User login
Stalked by a ‘patient’
CASE: Delusions and threats
For over 20 months, Ms. I, age 48, sends a psychiatric resident letters and postcards that total approximately 3,000 pages and come from dozens of return addresses. Ms. I expresses romantic feelings toward the resident and believes that he was her physician and prescribed medications, including “mood stabilizers.” The resident never treated Ms. I; to his knowledge, he has never interacted with her.
Ms. I describes the resident’s refusal to continue treating her as “abandonment” and states that she is contemplating self-harm because of this rejection. In her letters, Ms. I admits that she was a long-term patient in a state psychiatric hospital in her home state and suffers from persistent auditory hallucinations. She also wants a romantic relationship with the resident and repeatedly threatens the resident’s female acquaintances and former romantic partners whose relationships she had surmised from news articles available on the Internet. Ms. I also threatens to strangle the resident. The resident sends her multiple written requests that she cease contact, but they are not acknowledged.
The authors’ observations
Stalking—repeated, unwanted attention or communication that would cause a reasonable person fear—is a serious threat for many psychiatric clinicians.1 Prevalence rates among mental health care providers range from 3% to 21%.2,3 Most stalkers have engaged in previous stalking behavior.3
Being stalked is highly distressing,4 and mental health professionals often do not reveal such experiences to colleagues.5 Irrational feelings of guilt or embarrassment, such as being thought to have poorly managed interactions with the stalker, often motivate a self-imposed silence (Table 1).6 This isolation may foster anxiety, interfere with receiving problem-solving advice, and increase physical vulnerability. In the case involving Ms. I, the psychiatric resident’s primary responsibility is safeguarding his own physical and psychological welfare.
Clinicians who work in a hospital or other institutional setting who are being stalked should inform their supervisors and the facility’s security personnel. Security personnel may be able to gather data about the stalker, decrease the stalker’s ability to communicate with the victim, and reduce unwanted physical access to the victim by distributing a photo of the stalker or installing a camera or receptionist-controlled door lock in patient entryways. Security personnel also may collaborate with local law enforcement. Having a third party respond to a stalker’s aggressive behavior—rather than the victim responding directly—avoids rewarding the stalker, which may generate further unwanted contact.7 Any intervention by the victim may increase the risk of violence, creating an “intervention dilemma.” Resnick8 argues that before deciding how best to address the stalker’s behavior, a stalking victim must “first separate the risk of continued stalking from the risk that the stalker will commit a violent act.”
Mental health professionals in private practice who are being stalked should consider retaining an attorney. An attorney often can maintain privacy of communications regarding the stalker via the attorney-client and attorney-work product privileges, which may help during legal proceedings.
Table 1
Factors that can impede psychiatrists from reporting stalking
| Fear of being perceived as a failure |
| Embarrassment |
| High professional tolerance for antisocial and threatening behavior |
| Misplaced sense of duty |
| Source: Reference 6 |
RESPONSE: Involving police
Over 2 months, Ms. I phones the resident’s home 105 times (the resident screens the calls). During 1 call, she states that she is hidden in a closet in her home and will hurt herself unless the resident “resumes” her psychiatric care. The resident contacts police in his city and Ms. I’s community, but authorities are reluctant to act when he acknowledges that he is not Ms. I’s psychiatrist and does not know her. Police officers in Ms. I’s hometown tell the resident no one answered the door when they visited her home. They state that they would enter the residence forcibly only if Ms. I’s physician or a family member asked them to do so, and because the resident admits that he is not her psychiatrist, they cannot take further action. Ms. I leaves the resident a phone message several hours later to inform him she is safe.
The authors’ observations
Stalking-induced countertransference responses may lead a psychiatrist to unwittingly place himself in harm’s way. For example, intense rage at a stalker’s request for treatment may generate guilt that motivates the psychiatrist to agree to treat the stalker. Feelings of helplessness may produce a frantic desire to do something even when such activity is ill-advised. Psychiatrists may develop a tolerance for antisocial or threatening behavior—which is common in mental health settings—and could accept unnecessary risks.
A psychiatrist who is being stalked may be able to assist a mentally ill stalker in a way that does not create a duty to treat and does not expose the psychiatrist to harm, such as contacting a mobile crisis intervention team, a mental health professional who recently treated the stalker, a family member of the stalker, or law enforcement personnel. A psychiatrist who is thrust from the role of helper to victim and must protect his or her own well-being instead of attending to a patient’s welfare is prone to suffer substantial countertransference distress.
The situation with Ms. I was particularly challenging because the resident did not know her complete history and therefore had little information to gauge how likely she was to act on her aggressive threats. Factors that predict future violence include:
- a history of violence
- significant prior criminality
- young age at first arrest
- concomitant substance abuse
- male sex.9
Unfortunately, other than sex, this data regarding Ms. I could not be readily obtained.
A psychiatrist’s duty
Although sympathetic to his stalker’s distress, the resident did not want to treat this woman, nor was he ethically or legally obligated to do so. An individual’s wish to be treated by a particular psychiatrist does not create a duty for the psychiatrist to satisfy this wish.10 State-based “Good Samaritan” laws encourage physicians to assist those in acute need by shielding them from liability, as long as they reasonably act within the scope of their expertise.11 However, they do not require a physician to care for an individual in acute need. A delusional wish for treatment or a false belief of already being in treatment does not create a duty to care for a person.
OUTCOME: Seeking help
Ms. I’s phone calls and letters continue. The resident discusses the situation with his associate residency director, who refers him to the hospital’s legal and investigative staffs. Based on advice from the hospital’s private investigator, the resident sends Ms. I a formal “cease and desist” letter that threatens her with legal action and possible jail time. The staff at the front desk of the clinic where the resident works and the hospital’s security department are instructed to watch for a visitor with Ms. I’s name and description, although the hospital’s investigator is unable to obtain a photograph of her. Shortly after the resident sends the letter, Ms. I ceases communication.
The authors’ observations
This case is unusual because most stalking victims know their stalkers. Identifying a stalker’s motivation can be helpful in formulating a risk assessment. One classification system recognizes 5 categories of stalkers: rejected, intimacy seeking, incompetent, resentful, and predatory (Table 2).1 Rejected stalkers appear to pose the greatest risk of violence and homicide.8 However, all stalkers may pose a risk of violence and therefore all stalking behavior should be treated seriously.
Table 2
Classification of stalkers
| Category | Common features |
|---|---|
| Rejected | Most have a personality disorder; often seeking reconciliation and revenge; most frequent victims are ex-romantic partners, but also target estranged relatives, former friends |
| Intimacy seeking | Erotomania; “morbid infatuation” |
| Incompetent | Lacking social skills; often have stalked others |
| Resentful | Pursuing a vendetta; generally feeling aggrieved |
| Predatory | Often comorbid with paraphilias; may have past convictions for sex offenses |
| Source: Adapted from reference 1 | |
Responding to a stalker
The approach should be tailored to the stalker’s characteristics.12 Silence—ie, lack of acknowledgement of a stalker’s intrusions—is one tactic.13 Consistent and persistent lack of engagement may bore the stalker, but also may provoke frustration or narcissistic or paranoia-fueled rage, and increased efforts to interact with the mental health professional. Other responses include:
- obtaining a protection or restraining order
- promoting the stalker’s participation in adversarial civil litigation, such as a lawsuit
- issuing verbal counterthreats.
Restraining orders are controversial and assessments of their effectiveness vary.14 How well a restraining order works may depend on the stalker’s:
- ability to appreciate reality, and how likely he or she is to experience anxiety when confronted with adverse consequences of his or her actions
- how consistently, rapidly, and harshly the criminal justice system responds to violations of restraining orders.
Restraining orders also may provide the victim a false sense of security.15 One of her letters revealed that Ms. I violated a criminal plea arrangement years earlier, which suggests she was capable of violating a restraining order.
Litigation. A stalker may initiate civil litigation against the victim to feel that he or she has an impact on the victim, which may reduce the stalker’s risk of violence if he or she is emotionally engaged in the litigation. Based on the authors’ experience, as long as the stalker is talking, he or she generally is less likely to act out violently and terminate a satisfying process. Adversarial civil litigation could give a stalker the opportunity to be “close” to the victim and a means of expressing aggressive wishes. The benefit of litigation lasts only as long as the case persists and the stalker believes he or she may prevail. In one of her letters, Ms. I bragged that she had represented herself as a pro se litigant in a complex civil matter, suggesting that she might be constructively channeled into litigation.
Promoting litigation carries significant risk.16 Being a defendant in pro se litigation may be emotionally and financially stressful. This approach may be desirable if the psychiatrist’s institution is willing to offer substantial support. For example, an institution may provide legal assistance—including helping to defray the cost of litigation—and litigation-related scheduling flexibility. An attorney may serve as a boundary between the victim and the pro se litigant’s sometimes ceaseless, time-devouring, anxiety-inducing legal maneuvers.
Counterthreats. Warning a stalker that he or she will face severe civil and criminal consequences if his or her behavior continues can make clear that his or her conduct is unacceptable.17 Such warnings may be delivered verbally or in writing by a legal representative, law enforcement personnel, a private security agent, or the victim.
Issuing a counterthreat can be risky. Stalkers with antisocial or narcissistic personality features may perceive a counterthreat as narcissistically diminishing, and to save face will escalate their stalking in retaliation. Avoid counterthreats if you believe the stalker might be psychotic because destabilizing such an individual—such as by precipitating a short psychotic episode—may increase unpredictability and diminish their responsive to interventions.
Ms. I’s contact with the resident lasted approximately 20 months, slightly less than the average 26 months reported in a survey of mental health professionals.3 Because stalkers are unpredictable, the psychiatric resident remains cautious.
Related Resources
- National Center for Victims of Crime. Stalking resource center. www.victimsofcrime.org/our-programs/stalking-resource-center.
- Mullen PE, Pathé M, Purcell R. Stalkers and their victims. New York, NY: Cambridge University Press; 2009.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mullen PE, Pathé M, Purcell R, et al. Study of stalkers. Am J Psychiatry. 1999;156(8):1244-1249.
2. Sandberg DA, McNiel DE, Binder RL. Stalking threatening, and harassing behavior by psychiatric patients toward clinicians. J Am Acad Psychiatry Law. 2002;30(2):221-229.
3. McIvor R, Potter L, Davies L. Stalking behavior by patients towards psychiatrists in a large mental health organization. Int J Soc Psychiatry. 2008;54(4):350-357.
4. Mullen PE, Pathé M. Stalking. Crime and Justice. 2002;29:273-318.
5. Bird S. Strategies for managing and minimizing the impact of harassment and stalking by patients. ANZ J Surg. 2009;79(7-8):537-538.
6. Sinwelski SA, Vinton L. Stalking: the constant threat of violence. Affilia. 2001;16(1):46-65.
7. Meloy JR. Commentary: stalking threatening, and harassing behavior by patients—the risk-management response. J Am Acad Psychiatry Law. 2002;30(2):230-231.
8. Resnick PJ. Stalking risk assessment. In: Pinals DA, ed. Stalking: psychiatric perspectives and practical approaches. New York, NY: Oxford University Press; 2007:61–84.
9. Dietz PE. Defenses against dangerous people when arrest and commitment fail. In: Simon RI, ed. American Psychiatric Press review of clinical psychiatry and the law. 1st ed. Washington, DC: American Psychiatric Press; 1989:205–219.
10. Hilliard J. Termination of treatment with troublesome patients. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law: a comprehensive handbook. Cambridge, MA: Harvard University Press; 1998:216–224.
11. Paterick TJ, Paterick BB, Paterick TE. Implications of Good Samaritan laws for physicians. J Med Pract Manage. 2008;23(6):372-375.
12. MacKenzie RD, James DV. Management and treatment of stalkers: problems options, and solutions. Behav Sci Law. 2011;29(2):220-239.
13. Fremouw WJ, Westrup D, Pennypacker J. Stalking on campus: the prevalence and strategies for coping with stalking. J Forensic Sci. 1997;42(4):666-669.
14. Nicastro AM, Cousins AV, Spitzberg BH. The tactical face of stalking. Journal of Criminal Justice. 2000;28(1):69-82.
15. Spitzberg BH. The tactical topography of stalking victimization and management. Trauma Violence Abuse. 2002;3(4):261-288.
16. Pathé M, MacKenzie R, Mullen PE. Stalking by law: damaging victims and rewarding offenders. J Law Med. 2004;12(1):103-111.
17. Lion JR, Herschler JA. The stalking of physicians by their patients. In: Meloy JR. The psychology of stalking: clinical and forensic perspectives. San Diego, CA: Academic Press; 1998:163–173.
CASE: Delusions and threats
For over 20 months, Ms. I, age 48, sends a psychiatric resident letters and postcards that total approximately 3,000 pages and come from dozens of return addresses. Ms. I expresses romantic feelings toward the resident and believes that he was her physician and prescribed medications, including “mood stabilizers.” The resident never treated Ms. I; to his knowledge, he has never interacted with her.
Ms. I describes the resident’s refusal to continue treating her as “abandonment” and states that she is contemplating self-harm because of this rejection. In her letters, Ms. I admits that she was a long-term patient in a state psychiatric hospital in her home state and suffers from persistent auditory hallucinations. She also wants a romantic relationship with the resident and repeatedly threatens the resident’s female acquaintances and former romantic partners whose relationships she had surmised from news articles available on the Internet. Ms. I also threatens to strangle the resident. The resident sends her multiple written requests that she cease contact, but they are not acknowledged.
The authors’ observations
Stalking—repeated, unwanted attention or communication that would cause a reasonable person fear—is a serious threat for many psychiatric clinicians.1 Prevalence rates among mental health care providers range from 3% to 21%.2,3 Most stalkers have engaged in previous stalking behavior.3
Being stalked is highly distressing,4 and mental health professionals often do not reveal such experiences to colleagues.5 Irrational feelings of guilt or embarrassment, such as being thought to have poorly managed interactions with the stalker, often motivate a self-imposed silence (Table 1).6 This isolation may foster anxiety, interfere with receiving problem-solving advice, and increase physical vulnerability. In the case involving Ms. I, the psychiatric resident’s primary responsibility is safeguarding his own physical and psychological welfare.
Clinicians who work in a hospital or other institutional setting who are being stalked should inform their supervisors and the facility’s security personnel. Security personnel may be able to gather data about the stalker, decrease the stalker’s ability to communicate with the victim, and reduce unwanted physical access to the victim by distributing a photo of the stalker or installing a camera or receptionist-controlled door lock in patient entryways. Security personnel also may collaborate with local law enforcement. Having a third party respond to a stalker’s aggressive behavior—rather than the victim responding directly—avoids rewarding the stalker, which may generate further unwanted contact.7 Any intervention by the victim may increase the risk of violence, creating an “intervention dilemma.” Resnick8 argues that before deciding how best to address the stalker’s behavior, a stalking victim must “first separate the risk of continued stalking from the risk that the stalker will commit a violent act.”
Mental health professionals in private practice who are being stalked should consider retaining an attorney. An attorney often can maintain privacy of communications regarding the stalker via the attorney-client and attorney-work product privileges, which may help during legal proceedings.
Table 1
Factors that can impede psychiatrists from reporting stalking
| Fear of being perceived as a failure |
| Embarrassment |
| High professional tolerance for antisocial and threatening behavior |
| Misplaced sense of duty |
| Source: Reference 6 |
RESPONSE: Involving police
Over 2 months, Ms. I phones the resident’s home 105 times (the resident screens the calls). During 1 call, she states that she is hidden in a closet in her home and will hurt herself unless the resident “resumes” her psychiatric care. The resident contacts police in his city and Ms. I’s community, but authorities are reluctant to act when he acknowledges that he is not Ms. I’s psychiatrist and does not know her. Police officers in Ms. I’s hometown tell the resident no one answered the door when they visited her home. They state that they would enter the residence forcibly only if Ms. I’s physician or a family member asked them to do so, and because the resident admits that he is not her psychiatrist, they cannot take further action. Ms. I leaves the resident a phone message several hours later to inform him she is safe.
The authors’ observations
Stalking-induced countertransference responses may lead a psychiatrist to unwittingly place himself in harm’s way. For example, intense rage at a stalker’s request for treatment may generate guilt that motivates the psychiatrist to agree to treat the stalker. Feelings of helplessness may produce a frantic desire to do something even when such activity is ill-advised. Psychiatrists may develop a tolerance for antisocial or threatening behavior—which is common in mental health settings—and could accept unnecessary risks.
A psychiatrist who is being stalked may be able to assist a mentally ill stalker in a way that does not create a duty to treat and does not expose the psychiatrist to harm, such as contacting a mobile crisis intervention team, a mental health professional who recently treated the stalker, a family member of the stalker, or law enforcement personnel. A psychiatrist who is thrust from the role of helper to victim and must protect his or her own well-being instead of attending to a patient’s welfare is prone to suffer substantial countertransference distress.
The situation with Ms. I was particularly challenging because the resident did not know her complete history and therefore had little information to gauge how likely she was to act on her aggressive threats. Factors that predict future violence include:
- a history of violence
- significant prior criminality
- young age at first arrest
- concomitant substance abuse
- male sex.9
Unfortunately, other than sex, this data regarding Ms. I could not be readily obtained.
A psychiatrist’s duty
Although sympathetic to his stalker’s distress, the resident did not want to treat this woman, nor was he ethically or legally obligated to do so. An individual’s wish to be treated by a particular psychiatrist does not create a duty for the psychiatrist to satisfy this wish.10 State-based “Good Samaritan” laws encourage physicians to assist those in acute need by shielding them from liability, as long as they reasonably act within the scope of their expertise.11 However, they do not require a physician to care for an individual in acute need. A delusional wish for treatment or a false belief of already being in treatment does not create a duty to care for a person.
OUTCOME: Seeking help
Ms. I’s phone calls and letters continue. The resident discusses the situation with his associate residency director, who refers him to the hospital’s legal and investigative staffs. Based on advice from the hospital’s private investigator, the resident sends Ms. I a formal “cease and desist” letter that threatens her with legal action and possible jail time. The staff at the front desk of the clinic where the resident works and the hospital’s security department are instructed to watch for a visitor with Ms. I’s name and description, although the hospital’s investigator is unable to obtain a photograph of her. Shortly after the resident sends the letter, Ms. I ceases communication.
The authors’ observations
This case is unusual because most stalking victims know their stalkers. Identifying a stalker’s motivation can be helpful in formulating a risk assessment. One classification system recognizes 5 categories of stalkers: rejected, intimacy seeking, incompetent, resentful, and predatory (Table 2).1 Rejected stalkers appear to pose the greatest risk of violence and homicide.8 However, all stalkers may pose a risk of violence and therefore all stalking behavior should be treated seriously.
Table 2
Classification of stalkers
| Category | Common features |
|---|---|
| Rejected | Most have a personality disorder; often seeking reconciliation and revenge; most frequent victims are ex-romantic partners, but also target estranged relatives, former friends |
| Intimacy seeking | Erotomania; “morbid infatuation” |
| Incompetent | Lacking social skills; often have stalked others |
| Resentful | Pursuing a vendetta; generally feeling aggrieved |
| Predatory | Often comorbid with paraphilias; may have past convictions for sex offenses |
| Source: Adapted from reference 1 | |
Responding to a stalker
The approach should be tailored to the stalker’s characteristics.12 Silence—ie, lack of acknowledgement of a stalker’s intrusions—is one tactic.13 Consistent and persistent lack of engagement may bore the stalker, but also may provoke frustration or narcissistic or paranoia-fueled rage, and increased efforts to interact with the mental health professional. Other responses include:
- obtaining a protection or restraining order
- promoting the stalker’s participation in adversarial civil litigation, such as a lawsuit
- issuing verbal counterthreats.
Restraining orders are controversial and assessments of their effectiveness vary.14 How well a restraining order works may depend on the stalker’s:
- ability to appreciate reality, and how likely he or she is to experience anxiety when confronted with adverse consequences of his or her actions
- how consistently, rapidly, and harshly the criminal justice system responds to violations of restraining orders.
Restraining orders also may provide the victim a false sense of security.15 One of her letters revealed that Ms. I violated a criminal plea arrangement years earlier, which suggests she was capable of violating a restraining order.
Litigation. A stalker may initiate civil litigation against the victim to feel that he or she has an impact on the victim, which may reduce the stalker’s risk of violence if he or she is emotionally engaged in the litigation. Based on the authors’ experience, as long as the stalker is talking, he or she generally is less likely to act out violently and terminate a satisfying process. Adversarial civil litigation could give a stalker the opportunity to be “close” to the victim and a means of expressing aggressive wishes. The benefit of litigation lasts only as long as the case persists and the stalker believes he or she may prevail. In one of her letters, Ms. I bragged that she had represented herself as a pro se litigant in a complex civil matter, suggesting that she might be constructively channeled into litigation.
Promoting litigation carries significant risk.16 Being a defendant in pro se litigation may be emotionally and financially stressful. This approach may be desirable if the psychiatrist’s institution is willing to offer substantial support. For example, an institution may provide legal assistance—including helping to defray the cost of litigation—and litigation-related scheduling flexibility. An attorney may serve as a boundary between the victim and the pro se litigant’s sometimes ceaseless, time-devouring, anxiety-inducing legal maneuvers.
Counterthreats. Warning a stalker that he or she will face severe civil and criminal consequences if his or her behavior continues can make clear that his or her conduct is unacceptable.17 Such warnings may be delivered verbally or in writing by a legal representative, law enforcement personnel, a private security agent, or the victim.
Issuing a counterthreat can be risky. Stalkers with antisocial or narcissistic personality features may perceive a counterthreat as narcissistically diminishing, and to save face will escalate their stalking in retaliation. Avoid counterthreats if you believe the stalker might be psychotic because destabilizing such an individual—such as by precipitating a short psychotic episode—may increase unpredictability and diminish their responsive to interventions.
Ms. I’s contact with the resident lasted approximately 20 months, slightly less than the average 26 months reported in a survey of mental health professionals.3 Because stalkers are unpredictable, the psychiatric resident remains cautious.
Related Resources
- National Center for Victims of Crime. Stalking resource center. www.victimsofcrime.org/our-programs/stalking-resource-center.
- Mullen PE, Pathé M, Purcell R. Stalkers and their victims. New York, NY: Cambridge University Press; 2009.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Delusions and threats
For over 20 months, Ms. I, age 48, sends a psychiatric resident letters and postcards that total approximately 3,000 pages and come from dozens of return addresses. Ms. I expresses romantic feelings toward the resident and believes that he was her physician and prescribed medications, including “mood stabilizers.” The resident never treated Ms. I; to his knowledge, he has never interacted with her.
Ms. I describes the resident’s refusal to continue treating her as “abandonment” and states that she is contemplating self-harm because of this rejection. In her letters, Ms. I admits that she was a long-term patient in a state psychiatric hospital in her home state and suffers from persistent auditory hallucinations. She also wants a romantic relationship with the resident and repeatedly threatens the resident’s female acquaintances and former romantic partners whose relationships she had surmised from news articles available on the Internet. Ms. I also threatens to strangle the resident. The resident sends her multiple written requests that she cease contact, but they are not acknowledged.
The authors’ observations
Stalking—repeated, unwanted attention or communication that would cause a reasonable person fear—is a serious threat for many psychiatric clinicians.1 Prevalence rates among mental health care providers range from 3% to 21%.2,3 Most stalkers have engaged in previous stalking behavior.3
Being stalked is highly distressing,4 and mental health professionals often do not reveal such experiences to colleagues.5 Irrational feelings of guilt or embarrassment, such as being thought to have poorly managed interactions with the stalker, often motivate a self-imposed silence (Table 1).6 This isolation may foster anxiety, interfere with receiving problem-solving advice, and increase physical vulnerability. In the case involving Ms. I, the psychiatric resident’s primary responsibility is safeguarding his own physical and psychological welfare.
Clinicians who work in a hospital or other institutional setting who are being stalked should inform their supervisors and the facility’s security personnel. Security personnel may be able to gather data about the stalker, decrease the stalker’s ability to communicate with the victim, and reduce unwanted physical access to the victim by distributing a photo of the stalker or installing a camera or receptionist-controlled door lock in patient entryways. Security personnel also may collaborate with local law enforcement. Having a third party respond to a stalker’s aggressive behavior—rather than the victim responding directly—avoids rewarding the stalker, which may generate further unwanted contact.7 Any intervention by the victim may increase the risk of violence, creating an “intervention dilemma.” Resnick8 argues that before deciding how best to address the stalker’s behavior, a stalking victim must “first separate the risk of continued stalking from the risk that the stalker will commit a violent act.”
Mental health professionals in private practice who are being stalked should consider retaining an attorney. An attorney often can maintain privacy of communications regarding the stalker via the attorney-client and attorney-work product privileges, which may help during legal proceedings.
Table 1
Factors that can impede psychiatrists from reporting stalking
| Fear of being perceived as a failure |
| Embarrassment |
| High professional tolerance for antisocial and threatening behavior |
| Misplaced sense of duty |
| Source: Reference 6 |
RESPONSE: Involving police
Over 2 months, Ms. I phones the resident’s home 105 times (the resident screens the calls). During 1 call, she states that she is hidden in a closet in her home and will hurt herself unless the resident “resumes” her psychiatric care. The resident contacts police in his city and Ms. I’s community, but authorities are reluctant to act when he acknowledges that he is not Ms. I’s psychiatrist and does not know her. Police officers in Ms. I’s hometown tell the resident no one answered the door when they visited her home. They state that they would enter the residence forcibly only if Ms. I’s physician or a family member asked them to do so, and because the resident admits that he is not her psychiatrist, they cannot take further action. Ms. I leaves the resident a phone message several hours later to inform him she is safe.
The authors’ observations
Stalking-induced countertransference responses may lead a psychiatrist to unwittingly place himself in harm’s way. For example, intense rage at a stalker’s request for treatment may generate guilt that motivates the psychiatrist to agree to treat the stalker. Feelings of helplessness may produce a frantic desire to do something even when such activity is ill-advised. Psychiatrists may develop a tolerance for antisocial or threatening behavior—which is common in mental health settings—and could accept unnecessary risks.
A psychiatrist who is being stalked may be able to assist a mentally ill stalker in a way that does not create a duty to treat and does not expose the psychiatrist to harm, such as contacting a mobile crisis intervention team, a mental health professional who recently treated the stalker, a family member of the stalker, or law enforcement personnel. A psychiatrist who is thrust from the role of helper to victim and must protect his or her own well-being instead of attending to a patient’s welfare is prone to suffer substantial countertransference distress.
The situation with Ms. I was particularly challenging because the resident did not know her complete history and therefore had little information to gauge how likely she was to act on her aggressive threats. Factors that predict future violence include:
- a history of violence
- significant prior criminality
- young age at first arrest
- concomitant substance abuse
- male sex.9
Unfortunately, other than sex, this data regarding Ms. I could not be readily obtained.
A psychiatrist’s duty
Although sympathetic to his stalker’s distress, the resident did not want to treat this woman, nor was he ethically or legally obligated to do so. An individual’s wish to be treated by a particular psychiatrist does not create a duty for the psychiatrist to satisfy this wish.10 State-based “Good Samaritan” laws encourage physicians to assist those in acute need by shielding them from liability, as long as they reasonably act within the scope of their expertise.11 However, they do not require a physician to care for an individual in acute need. A delusional wish for treatment or a false belief of already being in treatment does not create a duty to care for a person.
OUTCOME: Seeking help
Ms. I’s phone calls and letters continue. The resident discusses the situation with his associate residency director, who refers him to the hospital’s legal and investigative staffs. Based on advice from the hospital’s private investigator, the resident sends Ms. I a formal “cease and desist” letter that threatens her with legal action and possible jail time. The staff at the front desk of the clinic where the resident works and the hospital’s security department are instructed to watch for a visitor with Ms. I’s name and description, although the hospital’s investigator is unable to obtain a photograph of her. Shortly after the resident sends the letter, Ms. I ceases communication.
The authors’ observations
This case is unusual because most stalking victims know their stalkers. Identifying a stalker’s motivation can be helpful in formulating a risk assessment. One classification system recognizes 5 categories of stalkers: rejected, intimacy seeking, incompetent, resentful, and predatory (Table 2).1 Rejected stalkers appear to pose the greatest risk of violence and homicide.8 However, all stalkers may pose a risk of violence and therefore all stalking behavior should be treated seriously.
Table 2
Classification of stalkers
| Category | Common features |
|---|---|
| Rejected | Most have a personality disorder; often seeking reconciliation and revenge; most frequent victims are ex-romantic partners, but also target estranged relatives, former friends |
| Intimacy seeking | Erotomania; “morbid infatuation” |
| Incompetent | Lacking social skills; often have stalked others |
| Resentful | Pursuing a vendetta; generally feeling aggrieved |
| Predatory | Often comorbid with paraphilias; may have past convictions for sex offenses |
| Source: Adapted from reference 1 | |
Responding to a stalker
The approach should be tailored to the stalker’s characteristics.12 Silence—ie, lack of acknowledgement of a stalker’s intrusions—is one tactic.13 Consistent and persistent lack of engagement may bore the stalker, but also may provoke frustration or narcissistic or paranoia-fueled rage, and increased efforts to interact with the mental health professional. Other responses include:
- obtaining a protection or restraining order
- promoting the stalker’s participation in adversarial civil litigation, such as a lawsuit
- issuing verbal counterthreats.
Restraining orders are controversial and assessments of their effectiveness vary.14 How well a restraining order works may depend on the stalker’s:
- ability to appreciate reality, and how likely he or she is to experience anxiety when confronted with adverse consequences of his or her actions
- how consistently, rapidly, and harshly the criminal justice system responds to violations of restraining orders.
Restraining orders also may provide the victim a false sense of security.15 One of her letters revealed that Ms. I violated a criminal plea arrangement years earlier, which suggests she was capable of violating a restraining order.
Litigation. A stalker may initiate civil litigation against the victim to feel that he or she has an impact on the victim, which may reduce the stalker’s risk of violence if he or she is emotionally engaged in the litigation. Based on the authors’ experience, as long as the stalker is talking, he or she generally is less likely to act out violently and terminate a satisfying process. Adversarial civil litigation could give a stalker the opportunity to be “close” to the victim and a means of expressing aggressive wishes. The benefit of litigation lasts only as long as the case persists and the stalker believes he or she may prevail. In one of her letters, Ms. I bragged that she had represented herself as a pro se litigant in a complex civil matter, suggesting that she might be constructively channeled into litigation.
Promoting litigation carries significant risk.16 Being a defendant in pro se litigation may be emotionally and financially stressful. This approach may be desirable if the psychiatrist’s institution is willing to offer substantial support. For example, an institution may provide legal assistance—including helping to defray the cost of litigation—and litigation-related scheduling flexibility. An attorney may serve as a boundary between the victim and the pro se litigant’s sometimes ceaseless, time-devouring, anxiety-inducing legal maneuvers.
Counterthreats. Warning a stalker that he or she will face severe civil and criminal consequences if his or her behavior continues can make clear that his or her conduct is unacceptable.17 Such warnings may be delivered verbally or in writing by a legal representative, law enforcement personnel, a private security agent, or the victim.
Issuing a counterthreat can be risky. Stalkers with antisocial or narcissistic personality features may perceive a counterthreat as narcissistically diminishing, and to save face will escalate their stalking in retaliation. Avoid counterthreats if you believe the stalker might be psychotic because destabilizing such an individual—such as by precipitating a short psychotic episode—may increase unpredictability and diminish their responsive to interventions.
Ms. I’s contact with the resident lasted approximately 20 months, slightly less than the average 26 months reported in a survey of mental health professionals.3 Because stalkers are unpredictable, the psychiatric resident remains cautious.
Related Resources
- National Center for Victims of Crime. Stalking resource center. www.victimsofcrime.org/our-programs/stalking-resource-center.
- Mullen PE, Pathé M, Purcell R. Stalkers and their victims. New York, NY: Cambridge University Press; 2009.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mullen PE, Pathé M, Purcell R, et al. Study of stalkers. Am J Psychiatry. 1999;156(8):1244-1249.
2. Sandberg DA, McNiel DE, Binder RL. Stalking threatening, and harassing behavior by psychiatric patients toward clinicians. J Am Acad Psychiatry Law. 2002;30(2):221-229.
3. McIvor R, Potter L, Davies L. Stalking behavior by patients towards psychiatrists in a large mental health organization. Int J Soc Psychiatry. 2008;54(4):350-357.
4. Mullen PE, Pathé M. Stalking. Crime and Justice. 2002;29:273-318.
5. Bird S. Strategies for managing and minimizing the impact of harassment and stalking by patients. ANZ J Surg. 2009;79(7-8):537-538.
6. Sinwelski SA, Vinton L. Stalking: the constant threat of violence. Affilia. 2001;16(1):46-65.
7. Meloy JR. Commentary: stalking threatening, and harassing behavior by patients—the risk-management response. J Am Acad Psychiatry Law. 2002;30(2):230-231.
8. Resnick PJ. Stalking risk assessment. In: Pinals DA, ed. Stalking: psychiatric perspectives and practical approaches. New York, NY: Oxford University Press; 2007:61–84.
9. Dietz PE. Defenses against dangerous people when arrest and commitment fail. In: Simon RI, ed. American Psychiatric Press review of clinical psychiatry and the law. 1st ed. Washington, DC: American Psychiatric Press; 1989:205–219.
10. Hilliard J. Termination of treatment with troublesome patients. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law: a comprehensive handbook. Cambridge, MA: Harvard University Press; 1998:216–224.
11. Paterick TJ, Paterick BB, Paterick TE. Implications of Good Samaritan laws for physicians. J Med Pract Manage. 2008;23(6):372-375.
12. MacKenzie RD, James DV. Management and treatment of stalkers: problems options, and solutions. Behav Sci Law. 2011;29(2):220-239.
13. Fremouw WJ, Westrup D, Pennypacker J. Stalking on campus: the prevalence and strategies for coping with stalking. J Forensic Sci. 1997;42(4):666-669.
14. Nicastro AM, Cousins AV, Spitzberg BH. The tactical face of stalking. Journal of Criminal Justice. 2000;28(1):69-82.
15. Spitzberg BH. The tactical topography of stalking victimization and management. Trauma Violence Abuse. 2002;3(4):261-288.
16. Pathé M, MacKenzie R, Mullen PE. Stalking by law: damaging victims and rewarding offenders. J Law Med. 2004;12(1):103-111.
17. Lion JR, Herschler JA. The stalking of physicians by their patients. In: Meloy JR. The psychology of stalking: clinical and forensic perspectives. San Diego, CA: Academic Press; 1998:163–173.
1. Mullen PE, Pathé M, Purcell R, et al. Study of stalkers. Am J Psychiatry. 1999;156(8):1244-1249.
2. Sandberg DA, McNiel DE, Binder RL. Stalking threatening, and harassing behavior by psychiatric patients toward clinicians. J Am Acad Psychiatry Law. 2002;30(2):221-229.
3. McIvor R, Potter L, Davies L. Stalking behavior by patients towards psychiatrists in a large mental health organization. Int J Soc Psychiatry. 2008;54(4):350-357.
4. Mullen PE, Pathé M. Stalking. Crime and Justice. 2002;29:273-318.
5. Bird S. Strategies for managing and minimizing the impact of harassment and stalking by patients. ANZ J Surg. 2009;79(7-8):537-538.
6. Sinwelski SA, Vinton L. Stalking: the constant threat of violence. Affilia. 2001;16(1):46-65.
7. Meloy JR. Commentary: stalking threatening, and harassing behavior by patients—the risk-management response. J Am Acad Psychiatry Law. 2002;30(2):230-231.
8. Resnick PJ. Stalking risk assessment. In: Pinals DA, ed. Stalking: psychiatric perspectives and practical approaches. New York, NY: Oxford University Press; 2007:61–84.
9. Dietz PE. Defenses against dangerous people when arrest and commitment fail. In: Simon RI, ed. American Psychiatric Press review of clinical psychiatry and the law. 1st ed. Washington, DC: American Psychiatric Press; 1989:205–219.
10. Hilliard J. Termination of treatment with troublesome patients. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law: a comprehensive handbook. Cambridge, MA: Harvard University Press; 1998:216–224.
11. Paterick TJ, Paterick BB, Paterick TE. Implications of Good Samaritan laws for physicians. J Med Pract Manage. 2008;23(6):372-375.
12. MacKenzie RD, James DV. Management and treatment of stalkers: problems options, and solutions. Behav Sci Law. 2011;29(2):220-239.
13. Fremouw WJ, Westrup D, Pennypacker J. Stalking on campus: the prevalence and strategies for coping with stalking. J Forensic Sci. 1997;42(4):666-669.
14. Nicastro AM, Cousins AV, Spitzberg BH. The tactical face of stalking. Journal of Criminal Justice. 2000;28(1):69-82.
15. Spitzberg BH. The tactical topography of stalking victimization and management. Trauma Violence Abuse. 2002;3(4):261-288.
16. Pathé M, MacKenzie R, Mullen PE. Stalking by law: damaging victims and rewarding offenders. J Law Med. 2004;12(1):103-111.
17. Lion JR, Herschler JA. The stalking of physicians by their patients. In: Meloy JR. The psychology of stalking: clinical and forensic perspectives. San Diego, CA: Academic Press; 1998:163–173.
Which psychotropics carry the greatest risk of QTc prolongation?
- Screen patients for risk factors for prolonged QTc interval, such as congenital long QT syndrome, family history of cardiac conduction abnormalities, and previous occurrences of medication-mediated QTc prolongation.
- Obtain baseline and steady state ECG when initiating high-risk agents, particularly when administering combination therapy.
- Use the lowest effective dose of antidepressants and antipsychotics and monitor symptoms closely.
Mrs. A, age 68, has a 40-year history of schizoaffective disorder with comorbid anxiety disorder not otherwise specified, type 2 diabetes mellitus, and hypertension. She takes furosemide, 40 mg/d, lisinopril, 20 mg/d, and metformin, 2,000 mg/d, for hypertension and diabetes; lorazepam, 1.5 mg/d, and paroxetine, 40 mg/d, for anxiety; and quetiapine extended release, 800 mg/d, for psychotic features and mood dysregulation with schizoaffective disorder. Mrs. A’s husband died 5 years ago and she lives alone in a senior care facility. Mrs. A uses a weekly pill reminder box because her residential facility does not monitor medication adherence. She sees her psychiatrist once a month and her primary care provider every 3 months. She has no history of illicit drug, alcohol, or tobacco use.
Two weeks ago, Mrs. A was found leaning against the wall in a hallway, complaining of dizziness and disorientation, and unable to find her way back to her apartment. In the emergency department, her serum potassium is low (3.0 mEq/L; normal range: 3.5 to 5.0), fasting glucose is elevated (110 mg/dL; range: 65 to 99), and ECG reveals a prolonged QTc interval of 530 milliseconds. Before this episode, Mrs. A had been medically stable without mood or psychotic symptoms, although her daughter reported medication self-administration was becoming difficult.
Exposure to psychotropics carries a risk of QTc prolongation. The QT interval is an ECG measure of ventricular depolarization and repolarization. The QTc designation indicates a correction for heart rate with increasing heart rate correlating with a shorter QT interval. Readings of 440 milliseconds are considered normal.1 QTc prolongation is defined as >450 milliseconds for men and >470 milliseconds for women.2 An increase in the QT interval is a predictor of serious cardiac events.3
Antidepressants and antipsychotics have been associated with QTc prolongation. When identifying agents that could disrupt cardiac conduction, clinicians need to consider whether the drug’s molecular structure, receptor affinity, or pharmacologic effects are most critical.2 Although these may be important, patient-specific variables that increase the risk of QTc prolongation may have greater impact. These include:
- age >65
- female sex
- electrolyte imbalances (specifically low serum potassium and magnesium levels)
- high or toxic serum levels of the suspected drug
- preexisting cardiovascular impairment, such as bradycardia.4,5
Other risk factors include concurrent use of an agent with similar cardiovascular effects or one that competes for metabolism (either enzymatic or at the binding site), physiologic limitations such as renal insufficiency, and medication changes that may increase or decrease psychotropic clearance.4,6 Geriatric patients with dementia have an increased risk for cardiovascular-related death.7,8
Antidepressants
Among tricyclic antidepressants, most reports of QTc prolongation involve amitriptyline and maprotiline.9 Risk factors include demographics (eg, female sex, age), personal or family history (congenital long QT syndrome, cardiovascular disease), and concurrent conditions or drug use, particularly those associated with QTc prolongation.3 Desipramine and nortriptyline also have been identified as high-risk agents.10
QTc prolongation has been reported with all selective serotonin reuptake inhibitors at plasma concentrations above the therapeutic level.11 Fluoxetine-associated QTc prolongation was limited to cases of overdose or when additional risk factors were reported.4 QTc prolongation from psychotropics could increase the risk of torsades de pointes, according to an analysis of the FDA Adverse Event Reporting System.12 In 2011, the FDA reported an increased risk of abnormal heart rhythms—including QTc prolongation—with citalopram doses >40 mg/d.13 Although cases of QTc prolongation with paroxetine have not been reported,11 the Arizona Center for Education and Research on Therapeutics lists paroxetine with other agents that may increase the risk for QTc prolongation with concurrent use of medications that may prolong QTc interval.14 Venlafaxine doses >300 mg/d may require additional cardiac monitoring.5,12 Data from venlafaxine poisoning case reports found a positive correlation between dose and QTc prolongation.15 In a review of toxicology database information, Wenzel-Seifert et al4 found extended QT interval with citalopram, fluoxetine, and venlafaxine at toxic doses or in the presence of additional risk factors such as sex, older age, or personal or family history of congenital long QT syndrome or cardiovascular disease.
Antipsychotics
Case reports, case series, and research trials have evaluated the risk of QTc prolongation with antipsychotics (Table).1,2,4,16,17 The first-generation antipsychotics thioridazine,4,16,18 mesoridazine,16,18 chlorpromazine,19 and haloperidol3 warrant cardiac monitoring. The QTc prolongation effects of thioridazine and its active metabolite mesoridazine are well-documented and thioridazine-mediated QTc prolongation increases are dose-dependent.4,18 ECG monitoring is recommended with IV haloperidol, which is used for delirium in adults.20 QTc prolongation has been associated with long-term ziprasidone use more often than with risperidone, olanzapine, or quetiapine.19 Ziprasidone prolongs the QTc interval an average of 20 milliseconds,21 which could represent a clinically significant change. QTc prolongation for iloperidone is comparable to ziprasidone and haloperidol.22 There is some evidence that aripiprazole may shorten, rather than prolong, the QTc interval.4,17
Cardiovascular adverse effects associated with clozapine—including QTc prolongation—are dose-dependent.3 Olanzapine prolongs QTc interval, although the mean change is less than with other agents unless other variables were present, such as:
- concomitant use of medications that may prolong QTc interval (ie, amantadine, hydroxyzine, or tamoxifen2)
- preexisting cardiovascular conduction disorders
- higher doses (>40 mg/d).3,23
In 17 case reports of cardiac changes associated with quetiapine use, doses ranged from 100 mg/d24 to an overdose of 36 g/d.25 Only 1 patient death was reported secondary to overdose and preexisting dysrhythmia and hypertension.26 QTc prolongation associated with risperidone was minor1 based on oral doses in the normal therapeutic range and incidences of overdose.10 Paliperidone27 and lurasidone28 are associated with clinically insignificant QTc prolongation. Changes in QTc interval were positively correlated with asenapine dose, although at the highest dose of 40 mg/d, the increase was <5 milliseconds.29
Mrs. A presents with a number of risk factors for QTc prolongation, including older age, female sex, and psychiatric and medical comorbidities that require medication. A pill count revealed that she was taking more than the prescribed daily doses of her medications. During the interview, Mrs. A said that if she missed her medication time, she would take them when she remembered. If she could not remember if she took her pills, she would take them again. Her physicians will explore strategies to increase medication adherence.
Table
Examples of QTc prolongation associated with select antipsychoticsa
| Antipsychotic | Approximate QTc interval prolongation in millisecondsb |
|---|---|
| Aripiprazole4,17 | -1 to -4 |
| Clozapine4 | 10 |
| Haloperidol1,2 | 7 to 15 |
| Mesoridazine16 | 39 to 53 |
| Olanzapine1 | 2 to 6.5 |
| Paliperidone4 | 2 to 4 |
| Pimozide2 | 19 |
| Quetiapine1,2 | 6 to 15 |
| Risperidone1,2 | 3.5 to 10 |
| Sertindole1 | 30 |
| Thioridazine2,16 | 33 to 41 |
| Ziprasidone1,2 | 16 to 21 |
| aList is not comprehensive. Other antipsychotics may be associated with QTc prolongation bQTc prolongation interval may depend on the route of administration | |
Related Resources
- De Hert M, Detraux J, van Winkel R, et al. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol. 2011;8(2):114-126.
- Vieweg WV, Wood MA, Fernandez A, et al. Proarrhythmic risk with antipsychotic and antidepressant drugs: implications in the elderly. Drugs Aging. 2009;26(12):997-1012.
- Sandson NB, Armstrong SC, Cozza KL. An overview of psychotropic drug-drug interactions. Psychosomatics. 2005;46(5):464-494.
Drug Brand Names
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Asenapine • Saphris
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clozapine • Clozaril
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Furosemide • Lasix
- Haloperidol • Haldol
- Hydroxyzine • Atarax, Vistaril
- Iloperidone • Fanapt
- Lisinopril • Prinivil, Zestril
- Lorazepam • Ativan
- Lurasidone • Latuda
- Maprotiline • Ludiomil
- Mesoridazine • Serentil
- Metformin • Glucophage
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paliperidone • Invega
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Tamoxifen • Nolvadex, Soltamox
- Thioridazine • Mellaril
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. No similar work by the authors is under review or in press. No funding was requested or received in conjunction with this manuscript.
1. Muscatello MR, Bruno A, Pandolfo G, et al. Emerging treatments in the management of schizophrenia - focus on sertindole. Drug Des Devel Ther. 2010;4:187-201.
2. Taylor DM. Antipsychotics and QT prolongation. Acta Psychiatr Scand. 2003;107(2):85-95.
3. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
4. Wenzel-Seifert K, Wittmann M, Haen E. QTc prolongation by psychotropic drugs and the risk of torsade de pointes. Dtsch Arztebl Int. 2011;108(41):687-693.
5. Vieweg WV. New generation antipsychotic drugs and QTc interval prolongation. Prim Care Companion J Clin Psychiatry. 2003;5(5):205-215.
6. Nielsen J, Graff C, Kanters JK, et al. Assessing QT interval prolongation and its associated risks with antipsychotics. CNS Drugs. 2011;25(6):473-490.
7. Gill SS, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007;146(11):775-786.
8. Schneeweiss S, Setoguchi S, Brookhart A, et al. Risk of death associated with the use of conventional versus atypical antipsychotic drugs among elderly patients. CMAJ. 2007;176(5):627-632.
9. Vieweg WV, Wood MA. Tricyclic antidepressants QT interval prolongation, and torsade de pointes. Psychosomatics. 2004;45(5):371-377.
10. Jeon SH, Jaekal J, Lee SH, et al. Effects of nortriptyline on QT prolongation: a safety pharmacology study. Hum Exp Toxicol. 2011;30(10):1649-1656.
11. Wenzel-Seifert K, Wittmann M, Haen E. Torsade de pointes episodes under treatment with selective serotonin reuptake inhibitors. Pharmacopsychiatry. 2010;43(7):279-281.
12. Poluzzi E, Raschi E, Moretti U, et al. Drug-induced torsades de pointes: data mining of the public version of the FDA Adverse Event Reporting System (AERS). Pharmacoepidemiol Drug Saf. 2009;18(6):512-518.
13. U.S. Food and Drug Administration. FDA drug safety communication: revised recommendations for Celexa (citalopram hydrobromide) related to a potential risk of abnormal heart rhythms with high doses. http://www.fda.gov/Drugs/DrugSafety/ucm297391.htm. Published March 28, 2012. Accessed June 26, 2012.
14. Arizona CERT-QT Center for Education and Research on Therapeutics. QT drug lists by risk groups. http://www.azcert.org/medical-pros/drug-lists/drug-lists.cfm. Accessed June 26 2012.
15. Howell C, Wilson AD, Waring WS. Cardiovascular toxicity due to venlafaxine poisoning in adults: a review of 235 consecutive cases. Br J Clin Pharmacol. 2007;64(2):192-197.
16. Salih IS, Thanacoody RH, McKay GA, et al. Comparison of the effects of thioridazine and mesoridazine on the QT interval in healthy adults after single oral doses. Clin Pharmacol Ther. 2007;82(5):548-554.
17. Goodnick PJ, Jerry J, Parra F. Psychotropic drugs and the ECG: focus on the QTc interval. Expert Opin Pharmacother. 2002;3(5):479-498.
18. Dallaire S. Thioridazine (Mellaril) and mesoridazine (Serentil): prolongation of the QTc interval. CMAJ. 2001;164(1):91,95.-
19. Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation torsade de pointes and sudden death. Drugs. 2002;62(11):1649-1671.
20. Shapiro BA, Warren J, Egol AB, et al. Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: an executive summary. Crit Care Med. 1995;23(9):1596-1600.
21. Vieweg WV, Hasnain M. Question regarding ziprasidone and QTc interval prolongation in the ZODIAC Study. Am J Psychiatry. 2011;168(6):650-651.
22. Caccia S, Pasina L, Nobili A. New atypical antipsychotics for schizophrenia: iloperidone. Drug Des Devel Ther. 2010;4:33-48.
23. Dineen S, Withrow K, Voronovitch L, et al. QTc prolongation and high-dose olanzapine. Psychosomatics. 2003;44(2):174-175.
24. Vieweg WV, Schneider RK, Wood MA. Torsade de pointes in a patient with complex medical and psychiatric conditions receiving low-dose quetiapine. Acta Psychiatr Scand. 2005;112(4):318-322.
25. Capuano A, Ruggiero S, Vestini F, et al. Survival from coma induced by an intentional 36-g overdose of extended-release quetiapine. Drug Chem Toxicol. 2011;34(4):475-477.
26. Fernandes PP, Marcil WA. Death associated with quetiapine overdose. Am J Psychiatry. 2002;159(12):2114.-
27. Sedky K, Nazir R, Lindenmayer JP, et al. Paliperidone palmitate: once-monthly treatment option for schizophrenia. Current Psychiatry. 2010;9(3):48-50.
28. Citrome L. Lurasidone for schizophrenia: a review of the efficacy and safety profile for this newly approved second-generation antipsychotic. Int J Clin Pract. 2011;65(2):189-210.
29. Chapel S, Hutmacher MM, Haig G, et al. Exposure-response analysis in patients with schizophrenia to assess the effect of asenapine on QTc prolongation. J Clin Pharmacol. 2009;49(11):1297-1308.
Nicole B. Washington, DO
Dr. Washington is Assistant Professor, Department of Psychiatry, School of Community Medicine, University of Oklahoma, Tulsa, OK
Nancy C. Brahm, PharmD, MS, BCPP, CGP
Dr. Brahm is Clinical Professor, College of Pharmacy, University of Oklahoma, Tulsa, OK
Julie Kissack, PharmD, BCPP
Dr. Kissack is Professor and Chair, Department of Pharmacy Practice, Harding University College of Pharmacy, Searcy, AR
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Nicole B. Washington, DO
Dr. Washington is Assistant Professor, Department of Psychiatry, School of Community Medicine, University of Oklahoma, Tulsa, OK
Nancy C. Brahm, PharmD, MS, BCPP, CGP
Dr. Brahm is Clinical Professor, College of Pharmacy, University of Oklahoma, Tulsa, OK
Julie Kissack, PharmD, BCPP
Dr. Kissack is Professor and Chair, Department of Pharmacy Practice, Harding University College of Pharmacy, Searcy, AR
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Nicole B. Washington, DO
Dr. Washington is Assistant Professor, Department of Psychiatry, School of Community Medicine, University of Oklahoma, Tulsa, OK
Nancy C. Brahm, PharmD, MS, BCPP, CGP
Dr. Brahm is Clinical Professor, College of Pharmacy, University of Oklahoma, Tulsa, OK
Julie Kissack, PharmD, BCPP
Dr. Kissack is Professor and Chair, Department of Pharmacy Practice, Harding University College of Pharmacy, Searcy, AR
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
- Screen patients for risk factors for prolonged QTc interval, such as congenital long QT syndrome, family history of cardiac conduction abnormalities, and previous occurrences of medication-mediated QTc prolongation.
- Obtain baseline and steady state ECG when initiating high-risk agents, particularly when administering combination therapy.
- Use the lowest effective dose of antidepressants and antipsychotics and monitor symptoms closely.
Mrs. A, age 68, has a 40-year history of schizoaffective disorder with comorbid anxiety disorder not otherwise specified, type 2 diabetes mellitus, and hypertension. She takes furosemide, 40 mg/d, lisinopril, 20 mg/d, and metformin, 2,000 mg/d, for hypertension and diabetes; lorazepam, 1.5 mg/d, and paroxetine, 40 mg/d, for anxiety; and quetiapine extended release, 800 mg/d, for psychotic features and mood dysregulation with schizoaffective disorder. Mrs. A’s husband died 5 years ago and she lives alone in a senior care facility. Mrs. A uses a weekly pill reminder box because her residential facility does not monitor medication adherence. She sees her psychiatrist once a month and her primary care provider every 3 months. She has no history of illicit drug, alcohol, or tobacco use.
Two weeks ago, Mrs. A was found leaning against the wall in a hallway, complaining of dizziness and disorientation, and unable to find her way back to her apartment. In the emergency department, her serum potassium is low (3.0 mEq/L; normal range: 3.5 to 5.0), fasting glucose is elevated (110 mg/dL; range: 65 to 99), and ECG reveals a prolonged QTc interval of 530 milliseconds. Before this episode, Mrs. A had been medically stable without mood or psychotic symptoms, although her daughter reported medication self-administration was becoming difficult.
Exposure to psychotropics carries a risk of QTc prolongation. The QT interval is an ECG measure of ventricular depolarization and repolarization. The QTc designation indicates a correction for heart rate with increasing heart rate correlating with a shorter QT interval. Readings of 440 milliseconds are considered normal.1 QTc prolongation is defined as >450 milliseconds for men and >470 milliseconds for women.2 An increase in the QT interval is a predictor of serious cardiac events.3
Antidepressants and antipsychotics have been associated with QTc prolongation. When identifying agents that could disrupt cardiac conduction, clinicians need to consider whether the drug’s molecular structure, receptor affinity, or pharmacologic effects are most critical.2 Although these may be important, patient-specific variables that increase the risk of QTc prolongation may have greater impact. These include:
- age >65
- female sex
- electrolyte imbalances (specifically low serum potassium and magnesium levels)
- high or toxic serum levels of the suspected drug
- preexisting cardiovascular impairment, such as bradycardia.4,5
Other risk factors include concurrent use of an agent with similar cardiovascular effects or one that competes for metabolism (either enzymatic or at the binding site), physiologic limitations such as renal insufficiency, and medication changes that may increase or decrease psychotropic clearance.4,6 Geriatric patients with dementia have an increased risk for cardiovascular-related death.7,8
Antidepressants
Among tricyclic antidepressants, most reports of QTc prolongation involve amitriptyline and maprotiline.9 Risk factors include demographics (eg, female sex, age), personal or family history (congenital long QT syndrome, cardiovascular disease), and concurrent conditions or drug use, particularly those associated with QTc prolongation.3 Desipramine and nortriptyline also have been identified as high-risk agents.10
QTc prolongation has been reported with all selective serotonin reuptake inhibitors at plasma concentrations above the therapeutic level.11 Fluoxetine-associated QTc prolongation was limited to cases of overdose or when additional risk factors were reported.4 QTc prolongation from psychotropics could increase the risk of torsades de pointes, according to an analysis of the FDA Adverse Event Reporting System.12 In 2011, the FDA reported an increased risk of abnormal heart rhythms—including QTc prolongation—with citalopram doses >40 mg/d.13 Although cases of QTc prolongation with paroxetine have not been reported,11 the Arizona Center for Education and Research on Therapeutics lists paroxetine with other agents that may increase the risk for QTc prolongation with concurrent use of medications that may prolong QTc interval.14 Venlafaxine doses >300 mg/d may require additional cardiac monitoring.5,12 Data from venlafaxine poisoning case reports found a positive correlation between dose and QTc prolongation.15 In a review of toxicology database information, Wenzel-Seifert et al4 found extended QT interval with citalopram, fluoxetine, and venlafaxine at toxic doses or in the presence of additional risk factors such as sex, older age, or personal or family history of congenital long QT syndrome or cardiovascular disease.
Antipsychotics
Case reports, case series, and research trials have evaluated the risk of QTc prolongation with antipsychotics (Table).1,2,4,16,17 The first-generation antipsychotics thioridazine,4,16,18 mesoridazine,16,18 chlorpromazine,19 and haloperidol3 warrant cardiac monitoring. The QTc prolongation effects of thioridazine and its active metabolite mesoridazine are well-documented and thioridazine-mediated QTc prolongation increases are dose-dependent.4,18 ECG monitoring is recommended with IV haloperidol, which is used for delirium in adults.20 QTc prolongation has been associated with long-term ziprasidone use more often than with risperidone, olanzapine, or quetiapine.19 Ziprasidone prolongs the QTc interval an average of 20 milliseconds,21 which could represent a clinically significant change. QTc prolongation for iloperidone is comparable to ziprasidone and haloperidol.22 There is some evidence that aripiprazole may shorten, rather than prolong, the QTc interval.4,17
Cardiovascular adverse effects associated with clozapine—including QTc prolongation—are dose-dependent.3 Olanzapine prolongs QTc interval, although the mean change is less than with other agents unless other variables were present, such as:
- concomitant use of medications that may prolong QTc interval (ie, amantadine, hydroxyzine, or tamoxifen2)
- preexisting cardiovascular conduction disorders
- higher doses (>40 mg/d).3,23
In 17 case reports of cardiac changes associated with quetiapine use, doses ranged from 100 mg/d24 to an overdose of 36 g/d.25 Only 1 patient death was reported secondary to overdose and preexisting dysrhythmia and hypertension.26 QTc prolongation associated with risperidone was minor1 based on oral doses in the normal therapeutic range and incidences of overdose.10 Paliperidone27 and lurasidone28 are associated with clinically insignificant QTc prolongation. Changes in QTc interval were positively correlated with asenapine dose, although at the highest dose of 40 mg/d, the increase was <5 milliseconds.29
Mrs. A presents with a number of risk factors for QTc prolongation, including older age, female sex, and psychiatric and medical comorbidities that require medication. A pill count revealed that she was taking more than the prescribed daily doses of her medications. During the interview, Mrs. A said that if she missed her medication time, she would take them when she remembered. If she could not remember if she took her pills, she would take them again. Her physicians will explore strategies to increase medication adherence.
Table
Examples of QTc prolongation associated with select antipsychoticsa
| Antipsychotic | Approximate QTc interval prolongation in millisecondsb |
|---|---|
| Aripiprazole4,17 | -1 to -4 |
| Clozapine4 | 10 |
| Haloperidol1,2 | 7 to 15 |
| Mesoridazine16 | 39 to 53 |
| Olanzapine1 | 2 to 6.5 |
| Paliperidone4 | 2 to 4 |
| Pimozide2 | 19 |
| Quetiapine1,2 | 6 to 15 |
| Risperidone1,2 | 3.5 to 10 |
| Sertindole1 | 30 |
| Thioridazine2,16 | 33 to 41 |
| Ziprasidone1,2 | 16 to 21 |
| aList is not comprehensive. Other antipsychotics may be associated with QTc prolongation bQTc prolongation interval may depend on the route of administration | |
Related Resources
- De Hert M, Detraux J, van Winkel R, et al. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol. 2011;8(2):114-126.
- Vieweg WV, Wood MA, Fernandez A, et al. Proarrhythmic risk with antipsychotic and antidepressant drugs: implications in the elderly. Drugs Aging. 2009;26(12):997-1012.
- Sandson NB, Armstrong SC, Cozza KL. An overview of psychotropic drug-drug interactions. Psychosomatics. 2005;46(5):464-494.
Drug Brand Names
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Asenapine • Saphris
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clozapine • Clozaril
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Furosemide • Lasix
- Haloperidol • Haldol
- Hydroxyzine • Atarax, Vistaril
- Iloperidone • Fanapt
- Lisinopril • Prinivil, Zestril
- Lorazepam • Ativan
- Lurasidone • Latuda
- Maprotiline • Ludiomil
- Mesoridazine • Serentil
- Metformin • Glucophage
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paliperidone • Invega
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Tamoxifen • Nolvadex, Soltamox
- Thioridazine • Mellaril
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. No similar work by the authors is under review or in press. No funding was requested or received in conjunction with this manuscript.
- Screen patients for risk factors for prolonged QTc interval, such as congenital long QT syndrome, family history of cardiac conduction abnormalities, and previous occurrences of medication-mediated QTc prolongation.
- Obtain baseline and steady state ECG when initiating high-risk agents, particularly when administering combination therapy.
- Use the lowest effective dose of antidepressants and antipsychotics and monitor symptoms closely.
Mrs. A, age 68, has a 40-year history of schizoaffective disorder with comorbid anxiety disorder not otherwise specified, type 2 diabetes mellitus, and hypertension. She takes furosemide, 40 mg/d, lisinopril, 20 mg/d, and metformin, 2,000 mg/d, for hypertension and diabetes; lorazepam, 1.5 mg/d, and paroxetine, 40 mg/d, for anxiety; and quetiapine extended release, 800 mg/d, for psychotic features and mood dysregulation with schizoaffective disorder. Mrs. A’s husband died 5 years ago and she lives alone in a senior care facility. Mrs. A uses a weekly pill reminder box because her residential facility does not monitor medication adherence. She sees her psychiatrist once a month and her primary care provider every 3 months. She has no history of illicit drug, alcohol, or tobacco use.
Two weeks ago, Mrs. A was found leaning against the wall in a hallway, complaining of dizziness and disorientation, and unable to find her way back to her apartment. In the emergency department, her serum potassium is low (3.0 mEq/L; normal range: 3.5 to 5.0), fasting glucose is elevated (110 mg/dL; range: 65 to 99), and ECG reveals a prolonged QTc interval of 530 milliseconds. Before this episode, Mrs. A had been medically stable without mood or psychotic symptoms, although her daughter reported medication self-administration was becoming difficult.
Exposure to psychotropics carries a risk of QTc prolongation. The QT interval is an ECG measure of ventricular depolarization and repolarization. The QTc designation indicates a correction for heart rate with increasing heart rate correlating with a shorter QT interval. Readings of 440 milliseconds are considered normal.1 QTc prolongation is defined as >450 milliseconds for men and >470 milliseconds for women.2 An increase in the QT interval is a predictor of serious cardiac events.3
Antidepressants and antipsychotics have been associated with QTc prolongation. When identifying agents that could disrupt cardiac conduction, clinicians need to consider whether the drug’s molecular structure, receptor affinity, or pharmacologic effects are most critical.2 Although these may be important, patient-specific variables that increase the risk of QTc prolongation may have greater impact. These include:
- age >65
- female sex
- electrolyte imbalances (specifically low serum potassium and magnesium levels)
- high or toxic serum levels of the suspected drug
- preexisting cardiovascular impairment, such as bradycardia.4,5
Other risk factors include concurrent use of an agent with similar cardiovascular effects or one that competes for metabolism (either enzymatic or at the binding site), physiologic limitations such as renal insufficiency, and medication changes that may increase or decrease psychotropic clearance.4,6 Geriatric patients with dementia have an increased risk for cardiovascular-related death.7,8
Antidepressants
Among tricyclic antidepressants, most reports of QTc prolongation involve amitriptyline and maprotiline.9 Risk factors include demographics (eg, female sex, age), personal or family history (congenital long QT syndrome, cardiovascular disease), and concurrent conditions or drug use, particularly those associated with QTc prolongation.3 Desipramine and nortriptyline also have been identified as high-risk agents.10
QTc prolongation has been reported with all selective serotonin reuptake inhibitors at plasma concentrations above the therapeutic level.11 Fluoxetine-associated QTc prolongation was limited to cases of overdose or when additional risk factors were reported.4 QTc prolongation from psychotropics could increase the risk of torsades de pointes, according to an analysis of the FDA Adverse Event Reporting System.12 In 2011, the FDA reported an increased risk of abnormal heart rhythms—including QTc prolongation—with citalopram doses >40 mg/d.13 Although cases of QTc prolongation with paroxetine have not been reported,11 the Arizona Center for Education and Research on Therapeutics lists paroxetine with other agents that may increase the risk for QTc prolongation with concurrent use of medications that may prolong QTc interval.14 Venlafaxine doses >300 mg/d may require additional cardiac monitoring.5,12 Data from venlafaxine poisoning case reports found a positive correlation between dose and QTc prolongation.15 In a review of toxicology database information, Wenzel-Seifert et al4 found extended QT interval with citalopram, fluoxetine, and venlafaxine at toxic doses or in the presence of additional risk factors such as sex, older age, or personal or family history of congenital long QT syndrome or cardiovascular disease.
Antipsychotics
Case reports, case series, and research trials have evaluated the risk of QTc prolongation with antipsychotics (Table).1,2,4,16,17 The first-generation antipsychotics thioridazine,4,16,18 mesoridazine,16,18 chlorpromazine,19 and haloperidol3 warrant cardiac monitoring. The QTc prolongation effects of thioridazine and its active metabolite mesoridazine are well-documented and thioridazine-mediated QTc prolongation increases are dose-dependent.4,18 ECG monitoring is recommended with IV haloperidol, which is used for delirium in adults.20 QTc prolongation has been associated with long-term ziprasidone use more often than with risperidone, olanzapine, or quetiapine.19 Ziprasidone prolongs the QTc interval an average of 20 milliseconds,21 which could represent a clinically significant change. QTc prolongation for iloperidone is comparable to ziprasidone and haloperidol.22 There is some evidence that aripiprazole may shorten, rather than prolong, the QTc interval.4,17
Cardiovascular adverse effects associated with clozapine—including QTc prolongation—are dose-dependent.3 Olanzapine prolongs QTc interval, although the mean change is less than with other agents unless other variables were present, such as:
- concomitant use of medications that may prolong QTc interval (ie, amantadine, hydroxyzine, or tamoxifen2)
- preexisting cardiovascular conduction disorders
- higher doses (>40 mg/d).3,23
In 17 case reports of cardiac changes associated with quetiapine use, doses ranged from 100 mg/d24 to an overdose of 36 g/d.25 Only 1 patient death was reported secondary to overdose and preexisting dysrhythmia and hypertension.26 QTc prolongation associated with risperidone was minor1 based on oral doses in the normal therapeutic range and incidences of overdose.10 Paliperidone27 and lurasidone28 are associated with clinically insignificant QTc prolongation. Changes in QTc interval were positively correlated with asenapine dose, although at the highest dose of 40 mg/d, the increase was <5 milliseconds.29
Mrs. A presents with a number of risk factors for QTc prolongation, including older age, female sex, and psychiatric and medical comorbidities that require medication. A pill count revealed that she was taking more than the prescribed daily doses of her medications. During the interview, Mrs. A said that if she missed her medication time, she would take them when she remembered. If she could not remember if she took her pills, she would take them again. Her physicians will explore strategies to increase medication adherence.
Table
Examples of QTc prolongation associated with select antipsychoticsa
| Antipsychotic | Approximate QTc interval prolongation in millisecondsb |
|---|---|
| Aripiprazole4,17 | -1 to -4 |
| Clozapine4 | 10 |
| Haloperidol1,2 | 7 to 15 |
| Mesoridazine16 | 39 to 53 |
| Olanzapine1 | 2 to 6.5 |
| Paliperidone4 | 2 to 4 |
| Pimozide2 | 19 |
| Quetiapine1,2 | 6 to 15 |
| Risperidone1,2 | 3.5 to 10 |
| Sertindole1 | 30 |
| Thioridazine2,16 | 33 to 41 |
| Ziprasidone1,2 | 16 to 21 |
| aList is not comprehensive. Other antipsychotics may be associated with QTc prolongation bQTc prolongation interval may depend on the route of administration | |
Related Resources
- De Hert M, Detraux J, van Winkel R, et al. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol. 2011;8(2):114-126.
- Vieweg WV, Wood MA, Fernandez A, et al. Proarrhythmic risk with antipsychotic and antidepressant drugs: implications in the elderly. Drugs Aging. 2009;26(12):997-1012.
- Sandson NB, Armstrong SC, Cozza KL. An overview of psychotropic drug-drug interactions. Psychosomatics. 2005;46(5):464-494.
Drug Brand Names
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Asenapine • Saphris
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clozapine • Clozaril
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Furosemide • Lasix
- Haloperidol • Haldol
- Hydroxyzine • Atarax, Vistaril
- Iloperidone • Fanapt
- Lisinopril • Prinivil, Zestril
- Lorazepam • Ativan
- Lurasidone • Latuda
- Maprotiline • Ludiomil
- Mesoridazine • Serentil
- Metformin • Glucophage
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paliperidone • Invega
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Tamoxifen • Nolvadex, Soltamox
- Thioridazine • Mellaril
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. No similar work by the authors is under review or in press. No funding was requested or received in conjunction with this manuscript.
1. Muscatello MR, Bruno A, Pandolfo G, et al. Emerging treatments in the management of schizophrenia - focus on sertindole. Drug Des Devel Ther. 2010;4:187-201.
2. Taylor DM. Antipsychotics and QT prolongation. Acta Psychiatr Scand. 2003;107(2):85-95.
3. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
4. Wenzel-Seifert K, Wittmann M, Haen E. QTc prolongation by psychotropic drugs and the risk of torsade de pointes. Dtsch Arztebl Int. 2011;108(41):687-693.
5. Vieweg WV. New generation antipsychotic drugs and QTc interval prolongation. Prim Care Companion J Clin Psychiatry. 2003;5(5):205-215.
6. Nielsen J, Graff C, Kanters JK, et al. Assessing QT interval prolongation and its associated risks with antipsychotics. CNS Drugs. 2011;25(6):473-490.
7. Gill SS, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007;146(11):775-786.
8. Schneeweiss S, Setoguchi S, Brookhart A, et al. Risk of death associated with the use of conventional versus atypical antipsychotic drugs among elderly patients. CMAJ. 2007;176(5):627-632.
9. Vieweg WV, Wood MA. Tricyclic antidepressants QT interval prolongation, and torsade de pointes. Psychosomatics. 2004;45(5):371-377.
10. Jeon SH, Jaekal J, Lee SH, et al. Effects of nortriptyline on QT prolongation: a safety pharmacology study. Hum Exp Toxicol. 2011;30(10):1649-1656.
11. Wenzel-Seifert K, Wittmann M, Haen E. Torsade de pointes episodes under treatment with selective serotonin reuptake inhibitors. Pharmacopsychiatry. 2010;43(7):279-281.
12. Poluzzi E, Raschi E, Moretti U, et al. Drug-induced torsades de pointes: data mining of the public version of the FDA Adverse Event Reporting System (AERS). Pharmacoepidemiol Drug Saf. 2009;18(6):512-518.
13. U.S. Food and Drug Administration. FDA drug safety communication: revised recommendations for Celexa (citalopram hydrobromide) related to a potential risk of abnormal heart rhythms with high doses. http://www.fda.gov/Drugs/DrugSafety/ucm297391.htm. Published March 28, 2012. Accessed June 26, 2012.
14. Arizona CERT-QT Center for Education and Research on Therapeutics. QT drug lists by risk groups. http://www.azcert.org/medical-pros/drug-lists/drug-lists.cfm. Accessed June 26 2012.
15. Howell C, Wilson AD, Waring WS. Cardiovascular toxicity due to venlafaxine poisoning in adults: a review of 235 consecutive cases. Br J Clin Pharmacol. 2007;64(2):192-197.
16. Salih IS, Thanacoody RH, McKay GA, et al. Comparison of the effects of thioridazine and mesoridazine on the QT interval in healthy adults after single oral doses. Clin Pharmacol Ther. 2007;82(5):548-554.
17. Goodnick PJ, Jerry J, Parra F. Psychotropic drugs and the ECG: focus on the QTc interval. Expert Opin Pharmacother. 2002;3(5):479-498.
18. Dallaire S. Thioridazine (Mellaril) and mesoridazine (Serentil): prolongation of the QTc interval. CMAJ. 2001;164(1):91,95.-
19. Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation torsade de pointes and sudden death. Drugs. 2002;62(11):1649-1671.
20. Shapiro BA, Warren J, Egol AB, et al. Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: an executive summary. Crit Care Med. 1995;23(9):1596-1600.
21. Vieweg WV, Hasnain M. Question regarding ziprasidone and QTc interval prolongation in the ZODIAC Study. Am J Psychiatry. 2011;168(6):650-651.
22. Caccia S, Pasina L, Nobili A. New atypical antipsychotics for schizophrenia: iloperidone. Drug Des Devel Ther. 2010;4:33-48.
23. Dineen S, Withrow K, Voronovitch L, et al. QTc prolongation and high-dose olanzapine. Psychosomatics. 2003;44(2):174-175.
24. Vieweg WV, Schneider RK, Wood MA. Torsade de pointes in a patient with complex medical and psychiatric conditions receiving low-dose quetiapine. Acta Psychiatr Scand. 2005;112(4):318-322.
25. Capuano A, Ruggiero S, Vestini F, et al. Survival from coma induced by an intentional 36-g overdose of extended-release quetiapine. Drug Chem Toxicol. 2011;34(4):475-477.
26. Fernandes PP, Marcil WA. Death associated with quetiapine overdose. Am J Psychiatry. 2002;159(12):2114.-
27. Sedky K, Nazir R, Lindenmayer JP, et al. Paliperidone palmitate: once-monthly treatment option for schizophrenia. Current Psychiatry. 2010;9(3):48-50.
28. Citrome L. Lurasidone for schizophrenia: a review of the efficacy and safety profile for this newly approved second-generation antipsychotic. Int J Clin Pract. 2011;65(2):189-210.
29. Chapel S, Hutmacher MM, Haig G, et al. Exposure-response analysis in patients with schizophrenia to assess the effect of asenapine on QTc prolongation. J Clin Pharmacol. 2009;49(11):1297-1308.
1. Muscatello MR, Bruno A, Pandolfo G, et al. Emerging treatments in the management of schizophrenia - focus on sertindole. Drug Des Devel Ther. 2010;4:187-201.
2. Taylor DM. Antipsychotics and QT prolongation. Acta Psychiatr Scand. 2003;107(2):85-95.
3. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
4. Wenzel-Seifert K, Wittmann M, Haen E. QTc prolongation by psychotropic drugs and the risk of torsade de pointes. Dtsch Arztebl Int. 2011;108(41):687-693.
5. Vieweg WV. New generation antipsychotic drugs and QTc interval prolongation. Prim Care Companion J Clin Psychiatry. 2003;5(5):205-215.
6. Nielsen J, Graff C, Kanters JK, et al. Assessing QT interval prolongation and its associated risks with antipsychotics. CNS Drugs. 2011;25(6):473-490.
7. Gill SS, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007;146(11):775-786.
8. Schneeweiss S, Setoguchi S, Brookhart A, et al. Risk of death associated with the use of conventional versus atypical antipsychotic drugs among elderly patients. CMAJ. 2007;176(5):627-632.
9. Vieweg WV, Wood MA. Tricyclic antidepressants QT interval prolongation, and torsade de pointes. Psychosomatics. 2004;45(5):371-377.
10. Jeon SH, Jaekal J, Lee SH, et al. Effects of nortriptyline on QT prolongation: a safety pharmacology study. Hum Exp Toxicol. 2011;30(10):1649-1656.
11. Wenzel-Seifert K, Wittmann M, Haen E. Torsade de pointes episodes under treatment with selective serotonin reuptake inhibitors. Pharmacopsychiatry. 2010;43(7):279-281.
12. Poluzzi E, Raschi E, Moretti U, et al. Drug-induced torsades de pointes: data mining of the public version of the FDA Adverse Event Reporting System (AERS). Pharmacoepidemiol Drug Saf. 2009;18(6):512-518.
13. U.S. Food and Drug Administration. FDA drug safety communication: revised recommendations for Celexa (citalopram hydrobromide) related to a potential risk of abnormal heart rhythms with high doses. http://www.fda.gov/Drugs/DrugSafety/ucm297391.htm. Published March 28, 2012. Accessed June 26, 2012.
14. Arizona CERT-QT Center for Education and Research on Therapeutics. QT drug lists by risk groups. http://www.azcert.org/medical-pros/drug-lists/drug-lists.cfm. Accessed June 26 2012.
15. Howell C, Wilson AD, Waring WS. Cardiovascular toxicity due to venlafaxine poisoning in adults: a review of 235 consecutive cases. Br J Clin Pharmacol. 2007;64(2):192-197.
16. Salih IS, Thanacoody RH, McKay GA, et al. Comparison of the effects of thioridazine and mesoridazine on the QT interval in healthy adults after single oral doses. Clin Pharmacol Ther. 2007;82(5):548-554.
17. Goodnick PJ, Jerry J, Parra F. Psychotropic drugs and the ECG: focus on the QTc interval. Expert Opin Pharmacother. 2002;3(5):479-498.
18. Dallaire S. Thioridazine (Mellaril) and mesoridazine (Serentil): prolongation of the QTc interval. CMAJ. 2001;164(1):91,95.-
19. Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation torsade de pointes and sudden death. Drugs. 2002;62(11):1649-1671.
20. Shapiro BA, Warren J, Egol AB, et al. Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: an executive summary. Crit Care Med. 1995;23(9):1596-1600.
21. Vieweg WV, Hasnain M. Question regarding ziprasidone and QTc interval prolongation in the ZODIAC Study. Am J Psychiatry. 2011;168(6):650-651.
22. Caccia S, Pasina L, Nobili A. New atypical antipsychotics for schizophrenia: iloperidone. Drug Des Devel Ther. 2010;4:33-48.
23. Dineen S, Withrow K, Voronovitch L, et al. QTc prolongation and high-dose olanzapine. Psychosomatics. 2003;44(2):174-175.
24. Vieweg WV, Schneider RK, Wood MA. Torsade de pointes in a patient with complex medical and psychiatric conditions receiving low-dose quetiapine. Acta Psychiatr Scand. 2005;112(4):318-322.
25. Capuano A, Ruggiero S, Vestini F, et al. Survival from coma induced by an intentional 36-g overdose of extended-release quetiapine. Drug Chem Toxicol. 2011;34(4):475-477.
26. Fernandes PP, Marcil WA. Death associated with quetiapine overdose. Am J Psychiatry. 2002;159(12):2114.-
27. Sedky K, Nazir R, Lindenmayer JP, et al. Paliperidone palmitate: once-monthly treatment option for schizophrenia. Current Psychiatry. 2010;9(3):48-50.
28. Citrome L. Lurasidone for schizophrenia: a review of the efficacy and safety profile for this newly approved second-generation antipsychotic. Int J Clin Pract. 2011;65(2):189-210.
29. Chapel S, Hutmacher MM, Haig G, et al. Exposure-response analysis in patients with schizophrenia to assess the effect of asenapine on QTc prolongation. J Clin Pharmacol. 2009;49(11):1297-1308.
Epilepsy or something else?
CASE: Seizure-like symptoms
Ms. T, age 20, is brought to the emergency room (ER) by her father because she refuses to eat and drink, is unable to function at home, lies in bed all day, and does not attend to her activities of daily living (ADLs). Ms. T lives with her family, is not enrolled in school, and is unemployed. In the ER she initially is uncooperative and mute and then suddenly becomes agitated and has a seizure-like episode characterized by jerking of her trunk followed by random, asymmetrical movements of her legs and arms, closing both eyes, weeping, foaming at the mouth, moaning, and marked unresponsiveness. The episode lasts for >5 minutes.
The authors’ observations
Based on Ms. T’s presentation, the medical team considered acute epileptic seizures. Asymmetrical jerking of the body may be seen in frontal lobe epilepsy or seizures of the supplementary sensorimotor area. Frontal lobe epilepsy can present with bilateral asynchronous motor activity with consciousness during the event and a lack of postictal confusion.1 Seizures of the supplementary sensorimotor area—also known as the secondary motor area—are particularly problematic because typically they present with bilateral asymmetric tonic posturing followed by a few clonic movements, intact consciousness, and rarely postictal confusion. Adding to the diagnostic uncertainty, some “soft signs” thought to indicate PNES (eg, pelvic thrusting, crying) are common with frontal lobe epilepsy.1,2
PNES are episodes of altered movement, sensation, or experience that may be mistaken for epileptic seizures but are not a consequence of abnormal cortical discharges. Instead they are caused by physiological or psychological factors.3 Behaviors or signs that strongly suggest PNES include:
- gradual onset or termination
- pseudosleep, when the patient appears to be asleep but electroencephalography (EEG) findings indicate he or she is awake
- discontinuous (stop-and-go), irregular, or asynchronous (out-of-phase) activity—including side-to-side head movement, pelvic thrusting, and opisthotonic posturing—stuttering, and weeping4
- eye closure.5
Ms. T’s father said his daughter had been hospitalized several times for episodes characterized by pelvic thrusting, stuttering, and pseudosleep, which raised the possibility of PNES. Definitive diagnosis of PNES comes from video EEG when a patient is observed having typical seizures without accompanying EEG abnormalities.6
EVALUATION: Inconclusive data
Ms. T is admitted to the medical unit to rule out a seizure disorder. Physical examination is unremarkable and laboratory tests are within normal limits. The neurology service requests a head MRI, which is inconclusive. Inpatient video EEG with 24-hour monitoring does not indicate acute epileptic seizures. Ms. T’s father says that she has experienced many paroxysmal motor episodes and all neurologic tests, exams, and labs have failed to find a cause for these episodes. She did not receive any antiepileptic medications. A psychiatric consult is requested to clarify the diagnosis. Ms. T is transferred to an inpatient psychiatric unit for further evaluation and management.
The authors’ observations
Fleisher et al7 suggested that traumatic events may lead to presentations similar to PNES. Because Ms. T was molested by a family friend as a child, we considered posttraumatic stress disorder (PTSD) in the differential diagnosis, although she has not reported symptoms of intrusive recollections, avoidance, numbing, or hyperarousal.
We also considered conversion disorder and dissociative disorder. Patients with conversion disorder have ≥1 symptoms or signs that affect voluntary motor or sensory function that cannot be explained by a neurologic or general medical condition.8 Dissociative disorder is a disruption in usually integrated functions of consciousness, memory, identity, or perception of the environment.8 The presentation of patients with PNES may resemble that of patients with dissociative disorder.8 In a study of 45 adult PNES patients, Bowman et al8 found that PNES often are comorbid with other psychiatric disorders, including somatoform disorders (89%), dissociative disorders (91%), affective disorders (64%), personality disorders (62%), PTSD (49%), and other anxiety disorders (47%).
TREATMENT: Managing aggression
In the psychiatric unit, Ms. T initially is irritable and disorganized with poor oral intake and regressed behavior; she often is found in the fetal position, crying and talking in a childish manner. Throughout her admission, she receives several anxiolytics and antipsychotics—including lorazepam, up to 6 mg/d, clonazepam, up to 3 mg/d, haloperidol, up to 10 mg/d, and quetiapine, up to 200 mg/d—to help manage her aggressive behaviors after her seizure-like episodes. Further evaluation reveals that Ms. T has no psychotic symptoms, overt delusions, or perceptual disturbances and her thought process is coherent and clear. She has no history of substance abuse. Her ability to perform ADLs improves within a few days. She complains of depressed mood and engages in head banging, which requires close observation.
Ms. T has a history of mood and behavioral problems since early childhood characterized by episodic dysphoric mood, anxiety, and agitation. She has had trials of several antidepressants, including sertraline, fluoxetine, venlafaxine, and escitalopram, and anxiolytics, including lorazepam, clonazepam, and alprazolam. Her outpatient psychiatrist describes a history of physical and sexual abuse starting at age 7. At age 9, after her mother died from breast cancer, Ms. T and her siblings were moved to foster care, where she was physically abused by the staff. She remained in foster care until age 18.
The authors’ observations
PNES pose a diagnostic and therapeutic challenge. Many PNES patients seek medical attention for their seizures. PNES patients misdiagnosed as having epilepsy have a worse prognosis because they do not receive appropriate treatment9 and may experience side effects if antiepileptics are prescribed.10 Finally, the financial burden of medical care can be significant. Ms. T had several hospitalizations, including extensive neurologic workup, intensive care unit admissions for intubation, and use of antiepileptics with almost no benefit.
Psychosocial assessments of PNES patients have revealed that sexual abuse, family conflicts, and death of a family member often play an important role.11 It is possible that as a result of childhood trauma, Ms. T exhibited a regressed and primitive defense mechanism to deal with the trauma. PNES usually are considered when a patient presents with:
- absence of therapeutic response to antiepileptics
- loss of response (therapeutic failure) to antiepileptics
- paradoxical response to antiepileptics (worsening or unexpected responses)
- atypical, multiple, or inconsistent seizures
- seizures that occur soon after emotional stress.12
We concluded Ms. T had PNES because of the unusual presentations of her seizures, negative video EEG findings, failure to respond to antiepileptics, lack of risk factors for epilepsy, and aggressive behaviors before or after the seizures ( Table ).4,10,11,13 Diagnosing PNES early allows clinicians to focus on appropriate treatment modalities (eg, psychotherapy, antidepressants), prevents costly neurologic workups and treatments (eg, routine EEGs, trials of several antiepileptics), and provides patients with diagnostic assurance.10
Table
Characteristics of psychogenic nonepileptic seizures
| Characteristic | Comment |
|---|---|
| Duration | May be prolonged |
| Timing | Usually occur only during the day |
| Physical harm | Rare |
| Tongue biting | Rare |
| Urinary incontinence | Rare |
| Motor activity | Prolonged |
| Cyanosis | No |
| Postictal confusion | Rare |
| Related to medication changes | No |
| Interictal EEG | Normal |
| Ictal EEG | Normal |
| Presence of secondary gain | Common |
| EEG: electroencephalography Source: References 4,10,11,13 | |
3 components of treatment
Presenting the PNES diagnosis to the patient. The neurologist and the psychiatrist should convey to the patient that they see the symptoms as “real” and not “all in your head.”14
Withdrawing antiepileptic medications. Antiepileptic medication withdrawal is recommended when a thorough diagnostic workup shows no evidence of epileptic seizures.15 Oto et al16 reported 49% of PNES patients became seizure-free 12 months after discontinuing antiepileptics.
Psychotherapy and pharmacotherapy. Open-label studies of psychological treatments for PNES have demonstrated that a cognitive-behavioral therapy-based approach and brief augmented psychodynamic interpersonal therapy could reduce seizures.17 In a pilot, randomized, placebo-controlled trial, PNES patients who received flexibly dosed sertraline reported a 45% reduction in seizures compared with an 8% increase in the placebo group.18 Similar improvements in seizure frequency have been reported in PNES patients with anxiety or depression treated with venlafaxine.19
OUTCOME: Support, improvement
During the next several days, Ms. T has random episodes of seizures with foaming of the mouth and unresponsiveness. These episodes last from 5 to 30 minutes and require transfer to the ER. After each episode, Ms. T is medically cleared and sent back to the psychiatric unit. The neurologist recommends avoiding antiepileptics. Ms. T responds well to the structured inpatient setting and supportive psychotherapy. Her episodes decrease and her mood becomes more stable. She refrains from self-injurious behaviors and is discharged home with outpatient follow-up.
Related Resource
- Marsh P, Benbadis S, Fernandez F. Psychogenic nonepileptic seizures: ways to win over skeptical patients. Current Psychiatry. 2008;7(1):21-35.
Drug Brand Names
- Alprazolam • Xanax
- Clonazepam • Klonopin
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Lorazepam • Ativan
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kellinghaus C, Lüders HO. Frontal lobe epilepsy. Epileptic Disord. 2004;6(4):223-239.
2. Kanner AM, Morris HH, Lüders H, et al. Supplementary motor seizures mimicking pseudoseizures: some clinical differences. Neurology. 1990;40(9):1404-1407.
3. Hall-Patch L, Brown R, House A, et al. Acceptability and effectiveness of a strategy for the communication of the diagnosis of psychogenic nonepileptic seizures. Epilepsia. 2010;51(1):70-78.
4. Reuber M, Elger CE. Psychogenic nonepileptic seizures: review and update. Epilepsy Behav. 2003;4(3):205-216.
5. Chung SS, Gerber P, Kirlin KA. Ictal eye closure is a reliable indicator for psychogenic nonepileptic seizures. Neurology. 2006;66(11):1730-1731.
6. Mostacci B, Bisulli F, Alvisi L, et al. Ictal characteristics of psychogenic nonepileptic seizures: what we have learned from video/EEG recordings—a literature review. Epilepsy Behav. 2011;22(2):144-153.
7. Fleisher W, Staley D, Krawetz P, et al. Comparative study of trauma-related phenomena in subjects with pseudoseizures and subjects with epilepsy. Am J Psychiatry. 2002;159(4):660-663.
8. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry. 1996;153(1):57-63.
9. Benbadis SR. The EEG in nonepileptic seizures. J Clin Neurophysiol. 2006;23(4):340-352.
10. Brown RJ, Syed TU, Benbadis S, et al. Psychogenic nonepileptic seizures. Epilepsy Behav. 2011;22(1):85-93.
11. Bodde NM, Brooks JL, Baker GA, et al. Psychogenic non-epileptic seizures—definition, etiology, treatment and prognostic issues: a critical review. Seizure. 2009;18(8):543-553.
12. Alsaadi TM, Marquez AV. Psychogenic nonepileptic seizures. Am Fam Physician. 2005;72(5):849-856.
13. Bradley WG, Daroff RB, Fenichel GM, et al. eds. Neurology in clinical practice: principles of diagnosis and management. 4th ed. Philadelphia, PA: Butterworth Heinemann; 2004:19-20, 1971–1972.
14. Harden CL, Ferrando SJ. Delivering the diagnosis of psychogenic pseudoseizures: should the neurologist or the psychiatrist be responsible? Epilepsy Behav. 2001;2(6):519-523.
15. Oto M, Espie CA, Duncan R. An exploratory randomized controlled trial of immediate versus delayed withdrawal of antiepileptic drugs in patients with psychogenic nonepileptic attacks (PNEAs). Epilepsia. 2010;51(10):1994-1999.
16. Oto M, Espie C, Pelosi A, et al. The safety of antiepileptic drug withdrawal in patients with non-epileptic seizures. J Neurol Neurosurg Psychiatry. 2005;76(12):1682-1685.
17. Goldstein LH, Mellers JD. Recent developments in our understanding of the semiology and treatment of psychogenic nonepileptic seizures. Curr Neurol Neurosci Rep. 2012;12(4):436-444.
18. LaFrance WC, Jr, Keitner GI, Papandonatos GD, et al. Pilot pharmacologic randomized controlled trial for psychogenic nonepileptic seizures. Neurology. 2010;75(13):1166-1173.
19. Pintor L, Baillés E, Matrai S, et al. Efficiency of venlafaxine in patients with psychogenic nonepileptic seizures and anxiety and/or depressive disorders. J Neuropsychiatry Clin Neurosci. 2010;22(4):401-408.
CASE: Seizure-like symptoms
Ms. T, age 20, is brought to the emergency room (ER) by her father because she refuses to eat and drink, is unable to function at home, lies in bed all day, and does not attend to her activities of daily living (ADLs). Ms. T lives with her family, is not enrolled in school, and is unemployed. In the ER she initially is uncooperative and mute and then suddenly becomes agitated and has a seizure-like episode characterized by jerking of her trunk followed by random, asymmetrical movements of her legs and arms, closing both eyes, weeping, foaming at the mouth, moaning, and marked unresponsiveness. The episode lasts for >5 minutes.
The authors’ observations
Based on Ms. T’s presentation, the medical team considered acute epileptic seizures. Asymmetrical jerking of the body may be seen in frontal lobe epilepsy or seizures of the supplementary sensorimotor area. Frontal lobe epilepsy can present with bilateral asynchronous motor activity with consciousness during the event and a lack of postictal confusion.1 Seizures of the supplementary sensorimotor area—also known as the secondary motor area—are particularly problematic because typically they present with bilateral asymmetric tonic posturing followed by a few clonic movements, intact consciousness, and rarely postictal confusion. Adding to the diagnostic uncertainty, some “soft signs” thought to indicate PNES (eg, pelvic thrusting, crying) are common with frontal lobe epilepsy.1,2
PNES are episodes of altered movement, sensation, or experience that may be mistaken for epileptic seizures but are not a consequence of abnormal cortical discharges. Instead they are caused by physiological or psychological factors.3 Behaviors or signs that strongly suggest PNES include:
- gradual onset or termination
- pseudosleep, when the patient appears to be asleep but electroencephalography (EEG) findings indicate he or she is awake
- discontinuous (stop-and-go), irregular, or asynchronous (out-of-phase) activity—including side-to-side head movement, pelvic thrusting, and opisthotonic posturing—stuttering, and weeping4
- eye closure.5
Ms. T’s father said his daughter had been hospitalized several times for episodes characterized by pelvic thrusting, stuttering, and pseudosleep, which raised the possibility of PNES. Definitive diagnosis of PNES comes from video EEG when a patient is observed having typical seizures without accompanying EEG abnormalities.6
EVALUATION: Inconclusive data
Ms. T is admitted to the medical unit to rule out a seizure disorder. Physical examination is unremarkable and laboratory tests are within normal limits. The neurology service requests a head MRI, which is inconclusive. Inpatient video EEG with 24-hour monitoring does not indicate acute epileptic seizures. Ms. T’s father says that she has experienced many paroxysmal motor episodes and all neurologic tests, exams, and labs have failed to find a cause for these episodes. She did not receive any antiepileptic medications. A psychiatric consult is requested to clarify the diagnosis. Ms. T is transferred to an inpatient psychiatric unit for further evaluation and management.
The authors’ observations
Fleisher et al7 suggested that traumatic events may lead to presentations similar to PNES. Because Ms. T was molested by a family friend as a child, we considered posttraumatic stress disorder (PTSD) in the differential diagnosis, although she has not reported symptoms of intrusive recollections, avoidance, numbing, or hyperarousal.
We also considered conversion disorder and dissociative disorder. Patients with conversion disorder have ≥1 symptoms or signs that affect voluntary motor or sensory function that cannot be explained by a neurologic or general medical condition.8 Dissociative disorder is a disruption in usually integrated functions of consciousness, memory, identity, or perception of the environment.8 The presentation of patients with PNES may resemble that of patients with dissociative disorder.8 In a study of 45 adult PNES patients, Bowman et al8 found that PNES often are comorbid with other psychiatric disorders, including somatoform disorders (89%), dissociative disorders (91%), affective disorders (64%), personality disorders (62%), PTSD (49%), and other anxiety disorders (47%).
TREATMENT: Managing aggression
In the psychiatric unit, Ms. T initially is irritable and disorganized with poor oral intake and regressed behavior; she often is found in the fetal position, crying and talking in a childish manner. Throughout her admission, she receives several anxiolytics and antipsychotics—including lorazepam, up to 6 mg/d, clonazepam, up to 3 mg/d, haloperidol, up to 10 mg/d, and quetiapine, up to 200 mg/d—to help manage her aggressive behaviors after her seizure-like episodes. Further evaluation reveals that Ms. T has no psychotic symptoms, overt delusions, or perceptual disturbances and her thought process is coherent and clear. She has no history of substance abuse. Her ability to perform ADLs improves within a few days. She complains of depressed mood and engages in head banging, which requires close observation.
Ms. T has a history of mood and behavioral problems since early childhood characterized by episodic dysphoric mood, anxiety, and agitation. She has had trials of several antidepressants, including sertraline, fluoxetine, venlafaxine, and escitalopram, and anxiolytics, including lorazepam, clonazepam, and alprazolam. Her outpatient psychiatrist describes a history of physical and sexual abuse starting at age 7. At age 9, after her mother died from breast cancer, Ms. T and her siblings were moved to foster care, where she was physically abused by the staff. She remained in foster care until age 18.
The authors’ observations
PNES pose a diagnostic and therapeutic challenge. Many PNES patients seek medical attention for their seizures. PNES patients misdiagnosed as having epilepsy have a worse prognosis because they do not receive appropriate treatment9 and may experience side effects if antiepileptics are prescribed.10 Finally, the financial burden of medical care can be significant. Ms. T had several hospitalizations, including extensive neurologic workup, intensive care unit admissions for intubation, and use of antiepileptics with almost no benefit.
Psychosocial assessments of PNES patients have revealed that sexual abuse, family conflicts, and death of a family member often play an important role.11 It is possible that as a result of childhood trauma, Ms. T exhibited a regressed and primitive defense mechanism to deal with the trauma. PNES usually are considered when a patient presents with:
- absence of therapeutic response to antiepileptics
- loss of response (therapeutic failure) to antiepileptics
- paradoxical response to antiepileptics (worsening or unexpected responses)
- atypical, multiple, or inconsistent seizures
- seizures that occur soon after emotional stress.12
We concluded Ms. T had PNES because of the unusual presentations of her seizures, negative video EEG findings, failure to respond to antiepileptics, lack of risk factors for epilepsy, and aggressive behaviors before or after the seizures ( Table ).4,10,11,13 Diagnosing PNES early allows clinicians to focus on appropriate treatment modalities (eg, psychotherapy, antidepressants), prevents costly neurologic workups and treatments (eg, routine EEGs, trials of several antiepileptics), and provides patients with diagnostic assurance.10
Table
Characteristics of psychogenic nonepileptic seizures
| Characteristic | Comment |
|---|---|
| Duration | May be prolonged |
| Timing | Usually occur only during the day |
| Physical harm | Rare |
| Tongue biting | Rare |
| Urinary incontinence | Rare |
| Motor activity | Prolonged |
| Cyanosis | No |
| Postictal confusion | Rare |
| Related to medication changes | No |
| Interictal EEG | Normal |
| Ictal EEG | Normal |
| Presence of secondary gain | Common |
| EEG: electroencephalography Source: References 4,10,11,13 | |
3 components of treatment
Presenting the PNES diagnosis to the patient. The neurologist and the psychiatrist should convey to the patient that they see the symptoms as “real” and not “all in your head.”14
Withdrawing antiepileptic medications. Antiepileptic medication withdrawal is recommended when a thorough diagnostic workup shows no evidence of epileptic seizures.15 Oto et al16 reported 49% of PNES patients became seizure-free 12 months after discontinuing antiepileptics.
Psychotherapy and pharmacotherapy. Open-label studies of psychological treatments for PNES have demonstrated that a cognitive-behavioral therapy-based approach and brief augmented psychodynamic interpersonal therapy could reduce seizures.17 In a pilot, randomized, placebo-controlled trial, PNES patients who received flexibly dosed sertraline reported a 45% reduction in seizures compared with an 8% increase in the placebo group.18 Similar improvements in seizure frequency have been reported in PNES patients with anxiety or depression treated with venlafaxine.19
OUTCOME: Support, improvement
During the next several days, Ms. T has random episodes of seizures with foaming of the mouth and unresponsiveness. These episodes last from 5 to 30 minutes and require transfer to the ER. After each episode, Ms. T is medically cleared and sent back to the psychiatric unit. The neurologist recommends avoiding antiepileptics. Ms. T responds well to the structured inpatient setting and supportive psychotherapy. Her episodes decrease and her mood becomes more stable. She refrains from self-injurious behaviors and is discharged home with outpatient follow-up.
Related Resource
- Marsh P, Benbadis S, Fernandez F. Psychogenic nonepileptic seizures: ways to win over skeptical patients. Current Psychiatry. 2008;7(1):21-35.
Drug Brand Names
- Alprazolam • Xanax
- Clonazepam • Klonopin
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Lorazepam • Ativan
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Seizure-like symptoms
Ms. T, age 20, is brought to the emergency room (ER) by her father because she refuses to eat and drink, is unable to function at home, lies in bed all day, and does not attend to her activities of daily living (ADLs). Ms. T lives with her family, is not enrolled in school, and is unemployed. In the ER she initially is uncooperative and mute and then suddenly becomes agitated and has a seizure-like episode characterized by jerking of her trunk followed by random, asymmetrical movements of her legs and arms, closing both eyes, weeping, foaming at the mouth, moaning, and marked unresponsiveness. The episode lasts for >5 minutes.
The authors’ observations
Based on Ms. T’s presentation, the medical team considered acute epileptic seizures. Asymmetrical jerking of the body may be seen in frontal lobe epilepsy or seizures of the supplementary sensorimotor area. Frontal lobe epilepsy can present with bilateral asynchronous motor activity with consciousness during the event and a lack of postictal confusion.1 Seizures of the supplementary sensorimotor area—also known as the secondary motor area—are particularly problematic because typically they present with bilateral asymmetric tonic posturing followed by a few clonic movements, intact consciousness, and rarely postictal confusion. Adding to the diagnostic uncertainty, some “soft signs” thought to indicate PNES (eg, pelvic thrusting, crying) are common with frontal lobe epilepsy.1,2
PNES are episodes of altered movement, sensation, or experience that may be mistaken for epileptic seizures but are not a consequence of abnormal cortical discharges. Instead they are caused by physiological or psychological factors.3 Behaviors or signs that strongly suggest PNES include:
- gradual onset or termination
- pseudosleep, when the patient appears to be asleep but electroencephalography (EEG) findings indicate he or she is awake
- discontinuous (stop-and-go), irregular, or asynchronous (out-of-phase) activity—including side-to-side head movement, pelvic thrusting, and opisthotonic posturing—stuttering, and weeping4
- eye closure.5
Ms. T’s father said his daughter had been hospitalized several times for episodes characterized by pelvic thrusting, stuttering, and pseudosleep, which raised the possibility of PNES. Definitive diagnosis of PNES comes from video EEG when a patient is observed having typical seizures without accompanying EEG abnormalities.6
EVALUATION: Inconclusive data
Ms. T is admitted to the medical unit to rule out a seizure disorder. Physical examination is unremarkable and laboratory tests are within normal limits. The neurology service requests a head MRI, which is inconclusive. Inpatient video EEG with 24-hour monitoring does not indicate acute epileptic seizures. Ms. T’s father says that she has experienced many paroxysmal motor episodes and all neurologic tests, exams, and labs have failed to find a cause for these episodes. She did not receive any antiepileptic medications. A psychiatric consult is requested to clarify the diagnosis. Ms. T is transferred to an inpatient psychiatric unit for further evaluation and management.
The authors’ observations
Fleisher et al7 suggested that traumatic events may lead to presentations similar to PNES. Because Ms. T was molested by a family friend as a child, we considered posttraumatic stress disorder (PTSD) in the differential diagnosis, although she has not reported symptoms of intrusive recollections, avoidance, numbing, or hyperarousal.
We also considered conversion disorder and dissociative disorder. Patients with conversion disorder have ≥1 symptoms or signs that affect voluntary motor or sensory function that cannot be explained by a neurologic or general medical condition.8 Dissociative disorder is a disruption in usually integrated functions of consciousness, memory, identity, or perception of the environment.8 The presentation of patients with PNES may resemble that of patients with dissociative disorder.8 In a study of 45 adult PNES patients, Bowman et al8 found that PNES often are comorbid with other psychiatric disorders, including somatoform disorders (89%), dissociative disorders (91%), affective disorders (64%), personality disorders (62%), PTSD (49%), and other anxiety disorders (47%).
TREATMENT: Managing aggression
In the psychiatric unit, Ms. T initially is irritable and disorganized with poor oral intake and regressed behavior; she often is found in the fetal position, crying and talking in a childish manner. Throughout her admission, she receives several anxiolytics and antipsychotics—including lorazepam, up to 6 mg/d, clonazepam, up to 3 mg/d, haloperidol, up to 10 mg/d, and quetiapine, up to 200 mg/d—to help manage her aggressive behaviors after her seizure-like episodes. Further evaluation reveals that Ms. T has no psychotic symptoms, overt delusions, or perceptual disturbances and her thought process is coherent and clear. She has no history of substance abuse. Her ability to perform ADLs improves within a few days. She complains of depressed mood and engages in head banging, which requires close observation.
Ms. T has a history of mood and behavioral problems since early childhood characterized by episodic dysphoric mood, anxiety, and agitation. She has had trials of several antidepressants, including sertraline, fluoxetine, venlafaxine, and escitalopram, and anxiolytics, including lorazepam, clonazepam, and alprazolam. Her outpatient psychiatrist describes a history of physical and sexual abuse starting at age 7. At age 9, after her mother died from breast cancer, Ms. T and her siblings were moved to foster care, where she was physically abused by the staff. She remained in foster care until age 18.
The authors’ observations
PNES pose a diagnostic and therapeutic challenge. Many PNES patients seek medical attention for their seizures. PNES patients misdiagnosed as having epilepsy have a worse prognosis because they do not receive appropriate treatment9 and may experience side effects if antiepileptics are prescribed.10 Finally, the financial burden of medical care can be significant. Ms. T had several hospitalizations, including extensive neurologic workup, intensive care unit admissions for intubation, and use of antiepileptics with almost no benefit.
Psychosocial assessments of PNES patients have revealed that sexual abuse, family conflicts, and death of a family member often play an important role.11 It is possible that as a result of childhood trauma, Ms. T exhibited a regressed and primitive defense mechanism to deal with the trauma. PNES usually are considered when a patient presents with:
- absence of therapeutic response to antiepileptics
- loss of response (therapeutic failure) to antiepileptics
- paradoxical response to antiepileptics (worsening or unexpected responses)
- atypical, multiple, or inconsistent seizures
- seizures that occur soon after emotional stress.12
We concluded Ms. T had PNES because of the unusual presentations of her seizures, negative video EEG findings, failure to respond to antiepileptics, lack of risk factors for epilepsy, and aggressive behaviors before or after the seizures ( Table ).4,10,11,13 Diagnosing PNES early allows clinicians to focus on appropriate treatment modalities (eg, psychotherapy, antidepressants), prevents costly neurologic workups and treatments (eg, routine EEGs, trials of several antiepileptics), and provides patients with diagnostic assurance.10
Table
Characteristics of psychogenic nonepileptic seizures
| Characteristic | Comment |
|---|---|
| Duration | May be prolonged |
| Timing | Usually occur only during the day |
| Physical harm | Rare |
| Tongue biting | Rare |
| Urinary incontinence | Rare |
| Motor activity | Prolonged |
| Cyanosis | No |
| Postictal confusion | Rare |
| Related to medication changes | No |
| Interictal EEG | Normal |
| Ictal EEG | Normal |
| Presence of secondary gain | Common |
| EEG: electroencephalography Source: References 4,10,11,13 | |
3 components of treatment
Presenting the PNES diagnosis to the patient. The neurologist and the psychiatrist should convey to the patient that they see the symptoms as “real” and not “all in your head.”14
Withdrawing antiepileptic medications. Antiepileptic medication withdrawal is recommended when a thorough diagnostic workup shows no evidence of epileptic seizures.15 Oto et al16 reported 49% of PNES patients became seizure-free 12 months after discontinuing antiepileptics.
Psychotherapy and pharmacotherapy. Open-label studies of psychological treatments for PNES have demonstrated that a cognitive-behavioral therapy-based approach and brief augmented psychodynamic interpersonal therapy could reduce seizures.17 In a pilot, randomized, placebo-controlled trial, PNES patients who received flexibly dosed sertraline reported a 45% reduction in seizures compared with an 8% increase in the placebo group.18 Similar improvements in seizure frequency have been reported in PNES patients with anxiety or depression treated with venlafaxine.19
OUTCOME: Support, improvement
During the next several days, Ms. T has random episodes of seizures with foaming of the mouth and unresponsiveness. These episodes last from 5 to 30 minutes and require transfer to the ER. After each episode, Ms. T is medically cleared and sent back to the psychiatric unit. The neurologist recommends avoiding antiepileptics. Ms. T responds well to the structured inpatient setting and supportive psychotherapy. Her episodes decrease and her mood becomes more stable. She refrains from self-injurious behaviors and is discharged home with outpatient follow-up.
Related Resource
- Marsh P, Benbadis S, Fernandez F. Psychogenic nonepileptic seizures: ways to win over skeptical patients. Current Psychiatry. 2008;7(1):21-35.
Drug Brand Names
- Alprazolam • Xanax
- Clonazepam • Klonopin
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Lorazepam • Ativan
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kellinghaus C, Lüders HO. Frontal lobe epilepsy. Epileptic Disord. 2004;6(4):223-239.
2. Kanner AM, Morris HH, Lüders H, et al. Supplementary motor seizures mimicking pseudoseizures: some clinical differences. Neurology. 1990;40(9):1404-1407.
3. Hall-Patch L, Brown R, House A, et al. Acceptability and effectiveness of a strategy for the communication of the diagnosis of psychogenic nonepileptic seizures. Epilepsia. 2010;51(1):70-78.
4. Reuber M, Elger CE. Psychogenic nonepileptic seizures: review and update. Epilepsy Behav. 2003;4(3):205-216.
5. Chung SS, Gerber P, Kirlin KA. Ictal eye closure is a reliable indicator for psychogenic nonepileptic seizures. Neurology. 2006;66(11):1730-1731.
6. Mostacci B, Bisulli F, Alvisi L, et al. Ictal characteristics of psychogenic nonepileptic seizures: what we have learned from video/EEG recordings—a literature review. Epilepsy Behav. 2011;22(2):144-153.
7. Fleisher W, Staley D, Krawetz P, et al. Comparative study of trauma-related phenomena in subjects with pseudoseizures and subjects with epilepsy. Am J Psychiatry. 2002;159(4):660-663.
8. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry. 1996;153(1):57-63.
9. Benbadis SR. The EEG in nonepileptic seizures. J Clin Neurophysiol. 2006;23(4):340-352.
10. Brown RJ, Syed TU, Benbadis S, et al. Psychogenic nonepileptic seizures. Epilepsy Behav. 2011;22(1):85-93.
11. Bodde NM, Brooks JL, Baker GA, et al. Psychogenic non-epileptic seizures—definition, etiology, treatment and prognostic issues: a critical review. Seizure. 2009;18(8):543-553.
12. Alsaadi TM, Marquez AV. Psychogenic nonepileptic seizures. Am Fam Physician. 2005;72(5):849-856.
13. Bradley WG, Daroff RB, Fenichel GM, et al. eds. Neurology in clinical practice: principles of diagnosis and management. 4th ed. Philadelphia, PA: Butterworth Heinemann; 2004:19-20, 1971–1972.
14. Harden CL, Ferrando SJ. Delivering the diagnosis of psychogenic pseudoseizures: should the neurologist or the psychiatrist be responsible? Epilepsy Behav. 2001;2(6):519-523.
15. Oto M, Espie CA, Duncan R. An exploratory randomized controlled trial of immediate versus delayed withdrawal of antiepileptic drugs in patients with psychogenic nonepileptic attacks (PNEAs). Epilepsia. 2010;51(10):1994-1999.
16. Oto M, Espie C, Pelosi A, et al. The safety of antiepileptic drug withdrawal in patients with non-epileptic seizures. J Neurol Neurosurg Psychiatry. 2005;76(12):1682-1685.
17. Goldstein LH, Mellers JD. Recent developments in our understanding of the semiology and treatment of psychogenic nonepileptic seizures. Curr Neurol Neurosci Rep. 2012;12(4):436-444.
18. LaFrance WC, Jr, Keitner GI, Papandonatos GD, et al. Pilot pharmacologic randomized controlled trial for psychogenic nonepileptic seizures. Neurology. 2010;75(13):1166-1173.
19. Pintor L, Baillés E, Matrai S, et al. Efficiency of venlafaxine in patients with psychogenic nonepileptic seizures and anxiety and/or depressive disorders. J Neuropsychiatry Clin Neurosci. 2010;22(4):401-408.
1. Kellinghaus C, Lüders HO. Frontal lobe epilepsy. Epileptic Disord. 2004;6(4):223-239.
2. Kanner AM, Morris HH, Lüders H, et al. Supplementary motor seizures mimicking pseudoseizures: some clinical differences. Neurology. 1990;40(9):1404-1407.
3. Hall-Patch L, Brown R, House A, et al. Acceptability and effectiveness of a strategy for the communication of the diagnosis of psychogenic nonepileptic seizures. Epilepsia. 2010;51(1):70-78.
4. Reuber M, Elger CE. Psychogenic nonepileptic seizures: review and update. Epilepsy Behav. 2003;4(3):205-216.
5. Chung SS, Gerber P, Kirlin KA. Ictal eye closure is a reliable indicator for psychogenic nonepileptic seizures. Neurology. 2006;66(11):1730-1731.
6. Mostacci B, Bisulli F, Alvisi L, et al. Ictal characteristics of psychogenic nonepileptic seizures: what we have learned from video/EEG recordings—a literature review. Epilepsy Behav. 2011;22(2):144-153.
7. Fleisher W, Staley D, Krawetz P, et al. Comparative study of trauma-related phenomena in subjects with pseudoseizures and subjects with epilepsy. Am J Psychiatry. 2002;159(4):660-663.
8. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry. 1996;153(1):57-63.
9. Benbadis SR. The EEG in nonepileptic seizures. J Clin Neurophysiol. 2006;23(4):340-352.
10. Brown RJ, Syed TU, Benbadis S, et al. Psychogenic nonepileptic seizures. Epilepsy Behav. 2011;22(1):85-93.
11. Bodde NM, Brooks JL, Baker GA, et al. Psychogenic non-epileptic seizures—definition, etiology, treatment and prognostic issues: a critical review. Seizure. 2009;18(8):543-553.
12. Alsaadi TM, Marquez AV. Psychogenic nonepileptic seizures. Am Fam Physician. 2005;72(5):849-856.
13. Bradley WG, Daroff RB, Fenichel GM, et al. eds. Neurology in clinical practice: principles of diagnosis and management. 4th ed. Philadelphia, PA: Butterworth Heinemann; 2004:19-20, 1971–1972.
14. Harden CL, Ferrando SJ. Delivering the diagnosis of psychogenic pseudoseizures: should the neurologist or the psychiatrist be responsible? Epilepsy Behav. 2001;2(6):519-523.
15. Oto M, Espie CA, Duncan R. An exploratory randomized controlled trial of immediate versus delayed withdrawal of antiepileptic drugs in patients with psychogenic nonepileptic attacks (PNEAs). Epilepsia. 2010;51(10):1994-1999.
16. Oto M, Espie C, Pelosi A, et al. The safety of antiepileptic drug withdrawal in patients with non-epileptic seizures. J Neurol Neurosurg Psychiatry. 2005;76(12):1682-1685.
17. Goldstein LH, Mellers JD. Recent developments in our understanding of the semiology and treatment of psychogenic nonepileptic seizures. Curr Neurol Neurosci Rep. 2012;12(4):436-444.
18. LaFrance WC, Jr, Keitner GI, Papandonatos GD, et al. Pilot pharmacologic randomized controlled trial for psychogenic nonepileptic seizures. Neurology. 2010;75(13):1166-1173.
19. Pintor L, Baillés E, Matrai S, et al. Efficiency of venlafaxine in patients with psychogenic nonepileptic seizures and anxiety and/or depressive disorders. J Neuropsychiatry Clin Neurosci. 2010;22(4):401-408.
The avoidant psychotherapy patient
CASE: Unexplained panic
Mr. J, age 35, is a married, unemployed musician who presents for outpatient treatment for panic attacks. He experienced his first panic attack at his oldest son’s baptism 12 years ago, but does not know why it occurred at that moment. He rarely has panic attacks now, but wants to continue medication management. He denies depressive symptoms, saying, “I’m the most optimistic person in the world.” Mr. J tried several medications for his panic attacks before clonazepam, 2 mg/d, proved effective, but always has been vehemently opposed to antidepressants. Despite his insistence that he needs only medication management, Mr. J chooses to enroll in a resident-run psychotherapy clinic.
In sessions, Mr. J describes his father, who also has panic disorder, as a powerful figure who is physically and emotionally abusive, but also charismatic, charming, and “impossible not to love.” However, Mr. J felt his father was impossible to live with, and moved out at age 18 to marry his high school sweetheart. They have 3 children, ages 12, 10, and 8. Mr. J worked for his father at his construction company, but was not able to satisfy him or live up to his standards so he quit because he was tired of being cut down and emasculated.
Mr. J’s parents divorced 15 years ago after his mother had an affair with her husband’s friend. His father learned of the affair and threatened his wife with a handgun. Although Mr. J and his mother were close before her affair, he has been unable to forgive or empathize with her, and rarely speaks to her. Mr. J’s mother could not protect him from his father’s abuse, and later compounded her failure by abandoning her husband and son through her sexual affair. Growing up with a father he did not respect or get comfort from and sharing a common fear and alliance with his mother likely made it difficult for Mr. J to navigate his Oedipal phase,1 and made her abandonment even more painful.
When Mr. J was 6 years old, he was molested by one of his father’s friends. His father stabbed the man in the shoulder when he found out about the molestation and received probation. Although Mr. J knows he was molested, he does not remember it and has repressed most of his childhood.
The authors’ observations
I (JF) wanted to discuss with Mr. J why his first panic attack occurred during such a symbolic occasion. His panic could be the result of a struggle between a murderous wish toward his father and paternal protective instinct toward his son. The baptism placed his son in a highly vulnerable position, which reminded Mr. J of his own vulnerability and impotent rage toward his father. Anxiety often results when an individual has 2 opposing wishes,2 and a murderous wish often is involved when anxiety progresses to panic. Getting to the root of this with Mr. J could allow for further psychological growth.3 His murderous wishes and fantasies are ego-dystonic, and panic could be a way of punishing himself for these thoughts. When Mr. J identified himself as his son during the baptism, he likely was flooded with thoughts that his defenses were no longer able to repress. Seeing his son submerged in the baptismal font brought back an aspect of his own life that he had completely split off from consciousness, and likely will take time to process. Considering the current therapeutic dynamic, I decided that it was not the best time to address this potential conflict; however, I could have chosen a manualized form of psychodynamic psychotherapy for panic disorder.4 See Table 1 for an outline of the phases of psychodynamic psychotherapy for panic disorder.
Although Mr. J’s initial willingness to discuss his past was encouraging, he refused to schedule more than 1 session every 4 weeks. He also began to keep the content of our sessions superficial, which caused me angst because he seemed to be withholding information and would not come more frequently. Although I was not proud of my feelings, I had to be honest with myself that I had started to dislike Mr. J.
Table 1
Psychodynamic psychotherapy for panic disorder
| Phase | Comments |
|---|---|
| Treatment of acute panic | Therapy focuses on discovering the conscious and unconscious meaning of panic symptoms |
| Treatment of panic vulnerability | Core dynamic conflicts related to panic are understood and altered. Tasks include addressing the nature of the transference and working through them |
| Termination | The therapist directly addresses patients’ difficulties with separation and independence as they emerge in treatment. After treatment, patients may be better able to manage separations, anger, and independence |
| Source: Adapted from reference 4 | |
Countertransference reactions
Countertransference is a therapist's emotional reaction to a patient. Just as patients form reactions based on past relationships brought to present, therapists develop similar reactions.5 Noting one’s countertransference provides a window into how the patient’s thoughts and actions evoke feelings in others. It also can shed light on an aspect of the doctor-patient relationship that may have gone unnoticed.2
Countertransference hatred can occur when a therapist begins to dislike a patient. Typically, patients with borderline personality disorder, masochistic tendencies, or suicidality arouse strong countertransference reactions6; however, any patient can evoke these emotions. This type of hateful patient can precipitate antitherapeutic feelings such as aversion or malice that can be a major obstacle to treatment.7 Aversion leads the therapist to withdraw from the patient, and malice can trigger cruel impulses.
Maltsberger and Buie7 identified 5 defenses therapists may use to combat countertransference hatred (Table 2). When treating Mr. J, I used several of these defenses, including projection and turning against the self to protect myself from this challenging patient. In turning against the self, I became doubtful and critical of my skills and increasingly submissive to Mr. J. Additionally, I projected this countertransference hatred onto Mr. J, focusing on the negative transference that he brought to our therapeutic encounters. On an unconscious level, I may have feared retribution from Mr. J.
I became so frustrated with Mr. J that I reduced the frequency of our sessions to once every 6 weeks, which I realized could be evidence of my feelings regarding Mr. J’s minimization and avoidant style.
Table 2
Defenses against countertransference hate
| Defense mechanism | Description |
|---|---|
| Repression | Remaining unconscious of feelings of hate; may manifest as difficulty paying attention to what the patient is saying or feeling bored or tired |
| Turning against oneself | Doubting one’s capacity to help the patient; may feel inadequate, helpless, and hopeless. May lead to giving up on the patient because the therapist feels incompetent |
| Reaction formation | Turning hatred into the opposite emotion. The therapist may be too preoccupied with being helpful or overly concerned about the patient’s welfare and comfort |
| Projection | Feeling that the patient hates the therapist, leading to feelings of dread and fear |
| Distortion of reality | Devaluing the patient and seeing the patient as a hopeless case or a dangerous person. The therapist may feel indifference, pity, or anger toward the patient |
| Source: Reference 7 | |
TREATMENT: A breakthrough
Mr. J presents with obvious unease at the first visit after we had decreased the frequency of our sessions. At this point, Mr. J opens up to me. He says he has not been truthful with me, and has had worsening depression, anhedonia, and agoraphobia over the past year. He also reveals that he has homosexual fantasies that he cannot stop, which disturb him because he says he is heterosexual. He agrees to come once a week, and reluctantly admits that he desperately needs help.
Although Mr. J only takes clonazepam and citalopram, 20 mg/d, which I prescribed after he admitted to depression and anxiety, he has hyperlipidemia and a family history of heart disease. In addition to being a musician and working at his father’s construction company, he has worked as a security guard, bounty hunter, and computer technician. His careers have been solitary in nature, and, with the exception of computer work, permitted an outlet for aggression. However, he recently started taking online college classes and wants to become a music teacher because he feels he has a lot to offer children as a result of his life experiences. His fantasy of being a teacher shows considerably less aggression, and could be a sign of psychological growth.
Mr. J is struggling financially and his home is on the verge of foreclosure. Early in treatment he told me that he stopped paying his mortgage, but demonstrated blind optimism that things would “work out.” I asked if this was a wise decision, but he seemed confident and dismissive of my concerns. Although he now struggles with this situation, I consider this healthier than his constant pseudo-happy state, and a sign of psychological development.8 Despite his financial stressors, he wants to pursue his dream of being a famous musician, and says he “could never work a 9-to-5 job in a cubicle.”
The authors’ observations
I do not think it’s a coincidence that Mr. J stopped minimizing his symptoms when we decreased the frequency of his sessions. I had viewed our sessions as unproductive and blamed Mr. J for wasting both of our time with his resistance and minimization and had begun to dislike him. I felt impotent because he had been controlling each session with long, elaborate stories that had little relevance to his panic attacks, and I could not redirect him or get him to focus on pertinent issues. It was as if I was an audience for him, and provided nothing useful. However, I was interested in these superficial stories because Mr. J was charming and engaging. He likely reenacted his relationship with his father with me. Mr. J’s superficial relationship with me caused me to dislike him, and, similar to his father, reject him. This rejection likely was damaging because I was unable to anticipate his needs, which would have been to increase—rather than decrease—the frequency of our sessions. Just like his father, I was not able to take care of him.
Mr. J is deeply conflicted about his father. He states that his father “is a monster who instills fear and intimidation into everyone around him, but he’s charismatic, and I’ll always love him.” His view of his domineering father likely developed into a castration anxiety because he was afraid of competing for his mother’s love, contributing to a muddled sexual identity. This was intensified when Mr. J was sexually abused; he may have been stimulated by the molestation, adding to his confusion. Although Mr. J has repressed the abuse and split off most of his childhood, he suffers from shame, guilt, and depression because of his ego-dystonic homosexual fantasies. Homosexuality is at odds with his self-image and contributes to his anxiety and panic attacks. He cannot adequately discharge this dangerous libidinal energy, and as he becomes more conscious of it, his anxiety intensifies.
OUTCOME: Overcoming fear
As Mr. J sits crying in my office, he says he hasn’t cried in front of another man in years. I wonder aloud what his father would think of this situation. His states that his father does not respect any type of weakness and probably would “knock his teeth in.” Overcoming this fear of opening up will be a goal of Mr. J’s treatment. His unbridled optimism borders on pathologic, and is a defense against reality.8 Additionally, his reluctance to accept that he is suffering from depression, which he perceives as a weakness, will be a struggle throughout therapy. He likely will continue to minimize his symptoms when possible, making the true depths of his illness difficult to grasp.
Related Resources
- Waska R. Using countertransference: analytic contact, projective identification, and transference phantasy states. Am J Psychother. 2008;62(4):333-351.
- Gabbard GO, Litowitz BE, Williams P. Textbook of psychoanalysis. Arlington, VA: American Psychiatric Publishing, Inc; 2011.
Drug Brand Names
- Citalopram • Celexa
- Clonazepam • Klonopin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Blos P. Son and father: before and beyond the Oedipus complex. New York NY: Free Press/Macmillan; 1985.
2. Ursano RJ, Sonnenberg SM, Lazar SG. Concise guide to psychodynamic psychotherapy. Arlington VA: American Psychiatric Publishing; 2004.
3. Akhtar S. Comprehensive dictionary of psychoanalysis. London United Kingdom: Kamac Books; 2009.
4. Busch FN, Milrod BL, Singer MB. Theory and technique in psychodynamic treatment of panic disorder. J Psychother Pract Res. 1999;8(3):234-242.
5. Freud S. The future prospects of psycho-analytic therapy. The standard edition of the complete psychological works of Sigmund Freud volume XI (1910): five lectures on psycho-analysis, Leonardo da Vinci and other works. London, United Kingdom: Hogarth Press; 1957:139–152.
6. Winnicott DW. Hate in the counter-transference. J Psychother Pract Res. 1994;3(4):348-356.
7. Maltsberger JT, Buie DH. Countertransference hate in the treatment of suicidal patients. Arch Gen Psychiatry. 1974;30(5):625-633.
8. Akhtar S. “Someday…” and “if only…” fantasies: pathological optimism and inordinate nostalgia as related forms of idealization. J Am Psychoanal Assoc. 1996;44(3):723-753.
CASE: Unexplained panic
Mr. J, age 35, is a married, unemployed musician who presents for outpatient treatment for panic attacks. He experienced his first panic attack at his oldest son’s baptism 12 years ago, but does not know why it occurred at that moment. He rarely has panic attacks now, but wants to continue medication management. He denies depressive symptoms, saying, “I’m the most optimistic person in the world.” Mr. J tried several medications for his panic attacks before clonazepam, 2 mg/d, proved effective, but always has been vehemently opposed to antidepressants. Despite his insistence that he needs only medication management, Mr. J chooses to enroll in a resident-run psychotherapy clinic.
In sessions, Mr. J describes his father, who also has panic disorder, as a powerful figure who is physically and emotionally abusive, but also charismatic, charming, and “impossible not to love.” However, Mr. J felt his father was impossible to live with, and moved out at age 18 to marry his high school sweetheart. They have 3 children, ages 12, 10, and 8. Mr. J worked for his father at his construction company, but was not able to satisfy him or live up to his standards so he quit because he was tired of being cut down and emasculated.
Mr. J’s parents divorced 15 years ago after his mother had an affair with her husband’s friend. His father learned of the affair and threatened his wife with a handgun. Although Mr. J and his mother were close before her affair, he has been unable to forgive or empathize with her, and rarely speaks to her. Mr. J’s mother could not protect him from his father’s abuse, and later compounded her failure by abandoning her husband and son through her sexual affair. Growing up with a father he did not respect or get comfort from and sharing a common fear and alliance with his mother likely made it difficult for Mr. J to navigate his Oedipal phase,1 and made her abandonment even more painful.
When Mr. J was 6 years old, he was molested by one of his father’s friends. His father stabbed the man in the shoulder when he found out about the molestation and received probation. Although Mr. J knows he was molested, he does not remember it and has repressed most of his childhood.
The authors’ observations
I (JF) wanted to discuss with Mr. J why his first panic attack occurred during such a symbolic occasion. His panic could be the result of a struggle between a murderous wish toward his father and paternal protective instinct toward his son. The baptism placed his son in a highly vulnerable position, which reminded Mr. J of his own vulnerability and impotent rage toward his father. Anxiety often results when an individual has 2 opposing wishes,2 and a murderous wish often is involved when anxiety progresses to panic. Getting to the root of this with Mr. J could allow for further psychological growth.3 His murderous wishes and fantasies are ego-dystonic, and panic could be a way of punishing himself for these thoughts. When Mr. J identified himself as his son during the baptism, he likely was flooded with thoughts that his defenses were no longer able to repress. Seeing his son submerged in the baptismal font brought back an aspect of his own life that he had completely split off from consciousness, and likely will take time to process. Considering the current therapeutic dynamic, I decided that it was not the best time to address this potential conflict; however, I could have chosen a manualized form of psychodynamic psychotherapy for panic disorder.4 See Table 1 for an outline of the phases of psychodynamic psychotherapy for panic disorder.
Although Mr. J’s initial willingness to discuss his past was encouraging, he refused to schedule more than 1 session every 4 weeks. He also began to keep the content of our sessions superficial, which caused me angst because he seemed to be withholding information and would not come more frequently. Although I was not proud of my feelings, I had to be honest with myself that I had started to dislike Mr. J.
Table 1
Psychodynamic psychotherapy for panic disorder
| Phase | Comments |
|---|---|
| Treatment of acute panic | Therapy focuses on discovering the conscious and unconscious meaning of panic symptoms |
| Treatment of panic vulnerability | Core dynamic conflicts related to panic are understood and altered. Tasks include addressing the nature of the transference and working through them |
| Termination | The therapist directly addresses patients’ difficulties with separation and independence as they emerge in treatment. After treatment, patients may be better able to manage separations, anger, and independence |
| Source: Adapted from reference 4 | |
Countertransference reactions
Countertransference is a therapist's emotional reaction to a patient. Just as patients form reactions based on past relationships brought to present, therapists develop similar reactions.5 Noting one’s countertransference provides a window into how the patient’s thoughts and actions evoke feelings in others. It also can shed light on an aspect of the doctor-patient relationship that may have gone unnoticed.2
Countertransference hatred can occur when a therapist begins to dislike a patient. Typically, patients with borderline personality disorder, masochistic tendencies, or suicidality arouse strong countertransference reactions6; however, any patient can evoke these emotions. This type of hateful patient can precipitate antitherapeutic feelings such as aversion or malice that can be a major obstacle to treatment.7 Aversion leads the therapist to withdraw from the patient, and malice can trigger cruel impulses.
Maltsberger and Buie7 identified 5 defenses therapists may use to combat countertransference hatred (Table 2). When treating Mr. J, I used several of these defenses, including projection and turning against the self to protect myself from this challenging patient. In turning against the self, I became doubtful and critical of my skills and increasingly submissive to Mr. J. Additionally, I projected this countertransference hatred onto Mr. J, focusing on the negative transference that he brought to our therapeutic encounters. On an unconscious level, I may have feared retribution from Mr. J.
I became so frustrated with Mr. J that I reduced the frequency of our sessions to once every 6 weeks, which I realized could be evidence of my feelings regarding Mr. J’s minimization and avoidant style.
Table 2
Defenses against countertransference hate
| Defense mechanism | Description |
|---|---|
| Repression | Remaining unconscious of feelings of hate; may manifest as difficulty paying attention to what the patient is saying or feeling bored or tired |
| Turning against oneself | Doubting one’s capacity to help the patient; may feel inadequate, helpless, and hopeless. May lead to giving up on the patient because the therapist feels incompetent |
| Reaction formation | Turning hatred into the opposite emotion. The therapist may be too preoccupied with being helpful or overly concerned about the patient’s welfare and comfort |
| Projection | Feeling that the patient hates the therapist, leading to feelings of dread and fear |
| Distortion of reality | Devaluing the patient and seeing the patient as a hopeless case or a dangerous person. The therapist may feel indifference, pity, or anger toward the patient |
| Source: Reference 7 | |
TREATMENT: A breakthrough
Mr. J presents with obvious unease at the first visit after we had decreased the frequency of our sessions. At this point, Mr. J opens up to me. He says he has not been truthful with me, and has had worsening depression, anhedonia, and agoraphobia over the past year. He also reveals that he has homosexual fantasies that he cannot stop, which disturb him because he says he is heterosexual. He agrees to come once a week, and reluctantly admits that he desperately needs help.
Although Mr. J only takes clonazepam and citalopram, 20 mg/d, which I prescribed after he admitted to depression and anxiety, he has hyperlipidemia and a family history of heart disease. In addition to being a musician and working at his father’s construction company, he has worked as a security guard, bounty hunter, and computer technician. His careers have been solitary in nature, and, with the exception of computer work, permitted an outlet for aggression. However, he recently started taking online college classes and wants to become a music teacher because he feels he has a lot to offer children as a result of his life experiences. His fantasy of being a teacher shows considerably less aggression, and could be a sign of psychological growth.
Mr. J is struggling financially and his home is on the verge of foreclosure. Early in treatment he told me that he stopped paying his mortgage, but demonstrated blind optimism that things would “work out.” I asked if this was a wise decision, but he seemed confident and dismissive of my concerns. Although he now struggles with this situation, I consider this healthier than his constant pseudo-happy state, and a sign of psychological development.8 Despite his financial stressors, he wants to pursue his dream of being a famous musician, and says he “could never work a 9-to-5 job in a cubicle.”
The authors’ observations
I do not think it’s a coincidence that Mr. J stopped minimizing his symptoms when we decreased the frequency of his sessions. I had viewed our sessions as unproductive and blamed Mr. J for wasting both of our time with his resistance and minimization and had begun to dislike him. I felt impotent because he had been controlling each session with long, elaborate stories that had little relevance to his panic attacks, and I could not redirect him or get him to focus on pertinent issues. It was as if I was an audience for him, and provided nothing useful. However, I was interested in these superficial stories because Mr. J was charming and engaging. He likely reenacted his relationship with his father with me. Mr. J’s superficial relationship with me caused me to dislike him, and, similar to his father, reject him. This rejection likely was damaging because I was unable to anticipate his needs, which would have been to increase—rather than decrease—the frequency of our sessions. Just like his father, I was not able to take care of him.
Mr. J is deeply conflicted about his father. He states that his father “is a monster who instills fear and intimidation into everyone around him, but he’s charismatic, and I’ll always love him.” His view of his domineering father likely developed into a castration anxiety because he was afraid of competing for his mother’s love, contributing to a muddled sexual identity. This was intensified when Mr. J was sexually abused; he may have been stimulated by the molestation, adding to his confusion. Although Mr. J has repressed the abuse and split off most of his childhood, he suffers from shame, guilt, and depression because of his ego-dystonic homosexual fantasies. Homosexuality is at odds with his self-image and contributes to his anxiety and panic attacks. He cannot adequately discharge this dangerous libidinal energy, and as he becomes more conscious of it, his anxiety intensifies.
OUTCOME: Overcoming fear
As Mr. J sits crying in my office, he says he hasn’t cried in front of another man in years. I wonder aloud what his father would think of this situation. His states that his father does not respect any type of weakness and probably would “knock his teeth in.” Overcoming this fear of opening up will be a goal of Mr. J’s treatment. His unbridled optimism borders on pathologic, and is a defense against reality.8 Additionally, his reluctance to accept that he is suffering from depression, which he perceives as a weakness, will be a struggle throughout therapy. He likely will continue to minimize his symptoms when possible, making the true depths of his illness difficult to grasp.
Related Resources
- Waska R. Using countertransference: analytic contact, projective identification, and transference phantasy states. Am J Psychother. 2008;62(4):333-351.
- Gabbard GO, Litowitz BE, Williams P. Textbook of psychoanalysis. Arlington, VA: American Psychiatric Publishing, Inc; 2011.
Drug Brand Names
- Citalopram • Celexa
- Clonazepam • Klonopin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Unexplained panic
Mr. J, age 35, is a married, unemployed musician who presents for outpatient treatment for panic attacks. He experienced his first panic attack at his oldest son’s baptism 12 years ago, but does not know why it occurred at that moment. He rarely has panic attacks now, but wants to continue medication management. He denies depressive symptoms, saying, “I’m the most optimistic person in the world.” Mr. J tried several medications for his panic attacks before clonazepam, 2 mg/d, proved effective, but always has been vehemently opposed to antidepressants. Despite his insistence that he needs only medication management, Mr. J chooses to enroll in a resident-run psychotherapy clinic.
In sessions, Mr. J describes his father, who also has panic disorder, as a powerful figure who is physically and emotionally abusive, but also charismatic, charming, and “impossible not to love.” However, Mr. J felt his father was impossible to live with, and moved out at age 18 to marry his high school sweetheart. They have 3 children, ages 12, 10, and 8. Mr. J worked for his father at his construction company, but was not able to satisfy him or live up to his standards so he quit because he was tired of being cut down and emasculated.
Mr. J’s parents divorced 15 years ago after his mother had an affair with her husband’s friend. His father learned of the affair and threatened his wife with a handgun. Although Mr. J and his mother were close before her affair, he has been unable to forgive or empathize with her, and rarely speaks to her. Mr. J’s mother could not protect him from his father’s abuse, and later compounded her failure by abandoning her husband and son through her sexual affair. Growing up with a father he did not respect or get comfort from and sharing a common fear and alliance with his mother likely made it difficult for Mr. J to navigate his Oedipal phase,1 and made her abandonment even more painful.
When Mr. J was 6 years old, he was molested by one of his father’s friends. His father stabbed the man in the shoulder when he found out about the molestation and received probation. Although Mr. J knows he was molested, he does not remember it and has repressed most of his childhood.
The authors’ observations
I (JF) wanted to discuss with Mr. J why his first panic attack occurred during such a symbolic occasion. His panic could be the result of a struggle between a murderous wish toward his father and paternal protective instinct toward his son. The baptism placed his son in a highly vulnerable position, which reminded Mr. J of his own vulnerability and impotent rage toward his father. Anxiety often results when an individual has 2 opposing wishes,2 and a murderous wish often is involved when anxiety progresses to panic. Getting to the root of this with Mr. J could allow for further psychological growth.3 His murderous wishes and fantasies are ego-dystonic, and panic could be a way of punishing himself for these thoughts. When Mr. J identified himself as his son during the baptism, he likely was flooded with thoughts that his defenses were no longer able to repress. Seeing his son submerged in the baptismal font brought back an aspect of his own life that he had completely split off from consciousness, and likely will take time to process. Considering the current therapeutic dynamic, I decided that it was not the best time to address this potential conflict; however, I could have chosen a manualized form of psychodynamic psychotherapy for panic disorder.4 See Table 1 for an outline of the phases of psychodynamic psychotherapy for panic disorder.
Although Mr. J’s initial willingness to discuss his past was encouraging, he refused to schedule more than 1 session every 4 weeks. He also began to keep the content of our sessions superficial, which caused me angst because he seemed to be withholding information and would not come more frequently. Although I was not proud of my feelings, I had to be honest with myself that I had started to dislike Mr. J.
Table 1
Psychodynamic psychotherapy for panic disorder
| Phase | Comments |
|---|---|
| Treatment of acute panic | Therapy focuses on discovering the conscious and unconscious meaning of panic symptoms |
| Treatment of panic vulnerability | Core dynamic conflicts related to panic are understood and altered. Tasks include addressing the nature of the transference and working through them |
| Termination | The therapist directly addresses patients’ difficulties with separation and independence as they emerge in treatment. After treatment, patients may be better able to manage separations, anger, and independence |
| Source: Adapted from reference 4 | |
Countertransference reactions
Countertransference is a therapist's emotional reaction to a patient. Just as patients form reactions based on past relationships brought to present, therapists develop similar reactions.5 Noting one’s countertransference provides a window into how the patient’s thoughts and actions evoke feelings in others. It also can shed light on an aspect of the doctor-patient relationship that may have gone unnoticed.2
Countertransference hatred can occur when a therapist begins to dislike a patient. Typically, patients with borderline personality disorder, masochistic tendencies, or suicidality arouse strong countertransference reactions6; however, any patient can evoke these emotions. This type of hateful patient can precipitate antitherapeutic feelings such as aversion or malice that can be a major obstacle to treatment.7 Aversion leads the therapist to withdraw from the patient, and malice can trigger cruel impulses.
Maltsberger and Buie7 identified 5 defenses therapists may use to combat countertransference hatred (Table 2). When treating Mr. J, I used several of these defenses, including projection and turning against the self to protect myself from this challenging patient. In turning against the self, I became doubtful and critical of my skills and increasingly submissive to Mr. J. Additionally, I projected this countertransference hatred onto Mr. J, focusing on the negative transference that he brought to our therapeutic encounters. On an unconscious level, I may have feared retribution from Mr. J.
I became so frustrated with Mr. J that I reduced the frequency of our sessions to once every 6 weeks, which I realized could be evidence of my feelings regarding Mr. J’s minimization and avoidant style.
Table 2
Defenses against countertransference hate
| Defense mechanism | Description |
|---|---|
| Repression | Remaining unconscious of feelings of hate; may manifest as difficulty paying attention to what the patient is saying or feeling bored or tired |
| Turning against oneself | Doubting one’s capacity to help the patient; may feel inadequate, helpless, and hopeless. May lead to giving up on the patient because the therapist feels incompetent |
| Reaction formation | Turning hatred into the opposite emotion. The therapist may be too preoccupied with being helpful or overly concerned about the patient’s welfare and comfort |
| Projection | Feeling that the patient hates the therapist, leading to feelings of dread and fear |
| Distortion of reality | Devaluing the patient and seeing the patient as a hopeless case or a dangerous person. The therapist may feel indifference, pity, or anger toward the patient |
| Source: Reference 7 | |
TREATMENT: A breakthrough
Mr. J presents with obvious unease at the first visit after we had decreased the frequency of our sessions. At this point, Mr. J opens up to me. He says he has not been truthful with me, and has had worsening depression, anhedonia, and agoraphobia over the past year. He also reveals that he has homosexual fantasies that he cannot stop, which disturb him because he says he is heterosexual. He agrees to come once a week, and reluctantly admits that he desperately needs help.
Although Mr. J only takes clonazepam and citalopram, 20 mg/d, which I prescribed after he admitted to depression and anxiety, he has hyperlipidemia and a family history of heart disease. In addition to being a musician and working at his father’s construction company, he has worked as a security guard, bounty hunter, and computer technician. His careers have been solitary in nature, and, with the exception of computer work, permitted an outlet for aggression. However, he recently started taking online college classes and wants to become a music teacher because he feels he has a lot to offer children as a result of his life experiences. His fantasy of being a teacher shows considerably less aggression, and could be a sign of psychological growth.
Mr. J is struggling financially and his home is on the verge of foreclosure. Early in treatment he told me that he stopped paying his mortgage, but demonstrated blind optimism that things would “work out.” I asked if this was a wise decision, but he seemed confident and dismissive of my concerns. Although he now struggles with this situation, I consider this healthier than his constant pseudo-happy state, and a sign of psychological development.8 Despite his financial stressors, he wants to pursue his dream of being a famous musician, and says he “could never work a 9-to-5 job in a cubicle.”
The authors’ observations
I do not think it’s a coincidence that Mr. J stopped minimizing his symptoms when we decreased the frequency of his sessions. I had viewed our sessions as unproductive and blamed Mr. J for wasting both of our time with his resistance and minimization and had begun to dislike him. I felt impotent because he had been controlling each session with long, elaborate stories that had little relevance to his panic attacks, and I could not redirect him or get him to focus on pertinent issues. It was as if I was an audience for him, and provided nothing useful. However, I was interested in these superficial stories because Mr. J was charming and engaging. He likely reenacted his relationship with his father with me. Mr. J’s superficial relationship with me caused me to dislike him, and, similar to his father, reject him. This rejection likely was damaging because I was unable to anticipate his needs, which would have been to increase—rather than decrease—the frequency of our sessions. Just like his father, I was not able to take care of him.
Mr. J is deeply conflicted about his father. He states that his father “is a monster who instills fear and intimidation into everyone around him, but he’s charismatic, and I’ll always love him.” His view of his domineering father likely developed into a castration anxiety because he was afraid of competing for his mother’s love, contributing to a muddled sexual identity. This was intensified when Mr. J was sexually abused; he may have been stimulated by the molestation, adding to his confusion. Although Mr. J has repressed the abuse and split off most of his childhood, he suffers from shame, guilt, and depression because of his ego-dystonic homosexual fantasies. Homosexuality is at odds with his self-image and contributes to his anxiety and panic attacks. He cannot adequately discharge this dangerous libidinal energy, and as he becomes more conscious of it, his anxiety intensifies.
OUTCOME: Overcoming fear
As Mr. J sits crying in my office, he says he hasn’t cried in front of another man in years. I wonder aloud what his father would think of this situation. His states that his father does not respect any type of weakness and probably would “knock his teeth in.” Overcoming this fear of opening up will be a goal of Mr. J’s treatment. His unbridled optimism borders on pathologic, and is a defense against reality.8 Additionally, his reluctance to accept that he is suffering from depression, which he perceives as a weakness, will be a struggle throughout therapy. He likely will continue to minimize his symptoms when possible, making the true depths of his illness difficult to grasp.
Related Resources
- Waska R. Using countertransference: analytic contact, projective identification, and transference phantasy states. Am J Psychother. 2008;62(4):333-351.
- Gabbard GO, Litowitz BE, Williams P. Textbook of psychoanalysis. Arlington, VA: American Psychiatric Publishing, Inc; 2011.
Drug Brand Names
- Citalopram • Celexa
- Clonazepam • Klonopin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Blos P. Son and father: before and beyond the Oedipus complex. New York NY: Free Press/Macmillan; 1985.
2. Ursano RJ, Sonnenberg SM, Lazar SG. Concise guide to psychodynamic psychotherapy. Arlington VA: American Psychiatric Publishing; 2004.
3. Akhtar S. Comprehensive dictionary of psychoanalysis. London United Kingdom: Kamac Books; 2009.
4. Busch FN, Milrod BL, Singer MB. Theory and technique in psychodynamic treatment of panic disorder. J Psychother Pract Res. 1999;8(3):234-242.
5. Freud S. The future prospects of psycho-analytic therapy. The standard edition of the complete psychological works of Sigmund Freud volume XI (1910): five lectures on psycho-analysis, Leonardo da Vinci and other works. London, United Kingdom: Hogarth Press; 1957:139–152.
6. Winnicott DW. Hate in the counter-transference. J Psychother Pract Res. 1994;3(4):348-356.
7. Maltsberger JT, Buie DH. Countertransference hate in the treatment of suicidal patients. Arch Gen Psychiatry. 1974;30(5):625-633.
8. Akhtar S. “Someday…” and “if only…” fantasies: pathological optimism and inordinate nostalgia as related forms of idealization. J Am Psychoanal Assoc. 1996;44(3):723-753.
1. Blos P. Son and father: before and beyond the Oedipus complex. New York NY: Free Press/Macmillan; 1985.
2. Ursano RJ, Sonnenberg SM, Lazar SG. Concise guide to psychodynamic psychotherapy. Arlington VA: American Psychiatric Publishing; 2004.
3. Akhtar S. Comprehensive dictionary of psychoanalysis. London United Kingdom: Kamac Books; 2009.
4. Busch FN, Milrod BL, Singer MB. Theory and technique in psychodynamic treatment of panic disorder. J Psychother Pract Res. 1999;8(3):234-242.
5. Freud S. The future prospects of psycho-analytic therapy. The standard edition of the complete psychological works of Sigmund Freud volume XI (1910): five lectures on psycho-analysis, Leonardo da Vinci and other works. London, United Kingdom: Hogarth Press; 1957:139–152.
6. Winnicott DW. Hate in the counter-transference. J Psychother Pract Res. 1994;3(4):348-356.
7. Maltsberger JT, Buie DH. Countertransference hate in the treatment of suicidal patients. Arch Gen Psychiatry. 1974;30(5):625-633.
8. Akhtar S. “Someday…” and “if only…” fantasies: pathological optimism and inordinate nostalgia as related forms of idealization. J Am Psychoanal Assoc. 1996;44(3):723-753.
When and how to use long-acting injectable antipsychotics
Discuss this article at www.facebook.com/CurrentPsychiatry
• Long-acting injectable antipsychotics (LAIs) are an important therapeutic option for patients with schizophrenia that allows clinicians to tailor pharmacotherapy to each patient’s needs.
• When selecting a specific LAI, consider class similarities and individual antipsychotic differences.
• Although some LAIs are expensive, they potentially reduce the financial burden of schizophrenia and improve quality of life.
Long-acting injectable antipsychotics (LAIs) are a pharmacotherapeutic option to help clinicians individualize schizophrenia treatment. LAIs have been available since the 1960s, starting with fluphenazine and later haloperidol; however, second-generation antipsychotics were not available in the United States until 20071,2 and more are in development (Box).3,4
Aripiprazole microsphere long-acting injectable (LAI) is a phase III investigational drug that at press time was being reviewed by the FDA. This formulation appears to be similar to risperidone LAI. The active antipsychotic differs in side effect profile and pharmacokinetics. Because the pharmaceutical science of microsphere construction allows many variations, it is not possible to determine the strengths and weaknesses of aripiprazole LAI compared with risperidone LAI microspheres at this time. The dosing intervals currently under investigation are 14 and 28 days.3
Iloperidone crystalline LAI is a phase II-III investigational drug. FDA registration documents and early publication and presentation data report that iloperidone LAI will be a crystalline salt structure pharmaceutically similar to paliperidone and olanzapine LAI formulations.4 The dosing interval under investigation is 28 days.
Up to one-half of patients with schizophrenia do not adhere to their medications.5 LAI use may mitigate relapse in acute schizophrenia that is caused by poor adherence to oral medications. LAIs may have a lower risk of dose-related adverse effects because of lower peak antipsychotic plasma levels and less variation between peak and trough plasma levels. LAIs may decrease the financial burden of schizophrenia and increase individual quality of life because patients spend fewer days hospitalized due to acute exacerbations.6
Some widely used schizophrenia treatment algorithms, such as the Harvard Schizophrenia Algorithm, neglect LAIs. Also, LAIs have not been well studied for maintenance treatment of bipolar disorder (BD) even though nonadherence is a substantial problem in these patients. Patients, families, and legal guardians may choose LAI antipsychotics over oral formulations to decrease the frequency and severity of psychotic relapse or for convenience because patients who receive LAIs do not need to take a medication every day.
Understanding the similarities and differences among LAIs7 and potential interpatient variability of each LAI allows prescribers to tailor the dosing regimen to the patient more safely and efficiently (Table).1,8-11 All LAI antipsychotic formulations rely on absorption pharmacokinetics (PK) rather than elimination PK, which generally is true for sustained-release oral formulations as well. Absorption half-life duration and absorption half-life variability are key concepts in LAI dosing.
Table
Characteristics of long-acting injectable antipsychotics
| Antipsychotic | Oral elimination half-life | Formulation | Absorption half-life | Time between injections | Clinically relevant PK/PD variabilitya | Oral overlapping taper necessary? | Loading dose possible? |
|---|---|---|---|---|---|---|---|
| Fluphenazine | 1 day | Decanoate in organic oil | 14 days | 7 to 21 days | +++ | Yes | No |
| Haloperidol | 1 day | Decanoate in organic oil | 21 days | 28 days | +/- | No | Yes |
| Olanzapine | 1.5 days | Pamoate crystalline | 30 days | 14 to 28 days | ++ | Maybe | No |
| Risperidone | 1 day | Microspheres | 5 days | 14 days | ++ | Yes | No |
| Paliperidone | 1 day | Palmitate crystalline | 45 days | 28 days | + | No | Yes |
| aMore + indicates greater variability among patients PD: pharmacodynamics; PK: pharmacokinetics Source: References 1,8-11 | |||||||
Clinical pearls
Before prescribing an LAI, check that your patient has no known contraindications to the active drug or delivery method. Peak-related adverse effects typically are not contraindications, although they may prompt you to start at a lower dose.
Ensure that your patient will have long-term outpatient access to the LAI and the entire treatment team—inpatient and outpatient—is committed to LAI treatment.
Do not rule out first-generation LAIs such as haloperidol and fluphenazine. The Clinical Antipsychotic Trials of Intervention Effectiveness study, Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study, and other published data suggest older antipsychotics are not inferior to newer medications.12,13
Verify that your patient has had an oral trial of the active drug—ideally in the last 12 months—that resulted in at least partial positive response and no serious adverse drug effects (ADEs). Oral medications’ shorter duration of action may help identify ADEs before administering an LAI.1
Discontinue the oral medication as quickly as evidence, guidance, and good clinical judgment allow. Develop a plan to transition from oral to LAI that you will follow unless the patient develops intolerable ADEs or other problems. There is no evidence to suggest that patients who receive partial LAI therapy decompensate less frequently or less severely than those who take oral medication.
If antipsychotic polypharmacy is necessary, document your rationale.
In patients who are naïve to a specific LAI dosage form, ensure that the first dose does not exceed FDA and evidence-based guidelines for the initial dose (eg, 100 mg intramuscular [IM] for haloperidol decanoate).1
Consider a loading dose strategy to minimize the time a patient has to take an oral and LAI antipsychotic combination.14
Ensure that the total volume injected intramuscularly is not >3 ml per injection site per dose.
Use the recommended injection technique for the particular LAI (eg, Z-tract).1,15
Individualize the dose and dosing interval based on patient response, peak-related adverse effects (time to peak is approximately 5 half-lives for most drugs), and possible reduced symptom control at the end of the dosing interval.8
If your patient does not respond as expected, taking an antipsychotic plasma level to assess drug metabolism and other PK factors and characteristics may be useful.
LAI options
Fluphenazine decanoate is an older, inexpensive LAI with considerable interpatient variability in absorption rate and peak effects, and a relatively short duration of action. Dosing every 7 days may be necessary to avoid peak plasma level adverse effects or symptom recurrence. Variable PK make it difficult to accurately calculate an empiric conversion dose from oral to LAI; therefore, start at the low end (eg, 1.2 to 1.6 times the total daily oral dose) or 12.5 or 25 mg for the initial IM fluphenazine decanoate dose. A short overlap period—usually 1 to 2 weeks—may be necessary. Successful subcutaneous administration is possible.2
Haloperidol decanoate. A 28-day dosing interval is effective for most patients. It is possible to administer a loading dose so that no overlapping taper is required. My team has had good results using an initial loading dose 15 to 20 times the effective oral dose and a second dose 28 days later of 10 times the oral daily maintenance dose, with the same dose every month thereafter. If a patient is receiving his or her first haloperidol decanoate injection, the initial dose should not exceed 100 mg. The remainder of the loading dose may be administered 3 to 7 days later if no adverse effects occur. Similar to fluphenazine decanoate, haloperidol decanoate is relatively inexpensive. When considering giving a haloperidol decanoate loading dose >400 mg or a maintenance dose >200 mg every 28 days, carefully document the rationale (eg, rapid metabolism).16
Olanzapine pamoate. Clinicians who administer olanzapine pamoate must enroll in a national registry that documents the incidence of rare but serious ADEs, particularly hypotension, orthostatis, and post-injection delirium/sedation syndrome (0.1% incidence) at every injection, not just for drug-naïve patients. Patients should be observed for 3 hours after every dose and oral medication overlap may be necessary in some cases.10 Similar to clozapine, these monitoring difficulties and the expense may have inhibited olanzapine LAI use, even in patients who are likely to benefit.
Risperidone microspheres. This agent has been evolutionary, if not revolutionary, in schizophrenia treatment and data on its efficacy for BD will be available soon. Its 2-week dosing interval, necessity of oral overlap, and anecdotal reports of “dose dumping” possibly because of fragility of the microsphere formulation suggest the need for an improved version, which was addressed by the introduction of paliperidone palmitate.10,17,18
Paliperidone palmitate has a 28-day dosing interval. No overlapping oral taper is necessary. Details of a week-long, 2-dose loading dose strategy is provided in the package insert.11 It may be safe to use a more aggressive loading dose strategy.15,19
Related Resources
- Rothschild AJ. The evidence-based guide to antipsychotic medications. Arlington, VA: American Psychiatric Publishing, Inc.; 2010.
- Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683-697.
Drug Brand Names
- Aripiprazole • Abilify
- Fluphenazine deconoate • Prolixin Deconoate
- Haloperidol deconoate • Haldol Deconoate
- Iloperidone • Fanapt
- Olanzapine pamoate • Zyprexa Relprevv
- Paliperidone palmitate • Invega Sustenna
- Risperidone • Risperdal Consta
Disclosures
Dr. Kennedy receives grant or research support from Janssen and Johnson and Johnson.
1. Haloperidol decanoate [package insert]. Irvine CA: Teva Parenteral Medicines, Inc; 2009.
2. Fluphenazine decanoate [package insert]. Schaumburg IL: APP Pharmaceuticals, LLC; 2010.
3. A study of ALKS 9072 in subjects with chronic stable schizophrenia. http://clinicaltrials.gov/ct2/show/NCT01493726. Published December 12 2011. Accessed December 16, 2011.
4. Hill CL, Phadke D, Boyce KM. Four-week iloperidone depot injectable: safety and pharmacokinetic profile in patients with schizophrenia and schizoaffective disorder. Poster presented at: 161st annual meeting of the American Psychiatric Association; May 3-8 2008; Washington, DC.
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892-909.
6. Keith SJ, Kane JM, Turner M, et al. Academic highlights: guidelines for the use of long-acting injectable atypical antipsychotics. J Clin Psychiatry. 2004;65(1):120-131.
7. McEvoy JP. Risks versus benefits of different types of long-acting injectable antipsychotics. J Clin Psychiatry. 2006;67 (suppl 5):15-18.
8. Gitlin M, Midha KK, Fogelson D, et al. Persistence of fluphenazine in plasma after decanoate withdrawal. J Clin Psychopharmacol. 1988;8(1):53-56.
9. Wilson WH. A visual guide to expected blood levels of long-acting injectable risperidone in clinical practice. J Psychiatr Pract. 2004;10(6):393-401.
10. Zyprexa Relprevv [package insert]. Indianapolis IN: Eli Lilly and Company; 2011.
11. Invega Sustenna [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
12. Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
13. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia. Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63(10):1079-1087.
14. Wei FC, Jann MW, Lin HN, et al. A practical loading dose method for converting schizophrenic patients from oral to depot haloperidol therapy. J Clin Psychiatry. 1996;57(7):298-302.
15. Samtani MN, Vermeulen A, Stuyckens K. Population pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. 2009;48(9):585-600.
16. Kapur SJ, Zipursky R, Jones C, et al. Relationship between dopamine D2 occupancy, clinical response and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. 2000;157(4):514-520.
17. Deeks ED. Risperidone long-acting injection: in bipolar I disorder. Drugs. 2010;70(8):1001-1012.
18. Risperdal Consta [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
19. Samtani MN, Haskins JT, Alphs L, et al. Initiation dosing of deltoid intramuscular paliperidone palmitate in schizophrenia – pharmacokinetic rationale based on modeling and simulation. Poster presented at: 49th annual NCDEU meeting; June 29-July 2, 2009; Hollywood, FL.
William Klugh Kennedy, PharmD, BCPP, FASHP
Dr. Kennedy is Clinical Associate Professor of Pharmacy Practice and Psychiatry, Mercer University, Memorial University Medical Center, Savannah, GA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
William Klugh Kennedy, PharmD, BCPP, FASHP
Dr. Kennedy is Clinical Associate Professor of Pharmacy Practice and Psychiatry, Mercer University, Memorial University Medical Center, Savannah, GA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
William Klugh Kennedy, PharmD, BCPP, FASHP
Dr. Kennedy is Clinical Associate Professor of Pharmacy Practice and Psychiatry, Mercer University, Memorial University Medical Center, Savannah, GA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Discuss this article at www.facebook.com/CurrentPsychiatry
• Long-acting injectable antipsychotics (LAIs) are an important therapeutic option for patients with schizophrenia that allows clinicians to tailor pharmacotherapy to each patient’s needs.
• When selecting a specific LAI, consider class similarities and individual antipsychotic differences.
• Although some LAIs are expensive, they potentially reduce the financial burden of schizophrenia and improve quality of life.
Long-acting injectable antipsychotics (LAIs) are a pharmacotherapeutic option to help clinicians individualize schizophrenia treatment. LAIs have been available since the 1960s, starting with fluphenazine and later haloperidol; however, second-generation antipsychotics were not available in the United States until 20071,2 and more are in development (Box).3,4
Aripiprazole microsphere long-acting injectable (LAI) is a phase III investigational drug that at press time was being reviewed by the FDA. This formulation appears to be similar to risperidone LAI. The active antipsychotic differs in side effect profile and pharmacokinetics. Because the pharmaceutical science of microsphere construction allows many variations, it is not possible to determine the strengths and weaknesses of aripiprazole LAI compared with risperidone LAI microspheres at this time. The dosing intervals currently under investigation are 14 and 28 days.3
Iloperidone crystalline LAI is a phase II-III investigational drug. FDA registration documents and early publication and presentation data report that iloperidone LAI will be a crystalline salt structure pharmaceutically similar to paliperidone and olanzapine LAI formulations.4 The dosing interval under investigation is 28 days.
Up to one-half of patients with schizophrenia do not adhere to their medications.5 LAI use may mitigate relapse in acute schizophrenia that is caused by poor adherence to oral medications. LAIs may have a lower risk of dose-related adverse effects because of lower peak antipsychotic plasma levels and less variation between peak and trough plasma levels. LAIs may decrease the financial burden of schizophrenia and increase individual quality of life because patients spend fewer days hospitalized due to acute exacerbations.6
Some widely used schizophrenia treatment algorithms, such as the Harvard Schizophrenia Algorithm, neglect LAIs. Also, LAIs have not been well studied for maintenance treatment of bipolar disorder (BD) even though nonadherence is a substantial problem in these patients. Patients, families, and legal guardians may choose LAI antipsychotics over oral formulations to decrease the frequency and severity of psychotic relapse or for convenience because patients who receive LAIs do not need to take a medication every day.
Understanding the similarities and differences among LAIs7 and potential interpatient variability of each LAI allows prescribers to tailor the dosing regimen to the patient more safely and efficiently (Table).1,8-11 All LAI antipsychotic formulations rely on absorption pharmacokinetics (PK) rather than elimination PK, which generally is true for sustained-release oral formulations as well. Absorption half-life duration and absorption half-life variability are key concepts in LAI dosing.
Table
Characteristics of long-acting injectable antipsychotics
| Antipsychotic | Oral elimination half-life | Formulation | Absorption half-life | Time between injections | Clinically relevant PK/PD variabilitya | Oral overlapping taper necessary? | Loading dose possible? |
|---|---|---|---|---|---|---|---|
| Fluphenazine | 1 day | Decanoate in organic oil | 14 days | 7 to 21 days | +++ | Yes | No |
| Haloperidol | 1 day | Decanoate in organic oil | 21 days | 28 days | +/- | No | Yes |
| Olanzapine | 1.5 days | Pamoate crystalline | 30 days | 14 to 28 days | ++ | Maybe | No |
| Risperidone | 1 day | Microspheres | 5 days | 14 days | ++ | Yes | No |
| Paliperidone | 1 day | Palmitate crystalline | 45 days | 28 days | + | No | Yes |
| aMore + indicates greater variability among patients PD: pharmacodynamics; PK: pharmacokinetics Source: References 1,8-11 | |||||||
Clinical pearls
Before prescribing an LAI, check that your patient has no known contraindications to the active drug or delivery method. Peak-related adverse effects typically are not contraindications, although they may prompt you to start at a lower dose.
Ensure that your patient will have long-term outpatient access to the LAI and the entire treatment team—inpatient and outpatient—is committed to LAI treatment.
Do not rule out first-generation LAIs such as haloperidol and fluphenazine. The Clinical Antipsychotic Trials of Intervention Effectiveness study, Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study, and other published data suggest older antipsychotics are not inferior to newer medications.12,13
Verify that your patient has had an oral trial of the active drug—ideally in the last 12 months—that resulted in at least partial positive response and no serious adverse drug effects (ADEs). Oral medications’ shorter duration of action may help identify ADEs before administering an LAI.1
Discontinue the oral medication as quickly as evidence, guidance, and good clinical judgment allow. Develop a plan to transition from oral to LAI that you will follow unless the patient develops intolerable ADEs or other problems. There is no evidence to suggest that patients who receive partial LAI therapy decompensate less frequently or less severely than those who take oral medication.
If antipsychotic polypharmacy is necessary, document your rationale.
In patients who are naïve to a specific LAI dosage form, ensure that the first dose does not exceed FDA and evidence-based guidelines for the initial dose (eg, 100 mg intramuscular [IM] for haloperidol decanoate).1
Consider a loading dose strategy to minimize the time a patient has to take an oral and LAI antipsychotic combination.14
Ensure that the total volume injected intramuscularly is not >3 ml per injection site per dose.
Use the recommended injection technique for the particular LAI (eg, Z-tract).1,15
Individualize the dose and dosing interval based on patient response, peak-related adverse effects (time to peak is approximately 5 half-lives for most drugs), and possible reduced symptom control at the end of the dosing interval.8
If your patient does not respond as expected, taking an antipsychotic plasma level to assess drug metabolism and other PK factors and characteristics may be useful.
LAI options
Fluphenazine decanoate is an older, inexpensive LAI with considerable interpatient variability in absorption rate and peak effects, and a relatively short duration of action. Dosing every 7 days may be necessary to avoid peak plasma level adverse effects or symptom recurrence. Variable PK make it difficult to accurately calculate an empiric conversion dose from oral to LAI; therefore, start at the low end (eg, 1.2 to 1.6 times the total daily oral dose) or 12.5 or 25 mg for the initial IM fluphenazine decanoate dose. A short overlap period—usually 1 to 2 weeks—may be necessary. Successful subcutaneous administration is possible.2
Haloperidol decanoate. A 28-day dosing interval is effective for most patients. It is possible to administer a loading dose so that no overlapping taper is required. My team has had good results using an initial loading dose 15 to 20 times the effective oral dose and a second dose 28 days later of 10 times the oral daily maintenance dose, with the same dose every month thereafter. If a patient is receiving his or her first haloperidol decanoate injection, the initial dose should not exceed 100 mg. The remainder of the loading dose may be administered 3 to 7 days later if no adverse effects occur. Similar to fluphenazine decanoate, haloperidol decanoate is relatively inexpensive. When considering giving a haloperidol decanoate loading dose >400 mg or a maintenance dose >200 mg every 28 days, carefully document the rationale (eg, rapid metabolism).16
Olanzapine pamoate. Clinicians who administer olanzapine pamoate must enroll in a national registry that documents the incidence of rare but serious ADEs, particularly hypotension, orthostatis, and post-injection delirium/sedation syndrome (0.1% incidence) at every injection, not just for drug-naïve patients. Patients should be observed for 3 hours after every dose and oral medication overlap may be necessary in some cases.10 Similar to clozapine, these monitoring difficulties and the expense may have inhibited olanzapine LAI use, even in patients who are likely to benefit.
Risperidone microspheres. This agent has been evolutionary, if not revolutionary, in schizophrenia treatment and data on its efficacy for BD will be available soon. Its 2-week dosing interval, necessity of oral overlap, and anecdotal reports of “dose dumping” possibly because of fragility of the microsphere formulation suggest the need for an improved version, which was addressed by the introduction of paliperidone palmitate.10,17,18
Paliperidone palmitate has a 28-day dosing interval. No overlapping oral taper is necessary. Details of a week-long, 2-dose loading dose strategy is provided in the package insert.11 It may be safe to use a more aggressive loading dose strategy.15,19
Related Resources
- Rothschild AJ. The evidence-based guide to antipsychotic medications. Arlington, VA: American Psychiatric Publishing, Inc.; 2010.
- Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683-697.
Drug Brand Names
- Aripiprazole • Abilify
- Fluphenazine deconoate • Prolixin Deconoate
- Haloperidol deconoate • Haldol Deconoate
- Iloperidone • Fanapt
- Olanzapine pamoate • Zyprexa Relprevv
- Paliperidone palmitate • Invega Sustenna
- Risperidone • Risperdal Consta
Disclosures
Dr. Kennedy receives grant or research support from Janssen and Johnson and Johnson.
Discuss this article at www.facebook.com/CurrentPsychiatry
• Long-acting injectable antipsychotics (LAIs) are an important therapeutic option for patients with schizophrenia that allows clinicians to tailor pharmacotherapy to each patient’s needs.
• When selecting a specific LAI, consider class similarities and individual antipsychotic differences.
• Although some LAIs are expensive, they potentially reduce the financial burden of schizophrenia and improve quality of life.
Long-acting injectable antipsychotics (LAIs) are a pharmacotherapeutic option to help clinicians individualize schizophrenia treatment. LAIs have been available since the 1960s, starting with fluphenazine and later haloperidol; however, second-generation antipsychotics were not available in the United States until 20071,2 and more are in development (Box).3,4
Aripiprazole microsphere long-acting injectable (LAI) is a phase III investigational drug that at press time was being reviewed by the FDA. This formulation appears to be similar to risperidone LAI. The active antipsychotic differs in side effect profile and pharmacokinetics. Because the pharmaceutical science of microsphere construction allows many variations, it is not possible to determine the strengths and weaknesses of aripiprazole LAI compared with risperidone LAI microspheres at this time. The dosing intervals currently under investigation are 14 and 28 days.3
Iloperidone crystalline LAI is a phase II-III investigational drug. FDA registration documents and early publication and presentation data report that iloperidone LAI will be a crystalline salt structure pharmaceutically similar to paliperidone and olanzapine LAI formulations.4 The dosing interval under investigation is 28 days.
Up to one-half of patients with schizophrenia do not adhere to their medications.5 LAI use may mitigate relapse in acute schizophrenia that is caused by poor adherence to oral medications. LAIs may have a lower risk of dose-related adverse effects because of lower peak antipsychotic plasma levels and less variation between peak and trough plasma levels. LAIs may decrease the financial burden of schizophrenia and increase individual quality of life because patients spend fewer days hospitalized due to acute exacerbations.6
Some widely used schizophrenia treatment algorithms, such as the Harvard Schizophrenia Algorithm, neglect LAIs. Also, LAIs have not been well studied for maintenance treatment of bipolar disorder (BD) even though nonadherence is a substantial problem in these patients. Patients, families, and legal guardians may choose LAI antipsychotics over oral formulations to decrease the frequency and severity of psychotic relapse or for convenience because patients who receive LAIs do not need to take a medication every day.
Understanding the similarities and differences among LAIs7 and potential interpatient variability of each LAI allows prescribers to tailor the dosing regimen to the patient more safely and efficiently (Table).1,8-11 All LAI antipsychotic formulations rely on absorption pharmacokinetics (PK) rather than elimination PK, which generally is true for sustained-release oral formulations as well. Absorption half-life duration and absorption half-life variability are key concepts in LAI dosing.
Table
Characteristics of long-acting injectable antipsychotics
| Antipsychotic | Oral elimination half-life | Formulation | Absorption half-life | Time between injections | Clinically relevant PK/PD variabilitya | Oral overlapping taper necessary? | Loading dose possible? |
|---|---|---|---|---|---|---|---|
| Fluphenazine | 1 day | Decanoate in organic oil | 14 days | 7 to 21 days | +++ | Yes | No |
| Haloperidol | 1 day | Decanoate in organic oil | 21 days | 28 days | +/- | No | Yes |
| Olanzapine | 1.5 days | Pamoate crystalline | 30 days | 14 to 28 days | ++ | Maybe | No |
| Risperidone | 1 day | Microspheres | 5 days | 14 days | ++ | Yes | No |
| Paliperidone | 1 day | Palmitate crystalline | 45 days | 28 days | + | No | Yes |
| aMore + indicates greater variability among patients PD: pharmacodynamics; PK: pharmacokinetics Source: References 1,8-11 | |||||||
Clinical pearls
Before prescribing an LAI, check that your patient has no known contraindications to the active drug or delivery method. Peak-related adverse effects typically are not contraindications, although they may prompt you to start at a lower dose.
Ensure that your patient will have long-term outpatient access to the LAI and the entire treatment team—inpatient and outpatient—is committed to LAI treatment.
Do not rule out first-generation LAIs such as haloperidol and fluphenazine. The Clinical Antipsychotic Trials of Intervention Effectiveness study, Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study, and other published data suggest older antipsychotics are not inferior to newer medications.12,13
Verify that your patient has had an oral trial of the active drug—ideally in the last 12 months—that resulted in at least partial positive response and no serious adverse drug effects (ADEs). Oral medications’ shorter duration of action may help identify ADEs before administering an LAI.1
Discontinue the oral medication as quickly as evidence, guidance, and good clinical judgment allow. Develop a plan to transition from oral to LAI that you will follow unless the patient develops intolerable ADEs or other problems. There is no evidence to suggest that patients who receive partial LAI therapy decompensate less frequently or less severely than those who take oral medication.
If antipsychotic polypharmacy is necessary, document your rationale.
In patients who are naïve to a specific LAI dosage form, ensure that the first dose does not exceed FDA and evidence-based guidelines for the initial dose (eg, 100 mg intramuscular [IM] for haloperidol decanoate).1
Consider a loading dose strategy to minimize the time a patient has to take an oral and LAI antipsychotic combination.14
Ensure that the total volume injected intramuscularly is not >3 ml per injection site per dose.
Use the recommended injection technique for the particular LAI (eg, Z-tract).1,15
Individualize the dose and dosing interval based on patient response, peak-related adverse effects (time to peak is approximately 5 half-lives for most drugs), and possible reduced symptom control at the end of the dosing interval.8
If your patient does not respond as expected, taking an antipsychotic plasma level to assess drug metabolism and other PK factors and characteristics may be useful.
LAI options
Fluphenazine decanoate is an older, inexpensive LAI with considerable interpatient variability in absorption rate and peak effects, and a relatively short duration of action. Dosing every 7 days may be necessary to avoid peak plasma level adverse effects or symptom recurrence. Variable PK make it difficult to accurately calculate an empiric conversion dose from oral to LAI; therefore, start at the low end (eg, 1.2 to 1.6 times the total daily oral dose) or 12.5 or 25 mg for the initial IM fluphenazine decanoate dose. A short overlap period—usually 1 to 2 weeks—may be necessary. Successful subcutaneous administration is possible.2
Haloperidol decanoate. A 28-day dosing interval is effective for most patients. It is possible to administer a loading dose so that no overlapping taper is required. My team has had good results using an initial loading dose 15 to 20 times the effective oral dose and a second dose 28 days later of 10 times the oral daily maintenance dose, with the same dose every month thereafter. If a patient is receiving his or her first haloperidol decanoate injection, the initial dose should not exceed 100 mg. The remainder of the loading dose may be administered 3 to 7 days later if no adverse effects occur. Similar to fluphenazine decanoate, haloperidol decanoate is relatively inexpensive. When considering giving a haloperidol decanoate loading dose >400 mg or a maintenance dose >200 mg every 28 days, carefully document the rationale (eg, rapid metabolism).16
Olanzapine pamoate. Clinicians who administer olanzapine pamoate must enroll in a national registry that documents the incidence of rare but serious ADEs, particularly hypotension, orthostatis, and post-injection delirium/sedation syndrome (0.1% incidence) at every injection, not just for drug-naïve patients. Patients should be observed for 3 hours after every dose and oral medication overlap may be necessary in some cases.10 Similar to clozapine, these monitoring difficulties and the expense may have inhibited olanzapine LAI use, even in patients who are likely to benefit.
Risperidone microspheres. This agent has been evolutionary, if not revolutionary, in schizophrenia treatment and data on its efficacy for BD will be available soon. Its 2-week dosing interval, necessity of oral overlap, and anecdotal reports of “dose dumping” possibly because of fragility of the microsphere formulation suggest the need for an improved version, which was addressed by the introduction of paliperidone palmitate.10,17,18
Paliperidone palmitate has a 28-day dosing interval. No overlapping oral taper is necessary. Details of a week-long, 2-dose loading dose strategy is provided in the package insert.11 It may be safe to use a more aggressive loading dose strategy.15,19
Related Resources
- Rothschild AJ. The evidence-based guide to antipsychotic medications. Arlington, VA: American Psychiatric Publishing, Inc.; 2010.
- Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683-697.
Drug Brand Names
- Aripiprazole • Abilify
- Fluphenazine deconoate • Prolixin Deconoate
- Haloperidol deconoate • Haldol Deconoate
- Iloperidone • Fanapt
- Olanzapine pamoate • Zyprexa Relprevv
- Paliperidone palmitate • Invega Sustenna
- Risperidone • Risperdal Consta
Disclosures
Dr. Kennedy receives grant or research support from Janssen and Johnson and Johnson.
1. Haloperidol decanoate [package insert]. Irvine CA: Teva Parenteral Medicines, Inc; 2009.
2. Fluphenazine decanoate [package insert]. Schaumburg IL: APP Pharmaceuticals, LLC; 2010.
3. A study of ALKS 9072 in subjects with chronic stable schizophrenia. http://clinicaltrials.gov/ct2/show/NCT01493726. Published December 12 2011. Accessed December 16, 2011.
4. Hill CL, Phadke D, Boyce KM. Four-week iloperidone depot injectable: safety and pharmacokinetic profile in patients with schizophrenia and schizoaffective disorder. Poster presented at: 161st annual meeting of the American Psychiatric Association; May 3-8 2008; Washington, DC.
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892-909.
6. Keith SJ, Kane JM, Turner M, et al. Academic highlights: guidelines for the use of long-acting injectable atypical antipsychotics. J Clin Psychiatry. 2004;65(1):120-131.
7. McEvoy JP. Risks versus benefits of different types of long-acting injectable antipsychotics. J Clin Psychiatry. 2006;67 (suppl 5):15-18.
8. Gitlin M, Midha KK, Fogelson D, et al. Persistence of fluphenazine in plasma after decanoate withdrawal. J Clin Psychopharmacol. 1988;8(1):53-56.
9. Wilson WH. A visual guide to expected blood levels of long-acting injectable risperidone in clinical practice. J Psychiatr Pract. 2004;10(6):393-401.
10. Zyprexa Relprevv [package insert]. Indianapolis IN: Eli Lilly and Company; 2011.
11. Invega Sustenna [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
12. Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
13. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia. Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63(10):1079-1087.
14. Wei FC, Jann MW, Lin HN, et al. A practical loading dose method for converting schizophrenic patients from oral to depot haloperidol therapy. J Clin Psychiatry. 1996;57(7):298-302.
15. Samtani MN, Vermeulen A, Stuyckens K. Population pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. 2009;48(9):585-600.
16. Kapur SJ, Zipursky R, Jones C, et al. Relationship between dopamine D2 occupancy, clinical response and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. 2000;157(4):514-520.
17. Deeks ED. Risperidone long-acting injection: in bipolar I disorder. Drugs. 2010;70(8):1001-1012.
18. Risperdal Consta [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
19. Samtani MN, Haskins JT, Alphs L, et al. Initiation dosing of deltoid intramuscular paliperidone palmitate in schizophrenia – pharmacokinetic rationale based on modeling and simulation. Poster presented at: 49th annual NCDEU meeting; June 29-July 2, 2009; Hollywood, FL.
1. Haloperidol decanoate [package insert]. Irvine CA: Teva Parenteral Medicines, Inc; 2009.
2. Fluphenazine decanoate [package insert]. Schaumburg IL: APP Pharmaceuticals, LLC; 2010.
3. A study of ALKS 9072 in subjects with chronic stable schizophrenia. http://clinicaltrials.gov/ct2/show/NCT01493726. Published December 12 2011. Accessed December 16, 2011.
4. Hill CL, Phadke D, Boyce KM. Four-week iloperidone depot injectable: safety and pharmacokinetic profile in patients with schizophrenia and schizoaffective disorder. Poster presented at: 161st annual meeting of the American Psychiatric Association; May 3-8 2008; Washington, DC.
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892-909.
6. Keith SJ, Kane JM, Turner M, et al. Academic highlights: guidelines for the use of long-acting injectable atypical antipsychotics. J Clin Psychiatry. 2004;65(1):120-131.
7. McEvoy JP. Risks versus benefits of different types of long-acting injectable antipsychotics. J Clin Psychiatry. 2006;67 (suppl 5):15-18.
8. Gitlin M, Midha KK, Fogelson D, et al. Persistence of fluphenazine in plasma after decanoate withdrawal. J Clin Psychopharmacol. 1988;8(1):53-56.
9. Wilson WH. A visual guide to expected blood levels of long-acting injectable risperidone in clinical practice. J Psychiatr Pract. 2004;10(6):393-401.
10. Zyprexa Relprevv [package insert]. Indianapolis IN: Eli Lilly and Company; 2011.
11. Invega Sustenna [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
12. Lieberman JA, Stroup TS, McEvoy JP, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
13. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia. Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63(10):1079-1087.
14. Wei FC, Jann MW, Lin HN, et al. A practical loading dose method for converting schizophrenic patients from oral to depot haloperidol therapy. J Clin Psychiatry. 1996;57(7):298-302.
15. Samtani MN, Vermeulen A, Stuyckens K. Population pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. 2009;48(9):585-600.
16. Kapur SJ, Zipursky R, Jones C, et al. Relationship between dopamine D2 occupancy, clinical response and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. 2000;157(4):514-520.
17. Deeks ED. Risperidone long-acting injection: in bipolar I disorder. Drugs. 2010;70(8):1001-1012.
18. Risperdal Consta [package insert]. Titusville NJ: Janssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc; 2011.
19. Samtani MN, Haskins JT, Alphs L, et al. Initiation dosing of deltoid intramuscular paliperidone palmitate in schizophrenia – pharmacokinetic rationale based on modeling and simulation. Poster presented at: 49th annual NCDEU meeting; June 29-July 2, 2009; Hollywood, FL.
A perplexing case of altered mental status
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Agitated and paranoid
Mr. E, age 55, presents to the emergency department (ED) with a 2-week history of altered mental status (AMS). His wife reports, “He was normal one day and the next day he was not.” Mr. E also presents with sleep disturbance, decreased appetite and speech, and a 20-lb weight loss. His family reports no recent stressors or head trauma. Mr. E is agitated in the ED and receives a single dose of IV haloperidol, 5 mg. He exhibits paranoia and is afraid to get a CT scan. The medical team attempts a lumbar puncture (LP), but Mr. E does not cooperate.
His laboratory values are: potassium, 3.0 mEq/L; creatinine, 1.60 mg/dL; calcium, 10.6 mg/dL; thyroid-stimulating hormone, 0.177 IU/L; vitamin B12, >1500 pg/mL; folate, >20 ng/mL; and creatine kinase, 281 U/L. Urine drug screen is positive for benzodiazepines and opiates, neither of which was prescribed, and blood alcohol is negative.
Mr. E is admitted for further workup of AMS. His daughter-in-law states that Mr. E is an alcoholic and she is concerned that he may have mixed drugs and alcohol. The medical service starts Mr. E on empiric antimicrobials—vancomycin, ceftriaxone, and acyclovir—because of his AMS, and performs an LP to rule out intracranial pathology. His LP results are unremarkable.
Mr. E appears to be confused during psychiatric evaluation. He requests to be “hypnotized on a helicopter to find out what is wrong with me.” His wife states that Mr. E drank vodka daily but decreased his alcohol consumption after surgery 5 months ago. Before his current admission, he was drinking approximately half a glass of vodka every few days, according to his wife. Mr. E says he has no prior psychiatric admissions. During the mental status exam, his eye contact is poor, with latency of response to questions, thought blocking, and psychomotor retardation. He is alert, oriented to time, place, and person, and cooperative. He cannot concentrate or focus during the interview. He denies suicidal or homicidal ideation.
The authors’ observations
Mr. E appeared to be delirious, as evidenced by the sudden onset of waxing and waning changes in consciousness, attention deficits, and cognition. He also had a history of daily alcohol use and decreased his alcohol intake after a surgery 5 months ago, which puts him at risk for Wernicke’s encephalopathy.1-3 The type of surgery and whether he received adequate thiamine supplementation at that time was unclear. Because Mr. E is older, he has a higher risk of mortality and morbidity from delirium.4,5 We started Mr. E on quetiapine, 50 mg/d, for delirium and an IV lorazepam taper, starting at 2 mg every 8 hours, because the extent of his alcohol and benzodiazepine use was unclear—we weren’t sure how forthcoming he was about his alcohol use. He received IV thiamine supplementation followed by oral thiamine, 100 mg/d.
The authors’ recommendations
We requested a neurology consult, EEG, CSF cultures, and brain MRI (Table 1).6 EEG, chest radiography, thyroid scan, and CT scan were normal and MRI showed no acute intracranial process. However, there was a redemonstration of increased T1 signal seen within the bilateral basal ganglia and relative diminutive appearance to the bilateral mamillary bodies, which suggests possible liver disease and/or alcohol abuse. These findings were unchanged from an MRI Mr. E received 10 years ago, were consistent with his history of alcohol abuse, and may indicate an underlying predisposition to delirium. A CT scan of the abdomen showed hepatic cirrhosis with prominent, tortuous vessels of the upper abdomen, subtle ill-defined hypodensity of the anterior aspect of the liver, and an enlarged spleen.
Mr. E’s mental functioning did not improve with quetiapine and lorazepam. Further evaluation revealed a negative human immunodeficiency virus test and normal heavy metals, ammonia, ceruloplasmin, and thiamine. We suspected limbic encephalitis because of Mr. E’s memory problems and behavioral and psychiatric manifestations,7 but CSF was unremarkable and limbic encephalitis workup of CSF and paraneoplastic antibody panel were negative.
Mr. E’s primary care physician stated that at an appointment 1 month ago, Mr. E was alert, oriented, and conversational with normal thought processing. At that time he had presented with rectal bleeding, occult blood in his stool, and an unintentional 25-lb weight loss over 2 months. It was not clear if his weight loss was caused by poor nutrition—which is common among chronic alcoholics—or an occult disease process.
After 10 days, Mr. E was discharged home from the medicine service with no clear cause of his AMS.
Table 1
Suggested workup for altered mental status
| Complete blood count, basic metabolic profile, creatine kinase |
| Thyroid-stimulating hormone, thyroid scan |
| Vitamin B12, folate, thiamine |
| Blood alcohol, urine drug screen |
| Urine analysis and cultures |
| Lumbar puncture—CSF staining and cultures |
| Chest radiography |
| CT and MRI scan of brain |
| Electroencephalography |
| Neuropsychiatric testing |
| CSF: cerebrospinal fluid Source: Reference 6 |
EVALUATION: Worsening behavior
One week later, Mr. E presents to the ED with continued AMS and worsening behavior at home. Two days ago, he attempted to strangle his dog and cut himself with a knife. His paranoia was worsening and his oral intake continued to decrease. In the ED, Mr. E does not want a chest radiograph because, “I don’t like radiation contaminating my body”; his family stated that he had been suspicious of radiography all of his life. He receives empiric ceftriaxone because of a possible urinary tract infection. Urine culture is positive for Pseudomonas aeruginosa and he is switched to ciprofloxacin. Mr. E is admitted for further workup.
Mr. E’s mother states, “I think this change in behavior is related to my son drinking alcohol for 20 years. This is exactly how he acted when he was on drugs. I think he is having a flashback.” She also reports her son purchased multiple chemicals—the details of which are unclear—that he left lying around the house.
His wife says that after discharge a week ago, Mr. E was stable for 1 or 2 days and then “he started going downhill.” He became more paranoid and he started talking about cameras watching him in his house. Mr. E took quetiapine, 50 mg/d, for a few days, then refused because he thought there was something in the medication. Mr. E’s family feels that at times he is responding to internal stimuli. He makes statements about his DNA being changed and reports that he has 2 wives and the wife in the room was not the real one, which suggests Capgras syndrome. His wife provides a home medication list that includes vitamin B complex, vitamins B12, E, and C, a multivitamin, zinc, magnesium, fish oil, garlic, calcium, glucosamine, chondroitin, herbal supplements, and gingko. The psychiatry team recommends switching from quetiapine to olanzapine, 15 mg/d, because Mr. E was paranoid about taking quetiapine.
We determine that Mr. E does not have medical decision-making capacity.
Because his symptoms do not improve, Mr. E is transferred to the psychiatric intensive care unit. His mental status shows little change while there. Neuropsychiatric testing shows only “cognitive deficits.” He shows signs consistent with neurologic dysfunction in terms of stimulus-bound responding and perseveration, which is compatible with the bilateral basal ganglia lesion seen on MRI. However, some of his behaviors suggest psychiatric and motivationally driven or manipulative etiology. During this testing he was difficult to evaluate and needed to be convinced to engage. At times he was illogical and at other times he showed good focus and recall. It is difficult to draw more definitive conclusions and Mr. E is discharged home with minor improvement in his symptoms. He didn’t attend follow-up appointments. During a courtesy call a few months after his admission, his wife revealed that Mr. E had died after shooting himself. It is unclear if it was an accident or suicide.
The authors’ observations
Mr. E’s diagnosis remains unclear (for a summary of his clinical course, see Table 2). Although his initial presentation was consistent with delirium, the lack of an identifiable medical cause, prolonged time course, and lack of improvement with dopamine blocking agents suggest additional diagnoses such as Wernicke-Korsakoff syndrome, rapidly progressive dementia, or a substance-induced disorder. He displayed paranoia and bizarre delusions, which would suggest a thought disorder. However, he also had a history of substance use. A few months after we saw Mr. E, “bath salt” (methylenedioxypyrovalerone) abuse gained national attention. Patients with bath salt intoxication present with confusion, paranoia, and behavioral disturbances as well as a prolonged course.8
Mr. E’s CT and MRI scans, history of alcohol use, and cirrhosis also point to Wernicke-Korsakoff syndrome as an underlying diagnosis. It is unclear whether Mr. E experienced alcohol withdrawal and IV glucose without adequate thiamine replacement during a prior surgery. However, MRI findings were unchanged from a previous study 10 years ago.
It is puzzling whether Mr. E’s AMS was a first psychotic break, a result of drug and alcohol use, rapidly progressing dementia, or another neurologic problem that we have not identified. Our tentative diagnosis was Wernicke-Korsakoff syndrome because of his history of alcohol use and imaging findings.
Although we used a multidisciplinary team approach that included psychiatry, internal medicine, neurology, neuropsychology, and an aggressive and thorough workup, we could not establish a definitive diagnosis. Unsolved cases such as this can leave patients and clinicians frustrated and may lead to unfavorable outcomes. Additional resources such as a telephone call after the first missed appointment may have been warranted.
Table 2
Mr. E’s clinical course
| Symptoms | Treatment | |
|---|---|---|
| First ED visit | Agitation Confusion Sleep disturbance Decreased appetite and speech 20-lb weight loss | Empiric antimicrobials for possible meningitis Haloperidol for agitation Quetiapine for delirium Lorazepam taper Thiamine supplementation |
| Second ED visit | Violent behavior Worsening paranoia Responding to internal stimuli Mr. E believes he has 2 wives, but the wife in the room is not the real one, which suggests possible Capgras syndrome Cognitive deficits on mental status exam | Switch from ceftriaxone to ciprofloxacin for Pseudomonas aeruginosa Switch from quetiapine to olanzapine |
| ED: emergency department | ||
Related Resources
- Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders Elsevier; 2007.
- Sidhu KS, Balon R, Ajluni V, et al. Standard EEG and the difficult-to-assess mental status. Ann Clin Psychiatry. 2009;21(2):103-108.
Drug Brand Names
- Acyclovir • Zovirax
- Ceftriaxone • Rocephin
- Ciprofloxacin • Cipro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Thiamine • Betaxin
- Vancomycin • Vancocin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Jiang W, Gagliardi JP, Raj YP, et al. Acute psychotic disorder after gastric bypass surgery: differential diagnosis and treatment. Am J Psychiatry. 2006;163(1):15-19.
2. Harrison RA, Vu T, Hunter AJ. Wernicke’s encephalopathy in a patient with schizophrenia. J Gen Intern Med. 2006;21(12):C8-C11.
3. Sechi GP, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and treatment. Lancet Neurol. 2007;6(5):442-455.
4. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry. 1999;156(5 suppl):1-20.
5. Sharon KI, Fearing MA, Marcantonio RA. Delirium. In: Halter JB Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill Medical; 2009:647–658.
6. Sadock BJ, Sadock VA. Delirium dementia, and amnestic and other cognitive disorders. In: Sadock BJ, Kaplan HI, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:319–372.
7. Ahmad SA, Archer HA, Rice CM, et al. Seronegative limbic encephalitis: case report, literature review and proposed treatment algorithm. Pract Neurol. 2011;11(6):355-361.
8. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Agitated and paranoid
Mr. E, age 55, presents to the emergency department (ED) with a 2-week history of altered mental status (AMS). His wife reports, “He was normal one day and the next day he was not.” Mr. E also presents with sleep disturbance, decreased appetite and speech, and a 20-lb weight loss. His family reports no recent stressors or head trauma. Mr. E is agitated in the ED and receives a single dose of IV haloperidol, 5 mg. He exhibits paranoia and is afraid to get a CT scan. The medical team attempts a lumbar puncture (LP), but Mr. E does not cooperate.
His laboratory values are: potassium, 3.0 mEq/L; creatinine, 1.60 mg/dL; calcium, 10.6 mg/dL; thyroid-stimulating hormone, 0.177 IU/L; vitamin B12, >1500 pg/mL; folate, >20 ng/mL; and creatine kinase, 281 U/L. Urine drug screen is positive for benzodiazepines and opiates, neither of which was prescribed, and blood alcohol is negative.
Mr. E is admitted for further workup of AMS. His daughter-in-law states that Mr. E is an alcoholic and she is concerned that he may have mixed drugs and alcohol. The medical service starts Mr. E on empiric antimicrobials—vancomycin, ceftriaxone, and acyclovir—because of his AMS, and performs an LP to rule out intracranial pathology. His LP results are unremarkable.
Mr. E appears to be confused during psychiatric evaluation. He requests to be “hypnotized on a helicopter to find out what is wrong with me.” His wife states that Mr. E drank vodka daily but decreased his alcohol consumption after surgery 5 months ago. Before his current admission, he was drinking approximately half a glass of vodka every few days, according to his wife. Mr. E says he has no prior psychiatric admissions. During the mental status exam, his eye contact is poor, with latency of response to questions, thought blocking, and psychomotor retardation. He is alert, oriented to time, place, and person, and cooperative. He cannot concentrate or focus during the interview. He denies suicidal or homicidal ideation.
The authors’ observations
Mr. E appeared to be delirious, as evidenced by the sudden onset of waxing and waning changes in consciousness, attention deficits, and cognition. He also had a history of daily alcohol use and decreased his alcohol intake after a surgery 5 months ago, which puts him at risk for Wernicke’s encephalopathy.1-3 The type of surgery and whether he received adequate thiamine supplementation at that time was unclear. Because Mr. E is older, he has a higher risk of mortality and morbidity from delirium.4,5 We started Mr. E on quetiapine, 50 mg/d, for delirium and an IV lorazepam taper, starting at 2 mg every 8 hours, because the extent of his alcohol and benzodiazepine use was unclear—we weren’t sure how forthcoming he was about his alcohol use. He received IV thiamine supplementation followed by oral thiamine, 100 mg/d.
The authors’ recommendations
We requested a neurology consult, EEG, CSF cultures, and brain MRI (Table 1).6 EEG, chest radiography, thyroid scan, and CT scan were normal and MRI showed no acute intracranial process. However, there was a redemonstration of increased T1 signal seen within the bilateral basal ganglia and relative diminutive appearance to the bilateral mamillary bodies, which suggests possible liver disease and/or alcohol abuse. These findings were unchanged from an MRI Mr. E received 10 years ago, were consistent with his history of alcohol abuse, and may indicate an underlying predisposition to delirium. A CT scan of the abdomen showed hepatic cirrhosis with prominent, tortuous vessels of the upper abdomen, subtle ill-defined hypodensity of the anterior aspect of the liver, and an enlarged spleen.
Mr. E’s mental functioning did not improve with quetiapine and lorazepam. Further evaluation revealed a negative human immunodeficiency virus test and normal heavy metals, ammonia, ceruloplasmin, and thiamine. We suspected limbic encephalitis because of Mr. E’s memory problems and behavioral and psychiatric manifestations,7 but CSF was unremarkable and limbic encephalitis workup of CSF and paraneoplastic antibody panel were negative.
Mr. E’s primary care physician stated that at an appointment 1 month ago, Mr. E was alert, oriented, and conversational with normal thought processing. At that time he had presented with rectal bleeding, occult blood in his stool, and an unintentional 25-lb weight loss over 2 months. It was not clear if his weight loss was caused by poor nutrition—which is common among chronic alcoholics—or an occult disease process.
After 10 days, Mr. E was discharged home from the medicine service with no clear cause of his AMS.
Table 1
Suggested workup for altered mental status
| Complete blood count, basic metabolic profile, creatine kinase |
| Thyroid-stimulating hormone, thyroid scan |
| Vitamin B12, folate, thiamine |
| Blood alcohol, urine drug screen |
| Urine analysis and cultures |
| Lumbar puncture—CSF staining and cultures |
| Chest radiography |
| CT and MRI scan of brain |
| Electroencephalography |
| Neuropsychiatric testing |
| CSF: cerebrospinal fluid Source: Reference 6 |
EVALUATION: Worsening behavior
One week later, Mr. E presents to the ED with continued AMS and worsening behavior at home. Two days ago, he attempted to strangle his dog and cut himself with a knife. His paranoia was worsening and his oral intake continued to decrease. In the ED, Mr. E does not want a chest radiograph because, “I don’t like radiation contaminating my body”; his family stated that he had been suspicious of radiography all of his life. He receives empiric ceftriaxone because of a possible urinary tract infection. Urine culture is positive for Pseudomonas aeruginosa and he is switched to ciprofloxacin. Mr. E is admitted for further workup.
Mr. E’s mother states, “I think this change in behavior is related to my son drinking alcohol for 20 years. This is exactly how he acted when he was on drugs. I think he is having a flashback.” She also reports her son purchased multiple chemicals—the details of which are unclear—that he left lying around the house.
His wife says that after discharge a week ago, Mr. E was stable for 1 or 2 days and then “he started going downhill.” He became more paranoid and he started talking about cameras watching him in his house. Mr. E took quetiapine, 50 mg/d, for a few days, then refused because he thought there was something in the medication. Mr. E’s family feels that at times he is responding to internal stimuli. He makes statements about his DNA being changed and reports that he has 2 wives and the wife in the room was not the real one, which suggests Capgras syndrome. His wife provides a home medication list that includes vitamin B complex, vitamins B12, E, and C, a multivitamin, zinc, magnesium, fish oil, garlic, calcium, glucosamine, chondroitin, herbal supplements, and gingko. The psychiatry team recommends switching from quetiapine to olanzapine, 15 mg/d, because Mr. E was paranoid about taking quetiapine.
We determine that Mr. E does not have medical decision-making capacity.
Because his symptoms do not improve, Mr. E is transferred to the psychiatric intensive care unit. His mental status shows little change while there. Neuropsychiatric testing shows only “cognitive deficits.” He shows signs consistent with neurologic dysfunction in terms of stimulus-bound responding and perseveration, which is compatible with the bilateral basal ganglia lesion seen on MRI. However, some of his behaviors suggest psychiatric and motivationally driven or manipulative etiology. During this testing he was difficult to evaluate and needed to be convinced to engage. At times he was illogical and at other times he showed good focus and recall. It is difficult to draw more definitive conclusions and Mr. E is discharged home with minor improvement in his symptoms. He didn’t attend follow-up appointments. During a courtesy call a few months after his admission, his wife revealed that Mr. E had died after shooting himself. It is unclear if it was an accident or suicide.
The authors’ observations
Mr. E’s diagnosis remains unclear (for a summary of his clinical course, see Table 2). Although his initial presentation was consistent with delirium, the lack of an identifiable medical cause, prolonged time course, and lack of improvement with dopamine blocking agents suggest additional diagnoses such as Wernicke-Korsakoff syndrome, rapidly progressive dementia, or a substance-induced disorder. He displayed paranoia and bizarre delusions, which would suggest a thought disorder. However, he also had a history of substance use. A few months after we saw Mr. E, “bath salt” (methylenedioxypyrovalerone) abuse gained national attention. Patients with bath salt intoxication present with confusion, paranoia, and behavioral disturbances as well as a prolonged course.8
Mr. E’s CT and MRI scans, history of alcohol use, and cirrhosis also point to Wernicke-Korsakoff syndrome as an underlying diagnosis. It is unclear whether Mr. E experienced alcohol withdrawal and IV glucose without adequate thiamine replacement during a prior surgery. However, MRI findings were unchanged from a previous study 10 years ago.
It is puzzling whether Mr. E’s AMS was a first psychotic break, a result of drug and alcohol use, rapidly progressing dementia, or another neurologic problem that we have not identified. Our tentative diagnosis was Wernicke-Korsakoff syndrome because of his history of alcohol use and imaging findings.
Although we used a multidisciplinary team approach that included psychiatry, internal medicine, neurology, neuropsychology, and an aggressive and thorough workup, we could not establish a definitive diagnosis. Unsolved cases such as this can leave patients and clinicians frustrated and may lead to unfavorable outcomes. Additional resources such as a telephone call after the first missed appointment may have been warranted.
Table 2
Mr. E’s clinical course
| Symptoms | Treatment | |
|---|---|---|
| First ED visit | Agitation Confusion Sleep disturbance Decreased appetite and speech 20-lb weight loss | Empiric antimicrobials for possible meningitis Haloperidol for agitation Quetiapine for delirium Lorazepam taper Thiamine supplementation |
| Second ED visit | Violent behavior Worsening paranoia Responding to internal stimuli Mr. E believes he has 2 wives, but the wife in the room is not the real one, which suggests possible Capgras syndrome Cognitive deficits on mental status exam | Switch from ceftriaxone to ciprofloxacin for Pseudomonas aeruginosa Switch from quetiapine to olanzapine |
| ED: emergency department | ||
Related Resources
- Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders Elsevier; 2007.
- Sidhu KS, Balon R, Ajluni V, et al. Standard EEG and the difficult-to-assess mental status. Ann Clin Psychiatry. 2009;21(2):103-108.
Drug Brand Names
- Acyclovir • Zovirax
- Ceftriaxone • Rocephin
- Ciprofloxacin • Cipro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Thiamine • Betaxin
- Vancomycin • Vancocin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Agitated and paranoid
Mr. E, age 55, presents to the emergency department (ED) with a 2-week history of altered mental status (AMS). His wife reports, “He was normal one day and the next day he was not.” Mr. E also presents with sleep disturbance, decreased appetite and speech, and a 20-lb weight loss. His family reports no recent stressors or head trauma. Mr. E is agitated in the ED and receives a single dose of IV haloperidol, 5 mg. He exhibits paranoia and is afraid to get a CT scan. The medical team attempts a lumbar puncture (LP), but Mr. E does not cooperate.
His laboratory values are: potassium, 3.0 mEq/L; creatinine, 1.60 mg/dL; calcium, 10.6 mg/dL; thyroid-stimulating hormone, 0.177 IU/L; vitamin B12, >1500 pg/mL; folate, >20 ng/mL; and creatine kinase, 281 U/L. Urine drug screen is positive for benzodiazepines and opiates, neither of which was prescribed, and blood alcohol is negative.
Mr. E is admitted for further workup of AMS. His daughter-in-law states that Mr. E is an alcoholic and she is concerned that he may have mixed drugs and alcohol. The medical service starts Mr. E on empiric antimicrobials—vancomycin, ceftriaxone, and acyclovir—because of his AMS, and performs an LP to rule out intracranial pathology. His LP results are unremarkable.
Mr. E appears to be confused during psychiatric evaluation. He requests to be “hypnotized on a helicopter to find out what is wrong with me.” His wife states that Mr. E drank vodka daily but decreased his alcohol consumption after surgery 5 months ago. Before his current admission, he was drinking approximately half a glass of vodka every few days, according to his wife. Mr. E says he has no prior psychiatric admissions. During the mental status exam, his eye contact is poor, with latency of response to questions, thought blocking, and psychomotor retardation. He is alert, oriented to time, place, and person, and cooperative. He cannot concentrate or focus during the interview. He denies suicidal or homicidal ideation.
The authors’ observations
Mr. E appeared to be delirious, as evidenced by the sudden onset of waxing and waning changes in consciousness, attention deficits, and cognition. He also had a history of daily alcohol use and decreased his alcohol intake after a surgery 5 months ago, which puts him at risk for Wernicke’s encephalopathy.1-3 The type of surgery and whether he received adequate thiamine supplementation at that time was unclear. Because Mr. E is older, he has a higher risk of mortality and morbidity from delirium.4,5 We started Mr. E on quetiapine, 50 mg/d, for delirium and an IV lorazepam taper, starting at 2 mg every 8 hours, because the extent of his alcohol and benzodiazepine use was unclear—we weren’t sure how forthcoming he was about his alcohol use. He received IV thiamine supplementation followed by oral thiamine, 100 mg/d.
The authors’ recommendations
We requested a neurology consult, EEG, CSF cultures, and brain MRI (Table 1).6 EEG, chest radiography, thyroid scan, and CT scan were normal and MRI showed no acute intracranial process. However, there was a redemonstration of increased T1 signal seen within the bilateral basal ganglia and relative diminutive appearance to the bilateral mamillary bodies, which suggests possible liver disease and/or alcohol abuse. These findings were unchanged from an MRI Mr. E received 10 years ago, were consistent with his history of alcohol abuse, and may indicate an underlying predisposition to delirium. A CT scan of the abdomen showed hepatic cirrhosis with prominent, tortuous vessels of the upper abdomen, subtle ill-defined hypodensity of the anterior aspect of the liver, and an enlarged spleen.
Mr. E’s mental functioning did not improve with quetiapine and lorazepam. Further evaluation revealed a negative human immunodeficiency virus test and normal heavy metals, ammonia, ceruloplasmin, and thiamine. We suspected limbic encephalitis because of Mr. E’s memory problems and behavioral and psychiatric manifestations,7 but CSF was unremarkable and limbic encephalitis workup of CSF and paraneoplastic antibody panel were negative.
Mr. E’s primary care physician stated that at an appointment 1 month ago, Mr. E was alert, oriented, and conversational with normal thought processing. At that time he had presented with rectal bleeding, occult blood in his stool, and an unintentional 25-lb weight loss over 2 months. It was not clear if his weight loss was caused by poor nutrition—which is common among chronic alcoholics—or an occult disease process.
After 10 days, Mr. E was discharged home from the medicine service with no clear cause of his AMS.
Table 1
Suggested workup for altered mental status
| Complete blood count, basic metabolic profile, creatine kinase |
| Thyroid-stimulating hormone, thyroid scan |
| Vitamin B12, folate, thiamine |
| Blood alcohol, urine drug screen |
| Urine analysis and cultures |
| Lumbar puncture—CSF staining and cultures |
| Chest radiography |
| CT and MRI scan of brain |
| Electroencephalography |
| Neuropsychiatric testing |
| CSF: cerebrospinal fluid Source: Reference 6 |
EVALUATION: Worsening behavior
One week later, Mr. E presents to the ED with continued AMS and worsening behavior at home. Two days ago, he attempted to strangle his dog and cut himself with a knife. His paranoia was worsening and his oral intake continued to decrease. In the ED, Mr. E does not want a chest radiograph because, “I don’t like radiation contaminating my body”; his family stated that he had been suspicious of radiography all of his life. He receives empiric ceftriaxone because of a possible urinary tract infection. Urine culture is positive for Pseudomonas aeruginosa and he is switched to ciprofloxacin. Mr. E is admitted for further workup.
Mr. E’s mother states, “I think this change in behavior is related to my son drinking alcohol for 20 years. This is exactly how he acted when he was on drugs. I think he is having a flashback.” She also reports her son purchased multiple chemicals—the details of which are unclear—that he left lying around the house.
His wife says that after discharge a week ago, Mr. E was stable for 1 or 2 days and then “he started going downhill.” He became more paranoid and he started talking about cameras watching him in his house. Mr. E took quetiapine, 50 mg/d, for a few days, then refused because he thought there was something in the medication. Mr. E’s family feels that at times he is responding to internal stimuli. He makes statements about his DNA being changed and reports that he has 2 wives and the wife in the room was not the real one, which suggests Capgras syndrome. His wife provides a home medication list that includes vitamin B complex, vitamins B12, E, and C, a multivitamin, zinc, magnesium, fish oil, garlic, calcium, glucosamine, chondroitin, herbal supplements, and gingko. The psychiatry team recommends switching from quetiapine to olanzapine, 15 mg/d, because Mr. E was paranoid about taking quetiapine.
We determine that Mr. E does not have medical decision-making capacity.
Because his symptoms do not improve, Mr. E is transferred to the psychiatric intensive care unit. His mental status shows little change while there. Neuropsychiatric testing shows only “cognitive deficits.” He shows signs consistent with neurologic dysfunction in terms of stimulus-bound responding and perseveration, which is compatible with the bilateral basal ganglia lesion seen on MRI. However, some of his behaviors suggest psychiatric and motivationally driven or manipulative etiology. During this testing he was difficult to evaluate and needed to be convinced to engage. At times he was illogical and at other times he showed good focus and recall. It is difficult to draw more definitive conclusions and Mr. E is discharged home with minor improvement in his symptoms. He didn’t attend follow-up appointments. During a courtesy call a few months after his admission, his wife revealed that Mr. E had died after shooting himself. It is unclear if it was an accident or suicide.
The authors’ observations
Mr. E’s diagnosis remains unclear (for a summary of his clinical course, see Table 2). Although his initial presentation was consistent with delirium, the lack of an identifiable medical cause, prolonged time course, and lack of improvement with dopamine blocking agents suggest additional diagnoses such as Wernicke-Korsakoff syndrome, rapidly progressive dementia, or a substance-induced disorder. He displayed paranoia and bizarre delusions, which would suggest a thought disorder. However, he also had a history of substance use. A few months after we saw Mr. E, “bath salt” (methylenedioxypyrovalerone) abuse gained national attention. Patients with bath salt intoxication present with confusion, paranoia, and behavioral disturbances as well as a prolonged course.8
Mr. E’s CT and MRI scans, history of alcohol use, and cirrhosis also point to Wernicke-Korsakoff syndrome as an underlying diagnosis. It is unclear whether Mr. E experienced alcohol withdrawal and IV glucose without adequate thiamine replacement during a prior surgery. However, MRI findings were unchanged from a previous study 10 years ago.
It is puzzling whether Mr. E’s AMS was a first psychotic break, a result of drug and alcohol use, rapidly progressing dementia, or another neurologic problem that we have not identified. Our tentative diagnosis was Wernicke-Korsakoff syndrome because of his history of alcohol use and imaging findings.
Although we used a multidisciplinary team approach that included psychiatry, internal medicine, neurology, neuropsychology, and an aggressive and thorough workup, we could not establish a definitive diagnosis. Unsolved cases such as this can leave patients and clinicians frustrated and may lead to unfavorable outcomes. Additional resources such as a telephone call after the first missed appointment may have been warranted.
Table 2
Mr. E’s clinical course
| Symptoms | Treatment | |
|---|---|---|
| First ED visit | Agitation Confusion Sleep disturbance Decreased appetite and speech 20-lb weight loss | Empiric antimicrobials for possible meningitis Haloperidol for agitation Quetiapine for delirium Lorazepam taper Thiamine supplementation |
| Second ED visit | Violent behavior Worsening paranoia Responding to internal stimuli Mr. E believes he has 2 wives, but the wife in the room is not the real one, which suggests possible Capgras syndrome Cognitive deficits on mental status exam | Switch from ceftriaxone to ciprofloxacin for Pseudomonas aeruginosa Switch from quetiapine to olanzapine |
| ED: emergency department | ||
Related Resources
- Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders Elsevier; 2007.
- Sidhu KS, Balon R, Ajluni V, et al. Standard EEG and the difficult-to-assess mental status. Ann Clin Psychiatry. 2009;21(2):103-108.
Drug Brand Names
- Acyclovir • Zovirax
- Ceftriaxone • Rocephin
- Ciprofloxacin • Cipro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Thiamine • Betaxin
- Vancomycin • Vancocin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Jiang W, Gagliardi JP, Raj YP, et al. Acute psychotic disorder after gastric bypass surgery: differential diagnosis and treatment. Am J Psychiatry. 2006;163(1):15-19.
2. Harrison RA, Vu T, Hunter AJ. Wernicke’s encephalopathy in a patient with schizophrenia. J Gen Intern Med. 2006;21(12):C8-C11.
3. Sechi GP, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and treatment. Lancet Neurol. 2007;6(5):442-455.
4. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry. 1999;156(5 suppl):1-20.
5. Sharon KI, Fearing MA, Marcantonio RA. Delirium. In: Halter JB Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill Medical; 2009:647–658.
6. Sadock BJ, Sadock VA. Delirium dementia, and amnestic and other cognitive disorders. In: Sadock BJ, Kaplan HI, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:319–372.
7. Ahmad SA, Archer HA, Rice CM, et al. Seronegative limbic encephalitis: case report, literature review and proposed treatment algorithm. Pract Neurol. 2011;11(6):355-361.
8. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
1. Jiang W, Gagliardi JP, Raj YP, et al. Acute psychotic disorder after gastric bypass surgery: differential diagnosis and treatment. Am J Psychiatry. 2006;163(1):15-19.
2. Harrison RA, Vu T, Hunter AJ. Wernicke’s encephalopathy in a patient with schizophrenia. J Gen Intern Med. 2006;21(12):C8-C11.
3. Sechi GP, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and treatment. Lancet Neurol. 2007;6(5):442-455.
4. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry. 1999;156(5 suppl):1-20.
5. Sharon KI, Fearing MA, Marcantonio RA. Delirium. In: Halter JB Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill Medical; 2009:647–658.
6. Sadock BJ, Sadock VA. Delirium dementia, and amnestic and other cognitive disorders. In: Sadock BJ, Kaplan HI, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:319–372.
7. Ahmad SA, Archer HA, Rice CM, et al. Seronegative limbic encephalitis: case report, literature review and proposed treatment algorithm. Pract Neurol. 2011;11(6):355-361.
8. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
Overwhelmed by side effects
CASE: Medication sensitivity
Mrs. C, age 48, is admitted to a tertiary care inpatient mood disorder unit for evaluation of severe depression characterized by depressed mood, anhedonia, and insomnia. Her initial Hamilton Rating Scale for Depression 17-Item (HRSD-17) score is 30, indicating severe depression. Her medications are fluoxetine, 10 mg/d, and diazepam, 0.5 mg/d.
Mrs. C describes a 10-month history of depression and extreme anxiety in the context of several psychosocial stressors. Her father recently died and she is having difficulty with the demands of administering her father’s estate. She is intensely obsessive and focused on nihilistic themes, her diagnosis, somatic themes, and medications side effects. Her husband confirms our observations. No history or current symptoms of typical compulsions (eg, washing hands or checking doors) are elicited. She has limited insight into her obsessive tendencies.
Mrs. C had no psychiatric history before her depressive and obsessive symptoms developed 10 months ago. However, in the past 10 months, she has been hospitalized in a psychiatric facility twice. She also received a series of 8 electroconvulsive therapy treatments, but reported minimal improvement of her depressive symptoms. Mrs. C had a few cognitive-behavioral therapy (CBT) sessions with a psychotherapist, but she said they didn’t help much.
Mrs. C has substantial difficulty adhering to medications, even at subtherapeutic doses. She states she is “extremely sensitive” to all medications. Mrs. C says she develops dizziness, increased anxiety, insomnia, nausea, and other vague reactions whenever she attempts to increase her psychotropics to therapeutic doses. She took sertraline, 10 mg/d, for 4 days, but discontinued it because of unspecified side effects. She then received escitalopram, 2.5 mg/d, for 10 days, but again stopped it because of vague side effects. She was taking paroxetine, 10 mg/d, for 2 days, but experienced vomiting and discontinued the drug. She tried venlafaxine at a low dose and also discontinued it because of vomiting. Mrs. C stayed on mirtazapine, 22.5 mg/d, for 3 months, but stopped it because of lack of efficacy and she was unwilling to increase the dose. Other unsuccessful trials include citalopram and doxepin. Mrs. C is hesitant to try another medication or increase to therapeutic doses any of the previous medications.
The authors’ observations
Before initiating another treatment, the treatment team considered Mrs. C’s pervasive medication intolerance. Her enzymatic activity may be genetically compromised, which could lead to high blood levels of medications and significant side effects when she takes very low doses. Individual variations in response to psychotropics are influenced by genetic factors.1 Variants in the cytochrome P450 (CYP450) genes produce enzymes with increased activity, normal activity, reduced activity, or no activity, creating phenotypes of ultrarapid metabolizers, extensive metabolizers, intermediate metabolizers, and poor metabolizers, respectively. These genetic variations can affect blood levels of medications that employ these enzymes in their metabolic pathways.2 Mrs. C could be a poor metabolizer of common CYP450 variant enzymes, which led to her exquisite sensitivity to psychotropics. We felt this was a reasonable hypothesis given her tumultuous 10-month course of psychiatric treatment and multiple failed medication trials.
An alternative hypothesis is that Mrs. C’s somatic obsessions about drug side effects were the primary clinical issue that led to her severe medication intolerance. Mrs. C spends hours questioning the inpatient staff about her diagnosis (eg, “Are you sure I don’t have bipolar disorder?”), medications (eg, “Are you sure this medication won’t make me sick?”), somatic themes (eg, “Are you sure I don’t have Meniere’s disease with all my dizziness?”), and nihilistic themes (eg, “What if I never get better?”). Mrs. C’s husband attested that she has spent hours researching her new medications on the Internet and reading the medication handouts from the pharmacy. She admits to mentally cycling through the DSM-IV-TR criteria for hours at a time to “figure out” if she has bipolar disorder (BD).
We initiated pharmacogenomic testing to help distinguish between these hypotheses. Mrs. C’s results are presented in Table 1. Genotype results were applied using an interpretive algorithm (Figure) in which 26 psychiatric medications were placed in categories of “use as directed” (green column), “use with caution” (yellow column), and “use with caution or more frequent monitoring” (red column). The algorithm incorporates the genetic information with the known pharmacologic profile for each of the medications in the panel. Highlights of Mrs. C’s interpretive report are shown in Table 2.
Table 1
Mrs. C’s genotype results
| Gene | Allele | Predicted phenotype |
|---|---|---|
| CYP2D6 | *1/*4 | Intermediate metabolizer |
| CYP2C19 | *1/*1 | Extensive metabolizer |
| SLC6A4 | S/S | Low activity |
| 5HTR2A | G/G | Reduced activity |
Figure
Genotype-phenotype integration into Mrs. C’s interpretive report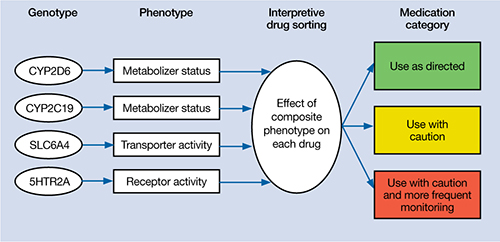
Table 2
Mrs. C’s pharmacogenomic-based interpretive report
| Use as directed | Use with caution | Use with caution and more frequent monitoring |
|---|---|---|
| Antidepressants: Duloxetine, mirtazapine Antipsychotics: Clozapine, olanzapine, quetiapine, ziprasidone | Antidepressants: Amitriptyline,a,b bupropion,a citalopram,c clomipramine,a,b desipramine,a,b escitalopram,c fluoxetine,a fluvoxamine,c imipramine,a,b nortriptyline,a,b sertraline,c paroxetine,c trazodone,a venlafaxinea Antipsychotics: Aripiprazole,a haloperidol,a perphenazine,a risperidonea | None |
| aSerum level may be too high, lower doses may be required bSerum levels may be outside of optimal range cGenotype suggests less than optimal response | ||
The authors’ observations
Mrs. C’s genotype might explain some sensitivity to medications metabolized by CYP2D6 (eg, venlafaxine, paroxetine, fluoxetine), but does not explain her acute sensitivity to all of the medications she has taken. For example, she is an extensive metabolizer for CYP2C19, which metabolizes escitalopram; therefore, it is unlikely escitalopram, 2.5 mg/d, would result in high blood levels and side effects.3 Regardless of the next step in treatment, we deemed her somatic obsessions to be the most important clinical issue. It seems unlikely that Mrs. C would adhere to any medication regimen until this underlying problem was addressed.
The focus of treatment shifted to Mrs. C’s obsessions about her medications and their side effects. Mrs. C was fixated on the content of her obsessions (eg, medications, side effects) rather than the process of her obsessional thinking. The goal was to help Mrs. C identify, label, and ultimately create distance from her obsessive thoughts associated with side effects. The treatment team employed an acceptance and commitment therapy (ACT) model of observing and defusing thoughts in the inpatient setting (Table 3).4 ACT is based on mindfulness and committed, values-based action.5 When patients are “fused” with their thoughts, they believe these thoughts are important and representative of reality. In Mrs. C’s case, she fused with the concept that her medications were making her sick and the idea that she may have BD. The treatment team thought these fused thoughts were the major problem that resulted in 10 months of protracted illness.
Conversely, in a “defused” state, patients can separate from their thoughts and observe them as disparate sounds, words, stories, or bits of language. The goal is to observe and allow the patient’s thoughts to simply be thoughts rather than trying to determine if they are “true.” Mrs. C was fused with the idea that her medications were making her ill, so this belief became the story underlying her obsessional thinking. Helping her disengage from this story became the focus of her treatment.
Table 3
6 core principles of acceptance and commitment therapy
| Defusion | Learning to step back and observe thoughts as separate from the self |
| Acceptance | Allowing unpleasant thoughts to come and go without trying to control them |
| Contact with the present moment | Full awareness and engagement with present experiences |
| Observing the present self | Accessing a transcendent sense of self |
| Values | Clarifying what is most important to the patient |
| Committed action | Setting goals and taking action to achieve them |
| Source: Reference 4 | |
Results guide pharmacotherapy
In addition to helping change the focus of Mrs. C’s psychotherapy, we used the pharmacogenomic results to guide medication treatment. We initially prescribed fluvoxamine, 50 mg/d, because her partially compromised CYP2D6 pathway probably would play only a minor role in metabolizing the drug.1 Smoking induces CYP1A2, which is fluvoxamine’s primary metabolic pathway; however, Mrs. C does not smoke.6 When we saw Mrs. C in January 2009, the author (JGW) was unaware of any available genetic testing for CYP1A2, although now such testing is clinically available.
Mirtazapine is in the “use as directed” category for Mrs. C’s genotype (Table 2) and was the only medication she had adhered to at a therapeutic dose for more than a few days. However, she indicated that she would not adhere to this medication if we prescribed it again. Duloxetine also is in the “use as directed” category; however, given the entire clinical picture, we chose fluvoxamine because of Mrs. C’s obsessive symptomatology and because she had never reached a therapeutic dose of a selective serotonin reuptake inhibitor.
OUTCOME: Obsessions abate
Given Mrs. C’s lack of insight, we initiate a family approach to help broach the topic of obsessions as the focus of treatment. With her husband’s help, she participates in defusion techniques as an inpatient and follows up with an acceptance-based psychotherapist after discharge. After we share the pharmacogenomic information with Mrs. C, she agrees to try fluvoxamine, which is titrated to 100 mg/d. She maintains this dose at her 4-week follow-up visit. Notably, this was only the second time Mrs. C adhered to a medication trial since illness onset. Upon admission, Mrs. C had an HRSD-17 score of 30, indicating severe depression; at 4 weeks, her HRSD-17 score is 8, indicating mild depression.
The authors’ observations
In a complementary case, the author (JGW) consulted on a patient who was taking paroxetine and experiencing anorgasmia, weight gain, and loss of libido. Pharmacogenomic testing revealed that the patient was a poor metabolizer of CYP2D6. Paroxetine is substantially metabolized by CYP2D6; therefore, it was likely that high blood levels were contributing to the side effects.3,7 The key clinical distinction is that although this patient was bothered by intrusive side effects, he was not fixated on them like Mrs. C. His pharmacogenomic test results were used to identify a metabolic issue that was causing the side effects. This is in contrast with Mrs. C, for whom the pharmacogenomic information ruled out a metabolic issue as the primary problem and helped guide the next step in treatment.
Mrs. C’s case illustrates how pharmacogenomics and ACT complemented each other to create a desirable outcome. Pharmacogenomic testing originally was developed as a safety mechanism for medication choice and dosing, but clinical applications have grown as astute clinicians utilize it to help care for their patients.8 ACT can be a powerful tool for patients who have difficulties creating distance from their thoughts. Both pharmacogenomic testing and ACT are noninvasive interventions that can be implemented as part of a multi-faceted treatment approach.
Related Resources
- Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: The process and practice of mindful change. 2nd ed. New York, NY: The Guilford Press; 2011.
- Mrazek DA. Psychiatric pharmacogenomics. New York, NY: Oxford University Press; 2010.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Desipramine • Norpramin
- Diazepam • Valium
- Doxepin • Adapin, Silenor
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lithium • Eskalith, Lithobid
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel, Oleptro
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors are employed by AssureRx Health, Inc., the provider of the pharmacogenomic testing used in this article.
1. Mrazek DA. Psychiatric pharmacogenomics. New York, NY: Oxford University Press; 2010.
2. Kirchheiner J, Nickchen K, Bauer M, et al. Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response. Mol Psychiatry. 2004;9(5):442-473.
3. Kircheiner J, Brøsen K, Dahl ML, et al. CYP2D6 and CYP2C19 genotype-based dose recommendations for antidepressants: a first step towards subpopulation-specific dosages. Acta Psychiatr Scand. 2001;104(3):173-192.
4. Harris R. Embracing your demons: an overview of acceptance and commitment therapy. Psychotherapy in Australia. 2006;12(4):2-8.
5. Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: an experiential approach to behavior change. New York, NY: Guilford Press; 2003.
6. Luvox CR [package insert] Palo Alto CA: Jazz Pharmaceuticals, Inc.; 2011.
7. Kaneda Y, Kawamura I, Fujii A, et al. Serotonin syndrome– ‘potential’ role of the CYP2D6 genetic polymorphism in Asians. Int J Neuropsychopharmacol. 2002;5(1):105-106.
8. Kung S, Li X. The clinical use of pharmacogenomic testing in treatment-resistant depression. Primary Psychiatry. 2010;17(5):46-51.
CASE: Medication sensitivity
Mrs. C, age 48, is admitted to a tertiary care inpatient mood disorder unit for evaluation of severe depression characterized by depressed mood, anhedonia, and insomnia. Her initial Hamilton Rating Scale for Depression 17-Item (HRSD-17) score is 30, indicating severe depression. Her medications are fluoxetine, 10 mg/d, and diazepam, 0.5 mg/d.
Mrs. C describes a 10-month history of depression and extreme anxiety in the context of several psychosocial stressors. Her father recently died and she is having difficulty with the demands of administering her father’s estate. She is intensely obsessive and focused on nihilistic themes, her diagnosis, somatic themes, and medications side effects. Her husband confirms our observations. No history or current symptoms of typical compulsions (eg, washing hands or checking doors) are elicited. She has limited insight into her obsessive tendencies.
Mrs. C had no psychiatric history before her depressive and obsessive symptoms developed 10 months ago. However, in the past 10 months, she has been hospitalized in a psychiatric facility twice. She also received a series of 8 electroconvulsive therapy treatments, but reported minimal improvement of her depressive symptoms. Mrs. C had a few cognitive-behavioral therapy (CBT) sessions with a psychotherapist, but she said they didn’t help much.
Mrs. C has substantial difficulty adhering to medications, even at subtherapeutic doses. She states she is “extremely sensitive” to all medications. Mrs. C says she develops dizziness, increased anxiety, insomnia, nausea, and other vague reactions whenever she attempts to increase her psychotropics to therapeutic doses. She took sertraline, 10 mg/d, for 4 days, but discontinued it because of unspecified side effects. She then received escitalopram, 2.5 mg/d, for 10 days, but again stopped it because of vague side effects. She was taking paroxetine, 10 mg/d, for 2 days, but experienced vomiting and discontinued the drug. She tried venlafaxine at a low dose and also discontinued it because of vomiting. Mrs. C stayed on mirtazapine, 22.5 mg/d, for 3 months, but stopped it because of lack of efficacy and she was unwilling to increase the dose. Other unsuccessful trials include citalopram and doxepin. Mrs. C is hesitant to try another medication or increase to therapeutic doses any of the previous medications.
The authors’ observations
Before initiating another treatment, the treatment team considered Mrs. C’s pervasive medication intolerance. Her enzymatic activity may be genetically compromised, which could lead to high blood levels of medications and significant side effects when she takes very low doses. Individual variations in response to psychotropics are influenced by genetic factors.1 Variants in the cytochrome P450 (CYP450) genes produce enzymes with increased activity, normal activity, reduced activity, or no activity, creating phenotypes of ultrarapid metabolizers, extensive metabolizers, intermediate metabolizers, and poor metabolizers, respectively. These genetic variations can affect blood levels of medications that employ these enzymes in their metabolic pathways.2 Mrs. C could be a poor metabolizer of common CYP450 variant enzymes, which led to her exquisite sensitivity to psychotropics. We felt this was a reasonable hypothesis given her tumultuous 10-month course of psychiatric treatment and multiple failed medication trials.
An alternative hypothesis is that Mrs. C’s somatic obsessions about drug side effects were the primary clinical issue that led to her severe medication intolerance. Mrs. C spends hours questioning the inpatient staff about her diagnosis (eg, “Are you sure I don’t have bipolar disorder?”), medications (eg, “Are you sure this medication won’t make me sick?”), somatic themes (eg, “Are you sure I don’t have Meniere’s disease with all my dizziness?”), and nihilistic themes (eg, “What if I never get better?”). Mrs. C’s husband attested that she has spent hours researching her new medications on the Internet and reading the medication handouts from the pharmacy. She admits to mentally cycling through the DSM-IV-TR criteria for hours at a time to “figure out” if she has bipolar disorder (BD).
We initiated pharmacogenomic testing to help distinguish between these hypotheses. Mrs. C’s results are presented in Table 1. Genotype results were applied using an interpretive algorithm (Figure) in which 26 psychiatric medications were placed in categories of “use as directed” (green column), “use with caution” (yellow column), and “use with caution or more frequent monitoring” (red column). The algorithm incorporates the genetic information with the known pharmacologic profile for each of the medications in the panel. Highlights of Mrs. C’s interpretive report are shown in Table 2.
Table 1
Mrs. C’s genotype results
| Gene | Allele | Predicted phenotype |
|---|---|---|
| CYP2D6 | *1/*4 | Intermediate metabolizer |
| CYP2C19 | *1/*1 | Extensive metabolizer |
| SLC6A4 | S/S | Low activity |
| 5HTR2A | G/G | Reduced activity |
Figure
Genotype-phenotype integration into Mrs. C’s interpretive report
Table 2
Mrs. C’s pharmacogenomic-based interpretive report
| Use as directed | Use with caution | Use with caution and more frequent monitoring |
|---|---|---|
| Antidepressants: Duloxetine, mirtazapine Antipsychotics: Clozapine, olanzapine, quetiapine, ziprasidone | Antidepressants: Amitriptyline,a,b bupropion,a citalopram,c clomipramine,a,b desipramine,a,b escitalopram,c fluoxetine,a fluvoxamine,c imipramine,a,b nortriptyline,a,b sertraline,c paroxetine,c trazodone,a venlafaxinea Antipsychotics: Aripiprazole,a haloperidol,a perphenazine,a risperidonea | None |
| aSerum level may be too high, lower doses may be required bSerum levels may be outside of optimal range cGenotype suggests less than optimal response | ||
The authors’ observations
Mrs. C’s genotype might explain some sensitivity to medications metabolized by CYP2D6 (eg, venlafaxine, paroxetine, fluoxetine), but does not explain her acute sensitivity to all of the medications she has taken. For example, she is an extensive metabolizer for CYP2C19, which metabolizes escitalopram; therefore, it is unlikely escitalopram, 2.5 mg/d, would result in high blood levels and side effects.3 Regardless of the next step in treatment, we deemed her somatic obsessions to be the most important clinical issue. It seems unlikely that Mrs. C would adhere to any medication regimen until this underlying problem was addressed.
The focus of treatment shifted to Mrs. C’s obsessions about her medications and their side effects. Mrs. C was fixated on the content of her obsessions (eg, medications, side effects) rather than the process of her obsessional thinking. The goal was to help Mrs. C identify, label, and ultimately create distance from her obsessive thoughts associated with side effects. The treatment team employed an acceptance and commitment therapy (ACT) model of observing and defusing thoughts in the inpatient setting (Table 3).4 ACT is based on mindfulness and committed, values-based action.5 When patients are “fused” with their thoughts, they believe these thoughts are important and representative of reality. In Mrs. C’s case, she fused with the concept that her medications were making her sick and the idea that she may have BD. The treatment team thought these fused thoughts were the major problem that resulted in 10 months of protracted illness.
Conversely, in a “defused” state, patients can separate from their thoughts and observe them as disparate sounds, words, stories, or bits of language. The goal is to observe and allow the patient’s thoughts to simply be thoughts rather than trying to determine if they are “true.” Mrs. C was fused with the idea that her medications were making her ill, so this belief became the story underlying her obsessional thinking. Helping her disengage from this story became the focus of her treatment.
Table 3
6 core principles of acceptance and commitment therapy
| Defusion | Learning to step back and observe thoughts as separate from the self |
| Acceptance | Allowing unpleasant thoughts to come and go without trying to control them |
| Contact with the present moment | Full awareness and engagement with present experiences |
| Observing the present self | Accessing a transcendent sense of self |
| Values | Clarifying what is most important to the patient |
| Committed action | Setting goals and taking action to achieve them |
| Source: Reference 4 | |
Results guide pharmacotherapy
In addition to helping change the focus of Mrs. C’s psychotherapy, we used the pharmacogenomic results to guide medication treatment. We initially prescribed fluvoxamine, 50 mg/d, because her partially compromised CYP2D6 pathway probably would play only a minor role in metabolizing the drug.1 Smoking induces CYP1A2, which is fluvoxamine’s primary metabolic pathway; however, Mrs. C does not smoke.6 When we saw Mrs. C in January 2009, the author (JGW) was unaware of any available genetic testing for CYP1A2, although now such testing is clinically available.
Mirtazapine is in the “use as directed” category for Mrs. C’s genotype (Table 2) and was the only medication she had adhered to at a therapeutic dose for more than a few days. However, she indicated that she would not adhere to this medication if we prescribed it again. Duloxetine also is in the “use as directed” category; however, given the entire clinical picture, we chose fluvoxamine because of Mrs. C’s obsessive symptomatology and because she had never reached a therapeutic dose of a selective serotonin reuptake inhibitor.
OUTCOME: Obsessions abate
Given Mrs. C’s lack of insight, we initiate a family approach to help broach the topic of obsessions as the focus of treatment. With her husband’s help, she participates in defusion techniques as an inpatient and follows up with an acceptance-based psychotherapist after discharge. After we share the pharmacogenomic information with Mrs. C, she agrees to try fluvoxamine, which is titrated to 100 mg/d. She maintains this dose at her 4-week follow-up visit. Notably, this was only the second time Mrs. C adhered to a medication trial since illness onset. Upon admission, Mrs. C had an HRSD-17 score of 30, indicating severe depression; at 4 weeks, her HRSD-17 score is 8, indicating mild depression.
The authors’ observations
In a complementary case, the author (JGW) consulted on a patient who was taking paroxetine and experiencing anorgasmia, weight gain, and loss of libido. Pharmacogenomic testing revealed that the patient was a poor metabolizer of CYP2D6. Paroxetine is substantially metabolized by CYP2D6; therefore, it was likely that high blood levels were contributing to the side effects.3,7 The key clinical distinction is that although this patient was bothered by intrusive side effects, he was not fixated on them like Mrs. C. His pharmacogenomic test results were used to identify a metabolic issue that was causing the side effects. This is in contrast with Mrs. C, for whom the pharmacogenomic information ruled out a metabolic issue as the primary problem and helped guide the next step in treatment.
Mrs. C’s case illustrates how pharmacogenomics and ACT complemented each other to create a desirable outcome. Pharmacogenomic testing originally was developed as a safety mechanism for medication choice and dosing, but clinical applications have grown as astute clinicians utilize it to help care for their patients.8 ACT can be a powerful tool for patients who have difficulties creating distance from their thoughts. Both pharmacogenomic testing and ACT are noninvasive interventions that can be implemented as part of a multi-faceted treatment approach.
Related Resources
- Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: The process and practice of mindful change. 2nd ed. New York, NY: The Guilford Press; 2011.
- Mrazek DA. Psychiatric pharmacogenomics. New York, NY: Oxford University Press; 2010.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Desipramine • Norpramin
- Diazepam • Valium
- Doxepin • Adapin, Silenor
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lithium • Eskalith, Lithobid
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel, Oleptro
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors are employed by AssureRx Health, Inc., the provider of the pharmacogenomic testing used in this article.
CASE: Medication sensitivity
Mrs. C, age 48, is admitted to a tertiary care inpatient mood disorder unit for evaluation of severe depression characterized by depressed mood, anhedonia, and insomnia. Her initial Hamilton Rating Scale for Depression 17-Item (HRSD-17) score is 30, indicating severe depression. Her medications are fluoxetine, 10 mg/d, and diazepam, 0.5 mg/d.
Mrs. C describes a 10-month history of depression and extreme anxiety in the context of several psychosocial stressors. Her father recently died and she is having difficulty with the demands of administering her father’s estate. She is intensely obsessive and focused on nihilistic themes, her diagnosis, somatic themes, and medications side effects. Her husband confirms our observations. No history or current symptoms of typical compulsions (eg, washing hands or checking doors) are elicited. She has limited insight into her obsessive tendencies.
Mrs. C had no psychiatric history before her depressive and obsessive symptoms developed 10 months ago. However, in the past 10 months, she has been hospitalized in a psychiatric facility twice. She also received a series of 8 electroconvulsive therapy treatments, but reported minimal improvement of her depressive symptoms. Mrs. C had a few cognitive-behavioral therapy (CBT) sessions with a psychotherapist, but she said they didn’t help much.
Mrs. C has substantial difficulty adhering to medications, even at subtherapeutic doses. She states she is “extremely sensitive” to all medications. Mrs. C says she develops dizziness, increased anxiety, insomnia, nausea, and other vague reactions whenever she attempts to increase her psychotropics to therapeutic doses. She took sertraline, 10 mg/d, for 4 days, but discontinued it because of unspecified side effects. She then received escitalopram, 2.5 mg/d, for 10 days, but again stopped it because of vague side effects. She was taking paroxetine, 10 mg/d, for 2 days, but experienced vomiting and discontinued the drug. She tried venlafaxine at a low dose and also discontinued it because of vomiting. Mrs. C stayed on mirtazapine, 22.5 mg/d, for 3 months, but stopped it because of lack of efficacy and she was unwilling to increase the dose. Other unsuccessful trials include citalopram and doxepin. Mrs. C is hesitant to try another medication or increase to therapeutic doses any of the previous medications.
The authors’ observations
Before initiating another treatment, the treatment team considered Mrs. C’s pervasive medication intolerance. Her enzymatic activity may be genetically compromised, which could lead to high blood levels of medications and significant side effects when she takes very low doses. Individual variations in response to psychotropics are influenced by genetic factors.1 Variants in the cytochrome P450 (CYP450) genes produce enzymes with increased activity, normal activity, reduced activity, or no activity, creating phenotypes of ultrarapid metabolizers, extensive metabolizers, intermediate metabolizers, and poor metabolizers, respectively. These genetic variations can affect blood levels of medications that employ these enzymes in their metabolic pathways.2 Mrs. C could be a poor metabolizer of common CYP450 variant enzymes, which led to her exquisite sensitivity to psychotropics. We felt this was a reasonable hypothesis given her tumultuous 10-month course of psychiatric treatment and multiple failed medication trials.
An alternative hypothesis is that Mrs. C’s somatic obsessions about drug side effects were the primary clinical issue that led to her severe medication intolerance. Mrs. C spends hours questioning the inpatient staff about her diagnosis (eg, “Are you sure I don’t have bipolar disorder?”), medications (eg, “Are you sure this medication won’t make me sick?”), somatic themes (eg, “Are you sure I don’t have Meniere’s disease with all my dizziness?”), and nihilistic themes (eg, “What if I never get better?”). Mrs. C’s husband attested that she has spent hours researching her new medications on the Internet and reading the medication handouts from the pharmacy. She admits to mentally cycling through the DSM-IV-TR criteria for hours at a time to “figure out” if she has bipolar disorder (BD).
We initiated pharmacogenomic testing to help distinguish between these hypotheses. Mrs. C’s results are presented in Table 1. Genotype results were applied using an interpretive algorithm (Figure) in which 26 psychiatric medications were placed in categories of “use as directed” (green column), “use with caution” (yellow column), and “use with caution or more frequent monitoring” (red column). The algorithm incorporates the genetic information with the known pharmacologic profile for each of the medications in the panel. Highlights of Mrs. C’s interpretive report are shown in Table 2.
Table 1
Mrs. C’s genotype results
| Gene | Allele | Predicted phenotype |
|---|---|---|
| CYP2D6 | *1/*4 | Intermediate metabolizer |
| CYP2C19 | *1/*1 | Extensive metabolizer |
| SLC6A4 | S/S | Low activity |
| 5HTR2A | G/G | Reduced activity |
Figure
Genotype-phenotype integration into Mrs. C’s interpretive report
Table 2
Mrs. C’s pharmacogenomic-based interpretive report
| Use as directed | Use with caution | Use with caution and more frequent monitoring |
|---|---|---|
| Antidepressants: Duloxetine, mirtazapine Antipsychotics: Clozapine, olanzapine, quetiapine, ziprasidone | Antidepressants: Amitriptyline,a,b bupropion,a citalopram,c clomipramine,a,b desipramine,a,b escitalopram,c fluoxetine,a fluvoxamine,c imipramine,a,b nortriptyline,a,b sertraline,c paroxetine,c trazodone,a venlafaxinea Antipsychotics: Aripiprazole,a haloperidol,a perphenazine,a risperidonea | None |
| aSerum level may be too high, lower doses may be required bSerum levels may be outside of optimal range cGenotype suggests less than optimal response | ||
The authors’ observations
Mrs. C’s genotype might explain some sensitivity to medications metabolized by CYP2D6 (eg, venlafaxine, paroxetine, fluoxetine), but does not explain her acute sensitivity to all of the medications she has taken. For example, she is an extensive metabolizer for CYP2C19, which metabolizes escitalopram; therefore, it is unlikely escitalopram, 2.5 mg/d, would result in high blood levels and side effects.3 Regardless of the next step in treatment, we deemed her somatic obsessions to be the most important clinical issue. It seems unlikely that Mrs. C would adhere to any medication regimen until this underlying problem was addressed.
The focus of treatment shifted to Mrs. C’s obsessions about her medications and their side effects. Mrs. C was fixated on the content of her obsessions (eg, medications, side effects) rather than the process of her obsessional thinking. The goal was to help Mrs. C identify, label, and ultimately create distance from her obsessive thoughts associated with side effects. The treatment team employed an acceptance and commitment therapy (ACT) model of observing and defusing thoughts in the inpatient setting (Table 3).4 ACT is based on mindfulness and committed, values-based action.5 When patients are “fused” with their thoughts, they believe these thoughts are important and representative of reality. In Mrs. C’s case, she fused with the concept that her medications were making her sick and the idea that she may have BD. The treatment team thought these fused thoughts were the major problem that resulted in 10 months of protracted illness.
Conversely, in a “defused” state, patients can separate from their thoughts and observe them as disparate sounds, words, stories, or bits of language. The goal is to observe and allow the patient’s thoughts to simply be thoughts rather than trying to determine if they are “true.” Mrs. C was fused with the idea that her medications were making her ill, so this belief became the story underlying her obsessional thinking. Helping her disengage from this story became the focus of her treatment.
Table 3
6 core principles of acceptance and commitment therapy
| Defusion | Learning to step back and observe thoughts as separate from the self |
| Acceptance | Allowing unpleasant thoughts to come and go without trying to control them |
| Contact with the present moment | Full awareness and engagement with present experiences |
| Observing the present self | Accessing a transcendent sense of self |
| Values | Clarifying what is most important to the patient |
| Committed action | Setting goals and taking action to achieve them |
| Source: Reference 4 | |
Results guide pharmacotherapy
In addition to helping change the focus of Mrs. C’s psychotherapy, we used the pharmacogenomic results to guide medication treatment. We initially prescribed fluvoxamine, 50 mg/d, because her partially compromised CYP2D6 pathway probably would play only a minor role in metabolizing the drug.1 Smoking induces CYP1A2, which is fluvoxamine’s primary metabolic pathway; however, Mrs. C does not smoke.6 When we saw Mrs. C in January 2009, the author (JGW) was unaware of any available genetic testing for CYP1A2, although now such testing is clinically available.
Mirtazapine is in the “use as directed” category for Mrs. C’s genotype (Table 2) and was the only medication she had adhered to at a therapeutic dose for more than a few days. However, she indicated that she would not adhere to this medication if we prescribed it again. Duloxetine also is in the “use as directed” category; however, given the entire clinical picture, we chose fluvoxamine because of Mrs. C’s obsessive symptomatology and because she had never reached a therapeutic dose of a selective serotonin reuptake inhibitor.
OUTCOME: Obsessions abate
Given Mrs. C’s lack of insight, we initiate a family approach to help broach the topic of obsessions as the focus of treatment. With her husband’s help, she participates in defusion techniques as an inpatient and follows up with an acceptance-based psychotherapist after discharge. After we share the pharmacogenomic information with Mrs. C, she agrees to try fluvoxamine, which is titrated to 100 mg/d. She maintains this dose at her 4-week follow-up visit. Notably, this was only the second time Mrs. C adhered to a medication trial since illness onset. Upon admission, Mrs. C had an HRSD-17 score of 30, indicating severe depression; at 4 weeks, her HRSD-17 score is 8, indicating mild depression.
The authors’ observations
In a complementary case, the author (JGW) consulted on a patient who was taking paroxetine and experiencing anorgasmia, weight gain, and loss of libido. Pharmacogenomic testing revealed that the patient was a poor metabolizer of CYP2D6. Paroxetine is substantially metabolized by CYP2D6; therefore, it was likely that high blood levels were contributing to the side effects.3,7 The key clinical distinction is that although this patient was bothered by intrusive side effects, he was not fixated on them like Mrs. C. His pharmacogenomic test results were used to identify a metabolic issue that was causing the side effects. This is in contrast with Mrs. C, for whom the pharmacogenomic information ruled out a metabolic issue as the primary problem and helped guide the next step in treatment.
Mrs. C’s case illustrates how pharmacogenomics and ACT complemented each other to create a desirable outcome. Pharmacogenomic testing originally was developed as a safety mechanism for medication choice and dosing, but clinical applications have grown as astute clinicians utilize it to help care for their patients.8 ACT can be a powerful tool for patients who have difficulties creating distance from their thoughts. Both pharmacogenomic testing and ACT are noninvasive interventions that can be implemented as part of a multi-faceted treatment approach.
Related Resources
- Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: The process and practice of mindful change. 2nd ed. New York, NY: The Guilford Press; 2011.
- Mrazek DA. Psychiatric pharmacogenomics. New York, NY: Oxford University Press; 2010.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Desipramine • Norpramin
- Diazepam • Valium
- Doxepin • Adapin, Silenor
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lithium • Eskalith, Lithobid
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel, Oleptro
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors are employed by AssureRx Health, Inc., the provider of the pharmacogenomic testing used in this article.
1. Mrazek DA. Psychiatric pharmacogenomics. New York, NY: Oxford University Press; 2010.
2. Kirchheiner J, Nickchen K, Bauer M, et al. Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response. Mol Psychiatry. 2004;9(5):442-473.
3. Kircheiner J, Brøsen K, Dahl ML, et al. CYP2D6 and CYP2C19 genotype-based dose recommendations for antidepressants: a first step towards subpopulation-specific dosages. Acta Psychiatr Scand. 2001;104(3):173-192.
4. Harris R. Embracing your demons: an overview of acceptance and commitment therapy. Psychotherapy in Australia. 2006;12(4):2-8.
5. Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: an experiential approach to behavior change. New York, NY: Guilford Press; 2003.
6. Luvox CR [package insert] Palo Alto CA: Jazz Pharmaceuticals, Inc.; 2011.
7. Kaneda Y, Kawamura I, Fujii A, et al. Serotonin syndrome– ‘potential’ role of the CYP2D6 genetic polymorphism in Asians. Int J Neuropsychopharmacol. 2002;5(1):105-106.
8. Kung S, Li X. The clinical use of pharmacogenomic testing in treatment-resistant depression. Primary Psychiatry. 2010;17(5):46-51.
1. Mrazek DA. Psychiatric pharmacogenomics. New York, NY: Oxford University Press; 2010.
2. Kirchheiner J, Nickchen K, Bauer M, et al. Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response. Mol Psychiatry. 2004;9(5):442-473.
3. Kircheiner J, Brøsen K, Dahl ML, et al. CYP2D6 and CYP2C19 genotype-based dose recommendations for antidepressants: a first step towards subpopulation-specific dosages. Acta Psychiatr Scand. 2001;104(3):173-192.
4. Harris R. Embracing your demons: an overview of acceptance and commitment therapy. Psychotherapy in Australia. 2006;12(4):2-8.
5. Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: an experiential approach to behavior change. New York, NY: Guilford Press; 2003.
6. Luvox CR [package insert] Palo Alto CA: Jazz Pharmaceuticals, Inc.; 2011.
7. Kaneda Y, Kawamura I, Fujii A, et al. Serotonin syndrome– ‘potential’ role of the CYP2D6 genetic polymorphism in Asians. Int J Neuropsychopharmacol. 2002;5(1):105-106.
8. Kung S, Li X. The clinical use of pharmacogenomic testing in treatment-resistant depression. Primary Psychiatry. 2010;17(5):46-51.
PTSD nightmares: Prazosin and atypical antipsychotics
• Prazosin is recommended as a first-line therapy for nighttime PTSD symptoms, such as nightmares or sleep disturbances—especially among veterans—because of superior long-term effectiveness.
• Risk of metabolic syndrome, which has been reported with low-dose atypical antipsychotics used for treating insomnia, limits their use for PTSD-related nightmares.
Mr. S, a 45-year-old veteran, was diagnosed with posttraumatic stress disorder (PTSD) 18 years ago after a tour of duty in the Persian Gulf. He had combat-related flashbacks triggered by the smell of gasoline or smoke from a fire, was easily startled, and began to isolate himself socially. However, his symptoms improved when he started volunteering at his local Veterans Affairs Medical Center. After he lost his job 3 years ago, Mr. S started experiencing flashbacks. He was irritable, easily startled, and avoided things that reminded him of his time in the Persian Gulf. His psychiatrist prescribed sertraline, titrated to 200 mg/d. The drug reduced the severity of his avoidance and hyperarousal symptoms and improved his mood.
During a clinic visit, Mr. S says he is doing well and can fall asleep at night but is having recurring nightmares about traumatic events that occurred during combat. These nightmares wake him up and have become more frequent, occurring once per night for the past month. Mr. S says he has been watching more news programs about conflicts in Afghanistan and Iraq since the nightmares began. His psychiatrist starts quetiapine, 50 mg at bedtime for 7 nights then 100 mg at bedtime, but after 6 weeks Mr. S says his nightmares continue.
PTSD occurs in approximately 19% of Vietnam war combat veterans1 and 14% of service members returning from Iraq and Afghanistan.2 PTSD symptoms are classified into clusters: intrusive/re-experiencing; avoidant/numbing; and hyperarousal.3 Nightmares are part of the intrusive/re-experiencing cluster, which is Criterion B in DSM-IV-TR. See Table 1 for a description of DSM-IV-TR PTSD criteria. Among PTSD patients, 50% to 70% report PTSD-associated nightmares.4 Despite adequate treatment targeted to improve PTSD’s core symptoms, symptoms such as sleep disturbances or nightmares often persist.
Table 1
DSM-IV-TR diagnostic criteria for posttraumatic stress disorder
|
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Nightmares and other sleep disturbances are associated with significant distress and daytime impairment and can interfere with PTSD recovery4-8 by disrupting sleep-dependent processing of emotional experiences and causing repeated resensitization to trauma cues (Table 2).8
Table 2
Psychosocial consequences of sleep disruption in PTSD
| Increased reactivity to emotional cues |
| Compromised ability to function in social and occupational roles |
| Negative psychiatric outcomes, including suicidal ideation or worsening of depression or psychosis |
| Interference of natural recovery from trauma exposure |
| Repeated resensitization to trauma cues |
| Neurocognitive deficits |
| Neuroendocrine abnormalities |
| PTSD: posttraumatic stress disorder Source: Adapted from reference 8 |
Few randomized controlled medication trials specifically address PTSD-related nightmares. Most PTSD studies do not examine sleep outcomes as a primary measure, and comprehensive literature reviews could not offer evidence-based recommendations.9,10 The American Academy of Sleep Medicine (AASM) also noted a paucity of PTSD studies that identified nightmares as a primary outcome measure.11 See Table 3 for a list of recommended medication options for PTSD-associated nightmares.
Table 3
Recommended medication treatments for PTSD-associated nightmares
| Evidence level | Medication | Evidence |
|---|---|---|
| Recommended for treating PTSD-associated nightmares | ||
| 1, 4 | Prazosin | In 3 level 1 studies, adding prazosin (mean dose 3 mg/d) significantly decreased trauma-related nightmares according to the CAPS “recurrent distressing dreams” item after 3 to 9 weeks of treatment vs placebo in veteran and civilian patients (N = 57) |
| Not suggested for treating PTSD-associated nightmares | ||
| 1 | Venlafaxine | No difference between extended-release venlafaxine (37.5 to 300 mg/d) and placebo in the CAPS-SX17 “distressing dreams” item at 12 weeks in 340 PTSD patients |
| May be considered for treating PTSD-associated nightmares | ||
| 4 | Clonidine | Reduced the number of nightmares in 11 of 13 refugees for 2 weeks to 3 months (dose: 0.2 to 0.6 mg/d) |
| May be considered for treating PTSD-associated nightmares, but data are low grade and sparse | ||
| 4 | Trazodone | Although trazodone (25 to 600 mg) significantly decreased nightmare frequency in veteran patients during an 8-week hospital stay (N = 60), 19% discontinued therapy because of side effects |
| 4 | Olanzapine | Adjunctive olanzapine (10 to 20 mg) rapidly improved sleep in a case series of combat-related PTSD patients resistant to SSRIs and benzodiazepines (N = 5) |
| 4 | Risperidone | In case series, risperidone (0.5 to 3 mg) significantly decreased CAPS scores for recurrent distressing dreams and proportion of traumatic dreams documented in diaries of combat veterans over 6 weeks (N = 17), and improved nightmares in adult burn patients taking pain medications after 1 to 2 days (N = 10) |
| 4 | Aripiprazole | In a case series, aripiprazole (15 to 30 mg at bedtime) with CBT or sertraline significantly improved nightmares in 4 of 5 combat-related PTSD patients |
| 4 | Topiramate | Topiramate reduced nightmares in 79% of civilians with PTSD and fully suppressed nightmares in 50% of patients in a case series (N = 35) |
| 4 | Low-dose cortisol | Significant decrease in frequency but not intensity of nightmares with low-dose cortisol (10 mg/d) in civilians with PTSD (N = 3) |
| 4 | Fluvoxamine | In 2 case series, fluvoxamine (up to 300 mg/d) significantly decreased the IES-R level of “dreams about combat trauma” but not the SRRS “bad dreams” rating at 10 weeks (N = 21). During 4 to 12 weeks of follow-up there was a qualitative decrease in reported nightmares in veteran patients (n = 12) |
| 2 | Triazolam/nitrazepam | Limited data showed triazolam (0.5 mg) and nitrazepam (5 mg) provide equal efficacy in decreasing the number of patients who experience unpleasant dreams over 1 night |
| 4 | Phenelzine | One study showed phenelzine monotherapy (30 to 90 mg) resulted in elimination of nightmares within 1 month (N = 5); another reported “moderately reduced traumatic dreams” (N = 21) in veterans. Therapy was discontinued because of short-lived efficacy or plateau effect |
| 4 | Gabapentin | Adjunctive gabapentin (300 to 3,600 mg/d) improved insomnia and decreased nightmare frequency and/or intensity over 1 to 36 months in 30 veterans with PTSD |
| 4 | Cyproheptadine | Conflicting data ranges from eliminating nightmares to no changes in the presence or intensity of nightmares |
| 4 | TCAs | Among 10 Cambodian concentration camp survivors treated with TCAs, 4 reported their nightmares ceased and 4 reported improvement after 1-year follow-up |
| 4 | Nefazodone | Reduced nightmare occurrence in 3 open-label studies as monotherapy (386 to 600 mg/d). Not recommended first line because of hepatotoxicity risk |
| No recommendation because of sparse data | ||
| 2 | Clonazepam | Clonazepam (1 to 2 mg/d) was ineffective in decreasing frequency or intensity of combat-related PTSD nightmares in veterans (N = 6) |
Evidence levels:
| ||
| CAPS: Clinician-Administered PTSD Scale; CAPS-SX17: 17-item Clinician-Administered PTSD Scale; CBT: cognitive-behavioral therapy; IES-R: Impact of Event Scale-Revised; PTSD: posttraumatic stress disorder; SRRS: Stress Response Rating Scale; SSRI: selective serotonin reuptake inhibitor; TCAs: tricyclic antidepressants Source: Adapted from Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401 | ||
CASE CONTINUED: Medication change, improvement
After reviewing AASM’s treatment recommendations, we prescribe prazosin, 1 mg at bedtime for 7 nights, then increase by 1 mg at bedtime each week until Mr. S’s nightmares improve. He reports a substantial improvement in nightmare severity and frequency after a few weeks of treatment with prazosin, 5 mg at bedtime.
Prazosin
Prazosin is an α1-adrenergic receptor antagonist with good CNS penetrability. The rationale for reducing adrenergic activity to address intrusive PTSD symptoms has been well documented.12,13 In open-label trials,14-18 a chart review,19 and placebo-controlled trials,20-22prazosin reduced trauma nightmares and improved sleep quality and global clinical status more than placebo (Table 4). In these studies, prazosin doses ranged from 1 to 20 mg/d, with an average of 3 mg at bedtime and a starting dose of 1 mg. Prazosin is the only agent recommended in the AASM’s Best Practice Guide for treating PTSD-related nightmares.11
Table 4
RCTs of prazosin for trauma-related nightmares
| Study | Design | Patients | Results |
|---|---|---|---|
| Raskind et al, 200320 | 20-week, double-blind, placebo-controlled, crossover study (mean dose 9.5 mg/d at bedtime) | 10 Vietnam veterans with chronic PTSD and severe trauma-related nightmares | Prazosin was superior to placebo on scores on the recurrent distressing dreams item and difficulty falling/staying asleep item of the CAPS and change in PTSD severity and functional status on the CGI-C |
| Raskind et al, 200721 | 8-week, placebo-controlled, parallel study (mean dose 13.3 ± 3 mg/d in the evening) | 40 veterans with chronic PTSD, distressing trauma nightmares, and sleep disturbance | Prazosin was superior to placebo in reducing trauma nightmares and improving sleep quality and global clinical status; prazosin also shifted dream characteristics of trauma-related nightmares to those typical of normal dreams |
| Taylor et al, 200822 | 7-week, randomized, placebo-controlled, crossover trial (mean dose 3.1 ± 1.3 mg) | 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance | Prazosin significantly increased total sleep time and REM sleep time; reduced trauma-related nightmares, distressed awakenings, and total PCL-C scores; improved CGI-I scores; and changed PDRS scores toward normal dreaming |
| CAPS: Clinician-Administered PTSD Scale; CGI-C: Clinical Global Impression of Change; CGI-I: Clinical Global Impression of Improvement; PCL-C: PTSD Checklist-Civilian; PDRS: PTSD Dream Rating Scale; PTSD: posttraumatic stress disorder; RCTs: randomized controlled trials; REM: rapid eye movement | |||
Atypical antipsychotics
Atypical antipsychotics have been used to reduce nightmares in PTSD; however, most of the evidence from studies evaluated in the AASM’s Best Practice Guide were considered to be low quality.11 Quetiapine and ziprasidone were not included in the AASM review. See (Table 5) for a review of the evidence for atypical antipsychotics for treating PTSD nightmares.
Table 5
Combat-related nightmares: Evidence for atypical antipsychotics
| Study | Design | Patients/dosage | Results |
|---|---|---|---|
| Aripiprazole | |||
| Lambert, 2006 a | Case report | 4 veterans with combat-related PTSD (3 male, 1 female; age 22 to 24); dose: 15 to 30 mg; concurrent treatment sertraline or CBT | Decreased frequency of weekly nightmares and agitated sleep by at least 50% |
| Olanzapine | |||
| Stein et al, 2002 b | 8-week, double-blind, placebo-controlled study | 19 male veterans with combat-related PTSD (olanzapine group mean age: 55.2 ± 6.6; placebo group 51.1 ± 8.1); mean dose: 15 mg/d | Significantly greater reduction in sleep disturbances (PSQI: -3.29 vs 1.57; P = .01); significantly higher weight gain (13.2 lbs vs -3 lbs; P = .001) |
| Jakovljevic et al, 2003 c | Case reports | 5 veterans with combat-related PTSD for 6 to 7 years (age: 28 to 50); dose: 10 to 20 mg; adjunct treatment | Decreased frequency of nightmares within 3 days |
| Labbate et al, 2000 d | Case report | 1 male veteran (age: 58) with a 20-year history of combat-related PTSD; dose: 5 mg at bedtime; concurrent treatment with sertraline (200 mg/d), bupropion (150 mg/d), and diazepam (15 mg/d) | Eliminated nightmares after 1 week and improved sleep quality |
| Quetiapine | |||
| Ahearn et al, 2006 e | 8-week, open-label trial | 15 PTSD patients (8 male; 7 female; 5 with combat-related PTSD; mean age: 49); mean dose: 216 mg/d (100 to 400 mg/d) | Significantly improved re-experiencing (CAPS: 10 vs 23; P = .0012) and sleep (PSQI: 17.5 vs 30; P = .0044) at 8 weeks compared with baseline |
| Robert et al, 2005 f | 6-week, open-label trial | 19 combat veterans; mean dose: 100 ± 70 mg/d (25 to 300 mg/d); adjunct treatment | Significantly improved sleep quality (PSQI: 1.67 vs 2.41; P = .006), latency (PSQI: 1.5 vs 2.65; P = .002), duration (PSQI: 1.31 vs 2.71; P < .001), and sleep disturbances (PSQI: 1.22 vs 1.71; P = .034) and decreased terror episodes (PSQI-A: 0.73 vs 0.91; P = .040) and acting out dreams (PSQI-A: 1.07 vs 1.35; P = .013); however, no difference in nightmares caused by trauma (PSQI-A: 1.53 vs 2.06) |
| Sokolski et al, 2003 g | Retrospective chart review | 68 male Vietnam War combat veterans (mean age: 55 ± 3.5); mean dose: 155 ± 130 mg (25 to 700 mg); adjunct treatment | Improved sleep disturbances in 62% and nightmares in 25% of patients |
| Ahearn et al, 2003 h | Case report | 2 male patients with combat-related PTSD (age 53, 72); dose: 25 to 50 mg; adjunct to SSRI therapy | Decreased frequency of nightmares with increased sleep duration |
| Risperidone | |||
| David et al, 2006 i | 6-week, open-label trial | 17 male veterans with combat-related PTSD (mean age: 53.7 ± 3.8); mean maximum dose: 2.3 ± 0.6 mg (range: 1 to 3 mg) | Improved recurrent distressing dreams (CAPS B-2: 3.8 vs 5.4; P = .04), but not with the PSQI subscale (PSQI bad dreams: 2.5 vs 2.7; NS). Decreased nighttime awakenings (1.9 vs 2.8; P = .003) and trauma dreams (19% vs 38%; P = .04) |
| Leyba et al, 1998 j | Case reports | 3 male patients (age 43 to 46); dose: 1 to 3 mg; adjunct therapy | Decreased occurrence of nightmares |
| Ziprasidone | |||
| Siddiqui et al, 2005 k | Case report | 1 male veteran with chronic combat-related PTSD (age 55); dose: 80 to 120 mg/d; adjunct with trazodone (100 mg) and topiramate | Improved occurrence of nightmares up to 4 months |
CAPS: Clinician-Administered PTSD Scale; CAPS B-2: Clinician-Administered PTSD Scale B-2 (recurrent distressing dreams of the event); CBT: cognitive-behavioral therapy; PSQI: Pittsburgh Sleep Quality Index; PSQI-A: Pittsburgh Sleep Quality Index Addendum for PTSD; NS: not significant; PTSD: posttraumatic stress disorder; SSRI: selective serotonin reuptake inhibitor References
| |||
Comparing prazosin and quetiapine. A historical prospective cohort study of 237 veterans with PTSD receiving prazosin or quetiapine for nighttime PTSD symptoms demonstrated that although the 2 drugs have similar efficacy (defined as symptomatic improvement) for short-term, 6-month treatment (61% vs 62%; P=.54), a higher percentage of patients continued prazosin long-term (3 to 6 years) than those taking quetiapine (48% vs 24%; P < .001).23 Twenty-five percent of patients taking quetiapine switched to prazosin during the study, and approximately one-half of these patients remained on prazosin until the study’s end. Only 8% of prazosin patients switched to quetiapine, and none continued this therapy until study end.23 Patients in the quetiapine group were more likely to discontinue the drug because of lack of efficacy (13% vs 3%; P=.03) and adverse effects (35% vs 18%; P=.008), specifically sedation (21% vs 2%; P < .001) and metabolic effects (9% vs 0%; P=.014), compared with prazosin. Although this trial may be the only published comparison study of prazosin and quetiapine, its methodological quality has been questioned, which makes it difficult to draw definitive conclusions.
Metabolic syndrome—elevated diastolic blood pressure, increased waist circumference, and low high-density lipoprotein cholesterol—is common among PTSD patients treated with antipsychotics.24 This syndrome may be caused by medications, lifestyle factors, or long-term overactivation of stress-response pathways. A retrospective chart review at a community mental health center revealed that patients taking even low doses of quetiapine for insomnia gained an average of 5 lbs (P=.037).25 Another retrospective chart review at 2 military hospitals reported that patients receiving low-dose quetiapine (≤100 mg/d) gained an average of slightly less than 1 lb per month, which adds up to approximately 10 lbs per year (P < .001).26 The benefit of using atypical antipsychotics may be outweighed by metabolic risks such as obesity, new-onset diabetes, and dyslipidemia.27
Prazosin is considered a first-line treatment for sleep disturbances and nightmares in PTSD because of its superior long-term efficacy and decreased adverse effects compared with quetiapine.
Related Resources
- American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
- Veterans Affairs/Department of Defense clinical practice guidelines. Management of traumatic stress disorder and acute stress reaction. www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp.
Drug Brand Names
- Prazosin • Minipress
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Dohrenwend BP, Turner JB, Turse NA, et al. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313(5789):979-982.
2. Tanielian T, Jaycox L. eds. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
4. Wittmann L, Schredl M, Kramer M. Dreaming in posttraumatic stress disorder: a critical review of phenomenology psychophysiology and treatment. Psychother Psychosom. 2007;76(1):25-39.
5. Clum GA, Nishith P, Resick PA. Trauma-related sleep disturbance and self-reported physical health symptoms in treatment-seeking female rape victims. J Nerv Ment Dis. 2001;189(9):618-622.
6. Kramer TL, Booth BM, Han X, et al. Service utilization and outcomes in medically ill veterans with posttraumatic stress and depressive disorders. J Trauma Stress. 2003;16(3):211-219.
7. Neylan TC, Marmar CR, Metzler TJ, et al. Sleep disturbances in the Vietnam generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry. 1998;155(7):929-933.
8. Nappi CM, Drummond SP, Hall JM. Treating nightmares and insomnia in posttraumatic stress disorder: a review of current evidence. Neuropharmacology. 2012;62(2):576-585.
9. Maher MJ, Rego SA, Asnis GM. Sleep disturbances in patients with post-traumatic stress disorder: epidemiology impact and approaches to management. CNS Drugs. 2006;20(7):567-590.
10. van Liempt S, Vermetten E, Geuze E, et al. Pharmacotherapy for disordered sleep in post-traumatic stress disorder: a systematic review. Int Clin Psychopharmacol. 2006;21(4):193-202.
11. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401.
12. Boehnlein JK, Kinzie JD. Pharmacologic reduction of CNS noradrenergic activity in PTSD: the case for clonidine and prazosin. J Psychiatr Pract. 2007;13(2):72-78.
13. Strawn JR, Geracioti TD, Jr. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety. 2008;25(3):260-271.
14. Calohan J, Peterson K, Peskind ER, et al. Prazosin treatment of trauma nightmares and sleep disturbance in soldiers deployed in Iraq. J Trauma Stress. 2010;23(5):645-648.
15. Daly CM, Doyle ME, Radkind M, et al. Clinical case series: the use of Prazosin for combat-related recurrent nightmares among Operation Iraqi Freedom combat veterans. Mil Med. 2005;170(6):513-515.
16. Peskind ER, Bonner LT, Hoff DJ, et al. Prazosin reduces trauma-related nightmares in older men with chronic posttraumatic stress disorder. J Geriatr Psychiatry Neurol. 2003;16(3):165-171.
17. Raskind MA, Dobie DJ, Kanter ED, et al. The alpha1-adrenergic antagonist prazosin ameliorates combat trauma nightmares in veterans with posttraumatic stress disorder: a report of 4 cases. J Clin Psychiatry. 2000;61(2):129-133.
18. Taylor F, Raskind MA. The alpha1-adrenergic antagonist prazosin improves sleep and nightmares in civilian trauma posttraumatic stress disorder. J Clin Psychopharmacol. 2002;22(1):82-85.
19. Raskind MA, Thompson C, Petrie EC, et al. Prazosin reduces nightmares in combat veterans with posttraumatic stress disorder. J Clin Psychiatry. 2002;63(7):565-568.
20. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry. 2003;160(2):371-373.
21. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry. 2007;61(8):928-934.
22. Taylor FB, Martin P, Thompson C, et al. Prazosin effects on objective sleep measures and clinical symptoms in civilian trauma posttraumatic stress disorder: a placebo-controlled study. Biol Psychiatry. 2008;63(6):629-632.
23. Byers MG, Allison KM, Wendel CS, et al. Prazosin versus quetiapine for nighttime posttraumatic stress disorder symptoms in veterans: an assessment of long-term comparative effectiveness and safety. J Clin Psychopharmacol. 2010;30(3):225-229.
24. Jin H, Lanouette NM, Mudaliar S, et al. Association of posttraumatic stress disorder with increased prevalence of metabolic syndrome. J Clin Psychopharmacol. 2009;29(3):210-215.
25. Cates ME, Jackson CW, Feldman JM, et al. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Ment Health J. 2009;45(4):251-254.
26. Williams SG, Alinejad NA, Williams JA, et al. Statistically significant increase in weight caused by low-dose quetiapine. Pharmacotherapy. 2010;30(10):1011-1015.
27. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65(2):267-272.
Rebecca L. Graham, PharmD
Dr. Graham is a Second-Year Psychiatric Pharmacy Resident, Veterans Affairs San Diego Healthcare System (VASDHS)
Susan G. Leckband, RPh, BCPP
Ms. Leckband is a Clinical Psychiatric Pharmacist Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Dr. Endow-Eyer is Psychiatric Clinical Pharmacy Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego, San Diego, CA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Rebecca L. Graham, PharmD
Dr. Graham is a Second-Year Psychiatric Pharmacy Resident, Veterans Affairs San Diego Healthcare System (VASDHS)
Susan G. Leckband, RPh, BCPP
Ms. Leckband is a Clinical Psychiatric Pharmacist Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Dr. Endow-Eyer is Psychiatric Clinical Pharmacy Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego, San Diego, CA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Rebecca L. Graham, PharmD
Dr. Graham is a Second-Year Psychiatric Pharmacy Resident, Veterans Affairs San Diego Healthcare System (VASDHS)
Susan G. Leckband, RPh, BCPP
Ms. Leckband is a Clinical Psychiatric Pharmacist Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Dr. Endow-Eyer is Psychiatric Clinical Pharmacy Specialist, VASDHS, and Assistant Clinical Professor through Skaggs School of Pharmacy and Pharmaceutical Sciences and Department of Psychiatry, University of California, San Diego, San Diego, CA
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
• Prazosin is recommended as a first-line therapy for nighttime PTSD symptoms, such as nightmares or sleep disturbances—especially among veterans—because of superior long-term effectiveness.
• Risk of metabolic syndrome, which has been reported with low-dose atypical antipsychotics used for treating insomnia, limits their use for PTSD-related nightmares.
Mr. S, a 45-year-old veteran, was diagnosed with posttraumatic stress disorder (PTSD) 18 years ago after a tour of duty in the Persian Gulf. He had combat-related flashbacks triggered by the smell of gasoline or smoke from a fire, was easily startled, and began to isolate himself socially. However, his symptoms improved when he started volunteering at his local Veterans Affairs Medical Center. After he lost his job 3 years ago, Mr. S started experiencing flashbacks. He was irritable, easily startled, and avoided things that reminded him of his time in the Persian Gulf. His psychiatrist prescribed sertraline, titrated to 200 mg/d. The drug reduced the severity of his avoidance and hyperarousal symptoms and improved his mood.
During a clinic visit, Mr. S says he is doing well and can fall asleep at night but is having recurring nightmares about traumatic events that occurred during combat. These nightmares wake him up and have become more frequent, occurring once per night for the past month. Mr. S says he has been watching more news programs about conflicts in Afghanistan and Iraq since the nightmares began. His psychiatrist starts quetiapine, 50 mg at bedtime for 7 nights then 100 mg at bedtime, but after 6 weeks Mr. S says his nightmares continue.
PTSD occurs in approximately 19% of Vietnam war combat veterans1 and 14% of service members returning from Iraq and Afghanistan.2 PTSD symptoms are classified into clusters: intrusive/re-experiencing; avoidant/numbing; and hyperarousal.3 Nightmares are part of the intrusive/re-experiencing cluster, which is Criterion B in DSM-IV-TR. See Table 1 for a description of DSM-IV-TR PTSD criteria. Among PTSD patients, 50% to 70% report PTSD-associated nightmares.4 Despite adequate treatment targeted to improve PTSD’s core symptoms, symptoms such as sleep disturbances or nightmares often persist.
Table 1
DSM-IV-TR diagnostic criteria for posttraumatic stress disorder
|
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Nightmares and other sleep disturbances are associated with significant distress and daytime impairment and can interfere with PTSD recovery4-8 by disrupting sleep-dependent processing of emotional experiences and causing repeated resensitization to trauma cues (Table 2).8
Table 2
Psychosocial consequences of sleep disruption in PTSD
| Increased reactivity to emotional cues |
| Compromised ability to function in social and occupational roles |
| Negative psychiatric outcomes, including suicidal ideation or worsening of depression or psychosis |
| Interference of natural recovery from trauma exposure |
| Repeated resensitization to trauma cues |
| Neurocognitive deficits |
| Neuroendocrine abnormalities |
| PTSD: posttraumatic stress disorder Source: Adapted from reference 8 |
Few randomized controlled medication trials specifically address PTSD-related nightmares. Most PTSD studies do not examine sleep outcomes as a primary measure, and comprehensive literature reviews could not offer evidence-based recommendations.9,10 The American Academy of Sleep Medicine (AASM) also noted a paucity of PTSD studies that identified nightmares as a primary outcome measure.11 See Table 3 for a list of recommended medication options for PTSD-associated nightmares.
Table 3
Recommended medication treatments for PTSD-associated nightmares
| Evidence level | Medication | Evidence |
|---|---|---|
| Recommended for treating PTSD-associated nightmares | ||
| 1, 4 | Prazosin | In 3 level 1 studies, adding prazosin (mean dose 3 mg/d) significantly decreased trauma-related nightmares according to the CAPS “recurrent distressing dreams” item after 3 to 9 weeks of treatment vs placebo in veteran and civilian patients (N = 57) |
| Not suggested for treating PTSD-associated nightmares | ||
| 1 | Venlafaxine | No difference between extended-release venlafaxine (37.5 to 300 mg/d) and placebo in the CAPS-SX17 “distressing dreams” item at 12 weeks in 340 PTSD patients |
| May be considered for treating PTSD-associated nightmares | ||
| 4 | Clonidine | Reduced the number of nightmares in 11 of 13 refugees for 2 weeks to 3 months (dose: 0.2 to 0.6 mg/d) |
| May be considered for treating PTSD-associated nightmares, but data are low grade and sparse | ||
| 4 | Trazodone | Although trazodone (25 to 600 mg) significantly decreased nightmare frequency in veteran patients during an 8-week hospital stay (N = 60), 19% discontinued therapy because of side effects |
| 4 | Olanzapine | Adjunctive olanzapine (10 to 20 mg) rapidly improved sleep in a case series of combat-related PTSD patients resistant to SSRIs and benzodiazepines (N = 5) |
| 4 | Risperidone | In case series, risperidone (0.5 to 3 mg) significantly decreased CAPS scores for recurrent distressing dreams and proportion of traumatic dreams documented in diaries of combat veterans over 6 weeks (N = 17), and improved nightmares in adult burn patients taking pain medications after 1 to 2 days (N = 10) |
| 4 | Aripiprazole | In a case series, aripiprazole (15 to 30 mg at bedtime) with CBT or sertraline significantly improved nightmares in 4 of 5 combat-related PTSD patients |
| 4 | Topiramate | Topiramate reduced nightmares in 79% of civilians with PTSD and fully suppressed nightmares in 50% of patients in a case series (N = 35) |
| 4 | Low-dose cortisol | Significant decrease in frequency but not intensity of nightmares with low-dose cortisol (10 mg/d) in civilians with PTSD (N = 3) |
| 4 | Fluvoxamine | In 2 case series, fluvoxamine (up to 300 mg/d) significantly decreased the IES-R level of “dreams about combat trauma” but not the SRRS “bad dreams” rating at 10 weeks (N = 21). During 4 to 12 weeks of follow-up there was a qualitative decrease in reported nightmares in veteran patients (n = 12) |
| 2 | Triazolam/nitrazepam | Limited data showed triazolam (0.5 mg) and nitrazepam (5 mg) provide equal efficacy in decreasing the number of patients who experience unpleasant dreams over 1 night |
| 4 | Phenelzine | One study showed phenelzine monotherapy (30 to 90 mg) resulted in elimination of nightmares within 1 month (N = 5); another reported “moderately reduced traumatic dreams” (N = 21) in veterans. Therapy was discontinued because of short-lived efficacy or plateau effect |
| 4 | Gabapentin | Adjunctive gabapentin (300 to 3,600 mg/d) improved insomnia and decreased nightmare frequency and/or intensity over 1 to 36 months in 30 veterans with PTSD |
| 4 | Cyproheptadine | Conflicting data ranges from eliminating nightmares to no changes in the presence or intensity of nightmares |
| 4 | TCAs | Among 10 Cambodian concentration camp survivors treated with TCAs, 4 reported their nightmares ceased and 4 reported improvement after 1-year follow-up |
| 4 | Nefazodone | Reduced nightmare occurrence in 3 open-label studies as monotherapy (386 to 600 mg/d). Not recommended first line because of hepatotoxicity risk |
| No recommendation because of sparse data | ||
| 2 | Clonazepam | Clonazepam (1 to 2 mg/d) was ineffective in decreasing frequency or intensity of combat-related PTSD nightmares in veterans (N = 6) |
Evidence levels:
| ||
| CAPS: Clinician-Administered PTSD Scale; CAPS-SX17: 17-item Clinician-Administered PTSD Scale; CBT: cognitive-behavioral therapy; IES-R: Impact of Event Scale-Revised; PTSD: posttraumatic stress disorder; SRRS: Stress Response Rating Scale; SSRI: selective serotonin reuptake inhibitor; TCAs: tricyclic antidepressants Source: Adapted from Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401 | ||
CASE CONTINUED: Medication change, improvement
After reviewing AASM’s treatment recommendations, we prescribe prazosin, 1 mg at bedtime for 7 nights, then increase by 1 mg at bedtime each week until Mr. S’s nightmares improve. He reports a substantial improvement in nightmare severity and frequency after a few weeks of treatment with prazosin, 5 mg at bedtime.
Prazosin
Prazosin is an α1-adrenergic receptor antagonist with good CNS penetrability. The rationale for reducing adrenergic activity to address intrusive PTSD symptoms has been well documented.12,13 In open-label trials,14-18 a chart review,19 and placebo-controlled trials,20-22prazosin reduced trauma nightmares and improved sleep quality and global clinical status more than placebo (Table 4). In these studies, prazosin doses ranged from 1 to 20 mg/d, with an average of 3 mg at bedtime and a starting dose of 1 mg. Prazosin is the only agent recommended in the AASM’s Best Practice Guide for treating PTSD-related nightmares.11
Table 4
RCTs of prazosin for trauma-related nightmares
| Study | Design | Patients | Results |
|---|---|---|---|
| Raskind et al, 200320 | 20-week, double-blind, placebo-controlled, crossover study (mean dose 9.5 mg/d at bedtime) | 10 Vietnam veterans with chronic PTSD and severe trauma-related nightmares | Prazosin was superior to placebo on scores on the recurrent distressing dreams item and difficulty falling/staying asleep item of the CAPS and change in PTSD severity and functional status on the CGI-C |
| Raskind et al, 200721 | 8-week, placebo-controlled, parallel study (mean dose 13.3 ± 3 mg/d in the evening) | 40 veterans with chronic PTSD, distressing trauma nightmares, and sleep disturbance | Prazosin was superior to placebo in reducing trauma nightmares and improving sleep quality and global clinical status; prazosin also shifted dream characteristics of trauma-related nightmares to those typical of normal dreams |
| Taylor et al, 200822 | 7-week, randomized, placebo-controlled, crossover trial (mean dose 3.1 ± 1.3 mg) | 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance | Prazosin significantly increased total sleep time and REM sleep time; reduced trauma-related nightmares, distressed awakenings, and total PCL-C scores; improved CGI-I scores; and changed PDRS scores toward normal dreaming |
| CAPS: Clinician-Administered PTSD Scale; CGI-C: Clinical Global Impression of Change; CGI-I: Clinical Global Impression of Improvement; PCL-C: PTSD Checklist-Civilian; PDRS: PTSD Dream Rating Scale; PTSD: posttraumatic stress disorder; RCTs: randomized controlled trials; REM: rapid eye movement | |||
Atypical antipsychotics
Atypical antipsychotics have been used to reduce nightmares in PTSD; however, most of the evidence from studies evaluated in the AASM’s Best Practice Guide were considered to be low quality.11 Quetiapine and ziprasidone were not included in the AASM review. See (Table 5) for a review of the evidence for atypical antipsychotics for treating PTSD nightmares.
Table 5
Combat-related nightmares: Evidence for atypical antipsychotics
| Study | Design | Patients/dosage | Results |
|---|---|---|---|
| Aripiprazole | |||
| Lambert, 2006 a | Case report | 4 veterans with combat-related PTSD (3 male, 1 female; age 22 to 24); dose: 15 to 30 mg; concurrent treatment sertraline or CBT | Decreased frequency of weekly nightmares and agitated sleep by at least 50% |
| Olanzapine | |||
| Stein et al, 2002 b | 8-week, double-blind, placebo-controlled study | 19 male veterans with combat-related PTSD (olanzapine group mean age: 55.2 ± 6.6; placebo group 51.1 ± 8.1); mean dose: 15 mg/d | Significantly greater reduction in sleep disturbances (PSQI: -3.29 vs 1.57; P = .01); significantly higher weight gain (13.2 lbs vs -3 lbs; P = .001) |
| Jakovljevic et al, 2003 c | Case reports | 5 veterans with combat-related PTSD for 6 to 7 years (age: 28 to 50); dose: 10 to 20 mg; adjunct treatment | Decreased frequency of nightmares within 3 days |
| Labbate et al, 2000 d | Case report | 1 male veteran (age: 58) with a 20-year history of combat-related PTSD; dose: 5 mg at bedtime; concurrent treatment with sertraline (200 mg/d), bupropion (150 mg/d), and diazepam (15 mg/d) | Eliminated nightmares after 1 week and improved sleep quality |
| Quetiapine | |||
| Ahearn et al, 2006 e | 8-week, open-label trial | 15 PTSD patients (8 male; 7 female; 5 with combat-related PTSD; mean age: 49); mean dose: 216 mg/d (100 to 400 mg/d) | Significantly improved re-experiencing (CAPS: 10 vs 23; P = .0012) and sleep (PSQI: 17.5 vs 30; P = .0044) at 8 weeks compared with baseline |
| Robert et al, 2005 f | 6-week, open-label trial | 19 combat veterans; mean dose: 100 ± 70 mg/d (25 to 300 mg/d); adjunct treatment | Significantly improved sleep quality (PSQI: 1.67 vs 2.41; P = .006), latency (PSQI: 1.5 vs 2.65; P = .002), duration (PSQI: 1.31 vs 2.71; P < .001), and sleep disturbances (PSQI: 1.22 vs 1.71; P = .034) and decreased terror episodes (PSQI-A: 0.73 vs 0.91; P = .040) and acting out dreams (PSQI-A: 1.07 vs 1.35; P = .013); however, no difference in nightmares caused by trauma (PSQI-A: 1.53 vs 2.06) |
| Sokolski et al, 2003 g | Retrospective chart review | 68 male Vietnam War combat veterans (mean age: 55 ± 3.5); mean dose: 155 ± 130 mg (25 to 700 mg); adjunct treatment | Improved sleep disturbances in 62% and nightmares in 25% of patients |
| Ahearn et al, 2003 h | Case report | 2 male patients with combat-related PTSD (age 53, 72); dose: 25 to 50 mg; adjunct to SSRI therapy | Decreased frequency of nightmares with increased sleep duration |
| Risperidone | |||
| David et al, 2006 i | 6-week, open-label trial | 17 male veterans with combat-related PTSD (mean age: 53.7 ± 3.8); mean maximum dose: 2.3 ± 0.6 mg (range: 1 to 3 mg) | Improved recurrent distressing dreams (CAPS B-2: 3.8 vs 5.4; P = .04), but not with the PSQI subscale (PSQI bad dreams: 2.5 vs 2.7; NS). Decreased nighttime awakenings (1.9 vs 2.8; P = .003) and trauma dreams (19% vs 38%; P = .04) |
| Leyba et al, 1998 j | Case reports | 3 male patients (age 43 to 46); dose: 1 to 3 mg; adjunct therapy | Decreased occurrence of nightmares |
| Ziprasidone | |||
| Siddiqui et al, 2005 k | Case report | 1 male veteran with chronic combat-related PTSD (age 55); dose: 80 to 120 mg/d; adjunct with trazodone (100 mg) and topiramate | Improved occurrence of nightmares up to 4 months |
CAPS: Clinician-Administered PTSD Scale; CAPS B-2: Clinician-Administered PTSD Scale B-2 (recurrent distressing dreams of the event); CBT: cognitive-behavioral therapy; PSQI: Pittsburgh Sleep Quality Index; PSQI-A: Pittsburgh Sleep Quality Index Addendum for PTSD; NS: not significant; PTSD: posttraumatic stress disorder; SSRI: selective serotonin reuptake inhibitor References
| |||
Comparing prazosin and quetiapine. A historical prospective cohort study of 237 veterans with PTSD receiving prazosin or quetiapine for nighttime PTSD symptoms demonstrated that although the 2 drugs have similar efficacy (defined as symptomatic improvement) for short-term, 6-month treatment (61% vs 62%; P=.54), a higher percentage of patients continued prazosin long-term (3 to 6 years) than those taking quetiapine (48% vs 24%; P < .001).23 Twenty-five percent of patients taking quetiapine switched to prazosin during the study, and approximately one-half of these patients remained on prazosin until the study’s end. Only 8% of prazosin patients switched to quetiapine, and none continued this therapy until study end.23 Patients in the quetiapine group were more likely to discontinue the drug because of lack of efficacy (13% vs 3%; P=.03) and adverse effects (35% vs 18%; P=.008), specifically sedation (21% vs 2%; P < .001) and metabolic effects (9% vs 0%; P=.014), compared with prazosin. Although this trial may be the only published comparison study of prazosin and quetiapine, its methodological quality has been questioned, which makes it difficult to draw definitive conclusions.
Metabolic syndrome—elevated diastolic blood pressure, increased waist circumference, and low high-density lipoprotein cholesterol—is common among PTSD patients treated with antipsychotics.24 This syndrome may be caused by medications, lifestyle factors, or long-term overactivation of stress-response pathways. A retrospective chart review at a community mental health center revealed that patients taking even low doses of quetiapine for insomnia gained an average of 5 lbs (P=.037).25 Another retrospective chart review at 2 military hospitals reported that patients receiving low-dose quetiapine (≤100 mg/d) gained an average of slightly less than 1 lb per month, which adds up to approximately 10 lbs per year (P < .001).26 The benefit of using atypical antipsychotics may be outweighed by metabolic risks such as obesity, new-onset diabetes, and dyslipidemia.27
Prazosin is considered a first-line treatment for sleep disturbances and nightmares in PTSD because of its superior long-term efficacy and decreased adverse effects compared with quetiapine.
Related Resources
- American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
- Veterans Affairs/Department of Defense clinical practice guidelines. Management of traumatic stress disorder and acute stress reaction. www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp.
Drug Brand Names
- Prazosin • Minipress
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
• Prazosin is recommended as a first-line therapy for nighttime PTSD symptoms, such as nightmares or sleep disturbances—especially among veterans—because of superior long-term effectiveness.
• Risk of metabolic syndrome, which has been reported with low-dose atypical antipsychotics used for treating insomnia, limits their use for PTSD-related nightmares.
Mr. S, a 45-year-old veteran, was diagnosed with posttraumatic stress disorder (PTSD) 18 years ago after a tour of duty in the Persian Gulf. He had combat-related flashbacks triggered by the smell of gasoline or smoke from a fire, was easily startled, and began to isolate himself socially. However, his symptoms improved when he started volunteering at his local Veterans Affairs Medical Center. After he lost his job 3 years ago, Mr. S started experiencing flashbacks. He was irritable, easily startled, and avoided things that reminded him of his time in the Persian Gulf. His psychiatrist prescribed sertraline, titrated to 200 mg/d. The drug reduced the severity of his avoidance and hyperarousal symptoms and improved his mood.
During a clinic visit, Mr. S says he is doing well and can fall asleep at night but is having recurring nightmares about traumatic events that occurred during combat. These nightmares wake him up and have become more frequent, occurring once per night for the past month. Mr. S says he has been watching more news programs about conflicts in Afghanistan and Iraq since the nightmares began. His psychiatrist starts quetiapine, 50 mg at bedtime for 7 nights then 100 mg at bedtime, but after 6 weeks Mr. S says his nightmares continue.
PTSD occurs in approximately 19% of Vietnam war combat veterans1 and 14% of service members returning from Iraq and Afghanistan.2 PTSD symptoms are classified into clusters: intrusive/re-experiencing; avoidant/numbing; and hyperarousal.3 Nightmares are part of the intrusive/re-experiencing cluster, which is Criterion B in DSM-IV-TR. See Table 1 for a description of DSM-IV-TR PTSD criteria. Among PTSD patients, 50% to 70% report PTSD-associated nightmares.4 Despite adequate treatment targeted to improve PTSD’s core symptoms, symptoms such as sleep disturbances or nightmares often persist.
Table 1
DSM-IV-TR diagnostic criteria for posttraumatic stress disorder
|
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Nightmares and other sleep disturbances are associated with significant distress and daytime impairment and can interfere with PTSD recovery4-8 by disrupting sleep-dependent processing of emotional experiences and causing repeated resensitization to trauma cues (Table 2).8
Table 2
Psychosocial consequences of sleep disruption in PTSD
| Increased reactivity to emotional cues |
| Compromised ability to function in social and occupational roles |
| Negative psychiatric outcomes, including suicidal ideation or worsening of depression or psychosis |
| Interference of natural recovery from trauma exposure |
| Repeated resensitization to trauma cues |
| Neurocognitive deficits |
| Neuroendocrine abnormalities |
| PTSD: posttraumatic stress disorder Source: Adapted from reference 8 |
Few randomized controlled medication trials specifically address PTSD-related nightmares. Most PTSD studies do not examine sleep outcomes as a primary measure, and comprehensive literature reviews could not offer evidence-based recommendations.9,10 The American Academy of Sleep Medicine (AASM) also noted a paucity of PTSD studies that identified nightmares as a primary outcome measure.11 See Table 3 for a list of recommended medication options for PTSD-associated nightmares.
Table 3
Recommended medication treatments for PTSD-associated nightmares
| Evidence level | Medication | Evidence |
|---|---|---|
| Recommended for treating PTSD-associated nightmares | ||
| 1, 4 | Prazosin | In 3 level 1 studies, adding prazosin (mean dose 3 mg/d) significantly decreased trauma-related nightmares according to the CAPS “recurrent distressing dreams” item after 3 to 9 weeks of treatment vs placebo in veteran and civilian patients (N = 57) |
| Not suggested for treating PTSD-associated nightmares | ||
| 1 | Venlafaxine | No difference between extended-release venlafaxine (37.5 to 300 mg/d) and placebo in the CAPS-SX17 “distressing dreams” item at 12 weeks in 340 PTSD patients |
| May be considered for treating PTSD-associated nightmares | ||
| 4 | Clonidine | Reduced the number of nightmares in 11 of 13 refugees for 2 weeks to 3 months (dose: 0.2 to 0.6 mg/d) |
| May be considered for treating PTSD-associated nightmares, but data are low grade and sparse | ||
| 4 | Trazodone | Although trazodone (25 to 600 mg) significantly decreased nightmare frequency in veteran patients during an 8-week hospital stay (N = 60), 19% discontinued therapy because of side effects |
| 4 | Olanzapine | Adjunctive olanzapine (10 to 20 mg) rapidly improved sleep in a case series of combat-related PTSD patients resistant to SSRIs and benzodiazepines (N = 5) |
| 4 | Risperidone | In case series, risperidone (0.5 to 3 mg) significantly decreased CAPS scores for recurrent distressing dreams and proportion of traumatic dreams documented in diaries of combat veterans over 6 weeks (N = 17), and improved nightmares in adult burn patients taking pain medications after 1 to 2 days (N = 10) |
| 4 | Aripiprazole | In a case series, aripiprazole (15 to 30 mg at bedtime) with CBT or sertraline significantly improved nightmares in 4 of 5 combat-related PTSD patients |
| 4 | Topiramate | Topiramate reduced nightmares in 79% of civilians with PTSD and fully suppressed nightmares in 50% of patients in a case series (N = 35) |
| 4 | Low-dose cortisol | Significant decrease in frequency but not intensity of nightmares with low-dose cortisol (10 mg/d) in civilians with PTSD (N = 3) |
| 4 | Fluvoxamine | In 2 case series, fluvoxamine (up to 300 mg/d) significantly decreased the IES-R level of “dreams about combat trauma” but not the SRRS “bad dreams” rating at 10 weeks (N = 21). During 4 to 12 weeks of follow-up there was a qualitative decrease in reported nightmares in veteran patients (n = 12) |
| 2 | Triazolam/nitrazepam | Limited data showed triazolam (0.5 mg) and nitrazepam (5 mg) provide equal efficacy in decreasing the number of patients who experience unpleasant dreams over 1 night |
| 4 | Phenelzine | One study showed phenelzine monotherapy (30 to 90 mg) resulted in elimination of nightmares within 1 month (N = 5); another reported “moderately reduced traumatic dreams” (N = 21) in veterans. Therapy was discontinued because of short-lived efficacy or plateau effect |
| 4 | Gabapentin | Adjunctive gabapentin (300 to 3,600 mg/d) improved insomnia and decreased nightmare frequency and/or intensity over 1 to 36 months in 30 veterans with PTSD |
| 4 | Cyproheptadine | Conflicting data ranges from eliminating nightmares to no changes in the presence or intensity of nightmares |
| 4 | TCAs | Among 10 Cambodian concentration camp survivors treated with TCAs, 4 reported their nightmares ceased and 4 reported improvement after 1-year follow-up |
| 4 | Nefazodone | Reduced nightmare occurrence in 3 open-label studies as monotherapy (386 to 600 mg/d). Not recommended first line because of hepatotoxicity risk |
| No recommendation because of sparse data | ||
| 2 | Clonazepam | Clonazepam (1 to 2 mg/d) was ineffective in decreasing frequency or intensity of combat-related PTSD nightmares in veterans (N = 6) |
Evidence levels:
| ||
| CAPS: Clinician-Administered PTSD Scale; CAPS-SX17: 17-item Clinician-Administered PTSD Scale; CBT: cognitive-behavioral therapy; IES-R: Impact of Event Scale-Revised; PTSD: posttraumatic stress disorder; SRRS: Stress Response Rating Scale; SSRI: selective serotonin reuptake inhibitor; TCAs: tricyclic antidepressants Source: Adapted from Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401 | ||
CASE CONTINUED: Medication change, improvement
After reviewing AASM’s treatment recommendations, we prescribe prazosin, 1 mg at bedtime for 7 nights, then increase by 1 mg at bedtime each week until Mr. S’s nightmares improve. He reports a substantial improvement in nightmare severity and frequency after a few weeks of treatment with prazosin, 5 mg at bedtime.
Prazosin
Prazosin is an α1-adrenergic receptor antagonist with good CNS penetrability. The rationale for reducing adrenergic activity to address intrusive PTSD symptoms has been well documented.12,13 In open-label trials,14-18 a chart review,19 and placebo-controlled trials,20-22prazosin reduced trauma nightmares and improved sleep quality and global clinical status more than placebo (Table 4). In these studies, prazosin doses ranged from 1 to 20 mg/d, with an average of 3 mg at bedtime and a starting dose of 1 mg. Prazosin is the only agent recommended in the AASM’s Best Practice Guide for treating PTSD-related nightmares.11
Table 4
RCTs of prazosin for trauma-related nightmares
| Study | Design | Patients | Results |
|---|---|---|---|
| Raskind et al, 200320 | 20-week, double-blind, placebo-controlled, crossover study (mean dose 9.5 mg/d at bedtime) | 10 Vietnam veterans with chronic PTSD and severe trauma-related nightmares | Prazosin was superior to placebo on scores on the recurrent distressing dreams item and difficulty falling/staying asleep item of the CAPS and change in PTSD severity and functional status on the CGI-C |
| Raskind et al, 200721 | 8-week, placebo-controlled, parallel study (mean dose 13.3 ± 3 mg/d in the evening) | 40 veterans with chronic PTSD, distressing trauma nightmares, and sleep disturbance | Prazosin was superior to placebo in reducing trauma nightmares and improving sleep quality and global clinical status; prazosin also shifted dream characteristics of trauma-related nightmares to those typical of normal dreams |
| Taylor et al, 200822 | 7-week, randomized, placebo-controlled, crossover trial (mean dose 3.1 ± 1.3 mg) | 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance | Prazosin significantly increased total sleep time and REM sleep time; reduced trauma-related nightmares, distressed awakenings, and total PCL-C scores; improved CGI-I scores; and changed PDRS scores toward normal dreaming |
| CAPS: Clinician-Administered PTSD Scale; CGI-C: Clinical Global Impression of Change; CGI-I: Clinical Global Impression of Improvement; PCL-C: PTSD Checklist-Civilian; PDRS: PTSD Dream Rating Scale; PTSD: posttraumatic stress disorder; RCTs: randomized controlled trials; REM: rapid eye movement | |||
Atypical antipsychotics
Atypical antipsychotics have been used to reduce nightmares in PTSD; however, most of the evidence from studies evaluated in the AASM’s Best Practice Guide were considered to be low quality.11 Quetiapine and ziprasidone were not included in the AASM review. See (Table 5) for a review of the evidence for atypical antipsychotics for treating PTSD nightmares.
Table 5
Combat-related nightmares: Evidence for atypical antipsychotics
| Study | Design | Patients/dosage | Results |
|---|---|---|---|
| Aripiprazole | |||
| Lambert, 2006 a | Case report | 4 veterans with combat-related PTSD (3 male, 1 female; age 22 to 24); dose: 15 to 30 mg; concurrent treatment sertraline or CBT | Decreased frequency of weekly nightmares and agitated sleep by at least 50% |
| Olanzapine | |||
| Stein et al, 2002 b | 8-week, double-blind, placebo-controlled study | 19 male veterans with combat-related PTSD (olanzapine group mean age: 55.2 ± 6.6; placebo group 51.1 ± 8.1); mean dose: 15 mg/d | Significantly greater reduction in sleep disturbances (PSQI: -3.29 vs 1.57; P = .01); significantly higher weight gain (13.2 lbs vs -3 lbs; P = .001) |
| Jakovljevic et al, 2003 c | Case reports | 5 veterans with combat-related PTSD for 6 to 7 years (age: 28 to 50); dose: 10 to 20 mg; adjunct treatment | Decreased frequency of nightmares within 3 days |
| Labbate et al, 2000 d | Case report | 1 male veteran (age: 58) with a 20-year history of combat-related PTSD; dose: 5 mg at bedtime; concurrent treatment with sertraline (200 mg/d), bupropion (150 mg/d), and diazepam (15 mg/d) | Eliminated nightmares after 1 week and improved sleep quality |
| Quetiapine | |||
| Ahearn et al, 2006 e | 8-week, open-label trial | 15 PTSD patients (8 male; 7 female; 5 with combat-related PTSD; mean age: 49); mean dose: 216 mg/d (100 to 400 mg/d) | Significantly improved re-experiencing (CAPS: 10 vs 23; P = .0012) and sleep (PSQI: 17.5 vs 30; P = .0044) at 8 weeks compared with baseline |
| Robert et al, 2005 f | 6-week, open-label trial | 19 combat veterans; mean dose: 100 ± 70 mg/d (25 to 300 mg/d); adjunct treatment | Significantly improved sleep quality (PSQI: 1.67 vs 2.41; P = .006), latency (PSQI: 1.5 vs 2.65; P = .002), duration (PSQI: 1.31 vs 2.71; P < .001), and sleep disturbances (PSQI: 1.22 vs 1.71; P = .034) and decreased terror episodes (PSQI-A: 0.73 vs 0.91; P = .040) and acting out dreams (PSQI-A: 1.07 vs 1.35; P = .013); however, no difference in nightmares caused by trauma (PSQI-A: 1.53 vs 2.06) |
| Sokolski et al, 2003 g | Retrospective chart review | 68 male Vietnam War combat veterans (mean age: 55 ± 3.5); mean dose: 155 ± 130 mg (25 to 700 mg); adjunct treatment | Improved sleep disturbances in 62% and nightmares in 25% of patients |
| Ahearn et al, 2003 h | Case report | 2 male patients with combat-related PTSD (age 53, 72); dose: 25 to 50 mg; adjunct to SSRI therapy | Decreased frequency of nightmares with increased sleep duration |
| Risperidone | |||
| David et al, 2006 i | 6-week, open-label trial | 17 male veterans with combat-related PTSD (mean age: 53.7 ± 3.8); mean maximum dose: 2.3 ± 0.6 mg (range: 1 to 3 mg) | Improved recurrent distressing dreams (CAPS B-2: 3.8 vs 5.4; P = .04), but not with the PSQI subscale (PSQI bad dreams: 2.5 vs 2.7; NS). Decreased nighttime awakenings (1.9 vs 2.8; P = .003) and trauma dreams (19% vs 38%; P = .04) |
| Leyba et al, 1998 j | Case reports | 3 male patients (age 43 to 46); dose: 1 to 3 mg; adjunct therapy | Decreased occurrence of nightmares |
| Ziprasidone | |||
| Siddiqui et al, 2005 k | Case report | 1 male veteran with chronic combat-related PTSD (age 55); dose: 80 to 120 mg/d; adjunct with trazodone (100 mg) and topiramate | Improved occurrence of nightmares up to 4 months |
CAPS: Clinician-Administered PTSD Scale; CAPS B-2: Clinician-Administered PTSD Scale B-2 (recurrent distressing dreams of the event); CBT: cognitive-behavioral therapy; PSQI: Pittsburgh Sleep Quality Index; PSQI-A: Pittsburgh Sleep Quality Index Addendum for PTSD; NS: not significant; PTSD: posttraumatic stress disorder; SSRI: selective serotonin reuptake inhibitor References
| |||
Comparing prazosin and quetiapine. A historical prospective cohort study of 237 veterans with PTSD receiving prazosin or quetiapine for nighttime PTSD symptoms demonstrated that although the 2 drugs have similar efficacy (defined as symptomatic improvement) for short-term, 6-month treatment (61% vs 62%; P=.54), a higher percentage of patients continued prazosin long-term (3 to 6 years) than those taking quetiapine (48% vs 24%; P < .001).23 Twenty-five percent of patients taking quetiapine switched to prazosin during the study, and approximately one-half of these patients remained on prazosin until the study’s end. Only 8% of prazosin patients switched to quetiapine, and none continued this therapy until study end.23 Patients in the quetiapine group were more likely to discontinue the drug because of lack of efficacy (13% vs 3%; P=.03) and adverse effects (35% vs 18%; P=.008), specifically sedation (21% vs 2%; P < .001) and metabolic effects (9% vs 0%; P=.014), compared with prazosin. Although this trial may be the only published comparison study of prazosin and quetiapine, its methodological quality has been questioned, which makes it difficult to draw definitive conclusions.
Metabolic syndrome—elevated diastolic blood pressure, increased waist circumference, and low high-density lipoprotein cholesterol—is common among PTSD patients treated with antipsychotics.24 This syndrome may be caused by medications, lifestyle factors, or long-term overactivation of stress-response pathways. A retrospective chart review at a community mental health center revealed that patients taking even low doses of quetiapine for insomnia gained an average of 5 lbs (P=.037).25 Another retrospective chart review at 2 military hospitals reported that patients receiving low-dose quetiapine (≤100 mg/d) gained an average of slightly less than 1 lb per month, which adds up to approximately 10 lbs per year (P < .001).26 The benefit of using atypical antipsychotics may be outweighed by metabolic risks such as obesity, new-onset diabetes, and dyslipidemia.27
Prazosin is considered a first-line treatment for sleep disturbances and nightmares in PTSD because of its superior long-term efficacy and decreased adverse effects compared with quetiapine.
Related Resources
- American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
- Veterans Affairs/Department of Defense clinical practice guidelines. Management of traumatic stress disorder and acute stress reaction. www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp.
Drug Brand Names
- Prazosin • Minipress
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Dohrenwend BP, Turner JB, Turse NA, et al. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313(5789):979-982.
2. Tanielian T, Jaycox L. eds. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
4. Wittmann L, Schredl M, Kramer M. Dreaming in posttraumatic stress disorder: a critical review of phenomenology psychophysiology and treatment. Psychother Psychosom. 2007;76(1):25-39.
5. Clum GA, Nishith P, Resick PA. Trauma-related sleep disturbance and self-reported physical health symptoms in treatment-seeking female rape victims. J Nerv Ment Dis. 2001;189(9):618-622.
6. Kramer TL, Booth BM, Han X, et al. Service utilization and outcomes in medically ill veterans with posttraumatic stress and depressive disorders. J Trauma Stress. 2003;16(3):211-219.
7. Neylan TC, Marmar CR, Metzler TJ, et al. Sleep disturbances in the Vietnam generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry. 1998;155(7):929-933.
8. Nappi CM, Drummond SP, Hall JM. Treating nightmares and insomnia in posttraumatic stress disorder: a review of current evidence. Neuropharmacology. 2012;62(2):576-585.
9. Maher MJ, Rego SA, Asnis GM. Sleep disturbances in patients with post-traumatic stress disorder: epidemiology impact and approaches to management. CNS Drugs. 2006;20(7):567-590.
10. van Liempt S, Vermetten E, Geuze E, et al. Pharmacotherapy for disordered sleep in post-traumatic stress disorder: a systematic review. Int Clin Psychopharmacol. 2006;21(4):193-202.
11. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401.
12. Boehnlein JK, Kinzie JD. Pharmacologic reduction of CNS noradrenergic activity in PTSD: the case for clonidine and prazosin. J Psychiatr Pract. 2007;13(2):72-78.
13. Strawn JR, Geracioti TD, Jr. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety. 2008;25(3):260-271.
14. Calohan J, Peterson K, Peskind ER, et al. Prazosin treatment of trauma nightmares and sleep disturbance in soldiers deployed in Iraq. J Trauma Stress. 2010;23(5):645-648.
15. Daly CM, Doyle ME, Radkind M, et al. Clinical case series: the use of Prazosin for combat-related recurrent nightmares among Operation Iraqi Freedom combat veterans. Mil Med. 2005;170(6):513-515.
16. Peskind ER, Bonner LT, Hoff DJ, et al. Prazosin reduces trauma-related nightmares in older men with chronic posttraumatic stress disorder. J Geriatr Psychiatry Neurol. 2003;16(3):165-171.
17. Raskind MA, Dobie DJ, Kanter ED, et al. The alpha1-adrenergic antagonist prazosin ameliorates combat trauma nightmares in veterans with posttraumatic stress disorder: a report of 4 cases. J Clin Psychiatry. 2000;61(2):129-133.
18. Taylor F, Raskind MA. The alpha1-adrenergic antagonist prazosin improves sleep and nightmares in civilian trauma posttraumatic stress disorder. J Clin Psychopharmacol. 2002;22(1):82-85.
19. Raskind MA, Thompson C, Petrie EC, et al. Prazosin reduces nightmares in combat veterans with posttraumatic stress disorder. J Clin Psychiatry. 2002;63(7):565-568.
20. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry. 2003;160(2):371-373.
21. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry. 2007;61(8):928-934.
22. Taylor FB, Martin P, Thompson C, et al. Prazosin effects on objective sleep measures and clinical symptoms in civilian trauma posttraumatic stress disorder: a placebo-controlled study. Biol Psychiatry. 2008;63(6):629-632.
23. Byers MG, Allison KM, Wendel CS, et al. Prazosin versus quetiapine for nighttime posttraumatic stress disorder symptoms in veterans: an assessment of long-term comparative effectiveness and safety. J Clin Psychopharmacol. 2010;30(3):225-229.
24. Jin H, Lanouette NM, Mudaliar S, et al. Association of posttraumatic stress disorder with increased prevalence of metabolic syndrome. J Clin Psychopharmacol. 2009;29(3):210-215.
25. Cates ME, Jackson CW, Feldman JM, et al. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Ment Health J. 2009;45(4):251-254.
26. Williams SG, Alinejad NA, Williams JA, et al. Statistically significant increase in weight caused by low-dose quetiapine. Pharmacotherapy. 2010;30(10):1011-1015.
27. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65(2):267-272.
1. Dohrenwend BP, Turner JB, Turse NA, et al. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods. Science. 2006;313(5789):979-982.
2. Tanielian T, Jaycox L. eds. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
4. Wittmann L, Schredl M, Kramer M. Dreaming in posttraumatic stress disorder: a critical review of phenomenology psychophysiology and treatment. Psychother Psychosom. 2007;76(1):25-39.
5. Clum GA, Nishith P, Resick PA. Trauma-related sleep disturbance and self-reported physical health symptoms in treatment-seeking female rape victims. J Nerv Ment Dis. 2001;189(9):618-622.
6. Kramer TL, Booth BM, Han X, et al. Service utilization and outcomes in medically ill veterans with posttraumatic stress and depressive disorders. J Trauma Stress. 2003;16(3):211-219.
7. Neylan TC, Marmar CR, Metzler TJ, et al. Sleep disturbances in the Vietnam generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry. 1998;155(7):929-933.
8. Nappi CM, Drummond SP, Hall JM. Treating nightmares and insomnia in posttraumatic stress disorder: a review of current evidence. Neuropharmacology. 2012;62(2):576-585.
9. Maher MJ, Rego SA, Asnis GM. Sleep disturbances in patients with post-traumatic stress disorder: epidemiology impact and approaches to management. CNS Drugs. 2006;20(7):567-590.
10. van Liempt S, Vermetten E, Geuze E, et al. Pharmacotherapy for disordered sleep in post-traumatic stress disorder: a systematic review. Int Clin Psychopharmacol. 2006;21(4):193-202.
11. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389-401.
12. Boehnlein JK, Kinzie JD. Pharmacologic reduction of CNS noradrenergic activity in PTSD: the case for clonidine and prazosin. J Psychiatr Pract. 2007;13(2):72-78.
13. Strawn JR, Geracioti TD, Jr. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety. 2008;25(3):260-271.
14. Calohan J, Peterson K, Peskind ER, et al. Prazosin treatment of trauma nightmares and sleep disturbance in soldiers deployed in Iraq. J Trauma Stress. 2010;23(5):645-648.
15. Daly CM, Doyle ME, Radkind M, et al. Clinical case series: the use of Prazosin for combat-related recurrent nightmares among Operation Iraqi Freedom combat veterans. Mil Med. 2005;170(6):513-515.
16. Peskind ER, Bonner LT, Hoff DJ, et al. Prazosin reduces trauma-related nightmares in older men with chronic posttraumatic stress disorder. J Geriatr Psychiatry Neurol. 2003;16(3):165-171.
17. Raskind MA, Dobie DJ, Kanter ED, et al. The alpha1-adrenergic antagonist prazosin ameliorates combat trauma nightmares in veterans with posttraumatic stress disorder: a report of 4 cases. J Clin Psychiatry. 2000;61(2):129-133.
18. Taylor F, Raskind MA. The alpha1-adrenergic antagonist prazosin improves sleep and nightmares in civilian trauma posttraumatic stress disorder. J Clin Psychopharmacol. 2002;22(1):82-85.
19. Raskind MA, Thompson C, Petrie EC, et al. Prazosin reduces nightmares in combat veterans with posttraumatic stress disorder. J Clin Psychiatry. 2002;63(7):565-568.
20. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry. 2003;160(2):371-373.
21. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry. 2007;61(8):928-934.
22. Taylor FB, Martin P, Thompson C, et al. Prazosin effects on objective sleep measures and clinical symptoms in civilian trauma posttraumatic stress disorder: a placebo-controlled study. Biol Psychiatry. 2008;63(6):629-632.
23. Byers MG, Allison KM, Wendel CS, et al. Prazosin versus quetiapine for nighttime posttraumatic stress disorder symptoms in veterans: an assessment of long-term comparative effectiveness and safety. J Clin Psychopharmacol. 2010;30(3):225-229.
24. Jin H, Lanouette NM, Mudaliar S, et al. Association of posttraumatic stress disorder with increased prevalence of metabolic syndrome. J Clin Psychopharmacol. 2009;29(3):210-215.
25. Cates ME, Jackson CW, Feldman JM, et al. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Ment Health J. 2009;45(4):251-254.
26. Williams SG, Alinejad NA, Williams JA, et al. Statistically significant increase in weight caused by low-dose quetiapine. Pharmacotherapy. 2010;30(10):1011-1015.
27. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65(2):267-272.
Epileptic and depressed
CASE: New-onset seizures
Ms. R, age 33, is referred by her neurologist for treatment of depressive symptoms that have intensified after she was diagnosed with epilepsy 1 year ago. She has a history of bulimia and ongoing anxiety and depression. She also has long-standing neuropathic pain in her left lateral shin and ankle that started after her foot was amputated in a lawn mower accident at age 5. Ms. R says she didn’t take pain medication until age 24, when her pain specialist prescribed tramadol, 300 to 400 mg/d, which she continues to take.
Ms. R’s first seizure occurred 1 year ago. Despite trials of several antiepileptics, her seizures persist; she is taking lamotrigine, 200 mg/d, when she presents for treatment. She has no history of brain injuries or strokes to explain her epilepsy. An MRI and 3 electroencephalograms show no signs of focal, potentially epileptogenic lesions.
Ms. R reports worsening depressive symptoms—particularly impaired attention and concentration—over several months that interfere with her housekeeping and ability to finish simple tasks at work. She says she drinks alcohol occasionally, but denies substance abuse. We initiate venlafaxine, titrated to 300 mg/d, because Ms. R has a history of intolerable side effects with fluoxetine (gastrointestinal distress) and citalopram (weight gain).
The authors’ observations
Tramadol, a centrally acting synthetic analgesic, consists of 2 enantiomers that act as weak agonists at μ-opioid receptors while also inhibiting serotonin and norepinephrine reuptake.1 Euphoria associated with μ receptor activation often is considered a “high.” Most abused opioids are prototypical μ agonists. When opioids are injected or inhaled, drug levels in the brain rise rapidly, causing a “rush”—a brief, intense, pleasurable sensation—followed by a longer-lasting high. Tolerance and physical dependence occur when opioids are used chronically.
Despite tramadol’s μ-opioid activity, the FDA approved it as an unscheduled analgesic in 1994 based on several human studies.2 Experience with tramadol has confirmed it has low abuse potential, yet human laboratory data—and some epidemiologic data—show that repeated use can lead to physical dependence. Although tramadol is considered a relatively weak opioid, human studies suggest that it possesses μ-agonist activity. The Drug Abuse Warning Network reported >15,000 emergency department (ED) visits for nonmedical tramadol use in 2009, which was more than the number of ED visits for codeine products (7,958) or propoxyphene products (9,526), but much fewer than visits for hydrocodone (86,258) or oxycodone (148,449) products.3
The recommended tramadol dose is 50 to 100 mg every 4 to 6 hours (maximum 400 mg/d). Adverse effects range from dysphoria, constipation, and nausea to agitation, seizures, respiratory depression, and coma.4 Tramadol withdrawal is similar to opioid withdrawal, and is characterized by anxiety, restlessness, insomnia, yawning, rhinorrhea, lacrimation, diaphoresis, tremor, muscle spasms, vomiting, diarrhea, and tachycardia. Rarely, psychomotor agitation and confusion may occur.5
Tramadol and seizures
At clinically appropriate doses, tramadol slightly suppresses seizure severity,6 but higher doses can induce seizures.7-12 This paradox is explained by tramadol’s effect on γ-aminobutyric acid (GABA) receptors. Although at clinical doses tramadol does not affect GABA, which could precipitate seizures, at higher doses it has been shown to have an inhibitory effect on GABA receptors.13,14 No prospective studies have assessed how often tramadol-induced seizures occur. Case reports12,15 suggest that seizures are more likely with acute tramadol intoxication, in patients with a history of alcohol abuse, or with pharmacologic regimens that include other medications that may cause seizures. Tramadol-induced seizures are generalized tonic-clonic in nature, and typically occur within 24 hours of the last dose.16
HISTORY: Worsening seizures
Two months after she presents for psychiatric evaluation, Ms. R experiences 6 generalized convulsions lasting from 15 minutes to 1 hour with no identifiable precipitant. Because oxcarbazepine and lamotrigine have failed to suppress her seizures, her neurologist adds phenytoin, 200 mg/d, and increases lamotrigine from 200 to 300 mg/d. Her depression continues to worsen. She reports severe insomnia, anhedonia, restlessness, and hopelessness, so we add sertraline, 50 mg/d, to venlafaxine. Ms. R says the seizures are terrifying and she cannot work. She moves in with her parents because she is unable to care for herself.
During a psychiatric appointment, Ms. R confesses that for 2 years her pain has been so unbearable that she has been buying extra tramadol from Internet retailers and taking 600 to 800 mg/d in addition to the prescribed 400 mg/d.
The authors’ observations
Ms. R had a history of chronic pain Table 117 and developed seizures after escalating her tramadol use. After her first epilepsy attack, she did not tell her physicians she was taking additional tramadol nor did she stop taking it. Treatment with several antiepileptics was unsuccessful. Her seizures persisted as long as her tramadol addiction continued.
Table 1
DSM-IV-TR criteria for pain disorder
|
| Source: Reference 17 |
Spiller et al18 reported the lowest daily tramadol dose associated with seizures is 500 mg/d, although Talaie et al16 observed seizures at doses as low as 100 mg/d. Additionally, seizure risk may increase through tramadol’s interactions with several medications, including tricyclic antidepressants, selective serotonin reuptake inhibitors, phenothiazines, fluoroquinolone antibiotics, meperidine, clozapine, buspirone, bupropion, phenylephrine, guaifenesin, tripelennamine, thioridazine, theophylline, and acetaminophen, butalbital, and caffeine combination (Table 2).19 Transdermal selegiline is contraindicated with tramadol. For Ms. R, the sertraline and venlafaxine she was taking may have augmented tramadol’s seizure potential.
Table 2
Tramadol: Major drug-drug interactions
| Drug | Symptoms |
|---|---|
| Selegiline | Nausea, vomiting, cardiovascular collapse, respiratory depression, seizures, or serotonin syndrome (hypertension, hyperthermia, myoclonus, mental status changes); use of the transdermal formulation with tramadol is contraindicated |
| Carbamazepine | Decreased tramadol efficacy and increased seizure risk |
| Venlafaxine | Increased risk of serotonin syndrome |
| Linezolid | Increased risk of serotonin syndrome |
| Fluoxetine | Increased risk of seizures and serotonin syndrome; increased concentrations of tramadol and decreased concentrations of tramadol active metabolite, O-desmethyltramadol (M1) |
| Olanzapine | Increased risk of serotonin syndrome |
| Mirtazapine | Increased risk of serotonin syndrome |
| Haloperidol | Increased risk of seizures |
| Escitalopram | Increased risk of seizures and serotonin syndrome |
| Clomipramine | Increased risk of seizures |
| Risperidone | Increased risk of seizures |
| Ketamine | Increased risk of respiratory depression and excessive CNS depression |
| Imipramine | Increased risk of seizures |
| Duloxetine | Increased risk of serotonin syndrome |
| Nortriptyline | Increased risk of seizures |
| Clozapine | Increased risk of seizures |
| Sertraline | Increased risk of seizures and serotonin syndrome |
| Paroxetine | Increased risk of seizures and serotonin syndrome; decrease in the analgesic effect of tramadol |
| Amitriptyline | Increased risk of seizures; increased concentrations of tramadol and decreased concentrations of tramadol active metabolite, M1 |
| Desipramine | Increased risk of seizures |
| Doxepin | Increased risk of seizures |
| Citalopram | Increased risk of seizures and serotonin syndrome |
| Fluvoxamine | Increased risk of seizures and serotonin syndrome |
| Source: Reference 19 | |
It is important to avoid polypharmacy in patients taking tramadol.20 Most psychiatrists are aware of the risk of serotonin syndrome with antidepressants, but may be less likely to attribute serotonergic additive effects from other medication classes such as analgesics. Recognizing tramadol’s potential to contribute to serotonin syndrome—especially in light of concomitant usage with other serotonergic medications such as antidepressants—is essential.
Tramadol toxicity appears to be caused by monoamine uptake inhibition rather than its opioid effects.21 The most frequent pharmacokinetic drug-drug interactions that lead to side effects such as serotonin syndrome or seizures involve several isoenzymes of the hepatic cytochrome P450 (CYP). The isoenzymes CYP2D6 (substrates—eg, amitriptyline, tramadol, and venlafaxine; inhibitors—eg, fluoxetine and duloxetine) and CYP3A4 (substrates—eg, carbamazepine, oxycodone, and venlafaxine; inductors—eg, carbamazepine; inhibitors, eg—grapefruit juice) are most important clinically.22
Ms. R readily obtained tramadol from Internet retailers. In a 2004 report, a Google search yielded 2,150,000 sources for acquiring tramadol, most of which did not require a prescription.23 Chronic pain patients have a higher prevalence of substance abuse than the general population.24 Because Ms. R did not have a documented substance abuse history, none of her physicians screened her for drug abuse, although toxicology screening wouldn’t have helped because the tramadol had been prescribed. We didn’t think to directly ask Ms. R about medication misuse, but if we had, she might have revealed it sooner.
OUTCOME: Seizure free
With Ms. R’s permission, we speak to her neurologist, who agrees that excess tramadol likely induced her seizures. The seizures stop after Ms. R discontinues tramadol. After 3 months without seizures, phenytoin is discontinued and lamotrigine is tapered to 200 mg/d. Ms. R participates in a pain rehabilitation program and continues to take venlafaxine, 300 mg/d, and sertraline, 50 mg/d. Her mood improves and she returns to work. Her pain is managed by non-steroidal anti-inflammatory drugs because she decides to decrease her activity level. Ms. R also is trying alternative medicine modalities such as acupuncture and acupressure.
Related Resource
- Clark MR, Treisman GJ. Chronic pain and addiction. Basel, Switzerland: Karger; 2011.
Drug Brand Names
- Acetaminophen, butalbital, and caffeine • Fioricet
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Carbamazepine • Tegretol, Carbatrol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Desipramine • Norpramin
- Doxepin • Adapin, Silenor
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guaifenesin • Tenex
- Haloperidol • Haldol
- Imipramine • Tofranil
- Ketamine • Ketalar
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Meperidine • Demerol
- Mirtazapine • Remeron
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Oxycodone • Percolone, OxyContin
- Paroxetine • Paxil
- Phenylephrine • Lusonal
- Phenytoin • Dilantin
- Propoxyphene • Darvon
- Risperidone • Risperdal
- Selegiline • Eldepryl, EMSAM
- Sertraline • Zoloft
- Theophylline • Aerolate
- Thioridazine • Mellaril
- Tramadol • Ultram
- Tripelennamine • Pyribenzamine
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufactur-ers of competing products.
1. Katz KD. Tramadol is an opioid. J Med Toxicol. 2008;4(2):145-
2. Preston KL, Jasinski DR, Testa M. Abuse potential and pharmacological comparison of tramadol and morphine. Drug Alcohol Depend. 1991;27(1):7-17.
3. U.S. Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. Drug abuse warning network, 2009: national estimates of drug-related emergency department visits. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2011. HHS publication (SMA) 11-4659, DAWN Series D-35.
4. Afshari R, Ghooshkhanehee H. Tramadol overdose induced seizure dramatic rise of CPK and acute renal failure. J Pak Med Assoc. 2009;59(3):178.-
5. Rodriguez Villamañan JC, Albaladejo Blanco C, Sanchez Sanchez A, et al. Withdrawal syndrome after long-term treatment with tramadol. Br J Gen Pract. 2000;50(454):406.-
6. Manocha A, Sharma KK, Mediratta PK. On the mechanism of anticonvulsant effect of tramadol in mice. Pharmacol Biochem Behav. 2005;82(1):74-81.
7. Boyd IW. Tramadol and seizures. Med J Aust. 2005;182(11):595-596.
8. Labate A, Newton MR, Vernon GM, et al. Tramadol and new-onset seizures. Med J Aust. 2005;182(1):42-43.
9. Gasse C, Derby L, Vasilakis-Scaramozza C, et al. Incidence of first-time idiopathic seizures in users of tramadol. Pharmacotherapy. 2000;20(6):629-634.
10. Kahn LH, Alderfer RJ, Graham DJ. Seizures reported with tramadol. JAMA. 1997;278(20):1661.-
11. Mazor SS, Feldman KW, Sugar NF, et al. Pediatric tramadol ingestion resulting in seizurelike activity: a case series. Pediatr Emerg Care. 2008;24(6):380-381.
12. Raffa RB, Stone DJ, Jr. Unexceptional seizure potential of tramadol or its enantiomers or metabolites in mice. J Pharmacol Exp Ther. 2008;325(2):500-506.
13. Rehni AK, Singh TG, Singh N, et al. Tramadol-induced seizurogenic effect: a possible role of opioid-dependent histamine H1 receptor activation-linked mechanism. Naunyn Schmiedebergs Arch Pharmacol. 2010;381(1):11-19.
14. Rehni AK, Singh I, Kumar M. Tramadol-induced seizurogenic effect: a possible role of opioid-dependent gamma-aminobutyric acid inhibitory pathway. Basic Clin Pharmacol Toxicol. 2008;103(3):262-266.
15. Jovanović-Cupić V, Martinović Z, Nesić N. Seizures associated with intoxication and abuse of tramadol. Clin Toxicol (Phila). 2006;44(2):143-146.
16. Talaie H, Panahandeh R, Fayaznouri M, et al. Dose-independent occurrence of seizure with tramadol. J Med Toxicol. 2009;5(2):63-67.
17. Diagnostic and statistical manual of mental disorders 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
18. Spiller HA, Gorman SE, Villalobos D, et al. Prospective multicenter evaluation of tramadol exposure. J Toxicol Clin Toxicol. 1997;35(4):361-364.
19. Reus VI, Rawitscher L. Possible interaction of tramadol and antidepressants. Am J Psychiatry. 2000;157(5):839.-
20. Thundiyil JG, Kearney TE, Olson KR. Evolving epidemiology of drug-induced seizures reported to a Poison Control Center System. J Med Toxicol. 2007;3(1):15-19.
21. Looper KJ. Potential medical and surgical complications of serotonergic antidepressant medications. Psychosomatics. 2007;48(1):1-9.
22. Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879-923.
23. Lineberry TW, Bostwick JM. Taking the physician out of “physician shopping”: a case series of clinical problems associated with Internet purchases of medication. Mayo Clin Proc. 2004;79(8):1031-1034.
24. Savage SR. Assessment for addiction in pain-treatment settings. Clin J Pain. 2002;18(4 suppl):S28-S38.
CASE: New-onset seizures
Ms. R, age 33, is referred by her neurologist for treatment of depressive symptoms that have intensified after she was diagnosed with epilepsy 1 year ago. She has a history of bulimia and ongoing anxiety and depression. She also has long-standing neuropathic pain in her left lateral shin and ankle that started after her foot was amputated in a lawn mower accident at age 5. Ms. R says she didn’t take pain medication until age 24, when her pain specialist prescribed tramadol, 300 to 400 mg/d, which she continues to take.
Ms. R’s first seizure occurred 1 year ago. Despite trials of several antiepileptics, her seizures persist; she is taking lamotrigine, 200 mg/d, when she presents for treatment. She has no history of brain injuries or strokes to explain her epilepsy. An MRI and 3 electroencephalograms show no signs of focal, potentially epileptogenic lesions.
Ms. R reports worsening depressive symptoms—particularly impaired attention and concentration—over several months that interfere with her housekeeping and ability to finish simple tasks at work. She says she drinks alcohol occasionally, but denies substance abuse. We initiate venlafaxine, titrated to 300 mg/d, because Ms. R has a history of intolerable side effects with fluoxetine (gastrointestinal distress) and citalopram (weight gain).
The authors’ observations
Tramadol, a centrally acting synthetic analgesic, consists of 2 enantiomers that act as weak agonists at μ-opioid receptors while also inhibiting serotonin and norepinephrine reuptake.1 Euphoria associated with μ receptor activation often is considered a “high.” Most abused opioids are prototypical μ agonists. When opioids are injected or inhaled, drug levels in the brain rise rapidly, causing a “rush”—a brief, intense, pleasurable sensation—followed by a longer-lasting high. Tolerance and physical dependence occur when opioids are used chronically.
Despite tramadol’s μ-opioid activity, the FDA approved it as an unscheduled analgesic in 1994 based on several human studies.2 Experience with tramadol has confirmed it has low abuse potential, yet human laboratory data—and some epidemiologic data—show that repeated use can lead to physical dependence. Although tramadol is considered a relatively weak opioid, human studies suggest that it possesses μ-agonist activity. The Drug Abuse Warning Network reported >15,000 emergency department (ED) visits for nonmedical tramadol use in 2009, which was more than the number of ED visits for codeine products (7,958) or propoxyphene products (9,526), but much fewer than visits for hydrocodone (86,258) or oxycodone (148,449) products.3
The recommended tramadol dose is 50 to 100 mg every 4 to 6 hours (maximum 400 mg/d). Adverse effects range from dysphoria, constipation, and nausea to agitation, seizures, respiratory depression, and coma.4 Tramadol withdrawal is similar to opioid withdrawal, and is characterized by anxiety, restlessness, insomnia, yawning, rhinorrhea, lacrimation, diaphoresis, tremor, muscle spasms, vomiting, diarrhea, and tachycardia. Rarely, psychomotor agitation and confusion may occur.5
Tramadol and seizures
At clinically appropriate doses, tramadol slightly suppresses seizure severity,6 but higher doses can induce seizures.7-12 This paradox is explained by tramadol’s effect on γ-aminobutyric acid (GABA) receptors. Although at clinical doses tramadol does not affect GABA, which could precipitate seizures, at higher doses it has been shown to have an inhibitory effect on GABA receptors.13,14 No prospective studies have assessed how often tramadol-induced seizures occur. Case reports12,15 suggest that seizures are more likely with acute tramadol intoxication, in patients with a history of alcohol abuse, or with pharmacologic regimens that include other medications that may cause seizures. Tramadol-induced seizures are generalized tonic-clonic in nature, and typically occur within 24 hours of the last dose.16
HISTORY: Worsening seizures
Two months after she presents for psychiatric evaluation, Ms. R experiences 6 generalized convulsions lasting from 15 minutes to 1 hour with no identifiable precipitant. Because oxcarbazepine and lamotrigine have failed to suppress her seizures, her neurologist adds phenytoin, 200 mg/d, and increases lamotrigine from 200 to 300 mg/d. Her depression continues to worsen. She reports severe insomnia, anhedonia, restlessness, and hopelessness, so we add sertraline, 50 mg/d, to venlafaxine. Ms. R says the seizures are terrifying and she cannot work. She moves in with her parents because she is unable to care for herself.
During a psychiatric appointment, Ms. R confesses that for 2 years her pain has been so unbearable that she has been buying extra tramadol from Internet retailers and taking 600 to 800 mg/d in addition to the prescribed 400 mg/d.
The authors’ observations
Ms. R had a history of chronic pain Table 117 and developed seizures after escalating her tramadol use. After her first epilepsy attack, she did not tell her physicians she was taking additional tramadol nor did she stop taking it. Treatment with several antiepileptics was unsuccessful. Her seizures persisted as long as her tramadol addiction continued.
Table 1
DSM-IV-TR criteria for pain disorder
|
| Source: Reference 17 |
Spiller et al18 reported the lowest daily tramadol dose associated with seizures is 500 mg/d, although Talaie et al16 observed seizures at doses as low as 100 mg/d. Additionally, seizure risk may increase through tramadol’s interactions with several medications, including tricyclic antidepressants, selective serotonin reuptake inhibitors, phenothiazines, fluoroquinolone antibiotics, meperidine, clozapine, buspirone, bupropion, phenylephrine, guaifenesin, tripelennamine, thioridazine, theophylline, and acetaminophen, butalbital, and caffeine combination (Table 2).19 Transdermal selegiline is contraindicated with tramadol. For Ms. R, the sertraline and venlafaxine she was taking may have augmented tramadol’s seizure potential.
Table 2
Tramadol: Major drug-drug interactions
| Drug | Symptoms |
|---|---|
| Selegiline | Nausea, vomiting, cardiovascular collapse, respiratory depression, seizures, or serotonin syndrome (hypertension, hyperthermia, myoclonus, mental status changes); use of the transdermal formulation with tramadol is contraindicated |
| Carbamazepine | Decreased tramadol efficacy and increased seizure risk |
| Venlafaxine | Increased risk of serotonin syndrome |
| Linezolid | Increased risk of serotonin syndrome |
| Fluoxetine | Increased risk of seizures and serotonin syndrome; increased concentrations of tramadol and decreased concentrations of tramadol active metabolite, O-desmethyltramadol (M1) |
| Olanzapine | Increased risk of serotonin syndrome |
| Mirtazapine | Increased risk of serotonin syndrome |
| Haloperidol | Increased risk of seizures |
| Escitalopram | Increased risk of seizures and serotonin syndrome |
| Clomipramine | Increased risk of seizures |
| Risperidone | Increased risk of seizures |
| Ketamine | Increased risk of respiratory depression and excessive CNS depression |
| Imipramine | Increased risk of seizures |
| Duloxetine | Increased risk of serotonin syndrome |
| Nortriptyline | Increased risk of seizures |
| Clozapine | Increased risk of seizures |
| Sertraline | Increased risk of seizures and serotonin syndrome |
| Paroxetine | Increased risk of seizures and serotonin syndrome; decrease in the analgesic effect of tramadol |
| Amitriptyline | Increased risk of seizures; increased concentrations of tramadol and decreased concentrations of tramadol active metabolite, M1 |
| Desipramine | Increased risk of seizures |
| Doxepin | Increased risk of seizures |
| Citalopram | Increased risk of seizures and serotonin syndrome |
| Fluvoxamine | Increased risk of seizures and serotonin syndrome |
| Source: Reference 19 | |
It is important to avoid polypharmacy in patients taking tramadol.20 Most psychiatrists are aware of the risk of serotonin syndrome with antidepressants, but may be less likely to attribute serotonergic additive effects from other medication classes such as analgesics. Recognizing tramadol’s potential to contribute to serotonin syndrome—especially in light of concomitant usage with other serotonergic medications such as antidepressants—is essential.
Tramadol toxicity appears to be caused by monoamine uptake inhibition rather than its opioid effects.21 The most frequent pharmacokinetic drug-drug interactions that lead to side effects such as serotonin syndrome or seizures involve several isoenzymes of the hepatic cytochrome P450 (CYP). The isoenzymes CYP2D6 (substrates—eg, amitriptyline, tramadol, and venlafaxine; inhibitors—eg, fluoxetine and duloxetine) and CYP3A4 (substrates—eg, carbamazepine, oxycodone, and venlafaxine; inductors—eg, carbamazepine; inhibitors, eg—grapefruit juice) are most important clinically.22
Ms. R readily obtained tramadol from Internet retailers. In a 2004 report, a Google search yielded 2,150,000 sources for acquiring tramadol, most of which did not require a prescription.23 Chronic pain patients have a higher prevalence of substance abuse than the general population.24 Because Ms. R did not have a documented substance abuse history, none of her physicians screened her for drug abuse, although toxicology screening wouldn’t have helped because the tramadol had been prescribed. We didn’t think to directly ask Ms. R about medication misuse, but if we had, she might have revealed it sooner.
OUTCOME: Seizure free
With Ms. R’s permission, we speak to her neurologist, who agrees that excess tramadol likely induced her seizures. The seizures stop after Ms. R discontinues tramadol. After 3 months without seizures, phenytoin is discontinued and lamotrigine is tapered to 200 mg/d. Ms. R participates in a pain rehabilitation program and continues to take venlafaxine, 300 mg/d, and sertraline, 50 mg/d. Her mood improves and she returns to work. Her pain is managed by non-steroidal anti-inflammatory drugs because she decides to decrease her activity level. Ms. R also is trying alternative medicine modalities such as acupuncture and acupressure.
Related Resource
- Clark MR, Treisman GJ. Chronic pain and addiction. Basel, Switzerland: Karger; 2011.
Drug Brand Names
- Acetaminophen, butalbital, and caffeine • Fioricet
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Carbamazepine • Tegretol, Carbatrol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Desipramine • Norpramin
- Doxepin • Adapin, Silenor
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guaifenesin • Tenex
- Haloperidol • Haldol
- Imipramine • Tofranil
- Ketamine • Ketalar
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Meperidine • Demerol
- Mirtazapine • Remeron
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Oxycodone • Percolone, OxyContin
- Paroxetine • Paxil
- Phenylephrine • Lusonal
- Phenytoin • Dilantin
- Propoxyphene • Darvon
- Risperidone • Risperdal
- Selegiline • Eldepryl, EMSAM
- Sertraline • Zoloft
- Theophylline • Aerolate
- Thioridazine • Mellaril
- Tramadol • Ultram
- Tripelennamine • Pyribenzamine
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufactur-ers of competing products.
CASE: New-onset seizures
Ms. R, age 33, is referred by her neurologist for treatment of depressive symptoms that have intensified after she was diagnosed with epilepsy 1 year ago. She has a history of bulimia and ongoing anxiety and depression. She also has long-standing neuropathic pain in her left lateral shin and ankle that started after her foot was amputated in a lawn mower accident at age 5. Ms. R says she didn’t take pain medication until age 24, when her pain specialist prescribed tramadol, 300 to 400 mg/d, which she continues to take.
Ms. R’s first seizure occurred 1 year ago. Despite trials of several antiepileptics, her seizures persist; she is taking lamotrigine, 200 mg/d, when she presents for treatment. She has no history of brain injuries or strokes to explain her epilepsy. An MRI and 3 electroencephalograms show no signs of focal, potentially epileptogenic lesions.
Ms. R reports worsening depressive symptoms—particularly impaired attention and concentration—over several months that interfere with her housekeeping and ability to finish simple tasks at work. She says she drinks alcohol occasionally, but denies substance abuse. We initiate venlafaxine, titrated to 300 mg/d, because Ms. R has a history of intolerable side effects with fluoxetine (gastrointestinal distress) and citalopram (weight gain).
The authors’ observations
Tramadol, a centrally acting synthetic analgesic, consists of 2 enantiomers that act as weak agonists at μ-opioid receptors while also inhibiting serotonin and norepinephrine reuptake.1 Euphoria associated with μ receptor activation often is considered a “high.” Most abused opioids are prototypical μ agonists. When opioids are injected or inhaled, drug levels in the brain rise rapidly, causing a “rush”—a brief, intense, pleasurable sensation—followed by a longer-lasting high. Tolerance and physical dependence occur when opioids are used chronically.
Despite tramadol’s μ-opioid activity, the FDA approved it as an unscheduled analgesic in 1994 based on several human studies.2 Experience with tramadol has confirmed it has low abuse potential, yet human laboratory data—and some epidemiologic data—show that repeated use can lead to physical dependence. Although tramadol is considered a relatively weak opioid, human studies suggest that it possesses μ-agonist activity. The Drug Abuse Warning Network reported >15,000 emergency department (ED) visits for nonmedical tramadol use in 2009, which was more than the number of ED visits for codeine products (7,958) or propoxyphene products (9,526), but much fewer than visits for hydrocodone (86,258) or oxycodone (148,449) products.3
The recommended tramadol dose is 50 to 100 mg every 4 to 6 hours (maximum 400 mg/d). Adverse effects range from dysphoria, constipation, and nausea to agitation, seizures, respiratory depression, and coma.4 Tramadol withdrawal is similar to opioid withdrawal, and is characterized by anxiety, restlessness, insomnia, yawning, rhinorrhea, lacrimation, diaphoresis, tremor, muscle spasms, vomiting, diarrhea, and tachycardia. Rarely, psychomotor agitation and confusion may occur.5
Tramadol and seizures
At clinically appropriate doses, tramadol slightly suppresses seizure severity,6 but higher doses can induce seizures.7-12 This paradox is explained by tramadol’s effect on γ-aminobutyric acid (GABA) receptors. Although at clinical doses tramadol does not affect GABA, which could precipitate seizures, at higher doses it has been shown to have an inhibitory effect on GABA receptors.13,14 No prospective studies have assessed how often tramadol-induced seizures occur. Case reports12,15 suggest that seizures are more likely with acute tramadol intoxication, in patients with a history of alcohol abuse, or with pharmacologic regimens that include other medications that may cause seizures. Tramadol-induced seizures are generalized tonic-clonic in nature, and typically occur within 24 hours of the last dose.16
HISTORY: Worsening seizures
Two months after she presents for psychiatric evaluation, Ms. R experiences 6 generalized convulsions lasting from 15 minutes to 1 hour with no identifiable precipitant. Because oxcarbazepine and lamotrigine have failed to suppress her seizures, her neurologist adds phenytoin, 200 mg/d, and increases lamotrigine from 200 to 300 mg/d. Her depression continues to worsen. She reports severe insomnia, anhedonia, restlessness, and hopelessness, so we add sertraline, 50 mg/d, to venlafaxine. Ms. R says the seizures are terrifying and she cannot work. She moves in with her parents because she is unable to care for herself.
During a psychiatric appointment, Ms. R confesses that for 2 years her pain has been so unbearable that she has been buying extra tramadol from Internet retailers and taking 600 to 800 mg/d in addition to the prescribed 400 mg/d.
The authors’ observations
Ms. R had a history of chronic pain Table 117 and developed seizures after escalating her tramadol use. After her first epilepsy attack, she did not tell her physicians she was taking additional tramadol nor did she stop taking it. Treatment with several antiepileptics was unsuccessful. Her seizures persisted as long as her tramadol addiction continued.
Table 1
DSM-IV-TR criteria for pain disorder
|
| Source: Reference 17 |
Spiller et al18 reported the lowest daily tramadol dose associated with seizures is 500 mg/d, although Talaie et al16 observed seizures at doses as low as 100 mg/d. Additionally, seizure risk may increase through tramadol’s interactions with several medications, including tricyclic antidepressants, selective serotonin reuptake inhibitors, phenothiazines, fluoroquinolone antibiotics, meperidine, clozapine, buspirone, bupropion, phenylephrine, guaifenesin, tripelennamine, thioridazine, theophylline, and acetaminophen, butalbital, and caffeine combination (Table 2).19 Transdermal selegiline is contraindicated with tramadol. For Ms. R, the sertraline and venlafaxine she was taking may have augmented tramadol’s seizure potential.
Table 2
Tramadol: Major drug-drug interactions
| Drug | Symptoms |
|---|---|
| Selegiline | Nausea, vomiting, cardiovascular collapse, respiratory depression, seizures, or serotonin syndrome (hypertension, hyperthermia, myoclonus, mental status changes); use of the transdermal formulation with tramadol is contraindicated |
| Carbamazepine | Decreased tramadol efficacy and increased seizure risk |
| Venlafaxine | Increased risk of serotonin syndrome |
| Linezolid | Increased risk of serotonin syndrome |
| Fluoxetine | Increased risk of seizures and serotonin syndrome; increased concentrations of tramadol and decreased concentrations of tramadol active metabolite, O-desmethyltramadol (M1) |
| Olanzapine | Increased risk of serotonin syndrome |
| Mirtazapine | Increased risk of serotonin syndrome |
| Haloperidol | Increased risk of seizures |
| Escitalopram | Increased risk of seizures and serotonin syndrome |
| Clomipramine | Increased risk of seizures |
| Risperidone | Increased risk of seizures |
| Ketamine | Increased risk of respiratory depression and excessive CNS depression |
| Imipramine | Increased risk of seizures |
| Duloxetine | Increased risk of serotonin syndrome |
| Nortriptyline | Increased risk of seizures |
| Clozapine | Increased risk of seizures |
| Sertraline | Increased risk of seizures and serotonin syndrome |
| Paroxetine | Increased risk of seizures and serotonin syndrome; decrease in the analgesic effect of tramadol |
| Amitriptyline | Increased risk of seizures; increased concentrations of tramadol and decreased concentrations of tramadol active metabolite, M1 |
| Desipramine | Increased risk of seizures |
| Doxepin | Increased risk of seizures |
| Citalopram | Increased risk of seizures and serotonin syndrome |
| Fluvoxamine | Increased risk of seizures and serotonin syndrome |
| Source: Reference 19 | |
It is important to avoid polypharmacy in patients taking tramadol.20 Most psychiatrists are aware of the risk of serotonin syndrome with antidepressants, but may be less likely to attribute serotonergic additive effects from other medication classes such as analgesics. Recognizing tramadol’s potential to contribute to serotonin syndrome—especially in light of concomitant usage with other serotonergic medications such as antidepressants—is essential.
Tramadol toxicity appears to be caused by monoamine uptake inhibition rather than its opioid effects.21 The most frequent pharmacokinetic drug-drug interactions that lead to side effects such as serotonin syndrome or seizures involve several isoenzymes of the hepatic cytochrome P450 (CYP). The isoenzymes CYP2D6 (substrates—eg, amitriptyline, tramadol, and venlafaxine; inhibitors—eg, fluoxetine and duloxetine) and CYP3A4 (substrates—eg, carbamazepine, oxycodone, and venlafaxine; inductors—eg, carbamazepine; inhibitors, eg—grapefruit juice) are most important clinically.22
Ms. R readily obtained tramadol from Internet retailers. In a 2004 report, a Google search yielded 2,150,000 sources for acquiring tramadol, most of which did not require a prescription.23 Chronic pain patients have a higher prevalence of substance abuse than the general population.24 Because Ms. R did not have a documented substance abuse history, none of her physicians screened her for drug abuse, although toxicology screening wouldn’t have helped because the tramadol had been prescribed. We didn’t think to directly ask Ms. R about medication misuse, but if we had, she might have revealed it sooner.
OUTCOME: Seizure free
With Ms. R’s permission, we speak to her neurologist, who agrees that excess tramadol likely induced her seizures. The seizures stop after Ms. R discontinues tramadol. After 3 months without seizures, phenytoin is discontinued and lamotrigine is tapered to 200 mg/d. Ms. R participates in a pain rehabilitation program and continues to take venlafaxine, 300 mg/d, and sertraline, 50 mg/d. Her mood improves and she returns to work. Her pain is managed by non-steroidal anti-inflammatory drugs because she decides to decrease her activity level. Ms. R also is trying alternative medicine modalities such as acupuncture and acupressure.
Related Resource
- Clark MR, Treisman GJ. Chronic pain and addiction. Basel, Switzerland: Karger; 2011.
Drug Brand Names
- Acetaminophen, butalbital, and caffeine • Fioricet
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Carbamazepine • Tegretol, Carbatrol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Desipramine • Norpramin
- Doxepin • Adapin, Silenor
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guaifenesin • Tenex
- Haloperidol • Haldol
- Imipramine • Tofranil
- Ketamine • Ketalar
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Meperidine • Demerol
- Mirtazapine • Remeron
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Oxycodone • Percolone, OxyContin
- Paroxetine • Paxil
- Phenylephrine • Lusonal
- Phenytoin • Dilantin
- Propoxyphene • Darvon
- Risperidone • Risperdal
- Selegiline • Eldepryl, EMSAM
- Sertraline • Zoloft
- Theophylline • Aerolate
- Thioridazine • Mellaril
- Tramadol • Ultram
- Tripelennamine • Pyribenzamine
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufactur-ers of competing products.
1. Katz KD. Tramadol is an opioid. J Med Toxicol. 2008;4(2):145-
2. Preston KL, Jasinski DR, Testa M. Abuse potential and pharmacological comparison of tramadol and morphine. Drug Alcohol Depend. 1991;27(1):7-17.
3. U.S. Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. Drug abuse warning network, 2009: national estimates of drug-related emergency department visits. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2011. HHS publication (SMA) 11-4659, DAWN Series D-35.
4. Afshari R, Ghooshkhanehee H. Tramadol overdose induced seizure dramatic rise of CPK and acute renal failure. J Pak Med Assoc. 2009;59(3):178.-
5. Rodriguez Villamañan JC, Albaladejo Blanco C, Sanchez Sanchez A, et al. Withdrawal syndrome after long-term treatment with tramadol. Br J Gen Pract. 2000;50(454):406.-
6. Manocha A, Sharma KK, Mediratta PK. On the mechanism of anticonvulsant effect of tramadol in mice. Pharmacol Biochem Behav. 2005;82(1):74-81.
7. Boyd IW. Tramadol and seizures. Med J Aust. 2005;182(11):595-596.
8. Labate A, Newton MR, Vernon GM, et al. Tramadol and new-onset seizures. Med J Aust. 2005;182(1):42-43.
9. Gasse C, Derby L, Vasilakis-Scaramozza C, et al. Incidence of first-time idiopathic seizures in users of tramadol. Pharmacotherapy. 2000;20(6):629-634.
10. Kahn LH, Alderfer RJ, Graham DJ. Seizures reported with tramadol. JAMA. 1997;278(20):1661.-
11. Mazor SS, Feldman KW, Sugar NF, et al. Pediatric tramadol ingestion resulting in seizurelike activity: a case series. Pediatr Emerg Care. 2008;24(6):380-381.
12. Raffa RB, Stone DJ, Jr. Unexceptional seizure potential of tramadol or its enantiomers or metabolites in mice. J Pharmacol Exp Ther. 2008;325(2):500-506.
13. Rehni AK, Singh TG, Singh N, et al. Tramadol-induced seizurogenic effect: a possible role of opioid-dependent histamine H1 receptor activation-linked mechanism. Naunyn Schmiedebergs Arch Pharmacol. 2010;381(1):11-19.
14. Rehni AK, Singh I, Kumar M. Tramadol-induced seizurogenic effect: a possible role of opioid-dependent gamma-aminobutyric acid inhibitory pathway. Basic Clin Pharmacol Toxicol. 2008;103(3):262-266.
15. Jovanović-Cupić V, Martinović Z, Nesić N. Seizures associated with intoxication and abuse of tramadol. Clin Toxicol (Phila). 2006;44(2):143-146.
16. Talaie H, Panahandeh R, Fayaznouri M, et al. Dose-independent occurrence of seizure with tramadol. J Med Toxicol. 2009;5(2):63-67.
17. Diagnostic and statistical manual of mental disorders 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
18. Spiller HA, Gorman SE, Villalobos D, et al. Prospective multicenter evaluation of tramadol exposure. J Toxicol Clin Toxicol. 1997;35(4):361-364.
19. Reus VI, Rawitscher L. Possible interaction of tramadol and antidepressants. Am J Psychiatry. 2000;157(5):839.-
20. Thundiyil JG, Kearney TE, Olson KR. Evolving epidemiology of drug-induced seizures reported to a Poison Control Center System. J Med Toxicol. 2007;3(1):15-19.
21. Looper KJ. Potential medical and surgical complications of serotonergic antidepressant medications. Psychosomatics. 2007;48(1):1-9.
22. Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879-923.
23. Lineberry TW, Bostwick JM. Taking the physician out of “physician shopping”: a case series of clinical problems associated with Internet purchases of medication. Mayo Clin Proc. 2004;79(8):1031-1034.
24. Savage SR. Assessment for addiction in pain-treatment settings. Clin J Pain. 2002;18(4 suppl):S28-S38.
1. Katz KD. Tramadol is an opioid. J Med Toxicol. 2008;4(2):145-
2. Preston KL, Jasinski DR, Testa M. Abuse potential and pharmacological comparison of tramadol and morphine. Drug Alcohol Depend. 1991;27(1):7-17.
3. U.S. Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. Drug abuse warning network, 2009: national estimates of drug-related emergency department visits. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2011. HHS publication (SMA) 11-4659, DAWN Series D-35.
4. Afshari R, Ghooshkhanehee H. Tramadol overdose induced seizure dramatic rise of CPK and acute renal failure. J Pak Med Assoc. 2009;59(3):178.-
5. Rodriguez Villamañan JC, Albaladejo Blanco C, Sanchez Sanchez A, et al. Withdrawal syndrome after long-term treatment with tramadol. Br J Gen Pract. 2000;50(454):406.-
6. Manocha A, Sharma KK, Mediratta PK. On the mechanism of anticonvulsant effect of tramadol in mice. Pharmacol Biochem Behav. 2005;82(1):74-81.
7. Boyd IW. Tramadol and seizures. Med J Aust. 2005;182(11):595-596.
8. Labate A, Newton MR, Vernon GM, et al. Tramadol and new-onset seizures. Med J Aust. 2005;182(1):42-43.
9. Gasse C, Derby L, Vasilakis-Scaramozza C, et al. Incidence of first-time idiopathic seizures in users of tramadol. Pharmacotherapy. 2000;20(6):629-634.
10. Kahn LH, Alderfer RJ, Graham DJ. Seizures reported with tramadol. JAMA. 1997;278(20):1661.-
11. Mazor SS, Feldman KW, Sugar NF, et al. Pediatric tramadol ingestion resulting in seizurelike activity: a case series. Pediatr Emerg Care. 2008;24(6):380-381.
12. Raffa RB, Stone DJ, Jr. Unexceptional seizure potential of tramadol or its enantiomers or metabolites in mice. J Pharmacol Exp Ther. 2008;325(2):500-506.
13. Rehni AK, Singh TG, Singh N, et al. Tramadol-induced seizurogenic effect: a possible role of opioid-dependent histamine H1 receptor activation-linked mechanism. Naunyn Schmiedebergs Arch Pharmacol. 2010;381(1):11-19.
14. Rehni AK, Singh I, Kumar M. Tramadol-induced seizurogenic effect: a possible role of opioid-dependent gamma-aminobutyric acid inhibitory pathway. Basic Clin Pharmacol Toxicol. 2008;103(3):262-266.
15. Jovanović-Cupić V, Martinović Z, Nesić N. Seizures associated with intoxication and abuse of tramadol. Clin Toxicol (Phila). 2006;44(2):143-146.
16. Talaie H, Panahandeh R, Fayaznouri M, et al. Dose-independent occurrence of seizure with tramadol. J Med Toxicol. 2009;5(2):63-67.
17. Diagnostic and statistical manual of mental disorders 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
18. Spiller HA, Gorman SE, Villalobos D, et al. Prospective multicenter evaluation of tramadol exposure. J Toxicol Clin Toxicol. 1997;35(4):361-364.
19. Reus VI, Rawitscher L. Possible interaction of tramadol and antidepressants. Am J Psychiatry. 2000;157(5):839.-
20. Thundiyil JG, Kearney TE, Olson KR. Evolving epidemiology of drug-induced seizures reported to a Poison Control Center System. J Med Toxicol. 2007;3(1):15-19.
21. Looper KJ. Potential medical and surgical complications of serotonergic antidepressant medications. Psychosomatics. 2007;48(1):1-9.
22. Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879-923.
23. Lineberry TW, Bostwick JM. Taking the physician out of “physician shopping”: a case series of clinical problems associated with Internet purchases of medication. Mayo Clin Proc. 2004;79(8):1031-1034.
24. Savage SR. Assessment for addiction in pain-treatment settings. Clin J Pain. 2002;18(4 suppl):S28-S38.
Psychotic and in pain
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Depressed and delusional
Mrs. P, age 58, is a retired art teacher who presents for inpatient psychiatric admission after an 8-month depressive and psychotic illness. She reports profound feelings of worthlessness, anhedonia, psychomotor retardation, daily spontaneous crying spells, and worsening suicidal ideation. She is unkempt, disheveled, and makes limited eye contact. She is floridly psychotic, exhibits hebephrenia at times, and appears to be having conversations with people who are not there. Mrs. P reports derogatory intracranial auditory hallucinations of her brother’s and father’s voices. She also describes a complex delusional system relating to sexual trauma she experienced as a child perpetrated by her brother. Her family corroborates some details of the trauma; however, she says her father, neighbors, pastor, and outpatient psychiatrist are involved. Mrs. P believes these individuals are members of a cult, she has been the victim of a satanic sexual rite, and a television news personality knows about this conspiracy and has been attempting to contact her.
Mrs. P suffers from severe, debilitating chronic pain experienced as shock-like pain lasting for several minutes that starts in her throat and radiates to her left ear. Her pain began several years ago and prompted a neurologic workup, including MRI of the head and somatosensory evoked potentials of the glossopharyngeal nerve. She was diagnosed with “probable” glossopharyngeal neuralgia and failed multiple medication trials, including carbamazepine, phenytoin, gabapentin, and amitriptyline. She underwent microvascular decompression surgery 3 years ago. The operation, which has an 80% to 90% success rate for neuralgias,1,2 offered only brief symptomatic relief. She was maintained on immediate-release opiates until the pain became “unbearable” 8 months ago. This prompted a second neurologic workup, which was unremarkable. Mrs. P was diagnosed with pain disorder associated with psychological factors and a general medical condition.
Ten years ago she had 2 major depressive episodes with inpatient hospitalization and 2 suicide attempts within 1 year, but no history of psychosis before 8 months ago. Mrs. P’s husband says his wife has no history of manic or hypomanic episodes. Her medications are ziprasidone, 20 mg/d, thiothixene, 10 mg/d, benztropine, 3 mg/d, and escitalopram, 30 mg/d. She also receives oxycodone/acetaminophen, 5 mg/325 mg as needed for facial pain and headaches, and clonazepam, 1 mg as needed for panic attacks.
The authors’ observations
Psychosis can be a feature of any of the disorders listed in Table 13; however, several features of Mrs. P’s illness led us to diagnose MDD, recurrent, severe with psychotic features.4 Mrs. P and her husband described several discreet episodes of major debilitating depression without alternating periods of hypomanic or manic symptoms (Table 2).4 Comorbid depressive symptoms and a timeline indicating persistence of psychotic symptoms make a brief psychotic episode less likely. Although uncommon, patients can develop psychotic or mood disorders as a result of opiate abuse or dependence. However, Mrs. P was taking opiates as prescribed and not asking for early refills, which makes substance abuse an unlikely cause of her psychosis. In addition, because Mrs. P had 2 major depressive episodes in the absence of opiate use, a primary mood disorder seemed the more appropriate diagnosis. Schizophrenia is ruled out based on history. Although Mrs. P was suffering from complex delusional constructs, auditory hallucinations, and grossly disorganized behavior, these symptoms occurred only within the context of her depressive episode. New-onset delusional guilt relating to her childhood sexual trauma and hypochondriacal preoccupations within the context of pain complaints make psychotic depression more likely.5
Table 1
Psychiatric diseases in which patients may present with psychotic symptoms
| Bipolar depression |
| Borderline personality disorder |
| Brief psychotic disorder |
| Delirium |
| Delusional disorder |
| Dementia |
| Major depressive disorder |
| Psychotic disorder due to a general medical condition |
| Schizoaffective disorder |
| Schizophrenia |
| Shared psychotic disorder |
| Substance-induced psychosis |
| Source: Reference 3 |
Table 2
DSM-IV-TR criteria for major depressive episode
|
| Source: Reference 4 |
Depression, psychosis, and pain
From the beginning of Mrs. P’s treatment, we considered psychotic depression worsened—if not completely explained—her pain. Her somatic complaints appeared to be subtly woven into her delusional constructs. For instance, she complained that a device had been implanted in her head and she had the scar to prove it, pointing to the scar from her microvascular decompression surgery. Research indicates that depressive illness and chronic pain syndromes are highly comorbid and depressive illness can worsen pain syndromes.6,7 In addition, Mrs. P failed several medical and 1 surgical interventions for her pain condition that had high success rates. Her husband notes that when her outpatient psychiatrist started olanzapine 3 months ago for emerging psychotic symptoms, her pain complaints initially decreased with her psychotic symptoms, and she used less opiate medication during that time. Several months later Mrs. P’s pain complaints increased as her psychotic symptoms worsened. Second-generation antipsychotics have been evaluated as treatment for chronic pain syndromes, and may exert a primary analgesic effect.8,9 However, because of the correlation between her fluctuating psychotic symptoms and pain complaints, the more plausible explanation for olanzapine’s initial efficacy in treating Mrs. P’s pain is a secondary analgesic effect from decreased psychotic somatic preoccupation.
TREATMENT: ECT
Mrs. P is admitted to the inpatient psychiatric unit and placed on suicide precautions. Oxycodone/acetaminophen and clonazepam are tapered and limited to twice daily as needed. Escitalopram is tapered and discontinued. Thiothixene is tapered and replaced by olanzapine, 5 mg/d. Mrs. P receives 3 bifrontal, brief pulse-width ECT treatments. These result in marked improvement in her depressive and psychotic symptoms. In addition, her pain complaints become minimal. She becomes less preoccupied with her sexual trauma and grows to trust many staff members whom she previously believed were part of her traumatic childhood events. Mrs. P is no longer suicidal and asks to continue ECT treatments as an outpatient. She is discharged on olanzapine, 5 mg/d, trazodone, 100 mg/d for insomnia, benztropine, 2 mg/d, clonazepam 0.5 mg twice daily as needed for panic attacks, and oxycodone/acetaminophen, 5 mg/325 mg twice daily as needed for pain.
The authors’ observations
According to the Harvard South Shore Algorithm, treatment strategies for psychotic depression include antidepressant and antipsychotic combinations, lithium augmentation, clozapine, and ECT.10 Several factors made ECT the best option for Mrs. P. She had failed multiple treatment strategies and was suicidal. ECT is an effective treatment for MDD with psychotic features, single or recurrent episode.11 ECT can be used as a primary treatment before psychotropic medications or secondarily when there has been lack of clinical response to medications, intolerable side effects, deterioration in psychiatric condition, or suicidality.11,12 In addition, when treated with ECT, psychotic depression has a significantly higher remission rate than major depression without psychosis.12 Delusional guilt, psychomotor retardation, hypochondriacal preoccupations, loss of insight, paranoia, and obsessive-compulsive symptoms predict a favorable response.12 ECT also has demonstrated efficacy for treating pain secondary to psychotic depression or melancholic depression.13 In addition, ECT has been shown to have analgesic properties beyond treating underlying depression.14 Our primary focus was not to treat Mrs. P’s pain syndrome with ECT; however, in treating her psychotic depression we had hoped that her pain tolerance would improve and she would rely less on opiates.
OUTCOME: Pain relief
As an outpatient, Mrs. P receives 11 bifrontal ECT treatments in her initial series, followed by 7 bifrontal maintenance treatments. Her speech is more spontaneous, her grooming and hygiene improve, and she exhibits a brighter and more reactive affect. Suicidal ideation has resolved. Pain improves from a “10 out of 10” to a “2 out of 10.” Mrs. P consistently requires less oxycodone/acetaminophen. She relates better to her family and begins exploring new hobbies such as pottery. In addition to monthly maintenance bifrontal ECT treatments, she is stable on citalopram, 60 mg/d, and trazodone, 50 mg/d as needed for insomnia.
The authors’ observations
The relationship between depressive illness and chronic pain is complex. Treating a primary depressive illness can lead to improved functional outcomes and decreased disability from chronic pain complaints.15 Patients with comorbid chronic pain and depressive illness are more likely to suffer from unremitting pain despite compliance with evidence-based treatment strategies.16 Mrs. P had 2 co-occurring disorders: psychotic depression and chronic pain disorder secondary to glossopharyngeal neuralgia. Our opinion is that Mrs. P’s psychotic depression worsened her experience of pain.
Treatment strategies that address both depressive symptoms and chronic pain are ideal.17 These treatment modalities include psychotherapeutic techniques such as cognitive-behavioral therapy, medications, and somatic treatments such as ECT.18 In Mrs. P’s case, ECT was an effective treatment that caused remission of psychotic depressive symptoms, which lead to improved pain control and restored social and occupational functioning.
Related Resources
- Schreiber S, Shmueli D, Grunhaus L, et al. The influence of electroconvulsive therapy on pain threshold and pain tolerance in major depression patients before, during and after treatment. Eur J Pain. 2003;7(5):419-424.
- Suzuki K, Ebina Y, Shindo T, et al. Repeated electroconvulsive therapy courses improved chronic regional pain with depression caused by failed back syndrome. Med Sci Monit. 2009;15(4):CS77-CS79.
- Giesecke T, Gracely RH, Williams DA, et al. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005;52(5):1577-1584.
Drug Brand Names
- Amitriptyline • Elavil
- Benztropine • Cogentin
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Escitalopram • Lexapro
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Olanzapine • Zyprexa
- Oxycodone/ acetaminophen • Vicodin
- Phenytoin • Dilantin
- Thiothixene • Navane
- Trazodone • Desyrel, Oleptro
- Ziprasidone • Geodon
Disclosures
Dr. Kugler reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Magid receives NARSAD grant support.
1. Kawashima M, Matsushima T, Inoue T, et al. Microvascular decompression for glossopharyngeal neuralgia through the transcondylar fossa (supracondylar transjugular tubercle) approach. Neurosurgery. 2010;66(6 suppl operative):275-280.
2. Ferroli P, Fioravanti A, Schiariti M, et al. Microvascular decompression for glossopharyngeal neuralgia: a long-term retrospective review of the Milan-Bologna experience in 31 consecutive cases. Acta Neurochir (Wien). 2009;151(10):1245-1250.
3. Stahl SM. Stahl’s essential psychopharmacology: neuroscientific basis and practical applications. 3rd ed. New York NY: Cambridge University Press; 2008.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev.Washington DC: American Psychiatric Association; 2000.
5. Rothschild AJ. Diagnosis and assessment. In: Rothschild AJ. Clinical manual for diagnosis and treatment of psychotic depression. Arlington VA: American Psychiatric Publishing Inc.; 2009:57-71.
6. Tunks ER, Crook J, Weir R. Epidemiology of chronic pain with psychological comorbidity: prevalence risk, course and prognosis. Can J Psychiatry. 2008;53(4):235-242.
7. Hooten MW, Shi Y, Gazelka HM, et al. The effects of depression and smoking on pain severity and opioid use in patients with chronic pain. Pain. 2011;152(1):223-229.
8. Rico-Villademoros F, Hidalgo J, Dominguez I, et al. Atypical antipsychotics in the treatment of fibromyalgia: a case series with olanzapine. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):161-164.
9. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. J Pain Symptom Manage. 2010;39(4):768-778.
10. Hamoda HM, Osser DN. The Psychopharmacology Algorithm Project at the Harvard South Shore Program: an update on psychotic depression. Harv Rev Psychiatry. 2008;16(4):235-247.
11. American Psychiatric Association. Committee on Electroconvulsive Therapy, Weiner RD, eds. The practice of electroconvulsive therapy: recommendations for treatment, training and privileging. 2nd ed. Washington DC: American Psychiatric Association; 2001.
12. Petrides G, Fink M, Husain MM, et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: a report from CORE. J ECT. 2001;17(4):244-253.
13. Rasmussen KG, Rummans TA. Electroconvulsive therapy in the management of chronic pain. Curr Pain Headache Rep. 2002;6(1):17-22.
14. Wasan AD, Artin K, Clark MR. A case-matching study of the analgesic properties of electroconvulsive therapy. Pain Med. 2004;5(1):50-58.
15. Teh FC, Zaslavsky AM, Reynolds CF, 3rd, et al. Effect of depression treatment on chronic pain outcomes. Psychosom Med. 2010;72(1):61-67.
16. Sertel Berk HO. The biopsychosocial factors that serve as predictors of the outcome of surgical modalities for chronic pain. Agri. 2010;22(3):93-97.
17. Bair MJ, Robinson RL, Katon W, et al. Depression and pain comorbidity. Arch Intern Med. 2003;163(20):2433-2445.
18. Veehof MM, Oskam MJ, Schreurs KM, et al. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis. Pain. 2011;152(3):533-542.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Depressed and delusional
Mrs. P, age 58, is a retired art teacher who presents for inpatient psychiatric admission after an 8-month depressive and psychotic illness. She reports profound feelings of worthlessness, anhedonia, psychomotor retardation, daily spontaneous crying spells, and worsening suicidal ideation. She is unkempt, disheveled, and makes limited eye contact. She is floridly psychotic, exhibits hebephrenia at times, and appears to be having conversations with people who are not there. Mrs. P reports derogatory intracranial auditory hallucinations of her brother’s and father’s voices. She also describes a complex delusional system relating to sexual trauma she experienced as a child perpetrated by her brother. Her family corroborates some details of the trauma; however, she says her father, neighbors, pastor, and outpatient psychiatrist are involved. Mrs. P believes these individuals are members of a cult, she has been the victim of a satanic sexual rite, and a television news personality knows about this conspiracy and has been attempting to contact her.
Mrs. P suffers from severe, debilitating chronic pain experienced as shock-like pain lasting for several minutes that starts in her throat and radiates to her left ear. Her pain began several years ago and prompted a neurologic workup, including MRI of the head and somatosensory evoked potentials of the glossopharyngeal nerve. She was diagnosed with “probable” glossopharyngeal neuralgia and failed multiple medication trials, including carbamazepine, phenytoin, gabapentin, and amitriptyline. She underwent microvascular decompression surgery 3 years ago. The operation, which has an 80% to 90% success rate for neuralgias,1,2 offered only brief symptomatic relief. She was maintained on immediate-release opiates until the pain became “unbearable” 8 months ago. This prompted a second neurologic workup, which was unremarkable. Mrs. P was diagnosed with pain disorder associated with psychological factors and a general medical condition.
Ten years ago she had 2 major depressive episodes with inpatient hospitalization and 2 suicide attempts within 1 year, but no history of psychosis before 8 months ago. Mrs. P’s husband says his wife has no history of manic or hypomanic episodes. Her medications are ziprasidone, 20 mg/d, thiothixene, 10 mg/d, benztropine, 3 mg/d, and escitalopram, 30 mg/d. She also receives oxycodone/acetaminophen, 5 mg/325 mg as needed for facial pain and headaches, and clonazepam, 1 mg as needed for panic attacks.
The authors’ observations
Psychosis can be a feature of any of the disorders listed in Table 13; however, several features of Mrs. P’s illness led us to diagnose MDD, recurrent, severe with psychotic features.4 Mrs. P and her husband described several discreet episodes of major debilitating depression without alternating periods of hypomanic or manic symptoms (Table 2).4 Comorbid depressive symptoms and a timeline indicating persistence of psychotic symptoms make a brief psychotic episode less likely. Although uncommon, patients can develop psychotic or mood disorders as a result of opiate abuse or dependence. However, Mrs. P was taking opiates as prescribed and not asking for early refills, which makes substance abuse an unlikely cause of her psychosis. In addition, because Mrs. P had 2 major depressive episodes in the absence of opiate use, a primary mood disorder seemed the more appropriate diagnosis. Schizophrenia is ruled out based on history. Although Mrs. P was suffering from complex delusional constructs, auditory hallucinations, and grossly disorganized behavior, these symptoms occurred only within the context of her depressive episode. New-onset delusional guilt relating to her childhood sexual trauma and hypochondriacal preoccupations within the context of pain complaints make psychotic depression more likely.5
Table 1
Psychiatric diseases in which patients may present with psychotic symptoms
| Bipolar depression |
| Borderline personality disorder |
| Brief psychotic disorder |
| Delirium |
| Delusional disorder |
| Dementia |
| Major depressive disorder |
| Psychotic disorder due to a general medical condition |
| Schizoaffective disorder |
| Schizophrenia |
| Shared psychotic disorder |
| Substance-induced psychosis |
| Source: Reference 3 |
Table 2
DSM-IV-TR criteria for major depressive episode
|
| Source: Reference 4 |
Depression, psychosis, and pain
From the beginning of Mrs. P’s treatment, we considered psychotic depression worsened—if not completely explained—her pain. Her somatic complaints appeared to be subtly woven into her delusional constructs. For instance, she complained that a device had been implanted in her head and she had the scar to prove it, pointing to the scar from her microvascular decompression surgery. Research indicates that depressive illness and chronic pain syndromes are highly comorbid and depressive illness can worsen pain syndromes.6,7 In addition, Mrs. P failed several medical and 1 surgical interventions for her pain condition that had high success rates. Her husband notes that when her outpatient psychiatrist started olanzapine 3 months ago for emerging psychotic symptoms, her pain complaints initially decreased with her psychotic symptoms, and she used less opiate medication during that time. Several months later Mrs. P’s pain complaints increased as her psychotic symptoms worsened. Second-generation antipsychotics have been evaluated as treatment for chronic pain syndromes, and may exert a primary analgesic effect.8,9 However, because of the correlation between her fluctuating psychotic symptoms and pain complaints, the more plausible explanation for olanzapine’s initial efficacy in treating Mrs. P’s pain is a secondary analgesic effect from decreased psychotic somatic preoccupation.
TREATMENT: ECT
Mrs. P is admitted to the inpatient psychiatric unit and placed on suicide precautions. Oxycodone/acetaminophen and clonazepam are tapered and limited to twice daily as needed. Escitalopram is tapered and discontinued. Thiothixene is tapered and replaced by olanzapine, 5 mg/d. Mrs. P receives 3 bifrontal, brief pulse-width ECT treatments. These result in marked improvement in her depressive and psychotic symptoms. In addition, her pain complaints become minimal. She becomes less preoccupied with her sexual trauma and grows to trust many staff members whom she previously believed were part of her traumatic childhood events. Mrs. P is no longer suicidal and asks to continue ECT treatments as an outpatient. She is discharged on olanzapine, 5 mg/d, trazodone, 100 mg/d for insomnia, benztropine, 2 mg/d, clonazepam 0.5 mg twice daily as needed for panic attacks, and oxycodone/acetaminophen, 5 mg/325 mg twice daily as needed for pain.
The authors’ observations
According to the Harvard South Shore Algorithm, treatment strategies for psychotic depression include antidepressant and antipsychotic combinations, lithium augmentation, clozapine, and ECT.10 Several factors made ECT the best option for Mrs. P. She had failed multiple treatment strategies and was suicidal. ECT is an effective treatment for MDD with psychotic features, single or recurrent episode.11 ECT can be used as a primary treatment before psychotropic medications or secondarily when there has been lack of clinical response to medications, intolerable side effects, deterioration in psychiatric condition, or suicidality.11,12 In addition, when treated with ECT, psychotic depression has a significantly higher remission rate than major depression without psychosis.12 Delusional guilt, psychomotor retardation, hypochondriacal preoccupations, loss of insight, paranoia, and obsessive-compulsive symptoms predict a favorable response.12 ECT also has demonstrated efficacy for treating pain secondary to psychotic depression or melancholic depression.13 In addition, ECT has been shown to have analgesic properties beyond treating underlying depression.14 Our primary focus was not to treat Mrs. P’s pain syndrome with ECT; however, in treating her psychotic depression we had hoped that her pain tolerance would improve and she would rely less on opiates.
OUTCOME: Pain relief
As an outpatient, Mrs. P receives 11 bifrontal ECT treatments in her initial series, followed by 7 bifrontal maintenance treatments. Her speech is more spontaneous, her grooming and hygiene improve, and she exhibits a brighter and more reactive affect. Suicidal ideation has resolved. Pain improves from a “10 out of 10” to a “2 out of 10.” Mrs. P consistently requires less oxycodone/acetaminophen. She relates better to her family and begins exploring new hobbies such as pottery. In addition to monthly maintenance bifrontal ECT treatments, she is stable on citalopram, 60 mg/d, and trazodone, 50 mg/d as needed for insomnia.
The authors’ observations
The relationship between depressive illness and chronic pain is complex. Treating a primary depressive illness can lead to improved functional outcomes and decreased disability from chronic pain complaints.15 Patients with comorbid chronic pain and depressive illness are more likely to suffer from unremitting pain despite compliance with evidence-based treatment strategies.16 Mrs. P had 2 co-occurring disorders: psychotic depression and chronic pain disorder secondary to glossopharyngeal neuralgia. Our opinion is that Mrs. P’s psychotic depression worsened her experience of pain.
Treatment strategies that address both depressive symptoms and chronic pain are ideal.17 These treatment modalities include psychotherapeutic techniques such as cognitive-behavioral therapy, medications, and somatic treatments such as ECT.18 In Mrs. P’s case, ECT was an effective treatment that caused remission of psychotic depressive symptoms, which lead to improved pain control and restored social and occupational functioning.
Related Resources
- Schreiber S, Shmueli D, Grunhaus L, et al. The influence of electroconvulsive therapy on pain threshold and pain tolerance in major depression patients before, during and after treatment. Eur J Pain. 2003;7(5):419-424.
- Suzuki K, Ebina Y, Shindo T, et al. Repeated electroconvulsive therapy courses improved chronic regional pain with depression caused by failed back syndrome. Med Sci Monit. 2009;15(4):CS77-CS79.
- Giesecke T, Gracely RH, Williams DA, et al. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005;52(5):1577-1584.
Drug Brand Names
- Amitriptyline • Elavil
- Benztropine • Cogentin
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Escitalopram • Lexapro
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Olanzapine • Zyprexa
- Oxycodone/ acetaminophen • Vicodin
- Phenytoin • Dilantin
- Thiothixene • Navane
- Trazodone • Desyrel, Oleptro
- Ziprasidone • Geodon
Disclosures
Dr. Kugler reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Magid receives NARSAD grant support.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Depressed and delusional
Mrs. P, age 58, is a retired art teacher who presents for inpatient psychiatric admission after an 8-month depressive and psychotic illness. She reports profound feelings of worthlessness, anhedonia, psychomotor retardation, daily spontaneous crying spells, and worsening suicidal ideation. She is unkempt, disheveled, and makes limited eye contact. She is floridly psychotic, exhibits hebephrenia at times, and appears to be having conversations with people who are not there. Mrs. P reports derogatory intracranial auditory hallucinations of her brother’s and father’s voices. She also describes a complex delusional system relating to sexual trauma she experienced as a child perpetrated by her brother. Her family corroborates some details of the trauma; however, she says her father, neighbors, pastor, and outpatient psychiatrist are involved. Mrs. P believes these individuals are members of a cult, she has been the victim of a satanic sexual rite, and a television news personality knows about this conspiracy and has been attempting to contact her.
Mrs. P suffers from severe, debilitating chronic pain experienced as shock-like pain lasting for several minutes that starts in her throat and radiates to her left ear. Her pain began several years ago and prompted a neurologic workup, including MRI of the head and somatosensory evoked potentials of the glossopharyngeal nerve. She was diagnosed with “probable” glossopharyngeal neuralgia and failed multiple medication trials, including carbamazepine, phenytoin, gabapentin, and amitriptyline. She underwent microvascular decompression surgery 3 years ago. The operation, which has an 80% to 90% success rate for neuralgias,1,2 offered only brief symptomatic relief. She was maintained on immediate-release opiates until the pain became “unbearable” 8 months ago. This prompted a second neurologic workup, which was unremarkable. Mrs. P was diagnosed with pain disorder associated with psychological factors and a general medical condition.
Ten years ago she had 2 major depressive episodes with inpatient hospitalization and 2 suicide attempts within 1 year, but no history of psychosis before 8 months ago. Mrs. P’s husband says his wife has no history of manic or hypomanic episodes. Her medications are ziprasidone, 20 mg/d, thiothixene, 10 mg/d, benztropine, 3 mg/d, and escitalopram, 30 mg/d. She also receives oxycodone/acetaminophen, 5 mg/325 mg as needed for facial pain and headaches, and clonazepam, 1 mg as needed for panic attacks.
The authors’ observations
Psychosis can be a feature of any of the disorders listed in Table 13; however, several features of Mrs. P’s illness led us to diagnose MDD, recurrent, severe with psychotic features.4 Mrs. P and her husband described several discreet episodes of major debilitating depression without alternating periods of hypomanic or manic symptoms (Table 2).4 Comorbid depressive symptoms and a timeline indicating persistence of psychotic symptoms make a brief psychotic episode less likely. Although uncommon, patients can develop psychotic or mood disorders as a result of opiate abuse or dependence. However, Mrs. P was taking opiates as prescribed and not asking for early refills, which makes substance abuse an unlikely cause of her psychosis. In addition, because Mrs. P had 2 major depressive episodes in the absence of opiate use, a primary mood disorder seemed the more appropriate diagnosis. Schizophrenia is ruled out based on history. Although Mrs. P was suffering from complex delusional constructs, auditory hallucinations, and grossly disorganized behavior, these symptoms occurred only within the context of her depressive episode. New-onset delusional guilt relating to her childhood sexual trauma and hypochondriacal preoccupations within the context of pain complaints make psychotic depression more likely.5
Table 1
Psychiatric diseases in which patients may present with psychotic symptoms
| Bipolar depression |
| Borderline personality disorder |
| Brief psychotic disorder |
| Delirium |
| Delusional disorder |
| Dementia |
| Major depressive disorder |
| Psychotic disorder due to a general medical condition |
| Schizoaffective disorder |
| Schizophrenia |
| Shared psychotic disorder |
| Substance-induced psychosis |
| Source: Reference 3 |
Table 2
DSM-IV-TR criteria for major depressive episode
|
| Source: Reference 4 |
Depression, psychosis, and pain
From the beginning of Mrs. P’s treatment, we considered psychotic depression worsened—if not completely explained—her pain. Her somatic complaints appeared to be subtly woven into her delusional constructs. For instance, she complained that a device had been implanted in her head and she had the scar to prove it, pointing to the scar from her microvascular decompression surgery. Research indicates that depressive illness and chronic pain syndromes are highly comorbid and depressive illness can worsen pain syndromes.6,7 In addition, Mrs. P failed several medical and 1 surgical interventions for her pain condition that had high success rates. Her husband notes that when her outpatient psychiatrist started olanzapine 3 months ago for emerging psychotic symptoms, her pain complaints initially decreased with her psychotic symptoms, and she used less opiate medication during that time. Several months later Mrs. P’s pain complaints increased as her psychotic symptoms worsened. Second-generation antipsychotics have been evaluated as treatment for chronic pain syndromes, and may exert a primary analgesic effect.8,9 However, because of the correlation between her fluctuating psychotic symptoms and pain complaints, the more plausible explanation for olanzapine’s initial efficacy in treating Mrs. P’s pain is a secondary analgesic effect from decreased psychotic somatic preoccupation.
TREATMENT: ECT
Mrs. P is admitted to the inpatient psychiatric unit and placed on suicide precautions. Oxycodone/acetaminophen and clonazepam are tapered and limited to twice daily as needed. Escitalopram is tapered and discontinued. Thiothixene is tapered and replaced by olanzapine, 5 mg/d. Mrs. P receives 3 bifrontal, brief pulse-width ECT treatments. These result in marked improvement in her depressive and psychotic symptoms. In addition, her pain complaints become minimal. She becomes less preoccupied with her sexual trauma and grows to trust many staff members whom she previously believed were part of her traumatic childhood events. Mrs. P is no longer suicidal and asks to continue ECT treatments as an outpatient. She is discharged on olanzapine, 5 mg/d, trazodone, 100 mg/d for insomnia, benztropine, 2 mg/d, clonazepam 0.5 mg twice daily as needed for panic attacks, and oxycodone/acetaminophen, 5 mg/325 mg twice daily as needed for pain.
The authors’ observations
According to the Harvard South Shore Algorithm, treatment strategies for psychotic depression include antidepressant and antipsychotic combinations, lithium augmentation, clozapine, and ECT.10 Several factors made ECT the best option for Mrs. P. She had failed multiple treatment strategies and was suicidal. ECT is an effective treatment for MDD with psychotic features, single or recurrent episode.11 ECT can be used as a primary treatment before psychotropic medications or secondarily when there has been lack of clinical response to medications, intolerable side effects, deterioration in psychiatric condition, or suicidality.11,12 In addition, when treated with ECT, psychotic depression has a significantly higher remission rate than major depression without psychosis.12 Delusional guilt, psychomotor retardation, hypochondriacal preoccupations, loss of insight, paranoia, and obsessive-compulsive symptoms predict a favorable response.12 ECT also has demonstrated efficacy for treating pain secondary to psychotic depression or melancholic depression.13 In addition, ECT has been shown to have analgesic properties beyond treating underlying depression.14 Our primary focus was not to treat Mrs. P’s pain syndrome with ECT; however, in treating her psychotic depression we had hoped that her pain tolerance would improve and she would rely less on opiates.
OUTCOME: Pain relief
As an outpatient, Mrs. P receives 11 bifrontal ECT treatments in her initial series, followed by 7 bifrontal maintenance treatments. Her speech is more spontaneous, her grooming and hygiene improve, and she exhibits a brighter and more reactive affect. Suicidal ideation has resolved. Pain improves from a “10 out of 10” to a “2 out of 10.” Mrs. P consistently requires less oxycodone/acetaminophen. She relates better to her family and begins exploring new hobbies such as pottery. In addition to monthly maintenance bifrontal ECT treatments, she is stable on citalopram, 60 mg/d, and trazodone, 50 mg/d as needed for insomnia.
The authors’ observations
The relationship between depressive illness and chronic pain is complex. Treating a primary depressive illness can lead to improved functional outcomes and decreased disability from chronic pain complaints.15 Patients with comorbid chronic pain and depressive illness are more likely to suffer from unremitting pain despite compliance with evidence-based treatment strategies.16 Mrs. P had 2 co-occurring disorders: psychotic depression and chronic pain disorder secondary to glossopharyngeal neuralgia. Our opinion is that Mrs. P’s psychotic depression worsened her experience of pain.
Treatment strategies that address both depressive symptoms and chronic pain are ideal.17 These treatment modalities include psychotherapeutic techniques such as cognitive-behavioral therapy, medications, and somatic treatments such as ECT.18 In Mrs. P’s case, ECT was an effective treatment that caused remission of psychotic depressive symptoms, which lead to improved pain control and restored social and occupational functioning.
Related Resources
- Schreiber S, Shmueli D, Grunhaus L, et al. The influence of electroconvulsive therapy on pain threshold and pain tolerance in major depression patients before, during and after treatment. Eur J Pain. 2003;7(5):419-424.
- Suzuki K, Ebina Y, Shindo T, et al. Repeated electroconvulsive therapy courses improved chronic regional pain with depression caused by failed back syndrome. Med Sci Monit. 2009;15(4):CS77-CS79.
- Giesecke T, Gracely RH, Williams DA, et al. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005;52(5):1577-1584.
Drug Brand Names
- Amitriptyline • Elavil
- Benztropine • Cogentin
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Escitalopram • Lexapro
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Olanzapine • Zyprexa
- Oxycodone/ acetaminophen • Vicodin
- Phenytoin • Dilantin
- Thiothixene • Navane
- Trazodone • Desyrel, Oleptro
- Ziprasidone • Geodon
Disclosures
Dr. Kugler reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Magid receives NARSAD grant support.
1. Kawashima M, Matsushima T, Inoue T, et al. Microvascular decompression for glossopharyngeal neuralgia through the transcondylar fossa (supracondylar transjugular tubercle) approach. Neurosurgery. 2010;66(6 suppl operative):275-280.
2. Ferroli P, Fioravanti A, Schiariti M, et al. Microvascular decompression for glossopharyngeal neuralgia: a long-term retrospective review of the Milan-Bologna experience in 31 consecutive cases. Acta Neurochir (Wien). 2009;151(10):1245-1250.
3. Stahl SM. Stahl’s essential psychopharmacology: neuroscientific basis and practical applications. 3rd ed. New York NY: Cambridge University Press; 2008.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev.Washington DC: American Psychiatric Association; 2000.
5. Rothschild AJ. Diagnosis and assessment. In: Rothschild AJ. Clinical manual for diagnosis and treatment of psychotic depression. Arlington VA: American Psychiatric Publishing Inc.; 2009:57-71.
6. Tunks ER, Crook J, Weir R. Epidemiology of chronic pain with psychological comorbidity: prevalence risk, course and prognosis. Can J Psychiatry. 2008;53(4):235-242.
7. Hooten MW, Shi Y, Gazelka HM, et al. The effects of depression and smoking on pain severity and opioid use in patients with chronic pain. Pain. 2011;152(1):223-229.
8. Rico-Villademoros F, Hidalgo J, Dominguez I, et al. Atypical antipsychotics in the treatment of fibromyalgia: a case series with olanzapine. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):161-164.
9. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. J Pain Symptom Manage. 2010;39(4):768-778.
10. Hamoda HM, Osser DN. The Psychopharmacology Algorithm Project at the Harvard South Shore Program: an update on psychotic depression. Harv Rev Psychiatry. 2008;16(4):235-247.
11. American Psychiatric Association. Committee on Electroconvulsive Therapy, Weiner RD, eds. The practice of electroconvulsive therapy: recommendations for treatment, training and privileging. 2nd ed. Washington DC: American Psychiatric Association; 2001.
12. Petrides G, Fink M, Husain MM, et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: a report from CORE. J ECT. 2001;17(4):244-253.
13. Rasmussen KG, Rummans TA. Electroconvulsive therapy in the management of chronic pain. Curr Pain Headache Rep. 2002;6(1):17-22.
14. Wasan AD, Artin K, Clark MR. A case-matching study of the analgesic properties of electroconvulsive therapy. Pain Med. 2004;5(1):50-58.
15. Teh FC, Zaslavsky AM, Reynolds CF, 3rd, et al. Effect of depression treatment on chronic pain outcomes. Psychosom Med. 2010;72(1):61-67.
16. Sertel Berk HO. The biopsychosocial factors that serve as predictors of the outcome of surgical modalities for chronic pain. Agri. 2010;22(3):93-97.
17. Bair MJ, Robinson RL, Katon W, et al. Depression and pain comorbidity. Arch Intern Med. 2003;163(20):2433-2445.
18. Veehof MM, Oskam MJ, Schreurs KM, et al. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis. Pain. 2011;152(3):533-542.
1. Kawashima M, Matsushima T, Inoue T, et al. Microvascular decompression for glossopharyngeal neuralgia through the transcondylar fossa (supracondylar transjugular tubercle) approach. Neurosurgery. 2010;66(6 suppl operative):275-280.
2. Ferroli P, Fioravanti A, Schiariti M, et al. Microvascular decompression for glossopharyngeal neuralgia: a long-term retrospective review of the Milan-Bologna experience in 31 consecutive cases. Acta Neurochir (Wien). 2009;151(10):1245-1250.
3. Stahl SM. Stahl’s essential psychopharmacology: neuroscientific basis and practical applications. 3rd ed. New York NY: Cambridge University Press; 2008.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev.Washington DC: American Psychiatric Association; 2000.
5. Rothschild AJ. Diagnosis and assessment. In: Rothschild AJ. Clinical manual for diagnosis and treatment of psychotic depression. Arlington VA: American Psychiatric Publishing Inc.; 2009:57-71.
6. Tunks ER, Crook J, Weir R. Epidemiology of chronic pain with psychological comorbidity: prevalence risk, course and prognosis. Can J Psychiatry. 2008;53(4):235-242.
7. Hooten MW, Shi Y, Gazelka HM, et al. The effects of depression and smoking on pain severity and opioid use in patients with chronic pain. Pain. 2011;152(1):223-229.
8. Rico-Villademoros F, Hidalgo J, Dominguez I, et al. Atypical antipsychotics in the treatment of fibromyalgia: a case series with olanzapine. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):161-164.
9. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. J Pain Symptom Manage. 2010;39(4):768-778.
10. Hamoda HM, Osser DN. The Psychopharmacology Algorithm Project at the Harvard South Shore Program: an update on psychotic depression. Harv Rev Psychiatry. 2008;16(4):235-247.
11. American Psychiatric Association. Committee on Electroconvulsive Therapy, Weiner RD, eds. The practice of electroconvulsive therapy: recommendations for treatment, training and privileging. 2nd ed. Washington DC: American Psychiatric Association; 2001.
12. Petrides G, Fink M, Husain MM, et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: a report from CORE. J ECT. 2001;17(4):244-253.
13. Rasmussen KG, Rummans TA. Electroconvulsive therapy in the management of chronic pain. Curr Pain Headache Rep. 2002;6(1):17-22.
14. Wasan AD, Artin K, Clark MR. A case-matching study of the analgesic properties of electroconvulsive therapy. Pain Med. 2004;5(1):50-58.
15. Teh FC, Zaslavsky AM, Reynolds CF, 3rd, et al. Effect of depression treatment on chronic pain outcomes. Psychosom Med. 2010;72(1):61-67.
16. Sertel Berk HO. The biopsychosocial factors that serve as predictors of the outcome of surgical modalities for chronic pain. Agri. 2010;22(3):93-97.
17. Bair MJ, Robinson RL, Katon W, et al. Depression and pain comorbidity. Arch Intern Med. 2003;163(20):2433-2445.
18. Veehof MM, Oskam MJ, Schreurs KM, et al. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis. Pain. 2011;152(3):533-542.