User login
Do inhaled steroids increase the risk of osteoporosis?
The use of inhaled corticosteroids at conventional doses for asthma and chronic obstructive pulmonary disease (COPD) does not appear to be associated with significant bone loss at 2 to 3 years of follow-up (strength of recommendation [SOR]: A, systematic reviews and randomized controlled trials [RCTs]). However, higher doses of inhaled corticosteroids may be associated with negative bone density changes at up to 4 years of follow-up (SOR: C, RCTs without change in fracture rates). No evidence exists to evaluate whether nasal steroids increase the risks of bone loss. Longer-term effects of prolonged use of inhaled steroids on BMD or fracture risk are undetermined with current evidence.
Encourage weight-bearing and aerobic exercise to all asthma or COPD patients
José E. Rodríguez, MD
Florida State University College of Medicine, Tallahassee
Asthma and COPD are prevalent among the underserved patients I see. Inhaled steroids are difficult for these patients to obtain. Once they feel better, many stop using the steroid until symptoms return.
Although we do not usually prescribe at the higher doses described in the review, our goal has always been long-term treatment. If these medications can cause osteoporosis with longer use, it may become an additional deterrent to adherence. However, consistent use may reduce the use of oral steroids for acute exacerbations, potentially even reducing bone loss.
Encourage weight-bearing and aerobic exercise for osteoporosis prevention and balance exercises to prevent falls for all asthma or COPD patients. These exercises may be prudent prevention for both lung disease and osteoporotic fractures.
Evidence summary
Inhaled corticosteroids are the primary therapy for asthma and are commonly prescribed for chronic obstructive pulmonary disease. The use of oral steroids is a well-known risk factor for osteoporosis, but the effects of inhaled corticosteroids on bone mineral density (BMD) are not well defined.
No significant changes seen in BMD at moderate doses
Our search found evidence pertaining to the use of inhaled pulmonary steroids, but no evidence meeting our inclusion criteria about the effect of inhaled nasal steroids. We located a Cochrane review, 1 other meta-analysis, and 2 individual RCTs that were not included in the systematic reviews. Three of the 7 RCTs included in the 2002 Cochrane review met our inclusion criteria for evaluating the impact of inhaled corticosteroids on BMD or fracture rate for adults with asthma or COPD.
All 3 RCTs (792 subjects total) examined the effect of conventional doses of inhaled corticosteroids on BMD and 2 of the RCTs (892 participants total) collected fracture data. No demonstrable effect was seen on vertebral fracture (odds ratio [OR]=1.87; 95% confidence interval [CI], 0.5–7.03) or BMD at 2 years follow-up.1 The subjects were otherwise healthy people with asthma or COPD with an average age of 40 years; men outnumbered women 2 to 1.
A fair-quality 2004 meta-analysis of 14 randomized trials (2300 participants) included 2 studies (448 subjects) that overlapped with the Cochrane review. There were no significant changes in BMD with moderately high doses of inhaled corticosteroids at 1 to 3 years follow-up.2
Annual changes in lumbar and femoral neck BMD (–0.23% and –0.17%, respectively) were not statistically significant. Mean changes in lumbar BMD were not significantly different from controls (–0.02). A fair-quality 2004 RCT did not demonstrate any clinically relevant effect on BMD at 2 years follow-up. This study used 800 mcg/day of fluticasone for patients with mild asthma.3
BMD changes found at higher doses
There is, however, some evidence that higher doses of inhaled corticosteroids can result in adverse BMD changes. In a high-quality RCT of 412 participants, aged 40 to 69 years, with mild to moderate COPD, use of higher-dose triamcinolone (1200 mcg/day) was associated with decreased lumbar and femoral neck BMD over 3 to 4 years.4 The differences in BMD between the inhaled corticosteroids and placebo groups at the femoral neck and lumbar spine were 1.78% (P<.001) and 1.33% (P=.007), respectively. However, the risk of fracture or height loss did not increase at follow-up.
A large fair-quality RCT from 2001 included in both meta-analyses demonstrated a dose-related fall in BMD within the subjects over 2 years at the lumbar spine (standard deviation, 3.4%; P<.010). This finding remained statistically significant after adjusting for asthma severity, but BMD changes were not different between the inhaled corticosteroids and placebo groups. However, this finding may be the result of higher oral corticosteroids use in the reference group.5
Limitations of these studies
These studies, though, have limitations. The follow-up periods for all of these studies are less than 5 years, and thus the longer-term effects of prolonged use of inhaled corticosteroids on BMD or fracture risk cannot be determined with this evidence. Furthermore, the study populations were relatively young, with few other risk factors (they were, for example, predominantly male) than populations at highest risk for osteoporosis and fracture. These factors limit interpretation of the data for long-term inhaled corticosteroids use, particularly in populations with higher baseline osteoporosis risk—older persons with chronic lung disease who take inhaled corticosteroids for more than 2 to 3 years. We need better and longer-term studies to help advise our patients about the risks and benefits of inhaled corticosteroids therapy.
Recommendations from others
The New Zealand Guideline Group says the risk of reduced BMD increased with long-term, high-dose inhaled corticosteroids.6 The Institute for Clinical Systems Improvement guidelines recommends considering osteoporosis prevention measures for those who have been (or will be) taking a daily high-dose inhaled glucocorticoid for several years as glucocorticoid use compounds fracture risk beyond that determined solely by BMD.7
1. Jones A, Fay JK, Burr M, et al. Inhaled corticosteroid effects on bone metabolism in asthma and chronic obstructive pulmonary disease. Cochrane Database Syst Rev 1, 2006.
2. Halpern MT, Schmier JK, Van Kerkhove MD, et al. Impact of long term inhaled corticosteroid therapy on bone mineral density results of a meta-analysis. Ann Allergy Asthma Immunol 2004;92:201-207.
3. Kemp JP, Osur S, Shrewsburry SB, et al. Potential effects of fluticasone propionate on bone mineral density in patients with asthma: A 2-year randomized, double-blind, placebo-controlled trial. Mayo Clin Proc 2004;79:458-466.
4. Scanlon PD, Connett JE, Wise RA, et al. Loss of bone density with inhaled triamcinolone in Lung Health Study II. Am J Respir Crit Care Med 2004;170:1302-1309.
5. Tattersfield AE, Town GI, Johnell O, et al. Bone mineral density in subjects with mild asthma randomized to treatment with inhaled corticosteroids or non-corticosteroid treatment for two years. Thorax 2001;56:272-278.
6. New Zealand Guidelines Group. The diagnosis and treatment of adult asthma. Wellington, NZ: New Zealand Guidelines Group; 2002 Sep. 101 p. Available at: www.guideline.gov/summary/summary.aspx?doc_id=3462 (NCG: 2688). Accessed on January 18, 2007.
7. Institute for Clinical Systems Improvement. Diagnosis and treatment of osteoporosis. Bloomington, Minn: Institute for Clinical Systems Improvement; 2005 Sep. 61 p. Available at: www.guideline.gov/summary/summary.aspx?doc_id=9626 (NCG: 5146). Accessed on January 18, 2007.
The use of inhaled corticosteroids at conventional doses for asthma and chronic obstructive pulmonary disease (COPD) does not appear to be associated with significant bone loss at 2 to 3 years of follow-up (strength of recommendation [SOR]: A, systematic reviews and randomized controlled trials [RCTs]). However, higher doses of inhaled corticosteroids may be associated with negative bone density changes at up to 4 years of follow-up (SOR: C, RCTs without change in fracture rates). No evidence exists to evaluate whether nasal steroids increase the risks of bone loss. Longer-term effects of prolonged use of inhaled steroids on BMD or fracture risk are undetermined with current evidence.
Encourage weight-bearing and aerobic exercise to all asthma or COPD patients
José E. Rodríguez, MD
Florida State University College of Medicine, Tallahassee
Asthma and COPD are prevalent among the underserved patients I see. Inhaled steroids are difficult for these patients to obtain. Once they feel better, many stop using the steroid until symptoms return.
Although we do not usually prescribe at the higher doses described in the review, our goal has always been long-term treatment. If these medications can cause osteoporosis with longer use, it may become an additional deterrent to adherence. However, consistent use may reduce the use of oral steroids for acute exacerbations, potentially even reducing bone loss.
Encourage weight-bearing and aerobic exercise for osteoporosis prevention and balance exercises to prevent falls for all asthma or COPD patients. These exercises may be prudent prevention for both lung disease and osteoporotic fractures.
Evidence summary
Inhaled corticosteroids are the primary therapy for asthma and are commonly prescribed for chronic obstructive pulmonary disease. The use of oral steroids is a well-known risk factor for osteoporosis, but the effects of inhaled corticosteroids on bone mineral density (BMD) are not well defined.
No significant changes seen in BMD at moderate doses
Our search found evidence pertaining to the use of inhaled pulmonary steroids, but no evidence meeting our inclusion criteria about the effect of inhaled nasal steroids. We located a Cochrane review, 1 other meta-analysis, and 2 individual RCTs that were not included in the systematic reviews. Three of the 7 RCTs included in the 2002 Cochrane review met our inclusion criteria for evaluating the impact of inhaled corticosteroids on BMD or fracture rate for adults with asthma or COPD.
All 3 RCTs (792 subjects total) examined the effect of conventional doses of inhaled corticosteroids on BMD and 2 of the RCTs (892 participants total) collected fracture data. No demonstrable effect was seen on vertebral fracture (odds ratio [OR]=1.87; 95% confidence interval [CI], 0.5–7.03) or BMD at 2 years follow-up.1 The subjects were otherwise healthy people with asthma or COPD with an average age of 40 years; men outnumbered women 2 to 1.
A fair-quality 2004 meta-analysis of 14 randomized trials (2300 participants) included 2 studies (448 subjects) that overlapped with the Cochrane review. There were no significant changes in BMD with moderately high doses of inhaled corticosteroids at 1 to 3 years follow-up.2
Annual changes in lumbar and femoral neck BMD (–0.23% and –0.17%, respectively) were not statistically significant. Mean changes in lumbar BMD were not significantly different from controls (–0.02). A fair-quality 2004 RCT did not demonstrate any clinically relevant effect on BMD at 2 years follow-up. This study used 800 mcg/day of fluticasone for patients with mild asthma.3
BMD changes found at higher doses
There is, however, some evidence that higher doses of inhaled corticosteroids can result in adverse BMD changes. In a high-quality RCT of 412 participants, aged 40 to 69 years, with mild to moderate COPD, use of higher-dose triamcinolone (1200 mcg/day) was associated with decreased lumbar and femoral neck BMD over 3 to 4 years.4 The differences in BMD between the inhaled corticosteroids and placebo groups at the femoral neck and lumbar spine were 1.78% (P<.001) and 1.33% (P=.007), respectively. However, the risk of fracture or height loss did not increase at follow-up.
A large fair-quality RCT from 2001 included in both meta-analyses demonstrated a dose-related fall in BMD within the subjects over 2 years at the lumbar spine (standard deviation, 3.4%; P<.010). This finding remained statistically significant after adjusting for asthma severity, but BMD changes were not different between the inhaled corticosteroids and placebo groups. However, this finding may be the result of higher oral corticosteroids use in the reference group.5
Limitations of these studies
These studies, though, have limitations. The follow-up periods for all of these studies are less than 5 years, and thus the longer-term effects of prolonged use of inhaled corticosteroids on BMD or fracture risk cannot be determined with this evidence. Furthermore, the study populations were relatively young, with few other risk factors (they were, for example, predominantly male) than populations at highest risk for osteoporosis and fracture. These factors limit interpretation of the data for long-term inhaled corticosteroids use, particularly in populations with higher baseline osteoporosis risk—older persons with chronic lung disease who take inhaled corticosteroids for more than 2 to 3 years. We need better and longer-term studies to help advise our patients about the risks and benefits of inhaled corticosteroids therapy.
Recommendations from others
The New Zealand Guideline Group says the risk of reduced BMD increased with long-term, high-dose inhaled corticosteroids.6 The Institute for Clinical Systems Improvement guidelines recommends considering osteoporosis prevention measures for those who have been (or will be) taking a daily high-dose inhaled glucocorticoid for several years as glucocorticoid use compounds fracture risk beyond that determined solely by BMD.7
The use of inhaled corticosteroids at conventional doses for asthma and chronic obstructive pulmonary disease (COPD) does not appear to be associated with significant bone loss at 2 to 3 years of follow-up (strength of recommendation [SOR]: A, systematic reviews and randomized controlled trials [RCTs]). However, higher doses of inhaled corticosteroids may be associated with negative bone density changes at up to 4 years of follow-up (SOR: C, RCTs without change in fracture rates). No evidence exists to evaluate whether nasal steroids increase the risks of bone loss. Longer-term effects of prolonged use of inhaled steroids on BMD or fracture risk are undetermined with current evidence.
Encourage weight-bearing and aerobic exercise to all asthma or COPD patients
José E. Rodríguez, MD
Florida State University College of Medicine, Tallahassee
Asthma and COPD are prevalent among the underserved patients I see. Inhaled steroids are difficult for these patients to obtain. Once they feel better, many stop using the steroid until symptoms return.
Although we do not usually prescribe at the higher doses described in the review, our goal has always been long-term treatment. If these medications can cause osteoporosis with longer use, it may become an additional deterrent to adherence. However, consistent use may reduce the use of oral steroids for acute exacerbations, potentially even reducing bone loss.
Encourage weight-bearing and aerobic exercise for osteoporosis prevention and balance exercises to prevent falls for all asthma or COPD patients. These exercises may be prudent prevention for both lung disease and osteoporotic fractures.
Evidence summary
Inhaled corticosteroids are the primary therapy for asthma and are commonly prescribed for chronic obstructive pulmonary disease. The use of oral steroids is a well-known risk factor for osteoporosis, but the effects of inhaled corticosteroids on bone mineral density (BMD) are not well defined.
No significant changes seen in BMD at moderate doses
Our search found evidence pertaining to the use of inhaled pulmonary steroids, but no evidence meeting our inclusion criteria about the effect of inhaled nasal steroids. We located a Cochrane review, 1 other meta-analysis, and 2 individual RCTs that were not included in the systematic reviews. Three of the 7 RCTs included in the 2002 Cochrane review met our inclusion criteria for evaluating the impact of inhaled corticosteroids on BMD or fracture rate for adults with asthma or COPD.
All 3 RCTs (792 subjects total) examined the effect of conventional doses of inhaled corticosteroids on BMD and 2 of the RCTs (892 participants total) collected fracture data. No demonstrable effect was seen on vertebral fracture (odds ratio [OR]=1.87; 95% confidence interval [CI], 0.5–7.03) or BMD at 2 years follow-up.1 The subjects were otherwise healthy people with asthma or COPD with an average age of 40 years; men outnumbered women 2 to 1.
A fair-quality 2004 meta-analysis of 14 randomized trials (2300 participants) included 2 studies (448 subjects) that overlapped with the Cochrane review. There were no significant changes in BMD with moderately high doses of inhaled corticosteroids at 1 to 3 years follow-up.2
Annual changes in lumbar and femoral neck BMD (–0.23% and –0.17%, respectively) were not statistically significant. Mean changes in lumbar BMD were not significantly different from controls (–0.02). A fair-quality 2004 RCT did not demonstrate any clinically relevant effect on BMD at 2 years follow-up. This study used 800 mcg/day of fluticasone for patients with mild asthma.3
BMD changes found at higher doses
There is, however, some evidence that higher doses of inhaled corticosteroids can result in adverse BMD changes. In a high-quality RCT of 412 participants, aged 40 to 69 years, with mild to moderate COPD, use of higher-dose triamcinolone (1200 mcg/day) was associated with decreased lumbar and femoral neck BMD over 3 to 4 years.4 The differences in BMD between the inhaled corticosteroids and placebo groups at the femoral neck and lumbar spine were 1.78% (P<.001) and 1.33% (P=.007), respectively. However, the risk of fracture or height loss did not increase at follow-up.
A large fair-quality RCT from 2001 included in both meta-analyses demonstrated a dose-related fall in BMD within the subjects over 2 years at the lumbar spine (standard deviation, 3.4%; P<.010). This finding remained statistically significant after adjusting for asthma severity, but BMD changes were not different between the inhaled corticosteroids and placebo groups. However, this finding may be the result of higher oral corticosteroids use in the reference group.5
Limitations of these studies
These studies, though, have limitations. The follow-up periods for all of these studies are less than 5 years, and thus the longer-term effects of prolonged use of inhaled corticosteroids on BMD or fracture risk cannot be determined with this evidence. Furthermore, the study populations were relatively young, with few other risk factors (they were, for example, predominantly male) than populations at highest risk for osteoporosis and fracture. These factors limit interpretation of the data for long-term inhaled corticosteroids use, particularly in populations with higher baseline osteoporosis risk—older persons with chronic lung disease who take inhaled corticosteroids for more than 2 to 3 years. We need better and longer-term studies to help advise our patients about the risks and benefits of inhaled corticosteroids therapy.
Recommendations from others
The New Zealand Guideline Group says the risk of reduced BMD increased with long-term, high-dose inhaled corticosteroids.6 The Institute for Clinical Systems Improvement guidelines recommends considering osteoporosis prevention measures for those who have been (or will be) taking a daily high-dose inhaled glucocorticoid for several years as glucocorticoid use compounds fracture risk beyond that determined solely by BMD.7
1. Jones A, Fay JK, Burr M, et al. Inhaled corticosteroid effects on bone metabolism in asthma and chronic obstructive pulmonary disease. Cochrane Database Syst Rev 1, 2006.
2. Halpern MT, Schmier JK, Van Kerkhove MD, et al. Impact of long term inhaled corticosteroid therapy on bone mineral density results of a meta-analysis. Ann Allergy Asthma Immunol 2004;92:201-207.
3. Kemp JP, Osur S, Shrewsburry SB, et al. Potential effects of fluticasone propionate on bone mineral density in patients with asthma: A 2-year randomized, double-blind, placebo-controlled trial. Mayo Clin Proc 2004;79:458-466.
4. Scanlon PD, Connett JE, Wise RA, et al. Loss of bone density with inhaled triamcinolone in Lung Health Study II. Am J Respir Crit Care Med 2004;170:1302-1309.
5. Tattersfield AE, Town GI, Johnell O, et al. Bone mineral density in subjects with mild asthma randomized to treatment with inhaled corticosteroids or non-corticosteroid treatment for two years. Thorax 2001;56:272-278.
6. New Zealand Guidelines Group. The diagnosis and treatment of adult asthma. Wellington, NZ: New Zealand Guidelines Group; 2002 Sep. 101 p. Available at: www.guideline.gov/summary/summary.aspx?doc_id=3462 (NCG: 2688). Accessed on January 18, 2007.
7. Institute for Clinical Systems Improvement. Diagnosis and treatment of osteoporosis. Bloomington, Minn: Institute for Clinical Systems Improvement; 2005 Sep. 61 p. Available at: www.guideline.gov/summary/summary.aspx?doc_id=9626 (NCG: 5146). Accessed on January 18, 2007.
1. Jones A, Fay JK, Burr M, et al. Inhaled corticosteroid effects on bone metabolism in asthma and chronic obstructive pulmonary disease. Cochrane Database Syst Rev 1, 2006.
2. Halpern MT, Schmier JK, Van Kerkhove MD, et al. Impact of long term inhaled corticosteroid therapy on bone mineral density results of a meta-analysis. Ann Allergy Asthma Immunol 2004;92:201-207.
3. Kemp JP, Osur S, Shrewsburry SB, et al. Potential effects of fluticasone propionate on bone mineral density in patients with asthma: A 2-year randomized, double-blind, placebo-controlled trial. Mayo Clin Proc 2004;79:458-466.
4. Scanlon PD, Connett JE, Wise RA, et al. Loss of bone density with inhaled triamcinolone in Lung Health Study II. Am J Respir Crit Care Med 2004;170:1302-1309.
5. Tattersfield AE, Town GI, Johnell O, et al. Bone mineral density in subjects with mild asthma randomized to treatment with inhaled corticosteroids or non-corticosteroid treatment for two years. Thorax 2001;56:272-278.
6. New Zealand Guidelines Group. The diagnosis and treatment of adult asthma. Wellington, NZ: New Zealand Guidelines Group; 2002 Sep. 101 p. Available at: www.guideline.gov/summary/summary.aspx?doc_id=3462 (NCG: 2688). Accessed on January 18, 2007.
7. Institute for Clinical Systems Improvement. Diagnosis and treatment of osteoporosis. Bloomington, Minn: Institute for Clinical Systems Improvement; 2005 Sep. 61 p. Available at: www.guideline.gov/summary/summary.aspx?doc_id=9626 (NCG: 5146). Accessed on January 18, 2007.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best treatment for hypertension in African Americans?
In African Americans with hypertension, therapy is best initiated with the low-sodium Dietary Approaches to Stop Hypertension (DASH) diet and a thiazide-type diuretic (strength of recommendation [SOR]: A, based on randomized controlled trials). If the blood pressure goal is not achieved with thiazide monotherapy, a calcium channel blocker, angiotensin-converting enzyme (ACE) inhibitor, angiotensin II receptor blocker (ARB), or a beta-blocker can be added. An initial combination treatment is recommended for patients with systolic blood pressure >15 mm Hg or diastolic blood pressure >10 mm Hg above target (SOR: C, expert opinion).
African Americans have reduced blood pressure responses to monotherapy with beta-blocker, ACE inhibitor, or ARBs when compared to diuretics or calcium channel blockers (SOR: A, randomized controlled trials). However, cardiac and renal indications for prescribing these medications should be equally applied to African American patients (SOR: C, expert opinion).
African Americans respond better to combination ACE inhibitor plus diuretic
Mandi Sehgal, MD
University of Cincinnati
Treat African American patients with hypertension according to the Joint National Committee on Prevention, Detection, and Treatment of High blood Pressure (JNC 7) guidelines. These guidelines state that patients with stage 1 hypertension, regardless of race, should be treated with lifestyle modification (to include a low-salt diet and weight loss) for 3 months. If, after a trial of lifestyle modification, these patients still have hypertension, then start diuretic therapy while continuing lifestyle modifications.
If patients present with stage-2 hypertension, started them on a diuretic plus another agent. African American patients do not respond to ACE inhibitor monotherapy well, but do respond to the combination of an ACE inhibitor plus diuretic. If patients, regardless of race, have comorbid conditions that lend themselves to alternate antihypertensive treatment (ie, beta-blocker therapy post–myocardial infarction), then use these therapies first-line.
Evidence summary
Three large cohort studies determined that African Americans have a higher prevalence of hypertension and worse cardiovascular and renal outcomes when compared with white Americans. For African American patients, the standard blood pressure goals apply: below 140/90 mm Hg with uncomplicated hypertension and below 130/80 with diabetes or renal disease.1
Dietary interventions
An RCT compared the effects of consuming the DASH diet (consisting of 4–5 servings of fruit, 4–5 servings of vegetables, 2–3 servings of low-fat dairy per day, and <25% fat) with a typical high-fat control diet among 459 adults with normal or elevated blood pressure.2 Among 133 patients with hypertension, the DASH diet reduced systolic and diastolic blood pressure by 11.4 mm Hg (97.5% confidence interval [CI], –15.9 to –6.9) and 5.5 mm Hg (97.5% CI, –8.2 to –2.7) respectively when compared with the control diet. Among African Americans with hypertension, the DASH diet was even more beneficial, reducing their systolic and diastolic blood pressure by 13.2 mm Hg and 6.1 mm Hg respectively.1
Another RCT studied the effect of different levels of dietary sodium in conjunction with the DASH diet.3 A total of 412 participants were randomly assigned to eat either a control diet or the DASH diet. Within the assigned diet, participants ate foods with high (150 mmol/d), intermediate (100 mmol/d), and low (50 mmol/d) levels of sodium in random order. In this study, low-sodium DASH diet was associated with additional lowering of blood pressure, an effect that was also found to be stronger for African Americans patients than others.3 When compared with the combination of the control diet and a high level of sodium, the DASH diet and a low level of sodium lowered systolic blood pressure by 11.5 mm Hg for participants with hypertension (12.6 mm Hg for blacks; 9.5 mm Hg for others), and by 7.1 mm Hg for participants without hypertension (7.2 mm Hg for blacks; 6.9 mm Hg for others).3
Medical interventions
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial4 (ALLHAT) and African American Study of Kidney Disease and Hypertension5 (AASK) have demonstrated the benefit of blood pressure reduction using specific classes of antihypertensive agents.
The ALLHAT trial, a double-blind RCT of 42,448 high-risk hypertensive patients aged >55 years, compared chlorthalidone (a thiazide-type diuretic) with amlodipine (Norvasc), lisinopril (Prinivil, Zestril), or doxazosin (Cardura). In this study, which included 36% African Americans, chlorthalidone, lisinopril, and amlodipine did not differ in preventing major cardiovascular events. However, lisinopril was associated with an increased risk for heart failure (relative risk [RR] for African Americans=1.32; 95% CI, 1.11–1.58) and stroke (RR for African Americans=1.4; 95% CI, 1.17–1.68), and amlodipine was associated with a higher risk of heart failure (RR in African Americans=1.47; 95% CI, 1.24–1.74). Additionally, ACE inhibitor–induced angioedema or cough occurred more frequently among African American patients than white patients.4
Although a randomized controlled trial5 and a review of multiple studies6 demonstrated that African Americans may be less responsive to monotherapy with ACE inhibitors, the AASK trial confirmed that ACE inhibitors can provide significant clinical benefits for African Americans with hypertensive renal disease. AASK, a double-blind RCT of 1094 African American patients with renal insufficiency, compared the effects of an ACE inhibitor (ramipril [Altace]), a dihydropyridine calcium channel blocker (amlodipine), or a beta blocker (metoprolol [Lopressor]) on the progression of hypertensive renal disease.
The study showed a 44% relative risk reduction (95% CI, 13%–65%; number needed to treat [NNT]=25) in progression to end-stage renal disease, and a significant decrease in the combined endpoints of glomerular filtration rate events (decrease >50%), end-stage renal disease, and death (decreased by 38%) in the ramipril group compared with the amlodipine group (95% CI, 13%–56%; NNT=56 per patient-year).5,7 Metoprolol appeared to have intermediate outcomes.8
Recommendations from others
Both the International Society on Hypertension in Blacks (ISHIB) guidelines1 and the JNC 79 recommend therapeutic lifestyle modification that includes DASH diet, dietary sodium restriction, and weight reduction. Both guidelines recognize the importance of thiazide diuretics and recommend its use as first-line therapy or as a part of combination therapy for hypertension among African Americans. They also recommend initiating therapy with 2 agents for blood pressure significantly above target level (20/10 mm Hg above target per JNC 7, 15/10 mm Hg above target per ISHIB).
The ISHIB report emphasizes the need for not overlooking renal protection with an ACE inhibitor for African Americans with renal disease. The American Diabetes Association recommends that all patients with diabetes and hypertension be treated with a regimen that includes either an ACE inhibitor or an ARB.10
1. Americans: consensus statement of the Hypertension in African Americans Working Group of the International Society on Hypertension in Blacks. Arch Intern Med 2003;163:525-541.
2. Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative research Group. N Engl J Med 1997;336:1117-1124.
3. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001;344:3-10.
4. ALLHAT Officers and Coordinators for the ALLHAT Collaborative research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002;288:2981-2997.
5. Agodoa LY, Appel L, Bakris GL, et al. and the African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001;285:2719-2728.
6. Richardson AD, Piepho RW. Effect of race on hypertension and antihypertensive therapy. Int J Clin Pharmacol Ther 2000;38:75-79.
7. McConaghy J. What is the best treatment for slowing the progression to end-stage renal disease (ESRD) in African Americans with hypertensive nephropathy? J Fam Pract 2001;50:744.-
8. Wright JT, Bakris G, Greene T, et al. and the African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: Results of the AASK trial. JAMA 2002;288:2421-2431.
9. Chobanian AV, Bakris GL, Black HR, et al. and the National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High blood Pressure: the JNC 7 report. JAMA 2003;289:2560-2572.
10. American Diabetes Association. Standards of Medical Care in Diabetes—2006. Diabetes Care 2006;29:S4-S42.
In African Americans with hypertension, therapy is best initiated with the low-sodium Dietary Approaches to Stop Hypertension (DASH) diet and a thiazide-type diuretic (strength of recommendation [SOR]: A, based on randomized controlled trials). If the blood pressure goal is not achieved with thiazide monotherapy, a calcium channel blocker, angiotensin-converting enzyme (ACE) inhibitor, angiotensin II receptor blocker (ARB), or a beta-blocker can be added. An initial combination treatment is recommended for patients with systolic blood pressure >15 mm Hg or diastolic blood pressure >10 mm Hg above target (SOR: C, expert opinion).
African Americans have reduced blood pressure responses to monotherapy with beta-blocker, ACE inhibitor, or ARBs when compared to diuretics or calcium channel blockers (SOR: A, randomized controlled trials). However, cardiac and renal indications for prescribing these medications should be equally applied to African American patients (SOR: C, expert opinion).
African Americans respond better to combination ACE inhibitor plus diuretic
Mandi Sehgal, MD
University of Cincinnati
Treat African American patients with hypertension according to the Joint National Committee on Prevention, Detection, and Treatment of High blood Pressure (JNC 7) guidelines. These guidelines state that patients with stage 1 hypertension, regardless of race, should be treated with lifestyle modification (to include a low-salt diet and weight loss) for 3 months. If, after a trial of lifestyle modification, these patients still have hypertension, then start diuretic therapy while continuing lifestyle modifications.
If patients present with stage-2 hypertension, started them on a diuretic plus another agent. African American patients do not respond to ACE inhibitor monotherapy well, but do respond to the combination of an ACE inhibitor plus diuretic. If patients, regardless of race, have comorbid conditions that lend themselves to alternate antihypertensive treatment (ie, beta-blocker therapy post–myocardial infarction), then use these therapies first-line.
Evidence summary
Three large cohort studies determined that African Americans have a higher prevalence of hypertension and worse cardiovascular and renal outcomes when compared with white Americans. For African American patients, the standard blood pressure goals apply: below 140/90 mm Hg with uncomplicated hypertension and below 130/80 with diabetes or renal disease.1
Dietary interventions
An RCT compared the effects of consuming the DASH diet (consisting of 4–5 servings of fruit, 4–5 servings of vegetables, 2–3 servings of low-fat dairy per day, and <25% fat) with a typical high-fat control diet among 459 adults with normal or elevated blood pressure.2 Among 133 patients with hypertension, the DASH diet reduced systolic and diastolic blood pressure by 11.4 mm Hg (97.5% confidence interval [CI], –15.9 to –6.9) and 5.5 mm Hg (97.5% CI, –8.2 to –2.7) respectively when compared with the control diet. Among African Americans with hypertension, the DASH diet was even more beneficial, reducing their systolic and diastolic blood pressure by 13.2 mm Hg and 6.1 mm Hg respectively.1
Another RCT studied the effect of different levels of dietary sodium in conjunction with the DASH diet.3 A total of 412 participants were randomly assigned to eat either a control diet or the DASH diet. Within the assigned diet, participants ate foods with high (150 mmol/d), intermediate (100 mmol/d), and low (50 mmol/d) levels of sodium in random order. In this study, low-sodium DASH diet was associated with additional lowering of blood pressure, an effect that was also found to be stronger for African Americans patients than others.3 When compared with the combination of the control diet and a high level of sodium, the DASH diet and a low level of sodium lowered systolic blood pressure by 11.5 mm Hg for participants with hypertension (12.6 mm Hg for blacks; 9.5 mm Hg for others), and by 7.1 mm Hg for participants without hypertension (7.2 mm Hg for blacks; 6.9 mm Hg for others).3
Medical interventions
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial4 (ALLHAT) and African American Study of Kidney Disease and Hypertension5 (AASK) have demonstrated the benefit of blood pressure reduction using specific classes of antihypertensive agents.
The ALLHAT trial, a double-blind RCT of 42,448 high-risk hypertensive patients aged >55 years, compared chlorthalidone (a thiazide-type diuretic) with amlodipine (Norvasc), lisinopril (Prinivil, Zestril), or doxazosin (Cardura). In this study, which included 36% African Americans, chlorthalidone, lisinopril, and amlodipine did not differ in preventing major cardiovascular events. However, lisinopril was associated with an increased risk for heart failure (relative risk [RR] for African Americans=1.32; 95% CI, 1.11–1.58) and stroke (RR for African Americans=1.4; 95% CI, 1.17–1.68), and amlodipine was associated with a higher risk of heart failure (RR in African Americans=1.47; 95% CI, 1.24–1.74). Additionally, ACE inhibitor–induced angioedema or cough occurred more frequently among African American patients than white patients.4
Although a randomized controlled trial5 and a review of multiple studies6 demonstrated that African Americans may be less responsive to monotherapy with ACE inhibitors, the AASK trial confirmed that ACE inhibitors can provide significant clinical benefits for African Americans with hypertensive renal disease. AASK, a double-blind RCT of 1094 African American patients with renal insufficiency, compared the effects of an ACE inhibitor (ramipril [Altace]), a dihydropyridine calcium channel blocker (amlodipine), or a beta blocker (metoprolol [Lopressor]) on the progression of hypertensive renal disease.
The study showed a 44% relative risk reduction (95% CI, 13%–65%; number needed to treat [NNT]=25) in progression to end-stage renal disease, and a significant decrease in the combined endpoints of glomerular filtration rate events (decrease >50%), end-stage renal disease, and death (decreased by 38%) in the ramipril group compared with the amlodipine group (95% CI, 13%–56%; NNT=56 per patient-year).5,7 Metoprolol appeared to have intermediate outcomes.8
Recommendations from others
Both the International Society on Hypertension in Blacks (ISHIB) guidelines1 and the JNC 79 recommend therapeutic lifestyle modification that includes DASH diet, dietary sodium restriction, and weight reduction. Both guidelines recognize the importance of thiazide diuretics and recommend its use as first-line therapy or as a part of combination therapy for hypertension among African Americans. They also recommend initiating therapy with 2 agents for blood pressure significantly above target level (20/10 mm Hg above target per JNC 7, 15/10 mm Hg above target per ISHIB).
The ISHIB report emphasizes the need for not overlooking renal protection with an ACE inhibitor for African Americans with renal disease. The American Diabetes Association recommends that all patients with diabetes and hypertension be treated with a regimen that includes either an ACE inhibitor or an ARB.10
In African Americans with hypertension, therapy is best initiated with the low-sodium Dietary Approaches to Stop Hypertension (DASH) diet and a thiazide-type diuretic (strength of recommendation [SOR]: A, based on randomized controlled trials). If the blood pressure goal is not achieved with thiazide monotherapy, a calcium channel blocker, angiotensin-converting enzyme (ACE) inhibitor, angiotensin II receptor blocker (ARB), or a beta-blocker can be added. An initial combination treatment is recommended for patients with systolic blood pressure >15 mm Hg or diastolic blood pressure >10 mm Hg above target (SOR: C, expert opinion).
African Americans have reduced blood pressure responses to monotherapy with beta-blocker, ACE inhibitor, or ARBs when compared to diuretics or calcium channel blockers (SOR: A, randomized controlled trials). However, cardiac and renal indications for prescribing these medications should be equally applied to African American patients (SOR: C, expert opinion).
African Americans respond better to combination ACE inhibitor plus diuretic
Mandi Sehgal, MD
University of Cincinnati
Treat African American patients with hypertension according to the Joint National Committee on Prevention, Detection, and Treatment of High blood Pressure (JNC 7) guidelines. These guidelines state that patients with stage 1 hypertension, regardless of race, should be treated with lifestyle modification (to include a low-salt diet and weight loss) for 3 months. If, after a trial of lifestyle modification, these patients still have hypertension, then start diuretic therapy while continuing lifestyle modifications.
If patients present with stage-2 hypertension, started them on a diuretic plus another agent. African American patients do not respond to ACE inhibitor monotherapy well, but do respond to the combination of an ACE inhibitor plus diuretic. If patients, regardless of race, have comorbid conditions that lend themselves to alternate antihypertensive treatment (ie, beta-blocker therapy post–myocardial infarction), then use these therapies first-line.
Evidence summary
Three large cohort studies determined that African Americans have a higher prevalence of hypertension and worse cardiovascular and renal outcomes when compared with white Americans. For African American patients, the standard blood pressure goals apply: below 140/90 mm Hg with uncomplicated hypertension and below 130/80 with diabetes or renal disease.1
Dietary interventions
An RCT compared the effects of consuming the DASH diet (consisting of 4–5 servings of fruit, 4–5 servings of vegetables, 2–3 servings of low-fat dairy per day, and <25% fat) with a typical high-fat control diet among 459 adults with normal or elevated blood pressure.2 Among 133 patients with hypertension, the DASH diet reduced systolic and diastolic blood pressure by 11.4 mm Hg (97.5% confidence interval [CI], –15.9 to –6.9) and 5.5 mm Hg (97.5% CI, –8.2 to –2.7) respectively when compared with the control diet. Among African Americans with hypertension, the DASH diet was even more beneficial, reducing their systolic and diastolic blood pressure by 13.2 mm Hg and 6.1 mm Hg respectively.1
Another RCT studied the effect of different levels of dietary sodium in conjunction with the DASH diet.3 A total of 412 participants were randomly assigned to eat either a control diet or the DASH diet. Within the assigned diet, participants ate foods with high (150 mmol/d), intermediate (100 mmol/d), and low (50 mmol/d) levels of sodium in random order. In this study, low-sodium DASH diet was associated with additional lowering of blood pressure, an effect that was also found to be stronger for African Americans patients than others.3 When compared with the combination of the control diet and a high level of sodium, the DASH diet and a low level of sodium lowered systolic blood pressure by 11.5 mm Hg for participants with hypertension (12.6 mm Hg for blacks; 9.5 mm Hg for others), and by 7.1 mm Hg for participants without hypertension (7.2 mm Hg for blacks; 6.9 mm Hg for others).3
Medical interventions
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial4 (ALLHAT) and African American Study of Kidney Disease and Hypertension5 (AASK) have demonstrated the benefit of blood pressure reduction using specific classes of antihypertensive agents.
The ALLHAT trial, a double-blind RCT of 42,448 high-risk hypertensive patients aged >55 years, compared chlorthalidone (a thiazide-type diuretic) with amlodipine (Norvasc), lisinopril (Prinivil, Zestril), or doxazosin (Cardura). In this study, which included 36% African Americans, chlorthalidone, lisinopril, and amlodipine did not differ in preventing major cardiovascular events. However, lisinopril was associated with an increased risk for heart failure (relative risk [RR] for African Americans=1.32; 95% CI, 1.11–1.58) and stroke (RR for African Americans=1.4; 95% CI, 1.17–1.68), and amlodipine was associated with a higher risk of heart failure (RR in African Americans=1.47; 95% CI, 1.24–1.74). Additionally, ACE inhibitor–induced angioedema or cough occurred more frequently among African American patients than white patients.4
Although a randomized controlled trial5 and a review of multiple studies6 demonstrated that African Americans may be less responsive to monotherapy with ACE inhibitors, the AASK trial confirmed that ACE inhibitors can provide significant clinical benefits for African Americans with hypertensive renal disease. AASK, a double-blind RCT of 1094 African American patients with renal insufficiency, compared the effects of an ACE inhibitor (ramipril [Altace]), a dihydropyridine calcium channel blocker (amlodipine), or a beta blocker (metoprolol [Lopressor]) on the progression of hypertensive renal disease.
The study showed a 44% relative risk reduction (95% CI, 13%–65%; number needed to treat [NNT]=25) in progression to end-stage renal disease, and a significant decrease in the combined endpoints of glomerular filtration rate events (decrease >50%), end-stage renal disease, and death (decreased by 38%) in the ramipril group compared with the amlodipine group (95% CI, 13%–56%; NNT=56 per patient-year).5,7 Metoprolol appeared to have intermediate outcomes.8
Recommendations from others
Both the International Society on Hypertension in Blacks (ISHIB) guidelines1 and the JNC 79 recommend therapeutic lifestyle modification that includes DASH diet, dietary sodium restriction, and weight reduction. Both guidelines recognize the importance of thiazide diuretics and recommend its use as first-line therapy or as a part of combination therapy for hypertension among African Americans. They also recommend initiating therapy with 2 agents for blood pressure significantly above target level (20/10 mm Hg above target per JNC 7, 15/10 mm Hg above target per ISHIB).
The ISHIB report emphasizes the need for not overlooking renal protection with an ACE inhibitor for African Americans with renal disease. The American Diabetes Association recommends that all patients with diabetes and hypertension be treated with a regimen that includes either an ACE inhibitor or an ARB.10
1. Americans: consensus statement of the Hypertension in African Americans Working Group of the International Society on Hypertension in Blacks. Arch Intern Med 2003;163:525-541.
2. Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative research Group. N Engl J Med 1997;336:1117-1124.
3. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001;344:3-10.
4. ALLHAT Officers and Coordinators for the ALLHAT Collaborative research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002;288:2981-2997.
5. Agodoa LY, Appel L, Bakris GL, et al. and the African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001;285:2719-2728.
6. Richardson AD, Piepho RW. Effect of race on hypertension and antihypertensive therapy. Int J Clin Pharmacol Ther 2000;38:75-79.
7. McConaghy J. What is the best treatment for slowing the progression to end-stage renal disease (ESRD) in African Americans with hypertensive nephropathy? J Fam Pract 2001;50:744.-
8. Wright JT, Bakris G, Greene T, et al. and the African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: Results of the AASK trial. JAMA 2002;288:2421-2431.
9. Chobanian AV, Bakris GL, Black HR, et al. and the National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High blood Pressure: the JNC 7 report. JAMA 2003;289:2560-2572.
10. American Diabetes Association. Standards of Medical Care in Diabetes—2006. Diabetes Care 2006;29:S4-S42.
1. Americans: consensus statement of the Hypertension in African Americans Working Group of the International Society on Hypertension in Blacks. Arch Intern Med 2003;163:525-541.
2. Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative research Group. N Engl J Med 1997;336:1117-1124.
3. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001;344:3-10.
4. ALLHAT Officers and Coordinators for the ALLHAT Collaborative research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002;288:2981-2997.
5. Agodoa LY, Appel L, Bakris GL, et al. and the African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001;285:2719-2728.
6. Richardson AD, Piepho RW. Effect of race on hypertension and antihypertensive therapy. Int J Clin Pharmacol Ther 2000;38:75-79.
7. McConaghy J. What is the best treatment for slowing the progression to end-stage renal disease (ESRD) in African Americans with hypertensive nephropathy? J Fam Pract 2001;50:744.-
8. Wright JT, Bakris G, Greene T, et al. and the African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: Results of the AASK trial. JAMA 2002;288:2421-2431.
9. Chobanian AV, Bakris GL, Black HR, et al. and the National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High blood Pressure: the JNC 7 report. JAMA 2003;289:2560-2572.
10. American Diabetes Association. Standards of Medical Care in Diabetes—2006. Diabetes Care 2006;29:S4-S42.
Evidence-based answers from the Family Physicians Inquiries Network
What evaluation is best for an isolated, enlarged cervical lymph node?
The evaluation and follow-up of an isolated, enlarged cervical lymph node is determined by the presence of inflammation, duration, size, and associated symptoms. For patients with inflammatory symptoms (ie, fever, pain, erythema, and recent infection), a single course of broad-spectrum antibiotic and reassessment in 1 to 2 weeks is reasonable (strength of recommendation [SOR]: C, expert opinion). If lymph node enlargement persists despite antibiotics, yet an infectious or inflammatory cause is still suspected, further evaluation may include a PPD skin test and chest radiograph1 (SOR: C, expert opinion). For patients without initial inflammatory symptoms, biopsy is recommended if the lymph node enlargement persists beyond 4 to 6 weeks, continues to enlarge, or is >3 cm1 (SOR: C, expert opinion). Biopsy is also indicated if there is a supraclavicular lymph node or concomitant constitutional symptoms (weight loss or night sweats)2 (SOR: B, case series). Ultrasound or computerized tomography (CT) can also be helpful in determining which method of biopsy to choose3 (SOR: B, case series). Fine-needle aspiration is a minimally invasive method for obtaining a tissue sample, but excisional biopsy can provide a definitive diagnosis2-6 (SOR: B, case series).
For those with no risk factors and an uncomplicated exam, counsel “tincture of time”
Paul Crawford, MD
US Air Force–Eglin Family Practice Residency, Eglin, Air Force Base, Fla
The foundation of managing solitary enlarged cervical nodes is a good history and physical. For patients with a benign story, no risk factors, and an uncomplicated exam, I always counsel “tincture of time” as the first-line diagnostic test.
However, this changes when patients present with risk factors for malignancy (such as being older, male, white. or with a supraclavicular node) and a worrisome story or exam finding. In these cases, watchful waiting may delay diagnosis. Sometimes, in spite of my best efforts to reassure low-risk patients, their fear and anxiety derail my attempts to practice good medicine. For these patients, the only harm an ultra-sound does is to the wallet.
Evidence summary
Limited research exists in this area. Practice today is guided by clinical judgment, anecdotal evidence, and historical teaching. Assessment for inflammation and malignancy risk factors contributes to the diagnosis.
Lymph nodes with concomitant malignancy risk factors warrant immediate evaluation. For lymph nodes without signs or symptoms of inflammation or malignancy, observation for 4 to 6 weeks has been recommended. Further evaluation with imaging or biopsy is indicated if the node persists beyond 4 to 6 weeks, continues to enlarge, is located within the supraclavicular fossa, or is >3 cm.1
A study of 550 patients identified 5 significant predictors of malignancy: male gender (risk ratio [RR]=2.72; 95% confidence interval [CI], 1.63–4.56), increasing age (RR=1.05; 95% CI, 1.04–1.07), white ethnicity (RR=3.01; 95% CI, 1.19–7.6), supraclavicular lymph nodes (RR=3.72; 95% CI, 1.52–9.12), and 2 or more regions of lymph nodes (RR=6.41; 95% CI, 2.82–14.58).5
For lymph nodes with inflammatory symptoms, further evaluation (including imaging) is indicated if there is no response to antibiotics. CT with contrast is considered the gold standard. However, a study of 50 patients with lymphadenopathy on CT demonstrated the sensitivity of ultrasound was 92% in identifying the same nodes.3 Another study demonstrated an ultrasound sensitivity of 100% and specificity of 97% for 154 patients with lymphadenopathy.5
Histologic evaluation after excisional biopsy is the gold standard for diagnosis. Fine-needle aspiration is an alternate, minimally invasive option for further work-up. Fine-needle aspiration had a sensitivity of 49% and specificity of 97% in a study of 550 patients.5 In a study of 309 patients with supraclavicular lymphadenopathy, fine-needle aspiration had a sensitivity of 97%, a specificity of 98%, and a positive predictive value of 98%. A study of 94 patients found that clinical exam alone was 78% sensitive in diagnosing the cause of lymphadenopathy; this improved to 93% sensitivity with fine-needle aspiration.6
Fine-needle aspiration has a higher rate of false negatives. A study of 1103 patients found a 97% sensitivity (3.4% false-negative rate) and a 99% specificity (0.9% false-positive rate) for fine-needle aspiration.4 In cases where pathology is equivocal, or where concern for malignancy is exceptionally high, excisional biopsy provides a more definitive diagnosis.
Recommendations from others
Cecil’s Textbook of Medicine recommends observing the nodes when they are soft and smaller than 2 to 3 cm and the patient has no obvious systemic illness. They note that performing a complete blood count and peripheral smear exam can aid in diagnosing systemic illness and that antibiotics are often given. They suggest performing a biopsy if the lymph node does not regress within a few weeks or if it grows. They also say the art of medicine is at play here and that if patients are particularly anxious, biopsy may be done more quickly.7
Harrison’s Manual of Medicine specifies that nodes >4 cm located in the subclavicular or scalene area or hard nodes fixed to surrounding tissues should be biopsied immediately, and that tender nodes are most often benign.8
1. Schwetschenau E, Kelley DJ. The adult neck mass. Am Fam Physician 2002;66:831-838.
2. Ellison E, LaPuerta P, Martin SE. Supraclavicular masses: Results of a series of 309 cases biopsied by fine needle aspiration. Head Neck 1999;21:239-246.
3. Beissert M, Jenett M, Wetzler T, Hinterseher I, Kessler C, Hahn D. Enlarged lymph nodes of the neck: evaluation with parallel extended field-of-view sonographic sequences. J Ultrasound Med 2000;19:195-200.
4. Steel BL, Schwartz MR, Ramzy I. Fine needle aspiration biopsy in the diagnosis of lymphadenopathy in 1,103 patients. Role, limitations and analysis of diagnostic pitfalls. Acta Cytol 1995;39:76-81.
5. Chau I, Kelleher MT, Cunningham D, et al. Rapid access multidisciplinary lymph node diagnostic clinic: Analysis of 550 patients. Br J Cancer 2003;88:354-361.
6. Al-Mulhim AS, Al-Ghamdi AM, Al-Marzooq YM, et al. The role of fine needle aspiration cytology and imprint cytology in cervical lymphadenopathy. Saudi Med J 2004;25:862-865.
7. Armitage JO. Approach to the patient with lymphadenopathy and splenomegaly. In Goldman L, Ausiello A (eds), Cecil Textbook of Medicine, 22nd ed. Chapter 164. Philadelphia, Pa: WB Saunders Co; 2004.
8. Braunwald E, Fauci AS, Kasper DL, et al. Harrison’s Manual of Medicine. Chapter 28. New york: McGraw-Hill Professional; 2002.
The evaluation and follow-up of an isolated, enlarged cervical lymph node is determined by the presence of inflammation, duration, size, and associated symptoms. For patients with inflammatory symptoms (ie, fever, pain, erythema, and recent infection), a single course of broad-spectrum antibiotic and reassessment in 1 to 2 weeks is reasonable (strength of recommendation [SOR]: C, expert opinion). If lymph node enlargement persists despite antibiotics, yet an infectious or inflammatory cause is still suspected, further evaluation may include a PPD skin test and chest radiograph1 (SOR: C, expert opinion). For patients without initial inflammatory symptoms, biopsy is recommended if the lymph node enlargement persists beyond 4 to 6 weeks, continues to enlarge, or is >3 cm1 (SOR: C, expert opinion). Biopsy is also indicated if there is a supraclavicular lymph node or concomitant constitutional symptoms (weight loss or night sweats)2 (SOR: B, case series). Ultrasound or computerized tomography (CT) can also be helpful in determining which method of biopsy to choose3 (SOR: B, case series). Fine-needle aspiration is a minimally invasive method for obtaining a tissue sample, but excisional biopsy can provide a definitive diagnosis2-6 (SOR: B, case series).
For those with no risk factors and an uncomplicated exam, counsel “tincture of time”
Paul Crawford, MD
US Air Force–Eglin Family Practice Residency, Eglin, Air Force Base, Fla
The foundation of managing solitary enlarged cervical nodes is a good history and physical. For patients with a benign story, no risk factors, and an uncomplicated exam, I always counsel “tincture of time” as the first-line diagnostic test.
However, this changes when patients present with risk factors for malignancy (such as being older, male, white. or with a supraclavicular node) and a worrisome story or exam finding. In these cases, watchful waiting may delay diagnosis. Sometimes, in spite of my best efforts to reassure low-risk patients, their fear and anxiety derail my attempts to practice good medicine. For these patients, the only harm an ultra-sound does is to the wallet.
Evidence summary
Limited research exists in this area. Practice today is guided by clinical judgment, anecdotal evidence, and historical teaching. Assessment for inflammation and malignancy risk factors contributes to the diagnosis.
Lymph nodes with concomitant malignancy risk factors warrant immediate evaluation. For lymph nodes without signs or symptoms of inflammation or malignancy, observation for 4 to 6 weeks has been recommended. Further evaluation with imaging or biopsy is indicated if the node persists beyond 4 to 6 weeks, continues to enlarge, is located within the supraclavicular fossa, or is >3 cm.1
A study of 550 patients identified 5 significant predictors of malignancy: male gender (risk ratio [RR]=2.72; 95% confidence interval [CI], 1.63–4.56), increasing age (RR=1.05; 95% CI, 1.04–1.07), white ethnicity (RR=3.01; 95% CI, 1.19–7.6), supraclavicular lymph nodes (RR=3.72; 95% CI, 1.52–9.12), and 2 or more regions of lymph nodes (RR=6.41; 95% CI, 2.82–14.58).5
For lymph nodes with inflammatory symptoms, further evaluation (including imaging) is indicated if there is no response to antibiotics. CT with contrast is considered the gold standard. However, a study of 50 patients with lymphadenopathy on CT demonstrated the sensitivity of ultrasound was 92% in identifying the same nodes.3 Another study demonstrated an ultrasound sensitivity of 100% and specificity of 97% for 154 patients with lymphadenopathy.5
Histologic evaluation after excisional biopsy is the gold standard for diagnosis. Fine-needle aspiration is an alternate, minimally invasive option for further work-up. Fine-needle aspiration had a sensitivity of 49% and specificity of 97% in a study of 550 patients.5 In a study of 309 patients with supraclavicular lymphadenopathy, fine-needle aspiration had a sensitivity of 97%, a specificity of 98%, and a positive predictive value of 98%. A study of 94 patients found that clinical exam alone was 78% sensitive in diagnosing the cause of lymphadenopathy; this improved to 93% sensitivity with fine-needle aspiration.6
Fine-needle aspiration has a higher rate of false negatives. A study of 1103 patients found a 97% sensitivity (3.4% false-negative rate) and a 99% specificity (0.9% false-positive rate) for fine-needle aspiration.4 In cases where pathology is equivocal, or where concern for malignancy is exceptionally high, excisional biopsy provides a more definitive diagnosis.
Recommendations from others
Cecil’s Textbook of Medicine recommends observing the nodes when they are soft and smaller than 2 to 3 cm and the patient has no obvious systemic illness. They note that performing a complete blood count and peripheral smear exam can aid in diagnosing systemic illness and that antibiotics are often given. They suggest performing a biopsy if the lymph node does not regress within a few weeks or if it grows. They also say the art of medicine is at play here and that if patients are particularly anxious, biopsy may be done more quickly.7
Harrison’s Manual of Medicine specifies that nodes >4 cm located in the subclavicular or scalene area or hard nodes fixed to surrounding tissues should be biopsied immediately, and that tender nodes are most often benign.8
The evaluation and follow-up of an isolated, enlarged cervical lymph node is determined by the presence of inflammation, duration, size, and associated symptoms. For patients with inflammatory symptoms (ie, fever, pain, erythema, and recent infection), a single course of broad-spectrum antibiotic and reassessment in 1 to 2 weeks is reasonable (strength of recommendation [SOR]: C, expert opinion). If lymph node enlargement persists despite antibiotics, yet an infectious or inflammatory cause is still suspected, further evaluation may include a PPD skin test and chest radiograph1 (SOR: C, expert opinion). For patients without initial inflammatory symptoms, biopsy is recommended if the lymph node enlargement persists beyond 4 to 6 weeks, continues to enlarge, or is >3 cm1 (SOR: C, expert opinion). Biopsy is also indicated if there is a supraclavicular lymph node or concomitant constitutional symptoms (weight loss or night sweats)2 (SOR: B, case series). Ultrasound or computerized tomography (CT) can also be helpful in determining which method of biopsy to choose3 (SOR: B, case series). Fine-needle aspiration is a minimally invasive method for obtaining a tissue sample, but excisional biopsy can provide a definitive diagnosis2-6 (SOR: B, case series).
For those with no risk factors and an uncomplicated exam, counsel “tincture of time”
Paul Crawford, MD
US Air Force–Eglin Family Practice Residency, Eglin, Air Force Base, Fla
The foundation of managing solitary enlarged cervical nodes is a good history and physical. For patients with a benign story, no risk factors, and an uncomplicated exam, I always counsel “tincture of time” as the first-line diagnostic test.
However, this changes when patients present with risk factors for malignancy (such as being older, male, white. or with a supraclavicular node) and a worrisome story or exam finding. In these cases, watchful waiting may delay diagnosis. Sometimes, in spite of my best efforts to reassure low-risk patients, their fear and anxiety derail my attempts to practice good medicine. For these patients, the only harm an ultra-sound does is to the wallet.
Evidence summary
Limited research exists in this area. Practice today is guided by clinical judgment, anecdotal evidence, and historical teaching. Assessment for inflammation and malignancy risk factors contributes to the diagnosis.
Lymph nodes with concomitant malignancy risk factors warrant immediate evaluation. For lymph nodes without signs or symptoms of inflammation or malignancy, observation for 4 to 6 weeks has been recommended. Further evaluation with imaging or biopsy is indicated if the node persists beyond 4 to 6 weeks, continues to enlarge, is located within the supraclavicular fossa, or is >3 cm.1
A study of 550 patients identified 5 significant predictors of malignancy: male gender (risk ratio [RR]=2.72; 95% confidence interval [CI], 1.63–4.56), increasing age (RR=1.05; 95% CI, 1.04–1.07), white ethnicity (RR=3.01; 95% CI, 1.19–7.6), supraclavicular lymph nodes (RR=3.72; 95% CI, 1.52–9.12), and 2 or more regions of lymph nodes (RR=6.41; 95% CI, 2.82–14.58).5
For lymph nodes with inflammatory symptoms, further evaluation (including imaging) is indicated if there is no response to antibiotics. CT with contrast is considered the gold standard. However, a study of 50 patients with lymphadenopathy on CT demonstrated the sensitivity of ultrasound was 92% in identifying the same nodes.3 Another study demonstrated an ultrasound sensitivity of 100% and specificity of 97% for 154 patients with lymphadenopathy.5
Histologic evaluation after excisional biopsy is the gold standard for diagnosis. Fine-needle aspiration is an alternate, minimally invasive option for further work-up. Fine-needle aspiration had a sensitivity of 49% and specificity of 97% in a study of 550 patients.5 In a study of 309 patients with supraclavicular lymphadenopathy, fine-needle aspiration had a sensitivity of 97%, a specificity of 98%, and a positive predictive value of 98%. A study of 94 patients found that clinical exam alone was 78% sensitive in diagnosing the cause of lymphadenopathy; this improved to 93% sensitivity with fine-needle aspiration.6
Fine-needle aspiration has a higher rate of false negatives. A study of 1103 patients found a 97% sensitivity (3.4% false-negative rate) and a 99% specificity (0.9% false-positive rate) for fine-needle aspiration.4 In cases where pathology is equivocal, or where concern for malignancy is exceptionally high, excisional biopsy provides a more definitive diagnosis.
Recommendations from others
Cecil’s Textbook of Medicine recommends observing the nodes when they are soft and smaller than 2 to 3 cm and the patient has no obvious systemic illness. They note that performing a complete blood count and peripheral smear exam can aid in diagnosing systemic illness and that antibiotics are often given. They suggest performing a biopsy if the lymph node does not regress within a few weeks or if it grows. They also say the art of medicine is at play here and that if patients are particularly anxious, biopsy may be done more quickly.7
Harrison’s Manual of Medicine specifies that nodes >4 cm located in the subclavicular or scalene area or hard nodes fixed to surrounding tissues should be biopsied immediately, and that tender nodes are most often benign.8
1. Schwetschenau E, Kelley DJ. The adult neck mass. Am Fam Physician 2002;66:831-838.
2. Ellison E, LaPuerta P, Martin SE. Supraclavicular masses: Results of a series of 309 cases biopsied by fine needle aspiration. Head Neck 1999;21:239-246.
3. Beissert M, Jenett M, Wetzler T, Hinterseher I, Kessler C, Hahn D. Enlarged lymph nodes of the neck: evaluation with parallel extended field-of-view sonographic sequences. J Ultrasound Med 2000;19:195-200.
4. Steel BL, Schwartz MR, Ramzy I. Fine needle aspiration biopsy in the diagnosis of lymphadenopathy in 1,103 patients. Role, limitations and analysis of diagnostic pitfalls. Acta Cytol 1995;39:76-81.
5. Chau I, Kelleher MT, Cunningham D, et al. Rapid access multidisciplinary lymph node diagnostic clinic: Analysis of 550 patients. Br J Cancer 2003;88:354-361.
6. Al-Mulhim AS, Al-Ghamdi AM, Al-Marzooq YM, et al. The role of fine needle aspiration cytology and imprint cytology in cervical lymphadenopathy. Saudi Med J 2004;25:862-865.
7. Armitage JO. Approach to the patient with lymphadenopathy and splenomegaly. In Goldman L, Ausiello A (eds), Cecil Textbook of Medicine, 22nd ed. Chapter 164. Philadelphia, Pa: WB Saunders Co; 2004.
8. Braunwald E, Fauci AS, Kasper DL, et al. Harrison’s Manual of Medicine. Chapter 28. New york: McGraw-Hill Professional; 2002.
1. Schwetschenau E, Kelley DJ. The adult neck mass. Am Fam Physician 2002;66:831-838.
2. Ellison E, LaPuerta P, Martin SE. Supraclavicular masses: Results of a series of 309 cases biopsied by fine needle aspiration. Head Neck 1999;21:239-246.
3. Beissert M, Jenett M, Wetzler T, Hinterseher I, Kessler C, Hahn D. Enlarged lymph nodes of the neck: evaluation with parallel extended field-of-view sonographic sequences. J Ultrasound Med 2000;19:195-200.
4. Steel BL, Schwartz MR, Ramzy I. Fine needle aspiration biopsy in the diagnosis of lymphadenopathy in 1,103 patients. Role, limitations and analysis of diagnostic pitfalls. Acta Cytol 1995;39:76-81.
5. Chau I, Kelleher MT, Cunningham D, et al. Rapid access multidisciplinary lymph node diagnostic clinic: Analysis of 550 patients. Br J Cancer 2003;88:354-361.
6. Al-Mulhim AS, Al-Ghamdi AM, Al-Marzooq YM, et al. The role of fine needle aspiration cytology and imprint cytology in cervical lymphadenopathy. Saudi Med J 2004;25:862-865.
7. Armitage JO. Approach to the patient with lymphadenopathy and splenomegaly. In Goldman L, Ausiello A (eds), Cecil Textbook of Medicine, 22nd ed. Chapter 164. Philadelphia, Pa: WB Saunders Co; 2004.
8. Braunwald E, Fauci AS, Kasper DL, et al. Harrison’s Manual of Medicine. Chapter 28. New york: McGraw-Hill Professional; 2002.
Evidence-based answers from the Family Physicians Inquiries Network
Angiotensin blockade for diabetes: Monitor microalbuminuria?
No studies address whether continued screening for microalbuminuria once a patient is taking an angiotensin-converting enzyme (ACE) inhibitor or angiotensin-2 receptor blocker (ARB) improves outcomes. Indirect evidence and expert opinion suggest that it may be beneficial to continue microalbuminuria surveillance to assess response to therapy and monitor disease progression (strength of recommendation: C, based on expert opinion).
It is unclear whether microalbuminuria tests in these cases is money well spent
Chris Vincent, MD
Swedish Family Medicine Residency, University of Washington, Seattle
At the residency where I teach, clinicians routinely try to get to the evidence behind the expert opinions, and faculty are discouraged from giving off the cuff or experiential answers. When asked whether to monitor microalbuminuria for patients with diabetes receiving ACE inhibitors or ARBs, it is frustrating to discover that no direct evidence supports the experts’ advice.
The screening test for urine microalbuminuria at our hospital costs $90. Since most patients with diabetes are being treated with ACE inhibitors or ARBs, it would be nice to know that the money for the testing is well spent. Unfortunately, in this instance, we can only continue to practice the “standard of care” and hope for future research to definitively answer this question.
Evidence Summary
Our comprehensive literature search found no studies that provide direct evidence for or against continuing to monitor microalbuminuria among patients with diabetes already on ACE inhibitor or ARB therapy. We reviewed and included indirect evidence and expert opinion to answer this clinical question.
Diabetes mellitus is the leading cause of end-stage renal disease in the Western world.1 The prevalence of diabetic nephropathy continues to rise along with the rapidly rising prevalence of obesity and diabetes, with 40% of patients with diabetes at risk of developing nephropathy. One study that followed 5097 patients with type 2 diabetes over a median of 10.4 years found that 2% of patients progressed from normal levels of urinary protein to microalbuminuria; 2.8% changed from microalbuminuria to macroalbuminuria (urine albumin >300 mg in a 24-hour period); and 2.3% progressed to chronic renal disease (creatinine ≥2 mg/dL) from macroalbuminuria per year.2 Chronic renal disease is more likely to occur in those patients whose hypertension or hyperglycemia is poorly controlled.
For patients with diabetes who develop microalbuminuria, the evidence is good for starting ACE inhibitors or ARBs for renal protection.3,4 The American Diabetes Association (ADA) also recommends that patients with diabetes and hypertension and those aged >55 years with other cardiovascular risk factors (history of cardiovascular disease, dyslipidemia, or tobacco use) be started on ACE inhibitors or ARBs.1 There is also good evidence that screening for microalbuminuria can identify those who might benefit from treatments that delay the onset of nephropathy.5
Recent studies have raised the possibility of further benefit in prevention and treatment of diabetic nephropathy by maximizing doses of ACE inhibitors or ARBs, and even from the dual blockade attained from using both. For example, during a 2-year trial—in which 590 patients with diabetes and microalbuminuria were randomized to receive placebo, 150 mg irbesartan, or 300 mg irbesartan—14.9% of the placebo group, 9.7% of the 150-mg group, and only 5.2% of the 300-mg group progressed to overt nephropathy.6 In very small randomized trial of 20 patients with type 2 diabetes, adding 16 mg of candesartan to the maximal dose of an ACE inhibitor decreased albuminuria an additional 28%.7
Experts argue that it may benefit patients to continue regular surveillance for the presence or progression of microalbuminuria even if they are already taking an ACE inhibitor or ARB so that therapy can be maximized.1,8 However, no direct evidence supports this recommendation.
Recommendations from others
The ADA suggests that clinicians perform a test each year for microalbuminuria among patients with type 1 diabetes of ≥5 years duration, and in all patients with type 2 diabetes at diagnosis and during pregnancy. They also recommend continued surveillance of proteinuria to assess both response to therapy and progression of disease.1
The National Kidney Foundation recommends continued surveillance of microalbuminuria to assess progression of chronic kidney disease and response to therapy.8
1. American Diabetes Association. Standards of Medical Care in Diabetes—2006. Diabetes Care 2006;29:S4-S42.
2. Adler AI, Stevens RJ, Manley SE. Development and progression of nephropathy in type 2 diabetes: The united Kingdom Prospective Diabetes study (UKPDS 64). Kidney Intl 2003;63:225-232.
3. Sferra L, Kelsberg G. Do ACE inhibitors prevent nephropathy in type 2 diabetes without proteinuria? J Fam Pract 2004;53:68-69.
4. Foreman BH, Chambliss ML. Are ARBs or ACE inhibitors preferred for nephropathy in diabetes? J Fam Pract 2004;53:241-242.
5. Hale WA, Nashelsky J. Does microalbuminuria screening in diabetes prevent complications? J Fam Pract 2003;52:229-230.
6. Parving HH, Lehnart H, et al. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 2001;345:870-878.
7. Rossing K, Jacobsen P, et al. Renoprotective effects of adding angiotensin II receptor blocker to maximal recommended doses of ACE inhibitor in diabetic nephropathy: a randomized double-blind crossover trial. Diabetes Care 2003;26:2268-2274.
8. Eknoyan G, Hostetter T, Bakris GL, et al. Proteinuria and other Markers of Chronic Kidney Disease: A Position statement of the National Kidney foundation (NKF) and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Am J Kidney Dis 2003;42:617-622.
No studies address whether continued screening for microalbuminuria once a patient is taking an angiotensin-converting enzyme (ACE) inhibitor or angiotensin-2 receptor blocker (ARB) improves outcomes. Indirect evidence and expert opinion suggest that it may be beneficial to continue microalbuminuria surveillance to assess response to therapy and monitor disease progression (strength of recommendation: C, based on expert opinion).
It is unclear whether microalbuminuria tests in these cases is money well spent
Chris Vincent, MD
Swedish Family Medicine Residency, University of Washington, Seattle
At the residency where I teach, clinicians routinely try to get to the evidence behind the expert opinions, and faculty are discouraged from giving off the cuff or experiential answers. When asked whether to monitor microalbuminuria for patients with diabetes receiving ACE inhibitors or ARBs, it is frustrating to discover that no direct evidence supports the experts’ advice.
The screening test for urine microalbuminuria at our hospital costs $90. Since most patients with diabetes are being treated with ACE inhibitors or ARBs, it would be nice to know that the money for the testing is well spent. Unfortunately, in this instance, we can only continue to practice the “standard of care” and hope for future research to definitively answer this question.
Evidence Summary
Our comprehensive literature search found no studies that provide direct evidence for or against continuing to monitor microalbuminuria among patients with diabetes already on ACE inhibitor or ARB therapy. We reviewed and included indirect evidence and expert opinion to answer this clinical question.
Diabetes mellitus is the leading cause of end-stage renal disease in the Western world.1 The prevalence of diabetic nephropathy continues to rise along with the rapidly rising prevalence of obesity and diabetes, with 40% of patients with diabetes at risk of developing nephropathy. One study that followed 5097 patients with type 2 diabetes over a median of 10.4 years found that 2% of patients progressed from normal levels of urinary protein to microalbuminuria; 2.8% changed from microalbuminuria to macroalbuminuria (urine albumin >300 mg in a 24-hour period); and 2.3% progressed to chronic renal disease (creatinine ≥2 mg/dL) from macroalbuminuria per year.2 Chronic renal disease is more likely to occur in those patients whose hypertension or hyperglycemia is poorly controlled.
For patients with diabetes who develop microalbuminuria, the evidence is good for starting ACE inhibitors or ARBs for renal protection.3,4 The American Diabetes Association (ADA) also recommends that patients with diabetes and hypertension and those aged >55 years with other cardiovascular risk factors (history of cardiovascular disease, dyslipidemia, or tobacco use) be started on ACE inhibitors or ARBs.1 There is also good evidence that screening for microalbuminuria can identify those who might benefit from treatments that delay the onset of nephropathy.5
Recent studies have raised the possibility of further benefit in prevention and treatment of diabetic nephropathy by maximizing doses of ACE inhibitors or ARBs, and even from the dual blockade attained from using both. For example, during a 2-year trial—in which 590 patients with diabetes and microalbuminuria were randomized to receive placebo, 150 mg irbesartan, or 300 mg irbesartan—14.9% of the placebo group, 9.7% of the 150-mg group, and only 5.2% of the 300-mg group progressed to overt nephropathy.6 In very small randomized trial of 20 patients with type 2 diabetes, adding 16 mg of candesartan to the maximal dose of an ACE inhibitor decreased albuminuria an additional 28%.7
Experts argue that it may benefit patients to continue regular surveillance for the presence or progression of microalbuminuria even if they are already taking an ACE inhibitor or ARB so that therapy can be maximized.1,8 However, no direct evidence supports this recommendation.
Recommendations from others
The ADA suggests that clinicians perform a test each year for microalbuminuria among patients with type 1 diabetes of ≥5 years duration, and in all patients with type 2 diabetes at diagnosis and during pregnancy. They also recommend continued surveillance of proteinuria to assess both response to therapy and progression of disease.1
The National Kidney Foundation recommends continued surveillance of microalbuminuria to assess progression of chronic kidney disease and response to therapy.8
No studies address whether continued screening for microalbuminuria once a patient is taking an angiotensin-converting enzyme (ACE) inhibitor or angiotensin-2 receptor blocker (ARB) improves outcomes. Indirect evidence and expert opinion suggest that it may be beneficial to continue microalbuminuria surveillance to assess response to therapy and monitor disease progression (strength of recommendation: C, based on expert opinion).
It is unclear whether microalbuminuria tests in these cases is money well spent
Chris Vincent, MD
Swedish Family Medicine Residency, University of Washington, Seattle
At the residency where I teach, clinicians routinely try to get to the evidence behind the expert opinions, and faculty are discouraged from giving off the cuff or experiential answers. When asked whether to monitor microalbuminuria for patients with diabetes receiving ACE inhibitors or ARBs, it is frustrating to discover that no direct evidence supports the experts’ advice.
The screening test for urine microalbuminuria at our hospital costs $90. Since most patients with diabetes are being treated with ACE inhibitors or ARBs, it would be nice to know that the money for the testing is well spent. Unfortunately, in this instance, we can only continue to practice the “standard of care” and hope for future research to definitively answer this question.
Evidence Summary
Our comprehensive literature search found no studies that provide direct evidence for or against continuing to monitor microalbuminuria among patients with diabetes already on ACE inhibitor or ARB therapy. We reviewed and included indirect evidence and expert opinion to answer this clinical question.
Diabetes mellitus is the leading cause of end-stage renal disease in the Western world.1 The prevalence of diabetic nephropathy continues to rise along with the rapidly rising prevalence of obesity and diabetes, with 40% of patients with diabetes at risk of developing nephropathy. One study that followed 5097 patients with type 2 diabetes over a median of 10.4 years found that 2% of patients progressed from normal levels of urinary protein to microalbuminuria; 2.8% changed from microalbuminuria to macroalbuminuria (urine albumin >300 mg in a 24-hour period); and 2.3% progressed to chronic renal disease (creatinine ≥2 mg/dL) from macroalbuminuria per year.2 Chronic renal disease is more likely to occur in those patients whose hypertension or hyperglycemia is poorly controlled.
For patients with diabetes who develop microalbuminuria, the evidence is good for starting ACE inhibitors or ARBs for renal protection.3,4 The American Diabetes Association (ADA) also recommends that patients with diabetes and hypertension and those aged >55 years with other cardiovascular risk factors (history of cardiovascular disease, dyslipidemia, or tobacco use) be started on ACE inhibitors or ARBs.1 There is also good evidence that screening for microalbuminuria can identify those who might benefit from treatments that delay the onset of nephropathy.5
Recent studies have raised the possibility of further benefit in prevention and treatment of diabetic nephropathy by maximizing doses of ACE inhibitors or ARBs, and even from the dual blockade attained from using both. For example, during a 2-year trial—in which 590 patients with diabetes and microalbuminuria were randomized to receive placebo, 150 mg irbesartan, or 300 mg irbesartan—14.9% of the placebo group, 9.7% of the 150-mg group, and only 5.2% of the 300-mg group progressed to overt nephropathy.6 In very small randomized trial of 20 patients with type 2 diabetes, adding 16 mg of candesartan to the maximal dose of an ACE inhibitor decreased albuminuria an additional 28%.7
Experts argue that it may benefit patients to continue regular surveillance for the presence or progression of microalbuminuria even if they are already taking an ACE inhibitor or ARB so that therapy can be maximized.1,8 However, no direct evidence supports this recommendation.
Recommendations from others
The ADA suggests that clinicians perform a test each year for microalbuminuria among patients with type 1 diabetes of ≥5 years duration, and in all patients with type 2 diabetes at diagnosis and during pregnancy. They also recommend continued surveillance of proteinuria to assess both response to therapy and progression of disease.1
The National Kidney Foundation recommends continued surveillance of microalbuminuria to assess progression of chronic kidney disease and response to therapy.8
1. American Diabetes Association. Standards of Medical Care in Diabetes—2006. Diabetes Care 2006;29:S4-S42.
2. Adler AI, Stevens RJ, Manley SE. Development and progression of nephropathy in type 2 diabetes: The united Kingdom Prospective Diabetes study (UKPDS 64). Kidney Intl 2003;63:225-232.
3. Sferra L, Kelsberg G. Do ACE inhibitors prevent nephropathy in type 2 diabetes without proteinuria? J Fam Pract 2004;53:68-69.
4. Foreman BH, Chambliss ML. Are ARBs or ACE inhibitors preferred for nephropathy in diabetes? J Fam Pract 2004;53:241-242.
5. Hale WA, Nashelsky J. Does microalbuminuria screening in diabetes prevent complications? J Fam Pract 2003;52:229-230.
6. Parving HH, Lehnart H, et al. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 2001;345:870-878.
7. Rossing K, Jacobsen P, et al. Renoprotective effects of adding angiotensin II receptor blocker to maximal recommended doses of ACE inhibitor in diabetic nephropathy: a randomized double-blind crossover trial. Diabetes Care 2003;26:2268-2274.
8. Eknoyan G, Hostetter T, Bakris GL, et al. Proteinuria and other Markers of Chronic Kidney Disease: A Position statement of the National Kidney foundation (NKF) and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Am J Kidney Dis 2003;42:617-622.
1. American Diabetes Association. Standards of Medical Care in Diabetes—2006. Diabetes Care 2006;29:S4-S42.
2. Adler AI, Stevens RJ, Manley SE. Development and progression of nephropathy in type 2 diabetes: The united Kingdom Prospective Diabetes study (UKPDS 64). Kidney Intl 2003;63:225-232.
3. Sferra L, Kelsberg G. Do ACE inhibitors prevent nephropathy in type 2 diabetes without proteinuria? J Fam Pract 2004;53:68-69.
4. Foreman BH, Chambliss ML. Are ARBs or ACE inhibitors preferred for nephropathy in diabetes? J Fam Pract 2004;53:241-242.
5. Hale WA, Nashelsky J. Does microalbuminuria screening in diabetes prevent complications? J Fam Pract 2003;52:229-230.
6. Parving HH, Lehnart H, et al. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 2001;345:870-878.
7. Rossing K, Jacobsen P, et al. Renoprotective effects of adding angiotensin II receptor blocker to maximal recommended doses of ACE inhibitor in diabetic nephropathy: a randomized double-blind crossover trial. Diabetes Care 2003;26:2268-2274.
8. Eknoyan G, Hostetter T, Bakris GL, et al. Proteinuria and other Markers of Chronic Kidney Disease: A Position statement of the National Kidney foundation (NKF) and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Am J Kidney Dis 2003;42:617-622.
Evidence-based answers from the Family Physicians Inquiries Network
Do topical antibiotics improve wound healing?
The use of topical triple-antibiotic ointments significantly decreases infection rates in minor contaminated wounds compared with a petrolatum control. Plain petrolatum ointment is equivalent to triple-antibiotic ointments for sterile wounds as a post-procedure wound dressing (strength of recommendation [SOR]: A, based on randomized controlled trials [RCTs]).
Mupirocin cream is as effective as oral cephalexin in the treatment of secondarily infected minor wounds and, because of better tolerability, is the treatment of choice for the prevention and treatment of Staphylococcus aureus and Staphylococcus pyogenes infections. Emerging resistance, including methicillin-resistant S aureus (MRSA), makes it prudent to check for clinical response in 24 to 48 hours. Major contaminated wounds requiring parenteral antibiotics do not appear to additionally benefit from topical antibiotics (SOR: A, based on RCTs).
Topical antibiotics may also aid in the healing of chronic wounds (SOR: B, based on a systematic review of low-quality RCTs), as does the application of honey (SOR: B, based on a systematic review of cohort studies).
It would be helpful to have objective criteria to properly classify skin wounds
Michael Mendoza, MD, MPH
Pritzker School of Medicine, University of Chicago
These results are encouraging, but they do not fully account for variability in the diagnosis of skin wounds or in the practical use of topical agents. The evaluation of skin wounds is inherently subjective. In order to properly apply these findings to my practice, it would be helpful to have more objective diagnostic criteria to properly classify skin wounds.
Furthermore, how patients use topical agents varies considerably. Patients apply topical agents differently, due to individual preference or perhaps inconsistent recommendations from their physician. Used improperly, topical agents may not provide the same potential for clinical improvement.
Evidence summary
Topical antibiotics for prophylaxis
Numerous studies support the prophylactic application of topical antibiotics to wounds that are clean. Topical bacitracin zinc (Bacitracin), a triple ointment of neomycin sulfate, bacitracin zinc, and polymyxin B sulfate (Neosporin), and silver sulfadiazine (Silvadene) were compared with petrolatum as a control in a well-conducted RCT of 426 patients with uncomplicated wounds seen at a military community hospital. Wound infection rates were 17.6% (19/108) for petrolatum, 5.5% (6/109) for Bacitracin (number needed to treat [NNT]=8), 4.5% (5/110) for Neosporin (NNT=8), and 12.1% (12/99) for Silvadene (NNT=18).1 Most (60%) of the infections were “stitch abscesses” and were treated with local care only. There was no difference in rates of more serious infections between groups. One patient (0.9%) developed a hypersensitivity reaction to Neosporin.
A clinical trial compared the efficacy of a cetrimide, bacitracin zinc, and polymyxin B sulfate gel (a combination not available in the US) with placebo and povidone-iodine cream in preventing infections in 177 minor wounds (cuts, grazes, scrapes, and scratches) among children. The antibiotic gel was found to be superior to placebo and equivalent to povidone-iodine, in that it reduced clinical infections from 12.5% to 1.6% (absolute risk reduction [ARR]=0.109; 95% confidence interval [CI], 0.011–0.207; NNT=11).2
A double-blind study of 59 patients found Neosporin superior to placebo ointment in the prevention of streptococcal pyoderma for children with minor wounds. Infection occurred in 47% of placebo-treated children compared with 15% treated with the triple-antibiotic ointment (NNT=32; P=.01).3
A small randomized prospective trial of 99 patients, who self-reported compliance with wound care and dressing changes, compared Neosporin with mupirocin (Bactroban) in preventing infections in uncomplicated soft tissue wounds. The study found no statistical difference in infection rates, and the authors recommend the more cost-effective Neosporin, as well as a larger trial to confirm the results.4
Another randomized controlled trial of 933 outpatients—with a total of 1249 wounds from sterile dermatologic surgeries—compared white petrolatum with bacitracin zinc ointment prophylaxis. The study found no statistically significant differences in post-procedure infection rates, though only 13 patients developed an infection (2% in petrolatum group vs. 0.9% in bacitracin zinc group; 95% CI for the difference, –0.4 to 2.7).5
Topical antibiotics for treatment
Topical antimicrobials are appealing for the treatment of secondarily infected wounds for the sake of convenience and because they may reduce the risk of adverse effects.
An open randomized trial with 48 volunteers compared the effects of Neosporin with several antiseptics (3% hydrogen peroxide, 1% povidone-iodine, 0.25% acetic acid, 0.5% sodium hydrochloride) and a wound protectant (Johnson & Johnson First Aid Cream without antimicrobial agent) on blister wounds (6 blisters per volunteer) intentionally contaminated with S aureus. Only Neosporin eliminated the infection after 2 applications (at 16 and 24 hours). Both the antibiotic ointment and the wound protectant led to faster wound healing by about 4 days compared with the antiseptics or no treatment.6
Another study with 2 parallel, identical RCTs of a total of 706 patients found mupirocin cream (Bactroban) to be equivalent to oral cephalexin in the treatment of secondarily infected minor wounds, such as small lacerations, abrasions, or sutured wounds. Clinical success (95.1% for mupirocin and 95.3% for cephalexin), bacteriologic success (96.9% for mupirocin and 98.9% for cephalexin), as well as the intention-to-treat success rate of 83% at follow-up were equivalent in the 2 groups.7
A small but well-designed study of 62 patients with major contaminated wounds failed to show any additional benefit when topical piperacillin/tazobactam (not available in US as a topical agent) was added to parenteral piperacillin/tazobactam (Zosyn) alone. Two of 31 patients on just parenteral antibiotics and 3 of 31 patients on both topical and parenteral antibiotics developed wound infections (P>.05).8
Finally, topical antibiotics also appear to aid in the healing of chronic wounds. However, these findings are difficult to interpret in light of small sample size and other methodological problems. A systematic review of the treatment of chronic wounds, such as diabetic foot ulcers, found 30 trials, including 25 RCTs, mostly of low quality. Little evidence supports the routine use of systemic antibiotics for patients with chronic wounds; however, some topical antiseptic and antimicrobial agents may hasten the healing of these wounds. Topical preparations that may be helpful include dimethyl sulfoxide (Rimso-50), silver sulfadiazine (Silvadene), benzoyl peroxide (Benzac, Brevoxyl, Desquam, Triaz, ZoDerm), oxyquinoline (Trimo-san Vaginal Jelly), and gentamicin (Garamycin).9
Honey may also make an acceptable wound dressing for chronic wounds, as it has been repeatedly shown to suppress bacterial growth. Infection with Clostridium spores does not appear to be a concern when treating chronic wounds with honey.10,11
Recommendations from others
Guidelines for antibiotic prophylaxis of surgical wounds uniformly recommend prophylaxis for all clean-contaminated, contaminated, and dirty procedures. Prophylaxis is considered optional for most clean procedures, although it may be indicated for certain at-risk patients and for clean procedures that fulfill specific risk criteria.12
The Infectious Diseases Society of America recommends mupirocin as the best topical agent for the treatment and prevention of S aureus and S pyogenes infections, followed by bacitracin zinc and neomycin, although resistance is emerging.13 Expert and consensus opinion from the Canadian Chronic Wound Advisory Board and the International Wound Bed Preparation Advisory Board for wound care management of infected chronic wounds recommend that since bacterial infection can develop gradually, good-quality wound cultures should be used in conjunction with clinical assessment. Iodine and silver-based dressings, topical antibiotics, and systemic antibiotics can be helpful.14
1. Dire DJ, Coppola M, Dwyer DA, Lorette JJ, Karr JL. Prospective evaluation of topical antibiotics for preventing infections in uncomplicated soft-tissue wounds repaired in the ED. Acad Emerg Med 1995;2:4-10.
2. Langford JH, Artemi P, Benrimoj SI. Topical antimicrobial prophylaxis in minor wounds. Ann Pharmacotherapy 1997;31:559-563.
3. Maddox JS, Ware JC, Dillon HC, Jr. The natural history of streptococcal skin infection: prevention with topical antibiotics. J Am Acad Derm 1985;13:207-212.
4. Hood R, Shermock KM, Emerman C. A prospective, randomized pilot evaluation of topical triple antibiotic versus mupirocin for the prevention of uncomplicated soft tissue wound infections. Am J Emerg Med 2005;22:1-3.
5. Smack DP, Harrington AC, Dunn C, et al. Infection and allergic incidence in ambulatory surgery patients using white petrolatum vs bacitracin ointment. A randomized controlled trial. JAMA 1996;276:972-977.
6. Leyden JJ, Bartelt NM. Comparison of topical antibiotic ointment, a wound protectant and antiseptic for the treatment of human blister wounds contaminated with Staphylococcus aureus. J Fam Pract 1987;24:601-604.
7. Kraus SJ, Eron LJ, Bottenfield GW, Drehobl MA, Bushnell WD, Cupo MA. Mupirocin cream is as effective as oral cephalexin in the treatment of secondarily infected wounds. J Fam Pract 1998;47:429-433.
8. Simons JP, Johnson JT, Yu VL, et al. The role of topical antimicrobial prophylaxis in patients undergoing contaminated head and neck surgery with flap reconstruction. Laryngoscope 2001;111:329-335.
9. O’Meara SM, Cullum NA, Majid M, Sheldon TA. Systematic review of antimicrobial agents used for chronic wounds. Br J Surg 2001;88:4-21.
10. Molan PC. The evidence supporting the use of honey as a wound dressing. Int J Low Extrem Wounds 2005;5:40-54.
11. Molan PC. Potential of honey in the treatment of wounds and burns. Am J Clin Dermatology 2001;2:13-19.
12. Woods RK, Dellinger EP. Current guidelines for antibiotic prophylaxis of surgical wounds. Am Fam Physician 1998;57:2731-2740.
13. Stevens DL, Bisno AL, Chambers HF, et al. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of soft-tissue infections. Clin Infect Dis 2005;41:1373-1406.
14. Frank C, Bayoumi I, Westendorp C. Approach to infected skin ulcers. Can Fam Physician 2005;51:1352-1359.
The use of topical triple-antibiotic ointments significantly decreases infection rates in minor contaminated wounds compared with a petrolatum control. Plain petrolatum ointment is equivalent to triple-antibiotic ointments for sterile wounds as a post-procedure wound dressing (strength of recommendation [SOR]: A, based on randomized controlled trials [RCTs]).
Mupirocin cream is as effective as oral cephalexin in the treatment of secondarily infected minor wounds and, because of better tolerability, is the treatment of choice for the prevention and treatment of Staphylococcus aureus and Staphylococcus pyogenes infections. Emerging resistance, including methicillin-resistant S aureus (MRSA), makes it prudent to check for clinical response in 24 to 48 hours. Major contaminated wounds requiring parenteral antibiotics do not appear to additionally benefit from topical antibiotics (SOR: A, based on RCTs).
Topical antibiotics may also aid in the healing of chronic wounds (SOR: B, based on a systematic review of low-quality RCTs), as does the application of honey (SOR: B, based on a systematic review of cohort studies).
It would be helpful to have objective criteria to properly classify skin wounds
Michael Mendoza, MD, MPH
Pritzker School of Medicine, University of Chicago
These results are encouraging, but they do not fully account for variability in the diagnosis of skin wounds or in the practical use of topical agents. The evaluation of skin wounds is inherently subjective. In order to properly apply these findings to my practice, it would be helpful to have more objective diagnostic criteria to properly classify skin wounds.
Furthermore, how patients use topical agents varies considerably. Patients apply topical agents differently, due to individual preference or perhaps inconsistent recommendations from their physician. Used improperly, topical agents may not provide the same potential for clinical improvement.
Evidence summary
Topical antibiotics for prophylaxis
Numerous studies support the prophylactic application of topical antibiotics to wounds that are clean. Topical bacitracin zinc (Bacitracin), a triple ointment of neomycin sulfate, bacitracin zinc, and polymyxin B sulfate (Neosporin), and silver sulfadiazine (Silvadene) were compared with petrolatum as a control in a well-conducted RCT of 426 patients with uncomplicated wounds seen at a military community hospital. Wound infection rates were 17.6% (19/108) for petrolatum, 5.5% (6/109) for Bacitracin (number needed to treat [NNT]=8), 4.5% (5/110) for Neosporin (NNT=8), and 12.1% (12/99) for Silvadene (NNT=18).1 Most (60%) of the infections were “stitch abscesses” and were treated with local care only. There was no difference in rates of more serious infections between groups. One patient (0.9%) developed a hypersensitivity reaction to Neosporin.
A clinical trial compared the efficacy of a cetrimide, bacitracin zinc, and polymyxin B sulfate gel (a combination not available in the US) with placebo and povidone-iodine cream in preventing infections in 177 minor wounds (cuts, grazes, scrapes, and scratches) among children. The antibiotic gel was found to be superior to placebo and equivalent to povidone-iodine, in that it reduced clinical infections from 12.5% to 1.6% (absolute risk reduction [ARR]=0.109; 95% confidence interval [CI], 0.011–0.207; NNT=11).2
A double-blind study of 59 patients found Neosporin superior to placebo ointment in the prevention of streptococcal pyoderma for children with minor wounds. Infection occurred in 47% of placebo-treated children compared with 15% treated with the triple-antibiotic ointment (NNT=32; P=.01).3
A small randomized prospective trial of 99 patients, who self-reported compliance with wound care and dressing changes, compared Neosporin with mupirocin (Bactroban) in preventing infections in uncomplicated soft tissue wounds. The study found no statistical difference in infection rates, and the authors recommend the more cost-effective Neosporin, as well as a larger trial to confirm the results.4
Another randomized controlled trial of 933 outpatients—with a total of 1249 wounds from sterile dermatologic surgeries—compared white petrolatum with bacitracin zinc ointment prophylaxis. The study found no statistically significant differences in post-procedure infection rates, though only 13 patients developed an infection (2% in petrolatum group vs. 0.9% in bacitracin zinc group; 95% CI for the difference, –0.4 to 2.7).5
Topical antibiotics for treatment
Topical antimicrobials are appealing for the treatment of secondarily infected wounds for the sake of convenience and because they may reduce the risk of adverse effects.
An open randomized trial with 48 volunteers compared the effects of Neosporin with several antiseptics (3% hydrogen peroxide, 1% povidone-iodine, 0.25% acetic acid, 0.5% sodium hydrochloride) and a wound protectant (Johnson & Johnson First Aid Cream without antimicrobial agent) on blister wounds (6 blisters per volunteer) intentionally contaminated with S aureus. Only Neosporin eliminated the infection after 2 applications (at 16 and 24 hours). Both the antibiotic ointment and the wound protectant led to faster wound healing by about 4 days compared with the antiseptics or no treatment.6
Another study with 2 parallel, identical RCTs of a total of 706 patients found mupirocin cream (Bactroban) to be equivalent to oral cephalexin in the treatment of secondarily infected minor wounds, such as small lacerations, abrasions, or sutured wounds. Clinical success (95.1% for mupirocin and 95.3% for cephalexin), bacteriologic success (96.9% for mupirocin and 98.9% for cephalexin), as well as the intention-to-treat success rate of 83% at follow-up were equivalent in the 2 groups.7
A small but well-designed study of 62 patients with major contaminated wounds failed to show any additional benefit when topical piperacillin/tazobactam (not available in US as a topical agent) was added to parenteral piperacillin/tazobactam (Zosyn) alone. Two of 31 patients on just parenteral antibiotics and 3 of 31 patients on both topical and parenteral antibiotics developed wound infections (P>.05).8
Finally, topical antibiotics also appear to aid in the healing of chronic wounds. However, these findings are difficult to interpret in light of small sample size and other methodological problems. A systematic review of the treatment of chronic wounds, such as diabetic foot ulcers, found 30 trials, including 25 RCTs, mostly of low quality. Little evidence supports the routine use of systemic antibiotics for patients with chronic wounds; however, some topical antiseptic and antimicrobial agents may hasten the healing of these wounds. Topical preparations that may be helpful include dimethyl sulfoxide (Rimso-50), silver sulfadiazine (Silvadene), benzoyl peroxide (Benzac, Brevoxyl, Desquam, Triaz, ZoDerm), oxyquinoline (Trimo-san Vaginal Jelly), and gentamicin (Garamycin).9
Honey may also make an acceptable wound dressing for chronic wounds, as it has been repeatedly shown to suppress bacterial growth. Infection with Clostridium spores does not appear to be a concern when treating chronic wounds with honey.10,11
Recommendations from others
Guidelines for antibiotic prophylaxis of surgical wounds uniformly recommend prophylaxis for all clean-contaminated, contaminated, and dirty procedures. Prophylaxis is considered optional for most clean procedures, although it may be indicated for certain at-risk patients and for clean procedures that fulfill specific risk criteria.12
The Infectious Diseases Society of America recommends mupirocin as the best topical agent for the treatment and prevention of S aureus and S pyogenes infections, followed by bacitracin zinc and neomycin, although resistance is emerging.13 Expert and consensus opinion from the Canadian Chronic Wound Advisory Board and the International Wound Bed Preparation Advisory Board for wound care management of infected chronic wounds recommend that since bacterial infection can develop gradually, good-quality wound cultures should be used in conjunction with clinical assessment. Iodine and silver-based dressings, topical antibiotics, and systemic antibiotics can be helpful.14
The use of topical triple-antibiotic ointments significantly decreases infection rates in minor contaminated wounds compared with a petrolatum control. Plain petrolatum ointment is equivalent to triple-antibiotic ointments for sterile wounds as a post-procedure wound dressing (strength of recommendation [SOR]: A, based on randomized controlled trials [RCTs]).
Mupirocin cream is as effective as oral cephalexin in the treatment of secondarily infected minor wounds and, because of better tolerability, is the treatment of choice for the prevention and treatment of Staphylococcus aureus and Staphylococcus pyogenes infections. Emerging resistance, including methicillin-resistant S aureus (MRSA), makes it prudent to check for clinical response in 24 to 48 hours. Major contaminated wounds requiring parenteral antibiotics do not appear to additionally benefit from topical antibiotics (SOR: A, based on RCTs).
Topical antibiotics may also aid in the healing of chronic wounds (SOR: B, based on a systematic review of low-quality RCTs), as does the application of honey (SOR: B, based on a systematic review of cohort studies).
It would be helpful to have objective criteria to properly classify skin wounds
Michael Mendoza, MD, MPH
Pritzker School of Medicine, University of Chicago
These results are encouraging, but they do not fully account for variability in the diagnosis of skin wounds or in the practical use of topical agents. The evaluation of skin wounds is inherently subjective. In order to properly apply these findings to my practice, it would be helpful to have more objective diagnostic criteria to properly classify skin wounds.
Furthermore, how patients use topical agents varies considerably. Patients apply topical agents differently, due to individual preference or perhaps inconsistent recommendations from their physician. Used improperly, topical agents may not provide the same potential for clinical improvement.
Evidence summary
Topical antibiotics for prophylaxis
Numerous studies support the prophylactic application of topical antibiotics to wounds that are clean. Topical bacitracin zinc (Bacitracin), a triple ointment of neomycin sulfate, bacitracin zinc, and polymyxin B sulfate (Neosporin), and silver sulfadiazine (Silvadene) were compared with petrolatum as a control in a well-conducted RCT of 426 patients with uncomplicated wounds seen at a military community hospital. Wound infection rates were 17.6% (19/108) for petrolatum, 5.5% (6/109) for Bacitracin (number needed to treat [NNT]=8), 4.5% (5/110) for Neosporin (NNT=8), and 12.1% (12/99) for Silvadene (NNT=18).1 Most (60%) of the infections were “stitch abscesses” and were treated with local care only. There was no difference in rates of more serious infections between groups. One patient (0.9%) developed a hypersensitivity reaction to Neosporin.
A clinical trial compared the efficacy of a cetrimide, bacitracin zinc, and polymyxin B sulfate gel (a combination not available in the US) with placebo and povidone-iodine cream in preventing infections in 177 minor wounds (cuts, grazes, scrapes, and scratches) among children. The antibiotic gel was found to be superior to placebo and equivalent to povidone-iodine, in that it reduced clinical infections from 12.5% to 1.6% (absolute risk reduction [ARR]=0.109; 95% confidence interval [CI], 0.011–0.207; NNT=11).2
A double-blind study of 59 patients found Neosporin superior to placebo ointment in the prevention of streptococcal pyoderma for children with minor wounds. Infection occurred in 47% of placebo-treated children compared with 15% treated with the triple-antibiotic ointment (NNT=32; P=.01).3
A small randomized prospective trial of 99 patients, who self-reported compliance with wound care and dressing changes, compared Neosporin with mupirocin (Bactroban) in preventing infections in uncomplicated soft tissue wounds. The study found no statistical difference in infection rates, and the authors recommend the more cost-effective Neosporin, as well as a larger trial to confirm the results.4
Another randomized controlled trial of 933 outpatients—with a total of 1249 wounds from sterile dermatologic surgeries—compared white petrolatum with bacitracin zinc ointment prophylaxis. The study found no statistically significant differences in post-procedure infection rates, though only 13 patients developed an infection (2% in petrolatum group vs. 0.9% in bacitracin zinc group; 95% CI for the difference, –0.4 to 2.7).5
Topical antibiotics for treatment
Topical antimicrobials are appealing for the treatment of secondarily infected wounds for the sake of convenience and because they may reduce the risk of adverse effects.
An open randomized trial with 48 volunteers compared the effects of Neosporin with several antiseptics (3% hydrogen peroxide, 1% povidone-iodine, 0.25% acetic acid, 0.5% sodium hydrochloride) and a wound protectant (Johnson & Johnson First Aid Cream without antimicrobial agent) on blister wounds (6 blisters per volunteer) intentionally contaminated with S aureus. Only Neosporin eliminated the infection after 2 applications (at 16 and 24 hours). Both the antibiotic ointment and the wound protectant led to faster wound healing by about 4 days compared with the antiseptics or no treatment.6
Another study with 2 parallel, identical RCTs of a total of 706 patients found mupirocin cream (Bactroban) to be equivalent to oral cephalexin in the treatment of secondarily infected minor wounds, such as small lacerations, abrasions, or sutured wounds. Clinical success (95.1% for mupirocin and 95.3% for cephalexin), bacteriologic success (96.9% for mupirocin and 98.9% for cephalexin), as well as the intention-to-treat success rate of 83% at follow-up were equivalent in the 2 groups.7
A small but well-designed study of 62 patients with major contaminated wounds failed to show any additional benefit when topical piperacillin/tazobactam (not available in US as a topical agent) was added to parenteral piperacillin/tazobactam (Zosyn) alone. Two of 31 patients on just parenteral antibiotics and 3 of 31 patients on both topical and parenteral antibiotics developed wound infections (P>.05).8
Finally, topical antibiotics also appear to aid in the healing of chronic wounds. However, these findings are difficult to interpret in light of small sample size and other methodological problems. A systematic review of the treatment of chronic wounds, such as diabetic foot ulcers, found 30 trials, including 25 RCTs, mostly of low quality. Little evidence supports the routine use of systemic antibiotics for patients with chronic wounds; however, some topical antiseptic and antimicrobial agents may hasten the healing of these wounds. Topical preparations that may be helpful include dimethyl sulfoxide (Rimso-50), silver sulfadiazine (Silvadene), benzoyl peroxide (Benzac, Brevoxyl, Desquam, Triaz, ZoDerm), oxyquinoline (Trimo-san Vaginal Jelly), and gentamicin (Garamycin).9
Honey may also make an acceptable wound dressing for chronic wounds, as it has been repeatedly shown to suppress bacterial growth. Infection with Clostridium spores does not appear to be a concern when treating chronic wounds with honey.10,11
Recommendations from others
Guidelines for antibiotic prophylaxis of surgical wounds uniformly recommend prophylaxis for all clean-contaminated, contaminated, and dirty procedures. Prophylaxis is considered optional for most clean procedures, although it may be indicated for certain at-risk patients and for clean procedures that fulfill specific risk criteria.12
The Infectious Diseases Society of America recommends mupirocin as the best topical agent for the treatment and prevention of S aureus and S pyogenes infections, followed by bacitracin zinc and neomycin, although resistance is emerging.13 Expert and consensus opinion from the Canadian Chronic Wound Advisory Board and the International Wound Bed Preparation Advisory Board for wound care management of infected chronic wounds recommend that since bacterial infection can develop gradually, good-quality wound cultures should be used in conjunction with clinical assessment. Iodine and silver-based dressings, topical antibiotics, and systemic antibiotics can be helpful.14
1. Dire DJ, Coppola M, Dwyer DA, Lorette JJ, Karr JL. Prospective evaluation of topical antibiotics for preventing infections in uncomplicated soft-tissue wounds repaired in the ED. Acad Emerg Med 1995;2:4-10.
2. Langford JH, Artemi P, Benrimoj SI. Topical antimicrobial prophylaxis in minor wounds. Ann Pharmacotherapy 1997;31:559-563.
3. Maddox JS, Ware JC, Dillon HC, Jr. The natural history of streptococcal skin infection: prevention with topical antibiotics. J Am Acad Derm 1985;13:207-212.
4. Hood R, Shermock KM, Emerman C. A prospective, randomized pilot evaluation of topical triple antibiotic versus mupirocin for the prevention of uncomplicated soft tissue wound infections. Am J Emerg Med 2005;22:1-3.
5. Smack DP, Harrington AC, Dunn C, et al. Infection and allergic incidence in ambulatory surgery patients using white petrolatum vs bacitracin ointment. A randomized controlled trial. JAMA 1996;276:972-977.
6. Leyden JJ, Bartelt NM. Comparison of topical antibiotic ointment, a wound protectant and antiseptic for the treatment of human blister wounds contaminated with Staphylococcus aureus. J Fam Pract 1987;24:601-604.
7. Kraus SJ, Eron LJ, Bottenfield GW, Drehobl MA, Bushnell WD, Cupo MA. Mupirocin cream is as effective as oral cephalexin in the treatment of secondarily infected wounds. J Fam Pract 1998;47:429-433.
8. Simons JP, Johnson JT, Yu VL, et al. The role of topical antimicrobial prophylaxis in patients undergoing contaminated head and neck surgery with flap reconstruction. Laryngoscope 2001;111:329-335.
9. O’Meara SM, Cullum NA, Majid M, Sheldon TA. Systematic review of antimicrobial agents used for chronic wounds. Br J Surg 2001;88:4-21.
10. Molan PC. The evidence supporting the use of honey as a wound dressing. Int J Low Extrem Wounds 2005;5:40-54.
11. Molan PC. Potential of honey in the treatment of wounds and burns. Am J Clin Dermatology 2001;2:13-19.
12. Woods RK, Dellinger EP. Current guidelines for antibiotic prophylaxis of surgical wounds. Am Fam Physician 1998;57:2731-2740.
13. Stevens DL, Bisno AL, Chambers HF, et al. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of soft-tissue infections. Clin Infect Dis 2005;41:1373-1406.
14. Frank C, Bayoumi I, Westendorp C. Approach to infected skin ulcers. Can Fam Physician 2005;51:1352-1359.
1. Dire DJ, Coppola M, Dwyer DA, Lorette JJ, Karr JL. Prospective evaluation of topical antibiotics for preventing infections in uncomplicated soft-tissue wounds repaired in the ED. Acad Emerg Med 1995;2:4-10.
2. Langford JH, Artemi P, Benrimoj SI. Topical antimicrobial prophylaxis in minor wounds. Ann Pharmacotherapy 1997;31:559-563.
3. Maddox JS, Ware JC, Dillon HC, Jr. The natural history of streptococcal skin infection: prevention with topical antibiotics. J Am Acad Derm 1985;13:207-212.
4. Hood R, Shermock KM, Emerman C. A prospective, randomized pilot evaluation of topical triple antibiotic versus mupirocin for the prevention of uncomplicated soft tissue wound infections. Am J Emerg Med 2005;22:1-3.
5. Smack DP, Harrington AC, Dunn C, et al. Infection and allergic incidence in ambulatory surgery patients using white petrolatum vs bacitracin ointment. A randomized controlled trial. JAMA 1996;276:972-977.
6. Leyden JJ, Bartelt NM. Comparison of topical antibiotic ointment, a wound protectant and antiseptic for the treatment of human blister wounds contaminated with Staphylococcus aureus. J Fam Pract 1987;24:601-604.
7. Kraus SJ, Eron LJ, Bottenfield GW, Drehobl MA, Bushnell WD, Cupo MA. Mupirocin cream is as effective as oral cephalexin in the treatment of secondarily infected wounds. J Fam Pract 1998;47:429-433.
8. Simons JP, Johnson JT, Yu VL, et al. The role of topical antimicrobial prophylaxis in patients undergoing contaminated head and neck surgery with flap reconstruction. Laryngoscope 2001;111:329-335.
9. O’Meara SM, Cullum NA, Majid M, Sheldon TA. Systematic review of antimicrobial agents used for chronic wounds. Br J Surg 2001;88:4-21.
10. Molan PC. The evidence supporting the use of honey as a wound dressing. Int J Low Extrem Wounds 2005;5:40-54.
11. Molan PC. Potential of honey in the treatment of wounds and burns. Am J Clin Dermatology 2001;2:13-19.
12. Woods RK, Dellinger EP. Current guidelines for antibiotic prophylaxis of surgical wounds. Am Fam Physician 1998;57:2731-2740.
13. Stevens DL, Bisno AL, Chambers HF, et al. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of soft-tissue infections. Clin Infect Dis 2005;41:1373-1406.
14. Frank C, Bayoumi I, Westendorp C. Approach to infected skin ulcers. Can Fam Physician 2005;51:1352-1359.
Evidence-based answers from the Family Physicians Inquiries Network
What is the preferred treatment for a child with mild persistent asthma?
Low-dose inhaled corticosteroids are the preferred treatment for children with mild persistent asthma because they demonstrate superior reduction in severity and frequency of asthma exacerbations compared with alternatives (strength of recommendation [SOR]: A, based on multiple randomized controlled trials). As add-on therapy, nedocromil, theophylline, and cromolyn have all demonstrated a modest benefit in symptom control; leukotriene receptor antagonists are also recommended based on data from older children (SOR: B, cohort study). Unlike treatment of moderate or severe asthma, long-acting beta-agonists are not recommended (SOR: A, randomized trials).
Clear medication choices for mild asthma are supported by good evidence
John Heintzman, MD
Oregon Health and Science University, Portland
Physicians who routinely treat children with asthma are fortunate to have the body of evidence outlined in this review. Clear medication choices are supported in most instances by relatively clear comparisons with alternatives. In my practice, where many children can be classified in the “mild persistent” category, I am always surprised at how many patients’ families lack a clear understanding of the factors that trigger a child’s asthma and how to avoid them.
Another common clinical scenario among children and adolescents is exercise-induced asthma. Depending on the sport, the asthma can be classified as “mild persistent” or “mild intermittent.” for true intermittent symptoms, my clinical experience (and often parental preference) argues for pre-activity treatment with short acting beta-agonists as the most practical therapy.
Evidence summary
Mild persistent asthma is defined as forced expiratory volume over 1 second (FEV1) ≥80% predicted, with daytime symptoms more than twice per week but less than once daily, and nighttime symptoms more often than twice monthly.1
Low-dose inhaled corticosteroids
Two large randomized trials support using low-dose inhaled corticosteroids in these children. The Childhood Asthma Management Program (CAMP) study, which included 1041 children, evaluated treatment with either budesonide or nedocromil vs placebo. Patients taking budesonide had a lower rate of urgent care visits (absolute risk reduction [ARR]=10%; number needed to treat [NNT]=10; P=.02) compared with children taking nedocromil (ARR=6%; NNT=17; P=.02). The urgent care visits were reported as number of visits per 100 person-years.
In practical terms, this means that in order to decrease 1 urgent care visit, 1 patient would need to take budesonide for 10 years. However, because rates are not necessarily homogenous over time, the number of visits decreased during the first year may be different than the number of events decreased throughout the tenth year.
Children taking budesonide experienced 21.5% more episode-free days than those taking placebo (P=.01). No change was observed in the nedocromil group.2 In the inhaled Steroid Treatment As Regular Therapy (START) in early asthma study, budesonide demonstrated a 44% relative reduction in time to first severe asthma related event, compared with placebo (95% confidence interval [CI], 0.45–0.71; NNT=44; P=.0001).3
Theophylline
Theophylline is considered an alternative to inhaled corticosteroids. One study compared beclomethasone with theophylline in 195 children. This study found near-equivalent efficacy in doctor visits, hospitalizations, monthly peak expiratory flow rates, and FEV1; however, beclomethasone was superior to theophylline in maintaining symptom control and decreasing the use of inhaled bronchodilators and systemic steroids.
When compared with beclomethasone, theophylline was linked to 14% more central nervous system adverse effects (P<.001) and 17% more gastrointestinal disturbances (P<.001). Although beclomethasone induced more oral candidiasis compared with theophylline (8.9% vs 2.4%; P<.001), the incidence of this infection can be reduced by using a spacer.
Long-term systemic effects
The potential long-term adverse systemic effects of inhaled corticosteroids on growth, bone metabolism, and pituitary-adrenal function call for longer-term studies.4 A systematic review of 15 trials reported that the protective effect of leukotriene receptor antagonists is inferior to inhaled corticosteroids for adults (relative risk [RR]=1.71; 95% CI, 1.40–2.09); however, evidence is insufficient to extrapolate this to children.5
Beta-agonists
Evidence does not support use of long-acting beta-agonists as monotherapy or in combination with other medications for children with mild persistent asthma. Although 1 study showed an improvement in lung function for children taking budesonide plus formoterol compared with budesonide alone, the rate of severe exacerbations was lower for those taking budesonide alone (62% decrease vs 55.8% decrease; P=.001). Both groups had a 32% decrease in the number of rescue inhalations per day when compared with placebo (P=.0008).6
Recommendations from others
Recommendations are listed in the TABLE.1,7,8 Unlike the NAEPP and GINA asthma guidelines, the BTS/SIGN asthma guidelines define no objective measurement or staging classification to diagnose asthma among children. Diagnosis is determined by a child’s response to medication.8 Independent of any daily controller medication use, all children should have a short acting bronchodilator on hand in case of an acute attack.1,8
TABLE
Recommendations for treating mild persistent asthma
| GUIDELINE | DAILY CONTROLLER MEDICATION | ALTERNATIVE TREATMENT |
|---|---|---|
| National Asthma Education and Prevention Program (NAEPP)1 | Low-dose inhaled corticosteroids | Children <5: cromolyn, LTRAs Children >5: cromolyn, LTRAs, nedocromil, sustained release theophylline |
| Global initiative for asthma (GINA)7 | low-dose inhaled corticosteroids | All children: sustained released theophylline, Cromone, LTRAs |
| British Thoracic Society/Scottish intercollegiate Guidelines network (BTS/SIGN)8 | Inhaled steroids | All children: LTRAs, theophylline Children >5: cromones, nedocromil |
| LRTA leukotriene receptor antagonists. | ||
| Sources: NAEPP J Allergy Clin Immunol 20021; GINA Guidelines and Resources 20057 and BTS/SIGN, Thorax 2003.8 | ||
1. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma Update on Selected Topics—2002. National Asthma Education and Prevention Program. J Allergy Clin Immunol 2002;110:S141-S219.
2. Long-term effects of budesonide or nedocromil in children with asthma. The Childhood Asthma Management Program Research Group. N Engl J Med 2000;343:1054-1063.
3. Pauwels RA, Pedersen S, Busse WW, et al. START Investigators Group. Early intervention with budesonide in mild persistent asthma: a randomised, double-blind trial. Lancet 2003;361:1071-1076.
4. Reed CE, Offord KP, Nelson HS, Li JT, Tinkelman DG. Aerosol beclomethasone dipropionate spray compared with theophylline as primary treatment for chronic mild-to-moderate asthma. The American Academy of Allergy, Asthma and Immunology Beclomethasone Dipropionate-Theophylline Study Group. J Allergy Clin Immunol 1998;101:14-23.
5. Ducharme FM, Salvio F, Ducharme F. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children (Cochrane review). In: The Cochrane Library. 2006 Issue 2. Chichester, UK: John Wiley and Sons, Ltd.
6. O’byrne PM, Barnes PJ, Rodriguez-Roisin R, et al. Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med 2001;164:1392-1397.
7. The Global Initiative for Asthma. Guidelines and Resources: 2005 Update. Available at: www.ginasthma.com/Guidelineitem.asp??I1=2&I2=1&intId=60. Accessed January 9, 2007.
8. British Thoracic Society Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. Thorax 2003;58:i1-i94.
Low-dose inhaled corticosteroids are the preferred treatment for children with mild persistent asthma because they demonstrate superior reduction in severity and frequency of asthma exacerbations compared with alternatives (strength of recommendation [SOR]: A, based on multiple randomized controlled trials). As add-on therapy, nedocromil, theophylline, and cromolyn have all demonstrated a modest benefit in symptom control; leukotriene receptor antagonists are also recommended based on data from older children (SOR: B, cohort study). Unlike treatment of moderate or severe asthma, long-acting beta-agonists are not recommended (SOR: A, randomized trials).
Clear medication choices for mild asthma are supported by good evidence
John Heintzman, MD
Oregon Health and Science University, Portland
Physicians who routinely treat children with asthma are fortunate to have the body of evidence outlined in this review. Clear medication choices are supported in most instances by relatively clear comparisons with alternatives. In my practice, where many children can be classified in the “mild persistent” category, I am always surprised at how many patients’ families lack a clear understanding of the factors that trigger a child’s asthma and how to avoid them.
Another common clinical scenario among children and adolescents is exercise-induced asthma. Depending on the sport, the asthma can be classified as “mild persistent” or “mild intermittent.” for true intermittent symptoms, my clinical experience (and often parental preference) argues for pre-activity treatment with short acting beta-agonists as the most practical therapy.
Evidence summary
Mild persistent asthma is defined as forced expiratory volume over 1 second (FEV1) ≥80% predicted, with daytime symptoms more than twice per week but less than once daily, and nighttime symptoms more often than twice monthly.1
Low-dose inhaled corticosteroids
Two large randomized trials support using low-dose inhaled corticosteroids in these children. The Childhood Asthma Management Program (CAMP) study, which included 1041 children, evaluated treatment with either budesonide or nedocromil vs placebo. Patients taking budesonide had a lower rate of urgent care visits (absolute risk reduction [ARR]=10%; number needed to treat [NNT]=10; P=.02) compared with children taking nedocromil (ARR=6%; NNT=17; P=.02). The urgent care visits were reported as number of visits per 100 person-years.
In practical terms, this means that in order to decrease 1 urgent care visit, 1 patient would need to take budesonide for 10 years. However, because rates are not necessarily homogenous over time, the number of visits decreased during the first year may be different than the number of events decreased throughout the tenth year.
Children taking budesonide experienced 21.5% more episode-free days than those taking placebo (P=.01). No change was observed in the nedocromil group.2 In the inhaled Steroid Treatment As Regular Therapy (START) in early asthma study, budesonide demonstrated a 44% relative reduction in time to first severe asthma related event, compared with placebo (95% confidence interval [CI], 0.45–0.71; NNT=44; P=.0001).3
Theophylline
Theophylline is considered an alternative to inhaled corticosteroids. One study compared beclomethasone with theophylline in 195 children. This study found near-equivalent efficacy in doctor visits, hospitalizations, monthly peak expiratory flow rates, and FEV1; however, beclomethasone was superior to theophylline in maintaining symptom control and decreasing the use of inhaled bronchodilators and systemic steroids.
When compared with beclomethasone, theophylline was linked to 14% more central nervous system adverse effects (P<.001) and 17% more gastrointestinal disturbances (P<.001). Although beclomethasone induced more oral candidiasis compared with theophylline (8.9% vs 2.4%; P<.001), the incidence of this infection can be reduced by using a spacer.
Long-term systemic effects
The potential long-term adverse systemic effects of inhaled corticosteroids on growth, bone metabolism, and pituitary-adrenal function call for longer-term studies.4 A systematic review of 15 trials reported that the protective effect of leukotriene receptor antagonists is inferior to inhaled corticosteroids for adults (relative risk [RR]=1.71; 95% CI, 1.40–2.09); however, evidence is insufficient to extrapolate this to children.5
Beta-agonists
Evidence does not support use of long-acting beta-agonists as monotherapy or in combination with other medications for children with mild persistent asthma. Although 1 study showed an improvement in lung function for children taking budesonide plus formoterol compared with budesonide alone, the rate of severe exacerbations was lower for those taking budesonide alone (62% decrease vs 55.8% decrease; P=.001). Both groups had a 32% decrease in the number of rescue inhalations per day when compared with placebo (P=.0008).6
Recommendations from others
Recommendations are listed in the TABLE.1,7,8 Unlike the NAEPP and GINA asthma guidelines, the BTS/SIGN asthma guidelines define no objective measurement or staging classification to diagnose asthma among children. Diagnosis is determined by a child’s response to medication.8 Independent of any daily controller medication use, all children should have a short acting bronchodilator on hand in case of an acute attack.1,8
TABLE
Recommendations for treating mild persistent asthma
| GUIDELINE | DAILY CONTROLLER MEDICATION | ALTERNATIVE TREATMENT |
|---|---|---|
| National Asthma Education and Prevention Program (NAEPP)1 | Low-dose inhaled corticosteroids | Children <5: cromolyn, LTRAs Children >5: cromolyn, LTRAs, nedocromil, sustained release theophylline |
| Global initiative for asthma (GINA)7 | low-dose inhaled corticosteroids | All children: sustained released theophylline, Cromone, LTRAs |
| British Thoracic Society/Scottish intercollegiate Guidelines network (BTS/SIGN)8 | Inhaled steroids | All children: LTRAs, theophylline Children >5: cromones, nedocromil |
| LRTA leukotriene receptor antagonists. | ||
| Sources: NAEPP J Allergy Clin Immunol 20021; GINA Guidelines and Resources 20057 and BTS/SIGN, Thorax 2003.8 | ||
Low-dose inhaled corticosteroids are the preferred treatment for children with mild persistent asthma because they demonstrate superior reduction in severity and frequency of asthma exacerbations compared with alternatives (strength of recommendation [SOR]: A, based on multiple randomized controlled trials). As add-on therapy, nedocromil, theophylline, and cromolyn have all demonstrated a modest benefit in symptom control; leukotriene receptor antagonists are also recommended based on data from older children (SOR: B, cohort study). Unlike treatment of moderate or severe asthma, long-acting beta-agonists are not recommended (SOR: A, randomized trials).
Clear medication choices for mild asthma are supported by good evidence
John Heintzman, MD
Oregon Health and Science University, Portland
Physicians who routinely treat children with asthma are fortunate to have the body of evidence outlined in this review. Clear medication choices are supported in most instances by relatively clear comparisons with alternatives. In my practice, where many children can be classified in the “mild persistent” category, I am always surprised at how many patients’ families lack a clear understanding of the factors that trigger a child’s asthma and how to avoid them.
Another common clinical scenario among children and adolescents is exercise-induced asthma. Depending on the sport, the asthma can be classified as “mild persistent” or “mild intermittent.” for true intermittent symptoms, my clinical experience (and often parental preference) argues for pre-activity treatment with short acting beta-agonists as the most practical therapy.
Evidence summary
Mild persistent asthma is defined as forced expiratory volume over 1 second (FEV1) ≥80% predicted, with daytime symptoms more than twice per week but less than once daily, and nighttime symptoms more often than twice monthly.1
Low-dose inhaled corticosteroids
Two large randomized trials support using low-dose inhaled corticosteroids in these children. The Childhood Asthma Management Program (CAMP) study, which included 1041 children, evaluated treatment with either budesonide or nedocromil vs placebo. Patients taking budesonide had a lower rate of urgent care visits (absolute risk reduction [ARR]=10%; number needed to treat [NNT]=10; P=.02) compared with children taking nedocromil (ARR=6%; NNT=17; P=.02). The urgent care visits were reported as number of visits per 100 person-years.
In practical terms, this means that in order to decrease 1 urgent care visit, 1 patient would need to take budesonide for 10 years. However, because rates are not necessarily homogenous over time, the number of visits decreased during the first year may be different than the number of events decreased throughout the tenth year.
Children taking budesonide experienced 21.5% more episode-free days than those taking placebo (P=.01). No change was observed in the nedocromil group.2 In the inhaled Steroid Treatment As Regular Therapy (START) in early asthma study, budesonide demonstrated a 44% relative reduction in time to first severe asthma related event, compared with placebo (95% confidence interval [CI], 0.45–0.71; NNT=44; P=.0001).3
Theophylline
Theophylline is considered an alternative to inhaled corticosteroids. One study compared beclomethasone with theophylline in 195 children. This study found near-equivalent efficacy in doctor visits, hospitalizations, monthly peak expiratory flow rates, and FEV1; however, beclomethasone was superior to theophylline in maintaining symptom control and decreasing the use of inhaled bronchodilators and systemic steroids.
When compared with beclomethasone, theophylline was linked to 14% more central nervous system adverse effects (P<.001) and 17% more gastrointestinal disturbances (P<.001). Although beclomethasone induced more oral candidiasis compared with theophylline (8.9% vs 2.4%; P<.001), the incidence of this infection can be reduced by using a spacer.
Long-term systemic effects
The potential long-term adverse systemic effects of inhaled corticosteroids on growth, bone metabolism, and pituitary-adrenal function call for longer-term studies.4 A systematic review of 15 trials reported that the protective effect of leukotriene receptor antagonists is inferior to inhaled corticosteroids for adults (relative risk [RR]=1.71; 95% CI, 1.40–2.09); however, evidence is insufficient to extrapolate this to children.5
Beta-agonists
Evidence does not support use of long-acting beta-agonists as monotherapy or in combination with other medications for children with mild persistent asthma. Although 1 study showed an improvement in lung function for children taking budesonide plus formoterol compared with budesonide alone, the rate of severe exacerbations was lower for those taking budesonide alone (62% decrease vs 55.8% decrease; P=.001). Both groups had a 32% decrease in the number of rescue inhalations per day when compared with placebo (P=.0008).6
Recommendations from others
Recommendations are listed in the TABLE.1,7,8 Unlike the NAEPP and GINA asthma guidelines, the BTS/SIGN asthma guidelines define no objective measurement or staging classification to diagnose asthma among children. Diagnosis is determined by a child’s response to medication.8 Independent of any daily controller medication use, all children should have a short acting bronchodilator on hand in case of an acute attack.1,8
TABLE
Recommendations for treating mild persistent asthma
| GUIDELINE | DAILY CONTROLLER MEDICATION | ALTERNATIVE TREATMENT |
|---|---|---|
| National Asthma Education and Prevention Program (NAEPP)1 | Low-dose inhaled corticosteroids | Children <5: cromolyn, LTRAs Children >5: cromolyn, LTRAs, nedocromil, sustained release theophylline |
| Global initiative for asthma (GINA)7 | low-dose inhaled corticosteroids | All children: sustained released theophylline, Cromone, LTRAs |
| British Thoracic Society/Scottish intercollegiate Guidelines network (BTS/SIGN)8 | Inhaled steroids | All children: LTRAs, theophylline Children >5: cromones, nedocromil |
| LRTA leukotriene receptor antagonists. | ||
| Sources: NAEPP J Allergy Clin Immunol 20021; GINA Guidelines and Resources 20057 and BTS/SIGN, Thorax 2003.8 | ||
1. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma Update on Selected Topics—2002. National Asthma Education and Prevention Program. J Allergy Clin Immunol 2002;110:S141-S219.
2. Long-term effects of budesonide or nedocromil in children with asthma. The Childhood Asthma Management Program Research Group. N Engl J Med 2000;343:1054-1063.
3. Pauwels RA, Pedersen S, Busse WW, et al. START Investigators Group. Early intervention with budesonide in mild persistent asthma: a randomised, double-blind trial. Lancet 2003;361:1071-1076.
4. Reed CE, Offord KP, Nelson HS, Li JT, Tinkelman DG. Aerosol beclomethasone dipropionate spray compared with theophylline as primary treatment for chronic mild-to-moderate asthma. The American Academy of Allergy, Asthma and Immunology Beclomethasone Dipropionate-Theophylline Study Group. J Allergy Clin Immunol 1998;101:14-23.
5. Ducharme FM, Salvio F, Ducharme F. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children (Cochrane review). In: The Cochrane Library. 2006 Issue 2. Chichester, UK: John Wiley and Sons, Ltd.
6. O’byrne PM, Barnes PJ, Rodriguez-Roisin R, et al. Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med 2001;164:1392-1397.
7. The Global Initiative for Asthma. Guidelines and Resources: 2005 Update. Available at: www.ginasthma.com/Guidelineitem.asp??I1=2&I2=1&intId=60. Accessed January 9, 2007.
8. British Thoracic Society Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. Thorax 2003;58:i1-i94.
1. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma Update on Selected Topics—2002. National Asthma Education and Prevention Program. J Allergy Clin Immunol 2002;110:S141-S219.
2. Long-term effects of budesonide or nedocromil in children with asthma. The Childhood Asthma Management Program Research Group. N Engl J Med 2000;343:1054-1063.
3. Pauwels RA, Pedersen S, Busse WW, et al. START Investigators Group. Early intervention with budesonide in mild persistent asthma: a randomised, double-blind trial. Lancet 2003;361:1071-1076.
4. Reed CE, Offord KP, Nelson HS, Li JT, Tinkelman DG. Aerosol beclomethasone dipropionate spray compared with theophylline as primary treatment for chronic mild-to-moderate asthma. The American Academy of Allergy, Asthma and Immunology Beclomethasone Dipropionate-Theophylline Study Group. J Allergy Clin Immunol 1998;101:14-23.
5. Ducharme FM, Salvio F, Ducharme F. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children (Cochrane review). In: The Cochrane Library. 2006 Issue 2. Chichester, UK: John Wiley and Sons, Ltd.
6. O’byrne PM, Barnes PJ, Rodriguez-Roisin R, et al. Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med 2001;164:1392-1397.
7. The Global Initiative for Asthma. Guidelines and Resources: 2005 Update. Available at: www.ginasthma.com/Guidelineitem.asp??I1=2&I2=1&intId=60. Accessed January 9, 2007.
8. British Thoracic Society Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. Thorax 2003;58:i1-i94.
Evidence-based answers from the Family Physicians Inquiries Network
What other STI testing should we do for a patient with chlamydia?
Testing for gonorrhea is recommended for a patient with genital chlamydia; also test for gonorrhea and chlamydia in their sexual partner because of the high prevalence of coinfection, particularly among younger patients (strength of recommendation [SOR]: C, based on expert opinion and observational studies). Testing for syphilis and HIV is also recommended for the patient and their partner (SOR: C, based on expert opinion).
David B. , MD, FAAFP
Tacoma Family Medicine, Tacoma, Wash
Counsel younger adults and teens regarding the risks for STIs by taking an adequate sexual history Many outpatient labs offer combined upfront testing of chlamydia and gonorrhea—the information here supports that approach. More important, the recommendation to “screen” all patients seeking treatment for sexually transmitted infections (STIs) for HIV carries an essential underlying message: the need to talk with and counsel our patients, especially younger adults and teens, regarding their risks for STIs by taking an adequate sexual history.
The Centers for Disease Control and Prevention (CDC) suggests one organized approach using “The Five Ps”: Partners (gender, number), Prevention of pregnancy, Protection from STIs, Practices (type of sex and condom use), Past history of STIs. This important conversation not only guides decisions about completing testing for other STIs but provides an avenue for potentially life-saving conversations.
Evidence Summary
A pilot study evaluated the yield of testing patients for other STIs among patients with genital chlamydia diagnosed during opportunistic screening. The study screened patients of both sexes in primary health care settings, as well as men attending a genitourinary medicine clinic. All patients testing positive in the community were advised to attend the genitourinary medicine clinic for STI screening, partner notification, and testing of patients and their contacts. More than 90% of the patients testing positive for chlamydia attended the genitourinary medicine clinic for management (total numbers seen in the clinic; women n=1245 [957 screened in the community] and men n=490 [280 screened in the community]).
At the clinic, further workup included evaluation and testing for chlamydia, gonorrhea, trichomonas, and bacterial vaginosis. Of the patients whose initial screening was in the genitourinary medicine clinic, 28% had an additional STI. Of the patients initially screened in the community setting, 4% had another STI. Partner testing showed that 55% of male partners of female patients had an STI and 76% of female partners of male patients had one or more STI.1
The high prevalence of coinfection of chlamydia and gonorrhea has been shown in several studies. One cross-sectional study of new clients to a hospital-based STI clinic with gonorrhea, chlamydia, or both infections found 39% of 1239 women and 24% of 1141 heterosexual men with gonorrhea also had chlamydia. Thirteen percent of females and 19% of heterosexual males with chlamydia also had gonorrhea. More than half of the women and a third of the men aged 15 to 19 had both gonorrhea and chlamydia. Patients with both STIs tended to be younger than those with one.2 A study of the prevalence rate of chlamydia, gonorrhea, and their coinfection in an adolescent population (women n=131,915 and men n=71,074) of juvenile detention centers between 1997 and 2002 found that 18% of women and 13% of males with chlamydia were coinfected with gonorrhea.3 In non–STI clinic settings, gonorrhea has been found in 9% of men4,5 and 6% of women5 with chlamydia.
Recommendations from others
The American Academy of Family Physicians (AAFP) strongly recommends testing for chlamydia in all sexually active women aged 25 years or younger and those at increased risk. The AAFP recommends screening all sexually active women for gonorrhea if they are at increased risk for infection; strongly recommends screening persons at increased risk for syphilis infection; and strongly recommends screening for HIV for persons seeking treatment for STIs.6
The CDC guidelines recommend evaluation, testing and treatment of partners of persons with chlamydia. As well as testing for other STIs, the guidelines suggest Pap smear screening for women who have not been adequately screened, as they often are at high risk for later cervical cancer.7 All patients seeking treatment for STDs, including all patients attending STD clinics, should be screened routinely for HIV during each visit for a new complaint, regardless of whether the patient is known or suspected to have specific behavior risks for HIV infection.8
The Institute for Clinical Systems Improvement recommends screening for chlamydia and gonorrhea for all sexually active women aged 25 years and younger and other asymptomatic women at risk for infection. Routine screening for HIV is also recommended to all persons at high risk, including those seeking treatment for any STI.9
1. Harindra V, Tobin JM, Underhill G. Opportunistic chlamydia screening; should positive patients be screened for co-infections? Int J STD AIDS 2002;13:821-825
2. Creighton S, Tenant-Flowers M, Taylor CB, Miller R, Low N. Co-infection with gonorrhoea and chlamydia: how much is there and what does it mean? Int J STD AIDS 2003;14:109-113
3. Kahn RH, Mosure DJ, Blank S, et al for the jail STD Prevalence Monitoring Project. Chlamydia trachomatis and Neisseria gonorrhoeae Prevalence and Coinfection in adolescents entering selected US juvenile Detention Centers, 1997-2002. Sex Transm Dis 2005;32:255-259.
4. Gaydos CA, Kent CK, Rietmeijer CA, et al. Prevalence of Neisseria Gonorrheae among men screened for Chlamydia Trachomatis in four US cities, 1999-2003 Sex Transm D 2006;33:314-319.
5. KMiller WC, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the united states. JAMA 2004;291:2229-2236
6. American Academy of Family Physicians (AAFP). Summary of the recommendations for clinical preventive services. Revision 6.0. Leawood, Kan: AAFP; August 2005.
7. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep 2006;55(RR-11):1-94.
8. Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep 2006;55(RR-14):1-17.
9. Institute for Clinical systems Improvement Preventive services for adults. Bloomington, Minn: Institute for Clinical systems Improvement; 2004. Available online at www guideline.gov. Accessed on December 13, 2006.
Testing for gonorrhea is recommended for a patient with genital chlamydia; also test for gonorrhea and chlamydia in their sexual partner because of the high prevalence of coinfection, particularly among younger patients (strength of recommendation [SOR]: C, based on expert opinion and observational studies). Testing for syphilis and HIV is also recommended for the patient and their partner (SOR: C, based on expert opinion).
David B. , MD, FAAFP
Tacoma Family Medicine, Tacoma, Wash
Counsel younger adults and teens regarding the risks for STIs by taking an adequate sexual history Many outpatient labs offer combined upfront testing of chlamydia and gonorrhea—the information here supports that approach. More important, the recommendation to “screen” all patients seeking treatment for sexually transmitted infections (STIs) for HIV carries an essential underlying message: the need to talk with and counsel our patients, especially younger adults and teens, regarding their risks for STIs by taking an adequate sexual history.
The Centers for Disease Control and Prevention (CDC) suggests one organized approach using “The Five Ps”: Partners (gender, number), Prevention of pregnancy, Protection from STIs, Practices (type of sex and condom use), Past history of STIs. This important conversation not only guides decisions about completing testing for other STIs but provides an avenue for potentially life-saving conversations.
Evidence Summary
A pilot study evaluated the yield of testing patients for other STIs among patients with genital chlamydia diagnosed during opportunistic screening. The study screened patients of both sexes in primary health care settings, as well as men attending a genitourinary medicine clinic. All patients testing positive in the community were advised to attend the genitourinary medicine clinic for STI screening, partner notification, and testing of patients and their contacts. More than 90% of the patients testing positive for chlamydia attended the genitourinary medicine clinic for management (total numbers seen in the clinic; women n=1245 [957 screened in the community] and men n=490 [280 screened in the community]).
At the clinic, further workup included evaluation and testing for chlamydia, gonorrhea, trichomonas, and bacterial vaginosis. Of the patients whose initial screening was in the genitourinary medicine clinic, 28% had an additional STI. Of the patients initially screened in the community setting, 4% had another STI. Partner testing showed that 55% of male partners of female patients had an STI and 76% of female partners of male patients had one or more STI.1
The high prevalence of coinfection of chlamydia and gonorrhea has been shown in several studies. One cross-sectional study of new clients to a hospital-based STI clinic with gonorrhea, chlamydia, or both infections found 39% of 1239 women and 24% of 1141 heterosexual men with gonorrhea also had chlamydia. Thirteen percent of females and 19% of heterosexual males with chlamydia also had gonorrhea. More than half of the women and a third of the men aged 15 to 19 had both gonorrhea and chlamydia. Patients with both STIs tended to be younger than those with one.2 A study of the prevalence rate of chlamydia, gonorrhea, and their coinfection in an adolescent population (women n=131,915 and men n=71,074) of juvenile detention centers between 1997 and 2002 found that 18% of women and 13% of males with chlamydia were coinfected with gonorrhea.3 In non–STI clinic settings, gonorrhea has been found in 9% of men4,5 and 6% of women5 with chlamydia.
Recommendations from others
The American Academy of Family Physicians (AAFP) strongly recommends testing for chlamydia in all sexually active women aged 25 years or younger and those at increased risk. The AAFP recommends screening all sexually active women for gonorrhea if they are at increased risk for infection; strongly recommends screening persons at increased risk for syphilis infection; and strongly recommends screening for HIV for persons seeking treatment for STIs.6
The CDC guidelines recommend evaluation, testing and treatment of partners of persons with chlamydia. As well as testing for other STIs, the guidelines suggest Pap smear screening for women who have not been adequately screened, as they often are at high risk for later cervical cancer.7 All patients seeking treatment for STDs, including all patients attending STD clinics, should be screened routinely for HIV during each visit for a new complaint, regardless of whether the patient is known or suspected to have specific behavior risks for HIV infection.8
The Institute for Clinical Systems Improvement recommends screening for chlamydia and gonorrhea for all sexually active women aged 25 years and younger and other asymptomatic women at risk for infection. Routine screening for HIV is also recommended to all persons at high risk, including those seeking treatment for any STI.9
Testing for gonorrhea is recommended for a patient with genital chlamydia; also test for gonorrhea and chlamydia in their sexual partner because of the high prevalence of coinfection, particularly among younger patients (strength of recommendation [SOR]: C, based on expert opinion and observational studies). Testing for syphilis and HIV is also recommended for the patient and their partner (SOR: C, based on expert opinion).
David B. , MD, FAAFP
Tacoma Family Medicine, Tacoma, Wash
Counsel younger adults and teens regarding the risks for STIs by taking an adequate sexual history Many outpatient labs offer combined upfront testing of chlamydia and gonorrhea—the information here supports that approach. More important, the recommendation to “screen” all patients seeking treatment for sexually transmitted infections (STIs) for HIV carries an essential underlying message: the need to talk with and counsel our patients, especially younger adults and teens, regarding their risks for STIs by taking an adequate sexual history.
The Centers for Disease Control and Prevention (CDC) suggests one organized approach using “The Five Ps”: Partners (gender, number), Prevention of pregnancy, Protection from STIs, Practices (type of sex and condom use), Past history of STIs. This important conversation not only guides decisions about completing testing for other STIs but provides an avenue for potentially life-saving conversations.
Evidence Summary
A pilot study evaluated the yield of testing patients for other STIs among patients with genital chlamydia diagnosed during opportunistic screening. The study screened patients of both sexes in primary health care settings, as well as men attending a genitourinary medicine clinic. All patients testing positive in the community were advised to attend the genitourinary medicine clinic for STI screening, partner notification, and testing of patients and their contacts. More than 90% of the patients testing positive for chlamydia attended the genitourinary medicine clinic for management (total numbers seen in the clinic; women n=1245 [957 screened in the community] and men n=490 [280 screened in the community]).
At the clinic, further workup included evaluation and testing for chlamydia, gonorrhea, trichomonas, and bacterial vaginosis. Of the patients whose initial screening was in the genitourinary medicine clinic, 28% had an additional STI. Of the patients initially screened in the community setting, 4% had another STI. Partner testing showed that 55% of male partners of female patients had an STI and 76% of female partners of male patients had one or more STI.1
The high prevalence of coinfection of chlamydia and gonorrhea has been shown in several studies. One cross-sectional study of new clients to a hospital-based STI clinic with gonorrhea, chlamydia, or both infections found 39% of 1239 women and 24% of 1141 heterosexual men with gonorrhea also had chlamydia. Thirteen percent of females and 19% of heterosexual males with chlamydia also had gonorrhea. More than half of the women and a third of the men aged 15 to 19 had both gonorrhea and chlamydia. Patients with both STIs tended to be younger than those with one.2 A study of the prevalence rate of chlamydia, gonorrhea, and their coinfection in an adolescent population (women n=131,915 and men n=71,074) of juvenile detention centers between 1997 and 2002 found that 18% of women and 13% of males with chlamydia were coinfected with gonorrhea.3 In non–STI clinic settings, gonorrhea has been found in 9% of men4,5 and 6% of women5 with chlamydia.
Recommendations from others
The American Academy of Family Physicians (AAFP) strongly recommends testing for chlamydia in all sexually active women aged 25 years or younger and those at increased risk. The AAFP recommends screening all sexually active women for gonorrhea if they are at increased risk for infection; strongly recommends screening persons at increased risk for syphilis infection; and strongly recommends screening for HIV for persons seeking treatment for STIs.6
The CDC guidelines recommend evaluation, testing and treatment of partners of persons with chlamydia. As well as testing for other STIs, the guidelines suggest Pap smear screening for women who have not been adequately screened, as they often are at high risk for later cervical cancer.7 All patients seeking treatment for STDs, including all patients attending STD clinics, should be screened routinely for HIV during each visit for a new complaint, regardless of whether the patient is known or suspected to have specific behavior risks for HIV infection.8
The Institute for Clinical Systems Improvement recommends screening for chlamydia and gonorrhea for all sexually active women aged 25 years and younger and other asymptomatic women at risk for infection. Routine screening for HIV is also recommended to all persons at high risk, including those seeking treatment for any STI.9
1. Harindra V, Tobin JM, Underhill G. Opportunistic chlamydia screening; should positive patients be screened for co-infections? Int J STD AIDS 2002;13:821-825
2. Creighton S, Tenant-Flowers M, Taylor CB, Miller R, Low N. Co-infection with gonorrhoea and chlamydia: how much is there and what does it mean? Int J STD AIDS 2003;14:109-113
3. Kahn RH, Mosure DJ, Blank S, et al for the jail STD Prevalence Monitoring Project. Chlamydia trachomatis and Neisseria gonorrhoeae Prevalence and Coinfection in adolescents entering selected US juvenile Detention Centers, 1997-2002. Sex Transm Dis 2005;32:255-259.
4. Gaydos CA, Kent CK, Rietmeijer CA, et al. Prevalence of Neisseria Gonorrheae among men screened for Chlamydia Trachomatis in four US cities, 1999-2003 Sex Transm D 2006;33:314-319.
5. KMiller WC, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the united states. JAMA 2004;291:2229-2236
6. American Academy of Family Physicians (AAFP). Summary of the recommendations for clinical preventive services. Revision 6.0. Leawood, Kan: AAFP; August 2005.
7. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep 2006;55(RR-11):1-94.
8. Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep 2006;55(RR-14):1-17.
9. Institute for Clinical systems Improvement Preventive services for adults. Bloomington, Minn: Institute for Clinical systems Improvement; 2004. Available online at www guideline.gov. Accessed on December 13, 2006.
1. Harindra V, Tobin JM, Underhill G. Opportunistic chlamydia screening; should positive patients be screened for co-infections? Int J STD AIDS 2002;13:821-825
2. Creighton S, Tenant-Flowers M, Taylor CB, Miller R, Low N. Co-infection with gonorrhoea and chlamydia: how much is there and what does it mean? Int J STD AIDS 2003;14:109-113
3. Kahn RH, Mosure DJ, Blank S, et al for the jail STD Prevalence Monitoring Project. Chlamydia trachomatis and Neisseria gonorrhoeae Prevalence and Coinfection in adolescents entering selected US juvenile Detention Centers, 1997-2002. Sex Transm Dis 2005;32:255-259.
4. Gaydos CA, Kent CK, Rietmeijer CA, et al. Prevalence of Neisseria Gonorrheae among men screened for Chlamydia Trachomatis in four US cities, 1999-2003 Sex Transm D 2006;33:314-319.
5. KMiller WC, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the united states. JAMA 2004;291:2229-2236
6. American Academy of Family Physicians (AAFP). Summary of the recommendations for clinical preventive services. Revision 6.0. Leawood, Kan: AAFP; August 2005.
7. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep 2006;55(RR-11):1-94.
8. Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep 2006;55(RR-14):1-17.
9. Institute for Clinical systems Improvement Preventive services for adults. Bloomington, Minn: Institute for Clinical systems Improvement; 2004. Available online at www guideline.gov. Accessed on December 13, 2006.
Evidence-based answers from the Family Physicians Inquiries Network
How do we evaluate a marginally low B12 level?
The best way to evaluate a low-normal B12 level is to check serum methylmalonic acid and homocysteine levels1 (strength of recommendation [SOR]: B, based on consistent level 2 or 3 studies). Give 1 or 2 mg of oral vitamin B12 a day if levels are marginally low and either methylmalonic acid or both methylmalonic acid and homocysteine are elevated (SOR: A).
When faced with low-normal serum B12, either further evaluation or empiric treatment is warranted
Robert C. Oh, MD, MPH
Tripler Army Medical Center, Honolulu, Hawaii
With the advent of methylmalonic acid, homocysteine testing, and the proven efficacy of oral B12, medicine has come a long way from shilling tests and monthly intramuscular shots in the diagnosis and management of B12 deficiency. “Normal” serum B12 may not accurately reflect true tissue B12 stores. Therefore, if serum B12 is borderline low, I routinely get methylmalonic acid and homocysteine for patients in whom I need to “prove” deficiency (for myself, patients, or third-party agents) or monitor closely (ie, those with neurologic symptoms).
Once Deficiency is confirmed, search for a cause. Since 1000 mcg of oral B12 treats nearly all causes of B12 deficiency (including pernicious anemia and deficiency from gastric bypass surgery), empiric treatment is a reasonable alternative as long as serum B12 and symptoms are monitored for therapeutic response. Bottom line: since early detection and treatment could potentially prevent permanent neurologic sequelae, when faced with a low-normal serum B12, it should not be dismissed as “normal”—either further evaluation or empiric treatment is warranted.
Evidence Summary
A low-normal B12 level is 150 to 350 pg/mL. Levels less than 150 pg/mL indicate deficiency. Levels greater than 350 pg/mL indicate adequate B12 supply.2
Vitamin B12 is a necessary coenzyme in the metabolism of methylmalonic acid to succinyl choline, and is also a necessary coenzyme with folate in the metabolism of homocysteine to methionine. Therefore, a vitamin B12 deficiency leads to elevated levels of unmetabolized methylmalonic acid and homocysteine. At a local lab the normal range of methylmalonic acid is 0.00 to 0.40 umol/L, and homocysteine’s normal range is 4.0 to 10.0 mmol/L. Normal levels might vary by laboratory. Other conditions, such as renal insufficiency, may also cause elevation of methylmalonic acid and homocysteine.3
Holotranscobalamin may become a first-choice assay for diagnosing early vitamin B12 deficiency. Studies have shown that it compares favorably with current combined measures (B12 levels, methylmalonic acid, homocysteine). Like current assays, holotranscobalamin is also affected by renal function. It requires further investigation to establish relevant cutoff levels before it can be recommended as a diagnostic strategy.4
Oral vitamin B12 at doses of 1000 to 2000 mcg/d is a simple and cost-effective treatment option for any B12-deficient person, and may actually be superior to intramuscular replacement.5,6 A Cochrane Collaboration review of oral vitamin B12 replacement found that these high doses seemed as effective as intramuscular vitamin B12 in all B12-deficient patients—even those with pernicious anemia, Crohn’s disease, ileal resection, or malabsorption states. The authors of the review recommend a “further large, pragmatic trial in a primary care setting” to determine whether oral vitamin B12 is effective for patients with major common cases of malabsorption and to provide additional evidence for cost effectiveness.6
Recommendations from Others
Current guidelines recommend giving vitamin B12 if methylmalonic acid or both methylmalonic acid and homocysteine are elevated. Give folate if only homocysteine is elevated. Give vitamin B12 if homocysteine elevation persists in spite of adequate folate replacement.2
Monitor for correction of low-normal B12 and metabolites with follow-up blood test after 1 to 2 months of treatment. The negative predictive value of normal metabolites (methylmalonic acid and homocysteine) is unknown.
Individuals with normal vitamin B12 levels and metabolites but significant B12 deficiency signs and symptoms have responded dramatically to B12 replacement.7 Therefore, it is reasonable to treat and monitor for response as an alternative approach to the evaluation of a low-normal B12 level. Pennypacker et al2 state that “the ultimate gold standard for vitamin B12 deficiency may be the reduction in homocysteine and methylmalonic acid concentrations and improvement in clinical symptoms or signs in response to vitamin B12 treatment.”
1. Clarke R, Refsum H, Birks J, et al. Screening for vitamin B-12 and folate deficiency in older persons. Am J Clin Nutr 2003;77:1241-1247.
2. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly out-patients. J Am Geriatr Soc 1992;40:1197-1204.
3. Hvas AM, Juul S, Gerdes LU, Nexo E. The marker of cobalamin deficiency, plasma methylmalonic acid, correlates to plasma creatinine. J Intern Med 2000;247:507-512.
4. Hvas AM, Nexo E. Holotranscobalamin—a first choice assay for diagnosing early vitamin B deficiency? J Intern Med 2005;257:289-298.
5. Kuzminski AM, Del Giacco EJ, Sllen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood 1998;92:1191-1198.
6. Vidal-Alaball J, Butler CC, Cannings-John R, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev 2005;(3):CD004655.
7. Solomon LR. Cobalamin-responsive disorders in the ambulatory care setting: unreliability of cobalamin, methylmalonic acid, and homocysteine testing. Blood 2005;105:978-985.
The best way to evaluate a low-normal B12 level is to check serum methylmalonic acid and homocysteine levels1 (strength of recommendation [SOR]: B, based on consistent level 2 or 3 studies). Give 1 or 2 mg of oral vitamin B12 a day if levels are marginally low and either methylmalonic acid or both methylmalonic acid and homocysteine are elevated (SOR: A).
When faced with low-normal serum B12, either further evaluation or empiric treatment is warranted
Robert C. Oh, MD, MPH
Tripler Army Medical Center, Honolulu, Hawaii
With the advent of methylmalonic acid, homocysteine testing, and the proven efficacy of oral B12, medicine has come a long way from shilling tests and monthly intramuscular shots in the diagnosis and management of B12 deficiency. “Normal” serum B12 may not accurately reflect true tissue B12 stores. Therefore, if serum B12 is borderline low, I routinely get methylmalonic acid and homocysteine for patients in whom I need to “prove” deficiency (for myself, patients, or third-party agents) or monitor closely (ie, those with neurologic symptoms).
Once Deficiency is confirmed, search for a cause. Since 1000 mcg of oral B12 treats nearly all causes of B12 deficiency (including pernicious anemia and deficiency from gastric bypass surgery), empiric treatment is a reasonable alternative as long as serum B12 and symptoms are monitored for therapeutic response. Bottom line: since early detection and treatment could potentially prevent permanent neurologic sequelae, when faced with a low-normal serum B12, it should not be dismissed as “normal”—either further evaluation or empiric treatment is warranted.
Evidence Summary
A low-normal B12 level is 150 to 350 pg/mL. Levels less than 150 pg/mL indicate deficiency. Levels greater than 350 pg/mL indicate adequate B12 supply.2
Vitamin B12 is a necessary coenzyme in the metabolism of methylmalonic acid to succinyl choline, and is also a necessary coenzyme with folate in the metabolism of homocysteine to methionine. Therefore, a vitamin B12 deficiency leads to elevated levels of unmetabolized methylmalonic acid and homocysteine. At a local lab the normal range of methylmalonic acid is 0.00 to 0.40 umol/L, and homocysteine’s normal range is 4.0 to 10.0 mmol/L. Normal levels might vary by laboratory. Other conditions, such as renal insufficiency, may also cause elevation of methylmalonic acid and homocysteine.3
Holotranscobalamin may become a first-choice assay for diagnosing early vitamin B12 deficiency. Studies have shown that it compares favorably with current combined measures (B12 levels, methylmalonic acid, homocysteine). Like current assays, holotranscobalamin is also affected by renal function. It requires further investigation to establish relevant cutoff levels before it can be recommended as a diagnostic strategy.4
Oral vitamin B12 at doses of 1000 to 2000 mcg/d is a simple and cost-effective treatment option for any B12-deficient person, and may actually be superior to intramuscular replacement.5,6 A Cochrane Collaboration review of oral vitamin B12 replacement found that these high doses seemed as effective as intramuscular vitamin B12 in all B12-deficient patients—even those with pernicious anemia, Crohn’s disease, ileal resection, or malabsorption states. The authors of the review recommend a “further large, pragmatic trial in a primary care setting” to determine whether oral vitamin B12 is effective for patients with major common cases of malabsorption and to provide additional evidence for cost effectiveness.6
Recommendations from Others
Current guidelines recommend giving vitamin B12 if methylmalonic acid or both methylmalonic acid and homocysteine are elevated. Give folate if only homocysteine is elevated. Give vitamin B12 if homocysteine elevation persists in spite of adequate folate replacement.2
Monitor for correction of low-normal B12 and metabolites with follow-up blood test after 1 to 2 months of treatment. The negative predictive value of normal metabolites (methylmalonic acid and homocysteine) is unknown.
Individuals with normal vitamin B12 levels and metabolites but significant B12 deficiency signs and symptoms have responded dramatically to B12 replacement.7 Therefore, it is reasonable to treat and monitor for response as an alternative approach to the evaluation of a low-normal B12 level. Pennypacker et al2 state that “the ultimate gold standard for vitamin B12 deficiency may be the reduction in homocysteine and methylmalonic acid concentrations and improvement in clinical symptoms or signs in response to vitamin B12 treatment.”
The best way to evaluate a low-normal B12 level is to check serum methylmalonic acid and homocysteine levels1 (strength of recommendation [SOR]: B, based on consistent level 2 or 3 studies). Give 1 or 2 mg of oral vitamin B12 a day if levels are marginally low and either methylmalonic acid or both methylmalonic acid and homocysteine are elevated (SOR: A).
When faced with low-normal serum B12, either further evaluation or empiric treatment is warranted
Robert C. Oh, MD, MPH
Tripler Army Medical Center, Honolulu, Hawaii
With the advent of methylmalonic acid, homocysteine testing, and the proven efficacy of oral B12, medicine has come a long way from shilling tests and monthly intramuscular shots in the diagnosis and management of B12 deficiency. “Normal” serum B12 may not accurately reflect true tissue B12 stores. Therefore, if serum B12 is borderline low, I routinely get methylmalonic acid and homocysteine for patients in whom I need to “prove” deficiency (for myself, patients, or third-party agents) or monitor closely (ie, those with neurologic symptoms).
Once Deficiency is confirmed, search for a cause. Since 1000 mcg of oral B12 treats nearly all causes of B12 deficiency (including pernicious anemia and deficiency from gastric bypass surgery), empiric treatment is a reasonable alternative as long as serum B12 and symptoms are monitored for therapeutic response. Bottom line: since early detection and treatment could potentially prevent permanent neurologic sequelae, when faced with a low-normal serum B12, it should not be dismissed as “normal”—either further evaluation or empiric treatment is warranted.
Evidence Summary
A low-normal B12 level is 150 to 350 pg/mL. Levels less than 150 pg/mL indicate deficiency. Levels greater than 350 pg/mL indicate adequate B12 supply.2
Vitamin B12 is a necessary coenzyme in the metabolism of methylmalonic acid to succinyl choline, and is also a necessary coenzyme with folate in the metabolism of homocysteine to methionine. Therefore, a vitamin B12 deficiency leads to elevated levels of unmetabolized methylmalonic acid and homocysteine. At a local lab the normal range of methylmalonic acid is 0.00 to 0.40 umol/L, and homocysteine’s normal range is 4.0 to 10.0 mmol/L. Normal levels might vary by laboratory. Other conditions, such as renal insufficiency, may also cause elevation of methylmalonic acid and homocysteine.3
Holotranscobalamin may become a first-choice assay for diagnosing early vitamin B12 deficiency. Studies have shown that it compares favorably with current combined measures (B12 levels, methylmalonic acid, homocysteine). Like current assays, holotranscobalamin is also affected by renal function. It requires further investigation to establish relevant cutoff levels before it can be recommended as a diagnostic strategy.4
Oral vitamin B12 at doses of 1000 to 2000 mcg/d is a simple and cost-effective treatment option for any B12-deficient person, and may actually be superior to intramuscular replacement.5,6 A Cochrane Collaboration review of oral vitamin B12 replacement found that these high doses seemed as effective as intramuscular vitamin B12 in all B12-deficient patients—even those with pernicious anemia, Crohn’s disease, ileal resection, or malabsorption states. The authors of the review recommend a “further large, pragmatic trial in a primary care setting” to determine whether oral vitamin B12 is effective for patients with major common cases of malabsorption and to provide additional evidence for cost effectiveness.6
Recommendations from Others
Current guidelines recommend giving vitamin B12 if methylmalonic acid or both methylmalonic acid and homocysteine are elevated. Give folate if only homocysteine is elevated. Give vitamin B12 if homocysteine elevation persists in spite of adequate folate replacement.2
Monitor for correction of low-normal B12 and metabolites with follow-up blood test after 1 to 2 months of treatment. The negative predictive value of normal metabolites (methylmalonic acid and homocysteine) is unknown.
Individuals with normal vitamin B12 levels and metabolites but significant B12 deficiency signs and symptoms have responded dramatically to B12 replacement.7 Therefore, it is reasonable to treat and monitor for response as an alternative approach to the evaluation of a low-normal B12 level. Pennypacker et al2 state that “the ultimate gold standard for vitamin B12 deficiency may be the reduction in homocysteine and methylmalonic acid concentrations and improvement in clinical symptoms or signs in response to vitamin B12 treatment.”
1. Clarke R, Refsum H, Birks J, et al. Screening for vitamin B-12 and folate deficiency in older persons. Am J Clin Nutr 2003;77:1241-1247.
2. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly out-patients. J Am Geriatr Soc 1992;40:1197-1204.
3. Hvas AM, Juul S, Gerdes LU, Nexo E. The marker of cobalamin deficiency, plasma methylmalonic acid, correlates to plasma creatinine. J Intern Med 2000;247:507-512.
4. Hvas AM, Nexo E. Holotranscobalamin—a first choice assay for diagnosing early vitamin B deficiency? J Intern Med 2005;257:289-298.
5. Kuzminski AM, Del Giacco EJ, Sllen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood 1998;92:1191-1198.
6. Vidal-Alaball J, Butler CC, Cannings-John R, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev 2005;(3):CD004655.
7. Solomon LR. Cobalamin-responsive disorders in the ambulatory care setting: unreliability of cobalamin, methylmalonic acid, and homocysteine testing. Blood 2005;105:978-985.
1. Clarke R, Refsum H, Birks J, et al. Screening for vitamin B-12 and folate deficiency in older persons. Am J Clin Nutr 2003;77:1241-1247.
2. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly out-patients. J Am Geriatr Soc 1992;40:1197-1204.
3. Hvas AM, Juul S, Gerdes LU, Nexo E. The marker of cobalamin deficiency, plasma methylmalonic acid, correlates to plasma creatinine. J Intern Med 2000;247:507-512.
4. Hvas AM, Nexo E. Holotranscobalamin—a first choice assay for diagnosing early vitamin B deficiency? J Intern Med 2005;257:289-298.
5. Kuzminski AM, Del Giacco EJ, Sllen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood 1998;92:1191-1198.
6. Vidal-Alaball J, Butler CC, Cannings-John R, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev 2005;(3):CD004655.
7. Solomon LR. Cobalamin-responsive disorders in the ambulatory care setting: unreliability of cobalamin, methylmalonic acid, and homocysteine testing. Blood 2005;105:978-985.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best approach to the evaluation of resting tachycardia for an adult?
The best evidence about the diagnostic evaluation of resting tachycardias in adults is currently outlined by practice guidelines.1 Initial evaluation includes clinical history, physical examination, and 12-lead electrocardiogram (ECG). If the initial evaluation suggests a sinus tachycardia with narrow QRS complexes and no identifiable secondary cause, a 24-hour Holter monitor is usually recommended (strength of recommendation: C, based on expert opinion).
Wide-complex tachycardias and irregular heartbeats should be urgently managed
Laurel Woods, MD
Group Health Family Medicine Residency Program, Seattle, Wash
This Clinical Inquiry organizes a rational approach to tachycardia, which is frequently an incidental and asymptomatic finding on patient intake. The recommendation of evaluating a 12-lead ECG for sinus vs non-sinus tachycardia, then further investigating underlying causes, helps frame the workup in an approachable manner. Particularly helpful is the pointer that the wide-complex tachycardias and irregular heartbeats should be urgently managed, whereas the rest can be assessed at a more relaxed pace. For nonurgent cases it is important to keep in mind the differential diagnosis and rationally evaluate the likely causes. In my patient population, I tend to see sinus tachycardias in young healthy patients in whom no secondary cause aside from anxiety is identified. Oftentimes I follow up after initiating treatment for anxiety or its underlying cause and find that the tachycardia has resolved. In these cases, I have been less aggressive about ordering a 24-hour Holter monitor.
Evidence Summary
Heart rate varies by age; however, tachycardia in adults is usually defined as a rate exceeding 100 beats/minute.1 Tachycardia at rest requires a diagnostic evaluation. However, our search found no systematic reviews, randomized trials, or prospective cohort studies relevant to this question. The highest level of evidence we located was an international practice guideline developed by the American College of Cardiology, the American Heart Association Task Force on Practice Guidelines, and the European Society of Cardiology Committee for Practice Guidelines.1
This joint guideline recommends that the diagnostic evaluation of a hemodynamically stable patient should begin with a clinical history, physical examination with relevant labs, and 12-lead ECG.1 Many patients with tachycardia are asymptomatic; however, common symptoms and complaints include palpitations, fatigue, lightheadedness, chest discomfort, dyspnea, presyncope, or syncope.1 If the patient has experienced symptoms, it is of crucial importance to obtain a clinical history describing the pattern in terms of the number of episodes, duration, frequency, mode of onset, and possible triggers.1
The main goals of the physical examination, labs, and the 12-lead ECG are to determine if the patient has a sinus or non-sinus tachycardia and to look for other findings that may suggest either a cause for the tachycardia or any complications resulting from the tachycardia.
First, determine if the patient’s heartbeat is regular or irregular. Atrial flutter and atrial fibrillation are common causes of an irregular heartbeat that can easily be diagnosed with a 12-lead ECG. Second, determine the width of the QRS interval: narrow QRS complex tachycardias are supraventricular (from the sinus node, the atria, and the atrioventricular junction) in origin, and wide QRS complex tachycardias are usually ventricular (from all sites below the AV junction).2,3 If an irregular heartbeat or wide-complex tachycardia is detected, appropriate management (including possible urgent referrals) should begin immediately.1 A stable patient with a regular rhythm and a narrow QRS complex can be further investigated at a more relaxed pace.
Refer to the TABLE for a listing of common secondary causes for sinus tachycardia, which should direct lab investigations. If no secondary cause is easily identifiable, a 24-hour monitor is recommended as the next step.
TABLE
Potential secondary causes of resting sinus tachycardia5-7
| Hyperthyroidism |
| Fever |
| Sepsis |
| Anxiety |
| Pheochromocytoma |
| Anemia |
| Hypotension and shock |
| Pulmonary embolism |
| Acute coronary ischemia and myocardial infarction |
| Heart failure |
| Chronic pulmonary disease |
| Hypoxia exposure to medications, stimulants, or illicit drugs |
| Malignancy |
| Pregnancy |
Recommendations from others
Textbook chapters and other review articles regarding this topic describe a similar initial evaluation and provide further details about interpreting the 12-lead ECG.2-7 The most relevant and recent review article suggests that further investigation of narrow QRS complex tachycardias with a regular rate currently involves 4 diagnostic categories: normal sinus tachycardia (ie, secondary cause can be identified), inappropriate sinus tachycardia (IST), postural orthostatic tachycardia syndrome (POTS), and sinus node reentry tachycardia (SNRT).4
If a secondary cause is identified, it should be treated appropriately. If no underlying cause is discovered, a 24-hour Holter monitor is recommended.
Persistent sinus tachycardia (sometimes with nocturnal normalization of heart rate) is diagnosed as IST.4 If the monitor shows paroxysmal episodes of sinus tachycardia, determine if they are triggered by orthostasis and relieved by recumbency (confirm with head upright tilt test) to make the diagnosis of POTS. If it is not POTS, the recordings from the 24-hour Holter monitor help make the diagnosis of SNRT, which consists of sudden, paroxysmal, and usually nonsustained tachycardia.4 The FIGURE shows an algorithm of one common diagnostic strategy for evaluation of tachycardia.2-7
{kind=link}
FIGURE
Diagnostic algorithm for evaluating tachycardias4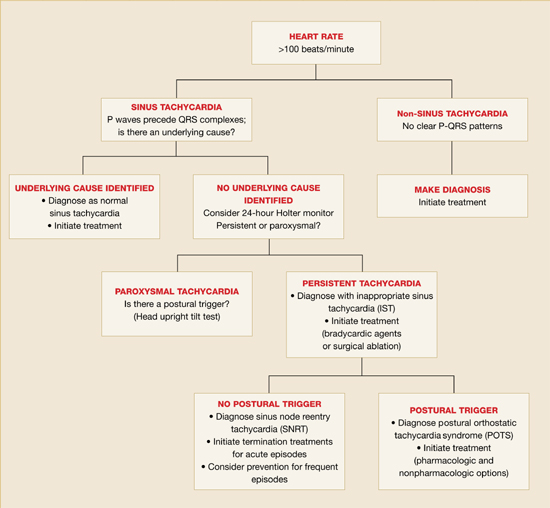
1. American College of Cardiology/American Heart association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (ACC/AHA/ESC). ACC/AHA/ESC guidelines for the management of patients with surpraventricular arrythmias-executive summary. J Am Coll Cardiol 2003;42:1493-1531.
2. Yusuf S, Camm JA. Deciphering the sinus tachycardias. Clin Cardiol 2005;28:267-276.
3. Martin DT. Arrhythmias. In: Noble J, Greene HL, eds. Textbook of Primary Care Medicine. 3rd ed. St. Louis, Mo: Mosby; 2001:528–537.
4. Stoenescu ML, Kowey PR. Tachycardias. In: Rakel RE, ed. Conn’s Current Therapy. 57th ed. Philadelphia, Pa: Saunders; 2005;354-355.
5. Olgin JE, Zipes DP. Specific arrhythmias: diagnosis and treatment. In: Braunwald E, ed. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia, Pa: Saunders; 2005;803-806.
6. Castellanos A, Moleiro F, Chakko S, et al. Heart rate variability in inappropriate sinus tachycardia. Am J Cardiol 1998;82:531-534.
7. Krahn AD, yee R, Klein GJ, Morillo C. Inappropriate sinus tachycardia: evaluation and treatment. J Cardiovasc Electrophysiol 1995;6:1124-1128.
The best evidence about the diagnostic evaluation of resting tachycardias in adults is currently outlined by practice guidelines.1 Initial evaluation includes clinical history, physical examination, and 12-lead electrocardiogram (ECG). If the initial evaluation suggests a sinus tachycardia with narrow QRS complexes and no identifiable secondary cause, a 24-hour Holter monitor is usually recommended (strength of recommendation: C, based on expert opinion).
Wide-complex tachycardias and irregular heartbeats should be urgently managed
Laurel Woods, MD
Group Health Family Medicine Residency Program, Seattle, Wash
This Clinical Inquiry organizes a rational approach to tachycardia, which is frequently an incidental and asymptomatic finding on patient intake. The recommendation of evaluating a 12-lead ECG for sinus vs non-sinus tachycardia, then further investigating underlying causes, helps frame the workup in an approachable manner. Particularly helpful is the pointer that the wide-complex tachycardias and irregular heartbeats should be urgently managed, whereas the rest can be assessed at a more relaxed pace. For nonurgent cases it is important to keep in mind the differential diagnosis and rationally evaluate the likely causes. In my patient population, I tend to see sinus tachycardias in young healthy patients in whom no secondary cause aside from anxiety is identified. Oftentimes I follow up after initiating treatment for anxiety or its underlying cause and find that the tachycardia has resolved. In these cases, I have been less aggressive about ordering a 24-hour Holter monitor.
Evidence Summary
Heart rate varies by age; however, tachycardia in adults is usually defined as a rate exceeding 100 beats/minute.1 Tachycardia at rest requires a diagnostic evaluation. However, our search found no systematic reviews, randomized trials, or prospective cohort studies relevant to this question. The highest level of evidence we located was an international practice guideline developed by the American College of Cardiology, the American Heart Association Task Force on Practice Guidelines, and the European Society of Cardiology Committee for Practice Guidelines.1
This joint guideline recommends that the diagnostic evaluation of a hemodynamically stable patient should begin with a clinical history, physical examination with relevant labs, and 12-lead ECG.1 Many patients with tachycardia are asymptomatic; however, common symptoms and complaints include palpitations, fatigue, lightheadedness, chest discomfort, dyspnea, presyncope, or syncope.1 If the patient has experienced symptoms, it is of crucial importance to obtain a clinical history describing the pattern in terms of the number of episodes, duration, frequency, mode of onset, and possible triggers.1
The main goals of the physical examination, labs, and the 12-lead ECG are to determine if the patient has a sinus or non-sinus tachycardia and to look for other findings that may suggest either a cause for the tachycardia or any complications resulting from the tachycardia.
First, determine if the patient’s heartbeat is regular or irregular. Atrial flutter and atrial fibrillation are common causes of an irregular heartbeat that can easily be diagnosed with a 12-lead ECG. Second, determine the width of the QRS interval: narrow QRS complex tachycardias are supraventricular (from the sinus node, the atria, and the atrioventricular junction) in origin, and wide QRS complex tachycardias are usually ventricular (from all sites below the AV junction).2,3 If an irregular heartbeat or wide-complex tachycardia is detected, appropriate management (including possible urgent referrals) should begin immediately.1 A stable patient with a regular rhythm and a narrow QRS complex can be further investigated at a more relaxed pace.
Refer to the TABLE for a listing of common secondary causes for sinus tachycardia, which should direct lab investigations. If no secondary cause is easily identifiable, a 24-hour monitor is recommended as the next step.
TABLE
Potential secondary causes of resting sinus tachycardia5-7
| Hyperthyroidism |
| Fever |
| Sepsis |
| Anxiety |
| Pheochromocytoma |
| Anemia |
| Hypotension and shock |
| Pulmonary embolism |
| Acute coronary ischemia and myocardial infarction |
| Heart failure |
| Chronic pulmonary disease |
| Hypoxia exposure to medications, stimulants, or illicit drugs |
| Malignancy |
| Pregnancy |
Recommendations from others
Textbook chapters and other review articles regarding this topic describe a similar initial evaluation and provide further details about interpreting the 12-lead ECG.2-7 The most relevant and recent review article suggests that further investigation of narrow QRS complex tachycardias with a regular rate currently involves 4 diagnostic categories: normal sinus tachycardia (ie, secondary cause can be identified), inappropriate sinus tachycardia (IST), postural orthostatic tachycardia syndrome (POTS), and sinus node reentry tachycardia (SNRT).4
If a secondary cause is identified, it should be treated appropriately. If no underlying cause is discovered, a 24-hour Holter monitor is recommended.
Persistent sinus tachycardia (sometimes with nocturnal normalization of heart rate) is diagnosed as IST.4 If the monitor shows paroxysmal episodes of sinus tachycardia, determine if they are triggered by orthostasis and relieved by recumbency (confirm with head upright tilt test) to make the diagnosis of POTS. If it is not POTS, the recordings from the 24-hour Holter monitor help make the diagnosis of SNRT, which consists of sudden, paroxysmal, and usually nonsustained tachycardia.4 The FIGURE shows an algorithm of one common diagnostic strategy for evaluation of tachycardia.2-7
FIGURE
Diagnostic algorithm for evaluating tachycardias4
The best evidence about the diagnostic evaluation of resting tachycardias in adults is currently outlined by practice guidelines.1 Initial evaluation includes clinical history, physical examination, and 12-lead electrocardiogram (ECG). If the initial evaluation suggests a sinus tachycardia with narrow QRS complexes and no identifiable secondary cause, a 24-hour Holter monitor is usually recommended (strength of recommendation: C, based on expert opinion).
Wide-complex tachycardias and irregular heartbeats should be urgently managed
Laurel Woods, MD
Group Health Family Medicine Residency Program, Seattle, Wash
This Clinical Inquiry organizes a rational approach to tachycardia, which is frequently an incidental and asymptomatic finding on patient intake. The recommendation of evaluating a 12-lead ECG for sinus vs non-sinus tachycardia, then further investigating underlying causes, helps frame the workup in an approachable manner. Particularly helpful is the pointer that the wide-complex tachycardias and irregular heartbeats should be urgently managed, whereas the rest can be assessed at a more relaxed pace. For nonurgent cases it is important to keep in mind the differential diagnosis and rationally evaluate the likely causes. In my patient population, I tend to see sinus tachycardias in young healthy patients in whom no secondary cause aside from anxiety is identified. Oftentimes I follow up after initiating treatment for anxiety or its underlying cause and find that the tachycardia has resolved. In these cases, I have been less aggressive about ordering a 24-hour Holter monitor.
Evidence Summary
Heart rate varies by age; however, tachycardia in adults is usually defined as a rate exceeding 100 beats/minute.1 Tachycardia at rest requires a diagnostic evaluation. However, our search found no systematic reviews, randomized trials, or prospective cohort studies relevant to this question. The highest level of evidence we located was an international practice guideline developed by the American College of Cardiology, the American Heart Association Task Force on Practice Guidelines, and the European Society of Cardiology Committee for Practice Guidelines.1
This joint guideline recommends that the diagnostic evaluation of a hemodynamically stable patient should begin with a clinical history, physical examination with relevant labs, and 12-lead ECG.1 Many patients with tachycardia are asymptomatic; however, common symptoms and complaints include palpitations, fatigue, lightheadedness, chest discomfort, dyspnea, presyncope, or syncope.1 If the patient has experienced symptoms, it is of crucial importance to obtain a clinical history describing the pattern in terms of the number of episodes, duration, frequency, mode of onset, and possible triggers.1
The main goals of the physical examination, labs, and the 12-lead ECG are to determine if the patient has a sinus or non-sinus tachycardia and to look for other findings that may suggest either a cause for the tachycardia or any complications resulting from the tachycardia.
First, determine if the patient’s heartbeat is regular or irregular. Atrial flutter and atrial fibrillation are common causes of an irregular heartbeat that can easily be diagnosed with a 12-lead ECG. Second, determine the width of the QRS interval: narrow QRS complex tachycardias are supraventricular (from the sinus node, the atria, and the atrioventricular junction) in origin, and wide QRS complex tachycardias are usually ventricular (from all sites below the AV junction).2,3 If an irregular heartbeat or wide-complex tachycardia is detected, appropriate management (including possible urgent referrals) should begin immediately.1 A stable patient with a regular rhythm and a narrow QRS complex can be further investigated at a more relaxed pace.
Refer to the TABLE for a listing of common secondary causes for sinus tachycardia, which should direct lab investigations. If no secondary cause is easily identifiable, a 24-hour monitor is recommended as the next step.
TABLE
Potential secondary causes of resting sinus tachycardia5-7
| Hyperthyroidism |
| Fever |
| Sepsis |
| Anxiety |
| Pheochromocytoma |
| Anemia |
| Hypotension and shock |
| Pulmonary embolism |
| Acute coronary ischemia and myocardial infarction |
| Heart failure |
| Chronic pulmonary disease |
| Hypoxia exposure to medications, stimulants, or illicit drugs |
| Malignancy |
| Pregnancy |
Recommendations from others
Textbook chapters and other review articles regarding this topic describe a similar initial evaluation and provide further details about interpreting the 12-lead ECG.2-7 The most relevant and recent review article suggests that further investigation of narrow QRS complex tachycardias with a regular rate currently involves 4 diagnostic categories: normal sinus tachycardia (ie, secondary cause can be identified), inappropriate sinus tachycardia (IST), postural orthostatic tachycardia syndrome (POTS), and sinus node reentry tachycardia (SNRT).4
If a secondary cause is identified, it should be treated appropriately. If no underlying cause is discovered, a 24-hour Holter monitor is recommended.
Persistent sinus tachycardia (sometimes with nocturnal normalization of heart rate) is diagnosed as IST.4 If the monitor shows paroxysmal episodes of sinus tachycardia, determine if they are triggered by orthostasis and relieved by recumbency (confirm with head upright tilt test) to make the diagnosis of POTS. If it is not POTS, the recordings from the 24-hour Holter monitor help make the diagnosis of SNRT, which consists of sudden, paroxysmal, and usually nonsustained tachycardia.4 The FIGURE shows an algorithm of one common diagnostic strategy for evaluation of tachycardia.2-7
FIGURE
Diagnostic algorithm for evaluating tachycardias4
1. American College of Cardiology/American Heart association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (ACC/AHA/ESC). ACC/AHA/ESC guidelines for the management of patients with surpraventricular arrythmias-executive summary. J Am Coll Cardiol 2003;42:1493-1531.
2. Yusuf S, Camm JA. Deciphering the sinus tachycardias. Clin Cardiol 2005;28:267-276.
3. Martin DT. Arrhythmias. In: Noble J, Greene HL, eds. Textbook of Primary Care Medicine. 3rd ed. St. Louis, Mo: Mosby; 2001:528–537.
4. Stoenescu ML, Kowey PR. Tachycardias. In: Rakel RE, ed. Conn’s Current Therapy. 57th ed. Philadelphia, Pa: Saunders; 2005;354-355.
5. Olgin JE, Zipes DP. Specific arrhythmias: diagnosis and treatment. In: Braunwald E, ed. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia, Pa: Saunders; 2005;803-806.
6. Castellanos A, Moleiro F, Chakko S, et al. Heart rate variability in inappropriate sinus tachycardia. Am J Cardiol 1998;82:531-534.
7. Krahn AD, yee R, Klein GJ, Morillo C. Inappropriate sinus tachycardia: evaluation and treatment. J Cardiovasc Electrophysiol 1995;6:1124-1128.
1. American College of Cardiology/American Heart association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (ACC/AHA/ESC). ACC/AHA/ESC guidelines for the management of patients with surpraventricular arrythmias-executive summary. J Am Coll Cardiol 2003;42:1493-1531.
2. Yusuf S, Camm JA. Deciphering the sinus tachycardias. Clin Cardiol 2005;28:267-276.
3. Martin DT. Arrhythmias. In: Noble J, Greene HL, eds. Textbook of Primary Care Medicine. 3rd ed. St. Louis, Mo: Mosby; 2001:528–537.
4. Stoenescu ML, Kowey PR. Tachycardias. In: Rakel RE, ed. Conn’s Current Therapy. 57th ed. Philadelphia, Pa: Saunders; 2005;354-355.
5. Olgin JE, Zipes DP. Specific arrhythmias: diagnosis and treatment. In: Braunwald E, ed. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia, Pa: Saunders; 2005;803-806.
6. Castellanos A, Moleiro F, Chakko S, et al. Heart rate variability in inappropriate sinus tachycardia. Am J Cardiol 1998;82:531-534.
7. Krahn AD, yee R, Klein GJ, Morillo C. Inappropriate sinus tachycardia: evaluation and treatment. J Cardiovasc Electrophysiol 1995;6:1124-1128.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best management for patients with evidence of asymptomatic ischemia on exercise stress testing?
Patients with intermediate- or high-risk Duke Treadmill score (DTS) on exercise stress testing (EST) should undergo myocardial perfusion imaging or exercise echocardiography, especially if they have abnormal values of Chronotropic Index or post-EST Heart Rate Recovery.
For patients who have a low-risk DTS, the 4-year mortality is less than 1% to 2%; therefore, risk-factor reduction without further investigation is appropriate (strength of recommendation: B, based on cohort studies and consensus guideline).
When a stress test is not normal, discuss with the patient and examine risk factors
Ronald L. Healy, MD
United Medical Center, Cheyenne, Wyoming
Exercise stress testing is performed to assess the risk of heart disease for asymptomatic patients. EST is relatively inexpensive, convenient, and, with the appropriate equipment, easily performed in a physician’s office. Although the test is limited in its predictive value, it can be reasonably sensitive when performed on the appropriate population groups.
When the EST result is normal, I review cardiovascular risk factors with the patient and use the opportunity to reinforce the importance of healthy lifestyle modifications. Difficulties arise, however, when an EST result is not normal. Since the patient is at increased risk of cardiovascular morbidity and mortality, I usually recommend further testing. Many options are available, including exercise stress echocardiography, thallium scan, and coronary catheterization. Newer technologies such as MRI and CT scan may be appropriate in some circumstances. I usually base my decision after discussion with the patient, examination of the patient’s risk factors, and the preferences and expertise of my local cardiology group.
Evidence summary
No randomized controlled trials have identified the optimal management of patients with asymptomatic ischemia on EST. EST is not generally recommended for asymptomatic persons because of its limited predictive value. EST may sometimes be useful for predicting mortality risk among patients who plan to begin exercise programs, or whose jobs affect public safety, or who have conditions such as diabetes or chronic renal insufficiency.1
For example, a prospective cohort study of 613 patients with suspected coronary artery disease investigated EST duration, presence of angina, and ST-segment depression as predictors of mortality.2 Patients with asymptomatic ischemia (2 mm of ischemic depression) whose EST lasted 15 minutes (DTS=+5, low risk) had a 5-year cardiac mortality of less than 1%, compared with 2% for those whose EST was tolerated for only 7 minutes (DTS=–3, intermediate risk).2 (See TABLE for DTS formula.)
Later prospective cohort studies3,4 confirmed that a low-risk DTS was associated with high 5-year survival—eg, 97% among 2758 patients (median age 49, 70% male, 30% prior myocardial infarction, 49% with angina).3 Those with an intermediate- or high-risk DTS had corresponding survival rates of 90% and 65%, respectively. The DTS was further analyzed in a 5-year follow-up of 9454 patients, 88% of whom were low-risk (75% undergoing screening EST).4 Most patients (1406 of 1477) with ST-segment depression ≥1 mm had asymptomatic ischemia, only 71 having EST-induced angina. A low-risk DTS was associated with 98% survival, compared with 92% for patients with an intermediate- or high-risk DTS.4
Patients with an intermediate-risk DTS, and normal or near-normal perfusion imaging without cardiomegaly, also comprised a low-risk group with 5-year cardiac survival of 99.5%.5 Post-EST heart rate recovery and the Chronotropic Index are enhancements to the DTS.6 Used singly or in combination, these tools provided more accurate estimates of 5-year all-cause mortality among 9454 patients referred for EST (TABLE).
Two other prospective cohort studies of middle-aged men with EST showing asymptomatic ischemia did not employ the above enhancements but reported major impact of cardiac risk factors on mortality. Among 25,927 healthy men followed for an average of 8.4 years, the age-adjusted risk of death from all causes of those with asymptomatic ischemia increased from 2-fold (95% confidence interval [CI], 1.1–3.8, P=.03) with no risk factors to 4 (95% CI, 2.7–5.4) with 1 risk factor, 5 (95% CI, 3.3–6.9) with 2 risk factors, and 8 (95% CI, 5.4–12.8) with 3 or more risk factors (P<.0001).7 Other investigators found increased mortality from coronary artery disease to be associated with smoking (relative risk [RR]=5.0 [95% CI, 2.1–11.9]), hypercholesterolemia (RR=7.6 [95% CI, 3.0–19.5]) and hypertension (RR=6.7 [95% CI, 2.9–16.0]).8
While risk factor reduction seems logical for all patients who have asymptomatic ischemia, actual evidence of benefit is limited. In the MRFIT study,9 high-risk men with asymptomatic ischemia were randomized to either usual care or a special intervention to reduce smoking, blood cholesterol, and diastolic blood pressure. The intervention group had lower cardiac mortality than men who received usual care (22 vs 53 per 1000, P<.002).9 As observed in 2 large prospective cohort studies, one of which documented abnormal EST in 17%, males who improved their fitness had 23% (95% CI, 4–42) and 44% (95% CI, 5–59) lower mortality over 18 years of mean follow-up, respectively.10,11 Smoking cessation is also important, associated with 41% lower mortality (95% CI, 20–57).11
Most of the evidence underlying the above recommendations derives from studies of men and hence may not apply directly to women. The American Heart Association’s guidelines12 for cardiovascular disease prevention in women do not consider EST results in risk assessment. They rely instead on the Framingham Risk Score to stratify women’s 10-year risk of coronary events as low (<10%), intermediate (10%–20%), and high (>20%), and prioritize recommendations for risk factor reduction according to these levels.12
TABLE
Duke Treadmill Scores: 5-year all-cause mortality
| ABNORMALITIES OBSERVED ON TREADMILL TESTING | |||||||
|---|---|---|---|---|---|---|---|
| NONE | DTS only | HRR only | CI only | HRR & CI | DTS & CI | HRR & DTS | CI, HRR, & DTS |
| 0.9 | 3.2 | 4.0 | 4.0 | 8.2 | 9.2 | 9.2 | 18.0 |
| Example: Patients having abnormal Duke Treadmill score and Chronotropic Index but normal Heart rate recovery sustained 5-year, all-cause mortality of 9.2%. Those with abnormal DTS and HRR but normal CI coincidentally had the same 9.2% mortality.6 | |||||||
| Duke Treadmill Test (DTS): Minutes in standard Bruce protocol –5 × (maximal ST deviation in mm) –4 × (0=no chest pain, 1=angina during EST, 2=EST stopped due to angina). | |||||||
| Heart Rate Recovery (HRR): abnormal if heart rate drops less than 12 bpm measured at least 2 minutes after stopping EST. | |||||||
| Chronotropic Index (CI): represents the ratio of heart rate reserve compared to metabolic reserve. | |||||||
| Normal is near 1. | |||||||
Recommendations from others
American College of Cardiology/American Heart Association (ACC/AHA) guidelines1 favor medical treatment for low-risk patients with asymptomatic ischemia (annual cardiac mortality ≤1%—ie, DTS ≥5, or normal HRR or normal CI). The ACC/AHA recommend perfusion imaging (or exercise echocardiography) for patients with asymptomatic ischemia who have intermediate or high-risk DTS.1 Such imaging can refine prognosis, guide therapy with aspirin, beta blockers, lipid-lowering agents, and angiotensin-converting enzyme inhibitors, and possibly identify patients who might benefit from coronary angiography and revascularization (AHA/ACC Recommendation Class IIa–IIb, Level of Evidence B–C).
1. Gibbons RJ, Balady GJ, Bricker JT, et al. AHA/ACC 2002 guideline update for exercise testing: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). 2002. American College of Cardiology Web site. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/dirindex.htm. Accessed on December 13, 2006.
2. Mark DB, Shaw L, Harrell FE, Jr, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med 1991;325:849-853.
3. Shaw LS, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying coronary artery disease subgroups. Circulation 1998;98:1622-1630.
4. Nishime EO, Cole CR, Blackstone EH, et al. Heart rate recovery and treadmill exercise score as predictors of mortality in patients referred for exercise ECG. JAMA 2000;284:1392-1398.
5. Gibbons RJ, Hodge DO, Berman DS, et al. Long-term outcome of patients with intermediate-risk exercise electrocardiograms who do not have myocardial perfusion defects on radionuclide imaging. Circulation 1999;100:2140-2145.
6. Lauer MS. Exercise electrocardiogram testing and prognosis. Novel markers and predictive instruments. Cardiol Clin 2001;19:401-414.
7. Gibbons LW, Mitchell TL, Wei M, et al. Maximal exercise testing as a predictor of risk for mortality from coronary heart disease in asymptomatic men. Am J Cardiol 2000;86:53-58.
8. Laukkanen JA, Kurl S, Lakka TA, et al. Exercise-induced silent myocardial ischemia can coronary morbidity and mortality in middle-aged men. J Am Coll Cardiol 2001;38:72-79.
9. Multiple Risk Factor Intervention Trial Research Group. Exercise electrocardiogram and coronary heart disease mortality in the Multiple Risk Factor Intervention Trial. Am J Cardiol 1985;55:16-24.
10. Paffenbarger RS, Hyde RT, Wing AL, et al. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med 1993;328:538-545.
11. Blair SN, Kohl HW, Barlow CE, et al. Changes in physical fitness and all-cause mortality: A prospective study of healthy and unhealthy men. JAMA 1995;272:1093-1098.
12. Mosca L, Appel LJ, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women. Circulation 2004;109:672-693.
Patients with intermediate- or high-risk Duke Treadmill score (DTS) on exercise stress testing (EST) should undergo myocardial perfusion imaging or exercise echocardiography, especially if they have abnormal values of Chronotropic Index or post-EST Heart Rate Recovery.
For patients who have a low-risk DTS, the 4-year mortality is less than 1% to 2%; therefore, risk-factor reduction without further investigation is appropriate (strength of recommendation: B, based on cohort studies and consensus guideline).
When a stress test is not normal, discuss with the patient and examine risk factors
Ronald L. Healy, MD
United Medical Center, Cheyenne, Wyoming
Exercise stress testing is performed to assess the risk of heart disease for asymptomatic patients. EST is relatively inexpensive, convenient, and, with the appropriate equipment, easily performed in a physician’s office. Although the test is limited in its predictive value, it can be reasonably sensitive when performed on the appropriate population groups.
When the EST result is normal, I review cardiovascular risk factors with the patient and use the opportunity to reinforce the importance of healthy lifestyle modifications. Difficulties arise, however, when an EST result is not normal. Since the patient is at increased risk of cardiovascular morbidity and mortality, I usually recommend further testing. Many options are available, including exercise stress echocardiography, thallium scan, and coronary catheterization. Newer technologies such as MRI and CT scan may be appropriate in some circumstances. I usually base my decision after discussion with the patient, examination of the patient’s risk factors, and the preferences and expertise of my local cardiology group.
Evidence summary
No randomized controlled trials have identified the optimal management of patients with asymptomatic ischemia on EST. EST is not generally recommended for asymptomatic persons because of its limited predictive value. EST may sometimes be useful for predicting mortality risk among patients who plan to begin exercise programs, or whose jobs affect public safety, or who have conditions such as diabetes or chronic renal insufficiency.1
For example, a prospective cohort study of 613 patients with suspected coronary artery disease investigated EST duration, presence of angina, and ST-segment depression as predictors of mortality.2 Patients with asymptomatic ischemia (2 mm of ischemic depression) whose EST lasted 15 minutes (DTS=+5, low risk) had a 5-year cardiac mortality of less than 1%, compared with 2% for those whose EST was tolerated for only 7 minutes (DTS=–3, intermediate risk).2 (See TABLE for DTS formula.)
Later prospective cohort studies3,4 confirmed that a low-risk DTS was associated with high 5-year survival—eg, 97% among 2758 patients (median age 49, 70% male, 30% prior myocardial infarction, 49% with angina).3 Those with an intermediate- or high-risk DTS had corresponding survival rates of 90% and 65%, respectively. The DTS was further analyzed in a 5-year follow-up of 9454 patients, 88% of whom were low-risk (75% undergoing screening EST).4 Most patients (1406 of 1477) with ST-segment depression ≥1 mm had asymptomatic ischemia, only 71 having EST-induced angina. A low-risk DTS was associated with 98% survival, compared with 92% for patients with an intermediate- or high-risk DTS.4
Patients with an intermediate-risk DTS, and normal or near-normal perfusion imaging without cardiomegaly, also comprised a low-risk group with 5-year cardiac survival of 99.5%.5 Post-EST heart rate recovery and the Chronotropic Index are enhancements to the DTS.6 Used singly or in combination, these tools provided more accurate estimates of 5-year all-cause mortality among 9454 patients referred for EST (TABLE).
Two other prospective cohort studies of middle-aged men with EST showing asymptomatic ischemia did not employ the above enhancements but reported major impact of cardiac risk factors on mortality. Among 25,927 healthy men followed for an average of 8.4 years, the age-adjusted risk of death from all causes of those with asymptomatic ischemia increased from 2-fold (95% confidence interval [CI], 1.1–3.8, P=.03) with no risk factors to 4 (95% CI, 2.7–5.4) with 1 risk factor, 5 (95% CI, 3.3–6.9) with 2 risk factors, and 8 (95% CI, 5.4–12.8) with 3 or more risk factors (P<.0001).7 Other investigators found increased mortality from coronary artery disease to be associated with smoking (relative risk [RR]=5.0 [95% CI, 2.1–11.9]), hypercholesterolemia (RR=7.6 [95% CI, 3.0–19.5]) and hypertension (RR=6.7 [95% CI, 2.9–16.0]).8
While risk factor reduction seems logical for all patients who have asymptomatic ischemia, actual evidence of benefit is limited. In the MRFIT study,9 high-risk men with asymptomatic ischemia were randomized to either usual care or a special intervention to reduce smoking, blood cholesterol, and diastolic blood pressure. The intervention group had lower cardiac mortality than men who received usual care (22 vs 53 per 1000, P<.002).9 As observed in 2 large prospective cohort studies, one of which documented abnormal EST in 17%, males who improved their fitness had 23% (95% CI, 4–42) and 44% (95% CI, 5–59) lower mortality over 18 years of mean follow-up, respectively.10,11 Smoking cessation is also important, associated with 41% lower mortality (95% CI, 20–57).11
Most of the evidence underlying the above recommendations derives from studies of men and hence may not apply directly to women. The American Heart Association’s guidelines12 for cardiovascular disease prevention in women do not consider EST results in risk assessment. They rely instead on the Framingham Risk Score to stratify women’s 10-year risk of coronary events as low (<10%), intermediate (10%–20%), and high (>20%), and prioritize recommendations for risk factor reduction according to these levels.12
TABLE
Duke Treadmill Scores: 5-year all-cause mortality
| ABNORMALITIES OBSERVED ON TREADMILL TESTING | |||||||
|---|---|---|---|---|---|---|---|
| NONE | DTS only | HRR only | CI only | HRR & CI | DTS & CI | HRR & DTS | CI, HRR, & DTS |
| 0.9 | 3.2 | 4.0 | 4.0 | 8.2 | 9.2 | 9.2 | 18.0 |
| Example: Patients having abnormal Duke Treadmill score and Chronotropic Index but normal Heart rate recovery sustained 5-year, all-cause mortality of 9.2%. Those with abnormal DTS and HRR but normal CI coincidentally had the same 9.2% mortality.6 | |||||||
| Duke Treadmill Test (DTS): Minutes in standard Bruce protocol –5 × (maximal ST deviation in mm) –4 × (0=no chest pain, 1=angina during EST, 2=EST stopped due to angina). | |||||||
| Heart Rate Recovery (HRR): abnormal if heart rate drops less than 12 bpm measured at least 2 minutes after stopping EST. | |||||||
| Chronotropic Index (CI): represents the ratio of heart rate reserve compared to metabolic reserve. | |||||||
| Normal is near 1. | |||||||
Recommendations from others
American College of Cardiology/American Heart Association (ACC/AHA) guidelines1 favor medical treatment for low-risk patients with asymptomatic ischemia (annual cardiac mortality ≤1%—ie, DTS ≥5, or normal HRR or normal CI). The ACC/AHA recommend perfusion imaging (or exercise echocardiography) for patients with asymptomatic ischemia who have intermediate or high-risk DTS.1 Such imaging can refine prognosis, guide therapy with aspirin, beta blockers, lipid-lowering agents, and angiotensin-converting enzyme inhibitors, and possibly identify patients who might benefit from coronary angiography and revascularization (AHA/ACC Recommendation Class IIa–IIb, Level of Evidence B–C).
Patients with intermediate- or high-risk Duke Treadmill score (DTS) on exercise stress testing (EST) should undergo myocardial perfusion imaging or exercise echocardiography, especially if they have abnormal values of Chronotropic Index or post-EST Heart Rate Recovery.
For patients who have a low-risk DTS, the 4-year mortality is less than 1% to 2%; therefore, risk-factor reduction without further investigation is appropriate (strength of recommendation: B, based on cohort studies and consensus guideline).
When a stress test is not normal, discuss with the patient and examine risk factors
Ronald L. Healy, MD
United Medical Center, Cheyenne, Wyoming
Exercise stress testing is performed to assess the risk of heart disease for asymptomatic patients. EST is relatively inexpensive, convenient, and, with the appropriate equipment, easily performed in a physician’s office. Although the test is limited in its predictive value, it can be reasonably sensitive when performed on the appropriate population groups.
When the EST result is normal, I review cardiovascular risk factors with the patient and use the opportunity to reinforce the importance of healthy lifestyle modifications. Difficulties arise, however, when an EST result is not normal. Since the patient is at increased risk of cardiovascular morbidity and mortality, I usually recommend further testing. Many options are available, including exercise stress echocardiography, thallium scan, and coronary catheterization. Newer technologies such as MRI and CT scan may be appropriate in some circumstances. I usually base my decision after discussion with the patient, examination of the patient’s risk factors, and the preferences and expertise of my local cardiology group.
Evidence summary
No randomized controlled trials have identified the optimal management of patients with asymptomatic ischemia on EST. EST is not generally recommended for asymptomatic persons because of its limited predictive value. EST may sometimes be useful for predicting mortality risk among patients who plan to begin exercise programs, or whose jobs affect public safety, or who have conditions such as diabetes or chronic renal insufficiency.1
For example, a prospective cohort study of 613 patients with suspected coronary artery disease investigated EST duration, presence of angina, and ST-segment depression as predictors of mortality.2 Patients with asymptomatic ischemia (2 mm of ischemic depression) whose EST lasted 15 minutes (DTS=+5, low risk) had a 5-year cardiac mortality of less than 1%, compared with 2% for those whose EST was tolerated for only 7 minutes (DTS=–3, intermediate risk).2 (See TABLE for DTS formula.)
Later prospective cohort studies3,4 confirmed that a low-risk DTS was associated with high 5-year survival—eg, 97% among 2758 patients (median age 49, 70% male, 30% prior myocardial infarction, 49% with angina).3 Those with an intermediate- or high-risk DTS had corresponding survival rates of 90% and 65%, respectively. The DTS was further analyzed in a 5-year follow-up of 9454 patients, 88% of whom were low-risk (75% undergoing screening EST).4 Most patients (1406 of 1477) with ST-segment depression ≥1 mm had asymptomatic ischemia, only 71 having EST-induced angina. A low-risk DTS was associated with 98% survival, compared with 92% for patients with an intermediate- or high-risk DTS.4
Patients with an intermediate-risk DTS, and normal or near-normal perfusion imaging without cardiomegaly, also comprised a low-risk group with 5-year cardiac survival of 99.5%.5 Post-EST heart rate recovery and the Chronotropic Index are enhancements to the DTS.6 Used singly or in combination, these tools provided more accurate estimates of 5-year all-cause mortality among 9454 patients referred for EST (TABLE).
Two other prospective cohort studies of middle-aged men with EST showing asymptomatic ischemia did not employ the above enhancements but reported major impact of cardiac risk factors on mortality. Among 25,927 healthy men followed for an average of 8.4 years, the age-adjusted risk of death from all causes of those with asymptomatic ischemia increased from 2-fold (95% confidence interval [CI], 1.1–3.8, P=.03) with no risk factors to 4 (95% CI, 2.7–5.4) with 1 risk factor, 5 (95% CI, 3.3–6.9) with 2 risk factors, and 8 (95% CI, 5.4–12.8) with 3 or more risk factors (P<.0001).7 Other investigators found increased mortality from coronary artery disease to be associated with smoking (relative risk [RR]=5.0 [95% CI, 2.1–11.9]), hypercholesterolemia (RR=7.6 [95% CI, 3.0–19.5]) and hypertension (RR=6.7 [95% CI, 2.9–16.0]).8
While risk factor reduction seems logical for all patients who have asymptomatic ischemia, actual evidence of benefit is limited. In the MRFIT study,9 high-risk men with asymptomatic ischemia were randomized to either usual care or a special intervention to reduce smoking, blood cholesterol, and diastolic blood pressure. The intervention group had lower cardiac mortality than men who received usual care (22 vs 53 per 1000, P<.002).9 As observed in 2 large prospective cohort studies, one of which documented abnormal EST in 17%, males who improved their fitness had 23% (95% CI, 4–42) and 44% (95% CI, 5–59) lower mortality over 18 years of mean follow-up, respectively.10,11 Smoking cessation is also important, associated with 41% lower mortality (95% CI, 20–57).11
Most of the evidence underlying the above recommendations derives from studies of men and hence may not apply directly to women. The American Heart Association’s guidelines12 for cardiovascular disease prevention in women do not consider EST results in risk assessment. They rely instead on the Framingham Risk Score to stratify women’s 10-year risk of coronary events as low (<10%), intermediate (10%–20%), and high (>20%), and prioritize recommendations for risk factor reduction according to these levels.12
TABLE
Duke Treadmill Scores: 5-year all-cause mortality
| ABNORMALITIES OBSERVED ON TREADMILL TESTING | |||||||
|---|---|---|---|---|---|---|---|
| NONE | DTS only | HRR only | CI only | HRR & CI | DTS & CI | HRR & DTS | CI, HRR, & DTS |
| 0.9 | 3.2 | 4.0 | 4.0 | 8.2 | 9.2 | 9.2 | 18.0 |
| Example: Patients having abnormal Duke Treadmill score and Chronotropic Index but normal Heart rate recovery sustained 5-year, all-cause mortality of 9.2%. Those with abnormal DTS and HRR but normal CI coincidentally had the same 9.2% mortality.6 | |||||||
| Duke Treadmill Test (DTS): Minutes in standard Bruce protocol –5 × (maximal ST deviation in mm) –4 × (0=no chest pain, 1=angina during EST, 2=EST stopped due to angina). | |||||||
| Heart Rate Recovery (HRR): abnormal if heart rate drops less than 12 bpm measured at least 2 minutes after stopping EST. | |||||||
| Chronotropic Index (CI): represents the ratio of heart rate reserve compared to metabolic reserve. | |||||||
| Normal is near 1. | |||||||
Recommendations from others
American College of Cardiology/American Heart Association (ACC/AHA) guidelines1 favor medical treatment for low-risk patients with asymptomatic ischemia (annual cardiac mortality ≤1%—ie, DTS ≥5, or normal HRR or normal CI). The ACC/AHA recommend perfusion imaging (or exercise echocardiography) for patients with asymptomatic ischemia who have intermediate or high-risk DTS.1 Such imaging can refine prognosis, guide therapy with aspirin, beta blockers, lipid-lowering agents, and angiotensin-converting enzyme inhibitors, and possibly identify patients who might benefit from coronary angiography and revascularization (AHA/ACC Recommendation Class IIa–IIb, Level of Evidence B–C).
1. Gibbons RJ, Balady GJ, Bricker JT, et al. AHA/ACC 2002 guideline update for exercise testing: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). 2002. American College of Cardiology Web site. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/dirindex.htm. Accessed on December 13, 2006.
2. Mark DB, Shaw L, Harrell FE, Jr, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med 1991;325:849-853.
3. Shaw LS, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying coronary artery disease subgroups. Circulation 1998;98:1622-1630.
4. Nishime EO, Cole CR, Blackstone EH, et al. Heart rate recovery and treadmill exercise score as predictors of mortality in patients referred for exercise ECG. JAMA 2000;284:1392-1398.
5. Gibbons RJ, Hodge DO, Berman DS, et al. Long-term outcome of patients with intermediate-risk exercise electrocardiograms who do not have myocardial perfusion defects on radionuclide imaging. Circulation 1999;100:2140-2145.
6. Lauer MS. Exercise electrocardiogram testing and prognosis. Novel markers and predictive instruments. Cardiol Clin 2001;19:401-414.
7. Gibbons LW, Mitchell TL, Wei M, et al. Maximal exercise testing as a predictor of risk for mortality from coronary heart disease in asymptomatic men. Am J Cardiol 2000;86:53-58.
8. Laukkanen JA, Kurl S, Lakka TA, et al. Exercise-induced silent myocardial ischemia can coronary morbidity and mortality in middle-aged men. J Am Coll Cardiol 2001;38:72-79.
9. Multiple Risk Factor Intervention Trial Research Group. Exercise electrocardiogram and coronary heart disease mortality in the Multiple Risk Factor Intervention Trial. Am J Cardiol 1985;55:16-24.
10. Paffenbarger RS, Hyde RT, Wing AL, et al. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med 1993;328:538-545.
11. Blair SN, Kohl HW, Barlow CE, et al. Changes in physical fitness and all-cause mortality: A prospective study of healthy and unhealthy men. JAMA 1995;272:1093-1098.
12. Mosca L, Appel LJ, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women. Circulation 2004;109:672-693.
1. Gibbons RJ, Balady GJ, Bricker JT, et al. AHA/ACC 2002 guideline update for exercise testing: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). 2002. American College of Cardiology Web site. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/dirindex.htm. Accessed on December 13, 2006.
2. Mark DB, Shaw L, Harrell FE, Jr, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med 1991;325:849-853.
3. Shaw LS, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying coronary artery disease subgroups. Circulation 1998;98:1622-1630.
4. Nishime EO, Cole CR, Blackstone EH, et al. Heart rate recovery and treadmill exercise score as predictors of mortality in patients referred for exercise ECG. JAMA 2000;284:1392-1398.
5. Gibbons RJ, Hodge DO, Berman DS, et al. Long-term outcome of patients with intermediate-risk exercise electrocardiograms who do not have myocardial perfusion defects on radionuclide imaging. Circulation 1999;100:2140-2145.
6. Lauer MS. Exercise electrocardiogram testing and prognosis. Novel markers and predictive instruments. Cardiol Clin 2001;19:401-414.
7. Gibbons LW, Mitchell TL, Wei M, et al. Maximal exercise testing as a predictor of risk for mortality from coronary heart disease in asymptomatic men. Am J Cardiol 2000;86:53-58.
8. Laukkanen JA, Kurl S, Lakka TA, et al. Exercise-induced silent myocardial ischemia can coronary morbidity and mortality in middle-aged men. J Am Coll Cardiol 2001;38:72-79.
9. Multiple Risk Factor Intervention Trial Research Group. Exercise electrocardiogram and coronary heart disease mortality in the Multiple Risk Factor Intervention Trial. Am J Cardiol 1985;55:16-24.
10. Paffenbarger RS, Hyde RT, Wing AL, et al. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med 1993;328:538-545.
11. Blair SN, Kohl HW, Barlow CE, et al. Changes in physical fitness and all-cause mortality: A prospective study of healthy and unhealthy men. JAMA 1995;272:1093-1098.
12. Mosca L, Appel LJ, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women. Circulation 2004;109:672-693.
Evidence-based answers from the Family Physicians Inquiries Network