the slack.
What are the other drawbacks to a rural hospital?
A: Our denominators are so small that, if we miss aspirin on arrival for one patient, it can pull us from first to the fourth in quality ratings. Everything has to be perfect. We can’t make any omissions. I think it certainly adds to perception. People in small towns talk a lot, and what people talk about are things that did not go well. They don’t talk about things that did go well.
What advice do you have for those considering a position at a rural hospital?
A: You have to be willing to work more than you would at a larger hospital, but I think you get to do more, which is more rewarding from my point of view.
What can rural hospitalists teach other hospitalists?
A: We probably can teach workload management a bit better. I think we can also talk about quality referral patterns. The things we need to do to make sure our quality numbers are good are probably a lot more stringent because our capture needs to be better. TH
Think a big hospital is where it’s at? Not according to Randy Ferrance, DC, MD, a hospitalist at Riverside Tappahanock Hospital, a 67-bed facility in rural Tappahannock, Va. The community is home to 2,172 residents and located about an hour east of Richmond, just up river from the Chesapeake Bay. Dr. Ferrance, a former chiropractor who has been practicing as a hospitalist at Riverside since 2002, recently spoke with The Hospitalist about why he enjoys the rural setting.
How is Riverside Tappahanock different from other hospitalist groups you’ve worked at?
Answer: The thing I like about it is I get to wear a lot of different hats. We don’t have intensivists; we manage our own ventilators and do our own critical care. And we’re also limited by the number of specialists we have, so of course, anything that is too difficult for us to do we transfer out. I don’t manage consultants, which seems like what hospitalists at a lot of big hospitals do. I’m often wondering what those hospitalists are left doing. Here we have cardiologists available to us, and as far as other specialists go, we have one gastroenterologist and a part-time nephrologist. I like the fact that I’m actually treating and not just stepping back and watching others treat. I especially like the ICU. This way I get to do critical care, and I think do it fairly well.
What are the challenges at a rural hospital?
A: A number of people just assume that, since we are just a small hospital, we can’t be giving good care. They come through the doors and they immediately want us to transfer them to a bigger hospital.
Is there a need for more rural hospitalists?
A: There have been times in the past when we’ve had trouble getting people [recruits] to look at us just because of the location, although I think we’re in a great location. We’re not far from Richmond, not far from good things to do.
Is there a solution to the recruitment problem?
A: The bottom line is we need more primary care physicians. We’re pretty selective and we’ve managed to do well despite that.
How many patients, on average, do you see?
A: We average about five admissions a day. We tend to follow about eight patients at a time. We don’t really do shifts. We take call a quarter of the time, doing admissions for a 24-hour stretch, averaging seven or eight calls in a month. Then we round on our post call days, as well, and the days in between. On average, we take every third day call, with a week off each month. We work 90 hours a week—pretty awful hours. So this is clearly a drawback. There are only four of us here, so if one of us were taken ill, we’d either have to get a [temporary doctor] or pick up the slack.
What are the other drawbacks to a rural hospital?
A: Our denominators are so small that, if we miss aspirin on arrival for one patient, it can pull us from first to the fourth in quality ratings. Everything has to be perfect. We can’t make any omissions. I think it certainly adds to perception. People in small towns talk a lot, and what people talk about are things that did not go well. They don’t talk about things that did go well.
What advice do you have for those considering a position at a rural hospital?
A: You have to be willing to work more than you would at a larger hospital, but I think you get to do more, which is more rewarding from my point of view.
What can rural hospitalists teach other hospitalists?
A: We probably can teach workload management a bit better. I think we can also talk about quality referral patterns. The things we need to do to make sure our quality numbers are good are probably a lot more stringent because our capture needs to be better. TH
When should a hospitalized patient be transfused?
Case
A 65-year-old male nursing home resident is sent to the emergency room with a productive cough, fever, and low blood pressure, and is diagnosed with community-acquired pneumonia. He has a history of tobacco abuse, hypertension, and a right middle cerebral artery stroke. His admission labs show a hemoglobin level of 9.0 g/dL. The day after admission his hypotension has resolved and he reports feeling much better after two liters of intravenous fluids and antibiotics. However, his hemoglobin level is 7.9 g/dL. There is no evidence of bleeding. Should this hospitalized patient be transfused?
Overview
When to give a red blood cell transfusion is a clinical question commonly encountered by hospitalists. Individuals with acute blood loss, chronic blood loss, anemia of chronic disease, and hemolytic anemia often are given transfusions. Hospitalists serving as consultants may be asked when to transfuse patients perioperatively.
It is estimated up to 25% of the red blood cells transfused in the U.S. are inappropriate.1-4 Many physicians transfuse based on a number, rather than on objective findings. Overuse is common because of the wide availability of red blood cells, the belief complications are infrequent, and an unfounded fear of adverse outcomes if a patient is not transfused.
Tachycardia, low blood pressure, and declining oxygen saturations are signs clinicians can use when making the decision to transfuse. Electrocardiographic changes associated with tissue hypoxia can occur at a hemoglobin level <5 g/dL in healthy adults. Studies show mortality and morbidity increase rapidly at levels <5.0 to 6.0 g/dL.5 Currently, no diagnostic serological test exists for tissue hypoxia, which is the physiologic reason to give red blood cells.
Red blood cell transfusion can be a life-saving therapy; however, it is not a benign intervention. It is estimated 10% of transfusion reactions will have some adverse event.6 Red blood cell use exposes patients to hemolytic transfusion reactions, infections, and transfusion related acute lung injury.7,8 Additionally, unnecessary economic expenses are incurred and a scarce resource is diverted from other patients.
Hospitalists should be able to describe the indications for red blood cell transfusion and understand the evidence for and against its use. Physicians who appreciate the risks and benefits of red blood cell use tend to transfuse less blood that those who less informed. 9, 10
Review of the Data
General outcomes: Despite the long history of red blood cell transfusion, which dates back to 1818, when James Blundell successfully saved a woman exsanguinating from a postpartum hemorrhage, little evidence has been accumulated for its appropriate use. In the 1980s, the discovery of the human immunodeficiency virus sparked blood product safety concerns. This stimulated research and a debate over red blood cell transfusion practices, with a growing body of literature unsupportive of transfusion for an arbitrary trigger, for example the “10/30 rule,” which referred to 10 g/dL hemoglobin or hematocrit of 30%.9
Observational studies have raised concerns by linking morbidity and mortality to red blood cell use. Among 1,958 surgical patients who refused blood transfusion on religious grounds, there was an increase in mortality when hemoglobin levels were <6.0 g/dL. Hemoglobin levels higher than 7.0 g/dL showed no increased mortality.11 A recent comprehensive review included 272,596 surgical, trauma, and ICU patients in 45 observational studies. The review included studies with end points, including mortality, infections, multiorgan dysfunction syndrome, and acute respiratory distress syndrome, and concluded transfusions are associated with a higher risk of morbidity and mortality.12 (see Figure 1, p. 20)
Higher rates of infection associated with transfusions occurred in patients with post-operative trauma, acute injuries, gastrointestinal cancer undergoing surgery, coronary bypass surgery, hip surgery, burns, critical illness, and patients requiring ventilation. (see Figure 2, p. 21)12 The increased infection risk likely is due to the transient depression of the immune system induced by red blood cell transfusion. Prolonged hospital stays in postoperative colorectal surgery patients and ICU patients have been associated with transfusions.13
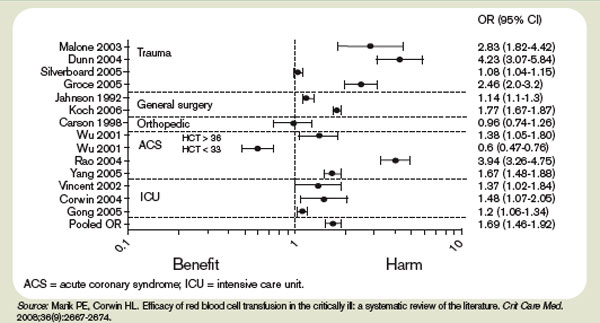
A meta-analysis of the few randomized controlled trials favors the restrictive use of red blood cells. The preponderance of the evidence comes from the Transfusion Requirements in Critical Care (TRICC) trial.14 This randomized control trial in critically ill medical and surgical patients demonstrated a restrictive strategy (transfusion trigger of <7.0 g/dL) and was as effective as a liberal transfusion strategy (transfusion trigger <10.0 g/dL). (see Figure 3, p. 22) Indeed, patients in the restrictive arm of the trial, who were less ill and under age 55 had a lower mortality rate than those who were transfused liberally.15 To date, there are no hospital-based randomized control trials that evaluate outcomes of anemic non-ICU medical patients.
This evidence has created a growing consensus that a restrictive use of blood results in improved patient outcomes. In patients without cardiovascular disease the evidence suggests most patients tolerate a hemoglobin level of 7.0 g/dL.5
Cardiac Patients
Experimental and clinical evidence suggests patients with cardiovascular disease are less tolerant of anemia. Patients with coronary disease are more likely to have adverse outcomes than those without coronary disease, if they do not have a red blood cell transfusion.11,16
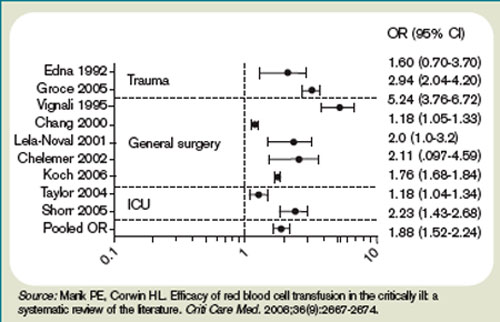
The myocardium has a higher oxygen extraction ratio compared to the tissue oxygen extraction ratio, making it more sensitive to anemia.17,18 The presence of cardiac disease may require a higher threshold to transfuse blood; however, the precise recommended threshold remains controversial. A restrictive red blood cell transfusion strategy (maintaining the hemoglobin between 7.0 g/dL and 9.0 g/dL) appeared to be safe in most critically ill patients with cardiovascular disease.14
The data is more conflicting for patients with an acute coronary syndrome (ACS). Some studies have found increased mortality and another concluded ACS decreased with red blood cell use.19-21 Further research is needed to determine when red blood cells should be given to patients with coronary disease.
Gastrointestinal Bleeding
The decision to transfuse for gastrointestinal (GI) bleeding takes into account the site and etiology of the bleeding, availability of treatments, and risk of continued bleeding. Once the blood loss is controlled, a decision must be made on how to treat the anemia. Currently, no studies have looked at outcomes for patients who did and did not receive blood for an acute or chronic GI bleed.
Additionally, no studies have been conducted to delineate when to transfuse patients with chronic GI blood loss. Studies of patients with an acute GI bleed and cardiovascular disease have shown an increase in mortality, but it is unknown if the use of specific transfusion triggers affects outcomes in this group.

In patients with GI bleeding, experts feel the use of red blood cells should be guided by available evidence. For patients without cardiac disease, red blood cell transfusion is rarely required following definitive treatment and cessation of blood loss unless the hemoglobin is <7.0 g/dL.22
Back to the Case
The patient described in our case should not be transfused unless he has clinical signs or symptoms of tissue hypoxemia. An appropriate workup for his anemia should be initiated and, if an etiology identified, definitive treatment or intervention applied.
Bottom Line
Unless there are clinical signs of tissue hypoxia, symptomatic anemia, or a hemoglobin of <7.0 g/dL, red blood cell transfusion is not recommended, unless the patient has active ACS or significant underlying coronary disease. TH
Dr. Dressler is associate program director, assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta. Dr. VanderEnde is assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta.
References
1. Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116(5):393-402.
2. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115.
3. Saxena S, Weiner JM, Rabinowitz A, Fridey J, Shulman IA, Carmel R. Transfusion practice in medical patients. Arch Int Med. 1993;153(22):2575-80.
4. Palermo G, Bove J, Katz AJ. Patterns of blood use in Connecticut. Transfusion. 1980;20(6):704-710.
5. Carson JL, Reynolds RC. In search of the transfusion threshold. Hematology. 2005;10(Suppl 1):86-88.
6. Walker RH. Special report: transfusion risks. Am J Clin Pathol. 1987;88(3):374-378.
7. Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355(13):1303-1305.
8. Spiess BD. Risks of transfusion: outcome focus. Transfusion. 2004;44(Suppl 12):4S-14S.
9. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision-making. JAMA. 1990;264(4):476-483.
10. Wilson K, MacDougall L, Fergusson D, Graham I, Tinmouth A, Hebert PC. The effectiveness of interventions to reduce physician’s levels of inappropriate transfusion: what can be learned from a systematic review of the literature. Transfusion. 2002;42(9):1224-1229.
11. Carson JL, Duff A, Poses RM, et al. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055-1060.
12. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667-2674.
13. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, and immunomodulation in the critically ill. Chest. 2005;127(1):295-307.
14. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion requirements in critical care investigators, Canadian critical care trials group. N Engl J Med. 1999;340(6):409-417.
15. Carson JL, Hill S, Carless P, Hebert P, Henry D. Transfusion triggers: a systematic review of the literature. Transfus Med Rev. 2002;16(3):187-199.
16. Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111(16):2042-2049.
17. Jan KM, Chien S. Effect of hematocrit variations on coronary hemodynamics and oxygen utilization. Am J Physiol. 1977;233(1):H106-H113.
18. Wilderson DK RASL, Gould SA, Sehgal HL, Moss GS. Limits of cardiac compensation in anemic baboons. Surgery. 1988;103(6):665-670.
19. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004; 292(13):1555-1562.
20. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345(17):1230-1236.
21. Hebert PC, Fergusson DA. Do transfusions get to the heart of the matter? JAMA. 2004;292(13):1610-1612.
22. Hearnshaw S, Travis S, Murphy M. The role of blood transfusion in the management of upper and lower intestinal tract bleeding. Best Pract Res Clin Gastroenterology. 2008;22(2):355-371.
Case
A 65-year-old male nursing home resident is sent to the emergency room with a productive cough, fever, and low blood pressure, and is diagnosed with community-acquired pneumonia. He has a history of tobacco abuse, hypertension, and a right middle cerebral artery stroke. His admission labs show a hemoglobin level of 9.0 g/dL. The day after admission his hypotension has resolved and he reports feeling much better after two liters of intravenous fluids and antibiotics. However, his hemoglobin level is 7.9 g/dL. There is no evidence of bleeding. Should this hospitalized patient be transfused?
Overview
When to give a red blood cell transfusion is a clinical question commonly encountered by hospitalists. Individuals with acute blood loss, chronic blood loss, anemia of chronic disease, and hemolytic anemia often are given transfusions. Hospitalists serving as consultants may be asked when to transfuse patients perioperatively.
It is estimated up to 25% of the red blood cells transfused in the U.S. are inappropriate.1-4 Many physicians transfuse based on a number, rather than on objective findings. Overuse is common because of the wide availability of red blood cells, the belief complications are infrequent, and an unfounded fear of adverse outcomes if a patient is not transfused.
Tachycardia, low blood pressure, and declining oxygen saturations are signs clinicians can use when making the decision to transfuse. Electrocardiographic changes associated with tissue hypoxia can occur at a hemoglobin level <5 g/dL in healthy adults. Studies show mortality and morbidity increase rapidly at levels <5.0 to 6.0 g/dL.5 Currently, no diagnostic serological test exists for tissue hypoxia, which is the physiologic reason to give red blood cells.
Red blood cell transfusion can be a life-saving therapy; however, it is not a benign intervention. It is estimated 10% of transfusion reactions will have some adverse event.6 Red blood cell use exposes patients to hemolytic transfusion reactions, infections, and transfusion related acute lung injury.7,8 Additionally, unnecessary economic expenses are incurred and a scarce resource is diverted from other patients.
Hospitalists should be able to describe the indications for red blood cell transfusion and understand the evidence for and against its use. Physicians who appreciate the risks and benefits of red blood cell use tend to transfuse less blood that those who less informed. 9, 10
Review of the Data
General outcomes: Despite the long history of red blood cell transfusion, which dates back to 1818, when James Blundell successfully saved a woman exsanguinating from a postpartum hemorrhage, little evidence has been accumulated for its appropriate use. In the 1980s, the discovery of the human immunodeficiency virus sparked blood product safety concerns. This stimulated research and a debate over red blood cell transfusion practices, with a growing body of literature unsupportive of transfusion for an arbitrary trigger, for example the “10/30 rule,” which referred to 10 g/dL hemoglobin or hematocrit of 30%.9
Observational studies have raised concerns by linking morbidity and mortality to red blood cell use. Among 1,958 surgical patients who refused blood transfusion on religious grounds, there was an increase in mortality when hemoglobin levels were <6.0 g/dL. Hemoglobin levels higher than 7.0 g/dL showed no increased mortality.11 A recent comprehensive review included 272,596 surgical, trauma, and ICU patients in 45 observational studies. The review included studies with end points, including mortality, infections, multiorgan dysfunction syndrome, and acute respiratory distress syndrome, and concluded transfusions are associated with a higher risk of morbidity and mortality.12 (see Figure 1, p. 20)
Higher rates of infection associated with transfusions occurred in patients with post-operative trauma, acute injuries, gastrointestinal cancer undergoing surgery, coronary bypass surgery, hip surgery, burns, critical illness, and patients requiring ventilation. (see Figure 2, p. 21)12 The increased infection risk likely is due to the transient depression of the immune system induced by red blood cell transfusion. Prolonged hospital stays in postoperative colorectal surgery patients and ICU patients have been associated with transfusions.13
A meta-analysis of the few randomized controlled trials favors the restrictive use of red blood cells. The preponderance of the evidence comes from the Transfusion Requirements in Critical Care (TRICC) trial.14 This randomized control trial in critically ill medical and surgical patients demonstrated a restrictive strategy (transfusion trigger of <7.0 g/dL) and was as effective as a liberal transfusion strategy (transfusion trigger <10.0 g/dL). (see Figure 3, p. 22) Indeed, patients in the restrictive arm of the trial, who were less ill and under age 55 had a lower mortality rate than those who were transfused liberally.15 To date, there are no hospital-based randomized control trials that evaluate outcomes of anemic non-ICU medical patients.
This evidence has created a growing consensus that a restrictive use of blood results in improved patient outcomes. In patients without cardiovascular disease the evidence suggests most patients tolerate a hemoglobin level of 7.0 g/dL.5
Cardiac Patients
Experimental and clinical evidence suggests patients with cardiovascular disease are less tolerant of anemia. Patients with coronary disease are more likely to have adverse outcomes than those without coronary disease, if they do not have a red blood cell transfusion.11,16
The myocardium has a higher oxygen extraction ratio compared to the tissue oxygen extraction ratio, making it more sensitive to anemia.17,18 The presence of cardiac disease may require a higher threshold to transfuse blood; however, the precise recommended threshold remains controversial. A restrictive red blood cell transfusion strategy (maintaining the hemoglobin between 7.0 g/dL and 9.0 g/dL) appeared to be safe in most critically ill patients with cardiovascular disease.14
The data is more conflicting for patients with an acute coronary syndrome (ACS). Some studies have found increased mortality and another concluded ACS decreased with red blood cell use.19-21 Further research is needed to determine when red blood cells should be given to patients with coronary disease.
Gastrointestinal Bleeding
The decision to transfuse for gastrointestinal (GI) bleeding takes into account the site and etiology of the bleeding, availability of treatments, and risk of continued bleeding. Once the blood loss is controlled, a decision must be made on how to treat the anemia. Currently, no studies have looked at outcomes for patients who did and did not receive blood for an acute or chronic GI bleed.
Additionally, no studies have been conducted to delineate when to transfuse patients with chronic GI blood loss. Studies of patients with an acute GI bleed and cardiovascular disease have shown an increase in mortality, but it is unknown if the use of specific transfusion triggers affects outcomes in this group.
In patients with GI bleeding, experts feel the use of red blood cells should be guided by available evidence. For patients without cardiac disease, red blood cell transfusion is rarely required following definitive treatment and cessation of blood loss unless the hemoglobin is <7.0 g/dL.22
Back to the Case
The patient described in our case should not be transfused unless he has clinical signs or symptoms of tissue hypoxemia. An appropriate workup for his anemia should be initiated and, if an etiology identified, definitive treatment or intervention applied.
Bottom Line
Unless there are clinical signs of tissue hypoxia, symptomatic anemia, or a hemoglobin of <7.0 g/dL, red blood cell transfusion is not recommended, unless the patient has active ACS or significant underlying coronary disease. TH
Dr. Dressler is associate program director, assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta. Dr. VanderEnde is assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta.
References
1. Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116(5):393-402.
2. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115.
3. Saxena S, Weiner JM, Rabinowitz A, Fridey J, Shulman IA, Carmel R. Transfusion practice in medical patients. Arch Int Med. 1993;153(22):2575-80.
4. Palermo G, Bove J, Katz AJ. Patterns of blood use in Connecticut. Transfusion. 1980;20(6):704-710.
5. Carson JL, Reynolds RC. In search of the transfusion threshold. Hematology. 2005;10(Suppl 1):86-88.
6. Walker RH. Special report: transfusion risks. Am J Clin Pathol. 1987;88(3):374-378.
7. Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355(13):1303-1305.
8. Spiess BD. Risks of transfusion: outcome focus. Transfusion. 2004;44(Suppl 12):4S-14S.
9. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision-making. JAMA. 1990;264(4):476-483.
10. Wilson K, MacDougall L, Fergusson D, Graham I, Tinmouth A, Hebert PC. The effectiveness of interventions to reduce physician’s levels of inappropriate transfusion: what can be learned from a systematic review of the literature. Transfusion. 2002;42(9):1224-1229.
11. Carson JL, Duff A, Poses RM, et al. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055-1060.
12. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667-2674.
13. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, and immunomodulation in the critically ill. Chest. 2005;127(1):295-307.
14. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion requirements in critical care investigators, Canadian critical care trials group. N Engl J Med. 1999;340(6):409-417.
15. Carson JL, Hill S, Carless P, Hebert P, Henry D. Transfusion triggers: a systematic review of the literature. Transfus Med Rev. 2002;16(3):187-199.
16. Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111(16):2042-2049.
17. Jan KM, Chien S. Effect of hematocrit variations on coronary hemodynamics and oxygen utilization. Am J Physiol. 1977;233(1):H106-H113.
18. Wilderson DK RASL, Gould SA, Sehgal HL, Moss GS. Limits of cardiac compensation in anemic baboons. Surgery. 1988;103(6):665-670.
19. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004; 292(13):1555-1562.
20. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345(17):1230-1236.
21. Hebert PC, Fergusson DA. Do transfusions get to the heart of the matter? JAMA. 2004;292(13):1610-1612.
22. Hearnshaw S, Travis S, Murphy M. The role of blood transfusion in the management of upper and lower intestinal tract bleeding. Best Pract Res Clin Gastroenterology. 2008;22(2):355-371.
Case
A 65-year-old male nursing home resident is sent to the emergency room with a productive cough, fever, and low blood pressure, and is diagnosed with community-acquired pneumonia. He has a history of tobacco abuse, hypertension, and a right middle cerebral artery stroke. His admission labs show a hemoglobin level of 9.0 g/dL. The day after admission his hypotension has resolved and he reports feeling much better after two liters of intravenous fluids and antibiotics. However, his hemoglobin level is 7.9 g/dL. There is no evidence of bleeding. Should this hospitalized patient be transfused?
Overview
When to give a red blood cell transfusion is a clinical question commonly encountered by hospitalists. Individuals with acute blood loss, chronic blood loss, anemia of chronic disease, and hemolytic anemia often are given transfusions. Hospitalists serving as consultants may be asked when to transfuse patients perioperatively.
It is estimated up to 25% of the red blood cells transfused in the U.S. are inappropriate.1-4 Many physicians transfuse based on a number, rather than on objective findings. Overuse is common because of the wide availability of red blood cells, the belief complications are infrequent, and an unfounded fear of adverse outcomes if a patient is not transfused.
Tachycardia, low blood pressure, and declining oxygen saturations are signs clinicians can use when making the decision to transfuse. Electrocardiographic changes associated with tissue hypoxia can occur at a hemoglobin level <5 g/dL in healthy adults. Studies show mortality and morbidity increase rapidly at levels <5.0 to 6.0 g/dL.5 Currently, no diagnostic serological test exists for tissue hypoxia, which is the physiologic reason to give red blood cells.
Red blood cell transfusion can be a life-saving therapy; however, it is not a benign intervention. It is estimated 10% of transfusion reactions will have some adverse event.6 Red blood cell use exposes patients to hemolytic transfusion reactions, infections, and transfusion related acute lung injury.7,8 Additionally, unnecessary economic expenses are incurred and a scarce resource is diverted from other patients.
Hospitalists should be able to describe the indications for red blood cell transfusion and understand the evidence for and against its use. Physicians who appreciate the risks and benefits of red blood cell use tend to transfuse less blood that those who less informed. 9, 10
Review of the Data
General outcomes: Despite the long history of red blood cell transfusion, which dates back to 1818, when James Blundell successfully saved a woman exsanguinating from a postpartum hemorrhage, little evidence has been accumulated for its appropriate use. In the 1980s, the discovery of the human immunodeficiency virus sparked blood product safety concerns. This stimulated research and a debate over red blood cell transfusion practices, with a growing body of literature unsupportive of transfusion for an arbitrary trigger, for example the “10/30 rule,” which referred to 10 g/dL hemoglobin or hematocrit of 30%.9
Observational studies have raised concerns by linking morbidity and mortality to red blood cell use. Among 1,958 surgical patients who refused blood transfusion on religious grounds, there was an increase in mortality when hemoglobin levels were <6.0 g/dL. Hemoglobin levels higher than 7.0 g/dL showed no increased mortality.11 A recent comprehensive review included 272,596 surgical, trauma, and ICU patients in 45 observational studies. The review included studies with end points, including mortality, infections, multiorgan dysfunction syndrome, and acute respiratory distress syndrome, and concluded transfusions are associated with a higher risk of morbidity and mortality.12 (see Figure 1, p. 20)
Higher rates of infection associated with transfusions occurred in patients with post-operative trauma, acute injuries, gastrointestinal cancer undergoing surgery, coronary bypass surgery, hip surgery, burns, critical illness, and patients requiring ventilation. (see Figure 2, p. 21)12 The increased infection risk likely is due to the transient depression of the immune system induced by red blood cell transfusion. Prolonged hospital stays in postoperative colorectal surgery patients and ICU patients have been associated with transfusions.13
A meta-analysis of the few randomized controlled trials favors the restrictive use of red blood cells. The preponderance of the evidence comes from the Transfusion Requirements in Critical Care (TRICC) trial.14 This randomized control trial in critically ill medical and surgical patients demonstrated a restrictive strategy (transfusion trigger of <7.0 g/dL) and was as effective as a liberal transfusion strategy (transfusion trigger <10.0 g/dL). (see Figure 3, p. 22) Indeed, patients in the restrictive arm of the trial, who were less ill and under age 55 had a lower mortality rate than those who were transfused liberally.15 To date, there are no hospital-based randomized control trials that evaluate outcomes of anemic non-ICU medical patients.
This evidence has created a growing consensus that a restrictive use of blood results in improved patient outcomes. In patients without cardiovascular disease the evidence suggests most patients tolerate a hemoglobin level of 7.0 g/dL.5
Cardiac Patients
Experimental and clinical evidence suggests patients with cardiovascular disease are less tolerant of anemia. Patients with coronary disease are more likely to have adverse outcomes than those without coronary disease, if they do not have a red blood cell transfusion.11,16
The myocardium has a higher oxygen extraction ratio compared to the tissue oxygen extraction ratio, making it more sensitive to anemia.17,18 The presence of cardiac disease may require a higher threshold to transfuse blood; however, the precise recommended threshold remains controversial. A restrictive red blood cell transfusion strategy (maintaining the hemoglobin between 7.0 g/dL and 9.0 g/dL) appeared to be safe in most critically ill patients with cardiovascular disease.14
The data is more conflicting for patients with an acute coronary syndrome (ACS). Some studies have found increased mortality and another concluded ACS decreased with red blood cell use.19-21 Further research is needed to determine when red blood cells should be given to patients with coronary disease.
Gastrointestinal Bleeding
The decision to transfuse for gastrointestinal (GI) bleeding takes into account the site and etiology of the bleeding, availability of treatments, and risk of continued bleeding. Once the blood loss is controlled, a decision must be made on how to treat the anemia. Currently, no studies have looked at outcomes for patients who did and did not receive blood for an acute or chronic GI bleed.
Additionally, no studies have been conducted to delineate when to transfuse patients with chronic GI blood loss. Studies of patients with an acute GI bleed and cardiovascular disease have shown an increase in mortality, but it is unknown if the use of specific transfusion triggers affects outcomes in this group.
In patients with GI bleeding, experts feel the use of red blood cells should be guided by available evidence. For patients without cardiac disease, red blood cell transfusion is rarely required following definitive treatment and cessation of blood loss unless the hemoglobin is <7.0 g/dL.22
Back to the Case
The patient described in our case should not be transfused unless he has clinical signs or symptoms of tissue hypoxemia. An appropriate workup for his anemia should be initiated and, if an etiology identified, definitive treatment or intervention applied.
Bottom Line
Unless there are clinical signs of tissue hypoxia, symptomatic anemia, or a hemoglobin of <7.0 g/dL, red blood cell transfusion is not recommended, unless the patient has active ACS or significant underlying coronary disease. TH
Dr. Dressler is associate program director, assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta. Dr. VanderEnde is assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta.
References
1. Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116(5):393-402.
2. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115.
3. Saxena S, Weiner JM, Rabinowitz A, Fridey J, Shulman IA, Carmel R. Transfusion practice in medical patients. Arch Int Med. 1993;153(22):2575-80.
4. Palermo G, Bove J, Katz AJ. Patterns of blood use in Connecticut. Transfusion. 1980;20(6):704-710.
5. Carson JL, Reynolds RC. In search of the transfusion threshold. Hematology. 2005;10(Suppl 1):86-88.
6. Walker RH. Special report: transfusion risks. Am J Clin Pathol. 1987;88(3):374-378.
7. Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355(13):1303-1305.
8. Spiess BD. Risks of transfusion: outcome focus. Transfusion. 2004;44(Suppl 12):4S-14S.
9. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision-making. JAMA. 1990;264(4):476-483.
10. Wilson K, MacDougall L, Fergusson D, Graham I, Tinmouth A, Hebert PC. The effectiveness of interventions to reduce physician’s levels of inappropriate transfusion: what can be learned from a systematic review of the literature. Transfusion. 2002;42(9):1224-1229.
11. Carson JL, Duff A, Poses RM, et al. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055-1060.
12. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667-2674.
13. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, and immunomodulation in the critically ill. Chest. 2005;127(1):295-307.
14. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion requirements in critical care investigators, Canadian critical care trials group. N Engl J Med. 1999;340(6):409-417.
15. Carson JL, Hill S, Carless P, Hebert P, Henry D. Transfusion triggers: a systematic review of the literature. Transfus Med Rev. 2002;16(3):187-199.
16. Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111(16):2042-2049.
17. Jan KM, Chien S. Effect of hematocrit variations on coronary hemodynamics and oxygen utilization. Am J Physiol. 1977;233(1):H106-H113.
18. Wilderson DK RASL, Gould SA, Sehgal HL, Moss GS. Limits of cardiac compensation in anemic baboons. Surgery. 1988;103(6):665-670.
19. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004; 292(13):1555-1562.
20. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345(17):1230-1236.
21. Hebert PC, Fergusson DA. Do transfusions get to the heart of the matter? JAMA. 2004;292(13):1610-1612.
22. Hearnshaw S, Travis S, Murphy M. The role of blood transfusion in the management of upper and lower intestinal tract bleeding. Best Pract Res Clin Gastroenterology. 2008;22(2):355-371.
Face-to-Face Improvement
The American Medical Association recently released Current Procedural Terminology (CPT) 2009. New, deleted, and revised codes went into effect Jan. 1. The biggest change to hospitalist billing involves prolonged care codes (99354-99357). CPT 2009 descriptor revisions make it possible for physicians to contribute non-face-to-face time toward prolonged care services.
Inpatient Prolonged Care
Previous versions of CPT defined code 99356 as the first hour of prolonged physician [inpatient] services requiring direct (face-to-face) patient contact beyond the usual services (reportable after the initial 30 minutes); and 99357 for each additional 30 minutes of prolonged [inpatient] care beyond the first hour (reportable after the first 15 minutes of each additional segment). CPT 2009 has changed prolonged care guidelines to be more consistent with other time-based services: all unit/floor time spent by the physician is considered when reporting 99356 and 99357.1
As with most other evaluation and management services, a face-to-face encounter still must occur. In addition to the time associated with the face-to-face encounter, count the time associated with all other physician activities occurring on the unit/floor (e.g., reviewing images, obtaining information involving overnight events, discussing management options with the family) directed toward an individual patient. The cumulative time spent by the billing provider on a single calendar day is considered for billing. Time spent by someone other than the billing provider cannot be credited toward prolonged care.
As example, a physician cares for a 65-year-old male with uncontrolled diabetes, diabetic nephropathy, and congestive heart failure. Early in the day, the physician rounds, spending a total of 20 minutes reviewing the overnight course of events on the unit, re-confirming the patient history, and performing an exam with the patient. Anticipating the patient’s needs, the physician discusses post-discharge options and care with the patient and his family for 45 minutes. After the discussion, the physician spends an additional 30 minutes relaying information to the team and coordinating care. Merely reporting the highest-level subsequent hospital care service (99233), does not capture the physician’s cumulative effort. It only would account for 40 of the 95 minutes spent throughout the day. In order to capture the remaining 55 minutes, the physician reports 99356 on the same claim form as 99233.
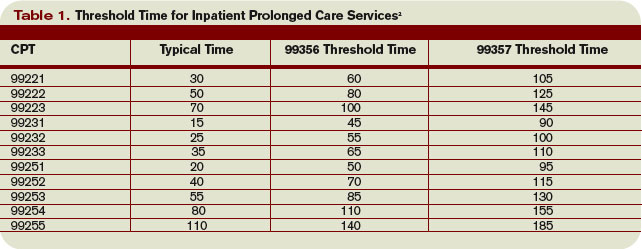
Do not report prolonged care codes on a separate claim form. Prolonged care codes do not represent an independent service. These codes are reported along with a primary service. They must appear as a separate line item on the claim form, which includes a code representing the primary service. For prolonged care in the inpatient setting, the primary service must be initial hospital care (99221-99223), subsequent hospital care (99231-99233), inpatient consultations (99251-99255), or nursing facility services (99304-99318). Additional examples of billable prolonged care services are in Section 30.6.15.1I of the Medicare manual, available at www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf.
Threshold Time
Prolonged care guidelines refer to “threshold” time. Threshold time requires the physician to exceed the time requirements associated with the “primary” codes before reporting prolonged care. Table 1 identifies the typical times associated with inpatient services qualifying for prolonged care. The physician must exceed the typical time by a minimum of 30 minutes. (For example, 99232 + 99356 = 25 minutes + 30 minutes = 55 total minutes). Additionally, the physician must document the total time spent during the face-to-face portion of the encounter, and the additional unit or floor time in one cumulative note or in separate notes representing the physician services provided to the patient throughout the day.
Prolonged Outpatient Services
Prolonged care (99354-99355) provided to outpatients remains unchanged. Physicians only report personally provided face-to-face time with the patient. Time spent by other staff members does not count toward prolonged care.
As with prolonged inpatient care, report 99354 and 99355 in addition to a primary service code. The companion outpatient codes are outpatient/office visits (99201-99205 or 99212–99215), outpatient consultation (99241–99245), domiciliary/custodial care (99324–99328 or 99334–99337), and home services (99341-99350). Hospitalists more often use outpatient prolonged care with office consultation codes for services provided in the emergency department, as appropriate.
Do not report 99354 or 99355 with observation care (99217-99220) or emergency department visits (99281-99288), since these service categories typically require prolonged periods of physician monitoring, thereby prohibiting use of prolonged care codes. As with inpatient-prolonged care, the concept of threshold time exists. Refer to Table 2 (pg. 25) for the typical threshold times associated with office consultation codes.
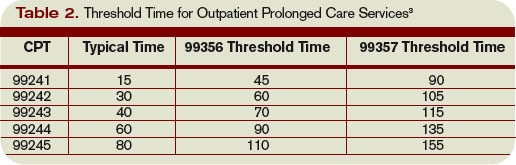
Medicare Consideration
Although CPT has offered revisions to this code, Medicare guidelines remain unchanged. The Medicare Claims Processing Manual still states: “In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.”4 It is yet to be determined if the Centers for Medicare and Medicaid Services (CMS) will issue a transmittal to revise the current description in the processing manual. Physicians and staff may access past and present transmittal information at www.cms.hhs.gov/ Transmittals/.
As always, be sure to query payers about prolonged care services, since some non-Medicare insurers may not recognize these codes.
Modifier 21
Modifier 21 has been deleted from the CPT. Modifier 21 was appended to an appropriate visit code (e.g., 99232-21) when the face-to-face or floor/unit service(s) provided is prolonged or otherwise greater than usually required for the highest level of evaluation and management service within a given category.5 Since the descriptors for codes 99354-99357 have been revised to more consistently reflect the description formerly associated with modifier 21, there is no need to maintain its existence. Additionally, Medicare and most other payers did not recognize this modifier.
Code This Case
Question: A newly diagnosed diabetic requires extensive counseling regarding lifestyle changes, medication regime, the disease process, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient (15 minutes), and performs an abbreviated service (problem-focused history and exam). The attending physician asks the resident to assist him with the remaining counseling efforts and coordination of care (30 minutes).
Each physician documents his or her portion of the service. What visit level can the hospitalist report?
Answer: When two billing providers (i.e., two attending physicians) from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service, since 99356 must be reported on the same invoice as the primary visit code (e.g., 99231).6
The example above involves the resident’s time as well as the attending physician’s time. Documentation must be very clear to demonstrate the attending physician actively participated in the entire 45-minute service. Otherwise, only the attending may report the amount of time he actually spent providing the service.
Billing options for this scenario can vary. When the physician performs and documents the key components of history, exam, and decision making for the primary encounter, report 99231 (0.76 physician work relative value units; $33.90) and 99356 (1.71 physician work relative value units; $76.46) for the cumulative service. Alternatively, in those evaluation and management services for which the [primary] code level is selected based on time alone (i.e., history and exam was not performed or required), prolonged services may only be reported with the highest code level in that family of codes as the companion code.7
Therefore, this 45-minute service may be reported as 99233 (2.0 physician work relative value units; $86.92) since more than half of the total visit time was dedicated to counseling/coordi-nation of care (see Section 30.6.1B-C available at www. cms.hhs.gov/manuals/ downloads/clm104c12.pdf for additional information on billing for counseling/coordination of care time).
If a payer does not recognize prolonged care codes, only the latter billing option is possible. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 25-26.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1G. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
3. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1F. www.cms.hhs.gov/manuals/dowloads/ clm104c12.pdf. Accessed November 19, 2008.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf. Accessed November 19, 2008.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 457.
6. Pohlig, C. Bill by time spent on case. The Hospitalist. Jul 2008;19.
7. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1H. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
The American Medical Association recently released Current Procedural Terminology (CPT) 2009. New, deleted, and revised codes went into effect Jan. 1. The biggest change to hospitalist billing involves prolonged care codes (99354-99357). CPT 2009 descriptor revisions make it possible for physicians to contribute non-face-to-face time toward prolonged care services.
Inpatient Prolonged Care
Previous versions of CPT defined code 99356 as the first hour of prolonged physician [inpatient] services requiring direct (face-to-face) patient contact beyond the usual services (reportable after the initial 30 minutes); and 99357 for each additional 30 minutes of prolonged [inpatient] care beyond the first hour (reportable after the first 15 minutes of each additional segment). CPT 2009 has changed prolonged care guidelines to be more consistent with other time-based services: all unit/floor time spent by the physician is considered when reporting 99356 and 99357.1
As with most other evaluation and management services, a face-to-face encounter still must occur. In addition to the time associated with the face-to-face encounter, count the time associated with all other physician activities occurring on the unit/floor (e.g., reviewing images, obtaining information involving overnight events, discussing management options with the family) directed toward an individual patient. The cumulative time spent by the billing provider on a single calendar day is considered for billing. Time spent by someone other than the billing provider cannot be credited toward prolonged care.
As example, a physician cares for a 65-year-old male with uncontrolled diabetes, diabetic nephropathy, and congestive heart failure. Early in the day, the physician rounds, spending a total of 20 minutes reviewing the overnight course of events on the unit, re-confirming the patient history, and performing an exam with the patient. Anticipating the patient’s needs, the physician discusses post-discharge options and care with the patient and his family for 45 minutes. After the discussion, the physician spends an additional 30 minutes relaying information to the team and coordinating care. Merely reporting the highest-level subsequent hospital care service (99233), does not capture the physician’s cumulative effort. It only would account for 40 of the 95 minutes spent throughout the day. In order to capture the remaining 55 minutes, the physician reports 99356 on the same claim form as 99233.
Do not report prolonged care codes on a separate claim form. Prolonged care codes do not represent an independent service. These codes are reported along with a primary service. They must appear as a separate line item on the claim form, which includes a code representing the primary service. For prolonged care in the inpatient setting, the primary service must be initial hospital care (99221-99223), subsequent hospital care (99231-99233), inpatient consultations (99251-99255), or nursing facility services (99304-99318). Additional examples of billable prolonged care services are in Section 30.6.15.1I of the Medicare manual, available at www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf.
Threshold Time
Prolonged care guidelines refer to “threshold” time. Threshold time requires the physician to exceed the time requirements associated with the “primary” codes before reporting prolonged care. Table 1 identifies the typical times associated with inpatient services qualifying for prolonged care. The physician must exceed the typical time by a minimum of 30 minutes. (For example, 99232 + 99356 = 25 minutes + 30 minutes = 55 total minutes). Additionally, the physician must document the total time spent during the face-to-face portion of the encounter, and the additional unit or floor time in one cumulative note or in separate notes representing the physician services provided to the patient throughout the day.
Prolonged Outpatient Services
Prolonged care (99354-99355) provided to outpatients remains unchanged. Physicians only report personally provided face-to-face time with the patient. Time spent by other staff members does not count toward prolonged care.
As with prolonged inpatient care, report 99354 and 99355 in addition to a primary service code. The companion outpatient codes are outpatient/office visits (99201-99205 or 99212–99215), outpatient consultation (99241–99245), domiciliary/custodial care (99324–99328 or 99334–99337), and home services (99341-99350). Hospitalists more often use outpatient prolonged care with office consultation codes for services provided in the emergency department, as appropriate.
Do not report 99354 or 99355 with observation care (99217-99220) or emergency department visits (99281-99288), since these service categories typically require prolonged periods of physician monitoring, thereby prohibiting use of prolonged care codes. As with inpatient-prolonged care, the concept of threshold time exists. Refer to Table 2 (pg. 25) for the typical threshold times associated with office consultation codes.
Medicare Consideration
Although CPT has offered revisions to this code, Medicare guidelines remain unchanged. The Medicare Claims Processing Manual still states: “In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.”4 It is yet to be determined if the Centers for Medicare and Medicaid Services (CMS) will issue a transmittal to revise the current description in the processing manual. Physicians and staff may access past and present transmittal information at www.cms.hhs.gov/ Transmittals/.
As always, be sure to query payers about prolonged care services, since some non-Medicare insurers may not recognize these codes.
Modifier 21
Modifier 21 has been deleted from the CPT. Modifier 21 was appended to an appropriate visit code (e.g., 99232-21) when the face-to-face or floor/unit service(s) provided is prolonged or otherwise greater than usually required for the highest level of evaluation and management service within a given category.5 Since the descriptors for codes 99354-99357 have been revised to more consistently reflect the description formerly associated with modifier 21, there is no need to maintain its existence. Additionally, Medicare and most other payers did not recognize this modifier.
Code This Case
Question: A newly diagnosed diabetic requires extensive counseling regarding lifestyle changes, medication regime, the disease process, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient (15 minutes), and performs an abbreviated service (problem-focused history and exam). The attending physician asks the resident to assist him with the remaining counseling efforts and coordination of care (30 minutes).
Each physician documents his or her portion of the service. What visit level can the hospitalist report?
Answer: When two billing providers (i.e., two attending physicians) from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service, since 99356 must be reported on the same invoice as the primary visit code (e.g., 99231).6
The example above involves the resident’s time as well as the attending physician’s time. Documentation must be very clear to demonstrate the attending physician actively participated in the entire 45-minute service. Otherwise, only the attending may report the amount of time he actually spent providing the service.
Billing options for this scenario can vary. When the physician performs and documents the key components of history, exam, and decision making for the primary encounter, report 99231 (0.76 physician work relative value units; $33.90) and 99356 (1.71 physician work relative value units; $76.46) for the cumulative service. Alternatively, in those evaluation and management services for which the [primary] code level is selected based on time alone (i.e., history and exam was not performed or required), prolonged services may only be reported with the highest code level in that family of codes as the companion code.7
Therefore, this 45-minute service may be reported as 99233 (2.0 physician work relative value units; $86.92) since more than half of the total visit time was dedicated to counseling/coordi-nation of care (see Section 30.6.1B-C available at www. cms.hhs.gov/manuals/ downloads/clm104c12.pdf for additional information on billing for counseling/coordination of care time).
If a payer does not recognize prolonged care codes, only the latter billing option is possible. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 25-26.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1G. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
3. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1F. www.cms.hhs.gov/manuals/dowloads/ clm104c12.pdf. Accessed November 19, 2008.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf. Accessed November 19, 2008.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 457.
6. Pohlig, C. Bill by time spent on case. The Hospitalist. Jul 2008;19.
7. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1H. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
The American Medical Association recently released Current Procedural Terminology (CPT) 2009. New, deleted, and revised codes went into effect Jan. 1. The biggest change to hospitalist billing involves prolonged care codes (99354-99357). CPT 2009 descriptor revisions make it possible for physicians to contribute non-face-to-face time toward prolonged care services.
Inpatient Prolonged Care
Previous versions of CPT defined code 99356 as the first hour of prolonged physician [inpatient] services requiring direct (face-to-face) patient contact beyond the usual services (reportable after the initial 30 minutes); and 99357 for each additional 30 minutes of prolonged [inpatient] care beyond the first hour (reportable after the first 15 minutes of each additional segment). CPT 2009 has changed prolonged care guidelines to be more consistent with other time-based services: all unit/floor time spent by the physician is considered when reporting 99356 and 99357.1
As with most other evaluation and management services, a face-to-face encounter still must occur. In addition to the time associated with the face-to-face encounter, count the time associated with all other physician activities occurring on the unit/floor (e.g., reviewing images, obtaining information involving overnight events, discussing management options with the family) directed toward an individual patient. The cumulative time spent by the billing provider on a single calendar day is considered for billing. Time spent by someone other than the billing provider cannot be credited toward prolonged care.
As example, a physician cares for a 65-year-old male with uncontrolled diabetes, diabetic nephropathy, and congestive heart failure. Early in the day, the physician rounds, spending a total of 20 minutes reviewing the overnight course of events on the unit, re-confirming the patient history, and performing an exam with the patient. Anticipating the patient’s needs, the physician discusses post-discharge options and care with the patient and his family for 45 minutes. After the discussion, the physician spends an additional 30 minutes relaying information to the team and coordinating care. Merely reporting the highest-level subsequent hospital care service (99233), does not capture the physician’s cumulative effort. It only would account for 40 of the 95 minutes spent throughout the day. In order to capture the remaining 55 minutes, the physician reports 99356 on the same claim form as 99233.
Do not report prolonged care codes on a separate claim form. Prolonged care codes do not represent an independent service. These codes are reported along with a primary service. They must appear as a separate line item on the claim form, which includes a code representing the primary service. For prolonged care in the inpatient setting, the primary service must be initial hospital care (99221-99223), subsequent hospital care (99231-99233), inpatient consultations (99251-99255), or nursing facility services (99304-99318). Additional examples of billable prolonged care services are in Section 30.6.15.1I of the Medicare manual, available at www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf.
Threshold Time
Prolonged care guidelines refer to “threshold” time. Threshold time requires the physician to exceed the time requirements associated with the “primary” codes before reporting prolonged care. Table 1 identifies the typical times associated with inpatient services qualifying for prolonged care. The physician must exceed the typical time by a minimum of 30 minutes. (For example, 99232 + 99356 = 25 minutes + 30 minutes = 55 total minutes). Additionally, the physician must document the total time spent during the face-to-face portion of the encounter, and the additional unit or floor time in one cumulative note or in separate notes representing the physician services provided to the patient throughout the day.
Prolonged Outpatient Services
Prolonged care (99354-99355) provided to outpatients remains unchanged. Physicians only report personally provided face-to-face time with the patient. Time spent by other staff members does not count toward prolonged care.
As with prolonged inpatient care, report 99354 and 99355 in addition to a primary service code. The companion outpatient codes are outpatient/office visits (99201-99205 or 99212–99215), outpatient consultation (99241–99245), domiciliary/custodial care (99324–99328 or 99334–99337), and home services (99341-99350). Hospitalists more often use outpatient prolonged care with office consultation codes for services provided in the emergency department, as appropriate.
Do not report 99354 or 99355 with observation care (99217-99220) or emergency department visits (99281-99288), since these service categories typically require prolonged periods of physician monitoring, thereby prohibiting use of prolonged care codes. As with inpatient-prolonged care, the concept of threshold time exists. Refer to Table 2 (pg. 25) for the typical threshold times associated with office consultation codes.
Medicare Consideration
Although CPT has offered revisions to this code, Medicare guidelines remain unchanged. The Medicare Claims Processing Manual still states: “In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.”4 It is yet to be determined if the Centers for Medicare and Medicaid Services (CMS) will issue a transmittal to revise the current description in the processing manual. Physicians and staff may access past and present transmittal information at www.cms.hhs.gov/ Transmittals/.
As always, be sure to query payers about prolonged care services, since some non-Medicare insurers may not recognize these codes.
Modifier 21
Modifier 21 has been deleted from the CPT. Modifier 21 was appended to an appropriate visit code (e.g., 99232-21) when the face-to-face or floor/unit service(s) provided is prolonged or otherwise greater than usually required for the highest level of evaluation and management service within a given category.5 Since the descriptors for codes 99354-99357 have been revised to more consistently reflect the description formerly associated with modifier 21, there is no need to maintain its existence. Additionally, Medicare and most other payers did not recognize this modifier.
Code This Case
Question: A newly diagnosed diabetic requires extensive counseling regarding lifestyle changes, medication regime, the disease process, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient (15 minutes), and performs an abbreviated service (problem-focused history and exam). The attending physician asks the resident to assist him with the remaining counseling efforts and coordination of care (30 minutes).
Each physician documents his or her portion of the service. What visit level can the hospitalist report?
Answer: When two billing providers (i.e., two attending physicians) from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service, since 99356 must be reported on the same invoice as the primary visit code (e.g., 99231).6
The example above involves the resident’s time as well as the attending physician’s time. Documentation must be very clear to demonstrate the attending physician actively participated in the entire 45-minute service. Otherwise, only the attending may report the amount of time he actually spent providing the service.
Billing options for this scenario can vary. When the physician performs and documents the key components of history, exam, and decision making for the primary encounter, report 99231 (0.76 physician work relative value units; $33.90) and 99356 (1.71 physician work relative value units; $76.46) for the cumulative service. Alternatively, in those evaluation and management services for which the [primary] code level is selected based on time alone (i.e., history and exam was not performed or required), prolonged services may only be reported with the highest code level in that family of codes as the companion code.7
Therefore, this 45-minute service may be reported as 99233 (2.0 physician work relative value units; $86.92) since more than half of the total visit time was dedicated to counseling/coordi-nation of care (see Section 30.6.1B-C available at www. cms.hhs.gov/manuals/ downloads/clm104c12.pdf for additional information on billing for counseling/coordination of care time).
If a payer does not recognize prolonged care codes, only the latter billing option is possible. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 25-26.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1G. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
3. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1F. www.cms.hhs.gov/manuals/dowloads/ clm104c12.pdf. Accessed November 19, 2008.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf. Accessed November 19, 2008.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 457.
6. Pohlig, C. Bill by time spent on case. The Hospitalist. Jul 2008;19.
7. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1H. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
Medicare Modifications
Physicians who count Medicare among their payers already know the government green-lighted a 1.1% increase in Medicare Part B payments to physicians last summer. The increase was made official by the Centers for Medicare and Medicaid Services (CMS) on Oct. 30, with the release of the Medicare Physician Fee Schedule Final Rule for fiscal year 2009. The Final Rule governs what services are reimbursed by Medicare, the reimbursement levels for those services, and other rules pertaining to Medicare. Many of these changes, additions, and deletions were dictated by the Medicare Improvements for Patients and Providers Act, or MIPPA. (See “MIPPA Matters,” December 2008, p. 18.)
The 2009 Final Rule not only makes official the short-term, 1.1% payment increase, it also marks significant increases in payments for inpatient evaluation and management services, higher bonuses for participation in the Physician Quality Reporting Initiative (PQRI), and new policies to help direct the future of healthcare.
Here is a look at a few of the key aspects of the Final Rule, of which you may not be aware:
Transparent Physicians
In a continued effort to make healthcare transparent, CMS will begin posting the names of physicians who successfully report through the 2009 PQRI on a physician compare Web site in 2010. (2007 and 2008 PQRI participants will not be included.) Just as the Hospital Compare site enables consumers to view data on facilities, this site will allow consumers to view data reported by individual doctors.
Although consumers may be interested in checking for information on their primary care physician, it is unlikely inpatients will check the site before agreeing to see a specific hospitalist. However, the Physician Compare site will have some impact on hospital medicine. “I think this is the beginning of physicians’ commitment to greater transparency,” says Eric Siegal, MD, chair of SHM’s Public Policy Committee. “In a very broad sense, physicians who agree to be listed on the Physician Compare site very clearly value transparency and quality of care. Their inclusion could be seen as a differentiator, though a small one.”
Another factor to consider regarding transparency: “Physician Compare is not just about patients,” Dr. Siegal points out. “Third-party payers will look at this, as well. If they’re looking for someone to help take care of their patients, this data might sway them in their decision.”
Telehealth and Inpatients
Medicare already reimburses for certain exchanges of medical information from off-site physicians or vendors via interactive electronic communications, also known as telehealth or telemedicine services. Under the 2009 Final Rule, CMS will create a new series of Healthcare Common Procedure Coding System (HCPCS) codes for follow-up inpatient telehealth consultations, allowing practitioners to bill for follow-up inpatient consultations delivered via telehealth.
These codes are intended for use by physicians or non-physician providers when an inpatient consultation is requested from an appropriate source, such as the patient’s attending physician. CMS emphasizes the codes are not intended for use in billing for the ongoing evaluation and management of a hospital inpatient.
E-prescribe Out of Reach
Much attention has been given to a new Medicare program, which promotes the widespread adoption of electronic prescribing (e-prescribing). Physicians who successfully participate in CMS’ Electronic Prescribing Incentive Program will earn an extra bonus; however, the program was designed for primary care programs and hospitalists are unlikely to be able to take advantage of this.
“We don’t even know if hospitalists will be able to participate,” Dr. Siegal explains. The only way a hospitalist can take part in the e-prescribing initiative is if the hospital already has an acceptable system. However, Dr. Siegal warns, “If you create a mandate requiring a system for medication reconciliation at discharge, and then require another, separate system for e-prescribing, you’ve got problems. The primary driver should be that the hospital’s system supports both. And as far as we can tell, most hospital systems don’t do this.”
In August, SHM and the American College of Emergency Physicians conducted a teleconference with CMS to voice concerns with the e-prescribe initiative. “What we wanted was an exception,” Dr. Siegal says. SHM’s concern: When CMS stops rewarding physicians for e-prescribing and begins to penalize those who don’t—currently scheduled for 2013—hospitalists who can’t participate will be penalized through their Medicare payments. The outcome of the meeting, Dr. Siegal says, is “CMS turned around and said ‘either you can participate or you can’t.’ But at least they are considering our points; they seem to understand them.”
The good news is there is time to work the problem out, “At the moment, while e-prescribing is all bonus and no penalty, there’s no urgency to address it,” Dr. Siegal says.
Patient Safety
The Final Rule also includes improvements to PQRI, which allows eligible professionals to report on 153 quality measures. Physicians who successfully report on cases during 2009 will be able to earn an incentive payment, which has been increased to 2% (up from 1.5% in 2008), of their total allowed charges for covered professional services.
“I hope that more hospitalists will get on board with this,” Dr. Siegal says. He believes PQRI will be around for a while, and any hospital medicine group waiting to see if it is worth investing in the program can safely do so. “My feeling is that there’s growing bi-partisan support for something like this. I think it’s here to stay,” Dr. Siegal says.
SHM’s Opinion Counts
One reason the Final Rule is especially hospitalist-friendly is because SHM submitted extensive comment on CMS’s proposals in August. “SHM had a fair amount to say, and there are things in the rule that dovetail with our comments,” Dr. Siegal explains. “Part of the challenge is picking which battles to fight; there is a lot covered in this rule. We ended up focusing on areas that were really important to us, and on items where we thought we had a unique voice where nobody else was going to articulate.”
The Final Rule is available at www.cms.hhs.gov/center/physician.asp under “CMS-1403-FC.” Fact sheets covering major provisions of the Final Rule are available at www.cms.hhs.gov/apps/media/ fact_sheets.asp. TH
Jane Jerrard is a medical writer based in Chicago.
Physicians who count Medicare among their payers already know the government green-lighted a 1.1% increase in Medicare Part B payments to physicians last summer. The increase was made official by the Centers for Medicare and Medicaid Services (CMS) on Oct. 30, with the release of the Medicare Physician Fee Schedule Final Rule for fiscal year 2009. The Final Rule governs what services are reimbursed by Medicare, the reimbursement levels for those services, and other rules pertaining to Medicare. Many of these changes, additions, and deletions were dictated by the Medicare Improvements for Patients and Providers Act, or MIPPA. (See “MIPPA Matters,” December 2008, p. 18.)
The 2009 Final Rule not only makes official the short-term, 1.1% payment increase, it also marks significant increases in payments for inpatient evaluation and management services, higher bonuses for participation in the Physician Quality Reporting Initiative (PQRI), and new policies to help direct the future of healthcare.
Here is a look at a few of the key aspects of the Final Rule, of which you may not be aware:
Transparent Physicians
In a continued effort to make healthcare transparent, CMS will begin posting the names of physicians who successfully report through the 2009 PQRI on a physician compare Web site in 2010. (2007 and 2008 PQRI participants will not be included.) Just as the Hospital Compare site enables consumers to view data on facilities, this site will allow consumers to view data reported by individual doctors.
Although consumers may be interested in checking for information on their primary care physician, it is unlikely inpatients will check the site before agreeing to see a specific hospitalist. However, the Physician Compare site will have some impact on hospital medicine. “I think this is the beginning of physicians’ commitment to greater transparency,” says Eric Siegal, MD, chair of SHM’s Public Policy Committee. “In a very broad sense, physicians who agree to be listed on the Physician Compare site very clearly value transparency and quality of care. Their inclusion could be seen as a differentiator, though a small one.”
Another factor to consider regarding transparency: “Physician Compare is not just about patients,” Dr. Siegal points out. “Third-party payers will look at this, as well. If they’re looking for someone to help take care of their patients, this data might sway them in their decision.”
Telehealth and Inpatients
Medicare already reimburses for certain exchanges of medical information from off-site physicians or vendors via interactive electronic communications, also known as telehealth or telemedicine services. Under the 2009 Final Rule, CMS will create a new series of Healthcare Common Procedure Coding System (HCPCS) codes for follow-up inpatient telehealth consultations, allowing practitioners to bill for follow-up inpatient consultations delivered via telehealth.
These codes are intended for use by physicians or non-physician providers when an inpatient consultation is requested from an appropriate source, such as the patient’s attending physician. CMS emphasizes the codes are not intended for use in billing for the ongoing evaluation and management of a hospital inpatient.
E-prescribe Out of Reach
Much attention has been given to a new Medicare program, which promotes the widespread adoption of electronic prescribing (e-prescribing). Physicians who successfully participate in CMS’ Electronic Prescribing Incentive Program will earn an extra bonus; however, the program was designed for primary care programs and hospitalists are unlikely to be able to take advantage of this.
“We don’t even know if hospitalists will be able to participate,” Dr. Siegal explains. The only way a hospitalist can take part in the e-prescribing initiative is if the hospital already has an acceptable system. However, Dr. Siegal warns, “If you create a mandate requiring a system for medication reconciliation at discharge, and then require another, separate system for e-prescribing, you’ve got problems. The primary driver should be that the hospital’s system supports both. And as far as we can tell, most hospital systems don’t do this.”
In August, SHM and the American College of Emergency Physicians conducted a teleconference with CMS to voice concerns with the e-prescribe initiative. “What we wanted was an exception,” Dr. Siegal says. SHM’s concern: When CMS stops rewarding physicians for e-prescribing and begins to penalize those who don’t—currently scheduled for 2013—hospitalists who can’t participate will be penalized through their Medicare payments. The outcome of the meeting, Dr. Siegal says, is “CMS turned around and said ‘either you can participate or you can’t.’ But at least they are considering our points; they seem to understand them.”
The good news is there is time to work the problem out, “At the moment, while e-prescribing is all bonus and no penalty, there’s no urgency to address it,” Dr. Siegal says.
Patient Safety
The Final Rule also includes improvements to PQRI, which allows eligible professionals to report on 153 quality measures. Physicians who successfully report on cases during 2009 will be able to earn an incentive payment, which has been increased to 2% (up from 1.5% in 2008), of their total allowed charges for covered professional services.
“I hope that more hospitalists will get on board with this,” Dr. Siegal says. He believes PQRI will be around for a while, and any hospital medicine group waiting to see if it is worth investing in the program can safely do so. “My feeling is that there’s growing bi-partisan support for something like this. I think it’s here to stay,” Dr. Siegal says.
SHM’s Opinion Counts
One reason the Final Rule is especially hospitalist-friendly is because SHM submitted extensive comment on CMS’s proposals in August. “SHM had a fair amount to say, and there are things in the rule that dovetail with our comments,” Dr. Siegal explains. “Part of the challenge is picking which battles to fight; there is a lot covered in this rule. We ended up focusing on areas that were really important to us, and on items where we thought we had a unique voice where nobody else was going to articulate.”
The Final Rule is available at www.cms.hhs.gov/center/physician.asp under “CMS-1403-FC.” Fact sheets covering major provisions of the Final Rule are available at www.cms.hhs.gov/apps/media/ fact_sheets.asp. TH
Jane Jerrard is a medical writer based in Chicago.
Physicians who count Medicare among their payers already know the government green-lighted a 1.1% increase in Medicare Part B payments to physicians last summer. The increase was made official by the Centers for Medicare and Medicaid Services (CMS) on Oct. 30, with the release of the Medicare Physician Fee Schedule Final Rule for fiscal year 2009. The Final Rule governs what services are reimbursed by Medicare, the reimbursement levels for those services, and other rules pertaining to Medicare. Many of these changes, additions, and deletions were dictated by the Medicare Improvements for Patients and Providers Act, or MIPPA. (See “MIPPA Matters,” December 2008, p. 18.)
The 2009 Final Rule not only makes official the short-term, 1.1% payment increase, it also marks significant increases in payments for inpatient evaluation and management services, higher bonuses for participation in the Physician Quality Reporting Initiative (PQRI), and new policies to help direct the future of healthcare.
Here is a look at a few of the key aspects of the Final Rule, of which you may not be aware:
Transparent Physicians
In a continued effort to make healthcare transparent, CMS will begin posting the names of physicians who successfully report through the 2009 PQRI on a physician compare Web site in 2010. (2007 and 2008 PQRI participants will not be included.) Just as the Hospital Compare site enables consumers to view data on facilities, this site will allow consumers to view data reported by individual doctors.
Although consumers may be interested in checking for information on their primary care physician, it is unlikely inpatients will check the site before agreeing to see a specific hospitalist. However, the Physician Compare site will have some impact on hospital medicine. “I think this is the beginning of physicians’ commitment to greater transparency,” says Eric Siegal, MD, chair of SHM’s Public Policy Committee. “In a very broad sense, physicians who agree to be listed on the Physician Compare site very clearly value transparency and quality of care. Their inclusion could be seen as a differentiator, though a small one.”
Another factor to consider regarding transparency: “Physician Compare is not just about patients,” Dr. Siegal points out. “Third-party payers will look at this, as well. If they’re looking for someone to help take care of their patients, this data might sway them in their decision.”
Telehealth and Inpatients
Medicare already reimburses for certain exchanges of medical information from off-site physicians or vendors via interactive electronic communications, also known as telehealth or telemedicine services. Under the 2009 Final Rule, CMS will create a new series of Healthcare Common Procedure Coding System (HCPCS) codes for follow-up inpatient telehealth consultations, allowing practitioners to bill for follow-up inpatient consultations delivered via telehealth.
These codes are intended for use by physicians or non-physician providers when an inpatient consultation is requested from an appropriate source, such as the patient’s attending physician. CMS emphasizes the codes are not intended for use in billing for the ongoing evaluation and management of a hospital inpatient.
E-prescribe Out of Reach
Much attention has been given to a new Medicare program, which promotes the widespread adoption of electronic prescribing (e-prescribing). Physicians who successfully participate in CMS’ Electronic Prescribing Incentive Program will earn an extra bonus; however, the program was designed for primary care programs and hospitalists are unlikely to be able to take advantage of this.
“We don’t even know if hospitalists will be able to participate,” Dr. Siegal explains. The only way a hospitalist can take part in the e-prescribing initiative is if the hospital already has an acceptable system. However, Dr. Siegal warns, “If you create a mandate requiring a system for medication reconciliation at discharge, and then require another, separate system for e-prescribing, you’ve got problems. The primary driver should be that the hospital’s system supports both. And as far as we can tell, most hospital systems don’t do this.”
In August, SHM and the American College of Emergency Physicians conducted a teleconference with CMS to voice concerns with the e-prescribe initiative. “What we wanted was an exception,” Dr. Siegal says. SHM’s concern: When CMS stops rewarding physicians for e-prescribing and begins to penalize those who don’t—currently scheduled for 2013—hospitalists who can’t participate will be penalized through their Medicare payments. The outcome of the meeting, Dr. Siegal says, is “CMS turned around and said ‘either you can participate or you can’t.’ But at least they are considering our points; they seem to understand them.”
The good news is there is time to work the problem out, “At the moment, while e-prescribing is all bonus and no penalty, there’s no urgency to address it,” Dr. Siegal says.
Patient Safety
The Final Rule also includes improvements to PQRI, which allows eligible professionals to report on 153 quality measures. Physicians who successfully report on cases during 2009 will be able to earn an incentive payment, which has been increased to 2% (up from 1.5% in 2008), of their total allowed charges for covered professional services.
“I hope that more hospitalists will get on board with this,” Dr. Siegal says. He believes PQRI will be around for a while, and any hospital medicine group waiting to see if it is worth investing in the program can safely do so. “My feeling is that there’s growing bi-partisan support for something like this. I think it’s here to stay,” Dr. Siegal says.
SHM’s Opinion Counts
One reason the Final Rule is especially hospitalist-friendly is because SHM submitted extensive comment on CMS’s proposals in August. “SHM had a fair amount to say, and there are things in the rule that dovetail with our comments,” Dr. Siegal explains. “Part of the challenge is picking which battles to fight; there is a lot covered in this rule. We ended up focusing on areas that were really important to us, and on items where we thought we had a unique voice where nobody else was going to articulate.”
The Final Rule is available at www.cms.hhs.gov/center/physician.asp under “CMS-1403-FC.” Fact sheets covering major provisions of the Final Rule are available at www.cms.hhs.gov/apps/media/ fact_sheets.asp. TH
Jane Jerrard is a medical writer based in Chicago.
Beware Office Politics
Hospitalists routinely confront clinical, administrative, and ethical issues. Sometimes they face less-identifiable issues, such as office politics. Webster’s Dictionary defines office politics as “factional scheming for power and status within a group.” Wikipedia describes office politics as “the use of one’s individual or assigned power within an employing organization for the purpose of obtaining advantages beyond one’s legitimate authority.”
How much does office politics affect hospital medicine?
“Of course there is office politics in any work environment,” says Heather A. Harris, MD, former director of Eden Inpatient Services in Castro Valley, Calif., and currently splitting time as a hospitalist at the University of California San Francisco and the Palo Alto Medical Foundation. Dr. Harris, however, believes office politics is rare within hospital medicine because, “It is a young field and a growing field; everyone is growing together, so things tend to be pretty democratic. This is especially true of newer groups.”
Then again, there are times hospitalists find themselves embroiled in office politics. When this happens, what should you do?
Take the High Ground
Although she’s encountered few cases of office politics in her career, Dr. Harris’ general advice for hospitalists is, “First, recognize it, and then try to be a good team player.” Stay above the fray and try to tread carefully around political situations, especially if you’re a manager or informal leader.
Mary Jo Gorman, MD, MBA, CEO of Advanced ICU Care in St. Louis, and former SHM president, advises hospitalists and group directors to “take the high ground, no matter how frustrated you become.” She stresses discretion: “You can talk about it to your spouse, but if you’re a leader, you can’t even [comment on someone’s behavior] in front of your group. You never know, especially if you’re in a relatively small community, when you’re going to need someone’s support. You need to stay on good terms with people.” Dr. Gorman’s advice for leaders holds true for individuals hospitalists caught up in office politics.
Power Struggles
The role hospital medicine groups play as change agents probably is the main reason office politics may develop. “Any time you’re introducing a new concept that somebody feels threatened by, you’re going to incur some defensive maneuvers,” Dr. Gorman warns. “Whether you’re introducing a new hospital medicine group, or trying to change something, like the admissions process in the emergency room, you’re going to disrupt someone’s actions. Then you’ll find a whole broad range of reactions. And the more a person feels threatened, the more aggressive they’ll become.”
Based on her experiences establishing Eden Inpatient Services in 2003, Dr. Harris knows bringing a hospital medicine group into a hospital for the first time can be “a very political situation.” You can be stepping on personal, professional, and financial toes. “When you’re part of a new hospital medicine group … you’re potentially poised to take a lot of business away from people,” Dr. Harris explains. “It’s difficult to navigate those waters and build relationships” with physicians you’re consulting with and with primary care physicians. “In a way, this even extends to nurses,” she says. “You’re suddenly going to be working with them on patient care, and changing the way they work.” Dr. Harris encourages hospitalists to be aware of touchy situations, so as not to inadvertently fuel the fire of office politics. “Especially for young physicians just starting out, there can be a lack of recognition of other people’s feelings and turfs,” she cautions.
Hospitalists faced with an office issue should combine the cautionary approach with a willingness to work with people, even those who are engaging in office politics. “When you’re implementing a change, regardless of what it is, you need to identify who will think it’s a good thing and who will not,” Dr. Gorman advises. “You need to speak with individuals in the latter group, or choose others to speak to them, to garner their support.”
Take, for example, proposing a new project for your hospital’s Quality Improvement committee. A cautionary approach and team building will go a long way. “You’ve got to get to the people on the committee ahead of time, explain what you want to do, and get their feedback and support,” Dr. Gorman says. “If you find someone who opposes it, make sure you have enough support to override them. Or, better yet, find someone who can approach them on the topic, maybe their partner or another member of their group. This is a very practical approach.”
Identify Informal Leadership
When considering this inclusive approach, don’t forget the indirect leadership. “You may have a member of the medical staff who has some informal authority or power, maybe they have the most years of experience, or bring a lot of patients to the hospital, or maybe they are a member of the same group as someone in power,” Dr. Gorman says. “These informal leaders can create a lot of disturbance.”
To avoid problems, either direct or indirect, with these types of people, identify them early and make it a point to include them in the plan. “Usually, you know who holds informal power within your organization or the hospital,” Dr. Gorman says. “All you have to do is talk to them and explain what you’re doing. No one likes to be surprised. You might have to make some changes to accommodate their concerns.”
If this tactic fails and you still face opposition, you might have to weigh how important the opposition is. “You may decide to move ahead, even if you have to make changes and the project takes more time,” she says. “For physicians working in hospitals, we’re all used to instant results. You have to understand that process change takes time and you may have to take something bit by bit, and not get immediate results or responses.”
Be tactful about other professionals’ territories and feelings. Keep communication open and avoid springing surprises on stakeholders. Most importantly, stick to the high ground. These simple steps can help you stay far from the minefield known as office politics. TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Hospitalists routinely confront clinical, administrative, and ethical issues. Sometimes they face less-identifiable issues, such as office politics. Webster’s Dictionary defines office politics as “factional scheming for power and status within a group.” Wikipedia describes office politics as “the use of one’s individual or assigned power within an employing organization for the purpose of obtaining advantages beyond one’s legitimate authority.”
How much does office politics affect hospital medicine?
“Of course there is office politics in any work environment,” says Heather A. Harris, MD, former director of Eden Inpatient Services in Castro Valley, Calif., and currently splitting time as a hospitalist at the University of California San Francisco and the Palo Alto Medical Foundation. Dr. Harris, however, believes office politics is rare within hospital medicine because, “It is a young field and a growing field; everyone is growing together, so things tend to be pretty democratic. This is especially true of newer groups.”
Then again, there are times hospitalists find themselves embroiled in office politics. When this happens, what should you do?
Take the High Ground
Although she’s encountered few cases of office politics in her career, Dr. Harris’ general advice for hospitalists is, “First, recognize it, and then try to be a good team player.” Stay above the fray and try to tread carefully around political situations, especially if you’re a manager or informal leader.
Mary Jo Gorman, MD, MBA, CEO of Advanced ICU Care in St. Louis, and former SHM president, advises hospitalists and group directors to “take the high ground, no matter how frustrated you become.” She stresses discretion: “You can talk about it to your spouse, but if you’re a leader, you can’t even [comment on someone’s behavior] in front of your group. You never know, especially if you’re in a relatively small community, when you’re going to need someone’s support. You need to stay on good terms with people.” Dr. Gorman’s advice for leaders holds true for individuals hospitalists caught up in office politics.
Power Struggles
The role hospital medicine groups play as change agents probably is the main reason office politics may develop. “Any time you’re introducing a new concept that somebody feels threatened by, you’re going to incur some defensive maneuvers,” Dr. Gorman warns. “Whether you’re introducing a new hospital medicine group, or trying to change something, like the admissions process in the emergency room, you’re going to disrupt someone’s actions. Then you’ll find a whole broad range of reactions. And the more a person feels threatened, the more aggressive they’ll become.”
Based on her experiences establishing Eden Inpatient Services in 2003, Dr. Harris knows bringing a hospital medicine group into a hospital for the first time can be “a very political situation.” You can be stepping on personal, professional, and financial toes. “When you’re part of a new hospital medicine group … you’re potentially poised to take a lot of business away from people,” Dr. Harris explains. “It’s difficult to navigate those waters and build relationships” with physicians you’re consulting with and with primary care physicians. “In a way, this even extends to nurses,” she says. “You’re suddenly going to be working with them on patient care, and changing the way they work.” Dr. Harris encourages hospitalists to be aware of touchy situations, so as not to inadvertently fuel the fire of office politics. “Especially for young physicians just starting out, there can be a lack of recognition of other people’s feelings and turfs,” she cautions.
Hospitalists faced with an office issue should combine the cautionary approach with a willingness to work with people, even those who are engaging in office politics. “When you’re implementing a change, regardless of what it is, you need to identify who will think it’s a good thing and who will not,” Dr. Gorman advises. “You need to speak with individuals in the latter group, or choose others to speak to them, to garner their support.”
Take, for example, proposing a new project for your hospital’s Quality Improvement committee. A cautionary approach and team building will go a long way. “You’ve got to get to the people on the committee ahead of time, explain what you want to do, and get their feedback and support,” Dr. Gorman says. “If you find someone who opposes it, make sure you have enough support to override them. Or, better yet, find someone who can approach them on the topic, maybe their partner or another member of their group. This is a very practical approach.”
Identify Informal Leadership
When considering this inclusive approach, don’t forget the indirect leadership. “You may have a member of the medical staff who has some informal authority or power, maybe they have the most years of experience, or bring a lot of patients to the hospital, or maybe they are a member of the same group as someone in power,” Dr. Gorman says. “These informal leaders can create a lot of disturbance.”
To avoid problems, either direct or indirect, with these types of people, identify them early and make it a point to include them in the plan. “Usually, you know who holds informal power within your organization or the hospital,” Dr. Gorman says. “All you have to do is talk to them and explain what you’re doing. No one likes to be surprised. You might have to make some changes to accommodate their concerns.”
If this tactic fails and you still face opposition, you might have to weigh how important the opposition is. “You may decide to move ahead, even if you have to make changes and the project takes more time,” she says. “For physicians working in hospitals, we’re all used to instant results. You have to understand that process change takes time and you may have to take something bit by bit, and not get immediate results or responses.”
Be tactful about other professionals’ territories and feelings. Keep communication open and avoid springing surprises on stakeholders. Most importantly, stick to the high ground. These simple steps can help you stay far from the minefield known as office politics. TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Hospitalists routinely confront clinical, administrative, and ethical issues. Sometimes they face less-identifiable issues, such as office politics. Webster’s Dictionary defines office politics as “factional scheming for power and status within a group.” Wikipedia describes office politics as “the use of one’s individual or assigned power within an employing organization for the purpose of obtaining advantages beyond one’s legitimate authority.”
How much does office politics affect hospital medicine?
“Of course there is office politics in any work environment,” says Heather A. Harris, MD, former director of Eden Inpatient Services in Castro Valley, Calif., and currently splitting time as a hospitalist at the University of California San Francisco and the Palo Alto Medical Foundation. Dr. Harris, however, believes office politics is rare within hospital medicine because, “It is a young field and a growing field; everyone is growing together, so things tend to be pretty democratic. This is especially true of newer groups.”
Then again, there are times hospitalists find themselves embroiled in office politics. When this happens, what should you do?
Take the High Ground
Although she’s encountered few cases of office politics in her career, Dr. Harris’ general advice for hospitalists is, “First, recognize it, and then try to be a good team player.” Stay above the fray and try to tread carefully around political situations, especially if you’re a manager or informal leader.
Mary Jo Gorman, MD, MBA, CEO of Advanced ICU Care in St. Louis, and former SHM president, advises hospitalists and group directors to “take the high ground, no matter how frustrated you become.” She stresses discretion: “You can talk about it to your spouse, but if you’re a leader, you can’t even [comment on someone’s behavior] in front of your group. You never know, especially if you’re in a relatively small community, when you’re going to need someone’s support. You need to stay on good terms with people.” Dr. Gorman’s advice for leaders holds true for individuals hospitalists caught up in office politics.
Power Struggles
The role hospital medicine groups play as change agents probably is the main reason office politics may develop. “Any time you’re introducing a new concept that somebody feels threatened by, you’re going to incur some defensive maneuvers,” Dr. Gorman warns. “Whether you’re introducing a new hospital medicine group, or trying to change something, like the admissions process in the emergency room, you’re going to disrupt someone’s actions. Then you’ll find a whole broad range of reactions. And the more a person feels threatened, the more aggressive they’ll become.”
Based on her experiences establishing Eden Inpatient Services in 2003, Dr. Harris knows bringing a hospital medicine group into a hospital for the first time can be “a very political situation.” You can be stepping on personal, professional, and financial toes. “When you’re part of a new hospital medicine group … you’re potentially poised to take a lot of business away from people,” Dr. Harris explains. “It’s difficult to navigate those waters and build relationships” with physicians you’re consulting with and with primary care physicians. “In a way, this even extends to nurses,” she says. “You’re suddenly going to be working with them on patient care, and changing the way they work.” Dr. Harris encourages hospitalists to be aware of touchy situations, so as not to inadvertently fuel the fire of office politics. “Especially for young physicians just starting out, there can be a lack of recognition of other people’s feelings and turfs,” she cautions.
Hospitalists faced with an office issue should combine the cautionary approach with a willingness to work with people, even those who are engaging in office politics. “When you’re implementing a change, regardless of what it is, you need to identify who will think it’s a good thing and who will not,” Dr. Gorman advises. “You need to speak with individuals in the latter group, or choose others to speak to them, to garner their support.”
Take, for example, proposing a new project for your hospital’s Quality Improvement committee. A cautionary approach and team building will go a long way. “You’ve got to get to the people on the committee ahead of time, explain what you want to do, and get their feedback and support,” Dr. Gorman says. “If you find someone who opposes it, make sure you have enough support to override them. Or, better yet, find someone who can approach them on the topic, maybe their partner or another member of their group. This is a very practical approach.”
Identify Informal Leadership
When considering this inclusive approach, don’t forget the indirect leadership. “You may have a member of the medical staff who has some informal authority or power, maybe they have the most years of experience, or bring a lot of patients to the hospital, or maybe they are a member of the same group as someone in power,” Dr. Gorman says. “These informal leaders can create a lot of disturbance.”
To avoid problems, either direct or indirect, with these types of people, identify them early and make it a point to include them in the plan. “Usually, you know who holds informal power within your organization or the hospital,” Dr. Gorman says. “All you have to do is talk to them and explain what you’re doing. No one likes to be surprised. You might have to make some changes to accommodate their concerns.”
If this tactic fails and you still face opposition, you might have to weigh how important the opposition is. “You may decide to move ahead, even if you have to make changes and the project takes more time,” she says. “For physicians working in hospitals, we’re all used to instant results. You have to understand that process change takes time and you may have to take something bit by bit, and not get immediate results or responses.”
Be tactful about other professionals’ territories and feelings. Keep communication open and avoid springing surprises on stakeholders. Most importantly, stick to the high ground. These simple steps can help you stay far from the minefield known as office politics. TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.