User login
Organize Your Samples—and Your Reps
Everybody, it seems, thinks they have too many samples, but you really don't. What you have is too much packaging.
If you doubt this, take a good look at the next set of samples that comes into your office. Each unit will probably consist of a big box or card, and somewhere within its depths, amid all the wasted space, will be a single tablet or 3-g tube.
All that space-wasting packaging is purposeful, of course. Bigger is better, after all, from a promotional standpoint. Bigger packages are more likely to be noticed, and there's more room for advertising. The marketing people figure that if they use up all of your available sample space, you won't have room for their competition.
As a result, you probably have sample packages taking up two or three closets' worth of expensive square footage—with the samples themselves occupying perhaps 5% of that space or less.
Not only that, but each time you need a particular sample, somebody has to go hunting for it. Sometimes you find it, sometimes you don't. And when you do, there's a fair chance it's expired. It's a waste of time, space, and energy, and it's not necessary.
Here's what you do: Create a “parts-bin system” for your samples.
Have a carpenter build some shelving in a central area of the office. Stock those shelves with cardboard or plastic parts bins, which are available in a variety of lengths, widths, shapes, and colors from many different sources. Three online examples are www.anytimeproducts.comwww.papermart.comwww.lkgoodwin.com
As samples come in, ask the representative who brings them to strip off all the space-wasting packaging, leaving only the tablet bubble-pack cards or the 3-g tubes. You'll be amazed at how much less space they take up. Store them in the bins, and arrange the bins on your shelving by whatever organizational system you fancy. We do it alphabetically.
You'll always know what samples you have, what you're out of, and what's close to its expiration date. You and your staff will waste far less time searching for the samples you want, and you can use all that freed-up sample space for something far more likely to generate revenue for your office.
A parts-bin system could be an even bigger boon to your office if the Food and Drug Administration ever makes good on its recurrent promise to require written paper trails for all samples entering and leaving a facility. Periodic inventories, as well as logging samples in and out, will be far easier with my system.
While you're organizing your samples, organize your pharmaceutical reps too. Many offices allow representatives to come and go as they please, and too many physicians, physician assistants, and nurse practitioners are all too willing to stop and chat with them, which disrupts efficient office flow. And if multiple reps show up in a single day, the chaos just multiplies.
Have your reps make appointments, just as your patients do. We allow only one rep appointment per day—during the lunch break, 10 minutes before the start of afternoon hours. That prevents disruption of the schedule, and it prevents me from chatting too long (which I have a tendency to do).
We also encourage reps not to make appointments at all unless they have something of significance to communicate. I'm happy to speak with reps, but not when all they have to offer is small talk.
Everybody, it seems, thinks they have too many samples, but you really don't. What you have is too much packaging.
If you doubt this, take a good look at the next set of samples that comes into your office. Each unit will probably consist of a big box or card, and somewhere within its depths, amid all the wasted space, will be a single tablet or 3-g tube.
All that space-wasting packaging is purposeful, of course. Bigger is better, after all, from a promotional standpoint. Bigger packages are more likely to be noticed, and there's more room for advertising. The marketing people figure that if they use up all of your available sample space, you won't have room for their competition.
As a result, you probably have sample packages taking up two or three closets' worth of expensive square footage—with the samples themselves occupying perhaps 5% of that space or less.
Not only that, but each time you need a particular sample, somebody has to go hunting for it. Sometimes you find it, sometimes you don't. And when you do, there's a fair chance it's expired. It's a waste of time, space, and energy, and it's not necessary.
Here's what you do: Create a “parts-bin system” for your samples.
Have a carpenter build some shelving in a central area of the office. Stock those shelves with cardboard or plastic parts bins, which are available in a variety of lengths, widths, shapes, and colors from many different sources. Three online examples are www.anytimeproducts.comwww.papermart.comwww.lkgoodwin.com
As samples come in, ask the representative who brings them to strip off all the space-wasting packaging, leaving only the tablet bubble-pack cards or the 3-g tubes. You'll be amazed at how much less space they take up. Store them in the bins, and arrange the bins on your shelving by whatever organizational system you fancy. We do it alphabetically.
You'll always know what samples you have, what you're out of, and what's close to its expiration date. You and your staff will waste far less time searching for the samples you want, and you can use all that freed-up sample space for something far more likely to generate revenue for your office.
A parts-bin system could be an even bigger boon to your office if the Food and Drug Administration ever makes good on its recurrent promise to require written paper trails for all samples entering and leaving a facility. Periodic inventories, as well as logging samples in and out, will be far easier with my system.
While you're organizing your samples, organize your pharmaceutical reps too. Many offices allow representatives to come and go as they please, and too many physicians, physician assistants, and nurse practitioners are all too willing to stop and chat with them, which disrupts efficient office flow. And if multiple reps show up in a single day, the chaos just multiplies.
Have your reps make appointments, just as your patients do. We allow only one rep appointment per day—during the lunch break, 10 minutes before the start of afternoon hours. That prevents disruption of the schedule, and it prevents me from chatting too long (which I have a tendency to do).
We also encourage reps not to make appointments at all unless they have something of significance to communicate. I'm happy to speak with reps, but not when all they have to offer is small talk.
Everybody, it seems, thinks they have too many samples, but you really don't. What you have is too much packaging.
If you doubt this, take a good look at the next set of samples that comes into your office. Each unit will probably consist of a big box or card, and somewhere within its depths, amid all the wasted space, will be a single tablet or 3-g tube.
All that space-wasting packaging is purposeful, of course. Bigger is better, after all, from a promotional standpoint. Bigger packages are more likely to be noticed, and there's more room for advertising. The marketing people figure that if they use up all of your available sample space, you won't have room for their competition.
As a result, you probably have sample packages taking up two or three closets' worth of expensive square footage—with the samples themselves occupying perhaps 5% of that space or less.
Not only that, but each time you need a particular sample, somebody has to go hunting for it. Sometimes you find it, sometimes you don't. And when you do, there's a fair chance it's expired. It's a waste of time, space, and energy, and it's not necessary.
Here's what you do: Create a “parts-bin system” for your samples.
Have a carpenter build some shelving in a central area of the office. Stock those shelves with cardboard or plastic parts bins, which are available in a variety of lengths, widths, shapes, and colors from many different sources. Three online examples are www.anytimeproducts.comwww.papermart.comwww.lkgoodwin.com
As samples come in, ask the representative who brings them to strip off all the space-wasting packaging, leaving only the tablet bubble-pack cards or the 3-g tubes. You'll be amazed at how much less space they take up. Store them in the bins, and arrange the bins on your shelving by whatever organizational system you fancy. We do it alphabetically.
You'll always know what samples you have, what you're out of, and what's close to its expiration date. You and your staff will waste far less time searching for the samples you want, and you can use all that freed-up sample space for something far more likely to generate revenue for your office.
A parts-bin system could be an even bigger boon to your office if the Food and Drug Administration ever makes good on its recurrent promise to require written paper trails for all samples entering and leaving a facility. Periodic inventories, as well as logging samples in and out, will be far easier with my system.
While you're organizing your samples, organize your pharmaceutical reps too. Many offices allow representatives to come and go as they please, and too many physicians, physician assistants, and nurse practitioners are all too willing to stop and chat with them, which disrupts efficient office flow. And if multiple reps show up in a single day, the chaos just multiplies.
Have your reps make appointments, just as your patients do. We allow only one rep appointment per day—during the lunch break, 10 minutes before the start of afternoon hours. That prevents disruption of the schedule, and it prevents me from chatting too long (which I have a tendency to do).
We also encourage reps not to make appointments at all unless they have something of significance to communicate. I'm happy to speak with reps, but not when all they have to offer is small talk.
Report Critical Care
Hospitalists often encounter patients who are or could become critically ill. The increased efforts while caring for these patients are best captured through critical-care service codes 99291 and 99292.
Although these codes yield higher reimbursement ($204.15 and $102.45, respectively, per national Medicare average payment), they are reported only under certain circumstances. The physician’s documentation must include enough detail to support critical-care claims: the patient’s condition, the nature of the physician’s care, and the time spent rendering care. Documentation of any other pertinent information is strongly encouraged because these services often come under payer scrutiny.
Condition and Care
A patient’s condition must meet the established criteria before the service qualifies as critical care. More specifically, the patient must have a critical illness or injury that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition.
The physician’s personal attention (i.e., care involving one critically ill patient at a time) is essential for rendering the highly complex decisions necessary to prevent the patient’s decline if left untreated. Given the seriousness of the patient’s condition, the physician is expected to focus only on the patient for whom critical-care time is reported.
Duration
Critical care is a time-based service. It constitutes the physician’s time spent providing direct care at the bedside and gathering and reviewing data on the patient’s unit or floor.
If the physician is not immediately available to the patient, the time associated with indirect care (e.g., reviewing data, calling the family from the office) is not counted in the overall critical-care service.
The physician keeps tracks of his/her total critical-care time throughout the day. A new period of critical-care time begins each calendar day. There is no prohibition against reporting multiple hours or days of critical care, as long as the patient’s condition prompts the service and documentation supports it.
Code 99291 represents the first “hour” of critical care, which physicians may report after accumulating the first 30 minutes of care. Alternately, physician management of the patient involving less than 30 minutes of critical-care time on a given day must be reported with the appropriate evaluation and management (E/M) code:
- Initial inpatient service (99221-99223);
- Subsequent hospital care (99231-99233); or
- Inpatient consultation (99251-99255).
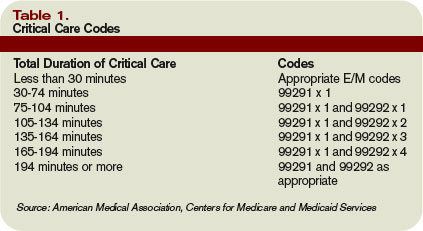
Once the physician achieves 75 minutes of critical-care time, he/she reports 99292 for the additional “30 minutes” of care beyond the first hour. Never report 99292 alone on the claim form. Code 99292 is considered an “add-on” code, which means it must be reported in addition to a primary code. Code 99291 is always the primary code (reported once per physician/group per day) for critical-care services. Code 99292 can be reported in multiple units per physician/group per day according to the number of minutes spent after the initial hour (see Table 1, p. 30).
Service Inclusions
Critical care involves highly complex decision making to manage the patient’s condition. This includes the physician’s performance and/or interpretation of labs, diagnostic studies, and procedures inherent in critical care.
Therefore, do not report the following services when billing 99291-99292:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762); and
- Blood gases (multiple codes).
Further, don’t report interpretation of data stored in computers:
- Electrocardiograms, blood pressures, hematologic data (99090);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).
Any other service or procedure provided by the physician can be billed in addition to 99291-99292.
Be sure not to add separately billable procedure time into the physician’s total critical-care time. A notation in the medical record should reflect this (e.g., time spent inserting a central line is not included in today’s critical-care time).
Location
Because a patient can become seriously ill in any setting, physicians often provide critical-care services in emergency departments (EDs) and on standard medical-surgical floors before the patient is transferred to the intensive care unit (ICU).
Bed location alone does not determine critical-care reporting. Patients assigned to an ICU might be critically ill or injured and meet the “condition” requirements for 99291-99292.
However, the care provided may not meet the remaining requirements. According to the American Medical Association’s Current Procedural Terminology 2008 (Professional Edition) and the Medicare Claims Processing Manual, payment can be made for critical-care services provided in any location as long as the care provided meets the definition of critical care. Services for a patient who is not critically ill and unstable but who happens to be receiving care in a critical-care, intensive-care, or other specialized-care unit are reported using subsequent hospital care codes 99231-99233 or hospital consultation codes 99251-99255. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Hospitalists often encounter patients who are or could become critically ill. The increased efforts while caring for these patients are best captured through critical-care service codes 99291 and 99292.
Although these codes yield higher reimbursement ($204.15 and $102.45, respectively, per national Medicare average payment), they are reported only under certain circumstances. The physician’s documentation must include enough detail to support critical-care claims: the patient’s condition, the nature of the physician’s care, and the time spent rendering care. Documentation of any other pertinent information is strongly encouraged because these services often come under payer scrutiny.
Condition and Care
A patient’s condition must meet the established criteria before the service qualifies as critical care. More specifically, the patient must have a critical illness or injury that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition.
The physician’s personal attention (i.e., care involving one critically ill patient at a time) is essential for rendering the highly complex decisions necessary to prevent the patient’s decline if left untreated. Given the seriousness of the patient’s condition, the physician is expected to focus only on the patient for whom critical-care time is reported.
Duration
Critical care is a time-based service. It constitutes the physician’s time spent providing direct care at the bedside and gathering and reviewing data on the patient’s unit or floor.
If the physician is not immediately available to the patient, the time associated with indirect care (e.g., reviewing data, calling the family from the office) is not counted in the overall critical-care service.
The physician keeps tracks of his/her total critical-care time throughout the day. A new period of critical-care time begins each calendar day. There is no prohibition against reporting multiple hours or days of critical care, as long as the patient’s condition prompts the service and documentation supports it.
Code 99291 represents the first “hour” of critical care, which physicians may report after accumulating the first 30 minutes of care. Alternately, physician management of the patient involving less than 30 minutes of critical-care time on a given day must be reported with the appropriate evaluation and management (E/M) code:
- Initial inpatient service (99221-99223);
- Subsequent hospital care (99231-99233); or
- Inpatient consultation (99251-99255).
Once the physician achieves 75 minutes of critical-care time, he/she reports 99292 for the additional “30 minutes” of care beyond the first hour. Never report 99292 alone on the claim form. Code 99292 is considered an “add-on” code, which means it must be reported in addition to a primary code. Code 99291 is always the primary code (reported once per physician/group per day) for critical-care services. Code 99292 can be reported in multiple units per physician/group per day according to the number of minutes spent after the initial hour (see Table 1, p. 30).
Service Inclusions
Critical care involves highly complex decision making to manage the patient’s condition. This includes the physician’s performance and/or interpretation of labs, diagnostic studies, and procedures inherent in critical care.
Therefore, do not report the following services when billing 99291-99292:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762); and
- Blood gases (multiple codes).
Further, don’t report interpretation of data stored in computers:
- Electrocardiograms, blood pressures, hematologic data (99090);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).
Any other service or procedure provided by the physician can be billed in addition to 99291-99292.
Be sure not to add separately billable procedure time into the physician’s total critical-care time. A notation in the medical record should reflect this (e.g., time spent inserting a central line is not included in today’s critical-care time).
Location
Because a patient can become seriously ill in any setting, physicians often provide critical-care services in emergency departments (EDs) and on standard medical-surgical floors before the patient is transferred to the intensive care unit (ICU).
Bed location alone does not determine critical-care reporting. Patients assigned to an ICU might be critically ill or injured and meet the “condition” requirements for 99291-99292.
However, the care provided may not meet the remaining requirements. According to the American Medical Association’s Current Procedural Terminology 2008 (Professional Edition) and the Medicare Claims Processing Manual, payment can be made for critical-care services provided in any location as long as the care provided meets the definition of critical care. Services for a patient who is not critically ill and unstable but who happens to be receiving care in a critical-care, intensive-care, or other specialized-care unit are reported using subsequent hospital care codes 99231-99233 or hospital consultation codes 99251-99255. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Hospitalists often encounter patients who are or could become critically ill. The increased efforts while caring for these patients are best captured through critical-care service codes 99291 and 99292.
Although these codes yield higher reimbursement ($204.15 and $102.45, respectively, per national Medicare average payment), they are reported only under certain circumstances. The physician’s documentation must include enough detail to support critical-care claims: the patient’s condition, the nature of the physician’s care, and the time spent rendering care. Documentation of any other pertinent information is strongly encouraged because these services often come under payer scrutiny.
Condition and Care
A patient’s condition must meet the established criteria before the service qualifies as critical care. More specifically, the patient must have a critical illness or injury that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition.
The physician’s personal attention (i.e., care involving one critically ill patient at a time) is essential for rendering the highly complex decisions necessary to prevent the patient’s decline if left untreated. Given the seriousness of the patient’s condition, the physician is expected to focus only on the patient for whom critical-care time is reported.
Duration
Critical care is a time-based service. It constitutes the physician’s time spent providing direct care at the bedside and gathering and reviewing data on the patient’s unit or floor.
If the physician is not immediately available to the patient, the time associated with indirect care (e.g., reviewing data, calling the family from the office) is not counted in the overall critical-care service.
The physician keeps tracks of his/her total critical-care time throughout the day. A new period of critical-care time begins each calendar day. There is no prohibition against reporting multiple hours or days of critical care, as long as the patient’s condition prompts the service and documentation supports it.
Code 99291 represents the first “hour” of critical care, which physicians may report after accumulating the first 30 minutes of care. Alternately, physician management of the patient involving less than 30 minutes of critical-care time on a given day must be reported with the appropriate evaluation and management (E/M) code:
- Initial inpatient service (99221-99223);
- Subsequent hospital care (99231-99233); or
- Inpatient consultation (99251-99255).
Once the physician achieves 75 minutes of critical-care time, he/she reports 99292 for the additional “30 minutes” of care beyond the first hour. Never report 99292 alone on the claim form. Code 99292 is considered an “add-on” code, which means it must be reported in addition to a primary code. Code 99291 is always the primary code (reported once per physician/group per day) for critical-care services. Code 99292 can be reported in multiple units per physician/group per day according to the number of minutes spent after the initial hour (see Table 1, p. 30).
Service Inclusions
Critical care involves highly complex decision making to manage the patient’s condition. This includes the physician’s performance and/or interpretation of labs, diagnostic studies, and procedures inherent in critical care.
Therefore, do not report the following services when billing 99291-99292:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762); and
- Blood gases (multiple codes).
Further, don’t report interpretation of data stored in computers:
- Electrocardiograms, blood pressures, hematologic data (99090);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).
Any other service or procedure provided by the physician can be billed in addition to 99291-99292.
Be sure not to add separately billable procedure time into the physician’s total critical-care time. A notation in the medical record should reflect this (e.g., time spent inserting a central line is not included in today’s critical-care time).
Location
Because a patient can become seriously ill in any setting, physicians often provide critical-care services in emergency departments (EDs) and on standard medical-surgical floors before the patient is transferred to the intensive care unit (ICU).
Bed location alone does not determine critical-care reporting. Patients assigned to an ICU might be critically ill or injured and meet the “condition” requirements for 99291-99292.
However, the care provided may not meet the remaining requirements. According to the American Medical Association’s Current Procedural Terminology 2008 (Professional Edition) and the Medicare Claims Processing Manual, payment can be made for critical-care services provided in any location as long as the care provided meets the definition of critical care. Services for a patient who is not critically ill and unstable but who happens to be receiving care in a critical-care, intensive-care, or other specialized-care unit are reported using subsequent hospital care codes 99231-99233 or hospital consultation codes 99251-99255. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
The Power of Paying Attention
Medical Verdicts
Difficult birth blamed for death at 1 year
A woman in labor had been pushing for 10 minutes when her OB began using a vacuum extractor to facilitate delivery. Shoulder dystocia occurred. The OB applied fundal pressure while a second physician dislodged the infant. At birth, the child was not breathing and had no heart rate. One year later, the child died because of birth-related complications.
Patient’s claim She never gave consent to use the vacuum extractor. The OB used fundal pressure at least twice before the infant’s head emerged.
Doctor’s defense There was no negligence.
Verdict $8,181,725 Maryland verdict, which included $7.5 million in noneconomic damages. The latter was expected to be reduced to $2.2 million pursuant to the statutory cap.
Genetic testing fails to detect Fabry’s disease
Unable to become pregnant despite trying for over 2 years, a woman decided on in vitro fertilization. A genetics consultation determined that she was a carrier for Fabry’s disease. Eggs and sperm were harvested and resulted in six fertilized embryos. It was recommended that each embryo be tested genetically by polymerase chain reaction (PCR). On day 3, single-cell biopsies were performed on the six developing embryos and the cells sent to a lab for PCR testing. Two embryos were found to be carriers of the mutation; two others were males with Fabry’s disease; and no results were obtained from the last two. Pregnancy occurred when the female carrier embryos were implanted. Ultrasonography showed the fetus to be male, a blood test suggested risk of Down’s syndrome, and amniocentesis indicated the fetus had Fabry’s disease. When the child was born, Fabry’s disease was confirmed.
Patient’s claim The fertility center was negligent for misrepresenting its experience with preimplantation genetic diagnosis. The lab failed to take precautions to avoid contamination and also failed to have a second person check that sample switching did not occur.
Doctor’s defense There was no evidence that samples were switched or that DNA contamination occurred during the testing and implantation. More likely, the problem was due to an unknown failure in the PCR testing technology, unavoidable DNA contamination, or mosaicism of the embryo tested.
Verdict California defense verdict.
Did surgery—or drugs—cause incontinence?
An ObGyn performed surgery on a 41-year-old woman with urinary incontinence to correct a cystocele. The patient developed chronic retention of urine and needed corrective surgery. She was referred to a urologist. All tests were normal, and she eventually had stoma surgery to allow her to empty her bladder with a catheter through the stoma.
Patient’s claim The surgery was premature and unnecessary, and the ObGyn used a negligent operative technique that led to chronic urinary retention and the need for a permanent stoma. Conservative treatment should have been used first.
Doctor’s defense Because of the anatomic cause of the patient’s stress urinary incontinence, surgery was necessary—and performed properly. Urinary retention was unrelated to the surgery, as cystoscopies showed there was no obstruction in the bladder or urethra. The patient’s psychiatric medication may have led to neurogenic bladder failure and her problems.
Verdict Virginia defense verdict.
Obese woman’s TAH incision heals—in a year
A 300-lb woman who had experienced intermittent heavy uterine bleeding for years underwent an open total abdominal hysterectomy (TAH), performed by an ObGyn. Bowel contents leaked into the abdominal wall, causing a wound infection that required several more procedures to repair the bowel and remove necrotic tissue from the abdomen. After 3 weeks in the hospital, the patient was discharged, but the surgical incision required about 1 year to heal completely. She has a 21-inch scar from hip to hip.
Patient’s claim The bowel was stitched to the peritoneum when the incision was closed, and the ObGyn failed to notice the error. The suture caused bowel contents to leak, causing the infection and need for further procedures.
Doctor’s defense Proper precautions were taken to avoid bowel injury, but it is a risk nonetheless of TAH—which the patient chose rather than a less invasive alternative. Her bowel was densely adhered to the peritoneum because of previous abdominal surgeries, making it impossible to distinguish bowel tissue from peritoneum when the incision was being closed.
Verdict Missouri defense verdict; an appeal was expected.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Difficult birth blamed for death at 1 year
A woman in labor had been pushing for 10 minutes when her OB began using a vacuum extractor to facilitate delivery. Shoulder dystocia occurred. The OB applied fundal pressure while a second physician dislodged the infant. At birth, the child was not breathing and had no heart rate. One year later, the child died because of birth-related complications.
Patient’s claim She never gave consent to use the vacuum extractor. The OB used fundal pressure at least twice before the infant’s head emerged.
Doctor’s defense There was no negligence.
Verdict $8,181,725 Maryland verdict, which included $7.5 million in noneconomic damages. The latter was expected to be reduced to $2.2 million pursuant to the statutory cap.
Genetic testing fails to detect Fabry’s disease
Unable to become pregnant despite trying for over 2 years, a woman decided on in vitro fertilization. A genetics consultation determined that she was a carrier for Fabry’s disease. Eggs and sperm were harvested and resulted in six fertilized embryos. It was recommended that each embryo be tested genetically by polymerase chain reaction (PCR). On day 3, single-cell biopsies were performed on the six developing embryos and the cells sent to a lab for PCR testing. Two embryos were found to be carriers of the mutation; two others were males with Fabry’s disease; and no results were obtained from the last two. Pregnancy occurred when the female carrier embryos were implanted. Ultrasonography showed the fetus to be male, a blood test suggested risk of Down’s syndrome, and amniocentesis indicated the fetus had Fabry’s disease. When the child was born, Fabry’s disease was confirmed.
Patient’s claim The fertility center was negligent for misrepresenting its experience with preimplantation genetic diagnosis. The lab failed to take precautions to avoid contamination and also failed to have a second person check that sample switching did not occur.
Doctor’s defense There was no evidence that samples were switched or that DNA contamination occurred during the testing and implantation. More likely, the problem was due to an unknown failure in the PCR testing technology, unavoidable DNA contamination, or mosaicism of the embryo tested.
Verdict California defense verdict.
Did surgery—or drugs—cause incontinence?
An ObGyn performed surgery on a 41-year-old woman with urinary incontinence to correct a cystocele. The patient developed chronic retention of urine and needed corrective surgery. She was referred to a urologist. All tests were normal, and she eventually had stoma surgery to allow her to empty her bladder with a catheter through the stoma.
Patient’s claim The surgery was premature and unnecessary, and the ObGyn used a negligent operative technique that led to chronic urinary retention and the need for a permanent stoma. Conservative treatment should have been used first.
Doctor’s defense Because of the anatomic cause of the patient’s stress urinary incontinence, surgery was necessary—and performed properly. Urinary retention was unrelated to the surgery, as cystoscopies showed there was no obstruction in the bladder or urethra. The patient’s psychiatric medication may have led to neurogenic bladder failure and her problems.
Verdict Virginia defense verdict.
Obese woman’s TAH incision heals—in a year
A 300-lb woman who had experienced intermittent heavy uterine bleeding for years underwent an open total abdominal hysterectomy (TAH), performed by an ObGyn. Bowel contents leaked into the abdominal wall, causing a wound infection that required several more procedures to repair the bowel and remove necrotic tissue from the abdomen. After 3 weeks in the hospital, the patient was discharged, but the surgical incision required about 1 year to heal completely. She has a 21-inch scar from hip to hip.
Patient’s claim The bowel was stitched to the peritoneum when the incision was closed, and the ObGyn failed to notice the error. The suture caused bowel contents to leak, causing the infection and need for further procedures.
Doctor’s defense Proper precautions were taken to avoid bowel injury, but it is a risk nonetheless of TAH—which the patient chose rather than a less invasive alternative. Her bowel was densely adhered to the peritoneum because of previous abdominal surgeries, making it impossible to distinguish bowel tissue from peritoneum when the incision was being closed.
Verdict Missouri defense verdict; an appeal was expected.
Difficult birth blamed for death at 1 year
A woman in labor had been pushing for 10 minutes when her OB began using a vacuum extractor to facilitate delivery. Shoulder dystocia occurred. The OB applied fundal pressure while a second physician dislodged the infant. At birth, the child was not breathing and had no heart rate. One year later, the child died because of birth-related complications.
Patient’s claim She never gave consent to use the vacuum extractor. The OB used fundal pressure at least twice before the infant’s head emerged.
Doctor’s defense There was no negligence.
Verdict $8,181,725 Maryland verdict, which included $7.5 million in noneconomic damages. The latter was expected to be reduced to $2.2 million pursuant to the statutory cap.
Genetic testing fails to detect Fabry’s disease
Unable to become pregnant despite trying for over 2 years, a woman decided on in vitro fertilization. A genetics consultation determined that she was a carrier for Fabry’s disease. Eggs and sperm were harvested and resulted in six fertilized embryos. It was recommended that each embryo be tested genetically by polymerase chain reaction (PCR). On day 3, single-cell biopsies were performed on the six developing embryos and the cells sent to a lab for PCR testing. Two embryos were found to be carriers of the mutation; two others were males with Fabry’s disease; and no results were obtained from the last two. Pregnancy occurred when the female carrier embryos were implanted. Ultrasonography showed the fetus to be male, a blood test suggested risk of Down’s syndrome, and amniocentesis indicated the fetus had Fabry’s disease. When the child was born, Fabry’s disease was confirmed.
Patient’s claim The fertility center was negligent for misrepresenting its experience with preimplantation genetic diagnosis. The lab failed to take precautions to avoid contamination and also failed to have a second person check that sample switching did not occur.
Doctor’s defense There was no evidence that samples were switched or that DNA contamination occurred during the testing and implantation. More likely, the problem was due to an unknown failure in the PCR testing technology, unavoidable DNA contamination, or mosaicism of the embryo tested.
Verdict California defense verdict.
Did surgery—or drugs—cause incontinence?
An ObGyn performed surgery on a 41-year-old woman with urinary incontinence to correct a cystocele. The patient developed chronic retention of urine and needed corrective surgery. She was referred to a urologist. All tests were normal, and she eventually had stoma surgery to allow her to empty her bladder with a catheter through the stoma.
Patient’s claim The surgery was premature and unnecessary, and the ObGyn used a negligent operative technique that led to chronic urinary retention and the need for a permanent stoma. Conservative treatment should have been used first.
Doctor’s defense Because of the anatomic cause of the patient’s stress urinary incontinence, surgery was necessary—and performed properly. Urinary retention was unrelated to the surgery, as cystoscopies showed there was no obstruction in the bladder or urethra. The patient’s psychiatric medication may have led to neurogenic bladder failure and her problems.
Verdict Virginia defense verdict.
Obese woman’s TAH incision heals—in a year
A 300-lb woman who had experienced intermittent heavy uterine bleeding for years underwent an open total abdominal hysterectomy (TAH), performed by an ObGyn. Bowel contents leaked into the abdominal wall, causing a wound infection that required several more procedures to repair the bowel and remove necrotic tissue from the abdomen. After 3 weeks in the hospital, the patient was discharged, but the surgical incision required about 1 year to heal completely. She has a 21-inch scar from hip to hip.
Patient’s claim The bowel was stitched to the peritoneum when the incision was closed, and the ObGyn failed to notice the error. The suture caused bowel contents to leak, causing the infection and need for further procedures.
Doctor’s defense Proper precautions were taken to avoid bowel injury, but it is a risk nonetheless of TAH—which the patient chose rather than a less invasive alternative. Her bowel was densely adhered to the peritoneum because of previous abdominal surgeries, making it impossible to distinguish bowel tissue from peritoneum when the incision was being closed.
Verdict Missouri defense verdict; an appeal was expected.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
The author reports no financial relationships relevant to this article.
The heightened risk of being sued for a poor outcome—even when you and the obstetric team have delivered excellent care—is a sad reality of ObGyn practice, especially when shoulder dystocia is involved. Not so long ago, some physicians viewed a lawsuit as one of the costs of doing business and considered settlement of claims to avoid disruption to their practice. Today, with insurance rates skyrocketing, settlement is not as palatable, unless a clear breach of the standard of care has occurred. And although only a small percentage of cases ever reach trial, and fewer still go to a jury verdict, don’t be lulled into a false sense of security. A single case can take 5 or more years to make its way through the system.
What can you do to avoid the appearance of negligence and prevent litigation? And what tangential actions on the part of the physician or staff can cast defensible cases into the abyss of negligence? This article addresses these questions, focusing on 10 keys to avert or win a lawsuit involving shoulder dystocia.
Before you begin. Here is one preliminary piece of advice: Be vigilant. Air crash investigators frequently note that a crash occurs when a number of small errors link together. To prevent a poor outcome, it is critical to be alert to even minor inconsistencies in the care you and the obstetric team provide so you can rectify the situation before the small errors link into a disastrous chain.
1. Don’t downplay the “D” word
There are three important rules in medicine: Document, document, document. Yes, you’ve heard many people stress the importance of good notation, and I can back them up: A well-documented chart is a defendant’s best friend. Time and again, I’ve heard defense counsel lamenting—and plaintiff’s counsel exhorting—“if it isn’t documented, it didn’t happen.”
Careful documentation begins early. If a child is expected to be large for gestational age (LGA) or macrosomic, clear documentation of that fact and a plan in the prenatal record to address it during labor and delivery is critical. It also is important to communicate the potential for a large infant to the labor and delivery staff. Consider using a stamp or other indicator to mark the prenatal chart for this potentiality.
Make it legible
Clear handwriting or typed notes add substantial benefit to the defense of a dystocia case. They also help prevent the uncomfortable silence that can overwhelm a courtroom as 12 jurors stare at a witness who is unable to decipher her own notes or those of a colleague. The inability to interpret a note is almost as damaging to a case as the complete lack of a note. If a detail is important enough to warrant documentation, it’s important enough to document legibly.
Sooner is always better
Any shoulder dystocia case that involves injury to the child—whether temporary or permanent—holds significant potential to blossom into litigation. It is important to document the diagnosis of dystocia, steps taken to resolve it, and the outcome—and to do so during the delivery or as soon thereafter as possible.
The importance of this recommendation cannot be overstated. A quick 8 pm summary of a delivery that took place at 1:30 pm is bound to be vague and, in some respects, inherently inaccurate. In contrast, a 1:45 pm note that consumes an entire page, noting the time of diagnosis, sequence of efforts to resolve the dystocia, use of vacuum or forceps, number of pop-offs, and who was present in the room is unquestionably superior.
Once mother and infant are stable and under the care of qualified personnel, take sufficient time—even as long as 1 hour—to draft your delivery note. Sit down. Calm down. Strive for clarity. The sequence and timing of events will be important.
The parents’ ability to recall the delivery will be blurred by emotion. If the case goes to trial, your well-documented note, combined with your accurate testimony, will have a significant advantage over what might be the understandably muddled recollections of the parents.
Call for a scrivener
If it seems as though it will be difficult to recall all the details of a delivery, consider calling a nurse or staff member into the room for the sole purpose of documentation once shoulder dystocia is diagnosed. Remember, once dystocia occurs, the risk of a poor outcome and years of litigation increases substantially. Having an extra staff member take notes is a small price to pay for documentation that may later establish your defense. The thinnest paper can sometimes extinguish the hottest litigation flame.
Prepare for a considerable lapse of time
Most states allow a claim to be filed on behalf of a child as late as 2 years after the child reaches the age of majority, which is 18 years in most states. Therefore, a child in many states can file suit as late as his or her 20th birthday. It is not uncommon for the events of an obstetrics case to be 10 or 15 years in the past by the time a claim is filed. Over such a long period, memories fade, radiographs and other imaging studies may get lost in storage, and so on. No matter how busy, tired, or hurried you may be from the events of the day, the most important 30 minutes you can spend are those in which you take time to sit, think, carefully draft, and proofread a delivery summary and check it for consistency against other documents generated during delivery. If necessary, call your partner in to cover you for an hour or two while you get the documentation right. If it helps your practice avoid a lawsuit, it is time well spent.
2. Educate your attorney
This point may seem rudimentary, but I have encountered a number of physicians who allowed their anger over being sued to taint their initial contacts with defense counsel.
A physician who sets aside 3 to 4 hours to meet with counsel, educate the attorney about medical issues, and review the medical literature is a cherished ally and is much more likely to be defended successfully. Physicians who treat the lawsuit as though it is an imposition on their personal or professional life and distance themselves from defense counsel do themselves a great disservice.
3. Be fluent in shoulder dystocia
If you are sued, and your case proceeds to trial—or even to depositions—a number of concepts particular to shoulder dystocia are very likely to arise, and you will be expected to address them coherently and to educate the jury and judge about their proper meaning.
Shoulder dystocia is unpredictable
Be conversant with the literature and statistics that show dystocia to be an unpredictable event.1
Fetal weight estimates are imprecise
Know the numbers. It is important to be conversant about projected birth weights and lines of demarcation for macrosomic and LGA fetuses. Plaintiff’s counsel and experts may try to obscure the lines between these definitions and terms. Keep your facts and definitions straight.
Also emphasize that ultrasonographic weight estimates are just that—estimates. There is no way to determine precise fetal weight in utero. Some studies suggest that ultrasonography (US) and physician weight estimation via palpation have similar accuracy rates. Do not allow the plaintiff’s attorney or expert to create the impression that US estimates are infallibly accurate.
Restitution of the head is a natural rotation
Understand the concept of “restitution of the head.” Do not allow plaintiff’s counsel to suggest that you turned the child’s head to one side or the other with your hands. Restitution is a natural rotation, and your hands merely guide and support the child’s head in this process. Gentle guiding of the head is appropriate.
The term “downward” is similarly misused. If ever there was a loaded term, it is “downward traction,” a favorite of plaintiff’s attorneys. Downward, as in “out of the birth canal,” versus downward, as in “90-degree angle to the birth canal and toward the floor,” are descriptions frequently misused in testimony and evidence. Be clear that any use of the term downward does not imply that the child’s neck was bent 45 to 90 degrees, with the top of the head inclined toward the floor. If a vague question regarding downward traction arises during the course of a legal case, ask for clarification of the term.
Degree of traction is another poorly understood concept. I am not aware of any reliable study that conclusively proves that major Erb’s palsy occurs when a greater degree of traction is applied and minor Erb’s palsy with a smaller degree of traction. Some counsel will use the fact that most brachial plexus injuries resolve over time to suggest that permanent Erb’s palsy is caused by overwhelming traction. Be prepared to dispute this argument!
Explain stations of the head
It is important that a jury understand that only a few inches separate –3 and +3 stations. Try to prevent plaintiff’s counsel from making the distance between these points seem like a long journey. Tissues stretch, caput occurs, and the station of the head may therefore become difficult to identify with pinpoint accuracy. A nurse’s estimate of –2 and a physician’s estimate of –1 for the same patient may, in fact, be consistent.
Use terminology precisely
If the infant develops a hematoma as a result of vacuum extraction or a similar device, be clear and concise about exactly what the injury is. Don’t let a subdural hematoma be described as a “brain bleed”!
Beware the magic gloves!
Studies in which physicians work on a model using pressure-sensitive gloves tend to suggest that excessive pressure is used. However, when the gloves are used in actual deliveries, pressure tends to be appropriate. Any mention of pressure-sensitive glove studies by plaintiff’s counsel should raise a red flag.
Growth charts are unreliable
Many shoulder dystocia–related trials use growth charts as exhibits. If you are confronted with one of these charts, be certain that you know what type of chart it is and the age and location of the children on whom it was based. Prenatal and postnatal growth charts are not the same. A child who is LGA on a postnatal chart might not be on a prenatal chart.
An expert witness once pointed out to me the existence of some charts from high-altitude cities; on these charts, the 95th percentile is slightly lower because children born at high altitude may be slightly smaller. Use of a high-altitude chart for a marginally LGA child in New York will make that child appear even larger than it is.
Triple-check each chart exhibit to make sure it is accurate and based on reliable data.
4. Don’t lose the case at deposition
You can’t win your case at deposition, but you certainly can lose it. Misplaced words and artless answers can damage your defense irreparably. Work with your attorney to fully explore any medical issues or terms on which the defense hinges. A simple misstatement of fact or misuse of a medically significant term can lock the defense into a difficult position.
Because the deposition is a major aspect of litigation, you should study for it and meet with your counsel well in advance of the date. A preparation session more than a week before your deposition will give you time to mull the issues and resolve any conflicts in your mind. A second session may be necessary to revisit difficult issues.
Know likely points of contention
Medical terminology and the sequence of events are two of the most likely areas of confusion. For example, although most physicians can readily distinguish between suprapubic and fundal pressure, many staff members confuse the two, as do many patients and lay witnesses to the birth. Fundal pressure may increase impaction of the shoulder; suprapubic pressure, correctly applied, is appropriate during the McRoberts maneuver (FIGURE).1
Some attorneys prefer to have the physician present when witnesses and parents are giving a deposition. This certainly conveys the message that the physician is committed to defense of the case.
If you choose to be present during a deposition, understand that lay witnesses may give inaccurate testimony. If this occurs while you are present, don’t get emotionally involved; do remain a passive observer. Remember, a deposition is not a trial. Although inaccurate testimony can be frustrating to the physician, it will ultimately trap the witness at trial and may be his (or her) undoing.
FIGURE Suprapubic vs fundal pressure
“Fundal pressure may increase impaction of the shoulder; suprapubic pressure (shown here), correctly applied, is appropriate during the McRoberts maneuver”
5. Retain the best expert you can find
Because the credentials and strength of expert opinions are critical to your defense, endeavor to retain the most highly qualified expert possible. Seek out an expert on the standard of care as soon as possible after filing of the lawsuit. Your counsel should be in consultation with this expert early in the case—certainly before your deposition. You don’t want to risk giving testimony that is inconsistent with your expert’s opinion or impossible for your expert to defend.
A highly qualified expert may be someone who has written about dystocia or participated in major studies. He or she also should be active in the delivery of babies and use any instrumentation or devices involved in your case. I recently cross-examined a plaintiff’s expert in a vacuum extraction case who hadn’t used the device since he finished his residency in 1974! This left several jurors with expressions of incredulity on their faces.
If you are practicing in a rural area, the availability of personnel or equipment may be an issue in your case. In such circumstances, an expert from a rural institution may be preferable to an expert from a major metropolitan area.
Scrutinize the expert’s credentials and communication style
Most defense counsel who practice in a specialized area of medicine will have access to the curriculum vitae of several potential experts. Review these documents with your attorney and investigate other cases in which the experts have testified.
If neither you nor your counsel has ever met or seen the expert, it may be helpful to explore whether the expert has ever given videotaped testimony. This will help you evaluate his or her physical appearance, demeanor, and general likeability, all of which influence the jury’s response to the testimony.
Remember, the plaintiff’s case is usually presented first. A jury may first be exposed to the facts of your case through the testimony of the plaintiff’s experts and witnesses, including emotional and at times weeping family members. Your expert will therefore need to refocus and reeducate the jury and dispel the opinions rendered by the plaintiff’s experts. To be successful, your expert must be able to create rapport with the jurors to keep them interested in his or her testimony and opinions. In this regard, your expert’s communication skills are paramount.
6. Be steadfast—the courtroom is a fishbowl!
At trial, you will be stared at, evaluated, and judged even while you are sitting in a chair at the defense table well before your testimony. This may seem unreasonable, capricious, and outrageous…and it is! However, until you take the witness stand, the jury has no other source of information about you.
Jurors are naturally curious. They begin to wonder about the case and, being human, may leap to conclusions. To protect yourself against unfair inferences, be mindful of your behavior, and assume that anything you say or do within two blocks of the courthouse will be seen by a juror. Here are some basic courtroom “don’ts,” culled from personal experience:
- Unless you are handicapped, do not park in a handicapped spot, even for a minute to unload a box of documents. A juror may see you and find your action inconsiderate.
- Don’t wear clothing or jewelry that is significantly more expensive than that worn by the plaintiffs or jurors.
- Be serious but not aloof.
- Remember to teach—not lecture—the jury.
- Take advantage of conference rooms.
Important discussions with counsel and experts should take place in private where there is no chance that a juror will accidentally observe or overhear the conversation.
7. Make exhibits informative, not disturbing
The purpose of a trial exhibit is to illustrate or demonstrate a point to the jurors. Any evidence that is presented must be accurate and based on facts already established in the case. The physician should assist defense counsel in the selection and preparation of exhibits. Here are a few tips:
- Make it easy to use. An exhibit—particularly a medical instrument—must be easy to use. Misusing, breaking, or fumbling with it on the stand is not only embarrassing, it casts doubt on the credibility of the witness. Have you ever seen a doctor accidentally fire a surgical staple into his own palm from an “empty” stapler while demonstrating the device in court? (I have.)
- Make it accurate. There are several types of vacuum extractors. If you choose to bring an exhibit—particularly a medical instrument—into the courtroom, it should be exactly the same type that was used in the delivery. Any variance should be insignificant. In a recent case, a plaintiff’s expert intended to use an outdated vacuum device that was rather large and ungainly and appeared to be far more ominous than the device that was actually used in the delivery. The court precluded its exhibition.
- Make sure it is unambiguous. There is great potential danger in using a defense exhibit that can be misinterpreted or reinterpreted to actually support the plaintiff’s position. Fetal growth charts, charts summarizing medical literature, and similar exhibits all have a potential for reinterpretation.
- Don’t send the wrong message. Photographs, medical instruments, and other exhibits can be gruesome or shocking to a jury. For example, if demonstration of a vacuum extractor is not critical to the defense of a case, the device may be inappropriate for courtroom demonstration. The reason? It may cause jurors to feel uncomfortable or place considerable focus on a minor issue. Any negative aspect of a potential exhibit should be evaluated in determining whether the exhibit will be used in front of the jury.
8. Get to the scene!
If at all possible, make a trip to the exact labor room where the events in question occurred, and take your counsel with you. Like Lieutenant Columbo wandering about, you never know what you might see. Suppose the family claims it was in the waiting room and heard the doctor shouting. How far away is the waiting room? How large is the labor room? Was the bed high enough that a 4-foot 7-inch nurse acted reasonably by standing on a stool to apply suprapubic pressure—despite how odd it seemed to the family?
The physical environment influences perceptions and recollections of witnesses. It’s impossible to know what you’ll find until you visit the location.
9. Never alter your records—never
A physician has a duty to keep accurate records. Never change your records to improve your position. I have seen several cases in which it was alleged that a physician went back and added a small notation to the record. That is a big mistake because many potential plaintiffs obtain their records before the child’s discharge.
If an error in a medical record merits a late correction, contact the risk-management staff and review the issue with them. A separate addendum note addressing and correcting the errant information may be preferred.
Whenever there are two versions of the labor record—especially when they are exhibited side by side in the courtroom—the die is cast, credibility is irreparably shattered, and the case may very well be lost.
10. You can pull a rabbit out of a hat!
The first lawyer I worked for asked me one day, “How do you get a rabbit out of a hat?” The answer? “First you put the rabbit into the hat.”
Preparation is essential to your testimony. Review the questions and responses to be covered during your testimony at length with your counsel. Be familiar with the issues and themes to be covered, and learn to phrase each answer truthfully, appropriately, and confidently.
The witness chair is charged with some invisible magic. Sitting there in front of a judge, jury, and packed courtroom can cause even the most confident and polished witness to become shaken and confused. Never underestimate your need to prepare.
Reference
1. American College of Obstetricians and Gynecologists. Shoulder Dystocia. Practice Bulletin No. 40. Washington, DC: ACOG; 2002.
The author reports no financial relationships relevant to this article.
The heightened risk of being sued for a poor outcome—even when you and the obstetric team have delivered excellent care—is a sad reality of ObGyn practice, especially when shoulder dystocia is involved. Not so long ago, some physicians viewed a lawsuit as one of the costs of doing business and considered settlement of claims to avoid disruption to their practice. Today, with insurance rates skyrocketing, settlement is not as palatable, unless a clear breach of the standard of care has occurred. And although only a small percentage of cases ever reach trial, and fewer still go to a jury verdict, don’t be lulled into a false sense of security. A single case can take 5 or more years to make its way through the system.
What can you do to avoid the appearance of negligence and prevent litigation? And what tangential actions on the part of the physician or staff can cast defensible cases into the abyss of negligence? This article addresses these questions, focusing on 10 keys to avert or win a lawsuit involving shoulder dystocia.
Before you begin. Here is one preliminary piece of advice: Be vigilant. Air crash investigators frequently note that a crash occurs when a number of small errors link together. To prevent a poor outcome, it is critical to be alert to even minor inconsistencies in the care you and the obstetric team provide so you can rectify the situation before the small errors link into a disastrous chain.
1. Don’t downplay the “D” word
There are three important rules in medicine: Document, document, document. Yes, you’ve heard many people stress the importance of good notation, and I can back them up: A well-documented chart is a defendant’s best friend. Time and again, I’ve heard defense counsel lamenting—and plaintiff’s counsel exhorting—“if it isn’t documented, it didn’t happen.”
Careful documentation begins early. If a child is expected to be large for gestational age (LGA) or macrosomic, clear documentation of that fact and a plan in the prenatal record to address it during labor and delivery is critical. It also is important to communicate the potential for a large infant to the labor and delivery staff. Consider using a stamp or other indicator to mark the prenatal chart for this potentiality.
Make it legible
Clear handwriting or typed notes add substantial benefit to the defense of a dystocia case. They also help prevent the uncomfortable silence that can overwhelm a courtroom as 12 jurors stare at a witness who is unable to decipher her own notes or those of a colleague. The inability to interpret a note is almost as damaging to a case as the complete lack of a note. If a detail is important enough to warrant documentation, it’s important enough to document legibly.
Sooner is always better
Any shoulder dystocia case that involves injury to the child—whether temporary or permanent—holds significant potential to blossom into litigation. It is important to document the diagnosis of dystocia, steps taken to resolve it, and the outcome—and to do so during the delivery or as soon thereafter as possible.
The importance of this recommendation cannot be overstated. A quick 8 pm summary of a delivery that took place at 1:30 pm is bound to be vague and, in some respects, inherently inaccurate. In contrast, a 1:45 pm note that consumes an entire page, noting the time of diagnosis, sequence of efforts to resolve the dystocia, use of vacuum or forceps, number of pop-offs, and who was present in the room is unquestionably superior.
Once mother and infant are stable and under the care of qualified personnel, take sufficient time—even as long as 1 hour—to draft your delivery note. Sit down. Calm down. Strive for clarity. The sequence and timing of events will be important.
The parents’ ability to recall the delivery will be blurred by emotion. If the case goes to trial, your well-documented note, combined with your accurate testimony, will have a significant advantage over what might be the understandably muddled recollections of the parents.
Call for a scrivener
If it seems as though it will be difficult to recall all the details of a delivery, consider calling a nurse or staff member into the room for the sole purpose of documentation once shoulder dystocia is diagnosed. Remember, once dystocia occurs, the risk of a poor outcome and years of litigation increases substantially. Having an extra staff member take notes is a small price to pay for documentation that may later establish your defense. The thinnest paper can sometimes extinguish the hottest litigation flame.
Prepare for a considerable lapse of time
Most states allow a claim to be filed on behalf of a child as late as 2 years after the child reaches the age of majority, which is 18 years in most states. Therefore, a child in many states can file suit as late as his or her 20th birthday. It is not uncommon for the events of an obstetrics case to be 10 or 15 years in the past by the time a claim is filed. Over such a long period, memories fade, radiographs and other imaging studies may get lost in storage, and so on. No matter how busy, tired, or hurried you may be from the events of the day, the most important 30 minutes you can spend are those in which you take time to sit, think, carefully draft, and proofread a delivery summary and check it for consistency against other documents generated during delivery. If necessary, call your partner in to cover you for an hour or two while you get the documentation right. If it helps your practice avoid a lawsuit, it is time well spent.
2. Educate your attorney
This point may seem rudimentary, but I have encountered a number of physicians who allowed their anger over being sued to taint their initial contacts with defense counsel.
A physician who sets aside 3 to 4 hours to meet with counsel, educate the attorney about medical issues, and review the medical literature is a cherished ally and is much more likely to be defended successfully. Physicians who treat the lawsuit as though it is an imposition on their personal or professional life and distance themselves from defense counsel do themselves a great disservice.
3. Be fluent in shoulder dystocia
If you are sued, and your case proceeds to trial—or even to depositions—a number of concepts particular to shoulder dystocia are very likely to arise, and you will be expected to address them coherently and to educate the jury and judge about their proper meaning.
Shoulder dystocia is unpredictable
Be conversant with the literature and statistics that show dystocia to be an unpredictable event.1
Fetal weight estimates are imprecise
Know the numbers. It is important to be conversant about projected birth weights and lines of demarcation for macrosomic and LGA fetuses. Plaintiff’s counsel and experts may try to obscure the lines between these definitions and terms. Keep your facts and definitions straight.
Also emphasize that ultrasonographic weight estimates are just that—estimates. There is no way to determine precise fetal weight in utero. Some studies suggest that ultrasonography (US) and physician weight estimation via palpation have similar accuracy rates. Do not allow the plaintiff’s attorney or expert to create the impression that US estimates are infallibly accurate.
Restitution of the head is a natural rotation
Understand the concept of “restitution of the head.” Do not allow plaintiff’s counsel to suggest that you turned the child’s head to one side or the other with your hands. Restitution is a natural rotation, and your hands merely guide and support the child’s head in this process. Gentle guiding of the head is appropriate.
The term “downward” is similarly misused. If ever there was a loaded term, it is “downward traction,” a favorite of plaintiff’s attorneys. Downward, as in “out of the birth canal,” versus downward, as in “90-degree angle to the birth canal and toward the floor,” are descriptions frequently misused in testimony and evidence. Be clear that any use of the term downward does not imply that the child’s neck was bent 45 to 90 degrees, with the top of the head inclined toward the floor. If a vague question regarding downward traction arises during the course of a legal case, ask for clarification of the term.
Degree of traction is another poorly understood concept. I am not aware of any reliable study that conclusively proves that major Erb’s palsy occurs when a greater degree of traction is applied and minor Erb’s palsy with a smaller degree of traction. Some counsel will use the fact that most brachial plexus injuries resolve over time to suggest that permanent Erb’s palsy is caused by overwhelming traction. Be prepared to dispute this argument!
Explain stations of the head
It is important that a jury understand that only a few inches separate –3 and +3 stations. Try to prevent plaintiff’s counsel from making the distance between these points seem like a long journey. Tissues stretch, caput occurs, and the station of the head may therefore become difficult to identify with pinpoint accuracy. A nurse’s estimate of –2 and a physician’s estimate of –1 for the same patient may, in fact, be consistent.
Use terminology precisely
If the infant develops a hematoma as a result of vacuum extraction or a similar device, be clear and concise about exactly what the injury is. Don’t let a subdural hematoma be described as a “brain bleed”!
Beware the magic gloves!
Studies in which physicians work on a model using pressure-sensitive gloves tend to suggest that excessive pressure is used. However, when the gloves are used in actual deliveries, pressure tends to be appropriate. Any mention of pressure-sensitive glove studies by plaintiff’s counsel should raise a red flag.
Growth charts are unreliable
Many shoulder dystocia–related trials use growth charts as exhibits. If you are confronted with one of these charts, be certain that you know what type of chart it is and the age and location of the children on whom it was based. Prenatal and postnatal growth charts are not the same. A child who is LGA on a postnatal chart might not be on a prenatal chart.
An expert witness once pointed out to me the existence of some charts from high-altitude cities; on these charts, the 95th percentile is slightly lower because children born at high altitude may be slightly smaller. Use of a high-altitude chart for a marginally LGA child in New York will make that child appear even larger than it is.
Triple-check each chart exhibit to make sure it is accurate and based on reliable data.
4. Don’t lose the case at deposition
You can’t win your case at deposition, but you certainly can lose it. Misplaced words and artless answers can damage your defense irreparably. Work with your attorney to fully explore any medical issues or terms on which the defense hinges. A simple misstatement of fact or misuse of a medically significant term can lock the defense into a difficult position.
Because the deposition is a major aspect of litigation, you should study for it and meet with your counsel well in advance of the date. A preparation session more than a week before your deposition will give you time to mull the issues and resolve any conflicts in your mind. A second session may be necessary to revisit difficult issues.
Know likely points of contention
Medical terminology and the sequence of events are two of the most likely areas of confusion. For example, although most physicians can readily distinguish between suprapubic and fundal pressure, many staff members confuse the two, as do many patients and lay witnesses to the birth. Fundal pressure may increase impaction of the shoulder; suprapubic pressure, correctly applied, is appropriate during the McRoberts maneuver (FIGURE).1
Some attorneys prefer to have the physician present when witnesses and parents are giving a deposition. This certainly conveys the message that the physician is committed to defense of the case.
If you choose to be present during a deposition, understand that lay witnesses may give inaccurate testimony. If this occurs while you are present, don’t get emotionally involved; do remain a passive observer. Remember, a deposition is not a trial. Although inaccurate testimony can be frustrating to the physician, it will ultimately trap the witness at trial and may be his (or her) undoing.
FIGURE Suprapubic vs fundal pressure
“Fundal pressure may increase impaction of the shoulder; suprapubic pressure (shown here), correctly applied, is appropriate during the McRoberts maneuver”
5. Retain the best expert you can find
Because the credentials and strength of expert opinions are critical to your defense, endeavor to retain the most highly qualified expert possible. Seek out an expert on the standard of care as soon as possible after filing of the lawsuit. Your counsel should be in consultation with this expert early in the case—certainly before your deposition. You don’t want to risk giving testimony that is inconsistent with your expert’s opinion or impossible for your expert to defend.
A highly qualified expert may be someone who has written about dystocia or participated in major studies. He or she also should be active in the delivery of babies and use any instrumentation or devices involved in your case. I recently cross-examined a plaintiff’s expert in a vacuum extraction case who hadn’t used the device since he finished his residency in 1974! This left several jurors with expressions of incredulity on their faces.
If you are practicing in a rural area, the availability of personnel or equipment may be an issue in your case. In such circumstances, an expert from a rural institution may be preferable to an expert from a major metropolitan area.
Scrutinize the expert’s credentials and communication style
Most defense counsel who practice in a specialized area of medicine will have access to the curriculum vitae of several potential experts. Review these documents with your attorney and investigate other cases in which the experts have testified.
If neither you nor your counsel has ever met or seen the expert, it may be helpful to explore whether the expert has ever given videotaped testimony. This will help you evaluate his or her physical appearance, demeanor, and general likeability, all of which influence the jury’s response to the testimony.
Remember, the plaintiff’s case is usually presented first. A jury may first be exposed to the facts of your case through the testimony of the plaintiff’s experts and witnesses, including emotional and at times weeping family members. Your expert will therefore need to refocus and reeducate the jury and dispel the opinions rendered by the plaintiff’s experts. To be successful, your expert must be able to create rapport with the jurors to keep them interested in his or her testimony and opinions. In this regard, your expert’s communication skills are paramount.
6. Be steadfast—the courtroom is a fishbowl!
At trial, you will be stared at, evaluated, and judged even while you are sitting in a chair at the defense table well before your testimony. This may seem unreasonable, capricious, and outrageous…and it is! However, until you take the witness stand, the jury has no other source of information about you.
Jurors are naturally curious. They begin to wonder about the case and, being human, may leap to conclusions. To protect yourself against unfair inferences, be mindful of your behavior, and assume that anything you say or do within two blocks of the courthouse will be seen by a juror. Here are some basic courtroom “don’ts,” culled from personal experience:
- Unless you are handicapped, do not park in a handicapped spot, even for a minute to unload a box of documents. A juror may see you and find your action inconsiderate.
- Don’t wear clothing or jewelry that is significantly more expensive than that worn by the plaintiffs or jurors.
- Be serious but not aloof.
- Remember to teach—not lecture—the jury.
- Take advantage of conference rooms.
Important discussions with counsel and experts should take place in private where there is no chance that a juror will accidentally observe or overhear the conversation.
7. Make exhibits informative, not disturbing
The purpose of a trial exhibit is to illustrate or demonstrate a point to the jurors. Any evidence that is presented must be accurate and based on facts already established in the case. The physician should assist defense counsel in the selection and preparation of exhibits. Here are a few tips:
- Make it easy to use. An exhibit—particularly a medical instrument—must be easy to use. Misusing, breaking, or fumbling with it on the stand is not only embarrassing, it casts doubt on the credibility of the witness. Have you ever seen a doctor accidentally fire a surgical staple into his own palm from an “empty” stapler while demonstrating the device in court? (I have.)
- Make it accurate. There are several types of vacuum extractors. If you choose to bring an exhibit—particularly a medical instrument—into the courtroom, it should be exactly the same type that was used in the delivery. Any variance should be insignificant. In a recent case, a plaintiff’s expert intended to use an outdated vacuum device that was rather large and ungainly and appeared to be far more ominous than the device that was actually used in the delivery. The court precluded its exhibition.
- Make sure it is unambiguous. There is great potential danger in using a defense exhibit that can be misinterpreted or reinterpreted to actually support the plaintiff’s position. Fetal growth charts, charts summarizing medical literature, and similar exhibits all have a potential for reinterpretation.
- Don’t send the wrong message. Photographs, medical instruments, and other exhibits can be gruesome or shocking to a jury. For example, if demonstration of a vacuum extractor is not critical to the defense of a case, the device may be inappropriate for courtroom demonstration. The reason? It may cause jurors to feel uncomfortable or place considerable focus on a minor issue. Any negative aspect of a potential exhibit should be evaluated in determining whether the exhibit will be used in front of the jury.
8. Get to the scene!
If at all possible, make a trip to the exact labor room where the events in question occurred, and take your counsel with you. Like Lieutenant Columbo wandering about, you never know what you might see. Suppose the family claims it was in the waiting room and heard the doctor shouting. How far away is the waiting room? How large is the labor room? Was the bed high enough that a 4-foot 7-inch nurse acted reasonably by standing on a stool to apply suprapubic pressure—despite how odd it seemed to the family?
The physical environment influences perceptions and recollections of witnesses. It’s impossible to know what you’ll find until you visit the location.
9. Never alter your records—never
A physician has a duty to keep accurate records. Never change your records to improve your position. I have seen several cases in which it was alleged that a physician went back and added a small notation to the record. That is a big mistake because many potential plaintiffs obtain their records before the child’s discharge.
If an error in a medical record merits a late correction, contact the risk-management staff and review the issue with them. A separate addendum note addressing and correcting the errant information may be preferred.
Whenever there are two versions of the labor record—especially when they are exhibited side by side in the courtroom—the die is cast, credibility is irreparably shattered, and the case may very well be lost.
10. You can pull a rabbit out of a hat!
The first lawyer I worked for asked me one day, “How do you get a rabbit out of a hat?” The answer? “First you put the rabbit into the hat.”
Preparation is essential to your testimony. Review the questions and responses to be covered during your testimony at length with your counsel. Be familiar with the issues and themes to be covered, and learn to phrase each answer truthfully, appropriately, and confidently.
The witness chair is charged with some invisible magic. Sitting there in front of a judge, jury, and packed courtroom can cause even the most confident and polished witness to become shaken and confused. Never underestimate your need to prepare.
The author reports no financial relationships relevant to this article.
The heightened risk of being sued for a poor outcome—even when you and the obstetric team have delivered excellent care—is a sad reality of ObGyn practice, especially when shoulder dystocia is involved. Not so long ago, some physicians viewed a lawsuit as one of the costs of doing business and considered settlement of claims to avoid disruption to their practice. Today, with insurance rates skyrocketing, settlement is not as palatable, unless a clear breach of the standard of care has occurred. And although only a small percentage of cases ever reach trial, and fewer still go to a jury verdict, don’t be lulled into a false sense of security. A single case can take 5 or more years to make its way through the system.
What can you do to avoid the appearance of negligence and prevent litigation? And what tangential actions on the part of the physician or staff can cast defensible cases into the abyss of negligence? This article addresses these questions, focusing on 10 keys to avert or win a lawsuit involving shoulder dystocia.
Before you begin. Here is one preliminary piece of advice: Be vigilant. Air crash investigators frequently note that a crash occurs when a number of small errors link together. To prevent a poor outcome, it is critical to be alert to even minor inconsistencies in the care you and the obstetric team provide so you can rectify the situation before the small errors link into a disastrous chain.
1. Don’t downplay the “D” word
There are three important rules in medicine: Document, document, document. Yes, you’ve heard many people stress the importance of good notation, and I can back them up: A well-documented chart is a defendant’s best friend. Time and again, I’ve heard defense counsel lamenting—and plaintiff’s counsel exhorting—“if it isn’t documented, it didn’t happen.”
Careful documentation begins early. If a child is expected to be large for gestational age (LGA) or macrosomic, clear documentation of that fact and a plan in the prenatal record to address it during labor and delivery is critical. It also is important to communicate the potential for a large infant to the labor and delivery staff. Consider using a stamp or other indicator to mark the prenatal chart for this potentiality.
Make it legible
Clear handwriting or typed notes add substantial benefit to the defense of a dystocia case. They also help prevent the uncomfortable silence that can overwhelm a courtroom as 12 jurors stare at a witness who is unable to decipher her own notes or those of a colleague. The inability to interpret a note is almost as damaging to a case as the complete lack of a note. If a detail is important enough to warrant documentation, it’s important enough to document legibly.
Sooner is always better
Any shoulder dystocia case that involves injury to the child—whether temporary or permanent—holds significant potential to blossom into litigation. It is important to document the diagnosis of dystocia, steps taken to resolve it, and the outcome—and to do so during the delivery or as soon thereafter as possible.
The importance of this recommendation cannot be overstated. A quick 8 pm summary of a delivery that took place at 1:30 pm is bound to be vague and, in some respects, inherently inaccurate. In contrast, a 1:45 pm note that consumes an entire page, noting the time of diagnosis, sequence of efforts to resolve the dystocia, use of vacuum or forceps, number of pop-offs, and who was present in the room is unquestionably superior.
Once mother and infant are stable and under the care of qualified personnel, take sufficient time—even as long as 1 hour—to draft your delivery note. Sit down. Calm down. Strive for clarity. The sequence and timing of events will be important.
The parents’ ability to recall the delivery will be blurred by emotion. If the case goes to trial, your well-documented note, combined with your accurate testimony, will have a significant advantage over what might be the understandably muddled recollections of the parents.
Call for a scrivener
If it seems as though it will be difficult to recall all the details of a delivery, consider calling a nurse or staff member into the room for the sole purpose of documentation once shoulder dystocia is diagnosed. Remember, once dystocia occurs, the risk of a poor outcome and years of litigation increases substantially. Having an extra staff member take notes is a small price to pay for documentation that may later establish your defense. The thinnest paper can sometimes extinguish the hottest litigation flame.
Prepare for a considerable lapse of time
Most states allow a claim to be filed on behalf of a child as late as 2 years after the child reaches the age of majority, which is 18 years in most states. Therefore, a child in many states can file suit as late as his or her 20th birthday. It is not uncommon for the events of an obstetrics case to be 10 or 15 years in the past by the time a claim is filed. Over such a long period, memories fade, radiographs and other imaging studies may get lost in storage, and so on. No matter how busy, tired, or hurried you may be from the events of the day, the most important 30 minutes you can spend are those in which you take time to sit, think, carefully draft, and proofread a delivery summary and check it for consistency against other documents generated during delivery. If necessary, call your partner in to cover you for an hour or two while you get the documentation right. If it helps your practice avoid a lawsuit, it is time well spent.
2. Educate your attorney
This point may seem rudimentary, but I have encountered a number of physicians who allowed their anger over being sued to taint their initial contacts with defense counsel.
A physician who sets aside 3 to 4 hours to meet with counsel, educate the attorney about medical issues, and review the medical literature is a cherished ally and is much more likely to be defended successfully. Physicians who treat the lawsuit as though it is an imposition on their personal or professional life and distance themselves from defense counsel do themselves a great disservice.
3. Be fluent in shoulder dystocia
If you are sued, and your case proceeds to trial—or even to depositions—a number of concepts particular to shoulder dystocia are very likely to arise, and you will be expected to address them coherently and to educate the jury and judge about their proper meaning.
Shoulder dystocia is unpredictable
Be conversant with the literature and statistics that show dystocia to be an unpredictable event.1
Fetal weight estimates are imprecise
Know the numbers. It is important to be conversant about projected birth weights and lines of demarcation for macrosomic and LGA fetuses. Plaintiff’s counsel and experts may try to obscure the lines between these definitions and terms. Keep your facts and definitions straight.
Also emphasize that ultrasonographic weight estimates are just that—estimates. There is no way to determine precise fetal weight in utero. Some studies suggest that ultrasonography (US) and physician weight estimation via palpation have similar accuracy rates. Do not allow the plaintiff’s attorney or expert to create the impression that US estimates are infallibly accurate.
Restitution of the head is a natural rotation
Understand the concept of “restitution of the head.” Do not allow plaintiff’s counsel to suggest that you turned the child’s head to one side or the other with your hands. Restitution is a natural rotation, and your hands merely guide and support the child’s head in this process. Gentle guiding of the head is appropriate.
The term “downward” is similarly misused. If ever there was a loaded term, it is “downward traction,” a favorite of plaintiff’s attorneys. Downward, as in “out of the birth canal,” versus downward, as in “90-degree angle to the birth canal and toward the floor,” are descriptions frequently misused in testimony and evidence. Be clear that any use of the term downward does not imply that the child’s neck was bent 45 to 90 degrees, with the top of the head inclined toward the floor. If a vague question regarding downward traction arises during the course of a legal case, ask for clarification of the term.
Degree of traction is another poorly understood concept. I am not aware of any reliable study that conclusively proves that major Erb’s palsy occurs when a greater degree of traction is applied and minor Erb’s palsy with a smaller degree of traction. Some counsel will use the fact that most brachial plexus injuries resolve over time to suggest that permanent Erb’s palsy is caused by overwhelming traction. Be prepared to dispute this argument!
Explain stations of the head
It is important that a jury understand that only a few inches separate –3 and +3 stations. Try to prevent plaintiff’s counsel from making the distance between these points seem like a long journey. Tissues stretch, caput occurs, and the station of the head may therefore become difficult to identify with pinpoint accuracy. A nurse’s estimate of –2 and a physician’s estimate of –1 for the same patient may, in fact, be consistent.
Use terminology precisely
If the infant develops a hematoma as a result of vacuum extraction or a similar device, be clear and concise about exactly what the injury is. Don’t let a subdural hematoma be described as a “brain bleed”!
Beware the magic gloves!
Studies in which physicians work on a model using pressure-sensitive gloves tend to suggest that excessive pressure is used. However, when the gloves are used in actual deliveries, pressure tends to be appropriate. Any mention of pressure-sensitive glove studies by plaintiff’s counsel should raise a red flag.
Growth charts are unreliable
Many shoulder dystocia–related trials use growth charts as exhibits. If you are confronted with one of these charts, be certain that you know what type of chart it is and the age and location of the children on whom it was based. Prenatal and postnatal growth charts are not the same. A child who is LGA on a postnatal chart might not be on a prenatal chart.
An expert witness once pointed out to me the existence of some charts from high-altitude cities; on these charts, the 95th percentile is slightly lower because children born at high altitude may be slightly smaller. Use of a high-altitude chart for a marginally LGA child in New York will make that child appear even larger than it is.
Triple-check each chart exhibit to make sure it is accurate and based on reliable data.
4. Don’t lose the case at deposition
You can’t win your case at deposition, but you certainly can lose it. Misplaced words and artless answers can damage your defense irreparably. Work with your attorney to fully explore any medical issues or terms on which the defense hinges. A simple misstatement of fact or misuse of a medically significant term can lock the defense into a difficult position.
Because the deposition is a major aspect of litigation, you should study for it and meet with your counsel well in advance of the date. A preparation session more than a week before your deposition will give you time to mull the issues and resolve any conflicts in your mind. A second session may be necessary to revisit difficult issues.
Know likely points of contention
Medical terminology and the sequence of events are two of the most likely areas of confusion. For example, although most physicians can readily distinguish between suprapubic and fundal pressure, many staff members confuse the two, as do many patients and lay witnesses to the birth. Fundal pressure may increase impaction of the shoulder; suprapubic pressure, correctly applied, is appropriate during the McRoberts maneuver (FIGURE).1
Some attorneys prefer to have the physician present when witnesses and parents are giving a deposition. This certainly conveys the message that the physician is committed to defense of the case.
If you choose to be present during a deposition, understand that lay witnesses may give inaccurate testimony. If this occurs while you are present, don’t get emotionally involved; do remain a passive observer. Remember, a deposition is not a trial. Although inaccurate testimony can be frustrating to the physician, it will ultimately trap the witness at trial and may be his (or her) undoing.
FIGURE Suprapubic vs fundal pressure
“Fundal pressure may increase impaction of the shoulder; suprapubic pressure (shown here), correctly applied, is appropriate during the McRoberts maneuver”
5. Retain the best expert you can find
Because the credentials and strength of expert opinions are critical to your defense, endeavor to retain the most highly qualified expert possible. Seek out an expert on the standard of care as soon as possible after filing of the lawsuit. Your counsel should be in consultation with this expert early in the case—certainly before your deposition. You don’t want to risk giving testimony that is inconsistent with your expert’s opinion or impossible for your expert to defend.
A highly qualified expert may be someone who has written about dystocia or participated in major studies. He or she also should be active in the delivery of babies and use any instrumentation or devices involved in your case. I recently cross-examined a plaintiff’s expert in a vacuum extraction case who hadn’t used the device since he finished his residency in 1974! This left several jurors with expressions of incredulity on their faces.
If you are practicing in a rural area, the availability of personnel or equipment may be an issue in your case. In such circumstances, an expert from a rural institution may be preferable to an expert from a major metropolitan area.
Scrutinize the expert’s credentials and communication style
Most defense counsel who practice in a specialized area of medicine will have access to the curriculum vitae of several potential experts. Review these documents with your attorney and investigate other cases in which the experts have testified.
If neither you nor your counsel has ever met or seen the expert, it may be helpful to explore whether the expert has ever given videotaped testimony. This will help you evaluate his or her physical appearance, demeanor, and general likeability, all of which influence the jury’s response to the testimony.
Remember, the plaintiff’s case is usually presented first. A jury may first be exposed to the facts of your case through the testimony of the plaintiff’s experts and witnesses, including emotional and at times weeping family members. Your expert will therefore need to refocus and reeducate the jury and dispel the opinions rendered by the plaintiff’s experts. To be successful, your expert must be able to create rapport with the jurors to keep them interested in his or her testimony and opinions. In this regard, your expert’s communication skills are paramount.
6. Be steadfast—the courtroom is a fishbowl!
At trial, you will be stared at, evaluated, and judged even while you are sitting in a chair at the defense table well before your testimony. This may seem unreasonable, capricious, and outrageous…and it is! However, until you take the witness stand, the jury has no other source of information about you.
Jurors are naturally curious. They begin to wonder about the case and, being human, may leap to conclusions. To protect yourself against unfair inferences, be mindful of your behavior, and assume that anything you say or do within two blocks of the courthouse will be seen by a juror. Here are some basic courtroom “don’ts,” culled from personal experience:
- Unless you are handicapped, do not park in a handicapped spot, even for a minute to unload a box of documents. A juror may see you and find your action inconsiderate.
- Don’t wear clothing or jewelry that is significantly more expensive than that worn by the plaintiffs or jurors.
- Be serious but not aloof.
- Remember to teach—not lecture—the jury.
- Take advantage of conference rooms.
Important discussions with counsel and experts should take place in private where there is no chance that a juror will accidentally observe or overhear the conversation.
7. Make exhibits informative, not disturbing
The purpose of a trial exhibit is to illustrate or demonstrate a point to the jurors. Any evidence that is presented must be accurate and based on facts already established in the case. The physician should assist defense counsel in the selection and preparation of exhibits. Here are a few tips:
- Make it easy to use. An exhibit—particularly a medical instrument—must be easy to use. Misusing, breaking, or fumbling with it on the stand is not only embarrassing, it casts doubt on the credibility of the witness. Have you ever seen a doctor accidentally fire a surgical staple into his own palm from an “empty” stapler while demonstrating the device in court? (I have.)
- Make it accurate. There are several types of vacuum extractors. If you choose to bring an exhibit—particularly a medical instrument—into the courtroom, it should be exactly the same type that was used in the delivery. Any variance should be insignificant. In a recent case, a plaintiff’s expert intended to use an outdated vacuum device that was rather large and ungainly and appeared to be far more ominous than the device that was actually used in the delivery. The court precluded its exhibition.
- Make sure it is unambiguous. There is great potential danger in using a defense exhibit that can be misinterpreted or reinterpreted to actually support the plaintiff’s position. Fetal growth charts, charts summarizing medical literature, and similar exhibits all have a potential for reinterpretation.
- Don’t send the wrong message. Photographs, medical instruments, and other exhibits can be gruesome or shocking to a jury. For example, if demonstration of a vacuum extractor is not critical to the defense of a case, the device may be inappropriate for courtroom demonstration. The reason? It may cause jurors to feel uncomfortable or place considerable focus on a minor issue. Any negative aspect of a potential exhibit should be evaluated in determining whether the exhibit will be used in front of the jury.
8. Get to the scene!
If at all possible, make a trip to the exact labor room where the events in question occurred, and take your counsel with you. Like Lieutenant Columbo wandering about, you never know what you might see. Suppose the family claims it was in the waiting room and heard the doctor shouting. How far away is the waiting room? How large is the labor room? Was the bed high enough that a 4-foot 7-inch nurse acted reasonably by standing on a stool to apply suprapubic pressure—despite how odd it seemed to the family?
The physical environment influences perceptions and recollections of witnesses. It’s impossible to know what you’ll find until you visit the location.
9. Never alter your records—never
A physician has a duty to keep accurate records. Never change your records to improve your position. I have seen several cases in which it was alleged that a physician went back and added a small notation to the record. That is a big mistake because many potential plaintiffs obtain their records before the child’s discharge.
If an error in a medical record merits a late correction, contact the risk-management staff and review the issue with them. A separate addendum note addressing and correcting the errant information may be preferred.
Whenever there are two versions of the labor record—especially when they are exhibited side by side in the courtroom—the die is cast, credibility is irreparably shattered, and the case may very well be lost.
10. You can pull a rabbit out of a hat!
The first lawyer I worked for asked me one day, “How do you get a rabbit out of a hat?” The answer? “First you put the rabbit into the hat.”
Preparation is essential to your testimony. Review the questions and responses to be covered during your testimony at length with your counsel. Be familiar with the issues and themes to be covered, and learn to phrase each answer truthfully, appropriately, and confidently.
The witness chair is charged with some invisible magic. Sitting there in front of a judge, jury, and packed courtroom can cause even the most confident and polished witness to become shaken and confused. Never underestimate your need to prepare.
Reference
1. American College of Obstetricians and Gynecologists. Shoulder Dystocia. Practice Bulletin No. 40. Washington, DC: ACOG; 2002.
Reference
1. American College of Obstetricians and Gynecologists. Shoulder Dystocia. Practice Bulletin No. 40. Washington, DC: ACOG; 2002.
Organize Your Samples—and Your Reps
My January column, a collection of possible New Year's resolutions, generated quite a few requests for elaboration on some of the suggestions. Hopefully, the next few columns will fulfill some of those requests.
The suggestion on organizing samples triggered the most feedback. Everybody, it seems, thinks they have too many samples, but you really don't. What you have is too much packaging.
If you doubt this, take a good look at the next set of samples that comes into your office. Each unit will probably consist of a big box or card, and somewhere within its depths, amid all the wasted space, will be a single tablet or 3-g tube.
All that space-wasting packaging is purposeful, of course. Bigger is better, after all, from a promotional standpoint anyway. Bigger packages are more likely to be noticed, and there's more room for advertising.
The marketing people figure that if they use up all of your available sample space, you won't have room for their competition.
As a result, you probably have sample packages taking up two or three closets' worth of expensive square footage—with the samples themselves occupying perhaps 5% of that space or less.
Not only that, but each time you need a particular sample, somebody has to go hunting for it. Sometimes you find it, sometimes you don't. And when you do, there's a fair chance it's expired. It's a waste of time, space, and energy, and it's not necessary.
Here's what you do: Create a “parts-bin system” for your samples.
Have a carpenter build you shelving in a central area of the office. Stock those shelves with cardboard or plastic parts bins, which are available in a variety of lengths, widths, shapes, and colors from many different sources.
Three online examples are: www.anytimeproducts.com, www.papermart.com, www.lkgoodwin.com
As samples come in, ask the representative who brings them to strip off all the space-wasting packaging, leaving only the tablet bubble-pack cards or the 3-g tubes. You'll be amazed at how much less space they take up. Store them in the bins, and arrange the bins on your shelving by whatever organizational system you fancy. We do it alphabetically.
You'll always know what samples you have, what you're out of, and what's close to its expiration date. You and your staff will waste far less time searching for the samples you want, and you can use all that freed-up sample space for something far more likely to generate revenue for your office.
A parts-bin system could be an even bigger boon to your office if the Food and Drug Administration ever makes good on its recurrent promise to require written paper trails for all samples entering and leaving a facility.
Periodic inventories, as well as logging samples in and out, will be far easier with my system.
While you're organizing your samples, consider organizing your pharmaceutical reps too.
Many offices allow representatives to come and go as they please, and too many physicians, physician assistants, and nurse practitioners are all too willing to stop and chat with them, which disrupts efficient office flow. And if multiple reps show up in a single day, the chaos just multiplies.
Have your reps make appointments, just as your patients do. We allow only one rep appointment per day—during the lunch break, 10 minutes before the start of afternoon hours. That prevents disruption of the schedule, and it prevents me from chatting too long (which I have a tendency to do).
We also encourage reps not to make appointments at all unless they have something of significance to communicate. I'm happy to speak with reps, but not when all they have to offer is small talk.
{kind=link}
A well-organized sample closet will save time, space, and energy.
Courtesy Dr. Joseph S. Eastern
My January column, a collection of possible New Year's resolutions, generated quite a few requests for elaboration on some of the suggestions. Hopefully, the next few columns will fulfill some of those requests.
The suggestion on organizing samples triggered the most feedback. Everybody, it seems, thinks they have too many samples, but you really don't. What you have is too much packaging.
If you doubt this, take a good look at the next set of samples that comes into your office. Each unit will probably consist of a big box or card, and somewhere within its depths, amid all the wasted space, will be a single tablet or 3-g tube.
All that space-wasting packaging is purposeful, of course. Bigger is better, after all, from a promotional standpoint anyway. Bigger packages are more likely to be noticed, and there's more room for advertising.
The marketing people figure that if they use up all of your available sample space, you won't have room for their competition.
As a result, you probably have sample packages taking up two or three closets' worth of expensive square footage—with the samples themselves occupying perhaps 5% of that space or less.
Not only that, but each time you need a particular sample, somebody has to go hunting for it. Sometimes you find it, sometimes you don't. And when you do, there's a fair chance it's expired. It's a waste of time, space, and energy, and it's not necessary.
Here's what you do: Create a “parts-bin system” for your samples.
Have a carpenter build you shelving in a central area of the office. Stock those shelves with cardboard or plastic parts bins, which are available in a variety of lengths, widths, shapes, and colors from many different sources.
Three online examples are: www.anytimeproducts.com, www.papermart.com, www.lkgoodwin.com
As samples come in, ask the representative who brings them to strip off all the space-wasting packaging, leaving only the tablet bubble-pack cards or the 3-g tubes. You'll be amazed at how much less space they take up. Store them in the bins, and arrange the bins on your shelving by whatever organizational system you fancy. We do it alphabetically.
You'll always know what samples you have, what you're out of, and what's close to its expiration date. You and your staff will waste far less time searching for the samples you want, and you can use all that freed-up sample space for something far more likely to generate revenue for your office.
A parts-bin system could be an even bigger boon to your office if the Food and Drug Administration ever makes good on its recurrent promise to require written paper trails for all samples entering and leaving a facility.
Periodic inventories, as well as logging samples in and out, will be far easier with my system.
While you're organizing your samples, consider organizing your pharmaceutical reps too.
Many offices allow representatives to come and go as they please, and too many physicians, physician assistants, and nurse practitioners are all too willing to stop and chat with them, which disrupts efficient office flow. And if multiple reps show up in a single day, the chaos just multiplies.
Have your reps make appointments, just as your patients do. We allow only one rep appointment per day—during the lunch break, 10 minutes before the start of afternoon hours. That prevents disruption of the schedule, and it prevents me from chatting too long (which I have a tendency to do).
We also encourage reps not to make appointments at all unless they have something of significance to communicate. I'm happy to speak with reps, but not when all they have to offer is small talk.
A well-organized sample closet will save time, space, and energy.
Courtesy Dr. Joseph S. Eastern
My January column, a collection of possible New Year's resolutions, generated quite a few requests for elaboration on some of the suggestions. Hopefully, the next few columns will fulfill some of those requests.
The suggestion on organizing samples triggered the most feedback. Everybody, it seems, thinks they have too many samples, but you really don't. What you have is too much packaging.
If you doubt this, take a good look at the next set of samples that comes into your office. Each unit will probably consist of a big box or card, and somewhere within its depths, amid all the wasted space, will be a single tablet or 3-g tube.
All that space-wasting packaging is purposeful, of course. Bigger is better, after all, from a promotional standpoint anyway. Bigger packages are more likely to be noticed, and there's more room for advertising.
The marketing people figure that if they use up all of your available sample space, you won't have room for their competition.
As a result, you probably have sample packages taking up two or three closets' worth of expensive square footage—with the samples themselves occupying perhaps 5% of that space or less.
Not only that, but each time you need a particular sample, somebody has to go hunting for it. Sometimes you find it, sometimes you don't. And when you do, there's a fair chance it's expired. It's a waste of time, space, and energy, and it's not necessary.
Here's what you do: Create a “parts-bin system” for your samples.
Have a carpenter build you shelving in a central area of the office. Stock those shelves with cardboard or plastic parts bins, which are available in a variety of lengths, widths, shapes, and colors from many different sources.
Three online examples are: www.anytimeproducts.com, www.papermart.com, www.lkgoodwin.com
As samples come in, ask the representative who brings them to strip off all the space-wasting packaging, leaving only the tablet bubble-pack cards or the 3-g tubes. You'll be amazed at how much less space they take up. Store them in the bins, and arrange the bins on your shelving by whatever organizational system you fancy. We do it alphabetically.
You'll always know what samples you have, what you're out of, and what's close to its expiration date. You and your staff will waste far less time searching for the samples you want, and you can use all that freed-up sample space for something far more likely to generate revenue for your office.
A parts-bin system could be an even bigger boon to your office if the Food and Drug Administration ever makes good on its recurrent promise to require written paper trails for all samples entering and leaving a facility.
Periodic inventories, as well as logging samples in and out, will be far easier with my system.
While you're organizing your samples, consider organizing your pharmaceutical reps too.
Many offices allow representatives to come and go as they please, and too many physicians, physician assistants, and nurse practitioners are all too willing to stop and chat with them, which disrupts efficient office flow. And if multiple reps show up in a single day, the chaos just multiplies.
Have your reps make appointments, just as your patients do. We allow only one rep appointment per day—during the lunch break, 10 minutes before the start of afternoon hours. That prevents disruption of the schedule, and it prevents me from chatting too long (which I have a tendency to do).
We also encourage reps not to make appointments at all unless they have something of significance to communicate. I'm happy to speak with reps, but not when all they have to offer is small talk.
A well-organized sample closet will save time, space, and energy.
Courtesy Dr. Joseph S. Eastern
Going Solo Wisely
Family practice provides us with a tremendous opportunity: We are among the few specialists who still commonly hang a shingle and go into private practice. About 7 years ago, I did just that and I'm satisfied with the autonomy I now have. I love not having to ask a boss if I can take vacation time, and I appreciate the flexibility to teach once a week and practice medicine 4 days a week. But there is a flip side to this independence for which our years in medical school could do a better job preparing us: By and large, family physicians are ill equipped to manage the business side of their practices.
This insight is nothing new. But here's a short list of things about managing a private practice that I wish I had known when I completed residency:
▸ Don't hire individuals based on the quality of their eye contact and hand shake. In three instances, I had employees take advantage of my trust. In two of the cases, employees stole prescriptions. In the other, an office worker used the credit card machine to embezzle money. In all three cases, the actions of the individuals involved seemed completely out of character, or so I thought. As painful as these experiences were, they taught me to be proactive, rather than reactive. I now take the time to do background checks on office staff candidates before I hire them. During preliminary phone interviews, I ask applicants if they would submit to a background check. Most people readily comply with this policy. People with problematic histories pull their hats out of the ring.
Anyone you are considering hiring should have to substantiate claims about themselves. If someone reports he or she had a 4.0 grade point average, ask for a transcript. As physicians, we are required to have and show our certification. We should expect the same from our employees.
▸ Take an active interest in all financial aspects of your practice. This might sound obvious, but how many times have you heard a colleague say the business side of running an office gets in the way of practicing medicine? As physicians, our impulse is to farm out it This is a big mistake. It pays to be a little bit of a control freak about your finances. I would not have realized my employee was embezzling money had I not been doing my own bookkeeping, because she withdrew funds in small amounts. Hiring someone to do your books costs about $20,000-$25,000 a year. Doing your own books is not difficult. It takes about an hour a week, and it builds confidence and peace of mind to know exactly how money is coming and going.
Other tips: Make all check deposits yourself, keep close track of the office credit card, and do not share with your employees sensitive information such as your social security number.
▸ Do you really need a practice manager? When I started out, I lacked confidence and felt I needed help building my practice, so I hired a manager. At 5% of my gross profit, his cut was the most expensive part of my practice. It was a solution that worked well, but it was an expensive one that in retrospect was not worth it. The bottom line is that if you want to go into private practice, jump in and do it. Get the crash course in building a practice from the ground up. Talk to colleagues about how best to advertise. Learn how to do your own coding; don't pay someone else to code. You'll gain more by taking the hard road and being self-sufficient from the outset.
Family practice provides us with a tremendous opportunity: We are among the few specialists who still commonly hang a shingle and go into private practice. About 7 years ago, I did just that and I'm satisfied with the autonomy I now have. I love not having to ask a boss if I can take vacation time, and I appreciate the flexibility to teach once a week and practice medicine 4 days a week. But there is a flip side to this independence for which our years in medical school could do a better job preparing us: By and large, family physicians are ill equipped to manage the business side of their practices.
This insight is nothing new. But here's a short list of things about managing a private practice that I wish I had known when I completed residency:
▸ Don't hire individuals based on the quality of their eye contact and hand shake. In three instances, I had employees take advantage of my trust. In two of the cases, employees stole prescriptions. In the other, an office worker used the credit card machine to embezzle money. In all three cases, the actions of the individuals involved seemed completely out of character, or so I thought. As painful as these experiences were, they taught me to be proactive, rather than reactive. I now take the time to do background checks on office staff candidates before I hire them. During preliminary phone interviews, I ask applicants if they would submit to a background check. Most people readily comply with this policy. People with problematic histories pull their hats out of the ring.
Anyone you are considering hiring should have to substantiate claims about themselves. If someone reports he or she had a 4.0 grade point average, ask for a transcript. As physicians, we are required to have and show our certification. We should expect the same from our employees.
▸ Take an active interest in all financial aspects of your practice. This might sound obvious, but how many times have you heard a colleague say the business side of running an office gets in the way of practicing medicine? As physicians, our impulse is to farm out it This is a big mistake. It pays to be a little bit of a control freak about your finances. I would not have realized my employee was embezzling money had I not been doing my own bookkeeping, because she withdrew funds in small amounts. Hiring someone to do your books costs about $20,000-$25,000 a year. Doing your own books is not difficult. It takes about an hour a week, and it builds confidence and peace of mind to know exactly how money is coming and going.
Other tips: Make all check deposits yourself, keep close track of the office credit card, and do not share with your employees sensitive information such as your social security number.
▸ Do you really need a practice manager? When I started out, I lacked confidence and felt I needed help building my practice, so I hired a manager. At 5% of my gross profit, his cut was the most expensive part of my practice. It was a solution that worked well, but it was an expensive one that in retrospect was not worth it. The bottom line is that if you want to go into private practice, jump in and do it. Get the crash course in building a practice from the ground up. Talk to colleagues about how best to advertise. Learn how to do your own coding; don't pay someone else to code. You'll gain more by taking the hard road and being self-sufficient from the outset.
Family practice provides us with a tremendous opportunity: We are among the few specialists who still commonly hang a shingle and go into private practice. About 7 years ago, I did just that and I'm satisfied with the autonomy I now have. I love not having to ask a boss if I can take vacation time, and I appreciate the flexibility to teach once a week and practice medicine 4 days a week. But there is a flip side to this independence for which our years in medical school could do a better job preparing us: By and large, family physicians are ill equipped to manage the business side of their practices.
This insight is nothing new. But here's a short list of things about managing a private practice that I wish I had known when I completed residency:
▸ Don't hire individuals based on the quality of their eye contact and hand shake. In three instances, I had employees take advantage of my trust. In two of the cases, employees stole prescriptions. In the other, an office worker used the credit card machine to embezzle money. In all three cases, the actions of the individuals involved seemed completely out of character, or so I thought. As painful as these experiences were, they taught me to be proactive, rather than reactive. I now take the time to do background checks on office staff candidates before I hire them. During preliminary phone interviews, I ask applicants if they would submit to a background check. Most people readily comply with this policy. People with problematic histories pull their hats out of the ring.
Anyone you are considering hiring should have to substantiate claims about themselves. If someone reports he or she had a 4.0 grade point average, ask for a transcript. As physicians, we are required to have and show our certification. We should expect the same from our employees.
▸ Take an active interest in all financial aspects of your practice. This might sound obvious, but how many times have you heard a colleague say the business side of running an office gets in the way of practicing medicine? As physicians, our impulse is to farm out it This is a big mistake. It pays to be a little bit of a control freak about your finances. I would not have realized my employee was embezzling money had I not been doing my own bookkeeping, because she withdrew funds in small amounts. Hiring someone to do your books costs about $20,000-$25,000 a year. Doing your own books is not difficult. It takes about an hour a week, and it builds confidence and peace of mind to know exactly how money is coming and going.
Other tips: Make all check deposits yourself, keep close track of the office credit card, and do not share with your employees sensitive information such as your social security number.
▸ Do you really need a practice manager? When I started out, I lacked confidence and felt I needed help building my practice, so I hired a manager. At 5% of my gross profit, his cut was the most expensive part of my practice. It was a solution that worked well, but it was an expensive one that in retrospect was not worth it. The bottom line is that if you want to go into private practice, jump in and do it. Get the crash course in building a practice from the ground up. Talk to colleagues about how best to advertise. Learn how to do your own coding; don't pay someone else to code. You'll gain more by taking the hard road and being self-sufficient from the outset.
Plan for Discharge
Discharge planning typically begins at the time of admission. Physicians and hospital staff manage the patient’s acute issues throughout the stay while simultaneously trying to anticipate the patient’s discharge needs. Physicians capture these associated efforts by reporting discharge day management codes 99238 or 99239.
Code Use
Use of discharge day management codes 99238-99239 is reserved for the admitting physician/group, unless a formal transfer of care occurs (e.g., patient is transferred from the intensive care unit by the critical care physician to the medical-surgical floor on the hospitalist’s service).
Report one discharge code per hospitalization, but only when the service occurs after the initial date of admission. Codes 99238 or 99239 are not permitted for use when the patient is admitted and discharged on the same calendar date. When this occurs, the physician selects from 99221-99223 (initial inpatient care) or 99234-99236 (admission and discharge on the same day). Choose 99234-99238 when the patient stay is eight or more hours on the same calendar day and the insurer accepts these codes.
Documentation must also reflect two components of service: the corresponding elements of both the admission and discharge. Alternately, if the patient stays less than eight hours, or the insurer does not recognize 99234-99236 (admission and discharge on the same day), report 9922x (initial inpatient care) as appropriate.
Don’t mistakenly report discharge services for merely dictating the discharge summary. Discharge day management, as with most payable evaluation and management (E/M) services, requires a face-to-face visit between the physician and the patient on discharge day.
The entire visit need not take place at the bedside and may include other discharge-related elements performed on the patient’s unit/floor such as discussions with other healthcare professionals, patient/caregiver instruction and coordination of follow-up care. The discharge code description indicates that a final examination of the patient is included, but only “as appropriate.” In other words, an exam may not occur, or may not be documented, yet this does not preclude the physician from reporting 99238-99239. However, inclusion of the exam in the discharge day documentation is the best way to justify that a face-to-face service occurred on discharge day. This may be included in the discharge summary or a separate progress note in the medical record.
Time-Based Service
Discharge day management codes reflect the time accumulated on a calendar date, ending when the patient physically leaves the hospital. Services performed in a location other than the patient’s unit/floor (e.g., dictating the discharge summary from the outpatient office), do not count toward the cumulative time. Additionally, discharge-related services performed by residents, students or ancillary staff (i.e., registered nurses), such as reviewing instructions with the patient, do not count toward the discharge service time.
To support the discharge day management claim, documentation should reference the discharge status and other clinically relevant information. Time is not required when documenting 99238 because this service code constitutes any amount of time up to and including 30 minutes. When reporting 99239, documentation must include the physician’s cumulative service time (more than 30 minutes).
Medicare currently initiates a prepayment review (i.e., request for documentation to review the service prior to any payment consideration) for claims involving 99239. Failure to respond to the prepayment request or failure to include the time component in the documentation often results in claim denial. Payment can be recovered only through the appeal process or claim correction, when applicable.
Rules For Surgery
Surgeons are prohibited from separately reporting inpatient postoperative services related to the surgery, including discharge day management (99238-99239). Additionally, when the surgeon admits a patient to the hospital and discharge services are performed postoperatively by the hospitalist, discharge day management is included in the surgical package.
The reasons are two-fold: If the surgeon transfers the remaining inpatient care to the hospitalist, these discharge services are considered part of the global surgical package.
If no transfer occurs (as the surgeon is typically responsible and paid for all care up to 90 days following surgery), only the admitting physician/group (i.e., the surgeon) may report discharge day management codes 99238-99239.
In the latter scenario, the hospitalist reports subsequent hospital care (99231-99233) for all medically necessary services involving the patient’s medical management, even if provided on the day of discharge.
Pronouncement of Death
One of the most underreported services involves pronouncement of death. A physician who performs this service may qualify to report discharge day management code 99238-99239. To pronounce death, the physician must examine the patient, thus satisfying the face-to-face visit requirement.
Additionally, the physician may have to coordinate the necessary services, speak with family members or other healthcare providers, and fill out the necessary documentation.
If performed on the patient’s unit/floor, these services count toward the cumulative discharge service time. Documentation must include the time (if reporting 99239) as well as the patient’s discharge status and clinically relevant information. Completion of the death certificate alone is not sufficient for billing. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Discharge planning typically begins at the time of admission. Physicians and hospital staff manage the patient’s acute issues throughout the stay while simultaneously trying to anticipate the patient’s discharge needs. Physicians capture these associated efforts by reporting discharge day management codes 99238 or 99239.
Code Use
Use of discharge day management codes 99238-99239 is reserved for the admitting physician/group, unless a formal transfer of care occurs (e.g., patient is transferred from the intensive care unit by the critical care physician to the medical-surgical floor on the hospitalist’s service).
Report one discharge code per hospitalization, but only when the service occurs after the initial date of admission. Codes 99238 or 99239 are not permitted for use when the patient is admitted and discharged on the same calendar date. When this occurs, the physician selects from 99221-99223 (initial inpatient care) or 99234-99236 (admission and discharge on the same day). Choose 99234-99238 when the patient stay is eight or more hours on the same calendar day and the insurer accepts these codes.
Documentation must also reflect two components of service: the corresponding elements of both the admission and discharge. Alternately, if the patient stays less than eight hours, or the insurer does not recognize 99234-99236 (admission and discharge on the same day), report 9922x (initial inpatient care) as appropriate.
Don’t mistakenly report discharge services for merely dictating the discharge summary. Discharge day management, as with most payable evaluation and management (E/M) services, requires a face-to-face visit between the physician and the patient on discharge day.
The entire visit need not take place at the bedside and may include other discharge-related elements performed on the patient’s unit/floor such as discussions with other healthcare professionals, patient/caregiver instruction and coordination of follow-up care. The discharge code description indicates that a final examination of the patient is included, but only “as appropriate.” In other words, an exam may not occur, or may not be documented, yet this does not preclude the physician from reporting 99238-99239. However, inclusion of the exam in the discharge day documentation is the best way to justify that a face-to-face service occurred on discharge day. This may be included in the discharge summary or a separate progress note in the medical record.
Time-Based Service
Discharge day management codes reflect the time accumulated on a calendar date, ending when the patient physically leaves the hospital. Services performed in a location other than the patient’s unit/floor (e.g., dictating the discharge summary from the outpatient office), do not count toward the cumulative time. Additionally, discharge-related services performed by residents, students or ancillary staff (i.e., registered nurses), such as reviewing instructions with the patient, do not count toward the discharge service time.
To support the discharge day management claim, documentation should reference the discharge status and other clinically relevant information. Time is not required when documenting 99238 because this service code constitutes any amount of time up to and including 30 minutes. When reporting 99239, documentation must include the physician’s cumulative service time (more than 30 minutes).
Medicare currently initiates a prepayment review (i.e., request for documentation to review the service prior to any payment consideration) for claims involving 99239. Failure to respond to the prepayment request or failure to include the time component in the documentation often results in claim denial. Payment can be recovered only through the appeal process or claim correction, when applicable.
Rules For Surgery
Surgeons are prohibited from separately reporting inpatient postoperative services related to the surgery, including discharge day management (99238-99239). Additionally, when the surgeon admits a patient to the hospital and discharge services are performed postoperatively by the hospitalist, discharge day management is included in the surgical package.
The reasons are two-fold: If the surgeon transfers the remaining inpatient care to the hospitalist, these discharge services are considered part of the global surgical package.
If no transfer occurs (as the surgeon is typically responsible and paid for all care up to 90 days following surgery), only the admitting physician/group (i.e., the surgeon) may report discharge day management codes 99238-99239.
In the latter scenario, the hospitalist reports subsequent hospital care (99231-99233) for all medically necessary services involving the patient’s medical management, even if provided on the day of discharge.
Pronouncement of Death
One of the most underreported services involves pronouncement of death. A physician who performs this service may qualify to report discharge day management code 99238-99239. To pronounce death, the physician must examine the patient, thus satisfying the face-to-face visit requirement.
Additionally, the physician may have to coordinate the necessary services, speak with family members or other healthcare providers, and fill out the necessary documentation.
If performed on the patient’s unit/floor, these services count toward the cumulative discharge service time. Documentation must include the time (if reporting 99239) as well as the patient’s discharge status and clinically relevant information. Completion of the death certificate alone is not sufficient for billing. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Discharge planning typically begins at the time of admission. Physicians and hospital staff manage the patient’s acute issues throughout the stay while simultaneously trying to anticipate the patient’s discharge needs. Physicians capture these associated efforts by reporting discharge day management codes 99238 or 99239.
Code Use
Use of discharge day management codes 99238-99239 is reserved for the admitting physician/group, unless a formal transfer of care occurs (e.g., patient is transferred from the intensive care unit by the critical care physician to the medical-surgical floor on the hospitalist’s service).
Report one discharge code per hospitalization, but only when the service occurs after the initial date of admission. Codes 99238 or 99239 are not permitted for use when the patient is admitted and discharged on the same calendar date. When this occurs, the physician selects from 99221-99223 (initial inpatient care) or 99234-99236 (admission and discharge on the same day). Choose 99234-99238 when the patient stay is eight or more hours on the same calendar day and the insurer accepts these codes.
Documentation must also reflect two components of service: the corresponding elements of both the admission and discharge. Alternately, if the patient stays less than eight hours, or the insurer does not recognize 99234-99236 (admission and discharge on the same day), report 9922x (initial inpatient care) as appropriate.
Don’t mistakenly report discharge services for merely dictating the discharge summary. Discharge day management, as with most payable evaluation and management (E/M) services, requires a face-to-face visit between the physician and the patient on discharge day.
The entire visit need not take place at the bedside and may include other discharge-related elements performed on the patient’s unit/floor such as discussions with other healthcare professionals, patient/caregiver instruction and coordination of follow-up care. The discharge code description indicates that a final examination of the patient is included, but only “as appropriate.” In other words, an exam may not occur, or may not be documented, yet this does not preclude the physician from reporting 99238-99239. However, inclusion of the exam in the discharge day documentation is the best way to justify that a face-to-face service occurred on discharge day. This may be included in the discharge summary or a separate progress note in the medical record.
Time-Based Service
Discharge day management codes reflect the time accumulated on a calendar date, ending when the patient physically leaves the hospital. Services performed in a location other than the patient’s unit/floor (e.g., dictating the discharge summary from the outpatient office), do not count toward the cumulative time. Additionally, discharge-related services performed by residents, students or ancillary staff (i.e., registered nurses), such as reviewing instructions with the patient, do not count toward the discharge service time.
To support the discharge day management claim, documentation should reference the discharge status and other clinically relevant information. Time is not required when documenting 99238 because this service code constitutes any amount of time up to and including 30 minutes. When reporting 99239, documentation must include the physician’s cumulative service time (more than 30 minutes).
Medicare currently initiates a prepayment review (i.e., request for documentation to review the service prior to any payment consideration) for claims involving 99239. Failure to respond to the prepayment request or failure to include the time component in the documentation often results in claim denial. Payment can be recovered only through the appeal process or claim correction, when applicable.
Rules For Surgery
Surgeons are prohibited from separately reporting inpatient postoperative services related to the surgery, including discharge day management (99238-99239). Additionally, when the surgeon admits a patient to the hospital and discharge services are performed postoperatively by the hospitalist, discharge day management is included in the surgical package.
The reasons are two-fold: If the surgeon transfers the remaining inpatient care to the hospitalist, these discharge services are considered part of the global surgical package.
If no transfer occurs (as the surgeon is typically responsible and paid for all care up to 90 days following surgery), only the admitting physician/group (i.e., the surgeon) may report discharge day management codes 99238-99239.
In the latter scenario, the hospitalist reports subsequent hospital care (99231-99233) for all medically necessary services involving the patient’s medical management, even if provided on the day of discharge.
Pronouncement of Death
One of the most underreported services involves pronouncement of death. A physician who performs this service may qualify to report discharge day management code 99238-99239. To pronounce death, the physician must examine the patient, thus satisfying the face-to-face visit requirement.
Additionally, the physician may have to coordinate the necessary services, speak with family members or other healthcare providers, and fill out the necessary documentation.
If performed on the patient’s unit/floor, these services count toward the cumulative discharge service time. Documentation must include the time (if reporting 99239) as well as the patient’s discharge status and clinically relevant information. Completion of the death certificate alone is not sufficient for billing. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Verdicts ONLY on the Web
Child is born with CP after oxytocin treatment
A woman who was given a diagnosis of eclampsia at the end of her pregnancy was admitted to the hospital and administered oxytocin with fetal monitoring. After 24 hours of labor, she was fully dilated and began pushing. Eventually, a cesarean delivery was performed. The child was born depressed and needed to be resuscitated, and was later transferred to another facility. The child has cerebral palsy, spastic quadriplegia, and a seizure disorder and requires 24-hour care.
Patient’s claim Oxytocin should have been discontinued and a cesarean section performed sooner. Also, the fetal monitor indicated tachycardia, evidence of uterine hyperstimulation, and other nonreassuring signs.
Doctor’s defense There was no hyperstimulation or fetal distress.
Verdict $9.5 million Illinois settlement.
Did midwife’s tugging cause birth trauma?
A woman in labor 9 days past her due date presented at the hospital, where fetal monitoring showed a fetal heart rate of 120 to 130 beats per minute. After 1.5 hours, the membranes were ruptured and the amniotic fluid was lightly stained with meconium. An hour later, the child was born weighing 8 lb 5 oz, with an Apgar score of 9.
For 4 days he appeared to be fine, despite not feeding well. On day 4, he was admitted to the NICU, because he displayed abnormal movements of the extremities and clenching of the fists. A CT scan performed on day 6 indicated axial hemorrhage associated with bony disruption and evidence of a right-sided subdural hemorrhage, consistent with birth trauma. An MRI later that day showed a subdural hemorrhage, but no bony disruption or evidence of birth trauma. The child has cerebral palsy with autistic features and has difficulty walking.
Patient’s claim Negligence during the delivery resulted in birth trauma and the child’s problems. The mother and her sister, also present at the birth, claimed the nurse midwife pulled, tugged, and had difficulty while delivering the child.
Doctor’s defense There was no birth trauma, and the Apgar Scores and MRI confirm that the birth occurred without incident and was nontraumatic.
Verdict A $1.1 million mediated settlement in New York.
D&C, perforations, then more surgery
When a 46-year-old woman experienced excessive bleeding during her last menstrual period, her gynecologist recommended a hysteroscopy with dilation and curettage. The operative report indicated a myomatous uterus and an endometrial polyp. A sharp curettage was done, the polyp was removed by polyp forceps, and the tissue was sent to pathology.
Initially stable following surgery, the patient began to suffer severe abdominal and pelvic pain. Oral oxycodone/acetaminophen and intravenous morphine sulfate were administered. The gynecologist was called but did not evaluate the patient. After she was discharged home, the patient called the gynecologist twice to complain of severe abdominal pain, and was advised to take acetaminophen. The pain persisted, and the patient was sent to the emergency room the next morning.
The pathologist discovered that the endometrial curettings were really small bowel fragments and the endometrial polyp was a loop of small bowel. Abdominal radiographs indicated free air in the abdomen. Diagnostic laparoscopy revealed a 5-mm serosal defect of the uterus, a 3-cm small bowel defect, and enteric bowel contents and filmy adhesions present intra-abdominally.
A general surgeon performed exploratory laparotomy, lysis of adhesions, resection of 36 cm of small bowel, and reanastamosic of the small bowel. Following surgery, intravenous antibiotics were administered for small bowel spillage, and the patient was hospitalized for 10 days, during which she continued to suffer severe abdominal pain, loss of bowel function, depression, and nightmares.
Patient’s claim The gynecologist perforated the small bowel and uterus during surgery, failed to recognize the uterine perforation while performing the hysteroscopy, and failed to investigate her complaints of severe abdominal and back pain.
Doctor’s defense Perforation of the uterus and small bowel are known complications of a dilation and curettage, and the perforations were properly diagnosed and treated. Also, the patient healed well, with a minor surgical scar.
Verdict $477,677 New York verdict against the physician; $120,000 settlement with the hospital.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Child is born with CP after oxytocin treatment
A woman who was given a diagnosis of eclampsia at the end of her pregnancy was admitted to the hospital and administered oxytocin with fetal monitoring. After 24 hours of labor, she was fully dilated and began pushing. Eventually, a cesarean delivery was performed. The child was born depressed and needed to be resuscitated, and was later transferred to another facility. The child has cerebral palsy, spastic quadriplegia, and a seizure disorder and requires 24-hour care.
Patient’s claim Oxytocin should have been discontinued and a cesarean section performed sooner. Also, the fetal monitor indicated tachycardia, evidence of uterine hyperstimulation, and other nonreassuring signs.
Doctor’s defense There was no hyperstimulation or fetal distress.
Verdict $9.5 million Illinois settlement.
Did midwife’s tugging cause birth trauma?
A woman in labor 9 days past her due date presented at the hospital, where fetal monitoring showed a fetal heart rate of 120 to 130 beats per minute. After 1.5 hours, the membranes were ruptured and the amniotic fluid was lightly stained with meconium. An hour later, the child was born weighing 8 lb 5 oz, with an Apgar score of 9.
For 4 days he appeared to be fine, despite not feeding well. On day 4, he was admitted to the NICU, because he displayed abnormal movements of the extremities and clenching of the fists. A CT scan performed on day 6 indicated axial hemorrhage associated with bony disruption and evidence of a right-sided subdural hemorrhage, consistent with birth trauma. An MRI later that day showed a subdural hemorrhage, but no bony disruption or evidence of birth trauma. The child has cerebral palsy with autistic features and has difficulty walking.
Patient’s claim Negligence during the delivery resulted in birth trauma and the child’s problems. The mother and her sister, also present at the birth, claimed the nurse midwife pulled, tugged, and had difficulty while delivering the child.
Doctor’s defense There was no birth trauma, and the Apgar Scores and MRI confirm that the birth occurred without incident and was nontraumatic.
Verdict A $1.1 million mediated settlement in New York.
D&C, perforations, then more surgery
When a 46-year-old woman experienced excessive bleeding during her last menstrual period, her gynecologist recommended a hysteroscopy with dilation and curettage. The operative report indicated a myomatous uterus and an endometrial polyp. A sharp curettage was done, the polyp was removed by polyp forceps, and the tissue was sent to pathology.
Initially stable following surgery, the patient began to suffer severe abdominal and pelvic pain. Oral oxycodone/acetaminophen and intravenous morphine sulfate were administered. The gynecologist was called but did not evaluate the patient. After she was discharged home, the patient called the gynecologist twice to complain of severe abdominal pain, and was advised to take acetaminophen. The pain persisted, and the patient was sent to the emergency room the next morning.
The pathologist discovered that the endometrial curettings were really small bowel fragments and the endometrial polyp was a loop of small bowel. Abdominal radiographs indicated free air in the abdomen. Diagnostic laparoscopy revealed a 5-mm serosal defect of the uterus, a 3-cm small bowel defect, and enteric bowel contents and filmy adhesions present intra-abdominally.
A general surgeon performed exploratory laparotomy, lysis of adhesions, resection of 36 cm of small bowel, and reanastamosic of the small bowel. Following surgery, intravenous antibiotics were administered for small bowel spillage, and the patient was hospitalized for 10 days, during which she continued to suffer severe abdominal pain, loss of bowel function, depression, and nightmares.
Patient’s claim The gynecologist perforated the small bowel and uterus during surgery, failed to recognize the uterine perforation while performing the hysteroscopy, and failed to investigate her complaints of severe abdominal and back pain.
Doctor’s defense Perforation of the uterus and small bowel are known complications of a dilation and curettage, and the perforations were properly diagnosed and treated. Also, the patient healed well, with a minor surgical scar.
Verdict $477,677 New York verdict against the physician; $120,000 settlement with the hospital.
Child is born with CP after oxytocin treatment
A woman who was given a diagnosis of eclampsia at the end of her pregnancy was admitted to the hospital and administered oxytocin with fetal monitoring. After 24 hours of labor, she was fully dilated and began pushing. Eventually, a cesarean delivery was performed. The child was born depressed and needed to be resuscitated, and was later transferred to another facility. The child has cerebral palsy, spastic quadriplegia, and a seizure disorder and requires 24-hour care.
Patient’s claim Oxytocin should have been discontinued and a cesarean section performed sooner. Also, the fetal monitor indicated tachycardia, evidence of uterine hyperstimulation, and other nonreassuring signs.
Doctor’s defense There was no hyperstimulation or fetal distress.
Verdict $9.5 million Illinois settlement.
Did midwife’s tugging cause birth trauma?
A woman in labor 9 days past her due date presented at the hospital, where fetal monitoring showed a fetal heart rate of 120 to 130 beats per minute. After 1.5 hours, the membranes were ruptured and the amniotic fluid was lightly stained with meconium. An hour later, the child was born weighing 8 lb 5 oz, with an Apgar score of 9.
For 4 days he appeared to be fine, despite not feeding well. On day 4, he was admitted to the NICU, because he displayed abnormal movements of the extremities and clenching of the fists. A CT scan performed on day 6 indicated axial hemorrhage associated with bony disruption and evidence of a right-sided subdural hemorrhage, consistent with birth trauma. An MRI later that day showed a subdural hemorrhage, but no bony disruption or evidence of birth trauma. The child has cerebral palsy with autistic features and has difficulty walking.
Patient’s claim Negligence during the delivery resulted in birth trauma and the child’s problems. The mother and her sister, also present at the birth, claimed the nurse midwife pulled, tugged, and had difficulty while delivering the child.
Doctor’s defense There was no birth trauma, and the Apgar Scores and MRI confirm that the birth occurred without incident and was nontraumatic.
Verdict A $1.1 million mediated settlement in New York.
D&C, perforations, then more surgery
When a 46-year-old woman experienced excessive bleeding during her last menstrual period, her gynecologist recommended a hysteroscopy with dilation and curettage. The operative report indicated a myomatous uterus and an endometrial polyp. A sharp curettage was done, the polyp was removed by polyp forceps, and the tissue was sent to pathology.
Initially stable following surgery, the patient began to suffer severe abdominal and pelvic pain. Oral oxycodone/acetaminophen and intravenous morphine sulfate were administered. The gynecologist was called but did not evaluate the patient. After she was discharged home, the patient called the gynecologist twice to complain of severe abdominal pain, and was advised to take acetaminophen. The pain persisted, and the patient was sent to the emergency room the next morning.
The pathologist discovered that the endometrial curettings were really small bowel fragments and the endometrial polyp was a loop of small bowel. Abdominal radiographs indicated free air in the abdomen. Diagnostic laparoscopy revealed a 5-mm serosal defect of the uterus, a 3-cm small bowel defect, and enteric bowel contents and filmy adhesions present intra-abdominally.
A general surgeon performed exploratory laparotomy, lysis of adhesions, resection of 36 cm of small bowel, and reanastamosic of the small bowel. Following surgery, intravenous antibiotics were administered for small bowel spillage, and the patient was hospitalized for 10 days, during which she continued to suffer severe abdominal pain, loss of bowel function, depression, and nightmares.
Patient’s claim The gynecologist perforated the small bowel and uterus during surgery, failed to recognize the uterine perforation while performing the hysteroscopy, and failed to investigate her complaints of severe abdominal and back pain.
Doctor’s defense Perforation of the uterus and small bowel are known complications of a dilation and curettage, and the perforations were properly diagnosed and treated. Also, the patient healed well, with a minor surgical scar.
Verdict $477,677 New York verdict against the physician; $120,000 settlement with the hospital.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Medical Verdicts
Several attempts, then laceration is repaired
A 45-year-old patient underwent a total abdominal hysterectomy. Near the end of the surgery, the nurse anesthetist noticed blood in the tubing of the urinary catheter bag, which the physician deemed a result of traumatic catheterization at the beginning of the procedure.
Despite the continued presence of blood in the urine and urinary leakage, a 4- to 5-cm laceration at the base of the bladder was not detected for 2 days. A vesicovaginal fistula developed. Over 8 months, several attempts to close the fistula surgically were unsuccessful. Eventually, it was repaired, and the patient has had no further leaks.
Patient’s claim Failure to detect and repair the laceration in a timely manner caused the fistula to develop. This condition lasted about 8 months.
Doctor’s defense The location of the laceration was difficult to find. Once it was discovered, the proper treatment was to drain the bladder with a catheter and wait several weeks to see if it could heal on its own. There was no reason for the repair attempts to fail.
Verdict $300,000 Illinois verdict.
Pain “like childbirth” is due to retained sponge
A 21-year-old woman suffered a perineal–vaginal tear during childbirth. This was repaired following delivery. A surgical sponge was inserted into the vagina to absorb blood during the repair. Two days later, the patient was discharged from the hospital and sent home.
Two days after that, she experienced pressure in the pelvic area that she likened to childbirth. When she felt something move inside her, she feared she was about to give birth to a second baby. She went to the emergency room, where the presence of the sponge was detected. According to the patient’s mother, who was also present, the pain was relieved almost instantly when the sponge was removed. In a phone call to the patient’s mother the next morning, the physician admitted he had neglected to tell the nursing staff that he had inserted the sponge and that he should have removed it.
Patient’s claim The physician was negligent for failing to remove the sponge.
Doctor’s defense There was no negligence.
Verdict Alabama defense verdict.
Perineal tear follows vacuum extraction
A 27-year-old primigravida experienced an essentially uncomplicated pregnancy during which she was monitored regularly by her ObGyn. When she went into labor and presented at the hospital, she was given an epidural, placed on a fetal monitor, examined regularly, and administered oxytocin. Because of normal progress to complete dilation and effacement, a vaginal delivery appeared likely. After 4.5 hours of second stage labor, a child weighing 8 lb 5 oz was delivered with the aid of a vacuum extractor.
During delivery of the shoulders, the mother suffered a third degree perineal tear extending to the rectal sphincter. This was noted immediately and repaired after completion of the delivery. Before the patient was discharged, she was examined and no problems were found at the site of the repairs.
At her 1-month postpartum visit, the woman informed her ObGyn of occasional fecal incontinence and was told the problem would probably resolve itself. The symptoms persisted, so she was referred to a colorectal surgeon. Dissatisfied with the surgical repair, the patient sought a second surgery from another physician.
Patient’s claim The ObGyn mismanaged the second stage of labor and should have performed a cesarean section rather than used vacuum extraction. Also, the defendant was negligent in the repair of the injury and failed to provide proper follow-up care.
Doctor’s defense There was no negligence. Both the delivery and repair of the tear were performed properly.
Verdict Georgia defense verdict.
During nerve ablation, ureter is damaged
A 39-year-old woman was being treated for low libido, painful intercourse, and heavy, painful menses. When conservative treatment failed to relieve the symptoms, the patient agreed to laparoscopy as recommended by her physician. Ablation of the uterosacral nerve was performed, because the physician believed it to be causing or contributing to the symptoms. The patient’s ureter was damaged and required repair surgery.
Patient’s claim There was lack of informed consent, and the physician was negligent for injuring the ureter.
Doctor’s defense There was no negligence.
Verdict California defense verdict.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Several attempts, then laceration is repaired
A 45-year-old patient underwent a total abdominal hysterectomy. Near the end of the surgery, the nurse anesthetist noticed blood in the tubing of the urinary catheter bag, which the physician deemed a result of traumatic catheterization at the beginning of the procedure.
Despite the continued presence of blood in the urine and urinary leakage, a 4- to 5-cm laceration at the base of the bladder was not detected for 2 days. A vesicovaginal fistula developed. Over 8 months, several attempts to close the fistula surgically were unsuccessful. Eventually, it was repaired, and the patient has had no further leaks.
Patient’s claim Failure to detect and repair the laceration in a timely manner caused the fistula to develop. This condition lasted about 8 months.
Doctor’s defense The location of the laceration was difficult to find. Once it was discovered, the proper treatment was to drain the bladder with a catheter and wait several weeks to see if it could heal on its own. There was no reason for the repair attempts to fail.
Verdict $300,000 Illinois verdict.
Pain “like childbirth” is due to retained sponge
A 21-year-old woman suffered a perineal–vaginal tear during childbirth. This was repaired following delivery. A surgical sponge was inserted into the vagina to absorb blood during the repair. Two days later, the patient was discharged from the hospital and sent home.
Two days after that, she experienced pressure in the pelvic area that she likened to childbirth. When she felt something move inside her, she feared she was about to give birth to a second baby. She went to the emergency room, where the presence of the sponge was detected. According to the patient’s mother, who was also present, the pain was relieved almost instantly when the sponge was removed. In a phone call to the patient’s mother the next morning, the physician admitted he had neglected to tell the nursing staff that he had inserted the sponge and that he should have removed it.
Patient’s claim The physician was negligent for failing to remove the sponge.
Doctor’s defense There was no negligence.
Verdict Alabama defense verdict.
Perineal tear follows vacuum extraction
A 27-year-old primigravida experienced an essentially uncomplicated pregnancy during which she was monitored regularly by her ObGyn. When she went into labor and presented at the hospital, she was given an epidural, placed on a fetal monitor, examined regularly, and administered oxytocin. Because of normal progress to complete dilation and effacement, a vaginal delivery appeared likely. After 4.5 hours of second stage labor, a child weighing 8 lb 5 oz was delivered with the aid of a vacuum extractor.
During delivery of the shoulders, the mother suffered a third degree perineal tear extending to the rectal sphincter. This was noted immediately and repaired after completion of the delivery. Before the patient was discharged, she was examined and no problems were found at the site of the repairs.
At her 1-month postpartum visit, the woman informed her ObGyn of occasional fecal incontinence and was told the problem would probably resolve itself. The symptoms persisted, so she was referred to a colorectal surgeon. Dissatisfied with the surgical repair, the patient sought a second surgery from another physician.
Patient’s claim The ObGyn mismanaged the second stage of labor and should have performed a cesarean section rather than used vacuum extraction. Also, the defendant was negligent in the repair of the injury and failed to provide proper follow-up care.
Doctor’s defense There was no negligence. Both the delivery and repair of the tear were performed properly.
Verdict Georgia defense verdict.
During nerve ablation, ureter is damaged
A 39-year-old woman was being treated for low libido, painful intercourse, and heavy, painful menses. When conservative treatment failed to relieve the symptoms, the patient agreed to laparoscopy as recommended by her physician. Ablation of the uterosacral nerve was performed, because the physician believed it to be causing or contributing to the symptoms. The patient’s ureter was damaged and required repair surgery.
Patient’s claim There was lack of informed consent, and the physician was negligent for injuring the ureter.
Doctor’s defense There was no negligence.
Verdict California defense verdict.
Several attempts, then laceration is repaired
A 45-year-old patient underwent a total abdominal hysterectomy. Near the end of the surgery, the nurse anesthetist noticed blood in the tubing of the urinary catheter bag, which the physician deemed a result of traumatic catheterization at the beginning of the procedure.
Despite the continued presence of blood in the urine and urinary leakage, a 4- to 5-cm laceration at the base of the bladder was not detected for 2 days. A vesicovaginal fistula developed. Over 8 months, several attempts to close the fistula surgically were unsuccessful. Eventually, it was repaired, and the patient has had no further leaks.
Patient’s claim Failure to detect and repair the laceration in a timely manner caused the fistula to develop. This condition lasted about 8 months.
Doctor’s defense The location of the laceration was difficult to find. Once it was discovered, the proper treatment was to drain the bladder with a catheter and wait several weeks to see if it could heal on its own. There was no reason for the repair attempts to fail.
Verdict $300,000 Illinois verdict.
Pain “like childbirth” is due to retained sponge
A 21-year-old woman suffered a perineal–vaginal tear during childbirth. This was repaired following delivery. A surgical sponge was inserted into the vagina to absorb blood during the repair. Two days later, the patient was discharged from the hospital and sent home.
Two days after that, she experienced pressure in the pelvic area that she likened to childbirth. When she felt something move inside her, she feared she was about to give birth to a second baby. She went to the emergency room, where the presence of the sponge was detected. According to the patient’s mother, who was also present, the pain was relieved almost instantly when the sponge was removed. In a phone call to the patient’s mother the next morning, the physician admitted he had neglected to tell the nursing staff that he had inserted the sponge and that he should have removed it.
Patient’s claim The physician was negligent for failing to remove the sponge.
Doctor’s defense There was no negligence.
Verdict Alabama defense verdict.
Perineal tear follows vacuum extraction
A 27-year-old primigravida experienced an essentially uncomplicated pregnancy during which she was monitored regularly by her ObGyn. When she went into labor and presented at the hospital, she was given an epidural, placed on a fetal monitor, examined regularly, and administered oxytocin. Because of normal progress to complete dilation and effacement, a vaginal delivery appeared likely. After 4.5 hours of second stage labor, a child weighing 8 lb 5 oz was delivered with the aid of a vacuum extractor.
During delivery of the shoulders, the mother suffered a third degree perineal tear extending to the rectal sphincter. This was noted immediately and repaired after completion of the delivery. Before the patient was discharged, she was examined and no problems were found at the site of the repairs.
At her 1-month postpartum visit, the woman informed her ObGyn of occasional fecal incontinence and was told the problem would probably resolve itself. The symptoms persisted, so she was referred to a colorectal surgeon. Dissatisfied with the surgical repair, the patient sought a second surgery from another physician.
Patient’s claim The ObGyn mismanaged the second stage of labor and should have performed a cesarean section rather than used vacuum extraction. Also, the defendant was negligent in the repair of the injury and failed to provide proper follow-up care.
Doctor’s defense There was no negligence. Both the delivery and repair of the tear were performed properly.
Verdict Georgia defense verdict.
During nerve ablation, ureter is damaged
A 39-year-old woman was being treated for low libido, painful intercourse, and heavy, painful menses. When conservative treatment failed to relieve the symptoms, the patient agreed to laparoscopy as recommended by her physician. Ablation of the uterosacral nerve was performed, because the physician believed it to be causing or contributing to the symptoms. The patient’s ureter was damaged and required repair surgery.
Patient’s claim There was lack of informed consent, and the physician was negligent for injuring the ureter.
Doctor’s defense There was no negligence.
Verdict California defense verdict.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska, of Nashville, Tenn (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; thus, pertinent details of a given situation may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.