User login
MDedge latest news is breaking news from medical conferences, journals, guidelines, the FDA and CDC.
AI Algorithm Predicts Transfusion Need, Mortality Risk in Acute GI Bleeds
SAN DIEGO — , researchers reported at Digestive Disease Week® (DDW) 2025.
Acute GI bleeding is the most common cause of digestive disease–related hospitalization, with an estimated 500,000 hospital admissions annually. It’s known that predicting the need for red blood cell transfusion in the first 24 hours may improve resuscitation and decrease both morbidity and mortality.
However, an existing clinical score known as the Rockall Score does not perform well for predicting mortality, Xi (Nicole) Zhang, an MD-PhD student at McGill University, Montreal, Quebec, Canada, told attendees at DDW. With an area under the curve of 0.65-0.75, better prediction is needed, said Zhang, whose coresearchers included Dennis Shung, MD, MHS, PhD, director of Applied Artificial Intelligence at Yale University School of Medicine, New Haven, Connecticut.

“We’d like to predict multiple outcomes in addition to mortality,” said Zhang, who is also a student at the Mila-Quebec Artificial Intelligence Institute.
As a result, the researchers turned to the TFM approach, applying it to ICU patients with acute GI bleeding to predict both the need for transfusion and in-hospital mortality risk. The all-cause mortality rate is up to 11%, according to a 2020 study by James Y. W. Lau, MD, and colleagues. The rebleeding rate of nonvariceal upper GI bleeds is up to 10.4%. Zhang said the rebleeding rate for variceal upper gastrointestinal bleeding is up to 65%.
The AI method the researchers used outperformed a standard deep learning model at predicting the need for transfusion and estimating mortality risk.
Defining the AI Framework
“Probabilistic flow matching is a class of generative artificial intelligence that learns how a simple distribution becomes a more complex distribution with ordinary differential equations,” Zhang told GI & Hepatology News. “For example, if you had a few lines and shapes you could learn how it could become a detailed portrait of a face. In our case, we start with a few blood pressure and heart rate measurements and learn the pattern of blood pressures and heart rates over time, particularly if they reflect clinical deterioration with hemodynamic instability.”
Another way to think about the underlying algorithm, Zhang said, is to think about a river with boats where the river flow determines where the boats end up. “We are trying to direct the boat to the correct dock by adjusting the flow of water in the canal. In this case we are mapping the distribution with the first few data points to the distribution with the entire patient trajectory.”
The information gained, she said, could be helpful in timing endoscopic evaluation or allocating red blood cell products for emergent transfusion.
Study Details
The researchers evaluated a cohort of 2602 patients admitted to the ICU, identified from the publicly available MIMIC-III database. They divided the patients into a training set of 2342 patients and an internal validation set of 260 patients. Input variables were severe liver disease comorbidity, administration of vasopressor medications, mean arterial blood pressure, and heart rate over the first 24 hours.
Excluded was hemoglobin, since the point was to test the trajectory of hemodynamic parameters independent of hemoglobin thresholds used to guide red blood cell transfusion.
The outcome measures were administration of packed red blood cell transfusion within 24 hours and all-cause hospital mortality.
The TFM was more accurate than a standard deep learning model in predicting red blood cell transfusion, with an accuracy of 93.6% vs 43.2%; P ≤ .001. It was also more accurate at predicting all-cause in-hospital mortality, with an accuracy of 89.5% vs 42.5%, P = .01.
The researchers concluded that the TFM approach was able to predict the hemodynamic trajectories of patients with acute GI bleeding defined as deviation and outperformed the baseline from the measured mean arterial pressure and heart rate.
Expert Perspective
“This is an exciting proof-of-concept study that shows generative AI methods may be applied to complex datasets in order to improve on our current predictive models and improve patient care,” said Jeremy Glissen Brown, MD, MSc, an assistant professor of medicine and a practicing gastroenterologist at Duke University who has published research on the use of AI in clinical practice. He reviewed the study for GI & Hepatology News but was not involved in the research.
“Future work will likely look into the implementation of a version of this model on real-time data.” he said. “We are at an exciting inflection point in predictive models within GI and clinical medicine. Predictive models based on deep learning and generative AI hold the promise of improving how we predict and treat disease states, but the excitement being generated with studies such as this needs to be balanced with the trade-offs inherent to the current paradigm of deep learning and generative models compared to more traditional regression-based models. These include many of the same ‘black box’ explainability questions that have risen in the age of convolutional neural networks as well as some method-specific questions due to the continuous and implicit nature of TFM.”
Elaborating on that, Glissen Brown said: “TFM, like many deep learning techniques, raises concerns about explainability that we’ve long seen with convolutional neural networks — the ‘black box’ problem, where it’s difficult to interpret exactly how and why the model arrives at a particular decision. But TFM also introduces unique challenges due to its continuous and implicit formulation. Since it often learns flows without explicitly defining intermediate representations or steps, it can be harder to trace the logic or pathways it uses to connect inputs to outputs. This makes standard interpretability tools less effective and calls for new techniques tailored to these continuous architectures.”
“This approach could have a real clinical impact,” said Robert Hirten, MD, associate professor of medicine and artificial intelligence, Icahn School of Medicine at Mount Sinai, New York City, who also reviewed the study. “Accurately predicting transfusion needs and mortality risk in real time could support earlier, more targeted interventions for high-risk patients. While these findings still need to be validated in prospective studies, it could enhance ICU decision-making and resource allocation.”

“For the practicing gastroenterologist, we envision this system could help them figure out when to perform endoscopy in a patient admitted with acute gastrointestinal bleeding in the ICU at very high risk of exsanguination,” Zhang told GI & Hepatology News.
The approach, the researchers said, will be useful in identifying unique patient characteristics, make possible the identification of high-risk patients and lead to more personalized medicine.
Hirten, Zhang, and Shung had no disclosures. Glissen Brown reported consulting relationships with Medtronic, OdinVision, Doximity, and Olympus. The National Institutes of Health funded this study.
A version of this article appeared on Medscape.com.
SAN DIEGO — , researchers reported at Digestive Disease Week® (DDW) 2025.
Acute GI bleeding is the most common cause of digestive disease–related hospitalization, with an estimated 500,000 hospital admissions annually. It’s known that predicting the need for red blood cell transfusion in the first 24 hours may improve resuscitation and decrease both morbidity and mortality.
However, an existing clinical score known as the Rockall Score does not perform well for predicting mortality, Xi (Nicole) Zhang, an MD-PhD student at McGill University, Montreal, Quebec, Canada, told attendees at DDW. With an area under the curve of 0.65-0.75, better prediction is needed, said Zhang, whose coresearchers included Dennis Shung, MD, MHS, PhD, director of Applied Artificial Intelligence at Yale University School of Medicine, New Haven, Connecticut.
“We’d like to predict multiple outcomes in addition to mortality,” said Zhang, who is also a student at the Mila-Quebec Artificial Intelligence Institute.
As a result, the researchers turned to the TFM approach, applying it to ICU patients with acute GI bleeding to predict both the need for transfusion and in-hospital mortality risk. The all-cause mortality rate is up to 11%, according to a 2020 study by James Y. W. Lau, MD, and colleagues. The rebleeding rate of nonvariceal upper GI bleeds is up to 10.4%. Zhang said the rebleeding rate for variceal upper gastrointestinal bleeding is up to 65%.
The AI method the researchers used outperformed a standard deep learning model at predicting the need for transfusion and estimating mortality risk.
Defining the AI Framework
“Probabilistic flow matching is a class of generative artificial intelligence that learns how a simple distribution becomes a more complex distribution with ordinary differential equations,” Zhang told GI & Hepatology News. “For example, if you had a few lines and shapes you could learn how it could become a detailed portrait of a face. In our case, we start with a few blood pressure and heart rate measurements and learn the pattern of blood pressures and heart rates over time, particularly if they reflect clinical deterioration with hemodynamic instability.”
Another way to think about the underlying algorithm, Zhang said, is to think about a river with boats where the river flow determines where the boats end up. “We are trying to direct the boat to the correct dock by adjusting the flow of water in the canal. In this case we are mapping the distribution with the first few data points to the distribution with the entire patient trajectory.”
The information gained, she said, could be helpful in timing endoscopic evaluation or allocating red blood cell products for emergent transfusion.
Study Details
The researchers evaluated a cohort of 2602 patients admitted to the ICU, identified from the publicly available MIMIC-III database. They divided the patients into a training set of 2342 patients and an internal validation set of 260 patients. Input variables were severe liver disease comorbidity, administration of vasopressor medications, mean arterial blood pressure, and heart rate over the first 24 hours.
Excluded was hemoglobin, since the point was to test the trajectory of hemodynamic parameters independent of hemoglobin thresholds used to guide red blood cell transfusion.
The outcome measures were administration of packed red blood cell transfusion within 24 hours and all-cause hospital mortality.
The TFM was more accurate than a standard deep learning model in predicting red blood cell transfusion, with an accuracy of 93.6% vs 43.2%; P ≤ .001. It was also more accurate at predicting all-cause in-hospital mortality, with an accuracy of 89.5% vs 42.5%, P = .01.
The researchers concluded that the TFM approach was able to predict the hemodynamic trajectories of patients with acute GI bleeding defined as deviation and outperformed the baseline from the measured mean arterial pressure and heart rate.
Expert Perspective
“This is an exciting proof-of-concept study that shows generative AI methods may be applied to complex datasets in order to improve on our current predictive models and improve patient care,” said Jeremy Glissen Brown, MD, MSc, an assistant professor of medicine and a practicing gastroenterologist at Duke University who has published research on the use of AI in clinical practice. He reviewed the study for GI & Hepatology News but was not involved in the research.
“Future work will likely look into the implementation of a version of this model on real-time data.” he said. “We are at an exciting inflection point in predictive models within GI and clinical medicine. Predictive models based on deep learning and generative AI hold the promise of improving how we predict and treat disease states, but the excitement being generated with studies such as this needs to be balanced with the trade-offs inherent to the current paradigm of deep learning and generative models compared to more traditional regression-based models. These include many of the same ‘black box’ explainability questions that have risen in the age of convolutional neural networks as well as some method-specific questions due to the continuous and implicit nature of TFM.”
Elaborating on that, Glissen Brown said: “TFM, like many deep learning techniques, raises concerns about explainability that we’ve long seen with convolutional neural networks — the ‘black box’ problem, where it’s difficult to interpret exactly how and why the model arrives at a particular decision. But TFM also introduces unique challenges due to its continuous and implicit formulation. Since it often learns flows without explicitly defining intermediate representations or steps, it can be harder to trace the logic or pathways it uses to connect inputs to outputs. This makes standard interpretability tools less effective and calls for new techniques tailored to these continuous architectures.”
“This approach could have a real clinical impact,” said Robert Hirten, MD, associate professor of medicine and artificial intelligence, Icahn School of Medicine at Mount Sinai, New York City, who also reviewed the study. “Accurately predicting transfusion needs and mortality risk in real time could support earlier, more targeted interventions for high-risk patients. While these findings still need to be validated in prospective studies, it could enhance ICU decision-making and resource allocation.”
“For the practicing gastroenterologist, we envision this system could help them figure out when to perform endoscopy in a patient admitted with acute gastrointestinal bleeding in the ICU at very high risk of exsanguination,” Zhang told GI & Hepatology News.
The approach, the researchers said, will be useful in identifying unique patient characteristics, make possible the identification of high-risk patients and lead to more personalized medicine.
Hirten, Zhang, and Shung had no disclosures. Glissen Brown reported consulting relationships with Medtronic, OdinVision, Doximity, and Olympus. The National Institutes of Health funded this study.
A version of this article appeared on Medscape.com.
SAN DIEGO — , researchers reported at Digestive Disease Week® (DDW) 2025.
Acute GI bleeding is the most common cause of digestive disease–related hospitalization, with an estimated 500,000 hospital admissions annually. It’s known that predicting the need for red blood cell transfusion in the first 24 hours may improve resuscitation and decrease both morbidity and mortality.
However, an existing clinical score known as the Rockall Score does not perform well for predicting mortality, Xi (Nicole) Zhang, an MD-PhD student at McGill University, Montreal, Quebec, Canada, told attendees at DDW. With an area under the curve of 0.65-0.75, better prediction is needed, said Zhang, whose coresearchers included Dennis Shung, MD, MHS, PhD, director of Applied Artificial Intelligence at Yale University School of Medicine, New Haven, Connecticut.
“We’d like to predict multiple outcomes in addition to mortality,” said Zhang, who is also a student at the Mila-Quebec Artificial Intelligence Institute.
As a result, the researchers turned to the TFM approach, applying it to ICU patients with acute GI bleeding to predict both the need for transfusion and in-hospital mortality risk. The all-cause mortality rate is up to 11%, according to a 2020 study by James Y. W. Lau, MD, and colleagues. The rebleeding rate of nonvariceal upper GI bleeds is up to 10.4%. Zhang said the rebleeding rate for variceal upper gastrointestinal bleeding is up to 65%.
The AI method the researchers used outperformed a standard deep learning model at predicting the need for transfusion and estimating mortality risk.
Defining the AI Framework
“Probabilistic flow matching is a class of generative artificial intelligence that learns how a simple distribution becomes a more complex distribution with ordinary differential equations,” Zhang told GI & Hepatology News. “For example, if you had a few lines and shapes you could learn how it could become a detailed portrait of a face. In our case, we start with a few blood pressure and heart rate measurements and learn the pattern of blood pressures and heart rates over time, particularly if they reflect clinical deterioration with hemodynamic instability.”
Another way to think about the underlying algorithm, Zhang said, is to think about a river with boats where the river flow determines where the boats end up. “We are trying to direct the boat to the correct dock by adjusting the flow of water in the canal. In this case we are mapping the distribution with the first few data points to the distribution with the entire patient trajectory.”
The information gained, she said, could be helpful in timing endoscopic evaluation or allocating red blood cell products for emergent transfusion.
Study Details
The researchers evaluated a cohort of 2602 patients admitted to the ICU, identified from the publicly available MIMIC-III database. They divided the patients into a training set of 2342 patients and an internal validation set of 260 patients. Input variables were severe liver disease comorbidity, administration of vasopressor medications, mean arterial blood pressure, and heart rate over the first 24 hours.
Excluded was hemoglobin, since the point was to test the trajectory of hemodynamic parameters independent of hemoglobin thresholds used to guide red blood cell transfusion.
The outcome measures were administration of packed red blood cell transfusion within 24 hours and all-cause hospital mortality.
The TFM was more accurate than a standard deep learning model in predicting red blood cell transfusion, with an accuracy of 93.6% vs 43.2%; P ≤ .001. It was also more accurate at predicting all-cause in-hospital mortality, with an accuracy of 89.5% vs 42.5%, P = .01.
The researchers concluded that the TFM approach was able to predict the hemodynamic trajectories of patients with acute GI bleeding defined as deviation and outperformed the baseline from the measured mean arterial pressure and heart rate.
Expert Perspective
“This is an exciting proof-of-concept study that shows generative AI methods may be applied to complex datasets in order to improve on our current predictive models and improve patient care,” said Jeremy Glissen Brown, MD, MSc, an assistant professor of medicine and a practicing gastroenterologist at Duke University who has published research on the use of AI in clinical practice. He reviewed the study for GI & Hepatology News but was not involved in the research.
“Future work will likely look into the implementation of a version of this model on real-time data.” he said. “We are at an exciting inflection point in predictive models within GI and clinical medicine. Predictive models based on deep learning and generative AI hold the promise of improving how we predict and treat disease states, but the excitement being generated with studies such as this needs to be balanced with the trade-offs inherent to the current paradigm of deep learning and generative models compared to more traditional regression-based models. These include many of the same ‘black box’ explainability questions that have risen in the age of convolutional neural networks as well as some method-specific questions due to the continuous and implicit nature of TFM.”
Elaborating on that, Glissen Brown said: “TFM, like many deep learning techniques, raises concerns about explainability that we’ve long seen with convolutional neural networks — the ‘black box’ problem, where it’s difficult to interpret exactly how and why the model arrives at a particular decision. But TFM also introduces unique challenges due to its continuous and implicit formulation. Since it often learns flows without explicitly defining intermediate representations or steps, it can be harder to trace the logic or pathways it uses to connect inputs to outputs. This makes standard interpretability tools less effective and calls for new techniques tailored to these continuous architectures.”
“This approach could have a real clinical impact,” said Robert Hirten, MD, associate professor of medicine and artificial intelligence, Icahn School of Medicine at Mount Sinai, New York City, who also reviewed the study. “Accurately predicting transfusion needs and mortality risk in real time could support earlier, more targeted interventions for high-risk patients. While these findings still need to be validated in prospective studies, it could enhance ICU decision-making and resource allocation.”
“For the practicing gastroenterologist, we envision this system could help them figure out when to perform endoscopy in a patient admitted with acute gastrointestinal bleeding in the ICU at very high risk of exsanguination,” Zhang told GI & Hepatology News.
The approach, the researchers said, will be useful in identifying unique patient characteristics, make possible the identification of high-risk patients and lead to more personalized medicine.
Hirten, Zhang, and Shung had no disclosures. Glissen Brown reported consulting relationships with Medtronic, OdinVision, Doximity, and Olympus. The National Institutes of Health funded this study.
A version of this article appeared on Medscape.com.
FROM DDW 2025
VA to Allow Veteran Referrals to Community Care Without Second Review
VA to Allow Veteran Referrals to Community Care Without Second Review
Veterans enrolled in the US Department of Veterans Affairs (VA) who have been referred to Community Care no longer need a second review from a VA clinician according to a new policy. The provision implements language from the Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act. VA officials hope that it will speed up access to community care.
The move expands on the 2019 MISSION Act, which allows eligible veterans to access health care from non-VA clinicians that is paid for by the VA when it is in their “best medical interest.” Those decisions, however, were not considered final until reviewed by a second VA doctor.
The Dole Act prohibits VA administrators from overriding a VA doctor’s referral for a patient to receive outside care. According to the law, the ban on administrative review will remain in place for 2 years, after which the VA must report on its effects to Congress. The VA announced it would begin training employees to ensure the community care referral process is followed in compliance with the Dole Act.
Analysis from the Veterans Healthcare Policy Institute claims the best medical interest criterion “is to be considered when a veteran's health and/or well-being would be compromised if they were not able to be seen in the community for the requested clinical service.”
During a March hearing, Rep. Julia Brownley (D-CA), ranking Democrat on the House Veterans’ Affairs subcommittee on health, said any veteran who seeks residential treatment should get it, but noted the VA has not developed a fee schedule for community treatment centers. In at least 1 case, she said, the department was charged up to $6000 a day for 1 patient. Brownley also noted that the VA doesn't track the timeliness or quality of medical care in community residential treatment facilities.
“We have no way of knowing the level of treatment or support they are getting,” she said. “We must find a balance between community care and VA direct care. In my opinion, we have not found that balance when it comes to residential rehabilitation treatment facilities.”
At the same hearing, chair of the House Veterans Affairs health subcommittee Rep. Mariannette Miller-Meeks (R-IA) said more change is needed—specifically to ensure that veterans also can access private residential substance abuse treatment centers. Some, she said, “are told they cannot access community care unless a VA facility fails to meet a 20-day threshold—forcing them to wait, even when immediate, alternative options exist."
The House of Representatives passed H.R. 1969, the No Wrong Door for Veterans Act, in May, which expands the VA suicide prevention grant program. However, the Senate has yet to take up the legislation. “I’ve seen firsthand how difficult it can be for veterans in crisis to navigate a complicated system when every second counts,” Miller-Meeks said. “The No Wrong Door for Veterans Act ensures that our heroes are never turned away or left without help. It streamlines access, strengthens coordination, and reaffirms our promise to those who served.”
Veterans enrolled in the US Department of Veterans Affairs (VA) who have been referred to Community Care no longer need a second review from a VA clinician according to a new policy. The provision implements language from the Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act. VA officials hope that it will speed up access to community care.
The move expands on the 2019 MISSION Act, which allows eligible veterans to access health care from non-VA clinicians that is paid for by the VA when it is in their “best medical interest.” Those decisions, however, were not considered final until reviewed by a second VA doctor.
The Dole Act prohibits VA administrators from overriding a VA doctor’s referral for a patient to receive outside care. According to the law, the ban on administrative review will remain in place for 2 years, after which the VA must report on its effects to Congress. The VA announced it would begin training employees to ensure the community care referral process is followed in compliance with the Dole Act.
Analysis from the Veterans Healthcare Policy Institute claims the best medical interest criterion “is to be considered when a veteran's health and/or well-being would be compromised if they were not able to be seen in the community for the requested clinical service.”
During a March hearing, Rep. Julia Brownley (D-CA), ranking Democrat on the House Veterans’ Affairs subcommittee on health, said any veteran who seeks residential treatment should get it, but noted the VA has not developed a fee schedule for community treatment centers. In at least 1 case, she said, the department was charged up to $6000 a day for 1 patient. Brownley also noted that the VA doesn't track the timeliness or quality of medical care in community residential treatment facilities.
“We have no way of knowing the level of treatment or support they are getting,” she said. “We must find a balance between community care and VA direct care. In my opinion, we have not found that balance when it comes to residential rehabilitation treatment facilities.”
At the same hearing, chair of the House Veterans Affairs health subcommittee Rep. Mariannette Miller-Meeks (R-IA) said more change is needed—specifically to ensure that veterans also can access private residential substance abuse treatment centers. Some, she said, “are told they cannot access community care unless a VA facility fails to meet a 20-day threshold—forcing them to wait, even when immediate, alternative options exist."
The House of Representatives passed H.R. 1969, the No Wrong Door for Veterans Act, in May, which expands the VA suicide prevention grant program. However, the Senate has yet to take up the legislation. “I’ve seen firsthand how difficult it can be for veterans in crisis to navigate a complicated system when every second counts,” Miller-Meeks said. “The No Wrong Door for Veterans Act ensures that our heroes are never turned away or left without help. It streamlines access, strengthens coordination, and reaffirms our promise to those who served.”
Veterans enrolled in the US Department of Veterans Affairs (VA) who have been referred to Community Care no longer need a second review from a VA clinician according to a new policy. The provision implements language from the Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act. VA officials hope that it will speed up access to community care.
The move expands on the 2019 MISSION Act, which allows eligible veterans to access health care from non-VA clinicians that is paid for by the VA when it is in their “best medical interest.” Those decisions, however, were not considered final until reviewed by a second VA doctor.
The Dole Act prohibits VA administrators from overriding a VA doctor’s referral for a patient to receive outside care. According to the law, the ban on administrative review will remain in place for 2 years, after which the VA must report on its effects to Congress. The VA announced it would begin training employees to ensure the community care referral process is followed in compliance with the Dole Act.
Analysis from the Veterans Healthcare Policy Institute claims the best medical interest criterion “is to be considered when a veteran's health and/or well-being would be compromised if they were not able to be seen in the community for the requested clinical service.”
During a March hearing, Rep. Julia Brownley (D-CA), ranking Democrat on the House Veterans’ Affairs subcommittee on health, said any veteran who seeks residential treatment should get it, but noted the VA has not developed a fee schedule for community treatment centers. In at least 1 case, she said, the department was charged up to $6000 a day for 1 patient. Brownley also noted that the VA doesn't track the timeliness or quality of medical care in community residential treatment facilities.
“We have no way of knowing the level of treatment or support they are getting,” she said. “We must find a balance between community care and VA direct care. In my opinion, we have not found that balance when it comes to residential rehabilitation treatment facilities.”
At the same hearing, chair of the House Veterans Affairs health subcommittee Rep. Mariannette Miller-Meeks (R-IA) said more change is needed—specifically to ensure that veterans also can access private residential substance abuse treatment centers. Some, she said, “are told they cannot access community care unless a VA facility fails to meet a 20-day threshold—forcing them to wait, even when immediate, alternative options exist."
The House of Representatives passed H.R. 1969, the No Wrong Door for Veterans Act, in May, which expands the VA suicide prevention grant program. However, the Senate has yet to take up the legislation. “I’ve seen firsthand how difficult it can be for veterans in crisis to navigate a complicated system when every second counts,” Miller-Meeks said. “The No Wrong Door for Veterans Act ensures that our heroes are never turned away or left without help. It streamlines access, strengthens coordination, and reaffirms our promise to those who served.”
VA to Allow Veteran Referrals to Community Care Without Second Review
VA to Allow Veteran Referrals to Community Care Without Second Review
Suicide Prevention Grant Program Reauthorized
Suicide Prevention Grant Program Reauthorized
Community-based organizations that provide suicide-prevention services can now access about $52.5 million in US Department of Veterans Affairs (VA) grants. The grant is part of the 3-year Staff Sergeant Fox Suicide Prevention Grant Program, which honors Parker Gordon Fox, a sniper instructor at the U.S. Army Infantry School at Fort Benning, Georgia, who died by suicide in 2020. In consecutive Congressional hearings, lawmakers called for the reauthorization of the program to address gaps in VA care.
“It has been a game-changer for so many veterans,” Sen. Richard Blumenthal (D-CT) said.
The money provides or coordinates primarily nonclinical suicide prevention services, including outreach and linkage to VA and community resources. Services also may include baseline mental health screenings, case management and peer support, education on suicide risk, VA benefits assistance, and emergency clinical services.
Since its inception in 2022, the program has awarded $157.5 million to 95 organizations in 43 states, US territories, and tribal lands. Speaking before the House Committee on Veterans’ Affairs on May 15, VA Secretary Doug Collins praised the Fox program for bringing “different voices into the conversation,” but added it wasn’t enough. He noted that the veteran suicide rate has not changed since 2008, despite the VA annually spending $588 million on suicide prevention over the past few years.
In an op-ed, Russell Lemle, a senior policy analyst at the Veterans Healthcare Policy Institute, disputed Collins' characterization of veteran suicides. Between 2008 and 2022 (the last year for which complete data is available), US deaths by suicide increased 37% while the number of veteran deaths by suicide fell 2%. “This data collection was the single best part of the program,” he argued, calling for reauthorization to continue requiring data-targeted solutions.
According to a 2024 VA interim report on the Fox grant program, grantees had completed > 16,590 outreach contacts and engaged 3204 participants as of September 30, 2023. An additional 864 individuals were onboarding at the time of the report.
The current version of the grant program requires grantees to use validated tools, including the VA Data Collection Tool, and other assessments furnished by VA to determine the effectiveness of the suicide prevention services. They must also provide each participant with a satisfaction survey and submit periodic and annual financial and performance reports.
Despite the Trump administration’s cuts and cancellations to the federal workforce and federal programs, Collins told the Senate committee he is firmly on the side of working with community-based organizations like the Fox grant program to broaden the VA’s reach: “I want to use grants and programs like [the Fox grant program] to reach out beyond the scope of where we’re currently reaching, to say how can we actually touch the veteran that’s not being touched right now by these programs,” Collins said. “We’ve got to do better at using the grants, using our programs to go outside the normal bubble and use others to help get the word out.”
Grant applications are due in July and VA will choose awardees in September. Organizations can apply for grants worth up to $750,000 and may apply to renew awards from year to year throughout the length of the program.
Community-based organizations that provide suicide-prevention services can now access about $52.5 million in US Department of Veterans Affairs (VA) grants. The grant is part of the 3-year Staff Sergeant Fox Suicide Prevention Grant Program, which honors Parker Gordon Fox, a sniper instructor at the U.S. Army Infantry School at Fort Benning, Georgia, who died by suicide in 2020. In consecutive Congressional hearings, lawmakers called for the reauthorization of the program to address gaps in VA care.
“It has been a game-changer for so many veterans,” Sen. Richard Blumenthal (D-CT) said.
The money provides or coordinates primarily nonclinical suicide prevention services, including outreach and linkage to VA and community resources. Services also may include baseline mental health screenings, case management and peer support, education on suicide risk, VA benefits assistance, and emergency clinical services.
Since its inception in 2022, the program has awarded $157.5 million to 95 organizations in 43 states, US territories, and tribal lands. Speaking before the House Committee on Veterans’ Affairs on May 15, VA Secretary Doug Collins praised the Fox program for bringing “different voices into the conversation,” but added it wasn’t enough. He noted that the veteran suicide rate has not changed since 2008, despite the VA annually spending $588 million on suicide prevention over the past few years.
In an op-ed, Russell Lemle, a senior policy analyst at the Veterans Healthcare Policy Institute, disputed Collins' characterization of veteran suicides. Between 2008 and 2022 (the last year for which complete data is available), US deaths by suicide increased 37% while the number of veteran deaths by suicide fell 2%. “This data collection was the single best part of the program,” he argued, calling for reauthorization to continue requiring data-targeted solutions.
According to a 2024 VA interim report on the Fox grant program, grantees had completed > 16,590 outreach contacts and engaged 3204 participants as of September 30, 2023. An additional 864 individuals were onboarding at the time of the report.
The current version of the grant program requires grantees to use validated tools, including the VA Data Collection Tool, and other assessments furnished by VA to determine the effectiveness of the suicide prevention services. They must also provide each participant with a satisfaction survey and submit periodic and annual financial and performance reports.
Despite the Trump administration’s cuts and cancellations to the federal workforce and federal programs, Collins told the Senate committee he is firmly on the side of working with community-based organizations like the Fox grant program to broaden the VA’s reach: “I want to use grants and programs like [the Fox grant program] to reach out beyond the scope of where we’re currently reaching, to say how can we actually touch the veteran that’s not being touched right now by these programs,” Collins said. “We’ve got to do better at using the grants, using our programs to go outside the normal bubble and use others to help get the word out.”
Grant applications are due in July and VA will choose awardees in September. Organizations can apply for grants worth up to $750,000 and may apply to renew awards from year to year throughout the length of the program.
Community-based organizations that provide suicide-prevention services can now access about $52.5 million in US Department of Veterans Affairs (VA) grants. The grant is part of the 3-year Staff Sergeant Fox Suicide Prevention Grant Program, which honors Parker Gordon Fox, a sniper instructor at the U.S. Army Infantry School at Fort Benning, Georgia, who died by suicide in 2020. In consecutive Congressional hearings, lawmakers called for the reauthorization of the program to address gaps in VA care.
“It has been a game-changer for so many veterans,” Sen. Richard Blumenthal (D-CT) said.
The money provides or coordinates primarily nonclinical suicide prevention services, including outreach and linkage to VA and community resources. Services also may include baseline mental health screenings, case management and peer support, education on suicide risk, VA benefits assistance, and emergency clinical services.
Since its inception in 2022, the program has awarded $157.5 million to 95 organizations in 43 states, US territories, and tribal lands. Speaking before the House Committee on Veterans’ Affairs on May 15, VA Secretary Doug Collins praised the Fox program for bringing “different voices into the conversation,” but added it wasn’t enough. He noted that the veteran suicide rate has not changed since 2008, despite the VA annually spending $588 million on suicide prevention over the past few years.
In an op-ed, Russell Lemle, a senior policy analyst at the Veterans Healthcare Policy Institute, disputed Collins' characterization of veteran suicides. Between 2008 and 2022 (the last year for which complete data is available), US deaths by suicide increased 37% while the number of veteran deaths by suicide fell 2%. “This data collection was the single best part of the program,” he argued, calling for reauthorization to continue requiring data-targeted solutions.
According to a 2024 VA interim report on the Fox grant program, grantees had completed > 16,590 outreach contacts and engaged 3204 participants as of September 30, 2023. An additional 864 individuals were onboarding at the time of the report.
The current version of the grant program requires grantees to use validated tools, including the VA Data Collection Tool, and other assessments furnished by VA to determine the effectiveness of the suicide prevention services. They must also provide each participant with a satisfaction survey and submit periodic and annual financial and performance reports.
Despite the Trump administration’s cuts and cancellations to the federal workforce and federal programs, Collins told the Senate committee he is firmly on the side of working with community-based organizations like the Fox grant program to broaden the VA’s reach: “I want to use grants and programs like [the Fox grant program] to reach out beyond the scope of where we’re currently reaching, to say how can we actually touch the veteran that’s not being touched right now by these programs,” Collins said. “We’ve got to do better at using the grants, using our programs to go outside the normal bubble and use others to help get the word out.”
Grant applications are due in July and VA will choose awardees in September. Organizations can apply for grants worth up to $750,000 and may apply to renew awards from year to year throughout the length of the program.
Suicide Prevention Grant Program Reauthorized
Suicide Prevention Grant Program Reauthorized
GLP-1s Treat and Even Reverse Some Forms of Liver Disease
In the past two decades, the global prevalence of metabolic dysfunction–associated steatohepatitis (MASH) has increased dramatically as a result of the obesity epidemic. Researchers project that by 2040, rates of MASH will increase by 55%. Prior to that most liver diseases were caused by alcohol use and hepatitis C, a viral infection that primarily affects the liver.
MASH, a preventable form of liver disease previously called nonalcoholic fatty liver disease, is caused by a buildup of visceral fat cells that accumulate on top of the internal organs, in this case the liver, and keep it from functioning properly. The liver’s primary role is to filter blood, nutrients, and bile used for digestion, as well as to remove toxins from the body. Excess fat cells blanket the liver and keep it from working at full capacity.
Fat cells are also metabolically active and can cause a chronic state of inflammation in the part of the body where they reside. Over time, these fat cells can cause cirrhosis of the liver, or permanent scarring. Once patients reach this stage, the only option is a liver transplant.
New Research on GLP-1 Agonists and MASH
Until recently, the lone treatment for early-stage MASH was weight loss to reduce the number of fat cells that surround the internal organs. But new research has shown that glucagon-like peptide 1 (GLP-1) agonists can reduce and even reverse the condition. In a study published in April, researchers were able to show that semaglutide resolved fatty liver and inflammation in over 60% of cases and decreased scar tissue in just over a third of patients.
“These findings suggest that semaglutide may prevent fatty liver disease from progressing to cirrhosis and can indeed reverse the course of the disease,” said Arun J. Sanyal, MD, study author and director of the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health at Virginia Commonwealth University in Richmond, Virginia.
Another study published last year had a similar finding, showing that GLP-1 agonists were associated with less progression of the disease and reduced mortality in patients with MASH and diabetes. Another large-scale observational study found that GLP-1s reduced the risk for hepatic failure, which occurs when the liver is unable to perform basic functions, as well as liver cancer, both of which are downstream consequences of MASH.
How GLP-1s Improve Liver Function
“These medications reduce fat burden, which results in fat loss everywhere, including around the liver,” said Ziyad Al-Aly, MD, an assistant professor in the Division of General Medicine & Geriatrics at Washington University School of Medicine in St. Louis. “When fat cells are reduced in size and volume, the normal liver cells have more room to grow and function.”
These medications also seem to work on reducing the inflammation and oxidative stress caused by metabolic disease, which allows for a better environment for the liver to function.
“Fat is not an inert tissue, it’s metabolically active, causing a slow burn to all the cells surrounding it,” said Al-Aly. These medications keep the disease from progressing and reduce scarring, which improves the damage that’s already been done, he said.
Changing How Liver Disease Is Diagnosed
Physicians need to be vigilant in the way that they screen for the condition, said Charu Sawhney, DO, MPH, of Harbor Health in Round Rock, Texas. She said that if liver enzymes appear even slightly elevated, there still could be a reason to utilize GLP-1s to prevent later-stage MASH.
“Normal levels for liver enzymes in some patients can be lower than what labs show,” said Sawhney. This is especially true if a patient has other metabolic risk factors such as diabetes, obesity, or high cholesterol.
If liver enzymes continue to go up even after diet and lifestyle changes, patients might require liver imaging, specifically a wave-based ultrasound called elastography, which measures the elasticity or stiffness of tissues on the liver and can judge if certain portions of it have scarred or hardened. When liver cells change texture and become harder, the scan can estimate levels of fibrosis and, therefore, the stage of MASH that a patient is in.
Additionally, the severity of fatty liver disease depends on other factors besides weight and can sometimes be surprising.
“How bad fatty liver disease is in a patient isn’t always related to how much weight someone has gained,” said Carolynn Francavilla, MD, a nationally recognized obesity physician who owns and operates Green Mountain Partners for Health and Colorado Weight Care, both in Denver.
It’s important for physicians to realize that some patients with fatty liver disease might not have obesity as would be expected. For these patients, adipose tissue seems to accumulate on the liver before it does on other parts of the body. This could be related to the quality of our food system, including the use of sugar substitutes like high fructose corn syrup, which research has shown is even harder on the liver. There might also be a genetic propensity toward fat storage around the organs.
A New Way to Treat MASH
, said Francavilla. Right now, there’s not an official approval from the US Food and Drug Administration (FDA) for prescribing GLP-1s in patients with MASH, but Francavilla hopes that it’s forthcoming.
“It will be really exciting to have these medications as a treatment option because right now there’s only one medication, and it’s for people who have pretty advanced fatty liver disease,” said Francavilla. This medication, called resmetirom, is approved by the FDA to target a protein in the liver to reduce fat and inflammation and scarring. But GLP-1s can be used much earlier to prevent the condition.
“With so many cases of MASH happening so much younger, it’s a disease that physicians really need to take seriously,” said Sawhney.
A version of this article appeared on Medscape.com.
In the past two decades, the global prevalence of metabolic dysfunction–associated steatohepatitis (MASH) has increased dramatically as a result of the obesity epidemic. Researchers project that by 2040, rates of MASH will increase by 55%. Prior to that most liver diseases were caused by alcohol use and hepatitis C, a viral infection that primarily affects the liver.
MASH, a preventable form of liver disease previously called nonalcoholic fatty liver disease, is caused by a buildup of visceral fat cells that accumulate on top of the internal organs, in this case the liver, and keep it from functioning properly. The liver’s primary role is to filter blood, nutrients, and bile used for digestion, as well as to remove toxins from the body. Excess fat cells blanket the liver and keep it from working at full capacity.
Fat cells are also metabolically active and can cause a chronic state of inflammation in the part of the body where they reside. Over time, these fat cells can cause cirrhosis of the liver, or permanent scarring. Once patients reach this stage, the only option is a liver transplant.
New Research on GLP-1 Agonists and MASH
Until recently, the lone treatment for early-stage MASH was weight loss to reduce the number of fat cells that surround the internal organs. But new research has shown that glucagon-like peptide 1 (GLP-1) agonists can reduce and even reverse the condition. In a study published in April, researchers were able to show that semaglutide resolved fatty liver and inflammation in over 60% of cases and decreased scar tissue in just over a third of patients.
“These findings suggest that semaglutide may prevent fatty liver disease from progressing to cirrhosis and can indeed reverse the course of the disease,” said Arun J. Sanyal, MD, study author and director of the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health at Virginia Commonwealth University in Richmond, Virginia.
Another study published last year had a similar finding, showing that GLP-1 agonists were associated with less progression of the disease and reduced mortality in patients with MASH and diabetes. Another large-scale observational study found that GLP-1s reduced the risk for hepatic failure, which occurs when the liver is unable to perform basic functions, as well as liver cancer, both of which are downstream consequences of MASH.
How GLP-1s Improve Liver Function
“These medications reduce fat burden, which results in fat loss everywhere, including around the liver,” said Ziyad Al-Aly, MD, an assistant professor in the Division of General Medicine & Geriatrics at Washington University School of Medicine in St. Louis. “When fat cells are reduced in size and volume, the normal liver cells have more room to grow and function.”
These medications also seem to work on reducing the inflammation and oxidative stress caused by metabolic disease, which allows for a better environment for the liver to function.
“Fat is not an inert tissue, it’s metabolically active, causing a slow burn to all the cells surrounding it,” said Al-Aly. These medications keep the disease from progressing and reduce scarring, which improves the damage that’s already been done, he said.
Changing How Liver Disease Is Diagnosed
Physicians need to be vigilant in the way that they screen for the condition, said Charu Sawhney, DO, MPH, of Harbor Health in Round Rock, Texas. She said that if liver enzymes appear even slightly elevated, there still could be a reason to utilize GLP-1s to prevent later-stage MASH.
“Normal levels for liver enzymes in some patients can be lower than what labs show,” said Sawhney. This is especially true if a patient has other metabolic risk factors such as diabetes, obesity, or high cholesterol.
If liver enzymes continue to go up even after diet and lifestyle changes, patients might require liver imaging, specifically a wave-based ultrasound called elastography, which measures the elasticity or stiffness of tissues on the liver and can judge if certain portions of it have scarred or hardened. When liver cells change texture and become harder, the scan can estimate levels of fibrosis and, therefore, the stage of MASH that a patient is in.
Additionally, the severity of fatty liver disease depends on other factors besides weight and can sometimes be surprising.
“How bad fatty liver disease is in a patient isn’t always related to how much weight someone has gained,” said Carolynn Francavilla, MD, a nationally recognized obesity physician who owns and operates Green Mountain Partners for Health and Colorado Weight Care, both in Denver.
It’s important for physicians to realize that some patients with fatty liver disease might not have obesity as would be expected. For these patients, adipose tissue seems to accumulate on the liver before it does on other parts of the body. This could be related to the quality of our food system, including the use of sugar substitutes like high fructose corn syrup, which research has shown is even harder on the liver. There might also be a genetic propensity toward fat storage around the organs.
A New Way to Treat MASH
, said Francavilla. Right now, there’s not an official approval from the US Food and Drug Administration (FDA) for prescribing GLP-1s in patients with MASH, but Francavilla hopes that it’s forthcoming.
“It will be really exciting to have these medications as a treatment option because right now there’s only one medication, and it’s for people who have pretty advanced fatty liver disease,” said Francavilla. This medication, called resmetirom, is approved by the FDA to target a protein in the liver to reduce fat and inflammation and scarring. But GLP-1s can be used much earlier to prevent the condition.
“With so many cases of MASH happening so much younger, it’s a disease that physicians really need to take seriously,” said Sawhney.
A version of this article appeared on Medscape.com.
In the past two decades, the global prevalence of metabolic dysfunction–associated steatohepatitis (MASH) has increased dramatically as a result of the obesity epidemic. Researchers project that by 2040, rates of MASH will increase by 55%. Prior to that most liver diseases were caused by alcohol use and hepatitis C, a viral infection that primarily affects the liver.
MASH, a preventable form of liver disease previously called nonalcoholic fatty liver disease, is caused by a buildup of visceral fat cells that accumulate on top of the internal organs, in this case the liver, and keep it from functioning properly. The liver’s primary role is to filter blood, nutrients, and bile used for digestion, as well as to remove toxins from the body. Excess fat cells blanket the liver and keep it from working at full capacity.
Fat cells are also metabolically active and can cause a chronic state of inflammation in the part of the body where they reside. Over time, these fat cells can cause cirrhosis of the liver, or permanent scarring. Once patients reach this stage, the only option is a liver transplant.
New Research on GLP-1 Agonists and MASH
Until recently, the lone treatment for early-stage MASH was weight loss to reduce the number of fat cells that surround the internal organs. But new research has shown that glucagon-like peptide 1 (GLP-1) agonists can reduce and even reverse the condition. In a study published in April, researchers were able to show that semaglutide resolved fatty liver and inflammation in over 60% of cases and decreased scar tissue in just over a third of patients.
“These findings suggest that semaglutide may prevent fatty liver disease from progressing to cirrhosis and can indeed reverse the course of the disease,” said Arun J. Sanyal, MD, study author and director of the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health at Virginia Commonwealth University in Richmond, Virginia.
Another study published last year had a similar finding, showing that GLP-1 agonists were associated with less progression of the disease and reduced mortality in patients with MASH and diabetes. Another large-scale observational study found that GLP-1s reduced the risk for hepatic failure, which occurs when the liver is unable to perform basic functions, as well as liver cancer, both of which are downstream consequences of MASH.
How GLP-1s Improve Liver Function
“These medications reduce fat burden, which results in fat loss everywhere, including around the liver,” said Ziyad Al-Aly, MD, an assistant professor in the Division of General Medicine & Geriatrics at Washington University School of Medicine in St. Louis. “When fat cells are reduced in size and volume, the normal liver cells have more room to grow and function.”
These medications also seem to work on reducing the inflammation and oxidative stress caused by metabolic disease, which allows for a better environment for the liver to function.
“Fat is not an inert tissue, it’s metabolically active, causing a slow burn to all the cells surrounding it,” said Al-Aly. These medications keep the disease from progressing and reduce scarring, which improves the damage that’s already been done, he said.
Changing How Liver Disease Is Diagnosed
Physicians need to be vigilant in the way that they screen for the condition, said Charu Sawhney, DO, MPH, of Harbor Health in Round Rock, Texas. She said that if liver enzymes appear even slightly elevated, there still could be a reason to utilize GLP-1s to prevent later-stage MASH.
“Normal levels for liver enzymes in some patients can be lower than what labs show,” said Sawhney. This is especially true if a patient has other metabolic risk factors such as diabetes, obesity, or high cholesterol.
If liver enzymes continue to go up even after diet and lifestyle changes, patients might require liver imaging, specifically a wave-based ultrasound called elastography, which measures the elasticity or stiffness of tissues on the liver and can judge if certain portions of it have scarred or hardened. When liver cells change texture and become harder, the scan can estimate levels of fibrosis and, therefore, the stage of MASH that a patient is in.
Additionally, the severity of fatty liver disease depends on other factors besides weight and can sometimes be surprising.
“How bad fatty liver disease is in a patient isn’t always related to how much weight someone has gained,” said Carolynn Francavilla, MD, a nationally recognized obesity physician who owns and operates Green Mountain Partners for Health and Colorado Weight Care, both in Denver.
It’s important for physicians to realize that some patients with fatty liver disease might not have obesity as would be expected. For these patients, adipose tissue seems to accumulate on the liver before it does on other parts of the body. This could be related to the quality of our food system, including the use of sugar substitutes like high fructose corn syrup, which research has shown is even harder on the liver. There might also be a genetic propensity toward fat storage around the organs.
A New Way to Treat MASH
, said Francavilla. Right now, there’s not an official approval from the US Food and Drug Administration (FDA) for prescribing GLP-1s in patients with MASH, but Francavilla hopes that it’s forthcoming.
“It will be really exciting to have these medications as a treatment option because right now there’s only one medication, and it’s for people who have pretty advanced fatty liver disease,” said Francavilla. This medication, called resmetirom, is approved by the FDA to target a protein in the liver to reduce fat and inflammation and scarring. But GLP-1s can be used much earlier to prevent the condition.
“With so many cases of MASH happening so much younger, it’s a disease that physicians really need to take seriously,” said Sawhney.
A version of this article appeared on Medscape.com.
Ostomy Innovation Grabs ‘Shark Tank’ Win
The “Shark Tank” winning innovation at the American Gastroenterological Association (AGA) Tech Summit in Chicago this April has “life-altering” potential for ostomy patients, according to one of the judges, and eliminates the need for constant pouch wear.
The innovation is called Twistomy and it is designed to replace current ostomy-pouch systems that can cause leaks, odor, skin irritation, embarrassment, and social and emotional distress. The AGA Committee for GI Innovation and Technology (CGIT) organizes the annual Tech Summit.

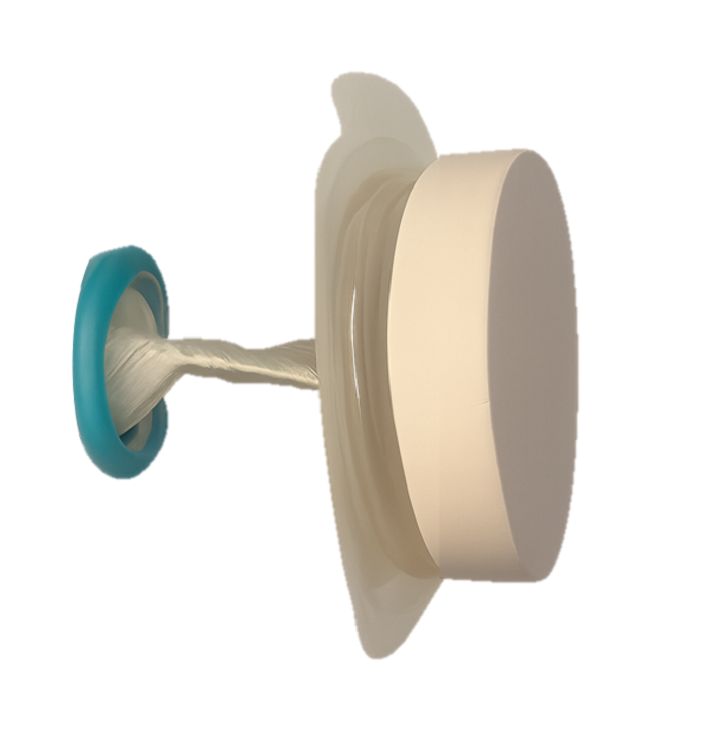
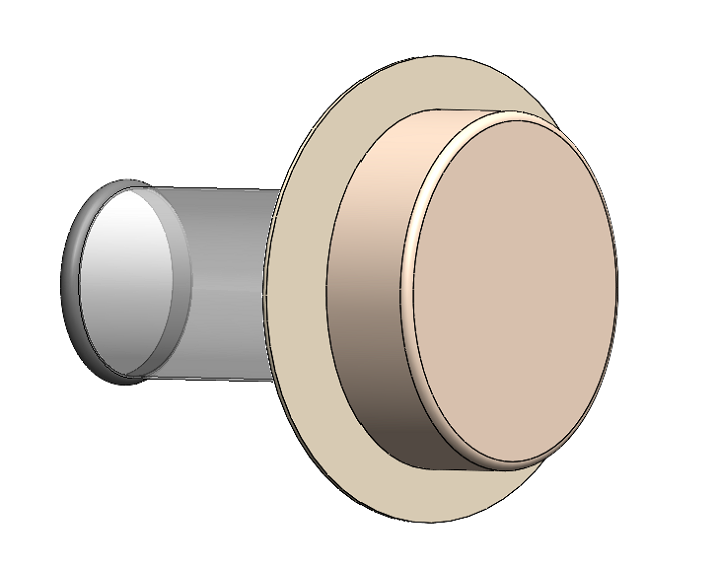
Twistomy’s winning design includes a flexible ring and sleeve, which are inserted into the stoma and secured on the outside with a set of rings that make up the housing unit attached to a standard wafer. The housing unit twists the sleeve closed, allowing the user to control fecal output. For evacuation, the user attaches a pouch, untwists the sleeve, evacuates cleanly and effectively, and then discards the pouch.
Twistomy cofounders Devon Horton, BS, senior bioengineer, and Lily Williams, BS, biomedical researcher and engineer, both work for the department of surgery at University of Colorado, Denver.

Horton said in an interview that when he was approached with the idea to create a better ostomy solution for a senior-year capstone project he was intrigued because the traditional ostomy system “has not changed in more than 70 years. It was crazy that no one had done anything to change that.”
The Twistomy team also won the Grand Prize this spring at the Emerging Medical Innovation Valuation Competition at the Design of Medical Devices Conference held at the University of Minnesota, Minneapolis.
Witnessing the Struggle as a CNA
Horton also works as a certified nursing assistant at an inpatient unit at University of Colorado Hospital and the ostomy patients he sees there every shift help drive his passion to find a better solution.
He hears the emotional stories of people who manage their ostomy daily.
“Many express feelings of depression and anxiety, feeling isolated with their severe inability to go out and do things because of the fear of the noise the stoma makes, or the crinkling of the plastic bag in a yoga class,” he said. “We want to help them regain that control of quality of life.”
They also hope to cut down on the ostomy management time. “Initial user testing [for Twistomy] was less than 75 seconds to insert and assemble,” he said. “I did an interview with a patient yesterday who said they probably spend an hour a day managing their ostomy,” including cleaning and replacing.
Horton and Williams have a patent on the device and currently use three-dimensional printing for the prototypes.
Williams said they are now conducting consumer discovery studies through the National Science Foundation and are interviewing 30 stakeholders — “anyone who has a relationship with an ostomy,” whether a colorectal surgeon, a gastrointestinal nurse, ostomy patients, or insurers.
Those interviews will help in refining the device so they can start consulting with manufacturers and work toward approval as a Class II medical device from the US Food and Drug Administration (FDA), Williams said.
Saving Healthcare Costs
Another potential benefit for Twistomy is its ability to cut healthcare costs, Horton said. Traditional ostomies are prone to leakage, which can lead to peristomal skin complications.
He pointed to a National Institutes of Health analysis that found that on average peristomal skin complications caused upwards of $80,000 more per ostomy patient in increased healthcare costs over a 3-month period than for those without the complications.
“With Twistomy, we are reducing leakage most likely to zero,” Horton said. “We set out to say if we could reduce [infections] by half or a little less than half, we can cut out those tens of thousands of dollars that insurance companies and payers are spending.”
Permanent and Temporary Ostomy Markets
He pointed out that not all ostomies are permanent ostomies, adding that the reversal rate “is about 65%.” Often those reversal surgeries cannot take place until peristomal skin complications have been healed.
“We’re not only hoping to market to the permanent stoma patients, but the patients with temporary stomas as well,” he said.
The team estimates it will need $4 million–$6 million in funding for manufacturing and consultation costs as well as costs involved in seeking FDA approval.
Horton and Williams project the housing unit cost will be $399 based on known out-of-pocket expenses for patients with ostomy care products and the unit would be replaced annually. Disposable elements would be an additional cost.
Assuming insurance acceptance of the product, he said, “With about an 80/20 insurance coverage, typical for many patients, it would be about $100 in out-of-pocket expenses per month to use our device, which is around the lower end of what a lot of patients are spending out of pocket.”
One of the Tech Summit judges, Somaya Albhaisi, MD, a gastroenterology/hepatology fellow at University of Southern California, Los Angeles, said in an interview that the Shark Tank results were unanimous among the five judges and Twistomy also took the fan favorite vote.
She said the teams were judged on quality of pitch, potential clinical impact, and feasibility of business plan. Teams got 5-7 minutes to pitch and answered questions afterward.
“Deep Understanding” of Patient Need
“They combined smart engineering with deep understanding of patient need, which is restoring control, dignity, and quality of life for ostomy users while also reducing healthcare costs. It is rare to see a solution this scalable and impactful. It was a deeply empathetic solution overall.” She noted that nearly 1 million people in the United States currently use an ostomy.
Ostomy users’ quality of life is compromised, and they often have mental health challenges, Albhaisi said. This innovation appears to offer easy use, more dignity and control.
The other four Shark Tank finalists were:
- AI Lumen, which developed a retroview camera system, which attaches to the colonoscope and enhances imaging to detect hidden polyps that may evade conventional endoscopes.
- Amplified Sciences, which developed an ultrasensitive diagnostic platform that detects biomarker activities in minute volumes of fluid from pancreatic cystic lesions, helping to stratify patients into low risk or potential malignancy, reducing unneeded surgeries, costs, and comorbidities.
- KITE Endoscopic Innovations, which designed the Dynaflex TruCut needle to offer a simpler endoscopic ultrasound (EUS)–guided biopsy procedure with fewer needle passes, deeper insights into tumor pathology, and more tissue for geonomic analysis.
- MicroSteer, which designed a device to facilitate semiautomated endoscopic submucosal dissection (ESD) by decoupling the dissecting knife from the endoscope, enhancing safety and effectiveness during the procedure.
The Twistomy Team “Surprised Everyone”
The competitors’ scores were “very close,” one of the judges, Kevin Berliner, said in an interview. “The Twistomy team surprised everyone — the judges and the crowd — with their succinct, informative, and impactful pitch. That presentation disparity was the tiebreaker for me,” said Berliner, who works for Medtronic, a sponsor of the competition, in Chicago.
He said Horton and Williams were the youngest presenters and had the earliest stage pitch they judged, but they “outpresented other competitors in clarity, simplification, and storytelling.”
Also impressive was their description of their “commercially viable path to success” and their plan for the challenges ahead, he said.
Those challenges to get Twistomy to market center “on the ongoing changing climate we have with research funds lately,” Horton said. “We’re giving it an estimate of 3-5 years.”
Horton, Williams, Albhaisi, and Berliner reported no relevant financial relationships.
The “Shark Tank” winning innovation at the American Gastroenterological Association (AGA) Tech Summit in Chicago this April has “life-altering” potential for ostomy patients, according to one of the judges, and eliminates the need for constant pouch wear.
The innovation is called Twistomy and it is designed to replace current ostomy-pouch systems that can cause leaks, odor, skin irritation, embarrassment, and social and emotional distress. The AGA Committee for GI Innovation and Technology (CGIT) organizes the annual Tech Summit.
Twistomy’s winning design includes a flexible ring and sleeve, which are inserted into the stoma and secured on the outside with a set of rings that make up the housing unit attached to a standard wafer. The housing unit twists the sleeve closed, allowing the user to control fecal output. For evacuation, the user attaches a pouch, untwists the sleeve, evacuates cleanly and effectively, and then discards the pouch.
Twistomy cofounders Devon Horton, BS, senior bioengineer, and Lily Williams, BS, biomedical researcher and engineer, both work for the department of surgery at University of Colorado, Denver.
Horton said in an interview that when he was approached with the idea to create a better ostomy solution for a senior-year capstone project he was intrigued because the traditional ostomy system “has not changed in more than 70 years. It was crazy that no one had done anything to change that.”
The Twistomy team also won the Grand Prize this spring at the Emerging Medical Innovation Valuation Competition at the Design of Medical Devices Conference held at the University of Minnesota, Minneapolis.
Witnessing the Struggle as a CNA
Horton also works as a certified nursing assistant at an inpatient unit at University of Colorado Hospital and the ostomy patients he sees there every shift help drive his passion to find a better solution.
He hears the emotional stories of people who manage their ostomy daily.
“Many express feelings of depression and anxiety, feeling isolated with their severe inability to go out and do things because of the fear of the noise the stoma makes, or the crinkling of the plastic bag in a yoga class,” he said. “We want to help them regain that control of quality of life.”
They also hope to cut down on the ostomy management time. “Initial user testing [for Twistomy] was less than 75 seconds to insert and assemble,” he said. “I did an interview with a patient yesterday who said they probably spend an hour a day managing their ostomy,” including cleaning and replacing.
Horton and Williams have a patent on the device and currently use three-dimensional printing for the prototypes.
Williams said they are now conducting consumer discovery studies through the National Science Foundation and are interviewing 30 stakeholders — “anyone who has a relationship with an ostomy,” whether a colorectal surgeon, a gastrointestinal nurse, ostomy patients, or insurers.
Those interviews will help in refining the device so they can start consulting with manufacturers and work toward approval as a Class II medical device from the US Food and Drug Administration (FDA), Williams said.
Saving Healthcare Costs
Another potential benefit for Twistomy is its ability to cut healthcare costs, Horton said. Traditional ostomies are prone to leakage, which can lead to peristomal skin complications.
He pointed to a National Institutes of Health analysis that found that on average peristomal skin complications caused upwards of $80,000 more per ostomy patient in increased healthcare costs over a 3-month period than for those without the complications.
“With Twistomy, we are reducing leakage most likely to zero,” Horton said. “We set out to say if we could reduce [infections] by half or a little less than half, we can cut out those tens of thousands of dollars that insurance companies and payers are spending.”
Permanent and Temporary Ostomy Markets
He pointed out that not all ostomies are permanent ostomies, adding that the reversal rate “is about 65%.” Often those reversal surgeries cannot take place until peristomal skin complications have been healed.
“We’re not only hoping to market to the permanent stoma patients, but the patients with temporary stomas as well,” he said.
The team estimates it will need $4 million–$6 million in funding for manufacturing and consultation costs as well as costs involved in seeking FDA approval.
Horton and Williams project the housing unit cost will be $399 based on known out-of-pocket expenses for patients with ostomy care products and the unit would be replaced annually. Disposable elements would be an additional cost.
Assuming insurance acceptance of the product, he said, “With about an 80/20 insurance coverage, typical for many patients, it would be about $100 in out-of-pocket expenses per month to use our device, which is around the lower end of what a lot of patients are spending out of pocket.”
One of the Tech Summit judges, Somaya Albhaisi, MD, a gastroenterology/hepatology fellow at University of Southern California, Los Angeles, said in an interview that the Shark Tank results were unanimous among the five judges and Twistomy also took the fan favorite vote.
She said the teams were judged on quality of pitch, potential clinical impact, and feasibility of business plan. Teams got 5-7 minutes to pitch and answered questions afterward.
“Deep Understanding” of Patient Need
“They combined smart engineering with deep understanding of patient need, which is restoring control, dignity, and quality of life for ostomy users while also reducing healthcare costs. It is rare to see a solution this scalable and impactful. It was a deeply empathetic solution overall.” She noted that nearly 1 million people in the United States currently use an ostomy.
Ostomy users’ quality of life is compromised, and they often have mental health challenges, Albhaisi said. This innovation appears to offer easy use, more dignity and control.
The other four Shark Tank finalists were:
- AI Lumen, which developed a retroview camera system, which attaches to the colonoscope and enhances imaging to detect hidden polyps that may evade conventional endoscopes.
- Amplified Sciences, which developed an ultrasensitive diagnostic platform that detects biomarker activities in minute volumes of fluid from pancreatic cystic lesions, helping to stratify patients into low risk or potential malignancy, reducing unneeded surgeries, costs, and comorbidities.
- KITE Endoscopic Innovations, which designed the Dynaflex TruCut needle to offer a simpler endoscopic ultrasound (EUS)–guided biopsy procedure with fewer needle passes, deeper insights into tumor pathology, and more tissue for geonomic analysis.
- MicroSteer, which designed a device to facilitate semiautomated endoscopic submucosal dissection (ESD) by decoupling the dissecting knife from the endoscope, enhancing safety and effectiveness during the procedure.
The Twistomy Team “Surprised Everyone”
The competitors’ scores were “very close,” one of the judges, Kevin Berliner, said in an interview. “The Twistomy team surprised everyone — the judges and the crowd — with their succinct, informative, and impactful pitch. That presentation disparity was the tiebreaker for me,” said Berliner, who works for Medtronic, a sponsor of the competition, in Chicago.
He said Horton and Williams were the youngest presenters and had the earliest stage pitch they judged, but they “outpresented other competitors in clarity, simplification, and storytelling.”
Also impressive was their description of their “commercially viable path to success” and their plan for the challenges ahead, he said.
Those challenges to get Twistomy to market center “on the ongoing changing climate we have with research funds lately,” Horton said. “We’re giving it an estimate of 3-5 years.”
Horton, Williams, Albhaisi, and Berliner reported no relevant financial relationships.
The “Shark Tank” winning innovation at the American Gastroenterological Association (AGA) Tech Summit in Chicago this April has “life-altering” potential for ostomy patients, according to one of the judges, and eliminates the need for constant pouch wear.
The innovation is called Twistomy and it is designed to replace current ostomy-pouch systems that can cause leaks, odor, skin irritation, embarrassment, and social and emotional distress. The AGA Committee for GI Innovation and Technology (CGIT) organizes the annual Tech Summit.
Twistomy’s winning design includes a flexible ring and sleeve, which are inserted into the stoma and secured on the outside with a set of rings that make up the housing unit attached to a standard wafer. The housing unit twists the sleeve closed, allowing the user to control fecal output. For evacuation, the user attaches a pouch, untwists the sleeve, evacuates cleanly and effectively, and then discards the pouch.
Twistomy cofounders Devon Horton, BS, senior bioengineer, and Lily Williams, BS, biomedical researcher and engineer, both work for the department of surgery at University of Colorado, Denver.
Horton said in an interview that when he was approached with the idea to create a better ostomy solution for a senior-year capstone project he was intrigued because the traditional ostomy system “has not changed in more than 70 years. It was crazy that no one had done anything to change that.”
The Twistomy team also won the Grand Prize this spring at the Emerging Medical Innovation Valuation Competition at the Design of Medical Devices Conference held at the University of Minnesota, Minneapolis.
Witnessing the Struggle as a CNA
Horton also works as a certified nursing assistant at an inpatient unit at University of Colorado Hospital and the ostomy patients he sees there every shift help drive his passion to find a better solution.
He hears the emotional stories of people who manage their ostomy daily.
“Many express feelings of depression and anxiety, feeling isolated with their severe inability to go out and do things because of the fear of the noise the stoma makes, or the crinkling of the plastic bag in a yoga class,” he said. “We want to help them regain that control of quality of life.”
They also hope to cut down on the ostomy management time. “Initial user testing [for Twistomy] was less than 75 seconds to insert and assemble,” he said. “I did an interview with a patient yesterday who said they probably spend an hour a day managing their ostomy,” including cleaning and replacing.
Horton and Williams have a patent on the device and currently use three-dimensional printing for the prototypes.
Williams said they are now conducting consumer discovery studies through the National Science Foundation and are interviewing 30 stakeholders — “anyone who has a relationship with an ostomy,” whether a colorectal surgeon, a gastrointestinal nurse, ostomy patients, or insurers.
Those interviews will help in refining the device so they can start consulting with manufacturers and work toward approval as a Class II medical device from the US Food and Drug Administration (FDA), Williams said.
Saving Healthcare Costs
Another potential benefit for Twistomy is its ability to cut healthcare costs, Horton said. Traditional ostomies are prone to leakage, which can lead to peristomal skin complications.
He pointed to a National Institutes of Health analysis that found that on average peristomal skin complications caused upwards of $80,000 more per ostomy patient in increased healthcare costs over a 3-month period than for those without the complications.
“With Twistomy, we are reducing leakage most likely to zero,” Horton said. “We set out to say if we could reduce [infections] by half or a little less than half, we can cut out those tens of thousands of dollars that insurance companies and payers are spending.”
Permanent and Temporary Ostomy Markets
He pointed out that not all ostomies are permanent ostomies, adding that the reversal rate “is about 65%.” Often those reversal surgeries cannot take place until peristomal skin complications have been healed.
“We’re not only hoping to market to the permanent stoma patients, but the patients with temporary stomas as well,” he said.
The team estimates it will need $4 million–$6 million in funding for manufacturing and consultation costs as well as costs involved in seeking FDA approval.
Horton and Williams project the housing unit cost will be $399 based on known out-of-pocket expenses for patients with ostomy care products and the unit would be replaced annually. Disposable elements would be an additional cost.
Assuming insurance acceptance of the product, he said, “With about an 80/20 insurance coverage, typical for many patients, it would be about $100 in out-of-pocket expenses per month to use our device, which is around the lower end of what a lot of patients are spending out of pocket.”
One of the Tech Summit judges, Somaya Albhaisi, MD, a gastroenterology/hepatology fellow at University of Southern California, Los Angeles, said in an interview that the Shark Tank results were unanimous among the five judges and Twistomy also took the fan favorite vote.
She said the teams were judged on quality of pitch, potential clinical impact, and feasibility of business plan. Teams got 5-7 minutes to pitch and answered questions afterward.
“Deep Understanding” of Patient Need
“They combined smart engineering with deep understanding of patient need, which is restoring control, dignity, and quality of life for ostomy users while also reducing healthcare costs. It is rare to see a solution this scalable and impactful. It was a deeply empathetic solution overall.” She noted that nearly 1 million people in the United States currently use an ostomy.
Ostomy users’ quality of life is compromised, and they often have mental health challenges, Albhaisi said. This innovation appears to offer easy use, more dignity and control.
The other four Shark Tank finalists were:
- AI Lumen, which developed a retroview camera system, which attaches to the colonoscope and enhances imaging to detect hidden polyps that may evade conventional endoscopes.
- Amplified Sciences, which developed an ultrasensitive diagnostic platform that detects biomarker activities in minute volumes of fluid from pancreatic cystic lesions, helping to stratify patients into low risk or potential malignancy, reducing unneeded surgeries, costs, and comorbidities.
- KITE Endoscopic Innovations, which designed the Dynaflex TruCut needle to offer a simpler endoscopic ultrasound (EUS)–guided biopsy procedure with fewer needle passes, deeper insights into tumor pathology, and more tissue for geonomic analysis.
- MicroSteer, which designed a device to facilitate semiautomated endoscopic submucosal dissection (ESD) by decoupling the dissecting knife from the endoscope, enhancing safety and effectiveness during the procedure.
The Twistomy Team “Surprised Everyone”
The competitors’ scores were “very close,” one of the judges, Kevin Berliner, said in an interview. “The Twistomy team surprised everyone — the judges and the crowd — with their succinct, informative, and impactful pitch. That presentation disparity was the tiebreaker for me,” said Berliner, who works for Medtronic, a sponsor of the competition, in Chicago.
He said Horton and Williams were the youngest presenters and had the earliest stage pitch they judged, but they “outpresented other competitors in clarity, simplification, and storytelling.”
Also impressive was their description of their “commercially viable path to success” and their plan for the challenges ahead, he said.
Those challenges to get Twistomy to market center “on the ongoing changing climate we have with research funds lately,” Horton said. “We’re giving it an estimate of 3-5 years.”
Horton, Williams, Albhaisi, and Berliner reported no relevant financial relationships.
Blood-Based Test May Predict Crohn’s Disease 2 Years Before Onset
SAN DIEGO — Crohn’s disease (CD) has become more common in the United States, and an estimated 1 million Americans have the condition. Still, much is unknown about how to evaluate the individual risk for the disease.
“It’s pretty much accepted that Crohn’s disease does not begin at diagnosis,” said Ryan Ungaro, MD, associate professor of medicine at the Icahn School of Medicine at Mount Sinai, New York City, speaking at Digestive Disease Week (DDW)® 2025.

Although individual blood markers have been associated with the future risk for CD, what’s needed, he said, is to understand which combination of biomarkers are most predictive.
Now, .
It’s an early version that will likely be further improved and needs additional validation, Ungaro told GI & Hepatology News.
“Once we can accurately identify individuals at risk for developing Crohn’s disease, we can then imagine a number of potential interventions,” Ungaro said.
Approaches would vary depending on how far away the onset is estimated to be. For people who likely wouldn’t develop disease for many years, one intervention might be close monitoring to enable diagnosis in the earliest stages, when treatment works best, he said. Someone at a high risk of developing CD in the next 2 or 3 years, on the other hand, might be offered a pharmaceutical intervention.
Developing and Testing the Risk Score
To develop the risk score, Ungaro and colleagues analyzed data of 200 patients with CD and 100 healthy control participants from PREDICTS, a nested case-controlled study of active US military service members. The study is within the larger Department of Defense Serum Repository, which began in 1985 and has more than 62.5 million samples, all stored at −30 °C.
The researchers collected serum samples at four timepoints up to 6 or more years before the diagnosis. They assayed antimicrobial antibodies using the Prometheus Laboratories platform, proteomic markers using the Olink inflammation panel, and anti–granulocyte macrophage colony-stimulating factor autoantibodies using enzyme-linked immunosorbent assay.
Participants (median age, 33 years for both groups) were randomly divided into equally sized training and testing sets. In both the group, 83% of patients were White and about 90% were men.
Time-varying trajectories of marker abundance were estimated for each biomarker. Then, logistic regression modeled disease status as a function of each marker for different timepoints and multivariate modeling was performed via logistic LASSO regression.
A risk score to predict CD onset within 2 years was developed. Prediction models were fit on the testing set and predictive performance evaluated using receiver operating characteristic curves and area under the curve (AUC).
Blood proteins and antibodies have differing associations with CD depending on the time before diagnosis, the researchers found.
The integrative model to predict CD onset within 2 years incorporated 10 biomarkers associated significantly with CD onset.
The AUC for the model was 0.87 (considered good, with 1 indicating perfect discrimination). It produced a specificity of 99% and a positive predictive value of 84%.
The researchers stratified the model scores into quartiles and found the CD incidence within 2 years increased from 2% in the first quartile to 57.7% in the fourth. The relative risk of developing CD in the top quartile individuals vs lower quartile individuals was 10.4.
The serologic and proteomic markers show dynamic changes years before the diagnosis, Ungaro said.
A Strong Start
The research represents “an ambitious and exciting frontier for the future of IBD [inflammatory bowel disease] care,” said Victor G. Chedid, MD, MS, consultant and assistant professor of medicine at Mayo Clinic, Rochester, Minnesota, who reviewed the findings but was not involved in the study.

Currently, physicians treat IBD once it manifests, and it’s difficult to predict who will get CD, he said.
The integrative model’s AUC of 0.87 is impressive, and its specificity and positive predictive value levels show it is highly accurate in predicting the onset of CD within 2 years, Chedid added.
Further validation in larger and more diverse population is needed, Chedid said, but he sees the potential for the model to be practical in clinical practice.
“Additionally, the use of blood-based biomarkers makes the model relatively noninvasive and easy to implement in a clinical setting,” he said.
Now, the research goal is to understand the best biomarkers for characterizing the different preclinical phases of CD and to test different interventions in prevention trials, Ungaro told GI & Hepatology News.
A few trials are planned or ongoing, he noted. The trial PIONIR trial will look at the impact of a specific diet on the risk of developing CD, and the INTERCEPT trial aims to develop a blood-based risk score that can identify individuals with a high risk of developing CD within 5 years after initial evaluation.
Ungaro reported being on the advisory board of and/or receiving speaker or consulting fees from AbbVie, Bristol Myer Squibb, Celltrion, ECM Therapeutics, Genentech, Jansen, Eli Lilly, Pfizer, Roivant, Sanofi, and Takeda. Chedid reported having no relevant disclosures.
The PROMISE Consortium is funded by the Helmsley Charitable Trust.
A version of this article appeared on Medscape.com.
SAN DIEGO — Crohn’s disease (CD) has become more common in the United States, and an estimated 1 million Americans have the condition. Still, much is unknown about how to evaluate the individual risk for the disease.
“It’s pretty much accepted that Crohn’s disease does not begin at diagnosis,” said Ryan Ungaro, MD, associate professor of medicine at the Icahn School of Medicine at Mount Sinai, New York City, speaking at Digestive Disease Week (DDW)® 2025.
Although individual blood markers have been associated with the future risk for CD, what’s needed, he said, is to understand which combination of biomarkers are most predictive.
Now, .
It’s an early version that will likely be further improved and needs additional validation, Ungaro told GI & Hepatology News.
“Once we can accurately identify individuals at risk for developing Crohn’s disease, we can then imagine a number of potential interventions,” Ungaro said.
Approaches would vary depending on how far away the onset is estimated to be. For people who likely wouldn’t develop disease for many years, one intervention might be close monitoring to enable diagnosis in the earliest stages, when treatment works best, he said. Someone at a high risk of developing CD in the next 2 or 3 years, on the other hand, might be offered a pharmaceutical intervention.
Developing and Testing the Risk Score
To develop the risk score, Ungaro and colleagues analyzed data of 200 patients with CD and 100 healthy control participants from PREDICTS, a nested case-controlled study of active US military service members. The study is within the larger Department of Defense Serum Repository, which began in 1985 and has more than 62.5 million samples, all stored at −30 °C.
The researchers collected serum samples at four timepoints up to 6 or more years before the diagnosis. They assayed antimicrobial antibodies using the Prometheus Laboratories platform, proteomic markers using the Olink inflammation panel, and anti–granulocyte macrophage colony-stimulating factor autoantibodies using enzyme-linked immunosorbent assay.
Participants (median age, 33 years for both groups) were randomly divided into equally sized training and testing sets. In both the group, 83% of patients were White and about 90% were men.
Time-varying trajectories of marker abundance were estimated for each biomarker. Then, logistic regression modeled disease status as a function of each marker for different timepoints and multivariate modeling was performed via logistic LASSO regression.
A risk score to predict CD onset within 2 years was developed. Prediction models were fit on the testing set and predictive performance evaluated using receiver operating characteristic curves and area under the curve (AUC).
Blood proteins and antibodies have differing associations with CD depending on the time before diagnosis, the researchers found.
The integrative model to predict CD onset within 2 years incorporated 10 biomarkers associated significantly with CD onset.
The AUC for the model was 0.87 (considered good, with 1 indicating perfect discrimination). It produced a specificity of 99% and a positive predictive value of 84%.
The researchers stratified the model scores into quartiles and found the CD incidence within 2 years increased from 2% in the first quartile to 57.7% in the fourth. The relative risk of developing CD in the top quartile individuals vs lower quartile individuals was 10.4.
The serologic and proteomic markers show dynamic changes years before the diagnosis, Ungaro said.
A Strong Start
The research represents “an ambitious and exciting frontier for the future of IBD [inflammatory bowel disease] care,” said Victor G. Chedid, MD, MS, consultant and assistant professor of medicine at Mayo Clinic, Rochester, Minnesota, who reviewed the findings but was not involved in the study.
Currently, physicians treat IBD once it manifests, and it’s difficult to predict who will get CD, he said.
The integrative model’s AUC of 0.87 is impressive, and its specificity and positive predictive value levels show it is highly accurate in predicting the onset of CD within 2 years, Chedid added.
Further validation in larger and more diverse population is needed, Chedid said, but he sees the potential for the model to be practical in clinical practice.
“Additionally, the use of blood-based biomarkers makes the model relatively noninvasive and easy to implement in a clinical setting,” he said.
Now, the research goal is to understand the best biomarkers for characterizing the different preclinical phases of CD and to test different interventions in prevention trials, Ungaro told GI & Hepatology News.
A few trials are planned or ongoing, he noted. The trial PIONIR trial will look at the impact of a specific diet on the risk of developing CD, and the INTERCEPT trial aims to develop a blood-based risk score that can identify individuals with a high risk of developing CD within 5 years after initial evaluation.
Ungaro reported being on the advisory board of and/or receiving speaker or consulting fees from AbbVie, Bristol Myer Squibb, Celltrion, ECM Therapeutics, Genentech, Jansen, Eli Lilly, Pfizer, Roivant, Sanofi, and Takeda. Chedid reported having no relevant disclosures.
The PROMISE Consortium is funded by the Helmsley Charitable Trust.
A version of this article appeared on Medscape.com.
SAN DIEGO — Crohn’s disease (CD) has become more common in the United States, and an estimated 1 million Americans have the condition. Still, much is unknown about how to evaluate the individual risk for the disease.
“It’s pretty much accepted that Crohn’s disease does not begin at diagnosis,” said Ryan Ungaro, MD, associate professor of medicine at the Icahn School of Medicine at Mount Sinai, New York City, speaking at Digestive Disease Week (DDW)® 2025.
Although individual blood markers have been associated with the future risk for CD, what’s needed, he said, is to understand which combination of biomarkers are most predictive.
Now, .
It’s an early version that will likely be further improved and needs additional validation, Ungaro told GI & Hepatology News.
“Once we can accurately identify individuals at risk for developing Crohn’s disease, we can then imagine a number of potential interventions,” Ungaro said.
Approaches would vary depending on how far away the onset is estimated to be. For people who likely wouldn’t develop disease for many years, one intervention might be close monitoring to enable diagnosis in the earliest stages, when treatment works best, he said. Someone at a high risk of developing CD in the next 2 or 3 years, on the other hand, might be offered a pharmaceutical intervention.
Developing and Testing the Risk Score
To develop the risk score, Ungaro and colleagues analyzed data of 200 patients with CD and 100 healthy control participants from PREDICTS, a nested case-controlled study of active US military service members. The study is within the larger Department of Defense Serum Repository, which began in 1985 and has more than 62.5 million samples, all stored at −30 °C.
The researchers collected serum samples at four timepoints up to 6 or more years before the diagnosis. They assayed antimicrobial antibodies using the Prometheus Laboratories platform, proteomic markers using the Olink inflammation panel, and anti–granulocyte macrophage colony-stimulating factor autoantibodies using enzyme-linked immunosorbent assay.
Participants (median age, 33 years for both groups) were randomly divided into equally sized training and testing sets. In both the group, 83% of patients were White and about 90% were men.
Time-varying trajectories of marker abundance were estimated for each biomarker. Then, logistic regression modeled disease status as a function of each marker for different timepoints and multivariate modeling was performed via logistic LASSO regression.
A risk score to predict CD onset within 2 years was developed. Prediction models were fit on the testing set and predictive performance evaluated using receiver operating characteristic curves and area under the curve (AUC).
Blood proteins and antibodies have differing associations with CD depending on the time before diagnosis, the researchers found.
The integrative model to predict CD onset within 2 years incorporated 10 biomarkers associated significantly with CD onset.
The AUC for the model was 0.87 (considered good, with 1 indicating perfect discrimination). It produced a specificity of 99% and a positive predictive value of 84%.
The researchers stratified the model scores into quartiles and found the CD incidence within 2 years increased from 2% in the first quartile to 57.7% in the fourth. The relative risk of developing CD in the top quartile individuals vs lower quartile individuals was 10.4.
The serologic and proteomic markers show dynamic changes years before the diagnosis, Ungaro said.
A Strong Start
The research represents “an ambitious and exciting frontier for the future of IBD [inflammatory bowel disease] care,” said Victor G. Chedid, MD, MS, consultant and assistant professor of medicine at Mayo Clinic, Rochester, Minnesota, who reviewed the findings but was not involved in the study.
Currently, physicians treat IBD once it manifests, and it’s difficult to predict who will get CD, he said.
The integrative model’s AUC of 0.87 is impressive, and its specificity and positive predictive value levels show it is highly accurate in predicting the onset of CD within 2 years, Chedid added.
Further validation in larger and more diverse population is needed, Chedid said, but he sees the potential for the model to be practical in clinical practice.
“Additionally, the use of blood-based biomarkers makes the model relatively noninvasive and easy to implement in a clinical setting,” he said.
Now, the research goal is to understand the best biomarkers for characterizing the different preclinical phases of CD and to test different interventions in prevention trials, Ungaro told GI & Hepatology News.
A few trials are planned or ongoing, he noted. The trial PIONIR trial will look at the impact of a specific diet on the risk of developing CD, and the INTERCEPT trial aims to develop a blood-based risk score that can identify individuals with a high risk of developing CD within 5 years after initial evaluation.
Ungaro reported being on the advisory board of and/or receiving speaker or consulting fees from AbbVie, Bristol Myer Squibb, Celltrion, ECM Therapeutics, Genentech, Jansen, Eli Lilly, Pfizer, Roivant, Sanofi, and Takeda. Chedid reported having no relevant disclosures.
The PROMISE Consortium is funded by the Helmsley Charitable Trust.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Winning Strategies to Retain Private Practice Gastroenterologists
SAN DIEGO — With the recently updated recommendations by the US Preventive Services Task Force lowering the age for colorectal cancer screening to 45 instead of 50, an additional 19 million patients now require screening, Asma Khapra, MD, AGAF, a gastroenterologist at Gastro Health in Fairfax, Virginia, told attendees at Digestive Disease Week® (DDW) 2025.

That change, coupled with the expected shortage of gastroenterologists, means one thing: The current workforce can’t meet patient demand, she said. , Khapra added.
The private practice model is already declining, she said. The fraction of US gastroenterologists in “fully independent” private practice was about 30% in 2019, Khapra noted. Then, “COVID really changed the landscape even more.” By 2022, “that number has shrunk to 13%.” Meanwhile, 67% are employed gastroenterologists (not in private practice), 7% work in large group practices, and 13% are private equity (PE) backed.
That makes effective retention strategies crucial for private practices, Khapra said. She first addressed the common attractions of private practices, then the challenges, and finally the winning strategies to retain and keep a viable private practice gastroenterology workforce.
The Attractions of Private Practice
The reasons for choosing private practice are many, Khapra said, including:
- Autonomy,
- Flexibility,
- Competitive compensation,
- Ownership mindset,
- Partnership paths, and
- Work-life balance including involvement in community and culture.
On the other hand, private practices have unique challenges, including:
- Administrative burdens such as EHR documentation, paperwork, prior authorizations, and staffing issues,
- Financial pressures, including competition with the employment packages offered by hospitals, as reimbursements continue to drop and staffing costs increase,
- Burnout,
- Variety of buy-ins and partnership tracks,
- Limited career development, and
- The strains of aging and endoscopy. “We used to joke in our practice that at any given time, three staff members are in physical therapy due to injuries and disabilities.”
Employing the Iceberg Model
One strategy, Khapra said, is to follow Edward T. Hall’s Iceberg Model of Culture , which focuses on the importance of both visible and invisible elements.
“The key to retention in private practice is to develop a value system where everyone is treated well and respected and compensated fairly,” she said. “That doesn’t mean you split the pie [equally].”
“Visible” elements of the model include the physical environment, policies and practices, symbols and behaviors, she said. While under the surface (“invisible” elements) are shared values, perceptions and attitudes, leadership style, conflict resolution, decision making and unwritten rules.
The key, she said, is to provide physicians an actual voice in decision making and to avoid favouritism, thus avoiding comments such as “Why do the same two people always get the prime scoping blocks?”
Financial transparency is also important, Khapra said. And people want flexibility without it being called special treatment. She provided several practical suggestions to accomplish the invisible Iceberg goals.
For instance, she suggested paying for activities outside the practice that physicians do, such as serving on committees. If the practice can’t afford that, she suggested asking the affiliated hospitals to do so, noting that such an initiative can often build community support.
Paying more attention to early associates than is typical can also benefit the practice, Khapra said. “So much effort is made to recruit them, and then once there, we’re on to the next [recruits].” Instead, she suggested, “pay attention to their needs.”
Providing support to physicians who are injured is also crucial and can foster a community culture, she said. For example, one Gastro Health physician was out for 4 weeks due to complications from surgery. “Everyone jumped in” to help fill the injured physician’s shifts, she said, reassuring the physician that the money would be figured out later. “That’s the culture you want to instill.”
To prevent burnout, another key to retaining physicians, “you have to provide support staff.” And offering good benefits, including parental and maternal leave and disability benefits, is also crucial, Khapra said. Consider practices such as having social dinners, another way to build a sense of community.
Finally, bring in national and local gastroenterologist organizations for discussions, including advocating for fair reimbursement for private practice. Consider working with the Digestive Health Physicians Alliance, which describes itself as the voice of independent gastroenterology, she suggested.
More Perspectives
Jami Kinnucan, MD, AGAF, a gastroenterologist and associate professor of medicine at Mayo Clinic, Jacksonville , Florida, spoke about optimizing recruitment of young gastroenterologists and provided perspective on Khapra’s talk.

“I think there’s a lot of overlap” with her topic and retaining private practice gastroenterologists, she said in an interview with GI & Hepatology News. Most important, she said, is having an efficient system in which the administrative flow is left to digital tools or other staff, not physicians. “That will also help to reduce burnout,” she said, and allow physicians to do what they most want to do, which is to focus on providing care to patients.
“People want to feel valued for their work,” she agreed. “People want opportunity for career development, opportunities for growth.”
As gastroenterologists age, flexibility is important, as it in in general for all physicians, Kinnucan said. She suggested schedule flexibility as one way. For instance, “if I tell 10 providers, ‘I need you to see 100 patients this week, but you can do it however you want,’ that promotes flexibility. They might want to see all of them on Monday and Tuesday, for instance. If you give people choice and autonomy, they are more likely to feel like they are part of the decision.”
How do you build a high-functioning team? “You do it by letting them operate autonomously,” and “you let people do the things they are really excited about.” And always, as Khapra said, focus on the invisible elements that are so crucial.
Khapra and Kinnucan had no relevant disclosures. Khapra received no funding for her presentation.
A version of this article appeared on Medscape.com.
SAN DIEGO — With the recently updated recommendations by the US Preventive Services Task Force lowering the age for colorectal cancer screening to 45 instead of 50, an additional 19 million patients now require screening, Asma Khapra, MD, AGAF, a gastroenterologist at Gastro Health in Fairfax, Virginia, told attendees at Digestive Disease Week® (DDW) 2025.
That change, coupled with the expected shortage of gastroenterologists, means one thing: The current workforce can’t meet patient demand, she said. , Khapra added.
The private practice model is already declining, she said. The fraction of US gastroenterologists in “fully independent” private practice was about 30% in 2019, Khapra noted. Then, “COVID really changed the landscape even more.” By 2022, “that number has shrunk to 13%.” Meanwhile, 67% are employed gastroenterologists (not in private practice), 7% work in large group practices, and 13% are private equity (PE) backed.
That makes effective retention strategies crucial for private practices, Khapra said. She first addressed the common attractions of private practices, then the challenges, and finally the winning strategies to retain and keep a viable private practice gastroenterology workforce.
The Attractions of Private Practice
The reasons for choosing private practice are many, Khapra said, including:
- Autonomy,
- Flexibility,
- Competitive compensation,
- Ownership mindset,
- Partnership paths, and
- Work-life balance including involvement in community and culture.
On the other hand, private practices have unique challenges, including:
- Administrative burdens such as EHR documentation, paperwork, prior authorizations, and staffing issues,
- Financial pressures, including competition with the employment packages offered by hospitals, as reimbursements continue to drop and staffing costs increase,
- Burnout,
- Variety of buy-ins and partnership tracks,
- Limited career development, and
- The strains of aging and endoscopy. “We used to joke in our practice that at any given time, three staff members are in physical therapy due to injuries and disabilities.”
Employing the Iceberg Model
One strategy, Khapra said, is to follow Edward T. Hall’s Iceberg Model of Culture , which focuses on the importance of both visible and invisible elements.
“The key to retention in private practice is to develop a value system where everyone is treated well and respected and compensated fairly,” she said. “That doesn’t mean you split the pie [equally].”
“Visible” elements of the model include the physical environment, policies and practices, symbols and behaviors, she said. While under the surface (“invisible” elements) are shared values, perceptions and attitudes, leadership style, conflict resolution, decision making and unwritten rules.
The key, she said, is to provide physicians an actual voice in decision making and to avoid favouritism, thus avoiding comments such as “Why do the same two people always get the prime scoping blocks?”
Financial transparency is also important, Khapra said. And people want flexibility without it being called special treatment. She provided several practical suggestions to accomplish the invisible Iceberg goals.
For instance, she suggested paying for activities outside the practice that physicians do, such as serving on committees. If the practice can’t afford that, she suggested asking the affiliated hospitals to do so, noting that such an initiative can often build community support.
Paying more attention to early associates than is typical can also benefit the practice, Khapra said. “So much effort is made to recruit them, and then once there, we’re on to the next [recruits].” Instead, she suggested, “pay attention to their needs.”
Providing support to physicians who are injured is also crucial and can foster a community culture, she said. For example, one Gastro Health physician was out for 4 weeks due to complications from surgery. “Everyone jumped in” to help fill the injured physician’s shifts, she said, reassuring the physician that the money would be figured out later. “That’s the culture you want to instill.”
To prevent burnout, another key to retaining physicians, “you have to provide support staff.” And offering good benefits, including parental and maternal leave and disability benefits, is also crucial, Khapra said. Consider practices such as having social dinners, another way to build a sense of community.
Finally, bring in national and local gastroenterologist organizations for discussions, including advocating for fair reimbursement for private practice. Consider working with the Digestive Health Physicians Alliance, which describes itself as the voice of independent gastroenterology, she suggested.
More Perspectives
Jami Kinnucan, MD, AGAF, a gastroenterologist and associate professor of medicine at Mayo Clinic, Jacksonville , Florida, spoke about optimizing recruitment of young gastroenterologists and provided perspective on Khapra’s talk.
“I think there’s a lot of overlap” with her topic and retaining private practice gastroenterologists, she said in an interview with GI & Hepatology News. Most important, she said, is having an efficient system in which the administrative flow is left to digital tools or other staff, not physicians. “That will also help to reduce burnout,” she said, and allow physicians to do what they most want to do, which is to focus on providing care to patients.
“People want to feel valued for their work,” she agreed. “People want opportunity for career development, opportunities for growth.”
As gastroenterologists age, flexibility is important, as it in in general for all physicians, Kinnucan said. She suggested schedule flexibility as one way. For instance, “if I tell 10 providers, ‘I need you to see 100 patients this week, but you can do it however you want,’ that promotes flexibility. They might want to see all of them on Monday and Tuesday, for instance. If you give people choice and autonomy, they are more likely to feel like they are part of the decision.”
How do you build a high-functioning team? “You do it by letting them operate autonomously,” and “you let people do the things they are really excited about.” And always, as Khapra said, focus on the invisible elements that are so crucial.
Khapra and Kinnucan had no relevant disclosures. Khapra received no funding for her presentation.
A version of this article appeared on Medscape.com.
SAN DIEGO — With the recently updated recommendations by the US Preventive Services Task Force lowering the age for colorectal cancer screening to 45 instead of 50, an additional 19 million patients now require screening, Asma Khapra, MD, AGAF, a gastroenterologist at Gastro Health in Fairfax, Virginia, told attendees at Digestive Disease Week® (DDW) 2025.
That change, coupled with the expected shortage of gastroenterologists, means one thing: The current workforce can’t meet patient demand, she said. , Khapra added.
The private practice model is already declining, she said. The fraction of US gastroenterologists in “fully independent” private practice was about 30% in 2019, Khapra noted. Then, “COVID really changed the landscape even more.” By 2022, “that number has shrunk to 13%.” Meanwhile, 67% are employed gastroenterologists (not in private practice), 7% work in large group practices, and 13% are private equity (PE) backed.
That makes effective retention strategies crucial for private practices, Khapra said. She first addressed the common attractions of private practices, then the challenges, and finally the winning strategies to retain and keep a viable private practice gastroenterology workforce.
The Attractions of Private Practice
The reasons for choosing private practice are many, Khapra said, including:
- Autonomy,
- Flexibility,
- Competitive compensation,
- Ownership mindset,
- Partnership paths, and
- Work-life balance including involvement in community and culture.
On the other hand, private practices have unique challenges, including:
- Administrative burdens such as EHR documentation, paperwork, prior authorizations, and staffing issues,
- Financial pressures, including competition with the employment packages offered by hospitals, as reimbursements continue to drop and staffing costs increase,
- Burnout,
- Variety of buy-ins and partnership tracks,
- Limited career development, and
- The strains of aging and endoscopy. “We used to joke in our practice that at any given time, three staff members are in physical therapy due to injuries and disabilities.”
Employing the Iceberg Model
One strategy, Khapra said, is to follow Edward T. Hall’s Iceberg Model of Culture , which focuses on the importance of both visible and invisible elements.
“The key to retention in private practice is to develop a value system where everyone is treated well and respected and compensated fairly,” she said. “That doesn’t mean you split the pie [equally].”
“Visible” elements of the model include the physical environment, policies and practices, symbols and behaviors, she said. While under the surface (“invisible” elements) are shared values, perceptions and attitudes, leadership style, conflict resolution, decision making and unwritten rules.
The key, she said, is to provide physicians an actual voice in decision making and to avoid favouritism, thus avoiding comments such as “Why do the same two people always get the prime scoping blocks?”
Financial transparency is also important, Khapra said. And people want flexibility without it being called special treatment. She provided several practical suggestions to accomplish the invisible Iceberg goals.
For instance, she suggested paying for activities outside the practice that physicians do, such as serving on committees. If the practice can’t afford that, she suggested asking the affiliated hospitals to do so, noting that such an initiative can often build community support.
Paying more attention to early associates than is typical can also benefit the practice, Khapra said. “So much effort is made to recruit them, and then once there, we’re on to the next [recruits].” Instead, she suggested, “pay attention to their needs.”
Providing support to physicians who are injured is also crucial and can foster a community culture, she said. For example, one Gastro Health physician was out for 4 weeks due to complications from surgery. “Everyone jumped in” to help fill the injured physician’s shifts, she said, reassuring the physician that the money would be figured out later. “That’s the culture you want to instill.”
To prevent burnout, another key to retaining physicians, “you have to provide support staff.” And offering good benefits, including parental and maternal leave and disability benefits, is also crucial, Khapra said. Consider practices such as having social dinners, another way to build a sense of community.
Finally, bring in national and local gastroenterologist organizations for discussions, including advocating for fair reimbursement for private practice. Consider working with the Digestive Health Physicians Alliance, which describes itself as the voice of independent gastroenterology, she suggested.
More Perspectives
Jami Kinnucan, MD, AGAF, a gastroenterologist and associate professor of medicine at Mayo Clinic, Jacksonville , Florida, spoke about optimizing recruitment of young gastroenterologists and provided perspective on Khapra’s talk.
“I think there’s a lot of overlap” with her topic and retaining private practice gastroenterologists, she said in an interview with GI & Hepatology News. Most important, she said, is having an efficient system in which the administrative flow is left to digital tools or other staff, not physicians. “That will also help to reduce burnout,” she said, and allow physicians to do what they most want to do, which is to focus on providing care to patients.
“People want to feel valued for their work,” she agreed. “People want opportunity for career development, opportunities for growth.”
As gastroenterologists age, flexibility is important, as it in in general for all physicians, Kinnucan said. She suggested schedule flexibility as one way. For instance, “if I tell 10 providers, ‘I need you to see 100 patients this week, but you can do it however you want,’ that promotes flexibility. They might want to see all of them on Monday and Tuesday, for instance. If you give people choice and autonomy, they are more likely to feel like they are part of the decision.”
How do you build a high-functioning team? “You do it by letting them operate autonomously,” and “you let people do the things they are really excited about.” And always, as Khapra said, focus on the invisible elements that are so crucial.
Khapra and Kinnucan had no relevant disclosures. Khapra received no funding for her presentation.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Blood Detection Capsule Helpful in Suspected Upper GI Bleeding
SAN DIEGO — , a study found.
Notably, patients with negative capsule results had shorter hospital stays and lower acuity markers, and in more than one third of cases, an esophagogastroduodenoscopy (EGD) was avoided altogether without any observed adverse events or readmissions, the study team found.
“Our study shows that this novel capsule that detects blood in the upper GI tract (PillSense) was highly sensitive and specific (> 90%) for detecting recent or active upper GI blood, influenced clinical management in 80% of cases and allowed about one third of patients to be safely discharged from the emergency department, with close outpatient follow-up,” Linda Lee, MD, AGAF, medical director of endoscopy, Brigham and Women’s Hospital and associate professor of medicine, Harvard Medical School, Boston, told GI & Hepatology News.
The study was presented at Digestive Disease Week® (DDW) 2025.
Real-World Insights
EGD is the gold standard for diagnosing suspected upper GI bleeding, but limited access to timely EGD complicates diagnosis and resource allocation.
Approved by the US Food and Drug Administration, PillSense (EnteraSense) is an ingestible capsule with a reusable receiver that provides a rapid, noninvasive method for detecting upper GI bleeding. The capsule analyzes light absorption to identify blood and transmits the result within 10 minutes.
Lee and colleagues evaluated the real-world impact of this point-of-care device on clinical triage and resource allocation, while assessing its safety profile.
They analyzed data on 43 patients (mean age 60 years; 72% men) with clinical suspicion of upper GI bleeding in whom the device was used. The most common symptoms were symptomatic anemia (70%), melena (67%), and hematemesis (33%).
Sixteen PillSense studies (37%) were positive for blood detection, and 27 (63%) were negative.
Compared to patients with a positive capsule results, those without blood detected by the capsule had shorter hospital stays (mean, 3.8 vs 13.4 days, P = .02), lower GBS scores (mean, 7.93 vs 12.81; P = .005), and fewer units of blood transfused (mean, 1.19 vs 10.94; P = .01) and were less apt to be hemodynamically unstable (5 vs 8 patients; P = .03).
Capsule results influenced clinical management in 80% of cases, leading to avoidance of EGD in 37% and prioritization of urgent EGD in 18% (all had active bleeding on EGD).
Capsule use improved resource allocation in 51% of cases. This included 12 patients who were discharged from the ED, six who were assigned an inpatient bed early, and four who underwent expedited colonoscopy as upper GI bleeding was ruled out, they noted.
Among the eight patients who did not undergo EGD, there were no readmissions within 30 days and no adverse events. There were no capsule-related adverse events.
“Clinicians should consider using this novel capsule PillSense as another data point in the management of suspected upper GI bleed,” Lee told GI & Hepatology News.
“This could include in helping to triage patients for safe discharge from the ED or to more urgent endoscopy, to differentiate between upper vs lower GI bleed and to manage ICU patients with possible rebleeding,” Lee said.
Important Real-World Evidence
Reached for comment, Shahin Ayazi, MD, esophageal surgeon, Director, Allegheny Health Network Chevalier Jackson Esophageal Research Center, Pittsburgh, Pennsylvania, said this study is important for several reasons.
“Prior investigations have established that PillSense possesses a high negative predictive value for detecting upper GI bleeding and have speculated on its utility in triage, decision-making, and potentially avoiding unnecessary endoscopy. This study is important because it substantiates that speculation with clinical data,” Ayazi, who wasn’t involved in the study, told GI & Hepatology News.
“These findings support the capsule’s practical application in patient stratification and clinical workflow, particularly when diagnostic uncertainty is high and endoscopic resources are limited,” Ayazi noted.
In his experience, PillSense is “highly useful as a triage adjunct in the evaluation of suspected upper GI bleeding. It provides direct and objective evidence as to whether blood is currently present in the stomach,” he said.
“In patients whose presentation is ambiguous or whose clinical scores fall into an intermediate risk zone, this binary result can provide clarity that subjective assessment alone may not achieve. This is particularly relevant in settings where the goal is to perform endoscopy within 24 hours, but the volume of consults exceeds procedural capacity,” Ayazi explained.
“In such scenarios, PillSense enables physicians to stratify patients based on objective evidence of active bleeding, helping to prioritize those who require urgent endoscopy and defer or even avoid endoscopic evaluation in those who do not. The result is a more efficient allocation of endoscopic resources without compromising patient safety,” he added.
Ayazi cautioned that the PillSense capsule should not be used as a replacement for clinical evaluation or established risk stratification protocols.
“It is intended for hemodynamically stable patients and has not been validated in cases of active or massive bleeding. Its diagnostic yield depends on the presence of blood in the stomach at the time of capsule transit; intermittent or proximal bleeding that has ceased may not be detected, introducing the potential for false-negative results,” Ayazi told GI & Hepatology News.
“However, in prior studies, the negative predictive value was high, and in the present study, no adverse outcomes were observed in patients who did not undergo endoscopy following a negative PillSense result,” Ayazi noted.
“It must also be understood that PillSense does not localize the source of bleeding or replace endoscopy in patients with a high likelihood of active hemorrhage. It is not designed to detect bleeding from the lower GI tract or distal small bowel. Rather, it serves as an adjunct that can provide immediate clarity when the need for endoscopy is uncertain, and should be interpreted within the broader context of clinical findings, laboratory data, and established risk stratification tools,” he added.
The study had no specific funding. Lee and Ayazi had no relevant disclosures.
A version of this article appeared on Medscape.com.
SAN DIEGO — , a study found.
Notably, patients with negative capsule results had shorter hospital stays and lower acuity markers, and in more than one third of cases, an esophagogastroduodenoscopy (EGD) was avoided altogether without any observed adverse events or readmissions, the study team found.
“Our study shows that this novel capsule that detects blood in the upper GI tract (PillSense) was highly sensitive and specific (> 90%) for detecting recent or active upper GI blood, influenced clinical management in 80% of cases and allowed about one third of patients to be safely discharged from the emergency department, with close outpatient follow-up,” Linda Lee, MD, AGAF, medical director of endoscopy, Brigham and Women’s Hospital and associate professor of medicine, Harvard Medical School, Boston, told GI & Hepatology News.
The study was presented at Digestive Disease Week® (DDW) 2025.
Real-World Insights
EGD is the gold standard for diagnosing suspected upper GI bleeding, but limited access to timely EGD complicates diagnosis and resource allocation.
Approved by the US Food and Drug Administration, PillSense (EnteraSense) is an ingestible capsule with a reusable receiver that provides a rapid, noninvasive method for detecting upper GI bleeding. The capsule analyzes light absorption to identify blood and transmits the result within 10 minutes.
Lee and colleagues evaluated the real-world impact of this point-of-care device on clinical triage and resource allocation, while assessing its safety profile.
They analyzed data on 43 patients (mean age 60 years; 72% men) with clinical suspicion of upper GI bleeding in whom the device was used. The most common symptoms were symptomatic anemia (70%), melena (67%), and hematemesis (33%).
Sixteen PillSense studies (37%) were positive for blood detection, and 27 (63%) were negative.
Compared to patients with a positive capsule results, those without blood detected by the capsule had shorter hospital stays (mean, 3.8 vs 13.4 days, P = .02), lower GBS scores (mean, 7.93 vs 12.81; P = .005), and fewer units of blood transfused (mean, 1.19 vs 10.94; P = .01) and were less apt to be hemodynamically unstable (5 vs 8 patients; P = .03).
Capsule results influenced clinical management in 80% of cases, leading to avoidance of EGD in 37% and prioritization of urgent EGD in 18% (all had active bleeding on EGD).
Capsule use improved resource allocation in 51% of cases. This included 12 patients who were discharged from the ED, six who were assigned an inpatient bed early, and four who underwent expedited colonoscopy as upper GI bleeding was ruled out, they noted.
Among the eight patients who did not undergo EGD, there were no readmissions within 30 days and no adverse events. There were no capsule-related adverse events.
“Clinicians should consider using this novel capsule PillSense as another data point in the management of suspected upper GI bleed,” Lee told GI & Hepatology News.
“This could include in helping to triage patients for safe discharge from the ED or to more urgent endoscopy, to differentiate between upper vs lower GI bleed and to manage ICU patients with possible rebleeding,” Lee said.
Important Real-World Evidence
Reached for comment, Shahin Ayazi, MD, esophageal surgeon, Director, Allegheny Health Network Chevalier Jackson Esophageal Research Center, Pittsburgh, Pennsylvania, said this study is important for several reasons.
“Prior investigations have established that PillSense possesses a high negative predictive value for detecting upper GI bleeding and have speculated on its utility in triage, decision-making, and potentially avoiding unnecessary endoscopy. This study is important because it substantiates that speculation with clinical data,” Ayazi, who wasn’t involved in the study, told GI & Hepatology News.
“These findings support the capsule’s practical application in patient stratification and clinical workflow, particularly when diagnostic uncertainty is high and endoscopic resources are limited,” Ayazi noted.
In his experience, PillSense is “highly useful as a triage adjunct in the evaluation of suspected upper GI bleeding. It provides direct and objective evidence as to whether blood is currently present in the stomach,” he said.
“In patients whose presentation is ambiguous or whose clinical scores fall into an intermediate risk zone, this binary result can provide clarity that subjective assessment alone may not achieve. This is particularly relevant in settings where the goal is to perform endoscopy within 24 hours, but the volume of consults exceeds procedural capacity,” Ayazi explained.
“In such scenarios, PillSense enables physicians to stratify patients based on objective evidence of active bleeding, helping to prioritize those who require urgent endoscopy and defer or even avoid endoscopic evaluation in those who do not. The result is a more efficient allocation of endoscopic resources without compromising patient safety,” he added.
Ayazi cautioned that the PillSense capsule should not be used as a replacement for clinical evaluation or established risk stratification protocols.
“It is intended for hemodynamically stable patients and has not been validated in cases of active or massive bleeding. Its diagnostic yield depends on the presence of blood in the stomach at the time of capsule transit; intermittent or proximal bleeding that has ceased may not be detected, introducing the potential for false-negative results,” Ayazi told GI & Hepatology News.
“However, in prior studies, the negative predictive value was high, and in the present study, no adverse outcomes were observed in patients who did not undergo endoscopy following a negative PillSense result,” Ayazi noted.
“It must also be understood that PillSense does not localize the source of bleeding or replace endoscopy in patients with a high likelihood of active hemorrhage. It is not designed to detect bleeding from the lower GI tract or distal small bowel. Rather, it serves as an adjunct that can provide immediate clarity when the need for endoscopy is uncertain, and should be interpreted within the broader context of clinical findings, laboratory data, and established risk stratification tools,” he added.
The study had no specific funding. Lee and Ayazi had no relevant disclosures.
A version of this article appeared on Medscape.com.
SAN DIEGO — , a study found.
Notably, patients with negative capsule results had shorter hospital stays and lower acuity markers, and in more than one third of cases, an esophagogastroduodenoscopy (EGD) was avoided altogether without any observed adverse events or readmissions, the study team found.
“Our study shows that this novel capsule that detects blood in the upper GI tract (PillSense) was highly sensitive and specific (> 90%) for detecting recent or active upper GI blood, influenced clinical management in 80% of cases and allowed about one third of patients to be safely discharged from the emergency department, with close outpatient follow-up,” Linda Lee, MD, AGAF, medical director of endoscopy, Brigham and Women’s Hospital and associate professor of medicine, Harvard Medical School, Boston, told GI & Hepatology News.
The study was presented at Digestive Disease Week® (DDW) 2025.
Real-World Insights
EGD is the gold standard for diagnosing suspected upper GI bleeding, but limited access to timely EGD complicates diagnosis and resource allocation.
Approved by the US Food and Drug Administration, PillSense (EnteraSense) is an ingestible capsule with a reusable receiver that provides a rapid, noninvasive method for detecting upper GI bleeding. The capsule analyzes light absorption to identify blood and transmits the result within 10 minutes.
Lee and colleagues evaluated the real-world impact of this point-of-care device on clinical triage and resource allocation, while assessing its safety profile.
They analyzed data on 43 patients (mean age 60 years; 72% men) with clinical suspicion of upper GI bleeding in whom the device was used. The most common symptoms were symptomatic anemia (70%), melena (67%), and hematemesis (33%).
Sixteen PillSense studies (37%) were positive for blood detection, and 27 (63%) were negative.
Compared to patients with a positive capsule results, those without blood detected by the capsule had shorter hospital stays (mean, 3.8 vs 13.4 days, P = .02), lower GBS scores (mean, 7.93 vs 12.81; P = .005), and fewer units of blood transfused (mean, 1.19 vs 10.94; P = .01) and were less apt to be hemodynamically unstable (5 vs 8 patients; P = .03).
Capsule results influenced clinical management in 80% of cases, leading to avoidance of EGD in 37% and prioritization of urgent EGD in 18% (all had active bleeding on EGD).
Capsule use improved resource allocation in 51% of cases. This included 12 patients who were discharged from the ED, six who were assigned an inpatient bed early, and four who underwent expedited colonoscopy as upper GI bleeding was ruled out, they noted.
Among the eight patients who did not undergo EGD, there were no readmissions within 30 days and no adverse events. There were no capsule-related adverse events.
“Clinicians should consider using this novel capsule PillSense as another data point in the management of suspected upper GI bleed,” Lee told GI & Hepatology News.
“This could include in helping to triage patients for safe discharge from the ED or to more urgent endoscopy, to differentiate between upper vs lower GI bleed and to manage ICU patients with possible rebleeding,” Lee said.
Important Real-World Evidence
Reached for comment, Shahin Ayazi, MD, esophageal surgeon, Director, Allegheny Health Network Chevalier Jackson Esophageal Research Center, Pittsburgh, Pennsylvania, said this study is important for several reasons.
“Prior investigations have established that PillSense possesses a high negative predictive value for detecting upper GI bleeding and have speculated on its utility in triage, decision-making, and potentially avoiding unnecessary endoscopy. This study is important because it substantiates that speculation with clinical data,” Ayazi, who wasn’t involved in the study, told GI & Hepatology News.
“These findings support the capsule’s practical application in patient stratification and clinical workflow, particularly when diagnostic uncertainty is high and endoscopic resources are limited,” Ayazi noted.
In his experience, PillSense is “highly useful as a triage adjunct in the evaluation of suspected upper GI bleeding. It provides direct and objective evidence as to whether blood is currently present in the stomach,” he said.
“In patients whose presentation is ambiguous or whose clinical scores fall into an intermediate risk zone, this binary result can provide clarity that subjective assessment alone may not achieve. This is particularly relevant in settings where the goal is to perform endoscopy within 24 hours, but the volume of consults exceeds procedural capacity,” Ayazi explained.
“In such scenarios, PillSense enables physicians to stratify patients based on objective evidence of active bleeding, helping to prioritize those who require urgent endoscopy and defer or even avoid endoscopic evaluation in those who do not. The result is a more efficient allocation of endoscopic resources without compromising patient safety,” he added.
Ayazi cautioned that the PillSense capsule should not be used as a replacement for clinical evaluation or established risk stratification protocols.
“It is intended for hemodynamically stable patients and has not been validated in cases of active or massive bleeding. Its diagnostic yield depends on the presence of blood in the stomach at the time of capsule transit; intermittent or proximal bleeding that has ceased may not be detected, introducing the potential for false-negative results,” Ayazi told GI & Hepatology News.
“However, in prior studies, the negative predictive value was high, and in the present study, no adverse outcomes were observed in patients who did not undergo endoscopy following a negative PillSense result,” Ayazi noted.
“It must also be understood that PillSense does not localize the source of bleeding or replace endoscopy in patients with a high likelihood of active hemorrhage. It is not designed to detect bleeding from the lower GI tract or distal small bowel. Rather, it serves as an adjunct that can provide immediate clarity when the need for endoscopy is uncertain, and should be interpreted within the broader context of clinical findings, laboratory data, and established risk stratification tools,” he added.
The study had no specific funding. Lee and Ayazi had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Are Your Patients With COPD Inhaling Eucalyptus Oil? Know the Risks
There’s been renewed interest in recent years for concentrated essential oils to replace or complement pharmaceutical treatments. This is especially concerning among patients with chronic obstructive pulmonary disease (COPD), who might be eager to turn to alternatives but are unaware that COPD increases sensitivity to lung irritants like essential oils.
Eucalyptus oil might be at or near the top of the essential oils list for these patients, given its storied history in both ancient and modern medicine for treating colds and respiratory illnesses. Its inclusion in the United States and European pharmacopoeias has also reinforced its legitimacy. And, today, patients are at risk of confusing the primary active ingredient in eucalyptus — the monoterpene 1,8-cineole (eucalyptol, which has been shown to reduce COPD exacerbations when used adjunctively) — with concentrated essential oils that can be purchased online and in stores here in the United States.
“The more potent active ingredient, eucalyptol (in capsule form), is approved in Germany — not the essential oil of eucalyptus, which contains other compounds. I recommend against using any sort of inhaled essential oils for patients with chronic respiratory illnesses, mainly because they are unregulated and unstandardized,” explained Ni-Chen Liang, MD, an integrative pulmonologist affiliated with Scripps Memorial Hospital Encinitas in Encinitas, California.
“The substances that come out when you create eucalyptus oil are a ‘gamash’ of all sorts of chemicals — some benign, some which taste good, and some that may be irritating or even dangerous,” said Neil Schachter, MD, pulmonologist and professor of medicine (pulmonary, critical care, and sleep medicine) at the Icahn School of Medicine at Mount Sinai, New York City.
“They can also produce volatile organic compounds (VOCs) related to their formulas, which contain fillers and other constituents,” Liang said.
Hidden Dangers
Eucalyptus oil was first used by Aboriginal Australians, who crushed the leaves for their antiseptic properties or steamed them for their expectorant activity. Today, eucalyptus oil can be found in mouthwash and soap, used topically to relieve pain or repel insects, or added to cleaning products due to its disinfectant properties.
However, inhalation via diffusers or directly from the bottle can trigger different respiratory reactions, including cough, wheezing, shortness of breath, as well as respiratory distress.
“The vapors contain oil, ie, fatty products that can be irritating in and of themselves,” said Schachter. “There are cases where people have inhaled these oils and developed lipid pneumonia, which is very hard to treat,” he said.
Anything inhaled into the lungs is a risk, said Juan Rojas, MD, assistant professor, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine at Rush University Medical Center in Chicago. Rojas compared inhaling essential oils to e-cigarettes, which, in addition to tobacco, contain a variety of chemicals and additives that cause a lung reaction in the short term and create inflammatory patterns in the medium and long term.
“Another problem is that when ingested, eucalyptus oil can be distressing to the gastrointestinal tract. In larger doses, it can actually have some neurological impact as well, including seizures,” said Kalilah L. Gates, MD, associate professor of medicine (pulmonary and critical care) and assistant dean of medical education at Northwestern Feinberg School of Medicine in Chicago.
Clinical trial data have also shown a significant association between long-term exposure to essential oils and cardiopulmonary effects such as increased heart rate and blood pressure and a decline in percentage predicted peak expiratory flow rate in healthy volunteers. In the study of 200 participants (who were homemakers), long-term exposure referred to daily hours (> 4/d) and the study period, which was 10 years.
About Eucalyptol
Eucalyptol is rapidly absorbed and quickly distributed throughout the bloodstream, which allows it to reach the bronchial system, where it is expelled by the lungs. It’s been shown in various preclinical studies to have anti-inflammatory, antioxidant, mucolytic, and bronchodilatory activity, as well as antimicrobial effects.
For the past decade, enteric-coated eucalyptol capsules containing 100 mg or 200 mg of 1,8-cineole have been available in Germany for adjunctive treatment of inflammatory respiratory disorders, including asthma and COPD. Due to its limited bioactivity, frequent administration is required.
Clinical evidence of eucalyptol’s effectiveness is somewhat limited. Findings from a 2009 double-blind, placebo-controlled, multicenter study also demonstrated that when used along with beta-agonists, anticholinergics, corticosteroids, or combinations in patients with stable COPD, severity and duration of exacerbations over 6 months were significantly decreased compared with placebo.
However, Liang was quick to point out that studies of oral eucalyptol preparations in pulmonary patients have not been robust enough.
“I haven’t been able to find anything written by a multitude of different authors, which, to me, is a red flag. We want naturally occurring substances to be well tested in multicenter studies across a variety of different patient populations outside of Germany to ensure that results are reproducible,” she said.
Rojas concurred. “Even with the data in Europe, I would say that the studies have been underpowered to support large-scale adoption or suggest that the active ingredient for patients with moderate or severe COPD could be considered an adjunctive therapy with traditional medications,” he said.
“It would be difficult for me to make a recommendation without knowing the full impact,” said Rojas.
Open Dialogue
Like many chronic diseases, it’s important to meet patients where they are, including their use of unapproved or unwise treatment strategies.
“More times than not, they’ve already figured out their triggers for worsening respiratory symptoms, what does and doesn’t work for them, and what predicts a good vs a bad day from a respiratory standpoint,” said Liang.
“There’s a lot of popularity and claims related to essential oil use, and ultimately, we need to partner to find healing modalities (which may or may not include essential oils) that are ultimately helpful and minimize harm,” she said.
Gates suggested that when it comes to eucalyptus essential oil vs eucalyptol, education of both patients and doctors is key.
“The issue is that we had a study showing that a particular component — the active ingredient of eucalyptus oil was isolated and put into the capsule form and showed benefit. And then we extrapolated and said, ‘well, let’s just take (or inhale) eucalyptus oil. It’s not the same thing,” she said.
“I feel that it’s my responsibility to make sure that patients have the information they need to make informed decisions. It’s about being willing to communicate and have open conversations about what they may be taking in addition to medications that I prescribe,” said Gates.
Liang, Schachter, Rojas, and Gates reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There’s been renewed interest in recent years for concentrated essential oils to replace or complement pharmaceutical treatments. This is especially concerning among patients with chronic obstructive pulmonary disease (COPD), who might be eager to turn to alternatives but are unaware that COPD increases sensitivity to lung irritants like essential oils.
Eucalyptus oil might be at or near the top of the essential oils list for these patients, given its storied history in both ancient and modern medicine for treating colds and respiratory illnesses. Its inclusion in the United States and European pharmacopoeias has also reinforced its legitimacy. And, today, patients are at risk of confusing the primary active ingredient in eucalyptus — the monoterpene 1,8-cineole (eucalyptol, which has been shown to reduce COPD exacerbations when used adjunctively) — with concentrated essential oils that can be purchased online and in stores here in the United States.
“The more potent active ingredient, eucalyptol (in capsule form), is approved in Germany — not the essential oil of eucalyptus, which contains other compounds. I recommend against using any sort of inhaled essential oils for patients with chronic respiratory illnesses, mainly because they are unregulated and unstandardized,” explained Ni-Chen Liang, MD, an integrative pulmonologist affiliated with Scripps Memorial Hospital Encinitas in Encinitas, California.
“The substances that come out when you create eucalyptus oil are a ‘gamash’ of all sorts of chemicals — some benign, some which taste good, and some that may be irritating or even dangerous,” said Neil Schachter, MD, pulmonologist and professor of medicine (pulmonary, critical care, and sleep medicine) at the Icahn School of Medicine at Mount Sinai, New York City.
“They can also produce volatile organic compounds (VOCs) related to their formulas, which contain fillers and other constituents,” Liang said.
Hidden Dangers
Eucalyptus oil was first used by Aboriginal Australians, who crushed the leaves for their antiseptic properties or steamed them for their expectorant activity. Today, eucalyptus oil can be found in mouthwash and soap, used topically to relieve pain or repel insects, or added to cleaning products due to its disinfectant properties.
However, inhalation via diffusers or directly from the bottle can trigger different respiratory reactions, including cough, wheezing, shortness of breath, as well as respiratory distress.
“The vapors contain oil, ie, fatty products that can be irritating in and of themselves,” said Schachter. “There are cases where people have inhaled these oils and developed lipid pneumonia, which is very hard to treat,” he said.
Anything inhaled into the lungs is a risk, said Juan Rojas, MD, assistant professor, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine at Rush University Medical Center in Chicago. Rojas compared inhaling essential oils to e-cigarettes, which, in addition to tobacco, contain a variety of chemicals and additives that cause a lung reaction in the short term and create inflammatory patterns in the medium and long term.
“Another problem is that when ingested, eucalyptus oil can be distressing to the gastrointestinal tract. In larger doses, it can actually have some neurological impact as well, including seizures,” said Kalilah L. Gates, MD, associate professor of medicine (pulmonary and critical care) and assistant dean of medical education at Northwestern Feinberg School of Medicine in Chicago.
Clinical trial data have also shown a significant association between long-term exposure to essential oils and cardiopulmonary effects such as increased heart rate and blood pressure and a decline in percentage predicted peak expiratory flow rate in healthy volunteers. In the study of 200 participants (who were homemakers), long-term exposure referred to daily hours (> 4/d) and the study period, which was 10 years.
About Eucalyptol
Eucalyptol is rapidly absorbed and quickly distributed throughout the bloodstream, which allows it to reach the bronchial system, where it is expelled by the lungs. It’s been shown in various preclinical studies to have anti-inflammatory, antioxidant, mucolytic, and bronchodilatory activity, as well as antimicrobial effects.
For the past decade, enteric-coated eucalyptol capsules containing 100 mg or 200 mg of 1,8-cineole have been available in Germany for adjunctive treatment of inflammatory respiratory disorders, including asthma and COPD. Due to its limited bioactivity, frequent administration is required.
Clinical evidence of eucalyptol’s effectiveness is somewhat limited. Findings from a 2009 double-blind, placebo-controlled, multicenter study also demonstrated that when used along with beta-agonists, anticholinergics, corticosteroids, or combinations in patients with stable COPD, severity and duration of exacerbations over 6 months were significantly decreased compared with placebo.
However, Liang was quick to point out that studies of oral eucalyptol preparations in pulmonary patients have not been robust enough.
“I haven’t been able to find anything written by a multitude of different authors, which, to me, is a red flag. We want naturally occurring substances to be well tested in multicenter studies across a variety of different patient populations outside of Germany to ensure that results are reproducible,” she said.
Rojas concurred. “Even with the data in Europe, I would say that the studies have been underpowered to support large-scale adoption or suggest that the active ingredient for patients with moderate or severe COPD could be considered an adjunctive therapy with traditional medications,” he said.
“It would be difficult for me to make a recommendation without knowing the full impact,” said Rojas.
Open Dialogue
Like many chronic diseases, it’s important to meet patients where they are, including their use of unapproved or unwise treatment strategies.
“More times than not, they’ve already figured out their triggers for worsening respiratory symptoms, what does and doesn’t work for them, and what predicts a good vs a bad day from a respiratory standpoint,” said Liang.
“There’s a lot of popularity and claims related to essential oil use, and ultimately, we need to partner to find healing modalities (which may or may not include essential oils) that are ultimately helpful and minimize harm,” she said.
Gates suggested that when it comes to eucalyptus essential oil vs eucalyptol, education of both patients and doctors is key.
“The issue is that we had a study showing that a particular component — the active ingredient of eucalyptus oil was isolated and put into the capsule form and showed benefit. And then we extrapolated and said, ‘well, let’s just take (or inhale) eucalyptus oil. It’s not the same thing,” she said.
“I feel that it’s my responsibility to make sure that patients have the information they need to make informed decisions. It’s about being willing to communicate and have open conversations about what they may be taking in addition to medications that I prescribe,” said Gates.
Liang, Schachter, Rojas, and Gates reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There’s been renewed interest in recent years for concentrated essential oils to replace or complement pharmaceutical treatments. This is especially concerning among patients with chronic obstructive pulmonary disease (COPD), who might be eager to turn to alternatives but are unaware that COPD increases sensitivity to lung irritants like essential oils.
Eucalyptus oil might be at or near the top of the essential oils list for these patients, given its storied history in both ancient and modern medicine for treating colds and respiratory illnesses. Its inclusion in the United States and European pharmacopoeias has also reinforced its legitimacy. And, today, patients are at risk of confusing the primary active ingredient in eucalyptus — the monoterpene 1,8-cineole (eucalyptol, which has been shown to reduce COPD exacerbations when used adjunctively) — with concentrated essential oils that can be purchased online and in stores here in the United States.
“The more potent active ingredient, eucalyptol (in capsule form), is approved in Germany — not the essential oil of eucalyptus, which contains other compounds. I recommend against using any sort of inhaled essential oils for patients with chronic respiratory illnesses, mainly because they are unregulated and unstandardized,” explained Ni-Chen Liang, MD, an integrative pulmonologist affiliated with Scripps Memorial Hospital Encinitas in Encinitas, California.
“The substances that come out when you create eucalyptus oil are a ‘gamash’ of all sorts of chemicals — some benign, some which taste good, and some that may be irritating or even dangerous,” said Neil Schachter, MD, pulmonologist and professor of medicine (pulmonary, critical care, and sleep medicine) at the Icahn School of Medicine at Mount Sinai, New York City.
“They can also produce volatile organic compounds (VOCs) related to their formulas, which contain fillers and other constituents,” Liang said.
Hidden Dangers
Eucalyptus oil was first used by Aboriginal Australians, who crushed the leaves for their antiseptic properties or steamed them for their expectorant activity. Today, eucalyptus oil can be found in mouthwash and soap, used topically to relieve pain or repel insects, or added to cleaning products due to its disinfectant properties.
However, inhalation via diffusers or directly from the bottle can trigger different respiratory reactions, including cough, wheezing, shortness of breath, as well as respiratory distress.
“The vapors contain oil, ie, fatty products that can be irritating in and of themselves,” said Schachter. “There are cases where people have inhaled these oils and developed lipid pneumonia, which is very hard to treat,” he said.
Anything inhaled into the lungs is a risk, said Juan Rojas, MD, assistant professor, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine at Rush University Medical Center in Chicago. Rojas compared inhaling essential oils to e-cigarettes, which, in addition to tobacco, contain a variety of chemicals and additives that cause a lung reaction in the short term and create inflammatory patterns in the medium and long term.
“Another problem is that when ingested, eucalyptus oil can be distressing to the gastrointestinal tract. In larger doses, it can actually have some neurological impact as well, including seizures,” said Kalilah L. Gates, MD, associate professor of medicine (pulmonary and critical care) and assistant dean of medical education at Northwestern Feinberg School of Medicine in Chicago.
Clinical trial data have also shown a significant association between long-term exposure to essential oils and cardiopulmonary effects such as increased heart rate and blood pressure and a decline in percentage predicted peak expiratory flow rate in healthy volunteers. In the study of 200 participants (who were homemakers), long-term exposure referred to daily hours (> 4/d) and the study period, which was 10 years.
About Eucalyptol
Eucalyptol is rapidly absorbed and quickly distributed throughout the bloodstream, which allows it to reach the bronchial system, where it is expelled by the lungs. It’s been shown in various preclinical studies to have anti-inflammatory, antioxidant, mucolytic, and bronchodilatory activity, as well as antimicrobial effects.
For the past decade, enteric-coated eucalyptol capsules containing 100 mg or 200 mg of 1,8-cineole have been available in Germany for adjunctive treatment of inflammatory respiratory disorders, including asthma and COPD. Due to its limited bioactivity, frequent administration is required.
Clinical evidence of eucalyptol’s effectiveness is somewhat limited. Findings from a 2009 double-blind, placebo-controlled, multicenter study also demonstrated that when used along with beta-agonists, anticholinergics, corticosteroids, or combinations in patients with stable COPD, severity and duration of exacerbations over 6 months were significantly decreased compared with placebo.
However, Liang was quick to point out that studies of oral eucalyptol preparations in pulmonary patients have not been robust enough.
“I haven’t been able to find anything written by a multitude of different authors, which, to me, is a red flag. We want naturally occurring substances to be well tested in multicenter studies across a variety of different patient populations outside of Germany to ensure that results are reproducible,” she said.
Rojas concurred. “Even with the data in Europe, I would say that the studies have been underpowered to support large-scale adoption or suggest that the active ingredient for patients with moderate or severe COPD could be considered an adjunctive therapy with traditional medications,” he said.
“It would be difficult for me to make a recommendation without knowing the full impact,” said Rojas.
Open Dialogue
Like many chronic diseases, it’s important to meet patients where they are, including their use of unapproved or unwise treatment strategies.
“More times than not, they’ve already figured out their triggers for worsening respiratory symptoms, what does and doesn’t work for them, and what predicts a good vs a bad day from a respiratory standpoint,” said Liang.
“There’s a lot of popularity and claims related to essential oil use, and ultimately, we need to partner to find healing modalities (which may or may not include essential oils) that are ultimately helpful and minimize harm,” she said.
Gates suggested that when it comes to eucalyptus essential oil vs eucalyptol, education of both patients and doctors is key.
“The issue is that we had a study showing that a particular component — the active ingredient of eucalyptus oil was isolated and put into the capsule form and showed benefit. And then we extrapolated and said, ‘well, let’s just take (or inhale) eucalyptus oil. It’s not the same thing,” she said.
“I feel that it’s my responsibility to make sure that patients have the information they need to make informed decisions. It’s about being willing to communicate and have open conversations about what they may be taking in addition to medications that I prescribe,” said Gates.
Liang, Schachter, Rojas, and Gates reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hurricanes, Fires, Floods: A Rising Threat to Cancer Care
As Hurricane Helene approached western North Carolina, Martin Palmeri, MD, MBA, didn’t anticipate the storm would disrupt practice operations for more than a day or so.
But the massive rainfall and flooding damage last September proved to be far more challenging. Despite best efforts by the 13-physician practice, basic treatments for most patients were interrupted for about a week.
Flooding washed out some of the major roads leading to the main Asheville clinic and affiliated rural sites, limiting travel and slowing delivery of medications, intravenous (IV) fluids, and other supplies, Palmeri said. Some patients and employees weren’t initially reachable due to the loss of the internet and cell phone service. The storm-related fallout even forced patients to relocate elsewhere for weeks or longer.
During the storm, backup generators kept power on at the Asheville clinic, protecting chemotherapy and other refrigerated drugs, but the storm damaged the municipal water supply.
“Water was the number one thing — how do you get water to the office?” Palmeri said. “You can’t give someone an 8-hour infusion if they don’t have means of going to the toilet or having something to drink.”
Hurricanes. Wildfires. Heat waves. As climate-driven extreme weather has become more common, researchers, oncologists, and patients are increasingly being forced to consider the consequences of these disruptions.
Along with preventing patients and providers from reaching treatment sites, experts said, extreme weather can undercut patients’ health and care in other ways. Patients with more limited lung capacity following lung cancer surgery, for instance, may struggle with breathing during wildfires. Extreme heat can prove risky for patients already dehydrated or weakened by treatment-related side effects. Power outages and severe flooding can affect vital infrastructure, disrupting operations at facilities that manufacture essential drugs. Power outages can also impede radiotherapy, which requires machines powered by electricity.
“Any of these [weather] events can disrupt this critical cancer care continuum among a population of people that already are very vulnerable,” said Joan Casey, PhD, an environmental epidemiologist and associate professor at the University of Washington in Seattle.
Extreme Weather and Cancer Survival
For patients with cancer, survival often relies on highly regimented protocols, which may require surgery plus frequent visits for radiation, chemotherapy, or immunotherapy that can last months, said Eric Bernicker, MD, a Colorado oncologist and lead author of a 2023 American Society of Clinical Oncology position statement about the impact of climate change on cancer care.
Interruptions to care, regardless of the cause, can lead to worse outcomes for patients, Bernicker said. “If you’re in the middle of your post-lumpectomy radiation and your radiation center shuts for 2 weeks,” he said, “that is not good.”
Research indicated that even short treatment disruptions can affect outcomes for patients with cancer and that delays caused by extreme weather — which may last for weeks — can affect survival for these patients.
One analysis, published in JAMA Oncology in 2023, found that patients exposed to wildfire within the first year after potentially curative lung cancer surgery had worse survival outcomes than those who weren’t exposed during their recovery.
In another study, patients with lung cancer who had their radiation interrupted when a hurricane struck had a 19% greater risk of dying overall compared with similar patients who were not affected. Another analysis found that patients with breast cancer who were partway through treatment when Hurricane Katrina hit the Louisiana coastline had a significantly greater risk of dying over a 10-year period compared with patients who lived elsewhere.
The potential threats to survival highlighted the impacts of extreme weather on carefully orchestrated systems of care that place patients facing already fragile situations in impossible binds, Casey said.
Douglas Flora, MD, a Kentucky oncologist and president-elect of the Association of Cancer Care Centers, Rockville, Maryland, agreed.
“We’ve seen this with an increasing frequency over the last several years,” Flora said. “It’s one thing if it’s routine follow-up or surveillance care, but many cancer patients’ survivals are directly related to not having interruptions in their care.”
Challenging Realities
Following Helene, the most pressing issue was the lack of water, Palmeri said.
The lack of reliable clean water created challenges for patients receiving radiation or chemotherapy infusions, which can cause vomiting and diarrhea that leave patients dehydrated. Toilets were also unusable.
Even when the city of Asheville said the water was likely safe enough to bathe in, local leaders still reported potential risks from bacteria and other contaminants in the water, Palmeri said. Those with a fragile immune system or breaks in the skin “could get serious and life-threatening infections,” he explained.
To make matters worse, damage to a North Carolina facility manufacturing IV fluids left the United States in shortage for months. IV fluids are key not only for providing hydration but also for easing nausea, fatigue, and other issues caused by cancer therapies.
With wildfires, as occurred in southern California early this year, patients undergoing cancer treatment might feel they have no option but to remain near home to continue getting care, Casey said. “It’s restricting their agency in the kinds of choices that they have to make during these severe weather events.”
Meanwhile, thick wildfire smoke can confine patients to their homes, said Lawrence Wagman, MD, a surgical oncologist and a regional medical director at the City of Hope network, who described its main facility in Duarte, California, coming within a dozen miles of the Eaton fire. “One of the biggest problems was so much smoke in the air,” he said. “And the air quality was so low that it was, in many ways, dangerous for patients to travel.”
“These fires were so aggressive, and they kept popping up,” Wagman said. Plus, the emotional strain of looming wildfires persisted for both patients and cancer clinicians for weeks on end, he added.
For those who evacuate, the logistics can be complex.
Not only are cancer treatment plans highly structured, but switching care to another facility is far from easy, Bernicker said. The new facility will likely need to submit a treatment plan and get insurance coverage before moving forward.
“I’m not saying that takes forever,” he said. “But what I’m saying is that it’s not like you just roll in and they hang the [infusion] bag.”
Neither is a shelter typically an option for patients during treatment, said Seth Berkowitz, a licensed clinical social worker and director of Strategic Healthcare Partnerships at The Leukemia & Lymphoma Society. “They have to have a place to go that’s safe and germ-free.”
In western North Carolina, the strain on already ill patients and their caregivers could be overwhelming, Palmeri said. He recounted how the husband of one patient with advanced cancer died after the storm came through.
“He tried to go out there with a chainsaw to clear a way out so that they could get out of their house in case he needed to take her to the hospital,” Palmeri said. “And he had a heart attack there in the driveway.”
Rebuilding and Planning Ahead
Experts are only at the early stages of grasping the magnitude of extreme weather on cancer care and developing strategies to curtail care gaps and potential harm to patients, said Katie Lichter, MD, a radiation oncologist at the University of California San Francisco, who studies extreme weather and cancer treatment.
“How does it impact health care delivery services at every step, from prevention to screening to treatment and survivorship?” Lichter asked. “We’re just starting to understand and to even quantify that,” she said, which included identifying patients who are most vulnerable. She worries, in particular, about patients living in rural areas who already travel longer distances and often face more difficulties accessing care.
The gap between research and reality still looms large. A recent analysis, led by Lichter, looked at 176 California radiation oncology clinics and found that all of them were located within 25 miles of a wildfire that had occurred within the prior 5 years. Yet among the 51 clinics that responded to a 2022 survey,just 47% reported that their clinic had a wildfire emergency preparedness plan.
The American Cancer Society does provide some guidance on how patients can prepare for a weather-related crisis, including having extra supplies of medications or special equipment on hand.
Still, providers are often in reaction mode when extreme weather strikes.
Without adequate clean water after Helene, leaders at Palmeri’s practice moved swiftly, purchasing 40,000-50,000 bottles of water and bringing in porta potties from elsewhere.
“I think we were able to get things up and going very quickly,” said Palmeri, who noted that full services resumed about 10 days after the storm. “For most patients, missing a week of treatment would not do a disservice to their well-being or outcome.”
Going forward, to provide a more comprehensive strategy, Lichter is working with colleagues to develop clinical tool kits to help oncology practices and patients prepare for severe weather events, such as outlining backup treatment contingency plans, ensuring early medication refills, and boosting communication with patient alert systems.
Clinicians are also implementing their own strategies. To limit communication gaps during power outages, Palmeri said that, since Helene, his practice has made sure that their clinic sites, physicians, and other key people now have cell phone service through satellite via Starlink.
“No one has phone books anymore,” he said, so cancer clinicians should keep crucial contact information on paper, such as details about businesses that distribute water and porta potties, given that online searches may not be feasible.
Clinicians should also advise patients to keep a hard copy of recent medical findings handy, including medications and lab results, in case they arrive at an emergency room far from home and physicians can’t access their electronic health record, Bernicker said.
When there is enough advance warning of an approaching weather event, clinicians can help patients keep at least a week’s worth of medication on hand for symptom-related issues, such as nausea or pain, as well as antibiotics so patients don’t have to seek out emergency care during the crisis, Bernicker said. However, Bernicker noted, some insurers may be reluctant to fill certain prescriptions in advance, like those for opioids.
Making headway on more robust preparedness strategies may be slowed. As of March, the National Institutes of Health will no longer fund research about the health effects of climate change.
Bernicker hoped that such cutbacks would be rolled back. What’s on the line, he stressed, is maintaining the highest quality of care for patients with cancer.
“We really are in a golden age of oncology therapeutics,” he said. “We have patients living longer than anyone would have predicted 20 or 25 years ago. But all those advances are contingent on people having access to their centers and not having that interrupted.”
A version of this article first appeared on Medscape.com.
As Hurricane Helene approached western North Carolina, Martin Palmeri, MD, MBA, didn’t anticipate the storm would disrupt practice operations for more than a day or so.
But the massive rainfall and flooding damage last September proved to be far more challenging. Despite best efforts by the 13-physician practice, basic treatments for most patients were interrupted for about a week.
Flooding washed out some of the major roads leading to the main Asheville clinic and affiliated rural sites, limiting travel and slowing delivery of medications, intravenous (IV) fluids, and other supplies, Palmeri said. Some patients and employees weren’t initially reachable due to the loss of the internet and cell phone service. The storm-related fallout even forced patients to relocate elsewhere for weeks or longer.
During the storm, backup generators kept power on at the Asheville clinic, protecting chemotherapy and other refrigerated drugs, but the storm damaged the municipal water supply.
“Water was the number one thing — how do you get water to the office?” Palmeri said. “You can’t give someone an 8-hour infusion if they don’t have means of going to the toilet or having something to drink.”
Hurricanes. Wildfires. Heat waves. As climate-driven extreme weather has become more common, researchers, oncologists, and patients are increasingly being forced to consider the consequences of these disruptions.
Along with preventing patients and providers from reaching treatment sites, experts said, extreme weather can undercut patients’ health and care in other ways. Patients with more limited lung capacity following lung cancer surgery, for instance, may struggle with breathing during wildfires. Extreme heat can prove risky for patients already dehydrated or weakened by treatment-related side effects. Power outages and severe flooding can affect vital infrastructure, disrupting operations at facilities that manufacture essential drugs. Power outages can also impede radiotherapy, which requires machines powered by electricity.
“Any of these [weather] events can disrupt this critical cancer care continuum among a population of people that already are very vulnerable,” said Joan Casey, PhD, an environmental epidemiologist and associate professor at the University of Washington in Seattle.
Extreme Weather and Cancer Survival
For patients with cancer, survival often relies on highly regimented protocols, which may require surgery plus frequent visits for radiation, chemotherapy, or immunotherapy that can last months, said Eric Bernicker, MD, a Colorado oncologist and lead author of a 2023 American Society of Clinical Oncology position statement about the impact of climate change on cancer care.
Interruptions to care, regardless of the cause, can lead to worse outcomes for patients, Bernicker said. “If you’re in the middle of your post-lumpectomy radiation and your radiation center shuts for 2 weeks,” he said, “that is not good.”
Research indicated that even short treatment disruptions can affect outcomes for patients with cancer and that delays caused by extreme weather — which may last for weeks — can affect survival for these patients.
One analysis, published in JAMA Oncology in 2023, found that patients exposed to wildfire within the first year after potentially curative lung cancer surgery had worse survival outcomes than those who weren’t exposed during their recovery.
In another study, patients with lung cancer who had their radiation interrupted when a hurricane struck had a 19% greater risk of dying overall compared with similar patients who were not affected. Another analysis found that patients with breast cancer who were partway through treatment when Hurricane Katrina hit the Louisiana coastline had a significantly greater risk of dying over a 10-year period compared with patients who lived elsewhere.
The potential threats to survival highlighted the impacts of extreme weather on carefully orchestrated systems of care that place patients facing already fragile situations in impossible binds, Casey said.
Douglas Flora, MD, a Kentucky oncologist and president-elect of the Association of Cancer Care Centers, Rockville, Maryland, agreed.
“We’ve seen this with an increasing frequency over the last several years,” Flora said. “It’s one thing if it’s routine follow-up or surveillance care, but many cancer patients’ survivals are directly related to not having interruptions in their care.”
Challenging Realities
Following Helene, the most pressing issue was the lack of water, Palmeri said.
The lack of reliable clean water created challenges for patients receiving radiation or chemotherapy infusions, which can cause vomiting and diarrhea that leave patients dehydrated. Toilets were also unusable.
Even when the city of Asheville said the water was likely safe enough to bathe in, local leaders still reported potential risks from bacteria and other contaminants in the water, Palmeri said. Those with a fragile immune system or breaks in the skin “could get serious and life-threatening infections,” he explained.
To make matters worse, damage to a North Carolina facility manufacturing IV fluids left the United States in shortage for months. IV fluids are key not only for providing hydration but also for easing nausea, fatigue, and other issues caused by cancer therapies.
With wildfires, as occurred in southern California early this year, patients undergoing cancer treatment might feel they have no option but to remain near home to continue getting care, Casey said. “It’s restricting their agency in the kinds of choices that they have to make during these severe weather events.”
Meanwhile, thick wildfire smoke can confine patients to their homes, said Lawrence Wagman, MD, a surgical oncologist and a regional medical director at the City of Hope network, who described its main facility in Duarte, California, coming within a dozen miles of the Eaton fire. “One of the biggest problems was so much smoke in the air,” he said. “And the air quality was so low that it was, in many ways, dangerous for patients to travel.”
“These fires were so aggressive, and they kept popping up,” Wagman said. Plus, the emotional strain of looming wildfires persisted for both patients and cancer clinicians for weeks on end, he added.
For those who evacuate, the logistics can be complex.
Not only are cancer treatment plans highly structured, but switching care to another facility is far from easy, Bernicker said. The new facility will likely need to submit a treatment plan and get insurance coverage before moving forward.
“I’m not saying that takes forever,” he said. “But what I’m saying is that it’s not like you just roll in and they hang the [infusion] bag.”
Neither is a shelter typically an option for patients during treatment, said Seth Berkowitz, a licensed clinical social worker and director of Strategic Healthcare Partnerships at The Leukemia & Lymphoma Society. “They have to have a place to go that’s safe and germ-free.”
In western North Carolina, the strain on already ill patients and their caregivers could be overwhelming, Palmeri said. He recounted how the husband of one patient with advanced cancer died after the storm came through.
“He tried to go out there with a chainsaw to clear a way out so that they could get out of their house in case he needed to take her to the hospital,” Palmeri said. “And he had a heart attack there in the driveway.”
Rebuilding and Planning Ahead
Experts are only at the early stages of grasping the magnitude of extreme weather on cancer care and developing strategies to curtail care gaps and potential harm to patients, said Katie Lichter, MD, a radiation oncologist at the University of California San Francisco, who studies extreme weather and cancer treatment.
“How does it impact health care delivery services at every step, from prevention to screening to treatment and survivorship?” Lichter asked. “We’re just starting to understand and to even quantify that,” she said, which included identifying patients who are most vulnerable. She worries, in particular, about patients living in rural areas who already travel longer distances and often face more difficulties accessing care.
The gap between research and reality still looms large. A recent analysis, led by Lichter, looked at 176 California radiation oncology clinics and found that all of them were located within 25 miles of a wildfire that had occurred within the prior 5 years. Yet among the 51 clinics that responded to a 2022 survey,just 47% reported that their clinic had a wildfire emergency preparedness plan.
The American Cancer Society does provide some guidance on how patients can prepare for a weather-related crisis, including having extra supplies of medications or special equipment on hand.
Still, providers are often in reaction mode when extreme weather strikes.
Without adequate clean water after Helene, leaders at Palmeri’s practice moved swiftly, purchasing 40,000-50,000 bottles of water and bringing in porta potties from elsewhere.
“I think we were able to get things up and going very quickly,” said Palmeri, who noted that full services resumed about 10 days after the storm. “For most patients, missing a week of treatment would not do a disservice to their well-being or outcome.”
Going forward, to provide a more comprehensive strategy, Lichter is working with colleagues to develop clinical tool kits to help oncology practices and patients prepare for severe weather events, such as outlining backup treatment contingency plans, ensuring early medication refills, and boosting communication with patient alert systems.
Clinicians are also implementing their own strategies. To limit communication gaps during power outages, Palmeri said that, since Helene, his practice has made sure that their clinic sites, physicians, and other key people now have cell phone service through satellite via Starlink.
“No one has phone books anymore,” he said, so cancer clinicians should keep crucial contact information on paper, such as details about businesses that distribute water and porta potties, given that online searches may not be feasible.
Clinicians should also advise patients to keep a hard copy of recent medical findings handy, including medications and lab results, in case they arrive at an emergency room far from home and physicians can’t access their electronic health record, Bernicker said.
When there is enough advance warning of an approaching weather event, clinicians can help patients keep at least a week’s worth of medication on hand for symptom-related issues, such as nausea or pain, as well as antibiotics so patients don’t have to seek out emergency care during the crisis, Bernicker said. However, Bernicker noted, some insurers may be reluctant to fill certain prescriptions in advance, like those for opioids.
Making headway on more robust preparedness strategies may be slowed. As of March, the National Institutes of Health will no longer fund research about the health effects of climate change.
Bernicker hoped that such cutbacks would be rolled back. What’s on the line, he stressed, is maintaining the highest quality of care for patients with cancer.
“We really are in a golden age of oncology therapeutics,” he said. “We have patients living longer than anyone would have predicted 20 or 25 years ago. But all those advances are contingent on people having access to their centers and not having that interrupted.”
A version of this article first appeared on Medscape.com.
As Hurricane Helene approached western North Carolina, Martin Palmeri, MD, MBA, didn’t anticipate the storm would disrupt practice operations for more than a day or so.
But the massive rainfall and flooding damage last September proved to be far more challenging. Despite best efforts by the 13-physician practice, basic treatments for most patients were interrupted for about a week.
Flooding washed out some of the major roads leading to the main Asheville clinic and affiliated rural sites, limiting travel and slowing delivery of medications, intravenous (IV) fluids, and other supplies, Palmeri said. Some patients and employees weren’t initially reachable due to the loss of the internet and cell phone service. The storm-related fallout even forced patients to relocate elsewhere for weeks or longer.
During the storm, backup generators kept power on at the Asheville clinic, protecting chemotherapy and other refrigerated drugs, but the storm damaged the municipal water supply.
“Water was the number one thing — how do you get water to the office?” Palmeri said. “You can’t give someone an 8-hour infusion if they don’t have means of going to the toilet or having something to drink.”
Hurricanes. Wildfires. Heat waves. As climate-driven extreme weather has become more common, researchers, oncologists, and patients are increasingly being forced to consider the consequences of these disruptions.
Along with preventing patients and providers from reaching treatment sites, experts said, extreme weather can undercut patients’ health and care in other ways. Patients with more limited lung capacity following lung cancer surgery, for instance, may struggle with breathing during wildfires. Extreme heat can prove risky for patients already dehydrated or weakened by treatment-related side effects. Power outages and severe flooding can affect vital infrastructure, disrupting operations at facilities that manufacture essential drugs. Power outages can also impede radiotherapy, which requires machines powered by electricity.
“Any of these [weather] events can disrupt this critical cancer care continuum among a population of people that already are very vulnerable,” said Joan Casey, PhD, an environmental epidemiologist and associate professor at the University of Washington in Seattle.
Extreme Weather and Cancer Survival
For patients with cancer, survival often relies on highly regimented protocols, which may require surgery plus frequent visits for radiation, chemotherapy, or immunotherapy that can last months, said Eric Bernicker, MD, a Colorado oncologist and lead author of a 2023 American Society of Clinical Oncology position statement about the impact of climate change on cancer care.
Interruptions to care, regardless of the cause, can lead to worse outcomes for patients, Bernicker said. “If you’re in the middle of your post-lumpectomy radiation and your radiation center shuts for 2 weeks,” he said, “that is not good.”
Research indicated that even short treatment disruptions can affect outcomes for patients with cancer and that delays caused by extreme weather — which may last for weeks — can affect survival for these patients.
One analysis, published in JAMA Oncology in 2023, found that patients exposed to wildfire within the first year after potentially curative lung cancer surgery had worse survival outcomes than those who weren’t exposed during their recovery.
In another study, patients with lung cancer who had their radiation interrupted when a hurricane struck had a 19% greater risk of dying overall compared with similar patients who were not affected. Another analysis found that patients with breast cancer who were partway through treatment when Hurricane Katrina hit the Louisiana coastline had a significantly greater risk of dying over a 10-year period compared with patients who lived elsewhere.
The potential threats to survival highlighted the impacts of extreme weather on carefully orchestrated systems of care that place patients facing already fragile situations in impossible binds, Casey said.
Douglas Flora, MD, a Kentucky oncologist and president-elect of the Association of Cancer Care Centers, Rockville, Maryland, agreed.
“We’ve seen this with an increasing frequency over the last several years,” Flora said. “It’s one thing if it’s routine follow-up or surveillance care, but many cancer patients’ survivals are directly related to not having interruptions in their care.”
Challenging Realities
Following Helene, the most pressing issue was the lack of water, Palmeri said.
The lack of reliable clean water created challenges for patients receiving radiation or chemotherapy infusions, which can cause vomiting and diarrhea that leave patients dehydrated. Toilets were also unusable.
Even when the city of Asheville said the water was likely safe enough to bathe in, local leaders still reported potential risks from bacteria and other contaminants in the water, Palmeri said. Those with a fragile immune system or breaks in the skin “could get serious and life-threatening infections,” he explained.
To make matters worse, damage to a North Carolina facility manufacturing IV fluids left the United States in shortage for months. IV fluids are key not only for providing hydration but also for easing nausea, fatigue, and other issues caused by cancer therapies.
With wildfires, as occurred in southern California early this year, patients undergoing cancer treatment might feel they have no option but to remain near home to continue getting care, Casey said. “It’s restricting their agency in the kinds of choices that they have to make during these severe weather events.”
Meanwhile, thick wildfire smoke can confine patients to their homes, said Lawrence Wagman, MD, a surgical oncologist and a regional medical director at the City of Hope network, who described its main facility in Duarte, California, coming within a dozen miles of the Eaton fire. “One of the biggest problems was so much smoke in the air,” he said. “And the air quality was so low that it was, in many ways, dangerous for patients to travel.”
“These fires were so aggressive, and they kept popping up,” Wagman said. Plus, the emotional strain of looming wildfires persisted for both patients and cancer clinicians for weeks on end, he added.
For those who evacuate, the logistics can be complex.
Not only are cancer treatment plans highly structured, but switching care to another facility is far from easy, Bernicker said. The new facility will likely need to submit a treatment plan and get insurance coverage before moving forward.
“I’m not saying that takes forever,” he said. “But what I’m saying is that it’s not like you just roll in and they hang the [infusion] bag.”
Neither is a shelter typically an option for patients during treatment, said Seth Berkowitz, a licensed clinical social worker and director of Strategic Healthcare Partnerships at The Leukemia & Lymphoma Society. “They have to have a place to go that’s safe and germ-free.”
In western North Carolina, the strain on already ill patients and their caregivers could be overwhelming, Palmeri said. He recounted how the husband of one patient with advanced cancer died after the storm came through.
“He tried to go out there with a chainsaw to clear a way out so that they could get out of their house in case he needed to take her to the hospital,” Palmeri said. “And he had a heart attack there in the driveway.”
Rebuilding and Planning Ahead
Experts are only at the early stages of grasping the magnitude of extreme weather on cancer care and developing strategies to curtail care gaps and potential harm to patients, said Katie Lichter, MD, a radiation oncologist at the University of California San Francisco, who studies extreme weather and cancer treatment.
“How does it impact health care delivery services at every step, from prevention to screening to treatment and survivorship?” Lichter asked. “We’re just starting to understand and to even quantify that,” she said, which included identifying patients who are most vulnerable. She worries, in particular, about patients living in rural areas who already travel longer distances and often face more difficulties accessing care.
The gap between research and reality still looms large. A recent analysis, led by Lichter, looked at 176 California radiation oncology clinics and found that all of them were located within 25 miles of a wildfire that had occurred within the prior 5 years. Yet among the 51 clinics that responded to a 2022 survey,just 47% reported that their clinic had a wildfire emergency preparedness plan.
The American Cancer Society does provide some guidance on how patients can prepare for a weather-related crisis, including having extra supplies of medications or special equipment on hand.
Still, providers are often in reaction mode when extreme weather strikes.
Without adequate clean water after Helene, leaders at Palmeri’s practice moved swiftly, purchasing 40,000-50,000 bottles of water and bringing in porta potties from elsewhere.
“I think we were able to get things up and going very quickly,” said Palmeri, who noted that full services resumed about 10 days after the storm. “For most patients, missing a week of treatment would not do a disservice to their well-being or outcome.”
Going forward, to provide a more comprehensive strategy, Lichter is working with colleagues to develop clinical tool kits to help oncology practices and patients prepare for severe weather events, such as outlining backup treatment contingency plans, ensuring early medication refills, and boosting communication with patient alert systems.
Clinicians are also implementing their own strategies. To limit communication gaps during power outages, Palmeri said that, since Helene, his practice has made sure that their clinic sites, physicians, and other key people now have cell phone service through satellite via Starlink.
“No one has phone books anymore,” he said, so cancer clinicians should keep crucial contact information on paper, such as details about businesses that distribute water and porta potties, given that online searches may not be feasible.
Clinicians should also advise patients to keep a hard copy of recent medical findings handy, including medications and lab results, in case they arrive at an emergency room far from home and physicians can’t access their electronic health record, Bernicker said.
When there is enough advance warning of an approaching weather event, clinicians can help patients keep at least a week’s worth of medication on hand for symptom-related issues, such as nausea or pain, as well as antibiotics so patients don’t have to seek out emergency care during the crisis, Bernicker said. However, Bernicker noted, some insurers may be reluctant to fill certain prescriptions in advance, like those for opioids.
Making headway on more robust preparedness strategies may be slowed. As of March, the National Institutes of Health will no longer fund research about the health effects of climate change.
Bernicker hoped that such cutbacks would be rolled back. What’s on the line, he stressed, is maintaining the highest quality of care for patients with cancer.
“We really are in a golden age of oncology therapeutics,” he said. “We have patients living longer than anyone would have predicted 20 or 25 years ago. But all those advances are contingent on people having access to their centers and not having that interrupted.”
A version of this article first appeared on Medscape.com.