User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
PsA tied with higher prevalence of coronary calcification
Key clinical point: In a cohort of at-risk patients with symptoms suggestive of coronary artery disease (CAD), the prevalence of coronary artery calcification (CAC) was higher in patients with psoriatic arthritis (PsA) compared with those without psoriasis or PsA.
Major finding: The prevalence of CAC score greater than 0 was significantly higher in patients with PsA vs. those without psoriasis or PsA (adjusted odds ratio, 1.28; 95% confidence interval, 1.00-1.64).
Study details: This was a cross-sectional study of 46,022 patient’s at-risk patients with symptoms suggestive of CAD from the Danish national computed tomography angiography registry, among which 1,356 had psoriasis, 370 had PsA whereas, 44,296 patients formed the reference nonpsoriasis/PsA cohort.
Disclosures: The study did not report any source of funding. No conflicts of interest were reported.
Source: Tinggaard AB et al. J Intern Med. 2021 May 12. doi: 10.1111/joim.13311.
Key clinical point: In a cohort of at-risk patients with symptoms suggestive of coronary artery disease (CAD), the prevalence of coronary artery calcification (CAC) was higher in patients with psoriatic arthritis (PsA) compared with those without psoriasis or PsA.
Major finding: The prevalence of CAC score greater than 0 was significantly higher in patients with PsA vs. those without psoriasis or PsA (adjusted odds ratio, 1.28; 95% confidence interval, 1.00-1.64).
Study details: This was a cross-sectional study of 46,022 patient’s at-risk patients with symptoms suggestive of CAD from the Danish national computed tomography angiography registry, among which 1,356 had psoriasis, 370 had PsA whereas, 44,296 patients formed the reference nonpsoriasis/PsA cohort.
Disclosures: The study did not report any source of funding. No conflicts of interest were reported.
Source: Tinggaard AB et al. J Intern Med. 2021 May 12. doi: 10.1111/joim.13311.
Key clinical point: In a cohort of at-risk patients with symptoms suggestive of coronary artery disease (CAD), the prevalence of coronary artery calcification (CAC) was higher in patients with psoriatic arthritis (PsA) compared with those without psoriasis or PsA.
Major finding: The prevalence of CAC score greater than 0 was significantly higher in patients with PsA vs. those without psoriasis or PsA (adjusted odds ratio, 1.28; 95% confidence interval, 1.00-1.64).
Study details: This was a cross-sectional study of 46,022 patient’s at-risk patients with symptoms suggestive of CAD from the Danish national computed tomography angiography registry, among which 1,356 had psoriasis, 370 had PsA whereas, 44,296 patients formed the reference nonpsoriasis/PsA cohort.
Disclosures: The study did not report any source of funding. No conflicts of interest were reported.
Source: Tinggaard AB et al. J Intern Med. 2021 May 12. doi: 10.1111/joim.13311.
PsA: Rates of hospitalized serious infections lower with ustekinumab vs. other biologics
Key clinical point: In patients with psoriasis or psoriatic arthritis (PsA), the risk for hospitalized serious infection was lower among those who initiated ustekinumab than other biologics and apremilast.
Major finding: Compared with ustekinumab, the risk for hospitalized serious infection was higher for adalimumab (combined weighted hazard ratio [HR], 1.66; 95% confidence interval [CI], 1.34-2.06), apremilast (HR, 1.42; 95% CI, 1.02-1.96), certolizumab (HR, 1.09; 95% CI, 0.68-1.75), etanercept (HR, 1.39; 95% CI, 1.01-1.90), golimumab (HR, 1.74; 95% CI, 1.00-3.03), infliximab (HR, 2.92; 95% CI, 1.80-4.72), ixekizumab (HR, 2.98; 95% CI, 1.20-7.41), and secukinumab (HR, 1.84; 95% CI, 1.24-2.72).
Study details: Findings are from a population-based cohort study of 123,383 patients with psoriasis/PsA who initiated 1 among ustekinumab, adalimumab, apremilast, certolizumab, etanercept, golimumab, ixekizumab, or secukinumab between 2009 and 2018.
Disclosures: This study was sponsored by the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. SC Kim, RJ Desai, and JF Merola reported receiving research grants from and/or working as consultants/investigators for various sources. The remaining authors declared no conflicts of interest.
Source: Jin Y et al. Arthritis Care Res (Hoboken). 2021 May 10. doi: 10.1002/acr.24630.
Key clinical point: In patients with psoriasis or psoriatic arthritis (PsA), the risk for hospitalized serious infection was lower among those who initiated ustekinumab than other biologics and apremilast.
Major finding: Compared with ustekinumab, the risk for hospitalized serious infection was higher for adalimumab (combined weighted hazard ratio [HR], 1.66; 95% confidence interval [CI], 1.34-2.06), apremilast (HR, 1.42; 95% CI, 1.02-1.96), certolizumab (HR, 1.09; 95% CI, 0.68-1.75), etanercept (HR, 1.39; 95% CI, 1.01-1.90), golimumab (HR, 1.74; 95% CI, 1.00-3.03), infliximab (HR, 2.92; 95% CI, 1.80-4.72), ixekizumab (HR, 2.98; 95% CI, 1.20-7.41), and secukinumab (HR, 1.84; 95% CI, 1.24-2.72).
Study details: Findings are from a population-based cohort study of 123,383 patients with psoriasis/PsA who initiated 1 among ustekinumab, adalimumab, apremilast, certolizumab, etanercept, golimumab, ixekizumab, or secukinumab between 2009 and 2018.
Disclosures: This study was sponsored by the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. SC Kim, RJ Desai, and JF Merola reported receiving research grants from and/or working as consultants/investigators for various sources. The remaining authors declared no conflicts of interest.
Source: Jin Y et al. Arthritis Care Res (Hoboken). 2021 May 10. doi: 10.1002/acr.24630.
Key clinical point: In patients with psoriasis or psoriatic arthritis (PsA), the risk for hospitalized serious infection was lower among those who initiated ustekinumab than other biologics and apremilast.
Major finding: Compared with ustekinumab, the risk for hospitalized serious infection was higher for adalimumab (combined weighted hazard ratio [HR], 1.66; 95% confidence interval [CI], 1.34-2.06), apremilast (HR, 1.42; 95% CI, 1.02-1.96), certolizumab (HR, 1.09; 95% CI, 0.68-1.75), etanercept (HR, 1.39; 95% CI, 1.01-1.90), golimumab (HR, 1.74; 95% CI, 1.00-3.03), infliximab (HR, 2.92; 95% CI, 1.80-4.72), ixekizumab (HR, 2.98; 95% CI, 1.20-7.41), and secukinumab (HR, 1.84; 95% CI, 1.24-2.72).
Study details: Findings are from a population-based cohort study of 123,383 patients with psoriasis/PsA who initiated 1 among ustekinumab, adalimumab, apremilast, certolizumab, etanercept, golimumab, ixekizumab, or secukinumab between 2009 and 2018.
Disclosures: This study was sponsored by the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. SC Kim, RJ Desai, and JF Merola reported receiving research grants from and/or working as consultants/investigators for various sources. The remaining authors declared no conflicts of interest.
Source: Jin Y et al. Arthritis Care Res (Hoboken). 2021 May 10. doi: 10.1002/acr.24630.
PsA: Swapping biologics gives no remarkable advantage over cycling
Key clinical point: In a real-life cohort of patients with psoriatic arthritis (PsA), using drugs with the same (cycling) mode of action (MoA) after the failure of the previous one was not remarkably better than using the drug with a different MoA (swapping) than the previously failed drug.
Major finding: Drug retention rate was not significantly different between the group that underwent swapping vs. cycling (hazard ratio [HR] 0.95; 95% confidence interval [CI], 0.52-1.74), and effectiveness of swapping was not different from that observed in the first-line prescription group (HR, 1.45; 95% CI, 0.83-2.52).
Study details: This was a monocentric medical records review study of 183 patients with PsA treated with biologic disease-modifying antirheumatic drugs (DMARDs) or targeted synthetic DMARDs. The medical records were grouped into cycling, swapping, or first-line groups.
Disclosures: The authors did not identify any source of funding. The authors declared no conflicts of interest.
Source: Ariani A et al. Medicine (Baltimore). 2021 Apr 23. doi: 10.1097/MD.0000000000025300.
Key clinical point: In a real-life cohort of patients with psoriatic arthritis (PsA), using drugs with the same (cycling) mode of action (MoA) after the failure of the previous one was not remarkably better than using the drug with a different MoA (swapping) than the previously failed drug.
Major finding: Drug retention rate was not significantly different between the group that underwent swapping vs. cycling (hazard ratio [HR] 0.95; 95% confidence interval [CI], 0.52-1.74), and effectiveness of swapping was not different from that observed in the first-line prescription group (HR, 1.45; 95% CI, 0.83-2.52).
Study details: This was a monocentric medical records review study of 183 patients with PsA treated with biologic disease-modifying antirheumatic drugs (DMARDs) or targeted synthetic DMARDs. The medical records were grouped into cycling, swapping, or first-line groups.
Disclosures: The authors did not identify any source of funding. The authors declared no conflicts of interest.
Source: Ariani A et al. Medicine (Baltimore). 2021 Apr 23. doi: 10.1097/MD.0000000000025300.
Key clinical point: In a real-life cohort of patients with psoriatic arthritis (PsA), using drugs with the same (cycling) mode of action (MoA) after the failure of the previous one was not remarkably better than using the drug with a different MoA (swapping) than the previously failed drug.
Major finding: Drug retention rate was not significantly different between the group that underwent swapping vs. cycling (hazard ratio [HR] 0.95; 95% confidence interval [CI], 0.52-1.74), and effectiveness of swapping was not different from that observed in the first-line prescription group (HR, 1.45; 95% CI, 0.83-2.52).
Study details: This was a monocentric medical records review study of 183 patients with PsA treated with biologic disease-modifying antirheumatic drugs (DMARDs) or targeted synthetic DMARDs. The medical records were grouped into cycling, swapping, or first-line groups.
Disclosures: The authors did not identify any source of funding. The authors declared no conflicts of interest.
Source: Ariani A et al. Medicine (Baltimore). 2021 Apr 23. doi: 10.1097/MD.0000000000025300.
PsA: Upadacitinib shows consistent efficacy and safety in patients with inadequate response to biologics
Key clinical point: Upadacitinib showed consistent improvement in signs and symptoms of psoriatic arthritis (PsA) with no new significant safety signals in patients with an inadequate response to biologic disease-modifying antirheumatic drugs (bDMARDs).
Major finding: At 56 weeks, the proportion of patients achieving American College of Rheumatology 20/50/70 and Psoriasis Area Severity Index 75/90/100 responses was 59.7%/40.8%/24.2% and 52.3%/40.8%/26.9%, respectively, with upadacitinib 15 mg and 59.2%/38.5%/26.6% and 58.8%/47.3%/35.1%, respectively, with upadacitinib 30 mg. Improvement was consistent through the study period with both upadacitinib doses with a safety profile consistent with that known previously.
Study details: Findings are from phase 3 SELECT-PsA 2 study, involving 641 patients with PsA who had an inadequate response to at least 1 bDMARD and were randomly allocated to receive upadacitinib 15 mg, 30 mg once daily (OD), or placebo switched to upadacitinib 15 mg or 30 mg OD at week 24.
Disclosures: SELECT-PsA 2 trial was funded by AbbVie. The authors reported receiving grants/consulting fees, speaker fees from, being employees of, and stockholder from various sources including AbbVie.
Source: Mease PJ et al. Rheumatol Ther. 2021 Apr 28. doi: 10.1007/s40744-021-00305-z.
Key clinical point: Upadacitinib showed consistent improvement in signs and symptoms of psoriatic arthritis (PsA) with no new significant safety signals in patients with an inadequate response to biologic disease-modifying antirheumatic drugs (bDMARDs).
Major finding: At 56 weeks, the proportion of patients achieving American College of Rheumatology 20/50/70 and Psoriasis Area Severity Index 75/90/100 responses was 59.7%/40.8%/24.2% and 52.3%/40.8%/26.9%, respectively, with upadacitinib 15 mg and 59.2%/38.5%/26.6% and 58.8%/47.3%/35.1%, respectively, with upadacitinib 30 mg. Improvement was consistent through the study period with both upadacitinib doses with a safety profile consistent with that known previously.
Study details: Findings are from phase 3 SELECT-PsA 2 study, involving 641 patients with PsA who had an inadequate response to at least 1 bDMARD and were randomly allocated to receive upadacitinib 15 mg, 30 mg once daily (OD), or placebo switched to upadacitinib 15 mg or 30 mg OD at week 24.
Disclosures: SELECT-PsA 2 trial was funded by AbbVie. The authors reported receiving grants/consulting fees, speaker fees from, being employees of, and stockholder from various sources including AbbVie.
Source: Mease PJ et al. Rheumatol Ther. 2021 Apr 28. doi: 10.1007/s40744-021-00305-z.
Key clinical point: Upadacitinib showed consistent improvement in signs and symptoms of psoriatic arthritis (PsA) with no new significant safety signals in patients with an inadequate response to biologic disease-modifying antirheumatic drugs (bDMARDs).
Major finding: At 56 weeks, the proportion of patients achieving American College of Rheumatology 20/50/70 and Psoriasis Area Severity Index 75/90/100 responses was 59.7%/40.8%/24.2% and 52.3%/40.8%/26.9%, respectively, with upadacitinib 15 mg and 59.2%/38.5%/26.6% and 58.8%/47.3%/35.1%, respectively, with upadacitinib 30 mg. Improvement was consistent through the study period with both upadacitinib doses with a safety profile consistent with that known previously.
Study details: Findings are from phase 3 SELECT-PsA 2 study, involving 641 patients with PsA who had an inadequate response to at least 1 bDMARD and were randomly allocated to receive upadacitinib 15 mg, 30 mg once daily (OD), or placebo switched to upadacitinib 15 mg or 30 mg OD at week 24.
Disclosures: SELECT-PsA 2 trial was funded by AbbVie. The authors reported receiving grants/consulting fees, speaker fees from, being employees of, and stockholder from various sources including AbbVie.
Source: Mease PJ et al. Rheumatol Ther. 2021 Apr 28. doi: 10.1007/s40744-021-00305-z.
PsA: No substantial change in body composition with ustekinumab treatment
Key clinical point: Patients with psoriatic arthritis (PsA) have higher adiposity and lower lean mass than healthy controls. Treatment with ustekinumab for 6-months decreased total lean mass slightly with no significant change in body composition.
Major finding: Patients with PsA had significantly lower total (P = .013) and appendicular (P = .010) lean mass and a significantly higher total fat mass and body fat percentage (both, P less than .001) compared with matched controls. After 6 months of ustekinumab treatment, total lean mass decreased significantly (P = .046) with no significant changes in body mass index.
Study details: This was a cross-sectional analysis of patients with established PsA (n=30) and matched non-PsA healthy controls (n=60). Patients with PsA who subsequently initiated ustekinumab were enrolled in a 6-month open-label follow-up study.
Disclosures: This study received an unrestricted grant from Janssen France. The authors declared no conflicts of interest.
Source: Paccou J et al. Arthritis Care Res (Hoboken). 2021 May 10. doi: 10.1002/acr.24623.
Key clinical point: Patients with psoriatic arthritis (PsA) have higher adiposity and lower lean mass than healthy controls. Treatment with ustekinumab for 6-months decreased total lean mass slightly with no significant change in body composition.
Major finding: Patients with PsA had significantly lower total (P = .013) and appendicular (P = .010) lean mass and a significantly higher total fat mass and body fat percentage (both, P less than .001) compared with matched controls. After 6 months of ustekinumab treatment, total lean mass decreased significantly (P = .046) with no significant changes in body mass index.
Study details: This was a cross-sectional analysis of patients with established PsA (n=30) and matched non-PsA healthy controls (n=60). Patients with PsA who subsequently initiated ustekinumab were enrolled in a 6-month open-label follow-up study.
Disclosures: This study received an unrestricted grant from Janssen France. The authors declared no conflicts of interest.
Source: Paccou J et al. Arthritis Care Res (Hoboken). 2021 May 10. doi: 10.1002/acr.24623.
Key clinical point: Patients with psoriatic arthritis (PsA) have higher adiposity and lower lean mass than healthy controls. Treatment with ustekinumab for 6-months decreased total lean mass slightly with no significant change in body composition.
Major finding: Patients with PsA had significantly lower total (P = .013) and appendicular (P = .010) lean mass and a significantly higher total fat mass and body fat percentage (both, P less than .001) compared with matched controls. After 6 months of ustekinumab treatment, total lean mass decreased significantly (P = .046) with no significant changes in body mass index.
Study details: This was a cross-sectional analysis of patients with established PsA (n=30) and matched non-PsA healthy controls (n=60). Patients with PsA who subsequently initiated ustekinumab were enrolled in a 6-month open-label follow-up study.
Disclosures: This study received an unrestricted grant from Janssen France. The authors declared no conflicts of interest.
Source: Paccou J et al. Arthritis Care Res (Hoboken). 2021 May 10. doi: 10.1002/acr.24623.
Secukinumab, a comprehensive biologic treatment for management of concomitant PsA and psoriasis
Key clinical point: Interleukin 17A inhibitor, secukinumab provides a comprehensive biologic treatment profile for management of concomitant features of psoriasis and psoriatic arthritis (PsA).
Major finding: At 52 weeks, the proportion of patients who achieved 20% or more improvement in the American College of Rheumatology response criteria was not significantly different between secukinumab and adalimumab (76.4% vs. 68.3%; P = .1752) groups. Psoriasis Area and Severity Index 90 response was higher with secukinumab vs. adalimumab (68.6% vs. 41.7%; P less than .0001).
Study details: Findings are from a prespecified analysis of 853 patients with active PsA having concomitant moderate-to-severe plaque psoriasis from phase 3b EXCEED study. Patients were randomly allocated to either subcutaneous secukinumab 300 mg (n=426) or adalimumab 40 mg (n=427).
Disclosures: EXCEED trial was funded by Novartis Pharma AG, Basel, Switzerland. The authors including the lead author reported receiving research/educational grants, consulting/speaker fees, and/or honoraria from various sources including Novartis. Three of the authors reported being employees and shareholders of Novartis.
Source: Gottlieb AB et al. Br J Dermatol. 2021 Apr 29. doi: 10.1111/bjd.20413.
Key clinical point: Interleukin 17A inhibitor, secukinumab provides a comprehensive biologic treatment profile for management of concomitant features of psoriasis and psoriatic arthritis (PsA).
Major finding: At 52 weeks, the proportion of patients who achieved 20% or more improvement in the American College of Rheumatology response criteria was not significantly different between secukinumab and adalimumab (76.4% vs. 68.3%; P = .1752) groups. Psoriasis Area and Severity Index 90 response was higher with secukinumab vs. adalimumab (68.6% vs. 41.7%; P less than .0001).
Study details: Findings are from a prespecified analysis of 853 patients with active PsA having concomitant moderate-to-severe plaque psoriasis from phase 3b EXCEED study. Patients were randomly allocated to either subcutaneous secukinumab 300 mg (n=426) or adalimumab 40 mg (n=427).
Disclosures: EXCEED trial was funded by Novartis Pharma AG, Basel, Switzerland. The authors including the lead author reported receiving research/educational grants, consulting/speaker fees, and/or honoraria from various sources including Novartis. Three of the authors reported being employees and shareholders of Novartis.
Source: Gottlieb AB et al. Br J Dermatol. 2021 Apr 29. doi: 10.1111/bjd.20413.
Key clinical point: Interleukin 17A inhibitor, secukinumab provides a comprehensive biologic treatment profile for management of concomitant features of psoriasis and psoriatic arthritis (PsA).
Major finding: At 52 weeks, the proportion of patients who achieved 20% or more improvement in the American College of Rheumatology response criteria was not significantly different between secukinumab and adalimumab (76.4% vs. 68.3%; P = .1752) groups. Psoriasis Area and Severity Index 90 response was higher with secukinumab vs. adalimumab (68.6% vs. 41.7%; P less than .0001).
Study details: Findings are from a prespecified analysis of 853 patients with active PsA having concomitant moderate-to-severe plaque psoriasis from phase 3b EXCEED study. Patients were randomly allocated to either subcutaneous secukinumab 300 mg (n=426) or adalimumab 40 mg (n=427).
Disclosures: EXCEED trial was funded by Novartis Pharma AG, Basel, Switzerland. The authors including the lead author reported receiving research/educational grants, consulting/speaker fees, and/or honoraria from various sources including Novartis. Three of the authors reported being employees and shareholders of Novartis.
Source: Gottlieb AB et al. Br J Dermatol. 2021 Apr 29. doi: 10.1111/bjd.20413.
PsA: Guselkumab well tolerated with no new safety signals
Key clinical point: Guselkumab 100 mg every 4 weeks (Q4W) and every 8 weeks (Q8W) was well tolerated in patients with psoriatic arthritis (PsA) without any new safety concerns through 1 year of DISCOVER trials.
Major finding: At 24 weeks, combined guselkumab- and placebo-treated patients showed a similar incidence of serious adverse events (SAEs; 4.4 and 7.1/100 patient-years [PY]), adverse events (AEs) leading to discontinuation of study agent (3.8 and 4.1/100 PY), infections (49.5 and 49.9/100 PY), and serious infections (1.2 and 1.7/100 PY), respectively. At 52 weeks, the time-adjusted incidence of SAEs and AEs remained stable with both guselkumab regimens.
Study details: This was a pooled analysis of phase 3 trials DISCOVER-1, and DISCOVER-2 including 1,120 patients with active PsA who had inadequate responses to standard therapies. Patients were randomly allocated to receive subcutaneous guselkumab 100 mg at week 0, then Q4W; guselkumab 100 mg at weeks 0, 4, then Q8W; or placebo at Q4W.
Disclosures: This study was funded by Janssen Research & Development, LLC. The authors reported receiving research support, speaker bureau support, consultant fees, honoraria, and being an employee of and/or holding stocks/stock options in various sources including Janssen and Johnson & Johnson.
Source: Rahman P et al. J Rheumatol. 2021 May 1. doi: 10.3899/jrheum.201532.
Key clinical point: Guselkumab 100 mg every 4 weeks (Q4W) and every 8 weeks (Q8W) was well tolerated in patients with psoriatic arthritis (PsA) without any new safety concerns through 1 year of DISCOVER trials.
Major finding: At 24 weeks, combined guselkumab- and placebo-treated patients showed a similar incidence of serious adverse events (SAEs; 4.4 and 7.1/100 patient-years [PY]), adverse events (AEs) leading to discontinuation of study agent (3.8 and 4.1/100 PY), infections (49.5 and 49.9/100 PY), and serious infections (1.2 and 1.7/100 PY), respectively. At 52 weeks, the time-adjusted incidence of SAEs and AEs remained stable with both guselkumab regimens.
Study details: This was a pooled analysis of phase 3 trials DISCOVER-1, and DISCOVER-2 including 1,120 patients with active PsA who had inadequate responses to standard therapies. Patients were randomly allocated to receive subcutaneous guselkumab 100 mg at week 0, then Q4W; guselkumab 100 mg at weeks 0, 4, then Q8W; or placebo at Q4W.
Disclosures: This study was funded by Janssen Research & Development, LLC. The authors reported receiving research support, speaker bureau support, consultant fees, honoraria, and being an employee of and/or holding stocks/stock options in various sources including Janssen and Johnson & Johnson.
Source: Rahman P et al. J Rheumatol. 2021 May 1. doi: 10.3899/jrheum.201532.
Key clinical point: Guselkumab 100 mg every 4 weeks (Q4W) and every 8 weeks (Q8W) was well tolerated in patients with psoriatic arthritis (PsA) without any new safety concerns through 1 year of DISCOVER trials.
Major finding: At 24 weeks, combined guselkumab- and placebo-treated patients showed a similar incidence of serious adverse events (SAEs; 4.4 and 7.1/100 patient-years [PY]), adverse events (AEs) leading to discontinuation of study agent (3.8 and 4.1/100 PY), infections (49.5 and 49.9/100 PY), and serious infections (1.2 and 1.7/100 PY), respectively. At 52 weeks, the time-adjusted incidence of SAEs and AEs remained stable with both guselkumab regimens.
Study details: This was a pooled analysis of phase 3 trials DISCOVER-1, and DISCOVER-2 including 1,120 patients with active PsA who had inadequate responses to standard therapies. Patients were randomly allocated to receive subcutaneous guselkumab 100 mg at week 0, then Q4W; guselkumab 100 mg at weeks 0, 4, then Q8W; or placebo at Q4W.
Disclosures: This study was funded by Janssen Research & Development, LLC. The authors reported receiving research support, speaker bureau support, consultant fees, honoraria, and being an employee of and/or holding stocks/stock options in various sources including Janssen and Johnson & Johnson.
Source: Rahman P et al. J Rheumatol. 2021 May 1. doi: 10.3899/jrheum.201532.
Is fecal microbiota transplantation beneficial in active peripheral PsA?
Key clinical point: Fecal microbiota transplantation (FMT) was safe but appeared inferior to sham in reducing disease activity in patients with active peripheral psoriatic arthritis (PsA) concomitantly treated with methotrexate.
Major finding: At 6 months, the treatment failure rate was significantly higher in FMT vs. sham group (60% vs. 19%; P = .018). Improvement in Health Assessment Questionnaire Disability Index favored sham vs. FMT by 0.23 points (P = .031) while the proportion of American College of Rheumatology 20 respondents was similar (between-group difference, 0.93; 95% confidence interval, 0.45-1.94). No serious adverse events or deaths were observed.
Study details: The findings are from a 26-week, double-blind, superiority trial of 31 participants with active peripheral PsA despite ongoing treatment with methotrexate who were randomly allocated to either gastroscopic-guided FMT (n=15) or sham transplantation (n=16) into the duodenum.
Disclosures: This study was supported by the Danish Rheumatism Association, Danish Psoriasis Research Foundation, Novartis Healthcare, and others. V Andersen and R Christensen declared receiving personal fees and grants/honoraria from Merck, Janssen, and other sources.
Source: Kragsnaes MS et al. Ann Rheum Dis. 2021 Apr 29. doi: 10.1136/annrheumdis-2020-219511.
Key clinical point: Fecal microbiota transplantation (FMT) was safe but appeared inferior to sham in reducing disease activity in patients with active peripheral psoriatic arthritis (PsA) concomitantly treated with methotrexate.
Major finding: At 6 months, the treatment failure rate was significantly higher in FMT vs. sham group (60% vs. 19%; P = .018). Improvement in Health Assessment Questionnaire Disability Index favored sham vs. FMT by 0.23 points (P = .031) while the proportion of American College of Rheumatology 20 respondents was similar (between-group difference, 0.93; 95% confidence interval, 0.45-1.94). No serious adverse events or deaths were observed.
Study details: The findings are from a 26-week, double-blind, superiority trial of 31 participants with active peripheral PsA despite ongoing treatment with methotrexate who were randomly allocated to either gastroscopic-guided FMT (n=15) or sham transplantation (n=16) into the duodenum.
Disclosures: This study was supported by the Danish Rheumatism Association, Danish Psoriasis Research Foundation, Novartis Healthcare, and others. V Andersen and R Christensen declared receiving personal fees and grants/honoraria from Merck, Janssen, and other sources.
Source: Kragsnaes MS et al. Ann Rheum Dis. 2021 Apr 29. doi: 10.1136/annrheumdis-2020-219511.
Key clinical point: Fecal microbiota transplantation (FMT) was safe but appeared inferior to sham in reducing disease activity in patients with active peripheral psoriatic arthritis (PsA) concomitantly treated with methotrexate.
Major finding: At 6 months, the treatment failure rate was significantly higher in FMT vs. sham group (60% vs. 19%; P = .018). Improvement in Health Assessment Questionnaire Disability Index favored sham vs. FMT by 0.23 points (P = .031) while the proportion of American College of Rheumatology 20 respondents was similar (between-group difference, 0.93; 95% confidence interval, 0.45-1.94). No serious adverse events or deaths were observed.
Study details: The findings are from a 26-week, double-blind, superiority trial of 31 participants with active peripheral PsA despite ongoing treatment with methotrexate who were randomly allocated to either gastroscopic-guided FMT (n=15) or sham transplantation (n=16) into the duodenum.
Disclosures: This study was supported by the Danish Rheumatism Association, Danish Psoriasis Research Foundation, Novartis Healthcare, and others. V Andersen and R Christensen declared receiving personal fees and grants/honoraria from Merck, Janssen, and other sources.
Source: Kragsnaes MS et al. Ann Rheum Dis. 2021 Apr 29. doi: 10.1136/annrheumdis-2020-219511.
Clinical Edge Journal Scan Commentary: PsA June 2021

Several important studies on psoriatic arthritis (PsA) were published in the month of May 2021. Although, 50% of patients with PsA are women, many of them being in the child-beaing age, few studies have investigated pregnancy outcomes in women with psoriatic disease. Xie et al, report the results of their systematic review and meta-analysis of observational studies evaluating the impact of psoriasis and PsA on pregnancy outcomes. They retrieved 16 articles that met their study criteria. They demonstrate that pregnant women with psoriatic disease have significantly higher risk of adverse maternal outcomes (caesarean delivery, preterm birth, (pre)eclampsia, gestational diabetes, or gestational hypertension) compared with general population. However, no increased risk of fetal complications was observed. The authors recommend close monitoring of the mothers’ clinical status before and during pregnancy.
Despite availability of multiple targeted therapies, only about 60% of patients achieve a meaningful response to therapy in randomized trials and only a quarter of patients achieve a state of minimal disease activity. The assessment of musculoskeletal inflammation is heavily dependent on assessment of tender and swollen joints. However, whether tender or swollen joints, especially tender joints, truly reflect joint inflammation is a matter of debate. Felbo et al investigated the association between clinical joint tenderness and intra- and periarticular inflammation as assessed by ultrasound and magnetic resonance imaging (MRI) in patients with active PsA. They found that tender joints poorly reflect intra- and periarticular inflammation assessed by imaging. The association between swollen joints and ultrasound and MRI assessed inflammation was stronger but still only low-to-moderate. The agreement between joint tenderness and imaging assessed inflammation was even weaker in patients with high overall pain scores, high disability scores, or nonerosive disease. Therefore, it is recommended that imaging be used to supplement clinical examination in patients with PsA and high overall pain, disability, and/or nonerosive disease.
With regard to PsA treatment, Rahman et al reported the pooled safety results through one year of two phase 3 trials with guselkumab in PsA. This drug inhibits IL-23, has proven efficacy in PsA and psoriasis, and was recently approved for the treatment of PsA. No active tuberculosis, opportunistic infections, or inflammatory bowel disease, and low rates of malignancy and major adverse cardiovascular events, were observed in guselkumab-treated patients. In another study, using data from 2 large US claims databases, MarketScan and Optum’s De-identified Clinformatics® Data Mart, Jin et al demonstrated that other biologics and apremilast were associated with 1.4- to 3-times higher risk of hospitalized serious infections in patients with psoriatic disease when compared with ustekinumab. Ustekinumab is a biologic agent that inhibits IL-12 and IL-23 and is approved for the treatment of psoriasis, PsA, and ulcerative colitis. The two studies speak to the safety of targeting IL-23 with biologics in psoriatic disease.
Finally, an exploratory, proof-of-concept study explored whether fecal microbiota transplantation (FMT) improves the signs and symptoms of PsA. Kragsnaes et al conducted a double-blind, parallel-group, placebo-controlled, superiority trial, randomly allocating adults with active PsA despite ongoing treatment with methotrexate to one gastroscopic-guided FMT (15 patients) or sham transplantation (16 patients) into the duodenum. Surprisingly, treatment failure occurred more frequently in the FMT group than in the sham group (9 [60%] vs 3 [19%]; risk ratio, 3.20; 95% CI 1.06 to 9.62; P = 0.018). Improvement in HAQ-DI favoured sham treatment. There was no difference in the proportion of ACR20 responders between groups. No serious adverse events were observed. This study highlights that such studies are feasible but indicates that such interventions may not provide significant benefit. Further investigations including careful selection of donors, patients and concomitant therapy is required.
Several important studies on psoriatic arthritis (PsA) were published in the month of May 2021. Although, 50% of patients with PsA are women, many of them being in the child-beaing age, few studies have investigated pregnancy outcomes in women with psoriatic disease. Xie et al, report the results of their systematic review and meta-analysis of observational studies evaluating the impact of psoriasis and PsA on pregnancy outcomes. They retrieved 16 articles that met their study criteria. They demonstrate that pregnant women with psoriatic disease have significantly higher risk of adverse maternal outcomes (caesarean delivery, preterm birth, (pre)eclampsia, gestational diabetes, or gestational hypertension) compared with general population. However, no increased risk of fetal complications was observed. The authors recommend close monitoring of the mothers’ clinical status before and during pregnancy.
Despite availability of multiple targeted therapies, only about 60% of patients achieve a meaningful response to therapy in randomized trials and only a quarter of patients achieve a state of minimal disease activity. The assessment of musculoskeletal inflammation is heavily dependent on assessment of tender and swollen joints. However, whether tender or swollen joints, especially tender joints, truly reflect joint inflammation is a matter of debate. Felbo et al investigated the association between clinical joint tenderness and intra- and periarticular inflammation as assessed by ultrasound and magnetic resonance imaging (MRI) in patients with active PsA. They found that tender joints poorly reflect intra- and periarticular inflammation assessed by imaging. The association between swollen joints and ultrasound and MRI assessed inflammation was stronger but still only low-to-moderate. The agreement between joint tenderness and imaging assessed inflammation was even weaker in patients with high overall pain scores, high disability scores, or nonerosive disease. Therefore, it is recommended that imaging be used to supplement clinical examination in patients with PsA and high overall pain, disability, and/or nonerosive disease.
With regard to PsA treatment, Rahman et al reported the pooled safety results through one year of two phase 3 trials with guselkumab in PsA. This drug inhibits IL-23, has proven efficacy in PsA and psoriasis, and was recently approved for the treatment of PsA. No active tuberculosis, opportunistic infections, or inflammatory bowel disease, and low rates of malignancy and major adverse cardiovascular events, were observed in guselkumab-treated patients. In another study, using data from 2 large US claims databases, MarketScan and Optum’s De-identified Clinformatics® Data Mart, Jin et al demonstrated that other biologics and apremilast were associated with 1.4- to 3-times higher risk of hospitalized serious infections in patients with psoriatic disease when compared with ustekinumab. Ustekinumab is a biologic agent that inhibits IL-12 and IL-23 and is approved for the treatment of psoriasis, PsA, and ulcerative colitis. The two studies speak to the safety of targeting IL-23 with biologics in psoriatic disease.
Finally, an exploratory, proof-of-concept study explored whether fecal microbiota transplantation (FMT) improves the signs and symptoms of PsA. Kragsnaes et al conducted a double-blind, parallel-group, placebo-controlled, superiority trial, randomly allocating adults with active PsA despite ongoing treatment with methotrexate to one gastroscopic-guided FMT (15 patients) or sham transplantation (16 patients) into the duodenum. Surprisingly, treatment failure occurred more frequently in the FMT group than in the sham group (9 [60%] vs 3 [19%]; risk ratio, 3.20; 95% CI 1.06 to 9.62; P = 0.018). Improvement in HAQ-DI favoured sham treatment. There was no difference in the proportion of ACR20 responders between groups. No serious adverse events were observed. This study highlights that such studies are feasible but indicates that such interventions may not provide significant benefit. Further investigations including careful selection of donors, patients and concomitant therapy is required.
Several important studies on psoriatic arthritis (PsA) were published in the month of May 2021. Although, 50% of patients with PsA are women, many of them being in the child-beaing age, few studies have investigated pregnancy outcomes in women with psoriatic disease. Xie et al, report the results of their systematic review and meta-analysis of observational studies evaluating the impact of psoriasis and PsA on pregnancy outcomes. They retrieved 16 articles that met their study criteria. They demonstrate that pregnant women with psoriatic disease have significantly higher risk of adverse maternal outcomes (caesarean delivery, preterm birth, (pre)eclampsia, gestational diabetes, or gestational hypertension) compared with general population. However, no increased risk of fetal complications was observed. The authors recommend close monitoring of the mothers’ clinical status before and during pregnancy.
Despite availability of multiple targeted therapies, only about 60% of patients achieve a meaningful response to therapy in randomized trials and only a quarter of patients achieve a state of minimal disease activity. The assessment of musculoskeletal inflammation is heavily dependent on assessment of tender and swollen joints. However, whether tender or swollen joints, especially tender joints, truly reflect joint inflammation is a matter of debate. Felbo et al investigated the association between clinical joint tenderness and intra- and periarticular inflammation as assessed by ultrasound and magnetic resonance imaging (MRI) in patients with active PsA. They found that tender joints poorly reflect intra- and periarticular inflammation assessed by imaging. The association between swollen joints and ultrasound and MRI assessed inflammation was stronger but still only low-to-moderate. The agreement between joint tenderness and imaging assessed inflammation was even weaker in patients with high overall pain scores, high disability scores, or nonerosive disease. Therefore, it is recommended that imaging be used to supplement clinical examination in patients with PsA and high overall pain, disability, and/or nonerosive disease.
With regard to PsA treatment, Rahman et al reported the pooled safety results through one year of two phase 3 trials with guselkumab in PsA. This drug inhibits IL-23, has proven efficacy in PsA and psoriasis, and was recently approved for the treatment of PsA. No active tuberculosis, opportunistic infections, or inflammatory bowel disease, and low rates of malignancy and major adverse cardiovascular events, were observed in guselkumab-treated patients. In another study, using data from 2 large US claims databases, MarketScan and Optum’s De-identified Clinformatics® Data Mart, Jin et al demonstrated that other biologics and apremilast were associated with 1.4- to 3-times higher risk of hospitalized serious infections in patients with psoriatic disease when compared with ustekinumab. Ustekinumab is a biologic agent that inhibits IL-12 and IL-23 and is approved for the treatment of psoriasis, PsA, and ulcerative colitis. The two studies speak to the safety of targeting IL-23 with biologics in psoriatic disease.
Finally, an exploratory, proof-of-concept study explored whether fecal microbiota transplantation (FMT) improves the signs and symptoms of PsA. Kragsnaes et al conducted a double-blind, parallel-group, placebo-controlled, superiority trial, randomly allocating adults with active PsA despite ongoing treatment with methotrexate to one gastroscopic-guided FMT (15 patients) or sham transplantation (16 patients) into the duodenum. Surprisingly, treatment failure occurred more frequently in the FMT group than in the sham group (9 [60%] vs 3 [19%]; risk ratio, 3.20; 95% CI 1.06 to 9.62; P = 0.018). Improvement in HAQ-DI favoured sham treatment. There was no difference in the proportion of ACR20 responders between groups. No serious adverse events were observed. This study highlights that such studies are feasible but indicates that such interventions may not provide significant benefit. Further investigations including careful selection of donors, patients and concomitant therapy is required.
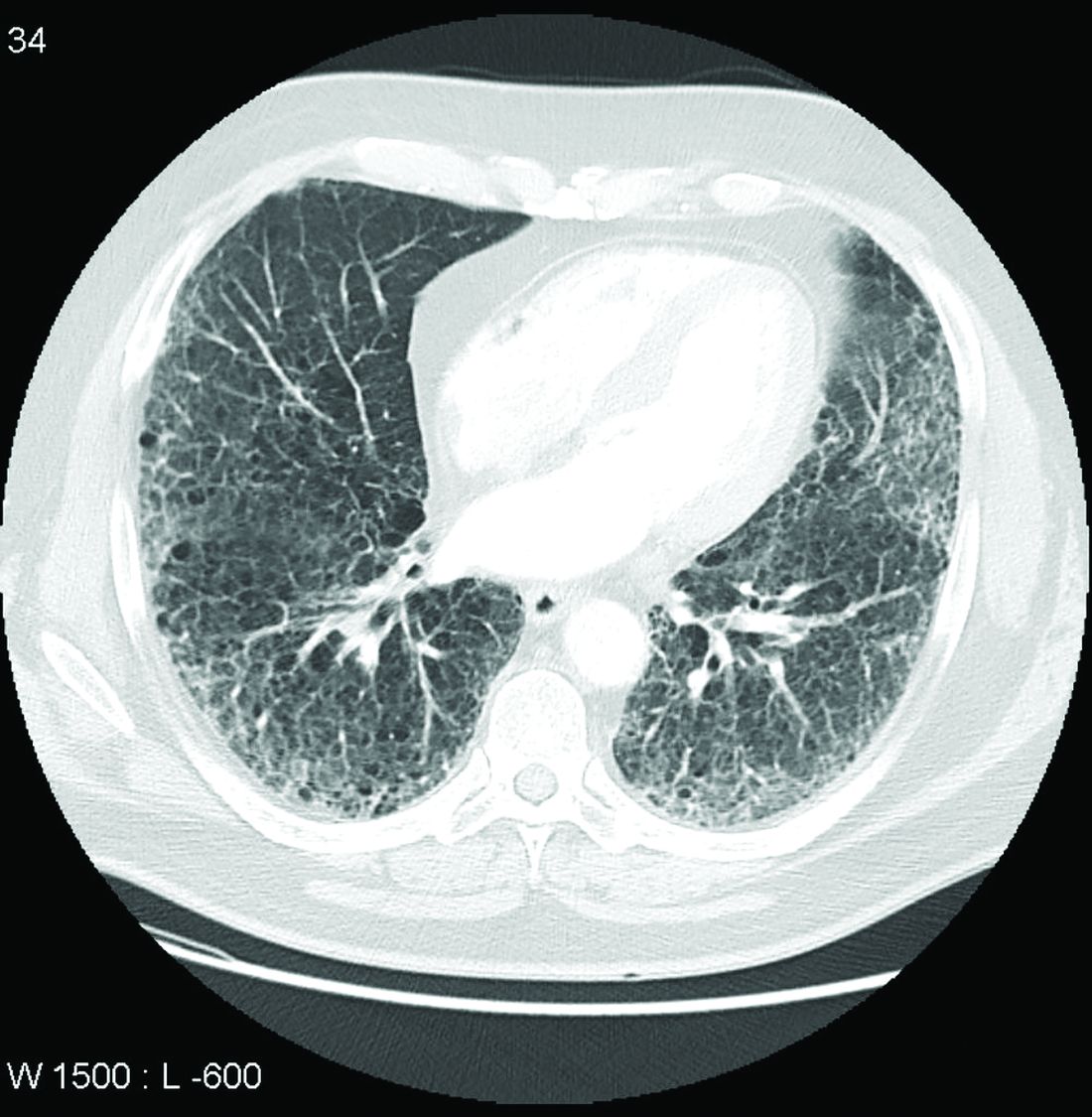
Nintedanib slows interstitial lung disease in RA patients
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.

“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.
“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.
“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
FROM THE EULAR 2021 CONGRESS