User login
Splitting treatment: How to limit liability risk when you share a patient’s care
Dear Drs. Mossman and Weston:
In my psychiatric practice, I sometimes provide pharmacotherapy for patients treated by psychotherapists who practice independently. Am I liable for what these therapists do or don’t do—for example, not contacting me if a patient is suicidal or experiences a medication side effect? How much communication should occur between us? Sometimes—after a patient signs a release—I call the therapist and leave messages, but my calls are not returned. What should I do?—Submitted by “Dr. B”
Pharmacologic advances and altered reimbursement patterns have drastically changed how psychiatrists understand and manage mental problems. Not long ago, insight-oriented psychotherapy was the primary treatment—and often the only one—psychiatrists provided for outpatients. Nowadays, most visits to psychiatrists involve little or no in-depth psychotherapy,1 and many patients receive “joint treatment”—a psychiatrist performs the diagnostic and medical assessment and prescribes medications where appropriate, and a nonphysician provides other treatment services.
Psychiatrists need to be clear about their responsibilities for patients whom they “share” with other mental health professionals. In this article, we’ll discuss:
- forces that promote split treatment
- types of split-treatment relationships
- how to limit liability risk when you split treatment with an nonphysician mental health practitioner.
Dollars and cents reasons
Since the 1980s, psychiatrists have spent less time with their patients, provided less psychotherapy, and prescribed medications more frequently.2 An estimated 70% of outpatient visits to psychiatrists involve no psychotherapy.1
Market conditions are a major factor in these changes. Cost-containment policies and reduced private insurance payments for psychotherapy visits have incentivized psychiatrists to collaborate with less-well-paid psychotherapists. Combining medication and psychotherapy may be the best and most cost-effective treatment for mentally ill patients, but psychiatrists get paid more for three 15-minute “med checks” than for one 45-minute psychotherapy session.3-5
Although managed care payment patterns may be “perversely influencing” psychiatry (as one psychiatrist puts it)6 other factors contributing to the decline of psychotherapy include:
- new medications with fewer side effects
- aggressive pharmaceutical company promotions of psychotropics
- greater public acceptance of mental illness and its treatment
- an increasingly cohort of psychiatrists trained by teachers and mentors who emphasized biologic therapies.1
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
Forms of split treatment
Psychiatrists engage in several types of professional relationships that split the care provided to mentally ill patients (Table 1),7 and Dr. B has asked us to focus on one type of split-care relationship: a physician and psychotherapist treat the same patient, ideally collaborating to provide good clinical care.
Split, collaborative care is common throughout medicine. Most of us see medical specialists who treat different illnesses, but each doctor is responsible for the care he or she provides. An allergist knows what orthopedic surgery is, but we don’t expect our allergist to provide follow-up after arthroscopic surgery—and neither does our orthopedist.
The same considerations apply when a psychiatrist’s patient sees an independent nonphysician therapist. The psychiatrist provides the same care that a patient receiving only pharmacotherapy would need. The psychiatrist should not expect the collaborating therapist to monitor the patient’s pharmacotherapy—for example, by checking lab tests or asking about medication side effects—although the therapist is welcome to tell the psychiatrist about pharmacotherapy matters or encourage the patient to do so.
Table 1
Types of split-care relationships
| Type | Characteristics |
|---|---|
| Consultative | Develops when one licensed practitioner asks for the opinion of another |
| Informal (‘curbside’) | One practitioner describes clinical characteristics to another; patient’s identity is unknown to consultant |
| Formal | Consultant documents findings after reviewing record and/or examining patient; consultant knows patient’s identity |
| Supervisory | Mandated relationship between 2 professionals in which supervisee should follow supervisor’s recommendations |
| Collaborative | Credentialed professionals share ongoing responsibility for care and complementary aspects of a patient’s treatment |
| Same agency | Practitioners have distinct treatment roles (eg, therapist and prescriber) in several patients’ care and may have regular contact with each other; shared medical record |
| Independent | Practitioners lack regular contact; scope of treatment duties is established for the individual shared patient |
| Source: Reference 7 | |
Limiting liability
Psychiatrists who share patients with independent nonphysicians can take several steps to promote better care and limit potential liability.
Delegation. Do not delegate essential aspects of medical care. For example, tell young patients starting antidepressants (and minors’ legal guardians) about the risk of increased suicidal ideation, and provide close monitoring. Although it is acceptable for a patient to tell his or her therapist about worsening suicidal thoughts, instruct the patient to inform you as well.
Check them out. Before agreeing to split care, find out if the potential collaborator is credentialed, and respectfully inquire about his or her training and clinical approaches.8 Because unlicensed or uncredentialed therapists might not be held to the same practice standards as physicians and often have little or no malpractice insurance, psychiatrists who work with them may be assuming most of the clinical and legal liability.9 If a court is looking for a way to compensate an injured patient, it may hold the psychiatrist accountable for not knowing the therapist’s qualifications, failing to supervise the therapist, or failing to inform the patient of the therapist’s lack of qualifications.7,10
Establish the collaboration. Psychiatrists have a duty to ensure that their patients receive good care. Split treatment can help patients—who get 2 pairs of eyes monitoring them, plus 2 clinicians’ combined areas of skill—if the clinicians work together satisfactorily. Some psychiatrists recommend using initial consultation forms8 or contracts to spell out mutual expectations and establish important components of the relationship (Table 2).11,12 Other psychiatrists are comfortable with brief discussions with potential collaborators that cover:
- how the clinicians will divide treatment responsibilities
- circumstances when they will communicate
- patient coverage during each other’s vacations
- availability to patients during crises
- types of problems that would prompt the patient to contact the psychiatrist or therapist first.
Table 2
7 C’s of effective collaborative treatment
| Clarity about the relationship (collaborative, supervisory) and what each provider will do |
| Contract. A written agreement about duties and roles may help to dispel an assumption that the psychiatrist had supervisory responsibilities |
| Communication that occurs routinely between caregivers, even when treatment is going well |
| Consent by the patient, which requires that the patient knows, understands, and accepts each provider’s role |
| Comprehensive review of what’s happened in therapy, especially if the psychiatrist sees the patient infrequently |
| Credentialing. If the parties don’t know each other well, they should check out each other’s background |
| Consultation. Seek when problems arise in treatment or with the above arrangements |
| Source: References 11,12 |
Be sure to document these discussions as well as written consent for initial and ongoing communication in the patient’s medical record. Major treatment advances or setbacks, nonadherence, or termination of treatment by/with one clinician should prompt contact with the other clinician. Collaborating clinicians should communicate regularly even when treatment is going well, not only when big changes occur.8
Back to Dr. B
What should you do if a patient seeks pharmacotherapy and the therapist hasn’t contacted you? First, you probably should speak with your patient about the absence of interclinician communication, explain that it is important, and get the patient’s written permission to initiate contact. After contacting the therapist, you will be in a better position to determine how often you should see the patient and how often you need to share information with the therapist.
If you are uncomfortable sharing care with some or all nonphysician therapists, tell your patients. You might refer prospective patients to psychotherapists with whom you’re comfortable providing collaborative care or to other psychiatrists who accept split relationships.
Ideally, get patients’ written consent to share confidential information before you agree to participate in a shared treatment relationship. If patients refuse, you will not have access to all treatment information. This may adversely affect the quality of care and increase your liability risk.
In some cases, your discomfort with a split-treatment situation may make you decide to decline or terminate the treatment relationship. This is permissible if you give the patient proper notice, suggest other psychiatrists who might see the patient, and remain available for urgent matters for a reasonable time—usually 30 to 60 days—to allow the patient to contact another psychiatrist.10 When you discuss potential providers, explain that you don’t know these clinicians (if that’s the case) or whether they will agree to treat the patient.12
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Olfson M, Marcus SC, Pincus HA. Trends in office-based psychiatric practice. Am J Psychiatry. 1999;156:451-457.
3. Rosack J. Researchers learning why treatment combo is best. Psychiatr News. 2004;39(12):37.-
4. Thase ME, Greenhouse JB, Frank E, et al. Treatment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations. Arch Gen Psychiatry. 1997;54:1009-1015.
5. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus split treatment. Am J Psychiatry. 1999;156:324-326.
6. Clemens NA, MacKenzie KR, Griffith JL, et al. Psychotherapy by psychiatrists in a managed care environment: must it be an oxymoron? A forum from the APA commission on psychotherapy by psychiatrists. J Psychother Pract Res. 2001;10:53-62.
7. Sederer LI, Ellison J, Keyes C. Guidelines for prescribing psychiatrists in consultative, collaborative, and supervisory relationships. Psychiatr Serv. 1998;49:1197-1202.
8. Ellison JM. Teaching collaboration between pharmacotherapist and psychotherapist. Acad Psychiatry. 2005;29:195-202.
9. Sederer LI, Ellison J, Badaracco M, et al. Guidelines for prescribing psychiatrists in consultative, collaborative, or supervisory relationships. Cambridge, MA: Risk Management Foundation of the Harvard Medical Institutions; 1998. Available at: http://www.rmf.harvard.edu/files/documents/psychPr.pdf. Accessed January 4, 2010.
10. Melonas JM. Split treatment: does managed care change the risk to psychiatrists? Psychiatric Practice and Managed Care. 1999;5:5.-Available at: http://www.psychprogram.com/Risk_Management/news_splittreatment1.htm. Accessed January 4, 2010.
11. Gutheil TG, Simon RI. Abandonment of patients in split treatment. Harv Rev Psychiatry. 2003;11:175-179.
12. Reid WH. Organization liability: beyond respondeat superior. J Psychiatr Pract. 2004;4:258-262.

Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director, division of forensic psychiatry, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director, division of forensic psychiatry, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director, division of forensic psychiatry, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Dear Drs. Mossman and Weston:
In my psychiatric practice, I sometimes provide pharmacotherapy for patients treated by psychotherapists who practice independently. Am I liable for what these therapists do or don’t do—for example, not contacting me if a patient is suicidal or experiences a medication side effect? How much communication should occur between us? Sometimes—after a patient signs a release—I call the therapist and leave messages, but my calls are not returned. What should I do?—Submitted by “Dr. B”
Pharmacologic advances and altered reimbursement patterns have drastically changed how psychiatrists understand and manage mental problems. Not long ago, insight-oriented psychotherapy was the primary treatment—and often the only one—psychiatrists provided for outpatients. Nowadays, most visits to psychiatrists involve little or no in-depth psychotherapy,1 and many patients receive “joint treatment”—a psychiatrist performs the diagnostic and medical assessment and prescribes medications where appropriate, and a nonphysician provides other treatment services.
Psychiatrists need to be clear about their responsibilities for patients whom they “share” with other mental health professionals. In this article, we’ll discuss:
- forces that promote split treatment
- types of split-treatment relationships
- how to limit liability risk when you split treatment with an nonphysician mental health practitioner.
Dollars and cents reasons
Since the 1980s, psychiatrists have spent less time with their patients, provided less psychotherapy, and prescribed medications more frequently.2 An estimated 70% of outpatient visits to psychiatrists involve no psychotherapy.1
Market conditions are a major factor in these changes. Cost-containment policies and reduced private insurance payments for psychotherapy visits have incentivized psychiatrists to collaborate with less-well-paid psychotherapists. Combining medication and psychotherapy may be the best and most cost-effective treatment for mentally ill patients, but psychiatrists get paid more for three 15-minute “med checks” than for one 45-minute psychotherapy session.3-5
Although managed care payment patterns may be “perversely influencing” psychiatry (as one psychiatrist puts it)6 other factors contributing to the decline of psychotherapy include:
- new medications with fewer side effects
- aggressive pharmaceutical company promotions of psychotropics
- greater public acceptance of mental illness and its treatment
- an increasingly cohort of psychiatrists trained by teachers and mentors who emphasized biologic therapies.1
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
Forms of split treatment
Psychiatrists engage in several types of professional relationships that split the care provided to mentally ill patients (Table 1),7 and Dr. B has asked us to focus on one type of split-care relationship: a physician and psychotherapist treat the same patient, ideally collaborating to provide good clinical care.
Split, collaborative care is common throughout medicine. Most of us see medical specialists who treat different illnesses, but each doctor is responsible for the care he or she provides. An allergist knows what orthopedic surgery is, but we don’t expect our allergist to provide follow-up after arthroscopic surgery—and neither does our orthopedist.
The same considerations apply when a psychiatrist’s patient sees an independent nonphysician therapist. The psychiatrist provides the same care that a patient receiving only pharmacotherapy would need. The psychiatrist should not expect the collaborating therapist to monitor the patient’s pharmacotherapy—for example, by checking lab tests or asking about medication side effects—although the therapist is welcome to tell the psychiatrist about pharmacotherapy matters or encourage the patient to do so.
Table 1
Types of split-care relationships
| Type | Characteristics |
|---|---|
| Consultative | Develops when one licensed practitioner asks for the opinion of another |
| Informal (‘curbside’) | One practitioner describes clinical characteristics to another; patient’s identity is unknown to consultant |
| Formal | Consultant documents findings after reviewing record and/or examining patient; consultant knows patient’s identity |
| Supervisory | Mandated relationship between 2 professionals in which supervisee should follow supervisor’s recommendations |
| Collaborative | Credentialed professionals share ongoing responsibility for care and complementary aspects of a patient’s treatment |
| Same agency | Practitioners have distinct treatment roles (eg, therapist and prescriber) in several patients’ care and may have regular contact with each other; shared medical record |
| Independent | Practitioners lack regular contact; scope of treatment duties is established for the individual shared patient |
| Source: Reference 7 | |
Limiting liability
Psychiatrists who share patients with independent nonphysicians can take several steps to promote better care and limit potential liability.
Delegation. Do not delegate essential aspects of medical care. For example, tell young patients starting antidepressants (and minors’ legal guardians) about the risk of increased suicidal ideation, and provide close monitoring. Although it is acceptable for a patient to tell his or her therapist about worsening suicidal thoughts, instruct the patient to inform you as well.
Check them out. Before agreeing to split care, find out if the potential collaborator is credentialed, and respectfully inquire about his or her training and clinical approaches.8 Because unlicensed or uncredentialed therapists might not be held to the same practice standards as physicians and often have little or no malpractice insurance, psychiatrists who work with them may be assuming most of the clinical and legal liability.9 If a court is looking for a way to compensate an injured patient, it may hold the psychiatrist accountable for not knowing the therapist’s qualifications, failing to supervise the therapist, or failing to inform the patient of the therapist’s lack of qualifications.7,10
Establish the collaboration. Psychiatrists have a duty to ensure that their patients receive good care. Split treatment can help patients—who get 2 pairs of eyes monitoring them, plus 2 clinicians’ combined areas of skill—if the clinicians work together satisfactorily. Some psychiatrists recommend using initial consultation forms8 or contracts to spell out mutual expectations and establish important components of the relationship (Table 2).11,12 Other psychiatrists are comfortable with brief discussions with potential collaborators that cover:
- how the clinicians will divide treatment responsibilities
- circumstances when they will communicate
- patient coverage during each other’s vacations
- availability to patients during crises
- types of problems that would prompt the patient to contact the psychiatrist or therapist first.
Table 2
7 C’s of effective collaborative treatment
| Clarity about the relationship (collaborative, supervisory) and what each provider will do |
| Contract. A written agreement about duties and roles may help to dispel an assumption that the psychiatrist had supervisory responsibilities |
| Communication that occurs routinely between caregivers, even when treatment is going well |
| Consent by the patient, which requires that the patient knows, understands, and accepts each provider’s role |
| Comprehensive review of what’s happened in therapy, especially if the psychiatrist sees the patient infrequently |
| Credentialing. If the parties don’t know each other well, they should check out each other’s background |
| Consultation. Seek when problems arise in treatment or with the above arrangements |
| Source: References 11,12 |
Be sure to document these discussions as well as written consent for initial and ongoing communication in the patient’s medical record. Major treatment advances or setbacks, nonadherence, or termination of treatment by/with one clinician should prompt contact with the other clinician. Collaborating clinicians should communicate regularly even when treatment is going well, not only when big changes occur.8
Back to Dr. B
What should you do if a patient seeks pharmacotherapy and the therapist hasn’t contacted you? First, you probably should speak with your patient about the absence of interclinician communication, explain that it is important, and get the patient’s written permission to initiate contact. After contacting the therapist, you will be in a better position to determine how often you should see the patient and how often you need to share information with the therapist.
If you are uncomfortable sharing care with some or all nonphysician therapists, tell your patients. You might refer prospective patients to psychotherapists with whom you’re comfortable providing collaborative care or to other psychiatrists who accept split relationships.
Ideally, get patients’ written consent to share confidential information before you agree to participate in a shared treatment relationship. If patients refuse, you will not have access to all treatment information. This may adversely affect the quality of care and increase your liability risk.
In some cases, your discomfort with a split-treatment situation may make you decide to decline or terminate the treatment relationship. This is permissible if you give the patient proper notice, suggest other psychiatrists who might see the patient, and remain available for urgent matters for a reasonable time—usually 30 to 60 days—to allow the patient to contact another psychiatrist.10 When you discuss potential providers, explain that you don’t know these clinicians (if that’s the case) or whether they will agree to treat the patient.12
Dear Drs. Mossman and Weston:
In my psychiatric practice, I sometimes provide pharmacotherapy for patients treated by psychotherapists who practice independently. Am I liable for what these therapists do or don’t do—for example, not contacting me if a patient is suicidal or experiences a medication side effect? How much communication should occur between us? Sometimes—after a patient signs a release—I call the therapist and leave messages, but my calls are not returned. What should I do?—Submitted by “Dr. B”
Pharmacologic advances and altered reimbursement patterns have drastically changed how psychiatrists understand and manage mental problems. Not long ago, insight-oriented psychotherapy was the primary treatment—and often the only one—psychiatrists provided for outpatients. Nowadays, most visits to psychiatrists involve little or no in-depth psychotherapy,1 and many patients receive “joint treatment”—a psychiatrist performs the diagnostic and medical assessment and prescribes medications where appropriate, and a nonphysician provides other treatment services.
Psychiatrists need to be clear about their responsibilities for patients whom they “share” with other mental health professionals. In this article, we’ll discuss:
- forces that promote split treatment
- types of split-treatment relationships
- how to limit liability risk when you split treatment with an nonphysician mental health practitioner.
Dollars and cents reasons
Since the 1980s, psychiatrists have spent less time with their patients, provided less psychotherapy, and prescribed medications more frequently.2 An estimated 70% of outpatient visits to psychiatrists involve no psychotherapy.1
Market conditions are a major factor in these changes. Cost-containment policies and reduced private insurance payments for psychotherapy visits have incentivized psychiatrists to collaborate with less-well-paid psychotherapists. Combining medication and psychotherapy may be the best and most cost-effective treatment for mentally ill patients, but psychiatrists get paid more for three 15-minute “med checks” than for one 45-minute psychotherapy session.3-5
Although managed care payment patterns may be “perversely influencing” psychiatry (as one psychiatrist puts it)6 other factors contributing to the decline of psychotherapy include:
- new medications with fewer side effects
- aggressive pharmaceutical company promotions of psychotropics
- greater public acceptance of mental illness and its treatment
- an increasingly cohort of psychiatrists trained by teachers and mentors who emphasized biologic therapies.1
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
Forms of split treatment
Psychiatrists engage in several types of professional relationships that split the care provided to mentally ill patients (Table 1),7 and Dr. B has asked us to focus on one type of split-care relationship: a physician and psychotherapist treat the same patient, ideally collaborating to provide good clinical care.
Split, collaborative care is common throughout medicine. Most of us see medical specialists who treat different illnesses, but each doctor is responsible for the care he or she provides. An allergist knows what orthopedic surgery is, but we don’t expect our allergist to provide follow-up after arthroscopic surgery—and neither does our orthopedist.
The same considerations apply when a psychiatrist’s patient sees an independent nonphysician therapist. The psychiatrist provides the same care that a patient receiving only pharmacotherapy would need. The psychiatrist should not expect the collaborating therapist to monitor the patient’s pharmacotherapy—for example, by checking lab tests or asking about medication side effects—although the therapist is welcome to tell the psychiatrist about pharmacotherapy matters or encourage the patient to do so.
Table 1
Types of split-care relationships
| Type | Characteristics |
|---|---|
| Consultative | Develops when one licensed practitioner asks for the opinion of another |
| Informal (‘curbside’) | One practitioner describes clinical characteristics to another; patient’s identity is unknown to consultant |
| Formal | Consultant documents findings after reviewing record and/or examining patient; consultant knows patient’s identity |
| Supervisory | Mandated relationship between 2 professionals in which supervisee should follow supervisor’s recommendations |
| Collaborative | Credentialed professionals share ongoing responsibility for care and complementary aspects of a patient’s treatment |
| Same agency | Practitioners have distinct treatment roles (eg, therapist and prescriber) in several patients’ care and may have regular contact with each other; shared medical record |
| Independent | Practitioners lack regular contact; scope of treatment duties is established for the individual shared patient |
| Source: Reference 7 | |
Limiting liability
Psychiatrists who share patients with independent nonphysicians can take several steps to promote better care and limit potential liability.
Delegation. Do not delegate essential aspects of medical care. For example, tell young patients starting antidepressants (and minors’ legal guardians) about the risk of increased suicidal ideation, and provide close monitoring. Although it is acceptable for a patient to tell his or her therapist about worsening suicidal thoughts, instruct the patient to inform you as well.
Check them out. Before agreeing to split care, find out if the potential collaborator is credentialed, and respectfully inquire about his or her training and clinical approaches.8 Because unlicensed or uncredentialed therapists might not be held to the same practice standards as physicians and often have little or no malpractice insurance, psychiatrists who work with them may be assuming most of the clinical and legal liability.9 If a court is looking for a way to compensate an injured patient, it may hold the psychiatrist accountable for not knowing the therapist’s qualifications, failing to supervise the therapist, or failing to inform the patient of the therapist’s lack of qualifications.7,10
Establish the collaboration. Psychiatrists have a duty to ensure that their patients receive good care. Split treatment can help patients—who get 2 pairs of eyes monitoring them, plus 2 clinicians’ combined areas of skill—if the clinicians work together satisfactorily. Some psychiatrists recommend using initial consultation forms8 or contracts to spell out mutual expectations and establish important components of the relationship (Table 2).11,12 Other psychiatrists are comfortable with brief discussions with potential collaborators that cover:
- how the clinicians will divide treatment responsibilities
- circumstances when they will communicate
- patient coverage during each other’s vacations
- availability to patients during crises
- types of problems that would prompt the patient to contact the psychiatrist or therapist first.
Table 2
7 C’s of effective collaborative treatment
| Clarity about the relationship (collaborative, supervisory) and what each provider will do |
| Contract. A written agreement about duties and roles may help to dispel an assumption that the psychiatrist had supervisory responsibilities |
| Communication that occurs routinely between caregivers, even when treatment is going well |
| Consent by the patient, which requires that the patient knows, understands, and accepts each provider’s role |
| Comprehensive review of what’s happened in therapy, especially if the psychiatrist sees the patient infrequently |
| Credentialing. If the parties don’t know each other well, they should check out each other’s background |
| Consultation. Seek when problems arise in treatment or with the above arrangements |
| Source: References 11,12 |
Be sure to document these discussions as well as written consent for initial and ongoing communication in the patient’s medical record. Major treatment advances or setbacks, nonadherence, or termination of treatment by/with one clinician should prompt contact with the other clinician. Collaborating clinicians should communicate regularly even when treatment is going well, not only when big changes occur.8
Back to Dr. B
What should you do if a patient seeks pharmacotherapy and the therapist hasn’t contacted you? First, you probably should speak with your patient about the absence of interclinician communication, explain that it is important, and get the patient’s written permission to initiate contact. After contacting the therapist, you will be in a better position to determine how often you should see the patient and how often you need to share information with the therapist.
If you are uncomfortable sharing care with some or all nonphysician therapists, tell your patients. You might refer prospective patients to psychotherapists with whom you’re comfortable providing collaborative care or to other psychiatrists who accept split relationships.
Ideally, get patients’ written consent to share confidential information before you agree to participate in a shared treatment relationship. If patients refuse, you will not have access to all treatment information. This may adversely affect the quality of care and increase your liability risk.
In some cases, your discomfort with a split-treatment situation may make you decide to decline or terminate the treatment relationship. This is permissible if you give the patient proper notice, suggest other psychiatrists who might see the patient, and remain available for urgent matters for a reasonable time—usually 30 to 60 days—to allow the patient to contact another psychiatrist.10 When you discuss potential providers, explain that you don’t know these clinicians (if that’s the case) or whether they will agree to treat the patient.12
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Olfson M, Marcus SC, Pincus HA. Trends in office-based psychiatric practice. Am J Psychiatry. 1999;156:451-457.
3. Rosack J. Researchers learning why treatment combo is best. Psychiatr News. 2004;39(12):37.-
4. Thase ME, Greenhouse JB, Frank E, et al. Treatment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations. Arch Gen Psychiatry. 1997;54:1009-1015.
5. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus split treatment. Am J Psychiatry. 1999;156:324-326.
6. Clemens NA, MacKenzie KR, Griffith JL, et al. Psychotherapy by psychiatrists in a managed care environment: must it be an oxymoron? A forum from the APA commission on psychotherapy by psychiatrists. J Psychother Pract Res. 2001;10:53-62.
7. Sederer LI, Ellison J, Keyes C. Guidelines for prescribing psychiatrists in consultative, collaborative, and supervisory relationships. Psychiatr Serv. 1998;49:1197-1202.
8. Ellison JM. Teaching collaboration between pharmacotherapist and psychotherapist. Acad Psychiatry. 2005;29:195-202.
9. Sederer LI, Ellison J, Badaracco M, et al. Guidelines for prescribing psychiatrists in consultative, collaborative, or supervisory relationships. Cambridge, MA: Risk Management Foundation of the Harvard Medical Institutions; 1998. Available at: http://www.rmf.harvard.edu/files/documents/psychPr.pdf. Accessed January 4, 2010.
10. Melonas JM. Split treatment: does managed care change the risk to psychiatrists? Psychiatric Practice and Managed Care. 1999;5:5.-Available at: http://www.psychprogram.com/Risk_Management/news_splittreatment1.htm. Accessed January 4, 2010.
11. Gutheil TG, Simon RI. Abandonment of patients in split treatment. Harv Rev Psychiatry. 2003;11:175-179.
12. Reid WH. Organization liability: beyond respondeat superior. J Psychiatr Pract. 2004;4:258-262.
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Olfson M, Marcus SC, Pincus HA. Trends in office-based psychiatric practice. Am J Psychiatry. 1999;156:451-457.
3. Rosack J. Researchers learning why treatment combo is best. Psychiatr News. 2004;39(12):37.-
4. Thase ME, Greenhouse JB, Frank E, et al. Treatment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations. Arch Gen Psychiatry. 1997;54:1009-1015.
5. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus split treatment. Am J Psychiatry. 1999;156:324-326.
6. Clemens NA, MacKenzie KR, Griffith JL, et al. Psychotherapy by psychiatrists in a managed care environment: must it be an oxymoron? A forum from the APA commission on psychotherapy by psychiatrists. J Psychother Pract Res. 2001;10:53-62.
7. Sederer LI, Ellison J, Keyes C. Guidelines for prescribing psychiatrists in consultative, collaborative, and supervisory relationships. Psychiatr Serv. 1998;49:1197-1202.
8. Ellison JM. Teaching collaboration between pharmacotherapist and psychotherapist. Acad Psychiatry. 2005;29:195-202.
9. Sederer LI, Ellison J, Badaracco M, et al. Guidelines for prescribing psychiatrists in consultative, collaborative, or supervisory relationships. Cambridge, MA: Risk Management Foundation of the Harvard Medical Institutions; 1998. Available at: http://www.rmf.harvard.edu/files/documents/psychPr.pdf. Accessed January 4, 2010.
10. Melonas JM. Split treatment: does managed care change the risk to psychiatrists? Psychiatric Practice and Managed Care. 1999;5:5.-Available at: http://www.psychprogram.com/Risk_Management/news_splittreatment1.htm. Accessed January 4, 2010.
11. Gutheil TG, Simon RI. Abandonment of patients in split treatment. Harv Rev Psychiatry. 2003;11:175-179.
12. Reid WH. Organization liability: beyond respondeat superior. J Psychiatr Pract. 2004;4:258-262.
The Year Ahead
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Malpractice Chronicle
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Breast Malignancy Dismissed as Cyst
A 23-year-old woman called the defendant obstetrician/gynecologist’s office in July 2003 and reported to the receptionist that she had found a lump in her breast; it had been present for two months, she said, with possible dimpling. She asked to be seen immediately. Upon receiving the patient’s message, Dr. M. told the nurse to instruct the patient to wait until her next scheduled appointment, two weeks away; she also declined to schedule a mammogram.
At the patient’s scheduled appointment, Dr. M. performed the standard gynecologic examination and needed to be reminded to examine the lump before the patient left her office. Dr. M. diagnosed the lump as a cyst and told the patient it was nothing to worry about. No testing was performed, and no follow-up was recommended. Dr. M. did not document her findings in the patient’s record, nor did she note any self-reminders to reevaluate the lump at a later date.
The patient subsequently became pregnant and was seen in the defendant’s office on 16 subsequent occasions without further evaluation or testing for the breast lump.
After the delivery of her child, the patient noted that the lump had become larger and painful. When she could not be seen by Dr. M., she was seen by her partner, Dr. P., in February 2005. Dr. P. found a suspicious mass and immediately ordered a mammogram and ultrasonography, which confirmed the presence of a 4.0-cm mass. Biopsy the next day led to a diagnosis of breast cancer. Through positron emission tomography and CT later that week and an additional biopsy, it was found that the cancer had metastasized to the patient’s liver.
She underwent 10 rounds of chemotherapy, a lumpectomy, a complete hysterectomy, and radiation treatment. She was given no chance for a cure, however.
The defendant denied any negligence, maintaining that the lump brought to her attention in July 2003 was not the same lump found in 2005. Even if the lump in 2003 had been found to be cancerous, the defendant argued, it had probably metastasized by that time, making any delay in treatment of no consequence.
A jury awarded $23.6 million to the plaintiff, which included $11,750,000 for the plaintiff’s husband.
Reaction to Radiologic Dye Blamed for Stroke Symptoms
An elderly woman presented to a hospital emergency department (ED) with left-side weakness and slurred speech; a stroke was suspected. The defendant ED physician evaluated the patient and made a diagnosis of an allergic reaction to a dye she had been given during IV pyelography the previous day. The patient was given diphenhydramine and discharged.
She returned to the ED the following day with indisputable symptoms of a stroke: left-side weakness affecting her hand and leg, diminished speech, and loss of bladder control.
The plaintiff alleged negligence in the failure of the ED physician to diagnose the stroke at her first visit.
The defendant claimed that in light of the plaintiff’s constellation of symptoms at the first visit, his diagnosis of an allergic reaction was reasonable. The defendant argued that the stroke had occurred after the patient’s first visit and that she would not have been a good candidate to receive tissue plasminogen activator therapy.
The jury was unable to reach a unanimous verdict, and the parties agreed to accept a less-than-unanimous verdict. The jury returned an eight-to-four verdict in favor of the defendant, and a defense judgment was entered.
Possible Fluid Overload for Child With Complex Medical History
A 7-year-old girl was brought into a hospital emergency department (ED) with congestion and several episodes of vomiting. Born prematurely, she had a history of hydroencephalitis requiring a ventriculoperitoneal shunt. As an infant, she had also experienced spastic cerebral palsy, developmental delays, and a chronic lung condition. She had spent her first three years in a hospital’s pediatric ICU.
At the ED, the child was examined by a PA, who then consulted with the ED physician. Pneumonitis, bronchiolitis, mild dehydration, and viral illness were diagnosed, with possible early-stage pneumonia. The child was sent home after being given 800 mL of IV normal saline infusion with 900 mg of ceftriaxone.
About two hours later, she was found by her father not breathing. She was taken back to the ED, where she was pronounced dead.
The plaintiff claimed that the child’s death was due to fluid overload, which caused pulmonary edema. The plaintiff also claimed that the ED staff failed to properly treat her complex medical condition or to monitor and observe her for a reasonable time.
The defendant claimed that the girl’s death was due to her chronic interstitial pneumonitis secondary to bronchopulmonary dysplasia.
According to a published account, the court found in favor of the defendant.
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Breast Malignancy Dismissed as Cyst
A 23-year-old woman called the defendant obstetrician/gynecologist’s office in July 2003 and reported to the receptionist that she had found a lump in her breast; it had been present for two months, she said, with possible dimpling. She asked to be seen immediately. Upon receiving the patient’s message, Dr. M. told the nurse to instruct the patient to wait until her next scheduled appointment, two weeks away; she also declined to schedule a mammogram.
At the patient’s scheduled appointment, Dr. M. performed the standard gynecologic examination and needed to be reminded to examine the lump before the patient left her office. Dr. M. diagnosed the lump as a cyst and told the patient it was nothing to worry about. No testing was performed, and no follow-up was recommended. Dr. M. did not document her findings in the patient’s record, nor did she note any self-reminders to reevaluate the lump at a later date.
The patient subsequently became pregnant and was seen in the defendant’s office on 16 subsequent occasions without further evaluation or testing for the breast lump.
After the delivery of her child, the patient noted that the lump had become larger and painful. When she could not be seen by Dr. M., she was seen by her partner, Dr. P., in February 2005. Dr. P. found a suspicious mass and immediately ordered a mammogram and ultrasonography, which confirmed the presence of a 4.0-cm mass. Biopsy the next day led to a diagnosis of breast cancer. Through positron emission tomography and CT later that week and an additional biopsy, it was found that the cancer had metastasized to the patient’s liver.
She underwent 10 rounds of chemotherapy, a lumpectomy, a complete hysterectomy, and radiation treatment. She was given no chance for a cure, however.
The defendant denied any negligence, maintaining that the lump brought to her attention in July 2003 was not the same lump found in 2005. Even if the lump in 2003 had been found to be cancerous, the defendant argued, it had probably metastasized by that time, making any delay in treatment of no consequence.
A jury awarded $23.6 million to the plaintiff, which included $11,750,000 for the plaintiff’s husband.
Reaction to Radiologic Dye Blamed for Stroke Symptoms
An elderly woman presented to a hospital emergency department (ED) with left-side weakness and slurred speech; a stroke was suspected. The defendant ED physician evaluated the patient and made a diagnosis of an allergic reaction to a dye she had been given during IV pyelography the previous day. The patient was given diphenhydramine and discharged.
She returned to the ED the following day with indisputable symptoms of a stroke: left-side weakness affecting her hand and leg, diminished speech, and loss of bladder control.
The plaintiff alleged negligence in the failure of the ED physician to diagnose the stroke at her first visit.
The defendant claimed that in light of the plaintiff’s constellation of symptoms at the first visit, his diagnosis of an allergic reaction was reasonable. The defendant argued that the stroke had occurred after the patient’s first visit and that she would not have been a good candidate to receive tissue plasminogen activator therapy.
The jury was unable to reach a unanimous verdict, and the parties agreed to accept a less-than-unanimous verdict. The jury returned an eight-to-four verdict in favor of the defendant, and a defense judgment was entered.
Possible Fluid Overload for Child With Complex Medical History
A 7-year-old girl was brought into a hospital emergency department (ED) with congestion and several episodes of vomiting. Born prematurely, she had a history of hydroencephalitis requiring a ventriculoperitoneal shunt. As an infant, she had also experienced spastic cerebral palsy, developmental delays, and a chronic lung condition. She had spent her first three years in a hospital’s pediatric ICU.
At the ED, the child was examined by a PA, who then consulted with the ED physician. Pneumonitis, bronchiolitis, mild dehydration, and viral illness were diagnosed, with possible early-stage pneumonia. The child was sent home after being given 800 mL of IV normal saline infusion with 900 mg of ceftriaxone.
About two hours later, she was found by her father not breathing. She was taken back to the ED, where she was pronounced dead.
The plaintiff claimed that the child’s death was due to fluid overload, which caused pulmonary edema. The plaintiff also claimed that the ED staff failed to properly treat her complex medical condition or to monitor and observe her for a reasonable time.
The defendant claimed that the girl’s death was due to her chronic interstitial pneumonitis secondary to bronchopulmonary dysplasia.
According to a published account, the court found in favor of the defendant.
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Breast Malignancy Dismissed as Cyst
A 23-year-old woman called the defendant obstetrician/gynecologist’s office in July 2003 and reported to the receptionist that she had found a lump in her breast; it had been present for two months, she said, with possible dimpling. She asked to be seen immediately. Upon receiving the patient’s message, Dr. M. told the nurse to instruct the patient to wait until her next scheduled appointment, two weeks away; she also declined to schedule a mammogram.
At the patient’s scheduled appointment, Dr. M. performed the standard gynecologic examination and needed to be reminded to examine the lump before the patient left her office. Dr. M. diagnosed the lump as a cyst and told the patient it was nothing to worry about. No testing was performed, and no follow-up was recommended. Dr. M. did not document her findings in the patient’s record, nor did she note any self-reminders to reevaluate the lump at a later date.
The patient subsequently became pregnant and was seen in the defendant’s office on 16 subsequent occasions without further evaluation or testing for the breast lump.
After the delivery of her child, the patient noted that the lump had become larger and painful. When she could not be seen by Dr. M., she was seen by her partner, Dr. P., in February 2005. Dr. P. found a suspicious mass and immediately ordered a mammogram and ultrasonography, which confirmed the presence of a 4.0-cm mass. Biopsy the next day led to a diagnosis of breast cancer. Through positron emission tomography and CT later that week and an additional biopsy, it was found that the cancer had metastasized to the patient’s liver.
She underwent 10 rounds of chemotherapy, a lumpectomy, a complete hysterectomy, and radiation treatment. She was given no chance for a cure, however.
The defendant denied any negligence, maintaining that the lump brought to her attention in July 2003 was not the same lump found in 2005. Even if the lump in 2003 had been found to be cancerous, the defendant argued, it had probably metastasized by that time, making any delay in treatment of no consequence.
A jury awarded $23.6 million to the plaintiff, which included $11,750,000 for the plaintiff’s husband.
Reaction to Radiologic Dye Blamed for Stroke Symptoms
An elderly woman presented to a hospital emergency department (ED) with left-side weakness and slurred speech; a stroke was suspected. The defendant ED physician evaluated the patient and made a diagnosis of an allergic reaction to a dye she had been given during IV pyelography the previous day. The patient was given diphenhydramine and discharged.
She returned to the ED the following day with indisputable symptoms of a stroke: left-side weakness affecting her hand and leg, diminished speech, and loss of bladder control.
The plaintiff alleged negligence in the failure of the ED physician to diagnose the stroke at her first visit.
The defendant claimed that in light of the plaintiff’s constellation of symptoms at the first visit, his diagnosis of an allergic reaction was reasonable. The defendant argued that the stroke had occurred after the patient’s first visit and that she would not have been a good candidate to receive tissue plasminogen activator therapy.
The jury was unable to reach a unanimous verdict, and the parties agreed to accept a less-than-unanimous verdict. The jury returned an eight-to-four verdict in favor of the defendant, and a defense judgment was entered.
Possible Fluid Overload for Child With Complex Medical History
A 7-year-old girl was brought into a hospital emergency department (ED) with congestion and several episodes of vomiting. Born prematurely, she had a history of hydroencephalitis requiring a ventriculoperitoneal shunt. As an infant, she had also experienced spastic cerebral palsy, developmental delays, and a chronic lung condition. She had spent her first three years in a hospital’s pediatric ICU.
At the ED, the child was examined by a PA, who then consulted with the ED physician. Pneumonitis, bronchiolitis, mild dehydration, and viral illness were diagnosed, with possible early-stage pneumonia. The child was sent home after being given 800 mL of IV normal saline infusion with 900 mg of ceftriaxone.
About two hours later, she was found by her father not breathing. She was taken back to the ED, where she was pronounced dead.
The plaintiff claimed that the child’s death was due to fluid overload, which caused pulmonary edema. The plaintiff also claimed that the ED staff failed to properly treat her complex medical condition or to monitor and observe her for a reasonable time.
The defendant claimed that the girl’s death was due to her chronic interstitial pneumonitis secondary to bronchopulmonary dysplasia.
According to a published account, the court found in favor of the defendant.
Because of migraines, severe preeclampsia diagnosis is delayed ...
Because of migraines, severe preeclampsia diagnosis is delayed
A WOMAN IN HER 35TH WEEK OF PREGNANCY awoke with what she thought was a migraine headache. When home remedies did not provide relief, she called her ObGyn. He sent her to the hospital for testing. The results suggested preeclampsia, and her blood pressure was at a level that would not cause bleeding in the brain, he believed. It was decided to admit the patient overnight, and then reassess her condition and consider a cesarean delivery on the following day. When the patient reported her headache was severe and the pain radiated to the back of her neck, she was administered Demerol. Her blood pressure and pain decreased. Two hours later, she was unresponsive and the fetal heart rate had dropped. An emergent cesarean delivery was performed, resulting in the birth of a healthy infant.
Following transfer of the mother to another hospital, a CT scan indicated acute intracranial bleeding at the left basal ganglia and frontal lobes. An emergency craniotomy left her semicomatose. During a 6-month stay at a rehabilitation hospital, a shunt placed in her head became infected and required several procedures to treat the infection and replace the shunt. At discharge, she required 24-hour care because of cognitive and physical impairments. She suffers severe memory lapses and poor vision and is unable to walk without a brace.
PATIENT’S CLAIM The ObGyn was negligent for failing to diagnose and treat severe preeclampsia in a timely manner.
PHYSICIAN’S DEFENSE Considering the patient’s history of migraines, the diagnosis and treatment were reasonable. The patient and her husband were informed of the benefits and risks of overnight observation at the hospital. They also wanted to delay the child’s delivery to avoid the complications of a premature birth.
VERDICT $6,420,000 Massachusetts verdict.
After removing right ovary, Gyn discovers no ovary on the left
BECAUSE OF A PAINFUL CYST, a gynecologist removed the right ovary of a 33-year-old patient. During the procedure, adhesions were found on the patient’s left side—but not the left ovary or fallopian tube. Postoperatively, the patient was found to be menopausal, suggesting the absence of a left ovary.
PATIENT’S CLAIM She did not give informed consent. The gynecologist was negligent for removing the right ovary before checking for the presence of the left ovary and for removing the right ovary rather than limiting surgery to removal of the cyst.
PHYSICIAN’S DEFENSE It was necessary to remove the right ovary, whether or not the patient had a left ovary.
VERDICT Texas defense verdict. Prior to trial, the radiologist settled for an undisclosed amount.
$11.5 million for waterbirth dystocia case; infant has CP
DURING A WATERBIRTH in a birthing tub, shoulder dystocia was encountered. The child has cerebral palsy as a result of oxygen deprivation and brain damage.
PATIENT’S CLAIM The birthing tub was not drained quickly enough to use the standard maneuvers for resolving shoulder dystocia.
PHYSICIAN’S DEFENSE The injuries resulted from an infection in the placenta. The maneuvers to resolve the dystocia were performed as quickly as if the mother had not been in a tub.
VERDICT $11.5 million Illinois settlement.
Patient needs vaginal sling, cystocele repair; suffers foot drop
A WOMAN WENT TO THE HOSPITAL for a vaginal sling procedure and repair of a cystocele. Two surgeons, Dr. A and Dr. B, performed the urology part of the surgery. Then an ObGyn, Dr. C, performed the sacrospinous vaginal vault suspension, which included placement of two sutures. Postoperatively, the patient suffered right foot drop. Four days later, Dr. C removed the sutures. The foot drop persisted. At first, she sued several parties. Only Dr. C and his group went to trial.
PATIENT’S CLAIM Not reported.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Alabama settlement. The first trial ended in a mistrial by the court. The second trial resulted in a $1 million verdict, but the court set it aside and ordered a new trial. Then the parties settled.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Because of migraines, severe preeclampsia diagnosis is delayed
A WOMAN IN HER 35TH WEEK OF PREGNANCY awoke with what she thought was a migraine headache. When home remedies did not provide relief, she called her ObGyn. He sent her to the hospital for testing. The results suggested preeclampsia, and her blood pressure was at a level that would not cause bleeding in the brain, he believed. It was decided to admit the patient overnight, and then reassess her condition and consider a cesarean delivery on the following day. When the patient reported her headache was severe and the pain radiated to the back of her neck, she was administered Demerol. Her blood pressure and pain decreased. Two hours later, she was unresponsive and the fetal heart rate had dropped. An emergent cesarean delivery was performed, resulting in the birth of a healthy infant.
Following transfer of the mother to another hospital, a CT scan indicated acute intracranial bleeding at the left basal ganglia and frontal lobes. An emergency craniotomy left her semicomatose. During a 6-month stay at a rehabilitation hospital, a shunt placed in her head became infected and required several procedures to treat the infection and replace the shunt. At discharge, she required 24-hour care because of cognitive and physical impairments. She suffers severe memory lapses and poor vision and is unable to walk without a brace.
PATIENT’S CLAIM The ObGyn was negligent for failing to diagnose and treat severe preeclampsia in a timely manner.
PHYSICIAN’S DEFENSE Considering the patient’s history of migraines, the diagnosis and treatment were reasonable. The patient and her husband were informed of the benefits and risks of overnight observation at the hospital. They also wanted to delay the child’s delivery to avoid the complications of a premature birth.
VERDICT $6,420,000 Massachusetts verdict.
After removing right ovary, Gyn discovers no ovary on the left
BECAUSE OF A PAINFUL CYST, a gynecologist removed the right ovary of a 33-year-old patient. During the procedure, adhesions were found on the patient’s left side—but not the left ovary or fallopian tube. Postoperatively, the patient was found to be menopausal, suggesting the absence of a left ovary.
PATIENT’S CLAIM She did not give informed consent. The gynecologist was negligent for removing the right ovary before checking for the presence of the left ovary and for removing the right ovary rather than limiting surgery to removal of the cyst.
PHYSICIAN’S DEFENSE It was necessary to remove the right ovary, whether or not the patient had a left ovary.
VERDICT Texas defense verdict. Prior to trial, the radiologist settled for an undisclosed amount.
$11.5 million for waterbirth dystocia case; infant has CP
DURING A WATERBIRTH in a birthing tub, shoulder dystocia was encountered. The child has cerebral palsy as a result of oxygen deprivation and brain damage.
PATIENT’S CLAIM The birthing tub was not drained quickly enough to use the standard maneuvers for resolving shoulder dystocia.
PHYSICIAN’S DEFENSE The injuries resulted from an infection in the placenta. The maneuvers to resolve the dystocia were performed as quickly as if the mother had not been in a tub.
VERDICT $11.5 million Illinois settlement.
Patient needs vaginal sling, cystocele repair; suffers foot drop
A WOMAN WENT TO THE HOSPITAL for a vaginal sling procedure and repair of a cystocele. Two surgeons, Dr. A and Dr. B, performed the urology part of the surgery. Then an ObGyn, Dr. C, performed the sacrospinous vaginal vault suspension, which included placement of two sutures. Postoperatively, the patient suffered right foot drop. Four days later, Dr. C removed the sutures. The foot drop persisted. At first, she sued several parties. Only Dr. C and his group went to trial.
PATIENT’S CLAIM Not reported.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Alabama settlement. The first trial ended in a mistrial by the court. The second trial resulted in a $1 million verdict, but the court set it aside and ordered a new trial. Then the parties settled.
Because of migraines, severe preeclampsia diagnosis is delayed
A WOMAN IN HER 35TH WEEK OF PREGNANCY awoke with what she thought was a migraine headache. When home remedies did not provide relief, she called her ObGyn. He sent her to the hospital for testing. The results suggested preeclampsia, and her blood pressure was at a level that would not cause bleeding in the brain, he believed. It was decided to admit the patient overnight, and then reassess her condition and consider a cesarean delivery on the following day. When the patient reported her headache was severe and the pain radiated to the back of her neck, she was administered Demerol. Her blood pressure and pain decreased. Two hours later, she was unresponsive and the fetal heart rate had dropped. An emergent cesarean delivery was performed, resulting in the birth of a healthy infant.
Following transfer of the mother to another hospital, a CT scan indicated acute intracranial bleeding at the left basal ganglia and frontal lobes. An emergency craniotomy left her semicomatose. During a 6-month stay at a rehabilitation hospital, a shunt placed in her head became infected and required several procedures to treat the infection and replace the shunt. At discharge, she required 24-hour care because of cognitive and physical impairments. She suffers severe memory lapses and poor vision and is unable to walk without a brace.
PATIENT’S CLAIM The ObGyn was negligent for failing to diagnose and treat severe preeclampsia in a timely manner.
PHYSICIAN’S DEFENSE Considering the patient’s history of migraines, the diagnosis and treatment were reasonable. The patient and her husband were informed of the benefits and risks of overnight observation at the hospital. They also wanted to delay the child’s delivery to avoid the complications of a premature birth.
VERDICT $6,420,000 Massachusetts verdict.
After removing right ovary, Gyn discovers no ovary on the left
BECAUSE OF A PAINFUL CYST, a gynecologist removed the right ovary of a 33-year-old patient. During the procedure, adhesions were found on the patient’s left side—but not the left ovary or fallopian tube. Postoperatively, the patient was found to be menopausal, suggesting the absence of a left ovary.
PATIENT’S CLAIM She did not give informed consent. The gynecologist was negligent for removing the right ovary before checking for the presence of the left ovary and for removing the right ovary rather than limiting surgery to removal of the cyst.
PHYSICIAN’S DEFENSE It was necessary to remove the right ovary, whether or not the patient had a left ovary.
VERDICT Texas defense verdict. Prior to trial, the radiologist settled for an undisclosed amount.
$11.5 million for waterbirth dystocia case; infant has CP
DURING A WATERBIRTH in a birthing tub, shoulder dystocia was encountered. The child has cerebral palsy as a result of oxygen deprivation and brain damage.
PATIENT’S CLAIM The birthing tub was not drained quickly enough to use the standard maneuvers for resolving shoulder dystocia.
PHYSICIAN’S DEFENSE The injuries resulted from an infection in the placenta. The maneuvers to resolve the dystocia were performed as quickly as if the mother had not been in a tub.
VERDICT $11.5 million Illinois settlement.
Patient needs vaginal sling, cystocele repair; suffers foot drop
A WOMAN WENT TO THE HOSPITAL for a vaginal sling procedure and repair of a cystocele. Two surgeons, Dr. A and Dr. B, performed the urology part of the surgery. Then an ObGyn, Dr. C, performed the sacrospinous vaginal vault suspension, which included placement of two sutures. Postoperatively, the patient suffered right foot drop. Four days later, Dr. C removed the sutures. The foot drop persisted. At first, she sued several parties. Only Dr. C and his group went to trial.
PATIENT’S CLAIM Not reported.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Alabama settlement. The first trial ended in a mistrial by the court. The second trial resulted in a $1 million verdict, but the court set it aside and ordered a new trial. Then the parties settled.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Necessary Evil: Change

The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Was gastroschisis of late onset—or visible on sonograms?... and more
Was gastroschisis of late onset—or visible on sonograms?
BECAUSE OF ADVANCED AGE and the presence of uterine fibroids, a woman underwent prenatal ultrasonography in the fifth, sixth, and seventh months of pregnancy. The sonograms were performed and interpreted by a specialist in maternal–fetal medicine. The baby was born with most of his intestines outside his abdomen and was transferred to another hospital, where surgery was performed nearly 4 hours after birth, revealing necrosis of a significant length of bowel. The child suffered short-gut syndrome and required intravenous catheter and tube feeding until the age of 5 years. His growth was stunted.
PATIENT’S CLAIM The sonograms showed gastroschisis. If this had been recognized at that time, the birth could have taken place in a hospital where surgical repair could be performed within 2 hours of birth. Because of the delay in surgery, necrosis of most of the small intestine occurred.
PHYSICIAN’S DEFENSE The child suffered late-onset gastroschisis, or ruptured umbilical hernia, which the sonograms did not show. No matter where the child was born, the outcome would have been the same.
VERDICT Illinois defense verdict for the specialist in maternal–fetal medicine. Prior to trial, the hospital and radiologist settled for $35,000 and $200,000, respectively.
Unsigned death certificate delays cremation of stillborn
FOLLOWING THE STILLBIRTH of their child, a couple waited 3 weeks for the death certificate to be signed. Only then were they given the body for cremation.
PLAINTIFFS’ CLAIM Dr. A, the attending physician, was negligent for not signing the baby’s death certificate in a timely manner, thus delaying the cremation and causing emotional distress. A death certificate should be signed within 1 day of determining the cause of death or knowing that there will be no further information about the cause.
PHYSICIAN’S DEFENSE According to Dr. A, his stated cause of death was rejected initially. While he was waiting for additional clinical information, Dr. B signed the certificate, giving only a general cause of death. Dr. A claimed his own actions caused no damages.
VERDICT $11,000 California verdict.
MDs find ovarian cyst, then, 7 months later, peritoneal cancer
A 49-YEAR-OLD WOMAN with an ovarian cyst underwent laparoscopy. Dr. C, the ObGyn who performed the surgery, found ovaries that were normal, but also the presence of endometriosis and adhesions. Dr. D and Dr. E provided follow-up care. When the patient visited Dr. E 5 months later complaining of bloating and gastrointestinal pain, ultrasonography was performed. She then followed up with her primary care physician and a gastroenterologist. Three months later, she underwent emergency surgery. Stage IIIC primary papillary serous carcinoma of the peritoneum was discovered in her pelvis and abdomen. Despite multiple surgeries and chemotherapy over the next year and a half, the patient died.
PLAINTIFF’S CLAIM Dr. C should have performed a biopsy during the original laparoscopy; this would have allowed an earlier diagnosis with a better prognosis.
PHYSICIAN’S DEFENSE A biopsy was not required initially; in fact, the cancer was probably either not present or microscopic at that time. Even with a diagnosis then, the odds of survival would have been much the same.
VERDICT Illinois defense verdict. The jury deadlocked, 11 to 1. The parties agreed to a less than unanimous verdict and a high/low agreement of $750,000/$100,000. Then the jury returned a defense verdict.
Still incontinent after undergoing retropubic urethropexy
A 43-YEAR-OLD WOMAN was experiencing urinary incontinence, gynecological pain, and bleeding. Her ObGyn diagnosed pelvic organ prolapse. A month later, the patient underwent a total abdominal hysterectomy with retropubic urethropexy. Following the surgery, the patient continued to be incontinent.
PATIENT’S CLAIM A sling procedure to correct the incontinence should have been performed.
PHYSICIAN’S DEFENSE The proper procedure and technique were used. As the patient was undergoing an abdominal hysterectomy, it was reasonable to perform a retropubic urethropexy at the same time.
VERDICT Texas defense verdict.
A $30.9 million verdict in the case of induced VBAC
ATTEMPTING A VAGINAL BIRTH after cesarean (VBAC), a woman arrived at the hospital for induced delivery of her child. During labor, the uterus ruptured and placental abruption occurred. For approximately 20 minutes, the fetus was deprived of oxygen. A cesarean delivery was performed, and the child was diagnosed with severe brain damage and cerebral palsy.
PATIENT’S CLAIM Uterine rupture was caused by hyperstimulation with oxytocin. After the loss of the fetal heart rate, the nurses delayed more than 15 minutes before notifying a physician.
PHYSICIAN’S DEFENSE The patient was informed of the increased risk of rupture when attempting VBAC. The nurses were following physician orders regarding use of oxytocin. Until the time of rupture and abruption, the uterus was not hyperstimulated and the heart rate was normal.
VERDICT $30,953,181 Ohio verdict against the hospital only. The case was settled under a confidential high/low agreement reached before the verdict.
While on HRT, patient with serious health concerns has stroke
DR. F PRESCRIBED oral hormone replacement therapy (HRT) to treat the menopausal symptoms of a 46-year-old patient. The following year he prescribed an estrogen patch and continued treating her for another 3 years until he died. Then Dr. G took over the patient’s care. She remained on some form of HRT until she suffered a stroke 2 years later. She suffered significant cognitive impairment and could no longer drive or work.
PATIENT’S CLAIM She should have been evaluated more thoroughly and weaned from artificial hormones. She had high blood pressure and high cholesterol, was overweight, and had a family history of cardiovascular problems.
PHYSICIAN’S DEFENSE The patient’s stroke was not necessarily related to HRT. In fact, it could have been caused by her cardiac condition.
VERDICT Missouri defense verdict.
Was laparoscopy to remove an ovary contraindicated?
A 39-YEAR-OLD WOMAN underwent multiple surgeries performed by her ObGyn: tubal ligation, dilation and curettage, hysteroscopy, and emergent hysterectomy. Following the hysterectomy, during which the ovaries were not removed, she had significant left upper quadrant pain. Ultrasonography revealed two cysts on the left ovary. During recommended surgery to remove the ovary, the physician continued laparoscopic dissection despite complications caused by extensive omental adhesions. The surgery lasted 5 hours, after which the patient required 2 days of hospitalization. Within 24 hours of leaving the hospital, she returned to the emergency room with fever, nausea, vomiting, and abdominal pain. A CT scan indicated a probable leak from the sigmoid colon. Follow-up surgery showed perforation of the sigmoid colon and a colostomy was placed. The patient developed acute respiratory distress syndrome and required intubation and mechanical ventilation during a 2-week hospitalization.
PATIENT’S CLAIM Because of her prior abdominal surgeries, laparoscopic surgery was contraindicated. Once begun, it should have been converted to an open procedure. Also, the physician should have recognized the injury to the sigmoid colon and treated it immediately.
PHYSICIAN’S DEFENSE Perforation is a known risk of laparoscopy, and the patient was informed of this.
VERDICT $437,438 Maryland verdict.
Nephrectomy is necessary after ureteral injury
A 52-YEAR-OLD WOMAN with a history of fibroids was told by her ObGyn, Dr. H, that the tumors had grown. After undergoing a recommended hysterectomy performed by Dr. H, the patient experienced ongoing pain. Three months after the surgery, she consulted Dr. J, who diagnosed ureteral obstruction. The patient then underwent surgical repair of the obstruction, but suffered permanent kidney damage. Nephrectomy was performed a month later.
PATIENT’S CLAIM Dr. H was negligent because he injured the ureter during the hysterectomy and was also negligent for failing to recognize the injury.
PHYSICIAN’S DEFENSE Ureteral injury is a known complication of the procedure. Also, the patient’s symptoms were inconsistent with such an injury.
VERDICT Tennessee defense verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Was gastroschisis of late onset—or visible on sonograms?
BECAUSE OF ADVANCED AGE and the presence of uterine fibroids, a woman underwent prenatal ultrasonography in the fifth, sixth, and seventh months of pregnancy. The sonograms were performed and interpreted by a specialist in maternal–fetal medicine. The baby was born with most of his intestines outside his abdomen and was transferred to another hospital, where surgery was performed nearly 4 hours after birth, revealing necrosis of a significant length of bowel. The child suffered short-gut syndrome and required intravenous catheter and tube feeding until the age of 5 years. His growth was stunted.
PATIENT’S CLAIM The sonograms showed gastroschisis. If this had been recognized at that time, the birth could have taken place in a hospital where surgical repair could be performed within 2 hours of birth. Because of the delay in surgery, necrosis of most of the small intestine occurred.
PHYSICIAN’S DEFENSE The child suffered late-onset gastroschisis, or ruptured umbilical hernia, which the sonograms did not show. No matter where the child was born, the outcome would have been the same.
VERDICT Illinois defense verdict for the specialist in maternal–fetal medicine. Prior to trial, the hospital and radiologist settled for $35,000 and $200,000, respectively.
Unsigned death certificate delays cremation of stillborn
FOLLOWING THE STILLBIRTH of their child, a couple waited 3 weeks for the death certificate to be signed. Only then were they given the body for cremation.
PLAINTIFFS’ CLAIM Dr. A, the attending physician, was negligent for not signing the baby’s death certificate in a timely manner, thus delaying the cremation and causing emotional distress. A death certificate should be signed within 1 day of determining the cause of death or knowing that there will be no further information about the cause.
PHYSICIAN’S DEFENSE According to Dr. A, his stated cause of death was rejected initially. While he was waiting for additional clinical information, Dr. B signed the certificate, giving only a general cause of death. Dr. A claimed his own actions caused no damages.
VERDICT $11,000 California verdict.
MDs find ovarian cyst, then, 7 months later, peritoneal cancer
A 49-YEAR-OLD WOMAN with an ovarian cyst underwent laparoscopy. Dr. C, the ObGyn who performed the surgery, found ovaries that were normal, but also the presence of endometriosis and adhesions. Dr. D and Dr. E provided follow-up care. When the patient visited Dr. E 5 months later complaining of bloating and gastrointestinal pain, ultrasonography was performed. She then followed up with her primary care physician and a gastroenterologist. Three months later, she underwent emergency surgery. Stage IIIC primary papillary serous carcinoma of the peritoneum was discovered in her pelvis and abdomen. Despite multiple surgeries and chemotherapy over the next year and a half, the patient died.
PLAINTIFF’S CLAIM Dr. C should have performed a biopsy during the original laparoscopy; this would have allowed an earlier diagnosis with a better prognosis.
PHYSICIAN’S DEFENSE A biopsy was not required initially; in fact, the cancer was probably either not present or microscopic at that time. Even with a diagnosis then, the odds of survival would have been much the same.
VERDICT Illinois defense verdict. The jury deadlocked, 11 to 1. The parties agreed to a less than unanimous verdict and a high/low agreement of $750,000/$100,000. Then the jury returned a defense verdict.
Still incontinent after undergoing retropubic urethropexy
A 43-YEAR-OLD WOMAN was experiencing urinary incontinence, gynecological pain, and bleeding. Her ObGyn diagnosed pelvic organ prolapse. A month later, the patient underwent a total abdominal hysterectomy with retropubic urethropexy. Following the surgery, the patient continued to be incontinent.
PATIENT’S CLAIM A sling procedure to correct the incontinence should have been performed.
PHYSICIAN’S DEFENSE The proper procedure and technique were used. As the patient was undergoing an abdominal hysterectomy, it was reasonable to perform a retropubic urethropexy at the same time.
VERDICT Texas defense verdict.
A $30.9 million verdict in the case of induced VBAC
ATTEMPTING A VAGINAL BIRTH after cesarean (VBAC), a woman arrived at the hospital for induced delivery of her child. During labor, the uterus ruptured and placental abruption occurred. For approximately 20 minutes, the fetus was deprived of oxygen. A cesarean delivery was performed, and the child was diagnosed with severe brain damage and cerebral palsy.
PATIENT’S CLAIM Uterine rupture was caused by hyperstimulation with oxytocin. After the loss of the fetal heart rate, the nurses delayed more than 15 minutes before notifying a physician.
PHYSICIAN’S DEFENSE The patient was informed of the increased risk of rupture when attempting VBAC. The nurses were following physician orders regarding use of oxytocin. Until the time of rupture and abruption, the uterus was not hyperstimulated and the heart rate was normal.
VERDICT $30,953,181 Ohio verdict against the hospital only. The case was settled under a confidential high/low agreement reached before the verdict.
While on HRT, patient with serious health concerns has stroke
DR. F PRESCRIBED oral hormone replacement therapy (HRT) to treat the menopausal symptoms of a 46-year-old patient. The following year he prescribed an estrogen patch and continued treating her for another 3 years until he died. Then Dr. G took over the patient’s care. She remained on some form of HRT until she suffered a stroke 2 years later. She suffered significant cognitive impairment and could no longer drive or work.
PATIENT’S CLAIM She should have been evaluated more thoroughly and weaned from artificial hormones. She had high blood pressure and high cholesterol, was overweight, and had a family history of cardiovascular problems.
PHYSICIAN’S DEFENSE The patient’s stroke was not necessarily related to HRT. In fact, it could have been caused by her cardiac condition.
VERDICT Missouri defense verdict.
Was laparoscopy to remove an ovary contraindicated?
A 39-YEAR-OLD WOMAN underwent multiple surgeries performed by her ObGyn: tubal ligation, dilation and curettage, hysteroscopy, and emergent hysterectomy. Following the hysterectomy, during which the ovaries were not removed, she had significant left upper quadrant pain. Ultrasonography revealed two cysts on the left ovary. During recommended surgery to remove the ovary, the physician continued laparoscopic dissection despite complications caused by extensive omental adhesions. The surgery lasted 5 hours, after which the patient required 2 days of hospitalization. Within 24 hours of leaving the hospital, she returned to the emergency room with fever, nausea, vomiting, and abdominal pain. A CT scan indicated a probable leak from the sigmoid colon. Follow-up surgery showed perforation of the sigmoid colon and a colostomy was placed. The patient developed acute respiratory distress syndrome and required intubation and mechanical ventilation during a 2-week hospitalization.
PATIENT’S CLAIM Because of her prior abdominal surgeries, laparoscopic surgery was contraindicated. Once begun, it should have been converted to an open procedure. Also, the physician should have recognized the injury to the sigmoid colon and treated it immediately.
PHYSICIAN’S DEFENSE Perforation is a known risk of laparoscopy, and the patient was informed of this.
VERDICT $437,438 Maryland verdict.
Nephrectomy is necessary after ureteral injury
A 52-YEAR-OLD WOMAN with a history of fibroids was told by her ObGyn, Dr. H, that the tumors had grown. After undergoing a recommended hysterectomy performed by Dr. H, the patient experienced ongoing pain. Three months after the surgery, she consulted Dr. J, who diagnosed ureteral obstruction. The patient then underwent surgical repair of the obstruction, but suffered permanent kidney damage. Nephrectomy was performed a month later.
PATIENT’S CLAIM Dr. H was negligent because he injured the ureter during the hysterectomy and was also negligent for failing to recognize the injury.
PHYSICIAN’S DEFENSE Ureteral injury is a known complication of the procedure. Also, the patient’s symptoms were inconsistent with such an injury.
VERDICT Tennessee defense verdict.
Was gastroschisis of late onset—or visible on sonograms?
BECAUSE OF ADVANCED AGE and the presence of uterine fibroids, a woman underwent prenatal ultrasonography in the fifth, sixth, and seventh months of pregnancy. The sonograms were performed and interpreted by a specialist in maternal–fetal medicine. The baby was born with most of his intestines outside his abdomen and was transferred to another hospital, where surgery was performed nearly 4 hours after birth, revealing necrosis of a significant length of bowel. The child suffered short-gut syndrome and required intravenous catheter and tube feeding until the age of 5 years. His growth was stunted.
PATIENT’S CLAIM The sonograms showed gastroschisis. If this had been recognized at that time, the birth could have taken place in a hospital where surgical repair could be performed within 2 hours of birth. Because of the delay in surgery, necrosis of most of the small intestine occurred.
PHYSICIAN’S DEFENSE The child suffered late-onset gastroschisis, or ruptured umbilical hernia, which the sonograms did not show. No matter where the child was born, the outcome would have been the same.
VERDICT Illinois defense verdict for the specialist in maternal–fetal medicine. Prior to trial, the hospital and radiologist settled for $35,000 and $200,000, respectively.
Unsigned death certificate delays cremation of stillborn
FOLLOWING THE STILLBIRTH of their child, a couple waited 3 weeks for the death certificate to be signed. Only then were they given the body for cremation.
PLAINTIFFS’ CLAIM Dr. A, the attending physician, was negligent for not signing the baby’s death certificate in a timely manner, thus delaying the cremation and causing emotional distress. A death certificate should be signed within 1 day of determining the cause of death or knowing that there will be no further information about the cause.
PHYSICIAN’S DEFENSE According to Dr. A, his stated cause of death was rejected initially. While he was waiting for additional clinical information, Dr. B signed the certificate, giving only a general cause of death. Dr. A claimed his own actions caused no damages.
VERDICT $11,000 California verdict.
MDs find ovarian cyst, then, 7 months later, peritoneal cancer
A 49-YEAR-OLD WOMAN with an ovarian cyst underwent laparoscopy. Dr. C, the ObGyn who performed the surgery, found ovaries that were normal, but also the presence of endometriosis and adhesions. Dr. D and Dr. E provided follow-up care. When the patient visited Dr. E 5 months later complaining of bloating and gastrointestinal pain, ultrasonography was performed. She then followed up with her primary care physician and a gastroenterologist. Three months later, she underwent emergency surgery. Stage IIIC primary papillary serous carcinoma of the peritoneum was discovered in her pelvis and abdomen. Despite multiple surgeries and chemotherapy over the next year and a half, the patient died.
PLAINTIFF’S CLAIM Dr. C should have performed a biopsy during the original laparoscopy; this would have allowed an earlier diagnosis with a better prognosis.
PHYSICIAN’S DEFENSE A biopsy was not required initially; in fact, the cancer was probably either not present or microscopic at that time. Even with a diagnosis then, the odds of survival would have been much the same.
VERDICT Illinois defense verdict. The jury deadlocked, 11 to 1. The parties agreed to a less than unanimous verdict and a high/low agreement of $750,000/$100,000. Then the jury returned a defense verdict.
Still incontinent after undergoing retropubic urethropexy
A 43-YEAR-OLD WOMAN was experiencing urinary incontinence, gynecological pain, and bleeding. Her ObGyn diagnosed pelvic organ prolapse. A month later, the patient underwent a total abdominal hysterectomy with retropubic urethropexy. Following the surgery, the patient continued to be incontinent.
PATIENT’S CLAIM A sling procedure to correct the incontinence should have been performed.
PHYSICIAN’S DEFENSE The proper procedure and technique were used. As the patient was undergoing an abdominal hysterectomy, it was reasonable to perform a retropubic urethropexy at the same time.
VERDICT Texas defense verdict.
A $30.9 million verdict in the case of induced VBAC
ATTEMPTING A VAGINAL BIRTH after cesarean (VBAC), a woman arrived at the hospital for induced delivery of her child. During labor, the uterus ruptured and placental abruption occurred. For approximately 20 minutes, the fetus was deprived of oxygen. A cesarean delivery was performed, and the child was diagnosed with severe brain damage and cerebral palsy.
PATIENT’S CLAIM Uterine rupture was caused by hyperstimulation with oxytocin. After the loss of the fetal heart rate, the nurses delayed more than 15 minutes before notifying a physician.
PHYSICIAN’S DEFENSE The patient was informed of the increased risk of rupture when attempting VBAC. The nurses were following physician orders regarding use of oxytocin. Until the time of rupture and abruption, the uterus was not hyperstimulated and the heart rate was normal.
VERDICT $30,953,181 Ohio verdict against the hospital only. The case was settled under a confidential high/low agreement reached before the verdict.
While on HRT, patient with serious health concerns has stroke
DR. F PRESCRIBED oral hormone replacement therapy (HRT) to treat the menopausal symptoms of a 46-year-old patient. The following year he prescribed an estrogen patch and continued treating her for another 3 years until he died. Then Dr. G took over the patient’s care. She remained on some form of HRT until she suffered a stroke 2 years later. She suffered significant cognitive impairment and could no longer drive or work.
PATIENT’S CLAIM She should have been evaluated more thoroughly and weaned from artificial hormones. She had high blood pressure and high cholesterol, was overweight, and had a family history of cardiovascular problems.
PHYSICIAN’S DEFENSE The patient’s stroke was not necessarily related to HRT. In fact, it could have been caused by her cardiac condition.
VERDICT Missouri defense verdict.
Was laparoscopy to remove an ovary contraindicated?
A 39-YEAR-OLD WOMAN underwent multiple surgeries performed by her ObGyn: tubal ligation, dilation and curettage, hysteroscopy, and emergent hysterectomy. Following the hysterectomy, during which the ovaries were not removed, she had significant left upper quadrant pain. Ultrasonography revealed two cysts on the left ovary. During recommended surgery to remove the ovary, the physician continued laparoscopic dissection despite complications caused by extensive omental adhesions. The surgery lasted 5 hours, after which the patient required 2 days of hospitalization. Within 24 hours of leaving the hospital, she returned to the emergency room with fever, nausea, vomiting, and abdominal pain. A CT scan indicated a probable leak from the sigmoid colon. Follow-up surgery showed perforation of the sigmoid colon and a colostomy was placed. The patient developed acute respiratory distress syndrome and required intubation and mechanical ventilation during a 2-week hospitalization.
PATIENT’S CLAIM Because of her prior abdominal surgeries, laparoscopic surgery was contraindicated. Once begun, it should have been converted to an open procedure. Also, the physician should have recognized the injury to the sigmoid colon and treated it immediately.
PHYSICIAN’S DEFENSE Perforation is a known risk of laparoscopy, and the patient was informed of this.
VERDICT $437,438 Maryland verdict.
Nephrectomy is necessary after ureteral injury
A 52-YEAR-OLD WOMAN with a history of fibroids was told by her ObGyn, Dr. H, that the tumors had grown. After undergoing a recommended hysterectomy performed by Dr. H, the patient experienced ongoing pain. Three months after the surgery, she consulted Dr. J, who diagnosed ureteral obstruction. The patient then underwent surgical repair of the obstruction, but suffered permanent kidney damage. Nephrectomy was performed a month later.
PATIENT’S CLAIM Dr. H was negligent because he injured the ureter during the hysterectomy and was also negligent for failing to recognize the injury.
PHYSICIAN’S DEFENSE Ureteral injury is a known complication of the procedure. Also, the patient’s symptoms were inconsistent with such an injury.
VERDICT Tennessee defense verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Quality over Quantity
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
Submission Support
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
What is the best initial treatment of an adult patient with healthcare-associated pneumonia?
Case
A 68-year-old man with hypertension, diabetes, and recent hip fracture with poor functional status presents from a nursing home with a productive cough, shortness of breath, and chills of two-day duration. He finished a five-day course of cephalexin for a urinary tract infection one week ago. His vital signs reveal a blood pressure of 162/80 mm/Hg, temperature of 101.9°F, respirations of 26 breaths per minute, and oxygen saturation of 88% on room air. Coarse breath sounds are noted in the right lung field and his chest X-ray reveals a right-middle-lobe infiltrate.
He is admitted to the hospital with a diagnosis of healthcare-associated pneumonia. What is the best empiric antibiotic coverage for this patient?

Overview
Modern medicine exists over a continuum of care that is delivered in a manifold of different settings. Patients routinely receive complex medical care at home, including wound care and infusion of intravenous antibiotics. Additionally, many patients are interfacing with the healthcare system on a regular basis via hemodialysis centers or sub-acute rehabilitation centers. As a result of these interactions, patients are exposed to—and colonized by—different bacterial pathogens that can result in a variety of infections.1
While patients with healthcare-associated pneumonia (HCAP) can present similarly to those with community-acquired pneumonia (CAP)—patients with CAP normally present with a lower-respiratory-tract infection—the differences in the likely etiological pathogens dictate that these patients be considered for broader-spectrum empiric antibiotics. Hospitalists will continue to be responsible for choosing the initial antibiotic regimen for these patients, and they need to be able to recognize this disease process in order to treat it appropriately.
The joint American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guidelines released in 2005 emphasize that certain clinical HCAP risk factors center on increased interactions and encounters with healthcare facilities.2 These risk factors are evolving over time to include a patient’s functional status, recent antibiotic use, and clinical severity.
Review of the Data
Differences between HCAP and CAP
HCAP represents a diagnostic category of pneumonia created to differentiate patients with infections caused by a different microbiological subset of bacteria, including possible multi-drug-resistant (MDR) organisms, from patients with CAP. Thus far, culture data support this dichotomy.3,4
Kollef and colleagues performed a multicenter, retrospective cohort study of 4,543 patients with bacterial respiratory culture-positive pneumonia between 2002 and 2003. The study examined the bacteriological differences between CAP and HCAP. In this study, HCAP patients were defined as having: transfer from another healthcare facility; long-term hemodialysis; or prior hospitalization within 30 days in which they had non-ventilator-associated pneumonia (VAP). CAP patients were defined as having non-VAP and non-HCAP.
The study showed that the frequency of Pseudomonas aeurginosa (25% HCAP vs. 17% CAP) and Staphylococcus aureus (46% vs. 25%), which included methicillin-resistant Staphylococcus aureus (MRSA) (18% vs. 6%), was significantly higher in patients with HCAP than those with CAP. Additionally, frequency of Streptococcus pneumoniae (5% vs. 16%) and Haemophilus influenza (5% vs. 16%) infections were noted as significantly lower.3
A single-center, retrospective cohort analysis of 639 patients done by Micek et al yielded similar culture differences between CAP and HCAP patients. In this study, criteria for HCAP were defined as hospitalization in the past year, immunosuppression, nursing-home resident, or hemodialysis. The study authors found that a significantly higher percentage of HCAP patients were infected with MRSA (30% vs. 12%), Pseudomonas aeurginosa (25% vs. 4%), and other non-fermenting gram-negative rods (GNR) (10% vs. 2%). HCAP patients again were noted as having significantly fewer infections with S. pneumoniae (10% vs. 40%) and Haemophilus influenza (4% vs. 17%).
In addition to showing a difference in the bacteriology of CAP and HCAP, the Kollef study also evaluated mortality rates, length of stay, and hospital charges. Mortality rates for HCAP (19.8%) were similar to those of hospital-acquired pneumonia (HAP) (18.8%), and both of these were significantly higher than CAP (10%). Length of stay and hospital cost increased across the spectrum, from CAP to HCAP to HAP, with significant differences between each.3
ATS/IDSA Guidelines
In 2005, a joint committee of the ATS and ISDA updated its initial 1996 nosocomial pneumonia guidelines. The guideline update included the new HCAP category.2 The No. 1 goal of these guidelines was to emphasize early and appropriate antibiotics, followed by tailoring of the treatment regimen based upon culture and clinical data. To this end, HCAP risk factors were developed via extrapolation from observational data generated from HAP and VAP patients.5,6,7
The risk factors are summarized in Table 1 (see p. 19).2 Guidelines dictated that the identification of any of these risk factors in pneumonia patients at the time of admission indicates increased risk for infection with an MDR organism. These high-risk patients require placement into the diagnostic category of HCAP.
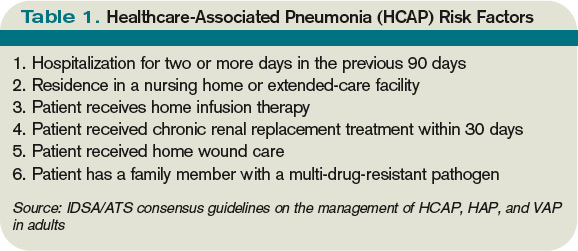
Once a patient has been diagnosed with HCAP, the guidelines recommended obtaining lower-respiratory-tract cultures and initiating broad-spectrum antibiotic therapy. Appropriate empiric antibiotic therapy was suggested to be the same as for HAP. This regimen requires coverage with two anti-pseudomonal agents, as well as an agent with activity against MRSA.
The rationale behind initial coverage with two anti-pseudomonal agents stems from the finding that pseudomonas has a high rate of resistance to many antibiotics, and that if two agents are empirically started, chances of appropriate coverage increase from the outset. This is important, as timely administration of appropriate antibiotics has been shown to decrease mortality in infections.8
Additional considerations for empiric antibiotic treatment include sensitivities of local microbiologic data, as well as any recent antibiotic regimens given to the patient. Following this broad primary antibiotic coverage, de-escalation was recommended based on results of lower respiratory cultures and clinical improvement.2
Evolution of Diagnostic Criteria and Empiric Antibiotic Coverage
Since the publication of the 2005 ATS/IDSA guidelines, the aforementioned risk factors for HCAP have been brought into question, as they have yet to be validated by prospective trials. There is a growing concern that these criteria may not be adequately specific and, therefore, might call for too many patients to be treated with a broader spectrum of antibiotic coverage, thereby increasing the likelihood of developing MDR bacteria.
In order to further analyze HCAP criteria, Poch and Ost wrote a review earlier this year examining the data behind each of the risk factors cited in the ATS/IDSA guidelines; they found considerable heterogeneity in magnitude of MDR infection risk for these criteria.9 The authors also reviewed studies looking at other risk factors for MDR infections in patients living in nursing homes or afflicted with CAP. They proposed that such additional factors as patient specific risks (including functional status and previous antibiotic exposure) and contextual risks (including nurse-to-patient ratio) be evaluated and possibly incorporated into criteria.
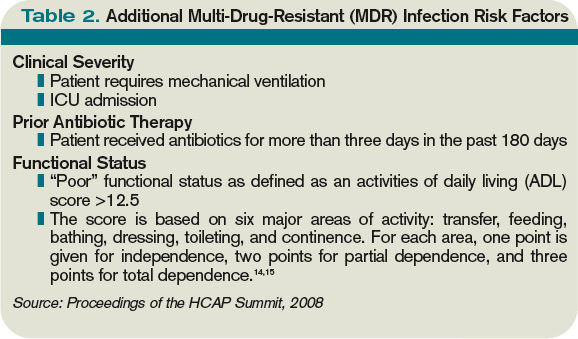
Of all the patients with HCAP criteria, residents in nursing homes have been studied the best. Loeb et al, while looking for a way to decrease hospitalizations for nursing-home residents, showed that patients who get pneumonia (by guideline definition HCAP) can be effectively treated as outpatients with a single antibiotic agent.10 This randomized controlled trial of 680 patients, all with HCAP, were treated with oral levofloxacin at the nursing home or admitted to the hospital. There were no significant differences between mortality (8% vs. 9%) and quality-of-life measures between the two groups. Furthermore, analysis of data from the 1980s showed that nursing-home-acquired pneumonia could be treated effectively with single agents.11,12
To address some of the questions regarding HCAP, national infectious-disease leaders were brought together to respond to a number of HCAP questions.13 One of the questions centered on the recommended empiric coverage for HCAP. Given the above noted studies in nursing-home patients, disagreement emerged about the need to empirically treat all HCAP patients with broad-spectrum antibiotics. Therefore, another assessment of risk factors for MDR infections was proposed (see Table 2, p. 20) and a consensus was reached, resulting in the current recommendations. The current guidelines state that once a patient has met HCAP criteria, if they have additional MDR risk factors, then broad antibiotic coverage is recommended; however, if no additional MDR risk is found, then more conservative, narrower coverage could be given (see Table 3, p. 31).13
Additional considerations
More studies are needed to refine and validate the specific diagnostic criteria for HCAP, as well as the MDR infectious risk factors. Moreover, current recommendations are for lower respiratory cultures to be obtained on all patients with pneumonia and antibiotic coverage to be titrated according to these results. This practice, however, appears to be uncommon. More data are needed to further guide treatment following initiation of empiric antibiotic coverage without the guidance of culture data, with reliance upon clinical parameters instead.
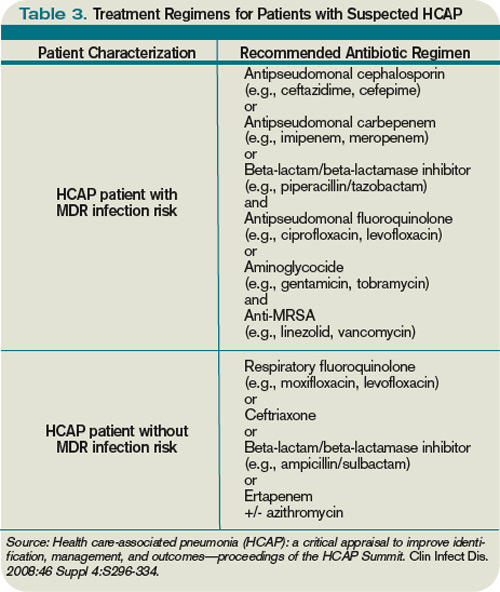
Back to the Case
This patient met initial criteria for HCAP because he was a nursing home resident, and was found to have additional MDR risk factors (poor functional status and a recent course of antibiotics). Therefore, lower respiratory cultures were obtained, supplemental oxygen was started, and piperacillin/tazobactam plus levofloxacin and vancomycin (with consideration made for local resistance patterns) was administered. He clinically improved over the next two days. His sputum cultures grew Pseudomonas aeuroginosa, which was sensitive to piperacillin/tazobactam but resistant to levofloxacin.
The vancomycin and levofloxacin were discontinued, and he was treated with a seven-day course of piperacillin/tazobactam.
Bottom Line
For adults who present with pneumonia from the community, special attention must be paid to certain parts of the patient’s history to determine if they have HCAP.
Patients who have HCAP can benefit from broad-spectrum empiric antibiotic coverage, which current expert consensus believes is dependent upon further MDR infection risk factors. TH
Dr. Rohde is medicine faculty hospitalist at the University of Michigan in Ann Arbor.
References
- Jernigan JA, Pullen AL, Flowers L, Bell M, Jarvis WR. Prevalence of and risk factors for colonization with methicillin-resistant Staphylococcus aureus at the time of hospital admission. Infect Control Hosp Epidemiol. 2003;24(6):409-414.
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005;128(5):3854-3862.
- Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother. 2007;51(10):3568-3573.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903.
- Celis R, Torres A, Gatell JM, Almela M, Rodríguez-Roisin R, Augustí-Vidal A. Nosocomial pneumonia: a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318-324.
- Lim WS, Macfarlane JT. A prospective comparison of nursing home acquired pneumonia with community acquired pneumonia. Eur Respir J. 2001;18(2):362-368.
- Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31 Supple 4:S131-S138.
- Poch DS, Ost DE. What are the important risk factors for healthcare-associated pneumonia? Semin Respir Crit Care Med. 2009;30(1):26-35.
- Loeb M, Carusone SC, Goeree R, et al. Effect of clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial. JAMA. 2006;295(21):2503-2510.
- Peterson PK, Stein D, Guay DR, et al. Prospective study of lower respiratory tract infections in an extended-care nursing home program: potential role of oral ciprofloxacin. Am J Med. 1988;85(2):164-171.
- Trenholme GM, Schmitt BA, Spear J, Gvazdinskas LC, Levin S. Randomized study of intravenous/oral ciprofloxacin versus ceftazidime in the treatment of hospital and nursing home patients with lower respiratory tract infections. Am J Med. 1989(5A);87:116S-118S.
- Kollef MH, Morrow LE, Baughman RP, et al. Healthcare-associated pneumonia (HCAP): a critical appraisal to improve identification, management and outcomes—proceedings of the HCAP summit. Clin Infect Dis. 2008;46 Suppl 4:S296-S334.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919.
- El Solh AA, Pietrantoni C, Bhat A, Bhora M, Berbary E. Indicators of potentially drug-resistant bacteria in severe nursing home-acquired pneumonia. Clin Infect Dis. 2004;39(4):474-480.
If you are interested in joining our reader-involvement program, e-mail Editor Jason Carris at [email protected].
Case
A 68-year-old man with hypertension, diabetes, and recent hip fracture with poor functional status presents from a nursing home with a productive cough, shortness of breath, and chills of two-day duration. He finished a five-day course of cephalexin for a urinary tract infection one week ago. His vital signs reveal a blood pressure of 162/80 mm/Hg, temperature of 101.9°F, respirations of 26 breaths per minute, and oxygen saturation of 88% on room air. Coarse breath sounds are noted in the right lung field and his chest X-ray reveals a right-middle-lobe infiltrate.
He is admitted to the hospital with a diagnosis of healthcare-associated pneumonia. What is the best empiric antibiotic coverage for this patient?
Overview
Modern medicine exists over a continuum of care that is delivered in a manifold of different settings. Patients routinely receive complex medical care at home, including wound care and infusion of intravenous antibiotics. Additionally, many patients are interfacing with the healthcare system on a regular basis via hemodialysis centers or sub-acute rehabilitation centers. As a result of these interactions, patients are exposed to—and colonized by—different bacterial pathogens that can result in a variety of infections.1
While patients with healthcare-associated pneumonia (HCAP) can present similarly to those with community-acquired pneumonia (CAP)—patients with CAP normally present with a lower-respiratory-tract infection—the differences in the likely etiological pathogens dictate that these patients be considered for broader-spectrum empiric antibiotics. Hospitalists will continue to be responsible for choosing the initial antibiotic regimen for these patients, and they need to be able to recognize this disease process in order to treat it appropriately.
The joint American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guidelines released in 2005 emphasize that certain clinical HCAP risk factors center on increased interactions and encounters with healthcare facilities.2 These risk factors are evolving over time to include a patient’s functional status, recent antibiotic use, and clinical severity.
Review of the Data
Differences between HCAP and CAP
HCAP represents a diagnostic category of pneumonia created to differentiate patients with infections caused by a different microbiological subset of bacteria, including possible multi-drug-resistant (MDR) organisms, from patients with CAP. Thus far, culture data support this dichotomy.3,4
Kollef and colleagues performed a multicenter, retrospective cohort study of 4,543 patients with bacterial respiratory culture-positive pneumonia between 2002 and 2003. The study examined the bacteriological differences between CAP and HCAP. In this study, HCAP patients were defined as having: transfer from another healthcare facility; long-term hemodialysis; or prior hospitalization within 30 days in which they had non-ventilator-associated pneumonia (VAP). CAP patients were defined as having non-VAP and non-HCAP.
The study showed that the frequency of Pseudomonas aeurginosa (25% HCAP vs. 17% CAP) and Staphylococcus aureus (46% vs. 25%), which included methicillin-resistant Staphylococcus aureus (MRSA) (18% vs. 6%), was significantly higher in patients with HCAP than those with CAP. Additionally, frequency of Streptococcus pneumoniae (5% vs. 16%) and Haemophilus influenza (5% vs. 16%) infections were noted as significantly lower.3
A single-center, retrospective cohort analysis of 639 patients done by Micek et al yielded similar culture differences between CAP and HCAP patients. In this study, criteria for HCAP were defined as hospitalization in the past year, immunosuppression, nursing-home resident, or hemodialysis. The study authors found that a significantly higher percentage of HCAP patients were infected with MRSA (30% vs. 12%), Pseudomonas aeurginosa (25% vs. 4%), and other non-fermenting gram-negative rods (GNR) (10% vs. 2%). HCAP patients again were noted as having significantly fewer infections with S. pneumoniae (10% vs. 40%) and Haemophilus influenza (4% vs. 17%).
In addition to showing a difference in the bacteriology of CAP and HCAP, the Kollef study also evaluated mortality rates, length of stay, and hospital charges. Mortality rates for HCAP (19.8%) were similar to those of hospital-acquired pneumonia (HAP) (18.8%), and both of these were significantly higher than CAP (10%). Length of stay and hospital cost increased across the spectrum, from CAP to HCAP to HAP, with significant differences between each.3
ATS/IDSA Guidelines
In 2005, a joint committee of the ATS and ISDA updated its initial 1996 nosocomial pneumonia guidelines. The guideline update included the new HCAP category.2 The No. 1 goal of these guidelines was to emphasize early and appropriate antibiotics, followed by tailoring of the treatment regimen based upon culture and clinical data. To this end, HCAP risk factors were developed via extrapolation from observational data generated from HAP and VAP patients.5,6,7
The risk factors are summarized in Table 1 (see p. 19).2 Guidelines dictated that the identification of any of these risk factors in pneumonia patients at the time of admission indicates increased risk for infection with an MDR organism. These high-risk patients require placement into the diagnostic category of HCAP.
Once a patient has been diagnosed with HCAP, the guidelines recommended obtaining lower-respiratory-tract cultures and initiating broad-spectrum antibiotic therapy. Appropriate empiric antibiotic therapy was suggested to be the same as for HAP. This regimen requires coverage with two anti-pseudomonal agents, as well as an agent with activity against MRSA.
The rationale behind initial coverage with two anti-pseudomonal agents stems from the finding that pseudomonas has a high rate of resistance to many antibiotics, and that if two agents are empirically started, chances of appropriate coverage increase from the outset. This is important, as timely administration of appropriate antibiotics has been shown to decrease mortality in infections.8
Additional considerations for empiric antibiotic treatment include sensitivities of local microbiologic data, as well as any recent antibiotic regimens given to the patient. Following this broad primary antibiotic coverage, de-escalation was recommended based on results of lower respiratory cultures and clinical improvement.2
Evolution of Diagnostic Criteria and Empiric Antibiotic Coverage
Since the publication of the 2005 ATS/IDSA guidelines, the aforementioned risk factors for HCAP have been brought into question, as they have yet to be validated by prospective trials. There is a growing concern that these criteria may not be adequately specific and, therefore, might call for too many patients to be treated with a broader spectrum of antibiotic coverage, thereby increasing the likelihood of developing MDR bacteria.
In order to further analyze HCAP criteria, Poch and Ost wrote a review earlier this year examining the data behind each of the risk factors cited in the ATS/IDSA guidelines; they found considerable heterogeneity in magnitude of MDR infection risk for these criteria.9 The authors also reviewed studies looking at other risk factors for MDR infections in patients living in nursing homes or afflicted with CAP. They proposed that such additional factors as patient specific risks (including functional status and previous antibiotic exposure) and contextual risks (including nurse-to-patient ratio) be evaluated and possibly incorporated into criteria.
Of all the patients with HCAP criteria, residents in nursing homes have been studied the best. Loeb et al, while looking for a way to decrease hospitalizations for nursing-home residents, showed that patients who get pneumonia (by guideline definition HCAP) can be effectively treated as outpatients with a single antibiotic agent.10 This randomized controlled trial of 680 patients, all with HCAP, were treated with oral levofloxacin at the nursing home or admitted to the hospital. There were no significant differences between mortality (8% vs. 9%) and quality-of-life measures between the two groups. Furthermore, analysis of data from the 1980s showed that nursing-home-acquired pneumonia could be treated effectively with single agents.11,12
To address some of the questions regarding HCAP, national infectious-disease leaders were brought together to respond to a number of HCAP questions.13 One of the questions centered on the recommended empiric coverage for HCAP. Given the above noted studies in nursing-home patients, disagreement emerged about the need to empirically treat all HCAP patients with broad-spectrum antibiotics. Therefore, another assessment of risk factors for MDR infections was proposed (see Table 2, p. 20) and a consensus was reached, resulting in the current recommendations. The current guidelines state that once a patient has met HCAP criteria, if they have additional MDR risk factors, then broad antibiotic coverage is recommended; however, if no additional MDR risk is found, then more conservative, narrower coverage could be given (see Table 3, p. 31).13
Additional considerations
More studies are needed to refine and validate the specific diagnostic criteria for HCAP, as well as the MDR infectious risk factors. Moreover, current recommendations are for lower respiratory cultures to be obtained on all patients with pneumonia and antibiotic coverage to be titrated according to these results. This practice, however, appears to be uncommon. More data are needed to further guide treatment following initiation of empiric antibiotic coverage without the guidance of culture data, with reliance upon clinical parameters instead.
Back to the Case
This patient met initial criteria for HCAP because he was a nursing home resident, and was found to have additional MDR risk factors (poor functional status and a recent course of antibiotics). Therefore, lower respiratory cultures were obtained, supplemental oxygen was started, and piperacillin/tazobactam plus levofloxacin and vancomycin (with consideration made for local resistance patterns) was administered. He clinically improved over the next two days. His sputum cultures grew Pseudomonas aeuroginosa, which was sensitive to piperacillin/tazobactam but resistant to levofloxacin.
The vancomycin and levofloxacin were discontinued, and he was treated with a seven-day course of piperacillin/tazobactam.
Bottom Line
For adults who present with pneumonia from the community, special attention must be paid to certain parts of the patient’s history to determine if they have HCAP.
Patients who have HCAP can benefit from broad-spectrum empiric antibiotic coverage, which current expert consensus believes is dependent upon further MDR infection risk factors. TH
Dr. Rohde is medicine faculty hospitalist at the University of Michigan in Ann Arbor.
References
- Jernigan JA, Pullen AL, Flowers L, Bell M, Jarvis WR. Prevalence of and risk factors for colonization with methicillin-resistant Staphylococcus aureus at the time of hospital admission. Infect Control Hosp Epidemiol. 2003;24(6):409-414.
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005;128(5):3854-3862.
- Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother. 2007;51(10):3568-3573.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903.
- Celis R, Torres A, Gatell JM, Almela M, Rodríguez-Roisin R, Augustí-Vidal A. Nosocomial pneumonia: a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318-324.
- Lim WS, Macfarlane JT. A prospective comparison of nursing home acquired pneumonia with community acquired pneumonia. Eur Respir J. 2001;18(2):362-368.
- Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31 Supple 4:S131-S138.
- Poch DS, Ost DE. What are the important risk factors for healthcare-associated pneumonia? Semin Respir Crit Care Med. 2009;30(1):26-35.
- Loeb M, Carusone SC, Goeree R, et al. Effect of clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial. JAMA. 2006;295(21):2503-2510.
- Peterson PK, Stein D, Guay DR, et al. Prospective study of lower respiratory tract infections in an extended-care nursing home program: potential role of oral ciprofloxacin. Am J Med. 1988;85(2):164-171.
- Trenholme GM, Schmitt BA, Spear J, Gvazdinskas LC, Levin S. Randomized study of intravenous/oral ciprofloxacin versus ceftazidime in the treatment of hospital and nursing home patients with lower respiratory tract infections. Am J Med. 1989(5A);87:116S-118S.
- Kollef MH, Morrow LE, Baughman RP, et al. Healthcare-associated pneumonia (HCAP): a critical appraisal to improve identification, management and outcomes—proceedings of the HCAP summit. Clin Infect Dis. 2008;46 Suppl 4:S296-S334.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919.
- El Solh AA, Pietrantoni C, Bhat A, Bhora M, Berbary E. Indicators of potentially drug-resistant bacteria in severe nursing home-acquired pneumonia. Clin Infect Dis. 2004;39(4):474-480.
If you are interested in joining our reader-involvement program, e-mail Editor Jason Carris at [email protected].
Case
A 68-year-old man with hypertension, diabetes, and recent hip fracture with poor functional status presents from a nursing home with a productive cough, shortness of breath, and chills of two-day duration. He finished a five-day course of cephalexin for a urinary tract infection one week ago. His vital signs reveal a blood pressure of 162/80 mm/Hg, temperature of 101.9°F, respirations of 26 breaths per minute, and oxygen saturation of 88% on room air. Coarse breath sounds are noted in the right lung field and his chest X-ray reveals a right-middle-lobe infiltrate.
He is admitted to the hospital with a diagnosis of healthcare-associated pneumonia. What is the best empiric antibiotic coverage for this patient?
Overview
Modern medicine exists over a continuum of care that is delivered in a manifold of different settings. Patients routinely receive complex medical care at home, including wound care and infusion of intravenous antibiotics. Additionally, many patients are interfacing with the healthcare system on a regular basis via hemodialysis centers or sub-acute rehabilitation centers. As a result of these interactions, patients are exposed to—and colonized by—different bacterial pathogens that can result in a variety of infections.1
While patients with healthcare-associated pneumonia (HCAP) can present similarly to those with community-acquired pneumonia (CAP)—patients with CAP normally present with a lower-respiratory-tract infection—the differences in the likely etiological pathogens dictate that these patients be considered for broader-spectrum empiric antibiotics. Hospitalists will continue to be responsible for choosing the initial antibiotic regimen for these patients, and they need to be able to recognize this disease process in order to treat it appropriately.
The joint American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guidelines released in 2005 emphasize that certain clinical HCAP risk factors center on increased interactions and encounters with healthcare facilities.2 These risk factors are evolving over time to include a patient’s functional status, recent antibiotic use, and clinical severity.
Review of the Data
Differences between HCAP and CAP
HCAP represents a diagnostic category of pneumonia created to differentiate patients with infections caused by a different microbiological subset of bacteria, including possible multi-drug-resistant (MDR) organisms, from patients with CAP. Thus far, culture data support this dichotomy.3,4
Kollef and colleagues performed a multicenter, retrospective cohort study of 4,543 patients with bacterial respiratory culture-positive pneumonia between 2002 and 2003. The study examined the bacteriological differences between CAP and HCAP. In this study, HCAP patients were defined as having: transfer from another healthcare facility; long-term hemodialysis; or prior hospitalization within 30 days in which they had non-ventilator-associated pneumonia (VAP). CAP patients were defined as having non-VAP and non-HCAP.
The study showed that the frequency of Pseudomonas aeurginosa (25% HCAP vs. 17% CAP) and Staphylococcus aureus (46% vs. 25%), which included methicillin-resistant Staphylococcus aureus (MRSA) (18% vs. 6%), was significantly higher in patients with HCAP than those with CAP. Additionally, frequency of Streptococcus pneumoniae (5% vs. 16%) and Haemophilus influenza (5% vs. 16%) infections were noted as significantly lower.3
A single-center, retrospective cohort analysis of 639 patients done by Micek et al yielded similar culture differences between CAP and HCAP patients. In this study, criteria for HCAP were defined as hospitalization in the past year, immunosuppression, nursing-home resident, or hemodialysis. The study authors found that a significantly higher percentage of HCAP patients were infected with MRSA (30% vs. 12%), Pseudomonas aeurginosa (25% vs. 4%), and other non-fermenting gram-negative rods (GNR) (10% vs. 2%). HCAP patients again were noted as having significantly fewer infections with S. pneumoniae (10% vs. 40%) and Haemophilus influenza (4% vs. 17%).
In addition to showing a difference in the bacteriology of CAP and HCAP, the Kollef study also evaluated mortality rates, length of stay, and hospital charges. Mortality rates for HCAP (19.8%) were similar to those of hospital-acquired pneumonia (HAP) (18.8%), and both of these were significantly higher than CAP (10%). Length of stay and hospital cost increased across the spectrum, from CAP to HCAP to HAP, with significant differences between each.3
ATS/IDSA Guidelines
In 2005, a joint committee of the ATS and ISDA updated its initial 1996 nosocomial pneumonia guidelines. The guideline update included the new HCAP category.2 The No. 1 goal of these guidelines was to emphasize early and appropriate antibiotics, followed by tailoring of the treatment regimen based upon culture and clinical data. To this end, HCAP risk factors were developed via extrapolation from observational data generated from HAP and VAP patients.5,6,7
The risk factors are summarized in Table 1 (see p. 19).2 Guidelines dictated that the identification of any of these risk factors in pneumonia patients at the time of admission indicates increased risk for infection with an MDR organism. These high-risk patients require placement into the diagnostic category of HCAP.
Once a patient has been diagnosed with HCAP, the guidelines recommended obtaining lower-respiratory-tract cultures and initiating broad-spectrum antibiotic therapy. Appropriate empiric antibiotic therapy was suggested to be the same as for HAP. This regimen requires coverage with two anti-pseudomonal agents, as well as an agent with activity against MRSA.
The rationale behind initial coverage with two anti-pseudomonal agents stems from the finding that pseudomonas has a high rate of resistance to many antibiotics, and that if two agents are empirically started, chances of appropriate coverage increase from the outset. This is important, as timely administration of appropriate antibiotics has been shown to decrease mortality in infections.8
Additional considerations for empiric antibiotic treatment include sensitivities of local microbiologic data, as well as any recent antibiotic regimens given to the patient. Following this broad primary antibiotic coverage, de-escalation was recommended based on results of lower respiratory cultures and clinical improvement.2
Evolution of Diagnostic Criteria and Empiric Antibiotic Coverage
Since the publication of the 2005 ATS/IDSA guidelines, the aforementioned risk factors for HCAP have been brought into question, as they have yet to be validated by prospective trials. There is a growing concern that these criteria may not be adequately specific and, therefore, might call for too many patients to be treated with a broader spectrum of antibiotic coverage, thereby increasing the likelihood of developing MDR bacteria.
In order to further analyze HCAP criteria, Poch and Ost wrote a review earlier this year examining the data behind each of the risk factors cited in the ATS/IDSA guidelines; they found considerable heterogeneity in magnitude of MDR infection risk for these criteria.9 The authors also reviewed studies looking at other risk factors for MDR infections in patients living in nursing homes or afflicted with CAP. They proposed that such additional factors as patient specific risks (including functional status and previous antibiotic exposure) and contextual risks (including nurse-to-patient ratio) be evaluated and possibly incorporated into criteria.
Of all the patients with HCAP criteria, residents in nursing homes have been studied the best. Loeb et al, while looking for a way to decrease hospitalizations for nursing-home residents, showed that patients who get pneumonia (by guideline definition HCAP) can be effectively treated as outpatients with a single antibiotic agent.10 This randomized controlled trial of 680 patients, all with HCAP, were treated with oral levofloxacin at the nursing home or admitted to the hospital. There were no significant differences between mortality (8% vs. 9%) and quality-of-life measures between the two groups. Furthermore, analysis of data from the 1980s showed that nursing-home-acquired pneumonia could be treated effectively with single agents.11,12
To address some of the questions regarding HCAP, national infectious-disease leaders were brought together to respond to a number of HCAP questions.13 One of the questions centered on the recommended empiric coverage for HCAP. Given the above noted studies in nursing-home patients, disagreement emerged about the need to empirically treat all HCAP patients with broad-spectrum antibiotics. Therefore, another assessment of risk factors for MDR infections was proposed (see Table 2, p. 20) and a consensus was reached, resulting in the current recommendations. The current guidelines state that once a patient has met HCAP criteria, if they have additional MDR risk factors, then broad antibiotic coverage is recommended; however, if no additional MDR risk is found, then more conservative, narrower coverage could be given (see Table 3, p. 31).13
Additional considerations
More studies are needed to refine and validate the specific diagnostic criteria for HCAP, as well as the MDR infectious risk factors. Moreover, current recommendations are for lower respiratory cultures to be obtained on all patients with pneumonia and antibiotic coverage to be titrated according to these results. This practice, however, appears to be uncommon. More data are needed to further guide treatment following initiation of empiric antibiotic coverage without the guidance of culture data, with reliance upon clinical parameters instead.
Back to the Case
This patient met initial criteria for HCAP because he was a nursing home resident, and was found to have additional MDR risk factors (poor functional status and a recent course of antibiotics). Therefore, lower respiratory cultures were obtained, supplemental oxygen was started, and piperacillin/tazobactam plus levofloxacin and vancomycin (with consideration made for local resistance patterns) was administered. He clinically improved over the next two days. His sputum cultures grew Pseudomonas aeuroginosa, which was sensitive to piperacillin/tazobactam but resistant to levofloxacin.
The vancomycin and levofloxacin were discontinued, and he was treated with a seven-day course of piperacillin/tazobactam.
Bottom Line
For adults who present with pneumonia from the community, special attention must be paid to certain parts of the patient’s history to determine if they have HCAP.
Patients who have HCAP can benefit from broad-spectrum empiric antibiotic coverage, which current expert consensus believes is dependent upon further MDR infection risk factors. TH
Dr. Rohde is medicine faculty hospitalist at the University of Michigan in Ann Arbor.
References
- Jernigan JA, Pullen AL, Flowers L, Bell M, Jarvis WR. Prevalence of and risk factors for colonization with methicillin-resistant Staphylococcus aureus at the time of hospital admission. Infect Control Hosp Epidemiol. 2003;24(6):409-414.
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005;128(5):3854-3862.
- Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother. 2007;51(10):3568-3573.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903.
- Celis R, Torres A, Gatell JM, Almela M, Rodríguez-Roisin R, Augustí-Vidal A. Nosocomial pneumonia: a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318-324.
- Lim WS, Macfarlane JT. A prospective comparison of nursing home acquired pneumonia with community acquired pneumonia. Eur Respir J. 2001;18(2):362-368.
- Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31 Supple 4:S131-S138.
- Poch DS, Ost DE. What are the important risk factors for healthcare-associated pneumonia? Semin Respir Crit Care Med. 2009;30(1):26-35.
- Loeb M, Carusone SC, Goeree R, et al. Effect of clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial. JAMA. 2006;295(21):2503-2510.
- Peterson PK, Stein D, Guay DR, et al. Prospective study of lower respiratory tract infections in an extended-care nursing home program: potential role of oral ciprofloxacin. Am J Med. 1988;85(2):164-171.
- Trenholme GM, Schmitt BA, Spear J, Gvazdinskas LC, Levin S. Randomized study of intravenous/oral ciprofloxacin versus ceftazidime in the treatment of hospital and nursing home patients with lower respiratory tract infections. Am J Med. 1989(5A);87:116S-118S.
- Kollef MH, Morrow LE, Baughman RP, et al. Healthcare-associated pneumonia (HCAP): a critical appraisal to improve identification, management and outcomes—proceedings of the HCAP summit. Clin Infect Dis. 2008;46 Suppl 4:S296-S334.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919.
- El Solh AA, Pietrantoni C, Bhat A, Bhora M, Berbary E. Indicators of potentially drug-resistant bacteria in severe nursing home-acquired pneumonia. Clin Infect Dis. 2004;39(4):474-480.
If you are interested in joining our reader-involvement program, e-mail Editor Jason Carris at [email protected].
Should group directors continue clinical practice?
PRO
Clinical practice is beneficial to patients, the group, and your career

Finding a balance between clinical care and leadership duties truly is a challenge for hospitalist directors. Changes in the landscape of inpatient care delivery, rapid growth of HM groups, and expansion of hospitalist roles have resulted in a substantial increase in a director’s responsibilities. Today’s hospitalist leader squarely faces the dilemma of continuing clinical practice and performing administrative efforts while demonstrating competence in each. To be effective, this is precisely what physician leaders must strive to do.
Maintaining clinical practice alongside directorship duties conveys advantages in critical leadership areas. You must consider the benefits to your patient, your career, and the hospitalist group.
The Patient, Director, Group
Physician leaders offer clinical experience combined with a unique perspective on systems of care, or “the big picture.”
Likewise, caring for patients provides the opportunity to interact with and listen to the customer, which is necessary for important outcomes, such as patient satisfaction. It reminds us that we are here to care for and about patients, keeping our efforts patient-centered.
Direct patient care refocuses directors on the fundamental reason they are in leadership. It offers intrinsic professional rewards and intellectual satisfaction that will sustain and strengthen the leadership role. The effective leader strategically finds balance by delegating, prioritizing, and focusing on time management.
Continuing your clinical practice affords physician leaders leverage with their constituents—the hospitalists. Working in the trenches, especially during critical times, yields legitimacy and credibility. It also allows the leader to identify with and respond to concerns raised by members. This can connect the leader to the group, avoiding the “suit vs. white coat” dynamic. The same principle extends to other stakeholders who are part of the care team, such as nurses and referring physicians.
Other Factors
Maintaining clinical aptitude ensures that leaders stay apprised of current practices, and are aware of the latest techniques, data, and evidence. This is critical for ensuring group performance in quality initiatives, and for setting standards of clinical excellence in the group practice.
In academic centers, ward teaching allows leaders to train future physicians, pass on knowledge, and gain an understanding of the next generation and its priorities, thus keeping an eye on the future and having a clear vision.
Perhaps the most important benefit direct patient care provides in leadership is the ability to accomplish the group’s mission. A firsthand experience brings understanding of issues around workflow, efficiency, and career satisfaction. It allows leaders to audit best practices. It inspires innovative ideas for healthcare delivery and processing improvement changes.
The model of successful physician leadership is based on clinical excellence. The construct of a separation between clinical and administrative roles is a false dichotomy; the two are interdependent. HM directors have a duty to perform both, as it is the combination that makes leaders successful. TH
Dr. Wright is associate clinical professor and chief of the division of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
CON
Physician leaders should relinquish clinical practice, focus on leading

I believe the vast majority of hospitalists agree with the “pro” side of this debate, but I also believe that this kind of knee-jerk reaction reflects the core deficiency that plagues physicians’ thinking regarding leadership.
The way medicine is being practiced and delivered in the hospital setting is rapidly changing. In fact, our specialty is based on this premise. Yet hospitalists still have a stone-age mentality when it comes to physician leaders. The concept of leadership, in most cases, is an afterthought.
Our Role as Leaders
The HM leader is expected to act as a caretaker: set the schedule, organize and implement QI programs, and represent the hospitalists to administration. Most HM directors are accidental leaders who sheepishly step into a position when the opportunity presents itself. This usually happens as programs grow. Few industries would accept this business model. Leadership should be considered critical and given its due respect in terms of resources, training, and experience. Rarely are supervisory positions rewarded to accidental, part-time volunteers. Leaders are chosen, groomed, and given the sufficient time and resources to carry out their mandate.
When HM programs become dysfunctional, hospitalists are quick to blame the administration—some refer to it as the “evil empire” or “the dark side.” But interesting research by Gallup Inc. has shown that the majority of employees who leave their jobs actually are leaving their manager.1
Wants vs. Needs
Leaders face dilemmas every work day. For instance, leaders need to communicate the administration’s goals and weave them into HM department systems and policies. Conversely, HM leaders have to negotiate with administration to secure the resources they need to execute those goals. Technologies are mere facilitators; people actually produce results. Yet many administrators and HM leaders are fixated on the latest software without giving much thought about how staff will implement the changes.
HM leaders need time and resources to be effective. As hospitalists, we’ve been bombarded by the evidence-based medicine mantra. But most hospitalists have never heard of, or they laugh at, evidence-based techniques that were first documented in the 1970s.2 Data is available regarding management skills that can be used to effect positive organization behavior.
We also need to be authentic leaders to combat internal disruptions from medical staff. Gallup Management research has shown that 42% of physicians on medical staffs are actively disengaged.3 Physicians not only are distant, they also actively sabotage and poison new efforts introduced by administration or physician leaders.
The hospitalist leader should only perform clinical responsibilities if they are absolutely necessary. The HM director should be given all the time, resources, due respect, and training to be a dynamic leader. The hospitalist movement would be better for it. TH
References
- Buckingham, M, Coffman C. First, Break All the Rules: How Managers Trump Companies. 1999. New York City: Simon & Schuster.
- Luthans F. Organizational Behavior. 1973. New York City: McGraw-Hill.
- Paller D. What the doctor ordered. Gallup Management Web site. Available at: http://gmj.gallup.com/content/18361/What-Doctor-Ordered.aspx. Accessed Nov. 9, 2009.
Dr. Yu is medical director of hospitalist services at Decatur (Ill.) Memorial Hospital.
PRO
Clinical practice is beneficial to patients, the group, and your career
Finding a balance between clinical care and leadership duties truly is a challenge for hospitalist directors. Changes in the landscape of inpatient care delivery, rapid growth of HM groups, and expansion of hospitalist roles have resulted in a substantial increase in a director’s responsibilities. Today’s hospitalist leader squarely faces the dilemma of continuing clinical practice and performing administrative efforts while demonstrating competence in each. To be effective, this is precisely what physician leaders must strive to do.
Maintaining clinical practice alongside directorship duties conveys advantages in critical leadership areas. You must consider the benefits to your patient, your career, and the hospitalist group.
The Patient, Director, Group
Physician leaders offer clinical experience combined with a unique perspective on systems of care, or “the big picture.”
Likewise, caring for patients provides the opportunity to interact with and listen to the customer, which is necessary for important outcomes, such as patient satisfaction. It reminds us that we are here to care for and about patients, keeping our efforts patient-centered.
Direct patient care refocuses directors on the fundamental reason they are in leadership. It offers intrinsic professional rewards and intellectual satisfaction that will sustain and strengthen the leadership role. The effective leader strategically finds balance by delegating, prioritizing, and focusing on time management.
Continuing your clinical practice affords physician leaders leverage with their constituents—the hospitalists. Working in the trenches, especially during critical times, yields legitimacy and credibility. It also allows the leader to identify with and respond to concerns raised by members. This can connect the leader to the group, avoiding the “suit vs. white coat” dynamic. The same principle extends to other stakeholders who are part of the care team, such as nurses and referring physicians.
Other Factors
Maintaining clinical aptitude ensures that leaders stay apprised of current practices, and are aware of the latest techniques, data, and evidence. This is critical for ensuring group performance in quality initiatives, and for setting standards of clinical excellence in the group practice.
In academic centers, ward teaching allows leaders to train future physicians, pass on knowledge, and gain an understanding of the next generation and its priorities, thus keeping an eye on the future and having a clear vision.
Perhaps the most important benefit direct patient care provides in leadership is the ability to accomplish the group’s mission. A firsthand experience brings understanding of issues around workflow, efficiency, and career satisfaction. It allows leaders to audit best practices. It inspires innovative ideas for healthcare delivery and processing improvement changes.
The model of successful physician leadership is based on clinical excellence. The construct of a separation between clinical and administrative roles is a false dichotomy; the two are interdependent. HM directors have a duty to perform both, as it is the combination that makes leaders successful. TH
Dr. Wright is associate clinical professor and chief of the division of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
CON
Physician leaders should relinquish clinical practice, focus on leading
I believe the vast majority of hospitalists agree with the “pro” side of this debate, but I also believe that this kind of knee-jerk reaction reflects the core deficiency that plagues physicians’ thinking regarding leadership.
The way medicine is being practiced and delivered in the hospital setting is rapidly changing. In fact, our specialty is based on this premise. Yet hospitalists still have a stone-age mentality when it comes to physician leaders. The concept of leadership, in most cases, is an afterthought.
Our Role as Leaders
The HM leader is expected to act as a caretaker: set the schedule, organize and implement QI programs, and represent the hospitalists to administration. Most HM directors are accidental leaders who sheepishly step into a position when the opportunity presents itself. This usually happens as programs grow. Few industries would accept this business model. Leadership should be considered critical and given its due respect in terms of resources, training, and experience. Rarely are supervisory positions rewarded to accidental, part-time volunteers. Leaders are chosen, groomed, and given the sufficient time and resources to carry out their mandate.
When HM programs become dysfunctional, hospitalists are quick to blame the administration—some refer to it as the “evil empire” or “the dark side.” But interesting research by Gallup Inc. has shown that the majority of employees who leave their jobs actually are leaving their manager.1
Wants vs. Needs
Leaders face dilemmas every work day. For instance, leaders need to communicate the administration’s goals and weave them into HM department systems and policies. Conversely, HM leaders have to negotiate with administration to secure the resources they need to execute those goals. Technologies are mere facilitators; people actually produce results. Yet many administrators and HM leaders are fixated on the latest software without giving much thought about how staff will implement the changes.
HM leaders need time and resources to be effective. As hospitalists, we’ve been bombarded by the evidence-based medicine mantra. But most hospitalists have never heard of, or they laugh at, evidence-based techniques that were first documented in the 1970s.2 Data is available regarding management skills that can be used to effect positive organization behavior.
We also need to be authentic leaders to combat internal disruptions from medical staff. Gallup Management research has shown that 42% of physicians on medical staffs are actively disengaged.3 Physicians not only are distant, they also actively sabotage and poison new efforts introduced by administration or physician leaders.
The hospitalist leader should only perform clinical responsibilities if they are absolutely necessary. The HM director should be given all the time, resources, due respect, and training to be a dynamic leader. The hospitalist movement would be better for it. TH
References
- Buckingham, M, Coffman C. First, Break All the Rules: How Managers Trump Companies. 1999. New York City: Simon & Schuster.
- Luthans F. Organizational Behavior. 1973. New York City: McGraw-Hill.
- Paller D. What the doctor ordered. Gallup Management Web site. Available at: http://gmj.gallup.com/content/18361/What-Doctor-Ordered.aspx. Accessed Nov. 9, 2009.
Dr. Yu is medical director of hospitalist services at Decatur (Ill.) Memorial Hospital.
PRO
Clinical practice is beneficial to patients, the group, and your career
Finding a balance between clinical care and leadership duties truly is a challenge for hospitalist directors. Changes in the landscape of inpatient care delivery, rapid growth of HM groups, and expansion of hospitalist roles have resulted in a substantial increase in a director’s responsibilities. Today’s hospitalist leader squarely faces the dilemma of continuing clinical practice and performing administrative efforts while demonstrating competence in each. To be effective, this is precisely what physician leaders must strive to do.
Maintaining clinical practice alongside directorship duties conveys advantages in critical leadership areas. You must consider the benefits to your patient, your career, and the hospitalist group.
The Patient, Director, Group
Physician leaders offer clinical experience combined with a unique perspective on systems of care, or “the big picture.”
Likewise, caring for patients provides the opportunity to interact with and listen to the customer, which is necessary for important outcomes, such as patient satisfaction. It reminds us that we are here to care for and about patients, keeping our efforts patient-centered.
Direct patient care refocuses directors on the fundamental reason they are in leadership. It offers intrinsic professional rewards and intellectual satisfaction that will sustain and strengthen the leadership role. The effective leader strategically finds balance by delegating, prioritizing, and focusing on time management.
Continuing your clinical practice affords physician leaders leverage with their constituents—the hospitalists. Working in the trenches, especially during critical times, yields legitimacy and credibility. It also allows the leader to identify with and respond to concerns raised by members. This can connect the leader to the group, avoiding the “suit vs. white coat” dynamic. The same principle extends to other stakeholders who are part of the care team, such as nurses and referring physicians.
Other Factors
Maintaining clinical aptitude ensures that leaders stay apprised of current practices, and are aware of the latest techniques, data, and evidence. This is critical for ensuring group performance in quality initiatives, and for setting standards of clinical excellence in the group practice.
In academic centers, ward teaching allows leaders to train future physicians, pass on knowledge, and gain an understanding of the next generation and its priorities, thus keeping an eye on the future and having a clear vision.
Perhaps the most important benefit direct patient care provides in leadership is the ability to accomplish the group’s mission. A firsthand experience brings understanding of issues around workflow, efficiency, and career satisfaction. It allows leaders to audit best practices. It inspires innovative ideas for healthcare delivery and processing improvement changes.
The model of successful physician leadership is based on clinical excellence. The construct of a separation between clinical and administrative roles is a false dichotomy; the two are interdependent. HM directors have a duty to perform both, as it is the combination that makes leaders successful. TH
Dr. Wright is associate clinical professor and chief of the division of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
CON
Physician leaders should relinquish clinical practice, focus on leading
I believe the vast majority of hospitalists agree with the “pro” side of this debate, but I also believe that this kind of knee-jerk reaction reflects the core deficiency that plagues physicians’ thinking regarding leadership.
The way medicine is being practiced and delivered in the hospital setting is rapidly changing. In fact, our specialty is based on this premise. Yet hospitalists still have a stone-age mentality when it comes to physician leaders. The concept of leadership, in most cases, is an afterthought.
Our Role as Leaders
The HM leader is expected to act as a caretaker: set the schedule, organize and implement QI programs, and represent the hospitalists to administration. Most HM directors are accidental leaders who sheepishly step into a position when the opportunity presents itself. This usually happens as programs grow. Few industries would accept this business model. Leadership should be considered critical and given its due respect in terms of resources, training, and experience. Rarely are supervisory positions rewarded to accidental, part-time volunteers. Leaders are chosen, groomed, and given the sufficient time and resources to carry out their mandate.
When HM programs become dysfunctional, hospitalists are quick to blame the administration—some refer to it as the “evil empire” or “the dark side.” But interesting research by Gallup Inc. has shown that the majority of employees who leave their jobs actually are leaving their manager.1
Wants vs. Needs
Leaders face dilemmas every work day. For instance, leaders need to communicate the administration’s goals and weave them into HM department systems and policies. Conversely, HM leaders have to negotiate with administration to secure the resources they need to execute those goals. Technologies are mere facilitators; people actually produce results. Yet many administrators and HM leaders are fixated on the latest software without giving much thought about how staff will implement the changes.
HM leaders need time and resources to be effective. As hospitalists, we’ve been bombarded by the evidence-based medicine mantra. But most hospitalists have never heard of, or they laugh at, evidence-based techniques that were first documented in the 1970s.2 Data is available regarding management skills that can be used to effect positive organization behavior.
We also need to be authentic leaders to combat internal disruptions from medical staff. Gallup Management research has shown that 42% of physicians on medical staffs are actively disengaged.3 Physicians not only are distant, they also actively sabotage and poison new efforts introduced by administration or physician leaders.
The hospitalist leader should only perform clinical responsibilities if they are absolutely necessary. The HM director should be given all the time, resources, due respect, and training to be a dynamic leader. The hospitalist movement would be better for it. TH
References
- Buckingham, M, Coffman C. First, Break All the Rules: How Managers Trump Companies. 1999. New York City: Simon & Schuster.
- Luthans F. Organizational Behavior. 1973. New York City: McGraw-Hill.
- Paller D. What the doctor ordered. Gallup Management Web site. Available at: http://gmj.gallup.com/content/18361/What-Doctor-Ordered.aspx. Accessed Nov. 9, 2009.
Dr. Yu is medical director of hospitalist services at Decatur (Ill.) Memorial Hospital.