User login
PHM15: Effective Intranasal Sedation
Presenters: Kelly Basaldua, MD; Daniel Sedillo, MD, MBA, and Jason Reynolds, MD
Summary:
In an environment where medicine is becoming ever more specialized and the scope of practice for many is ever narrowing into corridors of expertise, the hospitalist remains a bastion of generalism with an ever-diversifying skill set. One of the skills acquired by many hospitalists to aid in the overall efficiency of the hospital is intranasal (IN) sedation.
Intranasal sedation is becoming more popular given the rapid onset and offset and the relative safety of the sedation of patients without the need for intravenous catheters. This phenomenon is accomplished by avoiding the gut and thus avoiding first-pass metabolism. This allows for greatly increased bioavailability compared with oral administration. In addition, the nasal mucosa is in near direct contact with the CSF via the cribriform plate, allowing for rapid and effective action.
To maximize the effectiveness of intranasal sedation, low volumes with high concentrations, atomization, and minimal nasal occlusion are vital. The ideal volume per nostril is approximately 0.5 ml as using any greater volume results in oversaturation and minimal additional absorption. Thus, concentrating the medications into minimal volumes provides for more efficacious usage. Atomization aids in ensuring thorough surface area coverage and higher absorption. This is a far more efficacious method of delivery than liquid/drop administration.
Because intranasally administered agents have a delayed and widened serum peak compared to IV, IN sedation carries less of a chance to reach serum levels high enough to cause respiratory depression, though monitoring is still necessary. When compared to IV sedation, IN does have a delay in onset, but also provides for a more gentle recovery process, often resulting in a less disorienting recovery for the patient, while also providing for a wider safety profile.
The presenters covered three primary agents:
- midazolam,
- dexmedetomidine, and
- fentanyl
Midazolam is useful for non-painful, minimally invasive procedures. Fentanyl is more useful for painful or more invasive procedures. Dexmedetomidine is off-label use for intranasal sedation at this time, but has promising initial research given its safety profile and longer duration of action compared to most intranasal agents. Also, dexmedetomidine works extremely effectively in combination with other agents, particularly midazolam, to prolong sedations, making it very useful for longer procedures like combination MRIs.
The presenters then provided a practical workshop to practice the delivery of intranasal medication effectively. One of the pearls provided involved proper positioning of the patient in a reclined position as sitting to erect will cause the medication to drip out and having the patient lying flat will result in the medication dripping down the posterior pharynx. This position should be held for 30 seconds after delivery of the medication. Practicing with atomizers to achieve effective aerosolization was discussed. The target of medication should avoid the nasal septum given its poor absorption.
Key Takeaway:
With hospitalists being called to assist in ever-expanding roles within the hospital system while improving efficiency and throughput, intranasal sedation may provide reduced imaging wait times, bedside and ED procedure times in a safe and effective manner. TH
Dr. Crook is a hospitalist in the division of hospitalist medicine, assistant professor of pediatrics, and assistant pediatric clerkship director in the Department of Pediatrics at Vanderbilt University School of Medicine and Monroe Carell Jr. Children's Hospital at Vanderbilt in Nashville.
Presenters: Kelly Basaldua, MD; Daniel Sedillo, MD, MBA, and Jason Reynolds, MD
Summary:
In an environment where medicine is becoming ever more specialized and the scope of practice for many is ever narrowing into corridors of expertise, the hospitalist remains a bastion of generalism with an ever-diversifying skill set. One of the skills acquired by many hospitalists to aid in the overall efficiency of the hospital is intranasal (IN) sedation.
Intranasal sedation is becoming more popular given the rapid onset and offset and the relative safety of the sedation of patients without the need for intravenous catheters. This phenomenon is accomplished by avoiding the gut and thus avoiding first-pass metabolism. This allows for greatly increased bioavailability compared with oral administration. In addition, the nasal mucosa is in near direct contact with the CSF via the cribriform plate, allowing for rapid and effective action.
To maximize the effectiveness of intranasal sedation, low volumes with high concentrations, atomization, and minimal nasal occlusion are vital. The ideal volume per nostril is approximately 0.5 ml as using any greater volume results in oversaturation and minimal additional absorption. Thus, concentrating the medications into minimal volumes provides for more efficacious usage. Atomization aids in ensuring thorough surface area coverage and higher absorption. This is a far more efficacious method of delivery than liquid/drop administration.
Because intranasally administered agents have a delayed and widened serum peak compared to IV, IN sedation carries less of a chance to reach serum levels high enough to cause respiratory depression, though monitoring is still necessary. When compared to IV sedation, IN does have a delay in onset, but also provides for a more gentle recovery process, often resulting in a less disorienting recovery for the patient, while also providing for a wider safety profile.
The presenters covered three primary agents:
- midazolam,
- dexmedetomidine, and
- fentanyl
Midazolam is useful for non-painful, minimally invasive procedures. Fentanyl is more useful for painful or more invasive procedures. Dexmedetomidine is off-label use for intranasal sedation at this time, but has promising initial research given its safety profile and longer duration of action compared to most intranasal agents. Also, dexmedetomidine works extremely effectively in combination with other agents, particularly midazolam, to prolong sedations, making it very useful for longer procedures like combination MRIs.
The presenters then provided a practical workshop to practice the delivery of intranasal medication effectively. One of the pearls provided involved proper positioning of the patient in a reclined position as sitting to erect will cause the medication to drip out and having the patient lying flat will result in the medication dripping down the posterior pharynx. This position should be held for 30 seconds after delivery of the medication. Practicing with atomizers to achieve effective aerosolization was discussed. The target of medication should avoid the nasal septum given its poor absorption.
Key Takeaway:
With hospitalists being called to assist in ever-expanding roles within the hospital system while improving efficiency and throughput, intranasal sedation may provide reduced imaging wait times, bedside and ED procedure times in a safe and effective manner. TH
Dr. Crook is a hospitalist in the division of hospitalist medicine, assistant professor of pediatrics, and assistant pediatric clerkship director in the Department of Pediatrics at Vanderbilt University School of Medicine and Monroe Carell Jr. Children's Hospital at Vanderbilt in Nashville.
Presenters: Kelly Basaldua, MD; Daniel Sedillo, MD, MBA, and Jason Reynolds, MD
Summary:
In an environment where medicine is becoming ever more specialized and the scope of practice for many is ever narrowing into corridors of expertise, the hospitalist remains a bastion of generalism with an ever-diversifying skill set. One of the skills acquired by many hospitalists to aid in the overall efficiency of the hospital is intranasal (IN) sedation.
Intranasal sedation is becoming more popular given the rapid onset and offset and the relative safety of the sedation of patients without the need for intravenous catheters. This phenomenon is accomplished by avoiding the gut and thus avoiding first-pass metabolism. This allows for greatly increased bioavailability compared with oral administration. In addition, the nasal mucosa is in near direct contact with the CSF via the cribriform plate, allowing for rapid and effective action.
To maximize the effectiveness of intranasal sedation, low volumes with high concentrations, atomization, and minimal nasal occlusion are vital. The ideal volume per nostril is approximately 0.5 ml as using any greater volume results in oversaturation and minimal additional absorption. Thus, concentrating the medications into minimal volumes provides for more efficacious usage. Atomization aids in ensuring thorough surface area coverage and higher absorption. This is a far more efficacious method of delivery than liquid/drop administration.
Because intranasally administered agents have a delayed and widened serum peak compared to IV, IN sedation carries less of a chance to reach serum levels high enough to cause respiratory depression, though monitoring is still necessary. When compared to IV sedation, IN does have a delay in onset, but also provides for a more gentle recovery process, often resulting in a less disorienting recovery for the patient, while also providing for a wider safety profile.
The presenters covered three primary agents:
- midazolam,
- dexmedetomidine, and
- fentanyl
Midazolam is useful for non-painful, minimally invasive procedures. Fentanyl is more useful for painful or more invasive procedures. Dexmedetomidine is off-label use for intranasal sedation at this time, but has promising initial research given its safety profile and longer duration of action compared to most intranasal agents. Also, dexmedetomidine works extremely effectively in combination with other agents, particularly midazolam, to prolong sedations, making it very useful for longer procedures like combination MRIs.
The presenters then provided a practical workshop to practice the delivery of intranasal medication effectively. One of the pearls provided involved proper positioning of the patient in a reclined position as sitting to erect will cause the medication to drip out and having the patient lying flat will result in the medication dripping down the posterior pharynx. This position should be held for 30 seconds after delivery of the medication. Practicing with atomizers to achieve effective aerosolization was discussed. The target of medication should avoid the nasal septum given its poor absorption.
Key Takeaway:
With hospitalists being called to assist in ever-expanding roles within the hospital system while improving efficiency and throughput, intranasal sedation may provide reduced imaging wait times, bedside and ED procedure times in a safe and effective manner. TH
Dr. Crook is a hospitalist in the division of hospitalist medicine, assistant professor of pediatrics, and assistant pediatric clerkship director in the Department of Pediatrics at Vanderbilt University School of Medicine and Monroe Carell Jr. Children's Hospital at Vanderbilt in Nashville.
PHM15: Preparing for Global Health Experiences
Presenters: Gitanjli Arora, Phuc Le, and Christiana Russ
Summary:
Overseas medical missions can be rewarding experiences for both trainees as part of a supervised program and attending physicians. There is substantial inequity in the global distribution of disease versus health care providers with most providers being located in developed countries and higher disease burdens in underdeveloped countries. The goal of global healthcare training is mutual benefit, where the provider gains clinical experience and the host country gains enhanced medical care. Both provider and hosts gain increased cultural awareness.
The American Academy of Pediatrics guidelines for a meaningful international experience recommend 4 components:
- Pre-trip Training. Don’t go without some idea of what to expect
- Pre-travel preparations. Get your vaccines, travel plans, licensure, scope of practice taken care of.
- Preceptorship by host and US faculty
- Post-travel evaluation and feedback
Key Takeaways:
Providers in overseas medical missions will encounter challenging situations—culturally, ethically and medically. Get as much information beforehand. Be respectful of different cultural norms. Get a cultural ambassador. Keep in mind the Serenity Prayer. TH
Presenters: Gitanjli Arora, Phuc Le, and Christiana Russ
Summary:
Overseas medical missions can be rewarding experiences for both trainees as part of a supervised program and attending physicians. There is substantial inequity in the global distribution of disease versus health care providers with most providers being located in developed countries and higher disease burdens in underdeveloped countries. The goal of global healthcare training is mutual benefit, where the provider gains clinical experience and the host country gains enhanced medical care. Both provider and hosts gain increased cultural awareness.
The American Academy of Pediatrics guidelines for a meaningful international experience recommend 4 components:
- Pre-trip Training. Don’t go without some idea of what to expect
- Pre-travel preparations. Get your vaccines, travel plans, licensure, scope of practice taken care of.
- Preceptorship by host and US faculty
- Post-travel evaluation and feedback
Key Takeaways:
Providers in overseas medical missions will encounter challenging situations—culturally, ethically and medically. Get as much information beforehand. Be respectful of different cultural norms. Get a cultural ambassador. Keep in mind the Serenity Prayer. TH
Presenters: Gitanjli Arora, Phuc Le, and Christiana Russ
Summary:
Overseas medical missions can be rewarding experiences for both trainees as part of a supervised program and attending physicians. There is substantial inequity in the global distribution of disease versus health care providers with most providers being located in developed countries and higher disease burdens in underdeveloped countries. The goal of global healthcare training is mutual benefit, where the provider gains clinical experience and the host country gains enhanced medical care. Both provider and hosts gain increased cultural awareness.
The American Academy of Pediatrics guidelines for a meaningful international experience recommend 4 components:
- Pre-trip Training. Don’t go without some idea of what to expect
- Pre-travel preparations. Get your vaccines, travel plans, licensure, scope of practice taken care of.
- Preceptorship by host and US faculty
- Post-travel evaluation and feedback
Key Takeaways:
Providers in overseas medical missions will encounter challenging situations—culturally, ethically and medically. Get as much information beforehand. Be respectful of different cultural norms. Get a cultural ambassador. Keep in mind the Serenity Prayer. TH
PHM15: New Quality Measures for Children with Medical Complexity
Pediatric Hospital Medicine 2015's keynote speaker, Rita Mangione-Smith, MD, MPH, reviewed quality measures being developed for medically complex patients by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN). As one of the most challenging groups to not only provide care but to determine if the management provided brings value, the importance of quality measures was emphasized.
Dr. Mangione-Smith, of Seattle Children’s Hospital, reviewed the need for quality measures, as well as the process of developing these measures. Quality measures help to quantify outcomes from care practices, stated Dr. Mangione-Smith, to compare similar settings, and also to set possible benchmarks. The processes range from identifying and prioritizing measures to how they are validated as true value added outcomes. Data sources, sample size, and reliability/validity of the measures are considered important components to ensure that answers or results acquired are applicable and relevant to the population. Another important component is to clearly define a child with medical complexity.
Some reasons why medically complex patients require this focus:
- The low amount of information about their quality of care, investment, and need for coordination;
- Lack of understanding of which care practices make the biggest differences on their outcomes; and
- Their high rate of resource utilization.
The objective was to see which areas of care, such as care coordination, have the highest benefit/improvement on outcomes so as to prioritize resources more effectively. Dr. Mangione-Smith also touched on some obstacles and challenges, such as lack of insurance coverage leading to use of emergency resources as their primary care and its effect on increasing resource utilization.
Measures were determined via a multi-component methodology. Surveys using a binary and linear mean scoring tool were used. This provided multiple types of information such as assessing family’s perception of care, their understanding of medical information and care plans, and their accessibility to medical care services or information about their child.
Currently there is very little evidence on which management methods have the most significant, or any, effect on children with medical complexity. The use of quality measures to help guide which practices may have the highest positive impact on their outcomes greatly adds to the challenging care of this population and can be “used to assess quality of care coordination over time.” TH
Dr. Alvarez is a pediatric hospitalist and medical director of community hospital services at Children’s National Health System in Washington, D.C.
Pediatric Hospital Medicine 2015's keynote speaker, Rita Mangione-Smith, MD, MPH, reviewed quality measures being developed for medically complex patients by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN). As one of the most challenging groups to not only provide care but to determine if the management provided brings value, the importance of quality measures was emphasized.
Dr. Mangione-Smith, of Seattle Children’s Hospital, reviewed the need for quality measures, as well as the process of developing these measures. Quality measures help to quantify outcomes from care practices, stated Dr. Mangione-Smith, to compare similar settings, and also to set possible benchmarks. The processes range from identifying and prioritizing measures to how they are validated as true value added outcomes. Data sources, sample size, and reliability/validity of the measures are considered important components to ensure that answers or results acquired are applicable and relevant to the population. Another important component is to clearly define a child with medical complexity.
Some reasons why medically complex patients require this focus:
- The low amount of information about their quality of care, investment, and need for coordination;
- Lack of understanding of which care practices make the biggest differences on their outcomes; and
- Their high rate of resource utilization.
The objective was to see which areas of care, such as care coordination, have the highest benefit/improvement on outcomes so as to prioritize resources more effectively. Dr. Mangione-Smith also touched on some obstacles and challenges, such as lack of insurance coverage leading to use of emergency resources as their primary care and its effect on increasing resource utilization.
Measures were determined via a multi-component methodology. Surveys using a binary and linear mean scoring tool were used. This provided multiple types of information such as assessing family’s perception of care, their understanding of medical information and care plans, and their accessibility to medical care services or information about their child.
Currently there is very little evidence on which management methods have the most significant, or any, effect on children with medical complexity. The use of quality measures to help guide which practices may have the highest positive impact on their outcomes greatly adds to the challenging care of this population and can be “used to assess quality of care coordination over time.” TH
Dr. Alvarez is a pediatric hospitalist and medical director of community hospital services at Children’s National Health System in Washington, D.C.
Pediatric Hospital Medicine 2015's keynote speaker, Rita Mangione-Smith, MD, MPH, reviewed quality measures being developed for medically complex patients by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN). As one of the most challenging groups to not only provide care but to determine if the management provided brings value, the importance of quality measures was emphasized.
Dr. Mangione-Smith, of Seattle Children’s Hospital, reviewed the need for quality measures, as well as the process of developing these measures. Quality measures help to quantify outcomes from care practices, stated Dr. Mangione-Smith, to compare similar settings, and also to set possible benchmarks. The processes range from identifying and prioritizing measures to how they are validated as true value added outcomes. Data sources, sample size, and reliability/validity of the measures are considered important components to ensure that answers or results acquired are applicable and relevant to the population. Another important component is to clearly define a child with medical complexity.
Some reasons why medically complex patients require this focus:
- The low amount of information about their quality of care, investment, and need for coordination;
- Lack of understanding of which care practices make the biggest differences on their outcomes; and
- Their high rate of resource utilization.
The objective was to see which areas of care, such as care coordination, have the highest benefit/improvement on outcomes so as to prioritize resources more effectively. Dr. Mangione-Smith also touched on some obstacles and challenges, such as lack of insurance coverage leading to use of emergency resources as their primary care and its effect on increasing resource utilization.
Measures were determined via a multi-component methodology. Surveys using a binary and linear mean scoring tool were used. This provided multiple types of information such as assessing family’s perception of care, their understanding of medical information and care plans, and their accessibility to medical care services or information about their child.
Currently there is very little evidence on which management methods have the most significant, or any, effect on children with medical complexity. The use of quality measures to help guide which practices may have the highest positive impact on their outcomes greatly adds to the challenging care of this population and can be “used to assess quality of care coordination over time.” TH
Dr. Alvarez is a pediatric hospitalist and medical director of community hospital services at Children’s National Health System in Washington, D.C.
Fecal Microbiotia Transplantation in Treatment of Recurrent Clostridium difficile Infection
Clinical question: Does fecal microbiotia transplantation (FMT) effectively treat patients with recurrent Clostridium difficile infection (CDI)?
Background: Patients with initial CDI have increased rates of recurrence (15%–30%), with variable success noted in treatment of recurrent disease. Increased interest in the use of FMT as a treatment strategy for CDI has led to various studies evaluating its efficacy.
Study design: Systematic review.
Setting: Multiple settings from studies obtained from MEDLINE, Cochrane Library, and ClinicalTrials.gov.
Synopsis: Literature search and review yielded a total of 35 included articles for analysis, mostly case-series studies (28), with only two randomized controlled trials (RCTs). Primary outcome was defined as symptom resolution, with a secondary outcome of recurrence. Although studies included assessed FMT as treatment for initial, recurrent, and refractory CDI, the majority of the evidence was focused on recurrent CDI. Among the studies analyzed, FMT was found to have a substantial effect on primary outcome of symptom resolution (85% of cases) among all pooled studies for recurrent CDI.
Although this review provided evidence suggestive of the efficacy of FMT in recurrent CDI, the paucity of RCT data was well documented and noted as a limitation in providing high-quality recommendations on FMT as a treatment option. Further high-quality research is recommended, and hospitalists caring for patients with recurrent CDI should be wary of treatment with FMT based on these data alone.
Bottom line: Studies evaluating FMT as a treatment option for recurrent CDI demonstrate significant benefit in symptom resolution, but further high-quality research is needed.
Citation: Drekonja D, Reich J, Gezahegn S, et al. Fecal microbiota transplantation for Clostridium difficile infection: a systematic review of the evidence. Ann Intern Med. 2015;162:630-638. doi:10.7326/M14-2693.
Visit our website for more hospitalist-focused literature reviews.
Clinical question: Does fecal microbiotia transplantation (FMT) effectively treat patients with recurrent Clostridium difficile infection (CDI)?
Background: Patients with initial CDI have increased rates of recurrence (15%–30%), with variable success noted in treatment of recurrent disease. Increased interest in the use of FMT as a treatment strategy for CDI has led to various studies evaluating its efficacy.
Study design: Systematic review.
Setting: Multiple settings from studies obtained from MEDLINE, Cochrane Library, and ClinicalTrials.gov.
Synopsis: Literature search and review yielded a total of 35 included articles for analysis, mostly case-series studies (28), with only two randomized controlled trials (RCTs). Primary outcome was defined as symptom resolution, with a secondary outcome of recurrence. Although studies included assessed FMT as treatment for initial, recurrent, and refractory CDI, the majority of the evidence was focused on recurrent CDI. Among the studies analyzed, FMT was found to have a substantial effect on primary outcome of symptom resolution (85% of cases) among all pooled studies for recurrent CDI.
Although this review provided evidence suggestive of the efficacy of FMT in recurrent CDI, the paucity of RCT data was well documented and noted as a limitation in providing high-quality recommendations on FMT as a treatment option. Further high-quality research is recommended, and hospitalists caring for patients with recurrent CDI should be wary of treatment with FMT based on these data alone.
Bottom line: Studies evaluating FMT as a treatment option for recurrent CDI demonstrate significant benefit in symptom resolution, but further high-quality research is needed.
Citation: Drekonja D, Reich J, Gezahegn S, et al. Fecal microbiota transplantation for Clostridium difficile infection: a systematic review of the evidence. Ann Intern Med. 2015;162:630-638. doi:10.7326/M14-2693.
Visit our website for more hospitalist-focused literature reviews.
Clinical question: Does fecal microbiotia transplantation (FMT) effectively treat patients with recurrent Clostridium difficile infection (CDI)?
Background: Patients with initial CDI have increased rates of recurrence (15%–30%), with variable success noted in treatment of recurrent disease. Increased interest in the use of FMT as a treatment strategy for CDI has led to various studies evaluating its efficacy.
Study design: Systematic review.
Setting: Multiple settings from studies obtained from MEDLINE, Cochrane Library, and ClinicalTrials.gov.
Synopsis: Literature search and review yielded a total of 35 included articles for analysis, mostly case-series studies (28), with only two randomized controlled trials (RCTs). Primary outcome was defined as symptom resolution, with a secondary outcome of recurrence. Although studies included assessed FMT as treatment for initial, recurrent, and refractory CDI, the majority of the evidence was focused on recurrent CDI. Among the studies analyzed, FMT was found to have a substantial effect on primary outcome of symptom resolution (85% of cases) among all pooled studies for recurrent CDI.
Although this review provided evidence suggestive of the efficacy of FMT in recurrent CDI, the paucity of RCT data was well documented and noted as a limitation in providing high-quality recommendations on FMT as a treatment option. Further high-quality research is recommended, and hospitalists caring for patients with recurrent CDI should be wary of treatment with FMT based on these data alone.
Bottom line: Studies evaluating FMT as a treatment option for recurrent CDI demonstrate significant benefit in symptom resolution, but further high-quality research is needed.
Citation: Drekonja D, Reich J, Gezahegn S, et al. Fecal microbiota transplantation for Clostridium difficile infection: a systematic review of the evidence. Ann Intern Med. 2015;162:630-638. doi:10.7326/M14-2693.
Visit our website for more hospitalist-focused literature reviews.
ProMISe Trial Adds Skepticism to Early Goal-Directed Therapy for Sepsis
Clinical question: Does EGDT for sepsis reduce mortality at 90 days compared with standard therapy?
Background: EGDT is recommended in international guidelines for the resuscitation of patients presenting with early septic shock; however, adoption has been limited, and uncertainty about its effectiveness remains.
Study design: Pragmatic, multicenter, randomized controlled trial (RCT) with intention to treat analysis.
Setting: Fifty-six National Health Service EDs in the United Kingdom.
Synopsis: ProMISe trial enrolled 1,251 patients with severe sepsis or septic shock and patients were randomized to usual-care group (as determined by the treating clinicians) or algorithm-driven EGDT, which included continuous central venous oxygen saturation (ScvO2) using the original EGDT protocol. The primary outcome of all-cause mortality at 90 days was not significantly different between the two groups: 29.5% in EGDT and 29.2% in the usual-care group (P=0.9). This translated into a relative risk of 1.01% (95% CI 0.85-1.20) in the EGDT group. There were no meaningful differences in secondary outcomes.
Both groups in this study were actually well matched for most interventions. The main difference was in the use of continuous ScvO2 measurement and central venous pressure to guide management. Perhaps we should not completely dismiss the term EGDT. Most of our “usual care” consists of early intervention and goal-directed therapy.
Bottom line: In patients identified early with septic shock, the use of EGDT vs. “usual” care did not result in a statistical difference in 90-day mortality.
Citation: Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301-1311.
Clinical question: Does EGDT for sepsis reduce mortality at 90 days compared with standard therapy?
Background: EGDT is recommended in international guidelines for the resuscitation of patients presenting with early septic shock; however, adoption has been limited, and uncertainty about its effectiveness remains.
Study design: Pragmatic, multicenter, randomized controlled trial (RCT) with intention to treat analysis.
Setting: Fifty-six National Health Service EDs in the United Kingdom.
Synopsis: ProMISe trial enrolled 1,251 patients with severe sepsis or septic shock and patients were randomized to usual-care group (as determined by the treating clinicians) or algorithm-driven EGDT, which included continuous central venous oxygen saturation (ScvO2) using the original EGDT protocol. The primary outcome of all-cause mortality at 90 days was not significantly different between the two groups: 29.5% in EGDT and 29.2% in the usual-care group (P=0.9). This translated into a relative risk of 1.01% (95% CI 0.85-1.20) in the EGDT group. There were no meaningful differences in secondary outcomes.
Both groups in this study were actually well matched for most interventions. The main difference was in the use of continuous ScvO2 measurement and central venous pressure to guide management. Perhaps we should not completely dismiss the term EGDT. Most of our “usual care” consists of early intervention and goal-directed therapy.
Bottom line: In patients identified early with septic shock, the use of EGDT vs. “usual” care did not result in a statistical difference in 90-day mortality.
Citation: Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301-1311.
Clinical question: Does EGDT for sepsis reduce mortality at 90 days compared with standard therapy?
Background: EGDT is recommended in international guidelines for the resuscitation of patients presenting with early septic shock; however, adoption has been limited, and uncertainty about its effectiveness remains.
Study design: Pragmatic, multicenter, randomized controlled trial (RCT) with intention to treat analysis.
Setting: Fifty-six National Health Service EDs in the United Kingdom.
Synopsis: ProMISe trial enrolled 1,251 patients with severe sepsis or septic shock and patients were randomized to usual-care group (as determined by the treating clinicians) or algorithm-driven EGDT, which included continuous central venous oxygen saturation (ScvO2) using the original EGDT protocol. The primary outcome of all-cause mortality at 90 days was not significantly different between the two groups: 29.5% in EGDT and 29.2% in the usual-care group (P=0.9). This translated into a relative risk of 1.01% (95% CI 0.85-1.20) in the EGDT group. There were no meaningful differences in secondary outcomes.
Both groups in this study were actually well matched for most interventions. The main difference was in the use of continuous ScvO2 measurement and central venous pressure to guide management. Perhaps we should not completely dismiss the term EGDT. Most of our “usual care” consists of early intervention and goal-directed therapy.
Bottom line: In patients identified early with septic shock, the use of EGDT vs. “usual” care did not result in a statistical difference in 90-day mortality.
Citation: Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301-1311.
Effectiveness of Multicomponent Nonpharmacological Delirium Interventions
Clinical question: How effective are multicomponent, nonpharmacological interventions at reducing delirium and preventing poor outcomes?
Background: Delirium is an acute disorder with significant morbidity and mortality. Systemic reviews and clinical guidelines recommend targeted, multicomponent, nonpharmacologic strategies for prevention. The Hospital Elder Life Program (HELP) uses an interdisciplinary team to implement nonpharmacologic interventions, such as reorientation, early mobilization, therapeutic activities, hydration, nutrition, sleep strategies, and hearing and vision adaptation. Trials of nonpharmacological strategies to prevent this disorder have been limited to small-scale studies.
Study design: Systemic literature review and meta-analysis.
Synopsis: Fourteen studies involving 12 unique interventions were identified and results were pooled for meta-analysis, with primary outcomes being incidence and falls. Secondary outcomes were length of stay, institutionalization, and change in functional or cognitive status. Eleven studies were found to have demonstrated significant reductions in delirium incidence (odds ratio [OR], 0.47; 95% CI, 0.38-0.58), with four trials reducing delirium incidence by 44% (OR, 0.56; 95%CI, 0.42-0.76). Four studies demonstrated a significant decrease in the rate of falls (OR, 0.38; 95% CI, 0.25-0.60), with two studies reducing falls by 64% (OR, 0.36; 95% CI, 0.22-0.61). Institutionalization and length of stay did not demonstrate statistical significance between the two groups.
Bottom line: Multicomponent, nonpharmacological delirium prevention interventions were found to be effective in decreasing the occurrence of both delirium and falls during hospitalization in older persons.
Citation: Hshieh TT, Yue J, Oh E, et al. Effectiveness of multicomponent nonpharmacological delirium interventions. JAMA. 2015;175(4):512-520.
Clinical question: How effective are multicomponent, nonpharmacological interventions at reducing delirium and preventing poor outcomes?
Background: Delirium is an acute disorder with significant morbidity and mortality. Systemic reviews and clinical guidelines recommend targeted, multicomponent, nonpharmacologic strategies for prevention. The Hospital Elder Life Program (HELP) uses an interdisciplinary team to implement nonpharmacologic interventions, such as reorientation, early mobilization, therapeutic activities, hydration, nutrition, sleep strategies, and hearing and vision adaptation. Trials of nonpharmacological strategies to prevent this disorder have been limited to small-scale studies.
Study design: Systemic literature review and meta-analysis.
Synopsis: Fourteen studies involving 12 unique interventions were identified and results were pooled for meta-analysis, with primary outcomes being incidence and falls. Secondary outcomes were length of stay, institutionalization, and change in functional or cognitive status. Eleven studies were found to have demonstrated significant reductions in delirium incidence (odds ratio [OR], 0.47; 95% CI, 0.38-0.58), with four trials reducing delirium incidence by 44% (OR, 0.56; 95%CI, 0.42-0.76). Four studies demonstrated a significant decrease in the rate of falls (OR, 0.38; 95% CI, 0.25-0.60), with two studies reducing falls by 64% (OR, 0.36; 95% CI, 0.22-0.61). Institutionalization and length of stay did not demonstrate statistical significance between the two groups.
Bottom line: Multicomponent, nonpharmacological delirium prevention interventions were found to be effective in decreasing the occurrence of both delirium and falls during hospitalization in older persons.
Citation: Hshieh TT, Yue J, Oh E, et al. Effectiveness of multicomponent nonpharmacological delirium interventions. JAMA. 2015;175(4):512-520.
Clinical question: How effective are multicomponent, nonpharmacological interventions at reducing delirium and preventing poor outcomes?
Background: Delirium is an acute disorder with significant morbidity and mortality. Systemic reviews and clinical guidelines recommend targeted, multicomponent, nonpharmacologic strategies for prevention. The Hospital Elder Life Program (HELP) uses an interdisciplinary team to implement nonpharmacologic interventions, such as reorientation, early mobilization, therapeutic activities, hydration, nutrition, sleep strategies, and hearing and vision adaptation. Trials of nonpharmacological strategies to prevent this disorder have been limited to small-scale studies.
Study design: Systemic literature review and meta-analysis.
Synopsis: Fourteen studies involving 12 unique interventions were identified and results were pooled for meta-analysis, with primary outcomes being incidence and falls. Secondary outcomes were length of stay, institutionalization, and change in functional or cognitive status. Eleven studies were found to have demonstrated significant reductions in delirium incidence (odds ratio [OR], 0.47; 95% CI, 0.38-0.58), with four trials reducing delirium incidence by 44% (OR, 0.56; 95%CI, 0.42-0.76). Four studies demonstrated a significant decrease in the rate of falls (OR, 0.38; 95% CI, 0.25-0.60), with two studies reducing falls by 64% (OR, 0.36; 95% CI, 0.22-0.61). Institutionalization and length of stay did not demonstrate statistical significance between the two groups.
Bottom line: Multicomponent, nonpharmacological delirium prevention interventions were found to be effective in decreasing the occurrence of both delirium and falls during hospitalization in older persons.
Citation: Hshieh TT, Yue J, Oh E, et al. Effectiveness of multicomponent nonpharmacological delirium interventions. JAMA. 2015;175(4):512-520.
Post-Acute Patient Care Offers Opportunities for Non-Physicians
More than in the inpatient setting, post-acute care offers opportunities for nurse practitioners and physician assistants to play important clinical and administrative roles. Physician assistant (PA) Edwin Lopez, PA-C, is chief of an eight-member HM group—four doctors, four PAs—that provides coverage at St. Elizabeth, a rural critical access hospital in Enumclaw, Wash., population 10,669, and in the 80-bed SNF located across the street. Lopez was recruited to establish the HM group “in the shadow of Mt. Rainier” about eight years ago, at a time when the hospital’s parent, CHI Franciscan Health System, was trying to rebuild its quality and reputation while planning a new building.
He succeeded, dramatically improving its performance on HCAHPS surveys and other metrics; however, hospital readmissions then emerged as an issue.
“I began to realize, with our little facility’s large population of elderly patients with multiple chronic problems—typically the highest cohort for readmissions—all the gains we had made could be lost if we didn’t do something about this problem,” Lopez says. “I ran the numbers and found that the nursing home across the street readmitted 35% of patients discharged from our hospital.”
It took a year to get the larger system’s approval, but Lopez’s hospitalist group manages all the patients transferred to the nearby nursing home, with daily visits by the doctor and/or PA on duty.
“We started the program in January 2014, and, in one year, readmissions went from 35% down to 7%,” he says. “We developed culturally from the very beginning as a PA/MD collaborative model. The doctor doesn’t need to see the more routine patients with more common conditions but instead is freed up to focus on higher-acuity, more complex patients.”
In Dr. Tollman’s opinion, physician extenders “own” the post-acute realm, because of the demand for their care.
“There just aren’t going to be enough doctors for all of the patients who need to be seen,” he says, “and the amount of money for this care isn’t enough for these facilities to employ groups of doctors.”
Emily Rosenbaum, PA-C, works for Northwest Community Healthcare in Arlington Heights, Ill. She is the lone PA working with eight physician hospitalists. Much of her work is in a rehabilitation facility across the street from Northwest Community Hospital.
“I see all of the new admissions, although under my scope of practice I can’t bill for the initial visit. But I do the follow-ups, see patients that have been in rehab for 30 days or less, and put out [clinical] fires in the facility,” she says.
Rosenbaum works at the hospital part of her day taking care of acute patients, then works with the hospitalist assigned to the rehabilitation facility.
“It’s easier for me to go back and forth and keep my finger on the patients’ pulse,” she says. “As there are more demands on doctors on the acute side, it’s natural for the NP and PA to step up and take a larger role on the post-acute side.”
More than in the inpatient setting, post-acute care offers opportunities for nurse practitioners and physician assistants to play important clinical and administrative roles. Physician assistant (PA) Edwin Lopez, PA-C, is chief of an eight-member HM group—four doctors, four PAs—that provides coverage at St. Elizabeth, a rural critical access hospital in Enumclaw, Wash., population 10,669, and in the 80-bed SNF located across the street. Lopez was recruited to establish the HM group “in the shadow of Mt. Rainier” about eight years ago, at a time when the hospital’s parent, CHI Franciscan Health System, was trying to rebuild its quality and reputation while planning a new building.
He succeeded, dramatically improving its performance on HCAHPS surveys and other metrics; however, hospital readmissions then emerged as an issue.
“I began to realize, with our little facility’s large population of elderly patients with multiple chronic problems—typically the highest cohort for readmissions—all the gains we had made could be lost if we didn’t do something about this problem,” Lopez says. “I ran the numbers and found that the nursing home across the street readmitted 35% of patients discharged from our hospital.”
It took a year to get the larger system’s approval, but Lopez’s hospitalist group manages all the patients transferred to the nearby nursing home, with daily visits by the doctor and/or PA on duty.
“We started the program in January 2014, and, in one year, readmissions went from 35% down to 7%,” he says. “We developed culturally from the very beginning as a PA/MD collaborative model. The doctor doesn’t need to see the more routine patients with more common conditions but instead is freed up to focus on higher-acuity, more complex patients.”
In Dr. Tollman’s opinion, physician extenders “own” the post-acute realm, because of the demand for their care.
“There just aren’t going to be enough doctors for all of the patients who need to be seen,” he says, “and the amount of money for this care isn’t enough for these facilities to employ groups of doctors.”
Emily Rosenbaum, PA-C, works for Northwest Community Healthcare in Arlington Heights, Ill. She is the lone PA working with eight physician hospitalists. Much of her work is in a rehabilitation facility across the street from Northwest Community Hospital.
“I see all of the new admissions, although under my scope of practice I can’t bill for the initial visit. But I do the follow-ups, see patients that have been in rehab for 30 days or less, and put out [clinical] fires in the facility,” she says.
Rosenbaum works at the hospital part of her day taking care of acute patients, then works with the hospitalist assigned to the rehabilitation facility.
“It’s easier for me to go back and forth and keep my finger on the patients’ pulse,” she says. “As there are more demands on doctors on the acute side, it’s natural for the NP and PA to step up and take a larger role on the post-acute side.”
More than in the inpatient setting, post-acute care offers opportunities for nurse practitioners and physician assistants to play important clinical and administrative roles. Physician assistant (PA) Edwin Lopez, PA-C, is chief of an eight-member HM group—four doctors, four PAs—that provides coverage at St. Elizabeth, a rural critical access hospital in Enumclaw, Wash., population 10,669, and in the 80-bed SNF located across the street. Lopez was recruited to establish the HM group “in the shadow of Mt. Rainier” about eight years ago, at a time when the hospital’s parent, CHI Franciscan Health System, was trying to rebuild its quality and reputation while planning a new building.
He succeeded, dramatically improving its performance on HCAHPS surveys and other metrics; however, hospital readmissions then emerged as an issue.
“I began to realize, with our little facility’s large population of elderly patients with multiple chronic problems—typically the highest cohort for readmissions—all the gains we had made could be lost if we didn’t do something about this problem,” Lopez says. “I ran the numbers and found that the nursing home across the street readmitted 35% of patients discharged from our hospital.”
It took a year to get the larger system’s approval, but Lopez’s hospitalist group manages all the patients transferred to the nearby nursing home, with daily visits by the doctor and/or PA on duty.
“We started the program in January 2014, and, in one year, readmissions went from 35% down to 7%,” he says. “We developed culturally from the very beginning as a PA/MD collaborative model. The doctor doesn’t need to see the more routine patients with more common conditions but instead is freed up to focus on higher-acuity, more complex patients.”
In Dr. Tollman’s opinion, physician extenders “own” the post-acute realm, because of the demand for their care.
“There just aren’t going to be enough doctors for all of the patients who need to be seen,” he says, “and the amount of money for this care isn’t enough for these facilities to employ groups of doctors.”
Emily Rosenbaum, PA-C, works for Northwest Community Healthcare in Arlington Heights, Ill. She is the lone PA working with eight physician hospitalists. Much of her work is in a rehabilitation facility across the street from Northwest Community Hospital.
“I see all of the new admissions, although under my scope of practice I can’t bill for the initial visit. But I do the follow-ups, see patients that have been in rehab for 30 days or less, and put out [clinical] fires in the facility,” she says.
Rosenbaum works at the hospital part of her day taking care of acute patients, then works with the hospitalist assigned to the rehabilitation facility.
“It’s easier for me to go back and forth and keep my finger on the patients’ pulse,” she says. “As there are more demands on doctors on the acute side, it’s natural for the NP and PA to step up and take a larger role on the post-acute side.”
11 Things Gastroenterologists Think Hospitalists Need to Know
So many symptoms that are staples of gastroenterology—chest pain, nausea, diarrhea—are mainstay causes for hospitalization that it might be worth fine-tuning how well you handle patients with gastroenterology disorders.
The Hospitalist asked several gastroenterologists for their guidance on better care and their suggestions for correcting some common mistakes that they encounter. Here are their tips:
1 Fluid resuscitation is crucial for pancreatitis patients.
It’s very important to rehydrate these patients within the first 24 hours, because those who remain underhydrated can have a worse prognosis, says Robert Coben, MD, academic coordinator for the Gastroentestinal Fellowship Program at Thomas Jefferson University Hospital in Philadelphia. On occasion, physicians are reluctant to give extra fluids to these patients, he says, particularly if they have heart failure or suffer kidney problems. A 70-kg patient should be receiving about 200 cc per hour, he notes.
“Sometimes we’ll walk in the room and they’re getting 80 cc an hour,” Dr. Coben says.
“These patients…need to be flooded with fluids,” says Rajeev Jain, MD, chief of gastroenterology at Presbyterian Hospital of Dallas, partner at Texas Digestive Disease Consultants, and chair of the Practice Management and Economics Committee of the American Gastroenterological Association. “We’re talking sometimes liters and liters of IV normal saline or lactated Ringer’s (solution) in a 24-hour period.”1
Marcelo Vela, MD, a gastroenterologist and hepatologist at the Mayo Clinic in Scottsdale, Ariz., and an associate editor with Clinical Gastroenterology and Hepatology, says Ringer’s solution is a better choice than normal saline.2
“If you’re going to start IV fluids on somebody who’s coming in with acute pancreatitis, Ringer’s solution has been shown to be superior to saline in randomized controlled trials,” Dr. Vela says. “It reduces systemic inflammation.”
2 Gastrointestinal bleeding decisions
When inpatients have gastrointestinal bleeding, the hospitalist often has to assess its severity and make the call on whether a patient needs the ICU.
“The most important thing for that is obviously the vital signs,” says John Pandolfino, MD, chief of the division of medicine–gastroenterology and hepatology at Northwestern University Feinberg School of Medicine in Chicago. “If people are tachycardic and they’re not responding to hydration and blood transfusion, that usually means it’s a pretty active bleed and they need to go to the intensive care unit. If you have somebody who’s GI bleeding and they’re coagulopathic (i.e., they’re on anti-coagulation because they have a valve and they need anti-coagulation or they have cancer or bad cardiovascular disease), those are the people that you should have a low threshold for sending to the intensive care unit with a GI bleed; those are the people who are at a very high mortality [risk].”
He added that those with an ulcer, with a visible vessel, are at a high-risk of a rebleed and should spend some time in the ICU.
“Those people should be evaluated in the intensive care unit for at least 24 hours, maybe even 72 hours,” Dr. Pandolfino says, “and they should have IV PPI [proton pump inhibitor] therapy.”
3 Endoscopy has very low yield for diagnosis of reflux.
“Endoscopy has good yield for mucosa abnormalities on inspection of the esophageal mucosa, but it does not give you a diagnosis of reflux, especially on patients who have already been treated with a PPI,” says Prakash Gyawali, MD, MRCP, professor of gastroenterology at Washington University in St. Louis, Mo. “So, usually, in those settings, obtaining a consult or trying to decide exactly what you’re looking for to explain the symptoms has better yield than an endoscopy.”
Sometimes a pH study is needed, but that has to be planned, because patients may have to be taken off of a PPI in advance. That means those studies are not easy to set up in the hospital and might best be arranged by the gastroenterologist, Dr. Gyawali says.
4 In cases of acute diarrhea, order a stool sample right away.
That will help guide care from the gastroenterologist, if and when the gastroenterologist is called in, Dr. Pandolfino says.
“One of the things that is frustrating for the gastroenterologist is that we get called initially, but really the hospitalist should be getting stool studies, and they should have at least a very good idea of what they need from us,” he says. “Because, really, endoscopy is not usually needed very often in diagnosis of acute diarrhea.”
Broad-range stool studies, a good history and physical, and examining labs for a possible chronic inflammatory process or anemia are good ways to begin to assess patients with diarrhea, he says. Clostridium difficile colitis has to be considered as well, Dr. Pandolfino says.
Endoscopy is more helpful in evaluating acute diarrhea in those with bloody diarrhea suspected of having inflammatory bowel disease or an infectious diarrhea but on whom cultures have come back negative. For those with compromised immune systems, endoscopy could be done earlier, as well.
“So for us, I think we really need to get into the picture a little bit after the patient has been brought into the hospital and the stool study is negative, unless they’re an immune-compromised patient,” Dr. Pandolfino says.
5 When—and how—to test the stool.
If a patient develops diarrhea while already in the hospital, the only stool test needed is C. diff.
“They shouldn’t be developing a viral diarrhea, they shouldn’t be developing an infectious diarrhea—let’s say, from E. coli or Salmonella—unless they literally developed it a couple hours after getting in,” Dr. Jain says. “It should either be C. diff or a side effect of some medication. … We don’t need to spend the extra money, which is of low-value care to send for OVA and parasites, or bacterial pathogens and so forth.”
Dr. Jain says he thinks such testing is being done more appropriately of late.
“But I still will see multiple stool tests sent on somebody who’s been in the hospital for a week and then develops diarrhea,” he explains.
6 Gastroenterologists do not need to be consulted for every C. diff infection.
“I think that we really should get involved when patients are either not responding or when they’re very ill,” Dr. Pandolfino says.
Hospitalists should consider whether patients are on antibiotics or a PPI and whether or not they need to stay on those medications. Also, medications that slow motility (i.e., loperamide) should be avoided, if possible.
“We don’t want it to linger,” Dr. Pandolfino says. “One of the basic mechanisms of how we get rid of pathogens is to expel them with diarrhea.
“But you certainly don’t want the patient to be uncomfortable to the point where they’re having 20 to 30 bowel movements a day.”
In non-severe patients who have some diarrhea, abdominal pain, nausea, and vomiting—but are able to keep food down—the specialists might not have to be called in, and patients can just be treated with oral metronidazole or oral vancomycin fairly simply, he says.
For those who seem severely ill with a dilating colon, are in nearly a septic state, and have very severe diarrhea, the gastroenterologist should probably be called in, he says.

7 For patients with a possible GI bleed and black stools, do an exam before calling in the gastroenterologist.
The exam should determine what the stool color is and whether it is heme-positive, and the patient’s blood count should be evaluated, Dr. Coben says.
Frequently, “the consultant’s the one who ends up doing the rectal exam and checking that,” he says. “Sometimes we find that [the patient is] really not bleeding,” and it was just a case of a hospitalist taking the patient’s word that they were bleeding.
Being on iron therapy or taking Pepto-Bismol can turn the stool black, and the stool might not really be black; colors can sometimes be open to interpretation.
But he cautions that colon cancer could be the cause for a GI bleed.
“We’ve had it happen a few times where this occurred,” he says. “The patient was discharged, and they really didn’t get proper follow-up, and it ended up that they had a colon cancer. It kind of delayed that diagnosis. So I think you have to be aware of [the fact that], especially in somebody over the age of 40 or 50, if they have an iron-deficiency, anemia, or heme-positive stool, the first thing you really need to exclude is a colon cancer.”
8 Minimize CT scans in early evaluation and management of acute pancreatitis patients.
“The reason for that is they tend to be intravascularly volume-depleted,” Dr. Jain says. “So [with] the IV contrast, there’s an increased risk of developing kidney failure. It’s also been associated with increased risk of necrotizing pancreatitis.”
Dr. Jain notes that when he is consulted on this kind of patient, he will order a sonogram. If it doesn’t show gallstones, and there’s no clear reason for the pancreatitis, he will want a CT scan, but he will wait a few days until the patient is fluid-resuscitated.
Dr. Jain says that this is a problem more often seen in the ED—where 90% of patients with acute pancreatitis have already gotten the CT scan—and less so among hospitalists, but it’s still worth the reminder.
A CT scan right away is justified to rule out something such as a perforation, but not in the case of classic symptoms of acute pancreatitis, he adds.
9 Actively bleeding patients?
It’s smart to give patients a unit of packed red blood cells more quickly if they’re actively bleeding. Even over just one hour is OK, Dr. Jain says.
“Even if they have underlying heart failure, if they’re volume-depleted, they need that volume,” Dr. Jain explains. “Sometimes you’ll see that it takes eight hours to get two units of blood in. That’s inadequate.”
Another point worth a reminder, he says: Two large-bore peripheral IV’s are “much, much better” than a central or PICC line to deliver IV fluid resuscitation.

“Sometimes hospitalists order barium studies because these can be done the same day, whereas with endoscopy, patients need to be put on a schedule and have to be NPO [nothing by mouth] overnight.” —Prakash Gyawali, MD, MRCP
10 Don’t be too quick to order barium studies, especially in patients with dysphagia.
“The problem with that is it takes much longer to do an endoscopy if barium is put in the esophagus, because we usually wait until the barium clears,” Dr. Gyawali says. “And inpatient evaluation of new-onset dysphagia should be endoscopy first, and not barium, because biopsies need to be taken to rule out eosinophilic esophagitis.
“Sometimes hospitalists order barium studies because these can be done the same day, whereas with endoscopy, patients need to be put on a schedule and have to be NPO [nothing by mouth] overnight.”
11 Gastric-emptying studies should be outpatient.
Gastric-emptying studies are often better done when patients are not in a hospital, experts say, because they might be on medications that would interfere with the study.
“A common issue, not just among hospitalists but also gastroenterologists, is that patients may be on a bunch of medicines that would affect stomach-emptying while they are in-house for some other problem,” Dr. Gyawali says. “A lot of times, these patients with pain may get narcotics. They may be on medicines to prevent them from throwing up. … And all of these will slow down gastric emptying.”
With an abnormal test result, “you are left to decide whether that is a real abnormality or whether the medicines the patients were on impacted the abnormality.”
If emptying was significantly prolonged, the test may have some value, “but then it probably will need to be corroborated with symptoms and with endoscopic findings.”
Thomas Collins is a freelance writer in South Florida.
References
- Warndorf MG, Kurtzman JT, Bartel MJ, et al. Early fluid resuscitation reduces morbidity among patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):705-709.
- Wu BU, Hwang JQ, Gardner TH, et al. Lactated Ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):710-717.
So many symptoms that are staples of gastroenterology—chest pain, nausea, diarrhea—are mainstay causes for hospitalization that it might be worth fine-tuning how well you handle patients with gastroenterology disorders.
The Hospitalist asked several gastroenterologists for their guidance on better care and their suggestions for correcting some common mistakes that they encounter. Here are their tips:
1 Fluid resuscitation is crucial for pancreatitis patients.
It’s very important to rehydrate these patients within the first 24 hours, because those who remain underhydrated can have a worse prognosis, says Robert Coben, MD, academic coordinator for the Gastroentestinal Fellowship Program at Thomas Jefferson University Hospital in Philadelphia. On occasion, physicians are reluctant to give extra fluids to these patients, he says, particularly if they have heart failure or suffer kidney problems. A 70-kg patient should be receiving about 200 cc per hour, he notes.
“Sometimes we’ll walk in the room and they’re getting 80 cc an hour,” Dr. Coben says.
“These patients…need to be flooded with fluids,” says Rajeev Jain, MD, chief of gastroenterology at Presbyterian Hospital of Dallas, partner at Texas Digestive Disease Consultants, and chair of the Practice Management and Economics Committee of the American Gastroenterological Association. “We’re talking sometimes liters and liters of IV normal saline or lactated Ringer’s (solution) in a 24-hour period.”1
Marcelo Vela, MD, a gastroenterologist and hepatologist at the Mayo Clinic in Scottsdale, Ariz., and an associate editor with Clinical Gastroenterology and Hepatology, says Ringer’s solution is a better choice than normal saline.2
“If you’re going to start IV fluids on somebody who’s coming in with acute pancreatitis, Ringer’s solution has been shown to be superior to saline in randomized controlled trials,” Dr. Vela says. “It reduces systemic inflammation.”
2 Gastrointestinal bleeding decisions
When inpatients have gastrointestinal bleeding, the hospitalist often has to assess its severity and make the call on whether a patient needs the ICU.
“The most important thing for that is obviously the vital signs,” says John Pandolfino, MD, chief of the division of medicine–gastroenterology and hepatology at Northwestern University Feinberg School of Medicine in Chicago. “If people are tachycardic and they’re not responding to hydration and blood transfusion, that usually means it’s a pretty active bleed and they need to go to the intensive care unit. If you have somebody who’s GI bleeding and they’re coagulopathic (i.e., they’re on anti-coagulation because they have a valve and they need anti-coagulation or they have cancer or bad cardiovascular disease), those are the people that you should have a low threshold for sending to the intensive care unit with a GI bleed; those are the people who are at a very high mortality [risk].”
He added that those with an ulcer, with a visible vessel, are at a high-risk of a rebleed and should spend some time in the ICU.
“Those people should be evaluated in the intensive care unit for at least 24 hours, maybe even 72 hours,” Dr. Pandolfino says, “and they should have IV PPI [proton pump inhibitor] therapy.”
3 Endoscopy has very low yield for diagnosis of reflux.
“Endoscopy has good yield for mucosa abnormalities on inspection of the esophageal mucosa, but it does not give you a diagnosis of reflux, especially on patients who have already been treated with a PPI,” says Prakash Gyawali, MD, MRCP, professor of gastroenterology at Washington University in St. Louis, Mo. “So, usually, in those settings, obtaining a consult or trying to decide exactly what you’re looking for to explain the symptoms has better yield than an endoscopy.”
Sometimes a pH study is needed, but that has to be planned, because patients may have to be taken off of a PPI in advance. That means those studies are not easy to set up in the hospital and might best be arranged by the gastroenterologist, Dr. Gyawali says.
4 In cases of acute diarrhea, order a stool sample right away.
That will help guide care from the gastroenterologist, if and when the gastroenterologist is called in, Dr. Pandolfino says.
“One of the things that is frustrating for the gastroenterologist is that we get called initially, but really the hospitalist should be getting stool studies, and they should have at least a very good idea of what they need from us,” he says. “Because, really, endoscopy is not usually needed very often in diagnosis of acute diarrhea.”
Broad-range stool studies, a good history and physical, and examining labs for a possible chronic inflammatory process or anemia are good ways to begin to assess patients with diarrhea, he says. Clostridium difficile colitis has to be considered as well, Dr. Pandolfino says.
Endoscopy is more helpful in evaluating acute diarrhea in those with bloody diarrhea suspected of having inflammatory bowel disease or an infectious diarrhea but on whom cultures have come back negative. For those with compromised immune systems, endoscopy could be done earlier, as well.
“So for us, I think we really need to get into the picture a little bit after the patient has been brought into the hospital and the stool study is negative, unless they’re an immune-compromised patient,” Dr. Pandolfino says.
5 When—and how—to test the stool.
If a patient develops diarrhea while already in the hospital, the only stool test needed is C. diff.
“They shouldn’t be developing a viral diarrhea, they shouldn’t be developing an infectious diarrhea—let’s say, from E. coli or Salmonella—unless they literally developed it a couple hours after getting in,” Dr. Jain says. “It should either be C. diff or a side effect of some medication. … We don’t need to spend the extra money, which is of low-value care to send for OVA and parasites, or bacterial pathogens and so forth.”
Dr. Jain says he thinks such testing is being done more appropriately of late.
“But I still will see multiple stool tests sent on somebody who’s been in the hospital for a week and then develops diarrhea,” he explains.
6 Gastroenterologists do not need to be consulted for every C. diff infection.
“I think that we really should get involved when patients are either not responding or when they’re very ill,” Dr. Pandolfino says.
Hospitalists should consider whether patients are on antibiotics or a PPI and whether or not they need to stay on those medications. Also, medications that slow motility (i.e., loperamide) should be avoided, if possible.
“We don’t want it to linger,” Dr. Pandolfino says. “One of the basic mechanisms of how we get rid of pathogens is to expel them with diarrhea.
“But you certainly don’t want the patient to be uncomfortable to the point where they’re having 20 to 30 bowel movements a day.”
In non-severe patients who have some diarrhea, abdominal pain, nausea, and vomiting—but are able to keep food down—the specialists might not have to be called in, and patients can just be treated with oral metronidazole or oral vancomycin fairly simply, he says.
For those who seem severely ill with a dilating colon, are in nearly a septic state, and have very severe diarrhea, the gastroenterologist should probably be called in, he says.
7 For patients with a possible GI bleed and black stools, do an exam before calling in the gastroenterologist.
The exam should determine what the stool color is and whether it is heme-positive, and the patient’s blood count should be evaluated, Dr. Coben says.
Frequently, “the consultant’s the one who ends up doing the rectal exam and checking that,” he says. “Sometimes we find that [the patient is] really not bleeding,” and it was just a case of a hospitalist taking the patient’s word that they were bleeding.
Being on iron therapy or taking Pepto-Bismol can turn the stool black, and the stool might not really be black; colors can sometimes be open to interpretation.
But he cautions that colon cancer could be the cause for a GI bleed.
“We’ve had it happen a few times where this occurred,” he says. “The patient was discharged, and they really didn’t get proper follow-up, and it ended up that they had a colon cancer. It kind of delayed that diagnosis. So I think you have to be aware of [the fact that], especially in somebody over the age of 40 or 50, if they have an iron-deficiency, anemia, or heme-positive stool, the first thing you really need to exclude is a colon cancer.”
8 Minimize CT scans in early evaluation and management of acute pancreatitis patients.
“The reason for that is they tend to be intravascularly volume-depleted,” Dr. Jain says. “So [with] the IV contrast, there’s an increased risk of developing kidney failure. It’s also been associated with increased risk of necrotizing pancreatitis.”
Dr. Jain notes that when he is consulted on this kind of patient, he will order a sonogram. If it doesn’t show gallstones, and there’s no clear reason for the pancreatitis, he will want a CT scan, but he will wait a few days until the patient is fluid-resuscitated.
Dr. Jain says that this is a problem more often seen in the ED—where 90% of patients with acute pancreatitis have already gotten the CT scan—and less so among hospitalists, but it’s still worth the reminder.
A CT scan right away is justified to rule out something such as a perforation, but not in the case of classic symptoms of acute pancreatitis, he adds.
9 Actively bleeding patients?
It’s smart to give patients a unit of packed red blood cells more quickly if they’re actively bleeding. Even over just one hour is OK, Dr. Jain says.
“Even if they have underlying heart failure, if they’re volume-depleted, they need that volume,” Dr. Jain explains. “Sometimes you’ll see that it takes eight hours to get two units of blood in. That’s inadequate.”
Another point worth a reminder, he says: Two large-bore peripheral IV’s are “much, much better” than a central or PICC line to deliver IV fluid resuscitation.
“Sometimes hospitalists order barium studies because these can be done the same day, whereas with endoscopy, patients need to be put on a schedule and have to be NPO [nothing by mouth] overnight.” —Prakash Gyawali, MD, MRCP
10 Don’t be too quick to order barium studies, especially in patients with dysphagia.
“The problem with that is it takes much longer to do an endoscopy if barium is put in the esophagus, because we usually wait until the barium clears,” Dr. Gyawali says. “And inpatient evaluation of new-onset dysphagia should be endoscopy first, and not barium, because biopsies need to be taken to rule out eosinophilic esophagitis.
“Sometimes hospitalists order barium studies because these can be done the same day, whereas with endoscopy, patients need to be put on a schedule and have to be NPO [nothing by mouth] overnight.”
11 Gastric-emptying studies should be outpatient.
Gastric-emptying studies are often better done when patients are not in a hospital, experts say, because they might be on medications that would interfere with the study.
“A common issue, not just among hospitalists but also gastroenterologists, is that patients may be on a bunch of medicines that would affect stomach-emptying while they are in-house for some other problem,” Dr. Gyawali says. “A lot of times, these patients with pain may get narcotics. They may be on medicines to prevent them from throwing up. … And all of these will slow down gastric emptying.”
With an abnormal test result, “you are left to decide whether that is a real abnormality or whether the medicines the patients were on impacted the abnormality.”
If emptying was significantly prolonged, the test may have some value, “but then it probably will need to be corroborated with symptoms and with endoscopic findings.”
Thomas Collins is a freelance writer in South Florida.
References
- Warndorf MG, Kurtzman JT, Bartel MJ, et al. Early fluid resuscitation reduces morbidity among patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):705-709.
- Wu BU, Hwang JQ, Gardner TH, et al. Lactated Ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):710-717.
So many symptoms that are staples of gastroenterology—chest pain, nausea, diarrhea—are mainstay causes for hospitalization that it might be worth fine-tuning how well you handle patients with gastroenterology disorders.
The Hospitalist asked several gastroenterologists for their guidance on better care and their suggestions for correcting some common mistakes that they encounter. Here are their tips:
1 Fluid resuscitation is crucial for pancreatitis patients.
It’s very important to rehydrate these patients within the first 24 hours, because those who remain underhydrated can have a worse prognosis, says Robert Coben, MD, academic coordinator for the Gastroentestinal Fellowship Program at Thomas Jefferson University Hospital in Philadelphia. On occasion, physicians are reluctant to give extra fluids to these patients, he says, particularly if they have heart failure or suffer kidney problems. A 70-kg patient should be receiving about 200 cc per hour, he notes.
“Sometimes we’ll walk in the room and they’re getting 80 cc an hour,” Dr. Coben says.
“These patients…need to be flooded with fluids,” says Rajeev Jain, MD, chief of gastroenterology at Presbyterian Hospital of Dallas, partner at Texas Digestive Disease Consultants, and chair of the Practice Management and Economics Committee of the American Gastroenterological Association. “We’re talking sometimes liters and liters of IV normal saline or lactated Ringer’s (solution) in a 24-hour period.”1
Marcelo Vela, MD, a gastroenterologist and hepatologist at the Mayo Clinic in Scottsdale, Ariz., and an associate editor with Clinical Gastroenterology and Hepatology, says Ringer’s solution is a better choice than normal saline.2
“If you’re going to start IV fluids on somebody who’s coming in with acute pancreatitis, Ringer’s solution has been shown to be superior to saline in randomized controlled trials,” Dr. Vela says. “It reduces systemic inflammation.”
2 Gastrointestinal bleeding decisions
When inpatients have gastrointestinal bleeding, the hospitalist often has to assess its severity and make the call on whether a patient needs the ICU.
“The most important thing for that is obviously the vital signs,” says John Pandolfino, MD, chief of the division of medicine–gastroenterology and hepatology at Northwestern University Feinberg School of Medicine in Chicago. “If people are tachycardic and they’re not responding to hydration and blood transfusion, that usually means it’s a pretty active bleed and they need to go to the intensive care unit. If you have somebody who’s GI bleeding and they’re coagulopathic (i.e., they’re on anti-coagulation because they have a valve and they need anti-coagulation or they have cancer or bad cardiovascular disease), those are the people that you should have a low threshold for sending to the intensive care unit with a GI bleed; those are the people who are at a very high mortality [risk].”
He added that those with an ulcer, with a visible vessel, are at a high-risk of a rebleed and should spend some time in the ICU.
“Those people should be evaluated in the intensive care unit for at least 24 hours, maybe even 72 hours,” Dr. Pandolfino says, “and they should have IV PPI [proton pump inhibitor] therapy.”
3 Endoscopy has very low yield for diagnosis of reflux.
“Endoscopy has good yield for mucosa abnormalities on inspection of the esophageal mucosa, but it does not give you a diagnosis of reflux, especially on patients who have already been treated with a PPI,” says Prakash Gyawali, MD, MRCP, professor of gastroenterology at Washington University in St. Louis, Mo. “So, usually, in those settings, obtaining a consult or trying to decide exactly what you’re looking for to explain the symptoms has better yield than an endoscopy.”
Sometimes a pH study is needed, but that has to be planned, because patients may have to be taken off of a PPI in advance. That means those studies are not easy to set up in the hospital and might best be arranged by the gastroenterologist, Dr. Gyawali says.
4 In cases of acute diarrhea, order a stool sample right away.
That will help guide care from the gastroenterologist, if and when the gastroenterologist is called in, Dr. Pandolfino says.
“One of the things that is frustrating for the gastroenterologist is that we get called initially, but really the hospitalist should be getting stool studies, and they should have at least a very good idea of what they need from us,” he says. “Because, really, endoscopy is not usually needed very often in diagnosis of acute diarrhea.”
Broad-range stool studies, a good history and physical, and examining labs for a possible chronic inflammatory process or anemia are good ways to begin to assess patients with diarrhea, he says. Clostridium difficile colitis has to be considered as well, Dr. Pandolfino says.
Endoscopy is more helpful in evaluating acute diarrhea in those with bloody diarrhea suspected of having inflammatory bowel disease or an infectious diarrhea but on whom cultures have come back negative. For those with compromised immune systems, endoscopy could be done earlier, as well.
“So for us, I think we really need to get into the picture a little bit after the patient has been brought into the hospital and the stool study is negative, unless they’re an immune-compromised patient,” Dr. Pandolfino says.
5 When—and how—to test the stool.
If a patient develops diarrhea while already in the hospital, the only stool test needed is C. diff.
“They shouldn’t be developing a viral diarrhea, they shouldn’t be developing an infectious diarrhea—let’s say, from E. coli or Salmonella—unless they literally developed it a couple hours after getting in,” Dr. Jain says. “It should either be C. diff or a side effect of some medication. … We don’t need to spend the extra money, which is of low-value care to send for OVA and parasites, or bacterial pathogens and so forth.”
Dr. Jain says he thinks such testing is being done more appropriately of late.
“But I still will see multiple stool tests sent on somebody who’s been in the hospital for a week and then develops diarrhea,” he explains.
6 Gastroenterologists do not need to be consulted for every C. diff infection.
“I think that we really should get involved when patients are either not responding or when they’re very ill,” Dr. Pandolfino says.
Hospitalists should consider whether patients are on antibiotics or a PPI and whether or not they need to stay on those medications. Also, medications that slow motility (i.e., loperamide) should be avoided, if possible.
“We don’t want it to linger,” Dr. Pandolfino says. “One of the basic mechanisms of how we get rid of pathogens is to expel them with diarrhea.
“But you certainly don’t want the patient to be uncomfortable to the point where they’re having 20 to 30 bowel movements a day.”
In non-severe patients who have some diarrhea, abdominal pain, nausea, and vomiting—but are able to keep food down—the specialists might not have to be called in, and patients can just be treated with oral metronidazole or oral vancomycin fairly simply, he says.
For those who seem severely ill with a dilating colon, are in nearly a septic state, and have very severe diarrhea, the gastroenterologist should probably be called in, he says.
7 For patients with a possible GI bleed and black stools, do an exam before calling in the gastroenterologist.
The exam should determine what the stool color is and whether it is heme-positive, and the patient’s blood count should be evaluated, Dr. Coben says.
Frequently, “the consultant’s the one who ends up doing the rectal exam and checking that,” he says. “Sometimes we find that [the patient is] really not bleeding,” and it was just a case of a hospitalist taking the patient’s word that they were bleeding.
Being on iron therapy or taking Pepto-Bismol can turn the stool black, and the stool might not really be black; colors can sometimes be open to interpretation.
But he cautions that colon cancer could be the cause for a GI bleed.
“We’ve had it happen a few times where this occurred,” he says. “The patient was discharged, and they really didn’t get proper follow-up, and it ended up that they had a colon cancer. It kind of delayed that diagnosis. So I think you have to be aware of [the fact that], especially in somebody over the age of 40 or 50, if they have an iron-deficiency, anemia, or heme-positive stool, the first thing you really need to exclude is a colon cancer.”
8 Minimize CT scans in early evaluation and management of acute pancreatitis patients.
“The reason for that is they tend to be intravascularly volume-depleted,” Dr. Jain says. “So [with] the IV contrast, there’s an increased risk of developing kidney failure. It’s also been associated with increased risk of necrotizing pancreatitis.”
Dr. Jain notes that when he is consulted on this kind of patient, he will order a sonogram. If it doesn’t show gallstones, and there’s no clear reason for the pancreatitis, he will want a CT scan, but he will wait a few days until the patient is fluid-resuscitated.
Dr. Jain says that this is a problem more often seen in the ED—where 90% of patients with acute pancreatitis have already gotten the CT scan—and less so among hospitalists, but it’s still worth the reminder.
A CT scan right away is justified to rule out something such as a perforation, but not in the case of classic symptoms of acute pancreatitis, he adds.
9 Actively bleeding patients?
It’s smart to give patients a unit of packed red blood cells more quickly if they’re actively bleeding. Even over just one hour is OK, Dr. Jain says.
“Even if they have underlying heart failure, if they’re volume-depleted, they need that volume,” Dr. Jain explains. “Sometimes you’ll see that it takes eight hours to get two units of blood in. That’s inadequate.”
Another point worth a reminder, he says: Two large-bore peripheral IV’s are “much, much better” than a central or PICC line to deliver IV fluid resuscitation.
“Sometimes hospitalists order barium studies because these can be done the same day, whereas with endoscopy, patients need to be put on a schedule and have to be NPO [nothing by mouth] overnight.” —Prakash Gyawali, MD, MRCP
10 Don’t be too quick to order barium studies, especially in patients with dysphagia.
“The problem with that is it takes much longer to do an endoscopy if barium is put in the esophagus, because we usually wait until the barium clears,” Dr. Gyawali says. “And inpatient evaluation of new-onset dysphagia should be endoscopy first, and not barium, because biopsies need to be taken to rule out eosinophilic esophagitis.
“Sometimes hospitalists order barium studies because these can be done the same day, whereas with endoscopy, patients need to be put on a schedule and have to be NPO [nothing by mouth] overnight.”
11 Gastric-emptying studies should be outpatient.
Gastric-emptying studies are often better done when patients are not in a hospital, experts say, because they might be on medications that would interfere with the study.
“A common issue, not just among hospitalists but also gastroenterologists, is that patients may be on a bunch of medicines that would affect stomach-emptying while they are in-house for some other problem,” Dr. Gyawali says. “A lot of times, these patients with pain may get narcotics. They may be on medicines to prevent them from throwing up. … And all of these will slow down gastric emptying.”
With an abnormal test result, “you are left to decide whether that is a real abnormality or whether the medicines the patients were on impacted the abnormality.”
If emptying was significantly prolonged, the test may have some value, “but then it probably will need to be corroborated with symptoms and with endoscopic findings.”
Thomas Collins is a freelance writer in South Florida.
References
- Warndorf MG, Kurtzman JT, Bartel MJ, et al. Early fluid resuscitation reduces morbidity among patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):705-709.
- Wu BU, Hwang JQ, Gardner TH, et al. Lactated Ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9(8):710-717.
Childhood Bacteremia and Antibiotics Usage in the Emergency Department
Clinical question: Have the causative organisms in pediatric bacteremia changed over time concurrent with introduction of the pneumococcal conjugate vaccine?
Background: Previous research has shown introduction of polyvalent pneumococcal conjugate vaccine led to changes in the organisms causing meningitis and otitis media, and patterns of nasopharyngeal colonization. Pneumococcus, historically, was a common cause of bacteremia. The availability of pneumococcal conjugate vaccine may have changed the organisms causing bacteremia in children.
Study design: Retrospective chart review and time series.
Setting: Children presenting to the ED of Alder Hey Children’s Hospital in Liverpool, England, from 2001 to 2011.
Synopsis: Five hundred seventy-five episodes of bacteremia were found in 525 children. Infants most commonly had E. coli and Group B streptococcal infections; children over age five most commonly had S. aureus. The introduction of the pneumococcal conjugate vaccine decreased pneumococcal bacteremia by 49% over the study period. This decrease was accompanied by an increase in Gram-negative bacteremia. Susceptibility to empiric antibiotics (third-generation cephalosporins) dropped from 96% to 83%. Over the study period, more children presented with central venous lines, which was felt to be due to increasing outpatient use of total parenteral nutrition (TPN).
Bottom line: Vaccination against pneumococcus is changing the microbiology of pediatric bacteremia, with fewer vaccine-preventable Gram-positive infections and more Gram-negative infections. This increases the likelihood of resistance to third-generation cephalosporins as empiric antibiotic.
Citation: Irwin AD, Drew RJ, Marshall P, et al. Etiology of childhood bacteremia and timely antibiotics administration in the emergency department. Pediatrics. 2015;135(4): 635-642.

Clinical question: Have the causative organisms in pediatric bacteremia changed over time concurrent with introduction of the pneumococcal conjugate vaccine?
Background: Previous research has shown introduction of polyvalent pneumococcal conjugate vaccine led to changes in the organisms causing meningitis and otitis media, and patterns of nasopharyngeal colonization. Pneumococcus, historically, was a common cause of bacteremia. The availability of pneumococcal conjugate vaccine may have changed the organisms causing bacteremia in children.
Study design: Retrospective chart review and time series.
Setting: Children presenting to the ED of Alder Hey Children’s Hospital in Liverpool, England, from 2001 to 2011.
Synopsis: Five hundred seventy-five episodes of bacteremia were found in 525 children. Infants most commonly had E. coli and Group B streptococcal infections; children over age five most commonly had S. aureus. The introduction of the pneumococcal conjugate vaccine decreased pneumococcal bacteremia by 49% over the study period. This decrease was accompanied by an increase in Gram-negative bacteremia. Susceptibility to empiric antibiotics (third-generation cephalosporins) dropped from 96% to 83%. Over the study period, more children presented with central venous lines, which was felt to be due to increasing outpatient use of total parenteral nutrition (TPN).
Bottom line: Vaccination against pneumococcus is changing the microbiology of pediatric bacteremia, with fewer vaccine-preventable Gram-positive infections and more Gram-negative infections. This increases the likelihood of resistance to third-generation cephalosporins as empiric antibiotic.
Citation: Irwin AD, Drew RJ, Marshall P, et al. Etiology of childhood bacteremia and timely antibiotics administration in the emergency department. Pediatrics. 2015;135(4): 635-642.
Clinical question: Have the causative organisms in pediatric bacteremia changed over time concurrent with introduction of the pneumococcal conjugate vaccine?
Background: Previous research has shown introduction of polyvalent pneumococcal conjugate vaccine led to changes in the organisms causing meningitis and otitis media, and patterns of nasopharyngeal colonization. Pneumococcus, historically, was a common cause of bacteremia. The availability of pneumococcal conjugate vaccine may have changed the organisms causing bacteremia in children.
Study design: Retrospective chart review and time series.
Setting: Children presenting to the ED of Alder Hey Children’s Hospital in Liverpool, England, from 2001 to 2011.
Synopsis: Five hundred seventy-five episodes of bacteremia were found in 525 children. Infants most commonly had E. coli and Group B streptococcal infections; children over age five most commonly had S. aureus. The introduction of the pneumococcal conjugate vaccine decreased pneumococcal bacteremia by 49% over the study period. This decrease was accompanied by an increase in Gram-negative bacteremia. Susceptibility to empiric antibiotics (third-generation cephalosporins) dropped from 96% to 83%. Over the study period, more children presented with central venous lines, which was felt to be due to increasing outpatient use of total parenteral nutrition (TPN).
Bottom line: Vaccination against pneumococcus is changing the microbiology of pediatric bacteremia, with fewer vaccine-preventable Gram-positive infections and more Gram-negative infections. This increases the likelihood of resistance to third-generation cephalosporins as empiric antibiotic.
Citation: Irwin AD, Drew RJ, Marshall P, et al. Etiology of childhood bacteremia and timely antibiotics administration in the emergency department. Pediatrics. 2015;135(4): 635-642.
What Should You Do If You Get a Needlestick?
EDITOR’S NOTE: This month’s KCQ first appeared in October 2010 and since that time has been one of our website’s most-read articles, generating nearly 35,000-plus page views. Enjoy it again this month!
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?

Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center, approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione and colleagues surveyed internal medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the CDC in 2004 suggests that because these numbers represent only self-reported injuries, the annual incidence of such injuries is much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
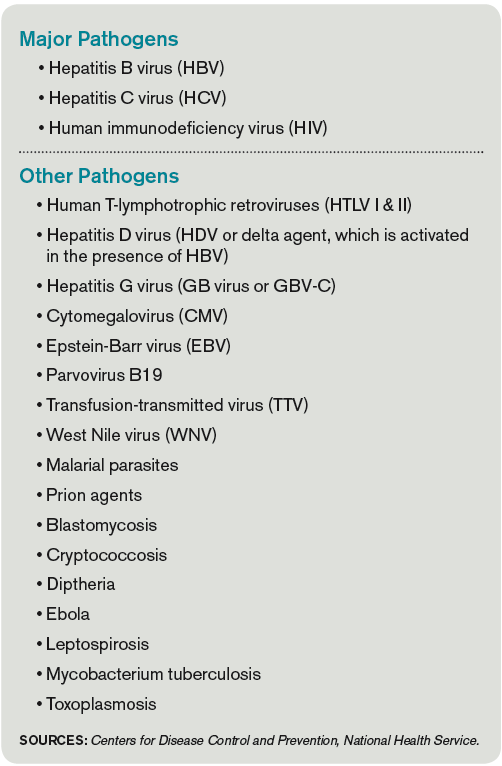
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
Because decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should be encouraged and supported in reporting all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
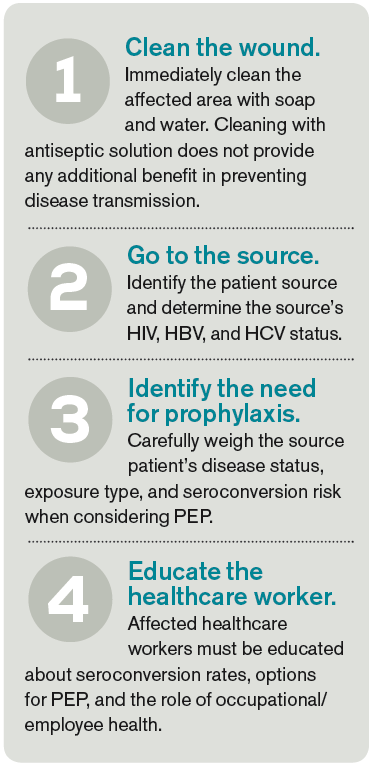
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Widespread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this improvement, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler and colleagues reported that, following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis (PEP), an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, PEP with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.

Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source ranges from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, because no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin; however, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
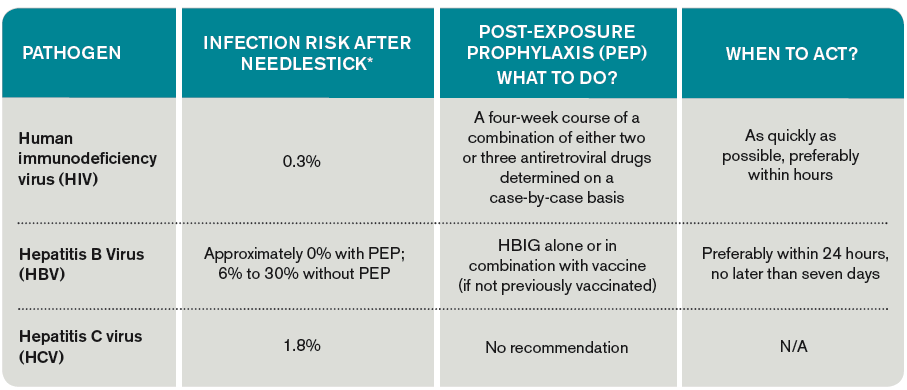
When testing is indicated, it should be done following institutional and state-specific exposure control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing the benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated and should be started as quickly as possible.3,8,10
The 2013 U.S. Public Health Service recommendations for PEP call for initiating three (or more) antiretroviral drugs for all occupational exposures. Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.10
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HBIG prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP.
Dr. Zehnder is a hospitalist and assistant professor of medicine at the University of Colorado Denver in Aurora.
References
- Mangione CM, Gerberding JL, Cummings SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, Cobden D, Pashos CL. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opin. 2005;21(5):741-747.
- Centers for Disease Control and Prevention. Workbook for designing, implementing, and evaluating a sharps injury prevention program. CDC website. Accessed May 31, 2015.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Centers for Disease Control and Prevention. Exposure to blood: What healthcare personnel need to know. CDC website. Accessed May 31, 2015.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Centers for Disease Control and Prevention. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Accessed May 31, 2015.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
- Updated US Public Health Service Guidelines for the management of occupational exposures to Human Immunodeficiency Virus and Recommendations for Postexposure Prophylaxis. Accessed May 31, 2015.
EDITOR’S NOTE: This month’s KCQ first appeared in October 2010 and since that time has been one of our website’s most-read articles, generating nearly 35,000-plus page views. Enjoy it again this month!
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center, approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione and colleagues surveyed internal medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the CDC in 2004 suggests that because these numbers represent only self-reported injuries, the annual incidence of such injuries is much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
Because decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should be encouraged and supported in reporting all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Widespread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this improvement, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler and colleagues reported that, following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis (PEP), an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, PEP with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source ranges from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, because no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin; however, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing the benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated and should be started as quickly as possible.3,8,10
The 2013 U.S. Public Health Service recommendations for PEP call for initiating three (or more) antiretroviral drugs for all occupational exposures. Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.10
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HBIG prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP.
Dr. Zehnder is a hospitalist and assistant professor of medicine at the University of Colorado Denver in Aurora.
References
- Mangione CM, Gerberding JL, Cummings SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, Cobden D, Pashos CL. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opin. 2005;21(5):741-747.
- Centers for Disease Control and Prevention. Workbook for designing, implementing, and evaluating a sharps injury prevention program. CDC website. Accessed May 31, 2015.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Centers for Disease Control and Prevention. Exposure to blood: What healthcare personnel need to know. CDC website. Accessed May 31, 2015.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Centers for Disease Control and Prevention. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Accessed May 31, 2015.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
- Updated US Public Health Service Guidelines for the management of occupational exposures to Human Immunodeficiency Virus and Recommendations for Postexposure Prophylaxis. Accessed May 31, 2015.
EDITOR’S NOTE: This month’s KCQ first appeared in October 2010 and since that time has been one of our website’s most-read articles, generating nearly 35,000-plus page views. Enjoy it again this month!
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center, approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione and colleagues surveyed internal medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the CDC in 2004 suggests that because these numbers represent only self-reported injuries, the annual incidence of such injuries is much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
Because decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should be encouraged and supported in reporting all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Widespread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this improvement, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler and colleagues reported that, following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis (PEP), an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, PEP with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source ranges from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, because no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin; however, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing the benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated and should be started as quickly as possible.3,8,10
The 2013 U.S. Public Health Service recommendations for PEP call for initiating three (or more) antiretroviral drugs for all occupational exposures. Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.10
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HBIG prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP.
Dr. Zehnder is a hospitalist and assistant professor of medicine at the University of Colorado Denver in Aurora.
References
- Mangione CM, Gerberding JL, Cummings SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, Cobden D, Pashos CL. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opin. 2005;21(5):741-747.
- Centers for Disease Control and Prevention. Workbook for designing, implementing, and evaluating a sharps injury prevention program. CDC website. Accessed May 31, 2015.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Centers for Disease Control and Prevention. Exposure to blood: What healthcare personnel need to know. CDC website. Accessed May 31, 2015.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Centers for Disease Control and Prevention. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Accessed May 31, 2015.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
- Updated US Public Health Service Guidelines for the management of occupational exposures to Human Immunodeficiency Virus and Recommendations for Postexposure Prophylaxis. Accessed May 31, 2015.