User login
Gettin’ Dirty

Several months ago, my toilet broke. You should also know that I’m not particularly handy. So when I first realized that the toilet bowl seemed to fill constantly, I got a little stressed out.
How much was it going cost to call in a plumber on the weekend?
What kind of a water bill was I going to have?
Was this a serious problem?
I took a quick peek in the tank, but that just made me more confused. I was paralyzed by a lack of know-how.
Normally, I would have just Googled a local plumber. But that day, I decided to do something different. Maybe it was because it was the fantasy football offseason. Maybe it was because my wife had started to ask my father-in-law to change light bulbs around the house. Or, maybe, I wanted to learn to actually fix the problem. A few hours later, after an Internet lesson in toilet physiology, a $4.12 trip to Home Depot, and a wet pair of hands, I had replaced my first toilet flapper.
This wasn’t the rebuilding of a car engine, but it was a clear DIY step toward self-improvement. Easily the most memorable moment here was my sense of accomplishment.
I felt empowered.
One Part Science, One Part Art
It’s taken me a while to realize this, but I’ve begun to take advantage of improvement opportunities at work as well. No, I haven’t been moonlighting as a plumber for my hospital. I’ve just been fortunate to be part of a trifecta of rewarding quality-improvement (QI) projects over the past year. Before I’d gotten my hands dirty with these, my understanding of QI was fairly naive. I’d heard about Plan-Do-Study-Act many times. I had listened to a talk at a national conference. And I had kept up with the general medical literature on the subject.
But none of those activities had truly prepared me for experience of actually doing the work on my own.
By taking on a project, an ambitious attempt to reduce continuous pulse oximetry use, I experienced a crash course in both the science and the art of process improvement. I was forced to overcome my “I don’t know how” inertia. And with expert guidance in the form of a clinical safety and effectiveness class, I learned the importance of run charts (science) and a well-crafted multidisciplinary team (art) in changing established but inefficient behavior.
Our rates of continuous pulse oximetry usage dropped by 50%, and cost savings were $12,000 per year on one unit. These results made my prior attempts at change—years of complaining about ingrained nursing culture—look infantile. (OK, maybe it was ineffective, but who hasn’t complained about the overuse of continuous monitoring?)
I haven’t met a pediatric hospitalist who wouldn’t understand the symbolic importance of this success. But I know of many hospitalists who have not yet participated in meaningful QI project. Imagine calling a plumber who grasped the flush and fill mechanism of a toilet but had never touched real porcelain. Here’s an even better analogy: What if doctors could get licensed without having touched real patients?
If pediatric hospitalists are to transform the care delivery of hospitalized children, and quality learning only comes through hands-on training, then we need some more hands in the pot.
Discharge Improvement
On the heels of my first project, I was fortunate enough to augment my education through another effort—this time with a cohort of fellow pediatric hospitalists. This was a national collaborative to improve discharge handoffs, and I will admit that, at the outset, I was as puzzled as the first time I pulled the lid off the tank of the toilet. There were just too many permutations on PCP communication at the participating institutions, and some felt our aim of timely discharge handoffs was unattainable.
What carried me through, however, was the collective and infectious DIY—no, QIY (Quality Improve-it-Yourself) attitude of the group. We were all learning, and regular participation in the collaborative essentially guaranteed improvement. We achieved our aim of 90% communication with PCPs within two days of discharge. The secret was simple: The more you do, the more you learn.
Pediatric hospitalists can transform care delivery through a focus on safe and quality care, but the tools to accomplish this must come through post-residency, on-the-job learning. This QI know-how must efficiently spread among our ranks through practical and project-based educational efforts. It’s “see one, do one, teach one,” but we’re not talking about lumbar punctures anymore.
This is a journey in which we all take on the responsibility of rolling up our sleeves and simply learn by doing. And here is where the third leg of my as-yet-unfinished QI course unfolds.
Through my involvement with the Value in Inpatient Pediatrics (VIP) Network, I’ve gained a newfound vision for what the future might hold. VIP has evolved from a benchmarking project focused on bronchiolitis to an improvement network that will incorporate projects similar to the discharge handoff collaborative above.
In the process, a model for how to rapidly spread QI learning has emerged. The capacity lies in the network’s rapidly growing connectivity. The power comes from the individuals: motivated, card-carrying pediatric hospitalists from a wide array of sites. Collaborative learning harbors the potential to exponentially increase the pace at which we improve.
The future of our quality care is bright. I see an open network of improvement doers and learners. I see collaboration on quality and safety initiatives in all manner of hospitals and communities. I see that this will all be built upon a foundation of hard work and a QIY attitude.
You, too, will play a role.
Just don’t be afraid to get your hands a little dirty. TH
Dr. Shen is medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas. He is pediatric editor of The Hospitalist.
Several months ago, my toilet broke. You should also know that I’m not particularly handy. So when I first realized that the toilet bowl seemed to fill constantly, I got a little stressed out.
How much was it going cost to call in a plumber on the weekend?
What kind of a water bill was I going to have?
Was this a serious problem?
I took a quick peek in the tank, but that just made me more confused. I was paralyzed by a lack of know-how.
Normally, I would have just Googled a local plumber. But that day, I decided to do something different. Maybe it was because it was the fantasy football offseason. Maybe it was because my wife had started to ask my father-in-law to change light bulbs around the house. Or, maybe, I wanted to learn to actually fix the problem. A few hours later, after an Internet lesson in toilet physiology, a $4.12 trip to Home Depot, and a wet pair of hands, I had replaced my first toilet flapper.
This wasn’t the rebuilding of a car engine, but it was a clear DIY step toward self-improvement. Easily the most memorable moment here was my sense of accomplishment.
I felt empowered.
One Part Science, One Part Art
It’s taken me a while to realize this, but I’ve begun to take advantage of improvement opportunities at work as well. No, I haven’t been moonlighting as a plumber for my hospital. I’ve just been fortunate to be part of a trifecta of rewarding quality-improvement (QI) projects over the past year. Before I’d gotten my hands dirty with these, my understanding of QI was fairly naive. I’d heard about Plan-Do-Study-Act many times. I had listened to a talk at a national conference. And I had kept up with the general medical literature on the subject.
But none of those activities had truly prepared me for experience of actually doing the work on my own.
By taking on a project, an ambitious attempt to reduce continuous pulse oximetry use, I experienced a crash course in both the science and the art of process improvement. I was forced to overcome my “I don’t know how” inertia. And with expert guidance in the form of a clinical safety and effectiveness class, I learned the importance of run charts (science) and a well-crafted multidisciplinary team (art) in changing established but inefficient behavior.
Our rates of continuous pulse oximetry usage dropped by 50%, and cost savings were $12,000 per year on one unit. These results made my prior attempts at change—years of complaining about ingrained nursing culture—look infantile. (OK, maybe it was ineffective, but who hasn’t complained about the overuse of continuous monitoring?)
I haven’t met a pediatric hospitalist who wouldn’t understand the symbolic importance of this success. But I know of many hospitalists who have not yet participated in meaningful QI project. Imagine calling a plumber who grasped the flush and fill mechanism of a toilet but had never touched real porcelain. Here’s an even better analogy: What if doctors could get licensed without having touched real patients?
If pediatric hospitalists are to transform the care delivery of hospitalized children, and quality learning only comes through hands-on training, then we need some more hands in the pot.
Discharge Improvement
On the heels of my first project, I was fortunate enough to augment my education through another effort—this time with a cohort of fellow pediatric hospitalists. This was a national collaborative to improve discharge handoffs, and I will admit that, at the outset, I was as puzzled as the first time I pulled the lid off the tank of the toilet. There were just too many permutations on PCP communication at the participating institutions, and some felt our aim of timely discharge handoffs was unattainable.
What carried me through, however, was the collective and infectious DIY—no, QIY (Quality Improve-it-Yourself) attitude of the group. We were all learning, and regular participation in the collaborative essentially guaranteed improvement. We achieved our aim of 90% communication with PCPs within two days of discharge. The secret was simple: The more you do, the more you learn.
Pediatric hospitalists can transform care delivery through a focus on safe and quality care, but the tools to accomplish this must come through post-residency, on-the-job learning. This QI know-how must efficiently spread among our ranks through practical and project-based educational efforts. It’s “see one, do one, teach one,” but we’re not talking about lumbar punctures anymore.
This is a journey in which we all take on the responsibility of rolling up our sleeves and simply learn by doing. And here is where the third leg of my as-yet-unfinished QI course unfolds.
Through my involvement with the Value in Inpatient Pediatrics (VIP) Network, I’ve gained a newfound vision for what the future might hold. VIP has evolved from a benchmarking project focused on bronchiolitis to an improvement network that will incorporate projects similar to the discharge handoff collaborative above.
In the process, a model for how to rapidly spread QI learning has emerged. The capacity lies in the network’s rapidly growing connectivity. The power comes from the individuals: motivated, card-carrying pediatric hospitalists from a wide array of sites. Collaborative learning harbors the potential to exponentially increase the pace at which we improve.
The future of our quality care is bright. I see an open network of improvement doers and learners. I see collaboration on quality and safety initiatives in all manner of hospitals and communities. I see that this will all be built upon a foundation of hard work and a QIY attitude.
You, too, will play a role.
Just don’t be afraid to get your hands a little dirty. TH
Dr. Shen is medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas. He is pediatric editor of The Hospitalist.
Several months ago, my toilet broke. You should also know that I’m not particularly handy. So when I first realized that the toilet bowl seemed to fill constantly, I got a little stressed out.
How much was it going cost to call in a plumber on the weekend?
What kind of a water bill was I going to have?
Was this a serious problem?
I took a quick peek in the tank, but that just made me more confused. I was paralyzed by a lack of know-how.
Normally, I would have just Googled a local plumber. But that day, I decided to do something different. Maybe it was because it was the fantasy football offseason. Maybe it was because my wife had started to ask my father-in-law to change light bulbs around the house. Or, maybe, I wanted to learn to actually fix the problem. A few hours later, after an Internet lesson in toilet physiology, a $4.12 trip to Home Depot, and a wet pair of hands, I had replaced my first toilet flapper.
This wasn’t the rebuilding of a car engine, but it was a clear DIY step toward self-improvement. Easily the most memorable moment here was my sense of accomplishment.
I felt empowered.
One Part Science, One Part Art
It’s taken me a while to realize this, but I’ve begun to take advantage of improvement opportunities at work as well. No, I haven’t been moonlighting as a plumber for my hospital. I’ve just been fortunate to be part of a trifecta of rewarding quality-improvement (QI) projects over the past year. Before I’d gotten my hands dirty with these, my understanding of QI was fairly naive. I’d heard about Plan-Do-Study-Act many times. I had listened to a talk at a national conference. And I had kept up with the general medical literature on the subject.
But none of those activities had truly prepared me for experience of actually doing the work on my own.
By taking on a project, an ambitious attempt to reduce continuous pulse oximetry use, I experienced a crash course in both the science and the art of process improvement. I was forced to overcome my “I don’t know how” inertia. And with expert guidance in the form of a clinical safety and effectiveness class, I learned the importance of run charts (science) and a well-crafted multidisciplinary team (art) in changing established but inefficient behavior.
Our rates of continuous pulse oximetry usage dropped by 50%, and cost savings were $12,000 per year on one unit. These results made my prior attempts at change—years of complaining about ingrained nursing culture—look infantile. (OK, maybe it was ineffective, but who hasn’t complained about the overuse of continuous monitoring?)
I haven’t met a pediatric hospitalist who wouldn’t understand the symbolic importance of this success. But I know of many hospitalists who have not yet participated in meaningful QI project. Imagine calling a plumber who grasped the flush and fill mechanism of a toilet but had never touched real porcelain. Here’s an even better analogy: What if doctors could get licensed without having touched real patients?
If pediatric hospitalists are to transform the care delivery of hospitalized children, and quality learning only comes through hands-on training, then we need some more hands in the pot.
Discharge Improvement
On the heels of my first project, I was fortunate enough to augment my education through another effort—this time with a cohort of fellow pediatric hospitalists. This was a national collaborative to improve discharge handoffs, and I will admit that, at the outset, I was as puzzled as the first time I pulled the lid off the tank of the toilet. There were just too many permutations on PCP communication at the participating institutions, and some felt our aim of timely discharge handoffs was unattainable.
What carried me through, however, was the collective and infectious DIY—no, QIY (Quality Improve-it-Yourself) attitude of the group. We were all learning, and regular participation in the collaborative essentially guaranteed improvement. We achieved our aim of 90% communication with PCPs within two days of discharge. The secret was simple: The more you do, the more you learn.
Pediatric hospitalists can transform care delivery through a focus on safe and quality care, but the tools to accomplish this must come through post-residency, on-the-job learning. This QI know-how must efficiently spread among our ranks through practical and project-based educational efforts. It’s “see one, do one, teach one,” but we’re not talking about lumbar punctures anymore.
This is a journey in which we all take on the responsibility of rolling up our sleeves and simply learn by doing. And here is where the third leg of my as-yet-unfinished QI course unfolds.
Through my involvement with the Value in Inpatient Pediatrics (VIP) Network, I’ve gained a newfound vision for what the future might hold. VIP has evolved from a benchmarking project focused on bronchiolitis to an improvement network that will incorporate projects similar to the discharge handoff collaborative above.
In the process, a model for how to rapidly spread QI learning has emerged. The capacity lies in the network’s rapidly growing connectivity. The power comes from the individuals: motivated, card-carrying pediatric hospitalists from a wide array of sites. Collaborative learning harbors the potential to exponentially increase the pace at which we improve.
The future of our quality care is bright. I see an open network of improvement doers and learners. I see collaboration on quality and safety initiatives in all manner of hospitals and communities. I see that this will all be built upon a foundation of hard work and a QIY attitude.
You, too, will play a role.
Just don’t be afraid to get your hands a little dirty. TH
Dr. Shen is medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas. He is pediatric editor of The Hospitalist.
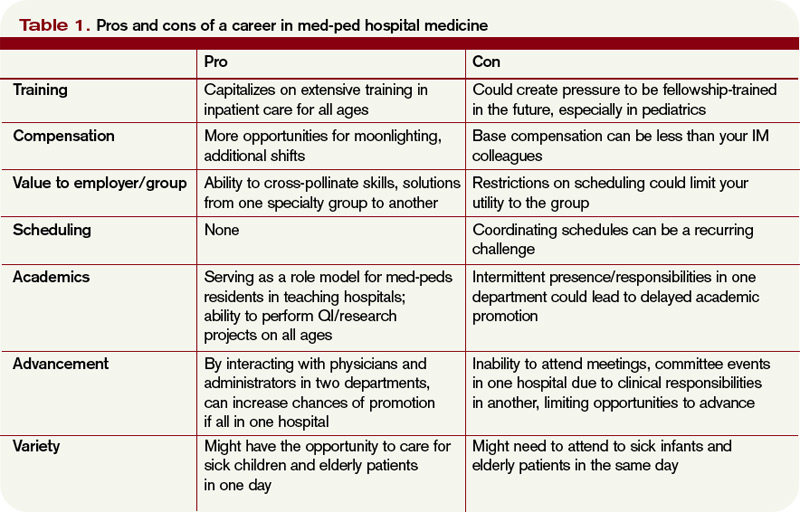
Split Personality
By the fourth year of residency, most in combined internal medicine/pediatrics (commonly known as “med-ped”) residencies come to realize that their training is heavily weighted toward inpatient and ICU settings. After all, med-ped residency programs require that all the inpatient and ICU requirements of both the American Board of Internal Medicine (ABIM) and the American Board of Pediatrics (ABP) be met. This allows med-ped graduates, numbering just over 300 each year, to sit for both boards, and potentially to be able to obtain admitting privileges for both adults and children. This seems to be the perfect training for a hospitalist-to-be, if one so desires.
But for hospitalists, there comes the dilemma: Should you concentrate on the adult or the pediatric population, or is it possible to be a med-ped hospitalist? By far, most HM job opportunities are for either purely adult hospitalists or purely pediatric hospitalists, although there are an increasing number of “off the shelf” med-ped hospitalist positions. Building a med-ped career as a hospitalist from shifts in adult and pediatric programs is a possibility but requires extra attention to scheduling, salary, and benefits.
Med-ped physicians are used to being creative about their work, but some might begin to ask themselves whether the additional effort is worth it. Seeking out knowledgeable administrators and department/division chiefs, following other med-ped hospitalists who have already blazed a trail, and being realistic about your “mix” of work are some solutions for the hybrid hospitalist.
Academia Fosters Cooperation—and Lack Thereof
An ever-increasing number of med-ped physicians seem to think being a med-peds hospitalist is possible, even desirable. Heather Toth, MD, program director for the med-ped residency program at Medical College of Wisconsin and a hospitalist at Children’s Hospital of Wisconsin, both in Milwaukee, doesn’t regret her decision to put in the extra work required to be a hospitalist for all age groups.
“[It is] absolutely a wonderful career and worth the effort to establish a combined position. There is much to be learned from each world [medicine and pediatrics] to enrich our patients’ care,” says Dr. Toth, who was a former chief resident for the med-ped program at the college. In her case, being close to the administrators of both departments played to her advantage and allowed her to craft her job “from the inside,” she says.

“The process was much smoother than anticipated,” Dr. Toth explains. “One concern was which department would own my time. This was overcome by splitting my time by months. For example, January is medicine wards, February is pediatric wards, etc., with corresponding overnight shifts/call.”
Others have experienced obstacles in carving out an academic med-peds hospitalist position. Susan Hunt, MD, a hospitalist at Brigham and Women’s Hospital in Boston, finished her med-ped residency at Duke University in 2008 and began her career as an adults-only hospitalist. However, the desire to work in pediatrics still burned, leading Dr. Hunt to seek pediatric hospitalist work within the Partners HealthCare system. Initially, her efforts were to no avail. More recently, she has been able to break into hospitalist work through the Children’s Hospital Boston’s outreach program at local community hospitals.
“Pediatric programs tend to be small and, in Boston, had very little turnover,” Dr. Hunt says. She also has a warning for pediatric hospitalist hopefuls. “Increasing pediatric time invariably results in decreased pay.”
For the most part, med-ped hospitalist positions in academic hospitals tend to be crafted from a combination of time from two distinct departments. But an academic setting does offer potential med-ped hospitalists a few advantages, such as:
- Typically more hospitalists in each department, leading to greater scheduling flexibility;
- Larger pediatric hospitalist programs that often encompass not only the “main” hospital, but also community hospitals; this leads to increased availability of hospitalist work; and
- The possibility of a med-ped residency program at the same site, which allows for the possibility of being a role model to med-ped residents.
Although the trends might be changing, there are multiple barriers to an academic med-ped hospitalist job. Often, the IM and pediatric departments are not used to working together. Determining who will pay the hospitalist’s salary and benefits, how the schedule will be coordinated, and to whom the hospitalist is responsible can be tricky. Moreover, it’s not always clear which department will take the lead in the promotion process. Departments expect hospitalists to act as good citizens by serving on committees, and it can be difficult to serve two masters.
As a result, many academic med-peds hospitalists have a primary appointment in one department and have their clinical salaries “bought down” by the other. A handful of hospital committees, including quality-improvement (QI) and information technology, allow med-ped hospitalists to serve on one committee and receive citizenship “credit” from both departments. Leonard Feldman, MD, FAAP, FACP, and Carrie Herzke, MD, have walked this tightrope at Johns Hopkins Hospital in Baltimore. Their successes in this arena have created more clinical and research opportunities for med-ped hospitalists, as the administrators and physicians have learned how to negotiate their relationship. One example of this success has been the Johns Hopkins Hospitalist Scholars Program, which provides up to $12,000 of annual funding to hospitalist faculty.
Although rare, the academic med-ped hospitalist program under a single administrative structure does exist. Allen Liles, MD, program director for the hospital medicine program at the University of North Carolina (UNC) Hospitals in Chapel Hill, has brought together a group of 17 hospitalists, six of whom are med-ped-trained.
“Both the pediatric portion and the medicine portion are administered within this one program,” states Dr. Liles. “I think this is a huge advantage to actually making it work. If I was not the director being med-peds-trained, I am not sure this would have happened.” According to Dr. Liles, it took six months of working closely with the CFO of UNC Hospitals to establish a program that he felt “managed to change the paradigm.”
“It is the hospital that derives the most benefit from a [combined] hospitalist program,” adds Dr. Liles. “And as such, they were easy to convince of the benefits of a med-ped model and expansion into pediatrics.”
The Community Setting: Challenges and Successes
Academic settings aren’t alone in their battles putting together med-ped hospitalist positions. Jacques-Bret Burgess, MD, MPH, FAAP, a hospitalist with Traverse City, Mich.-based Hospitalists of Northwest Michigan (HNM), began in April 2009 to establish a pediatric hospitalist program within his group of adult hospitalists. Since that time, med-ped-trained hospitalists have increased to five from just one out of the 30 hospitalists employed by HNM. But there have been growing pains.
“The majority of administrators and physicians just do not understand the potential, nor the efficiency, of a [med-ped] physician,” Dr. Burgess says. “Most frustrations come from trying to explain what an IM-ped physician is, what we are capable of, and then obtaining adequate support to practice both disciplines while at the same time maintaining some sense of self and family.”
In fact, it is not uncommon for med-ped hospitalists to work full time in one discipline—usually adult—and moonlight or work part time in pediatrics. Jeff Whittall, MD, a hospitalist for MultiCare Inpatient Services in Tacoma, Wash., works primarily as an adult hospitalist at Tacoma General Hospital but provides pediatric urgent care at Mary Bridge Children’s Hospital in Tacoma as well. “It is a fantastic mix,” Dr. Whittall says.
That said, other med-ped hospitalists consider such combinations to be a compromise. Many yearn for that perfect mix of adult and pediatric hospitalist work, and have even taken on additional training to do so.
Oliver Medzihradsy, MD, was a half-time adult hospitalist at Barton Memorial Hospital in South Lake Tahoe, Calif., with the other half spent in outpatient pediatrics for Tahoe Carson Valley Medical Group, until this year. In August, be became a first-year fellow at Rady Children’s Hospital in pediatric hospital medicine.
“Having been out [of] hospital-based peds for four years now, I decided that, if I wanted to get back into … [pediatrics] as a hospitalist, it would serve me well to go back for a peds hospital medicine fellowship,” said Dr. Medzihradsy. “Economically, it’s rather foolhardy to take such a salary cut, not to mention the philosophical change of becoming a trainee again, but from a clinical passion standpoint, it’s what I wish to do.”
In some cases, community hospitalist programs, many of which offer a less territorial work environment and organizational structure, have been more successful at establishing full-fledged combined med-ped hospitalist programs. Elliot Hospital in Manchester, N.H., has built from the ground up a hospitalist program utilizing both internal medicine and med-ped-trained hospitalists. Currently, Elliot Hospital employs four med-ped-trained hospitalists, who staff the pediatric inpatient unit but are available for adult inpatients when pediatric volume is low. Other community hospitalist programs utilize the pediatric skills of their med-ped hospitalists in urgent-care or ED coverage in times of low pediatric volume.
“From the perspective of our med-ped physicians, they feel that this is a unique employment opportunity that allows them to have a truly balanced 50-50 medicine/pediatrics inpatient experience,” said Anita Ritenour, MD, assistant vice president for medical affairs at Elliot Hospital. Although trained in internal medicine, her familiarity with community med-ped physicians made her an early advocate of med-ped hospitalists.
Amy Stone, MD, director of Elliot Hospital’s pediatric hospitalist program and a med-ped-trained physician, typically starts her day at 7 a.m. with sign-out from the overnight provider, then touches base with nurses about overnight events. Family-centered rounds follow, with the afternoons being occupied by ED or direct admissions and family meetings. Given their training, however, the med-ped-trained pediatric hospitalists can get called upon to help out on the internal-medicine side.
“As a med-ped hospitalist on the peds service, we get pulled occasionally to help with the internal-medicine service to admit, both during the day and at night,” adds Dr. Craig Widness, another med-peds-trained hospitalist at Elliot.
But the scope of practice and volume has ramped up for the pediatric hospitalist service at Elliot, as many community pediatric groups have opted to utilize their services. In addition, a new pediatric ICU has recently been established, managed by the pediatric hospitalist service.
As a result, the opportunities for the med-ped-trained pediatric hospitalists to help out on the adult hospitalist vortex have been increasingly rare, which seem to be a welcome development to the pediatric hospitalists.

Building the Perfect Beast
So how does a med-ped physician entering hospital medicine build a job that satisfies the need to care for both adults and children? In some cases, the perfect med-ped position is already available. More likely, however, hospitalist jobs in a specific location are limited to either one discipline or another.
In many, if not most, cases, practice in one discipline will have to be somewhat compromised to fulfill the staffing needs of the “primary” job, at least initially. In the interview and hiring process, however, hospitalists wishing to pursue med-peds must make known their desire to work in both medicine and pediatrics. The transparency will allow hospital and group administrators to build into your schedule time to work in both pursuits.
“Start trying to arrange for pediatrics early. I started before I finished residency and it took me over a year to set up,” Dr. Hunt says, noting her current position is in the academic arena. “Discuss your plans with any medicine group you intend to join. See if your FTE would be flexible or if they can help arrange things. Get in touch with local med-ped program directors, if possible, as they often know people on both sides and might be able to help get you in touch with the right people.”
When looking at community hospitalist jobs, it is critical to ensure your administrators are familiar with med-peds residency training. It helps them better understand your skills, your goals, and allows them to put you in position to care for patients in all age groups.
“When one finds administrators and leaders that understand and respect the concept [of med-peds], hold on to them,” Dr. Burgess advises. “Do not let anyone take your unique training for granted and try to categorize you as one or the other; rather, we are both. We have two sets of boards, with separate training and a unique overlap that provides synergy with our abilities. Find a group that understands the level of training you possess.”
Call Protection
As uncommon as it is to find med-ped hospitalist jobs that feature built-in coordination of work in both disciplines, one should pay attention to coordinating salary, call, vacation, and CME between the two disciplines.
“Talk with potential groups about how they cover you for call, how you will be reimbursed, and what data will they base your pay and incentives on,” Dr. Burgess says. “What will they base your CME on—two disciplines or one? What is your depth if you have a sick child and sick adult at the same time?”
Most important, med-peds must make sure administrators of both disciplines are aware of your activities on both sides. “We do not want double-call days,” Dr. Burgess adds. He also warns that overcoming the frustrations of med-pedwork “takes a great deal of patience and discussion.”
Salary might be an issue, especially as one tries to mold a position. SHM and the Medical Group Management Association (MGMA) State of Hospital Medicine: 2010 Report Based on 2009 Data lists the median national annual compensation for adult hospitalists as $215,000, and $160,038 for pediatric hospitalists. This also has implications when IM time is bought down by pediatrics in academic centers, as pediatrics might not pay as much for clinical time as medicine will.
Back Where You Belong
Either by necessity or choice, med-ped-trained hospitalists all across the country have taken jobs in one setting or another and now yearn to get back into the other discipline. It might not be as difficult as you think.
If hospitalist work in the other discipline is available in your institution, you could consider a reduction of FTE in your current job to expand into the other discipline. Keep in mind, however, the interdepartmental coordination difficulties (i.e. scheduling, benefits, maintaining privileges). Those can be even more pronounced if two or more employers are involved.
Additionally, a reduction of FTE in your current job could lead to increased clinical time on the part of your colleagues, or perhaps even hiring additional staff, so this change needs to be discussed thoroughly with administrators and colleagues well in advance of any changes.
Less dramatic changes can enable a med-ped hospitalist to get a taste of the other discipline without wholesale changes in salary and schedule. Moonlighting as an intermittent hospitalist or nocturnist, taking call in the other discipline’s call schedule, or filling in for urgent-care slots can keep skills and knowledge from getting rusty.
It also can prevent the loss of pediatric admitting and procedural privileges. A patchwork approach also could lead to a steady hospitalist job in the other discipline.
“I discussed my desire to do pediatrics with friends and acquaintances who worked as pediatricians in local community hospitals through Children’s Hospital Boston,” Dr. Hunt says. “Eventually, [it led] to the peds work.”
As is often the case in HM, med-ped programs tend to follow the tenet “if you build it, they will come.” Once a hospitalist director discovers the flexibility and skill set a med-ped hospitalist provides the group, they often look to expand—especially to staff smaller pediatric units.
Such was the case at Elliot Hospital; familiarity with med-ped moonlighters eventually led to a full-time med-ped hospitalist hire. Following the full-time hire, the HM group realized a dramatic increase in local pediatric groups referring patients to Elliot’s hospitalist group, including the largest pediatric group in Southern New Hampshire, Dartmouth-Hitchcock Clinic.
“Initial referral base from the community was sluggish as community [pediatricians] wanted to hold onto their patients,” Dr. Ritenour says. “As the acuity of what we could support as hospitalists grew, more referrals were made for kids that might have previously been transferred.”
The Future of Med-Ped Hospitalists
At the dawn of combined med-ped residencies in the early 1960s, the hospitalist movement was only a twinkle in the eye of house physicians of yore. Now that both movements have matured, will we see this hybrid of a hybrid flourish?
“I think med-peds is well suited for hospital medicine, based on solid training that includes numerous inpatient wards and critical care in both internal medicine and pediatrics,” says Dr. Toth, adding she hopes to bring additional med-ped hospitalists to her group in Milwaukee in the future.
It seems inevitable that the med-ped movement, which has grown into the largest combined residency specialty in the country, and the hospitalist movement, which has exploded as the fastest-growing medical specialty, will continue to intertwine, branch out, and evolve.
And every year, some of those med-ped residency program graduates will continue to climb those twisted trunks, as challenging as it might seem. TH
Dr. Chang is a med-peds hospitalist at the University of California at San Diego and Rady Children’s Hospital. He is a member of Team Hospitalist.
By the fourth year of residency, most in combined internal medicine/pediatrics (commonly known as “med-ped”) residencies come to realize that their training is heavily weighted toward inpatient and ICU settings. After all, med-ped residency programs require that all the inpatient and ICU requirements of both the American Board of Internal Medicine (ABIM) and the American Board of Pediatrics (ABP) be met. This allows med-ped graduates, numbering just over 300 each year, to sit for both boards, and potentially to be able to obtain admitting privileges for both adults and children. This seems to be the perfect training for a hospitalist-to-be, if one so desires.
But for hospitalists, there comes the dilemma: Should you concentrate on the adult or the pediatric population, or is it possible to be a med-ped hospitalist? By far, most HM job opportunities are for either purely adult hospitalists or purely pediatric hospitalists, although there are an increasing number of “off the shelf” med-ped hospitalist positions. Building a med-ped career as a hospitalist from shifts in adult and pediatric programs is a possibility but requires extra attention to scheduling, salary, and benefits.
Med-ped physicians are used to being creative about their work, but some might begin to ask themselves whether the additional effort is worth it. Seeking out knowledgeable administrators and department/division chiefs, following other med-ped hospitalists who have already blazed a trail, and being realistic about your “mix” of work are some solutions for the hybrid hospitalist.
Academia Fosters Cooperation—and Lack Thereof
An ever-increasing number of med-ped physicians seem to think being a med-peds hospitalist is possible, even desirable. Heather Toth, MD, program director for the med-ped residency program at Medical College of Wisconsin and a hospitalist at Children’s Hospital of Wisconsin, both in Milwaukee, doesn’t regret her decision to put in the extra work required to be a hospitalist for all age groups.
“[It is] absolutely a wonderful career and worth the effort to establish a combined position. There is much to be learned from each world [medicine and pediatrics] to enrich our patients’ care,” says Dr. Toth, who was a former chief resident for the med-ped program at the college. In her case, being close to the administrators of both departments played to her advantage and allowed her to craft her job “from the inside,” she says.
“The process was much smoother than anticipated,” Dr. Toth explains. “One concern was which department would own my time. This was overcome by splitting my time by months. For example, January is medicine wards, February is pediatric wards, etc., with corresponding overnight shifts/call.”
Others have experienced obstacles in carving out an academic med-peds hospitalist position. Susan Hunt, MD, a hospitalist at Brigham and Women’s Hospital in Boston, finished her med-ped residency at Duke University in 2008 and began her career as an adults-only hospitalist. However, the desire to work in pediatrics still burned, leading Dr. Hunt to seek pediatric hospitalist work within the Partners HealthCare system. Initially, her efforts were to no avail. More recently, she has been able to break into hospitalist work through the Children’s Hospital Boston’s outreach program at local community hospitals.
“Pediatric programs tend to be small and, in Boston, had very little turnover,” Dr. Hunt says. She also has a warning for pediatric hospitalist hopefuls. “Increasing pediatric time invariably results in decreased pay.”
For the most part, med-ped hospitalist positions in academic hospitals tend to be crafted from a combination of time from two distinct departments. But an academic setting does offer potential med-ped hospitalists a few advantages, such as:
- Typically more hospitalists in each department, leading to greater scheduling flexibility;
- Larger pediatric hospitalist programs that often encompass not only the “main” hospital, but also community hospitals; this leads to increased availability of hospitalist work; and
- The possibility of a med-ped residency program at the same site, which allows for the possibility of being a role model to med-ped residents.
Although the trends might be changing, there are multiple barriers to an academic med-ped hospitalist job. Often, the IM and pediatric departments are not used to working together. Determining who will pay the hospitalist’s salary and benefits, how the schedule will be coordinated, and to whom the hospitalist is responsible can be tricky. Moreover, it’s not always clear which department will take the lead in the promotion process. Departments expect hospitalists to act as good citizens by serving on committees, and it can be difficult to serve two masters.
As a result, many academic med-peds hospitalists have a primary appointment in one department and have their clinical salaries “bought down” by the other. A handful of hospital committees, including quality-improvement (QI) and information technology, allow med-ped hospitalists to serve on one committee and receive citizenship “credit” from both departments. Leonard Feldman, MD, FAAP, FACP, and Carrie Herzke, MD, have walked this tightrope at Johns Hopkins Hospital in Baltimore. Their successes in this arena have created more clinical and research opportunities for med-ped hospitalists, as the administrators and physicians have learned how to negotiate their relationship. One example of this success has been the Johns Hopkins Hospitalist Scholars Program, which provides up to $12,000 of annual funding to hospitalist faculty.
Although rare, the academic med-ped hospitalist program under a single administrative structure does exist. Allen Liles, MD, program director for the hospital medicine program at the University of North Carolina (UNC) Hospitals in Chapel Hill, has brought together a group of 17 hospitalists, six of whom are med-ped-trained.
“Both the pediatric portion and the medicine portion are administered within this one program,” states Dr. Liles. “I think this is a huge advantage to actually making it work. If I was not the director being med-peds-trained, I am not sure this would have happened.” According to Dr. Liles, it took six months of working closely with the CFO of UNC Hospitals to establish a program that he felt “managed to change the paradigm.”
“It is the hospital that derives the most benefit from a [combined] hospitalist program,” adds Dr. Liles. “And as such, they were easy to convince of the benefits of a med-ped model and expansion into pediatrics.”
The Community Setting: Challenges and Successes
Academic settings aren’t alone in their battles putting together med-ped hospitalist positions. Jacques-Bret Burgess, MD, MPH, FAAP, a hospitalist with Traverse City, Mich.-based Hospitalists of Northwest Michigan (HNM), began in April 2009 to establish a pediatric hospitalist program within his group of adult hospitalists. Since that time, med-ped-trained hospitalists have increased to five from just one out of the 30 hospitalists employed by HNM. But there have been growing pains.
“The majority of administrators and physicians just do not understand the potential, nor the efficiency, of a [med-ped] physician,” Dr. Burgess says. “Most frustrations come from trying to explain what an IM-ped physician is, what we are capable of, and then obtaining adequate support to practice both disciplines while at the same time maintaining some sense of self and family.”
In fact, it is not uncommon for med-ped hospitalists to work full time in one discipline—usually adult—and moonlight or work part time in pediatrics. Jeff Whittall, MD, a hospitalist for MultiCare Inpatient Services in Tacoma, Wash., works primarily as an adult hospitalist at Tacoma General Hospital but provides pediatric urgent care at Mary Bridge Children’s Hospital in Tacoma as well. “It is a fantastic mix,” Dr. Whittall says.
That said, other med-ped hospitalists consider such combinations to be a compromise. Many yearn for that perfect mix of adult and pediatric hospitalist work, and have even taken on additional training to do so.
Oliver Medzihradsy, MD, was a half-time adult hospitalist at Barton Memorial Hospital in South Lake Tahoe, Calif., with the other half spent in outpatient pediatrics for Tahoe Carson Valley Medical Group, until this year. In August, be became a first-year fellow at Rady Children’s Hospital in pediatric hospital medicine.
“Having been out [of] hospital-based peds for four years now, I decided that, if I wanted to get back into … [pediatrics] as a hospitalist, it would serve me well to go back for a peds hospital medicine fellowship,” said Dr. Medzihradsy. “Economically, it’s rather foolhardy to take such a salary cut, not to mention the philosophical change of becoming a trainee again, but from a clinical passion standpoint, it’s what I wish to do.”
In some cases, community hospitalist programs, many of which offer a less territorial work environment and organizational structure, have been more successful at establishing full-fledged combined med-ped hospitalist programs. Elliot Hospital in Manchester, N.H., has built from the ground up a hospitalist program utilizing both internal medicine and med-ped-trained hospitalists. Currently, Elliot Hospital employs four med-ped-trained hospitalists, who staff the pediatric inpatient unit but are available for adult inpatients when pediatric volume is low. Other community hospitalist programs utilize the pediatric skills of their med-ped hospitalists in urgent-care or ED coverage in times of low pediatric volume.
“From the perspective of our med-ped physicians, they feel that this is a unique employment opportunity that allows them to have a truly balanced 50-50 medicine/pediatrics inpatient experience,” said Anita Ritenour, MD, assistant vice president for medical affairs at Elliot Hospital. Although trained in internal medicine, her familiarity with community med-ped physicians made her an early advocate of med-ped hospitalists.
Amy Stone, MD, director of Elliot Hospital’s pediatric hospitalist program and a med-ped-trained physician, typically starts her day at 7 a.m. with sign-out from the overnight provider, then touches base with nurses about overnight events. Family-centered rounds follow, with the afternoons being occupied by ED or direct admissions and family meetings. Given their training, however, the med-ped-trained pediatric hospitalists can get called upon to help out on the internal-medicine side.
“As a med-ped hospitalist on the peds service, we get pulled occasionally to help with the internal-medicine service to admit, both during the day and at night,” adds Dr. Craig Widness, another med-peds-trained hospitalist at Elliot.
But the scope of practice and volume has ramped up for the pediatric hospitalist service at Elliot, as many community pediatric groups have opted to utilize their services. In addition, a new pediatric ICU has recently been established, managed by the pediatric hospitalist service.
As a result, the opportunities for the med-ped-trained pediatric hospitalists to help out on the adult hospitalist vortex have been increasingly rare, which seem to be a welcome development to the pediatric hospitalists.
Building the Perfect Beast
So how does a med-ped physician entering hospital medicine build a job that satisfies the need to care for both adults and children? In some cases, the perfect med-ped position is already available. More likely, however, hospitalist jobs in a specific location are limited to either one discipline or another.
In many, if not most, cases, practice in one discipline will have to be somewhat compromised to fulfill the staffing needs of the “primary” job, at least initially. In the interview and hiring process, however, hospitalists wishing to pursue med-peds must make known their desire to work in both medicine and pediatrics. The transparency will allow hospital and group administrators to build into your schedule time to work in both pursuits.
“Start trying to arrange for pediatrics early. I started before I finished residency and it took me over a year to set up,” Dr. Hunt says, noting her current position is in the academic arena. “Discuss your plans with any medicine group you intend to join. See if your FTE would be flexible or if they can help arrange things. Get in touch with local med-ped program directors, if possible, as they often know people on both sides and might be able to help get you in touch with the right people.”
When looking at community hospitalist jobs, it is critical to ensure your administrators are familiar with med-peds residency training. It helps them better understand your skills, your goals, and allows them to put you in position to care for patients in all age groups.
“When one finds administrators and leaders that understand and respect the concept [of med-peds], hold on to them,” Dr. Burgess advises. “Do not let anyone take your unique training for granted and try to categorize you as one or the other; rather, we are both. We have two sets of boards, with separate training and a unique overlap that provides synergy with our abilities. Find a group that understands the level of training you possess.”
Call Protection
As uncommon as it is to find med-ped hospitalist jobs that feature built-in coordination of work in both disciplines, one should pay attention to coordinating salary, call, vacation, and CME between the two disciplines.
“Talk with potential groups about how they cover you for call, how you will be reimbursed, and what data will they base your pay and incentives on,” Dr. Burgess says. “What will they base your CME on—two disciplines or one? What is your depth if you have a sick child and sick adult at the same time?”
Most important, med-peds must make sure administrators of both disciplines are aware of your activities on both sides. “We do not want double-call days,” Dr. Burgess adds. He also warns that overcoming the frustrations of med-pedwork “takes a great deal of patience and discussion.”
Salary might be an issue, especially as one tries to mold a position. SHM and the Medical Group Management Association (MGMA) State of Hospital Medicine: 2010 Report Based on 2009 Data lists the median national annual compensation for adult hospitalists as $215,000, and $160,038 for pediatric hospitalists. This also has implications when IM time is bought down by pediatrics in academic centers, as pediatrics might not pay as much for clinical time as medicine will.
Back Where You Belong
Either by necessity or choice, med-ped-trained hospitalists all across the country have taken jobs in one setting or another and now yearn to get back into the other discipline. It might not be as difficult as you think.
If hospitalist work in the other discipline is available in your institution, you could consider a reduction of FTE in your current job to expand into the other discipline. Keep in mind, however, the interdepartmental coordination difficulties (i.e. scheduling, benefits, maintaining privileges). Those can be even more pronounced if two or more employers are involved.
Additionally, a reduction of FTE in your current job could lead to increased clinical time on the part of your colleagues, or perhaps even hiring additional staff, so this change needs to be discussed thoroughly with administrators and colleagues well in advance of any changes.
Less dramatic changes can enable a med-ped hospitalist to get a taste of the other discipline without wholesale changes in salary and schedule. Moonlighting as an intermittent hospitalist or nocturnist, taking call in the other discipline’s call schedule, or filling in for urgent-care slots can keep skills and knowledge from getting rusty.
It also can prevent the loss of pediatric admitting and procedural privileges. A patchwork approach also could lead to a steady hospitalist job in the other discipline.
“I discussed my desire to do pediatrics with friends and acquaintances who worked as pediatricians in local community hospitals through Children’s Hospital Boston,” Dr. Hunt says. “Eventually, [it led] to the peds work.”
As is often the case in HM, med-ped programs tend to follow the tenet “if you build it, they will come.” Once a hospitalist director discovers the flexibility and skill set a med-ped hospitalist provides the group, they often look to expand—especially to staff smaller pediatric units.
Such was the case at Elliot Hospital; familiarity with med-ped moonlighters eventually led to a full-time med-ped hospitalist hire. Following the full-time hire, the HM group realized a dramatic increase in local pediatric groups referring patients to Elliot’s hospitalist group, including the largest pediatric group in Southern New Hampshire, Dartmouth-Hitchcock Clinic.
“Initial referral base from the community was sluggish as community [pediatricians] wanted to hold onto their patients,” Dr. Ritenour says. “As the acuity of what we could support as hospitalists grew, more referrals were made for kids that might have previously been transferred.”
The Future of Med-Ped Hospitalists
At the dawn of combined med-ped residencies in the early 1960s, the hospitalist movement was only a twinkle in the eye of house physicians of yore. Now that both movements have matured, will we see this hybrid of a hybrid flourish?
“I think med-peds is well suited for hospital medicine, based on solid training that includes numerous inpatient wards and critical care in both internal medicine and pediatrics,” says Dr. Toth, adding she hopes to bring additional med-ped hospitalists to her group in Milwaukee in the future.
It seems inevitable that the med-ped movement, which has grown into the largest combined residency specialty in the country, and the hospitalist movement, which has exploded as the fastest-growing medical specialty, will continue to intertwine, branch out, and evolve.
And every year, some of those med-ped residency program graduates will continue to climb those twisted trunks, as challenging as it might seem. TH
Dr. Chang is a med-peds hospitalist at the University of California at San Diego and Rady Children’s Hospital. He is a member of Team Hospitalist.
By the fourth year of residency, most in combined internal medicine/pediatrics (commonly known as “med-ped”) residencies come to realize that their training is heavily weighted toward inpatient and ICU settings. After all, med-ped residency programs require that all the inpatient and ICU requirements of both the American Board of Internal Medicine (ABIM) and the American Board of Pediatrics (ABP) be met. This allows med-ped graduates, numbering just over 300 each year, to sit for both boards, and potentially to be able to obtain admitting privileges for both adults and children. This seems to be the perfect training for a hospitalist-to-be, if one so desires.
But for hospitalists, there comes the dilemma: Should you concentrate on the adult or the pediatric population, or is it possible to be a med-ped hospitalist? By far, most HM job opportunities are for either purely adult hospitalists or purely pediatric hospitalists, although there are an increasing number of “off the shelf” med-ped hospitalist positions. Building a med-ped career as a hospitalist from shifts in adult and pediatric programs is a possibility but requires extra attention to scheduling, salary, and benefits.
Med-ped physicians are used to being creative about their work, but some might begin to ask themselves whether the additional effort is worth it. Seeking out knowledgeable administrators and department/division chiefs, following other med-ped hospitalists who have already blazed a trail, and being realistic about your “mix” of work are some solutions for the hybrid hospitalist.
Academia Fosters Cooperation—and Lack Thereof
An ever-increasing number of med-ped physicians seem to think being a med-peds hospitalist is possible, even desirable. Heather Toth, MD, program director for the med-ped residency program at Medical College of Wisconsin and a hospitalist at Children’s Hospital of Wisconsin, both in Milwaukee, doesn’t regret her decision to put in the extra work required to be a hospitalist for all age groups.
“[It is] absolutely a wonderful career and worth the effort to establish a combined position. There is much to be learned from each world [medicine and pediatrics] to enrich our patients’ care,” says Dr. Toth, who was a former chief resident for the med-ped program at the college. In her case, being close to the administrators of both departments played to her advantage and allowed her to craft her job “from the inside,” she says.
“The process was much smoother than anticipated,” Dr. Toth explains. “One concern was which department would own my time. This was overcome by splitting my time by months. For example, January is medicine wards, February is pediatric wards, etc., with corresponding overnight shifts/call.”
Others have experienced obstacles in carving out an academic med-peds hospitalist position. Susan Hunt, MD, a hospitalist at Brigham and Women’s Hospital in Boston, finished her med-ped residency at Duke University in 2008 and began her career as an adults-only hospitalist. However, the desire to work in pediatrics still burned, leading Dr. Hunt to seek pediatric hospitalist work within the Partners HealthCare system. Initially, her efforts were to no avail. More recently, she has been able to break into hospitalist work through the Children’s Hospital Boston’s outreach program at local community hospitals.
“Pediatric programs tend to be small and, in Boston, had very little turnover,” Dr. Hunt says. She also has a warning for pediatric hospitalist hopefuls. “Increasing pediatric time invariably results in decreased pay.”
For the most part, med-ped hospitalist positions in academic hospitals tend to be crafted from a combination of time from two distinct departments. But an academic setting does offer potential med-ped hospitalists a few advantages, such as:
- Typically more hospitalists in each department, leading to greater scheduling flexibility;
- Larger pediatric hospitalist programs that often encompass not only the “main” hospital, but also community hospitals; this leads to increased availability of hospitalist work; and
- The possibility of a med-ped residency program at the same site, which allows for the possibility of being a role model to med-ped residents.
Although the trends might be changing, there are multiple barriers to an academic med-ped hospitalist job. Often, the IM and pediatric departments are not used to working together. Determining who will pay the hospitalist’s salary and benefits, how the schedule will be coordinated, and to whom the hospitalist is responsible can be tricky. Moreover, it’s not always clear which department will take the lead in the promotion process. Departments expect hospitalists to act as good citizens by serving on committees, and it can be difficult to serve two masters.
As a result, many academic med-peds hospitalists have a primary appointment in one department and have their clinical salaries “bought down” by the other. A handful of hospital committees, including quality-improvement (QI) and information technology, allow med-ped hospitalists to serve on one committee and receive citizenship “credit” from both departments. Leonard Feldman, MD, FAAP, FACP, and Carrie Herzke, MD, have walked this tightrope at Johns Hopkins Hospital in Baltimore. Their successes in this arena have created more clinical and research opportunities for med-ped hospitalists, as the administrators and physicians have learned how to negotiate their relationship. One example of this success has been the Johns Hopkins Hospitalist Scholars Program, which provides up to $12,000 of annual funding to hospitalist faculty.
Although rare, the academic med-ped hospitalist program under a single administrative structure does exist. Allen Liles, MD, program director for the hospital medicine program at the University of North Carolina (UNC) Hospitals in Chapel Hill, has brought together a group of 17 hospitalists, six of whom are med-ped-trained.
“Both the pediatric portion and the medicine portion are administered within this one program,” states Dr. Liles. “I think this is a huge advantage to actually making it work. If I was not the director being med-peds-trained, I am not sure this would have happened.” According to Dr. Liles, it took six months of working closely with the CFO of UNC Hospitals to establish a program that he felt “managed to change the paradigm.”
“It is the hospital that derives the most benefit from a [combined] hospitalist program,” adds Dr. Liles. “And as such, they were easy to convince of the benefits of a med-ped model and expansion into pediatrics.”
The Community Setting: Challenges and Successes
Academic settings aren’t alone in their battles putting together med-ped hospitalist positions. Jacques-Bret Burgess, MD, MPH, FAAP, a hospitalist with Traverse City, Mich.-based Hospitalists of Northwest Michigan (HNM), began in April 2009 to establish a pediatric hospitalist program within his group of adult hospitalists. Since that time, med-ped-trained hospitalists have increased to five from just one out of the 30 hospitalists employed by HNM. But there have been growing pains.
“The majority of administrators and physicians just do not understand the potential, nor the efficiency, of a [med-ped] physician,” Dr. Burgess says. “Most frustrations come from trying to explain what an IM-ped physician is, what we are capable of, and then obtaining adequate support to practice both disciplines while at the same time maintaining some sense of self and family.”
In fact, it is not uncommon for med-ped hospitalists to work full time in one discipline—usually adult—and moonlight or work part time in pediatrics. Jeff Whittall, MD, a hospitalist for MultiCare Inpatient Services in Tacoma, Wash., works primarily as an adult hospitalist at Tacoma General Hospital but provides pediatric urgent care at Mary Bridge Children’s Hospital in Tacoma as well. “It is a fantastic mix,” Dr. Whittall says.
That said, other med-ped hospitalists consider such combinations to be a compromise. Many yearn for that perfect mix of adult and pediatric hospitalist work, and have even taken on additional training to do so.
Oliver Medzihradsy, MD, was a half-time adult hospitalist at Barton Memorial Hospital in South Lake Tahoe, Calif., with the other half spent in outpatient pediatrics for Tahoe Carson Valley Medical Group, until this year. In August, be became a first-year fellow at Rady Children’s Hospital in pediatric hospital medicine.
“Having been out [of] hospital-based peds for four years now, I decided that, if I wanted to get back into … [pediatrics] as a hospitalist, it would serve me well to go back for a peds hospital medicine fellowship,” said Dr. Medzihradsy. “Economically, it’s rather foolhardy to take such a salary cut, not to mention the philosophical change of becoming a trainee again, but from a clinical passion standpoint, it’s what I wish to do.”
In some cases, community hospitalist programs, many of which offer a less territorial work environment and organizational structure, have been more successful at establishing full-fledged combined med-ped hospitalist programs. Elliot Hospital in Manchester, N.H., has built from the ground up a hospitalist program utilizing both internal medicine and med-ped-trained hospitalists. Currently, Elliot Hospital employs four med-ped-trained hospitalists, who staff the pediatric inpatient unit but are available for adult inpatients when pediatric volume is low. Other community hospitalist programs utilize the pediatric skills of their med-ped hospitalists in urgent-care or ED coverage in times of low pediatric volume.
“From the perspective of our med-ped physicians, they feel that this is a unique employment opportunity that allows them to have a truly balanced 50-50 medicine/pediatrics inpatient experience,” said Anita Ritenour, MD, assistant vice president for medical affairs at Elliot Hospital. Although trained in internal medicine, her familiarity with community med-ped physicians made her an early advocate of med-ped hospitalists.
Amy Stone, MD, director of Elliot Hospital’s pediatric hospitalist program and a med-ped-trained physician, typically starts her day at 7 a.m. with sign-out from the overnight provider, then touches base with nurses about overnight events. Family-centered rounds follow, with the afternoons being occupied by ED or direct admissions and family meetings. Given their training, however, the med-ped-trained pediatric hospitalists can get called upon to help out on the internal-medicine side.
“As a med-ped hospitalist on the peds service, we get pulled occasionally to help with the internal-medicine service to admit, both during the day and at night,” adds Dr. Craig Widness, another med-peds-trained hospitalist at Elliot.
But the scope of practice and volume has ramped up for the pediatric hospitalist service at Elliot, as many community pediatric groups have opted to utilize their services. In addition, a new pediatric ICU has recently been established, managed by the pediatric hospitalist service.
As a result, the opportunities for the med-ped-trained pediatric hospitalists to help out on the adult hospitalist vortex have been increasingly rare, which seem to be a welcome development to the pediatric hospitalists.
Building the Perfect Beast
So how does a med-ped physician entering hospital medicine build a job that satisfies the need to care for both adults and children? In some cases, the perfect med-ped position is already available. More likely, however, hospitalist jobs in a specific location are limited to either one discipline or another.
In many, if not most, cases, practice in one discipline will have to be somewhat compromised to fulfill the staffing needs of the “primary” job, at least initially. In the interview and hiring process, however, hospitalists wishing to pursue med-peds must make known their desire to work in both medicine and pediatrics. The transparency will allow hospital and group administrators to build into your schedule time to work in both pursuits.
“Start trying to arrange for pediatrics early. I started before I finished residency and it took me over a year to set up,” Dr. Hunt says, noting her current position is in the academic arena. “Discuss your plans with any medicine group you intend to join. See if your FTE would be flexible or if they can help arrange things. Get in touch with local med-ped program directors, if possible, as they often know people on both sides and might be able to help get you in touch with the right people.”
When looking at community hospitalist jobs, it is critical to ensure your administrators are familiar with med-peds residency training. It helps them better understand your skills, your goals, and allows them to put you in position to care for patients in all age groups.
“When one finds administrators and leaders that understand and respect the concept [of med-peds], hold on to them,” Dr. Burgess advises. “Do not let anyone take your unique training for granted and try to categorize you as one or the other; rather, we are both. We have two sets of boards, with separate training and a unique overlap that provides synergy with our abilities. Find a group that understands the level of training you possess.”
Call Protection
As uncommon as it is to find med-ped hospitalist jobs that feature built-in coordination of work in both disciplines, one should pay attention to coordinating salary, call, vacation, and CME between the two disciplines.
“Talk with potential groups about how they cover you for call, how you will be reimbursed, and what data will they base your pay and incentives on,” Dr. Burgess says. “What will they base your CME on—two disciplines or one? What is your depth if you have a sick child and sick adult at the same time?”
Most important, med-peds must make sure administrators of both disciplines are aware of your activities on both sides. “We do not want double-call days,” Dr. Burgess adds. He also warns that overcoming the frustrations of med-pedwork “takes a great deal of patience and discussion.”
Salary might be an issue, especially as one tries to mold a position. SHM and the Medical Group Management Association (MGMA) State of Hospital Medicine: 2010 Report Based on 2009 Data lists the median national annual compensation for adult hospitalists as $215,000, and $160,038 for pediatric hospitalists. This also has implications when IM time is bought down by pediatrics in academic centers, as pediatrics might not pay as much for clinical time as medicine will.
Back Where You Belong
Either by necessity or choice, med-ped-trained hospitalists all across the country have taken jobs in one setting or another and now yearn to get back into the other discipline. It might not be as difficult as you think.
If hospitalist work in the other discipline is available in your institution, you could consider a reduction of FTE in your current job to expand into the other discipline. Keep in mind, however, the interdepartmental coordination difficulties (i.e. scheduling, benefits, maintaining privileges). Those can be even more pronounced if two or more employers are involved.
Additionally, a reduction of FTE in your current job could lead to increased clinical time on the part of your colleagues, or perhaps even hiring additional staff, so this change needs to be discussed thoroughly with administrators and colleagues well in advance of any changes.
Less dramatic changes can enable a med-ped hospitalist to get a taste of the other discipline without wholesale changes in salary and schedule. Moonlighting as an intermittent hospitalist or nocturnist, taking call in the other discipline’s call schedule, or filling in for urgent-care slots can keep skills and knowledge from getting rusty.
It also can prevent the loss of pediatric admitting and procedural privileges. A patchwork approach also could lead to a steady hospitalist job in the other discipline.
“I discussed my desire to do pediatrics with friends and acquaintances who worked as pediatricians in local community hospitals through Children’s Hospital Boston,” Dr. Hunt says. “Eventually, [it led] to the peds work.”
As is often the case in HM, med-ped programs tend to follow the tenet “if you build it, they will come.” Once a hospitalist director discovers the flexibility and skill set a med-ped hospitalist provides the group, they often look to expand—especially to staff smaller pediatric units.
Such was the case at Elliot Hospital; familiarity with med-ped moonlighters eventually led to a full-time med-ped hospitalist hire. Following the full-time hire, the HM group realized a dramatic increase in local pediatric groups referring patients to Elliot’s hospitalist group, including the largest pediatric group in Southern New Hampshire, Dartmouth-Hitchcock Clinic.
“Initial referral base from the community was sluggish as community [pediatricians] wanted to hold onto their patients,” Dr. Ritenour says. “As the acuity of what we could support as hospitalists grew, more referrals were made for kids that might have previously been transferred.”
The Future of Med-Ped Hospitalists
At the dawn of combined med-ped residencies in the early 1960s, the hospitalist movement was only a twinkle in the eye of house physicians of yore. Now that both movements have matured, will we see this hybrid of a hybrid flourish?
“I think med-peds is well suited for hospital medicine, based on solid training that includes numerous inpatient wards and critical care in both internal medicine and pediatrics,” says Dr. Toth, adding she hopes to bring additional med-ped hospitalists to her group in Milwaukee in the future.
It seems inevitable that the med-ped movement, which has grown into the largest combined residency specialty in the country, and the hospitalist movement, which has exploded as the fastest-growing medical specialty, will continue to intertwine, branch out, and evolve.
And every year, some of those med-ped residency program graduates will continue to climb those twisted trunks, as challenging as it might seem. TH
Dr. Chang is a med-peds hospitalist at the University of California at San Diego and Rady Children’s Hospital. He is a member of Team Hospitalist.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of infection with arterial and central venous catheters
- Rifaximin and prevention of hepatic encephalopathy
- Tracheotomy to prevent ventilator-associated pneumonia
- Coagulopathy and risk of VTE in patients with cirrhosis
- Use of age-adjusted D-dimer for PE diagnosis
- Continuation of anti-hypertensive medications after stroke
- Number of lumen cultures and detection of CRBSIs
- Timing of anticoagulation and outcomes in PE
Arterial and Central Venous Catheters Have Similar Rates of Colonization and Blood Stream Infections
Clinical question: Are arterial catheters (ACs) safer than central venous catheters (CVCs) in terms of colonization and catheter-related infections?
Background: Unlike CVCs, only a few studies have addressed blood-stream infections (BSI) related to AC usage, probably due to the traditional perception that ACs pose a lesser risk of colonization and BSI than CVC.
Study design: Randomized, controlled trial.
Setting: Three university hospitals and two general hospitals in France.
Synopsis: The study included 3,532 catheters (1,915 CVC and 1,617 AC) with 27,541 catheter-days from seven ICU settings. The same standard procedures were followed for catheter insertion and site dressing change at the various centers. Catheters were removed when they no longer were needed or when catheter-related infection (CRI) was suspected.
Colonization and CRI rates were similar in both arterial and venous catheters: 7.9% vs. 9.6% and 0.68% vs. 0.94%, respectively. The daily risk of colonization over time was stable for CVC, but appeared to increase for AC.
One important limitation to this study is that many patients had both arterial and venous catheters, leading to difficulty attributing infection to either one. Hospitalists caring for ICU patients should weigh the risks and benefits of prolonged use of AC due to similar rates of colonization and CRI as CVC.
Bottom line: Arterial and central venous catheters are equally prone to colonization and cause similar rates of CRI, but AC daily risk tends to increase with time; thus, AC should receive the same precautions as CVC.
Citation: Lucet JC, Bouadma L, Zahar JR, et. al. Infectious risk associated with arterial catheters compared with central venous catheters. Crit Care Med. 2010;38(4):1030-1005.
Rifaximin Prevents Recurrence of Hepatic Encephalopathy Episodes and Reduces Associated Risk for Hospitalization
Clinical question: What is the efficacy of rifaximin for the prevention of hepatic encephalopathy?
Background: Hepatic encephalopathy is a chronic, debilitating complication of liver cirrhosis. The efficacy of treatment of acute episodes with rifaximin is well documented in the literature; however, prevention of such episodes using rifaximin is poorly studied.
Study design: Randomized, double-blinded, placebo-controlled trial.
Setting: Seventy centers in the U.S., Canada, and Russia.
Synopsis: A total of 299 chronic liver disease patients, in remission from recurrent hepatic encephalopathy, randomly were assigned to receive either oral rifaximin (140 patients) or placebo (159 patients) for six months.
When compared to placebo, rifaximin reduced the risk of breakthrough episodes of hepatic encephalopathy over a six-month treatment period (22.1% vs 45.9%, HR 0.42; 95% confidence interval, 0.28-0.64, P<0.001), as well as risk of hospitalization involving hepatic encephalopathy (13.6% vs 22.6%, HR 0.50; 95% CI, 0.29-0.87, P=0.01).
The incidence of adverse effects was similar in both groups. More than 90% of patients received concomitant lactulose therapy.
Bottom line: Rifaximin treatment delays the first breakthrough episode of hepatic encephalopathy during a six-month period; moreover, it significantly reduces the associated risk for hospitalization.
Citation: Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
Early Tracheotomy Does Not Decrease the Incidence of Ventilator-Associated Pneumonia in ICU Patients
Clinical question: Does early tracheotomy decrease the incidence of ventilator-associated pneumonia (VAP) in mechanically ventilated adult ICU patients without existing lung infection?
Background: There is considerable variation in timing and incidence of tracheotomy across ICUs. Observational studies have reported that tracheotomy performed earlier might be associated with quicker weaning from mechanical ventilation; however, randomized, controlled trials have failed to confirm this finding.
Study design: Multicenter randomized controlled trial.
Setting: Adult ICU in Italy.
Synopsis: Between 2004 and 2008, 600 mechanically ventilated patients without lung infection were enrolled from 12 adult ICUs in Italy. Of these patients, 419 were randomized to early tracheotomy performed six to eight days after intubation (N=209) or to late tracheotomy performed 13-15 days after intubation (N=210).
VAP was diagnosed in 14% of patients in the early tracheotomy group, compared with 21% in the late tracheotomy group (P=0.07). Although the number of ventilator-free and ICU-free days was higher in the early tracheotomy group, long-term outcomes did not differ between the two groups.
Only 69% of patients in the early tracheotomy group and 57% of patients in the late tracheotomy group received tracheotomy, but all the patients were included in the final analysis due to the intention-to-treat design of the study, which might have diluted the effect of the intervention. In addition, the smaller sample size may have prevented the study from reaching statistical significance.
Bottom line: Early tracheotomy does not significantly decrease the incidence of VAP as compared to late tracheotomy.
Citation: Terragni PP, Antonelli M, Fumagalli R, et al. Early vs. late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients. JAMA. 2010;303(15): 1483-1489.
Coagulopathy in Cirrhotic Patients Is Not Protective against VTE
Clinical question: Does the degree of INR elevation affect the incidence of VTE in hospitalized patients with cirrhosis?
Background: Chronic liver disease (CLD) and subsequent development of cirrhosis renders patients coagulopathic. Historically, this has provided a sense of security to clinicians that these patients inherently possess a decreased VTE risk.
Study design: Retrospective cohort study.
Setting: University of Missouri Medical Center in Columbia.
Synopsis: Chart review of patients admitted with CLD and cirrhosis from Jan. 1, 2000, and Jan. 31, 2007, demonstrated an incidence rate of VTE of 6.3%, which is much higher than previous reports.
Most patients with CLD received no thrombosis prophylaxis; notably, there was no difference in VTE incidence between subgroups who received prophylaxis and those who did not. Five percent of VTE cases occurred in patients with an INR exceeding 1.6, with Child-Pugh class C patients having the highest thromboembolism incidence.
This retrospective chart review was limited by information and reporting bias and the inability to control confounding variables. Less than half of the patients were screened for VTE, which means that the true incidence of thrombus could actually be higher. Further studies are needed to provide proper risk assessment.
Bottom line: Patients with CLD and cirrhosis are at risk for VTE, even in the setting of coagulopathy, and might require VTE prophylaxis.
Citation: Dabbagh O, Oza A, Prakash S, Sunna R, Saettele TM. Coagulopathy does not protect against venous thromboembolism in hospitalized patients with chronic liver disease. Chest. 2010;137(5):1145-1149.
Pulmonary Embolism Can Be Safely Excluded Using Age-Adjusted D-dimer Cut-off Value
Clinical question: Does the new age-adjusted D-dimer cutoff value in older patients safely exclude pulmonary embolism (PE)?
Background: D-dimer is a useful blood test to exclude PE; however, D-dimer concentration increases with age, and hence the current cutoff of 500µg/l used in excluding a PE becomes less specific in older patients.
Study design: Retrospective multicenter cohort study.
Setting: General and teaching hospitals in Belgium, Switzerland, France, and Netherlands.
Synopsis: The study included 5,132 consecutive patients with clinically suspected PE. Patients were distributed into a derivation set (N=1,331) and two independent validation sets (N1=2,151 and N2=1,643). For patients older than 50, the use of the new age-adjusted D-dimer cutoff (patient age multiplied by 10µg/l) resulted in a combined 11% increase in the number of patients with negative results. This increase was more prominent in patients aged older than 70 (13% to 16%).
The new age-adjusted D-dimer cutoff point failed to detect PE in 0.2% of cases in the derivation set and in 0.6% and 0.3% of cases in the two validation sets, respectively. However, despite external validation, prospective studies are needed before implementing such criteria into clinical practice.
Bottom line: The age-adjusted D-dimer combined with clinical probability greatly increases the proportion of older patients in whom PE can be safely excluded.
Citation: Douma RA, Le Gal G, Söhne M, et al. Potential of an age adjusted D-dimer cut-off value to improve the exclusion of pulmonary embolism in older patients: a retrospective analysis of three large cohorts. BMJ. 2010;340:c1475.
Antihypertensive Drugs After Stroke Does Not Impact Cardiovascular Event Rate or Mortality at Six Months
Clinical question: Should antihypertensive medications be continued during the immediate post-stroke period in patients who previously were on such therapy?
Background: More than 50% of patients suffering from acute stroke are on antihypertensive therapy prior to admission. However, efficacy of such therapy in reducing cardiovascular event rates and mortality in the immediate post-stroke period is not well studied.
Study design: Prospective, randomized, open-blinded-endpoint trial.
Setting: Forty-nine UK National Institute for Health Research Stroke Centers.
Synopsis: From January 2003 and March 2009, 763 patients with pre-existing hypertension and diagnosis of mild to moderate acute stroke were recruited and assigned to continue or stop antihypertension drugs. The time limit for inclusion into the study was within 48 hours of the stroke and the endpoint was death or dependency (modified Rankin Scale >3) at the end of two weeks.
There was a statistically significant difference in the two groups at two weeks in both systolic and diastolic pressures, 13 mmHg and 8mmHg, respectively (P<0.0001). Seventy-two of 379 patients in the continuation group and 82 of 384 patients in the stop group reached the primary endpoint (P=0.3). The latter point is a major limitation to this trial, since it was underpowered because of early termination to detect differences in outcomes.
Bottom line: Antihypertensive therapy during the immediate post-stroke period did not reduce two-week death or dependency, cardiovascular event rate, or mortality at six months.
Citation: Robinson TG, Potter JF, Ford GA, et al. Effects of antihypertensive treatment after acute stroke in the continue or stop post-stroke antihypertensives collaborative study (COSSACS): a prospective, randomized, open, blinded-endpoint trial. Lancet Neurol. 2010;9:767-775.
All Lumens from Multi-Lumen Catheters Should Be Cultured to Diagnose Catheter-Related Bloodstream Infections
Clinical question: Do all lumens from multi-lumen catheters need to be cultured to best diagnose catheter-related bloodstream infections (CRBSIs)?
Background: The recent Infectious Diseases Society of America’s “Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infections” has not conclusively established the number of lumens to culture from multi-lumen catheters when attempting to diagnose CRBSIs.
Study design: Retrospective cohort study.
Setting: Large teaching institution in Spain.
Synopsis: From January 2003 until May 2009, 154 patients, mostly men, with a mean age of 58.1 years, were recruited to participate in the study. Of these, 171 episodes of proven CRBSIs were detected in 154 subjects. Of the 171 tested catheters (112 double lumen and 59 triple lumen), testing only one lumen from double catheters would have led to 27.2% of missed cases for CRBSIs. Additionally, testing only two or one lumen from triple lumen catheters would have led to 15.8% and 37.3% of missed cases for CRBSIs, respectively.
The study was limited by being conducted at a single test site and the need to withdraw catheters to perform endoluminal brushing and semi-quantitative techniques. Though diagnostic yield might significantly improve by culturing all multi-lumen sites, hospitalists should consider the time and cost expenditure for testing from more than one lumen.
Bottom line: Culturing all lumens from multi-lumen catheters could greatly increase diagnostic yield in CRBSIs.
Citation: Guembe M, Rodríguez-Créixems M, Sánchez-Carrillo C, Pérez-Parra A, Martín-Rabadán P, Bouza E. How many lumens should be cultured in the conservative diagnosis of catheter-related bloodstream infections? CID. 2010;50(12):1575-1579.
Early Anticoagulation Improves Survival after Acute PE
Clinical question: Does the timing of initial heparinization reduce mortality in patients with acute symptomatic PE?
Background: Acute PE is rapidly fatal if not diagnosed and treated. Studies have shown that intravenous heparin improves overall survival for patients with PE, and therapeutic anticoagulation reduces rates of recurrent VTE. However, studies investigating the relation between time to achieve therapeutic anticoagulation and mortality or PE recurrence are limited.
Study design: Retrospective cohort study.
Setting: Mayo Clinic, Rochester, Minn.
Synopsis: From June 2002 and September 2005, 400 patients were identified with PE using retrospective data from Mayo Clinic’s electronic medical records. Patients who received heparin in the ED had lower in-hospital mortality (OR 0.20, 95% CI, 0.06-0.69) and 30-day mortality (OR 0.25, 95% CI, 0.12-0.55) compared with patients who received heparin after admission. Similarly, patients who achieved a therapeutic aPTT within 24 hours also had lower 30-day mortality (OR 0.34, 95% CI, 0.14-0.84). Patients with COPD and malignancies had higher in-hospital and 30-day mortality, respectively.
Bottom line: It is difficult to draw a causal relationship from a retrospective review, but hospitalists should start immediate anticoagulation therapy when a PE is suspected.
Citation: Smith SB, Geske JB, Maguire JM, Zane NA, Carter RE, Morgenthaler TI. Early anticoagulation is associated with reduced mortality for acute pulmonary embolism. Chest. 2010;137(6): 1382-1390. TH
PEDIATRIC HM LITERATURE
Ibuprofen Use Associated with Complicated Pneumonia

Clinical question: What baseline characteristics are associated with suppurative complications in children hospitalized with community-acquired pneumonia?
Background: The prevalence of suppurative complications of community-acquired pneumonia (CAP) appears to be on the rise. Reasons for this increase remain unclear, although etiologic organism, older age, prior antibiotic, and nonsteroidal anti-inflammatory drug use have been implicated in a single prior retrospective study.
Study design: Retrospective cohort study.
Setting: Two hospitals in France.
Synopsis: Two physicians reviewed 1,184 charts based on ICD-10 discharge codes for pneumonia from 1995 to 2003. Children younger than 28 days and older than 15 years were excluded. Additionally, children with underlying or cardiorespiratory pathology were excluded. After applying predefined clinical criteria for pneumonia and suppurative complications, 677 children with CAP were compared to 90 with suppurative complications of pneumonia.
The incidence of suppurative complications increased to 13 per 100,000 from 0.5 per 100,000 over the time period. A minority of patients had etiologic microbes isolated, primarily Streptococcus pneumoniae, in both groups. Complicated pneumonia was more frequently seen in older children, and in children with prior antibiotic and anti-inflammatory medication use. After multivariable analysis, only ibuprofen use remained with an increased odds ratio (2.57, 95% confidence interval, 1.51-4.35) of complicated pneumonia.
The clear drawback of this study is an inability to draw a causal connection between ibuprofen use and the development of suppurative complications of pneumonia. The retrospective nature of the analysis further limits hypothesis generation. Nevertheless, it is notable that the results corroborate findings from a prior study in the U.S., in which ibuprofen was found to significantly increase the likelihood of parapneumonic empyema.
Bottom line: Ibuprofen use is associated with the development of suppurative complications of pneumonia.
Citation: François P, Desrumaux A, Cans C, Pin I, Pavese P, Labarère J. Prevalence and risk factors of suppurative complications in children with pneumonia. Acta Paediatr. 2010;99(6):861-866.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of infection with arterial and central venous catheters
- Rifaximin and prevention of hepatic encephalopathy
- Tracheotomy to prevent ventilator-associated pneumonia
- Coagulopathy and risk of VTE in patients with cirrhosis
- Use of age-adjusted D-dimer for PE diagnosis
- Continuation of anti-hypertensive medications after stroke
- Number of lumen cultures and detection of CRBSIs
- Timing of anticoagulation and outcomes in PE
Arterial and Central Venous Catheters Have Similar Rates of Colonization and Blood Stream Infections
Clinical question: Are arterial catheters (ACs) safer than central venous catheters (CVCs) in terms of colonization and catheter-related infections?
Background: Unlike CVCs, only a few studies have addressed blood-stream infections (BSI) related to AC usage, probably due to the traditional perception that ACs pose a lesser risk of colonization and BSI than CVC.
Study design: Randomized, controlled trial.
Setting: Three university hospitals and two general hospitals in France.
Synopsis: The study included 3,532 catheters (1,915 CVC and 1,617 AC) with 27,541 catheter-days from seven ICU settings. The same standard procedures were followed for catheter insertion and site dressing change at the various centers. Catheters were removed when they no longer were needed or when catheter-related infection (CRI) was suspected.
Colonization and CRI rates were similar in both arterial and venous catheters: 7.9% vs. 9.6% and 0.68% vs. 0.94%, respectively. The daily risk of colonization over time was stable for CVC, but appeared to increase for AC.
One important limitation to this study is that many patients had both arterial and venous catheters, leading to difficulty attributing infection to either one. Hospitalists caring for ICU patients should weigh the risks and benefits of prolonged use of AC due to similar rates of colonization and CRI as CVC.
Bottom line: Arterial and central venous catheters are equally prone to colonization and cause similar rates of CRI, but AC daily risk tends to increase with time; thus, AC should receive the same precautions as CVC.
Citation: Lucet JC, Bouadma L, Zahar JR, et. al. Infectious risk associated with arterial catheters compared with central venous catheters. Crit Care Med. 2010;38(4):1030-1005.
Rifaximin Prevents Recurrence of Hepatic Encephalopathy Episodes and Reduces Associated Risk for Hospitalization
Clinical question: What is the efficacy of rifaximin for the prevention of hepatic encephalopathy?
Background: Hepatic encephalopathy is a chronic, debilitating complication of liver cirrhosis. The efficacy of treatment of acute episodes with rifaximin is well documented in the literature; however, prevention of such episodes using rifaximin is poorly studied.
Study design: Randomized, double-blinded, placebo-controlled trial.
Setting: Seventy centers in the U.S., Canada, and Russia.
Synopsis: A total of 299 chronic liver disease patients, in remission from recurrent hepatic encephalopathy, randomly were assigned to receive either oral rifaximin (140 patients) or placebo (159 patients) for six months.
When compared to placebo, rifaximin reduced the risk of breakthrough episodes of hepatic encephalopathy over a six-month treatment period (22.1% vs 45.9%, HR 0.42; 95% confidence interval, 0.28-0.64, P<0.001), as well as risk of hospitalization involving hepatic encephalopathy (13.6% vs 22.6%, HR 0.50; 95% CI, 0.29-0.87, P=0.01).
The incidence of adverse effects was similar in both groups. More than 90% of patients received concomitant lactulose therapy.
Bottom line: Rifaximin treatment delays the first breakthrough episode of hepatic encephalopathy during a six-month period; moreover, it significantly reduces the associated risk for hospitalization.
Citation: Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
Early Tracheotomy Does Not Decrease the Incidence of Ventilator-Associated Pneumonia in ICU Patients
Clinical question: Does early tracheotomy decrease the incidence of ventilator-associated pneumonia (VAP) in mechanically ventilated adult ICU patients without existing lung infection?
Background: There is considerable variation in timing and incidence of tracheotomy across ICUs. Observational studies have reported that tracheotomy performed earlier might be associated with quicker weaning from mechanical ventilation; however, randomized, controlled trials have failed to confirm this finding.
Study design: Multicenter randomized controlled trial.
Setting: Adult ICU in Italy.
Synopsis: Between 2004 and 2008, 600 mechanically ventilated patients without lung infection were enrolled from 12 adult ICUs in Italy. Of these patients, 419 were randomized to early tracheotomy performed six to eight days after intubation (N=209) or to late tracheotomy performed 13-15 days after intubation (N=210).
VAP was diagnosed in 14% of patients in the early tracheotomy group, compared with 21% in the late tracheotomy group (P=0.07). Although the number of ventilator-free and ICU-free days was higher in the early tracheotomy group, long-term outcomes did not differ between the two groups.
Only 69% of patients in the early tracheotomy group and 57% of patients in the late tracheotomy group received tracheotomy, but all the patients were included in the final analysis due to the intention-to-treat design of the study, which might have diluted the effect of the intervention. In addition, the smaller sample size may have prevented the study from reaching statistical significance.
Bottom line: Early tracheotomy does not significantly decrease the incidence of VAP as compared to late tracheotomy.
Citation: Terragni PP, Antonelli M, Fumagalli R, et al. Early vs. late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients. JAMA. 2010;303(15): 1483-1489.
Coagulopathy in Cirrhotic Patients Is Not Protective against VTE
Clinical question: Does the degree of INR elevation affect the incidence of VTE in hospitalized patients with cirrhosis?
Background: Chronic liver disease (CLD) and subsequent development of cirrhosis renders patients coagulopathic. Historically, this has provided a sense of security to clinicians that these patients inherently possess a decreased VTE risk.
Study design: Retrospective cohort study.
Setting: University of Missouri Medical Center in Columbia.
Synopsis: Chart review of patients admitted with CLD and cirrhosis from Jan. 1, 2000, and Jan. 31, 2007, demonstrated an incidence rate of VTE of 6.3%, which is much higher than previous reports.
Most patients with CLD received no thrombosis prophylaxis; notably, there was no difference in VTE incidence between subgroups who received prophylaxis and those who did not. Five percent of VTE cases occurred in patients with an INR exceeding 1.6, with Child-Pugh class C patients having the highest thromboembolism incidence.
This retrospective chart review was limited by information and reporting bias and the inability to control confounding variables. Less than half of the patients were screened for VTE, which means that the true incidence of thrombus could actually be higher. Further studies are needed to provide proper risk assessment.
Bottom line: Patients with CLD and cirrhosis are at risk for VTE, even in the setting of coagulopathy, and might require VTE prophylaxis.
Citation: Dabbagh O, Oza A, Prakash S, Sunna R, Saettele TM. Coagulopathy does not protect against venous thromboembolism in hospitalized patients with chronic liver disease. Chest. 2010;137(5):1145-1149.
Pulmonary Embolism Can Be Safely Excluded Using Age-Adjusted D-dimer Cut-off Value
Clinical question: Does the new age-adjusted D-dimer cutoff value in older patients safely exclude pulmonary embolism (PE)?
Background: D-dimer is a useful blood test to exclude PE; however, D-dimer concentration increases with age, and hence the current cutoff of 500µg/l used in excluding a PE becomes less specific in older patients.
Study design: Retrospective multicenter cohort study.
Setting: General and teaching hospitals in Belgium, Switzerland, France, and Netherlands.
Synopsis: The study included 5,132 consecutive patients with clinically suspected PE. Patients were distributed into a derivation set (N=1,331) and two independent validation sets (N1=2,151 and N2=1,643). For patients older than 50, the use of the new age-adjusted D-dimer cutoff (patient age multiplied by 10µg/l) resulted in a combined 11% increase in the number of patients with negative results. This increase was more prominent in patients aged older than 70 (13% to 16%).
The new age-adjusted D-dimer cutoff point failed to detect PE in 0.2% of cases in the derivation set and in 0.6% and 0.3% of cases in the two validation sets, respectively. However, despite external validation, prospective studies are needed before implementing such criteria into clinical practice.
Bottom line: The age-adjusted D-dimer combined with clinical probability greatly increases the proportion of older patients in whom PE can be safely excluded.
Citation: Douma RA, Le Gal G, Söhne M, et al. Potential of an age adjusted D-dimer cut-off value to improve the exclusion of pulmonary embolism in older patients: a retrospective analysis of three large cohorts. BMJ. 2010;340:c1475.
Antihypertensive Drugs After Stroke Does Not Impact Cardiovascular Event Rate or Mortality at Six Months
Clinical question: Should antihypertensive medications be continued during the immediate post-stroke period in patients who previously were on such therapy?
Background: More than 50% of patients suffering from acute stroke are on antihypertensive therapy prior to admission. However, efficacy of such therapy in reducing cardiovascular event rates and mortality in the immediate post-stroke period is not well studied.
Study design: Prospective, randomized, open-blinded-endpoint trial.
Setting: Forty-nine UK National Institute for Health Research Stroke Centers.
Synopsis: From January 2003 and March 2009, 763 patients with pre-existing hypertension and diagnosis of mild to moderate acute stroke were recruited and assigned to continue or stop antihypertension drugs. The time limit for inclusion into the study was within 48 hours of the stroke and the endpoint was death or dependency (modified Rankin Scale >3) at the end of two weeks.
There was a statistically significant difference in the two groups at two weeks in both systolic and diastolic pressures, 13 mmHg and 8mmHg, respectively (P<0.0001). Seventy-two of 379 patients in the continuation group and 82 of 384 patients in the stop group reached the primary endpoint (P=0.3). The latter point is a major limitation to this trial, since it was underpowered because of early termination to detect differences in outcomes.
Bottom line: Antihypertensive therapy during the immediate post-stroke period did not reduce two-week death or dependency, cardiovascular event rate, or mortality at six months.
Citation: Robinson TG, Potter JF, Ford GA, et al. Effects of antihypertensive treatment after acute stroke in the continue or stop post-stroke antihypertensives collaborative study (COSSACS): a prospective, randomized, open, blinded-endpoint trial. Lancet Neurol. 2010;9:767-775.
All Lumens from Multi-Lumen Catheters Should Be Cultured to Diagnose Catheter-Related Bloodstream Infections
Clinical question: Do all lumens from multi-lumen catheters need to be cultured to best diagnose catheter-related bloodstream infections (CRBSIs)?
Background: The recent Infectious Diseases Society of America’s “Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infections” has not conclusively established the number of lumens to culture from multi-lumen catheters when attempting to diagnose CRBSIs.
Study design: Retrospective cohort study.
Setting: Large teaching institution in Spain.
Synopsis: From January 2003 until May 2009, 154 patients, mostly men, with a mean age of 58.1 years, were recruited to participate in the study. Of these, 171 episodes of proven CRBSIs were detected in 154 subjects. Of the 171 tested catheters (112 double lumen and 59 triple lumen), testing only one lumen from double catheters would have led to 27.2% of missed cases for CRBSIs. Additionally, testing only two or one lumen from triple lumen catheters would have led to 15.8% and 37.3% of missed cases for CRBSIs, respectively.
The study was limited by being conducted at a single test site and the need to withdraw catheters to perform endoluminal brushing and semi-quantitative techniques. Though diagnostic yield might significantly improve by culturing all multi-lumen sites, hospitalists should consider the time and cost expenditure for testing from more than one lumen.
Bottom line: Culturing all lumens from multi-lumen catheters could greatly increase diagnostic yield in CRBSIs.
Citation: Guembe M, Rodríguez-Créixems M, Sánchez-Carrillo C, Pérez-Parra A, Martín-Rabadán P, Bouza E. How many lumens should be cultured in the conservative diagnosis of catheter-related bloodstream infections? CID. 2010;50(12):1575-1579.
Early Anticoagulation Improves Survival after Acute PE
Clinical question: Does the timing of initial heparinization reduce mortality in patients with acute symptomatic PE?
Background: Acute PE is rapidly fatal if not diagnosed and treated. Studies have shown that intravenous heparin improves overall survival for patients with PE, and therapeutic anticoagulation reduces rates of recurrent VTE. However, studies investigating the relation between time to achieve therapeutic anticoagulation and mortality or PE recurrence are limited.
Study design: Retrospective cohort study.
Setting: Mayo Clinic, Rochester, Minn.
Synopsis: From June 2002 and September 2005, 400 patients were identified with PE using retrospective data from Mayo Clinic’s electronic medical records. Patients who received heparin in the ED had lower in-hospital mortality (OR 0.20, 95% CI, 0.06-0.69) and 30-day mortality (OR 0.25, 95% CI, 0.12-0.55) compared with patients who received heparin after admission. Similarly, patients who achieved a therapeutic aPTT within 24 hours also had lower 30-day mortality (OR 0.34, 95% CI, 0.14-0.84). Patients with COPD and malignancies had higher in-hospital and 30-day mortality, respectively.
Bottom line: It is difficult to draw a causal relationship from a retrospective review, but hospitalists should start immediate anticoagulation therapy when a PE is suspected.
Citation: Smith SB, Geske JB, Maguire JM, Zane NA, Carter RE, Morgenthaler TI. Early anticoagulation is associated with reduced mortality for acute pulmonary embolism. Chest. 2010;137(6): 1382-1390. TH
PEDIATRIC HM LITERATURE
Ibuprofen Use Associated with Complicated Pneumonia
Clinical question: What baseline characteristics are associated with suppurative complications in children hospitalized with community-acquired pneumonia?
Background: The prevalence of suppurative complications of community-acquired pneumonia (CAP) appears to be on the rise. Reasons for this increase remain unclear, although etiologic organism, older age, prior antibiotic, and nonsteroidal anti-inflammatory drug use have been implicated in a single prior retrospective study.
Study design: Retrospective cohort study.
Setting: Two hospitals in France.
Synopsis: Two physicians reviewed 1,184 charts based on ICD-10 discharge codes for pneumonia from 1995 to 2003. Children younger than 28 days and older than 15 years were excluded. Additionally, children with underlying or cardiorespiratory pathology were excluded. After applying predefined clinical criteria for pneumonia and suppurative complications, 677 children with CAP were compared to 90 with suppurative complications of pneumonia.
The incidence of suppurative complications increased to 13 per 100,000 from 0.5 per 100,000 over the time period. A minority of patients had etiologic microbes isolated, primarily Streptococcus pneumoniae, in both groups. Complicated pneumonia was more frequently seen in older children, and in children with prior antibiotic and anti-inflammatory medication use. After multivariable analysis, only ibuprofen use remained with an increased odds ratio (2.57, 95% confidence interval, 1.51-4.35) of complicated pneumonia.
The clear drawback of this study is an inability to draw a causal connection between ibuprofen use and the development of suppurative complications of pneumonia. The retrospective nature of the analysis further limits hypothesis generation. Nevertheless, it is notable that the results corroborate findings from a prior study in the U.S., in which ibuprofen was found to significantly increase the likelihood of parapneumonic empyema.
Bottom line: Ibuprofen use is associated with the development of suppurative complications of pneumonia.
Citation: François P, Desrumaux A, Cans C, Pin I, Pavese P, Labarère J. Prevalence and risk factors of suppurative complications in children with pneumonia. Acta Paediatr. 2010;99(6):861-866.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of infection with arterial and central venous catheters
- Rifaximin and prevention of hepatic encephalopathy
- Tracheotomy to prevent ventilator-associated pneumonia
- Coagulopathy and risk of VTE in patients with cirrhosis
- Use of age-adjusted D-dimer for PE diagnosis
- Continuation of anti-hypertensive medications after stroke
- Number of lumen cultures and detection of CRBSIs
- Timing of anticoagulation and outcomes in PE
Arterial and Central Venous Catheters Have Similar Rates of Colonization and Blood Stream Infections
Clinical question: Are arterial catheters (ACs) safer than central venous catheters (CVCs) in terms of colonization and catheter-related infections?
Background: Unlike CVCs, only a few studies have addressed blood-stream infections (BSI) related to AC usage, probably due to the traditional perception that ACs pose a lesser risk of colonization and BSI than CVC.
Study design: Randomized, controlled trial.
Setting: Three university hospitals and two general hospitals in France.
Synopsis: The study included 3,532 catheters (1,915 CVC and 1,617 AC) with 27,541 catheter-days from seven ICU settings. The same standard procedures were followed for catheter insertion and site dressing change at the various centers. Catheters were removed when they no longer were needed or when catheter-related infection (CRI) was suspected.
Colonization and CRI rates were similar in both arterial and venous catheters: 7.9% vs. 9.6% and 0.68% vs. 0.94%, respectively. The daily risk of colonization over time was stable for CVC, but appeared to increase for AC.
One important limitation to this study is that many patients had both arterial and venous catheters, leading to difficulty attributing infection to either one. Hospitalists caring for ICU patients should weigh the risks and benefits of prolonged use of AC due to similar rates of colonization and CRI as CVC.
Bottom line: Arterial and central venous catheters are equally prone to colonization and cause similar rates of CRI, but AC daily risk tends to increase with time; thus, AC should receive the same precautions as CVC.
Citation: Lucet JC, Bouadma L, Zahar JR, et. al. Infectious risk associated with arterial catheters compared with central venous catheters. Crit Care Med. 2010;38(4):1030-1005.
Rifaximin Prevents Recurrence of Hepatic Encephalopathy Episodes and Reduces Associated Risk for Hospitalization
Clinical question: What is the efficacy of rifaximin for the prevention of hepatic encephalopathy?
Background: Hepatic encephalopathy is a chronic, debilitating complication of liver cirrhosis. The efficacy of treatment of acute episodes with rifaximin is well documented in the literature; however, prevention of such episodes using rifaximin is poorly studied.
Study design: Randomized, double-blinded, placebo-controlled trial.
Setting: Seventy centers in the U.S., Canada, and Russia.
Synopsis: A total of 299 chronic liver disease patients, in remission from recurrent hepatic encephalopathy, randomly were assigned to receive either oral rifaximin (140 patients) or placebo (159 patients) for six months.
When compared to placebo, rifaximin reduced the risk of breakthrough episodes of hepatic encephalopathy over a six-month treatment period (22.1% vs 45.9%, HR 0.42; 95% confidence interval, 0.28-0.64, P<0.001), as well as risk of hospitalization involving hepatic encephalopathy (13.6% vs 22.6%, HR 0.50; 95% CI, 0.29-0.87, P=0.01).
The incidence of adverse effects was similar in both groups. More than 90% of patients received concomitant lactulose therapy.
Bottom line: Rifaximin treatment delays the first breakthrough episode of hepatic encephalopathy during a six-month period; moreover, it significantly reduces the associated risk for hospitalization.
Citation: Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362:1071-1081.
Early Tracheotomy Does Not Decrease the Incidence of Ventilator-Associated Pneumonia in ICU Patients
Clinical question: Does early tracheotomy decrease the incidence of ventilator-associated pneumonia (VAP) in mechanically ventilated adult ICU patients without existing lung infection?
Background: There is considerable variation in timing and incidence of tracheotomy across ICUs. Observational studies have reported that tracheotomy performed earlier might be associated with quicker weaning from mechanical ventilation; however, randomized, controlled trials have failed to confirm this finding.
Study design: Multicenter randomized controlled trial.
Setting: Adult ICU in Italy.
Synopsis: Between 2004 and 2008, 600 mechanically ventilated patients without lung infection were enrolled from 12 adult ICUs in Italy. Of these patients, 419 were randomized to early tracheotomy performed six to eight days after intubation (N=209) or to late tracheotomy performed 13-15 days after intubation (N=210).
VAP was diagnosed in 14% of patients in the early tracheotomy group, compared with 21% in the late tracheotomy group (P=0.07). Although the number of ventilator-free and ICU-free days was higher in the early tracheotomy group, long-term outcomes did not differ between the two groups.
Only 69% of patients in the early tracheotomy group and 57% of patients in the late tracheotomy group received tracheotomy, but all the patients were included in the final analysis due to the intention-to-treat design of the study, which might have diluted the effect of the intervention. In addition, the smaller sample size may have prevented the study from reaching statistical significance.
Bottom line: Early tracheotomy does not significantly decrease the incidence of VAP as compared to late tracheotomy.
Citation: Terragni PP, Antonelli M, Fumagalli R, et al. Early vs. late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients. JAMA. 2010;303(15): 1483-1489.
Coagulopathy in Cirrhotic Patients Is Not Protective against VTE
Clinical question: Does the degree of INR elevation affect the incidence of VTE in hospitalized patients with cirrhosis?
Background: Chronic liver disease (CLD) and subsequent development of cirrhosis renders patients coagulopathic. Historically, this has provided a sense of security to clinicians that these patients inherently possess a decreased VTE risk.
Study design: Retrospective cohort study.
Setting: University of Missouri Medical Center in Columbia.
Synopsis: Chart review of patients admitted with CLD and cirrhosis from Jan. 1, 2000, and Jan. 31, 2007, demonstrated an incidence rate of VTE of 6.3%, which is much higher than previous reports.
Most patients with CLD received no thrombosis prophylaxis; notably, there was no difference in VTE incidence between subgroups who received prophylaxis and those who did not. Five percent of VTE cases occurred in patients with an INR exceeding 1.6, with Child-Pugh class C patients having the highest thromboembolism incidence.
This retrospective chart review was limited by information and reporting bias and the inability to control confounding variables. Less than half of the patients were screened for VTE, which means that the true incidence of thrombus could actually be higher. Further studies are needed to provide proper risk assessment.
Bottom line: Patients with CLD and cirrhosis are at risk for VTE, even in the setting of coagulopathy, and might require VTE prophylaxis.
Citation: Dabbagh O, Oza A, Prakash S, Sunna R, Saettele TM. Coagulopathy does not protect against venous thromboembolism in hospitalized patients with chronic liver disease. Chest. 2010;137(5):1145-1149.
Pulmonary Embolism Can Be Safely Excluded Using Age-Adjusted D-dimer Cut-off Value
Clinical question: Does the new age-adjusted D-dimer cutoff value in older patients safely exclude pulmonary embolism (PE)?
Background: D-dimer is a useful blood test to exclude PE; however, D-dimer concentration increases with age, and hence the current cutoff of 500µg/l used in excluding a PE becomes less specific in older patients.
Study design: Retrospective multicenter cohort study.
Setting: General and teaching hospitals in Belgium, Switzerland, France, and Netherlands.
Synopsis: The study included 5,132 consecutive patients with clinically suspected PE. Patients were distributed into a derivation set (N=1,331) and two independent validation sets (N1=2,151 and N2=1,643). For patients older than 50, the use of the new age-adjusted D-dimer cutoff (patient age multiplied by 10µg/l) resulted in a combined 11% increase in the number of patients with negative results. This increase was more prominent in patients aged older than 70 (13% to 16%).
The new age-adjusted D-dimer cutoff point failed to detect PE in 0.2% of cases in the derivation set and in 0.6% and 0.3% of cases in the two validation sets, respectively. However, despite external validation, prospective studies are needed before implementing such criteria into clinical practice.
Bottom line: The age-adjusted D-dimer combined with clinical probability greatly increases the proportion of older patients in whom PE can be safely excluded.
Citation: Douma RA, Le Gal G, Söhne M, et al. Potential of an age adjusted D-dimer cut-off value to improve the exclusion of pulmonary embolism in older patients: a retrospective analysis of three large cohorts. BMJ. 2010;340:c1475.
Antihypertensive Drugs After Stroke Does Not Impact Cardiovascular Event Rate or Mortality at Six Months
Clinical question: Should antihypertensive medications be continued during the immediate post-stroke period in patients who previously were on such therapy?
Background: More than 50% of patients suffering from acute stroke are on antihypertensive therapy prior to admission. However, efficacy of such therapy in reducing cardiovascular event rates and mortality in the immediate post-stroke period is not well studied.
Study design: Prospective, randomized, open-blinded-endpoint trial.
Setting: Forty-nine UK National Institute for Health Research Stroke Centers.
Synopsis: From January 2003 and March 2009, 763 patients with pre-existing hypertension and diagnosis of mild to moderate acute stroke were recruited and assigned to continue or stop antihypertension drugs. The time limit for inclusion into the study was within 48 hours of the stroke and the endpoint was death or dependency (modified Rankin Scale >3) at the end of two weeks.
There was a statistically significant difference in the two groups at two weeks in both systolic and diastolic pressures, 13 mmHg and 8mmHg, respectively (P<0.0001). Seventy-two of 379 patients in the continuation group and 82 of 384 patients in the stop group reached the primary endpoint (P=0.3). The latter point is a major limitation to this trial, since it was underpowered because of early termination to detect differences in outcomes.
Bottom line: Antihypertensive therapy during the immediate post-stroke period did not reduce two-week death or dependency, cardiovascular event rate, or mortality at six months.
Citation: Robinson TG, Potter JF, Ford GA, et al. Effects of antihypertensive treatment after acute stroke in the continue or stop post-stroke antihypertensives collaborative study (COSSACS): a prospective, randomized, open, blinded-endpoint trial. Lancet Neurol. 2010;9:767-775.
All Lumens from Multi-Lumen Catheters Should Be Cultured to Diagnose Catheter-Related Bloodstream Infections
Clinical question: Do all lumens from multi-lumen catheters need to be cultured to best diagnose catheter-related bloodstream infections (CRBSIs)?
Background: The recent Infectious Diseases Society of America’s “Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infections” has not conclusively established the number of lumens to culture from multi-lumen catheters when attempting to diagnose CRBSIs.
Study design: Retrospective cohort study.
Setting: Large teaching institution in Spain.
Synopsis: From January 2003 until May 2009, 154 patients, mostly men, with a mean age of 58.1 years, were recruited to participate in the study. Of these, 171 episodes of proven CRBSIs were detected in 154 subjects. Of the 171 tested catheters (112 double lumen and 59 triple lumen), testing only one lumen from double catheters would have led to 27.2% of missed cases for CRBSIs. Additionally, testing only two or one lumen from triple lumen catheters would have led to 15.8% and 37.3% of missed cases for CRBSIs, respectively.
The study was limited by being conducted at a single test site and the need to withdraw catheters to perform endoluminal brushing and semi-quantitative techniques. Though diagnostic yield might significantly improve by culturing all multi-lumen sites, hospitalists should consider the time and cost expenditure for testing from more than one lumen.
Bottom line: Culturing all lumens from multi-lumen catheters could greatly increase diagnostic yield in CRBSIs.
Citation: Guembe M, Rodríguez-Créixems M, Sánchez-Carrillo C, Pérez-Parra A, Martín-Rabadán P, Bouza E. How many lumens should be cultured in the conservative diagnosis of catheter-related bloodstream infections? CID. 2010;50(12):1575-1579.
Early Anticoagulation Improves Survival after Acute PE
Clinical question: Does the timing of initial heparinization reduce mortality in patients with acute symptomatic PE?
Background: Acute PE is rapidly fatal if not diagnosed and treated. Studies have shown that intravenous heparin improves overall survival for patients with PE, and therapeutic anticoagulation reduces rates of recurrent VTE. However, studies investigating the relation between time to achieve therapeutic anticoagulation and mortality or PE recurrence are limited.
Study design: Retrospective cohort study.
Setting: Mayo Clinic, Rochester, Minn.
Synopsis: From June 2002 and September 2005, 400 patients were identified with PE using retrospective data from Mayo Clinic’s electronic medical records. Patients who received heparin in the ED had lower in-hospital mortality (OR 0.20, 95% CI, 0.06-0.69) and 30-day mortality (OR 0.25, 95% CI, 0.12-0.55) compared with patients who received heparin after admission. Similarly, patients who achieved a therapeutic aPTT within 24 hours also had lower 30-day mortality (OR 0.34, 95% CI, 0.14-0.84). Patients with COPD and malignancies had higher in-hospital and 30-day mortality, respectively.
Bottom line: It is difficult to draw a causal relationship from a retrospective review, but hospitalists should start immediate anticoagulation therapy when a PE is suspected.
Citation: Smith SB, Geske JB, Maguire JM, Zane NA, Carter RE, Morgenthaler TI. Early anticoagulation is associated with reduced mortality for acute pulmonary embolism. Chest. 2010;137(6): 1382-1390. TH
PEDIATRIC HM LITERATURE
Ibuprofen Use Associated with Complicated Pneumonia
Clinical question: What baseline characteristics are associated with suppurative complications in children hospitalized with community-acquired pneumonia?
Background: The prevalence of suppurative complications of community-acquired pneumonia (CAP) appears to be on the rise. Reasons for this increase remain unclear, although etiologic organism, older age, prior antibiotic, and nonsteroidal anti-inflammatory drug use have been implicated in a single prior retrospective study.
Study design: Retrospective cohort study.
Setting: Two hospitals in France.
Synopsis: Two physicians reviewed 1,184 charts based on ICD-10 discharge codes for pneumonia from 1995 to 2003. Children younger than 28 days and older than 15 years were excluded. Additionally, children with underlying or cardiorespiratory pathology were excluded. After applying predefined clinical criteria for pneumonia and suppurative complications, 677 children with CAP were compared to 90 with suppurative complications of pneumonia.
The incidence of suppurative complications increased to 13 per 100,000 from 0.5 per 100,000 over the time period. A minority of patients had etiologic microbes isolated, primarily Streptococcus pneumoniae, in both groups. Complicated pneumonia was more frequently seen in older children, and in children with prior antibiotic and anti-inflammatory medication use. After multivariable analysis, only ibuprofen use remained with an increased odds ratio (2.57, 95% confidence interval, 1.51-4.35) of complicated pneumonia.
The clear drawback of this study is an inability to draw a causal connection between ibuprofen use and the development of suppurative complications of pneumonia. The retrospective nature of the analysis further limits hypothesis generation. Nevertheless, it is notable that the results corroborate findings from a prior study in the U.S., in which ibuprofen was found to significantly increase the likelihood of parapneumonic empyema.
Bottom line: Ibuprofen use is associated with the development of suppurative complications of pneumonia.
Citation: François P, Desrumaux A, Cans C, Pin I, Pavese P, Labarère J. Prevalence and risk factors of suppurative complications in children with pneumonia. Acta Paediatr. 2010;99(6):861-866.
Market Watch
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
Concurrent Care
Let’s examine a documentation case for hospitalists providing daily care: A 65-year-old male patient is admitted with a left hip fracture. The patient also has hypertension and Type 2 diabetes, which might complicate his care. The orthopedic surgeon manages the patient’s perioperative course for the fracture while the hospitalist provides daily post-op care for hypertension and diabetes.
A common scenario is the hospitalist will provide concurrent care, along with a varying number of specialists, depending on the complexity of the patient’s presenting problems and existing comorbidities. Payors define concurrent care as more than one physician providing care to the same patient on the same date, or during the same hospitalization. Payors often consider two key principles before reimbursing concurrent care:
- Does the patient’s condition warrant more than one physician? and
- Are the services provided by each physician reasonable and necessary?1
When more than one medical condition exists and each physician actively treats the condition related to their expertise, each physician can demonstrate medical necessity. As in the above example, the orthopedic surgeon cares for the patient’s fracture while the hospitalist oversees diabetes and hypertension management. Claim submission follows the same logic. Report each subsequent hospital care code (99231-99233) with the corresponding diagnosis each physician primarily manages (i.e., orthopedic surgeon: 9923x with 820.8; hospitalist: 9923x with 250.00, 401.1).
When each physician assigns a different primary diagnosis code to the visit code, each is more likely to receive payment. Because each of these physicians are in different specialties and different provider groups, most payors do not require modifier 25 (separately identifiable E/M service on the same day as a procedure or other service) appended to the visit code. However, some managed-care payors require each physician to append modifier 25 to the concurrent E/M visit code (i.e., 99232-25) despite claim submission under different tax identification numbers.
Unfortunately, the physicians might not realize this until a claim rejection has been issued. Furthermore, payors might want to see the proof before rendering payment. In other words, they pay the first claim received and deny any subsequent claim in order to confirm medical necessity of the concurrent visit. Appeal denied such claims rejections with supporting documentation that distinguishes each physician visit, if possible. This assists the payors in understanding each physician’s contribution to care.
Reasons for Denial
Concurrent care services are more easily distinguished when separate diagnoses are reported with each service. Conversely, payors are likely to deny services that are hard to differentiate. Furthermore, payors frequently deny concurrent care services for the following reasons:
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate or overlap those of another provider without recognizable distinction.2
For example, a hospitalist might be involved in the post-op care of patients with fractures and no other identifiable chronic or acute conditions or complications. In these cases, the hospitalist’s continued involvement might constitute a facility policy (e.g., quality of care, risk reduction, etc.) rather than active clinical management. Claim submission could erroneously occur with each physician reporting 9923x for 820.8. Payors deny medically unnecessary services, or request refunds for inappropriate payments.
Hospitalists might attempt to negotiate other terms with the facility to account for the unpaid time and effort directed toward these types of cases.
Group Practice
Physicians in the same group practice with the same specialty designation must report, and are paid, as a single physician. Multiple visits to the same patient can occur on the same day by members of the same group (e.g., hospitalist A evaluates the patient in the morning, and hospitalist B reviews test results and the resulting course of treatment in the afternoon). However, only one subsequent hospital care service can be reported for the day.
The hospitalists should select the visit level representative of the combined services and submit one appropriately determined code (e.g., 99233), thereby capturing the medically necessary efforts of each physician. To complicate matters, the hospitalists must determine which name to report on the claim: the physician who provided the first encounter, or the physician who provided the most extensive or best-documented encounter.
Tracking productivity for these cases proves challenging. Some practices develop an internal accounting system and credit each physician for their medically necessary efforts (a labor-intensive task for administrators and physicians). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Medicare Benefit Policy Manual: Concurrent Care. Chapter 15, Section 30.E. CMS website. Available at: www.cms.gov/manuals/Downloads/bp102c15.pdf. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Physicians in Group Practice. Chapter 12, Section 30.6.5. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Pohlig, C. Daily care conundrums. The Hospitalist website. Available at: www.the-hospitalist.org/details/article/188735/Daily_Care_Conundrums_.html. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Hospital Visits Same Day But by Different Physicians. Chapter 12, Section 30.6.9.C. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:15.
Let’s examine a documentation case for hospitalists providing daily care: A 65-year-old male patient is admitted with a left hip fracture. The patient also has hypertension and Type 2 diabetes, which might complicate his care. The orthopedic surgeon manages the patient’s perioperative course for the fracture while the hospitalist provides daily post-op care for hypertension and diabetes.
A common scenario is the hospitalist will provide concurrent care, along with a varying number of specialists, depending on the complexity of the patient’s presenting problems and existing comorbidities. Payors define concurrent care as more than one physician providing care to the same patient on the same date, or during the same hospitalization. Payors often consider two key principles before reimbursing concurrent care:
- Does the patient’s condition warrant more than one physician? and
- Are the services provided by each physician reasonable and necessary?1
When more than one medical condition exists and each physician actively treats the condition related to their expertise, each physician can demonstrate medical necessity. As in the above example, the orthopedic surgeon cares for the patient’s fracture while the hospitalist oversees diabetes and hypertension management. Claim submission follows the same logic. Report each subsequent hospital care code (99231-99233) with the corresponding diagnosis each physician primarily manages (i.e., orthopedic surgeon: 9923x with 820.8; hospitalist: 9923x with 250.00, 401.1).
When each physician assigns a different primary diagnosis code to the visit code, each is more likely to receive payment. Because each of these physicians are in different specialties and different provider groups, most payors do not require modifier 25 (separately identifiable E/M service on the same day as a procedure or other service) appended to the visit code. However, some managed-care payors require each physician to append modifier 25 to the concurrent E/M visit code (i.e., 99232-25) despite claim submission under different tax identification numbers.
Unfortunately, the physicians might not realize this until a claim rejection has been issued. Furthermore, payors might want to see the proof before rendering payment. In other words, they pay the first claim received and deny any subsequent claim in order to confirm medical necessity of the concurrent visit. Appeal denied such claims rejections with supporting documentation that distinguishes each physician visit, if possible. This assists the payors in understanding each physician’s contribution to care.
Reasons for Denial
Concurrent care services are more easily distinguished when separate diagnoses are reported with each service. Conversely, payors are likely to deny services that are hard to differentiate. Furthermore, payors frequently deny concurrent care services for the following reasons:
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate or overlap those of another provider without recognizable distinction.2
For example, a hospitalist might be involved in the post-op care of patients with fractures and no other identifiable chronic or acute conditions or complications. In these cases, the hospitalist’s continued involvement might constitute a facility policy (e.g., quality of care, risk reduction, etc.) rather than active clinical management. Claim submission could erroneously occur with each physician reporting 9923x for 820.8. Payors deny medically unnecessary services, or request refunds for inappropriate payments.
Hospitalists might attempt to negotiate other terms with the facility to account for the unpaid time and effort directed toward these types of cases.
Group Practice
Physicians in the same group practice with the same specialty designation must report, and are paid, as a single physician. Multiple visits to the same patient can occur on the same day by members of the same group (e.g., hospitalist A evaluates the patient in the morning, and hospitalist B reviews test results and the resulting course of treatment in the afternoon). However, only one subsequent hospital care service can be reported for the day.
The hospitalists should select the visit level representative of the combined services and submit one appropriately determined code (e.g., 99233), thereby capturing the medically necessary efforts of each physician. To complicate matters, the hospitalists must determine which name to report on the claim: the physician who provided the first encounter, or the physician who provided the most extensive or best-documented encounter.
Tracking productivity for these cases proves challenging. Some practices develop an internal accounting system and credit each physician for their medically necessary efforts (a labor-intensive task for administrators and physicians). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Medicare Benefit Policy Manual: Concurrent Care. Chapter 15, Section 30.E. CMS website. Available at: www.cms.gov/manuals/Downloads/bp102c15.pdf. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Physicians in Group Practice. Chapter 12, Section 30.6.5. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Pohlig, C. Daily care conundrums. The Hospitalist website. Available at: www.the-hospitalist.org/details/article/188735/Daily_Care_Conundrums_.html. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Hospital Visits Same Day But by Different Physicians. Chapter 12, Section 30.6.9.C. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:15.
Let’s examine a documentation case for hospitalists providing daily care: A 65-year-old male patient is admitted with a left hip fracture. The patient also has hypertension and Type 2 diabetes, which might complicate his care. The orthopedic surgeon manages the patient’s perioperative course for the fracture while the hospitalist provides daily post-op care for hypertension and diabetes.
A common scenario is the hospitalist will provide concurrent care, along with a varying number of specialists, depending on the complexity of the patient’s presenting problems and existing comorbidities. Payors define concurrent care as more than one physician providing care to the same patient on the same date, or during the same hospitalization. Payors often consider two key principles before reimbursing concurrent care:
- Does the patient’s condition warrant more than one physician? and
- Are the services provided by each physician reasonable and necessary?1
When more than one medical condition exists and each physician actively treats the condition related to their expertise, each physician can demonstrate medical necessity. As in the above example, the orthopedic surgeon cares for the patient’s fracture while the hospitalist oversees diabetes and hypertension management. Claim submission follows the same logic. Report each subsequent hospital care code (99231-99233) with the corresponding diagnosis each physician primarily manages (i.e., orthopedic surgeon: 9923x with 820.8; hospitalist: 9923x with 250.00, 401.1).
When each physician assigns a different primary diagnosis code to the visit code, each is more likely to receive payment. Because each of these physicians are in different specialties and different provider groups, most payors do not require modifier 25 (separately identifiable E/M service on the same day as a procedure or other service) appended to the visit code. However, some managed-care payors require each physician to append modifier 25 to the concurrent E/M visit code (i.e., 99232-25) despite claim submission under different tax identification numbers.
Unfortunately, the physicians might not realize this until a claim rejection has been issued. Furthermore, payors might want to see the proof before rendering payment. In other words, they pay the first claim received and deny any subsequent claim in order to confirm medical necessity of the concurrent visit. Appeal denied such claims rejections with supporting documentation that distinguishes each physician visit, if possible. This assists the payors in understanding each physician’s contribution to care.
Reasons for Denial
Concurrent care services are more easily distinguished when separate diagnoses are reported with each service. Conversely, payors are likely to deny services that are hard to differentiate. Furthermore, payors frequently deny concurrent care services for the following reasons:
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate or overlap those of another provider without recognizable distinction.2
For example, a hospitalist might be involved in the post-op care of patients with fractures and no other identifiable chronic or acute conditions or complications. In these cases, the hospitalist’s continued involvement might constitute a facility policy (e.g., quality of care, risk reduction, etc.) rather than active clinical management. Claim submission could erroneously occur with each physician reporting 9923x for 820.8. Payors deny medically unnecessary services, or request refunds for inappropriate payments.
Hospitalists might attempt to negotiate other terms with the facility to account for the unpaid time and effort directed toward these types of cases.
Group Practice
Physicians in the same group practice with the same specialty designation must report, and are paid, as a single physician. Multiple visits to the same patient can occur on the same day by members of the same group (e.g., hospitalist A evaluates the patient in the morning, and hospitalist B reviews test results and the resulting course of treatment in the afternoon). However, only one subsequent hospital care service can be reported for the day.
The hospitalists should select the visit level representative of the combined services and submit one appropriately determined code (e.g., 99233), thereby capturing the medically necessary efforts of each physician. To complicate matters, the hospitalists must determine which name to report on the claim: the physician who provided the first encounter, or the physician who provided the most extensive or best-documented encounter.
Tracking productivity for these cases proves challenging. Some practices develop an internal accounting system and credit each physician for their medically necessary efforts (a labor-intensive task for administrators and physicians). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Medicare Benefit Policy Manual: Concurrent Care. Chapter 15, Section 30.E. CMS website. Available at: www.cms.gov/manuals/Downloads/bp102c15.pdf. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Physicians in Group Practice. Chapter 12, Section 30.6.5. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Pohlig, C. Daily care conundrums. The Hospitalist website. Available at: www.the-hospitalist.org/details/article/188735/Daily_Care_Conundrums_.html. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Hospital Visits Same Day But by Different Physicians. Chapter 12, Section 30.6.9.C. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:15.
ONLINE EXCLUSIVE: HM is a perfect fit for a palliative care service
John Harney, COO at University of Colorado Hospital, moved west in 2008 after working at New York University Hospitals Center. The East Coast hospital had used a grant to establish a palliative-care program and witnessed immediate results.
“We truly believed it resulted in reductions in length of stay, as well as humanistic benefits,” Harney says. “When I came out to Colorado, I was pleasantly surprised at the breadth and depth of the programs here.”
Harney says he believes HM is a logical place to advance palliative care to the next level, as most HM groups already possess an in-house presence and commitment to efficient throughput. Hospital administrators will be concerned with consistency, routines, and protocols, he says, as well as the palliative-care service’s commitment to quality improvement. Those same administrators appreciate the need for program and salary support, although he advises palliative-care advocates to do their homework and develop a viable business plan.
“Hospital administrators will quickly figure out the math,” Harney says. “If you’re coming to speak to us, you need to have your numbers in order. You also need some monitoring in place.”
The initial salvo should include confirmation that HM group leaders have done their homework: surveyed their HM staff and discussed the idea with oncologists and other specialists. “It’s also helpful to have real champions in nursing and social work,” Harney says. “It’s never easy to get financial support for a new program, but if you have those ducks lined up, it goes better.”
John Harney, COO at University of Colorado Hospital, moved west in 2008 after working at New York University Hospitals Center. The East Coast hospital had used a grant to establish a palliative-care program and witnessed immediate results.
“We truly believed it resulted in reductions in length of stay, as well as humanistic benefits,” Harney says. “When I came out to Colorado, I was pleasantly surprised at the breadth and depth of the programs here.”
Harney says he believes HM is a logical place to advance palliative care to the next level, as most HM groups already possess an in-house presence and commitment to efficient throughput. Hospital administrators will be concerned with consistency, routines, and protocols, he says, as well as the palliative-care service’s commitment to quality improvement. Those same administrators appreciate the need for program and salary support, although he advises palliative-care advocates to do their homework and develop a viable business plan.
“Hospital administrators will quickly figure out the math,” Harney says. “If you’re coming to speak to us, you need to have your numbers in order. You also need some monitoring in place.”
The initial salvo should include confirmation that HM group leaders have done their homework: surveyed their HM staff and discussed the idea with oncologists and other specialists. “It’s also helpful to have real champions in nursing and social work,” Harney says. “It’s never easy to get financial support for a new program, but if you have those ducks lined up, it goes better.”
John Harney, COO at University of Colorado Hospital, moved west in 2008 after working at New York University Hospitals Center. The East Coast hospital had used a grant to establish a palliative-care program and witnessed immediate results.
“We truly believed it resulted in reductions in length of stay, as well as humanistic benefits,” Harney says. “When I came out to Colorado, I was pleasantly surprised at the breadth and depth of the programs here.”
Harney says he believes HM is a logical place to advance palliative care to the next level, as most HM groups already possess an in-house presence and commitment to efficient throughput. Hospital administrators will be concerned with consistency, routines, and protocols, he says, as well as the palliative-care service’s commitment to quality improvement. Those same administrators appreciate the need for program and salary support, although he advises palliative-care advocates to do their homework and develop a viable business plan.
“Hospital administrators will quickly figure out the math,” Harney says. “If you’re coming to speak to us, you need to have your numbers in order. You also need some monitoring in place.”
The initial salvo should include confirmation that HM group leaders have done their homework: surveyed their HM staff and discussed the idea with oncologists and other specialists. “It’s also helpful to have real champions in nursing and social work,” Harney says. “It’s never easy to get financial support for a new program, but if you have those ducks lined up, it goes better.”
Innovative Use of Scribes in the Inpatient Setting
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Market Watch
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability

Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability
Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability
Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
What Should I Do If I Get a Needlestick?
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center (IHCWSC), approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione et al surveyed internal-medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the Centers for Disease Control and Prevention (CDC) in 2004 suggests that because these are only self-reported injuries, the annual incidence of such injuries is in fact much higher than the current estimates suggest.2,3,4

More than 20 bloodborne pathogens (see Table 1, right) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
As decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should always be encouraged and supported to report all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2, p. 19).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3, p. 19). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Wides-pread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler et al reported that following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons, and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis, an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, post-exposure prophylaxis (PEP) with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source is from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, as no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin. However, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational-health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure-control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated. Healthcare providers should be aware of rare cases in which the source patient initially tested HIV-seronegative but was subsequently found to have primary HIV infection.
Per 2004 CDC recommendations, PEP is indicated for all healthcare workers who sustain a percuanteous injury from a known HIV-positive source.3,8 For a less severe injury (e.g. solid needle or superficial injury), PEP with either a basic two-drug or three-drug regimen is indicated, depending on the source patient’s viral load.3,5,6,8
If the source patient has unknown HIV status, two-drug PEP is indicated based on the source patient’s HIV risk factors. In such patients, rapid HIV testing also is indicated to aid in determining the need for PEP. When the source HIV status is unknown, PEP is indicated in settings where exposure to HIV-infected persons is likely.
If PEP is indicated, it should be started as quickly as possible. The 2005 U.S. Public Health Service Recommendations for PEP recommend initiating two nucleosides for low-risk exposures and two nucleosides plus a boosted protease inhibitor for high-risk exposures.
Examples of commonly used dual nucleoside regimens are Zidovudine plus Lamivudine (coformulated as Combivir) or Tenofovir plus Emtricitabine (coformulated as Truvada). Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.
Hepatitis B virus. Numerous prospective studies have evaluated the post-exposure effectiveness of HBIG. When administered within 24 hours of exposure, HBIG might offer immediate passive protection against HBV infection. Additionally, if initiated within one week of percutaneous injury with a known HBV-positive source, multiple doses of HGIB provide an estimated 75% protection from transmission.
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
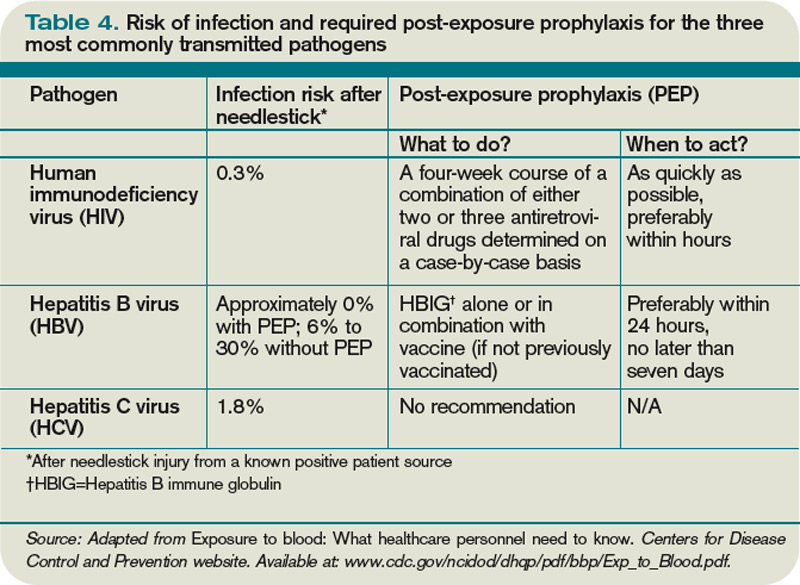
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HGIB prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP. TH
Dr. Zehnder is a hospitalist in the Section of Hospital Medicine at the University of Colorado Denver.
References
- Mangione CM, Gerberding JL, Cummings, SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, et al. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opinion. 2005;21(5):741-747.
- Workbook for designing, implementing, and evaluating a sharps injury prevention program. Centers for Disease Control and Prevention website. Available at: www.cdc.gov/sharpssafety/pdf/WorkbookComplete.pdf. Accessed Sept. 13, 2010.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Exposure to blood: What healthcare personnel need to know. CDC website. Available at: www.cdc.gov/ncidod /dhqp/pdf/bbp/Exp_to_Blood.pdf. Accessed Aug. 31, 2010.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed Aug. 31, 2010.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center (IHCWSC), approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione et al surveyed internal-medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the Centers for Disease Control and Prevention (CDC) in 2004 suggests that because these are only self-reported injuries, the annual incidence of such injuries is in fact much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1, right) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
As decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should always be encouraged and supported to report all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2, p. 19).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3, p. 19). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Wides-pread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler et al reported that following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons, and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis, an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, post-exposure prophylaxis (PEP) with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source is from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, as no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin. However, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational-health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure-control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated. Healthcare providers should be aware of rare cases in which the source patient initially tested HIV-seronegative but was subsequently found to have primary HIV infection.
Per 2004 CDC recommendations, PEP is indicated for all healthcare workers who sustain a percuanteous injury from a known HIV-positive source.3,8 For a less severe injury (e.g. solid needle or superficial injury), PEP with either a basic two-drug or three-drug regimen is indicated, depending on the source patient’s viral load.3,5,6,8
If the source patient has unknown HIV status, two-drug PEP is indicated based on the source patient’s HIV risk factors. In such patients, rapid HIV testing also is indicated to aid in determining the need for PEP. When the source HIV status is unknown, PEP is indicated in settings where exposure to HIV-infected persons is likely.
If PEP is indicated, it should be started as quickly as possible. The 2005 U.S. Public Health Service Recommendations for PEP recommend initiating two nucleosides for low-risk exposures and two nucleosides plus a boosted protease inhibitor for high-risk exposures.
Examples of commonly used dual nucleoside regimens are Zidovudine plus Lamivudine (coformulated as Combivir) or Tenofovir plus Emtricitabine (coformulated as Truvada). Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.
Hepatitis B virus. Numerous prospective studies have evaluated the post-exposure effectiveness of HBIG. When administered within 24 hours of exposure, HBIG might offer immediate passive protection against HBV infection. Additionally, if initiated within one week of percutaneous injury with a known HBV-positive source, multiple doses of HGIB provide an estimated 75% protection from transmission.
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HGIB prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP. TH
Dr. Zehnder is a hospitalist in the Section of Hospital Medicine at the University of Colorado Denver.
References
- Mangione CM, Gerberding JL, Cummings, SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, et al. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opinion. 2005;21(5):741-747.
- Workbook for designing, implementing, and evaluating a sharps injury prevention program. Centers for Disease Control and Prevention website. Available at: www.cdc.gov/sharpssafety/pdf/WorkbookComplete.pdf. Accessed Sept. 13, 2010.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Exposure to blood: What healthcare personnel need to know. CDC website. Available at: www.cdc.gov/ncidod /dhqp/pdf/bbp/Exp_to_Blood.pdf. Accessed Aug. 31, 2010.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed Aug. 31, 2010.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center (IHCWSC), approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione et al surveyed internal-medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the Centers for Disease Control and Prevention (CDC) in 2004 suggests that because these are only self-reported injuries, the annual incidence of such injuries is in fact much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1, right) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
As decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should always be encouraged and supported to report all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2, p. 19).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3, p. 19). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Wides-pread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler et al reported that following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons, and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis, an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, post-exposure prophylaxis (PEP) with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source is from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, as no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin. However, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational-health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure-control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated. Healthcare providers should be aware of rare cases in which the source patient initially tested HIV-seronegative but was subsequently found to have primary HIV infection.
Per 2004 CDC recommendations, PEP is indicated for all healthcare workers who sustain a percuanteous injury from a known HIV-positive source.3,8 For a less severe injury (e.g. solid needle or superficial injury), PEP with either a basic two-drug or three-drug regimen is indicated, depending on the source patient’s viral load.3,5,6,8
If the source patient has unknown HIV status, two-drug PEP is indicated based on the source patient’s HIV risk factors. In such patients, rapid HIV testing also is indicated to aid in determining the need for PEP. When the source HIV status is unknown, PEP is indicated in settings where exposure to HIV-infected persons is likely.
If PEP is indicated, it should be started as quickly as possible. The 2005 U.S. Public Health Service Recommendations for PEP recommend initiating two nucleosides for low-risk exposures and two nucleosides plus a boosted protease inhibitor for high-risk exposures.
Examples of commonly used dual nucleoside regimens are Zidovudine plus Lamivudine (coformulated as Combivir) or Tenofovir plus Emtricitabine (coformulated as Truvada). Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.
Hepatitis B virus. Numerous prospective studies have evaluated the post-exposure effectiveness of HBIG. When administered within 24 hours of exposure, HBIG might offer immediate passive protection against HBV infection. Additionally, if initiated within one week of percutaneous injury with a known HBV-positive source, multiple doses of HGIB provide an estimated 75% protection from transmission.
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HGIB prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP. TH
Dr. Zehnder is a hospitalist in the Section of Hospital Medicine at the University of Colorado Denver.
References
- Mangione CM, Gerberding JL, Cummings, SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, et al. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opinion. 2005;21(5):741-747.
- Workbook for designing, implementing, and evaluating a sharps injury prevention program. Centers for Disease Control and Prevention website. Available at: www.cdc.gov/sharpssafety/pdf/WorkbookComplete.pdf. Accessed Sept. 13, 2010.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Exposure to blood: What healthcare personnel need to know. CDC website. Available at: www.cdc.gov/ncidod /dhqp/pdf/bbp/Exp_to_Blood.pdf. Accessed Aug. 31, 2010.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed Aug. 31, 2010.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.