User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Your practice was bought out by private equity: Now what?
After her emergency medicine group was acquired by a staffing firm backed by a large private equity (PE) firm, Michelle Wiener, MD, said the workflow changes came swiftly.
“Our staffing has been greatly reduced,” the Detroit physician said. “At this point, we have no say in anything. We have no say in the scheduling. We aren’t allowed to see what is billed under our name. The morale has really gone down.”
Dr. Wiener, who practices at Ascension St. John Hospital, said she and fellow physicians have repeatedly brought their concerns to TeamHealth, which in 2015 took over St. John Emergency Services PC. TeamHealth is owned by PE giant Blackstone.
“It’s very frustrating,” Dr. Wiener said. “We’re taking it from all sides.”
Blackstone and Ascension St. John did not respond to this news organization’s request for comment.
TeamHealth would not respond directly to questions about the Ascension St. John Hospital physicians or their concerns.
Spokesman Josh Hopson provided only a general statement: “TeamHealth is committed to making sure that clinicians have the resources and support needed to provide first-class care to patients, particularly with regard to staffing and compensation. TeamHealth has and will always put patient care first, and that is not impacted by its ownership model.”
Acquisitions of medical practices and hospitals by PE firms are rapidly growing, with more than 1,400 PE deals in health care in 2021 totaling upwards of $208 billion, according to PitchBook Data Inc., a Seattle-based firm that tracks mergers and acquisitions.
Some physicians praise the partnerships as an opportunity to improve technology and efficiency, whereas others decry them as raising patient costs and lowering the quality of care. A recent UC Berkeley study found that PE ownership of medical practices was linked to consumer price increases for 8 of 10 specialties, most notably oncology and gastroenterology.
What should you expect after PE acquisition?
Since his practice partnered with a PE firm in 2020, Milwaukee-based otolaryngologist Madan Kandula, MD, said he has found the changes positive. The practice has grown and improved operations in finance, accounting, compliance, and information technology, said Dr. Kandula, founder and CEO of Advent, an ENT practice with 15 clinics in four Midwestern states.
Dr. Kandula said his group already had a sound business practice, and that the goal of partnering with a PE firm wasn’t to change day-to-day operations but to propel the organization forward.
“From patient load to visit time to how we staff our clinics, there has been no change,” he said. “My private equity firm does not, [and] cannot, impose their will on our clinical decisions.”
Experts say the impact of PE acquisitions on individual physicians often depends on where a doctor ranks in the organization, what stage they are in their career, and how much control they had over the deal.
“It’s the older physicians who are usually selling the practice and getting the big payout,” said Anjali Dooley, a St. Louis–based health law attorney who counsels physicians about PE deals. “The younger doctors are usually not part of the deal, as they may still be employees. They don’t have any negotiating power. Hopefully, there is some transparency, but sometimes there is not, and they are blindsided by the deal.”
When it comes to workload, most PE-owned groups are put on a production-based model, such as a wRVU-based model, said Roger Strode, a Chicago-based health law attorney who focuses on health care mergers and acquisitions. Most already operate under such a model, but there might be some changes after a buyout.
Staffing may also change, added Ms. Dooley. The PE firms may want to add partners or companies already in their portfolios to create efficiencies, causing training or workflow changes.
In a hospital buyout, changes may depend on whether a department is a significant revenue generator for the hospital, Ms. Dooley noted.
PE firms frequently favor higher revenue–generating specialties, such as neurosurgery, cardiology, orthopedics, gastroenterology, and plastic surgery. They closely scrutinize departments said that make less money, such as the emergency department or primary care, Ms. Dooley said. Physicians or teams that don’t fit the firm’s cost-efficiency plans may be terminated or replaced.
On the other hand, Mr. Strode said physicians may see improved electronic health records and collections.
“Some of your overall overhead costs may be reduced, because they’re better at it,” Mr. Strode said. “When you’ve got more scale, the cost per patient, the cost per hour, the cost per procedure, goes down, and the cost that’s applied against your production will go down. As [practices grow], they have more bargaining power with payers and you can potentially get better rates. At least, that’s the promise.”
Analysts note that PE health care acquisitions show no signs of slowing and that it pays for physicians to know what to expect and how to cope if their practice or hospital is acquired. Whether physicians have some control over a buyout or are blindsided by the transition, it’s critical to know what to consider, how workloads might change, and your options for settling in or settling up.
The PE industry has about $2 trillion lined up for potential investments in 2023, said Ms. Dooley.
“PE firms are looking at health care to expend some of this dry powder,” Ms. Dooley continued. “If done correctly, PE firms that are aware of health care regulations, compliance, and patient care issues can ... remove redundant services and improve ... efficiencies, but the bad is when that doesn’t happen, and the quality of care goes down or there are patient safety risks.”
How to prepare for and cope with PE partnerships
If your practice is considering a PE partnership, it’s important to explore the terms and conditions and carefully weigh the pros and cons, said Gary Herschman, a Newark, N.J.–based attorney who advises PE-owned physician groups.
“My recommendation is that physicians at a minimum conduct due diligence on all potential strategic options for their groups, and then make an informed decision regarding whether a partnership transaction is right for their group, as it’s not right for every group,” he said.
When Texas cardiologist Rick Snyder, MD, was considering PE partnerships, he spoke with physicians who made similar deals to determine whether they were satisfied years later, he said. In April, Snyder’s practice, HeartPlace, the largest physician-owned cardiology practice in Texas, was acquired by US Heart & Vascular, a practice management platform backed by PE firm Ares Management.
“I called every group that I knew that had done private equity for any meaningful amount of time,” Dr. Snyder said. “For the first year or two, everybody is in the honeymoon period. If the model is going to succeed or break down, it’s not going to be in the first year or two. So I wanted to talk to groups that had done this for a longer amount of time and find out what their pitfalls were. What would they have done differently? Has it been a productive relationship? Did they grow?”
Dr. Snyder, president of the Texas Medical Association, said his practice met with seven or eight firms before choosing one that best met their needs. His group wanted a platform that preserved their clinical autonomy, governance, and culture, he said. They also wanted to ensure they were not entering into a “buy and flip” scenario, but rather a “buy and build” plan.
“Thus, financial capital was not sufficient, they also had to have intellectual capital and relationship capital on their bench,” he said. “When we found the partner that embraced all of these factors as well as a history of buying and long-term building, we pulled the trigger and partnered with Ares and US Heart & Vascular Management. The partner we chose did not offer us the most money. We put a premium on these other criteria.”
“I always tell docs, know the culture of your group and your vision,” he said. “Before you go down that route, ask yourself what you want to accomplish and if it makes sense having a private equity partner to accomplish that vision with.”
For younger physicians or those with little control over buyouts, experts recommend they review their contracts and consider consulting with an attorney to better understand how the deal may affect their earnings and career prospects.
Those who have a much longer career runway need to weigh whether they want to work for a PE-linked practice, Mr. Strode said. For some, it’s time to check when their noncompete agreements end and find a position elsewhere.
Also, physicians should know their rights and the laws in their states regarding the corporate practice of medicine. Statutes vary by state, and knowing the provisions in your state helps doctors recognize their legal rights, learn possible exceptions to the requirements, and know the penalties for violations.
In Michigan, a group of physicians and other health professionals at Ascension St. John has voted to unionize. Doctors hope that the union, which includes advanced practice clinicians, nurse practitioners, and physician assistants, will help improve patient care and protect working conditions for staff, Dr. Wiener said.
She advises physicians who are unhappy after acquisitions to speak up and stick together.
“That’s the biggest thing I think physicians should start doing,” she said. “Support each other and stand up. You are stronger together.”
Why is PE so attracted to health care?
PE firms typically buy practices or hospitals, work to make the entities more profitable, and then sell them, with the goal of doubling or tripling their investment over a short period. In general, PE firms aim for annual returns exceeding 20% after 3-7 years.
These firms know that health care is relatively recession-proof, that providers have third-party payers, and that the industry is fragmented and requires more efficiency, Ms. Dooley said.
When PE practice acquisitions started gaining momentum about 12 years ago, traditional hospital-based specialties such as anesthesiology and radiology were prime targets, said Mr. Strode.
At the same time, increasing challenges in private practice, such as declining compensation from payers, pressure to participate in value-based care programs, and rising regional competitors have fueled more physician groups to partner with PE firms, Mr. Herschman noted.
Physicians who partner with PE firms often benefit by having new access to capital to grow their practices, cost savings through group purchasing, and the ability to compete with larger health groups, Mr. Herschman said.
Questions remain, however, about how PE involvement affects health care use and spending. An April 2023 JAMA Viewpoint article called out the lack of oversight and regulation in the health care/PE space, suggesting that a stronger framework for regulation and transparency is needed.
A 2022 study in JAMA Health Forum that examined changes in prices and utilization associated with the PE acquisitions of 578 dermatology, gastroenterology, and ophthalmology physician practices from 2016 to 2020 found that prices increased by an average of 11%, and volume rose by 16%, after acquisition.
“We found that acquisitions were associated with increases in health care spending and utilization, as well as some other patterns of care like potential upcoding,” said Jane M. Zhu, MD, an author of the study and assistant professor at Oregon Health & Science University in Portland.
Another recent study that Dr. Zhu coauthored, published in Health Affairs, found that physician practices acquired by PE firms experience greater staff turnover and rely more heavily on advanced practice professionals than doctors.
“To the extent that that turnover indicates physicians are dissatisfied after private equity comes in, that’s really important to investigate further,” Dr. Zhu said.
PE firms owned 4% of U.S. hospitals in 2021 and 11% of nursing homes, according to a Medicare Payment Advisory Commission (MedPAC) report. The report does not include 2021 data on medical practices but notes that from 2013 to 2016, PE firms acquired at least 2% of physician practices. Estimates of PE deals are probably lower than actual numbers because of the lack of comprehensive information sources, according to the MedPAC report.
A version of this article appeared on Medscape.com.
After her emergency medicine group was acquired by a staffing firm backed by a large private equity (PE) firm, Michelle Wiener, MD, said the workflow changes came swiftly.
“Our staffing has been greatly reduced,” the Detroit physician said. “At this point, we have no say in anything. We have no say in the scheduling. We aren’t allowed to see what is billed under our name. The morale has really gone down.”
Dr. Wiener, who practices at Ascension St. John Hospital, said she and fellow physicians have repeatedly brought their concerns to TeamHealth, which in 2015 took over St. John Emergency Services PC. TeamHealth is owned by PE giant Blackstone.
“It’s very frustrating,” Dr. Wiener said. “We’re taking it from all sides.”
Blackstone and Ascension St. John did not respond to this news organization’s request for comment.
TeamHealth would not respond directly to questions about the Ascension St. John Hospital physicians or their concerns.
Spokesman Josh Hopson provided only a general statement: “TeamHealth is committed to making sure that clinicians have the resources and support needed to provide first-class care to patients, particularly with regard to staffing and compensation. TeamHealth has and will always put patient care first, and that is not impacted by its ownership model.”
Acquisitions of medical practices and hospitals by PE firms are rapidly growing, with more than 1,400 PE deals in health care in 2021 totaling upwards of $208 billion, according to PitchBook Data Inc., a Seattle-based firm that tracks mergers and acquisitions.
Some physicians praise the partnerships as an opportunity to improve technology and efficiency, whereas others decry them as raising patient costs and lowering the quality of care. A recent UC Berkeley study found that PE ownership of medical practices was linked to consumer price increases for 8 of 10 specialties, most notably oncology and gastroenterology.
What should you expect after PE acquisition?
Since his practice partnered with a PE firm in 2020, Milwaukee-based otolaryngologist Madan Kandula, MD, said he has found the changes positive. The practice has grown and improved operations in finance, accounting, compliance, and information technology, said Dr. Kandula, founder and CEO of Advent, an ENT practice with 15 clinics in four Midwestern states.
Dr. Kandula said his group already had a sound business practice, and that the goal of partnering with a PE firm wasn’t to change day-to-day operations but to propel the organization forward.
“From patient load to visit time to how we staff our clinics, there has been no change,” he said. “My private equity firm does not, [and] cannot, impose their will on our clinical decisions.”
Experts say the impact of PE acquisitions on individual physicians often depends on where a doctor ranks in the organization, what stage they are in their career, and how much control they had over the deal.
“It’s the older physicians who are usually selling the practice and getting the big payout,” said Anjali Dooley, a St. Louis–based health law attorney who counsels physicians about PE deals. “The younger doctors are usually not part of the deal, as they may still be employees. They don’t have any negotiating power. Hopefully, there is some transparency, but sometimes there is not, and they are blindsided by the deal.”
When it comes to workload, most PE-owned groups are put on a production-based model, such as a wRVU-based model, said Roger Strode, a Chicago-based health law attorney who focuses on health care mergers and acquisitions. Most already operate under such a model, but there might be some changes after a buyout.
Staffing may also change, added Ms. Dooley. The PE firms may want to add partners or companies already in their portfolios to create efficiencies, causing training or workflow changes.
In a hospital buyout, changes may depend on whether a department is a significant revenue generator for the hospital, Ms. Dooley noted.
PE firms frequently favor higher revenue–generating specialties, such as neurosurgery, cardiology, orthopedics, gastroenterology, and plastic surgery. They closely scrutinize departments said that make less money, such as the emergency department or primary care, Ms. Dooley said. Physicians or teams that don’t fit the firm’s cost-efficiency plans may be terminated or replaced.
On the other hand, Mr. Strode said physicians may see improved electronic health records and collections.
“Some of your overall overhead costs may be reduced, because they’re better at it,” Mr. Strode said. “When you’ve got more scale, the cost per patient, the cost per hour, the cost per procedure, goes down, and the cost that’s applied against your production will go down. As [practices grow], they have more bargaining power with payers and you can potentially get better rates. At least, that’s the promise.”
Analysts note that PE health care acquisitions show no signs of slowing and that it pays for physicians to know what to expect and how to cope if their practice or hospital is acquired. Whether physicians have some control over a buyout or are blindsided by the transition, it’s critical to know what to consider, how workloads might change, and your options for settling in or settling up.
The PE industry has about $2 trillion lined up for potential investments in 2023, said Ms. Dooley.
“PE firms are looking at health care to expend some of this dry powder,” Ms. Dooley continued. “If done correctly, PE firms that are aware of health care regulations, compliance, and patient care issues can ... remove redundant services and improve ... efficiencies, but the bad is when that doesn’t happen, and the quality of care goes down or there are patient safety risks.”
How to prepare for and cope with PE partnerships
If your practice is considering a PE partnership, it’s important to explore the terms and conditions and carefully weigh the pros and cons, said Gary Herschman, a Newark, N.J.–based attorney who advises PE-owned physician groups.
“My recommendation is that physicians at a minimum conduct due diligence on all potential strategic options for their groups, and then make an informed decision regarding whether a partnership transaction is right for their group, as it’s not right for every group,” he said.
When Texas cardiologist Rick Snyder, MD, was considering PE partnerships, he spoke with physicians who made similar deals to determine whether they were satisfied years later, he said. In April, Snyder’s practice, HeartPlace, the largest physician-owned cardiology practice in Texas, was acquired by US Heart & Vascular, a practice management platform backed by PE firm Ares Management.
“I called every group that I knew that had done private equity for any meaningful amount of time,” Dr. Snyder said. “For the first year or two, everybody is in the honeymoon period. If the model is going to succeed or break down, it’s not going to be in the first year or two. So I wanted to talk to groups that had done this for a longer amount of time and find out what their pitfalls were. What would they have done differently? Has it been a productive relationship? Did they grow?”
Dr. Snyder, president of the Texas Medical Association, said his practice met with seven or eight firms before choosing one that best met their needs. His group wanted a platform that preserved their clinical autonomy, governance, and culture, he said. They also wanted to ensure they were not entering into a “buy and flip” scenario, but rather a “buy and build” plan.
“Thus, financial capital was not sufficient, they also had to have intellectual capital and relationship capital on their bench,” he said. “When we found the partner that embraced all of these factors as well as a history of buying and long-term building, we pulled the trigger and partnered with Ares and US Heart & Vascular Management. The partner we chose did not offer us the most money. We put a premium on these other criteria.”
“I always tell docs, know the culture of your group and your vision,” he said. “Before you go down that route, ask yourself what you want to accomplish and if it makes sense having a private equity partner to accomplish that vision with.”
For younger physicians or those with little control over buyouts, experts recommend they review their contracts and consider consulting with an attorney to better understand how the deal may affect their earnings and career prospects.
Those who have a much longer career runway need to weigh whether they want to work for a PE-linked practice, Mr. Strode said. For some, it’s time to check when their noncompete agreements end and find a position elsewhere.
Also, physicians should know their rights and the laws in their states regarding the corporate practice of medicine. Statutes vary by state, and knowing the provisions in your state helps doctors recognize their legal rights, learn possible exceptions to the requirements, and know the penalties for violations.
In Michigan, a group of physicians and other health professionals at Ascension St. John has voted to unionize. Doctors hope that the union, which includes advanced practice clinicians, nurse practitioners, and physician assistants, will help improve patient care and protect working conditions for staff, Dr. Wiener said.
She advises physicians who are unhappy after acquisitions to speak up and stick together.
“That’s the biggest thing I think physicians should start doing,” she said. “Support each other and stand up. You are stronger together.”
Why is PE so attracted to health care?
PE firms typically buy practices or hospitals, work to make the entities more profitable, and then sell them, with the goal of doubling or tripling their investment over a short period. In general, PE firms aim for annual returns exceeding 20% after 3-7 years.
These firms know that health care is relatively recession-proof, that providers have third-party payers, and that the industry is fragmented and requires more efficiency, Ms. Dooley said.
When PE practice acquisitions started gaining momentum about 12 years ago, traditional hospital-based specialties such as anesthesiology and radiology were prime targets, said Mr. Strode.
At the same time, increasing challenges in private practice, such as declining compensation from payers, pressure to participate in value-based care programs, and rising regional competitors have fueled more physician groups to partner with PE firms, Mr. Herschman noted.
Physicians who partner with PE firms often benefit by having new access to capital to grow their practices, cost savings through group purchasing, and the ability to compete with larger health groups, Mr. Herschman said.
Questions remain, however, about how PE involvement affects health care use and spending. An April 2023 JAMA Viewpoint article called out the lack of oversight and regulation in the health care/PE space, suggesting that a stronger framework for regulation and transparency is needed.
A 2022 study in JAMA Health Forum that examined changes in prices and utilization associated with the PE acquisitions of 578 dermatology, gastroenterology, and ophthalmology physician practices from 2016 to 2020 found that prices increased by an average of 11%, and volume rose by 16%, after acquisition.
“We found that acquisitions were associated with increases in health care spending and utilization, as well as some other patterns of care like potential upcoding,” said Jane M. Zhu, MD, an author of the study and assistant professor at Oregon Health & Science University in Portland.
Another recent study that Dr. Zhu coauthored, published in Health Affairs, found that physician practices acquired by PE firms experience greater staff turnover and rely more heavily on advanced practice professionals than doctors.
“To the extent that that turnover indicates physicians are dissatisfied after private equity comes in, that’s really important to investigate further,” Dr. Zhu said.
PE firms owned 4% of U.S. hospitals in 2021 and 11% of nursing homes, according to a Medicare Payment Advisory Commission (MedPAC) report. The report does not include 2021 data on medical practices but notes that from 2013 to 2016, PE firms acquired at least 2% of physician practices. Estimates of PE deals are probably lower than actual numbers because of the lack of comprehensive information sources, according to the MedPAC report.
A version of this article appeared on Medscape.com.
After her emergency medicine group was acquired by a staffing firm backed by a large private equity (PE) firm, Michelle Wiener, MD, said the workflow changes came swiftly.
“Our staffing has been greatly reduced,” the Detroit physician said. “At this point, we have no say in anything. We have no say in the scheduling. We aren’t allowed to see what is billed under our name. The morale has really gone down.”
Dr. Wiener, who practices at Ascension St. John Hospital, said she and fellow physicians have repeatedly brought their concerns to TeamHealth, which in 2015 took over St. John Emergency Services PC. TeamHealth is owned by PE giant Blackstone.
“It’s very frustrating,” Dr. Wiener said. “We’re taking it from all sides.”
Blackstone and Ascension St. John did not respond to this news organization’s request for comment.
TeamHealth would not respond directly to questions about the Ascension St. John Hospital physicians or their concerns.
Spokesman Josh Hopson provided only a general statement: “TeamHealth is committed to making sure that clinicians have the resources and support needed to provide first-class care to patients, particularly with regard to staffing and compensation. TeamHealth has and will always put patient care first, and that is not impacted by its ownership model.”
Acquisitions of medical practices and hospitals by PE firms are rapidly growing, with more than 1,400 PE deals in health care in 2021 totaling upwards of $208 billion, according to PitchBook Data Inc., a Seattle-based firm that tracks mergers and acquisitions.
Some physicians praise the partnerships as an opportunity to improve technology and efficiency, whereas others decry them as raising patient costs and lowering the quality of care. A recent UC Berkeley study found that PE ownership of medical practices was linked to consumer price increases for 8 of 10 specialties, most notably oncology and gastroenterology.
What should you expect after PE acquisition?
Since his practice partnered with a PE firm in 2020, Milwaukee-based otolaryngologist Madan Kandula, MD, said he has found the changes positive. The practice has grown and improved operations in finance, accounting, compliance, and information technology, said Dr. Kandula, founder and CEO of Advent, an ENT practice with 15 clinics in four Midwestern states.
Dr. Kandula said his group already had a sound business practice, and that the goal of partnering with a PE firm wasn’t to change day-to-day operations but to propel the organization forward.
“From patient load to visit time to how we staff our clinics, there has been no change,” he said. “My private equity firm does not, [and] cannot, impose their will on our clinical decisions.”
Experts say the impact of PE acquisitions on individual physicians often depends on where a doctor ranks in the organization, what stage they are in their career, and how much control they had over the deal.
“It’s the older physicians who are usually selling the practice and getting the big payout,” said Anjali Dooley, a St. Louis–based health law attorney who counsels physicians about PE deals. “The younger doctors are usually not part of the deal, as they may still be employees. They don’t have any negotiating power. Hopefully, there is some transparency, but sometimes there is not, and they are blindsided by the deal.”
When it comes to workload, most PE-owned groups are put on a production-based model, such as a wRVU-based model, said Roger Strode, a Chicago-based health law attorney who focuses on health care mergers and acquisitions. Most already operate under such a model, but there might be some changes after a buyout.
Staffing may also change, added Ms. Dooley. The PE firms may want to add partners or companies already in their portfolios to create efficiencies, causing training or workflow changes.
In a hospital buyout, changes may depend on whether a department is a significant revenue generator for the hospital, Ms. Dooley noted.
PE firms frequently favor higher revenue–generating specialties, such as neurosurgery, cardiology, orthopedics, gastroenterology, and plastic surgery. They closely scrutinize departments said that make less money, such as the emergency department or primary care, Ms. Dooley said. Physicians or teams that don’t fit the firm’s cost-efficiency plans may be terminated or replaced.
On the other hand, Mr. Strode said physicians may see improved electronic health records and collections.
“Some of your overall overhead costs may be reduced, because they’re better at it,” Mr. Strode said. “When you’ve got more scale, the cost per patient, the cost per hour, the cost per procedure, goes down, and the cost that’s applied against your production will go down. As [practices grow], they have more bargaining power with payers and you can potentially get better rates. At least, that’s the promise.”
Analysts note that PE health care acquisitions show no signs of slowing and that it pays for physicians to know what to expect and how to cope if their practice or hospital is acquired. Whether physicians have some control over a buyout or are blindsided by the transition, it’s critical to know what to consider, how workloads might change, and your options for settling in or settling up.
The PE industry has about $2 trillion lined up for potential investments in 2023, said Ms. Dooley.
“PE firms are looking at health care to expend some of this dry powder,” Ms. Dooley continued. “If done correctly, PE firms that are aware of health care regulations, compliance, and patient care issues can ... remove redundant services and improve ... efficiencies, but the bad is when that doesn’t happen, and the quality of care goes down or there are patient safety risks.”
How to prepare for and cope with PE partnerships
If your practice is considering a PE partnership, it’s important to explore the terms and conditions and carefully weigh the pros and cons, said Gary Herschman, a Newark, N.J.–based attorney who advises PE-owned physician groups.
“My recommendation is that physicians at a minimum conduct due diligence on all potential strategic options for their groups, and then make an informed decision regarding whether a partnership transaction is right for their group, as it’s not right for every group,” he said.
When Texas cardiologist Rick Snyder, MD, was considering PE partnerships, he spoke with physicians who made similar deals to determine whether they were satisfied years later, he said. In April, Snyder’s practice, HeartPlace, the largest physician-owned cardiology practice in Texas, was acquired by US Heart & Vascular, a practice management platform backed by PE firm Ares Management.
“I called every group that I knew that had done private equity for any meaningful amount of time,” Dr. Snyder said. “For the first year or two, everybody is in the honeymoon period. If the model is going to succeed or break down, it’s not going to be in the first year or two. So I wanted to talk to groups that had done this for a longer amount of time and find out what their pitfalls were. What would they have done differently? Has it been a productive relationship? Did they grow?”
Dr. Snyder, president of the Texas Medical Association, said his practice met with seven or eight firms before choosing one that best met their needs. His group wanted a platform that preserved their clinical autonomy, governance, and culture, he said. They also wanted to ensure they were not entering into a “buy and flip” scenario, but rather a “buy and build” plan.
“Thus, financial capital was not sufficient, they also had to have intellectual capital and relationship capital on their bench,” he said. “When we found the partner that embraced all of these factors as well as a history of buying and long-term building, we pulled the trigger and partnered with Ares and US Heart & Vascular Management. The partner we chose did not offer us the most money. We put a premium on these other criteria.”
“I always tell docs, know the culture of your group and your vision,” he said. “Before you go down that route, ask yourself what you want to accomplish and if it makes sense having a private equity partner to accomplish that vision with.”
For younger physicians or those with little control over buyouts, experts recommend they review their contracts and consider consulting with an attorney to better understand how the deal may affect their earnings and career prospects.
Those who have a much longer career runway need to weigh whether they want to work for a PE-linked practice, Mr. Strode said. For some, it’s time to check when their noncompete agreements end and find a position elsewhere.
Also, physicians should know their rights and the laws in their states regarding the corporate practice of medicine. Statutes vary by state, and knowing the provisions in your state helps doctors recognize their legal rights, learn possible exceptions to the requirements, and know the penalties for violations.
In Michigan, a group of physicians and other health professionals at Ascension St. John has voted to unionize. Doctors hope that the union, which includes advanced practice clinicians, nurse practitioners, and physician assistants, will help improve patient care and protect working conditions for staff, Dr. Wiener said.
She advises physicians who are unhappy after acquisitions to speak up and stick together.
“That’s the biggest thing I think physicians should start doing,” she said. “Support each other and stand up. You are stronger together.”
Why is PE so attracted to health care?
PE firms typically buy practices or hospitals, work to make the entities more profitable, and then sell them, with the goal of doubling or tripling their investment over a short period. In general, PE firms aim for annual returns exceeding 20% after 3-7 years.
These firms know that health care is relatively recession-proof, that providers have third-party payers, and that the industry is fragmented and requires more efficiency, Ms. Dooley said.
When PE practice acquisitions started gaining momentum about 12 years ago, traditional hospital-based specialties such as anesthesiology and radiology were prime targets, said Mr. Strode.
At the same time, increasing challenges in private practice, such as declining compensation from payers, pressure to participate in value-based care programs, and rising regional competitors have fueled more physician groups to partner with PE firms, Mr. Herschman noted.
Physicians who partner with PE firms often benefit by having new access to capital to grow their practices, cost savings through group purchasing, and the ability to compete with larger health groups, Mr. Herschman said.
Questions remain, however, about how PE involvement affects health care use and spending. An April 2023 JAMA Viewpoint article called out the lack of oversight and regulation in the health care/PE space, suggesting that a stronger framework for regulation and transparency is needed.
A 2022 study in JAMA Health Forum that examined changes in prices and utilization associated with the PE acquisitions of 578 dermatology, gastroenterology, and ophthalmology physician practices from 2016 to 2020 found that prices increased by an average of 11%, and volume rose by 16%, after acquisition.
“We found that acquisitions were associated with increases in health care spending and utilization, as well as some other patterns of care like potential upcoding,” said Jane M. Zhu, MD, an author of the study and assistant professor at Oregon Health & Science University in Portland.
Another recent study that Dr. Zhu coauthored, published in Health Affairs, found that physician practices acquired by PE firms experience greater staff turnover and rely more heavily on advanced practice professionals than doctors.
“To the extent that that turnover indicates physicians are dissatisfied after private equity comes in, that’s really important to investigate further,” Dr. Zhu said.
PE firms owned 4% of U.S. hospitals in 2021 and 11% of nursing homes, according to a Medicare Payment Advisory Commission (MedPAC) report. The report does not include 2021 data on medical practices but notes that from 2013 to 2016, PE firms acquired at least 2% of physician practices. Estimates of PE deals are probably lower than actual numbers because of the lack of comprehensive information sources, according to the MedPAC report.
A version of this article appeared on Medscape.com.
Piroxicam boosts success of levonorgestrel for emergency contraception
Adding oral piroxicam to oral levonorgestrel significantly improved the efficacy of emergency contraception, based on data from 860 women.
Oral hormonal emergency contraception (EC) is the most widely used EC method worldwide, but the two currently available drugs, levonorgestrel and ulipristal acetate (UPA), are not effective when given after ovulation, wrote Raymond Hang Wun Li, MD, of the University of Hong Kong, and colleagues. Previous studies suggest that cyclo-oxygenase (COX) inhibitors may disrupt follicular rupture and prevent ovulation, but data on their use in combination with current oral ECs are lacking, the researchers said.
In a study published in The Lancet, the researchers randomized 430 women to receive a single oral dose of 1.5 mg levonorgestrel plus 40 mg of the COX-2 inhibitor piroxicam or 1.5 mg levonorgestrel plus a placebo. The study participants were women aged 18 years and older who requested EC within 72 hours of unprotected sex and who had regular menstrual cycles between 24 and 42 days long. The median age of the participants was 30 years; 97% were Chinese. The median time from intercourse to treatment was 18 hours for both groups.
The primary outcome was the percentage of pregnancies prevented, based on pregnancy status 1-2 weeks after treatment.
One pregnancy occurred in the piroxicam group, compared with seven pregnancies in the placebo group, which translated to a significant difference in the percentage of pregnancies prevented (94.7% vs. 63.4%, P < .0001).
No trend toward increased failure rates appeared based on the time elapsed between intercourse and EC use in either group, and no differences appeared in the return or delay of subsequent menstrual periods between the groups.
The most common adverse events (reported by more than 5% of participants in both groups) included fatigue or weakness, nausea, lower abdominal pain, dizziness, and headache.
The choice of piroxicam as the COX inhibitor in conjunction with levonorgestrel for the current study had several potential advantages, the researchers wrote in their discussion. These advantages include the widespread availability and long-acting characteristics of piroxicam, which is also true of levonorgestrel, they said.
The findings were limited by several factors including the generalizability to other settings and populations, the researchers noted. The efficacy of the levonorgestrel/piroxicam combination in women with a body mass index greater than 26 kg/m2 may be lower, but the current study population did not have enough women in this category to measure the potential effect, they said. The study also did not examine the effect of piroxicam in combination with ulipristal acetate.
However, the results are the first known to demonstrate the improved effectiveness of oral piroxicam coadministered with oral levonorgestrel for EC, they said.
“The strength of this recommendation and changes in clinical guidelines may be determined upon demonstration of reproducible results in further studies,” they added.
Pill combination shows potential and practicality
Oral emergency contraception on demand is an unmet need on a global level, Erica P. Cahill, MD, of the department of obstetrics and gynecology and division of family planning services at Stanford (Calif.) University, wrote in an accompanying editorial.
Dr. Cahill noted the longer half-life of piroxicam compared with other COX-2 inhibitors, which made it a practical choice. Although the study was not powered to evaluate secondary outcomes, bleeding patterns consistent with use of EC pills were observed. Documentation of these patterns is worthwhile, Dr. Cahill said, “because people using emergency contraceptive pills might also be using fertility awareness methods and need to know when they can be certain they are not pregnant.”
Overall, the study supports the addition of 40 mg piroxicam to 1.5 mg levonorgestrel as emergency contraception, said Dr. Cahill. Future studies can build on the current findings by evaluating repeat dosing of the piroxicam/levonorgestrel combination and by evaluating the combination of COX-2 inhibitors and ulipristal acetate to prevent pregnancy, she said.
The study received no outside funding. The researchers and Dr. Cahill had no financial conflicts to disclose.
Adding oral piroxicam to oral levonorgestrel significantly improved the efficacy of emergency contraception, based on data from 860 women.
Oral hormonal emergency contraception (EC) is the most widely used EC method worldwide, but the two currently available drugs, levonorgestrel and ulipristal acetate (UPA), are not effective when given after ovulation, wrote Raymond Hang Wun Li, MD, of the University of Hong Kong, and colleagues. Previous studies suggest that cyclo-oxygenase (COX) inhibitors may disrupt follicular rupture and prevent ovulation, but data on their use in combination with current oral ECs are lacking, the researchers said.
In a study published in The Lancet, the researchers randomized 430 women to receive a single oral dose of 1.5 mg levonorgestrel plus 40 mg of the COX-2 inhibitor piroxicam or 1.5 mg levonorgestrel plus a placebo. The study participants were women aged 18 years and older who requested EC within 72 hours of unprotected sex and who had regular menstrual cycles between 24 and 42 days long. The median age of the participants was 30 years; 97% were Chinese. The median time from intercourse to treatment was 18 hours for both groups.
The primary outcome was the percentage of pregnancies prevented, based on pregnancy status 1-2 weeks after treatment.
One pregnancy occurred in the piroxicam group, compared with seven pregnancies in the placebo group, which translated to a significant difference in the percentage of pregnancies prevented (94.7% vs. 63.4%, P < .0001).
No trend toward increased failure rates appeared based on the time elapsed between intercourse and EC use in either group, and no differences appeared in the return or delay of subsequent menstrual periods between the groups.
The most common adverse events (reported by more than 5% of participants in both groups) included fatigue or weakness, nausea, lower abdominal pain, dizziness, and headache.
The choice of piroxicam as the COX inhibitor in conjunction with levonorgestrel for the current study had several potential advantages, the researchers wrote in their discussion. These advantages include the widespread availability and long-acting characteristics of piroxicam, which is also true of levonorgestrel, they said.
The findings were limited by several factors including the generalizability to other settings and populations, the researchers noted. The efficacy of the levonorgestrel/piroxicam combination in women with a body mass index greater than 26 kg/m2 may be lower, but the current study population did not have enough women in this category to measure the potential effect, they said. The study also did not examine the effect of piroxicam in combination with ulipristal acetate.
However, the results are the first known to demonstrate the improved effectiveness of oral piroxicam coadministered with oral levonorgestrel for EC, they said.
“The strength of this recommendation and changes in clinical guidelines may be determined upon demonstration of reproducible results in further studies,” they added.
Pill combination shows potential and practicality
Oral emergency contraception on demand is an unmet need on a global level, Erica P. Cahill, MD, of the department of obstetrics and gynecology and division of family planning services at Stanford (Calif.) University, wrote in an accompanying editorial.
Dr. Cahill noted the longer half-life of piroxicam compared with other COX-2 inhibitors, which made it a practical choice. Although the study was not powered to evaluate secondary outcomes, bleeding patterns consistent with use of EC pills were observed. Documentation of these patterns is worthwhile, Dr. Cahill said, “because people using emergency contraceptive pills might also be using fertility awareness methods and need to know when they can be certain they are not pregnant.”
Overall, the study supports the addition of 40 mg piroxicam to 1.5 mg levonorgestrel as emergency contraception, said Dr. Cahill. Future studies can build on the current findings by evaluating repeat dosing of the piroxicam/levonorgestrel combination and by evaluating the combination of COX-2 inhibitors and ulipristal acetate to prevent pregnancy, she said.
The study received no outside funding. The researchers and Dr. Cahill had no financial conflicts to disclose.
Adding oral piroxicam to oral levonorgestrel significantly improved the efficacy of emergency contraception, based on data from 860 women.
Oral hormonal emergency contraception (EC) is the most widely used EC method worldwide, but the two currently available drugs, levonorgestrel and ulipristal acetate (UPA), are not effective when given after ovulation, wrote Raymond Hang Wun Li, MD, of the University of Hong Kong, and colleagues. Previous studies suggest that cyclo-oxygenase (COX) inhibitors may disrupt follicular rupture and prevent ovulation, but data on their use in combination with current oral ECs are lacking, the researchers said.
In a study published in The Lancet, the researchers randomized 430 women to receive a single oral dose of 1.5 mg levonorgestrel plus 40 mg of the COX-2 inhibitor piroxicam or 1.5 mg levonorgestrel plus a placebo. The study participants were women aged 18 years and older who requested EC within 72 hours of unprotected sex and who had regular menstrual cycles between 24 and 42 days long. The median age of the participants was 30 years; 97% were Chinese. The median time from intercourse to treatment was 18 hours for both groups.
The primary outcome was the percentage of pregnancies prevented, based on pregnancy status 1-2 weeks after treatment.
One pregnancy occurred in the piroxicam group, compared with seven pregnancies in the placebo group, which translated to a significant difference in the percentage of pregnancies prevented (94.7% vs. 63.4%, P < .0001).
No trend toward increased failure rates appeared based on the time elapsed between intercourse and EC use in either group, and no differences appeared in the return or delay of subsequent menstrual periods between the groups.
The most common adverse events (reported by more than 5% of participants in both groups) included fatigue or weakness, nausea, lower abdominal pain, dizziness, and headache.
The choice of piroxicam as the COX inhibitor in conjunction with levonorgestrel for the current study had several potential advantages, the researchers wrote in their discussion. These advantages include the widespread availability and long-acting characteristics of piroxicam, which is also true of levonorgestrel, they said.
The findings were limited by several factors including the generalizability to other settings and populations, the researchers noted. The efficacy of the levonorgestrel/piroxicam combination in women with a body mass index greater than 26 kg/m2 may be lower, but the current study population did not have enough women in this category to measure the potential effect, they said. The study also did not examine the effect of piroxicam in combination with ulipristal acetate.
However, the results are the first known to demonstrate the improved effectiveness of oral piroxicam coadministered with oral levonorgestrel for EC, they said.
“The strength of this recommendation and changes in clinical guidelines may be determined upon demonstration of reproducible results in further studies,” they added.
Pill combination shows potential and practicality
Oral emergency contraception on demand is an unmet need on a global level, Erica P. Cahill, MD, of the department of obstetrics and gynecology and division of family planning services at Stanford (Calif.) University, wrote in an accompanying editorial.
Dr. Cahill noted the longer half-life of piroxicam compared with other COX-2 inhibitors, which made it a practical choice. Although the study was not powered to evaluate secondary outcomes, bleeding patterns consistent with use of EC pills were observed. Documentation of these patterns is worthwhile, Dr. Cahill said, “because people using emergency contraceptive pills might also be using fertility awareness methods and need to know when they can be certain they are not pregnant.”
Overall, the study supports the addition of 40 mg piroxicam to 1.5 mg levonorgestrel as emergency contraception, said Dr. Cahill. Future studies can build on the current findings by evaluating repeat dosing of the piroxicam/levonorgestrel combination and by evaluating the combination of COX-2 inhibitors and ulipristal acetate to prevent pregnancy, she said.
The study received no outside funding. The researchers and Dr. Cahill had no financial conflicts to disclose.
FROM THE LANCET
Cancer rates rise among people under age 50
From 2010 to 2019, the rate of cancer diagnoses rose from 100 to 103 cases per 100,000 people, according to the study, published in JAMA Network Open. The increases were driven by jumps in certain types of cancer and within specific age, racial, and ethnic groups. Researchers analyzed data for more than 560,000 people under age 50 who were diagnosed with cancer during the 9-year period.
Breast cancer remained the most common type of cancer to affect younger people, while the most striking increase was seen in gastrointestinal cancers. The rate of people with GI cancers rose 15%.
Women were more likely to be diagnosed with cancer, whereas the rate of cancer among men under age 50 declined by 5%. When the researchers analyzed the data based on a person’s race or ethnicity, they found that cancer rates were increasing among people who are Asian, Pacific Islander, Hispanic, American Indian, or Alaska Native. The rate of cancer among Black people declined and was steady among White people.
The only age group that saw cancer rates increase was 30- to 39-year-olds. One of the top concerns for younger people with cancer is that there is a greater risk for the cancer to spread.
The cancer rate has been declining among older people, the researchers noted. One doctor told The Washington Post that it’s urgent that the reasons for the increases among young people be understood.
“If we don’t understand what’s causing this risk and we can’t do something to change it, we’re afraid that as time goes on, it’s going to become a bigger and bigger challenge,” said Paul Oberstein, MD, director of the gastrointestinal medical oncology program at NYU Langone’s Perlmutter Cancer Center, New York. He was not involved in the study.
It’s unclear why cancer rates are rising among young people, but some possible reasons are obesity, alcohol use, smoking, poor sleep, sedentary lifestyle, and things in the environment like pollution and carcinogens, the Post reported.
A version of this article first appeared on WebMD.com.
From 2010 to 2019, the rate of cancer diagnoses rose from 100 to 103 cases per 100,000 people, according to the study, published in JAMA Network Open. The increases were driven by jumps in certain types of cancer and within specific age, racial, and ethnic groups. Researchers analyzed data for more than 560,000 people under age 50 who were diagnosed with cancer during the 9-year period.
Breast cancer remained the most common type of cancer to affect younger people, while the most striking increase was seen in gastrointestinal cancers. The rate of people with GI cancers rose 15%.
Women were more likely to be diagnosed with cancer, whereas the rate of cancer among men under age 50 declined by 5%. When the researchers analyzed the data based on a person’s race or ethnicity, they found that cancer rates were increasing among people who are Asian, Pacific Islander, Hispanic, American Indian, or Alaska Native. The rate of cancer among Black people declined and was steady among White people.
The only age group that saw cancer rates increase was 30- to 39-year-olds. One of the top concerns for younger people with cancer is that there is a greater risk for the cancer to spread.
The cancer rate has been declining among older people, the researchers noted. One doctor told The Washington Post that it’s urgent that the reasons for the increases among young people be understood.
“If we don’t understand what’s causing this risk and we can’t do something to change it, we’re afraid that as time goes on, it’s going to become a bigger and bigger challenge,” said Paul Oberstein, MD, director of the gastrointestinal medical oncology program at NYU Langone’s Perlmutter Cancer Center, New York. He was not involved in the study.
It’s unclear why cancer rates are rising among young people, but some possible reasons are obesity, alcohol use, smoking, poor sleep, sedentary lifestyle, and things in the environment like pollution and carcinogens, the Post reported.
A version of this article first appeared on WebMD.com.
From 2010 to 2019, the rate of cancer diagnoses rose from 100 to 103 cases per 100,000 people, according to the study, published in JAMA Network Open. The increases were driven by jumps in certain types of cancer and within specific age, racial, and ethnic groups. Researchers analyzed data for more than 560,000 people under age 50 who were diagnosed with cancer during the 9-year period.
Breast cancer remained the most common type of cancer to affect younger people, while the most striking increase was seen in gastrointestinal cancers. The rate of people with GI cancers rose 15%.
Women were more likely to be diagnosed with cancer, whereas the rate of cancer among men under age 50 declined by 5%. When the researchers analyzed the data based on a person’s race or ethnicity, they found that cancer rates were increasing among people who are Asian, Pacific Islander, Hispanic, American Indian, or Alaska Native. The rate of cancer among Black people declined and was steady among White people.
The only age group that saw cancer rates increase was 30- to 39-year-olds. One of the top concerns for younger people with cancer is that there is a greater risk for the cancer to spread.
The cancer rate has been declining among older people, the researchers noted. One doctor told The Washington Post that it’s urgent that the reasons for the increases among young people be understood.
“If we don’t understand what’s causing this risk and we can’t do something to change it, we’re afraid that as time goes on, it’s going to become a bigger and bigger challenge,” said Paul Oberstein, MD, director of the gastrointestinal medical oncology program at NYU Langone’s Perlmutter Cancer Center, New York. He was not involved in the study.
It’s unclear why cancer rates are rising among young people, but some possible reasons are obesity, alcohol use, smoking, poor sleep, sedentary lifestyle, and things in the environment like pollution and carcinogens, the Post reported.
A version of this article first appeared on WebMD.com.
FROM JAMA NETWORK OPEN
Ob.gyn. organizations opt for new residency application platform
In a recent joint announcement, the American College of Obstetricians and Gynecologists and the Association of Professors of Gynecology and Obstetrics said the new system, ResidencyCAS, offered by Liaison Centralized Application Service, will replace the Electronic Residency Application Service (ERAS). ERAS was implemented some 25 years ago by the Association of American Medical Colleges.
Efficiencies and lower costs
Potential startup glitches aside, the transition will allegedly lower skyrocketing application fees and provide enhanced efficiencies and a better user experience than ERAS. So far, ob.gyn. is first and the only specialty to jump ship from the established platform. But if other specialties follow suit making the new software the norm, that will have a serious impact on ERAS’s revenues, said J. Bryan Carmody, MD, MPH, a pediatric nephrologist at the Children’s Hospital of the King’s Daughters, Norfolk, Va., who closely monitors and writes about residency selection and discussed the coming transition in a recent blog posting.

“My feeling is that the average program director thinks that ERAS is functional but there are not many, if any, who are in love with ERAS,” Dr. Carmody said in an interview. “I think ERAS will benefit from having a competitor.”
A major drawback for applicants with the removal of ob.gyn. from ERAS, which handles almost all medical specialties, is that those seeking acceptance in more than one specialty will now need to apply twice and incur two sets of costs. “A substantial fraction of applicants do that and now they’ll have to navigate two different systems and collect and format all their documents for both, which will be burdensome,” he said.
Holistic review
According to the ACOG announcement, the new technology promises to manage the deluge of applications more efficiently and, most important, to allow program directors to evaluate candidates holistically in order to better meet the specific needs of different communities.

“The platform makes it much easier to review applicants for important characteristics other than academic, and It will cost applicants about 20% less,” said Maya M. Hammoud, MD, MBA, professor and association chair for education, obstetrics, and gynecology at the University of Michigan, Ann Arbor, and past president of APGO.
So far the announced switch has been positively received. “People are very excited about the change, especially when they see the video,” Dr. Hammoud said.
For Adi Katz, MD, director of gynecology and director of the obstetrics and gynecology residency program at Lenox Hill Hospital, New York, the change signals a step in the right direction, especially when it comes to application reviewing. “The number of applications has been increasing tremendously in the past few years. We have four residency spots and we get almost 900 applications for them, ” she said. “Under the present system it’s hard to give a fair review to all the applicants, and we hope that with change we’ll be able to give each one the attention they deserve.”
An important feature, added Dr. Katz, is that the new software will allow directors to do intuitive, “gut-level” screenings with the help of AI. In this approach, large numbers of candidates can be screened based on intuition in relation to their formal criteria.
Residency program administrators have long sought more holistic ways of screening applicants, and AI has the potential to provide insights into who’s a good fit by finding patterns in very complex data.
“Of course, we won’t know for sure if it’s the right move until we start using the platform,” Dr. Katz said.

“There are many factors beyond academic standing that can help determine which individual applicants would be the best fit for each unique program,” AnnaMarie Connolly, MD, chief of education and academic affairs at ACOG, said in an interview. ”In particular, improved holistic review will allow programs and applicants to better ensure alignment that, for example, considers factors such as applicants’ clinical interests, academic interests, and past life experiences.”
Updated data science is expected better align ob.gyn. programs and applicants, and improve staff efficiency at no cost to programs, Dr. Connolly added. Good alignment of residents with programs is especially important in a patient-interactive specialty such as ob.gyn. Webinars will prepare users to apply the new system.
According to the promotional video, ResidencyCAS integrates all components of application from candidates’ letters and credentials to lists of program directors, applicant reviews, and specialty data analytics. Collecting recommendations and credentials is expected to be streamlined. The software is currently used by 31 U.S. health care professions and across 31,000 programs.
“It’s clear that ob.gyn. residency applicants and ob.gyn. programs have been frustrated by certain aspects of the former application system, one of which being high costs,” Dr. Connolly added. “The feedback we’ve received indicates that programs are excited about a more streamlined process.”
AAMC strikes back
Not all groups are so enthusiastic, however, including, understandably, the AAMC, which expressed “surprise and dismay” at the switch.

“While it is too early to fully understand the consequences of this development – intended and unintended – the AAMC remains committed to creating a fair and equitable process for learners, medical schools, and programs,” wrote AAMC spokespersons David J. Skorton, MD, AAMC’s CEO, and Alison J. Whelan, MD, chief academic officer in a statement. “We are concerned that ob.gyn. program data will no longer be part of the numerous and longstanding AAMC data and research efforts.”
Those efforts include the Residency Readiness Survey, multidecade institution-level data and analytics, and future cross-specialty innovations. Lost with the changeover, the AAMC warned, may be the cross-specialty data it has collected, analyzed, and shared since ERAS’s inception, in particular its advocacy, research, and data support for the ob.gyn. community following the 2022 Supreme Court ruling in Dobbs v. Jackson.
Evolution of specialty application
In a blog posting, Dr. Carmody outlined the evolution of the specialty residency application process. Pre-ERAS application was slow, cumbersome, and done by mail. With the introduction of ERAS, applicants were able to put their information on floppy discs and submit them to the dean’s office, hopefully triggering interview offers via email. The new approach was originally piloted in partnership with ob.gyn. program directors and now ERAS finds itself in a first-in, first-out situation.
Over the years, program directors suffocating under the weight of applications have periodically asked the AAMC to share data or make changes to ERAS protocols or policies, including those on the sharing of collected information. “Its my perception that frustration about the AAMC’s data sharing was one of the things that led to the change,” Dr. Carmody said. While acknowledging that data sharing must be carefully done, he noted that, when program directors asked to see ERAS data to answer important questions, they were often refused.
While it appears that AAMC’s improvement efforts have not gone far or fast enough, the association pointed to significant efforts to streamline applications. It stressed its ongoing commitment to cooperation “with learners, medical schools, and the ERAS program community to further consider the implications of ACOG’s announcement.” It recently announced a collaboration with Thalamus-connecting the docs, a new interview-management software system the AAMC expects will accelerate innovation across the transition-to-residency process.
“We have many questions and few answers at this time,” Dr. Skorton and Dr. Whelan wrote, “and we will work diligently to fully understand the consequences and keep open communication with all of our constituents.”
Financial impact
Ob.gyn., an important but relatively small specialty, represented only 2.8% of the 2022 residency applications on ERAS and $3,362,760 of its $120 million in revenue that year, Dr. Carmody noted. That’s with 2,613 ob.gyn. applicants submitting an average of 63-83 applications depending on their background.
But if the defection of ob.gyn. starts a stampede among program directors in other branches of medicine to ResidencyCAS or some other new platform, that would cost ERAS substantially more.
“The next few years are going to be very telling,” said Dr. Carmody. Although competition may act as a catalyst for needed improvements to ERAS, if momentum grows, the comfortable inertia of staying with a known system may soon be overcome. “And the more specialties that switch, the more that will deprive the AAMC of the revenue it needs to improve the product.”
Dr. Carmody and Dr. Katz disclosed no relevant conflicts of interest with regard to their comments.
In a recent joint announcement, the American College of Obstetricians and Gynecologists and the Association of Professors of Gynecology and Obstetrics said the new system, ResidencyCAS, offered by Liaison Centralized Application Service, will replace the Electronic Residency Application Service (ERAS). ERAS was implemented some 25 years ago by the Association of American Medical Colleges.
Efficiencies and lower costs
Potential startup glitches aside, the transition will allegedly lower skyrocketing application fees and provide enhanced efficiencies and a better user experience than ERAS. So far, ob.gyn. is first and the only specialty to jump ship from the established platform. But if other specialties follow suit making the new software the norm, that will have a serious impact on ERAS’s revenues, said J. Bryan Carmody, MD, MPH, a pediatric nephrologist at the Children’s Hospital of the King’s Daughters, Norfolk, Va., who closely monitors and writes about residency selection and discussed the coming transition in a recent blog posting.
“My feeling is that the average program director thinks that ERAS is functional but there are not many, if any, who are in love with ERAS,” Dr. Carmody said in an interview. “I think ERAS will benefit from having a competitor.”
A major drawback for applicants with the removal of ob.gyn. from ERAS, which handles almost all medical specialties, is that those seeking acceptance in more than one specialty will now need to apply twice and incur two sets of costs. “A substantial fraction of applicants do that and now they’ll have to navigate two different systems and collect and format all their documents for both, which will be burdensome,” he said.
Holistic review
According to the ACOG announcement, the new technology promises to manage the deluge of applications more efficiently and, most important, to allow program directors to evaluate candidates holistically in order to better meet the specific needs of different communities.
“The platform makes it much easier to review applicants for important characteristics other than academic, and It will cost applicants about 20% less,” said Maya M. Hammoud, MD, MBA, professor and association chair for education, obstetrics, and gynecology at the University of Michigan, Ann Arbor, and past president of APGO.
So far the announced switch has been positively received. “People are very excited about the change, especially when they see the video,” Dr. Hammoud said.
For Adi Katz, MD, director of gynecology and director of the obstetrics and gynecology residency program at Lenox Hill Hospital, New York, the change signals a step in the right direction, especially when it comes to application reviewing. “The number of applications has been increasing tremendously in the past few years. We have four residency spots and we get almost 900 applications for them, ” she said. “Under the present system it’s hard to give a fair review to all the applicants, and we hope that with change we’ll be able to give each one the attention they deserve.”
An important feature, added Dr. Katz, is that the new software will allow directors to do intuitive, “gut-level” screenings with the help of AI. In this approach, large numbers of candidates can be screened based on intuition in relation to their formal criteria.
Residency program administrators have long sought more holistic ways of screening applicants, and AI has the potential to provide insights into who’s a good fit by finding patterns in very complex data.
“Of course, we won’t know for sure if it’s the right move until we start using the platform,” Dr. Katz said.
“There are many factors beyond academic standing that can help determine which individual applicants would be the best fit for each unique program,” AnnaMarie Connolly, MD, chief of education and academic affairs at ACOG, said in an interview. ”In particular, improved holistic review will allow programs and applicants to better ensure alignment that, for example, considers factors such as applicants’ clinical interests, academic interests, and past life experiences.”
Updated data science is expected better align ob.gyn. programs and applicants, and improve staff efficiency at no cost to programs, Dr. Connolly added. Good alignment of residents with programs is especially important in a patient-interactive specialty such as ob.gyn. Webinars will prepare users to apply the new system.
According to the promotional video, ResidencyCAS integrates all components of application from candidates’ letters and credentials to lists of program directors, applicant reviews, and specialty data analytics. Collecting recommendations and credentials is expected to be streamlined. The software is currently used by 31 U.S. health care professions and across 31,000 programs.
“It’s clear that ob.gyn. residency applicants and ob.gyn. programs have been frustrated by certain aspects of the former application system, one of which being high costs,” Dr. Connolly added. “The feedback we’ve received indicates that programs are excited about a more streamlined process.”
AAMC strikes back
Not all groups are so enthusiastic, however, including, understandably, the AAMC, which expressed “surprise and dismay” at the switch.
“While it is too early to fully understand the consequences of this development – intended and unintended – the AAMC remains committed to creating a fair and equitable process for learners, medical schools, and programs,” wrote AAMC spokespersons David J. Skorton, MD, AAMC’s CEO, and Alison J. Whelan, MD, chief academic officer in a statement. “We are concerned that ob.gyn. program data will no longer be part of the numerous and longstanding AAMC data and research efforts.”
Those efforts include the Residency Readiness Survey, multidecade institution-level data and analytics, and future cross-specialty innovations. Lost with the changeover, the AAMC warned, may be the cross-specialty data it has collected, analyzed, and shared since ERAS’s inception, in particular its advocacy, research, and data support for the ob.gyn. community following the 2022 Supreme Court ruling in Dobbs v. Jackson.
Evolution of specialty application
In a blog posting, Dr. Carmody outlined the evolution of the specialty residency application process. Pre-ERAS application was slow, cumbersome, and done by mail. With the introduction of ERAS, applicants were able to put their information on floppy discs and submit them to the dean’s office, hopefully triggering interview offers via email. The new approach was originally piloted in partnership with ob.gyn. program directors and now ERAS finds itself in a first-in, first-out situation.
Over the years, program directors suffocating under the weight of applications have periodically asked the AAMC to share data or make changes to ERAS protocols or policies, including those on the sharing of collected information. “Its my perception that frustration about the AAMC’s data sharing was one of the things that led to the change,” Dr. Carmody said. While acknowledging that data sharing must be carefully done, he noted that, when program directors asked to see ERAS data to answer important questions, they were often refused.
While it appears that AAMC’s improvement efforts have not gone far or fast enough, the association pointed to significant efforts to streamline applications. It stressed its ongoing commitment to cooperation “with learners, medical schools, and the ERAS program community to further consider the implications of ACOG’s announcement.” It recently announced a collaboration with Thalamus-connecting the docs, a new interview-management software system the AAMC expects will accelerate innovation across the transition-to-residency process.
“We have many questions and few answers at this time,” Dr. Skorton and Dr. Whelan wrote, “and we will work diligently to fully understand the consequences and keep open communication with all of our constituents.”
Financial impact
Ob.gyn., an important but relatively small specialty, represented only 2.8% of the 2022 residency applications on ERAS and $3,362,760 of its $120 million in revenue that year, Dr. Carmody noted. That’s with 2,613 ob.gyn. applicants submitting an average of 63-83 applications depending on their background.
But if the defection of ob.gyn. starts a stampede among program directors in other branches of medicine to ResidencyCAS or some other new platform, that would cost ERAS substantially more.
“The next few years are going to be very telling,” said Dr. Carmody. Although competition may act as a catalyst for needed improvements to ERAS, if momentum grows, the comfortable inertia of staying with a known system may soon be overcome. “And the more specialties that switch, the more that will deprive the AAMC of the revenue it needs to improve the product.”
Dr. Carmody and Dr. Katz disclosed no relevant conflicts of interest with regard to their comments.
In a recent joint announcement, the American College of Obstetricians and Gynecologists and the Association of Professors of Gynecology and Obstetrics said the new system, ResidencyCAS, offered by Liaison Centralized Application Service, will replace the Electronic Residency Application Service (ERAS). ERAS was implemented some 25 years ago by the Association of American Medical Colleges.
Efficiencies and lower costs
Potential startup glitches aside, the transition will allegedly lower skyrocketing application fees and provide enhanced efficiencies and a better user experience than ERAS. So far, ob.gyn. is first and the only specialty to jump ship from the established platform. But if other specialties follow suit making the new software the norm, that will have a serious impact on ERAS’s revenues, said J. Bryan Carmody, MD, MPH, a pediatric nephrologist at the Children’s Hospital of the King’s Daughters, Norfolk, Va., who closely monitors and writes about residency selection and discussed the coming transition in a recent blog posting.
“My feeling is that the average program director thinks that ERAS is functional but there are not many, if any, who are in love with ERAS,” Dr. Carmody said in an interview. “I think ERAS will benefit from having a competitor.”
A major drawback for applicants with the removal of ob.gyn. from ERAS, which handles almost all medical specialties, is that those seeking acceptance in more than one specialty will now need to apply twice and incur two sets of costs. “A substantial fraction of applicants do that and now they’ll have to navigate two different systems and collect and format all their documents for both, which will be burdensome,” he said.
Holistic review
According to the ACOG announcement, the new technology promises to manage the deluge of applications more efficiently and, most important, to allow program directors to evaluate candidates holistically in order to better meet the specific needs of different communities.
“The platform makes it much easier to review applicants for important characteristics other than academic, and It will cost applicants about 20% less,” said Maya M. Hammoud, MD, MBA, professor and association chair for education, obstetrics, and gynecology at the University of Michigan, Ann Arbor, and past president of APGO.
So far the announced switch has been positively received. “People are very excited about the change, especially when they see the video,” Dr. Hammoud said.
For Adi Katz, MD, director of gynecology and director of the obstetrics and gynecology residency program at Lenox Hill Hospital, New York, the change signals a step in the right direction, especially when it comes to application reviewing. “The number of applications has been increasing tremendously in the past few years. We have four residency spots and we get almost 900 applications for them, ” she said. “Under the present system it’s hard to give a fair review to all the applicants, and we hope that with change we’ll be able to give each one the attention they deserve.”
An important feature, added Dr. Katz, is that the new software will allow directors to do intuitive, “gut-level” screenings with the help of AI. In this approach, large numbers of candidates can be screened based on intuition in relation to their formal criteria.
Residency program administrators have long sought more holistic ways of screening applicants, and AI has the potential to provide insights into who’s a good fit by finding patterns in very complex data.
“Of course, we won’t know for sure if it’s the right move until we start using the platform,” Dr. Katz said.
“There are many factors beyond academic standing that can help determine which individual applicants would be the best fit for each unique program,” AnnaMarie Connolly, MD, chief of education and academic affairs at ACOG, said in an interview. ”In particular, improved holistic review will allow programs and applicants to better ensure alignment that, for example, considers factors such as applicants’ clinical interests, academic interests, and past life experiences.”
Updated data science is expected better align ob.gyn. programs and applicants, and improve staff efficiency at no cost to programs, Dr. Connolly added. Good alignment of residents with programs is especially important in a patient-interactive specialty such as ob.gyn. Webinars will prepare users to apply the new system.
According to the promotional video, ResidencyCAS integrates all components of application from candidates’ letters and credentials to lists of program directors, applicant reviews, and specialty data analytics. Collecting recommendations and credentials is expected to be streamlined. The software is currently used by 31 U.S. health care professions and across 31,000 programs.
“It’s clear that ob.gyn. residency applicants and ob.gyn. programs have been frustrated by certain aspects of the former application system, one of which being high costs,” Dr. Connolly added. “The feedback we’ve received indicates that programs are excited about a more streamlined process.”
AAMC strikes back
Not all groups are so enthusiastic, however, including, understandably, the AAMC, which expressed “surprise and dismay” at the switch.
“While it is too early to fully understand the consequences of this development – intended and unintended – the AAMC remains committed to creating a fair and equitable process for learners, medical schools, and programs,” wrote AAMC spokespersons David J. Skorton, MD, AAMC’s CEO, and Alison J. Whelan, MD, chief academic officer in a statement. “We are concerned that ob.gyn. program data will no longer be part of the numerous and longstanding AAMC data and research efforts.”
Those efforts include the Residency Readiness Survey, multidecade institution-level data and analytics, and future cross-specialty innovations. Lost with the changeover, the AAMC warned, may be the cross-specialty data it has collected, analyzed, and shared since ERAS’s inception, in particular its advocacy, research, and data support for the ob.gyn. community following the 2022 Supreme Court ruling in Dobbs v. Jackson.
Evolution of specialty application
In a blog posting, Dr. Carmody outlined the evolution of the specialty residency application process. Pre-ERAS application was slow, cumbersome, and done by mail. With the introduction of ERAS, applicants were able to put their information on floppy discs and submit them to the dean’s office, hopefully triggering interview offers via email. The new approach was originally piloted in partnership with ob.gyn. program directors and now ERAS finds itself in a first-in, first-out situation.
Over the years, program directors suffocating under the weight of applications have periodically asked the AAMC to share data or make changes to ERAS protocols or policies, including those on the sharing of collected information. “Its my perception that frustration about the AAMC’s data sharing was one of the things that led to the change,” Dr. Carmody said. While acknowledging that data sharing must be carefully done, he noted that, when program directors asked to see ERAS data to answer important questions, they were often refused.
While it appears that AAMC’s improvement efforts have not gone far or fast enough, the association pointed to significant efforts to streamline applications. It stressed its ongoing commitment to cooperation “with learners, medical schools, and the ERAS program community to further consider the implications of ACOG’s announcement.” It recently announced a collaboration with Thalamus-connecting the docs, a new interview-management software system the AAMC expects will accelerate innovation across the transition-to-residency process.
“We have many questions and few answers at this time,” Dr. Skorton and Dr. Whelan wrote, “and we will work diligently to fully understand the consequences and keep open communication with all of our constituents.”
Financial impact
Ob.gyn., an important but relatively small specialty, represented only 2.8% of the 2022 residency applications on ERAS and $3,362,760 of its $120 million in revenue that year, Dr. Carmody noted. That’s with 2,613 ob.gyn. applicants submitting an average of 63-83 applications depending on their background.
But if the defection of ob.gyn. starts a stampede among program directors in other branches of medicine to ResidencyCAS or some other new platform, that would cost ERAS substantially more.
“The next few years are going to be very telling,” said Dr. Carmody. Although competition may act as a catalyst for needed improvements to ERAS, if momentum grows, the comfortable inertia of staying with a known system may soon be overcome. “And the more specialties that switch, the more that will deprive the AAMC of the revenue it needs to improve the product.”
Dr. Carmody and Dr. Katz disclosed no relevant conflicts of interest with regard to their comments.
Adenomyosis: Why we need to reassess our understanding of this condition
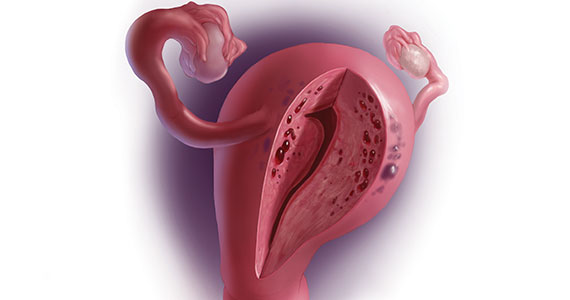
CASE Painful, heavy menstruation and recurrent pregnancy loss
A 37-year-old woman (G3P0030) with a history of recurrent pregnancy loss presents for evaluation. She had 3 losses—most recently a miscarriage at 22 weeks with a cerclage in place. She did not undergo any surgical procedures for these losses. Hormonal and thrombophilia workup is negative and semen analysis is normal. She reports a history of painful, heavy periods for many years, as well as dyspareunia and occasional post-coital bleeding. Past medical history was otherwise unremarkable. Pelvic magnetic resonance imaging (MRI) revealed focal thickening of the junctional zone up to 15 mm with 2 foci of T2 hyperintensities suggesting adenomyosis (FIGURE 1).
How do you counsel this patient regarding the MRI findings and their impact on her fertility?
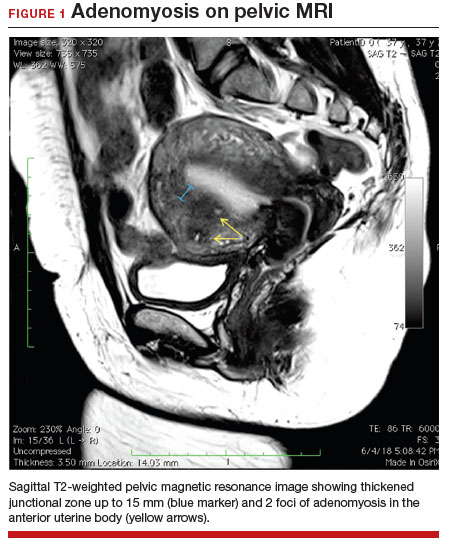
Adenomyosis is a condition in which endometrial glands and stroma are abnormally present in the uterine myometrium, resulting in smooth muscle hypertrophy and abnormal uterine contractility. Traditional teaching describes a woman in her 40s with heavy and painful menses, a “boggy uterus” on examination, who has completed childbearing and desires definitive treatment. Histologic diagnosis of adenomyosis is made from the uterine specimen at the time of hysterectomy, invariably confounding our understanding of the epidemiology of adenomyosis.
More recently, however, we are beginning to learn that this narrative is misguided. Imaging changes of adenomyosis can be seen in women who desire future fertility and in adolescents with severe dysmenorrhea, suggesting an earlier age of incidence.1 In a recent systematic review, prevalence estimates ranged from 15% to 67%, owing to varying diagnostic methods and patient inclusion criteria.2 It is increasingly being recognized as a primary contributor to infertility, with one study estimating a 30% prevalence of infertility in women with adenomyosis.3 Moreover, treatment with gonadotropin-releasing hormone agonists and/or surgical excision may improve fertility outcomes.4
As we learn more about this prevalent and life-altering condition, we owe it to our patients to consider this diagnosis when counseling on dysmenorrhea, heavy menstrual bleeding, or infertility.
Anatomy of the myometrium
The myometrium is composed of the inner and outer myometrium: the inner myometrium (IM) and endometrium are of Müllerian origin, and the outer myometrium (OM) is of mesenchymal origin. The IM thickens in response to steroid hormones during the menstrual cycle with metaplasia of endometrial stromal cells into myocytes and back again, whereas the OM is not responsive to hormones.5 Emerging literature suggests the OM is further divided into a middle and outer section based on different histologic morphologies, though the clinical implications of this are not understood.6 The term “junctional zone” (JZ) refers to the imaging appearance of what is thought to be the IM. Interestingly it cannot be identified on traditional hematoxylin and eosin staining. When the JZ is thickened or demonstrates irregular borders, it is used as a diagnostic marker for adenomyosis and is postulated to play an important role in adenomyosis pathophysiology, particularly heavy menstrual bleeding and infertility.7
Continue to: Subtypes of adenomyosis...
Subtypes of adenomyosis
While various disease classifications have been suggested for adenomyosis, to date there is no international consensus. Adenomyosis is typically described in 3 forms: diffuse, focal, or adenomyoma.8 As implied, the term focal adenomyosis refers to discrete lesions surrounded by normal myometrium, whereas abnormal glandular changes are pervasive throughout the myometrium in diffuse disease. Adenomyomas are a subgroup of focal adenomyosis that are thought to be surrounded by leiomyomatous smooth muscle and may be well demarcated on imaging.9
Recent research uses novel histologic imaging techniques to explore adenomyotic growth patterns in 3-dimensional (3D) reconstructions. Combining tissue-clearing methods with light-sheet fluorescence microscopy enables highly detailed 3D representations of the protein and nucleic acid structure of organs.10 For example, Yamaguchi and colleagues used this technology to explore the 3D morphological features of adenomyotic tissue and observed direct invasion of the endometrial glands into the myometrium and an “ant colony ̶ like network” of ectopic endometrial glands in the myometrium (FIGURE 2).11 These abnormal glandular networks have been visualized beyond the IM, which may not be captured on ultrasonography or MRI. While this work is still in its infancy, it has the potential to provide important insight into disease pathogenesis and to inform future therapy.
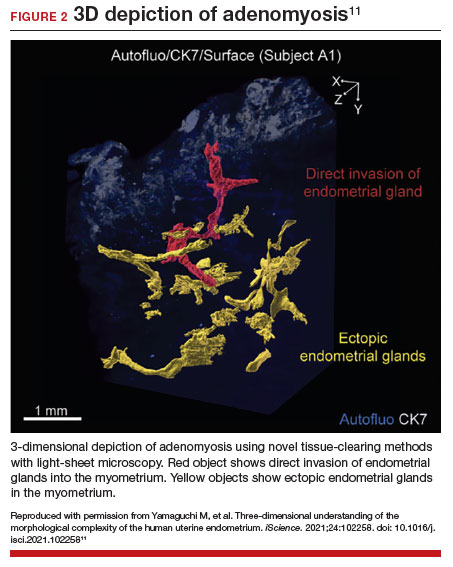
Pathogenesis
Proposed mechanisms for the development of adenomyosis include endometrial invasion, tissue injury and repair (TIAR) mechanisms, and the stem cell theory.12 According to the endometrial invasion theory, glandular epithelial cells from the basalis layer invaginate through an altered IM, slipping through weak muscle fibers and attracted by certain growth factors. In the TIAR mechanism theory, micro- or macro-trauma to the IM (whether from pregnancy, surgery, or infection) results in chronic proliferation and inflammation leading to the development of adenomyosis. Finally, the stem cell theory proposes that adenomyosis might develop from de novo ectopic endometrial tissue.
While the exact pathogenesis of adenomyosis is largely unknown, it has been associated with predictable molecular changes in the endometrium and surrounding myometrium.12 Myometrial hypercontractility is seen in patients with adenomyosis and dysmenorrhea, whereas neovascularization, high microvessel density, and abnormal uterine contractility are seen in those with abnormal uterine bleeding.13 In patients with infertility, increased inflammation, abnormal endometrial receptivity, and alterations in the myometrial architecture have been suggested to impair contractility and sperm transport.12,14
Differential growth factor expression and abnormal estrogen and progesterone signaling pathways have been observed in the IM in patients with adenomyosis, along with dysregulation of immune factors and increased inflammatory oxidative stress.12 This in turn results in myometrial hypertrophy and fibrosis, impairing normal uterine contractility patterns. This abnormal contractility may alter sperm transport and embryo implantation, and animal models that target pathways leading to fibrosis may improve endometrial receptivity.14,15 Further research is needed to elucidate specific molecular pathways and their complex interplay in this disease.
Continue to: Diagnosis...
Diagnosis
The gold standard for diagnosis of adenomyosis is histopathology from hysterectomy specimens, but specific definitions vary. Published criteria include endometrial glands within the myometrial layer greater than 0.5 to 1 low power field from the basal layer of the endometrium, endometrial glands extending deeper than 25% of the myometrial thickness, or endometrial glands a certain distance (ranging from 1-3 mm) from the basalis layer of the endometrium.16 Various methods of non-hysterectomy tissue sampling have been proposed for diagnosis, including needle, hysteroscopic, or laparoscopic sampling, but the sensitivity of these methods is poor.17 Limiting the diagnosis of adenomyosis to specimen pathology relies on invasive methods and clearly we cannot confirm the diagnosis by hysterectomy in patients with a desire for future fertility. It is for this reason that the prevalence of the disease is widely unknown.
The alternative to pathologic diagnosis is to identify radiologic changes that are associated with adenomyosis via either transvaginal ultrasound (TVUS) or MRI. Features suggestive of adenomyosis on MRI overlap with TVUS features, including uterine enlargement, anteroposterior myometrial asymmetry, T1- or T2-intense myometrial cysts or foci, and a thickened JZ.18 A JZ thicker than 12 mm has been thought to be predictive of adenomyosis, whereas a thickness of less than 8 mm is predictive of its absence, although the JZ may vary in thickness with the menstrual cycle.19,20 A 2021 systematic review and meta-analysis comparing MRI diagnosis with histopathologic findings reported a pooled sensitivity and specificity of 60% and 96%, respectively.21 The reported range for sensitivity and specificity is wide: 70% to 93% for sensitivity and 67% to 93% for specificity.22-24
Key TVUS features associated with adenomyosis were defined in 2015 in a consensus statement released by the Morphological Uterus Sonographic Assessment (MUSA) group.25 These include a globally enlarged uterus, anteroposterior myometrial asymmetry, myometrial cysts, fan-shaped shadowing, mixed myometrial echogenicity, translesional vascularity, echogenic subendometrial lines and buds, and a thickened, irregular or discontinuous JZ (FIGURES 3 and 4).25 The accuracy of ultrasonographic diagnosis of adenomyosis using these features has been investigated in multiple systematic reviews and meta-analyses, most recently by Liu and colleagues who found a pooled sensitivity of TVUS of 81% and pooled specificity of 87%.23 The range for ultrasonographic sensitivity and specificity is wide, however, ranging from 33% to 84% for sensitivity and 64% to 100% for specificity.22 Consensus is lacking as to which TVUS features are most predictive of adenomyosis, but in general, the combination of multiple MUSA criteria (particularly myometrial cysts and irregular JZ on 3D imaging) appears to be more accurate than any one feature alone.23 The presence of fibroids may decrease the sensitivity of TVUS, and one study suggested elastography may increase the accuracy of TVUS.24,26 Moreover, given that most radiologists receive limited training on the MUSA criteria, it behooves gynecologists to become familiar with these sonographic features to be able to identify adenomyosis in our patients.
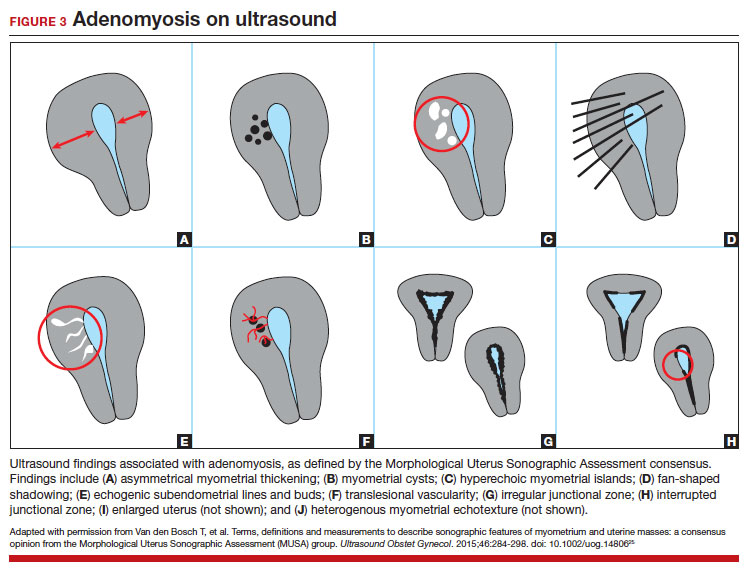

Adenomyosis also may be suspected based on hysteroscopic findings, although a normal hysteroscopy cannot rule out the disease and data are lacking to support these markers as diagnostic. Visual findings can include a “strawberry” pattern, mucosal elevation, cystic hemorrhagic lesions, localized vascularity, or endometrial defects.27 Hysteroscopy may be effective in the treatment of localized lesions, although that discussion is beyond the scope of this review.
Clinical presentation
While many women who are later diagnosed with adenomyosis are asymptomatic, the disease can present with heavy menstrual bleeding and dysmenorrhea, which occur in 50% and 30% of patients, respectively.28 Other symptoms include dyspareunia and infertility. Symptoms were previously reported to develop between the ages of 40 and 50 years; however, this is biased by diagnosis at the time of hysterectomy and the fact that younger patients are less likely to undergo definitive surgery. When using imaging criteria for diagnosis, adenomyosis might be more responsible for dysmenorrhea and chronic pelvic pain in younger patients than previously appreciated.1,29 In a recent study reviewing TVUS in 270 adolescents for any reason, adenomyosis was present in 5% of cases and this increased up to 44% in the presence of endometriosis.30
Adenomyosis often co-exists and shares similar clinical presentations with other gynecologic pathologies such as endometriosis and fibroids, making diagnosis on symptomatology alone challenging. Concurrent adenomyosis has been found in up to 73% and 57% of patients with suspected or diagnosed endometriosis and fibroids, respectively.31,32 Accumulating evidence suggests that pelvic pain previously attributed to endometriosis may in fact be a result of adenomyosis; for example, persistent pelvic pain after optimal resection of endometriosis may be confounded by the presence of adenomyosis.29 In one study of 155 patients with complete resection of deep infiltrating endometriosis, persistent pelvic pain was significantly associated with the presence of adenomyosis on imaging.33
Adenomyosis is increasingly being recognized at the time of infertility evaluation with an estimated prevalence of 30% in women with infertility.3 Among women with infertility, adenomyosis has been associated with a lower clinical pregnancy rate, higher miscarriage rate, and lower live birth rate, as well as obstetric complications such as abnormal placentation.34-36 A study of 37 baboons found the histologic diagnosis of adenomyosis alone at necropsy was associated with a 20-fold increased risk of lifelong infertility (odds ratio [OR], 20.1; 95% CI, 2.1-921), whereas presence of endometriosis was associated with a nonsignificant 3-fold risk of lifelong infertility (OR, 3.6; 95% CI, 0.9-15.8).37
In women with endometriosis and infertility, co-existing adenomyosis portends worse fertility outcomes. In a retrospective study of 244 women who underwent endometriosis surgery, more than five features of adenomyosis on imaging was associated with higher rates of infertility, in vitro fertilization treatments, and a higher number of in vitro fertilization cycles.31 Moreover, in women who underwent surgery for deep infiltrating endometriosis, the presence of adenomyosis on imaging was associated with a 68% reduction in likelihood of pregnancy after surgery.38
Conclusion
As we begin to learn about adenomyosis, our misconceptions become more evident. The notion that it largely affects women at the end of their reproductive lives is biased by using histopathology at hysterectomy as the gold standard for diagnosis. Lack of definitive histologic or imaging criteria and biopsy techniques add to the diagnostic challenge. This in turn leads to inaccurate estimates of incidence and prevalence, as we assume patients’ symptoms must be attributable to what we can see at the time of surgery (for example, Stage I or II endometriosis), rather than what we cannot see. We now know that adenomyosis is present in women of all ages, including adolescents, and can significantly contribute to reduced fertility and quality of life. We owe it to our patients to consider this condition in the differential diagnosis of dysmenorrhea, heavy menstrual bleeding, dyspareunia, and infertility.
CASE Resolved
The patient underwent targeted hysteroscopic resection of adenomyosis (FIGURE 5) and conceived spontaneously the following year. ●
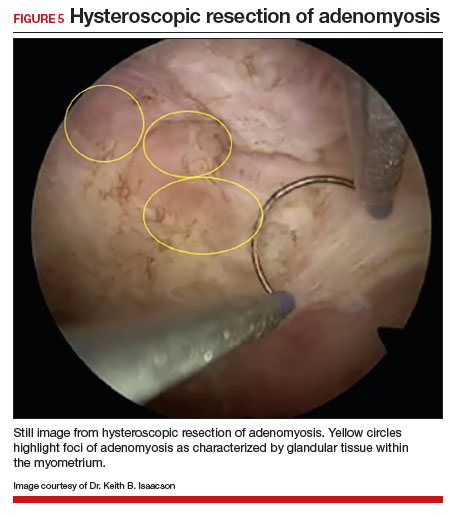
- Exacoustos C, Lazzeri L, Martire FG, et al. Ultrasound findings of adenomyosis in adolescents: type and grade of the disease. J Minim Invasive Gynecol. 2021;29:291.e1-299.e1. doi: 10.1016/j.jmig.2021.08.023
- Loring M, Chen TY, Isaacson KB. A systematic review of adenomyosis: it is time to reassess what we thought we knew about the disease. J Minim Invasive Gynecol. 2021;28:644655. doi: 10.1016/j.jmig.2020.10.012
- Bourdon M, Santulli P, Oliveira J, et al. Focal adenomyosis is associated with primary infertility. Fertil Steril. 2020;114:1271-1277. doi: 10.1016/j.fertnstert.2020.06.018
- Lan J, Wu Y, Wu Z, et al. Ultra-long GnRH agonist protocol during IVF/ICSI improves pregnancy outcomes in women with adenomyosis: a retrospective cohort study. Front Endocrinol (Lausanne). 2021;12:609771. doi: 10.3389 /fendo.2021.609771
- Gnecco JS, Brown AT, Kan EL, et al. Physiomimetic models of adenomyosis. Semin Reprod Med. 2020;38:179-196. doi: 10.1055/s-0040-1719084
- Harmsen MJ, Trommelen LM, de Leeuw RA, et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound Obstet Gynecol. 2023;62:42-60. doi: 10.1002/uog.26117
- Xie T, Xu X, Yang Y, et al. The role of abnormal uterine junction zone in the occurrence and development of adenomyosis. Reprod Sci. 2022;29:2719-2730. doi: 10.1007/s43032-021 -00684-2
- Lazzeri L, Morosetti G, Centini G, et al. A sonographic classification of adenomyosis: interobserver reproducibility in the evaluation of type and degree of the myometrial involvement. Fertil Steril. 2018;110:1154-1161.e3. doi: 10.1016 /j.fertnstert.2018.06.031
- Tahlan A, Nanda A, Mohan H. Uterine adenomyoma: a clinicopathologic review of 26 cases and a review of the literature. Int J Gynecol Pathol. 2006;25:361-365. doi: 10.1097/01.pgp.0000209570.08716.b3
- Chung K, Wallace J, Kim S-Y, et al. Structural and molecular interrogation of intact biological systems. Nature. 2013;497:332-337. doi: 10.1038/nature12107
- Yamaguchi M, Yoshihara K, Suda K, et al. Three-dimensional understanding of the morphological complexity of the human uterine endometrium. iScience. 2021;24:102258. doi: 10.1016/j.isci.2021.102258
- Vannuccini S, Tosti C, Carmona F, et al. Pathogenesis of adenomyosis: an update on molecular mechanisms. Reprod Biomed Online. 2017;35:592-601. doi: 10.1016 /j.rbmo.2017.06.016
- Zhai J, Vannuccini S, Petraglia F, et al. Adenomyosis: mechanisms and pathogenesis. Semin Reprod Med. 2020;38:129-143. doi: 10.1055/s-0040-1716687
- Munro MG. Uterine polyps, adenomyosis, leiomyomas, and endometrial receptivity. Fertil Steril. 2019;111:629-640. doi: 10.1016/j.fertnstert.2019.02.008
- Kay N, Huang C-Y, Shiu L-Y, et al. TGF-β1 neutralization improves pregnancy outcomes by restoring endometrial receptivity in mice with adenomyosis. Reprod Sci. 2021;28:877-887. doi: 10.1007/s43032-020-00308-1
- Habiba M, Benagiano G. Classifying adenomyosis: progress and challenges. Int J Environ Res Public Health. 2021;18:12386. doi: 10.3390/ijerph182312386
- Movilla P, Morris S, Isaacson K. A systematic review of tissue sampling techniques for the diagnosis of adenomyosis. J Minim Invasive Gynecol. 2020;27:344-351. doi: 10.1016 /j.jmig.2019.09.001
- Agostinho L, Cruz R, Osório F, et al. MRI for adenomyosis: a pictorial review. Insights Imaging. 2017;8:549-556. doi: 10.1007/s13244-017-0576-z
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod. 2001;16:2427-2433. doi: 10.1093/humrep/16.11.2427
- Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics. 1999;19:S147-S160. doi: 10.1148 /radiographics.19.suppl_1.g99oc13s147
- Rees CO, Nederend J, Mischi M, et al. Objective measures of adenomyosis on MRI and their diagnostic accuracy—a systematic review & meta-analysis. Acta Obstet Gynecol Scand. 2021;100:1377-1391.
- Chapron C, Vannuccini S, Santulli P, et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Hum Reprod Update. 2020;26:392-411. doi: 10.1093 /humupd/dmz049
- Liu L, Li W, Leonardi M, et al. Diagnostic accuracy of transvaginal ultrasound and magnetic resonance imaging for adenomyosis: systematic review and meta-analysis and review of sonographic diagnostic criteria. J Ultrasound Med. 2021;40:2289-2306. doi: 10.1002/jum.15635
- Bazot M, Daraï E. Role of transvaginal sonography and magnetic resonance imaging in the diagnosis of uterine adenomyosis. Fertil Steril. 2018;109:389-397. doi: 10.1016 /j.fertnstert.2018.01.024
- Van den Bosch T, Dueholm M, Leone FPG, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet Gynecol. 2015;46:284-298. doi: 10.1002/uog.14806
- Săsăran V, Turdean S, Gliga M, et al. Value of strainratio elastography in the diagnosis and differentiation of uterine fibroids and adenomyosis. J Pers Med. 2021;11:824. doi: 10.3390/jpm11080824
- Di Spiezio Sardo A, Calagna G, Santangelo F, et al. The role of hysteroscopy in the diagnosis and treatment of adenomyosis. Biomed Res Int. 2017;2017:2518396. doi: 10.1155/2017/2518396
- Azzi R. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-235.
- Parker JD, Leondires M, Sinaii N, et al. Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis. Fertil Steril. 2006;86:711-715. doi: 10.1016/j.fertnstert.2006.01.030
- Martire FG, Lazzeri L, Conway F, et al. Adolescence and endometriosis: symptoms, ultrasound signs and early diagnosis. Fertil Steril. 2020;114:1049-1057. doi: 10.1016 /j.fertnstert.2020.06.012
- Decter D, Arbib N, Markovitz H, et al. Sonographic signs of adenomyosis in women with endometriosis are associated with infertility. J Clin Med. 2021;10:2355. doi: 10.3390 /jcm10112355
- Brucker SY, Huebner M, Wallwiener M, et al. Clinical characteristics indicating adenomyosis coexisting with leiomyomas: a retrospective, questionnaire-based study. Fertil Steril. 2014;101:237-241.e1. doi: 10.1016 /j.fertnstert.2013.09.038
- Perelló MF, Martínez-Zamora MÁ, Torres X, et al. Endometriotic pain is associated with adenomyosis but not with the compartments affected by deep infiltrating endometriosis. Gynecol Obstet Invest. 2017;82:240-246. doi: 10.1159/000447633
- Younes G, Tulandi T. Effects of adenomyosis on in vitro fertilization treatment outcomes: a metaanalysis. Fertil Steril. 2017;108:483-490.e3. doi: 10.1016 /j.fertnstert.2017.06.025
- Nirgianakis K, Kalaitzopoulos DR, Schwartz ASK, et al. Fertility, pregnancy and neonatal outcomes of patients with adenomyosis: a systematic review and meta-analysis. Reprod BioMed Online. 2021;42:185-206. doi: 10.1016 /j.rbmo.2020.09.023
- Ono Y, Ota H, Takimoto K, et al. Perinatal outcomes associated with the positional relationship between the placenta and the adenomyosis lesion. J Gynecol Obstet Hum Reprod. 2021;50:102114. doi: 10.1016/j.jogoh.2021.102114
- Barrier BF, Malinowski MJ, Dick EJ Jr, et al. Adenomyosis in the baboon is associated with primary infertility. Fertil Steril. 2004;82(suppl 3):1091-1094. doi: 10.1016 /j.fertnstert.2003.11.065
- Vercellini P, Consonni D, Barbara G, et al. Adenomyosis and reproductive performance after surgery for rectovaginal and colorectal endometriosis: a systematic review and meta-analysis. Reprod Biomed Online. 2014;28:704-713. doi: 10.1016/j.rbmo.2014.02.006

Dr. Haber is Fellow, Minimally Invasive Gynecologic Surgery, Women’s Health Center, Newton-Wellesley Hospital, Newton, Massachusetts.

Dr. Fitzgerald is Resident, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, Boston, Massachusetts.

Dr. Isaacson is Associate Professor and Director of Minimally Invasive Gynecologic Surgery, Women’s Health Center, Newton-Wellesley Hospital.
The authors report no financial relationships relevant to this article.
Dr. Haber is Fellow, Minimally Invasive Gynecologic Surgery, Women’s Health Center, Newton-Wellesley Hospital, Newton, Massachusetts.
Dr. Fitzgerald is Resident, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, Boston, Massachusetts.
Dr. Isaacson is Associate Professor and Director of Minimally Invasive Gynecologic Surgery, Women’s Health Center, Newton-Wellesley Hospital.
The authors report no financial relationships relevant to this article.
Dr. Haber is Fellow, Minimally Invasive Gynecologic Surgery, Women’s Health Center, Newton-Wellesley Hospital, Newton, Massachusetts.
Dr. Fitzgerald is Resident, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, Boston, Massachusetts.
Dr. Isaacson is Associate Professor and Director of Minimally Invasive Gynecologic Surgery, Women’s Health Center, Newton-Wellesley Hospital.
The authors report no financial relationships relevant to this article.
CASE Painful, heavy menstruation and recurrent pregnancy loss
A 37-year-old woman (G3P0030) with a history of recurrent pregnancy loss presents for evaluation. She had 3 losses—most recently a miscarriage at 22 weeks with a cerclage in place. She did not undergo any surgical procedures for these losses. Hormonal and thrombophilia workup is negative and semen analysis is normal. She reports a history of painful, heavy periods for many years, as well as dyspareunia and occasional post-coital bleeding. Past medical history was otherwise unremarkable. Pelvic magnetic resonance imaging (MRI) revealed focal thickening of the junctional zone up to 15 mm with 2 foci of T2 hyperintensities suggesting adenomyosis (FIGURE 1).
How do you counsel this patient regarding the MRI findings and their impact on her fertility?
Adenomyosis is a condition in which endometrial glands and stroma are abnormally present in the uterine myometrium, resulting in smooth muscle hypertrophy and abnormal uterine contractility. Traditional teaching describes a woman in her 40s with heavy and painful menses, a “boggy uterus” on examination, who has completed childbearing and desires definitive treatment. Histologic diagnosis of adenomyosis is made from the uterine specimen at the time of hysterectomy, invariably confounding our understanding of the epidemiology of adenomyosis.
More recently, however, we are beginning to learn that this narrative is misguided. Imaging changes of adenomyosis can be seen in women who desire future fertility and in adolescents with severe dysmenorrhea, suggesting an earlier age of incidence.1 In a recent systematic review, prevalence estimates ranged from 15% to 67%, owing to varying diagnostic methods and patient inclusion criteria.2 It is increasingly being recognized as a primary contributor to infertility, with one study estimating a 30% prevalence of infertility in women with adenomyosis.3 Moreover, treatment with gonadotropin-releasing hormone agonists and/or surgical excision may improve fertility outcomes.4
As we learn more about this prevalent and life-altering condition, we owe it to our patients to consider this diagnosis when counseling on dysmenorrhea, heavy menstrual bleeding, or infertility.
Anatomy of the myometrium
The myometrium is composed of the inner and outer myometrium: the inner myometrium (IM) and endometrium are of Müllerian origin, and the outer myometrium (OM) is of mesenchymal origin. The IM thickens in response to steroid hormones during the menstrual cycle with metaplasia of endometrial stromal cells into myocytes and back again, whereas the OM is not responsive to hormones.5 Emerging literature suggests the OM is further divided into a middle and outer section based on different histologic morphologies, though the clinical implications of this are not understood.6 The term “junctional zone” (JZ) refers to the imaging appearance of what is thought to be the IM. Interestingly it cannot be identified on traditional hematoxylin and eosin staining. When the JZ is thickened or demonstrates irregular borders, it is used as a diagnostic marker for adenomyosis and is postulated to play an important role in adenomyosis pathophysiology, particularly heavy menstrual bleeding and infertility.7
Continue to: Subtypes of adenomyosis...
Subtypes of adenomyosis
While various disease classifications have been suggested for adenomyosis, to date there is no international consensus. Adenomyosis is typically described in 3 forms: diffuse, focal, or adenomyoma.8 As implied, the term focal adenomyosis refers to discrete lesions surrounded by normal myometrium, whereas abnormal glandular changes are pervasive throughout the myometrium in diffuse disease. Adenomyomas are a subgroup of focal adenomyosis that are thought to be surrounded by leiomyomatous smooth muscle and may be well demarcated on imaging.9
Recent research uses novel histologic imaging techniques to explore adenomyotic growth patterns in 3-dimensional (3D) reconstructions. Combining tissue-clearing methods with light-sheet fluorescence microscopy enables highly detailed 3D representations of the protein and nucleic acid structure of organs.10 For example, Yamaguchi and colleagues used this technology to explore the 3D morphological features of adenomyotic tissue and observed direct invasion of the endometrial glands into the myometrium and an “ant colony ̶ like network” of ectopic endometrial glands in the myometrium (FIGURE 2).11 These abnormal glandular networks have been visualized beyond the IM, which may not be captured on ultrasonography or MRI. While this work is still in its infancy, it has the potential to provide important insight into disease pathogenesis and to inform future therapy.
Pathogenesis
Proposed mechanisms for the development of adenomyosis include endometrial invasion, tissue injury and repair (TIAR) mechanisms, and the stem cell theory.12 According to the endometrial invasion theory, glandular epithelial cells from the basalis layer invaginate through an altered IM, slipping through weak muscle fibers and attracted by certain growth factors. In the TIAR mechanism theory, micro- or macro-trauma to the IM (whether from pregnancy, surgery, or infection) results in chronic proliferation and inflammation leading to the development of adenomyosis. Finally, the stem cell theory proposes that adenomyosis might develop from de novo ectopic endometrial tissue.
While the exact pathogenesis of adenomyosis is largely unknown, it has been associated with predictable molecular changes in the endometrium and surrounding myometrium.12 Myometrial hypercontractility is seen in patients with adenomyosis and dysmenorrhea, whereas neovascularization, high microvessel density, and abnormal uterine contractility are seen in those with abnormal uterine bleeding.13 In patients with infertility, increased inflammation, abnormal endometrial receptivity, and alterations in the myometrial architecture have been suggested to impair contractility and sperm transport.12,14
Differential growth factor expression and abnormal estrogen and progesterone signaling pathways have been observed in the IM in patients with adenomyosis, along with dysregulation of immune factors and increased inflammatory oxidative stress.12 This in turn results in myometrial hypertrophy and fibrosis, impairing normal uterine contractility patterns. This abnormal contractility may alter sperm transport and embryo implantation, and animal models that target pathways leading to fibrosis may improve endometrial receptivity.14,15 Further research is needed to elucidate specific molecular pathways and their complex interplay in this disease.
Continue to: Diagnosis...
Diagnosis
The gold standard for diagnosis of adenomyosis is histopathology from hysterectomy specimens, but specific definitions vary. Published criteria include endometrial glands within the myometrial layer greater than 0.5 to 1 low power field from the basal layer of the endometrium, endometrial glands extending deeper than 25% of the myometrial thickness, or endometrial glands a certain distance (ranging from 1-3 mm) from the basalis layer of the endometrium.16 Various methods of non-hysterectomy tissue sampling have been proposed for diagnosis, including needle, hysteroscopic, or laparoscopic sampling, but the sensitivity of these methods is poor.17 Limiting the diagnosis of adenomyosis to specimen pathology relies on invasive methods and clearly we cannot confirm the diagnosis by hysterectomy in patients with a desire for future fertility. It is for this reason that the prevalence of the disease is widely unknown.
The alternative to pathologic diagnosis is to identify radiologic changes that are associated with adenomyosis via either transvaginal ultrasound (TVUS) or MRI. Features suggestive of adenomyosis on MRI overlap with TVUS features, including uterine enlargement, anteroposterior myometrial asymmetry, T1- or T2-intense myometrial cysts or foci, and a thickened JZ.18 A JZ thicker than 12 mm has been thought to be predictive of adenomyosis, whereas a thickness of less than 8 mm is predictive of its absence, although the JZ may vary in thickness with the menstrual cycle.19,20 A 2021 systematic review and meta-analysis comparing MRI diagnosis with histopathologic findings reported a pooled sensitivity and specificity of 60% and 96%, respectively.21 The reported range for sensitivity and specificity is wide: 70% to 93% for sensitivity and 67% to 93% for specificity.22-24
Key TVUS features associated with adenomyosis were defined in 2015 in a consensus statement released by the Morphological Uterus Sonographic Assessment (MUSA) group.25 These include a globally enlarged uterus, anteroposterior myometrial asymmetry, myometrial cysts, fan-shaped shadowing, mixed myometrial echogenicity, translesional vascularity, echogenic subendometrial lines and buds, and a thickened, irregular or discontinuous JZ (FIGURES 3 and 4).25 The accuracy of ultrasonographic diagnosis of adenomyosis using these features has been investigated in multiple systematic reviews and meta-analyses, most recently by Liu and colleagues who found a pooled sensitivity of TVUS of 81% and pooled specificity of 87%.23 The range for ultrasonographic sensitivity and specificity is wide, however, ranging from 33% to 84% for sensitivity and 64% to 100% for specificity.22 Consensus is lacking as to which TVUS features are most predictive of adenomyosis, but in general, the combination of multiple MUSA criteria (particularly myometrial cysts and irregular JZ on 3D imaging) appears to be more accurate than any one feature alone.23 The presence of fibroids may decrease the sensitivity of TVUS, and one study suggested elastography may increase the accuracy of TVUS.24,26 Moreover, given that most radiologists receive limited training on the MUSA criteria, it behooves gynecologists to become familiar with these sonographic features to be able to identify adenomyosis in our patients.
Adenomyosis also may be suspected based on hysteroscopic findings, although a normal hysteroscopy cannot rule out the disease and data are lacking to support these markers as diagnostic. Visual findings can include a “strawberry” pattern, mucosal elevation, cystic hemorrhagic lesions, localized vascularity, or endometrial defects.27 Hysteroscopy may be effective in the treatment of localized lesions, although that discussion is beyond the scope of this review.
Clinical presentation
While many women who are later diagnosed with adenomyosis are asymptomatic, the disease can present with heavy menstrual bleeding and dysmenorrhea, which occur in 50% and 30% of patients, respectively.28 Other symptoms include dyspareunia and infertility. Symptoms were previously reported to develop between the ages of 40 and 50 years; however, this is biased by diagnosis at the time of hysterectomy and the fact that younger patients are less likely to undergo definitive surgery. When using imaging criteria for diagnosis, adenomyosis might be more responsible for dysmenorrhea and chronic pelvic pain in younger patients than previously appreciated.1,29 In a recent study reviewing TVUS in 270 adolescents for any reason, adenomyosis was present in 5% of cases and this increased up to 44% in the presence of endometriosis.30
Adenomyosis often co-exists and shares similar clinical presentations with other gynecologic pathologies such as endometriosis and fibroids, making diagnosis on symptomatology alone challenging. Concurrent adenomyosis has been found in up to 73% and 57% of patients with suspected or diagnosed endometriosis and fibroids, respectively.31,32 Accumulating evidence suggests that pelvic pain previously attributed to endometriosis may in fact be a result of adenomyosis; for example, persistent pelvic pain after optimal resection of endometriosis may be confounded by the presence of adenomyosis.29 In one study of 155 patients with complete resection of deep infiltrating endometriosis, persistent pelvic pain was significantly associated with the presence of adenomyosis on imaging.33
Adenomyosis is increasingly being recognized at the time of infertility evaluation with an estimated prevalence of 30% in women with infertility.3 Among women with infertility, adenomyosis has been associated with a lower clinical pregnancy rate, higher miscarriage rate, and lower live birth rate, as well as obstetric complications such as abnormal placentation.34-36 A study of 37 baboons found the histologic diagnosis of adenomyosis alone at necropsy was associated with a 20-fold increased risk of lifelong infertility (odds ratio [OR], 20.1; 95% CI, 2.1-921), whereas presence of endometriosis was associated with a nonsignificant 3-fold risk of lifelong infertility (OR, 3.6; 95% CI, 0.9-15.8).37
In women with endometriosis and infertility, co-existing adenomyosis portends worse fertility outcomes. In a retrospective study of 244 women who underwent endometriosis surgery, more than five features of adenomyosis on imaging was associated with higher rates of infertility, in vitro fertilization treatments, and a higher number of in vitro fertilization cycles.31 Moreover, in women who underwent surgery for deep infiltrating endometriosis, the presence of adenomyosis on imaging was associated with a 68% reduction in likelihood of pregnancy after surgery.38
Conclusion
As we begin to learn about adenomyosis, our misconceptions become more evident. The notion that it largely affects women at the end of their reproductive lives is biased by using histopathology at hysterectomy as the gold standard for diagnosis. Lack of definitive histologic or imaging criteria and biopsy techniques add to the diagnostic challenge. This in turn leads to inaccurate estimates of incidence and prevalence, as we assume patients’ symptoms must be attributable to what we can see at the time of surgery (for example, Stage I or II endometriosis), rather than what we cannot see. We now know that adenomyosis is present in women of all ages, including adolescents, and can significantly contribute to reduced fertility and quality of life. We owe it to our patients to consider this condition in the differential diagnosis of dysmenorrhea, heavy menstrual bleeding, dyspareunia, and infertility.
CASE Resolved
The patient underwent targeted hysteroscopic resection of adenomyosis (FIGURE 5) and conceived spontaneously the following year. ●
CASE Painful, heavy menstruation and recurrent pregnancy loss
A 37-year-old woman (G3P0030) with a history of recurrent pregnancy loss presents for evaluation. She had 3 losses—most recently a miscarriage at 22 weeks with a cerclage in place. She did not undergo any surgical procedures for these losses. Hormonal and thrombophilia workup is negative and semen analysis is normal. She reports a history of painful, heavy periods for many years, as well as dyspareunia and occasional post-coital bleeding. Past medical history was otherwise unremarkable. Pelvic magnetic resonance imaging (MRI) revealed focal thickening of the junctional zone up to 15 mm with 2 foci of T2 hyperintensities suggesting adenomyosis (FIGURE 1).
How do you counsel this patient regarding the MRI findings and their impact on her fertility?
Adenomyosis is a condition in which endometrial glands and stroma are abnormally present in the uterine myometrium, resulting in smooth muscle hypertrophy and abnormal uterine contractility. Traditional teaching describes a woman in her 40s with heavy and painful menses, a “boggy uterus” on examination, who has completed childbearing and desires definitive treatment. Histologic diagnosis of adenomyosis is made from the uterine specimen at the time of hysterectomy, invariably confounding our understanding of the epidemiology of adenomyosis.
More recently, however, we are beginning to learn that this narrative is misguided. Imaging changes of adenomyosis can be seen in women who desire future fertility and in adolescents with severe dysmenorrhea, suggesting an earlier age of incidence.1 In a recent systematic review, prevalence estimates ranged from 15% to 67%, owing to varying diagnostic methods and patient inclusion criteria.2 It is increasingly being recognized as a primary contributor to infertility, with one study estimating a 30% prevalence of infertility in women with adenomyosis.3 Moreover, treatment with gonadotropin-releasing hormone agonists and/or surgical excision may improve fertility outcomes.4
As we learn more about this prevalent and life-altering condition, we owe it to our patients to consider this diagnosis when counseling on dysmenorrhea, heavy menstrual bleeding, or infertility.
Anatomy of the myometrium
The myometrium is composed of the inner and outer myometrium: the inner myometrium (IM) and endometrium are of Müllerian origin, and the outer myometrium (OM) is of mesenchymal origin. The IM thickens in response to steroid hormones during the menstrual cycle with metaplasia of endometrial stromal cells into myocytes and back again, whereas the OM is not responsive to hormones.5 Emerging literature suggests the OM is further divided into a middle and outer section based on different histologic morphologies, though the clinical implications of this are not understood.6 The term “junctional zone” (JZ) refers to the imaging appearance of what is thought to be the IM. Interestingly it cannot be identified on traditional hematoxylin and eosin staining. When the JZ is thickened or demonstrates irregular borders, it is used as a diagnostic marker for adenomyosis and is postulated to play an important role in adenomyosis pathophysiology, particularly heavy menstrual bleeding and infertility.7
Continue to: Subtypes of adenomyosis...
Subtypes of adenomyosis
While various disease classifications have been suggested for adenomyosis, to date there is no international consensus. Adenomyosis is typically described in 3 forms: diffuse, focal, or adenomyoma.8 As implied, the term focal adenomyosis refers to discrete lesions surrounded by normal myometrium, whereas abnormal glandular changes are pervasive throughout the myometrium in diffuse disease. Adenomyomas are a subgroup of focal adenomyosis that are thought to be surrounded by leiomyomatous smooth muscle and may be well demarcated on imaging.9
Recent research uses novel histologic imaging techniques to explore adenomyotic growth patterns in 3-dimensional (3D) reconstructions. Combining tissue-clearing methods with light-sheet fluorescence microscopy enables highly detailed 3D representations of the protein and nucleic acid structure of organs.10 For example, Yamaguchi and colleagues used this technology to explore the 3D morphological features of adenomyotic tissue and observed direct invasion of the endometrial glands into the myometrium and an “ant colony ̶ like network” of ectopic endometrial glands in the myometrium (FIGURE 2).11 These abnormal glandular networks have been visualized beyond the IM, which may not be captured on ultrasonography or MRI. While this work is still in its infancy, it has the potential to provide important insight into disease pathogenesis and to inform future therapy.
Pathogenesis
Proposed mechanisms for the development of adenomyosis include endometrial invasion, tissue injury and repair (TIAR) mechanisms, and the stem cell theory.12 According to the endometrial invasion theory, glandular epithelial cells from the basalis layer invaginate through an altered IM, slipping through weak muscle fibers and attracted by certain growth factors. In the TIAR mechanism theory, micro- or macro-trauma to the IM (whether from pregnancy, surgery, or infection) results in chronic proliferation and inflammation leading to the development of adenomyosis. Finally, the stem cell theory proposes that adenomyosis might develop from de novo ectopic endometrial tissue.
While the exact pathogenesis of adenomyosis is largely unknown, it has been associated with predictable molecular changes in the endometrium and surrounding myometrium.12 Myometrial hypercontractility is seen in patients with adenomyosis and dysmenorrhea, whereas neovascularization, high microvessel density, and abnormal uterine contractility are seen in those with abnormal uterine bleeding.13 In patients with infertility, increased inflammation, abnormal endometrial receptivity, and alterations in the myometrial architecture have been suggested to impair contractility and sperm transport.12,14
Differential growth factor expression and abnormal estrogen and progesterone signaling pathways have been observed in the IM in patients with adenomyosis, along with dysregulation of immune factors and increased inflammatory oxidative stress.12 This in turn results in myometrial hypertrophy and fibrosis, impairing normal uterine contractility patterns. This abnormal contractility may alter sperm transport and embryo implantation, and animal models that target pathways leading to fibrosis may improve endometrial receptivity.14,15 Further research is needed to elucidate specific molecular pathways and their complex interplay in this disease.
Continue to: Diagnosis...
Diagnosis
The gold standard for diagnosis of adenomyosis is histopathology from hysterectomy specimens, but specific definitions vary. Published criteria include endometrial glands within the myometrial layer greater than 0.5 to 1 low power field from the basal layer of the endometrium, endometrial glands extending deeper than 25% of the myometrial thickness, or endometrial glands a certain distance (ranging from 1-3 mm) from the basalis layer of the endometrium.16 Various methods of non-hysterectomy tissue sampling have been proposed for diagnosis, including needle, hysteroscopic, or laparoscopic sampling, but the sensitivity of these methods is poor.17 Limiting the diagnosis of adenomyosis to specimen pathology relies on invasive methods and clearly we cannot confirm the diagnosis by hysterectomy in patients with a desire for future fertility. It is for this reason that the prevalence of the disease is widely unknown.
The alternative to pathologic diagnosis is to identify radiologic changes that are associated with adenomyosis via either transvaginal ultrasound (TVUS) or MRI. Features suggestive of adenomyosis on MRI overlap with TVUS features, including uterine enlargement, anteroposterior myometrial asymmetry, T1- or T2-intense myometrial cysts or foci, and a thickened JZ.18 A JZ thicker than 12 mm has been thought to be predictive of adenomyosis, whereas a thickness of less than 8 mm is predictive of its absence, although the JZ may vary in thickness with the menstrual cycle.19,20 A 2021 systematic review and meta-analysis comparing MRI diagnosis with histopathologic findings reported a pooled sensitivity and specificity of 60% and 96%, respectively.21 The reported range for sensitivity and specificity is wide: 70% to 93% for sensitivity and 67% to 93% for specificity.22-24
Key TVUS features associated with adenomyosis were defined in 2015 in a consensus statement released by the Morphological Uterus Sonographic Assessment (MUSA) group.25 These include a globally enlarged uterus, anteroposterior myometrial asymmetry, myometrial cysts, fan-shaped shadowing, mixed myometrial echogenicity, translesional vascularity, echogenic subendometrial lines and buds, and a thickened, irregular or discontinuous JZ (FIGURES 3 and 4).25 The accuracy of ultrasonographic diagnosis of adenomyosis using these features has been investigated in multiple systematic reviews and meta-analyses, most recently by Liu and colleagues who found a pooled sensitivity of TVUS of 81% and pooled specificity of 87%.23 The range for ultrasonographic sensitivity and specificity is wide, however, ranging from 33% to 84% for sensitivity and 64% to 100% for specificity.22 Consensus is lacking as to which TVUS features are most predictive of adenomyosis, but in general, the combination of multiple MUSA criteria (particularly myometrial cysts and irregular JZ on 3D imaging) appears to be more accurate than any one feature alone.23 The presence of fibroids may decrease the sensitivity of TVUS, and one study suggested elastography may increase the accuracy of TVUS.24,26 Moreover, given that most radiologists receive limited training on the MUSA criteria, it behooves gynecologists to become familiar with these sonographic features to be able to identify adenomyosis in our patients.
Adenomyosis also may be suspected based on hysteroscopic findings, although a normal hysteroscopy cannot rule out the disease and data are lacking to support these markers as diagnostic. Visual findings can include a “strawberry” pattern, mucosal elevation, cystic hemorrhagic lesions, localized vascularity, or endometrial defects.27 Hysteroscopy may be effective in the treatment of localized lesions, although that discussion is beyond the scope of this review.
Clinical presentation
While many women who are later diagnosed with adenomyosis are asymptomatic, the disease can present with heavy menstrual bleeding and dysmenorrhea, which occur in 50% and 30% of patients, respectively.28 Other symptoms include dyspareunia and infertility. Symptoms were previously reported to develop between the ages of 40 and 50 years; however, this is biased by diagnosis at the time of hysterectomy and the fact that younger patients are less likely to undergo definitive surgery. When using imaging criteria for diagnosis, adenomyosis might be more responsible for dysmenorrhea and chronic pelvic pain in younger patients than previously appreciated.1,29 In a recent study reviewing TVUS in 270 adolescents for any reason, adenomyosis was present in 5% of cases and this increased up to 44% in the presence of endometriosis.30
Adenomyosis often co-exists and shares similar clinical presentations with other gynecologic pathologies such as endometriosis and fibroids, making diagnosis on symptomatology alone challenging. Concurrent adenomyosis has been found in up to 73% and 57% of patients with suspected or diagnosed endometriosis and fibroids, respectively.31,32 Accumulating evidence suggests that pelvic pain previously attributed to endometriosis may in fact be a result of adenomyosis; for example, persistent pelvic pain after optimal resection of endometriosis may be confounded by the presence of adenomyosis.29 In one study of 155 patients with complete resection of deep infiltrating endometriosis, persistent pelvic pain was significantly associated with the presence of adenomyosis on imaging.33
Adenomyosis is increasingly being recognized at the time of infertility evaluation with an estimated prevalence of 30% in women with infertility.3 Among women with infertility, adenomyosis has been associated with a lower clinical pregnancy rate, higher miscarriage rate, and lower live birth rate, as well as obstetric complications such as abnormal placentation.34-36 A study of 37 baboons found the histologic diagnosis of adenomyosis alone at necropsy was associated with a 20-fold increased risk of lifelong infertility (odds ratio [OR], 20.1; 95% CI, 2.1-921), whereas presence of endometriosis was associated with a nonsignificant 3-fold risk of lifelong infertility (OR, 3.6; 95% CI, 0.9-15.8).37
In women with endometriosis and infertility, co-existing adenomyosis portends worse fertility outcomes. In a retrospective study of 244 women who underwent endometriosis surgery, more than five features of adenomyosis on imaging was associated with higher rates of infertility, in vitro fertilization treatments, and a higher number of in vitro fertilization cycles.31 Moreover, in women who underwent surgery for deep infiltrating endometriosis, the presence of adenomyosis on imaging was associated with a 68% reduction in likelihood of pregnancy after surgery.38
Conclusion
As we begin to learn about adenomyosis, our misconceptions become more evident. The notion that it largely affects women at the end of their reproductive lives is biased by using histopathology at hysterectomy as the gold standard for diagnosis. Lack of definitive histologic or imaging criteria and biopsy techniques add to the diagnostic challenge. This in turn leads to inaccurate estimates of incidence and prevalence, as we assume patients’ symptoms must be attributable to what we can see at the time of surgery (for example, Stage I or II endometriosis), rather than what we cannot see. We now know that adenomyosis is present in women of all ages, including adolescents, and can significantly contribute to reduced fertility and quality of life. We owe it to our patients to consider this condition in the differential diagnosis of dysmenorrhea, heavy menstrual bleeding, dyspareunia, and infertility.
CASE Resolved
The patient underwent targeted hysteroscopic resection of adenomyosis (FIGURE 5) and conceived spontaneously the following year. ●
- Exacoustos C, Lazzeri L, Martire FG, et al. Ultrasound findings of adenomyosis in adolescents: type and grade of the disease. J Minim Invasive Gynecol. 2021;29:291.e1-299.e1. doi: 10.1016/j.jmig.2021.08.023
- Loring M, Chen TY, Isaacson KB. A systematic review of adenomyosis: it is time to reassess what we thought we knew about the disease. J Minim Invasive Gynecol. 2021;28:644655. doi: 10.1016/j.jmig.2020.10.012
- Bourdon M, Santulli P, Oliveira J, et al. Focal adenomyosis is associated with primary infertility. Fertil Steril. 2020;114:1271-1277. doi: 10.1016/j.fertnstert.2020.06.018
- Lan J, Wu Y, Wu Z, et al. Ultra-long GnRH agonist protocol during IVF/ICSI improves pregnancy outcomes in women with adenomyosis: a retrospective cohort study. Front Endocrinol (Lausanne). 2021;12:609771. doi: 10.3389 /fendo.2021.609771
- Gnecco JS, Brown AT, Kan EL, et al. Physiomimetic models of adenomyosis. Semin Reprod Med. 2020;38:179-196. doi: 10.1055/s-0040-1719084
- Harmsen MJ, Trommelen LM, de Leeuw RA, et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound Obstet Gynecol. 2023;62:42-60. doi: 10.1002/uog.26117
- Xie T, Xu X, Yang Y, et al. The role of abnormal uterine junction zone in the occurrence and development of adenomyosis. Reprod Sci. 2022;29:2719-2730. doi: 10.1007/s43032-021 -00684-2
- Lazzeri L, Morosetti G, Centini G, et al. A sonographic classification of adenomyosis: interobserver reproducibility in the evaluation of type and degree of the myometrial involvement. Fertil Steril. 2018;110:1154-1161.e3. doi: 10.1016 /j.fertnstert.2018.06.031
- Tahlan A, Nanda A, Mohan H. Uterine adenomyoma: a clinicopathologic review of 26 cases and a review of the literature. Int J Gynecol Pathol. 2006;25:361-365. doi: 10.1097/01.pgp.0000209570.08716.b3
- Chung K, Wallace J, Kim S-Y, et al. Structural and molecular interrogation of intact biological systems. Nature. 2013;497:332-337. doi: 10.1038/nature12107
- Yamaguchi M, Yoshihara K, Suda K, et al. Three-dimensional understanding of the morphological complexity of the human uterine endometrium. iScience. 2021;24:102258. doi: 10.1016/j.isci.2021.102258
- Vannuccini S, Tosti C, Carmona F, et al. Pathogenesis of adenomyosis: an update on molecular mechanisms. Reprod Biomed Online. 2017;35:592-601. doi: 10.1016 /j.rbmo.2017.06.016
- Zhai J, Vannuccini S, Petraglia F, et al. Adenomyosis: mechanisms and pathogenesis. Semin Reprod Med. 2020;38:129-143. doi: 10.1055/s-0040-1716687
- Munro MG. Uterine polyps, adenomyosis, leiomyomas, and endometrial receptivity. Fertil Steril. 2019;111:629-640. doi: 10.1016/j.fertnstert.2019.02.008
- Kay N, Huang C-Y, Shiu L-Y, et al. TGF-β1 neutralization improves pregnancy outcomes by restoring endometrial receptivity in mice with adenomyosis. Reprod Sci. 2021;28:877-887. doi: 10.1007/s43032-020-00308-1
- Habiba M, Benagiano G. Classifying adenomyosis: progress and challenges. Int J Environ Res Public Health. 2021;18:12386. doi: 10.3390/ijerph182312386
- Movilla P, Morris S, Isaacson K. A systematic review of tissue sampling techniques for the diagnosis of adenomyosis. J Minim Invasive Gynecol. 2020;27:344-351. doi: 10.1016 /j.jmig.2019.09.001
- Agostinho L, Cruz R, Osório F, et al. MRI for adenomyosis: a pictorial review. Insights Imaging. 2017;8:549-556. doi: 10.1007/s13244-017-0576-z
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod. 2001;16:2427-2433. doi: 10.1093/humrep/16.11.2427
- Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics. 1999;19:S147-S160. doi: 10.1148 /radiographics.19.suppl_1.g99oc13s147
- Rees CO, Nederend J, Mischi M, et al. Objective measures of adenomyosis on MRI and their diagnostic accuracy—a systematic review & meta-analysis. Acta Obstet Gynecol Scand. 2021;100:1377-1391.
- Chapron C, Vannuccini S, Santulli P, et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Hum Reprod Update. 2020;26:392-411. doi: 10.1093 /humupd/dmz049
- Liu L, Li W, Leonardi M, et al. Diagnostic accuracy of transvaginal ultrasound and magnetic resonance imaging for adenomyosis: systematic review and meta-analysis and review of sonographic diagnostic criteria. J Ultrasound Med. 2021;40:2289-2306. doi: 10.1002/jum.15635
- Bazot M, Daraï E. Role of transvaginal sonography and magnetic resonance imaging in the diagnosis of uterine adenomyosis. Fertil Steril. 2018;109:389-397. doi: 10.1016 /j.fertnstert.2018.01.024
- Van den Bosch T, Dueholm M, Leone FPG, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet Gynecol. 2015;46:284-298. doi: 10.1002/uog.14806
- Săsăran V, Turdean S, Gliga M, et al. Value of strainratio elastography in the diagnosis and differentiation of uterine fibroids and adenomyosis. J Pers Med. 2021;11:824. doi: 10.3390/jpm11080824
- Di Spiezio Sardo A, Calagna G, Santangelo F, et al. The role of hysteroscopy in the diagnosis and treatment of adenomyosis. Biomed Res Int. 2017;2017:2518396. doi: 10.1155/2017/2518396
- Azzi R. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-235.
- Parker JD, Leondires M, Sinaii N, et al. Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis. Fertil Steril. 2006;86:711-715. doi: 10.1016/j.fertnstert.2006.01.030
- Martire FG, Lazzeri L, Conway F, et al. Adolescence and endometriosis: symptoms, ultrasound signs and early diagnosis. Fertil Steril. 2020;114:1049-1057. doi: 10.1016 /j.fertnstert.2020.06.012
- Decter D, Arbib N, Markovitz H, et al. Sonographic signs of adenomyosis in women with endometriosis are associated with infertility. J Clin Med. 2021;10:2355. doi: 10.3390 /jcm10112355
- Brucker SY, Huebner M, Wallwiener M, et al. Clinical characteristics indicating adenomyosis coexisting with leiomyomas: a retrospective, questionnaire-based study. Fertil Steril. 2014;101:237-241.e1. doi: 10.1016 /j.fertnstert.2013.09.038
- Perelló MF, Martínez-Zamora MÁ, Torres X, et al. Endometriotic pain is associated with adenomyosis but not with the compartments affected by deep infiltrating endometriosis. Gynecol Obstet Invest. 2017;82:240-246. doi: 10.1159/000447633
- Younes G, Tulandi T. Effects of adenomyosis on in vitro fertilization treatment outcomes: a metaanalysis. Fertil Steril. 2017;108:483-490.e3. doi: 10.1016 /j.fertnstert.2017.06.025
- Nirgianakis K, Kalaitzopoulos DR, Schwartz ASK, et al. Fertility, pregnancy and neonatal outcomes of patients with adenomyosis: a systematic review and meta-analysis. Reprod BioMed Online. 2021;42:185-206. doi: 10.1016 /j.rbmo.2020.09.023
- Ono Y, Ota H, Takimoto K, et al. Perinatal outcomes associated with the positional relationship between the placenta and the adenomyosis lesion. J Gynecol Obstet Hum Reprod. 2021;50:102114. doi: 10.1016/j.jogoh.2021.102114
- Barrier BF, Malinowski MJ, Dick EJ Jr, et al. Adenomyosis in the baboon is associated with primary infertility. Fertil Steril. 2004;82(suppl 3):1091-1094. doi: 10.1016 /j.fertnstert.2003.11.065
- Vercellini P, Consonni D, Barbara G, et al. Adenomyosis and reproductive performance after surgery for rectovaginal and colorectal endometriosis: a systematic review and meta-analysis. Reprod Biomed Online. 2014;28:704-713. doi: 10.1016/j.rbmo.2014.02.006
- Exacoustos C, Lazzeri L, Martire FG, et al. Ultrasound findings of adenomyosis in adolescents: type and grade of the disease. J Minim Invasive Gynecol. 2021;29:291.e1-299.e1. doi: 10.1016/j.jmig.2021.08.023
- Loring M, Chen TY, Isaacson KB. A systematic review of adenomyosis: it is time to reassess what we thought we knew about the disease. J Minim Invasive Gynecol. 2021;28:644655. doi: 10.1016/j.jmig.2020.10.012
- Bourdon M, Santulli P, Oliveira J, et al. Focal adenomyosis is associated with primary infertility. Fertil Steril. 2020;114:1271-1277. doi: 10.1016/j.fertnstert.2020.06.018
- Lan J, Wu Y, Wu Z, et al. Ultra-long GnRH agonist protocol during IVF/ICSI improves pregnancy outcomes in women with adenomyosis: a retrospective cohort study. Front Endocrinol (Lausanne). 2021;12:609771. doi: 10.3389 /fendo.2021.609771
- Gnecco JS, Brown AT, Kan EL, et al. Physiomimetic models of adenomyosis. Semin Reprod Med. 2020;38:179-196. doi: 10.1055/s-0040-1719084
- Harmsen MJ, Trommelen LM, de Leeuw RA, et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound Obstet Gynecol. 2023;62:42-60. doi: 10.1002/uog.26117
- Xie T, Xu X, Yang Y, et al. The role of abnormal uterine junction zone in the occurrence and development of adenomyosis. Reprod Sci. 2022;29:2719-2730. doi: 10.1007/s43032-021 -00684-2
- Lazzeri L, Morosetti G, Centini G, et al. A sonographic classification of adenomyosis: interobserver reproducibility in the evaluation of type and degree of the myometrial involvement. Fertil Steril. 2018;110:1154-1161.e3. doi: 10.1016 /j.fertnstert.2018.06.031
- Tahlan A, Nanda A, Mohan H. Uterine adenomyoma: a clinicopathologic review of 26 cases and a review of the literature. Int J Gynecol Pathol. 2006;25:361-365. doi: 10.1097/01.pgp.0000209570.08716.b3
- Chung K, Wallace J, Kim S-Y, et al. Structural and molecular interrogation of intact biological systems. Nature. 2013;497:332-337. doi: 10.1038/nature12107
- Yamaguchi M, Yoshihara K, Suda K, et al. Three-dimensional understanding of the morphological complexity of the human uterine endometrium. iScience. 2021;24:102258. doi: 10.1016/j.isci.2021.102258
- Vannuccini S, Tosti C, Carmona F, et al. Pathogenesis of adenomyosis: an update on molecular mechanisms. Reprod Biomed Online. 2017;35:592-601. doi: 10.1016 /j.rbmo.2017.06.016
- Zhai J, Vannuccini S, Petraglia F, et al. Adenomyosis: mechanisms and pathogenesis. Semin Reprod Med. 2020;38:129-143. doi: 10.1055/s-0040-1716687
- Munro MG. Uterine polyps, adenomyosis, leiomyomas, and endometrial receptivity. Fertil Steril. 2019;111:629-640. doi: 10.1016/j.fertnstert.2019.02.008
- Kay N, Huang C-Y, Shiu L-Y, et al. TGF-β1 neutralization improves pregnancy outcomes by restoring endometrial receptivity in mice with adenomyosis. Reprod Sci. 2021;28:877-887. doi: 10.1007/s43032-020-00308-1
- Habiba M, Benagiano G. Classifying adenomyosis: progress and challenges. Int J Environ Res Public Health. 2021;18:12386. doi: 10.3390/ijerph182312386
- Movilla P, Morris S, Isaacson K. A systematic review of tissue sampling techniques for the diagnosis of adenomyosis. J Minim Invasive Gynecol. 2020;27:344-351. doi: 10.1016 /j.jmig.2019.09.001
- Agostinho L, Cruz R, Osório F, et al. MRI for adenomyosis: a pictorial review. Insights Imaging. 2017;8:549-556. doi: 10.1007/s13244-017-0576-z
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod. 2001;16:2427-2433. doi: 10.1093/humrep/16.11.2427
- Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics. 1999;19:S147-S160. doi: 10.1148 /radiographics.19.suppl_1.g99oc13s147
- Rees CO, Nederend J, Mischi M, et al. Objective measures of adenomyosis on MRI and their diagnostic accuracy—a systematic review & meta-analysis. Acta Obstet Gynecol Scand. 2021;100:1377-1391.
- Chapron C, Vannuccini S, Santulli P, et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Hum Reprod Update. 2020;26:392-411. doi: 10.1093 /humupd/dmz049
- Liu L, Li W, Leonardi M, et al. Diagnostic accuracy of transvaginal ultrasound and magnetic resonance imaging for adenomyosis: systematic review and meta-analysis and review of sonographic diagnostic criteria. J Ultrasound Med. 2021;40:2289-2306. doi: 10.1002/jum.15635
- Bazot M, Daraï E. Role of transvaginal sonography and magnetic resonance imaging in the diagnosis of uterine adenomyosis. Fertil Steril. 2018;109:389-397. doi: 10.1016 /j.fertnstert.2018.01.024
- Van den Bosch T, Dueholm M, Leone FPG, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet Gynecol. 2015;46:284-298. doi: 10.1002/uog.14806
- Săsăran V, Turdean S, Gliga M, et al. Value of strainratio elastography in the diagnosis and differentiation of uterine fibroids and adenomyosis. J Pers Med. 2021;11:824. doi: 10.3390/jpm11080824
- Di Spiezio Sardo A, Calagna G, Santangelo F, et al. The role of hysteroscopy in the diagnosis and treatment of adenomyosis. Biomed Res Int. 2017;2017:2518396. doi: 10.1155/2017/2518396
- Azzi R. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-235.
- Parker JD, Leondires M, Sinaii N, et al. Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis. Fertil Steril. 2006;86:711-715. doi: 10.1016/j.fertnstert.2006.01.030
- Martire FG, Lazzeri L, Conway F, et al. Adolescence and endometriosis: symptoms, ultrasound signs and early diagnosis. Fertil Steril. 2020;114:1049-1057. doi: 10.1016 /j.fertnstert.2020.06.012
- Decter D, Arbib N, Markovitz H, et al. Sonographic signs of adenomyosis in women with endometriosis are associated with infertility. J Clin Med. 2021;10:2355. doi: 10.3390 /jcm10112355
- Brucker SY, Huebner M, Wallwiener M, et al. Clinical characteristics indicating adenomyosis coexisting with leiomyomas: a retrospective, questionnaire-based study. Fertil Steril. 2014;101:237-241.e1. doi: 10.1016 /j.fertnstert.2013.09.038
- Perelló MF, Martínez-Zamora MÁ, Torres X, et al. Endometriotic pain is associated with adenomyosis but not with the compartments affected by deep infiltrating endometriosis. Gynecol Obstet Invest. 2017;82:240-246. doi: 10.1159/000447633
- Younes G, Tulandi T. Effects of adenomyosis on in vitro fertilization treatment outcomes: a metaanalysis. Fertil Steril. 2017;108:483-490.e3. doi: 10.1016 /j.fertnstert.2017.06.025
- Nirgianakis K, Kalaitzopoulos DR, Schwartz ASK, et al. Fertility, pregnancy and neonatal outcomes of patients with adenomyosis: a systematic review and meta-analysis. Reprod BioMed Online. 2021;42:185-206. doi: 10.1016 /j.rbmo.2020.09.023
- Ono Y, Ota H, Takimoto K, et al. Perinatal outcomes associated with the positional relationship between the placenta and the adenomyosis lesion. J Gynecol Obstet Hum Reprod. 2021;50:102114. doi: 10.1016/j.jogoh.2021.102114
- Barrier BF, Malinowski MJ, Dick EJ Jr, et al. Adenomyosis in the baboon is associated with primary infertility. Fertil Steril. 2004;82(suppl 3):1091-1094. doi: 10.1016 /j.fertnstert.2003.11.065
- Vercellini P, Consonni D, Barbara G, et al. Adenomyosis and reproductive performance after surgery for rectovaginal and colorectal endometriosis: a systematic review and meta-analysis. Reprod Biomed Online. 2014;28:704-713. doi: 10.1016/j.rbmo.2014.02.006
Can we be too efficient?
“We were all of us cogs in a great machine which sometimes rolled forward, nobody knew where, sometimes backwards, nobody knew why.” – Ernst Toller
A nice feature of the Apple watch is the stopwatch. With it, I can discreetly click the timer and watch seconds tick away. Tap. There’s one lap. Tap. Two. Tap. That was a quick visit, 6 minutes and 42 seconds. Tap. Under 2 minutes to close the chart. Let’s see if I can beat it. Tap. Tap. What if I moved my Mayo stand over to this side of the room? How about a sign, “All patients must have clothes off if you want a skin exam.” You think ob.gyns. are quick from skin to baby in a stat C-section? You should see how fast I can go from alcohol wipe to Drysol on a biopsy. Seconds. Tick, tick, tap.
Every day I look for ways to go faster. This is not so I can be out the door by 3. Rather, it’s simply to make it through the day without having to log on after we put the kids to bed at night.
Speaking of bedtimes, another nice feature of the Apple watch is the timer. With it, I can set a timer and a lovely chimey alarm will go off. This comes in handy with 3-year-olds. “Sloan, in two minutes we are going to brush your teeth.” Ding. “Sloan, you have one minute to get your pajamas on.” Ding. “Sloanie, I’ll give you 3 more minutes to put the kitties away, then get into bed.” Ding, ding, ding ...
As you can see, using the stopwatch to time a bedtime routine would be demoralizing. If you’ve tried to put a toddler to bed in summer you know. They explore every option to avoid sleeping: one more book (that would make 3), “accidentally” putting their pajamas on backwards, offering to brush their teeth a second time. And once the light is off, “Papa, I have to potty.” No, bedtime routines cannot be standardized. They resist being made efficient.
In contrast, , Frederick Taylor. Taylor, a mechanical engineer, observed inefficiencies on the factory floor. His work was seminal in the development of the second industrial revolution. Before then no one had applied scientific rigor to productivity. His book, “The Principles of Scientific Management,” written in 1909, is considered the most influential management book of the 20th century. He was the first to use stopwatches to perform time studies, noting how long each task took with the belief that there was one best way. The worker was an extension of the machine, tuned by management such that he was as efficient as possible.

Others built on this idea including Frank and Lillian Gilbreth who added video recording, creating time and motion studies to further drive efficiency. This technique is still used in manufacturing and service industries today, including health care. In the 1980s, W. Edwards Deming modernized this effort, empowering workers with techniques taken from Japanese manufacturing. This, too, has been widely adopted in health care and evolved into the Lean and Lean Six Sigma quality movements about a decade ago. The common theme is to reduce waste to make health care as efficient as possible. Lately, this idea seems to have failed us.
The difficulty lies in the belief that efficient is always better. I’m unsure. Efficiency helps to reduce costs. It can also improve access. Yet, it comes at a cost. Eliminating slack concomitantly eliminates resilience. As such, when unexpected and significant changes impact a system, the gears of productivity jam. It’s in part why we are seeing rising wait times and patient dissatisfaction post pandemic. There was no slack and our system was too brittle.

A more insidious downside on the drive to efficiency lies in the nature of what we do. We aren’t factory workers punching out widgets, we’re physicians caring for people and people cannot be standardized. In this way, seeing patients is more like putting a toddler to bed than like assembling an iPhone. There will always be by-the-ways, basal cells hiding behind the ear, traffic jams, and bags of products that they want to review. Not sure how to use your fluorouracil? Let’s go over it again. Need to talk more about why you have granuloma annulare? Let me explain. Despite Taylor’s vision, some work simply cannot be optimized. And shouldn’t.
“Where’s my 11:30 patient who checked in half an hour ago?!” I asked my medical assistant. “Oh, she had to go to the bathroom.” Tap.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
“We were all of us cogs in a great machine which sometimes rolled forward, nobody knew where, sometimes backwards, nobody knew why.” – Ernst Toller
A nice feature of the Apple watch is the stopwatch. With it, I can discreetly click the timer and watch seconds tick away. Tap. There’s one lap. Tap. Two. Tap. That was a quick visit, 6 minutes and 42 seconds. Tap. Under 2 minutes to close the chart. Let’s see if I can beat it. Tap. Tap. What if I moved my Mayo stand over to this side of the room? How about a sign, “All patients must have clothes off if you want a skin exam.” You think ob.gyns. are quick from skin to baby in a stat C-section? You should see how fast I can go from alcohol wipe to Drysol on a biopsy. Seconds. Tick, tick, tap.
Every day I look for ways to go faster. This is not so I can be out the door by 3. Rather, it’s simply to make it through the day without having to log on after we put the kids to bed at night.
Speaking of bedtimes, another nice feature of the Apple watch is the timer. With it, I can set a timer and a lovely chimey alarm will go off. This comes in handy with 3-year-olds. “Sloan, in two minutes we are going to brush your teeth.” Ding. “Sloan, you have one minute to get your pajamas on.” Ding. “Sloanie, I’ll give you 3 more minutes to put the kitties away, then get into bed.” Ding, ding, ding ...
As you can see, using the stopwatch to time a bedtime routine would be demoralizing. If you’ve tried to put a toddler to bed in summer you know. They explore every option to avoid sleeping: one more book (that would make 3), “accidentally” putting their pajamas on backwards, offering to brush their teeth a second time. And once the light is off, “Papa, I have to potty.” No, bedtime routines cannot be standardized. They resist being made efficient.
In contrast, , Frederick Taylor. Taylor, a mechanical engineer, observed inefficiencies on the factory floor. His work was seminal in the development of the second industrial revolution. Before then no one had applied scientific rigor to productivity. His book, “The Principles of Scientific Management,” written in 1909, is considered the most influential management book of the 20th century. He was the first to use stopwatches to perform time studies, noting how long each task took with the belief that there was one best way. The worker was an extension of the machine, tuned by management such that he was as efficient as possible.
Others built on this idea including Frank and Lillian Gilbreth who added video recording, creating time and motion studies to further drive efficiency. This technique is still used in manufacturing and service industries today, including health care. In the 1980s, W. Edwards Deming modernized this effort, empowering workers with techniques taken from Japanese manufacturing. This, too, has been widely adopted in health care and evolved into the Lean and Lean Six Sigma quality movements about a decade ago. The common theme is to reduce waste to make health care as efficient as possible. Lately, this idea seems to have failed us.
The difficulty lies in the belief that efficient is always better. I’m unsure. Efficiency helps to reduce costs. It can also improve access. Yet, it comes at a cost. Eliminating slack concomitantly eliminates resilience. As such, when unexpected and significant changes impact a system, the gears of productivity jam. It’s in part why we are seeing rising wait times and patient dissatisfaction post pandemic. There was no slack and our system was too brittle.
A more insidious downside on the drive to efficiency lies in the nature of what we do. We aren’t factory workers punching out widgets, we’re physicians caring for people and people cannot be standardized. In this way, seeing patients is more like putting a toddler to bed than like assembling an iPhone. There will always be by-the-ways, basal cells hiding behind the ear, traffic jams, and bags of products that they want to review. Not sure how to use your fluorouracil? Let’s go over it again. Need to talk more about why you have granuloma annulare? Let me explain. Despite Taylor’s vision, some work simply cannot be optimized. And shouldn’t.
“Where’s my 11:30 patient who checked in half an hour ago?!” I asked my medical assistant. “Oh, she had to go to the bathroom.” Tap.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
“We were all of us cogs in a great machine which sometimes rolled forward, nobody knew where, sometimes backwards, nobody knew why.” – Ernst Toller
A nice feature of the Apple watch is the stopwatch. With it, I can discreetly click the timer and watch seconds tick away. Tap. There’s one lap. Tap. Two. Tap. That was a quick visit, 6 minutes and 42 seconds. Tap. Under 2 minutes to close the chart. Let’s see if I can beat it. Tap. Tap. What if I moved my Mayo stand over to this side of the room? How about a sign, “All patients must have clothes off if you want a skin exam.” You think ob.gyns. are quick from skin to baby in a stat C-section? You should see how fast I can go from alcohol wipe to Drysol on a biopsy. Seconds. Tick, tick, tap.
Every day I look for ways to go faster. This is not so I can be out the door by 3. Rather, it’s simply to make it through the day without having to log on after we put the kids to bed at night.
Speaking of bedtimes, another nice feature of the Apple watch is the timer. With it, I can set a timer and a lovely chimey alarm will go off. This comes in handy with 3-year-olds. “Sloan, in two minutes we are going to brush your teeth.” Ding. “Sloan, you have one minute to get your pajamas on.” Ding. “Sloanie, I’ll give you 3 more minutes to put the kitties away, then get into bed.” Ding, ding, ding ...
As you can see, using the stopwatch to time a bedtime routine would be demoralizing. If you’ve tried to put a toddler to bed in summer you know. They explore every option to avoid sleeping: one more book (that would make 3), “accidentally” putting their pajamas on backwards, offering to brush their teeth a second time. And once the light is off, “Papa, I have to potty.” No, bedtime routines cannot be standardized. They resist being made efficient.
In contrast, , Frederick Taylor. Taylor, a mechanical engineer, observed inefficiencies on the factory floor. His work was seminal in the development of the second industrial revolution. Before then no one had applied scientific rigor to productivity. His book, “The Principles of Scientific Management,” written in 1909, is considered the most influential management book of the 20th century. He was the first to use stopwatches to perform time studies, noting how long each task took with the belief that there was one best way. The worker was an extension of the machine, tuned by management such that he was as efficient as possible.
Others built on this idea including Frank and Lillian Gilbreth who added video recording, creating time and motion studies to further drive efficiency. This technique is still used in manufacturing and service industries today, including health care. In the 1980s, W. Edwards Deming modernized this effort, empowering workers with techniques taken from Japanese manufacturing. This, too, has been widely adopted in health care and evolved into the Lean and Lean Six Sigma quality movements about a decade ago. The common theme is to reduce waste to make health care as efficient as possible. Lately, this idea seems to have failed us.
The difficulty lies in the belief that efficient is always better. I’m unsure. Efficiency helps to reduce costs. It can also improve access. Yet, it comes at a cost. Eliminating slack concomitantly eliminates resilience. As such, when unexpected and significant changes impact a system, the gears of productivity jam. It’s in part why we are seeing rising wait times and patient dissatisfaction post pandemic. There was no slack and our system was too brittle.
A more insidious downside on the drive to efficiency lies in the nature of what we do. We aren’t factory workers punching out widgets, we’re physicians caring for people and people cannot be standardized. In this way, seeing patients is more like putting a toddler to bed than like assembling an iPhone. There will always be by-the-ways, basal cells hiding behind the ear, traffic jams, and bags of products that they want to review. Not sure how to use your fluorouracil? Let’s go over it again. Need to talk more about why you have granuloma annulare? Let me explain. Despite Taylor’s vision, some work simply cannot be optimized. And shouldn’t.
“Where’s my 11:30 patient who checked in half an hour ago?!” I asked my medical assistant. “Oh, she had to go to the bathroom.” Tap.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
What can you do during a mass shooting? This MD found out
Sunday night. Las Vegas. Jason Aldean had just started playing.
My wife and I were at the 2017 Route 91 Harvest Festival with three other couples; two of them were our close friends. We were sitting in the VIP section, a tented area right next to the stage. We started hearing what I was convinced were fireworks.
I’ve been in the Army for 20 some years. I’ve been deployed and shot at multiple times. But these shots were far away. And you don’t expect people to be shooting at you at a concert.
I was on the edge of the VIP area, so I could see around the corner of the tent. I looked up at the Mandalay Bay and saw the muzzle flash in the hotel window. That’s when I knew.
I screamed: “Somebody’s shooting at us! Everybody get down!”
It took a while for people to realize what was going on. When the first couple volleys sprayed into the crowd, nobody understood. But once enough people had been hit and dropped, everyone knew, and it was just mass exodus.
People screamed and ran everywhere. Some of them tried to jump over the front barrier so they could get underneath the stage. Others were trying to pick up loved ones who’d been shot.
The next 15 minutes are a little foggy. I was helping my wife and the people around us to get down. Funny things come back to you afterward. One of my friends was carrying a 16-ounce beer in his hand. Somebody’s shooting at him and he’s walking around with his beer like he’s afraid to put it down. It was so surreal.
We got everybody underneath the tent, and then we just sat there. There would be shooting and then a pause. You’d think it was over. And then there would be more shooting and another pause. It felt like it never was going to stop.
After a short period of time, somebody came in with an official badge, maybe FBI, who knows. They said: “Okay, everybody up. We’ve got to get you out of here.” So, we all got up and headed across the stage. The gate they were taking us to was in full view of the shooter, so it wasn’t very safe.
As I got up, I looked out at the field. Bodies were scattered everywhere. I’m a trauma surgeon by trade. I couldn’t just leave.
I told my two best friends to take my wife with them. My wife lost her mind at that point. She didn’t want me to run out on the field. But I had to. I saw the injured and they needed help. Another buddy and I jumped over the fence and started taking care of people.
The feeling of being out on the field was one of complete frustration. I was in sandals, shorts, and a t-shirt. We had no stretchers, no medical supplies, no nothing. I didn’t have a belt to use as a tourniquet. I didn’t even have a bandage.
Worse: We were seeing high-velocity gunshot wounds that I’ve seen for 20 years in the Army. I know how to take care of them. I know how to fix them. But there wasn’t a single thing I could do.
We had to get people off the field, so we started gathering up as many as we could. We didn’t know if we were going to get shot at again, so we were trying to hide behind things as we ran. Our main objective was just to get people to a place of safety.
A lot of it is a blur. But a few patients stick out in my mind.
A father and son. The father had been shot through the abdomen, exited out through his back. He was in severe pain and couldn’t walk.
A young girl shot in the arm. Her parents carrying her.
A group of people doing CPR on a young lady. She had a gunshot wound to the head or neck. She was obviously dead. But they were still doing chest compressions in the middle of the field. I had to say to them: “She’s dead. You can’t save her. You need to get off the field.” But they wouldn’t stop. We picked her up and took her out while they continued to do CPR.
Later, I realized I knew that woman. She was part of a group of friends that we would see at the festival. I hadn’t recognized her. I also didn’t know that my friend Marco was there. A month or 2 later, we figured out that he was one of the people doing CPR. And I was the guy who came up and said his friend was dead.
Some people were so badly injured we couldn’t lift them. We started tearing apart the fencing used to separate the crowd and slid sections of the barricades under the wounded to carry them. We also carried off a bunch of people who were dead.
We were moving patients to a covered bar area where we thought they would be safer. What we didn’t know was there was an ambulance rally point at the very far end of the field. Unfortunately, we had no idea it was there.
I saw a lot of other first responders out there, people from the fire department, corpsmen from the Navy, medics. I ran into an anesthesia provider and a series of nurses.
When we got everybody off the field, we started moving them into vehicles. People were bringing their trucks up. One guy even stole a truck so he could drive people to the ED. There wasn’t a lot of triage. We were just stacking whoever we could into the backs of these pickups.
I tried to help a nurse taking care of a lady who had been shot in the neck. She was sitting sort of half upright with the patient lying in her arms. When I reached to help her, she said: “You can’t move her.”
“We need to get her to the hospital,” I replied.
“This is the only position that this lady has an airway,” she said. “You’re going to have to move both of us together. If I move at all, she loses her airway.”
So, a group of us managed to slide something underneath and lift them into the back of a truck.
Loading the wounded went on for a while. And then, just like that, everybody was gone.
I walked back out onto this field which not too long ago held 30,000 people. It was as if aliens had just suddenly beamed everyone out.
There was stuff on the ground everywhere – blankets, clothing, single boots, wallets, purses. I walked past a food stand with food still cooking on the grill. There was a beer tap still running. It was the weirdest feeling I’d ever had in my life.
After that, things got a little crazy again. There had been a report of a second shooter, and no one knew if it was real or not. The police started herding a group of us across the street to the Tropicana. We were still trying to take cover as we walked there. We went past a big lion statue in front of one of the casinos. I have a picture from two years earlier of me sitting on the back of that lion. I remember thinking: Now I’m hunkered down behind the same lion hiding from a shooter. Times change.
They brought about 50 of us into a food court, which was closed. They wouldn’t tell us what was going on. And they wouldn’t let us leave. This went on for hours. Meanwhile, I had dropped my cell phone on the field, so my wife couldn’t get hold of me, and later she told me she assumed I’d been shot. I was just hoping that she was safe.
People were huddled together, crying, holding each other. Most were wearing Western concert–going stuff, which for a lot of them wasn’t very much clothing. The hotel eventually brought some blankets.
I was covered in blood. My shirt, shorts, and sandals were soaked. It was running down my legs. I couldn’t find anything to eat or drink. At one point, I sat down at a slot machine, put a hundred dollars in, and started playing slots. I didn’t know what else to do. It didn’t take me very long to lose it all.
Finally, I started looking for a way to get out. I checked all the exits, but there were security and police there. Then I ran into a guy who said he had found a fire exit. When we opened the fire door, there was a big security guard there, and he said: “You can’t leave.”
We said: “Try to stop us. We’re out of here.”
Another thing I’ll always remember – after I broke out of the Tropicana, I was low crawling through the bushes along the Strip toward my hotel. I got a block away and stood up to cross the street. I pushed the crosswalk button and waited. There were no cars, no people. I’ve just broken all the rules, violated police orders, and now I’m standing there waiting for a blinking light to allow me to cross the street!
I made it back to my hotel room around 3:30 or 4:00 in the morning. My wife was hysterical because I hadn’t been answering my cell phone. I came in, and she gave me a big hug, and I got in the shower. Our plane was leaving in a few hours, so we laid down, but didn’t sleep.
As we were getting ready to leave, my wife’s phone rang, and it was my number. A guy at the same hotel had found my phone on the field and called the “in case of emergency” number. So, I got my phone back.
It wasn’t easy to deal with the aftermath. It really affected everybody’s life. To this day, I’m particular about where we sit at concerts. My wife isn’t comfortable if she can’t see an exit. I now have a med bag in my car with tourniquets, pressure dressings, airway masks for CPR.
I’ll never forget that feeling of absolute frustration. That lady without an airway – I could’ve put a trach in her very quickly and made a difference. Were they able to keep her airway? Did she live?
The father and son – did the father make it? I have no idea what happened to any of them. Later, I went through and looked at the pictures of all the people who had died, but I couldn’t recognize anybody.
The hardest part was being there with my wife. I’ve been in places where people are shooting at you, in vehicles that are getting bombed. I’ve always believed that when it’s your time, it’s your time. If I get shot, well, okay, that happens. But if she got shot or my friends ... that would be really tough.
A year later, I gave a talk about it at a conference. I thought I had worked through everything. But all of those feelings, all of that helplessness, that anger, everything came roaring back to the surface again. They asked me how I deal with it, and I said: “Well ... poorly.” I’m the guy who sticks it in a box in the back of his brain, tucks it in and buries it with a bunch of other boxes, and hopes it never comes out again. But every once in a while, it does.
There were all kinds of people out on that field, some with medical training, some without, all determined to help, trying to get those injured people where they needed to be. In retrospect, it does make you feel good. Somebody was shooting at us, but people were still willing to stand up and risk their lives to help others.
We still talk with our friends about what happened that night. Over the years, it’s become less and less. But there’s still a text sent out every year on that day: “Today is the anniversary. Glad we’re all alive. Thanks for being our friends.”
Dr. Sebesta is a bariatric surgeon with MultiCare Health System in Tacoma, Wash.
A version of this article first appeared on Medscape.com.
Sunday night. Las Vegas. Jason Aldean had just started playing.
My wife and I were at the 2017 Route 91 Harvest Festival with three other couples; two of them were our close friends. We were sitting in the VIP section, a tented area right next to the stage. We started hearing what I was convinced were fireworks.
I’ve been in the Army for 20 some years. I’ve been deployed and shot at multiple times. But these shots were far away. And you don’t expect people to be shooting at you at a concert.
I was on the edge of the VIP area, so I could see around the corner of the tent. I looked up at the Mandalay Bay and saw the muzzle flash in the hotel window. That’s when I knew.
I screamed: “Somebody’s shooting at us! Everybody get down!”
It took a while for people to realize what was going on. When the first couple volleys sprayed into the crowd, nobody understood. But once enough people had been hit and dropped, everyone knew, and it was just mass exodus.
People screamed and ran everywhere. Some of them tried to jump over the front barrier so they could get underneath the stage. Others were trying to pick up loved ones who’d been shot.
The next 15 minutes are a little foggy. I was helping my wife and the people around us to get down. Funny things come back to you afterward. One of my friends was carrying a 16-ounce beer in his hand. Somebody’s shooting at him and he’s walking around with his beer like he’s afraid to put it down. It was so surreal.
We got everybody underneath the tent, and then we just sat there. There would be shooting and then a pause. You’d think it was over. And then there would be more shooting and another pause. It felt like it never was going to stop.
After a short period of time, somebody came in with an official badge, maybe FBI, who knows. They said: “Okay, everybody up. We’ve got to get you out of here.” So, we all got up and headed across the stage. The gate they were taking us to was in full view of the shooter, so it wasn’t very safe.
As I got up, I looked out at the field. Bodies were scattered everywhere. I’m a trauma surgeon by trade. I couldn’t just leave.
I told my two best friends to take my wife with them. My wife lost her mind at that point. She didn’t want me to run out on the field. But I had to. I saw the injured and they needed help. Another buddy and I jumped over the fence and started taking care of people.
The feeling of being out on the field was one of complete frustration. I was in sandals, shorts, and a t-shirt. We had no stretchers, no medical supplies, no nothing. I didn’t have a belt to use as a tourniquet. I didn’t even have a bandage.
Worse: We were seeing high-velocity gunshot wounds that I’ve seen for 20 years in the Army. I know how to take care of them. I know how to fix them. But there wasn’t a single thing I could do.
We had to get people off the field, so we started gathering up as many as we could. We didn’t know if we were going to get shot at again, so we were trying to hide behind things as we ran. Our main objective was just to get people to a place of safety.
A lot of it is a blur. But a few patients stick out in my mind.
A father and son. The father had been shot through the abdomen, exited out through his back. He was in severe pain and couldn’t walk.
A young girl shot in the arm. Her parents carrying her.
A group of people doing CPR on a young lady. She had a gunshot wound to the head or neck. She was obviously dead. But they were still doing chest compressions in the middle of the field. I had to say to them: “She’s dead. You can’t save her. You need to get off the field.” But they wouldn’t stop. We picked her up and took her out while they continued to do CPR.
Later, I realized I knew that woman. She was part of a group of friends that we would see at the festival. I hadn’t recognized her. I also didn’t know that my friend Marco was there. A month or 2 later, we figured out that he was one of the people doing CPR. And I was the guy who came up and said his friend was dead.
Some people were so badly injured we couldn’t lift them. We started tearing apart the fencing used to separate the crowd and slid sections of the barricades under the wounded to carry them. We also carried off a bunch of people who were dead.
We were moving patients to a covered bar area where we thought they would be safer. What we didn’t know was there was an ambulance rally point at the very far end of the field. Unfortunately, we had no idea it was there.
I saw a lot of other first responders out there, people from the fire department, corpsmen from the Navy, medics. I ran into an anesthesia provider and a series of nurses.
When we got everybody off the field, we started moving them into vehicles. People were bringing their trucks up. One guy even stole a truck so he could drive people to the ED. There wasn’t a lot of triage. We were just stacking whoever we could into the backs of these pickups.
I tried to help a nurse taking care of a lady who had been shot in the neck. She was sitting sort of half upright with the patient lying in her arms. When I reached to help her, she said: “You can’t move her.”
“We need to get her to the hospital,” I replied.
“This is the only position that this lady has an airway,” she said. “You’re going to have to move both of us together. If I move at all, she loses her airway.”
So, a group of us managed to slide something underneath and lift them into the back of a truck.
Loading the wounded went on for a while. And then, just like that, everybody was gone.
I walked back out onto this field which not too long ago held 30,000 people. It was as if aliens had just suddenly beamed everyone out.
There was stuff on the ground everywhere – blankets, clothing, single boots, wallets, purses. I walked past a food stand with food still cooking on the grill. There was a beer tap still running. It was the weirdest feeling I’d ever had in my life.
After that, things got a little crazy again. There had been a report of a second shooter, and no one knew if it was real or not. The police started herding a group of us across the street to the Tropicana. We were still trying to take cover as we walked there. We went past a big lion statue in front of one of the casinos. I have a picture from two years earlier of me sitting on the back of that lion. I remember thinking: Now I’m hunkered down behind the same lion hiding from a shooter. Times change.
They brought about 50 of us into a food court, which was closed. They wouldn’t tell us what was going on. And they wouldn’t let us leave. This went on for hours. Meanwhile, I had dropped my cell phone on the field, so my wife couldn’t get hold of me, and later she told me she assumed I’d been shot. I was just hoping that she was safe.
People were huddled together, crying, holding each other. Most were wearing Western concert–going stuff, which for a lot of them wasn’t very much clothing. The hotel eventually brought some blankets.
I was covered in blood. My shirt, shorts, and sandals were soaked. It was running down my legs. I couldn’t find anything to eat or drink. At one point, I sat down at a slot machine, put a hundred dollars in, and started playing slots. I didn’t know what else to do. It didn’t take me very long to lose it all.
Finally, I started looking for a way to get out. I checked all the exits, but there were security and police there. Then I ran into a guy who said he had found a fire exit. When we opened the fire door, there was a big security guard there, and he said: “You can’t leave.”
We said: “Try to stop us. We’re out of here.”
Another thing I’ll always remember – after I broke out of the Tropicana, I was low crawling through the bushes along the Strip toward my hotel. I got a block away and stood up to cross the street. I pushed the crosswalk button and waited. There were no cars, no people. I’ve just broken all the rules, violated police orders, and now I’m standing there waiting for a blinking light to allow me to cross the street!
I made it back to my hotel room around 3:30 or 4:00 in the morning. My wife was hysterical because I hadn’t been answering my cell phone. I came in, and she gave me a big hug, and I got in the shower. Our plane was leaving in a few hours, so we laid down, but didn’t sleep.
As we were getting ready to leave, my wife’s phone rang, and it was my number. A guy at the same hotel had found my phone on the field and called the “in case of emergency” number. So, I got my phone back.
It wasn’t easy to deal with the aftermath. It really affected everybody’s life. To this day, I’m particular about where we sit at concerts. My wife isn’t comfortable if she can’t see an exit. I now have a med bag in my car with tourniquets, pressure dressings, airway masks for CPR.
I’ll never forget that feeling of absolute frustration. That lady without an airway – I could’ve put a trach in her very quickly and made a difference. Were they able to keep her airway? Did she live?
The father and son – did the father make it? I have no idea what happened to any of them. Later, I went through and looked at the pictures of all the people who had died, but I couldn’t recognize anybody.
The hardest part was being there with my wife. I’ve been in places where people are shooting at you, in vehicles that are getting bombed. I’ve always believed that when it’s your time, it’s your time. If I get shot, well, okay, that happens. But if she got shot or my friends ... that would be really tough.
A year later, I gave a talk about it at a conference. I thought I had worked through everything. But all of those feelings, all of that helplessness, that anger, everything came roaring back to the surface again. They asked me how I deal with it, and I said: “Well ... poorly.” I’m the guy who sticks it in a box in the back of his brain, tucks it in and buries it with a bunch of other boxes, and hopes it never comes out again. But every once in a while, it does.
There were all kinds of people out on that field, some with medical training, some without, all determined to help, trying to get those injured people where they needed to be. In retrospect, it does make you feel good. Somebody was shooting at us, but people were still willing to stand up and risk their lives to help others.
We still talk with our friends about what happened that night. Over the years, it’s become less and less. But there’s still a text sent out every year on that day: “Today is the anniversary. Glad we’re all alive. Thanks for being our friends.”
Dr. Sebesta is a bariatric surgeon with MultiCare Health System in Tacoma, Wash.
A version of this article first appeared on Medscape.com.
Sunday night. Las Vegas. Jason Aldean had just started playing.
My wife and I were at the 2017 Route 91 Harvest Festival with three other couples; two of them were our close friends. We were sitting in the VIP section, a tented area right next to the stage. We started hearing what I was convinced were fireworks.
I’ve been in the Army for 20 some years. I’ve been deployed and shot at multiple times. But these shots were far away. And you don’t expect people to be shooting at you at a concert.
I was on the edge of the VIP area, so I could see around the corner of the tent. I looked up at the Mandalay Bay and saw the muzzle flash in the hotel window. That’s when I knew.
I screamed: “Somebody’s shooting at us! Everybody get down!”
It took a while for people to realize what was going on. When the first couple volleys sprayed into the crowd, nobody understood. But once enough people had been hit and dropped, everyone knew, and it was just mass exodus.
People screamed and ran everywhere. Some of them tried to jump over the front barrier so they could get underneath the stage. Others were trying to pick up loved ones who’d been shot.
The next 15 minutes are a little foggy. I was helping my wife and the people around us to get down. Funny things come back to you afterward. One of my friends was carrying a 16-ounce beer in his hand. Somebody’s shooting at him and he’s walking around with his beer like he’s afraid to put it down. It was so surreal.
We got everybody underneath the tent, and then we just sat there. There would be shooting and then a pause. You’d think it was over. And then there would be more shooting and another pause. It felt like it never was going to stop.
After a short period of time, somebody came in with an official badge, maybe FBI, who knows. They said: “Okay, everybody up. We’ve got to get you out of here.” So, we all got up and headed across the stage. The gate they were taking us to was in full view of the shooter, so it wasn’t very safe.
As I got up, I looked out at the field. Bodies were scattered everywhere. I’m a trauma surgeon by trade. I couldn’t just leave.
I told my two best friends to take my wife with them. My wife lost her mind at that point. She didn’t want me to run out on the field. But I had to. I saw the injured and they needed help. Another buddy and I jumped over the fence and started taking care of people.
The feeling of being out on the field was one of complete frustration. I was in sandals, shorts, and a t-shirt. We had no stretchers, no medical supplies, no nothing. I didn’t have a belt to use as a tourniquet. I didn’t even have a bandage.
Worse: We were seeing high-velocity gunshot wounds that I’ve seen for 20 years in the Army. I know how to take care of them. I know how to fix them. But there wasn’t a single thing I could do.
We had to get people off the field, so we started gathering up as many as we could. We didn’t know if we were going to get shot at again, so we were trying to hide behind things as we ran. Our main objective was just to get people to a place of safety.
A lot of it is a blur. But a few patients stick out in my mind.
A father and son. The father had been shot through the abdomen, exited out through his back. He was in severe pain and couldn’t walk.
A young girl shot in the arm. Her parents carrying her.
A group of people doing CPR on a young lady. She had a gunshot wound to the head or neck. She was obviously dead. But they were still doing chest compressions in the middle of the field. I had to say to them: “She’s dead. You can’t save her. You need to get off the field.” But they wouldn’t stop. We picked her up and took her out while they continued to do CPR.
Later, I realized I knew that woman. She was part of a group of friends that we would see at the festival. I hadn’t recognized her. I also didn’t know that my friend Marco was there. A month or 2 later, we figured out that he was one of the people doing CPR. And I was the guy who came up and said his friend was dead.
Some people were so badly injured we couldn’t lift them. We started tearing apart the fencing used to separate the crowd and slid sections of the barricades under the wounded to carry them. We also carried off a bunch of people who were dead.
We were moving patients to a covered bar area where we thought they would be safer. What we didn’t know was there was an ambulance rally point at the very far end of the field. Unfortunately, we had no idea it was there.
I saw a lot of other first responders out there, people from the fire department, corpsmen from the Navy, medics. I ran into an anesthesia provider and a series of nurses.
When we got everybody off the field, we started moving them into vehicles. People were bringing their trucks up. One guy even stole a truck so he could drive people to the ED. There wasn’t a lot of triage. We were just stacking whoever we could into the backs of these pickups.
I tried to help a nurse taking care of a lady who had been shot in the neck. She was sitting sort of half upright with the patient lying in her arms. When I reached to help her, she said: “You can’t move her.”
“We need to get her to the hospital,” I replied.
“This is the only position that this lady has an airway,” she said. “You’re going to have to move both of us together. If I move at all, she loses her airway.”
So, a group of us managed to slide something underneath and lift them into the back of a truck.
Loading the wounded went on for a while. And then, just like that, everybody was gone.
I walked back out onto this field which not too long ago held 30,000 people. It was as if aliens had just suddenly beamed everyone out.
There was stuff on the ground everywhere – blankets, clothing, single boots, wallets, purses. I walked past a food stand with food still cooking on the grill. There was a beer tap still running. It was the weirdest feeling I’d ever had in my life.
After that, things got a little crazy again. There had been a report of a second shooter, and no one knew if it was real or not. The police started herding a group of us across the street to the Tropicana. We were still trying to take cover as we walked there. We went past a big lion statue in front of one of the casinos. I have a picture from two years earlier of me sitting on the back of that lion. I remember thinking: Now I’m hunkered down behind the same lion hiding from a shooter. Times change.
They brought about 50 of us into a food court, which was closed. They wouldn’t tell us what was going on. And they wouldn’t let us leave. This went on for hours. Meanwhile, I had dropped my cell phone on the field, so my wife couldn’t get hold of me, and later she told me she assumed I’d been shot. I was just hoping that she was safe.
People were huddled together, crying, holding each other. Most were wearing Western concert–going stuff, which for a lot of them wasn’t very much clothing. The hotel eventually brought some blankets.
I was covered in blood. My shirt, shorts, and sandals were soaked. It was running down my legs. I couldn’t find anything to eat or drink. At one point, I sat down at a slot machine, put a hundred dollars in, and started playing slots. I didn’t know what else to do. It didn’t take me very long to lose it all.
Finally, I started looking for a way to get out. I checked all the exits, but there were security and police there. Then I ran into a guy who said he had found a fire exit. When we opened the fire door, there was a big security guard there, and he said: “You can’t leave.”
We said: “Try to stop us. We’re out of here.”
Another thing I’ll always remember – after I broke out of the Tropicana, I was low crawling through the bushes along the Strip toward my hotel. I got a block away and stood up to cross the street. I pushed the crosswalk button and waited. There were no cars, no people. I’ve just broken all the rules, violated police orders, and now I’m standing there waiting for a blinking light to allow me to cross the street!
I made it back to my hotel room around 3:30 or 4:00 in the morning. My wife was hysterical because I hadn’t been answering my cell phone. I came in, and she gave me a big hug, and I got in the shower. Our plane was leaving in a few hours, so we laid down, but didn’t sleep.
As we were getting ready to leave, my wife’s phone rang, and it was my number. A guy at the same hotel had found my phone on the field and called the “in case of emergency” number. So, I got my phone back.
It wasn’t easy to deal with the aftermath. It really affected everybody’s life. To this day, I’m particular about where we sit at concerts. My wife isn’t comfortable if she can’t see an exit. I now have a med bag in my car with tourniquets, pressure dressings, airway masks for CPR.
I’ll never forget that feeling of absolute frustration. That lady without an airway – I could’ve put a trach in her very quickly and made a difference. Were they able to keep her airway? Did she live?
The father and son – did the father make it? I have no idea what happened to any of them. Later, I went through and looked at the pictures of all the people who had died, but I couldn’t recognize anybody.
The hardest part was being there with my wife. I’ve been in places where people are shooting at you, in vehicles that are getting bombed. I’ve always believed that when it’s your time, it’s your time. If I get shot, well, okay, that happens. But if she got shot or my friends ... that would be really tough.
A year later, I gave a talk about it at a conference. I thought I had worked through everything. But all of those feelings, all of that helplessness, that anger, everything came roaring back to the surface again. They asked me how I deal with it, and I said: “Well ... poorly.” I’m the guy who sticks it in a box in the back of his brain, tucks it in and buries it with a bunch of other boxes, and hopes it never comes out again. But every once in a while, it does.
There were all kinds of people out on that field, some with medical training, some without, all determined to help, trying to get those injured people where they needed to be. In retrospect, it does make you feel good. Somebody was shooting at us, but people were still willing to stand up and risk their lives to help others.
We still talk with our friends about what happened that night. Over the years, it’s become less and less. But there’s still a text sent out every year on that day: “Today is the anniversary. Glad we’re all alive. Thanks for being our friends.”
Dr. Sebesta is a bariatric surgeon with MultiCare Health System in Tacoma, Wash.
A version of this article first appeared on Medscape.com.
The multitasking myth
, and that we are accomplishing more in less time. In fact, there is no credible evidence that this is true, and a mountain of evidence showing exactly the opposite.
According to this study and others, multitasking results in an average of 2 hours per day of lost productivity. It decreases the quality of work performed and increases cortisol levels, which impedes cognitive functioning, leading to a further decrease in productivity in a vicious cycle, making you increasingly ineffective and destroying your motivation and mood.

On the surface, the reasons for this are not intuitively obvious. After all, simple and routine tasks are easy to perform simultaneously; we can all walk and chew gum at the same time or eat a snack while watching TV. The problems arise when we try to multitask more complex tasks that require thought and decision-making.
It turns out that the pressures of our modern world have evolved faster than our brains. We are still hard-wired for monotasking. When we think we are completing two tasks simultaneously, we are actually performing individual actions in rapid succession. Each time you switch tasks, your brain must turn off the cognitive rules of the previous task and turn on new rules for the next one. When you switch back, the process repeats in reverse. Each of those mental gear shifts takes time and costs us productivity. According to one psychologist, even brief mental blocks created by shifting between tasks can cost as much as 40% of someone’s productive time. We are also far more likely to make mistakes while we are doing it.
Furthermore, you are stifling your creativity and innovation because you don’t focus on one task long enough to come up with original insights. Multitasking also slows down your general cognitive functions, in the same way that keeping many windows are open on your computer slows down the entire system. A study from my alma mater, the University of California, San Francisco, concluded that multitasking negativity affects memory in both younger and older adults (although the effects were greater in older adults) .
So, what to do? The fact remains that, all too often, there really are too many tasks and not enough hours in the day. How can you get through them without falling into the multitasking trap?
The first rule is to prioritize. In his book “The Seven Habits of Highly Effective People,” Stephen Covey makes an important distinction between tasks that are important and those that are merely urgent. Tasks that are important and urgent tend to make time for themselves, because they must be taken care of immediately.
Jobs that are important but not urgent are the ones we tend to try to multitask. Because there is no immediate deadline, we think we can do two or more of them simultaneously, or we fall into the other major productivity trap: procrastination. Neither of those strategies tends to end well. Identify those important but not urgent tasks and force yourself to go through them one by one.
Urgent but unimportant tasks are the productivity thieves. They demand your attention but are not worthy of it. Most tasks in this category can be delegated. I have written about physicians’ workaholic and perfectionist tendencies that drive our conviction that no one else can do anything as well as we can. Does that unimportant task, even if urgent, really demand your time, skills, education, and medical license? Is there someone in your office, or possibly an outside contractor, who could do it just as well, and maybe faster?
In fact, that is the question you should ask every time a project triggers your urge to multitask: “Who could be doing this job – or at least a major part of it – instead of me?”
If your multitasking urges are deeply ingrained – particularly those that involve phones, laptops, and the cloud – you might consider employing electronic aids. SelfControl, for example, is a free, open-sourced app that lets you block your own access to distracting websites, your email servers, social media, or anything else on the Internet. You list the sites you wish to block and set a period of time to block them. Until the set time expires, you will be unable to access those sites, even if you restart your computer or delete the application.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
, and that we are accomplishing more in less time. In fact, there is no credible evidence that this is true, and a mountain of evidence showing exactly the opposite.
According to this study and others, multitasking results in an average of 2 hours per day of lost productivity. It decreases the quality of work performed and increases cortisol levels, which impedes cognitive functioning, leading to a further decrease in productivity in a vicious cycle, making you increasingly ineffective and destroying your motivation and mood.
On the surface, the reasons for this are not intuitively obvious. After all, simple and routine tasks are easy to perform simultaneously; we can all walk and chew gum at the same time or eat a snack while watching TV. The problems arise when we try to multitask more complex tasks that require thought and decision-making.
It turns out that the pressures of our modern world have evolved faster than our brains. We are still hard-wired for monotasking. When we think we are completing two tasks simultaneously, we are actually performing individual actions in rapid succession. Each time you switch tasks, your brain must turn off the cognitive rules of the previous task and turn on new rules for the next one. When you switch back, the process repeats in reverse. Each of those mental gear shifts takes time and costs us productivity. According to one psychologist, even brief mental blocks created by shifting between tasks can cost as much as 40% of someone’s productive time. We are also far more likely to make mistakes while we are doing it.
Furthermore, you are stifling your creativity and innovation because you don’t focus on one task long enough to come up with original insights. Multitasking also slows down your general cognitive functions, in the same way that keeping many windows are open on your computer slows down the entire system. A study from my alma mater, the University of California, San Francisco, concluded that multitasking negativity affects memory in both younger and older adults (although the effects were greater in older adults) .
So, what to do? The fact remains that, all too often, there really are too many tasks and not enough hours in the day. How can you get through them without falling into the multitasking trap?
The first rule is to prioritize. In his book “The Seven Habits of Highly Effective People,” Stephen Covey makes an important distinction between tasks that are important and those that are merely urgent. Tasks that are important and urgent tend to make time for themselves, because they must be taken care of immediately.
Jobs that are important but not urgent are the ones we tend to try to multitask. Because there is no immediate deadline, we think we can do two or more of them simultaneously, or we fall into the other major productivity trap: procrastination. Neither of those strategies tends to end well. Identify those important but not urgent tasks and force yourself to go through them one by one.
Urgent but unimportant tasks are the productivity thieves. They demand your attention but are not worthy of it. Most tasks in this category can be delegated. I have written about physicians’ workaholic and perfectionist tendencies that drive our conviction that no one else can do anything as well as we can. Does that unimportant task, even if urgent, really demand your time, skills, education, and medical license? Is there someone in your office, or possibly an outside contractor, who could do it just as well, and maybe faster?
In fact, that is the question you should ask every time a project triggers your urge to multitask: “Who could be doing this job – or at least a major part of it – instead of me?”
If your multitasking urges are deeply ingrained – particularly those that involve phones, laptops, and the cloud – you might consider employing electronic aids. SelfControl, for example, is a free, open-sourced app that lets you block your own access to distracting websites, your email servers, social media, or anything else on the Internet. You list the sites you wish to block and set a period of time to block them. Until the set time expires, you will be unable to access those sites, even if you restart your computer or delete the application.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
, and that we are accomplishing more in less time. In fact, there is no credible evidence that this is true, and a mountain of evidence showing exactly the opposite.
According to this study and others, multitasking results in an average of 2 hours per day of lost productivity. It decreases the quality of work performed and increases cortisol levels, which impedes cognitive functioning, leading to a further decrease in productivity in a vicious cycle, making you increasingly ineffective and destroying your motivation and mood.
On the surface, the reasons for this are not intuitively obvious. After all, simple and routine tasks are easy to perform simultaneously; we can all walk and chew gum at the same time or eat a snack while watching TV. The problems arise when we try to multitask more complex tasks that require thought and decision-making.
It turns out that the pressures of our modern world have evolved faster than our brains. We are still hard-wired for monotasking. When we think we are completing two tasks simultaneously, we are actually performing individual actions in rapid succession. Each time you switch tasks, your brain must turn off the cognitive rules of the previous task and turn on new rules for the next one. When you switch back, the process repeats in reverse. Each of those mental gear shifts takes time and costs us productivity. According to one psychologist, even brief mental blocks created by shifting between tasks can cost as much as 40% of someone’s productive time. We are also far more likely to make mistakes while we are doing it.
Furthermore, you are stifling your creativity and innovation because you don’t focus on one task long enough to come up with original insights. Multitasking also slows down your general cognitive functions, in the same way that keeping many windows are open on your computer slows down the entire system. A study from my alma mater, the University of California, San Francisco, concluded that multitasking negativity affects memory in both younger and older adults (although the effects were greater in older adults) .
So, what to do? The fact remains that, all too often, there really are too many tasks and not enough hours in the day. How can you get through them without falling into the multitasking trap?
The first rule is to prioritize. In his book “The Seven Habits of Highly Effective People,” Stephen Covey makes an important distinction between tasks that are important and those that are merely urgent. Tasks that are important and urgent tend to make time for themselves, because they must be taken care of immediately.
Jobs that are important but not urgent are the ones we tend to try to multitask. Because there is no immediate deadline, we think we can do two or more of them simultaneously, or we fall into the other major productivity trap: procrastination. Neither of those strategies tends to end well. Identify those important but not urgent tasks and force yourself to go through them one by one.
Urgent but unimportant tasks are the productivity thieves. They demand your attention but are not worthy of it. Most tasks in this category can be delegated. I have written about physicians’ workaholic and perfectionist tendencies that drive our conviction that no one else can do anything as well as we can. Does that unimportant task, even if urgent, really demand your time, skills, education, and medical license? Is there someone in your office, or possibly an outside contractor, who could do it just as well, and maybe faster?
In fact, that is the question you should ask every time a project triggers your urge to multitask: “Who could be doing this job – or at least a major part of it – instead of me?”
If your multitasking urges are deeply ingrained – particularly those that involve phones, laptops, and the cloud – you might consider employing electronic aids. SelfControl, for example, is a free, open-sourced app that lets you block your own access to distracting websites, your email servers, social media, or anything else on the Internet. You list the sites you wish to block and set a period of time to block them. Until the set time expires, you will be unable to access those sites, even if you restart your computer or delete the application.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

New studies inform best practices for pelvic organ prolapse
“Approximately one in five women will undergo surgery for prolapse and/or urinary incontinence by the age of 80, which is more likely than the risk of developing breast cancer,” said David D. Rahn, MD, corresponding author of the study on perioperative vaginal estrogen, in an interview.

“About 13% of women will specifically undergo surgery to repair pelvic organ prolapse,” said Dr. Rahn, of the department of obstetrics and gynecology, University of Texas Southwestern Medical Center, Dallas. Reoperation for recurrent prolapse is not uncommon.
In their study, Dr. Rahn and colleagues examined whether the addition of perioperative vaginal estrogen cream in postmenopausal women with prolapse planning surgical correction could both strengthen the repair and lessen the likelihood of recurrence. The researchers randomized 206 postmenopausal women who were seeking surgical repair for bothersome anterior and apical vaginal prolapse to 1 gram of conjugated estrogen cream or a placebo for nightly vaginal insertion for 2 weeks, then twice weekly for at least 5 weeks of preoperative use. The treatment continued twice weekly for 12 months following surgery.
The primary outcome was the time to a failed prolapse repair by 12 months after surgery. Failure was defined by at least one of three criteria, “anatomical/objective prolapse of anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment,” the researchers wrote. The mean age of the patients was 65 years, and 90% and 92% of patients in the treatment and placebo groups, respectively, were White; 10% and 5%, respectively, were Black. Other baseline characteristics were similar between the groups.
After 12 months, the surgical failure incidence was not significantly different between the vaginal estrogen and placebo groups (19% vs. 9%, respectively; adjusted hazard ratio, 1.97).
Overall, anatomic recurrence was the most common outcome associated with surgical failure.
However, vaginal atrophy scores for most bothersome symptom was significantly better at 12 months in the vaginal estrogen group, compared with the placebo group, in a subset of 109 patients who reported vaginal atrophy that was at least “moderately bothersome,” the researchers said.
The findings were limited by several factors including the use of a nonvalidated instrument to assess secondary outcomes, the potentially short time period to the primary outcome, and the inclusion of the apex descending below one third total vaginal length as a criterion for surgical failure (which could be considered conservative), the researchers noted.
Unexpected results
“This work followed logically from a pilot study that similarly randomized postmenopausal women with prolapse planning surgical repair to vaginal estrogen cream versus placebo,” Dr. Rahn said. “In that smaller study, full thickness vaginal wall biopsies were collected at the time of surgery. Those participants who received the estrogen had a thicker vaginal epithelium, thicker underlying muscularis, and appeared to have a more robust concentration of strong connective tissue (i.e., type I collagen) with less of the proteases that break down connective tissue.”
This suggested that preoperative estrogen might optimize the vaginal tissue at the time of the repair. Dr. Rahn said. However, “despite evidence that the application of vaginal estrogen cream decreased the symptoms and signs of atrophic vaginal tissues, this did not lessen the likelihood of pelvic organ prolapse recurrence 12 months after surgical repair.”
The current study “would argue against routine prescription of vaginal estrogen to optimize vaginal tissue for prolapse repair, a practice that is recommended by some experts and commonly prescribed anecdotally,” said Dr. Rahn. “However, in those patients with prolapse and bothersome atrophy-related complaints such as vaginal dryness and pain with intercourse, vaginal estrogen may still be appropriate,” and vaginal estrogen also could be useful for postoperatively for patients prone to recurrent urinary tract infections.
Additional research from the study is underway, said Dr. Rahn. “All participants have now been followed to 3 years after surgery, and those clinical results are now being analyzed. In addition, full-thickness vaginal wall biopsies were collected at the time of all 186 surgeries; these are being analyzed and may yield important information regarding how biomarkers for connective tissue health could point to increased (or decreased) risk for prolapse recurrence.”
Manchester technique surpasses sacrospinous hysteropexy
In the second JAMA study, sacrospinous hysteropexy for uterine-sparing surgical management of uterine prolapse was less effective than the older Manchester procedure, based on data from nearly 400 individuals.
“Until now, the optimal uterus-sparing procedure for the treatment of uterine descent remained uncertain,” lead author Rosa Enklaar, MD, of Radboud (the Netherlands) University Medical Center, said in an interview.

“Globally, there has been a lack of scientific evidence comparing the efficacy of these two techniques, and this study aims to bridge that gap,” she said.
In their study, Dr. Enklaar and colleagues randomized 215 women to sacrospinous hysteropexy and 215 to the Manchester procedure. The mean age of the participants was 61.7 years.
The Manchester procedure involves “extraperitoneal plication of the uterosacral ligaments at the posterior side of the uterus and amputation of the cervix,” and “the cardinal ligaments are plicated on the anterior side of the cervix, “ the researchers wrote.
The primary outcome was a composite outcome of surgical success at 2 years after surgery, defined as the absence of three elements: absence of vaginal prolapse beyond the hymen, absence of bothersome bulge symptoms, and absence of retreatment of current prolapse.
Overall, 87.3% of patients in the Manchester group and 77.0% in the sacrospinous hysteropexy group met the primary outcome. At the end of the 2-year follow-up period, perioperative and patient-reported outcomes were not significantly different between the groups.
Dr. Enklaar said she was surprised by the findings. “At the start of this study, we hypothesized that there would be no difference between the two techniques,” as both have been used for a long period of time.
However, “based on the composite outcome of success at 2-year follow-up after the primary uterus-sparing surgery for uterine descent in patients with pelvic organ prolapse, these findings indicate that the sacrospinous hysteropexy is inferior to the Manchester procedure,” she said.
The study findings were limited by several factors including the lack of blinding and the applicability of the results only to women without uterine prolapse past the hymen, as well as the exclusion of patients with higher-stage prolapse, the researchers said. However, the results suggest that sacrospinous hysteropexy is inferior to the Manchester technique for uterine-sparing pelvic organ prolapse surgery.
As for additional research, few studies of prolapse surgery with long-term follow-up data are available, Dr. Enklaar said. “It is important that this current study will be continued to see the results after a longer follow-up period. Personalized health care is increasingly important, and we need to provide adequate information when counselling patients. With studies such as this one, we hope to improve the choices regarding surgical treatment of uterine descent.”
Studies challenge current prolapse protocols
The study by Dr. Rahn and colleagues contradicts the common clinical practice of preoperative vaginal estrogen to reduce recurrence of prolapse, wrote Charles W. Nager, MD, of the University of California San Diego Health, La Jolla, in an accompanying editorial that addressed both studies.
The results suggest that use of perioperative intravaginal estrogen had no impact on outcomes, “despite the surgeon assessment of less atrophy and better vaginal apex tissue in the estrogen group,” he noted. Although vaginal estrogen has other benefits in terms of patient symptoms and effects on the vaginal epithelium, “surgeons should not prescribe vaginal estrogen with the expectation that it will improve surgical success.”
The study by Dr. Enklaar and colleagues reflects the growing interest in uterine-conserving procedures, Dr. Nager wrote. The modified Manchester procedure conforms to professional society guidelines, and the composite outcome conforms to current standards for the treatment of pelvic organ prolapse.
Although suspension of the vaginal apex was quite successful, the researchers interpreted their noninferiority findings with caution, said Dr. Nager. However, they suggested that the modified Manchester procedure as performed in their study “has a role in modern prolapse surgical repair for women with uterine descent that does not protrude beyond the hymen.”
The vaginal estrogen study was supported by the National Institute on Aging, a Bridge Award from the American Board of Obstetrics & Gynecology and the American Association of Obstetricians and Gynecologists Foundation. Dr. Rahn disclosed grants from the National Institute on Aging, the American Board of Obstetrics & Gynecology, and the AAOGF bridge award, as well as nonfinancial support from National Center for Advancing Translational Sciences and Pfizer during the study. The uterine prolapse study was supported by the Netherlands Organisation for Health Research and Development. The researchers had no financial conflicts to disclose. Dr. Nager had no financial conflicts to disclose.
“Approximately one in five women will undergo surgery for prolapse and/or urinary incontinence by the age of 80, which is more likely than the risk of developing breast cancer,” said David D. Rahn, MD, corresponding author of the study on perioperative vaginal estrogen, in an interview.
“About 13% of women will specifically undergo surgery to repair pelvic organ prolapse,” said Dr. Rahn, of the department of obstetrics and gynecology, University of Texas Southwestern Medical Center, Dallas. Reoperation for recurrent prolapse is not uncommon.
In their study, Dr. Rahn and colleagues examined whether the addition of perioperative vaginal estrogen cream in postmenopausal women with prolapse planning surgical correction could both strengthen the repair and lessen the likelihood of recurrence. The researchers randomized 206 postmenopausal women who were seeking surgical repair for bothersome anterior and apical vaginal prolapse to 1 gram of conjugated estrogen cream or a placebo for nightly vaginal insertion for 2 weeks, then twice weekly for at least 5 weeks of preoperative use. The treatment continued twice weekly for 12 months following surgery.
The primary outcome was the time to a failed prolapse repair by 12 months after surgery. Failure was defined by at least one of three criteria, “anatomical/objective prolapse of anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment,” the researchers wrote. The mean age of the patients was 65 years, and 90% and 92% of patients in the treatment and placebo groups, respectively, were White; 10% and 5%, respectively, were Black. Other baseline characteristics were similar between the groups.
After 12 months, the surgical failure incidence was not significantly different between the vaginal estrogen and placebo groups (19% vs. 9%, respectively; adjusted hazard ratio, 1.97).
Overall, anatomic recurrence was the most common outcome associated with surgical failure.
However, vaginal atrophy scores for most bothersome symptom was significantly better at 12 months in the vaginal estrogen group, compared with the placebo group, in a subset of 109 patients who reported vaginal atrophy that was at least “moderately bothersome,” the researchers said.
The findings were limited by several factors including the use of a nonvalidated instrument to assess secondary outcomes, the potentially short time period to the primary outcome, and the inclusion of the apex descending below one third total vaginal length as a criterion for surgical failure (which could be considered conservative), the researchers noted.
Unexpected results
“This work followed logically from a pilot study that similarly randomized postmenopausal women with prolapse planning surgical repair to vaginal estrogen cream versus placebo,” Dr. Rahn said. “In that smaller study, full thickness vaginal wall biopsies were collected at the time of surgery. Those participants who received the estrogen had a thicker vaginal epithelium, thicker underlying muscularis, and appeared to have a more robust concentration of strong connective tissue (i.e., type I collagen) with less of the proteases that break down connective tissue.”
This suggested that preoperative estrogen might optimize the vaginal tissue at the time of the repair. Dr. Rahn said. However, “despite evidence that the application of vaginal estrogen cream decreased the symptoms and signs of atrophic vaginal tissues, this did not lessen the likelihood of pelvic organ prolapse recurrence 12 months after surgical repair.”
The current study “would argue against routine prescription of vaginal estrogen to optimize vaginal tissue for prolapse repair, a practice that is recommended by some experts and commonly prescribed anecdotally,” said Dr. Rahn. “However, in those patients with prolapse and bothersome atrophy-related complaints such as vaginal dryness and pain with intercourse, vaginal estrogen may still be appropriate,” and vaginal estrogen also could be useful for postoperatively for patients prone to recurrent urinary tract infections.
Additional research from the study is underway, said Dr. Rahn. “All participants have now been followed to 3 years after surgery, and those clinical results are now being analyzed. In addition, full-thickness vaginal wall biopsies were collected at the time of all 186 surgeries; these are being analyzed and may yield important information regarding how biomarkers for connective tissue health could point to increased (or decreased) risk for prolapse recurrence.”
Manchester technique surpasses sacrospinous hysteropexy
In the second JAMA study, sacrospinous hysteropexy for uterine-sparing surgical management of uterine prolapse was less effective than the older Manchester procedure, based on data from nearly 400 individuals.
“Until now, the optimal uterus-sparing procedure for the treatment of uterine descent remained uncertain,” lead author Rosa Enklaar, MD, of Radboud (the Netherlands) University Medical Center, said in an interview.
“Globally, there has been a lack of scientific evidence comparing the efficacy of these two techniques, and this study aims to bridge that gap,” she said.
In their study, Dr. Enklaar and colleagues randomized 215 women to sacrospinous hysteropexy and 215 to the Manchester procedure. The mean age of the participants was 61.7 years.
The Manchester procedure involves “extraperitoneal plication of the uterosacral ligaments at the posterior side of the uterus and amputation of the cervix,” and “the cardinal ligaments are plicated on the anterior side of the cervix, “ the researchers wrote.
The primary outcome was a composite outcome of surgical success at 2 years after surgery, defined as the absence of three elements: absence of vaginal prolapse beyond the hymen, absence of bothersome bulge symptoms, and absence of retreatment of current prolapse.
Overall, 87.3% of patients in the Manchester group and 77.0% in the sacrospinous hysteropexy group met the primary outcome. At the end of the 2-year follow-up period, perioperative and patient-reported outcomes were not significantly different between the groups.
Dr. Enklaar said she was surprised by the findings. “At the start of this study, we hypothesized that there would be no difference between the two techniques,” as both have been used for a long period of time.
However, “based on the composite outcome of success at 2-year follow-up after the primary uterus-sparing surgery for uterine descent in patients with pelvic organ prolapse, these findings indicate that the sacrospinous hysteropexy is inferior to the Manchester procedure,” she said.
The study findings were limited by several factors including the lack of blinding and the applicability of the results only to women without uterine prolapse past the hymen, as well as the exclusion of patients with higher-stage prolapse, the researchers said. However, the results suggest that sacrospinous hysteropexy is inferior to the Manchester technique for uterine-sparing pelvic organ prolapse surgery.
As for additional research, few studies of prolapse surgery with long-term follow-up data are available, Dr. Enklaar said. “It is important that this current study will be continued to see the results after a longer follow-up period. Personalized health care is increasingly important, and we need to provide adequate information when counselling patients. With studies such as this one, we hope to improve the choices regarding surgical treatment of uterine descent.”
Studies challenge current prolapse protocols
The study by Dr. Rahn and colleagues contradicts the common clinical practice of preoperative vaginal estrogen to reduce recurrence of prolapse, wrote Charles W. Nager, MD, of the University of California San Diego Health, La Jolla, in an accompanying editorial that addressed both studies.
The results suggest that use of perioperative intravaginal estrogen had no impact on outcomes, “despite the surgeon assessment of less atrophy and better vaginal apex tissue in the estrogen group,” he noted. Although vaginal estrogen has other benefits in terms of patient symptoms and effects on the vaginal epithelium, “surgeons should not prescribe vaginal estrogen with the expectation that it will improve surgical success.”
The study by Dr. Enklaar and colleagues reflects the growing interest in uterine-conserving procedures, Dr. Nager wrote. The modified Manchester procedure conforms to professional society guidelines, and the composite outcome conforms to current standards for the treatment of pelvic organ prolapse.
Although suspension of the vaginal apex was quite successful, the researchers interpreted their noninferiority findings with caution, said Dr. Nager. However, they suggested that the modified Manchester procedure as performed in their study “has a role in modern prolapse surgical repair for women with uterine descent that does not protrude beyond the hymen.”
The vaginal estrogen study was supported by the National Institute on Aging, a Bridge Award from the American Board of Obstetrics & Gynecology and the American Association of Obstetricians and Gynecologists Foundation. Dr. Rahn disclosed grants from the National Institute on Aging, the American Board of Obstetrics & Gynecology, and the AAOGF bridge award, as well as nonfinancial support from National Center for Advancing Translational Sciences and Pfizer during the study. The uterine prolapse study was supported by the Netherlands Organisation for Health Research and Development. The researchers had no financial conflicts to disclose. Dr. Nager had no financial conflicts to disclose.
“Approximately one in five women will undergo surgery for prolapse and/or urinary incontinence by the age of 80, which is more likely than the risk of developing breast cancer,” said David D. Rahn, MD, corresponding author of the study on perioperative vaginal estrogen, in an interview.
“About 13% of women will specifically undergo surgery to repair pelvic organ prolapse,” said Dr. Rahn, of the department of obstetrics and gynecology, University of Texas Southwestern Medical Center, Dallas. Reoperation for recurrent prolapse is not uncommon.
In their study, Dr. Rahn and colleagues examined whether the addition of perioperative vaginal estrogen cream in postmenopausal women with prolapse planning surgical correction could both strengthen the repair and lessen the likelihood of recurrence. The researchers randomized 206 postmenopausal women who were seeking surgical repair for bothersome anterior and apical vaginal prolapse to 1 gram of conjugated estrogen cream or a placebo for nightly vaginal insertion for 2 weeks, then twice weekly for at least 5 weeks of preoperative use. The treatment continued twice weekly for 12 months following surgery.
The primary outcome was the time to a failed prolapse repair by 12 months after surgery. Failure was defined by at least one of three criteria, “anatomical/objective prolapse of anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment,” the researchers wrote. The mean age of the patients was 65 years, and 90% and 92% of patients in the treatment and placebo groups, respectively, were White; 10% and 5%, respectively, were Black. Other baseline characteristics were similar between the groups.
After 12 months, the surgical failure incidence was not significantly different between the vaginal estrogen and placebo groups (19% vs. 9%, respectively; adjusted hazard ratio, 1.97).
Overall, anatomic recurrence was the most common outcome associated with surgical failure.
However, vaginal atrophy scores for most bothersome symptom was significantly better at 12 months in the vaginal estrogen group, compared with the placebo group, in a subset of 109 patients who reported vaginal atrophy that was at least “moderately bothersome,” the researchers said.
The findings were limited by several factors including the use of a nonvalidated instrument to assess secondary outcomes, the potentially short time period to the primary outcome, and the inclusion of the apex descending below one third total vaginal length as a criterion for surgical failure (which could be considered conservative), the researchers noted.
Unexpected results
“This work followed logically from a pilot study that similarly randomized postmenopausal women with prolapse planning surgical repair to vaginal estrogen cream versus placebo,” Dr. Rahn said. “In that smaller study, full thickness vaginal wall biopsies were collected at the time of surgery. Those participants who received the estrogen had a thicker vaginal epithelium, thicker underlying muscularis, and appeared to have a more robust concentration of strong connective tissue (i.e., type I collagen) with less of the proteases that break down connective tissue.”
This suggested that preoperative estrogen might optimize the vaginal tissue at the time of the repair. Dr. Rahn said. However, “despite evidence that the application of vaginal estrogen cream decreased the symptoms and signs of atrophic vaginal tissues, this did not lessen the likelihood of pelvic organ prolapse recurrence 12 months after surgical repair.”
The current study “would argue against routine prescription of vaginal estrogen to optimize vaginal tissue for prolapse repair, a practice that is recommended by some experts and commonly prescribed anecdotally,” said Dr. Rahn. “However, in those patients with prolapse and bothersome atrophy-related complaints such as vaginal dryness and pain with intercourse, vaginal estrogen may still be appropriate,” and vaginal estrogen also could be useful for postoperatively for patients prone to recurrent urinary tract infections.
Additional research from the study is underway, said Dr. Rahn. “All participants have now been followed to 3 years after surgery, and those clinical results are now being analyzed. In addition, full-thickness vaginal wall biopsies were collected at the time of all 186 surgeries; these are being analyzed and may yield important information regarding how biomarkers for connective tissue health could point to increased (or decreased) risk for prolapse recurrence.”
Manchester technique surpasses sacrospinous hysteropexy
In the second JAMA study, sacrospinous hysteropexy for uterine-sparing surgical management of uterine prolapse was less effective than the older Manchester procedure, based on data from nearly 400 individuals.
“Until now, the optimal uterus-sparing procedure for the treatment of uterine descent remained uncertain,” lead author Rosa Enklaar, MD, of Radboud (the Netherlands) University Medical Center, said in an interview.
“Globally, there has been a lack of scientific evidence comparing the efficacy of these two techniques, and this study aims to bridge that gap,” she said.
In their study, Dr. Enklaar and colleagues randomized 215 women to sacrospinous hysteropexy and 215 to the Manchester procedure. The mean age of the participants was 61.7 years.
The Manchester procedure involves “extraperitoneal plication of the uterosacral ligaments at the posterior side of the uterus and amputation of the cervix,” and “the cardinal ligaments are plicated on the anterior side of the cervix, “ the researchers wrote.
The primary outcome was a composite outcome of surgical success at 2 years after surgery, defined as the absence of three elements: absence of vaginal prolapse beyond the hymen, absence of bothersome bulge symptoms, and absence of retreatment of current prolapse.
Overall, 87.3% of patients in the Manchester group and 77.0% in the sacrospinous hysteropexy group met the primary outcome. At the end of the 2-year follow-up period, perioperative and patient-reported outcomes were not significantly different between the groups.
Dr. Enklaar said she was surprised by the findings. “At the start of this study, we hypothesized that there would be no difference between the two techniques,” as both have been used for a long period of time.
However, “based on the composite outcome of success at 2-year follow-up after the primary uterus-sparing surgery for uterine descent in patients with pelvic organ prolapse, these findings indicate that the sacrospinous hysteropexy is inferior to the Manchester procedure,” she said.
The study findings were limited by several factors including the lack of blinding and the applicability of the results only to women without uterine prolapse past the hymen, as well as the exclusion of patients with higher-stage prolapse, the researchers said. However, the results suggest that sacrospinous hysteropexy is inferior to the Manchester technique for uterine-sparing pelvic organ prolapse surgery.
As for additional research, few studies of prolapse surgery with long-term follow-up data are available, Dr. Enklaar said. “It is important that this current study will be continued to see the results after a longer follow-up period. Personalized health care is increasingly important, and we need to provide adequate information when counselling patients. With studies such as this one, we hope to improve the choices regarding surgical treatment of uterine descent.”
Studies challenge current prolapse protocols
The study by Dr. Rahn and colleagues contradicts the common clinical practice of preoperative vaginal estrogen to reduce recurrence of prolapse, wrote Charles W. Nager, MD, of the University of California San Diego Health, La Jolla, in an accompanying editorial that addressed both studies.
The results suggest that use of perioperative intravaginal estrogen had no impact on outcomes, “despite the surgeon assessment of less atrophy and better vaginal apex tissue in the estrogen group,” he noted. Although vaginal estrogen has other benefits in terms of patient symptoms and effects on the vaginal epithelium, “surgeons should not prescribe vaginal estrogen with the expectation that it will improve surgical success.”
The study by Dr. Enklaar and colleagues reflects the growing interest in uterine-conserving procedures, Dr. Nager wrote. The modified Manchester procedure conforms to professional society guidelines, and the composite outcome conforms to current standards for the treatment of pelvic organ prolapse.
Although suspension of the vaginal apex was quite successful, the researchers interpreted their noninferiority findings with caution, said Dr. Nager. However, they suggested that the modified Manchester procedure as performed in their study “has a role in modern prolapse surgical repair for women with uterine descent that does not protrude beyond the hymen.”
The vaginal estrogen study was supported by the National Institute on Aging, a Bridge Award from the American Board of Obstetrics & Gynecology and the American Association of Obstetricians and Gynecologists Foundation. Dr. Rahn disclosed grants from the National Institute on Aging, the American Board of Obstetrics & Gynecology, and the AAOGF bridge award, as well as nonfinancial support from National Center for Advancing Translational Sciences and Pfizer during the study. The uterine prolapse study was supported by the Netherlands Organisation for Health Research and Development. The researchers had no financial conflicts to disclose. Dr. Nager had no financial conflicts to disclose.
FROM JAMA
Intrauterine vacuum device treatment of postpartum hemorrhage
Postpartum hemorrhage (PPH) is a common complication of birth. In 2019, 4.3% of births in the United States were complicated by at least one episode of PPH.1 Major causes of PPH include uterine atony, retained products of conception, reproductive tract trauma, and coagulopathy.2 Active management of the third stage of labor with the routine administration of postpartum uterotonics reduces the risk of PPH.3,4
PPH treatment requires a systematic approach using appropriate uterotonic medications, tranexamic acid, and procedures performed in a timely sequence to resolve the hemorrhage. Following vaginal birth, procedures that do not require a laparotomy to treat PPH include uterine massage, uterine evacuation to remove retained placental tissue, repair of lacerations, uterine balloon tamponade (UBT), uterine packing, a vacuum-induced hemorrhage control device (VHCD; JADA, Organon), and uterine artery embolization. Following cesarean birth, with an open laparotomy incision, interventions to treat PPH due to atony include vascular ligation, uterine compression sutures, UBT, VHCD, hysterectomy, and pelvic packing.2
Over the past 2 decades, UBT has been widely used for the treatment of PPH with a success rate in observational studies of approximately 86%.5 The uterine balloon creates pressure against the wall of the uterus permitting accumulation of platelets at bleeding sites, enhancing the activity of the clotting system. The uterine balloon provides direct pressure on the bleeding site(s). It is well known in trauma care that the first step to treat a bleeding wound is to apply direct pressure to the bleeding site. During the third stage of labor, a natural process is tetanic uterine contraction, which constricts myometrial vessels and the placenta bed. Placing a balloon in the uterus and inflating the balloon to 200 mL to 500 mL may delay the involution of the uterus that should occur following birth. An observation of great interest is the insight that inducing a vacuum in the uterine cavity may enhance tetanic uterine contraction and constriction of the myometrial vessels. Vacuum-induced hemorrhage control is discussed in detail in this editorial.
Vacuum-induced hemorrhage control device
A new device for the treatment of PPH due to uterine atony is the JADA VHCD (FIGURE), which generates negative intrauterine pressure causing the uterus to contract, thereby constricting myometrial vessels and reducing uterine bleeding. The JADA VHCD system is indicated to provide control and treatment of abnormal postpartum uterine bleeding following vaginal or cesarean birth caused by uterine atony when conservative management is indicated.6
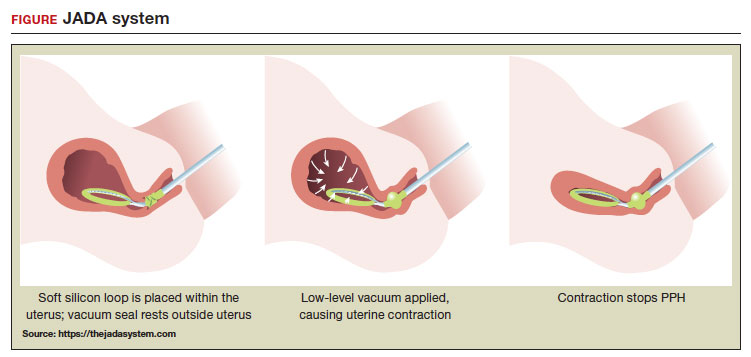 ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
System components
The JADA VHCD consists of a leading portion intended to be inserted into the uterine cavity, which consists of a silicone elliptical loop with 20 vacuum pores. A soft shield covers the vacuum loop to reduce the risk of the vacuum pores being clogged with biological material, including blood and clots. The elliptical loop is attached to a catheter intended for connection to a vacuum source set to 80 mm Hg ±10 mm Hg (hospital wall suction or portable suction device) with an in-line cannister to collect blood. Approximately 16 cm from the tip of the elliptical loop is a balloon that should be positioned in the upper vagina, not inside the cervix, and inflated with fluid (60 mL to 120 mL) through a dedicated port to occlude the vagina, thereby preserving a stable intrauterine vacuum.
Continue to: Correct usage...
Correct usage
A simple mnemonic to facilitate use of the JADA VHCD is “120/80”—fill the vaginal balloon with 120 mL of sterile fluid and attach the tubing to a source that is set to provide 80 mm Hg of vacuum with an in-line collection cannister. The VHCD may not work correctly if there is a substantial amount of blood in the uterus. Clinical experts advise that an important step prior to placing the elliptical loop in the uterus is to perform a sweep of the uterine cavity with a hand or instrument to remove clots and ensure there is no retained placental tissue. It is preferable to assemble the suction tubing, syringe, sterile fluid, and other instruments (eg, forceps, speculum) needed to insert the device prior to attempting to place the VHCD. When the elliptical loop is compressed for insertion, it is about 2 cm in diameter, necessitating that the cervix be dilated sufficiently to accommodate the device.
Immediately after placing the VHCD, contractions can be monitored by physical examination and the amount of ongoing bleeding can be estimated by observing the amount of blood accumulating in the cannister. Rapid onset of a palpable increase in uterine tone is a prominent feature of successful treatment of PPH with the VHCD. The VHCD should be kept in the uterus with active suction for at least 1 hour. Taping the tubing to the inner thigh may help stabilize the device. Once bleeding is controlled, prior to removing the device, the vacuum should be discontinued, and bleeding activityshould be assessed for at least 30 minutes. If the patient is stable, the vaginal balloon can be deflated, followed by removal of the device. The VHCD should be removed within 24 hours of placement.6
The JADA VHCD system should not be used with ongoing intrauterine pregnancy, untreated uterine rupture, unresolved uterine inversion, current cervical cancer, or serious infection of the uterus.6 The VHCD has not been evaluated for effectiveness in the treatment of placenta accreta or coagulopathy. The VHCD has not been specifically evaluated for safety and effectiveness in patients < 34 weeks’ duration, but clinicians report successful use of the device in cases of PPH that have occurred in the second and early-third trimesters. If the device can be appropriately placed with the elliptical loop in the uterus and the balloon in the vagina, it is theoretically possible to use the device for cases of PPH occurring before 34 weeks’ gestation.
When using the JADA VHCD system, it is important to simultaneously provide cardiovascular support, appropriate transfusion of blood products and timely surgical intervention, if indicated. All obstetricians know that in complicated cases of PPH, where conservative measures have not worked, uterine artery embolization or hysterectomy may be the only interventions that will prevent serious patient morbidity.
Effectiveness data
The VHCD has not been evaluated against an alternative approach, such as UBT, in published randomized clinical trials. However, prospective cohort studies have reported that the JADA is often successful in the treatment of PPH.7-10
In a multicenter cohort study of 107 patients with PPH, including 91 vaginal and 16 cesarean births, 100 patients (93%) were successfully treated with the JADA VHCD.7 Median blood loss before application of the system was 870 mL with vaginal birth and 1,300 mL with cesarean birth. Definitive control of the hemorrhage was observed at a median of 3 minutes after initiation of the intrauterine vacuum. In this study, 32% of patients had reproductive tract lacerations that needed to be repaired, and 2 patients required a hysterectomy. Forty patients required a blood transfusion.
Two patients were treated with a Bakri UBT when the VHCD did not resolve the PPH. In this cohort, the vacuum was applied for a median duration of 144 minutes, and a median total device dwell time was 191 minutes. Compared with UBT, the JADA VHCD intrauterine dwell time was shorter, facilitating patient progression and early transfer to the postpartum unit. The physicians who participated in the study reported that the device was easy to use. The complications reported in this cohort were minor and included endometritis (5 cases), vaginal infection (2 cases), and disruption of a vaginal laceration repair (1 case).7
Novel approaches to generating an intrauterine vacuum to treat PPH
The JADA VHCD is the only vacuum device approved by the US Food and Drug Administration (FDA) for treatment of PPH. However, clinical innovators have reported alternative approaches to generating an intrauterine vacuum using equipment designed for other purposes. In one study, a Bakri balloon was used to generate intrauterine vacuum tamponade to treat PPH.11 In this study, a Bakri balloon was inserted into the uterus, and the balloon was inflated to 50 mL to 100 mL to seal the vacuum. The main Bakri port was attached to a suction aspiration device set to generate a vacuum of 450 mm Hg to 525 mm Hg, a much greater vacuum than used with the JADA VHCD. This study included 44 cases of PPH due to uterine atony and 22 cases due to placental pathology, with successful treatment of PPH in 86% and 73% of the cases, respectively.
Another approach to generate intrauterine vacuum tamponade involves using a Levin stomach tube (FG24 or FG36), which has an open end and 4 side ports near the open tip.12-14 The Levin stomach tube is low cost and has many favorable design features, including a rounded tip, wide-bore, and circumferentially placed side ports. The FG36 Levin stomach tube is 12 mm in diameter and has 10 mm side ports. A vacuum device set to deliver 100 mm Hg to 200 mm Hgwas used in some of the studies evaluating the Levin stomach tube for the treatment of PPH. In 3 cases of severe PPH unresponsive to standard interventions, creation of vacuum tamponade with flexible suction tubing with side ports was successful in controlling the hemorrhage.13
Dr. T.N. Vasudeva Panicker invented an intrauterine cannula 12 mm in diameter and 25 cm in length, with dozens of 4 mm side ports over the distal 12 cm of the cannula.15 The cannula, which is made of stainless steel or plastic, is inserted into the uterus and 700 mm Hgvacuum is applied, a level much greater than the 80 mm Hg vacuum recommended for use with the JADA VHCD. When successful, the high suction clears the uterus of blood and causes uterine contraction. In 4 cases of severe PPH, the device successfully controlled the hemorrhage. In 2 of the 4 cases the device that was initially placed became clogged with blood and needed to be replaced.
UBT vs VHCD
To date there are no published randomized controlled trials comparing Bakri UBT to the JADA VHCD. In one retrospective study, the frequency of massive transfusion of red blood cells (RBCs), defined as the transfusion of 4 units or greater of RBCs, was assessed among 78 patients treated with the Bakri UBT and 36 patients treated with the JADA VHCD.9 In this study, at baseline there was a non ̶ statistically significant trend for JADA VHCD to be used more frequently than the Bakri UBT in cases of PPH occurring during repeat cesarean delivery (33% vs 14%). The Bakri UBT was used more frequently than the JADA VHCD among patients having a PPH following a vaginal delivery (51% vs 31%). Both devices were used at similar rates for operative vaginal delivery (6%) and primary cesarean birth (31% VHCD and 28% UBT).
In this retrospective study, the percentage of patients treated with VHCD or UBT who received 4 or more units of RBCs was 3% and 21%, respectively (P < .01). Among patients treated with VHCD and UBT, the estimated median blood loss was 1,500 mL and 1,850 mL (P=.02), respectively. The median hemoglobin concentration at discharge was similar in the VHCD and UBT groups, 8.8 g/dL and 8.6 g/dL, respectively.9 A randomized controlled trial is necessary to refine our understanding of the comparative effectiveness of UBT and VHCD in controlling PPH following vaginal and cesarean birth.
A welcome addition to treatment options
Every obstetrician knows that, in the next 12 months of their practice, they will encounter multiple cases of PPH. One or two of these cases may require the physician to use every medication and procedure available for the treatment of PPH to save the life of the patient. To prepare to treat the next case of PPH rapidly and effectively, it is important for every obstetrician to develop a standardized cognitive plan for using all available treatmentmodalities in an appropriate and timely sequence, including both the Bakri balloon and the JADA VHCD. The insight that inducing an intrauterine vacuum causes uterine contraction, which may resolve PPH, is an important discovery. The JADA VHCD is a welcome addition to our armamentarium of treatments for PPH. ●
- Corbetta-Rastelli CM, Friedman AM, Sobhani NC, et al. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstet Gynecol. 2023;141:152-161.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384:16351645.
- Salati JA, Leathersich SJ, Williams MJ, et al. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2019;CD001808.
- Begley CM, Gyte GMI, Devane D, et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;CD007412.
- Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222:293.e1-e52.
- US Food and Drug Administration. JADA system approval. Accessed July 25, 2023. https://www .accessdata.fda.gov/cdrh_docs/pdf21/K212757 .pdf
- D’Alton ME, Rood KM, Smid MC, et al. Intrauterine vacuum-induced hemorrhage control device for rapid treatment of postpartum hemorrhage. Obstet Gynecol. 2020;136:882-891.
- D’Alton M, Rood K, Simhan H, et al. Profile of the JADA System: the vacuum-induced hemorrhage control device for treating abnormal postpartum uterine bleeding and postpartum hemorrhage. Expert Rev Med Devices. 2021; 18:849-853.
- Gulersen M, Gerber RP, Rochelson B, et al. Vacuum-induced hemorrhage control versus uterine balloon tamponade for postpartum hemorrhage. J Obstet Gynaecol Can. 2023;45:267-272.
- Purwosunnu Y, Sarkoen W, Arulkumaran S, et al. Control of postpartum hemorrhage using vacuum-induced uterine tamponade. Obstet Gynecol. 2016;128:33-36.
- Haslinger C, Weber K, Zimmerman R. Vacuuminduced tamponade for treatment of postpartum hemorrhage. Obstet Gynecol. 2021;138:361-365.
- Hofmeyr GJ, Middleton K, Singata-Madliki M. Randomized feasibility study of suction-tube uterine tamponade for postpartum hemorrhage. Int J Gynaecol Obstet. 2019;146:339-343.
- Hofmeyr GJ, Singata-Madliki M. Novel suction tube uterine tamponade for treating intractable postpartum hemorrhage: description of technique and report of three cases. BJOG. 2020;127:1280-1283.
- Cebekhulu SN, Abdul H, Batting J, et al. Suction tube uterine tamponade for treatment of refractory postpartum hemorrhage: internal feasibility and acceptability pilot of a randomized clinical trial. Int J Gynaecol Obstet. 2022;158: 79-85.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum hemorrhage. J Obstet Gynaecol India. 2017;67:150-151.

Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Department of Obstetrics and Gynecology
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
The author reports no conflict of interest related to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Department of Obstetrics and Gynecology
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
The author reports no conflict of interest related to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Department of Obstetrics and Gynecology
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
The author reports no conflict of interest related to this article.
Postpartum hemorrhage (PPH) is a common complication of birth. In 2019, 4.3% of births in the United States were complicated by at least one episode of PPH.1 Major causes of PPH include uterine atony, retained products of conception, reproductive tract trauma, and coagulopathy.2 Active management of the third stage of labor with the routine administration of postpartum uterotonics reduces the risk of PPH.3,4
PPH treatment requires a systematic approach using appropriate uterotonic medications, tranexamic acid, and procedures performed in a timely sequence to resolve the hemorrhage. Following vaginal birth, procedures that do not require a laparotomy to treat PPH include uterine massage, uterine evacuation to remove retained placental tissue, repair of lacerations, uterine balloon tamponade (UBT), uterine packing, a vacuum-induced hemorrhage control device (VHCD; JADA, Organon), and uterine artery embolization. Following cesarean birth, with an open laparotomy incision, interventions to treat PPH due to atony include vascular ligation, uterine compression sutures, UBT, VHCD, hysterectomy, and pelvic packing.2
Over the past 2 decades, UBT has been widely used for the treatment of PPH with a success rate in observational studies of approximately 86%.5 The uterine balloon creates pressure against the wall of the uterus permitting accumulation of platelets at bleeding sites, enhancing the activity of the clotting system. The uterine balloon provides direct pressure on the bleeding site(s). It is well known in trauma care that the first step to treat a bleeding wound is to apply direct pressure to the bleeding site. During the third stage of labor, a natural process is tetanic uterine contraction, which constricts myometrial vessels and the placenta bed. Placing a balloon in the uterus and inflating the balloon to 200 mL to 500 mL may delay the involution of the uterus that should occur following birth. An observation of great interest is the insight that inducing a vacuum in the uterine cavity may enhance tetanic uterine contraction and constriction of the myometrial vessels. Vacuum-induced hemorrhage control is discussed in detail in this editorial.
Vacuum-induced hemorrhage control device
A new device for the treatment of PPH due to uterine atony is the JADA VHCD (FIGURE), which generates negative intrauterine pressure causing the uterus to contract, thereby constricting myometrial vessels and reducing uterine bleeding. The JADA VHCD system is indicated to provide control and treatment of abnormal postpartum uterine bleeding following vaginal or cesarean birth caused by uterine atony when conservative management is indicated.6
ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
System components
The JADA VHCD consists of a leading portion intended to be inserted into the uterine cavity, which consists of a silicone elliptical loop with 20 vacuum pores. A soft shield covers the vacuum loop to reduce the risk of the vacuum pores being clogged with biological material, including blood and clots. The elliptical loop is attached to a catheter intended for connection to a vacuum source set to 80 mm Hg ±10 mm Hg (hospital wall suction or portable suction device) with an in-line cannister to collect blood. Approximately 16 cm from the tip of the elliptical loop is a balloon that should be positioned in the upper vagina, not inside the cervix, and inflated with fluid (60 mL to 120 mL) through a dedicated port to occlude the vagina, thereby preserving a stable intrauterine vacuum.
Continue to: Correct usage...
Correct usage
A simple mnemonic to facilitate use of the JADA VHCD is “120/80”—fill the vaginal balloon with 120 mL of sterile fluid and attach the tubing to a source that is set to provide 80 mm Hg of vacuum with an in-line collection cannister. The VHCD may not work correctly if there is a substantial amount of blood in the uterus. Clinical experts advise that an important step prior to placing the elliptical loop in the uterus is to perform a sweep of the uterine cavity with a hand or instrument to remove clots and ensure there is no retained placental tissue. It is preferable to assemble the suction tubing, syringe, sterile fluid, and other instruments (eg, forceps, speculum) needed to insert the device prior to attempting to place the VHCD. When the elliptical loop is compressed for insertion, it is about 2 cm in diameter, necessitating that the cervix be dilated sufficiently to accommodate the device.
Immediately after placing the VHCD, contractions can be monitored by physical examination and the amount of ongoing bleeding can be estimated by observing the amount of blood accumulating in the cannister. Rapid onset of a palpable increase in uterine tone is a prominent feature of successful treatment of PPH with the VHCD. The VHCD should be kept in the uterus with active suction for at least 1 hour. Taping the tubing to the inner thigh may help stabilize the device. Once bleeding is controlled, prior to removing the device, the vacuum should be discontinued, and bleeding activityshould be assessed for at least 30 minutes. If the patient is stable, the vaginal balloon can be deflated, followed by removal of the device. The VHCD should be removed within 24 hours of placement.6
The JADA VHCD system should not be used with ongoing intrauterine pregnancy, untreated uterine rupture, unresolved uterine inversion, current cervical cancer, or serious infection of the uterus.6 The VHCD has not been evaluated for effectiveness in the treatment of placenta accreta or coagulopathy. The VHCD has not been specifically evaluated for safety and effectiveness in patients < 34 weeks’ duration, but clinicians report successful use of the device in cases of PPH that have occurred in the second and early-third trimesters. If the device can be appropriately placed with the elliptical loop in the uterus and the balloon in the vagina, it is theoretically possible to use the device for cases of PPH occurring before 34 weeks’ gestation.
When using the JADA VHCD system, it is important to simultaneously provide cardiovascular support, appropriate transfusion of blood products and timely surgical intervention, if indicated. All obstetricians know that in complicated cases of PPH, where conservative measures have not worked, uterine artery embolization or hysterectomy may be the only interventions that will prevent serious patient morbidity.
Effectiveness data
The VHCD has not been evaluated against an alternative approach, such as UBT, in published randomized clinical trials. However, prospective cohort studies have reported that the JADA is often successful in the treatment of PPH.7-10
In a multicenter cohort study of 107 patients with PPH, including 91 vaginal and 16 cesarean births, 100 patients (93%) were successfully treated with the JADA VHCD.7 Median blood loss before application of the system was 870 mL with vaginal birth and 1,300 mL with cesarean birth. Definitive control of the hemorrhage was observed at a median of 3 minutes after initiation of the intrauterine vacuum. In this study, 32% of patients had reproductive tract lacerations that needed to be repaired, and 2 patients required a hysterectomy. Forty patients required a blood transfusion.
Two patients were treated with a Bakri UBT when the VHCD did not resolve the PPH. In this cohort, the vacuum was applied for a median duration of 144 minutes, and a median total device dwell time was 191 minutes. Compared with UBT, the JADA VHCD intrauterine dwell time was shorter, facilitating patient progression and early transfer to the postpartum unit. The physicians who participated in the study reported that the device was easy to use. The complications reported in this cohort were minor and included endometritis (5 cases), vaginal infection (2 cases), and disruption of a vaginal laceration repair (1 case).7
Novel approaches to generating an intrauterine vacuum to treat PPH
The JADA VHCD is the only vacuum device approved by the US Food and Drug Administration (FDA) for treatment of PPH. However, clinical innovators have reported alternative approaches to generating an intrauterine vacuum using equipment designed for other purposes. In one study, a Bakri balloon was used to generate intrauterine vacuum tamponade to treat PPH.11 In this study, a Bakri balloon was inserted into the uterus, and the balloon was inflated to 50 mL to 100 mL to seal the vacuum. The main Bakri port was attached to a suction aspiration device set to generate a vacuum of 450 mm Hg to 525 mm Hg, a much greater vacuum than used with the JADA VHCD. This study included 44 cases of PPH due to uterine atony and 22 cases due to placental pathology, with successful treatment of PPH in 86% and 73% of the cases, respectively.
Another approach to generate intrauterine vacuum tamponade involves using a Levin stomach tube (FG24 or FG36), which has an open end and 4 side ports near the open tip.12-14 The Levin stomach tube is low cost and has many favorable design features, including a rounded tip, wide-bore, and circumferentially placed side ports. The FG36 Levin stomach tube is 12 mm in diameter and has 10 mm side ports. A vacuum device set to deliver 100 mm Hg to 200 mm Hgwas used in some of the studies evaluating the Levin stomach tube for the treatment of PPH. In 3 cases of severe PPH unresponsive to standard interventions, creation of vacuum tamponade with flexible suction tubing with side ports was successful in controlling the hemorrhage.13
Dr. T.N. Vasudeva Panicker invented an intrauterine cannula 12 mm in diameter and 25 cm in length, with dozens of 4 mm side ports over the distal 12 cm of the cannula.15 The cannula, which is made of stainless steel or plastic, is inserted into the uterus and 700 mm Hgvacuum is applied, a level much greater than the 80 mm Hg vacuum recommended for use with the JADA VHCD. When successful, the high suction clears the uterus of blood and causes uterine contraction. In 4 cases of severe PPH, the device successfully controlled the hemorrhage. In 2 of the 4 cases the device that was initially placed became clogged with blood and needed to be replaced.
UBT vs VHCD
To date there are no published randomized controlled trials comparing Bakri UBT to the JADA VHCD. In one retrospective study, the frequency of massive transfusion of red blood cells (RBCs), defined as the transfusion of 4 units or greater of RBCs, was assessed among 78 patients treated with the Bakri UBT and 36 patients treated with the JADA VHCD.9 In this study, at baseline there was a non ̶ statistically significant trend for JADA VHCD to be used more frequently than the Bakri UBT in cases of PPH occurring during repeat cesarean delivery (33% vs 14%). The Bakri UBT was used more frequently than the JADA VHCD among patients having a PPH following a vaginal delivery (51% vs 31%). Both devices were used at similar rates for operative vaginal delivery (6%) and primary cesarean birth (31% VHCD and 28% UBT).
In this retrospective study, the percentage of patients treated with VHCD or UBT who received 4 or more units of RBCs was 3% and 21%, respectively (P < .01). Among patients treated with VHCD and UBT, the estimated median blood loss was 1,500 mL and 1,850 mL (P=.02), respectively. The median hemoglobin concentration at discharge was similar in the VHCD and UBT groups, 8.8 g/dL and 8.6 g/dL, respectively.9 A randomized controlled trial is necessary to refine our understanding of the comparative effectiveness of UBT and VHCD in controlling PPH following vaginal and cesarean birth.
A welcome addition to treatment options
Every obstetrician knows that, in the next 12 months of their practice, they will encounter multiple cases of PPH. One or two of these cases may require the physician to use every medication and procedure available for the treatment of PPH to save the life of the patient. To prepare to treat the next case of PPH rapidly and effectively, it is important for every obstetrician to develop a standardized cognitive plan for using all available treatmentmodalities in an appropriate and timely sequence, including both the Bakri balloon and the JADA VHCD. The insight that inducing an intrauterine vacuum causes uterine contraction, which may resolve PPH, is an important discovery. The JADA VHCD is a welcome addition to our armamentarium of treatments for PPH. ●
Postpartum hemorrhage (PPH) is a common complication of birth. In 2019, 4.3% of births in the United States were complicated by at least one episode of PPH.1 Major causes of PPH include uterine atony, retained products of conception, reproductive tract trauma, and coagulopathy.2 Active management of the third stage of labor with the routine administration of postpartum uterotonics reduces the risk of PPH.3,4
PPH treatment requires a systematic approach using appropriate uterotonic medications, tranexamic acid, and procedures performed in a timely sequence to resolve the hemorrhage. Following vaginal birth, procedures that do not require a laparotomy to treat PPH include uterine massage, uterine evacuation to remove retained placental tissue, repair of lacerations, uterine balloon tamponade (UBT), uterine packing, a vacuum-induced hemorrhage control device (VHCD; JADA, Organon), and uterine artery embolization. Following cesarean birth, with an open laparotomy incision, interventions to treat PPH due to atony include vascular ligation, uterine compression sutures, UBT, VHCD, hysterectomy, and pelvic packing.2
Over the past 2 decades, UBT has been widely used for the treatment of PPH with a success rate in observational studies of approximately 86%.5 The uterine balloon creates pressure against the wall of the uterus permitting accumulation of platelets at bleeding sites, enhancing the activity of the clotting system. The uterine balloon provides direct pressure on the bleeding site(s). It is well known in trauma care that the first step to treat a bleeding wound is to apply direct pressure to the bleeding site. During the third stage of labor, a natural process is tetanic uterine contraction, which constricts myometrial vessels and the placenta bed. Placing a balloon in the uterus and inflating the balloon to 200 mL to 500 mL may delay the involution of the uterus that should occur following birth. An observation of great interest is the insight that inducing a vacuum in the uterine cavity may enhance tetanic uterine contraction and constriction of the myometrial vessels. Vacuum-induced hemorrhage control is discussed in detail in this editorial.
Vacuum-induced hemorrhage control device
A new device for the treatment of PPH due to uterine atony is the JADA VHCD (FIGURE), which generates negative intrauterine pressure causing the uterus to contract, thereby constricting myometrial vessels and reducing uterine bleeding. The JADA VHCD system is indicated to provide control and treatment of abnormal postpartum uterine bleeding following vaginal or cesarean birth caused by uterine atony when conservative management is indicated.6
ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
System components
The JADA VHCD consists of a leading portion intended to be inserted into the uterine cavity, which consists of a silicone elliptical loop with 20 vacuum pores. A soft shield covers the vacuum loop to reduce the risk of the vacuum pores being clogged with biological material, including blood and clots. The elliptical loop is attached to a catheter intended for connection to a vacuum source set to 80 mm Hg ±10 mm Hg (hospital wall suction or portable suction device) with an in-line cannister to collect blood. Approximately 16 cm from the tip of the elliptical loop is a balloon that should be positioned in the upper vagina, not inside the cervix, and inflated with fluid (60 mL to 120 mL) through a dedicated port to occlude the vagina, thereby preserving a stable intrauterine vacuum.
Continue to: Correct usage...
Correct usage
A simple mnemonic to facilitate use of the JADA VHCD is “120/80”—fill the vaginal balloon with 120 mL of sterile fluid and attach the tubing to a source that is set to provide 80 mm Hg of vacuum with an in-line collection cannister. The VHCD may not work correctly if there is a substantial amount of blood in the uterus. Clinical experts advise that an important step prior to placing the elliptical loop in the uterus is to perform a sweep of the uterine cavity with a hand or instrument to remove clots and ensure there is no retained placental tissue. It is preferable to assemble the suction tubing, syringe, sterile fluid, and other instruments (eg, forceps, speculum) needed to insert the device prior to attempting to place the VHCD. When the elliptical loop is compressed for insertion, it is about 2 cm in diameter, necessitating that the cervix be dilated sufficiently to accommodate the device.
Immediately after placing the VHCD, contractions can be monitored by physical examination and the amount of ongoing bleeding can be estimated by observing the amount of blood accumulating in the cannister. Rapid onset of a palpable increase in uterine tone is a prominent feature of successful treatment of PPH with the VHCD. The VHCD should be kept in the uterus with active suction for at least 1 hour. Taping the tubing to the inner thigh may help stabilize the device. Once bleeding is controlled, prior to removing the device, the vacuum should be discontinued, and bleeding activityshould be assessed for at least 30 minutes. If the patient is stable, the vaginal balloon can be deflated, followed by removal of the device. The VHCD should be removed within 24 hours of placement.6
The JADA VHCD system should not be used with ongoing intrauterine pregnancy, untreated uterine rupture, unresolved uterine inversion, current cervical cancer, or serious infection of the uterus.6 The VHCD has not been evaluated for effectiveness in the treatment of placenta accreta or coagulopathy. The VHCD has not been specifically evaluated for safety and effectiveness in patients < 34 weeks’ duration, but clinicians report successful use of the device in cases of PPH that have occurred in the second and early-third trimesters. If the device can be appropriately placed with the elliptical loop in the uterus and the balloon in the vagina, it is theoretically possible to use the device for cases of PPH occurring before 34 weeks’ gestation.
When using the JADA VHCD system, it is important to simultaneously provide cardiovascular support, appropriate transfusion of blood products and timely surgical intervention, if indicated. All obstetricians know that in complicated cases of PPH, where conservative measures have not worked, uterine artery embolization or hysterectomy may be the only interventions that will prevent serious patient morbidity.
Effectiveness data
The VHCD has not been evaluated against an alternative approach, such as UBT, in published randomized clinical trials. However, prospective cohort studies have reported that the JADA is often successful in the treatment of PPH.7-10
In a multicenter cohort study of 107 patients with PPH, including 91 vaginal and 16 cesarean births, 100 patients (93%) were successfully treated with the JADA VHCD.7 Median blood loss before application of the system was 870 mL with vaginal birth and 1,300 mL with cesarean birth. Definitive control of the hemorrhage was observed at a median of 3 minutes after initiation of the intrauterine vacuum. In this study, 32% of patients had reproductive tract lacerations that needed to be repaired, and 2 patients required a hysterectomy. Forty patients required a blood transfusion.
Two patients were treated with a Bakri UBT when the VHCD did not resolve the PPH. In this cohort, the vacuum was applied for a median duration of 144 minutes, and a median total device dwell time was 191 minutes. Compared with UBT, the JADA VHCD intrauterine dwell time was shorter, facilitating patient progression and early transfer to the postpartum unit. The physicians who participated in the study reported that the device was easy to use. The complications reported in this cohort were minor and included endometritis (5 cases), vaginal infection (2 cases), and disruption of a vaginal laceration repair (1 case).7
Novel approaches to generating an intrauterine vacuum to treat PPH
The JADA VHCD is the only vacuum device approved by the US Food and Drug Administration (FDA) for treatment of PPH. However, clinical innovators have reported alternative approaches to generating an intrauterine vacuum using equipment designed for other purposes. In one study, a Bakri balloon was used to generate intrauterine vacuum tamponade to treat PPH.11 In this study, a Bakri balloon was inserted into the uterus, and the balloon was inflated to 50 mL to 100 mL to seal the vacuum. The main Bakri port was attached to a suction aspiration device set to generate a vacuum of 450 mm Hg to 525 mm Hg, a much greater vacuum than used with the JADA VHCD. This study included 44 cases of PPH due to uterine atony and 22 cases due to placental pathology, with successful treatment of PPH in 86% and 73% of the cases, respectively.
Another approach to generate intrauterine vacuum tamponade involves using a Levin stomach tube (FG24 or FG36), which has an open end and 4 side ports near the open tip.12-14 The Levin stomach tube is low cost and has many favorable design features, including a rounded tip, wide-bore, and circumferentially placed side ports. The FG36 Levin stomach tube is 12 mm in diameter and has 10 mm side ports. A vacuum device set to deliver 100 mm Hg to 200 mm Hgwas used in some of the studies evaluating the Levin stomach tube for the treatment of PPH. In 3 cases of severe PPH unresponsive to standard interventions, creation of vacuum tamponade with flexible suction tubing with side ports was successful in controlling the hemorrhage.13
Dr. T.N. Vasudeva Panicker invented an intrauterine cannula 12 mm in diameter and 25 cm in length, with dozens of 4 mm side ports over the distal 12 cm of the cannula.15 The cannula, which is made of stainless steel or plastic, is inserted into the uterus and 700 mm Hgvacuum is applied, a level much greater than the 80 mm Hg vacuum recommended for use with the JADA VHCD. When successful, the high suction clears the uterus of blood and causes uterine contraction. In 4 cases of severe PPH, the device successfully controlled the hemorrhage. In 2 of the 4 cases the device that was initially placed became clogged with blood and needed to be replaced.
UBT vs VHCD
To date there are no published randomized controlled trials comparing Bakri UBT to the JADA VHCD. In one retrospective study, the frequency of massive transfusion of red blood cells (RBCs), defined as the transfusion of 4 units or greater of RBCs, was assessed among 78 patients treated with the Bakri UBT and 36 patients treated with the JADA VHCD.9 In this study, at baseline there was a non ̶ statistically significant trend for JADA VHCD to be used more frequently than the Bakri UBT in cases of PPH occurring during repeat cesarean delivery (33% vs 14%). The Bakri UBT was used more frequently than the JADA VHCD among patients having a PPH following a vaginal delivery (51% vs 31%). Both devices were used at similar rates for operative vaginal delivery (6%) and primary cesarean birth (31% VHCD and 28% UBT).
In this retrospective study, the percentage of patients treated with VHCD or UBT who received 4 or more units of RBCs was 3% and 21%, respectively (P < .01). Among patients treated with VHCD and UBT, the estimated median blood loss was 1,500 mL and 1,850 mL (P=.02), respectively. The median hemoglobin concentration at discharge was similar in the VHCD and UBT groups, 8.8 g/dL and 8.6 g/dL, respectively.9 A randomized controlled trial is necessary to refine our understanding of the comparative effectiveness of UBT and VHCD in controlling PPH following vaginal and cesarean birth.
A welcome addition to treatment options
Every obstetrician knows that, in the next 12 months of their practice, they will encounter multiple cases of PPH. One or two of these cases may require the physician to use every medication and procedure available for the treatment of PPH to save the life of the patient. To prepare to treat the next case of PPH rapidly and effectively, it is important for every obstetrician to develop a standardized cognitive plan for using all available treatmentmodalities in an appropriate and timely sequence, including both the Bakri balloon and the JADA VHCD. The insight that inducing an intrauterine vacuum causes uterine contraction, which may resolve PPH, is an important discovery. The JADA VHCD is a welcome addition to our armamentarium of treatments for PPH. ●
- Corbetta-Rastelli CM, Friedman AM, Sobhani NC, et al. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstet Gynecol. 2023;141:152-161.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384:16351645.
- Salati JA, Leathersich SJ, Williams MJ, et al. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2019;CD001808.
- Begley CM, Gyte GMI, Devane D, et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;CD007412.
- Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222:293.e1-e52.
- US Food and Drug Administration. JADA system approval. Accessed July 25, 2023. https://www .accessdata.fda.gov/cdrh_docs/pdf21/K212757 .pdf
- D’Alton ME, Rood KM, Smid MC, et al. Intrauterine vacuum-induced hemorrhage control device for rapid treatment of postpartum hemorrhage. Obstet Gynecol. 2020;136:882-891.
- D’Alton M, Rood K, Simhan H, et al. Profile of the JADA System: the vacuum-induced hemorrhage control device for treating abnormal postpartum uterine bleeding and postpartum hemorrhage. Expert Rev Med Devices. 2021; 18:849-853.
- Gulersen M, Gerber RP, Rochelson B, et al. Vacuum-induced hemorrhage control versus uterine balloon tamponade for postpartum hemorrhage. J Obstet Gynaecol Can. 2023;45:267-272.
- Purwosunnu Y, Sarkoen W, Arulkumaran S, et al. Control of postpartum hemorrhage using vacuum-induced uterine tamponade. Obstet Gynecol. 2016;128:33-36.
- Haslinger C, Weber K, Zimmerman R. Vacuuminduced tamponade for treatment of postpartum hemorrhage. Obstet Gynecol. 2021;138:361-365.
- Hofmeyr GJ, Middleton K, Singata-Madliki M. Randomized feasibility study of suction-tube uterine tamponade for postpartum hemorrhage. Int J Gynaecol Obstet. 2019;146:339-343.
- Hofmeyr GJ, Singata-Madliki M. Novel suction tube uterine tamponade for treating intractable postpartum hemorrhage: description of technique and report of three cases. BJOG. 2020;127:1280-1283.
- Cebekhulu SN, Abdul H, Batting J, et al. Suction tube uterine tamponade for treatment of refractory postpartum hemorrhage: internal feasibility and acceptability pilot of a randomized clinical trial. Int J Gynaecol Obstet. 2022;158: 79-85.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum hemorrhage. J Obstet Gynaecol India. 2017;67:150-151.
- Corbetta-Rastelli CM, Friedman AM, Sobhani NC, et al. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstet Gynecol. 2023;141:152-161.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384:16351645.
- Salati JA, Leathersich SJ, Williams MJ, et al. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2019;CD001808.
- Begley CM, Gyte GMI, Devane D, et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;CD007412.
- Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222:293.e1-e52.
- US Food and Drug Administration. JADA system approval. Accessed July 25, 2023. https://www .accessdata.fda.gov/cdrh_docs/pdf21/K212757 .pdf
- D’Alton ME, Rood KM, Smid MC, et al. Intrauterine vacuum-induced hemorrhage control device for rapid treatment of postpartum hemorrhage. Obstet Gynecol. 2020;136:882-891.
- D’Alton M, Rood K, Simhan H, et al. Profile of the JADA System: the vacuum-induced hemorrhage control device for treating abnormal postpartum uterine bleeding and postpartum hemorrhage. Expert Rev Med Devices. 2021; 18:849-853.
- Gulersen M, Gerber RP, Rochelson B, et al. Vacuum-induced hemorrhage control versus uterine balloon tamponade for postpartum hemorrhage. J Obstet Gynaecol Can. 2023;45:267-272.
- Purwosunnu Y, Sarkoen W, Arulkumaran S, et al. Control of postpartum hemorrhage using vacuum-induced uterine tamponade. Obstet Gynecol. 2016;128:33-36.
- Haslinger C, Weber K, Zimmerman R. Vacuuminduced tamponade for treatment of postpartum hemorrhage. Obstet Gynecol. 2021;138:361-365.
- Hofmeyr GJ, Middleton K, Singata-Madliki M. Randomized feasibility study of suction-tube uterine tamponade for postpartum hemorrhage. Int J Gynaecol Obstet. 2019;146:339-343.
- Hofmeyr GJ, Singata-Madliki M. Novel suction tube uterine tamponade for treating intractable postpartum hemorrhage: description of technique and report of three cases. BJOG. 2020;127:1280-1283.
- Cebekhulu SN, Abdul H, Batting J, et al. Suction tube uterine tamponade for treatment of refractory postpartum hemorrhage: internal feasibility and acceptability pilot of a randomized clinical trial. Int J Gynaecol Obstet. 2022;158: 79-85.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum hemorrhage. J Obstet Gynaecol India. 2017;67:150-151.