User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Which providers miss metabolic monitoring of children taking antipsychotics?
The number and types of providers involved in a child’s care are associated with the likelihood that the child will receive metabolic monitoring, according to the study, which was published in Pediatrics.
The results suggest that primary care providers and mental health providers should collaborate to monitor children taking antipsychotics, the researchers said.
“Shared care arrangements between primary care physicians and mental health specialists significantly increased the chances that metabolic monitoring would be done, compared with care delivered by one provider,” reported Elizabeth A. Shenkman, PhD, chair of the department of health outcomes and biomedical informatics at the University of Florida, Gainesville, and colleagues. “The results of our study point to the importance of state Medicaid agencies and Medicaid managed care plans in identifying all providers caring for the children taking antipsychotic medication and using this information to engage the providers in quality improvement efforts to improve metabolic monitoring rates.”
Comparing specialties
Children who take antipsychotic medication are at risk for obesity, impaired glucose metabolism, and hyperlipidemia, but less than 40% receive recommended metabolic monitoring with glucose and cholesterol tests.
To examine how health care provider specialty influences the receipt of metabolic monitoring, Dr. Shenkman and colleagues analyzed Medicaid enrollment and health care and pharmacy claims data from Florida and Texas.
They focused on 41,078 children who had an antipsychotic medication dispensed at least twice in 2017 and were eligible for inclusion in the Centers for Medicare & Medicaid Services metabolic monitoring measure. The Metabolic Monitoring for Children and Adolescents on Antipsychotics measure is a “priority nationally and is currently on the CMS Child Core Set, which is used to annually assess state-specific performance on pediatric quality measures,” the authors wrote.
About 65% were boys, and the children had an average age of 12 years. The researchers compared metabolic monitoring rates when children received outpatient care from a primary care provider, a mental health provider with prescribing privileges, or both.
Less than 40% of the children received metabolic monitoring, that is, at least one diabetes test and at least one cholesterol test, during the year.
Most of the children (61%) saw both primary care providers and mental health providers. Approximately one-third had a primary care provider prescribe antipsychotic medication the majority of the time, and 60% had a mental health provider prescribe antipsychotic medication the majority of the time.
Patients who saw both types of providers were significantly more likely to receive metabolic monitoring, relative to those who saw primary care providers only (adjusted odds ratio, 1.42). Those seeing a mental health provider alone had adjusted odds of metabolic monitoring that were 23% lower than those seeing a primary care provider alone.
Children who had a mental health provider prescribe the medication the majority of the time were 25% more likely to receive metabolic monitoring, compared with those who had a primary care provider prescribing the medication the majority of the time.
Slipping through the cracks
Child psychiatrist Fred Volkmar, MD, commented that the results are “sadly” unsurprising and reflect issues that pertain to other psychotropic drugs as well as antipsychotics and to adults as well as children.

The researchers “are quite right to point to it,” and “we really do need to develop better plans for improving” monitoring, said Dr. Volkmar, the Irving B. Harris Professor in the Child Study Center and professor of psychology at Yale University, New Haven, Conn.
“Increasingly we are asking primary care providers ... to take care of folks who have important either developmental or mental health problems,” Dr. Volkmar said. While they can do a good job, they increasingly are underpaid. Monitoring patients takes work, and they may be less familiar with the medications. “Either they prescribe these medications or they are asked to monitor them in place of the specialist provider who may have started them or suggested them,” he said. Metabolic monitoring may not be prioritized and can easily “slip through the cracks.” At the same time, doctors need to be aware of the risk of serious side effects of antipsychotic medications, such as malignant hyperthermia.
These medications can be overused and inappropriately used, which is a further complication. And when patients are taking multiple medications, there may be a need for additional monitoring and awareness of drug interactions.
“These medications are very complicated to use,” and there needs to be a way to connect primary care providers with child psychiatrists who are best trained in their use, said Dr. Volkmar.
A system with reminders can facilitate effective metabolic monitoring, he suggested. Dr. Volkmar has established a routine while providing care for a group home of adults with autism. Every 3 months, he reviews lab results. “You just have to force yourself to do it.”
Shared care arrangements may be another way to promote metabolic monitoring, Dr. Shenkman and colleagues said.
“Attributing care back to the multiple providers is important for care coordination and development of strategies to ensure that the evidence-based care is delivered and there is appropriate follow-up with the family and child to be sure care is received,” the study authors wrote. “Formalized shared care arrangements and adaptation of existing care delivery models to support integrated care, which can vary in degree from external coordination to on-site intervention and collaboration, are effective methods to promote partnership between primary and mental health providers.”
It is possible that clinicians in the study ordered metabolic monitoring but families did not take the children for testing, the investigators noted. In addition, it is not clear how much information providers have about other providers their patients are seeing.
The study authors and Dr. Volkmar had no disclosures.
The number and types of providers involved in a child’s care are associated with the likelihood that the child will receive metabolic monitoring, according to the study, which was published in Pediatrics.
The results suggest that primary care providers and mental health providers should collaborate to monitor children taking antipsychotics, the researchers said.
“Shared care arrangements between primary care physicians and mental health specialists significantly increased the chances that metabolic monitoring would be done, compared with care delivered by one provider,” reported Elizabeth A. Shenkman, PhD, chair of the department of health outcomes and biomedical informatics at the University of Florida, Gainesville, and colleagues. “The results of our study point to the importance of state Medicaid agencies and Medicaid managed care plans in identifying all providers caring for the children taking antipsychotic medication and using this information to engage the providers in quality improvement efforts to improve metabolic monitoring rates.”
Comparing specialties
Children who take antipsychotic medication are at risk for obesity, impaired glucose metabolism, and hyperlipidemia, but less than 40% receive recommended metabolic monitoring with glucose and cholesterol tests.
To examine how health care provider specialty influences the receipt of metabolic monitoring, Dr. Shenkman and colleagues analyzed Medicaid enrollment and health care and pharmacy claims data from Florida and Texas.
They focused on 41,078 children who had an antipsychotic medication dispensed at least twice in 2017 and were eligible for inclusion in the Centers for Medicare & Medicaid Services metabolic monitoring measure. The Metabolic Monitoring for Children and Adolescents on Antipsychotics measure is a “priority nationally and is currently on the CMS Child Core Set, which is used to annually assess state-specific performance on pediatric quality measures,” the authors wrote.
About 65% were boys, and the children had an average age of 12 years. The researchers compared metabolic monitoring rates when children received outpatient care from a primary care provider, a mental health provider with prescribing privileges, or both.
Less than 40% of the children received metabolic monitoring, that is, at least one diabetes test and at least one cholesterol test, during the year.
Most of the children (61%) saw both primary care providers and mental health providers. Approximately one-third had a primary care provider prescribe antipsychotic medication the majority of the time, and 60% had a mental health provider prescribe antipsychotic medication the majority of the time.
Patients who saw both types of providers were significantly more likely to receive metabolic monitoring, relative to those who saw primary care providers only (adjusted odds ratio, 1.42). Those seeing a mental health provider alone had adjusted odds of metabolic monitoring that were 23% lower than those seeing a primary care provider alone.
Children who had a mental health provider prescribe the medication the majority of the time were 25% more likely to receive metabolic monitoring, compared with those who had a primary care provider prescribing the medication the majority of the time.
Slipping through the cracks
Child psychiatrist Fred Volkmar, MD, commented that the results are “sadly” unsurprising and reflect issues that pertain to other psychotropic drugs as well as antipsychotics and to adults as well as children.
The researchers “are quite right to point to it,” and “we really do need to develop better plans for improving” monitoring, said Dr. Volkmar, the Irving B. Harris Professor in the Child Study Center and professor of psychology at Yale University, New Haven, Conn.
“Increasingly we are asking primary care providers ... to take care of folks who have important either developmental or mental health problems,” Dr. Volkmar said. While they can do a good job, they increasingly are underpaid. Monitoring patients takes work, and they may be less familiar with the medications. “Either they prescribe these medications or they are asked to monitor them in place of the specialist provider who may have started them or suggested them,” he said. Metabolic monitoring may not be prioritized and can easily “slip through the cracks.” At the same time, doctors need to be aware of the risk of serious side effects of antipsychotic medications, such as malignant hyperthermia.
These medications can be overused and inappropriately used, which is a further complication. And when patients are taking multiple medications, there may be a need for additional monitoring and awareness of drug interactions.
“These medications are very complicated to use,” and there needs to be a way to connect primary care providers with child psychiatrists who are best trained in their use, said Dr. Volkmar.
A system with reminders can facilitate effective metabolic monitoring, he suggested. Dr. Volkmar has established a routine while providing care for a group home of adults with autism. Every 3 months, he reviews lab results. “You just have to force yourself to do it.”
Shared care arrangements may be another way to promote metabolic monitoring, Dr. Shenkman and colleagues said.
“Attributing care back to the multiple providers is important for care coordination and development of strategies to ensure that the evidence-based care is delivered and there is appropriate follow-up with the family and child to be sure care is received,” the study authors wrote. “Formalized shared care arrangements and adaptation of existing care delivery models to support integrated care, which can vary in degree from external coordination to on-site intervention and collaboration, are effective methods to promote partnership between primary and mental health providers.”
It is possible that clinicians in the study ordered metabolic monitoring but families did not take the children for testing, the investigators noted. In addition, it is not clear how much information providers have about other providers their patients are seeing.
The study authors and Dr. Volkmar had no disclosures.
The number and types of providers involved in a child’s care are associated with the likelihood that the child will receive metabolic monitoring, according to the study, which was published in Pediatrics.
The results suggest that primary care providers and mental health providers should collaborate to monitor children taking antipsychotics, the researchers said.
“Shared care arrangements between primary care physicians and mental health specialists significantly increased the chances that metabolic monitoring would be done, compared with care delivered by one provider,” reported Elizabeth A. Shenkman, PhD, chair of the department of health outcomes and biomedical informatics at the University of Florida, Gainesville, and colleagues. “The results of our study point to the importance of state Medicaid agencies and Medicaid managed care plans in identifying all providers caring for the children taking antipsychotic medication and using this information to engage the providers in quality improvement efforts to improve metabolic monitoring rates.”
Comparing specialties
Children who take antipsychotic medication are at risk for obesity, impaired glucose metabolism, and hyperlipidemia, but less than 40% receive recommended metabolic monitoring with glucose and cholesterol tests.
To examine how health care provider specialty influences the receipt of metabolic monitoring, Dr. Shenkman and colleagues analyzed Medicaid enrollment and health care and pharmacy claims data from Florida and Texas.
They focused on 41,078 children who had an antipsychotic medication dispensed at least twice in 2017 and were eligible for inclusion in the Centers for Medicare & Medicaid Services metabolic monitoring measure. The Metabolic Monitoring for Children and Adolescents on Antipsychotics measure is a “priority nationally and is currently on the CMS Child Core Set, which is used to annually assess state-specific performance on pediatric quality measures,” the authors wrote.
About 65% were boys, and the children had an average age of 12 years. The researchers compared metabolic monitoring rates when children received outpatient care from a primary care provider, a mental health provider with prescribing privileges, or both.
Less than 40% of the children received metabolic monitoring, that is, at least one diabetes test and at least one cholesterol test, during the year.
Most of the children (61%) saw both primary care providers and mental health providers. Approximately one-third had a primary care provider prescribe antipsychotic medication the majority of the time, and 60% had a mental health provider prescribe antipsychotic medication the majority of the time.
Patients who saw both types of providers were significantly more likely to receive metabolic monitoring, relative to those who saw primary care providers only (adjusted odds ratio, 1.42). Those seeing a mental health provider alone had adjusted odds of metabolic monitoring that were 23% lower than those seeing a primary care provider alone.
Children who had a mental health provider prescribe the medication the majority of the time were 25% more likely to receive metabolic monitoring, compared with those who had a primary care provider prescribing the medication the majority of the time.
Slipping through the cracks
Child psychiatrist Fred Volkmar, MD, commented that the results are “sadly” unsurprising and reflect issues that pertain to other psychotropic drugs as well as antipsychotics and to adults as well as children.
The researchers “are quite right to point to it,” and “we really do need to develop better plans for improving” monitoring, said Dr. Volkmar, the Irving B. Harris Professor in the Child Study Center and professor of psychology at Yale University, New Haven, Conn.
“Increasingly we are asking primary care providers ... to take care of folks who have important either developmental or mental health problems,” Dr. Volkmar said. While they can do a good job, they increasingly are underpaid. Monitoring patients takes work, and they may be less familiar with the medications. “Either they prescribe these medications or they are asked to monitor them in place of the specialist provider who may have started them or suggested them,” he said. Metabolic monitoring may not be prioritized and can easily “slip through the cracks.” At the same time, doctors need to be aware of the risk of serious side effects of antipsychotic medications, such as malignant hyperthermia.
These medications can be overused and inappropriately used, which is a further complication. And when patients are taking multiple medications, there may be a need for additional monitoring and awareness of drug interactions.
“These medications are very complicated to use,” and there needs to be a way to connect primary care providers with child psychiatrists who are best trained in their use, said Dr. Volkmar.
A system with reminders can facilitate effective metabolic monitoring, he suggested. Dr. Volkmar has established a routine while providing care for a group home of adults with autism. Every 3 months, he reviews lab results. “You just have to force yourself to do it.”
Shared care arrangements may be another way to promote metabolic monitoring, Dr. Shenkman and colleagues said.
“Attributing care back to the multiple providers is important for care coordination and development of strategies to ensure that the evidence-based care is delivered and there is appropriate follow-up with the family and child to be sure care is received,” the study authors wrote. “Formalized shared care arrangements and adaptation of existing care delivery models to support integrated care, which can vary in degree from external coordination to on-site intervention and collaboration, are effective methods to promote partnership between primary and mental health providers.”
It is possible that clinicians in the study ordered metabolic monitoring but families did not take the children for testing, the investigators noted. In addition, it is not clear how much information providers have about other providers their patients are seeing.
The study authors and Dr. Volkmar had no disclosures.
FROM PEDIATRICS
Vaccines may not be as effective against variants
The current COVID-19 vaccines may not be as effective against new coronavirus variants, but they should be powerful enough to still be beneficial, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said during a news briefing on Jan. 21.
Both vaccines from Pfizer-BioNTech and Moderna have such high efficacy rates that it creates a “cushion effect,” he said, meaning that new variants will likely only diminish vaccine efficacy slightly.
“Bottom line: We’re paying very close attention to it,” he said. “There are alternative plans if we ever have to modify the vaccine.”
The U.S. has reported 144 cases of the B.1.1.7 variant, which was first identified in the United Kingdom, according to the latest update from the CDC. So far, no cases of the variant strain identified in South Africa have been reported in the U.S., but Dr. Fauci said public health officials are looking for it.
“We’re following very carefully the one in South Africa, which is a little bit more concerning, but nonetheless not something that we don’t think we can handle,” he said.
Despite challenges with vaccine distribution and administration, the U.S. “can and should” vaccinate 70% to 85% of adults by the end of the summer, Dr. Fauci told CNN. If that happens, people could begin to return to some sense of normalcy by the fall, he added.
“When you put ... the pedal to the floor, you can get it done,” he said.
If the U.S. administered one million shots per day, it would take until the end of 2021 to fully vaccine 75% of adults, according to a CNN analysis. Dr. Fauci said he believes the U.S. can give more than one million shots per day. An updated tally from the CDC showed that 1.6 million shots were given in the past 24 hours, which was the largest single-day increase yet reported.
“I’d like it to be a lot more,” Dr. Fauci told CNN. “If we can do better than that, which I personally think we likely will, then great.”
A version of this article first appeared on WebMD.com.
The current COVID-19 vaccines may not be as effective against new coronavirus variants, but they should be powerful enough to still be beneficial, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said during a news briefing on Jan. 21.
Both vaccines from Pfizer-BioNTech and Moderna have such high efficacy rates that it creates a “cushion effect,” he said, meaning that new variants will likely only diminish vaccine efficacy slightly.
“Bottom line: We’re paying very close attention to it,” he said. “There are alternative plans if we ever have to modify the vaccine.”
The U.S. has reported 144 cases of the B.1.1.7 variant, which was first identified in the United Kingdom, according to the latest update from the CDC. So far, no cases of the variant strain identified in South Africa have been reported in the U.S., but Dr. Fauci said public health officials are looking for it.
“We’re following very carefully the one in South Africa, which is a little bit more concerning, but nonetheless not something that we don’t think we can handle,” he said.
Despite challenges with vaccine distribution and administration, the U.S. “can and should” vaccinate 70% to 85% of adults by the end of the summer, Dr. Fauci told CNN. If that happens, people could begin to return to some sense of normalcy by the fall, he added.
“When you put ... the pedal to the floor, you can get it done,” he said.
If the U.S. administered one million shots per day, it would take until the end of 2021 to fully vaccine 75% of adults, according to a CNN analysis. Dr. Fauci said he believes the U.S. can give more than one million shots per day. An updated tally from the CDC showed that 1.6 million shots were given in the past 24 hours, which was the largest single-day increase yet reported.
“I’d like it to be a lot more,” Dr. Fauci told CNN. “If we can do better than that, which I personally think we likely will, then great.”
A version of this article first appeared on WebMD.com.
The current COVID-19 vaccines may not be as effective against new coronavirus variants, but they should be powerful enough to still be beneficial, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said during a news briefing on Jan. 21.
Both vaccines from Pfizer-BioNTech and Moderna have such high efficacy rates that it creates a “cushion effect,” he said, meaning that new variants will likely only diminish vaccine efficacy slightly.
“Bottom line: We’re paying very close attention to it,” he said. “There are alternative plans if we ever have to modify the vaccine.”
The U.S. has reported 144 cases of the B.1.1.7 variant, which was first identified in the United Kingdom, according to the latest update from the CDC. So far, no cases of the variant strain identified in South Africa have been reported in the U.S., but Dr. Fauci said public health officials are looking for it.
“We’re following very carefully the one in South Africa, which is a little bit more concerning, but nonetheless not something that we don’t think we can handle,” he said.
Despite challenges with vaccine distribution and administration, the U.S. “can and should” vaccinate 70% to 85% of adults by the end of the summer, Dr. Fauci told CNN. If that happens, people could begin to return to some sense of normalcy by the fall, he added.
“When you put ... the pedal to the floor, you can get it done,” he said.
If the U.S. administered one million shots per day, it would take until the end of 2021 to fully vaccine 75% of adults, according to a CNN analysis. Dr. Fauci said he believes the U.S. can give more than one million shots per day. An updated tally from the CDC showed that 1.6 million shots were given in the past 24 hours, which was the largest single-day increase yet reported.
“I’d like it to be a lot more,” Dr. Fauci told CNN. “If we can do better than that, which I personally think we likely will, then great.”
A version of this article first appeared on WebMD.com.
ColCORONA: Colchicine reduces complications in outpatient COVID-19
The oral, anti-inflammatory drug colchicine can prevent complications and hospitalizations in nonhospitalized patients newly diagnosed with COVID-19, according to a press release from the ColCORONA trial investigators.
After 1 month of therapy, there was a 21% risk reduction in the primary composite endpoint of death or hospitalizations that missed statistical significance, compared with placebo among 4,488 outpatients enrolled in the global, phase 3 trial.
After excluding 329 patients without a confirmatory polymerase chain reaction test, however, the use of colchicine was reported to significantly reduce hospitalizations by 25%, the need for mechanical ventilation by 50%, and deaths by 44%.
“We believe that this is a medical breakthrough. There’s no approved therapy to prevent complications of COVID-19 in outpatients, to prevent them from reaching the hospital,” lead investigator Jean-Claude Tardif, MD, from the Montreal Heart Institute, said in an interview.
“I know that several countries will be reviewing the data very rapidly and that Greece approved it today,” he said. “So this is providing hope for patients.”
Having been burned by hydroxychloroquine and other treatments brought forth without peer review, the response to the announcement was tempered by a desire for more details.
Asked for comment, Steven E. Nissen, MD, of the Cleveland Clinic Foundation, was cautious. “The press release about the trial is vague and lacks details such as hazard ratios, confidence intervals, and P values,” he said in an interview.
“It is impossible to evaluate the results of this trial without these details. It is also uncertain how rigorously data were collected,” he added. “We’ll need to see the manuscript to adequately interpret the results.”
The evidence in the press release is hard to interpret, but early intervention with anti-inflammatory therapy has considerable biologic appeal in COVID, said Paul Ridker, MD, MPH, who led the pivotal CANTOS trial of the anti-inflammatory drug canakinumab in the post-MI setting, and is also chair of the ACTIV-4B trial currently investigating anticoagulants and antithrombotics in outpatient COVID-19.
“Colchicine is both inexpensive and generally well tolerated, and the apparent benefits so far reported are substantial,” Dr. Ridker, from Brigham and Women’s Hospital in Boston, said in an interview. “We are eager to see the full data as rapidly as possible.”
The commonly used gout and rheumatic disease agent costs about 26 cents in Canada and between $4 and $6 in the United States. As previously reported, it reduced the time to clinical deterioration and hospital stay but not mortality in the 105-patient Greek Study in the Effects of Colchicine in COVID-19 Complications Prevention (GRECCO-19) study.
Dr. Tardif said he’s looking forward to having the data in the public domain and that they acted swiftly because the evidence was “clinically persuasive” and “the health system is congested now.”
“We received the results Friday, Jan. 22 at 5 p.m., an hour later we were in meetings with our data safety monitoring board [DSMB], 2 hours later we issued a press release, and a day later we’re submitting a full manuscript to a major scientific journal, so I don’t know if anyone has done this at this speed,” he said. “So we are actually very proud of what we did.”
ColCORONA was designed to enroll 6,000 outpatients, at least 40 years of age, who were diagnosed with COVID-19 infection within the previous 24 hours, and had a least one high-risk criterion, including age at least 70 years, body mass index of at least 30 kg/m2, diabetes mellitus, uncontrolled hypertension, known respiratory disease, heart failure or coronary disease, fever of at least 38.4° C within the last 48 hours, dyspnea at presentation, bicytopenia, pancytopenia, or the combination of high neutrophil count and low lymphocyte count.
Participants were randomly assigned to receive either placebo or colchicine 0.5 mg twice daily for 3 days and then once daily for another 27 days.
The number needed to prevent one COVID-19 complication is about 60 patients, Dr. Tardif said.
Colchicine was well tolerated and resulted in fewer serious adverse events than with placebo, he said. Diarrhea occurred more often with colchicine, but there was no increase in pneumonia. Caution should be used, however, in treating patients with severe renal disease.
Dr. Tardif said he would not prescribe colchicine to an 18-year-old COVID outpatient who doesn’t have any concomitant diseases, but would for those meeting the study protocol.
“As long as a patient appears to me to be at risk of a complication, I would prescribe it, without a doubt,” he said. “I can tell you that when we held the meeting with the DSMB Friday evening, I actually put each member on the spot and asked them: ‘If it were you – not even treating a patient, but if you had COVID today, would you take it based on the data you’ve seen?’ and all of the DSMB members said they would.
“So we’ll have that debate in the public domain when the paper is out, but I believe most physicians will use it to treat their patients.”
The trial was coordinated by the Montreal Heart Institute and funded by the government of Quebec; the U.S. National Heart, Lung, and Blood Institute; Montreal philanthropist Sophie Desmarais; and the COVID-19 Therapeutics Accelerator launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard. CGI, Dacima, and Pharmascience of Montreal were also collaborators.
A version of this article first appeared on Medscape.com.
The oral, anti-inflammatory drug colchicine can prevent complications and hospitalizations in nonhospitalized patients newly diagnosed with COVID-19, according to a press release from the ColCORONA trial investigators.
After 1 month of therapy, there was a 21% risk reduction in the primary composite endpoint of death or hospitalizations that missed statistical significance, compared with placebo among 4,488 outpatients enrolled in the global, phase 3 trial.
After excluding 329 patients without a confirmatory polymerase chain reaction test, however, the use of colchicine was reported to significantly reduce hospitalizations by 25%, the need for mechanical ventilation by 50%, and deaths by 44%.
“We believe that this is a medical breakthrough. There’s no approved therapy to prevent complications of COVID-19 in outpatients, to prevent them from reaching the hospital,” lead investigator Jean-Claude Tardif, MD, from the Montreal Heart Institute, said in an interview.
“I know that several countries will be reviewing the data very rapidly and that Greece approved it today,” he said. “So this is providing hope for patients.”
Having been burned by hydroxychloroquine and other treatments brought forth without peer review, the response to the announcement was tempered by a desire for more details.
Asked for comment, Steven E. Nissen, MD, of the Cleveland Clinic Foundation, was cautious. “The press release about the trial is vague and lacks details such as hazard ratios, confidence intervals, and P values,” he said in an interview.
“It is impossible to evaluate the results of this trial without these details. It is also uncertain how rigorously data were collected,” he added. “We’ll need to see the manuscript to adequately interpret the results.”
The evidence in the press release is hard to interpret, but early intervention with anti-inflammatory therapy has considerable biologic appeal in COVID, said Paul Ridker, MD, MPH, who led the pivotal CANTOS trial of the anti-inflammatory drug canakinumab in the post-MI setting, and is also chair of the ACTIV-4B trial currently investigating anticoagulants and antithrombotics in outpatient COVID-19.
“Colchicine is both inexpensive and generally well tolerated, and the apparent benefits so far reported are substantial,” Dr. Ridker, from Brigham and Women’s Hospital in Boston, said in an interview. “We are eager to see the full data as rapidly as possible.”
The commonly used gout and rheumatic disease agent costs about 26 cents in Canada and between $4 and $6 in the United States. As previously reported, it reduced the time to clinical deterioration and hospital stay but not mortality in the 105-patient Greek Study in the Effects of Colchicine in COVID-19 Complications Prevention (GRECCO-19) study.
Dr. Tardif said he’s looking forward to having the data in the public domain and that they acted swiftly because the evidence was “clinically persuasive” and “the health system is congested now.”
“We received the results Friday, Jan. 22 at 5 p.m., an hour later we were in meetings with our data safety monitoring board [DSMB], 2 hours later we issued a press release, and a day later we’re submitting a full manuscript to a major scientific journal, so I don’t know if anyone has done this at this speed,” he said. “So we are actually very proud of what we did.”
ColCORONA was designed to enroll 6,000 outpatients, at least 40 years of age, who were diagnosed with COVID-19 infection within the previous 24 hours, and had a least one high-risk criterion, including age at least 70 years, body mass index of at least 30 kg/m2, diabetes mellitus, uncontrolled hypertension, known respiratory disease, heart failure or coronary disease, fever of at least 38.4° C within the last 48 hours, dyspnea at presentation, bicytopenia, pancytopenia, or the combination of high neutrophil count and low lymphocyte count.
Participants were randomly assigned to receive either placebo or colchicine 0.5 mg twice daily for 3 days and then once daily for another 27 days.
The number needed to prevent one COVID-19 complication is about 60 patients, Dr. Tardif said.
Colchicine was well tolerated and resulted in fewer serious adverse events than with placebo, he said. Diarrhea occurred more often with colchicine, but there was no increase in pneumonia. Caution should be used, however, in treating patients with severe renal disease.
Dr. Tardif said he would not prescribe colchicine to an 18-year-old COVID outpatient who doesn’t have any concomitant diseases, but would for those meeting the study protocol.
“As long as a patient appears to me to be at risk of a complication, I would prescribe it, without a doubt,” he said. “I can tell you that when we held the meeting with the DSMB Friday evening, I actually put each member on the spot and asked them: ‘If it were you – not even treating a patient, but if you had COVID today, would you take it based on the data you’ve seen?’ and all of the DSMB members said they would.
“So we’ll have that debate in the public domain when the paper is out, but I believe most physicians will use it to treat their patients.”
The trial was coordinated by the Montreal Heart Institute and funded by the government of Quebec; the U.S. National Heart, Lung, and Blood Institute; Montreal philanthropist Sophie Desmarais; and the COVID-19 Therapeutics Accelerator launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard. CGI, Dacima, and Pharmascience of Montreal were also collaborators.
A version of this article first appeared on Medscape.com.
The oral, anti-inflammatory drug colchicine can prevent complications and hospitalizations in nonhospitalized patients newly diagnosed with COVID-19, according to a press release from the ColCORONA trial investigators.
After 1 month of therapy, there was a 21% risk reduction in the primary composite endpoint of death or hospitalizations that missed statistical significance, compared with placebo among 4,488 outpatients enrolled in the global, phase 3 trial.
After excluding 329 patients without a confirmatory polymerase chain reaction test, however, the use of colchicine was reported to significantly reduce hospitalizations by 25%, the need for mechanical ventilation by 50%, and deaths by 44%.
“We believe that this is a medical breakthrough. There’s no approved therapy to prevent complications of COVID-19 in outpatients, to prevent them from reaching the hospital,” lead investigator Jean-Claude Tardif, MD, from the Montreal Heart Institute, said in an interview.
“I know that several countries will be reviewing the data very rapidly and that Greece approved it today,” he said. “So this is providing hope for patients.”
Having been burned by hydroxychloroquine and other treatments brought forth without peer review, the response to the announcement was tempered by a desire for more details.
Asked for comment, Steven E. Nissen, MD, of the Cleveland Clinic Foundation, was cautious. “The press release about the trial is vague and lacks details such as hazard ratios, confidence intervals, and P values,” he said in an interview.
“It is impossible to evaluate the results of this trial without these details. It is also uncertain how rigorously data were collected,” he added. “We’ll need to see the manuscript to adequately interpret the results.”
The evidence in the press release is hard to interpret, but early intervention with anti-inflammatory therapy has considerable biologic appeal in COVID, said Paul Ridker, MD, MPH, who led the pivotal CANTOS trial of the anti-inflammatory drug canakinumab in the post-MI setting, and is also chair of the ACTIV-4B trial currently investigating anticoagulants and antithrombotics in outpatient COVID-19.
“Colchicine is both inexpensive and generally well tolerated, and the apparent benefits so far reported are substantial,” Dr. Ridker, from Brigham and Women’s Hospital in Boston, said in an interview. “We are eager to see the full data as rapidly as possible.”
The commonly used gout and rheumatic disease agent costs about 26 cents in Canada and between $4 and $6 in the United States. As previously reported, it reduced the time to clinical deterioration and hospital stay but not mortality in the 105-patient Greek Study in the Effects of Colchicine in COVID-19 Complications Prevention (GRECCO-19) study.
Dr. Tardif said he’s looking forward to having the data in the public domain and that they acted swiftly because the evidence was “clinically persuasive” and “the health system is congested now.”
“We received the results Friday, Jan. 22 at 5 p.m., an hour later we were in meetings with our data safety monitoring board [DSMB], 2 hours later we issued a press release, and a day later we’re submitting a full manuscript to a major scientific journal, so I don’t know if anyone has done this at this speed,” he said. “So we are actually very proud of what we did.”
ColCORONA was designed to enroll 6,000 outpatients, at least 40 years of age, who were diagnosed with COVID-19 infection within the previous 24 hours, and had a least one high-risk criterion, including age at least 70 years, body mass index of at least 30 kg/m2, diabetes mellitus, uncontrolled hypertension, known respiratory disease, heart failure or coronary disease, fever of at least 38.4° C within the last 48 hours, dyspnea at presentation, bicytopenia, pancytopenia, or the combination of high neutrophil count and low lymphocyte count.
Participants were randomly assigned to receive either placebo or colchicine 0.5 mg twice daily for 3 days and then once daily for another 27 days.
The number needed to prevent one COVID-19 complication is about 60 patients, Dr. Tardif said.
Colchicine was well tolerated and resulted in fewer serious adverse events than with placebo, he said. Diarrhea occurred more often with colchicine, but there was no increase in pneumonia. Caution should be used, however, in treating patients with severe renal disease.
Dr. Tardif said he would not prescribe colchicine to an 18-year-old COVID outpatient who doesn’t have any concomitant diseases, but would for those meeting the study protocol.
“As long as a patient appears to me to be at risk of a complication, I would prescribe it, without a doubt,” he said. “I can tell you that when we held the meeting with the DSMB Friday evening, I actually put each member on the spot and asked them: ‘If it were you – not even treating a patient, but if you had COVID today, would you take it based on the data you’ve seen?’ and all of the DSMB members said they would.
“So we’ll have that debate in the public domain when the paper is out, but I believe most physicians will use it to treat their patients.”
The trial was coordinated by the Montreal Heart Institute and funded by the government of Quebec; the U.S. National Heart, Lung, and Blood Institute; Montreal philanthropist Sophie Desmarais; and the COVID-19 Therapeutics Accelerator launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard. CGI, Dacima, and Pharmascience of Montreal were also collaborators.
A version of this article first appeared on Medscape.com.
Full-dose anticoagulation reduces need for life support in COVID-19
Full-dose anticoagulation was superior to low, prophylactic doses in reducing the need for vital organ support such as ventilation in moderately ill patients hospitalized for COVID-19, according to a report released Jan. 22 by the National Institutes of Health (NIH).
“This is a major advance for patients hospitalized with COVID. Full dose of anticoagulation in these non-ICU patients improved outcomes and there’s a trend toward a reduction in mortality,” Judith Hochman, MD, director of the Cardiovascular Clinical Research Center at NYU Langone Medical Center, New York, said in an interview.
“We have treatments that are improving outcomes but not as many that reduce mortality, so we’re hopeful when the full dataset comes in that will be confirmed,” she said.
The observation of increased rates of blood clots and inflammation among COVID-19 patients, which can lead to complications such as lung failure, heart attack, and stroke, has given rise to various anticoagulant treatment protocols and a need for randomized data on routinely administering increased doses of anticoagulation to hospitalized patients.
Today’s top-line findings come from three linked clinical trials – REMAP-CAP, ACTIV-4, and ATTACC – examining the safety and efficacy of full-dose anticoagulation to treat moderately ill or critically ill adults hospitalized with COVID-19 compared with a lower dose typically used to prevent blood clots in hospitalized patients.
In December 2020, all three trials paused enrollment of the critically ill subgroup after results showed that full-dose anticoagulation started in the intensive care unit (ICU) was not beneficial and may have been harmful in some patients.
Moderately ill patients with COVID-19, defined as those who did not require ICU care or organ support, made up 80% of participants at enrollment in the three trials, Dr. Hochman said.
Among more than 1,000 moderately ill patients reviewed as of the data cut with the data safety monitoring board, full doses of low molecular weight or unfractionated heparin were superior to low prophylactic doses for the primary endpoint of need for ventilation or other organ supportive interventions at 21 days after randomization.
This met the predefined threshold for 99% probability of superiority and recruitment was stopped, Dr. Hochman reported. “Obviously safety figured into this decision. The risk/benefit ratio was very clear.”
The results do not pertain to patients with a previous indication for anticoagulation, who were excluded from the trials.
Data from an additional 1,000 patients will be reviewed and the data published sometime in the next 2-3 months, she said.
With large numbers of COVID-19 patients requiring hospitalization, the outcomes could help reduce the overload on intensive care units around the world, the NIH noted.
The results also highlight the critical role of timing in the course of COVID-19.
“We believe that full anticoagulation is effective early in the disease course,” Dr. Hochman said. “Based on the results so far from these three platform trials, those that were very, very sick at the time of enrollment really didn’t benefit and we needed to have caught them at an earlier stage.
“It’s possible that the people in the ICU are just different and the minute they get sick they need the ICU; so we haven’t clearly demonstrated this time course and when to intervene, but that’s the implication of the findings.”
The question of even earlier treatment is being examined in the partner ACTIV-4B trial, which is enrolling patients with COVID-19 illness not requiring hospitalization and randomizing them to the direct oral anticoagulant apixaban or aspirin or placebo.
“It’s a very important trial and we really want to get the message out that patients should volunteer for it,” said Dr. Hochman, principal investigator of the ACTIV-4 trial.
In the United States, the ACTIV-4 trial is being led by a collaborative effort involving a number of universities, including the University of Pittsburgh and New York University.
The REMAP-CAP, ACTIV-4, and ATTACC study platforms span five continents in more than 300 hospitals and are supported by multiple international funding organizations including the National Institutes of Health, Canadian Institutes of Health Research, the National Institute for Health Research (United Kingdom), the National Health and Medical Research Council (Australia), and the PREPARE and RECOVER consortia (European Union).
A version of this article first appeared on Medscape.com.
Full-dose anticoagulation was superior to low, prophylactic doses in reducing the need for vital organ support such as ventilation in moderately ill patients hospitalized for COVID-19, according to a report released Jan. 22 by the National Institutes of Health (NIH).
“This is a major advance for patients hospitalized with COVID. Full dose of anticoagulation in these non-ICU patients improved outcomes and there’s a trend toward a reduction in mortality,” Judith Hochman, MD, director of the Cardiovascular Clinical Research Center at NYU Langone Medical Center, New York, said in an interview.
“We have treatments that are improving outcomes but not as many that reduce mortality, so we’re hopeful when the full dataset comes in that will be confirmed,” she said.
The observation of increased rates of blood clots and inflammation among COVID-19 patients, which can lead to complications such as lung failure, heart attack, and stroke, has given rise to various anticoagulant treatment protocols and a need for randomized data on routinely administering increased doses of anticoagulation to hospitalized patients.
Today’s top-line findings come from three linked clinical trials – REMAP-CAP, ACTIV-4, and ATTACC – examining the safety and efficacy of full-dose anticoagulation to treat moderately ill or critically ill adults hospitalized with COVID-19 compared with a lower dose typically used to prevent blood clots in hospitalized patients.
In December 2020, all three trials paused enrollment of the critically ill subgroup after results showed that full-dose anticoagulation started in the intensive care unit (ICU) was not beneficial and may have been harmful in some patients.
Moderately ill patients with COVID-19, defined as those who did not require ICU care or organ support, made up 80% of participants at enrollment in the three trials, Dr. Hochman said.
Among more than 1,000 moderately ill patients reviewed as of the data cut with the data safety monitoring board, full doses of low molecular weight or unfractionated heparin were superior to low prophylactic doses for the primary endpoint of need for ventilation or other organ supportive interventions at 21 days after randomization.
This met the predefined threshold for 99% probability of superiority and recruitment was stopped, Dr. Hochman reported. “Obviously safety figured into this decision. The risk/benefit ratio was very clear.”
The results do not pertain to patients with a previous indication for anticoagulation, who were excluded from the trials.
Data from an additional 1,000 patients will be reviewed and the data published sometime in the next 2-3 months, she said.
With large numbers of COVID-19 patients requiring hospitalization, the outcomes could help reduce the overload on intensive care units around the world, the NIH noted.
The results also highlight the critical role of timing in the course of COVID-19.
“We believe that full anticoagulation is effective early in the disease course,” Dr. Hochman said. “Based on the results so far from these three platform trials, those that were very, very sick at the time of enrollment really didn’t benefit and we needed to have caught them at an earlier stage.
“It’s possible that the people in the ICU are just different and the minute they get sick they need the ICU; so we haven’t clearly demonstrated this time course and when to intervene, but that’s the implication of the findings.”
The question of even earlier treatment is being examined in the partner ACTIV-4B trial, which is enrolling patients with COVID-19 illness not requiring hospitalization and randomizing them to the direct oral anticoagulant apixaban or aspirin or placebo.
“It’s a very important trial and we really want to get the message out that patients should volunteer for it,” said Dr. Hochman, principal investigator of the ACTIV-4 trial.
In the United States, the ACTIV-4 trial is being led by a collaborative effort involving a number of universities, including the University of Pittsburgh and New York University.
The REMAP-CAP, ACTIV-4, and ATTACC study platforms span five continents in more than 300 hospitals and are supported by multiple international funding organizations including the National Institutes of Health, Canadian Institutes of Health Research, the National Institute for Health Research (United Kingdom), the National Health and Medical Research Council (Australia), and the PREPARE and RECOVER consortia (European Union).
A version of this article first appeared on Medscape.com.
Full-dose anticoagulation was superior to low, prophylactic doses in reducing the need for vital organ support such as ventilation in moderately ill patients hospitalized for COVID-19, according to a report released Jan. 22 by the National Institutes of Health (NIH).
“This is a major advance for patients hospitalized with COVID. Full dose of anticoagulation in these non-ICU patients improved outcomes and there’s a trend toward a reduction in mortality,” Judith Hochman, MD, director of the Cardiovascular Clinical Research Center at NYU Langone Medical Center, New York, said in an interview.
“We have treatments that are improving outcomes but not as many that reduce mortality, so we’re hopeful when the full dataset comes in that will be confirmed,” she said.
The observation of increased rates of blood clots and inflammation among COVID-19 patients, which can lead to complications such as lung failure, heart attack, and stroke, has given rise to various anticoagulant treatment protocols and a need for randomized data on routinely administering increased doses of anticoagulation to hospitalized patients.
Today’s top-line findings come from three linked clinical trials – REMAP-CAP, ACTIV-4, and ATTACC – examining the safety and efficacy of full-dose anticoagulation to treat moderately ill or critically ill adults hospitalized with COVID-19 compared with a lower dose typically used to prevent blood clots in hospitalized patients.
In December 2020, all three trials paused enrollment of the critically ill subgroup after results showed that full-dose anticoagulation started in the intensive care unit (ICU) was not beneficial and may have been harmful in some patients.
Moderately ill patients with COVID-19, defined as those who did not require ICU care or organ support, made up 80% of participants at enrollment in the three trials, Dr. Hochman said.
Among more than 1,000 moderately ill patients reviewed as of the data cut with the data safety monitoring board, full doses of low molecular weight or unfractionated heparin were superior to low prophylactic doses for the primary endpoint of need for ventilation or other organ supportive interventions at 21 days after randomization.
This met the predefined threshold for 99% probability of superiority and recruitment was stopped, Dr. Hochman reported. “Obviously safety figured into this decision. The risk/benefit ratio was very clear.”
The results do not pertain to patients with a previous indication for anticoagulation, who were excluded from the trials.
Data from an additional 1,000 patients will be reviewed and the data published sometime in the next 2-3 months, she said.
With large numbers of COVID-19 patients requiring hospitalization, the outcomes could help reduce the overload on intensive care units around the world, the NIH noted.
The results also highlight the critical role of timing in the course of COVID-19.
“We believe that full anticoagulation is effective early in the disease course,” Dr. Hochman said. “Based on the results so far from these three platform trials, those that were very, very sick at the time of enrollment really didn’t benefit and we needed to have caught them at an earlier stage.
“It’s possible that the people in the ICU are just different and the minute they get sick they need the ICU; so we haven’t clearly demonstrated this time course and when to intervene, but that’s the implication of the findings.”
The question of even earlier treatment is being examined in the partner ACTIV-4B trial, which is enrolling patients with COVID-19 illness not requiring hospitalization and randomizing them to the direct oral anticoagulant apixaban or aspirin or placebo.
“It’s a very important trial and we really want to get the message out that patients should volunteer for it,” said Dr. Hochman, principal investigator of the ACTIV-4 trial.
In the United States, the ACTIV-4 trial is being led by a collaborative effort involving a number of universities, including the University of Pittsburgh and New York University.
The REMAP-CAP, ACTIV-4, and ATTACC study platforms span five continents in more than 300 hospitals and are supported by multiple international funding organizations including the National Institutes of Health, Canadian Institutes of Health Research, the National Institute for Health Research (United Kingdom), the National Health and Medical Research Council (Australia), and the PREPARE and RECOVER consortia (European Union).
A version of this article first appeared on Medscape.com.
COVID-19 drives physician burnout for some specialties
Physician burnout remains at a critical level, at 42% overall – the same percentage as last year – but COVID-19 has changed the specialties hit hardest, according to Medscape’s Death by 1,000 Cuts: Physician Burnout & Suicide Report.
Critical care physicians now top the list of those experiencing burnout, at 51%, up from 44% last year, followed by rheumatologists (50%, up from 46%) and infectious disease specialists (49%, up from 45%). Forty-nine percent of urologists reported burnout, but that was a reduction from 54% last year.
Last year, the specialties burdened most by burnout were urology, neurology, nephrology, endocrinology, and family medicine.
Women hit particularly hard
Women in medicine traditionally have experienced higher levels of burnout than men, and the pandemic seems to have widened that gap, with the divide now at 51% for women and 36% for men.
“Many women physicians are in families with children at home,” said Carol Bernstein, MD, psychiatrist at Montefiore Medical Center, New York. “It’s already known that women assume more responsibilities in the home than do men. The pressures have increased during COVID-19 – having to be their child’s teacher during home schooling, no child care, and the grandparents can’t babysit. In addition, all doctors and nurses are worried about bringing the virus home to their families.”
Data were collected from Aug. 30 through Nov. 5, 2020. More than 12,000 physicians from 29 specialties responded.
For many, (79%) burnout has been building over years, but for some (21%), it started with the pandemic. Factors cited include lack of adequate personal protective equipment, grief from losing patients, watching families suffer, long hours, and difficult working conditions.
More than 70% of those who responded feel that burnout has had at least a moderate impact on their lives.
“One-tenth consider it severe enough to consider leaving medicine,” survey authors wrote, “an unexpected outcome after having spent so many years in training to become a physician.”
Tragically, an estimated 300 physicians each year in the United States are consumed by the struggle and take their own lives.
One percent have attempted suicide
In this survey, 13% of physicians had thoughts of suicide, and 1% have attempted it; 81% said they had no thoughts of suicide; and 5% preferred not to answer.
By specialty, obstetricians/gynecologists were most likely to have thoughts of suicide (19%), followed by orthopedists (18%) and otolaryngologists and plastic surgeons (17%).
“I yell all the time, I am angry and frustrated all the time. I think about quitting all the time,” said an internist who admitted having suicidal thoughts. “No one in my organization cares about doing the right things for patients as much as I do.”
Yet, many with such thoughts tell no one. By age group, 32% of millennials, 40% of generation X physicians, and 41% of baby boomer physicians who had had thoughts of suicide said they had told no one about those thoughts.
Fear of being reported to the medical board, fear of colleagues finding out, and other factors perpetuate a cycle of burnout and depression, and most don’t seek help.
Top reasons physicians listed for not seeking help for burnout and depression include “symptoms are not severe enough” (52%); “I can deal with without help from a professional” (46%); and feeling “too busy” (40%).
Administrative tasks fuel burnout
The top driver of burnout continues to be “too many administrative tasks.” This year, 58% put it at the top. The next highest categories (named by 37%) were “spending too many hours at work” and “lack of respect from administrators/employers, colleagues or staff.” Others mentioned lack of control or insufficient compensation and government regulations.
Notably, only 8% said stress from treating COVID-19 patients was the top driver.
An internist said, “I’m working 6 days a week, nights, weekends, holidays!”
A general surgeon said, “Being forced to see four patients an hour when complicated patients and procedures are involved” was the biggest contributor to burnout.
One physician in the survey summarized it: “It’s all of these causes; it’s death by 1,000 cuts.”
Exercise tops coping list
Asked how they cope with stress and burnout, physicians put exercise at the top (48%). Next was talking with family and friends (43%), though 43% said they cope by isolating themselves.
Drinking alcohol and overeating junk food were up slightly in the past year: for alcohol, 26%, up from 24%; for junk food, 35%, up from 33%.
The action respondents said would help most to reduce burnout was “increased compensation to avoid financial stress,” chosen by 45%. Next, at 42%, was “more manageable work and schedule,” followed by greater respect from employers, colleagues, and staff (39%).
Asked whether their workplace offered programs to reduce stress and/or burnout, almost half (47%) of physicians said no; 35% said yes; and 18% didn’t know.
Participation in such programs has been low. Almost half (42%) of physicians in this survey said they would be unlikely to attend such a program. Thirty percent they would be likely to participate; 28% said they were neutral on the idea.
“Anti-stress/burnout programs focus on individual approaches to much larger problems,” Wendy K. Dean, MD, psychiatrist and president of Moral Injury of Healthcare, said in an interview. “The programs offer temporary symptomatic relief rather than lasting systemic change. Many physicians are frustrated by these approaches.”
A study last year by the Mayo Clinic found that “the most efficacious strategy to alleviate physician burnout will target organization-directed changes rather than the level of the individual.”
A version of this article first appeared on Medscape.com.
Physician burnout remains at a critical level, at 42% overall – the same percentage as last year – but COVID-19 has changed the specialties hit hardest, according to Medscape’s Death by 1,000 Cuts: Physician Burnout & Suicide Report.
Critical care physicians now top the list of those experiencing burnout, at 51%, up from 44% last year, followed by rheumatologists (50%, up from 46%) and infectious disease specialists (49%, up from 45%). Forty-nine percent of urologists reported burnout, but that was a reduction from 54% last year.
Last year, the specialties burdened most by burnout were urology, neurology, nephrology, endocrinology, and family medicine.
Women hit particularly hard
Women in medicine traditionally have experienced higher levels of burnout than men, and the pandemic seems to have widened that gap, with the divide now at 51% for women and 36% for men.
“Many women physicians are in families with children at home,” said Carol Bernstein, MD, psychiatrist at Montefiore Medical Center, New York. “It’s already known that women assume more responsibilities in the home than do men. The pressures have increased during COVID-19 – having to be their child’s teacher during home schooling, no child care, and the grandparents can’t babysit. In addition, all doctors and nurses are worried about bringing the virus home to their families.”
Data were collected from Aug. 30 through Nov. 5, 2020. More than 12,000 physicians from 29 specialties responded.
For many, (79%) burnout has been building over years, but for some (21%), it started with the pandemic. Factors cited include lack of adequate personal protective equipment, grief from losing patients, watching families suffer, long hours, and difficult working conditions.
More than 70% of those who responded feel that burnout has had at least a moderate impact on their lives.
“One-tenth consider it severe enough to consider leaving medicine,” survey authors wrote, “an unexpected outcome after having spent so many years in training to become a physician.”
Tragically, an estimated 300 physicians each year in the United States are consumed by the struggle and take their own lives.
One percent have attempted suicide
In this survey, 13% of physicians had thoughts of suicide, and 1% have attempted it; 81% said they had no thoughts of suicide; and 5% preferred not to answer.
By specialty, obstetricians/gynecologists were most likely to have thoughts of suicide (19%), followed by orthopedists (18%) and otolaryngologists and plastic surgeons (17%).
“I yell all the time, I am angry and frustrated all the time. I think about quitting all the time,” said an internist who admitted having suicidal thoughts. “No one in my organization cares about doing the right things for patients as much as I do.”
Yet, many with such thoughts tell no one. By age group, 32% of millennials, 40% of generation X physicians, and 41% of baby boomer physicians who had had thoughts of suicide said they had told no one about those thoughts.
Fear of being reported to the medical board, fear of colleagues finding out, and other factors perpetuate a cycle of burnout and depression, and most don’t seek help.
Top reasons physicians listed for not seeking help for burnout and depression include “symptoms are not severe enough” (52%); “I can deal with without help from a professional” (46%); and feeling “too busy” (40%).
Administrative tasks fuel burnout
The top driver of burnout continues to be “too many administrative tasks.” This year, 58% put it at the top. The next highest categories (named by 37%) were “spending too many hours at work” and “lack of respect from administrators/employers, colleagues or staff.” Others mentioned lack of control or insufficient compensation and government regulations.
Notably, only 8% said stress from treating COVID-19 patients was the top driver.
An internist said, “I’m working 6 days a week, nights, weekends, holidays!”
A general surgeon said, “Being forced to see four patients an hour when complicated patients and procedures are involved” was the biggest contributor to burnout.
One physician in the survey summarized it: “It’s all of these causes; it’s death by 1,000 cuts.”
Exercise tops coping list
Asked how they cope with stress and burnout, physicians put exercise at the top (48%). Next was talking with family and friends (43%), though 43% said they cope by isolating themselves.
Drinking alcohol and overeating junk food were up slightly in the past year: for alcohol, 26%, up from 24%; for junk food, 35%, up from 33%.
The action respondents said would help most to reduce burnout was “increased compensation to avoid financial stress,” chosen by 45%. Next, at 42%, was “more manageable work and schedule,” followed by greater respect from employers, colleagues, and staff (39%).
Asked whether their workplace offered programs to reduce stress and/or burnout, almost half (47%) of physicians said no; 35% said yes; and 18% didn’t know.
Participation in such programs has been low. Almost half (42%) of physicians in this survey said they would be unlikely to attend such a program. Thirty percent they would be likely to participate; 28% said they were neutral on the idea.
“Anti-stress/burnout programs focus on individual approaches to much larger problems,” Wendy K. Dean, MD, psychiatrist and president of Moral Injury of Healthcare, said in an interview. “The programs offer temporary symptomatic relief rather than lasting systemic change. Many physicians are frustrated by these approaches.”
A study last year by the Mayo Clinic found that “the most efficacious strategy to alleviate physician burnout will target organization-directed changes rather than the level of the individual.”
A version of this article first appeared on Medscape.com.
Physician burnout remains at a critical level, at 42% overall – the same percentage as last year – but COVID-19 has changed the specialties hit hardest, according to Medscape’s Death by 1,000 Cuts: Physician Burnout & Suicide Report.
Critical care physicians now top the list of those experiencing burnout, at 51%, up from 44% last year, followed by rheumatologists (50%, up from 46%) and infectious disease specialists (49%, up from 45%). Forty-nine percent of urologists reported burnout, but that was a reduction from 54% last year.
Last year, the specialties burdened most by burnout were urology, neurology, nephrology, endocrinology, and family medicine.
Women hit particularly hard
Women in medicine traditionally have experienced higher levels of burnout than men, and the pandemic seems to have widened that gap, with the divide now at 51% for women and 36% for men.
“Many women physicians are in families with children at home,” said Carol Bernstein, MD, psychiatrist at Montefiore Medical Center, New York. “It’s already known that women assume more responsibilities in the home than do men. The pressures have increased during COVID-19 – having to be their child’s teacher during home schooling, no child care, and the grandparents can’t babysit. In addition, all doctors and nurses are worried about bringing the virus home to their families.”
Data were collected from Aug. 30 through Nov. 5, 2020. More than 12,000 physicians from 29 specialties responded.
For many, (79%) burnout has been building over years, but for some (21%), it started with the pandemic. Factors cited include lack of adequate personal protective equipment, grief from losing patients, watching families suffer, long hours, and difficult working conditions.
More than 70% of those who responded feel that burnout has had at least a moderate impact on their lives.
“One-tenth consider it severe enough to consider leaving medicine,” survey authors wrote, “an unexpected outcome after having spent so many years in training to become a physician.”
Tragically, an estimated 300 physicians each year in the United States are consumed by the struggle and take their own lives.
One percent have attempted suicide
In this survey, 13% of physicians had thoughts of suicide, and 1% have attempted it; 81% said they had no thoughts of suicide; and 5% preferred not to answer.
By specialty, obstetricians/gynecologists were most likely to have thoughts of suicide (19%), followed by orthopedists (18%) and otolaryngologists and plastic surgeons (17%).
“I yell all the time, I am angry and frustrated all the time. I think about quitting all the time,” said an internist who admitted having suicidal thoughts. “No one in my organization cares about doing the right things for patients as much as I do.”
Yet, many with such thoughts tell no one. By age group, 32% of millennials, 40% of generation X physicians, and 41% of baby boomer physicians who had had thoughts of suicide said they had told no one about those thoughts.
Fear of being reported to the medical board, fear of colleagues finding out, and other factors perpetuate a cycle of burnout and depression, and most don’t seek help.
Top reasons physicians listed for not seeking help for burnout and depression include “symptoms are not severe enough” (52%); “I can deal with without help from a professional” (46%); and feeling “too busy” (40%).
Administrative tasks fuel burnout
The top driver of burnout continues to be “too many administrative tasks.” This year, 58% put it at the top. The next highest categories (named by 37%) were “spending too many hours at work” and “lack of respect from administrators/employers, colleagues or staff.” Others mentioned lack of control or insufficient compensation and government regulations.
Notably, only 8% said stress from treating COVID-19 patients was the top driver.
An internist said, “I’m working 6 days a week, nights, weekends, holidays!”
A general surgeon said, “Being forced to see four patients an hour when complicated patients and procedures are involved” was the biggest contributor to burnout.
One physician in the survey summarized it: “It’s all of these causes; it’s death by 1,000 cuts.”
Exercise tops coping list
Asked how they cope with stress and burnout, physicians put exercise at the top (48%). Next was talking with family and friends (43%), though 43% said they cope by isolating themselves.
Drinking alcohol and overeating junk food were up slightly in the past year: for alcohol, 26%, up from 24%; for junk food, 35%, up from 33%.
The action respondents said would help most to reduce burnout was “increased compensation to avoid financial stress,” chosen by 45%. Next, at 42%, was “more manageable work and schedule,” followed by greater respect from employers, colleagues, and staff (39%).
Asked whether their workplace offered programs to reduce stress and/or burnout, almost half (47%) of physicians said no; 35% said yes; and 18% didn’t know.
Participation in such programs has been low. Almost half (42%) of physicians in this survey said they would be unlikely to attend such a program. Thirty percent they would be likely to participate; 28% said they were neutral on the idea.
“Anti-stress/burnout programs focus on individual approaches to much larger problems,” Wendy K. Dean, MD, psychiatrist and president of Moral Injury of Healthcare, said in an interview. “The programs offer temporary symptomatic relief rather than lasting systemic change. Many physicians are frustrated by these approaches.”
A study last year by the Mayo Clinic found that “the most efficacious strategy to alleviate physician burnout will target organization-directed changes rather than the level of the individual.”
A version of this article first appeared on Medscape.com.
Daily moisturizers a bedrock of atopic dermatitis management
Mounting .

In an updated review of clinical evidence on the topic, Adelaide A. Hebert, MD, Noreen Heer Nicol, PhD, RN, FNP, and colleagues evaluated 13 trials that assessed daily moisturization for the treatment of AD published between 2006 and 2019. “The bottom line is, daily moisturization increased skin hydration and it decreased transepidermal water loss in all children and adults in the 13 studies we looked at,” Dr. Nicol, associate dean and associate professor of nursing at the University of Colorado, Denver, said at the Revolutionizing Atopic Dermatitis symposium.
Based on published evidence in the review, she and her coauthors assembled six points regarding the importance of essential skin repair in AD:
1. It strengthens the barrier that protects against environmental triggers such as skin irritants aeroallergens, dust mites, and pet dander.
2. It decreases moisture loss that perpetuates damage and can provoke inflammatory processes.
3. It promotes a healthy microbiome via induction of antimicrobial peptides.
4. It maintains stratum corneum acidification, which protects against pathogens.
5. It reduces recurrence of flares when used daily.
6. It prevents the onset of AD when applied early in life to at-risk children.
A separate review of optimal AD care authored by Dr. Nicol underscores the importance of foundational management, “meaning that we want you to use hydration and daily moisturizers as part of your everyday management,” she said. “Without good barrier repair, infections and allergens can break through. The intention is to have that barrier repair a key point of moisturizer use.”
In a 2014 published study, researchers investigated the role of proactive emollient therapy in preventing AD in 124 neonates in the United States and the United Kingdom with a first-degree relative with a history of allergic rhinitis, asthma, or AD. The treatment group received daily total body application of Aquaphor Healing Ointment, Cetaphil Cream, or sunflower seed oil, starting at 3 weeks of age, while the control group received no moisturizers. They found that daily emollient therapy significantly reduced the cumulative incidence of AD at 6 months (22% vs. 42% among controls). A follow-up study confirmed a protective but nonsignificant effect of daily moisturizer use at 12 months (AD was diagnosed in 13.2% of those in the treatment group vs. 25% in the control group), most likely due to the study being underpowered.
“The message here is simple,” Dr. Nicol said. “Wouldn’t it be wonderful if we could reduce the burden of AD by doing something as straightforward as moisturizer use in our neonates?”
With so many moisturizers on the market today, considerations include active ingredients, side effects, absorption, and amount required for efficacy. “On the average adult, head to toe, front to back, one time it takes about 30 grams or one ounce of something to cover them completely, so you want to make sure people are using enough,” Dr. Nicol said. “You don’t want to be prescribing people 15- and 30-gram tubes of product and hoping they have enough to cover their bodies multiple times.”
Ten years ago, a randomized, controlled trial found that Aquaphor Healing Ointment was 47 times more cost-effective than prescription barrier creams Atopiclair nonsteroidal cream and EpiCeram controlled release skin barrier emulsion. “The most expensive things do not have to be the best things to be used,” Dr. Nicol said. “Recognize what the properties of these products are and what the benefit is.”
A basic principle of skin care for AD patients recommended by Dr. Nicol and colleagues at National Jewish Health, Denver, includes applying a fragrance-free moisturizer within 3 minutes of finishing a bath or a shower. They recommend products sold in 1-pound jars or large tubes, such as Aquaphor Healing Ointment, Vaniply Ointment, Eucerin Creme (various formulations), Vanicream, CeraVe Cream, or Cetaphil cream. “Vaseline is a good occlusive preparation to seal in but is most effective after bath or shower,” the recommendations continue. “Topical maintenance medications may be used in place of moisturizers or sealer when prescribed.”
She recommends including a list of preferred moisturizers for patients to use into written action plans for skin care. “This adds a lot of benefit to patients,” she said. “Always put the patient at the center of your decision-making. Spend time listening to them, give them options of things that they are willing to use so that they can trust you.”
Dr. Nicol disclosed that she has served as an advisory board member for Eli Lilly & Co.
Mounting .
In an updated review of clinical evidence on the topic, Adelaide A. Hebert, MD, Noreen Heer Nicol, PhD, RN, FNP, and colleagues evaluated 13 trials that assessed daily moisturization for the treatment of AD published between 2006 and 2019. “The bottom line is, daily moisturization increased skin hydration and it decreased transepidermal water loss in all children and adults in the 13 studies we looked at,” Dr. Nicol, associate dean and associate professor of nursing at the University of Colorado, Denver, said at the Revolutionizing Atopic Dermatitis symposium.
Based on published evidence in the review, she and her coauthors assembled six points regarding the importance of essential skin repair in AD:
1. It strengthens the barrier that protects against environmental triggers such as skin irritants aeroallergens, dust mites, and pet dander.
2. It decreases moisture loss that perpetuates damage and can provoke inflammatory processes.
3. It promotes a healthy microbiome via induction of antimicrobial peptides.
4. It maintains stratum corneum acidification, which protects against pathogens.
5. It reduces recurrence of flares when used daily.
6. It prevents the onset of AD when applied early in life to at-risk children.
A separate review of optimal AD care authored by Dr. Nicol underscores the importance of foundational management, “meaning that we want you to use hydration and daily moisturizers as part of your everyday management,” she said. “Without good barrier repair, infections and allergens can break through. The intention is to have that barrier repair a key point of moisturizer use.”
In a 2014 published study, researchers investigated the role of proactive emollient therapy in preventing AD in 124 neonates in the United States and the United Kingdom with a first-degree relative with a history of allergic rhinitis, asthma, or AD. The treatment group received daily total body application of Aquaphor Healing Ointment, Cetaphil Cream, or sunflower seed oil, starting at 3 weeks of age, while the control group received no moisturizers. They found that daily emollient therapy significantly reduced the cumulative incidence of AD at 6 months (22% vs. 42% among controls). A follow-up study confirmed a protective but nonsignificant effect of daily moisturizer use at 12 months (AD was diagnosed in 13.2% of those in the treatment group vs. 25% in the control group), most likely due to the study being underpowered.
“The message here is simple,” Dr. Nicol said. “Wouldn’t it be wonderful if we could reduce the burden of AD by doing something as straightforward as moisturizer use in our neonates?”
With so many moisturizers on the market today, considerations include active ingredients, side effects, absorption, and amount required for efficacy. “On the average adult, head to toe, front to back, one time it takes about 30 grams or one ounce of something to cover them completely, so you want to make sure people are using enough,” Dr. Nicol said. “You don’t want to be prescribing people 15- and 30-gram tubes of product and hoping they have enough to cover their bodies multiple times.”
Ten years ago, a randomized, controlled trial found that Aquaphor Healing Ointment was 47 times more cost-effective than prescription barrier creams Atopiclair nonsteroidal cream and EpiCeram controlled release skin barrier emulsion. “The most expensive things do not have to be the best things to be used,” Dr. Nicol said. “Recognize what the properties of these products are and what the benefit is.”
A basic principle of skin care for AD patients recommended by Dr. Nicol and colleagues at National Jewish Health, Denver, includes applying a fragrance-free moisturizer within 3 minutes of finishing a bath or a shower. They recommend products sold in 1-pound jars or large tubes, such as Aquaphor Healing Ointment, Vaniply Ointment, Eucerin Creme (various formulations), Vanicream, CeraVe Cream, or Cetaphil cream. “Vaseline is a good occlusive preparation to seal in but is most effective after bath or shower,” the recommendations continue. “Topical maintenance medications may be used in place of moisturizers or sealer when prescribed.”
She recommends including a list of preferred moisturizers for patients to use into written action plans for skin care. “This adds a lot of benefit to patients,” she said. “Always put the patient at the center of your decision-making. Spend time listening to them, give them options of things that they are willing to use so that they can trust you.”
Dr. Nicol disclosed that she has served as an advisory board member for Eli Lilly & Co.
Mounting .
In an updated review of clinical evidence on the topic, Adelaide A. Hebert, MD, Noreen Heer Nicol, PhD, RN, FNP, and colleagues evaluated 13 trials that assessed daily moisturization for the treatment of AD published between 2006 and 2019. “The bottom line is, daily moisturization increased skin hydration and it decreased transepidermal water loss in all children and adults in the 13 studies we looked at,” Dr. Nicol, associate dean and associate professor of nursing at the University of Colorado, Denver, said at the Revolutionizing Atopic Dermatitis symposium.
Based on published evidence in the review, she and her coauthors assembled six points regarding the importance of essential skin repair in AD:
1. It strengthens the barrier that protects against environmental triggers such as skin irritants aeroallergens, dust mites, and pet dander.
2. It decreases moisture loss that perpetuates damage and can provoke inflammatory processes.
3. It promotes a healthy microbiome via induction of antimicrobial peptides.
4. It maintains stratum corneum acidification, which protects against pathogens.
5. It reduces recurrence of flares when used daily.
6. It prevents the onset of AD when applied early in life to at-risk children.
A separate review of optimal AD care authored by Dr. Nicol underscores the importance of foundational management, “meaning that we want you to use hydration and daily moisturizers as part of your everyday management,” she said. “Without good barrier repair, infections and allergens can break through. The intention is to have that barrier repair a key point of moisturizer use.”
In a 2014 published study, researchers investigated the role of proactive emollient therapy in preventing AD in 124 neonates in the United States and the United Kingdom with a first-degree relative with a history of allergic rhinitis, asthma, or AD. The treatment group received daily total body application of Aquaphor Healing Ointment, Cetaphil Cream, or sunflower seed oil, starting at 3 weeks of age, while the control group received no moisturizers. They found that daily emollient therapy significantly reduced the cumulative incidence of AD at 6 months (22% vs. 42% among controls). A follow-up study confirmed a protective but nonsignificant effect of daily moisturizer use at 12 months (AD was diagnosed in 13.2% of those in the treatment group vs. 25% in the control group), most likely due to the study being underpowered.
“The message here is simple,” Dr. Nicol said. “Wouldn’t it be wonderful if we could reduce the burden of AD by doing something as straightforward as moisturizer use in our neonates?”
With so many moisturizers on the market today, considerations include active ingredients, side effects, absorption, and amount required for efficacy. “On the average adult, head to toe, front to back, one time it takes about 30 grams or one ounce of something to cover them completely, so you want to make sure people are using enough,” Dr. Nicol said. “You don’t want to be prescribing people 15- and 30-gram tubes of product and hoping they have enough to cover their bodies multiple times.”
Ten years ago, a randomized, controlled trial found that Aquaphor Healing Ointment was 47 times more cost-effective than prescription barrier creams Atopiclair nonsteroidal cream and EpiCeram controlled release skin barrier emulsion. “The most expensive things do not have to be the best things to be used,” Dr. Nicol said. “Recognize what the properties of these products are and what the benefit is.”
A basic principle of skin care for AD patients recommended by Dr. Nicol and colleagues at National Jewish Health, Denver, includes applying a fragrance-free moisturizer within 3 minutes of finishing a bath or a shower. They recommend products sold in 1-pound jars or large tubes, such as Aquaphor Healing Ointment, Vaniply Ointment, Eucerin Creme (various formulations), Vanicream, CeraVe Cream, or Cetaphil cream. “Vaseline is a good occlusive preparation to seal in but is most effective after bath or shower,” the recommendations continue. “Topical maintenance medications may be used in place of moisturizers or sealer when prescribed.”
She recommends including a list of preferred moisturizers for patients to use into written action plans for skin care. “This adds a lot of benefit to patients,” she said. “Always put the patient at the center of your decision-making. Spend time listening to them, give them options of things that they are willing to use so that they can trust you.”
Dr. Nicol disclosed that she has served as an advisory board member for Eli Lilly & Co.
FROM REVOLUTIONIZING AD 2020
What we know and don’t know about virus variants and vaccines
About 20 states across the country have detected the more transmissible B.1.1.7 SARS-CoV-2 variant to date. Given the unknowns of the emerging situation, experts with the Infectious Diseases Society of America addressed vaccine effectiveness, how well equipped the United States is to track new mutations, and shared their impressions of President Joe Biden’s COVID-19 executive orders.
One of the major concerns remains the ability of COVID-19 vaccines to work on new strains. “All of our vaccines target the spike protein and try to elicit neutralizing antibodies that bind to that protein,” Mirella Salvatore, MD, assistant professor of medicine and population health sciences at Weill Cornell Medicine, New York, said during an IDSA press briefing on Thursday.
The B.1.1.7 mutation occurs in the “very important” spike protein, a component of the SARS-CoV-2 virus necessary for binding, which allows the virus to enter cells, added Dr. Salvatore, an IDSA fellow.
The evidence suggests that SARS-CoV-2 should be capable of producing one or two mutations per month. However, the B.1.1.7 variant surprised investigators in the United Kingdom when they first discovered the strain had 17 mutations, Dr. Salvatore said.
It’s still unknown why this particular strain is more transmissible, but Dr. Salvatore speculated that the mutation gives the virus an advantage and increases binding, allowing it to enter cells more easily. She added that the mutations might have arisen among immunocompromised people infected with SARS-CoV-2, but “that is just a hypothesis.”
On a positive note, Kathryn M. Edwards, MD, another IDSA fellow, explained at the briefing that the existing vaccines target more than one location on the virus’ spike protein. Therefore, “if there is a mutation that changes one structure of the spike protein, there will be other areas where the binding can occur.”
This polyclonal response “is why the vaccine can still be effective against this virus,” added Dr. Edwards, scientific director of the Vanderbilt Vaccine Research Program and professor of pediatrics at Vanderbilt University, Nashville, Tenn.
Dr. Salvatore emphasized that, although the new variant is more transmissible, it doesn’t appear to be more lethal. “This might affect overall mortality but not for the individual who gets the infection.”
Staying one step ahead
When asked for assurance that COVID-19 vaccines will work against emerging variants, Dr. Edwards said, “It may be we will have to change the vaccine so it is more responsive to new variants, but at this point that does not seem to be the case.”
Should the vaccines require an update, the messenger RNA vaccines have an advantage – researchers can rapidly revise them. “All you need to do is put all the little nucleotides together,” Dr. Edwards said.
“A number of us are looking at how this will work, and we look to influenza,” she added. Dr. Edwards drew an analogy to choosing – and sometimes updating – the influenza strains each year for the annual flu vaccine. With appropriate funding, the same system could be replicated to address any evolving changes to SARS-CoV-2.
On funding, Dr. Salvatore said more money would be required to optimize the surveillance system for emerging strains in the United States.
“We actually have this system – there is a wonderful network that sequences the influenza strains,” she said. “The structure exists, we just need the funding.”
“The CDC is getting the system tooled up to get more viruses to be sequenced,” Dr. Edwards said.
Both experts praised the CDC for its website with up-to-date surveillance information on emerging strains of SARS-CoV-2.
President Biden’s backing of science
A reporter asked each infectious disease expert to share their impression of President Biden’s newly signed COVID-19 executive orders.
“The biggest takeaway is the role of science and the lessons we’ve learned from masks, handwashing, and distancing,” Dr. Edwards said. “We need to heed the advice ... [especially] with a variant that is more contagious.
“It is encouraging that science will be listened to – that is the overall message,” she added.
Dr. Salvatore agreed, saying that the orders give “the feeling that we can now act by following science.”
“We have plenty of papers that show the effectiveness of masking,” for example, she said. Dr. Salvatore acknowledged that there are “a lot of contrasting ideas about masking” across the United States but stressed their importance.
“We should follow measures that we know work,” she said.
Both experts said more research is needed to stay ahead of this evolving scenario. “We still need a lot of basic science showing how this virus replicates in the cell,” Dr. Salvatore said. “We need to really characterize all these mutations and their functions.”
“We need to be concerned, do follow-up studies,” she added, “but we don’t need to panic.”
This article was based on an Infectious Diseases Society of America Media Briefing on Jan. 21, 2021. Dr. Salvatore disclosed that she is a site principal investigator on a study from Verily Life Sciences/Brin Foundation on Predictors of Severe COVID-19 Outcomes and principal investigator for an investigator-initiated study sponsored by Genentech on combination therapy in influenza. Dr. Edwards disclosed National Institutes of Health and Centers for Disease Control and Prevention grants; consulting for Bionet and IBM; and being a member of data safety and monitoring committees for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, and Merck.
A version of this article first appeared on Medscape.com.
About 20 states across the country have detected the more transmissible B.1.1.7 SARS-CoV-2 variant to date. Given the unknowns of the emerging situation, experts with the Infectious Diseases Society of America addressed vaccine effectiveness, how well equipped the United States is to track new mutations, and shared their impressions of President Joe Biden’s COVID-19 executive orders.
One of the major concerns remains the ability of COVID-19 vaccines to work on new strains. “All of our vaccines target the spike protein and try to elicit neutralizing antibodies that bind to that protein,” Mirella Salvatore, MD, assistant professor of medicine and population health sciences at Weill Cornell Medicine, New York, said during an IDSA press briefing on Thursday.
The B.1.1.7 mutation occurs in the “very important” spike protein, a component of the SARS-CoV-2 virus necessary for binding, which allows the virus to enter cells, added Dr. Salvatore, an IDSA fellow.
The evidence suggests that SARS-CoV-2 should be capable of producing one or two mutations per month. However, the B.1.1.7 variant surprised investigators in the United Kingdom when they first discovered the strain had 17 mutations, Dr. Salvatore said.
It’s still unknown why this particular strain is more transmissible, but Dr. Salvatore speculated that the mutation gives the virus an advantage and increases binding, allowing it to enter cells more easily. She added that the mutations might have arisen among immunocompromised people infected with SARS-CoV-2, but “that is just a hypothesis.”
On a positive note, Kathryn M. Edwards, MD, another IDSA fellow, explained at the briefing that the existing vaccines target more than one location on the virus’ spike protein. Therefore, “if there is a mutation that changes one structure of the spike protein, there will be other areas where the binding can occur.”
This polyclonal response “is why the vaccine can still be effective against this virus,” added Dr. Edwards, scientific director of the Vanderbilt Vaccine Research Program and professor of pediatrics at Vanderbilt University, Nashville, Tenn.
Dr. Salvatore emphasized that, although the new variant is more transmissible, it doesn’t appear to be more lethal. “This might affect overall mortality but not for the individual who gets the infection.”
Staying one step ahead
When asked for assurance that COVID-19 vaccines will work against emerging variants, Dr. Edwards said, “It may be we will have to change the vaccine so it is more responsive to new variants, but at this point that does not seem to be the case.”
Should the vaccines require an update, the messenger RNA vaccines have an advantage – researchers can rapidly revise them. “All you need to do is put all the little nucleotides together,” Dr. Edwards said.
“A number of us are looking at how this will work, and we look to influenza,” she added. Dr. Edwards drew an analogy to choosing – and sometimes updating – the influenza strains each year for the annual flu vaccine. With appropriate funding, the same system could be replicated to address any evolving changes to SARS-CoV-2.
On funding, Dr. Salvatore said more money would be required to optimize the surveillance system for emerging strains in the United States.
“We actually have this system – there is a wonderful network that sequences the influenza strains,” she said. “The structure exists, we just need the funding.”
“The CDC is getting the system tooled up to get more viruses to be sequenced,” Dr. Edwards said.
Both experts praised the CDC for its website with up-to-date surveillance information on emerging strains of SARS-CoV-2.
President Biden’s backing of science
A reporter asked each infectious disease expert to share their impression of President Biden’s newly signed COVID-19 executive orders.
“The biggest takeaway is the role of science and the lessons we’ve learned from masks, handwashing, and distancing,” Dr. Edwards said. “We need to heed the advice ... [especially] with a variant that is more contagious.
“It is encouraging that science will be listened to – that is the overall message,” she added.
Dr. Salvatore agreed, saying that the orders give “the feeling that we can now act by following science.”
“We have plenty of papers that show the effectiveness of masking,” for example, she said. Dr. Salvatore acknowledged that there are “a lot of contrasting ideas about masking” across the United States but stressed their importance.
“We should follow measures that we know work,” she said.
Both experts said more research is needed to stay ahead of this evolving scenario. “We still need a lot of basic science showing how this virus replicates in the cell,” Dr. Salvatore said. “We need to really characterize all these mutations and their functions.”
“We need to be concerned, do follow-up studies,” she added, “but we don’t need to panic.”
This article was based on an Infectious Diseases Society of America Media Briefing on Jan. 21, 2021. Dr. Salvatore disclosed that she is a site principal investigator on a study from Verily Life Sciences/Brin Foundation on Predictors of Severe COVID-19 Outcomes and principal investigator for an investigator-initiated study sponsored by Genentech on combination therapy in influenza. Dr. Edwards disclosed National Institutes of Health and Centers for Disease Control and Prevention grants; consulting for Bionet and IBM; and being a member of data safety and monitoring committees for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, and Merck.
A version of this article first appeared on Medscape.com.
About 20 states across the country have detected the more transmissible B.1.1.7 SARS-CoV-2 variant to date. Given the unknowns of the emerging situation, experts with the Infectious Diseases Society of America addressed vaccine effectiveness, how well equipped the United States is to track new mutations, and shared their impressions of President Joe Biden’s COVID-19 executive orders.
One of the major concerns remains the ability of COVID-19 vaccines to work on new strains. “All of our vaccines target the spike protein and try to elicit neutralizing antibodies that bind to that protein,” Mirella Salvatore, MD, assistant professor of medicine and population health sciences at Weill Cornell Medicine, New York, said during an IDSA press briefing on Thursday.
The B.1.1.7 mutation occurs in the “very important” spike protein, a component of the SARS-CoV-2 virus necessary for binding, which allows the virus to enter cells, added Dr. Salvatore, an IDSA fellow.
The evidence suggests that SARS-CoV-2 should be capable of producing one or two mutations per month. However, the B.1.1.7 variant surprised investigators in the United Kingdom when they first discovered the strain had 17 mutations, Dr. Salvatore said.
It’s still unknown why this particular strain is more transmissible, but Dr. Salvatore speculated that the mutation gives the virus an advantage and increases binding, allowing it to enter cells more easily. She added that the mutations might have arisen among immunocompromised people infected with SARS-CoV-2, but “that is just a hypothesis.”
On a positive note, Kathryn M. Edwards, MD, another IDSA fellow, explained at the briefing that the existing vaccines target more than one location on the virus’ spike protein. Therefore, “if there is a mutation that changes one structure of the spike protein, there will be other areas where the binding can occur.”
This polyclonal response “is why the vaccine can still be effective against this virus,” added Dr. Edwards, scientific director of the Vanderbilt Vaccine Research Program and professor of pediatrics at Vanderbilt University, Nashville, Tenn.
Dr. Salvatore emphasized that, although the new variant is more transmissible, it doesn’t appear to be more lethal. “This might affect overall mortality but not for the individual who gets the infection.”
Staying one step ahead
When asked for assurance that COVID-19 vaccines will work against emerging variants, Dr. Edwards said, “It may be we will have to change the vaccine so it is more responsive to new variants, but at this point that does not seem to be the case.”
Should the vaccines require an update, the messenger RNA vaccines have an advantage – researchers can rapidly revise them. “All you need to do is put all the little nucleotides together,” Dr. Edwards said.
“A number of us are looking at how this will work, and we look to influenza,” she added. Dr. Edwards drew an analogy to choosing – and sometimes updating – the influenza strains each year for the annual flu vaccine. With appropriate funding, the same system could be replicated to address any evolving changes to SARS-CoV-2.
On funding, Dr. Salvatore said more money would be required to optimize the surveillance system for emerging strains in the United States.
“We actually have this system – there is a wonderful network that sequences the influenza strains,” she said. “The structure exists, we just need the funding.”
“The CDC is getting the system tooled up to get more viruses to be sequenced,” Dr. Edwards said.
Both experts praised the CDC for its website with up-to-date surveillance information on emerging strains of SARS-CoV-2.
President Biden’s backing of science
A reporter asked each infectious disease expert to share their impression of President Biden’s newly signed COVID-19 executive orders.
“The biggest takeaway is the role of science and the lessons we’ve learned from masks, handwashing, and distancing,” Dr. Edwards said. “We need to heed the advice ... [especially] with a variant that is more contagious.
“It is encouraging that science will be listened to – that is the overall message,” she added.
Dr. Salvatore agreed, saying that the orders give “the feeling that we can now act by following science.”
“We have plenty of papers that show the effectiveness of masking,” for example, she said. Dr. Salvatore acknowledged that there are “a lot of contrasting ideas about masking” across the United States but stressed their importance.
“We should follow measures that we know work,” she said.
Both experts said more research is needed to stay ahead of this evolving scenario. “We still need a lot of basic science showing how this virus replicates in the cell,” Dr. Salvatore said. “We need to really characterize all these mutations and their functions.”
“We need to be concerned, do follow-up studies,” she added, “but we don’t need to panic.”
This article was based on an Infectious Diseases Society of America Media Briefing on Jan. 21, 2021. Dr. Salvatore disclosed that she is a site principal investigator on a study from Verily Life Sciences/Brin Foundation on Predictors of Severe COVID-19 Outcomes and principal investigator for an investigator-initiated study sponsored by Genentech on combination therapy in influenza. Dr. Edwards disclosed National Institutes of Health and Centers for Disease Control and Prevention grants; consulting for Bionet and IBM; and being a member of data safety and monitoring committees for Sanofi, X-4 Pharma, Seqirus, Moderna, Pfizer, and Merck.
A version of this article first appeared on Medscape.com.
Coronasomnia: Pervasive sleeplessness, self-medicating raise concerns of sleep experts
Among the many losses suffered by millions worldwide during the COVID-19 pandemic, the loss of sleep may be the most widespread, with potentially long-lasting, negative consequences on physical, mental, and emotional health, sleep researchers have found.
Results from multiple studies and surveys conducted during the pandemic show that a majority of subjects report clinically meaningful changes in sleep quality, sleep patterns, and sleep disturbances.

For example, a cross-sectional international survey conducted from late March through late April 2020 found that among more than 3,000 responders from 49 countries, 58% reported dissatisfaction with their sleep, and 40% reported a decrease in sleep quality during the pandemic, compared with pre-COVID-19 sleep, according to Uri Mandelkorn of the Natural Sleep Clinic in Jerusalem, and colleagues.
“In particular, this research raises the need to screen for worsening sleep patterns and use of sleeping aids in the more susceptible populations identified in this study, namely, women and people with insecure livelihoods or those subjected to strict quarantine. Health care providers should pay special attention to physical and psychological problems that this surge in sleep disturbances may cause,” they wrote. The report is in the Journal of Clinical Sleep Medicine.
Sleeping, more or less
A coauthor of that study, David Gozal, MD, FCCP, a pediatric pulmonologist and sleep medicine specialist at the University of Missouri in Columbia, said that the pandemic has had paradoxical effects on sleeps patterns for many.
“At the beginning, with the initial phases of lockdown for COVID, for most of the people whose jobs were not affected and who did not lose their jobs, [for whom] there was not the anxiety of being jobless and financially strapped, but who now were staying at home, there was actually a benefit. People started reporting getting more sleep and, more importantly, more vivid dreams and things of that nature,” he said in an interview.
“But as the lockdown progressed, we saw progressively and increasingly more people having difficulty falling asleep and staying asleep, using more medicines such as hypnotics to induce sleep, and we saw a 20% increase in the overall consumption of sleeping pills,” he said.
Similar results were seen in a cross-sectional survey of 843 adults in the United Kingdom, which showed that nearly 70% of participants reported a change in sleep patterns, only 45% reported having refreshing sleep, and 46% reported being sleepier during lockdown than before. Two-thirds of the respondents reported that the pandemic affected their mental health, and one-fourth reported increased alcohol consumption during lockdown. Those with suspected COVID-19 infections reported having more nightmares and abnormal sleep rhythms.
It is possible that the effects of COVID-19 infection on sleep may linger long after the infection itself has resolved, results of a cohort study from China suggest. As reported in The Lancet, among 1,655 patients discharged from the Jin Yin-tan hospital in Wuhan, 26% reported sleep disturbances 6 months after acute COVID-19 infection.
Self-medicating
Among 5,525 Canadians surveyed from April 3 through June 24, 2020, a large proportion reported the use of pharmacologic sleeps aids, said Tetyana Kendzerska, MD, PhD, assistant professor of medicine in the division of respirology at the University of Ottawa.
“At the time of the survey completion, 27% of participants reported taking sleeping aids (prescribed or [over] the counter); across the entire sample, 8% of respondents reported an increase in the frequency of sleeping medication use during the outbreak compared to before the outbreak,” she said in an interview.
Many people resort to self-medicating with over-the-counter preparations such as melatonin and pain-relief nighttime formulations containing diphenhydramine (Benadryl), a first-generation antihistamine with sedative properties, noted Kannan Ramar, MBBS, MD, a critical care, pulmonary, and sleep medicine specialist at the Mayo Clinic in Rochester, Minn., and current president of the American Academy of Sleep Medicine.
“When people are self-medicating for what they think is difficulty sleeping, the concern is that even if a diagnosis of insomnia has been established, there could be another, ongoing sleep disorder that may be undiagnosed, which might be causing the problem with insomnia,” he said in an interview.
“For example, obstructive sleep apnea might be causing people to wake up in the night or even contribute to difficulty falling asleep in the first place. So medicating for something without a known diagnosis may leave an underlying sleep disorder untreated, which won’t help the patient in either the short or the long term,” Dr. Ramar said.
Causes for concern
“For those people who have COVID, we have seen quite a few sleep issues develop. Those were not reported in the actual study, but in the clinic and subsequent studies published from other places,” Dr. Gozal said.
“People who suffered from COVID, and even people who supposedly did very well and were virtually asymptomatic or maybe had only a headache or fever but did not need to go to the hospital, many of those people reported either excessive sleepiness for a long period of time, and would sleep 2 or 3 hours more per night. Or the opposite was reported: There were those that after recovering reported that they couldn’t sleep – they were sleeping 4 or 5 hours when they normally sleep 7 or 8,” he said.
It’s also unclear from current evidence whether the reported uptick in sleep problems is related to stress or, in patients who have had COVID-19 infections, to physiologic causes.
Dr. Gozal said that insomnia in the time of COVID-19 could be attributed to a number of factors such as less daily exposure to natural light from people sheltering indoors, stress related to financial or health worries, depression, or other psychological factors.
It’s also, possible, however, that COVID-19-related physiological changes could contribute to sleep disorders, he said, pointing to a recent study in the Journal of Experimental Medicine showing that SARS-CoV-2, the virus that causes COVID-19, can bind to neurons and cause metabolic changes in both infected and neighboring cells.
“My guess is that some of it is related more to behavioral impacts – people develop depression, changes in mood, anxiety, and so on, and all of these can translate into difficulties with sleep,” he said.
“It could be that in some instances – not very commonly – the virus will affect areas that control sleep in our brain, and that therefore we may see too much or too little sleep, and how to differentiate between all of these is the area that clearly needs to be explored, particularly in light of the finding that the virus can bind to brain cells and can induce substantial issues in the brain cells.”
Compromised immunity
It has been well documented that in addition to being, as Shakespeare called it, “the balm of hurt minds,” sleep has an important role in supporting the immune system.
“Sleep and immunity go together,” Dr. Ramar said. “When people have adequate sleep, their immune system is boosted. We know that there are good data from hepatitis A and hepatitis B vaccinations, and recently on flu vaccination, that if people get sufficient duration of sleep before and after they receive the shot, their likelihood of building an immune response to that particular vaccination tends to go up.”
It’s reasonable to assume that the same would hold true for COVID-19 vaccinations, but this has yet to be shown, he added.
“We do know from the previous studies that persistent sleep problems can make people more susceptible to infection or impair recovery; not yet, I believe, from the COVID-19 infection perspective,” Dr. Kendzerska said. “In our study, we did find that, among other factors, having a chronic illness was associated with new sleep difficulties during the pandemic. We did not look separately if sleep difficulties were associated with the COVID-19 infection or symptoms, but this is a great question to address with longitudinal data we have.”
What to do?
All three sleep experts contacted for this article agreed that for patients with insomnia, mitigating stress through relaxation techniques or cognitive behavioral therapy is more beneficial than medication.
“Medications, even over-the-counter medications, all have side effects, and if one is taking a medication that has stimulants in place, such as pseudoephedrine in antihistamine combinations, that can potentially contribute to or exacerbate any underlying sleep disorders,” Dr. Ramar said.
Dr. Kendzerska recommended reserving medications such as melatonin, a chronobiotic therapy, for patients with sleep disorders related to circadian rhythm problems, including a sleep phase delay. Supplemental, short-term treatment with hypnotic agents such as zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) should be used only as a last resort, she said.
Sleep medicine specialists recommend good sleep hygiene as the best means of obtaining restful sleep, including regular bed and wake times, limited exposure to stressful news (including COVID-19 stories), reduced consumption of alcohol and stimulants such as coffee or caffeine drinks, avoiding use of electronic devices in bed or near bedtime, and healthy lifestyle, including diet and exercise.
They also frown on self-medication with over-the-counter aids, because these products may not be addressing the underlying issue, as noted before.
“It is also foreseeable that there may be an increase in individuals who may require professional guidance to taper off from sleeping medications started or increased during the pandemic. While some of these sleep problems may be transient, it should be a high priority to ensure they do not evolve into chronic sleep disorders,” Dr. Kendzerska and colleagues wrote.
Research avenues
If there’s anything that causes specialists to lose sleep, it’s the lack of data or evidence to guide clinical care and research. Dr. Gozal emphasized that little is still known about the potential central nervous system effects of COVID-19, and said that should be an important focus for research into the still novel coronavirus.
“What happens post COVID and how might that affect subsequent recovery is a great question, and I don’t think we have good data there,” Dr. Ramar said. “What we do know is that patients develop the symptoms of fatigue, disrupted sleep, even ongoing fever, and unfortunately, this may persist for a long period of time even among patients who have otherwise recovered from COVID-19. We know that leaving that untreated from a sleep disorder perspective can exacerbate their daytime symptoms, and that’s where I would strongly recommend that they seek help with a sleep provider or if there are symptoms other than insomnia at least with a primary care provider.”
Among the many losses suffered by millions worldwide during the COVID-19 pandemic, the loss of sleep may be the most widespread, with potentially long-lasting, negative consequences on physical, mental, and emotional health, sleep researchers have found.
Results from multiple studies and surveys conducted during the pandemic show that a majority of subjects report clinically meaningful changes in sleep quality, sleep patterns, and sleep disturbances.
For example, a cross-sectional international survey conducted from late March through late April 2020 found that among more than 3,000 responders from 49 countries, 58% reported dissatisfaction with their sleep, and 40% reported a decrease in sleep quality during the pandemic, compared with pre-COVID-19 sleep, according to Uri Mandelkorn of the Natural Sleep Clinic in Jerusalem, and colleagues.
“In particular, this research raises the need to screen for worsening sleep patterns and use of sleeping aids in the more susceptible populations identified in this study, namely, women and people with insecure livelihoods or those subjected to strict quarantine. Health care providers should pay special attention to physical and psychological problems that this surge in sleep disturbances may cause,” they wrote. The report is in the Journal of Clinical Sleep Medicine.
Sleeping, more or less
A coauthor of that study, David Gozal, MD, FCCP, a pediatric pulmonologist and sleep medicine specialist at the University of Missouri in Columbia, said that the pandemic has had paradoxical effects on sleeps patterns for many.
“At the beginning, with the initial phases of lockdown for COVID, for most of the people whose jobs were not affected and who did not lose their jobs, [for whom] there was not the anxiety of being jobless and financially strapped, but who now were staying at home, there was actually a benefit. People started reporting getting more sleep and, more importantly, more vivid dreams and things of that nature,” he said in an interview.
“But as the lockdown progressed, we saw progressively and increasingly more people having difficulty falling asleep and staying asleep, using more medicines such as hypnotics to induce sleep, and we saw a 20% increase in the overall consumption of sleeping pills,” he said.
Similar results were seen in a cross-sectional survey of 843 adults in the United Kingdom, which showed that nearly 70% of participants reported a change in sleep patterns, only 45% reported having refreshing sleep, and 46% reported being sleepier during lockdown than before. Two-thirds of the respondents reported that the pandemic affected their mental health, and one-fourth reported increased alcohol consumption during lockdown. Those with suspected COVID-19 infections reported having more nightmares and abnormal sleep rhythms.
It is possible that the effects of COVID-19 infection on sleep may linger long after the infection itself has resolved, results of a cohort study from China suggest. As reported in The Lancet, among 1,655 patients discharged from the Jin Yin-tan hospital in Wuhan, 26% reported sleep disturbances 6 months after acute COVID-19 infection.
Self-medicating
Among 5,525 Canadians surveyed from April 3 through June 24, 2020, a large proportion reported the use of pharmacologic sleeps aids, said Tetyana Kendzerska, MD, PhD, assistant professor of medicine in the division of respirology at the University of Ottawa.
“At the time of the survey completion, 27% of participants reported taking sleeping aids (prescribed or [over] the counter); across the entire sample, 8% of respondents reported an increase in the frequency of sleeping medication use during the outbreak compared to before the outbreak,” she said in an interview.
Many people resort to self-medicating with over-the-counter preparations such as melatonin and pain-relief nighttime formulations containing diphenhydramine (Benadryl), a first-generation antihistamine with sedative properties, noted Kannan Ramar, MBBS, MD, a critical care, pulmonary, and sleep medicine specialist at the Mayo Clinic in Rochester, Minn., and current president of the American Academy of Sleep Medicine.
“When people are self-medicating for what they think is difficulty sleeping, the concern is that even if a diagnosis of insomnia has been established, there could be another, ongoing sleep disorder that may be undiagnosed, which might be causing the problem with insomnia,” he said in an interview.
“For example, obstructive sleep apnea might be causing people to wake up in the night or even contribute to difficulty falling asleep in the first place. So medicating for something without a known diagnosis may leave an underlying sleep disorder untreated, which won’t help the patient in either the short or the long term,” Dr. Ramar said.
Causes for concern
“For those people who have COVID, we have seen quite a few sleep issues develop. Those were not reported in the actual study, but in the clinic and subsequent studies published from other places,” Dr. Gozal said.
“People who suffered from COVID, and even people who supposedly did very well and were virtually asymptomatic or maybe had only a headache or fever but did not need to go to the hospital, many of those people reported either excessive sleepiness for a long period of time, and would sleep 2 or 3 hours more per night. Or the opposite was reported: There were those that after recovering reported that they couldn’t sleep – they were sleeping 4 or 5 hours when they normally sleep 7 or 8,” he said.
It’s also unclear from current evidence whether the reported uptick in sleep problems is related to stress or, in patients who have had COVID-19 infections, to physiologic causes.
Dr. Gozal said that insomnia in the time of COVID-19 could be attributed to a number of factors such as less daily exposure to natural light from people sheltering indoors, stress related to financial or health worries, depression, or other psychological factors.
It’s also, possible, however, that COVID-19-related physiological changes could contribute to sleep disorders, he said, pointing to a recent study in the Journal of Experimental Medicine showing that SARS-CoV-2, the virus that causes COVID-19, can bind to neurons and cause metabolic changes in both infected and neighboring cells.
“My guess is that some of it is related more to behavioral impacts – people develop depression, changes in mood, anxiety, and so on, and all of these can translate into difficulties with sleep,” he said.
“It could be that in some instances – not very commonly – the virus will affect areas that control sleep in our brain, and that therefore we may see too much or too little sleep, and how to differentiate between all of these is the area that clearly needs to be explored, particularly in light of the finding that the virus can bind to brain cells and can induce substantial issues in the brain cells.”
Compromised immunity
It has been well documented that in addition to being, as Shakespeare called it, “the balm of hurt minds,” sleep has an important role in supporting the immune system.
“Sleep and immunity go together,” Dr. Ramar said. “When people have adequate sleep, their immune system is boosted. We know that there are good data from hepatitis A and hepatitis B vaccinations, and recently on flu vaccination, that if people get sufficient duration of sleep before and after they receive the shot, their likelihood of building an immune response to that particular vaccination tends to go up.”
It’s reasonable to assume that the same would hold true for COVID-19 vaccinations, but this has yet to be shown, he added.
“We do know from the previous studies that persistent sleep problems can make people more susceptible to infection or impair recovery; not yet, I believe, from the COVID-19 infection perspective,” Dr. Kendzerska said. “In our study, we did find that, among other factors, having a chronic illness was associated with new sleep difficulties during the pandemic. We did not look separately if sleep difficulties were associated with the COVID-19 infection or symptoms, but this is a great question to address with longitudinal data we have.”
What to do?
All three sleep experts contacted for this article agreed that for patients with insomnia, mitigating stress through relaxation techniques or cognitive behavioral therapy is more beneficial than medication.
“Medications, even over-the-counter medications, all have side effects, and if one is taking a medication that has stimulants in place, such as pseudoephedrine in antihistamine combinations, that can potentially contribute to or exacerbate any underlying sleep disorders,” Dr. Ramar said.
Dr. Kendzerska recommended reserving medications such as melatonin, a chronobiotic therapy, for patients with sleep disorders related to circadian rhythm problems, including a sleep phase delay. Supplemental, short-term treatment with hypnotic agents such as zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) should be used only as a last resort, she said.
Sleep medicine specialists recommend good sleep hygiene as the best means of obtaining restful sleep, including regular bed and wake times, limited exposure to stressful news (including COVID-19 stories), reduced consumption of alcohol and stimulants such as coffee or caffeine drinks, avoiding use of electronic devices in bed or near bedtime, and healthy lifestyle, including diet and exercise.
They also frown on self-medication with over-the-counter aids, because these products may not be addressing the underlying issue, as noted before.
“It is also foreseeable that there may be an increase in individuals who may require professional guidance to taper off from sleeping medications started or increased during the pandemic. While some of these sleep problems may be transient, it should be a high priority to ensure they do not evolve into chronic sleep disorders,” Dr. Kendzerska and colleagues wrote.
Research avenues
If there’s anything that causes specialists to lose sleep, it’s the lack of data or evidence to guide clinical care and research. Dr. Gozal emphasized that little is still known about the potential central nervous system effects of COVID-19, and said that should be an important focus for research into the still novel coronavirus.
“What happens post COVID and how might that affect subsequent recovery is a great question, and I don’t think we have good data there,” Dr. Ramar said. “What we do know is that patients develop the symptoms of fatigue, disrupted sleep, even ongoing fever, and unfortunately, this may persist for a long period of time even among patients who have otherwise recovered from COVID-19. We know that leaving that untreated from a sleep disorder perspective can exacerbate their daytime symptoms, and that’s where I would strongly recommend that they seek help with a sleep provider or if there are symptoms other than insomnia at least with a primary care provider.”
Among the many losses suffered by millions worldwide during the COVID-19 pandemic, the loss of sleep may be the most widespread, with potentially long-lasting, negative consequences on physical, mental, and emotional health, sleep researchers have found.
Results from multiple studies and surveys conducted during the pandemic show that a majority of subjects report clinically meaningful changes in sleep quality, sleep patterns, and sleep disturbances.
For example, a cross-sectional international survey conducted from late March through late April 2020 found that among more than 3,000 responders from 49 countries, 58% reported dissatisfaction with their sleep, and 40% reported a decrease in sleep quality during the pandemic, compared with pre-COVID-19 sleep, according to Uri Mandelkorn of the Natural Sleep Clinic in Jerusalem, and colleagues.
“In particular, this research raises the need to screen for worsening sleep patterns and use of sleeping aids in the more susceptible populations identified in this study, namely, women and people with insecure livelihoods or those subjected to strict quarantine. Health care providers should pay special attention to physical and psychological problems that this surge in sleep disturbances may cause,” they wrote. The report is in the Journal of Clinical Sleep Medicine.
Sleeping, more or less
A coauthor of that study, David Gozal, MD, FCCP, a pediatric pulmonologist and sleep medicine specialist at the University of Missouri in Columbia, said that the pandemic has had paradoxical effects on sleeps patterns for many.
“At the beginning, with the initial phases of lockdown for COVID, for most of the people whose jobs were not affected and who did not lose their jobs, [for whom] there was not the anxiety of being jobless and financially strapped, but who now were staying at home, there was actually a benefit. People started reporting getting more sleep and, more importantly, more vivid dreams and things of that nature,” he said in an interview.
“But as the lockdown progressed, we saw progressively and increasingly more people having difficulty falling asleep and staying asleep, using more medicines such as hypnotics to induce sleep, and we saw a 20% increase in the overall consumption of sleeping pills,” he said.
Similar results were seen in a cross-sectional survey of 843 adults in the United Kingdom, which showed that nearly 70% of participants reported a change in sleep patterns, only 45% reported having refreshing sleep, and 46% reported being sleepier during lockdown than before. Two-thirds of the respondents reported that the pandemic affected their mental health, and one-fourth reported increased alcohol consumption during lockdown. Those with suspected COVID-19 infections reported having more nightmares and abnormal sleep rhythms.
It is possible that the effects of COVID-19 infection on sleep may linger long after the infection itself has resolved, results of a cohort study from China suggest. As reported in The Lancet, among 1,655 patients discharged from the Jin Yin-tan hospital in Wuhan, 26% reported sleep disturbances 6 months after acute COVID-19 infection.
Self-medicating
Among 5,525 Canadians surveyed from April 3 through June 24, 2020, a large proportion reported the use of pharmacologic sleeps aids, said Tetyana Kendzerska, MD, PhD, assistant professor of medicine in the division of respirology at the University of Ottawa.
“At the time of the survey completion, 27% of participants reported taking sleeping aids (prescribed or [over] the counter); across the entire sample, 8% of respondents reported an increase in the frequency of sleeping medication use during the outbreak compared to before the outbreak,” she said in an interview.
Many people resort to self-medicating with over-the-counter preparations such as melatonin and pain-relief nighttime formulations containing diphenhydramine (Benadryl), a first-generation antihistamine with sedative properties, noted Kannan Ramar, MBBS, MD, a critical care, pulmonary, and sleep medicine specialist at the Mayo Clinic in Rochester, Minn., and current president of the American Academy of Sleep Medicine.
“When people are self-medicating for what they think is difficulty sleeping, the concern is that even if a diagnosis of insomnia has been established, there could be another, ongoing sleep disorder that may be undiagnosed, which might be causing the problem with insomnia,” he said in an interview.
“For example, obstructive sleep apnea might be causing people to wake up in the night or even contribute to difficulty falling asleep in the first place. So medicating for something without a known diagnosis may leave an underlying sleep disorder untreated, which won’t help the patient in either the short or the long term,” Dr. Ramar said.
Causes for concern
“For those people who have COVID, we have seen quite a few sleep issues develop. Those were not reported in the actual study, but in the clinic and subsequent studies published from other places,” Dr. Gozal said.
“People who suffered from COVID, and even people who supposedly did very well and were virtually asymptomatic or maybe had only a headache or fever but did not need to go to the hospital, many of those people reported either excessive sleepiness for a long period of time, and would sleep 2 or 3 hours more per night. Or the opposite was reported: There were those that after recovering reported that they couldn’t sleep – they were sleeping 4 or 5 hours when they normally sleep 7 or 8,” he said.
It’s also unclear from current evidence whether the reported uptick in sleep problems is related to stress or, in patients who have had COVID-19 infections, to physiologic causes.
Dr. Gozal said that insomnia in the time of COVID-19 could be attributed to a number of factors such as less daily exposure to natural light from people sheltering indoors, stress related to financial or health worries, depression, or other psychological factors.
It’s also, possible, however, that COVID-19-related physiological changes could contribute to sleep disorders, he said, pointing to a recent study in the Journal of Experimental Medicine showing that SARS-CoV-2, the virus that causes COVID-19, can bind to neurons and cause metabolic changes in both infected and neighboring cells.
“My guess is that some of it is related more to behavioral impacts – people develop depression, changes in mood, anxiety, and so on, and all of these can translate into difficulties with sleep,” he said.
“It could be that in some instances – not very commonly – the virus will affect areas that control sleep in our brain, and that therefore we may see too much or too little sleep, and how to differentiate between all of these is the area that clearly needs to be explored, particularly in light of the finding that the virus can bind to brain cells and can induce substantial issues in the brain cells.”
Compromised immunity
It has been well documented that in addition to being, as Shakespeare called it, “the balm of hurt minds,” sleep has an important role in supporting the immune system.
“Sleep and immunity go together,” Dr. Ramar said. “When people have adequate sleep, their immune system is boosted. We know that there are good data from hepatitis A and hepatitis B vaccinations, and recently on flu vaccination, that if people get sufficient duration of sleep before and after they receive the shot, their likelihood of building an immune response to that particular vaccination tends to go up.”
It’s reasonable to assume that the same would hold true for COVID-19 vaccinations, but this has yet to be shown, he added.
“We do know from the previous studies that persistent sleep problems can make people more susceptible to infection or impair recovery; not yet, I believe, from the COVID-19 infection perspective,” Dr. Kendzerska said. “In our study, we did find that, among other factors, having a chronic illness was associated with new sleep difficulties during the pandemic. We did not look separately if sleep difficulties were associated with the COVID-19 infection or symptoms, but this is a great question to address with longitudinal data we have.”
What to do?
All three sleep experts contacted for this article agreed that for patients with insomnia, mitigating stress through relaxation techniques or cognitive behavioral therapy is more beneficial than medication.
“Medications, even over-the-counter medications, all have side effects, and if one is taking a medication that has stimulants in place, such as pseudoephedrine in antihistamine combinations, that can potentially contribute to or exacerbate any underlying sleep disorders,” Dr. Ramar said.
Dr. Kendzerska recommended reserving medications such as melatonin, a chronobiotic therapy, for patients with sleep disorders related to circadian rhythm problems, including a sleep phase delay. Supplemental, short-term treatment with hypnotic agents such as zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) should be used only as a last resort, she said.
Sleep medicine specialists recommend good sleep hygiene as the best means of obtaining restful sleep, including regular bed and wake times, limited exposure to stressful news (including COVID-19 stories), reduced consumption of alcohol and stimulants such as coffee or caffeine drinks, avoiding use of electronic devices in bed or near bedtime, and healthy lifestyle, including diet and exercise.
They also frown on self-medication with over-the-counter aids, because these products may not be addressing the underlying issue, as noted before.
“It is also foreseeable that there may be an increase in individuals who may require professional guidance to taper off from sleeping medications started or increased during the pandemic. While some of these sleep problems may be transient, it should be a high priority to ensure they do not evolve into chronic sleep disorders,” Dr. Kendzerska and colleagues wrote.
Research avenues
If there’s anything that causes specialists to lose sleep, it’s the lack of data or evidence to guide clinical care and research. Dr. Gozal emphasized that little is still known about the potential central nervous system effects of COVID-19, and said that should be an important focus for research into the still novel coronavirus.
“What happens post COVID and how might that affect subsequent recovery is a great question, and I don’t think we have good data there,” Dr. Ramar said. “What we do know is that patients develop the symptoms of fatigue, disrupted sleep, even ongoing fever, and unfortunately, this may persist for a long period of time even among patients who have otherwise recovered from COVID-19. We know that leaving that untreated from a sleep disorder perspective can exacerbate their daytime symptoms, and that’s where I would strongly recommend that they seek help with a sleep provider or if there are symptoms other than insomnia at least with a primary care provider.”
Monoclonal antibody combo treatment reduces viral load in mild to moderate COVID-19
A combination treatment of neutralizing monoclonal antibodies bamlanivimab and etesevimab was associated with a statistically significant reduction in SARS-CoV-2 at day 11 compared with placebo among nonhospitalized patients who had mild to moderate COVID-19, new data indicate.
However, bamlanivimab alone in three different single-infusion doses showed no significant reduction in viral load, compared with placebo, according to the phase 2/3 study by Robert L. Gottlieb, MD, PhD, of the Baylor University Medical Center and the Baylor Scott & White Research Institute, both in Dallas, and colleagues.
Findings from the Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) study were published online Jan. 21 in JAMA. The results represent findings through Oct. 6, 2020.
BLAZE-1 was funded by Eli Lilly, which makes both of the antispike neutralizing antibodies. The trial was conducted at 49 U.S. centers and included 613 outpatients who tested positive for SARS-CoV-2 and had one or more mild to moderate symptoms.
Patients were randomized to one of five groups (four treatment groups and a placebo control), and researchers analyzed between-group differences.
All four treatment arms suggest a trend toward reduction in viral load, which was the primary endpoint of the trial, but only the combination showed a statistically significant reduction.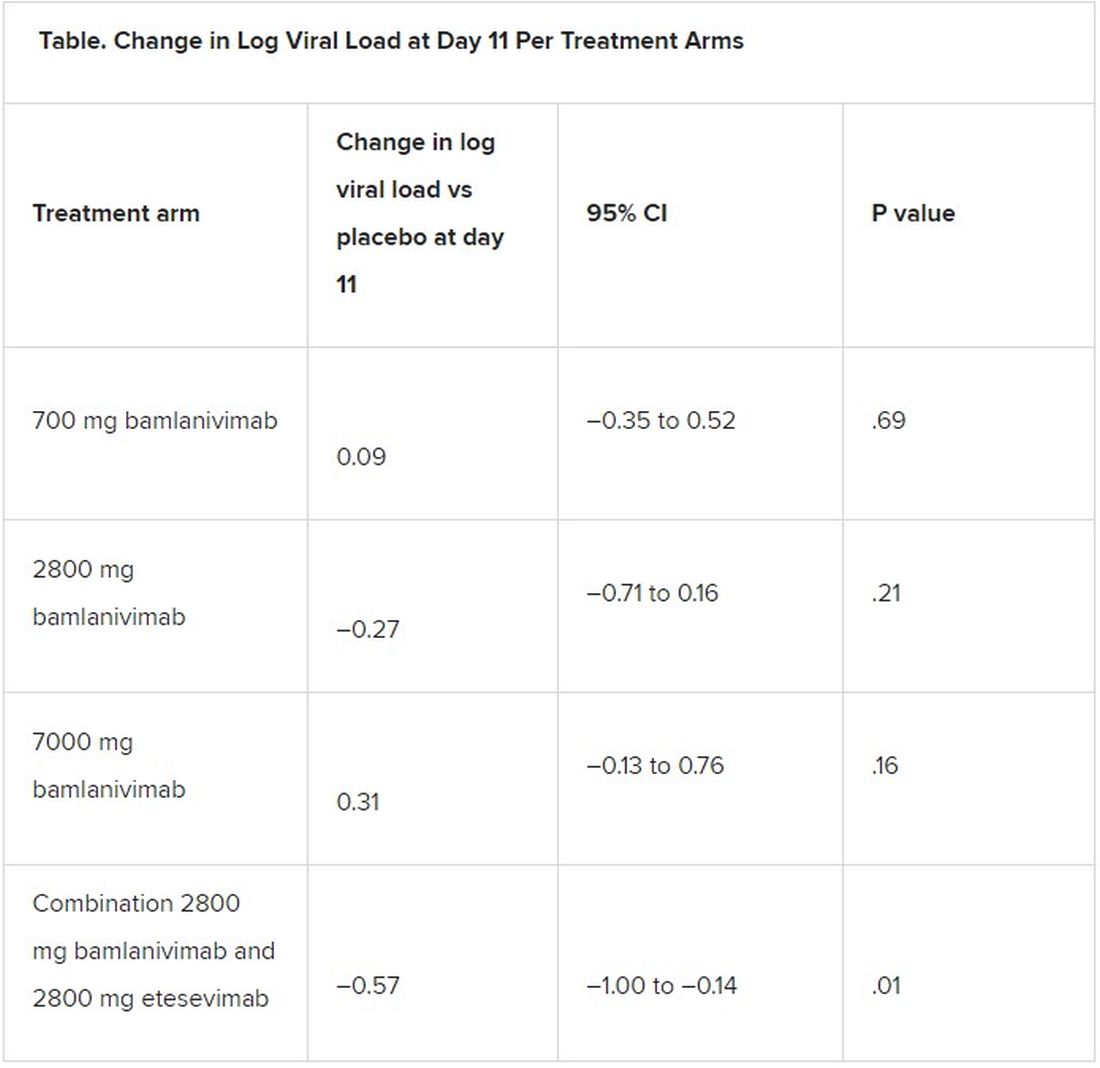
The average age of patients was 44.7 years, 54.6% were female, 42.5% were Hispanic, and 67.1% had at least one risk factor for severe COVID-19 (aged ≥55 years, body mass index of at least 30, or relevant comorbidity such as hypertension).
Among secondary outcomes, there were no consistent differences between the monotherapy groups or the combination group versus placebo for the other measures of viral load or clinical symptom scores.
The proportion of patients who had COVID-19–related hospitalizations or ED visits was 5.8% (nine events) for placebo; 1.0% (one event) for the 700-mg group; 1.9% (two events) for 2,800 mg; 2.0% (two events) for 7,000 mg; and 0.9% (one event) for combination treatment.
“Combining these two neutralizing monoclonal antibodies in clinical use may enhance viral load reduction and decrease treatment-emergent resistant variants,” the authors concluded.
Safety profile comparison
As for adverse events, immediate hypersensitivity reactions were reported in nine patients (six bamlanivimab, two combination treatment, and one placebo). No deaths occurred during the study.
Serious adverse events unrelated to SARS-CoV-2 infection or considered related to the study drug occurred in 0% (0/309) of patients in the bamlanivimab monotherapy groups; in 0.9% (1/112) of patients in the combination group; and in 0.6% (1/156) of patients in the placebo group.
The serious adverse event in the combination group was a urinary tract infection deemed unrelated to the study drug, the authors wrote.
The two most frequently reported side effects were nausea (3.0% for the 700-mg group; 3.7% for the 2,800-mg group; 5.0% for the 7,000-mg group; 3.6% for the combination group; and 3.8% for the placebo group) and diarrhea (1.0%, 1.9%, 5.9%, 0.9%, and 4.5%, respectively).
The authors included in the study’s limitations that the primary endpoint at day 11 may have been too late to best detect treatment effects.
“All patients, including those who received placebo, demonstrated substantial viral reduction by day 11,” they noted. “An earlier time point like day 3 or day 7 could possibly have been more appropriate to measure viral load.”
Currently, only remdesivir has been approved by the Food and Drug Administration for treating COVID-19, but convalescent plasma and neutralizing monoclonal antibodies have been granted emergency-use authorization.
In an accompanying editor’s note, Preeti N. Malani, MD, with the division of infectious diseases at the University of Michigan, Ann Arbor, and associate editor of JAMA, and Robert M. Golub, MD, deputy editor of JAMA, pointed out that these results differ from an earlier interim analysis of BLAZE-1 data.
A previous publication by Peter Chen, MD, with the department of medicine at Cedars Sinai Medical Center, Los Angeles, compared the three monotherapy groups (no combination group) with placebo, and in that study the 2,800-mg dose of bamlanivimab versus placebo achieved statistical significance for reduction in viral load from baseline at day 11, whereas the other two doses did not.
The editors explain that, in the study by Dr. Chen, “Follow-up for the placebo group was incomplete at the time of the database lock on Sept. 5, 2020. In the final analysis reported in the current article, the database was locked on Oct. 6, 2020, and the longer follow-up for the placebo group, which is now complete, resulted in changes in the primary outcome among that group.”
They concluded: “The comparison of the monotherapy groups against the final results for the placebo group led to changes in the effect sizes,” and the statistical significance of the 2,800-mg group was erased.
The editors pointed out that monoclonal antibodies are likely to benefit certain patients but definitive answers regarding which patients will benefit and under what circumstances will likely take more time than clinicians have to make decisions on treatment.
Meanwhile, as this news organization reported, the United States has spent $375 million on bamlanivimab and $450 million on Regeneron’s monoclonal antibody cocktail of casirivimab plus imdevimab, with the promise to spend billions more.
However, 80% of the 660,000 doses delivered by the two companies are still sitting on shelves, federal officials said in a press briefing last week, because of doubts about efficacy, lack of resources for infusion centers, and questions on reimbursement.
“While the world waits for widespread administration of effective vaccines and additional data on treatments, local efforts should work to improve testing access and turnaround time and reduce logistical barriers to ensure that monoclonal therapies can be provided to patients who are most likely to benefit,” Dr. Malani and Dr. Golub wrote.
This trial was sponsored and funded by Eli Lilly. Dr. Gottlieb disclosed personal fees and nonfinancial support (medication for another trial) from Gilead Sciences and serving on an advisory board for Sentinel. Several coauthors have financial ties to Eli Lilly. Dr. Malani reported serving on the National Institute of Allergy and Infectious Diseases COVID-19 Preventive Monoclonal Antibody data and safety monitoring board but was not compensated. Dr. Golub disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A combination treatment of neutralizing monoclonal antibodies bamlanivimab and etesevimab was associated with a statistically significant reduction in SARS-CoV-2 at day 11 compared with placebo among nonhospitalized patients who had mild to moderate COVID-19, new data indicate.
However, bamlanivimab alone in three different single-infusion doses showed no significant reduction in viral load, compared with placebo, according to the phase 2/3 study by Robert L. Gottlieb, MD, PhD, of the Baylor University Medical Center and the Baylor Scott & White Research Institute, both in Dallas, and colleagues.
Findings from the Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) study were published online Jan. 21 in JAMA. The results represent findings through Oct. 6, 2020.
BLAZE-1 was funded by Eli Lilly, which makes both of the antispike neutralizing antibodies. The trial was conducted at 49 U.S. centers and included 613 outpatients who tested positive for SARS-CoV-2 and had one or more mild to moderate symptoms.
Patients were randomized to one of five groups (four treatment groups and a placebo control), and researchers analyzed between-group differences.
All four treatment arms suggest a trend toward reduction in viral load, which was the primary endpoint of the trial, but only the combination showed a statistically significant reduction.
The average age of patients was 44.7 years, 54.6% were female, 42.5% were Hispanic, and 67.1% had at least one risk factor for severe COVID-19 (aged ≥55 years, body mass index of at least 30, or relevant comorbidity such as hypertension).
Among secondary outcomes, there were no consistent differences between the monotherapy groups or the combination group versus placebo for the other measures of viral load or clinical symptom scores.
The proportion of patients who had COVID-19–related hospitalizations or ED visits was 5.8% (nine events) for placebo; 1.0% (one event) for the 700-mg group; 1.9% (two events) for 2,800 mg; 2.0% (two events) for 7,000 mg; and 0.9% (one event) for combination treatment.
“Combining these two neutralizing monoclonal antibodies in clinical use may enhance viral load reduction and decrease treatment-emergent resistant variants,” the authors concluded.
Safety profile comparison
As for adverse events, immediate hypersensitivity reactions were reported in nine patients (six bamlanivimab, two combination treatment, and one placebo). No deaths occurred during the study.
Serious adverse events unrelated to SARS-CoV-2 infection or considered related to the study drug occurred in 0% (0/309) of patients in the bamlanivimab monotherapy groups; in 0.9% (1/112) of patients in the combination group; and in 0.6% (1/156) of patients in the placebo group.
The serious adverse event in the combination group was a urinary tract infection deemed unrelated to the study drug, the authors wrote.
The two most frequently reported side effects were nausea (3.0% for the 700-mg group; 3.7% for the 2,800-mg group; 5.0% for the 7,000-mg group; 3.6% for the combination group; and 3.8% for the placebo group) and diarrhea (1.0%, 1.9%, 5.9%, 0.9%, and 4.5%, respectively).
The authors included in the study’s limitations that the primary endpoint at day 11 may have been too late to best detect treatment effects.
“All patients, including those who received placebo, demonstrated substantial viral reduction by day 11,” they noted. “An earlier time point like day 3 or day 7 could possibly have been more appropriate to measure viral load.”
Currently, only remdesivir has been approved by the Food and Drug Administration for treating COVID-19, but convalescent plasma and neutralizing monoclonal antibodies have been granted emergency-use authorization.
In an accompanying editor’s note, Preeti N. Malani, MD, with the division of infectious diseases at the University of Michigan, Ann Arbor, and associate editor of JAMA, and Robert M. Golub, MD, deputy editor of JAMA, pointed out that these results differ from an earlier interim analysis of BLAZE-1 data.
A previous publication by Peter Chen, MD, with the department of medicine at Cedars Sinai Medical Center, Los Angeles, compared the three monotherapy groups (no combination group) with placebo, and in that study the 2,800-mg dose of bamlanivimab versus placebo achieved statistical significance for reduction in viral load from baseline at day 11, whereas the other two doses did not.
The editors explain that, in the study by Dr. Chen, “Follow-up for the placebo group was incomplete at the time of the database lock on Sept. 5, 2020. In the final analysis reported in the current article, the database was locked on Oct. 6, 2020, and the longer follow-up for the placebo group, which is now complete, resulted in changes in the primary outcome among that group.”
They concluded: “The comparison of the monotherapy groups against the final results for the placebo group led to changes in the effect sizes,” and the statistical significance of the 2,800-mg group was erased.
The editors pointed out that monoclonal antibodies are likely to benefit certain patients but definitive answers regarding which patients will benefit and under what circumstances will likely take more time than clinicians have to make decisions on treatment.
Meanwhile, as this news organization reported, the United States has spent $375 million on bamlanivimab and $450 million on Regeneron’s monoclonal antibody cocktail of casirivimab plus imdevimab, with the promise to spend billions more.
However, 80% of the 660,000 doses delivered by the two companies are still sitting on shelves, federal officials said in a press briefing last week, because of doubts about efficacy, lack of resources for infusion centers, and questions on reimbursement.
“While the world waits for widespread administration of effective vaccines and additional data on treatments, local efforts should work to improve testing access and turnaround time and reduce logistical barriers to ensure that monoclonal therapies can be provided to patients who are most likely to benefit,” Dr. Malani and Dr. Golub wrote.
This trial was sponsored and funded by Eli Lilly. Dr. Gottlieb disclosed personal fees and nonfinancial support (medication for another trial) from Gilead Sciences and serving on an advisory board for Sentinel. Several coauthors have financial ties to Eli Lilly. Dr. Malani reported serving on the National Institute of Allergy and Infectious Diseases COVID-19 Preventive Monoclonal Antibody data and safety monitoring board but was not compensated. Dr. Golub disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A combination treatment of neutralizing monoclonal antibodies bamlanivimab and etesevimab was associated with a statistically significant reduction in SARS-CoV-2 at day 11 compared with placebo among nonhospitalized patients who had mild to moderate COVID-19, new data indicate.
However, bamlanivimab alone in three different single-infusion doses showed no significant reduction in viral load, compared with placebo, according to the phase 2/3 study by Robert L. Gottlieb, MD, PhD, of the Baylor University Medical Center and the Baylor Scott & White Research Institute, both in Dallas, and colleagues.
Findings from the Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) study were published online Jan. 21 in JAMA. The results represent findings through Oct. 6, 2020.
BLAZE-1 was funded by Eli Lilly, which makes both of the antispike neutralizing antibodies. The trial was conducted at 49 U.S. centers and included 613 outpatients who tested positive for SARS-CoV-2 and had one or more mild to moderate symptoms.
Patients were randomized to one of five groups (four treatment groups and a placebo control), and researchers analyzed between-group differences.
All four treatment arms suggest a trend toward reduction in viral load, which was the primary endpoint of the trial, but only the combination showed a statistically significant reduction.
The average age of patients was 44.7 years, 54.6% were female, 42.5% were Hispanic, and 67.1% had at least one risk factor for severe COVID-19 (aged ≥55 years, body mass index of at least 30, or relevant comorbidity such as hypertension).
Among secondary outcomes, there were no consistent differences between the monotherapy groups or the combination group versus placebo for the other measures of viral load or clinical symptom scores.
The proportion of patients who had COVID-19–related hospitalizations or ED visits was 5.8% (nine events) for placebo; 1.0% (one event) for the 700-mg group; 1.9% (two events) for 2,800 mg; 2.0% (two events) for 7,000 mg; and 0.9% (one event) for combination treatment.
“Combining these two neutralizing monoclonal antibodies in clinical use may enhance viral load reduction and decrease treatment-emergent resistant variants,” the authors concluded.
Safety profile comparison
As for adverse events, immediate hypersensitivity reactions were reported in nine patients (six bamlanivimab, two combination treatment, and one placebo). No deaths occurred during the study.
Serious adverse events unrelated to SARS-CoV-2 infection or considered related to the study drug occurred in 0% (0/309) of patients in the bamlanivimab monotherapy groups; in 0.9% (1/112) of patients in the combination group; and in 0.6% (1/156) of patients in the placebo group.
The serious adverse event in the combination group was a urinary tract infection deemed unrelated to the study drug, the authors wrote.
The two most frequently reported side effects were nausea (3.0% for the 700-mg group; 3.7% for the 2,800-mg group; 5.0% for the 7,000-mg group; 3.6% for the combination group; and 3.8% for the placebo group) and diarrhea (1.0%, 1.9%, 5.9%, 0.9%, and 4.5%, respectively).
The authors included in the study’s limitations that the primary endpoint at day 11 may have been too late to best detect treatment effects.
“All patients, including those who received placebo, demonstrated substantial viral reduction by day 11,” they noted. “An earlier time point like day 3 or day 7 could possibly have been more appropriate to measure viral load.”
Currently, only remdesivir has been approved by the Food and Drug Administration for treating COVID-19, but convalescent plasma and neutralizing monoclonal antibodies have been granted emergency-use authorization.
In an accompanying editor’s note, Preeti N. Malani, MD, with the division of infectious diseases at the University of Michigan, Ann Arbor, and associate editor of JAMA, and Robert M. Golub, MD, deputy editor of JAMA, pointed out that these results differ from an earlier interim analysis of BLAZE-1 data.
A previous publication by Peter Chen, MD, with the department of medicine at Cedars Sinai Medical Center, Los Angeles, compared the three monotherapy groups (no combination group) with placebo, and in that study the 2,800-mg dose of bamlanivimab versus placebo achieved statistical significance for reduction in viral load from baseline at day 11, whereas the other two doses did not.
The editors explain that, in the study by Dr. Chen, “Follow-up for the placebo group was incomplete at the time of the database lock on Sept. 5, 2020. In the final analysis reported in the current article, the database was locked on Oct. 6, 2020, and the longer follow-up for the placebo group, which is now complete, resulted in changes in the primary outcome among that group.”
They concluded: “The comparison of the monotherapy groups against the final results for the placebo group led to changes in the effect sizes,” and the statistical significance of the 2,800-mg group was erased.
The editors pointed out that monoclonal antibodies are likely to benefit certain patients but definitive answers regarding which patients will benefit and under what circumstances will likely take more time than clinicians have to make decisions on treatment.
Meanwhile, as this news organization reported, the United States has spent $375 million on bamlanivimab and $450 million on Regeneron’s monoclonal antibody cocktail of casirivimab plus imdevimab, with the promise to spend billions more.
However, 80% of the 660,000 doses delivered by the two companies are still sitting on shelves, federal officials said in a press briefing last week, because of doubts about efficacy, lack of resources for infusion centers, and questions on reimbursement.
“While the world waits for widespread administration of effective vaccines and additional data on treatments, local efforts should work to improve testing access and turnaround time and reduce logistical barriers to ensure that monoclonal therapies can be provided to patients who are most likely to benefit,” Dr. Malani and Dr. Golub wrote.
This trial was sponsored and funded by Eli Lilly. Dr. Gottlieb disclosed personal fees and nonfinancial support (medication for another trial) from Gilead Sciences and serving on an advisory board for Sentinel. Several coauthors have financial ties to Eli Lilly. Dr. Malani reported serving on the National Institute of Allergy and Infectious Diseases COVID-19 Preventive Monoclonal Antibody data and safety monitoring board but was not compensated. Dr. Golub disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Biggest challenges practices faced from COVID last year: MGMA
according to a December 2020 report from the Medical Group Management Association.
The report was assembled from the results of weekly Stat polls by MGMA, which consists of 15,000 group practices representing more than 350,000 physicians. During the course of the year, more than 4,800 practice leaders were surveyed, but the individual polls had far fewer respondents.
The 2020 data represents snapshots from different points in the developing public health crisis. Still, much of what practices experienced earlier in the pandemic continues to apply, and it’s likely to persist this year as long as the coronavirus spreads and its toll deepens.
One top-line conclusion of the report: the economic pain felt by practices has resulted in layoffs, furloughs, and/or reduced compensation for providers and staff.
In the May 19 weekly survey, 82% of respondents said some or all of their providers’ compensation had been affected by the crisis. About 62% said every provider had been affected. Provider compensation was cut in several ways, including reduced hours and salaries, reduced or eliminated bonuses, and lower allowances for continuing medical education.
About 61% of health care leaders said in the June 26 poll that their own compensation had decreased.
In the following week’s survey, one in three managers said their organization had reduced staff compensation. Nearly all of the respondents in this category predicted the salary reductions would be temporary.
As of March 17, early in the pandemic, 40% of health care leaders said they were experiencing staff shortages. An April 21 poll found that 53% of health care leaders were taking steps to address their providers’ and staffers’ mental health.
“The mental and emotional toll on everyone continues to be a concern, as public health authorities continue to report alarming numbers of new [COVID-19] cases, hospitalizations, and deaths,” MGMA commented.
Telehealth and remote monitoring
Nearly all of the health care leaders surveyed on March 31 reported that their practices had expanded telehealth access because of COVID-19. The percentage of patient visits handled remotely had dropped substantially by the fall, according to a Harvard University/Commonwealth Fund/Phreesia survey. Still, it remains significantly higher than it was before the pandemic.
“At the end of 2020, telemedicine continues to play a vital role in everyday practice operations and long-term planning,” the MGMA report said. One indication of this, the association said, is that health care leaders are recognizing new best practices in specialty telemedicine, such as pediatrics and ob.gyn.
According to an April 28 poll, the top three coding/billing challenges for telehealth and telephone visits amid COVID-19 were inconsistent payer rules, pay parity and accuracy, and documentation of virtual visits.
While the Centers for Medicare & Medicaid Services has loosened its regulations to allow reimbursement of telehealth in all locations and at the same level as in-person visits, most of those changes will not last beyond the public health crisis without new legislation.
More health care leaders are considering the use of remote patient monitoring, MGMA said, but only 21% of practices offered such services as of Sept. 15. The report drew a connection between these plans and the current challenge of deferred care.
In the July 21 poll, 87% of health care leaders reported that safety concerns were the top reason that patients deferred care amid COVID-19. The MGMA report quoted JaeLynn Williams, CEO of Air Methods, which provides helicopter ambulance services, as saying that many people are staying home even when they face life-threatening conditions such as chest pain, drug symptoms, inflamed appendix, and gallbladder pain.
Operational issues
Overall, MGMA said, practices that have taken a financial risk have done better during the pandemic than fee-for-service practices because their monthly capitation revenue has continued unabated. In contrast, “most groups’ struggles to sustain visits and procedures meant less revenue and lower compensation,” the report said.
In the August 18 survey, one in three health care leaders reported their practices were changing their operational metrics and how often they looked at those measures because of the pandemic. “Practice managers are asking for dashboard data in weeks instead of months to measure the drop in charges and forecast the resulting change in collections,” MGMA noted. “The type of data practice managers are asking for has also changed.”
Among the new metrics that practices are interested in, according to an MGMA article, are measures that track telehealth visits, the productivity of staff working at home, and the number of ancillary services and procedures that new patients might need based on historical data.
Nearly all health care leaders surveyed on Aug. 11 said the cost of obtaining personal protective equipment had increased during 2020. MGMA said it expects this situation to worsen if the pandemic lasts through the summer of 2021.
While everyone is talking about the botched launch of the COVID-19 vaccination campaign, there were also problems with flu vaccination in 2020. In the Sept. 25 poll, 34% of health care leaders reported their practices were experiencing delays in getting the flu vaccine.
Looking ahead
Looking further ahead, the report recommended that practices make plans to boost staff morale by restoring bonuses.
In addition, MGMA suggested that physician groups reassess their space needs. “The equation is simple – fewer nonclinical staff members at your facility means you should repurpose that office space or consider finding a better fit for your new real estate needs in 2021.”
Finally, MGMA noted that the practices expanding rather than contracting their business are those increasing their value-based revenues by taking on more risk. For those groups, “growing the patient panel can help [them] seek better rates in contract negotiations.”
A version of this article first appeared on Medscape.com.
according to a December 2020 report from the Medical Group Management Association.
The report was assembled from the results of weekly Stat polls by MGMA, which consists of 15,000 group practices representing more than 350,000 physicians. During the course of the year, more than 4,800 practice leaders were surveyed, but the individual polls had far fewer respondents.
The 2020 data represents snapshots from different points in the developing public health crisis. Still, much of what practices experienced earlier in the pandemic continues to apply, and it’s likely to persist this year as long as the coronavirus spreads and its toll deepens.
One top-line conclusion of the report: the economic pain felt by practices has resulted in layoffs, furloughs, and/or reduced compensation for providers and staff.
In the May 19 weekly survey, 82% of respondents said some or all of their providers’ compensation had been affected by the crisis. About 62% said every provider had been affected. Provider compensation was cut in several ways, including reduced hours and salaries, reduced or eliminated bonuses, and lower allowances for continuing medical education.
About 61% of health care leaders said in the June 26 poll that their own compensation had decreased.
In the following week’s survey, one in three managers said their organization had reduced staff compensation. Nearly all of the respondents in this category predicted the salary reductions would be temporary.
As of March 17, early in the pandemic, 40% of health care leaders said they were experiencing staff shortages. An April 21 poll found that 53% of health care leaders were taking steps to address their providers’ and staffers’ mental health.
“The mental and emotional toll on everyone continues to be a concern, as public health authorities continue to report alarming numbers of new [COVID-19] cases, hospitalizations, and deaths,” MGMA commented.
Telehealth and remote monitoring
Nearly all of the health care leaders surveyed on March 31 reported that their practices had expanded telehealth access because of COVID-19. The percentage of patient visits handled remotely had dropped substantially by the fall, according to a Harvard University/Commonwealth Fund/Phreesia survey. Still, it remains significantly higher than it was before the pandemic.
“At the end of 2020, telemedicine continues to play a vital role in everyday practice operations and long-term planning,” the MGMA report said. One indication of this, the association said, is that health care leaders are recognizing new best practices in specialty telemedicine, such as pediatrics and ob.gyn.
According to an April 28 poll, the top three coding/billing challenges for telehealth and telephone visits amid COVID-19 were inconsistent payer rules, pay parity and accuracy, and documentation of virtual visits.
While the Centers for Medicare & Medicaid Services has loosened its regulations to allow reimbursement of telehealth in all locations and at the same level as in-person visits, most of those changes will not last beyond the public health crisis without new legislation.
More health care leaders are considering the use of remote patient monitoring, MGMA said, but only 21% of practices offered such services as of Sept. 15. The report drew a connection between these plans and the current challenge of deferred care.
In the July 21 poll, 87% of health care leaders reported that safety concerns were the top reason that patients deferred care amid COVID-19. The MGMA report quoted JaeLynn Williams, CEO of Air Methods, which provides helicopter ambulance services, as saying that many people are staying home even when they face life-threatening conditions such as chest pain, drug symptoms, inflamed appendix, and gallbladder pain.
Operational issues
Overall, MGMA said, practices that have taken a financial risk have done better during the pandemic than fee-for-service practices because their monthly capitation revenue has continued unabated. In contrast, “most groups’ struggles to sustain visits and procedures meant less revenue and lower compensation,” the report said.
In the August 18 survey, one in three health care leaders reported their practices were changing their operational metrics and how often they looked at those measures because of the pandemic. “Practice managers are asking for dashboard data in weeks instead of months to measure the drop in charges and forecast the resulting change in collections,” MGMA noted. “The type of data practice managers are asking for has also changed.”
Among the new metrics that practices are interested in, according to an MGMA article, are measures that track telehealth visits, the productivity of staff working at home, and the number of ancillary services and procedures that new patients might need based on historical data.
Nearly all health care leaders surveyed on Aug. 11 said the cost of obtaining personal protective equipment had increased during 2020. MGMA said it expects this situation to worsen if the pandemic lasts through the summer of 2021.
While everyone is talking about the botched launch of the COVID-19 vaccination campaign, there were also problems with flu vaccination in 2020. In the Sept. 25 poll, 34% of health care leaders reported their practices were experiencing delays in getting the flu vaccine.
Looking ahead
Looking further ahead, the report recommended that practices make plans to boost staff morale by restoring bonuses.
In addition, MGMA suggested that physician groups reassess their space needs. “The equation is simple – fewer nonclinical staff members at your facility means you should repurpose that office space or consider finding a better fit for your new real estate needs in 2021.”
Finally, MGMA noted that the practices expanding rather than contracting their business are those increasing their value-based revenues by taking on more risk. For those groups, “growing the patient panel can help [them] seek better rates in contract negotiations.”
A version of this article first appeared on Medscape.com.
according to a December 2020 report from the Medical Group Management Association.
The report was assembled from the results of weekly Stat polls by MGMA, which consists of 15,000 group practices representing more than 350,000 physicians. During the course of the year, more than 4,800 practice leaders were surveyed, but the individual polls had far fewer respondents.
The 2020 data represents snapshots from different points in the developing public health crisis. Still, much of what practices experienced earlier in the pandemic continues to apply, and it’s likely to persist this year as long as the coronavirus spreads and its toll deepens.
One top-line conclusion of the report: the economic pain felt by practices has resulted in layoffs, furloughs, and/or reduced compensation for providers and staff.
In the May 19 weekly survey, 82% of respondents said some or all of their providers’ compensation had been affected by the crisis. About 62% said every provider had been affected. Provider compensation was cut in several ways, including reduced hours and salaries, reduced or eliminated bonuses, and lower allowances for continuing medical education.
About 61% of health care leaders said in the June 26 poll that their own compensation had decreased.
In the following week’s survey, one in three managers said their organization had reduced staff compensation. Nearly all of the respondents in this category predicted the salary reductions would be temporary.
As of March 17, early in the pandemic, 40% of health care leaders said they were experiencing staff shortages. An April 21 poll found that 53% of health care leaders were taking steps to address their providers’ and staffers’ mental health.
“The mental and emotional toll on everyone continues to be a concern, as public health authorities continue to report alarming numbers of new [COVID-19] cases, hospitalizations, and deaths,” MGMA commented.
Telehealth and remote monitoring
Nearly all of the health care leaders surveyed on March 31 reported that their practices had expanded telehealth access because of COVID-19. The percentage of patient visits handled remotely had dropped substantially by the fall, according to a Harvard University/Commonwealth Fund/Phreesia survey. Still, it remains significantly higher than it was before the pandemic.
“At the end of 2020, telemedicine continues to play a vital role in everyday practice operations and long-term planning,” the MGMA report said. One indication of this, the association said, is that health care leaders are recognizing new best practices in specialty telemedicine, such as pediatrics and ob.gyn.
According to an April 28 poll, the top three coding/billing challenges for telehealth and telephone visits amid COVID-19 were inconsistent payer rules, pay parity and accuracy, and documentation of virtual visits.
While the Centers for Medicare & Medicaid Services has loosened its regulations to allow reimbursement of telehealth in all locations and at the same level as in-person visits, most of those changes will not last beyond the public health crisis without new legislation.
More health care leaders are considering the use of remote patient monitoring, MGMA said, but only 21% of practices offered such services as of Sept. 15. The report drew a connection between these plans and the current challenge of deferred care.
In the July 21 poll, 87% of health care leaders reported that safety concerns were the top reason that patients deferred care amid COVID-19. The MGMA report quoted JaeLynn Williams, CEO of Air Methods, which provides helicopter ambulance services, as saying that many people are staying home even when they face life-threatening conditions such as chest pain, drug symptoms, inflamed appendix, and gallbladder pain.
Operational issues
Overall, MGMA said, practices that have taken a financial risk have done better during the pandemic than fee-for-service practices because their monthly capitation revenue has continued unabated. In contrast, “most groups’ struggles to sustain visits and procedures meant less revenue and lower compensation,” the report said.
In the August 18 survey, one in three health care leaders reported their practices were changing their operational metrics and how often they looked at those measures because of the pandemic. “Practice managers are asking for dashboard data in weeks instead of months to measure the drop in charges and forecast the resulting change in collections,” MGMA noted. “The type of data practice managers are asking for has also changed.”
Among the new metrics that practices are interested in, according to an MGMA article, are measures that track telehealth visits, the productivity of staff working at home, and the number of ancillary services and procedures that new patients might need based on historical data.
Nearly all health care leaders surveyed on Aug. 11 said the cost of obtaining personal protective equipment had increased during 2020. MGMA said it expects this situation to worsen if the pandemic lasts through the summer of 2021.
While everyone is talking about the botched launch of the COVID-19 vaccination campaign, there were also problems with flu vaccination in 2020. In the Sept. 25 poll, 34% of health care leaders reported their practices were experiencing delays in getting the flu vaccine.
Looking ahead
Looking further ahead, the report recommended that practices make plans to boost staff morale by restoring bonuses.
In addition, MGMA suggested that physician groups reassess their space needs. “The equation is simple – fewer nonclinical staff members at your facility means you should repurpose that office space or consider finding a better fit for your new real estate needs in 2021.”
Finally, MGMA noted that the practices expanding rather than contracting their business are those increasing their value-based revenues by taking on more risk. For those groups, “growing the patient panel can help [them] seek better rates in contract negotiations.”
A version of this article first appeared on Medscape.com.