HM15 Session RAPID FIRE PANEL: Hot Topics in Practice Management Updates on Key Issues, Including the Key Characteristics of an Effective HMG
HM15 Presenters: Roy Sittig MD SFHM, Jeffrey Frank MD MBA, Jodi Braun
Summation: Speakers covered timely topics regarding the Accountable Care Act, namely Medicaid Expansion and Bundled Payment arrangements; and reviewed the seminal paper on “Key Principals and Characteristics of an Effective Hospitalist Medicine Group” and lessons learned in implementing those 10 Key Principles.
Medicaid Expansion: EDs serving the 29 Medicaid expansion states are reporting higher volumes, likely due to 11.4million new lives now insured under the ACA. While the ACA does provide for higher Medicaid payment rates thus far, only 34% of providers accept Medicaid, a 21% drop since the ACA went into effect.
Bundled Payment Arrangements:
Bundled Payment Care Initiative (BPCI) lexicon:
Model 2-Episode Anchor (anchor admission) AND 90days post d/c; Medicare pays 98% of usual cost
Model 3-90days post d/c AFTER anchor admission; Medicare pays 97% of usual cost
Convener-entity that brings providers together and enters into CMS agreement to bear risk for bundles
Awardee (entity having agreement with Medicare to assume risk and receive payment via BPCI) and Convener own the Bundle
Episode initiator (EI) triggers “bundle period”
Bundles based on DRG
10-Key Principles of an Effective Hospitalist Medicine Group:
Effective Leadership
Engaged Hospitalists
Adequate Resources
Planning and Management Infrastructure
Alignment with Hospital/Health System
Care Coordination Across Settings
Leadership in Key Clinical Issues in the Hospital/Health System
Thoughtful Approach to Scope of Activity
Patient/Family-Centered, Team-Based Care; Effective Communication
Recruiting/Retaining Qualified Clinicians
Key Points/HM Takeaways:
Medicaid Expansion- many of the 11.4M newly insured lives under the ACA have moved into Medicaid. Only about 1/3 of providers now accept Medicaid- 1 in 5 covered persons now have Medicaid, nearly 20% increase since 2013.
Bundled Payments- Majority of savings opportunity lies in Post-Acute Care. Awardee and Convener make profit is total cost is less than 98% of Target Price. In gainsharing agreements individuals can be reimbursed up to 150% usual Medicare rate. Pay occurs in usual Medicare fashion but is reconciled 60-90 days after end of bundle. For more information: http://innovation.cms.gov/initiatives/bundled-payments/
Effective HM Groups- Three important areas for focus when beginning to address group performance are: engaged hospitalists, planning and management infrastructure, care coordination across settings. These three topics have broad reaching implications into the hospitalist practice and patient care. [Cawley P, et al. Journal of Hospital Medicine 2014; 9(2):123-128]
HM15 Session RAPID FIRE PANEL: Hot Topics in Practice Management Updates on Key Issues, Including the Key Characteristics of an Effective HMG
HM15 Presenters: Roy Sittig MD SFHM, Jeffrey Frank MD MBA, Jodi Braun
Summation: Speakers covered timely topics regarding the Accountable Care Act, namely Medicaid Expansion and Bundled Payment arrangements; and reviewed the seminal paper on “Key Principals and Characteristics of an Effective Hospitalist Medicine Group” and lessons learned in implementing those 10 Key Principles.
Medicaid Expansion: EDs serving the 29 Medicaid expansion states are reporting higher volumes, likely due to 11.4million new lives now insured under the ACA. While the ACA does provide for higher Medicaid payment rates thus far, only 34% of providers accept Medicaid, a 21% drop since the ACA went into effect.
Bundled Payment Arrangements:
Bundled Payment Care Initiative (BPCI) lexicon:
Model 2-Episode Anchor (anchor admission) AND 90days post d/c; Medicare pays 98% of usual cost
Model 3-90days post d/c AFTER anchor admission; Medicare pays 97% of usual cost
Convener-entity that brings providers together and enters into CMS agreement to bear risk for bundles
Awardee (entity having agreement with Medicare to assume risk and receive payment via BPCI) and Convener own the Bundle
Episode initiator (EI) triggers “bundle period”
Bundles based on DRG
10-Key Principles of an Effective Hospitalist Medicine Group:
Effective Leadership
Engaged Hospitalists
Adequate Resources
Planning and Management Infrastructure
Alignment with Hospital/Health System
Care Coordination Across Settings
Leadership in Key Clinical Issues in the Hospital/Health System
Thoughtful Approach to Scope of Activity
Patient/Family-Centered, Team-Based Care; Effective Communication
Recruiting/Retaining Qualified Clinicians
Key Points/HM Takeaways:
Medicaid Expansion- many of the 11.4M newly insured lives under the ACA have moved into Medicaid. Only about 1/3 of providers now accept Medicaid- 1 in 5 covered persons now have Medicaid, nearly 20% increase since 2013.
Bundled Payments- Majority of savings opportunity lies in Post-Acute Care. Awardee and Convener make profit is total cost is less than 98% of Target Price. In gainsharing agreements individuals can be reimbursed up to 150% usual Medicare rate. Pay occurs in usual Medicare fashion but is reconciled 60-90 days after end of bundle. For more information: http://innovation.cms.gov/initiatives/bundled-payments/
Effective HM Groups- Three important areas for focus when beginning to address group performance are: engaged hospitalists, planning and management infrastructure, care coordination across settings. These three topics have broad reaching implications into the hospitalist practice and patient care. [Cawley P, et al. Journal of Hospital Medicine 2014; 9(2):123-128]
HM15 Session RAPID FIRE PANEL: Hot Topics in Practice Management Updates on Key Issues, Including the Key Characteristics of an Effective HMG
HM15 Presenters: Roy Sittig MD SFHM, Jeffrey Frank MD MBA, Jodi Braun
Summation: Speakers covered timely topics regarding the Accountable Care Act, namely Medicaid Expansion and Bundled Payment arrangements; and reviewed the seminal paper on “Key Principals and Characteristics of an Effective Hospitalist Medicine Group” and lessons learned in implementing those 10 Key Principles.
Medicaid Expansion: EDs serving the 29 Medicaid expansion states are reporting higher volumes, likely due to 11.4million new lives now insured under the ACA. While the ACA does provide for higher Medicaid payment rates thus far, only 34% of providers accept Medicaid, a 21% drop since the ACA went into effect.
Bundled Payment Arrangements:
Bundled Payment Care Initiative (BPCI) lexicon:
Model 2-Episode Anchor (anchor admission) AND 90days post d/c; Medicare pays 98% of usual cost
Model 3-90days post d/c AFTER anchor admission; Medicare pays 97% of usual cost
Convener-entity that brings providers together and enters into CMS agreement to bear risk for bundles
Awardee (entity having agreement with Medicare to assume risk and receive payment via BPCI) and Convener own the Bundle
Episode initiator (EI) triggers “bundle period”
Bundles based on DRG
10-Key Principles of an Effective Hospitalist Medicine Group:
Effective Leadership
Engaged Hospitalists
Adequate Resources
Planning and Management Infrastructure
Alignment with Hospital/Health System
Care Coordination Across Settings
Leadership in Key Clinical Issues in the Hospital/Health System
Thoughtful Approach to Scope of Activity
Patient/Family-Centered, Team-Based Care; Effective Communication
Recruiting/Retaining Qualified Clinicians
Key Points/HM Takeaways:
Medicaid Expansion- many of the 11.4M newly insured lives under the ACA have moved into Medicaid. Only about 1/3 of providers now accept Medicaid- 1 in 5 covered persons now have Medicaid, nearly 20% increase since 2013.
Bundled Payments- Majority of savings opportunity lies in Post-Acute Care. Awardee and Convener make profit is total cost is less than 98% of Target Price. In gainsharing agreements individuals can be reimbursed up to 150% usual Medicare rate. Pay occurs in usual Medicare fashion but is reconciled 60-90 days after end of bundle. For more information: http://innovation.cms.gov/initiatives/bundled-payments/
Effective HM Groups- Three important areas for focus when beginning to address group performance are: engaged hospitalists, planning and management infrastructure, care coordination across settings. These three topics have broad reaching implications into the hospitalist practice and patient care. [Cawley P, et al. Journal of Hospital Medicine 2014; 9(2):123-128]
Health care providers select Current Procedural Terminology codes based on the service provided and then document to support the level of service reported.1 According to the Office of Inspector General (OIG) for the US Department of Health and Human Services, “Medicare contractors have noted an increased frequency of medical records with identical documentation across services,” which may under certain circumstances be considered inappropriate.2 Regarding this practice, the OIG work plan for the 2014 fiscal year stated: "We will determine the extent to which selected payments for evaluation and management (E/M) services were inappropriate. We will also review multiple E/M services associated with the same providers and beneficiaries to determine the extent to which electronic or paper medical records had documentation vulnerabilities."2The OIG’s annual work plan reflects areas of concern that will be investigated in the coming years. These investigations may result in audits of specific Medicare and Medicaid providers, including physicians.
Concerns about physicians providing identical documentation across services has evinced an ongoing focus on the so-called cloning of medical records. Cloning is not well defined but generally refers to inappropriate use of the same exact documentation, perhaps via cutting and pasting, in different patient encounters. This type of cloning could occur in office visits with the same patient or different patients. The advent of electronic health records has made such duplication easier, and the concern is that duplicated notes in a medical record for a particular encounter may not accurately reflect the services that were provided in another encounter; in some cases, services may be overdocumented, with this creating a risk that that they may also be overcoded.
How can dermatologists minimize the risk for being flagged for cloning records? If you use templates for procedures, you may consider reviewing the completed template before filing the record to ensure that the details are consistent with the procedure that was performed. If you use abbreviations or other unique documentation that may not be easily understandable to an outside authority, you may want to keep a manual somewhere in your office that defines or describes such abbreviations and notations. Also, be aware that scribing is different than cloning, and scribing is not under scrutiny by OIG. A scribe writes word for word as a physician dictates and cannot act independently to alter or embellish the notes; once scribing is complete, both the scribe and the physician should sign the notes.
The American Academy of Dermatology has been concerned that an imprecise definition of so-called cloning can unfairly marginalize appropriate coding practices. In particular, when similar procedures or E/M services are performed by the same physician, the documentation may be very similar, even identical, while still being accurate and appropriately descriptive of the services provided. To help explain when similar notes are an acceptable practice in dermatology and when notes should be different, the American Academy of Dermatology has developed a guidance document that has been approved by its board of directors.3
Current Procedural Terminology coding guidelines clearly indicate that documentation cannot drive the level of coding and that excessive documentation cannot be used to justify a higher-level code, such as a higher-level E/M code. Instead, the level of service delivered should be appropriate for the patient’s condition and should be documented accordingly.4
It is important for dermatologists to document patient encounters as accurately and completely as is necessary for good patient care. Documentation will often vary substantially from patient to patient and encounter to encounter, but sometimes routine procedures or E/M visits may be coded similarly. For instance, a shave biopsy on the cheek to rule out nonmelanoma skin cancer may be performed by a particular practitioner with a standard instrument and after standard preparation and infiltration of local anesthetic; postoperative care may also be the same. To minimize regulatory scrutiny when similar descriptions are used, review the documentation for accuracy and to confirm that important specific information has not been inadvertently omitted or that wrong information has not been appended.
Unfortunately, there are dermatologists who have been audited for cloning during the last year. As with any audit, it is important to be vigilant regarding deadlines and to file appeals in a timely manner. Keep all the notifications you receive safely and explain to your staff that any communications should be promptly forwarded to you. If you are audited for suspected cloning, you may wish to contact the coding staff of professional dermatology societies for general guidance.
References
1. Centers for Medicare & Medicaid Services. Medicare claim processing manual: chapter 12 – physicians/nonphysician practitioners. http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf. Revised October 17, 2014. Accessed March 4, 2015.
2. Work plan for fiscal year 2014. Office of Inspector General, US Department of Health and Human Services Web site. https://oig.hhs.gov/reports-and-publications/archives/workplan/2014/Work-Plan-2014.pdf. Accessed March 4, 2015.
3. American Academy of Dermatology and AAD Association. Guidance statement: documentation of patient encounters and procedures. https://www.aad.org/forms/policies/Uploads/PS/Guidance%20Statement%20on%20Charting%20Practices.pdf. Approved October 23, 2014. Accessed March 6, 2015.
4. Evaluation and management services guide. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnproducts/downloads/eval_mgmt_serv_guide-icn006764.pdf. Published November 2014. Accessed March 5, 2015.
This article provides general information. Physicians should consult Current Procedural Terminology (CPT) guidelines, state regulations, and payer rules for coding and billing guidance relevant to specific cases. The opinions represented here are those of the author and have not been reviewed, endorsed, or approved by the American Medical Association, the American Academy of Dermatology, or any other coding or billing authority.
Correspondence: Murad Alam, MD, MSCI, 676 N Saint Clair St, Ste 1600, Chicago, IL 60611 ([email protected]).
Chart cloning, records, American Academy of Dermatology, chart similarity, coding, Current Procedural Terminology, CPT, e/m services, evaluation and management services
This article provides general information. Physicians should consult Current Procedural Terminology (CPT) guidelines, state regulations, and payer rules for coding and billing guidance relevant to specific cases. The opinions represented here are those of the author and have not been reviewed, endorsed, or approved by the American Medical Association, the American Academy of Dermatology, or any other coding or billing authority.
Correspondence: Murad Alam, MD, MSCI, 676 N Saint Clair St, Ste 1600, Chicago, IL 60611 ([email protected]).
Author and Disclosure Information
Murad Alam, MD, MSCI
From Northwestern University, Chicago, Illinois.
The author reports no conflict of interest.
This article provides general information. Physicians should consult Current Procedural Terminology (CPT) guidelines, state regulations, and payer rules for coding and billing guidance relevant to specific cases. The opinions represented here are those of the author and have not been reviewed, endorsed, or approved by the American Medical Association, the American Academy of Dermatology, or any other coding or billing authority.
Correspondence: Murad Alam, MD, MSCI, 676 N Saint Clair St, Ste 1600, Chicago, IL 60611 ([email protected]).
Health care providers select Current Procedural Terminology codes based on the service provided and then document to support the level of service reported.1 According to the Office of Inspector General (OIG) for the US Department of Health and Human Services, “Medicare contractors have noted an increased frequency of medical records with identical documentation across services,” which may under certain circumstances be considered inappropriate.2 Regarding this practice, the OIG work plan for the 2014 fiscal year stated: "We will determine the extent to which selected payments for evaluation and management (E/M) services were inappropriate. We will also review multiple E/M services associated with the same providers and beneficiaries to determine the extent to which electronic or paper medical records had documentation vulnerabilities."2The OIG’s annual work plan reflects areas of concern that will be investigated in the coming years. These investigations may result in audits of specific Medicare and Medicaid providers, including physicians.
Concerns about physicians providing identical documentation across services has evinced an ongoing focus on the so-called cloning of medical records. Cloning is not well defined but generally refers to inappropriate use of the same exact documentation, perhaps via cutting and pasting, in different patient encounters. This type of cloning could occur in office visits with the same patient or different patients. The advent of electronic health records has made such duplication easier, and the concern is that duplicated notes in a medical record for a particular encounter may not accurately reflect the services that were provided in another encounter; in some cases, services may be overdocumented, with this creating a risk that that they may also be overcoded.
How can dermatologists minimize the risk for being flagged for cloning records? If you use templates for procedures, you may consider reviewing the completed template before filing the record to ensure that the details are consistent with the procedure that was performed. If you use abbreviations or other unique documentation that may not be easily understandable to an outside authority, you may want to keep a manual somewhere in your office that defines or describes such abbreviations and notations. Also, be aware that scribing is different than cloning, and scribing is not under scrutiny by OIG. A scribe writes word for word as a physician dictates and cannot act independently to alter or embellish the notes; once scribing is complete, both the scribe and the physician should sign the notes.
The American Academy of Dermatology has been concerned that an imprecise definition of so-called cloning can unfairly marginalize appropriate coding practices. In particular, when similar procedures or E/M services are performed by the same physician, the documentation may be very similar, even identical, while still being accurate and appropriately descriptive of the services provided. To help explain when similar notes are an acceptable practice in dermatology and when notes should be different, the American Academy of Dermatology has developed a guidance document that has been approved by its board of directors.3
Current Procedural Terminology coding guidelines clearly indicate that documentation cannot drive the level of coding and that excessive documentation cannot be used to justify a higher-level code, such as a higher-level E/M code. Instead, the level of service delivered should be appropriate for the patient’s condition and should be documented accordingly.4
It is important for dermatologists to document patient encounters as accurately and completely as is necessary for good patient care. Documentation will often vary substantially from patient to patient and encounter to encounter, but sometimes routine procedures or E/M visits may be coded similarly. For instance, a shave biopsy on the cheek to rule out nonmelanoma skin cancer may be performed by a particular practitioner with a standard instrument and after standard preparation and infiltration of local anesthetic; postoperative care may also be the same. To minimize regulatory scrutiny when similar descriptions are used, review the documentation for accuracy and to confirm that important specific information has not been inadvertently omitted or that wrong information has not been appended.
Unfortunately, there are dermatologists who have been audited for cloning during the last year. As with any audit, it is important to be vigilant regarding deadlines and to file appeals in a timely manner. Keep all the notifications you receive safely and explain to your staff that any communications should be promptly forwarded to you. If you are audited for suspected cloning, you may wish to contact the coding staff of professional dermatology societies for general guidance.
Health care providers select Current Procedural Terminology codes based on the service provided and then document to support the level of service reported.1 According to the Office of Inspector General (OIG) for the US Department of Health and Human Services, “Medicare contractors have noted an increased frequency of medical records with identical documentation across services,” which may under certain circumstances be considered inappropriate.2 Regarding this practice, the OIG work plan for the 2014 fiscal year stated: "We will determine the extent to which selected payments for evaluation and management (E/M) services were inappropriate. We will also review multiple E/M services associated with the same providers and beneficiaries to determine the extent to which electronic or paper medical records had documentation vulnerabilities."2The OIG’s annual work plan reflects areas of concern that will be investigated in the coming years. These investigations may result in audits of specific Medicare and Medicaid providers, including physicians.
Concerns about physicians providing identical documentation across services has evinced an ongoing focus on the so-called cloning of medical records. Cloning is not well defined but generally refers to inappropriate use of the same exact documentation, perhaps via cutting and pasting, in different patient encounters. This type of cloning could occur in office visits with the same patient or different patients. The advent of electronic health records has made such duplication easier, and the concern is that duplicated notes in a medical record for a particular encounter may not accurately reflect the services that were provided in another encounter; in some cases, services may be overdocumented, with this creating a risk that that they may also be overcoded.
How can dermatologists minimize the risk for being flagged for cloning records? If you use templates for procedures, you may consider reviewing the completed template before filing the record to ensure that the details are consistent with the procedure that was performed. If you use abbreviations or other unique documentation that may not be easily understandable to an outside authority, you may want to keep a manual somewhere in your office that defines or describes such abbreviations and notations. Also, be aware that scribing is different than cloning, and scribing is not under scrutiny by OIG. A scribe writes word for word as a physician dictates and cannot act independently to alter or embellish the notes; once scribing is complete, both the scribe and the physician should sign the notes.
The American Academy of Dermatology has been concerned that an imprecise definition of so-called cloning can unfairly marginalize appropriate coding practices. In particular, when similar procedures or E/M services are performed by the same physician, the documentation may be very similar, even identical, while still being accurate and appropriately descriptive of the services provided. To help explain when similar notes are an acceptable practice in dermatology and when notes should be different, the American Academy of Dermatology has developed a guidance document that has been approved by its board of directors.3
Current Procedural Terminology coding guidelines clearly indicate that documentation cannot drive the level of coding and that excessive documentation cannot be used to justify a higher-level code, such as a higher-level E/M code. Instead, the level of service delivered should be appropriate for the patient’s condition and should be documented accordingly.4
It is important for dermatologists to document patient encounters as accurately and completely as is necessary for good patient care. Documentation will often vary substantially from patient to patient and encounter to encounter, but sometimes routine procedures or E/M visits may be coded similarly. For instance, a shave biopsy on the cheek to rule out nonmelanoma skin cancer may be performed by a particular practitioner with a standard instrument and after standard preparation and infiltration of local anesthetic; postoperative care may also be the same. To minimize regulatory scrutiny when similar descriptions are used, review the documentation for accuracy and to confirm that important specific information has not been inadvertently omitted or that wrong information has not been appended.
Unfortunately, there are dermatologists who have been audited for cloning during the last year. As with any audit, it is important to be vigilant regarding deadlines and to file appeals in a timely manner. Keep all the notifications you receive safely and explain to your staff that any communications should be promptly forwarded to you. If you are audited for suspected cloning, you may wish to contact the coding staff of professional dermatology societies for general guidance.
References
1. Centers for Medicare & Medicaid Services. Medicare claim processing manual: chapter 12 – physicians/nonphysician practitioners. http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf. Revised October 17, 2014. Accessed March 4, 2015.
2. Work plan for fiscal year 2014. Office of Inspector General, US Department of Health and Human Services Web site. https://oig.hhs.gov/reports-and-publications/archives/workplan/2014/Work-Plan-2014.pdf. Accessed March 4, 2015.
3. American Academy of Dermatology and AAD Association. Guidance statement: documentation of patient encounters and procedures. https://www.aad.org/forms/policies/Uploads/PS/Guidance%20Statement%20on%20Charting%20Practices.pdf. Approved October 23, 2014. Accessed March 6, 2015.
4. Evaluation and management services guide. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnproducts/downloads/eval_mgmt_serv_guide-icn006764.pdf. Published November 2014. Accessed March 5, 2015.
References
1. Centers for Medicare & Medicaid Services. Medicare claim processing manual: chapter 12 – physicians/nonphysician practitioners. http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf. Revised October 17, 2014. Accessed March 4, 2015.
2. Work plan for fiscal year 2014. Office of Inspector General, US Department of Health and Human Services Web site. https://oig.hhs.gov/reports-and-publications/archives/workplan/2014/Work-Plan-2014.pdf. Accessed March 4, 2015.
3. American Academy of Dermatology and AAD Association. Guidance statement: documentation of patient encounters and procedures. https://www.aad.org/forms/policies/Uploads/PS/Guidance%20Statement%20on%20Charting%20Practices.pdf. Approved October 23, 2014. Accessed March 6, 2015.
4. Evaluation and management services guide. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnproducts/downloads/eval_mgmt_serv_guide-icn006764.pdf. Published November 2014. Accessed March 5, 2015.
Chart cloning, records, American Academy of Dermatology, chart similarity, coding, Current Procedural Terminology, CPT, e/m services, evaluation and management services
Legacy Keywords
Chart cloning, records, American Academy of Dermatology, chart similarity, coding, Current Procedural Terminology, CPT, e/m services, evaluation and management services
Medical record documentation for evaluation and management services includes information relevant to the patient encounter. Providing identical documentation for different patients may under certain circumstances be considered cloning and hence inappropriate.
Following best practices can minimize the risk for being flagged for cloning.
In the article “Common Coding Mistakes Hospitalists Should Avoid” in the August 2014 issue of The Hospitalist, the author states:
“For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization.”
This definition contradicts what I have been told in other coding courses regarding new vs. established problems relative to the examiner. It has been my understanding that when [I am] rotating on service and I have not seen that particular patient during the current admission, all of the current problems are new to me, even if previously identified by another member of my group. This [situation] results in a higher complexity of medical decision-making, which is reflective of the increased time spent learning a new patient when coming on service. I would appreciate clarification from the author.
–Matt George, MD,
medical director, MBHS Hospitalists
Billing and coding expert Carol Pohlig, BSN, RN, CPC, ACS, explains:
Be mindful when attending coding courses that are not contractor sponsored, as they may not validate the geographical interpretations of the rules for providers. There are several factors to consider when crediting the physician with “new” or “established” problems.
CMS documentation guidelines state: “Decision making with respect to a diagnosed problem is easier than that for an identified but undiagnosed problem.1
For a presenting problem with an established diagnosis, the record should reflect whether the problem is:
Improved, well-controlled, resolving, or resolved or
Inadequately controlled, worsening, or failing to change as expected.
For a presenting problem without an established diagnosis, the assessment or clinical impression may be stated in the form of differential diagnoses or as a “possible,” “probable,” or “rule out” diagnosis.
Although Medicare contractors utilize the Marshfield Clinic Scoring Tool when reviewing evaluation and management (E/M) services, a tool that historically refers to the “examiner” when considering the patient’s diagnoses, not all accept this tool-inspired standard, particularly in the advent of electronic health record accessibility and the idea that same-specialty physicians in a group practice are viewed as an individual physician.2,3
Reviewing information and familiarization of patients is often considered pre-service work and factored into the payment for E/M services. More importantly, the feasibility of an auditor being able to distinguish new vs. established problems at the level of the “examiner” is decreased when auditing a single date of service. Non-Medicare payers who audit E/M services do not necessarily follow contractor-specific guidelines but, rather, general CMS guidelines.
Therefore, without knowing the insurer or their interpretation at the time of service or visit level selection, the CMS-developed standard is the most practical application when considering the complexity of the encounter.
In the article “Common Coding Mistakes Hospitalists Should Avoid” in the August 2014 issue of The Hospitalist, the author states:
“For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization.”
This definition contradicts what I have been told in other coding courses regarding new vs. established problems relative to the examiner. It has been my understanding that when [I am] rotating on service and I have not seen that particular patient during the current admission, all of the current problems are new to me, even if previously identified by another member of my group. This [situation] results in a higher complexity of medical decision-making, which is reflective of the increased time spent learning a new patient when coming on service. I would appreciate clarification from the author.
–Matt George, MD,
medical director, MBHS Hospitalists
Billing and coding expert Carol Pohlig, BSN, RN, CPC, ACS, explains:
Be mindful when attending coding courses that are not contractor sponsored, as they may not validate the geographical interpretations of the rules for providers. There are several factors to consider when crediting the physician with “new” or “established” problems.
CMS documentation guidelines state: “Decision making with respect to a diagnosed problem is easier than that for an identified but undiagnosed problem.1
For a presenting problem with an established diagnosis, the record should reflect whether the problem is:
Improved, well-controlled, resolving, or resolved or
Inadequately controlled, worsening, or failing to change as expected.
For a presenting problem without an established diagnosis, the assessment or clinical impression may be stated in the form of differential diagnoses or as a “possible,” “probable,” or “rule out” diagnosis.
Although Medicare contractors utilize the Marshfield Clinic Scoring Tool when reviewing evaluation and management (E/M) services, a tool that historically refers to the “examiner” when considering the patient’s diagnoses, not all accept this tool-inspired standard, particularly in the advent of electronic health record accessibility and the idea that same-specialty physicians in a group practice are viewed as an individual physician.2,3
Reviewing information and familiarization of patients is often considered pre-service work and factored into the payment for E/M services. More importantly, the feasibility of an auditor being able to distinguish new vs. established problems at the level of the “examiner” is decreased when auditing a single date of service. Non-Medicare payers who audit E/M services do not necessarily follow contractor-specific guidelines but, rather, general CMS guidelines.
Therefore, without knowing the insurer or their interpretation at the time of service or visit level selection, the CMS-developed standard is the most practical application when considering the complexity of the encounter.
In the article “Common Coding Mistakes Hospitalists Should Avoid” in the August 2014 issue of The Hospitalist, the author states:
“For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization.”
This definition contradicts what I have been told in other coding courses regarding new vs. established problems relative to the examiner. It has been my understanding that when [I am] rotating on service and I have not seen that particular patient during the current admission, all of the current problems are new to me, even if previously identified by another member of my group. This [situation] results in a higher complexity of medical decision-making, which is reflective of the increased time spent learning a new patient when coming on service. I would appreciate clarification from the author.
–Matt George, MD,
medical director, MBHS Hospitalists
Billing and coding expert Carol Pohlig, BSN, RN, CPC, ACS, explains:
Be mindful when attending coding courses that are not contractor sponsored, as they may not validate the geographical interpretations of the rules for providers. There are several factors to consider when crediting the physician with “new” or “established” problems.
CMS documentation guidelines state: “Decision making with respect to a diagnosed problem is easier than that for an identified but undiagnosed problem.1
For a presenting problem with an established diagnosis, the record should reflect whether the problem is:
Improved, well-controlled, resolving, or resolved or
Inadequately controlled, worsening, or failing to change as expected.
For a presenting problem without an established diagnosis, the assessment or clinical impression may be stated in the form of differential diagnoses or as a “possible,” “probable,” or “rule out” diagnosis.
Although Medicare contractors utilize the Marshfield Clinic Scoring Tool when reviewing evaluation and management (E/M) services, a tool that historically refers to the “examiner” when considering the patient’s diagnoses, not all accept this tool-inspired standard, particularly in the advent of electronic health record accessibility and the idea that same-specialty physicians in a group practice are viewed as an individual physician.2,3
Reviewing information and familiarization of patients is often considered pre-service work and factored into the payment for E/M services. More importantly, the feasibility of an auditor being able to distinguish new vs. established problems at the level of the “examiner” is decreased when auditing a single date of service. Non-Medicare payers who audit E/M services do not necessarily follow contractor-specific guidelines but, rather, general CMS guidelines.
Therefore, without knowing the insurer or their interpretation at the time of service or visit level selection, the CMS-developed standard is the most practical application when considering the complexity of the encounter.
Hospitalists often are tasked with coordinating and overseeing patient care throughout a hospitalization. Depending on the care model and the availability of varying specialists, a patient could see several specialists throughout the stay, and even during a single day. A recurring issue for many hospitalists is justifying the medical necessity of their services, because payers do not want to reimburse overlapping care (i.e., multiple providers caring for the same patient problem) when more than one physician provides care on the same service date.
Payers often consider two key principles before reimbursing multiple visits on the same date:1
Does the patient’s condition warrant the services of more than one physician?
Are the individual services provided by each physician reasonable and necessary?
Consider the following example: A 65-year-old female patient is admitted with a hip fracture (820.8) after slipping on the ice outside her home. The patient also has hypertension (401.1) and type II diabetes (250.00). The surgeon manages the patient’s peri-operative course for the fracture, while the hospitalist manages the patient’s medical issues.
Payers must be sure that the services of one physician do not duplicate those provided by another.1 For the above scenario, it is imperative that the hospitalist understand which services are considered the surgeon’s responsibility. The global surgical package includes payment for the surgical procedure and the completion of its corresponding facility-required paperwork (e.g. pre-operative history and physical exam, operative consent forms, pre-operative orders), in addition to the following services:2
Pre-operative visits after making the decision for surgery beginning one day prior to surgery;
All additional post-operative medical or surgical services provided by the surgeon related to complications but not requiring additional trips to the operating room;
Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes, local incisional care, removal of cutaneous sutures and staples, line removals, changes and removal of tracheostomy tubes, and discharge services; and
Post-operative pain management provided by the surgeon.
Another physician who performs any component of the global package will not receive separate payment unless the surgeon is willing to forego a portion of the payment. For example, a hospitalist admits a patient who has no other identifiable medical conditions aside from the problem prompting surgery. The hospitalist’s role may be dictated by facility policy—quality of care or risk reduction, for example—and administrative requirements (history and physical exam, discharge services, coordination of care) rather than what a payer would perceive as necessary “medical” management. Similarly, if the hospitalist’s post-op care is limited to ordering routine post-op labs or maintaining appropriate pain management, the hospitalist’s service will likely be denied as incidental to the surgical package.
The hospitalist’s role may be dictated by facility policy and administrative requirements history and physical exam, discharge services, coordination of care rather than what a payer would perceive as necessary “medical” management.
Remember, if the hospitalist’s claim is submitted and paid, it doesn’t mean that the payer won’t retract the payment upon review if an erroneous payment is suspected. A payer review may be triggered when the diagnosis listed on the hospitalist’s claim matches the diagnosis listed on the surgeon’s claim (e.g. 820.8). If too many claims are considered “not medically necessary” due to overlapping care, hospitalists may need to negotiate other terms of payment with the facility to recoup unpaid time and effort when involved in this type of care.
When more than one medical condition exists and several physicians participate in the patient’s care, medical necessity is easily established for each physician. Each physician manages the condition related to his/her expertise. In the above example, the surgeon cares for the patient’s fracture, while the hospitalist oversees diabetes and hypertension management. Service distinction is crucial during the claim submission process. The hospitalist should report a subsequent hospital care code (99231-99233) with a primary diagnosis corresponding to his/her specialty-related care (i.e., 9923x with 250.00, 401.1).3
When more specialists are involved, claim submission becomes more complex. A cardiologist who was also involved in patient management would report his or her service using 401.1. When a different primary diagnosis is assigned to the visit code to indicate the reason for each physician’s involvement, all claims are more likely to be paid.4 As long as the hospitalist maintains care over one of the patients’ conditions, concurrent care is justified.
Because these physicians are in different specialties and different provider groups, most payers do not require the modifier 25 (separately identifiable evaluation/management [E/M] service on the same day as a procedure or other service) with the visit code; however, some managed care payers may have a general claim edit that pays the first claim and denies the second unless modifier 25 is appended to the concurrent E/M visit code (i.e., 99232-25) as an attestation that the service is distinct from any other provider’s service that day, despite claim submission under different tax identification numbers. This may not be identified until the claim is rejected or denied. If appropriate modifier use does not yield payment, appeal the denied concurrent care claims with supporting documentation from each physician visit, if possible. This demonstrates each physician’s contribution to care.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Code This Case
A hospitalist providing night coverage admits a patient with chest pain after midnight on Day 1. Later that same day, the cardiologist is consulted and manages the patient’s care. If the hospitalist’s role is to provide “night coverage,” can each physician see the patient for management on Day 2?
If the patient does not have any noncardiac issues, it would be difficult to justify the hospitalist service on Day 2, since the cardiologist is managing the same patient. Medicare and other payers advise against separate reporting in this case. Payers only consider reimbursement for concurrent services involving different aspects of patient care and reimburse separate services when billed with different diagnoses.4
Circumstances become even more difficult when a hospitalist sees the patient after midnight, and an internist sees the patient during the day. Medicare acknowledges that there are circumstances in which concurrent care may be billed by physicians of the same specialty.4
In this situation, if the nocturnist was called to manage a change in the patient’s condition, a separate service is warranted and should be reported. Since both physicians are enrolled with the payer as “internists,” it is unlikely that payers will reimburse each service; therefore, the first claim received is paid. If the hospitalist submits the first claim, the payer is likely to pay the hospitalist and deny the internist; however, the hospitalist claim may not always be first, and an appeal using both the internist’s and the hospitalist’s notes is suggested.
To maintain costs and avoid internal conflict, some hospitalist groups contract with the facility and receive a stipend for night coverage instead of submitting claims. It is best to seek legal advice before pursuing this option in order to prevent any inappropriate arrangements.
—Carol Pohlig
SHM Offers Training
Want to get better at documentation and coding? Check out iCATT, SHM’s new Interactive Coding Audit and Training Tool. iCATT is:
A self-directed training tool (on documentation and coding) for hospitalists;
A tool for testing the coding/documentation competency of new hospitalists; and
A training tool for coders who conduct coding/documentation audits of hospital medicine groups.
Physicians in Group Practice
According to Medicare, “physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician. If more than one evaluation and management (face-to-face) service is provided on the same day to the same patient by the same physician, or more than one physician in the same specialty in the same group, only one E&M service may be reported unless the services are for unrelated problems. Instead of billing separately, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level.”5
For example, hospitalist A evaluates the patient in the morning and hospitalist B subsequently reviews test results and discusses the course of treatment with the family members who will be involved in the patient’s care upon returning home. The hospitalist group can submit only one subsequent hospital care service for the day; the selected visit level should represent the combined visits (e.g. 99233).
The hospitalists must determine which name to report on the claim, the physician who provided the initial encounter or the physician who provided the most extensive—or best documented—encounter.
Physicians who are in the same group practice and submit claims under the same tax identification number can still be paid if they are enrolled with the payers as different specialty providers. This requires accurately identifying the physician’s primary two-digit specialty code on the payer enrollment form. For example, a hospitalist is enrolled as an internist (code 11), and a cardiologist is enrolled using code 06.6
Physicians can declare two specialty codes on their enrollment forms, but the primary code is the most crucial for accurate claim submission.
Hospitalists often are tasked with coordinating and overseeing patient care throughout a hospitalization. Depending on the care model and the availability of varying specialists, a patient could see several specialists throughout the stay, and even during a single day. A recurring issue for many hospitalists is justifying the medical necessity of their services, because payers do not want to reimburse overlapping care (i.e., multiple providers caring for the same patient problem) when more than one physician provides care on the same service date.
Payers often consider two key principles before reimbursing multiple visits on the same date:1
Does the patient’s condition warrant the services of more than one physician?
Are the individual services provided by each physician reasonable and necessary?
Consider the following example: A 65-year-old female patient is admitted with a hip fracture (820.8) after slipping on the ice outside her home. The patient also has hypertension (401.1) and type II diabetes (250.00). The surgeon manages the patient’s peri-operative course for the fracture, while the hospitalist manages the patient’s medical issues.
Payers must be sure that the services of one physician do not duplicate those provided by another.1 For the above scenario, it is imperative that the hospitalist understand which services are considered the surgeon’s responsibility. The global surgical package includes payment for the surgical procedure and the completion of its corresponding facility-required paperwork (e.g. pre-operative history and physical exam, operative consent forms, pre-operative orders), in addition to the following services:2
Pre-operative visits after making the decision for surgery beginning one day prior to surgery;
All additional post-operative medical or surgical services provided by the surgeon related to complications but not requiring additional trips to the operating room;
Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes, local incisional care, removal of cutaneous sutures and staples, line removals, changes and removal of tracheostomy tubes, and discharge services; and
Post-operative pain management provided by the surgeon.
Another physician who performs any component of the global package will not receive separate payment unless the surgeon is willing to forego a portion of the payment. For example, a hospitalist admits a patient who has no other identifiable medical conditions aside from the problem prompting surgery. The hospitalist’s role may be dictated by facility policy—quality of care or risk reduction, for example—and administrative requirements (history and physical exam, discharge services, coordination of care) rather than what a payer would perceive as necessary “medical” management. Similarly, if the hospitalist’s post-op care is limited to ordering routine post-op labs or maintaining appropriate pain management, the hospitalist’s service will likely be denied as incidental to the surgical package.
The hospitalist’s role may be dictated by facility policy and administrative requirements history and physical exam, discharge services, coordination of care rather than what a payer would perceive as necessary “medical” management.
Remember, if the hospitalist’s claim is submitted and paid, it doesn’t mean that the payer won’t retract the payment upon review if an erroneous payment is suspected. A payer review may be triggered when the diagnosis listed on the hospitalist’s claim matches the diagnosis listed on the surgeon’s claim (e.g. 820.8). If too many claims are considered “not medically necessary” due to overlapping care, hospitalists may need to negotiate other terms of payment with the facility to recoup unpaid time and effort when involved in this type of care.
When more than one medical condition exists and several physicians participate in the patient’s care, medical necessity is easily established for each physician. Each physician manages the condition related to his/her expertise. In the above example, the surgeon cares for the patient’s fracture, while the hospitalist oversees diabetes and hypertension management. Service distinction is crucial during the claim submission process. The hospitalist should report a subsequent hospital care code (99231-99233) with a primary diagnosis corresponding to his/her specialty-related care (i.e., 9923x with 250.00, 401.1).3
When more specialists are involved, claim submission becomes more complex. A cardiologist who was also involved in patient management would report his or her service using 401.1. When a different primary diagnosis is assigned to the visit code to indicate the reason for each physician’s involvement, all claims are more likely to be paid.4 As long as the hospitalist maintains care over one of the patients’ conditions, concurrent care is justified.
Because these physicians are in different specialties and different provider groups, most payers do not require the modifier 25 (separately identifiable evaluation/management [E/M] service on the same day as a procedure or other service) with the visit code; however, some managed care payers may have a general claim edit that pays the first claim and denies the second unless modifier 25 is appended to the concurrent E/M visit code (i.e., 99232-25) as an attestation that the service is distinct from any other provider’s service that day, despite claim submission under different tax identification numbers. This may not be identified until the claim is rejected or denied. If appropriate modifier use does not yield payment, appeal the denied concurrent care claims with supporting documentation from each physician visit, if possible. This demonstrates each physician’s contribution to care.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Code This Case
A hospitalist providing night coverage admits a patient with chest pain after midnight on Day 1. Later that same day, the cardiologist is consulted and manages the patient’s care. If the hospitalist’s role is to provide “night coverage,” can each physician see the patient for management on Day 2?
If the patient does not have any noncardiac issues, it would be difficult to justify the hospitalist service on Day 2, since the cardiologist is managing the same patient. Medicare and other payers advise against separate reporting in this case. Payers only consider reimbursement for concurrent services involving different aspects of patient care and reimburse separate services when billed with different diagnoses.4
Circumstances become even more difficult when a hospitalist sees the patient after midnight, and an internist sees the patient during the day. Medicare acknowledges that there are circumstances in which concurrent care may be billed by physicians of the same specialty.4
In this situation, if the nocturnist was called to manage a change in the patient’s condition, a separate service is warranted and should be reported. Since both physicians are enrolled with the payer as “internists,” it is unlikely that payers will reimburse each service; therefore, the first claim received is paid. If the hospitalist submits the first claim, the payer is likely to pay the hospitalist and deny the internist; however, the hospitalist claim may not always be first, and an appeal using both the internist’s and the hospitalist’s notes is suggested.
To maintain costs and avoid internal conflict, some hospitalist groups contract with the facility and receive a stipend for night coverage instead of submitting claims. It is best to seek legal advice before pursuing this option in order to prevent any inappropriate arrangements.
—Carol Pohlig
SHM Offers Training
Want to get better at documentation and coding? Check out iCATT, SHM’s new Interactive Coding Audit and Training Tool. iCATT is:
A self-directed training tool (on documentation and coding) for hospitalists;
A tool for testing the coding/documentation competency of new hospitalists; and
A training tool for coders who conduct coding/documentation audits of hospital medicine groups.
Physicians in Group Practice
According to Medicare, “physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician. If more than one evaluation and management (face-to-face) service is provided on the same day to the same patient by the same physician, or more than one physician in the same specialty in the same group, only one E&M service may be reported unless the services are for unrelated problems. Instead of billing separately, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level.”5
For example, hospitalist A evaluates the patient in the morning and hospitalist B subsequently reviews test results and discusses the course of treatment with the family members who will be involved in the patient’s care upon returning home. The hospitalist group can submit only one subsequent hospital care service for the day; the selected visit level should represent the combined visits (e.g. 99233).
The hospitalists must determine which name to report on the claim, the physician who provided the initial encounter or the physician who provided the most extensive—or best documented—encounter.
Physicians who are in the same group practice and submit claims under the same tax identification number can still be paid if they are enrolled with the payers as different specialty providers. This requires accurately identifying the physician’s primary two-digit specialty code on the payer enrollment form. For example, a hospitalist is enrolled as an internist (code 11), and a cardiologist is enrolled using code 06.6
Physicians can declare two specialty codes on their enrollment forms, but the primary code is the most crucial for accurate claim submission.
Hospitalists often are tasked with coordinating and overseeing patient care throughout a hospitalization. Depending on the care model and the availability of varying specialists, a patient could see several specialists throughout the stay, and even during a single day. A recurring issue for many hospitalists is justifying the medical necessity of their services, because payers do not want to reimburse overlapping care (i.e., multiple providers caring for the same patient problem) when more than one physician provides care on the same service date.
Payers often consider two key principles before reimbursing multiple visits on the same date:1
Does the patient’s condition warrant the services of more than one physician?
Are the individual services provided by each physician reasonable and necessary?
Consider the following example: A 65-year-old female patient is admitted with a hip fracture (820.8) after slipping on the ice outside her home. The patient also has hypertension (401.1) and type II diabetes (250.00). The surgeon manages the patient’s peri-operative course for the fracture, while the hospitalist manages the patient’s medical issues.
Payers must be sure that the services of one physician do not duplicate those provided by another.1 For the above scenario, it is imperative that the hospitalist understand which services are considered the surgeon’s responsibility. The global surgical package includes payment for the surgical procedure and the completion of its corresponding facility-required paperwork (e.g. pre-operative history and physical exam, operative consent forms, pre-operative orders), in addition to the following services:2
Pre-operative visits after making the decision for surgery beginning one day prior to surgery;
All additional post-operative medical or surgical services provided by the surgeon related to complications but not requiring additional trips to the operating room;
Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes, local incisional care, removal of cutaneous sutures and staples, line removals, changes and removal of tracheostomy tubes, and discharge services; and
Post-operative pain management provided by the surgeon.
Another physician who performs any component of the global package will not receive separate payment unless the surgeon is willing to forego a portion of the payment. For example, a hospitalist admits a patient who has no other identifiable medical conditions aside from the problem prompting surgery. The hospitalist’s role may be dictated by facility policy—quality of care or risk reduction, for example—and administrative requirements (history and physical exam, discharge services, coordination of care) rather than what a payer would perceive as necessary “medical” management. Similarly, if the hospitalist’s post-op care is limited to ordering routine post-op labs or maintaining appropriate pain management, the hospitalist’s service will likely be denied as incidental to the surgical package.
The hospitalist’s role may be dictated by facility policy and administrative requirements history and physical exam, discharge services, coordination of care rather than what a payer would perceive as necessary “medical” management.
Remember, if the hospitalist’s claim is submitted and paid, it doesn’t mean that the payer won’t retract the payment upon review if an erroneous payment is suspected. A payer review may be triggered when the diagnosis listed on the hospitalist’s claim matches the diagnosis listed on the surgeon’s claim (e.g. 820.8). If too many claims are considered “not medically necessary” due to overlapping care, hospitalists may need to negotiate other terms of payment with the facility to recoup unpaid time and effort when involved in this type of care.
When more than one medical condition exists and several physicians participate in the patient’s care, medical necessity is easily established for each physician. Each physician manages the condition related to his/her expertise. In the above example, the surgeon cares for the patient’s fracture, while the hospitalist oversees diabetes and hypertension management. Service distinction is crucial during the claim submission process. The hospitalist should report a subsequent hospital care code (99231-99233) with a primary diagnosis corresponding to his/her specialty-related care (i.e., 9923x with 250.00, 401.1).3
When more specialists are involved, claim submission becomes more complex. A cardiologist who was also involved in patient management would report his or her service using 401.1. When a different primary diagnosis is assigned to the visit code to indicate the reason for each physician’s involvement, all claims are more likely to be paid.4 As long as the hospitalist maintains care over one of the patients’ conditions, concurrent care is justified.
Because these physicians are in different specialties and different provider groups, most payers do not require the modifier 25 (separately identifiable evaluation/management [E/M] service on the same day as a procedure or other service) with the visit code; however, some managed care payers may have a general claim edit that pays the first claim and denies the second unless modifier 25 is appended to the concurrent E/M visit code (i.e., 99232-25) as an attestation that the service is distinct from any other provider’s service that day, despite claim submission under different tax identification numbers. This may not be identified until the claim is rejected or denied. If appropriate modifier use does not yield payment, appeal the denied concurrent care claims with supporting documentation from each physician visit, if possible. This demonstrates each physician’s contribution to care.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Code This Case
A hospitalist providing night coverage admits a patient with chest pain after midnight on Day 1. Later that same day, the cardiologist is consulted and manages the patient’s care. If the hospitalist’s role is to provide “night coverage,” can each physician see the patient for management on Day 2?
If the patient does not have any noncardiac issues, it would be difficult to justify the hospitalist service on Day 2, since the cardiologist is managing the same patient. Medicare and other payers advise against separate reporting in this case. Payers only consider reimbursement for concurrent services involving different aspects of patient care and reimburse separate services when billed with different diagnoses.4
Circumstances become even more difficult when a hospitalist sees the patient after midnight, and an internist sees the patient during the day. Medicare acknowledges that there are circumstances in which concurrent care may be billed by physicians of the same specialty.4
In this situation, if the nocturnist was called to manage a change in the patient’s condition, a separate service is warranted and should be reported. Since both physicians are enrolled with the payer as “internists,” it is unlikely that payers will reimburse each service; therefore, the first claim received is paid. If the hospitalist submits the first claim, the payer is likely to pay the hospitalist and deny the internist; however, the hospitalist claim may not always be first, and an appeal using both the internist’s and the hospitalist’s notes is suggested.
To maintain costs and avoid internal conflict, some hospitalist groups contract with the facility and receive a stipend for night coverage instead of submitting claims. It is best to seek legal advice before pursuing this option in order to prevent any inappropriate arrangements.
—Carol Pohlig
SHM Offers Training
Want to get better at documentation and coding? Check out iCATT, SHM’s new Interactive Coding Audit and Training Tool. iCATT is:
A self-directed training tool (on documentation and coding) for hospitalists;
A tool for testing the coding/documentation competency of new hospitalists; and
A training tool for coders who conduct coding/documentation audits of hospital medicine groups.
Physicians in Group Practice
According to Medicare, “physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician. If more than one evaluation and management (face-to-face) service is provided on the same day to the same patient by the same physician, or more than one physician in the same specialty in the same group, only one E&M service may be reported unless the services are for unrelated problems. Instead of billing separately, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level.”5
For example, hospitalist A evaluates the patient in the morning and hospitalist B subsequently reviews test results and discusses the course of treatment with the family members who will be involved in the patient’s care upon returning home. The hospitalist group can submit only one subsequent hospital care service for the day; the selected visit level should represent the combined visits (e.g. 99233).
The hospitalists must determine which name to report on the claim, the physician who provided the initial encounter or the physician who provided the most extensive—or best documented—encounter.
Physicians who are in the same group practice and submit claims under the same tax identification number can still be paid if they are enrolled with the payers as different specialty providers. This requires accurately identifying the physician’s primary two-digit specialty code on the payer enrollment form. For example, a hospitalist is enrolled as an internist (code 11), and a cardiologist is enrolled using code 06.6
Physicians can declare two specialty codes on their enrollment forms, but the primary code is the most crucial for accurate claim submission.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
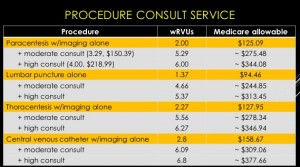
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
Gather baseline and follow-up data.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
Should the admitting physician or the discharge physician bill the CPT code (99234-99236) for a patient who is admitted and discharged in the same 24-hour period?
—Charlette
Dr. Hospitalist responds:
Assuming both physicians are part of the same group and specialty, they are considered one physician. Since it appears that both face-to-face encounters are separated by eight hours, you’re correct, only one physician can bill the bundled care code 99234-99236. The group must decide which physician gets the RVU credit for the bundled code. Our group gives the credit to the admitting physician.
Should the admitting physician or the discharge physician bill the CPT code (99234-99236) for a patient who is admitted and discharged in the same 24-hour period?
—Charlette
Dr. Hospitalist responds:
Assuming both physicians are part of the same group and specialty, they are considered one physician. Since it appears that both face-to-face encounters are separated by eight hours, you’re correct, only one physician can bill the bundled care code 99234-99236. The group must decide which physician gets the RVU credit for the bundled code. Our group gives the credit to the admitting physician.
Should the admitting physician or the discharge physician bill the CPT code (99234-99236) for a patient who is admitted and discharged in the same 24-hour period?
—Charlette
Dr. Hospitalist responds:
Assuming both physicians are part of the same group and specialty, they are considered one physician. Since it appears that both face-to-face encounters are separated by eight hours, you’re correct, only one physician can bill the bundled care code 99234-99236. The group must decide which physician gets the RVU credit for the bundled code. Our group gives the credit to the admitting physician.
It’s spring. Have you started your Meaningful Use reporting yet? More important, have you begun reporting at all?
“Say the words Meaningful Use to most orthopedists, and they usually roll their eyes or shake their heads,” says Cheyenne Brinson, MBA, CPA, a KarenZupko & Associates consultant who has been advising surgical practices on Meaningful Use since the program’s inception. Although many orthopedists are successfully using certified electronic health records (EHRs) to e-prescribe and enter radiology and laboratory orders, Brinson says many other requirements are misunderstood and perceived as overly complex. In many cases, practices are doing more work than they need to in order to attest.
“It’s actually not that complicated to meet Meaningful Use requirements,” she says. “The trick is to zero in on what’s relevant only for surgeons. This isn’t crystal clear in the CMS [Centers for Medicare & Medicaid Services] documents, and it’s not the forte of most EHR vendors or trainers either.” In fact, in Brinson’s experience, most EHR trainers present Meaningful Use to every practice as if it were primary care. Yet, the requirements for surgeons are different for primary care and are, frankly, less involved.
That’s good news. Because if you didn’t attest for Meaningful Use in 2014, the first year that reporting was required, you’re automatically getting dinged 2% on your Medicare payments in 2015. So, it’s time to get organized and get moving to avoid further penalties.
Avoid These Four Common Faux Pas
Brinson says the Clinical Quality Measures (CQMs) are hands down the most misunderstood component of Meaningful Use. “When I explain Meaningful Use to surgeons, I can’t jump up and down and wave my hands in the air enough to call attention to this,” she quips.
At issue: There are 64 CQMs, but very few are applicable to surgeons. Yet, many surgeons think they have to perform them for Meaningful Use. Not so, says Brinson. “Surgeons have to report a CQM only if it’s clinically relevant. If none of the CQMs are clinically relevant in your practice, it’s okay to report a zero value if you have not actually performed it.”
Here’s how this plays out. In Stage 2, physicians must report 9 CQMs across 3 domains; Population/Public Health, Patient Safety, and Efficient Use of Healthcare Resources are examples of domains that are most applicable to orthopedists. “If you choose Low Back Pain: Use of Imaging Studies as one of these, it’s possible an orthopedist would have a numeric value to report,” Brinson says. “But if you also choose Use of High-Risk Medications in the Elderly, an orthopedist will probably report a zero value. And that’s totally acceptable. You will not be penalized for reporting zero.”
Another common misconception is around the Vital Signs and Smoking Status measures. “We have worked with surgical practices that think Meaningful Use is requiring them to collect vital signs and smoking status at every visit, even though they may not be clinically relevant,” says Brinson. Again, not true.
“Height and/or weight and blood pressure, as well as smoking status measures, need to be reported only once per patient during the reporting period,” Brinson clarifies. “So from a practical standpoint, most orthopedic practices can collect this data from new patients and then again as clinically necessary,” adding there are even exclusions for physicians who attest that either height and weight and/or blood pressure has no relevance to their scope of practice at all.
Brinson also sees practices do more work than they need to when it comes to Patient Care Reminders. She recently worked with a surgery practice that sent reminders for colonoscopies. “Not exactly clinically relevant,” she says, “and an unnecessary step for staff.” That’s because physicians aren’t required to send reminders that aren’t relevant to their specialty.
The Federal Register states, “An eligible provider (EP) should use clinically relevant information stored within the [EHR] to identify patients who should receive reminders…. The EP is best positioned to decide which information is clinically relevant for this purpose.”
“In orthopedics, clinically relevant reminders could be for an outside referral, a follow-up on an MRI or other test, or a reminder to schedule a postoperative appointment,” Brinson explains. “Work with your EHR vendor to create the reminders that are most appropriate for your patient base.”
The final faux pas that Brinson finds: “Meaningful Use requires you to report data for all patients, not just Medicare patients. That seems to be a point of confusion for many.”
Three Cheers for the Patient Portal Requirement
Stage 2 saw the addition of the Patient Portal Requirement, and Brinson suggests that the benefits of this tool go far beyond Meaningful Use. “Patient portals are essential to a modern practice,” she says. “Patients use them to complete a health history prior to their appointment, pay their bill, schedule follow-up appointments, and more.” Further, the patient portal facilitates another Meaningful Use Stage 2 requirement: secure electronic messaging with patients. For both Meaningful Use and risk management, moving away from e-mail and texting and toward secure/encrypted messaging is a must. The patient portal has this feature already built in, and all messages are stored securely and archived—which meets the HIPAA (Health Insurance Portability and Accountability Act) Omnibus requirements, too.
So if you’ve implemented a patient portal, that’s good for your practice and your patients on many levels. But there is a caveat about meeting the Meaningful Use requirement. “For this requirement, 5% of the unique patients seen during the reporting period must ‘view, download, or transmit to a third party their health information,’” Brinson explains. “So the onus is on your practice to ‘sell’ the benefits of the patient portal and get patients to use it so you can achieve the 5% threshold.”
Clinical Decision Support and Summaries
The requirements of Clinical Decision Support Interventions and Clinical Summaries may seem daunting, but, if you think beyond Meaningful Use for a moment, both facilitate better care.
Take Clinical Decision Support Interventions. What would be helpful for you to know about a patient before surgery? What information would enable you to deliver better care?
“One surgeon told me that a family history of malignant hyperthermia would mean the difference between performing the case in the operating room versus the ambulatory surgery center,” Brinson says. “This is a good example of an intervention that a surgeon would work with their EHR vendor to set up.”
The objective states that each intervention is to be an evidence-based decision-support intervention based on each one and at least one combination of the following data: problem list, medication list, medication allergy list, demographics, laboratory tests and values/results, and vital signs. “Stage 1 requires physicians to implement 1 Clinical Decision Support Intervention, and Stage 2 requires 5,” reminds Brinson.
And here’s all you need to know about Clinical Summaries. Although there are 20 specific required elements of a clinical summary, physicians themselves need to provide details only for clinical instructions and the care plan, including goals and instructions. Ancillary staff can populate the other elements.
Brinson points out that surgeons are not expected to provide a copy of the patient’s note, or to complete the note, before the patient checks out. The requirement under Stage 2 is that the clinical summary is provided to the patient within 1 business day. “From a practical standpoint, practices can print the clinical summary for patients at checkout. A well-done clinical summary is a practice efficiency tool as much as a clinical document. It can reduce phone calls from patients asking, ‘Now what did the doctor tell me to do?’”
Often Overlooked
There are requirements that, Brinson says, surgeons often gloss over: Protect Electronic Health Information and Text-Searchable Progress Notes.
“Stage 2 requires physicians to conduct a privacy risk analysis to protect electronic health information,” she explains. “Most EHR vendors don’t offer this as part of their product, so it’s frequently overlooked.” Such an analysis typically requires an outside vendor, but there are free, do-it-yourself tools available, such as the Privacy and Security Toolkit for Small Provider Organizations,* from the Healthcare Information and Management Systems Society (HIMSS).
The analysis should follow HIPAA guidelines, and the most intensive part of this requirement is to conduct or review a privacy risk analysis of the clinical technology. “You’ve also got to address data encryption and security in the EHR, and ensure HIPAA policies and procedures are in place,” Brinson states.
Text-Searchable Progress Notes are also a new requirement in Stage 2. All progress notes must be text searchable—practices can no longer include progress notes as scanned attachments. “That means no more PDFs,” Brinson says. “Surgeons can still dictate, but the dictation must be entered into the EHR in such a way that it’s searchable. In Stage 2, 30% of unique patients must have a minimum of 1 text-searchable electronic progress note created, edited, and signed in the EHR.”
Conclusion
Meaningful Use does not have to be cumbersome. Focus on what surgical practices need to know, and attestation won’t be as complicated as you think.
american journal of orthopedics, AJO, practice management, health care, business, electronic health records, EHR, clinical quality measures, CQM, patient portal, meaningful use, surgeons, practices, technology, toth
It’s spring. Have you started your Meaningful Use reporting yet? More important, have you begun reporting at all?
“Say the words Meaningful Use to most orthopedists, and they usually roll their eyes or shake their heads,” says Cheyenne Brinson, MBA, CPA, a KarenZupko & Associates consultant who has been advising surgical practices on Meaningful Use since the program’s inception. Although many orthopedists are successfully using certified electronic health records (EHRs) to e-prescribe and enter radiology and laboratory orders, Brinson says many other requirements are misunderstood and perceived as overly complex. In many cases, practices are doing more work than they need to in order to attest.
“It’s actually not that complicated to meet Meaningful Use requirements,” she says. “The trick is to zero in on what’s relevant only for surgeons. This isn’t crystal clear in the CMS [Centers for Medicare & Medicaid Services] documents, and it’s not the forte of most EHR vendors or trainers either.” In fact, in Brinson’s experience, most EHR trainers present Meaningful Use to every practice as if it were primary care. Yet, the requirements for surgeons are different for primary care and are, frankly, less involved.
That’s good news. Because if you didn’t attest for Meaningful Use in 2014, the first year that reporting was required, you’re automatically getting dinged 2% on your Medicare payments in 2015. So, it’s time to get organized and get moving to avoid further penalties.
Avoid These Four Common Faux Pas
Brinson says the Clinical Quality Measures (CQMs) are hands down the most misunderstood component of Meaningful Use. “When I explain Meaningful Use to surgeons, I can’t jump up and down and wave my hands in the air enough to call attention to this,” she quips.
At issue: There are 64 CQMs, but very few are applicable to surgeons. Yet, many surgeons think they have to perform them for Meaningful Use. Not so, says Brinson. “Surgeons have to report a CQM only if it’s clinically relevant. If none of the CQMs are clinically relevant in your practice, it’s okay to report a zero value if you have not actually performed it.”
Here’s how this plays out. In Stage 2, physicians must report 9 CQMs across 3 domains; Population/Public Health, Patient Safety, and Efficient Use of Healthcare Resources are examples of domains that are most applicable to orthopedists. “If you choose Low Back Pain: Use of Imaging Studies as one of these, it’s possible an orthopedist would have a numeric value to report,” Brinson says. “But if you also choose Use of High-Risk Medications in the Elderly, an orthopedist will probably report a zero value. And that’s totally acceptable. You will not be penalized for reporting zero.”
Another common misconception is around the Vital Signs and Smoking Status measures. “We have worked with surgical practices that think Meaningful Use is requiring them to collect vital signs and smoking status at every visit, even though they may not be clinically relevant,” says Brinson. Again, not true.
“Height and/or weight and blood pressure, as well as smoking status measures, need to be reported only once per patient during the reporting period,” Brinson clarifies. “So from a practical standpoint, most orthopedic practices can collect this data from new patients and then again as clinically necessary,” adding there are even exclusions for physicians who attest that either height and weight and/or blood pressure has no relevance to their scope of practice at all.
Brinson also sees practices do more work than they need to when it comes to Patient Care Reminders. She recently worked with a surgery practice that sent reminders for colonoscopies. “Not exactly clinically relevant,” she says, “and an unnecessary step for staff.” That’s because physicians aren’t required to send reminders that aren’t relevant to their specialty.
The Federal Register states, “An eligible provider (EP) should use clinically relevant information stored within the [EHR] to identify patients who should receive reminders…. The EP is best positioned to decide which information is clinically relevant for this purpose.”
“In orthopedics, clinically relevant reminders could be for an outside referral, a follow-up on an MRI or other test, or a reminder to schedule a postoperative appointment,” Brinson explains. “Work with your EHR vendor to create the reminders that are most appropriate for your patient base.”
The final faux pas that Brinson finds: “Meaningful Use requires you to report data for all patients, not just Medicare patients. That seems to be a point of confusion for many.”
Three Cheers for the Patient Portal Requirement
Stage 2 saw the addition of the Patient Portal Requirement, and Brinson suggests that the benefits of this tool go far beyond Meaningful Use. “Patient portals are essential to a modern practice,” she says. “Patients use them to complete a health history prior to their appointment, pay their bill, schedule follow-up appointments, and more.” Further, the patient portal facilitates another Meaningful Use Stage 2 requirement: secure electronic messaging with patients. For both Meaningful Use and risk management, moving away from e-mail and texting and toward secure/encrypted messaging is a must. The patient portal has this feature already built in, and all messages are stored securely and archived—which meets the HIPAA (Health Insurance Portability and Accountability Act) Omnibus requirements, too.
So if you’ve implemented a patient portal, that’s good for your practice and your patients on many levels. But there is a caveat about meeting the Meaningful Use requirement. “For this requirement, 5% of the unique patients seen during the reporting period must ‘view, download, or transmit to a third party their health information,’” Brinson explains. “So the onus is on your practice to ‘sell’ the benefits of the patient portal and get patients to use it so you can achieve the 5% threshold.”
Clinical Decision Support and Summaries
The requirements of Clinical Decision Support Interventions and Clinical Summaries may seem daunting, but, if you think beyond Meaningful Use for a moment, both facilitate better care.
Take Clinical Decision Support Interventions. What would be helpful for you to know about a patient before surgery? What information would enable you to deliver better care?
“One surgeon told me that a family history of malignant hyperthermia would mean the difference between performing the case in the operating room versus the ambulatory surgery center,” Brinson says. “This is a good example of an intervention that a surgeon would work with their EHR vendor to set up.”
The objective states that each intervention is to be an evidence-based decision-support intervention based on each one and at least one combination of the following data: problem list, medication list, medication allergy list, demographics, laboratory tests and values/results, and vital signs. “Stage 1 requires physicians to implement 1 Clinical Decision Support Intervention, and Stage 2 requires 5,” reminds Brinson.
And here’s all you need to know about Clinical Summaries. Although there are 20 specific required elements of a clinical summary, physicians themselves need to provide details only for clinical instructions and the care plan, including goals and instructions. Ancillary staff can populate the other elements.
Brinson points out that surgeons are not expected to provide a copy of the patient’s note, or to complete the note, before the patient checks out. The requirement under Stage 2 is that the clinical summary is provided to the patient within 1 business day. “From a practical standpoint, practices can print the clinical summary for patients at checkout. A well-done clinical summary is a practice efficiency tool as much as a clinical document. It can reduce phone calls from patients asking, ‘Now what did the doctor tell me to do?’”
Often Overlooked
There are requirements that, Brinson says, surgeons often gloss over: Protect Electronic Health Information and Text-Searchable Progress Notes.
“Stage 2 requires physicians to conduct a privacy risk analysis to protect electronic health information,” she explains. “Most EHR vendors don’t offer this as part of their product, so it’s frequently overlooked.” Such an analysis typically requires an outside vendor, but there are free, do-it-yourself tools available, such as the Privacy and Security Toolkit for Small Provider Organizations,* from the Healthcare Information and Management Systems Society (HIMSS).
The analysis should follow HIPAA guidelines, and the most intensive part of this requirement is to conduct or review a privacy risk analysis of the clinical technology. “You’ve also got to address data encryption and security in the EHR, and ensure HIPAA policies and procedures are in place,” Brinson states.
Text-Searchable Progress Notes are also a new requirement in Stage 2. All progress notes must be text searchable—practices can no longer include progress notes as scanned attachments. “That means no more PDFs,” Brinson says. “Surgeons can still dictate, but the dictation must be entered into the EHR in such a way that it’s searchable. In Stage 2, 30% of unique patients must have a minimum of 1 text-searchable electronic progress note created, edited, and signed in the EHR.”
Conclusion
Meaningful Use does not have to be cumbersome. Focus on what surgical practices need to know, and attestation won’t be as complicated as you think.
It’s spring. Have you started your Meaningful Use reporting yet? More important, have you begun reporting at all?
“Say the words Meaningful Use to most orthopedists, and they usually roll their eyes or shake their heads,” says Cheyenne Brinson, MBA, CPA, a KarenZupko & Associates consultant who has been advising surgical practices on Meaningful Use since the program’s inception. Although many orthopedists are successfully using certified electronic health records (EHRs) to e-prescribe and enter radiology and laboratory orders, Brinson says many other requirements are misunderstood and perceived as overly complex. In many cases, practices are doing more work than they need to in order to attest.
“It’s actually not that complicated to meet Meaningful Use requirements,” she says. “The trick is to zero in on what’s relevant only for surgeons. This isn’t crystal clear in the CMS [Centers for Medicare & Medicaid Services] documents, and it’s not the forte of most EHR vendors or trainers either.” In fact, in Brinson’s experience, most EHR trainers present Meaningful Use to every practice as if it were primary care. Yet, the requirements for surgeons are different for primary care and are, frankly, less involved.
That’s good news. Because if you didn’t attest for Meaningful Use in 2014, the first year that reporting was required, you’re automatically getting dinged 2% on your Medicare payments in 2015. So, it’s time to get organized and get moving to avoid further penalties.
Avoid These Four Common Faux Pas
Brinson says the Clinical Quality Measures (CQMs) are hands down the most misunderstood component of Meaningful Use. “When I explain Meaningful Use to surgeons, I can’t jump up and down and wave my hands in the air enough to call attention to this,” she quips.
At issue: There are 64 CQMs, but very few are applicable to surgeons. Yet, many surgeons think they have to perform them for Meaningful Use. Not so, says Brinson. “Surgeons have to report a CQM only if it’s clinically relevant. If none of the CQMs are clinically relevant in your practice, it’s okay to report a zero value if you have not actually performed it.”
Here’s how this plays out. In Stage 2, physicians must report 9 CQMs across 3 domains; Population/Public Health, Patient Safety, and Efficient Use of Healthcare Resources are examples of domains that are most applicable to orthopedists. “If you choose Low Back Pain: Use of Imaging Studies as one of these, it’s possible an orthopedist would have a numeric value to report,” Brinson says. “But if you also choose Use of High-Risk Medications in the Elderly, an orthopedist will probably report a zero value. And that’s totally acceptable. You will not be penalized for reporting zero.”
Another common misconception is around the Vital Signs and Smoking Status measures. “We have worked with surgical practices that think Meaningful Use is requiring them to collect vital signs and smoking status at every visit, even though they may not be clinically relevant,” says Brinson. Again, not true.
“Height and/or weight and blood pressure, as well as smoking status measures, need to be reported only once per patient during the reporting period,” Brinson clarifies. “So from a practical standpoint, most orthopedic practices can collect this data from new patients and then again as clinically necessary,” adding there are even exclusions for physicians who attest that either height and weight and/or blood pressure has no relevance to their scope of practice at all.
Brinson also sees practices do more work than they need to when it comes to Patient Care Reminders. She recently worked with a surgery practice that sent reminders for colonoscopies. “Not exactly clinically relevant,” she says, “and an unnecessary step for staff.” That’s because physicians aren’t required to send reminders that aren’t relevant to their specialty.
The Federal Register states, “An eligible provider (EP) should use clinically relevant information stored within the [EHR] to identify patients who should receive reminders…. The EP is best positioned to decide which information is clinically relevant for this purpose.”
“In orthopedics, clinically relevant reminders could be for an outside referral, a follow-up on an MRI or other test, or a reminder to schedule a postoperative appointment,” Brinson explains. “Work with your EHR vendor to create the reminders that are most appropriate for your patient base.”
The final faux pas that Brinson finds: “Meaningful Use requires you to report data for all patients, not just Medicare patients. That seems to be a point of confusion for many.”
Three Cheers for the Patient Portal Requirement
Stage 2 saw the addition of the Patient Portal Requirement, and Brinson suggests that the benefits of this tool go far beyond Meaningful Use. “Patient portals are essential to a modern practice,” she says. “Patients use them to complete a health history prior to their appointment, pay their bill, schedule follow-up appointments, and more.” Further, the patient portal facilitates another Meaningful Use Stage 2 requirement: secure electronic messaging with patients. For both Meaningful Use and risk management, moving away from e-mail and texting and toward secure/encrypted messaging is a must. The patient portal has this feature already built in, and all messages are stored securely and archived—which meets the HIPAA (Health Insurance Portability and Accountability Act) Omnibus requirements, too.
So if you’ve implemented a patient portal, that’s good for your practice and your patients on many levels. But there is a caveat about meeting the Meaningful Use requirement. “For this requirement, 5% of the unique patients seen during the reporting period must ‘view, download, or transmit to a third party their health information,’” Brinson explains. “So the onus is on your practice to ‘sell’ the benefits of the patient portal and get patients to use it so you can achieve the 5% threshold.”
Clinical Decision Support and Summaries
The requirements of Clinical Decision Support Interventions and Clinical Summaries may seem daunting, but, if you think beyond Meaningful Use for a moment, both facilitate better care.
Take Clinical Decision Support Interventions. What would be helpful for you to know about a patient before surgery? What information would enable you to deliver better care?
“One surgeon told me that a family history of malignant hyperthermia would mean the difference between performing the case in the operating room versus the ambulatory surgery center,” Brinson says. “This is a good example of an intervention that a surgeon would work with their EHR vendor to set up.”
The objective states that each intervention is to be an evidence-based decision-support intervention based on each one and at least one combination of the following data: problem list, medication list, medication allergy list, demographics, laboratory tests and values/results, and vital signs. “Stage 1 requires physicians to implement 1 Clinical Decision Support Intervention, and Stage 2 requires 5,” reminds Brinson.
And here’s all you need to know about Clinical Summaries. Although there are 20 specific required elements of a clinical summary, physicians themselves need to provide details only for clinical instructions and the care plan, including goals and instructions. Ancillary staff can populate the other elements.
Brinson points out that surgeons are not expected to provide a copy of the patient’s note, or to complete the note, before the patient checks out. The requirement under Stage 2 is that the clinical summary is provided to the patient within 1 business day. “From a practical standpoint, practices can print the clinical summary for patients at checkout. A well-done clinical summary is a practice efficiency tool as much as a clinical document. It can reduce phone calls from patients asking, ‘Now what did the doctor tell me to do?’”
Often Overlooked
There are requirements that, Brinson says, surgeons often gloss over: Protect Electronic Health Information and Text-Searchable Progress Notes.
“Stage 2 requires physicians to conduct a privacy risk analysis to protect electronic health information,” she explains. “Most EHR vendors don’t offer this as part of their product, so it’s frequently overlooked.” Such an analysis typically requires an outside vendor, but there are free, do-it-yourself tools available, such as the Privacy and Security Toolkit for Small Provider Organizations,* from the Healthcare Information and Management Systems Society (HIMSS).
The analysis should follow HIPAA guidelines, and the most intensive part of this requirement is to conduct or review a privacy risk analysis of the clinical technology. “You’ve also got to address data encryption and security in the EHR, and ensure HIPAA policies and procedures are in place,” Brinson states.
Text-Searchable Progress Notes are also a new requirement in Stage 2. All progress notes must be text searchable—practices can no longer include progress notes as scanned attachments. “That means no more PDFs,” Brinson says. “Surgeons can still dictate, but the dictation must be entered into the EHR in such a way that it’s searchable. In Stage 2, 30% of unique patients must have a minimum of 1 text-searchable electronic progress note created, edited, and signed in the EHR.”
Conclusion
Meaningful Use does not have to be cumbersome. Focus on what surgical practices need to know, and attestation won’t be as complicated as you think.
Meaningful Use for Surgeons—It’s Not as Complicated as You Think
Display Headline
Meaningful Use for Surgeons—It’s Not as Complicated as You Think
Legacy Keywords
american journal of orthopedics, AJO, practice management, health care, business, electronic health records, EHR, clinical quality measures, CQM, patient portal, meaningful use, surgeons, practices, technology, toth
Legacy Keywords
american journal of orthopedics, AJO, practice management, health care, business, electronic health records, EHR, clinical quality measures, CQM, patient portal, meaningful use, surgeons, practices, technology, toth
According to Current Procedural Terminology (CPT), modifier -25 is to be used to identify “significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service.”1 Modifier -25 frequently is integral to the description of patient visits in dermatology. Dermatologists use modifier -25 more than physicians of any other specialty, and in recent years, more than 50% of dermatology evaluation and management (E/M) visits have been appended with this modifier.
When patients present for assessment and management of various skin findings, a dermatologist may deem it appropriate to proceed with a diagnostic or therapeutic procedure at the same visit after obtaining the patient’s medical history, completing a review of systems, and conducting a clinical examination. Most commonly, a skin biopsy or destruction of a benign or malignant lesion may be performed, but other simple procedures also may be appropriate. The ability to assess and intervene during the same visit is optimal for patients who subsequently may require fewer follow-up visits and experience more immediate relief from their symptoms.
When E/M Cannot Be Billed Separately
Regulatory guidance from the National Correct Coding Initiative (NCCI) dated January 2013 indicates that procedures with a global period of 90 days are major surgical procedures, and if an E/M service is performed on the same day as such a procedure to decide whether or not to perform that procedure, then the E/M service should be reported with modifier -57.2 On the other hand, CPT defines procedures with a 0- or 10-day global period as minor surgical procedures, and E/M services provided on the same day of service as these procedures are included in the procedure code and cannot be billed separately. For review, common dermatologic procedures with 0-day global periods include biopsies (CPT code 11000), shave removals (11300–11313), debridements (11000, 11011–11042), and Mohs micrographic surgery (17311–17315); procedures with 10-day global periods include destructions (17000–17286), excisions (11400–11646), and repairs (12001–13153). If an E/M service is performed on the same day as one of these procedures to decide whether to proceed with the minor surgical procedure, this E/M service cannot be reported separately. Additionally, the fact that the patient is new to the physician is not sufficient to allow reporting of an E/M with such a minor procedure.
When E/M Can Be Billed Separately
However, a “significant and separately identifiable E/M service unrelated to the decision to perform the minor procedure” is separately reportable with modifier -25. According to the NCCI, the minor procedure and the E/M do not require different diagnoses, but the E/M service must be above and beyond what is usually required for the minor surgical procedure.2 Because a certain amount of so-called preservice time is built into minor procedure codes, the implication is that substantially more E/M was needed than envisioned in this preservice time, necessitating inclusion of an E/M in addition to a minor procedure when there is a single diagnosis.
When there is a single diagnosis, the physician has to decide when such a significant and separately identifiable service exists. If the physician determines that it is appropriate to code for E/M in addition to the minor procedure, clear documentation of the additional E/M service provided will reduce the likelihood of this choice being questioned. Specifically, it may be helpful to describe the additional history, examination results, medical knowledge, professional skill, and work time above and beyond what is usually required for the minor surgical procedure.
When there are many diagnosis codes for a single visit and only a subset of them are associated with the minor procedure, as is common in dermatology, then the decision to include an E/M service is simpler. In this case, if E/M services were provided that pertained to a diagnosis or diagnoses other than the one(s) associated with the minor procedure(s), then these additional E/M services will clearly not be included in the preservice time for the procedure and an E/M can virtually always be coded separately. For instance, if a patient presents with a growing scaly bump (clinically apparent squamous cell carcinoma) on the leg that the dermatologist deems is appropriate for biopsy but concurrently notices nummular dermatitis of the legs, which the patient describes as itchy and uncomfortable, then the diagnosis and management of the dermatitis would clearly be a separate E/M service and would not be included in the workup for the biopsy. The E/M code that is applied should, of course, reflect the services provided exclusive of those integral to the minor procedure. To make it easier for regulators and auditors, it may be helpful to clearly itemize the additional diagnoses unrelated to the minor procedure and describe the specific E/M services provided for these diagnoses. Although it is certainly not necessary or required, it also may be helpful to physically separate the documentation for the minor procedure from the E/M services for the additional diagnoses within the medical chart.
Final Thoughts
It is clear that frequent use of modifier -25 is appropriate in routine, high-quality dermatologic practice. Simultaneous provision of E/M services and minor procedures often is in the patient’s best interest, as it minimizes unnecessary office visits and expedites treatment. When modifier -25 is appropriately appended, careful documentation by the dermatologist can help to clarify the precise basis for its use. Recent NCCI edits provide guidelines for use of this modifier that can be adapted by individual dermatologists for particular patient circumstances.2
References
1. CPT 2014 Professional Edition. Chicago, IL: American Medical Association; 2014.
2. National Correct Coding Initiative Policy Manual for Medicare Services. Carmel, IN: National Correct Coding Initiative; 2013.
This article provides general information. Physicians should consult Current Procedural Terminology (CPT) guidelines, state regulations, and payer rules for coding and billing guidance relevant to specific cases. The opinions represented here are those of the author and have not been reviewed, endorsed, or approved by the American Medical Association, the American Academy of Dermatology, or any other coding or billing authority.
Correspondence: Murad Alam, MD, MSCI, 676 N Saint Clair St, Ste 1600, Chicago, IL 60611 ([email protected]).
This article provides general information. Physicians should consult Current Procedural Terminology (CPT) guidelines, state regulations, and payer rules for coding and billing guidance relevant to specific cases. The opinions represented here are those of the author and have not been reviewed, endorsed, or approved by the American Medical Association, the American Academy of Dermatology, or any other coding or billing authority.
Correspondence: Murad Alam, MD, MSCI, 676 N Saint Clair St, Ste 1600, Chicago, IL 60611 ([email protected]).
Author and Disclosure Information
Murad Alam, MD, MSCI
From Northwestern University, Chicago, Illinois.
The author reports no conflict of interest.
This article provides general information. Physicians should consult Current Procedural Terminology (CPT) guidelines, state regulations, and payer rules for coding and billing guidance relevant to specific cases. The opinions represented here are those of the author and have not been reviewed, endorsed, or approved by the American Medical Association, the American Academy of Dermatology, or any other coding or billing authority.
Correspondence: Murad Alam, MD, MSCI, 676 N Saint Clair St, Ste 1600, Chicago, IL 60611 ([email protected]).
According to Current Procedural Terminology (CPT), modifier -25 is to be used to identify “significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service.”1 Modifier -25 frequently is integral to the description of patient visits in dermatology. Dermatologists use modifier -25 more than physicians of any other specialty, and in recent years, more than 50% of dermatology evaluation and management (E/M) visits have been appended with this modifier.
When patients present for assessment and management of various skin findings, a dermatologist may deem it appropriate to proceed with a diagnostic or therapeutic procedure at the same visit after obtaining the patient’s medical history, completing a review of systems, and conducting a clinical examination. Most commonly, a skin biopsy or destruction of a benign or malignant lesion may be performed, but other simple procedures also may be appropriate. The ability to assess and intervene during the same visit is optimal for patients who subsequently may require fewer follow-up visits and experience more immediate relief from their symptoms.
When E/M Cannot Be Billed Separately
Regulatory guidance from the National Correct Coding Initiative (NCCI) dated January 2013 indicates that procedures with a global period of 90 days are major surgical procedures, and if an E/M service is performed on the same day as such a procedure to decide whether or not to perform that procedure, then the E/M service should be reported with modifier -57.2 On the other hand, CPT defines procedures with a 0- or 10-day global period as minor surgical procedures, and E/M services provided on the same day of service as these procedures are included in the procedure code and cannot be billed separately. For review, common dermatologic procedures with 0-day global periods include biopsies (CPT code 11000), shave removals (11300–11313), debridements (11000, 11011–11042), and Mohs micrographic surgery (17311–17315); procedures with 10-day global periods include destructions (17000–17286), excisions (11400–11646), and repairs (12001–13153). If an E/M service is performed on the same day as one of these procedures to decide whether to proceed with the minor surgical procedure, this E/M service cannot be reported separately. Additionally, the fact that the patient is new to the physician is not sufficient to allow reporting of an E/M with such a minor procedure.
When E/M Can Be Billed Separately
However, a “significant and separately identifiable E/M service unrelated to the decision to perform the minor procedure” is separately reportable with modifier -25. According to the NCCI, the minor procedure and the E/M do not require different diagnoses, but the E/M service must be above and beyond what is usually required for the minor surgical procedure.2 Because a certain amount of so-called preservice time is built into minor procedure codes, the implication is that substantially more E/M was needed than envisioned in this preservice time, necessitating inclusion of an E/M in addition to a minor procedure when there is a single diagnosis.
When there is a single diagnosis, the physician has to decide when such a significant and separately identifiable service exists. If the physician determines that it is appropriate to code for E/M in addition to the minor procedure, clear documentation of the additional E/M service provided will reduce the likelihood of this choice being questioned. Specifically, it may be helpful to describe the additional history, examination results, medical knowledge, professional skill, and work time above and beyond what is usually required for the minor surgical procedure.
When there are many diagnosis codes for a single visit and only a subset of them are associated with the minor procedure, as is common in dermatology, then the decision to include an E/M service is simpler. In this case, if E/M services were provided that pertained to a diagnosis or diagnoses other than the one(s) associated with the minor procedure(s), then these additional E/M services will clearly not be included in the preservice time for the procedure and an E/M can virtually always be coded separately. For instance, if a patient presents with a growing scaly bump (clinically apparent squamous cell carcinoma) on the leg that the dermatologist deems is appropriate for biopsy but concurrently notices nummular dermatitis of the legs, which the patient describes as itchy and uncomfortable, then the diagnosis and management of the dermatitis would clearly be a separate E/M service and would not be included in the workup for the biopsy. The E/M code that is applied should, of course, reflect the services provided exclusive of those integral to the minor procedure. To make it easier for regulators and auditors, it may be helpful to clearly itemize the additional diagnoses unrelated to the minor procedure and describe the specific E/M services provided for these diagnoses. Although it is certainly not necessary or required, it also may be helpful to physically separate the documentation for the minor procedure from the E/M services for the additional diagnoses within the medical chart.
Final Thoughts
It is clear that frequent use of modifier -25 is appropriate in routine, high-quality dermatologic practice. Simultaneous provision of E/M services and minor procedures often is in the patient’s best interest, as it minimizes unnecessary office visits and expedites treatment. When modifier -25 is appropriately appended, careful documentation by the dermatologist can help to clarify the precise basis for its use. Recent NCCI edits provide guidelines for use of this modifier that can be adapted by individual dermatologists for particular patient circumstances.2
According to Current Procedural Terminology (CPT), modifier -25 is to be used to identify “significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service.”1 Modifier -25 frequently is integral to the description of patient visits in dermatology. Dermatologists use modifier -25 more than physicians of any other specialty, and in recent years, more than 50% of dermatology evaluation and management (E/M) visits have been appended with this modifier.
When patients present for assessment and management of various skin findings, a dermatologist may deem it appropriate to proceed with a diagnostic or therapeutic procedure at the same visit after obtaining the patient’s medical history, completing a review of systems, and conducting a clinical examination. Most commonly, a skin biopsy or destruction of a benign or malignant lesion may be performed, but other simple procedures also may be appropriate. The ability to assess and intervene during the same visit is optimal for patients who subsequently may require fewer follow-up visits and experience more immediate relief from their symptoms.
When E/M Cannot Be Billed Separately
Regulatory guidance from the National Correct Coding Initiative (NCCI) dated January 2013 indicates that procedures with a global period of 90 days are major surgical procedures, and if an E/M service is performed on the same day as such a procedure to decide whether or not to perform that procedure, then the E/M service should be reported with modifier -57.2 On the other hand, CPT defines procedures with a 0- or 10-day global period as minor surgical procedures, and E/M services provided on the same day of service as these procedures are included in the procedure code and cannot be billed separately. For review, common dermatologic procedures with 0-day global periods include biopsies (CPT code 11000), shave removals (11300–11313), debridements (11000, 11011–11042), and Mohs micrographic surgery (17311–17315); procedures with 10-day global periods include destructions (17000–17286), excisions (11400–11646), and repairs (12001–13153). If an E/M service is performed on the same day as one of these procedures to decide whether to proceed with the minor surgical procedure, this E/M service cannot be reported separately. Additionally, the fact that the patient is new to the physician is not sufficient to allow reporting of an E/M with such a minor procedure.
When E/M Can Be Billed Separately
However, a “significant and separately identifiable E/M service unrelated to the decision to perform the minor procedure” is separately reportable with modifier -25. According to the NCCI, the minor procedure and the E/M do not require different diagnoses, but the E/M service must be above and beyond what is usually required for the minor surgical procedure.2 Because a certain amount of so-called preservice time is built into minor procedure codes, the implication is that substantially more E/M was needed than envisioned in this preservice time, necessitating inclusion of an E/M in addition to a minor procedure when there is a single diagnosis.
When there is a single diagnosis, the physician has to decide when such a significant and separately identifiable service exists. If the physician determines that it is appropriate to code for E/M in addition to the minor procedure, clear documentation of the additional E/M service provided will reduce the likelihood of this choice being questioned. Specifically, it may be helpful to describe the additional history, examination results, medical knowledge, professional skill, and work time above and beyond what is usually required for the minor surgical procedure.
When there are many diagnosis codes for a single visit and only a subset of them are associated with the minor procedure, as is common in dermatology, then the decision to include an E/M service is simpler. In this case, if E/M services were provided that pertained to a diagnosis or diagnoses other than the one(s) associated with the minor procedure(s), then these additional E/M services will clearly not be included in the preservice time for the procedure and an E/M can virtually always be coded separately. For instance, if a patient presents with a growing scaly bump (clinically apparent squamous cell carcinoma) on the leg that the dermatologist deems is appropriate for biopsy but concurrently notices nummular dermatitis of the legs, which the patient describes as itchy and uncomfortable, then the diagnosis and management of the dermatitis would clearly be a separate E/M service and would not be included in the workup for the biopsy. The E/M code that is applied should, of course, reflect the services provided exclusive of those integral to the minor procedure. To make it easier for regulators and auditors, it may be helpful to clearly itemize the additional diagnoses unrelated to the minor procedure and describe the specific E/M services provided for these diagnoses. Although it is certainly not necessary or required, it also may be helpful to physically separate the documentation for the minor procedure from the E/M services for the additional diagnoses within the medical chart.
Final Thoughts
It is clear that frequent use of modifier -25 is appropriate in routine, high-quality dermatologic practice. Simultaneous provision of E/M services and minor procedures often is in the patient’s best interest, as it minimizes unnecessary office visits and expedites treatment. When modifier -25 is appropriately appended, careful documentation by the dermatologist can help to clarify the precise basis for its use. Recent NCCI edits provide guidelines for use of this modifier that can be adapted by individual dermatologists for particular patient circumstances.2
References
1. CPT 2014 Professional Edition. Chicago, IL: American Medical Association; 2014.
2. National Correct Coding Initiative Policy Manual for Medicare Services. Carmel, IN: National Correct Coding Initiative; 2013.
References
1. CPT 2014 Professional Edition. Chicago, IL: American Medical Association; 2014.
2. National Correct Coding Initiative Policy Manual for Medicare Services. Carmel, IN: National Correct Coding Initiative; 2013.
Frequent use of modifier -25 is appropriate in routine, high-quality dermatologic practice.
The global period (0, 10, or 90 days) of a procedure dictates if evaluation and management services provided on the same day of service as the original procedure can be billed separately.
Careful documentation by the dermatologist can help clarify the precise basis for the use of modifier -25.
Providers typically rely on the “key components” (history, exam, medical decision-making) when documenting in the medical record, and they often misunderstand the use of time when selecting visit levels. Sometimes providers may report a lower service level than warranted because they didn’t feel that they spent the required amount of time with the patient; however, the duration of the visit is an ancillary factor and does not control the level of service to be billed unless more than 50% of the face-to-face time (for non-inpatient services) or more than 50% of the floor time (for inpatient services) is spent providing counseling or coordination of care (C/CC).1 In these instances, providers may choose to document only a brief history and exam, or none at all. They should update the medical decision-making based on the discussion.
Consider the hospitalization of an elderly patient who is newly diagnosed with diabetes. In addition to stabilizing the patient’s glucose levels and devising the appropriate care plan, the patient and/or caregivers also require extensive counseling regarding disease management, lifestyle modification, and medication regime. Coordination of care for outpatient programs and resources is also crucial. To make sure that this qualifies as a time-based service, ensure that the documentation contains the duration, the issues addressed, and the signature of the service provider.
Duration of Counseling and/or Coordination of Care
Time is not used for visit level selection if C/CC is minimal (<50%) or absent from the patient encounter. For inpatient services, total visit time is identified as provider face-to-face time (i.e., at the bedside) combined with time spent on the patient’s unit/floor performing services that are directly related to that patient, such as reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers.
Time associated with activities performed in locations other than the patient’s unit/floor (e.g. reviewing current results or images from the physician’s office) is not allowable in calculating the total visit time. Time associated with teaching students/interns is also excluded, because this doesn’t reflect patient care activities. Once the provider documents all services rendered on a given calendar date, the provider selects the visit level that corresponds with the cumulative visit time documented in the chart (see Tables 1 and 2).
(click for larger image)Table 1. Initial and Subsequent Acute Care Service
Issues Addressed
When counseling and/or coordination of care dominate more than 50% of the time a physician spends with a patient during an evaluation and management (E/M) service, then time may be considered as the controlling factor to qualify the E/M service for a particular level of care.2 The following must be documented in the patient’s medical record in order to report an E/M service based on time:
The total length of time of the E/M visit;
Evidence that more than half of the total length of time of the E/M visit was spent in counseling and coordinating of care; and
The content of the counseling and coordination of care provided during the E/M visit.
History and exam, if performed or updated, should also be documented, along with the patient response or comprehension of information. An acceptable C/CC time entry may be noted as, “Total visit time = 35 minutes; > 50% spent counseling/coordinating care” or “20 of 35 minutes spent counseling/coordinating care.”
A payer may prefer one documentation style over another. It is always best to query payer policy and review local documentation standards to ensure compliance. Please remember that while this example constitutes the required elements for the notation of time, documentation must also include the details of counseling, care plan revisions, and any information that is pertinent to patient care and communication with other healthcare professionals.
(click for larger image)Table 2. Consultation Services (if recognized by payer)
Family Discussions
Family discussions are a typical event involved in taking care of patients and are appropriate to count as C/CC time. Special circumstances are considered when discussions must take place without the patient present. This type of counseling time is recognized but only counts towards C/CC time if the following criteria are met and documented:
The patient is unable or clinically incompetent to participate in discussions;
The time is spent on the unit/floor with the family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; and
The conversation bears directly on the management of the patient.3
Time cannot be counted if the discussion takes place in an area outside of the patient’s unit/floor (e.g. in the physician’s office) or if the time is spent counseling the family members through their grieving process.
It is fairly common for the family discussion to take place later in the day, after the physician has completed morning rounds. If the earlier encounter involved C/CC, the physician would report the cumulative time spent for that service date. If the earlier encounter was a typical patient assessment incorporating the components of an evaluation (i.e., history update and physical) and management (i.e., care plan review/revision) service, the meeting time may qualify for prolonged care services.
(click for larger image)Table 3. Threshold Time for Prolonged Care Services7
Service Provider
Be sure to count only the physician’s time spent in C/CC. Counseling time by the nursing staff, the social worker, or the resident cannot contribute toward the physician’s total visit time. When more than one physician is involved in services throughout the day, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level under one physician’s name.4
Consider the following example: The hospitalist takes a brief history about overnight events and reviews some of the pertinent information with the patient. He/she then leaves the room to coordinate the patient’s ongoing care in anticipation that the patient will be discharged over the next few days (25 minutes). The resident is asked to continue the assessment and counsel the patient on the patient’s current disease process (20 minutes).
In the above scenario, the hospitalist is only able to report 99232, because the time spent by the resident is “nonbillable time.”
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Prolonged Care Reminders
Prolonged care codes exist for both outpatient and inpatient services. Hospitalist opportunities for prolonged care mainly involve inpatient code series:
99356: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; first hour.
99357: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; each additional 30 minutes.
Both of these codes are considered “add-on” codes and cannot be reported without a primary service. In this case, the appropriate “inpatient” E/M code (e.g. 9922x, 9923x, 9925x) represents the “primary” service. Code 99356 is reported during the first hour of prolonged services, beyond the initial encounter time, and 99357 is used for each additional 30 minutes of prolonged care beyond the first prolonged care hour. Only one unit of 99356 may be reported per patient per physician group per day, whereas multiple units of 99357 may be reported in a single day.
The CPT definition of prolonged care varies from that of the Centers for Medicare and Medicaid Services (CMS). CPT recognizes the total duration spent by a physician on a given date, even if the time spent by the physician on that date is not continuous; the time involves both face-to-face time and unit/floor time.5 CMS only counts direct face-to-face time between the physician and the patient toward prolonged care billing. Time spent reviewing charts or discussion of a patient with house medical staff that does not involve direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities cannot be billed as prolonged services.6 This contradicts policy for C/CC services and makes prolonged care services an inefficient practice method.
Medicare also identifies “threshold” time (see Table 3).7 The total physician visit time must exceed the time requirements associated with the “primary codes by a thirty”-minute threshold (e.g. 99221 + 99356 = 30 minutes + 30 minutes = 60 minutes threshold time). The physician must document the total face-to-face time spent in separate notes throughout the day or in one cumulative note. The latter method is a more realistic option for physicians. When two providers from the same group and same specialty provide services on the same date (e.g. physician A saw the patient during morning rounds, and physician B spoke with the patient/family in the afternoon), only one physician can report the cumulative service.4 As always, query payers for coverage, because some non-Medicare insurers do not recognize these codes.—CP
Providers typically rely on the “key components” (history, exam, medical decision-making) when documenting in the medical record, and they often misunderstand the use of time when selecting visit levels. Sometimes providers may report a lower service level than warranted because they didn’t feel that they spent the required amount of time with the patient; however, the duration of the visit is an ancillary factor and does not control the level of service to be billed unless more than 50% of the face-to-face time (for non-inpatient services) or more than 50% of the floor time (for inpatient services) is spent providing counseling or coordination of care (C/CC).1 In these instances, providers may choose to document only a brief history and exam, or none at all. They should update the medical decision-making based on the discussion.
Consider the hospitalization of an elderly patient who is newly diagnosed with diabetes. In addition to stabilizing the patient’s glucose levels and devising the appropriate care plan, the patient and/or caregivers also require extensive counseling regarding disease management, lifestyle modification, and medication regime. Coordination of care for outpatient programs and resources is also crucial. To make sure that this qualifies as a time-based service, ensure that the documentation contains the duration, the issues addressed, and the signature of the service provider.
Duration of Counseling and/or Coordination of Care
Time is not used for visit level selection if C/CC is minimal (<50%) or absent from the patient encounter. For inpatient services, total visit time is identified as provider face-to-face time (i.e., at the bedside) combined with time spent on the patient’s unit/floor performing services that are directly related to that patient, such as reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers.
Time associated with activities performed in locations other than the patient’s unit/floor (e.g. reviewing current results or images from the physician’s office) is not allowable in calculating the total visit time. Time associated with teaching students/interns is also excluded, because this doesn’t reflect patient care activities. Once the provider documents all services rendered on a given calendar date, the provider selects the visit level that corresponds with the cumulative visit time documented in the chart (see Tables 1 and 2).
(click for larger image)Table 1. Initial and Subsequent Acute Care Service
Issues Addressed
When counseling and/or coordination of care dominate more than 50% of the time a physician spends with a patient during an evaluation and management (E/M) service, then time may be considered as the controlling factor to qualify the E/M service for a particular level of care.2 The following must be documented in the patient’s medical record in order to report an E/M service based on time:
The total length of time of the E/M visit;
Evidence that more than half of the total length of time of the E/M visit was spent in counseling and coordinating of care; and
The content of the counseling and coordination of care provided during the E/M visit.
History and exam, if performed or updated, should also be documented, along with the patient response or comprehension of information. An acceptable C/CC time entry may be noted as, “Total visit time = 35 minutes; > 50% spent counseling/coordinating care” or “20 of 35 minutes spent counseling/coordinating care.”
A payer may prefer one documentation style over another. It is always best to query payer policy and review local documentation standards to ensure compliance. Please remember that while this example constitutes the required elements for the notation of time, documentation must also include the details of counseling, care plan revisions, and any information that is pertinent to patient care and communication with other healthcare professionals.
(click for larger image)Table 2. Consultation Services (if recognized by payer)
Family Discussions
Family discussions are a typical event involved in taking care of patients and are appropriate to count as C/CC time. Special circumstances are considered when discussions must take place without the patient present. This type of counseling time is recognized but only counts towards C/CC time if the following criteria are met and documented:
The patient is unable or clinically incompetent to participate in discussions;
The time is spent on the unit/floor with the family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; and
The conversation bears directly on the management of the patient.3
Time cannot be counted if the discussion takes place in an area outside of the patient’s unit/floor (e.g. in the physician’s office) or if the time is spent counseling the family members through their grieving process.
It is fairly common for the family discussion to take place later in the day, after the physician has completed morning rounds. If the earlier encounter involved C/CC, the physician would report the cumulative time spent for that service date. If the earlier encounter was a typical patient assessment incorporating the components of an evaluation (i.e., history update and physical) and management (i.e., care plan review/revision) service, the meeting time may qualify for prolonged care services.
(click for larger image)Table 3. Threshold Time for Prolonged Care Services7
Service Provider
Be sure to count only the physician’s time spent in C/CC. Counseling time by the nursing staff, the social worker, or the resident cannot contribute toward the physician’s total visit time. When more than one physician is involved in services throughout the day, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level under one physician’s name.4
Consider the following example: The hospitalist takes a brief history about overnight events and reviews some of the pertinent information with the patient. He/she then leaves the room to coordinate the patient’s ongoing care in anticipation that the patient will be discharged over the next few days (25 minutes). The resident is asked to continue the assessment and counsel the patient on the patient’s current disease process (20 minutes).
In the above scenario, the hospitalist is only able to report 99232, because the time spent by the resident is “nonbillable time.”
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Prolonged Care Reminders
Prolonged care codes exist for both outpatient and inpatient services. Hospitalist opportunities for prolonged care mainly involve inpatient code series:
99356: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; first hour.
99357: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; each additional 30 minutes.
Both of these codes are considered “add-on” codes and cannot be reported without a primary service. In this case, the appropriate “inpatient” E/M code (e.g. 9922x, 9923x, 9925x) represents the “primary” service. Code 99356 is reported during the first hour of prolonged services, beyond the initial encounter time, and 99357 is used for each additional 30 minutes of prolonged care beyond the first prolonged care hour. Only one unit of 99356 may be reported per patient per physician group per day, whereas multiple units of 99357 may be reported in a single day.
The CPT definition of prolonged care varies from that of the Centers for Medicare and Medicaid Services (CMS). CPT recognizes the total duration spent by a physician on a given date, even if the time spent by the physician on that date is not continuous; the time involves both face-to-face time and unit/floor time.5 CMS only counts direct face-to-face time between the physician and the patient toward prolonged care billing. Time spent reviewing charts or discussion of a patient with house medical staff that does not involve direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities cannot be billed as prolonged services.6 This contradicts policy for C/CC services and makes prolonged care services an inefficient practice method.
Medicare also identifies “threshold” time (see Table 3).7 The total physician visit time must exceed the time requirements associated with the “primary codes by a thirty”-minute threshold (e.g. 99221 + 99356 = 30 minutes + 30 minutes = 60 minutes threshold time). The physician must document the total face-to-face time spent in separate notes throughout the day or in one cumulative note. The latter method is a more realistic option for physicians. When two providers from the same group and same specialty provide services on the same date (e.g. physician A saw the patient during morning rounds, and physician B spoke with the patient/family in the afternoon), only one physician can report the cumulative service.4 As always, query payers for coverage, because some non-Medicare insurers do not recognize these codes.—CP
Providers typically rely on the “key components” (history, exam, medical decision-making) when documenting in the medical record, and they often misunderstand the use of time when selecting visit levels. Sometimes providers may report a lower service level than warranted because they didn’t feel that they spent the required amount of time with the patient; however, the duration of the visit is an ancillary factor and does not control the level of service to be billed unless more than 50% of the face-to-face time (for non-inpatient services) or more than 50% of the floor time (for inpatient services) is spent providing counseling or coordination of care (C/CC).1 In these instances, providers may choose to document only a brief history and exam, or none at all. They should update the medical decision-making based on the discussion.
Consider the hospitalization of an elderly patient who is newly diagnosed with diabetes. In addition to stabilizing the patient’s glucose levels and devising the appropriate care plan, the patient and/or caregivers also require extensive counseling regarding disease management, lifestyle modification, and medication regime. Coordination of care for outpatient programs and resources is also crucial. To make sure that this qualifies as a time-based service, ensure that the documentation contains the duration, the issues addressed, and the signature of the service provider.
Duration of Counseling and/or Coordination of Care
Time is not used for visit level selection if C/CC is minimal (<50%) or absent from the patient encounter. For inpatient services, total visit time is identified as provider face-to-face time (i.e., at the bedside) combined with time spent on the patient’s unit/floor performing services that are directly related to that patient, such as reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers.
Time associated with activities performed in locations other than the patient’s unit/floor (e.g. reviewing current results or images from the physician’s office) is not allowable in calculating the total visit time. Time associated with teaching students/interns is also excluded, because this doesn’t reflect patient care activities. Once the provider documents all services rendered on a given calendar date, the provider selects the visit level that corresponds with the cumulative visit time documented in the chart (see Tables 1 and 2).
(click for larger image)Table 1. Initial and Subsequent Acute Care Service
Issues Addressed
When counseling and/or coordination of care dominate more than 50% of the time a physician spends with a patient during an evaluation and management (E/M) service, then time may be considered as the controlling factor to qualify the E/M service for a particular level of care.2 The following must be documented in the patient’s medical record in order to report an E/M service based on time:
The total length of time of the E/M visit;
Evidence that more than half of the total length of time of the E/M visit was spent in counseling and coordinating of care; and
The content of the counseling and coordination of care provided during the E/M visit.
History and exam, if performed or updated, should also be documented, along with the patient response or comprehension of information. An acceptable C/CC time entry may be noted as, “Total visit time = 35 minutes; > 50% spent counseling/coordinating care” or “20 of 35 minutes spent counseling/coordinating care.”
A payer may prefer one documentation style over another. It is always best to query payer policy and review local documentation standards to ensure compliance. Please remember that while this example constitutes the required elements for the notation of time, documentation must also include the details of counseling, care plan revisions, and any information that is pertinent to patient care and communication with other healthcare professionals.
(click for larger image)Table 2. Consultation Services (if recognized by payer)
Family Discussions
Family discussions are a typical event involved in taking care of patients and are appropriate to count as C/CC time. Special circumstances are considered when discussions must take place without the patient present. This type of counseling time is recognized but only counts towards C/CC time if the following criteria are met and documented:
The patient is unable or clinically incompetent to participate in discussions;
The time is spent on the unit/floor with the family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; and
The conversation bears directly on the management of the patient.3
Time cannot be counted if the discussion takes place in an area outside of the patient’s unit/floor (e.g. in the physician’s office) or if the time is spent counseling the family members through their grieving process.
It is fairly common for the family discussion to take place later in the day, after the physician has completed morning rounds. If the earlier encounter involved C/CC, the physician would report the cumulative time spent for that service date. If the earlier encounter was a typical patient assessment incorporating the components of an evaluation (i.e., history update and physical) and management (i.e., care plan review/revision) service, the meeting time may qualify for prolonged care services.
(click for larger image)Table 3. Threshold Time for Prolonged Care Services7
Service Provider
Be sure to count only the physician’s time spent in C/CC. Counseling time by the nursing staff, the social worker, or the resident cannot contribute toward the physician’s total visit time. When more than one physician is involved in services throughout the day, the physicians should select a level of service representative of the combined visits and submit the appropriate code for that level under one physician’s name.4
Consider the following example: The hospitalist takes a brief history about overnight events and reviews some of the pertinent information with the patient. He/she then leaves the room to coordinate the patient’s ongoing care in anticipation that the patient will be discharged over the next few days (25 minutes). The resident is asked to continue the assessment and counsel the patient on the patient’s current disease process (20 minutes).
In the above scenario, the hospitalist is only able to report 99232, because the time spent by the resident is “nonbillable time.”
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Prolonged Care Reminders
Prolonged care codes exist for both outpatient and inpatient services. Hospitalist opportunities for prolonged care mainly involve inpatient code series:
99356: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; first hour.
99357: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; each additional 30 minutes.
Both of these codes are considered “add-on” codes and cannot be reported without a primary service. In this case, the appropriate “inpatient” E/M code (e.g. 9922x, 9923x, 9925x) represents the “primary” service. Code 99356 is reported during the first hour of prolonged services, beyond the initial encounter time, and 99357 is used for each additional 30 minutes of prolonged care beyond the first prolonged care hour. Only one unit of 99356 may be reported per patient per physician group per day, whereas multiple units of 99357 may be reported in a single day.
The CPT definition of prolonged care varies from that of the Centers for Medicare and Medicaid Services (CMS). CPT recognizes the total duration spent by a physician on a given date, even if the time spent by the physician on that date is not continuous; the time involves both face-to-face time and unit/floor time.5 CMS only counts direct face-to-face time between the physician and the patient toward prolonged care billing. Time spent reviewing charts or discussion of a patient with house medical staff that does not involve direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities cannot be billed as prolonged services.6 This contradicts policy for C/CC services and makes prolonged care services an inefficient practice method.
Medicare also identifies “threshold” time (see Table 3).7 The total physician visit time must exceed the time requirements associated with the “primary codes by a thirty”-minute threshold (e.g. 99221 + 99356 = 30 minutes + 30 minutes = 60 minutes threshold time). The physician must document the total face-to-face time spent in separate notes throughout the day or in one cumulative note. The latter method is a more realistic option for physicians. When two providers from the same group and same specialty provide services on the same date (e.g. physician A saw the patient during morning rounds, and physician B spoke with the patient/family in the afternoon), only one physician can report the cumulative service.4 As always, query payers for coverage, because some non-Medicare insurers do not recognize these codes.—CP