User login
New consensus on inpatient opioid use
SHM’s new recommendations to improve opioid prescribing for acute, noncancer pain in hospitalized adults will be the focus of Monday (April 9) morning’s session, “Opioids: What Now?”
Many patients who wind up on opioids for chronic pain start on the medications in an acute pain setting, said presenter Shoshana J. Herzig, MD, MPH, director of hospital medicine research at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston.
“Our prescribing patterns in the setting of acute pain meaningfully impact downstream outcomes and prescribing practices,” she said. “The degree of importance related to this topic often is underestimated by hospitalists, because we think of it as a more straightforward situation – prescribing for acute pain. In reality, there are nuances to it, and we have data to show that it’s not done well a lot of the time. It’s a big problem.”

During the session, “we’re going to do a case-based review that highlights the main points of the SHM consensus statement, just published in the Journal of Hospital Medicine [April issue],” Dr. Herzig said. She led the working group that developed the consensus statement. It features 16 suggestions to help hospital-based physicians appropriately employ opioids as part of their acute pain management strategies.
The copresenter will be Teryl K. Nuckols, MD, FHM, associate professor of medicine at the University of California, Los Angeles, and director of the division of internal medicine and associate professor of medicine at Cedars-Sinai Medical Center, Los Angeles. Dr. Nuckols was senior author of the JHM articles.
The presentation will assess the state of opioid prescribing in hospitalized patients and the challenges to acute pain management in hospitalized adults and explain how to improve prescribing practices to prevent opioid-related adverse events, opioid-use disorder, and long-term opioid use. Dr. Herzig and Dr. Nuckols will discuss how their group developed the new consensus statement by culling the key points from other physician group guidelines and present several case studies for interactive discussion to showcase the consensus statement suggestions. They also will go over topics in need of future research.
“We hope that attending the session and reading over the consensus statement will help to improve the appropriateness as well as the safety of opioid prescribing in the setting of acute pain in the hospital and help physicians recognize common pitfalls,” Dr. Herzig said. These include not remembering to combine opioids with nonopioid-based pharmacologic therapy; inappropriately continuing a patient on intravenous opioids when oral opioids, which have a lower risk of adverse outcomes, would suffice; and being able to identify patients at increased risk for opioid-related adverse events for whom a dose reduction or increased monitoring may be warranted.
Hospitalists should continue to strive to achieve a proper balance with opioids between offering adequate analgesia for their patients and the risk of adverse events, she said. “The need for judicious prescribing is our main take-home message. I hope that people leave with a better understanding of what a reasonable amount of opioids to prescribe on discharge looks like.”
Dr. Herzig receives financial compensation from SHM for her role as senior deputy editor of the Journal of Hospital Medicine (unrelated to the present work).
Opioids: What Now?
Monday, April 10:35-11:35 a.m.
Crystal Ballroom G1/A&B
SHM’s new recommendations to improve opioid prescribing for acute, noncancer pain in hospitalized adults will be the focus of Monday (April 9) morning’s session, “Opioids: What Now?”
Many patients who wind up on opioids for chronic pain start on the medications in an acute pain setting, said presenter Shoshana J. Herzig, MD, MPH, director of hospital medicine research at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston.
“Our prescribing patterns in the setting of acute pain meaningfully impact downstream outcomes and prescribing practices,” she said. “The degree of importance related to this topic often is underestimated by hospitalists, because we think of it as a more straightforward situation – prescribing for acute pain. In reality, there are nuances to it, and we have data to show that it’s not done well a lot of the time. It’s a big problem.”
During the session, “we’re going to do a case-based review that highlights the main points of the SHM consensus statement, just published in the Journal of Hospital Medicine [April issue],” Dr. Herzig said. She led the working group that developed the consensus statement. It features 16 suggestions to help hospital-based physicians appropriately employ opioids as part of their acute pain management strategies.
The copresenter will be Teryl K. Nuckols, MD, FHM, associate professor of medicine at the University of California, Los Angeles, and director of the division of internal medicine and associate professor of medicine at Cedars-Sinai Medical Center, Los Angeles. Dr. Nuckols was senior author of the JHM articles.
The presentation will assess the state of opioid prescribing in hospitalized patients and the challenges to acute pain management in hospitalized adults and explain how to improve prescribing practices to prevent opioid-related adverse events, opioid-use disorder, and long-term opioid use. Dr. Herzig and Dr. Nuckols will discuss how their group developed the new consensus statement by culling the key points from other physician group guidelines and present several case studies for interactive discussion to showcase the consensus statement suggestions. They also will go over topics in need of future research.
“We hope that attending the session and reading over the consensus statement will help to improve the appropriateness as well as the safety of opioid prescribing in the setting of acute pain in the hospital and help physicians recognize common pitfalls,” Dr. Herzig said. These include not remembering to combine opioids with nonopioid-based pharmacologic therapy; inappropriately continuing a patient on intravenous opioids when oral opioids, which have a lower risk of adverse outcomes, would suffice; and being able to identify patients at increased risk for opioid-related adverse events for whom a dose reduction or increased monitoring may be warranted.
Hospitalists should continue to strive to achieve a proper balance with opioids between offering adequate analgesia for their patients and the risk of adverse events, she said. “The need for judicious prescribing is our main take-home message. I hope that people leave with a better understanding of what a reasonable amount of opioids to prescribe on discharge looks like.”
Dr. Herzig receives financial compensation from SHM for her role as senior deputy editor of the Journal of Hospital Medicine (unrelated to the present work).
Opioids: What Now?
Monday, April 10:35-11:35 a.m.
Crystal Ballroom G1/A&B
SHM’s new recommendations to improve opioid prescribing for acute, noncancer pain in hospitalized adults will be the focus of Monday (April 9) morning’s session, “Opioids: What Now?”
Many patients who wind up on opioids for chronic pain start on the medications in an acute pain setting, said presenter Shoshana J. Herzig, MD, MPH, director of hospital medicine research at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston.
“Our prescribing patterns in the setting of acute pain meaningfully impact downstream outcomes and prescribing practices,” she said. “The degree of importance related to this topic often is underestimated by hospitalists, because we think of it as a more straightforward situation – prescribing for acute pain. In reality, there are nuances to it, and we have data to show that it’s not done well a lot of the time. It’s a big problem.”
During the session, “we’re going to do a case-based review that highlights the main points of the SHM consensus statement, just published in the Journal of Hospital Medicine [April issue],” Dr. Herzig said. She led the working group that developed the consensus statement. It features 16 suggestions to help hospital-based physicians appropriately employ opioids as part of their acute pain management strategies.
The copresenter will be Teryl K. Nuckols, MD, FHM, associate professor of medicine at the University of California, Los Angeles, and director of the division of internal medicine and associate professor of medicine at Cedars-Sinai Medical Center, Los Angeles. Dr. Nuckols was senior author of the JHM articles.
The presentation will assess the state of opioid prescribing in hospitalized patients and the challenges to acute pain management in hospitalized adults and explain how to improve prescribing practices to prevent opioid-related adverse events, opioid-use disorder, and long-term opioid use. Dr. Herzig and Dr. Nuckols will discuss how their group developed the new consensus statement by culling the key points from other physician group guidelines and present several case studies for interactive discussion to showcase the consensus statement suggestions. They also will go over topics in need of future research.
“We hope that attending the session and reading over the consensus statement will help to improve the appropriateness as well as the safety of opioid prescribing in the setting of acute pain in the hospital and help physicians recognize common pitfalls,” Dr. Herzig said. These include not remembering to combine opioids with nonopioid-based pharmacologic therapy; inappropriately continuing a patient on intravenous opioids when oral opioids, which have a lower risk of adverse outcomes, would suffice; and being able to identify patients at increased risk for opioid-related adverse events for whom a dose reduction or increased monitoring may be warranted.
Hospitalists should continue to strive to achieve a proper balance with opioids between offering adequate analgesia for their patients and the risk of adverse events, she said. “The need for judicious prescribing is our main take-home message. I hope that people leave with a better understanding of what a reasonable amount of opioids to prescribe on discharge looks like.”
Dr. Herzig receives financial compensation from SHM for her role as senior deputy editor of the Journal of Hospital Medicine (unrelated to the present work).
Opioids: What Now?
Monday, April 10:35-11:35 a.m.
Crystal Ballroom G1/A&B
FDA advisors recommend lofexidine for opioid withdrawal
SILVER SPRING, MD. – Members of the Food and Drug Administration Psychopharmacologic Drugs Advisory Committee voted 11 to 1 to recommend approval of lofexidine as the first nonopioid treatment option for the symptomatic treatment of opioid withdrawal.
Opioid withdrawal symptoms are the largest barrier to discontinuing opioid use, according to Louis Baxter, MD, executive medical director of the Professional Assistance Program in Princeton, N.J., who presented on behalf of U.S. WorldMeds, which plans to market lofexidine as Lucemyra.

Lofexidine, a selective alpha2-adrenergic receptor agonist that regulates norepinephrine release has been approved for management of opioid withdrawal in the United Kingdom since 1992.
The advisory committee voted to recommend lofexidine on the strength of the results of two randomized, double-blind, and placebo controlled phase 3 studies on the safety and efficacy of lofexidine for symptomatic treatment of opioid withdrawal between days 1 through 7. One study randomized 264 patients to lofexidine (134) or placebo (130), with patients in the treatment arm received 3.2 mg of lofexidine on days 1-5, then placebo until day 7. The second study randomized 603 patients to three groups, comparing high dose (3.2 mg/day) and low dose (2.4 mg/day) regimens of lofexidine to placebo; patients in the treatment arms took four smaller doses of lofexidine throughout the day to achieve the cumulative dose.
Researchers enrolled heavy users of short-acting opioids; heroin was the predominant agent. Both studies were conducted in the scenario of abrupt withdrawal, or the most intense withdrawal situation.
Symptomatic benefit was measured using the Short Opiate Withdrawal Scale of Gossop (SOWS-Gossop), a patient reported outcome. Patients were asked to rank their symptoms as none, mild, moderate or severe across measures like feeling sick, stomach cramps, and heart pounding among other symptoms.
Lofexidine increased completion of withdrawal treatment compared to placebo. Patients in the first study had a 5-day completion rate of 53%, compared to 35% for the placebo group. Researchers observed similar results in the 7-day completion rates the second study, with low and high dose completion rates of 42% and 40%, respectively, both of which were much higher than placebo (28%).
Lofexidine also reduced patient withdrawal symptoms, according to SOWS-Gossop scores during peak withdrawal. In the first study, SOWS-Gossop scores were 2-4 points lower in the lofexidine group compared to placebo. Similarly, the scores were significantly better in both lofexidine groups in the second study, compared to placebo, particularly on days 1 to 4. Decreasing withdrawal symptoms during this period is particularly important because this is the most vulnerable window for patient dropout, briefing documents from US WorldMeds.
Several notable adverse events occurred during the study, particularly at higher doses of lofexidine. The risk of bradycardia and hypotension are prominent in patients taking lofexidine, but these are risks associated with this class of drug, according to Mark Pirner, MD, senior medical director at US WorldMeds, who noted that “the lower dose, if that’s what ultimately gets approved [by the FDA], is safe and effective too.”
Development of lofexidine was conducted in collaboration with the National Institute on Drug Abuse and the FDA, according to briefing documents from US WorldMeds.
The Prescription Drug User Fee Act (PDUFA) for lofexidine is May 26; FDA actions on new drug applications often occur at near the PDUFA date.
The FDA is not obligated to follow the recommendations of its advisory committees.
SILVER SPRING, MD. – Members of the Food and Drug Administration Psychopharmacologic Drugs Advisory Committee voted 11 to 1 to recommend approval of lofexidine as the first nonopioid treatment option for the symptomatic treatment of opioid withdrawal.
Opioid withdrawal symptoms are the largest barrier to discontinuing opioid use, according to Louis Baxter, MD, executive medical director of the Professional Assistance Program in Princeton, N.J., who presented on behalf of U.S. WorldMeds, which plans to market lofexidine as Lucemyra.
Lofexidine, a selective alpha2-adrenergic receptor agonist that regulates norepinephrine release has been approved for management of opioid withdrawal in the United Kingdom since 1992.
The advisory committee voted to recommend lofexidine on the strength of the results of two randomized, double-blind, and placebo controlled phase 3 studies on the safety and efficacy of lofexidine for symptomatic treatment of opioid withdrawal between days 1 through 7. One study randomized 264 patients to lofexidine (134) or placebo (130), with patients in the treatment arm received 3.2 mg of lofexidine on days 1-5, then placebo until day 7. The second study randomized 603 patients to three groups, comparing high dose (3.2 mg/day) and low dose (2.4 mg/day) regimens of lofexidine to placebo; patients in the treatment arms took four smaller doses of lofexidine throughout the day to achieve the cumulative dose.
Researchers enrolled heavy users of short-acting opioids; heroin was the predominant agent. Both studies were conducted in the scenario of abrupt withdrawal, or the most intense withdrawal situation.
Symptomatic benefit was measured using the Short Opiate Withdrawal Scale of Gossop (SOWS-Gossop), a patient reported outcome. Patients were asked to rank their symptoms as none, mild, moderate or severe across measures like feeling sick, stomach cramps, and heart pounding among other symptoms.
Lofexidine increased completion of withdrawal treatment compared to placebo. Patients in the first study had a 5-day completion rate of 53%, compared to 35% for the placebo group. Researchers observed similar results in the 7-day completion rates the second study, with low and high dose completion rates of 42% and 40%, respectively, both of which were much higher than placebo (28%).
Lofexidine also reduced patient withdrawal symptoms, according to SOWS-Gossop scores during peak withdrawal. In the first study, SOWS-Gossop scores were 2-4 points lower in the lofexidine group compared to placebo. Similarly, the scores were significantly better in both lofexidine groups in the second study, compared to placebo, particularly on days 1 to 4. Decreasing withdrawal symptoms during this period is particularly important because this is the most vulnerable window for patient dropout, briefing documents from US WorldMeds.
Several notable adverse events occurred during the study, particularly at higher doses of lofexidine. The risk of bradycardia and hypotension are prominent in patients taking lofexidine, but these are risks associated with this class of drug, according to Mark Pirner, MD, senior medical director at US WorldMeds, who noted that “the lower dose, if that’s what ultimately gets approved [by the FDA], is safe and effective too.”
Development of lofexidine was conducted in collaboration with the National Institute on Drug Abuse and the FDA, according to briefing documents from US WorldMeds.
The Prescription Drug User Fee Act (PDUFA) for lofexidine is May 26; FDA actions on new drug applications often occur at near the PDUFA date.
The FDA is not obligated to follow the recommendations of its advisory committees.
SILVER SPRING, MD. – Members of the Food and Drug Administration Psychopharmacologic Drugs Advisory Committee voted 11 to 1 to recommend approval of lofexidine as the first nonopioid treatment option for the symptomatic treatment of opioid withdrawal.
Opioid withdrawal symptoms are the largest barrier to discontinuing opioid use, according to Louis Baxter, MD, executive medical director of the Professional Assistance Program in Princeton, N.J., who presented on behalf of U.S. WorldMeds, which plans to market lofexidine as Lucemyra.
Lofexidine, a selective alpha2-adrenergic receptor agonist that regulates norepinephrine release has been approved for management of opioid withdrawal in the United Kingdom since 1992.
The advisory committee voted to recommend lofexidine on the strength of the results of two randomized, double-blind, and placebo controlled phase 3 studies on the safety and efficacy of lofexidine for symptomatic treatment of opioid withdrawal between days 1 through 7. One study randomized 264 patients to lofexidine (134) or placebo (130), with patients in the treatment arm received 3.2 mg of lofexidine on days 1-5, then placebo until day 7. The second study randomized 603 patients to three groups, comparing high dose (3.2 mg/day) and low dose (2.4 mg/day) regimens of lofexidine to placebo; patients in the treatment arms took four smaller doses of lofexidine throughout the day to achieve the cumulative dose.
Researchers enrolled heavy users of short-acting opioids; heroin was the predominant agent. Both studies were conducted in the scenario of abrupt withdrawal, or the most intense withdrawal situation.
Symptomatic benefit was measured using the Short Opiate Withdrawal Scale of Gossop (SOWS-Gossop), a patient reported outcome. Patients were asked to rank their symptoms as none, mild, moderate or severe across measures like feeling sick, stomach cramps, and heart pounding among other symptoms.
Lofexidine increased completion of withdrawal treatment compared to placebo. Patients in the first study had a 5-day completion rate of 53%, compared to 35% for the placebo group. Researchers observed similar results in the 7-day completion rates the second study, with low and high dose completion rates of 42% and 40%, respectively, both of which were much higher than placebo (28%).
Lofexidine also reduced patient withdrawal symptoms, according to SOWS-Gossop scores during peak withdrawal. In the first study, SOWS-Gossop scores were 2-4 points lower in the lofexidine group compared to placebo. Similarly, the scores were significantly better in both lofexidine groups in the second study, compared to placebo, particularly on days 1 to 4. Decreasing withdrawal symptoms during this period is particularly important because this is the most vulnerable window for patient dropout, briefing documents from US WorldMeds.
Several notable adverse events occurred during the study, particularly at higher doses of lofexidine. The risk of bradycardia and hypotension are prominent in patients taking lofexidine, but these are risks associated with this class of drug, according to Mark Pirner, MD, senior medical director at US WorldMeds, who noted that “the lower dose, if that’s what ultimately gets approved [by the FDA], is safe and effective too.”
Development of lofexidine was conducted in collaboration with the National Institute on Drug Abuse and the FDA, according to briefing documents from US WorldMeds.
The Prescription Drug User Fee Act (PDUFA) for lofexidine is May 26; FDA actions on new drug applications often occur at near the PDUFA date.
The FDA is not obligated to follow the recommendations of its advisory committees.
REPORTING FROM AN FDA ADVISORY COMMITTEE MEETING

Major message: Most heart failure is preventable
SNOWMASS, COLO. – More than 960,000 new cases of heart failure will occur in the United States this year – and most of them could have been prevented, Gregg C. Fonarow, MD, asserted at the Annual Cardiovascular Conference at Snowmass.
Preventing heart failure doesn’t require heroic measures. It entails identifying high-risk individuals while they are still asymptomatic and free of structural heart disease – that is, patients who are stage A, pre–heart failure, in the American College of Cardiology/American Heart Association classification system for heart failure – and then addressing their modifiable risk factors via evidence-based, guideline-directed medical therapy, said Dr. Fonarow, professor of cardiovascular medicine and cochief of cardiology at the University of California, Los Angeles, and director of the Ahmanson-UCLA Cardiomyopathy Center.
A special word about obesity: A Framingham Heart Study analysis concluded that, after controlling for other cardiovascular risk factors, obese individuals had double the risk of new-onset heart failure, compared with normal weight subjects, during a mean follow-up of 14 years. For each one-unit increase in body mass index, the adjusted risk of heart failure climbed by 5% in men and 7% in women (N Engl J Med. 2002 Aug 1;347[5]:305-13). And that spells trouble down the line.
“You can imagine, with the marked increase in overweight and obesity status now affecting over half of U.S. adults, what this will mean for a potential rise in heart failure prevalence and incidence unless we do something further to modify this,” the cardiologist observed.
Dr. Fonarow is a member of the writing group for the ACC/AHA guidelines on management of heart failure. They recommend as a risk reduction strategy identification of patients with stage A pre–heart failure and addressing their risk factors: treating their hypertension and lipid disorders, gaining control over metabolic syndrome, discouraging heavy alcohol intake, and encouraging smoking cessation and regular exercise (J Am Coll Cardiol. 2013 Oct 15;62[16]:e147-239).
What kind of reduction in heart failure risk can be expected via these measures?
Antihypertensive therapy
More than a quarter century ago, the landmark SHEP trial (Systolic Hypertension in the Elderly Program) in more than 4,700 hypertensive seniors showed that treatment with diuretics and beta-blockers resulted in a 49% reduction in heart failure events, compared with placebo. And this has been a consistent finding in other studies: A meta-analysis of all 12 major randomized trials of antihypertensive therapy conducted over a 20-year period showed that treatment resulted in a whopping 52% reduction in the risk of heart failure (J Am Coll Cardiol. 1995 Apr; 27[5]:1214-8).
“If you ask most people why they’re on antihypertensive medication, they say, ‘Oh, to prevent heart attacks and stroke.’ But in fact the greatest relative risk reduction that we see is this remarkable reduction in the risk of developing heart failure with blood pressure treatment,” Dr. Fonarow said.
There has been some argument within medicine as to whether aggressive blood pressure lowering is appropriate in individuals over age 80. But in the HYVET trial (Hypertension in the Very Elderly Trial) conducted in that age group, the use of diuretics and/or ACE inhibitors to lower systolic blood pressure from roughly 155 mm Hg to 145 mm Hg resulted in a dramatic 64% reduction in the rate of new-onset heart failure (N Engl J Med. 2008 May 1;358[18]:1887-98).
How low to go with blood pressure reduction in order to maximize the heart failure risk reduction benefit? In the SPRINT trial (Systolic Blood Pressure Intervention Trial) of 9,361 hypertensive patients with a history of cardiovascular disease or multiple risk factors, participants randomized to a goal of less than 120 mm Hg enjoyed a 38% lower risk of heart failure events, compared with those whose target was less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16).
A secondary analysis from SPRINT showed that the risk of acute decompensated heart failure was 37% lower in patients treated to the target of less than 120 mm Hg. That finding takes on particular importance because SPRINT participants who developed acute decompensated heart failure had a 27-fold increase in cardiovascular death (Circ Heart Fail. 2017 Apr; doi: 10.1161/CIRCHEARTFAILURE.116.003613).
Lipid lowering
A meta-analysis of four major, randomized clinical trials of intensive versus moderate statin therapy in 27,546 patients with stable coronary artery disease or acute coronary syndrome concluded that intensive therapy resulted in a 27% reduction in the risk of hospitalization for heart failure (J Am Coll Cardiol. 2006 Jun 6;47[11]:2326-31).
SGLT-2 inhibition
Until the randomized EMPA-REG OUTCOME trial of the sodium-glucose transporter 2 (SGLT-2) inhibitor empagliflozin(Jardiance), no glucose-lowering drug available for treatment of type 2 diabetes had shown any benefit in terms of reducing diabetic patients’ elevated risk of heart failure. Neither had weight loss. Abundant evidence showed that glycemic control had no impact on the risk of heart failure events. So EMPA-REG OUTCOME was cause for celebration among heart failure specialists, with its demonstration of a 35% reduction in the risk of hospitalization for heart failure, compared with placebo in more than 7,000 randomized patients. The risk of death because of heart failure was chopped by 68%. Sharp reductions in other cardiovascular events were also seen with empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
Similar benefits were subsequently documented with another SGLT-2 inhibitor, canagliflozin(Invokana), in the CANVAS study program (N Engl J Med. 2017 Aug 17;377:644-57).
The reduction in cardiovascular mortality achieved with empagliflozin in EMPA-REG OUTCOME was actually bigger than seen with ACE inhibitors and angiotensin-receptor blockers (ARBs) in earlier landmark heart failure trials (Eur J Heart Fail. 2017 Jan;19[1]:43-53).
Dr. Fonarow views these data as “compelling.” These trials mark a huge step forward in the prevention of heart failure.
“We now for the first time in patients with diabetes have the ability to markedly prevent heart failure as well as cardiovascular death,” the cardiologist commented. “It is critical for cardiologists and heart failure specialists to play an active role in this [pharmacologic diabetes] management, as choice of therapy is a key determinant of outcomes, including survival.”
ACE inhibitors and ARBs
The ACC/AHA heart failure guidelines give a Class I recommendation to the routine use of ACE inhibitors or ARBs in patients at high risk for developing heart failure because of a history of diabetes, hypertension with associated cardiovascular risk factors, or any form of atherosclerotic vascular disease.
Lifestyle modification
Heavy drinking is known to raise the risk of heart failure. However, moderate alcohol consumption may be protective. In a classic prospective cohort study, individuals who reported consuming 1.5-4 drinks per day in the previous month had a 47% reduction in subsequent new-onset heart failure, compared with teetotalers in a multivariate analysis adjusted for conventional cardiovascular risk factors. Those who drank less than 1.5 drinks per day had a 21% reduction in heart failure risk, compared with the nondrinkers (JAMA. 2001 Apr 18;285[15]:1971-7).
In the prospective observational Physicians’ Health Study of nearly 21,000 men, adherence to six modifiable healthy lifestyle factors was associated with an incremental stepwise reduction in lifetime risk of developing heart failure. The six lifestyle factors – a forerunner of the AHA’s Life’s Simple 7 – were maintaining a normal body weight, stopping smoking, getting exercise, drinking alcohol in moderation, consuming breakfast cereals, and eating fruits and vegetables. Male physicians who shunned all six had a 21.2% lifetime risk of heart failure; those who followed at least four of the healthy lifestyle factors had a 10.1% risk (JAMA 2009 Jul 22;302[4]:394-400).
In a separate analysis from the Physicians’ Health Study, men who engaged in vigorous exercise to the point of breaking a sweat as little as one to three times per month had an 18% lower risk of developing heart failure during follow-up, compared with inactive men (Circulation 2009 Jan 6;119[1]:44-52).
What’s next in prevention of heart failure
Heart failure is one of the most expensive health care problems in the United States, and one of the deadliest. Today an estimated 6.5 million Americans have symptomatic heart failure. But that’s just the tip of the iceberg.
“Countless millions more are likely to manifest heart failure in the future,” Dr. Fonarow warned, noting the vast prevalence of identifiable risk factors.
It’s time for a high-visibility public health campaign designed to foster community education and engagement regarding heart failure prevention, he added.
“We have a lot of action and events around preventing atherosclerotic cardiovascular disease. But can you think of any campaign you’ve seen focusing specifically on heart failure? Heart failure isn’t one of the endpoints in the ACC/AHA Atherosclerotic Cardiovascular Disease Risk Calculator or even the new hypertension risk calculator, so we need to take this a whole lot more seriously,” the cardiologist said.
The 2017 focused update of the ACC/AHA heart failure guidelines endorsed a novel strategy of primary care–centered, biomarker-based screening of patients with cardiovascular risk factors as a means of triggering early intervention to prevent heart failure (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803). This strategy, which received a Class IIa recommendation, involves screening measurement of a natriuretic peptide biomarker.
The recommendation was based on evidence including the STOP-HF randomized trial (St. Vincent’s Screening to Prevent Heart Failure Study), in which 1,374 asymptomatic Irish patients with cardiovascular risk factors were randomized to routine primary care or primary care plus screening with brain-type natriuretic peptide testing. Patients with a brain-type natriuretic peptide level of 50 pg/mL or more were directed to team-based care involving a collaboration between their primary care physician and a specialist cardiovascular service focused on optimizing guideline-directed medical therapy. During a mean follow-up of 4.2 years, the primary endpoint of new-onset left ventricular dysfunction occurred in 5.3% of the intervention group and 8.7% of controls, for a 45% relative risk reduction (JAMA 2013 Jul 3;310[1]:66-74).
Dr. Fonarow reported receiving research grants from and serving as a consultant to the National Heart, Lung, and Blood Institute and a handful of medical companies.
SNOWMASS, COLO. – More than 960,000 new cases of heart failure will occur in the United States this year – and most of them could have been prevented, Gregg C. Fonarow, MD, asserted at the Annual Cardiovascular Conference at Snowmass.
Preventing heart failure doesn’t require heroic measures. It entails identifying high-risk individuals while they are still asymptomatic and free of structural heart disease – that is, patients who are stage A, pre–heart failure, in the American College of Cardiology/American Heart Association classification system for heart failure – and then addressing their modifiable risk factors via evidence-based, guideline-directed medical therapy, said Dr. Fonarow, professor of cardiovascular medicine and cochief of cardiology at the University of California, Los Angeles, and director of the Ahmanson-UCLA Cardiomyopathy Center.
A special word about obesity: A Framingham Heart Study analysis concluded that, after controlling for other cardiovascular risk factors, obese individuals had double the risk of new-onset heart failure, compared with normal weight subjects, during a mean follow-up of 14 years. For each one-unit increase in body mass index, the adjusted risk of heart failure climbed by 5% in men and 7% in women (N Engl J Med. 2002 Aug 1;347[5]:305-13). And that spells trouble down the line.
“You can imagine, with the marked increase in overweight and obesity status now affecting over half of U.S. adults, what this will mean for a potential rise in heart failure prevalence and incidence unless we do something further to modify this,” the cardiologist observed.
Dr. Fonarow is a member of the writing group for the ACC/AHA guidelines on management of heart failure. They recommend as a risk reduction strategy identification of patients with stage A pre–heart failure and addressing their risk factors: treating their hypertension and lipid disorders, gaining control over metabolic syndrome, discouraging heavy alcohol intake, and encouraging smoking cessation and regular exercise (J Am Coll Cardiol. 2013 Oct 15;62[16]:e147-239).
What kind of reduction in heart failure risk can be expected via these measures?
Antihypertensive therapy
More than a quarter century ago, the landmark SHEP trial (Systolic Hypertension in the Elderly Program) in more than 4,700 hypertensive seniors showed that treatment with diuretics and beta-blockers resulted in a 49% reduction in heart failure events, compared with placebo. And this has been a consistent finding in other studies: A meta-analysis of all 12 major randomized trials of antihypertensive therapy conducted over a 20-year period showed that treatment resulted in a whopping 52% reduction in the risk of heart failure (J Am Coll Cardiol. 1995 Apr; 27[5]:1214-8).
“If you ask most people why they’re on antihypertensive medication, they say, ‘Oh, to prevent heart attacks and stroke.’ But in fact the greatest relative risk reduction that we see is this remarkable reduction in the risk of developing heart failure with blood pressure treatment,” Dr. Fonarow said.
There has been some argument within medicine as to whether aggressive blood pressure lowering is appropriate in individuals over age 80. But in the HYVET trial (Hypertension in the Very Elderly Trial) conducted in that age group, the use of diuretics and/or ACE inhibitors to lower systolic blood pressure from roughly 155 mm Hg to 145 mm Hg resulted in a dramatic 64% reduction in the rate of new-onset heart failure (N Engl J Med. 2008 May 1;358[18]:1887-98).
How low to go with blood pressure reduction in order to maximize the heart failure risk reduction benefit? In the SPRINT trial (Systolic Blood Pressure Intervention Trial) of 9,361 hypertensive patients with a history of cardiovascular disease or multiple risk factors, participants randomized to a goal of less than 120 mm Hg enjoyed a 38% lower risk of heart failure events, compared with those whose target was less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16).
A secondary analysis from SPRINT showed that the risk of acute decompensated heart failure was 37% lower in patients treated to the target of less than 120 mm Hg. That finding takes on particular importance because SPRINT participants who developed acute decompensated heart failure had a 27-fold increase in cardiovascular death (Circ Heart Fail. 2017 Apr; doi: 10.1161/CIRCHEARTFAILURE.116.003613).
Lipid lowering
A meta-analysis of four major, randomized clinical trials of intensive versus moderate statin therapy in 27,546 patients with stable coronary artery disease or acute coronary syndrome concluded that intensive therapy resulted in a 27% reduction in the risk of hospitalization for heart failure (J Am Coll Cardiol. 2006 Jun 6;47[11]:2326-31).
SGLT-2 inhibition
Until the randomized EMPA-REG OUTCOME trial of the sodium-glucose transporter 2 (SGLT-2) inhibitor empagliflozin(Jardiance), no glucose-lowering drug available for treatment of type 2 diabetes had shown any benefit in terms of reducing diabetic patients’ elevated risk of heart failure. Neither had weight loss. Abundant evidence showed that glycemic control had no impact on the risk of heart failure events. So EMPA-REG OUTCOME was cause for celebration among heart failure specialists, with its demonstration of a 35% reduction in the risk of hospitalization for heart failure, compared with placebo in more than 7,000 randomized patients. The risk of death because of heart failure was chopped by 68%. Sharp reductions in other cardiovascular events were also seen with empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
Similar benefits were subsequently documented with another SGLT-2 inhibitor, canagliflozin(Invokana), in the CANVAS study program (N Engl J Med. 2017 Aug 17;377:644-57).
The reduction in cardiovascular mortality achieved with empagliflozin in EMPA-REG OUTCOME was actually bigger than seen with ACE inhibitors and angiotensin-receptor blockers (ARBs) in earlier landmark heart failure trials (Eur J Heart Fail. 2017 Jan;19[1]:43-53).
Dr. Fonarow views these data as “compelling.” These trials mark a huge step forward in the prevention of heart failure.
“We now for the first time in patients with diabetes have the ability to markedly prevent heart failure as well as cardiovascular death,” the cardiologist commented. “It is critical for cardiologists and heart failure specialists to play an active role in this [pharmacologic diabetes] management, as choice of therapy is a key determinant of outcomes, including survival.”
ACE inhibitors and ARBs
The ACC/AHA heart failure guidelines give a Class I recommendation to the routine use of ACE inhibitors or ARBs in patients at high risk for developing heart failure because of a history of diabetes, hypertension with associated cardiovascular risk factors, or any form of atherosclerotic vascular disease.
Lifestyle modification
Heavy drinking is known to raise the risk of heart failure. However, moderate alcohol consumption may be protective. In a classic prospective cohort study, individuals who reported consuming 1.5-4 drinks per day in the previous month had a 47% reduction in subsequent new-onset heart failure, compared with teetotalers in a multivariate analysis adjusted for conventional cardiovascular risk factors. Those who drank less than 1.5 drinks per day had a 21% reduction in heart failure risk, compared with the nondrinkers (JAMA. 2001 Apr 18;285[15]:1971-7).
In the prospective observational Physicians’ Health Study of nearly 21,000 men, adherence to six modifiable healthy lifestyle factors was associated with an incremental stepwise reduction in lifetime risk of developing heart failure. The six lifestyle factors – a forerunner of the AHA’s Life’s Simple 7 – were maintaining a normal body weight, stopping smoking, getting exercise, drinking alcohol in moderation, consuming breakfast cereals, and eating fruits and vegetables. Male physicians who shunned all six had a 21.2% lifetime risk of heart failure; those who followed at least four of the healthy lifestyle factors had a 10.1% risk (JAMA 2009 Jul 22;302[4]:394-400).
In a separate analysis from the Physicians’ Health Study, men who engaged in vigorous exercise to the point of breaking a sweat as little as one to three times per month had an 18% lower risk of developing heart failure during follow-up, compared with inactive men (Circulation 2009 Jan 6;119[1]:44-52).
What’s next in prevention of heart failure
Heart failure is one of the most expensive health care problems in the United States, and one of the deadliest. Today an estimated 6.5 million Americans have symptomatic heart failure. But that’s just the tip of the iceberg.
“Countless millions more are likely to manifest heart failure in the future,” Dr. Fonarow warned, noting the vast prevalence of identifiable risk factors.
It’s time for a high-visibility public health campaign designed to foster community education and engagement regarding heart failure prevention, he added.
“We have a lot of action and events around preventing atherosclerotic cardiovascular disease. But can you think of any campaign you’ve seen focusing specifically on heart failure? Heart failure isn’t one of the endpoints in the ACC/AHA Atherosclerotic Cardiovascular Disease Risk Calculator or even the new hypertension risk calculator, so we need to take this a whole lot more seriously,” the cardiologist said.
The 2017 focused update of the ACC/AHA heart failure guidelines endorsed a novel strategy of primary care–centered, biomarker-based screening of patients with cardiovascular risk factors as a means of triggering early intervention to prevent heart failure (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803). This strategy, which received a Class IIa recommendation, involves screening measurement of a natriuretic peptide biomarker.
The recommendation was based on evidence including the STOP-HF randomized trial (St. Vincent’s Screening to Prevent Heart Failure Study), in which 1,374 asymptomatic Irish patients with cardiovascular risk factors were randomized to routine primary care or primary care plus screening with brain-type natriuretic peptide testing. Patients with a brain-type natriuretic peptide level of 50 pg/mL or more were directed to team-based care involving a collaboration between their primary care physician and a specialist cardiovascular service focused on optimizing guideline-directed medical therapy. During a mean follow-up of 4.2 years, the primary endpoint of new-onset left ventricular dysfunction occurred in 5.3% of the intervention group and 8.7% of controls, for a 45% relative risk reduction (JAMA 2013 Jul 3;310[1]:66-74).
Dr. Fonarow reported receiving research grants from and serving as a consultant to the National Heart, Lung, and Blood Institute and a handful of medical companies.
SNOWMASS, COLO. – More than 960,000 new cases of heart failure will occur in the United States this year – and most of them could have been prevented, Gregg C. Fonarow, MD, asserted at the Annual Cardiovascular Conference at Snowmass.
Preventing heart failure doesn’t require heroic measures. It entails identifying high-risk individuals while they are still asymptomatic and free of structural heart disease – that is, patients who are stage A, pre–heart failure, in the American College of Cardiology/American Heart Association classification system for heart failure – and then addressing their modifiable risk factors via evidence-based, guideline-directed medical therapy, said Dr. Fonarow, professor of cardiovascular medicine and cochief of cardiology at the University of California, Los Angeles, and director of the Ahmanson-UCLA Cardiomyopathy Center.
A special word about obesity: A Framingham Heart Study analysis concluded that, after controlling for other cardiovascular risk factors, obese individuals had double the risk of new-onset heart failure, compared with normal weight subjects, during a mean follow-up of 14 years. For each one-unit increase in body mass index, the adjusted risk of heart failure climbed by 5% in men and 7% in women (N Engl J Med. 2002 Aug 1;347[5]:305-13). And that spells trouble down the line.
“You can imagine, with the marked increase in overweight and obesity status now affecting over half of U.S. adults, what this will mean for a potential rise in heart failure prevalence and incidence unless we do something further to modify this,” the cardiologist observed.
Dr. Fonarow is a member of the writing group for the ACC/AHA guidelines on management of heart failure. They recommend as a risk reduction strategy identification of patients with stage A pre–heart failure and addressing their risk factors: treating their hypertension and lipid disorders, gaining control over metabolic syndrome, discouraging heavy alcohol intake, and encouraging smoking cessation and regular exercise (J Am Coll Cardiol. 2013 Oct 15;62[16]:e147-239).
What kind of reduction in heart failure risk can be expected via these measures?
Antihypertensive therapy
More than a quarter century ago, the landmark SHEP trial (Systolic Hypertension in the Elderly Program) in more than 4,700 hypertensive seniors showed that treatment with diuretics and beta-blockers resulted in a 49% reduction in heart failure events, compared with placebo. And this has been a consistent finding in other studies: A meta-analysis of all 12 major randomized trials of antihypertensive therapy conducted over a 20-year period showed that treatment resulted in a whopping 52% reduction in the risk of heart failure (J Am Coll Cardiol. 1995 Apr; 27[5]:1214-8).
“If you ask most people why they’re on antihypertensive medication, they say, ‘Oh, to prevent heart attacks and stroke.’ But in fact the greatest relative risk reduction that we see is this remarkable reduction in the risk of developing heart failure with blood pressure treatment,” Dr. Fonarow said.
There has been some argument within medicine as to whether aggressive blood pressure lowering is appropriate in individuals over age 80. But in the HYVET trial (Hypertension in the Very Elderly Trial) conducted in that age group, the use of diuretics and/or ACE inhibitors to lower systolic blood pressure from roughly 155 mm Hg to 145 mm Hg resulted in a dramatic 64% reduction in the rate of new-onset heart failure (N Engl J Med. 2008 May 1;358[18]:1887-98).
How low to go with blood pressure reduction in order to maximize the heart failure risk reduction benefit? In the SPRINT trial (Systolic Blood Pressure Intervention Trial) of 9,361 hypertensive patients with a history of cardiovascular disease or multiple risk factors, participants randomized to a goal of less than 120 mm Hg enjoyed a 38% lower risk of heart failure events, compared with those whose target was less than 140 mm Hg (N Engl J Med. 2015 Nov 26;373[22]:2103-16).
A secondary analysis from SPRINT showed that the risk of acute decompensated heart failure was 37% lower in patients treated to the target of less than 120 mm Hg. That finding takes on particular importance because SPRINT participants who developed acute decompensated heart failure had a 27-fold increase in cardiovascular death (Circ Heart Fail. 2017 Apr; doi: 10.1161/CIRCHEARTFAILURE.116.003613).
Lipid lowering
A meta-analysis of four major, randomized clinical trials of intensive versus moderate statin therapy in 27,546 patients with stable coronary artery disease or acute coronary syndrome concluded that intensive therapy resulted in a 27% reduction in the risk of hospitalization for heart failure (J Am Coll Cardiol. 2006 Jun 6;47[11]:2326-31).
SGLT-2 inhibition
Until the randomized EMPA-REG OUTCOME trial of the sodium-glucose transporter 2 (SGLT-2) inhibitor empagliflozin(Jardiance), no glucose-lowering drug available for treatment of type 2 diabetes had shown any benefit in terms of reducing diabetic patients’ elevated risk of heart failure. Neither had weight loss. Abundant evidence showed that glycemic control had no impact on the risk of heart failure events. So EMPA-REG OUTCOME was cause for celebration among heart failure specialists, with its demonstration of a 35% reduction in the risk of hospitalization for heart failure, compared with placebo in more than 7,000 randomized patients. The risk of death because of heart failure was chopped by 68%. Sharp reductions in other cardiovascular events were also seen with empagliflozin (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
Similar benefits were subsequently documented with another SGLT-2 inhibitor, canagliflozin(Invokana), in the CANVAS study program (N Engl J Med. 2017 Aug 17;377:644-57).
The reduction in cardiovascular mortality achieved with empagliflozin in EMPA-REG OUTCOME was actually bigger than seen with ACE inhibitors and angiotensin-receptor blockers (ARBs) in earlier landmark heart failure trials (Eur J Heart Fail. 2017 Jan;19[1]:43-53).
Dr. Fonarow views these data as “compelling.” These trials mark a huge step forward in the prevention of heart failure.
“We now for the first time in patients with diabetes have the ability to markedly prevent heart failure as well as cardiovascular death,” the cardiologist commented. “It is critical for cardiologists and heart failure specialists to play an active role in this [pharmacologic diabetes] management, as choice of therapy is a key determinant of outcomes, including survival.”
ACE inhibitors and ARBs
The ACC/AHA heart failure guidelines give a Class I recommendation to the routine use of ACE inhibitors or ARBs in patients at high risk for developing heart failure because of a history of diabetes, hypertension with associated cardiovascular risk factors, or any form of atherosclerotic vascular disease.
Lifestyle modification
Heavy drinking is known to raise the risk of heart failure. However, moderate alcohol consumption may be protective. In a classic prospective cohort study, individuals who reported consuming 1.5-4 drinks per day in the previous month had a 47% reduction in subsequent new-onset heart failure, compared with teetotalers in a multivariate analysis adjusted for conventional cardiovascular risk factors. Those who drank less than 1.5 drinks per day had a 21% reduction in heart failure risk, compared with the nondrinkers (JAMA. 2001 Apr 18;285[15]:1971-7).
In the prospective observational Physicians’ Health Study of nearly 21,000 men, adherence to six modifiable healthy lifestyle factors was associated with an incremental stepwise reduction in lifetime risk of developing heart failure. The six lifestyle factors – a forerunner of the AHA’s Life’s Simple 7 – were maintaining a normal body weight, stopping smoking, getting exercise, drinking alcohol in moderation, consuming breakfast cereals, and eating fruits and vegetables. Male physicians who shunned all six had a 21.2% lifetime risk of heart failure; those who followed at least four of the healthy lifestyle factors had a 10.1% risk (JAMA 2009 Jul 22;302[4]:394-400).
In a separate analysis from the Physicians’ Health Study, men who engaged in vigorous exercise to the point of breaking a sweat as little as one to three times per month had an 18% lower risk of developing heart failure during follow-up, compared with inactive men (Circulation 2009 Jan 6;119[1]:44-52).
What’s next in prevention of heart failure
Heart failure is one of the most expensive health care problems in the United States, and one of the deadliest. Today an estimated 6.5 million Americans have symptomatic heart failure. But that’s just the tip of the iceberg.
“Countless millions more are likely to manifest heart failure in the future,” Dr. Fonarow warned, noting the vast prevalence of identifiable risk factors.
It’s time for a high-visibility public health campaign designed to foster community education and engagement regarding heart failure prevention, he added.
“We have a lot of action and events around preventing atherosclerotic cardiovascular disease. But can you think of any campaign you’ve seen focusing specifically on heart failure? Heart failure isn’t one of the endpoints in the ACC/AHA Atherosclerotic Cardiovascular Disease Risk Calculator or even the new hypertension risk calculator, so we need to take this a whole lot more seriously,” the cardiologist said.
The 2017 focused update of the ACC/AHA heart failure guidelines endorsed a novel strategy of primary care–centered, biomarker-based screening of patients with cardiovascular risk factors as a means of triggering early intervention to prevent heart failure (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803). This strategy, which received a Class IIa recommendation, involves screening measurement of a natriuretic peptide biomarker.
The recommendation was based on evidence including the STOP-HF randomized trial (St. Vincent’s Screening to Prevent Heart Failure Study), in which 1,374 asymptomatic Irish patients with cardiovascular risk factors were randomized to routine primary care or primary care plus screening with brain-type natriuretic peptide testing. Patients with a brain-type natriuretic peptide level of 50 pg/mL or more were directed to team-based care involving a collaboration between their primary care physician and a specialist cardiovascular service focused on optimizing guideline-directed medical therapy. During a mean follow-up of 4.2 years, the primary endpoint of new-onset left ventricular dysfunction occurred in 5.3% of the intervention group and 8.7% of controls, for a 45% relative risk reduction (JAMA 2013 Jul 3;310[1]:66-74).
Dr. Fonarow reported receiving research grants from and serving as a consultant to the National Heart, Lung, and Blood Institute and a handful of medical companies.
EXPERT ANALYSIS FROM THE ANNUAL CARDIOVASCULAR CONFERENCE AT SNOWMASS
Top hospital heart failure performance translates to longer survival
ORLANDO – Hospitals in the first quartile of short-term performance in treating heart failure patients had higher long-term survival rates for those patients, based on data from 317 hospitals that participated in a voluntary quality improvement program.
The burden of heart failure remains substantial in the United States, and health policies are increasingly focused on improving care for heart failure patients, said Ambarish Pandey, MD, of the University of Texas, Dallas, in a presentation at the annual meeting of the American College of Cardiology.

The researchers assessed hospital performance based on 30-day risk-standardized mortality rates (RSMR) in hospitals participating in the Get With the Guidelines–Heart Failure (GWTG-HF) registry, using a hierarchical, logistic regression model to calculate hospital-specific 30-day RSMRs.
Get With the Guidelines is a voluntary, observational quality improvement program that has been linked with CMS to capture long-term follow-up data, Dr. Pandey explained.
The study included 106,304 heart failure patients older than 65 years at 317 GWTG hospitals across the United States during 2005-2013. The hospitals were divided into performance quartiles based on 30-day RSMR. The 30-day RSMRs were 8.6%, 9.4%, 9.9%, and 10.7% in the first, second, third, and fourth quartiles, respectively.
There was a strong association between the top-performing hospitals and long-term survival rates for the patients that persisted beyond 30 days, said Dr. Pandey. The mortality rates after 5 years were 75.6%, 76.2%, 76.9%, and 79.6%, in the first, second, third, and fourth quartiles, respectively.
The hospitals in the first quartile were more likely than those in the fourth quartile to have primary percutaneous coronary intervention capabilities (80% vs. 73%), in-house cardiac surgery (66% vs. 57%), and a heart transplant center (13% vs. 2%).
In addition, the hospitals in the highest quartile had higher rates of adherence than those in the lowest quartile to guideline-directed heart failure therapies, including evidence-based beta-blocker use, ACE inhibitor and angiotensin receptor blocker use, postdischarge heart failure follow-up, implantable cardioverter defibrillator placement prior to discharge, and cardiac resynchronization therapy prior to discharge.The study was limited by a possible lack of generalizability to hospitals not participating in the GWTG program, Dr. Pandey said. In addition, “we cannot establish causation between hospital performance based on 30-day RSMR and long-term survival.”
However, the long-term survival advantage for heart failure patients treated at hospitals with the highest measures of short-term performance suggests that the 30-day RSMR could be used as an incentive for quality care and the improvement of long-term outcomes, he said.
Dr. Pandey had no financial conflicts to disclose. The Get With the Guidelines–Heart Failure program is supported by the American Heart Association, and has been previously funded by Medtronic, GlaxoSmithKline, Ortho-McNeil, and the AHA Pharmaceutical Roundtable. The findings were published simultaneously in JAMA Cardiology (2018 Mar 12. doi:10.1001/jamacardio.2018.0579).
SOURCE: Pandy A. ACC 2018.
ORLANDO – Hospitals in the first quartile of short-term performance in treating heart failure patients had higher long-term survival rates for those patients, based on data from 317 hospitals that participated in a voluntary quality improvement program.
The burden of heart failure remains substantial in the United States, and health policies are increasingly focused on improving care for heart failure patients, said Ambarish Pandey, MD, of the University of Texas, Dallas, in a presentation at the annual meeting of the American College of Cardiology.
The researchers assessed hospital performance based on 30-day risk-standardized mortality rates (RSMR) in hospitals participating in the Get With the Guidelines–Heart Failure (GWTG-HF) registry, using a hierarchical, logistic regression model to calculate hospital-specific 30-day RSMRs.
Get With the Guidelines is a voluntary, observational quality improvement program that has been linked with CMS to capture long-term follow-up data, Dr. Pandey explained.
The study included 106,304 heart failure patients older than 65 years at 317 GWTG hospitals across the United States during 2005-2013. The hospitals were divided into performance quartiles based on 30-day RSMR. The 30-day RSMRs were 8.6%, 9.4%, 9.9%, and 10.7% in the first, second, third, and fourth quartiles, respectively.
There was a strong association between the top-performing hospitals and long-term survival rates for the patients that persisted beyond 30 days, said Dr. Pandey. The mortality rates after 5 years were 75.6%, 76.2%, 76.9%, and 79.6%, in the first, second, third, and fourth quartiles, respectively.
The hospitals in the first quartile were more likely than those in the fourth quartile to have primary percutaneous coronary intervention capabilities (80% vs. 73%), in-house cardiac surgery (66% vs. 57%), and a heart transplant center (13% vs. 2%).
In addition, the hospitals in the highest quartile had higher rates of adherence than those in the lowest quartile to guideline-directed heart failure therapies, including evidence-based beta-blocker use, ACE inhibitor and angiotensin receptor blocker use, postdischarge heart failure follow-up, implantable cardioverter defibrillator placement prior to discharge, and cardiac resynchronization therapy prior to discharge.The study was limited by a possible lack of generalizability to hospitals not participating in the GWTG program, Dr. Pandey said. In addition, “we cannot establish causation between hospital performance based on 30-day RSMR and long-term survival.”
However, the long-term survival advantage for heart failure patients treated at hospitals with the highest measures of short-term performance suggests that the 30-day RSMR could be used as an incentive for quality care and the improvement of long-term outcomes, he said.
Dr. Pandey had no financial conflicts to disclose. The Get With the Guidelines–Heart Failure program is supported by the American Heart Association, and has been previously funded by Medtronic, GlaxoSmithKline, Ortho-McNeil, and the AHA Pharmaceutical Roundtable. The findings were published simultaneously in JAMA Cardiology (2018 Mar 12. doi:10.1001/jamacardio.2018.0579).
SOURCE: Pandy A. ACC 2018.
ORLANDO – Hospitals in the first quartile of short-term performance in treating heart failure patients had higher long-term survival rates for those patients, based on data from 317 hospitals that participated in a voluntary quality improvement program.
The burden of heart failure remains substantial in the United States, and health policies are increasingly focused on improving care for heart failure patients, said Ambarish Pandey, MD, of the University of Texas, Dallas, in a presentation at the annual meeting of the American College of Cardiology.
The researchers assessed hospital performance based on 30-day risk-standardized mortality rates (RSMR) in hospitals participating in the Get With the Guidelines–Heart Failure (GWTG-HF) registry, using a hierarchical, logistic regression model to calculate hospital-specific 30-day RSMRs.
Get With the Guidelines is a voluntary, observational quality improvement program that has been linked with CMS to capture long-term follow-up data, Dr. Pandey explained.
The study included 106,304 heart failure patients older than 65 years at 317 GWTG hospitals across the United States during 2005-2013. The hospitals were divided into performance quartiles based on 30-day RSMR. The 30-day RSMRs were 8.6%, 9.4%, 9.9%, and 10.7% in the first, second, third, and fourth quartiles, respectively.
There was a strong association between the top-performing hospitals and long-term survival rates for the patients that persisted beyond 30 days, said Dr. Pandey. The mortality rates after 5 years were 75.6%, 76.2%, 76.9%, and 79.6%, in the first, second, third, and fourth quartiles, respectively.
The hospitals in the first quartile were more likely than those in the fourth quartile to have primary percutaneous coronary intervention capabilities (80% vs. 73%), in-house cardiac surgery (66% vs. 57%), and a heart transplant center (13% vs. 2%).
In addition, the hospitals in the highest quartile had higher rates of adherence than those in the lowest quartile to guideline-directed heart failure therapies, including evidence-based beta-blocker use, ACE inhibitor and angiotensin receptor blocker use, postdischarge heart failure follow-up, implantable cardioverter defibrillator placement prior to discharge, and cardiac resynchronization therapy prior to discharge.The study was limited by a possible lack of generalizability to hospitals not participating in the GWTG program, Dr. Pandey said. In addition, “we cannot establish causation between hospital performance based on 30-day RSMR and long-term survival.”
However, the long-term survival advantage for heart failure patients treated at hospitals with the highest measures of short-term performance suggests that the 30-day RSMR could be used as an incentive for quality care and the improvement of long-term outcomes, he said.
Dr. Pandey had no financial conflicts to disclose. The Get With the Guidelines–Heart Failure program is supported by the American Heart Association, and has been previously funded by Medtronic, GlaxoSmithKline, Ortho-McNeil, and the AHA Pharmaceutical Roundtable. The findings were published simultaneously in JAMA Cardiology (2018 Mar 12. doi:10.1001/jamacardio.2018.0579).
SOURCE: Pandy A. ACC 2018.
REPORTING FROM ACC 2018
Key clinical point:
Major finding: Hospitals in the lowest quartile had a 22% higher 5-year mortality rate for heart failure patients compared with the highest quartile hospitals.
Study details: The data come from 106,304 heart failure patients admitted to 317 hospitals participating in a voluntary quality improvement program.
Disclosures: Dr. Pandey had no financial conflicts to disclose. The Get With the Guidelines–Heart Failure program is supported by the American Heart Association, and has been previously funded by Medtronic, GlaxoSmithKline, Ortho-McNeil, and the AHA Pharmaceutical Roundtable.
Source: Pandey A. ACC 2018.
VIDEO: Andexanet alfa effectively reverses factor Xa anticoagulant
ORLANDO – Andexanet alfa, a new agent that reverses the anticoagulant effect of direct factor Xa inhibitors, showed an acceptable level of efficacy and safety in 227 patients who received the drug in the agent’s pivotal trial.
These results, which placed andexanet in the same ballpark for efficacy and safety as idarucizumab (Praxbind), approved in 2015 for reversing the anticoagulant dabigatran (Pradaxa), suggest that andexanet is likely on track for its own Food and Drug Administration marketing approval, Stuart Connolly, MD, said at the annual meeting of the American College of Cardiology.

Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa) previously announced that it expected Food and Drug Administration action on its marketing application by May 2018.
Andexanet reversal “has similar efficacy and safety as seen with other reversal agents” for other types of anticoagulants, said Dr. Connolly, a professor of medicine and an electrophysiologist at McMaster University in Hamilton, Ont. In the trial results he reported, andexanet treatment of patients who were bleeding while on treatment with a direct factor Xa inhibitor had an 83% rate of hemostatic efficacy and an 11% rate of thrombotic events. By comparison, idarucizumab, the FDA-approved reversal agent for the anticoagulant dabigatran, produced a 68% hemostatic efficacy and a 6% rate of thrombotic events in the idarucizumab pivotal trial, RE-VERSE AD (N Engl J Med. 2015 Aug 6;373[6]:511-20).

The Prospective, Open-Label Study of Andexanet Alfa in Patients Receiving a Factor Xa Inhibitor Who Have Acute Major Bleeding (ANNEXA-4) enrolled 227 patients at any of 60 centers, with efficacy data available from 132 of the patients. About 60% of the patients had an intracranial bleed, and about 30% had a gastrointestinal bleed, and their average age was 77 years. Roughly three-quarters of patients were on an anticoagulant for atrial fibrillation, with the rest treated for venous thromboembolism, with 4% having both conditions. The most commonly used direct factor Xa inhbitors in these patients were apixaban (Eliquis) in 105 and rivaroxaban (Xarelto) in 75. The ANNEXA-4 study has not enrolled patients treated with a direct factor Xa inhibitor anticoagulant and undergoing surgery, a setting that will be the subject of a future study, Dr. Connolly said.
Clinicians administered andexanet alfa as a bolus followed by a 2-hour continuous infusion, with hemostatic efficacy assessed 12 hours after the start of treatment. The results showed that factor Xa inhibition fell by about 75%-90% within minutes of starting the bolus and remained depressed at that level during the infusion but then began recovering by 2 hours after the stop of infusion. Andexanet is a factor Xa “decoy” molecule that acts by latching onto the inhibitor molecules and thereby preventing them from interacting with actual factor Xa, but andexanet also has a short half life and hence the effect quickly reduces once treatment stops.
“There is no doubt that andexanet rapidly decreases anti–factor Xa activity,” he said.
Adjudicated efficacy results were available for 132 patients and showed good or excellent hemostasis achieved on andexanet in 109 patients (83%), Dr. Connolly reported. The effect on hemostasis was consistent regardless of patient age, sex, bleeding site, type of anticoagulant, and dosage tested.
Thrombotic events during the 30 days following treatment occurred in 24 of 227 patients (11%) who received andexanet and were evaluable for safety. Notably, no clustering of thrombotic events occurred early, even among the 129 patients who restarted on an anticoagulant during the 30 days after treatment. Among the 129 patients who restarted on an anticoagulant, 9 (7%) had a thrombotic event during the 30-day follow-up, compared with 15 events among 98 patients (15%) who did not restart on an anticoagulant.
Dr. Connolly acknowledged that a limitation of the ANNEXA-4 study is the absence of a control group, but he added that he and his associates believed randomizing patients with a serious bleed to placebo control would not have been “practical, feasible, or ethical.”
ANNEXA-4 is sponsored by Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa). Dr. Connolly has been a consultant to Portola, and also to Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, and Sanofi-Aventis. Dr. Kirtane has received research support from several device manufacturers.
SOURCE: Connolly S. ACC 2018.
Treatment with andexanet alfa produced good or excellent hemostasis in 83% of patients in the ANNEXA-4 study, which is what matters when patients are bleeding. Clinicians want to know that you can restore coagulation to a level where you can stop bleeding, and that’s what the results show.
The lack of a reversal agent until now for direct-acting factor Xa inhibitor drugs has probably been a modest but real obstacle to widespread adoption of these agents. We can look at the example of another new oral anticoagulant, dabigatran (Pradaxa), which works by a different mechanism, specifically by inhibiting thrombin. After a reversal agent for dabigatran, idarucizumab (Praxbind) received Food and Drug Administration approval and became available in late 2015, an uptick in dabigatran prescriptions occurred. That experience shows that patients and providers want the safety net of a reversal agent. They want to know that, if there is bleeding or need for urgent surgery, there is a way to facilitate restoration of hemostasis.
It’s the same with direct factor Xa inhibitors: Some patients are concerned about the lack of a reversal agent, and having such an agent may help increase access to these agents for such patients. I think that, once andexanet becomes available for routine U.S. practice, we’ll see an uptick in prescribing of direct factor Xa inhibitors. Also, some patients who have opted for treatment with warfarin will switch to a safer class of drugs, the direct factor X a inhibitors. A myth exists that reversal agents can easily negate the anticoagulant effect of warfarin. The reality is that, despite having treatments that reverse warfarin’s effect, this is often not an easy process in actual practice.
On the safety side, there was no indication in the ANNEXA-4 results of rebound thrombosis with andexanet alfa treatment. Patients receiving a direct factor Xa inhibitor are prothrombotic – that’s why they are on an anticoagulant – so their risk for a thrombotic event is always there, especially when they are not fully anticoagulated, such as when a reversal agent is administered. We need to look to restarting treatment with an anticoagulant because these patients have a high thrombotic risk.
Gregory Piazza, MD , is a cardiologist at Brigham and Women’s Hospital in Boston. He has been an advisor to Portola Pharmaceuticals, the company developing andexanet alfa, as well as to Bayer and Pfizer, and he has received research funding from Bristol-Myers Squibb, Janssen, and Daiichi Sankyo. He made these comments in an interview .
Treatment with andexanet alfa produced good or excellent hemostasis in 83% of patients in the ANNEXA-4 study, which is what matters when patients are bleeding. Clinicians want to know that you can restore coagulation to a level where you can stop bleeding, and that’s what the results show.
The lack of a reversal agent until now for direct-acting factor Xa inhibitor drugs has probably been a modest but real obstacle to widespread adoption of these agents. We can look at the example of another new oral anticoagulant, dabigatran (Pradaxa), which works by a different mechanism, specifically by inhibiting thrombin. After a reversal agent for dabigatran, idarucizumab (Praxbind) received Food and Drug Administration approval and became available in late 2015, an uptick in dabigatran prescriptions occurred. That experience shows that patients and providers want the safety net of a reversal agent. They want to know that, if there is bleeding or need for urgent surgery, there is a way to facilitate restoration of hemostasis.
It’s the same with direct factor Xa inhibitors: Some patients are concerned about the lack of a reversal agent, and having such an agent may help increase access to these agents for such patients. I think that, once andexanet becomes available for routine U.S. practice, we’ll see an uptick in prescribing of direct factor Xa inhibitors. Also, some patients who have opted for treatment with warfarin will switch to a safer class of drugs, the direct factor X a inhibitors. A myth exists that reversal agents can easily negate the anticoagulant effect of warfarin. The reality is that, despite having treatments that reverse warfarin’s effect, this is often not an easy process in actual practice.
On the safety side, there was no indication in the ANNEXA-4 results of rebound thrombosis with andexanet alfa treatment. Patients receiving a direct factor Xa inhibitor are prothrombotic – that’s why they are on an anticoagulant – so their risk for a thrombotic event is always there, especially when they are not fully anticoagulated, such as when a reversal agent is administered. We need to look to restarting treatment with an anticoagulant because these patients have a high thrombotic risk.
Gregory Piazza, MD , is a cardiologist at Brigham and Women’s Hospital in Boston. He has been an advisor to Portola Pharmaceuticals, the company developing andexanet alfa, as well as to Bayer and Pfizer, and he has received research funding from Bristol-Myers Squibb, Janssen, and Daiichi Sankyo. He made these comments in an interview .
Treatment with andexanet alfa produced good or excellent hemostasis in 83% of patients in the ANNEXA-4 study, which is what matters when patients are bleeding. Clinicians want to know that you can restore coagulation to a level where you can stop bleeding, and that’s what the results show.
The lack of a reversal agent until now for direct-acting factor Xa inhibitor drugs has probably been a modest but real obstacle to widespread adoption of these agents. We can look at the example of another new oral anticoagulant, dabigatran (Pradaxa), which works by a different mechanism, specifically by inhibiting thrombin. After a reversal agent for dabigatran, idarucizumab (Praxbind) received Food and Drug Administration approval and became available in late 2015, an uptick in dabigatran prescriptions occurred. That experience shows that patients and providers want the safety net of a reversal agent. They want to know that, if there is bleeding or need for urgent surgery, there is a way to facilitate restoration of hemostasis.
It’s the same with direct factor Xa inhibitors: Some patients are concerned about the lack of a reversal agent, and having such an agent may help increase access to these agents for such patients. I think that, once andexanet becomes available for routine U.S. practice, we’ll see an uptick in prescribing of direct factor Xa inhibitors. Also, some patients who have opted for treatment with warfarin will switch to a safer class of drugs, the direct factor X a inhibitors. A myth exists that reversal agents can easily negate the anticoagulant effect of warfarin. The reality is that, despite having treatments that reverse warfarin’s effect, this is often not an easy process in actual practice.
On the safety side, there was no indication in the ANNEXA-4 results of rebound thrombosis with andexanet alfa treatment. Patients receiving a direct factor Xa inhibitor are prothrombotic – that’s why they are on an anticoagulant – so their risk for a thrombotic event is always there, especially when they are not fully anticoagulated, such as when a reversal agent is administered. We need to look to restarting treatment with an anticoagulant because these patients have a high thrombotic risk.
Gregory Piazza, MD , is a cardiologist at Brigham and Women’s Hospital in Boston. He has been an advisor to Portola Pharmaceuticals, the company developing andexanet alfa, as well as to Bayer and Pfizer, and he has received research funding from Bristol-Myers Squibb, Janssen, and Daiichi Sankyo. He made these comments in an interview .
ORLANDO – Andexanet alfa, a new agent that reverses the anticoagulant effect of direct factor Xa inhibitors, showed an acceptable level of efficacy and safety in 227 patients who received the drug in the agent’s pivotal trial.
These results, which placed andexanet in the same ballpark for efficacy and safety as idarucizumab (Praxbind), approved in 2015 for reversing the anticoagulant dabigatran (Pradaxa), suggest that andexanet is likely on track for its own Food and Drug Administration marketing approval, Stuart Connolly, MD, said at the annual meeting of the American College of Cardiology.
Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa) previously announced that it expected Food and Drug Administration action on its marketing application by May 2018.
Andexanet reversal “has similar efficacy and safety as seen with other reversal agents” for other types of anticoagulants, said Dr. Connolly, a professor of medicine and an electrophysiologist at McMaster University in Hamilton, Ont. In the trial results he reported, andexanet treatment of patients who were bleeding while on treatment with a direct factor Xa inhibitor had an 83% rate of hemostatic efficacy and an 11% rate of thrombotic events. By comparison, idarucizumab, the FDA-approved reversal agent for the anticoagulant dabigatran, produced a 68% hemostatic efficacy and a 6% rate of thrombotic events in the idarucizumab pivotal trial, RE-VERSE AD (N Engl J Med. 2015 Aug 6;373[6]:511-20).
The Prospective, Open-Label Study of Andexanet Alfa in Patients Receiving a Factor Xa Inhibitor Who Have Acute Major Bleeding (ANNEXA-4) enrolled 227 patients at any of 60 centers, with efficacy data available from 132 of the patients. About 60% of the patients had an intracranial bleed, and about 30% had a gastrointestinal bleed, and their average age was 77 years. Roughly three-quarters of patients were on an anticoagulant for atrial fibrillation, with the rest treated for venous thromboembolism, with 4% having both conditions. The most commonly used direct factor Xa inhbitors in these patients were apixaban (Eliquis) in 105 and rivaroxaban (Xarelto) in 75. The ANNEXA-4 study has not enrolled patients treated with a direct factor Xa inhibitor anticoagulant and undergoing surgery, a setting that will be the subject of a future study, Dr. Connolly said.
Clinicians administered andexanet alfa as a bolus followed by a 2-hour continuous infusion, with hemostatic efficacy assessed 12 hours after the start of treatment. The results showed that factor Xa inhibition fell by about 75%-90% within minutes of starting the bolus and remained depressed at that level during the infusion but then began recovering by 2 hours after the stop of infusion. Andexanet is a factor Xa “decoy” molecule that acts by latching onto the inhibitor molecules and thereby preventing them from interacting with actual factor Xa, but andexanet also has a short half life and hence the effect quickly reduces once treatment stops.
“There is no doubt that andexanet rapidly decreases anti–factor Xa activity,” he said.
Adjudicated efficacy results were available for 132 patients and showed good or excellent hemostasis achieved on andexanet in 109 patients (83%), Dr. Connolly reported. The effect on hemostasis was consistent regardless of patient age, sex, bleeding site, type of anticoagulant, and dosage tested.
Thrombotic events during the 30 days following treatment occurred in 24 of 227 patients (11%) who received andexanet and were evaluable for safety. Notably, no clustering of thrombotic events occurred early, even among the 129 patients who restarted on an anticoagulant during the 30 days after treatment. Among the 129 patients who restarted on an anticoagulant, 9 (7%) had a thrombotic event during the 30-day follow-up, compared with 15 events among 98 patients (15%) who did not restart on an anticoagulant.
Dr. Connolly acknowledged that a limitation of the ANNEXA-4 study is the absence of a control group, but he added that he and his associates believed randomizing patients with a serious bleed to placebo control would not have been “practical, feasible, or ethical.”
ANNEXA-4 is sponsored by Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa). Dr. Connolly has been a consultant to Portola, and also to Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, and Sanofi-Aventis. Dr. Kirtane has received research support from several device manufacturers.
SOURCE: Connolly S. ACC 2018.
ORLANDO – Andexanet alfa, a new agent that reverses the anticoagulant effect of direct factor Xa inhibitors, showed an acceptable level of efficacy and safety in 227 patients who received the drug in the agent’s pivotal trial.
These results, which placed andexanet in the same ballpark for efficacy and safety as idarucizumab (Praxbind), approved in 2015 for reversing the anticoagulant dabigatran (Pradaxa), suggest that andexanet is likely on track for its own Food and Drug Administration marketing approval, Stuart Connolly, MD, said at the annual meeting of the American College of Cardiology.
Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa) previously announced that it expected Food and Drug Administration action on its marketing application by May 2018.
Andexanet reversal “has similar efficacy and safety as seen with other reversal agents” for other types of anticoagulants, said Dr. Connolly, a professor of medicine and an electrophysiologist at McMaster University in Hamilton, Ont. In the trial results he reported, andexanet treatment of patients who were bleeding while on treatment with a direct factor Xa inhibitor had an 83% rate of hemostatic efficacy and an 11% rate of thrombotic events. By comparison, idarucizumab, the FDA-approved reversal agent for the anticoagulant dabigatran, produced a 68% hemostatic efficacy and a 6% rate of thrombotic events in the idarucizumab pivotal trial, RE-VERSE AD (N Engl J Med. 2015 Aug 6;373[6]:511-20).
The Prospective, Open-Label Study of Andexanet Alfa in Patients Receiving a Factor Xa Inhibitor Who Have Acute Major Bleeding (ANNEXA-4) enrolled 227 patients at any of 60 centers, with efficacy data available from 132 of the patients. About 60% of the patients had an intracranial bleed, and about 30% had a gastrointestinal bleed, and their average age was 77 years. Roughly three-quarters of patients were on an anticoagulant for atrial fibrillation, with the rest treated for venous thromboembolism, with 4% having both conditions. The most commonly used direct factor Xa inhbitors in these patients were apixaban (Eliquis) in 105 and rivaroxaban (Xarelto) in 75. The ANNEXA-4 study has not enrolled patients treated with a direct factor Xa inhibitor anticoagulant and undergoing surgery, a setting that will be the subject of a future study, Dr. Connolly said.
Clinicians administered andexanet alfa as a bolus followed by a 2-hour continuous infusion, with hemostatic efficacy assessed 12 hours after the start of treatment. The results showed that factor Xa inhibition fell by about 75%-90% within minutes of starting the bolus and remained depressed at that level during the infusion but then began recovering by 2 hours after the stop of infusion. Andexanet is a factor Xa “decoy” molecule that acts by latching onto the inhibitor molecules and thereby preventing them from interacting with actual factor Xa, but andexanet also has a short half life and hence the effect quickly reduces once treatment stops.
“There is no doubt that andexanet rapidly decreases anti–factor Xa activity,” he said.
Adjudicated efficacy results were available for 132 patients and showed good or excellent hemostasis achieved on andexanet in 109 patients (83%), Dr. Connolly reported. The effect on hemostasis was consistent regardless of patient age, sex, bleeding site, type of anticoagulant, and dosage tested.
Thrombotic events during the 30 days following treatment occurred in 24 of 227 patients (11%) who received andexanet and were evaluable for safety. Notably, no clustering of thrombotic events occurred early, even among the 129 patients who restarted on an anticoagulant during the 30 days after treatment. Among the 129 patients who restarted on an anticoagulant, 9 (7%) had a thrombotic event during the 30-day follow-up, compared with 15 events among 98 patients (15%) who did not restart on an anticoagulant.
Dr. Connolly acknowledged that a limitation of the ANNEXA-4 study is the absence of a control group, but he added that he and his associates believed randomizing patients with a serious bleed to placebo control would not have been “practical, feasible, or ethical.”
ANNEXA-4 is sponsored by Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa). Dr. Connolly has been a consultant to Portola, and also to Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, and Sanofi-Aventis. Dr. Kirtane has received research support from several device manufacturers.
SOURCE: Connolly S. ACC 2018.
REPORTING FROM ACC 18
Key clinical point:
Major finding: Hemostatic efficacy of andexanet alfa was 83%, and thrombotic events occurred in 11%.
Study details: ANNEXA-4, a single arm cohort study with 227 patients.
Disclosures: ANNEXA-4 is sponsored by Portola Pharmaceuticals, the company developing andexanet alfa (AndexXa). Dr. Connolly has been a consultant to Portola and also to Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, and Sanofi-Aventis.
Source: Connolly S. ACC 2018.
Beware of polypharmacy in patients taking warfarin
SAN DIEGO – The incidence of polypharmacy among patients on warfarin therapy appears to peak at age 75, with close to 10 concurrent active prescriptions on average, results from a single-center study showed.
“Beware of polypharmacy with these patients,” Alan Jacobson, MD, said in an interview at the biennial summit of the Thrombosis & Hemostasis Societies of North America. “Anticoagulation tends to be a high-risk area. If you don’t treat, people have strokes. If you treat, they can have bleeds. Warfarin is the number one drug that gets older patients into the ER and admitted. We know that warfarin has a lot of drug-drug interactions.”

For example, in the ARISTOTLE trial, patients used a median of six drugs, and 26% of patients used nine or more drugs (BMJ. 2016 Jun 15;353:i2868.
In an effort to determine the average and maximum number of concurrent prescription drugs for age-dependent brackets of patients on warfarin, Dr. Jacobson and his associates reviewed the electronic pharmacy records of 1,122 warfarin patients at the VA Loma Linda Healthcare System. They excluded medications that could be obtained over the counter and calculated the average number of concurrent drugs for each of 10 age brackets: under age 50, over age 90, and eight brackets between those limits.
The researchers reported that 9,885 prescriptions were tabulated for the study population, which translated into a per patient average of 8.8 concurrent active prescription drugs, independent of age. They observed an age-dependent increase in the number of concurrent drugs that peaked at 9.9 among patients aged 70-74 years, and tapered off in those older than age 75. One patient in the 70- to 74-year-old age group was on 28 active prescriptions.
“If you’re on 28 pills, your chance of a bleeding complication is high,” Dr. Jacobson said. “We try to be rigorous with all of our patients on education. With these patients, slow the conversation down more. Have a family member come in with them and go into more detail.”
He added that the maximum number of concurrent prescriptions for any single patient in each age bracket tended to be two to three times higher than that of the average patient.
Dr. Jacobson acknowledged certain limitations of the study, including its single-center design and relatively small sample size. There was also no comparison available as to the number of concurrent prescriptions for patients not receiving warfarin. He reported having no financial disclosures.
[email protected]
SOURCE: Jacobson M et al. THSNA 2018. Poster 2.
SAN DIEGO – The incidence of polypharmacy among patients on warfarin therapy appears to peak at age 75, with close to 10 concurrent active prescriptions on average, results from a single-center study showed.
“Beware of polypharmacy with these patients,” Alan Jacobson, MD, said in an interview at the biennial summit of the Thrombosis & Hemostasis Societies of North America. “Anticoagulation tends to be a high-risk area. If you don’t treat, people have strokes. If you treat, they can have bleeds. Warfarin is the number one drug that gets older patients into the ER and admitted. We know that warfarin has a lot of drug-drug interactions.”
For example, in the ARISTOTLE trial, patients used a median of six drugs, and 26% of patients used nine or more drugs (BMJ. 2016 Jun 15;353:i2868.
In an effort to determine the average and maximum number of concurrent prescription drugs for age-dependent brackets of patients on warfarin, Dr. Jacobson and his associates reviewed the electronic pharmacy records of 1,122 warfarin patients at the VA Loma Linda Healthcare System. They excluded medications that could be obtained over the counter and calculated the average number of concurrent drugs for each of 10 age brackets: under age 50, over age 90, and eight brackets between those limits.
The researchers reported that 9,885 prescriptions were tabulated for the study population, which translated into a per patient average of 8.8 concurrent active prescription drugs, independent of age. They observed an age-dependent increase in the number of concurrent drugs that peaked at 9.9 among patients aged 70-74 years, and tapered off in those older than age 75. One patient in the 70- to 74-year-old age group was on 28 active prescriptions.
“If you’re on 28 pills, your chance of a bleeding complication is high,” Dr. Jacobson said. “We try to be rigorous with all of our patients on education. With these patients, slow the conversation down more. Have a family member come in with them and go into more detail.”
He added that the maximum number of concurrent prescriptions for any single patient in each age bracket tended to be two to three times higher than that of the average patient.
Dr. Jacobson acknowledged certain limitations of the study, including its single-center design and relatively small sample size. There was also no comparison available as to the number of concurrent prescriptions for patients not receiving warfarin. He reported having no financial disclosures.
[email protected]
SOURCE: Jacobson M et al. THSNA 2018. Poster 2.
SAN DIEGO – The incidence of polypharmacy among patients on warfarin therapy appears to peak at age 75, with close to 10 concurrent active prescriptions on average, results from a single-center study showed.
“Beware of polypharmacy with these patients,” Alan Jacobson, MD, said in an interview at the biennial summit of the Thrombosis & Hemostasis Societies of North America. “Anticoagulation tends to be a high-risk area. If you don’t treat, people have strokes. If you treat, they can have bleeds. Warfarin is the number one drug that gets older patients into the ER and admitted. We know that warfarin has a lot of drug-drug interactions.”
For example, in the ARISTOTLE trial, patients used a median of six drugs, and 26% of patients used nine or more drugs (BMJ. 2016 Jun 15;353:i2868.
In an effort to determine the average and maximum number of concurrent prescription drugs for age-dependent brackets of patients on warfarin, Dr. Jacobson and his associates reviewed the electronic pharmacy records of 1,122 warfarin patients at the VA Loma Linda Healthcare System. They excluded medications that could be obtained over the counter and calculated the average number of concurrent drugs for each of 10 age brackets: under age 50, over age 90, and eight brackets between those limits.
The researchers reported that 9,885 prescriptions were tabulated for the study population, which translated into a per patient average of 8.8 concurrent active prescription drugs, independent of age. They observed an age-dependent increase in the number of concurrent drugs that peaked at 9.9 among patients aged 70-74 years, and tapered off in those older than age 75. One patient in the 70- to 74-year-old age group was on 28 active prescriptions.
“If you’re on 28 pills, your chance of a bleeding complication is high,” Dr. Jacobson said. “We try to be rigorous with all of our patients on education. With these patients, slow the conversation down more. Have a family member come in with them and go into more detail.”
He added that the maximum number of concurrent prescriptions for any single patient in each age bracket tended to be two to three times higher than that of the average patient.
Dr. Jacobson acknowledged certain limitations of the study, including its single-center design and relatively small sample size. There was also no comparison available as to the number of concurrent prescriptions for patients not receiving warfarin. He reported having no financial disclosures.
[email protected]
SOURCE: Jacobson M et al. THSNA 2018. Poster 2.
REPORTING FROM THSNA 2018
Key clinical point:
Major finding: On average, warfarin patients had 8.8 concurrent active prescription drugs.
Study details: A review of medical records from 1,122 warfarin patients.
Disclosures: Dr. Jacobson reported having no financial disclosures.
Source: Jacobson A et al. THSNA 2018. Poster 2.
Making structural improvements in health care
Every day, hospitalists devote time and energy to the best practices that can limit the spread of infection and the development of antibiotic resistance. Infection Prevention (IP) and Antimicrobial Stewardship (ASP) are two hospital programs that address that same goal.
But there may be a more effective approach possible, according to Jerome A. Leis, MD, MSc, FRCPC, of the Centre for Quality Improvement and Patient Safety at the University of Toronto.
“Despite the high-quality evidence supporting these IP/ASP interventions, our approach to adding these to our current practice sometimes feels like adding scaffolding to a rickety building,” he said. “It supports the underlying structure, but remove the scaffolding without fixing the building, and it may just come tumbling down.” Sometimes the work seems like an uphill battle, he added, as the same problems continue to recur.
That’s because there’s a systemic element to the problems. “Hospitalists know first hand about how the system that we work in makes it difficult to ensure that all the best IP/ASP practices are adhered to all the time,” Dr. Leis said. “Simply reminding staff to remove a urinary catheter in a timely fashion or clean their hands every single time they touch a patient or the environment can only get us so far.” That’s where improvement science comes in.
The relatively new field of improvement science provides a framework for research focused on health care improvement; its goal is to determine which improvement strategies are most effective. Dr. Leis argued that, “when our approach to IP and ASP incorporate principles of improvement science, we are more likely to be successful in achieving sustainable changes in practice.”
Rather than constantly adding extra steps and reminders for hospitalists about patient safety, he said, we need to recognize that there are systemic factors that lead to specific practices. “Our focus should be to use improvement-science methodology to understand these barriers and redesign the processes of care in a way that makes it easier for hospitalists to adhere to the best IP/ASP practices for our patients.”
These structural changes should come from collaboration among content experts in IP/ASP and those with training in improvement science, he said – many IP and ASP programs are already putting this in practice, using improvement science to create safer systems of care.
Reference
Leis J. Advancing infection prevention and antimicrobial stewardship through improvement science. BMJ Qual Saf. 2017 Jun 14. doi: 10.1136/bmjqs-2017-006793.
Every day, hospitalists devote time and energy to the best practices that can limit the spread of infection and the development of antibiotic resistance. Infection Prevention (IP) and Antimicrobial Stewardship (ASP) are two hospital programs that address that same goal.
But there may be a more effective approach possible, according to Jerome A. Leis, MD, MSc, FRCPC, of the Centre for Quality Improvement and Patient Safety at the University of Toronto.
“Despite the high-quality evidence supporting these IP/ASP interventions, our approach to adding these to our current practice sometimes feels like adding scaffolding to a rickety building,” he said. “It supports the underlying structure, but remove the scaffolding without fixing the building, and it may just come tumbling down.” Sometimes the work seems like an uphill battle, he added, as the same problems continue to recur.
That’s because there’s a systemic element to the problems. “Hospitalists know first hand about how the system that we work in makes it difficult to ensure that all the best IP/ASP practices are adhered to all the time,” Dr. Leis said. “Simply reminding staff to remove a urinary catheter in a timely fashion or clean their hands every single time they touch a patient or the environment can only get us so far.” That’s where improvement science comes in.
The relatively new field of improvement science provides a framework for research focused on health care improvement; its goal is to determine which improvement strategies are most effective. Dr. Leis argued that, “when our approach to IP and ASP incorporate principles of improvement science, we are more likely to be successful in achieving sustainable changes in practice.”
Rather than constantly adding extra steps and reminders for hospitalists about patient safety, he said, we need to recognize that there are systemic factors that lead to specific practices. “Our focus should be to use improvement-science methodology to understand these barriers and redesign the processes of care in a way that makes it easier for hospitalists to adhere to the best IP/ASP practices for our patients.”
These structural changes should come from collaboration among content experts in IP/ASP and those with training in improvement science, he said – many IP and ASP programs are already putting this in practice, using improvement science to create safer systems of care.
Reference
Leis J. Advancing infection prevention and antimicrobial stewardship through improvement science. BMJ Qual Saf. 2017 Jun 14. doi: 10.1136/bmjqs-2017-006793.
Every day, hospitalists devote time and energy to the best practices that can limit the spread of infection and the development of antibiotic resistance. Infection Prevention (IP) and Antimicrobial Stewardship (ASP) are two hospital programs that address that same goal.
But there may be a more effective approach possible, according to Jerome A. Leis, MD, MSc, FRCPC, of the Centre for Quality Improvement and Patient Safety at the University of Toronto.
“Despite the high-quality evidence supporting these IP/ASP interventions, our approach to adding these to our current practice sometimes feels like adding scaffolding to a rickety building,” he said. “It supports the underlying structure, but remove the scaffolding without fixing the building, and it may just come tumbling down.” Sometimes the work seems like an uphill battle, he added, as the same problems continue to recur.
That’s because there’s a systemic element to the problems. “Hospitalists know first hand about how the system that we work in makes it difficult to ensure that all the best IP/ASP practices are adhered to all the time,” Dr. Leis said. “Simply reminding staff to remove a urinary catheter in a timely fashion or clean their hands every single time they touch a patient or the environment can only get us so far.” That’s where improvement science comes in.
The relatively new field of improvement science provides a framework for research focused on health care improvement; its goal is to determine which improvement strategies are most effective. Dr. Leis argued that, “when our approach to IP and ASP incorporate principles of improvement science, we are more likely to be successful in achieving sustainable changes in practice.”
Rather than constantly adding extra steps and reminders for hospitalists about patient safety, he said, we need to recognize that there are systemic factors that lead to specific practices. “Our focus should be to use improvement-science methodology to understand these barriers and redesign the processes of care in a way that makes it easier for hospitalists to adhere to the best IP/ASP practices for our patients.”
These structural changes should come from collaboration among content experts in IP/ASP and those with training in improvement science, he said – many IP and ASP programs are already putting this in practice, using improvement science to create safer systems of care.
Reference
Leis J. Advancing infection prevention and antimicrobial stewardship through improvement science. BMJ Qual Saf. 2017 Jun 14. doi: 10.1136/bmjqs-2017-006793.
Abdominal pain with high transaminases
A 54-year-old woman presents with severe abdominal pain lasting 3 hours. The pain came on suddenly and was 10/10 in severity. It was in her right upper quadrant radiating to her back. She has had a 50-pound weight loss in the past year. Her medications include sertraline, phentermine-topiramate, and simvastatin.
She is evaluated in the emergency department, and labs show the following: aspartate aminotransferase, 450; alanine aminotransferase, 500; alkaline phosphatase, 100; bilirubin, 1.2. She receives morphine for her pain with minimal relief. An ultrasound shows no gallstones and no dilated common bile duct (CBD).
Her pain resolves 3 hours after arriving in the ED. Repeat labs 15 minutes after pain resolution show the following: AST, 900; ALT, 1,000; alk phos, 130; bili, 1.2.
What is the most likely diagnosis?
A. Acetaminophen toxicity.
B. Hepatitis A.
C. Ischemic hepatitis.
D. Simvastatin.
E. Passage of gallstone.
The correct answer in this case is passage of a gallstone.
The patient has had weight loss, which increases the risk of gallstone formation, and the pain pattern is consistent with passage of a gallstone through the common bile duct.
I have seen a number of cases where the diagnosis was missed when the lab pattern is similar to the labs in this case. The high transaminases and the absence of significant alkaline phosphatase elevation can be confusing. We are taught in our medical training that alkaline phosphatase is a lab value that goes up with obstruction, and that transaminases are liver injury labs. What are the data on liver labs in the setting of acute obstruction as seen with the passage of a gallstone?
Frederick Kiechle, MD, and colleagues reported that alkaline phosphatase levels, either alone or in conjunction with bilirubin levels, were not useful in determining the presence of common bile duct stones.1 Ming-Hsun Yang et al. found that normal gamma-glutamyl transferase results had the highest negative predictive value for the presence of a common bile duct stone (97%).2 The sensitivity for ultrasound detection of CBD stone in this study was only 35%.
Keun Soo Ahn and colleagues found that, in patients with symptomatic CBD stones, the average AST was 275, and the average ALT was 317 – about six to seven times the upper limit of normal for these lab tests.3 In the same study, the average alkaline phosphatase was 213, which is about twice the upper limit of normal.
Sometimes, extremely high transaminase elevations can occur with choledocholithiasis. Saroja Bangaru et al. reported on a case series of patients who all had transaminase values greater than 1,000 with symptomatic choledocholithiasis.4 All of the patients had normal or just mildly elevated alkaline phosphatase levels.
Rahul Nathwani, MD, and colleagues also reported on a series of 16 patients with choledocholithiasis and transaminase levels greater than 1,000.5 All patients were symptomatic, and the average alkaline phosphatase levels were 2.5 times the upper limit of normal.
Ala Sharara, MD, et al. looked at 40 patients in a retrospective study of patients found to have choledocholithiasis who presented within 12 hours of pain onset.6 Levels of AST and ALT both significantly correlated with duration of pain (P less than .001), whereas there was no significant correlation with alkaline phosphatase and bilirubin levels.

Pearl: AST and ALT elevations in patients with acute abdominal pain could be due to choledocholithiasis, even if there are minimal or no abnormalities in alkaline phosphatase. Marked elevations (greater than 1,000) can occur.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am J Emerg Med. 1985 Nov;3(6):556-60.
2. Surg Endosc. 2008 Jul;22(7):1620-4.
3. World J Surg. 2016 Aug;40(8):1925-31.
4. J Clin Gastroenterol. 2017 Sep;51(8):728-33.
5. Am J Gastroenterol. 2005 Feb;100(2):295-8.
6. Clin Gastroenterol Hepatol. 2010 Dec;8(12):1077-82.
A 54-year-old woman presents with severe abdominal pain lasting 3 hours. The pain came on suddenly and was 10/10 in severity. It was in her right upper quadrant radiating to her back. She has had a 50-pound weight loss in the past year. Her medications include sertraline, phentermine-topiramate, and simvastatin.
She is evaluated in the emergency department, and labs show the following: aspartate aminotransferase, 450; alanine aminotransferase, 500; alkaline phosphatase, 100; bilirubin, 1.2. She receives morphine for her pain with minimal relief. An ultrasound shows no gallstones and no dilated common bile duct (CBD).
Her pain resolves 3 hours after arriving in the ED. Repeat labs 15 minutes after pain resolution show the following: AST, 900; ALT, 1,000; alk phos, 130; bili, 1.2.
What is the most likely diagnosis?
A. Acetaminophen toxicity.
B. Hepatitis A.
C. Ischemic hepatitis.
D. Simvastatin.
E. Passage of gallstone.
The correct answer in this case is passage of a gallstone.
The patient has had weight loss, which increases the risk of gallstone formation, and the pain pattern is consistent with passage of a gallstone through the common bile duct.
I have seen a number of cases where the diagnosis was missed when the lab pattern is similar to the labs in this case. The high transaminases and the absence of significant alkaline phosphatase elevation can be confusing. We are taught in our medical training that alkaline phosphatase is a lab value that goes up with obstruction, and that transaminases are liver injury labs. What are the data on liver labs in the setting of acute obstruction as seen with the passage of a gallstone?
Frederick Kiechle, MD, and colleagues reported that alkaline phosphatase levels, either alone or in conjunction with bilirubin levels, were not useful in determining the presence of common bile duct stones.1 Ming-Hsun Yang et al. found that normal gamma-glutamyl transferase results had the highest negative predictive value for the presence of a common bile duct stone (97%).2 The sensitivity for ultrasound detection of CBD stone in this study was only 35%.
Keun Soo Ahn and colleagues found that, in patients with symptomatic CBD stones, the average AST was 275, and the average ALT was 317 – about six to seven times the upper limit of normal for these lab tests.3 In the same study, the average alkaline phosphatase was 213, which is about twice the upper limit of normal.
Sometimes, extremely high transaminase elevations can occur with choledocholithiasis. Saroja Bangaru et al. reported on a case series of patients who all had transaminase values greater than 1,000 with symptomatic choledocholithiasis.4 All of the patients had normal or just mildly elevated alkaline phosphatase levels.
Rahul Nathwani, MD, and colleagues also reported on a series of 16 patients with choledocholithiasis and transaminase levels greater than 1,000.5 All patients were symptomatic, and the average alkaline phosphatase levels were 2.5 times the upper limit of normal.
Ala Sharara, MD, et al. looked at 40 patients in a retrospective study of patients found to have choledocholithiasis who presented within 12 hours of pain onset.6 Levels of AST and ALT both significantly correlated with duration of pain (P less than .001), whereas there was no significant correlation with alkaline phosphatase and bilirubin levels.
Pearl: AST and ALT elevations in patients with acute abdominal pain could be due to choledocholithiasis, even if there are minimal or no abnormalities in alkaline phosphatase. Marked elevations (greater than 1,000) can occur.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am J Emerg Med. 1985 Nov;3(6):556-60.
2. Surg Endosc. 2008 Jul;22(7):1620-4.
3. World J Surg. 2016 Aug;40(8):1925-31.
4. J Clin Gastroenterol. 2017 Sep;51(8):728-33.
5. Am J Gastroenterol. 2005 Feb;100(2):295-8.
6. Clin Gastroenterol Hepatol. 2010 Dec;8(12):1077-82.
A 54-year-old woman presents with severe abdominal pain lasting 3 hours. The pain came on suddenly and was 10/10 in severity. It was in her right upper quadrant radiating to her back. She has had a 50-pound weight loss in the past year. Her medications include sertraline, phentermine-topiramate, and simvastatin.
She is evaluated in the emergency department, and labs show the following: aspartate aminotransferase, 450; alanine aminotransferase, 500; alkaline phosphatase, 100; bilirubin, 1.2. She receives morphine for her pain with minimal relief. An ultrasound shows no gallstones and no dilated common bile duct (CBD).
Her pain resolves 3 hours after arriving in the ED. Repeat labs 15 minutes after pain resolution show the following: AST, 900; ALT, 1,000; alk phos, 130; bili, 1.2.
What is the most likely diagnosis?
A. Acetaminophen toxicity.
B. Hepatitis A.
C. Ischemic hepatitis.
D. Simvastatin.
E. Passage of gallstone.
The correct answer in this case is passage of a gallstone.
The patient has had weight loss, which increases the risk of gallstone formation, and the pain pattern is consistent with passage of a gallstone through the common bile duct.
I have seen a number of cases where the diagnosis was missed when the lab pattern is similar to the labs in this case. The high transaminases and the absence of significant alkaline phosphatase elevation can be confusing. We are taught in our medical training that alkaline phosphatase is a lab value that goes up with obstruction, and that transaminases are liver injury labs. What are the data on liver labs in the setting of acute obstruction as seen with the passage of a gallstone?
Frederick Kiechle, MD, and colleagues reported that alkaline phosphatase levels, either alone or in conjunction with bilirubin levels, were not useful in determining the presence of common bile duct stones.1 Ming-Hsun Yang et al. found that normal gamma-glutamyl transferase results had the highest negative predictive value for the presence of a common bile duct stone (97%).2 The sensitivity for ultrasound detection of CBD stone in this study was only 35%.
Keun Soo Ahn and colleagues found that, in patients with symptomatic CBD stones, the average AST was 275, and the average ALT was 317 – about six to seven times the upper limit of normal for these lab tests.3 In the same study, the average alkaline phosphatase was 213, which is about twice the upper limit of normal.
Sometimes, extremely high transaminase elevations can occur with choledocholithiasis. Saroja Bangaru et al. reported on a case series of patients who all had transaminase values greater than 1,000 with symptomatic choledocholithiasis.4 All of the patients had normal or just mildly elevated alkaline phosphatase levels.
Rahul Nathwani, MD, and colleagues also reported on a series of 16 patients with choledocholithiasis and transaminase levels greater than 1,000.5 All patients were symptomatic, and the average alkaline phosphatase levels were 2.5 times the upper limit of normal.
Ala Sharara, MD, et al. looked at 40 patients in a retrospective study of patients found to have choledocholithiasis who presented within 12 hours of pain onset.6 Levels of AST and ALT both significantly correlated with duration of pain (P less than .001), whereas there was no significant correlation with alkaline phosphatase and bilirubin levels.
Pearl: AST and ALT elevations in patients with acute abdominal pain could be due to choledocholithiasis, even if there are minimal or no abnormalities in alkaline phosphatase. Marked elevations (greater than 1,000) can occur.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am J Emerg Med. 1985 Nov;3(6):556-60.
2. Surg Endosc. 2008 Jul;22(7):1620-4.
3. World J Surg. 2016 Aug;40(8):1925-31.
4. J Clin Gastroenterol. 2017 Sep;51(8):728-33.
5. Am J Gastroenterol. 2005 Feb;100(2):295-8.
6. Clin Gastroenterol Hepatol. 2010 Dec;8(12):1077-82.
DOACs may be beneficial in post-op atrial fib after CABG
SAN DIEGO – The use of direct oral anticoagulants were not significantly different from warfarin for safety and efficacy in cases of postoperative atrial fibrillation following coronary artery bypass grafting, according to results from a single-center study.
In fact, , which suggests a potential for reduced hospital stay-related costs. “There are several different niche populations for which the DOACs have not been studied,” one of the study authors, Ammie J. Patel, PharmD, said in an interview at the biennial summit of the Thrombosis & Hemostasis Societies of North America. “This provides the opportunity for institutions and hospitals to study the use of these drugs in non-traditional ways.”
Dr. Patel, of Temple University, Philadelphia, said that postoperative atrial fibrillation occurs in about 30% of patients following CABG and that new-onset postoperative atrial fibrillation after CABG has been linked to a 21% increase in relative mortality.
Noting that patients with planned major surgery were excluded from RE-LY, ROCKET AF, ARISTOTLE, and other pivotal clinical trials of DOACs, she and her research mentor, Rachael Durie, PharmD, retrospectively evaluated the safety and efficacy of DOACs in 285 cases of new-onset postoperative atrial fibrillation following CABG performed at Jersey Shore University Medical Center, Neptune, N.J., between July 1, 2014, and June 30, 2016. They hypothesized that using DOACs in this patient population might offer advantages over warfarin, including rapid onset and earlier hospital discharge, fewer drug interactions, and no coagulation monitoring.
Of the 146 patients on anticoagulants, 79 were discharged on warfarin, 43 on apixaban, 20 on rivaroxaban, and 4 on dabigatran. The other 139 patients were not anticoagulated for various reasons, one of which included normal sinus rhythm at discharge.
The researchers found that the DOACs were not significantly different from warfarin for efficacy endpoints in stroke (P = 0.23) or systemic embolism (P = 0.68). Safety endpoints also were similar among all groups for major bleeding (P = 0.57) or minor bleeding (P = 0.63). Median post-CABG length of stay was significantly longer in the warfarin group (8 days, P = 0.005), compared with dabigatran (7.5 days), rivaroxaban (6.5 days), and apixaban (6 days). In addition, the median total hospital length of stay was significantly longer with warfarin (11 days, P = 0.004), compared with rivaroxaban (8.5 days) and apixaban (9 days), but not compared with dabigatran (12 days).
Dr. Patel acknowledged that the study’s retrospective design and small sample size are limitations and said that larger prospective trials are warranted to confirm these results. She reported having no financial disclosures.
SOURCE: Patel AJ et al. THSNA 2018. Poster 64.
SAN DIEGO – The use of direct oral anticoagulants were not significantly different from warfarin for safety and efficacy in cases of postoperative atrial fibrillation following coronary artery bypass grafting, according to results from a single-center study.
In fact, , which suggests a potential for reduced hospital stay-related costs. “There are several different niche populations for which the DOACs have not been studied,” one of the study authors, Ammie J. Patel, PharmD, said in an interview at the biennial summit of the Thrombosis & Hemostasis Societies of North America. “This provides the opportunity for institutions and hospitals to study the use of these drugs in non-traditional ways.”
Dr. Patel, of Temple University, Philadelphia, said that postoperative atrial fibrillation occurs in about 30% of patients following CABG and that new-onset postoperative atrial fibrillation after CABG has been linked to a 21% increase in relative mortality.
Noting that patients with planned major surgery were excluded from RE-LY, ROCKET AF, ARISTOTLE, and other pivotal clinical trials of DOACs, she and her research mentor, Rachael Durie, PharmD, retrospectively evaluated the safety and efficacy of DOACs in 285 cases of new-onset postoperative atrial fibrillation following CABG performed at Jersey Shore University Medical Center, Neptune, N.J., between July 1, 2014, and June 30, 2016. They hypothesized that using DOACs in this patient population might offer advantages over warfarin, including rapid onset and earlier hospital discharge, fewer drug interactions, and no coagulation monitoring.
Of the 146 patients on anticoagulants, 79 were discharged on warfarin, 43 on apixaban, 20 on rivaroxaban, and 4 on dabigatran. The other 139 patients were not anticoagulated for various reasons, one of which included normal sinus rhythm at discharge.
The researchers found that the DOACs were not significantly different from warfarin for efficacy endpoints in stroke (P = 0.23) or systemic embolism (P = 0.68). Safety endpoints also were similar among all groups for major bleeding (P = 0.57) or minor bleeding (P = 0.63). Median post-CABG length of stay was significantly longer in the warfarin group (8 days, P = 0.005), compared with dabigatran (7.5 days), rivaroxaban (6.5 days), and apixaban (6 days). In addition, the median total hospital length of stay was significantly longer with warfarin (11 days, P = 0.004), compared with rivaroxaban (8.5 days) and apixaban (9 days), but not compared with dabigatran (12 days).
Dr. Patel acknowledged that the study’s retrospective design and small sample size are limitations and said that larger prospective trials are warranted to confirm these results. She reported having no financial disclosures.
SOURCE: Patel AJ et al. THSNA 2018. Poster 64.
SAN DIEGO – The use of direct oral anticoagulants were not significantly different from warfarin for safety and efficacy in cases of postoperative atrial fibrillation following coronary artery bypass grafting, according to results from a single-center study.
In fact, , which suggests a potential for reduced hospital stay-related costs. “There are several different niche populations for which the DOACs have not been studied,” one of the study authors, Ammie J. Patel, PharmD, said in an interview at the biennial summit of the Thrombosis & Hemostasis Societies of North America. “This provides the opportunity for institutions and hospitals to study the use of these drugs in non-traditional ways.”
Dr. Patel, of Temple University, Philadelphia, said that postoperative atrial fibrillation occurs in about 30% of patients following CABG and that new-onset postoperative atrial fibrillation after CABG has been linked to a 21% increase in relative mortality.
Noting that patients with planned major surgery were excluded from RE-LY, ROCKET AF, ARISTOTLE, and other pivotal clinical trials of DOACs, she and her research mentor, Rachael Durie, PharmD, retrospectively evaluated the safety and efficacy of DOACs in 285 cases of new-onset postoperative atrial fibrillation following CABG performed at Jersey Shore University Medical Center, Neptune, N.J., between July 1, 2014, and June 30, 2016. They hypothesized that using DOACs in this patient population might offer advantages over warfarin, including rapid onset and earlier hospital discharge, fewer drug interactions, and no coagulation monitoring.
Of the 146 patients on anticoagulants, 79 were discharged on warfarin, 43 on apixaban, 20 on rivaroxaban, and 4 on dabigatran. The other 139 patients were not anticoagulated for various reasons, one of which included normal sinus rhythm at discharge.
The researchers found that the DOACs were not significantly different from warfarin for efficacy endpoints in stroke (P = 0.23) or systemic embolism (P = 0.68). Safety endpoints also were similar among all groups for major bleeding (P = 0.57) or minor bleeding (P = 0.63). Median post-CABG length of stay was significantly longer in the warfarin group (8 days, P = 0.005), compared with dabigatran (7.5 days), rivaroxaban (6.5 days), and apixaban (6 days). In addition, the median total hospital length of stay was significantly longer with warfarin (11 days, P = 0.004), compared with rivaroxaban (8.5 days) and apixaban (9 days), but not compared with dabigatran (12 days).
Dr. Patel acknowledged that the study’s retrospective design and small sample size are limitations and said that larger prospective trials are warranted to confirm these results. She reported having no financial disclosures.
SOURCE: Patel AJ et al. THSNA 2018. Poster 64.
REPORTING FROM THSNA 2018
Key clinical point: DOACs may be safe and effective alternatives to warfarin in postoperative atrial fibrillation after CABG.
Major finding: DOACs were not significantly different from warfarin for efficacy endpoints in stroke (P = 0.23) or systemic embolism (P = 0.68).
Study details: A retrospective, single-center study of DOACs in 285 cases of new-onset postoperative atrial fibrillation following CABG.
Disclosures: Dr. Patel reported having no financial disclosures.
Source: Patel AJ et al. THSNA 2018. Poster 64.
When should nutritional support be implemented in a hospitalized patient?
Case
A 60-year-old male with a history of head & neck cancer, treated with radical neck dissection and radiation 5 years prior is admitted with community-acquired pneumonia and anasarca. Prior to admission, he was on a soft dysphagia diet and reports increased difficulty with solid foods and weight loss from 70 kg to 55 kg over 2.5 years. Should nutritional support be initiated?
Background
Malnutrition is associated with increased hospital mortality, decreased functional status and quality of life, infections, longer length of stay, higher hospital costs, and more frequent nonelective readmissions.1,2
Identifying patients who are malnourished or at risk for malnutrition
An international consensus committee recommended the following criteria for the diagnosis of undernutrition if two of six are present3:
- Insufficient energy intake.
- Weight loss.
- Loss of muscle mass.
- Loss of subcutaneous fat.
- Localized or generalized fluid accumulation that may sometimes mask weight loss.
- Diminished functional status as measured by handgrip strength.
The joint commission requires that all patients admitted to acute care hospitals be screened for risk of malnutrition within 24 hours. The American College of Gastroenterologists recommends using a validated score to assess nutritional risk, such as the Nutritional Risk Score (NRS) 2002 or the NUTRIC (Nutrition Risk in the Critically Ill) Score, which use a combination of nutritional status and diet-related factors – weight loss, body mass index, and food intake – and also severity of illness measurements.4

- Starvation-related malnutrition, such as anorexia nervosa, presents with a deficiency in calories and protein without inflammation, .
- Chronic disease–related malnutrition, such as that caused chronic obstructive pulmonary disease, cancer, and obesity, presents with mild to moderate inflammation.
- Acute disease or injury–related malnutrition, such as that caused by sepsis, burns, and trauma, presents with acute and severe inflammation.
Laboratory indicators such as albumin, prealbumin, and transferrin are not recommended for the determination of nutritional status. Instead, as negative acute-phase reactants, they can be used as surrogate markers of nutritional risk and degree of inflammation.4
Overview of the data
What are the indications for initiating nutritional support, and what is the optimal timing for initiation?
Patients who are malnourished or at significant risk for becoming malnourished should receive specialized nutrition support. Early enteral nutrition should be initiated within 24-48 hours of admission in critically ill patients with high nutritional risk who are unable to maintain volitional intake.6 In the absence of preexisting malnutrition, nutritional support should be provided for patients with inadequate oral intake for 7-14 days or for those in whom inadequate oral intake is expected over the same time period.7
How should nutritional support be administered?
Dietary modification and supplementation
In patients who can tolerate an oral diet, dietary modifications may be made in order to facilitate the provision of essential nutrients in a well-tolerated form. Modifications may include adjusting the consistency of foods, energy value of foods, types of nutrients consumed, and number and frequency of meals.8 Commercial meal replacement beverages are widely used to support a standard oral diet, but there is no data to support their routine use.7
Enteral nutrition
Enteral nutrition (EN) is the method of choice for administering nutrition support. Contraindications to enteral feeding include diffuse peritonitis, intestinal obstruction, and gastrointestinal ischemia.9 The potential advantages of EN over parenteral nutrition (PN) include decreased infection rate, decreased total complications, and shorter length of stay, but there has been no observed difference in mortality. EN is also suggested to have nonnutritional benefits related to providing luminal nutrients – these include maintaining gut integrity, beneficial immune responses, and favorable metabolic responses that help maintain euglycemia and enhance more physiologic fuel utilization.4
Enteral feeding can be administered through the following routes of access:
- Nasogastric tubes: A nasogastric or orogastric tube with radiologic confirmation of positioning is the first line of enteral access. Gastric feeding is preferred because it is well tolerated in the majority of patients, is more physiological, requires a lower level of expertise, and minimizes any delay in initiation of feeding.
- Postpyloric tubes: Postpyloric feeding tubes are indicated if gastric feeding is poorly tolerated or if the patient is at high risk for aspiration because jejunal feedings decrease the incidence of reflux, regurgitation, and aspiration.
- Percutaneous access: When long-term enteral access is required – that is, for greater than 4 weeks – a percutaneous enteral access device should be placed. Prolonged use of a nasoenteric tube may be associated with erosion of the nares and an increase in the incidence of aspiration pneumonia, sinusitis, and esophageal ulceration or stricture. Patients who have had a stroke are the most likely to benefit from percutaneous endoscopic gastrostomy placement, as 40% of patients can have continued dysphagia as long as 1 year after.4,10 Absolute contraindications for PEG placement include serious coagulation disorders (international normalized ratio greater than 1.5; fewer than 50,000 platelets/mcL), sepsis, abdominal wall infections, marked peritoneal carcinomatosis, peritonitis, severe gastroparesis, gastric outlet obstruction, or a history of total gastrectomy. Risks often outweigh benefits in patients who have cirrhosis with ascites, patients undergoing peritoneal dialysis, and patients who have portal hypertension with gastric varices, but PEG can be considered on a case-by-case basis.11
Parenteral nutrition
Parenteral nutrition is reserved for patients in whom enteral feeding is contraindicated or who fail to meet their nutritional needs with enteral feedings. If EN is not feasible, then parenteral nutrition should be initiated as soon as possible in patients who had high nutritional risk on admission. Otherwise, PN should not be initiated during the first week of hospitalization because there is evidence to suggest net harm when initiated early. Supplemental PN may be considered for patients already on EN who are unable to meet more than 60% of their energy and protein requirements by the enteral route alone, but again, this should only be considered after 7-10 days on EN. PN is generally stopped when the patients achieve more than 60% of their energy and protein goals from EN.4
How should patients be monitored while receiving nutritional support?
If a patient is severely malnourished and refeeding is initiated, serious complications can occur, which are summarized in Table 1; these complications can include severe electrolyte disorders, fluid shifts, and even death.12 Refeeding syndrome occurs in the first few days of initiating a diet in severely malnourished patients, and its severity is directly related to the severity of malnutrition prior to refeeding. The National Institute of Health and Clinical Excellence created criteria to identify patients at risk for refeeding syndrome; these criteria include having a BMI less than 18.5 kg/m2; unintentional weight loss of greater than 10% in the previous 3-6 months; little or no nutritional intake for more than 5 days; low levels of potassium, phosphorus, or magnesium before refeeding; and a history of alcohol misuse or taking certain drugs, such as insulin, chemotherapy, antacids, or diuretics.9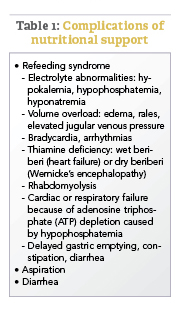
Aspiration is a risk with enteral feeding – the risk factors include being older than 70 years, altered mental status, supine position, and bolus rather than continuous infusion.4 Postpyloric feeding may reduce the risk of aspiration. Expert consensus suggests elevating the head of the bed by 30°-40° for all intubated patients receiving EN, as well as administering chlorhexidine mouthwash twice daily.6
Diarrhea is very common in patients receiving EN. After evaluating for other etiologies of diarrhea, tube feeding–associated diarrhea may be managed first by using a fiber-containing formulation. Fiber should be avoided in patients at risk for bowel ischemia or severe dysmotility. If diarrhea persists despite fiber, small peptide formulations, also known as elemental tube feeds, may be used.4,6
Gastric residual volume (GRV) is commonly monitored in patients receiving enteral nutrition. However, the American College of Gastroenterology does not recommend using GRVs to monitor EN feeding because it is a poor marker of clinically meaningful variables, such as gastric emptying, risk of aspiration, and risk of poor outcomes, and increases the risk of tube clogging and inadequate delivery of EN. If GRVs are being monitored, tube feedings should not be withheld because of high GRVs when there are no other signs of intolerance.4 Nausea may be managed by changing a patient from bolus to continuous feedings or by adding promotility agents such as metoclopramide or erythromycin.6
Special considerations in common conditions treated by hospitalists
The principles outlined above are general guidelines that are applicable to most patients requiring nutrition support. We have highlighted special considerations for common conditions in hospitalized patients who require nutritional support below.
Critical Illness
- Defer enteral nutrition until patient is fully resuscitated and hemodynamically stable.
- Severely malnourished or high nutritional-risk patients should be advanced toward goals as quickly as can be tolerated over 24-48 hours.
- Patients with acute respiratory distress syndrome or acute lung injury, or those expected to require mechanical ventilation for more than 72 hours, should receive trophic feeds or full nutrition by enteral route.6
Pancreatitis
- Oral feeding should be attempted as soon as abdominal pain is decreasing and inflammatory markers are improving.13
- A regular solid, low-fat diet should be initiated, rather than slowly advancing from a clear liquid diet.13
- In severe acute pancreatitis, initiation of enteral nutrition within 48 hours of presentation is associated with improved outcomes.13
- There is no difference in outcomes between gastric and postpyloric feeding.14
- Initiation of parenteral nutrition may be delayed for up to 5 days to allow for a trial of oral or enteral feeding.13
Surgical patients
- Consider postponing surgery to provide 7-10 days of preoperative nutrition supplementation in patients with risk of severe undernutrition.16
- Consider postoperative nutritional support if patients are at risk for severe undernutrition, are unable to eat for more than 7 days perioperatively, or are unable to maintain oral intake above 60% of recommended intake for more than 10 days.16
- Consider total parenteral nutrition in cases of impaired gastrointestinal function and absorption, high output enterocutaneous fistulae, obstructive lesions that do not allow enteral refeeding, or prolonged gastrointestinal failure.16
Prolonged Starvation
- Because of the high risk of refeeding syndrome, patients greater than 30% below ideal body weight should be hospitalized for close monitoring during refeeding.12
- Typical goal for weight gain is no greater than 2-3 pounds per week.10
- Total parenteral nutrition should be reserved for extreme cases, and if used, carbohydrate intake should not exceed 7 mg/kg/min.12
Stroke
- Enteral nutrition should be initiated within 24-48 hours of initial hospitalization if a patient is estimated to require feeding for more than 5 days and/or remain nil per os for 5-7 days.
- If a patient is intubated with increased intracranial pressure, this could delay gastric motility requiring a postpyloric tube placement.
- Initial placement of percutaneous endoscopic gastrostomy tubes can be considered if the hospitalized patient is expected to require nutritional support for greater than 30 days. Most patients will have improved dysphagia symptoms within 1 month of their acute stroke, although as many as 40% can have continued dysphagia up to 1 year.10
Back to the Case
The patient was admitted for a common general medical condition, but it is important to recognize that malnutrition was present on admission with weight loss and generalized fluid overload. Furthermore, he is at high nutritional risk because of his low body weight, poor oral intake, and dysphagia. Additionally, the acute inflammation from pneumonia places him in an increased catabolic state.
He was able to maintain some volitional oral intake, but after 7 days of close monitoring by a licensed dietician, it was determined that he was unable to meet his nutritional needs via the oral route. A percutaneous endoscopic gastrostomy tube was placed, and tube feeds were initiated, because his dysphagia – which was a significant factor contributing to his inability to meet his nutritional needs orally – was expected to persist for greater than 30 days.
Bottom Line
Nutrition support should be initiated in this patient with malnutrition on admission and high nutritional risk.
Dr. Abalos is an assistant professor at Georgetown University Medical Center in Washington. Dr. Corbett is an assistant professor at the University of Oklahoma Health Sciences Center in Oklahoma City.
References
1. Correia MI et al. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr. 2003 Jun;22(3):235-9.
2. Felder S et al. Association of nutritional risk and adverse medical outcomes across different medical inpatient populations. Nutrition. 2015 Nov-Dec;31(11-12):1385-93.
3. White JV et al. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad Nutr Diet. 2012 May;112(5):730-8.
4. McClave SA et al. ACG clinical guideline: Nutrition therapy in the adult hospitalized patient. Am J Gastroenterol. 2016 Mar;111(3):315-334.
5. Mueller C et al. A.S.P.E.N. clinical guidelines: Nutrition screening, assessment, and intervention in adults. JPEN J Parenter Enter Nutr. 2011 Jan;35(1):16-24.
6. McClave SA et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. JPEN J Parenter Enter Nutr. 2016 Feb;40(2):159-211.
7. August D et al. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN J Parenter Enter Nutr. 2002 Jan-Feb:26(1):SUPPL:1SA-138SA.
8. Kirkland LL et al. Nutrition in the hospitalized patient. J Hosp Med. 2013 Jan;8(1):52-8.
9. National Collaborating Centre for Acute Care, February 2006. Nutrition support in adults Oral nutrition support, enteral tube feeding and parenteral nutrition. National Collaborating Centre for Acute Care, London. Available from www.rcseng.ac.uk.
10. Corrigan ML et al. Nutrition in the stroke patient. Nutr Clin Pract. 2011 Jun;26(3):242-52.
11. Loser C et al. ESPEN guidelines on artificial enteral nutrition – Percutaneous endoscopic gastrostomy (PEG). Clin Nutr. 2005 Oct;24(5):848-61.
12. Mehler PS et al. Nutritional rehabilitation: Practical guidelines for refeeding the anorectic patient. J Nutr Metab. 2010. doi: 10.1155/2010/625782.
13. Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013 Jul-Aug;13(4 Suppl 2):e1-15.
14. Singh N et al. Evaluation of early enteral feeding through nasogastric and nasojejunal tube in severe acute pancreatitis: A noninferiority randomized controlled trial. Pancreas. 2012 Jan;41(1):153-9.
15. Braga M et al. ESPEN guidelines on parenteral nutrition: Surgery. Clin Nutr. 2009 Aug;28(4):378-86.
16. Weimann A et al. ESPEN Guidelines on enteral nutrition: Surgery including organ transplantation. Clin Nutr. 2006 Apr;25(2):224-44.
Additional reading
- Kirkland LL et al. Nutrition in the Hospitalized Patient. J Hosp Med. 2013 Jan;8(1):52-8.
- McClave SA et al. ACG Clinical Guideline: Nutrition Therapy in the Adult Hospitalized Patient. Am J Gastroenterol. 2016 Mar;111(3):315-334.
Quiz: Recognizing Malnutrition
Which of the following is not a criteria for the diagnosis of malnutrition?
A. Weight loss
B. Insufficient energy intake
C. Prealbumin
D. Diminished handgrip strength
Answer: C. Prealbumin. Laboratory indicators of nutrition, such as albumin, prealbumin, and transferrin, and markers of infection or inflammation are not recommended for the determination of nutritional status. Because negative acute-phase reactants, they instead can be used as surrogate markers of nutritional risk and degree of inflammation
Key Points
- At the time of admission to the hospital, malnutrition is present in 20-50% of patients. All hospitalized patients should be screened for nutritional risk and nutritional support should be considered if patients are not expected to be able to meet nutritional needs for more than 7 days.
- Patients with severe malnutrition on admission, severe critical illness, or severe acute pancreatitis should be provided nutritional support within 24-48 hours.
- Use the gut! Nutritional support should be provided via the most physiologic route possible. Total parenteral nutrition (TPN) should be reserved for patients in whom adequate nutrition cannot be provided enterally.
- Consider a percutaneous endoscopic gastrostomy (PEG) tube if the patient is expected to require tube feedings for more than 30 days.
- Patients with severe malnutrition who are given nutritional support are at high risk of developing refeeding syndrome, which manifests as electrolyte depletions and heart failure or volume overload.
Case
A 60-year-old male with a history of head & neck cancer, treated with radical neck dissection and radiation 5 years prior is admitted with community-acquired pneumonia and anasarca. Prior to admission, he was on a soft dysphagia diet and reports increased difficulty with solid foods and weight loss from 70 kg to 55 kg over 2.5 years. Should nutritional support be initiated?
Background
Malnutrition is associated with increased hospital mortality, decreased functional status and quality of life, infections, longer length of stay, higher hospital costs, and more frequent nonelective readmissions.1,2
Identifying patients who are malnourished or at risk for malnutrition
An international consensus committee recommended the following criteria for the diagnosis of undernutrition if two of six are present3:
- Insufficient energy intake.
- Weight loss.
- Loss of muscle mass.
- Loss of subcutaneous fat.
- Localized or generalized fluid accumulation that may sometimes mask weight loss.
- Diminished functional status as measured by handgrip strength.
The joint commission requires that all patients admitted to acute care hospitals be screened for risk of malnutrition within 24 hours. The American College of Gastroenterologists recommends using a validated score to assess nutritional risk, such as the Nutritional Risk Score (NRS) 2002 or the NUTRIC (Nutrition Risk in the Critically Ill) Score, which use a combination of nutritional status and diet-related factors – weight loss, body mass index, and food intake – and also severity of illness measurements.4
- Starvation-related malnutrition, such as anorexia nervosa, presents with a deficiency in calories and protein without inflammation, .
- Chronic disease–related malnutrition, such as that caused chronic obstructive pulmonary disease, cancer, and obesity, presents with mild to moderate inflammation.
- Acute disease or injury–related malnutrition, such as that caused by sepsis, burns, and trauma, presents with acute and severe inflammation.
Laboratory indicators such as albumin, prealbumin, and transferrin are not recommended for the determination of nutritional status. Instead, as negative acute-phase reactants, they can be used as surrogate markers of nutritional risk and degree of inflammation.4
Overview of the data
What are the indications for initiating nutritional support, and what is the optimal timing for initiation?
Patients who are malnourished or at significant risk for becoming malnourished should receive specialized nutrition support. Early enteral nutrition should be initiated within 24-48 hours of admission in critically ill patients with high nutritional risk who are unable to maintain volitional intake.6 In the absence of preexisting malnutrition, nutritional support should be provided for patients with inadequate oral intake for 7-14 days or for those in whom inadequate oral intake is expected over the same time period.7
How should nutritional support be administered?
Dietary modification and supplementation
In patients who can tolerate an oral diet, dietary modifications may be made in order to facilitate the provision of essential nutrients in a well-tolerated form. Modifications may include adjusting the consistency of foods, energy value of foods, types of nutrients consumed, and number and frequency of meals.8 Commercial meal replacement beverages are widely used to support a standard oral diet, but there is no data to support their routine use.7
Enteral nutrition
Enteral nutrition (EN) is the method of choice for administering nutrition support. Contraindications to enteral feeding include diffuse peritonitis, intestinal obstruction, and gastrointestinal ischemia.9 The potential advantages of EN over parenteral nutrition (PN) include decreased infection rate, decreased total complications, and shorter length of stay, but there has been no observed difference in mortality. EN is also suggested to have nonnutritional benefits related to providing luminal nutrients – these include maintaining gut integrity, beneficial immune responses, and favorable metabolic responses that help maintain euglycemia and enhance more physiologic fuel utilization.4
Enteral feeding can be administered through the following routes of access:
- Nasogastric tubes: A nasogastric or orogastric tube with radiologic confirmation of positioning is the first line of enteral access. Gastric feeding is preferred because it is well tolerated in the majority of patients, is more physiological, requires a lower level of expertise, and minimizes any delay in initiation of feeding.
- Postpyloric tubes: Postpyloric feeding tubes are indicated if gastric feeding is poorly tolerated or if the patient is at high risk for aspiration because jejunal feedings decrease the incidence of reflux, regurgitation, and aspiration.
- Percutaneous access: When long-term enteral access is required – that is, for greater than 4 weeks – a percutaneous enteral access device should be placed. Prolonged use of a nasoenteric tube may be associated with erosion of the nares and an increase in the incidence of aspiration pneumonia, sinusitis, and esophageal ulceration or stricture. Patients who have had a stroke are the most likely to benefit from percutaneous endoscopic gastrostomy placement, as 40% of patients can have continued dysphagia as long as 1 year after.4,10 Absolute contraindications for PEG placement include serious coagulation disorders (international normalized ratio greater than 1.5; fewer than 50,000 platelets/mcL), sepsis, abdominal wall infections, marked peritoneal carcinomatosis, peritonitis, severe gastroparesis, gastric outlet obstruction, or a history of total gastrectomy. Risks often outweigh benefits in patients who have cirrhosis with ascites, patients undergoing peritoneal dialysis, and patients who have portal hypertension with gastric varices, but PEG can be considered on a case-by-case basis.11
Parenteral nutrition
Parenteral nutrition is reserved for patients in whom enteral feeding is contraindicated or who fail to meet their nutritional needs with enteral feedings. If EN is not feasible, then parenteral nutrition should be initiated as soon as possible in patients who had high nutritional risk on admission. Otherwise, PN should not be initiated during the first week of hospitalization because there is evidence to suggest net harm when initiated early. Supplemental PN may be considered for patients already on EN who are unable to meet more than 60% of their energy and protein requirements by the enteral route alone, but again, this should only be considered after 7-10 days on EN. PN is generally stopped when the patients achieve more than 60% of their energy and protein goals from EN.4
How should patients be monitored while receiving nutritional support?
If a patient is severely malnourished and refeeding is initiated, serious complications can occur, which are summarized in Table 1; these complications can include severe electrolyte disorders, fluid shifts, and even death.12 Refeeding syndrome occurs in the first few days of initiating a diet in severely malnourished patients, and its severity is directly related to the severity of malnutrition prior to refeeding. The National Institute of Health and Clinical Excellence created criteria to identify patients at risk for refeeding syndrome; these criteria include having a BMI less than 18.5 kg/m2; unintentional weight loss of greater than 10% in the previous 3-6 months; little or no nutritional intake for more than 5 days; low levels of potassium, phosphorus, or magnesium before refeeding; and a history of alcohol misuse or taking certain drugs, such as insulin, chemotherapy, antacids, or diuretics.9
Aspiration is a risk with enteral feeding – the risk factors include being older than 70 years, altered mental status, supine position, and bolus rather than continuous infusion.4 Postpyloric feeding may reduce the risk of aspiration. Expert consensus suggests elevating the head of the bed by 30°-40° for all intubated patients receiving EN, as well as administering chlorhexidine mouthwash twice daily.6
Diarrhea is very common in patients receiving EN. After evaluating for other etiologies of diarrhea, tube feeding–associated diarrhea may be managed first by using a fiber-containing formulation. Fiber should be avoided in patients at risk for bowel ischemia or severe dysmotility. If diarrhea persists despite fiber, small peptide formulations, also known as elemental tube feeds, may be used.4,6
Gastric residual volume (GRV) is commonly monitored in patients receiving enteral nutrition. However, the American College of Gastroenterology does not recommend using GRVs to monitor EN feeding because it is a poor marker of clinically meaningful variables, such as gastric emptying, risk of aspiration, and risk of poor outcomes, and increases the risk of tube clogging and inadequate delivery of EN. If GRVs are being monitored, tube feedings should not be withheld because of high GRVs when there are no other signs of intolerance.4 Nausea may be managed by changing a patient from bolus to continuous feedings or by adding promotility agents such as metoclopramide or erythromycin.6
Special considerations in common conditions treated by hospitalists
The principles outlined above are general guidelines that are applicable to most patients requiring nutrition support. We have highlighted special considerations for common conditions in hospitalized patients who require nutritional support below.
Critical Illness
- Defer enteral nutrition until patient is fully resuscitated and hemodynamically stable.
- Severely malnourished or high nutritional-risk patients should be advanced toward goals as quickly as can be tolerated over 24-48 hours.
- Patients with acute respiratory distress syndrome or acute lung injury, or those expected to require mechanical ventilation for more than 72 hours, should receive trophic feeds or full nutrition by enteral route.6
Pancreatitis
- Oral feeding should be attempted as soon as abdominal pain is decreasing and inflammatory markers are improving.13
- A regular solid, low-fat diet should be initiated, rather than slowly advancing from a clear liquid diet.13
- In severe acute pancreatitis, initiation of enteral nutrition within 48 hours of presentation is associated with improved outcomes.13
- There is no difference in outcomes between gastric and postpyloric feeding.14
- Initiation of parenteral nutrition may be delayed for up to 5 days to allow for a trial of oral or enteral feeding.13
Surgical patients
- Consider postponing surgery to provide 7-10 days of preoperative nutrition supplementation in patients with risk of severe undernutrition.16
- Consider postoperative nutritional support if patients are at risk for severe undernutrition, are unable to eat for more than 7 days perioperatively, or are unable to maintain oral intake above 60% of recommended intake for more than 10 days.16
- Consider total parenteral nutrition in cases of impaired gastrointestinal function and absorption, high output enterocutaneous fistulae, obstructive lesions that do not allow enteral refeeding, or prolonged gastrointestinal failure.16
Prolonged Starvation
- Because of the high risk of refeeding syndrome, patients greater than 30% below ideal body weight should be hospitalized for close monitoring during refeeding.12
- Typical goal for weight gain is no greater than 2-3 pounds per week.10
- Total parenteral nutrition should be reserved for extreme cases, and if used, carbohydrate intake should not exceed 7 mg/kg/min.12
Stroke
- Enteral nutrition should be initiated within 24-48 hours of initial hospitalization if a patient is estimated to require feeding for more than 5 days and/or remain nil per os for 5-7 days.
- If a patient is intubated with increased intracranial pressure, this could delay gastric motility requiring a postpyloric tube placement.
- Initial placement of percutaneous endoscopic gastrostomy tubes can be considered if the hospitalized patient is expected to require nutritional support for greater than 30 days. Most patients will have improved dysphagia symptoms within 1 month of their acute stroke, although as many as 40% can have continued dysphagia up to 1 year.10
Back to the Case
The patient was admitted for a common general medical condition, but it is important to recognize that malnutrition was present on admission with weight loss and generalized fluid overload. Furthermore, he is at high nutritional risk because of his low body weight, poor oral intake, and dysphagia. Additionally, the acute inflammation from pneumonia places him in an increased catabolic state.
He was able to maintain some volitional oral intake, but after 7 days of close monitoring by a licensed dietician, it was determined that he was unable to meet his nutritional needs via the oral route. A percutaneous endoscopic gastrostomy tube was placed, and tube feeds were initiated, because his dysphagia – which was a significant factor contributing to his inability to meet his nutritional needs orally – was expected to persist for greater than 30 days.
Bottom Line
Nutrition support should be initiated in this patient with malnutrition on admission and high nutritional risk.
Dr. Abalos is an assistant professor at Georgetown University Medical Center in Washington. Dr. Corbett is an assistant professor at the University of Oklahoma Health Sciences Center in Oklahoma City.
References
1. Correia MI et al. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr. 2003 Jun;22(3):235-9.
2. Felder S et al. Association of nutritional risk and adverse medical outcomes across different medical inpatient populations. Nutrition. 2015 Nov-Dec;31(11-12):1385-93.
3. White JV et al. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad Nutr Diet. 2012 May;112(5):730-8.
4. McClave SA et al. ACG clinical guideline: Nutrition therapy in the adult hospitalized patient. Am J Gastroenterol. 2016 Mar;111(3):315-334.
5. Mueller C et al. A.S.P.E.N. clinical guidelines: Nutrition screening, assessment, and intervention in adults. JPEN J Parenter Enter Nutr. 2011 Jan;35(1):16-24.
6. McClave SA et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. JPEN J Parenter Enter Nutr. 2016 Feb;40(2):159-211.
7. August D et al. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN J Parenter Enter Nutr. 2002 Jan-Feb:26(1):SUPPL:1SA-138SA.
8. Kirkland LL et al. Nutrition in the hospitalized patient. J Hosp Med. 2013 Jan;8(1):52-8.
9. National Collaborating Centre for Acute Care, February 2006. Nutrition support in adults Oral nutrition support, enteral tube feeding and parenteral nutrition. National Collaborating Centre for Acute Care, London. Available from www.rcseng.ac.uk.
10. Corrigan ML et al. Nutrition in the stroke patient. Nutr Clin Pract. 2011 Jun;26(3):242-52.
11. Loser C et al. ESPEN guidelines on artificial enteral nutrition – Percutaneous endoscopic gastrostomy (PEG). Clin Nutr. 2005 Oct;24(5):848-61.
12. Mehler PS et al. Nutritional rehabilitation: Practical guidelines for refeeding the anorectic patient. J Nutr Metab. 2010. doi: 10.1155/2010/625782.
13. Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013 Jul-Aug;13(4 Suppl 2):e1-15.
14. Singh N et al. Evaluation of early enteral feeding through nasogastric and nasojejunal tube in severe acute pancreatitis: A noninferiority randomized controlled trial. Pancreas. 2012 Jan;41(1):153-9.
15. Braga M et al. ESPEN guidelines on parenteral nutrition: Surgery. Clin Nutr. 2009 Aug;28(4):378-86.
16. Weimann A et al. ESPEN Guidelines on enteral nutrition: Surgery including organ transplantation. Clin Nutr. 2006 Apr;25(2):224-44.
Additional reading
- Kirkland LL et al. Nutrition in the Hospitalized Patient. J Hosp Med. 2013 Jan;8(1):52-8.
- McClave SA et al. ACG Clinical Guideline: Nutrition Therapy in the Adult Hospitalized Patient. Am J Gastroenterol. 2016 Mar;111(3):315-334.
Quiz: Recognizing Malnutrition
Which of the following is not a criteria for the diagnosis of malnutrition?
A. Weight loss
B. Insufficient energy intake
C. Prealbumin
D. Diminished handgrip strength
Answer: C. Prealbumin. Laboratory indicators of nutrition, such as albumin, prealbumin, and transferrin, and markers of infection or inflammation are not recommended for the determination of nutritional status. Because negative acute-phase reactants, they instead can be used as surrogate markers of nutritional risk and degree of inflammation
Key Points
- At the time of admission to the hospital, malnutrition is present in 20-50% of patients. All hospitalized patients should be screened for nutritional risk and nutritional support should be considered if patients are not expected to be able to meet nutritional needs for more than 7 days.
- Patients with severe malnutrition on admission, severe critical illness, or severe acute pancreatitis should be provided nutritional support within 24-48 hours.
- Use the gut! Nutritional support should be provided via the most physiologic route possible. Total parenteral nutrition (TPN) should be reserved for patients in whom adequate nutrition cannot be provided enterally.
- Consider a percutaneous endoscopic gastrostomy (PEG) tube if the patient is expected to require tube feedings for more than 30 days.
- Patients with severe malnutrition who are given nutritional support are at high risk of developing refeeding syndrome, which manifests as electrolyte depletions and heart failure or volume overload.
Case
A 60-year-old male with a history of head & neck cancer, treated with radical neck dissection and radiation 5 years prior is admitted with community-acquired pneumonia and anasarca. Prior to admission, he was on a soft dysphagia diet and reports increased difficulty with solid foods and weight loss from 70 kg to 55 kg over 2.5 years. Should nutritional support be initiated?
Background
Malnutrition is associated with increased hospital mortality, decreased functional status and quality of life, infections, longer length of stay, higher hospital costs, and more frequent nonelective readmissions.1,2
Identifying patients who are malnourished or at risk for malnutrition
An international consensus committee recommended the following criteria for the diagnosis of undernutrition if two of six are present3:
- Insufficient energy intake.
- Weight loss.
- Loss of muscle mass.
- Loss of subcutaneous fat.
- Localized or generalized fluid accumulation that may sometimes mask weight loss.
- Diminished functional status as measured by handgrip strength.
The joint commission requires that all patients admitted to acute care hospitals be screened for risk of malnutrition within 24 hours. The American College of Gastroenterologists recommends using a validated score to assess nutritional risk, such as the Nutritional Risk Score (NRS) 2002 or the NUTRIC (Nutrition Risk in the Critically Ill) Score, which use a combination of nutritional status and diet-related factors – weight loss, body mass index, and food intake – and also severity of illness measurements.4
- Starvation-related malnutrition, such as anorexia nervosa, presents with a deficiency in calories and protein without inflammation, .
- Chronic disease–related malnutrition, such as that caused chronic obstructive pulmonary disease, cancer, and obesity, presents with mild to moderate inflammation.
- Acute disease or injury–related malnutrition, such as that caused by sepsis, burns, and trauma, presents with acute and severe inflammation.
Laboratory indicators such as albumin, prealbumin, and transferrin are not recommended for the determination of nutritional status. Instead, as negative acute-phase reactants, they can be used as surrogate markers of nutritional risk and degree of inflammation.4
Overview of the data
What are the indications for initiating nutritional support, and what is the optimal timing for initiation?
Patients who are malnourished or at significant risk for becoming malnourished should receive specialized nutrition support. Early enteral nutrition should be initiated within 24-48 hours of admission in critically ill patients with high nutritional risk who are unable to maintain volitional intake.6 In the absence of preexisting malnutrition, nutritional support should be provided for patients with inadequate oral intake for 7-14 days or for those in whom inadequate oral intake is expected over the same time period.7
How should nutritional support be administered?
Dietary modification and supplementation
In patients who can tolerate an oral diet, dietary modifications may be made in order to facilitate the provision of essential nutrients in a well-tolerated form. Modifications may include adjusting the consistency of foods, energy value of foods, types of nutrients consumed, and number and frequency of meals.8 Commercial meal replacement beverages are widely used to support a standard oral diet, but there is no data to support their routine use.7
Enteral nutrition
Enteral nutrition (EN) is the method of choice for administering nutrition support. Contraindications to enteral feeding include diffuse peritonitis, intestinal obstruction, and gastrointestinal ischemia.9 The potential advantages of EN over parenteral nutrition (PN) include decreased infection rate, decreased total complications, and shorter length of stay, but there has been no observed difference in mortality. EN is also suggested to have nonnutritional benefits related to providing luminal nutrients – these include maintaining gut integrity, beneficial immune responses, and favorable metabolic responses that help maintain euglycemia and enhance more physiologic fuel utilization.4
Enteral feeding can be administered through the following routes of access:
- Nasogastric tubes: A nasogastric or orogastric tube with radiologic confirmation of positioning is the first line of enteral access. Gastric feeding is preferred because it is well tolerated in the majority of patients, is more physiological, requires a lower level of expertise, and minimizes any delay in initiation of feeding.
- Postpyloric tubes: Postpyloric feeding tubes are indicated if gastric feeding is poorly tolerated or if the patient is at high risk for aspiration because jejunal feedings decrease the incidence of reflux, regurgitation, and aspiration.
- Percutaneous access: When long-term enteral access is required – that is, for greater than 4 weeks – a percutaneous enteral access device should be placed. Prolonged use of a nasoenteric tube may be associated with erosion of the nares and an increase in the incidence of aspiration pneumonia, sinusitis, and esophageal ulceration or stricture. Patients who have had a stroke are the most likely to benefit from percutaneous endoscopic gastrostomy placement, as 40% of patients can have continued dysphagia as long as 1 year after.4,10 Absolute contraindications for PEG placement include serious coagulation disorders (international normalized ratio greater than 1.5; fewer than 50,000 platelets/mcL), sepsis, abdominal wall infections, marked peritoneal carcinomatosis, peritonitis, severe gastroparesis, gastric outlet obstruction, or a history of total gastrectomy. Risks often outweigh benefits in patients who have cirrhosis with ascites, patients undergoing peritoneal dialysis, and patients who have portal hypertension with gastric varices, but PEG can be considered on a case-by-case basis.11
Parenteral nutrition
Parenteral nutrition is reserved for patients in whom enteral feeding is contraindicated or who fail to meet their nutritional needs with enteral feedings. If EN is not feasible, then parenteral nutrition should be initiated as soon as possible in patients who had high nutritional risk on admission. Otherwise, PN should not be initiated during the first week of hospitalization because there is evidence to suggest net harm when initiated early. Supplemental PN may be considered for patients already on EN who are unable to meet more than 60% of their energy and protein requirements by the enteral route alone, but again, this should only be considered after 7-10 days on EN. PN is generally stopped when the patients achieve more than 60% of their energy and protein goals from EN.4
How should patients be monitored while receiving nutritional support?
If a patient is severely malnourished and refeeding is initiated, serious complications can occur, which are summarized in Table 1; these complications can include severe electrolyte disorders, fluid shifts, and even death.12 Refeeding syndrome occurs in the first few days of initiating a diet in severely malnourished patients, and its severity is directly related to the severity of malnutrition prior to refeeding. The National Institute of Health and Clinical Excellence created criteria to identify patients at risk for refeeding syndrome; these criteria include having a BMI less than 18.5 kg/m2; unintentional weight loss of greater than 10% in the previous 3-6 months; little or no nutritional intake for more than 5 days; low levels of potassium, phosphorus, or magnesium before refeeding; and a history of alcohol misuse or taking certain drugs, such as insulin, chemotherapy, antacids, or diuretics.9
Aspiration is a risk with enteral feeding – the risk factors include being older than 70 years, altered mental status, supine position, and bolus rather than continuous infusion.4 Postpyloric feeding may reduce the risk of aspiration. Expert consensus suggests elevating the head of the bed by 30°-40° for all intubated patients receiving EN, as well as administering chlorhexidine mouthwash twice daily.6
Diarrhea is very common in patients receiving EN. After evaluating for other etiologies of diarrhea, tube feeding–associated diarrhea may be managed first by using a fiber-containing formulation. Fiber should be avoided in patients at risk for bowel ischemia or severe dysmotility. If diarrhea persists despite fiber, small peptide formulations, also known as elemental tube feeds, may be used.4,6
Gastric residual volume (GRV) is commonly monitored in patients receiving enteral nutrition. However, the American College of Gastroenterology does not recommend using GRVs to monitor EN feeding because it is a poor marker of clinically meaningful variables, such as gastric emptying, risk of aspiration, and risk of poor outcomes, and increases the risk of tube clogging and inadequate delivery of EN. If GRVs are being monitored, tube feedings should not be withheld because of high GRVs when there are no other signs of intolerance.4 Nausea may be managed by changing a patient from bolus to continuous feedings or by adding promotility agents such as metoclopramide or erythromycin.6
Special considerations in common conditions treated by hospitalists
The principles outlined above are general guidelines that are applicable to most patients requiring nutrition support. We have highlighted special considerations for common conditions in hospitalized patients who require nutritional support below.
Critical Illness
- Defer enteral nutrition until patient is fully resuscitated and hemodynamically stable.
- Severely malnourished or high nutritional-risk patients should be advanced toward goals as quickly as can be tolerated over 24-48 hours.
- Patients with acute respiratory distress syndrome or acute lung injury, or those expected to require mechanical ventilation for more than 72 hours, should receive trophic feeds or full nutrition by enteral route.6
Pancreatitis
- Oral feeding should be attempted as soon as abdominal pain is decreasing and inflammatory markers are improving.13
- A regular solid, low-fat diet should be initiated, rather than slowly advancing from a clear liquid diet.13
- In severe acute pancreatitis, initiation of enteral nutrition within 48 hours of presentation is associated with improved outcomes.13
- There is no difference in outcomes between gastric and postpyloric feeding.14
- Initiation of parenteral nutrition may be delayed for up to 5 days to allow for a trial of oral or enteral feeding.13
Surgical patients
- Consider postponing surgery to provide 7-10 days of preoperative nutrition supplementation in patients with risk of severe undernutrition.16
- Consider postoperative nutritional support if patients are at risk for severe undernutrition, are unable to eat for more than 7 days perioperatively, or are unable to maintain oral intake above 60% of recommended intake for more than 10 days.16
- Consider total parenteral nutrition in cases of impaired gastrointestinal function and absorption, high output enterocutaneous fistulae, obstructive lesions that do not allow enteral refeeding, or prolonged gastrointestinal failure.16
Prolonged Starvation
- Because of the high risk of refeeding syndrome, patients greater than 30% below ideal body weight should be hospitalized for close monitoring during refeeding.12
- Typical goal for weight gain is no greater than 2-3 pounds per week.10
- Total parenteral nutrition should be reserved for extreme cases, and if used, carbohydrate intake should not exceed 7 mg/kg/min.12
Stroke
- Enteral nutrition should be initiated within 24-48 hours of initial hospitalization if a patient is estimated to require feeding for more than 5 days and/or remain nil per os for 5-7 days.
- If a patient is intubated with increased intracranial pressure, this could delay gastric motility requiring a postpyloric tube placement.
- Initial placement of percutaneous endoscopic gastrostomy tubes can be considered if the hospitalized patient is expected to require nutritional support for greater than 30 days. Most patients will have improved dysphagia symptoms within 1 month of their acute stroke, although as many as 40% can have continued dysphagia up to 1 year.10
Back to the Case
The patient was admitted for a common general medical condition, but it is important to recognize that malnutrition was present on admission with weight loss and generalized fluid overload. Furthermore, he is at high nutritional risk because of his low body weight, poor oral intake, and dysphagia. Additionally, the acute inflammation from pneumonia places him in an increased catabolic state.
He was able to maintain some volitional oral intake, but after 7 days of close monitoring by a licensed dietician, it was determined that he was unable to meet his nutritional needs via the oral route. A percutaneous endoscopic gastrostomy tube was placed, and tube feeds were initiated, because his dysphagia – which was a significant factor contributing to his inability to meet his nutritional needs orally – was expected to persist for greater than 30 days.
Bottom Line
Nutrition support should be initiated in this patient with malnutrition on admission and high nutritional risk.
Dr. Abalos is an assistant professor at Georgetown University Medical Center in Washington. Dr. Corbett is an assistant professor at the University of Oklahoma Health Sciences Center in Oklahoma City.
References
1. Correia MI et al. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr. 2003 Jun;22(3):235-9.
2. Felder S et al. Association of nutritional risk and adverse medical outcomes across different medical inpatient populations. Nutrition. 2015 Nov-Dec;31(11-12):1385-93.
3. White JV et al. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad Nutr Diet. 2012 May;112(5):730-8.
4. McClave SA et al. ACG clinical guideline: Nutrition therapy in the adult hospitalized patient. Am J Gastroenterol. 2016 Mar;111(3):315-334.
5. Mueller C et al. A.S.P.E.N. clinical guidelines: Nutrition screening, assessment, and intervention in adults. JPEN J Parenter Enter Nutr. 2011 Jan;35(1):16-24.
6. McClave SA et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. JPEN J Parenter Enter Nutr. 2016 Feb;40(2):159-211.
7. August D et al. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN J Parenter Enter Nutr. 2002 Jan-Feb:26(1):SUPPL:1SA-138SA.
8. Kirkland LL et al. Nutrition in the hospitalized patient. J Hosp Med. 2013 Jan;8(1):52-8.
9. National Collaborating Centre for Acute Care, February 2006. Nutrition support in adults Oral nutrition support, enteral tube feeding and parenteral nutrition. National Collaborating Centre for Acute Care, London. Available from www.rcseng.ac.uk.
10. Corrigan ML et al. Nutrition in the stroke patient. Nutr Clin Pract. 2011 Jun;26(3):242-52.
11. Loser C et al. ESPEN guidelines on artificial enteral nutrition – Percutaneous endoscopic gastrostomy (PEG). Clin Nutr. 2005 Oct;24(5):848-61.
12. Mehler PS et al. Nutritional rehabilitation: Practical guidelines for refeeding the anorectic patient. J Nutr Metab. 2010. doi: 10.1155/2010/625782.
13. Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013 Jul-Aug;13(4 Suppl 2):e1-15.
14. Singh N et al. Evaluation of early enteral feeding through nasogastric and nasojejunal tube in severe acute pancreatitis: A noninferiority randomized controlled trial. Pancreas. 2012 Jan;41(1):153-9.
15. Braga M et al. ESPEN guidelines on parenteral nutrition: Surgery. Clin Nutr. 2009 Aug;28(4):378-86.
16. Weimann A et al. ESPEN Guidelines on enteral nutrition: Surgery including organ transplantation. Clin Nutr. 2006 Apr;25(2):224-44.
Additional reading
- Kirkland LL et al. Nutrition in the Hospitalized Patient. J Hosp Med. 2013 Jan;8(1):52-8.
- McClave SA et al. ACG Clinical Guideline: Nutrition Therapy in the Adult Hospitalized Patient. Am J Gastroenterol. 2016 Mar;111(3):315-334.
Quiz: Recognizing Malnutrition
Which of the following is not a criteria for the diagnosis of malnutrition?
A. Weight loss
B. Insufficient energy intake
C. Prealbumin
D. Diminished handgrip strength
Answer: C. Prealbumin. Laboratory indicators of nutrition, such as albumin, prealbumin, and transferrin, and markers of infection or inflammation are not recommended for the determination of nutritional status. Because negative acute-phase reactants, they instead can be used as surrogate markers of nutritional risk and degree of inflammation
Key Points
- At the time of admission to the hospital, malnutrition is present in 20-50% of patients. All hospitalized patients should be screened for nutritional risk and nutritional support should be considered if patients are not expected to be able to meet nutritional needs for more than 7 days.
- Patients with severe malnutrition on admission, severe critical illness, or severe acute pancreatitis should be provided nutritional support within 24-48 hours.
- Use the gut! Nutritional support should be provided via the most physiologic route possible. Total parenteral nutrition (TPN) should be reserved for patients in whom adequate nutrition cannot be provided enterally.
- Consider a percutaneous endoscopic gastrostomy (PEG) tube if the patient is expected to require tube feedings for more than 30 days.
- Patients with severe malnutrition who are given nutritional support are at high risk of developing refeeding syndrome, which manifests as electrolyte depletions and heart failure or volume overload.