User login
Correct coding when the patient goes to ER
Timing is everything. Although the codes for observation care do not stipulate a time period, the record must clearly show that she was observed before a determination could be made to send her home or admit her to the hospital. This would include being seen first by you and then having nursing staff observe for problems prior to your deciding to send her home.
The observation codes require, at a minimum, documentation of a detailed history and exam (with any level of medical decision making). If your patient was admitted and discharged on the same service date, the codes you would select from are 99234-99236 (observation or inpatient hospital care, for the evaluation and management of a patient including admission and discharge on the same date).
If, on the other hand, you saw the patient, treated her, and then immediately released her to go home or you left orders to send her home after a test had been performed such as a nonstress test, you should consider this to be an outpatient service and you would report one of the established patient problem codes (99212-99215).
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Timing is everything. Although the codes for observation care do not stipulate a time period, the record must clearly show that she was observed before a determination could be made to send her home or admit her to the hospital. This would include being seen first by you and then having nursing staff observe for problems prior to your deciding to send her home.
The observation codes require, at a minimum, documentation of a detailed history and exam (with any level of medical decision making). If your patient was admitted and discharged on the same service date, the codes you would select from are 99234-99236 (observation or inpatient hospital care, for the evaluation and management of a patient including admission and discharge on the same date).
If, on the other hand, you saw the patient, treated her, and then immediately released her to go home or you left orders to send her home after a test had been performed such as a nonstress test, you should consider this to be an outpatient service and you would report one of the established patient problem codes (99212-99215).
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Timing is everything. Although the codes for observation care do not stipulate a time period, the record must clearly show that she was observed before a determination could be made to send her home or admit her to the hospital. This would include being seen first by you and then having nursing staff observe for problems prior to your deciding to send her home.
The observation codes require, at a minimum, documentation of a detailed history and exam (with any level of medical decision making). If your patient was admitted and discharged on the same service date, the codes you would select from are 99234-99236 (observation or inpatient hospital care, for the evaluation and management of a patient including admission and discharge on the same date).
If, on the other hand, you saw the patient, treated her, and then immediately released her to go home or you left orders to send her home after a test had been performed such as a nonstress test, you should consider this to be an outpatient service and you would report one of the established patient problem codes (99212-99215).
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
ICD code depends on why labor was induced
In either case, report the ICD-9-CM code that supports the type of preeclampsia (eg, 642.51, severe preeclampsia; delivered with or without mention of antepartum condition). But if labor was induced, add code 644.21 (early onset of delivery; delivered with or without mention of antepartum condition). This code represents premature labor with delivery before 37 completed weeks of gestation.
If the delivery was accomplished by performing a cesarean, in addition to an outcome code such as V27.0 (single liveborn), you might add a code if the patient had a previous cesarean delivery (654.21).
If this was her first cesarean delivery, only the preeclampsia and outcome diagnosis codes would be assigned.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
In either case, report the ICD-9-CM code that supports the type of preeclampsia (eg, 642.51, severe preeclampsia; delivered with or without mention of antepartum condition). But if labor was induced, add code 644.21 (early onset of delivery; delivered with or without mention of antepartum condition). This code represents premature labor with delivery before 37 completed weeks of gestation.
If the delivery was accomplished by performing a cesarean, in addition to an outcome code such as V27.0 (single liveborn), you might add a code if the patient had a previous cesarean delivery (654.21).
If this was her first cesarean delivery, only the preeclampsia and outcome diagnosis codes would be assigned.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
In either case, report the ICD-9-CM code that supports the type of preeclampsia (eg, 642.51, severe preeclampsia; delivered with or without mention of antepartum condition). But if labor was induced, add code 644.21 (early onset of delivery; delivered with or without mention of antepartum condition). This code represents premature labor with delivery before 37 completed weeks of gestation.
If the delivery was accomplished by performing a cesarean, in addition to an outcome code such as V27.0 (single liveborn), you might add a code if the patient had a previous cesarean delivery (654.21).
If this was her first cesarean delivery, only the preeclampsia and outcome diagnosis codes would be assigned.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Use OB or GYN code if fetal pole is absent?
If the purpose of the ultrasound is only to check for fetal heart tones, then the correct code is 76815 (ultrasound, pregnant uterus, real time with image documentation limited [eg, fetal heart beat, placental location, fetal position and/or qualitative amniotic fluid volume], one or more fetuses).
While this scan could be performed transvaginally, the amount of work in checking only for fetal heart tones is significantly less than that involved in the OB transvaginal procedure.
Therefore, I recommend that you use the limited ultrasound code even if a vaginal probe was used.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
If the purpose of the ultrasound is only to check for fetal heart tones, then the correct code is 76815 (ultrasound, pregnant uterus, real time with image documentation limited [eg, fetal heart beat, placental location, fetal position and/or qualitative amniotic fluid volume], one or more fetuses).
While this scan could be performed transvaginally, the amount of work in checking only for fetal heart tones is significantly less than that involved in the OB transvaginal procedure.
Therefore, I recommend that you use the limited ultrasound code even if a vaginal probe was used.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
If the purpose of the ultrasound is only to check for fetal heart tones, then the correct code is 76815 (ultrasound, pregnant uterus, real time with image documentation limited [eg, fetal heart beat, placental location, fetal position and/or qualitative amniotic fluid volume], one or more fetuses).
While this scan could be performed transvaginally, the amount of work in checking only for fetal heart tones is significantly less than that involved in the OB transvaginal procedure.
Therefore, I recommend that you use the limited ultrasound code even if a vaginal probe was used.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
How do we code for new HPV vaccine?
- 90649 is the vaccine product code (human papilloma virus [HPV] vaccine, types 6, 11, 16, 18 [quadrivalent], 3-dose schedule, for intramuscular use). A 3-dose schedule means you will be billing for the procedure 3 times during a 6-month period.
- 90471 can also be reported for the administration of the vaccine. (Immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid])
Adding modifiers. CPT guidelines state that a modifier -51 (multiple procedure) would not be added to either of these codes, and of course if you provide a significant and separate evaluation and management (E/M) service at the time the vaccine is given, you may also bill an E/M code with a modifier -25 added to let the payer know that the E/M service was separate.
Note that almost no payers will pay separately for the E/M code 99211 plus an injection procedure because it represents a minimal, not a significant E/M service.
Insurance coverage unlikely, for now
Until such time as the CDC comes out with a recommendation for the vaccine, coverage is going to be a problem. Insurance plans can be expected to cover the cost of the vaccine only if the CDC Advisory Committee on Immunization Practices recommends HPV vaccination as standard.
Tell patients! Until then, you may want to advise your patients who are candidates for the vaccine that this vaccine may be an out-of-pocket expense for them. Merck, the company that produces the quadrivalent vaccine, has stated that the price will be $120 per injection. The company has indicated that they have created a new program to provide free vaccines including HPV vaccine, for uninsured adults unable to pay.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
- 90649 is the vaccine product code (human papilloma virus [HPV] vaccine, types 6, 11, 16, 18 [quadrivalent], 3-dose schedule, for intramuscular use). A 3-dose schedule means you will be billing for the procedure 3 times during a 6-month period.
- 90471 can also be reported for the administration of the vaccine. (Immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid])
Adding modifiers. CPT guidelines state that a modifier -51 (multiple procedure) would not be added to either of these codes, and of course if you provide a significant and separate evaluation and management (E/M) service at the time the vaccine is given, you may also bill an E/M code with a modifier -25 added to let the payer know that the E/M service was separate.
Note that almost no payers will pay separately for the E/M code 99211 plus an injection procedure because it represents a minimal, not a significant E/M service.
Insurance coverage unlikely, for now
Until such time as the CDC comes out with a recommendation for the vaccine, coverage is going to be a problem. Insurance plans can be expected to cover the cost of the vaccine only if the CDC Advisory Committee on Immunization Practices recommends HPV vaccination as standard.
Tell patients! Until then, you may want to advise your patients who are candidates for the vaccine that this vaccine may be an out-of-pocket expense for them. Merck, the company that produces the quadrivalent vaccine, has stated that the price will be $120 per injection. The company has indicated that they have created a new program to provide free vaccines including HPV vaccine, for uninsured adults unable to pay.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
- 90649 is the vaccine product code (human papilloma virus [HPV] vaccine, types 6, 11, 16, 18 [quadrivalent], 3-dose schedule, for intramuscular use). A 3-dose schedule means you will be billing for the procedure 3 times during a 6-month period.
- 90471 can also be reported for the administration of the vaccine. (Immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid])
Adding modifiers. CPT guidelines state that a modifier -51 (multiple procedure) would not be added to either of these codes, and of course if you provide a significant and separate evaluation and management (E/M) service at the time the vaccine is given, you may also bill an E/M code with a modifier -25 added to let the payer know that the E/M service was separate.
Note that almost no payers will pay separately for the E/M code 99211 plus an injection procedure because it represents a minimal, not a significant E/M service.
Insurance coverage unlikely, for now
Until such time as the CDC comes out with a recommendation for the vaccine, coverage is going to be a problem. Insurance plans can be expected to cover the cost of the vaccine only if the CDC Advisory Committee on Immunization Practices recommends HPV vaccination as standard.
Tell patients! Until then, you may want to advise your patients who are candidates for the vaccine that this vaccine may be an out-of-pocket expense for them. Merck, the company that produces the quadrivalent vaccine, has stated that the price will be $120 per injection. The company has indicated that they have created a new program to provide free vaccines including HPV vaccine, for uninsured adults unable to pay.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
When Can I Retire?
Retirement seems to be on a lot of readers' minds these days, and one of the more common questions I'm receiving is, “How will I know when I've accumulated enough money to safely retire?”
It's good that more physicians are turning their attention to this issue, because the road to retirement is fraught with many challenges.
The most common mistake made by physicians and other professionals is saving too little. We either never calculate or we underestimate how much we'll need to last through retirement.
We also tend to live longer than planned. As life expectancy increases, we run the risk of outliving our savings. And we don't face facts about long-term care. Not nearly enough of us have long-term-care insurance, or the means to self-fund an extended long-term-care situation.
Many people lack a clear idea of where their retirement income will come from, and even when they do, they don't know how to manage their savings correctly. Physicians in particular are notorious for not understanding investments. Many attempt to manage their practice's retirement plans with inadequate knowledge of how the investments within their plans work. Seeking the guidance of a qualified financial professional is often a far better strategy.
So, how will you know when you can safely retire? As with everything else, it depends. To arrive at any sort of reliable ballpark figure, you'll need to know three things: how much you realistically expect to spend annually after retirement, how much principal you'll need to generate that annual income, and how far your present savings are from that figure.
According to one oft-quoted rule of thumb, in retirement you should plan to spend about 70% of what you're spending now. That's nonsense. A few significant expenses, such as disability and malpractice insurance premiums, will be eliminated, but other expenses, such as travel, recreation, and medical care (including long-term-care insurance), will increase.
My wife and I are assuming we will spend about the same in retirement as we spend now, and I suggest you do, too.
Once you have an estimate of your annual retirement expenses, you'll need to determine how much you'll need—usually in fixed pensions and invested assets—to generate that income. Social Security can be included, if you're over 50. If you're younger, don't count on receiving any entitlements since no one can predict how they will fare in coming generations.
Most financial advisors use the 5% rule: Assume the best you'll do on your money is 5% a year. So if your annual retirement expense estimate is $100,000, you'll need $2 million in assets. If you want to spend $200,000 per year, you'll need $4 million. That rule has worked well in most years, allowing for reasonable taxes, inflation, and rates of return.
How do you accumulate that kind of money? Financial experts say that too many physicians invest too aggressively. For retirement, safety is the key. The most foolproof strategy—seldom employed, because it's boring—is to sock away a fixed amount per month (after your retirement plan has been funded) in a mutual fund. With the power of compounded interest working for you, $1,000 per month for 25 years with the market earning 10% overall comes to almost $2 million.
Of course, it goes without saying that debt can destroy the best-laid retirement plans. If you carry significant debt, pay it off as soon as possible.
For those of you who are early in your careers, it is never too soon to think about retirement. Young physicians often defer contributing to their retirement plans because they want to save for a new house or for college for their children. There are tangible tax benefits that you get now, though, because your contributions usually reduce your taxable income and your investment grows tax free until you take it out.
No matter what your age, it's hard to motivate yourself to save for retirement because it generally requires spending less money now. You can always pay a financial planner to help you get organized, but you still must motivate yourself to change and follow the planner's advice.
In the end, the strategy is very straightforward: Put as much money as you can in a tax-deductible retirement plan, let it stay there and grow tax deferred until you take it out, and invest for the long term with your target amount in mind. It really is that simple.
Retirement seems to be on a lot of readers' minds these days, and one of the more common questions I'm receiving is, “How will I know when I've accumulated enough money to safely retire?”
It's good that more physicians are turning their attention to this issue, because the road to retirement is fraught with many challenges.
The most common mistake made by physicians and other professionals is saving too little. We either never calculate or we underestimate how much we'll need to last through retirement.
We also tend to live longer than planned. As life expectancy increases, we run the risk of outliving our savings. And we don't face facts about long-term care. Not nearly enough of us have long-term-care insurance, or the means to self-fund an extended long-term-care situation.
Many people lack a clear idea of where their retirement income will come from, and even when they do, they don't know how to manage their savings correctly. Physicians in particular are notorious for not understanding investments. Many attempt to manage their practice's retirement plans with inadequate knowledge of how the investments within their plans work. Seeking the guidance of a qualified financial professional is often a far better strategy.
So, how will you know when you can safely retire? As with everything else, it depends. To arrive at any sort of reliable ballpark figure, you'll need to know three things: how much you realistically expect to spend annually after retirement, how much principal you'll need to generate that annual income, and how far your present savings are from that figure.
According to one oft-quoted rule of thumb, in retirement you should plan to spend about 70% of what you're spending now. That's nonsense. A few significant expenses, such as disability and malpractice insurance premiums, will be eliminated, but other expenses, such as travel, recreation, and medical care (including long-term-care insurance), will increase.
My wife and I are assuming we will spend about the same in retirement as we spend now, and I suggest you do, too.
Once you have an estimate of your annual retirement expenses, you'll need to determine how much you'll need—usually in fixed pensions and invested assets—to generate that income. Social Security can be included, if you're over 50. If you're younger, don't count on receiving any entitlements since no one can predict how they will fare in coming generations.
Most financial advisors use the 5% rule: Assume the best you'll do on your money is 5% a year. So if your annual retirement expense estimate is $100,000, you'll need $2 million in assets. If you want to spend $200,000 per year, you'll need $4 million. That rule has worked well in most years, allowing for reasonable taxes, inflation, and rates of return.
How do you accumulate that kind of money? Financial experts say that too many physicians invest too aggressively. For retirement, safety is the key. The most foolproof strategy—seldom employed, because it's boring—is to sock away a fixed amount per month (after your retirement plan has been funded) in a mutual fund. With the power of compounded interest working for you, $1,000 per month for 25 years with the market earning 10% overall comes to almost $2 million.
Of course, it goes without saying that debt can destroy the best-laid retirement plans. If you carry significant debt, pay it off as soon as possible.
For those of you who are early in your careers, it is never too soon to think about retirement. Young physicians often defer contributing to their retirement plans because they want to save for a new house or for college for their children. There are tangible tax benefits that you get now, though, because your contributions usually reduce your taxable income and your investment grows tax free until you take it out.
No matter what your age, it's hard to motivate yourself to save for retirement because it generally requires spending less money now. You can always pay a financial planner to help you get organized, but you still must motivate yourself to change and follow the planner's advice.
In the end, the strategy is very straightforward: Put as much money as you can in a tax-deductible retirement plan, let it stay there and grow tax deferred until you take it out, and invest for the long term with your target amount in mind. It really is that simple.
Retirement seems to be on a lot of readers' minds these days, and one of the more common questions I'm receiving is, “How will I know when I've accumulated enough money to safely retire?”
It's good that more physicians are turning their attention to this issue, because the road to retirement is fraught with many challenges.
The most common mistake made by physicians and other professionals is saving too little. We either never calculate or we underestimate how much we'll need to last through retirement.
We also tend to live longer than planned. As life expectancy increases, we run the risk of outliving our savings. And we don't face facts about long-term care. Not nearly enough of us have long-term-care insurance, or the means to self-fund an extended long-term-care situation.
Many people lack a clear idea of where their retirement income will come from, and even when they do, they don't know how to manage their savings correctly. Physicians in particular are notorious for not understanding investments. Many attempt to manage their practice's retirement plans with inadequate knowledge of how the investments within their plans work. Seeking the guidance of a qualified financial professional is often a far better strategy.
So, how will you know when you can safely retire? As with everything else, it depends. To arrive at any sort of reliable ballpark figure, you'll need to know three things: how much you realistically expect to spend annually after retirement, how much principal you'll need to generate that annual income, and how far your present savings are from that figure.
According to one oft-quoted rule of thumb, in retirement you should plan to spend about 70% of what you're spending now. That's nonsense. A few significant expenses, such as disability and malpractice insurance premiums, will be eliminated, but other expenses, such as travel, recreation, and medical care (including long-term-care insurance), will increase.
My wife and I are assuming we will spend about the same in retirement as we spend now, and I suggest you do, too.
Once you have an estimate of your annual retirement expenses, you'll need to determine how much you'll need—usually in fixed pensions and invested assets—to generate that income. Social Security can be included, if you're over 50. If you're younger, don't count on receiving any entitlements since no one can predict how they will fare in coming generations.
Most financial advisors use the 5% rule: Assume the best you'll do on your money is 5% a year. So if your annual retirement expense estimate is $100,000, you'll need $2 million in assets. If you want to spend $200,000 per year, you'll need $4 million. That rule has worked well in most years, allowing for reasonable taxes, inflation, and rates of return.
How do you accumulate that kind of money? Financial experts say that too many physicians invest too aggressively. For retirement, safety is the key. The most foolproof strategy—seldom employed, because it's boring—is to sock away a fixed amount per month (after your retirement plan has been funded) in a mutual fund. With the power of compounded interest working for you, $1,000 per month for 25 years with the market earning 10% overall comes to almost $2 million.
Of course, it goes without saying that debt can destroy the best-laid retirement plans. If you carry significant debt, pay it off as soon as possible.
For those of you who are early in your careers, it is never too soon to think about retirement. Young physicians often defer contributing to their retirement plans because they want to save for a new house or for college for their children. There are tangible tax benefits that you get now, though, because your contributions usually reduce your taxable income and your investment grows tax free until you take it out.
No matter what your age, it's hard to motivate yourself to save for retirement because it generally requires spending less money now. You can always pay a financial planner to help you get organized, but you still must motivate yourself to change and follow the planner's advice.
In the end, the strategy is very straightforward: Put as much money as you can in a tax-deductible retirement plan, let it stay there and grow tax deferred until you take it out, and invest for the long term with your target amount in mind. It really is that simple.
Medical Verdicts
Woman recants request for hysterectomy after she remarries
<court> Harris County (Tex) District Court </court>
Over the course of 12 years, a woman had various obstetric and gynecologic problems, among them adhesions, ovarian cysts, and possible endometriosis. She had ongoing pelvic pain, which was occasionally severe. She was treated with various medications and underwent several surgeries, including removal of her left fallopian tube and ovary due to infection.
After having 2 children, the woman had her remaining tube ligated. Six years later she presented to an emergency department complaining of severe pelvic pain. Three days after a surgical consult suggested the pelvic pain was gynecologic in origin, she requested and underwent a hysterectomy.
In suing, the woman, now divorced and remarried, contended the physician should have obtained more consults, including a psychiatry consult, prior to the hysterectomy to rule out other causes of the pelvic pain. She claimed her request for the hysterectomy did not justify the performance of the procedure. She noted that she had a new marriage and planned to have her tubal ligation reversed because of a desire to have more children.
- The jury returned a defense verdict.
Was Brannon pack “ too big to overlook ” ?
<court> Hillsborough County (Fla) Circuit Court </court>
After a total abdominal hysterectomy with bilateral salpingo-oophorectomy for abdominal pain and postmenstrual spotting, a 43-year-old woman had a temperature as high as 102 ° F and bilious projectile vomiting. An x-ray 3 days after surgery revealed a foreign object in the upper abdomen. During exploratory laparotomy, a lap sponge (Brannon pack) was removed.
In suing, the woman claimed the physician was negligent in failing to remove the Brannon pack. The defense asserted that the physician was entitled to rely on the hospital staff report that the sponge count was correct. The woman claimed the Brannon pack was so large that it should not have been overlooked.
- The hospital settled prior to the filing of the lawsuit for an undisclosed amount. The jury awarded the plaintiff $22,500.
Manifold errors charged in cerebral palsy case
<court> King ’ s County (NY) Supreme Court </court>
At 29 weeks ’ gestation, a woman with diabetes and a history of preterm delivery was admitted for mild-to-moderate contractions. Her physician and the perinatologist on staff ordered magnesium sulfate to stop contractions, but labor progressed. The infant was born with Apgar scores of 4 and 4. She was limp, blue, and not breathing. She was intubated for 4 days and discharged after 3 months, with a diagnosis of periventricular leukomalacia. The child has no use of her legs and little use of her right arm. She is wheel-chair bound and cannot attend to her daily needs. She has full cognition and above-average intelligence and is doing well in school.
In suing the hospital and the physicians, the woman claimed the physicians should have prescribed antibiotics because infection is a known cause of preterm labor. She also asserted that the hospital and the physician improperly reduced the magnesium sulfate, allowing labor to progress. She claimed the hospital staff failed to monitor the fetal heart tracings, which revealed variable decelerations, reduced accelerations, and reduced variability. She claimed failure to perform a cesarean section resulted in cerebral palsy and brain damage.
The hospital maintained the physician was in charge of the labor and delivery, and made all the decisions. The defendants claimed the care given was appropriate.
- The jury awarded the plaintiff $29.3 million, with fault divided 35% to the hospital and 65% to the physician. The plaintiff had agreed to a high/low settlement with the hospital only; a $5 million settlement was reached.
Defense: Consent form warned of dangers
<court> Fresno County (Calif) Superior Court </court>
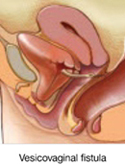
A 39-year-old woman with a 1-year history of pelvic pressure due to uterine fibroids under-went a hysterectomy. Five days after hospital discharge, she complained of urinary incontinence. A urologist diagnosed a vesicovaginal fistula and recommended surgery.
Ultrasound examination of the kidneys a month later was suggestive of a left ureter injury. The bladder leak and the ureter were repaired soon afterward.
In suing, the woman claimed the physician performed the hysterectomy negligently and failed to perform a postoperative intravenous pyelogram to reveal the bladder and ureter problems.
Denying negligence, the surgeon pointed out that the written consent form explained the risks posed to other organs by the surgery. He noted that the surgical field had substantial adhesions and scar tissue, complicating the procedure. He also claimed the woman would not consent to an intravenous pyelogram because of an iodine allergy.
- The jury returned a defense verdict.
Diabetes undiagnosed until emergency delivery
<court> Kings County (NY) Supreme Court </court>
Because traces of glucose were found in the urine of a 38-year-old pregnant woman, her ObGyn ordered a standard glucose tolerance test. She was unable to drink the liquid necessary for the test, however, and there was no follow-up.
Six months later the woman presented to a hospital complaining of decreased fetal movement, excessive thirst, dry mouth, and vomiting. The hospital physician placed her on a fetal monitor and discharged her several hours later. The next day after reviewing the fetal heart monitor results, her ObGyn asked that she return to the hospital. The hospital physician ordered an emergency cesarean section after an abnormal scalp pH test result.
At birth, the infant weighed 11 lb 14 oz and his Apgar scores were 1, 2, and 5. After a seizure the infant was given anticonvulsants and remained in ICU for 17 days. He was diagnosed with perinatal asphyxia, acidosis, and hypoglycemia. Now 12, the child has mild mental retardation and attention deficit disorder, as well as cognitive and learning disabilities.
The mother claimed the defendants failed to diagnose gestational diabetes in a timely manner, and failed to proceed to immediate cesarean section when the nonreactive and nonreassuring heart rate pattern was noted. The gynecologist asserted he ordered the glucose tolerance test to rule out diabetes, and that the diabetes was not the cause of the fetal distress.
- Damages were set at $4.1 million. The jury assigned fault 55% to the hospital, 25% to the hospital physician, and 20% to the gynecologist.
Abnormal fetal tracing and spastic quadriplegia
<court> Queens County (NY) Supreme Court </court>
In her 37th week of pregnancy, a 19-year-old woman presented to her hospital at 4 cm dilated. She was instructed to ambulate to help induce labor. Two hours later she was given an epidural and placed on a fetal heart monitor. Physicians ruptured her membranes and noticed meconium staining. During the next few hours, fetal distress was recorded; the fetus did not descend into the birth canal, but remained at minus-1 station.
The infant was delivered by cesarean section and had Apgar scores of 2, 4, and 5. After transfer to another facility, the child was diagnosed with microcephaly and spastic quadriplegia.
The woman asserted the delayed cesarean section led to oxygen deprivation that caused the infant ’ s injuries.
- The case settled for $2.95 million.
Unpredictable event to blame, jury agrees
<court> St. Louis County (Mo) Circuit Court </court>
A woman at 41 weeks ’ gestation arrived at the hospital with ruptured membranes and was given oxytocin at 5:25 PM. At about 6 PM the fetal heart rate fell from 130 to 90 and sometimes 70.
Because of difficulties with the fetal monitor, the nurse switched from an external monitor to an internal lead attached to the fetus ’ s scalp. Although the fetal heart rate improved, another deceleration was noted at 6:11 PM. The nurse adjusted the position of the mother, turned off the oxytocin at 6:23 PM, and called the physician 3 minutes later to alert him to the decreased fetal heart rate.
The physician suggested several interventions and told the nurse to call him back with another update. Although the nurse increased IV fluids, administered oxygen, and turned the mother to increase fetal circulation, the deceleration continued. The physician was called again at 6:37 PM; he arrived at the hospital at 6:50 PM for an immediate cesarean section.
The infant was delivered at 7:11 PM with no pulse or respirations. Cerebral palsy due to perinatal hypoxia was diagnosed. The child is confined to a wheelchair, unable to move any part of her body except for one arm. Now age 15, she cannot speak or swallow, and requires a feeding tube. The plaintiff faulted the nurse for failing to recognize signs of fetal distress in a timely manner, and the physician for failing to come to the hospital after the first phone call and failing to recognize the need for cesarean section sooner.
The defense denied any negligence and asserted the injury was caused by an unpredictable, profound, and sudden event.
- The jury returned a defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, Nashville, Tenn ( www.verdictslaska.com ).The available information about the cases is sometimes incomplete; pertinent details may be unavailable. Moreover, the cases may or may not have merit. Still, these cases represent types of clinical situations that may result in litigation and are meant to illustrate variation in verdicts and awards. Any illustrations are generic and do not represent a specific legal case.
Woman recants request for hysterectomy after she remarries
<court> Harris County (Tex) District Court </court>
Over the course of 12 years, a woman had various obstetric and gynecologic problems, among them adhesions, ovarian cysts, and possible endometriosis. She had ongoing pelvic pain, which was occasionally severe. She was treated with various medications and underwent several surgeries, including removal of her left fallopian tube and ovary due to infection.
After having 2 children, the woman had her remaining tube ligated. Six years later she presented to an emergency department complaining of severe pelvic pain. Three days after a surgical consult suggested the pelvic pain was gynecologic in origin, she requested and underwent a hysterectomy.
In suing, the woman, now divorced and remarried, contended the physician should have obtained more consults, including a psychiatry consult, prior to the hysterectomy to rule out other causes of the pelvic pain. She claimed her request for the hysterectomy did not justify the performance of the procedure. She noted that she had a new marriage and planned to have her tubal ligation reversed because of a desire to have more children.
- The jury returned a defense verdict.
Was Brannon pack “ too big to overlook ” ?
<court> Hillsborough County (Fla) Circuit Court </court>
After a total abdominal hysterectomy with bilateral salpingo-oophorectomy for abdominal pain and postmenstrual spotting, a 43-year-old woman had a temperature as high as 102 ° F and bilious projectile vomiting. An x-ray 3 days after surgery revealed a foreign object in the upper abdomen. During exploratory laparotomy, a lap sponge (Brannon pack) was removed.
In suing, the woman claimed the physician was negligent in failing to remove the Brannon pack. The defense asserted that the physician was entitled to rely on the hospital staff report that the sponge count was correct. The woman claimed the Brannon pack was so large that it should not have been overlooked.
- The hospital settled prior to the filing of the lawsuit for an undisclosed amount. The jury awarded the plaintiff $22,500.
Manifold errors charged in cerebral palsy case
<court> King ’ s County (NY) Supreme Court </court>
At 29 weeks ’ gestation, a woman with diabetes and a history of preterm delivery was admitted for mild-to-moderate contractions. Her physician and the perinatologist on staff ordered magnesium sulfate to stop contractions, but labor progressed. The infant was born with Apgar scores of 4 and 4. She was limp, blue, and not breathing. She was intubated for 4 days and discharged after 3 months, with a diagnosis of periventricular leukomalacia. The child has no use of her legs and little use of her right arm. She is wheel-chair bound and cannot attend to her daily needs. She has full cognition and above-average intelligence and is doing well in school.
In suing the hospital and the physicians, the woman claimed the physicians should have prescribed antibiotics because infection is a known cause of preterm labor. She also asserted that the hospital and the physician improperly reduced the magnesium sulfate, allowing labor to progress. She claimed the hospital staff failed to monitor the fetal heart tracings, which revealed variable decelerations, reduced accelerations, and reduced variability. She claimed failure to perform a cesarean section resulted in cerebral palsy and brain damage.
The hospital maintained the physician was in charge of the labor and delivery, and made all the decisions. The defendants claimed the care given was appropriate.
- The jury awarded the plaintiff $29.3 million, with fault divided 35% to the hospital and 65% to the physician. The plaintiff had agreed to a high/low settlement with the hospital only; a $5 million settlement was reached.
Defense: Consent form warned of dangers
<court> Fresno County (Calif) Superior Court </court>
A 39-year-old woman with a 1-year history of pelvic pressure due to uterine fibroids under-went a hysterectomy. Five days after hospital discharge, she complained of urinary incontinence. A urologist diagnosed a vesicovaginal fistula and recommended surgery.
Ultrasound examination of the kidneys a month later was suggestive of a left ureter injury. The bladder leak and the ureter were repaired soon afterward.
In suing, the woman claimed the physician performed the hysterectomy negligently and failed to perform a postoperative intravenous pyelogram to reveal the bladder and ureter problems.
Denying negligence, the surgeon pointed out that the written consent form explained the risks posed to other organs by the surgery. He noted that the surgical field had substantial adhesions and scar tissue, complicating the procedure. He also claimed the woman would not consent to an intravenous pyelogram because of an iodine allergy.
- The jury returned a defense verdict.
Diabetes undiagnosed until emergency delivery
<court> Kings County (NY) Supreme Court </court>
Because traces of glucose were found in the urine of a 38-year-old pregnant woman, her ObGyn ordered a standard glucose tolerance test. She was unable to drink the liquid necessary for the test, however, and there was no follow-up.
Six months later the woman presented to a hospital complaining of decreased fetal movement, excessive thirst, dry mouth, and vomiting. The hospital physician placed her on a fetal monitor and discharged her several hours later. The next day after reviewing the fetal heart monitor results, her ObGyn asked that she return to the hospital. The hospital physician ordered an emergency cesarean section after an abnormal scalp pH test result.
At birth, the infant weighed 11 lb 14 oz and his Apgar scores were 1, 2, and 5. After a seizure the infant was given anticonvulsants and remained in ICU for 17 days. He was diagnosed with perinatal asphyxia, acidosis, and hypoglycemia. Now 12, the child has mild mental retardation and attention deficit disorder, as well as cognitive and learning disabilities.
The mother claimed the defendants failed to diagnose gestational diabetes in a timely manner, and failed to proceed to immediate cesarean section when the nonreactive and nonreassuring heart rate pattern was noted. The gynecologist asserted he ordered the glucose tolerance test to rule out diabetes, and that the diabetes was not the cause of the fetal distress.
- Damages were set at $4.1 million. The jury assigned fault 55% to the hospital, 25% to the hospital physician, and 20% to the gynecologist.
Abnormal fetal tracing and spastic quadriplegia
<court> Queens County (NY) Supreme Court </court>
In her 37th week of pregnancy, a 19-year-old woman presented to her hospital at 4 cm dilated. She was instructed to ambulate to help induce labor. Two hours later she was given an epidural and placed on a fetal heart monitor. Physicians ruptured her membranes and noticed meconium staining. During the next few hours, fetal distress was recorded; the fetus did not descend into the birth canal, but remained at minus-1 station.
The infant was delivered by cesarean section and had Apgar scores of 2, 4, and 5. After transfer to another facility, the child was diagnosed with microcephaly and spastic quadriplegia.
The woman asserted the delayed cesarean section led to oxygen deprivation that caused the infant ’ s injuries.
- The case settled for $2.95 million.
Unpredictable event to blame, jury agrees
<court> St. Louis County (Mo) Circuit Court </court>
A woman at 41 weeks ’ gestation arrived at the hospital with ruptured membranes and was given oxytocin at 5:25 PM. At about 6 PM the fetal heart rate fell from 130 to 90 and sometimes 70.
Because of difficulties with the fetal monitor, the nurse switched from an external monitor to an internal lead attached to the fetus ’ s scalp. Although the fetal heart rate improved, another deceleration was noted at 6:11 PM. The nurse adjusted the position of the mother, turned off the oxytocin at 6:23 PM, and called the physician 3 minutes later to alert him to the decreased fetal heart rate.
The physician suggested several interventions and told the nurse to call him back with another update. Although the nurse increased IV fluids, administered oxygen, and turned the mother to increase fetal circulation, the deceleration continued. The physician was called again at 6:37 PM; he arrived at the hospital at 6:50 PM for an immediate cesarean section.
The infant was delivered at 7:11 PM with no pulse or respirations. Cerebral palsy due to perinatal hypoxia was diagnosed. The child is confined to a wheelchair, unable to move any part of her body except for one arm. Now age 15, she cannot speak or swallow, and requires a feeding tube. The plaintiff faulted the nurse for failing to recognize signs of fetal distress in a timely manner, and the physician for failing to come to the hospital after the first phone call and failing to recognize the need for cesarean section sooner.
The defense denied any negligence and asserted the injury was caused by an unpredictable, profound, and sudden event.
- The jury returned a defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, Nashville, Tenn ( www.verdictslaska.com ).The available information about the cases is sometimes incomplete; pertinent details may be unavailable. Moreover, the cases may or may not have merit. Still, these cases represent types of clinical situations that may result in litigation and are meant to illustrate variation in verdicts and awards. Any illustrations are generic and do not represent a specific legal case.
Woman recants request for hysterectomy after she remarries
<court> Harris County (Tex) District Court </court>
Over the course of 12 years, a woman had various obstetric and gynecologic problems, among them adhesions, ovarian cysts, and possible endometriosis. She had ongoing pelvic pain, which was occasionally severe. She was treated with various medications and underwent several surgeries, including removal of her left fallopian tube and ovary due to infection.
After having 2 children, the woman had her remaining tube ligated. Six years later she presented to an emergency department complaining of severe pelvic pain. Three days after a surgical consult suggested the pelvic pain was gynecologic in origin, she requested and underwent a hysterectomy.
In suing, the woman, now divorced and remarried, contended the physician should have obtained more consults, including a psychiatry consult, prior to the hysterectomy to rule out other causes of the pelvic pain. She claimed her request for the hysterectomy did not justify the performance of the procedure. She noted that she had a new marriage and planned to have her tubal ligation reversed because of a desire to have more children.
- The jury returned a defense verdict.
Was Brannon pack “ too big to overlook ” ?
<court> Hillsborough County (Fla) Circuit Court </court>
After a total abdominal hysterectomy with bilateral salpingo-oophorectomy for abdominal pain and postmenstrual spotting, a 43-year-old woman had a temperature as high as 102 ° F and bilious projectile vomiting. An x-ray 3 days after surgery revealed a foreign object in the upper abdomen. During exploratory laparotomy, a lap sponge (Brannon pack) was removed.
In suing, the woman claimed the physician was negligent in failing to remove the Brannon pack. The defense asserted that the physician was entitled to rely on the hospital staff report that the sponge count was correct. The woman claimed the Brannon pack was so large that it should not have been overlooked.
- The hospital settled prior to the filing of the lawsuit for an undisclosed amount. The jury awarded the plaintiff $22,500.
Manifold errors charged in cerebral palsy case
<court> King ’ s County (NY) Supreme Court </court>
At 29 weeks ’ gestation, a woman with diabetes and a history of preterm delivery was admitted for mild-to-moderate contractions. Her physician and the perinatologist on staff ordered magnesium sulfate to stop contractions, but labor progressed. The infant was born with Apgar scores of 4 and 4. She was limp, blue, and not breathing. She was intubated for 4 days and discharged after 3 months, with a diagnosis of periventricular leukomalacia. The child has no use of her legs and little use of her right arm. She is wheel-chair bound and cannot attend to her daily needs. She has full cognition and above-average intelligence and is doing well in school.
In suing the hospital and the physicians, the woman claimed the physicians should have prescribed antibiotics because infection is a known cause of preterm labor. She also asserted that the hospital and the physician improperly reduced the magnesium sulfate, allowing labor to progress. She claimed the hospital staff failed to monitor the fetal heart tracings, which revealed variable decelerations, reduced accelerations, and reduced variability. She claimed failure to perform a cesarean section resulted in cerebral palsy and brain damage.
The hospital maintained the physician was in charge of the labor and delivery, and made all the decisions. The defendants claimed the care given was appropriate.
- The jury awarded the plaintiff $29.3 million, with fault divided 35% to the hospital and 65% to the physician. The plaintiff had agreed to a high/low settlement with the hospital only; a $5 million settlement was reached.
Defense: Consent form warned of dangers
<court> Fresno County (Calif) Superior Court </court>
A 39-year-old woman with a 1-year history of pelvic pressure due to uterine fibroids under-went a hysterectomy. Five days after hospital discharge, she complained of urinary incontinence. A urologist diagnosed a vesicovaginal fistula and recommended surgery.
Ultrasound examination of the kidneys a month later was suggestive of a left ureter injury. The bladder leak and the ureter were repaired soon afterward.
In suing, the woman claimed the physician performed the hysterectomy negligently and failed to perform a postoperative intravenous pyelogram to reveal the bladder and ureter problems.
Denying negligence, the surgeon pointed out that the written consent form explained the risks posed to other organs by the surgery. He noted that the surgical field had substantial adhesions and scar tissue, complicating the procedure. He also claimed the woman would not consent to an intravenous pyelogram because of an iodine allergy.
- The jury returned a defense verdict.
Diabetes undiagnosed until emergency delivery
<court> Kings County (NY) Supreme Court </court>
Because traces of glucose were found in the urine of a 38-year-old pregnant woman, her ObGyn ordered a standard glucose tolerance test. She was unable to drink the liquid necessary for the test, however, and there was no follow-up.
Six months later the woman presented to a hospital complaining of decreased fetal movement, excessive thirst, dry mouth, and vomiting. The hospital physician placed her on a fetal monitor and discharged her several hours later. The next day after reviewing the fetal heart monitor results, her ObGyn asked that she return to the hospital. The hospital physician ordered an emergency cesarean section after an abnormal scalp pH test result.
At birth, the infant weighed 11 lb 14 oz and his Apgar scores were 1, 2, and 5. After a seizure the infant was given anticonvulsants and remained in ICU for 17 days. He was diagnosed with perinatal asphyxia, acidosis, and hypoglycemia. Now 12, the child has mild mental retardation and attention deficit disorder, as well as cognitive and learning disabilities.
The mother claimed the defendants failed to diagnose gestational diabetes in a timely manner, and failed to proceed to immediate cesarean section when the nonreactive and nonreassuring heart rate pattern was noted. The gynecologist asserted he ordered the glucose tolerance test to rule out diabetes, and that the diabetes was not the cause of the fetal distress.
- Damages were set at $4.1 million. The jury assigned fault 55% to the hospital, 25% to the hospital physician, and 20% to the gynecologist.
Abnormal fetal tracing and spastic quadriplegia
<court> Queens County (NY) Supreme Court </court>
In her 37th week of pregnancy, a 19-year-old woman presented to her hospital at 4 cm dilated. She was instructed to ambulate to help induce labor. Two hours later she was given an epidural and placed on a fetal heart monitor. Physicians ruptured her membranes and noticed meconium staining. During the next few hours, fetal distress was recorded; the fetus did not descend into the birth canal, but remained at minus-1 station.
The infant was delivered by cesarean section and had Apgar scores of 2, 4, and 5. After transfer to another facility, the child was diagnosed with microcephaly and spastic quadriplegia.
The woman asserted the delayed cesarean section led to oxygen deprivation that caused the infant ’ s injuries.
- The case settled for $2.95 million.
Unpredictable event to blame, jury agrees
<court> St. Louis County (Mo) Circuit Court </court>
A woman at 41 weeks ’ gestation arrived at the hospital with ruptured membranes and was given oxytocin at 5:25 PM. At about 6 PM the fetal heart rate fell from 130 to 90 and sometimes 70.
Because of difficulties with the fetal monitor, the nurse switched from an external monitor to an internal lead attached to the fetus ’ s scalp. Although the fetal heart rate improved, another deceleration was noted at 6:11 PM. The nurse adjusted the position of the mother, turned off the oxytocin at 6:23 PM, and called the physician 3 minutes later to alert him to the decreased fetal heart rate.
The physician suggested several interventions and told the nurse to call him back with another update. Although the nurse increased IV fluids, administered oxygen, and turned the mother to increase fetal circulation, the deceleration continued. The physician was called again at 6:37 PM; he arrived at the hospital at 6:50 PM for an immediate cesarean section.
The infant was delivered at 7:11 PM with no pulse or respirations. Cerebral palsy due to perinatal hypoxia was diagnosed. The child is confined to a wheelchair, unable to move any part of her body except for one arm. Now age 15, she cannot speak or swallow, and requires a feeding tube. The plaintiff faulted the nurse for failing to recognize signs of fetal distress in a timely manner, and the physician for failing to come to the hospital after the first phone call and failing to recognize the need for cesarean section sooner.
The defense denied any negligence and asserted the injury was caused by an unpredictable, profound, and sudden event.
- The jury returned a defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, Nashville, Tenn ( www.verdictslaska.com ).The available information about the cases is sometimes incomplete; pertinent details may be unavailable. Moreover, the cases may or may not have merit. Still, these cases represent types of clinical situations that may result in litigation and are meant to illustrate variation in verdicts and awards. Any illustrations are generic and do not represent a specific legal case.
New 3D ultrasound codes are not for routine use
Payment for services during miscarriage
Induction with IV oxytocin would be classified as medical management of an abortion. Under CPT rules and ACOG guidelines, you would bill only for the evaluation and management (E/M) services. However, this means you would be billing for the hospital admission, subsequent care, and, prior to delivery, prolonged physician services. In this case you would report the hospital prolonged care codes that account for the actual time you spent with the patient managing her labor, as long as that time exceeds by 30 minutes the typical time of the E/M code you reported (TABLE).
For instance, if she is admitted at 10 PM on day 1 and delivers on day 2 at 2 PM, with your having documented that you spent a total of 2 hours at the patient’s bedside on day 1 and 8 hours at the patient’s bedside on day 2, you could bill as follows:
Day 1: Hospital admission (eg, 99222, requiring comprehensive history and exam and moderate medical decision-making with a typical time of 50 minutes)
Prolonged services on day 1: 120 minutes total –50 minutes=70 minutes of prolonged service. Bill code 99356 (first 60 minutes), but no additional code for the last 10 minutes of prolonged service.
Day 2: Subsequent hospital care (eg, 99232 requiring an expanded problem, focused history or exam with moderate complexity of medical decision-making with a typical time of 25 minutes).
Prolonged services for 8 hours on day 2: 480 minutes total –25 minutes=455 minutes of prolonged service; bill code 99356 (first 60 minutes), and 99357 with a quantity of 13 for the remaining 395 minutes.
TABLE
You have to do the math: Coding prolonged physician services
| TOTAL TIME W/PATIENT | BASIC SERVICE | BILLABLE PROLONGED SERVICE | PROLONGED SERVICES WITH CODES REPORTED |
|---|---|---|---|
| Day 1 120 minutes | 99222 (50 minutes) | 120 min –50 min=70 minutes | 99356 for first 60 minutes, but no extra codes for last 10 minutes |
| Day 2 480 minutes | 99232 (25 minutes) | 480 min –25 min=455 minutes | 99356 for first 60 minutes; 455 min –60 minutes=395 minutes 99357×13 for remaining time (13 times for each 30-minute increment) |
Induction with IV oxytocin would be classified as medical management of an abortion. Under CPT rules and ACOG guidelines, you would bill only for the evaluation and management (E/M) services. However, this means you would be billing for the hospital admission, subsequent care, and, prior to delivery, prolonged physician services. In this case you would report the hospital prolonged care codes that account for the actual time you spent with the patient managing her labor, as long as that time exceeds by 30 minutes the typical time of the E/M code you reported (TABLE).
For instance, if she is admitted at 10 PM on day 1 and delivers on day 2 at 2 PM, with your having documented that you spent a total of 2 hours at the patient’s bedside on day 1 and 8 hours at the patient’s bedside on day 2, you could bill as follows:
Day 1: Hospital admission (eg, 99222, requiring comprehensive history and exam and moderate medical decision-making with a typical time of 50 minutes)
Prolonged services on day 1: 120 minutes total –50 minutes=70 minutes of prolonged service. Bill code 99356 (first 60 minutes), but no additional code for the last 10 minutes of prolonged service.
Day 2: Subsequent hospital care (eg, 99232 requiring an expanded problem, focused history or exam with moderate complexity of medical decision-making with a typical time of 25 minutes).
Prolonged services for 8 hours on day 2: 480 minutes total –25 minutes=455 minutes of prolonged service; bill code 99356 (first 60 minutes), and 99357 with a quantity of 13 for the remaining 395 minutes.
TABLE
You have to do the math: Coding prolonged physician services
| TOTAL TIME W/PATIENT | BASIC SERVICE | BILLABLE PROLONGED SERVICE | PROLONGED SERVICES WITH CODES REPORTED |
|---|---|---|---|
| Day 1 120 minutes | 99222 (50 minutes) | 120 min –50 min=70 minutes | 99356 for first 60 minutes, but no extra codes for last 10 minutes |
| Day 2 480 minutes | 99232 (25 minutes) | 480 min –25 min=455 minutes | 99356 for first 60 minutes; 455 min –60 minutes=395 minutes 99357×13 for remaining time (13 times for each 30-minute increment) |
Induction with IV oxytocin would be classified as medical management of an abortion. Under CPT rules and ACOG guidelines, you would bill only for the evaluation and management (E/M) services. However, this means you would be billing for the hospital admission, subsequent care, and, prior to delivery, prolonged physician services. In this case you would report the hospital prolonged care codes that account for the actual time you spent with the patient managing her labor, as long as that time exceeds by 30 minutes the typical time of the E/M code you reported (TABLE).
For instance, if she is admitted at 10 PM on day 1 and delivers on day 2 at 2 PM, with your having documented that you spent a total of 2 hours at the patient’s bedside on day 1 and 8 hours at the patient’s bedside on day 2, you could bill as follows:
Day 1: Hospital admission (eg, 99222, requiring comprehensive history and exam and moderate medical decision-making with a typical time of 50 minutes)
Prolonged services on day 1: 120 minutes total –50 minutes=70 minutes of prolonged service. Bill code 99356 (first 60 minutes), but no additional code for the last 10 minutes of prolonged service.
Day 2: Subsequent hospital care (eg, 99232 requiring an expanded problem, focused history or exam with moderate complexity of medical decision-making with a typical time of 25 minutes).
Prolonged services for 8 hours on day 2: 480 minutes total –25 minutes=455 minutes of prolonged service; bill code 99356 (first 60 minutes), and 99357 with a quantity of 13 for the remaining 395 minutes.
TABLE
You have to do the math: Coding prolonged physician services
| TOTAL TIME W/PATIENT | BASIC SERVICE | BILLABLE PROLONGED SERVICE | PROLONGED SERVICES WITH CODES REPORTED |
|---|---|---|---|
| Day 1 120 minutes | 99222 (50 minutes) | 120 min –50 min=70 minutes | 99356 for first 60 minutes, but no extra codes for last 10 minutes |
| Day 2 480 minutes | 99232 (25 minutes) | 480 min –25 min=455 minutes | 99356 for first 60 minutes; 455 min –60 minutes=395 minutes 99357×13 for remaining time (13 times for each 30-minute increment) |
Getting paid for pregnancy complications
Would it be appropriate to add a –57 modifier (decision to do surgery) to the admission, and if so, what modifier should be added to subsequent hospital visits?
But some payers will acknowledge that the patient is being treated for a complication of the pregnancy and not for admission for delivery and will allow both the admission and any subsequent visits except on the day of delivery.
The problem with any modifier prior to delivery with global obstetric care is that “delivery” is the inevitable outcome of the care, so the modifier –57, in my opinion, is not appropriate in this setting for the physician who is providing the global care. If the MFM specialist has not been providing maternity care and then determines that an emergency delivery must be performed, modifier –57 might be warranted. There are no other applicable modifiers for the care prior to delivery.
I suggest that you appeal the denial. Explain that the admission was not planned, and the reason for admission and care on the second day was for a complication of pregnancy, not labor management.
Would it be appropriate to add a –57 modifier (decision to do surgery) to the admission, and if so, what modifier should be added to subsequent hospital visits?
But some payers will acknowledge that the patient is being treated for a complication of the pregnancy and not for admission for delivery and will allow both the admission and any subsequent visits except on the day of delivery.
The problem with any modifier prior to delivery with global obstetric care is that “delivery” is the inevitable outcome of the care, so the modifier –57, in my opinion, is not appropriate in this setting for the physician who is providing the global care. If the MFM specialist has not been providing maternity care and then determines that an emergency delivery must be performed, modifier –57 might be warranted. There are no other applicable modifiers for the care prior to delivery.
I suggest that you appeal the denial. Explain that the admission was not planned, and the reason for admission and care on the second day was for a complication of pregnancy, not labor management.
Would it be appropriate to add a –57 modifier (decision to do surgery) to the admission, and if so, what modifier should be added to subsequent hospital visits?
But some payers will acknowledge that the patient is being treated for a complication of the pregnancy and not for admission for delivery and will allow both the admission and any subsequent visits except on the day of delivery.
The problem with any modifier prior to delivery with global obstetric care is that “delivery” is the inevitable outcome of the care, so the modifier –57, in my opinion, is not appropriate in this setting for the physician who is providing the global care. If the MFM specialist has not been providing maternity care and then determines that an emergency delivery must be performed, modifier –57 might be warranted. There are no other applicable modifiers for the care prior to delivery.
I suggest that you appeal the denial. Explain that the admission was not planned, and the reason for admission and care on the second day was for a complication of pregnancy, not labor management.
Code for perineoplasty depends on setting
If a repair only is documented, your other possibility is to use codes 12001–12004 (simple repair of superficial wounds of scalp, neck, axillae, external genitalia, trunk and/or extremities [including hands and feet]; 2.5 cm or less up to 12.5 cm). These codes do have a practice expense differential when the procedure is carried out in the office. Like the perineoplasty code, this code series has a 10-day global period.
If a repair only is documented, your other possibility is to use codes 12001–12004 (simple repair of superficial wounds of scalp, neck, axillae, external genitalia, trunk and/or extremities [including hands and feet]; 2.5 cm or less up to 12.5 cm). These codes do have a practice expense differential when the procedure is carried out in the office. Like the perineoplasty code, this code series has a 10-day global period.
If a repair only is documented, your other possibility is to use codes 12001–12004 (simple repair of superficial wounds of scalp, neck, axillae, external genitalia, trunk and/or extremities [including hands and feet]; 2.5 cm or less up to 12.5 cm). These codes do have a practice expense differential when the procedure is carried out in the office. Like the perineoplasty code, this code series has a 10-day global period.