User login
Choose Your Exam Rules
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
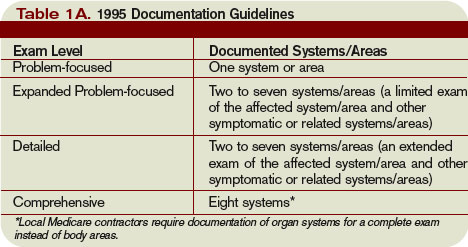
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Medical Verdicts
Missed meningitis—mother and twins die
A 46-year-old woman pregnant with twins presented to a high-risk ObGyn because of her age. She complained of having a fever for several days, cold-like symptoms, headache, and coughing. The ObGyn diagnosed an upper respiratory infection, prescribed Reglan, Pepcid, and Tussin, and asked her to return in 3 weeks. Her headache and fever continued. After a couple of weeks, she called the ObGyn three times on different days complaining of headache and fever and was advised to take over-the-counter medications. After another 2 days, she called again and was told to take Advil. The following day she died. The twins, at 30 weeks’ gestation, also died. An autopsy indicated that the woman died from untreated streptococcal meningitis.
Patient’s claim The ObGyn (1) failed to properly monitor, diagnose, and treat the patient’s condition; (2) failed to properly conduct testing that would have detected the bacterial infection; and (3) allowed her condition to worsen without treatment.
Doctor’s defense Not reported.
Verdict Florida defense verdict.
Undetected injury leads to extensive surgery
A 37-year-old woman with endometriosis that was causing pelvic pain underwent diagnostic laparoscopic surgery. During the surgery, a trocar perforated her right common iliac artery. The injury was noticed immediately, and assistance was requested. Following vascular repair surgery, the patient experienced a more complex recovery than expected.
Patient’s claim The physician was negligent in perforating the artery.
Doctor’s defense This type of injury is a known risk of the procedure. Its repair was properly handled.
Verdict $312,645 Tennessee verdict.
Alleged substance abuse hurts her infant
A 15-year-old girl with a history of smoking cigarettes, drinking alcohol, and using marijuana and crack was found to be pregnant. It was unclear if she had used the substances early in her pregnancy. When she was admitted to the hospital for delivery, oxytocin was administered over 1½ days until the infant was delivered using vacuum extraction. Neurological damage was apparent soon after delivery. The child suffers from cerebral palsy and microcephalia.
Patient’s claim Protracted labor and slow descent of the baby indicated cephalopelvic disproportion. A cesarean section should have been performed.
Doctor’s defense There was no negligence. As this was a first pregnancy, the slow progress of delivery was not unusual. The child’s neurological problems resulted from (1) maternal drug use early in the pregnancy and (2) maternal viral infection at the time of delivery.
Verdict Nebraska defense verdict.
Fetal distress or viral infection? Baby has CP
A pregnant woman several days past her due date was admitted to the hospital for induction of labor with oxytocin. Initially, the fetal heart tracing indicated no signs of distress. After a few hours, however, the heart rate pattern became irregular, and a significant deceleration occurred. As instructed, the mother began pushing. This continued for 4 hours. About 12 hours after admission, the mother gave birth to a severely depressed infant, whose Apgar score was 0 at 1 and 5 minutes. The child was resuscitated at 12 minutes and was later determined to have suffered severe asphyxia. He has cerebral palsy and spastic quadriplegia and needs 24-hour care.
Patient’s claim The defendants responded improperly to fetal distress and failed to perform a cesarean section.
Doctor’s defense Brain damage was caused by a prenatal viral infection. Also, the fetal heart tracings did not show fetal distress.
Verdict $18 million Illinois settlement: $14.5 million from the hospital; $1 million each from the obstetrician and her employer; and $1.5 million from the delivery nurse’s employer.
Second surgery rules out injury
A 51-year-old woman with a host of medical and physical problems—osteoarthritis, rheumatoid arthritis, ruptured and displaced spinal discs, irritable bowel syndrome—was taking 30 prescriptions each day, including eight for pain from providers other than her ObGyn, Dr. A. When she complained of postmenopausal bleeding and pain, but wanted to continue hormone therapy, Dr. A said that her only option was a hysterectomy. The surgery was performed. Immediately afterward, Dr. A left the practice and Dr. B, a second ObGyn, assumed the patient’s care. Following the hysterectomy, the patient suffered a postoperative abdominal hematoma, of which Dr. B was aware. For 2 to 3 days after the surgery, the patient was given hemoglobin and her blood count increased. On day 4, she began to show signs of confusion. A surgeon was called because septic infection from a perforated bowel was suspected. Laparoscopy was performed. As no source of bleeding was found in the abdomen or pelvis, her confusion was believed to be due to withdrawal from the pain medications. She acquired a hospital infection during her second hospitalization and required several weeks of inpatient therapy to recover.
Patient’s claim Dr. A injured a major artery, resulting in a hematoma. The second surgery should have been done sooner, or may even have been unnecessary.
Doctor’s defense There was no artery injury or bowel perforation. In order to rule out any bleed, the second surgery was necessary. Also, hospital infection is a known complication of surgery.
Verdict Michigan defense verdict.
Foot drop follows transvaginal taping
A 53-year-old woman underwent a transvaginal taping to correct urinary incontinence. Following surgery, she complained of pain along the side of her right leg—from her hip down to her foot. Right foot drop was diagnosed. She needs an ankle brace and cane to walk.
Patient’s claim The injury was a result of inappropriate positioning during surgery that caused pressure on her common peroneal nerve.
Doctor’s defense Most likely, the injury was secondary to a preexisting sciatic nerve dysfunction.
Verdict Illinois defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Missed meningitis—mother and twins die
A 46-year-old woman pregnant with twins presented to a high-risk ObGyn because of her age. She complained of having a fever for several days, cold-like symptoms, headache, and coughing. The ObGyn diagnosed an upper respiratory infection, prescribed Reglan, Pepcid, and Tussin, and asked her to return in 3 weeks. Her headache and fever continued. After a couple of weeks, she called the ObGyn three times on different days complaining of headache and fever and was advised to take over-the-counter medications. After another 2 days, she called again and was told to take Advil. The following day she died. The twins, at 30 weeks’ gestation, also died. An autopsy indicated that the woman died from untreated streptococcal meningitis.
Patient’s claim The ObGyn (1) failed to properly monitor, diagnose, and treat the patient’s condition; (2) failed to properly conduct testing that would have detected the bacterial infection; and (3) allowed her condition to worsen without treatment.
Doctor’s defense Not reported.
Verdict Florida defense verdict.
Undetected injury leads to extensive surgery
A 37-year-old woman with endometriosis that was causing pelvic pain underwent diagnostic laparoscopic surgery. During the surgery, a trocar perforated her right common iliac artery. The injury was noticed immediately, and assistance was requested. Following vascular repair surgery, the patient experienced a more complex recovery than expected.
Patient’s claim The physician was negligent in perforating the artery.
Doctor’s defense This type of injury is a known risk of the procedure. Its repair was properly handled.
Verdict $312,645 Tennessee verdict.
Alleged substance abuse hurts her infant
A 15-year-old girl with a history of smoking cigarettes, drinking alcohol, and using marijuana and crack was found to be pregnant. It was unclear if she had used the substances early in her pregnancy. When she was admitted to the hospital for delivery, oxytocin was administered over 1½ days until the infant was delivered using vacuum extraction. Neurological damage was apparent soon after delivery. The child suffers from cerebral palsy and microcephalia.
Patient’s claim Protracted labor and slow descent of the baby indicated cephalopelvic disproportion. A cesarean section should have been performed.
Doctor’s defense There was no negligence. As this was a first pregnancy, the slow progress of delivery was not unusual. The child’s neurological problems resulted from (1) maternal drug use early in the pregnancy and (2) maternal viral infection at the time of delivery.
Verdict Nebraska defense verdict.
Fetal distress or viral infection? Baby has CP
A pregnant woman several days past her due date was admitted to the hospital for induction of labor with oxytocin. Initially, the fetal heart tracing indicated no signs of distress. After a few hours, however, the heart rate pattern became irregular, and a significant deceleration occurred. As instructed, the mother began pushing. This continued for 4 hours. About 12 hours after admission, the mother gave birth to a severely depressed infant, whose Apgar score was 0 at 1 and 5 minutes. The child was resuscitated at 12 minutes and was later determined to have suffered severe asphyxia. He has cerebral palsy and spastic quadriplegia and needs 24-hour care.
Patient’s claim The defendants responded improperly to fetal distress and failed to perform a cesarean section.
Doctor’s defense Brain damage was caused by a prenatal viral infection. Also, the fetal heart tracings did not show fetal distress.
Verdict $18 million Illinois settlement: $14.5 million from the hospital; $1 million each from the obstetrician and her employer; and $1.5 million from the delivery nurse’s employer.
Second surgery rules out injury
A 51-year-old woman with a host of medical and physical problems—osteoarthritis, rheumatoid arthritis, ruptured and displaced spinal discs, irritable bowel syndrome—was taking 30 prescriptions each day, including eight for pain from providers other than her ObGyn, Dr. A. When she complained of postmenopausal bleeding and pain, but wanted to continue hormone therapy, Dr. A said that her only option was a hysterectomy. The surgery was performed. Immediately afterward, Dr. A left the practice and Dr. B, a second ObGyn, assumed the patient’s care. Following the hysterectomy, the patient suffered a postoperative abdominal hematoma, of which Dr. B was aware. For 2 to 3 days after the surgery, the patient was given hemoglobin and her blood count increased. On day 4, she began to show signs of confusion. A surgeon was called because septic infection from a perforated bowel was suspected. Laparoscopy was performed. As no source of bleeding was found in the abdomen or pelvis, her confusion was believed to be due to withdrawal from the pain medications. She acquired a hospital infection during her second hospitalization and required several weeks of inpatient therapy to recover.
Patient’s claim Dr. A injured a major artery, resulting in a hematoma. The second surgery should have been done sooner, or may even have been unnecessary.
Doctor’s defense There was no artery injury or bowel perforation. In order to rule out any bleed, the second surgery was necessary. Also, hospital infection is a known complication of surgery.
Verdict Michigan defense verdict.
Foot drop follows transvaginal taping
A 53-year-old woman underwent a transvaginal taping to correct urinary incontinence. Following surgery, she complained of pain along the side of her right leg—from her hip down to her foot. Right foot drop was diagnosed. She needs an ankle brace and cane to walk.
Patient’s claim The injury was a result of inappropriate positioning during surgery that caused pressure on her common peroneal nerve.
Doctor’s defense Most likely, the injury was secondary to a preexisting sciatic nerve dysfunction.
Verdict Illinois defense verdict.
Missed meningitis—mother and twins die
A 46-year-old woman pregnant with twins presented to a high-risk ObGyn because of her age. She complained of having a fever for several days, cold-like symptoms, headache, and coughing. The ObGyn diagnosed an upper respiratory infection, prescribed Reglan, Pepcid, and Tussin, and asked her to return in 3 weeks. Her headache and fever continued. After a couple of weeks, she called the ObGyn three times on different days complaining of headache and fever and was advised to take over-the-counter medications. After another 2 days, she called again and was told to take Advil. The following day she died. The twins, at 30 weeks’ gestation, also died. An autopsy indicated that the woman died from untreated streptococcal meningitis.
Patient’s claim The ObGyn (1) failed to properly monitor, diagnose, and treat the patient’s condition; (2) failed to properly conduct testing that would have detected the bacterial infection; and (3) allowed her condition to worsen without treatment.
Doctor’s defense Not reported.
Verdict Florida defense verdict.
Undetected injury leads to extensive surgery
A 37-year-old woman with endometriosis that was causing pelvic pain underwent diagnostic laparoscopic surgery. During the surgery, a trocar perforated her right common iliac artery. The injury was noticed immediately, and assistance was requested. Following vascular repair surgery, the patient experienced a more complex recovery than expected.
Patient’s claim The physician was negligent in perforating the artery.
Doctor’s defense This type of injury is a known risk of the procedure. Its repair was properly handled.
Verdict $312,645 Tennessee verdict.
Alleged substance abuse hurts her infant
A 15-year-old girl with a history of smoking cigarettes, drinking alcohol, and using marijuana and crack was found to be pregnant. It was unclear if she had used the substances early in her pregnancy. When she was admitted to the hospital for delivery, oxytocin was administered over 1½ days until the infant was delivered using vacuum extraction. Neurological damage was apparent soon after delivery. The child suffers from cerebral palsy and microcephalia.
Patient’s claim Protracted labor and slow descent of the baby indicated cephalopelvic disproportion. A cesarean section should have been performed.
Doctor’s defense There was no negligence. As this was a first pregnancy, the slow progress of delivery was not unusual. The child’s neurological problems resulted from (1) maternal drug use early in the pregnancy and (2) maternal viral infection at the time of delivery.
Verdict Nebraska defense verdict.
Fetal distress or viral infection? Baby has CP
A pregnant woman several days past her due date was admitted to the hospital for induction of labor with oxytocin. Initially, the fetal heart tracing indicated no signs of distress. After a few hours, however, the heart rate pattern became irregular, and a significant deceleration occurred. As instructed, the mother began pushing. This continued for 4 hours. About 12 hours after admission, the mother gave birth to a severely depressed infant, whose Apgar score was 0 at 1 and 5 minutes. The child was resuscitated at 12 minutes and was later determined to have suffered severe asphyxia. He has cerebral palsy and spastic quadriplegia and needs 24-hour care.
Patient’s claim The defendants responded improperly to fetal distress and failed to perform a cesarean section.
Doctor’s defense Brain damage was caused by a prenatal viral infection. Also, the fetal heart tracings did not show fetal distress.
Verdict $18 million Illinois settlement: $14.5 million from the hospital; $1 million each from the obstetrician and her employer; and $1.5 million from the delivery nurse’s employer.
Second surgery rules out injury
A 51-year-old woman with a host of medical and physical problems—osteoarthritis, rheumatoid arthritis, ruptured and displaced spinal discs, irritable bowel syndrome—was taking 30 prescriptions each day, including eight for pain from providers other than her ObGyn, Dr. A. When she complained of postmenopausal bleeding and pain, but wanted to continue hormone therapy, Dr. A said that her only option was a hysterectomy. The surgery was performed. Immediately afterward, Dr. A left the practice and Dr. B, a second ObGyn, assumed the patient’s care. Following the hysterectomy, the patient suffered a postoperative abdominal hematoma, of which Dr. B was aware. For 2 to 3 days after the surgery, the patient was given hemoglobin and her blood count increased. On day 4, she began to show signs of confusion. A surgeon was called because septic infection from a perforated bowel was suspected. Laparoscopy was performed. As no source of bleeding was found in the abdomen or pelvis, her confusion was believed to be due to withdrawal from the pain medications. She acquired a hospital infection during her second hospitalization and required several weeks of inpatient therapy to recover.
Patient’s claim Dr. A injured a major artery, resulting in a hematoma. The second surgery should have been done sooner, or may even have been unnecessary.
Doctor’s defense There was no artery injury or bowel perforation. In order to rule out any bleed, the second surgery was necessary. Also, hospital infection is a known complication of surgery.
Verdict Michigan defense verdict.
Foot drop follows transvaginal taping
A 53-year-old woman underwent a transvaginal taping to correct urinary incontinence. Following surgery, she complained of pain along the side of her right leg—from her hip down to her foot. Right foot drop was diagnosed. She needs an ankle brace and cane to walk.
Patient’s claim The injury was a result of inappropriate positioning during surgery that caused pressure on her common peroneal nerve.
Doctor’s defense Most likely, the injury was secondary to a preexisting sciatic nerve dysfunction.
Verdict Illinois defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Deposition Dos and Don’ts: How to answer 8 tricky questions
CASE Direct question at deposition
During your deposition in a malpractice suit, plaintiff’s counsel asks you: “Are you saying it was impossible to foresee Ms. Jones’s preterm premature rupture of membranes?”
How would you reply?
Ninety percent of malpractice cases are settled before trial, and the deposition often is the turning point in those cases.1-3 Your answer to tricky questions such as the one in the case fragment above could favorably affect a critical stage of litigation—or it might spur the plaintiff’s attorney to pursue the case more vigorously. Even if a case is settled in the plaintiff’s favor before trial, the effectiveness of the deposition may determine whether the settlement is $300,000 or $1 million.
Our central message in this article is: Don’t go to a deposition unprepared. We offer guidelines to help you anticipate many different scenarios, and we include examples of honest, skillful answers to difficult questions (see “Honest, skillful answers to 8 tricky questions at deposition”).3-7
Digging for pay dirt
Discovery begins after a formal complaint alleges malpractice. The parties to a lawsuit gather information through written interrogatories, requests for documents, and witness depositions—out-of-court testimony to be used later in court or for discovery purposes.8 The rationale for discovery is to reduce surprises at trial and encourage pretrial settlement. The witness being deposed is the deponent, and testimony is given under oath.9
A discovery deposition is designed to gather information, with almost all questions asked by opposing counsel. If you are sued for malpractice, this is the type of deposition you probably will encounter.
Rules of engagement. The plaintiff’s attorney initiates the discovery deposition. Ground rules vary by jurisdiction, but, in general, the Rules of Civil Procedure give deposing counsel substantial latitude in the questions that can be asked.10 The deponent and defending counsel, opposing counsel, and transcriptionist typically attend the deposition. To help you prepare appropriately, confirm with your defense counsel if other attorneys or the plaintiff will be present.
Not-so-hidden agendas. The plaintiff’s attorney’s primary goal is to gather as much information as possible about your side’s case4 (TABLE 1). No matter how accurate medical records may be, they require interpretation and follow-up questioning of key players to get the full story. Opposing counsel also wants to:
- “lock down” your testimony for use at trial (testimony captured at a deposition can be used to impeach a witness who gives inconsistent testimony at trial)9
- “size up” your potential impact on a jury by assessing your strengths and weaknesses as a witness.11
The impression you make may influence the opposing attorney’s decision about how far to pursue the case. Plaintiff’s attorney Bruce Fagel once told an interviewer that defense attorneys, too, may consider settling a case “if their client shows such arrogance in our deposition that they’re afraid to let him appear in front of a jury.”12
TABLE 1
Plaintiff’s attorney has 5 goals at deposition
| Lock down testimony for trial |
| Scrutinize the defendant’s qualifications |
| Size up the defendant’s effectiveness as a witness |
| Probe the defendant for bias, arrogance, or hostility |
| Learn as much as possible—known as “fishing” |
Choosing a site. Most depositions take place in a conference room in the law office of one of the attorneys or at a neutral site. Avoid any temptation to schedule the deposition in your office, even though meeting there might seem more expedient and comfortable for you.9 Scheduling the deposition at your site:
- might make you feel it is “just another day at the office” and dissuade you from preparing sufficiently or taking the deposition seriously
- allows opposing counsel to scrutinize diplomas, books, journals, and other materials in your office.
Questioning you about these materials during the deposition is not off-limits for the plaintiff’s attorney. You might find it difficult to explain why a book on your bookshelf is not “authoritative.”
Prepare, prepare, and…prepare some more
Your emotional stress will probably wax and wane during the lengthy litigation process.13,14 Knowing what to expect and being well-prepared for the deposition may relieve some anxiety.
Review the case. At least twice, carefully review the entire database—including medical records and other depositions. Perform one of these reviews just before the deposition.3 Having the details fresh in mind will help you if opposing counsel mischaracterizes information when questioning you.
Meet with your attorney. Insist on at least two predeposition conferences with defense counsel.
At the first conference, volunteer all pertinent information about the case as well as any noteworthy medical inconsistencies.2 Find out what documents to bring to the deposition, who will be present, and how long the deposition is expected to take. You might wish to prepare mentally by inquiring about the style and personality of opposing counsel.
Defense counsel does not control how long a deposition lasts but might be able to give a rough estimate. Plan accordingly, and allow for sufficient scheduling flexibility. Depositions typically last half a day but can last more than 1 day.
At a later predeposition conference, defense counsel might walk you through a mock deposition that involves difficult or anticipated questions. This is a good opportunity to master your anxiety and improve your effectiveness as a witness.
You also may wish to go over your curriculum vitae with defense counsel and check it for mistakes or other content that might raise problematic questions during the deposition (TABLE 2). Make sure your CV is up-to-date, and refresh your memory if it lists lectures given or articles written—no matter how long ago—on topics related to the litigation.
TABLE 2
Step by step, prepping for a deposition
| Thoroughly review case records |
| Master the case (memorize key names, dates, facts) |
| Meet with defense counsel at least twice to: |
| —find out where the deposition is being held, who will be present, and how long it is expected to take —learn what documents to bring —understand opposing counsel’s style and personality —prepare for difficult questions —consider holding a mock deposition |
| Double-check your curriculum vitae for accuracy and updating |
| Come to the deposition well-rested |
Don’t open Pandora’s box! Keep your answers to deposition questions brief and clear. Opposing counsel may ask broad questions, hoping to encourage rambling answers that reveal new facts. Answering questions succinctly and briefly is the best strategy under most circumstances.
One exception may involve scenarios in which the defense attorney instructs you, for various reasons, to provide information beyond the question asked. For example, when a case is close to settling, your attorney might instruct you to lay out all evidence that supports your professional judgment and clinical decisions in the case. Do not use this approach, however, unless your attorney specifically instructs you to do so.
You are under no obligation to make opposing counsel’s job easier. In a discovery deposition, volunteering information may:
- open up new areas for questioning
- equip the deposing attorney with more ammunition
- eliminate opportunities for your attorney to use surprise as a strategy, should the case go to trial.
Consider, for example, a scenario in which you and a hospital are sued in regard to a labor-and-delivery case. At deposition, you might be asked whether you can identify written evidence in the patient’s chart that the mother was checked every certain number of minutes.
The correct answer is “No,” even though you know such checks are documented in a log kept at the nursing station in that hospital. You might be tempted to reveal this information, but don’t—instead, leave the timing of its disclosure to the defense attorney. Your attorney’s strategy may be to reveal this critical piece of information at trial, when the plaintiff’s attorney has less opportunity to strategize ways to discredit the evidence.
Keep your cool. Attorneys have different styles of questioning. Some may be excessively friendly or polite to get you to let down your guard—only to set you up for a devastating blow at the end of the deposition (or to save this for trial). Other attorneys might employ a bullying style that seeks to intimidate. In responding, always remain composed and resist the urge to counterattack.
In all circumstances, strive for humility and dignified confidence. Opposing counsel gains the advantage when defendants lose composure or become angry, defensive, or arrogant. Indeed, experienced plaintiff’s attorneys may be testing for precisely this reaction in the hope that a defendant will “demonstrate his arrogance” during the deposition or later on the witness stand.12
In working as expert witnesses in malpractice cases, we have observed many instances in which a defendant physician’s arrogant or hostile remarks at deposition played a key role in causing the case to be prematurely settled in the plaintiff’s favor.
Avoid making jokes or sarcastic comments. Even a well-timed, self-deprecating joke may backfire should opposing counsel take the opportunity to point out that the case is a “serious matter.”
Listen carefully to each question during the deposition. Pause for a moment to consider the question and allow time for other attorneys to object.5 Your attorney’s objection may suggest the best way for you to respond to the question. Refrain from answering any questions when defense counsel advises you to do so (TABLE 3).
Don’t answer questions you don’t understand. Rather, ask for clarification. Avoid using adjectives and superlatives such as “never” and “always,” which may be used to distort or mischaracterize your testimony at trial.
Don’t guess. No rule prevents opposing counsel from asking a witness to speculate, but you should generally avoid doing so. You are required to tell the truth, not to speculate or to volunteer guesses. The best way to cause a jury to disbelieve your testimony is to make inaccurate or unfounded statements, which opposing counsel will surely point out at trial.
Don’t be tempted to “plumb the depths” of your memory for a forgotten piece of information, however. If you’re asked, for example, if a patient displayed a specific symptom during an appointment 4 years ago, the true answer is likely to be “Not that I recall,” rather than “No.” Qualify similar answers with statements such as “To the best of my recollection” or “Not that I recall at this time.”
If opposing counsel asks questions based on a particular document, ask to see the document. Review it carefully to determine:
- who signed or authored it
- when it was prepared and dated
- whether it is a draft copy
- whether it contains confidential information relating to patients other than the plaintiff
- whether it carries attorney–client privilege
- most important, whether opposing counsel has quoted it out of context.
TABLE 3
Deposition Dos and Don’ts
| Always tell the truth |
| Actively listen to questions, and pause before answering |
| Keep your cool; never lose composure |
| Answer only the question asked |
| Stop speaking and listen carefully if your attorney makes an objection |
| Avoid long narratives, and don’t volunteer information |
| Don’t speculate or guess |
| Avoid absolutes such as “never” or “always” |
| Avoid jokes, sarcasm, and edgy comments |
| Ask for breaks if needed to keep from becoming inattentive |
| Carefully examine documents, reports, etc., before answering opposing counsel’s questions about them |
| Ask for clarification of confusing questions |
| Remember: Nothing is “off the record” |
| Don’t waive your right to read and sign the deposition transcript |
Procedural pitfalls. Throughout the deposition, attorneys may periodically tell the court reporter that they wish to have a discussion “off the record.” Nothing is off the record for you, however. If you make a statement when the court reporter has been told to stop, opposing counsel can summarize on the record everything you said during that time.
At the beginning or end of the deposition, one of the attorneys may ask if you wish to waive the right to read and sign the deposition transcript. Seek your counsel’s advice, but defendants usually choose to retain this right. Typically, you have 30 days to read the transcript and correct errors. Keep in mind that substantive changes beyond typos are likely to be the subject of intense cross-examination if the case goes to trial.9
Depositions are sometimes videotaped, usually because a witness will not be available at the time of trial. Because the jury will hear and see you, approach a videotaped deposition as if it were an actual trial. Dress appropriately, speak clearly, and look directly into the camera. Don’t feel embarrassed about making sure that you are taped with the best possible lighting, camera angle, and background.
Keep your guard up!
Don’t allow yourself to be distracted if opposing counsel jumps from open-ended questions to clarification questions to “pinning-down” questions. An erratic approach could be part of opposing counsel’s strategy. Answer only the question asked, and give the shortest correct answer possible to each question.
Opposing counsel may ask a question in a way that suggests substantial confusion or misunderstanding. If this confusion does not affect your testimony, you don’t need to clear up matters for opposing counsel. If, for example, opposing counsel asserts that one of your statements is contradictory, an appropriate response may be simply, “No, it wasn’t.” It is opposing counsel’s job to explicate further details.11
Opposing counsel may approach the deposition with a particular demeanor—friendly, eager to learn—in an attempt to get you to let down your guard and speak more freely (see “Personae sometimes adopted by plaintiffs’ attorneys to obtain information at deposition”).
During a full-day deposition, particularly, the greatest likelihood of making a mistake begins around 4 pm. Some attorneys may reserve especially important questions for this time, hoping that the witness will be less guarded. Start the day well-rested and ask for breaks if fatigue begins to affect your concentration.
Be alert to questioning designed to elicit only “Yes” answers. This technique—often used by salespersons—makes it difficult to say “No” in response to an ambiguous question. Last, point out errors if opposing counsel misquotes earlier testimony or states facts incorrectly. These mistakes may be innocent, or an attempt to distort your testimony.
“Mr./Ms. Friendly” Some attorneys look for an opportunity, before the deposition begins, to show that they are “friendly” and not to be feared. Remember: Discussions with opposing counsel without defense counsel present are inappropriate.
“Eager Student” Opposing counsel may play the “eager student” to massage your ego and pave the way for long narratives and volunteered information.
“Counselor Clueless” Opposing counsel may appear so ignorant of certain facts that you can scarcely resist jumping in to educate him or her.
“Mr./Ms. Silent Treatment” After you give a brief, honest answer, opposing counsel may sit silently as if expecting a more substantive response. Resist the temptation to fill the silence.
CASE RESOLVED Direct question at deposition
You reply to plaintiff’s attorney: “I don’t know how the rupturing of membranes in this case could have been foreseen.”
THE IMPOSSIBLE DREAM
In law, there is a distinction between possibility and probability. The law considers anything possible, but something isn’t probable unless it is more likely than not—that is, when expressed mathematically, its chances are ≥51%.
Q. Doctor, are you saying it was impossible to foresee Ms. Jones’ preterm premature rupture of membranes?
A. I don’t know of any way that the rupturing of membranes could have been foreseen. It was an unfortunate event that was not possible to foresee.
THE HYPOTHETICAL
When confronted with questions containing a hypothetical, identify the hidden assumption before answering.
Q. Doctor, with a depressed pregnant patient, would you agree that the standard of care requires you to…?
A. I can’t agree with you that, in this case, we are talking about a depressed patient. Do you still want me to answer the question? OR
A. I can’t answer that based on the few facts you’ve given me. I’d need to examine that patient first.
INVITATION TO SPECULATE
Refrain from speculating, especially when you’ve been presented with an incomplete clinical picture.
Q. Doctor, is it fair to say that a patient with this history should be referred to a specialist in high-risk pregnancy?
A. I really can’t speculate based on that limited information—I’d just be guessing.
DID I SAY THAT?
Opposing counsel may mischaracterize or distort your testimony by attempting to paraphrase what you’ve said.
Q. Now doctor, as I understand it, what you’re really saying is that the patient…?
A. No. OR
A. No—that’s not an accurate summary of what I just said.
THE AUTHORITATIVE TREATISE
Opposing counsel wants you to acknowledge a specific piece of literature as ‘authoritative’ in gynecology, so that counsel can then impeach you at trial with points from the literature that contradict your testimony. Although you may be made to look foolish if you refuse to acknowledge anything as authoritative, that usually is the safest course.
Q. Doctor, do you accept Williams Obstetrics as an authoritative reference in your field?
A. It is certainly well-respected, but the entire text can’t be considered authoritative. OR
A. Significant portions may be authoritative, but I would need to see the portion in question to be able to answer your question.
THE TYRANNY OF YES OR NO
In an effort to control you, opposing counsel may demand only “Yes” or “No” answers. Listen closely to each question, and determine if you can convey the whole truth with “Yes” or “No.” Asking to further explain to avoid giving a misleading answer will make opposing counsel appear defensive if he (she) does not agree.
Q. Doctor, please answer the question; it requires only a simple “Yes” or “No.”
A. I cannot answer that question with only a “Yes” or “No.” Would you like me to explain? OR
A. A mere “Yes” or “No” answer to that question would be misleading. May I explain?
CONVOLUTED COMPOUNDS
When opposing counsel asks you a double- or triple-jointed question, ask her to reframe or break down the inquiry into simpler questions.
Q. Doctor, would you agree that a woman with a family history of diabetes who is taking…should be tested for…at least once a month, and that if there is evidence of…then the standard of care requires you to…?
A. Please repeat those questions again, one at a time.
GIVE ME MORE
Opposing counsel may try to “fish” for more information. You are under no obligation to make his job easier. Answers that contain a qualifier are useful.
Q. Doctor, to your knowledge, have you told me everything you consider important about your patient’s death after she hemorrhaged?
A. I have told you all the information I can remember at this time.
1. Babitsky S, Mangraviti J. The discovery process. In: How to Become a Dangerous Expert Witness: Advanced Techniques and Strategies. Falmouth, Mass: Seak Inc; 2005:4-9:113-139.
2. Clark A, Fox P. The defendant physician’s deposition: fighting back—at last! Mo Med. 2002;99(10):524-525.
3. Rice B. Malpractice: how to survive a deposition. Med Econ. 2005;82:45-48.
4. Babitsky S, Mangraviti J. How to Excel during Depositions: Techniques for Experts that Work. Falmouth, Mass: Seak Inc; 1998.
5. Gutheil T. The Psychiatrist as Expert Witness. Washington, DC: American Psychiatric Publishing, Inc; 1998.
6. Babitsky S, Mangraviti J. How to Excel during Cross-Examination: Techniques for Experts that Work. Falmouth, Mass: Seak Inc; 1997.
7. Hirsch C, Morris R, Moritz A. Handbook of Legal Medicine. 5th ed. St. Louis, Mo: CV Mosby Co; 1979.
8. Black H. Black’s Law Dictionary. 8th ed. St. Paul, Minn: West Publishing; 2004;440
9. Babitsky S, Mangraviti J. Depositions: The Comprehensive Guide for Expert Witnesses. Falmouth, Mass: Seak Inc; 2007.
10. Cornell Law School. Federal Rules of Civil Procedure. Depositions and discovery. Rule 26(5) B(1). Available at: http://www.law.cornell.edu/rules/frcp/Rule26.htm. Accessed April 10, 2008.
11. Culley CA, Jr, Spisak LJ. So you’re being sued: do’s and don’ts for the defendant. Cleve Clin J Med. 2002;69:752-760.
12. Rice B. How I pick the doctors I’ll sue. Med Econ. 2004;81:54.-
13. Charles S. Coping with a medical malpractice suit. West J Med. 2001;174:55-58.
14. Charles SC. Got malpractice distress? You can help yourself survive. OBG Management. 2008;20(2):38-51.
CASE Direct question at deposition
During your deposition in a malpractice suit, plaintiff’s counsel asks you: “Are you saying it was impossible to foresee Ms. Jones’s preterm premature rupture of membranes?”
How would you reply?
Ninety percent of malpractice cases are settled before trial, and the deposition often is the turning point in those cases.1-3 Your answer to tricky questions such as the one in the case fragment above could favorably affect a critical stage of litigation—or it might spur the plaintiff’s attorney to pursue the case more vigorously. Even if a case is settled in the plaintiff’s favor before trial, the effectiveness of the deposition may determine whether the settlement is $300,000 or $1 million.
Our central message in this article is: Don’t go to a deposition unprepared. We offer guidelines to help you anticipate many different scenarios, and we include examples of honest, skillful answers to difficult questions (see “Honest, skillful answers to 8 tricky questions at deposition”).3-7
Digging for pay dirt
Discovery begins after a formal complaint alleges malpractice. The parties to a lawsuit gather information through written interrogatories, requests for documents, and witness depositions—out-of-court testimony to be used later in court or for discovery purposes.8 The rationale for discovery is to reduce surprises at trial and encourage pretrial settlement. The witness being deposed is the deponent, and testimony is given under oath.9
A discovery deposition is designed to gather information, with almost all questions asked by opposing counsel. If you are sued for malpractice, this is the type of deposition you probably will encounter.
Rules of engagement. The plaintiff’s attorney initiates the discovery deposition. Ground rules vary by jurisdiction, but, in general, the Rules of Civil Procedure give deposing counsel substantial latitude in the questions that can be asked.10 The deponent and defending counsel, opposing counsel, and transcriptionist typically attend the deposition. To help you prepare appropriately, confirm with your defense counsel if other attorneys or the plaintiff will be present.
Not-so-hidden agendas. The plaintiff’s attorney’s primary goal is to gather as much information as possible about your side’s case4 (TABLE 1). No matter how accurate medical records may be, they require interpretation and follow-up questioning of key players to get the full story. Opposing counsel also wants to:
- “lock down” your testimony for use at trial (testimony captured at a deposition can be used to impeach a witness who gives inconsistent testimony at trial)9
- “size up” your potential impact on a jury by assessing your strengths and weaknesses as a witness.11
The impression you make may influence the opposing attorney’s decision about how far to pursue the case. Plaintiff’s attorney Bruce Fagel once told an interviewer that defense attorneys, too, may consider settling a case “if their client shows such arrogance in our deposition that they’re afraid to let him appear in front of a jury.”12
TABLE 1
Plaintiff’s attorney has 5 goals at deposition
| Lock down testimony for trial |
| Scrutinize the defendant’s qualifications |
| Size up the defendant’s effectiveness as a witness |
| Probe the defendant for bias, arrogance, or hostility |
| Learn as much as possible—known as “fishing” |
Choosing a site. Most depositions take place in a conference room in the law office of one of the attorneys or at a neutral site. Avoid any temptation to schedule the deposition in your office, even though meeting there might seem more expedient and comfortable for you.9 Scheduling the deposition at your site:
- might make you feel it is “just another day at the office” and dissuade you from preparing sufficiently or taking the deposition seriously
- allows opposing counsel to scrutinize diplomas, books, journals, and other materials in your office.
Questioning you about these materials during the deposition is not off-limits for the plaintiff’s attorney. You might find it difficult to explain why a book on your bookshelf is not “authoritative.”
Prepare, prepare, and…prepare some more
Your emotional stress will probably wax and wane during the lengthy litigation process.13,14 Knowing what to expect and being well-prepared for the deposition may relieve some anxiety.
Review the case. At least twice, carefully review the entire database—including medical records and other depositions. Perform one of these reviews just before the deposition.3 Having the details fresh in mind will help you if opposing counsel mischaracterizes information when questioning you.
Meet with your attorney. Insist on at least two predeposition conferences with defense counsel.
At the first conference, volunteer all pertinent information about the case as well as any noteworthy medical inconsistencies.2 Find out what documents to bring to the deposition, who will be present, and how long the deposition is expected to take. You might wish to prepare mentally by inquiring about the style and personality of opposing counsel.
Defense counsel does not control how long a deposition lasts but might be able to give a rough estimate. Plan accordingly, and allow for sufficient scheduling flexibility. Depositions typically last half a day but can last more than 1 day.
At a later predeposition conference, defense counsel might walk you through a mock deposition that involves difficult or anticipated questions. This is a good opportunity to master your anxiety and improve your effectiveness as a witness.
You also may wish to go over your curriculum vitae with defense counsel and check it for mistakes or other content that might raise problematic questions during the deposition (TABLE 2). Make sure your CV is up-to-date, and refresh your memory if it lists lectures given or articles written—no matter how long ago—on topics related to the litigation.
TABLE 2
Step by step, prepping for a deposition
| Thoroughly review case records |
| Master the case (memorize key names, dates, facts) |
| Meet with defense counsel at least twice to: |
| —find out where the deposition is being held, who will be present, and how long it is expected to take —learn what documents to bring —understand opposing counsel’s style and personality —prepare for difficult questions —consider holding a mock deposition |
| Double-check your curriculum vitae for accuracy and updating |
| Come to the deposition well-rested |
Don’t open Pandora’s box! Keep your answers to deposition questions brief and clear. Opposing counsel may ask broad questions, hoping to encourage rambling answers that reveal new facts. Answering questions succinctly and briefly is the best strategy under most circumstances.
One exception may involve scenarios in which the defense attorney instructs you, for various reasons, to provide information beyond the question asked. For example, when a case is close to settling, your attorney might instruct you to lay out all evidence that supports your professional judgment and clinical decisions in the case. Do not use this approach, however, unless your attorney specifically instructs you to do so.
You are under no obligation to make opposing counsel’s job easier. In a discovery deposition, volunteering information may:
- open up new areas for questioning
- equip the deposing attorney with more ammunition
- eliminate opportunities for your attorney to use surprise as a strategy, should the case go to trial.
Consider, for example, a scenario in which you and a hospital are sued in regard to a labor-and-delivery case. At deposition, you might be asked whether you can identify written evidence in the patient’s chart that the mother was checked every certain number of minutes.
The correct answer is “No,” even though you know such checks are documented in a log kept at the nursing station in that hospital. You might be tempted to reveal this information, but don’t—instead, leave the timing of its disclosure to the defense attorney. Your attorney’s strategy may be to reveal this critical piece of information at trial, when the plaintiff’s attorney has less opportunity to strategize ways to discredit the evidence.
Keep your cool. Attorneys have different styles of questioning. Some may be excessively friendly or polite to get you to let down your guard—only to set you up for a devastating blow at the end of the deposition (or to save this for trial). Other attorneys might employ a bullying style that seeks to intimidate. In responding, always remain composed and resist the urge to counterattack.
In all circumstances, strive for humility and dignified confidence. Opposing counsel gains the advantage when defendants lose composure or become angry, defensive, or arrogant. Indeed, experienced plaintiff’s attorneys may be testing for precisely this reaction in the hope that a defendant will “demonstrate his arrogance” during the deposition or later on the witness stand.12
In working as expert witnesses in malpractice cases, we have observed many instances in which a defendant physician’s arrogant or hostile remarks at deposition played a key role in causing the case to be prematurely settled in the plaintiff’s favor.
Avoid making jokes or sarcastic comments. Even a well-timed, self-deprecating joke may backfire should opposing counsel take the opportunity to point out that the case is a “serious matter.”
Listen carefully to each question during the deposition. Pause for a moment to consider the question and allow time for other attorneys to object.5 Your attorney’s objection may suggest the best way for you to respond to the question. Refrain from answering any questions when defense counsel advises you to do so (TABLE 3).
Don’t answer questions you don’t understand. Rather, ask for clarification. Avoid using adjectives and superlatives such as “never” and “always,” which may be used to distort or mischaracterize your testimony at trial.
Don’t guess. No rule prevents opposing counsel from asking a witness to speculate, but you should generally avoid doing so. You are required to tell the truth, not to speculate or to volunteer guesses. The best way to cause a jury to disbelieve your testimony is to make inaccurate or unfounded statements, which opposing counsel will surely point out at trial.
Don’t be tempted to “plumb the depths” of your memory for a forgotten piece of information, however. If you’re asked, for example, if a patient displayed a specific symptom during an appointment 4 years ago, the true answer is likely to be “Not that I recall,” rather than “No.” Qualify similar answers with statements such as “To the best of my recollection” or “Not that I recall at this time.”
If opposing counsel asks questions based on a particular document, ask to see the document. Review it carefully to determine:
- who signed or authored it
- when it was prepared and dated
- whether it is a draft copy
- whether it contains confidential information relating to patients other than the plaintiff
- whether it carries attorney–client privilege
- most important, whether opposing counsel has quoted it out of context.
TABLE 3
Deposition Dos and Don’ts
| Always tell the truth |
| Actively listen to questions, and pause before answering |
| Keep your cool; never lose composure |
| Answer only the question asked |
| Stop speaking and listen carefully if your attorney makes an objection |
| Avoid long narratives, and don’t volunteer information |
| Don’t speculate or guess |
| Avoid absolutes such as “never” or “always” |
| Avoid jokes, sarcasm, and edgy comments |
| Ask for breaks if needed to keep from becoming inattentive |
| Carefully examine documents, reports, etc., before answering opposing counsel’s questions about them |
| Ask for clarification of confusing questions |
| Remember: Nothing is “off the record” |
| Don’t waive your right to read and sign the deposition transcript |
Procedural pitfalls. Throughout the deposition, attorneys may periodically tell the court reporter that they wish to have a discussion “off the record.” Nothing is off the record for you, however. If you make a statement when the court reporter has been told to stop, opposing counsel can summarize on the record everything you said during that time.
At the beginning or end of the deposition, one of the attorneys may ask if you wish to waive the right to read and sign the deposition transcript. Seek your counsel’s advice, but defendants usually choose to retain this right. Typically, you have 30 days to read the transcript and correct errors. Keep in mind that substantive changes beyond typos are likely to be the subject of intense cross-examination if the case goes to trial.9
Depositions are sometimes videotaped, usually because a witness will not be available at the time of trial. Because the jury will hear and see you, approach a videotaped deposition as if it were an actual trial. Dress appropriately, speak clearly, and look directly into the camera. Don’t feel embarrassed about making sure that you are taped with the best possible lighting, camera angle, and background.
Keep your guard up!
Don’t allow yourself to be distracted if opposing counsel jumps from open-ended questions to clarification questions to “pinning-down” questions. An erratic approach could be part of opposing counsel’s strategy. Answer only the question asked, and give the shortest correct answer possible to each question.
Opposing counsel may ask a question in a way that suggests substantial confusion or misunderstanding. If this confusion does not affect your testimony, you don’t need to clear up matters for opposing counsel. If, for example, opposing counsel asserts that one of your statements is contradictory, an appropriate response may be simply, “No, it wasn’t.” It is opposing counsel’s job to explicate further details.11
Opposing counsel may approach the deposition with a particular demeanor—friendly, eager to learn—in an attempt to get you to let down your guard and speak more freely (see “Personae sometimes adopted by plaintiffs’ attorneys to obtain information at deposition”).
During a full-day deposition, particularly, the greatest likelihood of making a mistake begins around 4 pm. Some attorneys may reserve especially important questions for this time, hoping that the witness will be less guarded. Start the day well-rested and ask for breaks if fatigue begins to affect your concentration.
Be alert to questioning designed to elicit only “Yes” answers. This technique—often used by salespersons—makes it difficult to say “No” in response to an ambiguous question. Last, point out errors if opposing counsel misquotes earlier testimony or states facts incorrectly. These mistakes may be innocent, or an attempt to distort your testimony.
“Mr./Ms. Friendly” Some attorneys look for an opportunity, before the deposition begins, to show that they are “friendly” and not to be feared. Remember: Discussions with opposing counsel without defense counsel present are inappropriate.
“Eager Student” Opposing counsel may play the “eager student” to massage your ego and pave the way for long narratives and volunteered information.
“Counselor Clueless” Opposing counsel may appear so ignorant of certain facts that you can scarcely resist jumping in to educate him or her.
“Mr./Ms. Silent Treatment” After you give a brief, honest answer, opposing counsel may sit silently as if expecting a more substantive response. Resist the temptation to fill the silence.
CASE RESOLVED Direct question at deposition
You reply to plaintiff’s attorney: “I don’t know how the rupturing of membranes in this case could have been foreseen.”
THE IMPOSSIBLE DREAM
In law, there is a distinction between possibility and probability. The law considers anything possible, but something isn’t probable unless it is more likely than not—that is, when expressed mathematically, its chances are ≥51%.
Q. Doctor, are you saying it was impossible to foresee Ms. Jones’ preterm premature rupture of membranes?
A. I don’t know of any way that the rupturing of membranes could have been foreseen. It was an unfortunate event that was not possible to foresee.
THE HYPOTHETICAL
When confronted with questions containing a hypothetical, identify the hidden assumption before answering.
Q. Doctor, with a depressed pregnant patient, would you agree that the standard of care requires you to…?
A. I can’t agree with you that, in this case, we are talking about a depressed patient. Do you still want me to answer the question? OR
A. I can’t answer that based on the few facts you’ve given me. I’d need to examine that patient first.
INVITATION TO SPECULATE
Refrain from speculating, especially when you’ve been presented with an incomplete clinical picture.
Q. Doctor, is it fair to say that a patient with this history should be referred to a specialist in high-risk pregnancy?
A. I really can’t speculate based on that limited information—I’d just be guessing.
DID I SAY THAT?
Opposing counsel may mischaracterize or distort your testimony by attempting to paraphrase what you’ve said.
Q. Now doctor, as I understand it, what you’re really saying is that the patient…?
A. No. OR
A. No—that’s not an accurate summary of what I just said.
THE AUTHORITATIVE TREATISE
Opposing counsel wants you to acknowledge a specific piece of literature as ‘authoritative’ in gynecology, so that counsel can then impeach you at trial with points from the literature that contradict your testimony. Although you may be made to look foolish if you refuse to acknowledge anything as authoritative, that usually is the safest course.
Q. Doctor, do you accept Williams Obstetrics as an authoritative reference in your field?
A. It is certainly well-respected, but the entire text can’t be considered authoritative. OR
A. Significant portions may be authoritative, but I would need to see the portion in question to be able to answer your question.
THE TYRANNY OF YES OR NO
In an effort to control you, opposing counsel may demand only “Yes” or “No” answers. Listen closely to each question, and determine if you can convey the whole truth with “Yes” or “No.” Asking to further explain to avoid giving a misleading answer will make opposing counsel appear defensive if he (she) does not agree.
Q. Doctor, please answer the question; it requires only a simple “Yes” or “No.”
A. I cannot answer that question with only a “Yes” or “No.” Would you like me to explain? OR
A. A mere “Yes” or “No” answer to that question would be misleading. May I explain?
CONVOLUTED COMPOUNDS
When opposing counsel asks you a double- or triple-jointed question, ask her to reframe or break down the inquiry into simpler questions.
Q. Doctor, would you agree that a woman with a family history of diabetes who is taking…should be tested for…at least once a month, and that if there is evidence of…then the standard of care requires you to…?
A. Please repeat those questions again, one at a time.
GIVE ME MORE
Opposing counsel may try to “fish” for more information. You are under no obligation to make his job easier. Answers that contain a qualifier are useful.
Q. Doctor, to your knowledge, have you told me everything you consider important about your patient’s death after she hemorrhaged?
A. I have told you all the information I can remember at this time.
CASE Direct question at deposition
During your deposition in a malpractice suit, plaintiff’s counsel asks you: “Are you saying it was impossible to foresee Ms. Jones’s preterm premature rupture of membranes?”
How would you reply?
Ninety percent of malpractice cases are settled before trial, and the deposition often is the turning point in those cases.1-3 Your answer to tricky questions such as the one in the case fragment above could favorably affect a critical stage of litigation—or it might spur the plaintiff’s attorney to pursue the case more vigorously. Even if a case is settled in the plaintiff’s favor before trial, the effectiveness of the deposition may determine whether the settlement is $300,000 or $1 million.
Our central message in this article is: Don’t go to a deposition unprepared. We offer guidelines to help you anticipate many different scenarios, and we include examples of honest, skillful answers to difficult questions (see “Honest, skillful answers to 8 tricky questions at deposition”).3-7
Digging for pay dirt
Discovery begins after a formal complaint alleges malpractice. The parties to a lawsuit gather information through written interrogatories, requests for documents, and witness depositions—out-of-court testimony to be used later in court or for discovery purposes.8 The rationale for discovery is to reduce surprises at trial and encourage pretrial settlement. The witness being deposed is the deponent, and testimony is given under oath.9
A discovery deposition is designed to gather information, with almost all questions asked by opposing counsel. If you are sued for malpractice, this is the type of deposition you probably will encounter.
Rules of engagement. The plaintiff’s attorney initiates the discovery deposition. Ground rules vary by jurisdiction, but, in general, the Rules of Civil Procedure give deposing counsel substantial latitude in the questions that can be asked.10 The deponent and defending counsel, opposing counsel, and transcriptionist typically attend the deposition. To help you prepare appropriately, confirm with your defense counsel if other attorneys or the plaintiff will be present.
Not-so-hidden agendas. The plaintiff’s attorney’s primary goal is to gather as much information as possible about your side’s case4 (TABLE 1). No matter how accurate medical records may be, they require interpretation and follow-up questioning of key players to get the full story. Opposing counsel also wants to:
- “lock down” your testimony for use at trial (testimony captured at a deposition can be used to impeach a witness who gives inconsistent testimony at trial)9
- “size up” your potential impact on a jury by assessing your strengths and weaknesses as a witness.11
The impression you make may influence the opposing attorney’s decision about how far to pursue the case. Plaintiff’s attorney Bruce Fagel once told an interviewer that defense attorneys, too, may consider settling a case “if their client shows such arrogance in our deposition that they’re afraid to let him appear in front of a jury.”12
TABLE 1
Plaintiff’s attorney has 5 goals at deposition
| Lock down testimony for trial |
| Scrutinize the defendant’s qualifications |
| Size up the defendant’s effectiveness as a witness |
| Probe the defendant for bias, arrogance, or hostility |
| Learn as much as possible—known as “fishing” |
Choosing a site. Most depositions take place in a conference room in the law office of one of the attorneys or at a neutral site. Avoid any temptation to schedule the deposition in your office, even though meeting there might seem more expedient and comfortable for you.9 Scheduling the deposition at your site:
- might make you feel it is “just another day at the office” and dissuade you from preparing sufficiently or taking the deposition seriously
- allows opposing counsel to scrutinize diplomas, books, journals, and other materials in your office.
Questioning you about these materials during the deposition is not off-limits for the plaintiff’s attorney. You might find it difficult to explain why a book on your bookshelf is not “authoritative.”
Prepare, prepare, and…prepare some more
Your emotional stress will probably wax and wane during the lengthy litigation process.13,14 Knowing what to expect and being well-prepared for the deposition may relieve some anxiety.
Review the case. At least twice, carefully review the entire database—including medical records and other depositions. Perform one of these reviews just before the deposition.3 Having the details fresh in mind will help you if opposing counsel mischaracterizes information when questioning you.
Meet with your attorney. Insist on at least two predeposition conferences with defense counsel.
At the first conference, volunteer all pertinent information about the case as well as any noteworthy medical inconsistencies.2 Find out what documents to bring to the deposition, who will be present, and how long the deposition is expected to take. You might wish to prepare mentally by inquiring about the style and personality of opposing counsel.
Defense counsel does not control how long a deposition lasts but might be able to give a rough estimate. Plan accordingly, and allow for sufficient scheduling flexibility. Depositions typically last half a day but can last more than 1 day.
At a later predeposition conference, defense counsel might walk you through a mock deposition that involves difficult or anticipated questions. This is a good opportunity to master your anxiety and improve your effectiveness as a witness.
You also may wish to go over your curriculum vitae with defense counsel and check it for mistakes or other content that might raise problematic questions during the deposition (TABLE 2). Make sure your CV is up-to-date, and refresh your memory if it lists lectures given or articles written—no matter how long ago—on topics related to the litigation.
TABLE 2
Step by step, prepping for a deposition
| Thoroughly review case records |
| Master the case (memorize key names, dates, facts) |
| Meet with defense counsel at least twice to: |
| —find out where the deposition is being held, who will be present, and how long it is expected to take —learn what documents to bring —understand opposing counsel’s style and personality —prepare for difficult questions —consider holding a mock deposition |
| Double-check your curriculum vitae for accuracy and updating |
| Come to the deposition well-rested |
Don’t open Pandora’s box! Keep your answers to deposition questions brief and clear. Opposing counsel may ask broad questions, hoping to encourage rambling answers that reveal new facts. Answering questions succinctly and briefly is the best strategy under most circumstances.
One exception may involve scenarios in which the defense attorney instructs you, for various reasons, to provide information beyond the question asked. For example, when a case is close to settling, your attorney might instruct you to lay out all evidence that supports your professional judgment and clinical decisions in the case. Do not use this approach, however, unless your attorney specifically instructs you to do so.
You are under no obligation to make opposing counsel’s job easier. In a discovery deposition, volunteering information may:
- open up new areas for questioning
- equip the deposing attorney with more ammunition
- eliminate opportunities for your attorney to use surprise as a strategy, should the case go to trial.
Consider, for example, a scenario in which you and a hospital are sued in regard to a labor-and-delivery case. At deposition, you might be asked whether you can identify written evidence in the patient’s chart that the mother was checked every certain number of minutes.
The correct answer is “No,” even though you know such checks are documented in a log kept at the nursing station in that hospital. You might be tempted to reveal this information, but don’t—instead, leave the timing of its disclosure to the defense attorney. Your attorney’s strategy may be to reveal this critical piece of information at trial, when the plaintiff’s attorney has less opportunity to strategize ways to discredit the evidence.
Keep your cool. Attorneys have different styles of questioning. Some may be excessively friendly or polite to get you to let down your guard—only to set you up for a devastating blow at the end of the deposition (or to save this for trial). Other attorneys might employ a bullying style that seeks to intimidate. In responding, always remain composed and resist the urge to counterattack.
In all circumstances, strive for humility and dignified confidence. Opposing counsel gains the advantage when defendants lose composure or become angry, defensive, or arrogant. Indeed, experienced plaintiff’s attorneys may be testing for precisely this reaction in the hope that a defendant will “demonstrate his arrogance” during the deposition or later on the witness stand.12
In working as expert witnesses in malpractice cases, we have observed many instances in which a defendant physician’s arrogant or hostile remarks at deposition played a key role in causing the case to be prematurely settled in the plaintiff’s favor.
Avoid making jokes or sarcastic comments. Even a well-timed, self-deprecating joke may backfire should opposing counsel take the opportunity to point out that the case is a “serious matter.”
Listen carefully to each question during the deposition. Pause for a moment to consider the question and allow time for other attorneys to object.5 Your attorney’s objection may suggest the best way for you to respond to the question. Refrain from answering any questions when defense counsel advises you to do so (TABLE 3).
Don’t answer questions you don’t understand. Rather, ask for clarification. Avoid using adjectives and superlatives such as “never” and “always,” which may be used to distort or mischaracterize your testimony at trial.
Don’t guess. No rule prevents opposing counsel from asking a witness to speculate, but you should generally avoid doing so. You are required to tell the truth, not to speculate or to volunteer guesses. The best way to cause a jury to disbelieve your testimony is to make inaccurate or unfounded statements, which opposing counsel will surely point out at trial.
Don’t be tempted to “plumb the depths” of your memory for a forgotten piece of information, however. If you’re asked, for example, if a patient displayed a specific symptom during an appointment 4 years ago, the true answer is likely to be “Not that I recall,” rather than “No.” Qualify similar answers with statements such as “To the best of my recollection” or “Not that I recall at this time.”
If opposing counsel asks questions based on a particular document, ask to see the document. Review it carefully to determine:
- who signed or authored it
- when it was prepared and dated
- whether it is a draft copy
- whether it contains confidential information relating to patients other than the plaintiff
- whether it carries attorney–client privilege
- most important, whether opposing counsel has quoted it out of context.
TABLE 3
Deposition Dos and Don’ts
| Always tell the truth |
| Actively listen to questions, and pause before answering |
| Keep your cool; never lose composure |
| Answer only the question asked |
| Stop speaking and listen carefully if your attorney makes an objection |
| Avoid long narratives, and don’t volunteer information |
| Don’t speculate or guess |
| Avoid absolutes such as “never” or “always” |
| Avoid jokes, sarcasm, and edgy comments |
| Ask for breaks if needed to keep from becoming inattentive |
| Carefully examine documents, reports, etc., before answering opposing counsel’s questions about them |
| Ask for clarification of confusing questions |
| Remember: Nothing is “off the record” |
| Don’t waive your right to read and sign the deposition transcript |
Procedural pitfalls. Throughout the deposition, attorneys may periodically tell the court reporter that they wish to have a discussion “off the record.” Nothing is off the record for you, however. If you make a statement when the court reporter has been told to stop, opposing counsel can summarize on the record everything you said during that time.
At the beginning or end of the deposition, one of the attorneys may ask if you wish to waive the right to read and sign the deposition transcript. Seek your counsel’s advice, but defendants usually choose to retain this right. Typically, you have 30 days to read the transcript and correct errors. Keep in mind that substantive changes beyond typos are likely to be the subject of intense cross-examination if the case goes to trial.9
Depositions are sometimes videotaped, usually because a witness will not be available at the time of trial. Because the jury will hear and see you, approach a videotaped deposition as if it were an actual trial. Dress appropriately, speak clearly, and look directly into the camera. Don’t feel embarrassed about making sure that you are taped with the best possible lighting, camera angle, and background.
Keep your guard up!
Don’t allow yourself to be distracted if opposing counsel jumps from open-ended questions to clarification questions to “pinning-down” questions. An erratic approach could be part of opposing counsel’s strategy. Answer only the question asked, and give the shortest correct answer possible to each question.
Opposing counsel may ask a question in a way that suggests substantial confusion or misunderstanding. If this confusion does not affect your testimony, you don’t need to clear up matters for opposing counsel. If, for example, opposing counsel asserts that one of your statements is contradictory, an appropriate response may be simply, “No, it wasn’t.” It is opposing counsel’s job to explicate further details.11
Opposing counsel may approach the deposition with a particular demeanor—friendly, eager to learn—in an attempt to get you to let down your guard and speak more freely (see “Personae sometimes adopted by plaintiffs’ attorneys to obtain information at deposition”).
During a full-day deposition, particularly, the greatest likelihood of making a mistake begins around 4 pm. Some attorneys may reserve especially important questions for this time, hoping that the witness will be less guarded. Start the day well-rested and ask for breaks if fatigue begins to affect your concentration.
Be alert to questioning designed to elicit only “Yes” answers. This technique—often used by salespersons—makes it difficult to say “No” in response to an ambiguous question. Last, point out errors if opposing counsel misquotes earlier testimony or states facts incorrectly. These mistakes may be innocent, or an attempt to distort your testimony.
“Mr./Ms. Friendly” Some attorneys look for an opportunity, before the deposition begins, to show that they are “friendly” and not to be feared. Remember: Discussions with opposing counsel without defense counsel present are inappropriate.
“Eager Student” Opposing counsel may play the “eager student” to massage your ego and pave the way for long narratives and volunteered information.
“Counselor Clueless” Opposing counsel may appear so ignorant of certain facts that you can scarcely resist jumping in to educate him or her.
“Mr./Ms. Silent Treatment” After you give a brief, honest answer, opposing counsel may sit silently as if expecting a more substantive response. Resist the temptation to fill the silence.
CASE RESOLVED Direct question at deposition
You reply to plaintiff’s attorney: “I don’t know how the rupturing of membranes in this case could have been foreseen.”
THE IMPOSSIBLE DREAM
In law, there is a distinction between possibility and probability. The law considers anything possible, but something isn’t probable unless it is more likely than not—that is, when expressed mathematically, its chances are ≥51%.
Q. Doctor, are you saying it was impossible to foresee Ms. Jones’ preterm premature rupture of membranes?
A. I don’t know of any way that the rupturing of membranes could have been foreseen. It was an unfortunate event that was not possible to foresee.
THE HYPOTHETICAL
When confronted with questions containing a hypothetical, identify the hidden assumption before answering.
Q. Doctor, with a depressed pregnant patient, would you agree that the standard of care requires you to…?
A. I can’t agree with you that, in this case, we are talking about a depressed patient. Do you still want me to answer the question? OR
A. I can’t answer that based on the few facts you’ve given me. I’d need to examine that patient first.
INVITATION TO SPECULATE
Refrain from speculating, especially when you’ve been presented with an incomplete clinical picture.
Q. Doctor, is it fair to say that a patient with this history should be referred to a specialist in high-risk pregnancy?
A. I really can’t speculate based on that limited information—I’d just be guessing.
DID I SAY THAT?
Opposing counsel may mischaracterize or distort your testimony by attempting to paraphrase what you’ve said.
Q. Now doctor, as I understand it, what you’re really saying is that the patient…?
A. No. OR
A. No—that’s not an accurate summary of what I just said.
THE AUTHORITATIVE TREATISE
Opposing counsel wants you to acknowledge a specific piece of literature as ‘authoritative’ in gynecology, so that counsel can then impeach you at trial with points from the literature that contradict your testimony. Although you may be made to look foolish if you refuse to acknowledge anything as authoritative, that usually is the safest course.
Q. Doctor, do you accept Williams Obstetrics as an authoritative reference in your field?
A. It is certainly well-respected, but the entire text can’t be considered authoritative. OR
A. Significant portions may be authoritative, but I would need to see the portion in question to be able to answer your question.
THE TYRANNY OF YES OR NO
In an effort to control you, opposing counsel may demand only “Yes” or “No” answers. Listen closely to each question, and determine if you can convey the whole truth with “Yes” or “No.” Asking to further explain to avoid giving a misleading answer will make opposing counsel appear defensive if he (she) does not agree.
Q. Doctor, please answer the question; it requires only a simple “Yes” or “No.”
A. I cannot answer that question with only a “Yes” or “No.” Would you like me to explain? OR
A. A mere “Yes” or “No” answer to that question would be misleading. May I explain?
CONVOLUTED COMPOUNDS
When opposing counsel asks you a double- or triple-jointed question, ask her to reframe or break down the inquiry into simpler questions.
Q. Doctor, would you agree that a woman with a family history of diabetes who is taking…should be tested for…at least once a month, and that if there is evidence of…then the standard of care requires you to…?
A. Please repeat those questions again, one at a time.
GIVE ME MORE
Opposing counsel may try to “fish” for more information. You are under no obligation to make his job easier. Answers that contain a qualifier are useful.
Q. Doctor, to your knowledge, have you told me everything you consider important about your patient’s death after she hemorrhaged?
A. I have told you all the information I can remember at this time.
1. Babitsky S, Mangraviti J. The discovery process. In: How to Become a Dangerous Expert Witness: Advanced Techniques and Strategies. Falmouth, Mass: Seak Inc; 2005:4-9:113-139.
2. Clark A, Fox P. The defendant physician’s deposition: fighting back—at last! Mo Med. 2002;99(10):524-525.
3. Rice B. Malpractice: how to survive a deposition. Med Econ. 2005;82:45-48.
4. Babitsky S, Mangraviti J. How to Excel during Depositions: Techniques for Experts that Work. Falmouth, Mass: Seak Inc; 1998.
5. Gutheil T. The Psychiatrist as Expert Witness. Washington, DC: American Psychiatric Publishing, Inc; 1998.
6. Babitsky S, Mangraviti J. How to Excel during Cross-Examination: Techniques for Experts that Work. Falmouth, Mass: Seak Inc; 1997.
7. Hirsch C, Morris R, Moritz A. Handbook of Legal Medicine. 5th ed. St. Louis, Mo: CV Mosby Co; 1979.
8. Black H. Black’s Law Dictionary. 8th ed. St. Paul, Minn: West Publishing; 2004;440
9. Babitsky S, Mangraviti J. Depositions: The Comprehensive Guide for Expert Witnesses. Falmouth, Mass: Seak Inc; 2007.
10. Cornell Law School. Federal Rules of Civil Procedure. Depositions and discovery. Rule 26(5) B(1). Available at: http://www.law.cornell.edu/rules/frcp/Rule26.htm. Accessed April 10, 2008.
11. Culley CA, Jr, Spisak LJ. So you’re being sued: do’s and don’ts for the defendant. Cleve Clin J Med. 2002;69:752-760.
12. Rice B. How I pick the doctors I’ll sue. Med Econ. 2004;81:54.-
13. Charles S. Coping with a medical malpractice suit. West J Med. 2001;174:55-58.
14. Charles SC. Got malpractice distress? You can help yourself survive. OBG Management. 2008;20(2):38-51.
1. Babitsky S, Mangraviti J. The discovery process. In: How to Become a Dangerous Expert Witness: Advanced Techniques and Strategies. Falmouth, Mass: Seak Inc; 2005:4-9:113-139.
2. Clark A, Fox P. The defendant physician’s deposition: fighting back—at last! Mo Med. 2002;99(10):524-525.
3. Rice B. Malpractice: how to survive a deposition. Med Econ. 2005;82:45-48.
4. Babitsky S, Mangraviti J. How to Excel during Depositions: Techniques for Experts that Work. Falmouth, Mass: Seak Inc; 1998.
5. Gutheil T. The Psychiatrist as Expert Witness. Washington, DC: American Psychiatric Publishing, Inc; 1998.
6. Babitsky S, Mangraviti J. How to Excel during Cross-Examination: Techniques for Experts that Work. Falmouth, Mass: Seak Inc; 1997.
7. Hirsch C, Morris R, Moritz A. Handbook of Legal Medicine. 5th ed. St. Louis, Mo: CV Mosby Co; 1979.
8. Black H. Black’s Law Dictionary. 8th ed. St. Paul, Minn: West Publishing; 2004;440
9. Babitsky S, Mangraviti J. Depositions: The Comprehensive Guide for Expert Witnesses. Falmouth, Mass: Seak Inc; 2007.
10. Cornell Law School. Federal Rules of Civil Procedure. Depositions and discovery. Rule 26(5) B(1). Available at: http://www.law.cornell.edu/rules/frcp/Rule26.htm. Accessed April 10, 2008.
11. Culley CA, Jr, Spisak LJ. So you’re being sued: do’s and don’ts for the defendant. Cleve Clin J Med. 2002;69:752-760.
12. Rice B. How I pick the doctors I’ll sue. Med Econ. 2004;81:54.-
13. Charles S. Coping with a medical malpractice suit. West J Med. 2001;174:55-58.
14. Charles SC. Got malpractice distress? You can help yourself survive. OBG Management. 2008;20(2):38-51.
Adviser ONLY on the Web
BSO for breast Ca patient—OK to code as CIS surgery?
In any case, your primary diagnosis would be V50.42 (prophylactic organ removal, ovary), followed by V10.3, then followed by V86.1 because she is probably estrogen-receptor positive (meaning that taking anti-estrogens will not prevent the return of cancer).
If she is still being treated for cancer in situ, then 233.0 is correct but V50.42 needs to be the primary diagnosis because, otherwise, you get a mismatch between the diagnosis and the surgery (i.e., it appears that you are performing an oophorectomy because of breast cancer).
BSO for breast Ca patient—OK to code as CIS surgery?
In any case, your primary diagnosis would be V50.42 (prophylactic organ removal, ovary), followed by V10.3, then followed by V86.1 because she is probably estrogen-receptor positive (meaning that taking anti-estrogens will not prevent the return of cancer).
If she is still being treated for cancer in situ, then 233.0 is correct but V50.42 needs to be the primary diagnosis because, otherwise, you get a mismatch between the diagnosis and the surgery (i.e., it appears that you are performing an oophorectomy because of breast cancer).
BSO for breast Ca patient—OK to code as CIS surgery?
In any case, your primary diagnosis would be V50.42 (prophylactic organ removal, ovary), followed by V10.3, then followed by V86.1 because she is probably estrogen-receptor positive (meaning that taking anti-estrogens will not prevent the return of cancer).
If she is still being treated for cancer in situ, then 233.0 is correct but V50.42 needs to be the primary diagnosis because, otherwise, you get a mismatch between the diagnosis and the surgery (i.e., it appears that you are performing an oophorectomy because of breast cancer).
REIMBURSEMENT ADVISER
If the patient can pinpoint which quadrant the pain is in, a better option is to report 789.0X (abdominal pain; the fifth [X] digit reports the site, such as left lower-quadrant or right upper-quadrant, etc.). Using this code more specifically identifies the complaint and location; I have found that fewer payers deny a US scan when this code is reported.
Problem with -52 modifier for US follicle evaluation
Can you comment on our coding strategies for these services?
Among payers that recognize -52, almost all put the claim into manual review before payment. If you are being paid a reduced amount, have you compared it with the reimbursement you might be getting by reporting 76857 instead? Note that neither code 76857 (which specifies checking for follicles) nor code 76815 (which specifies a limited exam such as you would perform for a quick cervical check on a pregnant patient) specifies the approach—in other words, the word “pelvic” does not imply strictly a transabdominal approach. These codes can therefore be used to report either an abdominal or transvaginal scan. In my opinion, either code more accurately describes the procedures that you are performing.
Dx/procedure mismatch when checking for fibroids
Also, understand that the duplex procedures are only reported when you are trying to characterize the pattern and direction of blood flow in arteries or veins. This year, CPT clarified that, although evaluation of vascular structures using both color and spectral Doppler is reportable separately, color Doppler alone, when performed for identification of anatomic structures in conjunction with a real-time US exam, cannot be reported separately.
Last, the code you are billing, 93975, represents a complete study. Examination of a single fibroid within the uterus constitutes a limited study, billed using 93976.
If the patient can pinpoint which quadrant the pain is in, a better option is to report 789.0X (abdominal pain; the fifth [X] digit reports the site, such as left lower-quadrant or right upper-quadrant, etc.). Using this code more specifically identifies the complaint and location; I have found that fewer payers deny a US scan when this code is reported.
Problem with -52 modifier for US follicle evaluation
Can you comment on our coding strategies for these services?
Among payers that recognize -52, almost all put the claim into manual review before payment. If you are being paid a reduced amount, have you compared it with the reimbursement you might be getting by reporting 76857 instead? Note that neither code 76857 (which specifies checking for follicles) nor code 76815 (which specifies a limited exam such as you would perform for a quick cervical check on a pregnant patient) specifies the approach—in other words, the word “pelvic” does not imply strictly a transabdominal approach. These codes can therefore be used to report either an abdominal or transvaginal scan. In my opinion, either code more accurately describes the procedures that you are performing.
Dx/procedure mismatch when checking for fibroids
Also, understand that the duplex procedures are only reported when you are trying to characterize the pattern and direction of blood flow in arteries or veins. This year, CPT clarified that, although evaluation of vascular structures using both color and spectral Doppler is reportable separately, color Doppler alone, when performed for identification of anatomic structures in conjunction with a real-time US exam, cannot be reported separately.
Last, the code you are billing, 93975, represents a complete study. Examination of a single fibroid within the uterus constitutes a limited study, billed using 93976.
If the patient can pinpoint which quadrant the pain is in, a better option is to report 789.0X (abdominal pain; the fifth [X] digit reports the site, such as left lower-quadrant or right upper-quadrant, etc.). Using this code more specifically identifies the complaint and location; I have found that fewer payers deny a US scan when this code is reported.
Problem with -52 modifier for US follicle evaluation
Can you comment on our coding strategies for these services?
Among payers that recognize -52, almost all put the claim into manual review before payment. If you are being paid a reduced amount, have you compared it with the reimbursement you might be getting by reporting 76857 instead? Note that neither code 76857 (which specifies checking for follicles) nor code 76815 (which specifies a limited exam such as you would perform for a quick cervical check on a pregnant patient) specifies the approach—in other words, the word “pelvic” does not imply strictly a transabdominal approach. These codes can therefore be used to report either an abdominal or transvaginal scan. In my opinion, either code more accurately describes the procedures that you are performing.
Dx/procedure mismatch when checking for fibroids
Also, understand that the duplex procedures are only reported when you are trying to characterize the pattern and direction of blood flow in arteries or veins. This year, CPT clarified that, although evaluation of vascular structures using both color and spectral Doppler is reportable separately, color Doppler alone, when performed for identification of anatomic structures in conjunction with a real-time US exam, cannot be reported separately.
Last, the code you are billing, 93975, represents a complete study. Examination of a single fibroid within the uterus constitutes a limited study, billed using 93976.
Is Your Overhead Too Low?
I get a lot of questions and complaints from physicians about overhead. How should I define it? How do I calculate it? And, of course, how do I lower it?
Many physicians are surprised when I tell them that lowering their overhead isn't necessarily a good thing. In fact, it may be too low already.
Numerous studies have shown that practices with higher overhead generally produce higher net incomes for their physicians. The money has to be judiciously spent, of course, but keeping overhead costs too low can be counterproductive.
Too much cutting of operating expenses may be costing you revenue. Insufficient office space or too few staff may be crimping the office's efficiency and reducing the number of patients that can be seen.
Overhead is generally defined as the expense of maintaining your practice, not including depreciation, and is usually calculated first as an absolute number, then as total expenses as a percentage of total gross income. The percentage figure can be misleading, however.
If you're trying to decide whether your overhead is too high or too low, you'll need an itemized breakdown. That will require some “billable hours” from your accountant, but those hours will pay for themselves many times over because the itemization will allow you to see where you could be spending less and where you could be spending more.
It's important to understand that overhead is not always the enemy. It is an easy target because everyone can focus on it—and look for ways to decrease it. Compulsive attention to it, however, is often a sign that more important aspects of the practice are being neglected.
Consider revenue, for example. More often than not, it is better to increase gross receipts than to decrease overhead. As a famous businessman once told me, “Your ability to cut costs is limited, but your ability to increase revenue is unlimited.”
Negotiate better contracts with third-party payers. Improve collections, possibly with the credit card system I've discussed in several recent columns. Learn to code better and train your staff to do so as well. Use your time more efficiently. Don't worry so much about overhead. Would you rather keep 60% of $800,000 or 40% of $2 million?
I recently spoke with a prominent cosmetic dermatologist in New York City whose spa was bringing in a steady $1 million per year in revenue, but with 80% overhead. He was talking about closing it down because the overhead was too high! He didn't understand that his spa was making him money, regardless of the overhead percentage. By closing the spa, he would have traded a tidy profit of 20 cents on the dollar for zero cents on the dollar.
That's why you have to be careful when using percentage as a yardstick of your overhead. Overhead percentage doesn't reflect overhead; it reflects the ratio of overhead to revenue. Without looking at the numbers themselves, both revenue and overhead, you can get a distorted view.
Let's compare two hypothetical dermatology practices: One is primarily medical and the other is surgical. The medical practice has an overhead percentage of 60% and the surgical practice 40%, but in real dollars, their overheads are exactly the same. How can that be? Is one more efficient than the other? No, the difference is in total revenue; the surgical practice generates substantially higher gross receipts than does the medical practice. When the revenue goes up, the overhead percentage drops, even though the overhead in real dollars is the same. Once again, would you rather keep 60% of $800,000 or 40% of $2 million?
Don't get me wrong. Overhead is not something you should ignore, but neither should you obsess over it on a regular basis. You would be far better off seeing patients with that time. The incremental cost of seeing an additional patient is almost zero, and the revenue is almost pure profit, since you've already paid your overhead.
Concentrate on finding new ways to increase revenue or expand your practice, and your overhead will take care of itself.
I get a lot of questions and complaints from physicians about overhead. How should I define it? How do I calculate it? And, of course, how do I lower it?
Many physicians are surprised when I tell them that lowering their overhead isn't necessarily a good thing. In fact, it may be too low already.
Numerous studies have shown that practices with higher overhead generally produce higher net incomes for their physicians. The money has to be judiciously spent, of course, but keeping overhead costs too low can be counterproductive.
Too much cutting of operating expenses may be costing you revenue. Insufficient office space or too few staff may be crimping the office's efficiency and reducing the number of patients that can be seen.
Overhead is generally defined as the expense of maintaining your practice, not including depreciation, and is usually calculated first as an absolute number, then as total expenses as a percentage of total gross income. The percentage figure can be misleading, however.
If you're trying to decide whether your overhead is too high or too low, you'll need an itemized breakdown. That will require some “billable hours” from your accountant, but those hours will pay for themselves many times over because the itemization will allow you to see where you could be spending less and where you could be spending more.
It's important to understand that overhead is not always the enemy. It is an easy target because everyone can focus on it—and look for ways to decrease it. Compulsive attention to it, however, is often a sign that more important aspects of the practice are being neglected.
Consider revenue, for example. More often than not, it is better to increase gross receipts than to decrease overhead. As a famous businessman once told me, “Your ability to cut costs is limited, but your ability to increase revenue is unlimited.”
Negotiate better contracts with third-party payers. Improve collections, possibly with the credit card system I've discussed in several recent columns. Learn to code better and train your staff to do so as well. Use your time more efficiently. Don't worry so much about overhead. Would you rather keep 60% of $800,000 or 40% of $2 million?
I recently spoke with a prominent cosmetic dermatologist in New York City whose spa was bringing in a steady $1 million per year in revenue, but with 80% overhead. He was talking about closing it down because the overhead was too high! He didn't understand that his spa was making him money, regardless of the overhead percentage. By closing the spa, he would have traded a tidy profit of 20 cents on the dollar for zero cents on the dollar.
That's why you have to be careful when using percentage as a yardstick of your overhead. Overhead percentage doesn't reflect overhead; it reflects the ratio of overhead to revenue. Without looking at the numbers themselves, both revenue and overhead, you can get a distorted view.
Let's compare two hypothetical dermatology practices: One is primarily medical and the other is surgical. The medical practice has an overhead percentage of 60% and the surgical practice 40%, but in real dollars, their overheads are exactly the same. How can that be? Is one more efficient than the other? No, the difference is in total revenue; the surgical practice generates substantially higher gross receipts than does the medical practice. When the revenue goes up, the overhead percentage drops, even though the overhead in real dollars is the same. Once again, would you rather keep 60% of $800,000 or 40% of $2 million?
Don't get me wrong. Overhead is not something you should ignore, but neither should you obsess over it on a regular basis. You would be far better off seeing patients with that time. The incremental cost of seeing an additional patient is almost zero, and the revenue is almost pure profit, since you've already paid your overhead.
Concentrate on finding new ways to increase revenue or expand your practice, and your overhead will take care of itself.
I get a lot of questions and complaints from physicians about overhead. How should I define it? How do I calculate it? And, of course, how do I lower it?
Many physicians are surprised when I tell them that lowering their overhead isn't necessarily a good thing. In fact, it may be too low already.
Numerous studies have shown that practices with higher overhead generally produce higher net incomes for their physicians. The money has to be judiciously spent, of course, but keeping overhead costs too low can be counterproductive.
Too much cutting of operating expenses may be costing you revenue. Insufficient office space or too few staff may be crimping the office's efficiency and reducing the number of patients that can be seen.
Overhead is generally defined as the expense of maintaining your practice, not including depreciation, and is usually calculated first as an absolute number, then as total expenses as a percentage of total gross income. The percentage figure can be misleading, however.
If you're trying to decide whether your overhead is too high or too low, you'll need an itemized breakdown. That will require some “billable hours” from your accountant, but those hours will pay for themselves many times over because the itemization will allow you to see where you could be spending less and where you could be spending more.
It's important to understand that overhead is not always the enemy. It is an easy target because everyone can focus on it—and look for ways to decrease it. Compulsive attention to it, however, is often a sign that more important aspects of the practice are being neglected.
Consider revenue, for example. More often than not, it is better to increase gross receipts than to decrease overhead. As a famous businessman once told me, “Your ability to cut costs is limited, but your ability to increase revenue is unlimited.”
Negotiate better contracts with third-party payers. Improve collections, possibly with the credit card system I've discussed in several recent columns. Learn to code better and train your staff to do so as well. Use your time more efficiently. Don't worry so much about overhead. Would you rather keep 60% of $800,000 or 40% of $2 million?
I recently spoke with a prominent cosmetic dermatologist in New York City whose spa was bringing in a steady $1 million per year in revenue, but with 80% overhead. He was talking about closing it down because the overhead was too high! He didn't understand that his spa was making him money, regardless of the overhead percentage. By closing the spa, he would have traded a tidy profit of 20 cents on the dollar for zero cents on the dollar.
That's why you have to be careful when using percentage as a yardstick of your overhead. Overhead percentage doesn't reflect overhead; it reflects the ratio of overhead to revenue. Without looking at the numbers themselves, both revenue and overhead, you can get a distorted view.
Let's compare two hypothetical dermatology practices: One is primarily medical and the other is surgical. The medical practice has an overhead percentage of 60% and the surgical practice 40%, but in real dollars, their overheads are exactly the same. How can that be? Is one more efficient than the other? No, the difference is in total revenue; the surgical practice generates substantially higher gross receipts than does the medical practice. When the revenue goes up, the overhead percentage drops, even though the overhead in real dollars is the same. Once again, would you rather keep 60% of $800,000 or 40% of $2 million?
Don't get me wrong. Overhead is not something you should ignore, but neither should you obsess over it on a regular basis. You would be far better off seeing patients with that time. The incremental cost of seeing an additional patient is almost zero, and the revenue is almost pure profit, since you've already paid your overhead.
Concentrate on finding new ways to increase revenue or expand your practice, and your overhead will take care of itself.
Document Patient History
Documentation in the medical record serves many purposes: communication among healthcare professionals, evidence of patient care, and justification for provider claims.
Although these three aspects of documentation are intertwined, the first two prevent physicians from paying settlements involving malpractice allegations, while the last one assists in obtaining appropriate reimbursement for services rendered. This is the first of a three-part series that will focus on claim reporting and outline the documentation guidelines set forth by the Centers for Medicare and Medicaid Services (CMS) in conjunction with the American Medical Association (AMA).
1995, 1997 Guidelines
Two sets of documentation guidelines are in place, referred to as the 1995 and 1997 guidelines. Increased criticism of the ambiguity in the 1995 guidelines from auditors and providers inspired development of the 1997 guidelines.
While the 1997 guidelines were intended to create a more objective and unified approach to documentation, the level of specificity required brought criticism and frustration. But while the physician community balked, most auditors praised these efforts.
To satisfy all parties and allow physicians to document as they prefer, both sets of guidelines remain. Physicians can document according to either style, and auditors are obligated to review provider records against both sets of guidelines, selecting the final visit level with the set that best supports provider documentation.
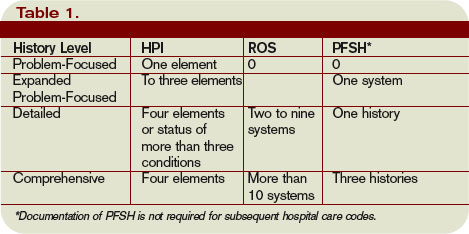
Elements of History
Chief complaint (CC): The CC is the reason for the visit as stated in the patient’s own words. This must be present for each encounter, and should reference a specific condition or complaint (e.g., patient complains of abdominal pain).
History of present illness (HPI): This is a description of the present illness as it developed. It is typically formatted and documented with reference to location, quality, severity, timing, context, modifying factors, and associated signs/symptoms as related to the chief complaint. The HPI may be classified as brief (a comment on fewer than HPI elements) or extended (a comment on more than four HPI elements). Sample documentation of an extended HPI is: “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
The 1997 guidelines offer an alternate format for documenting the HPI. In contrast to the standard method above, the physician may list and status the patient’s chronic or inactive conditions. An extended HPI consists of the status of at least three chronic or inactive conditions (e.g., “Diabetes controlled by oral medication; extrinsic asthma without acute exacerbation in past six months; hypertension stable with pressures ranging from 130-140/80-90”). Failing to document the status negates the opportunity for the physician to receive HPI credit. Instead, he will receive credit for a past medical history.
The HPI should never be documented by ancillary staff (e.g., registered nurse, medical assistant, students). HPI might be documented by residents (e.g., residents, fellows, interns) or nonphysician providers (nurse practitioners and physician assistants) when utilizing the Teaching Physician Rules or Split-Shared Billing Rules, respectively (teaching Physician Rules and Split-Shared Billing Rules will be addressed in an upcoming issue).
Review of systems (ROS): This is a series of questions used to elicit information about additional signs, symptoms, or problems currently or previously experienced by the patient:
- Constitutional;
- Eyes; ears, nose, mouth, throat;
- Cardiovascular;
- Respiratory;
- Gastrointestinal;
- Genitourinary;
- Musculoskeletal;
- Integumentary (including skin and/or breast);
- Neurological;
- Psychiatric;
- Endocrine;
- Hematologic/lymphatic; and
- Allergic/immunologic.
The ROS may be classified as brief (a comment on one system), expanded (a comment on two to nine systems), or complete (a comment on more than 10 systems).
Documentation of a complete ROS (more than 10 systems) can occur in two ways:
- The physician can individually document each system. For example: “No fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular); shortness of breath (respiratory); or belly pain (gastrointestinal); etc.”; or
- The physician can document the positive findings and pertinent negative findings related to the chief complaint, along with a comment that “all other systems are negative.” This latter statement is not accepted by all local Medicare contractors.
Information involving the ROS can be documented by anyone, including the patient. If documented by someone else (e.g., a medical student) other than residents under the Teaching Physician Rules or nonphysician providers under the Split-Shared Billing Rules, the physician should reference the documented ROS in his progress note. Re-documentation of the ROS is not necessary unless a revision is required.
Past, family, and social history (PFSH): Documentation of PFSH involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. The PFSH can be classified as pertinent (a comment on one history) or complete (a comment in each of the three histories). Documentation that exemplifies a complete PFSH is: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s esophagus; no tobacco or alcohol use.”
As with ROS, the PFSH can be documented by anyone, including the patient. If documented by someone else (e.g., a medical student) other than residents under the Teaching Physician Rules or nonphysician providers under the Split-Shared Billing Rules, the physician should reference the documented PFSH in his progress note. Re-documentation of the PFSH is not necessary unless a revision is required. It is important to note that while documentation of the PFSH is required when billing higher level consultations (99254-99255) or initial inpatient care (99221-99223), it is not required when reporting subsequent hospital care services (99231-99233).
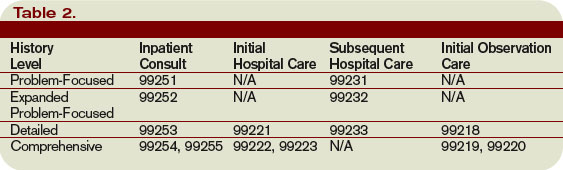
Levels of History
There are four levels of history, determined by the number of elements documented in the progress note (see Table 1, p. 21). The physician must meet all the requirements in a specific level of history before assigning it.
If all of the required elements in a given history level are not documented, the level assigned is that of the least documented element. For example, physician documentation may include four HPI elements and a complete PFSH, yet only eight ROS. The physician can only receive credit for a detailed history. If the physician submitted a claim for 99222 (initial hospital care requiring a comprehensive history, a comprehensive exam, and moderate-complexity decision making), documentation would not support the reported service due to the underdocumented ROS. Deficiencies in the ROS and family history are the most common physician documentation errors involving the history component.
A specific level of history is associated with each type of physician encounter, and must be documented accordingly (see Table 2, right). The most common visit categories provided by hospitalists that include documentation requirements for history are initial inpatient consultations, initial hospital care, subsequent hospital care, and initial observation care. Other visit categories, such as critical care and discharge day management, have neither associated levels of history nor documentation requirements for historical elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Documentation in the medical record serves many purposes: communication among healthcare professionals, evidence of patient care, and justification for provider claims.
Although these three aspects of documentation are intertwined, the first two prevent physicians from paying settlements involving malpractice allegations, while the last one assists in obtaining appropriate reimbursement for services rendered. This is the first of a three-part series that will focus on claim reporting and outline the documentation guidelines set forth by the Centers for Medicare and Medicaid Services (CMS) in conjunction with the American Medical Association (AMA).
1995, 1997 Guidelines
Two sets of documentation guidelines are in place, referred to as the 1995 and 1997 guidelines. Increased criticism of the ambiguity in the 1995 guidelines from auditors and providers inspired development of the 1997 guidelines.
While the 1997 guidelines were intended to create a more objective and unified approach to documentation, the level of specificity required brought criticism and frustration. But while the physician community balked, most auditors praised these efforts.
To satisfy all parties and allow physicians to document as they prefer, both sets of guidelines remain. Physicians can document according to either style, and auditors are obligated to review provider records against both sets of guidelines, selecting the final visit level with the set that best supports provider documentation.
Elements of History
Chief complaint (CC): The CC is the reason for the visit as stated in the patient’s own words. This must be present for each encounter, and should reference a specific condition or complaint (e.g., patient complains of abdominal pain).
History of present illness (HPI): This is a description of the present illness as it developed. It is typically formatted and documented with reference to location, quality, severity, timing, context, modifying factors, and associated signs/symptoms as related to the chief complaint. The HPI may be classified as brief (a comment on fewer than HPI elements) or extended (a comment on more than four HPI elements). Sample documentation of an extended HPI is: “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
The 1997 guidelines offer an alternate format for documenting the HPI. In contrast to the standard method above, the physician may list and status the patient’s chronic or inactive conditions. An extended HPI consists of the status of at least three chronic or inactive conditions (e.g., “Diabetes controlled by oral medication; extrinsic asthma without acute exacerbation in past six months; hypertension stable with pressures ranging from 130-140/80-90”). Failing to document the status negates the opportunity for the physician to receive HPI credit. Instead, he will receive credit for a past medical history.
The HPI should never be documented by ancillary staff (e.g., registered nurse, medical assistant, students). HPI might be documented by residents (e.g., residents, fellows, interns) or nonphysician providers (nurse practitioners and physician assistants) when utilizing the Teaching Physician Rules or Split-Shared Billing Rules, respectively (teaching Physician Rules and Split-Shared Billing Rules will be addressed in an upcoming issue).
Review of systems (ROS): This is a series of questions used to elicit information about additional signs, symptoms, or problems currently or previously experienced by the patient:
- Constitutional;
- Eyes; ears, nose, mouth, throat;
- Cardiovascular;
- Respiratory;
- Gastrointestinal;
- Genitourinary;
- Musculoskeletal;
- Integumentary (including skin and/or breast);
- Neurological;
- Psychiatric;
- Endocrine;
- Hematologic/lymphatic; and
- Allergic/immunologic.
The ROS may be classified as brief (a comment on one system), expanded (a comment on two to nine systems), or complete (a comment on more than 10 systems).
Documentation of a complete ROS (more than 10 systems) can occur in two ways:
- The physician can individually document each system. For example: “No fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular); shortness of breath (respiratory); or belly pain (gastrointestinal); etc.”; or
- The physician can document the positive findings and pertinent negative findings related to the chief complaint, along with a comment that “all other systems are negative.” This latter statement is not accepted by all local Medicare contractors.
Information involving the ROS can be documented by anyone, including the patient. If documented by someone else (e.g., a medical student) other than residents under the Teaching Physician Rules or nonphysician providers under the Split-Shared Billing Rules, the physician should reference the documented ROS in his progress note. Re-documentation of the ROS is not necessary unless a revision is required.
Past, family, and social history (PFSH): Documentation of PFSH involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. The PFSH can be classified as pertinent (a comment on one history) or complete (a comment in each of the three histories). Documentation that exemplifies a complete PFSH is: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s esophagus; no tobacco or alcohol use.”
As with ROS, the PFSH can be documented by anyone, including the patient. If documented by someone else (e.g., a medical student) other than residents under the Teaching Physician Rules or nonphysician providers under the Split-Shared Billing Rules, the physician should reference the documented PFSH in his progress note. Re-documentation of the PFSH is not necessary unless a revision is required. It is important to note that while documentation of the PFSH is required when billing higher level consultations (99254-99255) or initial inpatient care (99221-99223), it is not required when reporting subsequent hospital care services (99231-99233).
Levels of History
There are four levels of history, determined by the number of elements documented in the progress note (see Table 1, p. 21). The physician must meet all the requirements in a specific level of history before assigning it.
If all of the required elements in a given history level are not documented, the level assigned is that of the least documented element. For example, physician documentation may include four HPI elements and a complete PFSH, yet only eight ROS. The physician can only receive credit for a detailed history. If the physician submitted a claim for 99222 (initial hospital care requiring a comprehensive history, a comprehensive exam, and moderate-complexity decision making), documentation would not support the reported service due to the underdocumented ROS. Deficiencies in the ROS and family history are the most common physician documentation errors involving the history component.
A specific level of history is associated with each type of physician encounter, and must be documented accordingly (see Table 2, right). The most common visit categories provided by hospitalists that include documentation requirements for history are initial inpatient consultations, initial hospital care, subsequent hospital care, and initial observation care. Other visit categories, such as critical care and discharge day management, have neither associated levels of history nor documentation requirements for historical elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Documentation in the medical record serves many purposes: communication among healthcare professionals, evidence of patient care, and justification for provider claims.
Although these three aspects of documentation are intertwined, the first two prevent physicians from paying settlements involving malpractice allegations, while the last one assists in obtaining appropriate reimbursement for services rendered. This is the first of a three-part series that will focus on claim reporting and outline the documentation guidelines set forth by the Centers for Medicare and Medicaid Services (CMS) in conjunction with the American Medical Association (AMA).
1995, 1997 Guidelines
Two sets of documentation guidelines are in place, referred to as the 1995 and 1997 guidelines. Increased criticism of the ambiguity in the 1995 guidelines from auditors and providers inspired development of the 1997 guidelines.
While the 1997 guidelines were intended to create a more objective and unified approach to documentation, the level of specificity required brought criticism and frustration. But while the physician community balked, most auditors praised these efforts.
To satisfy all parties and allow physicians to document as they prefer, both sets of guidelines remain. Physicians can document according to either style, and auditors are obligated to review provider records against both sets of guidelines, selecting the final visit level with the set that best supports provider documentation.
Elements of History
Chief complaint (CC): The CC is the reason for the visit as stated in the patient’s own words. This must be present for each encounter, and should reference a specific condition or complaint (e.g., patient complains of abdominal pain).
History of present illness (HPI): This is a description of the present illness as it developed. It is typically formatted and documented with reference to location, quality, severity, timing, context, modifying factors, and associated signs/symptoms as related to the chief complaint. The HPI may be classified as brief (a comment on fewer than HPI elements) or extended (a comment on more than four HPI elements). Sample documentation of an extended HPI is: “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
The 1997 guidelines offer an alternate format for documenting the HPI. In contrast to the standard method above, the physician may list and status the patient’s chronic or inactive conditions. An extended HPI consists of the status of at least three chronic or inactive conditions (e.g., “Diabetes controlled by oral medication; extrinsic asthma without acute exacerbation in past six months; hypertension stable with pressures ranging from 130-140/80-90”). Failing to document the status negates the opportunity for the physician to receive HPI credit. Instead, he will receive credit for a past medical history.
The HPI should never be documented by ancillary staff (e.g., registered nurse, medical assistant, students). HPI might be documented by residents (e.g., residents, fellows, interns) or nonphysician providers (nurse practitioners and physician assistants) when utilizing the Teaching Physician Rules or Split-Shared Billing Rules, respectively (teaching Physician Rules and Split-Shared Billing Rules will be addressed in an upcoming issue).
Review of systems (ROS): This is a series of questions used to elicit information about additional signs, symptoms, or problems currently or previously experienced by the patient:
- Constitutional;
- Eyes; ears, nose, mouth, throat;
- Cardiovascular;
- Respiratory;
- Gastrointestinal;
- Genitourinary;
- Musculoskeletal;
- Integumentary (including skin and/or breast);
- Neurological;
- Psychiatric;
- Endocrine;
- Hematologic/lymphatic; and
- Allergic/immunologic.
The ROS may be classified as brief (a comment on one system), expanded (a comment on two to nine systems), or complete (a comment on more than 10 systems).
Documentation of a complete ROS (more than 10 systems) can occur in two ways:
- The physician can individually document each system. For example: “No fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular); shortness of breath (respiratory); or belly pain (gastrointestinal); etc.”; or
- The physician can document the positive findings and pertinent negative findings related to the chief complaint, along with a comment that “all other systems are negative.” This latter statement is not accepted by all local Medicare contractors.
Information involving the ROS can be documented by anyone, including the patient. If documented by someone else (e.g., a medical student) other than residents under the Teaching Physician Rules or nonphysician providers under the Split-Shared Billing Rules, the physician should reference the documented ROS in his progress note. Re-documentation of the ROS is not necessary unless a revision is required.
Past, family, and social history (PFSH): Documentation of PFSH involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. The PFSH can be classified as pertinent (a comment on one history) or complete (a comment in each of the three histories). Documentation that exemplifies a complete PFSH is: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s esophagus; no tobacco or alcohol use.”
As with ROS, the PFSH can be documented by anyone, including the patient. If documented by someone else (e.g., a medical student) other than residents under the Teaching Physician Rules or nonphysician providers under the Split-Shared Billing Rules, the physician should reference the documented PFSH in his progress note. Re-documentation of the PFSH is not necessary unless a revision is required. It is important to note that while documentation of the PFSH is required when billing higher level consultations (99254-99255) or initial inpatient care (99221-99223), it is not required when reporting subsequent hospital care services (99231-99233).
Levels of History
There are four levels of history, determined by the number of elements documented in the progress note (see Table 1, p. 21). The physician must meet all the requirements in a specific level of history before assigning it.
If all of the required elements in a given history level are not documented, the level assigned is that of the least documented element. For example, physician documentation may include four HPI elements and a complete PFSH, yet only eight ROS. The physician can only receive credit for a detailed history. If the physician submitted a claim for 99222 (initial hospital care requiring a comprehensive history, a comprehensive exam, and moderate-complexity decision making), documentation would not support the reported service due to the underdocumented ROS. Deficiencies in the ROS and family history are the most common physician documentation errors involving the history component.
A specific level of history is associated with each type of physician encounter, and must be documented accordingly (see Table 2, right). The most common visit categories provided by hospitalists that include documentation requirements for history are initial inpatient consultations, initial hospital care, subsequent hospital care, and initial observation care. Other visit categories, such as critical care and discharge day management, have neither associated levels of history nor documentation requirements for historical elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Medical Verdicts
Hospital discharge is followed by stillbirth
A 38-year-old woman’s pregnancy was proceeding uneventfully. After about 7 months of prenatal care, she presented to her physician with persistent vaginal bleeding and abdominal and back pain. One hour of monitoring at the hospital indicated that she was not in labor and the signs of fetal well-being were reassuring. Despite continued bleeding and abdominal pain, the woman was discharged. She returned to her physician’s office in early afternoon with increased bleeding and pain, and was sent to the hospital for delivery. On the way there, she suffered massive hemorrhaging due to placental abruption. Before an emergency cesarean section could be performed, the child was stillborn. The mother received transfusions for disseminated intravascular coagulation and blood loss.
Patient’s claim She was discharged without a proper workup for the bleeding and abdominal pain. A sonogram should have been ordered, and she should not have been discharged.
Doctor’s defense The mother’s condition had improved and delivery was not imminent, so the discharge was proper. The sudden massive placental abruption could not have been predicted.
Verdict $1,651,166 Illinois verdict.
Did MD cause kidney loss by injuring ureter?
A 36-year-old woman underwent a total hysterectomy performed by her ObGyn. A week later, she still complained about right flank pain. Additional surgery indicated an atrophied right kidney and an injured ureter, and a nephrectomy was performed.
Patient’s claim The physician injured the ureter during the hysterectomy, and this caused the loss of the kidney. He should have protected the ureter during the surgery—and identified the injury once it occurred.
Doctor’s defense The ureter was not injured during the surgery; rather, the patient had a slow-developing ureteral blockage.
Verdict $974,683 Kentucky verdict. Posttrial motions were pending.
$57 million verdict after admission of fault
A 39-year-old woman was in labor for 8 hours under the care of an ObGyn, an anesthesiologist, and a nurse midwife. When the child was eventually delivered by cesarean section, he was limp and pale, with no heart rate. He was diagnosed later as quadriplegic with cerebral palsy. He has global developmental delay and both bladder and bowel incontinence, and will never walk or live on his own.
Patient’s claim Despite significant abnormalities on the fetal heart monitor, labor was allowed to continue. A cesarean section should have been performed sooner. Also, it was negligent to not have specialists present at delivery; 11 minutes elapsed before a neonatologist arrived to resuscitate the infant.
Doctor’s defense Before the start of the trial, all defendants conceded liability.
Verdict $57,623,113 Pennsylvania verdict, which was reduced to $23,000,000 under a high-low agreement.
Was hysterectomy overly invasive?
Following laparoscopic surgery, a 33-year-old woman reported vaginal bleeding to her ObGyn. Three weeks later, he performed a total hysterectomy.
Patient’s claim The ObGyn made an improper diagnosis. Less invasive methods were available to address the vaginal bleeding.
Doctor’s defense Treatment with less invasive procedures was unsuccessful. Also, the patient was informed of the risks before the surgery.
Verdict Kentucky defense verdict.
Undetected injury leads to extensive surgery
A woman underwent endometrial ablation, performed by an ObGyn. During the procedure, the uterus was perforated. The physician did not recognize the perforation. The ablation device was acti vated, and a thermal injury to the bowel occurred. Ten days later, the patient returned to the hospital with extreme abdominal pain. She was diagnosed with peritonitis and taken to surgery, where the removal of 32 cm of small intestine and repair of the colon and uterus were performed. She returned to the hospital 2 weeks after this and was hospitalized for another 2 weeks for peritonitis.
Patient’s claim The physician was negligent for failing to recognize and treat the uterine perforation.
Doctor’s defense Not reported.
Verdict $245,000 Minnesota settlement was reached in mediation.
Mom blames injury on lack of cerclage
A woman who had already experienced preterm delivery was pregnant with twins and was being seen by both her ObGyn and a perinatologist. At 23 weeks’ gestation, she was admitted to a hospital for bed rest. A month later, due to signs of immediate delivery, she was transferred to a hospital with a better neonatal intensive care unit. She gave birth the following day to both a healthy twin and a twin suffering an intraventricular brain bleed, leading to diplegia, microcephaly, cognitive defects, and visual problems.
Patient’s claim She required cerclage for an incompetent cervix. If cerclage had been performed, the baby’s injuries would have been avoided. She disputed the defendants’ claim.
Doctor’s defense A cerclage had been offered, but the mother declined.
Verdict California defense verdict. A posttrial motion was pending.
Did mother’s behavior cause preterm births?
A woman pregnant with twins first sought prenatal care at 12 weeks’ gestation, at which time she was smoking half a pack of cigarettes a day. At 27 weeks, ultrasonography indicated that both twins were growing normally, although twin B had duodenal atresia and polyhydramnios. It also showed that the mother had a shortened cervix. To avoid preterm delivery, she was placed on strict bed rest. She presented at the hospital a few weeks later with vaginal pressure with contractions. She was placed on a fetal monitor, given tocolytics to stop contractions, and prescribed betamethasone to mature the twins’ lungs. Later records indicated that she had been non-compliant regarding bed rest and smoking cessation. She was discharged with no sign of contractions. Several weeks later, she was admitted to the hospital with diarrhea and contractions. Again she was administered tocolytics and betamethasone; a fetal monitor was placed and biophysical profiles were obtained. On day 4, the fetal monitor showed nonreassuring signs and did not always monitor both twins, so a cesarean section was scheduled for 4:10 pm. The delivering OB arrived at 5:20 pm and delivered the twins, now at 30 weeks’ gestation. Both showed signs of decreased oxygenation and were placed in the neonatal intensive care unit. Twin A developed meningitis 9 days later; a brain scan indicated hypoxic–ischemic encephalopathy. Twin B was discharged after 44 days, and twin A after 66 days.
Patient’s claim The babies suffered metabolic acidosis, so they should have been delivered a few days earlier. The fetal monitors were not functioning properly all of the time. Also, the mother was compliant while she was hospitalized.
Doctor’s defense Because of the twins’ prematurity, an earlier delivery was contra-indicated. Twin A’s brain injury occurred 10 to 14 days before birth. The twins’ deficits were due to both genetics and the mother’s smoking and noncompliance. Twin B had no brain injury, and her mild condition was a result of prematurity.
Verdict $2,250,000 Michigan settlement.
Midwife and nurse deliver CP baby
A 20-year-old primigravida went to the hospital in labor at term. A midwife and nurse examined her, conducted fetal monitoring, and administered oxytocin to enhance labor. The child was delivered about 24 hours later. He was diagnosed with spastic quadriplegic cerebral palsy, is almost blind, and will remain in diapers.
Patient’s claim Failure to recognize signs of fetal distress and summon an obstetrician was negligent. Oxytocin contributed to a fetal heart rate deceleration, at which time an obstetrician should have been called and oxytocin discontinued.
Doctor’s defense An obstetrician was not needed. The fetal heart rate never decreased to an unsafe level, and oxytocin did not affect the fetus. An infection caused the cerebral palsy, the onset of which occurred 24 hours prior to birth.
Verdict Pennsylvania defense verdict. A posttrial motion was pending.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Hospital discharge is followed by stillbirth
A 38-year-old woman’s pregnancy was proceeding uneventfully. After about 7 months of prenatal care, she presented to her physician with persistent vaginal bleeding and abdominal and back pain. One hour of monitoring at the hospital indicated that she was not in labor and the signs of fetal well-being were reassuring. Despite continued bleeding and abdominal pain, the woman was discharged. She returned to her physician’s office in early afternoon with increased bleeding and pain, and was sent to the hospital for delivery. On the way there, she suffered massive hemorrhaging due to placental abruption. Before an emergency cesarean section could be performed, the child was stillborn. The mother received transfusions for disseminated intravascular coagulation and blood loss.
Patient’s claim She was discharged without a proper workup for the bleeding and abdominal pain. A sonogram should have been ordered, and she should not have been discharged.
Doctor’s defense The mother’s condition had improved and delivery was not imminent, so the discharge was proper. The sudden massive placental abruption could not have been predicted.
Verdict $1,651,166 Illinois verdict.
Did MD cause kidney loss by injuring ureter?
A 36-year-old woman underwent a total hysterectomy performed by her ObGyn. A week later, she still complained about right flank pain. Additional surgery indicated an atrophied right kidney and an injured ureter, and a nephrectomy was performed.
Patient’s claim The physician injured the ureter during the hysterectomy, and this caused the loss of the kidney. He should have protected the ureter during the surgery—and identified the injury once it occurred.
Doctor’s defense The ureter was not injured during the surgery; rather, the patient had a slow-developing ureteral blockage.
Verdict $974,683 Kentucky verdict. Posttrial motions were pending.
$57 million verdict after admission of fault
A 39-year-old woman was in labor for 8 hours under the care of an ObGyn, an anesthesiologist, and a nurse midwife. When the child was eventually delivered by cesarean section, he was limp and pale, with no heart rate. He was diagnosed later as quadriplegic with cerebral palsy. He has global developmental delay and both bladder and bowel incontinence, and will never walk or live on his own.
Patient’s claim Despite significant abnormalities on the fetal heart monitor, labor was allowed to continue. A cesarean section should have been performed sooner. Also, it was negligent to not have specialists present at delivery; 11 minutes elapsed before a neonatologist arrived to resuscitate the infant.
Doctor’s defense Before the start of the trial, all defendants conceded liability.
Verdict $57,623,113 Pennsylvania verdict, which was reduced to $23,000,000 under a high-low agreement.
Was hysterectomy overly invasive?
Following laparoscopic surgery, a 33-year-old woman reported vaginal bleeding to her ObGyn. Three weeks later, he performed a total hysterectomy.
Patient’s claim The ObGyn made an improper diagnosis. Less invasive methods were available to address the vaginal bleeding.
Doctor’s defense Treatment with less invasive procedures was unsuccessful. Also, the patient was informed of the risks before the surgery.
Verdict Kentucky defense verdict.
Undetected injury leads to extensive surgery
A woman underwent endometrial ablation, performed by an ObGyn. During the procedure, the uterus was perforated. The physician did not recognize the perforation. The ablation device was acti vated, and a thermal injury to the bowel occurred. Ten days later, the patient returned to the hospital with extreme abdominal pain. She was diagnosed with peritonitis and taken to surgery, where the removal of 32 cm of small intestine and repair of the colon and uterus were performed. She returned to the hospital 2 weeks after this and was hospitalized for another 2 weeks for peritonitis.
Patient’s claim The physician was negligent for failing to recognize and treat the uterine perforation.
Doctor’s defense Not reported.
Verdict $245,000 Minnesota settlement was reached in mediation.
Mom blames injury on lack of cerclage
A woman who had already experienced preterm delivery was pregnant with twins and was being seen by both her ObGyn and a perinatologist. At 23 weeks’ gestation, she was admitted to a hospital for bed rest. A month later, due to signs of immediate delivery, she was transferred to a hospital with a better neonatal intensive care unit. She gave birth the following day to both a healthy twin and a twin suffering an intraventricular brain bleed, leading to diplegia, microcephaly, cognitive defects, and visual problems.
Patient’s claim She required cerclage for an incompetent cervix. If cerclage had been performed, the baby’s injuries would have been avoided. She disputed the defendants’ claim.
Doctor’s defense A cerclage had been offered, but the mother declined.
Verdict California defense verdict. A posttrial motion was pending.
Did mother’s behavior cause preterm births?
A woman pregnant with twins first sought prenatal care at 12 weeks’ gestation, at which time she was smoking half a pack of cigarettes a day. At 27 weeks, ultrasonography indicated that both twins were growing normally, although twin B had duodenal atresia and polyhydramnios. It also showed that the mother had a shortened cervix. To avoid preterm delivery, she was placed on strict bed rest. She presented at the hospital a few weeks later with vaginal pressure with contractions. She was placed on a fetal monitor, given tocolytics to stop contractions, and prescribed betamethasone to mature the twins’ lungs. Later records indicated that she had been non-compliant regarding bed rest and smoking cessation. She was discharged with no sign of contractions. Several weeks later, she was admitted to the hospital with diarrhea and contractions. Again she was administered tocolytics and betamethasone; a fetal monitor was placed and biophysical profiles were obtained. On day 4, the fetal monitor showed nonreassuring signs and did not always monitor both twins, so a cesarean section was scheduled for 4:10 pm. The delivering OB arrived at 5:20 pm and delivered the twins, now at 30 weeks’ gestation. Both showed signs of decreased oxygenation and were placed in the neonatal intensive care unit. Twin A developed meningitis 9 days later; a brain scan indicated hypoxic–ischemic encephalopathy. Twin B was discharged after 44 days, and twin A after 66 days.
Patient’s claim The babies suffered metabolic acidosis, so they should have been delivered a few days earlier. The fetal monitors were not functioning properly all of the time. Also, the mother was compliant while she was hospitalized.
Doctor’s defense Because of the twins’ prematurity, an earlier delivery was contra-indicated. Twin A’s brain injury occurred 10 to 14 days before birth. The twins’ deficits were due to both genetics and the mother’s smoking and noncompliance. Twin B had no brain injury, and her mild condition was a result of prematurity.
Verdict $2,250,000 Michigan settlement.
Midwife and nurse deliver CP baby
A 20-year-old primigravida went to the hospital in labor at term. A midwife and nurse examined her, conducted fetal monitoring, and administered oxytocin to enhance labor. The child was delivered about 24 hours later. He was diagnosed with spastic quadriplegic cerebral palsy, is almost blind, and will remain in diapers.
Patient’s claim Failure to recognize signs of fetal distress and summon an obstetrician was negligent. Oxytocin contributed to a fetal heart rate deceleration, at which time an obstetrician should have been called and oxytocin discontinued.
Doctor’s defense An obstetrician was not needed. The fetal heart rate never decreased to an unsafe level, and oxytocin did not affect the fetus. An infection caused the cerebral palsy, the onset of which occurred 24 hours prior to birth.
Verdict Pennsylvania defense verdict. A posttrial motion was pending.
Hospital discharge is followed by stillbirth
A 38-year-old woman’s pregnancy was proceeding uneventfully. After about 7 months of prenatal care, she presented to her physician with persistent vaginal bleeding and abdominal and back pain. One hour of monitoring at the hospital indicated that she was not in labor and the signs of fetal well-being were reassuring. Despite continued bleeding and abdominal pain, the woman was discharged. She returned to her physician’s office in early afternoon with increased bleeding and pain, and was sent to the hospital for delivery. On the way there, she suffered massive hemorrhaging due to placental abruption. Before an emergency cesarean section could be performed, the child was stillborn. The mother received transfusions for disseminated intravascular coagulation and blood loss.
Patient’s claim She was discharged without a proper workup for the bleeding and abdominal pain. A sonogram should have been ordered, and she should not have been discharged.
Doctor’s defense The mother’s condition had improved and delivery was not imminent, so the discharge was proper. The sudden massive placental abruption could not have been predicted.
Verdict $1,651,166 Illinois verdict.
Did MD cause kidney loss by injuring ureter?
A 36-year-old woman underwent a total hysterectomy performed by her ObGyn. A week later, she still complained about right flank pain. Additional surgery indicated an atrophied right kidney and an injured ureter, and a nephrectomy was performed.
Patient’s claim The physician injured the ureter during the hysterectomy, and this caused the loss of the kidney. He should have protected the ureter during the surgery—and identified the injury once it occurred.
Doctor’s defense The ureter was not injured during the surgery; rather, the patient had a slow-developing ureteral blockage.
Verdict $974,683 Kentucky verdict. Posttrial motions were pending.
$57 million verdict after admission of fault
A 39-year-old woman was in labor for 8 hours under the care of an ObGyn, an anesthesiologist, and a nurse midwife. When the child was eventually delivered by cesarean section, he was limp and pale, with no heart rate. He was diagnosed later as quadriplegic with cerebral palsy. He has global developmental delay and both bladder and bowel incontinence, and will never walk or live on his own.
Patient’s claim Despite significant abnormalities on the fetal heart monitor, labor was allowed to continue. A cesarean section should have been performed sooner. Also, it was negligent to not have specialists present at delivery; 11 minutes elapsed before a neonatologist arrived to resuscitate the infant.
Doctor’s defense Before the start of the trial, all defendants conceded liability.
Verdict $57,623,113 Pennsylvania verdict, which was reduced to $23,000,000 under a high-low agreement.
Was hysterectomy overly invasive?
Following laparoscopic surgery, a 33-year-old woman reported vaginal bleeding to her ObGyn. Three weeks later, he performed a total hysterectomy.
Patient’s claim The ObGyn made an improper diagnosis. Less invasive methods were available to address the vaginal bleeding.
Doctor’s defense Treatment with less invasive procedures was unsuccessful. Also, the patient was informed of the risks before the surgery.
Verdict Kentucky defense verdict.
Undetected injury leads to extensive surgery
A woman underwent endometrial ablation, performed by an ObGyn. During the procedure, the uterus was perforated. The physician did not recognize the perforation. The ablation device was acti vated, and a thermal injury to the bowel occurred. Ten days later, the patient returned to the hospital with extreme abdominal pain. She was diagnosed with peritonitis and taken to surgery, where the removal of 32 cm of small intestine and repair of the colon and uterus were performed. She returned to the hospital 2 weeks after this and was hospitalized for another 2 weeks for peritonitis.
Patient’s claim The physician was negligent for failing to recognize and treat the uterine perforation.
Doctor’s defense Not reported.
Verdict $245,000 Minnesota settlement was reached in mediation.
Mom blames injury on lack of cerclage
A woman who had already experienced preterm delivery was pregnant with twins and was being seen by both her ObGyn and a perinatologist. At 23 weeks’ gestation, she was admitted to a hospital for bed rest. A month later, due to signs of immediate delivery, she was transferred to a hospital with a better neonatal intensive care unit. She gave birth the following day to both a healthy twin and a twin suffering an intraventricular brain bleed, leading to diplegia, microcephaly, cognitive defects, and visual problems.
Patient’s claim She required cerclage for an incompetent cervix. If cerclage had been performed, the baby’s injuries would have been avoided. She disputed the defendants’ claim.
Doctor’s defense A cerclage had been offered, but the mother declined.
Verdict California defense verdict. A posttrial motion was pending.
Did mother’s behavior cause preterm births?
A woman pregnant with twins first sought prenatal care at 12 weeks’ gestation, at which time she was smoking half a pack of cigarettes a day. At 27 weeks, ultrasonography indicated that both twins were growing normally, although twin B had duodenal atresia and polyhydramnios. It also showed that the mother had a shortened cervix. To avoid preterm delivery, she was placed on strict bed rest. She presented at the hospital a few weeks later with vaginal pressure with contractions. She was placed on a fetal monitor, given tocolytics to stop contractions, and prescribed betamethasone to mature the twins’ lungs. Later records indicated that she had been non-compliant regarding bed rest and smoking cessation. She was discharged with no sign of contractions. Several weeks later, she was admitted to the hospital with diarrhea and contractions. Again she was administered tocolytics and betamethasone; a fetal monitor was placed and biophysical profiles were obtained. On day 4, the fetal monitor showed nonreassuring signs and did not always monitor both twins, so a cesarean section was scheduled for 4:10 pm. The delivering OB arrived at 5:20 pm and delivered the twins, now at 30 weeks’ gestation. Both showed signs of decreased oxygenation and were placed in the neonatal intensive care unit. Twin A developed meningitis 9 days later; a brain scan indicated hypoxic–ischemic encephalopathy. Twin B was discharged after 44 days, and twin A after 66 days.
Patient’s claim The babies suffered metabolic acidosis, so they should have been delivered a few days earlier. The fetal monitors were not functioning properly all of the time. Also, the mother was compliant while she was hospitalized.
Doctor’s defense Because of the twins’ prematurity, an earlier delivery was contra-indicated. Twin A’s brain injury occurred 10 to 14 days before birth. The twins’ deficits were due to both genetics and the mother’s smoking and noncompliance. Twin B had no brain injury, and her mild condition was a result of prematurity.
Verdict $2,250,000 Michigan settlement.
Midwife and nurse deliver CP baby
A 20-year-old primigravida went to the hospital in labor at term. A midwife and nurse examined her, conducted fetal monitoring, and administered oxytocin to enhance labor. The child was delivered about 24 hours later. He was diagnosed with spastic quadriplegic cerebral palsy, is almost blind, and will remain in diapers.
Patient’s claim Failure to recognize signs of fetal distress and summon an obstetrician was negligent. Oxytocin contributed to a fetal heart rate deceleration, at which time an obstetrician should have been called and oxytocin discontinued.
Doctor’s defense An obstetrician was not needed. The fetal heart rate never decreased to an unsafe level, and oxytocin did not affect the fetus. An infection caused the cerebral palsy, the onset of which occurred 24 hours prior to birth.
Verdict Pennsylvania defense verdict. A posttrial motion was pending.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Playing high-stakes poker: Do you fight—or settle—that malpractice lawsuit?
CASE Brachial plexus injury, then a summons
J.L., a 29-year-old primigravida, has gestational diabetes. When she goes into labor at term, she reports to the state-of-the-art hospital where you practice. Delivery is difficult and achieved using forceps. The infant weighs 9 lb 4 oz, and has obvious weakness in his right arm. A neurologist diagnoses Erb’s palsy, and the child undergoes brachial plexus exploration and repair of injured nerves.
Two years later, most arm function has returned. Soon thereafter, you receive a summons from the parents and their attorney demanding $3 million. Do you fight—or settle?
You could say there are two types of physicians: those who have been sued and those who will be.
This is an overstatement, of course, but not by much. In high-risk specialties such as obstetrics, most physicians will receive a summons at some point in their career. In fact, almost nine of every 10 ObGyns report that they have been sued at least once in their career, with an average of 2.6 claims each.Got malpractice distress? You can help yourself survive,” in the February 2008 issue of OBG Mangement, available at www.obgmanagment.comGiven how stressful litigation can be, there are a number of considerations that enter into the calculus of fight or settle. This article will focus on seven of those considerations (see the box above).
How consent-to-settle clauses can protect you
For years, many carriers curried favor with physicians by barring settlement of a case unless the physician agreed to it. If the physician balked, the carrier was obligated to defend the case to the end.
This clause is still found in professional liability policies, but the number of carriers offering such flexibility has decreased considerably. Many carriers now base the decision to settle on both the merits of a case and the cost of defense. If the carrier determines that it would be much less expensive to settle a case for nuisance value than to defend it through trial, the carrier is within its rights to settle. Obviously, this posture has ramifications for the insured physician.
A consent-to-settle clause—or its omission—is usually established contractually at the beginning of coverage. If the ability to demand consent for settling is important to you, look closely for such language when you purchase or renew coverage. State law can also determine whether such a clause is included.
In addition to a standard consent-to-settle provision, some carriers promote a “hammer clause,” by which an insurer’s liability is limited to a recommended settlement. Let’s say the carrier decides to settle a particular case for $100,000, the physician withholds consent, and a judgment of $300,000 is entered. The physician is individually liable for the “overage”—in this case, $200,000.
As if this were not complicated enough, there is also a modified hammer clause, which is a “kinder, gentler” approach. In this scenario, the physician is liable only for a percentage of any judgment above the recommended settlement. In the example just given, if the modified hammer provision were 50%, the carrier would pay its recommended settlement ($100,000) plus 50% of the overage—in this case, another $100,000, for a total of $200,000. The physician would be liable for the remaining $100,000.
Without a consent-to-settle clause, the physician is removed from decision-making. Further, a hammer clause or modified hammer clause should cause a physician to think long and hard before forgoing a recommended settlement.
When personal liability exceeds policy limits
Even if the carrier is bound, through its contract with you, to defend a case to the end, it will generally be limited to a maximum payout. Policy limits depend on the particular policy, with higher limits associated with higher premiums.
Carrying a very high limit can make you a more appealing target for a lawsuit, frivolous or otherwise. Many personal injury attorneys view medical malpractice as little more than a series of insurance transactions. If you have a high coverage limit, you will attract greater attention. This is of particular concern when there are multiple defendants and culpability varies significantly between the actors.
When negligence is proven in states that still allow joint and several liability, even 1% liability can leave you responsible for the entire amount. The solution is to have reasonable—but not excessive—coverage. Many believe this balance lies at $1 million/$3 million limits.
Desire for a payout may persuade a plaintiff to settle for policy limits
If you have coverage of up to $1 million and a court delivers a higher judgment, what happens?
It depends. In theory, you are liable for the overage; the carrier will pay up to the policy limit, and you are responsible for the rest. In reality, however, the situation is more complex.
You often have the right to demand a new trial or appeal the case. You may not prevail, but this approach creates new risks for the plaintiff right after “victory” is tasted. Rather than roll the dice, many plaintiffs, under the advice of their attorney, will reconsider and settle for the policy limit. It is in their interest to lock in a certain figure rather than prolong the case, exposing themselves to increased risk. And if the judgment makes it clear that bankruptcy is an option for the physician, a plaintiff will take pains to prevent that end game. Once bankruptcy is filed, the clock slows, and it may take years for the plaintiff to receive any funds. Even then, the plaintiff may have to wait in line behind more senior creditors.
Consider asset protection
Asset protection prior to litigation can affect the dynamics of posttrial settlement discussions. Asset protection means many things, and there are different degrees of protection. A limited number of attorneys are skilled in asset protection, and plaintiff’s attorneys generally have limited experience breaking through the shield.
With a robust asset-protection program in place, you can come to the table with greater leverage and engage in a more rational discussion about a just settlement in which most, if not all, of the settlement will be within the policy limit.
There are approximately 50,000 to 60,000 medicolegal cases open at any given moment, but the number of physicians involved is much higher because many suits name multiple defendants.3 In 2004, the National Practitioner Data Bank (NPDB) reported entries for more than 200,000 health-care providers since 1990, most of whom had been reported just one time.4 Again that number is low because not every physician who is sued is reported to the NPDB. Reporting is required only if payment is made by settlement or judgment related to a written demand by a plaintiff. If the case against the physician is dismissed, or the physician wins in court, no report is entered. So the 200,000 entries are just the tip of the iceberg. With roughly 700,000 physicians practicing in the United States, the number of physicians affected by liability litigation could be staggering.
When you want to settle, but the carrier doesn’t
Ordinarily, your interests and those of your carrier are aligned. You both want to win—or at least lose less—but there is one scenario in which your interests may diverge. That is when you believe you are at risk for a judgment that will exceed the policy limit. In such a situation, you want your carrier to tender the full limit, but the carrier faces a worst-case scenario: paying the maximum amount on the policy.
If the carrier believes the case is defensible, it may choose to fight, hoping to win or receive a judgment well below the policy limit. If the carrier’s strategy prevails, all parties will be better off. However, if the carrier gambles and loses, you will face the very scenario you hoped to avoid—exposure to a judgment beyond the policy limit.
The law generally provides that a carrier that wants to gamble must do so with its own money. To do otherwise constitutes action “in bad faith.” After judgment, many physicians sue their own insurance company on the basis of exactly that legal theory. It is even more common for a plaintiff, fresh from victory, to join forces with the doctor defendant and take action against the carrier.
This endgame is not automatic, however. If you want to minimize the risk that your pocket will be the only one left to pick after a high-stakes case ends, you must demand in writing that the case be settled up to the policy limit. Under such circumstances, it is best for your personal counsel to deliver that message because the carrier-appointed attorney faces something of a conflict, because she is an advocate for the physician but paid by the carrier.
Avoiding the National Practitioner Data Bank
In 1990, the National Practitioner Data Bank (NPDB) was launched with the goal of keeping dangerous physicians from migrating from state to state to escape accountability. A central database allows licensing agencies to quickly determine whether a doctor has a checkered past.
The NPDB labels a physician “as marked” if money is paid for a malpractice settlement or judgment. The NPDB lists hundreds of thousands of physicians, most of whom have a single entry. Many state licensing agencies have also begun listing physicians who have lost or settled a lawsuit; the only difference is that such information is posted online and is accessible to the public. In contrast, the NPDB remains confidential, accessible only by those who “need to know,” such as credentialing committees, hospitals, and licensing boards.
Even $1 can incur a listing
Many physicians wrongly believe that they will not be reported to the NPDB if they are involved in a case that settles for an amount under $30,000. Low-value settlements are often consummated for nuisance value, meaning that they have no legal merit. However, any payment—even $1—is reportable to the NPDB. It does not matter whether payment is made by settlement or judgment.
A written demand for money, whether as damages for an injury, money to see another physician, or a refund of cash tendered, can sometimes be construed as reportable.
Being joined to a corporate entity can help you
Seasoned plaintiff’s attorneys understand physicians’ deep aversion to being reported. They often take advantage of a well-known exception to reporting: payment made in the name of a corporate entity.
If a physician is employed by a corporation with at least two physicians, and the case is settled in the name of the corporation, the physician can be dismissed from the claim, and no reporting is required. In that case, the physician maintains his clean record in the data bank. That said, this can get complicated if one is obligated to report to state authorities. Because each state is different, these details should be addressed with your attorney.
High-low agreements can avert huge judgments
As discovery progresses, the plaintiff and defendant usually come to a better understanding of their respective risk—but not always. In some situations, the plaintiff may have a strong case in regard to one element of negligence, such as damages, but a weak case in regard to causation. Cerebral palsy cases fit this paradigm. In such cases, the infant has clear-cut medical and rehabilitation needs that can run easily into seven figures, but proving that a physician’s actions or omissions caused the injury can be difficult. Both sides can mitigate risk for one another by embracing a “high-low” agreement—a contract defining how a plaintiff will be paid based on a specific jury verdict.
For example, if the high-low agreement is $500,000/$100,000, the insurer is locked into one of two payments. If the jury returns a verdict for the defense, the carrier pays $100,000; if the verdict is for the plaintiff, the carrier pays $500,000, regardless of the amount of damages awarded by the jury. Without such an agreement, the range of potential judgments is no money at all to almost any amount.
When a high-low agreement is in effect, and the jury returns a verdict for the physician, the settlement is not reported to the NPDB even though the carrier must make a payment.
Why not?
The payment is being made pursuant to a separate agreement between the carrier and the plaintiff. The benefit to the insurer is the limitation of its liability, even if the plaintiff wins at trial and is awarded a higher amount. The benefit to the plaintiff is a guaranteed payment, even if there is no finding of liability against the practitioner.
How a reputation for settling can hurt
If you are so risk-averse that you demand that your carrier settle all cases—even those with no merit—two things will happen:
- Word will spread throughout the plaintiff’s bar that you are an easy target, and the threshold for filing suit against you will decline. And given how little work will be required to net a settlement, attorney’s summons will forever darken your door
- Your medical liability rates will climb—or coverage will be terminated. Settling meritorious cases makes sense, but settling all cases regardless of merit is ill-advised.
Stress is common on both sides of the equation
Lawsuits take a long time to percolate through the system, with an average time from medical event to claim resolution of about 5 years—longer in obstetrics.2
Attorneys are accustomed to this time frame; physicians are not. The lingering effects on doctors include stress, loss of job satisfaction, family strife, depression, substance abuse, and so on.
Because a lawsuit is a major stressful life event, a physician may be only too happy to be done with one. If there were absolutely no consequences to settling, that would be a smart move. But there are consequences, and living with them can also cause stress. The best way to minimize stress on either side of the equation is to think long and hard before settling any case.
1. Wilson N, Strunk A. Overview of the 2006 ACOG Survey on Professional Liability. Available at: www.acog.org/departments/professionalliability/2006surveyNatl.pdf. Accessed March 11, 2008.
2. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.
3. Mello MM, Studdert DM. The medical malpractice system: structure and performance. In: Sage WM, Kersh R, eds. Medical Malpractice and the U.S. Health Care System: New Century, Different Issues. 1st ed. New York: Cambridge University Press; 2006:11–29.
4. US Department of Health and Human Services. National Practitioner Data Bank. 2004 annual report. Available at: http://www.npdb-hipdb.hrsa.gov/pubs/stats/2004_NPDB_Annual_Report.pdf. Accessed March 11, 2008.
More about professional liability by this author. Prepare your defense of a cerebral palsy claim (and other claims) long beforehand—in the prenatal period. That’s what Dr. Segal advised readers in the July 2007 issue of OBG Mangement. Read his argument for obtaining patient contracts in the “Past Issues” archives at www.obgmanagement.com.
CASE Brachial plexus injury, then a summons
J.L., a 29-year-old primigravida, has gestational diabetes. When she goes into labor at term, she reports to the state-of-the-art hospital where you practice. Delivery is difficult and achieved using forceps. The infant weighs 9 lb 4 oz, and has obvious weakness in his right arm. A neurologist diagnoses Erb’s palsy, and the child undergoes brachial plexus exploration and repair of injured nerves.
Two years later, most arm function has returned. Soon thereafter, you receive a summons from the parents and their attorney demanding $3 million. Do you fight—or settle?
You could say there are two types of physicians: those who have been sued and those who will be.
This is an overstatement, of course, but not by much. In high-risk specialties such as obstetrics, most physicians will receive a summons at some point in their career. In fact, almost nine of every 10 ObGyns report that they have been sued at least once in their career, with an average of 2.6 claims each.Got malpractice distress? You can help yourself survive,” in the February 2008 issue of OBG Mangement, available at www.obgmanagment.comGiven how stressful litigation can be, there are a number of considerations that enter into the calculus of fight or settle. This article will focus on seven of those considerations (see the box above).
How consent-to-settle clauses can protect you
For years, many carriers curried favor with physicians by barring settlement of a case unless the physician agreed to it. If the physician balked, the carrier was obligated to defend the case to the end.
This clause is still found in professional liability policies, but the number of carriers offering such flexibility has decreased considerably. Many carriers now base the decision to settle on both the merits of a case and the cost of defense. If the carrier determines that it would be much less expensive to settle a case for nuisance value than to defend it through trial, the carrier is within its rights to settle. Obviously, this posture has ramifications for the insured physician.
A consent-to-settle clause—or its omission—is usually established contractually at the beginning of coverage. If the ability to demand consent for settling is important to you, look closely for such language when you purchase or renew coverage. State law can also determine whether such a clause is included.
In addition to a standard consent-to-settle provision, some carriers promote a “hammer clause,” by which an insurer’s liability is limited to a recommended settlement. Let’s say the carrier decides to settle a particular case for $100,000, the physician withholds consent, and a judgment of $300,000 is entered. The physician is individually liable for the “overage”—in this case, $200,000.
As if this were not complicated enough, there is also a modified hammer clause, which is a “kinder, gentler” approach. In this scenario, the physician is liable only for a percentage of any judgment above the recommended settlement. In the example just given, if the modified hammer provision were 50%, the carrier would pay its recommended settlement ($100,000) plus 50% of the overage—in this case, another $100,000, for a total of $200,000. The physician would be liable for the remaining $100,000.
Without a consent-to-settle clause, the physician is removed from decision-making. Further, a hammer clause or modified hammer clause should cause a physician to think long and hard before forgoing a recommended settlement.
When personal liability exceeds policy limits
Even if the carrier is bound, through its contract with you, to defend a case to the end, it will generally be limited to a maximum payout. Policy limits depend on the particular policy, with higher limits associated with higher premiums.
Carrying a very high limit can make you a more appealing target for a lawsuit, frivolous or otherwise. Many personal injury attorneys view medical malpractice as little more than a series of insurance transactions. If you have a high coverage limit, you will attract greater attention. This is of particular concern when there are multiple defendants and culpability varies significantly between the actors.
When negligence is proven in states that still allow joint and several liability, even 1% liability can leave you responsible for the entire amount. The solution is to have reasonable—but not excessive—coverage. Many believe this balance lies at $1 million/$3 million limits.
Desire for a payout may persuade a plaintiff to settle for policy limits
If you have coverage of up to $1 million and a court delivers a higher judgment, what happens?
It depends. In theory, you are liable for the overage; the carrier will pay up to the policy limit, and you are responsible for the rest. In reality, however, the situation is more complex.
You often have the right to demand a new trial or appeal the case. You may not prevail, but this approach creates new risks for the plaintiff right after “victory” is tasted. Rather than roll the dice, many plaintiffs, under the advice of their attorney, will reconsider and settle for the policy limit. It is in their interest to lock in a certain figure rather than prolong the case, exposing themselves to increased risk. And if the judgment makes it clear that bankruptcy is an option for the physician, a plaintiff will take pains to prevent that end game. Once bankruptcy is filed, the clock slows, and it may take years for the plaintiff to receive any funds. Even then, the plaintiff may have to wait in line behind more senior creditors.
Consider asset protection
Asset protection prior to litigation can affect the dynamics of posttrial settlement discussions. Asset protection means many things, and there are different degrees of protection. A limited number of attorneys are skilled in asset protection, and plaintiff’s attorneys generally have limited experience breaking through the shield.
With a robust asset-protection program in place, you can come to the table with greater leverage and engage in a more rational discussion about a just settlement in which most, if not all, of the settlement will be within the policy limit.
There are approximately 50,000 to 60,000 medicolegal cases open at any given moment, but the number of physicians involved is much higher because many suits name multiple defendants.3 In 2004, the National Practitioner Data Bank (NPDB) reported entries for more than 200,000 health-care providers since 1990, most of whom had been reported just one time.4 Again that number is low because not every physician who is sued is reported to the NPDB. Reporting is required only if payment is made by settlement or judgment related to a written demand by a plaintiff. If the case against the physician is dismissed, or the physician wins in court, no report is entered. So the 200,000 entries are just the tip of the iceberg. With roughly 700,000 physicians practicing in the United States, the number of physicians affected by liability litigation could be staggering.
When you want to settle, but the carrier doesn’t
Ordinarily, your interests and those of your carrier are aligned. You both want to win—or at least lose less—but there is one scenario in which your interests may diverge. That is when you believe you are at risk for a judgment that will exceed the policy limit. In such a situation, you want your carrier to tender the full limit, but the carrier faces a worst-case scenario: paying the maximum amount on the policy.
If the carrier believes the case is defensible, it may choose to fight, hoping to win or receive a judgment well below the policy limit. If the carrier’s strategy prevails, all parties will be better off. However, if the carrier gambles and loses, you will face the very scenario you hoped to avoid—exposure to a judgment beyond the policy limit.
The law generally provides that a carrier that wants to gamble must do so with its own money. To do otherwise constitutes action “in bad faith.” After judgment, many physicians sue their own insurance company on the basis of exactly that legal theory. It is even more common for a plaintiff, fresh from victory, to join forces with the doctor defendant and take action against the carrier.
This endgame is not automatic, however. If you want to minimize the risk that your pocket will be the only one left to pick after a high-stakes case ends, you must demand in writing that the case be settled up to the policy limit. Under such circumstances, it is best for your personal counsel to deliver that message because the carrier-appointed attorney faces something of a conflict, because she is an advocate for the physician but paid by the carrier.
Avoiding the National Practitioner Data Bank
In 1990, the National Practitioner Data Bank (NPDB) was launched with the goal of keeping dangerous physicians from migrating from state to state to escape accountability. A central database allows licensing agencies to quickly determine whether a doctor has a checkered past.
The NPDB labels a physician “as marked” if money is paid for a malpractice settlement or judgment. The NPDB lists hundreds of thousands of physicians, most of whom have a single entry. Many state licensing agencies have also begun listing physicians who have lost or settled a lawsuit; the only difference is that such information is posted online and is accessible to the public. In contrast, the NPDB remains confidential, accessible only by those who “need to know,” such as credentialing committees, hospitals, and licensing boards.
Even $1 can incur a listing
Many physicians wrongly believe that they will not be reported to the NPDB if they are involved in a case that settles for an amount under $30,000. Low-value settlements are often consummated for nuisance value, meaning that they have no legal merit. However, any payment—even $1—is reportable to the NPDB. It does not matter whether payment is made by settlement or judgment.
A written demand for money, whether as damages for an injury, money to see another physician, or a refund of cash tendered, can sometimes be construed as reportable.
Being joined to a corporate entity can help you
Seasoned plaintiff’s attorneys understand physicians’ deep aversion to being reported. They often take advantage of a well-known exception to reporting: payment made in the name of a corporate entity.
If a physician is employed by a corporation with at least two physicians, and the case is settled in the name of the corporation, the physician can be dismissed from the claim, and no reporting is required. In that case, the physician maintains his clean record in the data bank. That said, this can get complicated if one is obligated to report to state authorities. Because each state is different, these details should be addressed with your attorney.
High-low agreements can avert huge judgments
As discovery progresses, the plaintiff and defendant usually come to a better understanding of their respective risk—but not always. In some situations, the plaintiff may have a strong case in regard to one element of negligence, such as damages, but a weak case in regard to causation. Cerebral palsy cases fit this paradigm. In such cases, the infant has clear-cut medical and rehabilitation needs that can run easily into seven figures, but proving that a physician’s actions or omissions caused the injury can be difficult. Both sides can mitigate risk for one another by embracing a “high-low” agreement—a contract defining how a plaintiff will be paid based on a specific jury verdict.
For example, if the high-low agreement is $500,000/$100,000, the insurer is locked into one of two payments. If the jury returns a verdict for the defense, the carrier pays $100,000; if the verdict is for the plaintiff, the carrier pays $500,000, regardless of the amount of damages awarded by the jury. Without such an agreement, the range of potential judgments is no money at all to almost any amount.
When a high-low agreement is in effect, and the jury returns a verdict for the physician, the settlement is not reported to the NPDB even though the carrier must make a payment.
Why not?
The payment is being made pursuant to a separate agreement between the carrier and the plaintiff. The benefit to the insurer is the limitation of its liability, even if the plaintiff wins at trial and is awarded a higher amount. The benefit to the plaintiff is a guaranteed payment, even if there is no finding of liability against the practitioner.
How a reputation for settling can hurt
If you are so risk-averse that you demand that your carrier settle all cases—even those with no merit—two things will happen:
- Word will spread throughout the plaintiff’s bar that you are an easy target, and the threshold for filing suit against you will decline. And given how little work will be required to net a settlement, attorney’s summons will forever darken your door
- Your medical liability rates will climb—or coverage will be terminated. Settling meritorious cases makes sense, but settling all cases regardless of merit is ill-advised.
Stress is common on both sides of the equation
Lawsuits take a long time to percolate through the system, with an average time from medical event to claim resolution of about 5 years—longer in obstetrics.2
Attorneys are accustomed to this time frame; physicians are not. The lingering effects on doctors include stress, loss of job satisfaction, family strife, depression, substance abuse, and so on.
Because a lawsuit is a major stressful life event, a physician may be only too happy to be done with one. If there were absolutely no consequences to settling, that would be a smart move. But there are consequences, and living with them can also cause stress. The best way to minimize stress on either side of the equation is to think long and hard before settling any case.
CASE Brachial plexus injury, then a summons
J.L., a 29-year-old primigravida, has gestational diabetes. When she goes into labor at term, she reports to the state-of-the-art hospital where you practice. Delivery is difficult and achieved using forceps. The infant weighs 9 lb 4 oz, and has obvious weakness in his right arm. A neurologist diagnoses Erb’s palsy, and the child undergoes brachial plexus exploration and repair of injured nerves.
Two years later, most arm function has returned. Soon thereafter, you receive a summons from the parents and their attorney demanding $3 million. Do you fight—or settle?
You could say there are two types of physicians: those who have been sued and those who will be.
This is an overstatement, of course, but not by much. In high-risk specialties such as obstetrics, most physicians will receive a summons at some point in their career. In fact, almost nine of every 10 ObGyns report that they have been sued at least once in their career, with an average of 2.6 claims each.Got malpractice distress? You can help yourself survive,” in the February 2008 issue of OBG Mangement, available at www.obgmanagment.comGiven how stressful litigation can be, there are a number of considerations that enter into the calculus of fight or settle. This article will focus on seven of those considerations (see the box above).
How consent-to-settle clauses can protect you
For years, many carriers curried favor with physicians by barring settlement of a case unless the physician agreed to it. If the physician balked, the carrier was obligated to defend the case to the end.
This clause is still found in professional liability policies, but the number of carriers offering such flexibility has decreased considerably. Many carriers now base the decision to settle on both the merits of a case and the cost of defense. If the carrier determines that it would be much less expensive to settle a case for nuisance value than to defend it through trial, the carrier is within its rights to settle. Obviously, this posture has ramifications for the insured physician.
A consent-to-settle clause—or its omission—is usually established contractually at the beginning of coverage. If the ability to demand consent for settling is important to you, look closely for such language when you purchase or renew coverage. State law can also determine whether such a clause is included.
In addition to a standard consent-to-settle provision, some carriers promote a “hammer clause,” by which an insurer’s liability is limited to a recommended settlement. Let’s say the carrier decides to settle a particular case for $100,000, the physician withholds consent, and a judgment of $300,000 is entered. The physician is individually liable for the “overage”—in this case, $200,000.
As if this were not complicated enough, there is also a modified hammer clause, which is a “kinder, gentler” approach. In this scenario, the physician is liable only for a percentage of any judgment above the recommended settlement. In the example just given, if the modified hammer provision were 50%, the carrier would pay its recommended settlement ($100,000) plus 50% of the overage—in this case, another $100,000, for a total of $200,000. The physician would be liable for the remaining $100,000.
Without a consent-to-settle clause, the physician is removed from decision-making. Further, a hammer clause or modified hammer clause should cause a physician to think long and hard before forgoing a recommended settlement.
When personal liability exceeds policy limits
Even if the carrier is bound, through its contract with you, to defend a case to the end, it will generally be limited to a maximum payout. Policy limits depend on the particular policy, with higher limits associated with higher premiums.
Carrying a very high limit can make you a more appealing target for a lawsuit, frivolous or otherwise. Many personal injury attorneys view medical malpractice as little more than a series of insurance transactions. If you have a high coverage limit, you will attract greater attention. This is of particular concern when there are multiple defendants and culpability varies significantly between the actors.
When negligence is proven in states that still allow joint and several liability, even 1% liability can leave you responsible for the entire amount. The solution is to have reasonable—but not excessive—coverage. Many believe this balance lies at $1 million/$3 million limits.
Desire for a payout may persuade a plaintiff to settle for policy limits
If you have coverage of up to $1 million and a court delivers a higher judgment, what happens?
It depends. In theory, you are liable for the overage; the carrier will pay up to the policy limit, and you are responsible for the rest. In reality, however, the situation is more complex.
You often have the right to demand a new trial or appeal the case. You may not prevail, but this approach creates new risks for the plaintiff right after “victory” is tasted. Rather than roll the dice, many plaintiffs, under the advice of their attorney, will reconsider and settle for the policy limit. It is in their interest to lock in a certain figure rather than prolong the case, exposing themselves to increased risk. And if the judgment makes it clear that bankruptcy is an option for the physician, a plaintiff will take pains to prevent that end game. Once bankruptcy is filed, the clock slows, and it may take years for the plaintiff to receive any funds. Even then, the plaintiff may have to wait in line behind more senior creditors.
Consider asset protection
Asset protection prior to litigation can affect the dynamics of posttrial settlement discussions. Asset protection means many things, and there are different degrees of protection. A limited number of attorneys are skilled in asset protection, and plaintiff’s attorneys generally have limited experience breaking through the shield.
With a robust asset-protection program in place, you can come to the table with greater leverage and engage in a more rational discussion about a just settlement in which most, if not all, of the settlement will be within the policy limit.
There are approximately 50,000 to 60,000 medicolegal cases open at any given moment, but the number of physicians involved is much higher because many suits name multiple defendants.3 In 2004, the National Practitioner Data Bank (NPDB) reported entries for more than 200,000 health-care providers since 1990, most of whom had been reported just one time.4 Again that number is low because not every physician who is sued is reported to the NPDB. Reporting is required only if payment is made by settlement or judgment related to a written demand by a plaintiff. If the case against the physician is dismissed, or the physician wins in court, no report is entered. So the 200,000 entries are just the tip of the iceberg. With roughly 700,000 physicians practicing in the United States, the number of physicians affected by liability litigation could be staggering.
When you want to settle, but the carrier doesn’t
Ordinarily, your interests and those of your carrier are aligned. You both want to win—or at least lose less—but there is one scenario in which your interests may diverge. That is when you believe you are at risk for a judgment that will exceed the policy limit. In such a situation, you want your carrier to tender the full limit, but the carrier faces a worst-case scenario: paying the maximum amount on the policy.
If the carrier believes the case is defensible, it may choose to fight, hoping to win or receive a judgment well below the policy limit. If the carrier’s strategy prevails, all parties will be better off. However, if the carrier gambles and loses, you will face the very scenario you hoped to avoid—exposure to a judgment beyond the policy limit.
The law generally provides that a carrier that wants to gamble must do so with its own money. To do otherwise constitutes action “in bad faith.” After judgment, many physicians sue their own insurance company on the basis of exactly that legal theory. It is even more common for a plaintiff, fresh from victory, to join forces with the doctor defendant and take action against the carrier.
This endgame is not automatic, however. If you want to minimize the risk that your pocket will be the only one left to pick after a high-stakes case ends, you must demand in writing that the case be settled up to the policy limit. Under such circumstances, it is best for your personal counsel to deliver that message because the carrier-appointed attorney faces something of a conflict, because she is an advocate for the physician but paid by the carrier.
Avoiding the National Practitioner Data Bank
In 1990, the National Practitioner Data Bank (NPDB) was launched with the goal of keeping dangerous physicians from migrating from state to state to escape accountability. A central database allows licensing agencies to quickly determine whether a doctor has a checkered past.
The NPDB labels a physician “as marked” if money is paid for a malpractice settlement or judgment. The NPDB lists hundreds of thousands of physicians, most of whom have a single entry. Many state licensing agencies have also begun listing physicians who have lost or settled a lawsuit; the only difference is that such information is posted online and is accessible to the public. In contrast, the NPDB remains confidential, accessible only by those who “need to know,” such as credentialing committees, hospitals, and licensing boards.
Even $1 can incur a listing
Many physicians wrongly believe that they will not be reported to the NPDB if they are involved in a case that settles for an amount under $30,000. Low-value settlements are often consummated for nuisance value, meaning that they have no legal merit. However, any payment—even $1—is reportable to the NPDB. It does not matter whether payment is made by settlement or judgment.
A written demand for money, whether as damages for an injury, money to see another physician, or a refund of cash tendered, can sometimes be construed as reportable.
Being joined to a corporate entity can help you
Seasoned plaintiff’s attorneys understand physicians’ deep aversion to being reported. They often take advantage of a well-known exception to reporting: payment made in the name of a corporate entity.
If a physician is employed by a corporation with at least two physicians, and the case is settled in the name of the corporation, the physician can be dismissed from the claim, and no reporting is required. In that case, the physician maintains his clean record in the data bank. That said, this can get complicated if one is obligated to report to state authorities. Because each state is different, these details should be addressed with your attorney.
High-low agreements can avert huge judgments
As discovery progresses, the plaintiff and defendant usually come to a better understanding of their respective risk—but not always. In some situations, the plaintiff may have a strong case in regard to one element of negligence, such as damages, but a weak case in regard to causation. Cerebral palsy cases fit this paradigm. In such cases, the infant has clear-cut medical and rehabilitation needs that can run easily into seven figures, but proving that a physician’s actions or omissions caused the injury can be difficult. Both sides can mitigate risk for one another by embracing a “high-low” agreement—a contract defining how a plaintiff will be paid based on a specific jury verdict.
For example, if the high-low agreement is $500,000/$100,000, the insurer is locked into one of two payments. If the jury returns a verdict for the defense, the carrier pays $100,000; if the verdict is for the plaintiff, the carrier pays $500,000, regardless of the amount of damages awarded by the jury. Without such an agreement, the range of potential judgments is no money at all to almost any amount.
When a high-low agreement is in effect, and the jury returns a verdict for the physician, the settlement is not reported to the NPDB even though the carrier must make a payment.
Why not?
The payment is being made pursuant to a separate agreement between the carrier and the plaintiff. The benefit to the insurer is the limitation of its liability, even if the plaintiff wins at trial and is awarded a higher amount. The benefit to the plaintiff is a guaranteed payment, even if there is no finding of liability against the practitioner.
How a reputation for settling can hurt
If you are so risk-averse that you demand that your carrier settle all cases—even those with no merit—two things will happen:
- Word will spread throughout the plaintiff’s bar that you are an easy target, and the threshold for filing suit against you will decline. And given how little work will be required to net a settlement, attorney’s summons will forever darken your door
- Your medical liability rates will climb—or coverage will be terminated. Settling meritorious cases makes sense, but settling all cases regardless of merit is ill-advised.
Stress is common on both sides of the equation
Lawsuits take a long time to percolate through the system, with an average time from medical event to claim resolution of about 5 years—longer in obstetrics.2
Attorneys are accustomed to this time frame; physicians are not. The lingering effects on doctors include stress, loss of job satisfaction, family strife, depression, substance abuse, and so on.
Because a lawsuit is a major stressful life event, a physician may be only too happy to be done with one. If there were absolutely no consequences to settling, that would be a smart move. But there are consequences, and living with them can also cause stress. The best way to minimize stress on either side of the equation is to think long and hard before settling any case.
1. Wilson N, Strunk A. Overview of the 2006 ACOG Survey on Professional Liability. Available at: www.acog.org/departments/professionalliability/2006surveyNatl.pdf. Accessed March 11, 2008.
2. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.
3. Mello MM, Studdert DM. The medical malpractice system: structure and performance. In: Sage WM, Kersh R, eds. Medical Malpractice and the U.S. Health Care System: New Century, Different Issues. 1st ed. New York: Cambridge University Press; 2006:11–29.
4. US Department of Health and Human Services. National Practitioner Data Bank. 2004 annual report. Available at: http://www.npdb-hipdb.hrsa.gov/pubs/stats/2004_NPDB_Annual_Report.pdf. Accessed March 11, 2008.
More about professional liability by this author. Prepare your defense of a cerebral palsy claim (and other claims) long beforehand—in the prenatal period. That’s what Dr. Segal advised readers in the July 2007 issue of OBG Mangement. Read his argument for obtaining patient contracts in the “Past Issues” archives at www.obgmanagement.com.
1. Wilson N, Strunk A. Overview of the 2006 ACOG Survey on Professional Liability. Available at: www.acog.org/departments/professionalliability/2006surveyNatl.pdf. Accessed March 11, 2008.
2. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.
3. Mello MM, Studdert DM. The medical malpractice system: structure and performance. In: Sage WM, Kersh R, eds. Medical Malpractice and the U.S. Health Care System: New Century, Different Issues. 1st ed. New York: Cambridge University Press; 2006:11–29.
4. US Department of Health and Human Services. National Practitioner Data Bank. 2004 annual report. Available at: http://www.npdb-hipdb.hrsa.gov/pubs/stats/2004_NPDB_Annual_Report.pdf. Accessed March 11, 2008.
More about professional liability by this author. Prepare your defense of a cerebral palsy claim (and other claims) long beforehand—in the prenatal period. That’s what Dr. Segal advised readers in the July 2007 issue of OBG Mangement. Read his argument for obtaining patient contracts in the “Past Issues” archives at www.obgmanagement.com.
Hiring a Fee-Only Financial Planner
This is the second column to expand on the suggestions made in my January “New Year's Resolutions” column.
The suggestion on long-range financial planning generated a lot of feedback. It seems that many readers are concerned that all aspects of their finances might not be in the best possible shape, and several shared unsatisfactory experiences with financial planners.
Believe me, I've been there. The problem, as so many of us have learned the hard way, is that anyone can claim to be a financial planner. There are no officially sanctioned requirements, and there is no government agency to regulate them.
Of the estimated quarter-million people who call themselves financial planners, only a small percentage have any real training, qualifications, or expertise in financial matters. Most are just salespeople whose priority is to sell you financial instruments. Creating a plan consistent with your long-term investment and retirement goals is secondary.
Many have an annoying habit of “churning” accounts: buying and selling frequently to generate commissions and service charges for themselves, claiming they can “beat the market” (at the expense of the value of your portfolio).
Many of them know little or nothing about investing beyond the investments their employers tell them to sell, which may or may not be what you need. Ask about alternatives and you'll get a blank stare.
One solution is to hire a fee-only planner who will charge you a flat fee for his or her services rather than take a commission on everything you buy or sell. In addition to removing the obvious conflict of interest, fee-only planners tend to have more extensive training in a broad range of financial fields. Their role is that of adviser, helping you choose the instruments most consistent with your needs and goals.
You can find a fee-only planner by asking friends and colleagues for referrals, or by consulting one of several trade organizations. The National Association of Personal Financial Advisors www.napfa.org
Never hire an adviser who solicits you. Good fee-only planners are rare and busy, and they never have the time or need to make cold calls.
As with anyone else you hire, always ask for references and check qualifications and credentials. At the very least, an adviser should hold one of the three legitimate credentials of the industry: Certified Financial Planner (CFP), Chartered Financial Consultant (ChFC), or Personal Financial Specialist (PFS). None of these designations, however, carries a guarantee of adequate experience or education.
Ask to see the planner's ADV form, parts I and II. This document, which must be filed with the Securities and Exchange Commission, outlines the adviser's compensation, whether by commissions or straight fees. (Be sure you are not dealing with one of the few shifty advisers who accept both.) It also details disciplinary actions, if any. Be immediately wary of any adviser who does not freely offer this form upon request.
Once you've chosen an adviser, keep a close watch on the plan being built on your behalf. Make sure the investments are conservative and varied, not concentrated on a few of the adviser's favorites or the financial flavor of the week.
Your planner should be able to converse intelligently about alternatives to his or her recommendations. An adviser who can't or won't do so is lazy, or letting ego interfere with responsibility, and may need to be replaced.
Good financial planners keep their clients well diversified and they make sure that other aspects of clients' finances—budgets, credit ratings, insurance coverage, tax situations, education funds, estate plans, and retirement accounts—are in the best shape possible.
And unlike advisers-cum-salespeople trying to generate extra income for themselves, they won't try to convince you that you can amass a fortune quickly or easily.
This is the second column to expand on the suggestions made in my January “New Year's Resolutions” column.
The suggestion on long-range financial planning generated a lot of feedback. It seems that many readers are concerned that all aspects of their finances might not be in the best possible shape, and several shared unsatisfactory experiences with financial planners.
Believe me, I've been there. The problem, as so many of us have learned the hard way, is that anyone can claim to be a financial planner. There are no officially sanctioned requirements, and there is no government agency to regulate them.
Of the estimated quarter-million people who call themselves financial planners, only a small percentage have any real training, qualifications, or expertise in financial matters. Most are just salespeople whose priority is to sell you financial instruments. Creating a plan consistent with your long-term investment and retirement goals is secondary.
Many have an annoying habit of “churning” accounts: buying and selling frequently to generate commissions and service charges for themselves, claiming they can “beat the market” (at the expense of the value of your portfolio).
Many of them know little or nothing about investing beyond the investments their employers tell them to sell, which may or may not be what you need. Ask about alternatives and you'll get a blank stare.
One solution is to hire a fee-only planner who will charge you a flat fee for his or her services rather than take a commission on everything you buy or sell. In addition to removing the obvious conflict of interest, fee-only planners tend to have more extensive training in a broad range of financial fields. Their role is that of adviser, helping you choose the instruments most consistent with your needs and goals.
You can find a fee-only planner by asking friends and colleagues for referrals, or by consulting one of several trade organizations. The National Association of Personal Financial Advisors www.napfa.org
Never hire an adviser who solicits you. Good fee-only planners are rare and busy, and they never have the time or need to make cold calls.
As with anyone else you hire, always ask for references and check qualifications and credentials. At the very least, an adviser should hold one of the three legitimate credentials of the industry: Certified Financial Planner (CFP), Chartered Financial Consultant (ChFC), or Personal Financial Specialist (PFS). None of these designations, however, carries a guarantee of adequate experience or education.
Ask to see the planner's ADV form, parts I and II. This document, which must be filed with the Securities and Exchange Commission, outlines the adviser's compensation, whether by commissions or straight fees. (Be sure you are not dealing with one of the few shifty advisers who accept both.) It also details disciplinary actions, if any. Be immediately wary of any adviser who does not freely offer this form upon request.
Once you've chosen an adviser, keep a close watch on the plan being built on your behalf. Make sure the investments are conservative and varied, not concentrated on a few of the adviser's favorites or the financial flavor of the week.
Your planner should be able to converse intelligently about alternatives to his or her recommendations. An adviser who can't or won't do so is lazy, or letting ego interfere with responsibility, and may need to be replaced.
Good financial planners keep their clients well diversified and they make sure that other aspects of clients' finances—budgets, credit ratings, insurance coverage, tax situations, education funds, estate plans, and retirement accounts—are in the best shape possible.
And unlike advisers-cum-salespeople trying to generate extra income for themselves, they won't try to convince you that you can amass a fortune quickly or easily.
This is the second column to expand on the suggestions made in my January “New Year's Resolutions” column.
The suggestion on long-range financial planning generated a lot of feedback. It seems that many readers are concerned that all aspects of their finances might not be in the best possible shape, and several shared unsatisfactory experiences with financial planners.
Believe me, I've been there. The problem, as so many of us have learned the hard way, is that anyone can claim to be a financial planner. There are no officially sanctioned requirements, and there is no government agency to regulate them.
Of the estimated quarter-million people who call themselves financial planners, only a small percentage have any real training, qualifications, or expertise in financial matters. Most are just salespeople whose priority is to sell you financial instruments. Creating a plan consistent with your long-term investment and retirement goals is secondary.
Many have an annoying habit of “churning” accounts: buying and selling frequently to generate commissions and service charges for themselves, claiming they can “beat the market” (at the expense of the value of your portfolio).
Many of them know little or nothing about investing beyond the investments their employers tell them to sell, which may or may not be what you need. Ask about alternatives and you'll get a blank stare.
One solution is to hire a fee-only planner who will charge you a flat fee for his or her services rather than take a commission on everything you buy or sell. In addition to removing the obvious conflict of interest, fee-only planners tend to have more extensive training in a broad range of financial fields. Their role is that of adviser, helping you choose the instruments most consistent with your needs and goals.
You can find a fee-only planner by asking friends and colleagues for referrals, or by consulting one of several trade organizations. The National Association of Personal Financial Advisors www.napfa.org
Never hire an adviser who solicits you. Good fee-only planners are rare and busy, and they never have the time or need to make cold calls.
As with anyone else you hire, always ask for references and check qualifications and credentials. At the very least, an adviser should hold one of the three legitimate credentials of the industry: Certified Financial Planner (CFP), Chartered Financial Consultant (ChFC), or Personal Financial Specialist (PFS). None of these designations, however, carries a guarantee of adequate experience or education.
Ask to see the planner's ADV form, parts I and II. This document, which must be filed with the Securities and Exchange Commission, outlines the adviser's compensation, whether by commissions or straight fees. (Be sure you are not dealing with one of the few shifty advisers who accept both.) It also details disciplinary actions, if any. Be immediately wary of any adviser who does not freely offer this form upon request.
Once you've chosen an adviser, keep a close watch on the plan being built on your behalf. Make sure the investments are conservative and varied, not concentrated on a few of the adviser's favorites or the financial flavor of the week.
Your planner should be able to converse intelligently about alternatives to his or her recommendations. An adviser who can't or won't do so is lazy, or letting ego interfere with responsibility, and may need to be replaced.
Good financial planners keep their clients well diversified and they make sure that other aspects of clients' finances—budgets, credit ratings, insurance coverage, tax situations, education funds, estate plans, and retirement accounts—are in the best shape possible.
And unlike advisers-cum-salespeople trying to generate extra income for themselves, they won't try to convince you that you can amass a fortune quickly or easily.