User login
MDedge latest news is breaking news from medical conferences, journals, guidelines, the FDA and CDC.
GLP-1s May Improve Colon Cancer Outcomes
Treatment with a GLP-1 receptor agonist (RA) may offer a survival advantage in patients with colon cancer and obesity.
In a real-world analysis of nearly 7000 patients with colon cancer, those taking a GLP-1 RA were less than half as likely to die within 5 years compared with those who weren’t on a GLP-1 drug.
The association between GLP-1 exposure and lower 5–year mortality in colon cancer was “robust” and appeared to be concentrated in patients with severe obesity (BMI ≥ 35), lead investigator Raphael E. Cuomo, PhD, with University of California San Diego, told this news organization.
The apparent protective effect “persisted after controlling for differences in disease severity and demographics, as well as differences in circulating carcinoembryonic antigen, a biomarker of disease aggressiveness,” Cuomo said.
The study was published online in Cancer Investigation.
Effects Beyond Glucose-Lowering
Colon cancer remains a major global cause of cancer-related deaths, and obesity is both a risk factor and a driver of worse outcomes.
Beyond regulating blood sugar, GLP-1 drugs reduce systemic inflammation, improve insulin sensitivity, and promote weight loss. Prior preclinical work has also suggested they may prevent cancer cell growth, trigger cancer cell death, and reshape the tumor microenvironment.
To investigate further, Cuomo analyzed electronic health records of 6871 patients diagnosed with primary colon cancer before 2019 — of which 103 had at least 1 documented prescription for a GLP-1 drug within 5 years of diagnosis.
Five–year mortality was significantly lower in GLP-1 RA users than in nonusers (15.5% vs 37.1%; P < .001). A significant reduction in 5–year mortality among GLP-1 RA users was evident in an unadjusted model (odds ratio [OR], 0.38; P < .001) and persisted in fully adjusted models (OR, 0.28; P < .001).
When stratified by BMI, the odds of 5-year mortality with GLP-1 use was reduced only in patients with Class II obesity (BMI ≥ 35: fully adjusted hazard ratio [HR], 0.051; P = .004). In this group, fully adjusted hazard ratios suggested markedly lower risk for death (HR, 0.07; P = .009).
Beyond mortality, GLP-1 users also experienced fewer late cardiovascular events and had fewer markers of advanced colon cancer progression in the final months of follow-up, “which suggests that GLP-1 drugs exert benefits through both oncologic and cardiometabolic pathways,” Cuomo told this news organization.
Intriguing and Promising — but Further Studies Needed
“To further study the potential of GLP-1 therapy as an adjunct to standard care in colon cancer, randomized trials should be conducted with stratification by BMI, diabetes status, and disease severity, with endpoints spanning overall and cancerspecific survival and major cardiovascular events,” Cuomo said.
“We also need prospective translational studies integrating dosing/timing, adherence, tumor genomics, and serial biomarkers (including ctDNA and metabolic panels) to elucidate mechanisms, assess the role of adiposity and insulin resistance, and identify the patient subgroups most likely to benefit,” he noted.
For now, GLP1 medications are an option in “eligible colon cancer patients with severe obesity or diabetes who meet standard metabolic indications,” Cuomo told this news organization.
Commenting on this study for this news organization, David Greenwald, MD, director of Clinical Gastroenterology and Endoscopy at Icahn School of Medicine at Mount Sinai Hospital in New York City, noted “other studies have showed a lower risk of developing colorectal cancer in the first place and then improved survival.”
Greenwald cited a recent study that found people with diabetes who took GLP-1 RAs had a 44% lower risk of developing colorectal cancer than those who took insulin, and a 25% lower risk than those who took metformin.
The effects of GLP-1s in colon cancer are “very intriguing and very promising but more research is needed to confirm whether this is really true and the mechanisms behind it,” said Greenwald.
In terms of the lowering risk of developing colorectal cancer, “probably first and foremost is that the drugs are really effective in promoting weight loss. And if you can reduce obesity in the population, you do all sorts of good things — reduce diabetes, reduce heart disease, and maybe reduce colorectal cancer,” Greenwald said.
This study had no specific funding. Cuomo and Greenwald had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Treatment with a GLP-1 receptor agonist (RA) may offer a survival advantage in patients with colon cancer and obesity.
In a real-world analysis of nearly 7000 patients with colon cancer, those taking a GLP-1 RA were less than half as likely to die within 5 years compared with those who weren’t on a GLP-1 drug.
The association between GLP-1 exposure and lower 5–year mortality in colon cancer was “robust” and appeared to be concentrated in patients with severe obesity (BMI ≥ 35), lead investigator Raphael E. Cuomo, PhD, with University of California San Diego, told this news organization.
The apparent protective effect “persisted after controlling for differences in disease severity and demographics, as well as differences in circulating carcinoembryonic antigen, a biomarker of disease aggressiveness,” Cuomo said.
The study was published online in Cancer Investigation.
Effects Beyond Glucose-Lowering
Colon cancer remains a major global cause of cancer-related deaths, and obesity is both a risk factor and a driver of worse outcomes.
Beyond regulating blood sugar, GLP-1 drugs reduce systemic inflammation, improve insulin sensitivity, and promote weight loss. Prior preclinical work has also suggested they may prevent cancer cell growth, trigger cancer cell death, and reshape the tumor microenvironment.
To investigate further, Cuomo analyzed electronic health records of 6871 patients diagnosed with primary colon cancer before 2019 — of which 103 had at least 1 documented prescription for a GLP-1 drug within 5 years of diagnosis.
Five–year mortality was significantly lower in GLP-1 RA users than in nonusers (15.5% vs 37.1%; P < .001). A significant reduction in 5–year mortality among GLP-1 RA users was evident in an unadjusted model (odds ratio [OR], 0.38; P < .001) and persisted in fully adjusted models (OR, 0.28; P < .001).
When stratified by BMI, the odds of 5-year mortality with GLP-1 use was reduced only in patients with Class II obesity (BMI ≥ 35: fully adjusted hazard ratio [HR], 0.051; P = .004). In this group, fully adjusted hazard ratios suggested markedly lower risk for death (HR, 0.07; P = .009).
Beyond mortality, GLP-1 users also experienced fewer late cardiovascular events and had fewer markers of advanced colon cancer progression in the final months of follow-up, “which suggests that GLP-1 drugs exert benefits through both oncologic and cardiometabolic pathways,” Cuomo told this news organization.
Intriguing and Promising — but Further Studies Needed
“To further study the potential of GLP-1 therapy as an adjunct to standard care in colon cancer, randomized trials should be conducted with stratification by BMI, diabetes status, and disease severity, with endpoints spanning overall and cancerspecific survival and major cardiovascular events,” Cuomo said.
“We also need prospective translational studies integrating dosing/timing, adherence, tumor genomics, and serial biomarkers (including ctDNA and metabolic panels) to elucidate mechanisms, assess the role of adiposity and insulin resistance, and identify the patient subgroups most likely to benefit,” he noted.
For now, GLP1 medications are an option in “eligible colon cancer patients with severe obesity or diabetes who meet standard metabolic indications,” Cuomo told this news organization.
Commenting on this study for this news organization, David Greenwald, MD, director of Clinical Gastroenterology and Endoscopy at Icahn School of Medicine at Mount Sinai Hospital in New York City, noted “other studies have showed a lower risk of developing colorectal cancer in the first place and then improved survival.”
Greenwald cited a recent study that found people with diabetes who took GLP-1 RAs had a 44% lower risk of developing colorectal cancer than those who took insulin, and a 25% lower risk than those who took metformin.
The effects of GLP-1s in colon cancer are “very intriguing and very promising but more research is needed to confirm whether this is really true and the mechanisms behind it,” said Greenwald.
In terms of the lowering risk of developing colorectal cancer, “probably first and foremost is that the drugs are really effective in promoting weight loss. And if you can reduce obesity in the population, you do all sorts of good things — reduce diabetes, reduce heart disease, and maybe reduce colorectal cancer,” Greenwald said.
This study had no specific funding. Cuomo and Greenwald had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Treatment with a GLP-1 receptor agonist (RA) may offer a survival advantage in patients with colon cancer and obesity.
In a real-world analysis of nearly 7000 patients with colon cancer, those taking a GLP-1 RA were less than half as likely to die within 5 years compared with those who weren’t on a GLP-1 drug.
The association between GLP-1 exposure and lower 5–year mortality in colon cancer was “robust” and appeared to be concentrated in patients with severe obesity (BMI ≥ 35), lead investigator Raphael E. Cuomo, PhD, with University of California San Diego, told this news organization.
The apparent protective effect “persisted after controlling for differences in disease severity and demographics, as well as differences in circulating carcinoembryonic antigen, a biomarker of disease aggressiveness,” Cuomo said.
The study was published online in Cancer Investigation.
Effects Beyond Glucose-Lowering
Colon cancer remains a major global cause of cancer-related deaths, and obesity is both a risk factor and a driver of worse outcomes.
Beyond regulating blood sugar, GLP-1 drugs reduce systemic inflammation, improve insulin sensitivity, and promote weight loss. Prior preclinical work has also suggested they may prevent cancer cell growth, trigger cancer cell death, and reshape the tumor microenvironment.
To investigate further, Cuomo analyzed electronic health records of 6871 patients diagnosed with primary colon cancer before 2019 — of which 103 had at least 1 documented prescription for a GLP-1 drug within 5 years of diagnosis.
Five–year mortality was significantly lower in GLP-1 RA users than in nonusers (15.5% vs 37.1%; P < .001). A significant reduction in 5–year mortality among GLP-1 RA users was evident in an unadjusted model (odds ratio [OR], 0.38; P < .001) and persisted in fully adjusted models (OR, 0.28; P < .001).
When stratified by BMI, the odds of 5-year mortality with GLP-1 use was reduced only in patients with Class II obesity (BMI ≥ 35: fully adjusted hazard ratio [HR], 0.051; P = .004). In this group, fully adjusted hazard ratios suggested markedly lower risk for death (HR, 0.07; P = .009).
Beyond mortality, GLP-1 users also experienced fewer late cardiovascular events and had fewer markers of advanced colon cancer progression in the final months of follow-up, “which suggests that GLP-1 drugs exert benefits through both oncologic and cardiometabolic pathways,” Cuomo told this news organization.
Intriguing and Promising — but Further Studies Needed
“To further study the potential of GLP-1 therapy as an adjunct to standard care in colon cancer, randomized trials should be conducted with stratification by BMI, diabetes status, and disease severity, with endpoints spanning overall and cancerspecific survival and major cardiovascular events,” Cuomo said.
“We also need prospective translational studies integrating dosing/timing, adherence, tumor genomics, and serial biomarkers (including ctDNA and metabolic panels) to elucidate mechanisms, assess the role of adiposity and insulin resistance, and identify the patient subgroups most likely to benefit,” he noted.
For now, GLP1 medications are an option in “eligible colon cancer patients with severe obesity or diabetes who meet standard metabolic indications,” Cuomo told this news organization.
Commenting on this study for this news organization, David Greenwald, MD, director of Clinical Gastroenterology and Endoscopy at Icahn School of Medicine at Mount Sinai Hospital in New York City, noted “other studies have showed a lower risk of developing colorectal cancer in the first place and then improved survival.”
Greenwald cited a recent study that found people with diabetes who took GLP-1 RAs had a 44% lower risk of developing colorectal cancer than those who took insulin, and a 25% lower risk than those who took metformin.
The effects of GLP-1s in colon cancer are “very intriguing and very promising but more research is needed to confirm whether this is really true and the mechanisms behind it,” said Greenwald.
In terms of the lowering risk of developing colorectal cancer, “probably first and foremost is that the drugs are really effective in promoting weight loss. And if you can reduce obesity in the population, you do all sorts of good things — reduce diabetes, reduce heart disease, and maybe reduce colorectal cancer,” Greenwald said.
This study had no specific funding. Cuomo and Greenwald had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM CANCER INVESTIGATION
‘So You Have an Idea…’: A Practical Guide to Tech and Device Development for the Early Career GI

You are in the middle of a busy clinic day and think, “there has to be a better way to do this.” Suddenly, a better way to do something becomes obvious. Maybe it’s a tool that simplifies documentation, a device that improves patient comfort, or an app that bridges a clinical gap. Many physicians, especially early career gastroenterologists, have ideas like this, but few know what to do next.
This article is for the curious innovator at the beginning of their clinical career. It offers practical, real-world guidance on developing a clinical product: whether that be hardware, software, or a hybrid. It outlines what questions to ask, who to consult, and how to protect your work, using personal insights and business principles learned through lived experience.
1. Understand Intellectual Property (IP): Know Its Value and Ownership
What is IP?
Intellectual property refers to your original creations: inventions, designs, software, and more. This is what you want to protect legally through patents, trademarks, or copyrights.
Who owns your idea?
This is the first and most important question to ask. If you are employed (especially by a hospital or academic center), your contract may already give your employer rights to any inventions you create, even those developed in your personal time.

What to ask:
- Does my employment contract include an “assignment of inventions” clause?
- Does the institution claim rights to anything developed with institutional resources?
- Are there moonlighting or external activity policies that affect this?
If you are developing an idea on your personal time, with your own resources, and outside your scope of clinical duties, it might still be considered “theirs” under some contracts. Early legal consultation is critical. A specialized IP attorney can help you understand what you own and how to protect it. This should be done early, ideally before you start building anything.
2. Lawyers Aren’t Optional: They’re Essential Early Partners
You do not need a full legal team, but you do need a lawyer early. An early consultation with an IP attorney can clarify your rights, guide your filing process (e.g. provisional patents), and help you avoid costly missteps.
Do this before sharing your idea publicly, including in academic presentations, pitch competitions, or even on social media. Public disclosure can start a clock ticking for application to protect your IP.
3. Build a Founding Team with Intent

Think of your startup team like a long-term relationship: you’re committing to build something together through uncertainty, tension, and change.
Strong early-stage teams often include:
- The Visionary – understands the clinical need and vision
- The Builder – engineer, developer, or designer
- The Doer – project manager or operations lead
Before forming a company, clearly define:
- Ownership (equity percentages)
- Roles and responsibilities
- Time commitments
- What happens if someone exits
Have these discussions early and document your agreements. Avoid informal “handshake” deals that can lead to serious disputes later.
4. You Don’t Need to Know Everything on Day One
You do not need to know how to write code, build a prototype, or get FDA clearance on day one. Successful innovators are humble learners. Use a Minimum Viable Product (MVP), a simple, functional version of your idea, to test assumptions and gather feedback. Iterate based on what you learn. Do not chase perfection; pursue progress. Consider using online accelerators like Y Combinator’s startup school or AGA’s Center for GI Innovation and Technology.
5. Incubators: Use them Strategically
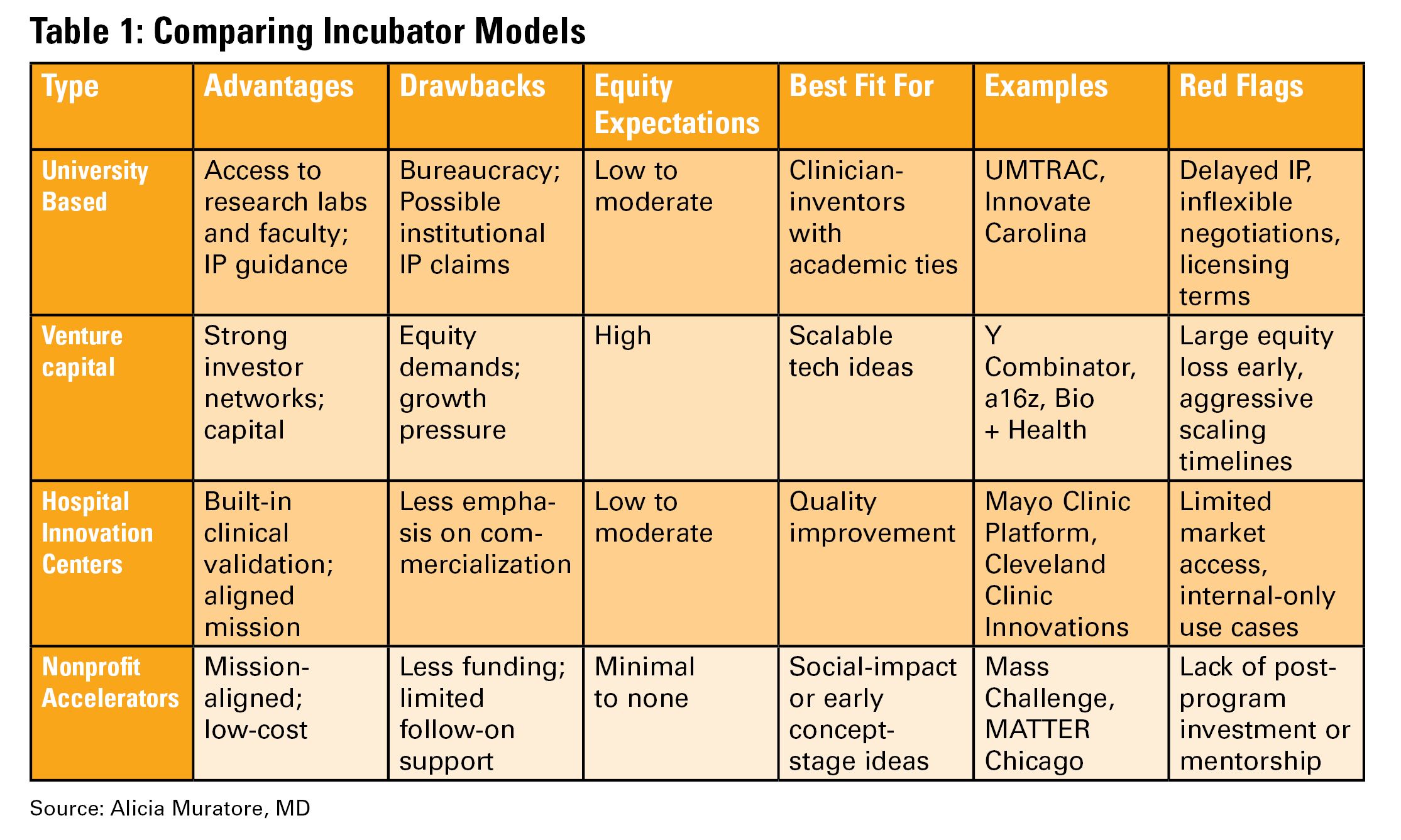
Incubators can offer mentorship, seed funding, legal support, and technical resources, but they vary widely in value (see Table 1). Many may want equity, and not all offer when you truly need.
Ask Yourself:
- Do I need technical help, business mentorship, or just accountability?
- What does this incubator offer in terms of IP protection, exposure, and connections?
- Do I understand the equity trade-off?
- What services and funding do they provide?
- Do they take equity? How much and when?
- What’s their track record with similar ventures?
- Are their incentives aligned with your vision?
6. Academic Institutions: Partners or Pitfalls?
Universities can provide credibility, resources, and early funding through their tech transfer office (TTO).
Key Questions to Ask:
- Will my IP be managed by the TTO?
- How much say do I have in licensing decisions?
- Are there royalty-sharing agreements in place?
- Can I form a startup while employed here?
You may need to negotiate if you want to commercialize your idea independently.
7. Do it for Purpose, Not Payday
Most founders end up owning only a small percentage of their company by the time a product reaches the market. Do not expect to get rich. Do it because it solves a problem you care about. If it happens to come with a nice paycheck, then that is an added bonus.
Your clinical training and insight give you a unique edge. You already know what’s broken. Use that as your compass.
Conclusion
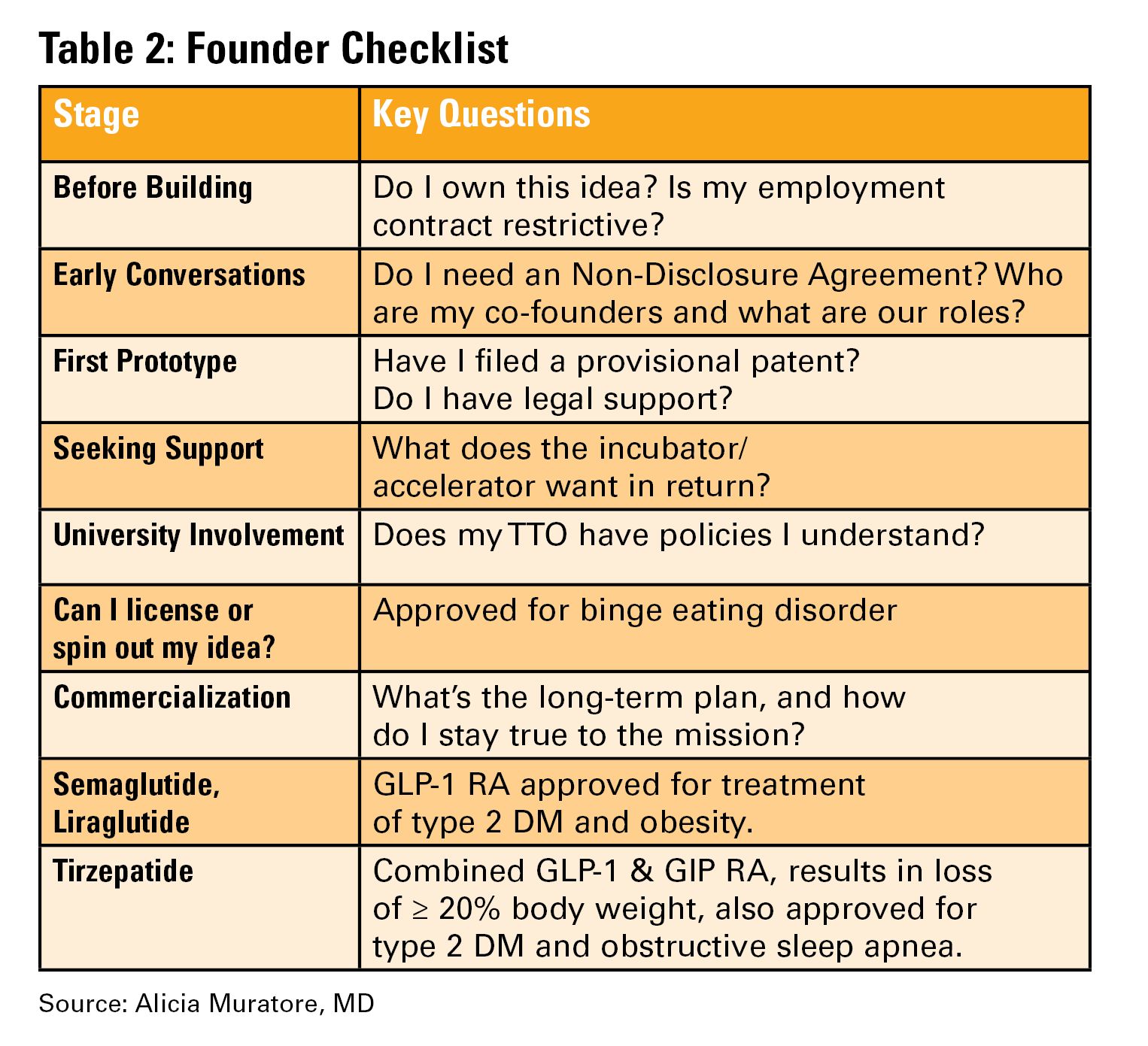
Innovation isn’t about brilliance, it’s about curiosity, structure, and tenacity (see Table 2). Start small. Protect your work. Choose the right partners. Most importantly, stay anchored in your mission to make GI care better.
Dr. Muratore is based at UNC Rex Digestive Health, Raleigh, North Carolina. She has no conflicts related to this article. Dr. Wechsler is based at the University of North Carolina at Chapel Hill, Chapel Hill, North Carolina. She holds a patent assigned to Trustees of Dartmouth College. Dr. Shah is based at the University of Michigan, Ann Arbor, Michigan. He consults for Ardelyx, Laborie, Neuraxis, Salix, Sanofi, and Takeda and holds a patent with the Regents of the University of Michigan.
You are in the middle of a busy clinic day and think, “there has to be a better way to do this.” Suddenly, a better way to do something becomes obvious. Maybe it’s a tool that simplifies documentation, a device that improves patient comfort, or an app that bridges a clinical gap. Many physicians, especially early career gastroenterologists, have ideas like this, but few know what to do next.
This article is for the curious innovator at the beginning of their clinical career. It offers practical, real-world guidance on developing a clinical product: whether that be hardware, software, or a hybrid. It outlines what questions to ask, who to consult, and how to protect your work, using personal insights and business principles learned through lived experience.
1. Understand Intellectual Property (IP): Know Its Value and Ownership
What is IP?
Intellectual property refers to your original creations: inventions, designs, software, and more. This is what you want to protect legally through patents, trademarks, or copyrights.
Who owns your idea?
This is the first and most important question to ask. If you are employed (especially by a hospital or academic center), your contract may already give your employer rights to any inventions you create, even those developed in your personal time.
What to ask:
- Does my employment contract include an “assignment of inventions” clause?
- Does the institution claim rights to anything developed with institutional resources?
- Are there moonlighting or external activity policies that affect this?
If you are developing an idea on your personal time, with your own resources, and outside your scope of clinical duties, it might still be considered “theirs” under some contracts. Early legal consultation is critical. A specialized IP attorney can help you understand what you own and how to protect it. This should be done early, ideally before you start building anything.
2. Lawyers Aren’t Optional: They’re Essential Early Partners
You do not need a full legal team, but you do need a lawyer early. An early consultation with an IP attorney can clarify your rights, guide your filing process (e.g. provisional patents), and help you avoid costly missteps.
Do this before sharing your idea publicly, including in academic presentations, pitch competitions, or even on social media. Public disclosure can start a clock ticking for application to protect your IP.
3. Build a Founding Team with Intent
Think of your startup team like a long-term relationship: you’re committing to build something together through uncertainty, tension, and change.
Strong early-stage teams often include:
- The Visionary – understands the clinical need and vision
- The Builder – engineer, developer, or designer
- The Doer – project manager or operations lead
Before forming a company, clearly define:
- Ownership (equity percentages)
- Roles and responsibilities
- Time commitments
- What happens if someone exits
Have these discussions early and document your agreements. Avoid informal “handshake” deals that can lead to serious disputes later.
4. You Don’t Need to Know Everything on Day One
You do not need to know how to write code, build a prototype, or get FDA clearance on day one. Successful innovators are humble learners. Use a Minimum Viable Product (MVP), a simple, functional version of your idea, to test assumptions and gather feedback. Iterate based on what you learn. Do not chase perfection; pursue progress. Consider using online accelerators like Y Combinator’s startup school or AGA’s Center for GI Innovation and Technology.
5. Incubators: Use them Strategically
Incubators can offer mentorship, seed funding, legal support, and technical resources, but they vary widely in value (see Table 1). Many may want equity, and not all offer when you truly need.
Ask Yourself:
- Do I need technical help, business mentorship, or just accountability?
- What does this incubator offer in terms of IP protection, exposure, and connections?
- Do I understand the equity trade-off?
- What services and funding do they provide?
- Do they take equity? How much and when?
- What’s their track record with similar ventures?
- Are their incentives aligned with your vision?
6. Academic Institutions: Partners or Pitfalls?
Universities can provide credibility, resources, and early funding through their tech transfer office (TTO).
Key Questions to Ask:
- Will my IP be managed by the TTO?
- How much say do I have in licensing decisions?
- Are there royalty-sharing agreements in place?
- Can I form a startup while employed here?
You may need to negotiate if you want to commercialize your idea independently.
7. Do it for Purpose, Not Payday
Most founders end up owning only a small percentage of their company by the time a product reaches the market. Do not expect to get rich. Do it because it solves a problem you care about. If it happens to come with a nice paycheck, then that is an added bonus.
Your clinical training and insight give you a unique edge. You already know what’s broken. Use that as your compass.
Conclusion
Innovation isn’t about brilliance, it’s about curiosity, structure, and tenacity (see Table 2). Start small. Protect your work. Choose the right partners. Most importantly, stay anchored in your mission to make GI care better.
Dr. Muratore is based at UNC Rex Digestive Health, Raleigh, North Carolina. She has no conflicts related to this article. Dr. Wechsler is based at the University of North Carolina at Chapel Hill, Chapel Hill, North Carolina. She holds a patent assigned to Trustees of Dartmouth College. Dr. Shah is based at the University of Michigan, Ann Arbor, Michigan. He consults for Ardelyx, Laborie, Neuraxis, Salix, Sanofi, and Takeda and holds a patent with the Regents of the University of Michigan.
You are in the middle of a busy clinic day and think, “there has to be a better way to do this.” Suddenly, a better way to do something becomes obvious. Maybe it’s a tool that simplifies documentation, a device that improves patient comfort, or an app that bridges a clinical gap. Many physicians, especially early career gastroenterologists, have ideas like this, but few know what to do next.
This article is for the curious innovator at the beginning of their clinical career. It offers practical, real-world guidance on developing a clinical product: whether that be hardware, software, or a hybrid. It outlines what questions to ask, who to consult, and how to protect your work, using personal insights and business principles learned through lived experience.
1. Understand Intellectual Property (IP): Know Its Value and Ownership
What is IP?
Intellectual property refers to your original creations: inventions, designs, software, and more. This is what you want to protect legally through patents, trademarks, or copyrights.
Who owns your idea?
This is the first and most important question to ask. If you are employed (especially by a hospital or academic center), your contract may already give your employer rights to any inventions you create, even those developed in your personal time.
What to ask:
- Does my employment contract include an “assignment of inventions” clause?
- Does the institution claim rights to anything developed with institutional resources?
- Are there moonlighting or external activity policies that affect this?
If you are developing an idea on your personal time, with your own resources, and outside your scope of clinical duties, it might still be considered “theirs” under some contracts. Early legal consultation is critical. A specialized IP attorney can help you understand what you own and how to protect it. This should be done early, ideally before you start building anything.
2. Lawyers Aren’t Optional: They’re Essential Early Partners
You do not need a full legal team, but you do need a lawyer early. An early consultation with an IP attorney can clarify your rights, guide your filing process (e.g. provisional patents), and help you avoid costly missteps.
Do this before sharing your idea publicly, including in academic presentations, pitch competitions, or even on social media. Public disclosure can start a clock ticking for application to protect your IP.
3. Build a Founding Team with Intent
Think of your startup team like a long-term relationship: you’re committing to build something together through uncertainty, tension, and change.
Strong early-stage teams often include:
- The Visionary – understands the clinical need and vision
- The Builder – engineer, developer, or designer
- The Doer – project manager or operations lead
Before forming a company, clearly define:
- Ownership (equity percentages)
- Roles and responsibilities
- Time commitments
- What happens if someone exits
Have these discussions early and document your agreements. Avoid informal “handshake” deals that can lead to serious disputes later.
4. You Don’t Need to Know Everything on Day One
You do not need to know how to write code, build a prototype, or get FDA clearance on day one. Successful innovators are humble learners. Use a Minimum Viable Product (MVP), a simple, functional version of your idea, to test assumptions and gather feedback. Iterate based on what you learn. Do not chase perfection; pursue progress. Consider using online accelerators like Y Combinator’s startup school or AGA’s Center for GI Innovation and Technology.
5. Incubators: Use them Strategically
Incubators can offer mentorship, seed funding, legal support, and technical resources, but they vary widely in value (see Table 1). Many may want equity, and not all offer when you truly need.
Ask Yourself:
- Do I need technical help, business mentorship, or just accountability?
- What does this incubator offer in terms of IP protection, exposure, and connections?
- Do I understand the equity trade-off?
- What services and funding do they provide?
- Do they take equity? How much and when?
- What’s their track record with similar ventures?
- Are their incentives aligned with your vision?
6. Academic Institutions: Partners or Pitfalls?
Universities can provide credibility, resources, and early funding through their tech transfer office (TTO).
Key Questions to Ask:
- Will my IP be managed by the TTO?
- How much say do I have in licensing decisions?
- Are there royalty-sharing agreements in place?
- Can I form a startup while employed here?
You may need to negotiate if you want to commercialize your idea independently.
7. Do it for Purpose, Not Payday
Most founders end up owning only a small percentage of their company by the time a product reaches the market. Do not expect to get rich. Do it because it solves a problem you care about. If it happens to come with a nice paycheck, then that is an added bonus.
Your clinical training and insight give you a unique edge. You already know what’s broken. Use that as your compass.
Conclusion
Innovation isn’t about brilliance, it’s about curiosity, structure, and tenacity (see Table 2). Start small. Protect your work. Choose the right partners. Most importantly, stay anchored in your mission to make GI care better.
Dr. Muratore is based at UNC Rex Digestive Health, Raleigh, North Carolina. She has no conflicts related to this article. Dr. Wechsler is based at the University of North Carolina at Chapel Hill, Chapel Hill, North Carolina. She holds a patent assigned to Trustees of Dartmouth College. Dr. Shah is based at the University of Michigan, Ann Arbor, Michigan. He consults for Ardelyx, Laborie, Neuraxis, Salix, Sanofi, and Takeda and holds a patent with the Regents of the University of Michigan.
When Your First Job Isn’t Forever: Lessons from My Journey and What Early-Career GIs Need to Know
Introduction
For many of us in gastroenterology, landing that first attending job feels like the ultimate victory lap — the reward for all those years of training. We sign the contract, relocate, and imagine this will be our “forever job.” Reality often plays out differently.
In fact, 43% of physicians change jobs within five years, while 83% changed employers at least once in their careers.1 Even within our field — which is always in demand — turnover is high; 1 in 3 gastroenterologists are planning to leave their current role within two years.2 Why does this happen? More importantly, how do we navigate this transition with clarity and confidence as an early-career GI?
My Story: When I Dared to Change My “Forever Job”
When I signed my first attending contract, I didn’t negotiate a single thing. My priorities were simple: family in Toronto and visa requirements. After a decade of medical school, residency, and fellowship, everything else felt secondary. I was happy to be back home.
The job itself was good — reasonable hours, flexible colleagues, and ample opportunity to enhance my procedural skills. As I started carving out my niche in endobariatrics, the support I needed to grow further was not there. I kept telling myself that this job fulfilled my values and I needed to be patient: “this is my forever job. I am close to my family and that’s what matters.”
Then, during a suturing course at the American Society of Gastrointestinal Endoscopy, I had a casual chat with the course director (now my boss). It took me by surprise, but as the conversation continued, he offered me a job. It was tempting: the chance to build my own endobariatrics program with real institutional backing. The catch? It was in a city I had never been to, with no family or friends around. I politely said “no, thank you, I can’t.” He smiled, gave me his number, and said, “think about it.”
For the first time, I allowed myself to ask, “could I really leave my forever job?”
The Power of a Circle and a Spreadsheet
I leaned on my circle — a close group of fellowship friends who each took a turn being someone’s lifeline. We have monthly Zoom calls to talk about jobs, family, and career aspirations. When I shared my dilemma, I realized I wasn’t alone; one friend was also unhappy with her first job. Suddenly, we were asking one another, “can we really leave?”
I hired a career consultant familiar with physician visa issues — hands down, the best money I ever invested. The job search felt like dating: each interview was a first date; some needed a second or third date before I knew if it could be a match.
After every interview, I’d jump on Zoom with my circle. We’d screen-share my giant Excel spreadsheet — our decision matrix — with columns for everything I cared about:
- Institute
- Administrative Time
- Endobariatric support
- Director Title
- Salary
- On-call
- Vacation
- Proximity to airport
- Cost of living
- RVU percentage
- Endoscopy center buy-in
- Contract duration
- Support staff
- CME
We scored each job, line by line, and not a single job checked all the boxes. As I sat there in a state of decision paralysis, it became clear that this was not a simple decision.
The GI Community: A Small, Supportive World
The GI community is incredibly close-knit and kind-hearted. At every conference, I made a point to chat with as many colleagues as I could, to hear their perspectives on jobs and how they made tough career moves. Those conversations were real — no Google search or Excel sheet could offer the perspective and insight I gained by simply asking and leaning on the GI community.
Meanwhile, the person who had first offered me that job kept checking in, catching up at conferences, and bonding over our love for food and baking. With him, I never felt like I was being ‘interviewed’ — I felt valued. It did not feel like he was trying to fill a position with just anyone to improve the call pool. He genuinely wanted to understand what my goals were and how I envisioned my future. Through those conversations, he reminded me of my original passions, which were sidelined when so immersed in the daily routine.
I’ve learned that feeling valued doesn’t come from grand gestures in recruitment. It’s in the quiet signs of respect, trust, and being seen. He wasn’t looking for just anyone; he was looking for someone whose goals aligned with his group’s and someone in whom he wanted to invest. While others might chase the highest salary, the most flexible schedule, or the strongest ancillary support, I realized I valued something I did not realize that I was lacking until then: mentorship.
What I Learned: There is No Such Thing As “The Perfect Job”
After a full year of spreadsheets, Zoom calls, conference chats, and overthinking, I came to a big realization: there’s no perfect job — there’s no such thing as an ideal “forever job.” The only constant for humans is change. Our circumstances change, our priorities shift, our interests shuffle, and our finances evolve. The best job is simply the one that fits the stage of life you’re in at that given moment. For me, mentorship and growth became my top priorities, even if it meant moving away from family.
What Physicians Value Most in a Second Job
After their first job, early-career gastroenterologists often reevaluate what really matters. Recent surveys highlight four key priorities:
- Work-life balance:
In a 2022 CompHealth Group healthcare survey, 85% of physicians ranked work-life balance as their top job priority.3
- Mentorship and growth:
Nearly 1 in 3 physicians cited lack of mentorship or career advancement as their reason for leaving a first job, per the 2023 MGMA/Jackson Physician Search report.4
- Compensation:
While not always the main reason for leaving, 77% of physicians now list compensation as a top priority — a big jump from prior years.3
- Practice support:
Poor infrastructure, administrative overload, or understaffed teams are common dealbreakers. In the second job, physicians look for well-run practices with solid support staff and reduced burnout risk.5
Conclusion
Welcome the uncertainty, talk to your circle, lean on your community, and use a spreadsheet if you need to — but don’t forget to trust your gut. There’s no forever job or the perfect path, only the next move that feels most true to who you are in that moment.
Dr. Ismail (@mayyismail) is Assistant Professor of Clinical Medicine (Gastroenterology) at Temple University in Philadelphia, Pennsylvania. She declares no conflicts of interest.
References
1. CHG Healthcare. Survey: 62% of physicians made a career change in the last two years. CHG Healthcare blog. June 10, 2024. Accessed August 5, 2025.
2. Berg S. Physicians in these 10 specialties are less likely to quit. AMA News. Published June 24, 2025. Accessed July 2025.
3. Saley C. Survey: Work/life balance is #1 priority in physicians’ job search. CHG Healthcare Insights. March 10, 2022. Accessed August 2025.
4. Medical Group Management Association; Jackson Physician Search. Early‑Career Physician Recruiting & Retention Playbook. October 23, 2023. Accessed August 2025.
5. Von Rosenvinge EC, et al. A crisis in scope: Recruitment and retention challenges reported by VA gastroenterology section chiefs. Fed Pract. 2024 Aug. doi:10.12788/fp.0504.
Introduction
For many of us in gastroenterology, landing that first attending job feels like the ultimate victory lap — the reward for all those years of training. We sign the contract, relocate, and imagine this will be our “forever job.” Reality often plays out differently.
In fact, 43% of physicians change jobs within five years, while 83% changed employers at least once in their careers.1 Even within our field — which is always in demand — turnover is high; 1 in 3 gastroenterologists are planning to leave their current role within two years.2 Why does this happen? More importantly, how do we navigate this transition with clarity and confidence as an early-career GI?
My Story: When I Dared to Change My “Forever Job”
When I signed my first attending contract, I didn’t negotiate a single thing. My priorities were simple: family in Toronto and visa requirements. After a decade of medical school, residency, and fellowship, everything else felt secondary. I was happy to be back home.
The job itself was good — reasonable hours, flexible colleagues, and ample opportunity to enhance my procedural skills. As I started carving out my niche in endobariatrics, the support I needed to grow further was not there. I kept telling myself that this job fulfilled my values and I needed to be patient: “this is my forever job. I am close to my family and that’s what matters.”
Then, during a suturing course at the American Society of Gastrointestinal Endoscopy, I had a casual chat with the course director (now my boss). It took me by surprise, but as the conversation continued, he offered me a job. It was tempting: the chance to build my own endobariatrics program with real institutional backing. The catch? It was in a city I had never been to, with no family or friends around. I politely said “no, thank you, I can’t.” He smiled, gave me his number, and said, “think about it.”
For the first time, I allowed myself to ask, “could I really leave my forever job?”
The Power of a Circle and a Spreadsheet
I leaned on my circle — a close group of fellowship friends who each took a turn being someone’s lifeline. We have monthly Zoom calls to talk about jobs, family, and career aspirations. When I shared my dilemma, I realized I wasn’t alone; one friend was also unhappy with her first job. Suddenly, we were asking one another, “can we really leave?”
I hired a career consultant familiar with physician visa issues — hands down, the best money I ever invested. The job search felt like dating: each interview was a first date; some needed a second or third date before I knew if it could be a match.
After every interview, I’d jump on Zoom with my circle. We’d screen-share my giant Excel spreadsheet — our decision matrix — with columns for everything I cared about:
- Institute
- Administrative Time
- Endobariatric support
- Director Title
- Salary
- On-call
- Vacation
- Proximity to airport
- Cost of living
- RVU percentage
- Endoscopy center buy-in
- Contract duration
- Support staff
- CME
We scored each job, line by line, and not a single job checked all the boxes. As I sat there in a state of decision paralysis, it became clear that this was not a simple decision.
The GI Community: A Small, Supportive World
The GI community is incredibly close-knit and kind-hearted. At every conference, I made a point to chat with as many colleagues as I could, to hear their perspectives on jobs and how they made tough career moves. Those conversations were real — no Google search or Excel sheet could offer the perspective and insight I gained by simply asking and leaning on the GI community.
Meanwhile, the person who had first offered me that job kept checking in, catching up at conferences, and bonding over our love for food and baking. With him, I never felt like I was being ‘interviewed’ — I felt valued. It did not feel like he was trying to fill a position with just anyone to improve the call pool. He genuinely wanted to understand what my goals were and how I envisioned my future. Through those conversations, he reminded me of my original passions, which were sidelined when so immersed in the daily routine.
I’ve learned that feeling valued doesn’t come from grand gestures in recruitment. It’s in the quiet signs of respect, trust, and being seen. He wasn’t looking for just anyone; he was looking for someone whose goals aligned with his group’s and someone in whom he wanted to invest. While others might chase the highest salary, the most flexible schedule, or the strongest ancillary support, I realized I valued something I did not realize that I was lacking until then: mentorship.
What I Learned: There is No Such Thing As “The Perfect Job”
After a full year of spreadsheets, Zoom calls, conference chats, and overthinking, I came to a big realization: there’s no perfect job — there’s no such thing as an ideal “forever job.” The only constant for humans is change. Our circumstances change, our priorities shift, our interests shuffle, and our finances evolve. The best job is simply the one that fits the stage of life you’re in at that given moment. For me, mentorship and growth became my top priorities, even if it meant moving away from family.
What Physicians Value Most in a Second Job
After their first job, early-career gastroenterologists often reevaluate what really matters. Recent surveys highlight four key priorities:
- Work-life balance:
In a 2022 CompHealth Group healthcare survey, 85% of physicians ranked work-life balance as their top job priority.3
- Mentorship and growth:
Nearly 1 in 3 physicians cited lack of mentorship or career advancement as their reason for leaving a first job, per the 2023 MGMA/Jackson Physician Search report.4
- Compensation:
While not always the main reason for leaving, 77% of physicians now list compensation as a top priority — a big jump from prior years.3
- Practice support:
Poor infrastructure, administrative overload, or understaffed teams are common dealbreakers. In the second job, physicians look for well-run practices with solid support staff and reduced burnout risk.5
Conclusion
Welcome the uncertainty, talk to your circle, lean on your community, and use a spreadsheet if you need to — but don’t forget to trust your gut. There’s no forever job or the perfect path, only the next move that feels most true to who you are in that moment.
Dr. Ismail (@mayyismail) is Assistant Professor of Clinical Medicine (Gastroenterology) at Temple University in Philadelphia, Pennsylvania. She declares no conflicts of interest.
References
1. CHG Healthcare. Survey: 62% of physicians made a career change in the last two years. CHG Healthcare blog. June 10, 2024. Accessed August 5, 2025.
2. Berg S. Physicians in these 10 specialties are less likely to quit. AMA News. Published June 24, 2025. Accessed July 2025.
3. Saley C. Survey: Work/life balance is #1 priority in physicians’ job search. CHG Healthcare Insights. March 10, 2022. Accessed August 2025.
4. Medical Group Management Association; Jackson Physician Search. Early‑Career Physician Recruiting & Retention Playbook. October 23, 2023. Accessed August 2025.
5. Von Rosenvinge EC, et al. A crisis in scope: Recruitment and retention challenges reported by VA gastroenterology section chiefs. Fed Pract. 2024 Aug. doi:10.12788/fp.0504.
Introduction
For many of us in gastroenterology, landing that first attending job feels like the ultimate victory lap — the reward for all those years of training. We sign the contract, relocate, and imagine this will be our “forever job.” Reality often plays out differently.
In fact, 43% of physicians change jobs within five years, while 83% changed employers at least once in their careers.1 Even within our field — which is always in demand — turnover is high; 1 in 3 gastroenterologists are planning to leave their current role within two years.2 Why does this happen? More importantly, how do we navigate this transition with clarity and confidence as an early-career GI?
My Story: When I Dared to Change My “Forever Job”
When I signed my first attending contract, I didn’t negotiate a single thing. My priorities were simple: family in Toronto and visa requirements. After a decade of medical school, residency, and fellowship, everything else felt secondary. I was happy to be back home.
The job itself was good — reasonable hours, flexible colleagues, and ample opportunity to enhance my procedural skills. As I started carving out my niche in endobariatrics, the support I needed to grow further was not there. I kept telling myself that this job fulfilled my values and I needed to be patient: “this is my forever job. I am close to my family and that’s what matters.”
Then, during a suturing course at the American Society of Gastrointestinal Endoscopy, I had a casual chat with the course director (now my boss). It took me by surprise, but as the conversation continued, he offered me a job. It was tempting: the chance to build my own endobariatrics program with real institutional backing. The catch? It was in a city I had never been to, with no family or friends around. I politely said “no, thank you, I can’t.” He smiled, gave me his number, and said, “think about it.”
For the first time, I allowed myself to ask, “could I really leave my forever job?”
The Power of a Circle and a Spreadsheet
I leaned on my circle — a close group of fellowship friends who each took a turn being someone’s lifeline. We have monthly Zoom calls to talk about jobs, family, and career aspirations. When I shared my dilemma, I realized I wasn’t alone; one friend was also unhappy with her first job. Suddenly, we were asking one another, “can we really leave?”
I hired a career consultant familiar with physician visa issues — hands down, the best money I ever invested. The job search felt like dating: each interview was a first date; some needed a second or third date before I knew if it could be a match.
After every interview, I’d jump on Zoom with my circle. We’d screen-share my giant Excel spreadsheet — our decision matrix — with columns for everything I cared about:
- Institute
- Administrative Time
- Endobariatric support
- Director Title
- Salary
- On-call
- Vacation
- Proximity to airport
- Cost of living
- RVU percentage
- Endoscopy center buy-in
- Contract duration
- Support staff
- CME
We scored each job, line by line, and not a single job checked all the boxes. As I sat there in a state of decision paralysis, it became clear that this was not a simple decision.
The GI Community: A Small, Supportive World
The GI community is incredibly close-knit and kind-hearted. At every conference, I made a point to chat with as many colleagues as I could, to hear their perspectives on jobs and how they made tough career moves. Those conversations were real — no Google search or Excel sheet could offer the perspective and insight I gained by simply asking and leaning on the GI community.
Meanwhile, the person who had first offered me that job kept checking in, catching up at conferences, and bonding over our love for food and baking. With him, I never felt like I was being ‘interviewed’ — I felt valued. It did not feel like he was trying to fill a position with just anyone to improve the call pool. He genuinely wanted to understand what my goals were and how I envisioned my future. Through those conversations, he reminded me of my original passions, which were sidelined when so immersed in the daily routine.
I’ve learned that feeling valued doesn’t come from grand gestures in recruitment. It’s in the quiet signs of respect, trust, and being seen. He wasn’t looking for just anyone; he was looking for someone whose goals aligned with his group’s and someone in whom he wanted to invest. While others might chase the highest salary, the most flexible schedule, or the strongest ancillary support, I realized I valued something I did not realize that I was lacking until then: mentorship.
What I Learned: There is No Such Thing As “The Perfect Job”
After a full year of spreadsheets, Zoom calls, conference chats, and overthinking, I came to a big realization: there’s no perfect job — there’s no such thing as an ideal “forever job.” The only constant for humans is change. Our circumstances change, our priorities shift, our interests shuffle, and our finances evolve. The best job is simply the one that fits the stage of life you’re in at that given moment. For me, mentorship and growth became my top priorities, even if it meant moving away from family.
What Physicians Value Most in a Second Job
After their first job, early-career gastroenterologists often reevaluate what really matters. Recent surveys highlight four key priorities:
- Work-life balance:
In a 2022 CompHealth Group healthcare survey, 85% of physicians ranked work-life balance as their top job priority.3
- Mentorship and growth:
Nearly 1 in 3 physicians cited lack of mentorship or career advancement as their reason for leaving a first job, per the 2023 MGMA/Jackson Physician Search report.4
- Compensation:
While not always the main reason for leaving, 77% of physicians now list compensation as a top priority — a big jump from prior years.3
- Practice support:
Poor infrastructure, administrative overload, or understaffed teams are common dealbreakers. In the second job, physicians look for well-run practices with solid support staff and reduced burnout risk.5
Conclusion
Welcome the uncertainty, talk to your circle, lean on your community, and use a spreadsheet if you need to — but don’t forget to trust your gut. There’s no forever job or the perfect path, only the next move that feels most true to who you are in that moment.
Dr. Ismail (@mayyismail) is Assistant Professor of Clinical Medicine (Gastroenterology) at Temple University in Philadelphia, Pennsylvania. She declares no conflicts of interest.
References
1. CHG Healthcare. Survey: 62% of physicians made a career change in the last two years. CHG Healthcare blog. June 10, 2024. Accessed August 5, 2025.
2. Berg S. Physicians in these 10 specialties are less likely to quit. AMA News. Published June 24, 2025. Accessed July 2025.
3. Saley C. Survey: Work/life balance is #1 priority in physicians’ job search. CHG Healthcare Insights. March 10, 2022. Accessed August 2025.
4. Medical Group Management Association; Jackson Physician Search. Early‑Career Physician Recruiting & Retention Playbook. October 23, 2023. Accessed August 2025.
5. Von Rosenvinge EC, et al. A crisis in scope: Recruitment and retention challenges reported by VA gastroenterology section chiefs. Fed Pract. 2024 Aug. doi:10.12788/fp.0504.
How Are The Most Vulnerable With Cancer Using Patient Portals?
TOPLINE:
Electronic health records patient portal signup rates were lower among vulnerable oncology patients at 64%, compared with 87% in nonvulnerable patients. Once adopted, both groups showed comparable meaningful use patterns. Non-English language emerged as a significant barrier to initial portal signup.
METHODOLOGY:
- Portal usage disparities persist across age, race, ethnicity, and health literacy groups, particularly at the initial signup stage.
- Oral anticancer medications represent a new frontier in cancer therapy, offering convenience but requiring high medication adherence and vigilant self-monitoring of symptoms.
- Researchers conducted a retrospective analysis of 280 patients who had recently started taking an oral anticancer medication at Tufts Medical Center, Boston, between October 2022 and March 2024.
- Vulnerability criteria included having an age ≥ 75 years, a non-English language preference, or subsidized insurance (Medicaid only or Medicare with Medicaid as secondary insurance).
- Analysis defined active portal use as having at least one message, while meaningful use was characterized by patient-provider bidirectional messaging.
- Portal messaging proxy use was determined through message content screening, particularly when non-English speaking patients sent messages in English or when message content indicated proxy use.
TAKEAWAY:
- Among the study population, 56% met vulnerability criteria, with 20% aged at least 75 years, 26% having a non-English language, and 30% having subsidized insurance.
- Non-English language was associated with lower portal signup rates (odds ratio [OR], 0.27; 95% CI, 0.15-0.49; P < .0001), whereas age and insurance status showed no significant association.
- Proxy messaging was utilized by 17% of vulnerable patients who signed up for the portal compared to 2.8% of nonvulnerable patients.
- Among patients who signed up for the portal, 31% used it specifically for communication about oral anticancer medications.
IN PRACTICE:
“Although patient portal signup was lower among vulnerable patients, once adopted, vulnerable patients demonstrated comparable meaningful use and greater proxy engagement. Fostering patient portal adoption requires a targeted approach with patient navigation and patient proxy engagement,” wrote the authors of the study.
SOURCE:
The study was led by Yenong Cao, MD, PhD, Boston Medical Center, Boston. It was published online on November 19 in JCO Oncology Practice.
LIMITATIONS:
The study was limited by its retrospective single-center design at Tufts Medical Center, which serves a large number of non-English, Chinese-speaking patients, potentially affecting the generalizability of findings. Additionally, formal proxy login identification was lacking in the Epic documentation during the study period, which may have led to underestimation of proxy portal use.
DISCLOSURES:
Cao reported being employed at Tufts Medical Center. Johnson Ching, PharmD, CSP, disclosed being employed at Duke University Hospital and SpeciaRx, LLC. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Electronic health records patient portal signup rates were lower among vulnerable oncology patients at 64%, compared with 87% in nonvulnerable patients. Once adopted, both groups showed comparable meaningful use patterns. Non-English language emerged as a significant barrier to initial portal signup.
METHODOLOGY:
- Portal usage disparities persist across age, race, ethnicity, and health literacy groups, particularly at the initial signup stage.
- Oral anticancer medications represent a new frontier in cancer therapy, offering convenience but requiring high medication adherence and vigilant self-monitoring of symptoms.
- Researchers conducted a retrospective analysis of 280 patients who had recently started taking an oral anticancer medication at Tufts Medical Center, Boston, between October 2022 and March 2024.
- Vulnerability criteria included having an age ≥ 75 years, a non-English language preference, or subsidized insurance (Medicaid only or Medicare with Medicaid as secondary insurance).
- Analysis defined active portal use as having at least one message, while meaningful use was characterized by patient-provider bidirectional messaging.
- Portal messaging proxy use was determined through message content screening, particularly when non-English speaking patients sent messages in English or when message content indicated proxy use.
TAKEAWAY:
- Among the study population, 56% met vulnerability criteria, with 20% aged at least 75 years, 26% having a non-English language, and 30% having subsidized insurance.
- Non-English language was associated with lower portal signup rates (odds ratio [OR], 0.27; 95% CI, 0.15-0.49; P < .0001), whereas age and insurance status showed no significant association.
- Proxy messaging was utilized by 17% of vulnerable patients who signed up for the portal compared to 2.8% of nonvulnerable patients.
- Among patients who signed up for the portal, 31% used it specifically for communication about oral anticancer medications.
IN PRACTICE:
“Although patient portal signup was lower among vulnerable patients, once adopted, vulnerable patients demonstrated comparable meaningful use and greater proxy engagement. Fostering patient portal adoption requires a targeted approach with patient navigation and patient proxy engagement,” wrote the authors of the study.
SOURCE:
The study was led by Yenong Cao, MD, PhD, Boston Medical Center, Boston. It was published online on November 19 in JCO Oncology Practice.
LIMITATIONS:
The study was limited by its retrospective single-center design at Tufts Medical Center, which serves a large number of non-English, Chinese-speaking patients, potentially affecting the generalizability of findings. Additionally, formal proxy login identification was lacking in the Epic documentation during the study period, which may have led to underestimation of proxy portal use.
DISCLOSURES:
Cao reported being employed at Tufts Medical Center. Johnson Ching, PharmD, CSP, disclosed being employed at Duke University Hospital and SpeciaRx, LLC. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Electronic health records patient portal signup rates were lower among vulnerable oncology patients at 64%, compared with 87% in nonvulnerable patients. Once adopted, both groups showed comparable meaningful use patterns. Non-English language emerged as a significant barrier to initial portal signup.
METHODOLOGY:
- Portal usage disparities persist across age, race, ethnicity, and health literacy groups, particularly at the initial signup stage.
- Oral anticancer medications represent a new frontier in cancer therapy, offering convenience but requiring high medication adherence and vigilant self-monitoring of symptoms.
- Researchers conducted a retrospective analysis of 280 patients who had recently started taking an oral anticancer medication at Tufts Medical Center, Boston, between October 2022 and March 2024.
- Vulnerability criteria included having an age ≥ 75 years, a non-English language preference, or subsidized insurance (Medicaid only or Medicare with Medicaid as secondary insurance).
- Analysis defined active portal use as having at least one message, while meaningful use was characterized by patient-provider bidirectional messaging.
- Portal messaging proxy use was determined through message content screening, particularly when non-English speaking patients sent messages in English or when message content indicated proxy use.
TAKEAWAY:
- Among the study population, 56% met vulnerability criteria, with 20% aged at least 75 years, 26% having a non-English language, and 30% having subsidized insurance.
- Non-English language was associated with lower portal signup rates (odds ratio [OR], 0.27; 95% CI, 0.15-0.49; P < .0001), whereas age and insurance status showed no significant association.
- Proxy messaging was utilized by 17% of vulnerable patients who signed up for the portal compared to 2.8% of nonvulnerable patients.
- Among patients who signed up for the portal, 31% used it specifically for communication about oral anticancer medications.
IN PRACTICE:
“Although patient portal signup was lower among vulnerable patients, once adopted, vulnerable patients demonstrated comparable meaningful use and greater proxy engagement. Fostering patient portal adoption requires a targeted approach with patient navigation and patient proxy engagement,” wrote the authors of the study.
SOURCE:
The study was led by Yenong Cao, MD, PhD, Boston Medical Center, Boston. It was published online on November 19 in JCO Oncology Practice.
LIMITATIONS:
The study was limited by its retrospective single-center design at Tufts Medical Center, which serves a large number of non-English, Chinese-speaking patients, potentially affecting the generalizability of findings. Additionally, formal proxy login identification was lacking in the Epic documentation during the study period, which may have led to underestimation of proxy portal use.
DISCLOSURES:
Cao reported being employed at Tufts Medical Center. Johnson Ching, PharmD, CSP, disclosed being employed at Duke University Hospital and SpeciaRx, LLC. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
YesRx: Michigan Program Turns Cancer Drug Waste Into Hope
Jerome Winegarden, MD, had bad news to deliver. A patient’s cancer was progressing, and the patient would need to stop his oral cancer medication.
That would normally mean tossing a 30-day supply of pills, said Winegarden, an oncologist with Trinity Health, a statewide health system in Michigan.
But not in this case.
Winegarden pointed to a sign on his exam room wall from YesRx, a nonprofit cancer drug repository program, that read: “Thank you, Michiganders! Donating cancer medication and supportive medication helps patients in Michigan.”
When Winegarden suggested donating the pills to YesRx, the patient was grateful. Turning a bad situation into hope for somebody else is “very powerful for patients,” Winegarden said. “We were going to be able to do something with [the medication], not just destroy it.”
In just 2 years of operation, YesRx has accepted donations and provided oral cancer or supportive care medications worth millions of dollars to nearly 1200 patients, at no cost to them, according to a recent analysis assessing the Michigan-based program. These patients couldn’t afford their prescribed medications or required immediate access and couldn’t wait for insurance approval, the researchers reported. The donated unopened or unused medications would otherwise have been wasted.
“This program is exactly what patients need: a safe way of recycling their unused prescriptions that actually benefits others with cancer,” said Fumiko Chino, MD, associate professor at MD Anderson Cancer Center, Houston, Texas, in a statement on YesRx.
Filling a Need
A growing body of research shows that patients with cancer face an increased risk for financial toxicity, given the high costs of oral cancer drugs as well as changes to insurance coverage that may require greater cost sharing by the patient. The financial burden on patients can be significant, with more than half reporting trouble affording their medications, an issue that can lead to persistent medical debt as well as gaps or delays in care that may impact patient outcomes.
Alongside the affordability problem is one of waste. A 2023 analysis found that the mean cost of drug waste associated with dose reductions or discontinuations of oral anticancer drugs came to $4290 per patient.
The YesRx program, however, turns that negative into a positive.
If YesRx has a relevant drug in stock, “we can get the medication into the patient’s hands within 24-to-48 hours,” said Maja Gibbons, PharmD, an oncology pharmacy specialist with Corewell Health in Grand Rapids, Michigan.
Facilitating quick access is one key goal of the program, said YesRx co-founder and chief medical officer Emily Mackler, PharmD, who led the recent analysis. “All the things we’re trying to do are to make sure that the patient doesn’t experience those gaps that can really be critical for their outcomes,” Mackler this news organization.
The drug repository concept has been around for decades. While there is no federal program, 29 states have general drug repository programs, according to the National Conference of State Legislatures.
One of the oldest repositories, Iowa’s SafeNetRx, which started in 2001, reports that it has given free medications worth $155 million to almost 161,000 patients. SafeNetRx also began a partnership with state cancer centers to boost oral anticancer drug donations. From 2016 to 2022, the repository donated 84,000 chemotherapy doses worth $15 million to patients in need, reported Natalie K. Heater and colleagues at Northwestern University in Health Affairs Scholar.
In addition to Iowa, four other states have cancer drug repositories: Florida, Montana, Nebraska, and Michigan.
Michigan enacted a drug repository law in 2006, but YesRx did not start until 2023. The Michigan Oncology Quality Consortium, Blue Cross Blue Shield of Michigan, Trinity Health, and the Michigan Society of Hematology and Oncology provided funding to get YesRx off the ground. YesRx, which grew from nine sites in 2023 to 105 in July 2025, helps new sites get certified as a repository by the state.
The program accepts donations of any room-temperature oral cancer or supportive care medication that is in its original, sealed manufacturer packaging and has at least 6 months before it expires. Controlled substances are not eligible, but medications such as anticoagulants and antiemetics are. Donations are sent by overnight delivery to Trinity Pharmacy at Reichert Health. Trinity receives and inspects donations, and redispenses medications for all YesRx participants.
Nearly 1600 people have donated oral cancer medications, valued at $28.6 million, according to the 2-year look at the program. “I am blown away by how many donations come in,” Mackler this news organization.
In the first 24 months, 1171 patients received, on average, a 1-month supply of a medication worth $18.4 million, at no cost. Slightly more than half (53%) were age 65 or older. The most common diagnoses among recipients were breast cancer (28%), leukemia (18%), lung cancer (12%), and prostate cancer (9%).
A survey about the program revealed that recipients spanned about 90% of Michigan counties, with around 40% living in rural areas. Survey respondents highlighted the value of YesRx, with most saying it was easy to use and that they could not have provided this assistance without support from the program.
“YesRx can kind of swoop in,” said Winegarden. When a new prescription presents an issue for a patient, Winegarden checks if YesRx has a 30-day supply of the drug. If it does, patients “can get started on their treatment while we figure out the financial piece of it.”
Gibbons connects with patients in need through oncologists and financial navigators, as well as education sessions she runs for patients starting treatment. The Corewell location in Grand Rapids also holds “YesRx Donation Days,” when patients and caregivers can drop off medications.
In just over a year, Corewell has provided “more than half a million dollars’ worth of medication to our cancer patients,” she said. “It’s just a large relief for patients to know that this is going to be able to help someone else out,” said Gibbons.
Many of the cancer drugs “can be challenging for patients to get rid of,” Gibbons said. YesRx “is helping make sure that these medications don’t end up in things like landfills and water systems where they should not be.”
Mackler says she has big plans for expanding access. Next on the agenda is to enlist more practices in rural areas, especially in Michigan’s Upper Peninsula.
“We want to be accessible to anyone in the state with cancer,” said Mackler. “We would love to be able to help other states get to this point as well.”
Winegarden and Gibbons have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jerome Winegarden, MD, had bad news to deliver. A patient’s cancer was progressing, and the patient would need to stop his oral cancer medication.
That would normally mean tossing a 30-day supply of pills, said Winegarden, an oncologist with Trinity Health, a statewide health system in Michigan.
But not in this case.
Winegarden pointed to a sign on his exam room wall from YesRx, a nonprofit cancer drug repository program, that read: “Thank you, Michiganders! Donating cancer medication and supportive medication helps patients in Michigan.”
When Winegarden suggested donating the pills to YesRx, the patient was grateful. Turning a bad situation into hope for somebody else is “very powerful for patients,” Winegarden said. “We were going to be able to do something with [the medication], not just destroy it.”
In just 2 years of operation, YesRx has accepted donations and provided oral cancer or supportive care medications worth millions of dollars to nearly 1200 patients, at no cost to them, according to a recent analysis assessing the Michigan-based program. These patients couldn’t afford their prescribed medications or required immediate access and couldn’t wait for insurance approval, the researchers reported. The donated unopened or unused medications would otherwise have been wasted.
“This program is exactly what patients need: a safe way of recycling their unused prescriptions that actually benefits others with cancer,” said Fumiko Chino, MD, associate professor at MD Anderson Cancer Center, Houston, Texas, in a statement on YesRx.
Filling a Need
A growing body of research shows that patients with cancer face an increased risk for financial toxicity, given the high costs of oral cancer drugs as well as changes to insurance coverage that may require greater cost sharing by the patient. The financial burden on patients can be significant, with more than half reporting trouble affording their medications, an issue that can lead to persistent medical debt as well as gaps or delays in care that may impact patient outcomes.
Alongside the affordability problem is one of waste. A 2023 analysis found that the mean cost of drug waste associated with dose reductions or discontinuations of oral anticancer drugs came to $4290 per patient.
The YesRx program, however, turns that negative into a positive.
If YesRx has a relevant drug in stock, “we can get the medication into the patient’s hands within 24-to-48 hours,” said Maja Gibbons, PharmD, an oncology pharmacy specialist with Corewell Health in Grand Rapids, Michigan.
Facilitating quick access is one key goal of the program, said YesRx co-founder and chief medical officer Emily Mackler, PharmD, who led the recent analysis. “All the things we’re trying to do are to make sure that the patient doesn’t experience those gaps that can really be critical for their outcomes,” Mackler this news organization.
The drug repository concept has been around for decades. While there is no federal program, 29 states have general drug repository programs, according to the National Conference of State Legislatures.
One of the oldest repositories, Iowa’s SafeNetRx, which started in 2001, reports that it has given free medications worth $155 million to almost 161,000 patients. SafeNetRx also began a partnership with state cancer centers to boost oral anticancer drug donations. From 2016 to 2022, the repository donated 84,000 chemotherapy doses worth $15 million to patients in need, reported Natalie K. Heater and colleagues at Northwestern University in Health Affairs Scholar.
In addition to Iowa, four other states have cancer drug repositories: Florida, Montana, Nebraska, and Michigan.
Michigan enacted a drug repository law in 2006, but YesRx did not start until 2023. The Michigan Oncology Quality Consortium, Blue Cross Blue Shield of Michigan, Trinity Health, and the Michigan Society of Hematology and Oncology provided funding to get YesRx off the ground. YesRx, which grew from nine sites in 2023 to 105 in July 2025, helps new sites get certified as a repository by the state.
The program accepts donations of any room-temperature oral cancer or supportive care medication that is in its original, sealed manufacturer packaging and has at least 6 months before it expires. Controlled substances are not eligible, but medications such as anticoagulants and antiemetics are. Donations are sent by overnight delivery to Trinity Pharmacy at Reichert Health. Trinity receives and inspects donations, and redispenses medications for all YesRx participants.
Nearly 1600 people have donated oral cancer medications, valued at $28.6 million, according to the 2-year look at the program. “I am blown away by how many donations come in,” Mackler this news organization.
In the first 24 months, 1171 patients received, on average, a 1-month supply of a medication worth $18.4 million, at no cost. Slightly more than half (53%) were age 65 or older. The most common diagnoses among recipients were breast cancer (28%), leukemia (18%), lung cancer (12%), and prostate cancer (9%).
A survey about the program revealed that recipients spanned about 90% of Michigan counties, with around 40% living in rural areas. Survey respondents highlighted the value of YesRx, with most saying it was easy to use and that they could not have provided this assistance without support from the program.
“YesRx can kind of swoop in,” said Winegarden. When a new prescription presents an issue for a patient, Winegarden checks if YesRx has a 30-day supply of the drug. If it does, patients “can get started on their treatment while we figure out the financial piece of it.”
Gibbons connects with patients in need through oncologists and financial navigators, as well as education sessions she runs for patients starting treatment. The Corewell location in Grand Rapids also holds “YesRx Donation Days,” when patients and caregivers can drop off medications.
In just over a year, Corewell has provided “more than half a million dollars’ worth of medication to our cancer patients,” she said. “It’s just a large relief for patients to know that this is going to be able to help someone else out,” said Gibbons.
Many of the cancer drugs “can be challenging for patients to get rid of,” Gibbons said. YesRx “is helping make sure that these medications don’t end up in things like landfills and water systems where they should not be.”
Mackler says she has big plans for expanding access. Next on the agenda is to enlist more practices in rural areas, especially in Michigan’s Upper Peninsula.
“We want to be accessible to anyone in the state with cancer,” said Mackler. “We would love to be able to help other states get to this point as well.”
Winegarden and Gibbons have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jerome Winegarden, MD, had bad news to deliver. A patient’s cancer was progressing, and the patient would need to stop his oral cancer medication.
That would normally mean tossing a 30-day supply of pills, said Winegarden, an oncologist with Trinity Health, a statewide health system in Michigan.
But not in this case.
Winegarden pointed to a sign on his exam room wall from YesRx, a nonprofit cancer drug repository program, that read: “Thank you, Michiganders! Donating cancer medication and supportive medication helps patients in Michigan.”
When Winegarden suggested donating the pills to YesRx, the patient was grateful. Turning a bad situation into hope for somebody else is “very powerful for patients,” Winegarden said. “We were going to be able to do something with [the medication], not just destroy it.”
In just 2 years of operation, YesRx has accepted donations and provided oral cancer or supportive care medications worth millions of dollars to nearly 1200 patients, at no cost to them, according to a recent analysis assessing the Michigan-based program. These patients couldn’t afford their prescribed medications or required immediate access and couldn’t wait for insurance approval, the researchers reported. The donated unopened or unused medications would otherwise have been wasted.
“This program is exactly what patients need: a safe way of recycling their unused prescriptions that actually benefits others with cancer,” said Fumiko Chino, MD, associate professor at MD Anderson Cancer Center, Houston, Texas, in a statement on YesRx.
Filling a Need
A growing body of research shows that patients with cancer face an increased risk for financial toxicity, given the high costs of oral cancer drugs as well as changes to insurance coverage that may require greater cost sharing by the patient. The financial burden on patients can be significant, with more than half reporting trouble affording their medications, an issue that can lead to persistent medical debt as well as gaps or delays in care that may impact patient outcomes.
Alongside the affordability problem is one of waste. A 2023 analysis found that the mean cost of drug waste associated with dose reductions or discontinuations of oral anticancer drugs came to $4290 per patient.
The YesRx program, however, turns that negative into a positive.
If YesRx has a relevant drug in stock, “we can get the medication into the patient’s hands within 24-to-48 hours,” said Maja Gibbons, PharmD, an oncology pharmacy specialist with Corewell Health in Grand Rapids, Michigan.
Facilitating quick access is one key goal of the program, said YesRx co-founder and chief medical officer Emily Mackler, PharmD, who led the recent analysis. “All the things we’re trying to do are to make sure that the patient doesn’t experience those gaps that can really be critical for their outcomes,” Mackler this news organization.
The drug repository concept has been around for decades. While there is no federal program, 29 states have general drug repository programs, according to the National Conference of State Legislatures.
One of the oldest repositories, Iowa’s SafeNetRx, which started in 2001, reports that it has given free medications worth $155 million to almost 161,000 patients. SafeNetRx also began a partnership with state cancer centers to boost oral anticancer drug donations. From 2016 to 2022, the repository donated 84,000 chemotherapy doses worth $15 million to patients in need, reported Natalie K. Heater and colleagues at Northwestern University in Health Affairs Scholar.
In addition to Iowa, four other states have cancer drug repositories: Florida, Montana, Nebraska, and Michigan.
Michigan enacted a drug repository law in 2006, but YesRx did not start until 2023. The Michigan Oncology Quality Consortium, Blue Cross Blue Shield of Michigan, Trinity Health, and the Michigan Society of Hematology and Oncology provided funding to get YesRx off the ground. YesRx, which grew from nine sites in 2023 to 105 in July 2025, helps new sites get certified as a repository by the state.
The program accepts donations of any room-temperature oral cancer or supportive care medication that is in its original, sealed manufacturer packaging and has at least 6 months before it expires. Controlled substances are not eligible, but medications such as anticoagulants and antiemetics are. Donations are sent by overnight delivery to Trinity Pharmacy at Reichert Health. Trinity receives and inspects donations, and redispenses medications for all YesRx participants.
Nearly 1600 people have donated oral cancer medications, valued at $28.6 million, according to the 2-year look at the program. “I am blown away by how many donations come in,” Mackler this news organization.
In the first 24 months, 1171 patients received, on average, a 1-month supply of a medication worth $18.4 million, at no cost. Slightly more than half (53%) were age 65 or older. The most common diagnoses among recipients were breast cancer (28%), leukemia (18%), lung cancer (12%), and prostate cancer (9%).
A survey about the program revealed that recipients spanned about 90% of Michigan counties, with around 40% living in rural areas. Survey respondents highlighted the value of YesRx, with most saying it was easy to use and that they could not have provided this assistance without support from the program.
“YesRx can kind of swoop in,” said Winegarden. When a new prescription presents an issue for a patient, Winegarden checks if YesRx has a 30-day supply of the drug. If it does, patients “can get started on their treatment while we figure out the financial piece of it.”
Gibbons connects with patients in need through oncologists and financial navigators, as well as education sessions she runs for patients starting treatment. The Corewell location in Grand Rapids also holds “YesRx Donation Days,” when patients and caregivers can drop off medications.
In just over a year, Corewell has provided “more than half a million dollars’ worth of medication to our cancer patients,” she said. “It’s just a large relief for patients to know that this is going to be able to help someone else out,” said Gibbons.
Many of the cancer drugs “can be challenging for patients to get rid of,” Gibbons said. YesRx “is helping make sure that these medications don’t end up in things like landfills and water systems where they should not be.”
Mackler says she has big plans for expanding access. Next on the agenda is to enlist more practices in rural areas, especially in Michigan’s Upper Peninsula.
“We want to be accessible to anyone in the state with cancer,” said Mackler. “We would love to be able to help other states get to this point as well.”
Winegarden and Gibbons have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Patient Portal That Patients Can’t Navigate
Beth Cavanaugh, 79, was starting a new medication when she ran into a modern hurdle: Her doctor’s office required all follow–up questions, even those about side effects of the drug, to go through the patient portal.
Cavanaugh said she did not know how to set up or use the system.
“I tried to explain that, but the receptionist said that was the only way to contact the doctor. I felt lost,” said Cavanaugh, a retired psychotherapist near Albany, New York.
Cavanaugh is far from alone. Many older people balk at the idea of communicating with their physicians over the internet. They may have limited digital skills, have physical challenges, or simply prefer human connection.
As medicine leans harder on electronic portals and telehealth, these patients are finding themselves shut out of their own care. Experts warn this approach deepens inequities in access to care and can worsen health outcomes.
Clinicians should “offer options for various types of communication, such as phone calls or texts, because whenever an older adult — or anyone, for that matter — is given a choice, they feel more empowered and more committed to their care,” said Susan Wehry, MD, associate clinical professor at the University of New England College of Osteopathic Medicine in Biddeford, Maine.
Tech Support
Use of medical communication tools varies among older adults. One study in JAMA Network Open found nearly two thirds of those older than 65 years who filled out surveys via phone or internet had used a patient portal, while a little under half used telehealth, and only 44% used a medical health application.
Older patients tend to fall into two camps, said Neela Patel, MD, MPH, CMD, chief of the Division of Geriatrics and Supportive Care at the UT Health San Antonio.
Her patients “are at two extremes of the spectrum — some technologically savvy and others with limited digital literacy or limited or no access to the Internet,” Patel, who is also the vice chair of the Health Systems Innovations and Technology Committee of the American Geriatric Society, said.
Patel’s practice has dedicated staff to help patients master certain technologies. For example, a pharmacist teaches patients how to use a glucometer and a blood pressure cuff. Other staff teach them how to use smartphone apps that track blood pressure or glucose.
She usually sees patients in person before offering telehealth as an option, ensuring the person has “enough digital literacy to utilize them and that the patient can see and hear the visit.”
If technological limitations impede a telehealth appointment, clinicians can help patients navigate their computer screen. Patel recounted the story of an older woman who was unable to come to the clinic in person, so had a telehealth visit instead.
“She had trouble hearing me, so I asked her to share her screen with me. I walked her through how to do that. Then I showed her where the ‘volume’ button was located. It turns out her volume was at zero,” Patel said. “Once that was adjusted, we were able to proceed with the appointment.”
Educating older adults on how to use health technology does not have to fall upon clinicians and their staff, according to Wehry. She routinely refers her patients to community resources to help them develop digital skills.
Local libraries and community centers often offer digital education. Some retirement communities and assisted living facilities also have tech support personnel or classes available to residents.
Wehry refers some of her patients to the National Digital Equity Center which teaches older adults how to hold a telehealth visit.
Roughly 90% of Patel’s patients are signed up for the patient portal, but they may not be operating the technology, she said. She advises these patients to ask their children or caregivers for help as appropriate.
Teaching patients to use the communication technology early on can also be helpful in other ways. If patients who have been technologically proficient start having difficulty, “it’s a clue there may be cognitive changes, and we follow up on those,” Patel said.
Additional resources to help older adults develop digital competence include Cyber Seniors, Older Adults Technology Services, AARP, AARP Find Digital Courses, Area Agencies on Aging, and Senior Navigator.
Human Touch
Some older adults may simply want a more traditional means of communicating with their clinician. A review of 29 papers, encompassing over 6200 adults older than 60 years, identified several domains affecting the adoption of healthcare technology, two of which were resistance to new technology and having family or friends that could help with.
Wehry said many older adults “don’t resist this technology because they’re unable to figure out how to use it. Instead, they see the technology as too impersonal.”
One study found many older adults fear technologies may end up replacing face-to-face contact.
“I’m beginning to encourage primary care providers to take a step back and refocus on the doctor-patient relationship. When communication is limited to the technological approach, it can erode trust in that relationship,” Wehry said.
The American Medical Association recommends clinicians “provide a method other than electronic communication for patients who are without technological proficiency or access.”
Some busy clinicians might be concerned phone calls will be too time-consuming, Wehry said. Patients should be informed of hours of phone availability, how much time is allotted to calls, and how many days or hours a response may take. Clinicians might also use tools that allow patients to use their cell phone to text their practice with medical questions.
Cavanaugh ended up finding technological help from a professional organizer whom she hired to help rearrange her closets.
“She’s knowledgeable and patient, and she’s helping me with the portal,” she said. “If I hadn’t serendipitously found the organizer, I’d still be struggling and unable to access proper medical care.”
Wehry and Patel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Beth Cavanaugh, 79, was starting a new medication when she ran into a modern hurdle: Her doctor’s office required all follow–up questions, even those about side effects of the drug, to go through the patient portal.
Cavanaugh said she did not know how to set up or use the system.
“I tried to explain that, but the receptionist said that was the only way to contact the doctor. I felt lost,” said Cavanaugh, a retired psychotherapist near Albany, New York.
Cavanaugh is far from alone. Many older people balk at the idea of communicating with their physicians over the internet. They may have limited digital skills, have physical challenges, or simply prefer human connection.
As medicine leans harder on electronic portals and telehealth, these patients are finding themselves shut out of their own care. Experts warn this approach deepens inequities in access to care and can worsen health outcomes.
Clinicians should “offer options for various types of communication, such as phone calls or texts, because whenever an older adult — or anyone, for that matter — is given a choice, they feel more empowered and more committed to their care,” said Susan Wehry, MD, associate clinical professor at the University of New England College of Osteopathic Medicine in Biddeford, Maine.
Tech Support
Use of medical communication tools varies among older adults. One study in JAMA Network Open found nearly two thirds of those older than 65 years who filled out surveys via phone or internet had used a patient portal, while a little under half used telehealth, and only 44% used a medical health application.
Older patients tend to fall into two camps, said Neela Patel, MD, MPH, CMD, chief of the Division of Geriatrics and Supportive Care at the UT Health San Antonio.
Her patients “are at two extremes of the spectrum — some technologically savvy and others with limited digital literacy or limited or no access to the Internet,” Patel, who is also the vice chair of the Health Systems Innovations and Technology Committee of the American Geriatric Society, said.
Patel’s practice has dedicated staff to help patients master certain technologies. For example, a pharmacist teaches patients how to use a glucometer and a blood pressure cuff. Other staff teach them how to use smartphone apps that track blood pressure or glucose.
She usually sees patients in person before offering telehealth as an option, ensuring the person has “enough digital literacy to utilize them and that the patient can see and hear the visit.”
If technological limitations impede a telehealth appointment, clinicians can help patients navigate their computer screen. Patel recounted the story of an older woman who was unable to come to the clinic in person, so had a telehealth visit instead.
“She had trouble hearing me, so I asked her to share her screen with me. I walked her through how to do that. Then I showed her where the ‘volume’ button was located. It turns out her volume was at zero,” Patel said. “Once that was adjusted, we were able to proceed with the appointment.”
Educating older adults on how to use health technology does not have to fall upon clinicians and their staff, according to Wehry. She routinely refers her patients to community resources to help them develop digital skills.
Local libraries and community centers often offer digital education. Some retirement communities and assisted living facilities also have tech support personnel or classes available to residents.
Wehry refers some of her patients to the National Digital Equity Center which teaches older adults how to hold a telehealth visit.
Roughly 90% of Patel’s patients are signed up for the patient portal, but they may not be operating the technology, she said. She advises these patients to ask their children or caregivers for help as appropriate.
Teaching patients to use the communication technology early on can also be helpful in other ways. If patients who have been technologically proficient start having difficulty, “it’s a clue there may be cognitive changes, and we follow up on those,” Patel said.
Additional resources to help older adults develop digital competence include Cyber Seniors, Older Adults Technology Services, AARP, AARP Find Digital Courses, Area Agencies on Aging, and Senior Navigator.
Human Touch
Some older adults may simply want a more traditional means of communicating with their clinician. A review of 29 papers, encompassing over 6200 adults older than 60 years, identified several domains affecting the adoption of healthcare technology, two of which were resistance to new technology and having family or friends that could help with.
Wehry said many older adults “don’t resist this technology because they’re unable to figure out how to use it. Instead, they see the technology as too impersonal.”
One study found many older adults fear technologies may end up replacing face-to-face contact.
“I’m beginning to encourage primary care providers to take a step back and refocus on the doctor-patient relationship. When communication is limited to the technological approach, it can erode trust in that relationship,” Wehry said.
The American Medical Association recommends clinicians “provide a method other than electronic communication for patients who are without technological proficiency or access.”
Some busy clinicians might be concerned phone calls will be too time-consuming, Wehry said. Patients should be informed of hours of phone availability, how much time is allotted to calls, and how many days or hours a response may take. Clinicians might also use tools that allow patients to use their cell phone to text their practice with medical questions.
Cavanaugh ended up finding technological help from a professional organizer whom she hired to help rearrange her closets.
“She’s knowledgeable and patient, and she’s helping me with the portal,” she said. “If I hadn’t serendipitously found the organizer, I’d still be struggling and unable to access proper medical care.”
Wehry and Patel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Beth Cavanaugh, 79, was starting a new medication when she ran into a modern hurdle: Her doctor’s office required all follow–up questions, even those about side effects of the drug, to go through the patient portal.
Cavanaugh said she did not know how to set up or use the system.
“I tried to explain that, but the receptionist said that was the only way to contact the doctor. I felt lost,” said Cavanaugh, a retired psychotherapist near Albany, New York.
Cavanaugh is far from alone. Many older people balk at the idea of communicating with their physicians over the internet. They may have limited digital skills, have physical challenges, or simply prefer human connection.
As medicine leans harder on electronic portals and telehealth, these patients are finding themselves shut out of their own care. Experts warn this approach deepens inequities in access to care and can worsen health outcomes.
Clinicians should “offer options for various types of communication, such as phone calls or texts, because whenever an older adult — or anyone, for that matter — is given a choice, they feel more empowered and more committed to their care,” said Susan Wehry, MD, associate clinical professor at the University of New England College of Osteopathic Medicine in Biddeford, Maine.
Tech Support
Use of medical communication tools varies among older adults. One study in JAMA Network Open found nearly two thirds of those older than 65 years who filled out surveys via phone or internet had used a patient portal, while a little under half used telehealth, and only 44% used a medical health application.
Older patients tend to fall into two camps, said Neela Patel, MD, MPH, CMD, chief of the Division of Geriatrics and Supportive Care at the UT Health San Antonio.
Her patients “are at two extremes of the spectrum — some technologically savvy and others with limited digital literacy or limited or no access to the Internet,” Patel, who is also the vice chair of the Health Systems Innovations and Technology Committee of the American Geriatric Society, said.
Patel’s practice has dedicated staff to help patients master certain technologies. For example, a pharmacist teaches patients how to use a glucometer and a blood pressure cuff. Other staff teach them how to use smartphone apps that track blood pressure or glucose.
She usually sees patients in person before offering telehealth as an option, ensuring the person has “enough digital literacy to utilize them and that the patient can see and hear the visit.”
If technological limitations impede a telehealth appointment, clinicians can help patients navigate their computer screen. Patel recounted the story of an older woman who was unable to come to the clinic in person, so had a telehealth visit instead.
“She had trouble hearing me, so I asked her to share her screen with me. I walked her through how to do that. Then I showed her where the ‘volume’ button was located. It turns out her volume was at zero,” Patel said. “Once that was adjusted, we were able to proceed with the appointment.”
Educating older adults on how to use health technology does not have to fall upon clinicians and their staff, according to Wehry. She routinely refers her patients to community resources to help them develop digital skills.
Local libraries and community centers often offer digital education. Some retirement communities and assisted living facilities also have tech support personnel or classes available to residents.
Wehry refers some of her patients to the National Digital Equity Center which teaches older adults how to hold a telehealth visit.
Roughly 90% of Patel’s patients are signed up for the patient portal, but they may not be operating the technology, she said. She advises these patients to ask their children or caregivers for help as appropriate.
Teaching patients to use the communication technology early on can also be helpful in other ways. If patients who have been technologically proficient start having difficulty, “it’s a clue there may be cognitive changes, and we follow up on those,” Patel said.
Additional resources to help older adults develop digital competence include Cyber Seniors, Older Adults Technology Services, AARP, AARP Find Digital Courses, Area Agencies on Aging, and Senior Navigator.
Human Touch
Some older adults may simply want a more traditional means of communicating with their clinician. A review of 29 papers, encompassing over 6200 adults older than 60 years, identified several domains affecting the adoption of healthcare technology, two of which were resistance to new technology and having family or friends that could help with.
Wehry said many older adults “don’t resist this technology because they’re unable to figure out how to use it. Instead, they see the technology as too impersonal.”
One study found many older adults fear technologies may end up replacing face-to-face contact.
“I’m beginning to encourage primary care providers to take a step back and refocus on the doctor-patient relationship. When communication is limited to the technological approach, it can erode trust in that relationship,” Wehry said.
The American Medical Association recommends clinicians “provide a method other than electronic communication for patients who are without technological proficiency or access.”
Some busy clinicians might be concerned phone calls will be too time-consuming, Wehry said. Patients should be informed of hours of phone availability, how much time is allotted to calls, and how many days or hours a response may take. Clinicians might also use tools that allow patients to use their cell phone to text their practice with medical questions.
Cavanaugh ended up finding technological help from a professional organizer whom she hired to help rearrange her closets.
“She’s knowledgeable and patient, and she’s helping me with the portal,” she said. “If I hadn’t serendipitously found the organizer, I’d still be struggling and unable to access proper medical care.”
Wehry and Patel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Famotidine Injection Recalled in US
, according to a company announcement posted on the FDA website.
The recall affects the following lot numbers 6133156 and 6133194, with expiration dates of August 2026, and lot number 6133388, with an expiration date of October 2026.
The recall stems from “out-of-specification endotoxin results in certain reserve samples of one lot,” the company said. The two additional lots are being recalled as a precaution.
Elevated endotoxin levels may lead to severe systemic reactions, including sepsis, septic shock, inflammatory and life-threatening immune responses, and potentially death.
Nonserious adverse events have been reported in association with lot 6133156, including chills, altered mental status, changes in respiratory status, fever/increased body temperature, shivering, and shaking.
Famotidine injection is indicated in some hospitalized patients with pathological hypersecretory conditions or intractable ulcers or as an alternative to the oral dosage forms for short-term use in patients unable to take oral medication for certain conditions, including active duodenal ulcer, benign gastric ulcer or gastroesophageal reflux disease, or maintenance therapy for duodenal ulcer patients at reduced dosage after healing of an active ulcer.
Clinicians should be alert for symptoms potentially related to endotoxin exposure in patients who have received the affected product; document use of the product in affected lots (if already administered) and monitor patients carefully; and inform prescribing clinicians and nursing staff so they can monitor for signs of endotoxin-related reaction.
Patients should be advised to contact their physician or healthcare provider if they experienced any problems that may be related to receiving the affected drug.
Clinicians should check their inventory for famotidine injection USP 20 mg/2 mL vials; discontinue use, dispensing, and distribution of affected lots; and segregate and quarantine any affected units to prevent inadvertent use.
For questions or product return coordination, contact Fresenius Kabi USA Quality Assurance at 1-866-716-2459 or email at [email protected].
Adverse events or quality issues related to this recall should be reported to Fresenius Kabi (1-800-551-7176) and to the FDA MedWatch program.
A version of this article appeared on Medscape.com.
, according to a company announcement posted on the FDA website.
The recall affects the following lot numbers 6133156 and 6133194, with expiration dates of August 2026, and lot number 6133388, with an expiration date of October 2026.
The recall stems from “out-of-specification endotoxin results in certain reserve samples of one lot,” the company said. The two additional lots are being recalled as a precaution.
Elevated endotoxin levels may lead to severe systemic reactions, including sepsis, septic shock, inflammatory and life-threatening immune responses, and potentially death.
Nonserious adverse events have been reported in association with lot 6133156, including chills, altered mental status, changes in respiratory status, fever/increased body temperature, shivering, and shaking.
Famotidine injection is indicated in some hospitalized patients with pathological hypersecretory conditions or intractable ulcers or as an alternative to the oral dosage forms for short-term use in patients unable to take oral medication for certain conditions, including active duodenal ulcer, benign gastric ulcer or gastroesophageal reflux disease, or maintenance therapy for duodenal ulcer patients at reduced dosage after healing of an active ulcer.
Clinicians should be alert for symptoms potentially related to endotoxin exposure in patients who have received the affected product; document use of the product in affected lots (if already administered) and monitor patients carefully; and inform prescribing clinicians and nursing staff so they can monitor for signs of endotoxin-related reaction.
Patients should be advised to contact their physician or healthcare provider if they experienced any problems that may be related to receiving the affected drug.
Clinicians should check their inventory for famotidine injection USP 20 mg/2 mL vials; discontinue use, dispensing, and distribution of affected lots; and segregate and quarantine any affected units to prevent inadvertent use.
For questions or product return coordination, contact Fresenius Kabi USA Quality Assurance at 1-866-716-2459 or email at [email protected].
Adverse events or quality issues related to this recall should be reported to Fresenius Kabi (1-800-551-7176) and to the FDA MedWatch program.
A version of this article appeared on Medscape.com.
, according to a company announcement posted on the FDA website.
The recall affects the following lot numbers 6133156 and 6133194, with expiration dates of August 2026, and lot number 6133388, with an expiration date of October 2026.
The recall stems from “out-of-specification endotoxin results in certain reserve samples of one lot,” the company said. The two additional lots are being recalled as a precaution.
Elevated endotoxin levels may lead to severe systemic reactions, including sepsis, septic shock, inflammatory and life-threatening immune responses, and potentially death.
Nonserious adverse events have been reported in association with lot 6133156, including chills, altered mental status, changes in respiratory status, fever/increased body temperature, shivering, and shaking.
Famotidine injection is indicated in some hospitalized patients with pathological hypersecretory conditions or intractable ulcers or as an alternative to the oral dosage forms for short-term use in patients unable to take oral medication for certain conditions, including active duodenal ulcer, benign gastric ulcer or gastroesophageal reflux disease, or maintenance therapy for duodenal ulcer patients at reduced dosage after healing of an active ulcer.
Clinicians should be alert for symptoms potentially related to endotoxin exposure in patients who have received the affected product; document use of the product in affected lots (if already administered) and monitor patients carefully; and inform prescribing clinicians and nursing staff so they can monitor for signs of endotoxin-related reaction.
Patients should be advised to contact their physician or healthcare provider if they experienced any problems that may be related to receiving the affected drug.
Clinicians should check their inventory for famotidine injection USP 20 mg/2 mL vials; discontinue use, dispensing, and distribution of affected lots; and segregate and quarantine any affected units to prevent inadvertent use.
For questions or product return coordination, contact Fresenius Kabi USA Quality Assurance at 1-866-716-2459 or email at [email protected].
Adverse events or quality issues related to this recall should be reported to Fresenius Kabi (1-800-551-7176) and to the FDA MedWatch program.
A version of this article appeared on Medscape.com.
Duodenal Mucosal Resurfacing Curbs Weight Gain Post-GLP-1
, initial results of the open-label, multistage REMAIN-1 trial showed.
In addition, “the procedure was well tolerated, with only minor, transient TEAEs [treatment-emergent adverse events] consistent with routine upper endoscopy,” said Shailendra Singh, MD, of West Virginia University in Morgantown, West Virginia, who presented the findings at The Obesity Society’s Obesity Week 2025 meeting in Atlanta.
DMR uses hydrothermal ablation to treat the duodenal mucosa, which may be dysfunctional in both obesity and impaired glucose tolerance. A previous pooled clinical trial analysis of more than 100 patients with type 2 diabetes demonstrated that DMR helped patients maintain body weight loss up to 48 weeks post-procedure.
Metabolic therapeutics company Fractyl Health, Burlington, Massachusetts, developed the procedure, called Revita, and is sponsoring the current study. The trial’s aim is to determine the effect of DMR on weight-loss maintenance in patients with ≥ 15% total body weight loss using a GLP-1 RA in both an open-label arm and a prospective, randomized, double-blind, sham-controlled multicenter arm.
‘Encouraging Preliminary Findings’
The open-label arm included 15 DMR-treated participants (mean age, 49 years, 87% female ), all of whom had taken tirzepatide for a minimum of 5 months and a maximum of 3 years prior to DMR and had lost at least 15% of their total body weight.
Participants had a mean pre-GLP-1 RA weight of 104.8 kg and a mean weight prior to DMR of 79.4 kg, for a mean total body weight loss from the start of GLP-1 RA of 23.8%. Weight loss was heterogeneous and reflective of the real-world patient population taking GLP-1 medications, according to the poster presentation.
Participants discontinued their GLP-1 medication, underwent the DMR procedure, and were followed for 3 months. A total of 12 of 13 patients maintained or lost weight at that point, with 6 of 13 losing additional weight.
Specifically, participants experienced a median of 0.46% weight change (approximately 1 lb) compared with the 5%-6% weight regain (10-15 lb) observed after GLP-1 discontinuation in the literature.
The procedure was well tolerated, with most patients experiencing no TEAEs and none experiencing an event greater than grade 1. Grade 1 events occurred in three patients; 23% were transient in nature, lasting 2-5 days, and were similar to those typically seen with a routine upper endoscopy.
“These encouraging preliminary findings suggest that DMR may safely achieve durable weight maintenance for patients who wish to discontinue GLP-1 RA therapy,” the study authors stated.
Randomization is anticipated in early 2026, with 6-month topline data and a potential premarket approval filing expected in the second half of 2026.
A version of this article appeared on Medscape.com.
, initial results of the open-label, multistage REMAIN-1 trial showed.
In addition, “the procedure was well tolerated, with only minor, transient TEAEs [treatment-emergent adverse events] consistent with routine upper endoscopy,” said Shailendra Singh, MD, of West Virginia University in Morgantown, West Virginia, who presented the findings at The Obesity Society’s Obesity Week 2025 meeting in Atlanta.
DMR uses hydrothermal ablation to treat the duodenal mucosa, which may be dysfunctional in both obesity and impaired glucose tolerance. A previous pooled clinical trial analysis of more than 100 patients with type 2 diabetes demonstrated that DMR helped patients maintain body weight loss up to 48 weeks post-procedure.
Metabolic therapeutics company Fractyl Health, Burlington, Massachusetts, developed the procedure, called Revita, and is sponsoring the current study. The trial’s aim is to determine the effect of DMR on weight-loss maintenance in patients with ≥ 15% total body weight loss using a GLP-1 RA in both an open-label arm and a prospective, randomized, double-blind, sham-controlled multicenter arm.
‘Encouraging Preliminary Findings’
The open-label arm included 15 DMR-treated participants (mean age, 49 years, 87% female ), all of whom had taken tirzepatide for a minimum of 5 months and a maximum of 3 years prior to DMR and had lost at least 15% of their total body weight.
Participants had a mean pre-GLP-1 RA weight of 104.8 kg and a mean weight prior to DMR of 79.4 kg, for a mean total body weight loss from the start of GLP-1 RA of 23.8%. Weight loss was heterogeneous and reflective of the real-world patient population taking GLP-1 medications, according to the poster presentation.
Participants discontinued their GLP-1 medication, underwent the DMR procedure, and were followed for 3 months. A total of 12 of 13 patients maintained or lost weight at that point, with 6 of 13 losing additional weight.
Specifically, participants experienced a median of 0.46% weight change (approximately 1 lb) compared with the 5%-6% weight regain (10-15 lb) observed after GLP-1 discontinuation in the literature.
The procedure was well tolerated, with most patients experiencing no TEAEs and none experiencing an event greater than grade 1. Grade 1 events occurred in three patients; 23% were transient in nature, lasting 2-5 days, and were similar to those typically seen with a routine upper endoscopy.
“These encouraging preliminary findings suggest that DMR may safely achieve durable weight maintenance for patients who wish to discontinue GLP-1 RA therapy,” the study authors stated.
Randomization is anticipated in early 2026, with 6-month topline data and a potential premarket approval filing expected in the second half of 2026.
A version of this article appeared on Medscape.com.
, initial results of the open-label, multistage REMAIN-1 trial showed.
In addition, “the procedure was well tolerated, with only minor, transient TEAEs [treatment-emergent adverse events] consistent with routine upper endoscopy,” said Shailendra Singh, MD, of West Virginia University in Morgantown, West Virginia, who presented the findings at The Obesity Society’s Obesity Week 2025 meeting in Atlanta.
DMR uses hydrothermal ablation to treat the duodenal mucosa, which may be dysfunctional in both obesity and impaired glucose tolerance. A previous pooled clinical trial analysis of more than 100 patients with type 2 diabetes demonstrated that DMR helped patients maintain body weight loss up to 48 weeks post-procedure.
Metabolic therapeutics company Fractyl Health, Burlington, Massachusetts, developed the procedure, called Revita, and is sponsoring the current study. The trial’s aim is to determine the effect of DMR on weight-loss maintenance in patients with ≥ 15% total body weight loss using a GLP-1 RA in both an open-label arm and a prospective, randomized, double-blind, sham-controlled multicenter arm.
‘Encouraging Preliminary Findings’
The open-label arm included 15 DMR-treated participants (mean age, 49 years, 87% female ), all of whom had taken tirzepatide for a minimum of 5 months and a maximum of 3 years prior to DMR and had lost at least 15% of their total body weight.
Participants had a mean pre-GLP-1 RA weight of 104.8 kg and a mean weight prior to DMR of 79.4 kg, for a mean total body weight loss from the start of GLP-1 RA of 23.8%. Weight loss was heterogeneous and reflective of the real-world patient population taking GLP-1 medications, according to the poster presentation.
Participants discontinued their GLP-1 medication, underwent the DMR procedure, and were followed for 3 months. A total of 12 of 13 patients maintained or lost weight at that point, with 6 of 13 losing additional weight.
Specifically, participants experienced a median of 0.46% weight change (approximately 1 lb) compared with the 5%-6% weight regain (10-15 lb) observed after GLP-1 discontinuation in the literature.
The procedure was well tolerated, with most patients experiencing no TEAEs and none experiencing an event greater than grade 1. Grade 1 events occurred in three patients; 23% were transient in nature, lasting 2-5 days, and were similar to those typically seen with a routine upper endoscopy.
“These encouraging preliminary findings suggest that DMR may safely achieve durable weight maintenance for patients who wish to discontinue GLP-1 RA therapy,” the study authors stated.
Randomization is anticipated in early 2026, with 6-month topline data and a potential premarket approval filing expected in the second half of 2026.
A version of this article appeared on Medscape.com.
Seladelpar Reduces Pruritus Measures in Primary Biliary Cholangitis
PHOENIX — , supporting the drug’s benefits for the large percentage of patients who may fail to improve with or become intolerant of standard PBC therapy.
“This pooled analysis demonstrated that seladelpar treatment for up to 6 months reduced pruritus to a greater extent vs placebo in patients with PBC who had moderate-to-severe pruritus at baseline,” said senior author Marlyn J. Mayo, MD, AGAF, of the Division of Digestive and Liver Diseases, University of Texas Southwestern, Dallas, in presenting the findings at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
In PBC, a rare, chronic liver disease that can progressively destroy the intrahepatic bile ducts, ursodeoxycholic acid (UDCA) has remained a highly effective standard of care; however, up to 40% of patients either fail to achieve a biochemical response or develop intolerances to the therapy.
Seladelpar, in addition to improving measures of PBC disease including liver function tests and markers of cholestasis, has been shown in clinical trials to reduce the symptoms of pruritus and related sleep disturbances.
The drug is approved by the FDA for the treatment of PBC in combination with UDCA when patients fail to have an adequate response to UDCA alone, or as monotherapy when patients are intolerant to UDCA.
With pruritus, or itching, representing a key detrimental symptom of PBC and affecting as many as 70% of patients, Mayo and her colleagues conducted a pooled analysis of two phase 3, placebo-controlled trials, the ENHANCE and RESPONSE trials, in order to delve deeper into the specifics of how seladelpar improves itching.
The studies both involved patients with PBC and moderate-to-severe pruritus at baseline who had an inadequate response to UDCA and received seladelpar as add-on therapy to the drug, if tolerant of UDCA.
In the ENHANCE trial, patients were randomized 1:1:1 to daily oral seladelpar 5 mg, 10 mg, or placebo for 52 weeks, and in the RESPONSE trial, they were randomized 2:1 to daily oral seladelpar 10 mg or placebo for 52 weeks.
The ENHANCE trial was terminated early with key endpoints amended to 3 months.
In total, the analysis included 126 patients with a pruritus numerical rating scale (NRS) score of at least 4 at baseline (indicative of moderate-to-severe itch), with 76 patients receiving seladelpar 10 mg and 50 receiving placebo.
Patients in the two groups had a mean age of 53 years; 96% were female; their mean age at PBC diagnosis was 47 years; and itch scores — including the NRS, PBC-40 itch domain, and 5-D itch scale scores — were similar across the treatment and placebo groups at baseline.
After 6 months, patients treated with seladelpar reported greater improvements than those receiving placebo across all measures.
For changes in pruritus NRS through month 6, greater decreases were observed with seladelpar 10 mg at months 1, 3, and 6, with a 6-month decrease from baseline of 3.33 in the seladelpar group vs 1.77 with placebo (P < .01).
For PBC-40 itch domain scores, the mean reduction from baseline at 6 months was 2.41 vs 0.98, although significance was lost at month 6 due to a reduction in numbers.
For the 5-D itch total scores, the mean reduction from baseline to 6 months was 5.09 vs 1.70 (P < .0001).
And for the 5-D itch degree, the domain scores were also improved with seladelpar (mean reduction from baseline to 6 months of 1.08 vs 0.47; P = .01).
Patients treated with seladelpar also showed greater improvement in the sleep disturbances that can accompany pruritus, including on the 5-D itch Sleep Item scale (P < .01 at 6 months) and the PBC-40 Sleep Disturbance Item (P < .0001 at 1 month vs placebo; not significant at 6 months).
There were no significant differences between the groups in safety or tolerability profiles overall, with any adverse events occurring in 57 of the 76 (75%) patients receiving seladelpar and 40 of 50 (80%) receiving placebo.
Grade 3 or higher adverse events occurred in 8% of seladelpar and 12% of placebo patients, and pruritus-specific adverse events occurred in 8% and 14%, respectively.
“We found that improvement versus placebo was evident at month 1 of treatment and was sustained through month 6 using three different measures of pruritus,” Mayo said.
“And improvements in sleep disturbance were also seen in patients receiving seladelpar vs placebo through month 6 using two different measures of (5-D itch and PBC-40).”
Mayo noted that seladelpar is currently the only FDA-approved second-line therapy for people who have not had an adequate biochemical response or cannot tolerate UDCA.
While the drug is not likely at a point where it could be positioned as a first-line itch therapy, Mayo suggested that, for those who have had a poor response to UDCA, “I think it makes sense to start with something like this and then see how patients’ itching is affected by the drug.”
“It’s possible it could help avoid having to add yet another drug to treat the itch, and the hope is that this will help reduce the issue of polypharmacy.”
Commenting on the study, Luis F. Lara, MD, Division Chief of Digestive Diseases at the University of Cincinnati in Cincinnati, who co-moderated the session, underscored the need for treatment among patients who fail to respond to standard therapy.
“I think this is very important research,” he told GI & Hepatology News. “First, the fact that so many patients suffer their pruritus without any therapy is actually disturbing.”
“And the fact that this medication seems to be extremely effective in treating this, likely tremendously affecting patients’ quality of life, is something to really highlight.”
Lara noted that the findings raise the question of “whether this should be considered earlier in the disease process, rather than waiting to use it as a second-line therapy, when pruritus has already become significant.”
Akwi W. Asombang, MD, interventional enterologist at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School in Boston, who was also a co-moderator, agreed that “having a disease process that results in itching all the time can represent profound discomfort and a significant quality of life issue.”
“So, to have a drug that could minimize or alleviate that process could be huge,” Asombang told GI & Hepatology News.
The ENHANCE and RESPONSE trials were funded by Gilead Sciences. Mayo’s disclosures included consulting and/or other relationships with CymaBay Therapeutics, GSK, Intra-Sana, Ipsen, Mirum Pharma, and Target PharmaSolutions. Lara disclosed having a relationship with AbbVie. Asombang reported having no disclosures.
A version of this article appeared on Medscape.com .
PHOENIX — , supporting the drug’s benefits for the large percentage of patients who may fail to improve with or become intolerant of standard PBC therapy.
“This pooled analysis demonstrated that seladelpar treatment for up to 6 months reduced pruritus to a greater extent vs placebo in patients with PBC who had moderate-to-severe pruritus at baseline,” said senior author Marlyn J. Mayo, MD, AGAF, of the Division of Digestive and Liver Diseases, University of Texas Southwestern, Dallas, in presenting the findings at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
In PBC, a rare, chronic liver disease that can progressively destroy the intrahepatic bile ducts, ursodeoxycholic acid (UDCA) has remained a highly effective standard of care; however, up to 40% of patients either fail to achieve a biochemical response or develop intolerances to the therapy.
Seladelpar, in addition to improving measures of PBC disease including liver function tests and markers of cholestasis, has been shown in clinical trials to reduce the symptoms of pruritus and related sleep disturbances.
The drug is approved by the FDA for the treatment of PBC in combination with UDCA when patients fail to have an adequate response to UDCA alone, or as monotherapy when patients are intolerant to UDCA.
With pruritus, or itching, representing a key detrimental symptom of PBC and affecting as many as 70% of patients, Mayo and her colleagues conducted a pooled analysis of two phase 3, placebo-controlled trials, the ENHANCE and RESPONSE trials, in order to delve deeper into the specifics of how seladelpar improves itching.
The studies both involved patients with PBC and moderate-to-severe pruritus at baseline who had an inadequate response to UDCA and received seladelpar as add-on therapy to the drug, if tolerant of UDCA.
In the ENHANCE trial, patients were randomized 1:1:1 to daily oral seladelpar 5 mg, 10 mg, or placebo for 52 weeks, and in the RESPONSE trial, they were randomized 2:1 to daily oral seladelpar 10 mg or placebo for 52 weeks.
The ENHANCE trial was terminated early with key endpoints amended to 3 months.
In total, the analysis included 126 patients with a pruritus numerical rating scale (NRS) score of at least 4 at baseline (indicative of moderate-to-severe itch), with 76 patients receiving seladelpar 10 mg and 50 receiving placebo.
Patients in the two groups had a mean age of 53 years; 96% were female; their mean age at PBC diagnosis was 47 years; and itch scores — including the NRS, PBC-40 itch domain, and 5-D itch scale scores — were similar across the treatment and placebo groups at baseline.
After 6 months, patients treated with seladelpar reported greater improvements than those receiving placebo across all measures.
For changes in pruritus NRS through month 6, greater decreases were observed with seladelpar 10 mg at months 1, 3, and 6, with a 6-month decrease from baseline of 3.33 in the seladelpar group vs 1.77 with placebo (P < .01).
For PBC-40 itch domain scores, the mean reduction from baseline at 6 months was 2.41 vs 0.98, although significance was lost at month 6 due to a reduction in numbers.
For the 5-D itch total scores, the mean reduction from baseline to 6 months was 5.09 vs 1.70 (P < .0001).
And for the 5-D itch degree, the domain scores were also improved with seladelpar (mean reduction from baseline to 6 months of 1.08 vs 0.47; P = .01).
Patients treated with seladelpar also showed greater improvement in the sleep disturbances that can accompany pruritus, including on the 5-D itch Sleep Item scale (P < .01 at 6 months) and the PBC-40 Sleep Disturbance Item (P < .0001 at 1 month vs placebo; not significant at 6 months).
There were no significant differences between the groups in safety or tolerability profiles overall, with any adverse events occurring in 57 of the 76 (75%) patients receiving seladelpar and 40 of 50 (80%) receiving placebo.
Grade 3 or higher adverse events occurred in 8% of seladelpar and 12% of placebo patients, and pruritus-specific adverse events occurred in 8% and 14%, respectively.
“We found that improvement versus placebo was evident at month 1 of treatment and was sustained through month 6 using three different measures of pruritus,” Mayo said.
“And improvements in sleep disturbance were also seen in patients receiving seladelpar vs placebo through month 6 using two different measures of (5-D itch and PBC-40).”
Mayo noted that seladelpar is currently the only FDA-approved second-line therapy for people who have not had an adequate biochemical response or cannot tolerate UDCA.
While the drug is not likely at a point where it could be positioned as a first-line itch therapy, Mayo suggested that, for those who have had a poor response to UDCA, “I think it makes sense to start with something like this and then see how patients’ itching is affected by the drug.”
“It’s possible it could help avoid having to add yet another drug to treat the itch, and the hope is that this will help reduce the issue of polypharmacy.”
Commenting on the study, Luis F. Lara, MD, Division Chief of Digestive Diseases at the University of Cincinnati in Cincinnati, who co-moderated the session, underscored the need for treatment among patients who fail to respond to standard therapy.
“I think this is very important research,” he told GI & Hepatology News. “First, the fact that so many patients suffer their pruritus without any therapy is actually disturbing.”
“And the fact that this medication seems to be extremely effective in treating this, likely tremendously affecting patients’ quality of life, is something to really highlight.”
Lara noted that the findings raise the question of “whether this should be considered earlier in the disease process, rather than waiting to use it as a second-line therapy, when pruritus has already become significant.”
Akwi W. Asombang, MD, interventional enterologist at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School in Boston, who was also a co-moderator, agreed that “having a disease process that results in itching all the time can represent profound discomfort and a significant quality of life issue.”
“So, to have a drug that could minimize or alleviate that process could be huge,” Asombang told GI & Hepatology News.
The ENHANCE and RESPONSE trials were funded by Gilead Sciences. Mayo’s disclosures included consulting and/or other relationships with CymaBay Therapeutics, GSK, Intra-Sana, Ipsen, Mirum Pharma, and Target PharmaSolutions. Lara disclosed having a relationship with AbbVie. Asombang reported having no disclosures.
A version of this article appeared on Medscape.com .
PHOENIX — , supporting the drug’s benefits for the large percentage of patients who may fail to improve with or become intolerant of standard PBC therapy.
“This pooled analysis demonstrated that seladelpar treatment for up to 6 months reduced pruritus to a greater extent vs placebo in patients with PBC who had moderate-to-severe pruritus at baseline,” said senior author Marlyn J. Mayo, MD, AGAF, of the Division of Digestive and Liver Diseases, University of Texas Southwestern, Dallas, in presenting the findings at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
In PBC, a rare, chronic liver disease that can progressively destroy the intrahepatic bile ducts, ursodeoxycholic acid (UDCA) has remained a highly effective standard of care; however, up to 40% of patients either fail to achieve a biochemical response or develop intolerances to the therapy.
Seladelpar, in addition to improving measures of PBC disease including liver function tests and markers of cholestasis, has been shown in clinical trials to reduce the symptoms of pruritus and related sleep disturbances.
The drug is approved by the FDA for the treatment of PBC in combination with UDCA when patients fail to have an adequate response to UDCA alone, or as monotherapy when patients are intolerant to UDCA.
With pruritus, or itching, representing a key detrimental symptom of PBC and affecting as many as 70% of patients, Mayo and her colleagues conducted a pooled analysis of two phase 3, placebo-controlled trials, the ENHANCE and RESPONSE trials, in order to delve deeper into the specifics of how seladelpar improves itching.
The studies both involved patients with PBC and moderate-to-severe pruritus at baseline who had an inadequate response to UDCA and received seladelpar as add-on therapy to the drug, if tolerant of UDCA.
In the ENHANCE trial, patients were randomized 1:1:1 to daily oral seladelpar 5 mg, 10 mg, or placebo for 52 weeks, and in the RESPONSE trial, they were randomized 2:1 to daily oral seladelpar 10 mg or placebo for 52 weeks.
The ENHANCE trial was terminated early with key endpoints amended to 3 months.
In total, the analysis included 126 patients with a pruritus numerical rating scale (NRS) score of at least 4 at baseline (indicative of moderate-to-severe itch), with 76 patients receiving seladelpar 10 mg and 50 receiving placebo.
Patients in the two groups had a mean age of 53 years; 96% were female; their mean age at PBC diagnosis was 47 years; and itch scores — including the NRS, PBC-40 itch domain, and 5-D itch scale scores — were similar across the treatment and placebo groups at baseline.
After 6 months, patients treated with seladelpar reported greater improvements than those receiving placebo across all measures.
For changes in pruritus NRS through month 6, greater decreases were observed with seladelpar 10 mg at months 1, 3, and 6, with a 6-month decrease from baseline of 3.33 in the seladelpar group vs 1.77 with placebo (P < .01).
For PBC-40 itch domain scores, the mean reduction from baseline at 6 months was 2.41 vs 0.98, although significance was lost at month 6 due to a reduction in numbers.
For the 5-D itch total scores, the mean reduction from baseline to 6 months was 5.09 vs 1.70 (P < .0001).
And for the 5-D itch degree, the domain scores were also improved with seladelpar (mean reduction from baseline to 6 months of 1.08 vs 0.47; P = .01).
Patients treated with seladelpar also showed greater improvement in the sleep disturbances that can accompany pruritus, including on the 5-D itch Sleep Item scale (P < .01 at 6 months) and the PBC-40 Sleep Disturbance Item (P < .0001 at 1 month vs placebo; not significant at 6 months).
There were no significant differences between the groups in safety or tolerability profiles overall, with any adverse events occurring in 57 of the 76 (75%) patients receiving seladelpar and 40 of 50 (80%) receiving placebo.
Grade 3 or higher adverse events occurred in 8% of seladelpar and 12% of placebo patients, and pruritus-specific adverse events occurred in 8% and 14%, respectively.
“We found that improvement versus placebo was evident at month 1 of treatment and was sustained through month 6 using three different measures of pruritus,” Mayo said.
“And improvements in sleep disturbance were also seen in patients receiving seladelpar vs placebo through month 6 using two different measures of (5-D itch and PBC-40).”
Mayo noted that seladelpar is currently the only FDA-approved second-line therapy for people who have not had an adequate biochemical response or cannot tolerate UDCA.
While the drug is not likely at a point where it could be positioned as a first-line itch therapy, Mayo suggested that, for those who have had a poor response to UDCA, “I think it makes sense to start with something like this and then see how patients’ itching is affected by the drug.”
“It’s possible it could help avoid having to add yet another drug to treat the itch, and the hope is that this will help reduce the issue of polypharmacy.”
Commenting on the study, Luis F. Lara, MD, Division Chief of Digestive Diseases at the University of Cincinnati in Cincinnati, who co-moderated the session, underscored the need for treatment among patients who fail to respond to standard therapy.
“I think this is very important research,” he told GI & Hepatology News. “First, the fact that so many patients suffer their pruritus without any therapy is actually disturbing.”
“And the fact that this medication seems to be extremely effective in treating this, likely tremendously affecting patients’ quality of life, is something to really highlight.”
Lara noted that the findings raise the question of “whether this should be considered earlier in the disease process, rather than waiting to use it as a second-line therapy, when pruritus has already become significant.”
Akwi W. Asombang, MD, interventional enterologist at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School in Boston, who was also a co-moderator, agreed that “having a disease process that results in itching all the time can represent profound discomfort and a significant quality of life issue.”
“So, to have a drug that could minimize or alleviate that process could be huge,” Asombang told GI & Hepatology News.
The ENHANCE and RESPONSE trials were funded by Gilead Sciences. Mayo’s disclosures included consulting and/or other relationships with CymaBay Therapeutics, GSK, Intra-Sana, Ipsen, Mirum Pharma, and Target PharmaSolutions. Lara disclosed having a relationship with AbbVie. Asombang reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM ACG 2025
Novel Anti-TL1a Antibody Shows Potential for Crohn’s Disease
PHOENIX — , according to results from the phase 2b RELIEVE UCCD study.
“Additional clinical and endoscopic endpoints supported the primary endpoint of endoscopic response observed with duvakitug,” study author Vipul Jairath, MB ChB, DPhil, MRCP, professor of medicine at the Schulich School of Medicine and Dentistry, Western University, London, Ontario, Canada, reported.
These findings “support further development of duvakitug as a treatment option” for these patients, said Jairath, who presented the data at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
In the 14-week randomized controlled induction study, 138 adults aged 18-75 years with moderately to severely active Crohn’s disease were randomized to receive a 2250-mg loading dose of duvakitug or placebo subcutaneously, followed by either duvakitug 450 mg, 900 mg, or placebo every 2 weeks. Each arm of the study contained 46 patients, with a mean age of about 40 years, and a mean duration of disease of 9-11 years. The mean Simple Endoscopic Score for Crohn’s Disease (SES-CD) score at baseline was 12.
Half to two thirds of the patients had taken advanced therapies, either approved or investigational. The trial participants were allowed to take concomitant corticosteroids, 5-aminosalicylic acid drugs, and immunosuppressants (including 6-mercaptopurine, azathioprine, and methotrexate).
Notably, the primary endpoint of endoscopic response — defined as ≥ 50% reduction from baseline in SES-CD score — was achieved in almost half of the patients taking the 900-mg higher dose (22 of 46 patients). The endoscopic response was achieved in 13 of 27 patients who had previous experience with advanced therapies, including approved biologics (anti-TNF, anti-integrins, anti-interleukin [IL]-12/23, or anti-IL-23), and JAK inhibitors.
In the high-dose arm, 26% of participants achieved endoscopic remission, and 54% achieved clinical remission.
Just 13% of patients in the duvakitug arms had a treatment-related adverse event, with serious adverse events slightly higher in the 450 mg arm than in the 900 mg arm (13% vs 2%). The most common side effects were anemia, headache, and nasopharyngitis. One patient in the 900 mg group and four in the lower-dose group discontinued due to an adverse event.
When asked to comment by GI & Hepatology News, Jordan Axelrad, MD, MPH, co-director of the Inflammatory Bowel Disease Center at the NYU Langone Health, New York City, said the “results demonstrate that duvakitug is a promising therapy for patients with Crohn’s disease, with 14-week induction placebo-adjusted endoscopic response rates rivaling or exceeding our currently FDA-approved advanced, effective therapies.”
The efficacy in patients with prior exposure to advanced therapies is especially noteworthy, as it is “a population in which most existing and investigational agents show limited clinical benefit,” said Axelrad, who is also an associate professor of medicine at the NYU Grossman School of Medicine, New York City.
Axelrad said there were no concerning safety signals, “which strengthens its appeal for clinical use.”
He said he sees promise in the anti-TL1a inhibitor class, noting that TL1A “is a key cytokine that spans innate and adaptive mucosal inflammation and also directly influences fibroblast and epithelial biology, contributing to intestinal fibrosis and barrier dysfunction.”
Because therapies in the class simultaneously target inflammatory and fibrotic pathways, “TL1A inhibition offers the potential for more durable disease control than conventional cytokine-directed therapies,” he said.
But, noted Axelrad, it is early in duvakitug’s development. “We certainly need a larger cohort in a phase 3 study with maintenance data,” he said.
Jairath disclosed having financial relationships with AbbVie, Alimentiv, Arena Pharmaceuticals, Asahi Kasei Pharma, Asieris Pharmaceuticals, AstraZeneca, Avoro Capital, Bristol Myers Squibb, Celltrion, Eli Lilly and Company, Endpoint Health, Enthera, Ferring Pharmaceuticals, Flagship Pioneering, Fresenius Kabi, Galapagos NV, Genentech, Gilde Healthcare, GlaxoSmithKline, Innomar, JAMP, Johnson & Johnson, Merck, Metacrine, Mylan, Pandion Therapeutics, Pendopharm, Pfizer, Prometheus Therapeutics and Diagnostics, Protagonist Therapeutics, Reistone Biopharma, Roche, Roivant, Sandoz, Second Genome, Shire, Sorriso Pharmaceuticals, Syndegen, Takeda, TD Securities, Teva, Topivert, Ventyx Biosciences, and Vividion Therapeutics. Axelrad reported receiving research grants from BioFire Diagnostics, Genentech, Janssen, and Takeda; consultant, advisory board fees or honorarium from Abbvie, Abviax, Adiso, BioFire Diagnostics, Biomerieux, Bristol-Myers Squibb, Celltrion, Eli Lilly, Ferring, Fresenius Kabi, Janssen, Merck, Pfizer, Sanofi, Takeda, and Vedanta.
A version of this article appeared on Medscape.com .
PHOENIX — , according to results from the phase 2b RELIEVE UCCD study.
“Additional clinical and endoscopic endpoints supported the primary endpoint of endoscopic response observed with duvakitug,” study author Vipul Jairath, MB ChB, DPhil, MRCP, professor of medicine at the Schulich School of Medicine and Dentistry, Western University, London, Ontario, Canada, reported.
These findings “support further development of duvakitug as a treatment option” for these patients, said Jairath, who presented the data at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
In the 14-week randomized controlled induction study, 138 adults aged 18-75 years with moderately to severely active Crohn’s disease were randomized to receive a 2250-mg loading dose of duvakitug or placebo subcutaneously, followed by either duvakitug 450 mg, 900 mg, or placebo every 2 weeks. Each arm of the study contained 46 patients, with a mean age of about 40 years, and a mean duration of disease of 9-11 years. The mean Simple Endoscopic Score for Crohn’s Disease (SES-CD) score at baseline was 12.
Half to two thirds of the patients had taken advanced therapies, either approved or investigational. The trial participants were allowed to take concomitant corticosteroids, 5-aminosalicylic acid drugs, and immunosuppressants (including 6-mercaptopurine, azathioprine, and methotrexate).
Notably, the primary endpoint of endoscopic response — defined as ≥ 50% reduction from baseline in SES-CD score — was achieved in almost half of the patients taking the 900-mg higher dose (22 of 46 patients). The endoscopic response was achieved in 13 of 27 patients who had previous experience with advanced therapies, including approved biologics (anti-TNF, anti-integrins, anti-interleukin [IL]-12/23, or anti-IL-23), and JAK inhibitors.
In the high-dose arm, 26% of participants achieved endoscopic remission, and 54% achieved clinical remission.
Just 13% of patients in the duvakitug arms had a treatment-related adverse event, with serious adverse events slightly higher in the 450 mg arm than in the 900 mg arm (13% vs 2%). The most common side effects were anemia, headache, and nasopharyngitis. One patient in the 900 mg group and four in the lower-dose group discontinued due to an adverse event.
When asked to comment by GI & Hepatology News, Jordan Axelrad, MD, MPH, co-director of the Inflammatory Bowel Disease Center at the NYU Langone Health, New York City, said the “results demonstrate that duvakitug is a promising therapy for patients with Crohn’s disease, with 14-week induction placebo-adjusted endoscopic response rates rivaling or exceeding our currently FDA-approved advanced, effective therapies.”
The efficacy in patients with prior exposure to advanced therapies is especially noteworthy, as it is “a population in which most existing and investigational agents show limited clinical benefit,” said Axelrad, who is also an associate professor of medicine at the NYU Grossman School of Medicine, New York City.
Axelrad said there were no concerning safety signals, “which strengthens its appeal for clinical use.”
He said he sees promise in the anti-TL1a inhibitor class, noting that TL1A “is a key cytokine that spans innate and adaptive mucosal inflammation and also directly influences fibroblast and epithelial biology, contributing to intestinal fibrosis and barrier dysfunction.”
Because therapies in the class simultaneously target inflammatory and fibrotic pathways, “TL1A inhibition offers the potential for more durable disease control than conventional cytokine-directed therapies,” he said.
But, noted Axelrad, it is early in duvakitug’s development. “We certainly need a larger cohort in a phase 3 study with maintenance data,” he said.
Jairath disclosed having financial relationships with AbbVie, Alimentiv, Arena Pharmaceuticals, Asahi Kasei Pharma, Asieris Pharmaceuticals, AstraZeneca, Avoro Capital, Bristol Myers Squibb, Celltrion, Eli Lilly and Company, Endpoint Health, Enthera, Ferring Pharmaceuticals, Flagship Pioneering, Fresenius Kabi, Galapagos NV, Genentech, Gilde Healthcare, GlaxoSmithKline, Innomar, JAMP, Johnson & Johnson, Merck, Metacrine, Mylan, Pandion Therapeutics, Pendopharm, Pfizer, Prometheus Therapeutics and Diagnostics, Protagonist Therapeutics, Reistone Biopharma, Roche, Roivant, Sandoz, Second Genome, Shire, Sorriso Pharmaceuticals, Syndegen, Takeda, TD Securities, Teva, Topivert, Ventyx Biosciences, and Vividion Therapeutics. Axelrad reported receiving research grants from BioFire Diagnostics, Genentech, Janssen, and Takeda; consultant, advisory board fees or honorarium from Abbvie, Abviax, Adiso, BioFire Diagnostics, Biomerieux, Bristol-Myers Squibb, Celltrion, Eli Lilly, Ferring, Fresenius Kabi, Janssen, Merck, Pfizer, Sanofi, Takeda, and Vedanta.
A version of this article appeared on Medscape.com .
PHOENIX — , according to results from the phase 2b RELIEVE UCCD study.
“Additional clinical and endoscopic endpoints supported the primary endpoint of endoscopic response observed with duvakitug,” study author Vipul Jairath, MB ChB, DPhil, MRCP, professor of medicine at the Schulich School of Medicine and Dentistry, Western University, London, Ontario, Canada, reported.
These findings “support further development of duvakitug as a treatment option” for these patients, said Jairath, who presented the data at the American College of Gastroenterology (ACG) 2025 Annual Scientific Meeting.
In the 14-week randomized controlled induction study, 138 adults aged 18-75 years with moderately to severely active Crohn’s disease were randomized to receive a 2250-mg loading dose of duvakitug or placebo subcutaneously, followed by either duvakitug 450 mg, 900 mg, or placebo every 2 weeks. Each arm of the study contained 46 patients, with a mean age of about 40 years, and a mean duration of disease of 9-11 years. The mean Simple Endoscopic Score for Crohn’s Disease (SES-CD) score at baseline was 12.
Half to two thirds of the patients had taken advanced therapies, either approved or investigational. The trial participants were allowed to take concomitant corticosteroids, 5-aminosalicylic acid drugs, and immunosuppressants (including 6-mercaptopurine, azathioprine, and methotrexate).
Notably, the primary endpoint of endoscopic response — defined as ≥ 50% reduction from baseline in SES-CD score — was achieved in almost half of the patients taking the 900-mg higher dose (22 of 46 patients). The endoscopic response was achieved in 13 of 27 patients who had previous experience with advanced therapies, including approved biologics (anti-TNF, anti-integrins, anti-interleukin [IL]-12/23, or anti-IL-23), and JAK inhibitors.
In the high-dose arm, 26% of participants achieved endoscopic remission, and 54% achieved clinical remission.
Just 13% of patients in the duvakitug arms had a treatment-related adverse event, with serious adverse events slightly higher in the 450 mg arm than in the 900 mg arm (13% vs 2%). The most common side effects were anemia, headache, and nasopharyngitis. One patient in the 900 mg group and four in the lower-dose group discontinued due to an adverse event.
When asked to comment by GI & Hepatology News, Jordan Axelrad, MD, MPH, co-director of the Inflammatory Bowel Disease Center at the NYU Langone Health, New York City, said the “results demonstrate that duvakitug is a promising therapy for patients with Crohn’s disease, with 14-week induction placebo-adjusted endoscopic response rates rivaling or exceeding our currently FDA-approved advanced, effective therapies.”
The efficacy in patients with prior exposure to advanced therapies is especially noteworthy, as it is “a population in which most existing and investigational agents show limited clinical benefit,” said Axelrad, who is also an associate professor of medicine at the NYU Grossman School of Medicine, New York City.
Axelrad said there were no concerning safety signals, “which strengthens its appeal for clinical use.”
He said he sees promise in the anti-TL1a inhibitor class, noting that TL1A “is a key cytokine that spans innate and adaptive mucosal inflammation and also directly influences fibroblast and epithelial biology, contributing to intestinal fibrosis and barrier dysfunction.”
Because therapies in the class simultaneously target inflammatory and fibrotic pathways, “TL1A inhibition offers the potential for more durable disease control than conventional cytokine-directed therapies,” he said.
But, noted Axelrad, it is early in duvakitug’s development. “We certainly need a larger cohort in a phase 3 study with maintenance data,” he said.
Jairath disclosed having financial relationships with AbbVie, Alimentiv, Arena Pharmaceuticals, Asahi Kasei Pharma, Asieris Pharmaceuticals, AstraZeneca, Avoro Capital, Bristol Myers Squibb, Celltrion, Eli Lilly and Company, Endpoint Health, Enthera, Ferring Pharmaceuticals, Flagship Pioneering, Fresenius Kabi, Galapagos NV, Genentech, Gilde Healthcare, GlaxoSmithKline, Innomar, JAMP, Johnson & Johnson, Merck, Metacrine, Mylan, Pandion Therapeutics, Pendopharm, Pfizer, Prometheus Therapeutics and Diagnostics, Protagonist Therapeutics, Reistone Biopharma, Roche, Roivant, Sandoz, Second Genome, Shire, Sorriso Pharmaceuticals, Syndegen, Takeda, TD Securities, Teva, Topivert, Ventyx Biosciences, and Vividion Therapeutics. Axelrad reported receiving research grants from BioFire Diagnostics, Genentech, Janssen, and Takeda; consultant, advisory board fees or honorarium from Abbvie, Abviax, Adiso, BioFire Diagnostics, Biomerieux, Bristol-Myers Squibb, Celltrion, Eli Lilly, Ferring, Fresenius Kabi, Janssen, Merck, Pfizer, Sanofi, Takeda, and Vedanta.
A version of this article appeared on Medscape.com .
FROM ACG 2025