User login
New Hypertension Approach Hits Multiple Targets at Low Dose
LONDON — , according to experts evaluating the new approach.
This multidrug strategy — in which ultralow-dose triple combinations can be used as a starting treatment and four full-dose combinations can be used to treat resistant hypertension — has shown an impressive ability to lower blood pressure in several new studies.
But will it catch on as a routine treatment recommendation in current practice?
Studies of treatment strategies that involve an ultralow quarter dose of three drugs that lower blood pressure and then escalation to a half-dose triple combination and then to a full-dose triple combination, all given as a single pill, were presented at the European Society of Cardiology (ESC) Congress 2024. Another strategy presented involves a four-drug full-dose combination in patients with resistant hypertension.
Start With Low Doses of Three Drugs
The triple-combination pill contains telmisartan (an angiotensin blocker), amlodipine (a calcium channel blocker), and indapamide (a diuretic). The three medications are used at three doses: Quarter, half, and standard.
“The idea is to start treatment with a little bit of the three main drug classes instead of the full dose of one drug and then to increase the triple-combination doses as required to get to blood pressure goal,” said Anthony Rodgers, PhD, from the team at The George Institute for Global Health, Sydney, Australia, that is developing this triple-combination product.
“Using three different mechanisms right from the beginning covers all the bases and leads to improved blood pressure reduction while just using very small doses of each agent. This represents a completely new approach that could transform the management of hypertension,” he reported.
Single-pill triple-combination antihypertensive formulations exist already, but the component drugs are all at standard doses. Such combinations were designed to improve adherence in patients with hard-to-control blood pressure who need more than two full-dose medications, he explained.
“We are suggesting a completely different concept using much lower doses of the triple combination right from the beginning of treatment,” Dr. Rodgers explained. “Convenience and adherence will be an added advantage, but there’s more to it than that. It’s about combining the different mechanisms of three separate drug classes to get a better antihypertensive effect and being able to do this right from the start of treatment in patients with mildly elevated blood pressure, as well as those with higher levels.”
Proof-of-concept trials of this approach have been conducted, but no commercial low-dose triple-combination product has been available.
The George Institute is now developing such a product — through George Medicines, its commercial arm — with the aim of bringing the triple-combination pill to market in both high- and low-income countries. An approval submission has been filed in the United States.
Dr. Rodgers presented two studies that assessed the triple combination. One showed that the quarter dose reduced blood pressure significantly better than placebo in patients with mildly elevated blood pressure. The second showed that half and standard doses of the three medications were more effective at lowering blood pressure than three dual combinations at the same doses.
The VERONICA Trial
The triple combination was also assessed in the VERONICA study, which showed that among Black adults in Nigeria with uncontrolled hypertension, blood pressure was lower and control was better with the low-dose triple-combination pill than with standard care, and tolerability was good.
In VERONICA, recently published in JAMA, 300 patients with a mean baseline blood pressure of 151/97 mm Hg at home and 156/97 mm Hg in the clinic were randomly assigned to receive the triple-combination pill or standard care.
In the triple-combination group, patients started with the quarter-dose pill, then accelerated, as necessary, to the half-dose and standard-dose pills.
In the standard care group, patients started with amlodipine (5 mg), which was stepped up at monthly intervals so patients could achieve a target blood pressure < 140/90 mm Hg as follows: Amlodipine (5 mg) plus losartan (50 mg); then amlodipine (10 mg) plus losartan (100 mg); then amlodipine (10 mg), losartan (100 mg), plus hydrochlorothiazide (25 mg); and finally referral to a specialist if the target blood pressure was still not achieved.
At month 6, mean home systolic blood pressure was, on average, 31 mm Hg lower in the triple-combination group and 26 mm Hg lower in the standard care group (adjusted difference, −5.8 mm Hg; P < .001).
More patients in the triple-combination group than in the standard care group achieved clinic blood pressure control, defined as blood pressure < 140/90 mm Hg (82% vs 72%), and more patients achieved home blood pressure control, defined as blood pressure below 130/80 mm Hg (62% vs 28%).
No participants discontinued treatment due to adverse events, and adverse events of special interest were reported by just 2% and 3% patients in the triple-combination and standard care groups, respectively.
At month 6, however, more participants in the triple-combination group than in the standard care group had serum potassium levels < 3.5 mmol/L (34% vs 18%), although fewer participants in both the groups had potassium levels < 3.0 mmol/L (10% vs 5%).
Hypokalemia may be the consequence of low dietary potassium intake in Africa, and co-administration with potassium-enriched salt substitution should be evaluated, said Dike Ojji, MBBS, PhD, University of Abuja, Nigeria, who was the lead investigator of VERONICA.
“These findings have broad clinical and public health implications, given that improved hypertension control is a priority in Africa and globally. The results underscore the need for combination therapy to be the cornerstone of effective treatment regimens,” Dr. Ojji said.
Missed Targets
“It has taken a long time for the penny to drop as to why the existing antihypertensive treatment paradigm does not work so well,” Dr. Rodgers pointed out. “What tends to happen in clinical practice is that people start on one drug and blood pressure falls a bit, then no further action is taken. But this is not usually enough to get to target. With our approach of using three drugs at low doses straight away, we can often get the blood pressure controlled to target much more quickly with one tablet.”
Low doses of the triple-combination pill should also have a favorable adverse-effect profile and fewer drug interactions, as these issues are generally seen much more frequently with higher doses of drugs, he explained.
This low-dose triple-combination approach could help manage the current epidemic of hypertension and cardiometabolic disease, said Pam Taub, MD, director of preventive cardiology at UC San Diego Health System.
“We are in a new era of cardiometabolic disease, and one of the fundamental drivers of atherosclerotic cardiovascular disease is hypertension, which is prevalent in patients with diabetes, in those with obesity, and is a contributor to chronic kidney disease,” she said.
“We really need to be addressing hypertension very early to prevent this end-organ damage, but because hypertension tends to occur alongside multiple other comorbidities, patients are often on many different medications and are overwhelmed by the burden of polypharmacy.”
Dr. Taub described this triple-combination approach as “looking at hypertension treatment through a new lens.”
“We’ve always been taught to maximize the dose of one agent before we go to a new agent,” she said. “These studies are fundamentally challenging that paradigm. From a pathophysiological and mechanistic perspective, we are seeing that lower doses of different medications can really harness some unique synergistic mechanisms, which can be beneficial for patients.”
But not all experts are convinced that this approach will be a popular option in all countries.
Although this approach makes sense, in that the different agents work synergistically to give a better antihypertensive effect, many physicians could be uncomfortable with the idea of giving multiple medications straight off as the first step of treatment, said Eugene Yang, MD, from the University of Washington in Seattle.
If the patient develops a side effect, it will not be clear which medication is causing it, making it difficult to know which one to stop, he pointed out.
“These studies confirm that a low-dose multidrug-combination pill is effective at lowering blood pressure, but we already have previous studies showing this,” he added. “The issue is how we translate this into patient care. It would be great if we could get people to use it, but I think concerns from both clinicians and patients about identifying the source of any side effects may be a stumbling block.”
The approach is more likely to be adopted in low- to middle-income countries, where there is limited access to healthcare and where the population-wide control of blood pressure makes sense, said Dr. Yang.
Most current guidelines now recommend initiating therapy with two agents, ideally, as a single-pill combination product. “We have finally acknowledged that the vast majority of patients need two drugs. That’s a good starting point. This low-dose triple combination could be an interesting new approach,” said Neil Poulter, MD, professor of preventive cardiovascular medicine at Imperial College London, England.
This approach is in line with the idea that single-pill combinations are the way forward for hypertension therapy, he added.
“The triple combination is attractive, in that you are never quite sure which particular mechanism is driving an individual’s elevated blood pressure, so if you can target three different mechanisms at the same time, you’ve got more chance of a good hit,” Dr. Poulter said.
“The VERONICA trial showed a very good result on lowering BP using this low-dose triple combination as a starting point and increasing quickly to single-pill combinations of triple half doses, then triple full doses, as required. But I think we need more evidence on how this compares to current practice than just this one study in Africa to make this an acceptable routine approach on a global level,” he said.
QUADRO: Four-Drug Combo in Resistant Hypertension
Another scenario in which single-pill antihypertensive combinations could be particularly useful is at the other end of the spectrum: The treatment of patients with resistant hypertension.
The QUADRO study showed that a single pill containing perindopril, indapamide, amlodipine, and bisoprolol is better at lowering blood pressure than the triple combination of perindopril, indapamide, and amlodipine.
The primary endpoint — office sitting systolic blood pressure at 16 weeks — was 8 mm Hg lower with the quadruple combination than with the triple combination. And mean ambulatory 24-hour systolic blood pressure was 7.5 mm Hg lower with the four-drug combination.
This was the first study of a single-pill quadruple combination in patients with resistant hypertension, which is a “difficult-to-treat condition demanding a high number of pills with not enough safe and practical options,” said Stefano Taddei, MD, from the University of Pisa, Italy, when he presented the study at the ESC meeting.
Using “four well-established drugs in a single-combination pill may improve adherence and should be an innovative solution for resistant and difficult-to-treat hypertensive patients,” he said.
Nonadherence is a big problem in patients with resistant hypertension. “It is really difficult to get patients to take three or four antihypertensive agents along with all the other medications they have for other comorbidities,” Dr. Taub pointed out. “We really need to think about combination formulations that reduce the pill burden for our patients.”
Around 10% patients with hypertension may require a fourth drug, so a four-drug single-pill combination therefore makes good sense, said Dr. Poulter.
But the choice of the fourth drug is the subject of debate. The PATHWAY trial showed spironolactone to be the most effective fourth agent, but it can cause side effects, such as gynecomastia and hyperkalemia.
“The beta-blocker in the four-drug combination product used in the QUADRO study may not be as effective as spironolactone at lowering blood pressure,” Dr. Poulter explained, noting that beta-blockers have known side effects. However, “they are often already recommended for patients with very common comorbidities, such as arrhythmias, history of MI, heart failure, angina. In that regard, it makes sense to have a beta-blocker in there.”
The four-drug combination used in the QUADRO study led to a bigger reduction — by 8 mm Hg — than the three-drug combination. “That’s pretty good. I thought this was a very useful and interesting study,” he said.
There could be a role for a four-drug combination product in resistant hypertension. “Whatever we can do to improve adherence and reduce blood pressure is good thing,” said Dr. Yang.
However, a mineralocorticoid receptor antagonist (such as spironolactone) might be better as the fourth drug; that is what is recommended in the resistant hypertension algorithm.
Lower Blood Pressure, Better Outcomes
“What we are seeing in these trials is that across a wide spectrum of patients with hypertension or resistant hypertension, combination pills are superior to standard practice for BP lowering, and that will lead to improved outcomes,” said Dr. Taub.
“For years, such single-pill combinations have been viewed as ‘bad medicine’ in hypertension,” Dr. Poulter added. “That is clearly not the case, as these studies are showing. And single-pill combination therapies are used extensively in practically every other area of medicine. We are starting to accept them now in the blood pressure community, and I think the use of triple and quadruple combinations, as in these studies, has a real logic to it. But for this approach to be useful, these single-pill combinations must be made available, cheaply, across the world, especially in low- and middle-income countries where hypertension rates are a particular problem.”
A version of this article appeared on Medscape.com.
LONDON — , according to experts evaluating the new approach.
This multidrug strategy — in which ultralow-dose triple combinations can be used as a starting treatment and four full-dose combinations can be used to treat resistant hypertension — has shown an impressive ability to lower blood pressure in several new studies.
But will it catch on as a routine treatment recommendation in current practice?
Studies of treatment strategies that involve an ultralow quarter dose of three drugs that lower blood pressure and then escalation to a half-dose triple combination and then to a full-dose triple combination, all given as a single pill, were presented at the European Society of Cardiology (ESC) Congress 2024. Another strategy presented involves a four-drug full-dose combination in patients with resistant hypertension.
Start With Low Doses of Three Drugs
The triple-combination pill contains telmisartan (an angiotensin blocker), amlodipine (a calcium channel blocker), and indapamide (a diuretic). The three medications are used at three doses: Quarter, half, and standard.
“The idea is to start treatment with a little bit of the three main drug classes instead of the full dose of one drug and then to increase the triple-combination doses as required to get to blood pressure goal,” said Anthony Rodgers, PhD, from the team at The George Institute for Global Health, Sydney, Australia, that is developing this triple-combination product.
“Using three different mechanisms right from the beginning covers all the bases and leads to improved blood pressure reduction while just using very small doses of each agent. This represents a completely new approach that could transform the management of hypertension,” he reported.
Single-pill triple-combination antihypertensive formulations exist already, but the component drugs are all at standard doses. Such combinations were designed to improve adherence in patients with hard-to-control blood pressure who need more than two full-dose medications, he explained.
“We are suggesting a completely different concept using much lower doses of the triple combination right from the beginning of treatment,” Dr. Rodgers explained. “Convenience and adherence will be an added advantage, but there’s more to it than that. It’s about combining the different mechanisms of three separate drug classes to get a better antihypertensive effect and being able to do this right from the start of treatment in patients with mildly elevated blood pressure, as well as those with higher levels.”
Proof-of-concept trials of this approach have been conducted, but no commercial low-dose triple-combination product has been available.
The George Institute is now developing such a product — through George Medicines, its commercial arm — with the aim of bringing the triple-combination pill to market in both high- and low-income countries. An approval submission has been filed in the United States.
Dr. Rodgers presented two studies that assessed the triple combination. One showed that the quarter dose reduced blood pressure significantly better than placebo in patients with mildly elevated blood pressure. The second showed that half and standard doses of the three medications were more effective at lowering blood pressure than three dual combinations at the same doses.
The VERONICA Trial
The triple combination was also assessed in the VERONICA study, which showed that among Black adults in Nigeria with uncontrolled hypertension, blood pressure was lower and control was better with the low-dose triple-combination pill than with standard care, and tolerability was good.
In VERONICA, recently published in JAMA, 300 patients with a mean baseline blood pressure of 151/97 mm Hg at home and 156/97 mm Hg in the clinic were randomly assigned to receive the triple-combination pill or standard care.
In the triple-combination group, patients started with the quarter-dose pill, then accelerated, as necessary, to the half-dose and standard-dose pills.
In the standard care group, patients started with amlodipine (5 mg), which was stepped up at monthly intervals so patients could achieve a target blood pressure < 140/90 mm Hg as follows: Amlodipine (5 mg) plus losartan (50 mg); then amlodipine (10 mg) plus losartan (100 mg); then amlodipine (10 mg), losartan (100 mg), plus hydrochlorothiazide (25 mg); and finally referral to a specialist if the target blood pressure was still not achieved.
At month 6, mean home systolic blood pressure was, on average, 31 mm Hg lower in the triple-combination group and 26 mm Hg lower in the standard care group (adjusted difference, −5.8 mm Hg; P < .001).
More patients in the triple-combination group than in the standard care group achieved clinic blood pressure control, defined as blood pressure < 140/90 mm Hg (82% vs 72%), and more patients achieved home blood pressure control, defined as blood pressure below 130/80 mm Hg (62% vs 28%).
No participants discontinued treatment due to adverse events, and adverse events of special interest were reported by just 2% and 3% patients in the triple-combination and standard care groups, respectively.
At month 6, however, more participants in the triple-combination group than in the standard care group had serum potassium levels < 3.5 mmol/L (34% vs 18%), although fewer participants in both the groups had potassium levels < 3.0 mmol/L (10% vs 5%).
Hypokalemia may be the consequence of low dietary potassium intake in Africa, and co-administration with potassium-enriched salt substitution should be evaluated, said Dike Ojji, MBBS, PhD, University of Abuja, Nigeria, who was the lead investigator of VERONICA.
“These findings have broad clinical and public health implications, given that improved hypertension control is a priority in Africa and globally. The results underscore the need for combination therapy to be the cornerstone of effective treatment regimens,” Dr. Ojji said.
Missed Targets
“It has taken a long time for the penny to drop as to why the existing antihypertensive treatment paradigm does not work so well,” Dr. Rodgers pointed out. “What tends to happen in clinical practice is that people start on one drug and blood pressure falls a bit, then no further action is taken. But this is not usually enough to get to target. With our approach of using three drugs at low doses straight away, we can often get the blood pressure controlled to target much more quickly with one tablet.”
Low doses of the triple-combination pill should also have a favorable adverse-effect profile and fewer drug interactions, as these issues are generally seen much more frequently with higher doses of drugs, he explained.
This low-dose triple-combination approach could help manage the current epidemic of hypertension and cardiometabolic disease, said Pam Taub, MD, director of preventive cardiology at UC San Diego Health System.
“We are in a new era of cardiometabolic disease, and one of the fundamental drivers of atherosclerotic cardiovascular disease is hypertension, which is prevalent in patients with diabetes, in those with obesity, and is a contributor to chronic kidney disease,” she said.
“We really need to be addressing hypertension very early to prevent this end-organ damage, but because hypertension tends to occur alongside multiple other comorbidities, patients are often on many different medications and are overwhelmed by the burden of polypharmacy.”
Dr. Taub described this triple-combination approach as “looking at hypertension treatment through a new lens.”
“We’ve always been taught to maximize the dose of one agent before we go to a new agent,” she said. “These studies are fundamentally challenging that paradigm. From a pathophysiological and mechanistic perspective, we are seeing that lower doses of different medications can really harness some unique synergistic mechanisms, which can be beneficial for patients.”
But not all experts are convinced that this approach will be a popular option in all countries.
Although this approach makes sense, in that the different agents work synergistically to give a better antihypertensive effect, many physicians could be uncomfortable with the idea of giving multiple medications straight off as the first step of treatment, said Eugene Yang, MD, from the University of Washington in Seattle.
If the patient develops a side effect, it will not be clear which medication is causing it, making it difficult to know which one to stop, he pointed out.
“These studies confirm that a low-dose multidrug-combination pill is effective at lowering blood pressure, but we already have previous studies showing this,” he added. “The issue is how we translate this into patient care. It would be great if we could get people to use it, but I think concerns from both clinicians and patients about identifying the source of any side effects may be a stumbling block.”
The approach is more likely to be adopted in low- to middle-income countries, where there is limited access to healthcare and where the population-wide control of blood pressure makes sense, said Dr. Yang.
Most current guidelines now recommend initiating therapy with two agents, ideally, as a single-pill combination product. “We have finally acknowledged that the vast majority of patients need two drugs. That’s a good starting point. This low-dose triple combination could be an interesting new approach,” said Neil Poulter, MD, professor of preventive cardiovascular medicine at Imperial College London, England.
This approach is in line with the idea that single-pill combinations are the way forward for hypertension therapy, he added.
“The triple combination is attractive, in that you are never quite sure which particular mechanism is driving an individual’s elevated blood pressure, so if you can target three different mechanisms at the same time, you’ve got more chance of a good hit,” Dr. Poulter said.
“The VERONICA trial showed a very good result on lowering BP using this low-dose triple combination as a starting point and increasing quickly to single-pill combinations of triple half doses, then triple full doses, as required. But I think we need more evidence on how this compares to current practice than just this one study in Africa to make this an acceptable routine approach on a global level,” he said.
QUADRO: Four-Drug Combo in Resistant Hypertension
Another scenario in which single-pill antihypertensive combinations could be particularly useful is at the other end of the spectrum: The treatment of patients with resistant hypertension.
The QUADRO study showed that a single pill containing perindopril, indapamide, amlodipine, and bisoprolol is better at lowering blood pressure than the triple combination of perindopril, indapamide, and amlodipine.
The primary endpoint — office sitting systolic blood pressure at 16 weeks — was 8 mm Hg lower with the quadruple combination than with the triple combination. And mean ambulatory 24-hour systolic blood pressure was 7.5 mm Hg lower with the four-drug combination.
This was the first study of a single-pill quadruple combination in patients with resistant hypertension, which is a “difficult-to-treat condition demanding a high number of pills with not enough safe and practical options,” said Stefano Taddei, MD, from the University of Pisa, Italy, when he presented the study at the ESC meeting.
Using “four well-established drugs in a single-combination pill may improve adherence and should be an innovative solution for resistant and difficult-to-treat hypertensive patients,” he said.
Nonadherence is a big problem in patients with resistant hypertension. “It is really difficult to get patients to take three or four antihypertensive agents along with all the other medications they have for other comorbidities,” Dr. Taub pointed out. “We really need to think about combination formulations that reduce the pill burden for our patients.”
Around 10% patients with hypertension may require a fourth drug, so a four-drug single-pill combination therefore makes good sense, said Dr. Poulter.
But the choice of the fourth drug is the subject of debate. The PATHWAY trial showed spironolactone to be the most effective fourth agent, but it can cause side effects, such as gynecomastia and hyperkalemia.
“The beta-blocker in the four-drug combination product used in the QUADRO study may not be as effective as spironolactone at lowering blood pressure,” Dr. Poulter explained, noting that beta-blockers have known side effects. However, “they are often already recommended for patients with very common comorbidities, such as arrhythmias, history of MI, heart failure, angina. In that regard, it makes sense to have a beta-blocker in there.”
The four-drug combination used in the QUADRO study led to a bigger reduction — by 8 mm Hg — than the three-drug combination. “That’s pretty good. I thought this was a very useful and interesting study,” he said.
There could be a role for a four-drug combination product in resistant hypertension. “Whatever we can do to improve adherence and reduce blood pressure is good thing,” said Dr. Yang.
However, a mineralocorticoid receptor antagonist (such as spironolactone) might be better as the fourth drug; that is what is recommended in the resistant hypertension algorithm.
Lower Blood Pressure, Better Outcomes
“What we are seeing in these trials is that across a wide spectrum of patients with hypertension or resistant hypertension, combination pills are superior to standard practice for BP lowering, and that will lead to improved outcomes,” said Dr. Taub.
“For years, such single-pill combinations have been viewed as ‘bad medicine’ in hypertension,” Dr. Poulter added. “That is clearly not the case, as these studies are showing. And single-pill combination therapies are used extensively in practically every other area of medicine. We are starting to accept them now in the blood pressure community, and I think the use of triple and quadruple combinations, as in these studies, has a real logic to it. But for this approach to be useful, these single-pill combinations must be made available, cheaply, across the world, especially in low- and middle-income countries where hypertension rates are a particular problem.”
A version of this article appeared on Medscape.com.
LONDON — , according to experts evaluating the new approach.
This multidrug strategy — in which ultralow-dose triple combinations can be used as a starting treatment and four full-dose combinations can be used to treat resistant hypertension — has shown an impressive ability to lower blood pressure in several new studies.
But will it catch on as a routine treatment recommendation in current practice?
Studies of treatment strategies that involve an ultralow quarter dose of three drugs that lower blood pressure and then escalation to a half-dose triple combination and then to a full-dose triple combination, all given as a single pill, were presented at the European Society of Cardiology (ESC) Congress 2024. Another strategy presented involves a four-drug full-dose combination in patients with resistant hypertension.
Start With Low Doses of Three Drugs
The triple-combination pill contains telmisartan (an angiotensin blocker), amlodipine (a calcium channel blocker), and indapamide (a diuretic). The three medications are used at three doses: Quarter, half, and standard.
“The idea is to start treatment with a little bit of the three main drug classes instead of the full dose of one drug and then to increase the triple-combination doses as required to get to blood pressure goal,” said Anthony Rodgers, PhD, from the team at The George Institute for Global Health, Sydney, Australia, that is developing this triple-combination product.
“Using three different mechanisms right from the beginning covers all the bases and leads to improved blood pressure reduction while just using very small doses of each agent. This represents a completely new approach that could transform the management of hypertension,” he reported.
Single-pill triple-combination antihypertensive formulations exist already, but the component drugs are all at standard doses. Such combinations were designed to improve adherence in patients with hard-to-control blood pressure who need more than two full-dose medications, he explained.
“We are suggesting a completely different concept using much lower doses of the triple combination right from the beginning of treatment,” Dr. Rodgers explained. “Convenience and adherence will be an added advantage, but there’s more to it than that. It’s about combining the different mechanisms of three separate drug classes to get a better antihypertensive effect and being able to do this right from the start of treatment in patients with mildly elevated blood pressure, as well as those with higher levels.”
Proof-of-concept trials of this approach have been conducted, but no commercial low-dose triple-combination product has been available.
The George Institute is now developing such a product — through George Medicines, its commercial arm — with the aim of bringing the triple-combination pill to market in both high- and low-income countries. An approval submission has been filed in the United States.
Dr. Rodgers presented two studies that assessed the triple combination. One showed that the quarter dose reduced blood pressure significantly better than placebo in patients with mildly elevated blood pressure. The second showed that half and standard doses of the three medications were more effective at lowering blood pressure than three dual combinations at the same doses.
The VERONICA Trial
The triple combination was also assessed in the VERONICA study, which showed that among Black adults in Nigeria with uncontrolled hypertension, blood pressure was lower and control was better with the low-dose triple-combination pill than with standard care, and tolerability was good.
In VERONICA, recently published in JAMA, 300 patients with a mean baseline blood pressure of 151/97 mm Hg at home and 156/97 mm Hg in the clinic were randomly assigned to receive the triple-combination pill or standard care.
In the triple-combination group, patients started with the quarter-dose pill, then accelerated, as necessary, to the half-dose and standard-dose pills.
In the standard care group, patients started with amlodipine (5 mg), which was stepped up at monthly intervals so patients could achieve a target blood pressure < 140/90 mm Hg as follows: Amlodipine (5 mg) plus losartan (50 mg); then amlodipine (10 mg) plus losartan (100 mg); then amlodipine (10 mg), losartan (100 mg), plus hydrochlorothiazide (25 mg); and finally referral to a specialist if the target blood pressure was still not achieved.
At month 6, mean home systolic blood pressure was, on average, 31 mm Hg lower in the triple-combination group and 26 mm Hg lower in the standard care group (adjusted difference, −5.8 mm Hg; P < .001).
More patients in the triple-combination group than in the standard care group achieved clinic blood pressure control, defined as blood pressure < 140/90 mm Hg (82% vs 72%), and more patients achieved home blood pressure control, defined as blood pressure below 130/80 mm Hg (62% vs 28%).
No participants discontinued treatment due to adverse events, and adverse events of special interest were reported by just 2% and 3% patients in the triple-combination and standard care groups, respectively.
At month 6, however, more participants in the triple-combination group than in the standard care group had serum potassium levels < 3.5 mmol/L (34% vs 18%), although fewer participants in both the groups had potassium levels < 3.0 mmol/L (10% vs 5%).
Hypokalemia may be the consequence of low dietary potassium intake in Africa, and co-administration with potassium-enriched salt substitution should be evaluated, said Dike Ojji, MBBS, PhD, University of Abuja, Nigeria, who was the lead investigator of VERONICA.
“These findings have broad clinical and public health implications, given that improved hypertension control is a priority in Africa and globally. The results underscore the need for combination therapy to be the cornerstone of effective treatment regimens,” Dr. Ojji said.
Missed Targets
“It has taken a long time for the penny to drop as to why the existing antihypertensive treatment paradigm does not work so well,” Dr. Rodgers pointed out. “What tends to happen in clinical practice is that people start on one drug and blood pressure falls a bit, then no further action is taken. But this is not usually enough to get to target. With our approach of using three drugs at low doses straight away, we can often get the blood pressure controlled to target much more quickly with one tablet.”
Low doses of the triple-combination pill should also have a favorable adverse-effect profile and fewer drug interactions, as these issues are generally seen much more frequently with higher doses of drugs, he explained.
This low-dose triple-combination approach could help manage the current epidemic of hypertension and cardiometabolic disease, said Pam Taub, MD, director of preventive cardiology at UC San Diego Health System.
“We are in a new era of cardiometabolic disease, and one of the fundamental drivers of atherosclerotic cardiovascular disease is hypertension, which is prevalent in patients with diabetes, in those with obesity, and is a contributor to chronic kidney disease,” she said.
“We really need to be addressing hypertension very early to prevent this end-organ damage, but because hypertension tends to occur alongside multiple other comorbidities, patients are often on many different medications and are overwhelmed by the burden of polypharmacy.”
Dr. Taub described this triple-combination approach as “looking at hypertension treatment through a new lens.”
“We’ve always been taught to maximize the dose of one agent before we go to a new agent,” she said. “These studies are fundamentally challenging that paradigm. From a pathophysiological and mechanistic perspective, we are seeing that lower doses of different medications can really harness some unique synergistic mechanisms, which can be beneficial for patients.”
But not all experts are convinced that this approach will be a popular option in all countries.
Although this approach makes sense, in that the different agents work synergistically to give a better antihypertensive effect, many physicians could be uncomfortable with the idea of giving multiple medications straight off as the first step of treatment, said Eugene Yang, MD, from the University of Washington in Seattle.
If the patient develops a side effect, it will not be clear which medication is causing it, making it difficult to know which one to stop, he pointed out.
“These studies confirm that a low-dose multidrug-combination pill is effective at lowering blood pressure, but we already have previous studies showing this,” he added. “The issue is how we translate this into patient care. It would be great if we could get people to use it, but I think concerns from both clinicians and patients about identifying the source of any side effects may be a stumbling block.”
The approach is more likely to be adopted in low- to middle-income countries, where there is limited access to healthcare and where the population-wide control of blood pressure makes sense, said Dr. Yang.
Most current guidelines now recommend initiating therapy with two agents, ideally, as a single-pill combination product. “We have finally acknowledged that the vast majority of patients need two drugs. That’s a good starting point. This low-dose triple combination could be an interesting new approach,” said Neil Poulter, MD, professor of preventive cardiovascular medicine at Imperial College London, England.
This approach is in line with the idea that single-pill combinations are the way forward for hypertension therapy, he added.
“The triple combination is attractive, in that you are never quite sure which particular mechanism is driving an individual’s elevated blood pressure, so if you can target three different mechanisms at the same time, you’ve got more chance of a good hit,” Dr. Poulter said.
“The VERONICA trial showed a very good result on lowering BP using this low-dose triple combination as a starting point and increasing quickly to single-pill combinations of triple half doses, then triple full doses, as required. But I think we need more evidence on how this compares to current practice than just this one study in Africa to make this an acceptable routine approach on a global level,” he said.
QUADRO: Four-Drug Combo in Resistant Hypertension
Another scenario in which single-pill antihypertensive combinations could be particularly useful is at the other end of the spectrum: The treatment of patients with resistant hypertension.
The QUADRO study showed that a single pill containing perindopril, indapamide, amlodipine, and bisoprolol is better at lowering blood pressure than the triple combination of perindopril, indapamide, and amlodipine.
The primary endpoint — office sitting systolic blood pressure at 16 weeks — was 8 mm Hg lower with the quadruple combination than with the triple combination. And mean ambulatory 24-hour systolic blood pressure was 7.5 mm Hg lower with the four-drug combination.
This was the first study of a single-pill quadruple combination in patients with resistant hypertension, which is a “difficult-to-treat condition demanding a high number of pills with not enough safe and practical options,” said Stefano Taddei, MD, from the University of Pisa, Italy, when he presented the study at the ESC meeting.
Using “four well-established drugs in a single-combination pill may improve adherence and should be an innovative solution for resistant and difficult-to-treat hypertensive patients,” he said.
Nonadherence is a big problem in patients with resistant hypertension. “It is really difficult to get patients to take three or four antihypertensive agents along with all the other medications they have for other comorbidities,” Dr. Taub pointed out. “We really need to think about combination formulations that reduce the pill burden for our patients.”
Around 10% patients with hypertension may require a fourth drug, so a four-drug single-pill combination therefore makes good sense, said Dr. Poulter.
But the choice of the fourth drug is the subject of debate. The PATHWAY trial showed spironolactone to be the most effective fourth agent, but it can cause side effects, such as gynecomastia and hyperkalemia.
“The beta-blocker in the four-drug combination product used in the QUADRO study may not be as effective as spironolactone at lowering blood pressure,” Dr. Poulter explained, noting that beta-blockers have known side effects. However, “they are often already recommended for patients with very common comorbidities, such as arrhythmias, history of MI, heart failure, angina. In that regard, it makes sense to have a beta-blocker in there.”
The four-drug combination used in the QUADRO study led to a bigger reduction — by 8 mm Hg — than the three-drug combination. “That’s pretty good. I thought this was a very useful and interesting study,” he said.
There could be a role for a four-drug combination product in resistant hypertension. “Whatever we can do to improve adherence and reduce blood pressure is good thing,” said Dr. Yang.
However, a mineralocorticoid receptor antagonist (such as spironolactone) might be better as the fourth drug; that is what is recommended in the resistant hypertension algorithm.
Lower Blood Pressure, Better Outcomes
“What we are seeing in these trials is that across a wide spectrum of patients with hypertension or resistant hypertension, combination pills are superior to standard practice for BP lowering, and that will lead to improved outcomes,” said Dr. Taub.
“For years, such single-pill combinations have been viewed as ‘bad medicine’ in hypertension,” Dr. Poulter added. “That is clearly not the case, as these studies are showing. And single-pill combination therapies are used extensively in practically every other area of medicine. We are starting to accept them now in the blood pressure community, and I think the use of triple and quadruple combinations, as in these studies, has a real logic to it. But for this approach to be useful, these single-pill combinations must be made available, cheaply, across the world, especially in low- and middle-income countries where hypertension rates are a particular problem.”
A version of this article appeared on Medscape.com.
FROM ESC CONGRESS 2024
Antidepressants Linked to Improved Verbal Memory
MILAN — , a clinical effect linked to changes in serotonin 4 (5-HT4) receptor levels in the brain, as shown on PET.
These findings suggested there is a role for specifically targeting the 5-HT4 receptor to improve verbal memory in depression, said investigator Vibeke H. Dam, PhD, from Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
“Verbal memory is often impaired in depression, and this has a lot of impact on patients’ ability to work and have a normal life. That’s why we’re so excited about this receptor in particular,” Dr. Dam said.
“If we can find a way to activate it more directly, we’re thinking this could be a way to treat this memory symptom that a lot of patients have and that currently we don’t really have a treatment for,” she added.
The findings were presented at the 37th European College of Neuropsychopharmacology (ECNP) Congress and recently published in Biological Psychiatry .
Largest Trial of Its Kind
The study is the largest single-site PET trial investigating serotonergic neurotransmission in major depressive disorder over the course of antidepressant treatment to date. It included 90 patients with moderate to severe depression who underwent baseline cognitive tests and brain scans to measure 5-HT4 receptor levels before starting their treatment with the selective serotonin reuptake inhibitor escitalopram.
Patients who showed no improvement in depressive symptoms after 4 weeks (n = 14), as assessed by the Hamilton Depression Rating Scale 6 (HAMD6), were switched to the serotonin-norepinephrine reuptake inhibitor duloxetine.
Both escitalopram and duloxetine inhibit the reuptake of 5-HT4, enhancing neurotransmitter activity; escitalopram primarily increases serotonin levels, while duloxetine increases both serotonin and norepinephrine levels.
The primary cognitive outcome measure was change in the Verbal Affective Memory Task 26. Secondary cognitive outcomes were change in working memory, reaction time, emotion recognition bias, and negative social emotion.
After 8 weeks of treatment, a subset of 40 patients repeated PET scans, and at 12 weeks, all patients repeated cognitive testing.
Matching neuroimaging and cognitive data were available for 88 patients at baseline and for 39 patients with rescan.
As expected, the study showed that antidepressant treatment resulted in the downregulation of 5-HT4 receptor levels. “One hypothesis is that if we increase the availability of serotonin [with treatment], downregulation of the receptors might be a response,” said Dr. Dam.
“What was interesting was that this was the effect across all patients, whether they [clinically] responded or not. So we see the medication does what it’s supposed to do in the brain.” But, she said, there was no association between 5-HT4 receptor levels and HAMD6 scores.
Gains in Verbal Memory
Although the downregulation of 5-HT4 did not correlate with somatic or mood symptoms, it did correlate with cognitive symptoms.
Interestingly, while most patients showed improvement in depressive symptoms — many reaching remission or recovery — they also experienced gains in verbal memory. However, these improvements were not correlated. It was possible for one to improve more than the other, with no apparent link between the two, said Dr. Dam.
“What was linked was how the brain responded to the medication for this particular receptor. So even though there is this downregulation of the receptor, there’s still a lot of activation of it, and our thinking is that it’s activation of the receptor that is the important bit.”
Work by other groups has shown that another medication, prucalopride, which is used to treat gastroparesis, can more directly activate the 5-HT4 receptor, and that the treatment of healthy volunteers with this medication can boost memory and learning, said Dr. Dam.
“We could repurpose this drug, and we’re currently looking for funding to test this in a wide variety of different groups such as concussion, diabetes, and depression.”
The study’s coinvestigator, Vibe G. Frokjaer, MD, said more research is required to understand the potential implications of the findings.
“Poor cognitive function is very hard to treat efficiently and may require extra treatment. This work points to the possibility of stimulating this specific receptor so that we can treat cognitive problems, even aside from whether or not the patient has overcome the core symptoms of depression,” she said in a release.
Commenting on the research, Philip Cowen, MD, professor of psychopharmacology at the University of Oxford, England, said in a release that in light of “recent controversies about the role of brain serotonin in clinical depression, it is noteworthy that the PET studies of the Copenhagen Group provide unequivocal evidence that brain 5-HT4 receptors are decreased in unmedicated depressed patients.
“Their work also demonstrates the intimate role of brain 5-HT4 receptors in cognitive function,” he added. “This confirms recent work from Oxford, showing that the 5-HT4 receptor stimulant, prucalopride — a drug licensed for the treatment of constipation — improves memory in both healthy participants and people at risk of depression,” he added.
The study was funded by the Innovation Fund Denmark, Research Fund of the Mental Health Services – Capital Region of Denmark, Independent Research Fund Denmark, Global Justice Foundation, Research Council of Rigshospitalet, Augustinus Foundation, Savværksejer Jeppe Juhl og hustru Ovita Juhls Mindelegat, Lundbeck Foundation, and H. Lundbeck A/S.
Dr. Dam reported serving as a speaker for H. Lundbeck. Frokjaer reported serving as a consultant for Sage Therapeutics and lecturer for H. Lundbeck, Janssen-Cilag, and Gedeon Richter. Study investigator Martin B. Jørgensen has given talks sponsored by Boehringer Ingelheim and Lundbeck Pharma. All other investigators reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN — , a clinical effect linked to changes in serotonin 4 (5-HT4) receptor levels in the brain, as shown on PET.
These findings suggested there is a role for specifically targeting the 5-HT4 receptor to improve verbal memory in depression, said investigator Vibeke H. Dam, PhD, from Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
“Verbal memory is often impaired in depression, and this has a lot of impact on patients’ ability to work and have a normal life. That’s why we’re so excited about this receptor in particular,” Dr. Dam said.
“If we can find a way to activate it more directly, we’re thinking this could be a way to treat this memory symptom that a lot of patients have and that currently we don’t really have a treatment for,” she added.
The findings were presented at the 37th European College of Neuropsychopharmacology (ECNP) Congress and recently published in Biological Psychiatry .
Largest Trial of Its Kind
The study is the largest single-site PET trial investigating serotonergic neurotransmission in major depressive disorder over the course of antidepressant treatment to date. It included 90 patients with moderate to severe depression who underwent baseline cognitive tests and brain scans to measure 5-HT4 receptor levels before starting their treatment with the selective serotonin reuptake inhibitor escitalopram.
Patients who showed no improvement in depressive symptoms after 4 weeks (n = 14), as assessed by the Hamilton Depression Rating Scale 6 (HAMD6), were switched to the serotonin-norepinephrine reuptake inhibitor duloxetine.
Both escitalopram and duloxetine inhibit the reuptake of 5-HT4, enhancing neurotransmitter activity; escitalopram primarily increases serotonin levels, while duloxetine increases both serotonin and norepinephrine levels.
The primary cognitive outcome measure was change in the Verbal Affective Memory Task 26. Secondary cognitive outcomes were change in working memory, reaction time, emotion recognition bias, and negative social emotion.
After 8 weeks of treatment, a subset of 40 patients repeated PET scans, and at 12 weeks, all patients repeated cognitive testing.
Matching neuroimaging and cognitive data were available for 88 patients at baseline and for 39 patients with rescan.
As expected, the study showed that antidepressant treatment resulted in the downregulation of 5-HT4 receptor levels. “One hypothesis is that if we increase the availability of serotonin [with treatment], downregulation of the receptors might be a response,” said Dr. Dam.
“What was interesting was that this was the effect across all patients, whether they [clinically] responded or not. So we see the medication does what it’s supposed to do in the brain.” But, she said, there was no association between 5-HT4 receptor levels and HAMD6 scores.
Gains in Verbal Memory
Although the downregulation of 5-HT4 did not correlate with somatic or mood symptoms, it did correlate with cognitive symptoms.
Interestingly, while most patients showed improvement in depressive symptoms — many reaching remission or recovery — they also experienced gains in verbal memory. However, these improvements were not correlated. It was possible for one to improve more than the other, with no apparent link between the two, said Dr. Dam.
“What was linked was how the brain responded to the medication for this particular receptor. So even though there is this downregulation of the receptor, there’s still a lot of activation of it, and our thinking is that it’s activation of the receptor that is the important bit.”
Work by other groups has shown that another medication, prucalopride, which is used to treat gastroparesis, can more directly activate the 5-HT4 receptor, and that the treatment of healthy volunteers with this medication can boost memory and learning, said Dr. Dam.
“We could repurpose this drug, and we’re currently looking for funding to test this in a wide variety of different groups such as concussion, diabetes, and depression.”
The study’s coinvestigator, Vibe G. Frokjaer, MD, said more research is required to understand the potential implications of the findings.
“Poor cognitive function is very hard to treat efficiently and may require extra treatment. This work points to the possibility of stimulating this specific receptor so that we can treat cognitive problems, even aside from whether or not the patient has overcome the core symptoms of depression,” she said in a release.
Commenting on the research, Philip Cowen, MD, professor of psychopharmacology at the University of Oxford, England, said in a release that in light of “recent controversies about the role of brain serotonin in clinical depression, it is noteworthy that the PET studies of the Copenhagen Group provide unequivocal evidence that brain 5-HT4 receptors are decreased in unmedicated depressed patients.
“Their work also demonstrates the intimate role of brain 5-HT4 receptors in cognitive function,” he added. “This confirms recent work from Oxford, showing that the 5-HT4 receptor stimulant, prucalopride — a drug licensed for the treatment of constipation — improves memory in both healthy participants and people at risk of depression,” he added.
The study was funded by the Innovation Fund Denmark, Research Fund of the Mental Health Services – Capital Region of Denmark, Independent Research Fund Denmark, Global Justice Foundation, Research Council of Rigshospitalet, Augustinus Foundation, Savværksejer Jeppe Juhl og hustru Ovita Juhls Mindelegat, Lundbeck Foundation, and H. Lundbeck A/S.
Dr. Dam reported serving as a speaker for H. Lundbeck. Frokjaer reported serving as a consultant for Sage Therapeutics and lecturer for H. Lundbeck, Janssen-Cilag, and Gedeon Richter. Study investigator Martin B. Jørgensen has given talks sponsored by Boehringer Ingelheim and Lundbeck Pharma. All other investigators reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN — , a clinical effect linked to changes in serotonin 4 (5-HT4) receptor levels in the brain, as shown on PET.
These findings suggested there is a role for specifically targeting the 5-HT4 receptor to improve verbal memory in depression, said investigator Vibeke H. Dam, PhD, from Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
“Verbal memory is often impaired in depression, and this has a lot of impact on patients’ ability to work and have a normal life. That’s why we’re so excited about this receptor in particular,” Dr. Dam said.
“If we can find a way to activate it more directly, we’re thinking this could be a way to treat this memory symptom that a lot of patients have and that currently we don’t really have a treatment for,” she added.
The findings were presented at the 37th European College of Neuropsychopharmacology (ECNP) Congress and recently published in Biological Psychiatry .
Largest Trial of Its Kind
The study is the largest single-site PET trial investigating serotonergic neurotransmission in major depressive disorder over the course of antidepressant treatment to date. It included 90 patients with moderate to severe depression who underwent baseline cognitive tests and brain scans to measure 5-HT4 receptor levels before starting their treatment with the selective serotonin reuptake inhibitor escitalopram.
Patients who showed no improvement in depressive symptoms after 4 weeks (n = 14), as assessed by the Hamilton Depression Rating Scale 6 (HAMD6), were switched to the serotonin-norepinephrine reuptake inhibitor duloxetine.
Both escitalopram and duloxetine inhibit the reuptake of 5-HT4, enhancing neurotransmitter activity; escitalopram primarily increases serotonin levels, while duloxetine increases both serotonin and norepinephrine levels.
The primary cognitive outcome measure was change in the Verbal Affective Memory Task 26. Secondary cognitive outcomes were change in working memory, reaction time, emotion recognition bias, and negative social emotion.
After 8 weeks of treatment, a subset of 40 patients repeated PET scans, and at 12 weeks, all patients repeated cognitive testing.
Matching neuroimaging and cognitive data were available for 88 patients at baseline and for 39 patients with rescan.
As expected, the study showed that antidepressant treatment resulted in the downregulation of 5-HT4 receptor levels. “One hypothesis is that if we increase the availability of serotonin [with treatment], downregulation of the receptors might be a response,” said Dr. Dam.
“What was interesting was that this was the effect across all patients, whether they [clinically] responded or not. So we see the medication does what it’s supposed to do in the brain.” But, she said, there was no association between 5-HT4 receptor levels and HAMD6 scores.
Gains in Verbal Memory
Although the downregulation of 5-HT4 did not correlate with somatic or mood symptoms, it did correlate with cognitive symptoms.
Interestingly, while most patients showed improvement in depressive symptoms — many reaching remission or recovery — they also experienced gains in verbal memory. However, these improvements were not correlated. It was possible for one to improve more than the other, with no apparent link between the two, said Dr. Dam.
“What was linked was how the brain responded to the medication for this particular receptor. So even though there is this downregulation of the receptor, there’s still a lot of activation of it, and our thinking is that it’s activation of the receptor that is the important bit.”
Work by other groups has shown that another medication, prucalopride, which is used to treat gastroparesis, can more directly activate the 5-HT4 receptor, and that the treatment of healthy volunteers with this medication can boost memory and learning, said Dr. Dam.
“We could repurpose this drug, and we’re currently looking for funding to test this in a wide variety of different groups such as concussion, diabetes, and depression.”
The study’s coinvestigator, Vibe G. Frokjaer, MD, said more research is required to understand the potential implications of the findings.
“Poor cognitive function is very hard to treat efficiently and may require extra treatment. This work points to the possibility of stimulating this specific receptor so that we can treat cognitive problems, even aside from whether or not the patient has overcome the core symptoms of depression,” she said in a release.
Commenting on the research, Philip Cowen, MD, professor of psychopharmacology at the University of Oxford, England, said in a release that in light of “recent controversies about the role of brain serotonin in clinical depression, it is noteworthy that the PET studies of the Copenhagen Group provide unequivocal evidence that brain 5-HT4 receptors are decreased in unmedicated depressed patients.
“Their work also demonstrates the intimate role of brain 5-HT4 receptors in cognitive function,” he added. “This confirms recent work from Oxford, showing that the 5-HT4 receptor stimulant, prucalopride — a drug licensed for the treatment of constipation — improves memory in both healthy participants and people at risk of depression,” he added.
The study was funded by the Innovation Fund Denmark, Research Fund of the Mental Health Services – Capital Region of Denmark, Independent Research Fund Denmark, Global Justice Foundation, Research Council of Rigshospitalet, Augustinus Foundation, Savværksejer Jeppe Juhl og hustru Ovita Juhls Mindelegat, Lundbeck Foundation, and H. Lundbeck A/S.
Dr. Dam reported serving as a speaker for H. Lundbeck. Frokjaer reported serving as a consultant for Sage Therapeutics and lecturer for H. Lundbeck, Janssen-Cilag, and Gedeon Richter. Study investigator Martin B. Jørgensen has given talks sponsored by Boehringer Ingelheim and Lundbeck Pharma. All other investigators reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ECNP 2024
An Rx for Burnout, Grief, and Illness: Dance
In 2012, Tara Rynders’ sister was diagnosed with acute disseminated encephalomyelitis. For Ms. Rynders, a registered nurse in Denver, Colorado, the news was devastating.
“She was this beautiful 26-year-old woman, strong and healthy, and within 12 hours, she went into a coma and couldn’t move or speak,” Ms. Rynders remembered. She flew to her sister in Reno, Nevada, and moved into her intensive care unit room. The helplessness she felt wasn’t just as a sister, but as a healthcare provider.
“As a nurse, we love to fix things,” Ms. Rynders said. “But when my sister was sick, I couldn’t do anything to fix her. The doctors didn’t even know what was going on.”
When Ms. Rynders’ sister woke from the coma, she couldn’t speak. The only comfort Ms. Rynders could provide was her presence and the ability to put a smile on her sister’s face. So, Ms. Rynders did what came naturally ...
She danced.
In that tiny hospital room, she blasted her sister’s favorite song — “Party in the U.S.A.” by Miley Cyrus — and danced around the room, doing anything she could to make her sister laugh.
And this patient who could not form words found her voice.
“She’d holler so deeply, it almost sounded like she was crying,” Ms. Rynders remembered. “The depths of her grief and the depths of her joy coming out simultaneously. It was really amazing and so healing for both of us.”
Do You Know How Powerful Dancing Really Is?
Ms. Rynders is far from the only healthcare professional who’s discovered the healing power of dance. In recent years, doctors and nurses across the country, from Los Angeles, California, to Atlanta, Georgia; from TikTok’s “Dancing Nurse,” Cindy Jones, to Max Chiu, Nebraska’s breakdancing oncologist, have demonstrated that finding new ways to move your body isn’t just good advice for patients but could be exactly what healthcare providers need to stay mentally and physically healthy.
It comes at a time when the field faces a “mental health crisis,” according to a 2023 report from the Centers for Disease Control and Prevention. Medscape Physician Burnout & Depression Report 2024 found current rates of 49% for burnout and 20% for depression.
And medical professionals are often hesitant about seeking help. Nearly 40% of physicians reported reluctance to seek out mental health treatment over fears of professional repercussions, according to 2024 recommendations by the Mayo Clinic.
The solution? It just might be dancing.
There’s ample evidence. A 2024 study from the University of Sydney, Australia, found that dancing offers more psychological and cognitive benefits — helping with everything from depression to motivation to emotional well-being — than any other type of exercise.
Another study, published in February by
Structured dance, where you learn specific movements, can offer a huge boost to mental health, according to a 2024 University of Sydney study. But so does unchoreographed dancing, where you’re basically just letting your limbs do their own thing. A 2021 study, published in Complementary Therapies in Clinical Practice, found that 95% of dancers who just moved their bodies, regardless of how it looked to the outside world, still had huge benefits with depression, anxiety, and trauma.
How to Turn a Mastectomy Into a Dance Party
Deborah Cohan, MD, 55, an obstetrician at Zuckerberg San Francisco General Hospital and Trauma Center, San Francisco, California, discovered firsthand the power of dance back in 2013. After finding a lump in her breast during a self-exam, Dr. Cohan feared the worst. Days later, her radiologist confirmed she had invasive ductal carcinoma.
“It was a complete shock,” Dr. Cohan remembered. “I took care of myself. I ate right. I had no obvious risk factors. I did work the night shift, and there’s actually an increased risk for breast cancer among ob.gyn. workers who do night shift work. But still, it took me completely by surprise. My kids were 5 and 8 at the time, and I was terrified that they’d grow up without a mom.”
So, Dr. Cohan turned to the only thing that gave her comfort — dance class. Dancing had been an escape for Dr. Cohan since she took her first ballet class at age 3. So, she skipped work and went to her weekly Soul Motion dance class, where she found herself doing the exact opposite of escaping. She embraced her fears.
“I visualized death as a dance partner,” Dr. Cohan said. “I felt a freedom come over my body. It didn’t make sense to me at the time, but it was almost joyful. Not that I was accepting death or anticipating death, but just that I acknowledged its presence. There’s so much pressure among people with cancer to be positive. [But] that’s something that needs to come from within a person, not from outside. Nobody can dictate how someone should be feeling. And as I danced, I was genuinely feeling joy even as I recognized my own fears and didn’t turn away from them. I was experiencing all the emotions at once. It was such a relief to realize this wasn’t all going to be about sadness.”
The experience was so healing for Dr. Cohan that she decided to see if she could bring those same feelings into her bilateral mastectomy. When meeting with her surgical team, Dr. Cohan made an unorthodox request: Could her pre-op include a dance party?
“I asked the anesthesiologist in the pre-op appointment if I could dance, and he said yes,” she remembered, laughing. “And then I checked with the surgeon, and he said yes. And then I asked the perioperative nurse, and he said yes, ‘but only if you don’t make me dance, too’. So somehow it all came together.”
Dr. Cohan decided on the Beyoncé song “Get Me Bodied,” which she says resonated with her because “it’s all about being in your body and being your full self. I was like, that is exactly how I want to show up in the operating room.” The moment the music kicked in and Dr. Cohan broke into dance, all of her stress melted away.
“Even though I’d been given permission to dance, I never expected anybody else to join in,” Dr. Cohan said. But that’s exactly what they did. A friend took a video, which shows Dr. Cohan in a hospital gown and bouffant cap, dancing alongside her surgical and anesthesia teams, all of whom are dressed in scrubs, at Mount Zion Hospital in San Francisco, California.
“It’s weird to say, especially about a mastectomy,” Dr. Cohan said, “but it was one of the most joyful moments of my life.”
The video’s been viewed 8.4 million times and is so inspirational — we dare you to watch it and not want to jump out of your chair to dance — that soon others were following Dr. Cohan’s lead.
- Sixteen-year-old Amari Hall danced to celebrate her successful heart transplant.
- Ana-Alecia Ayala, a 32-year-old uterine cancer survivor, danced along to “Juju on That Beat” to make chemotherapy more tolerable.
- Doreta Norris, a patient with breast cancer, chose “Gangnam Style” to serenade her into surgery.
Bringing Dance to Other Medical Pros
Ms. Rynders realized the true power of dance years before her sister’s illness, when her mother died of cancer. “I’ve always considered myself to be very resilient as a human, but I couldn’t bounce back after my mom died,” she said. “I was nursing full time in the emergency room, and I was sad all the time. And then one day I realized, you know what brings me joy? It’s always been dance.”
She went back to school to get her Master of Fine Arts in Dance from the University of Colorado at Boulder, which she believes helped her heal. “I was actually able to grieve instead of just pretending I was okay,” she said.
Inspired by these experiences, Ms. Rynders founded The Clinic in 2017, a company that provides dance workshops for healthcare professionals struggling with burnout and secondary traumatic stress.
“I see these nurses running down hospital hallways, covered in blood from patients whose lives are literally hanging on a thread,” she said. “They’re dealing with so much stress and grief and hardship. And then to see them with us, playing and laughing — those deep belly laughs that you haven’t done since you were a kid, the deep laughing that comes from deep in your soul. It can be transformational, for them and for you.”
Ms. Rynders remembers one especially healing workshop in which the participants pretended to be astronauts in deep space, using zero gravity to inform their movements. After the exercise, a veteran hospital nurse took Ms. Rynders aside to thank her, mentioning that she was still dealing with grief for her late son, who had died from suicide years earlier.
“She had a lot of guilt around it,” Ms. Rynders remembered. “And she said to me, ‘When I went to space, I felt closer to him.’ It was just this silly little game, but it gave her this lightness that she hadn’t felt in years. She was able to be free and laugh and play and feel close to her son again.”
Good Medicine
Dr. Cohan, who today is cancer free, said her experience made her completely rethink her relationship with patients. She has danced with more than a few of them, though she’s careful never to force it on them. “I never want to project my idea of joy onto others,” she said. “But more than anything, it’s changed my thinking on what it means to take ownership as a patient.”
The one thing Dr. Cohan never wanted as a patient, and the thing she never wants for her own patients, is the loss of agency. “When I danced, I didn’t feel like I was just handing over my body and begrudgingly accepting what was about to happen to me,” she said. “I was taking ownership around my decision, and I felt connected, really connected, to my surgical team.”
As a patient, Dr. Cohan experienced what she calls the “regimented” atmosphere of medicine. “You’re told where to go, what to do, and you have no control over any of it,” recalled Dr. Cohan, who’s now semiretired and runs retreats for women with breast cancer. “But by bringing in dance, it felt really radical that my healthcare team was doing my thing, not the other way around.”
(Re)Learning to Move More Consciously
Healthcare providers need these moments of escape just as much as patients living with disease. The difference is, as Ms. Rynders points out, those in the medical field aren’t always as aware of their emotional distress. “I think if you ask a nurse, ‘How can I help you? What do you need?’ They’re usually like, ‘I don’t know. I don’t even know what I need,’ ” Ms. Rynders said. “Even if they did know what they needed, I think it’s hard to ask for it and even harder to receive it.”
At Ms. Rynders’ workshops, not everybody is comfortable dancing, of course. So, new participants are always given the option just to witness, to be in the room and watch what happens. “But I also really encourage people to take advantage of this opportunity to do something different and disrupt the way we live on a daily basis,” Ms. Rynders said. “Let your brain try something new and be courageous. We’ve only had a few people who sat on the sidelines the whole time.”
It’s not always just about feelings, Dr. Cohan added, but physical relaxation. “Sometimes it’s just about remembering how to move consciously. When I was having surgery, I didn’t just dance to relax myself. I wanted my entire surgical team to be relaxed.”
For Ms. Rynders, every time she dances with her patients, or with fellow healthcare workers, she’s reminded of her sister and the comfort she was able to give her when no amount of medicine would make things better.
“We don’t always need to be fixed by things,” she said. “Sometimes we just need to be present with one another and be with each other. And sometimes, the best way to do that is by dancing till the tears roll down your cheeks.”
A version of this article appeared on Medscape.com.
In 2012, Tara Rynders’ sister was diagnosed with acute disseminated encephalomyelitis. For Ms. Rynders, a registered nurse in Denver, Colorado, the news was devastating.
“She was this beautiful 26-year-old woman, strong and healthy, and within 12 hours, she went into a coma and couldn’t move or speak,” Ms. Rynders remembered. She flew to her sister in Reno, Nevada, and moved into her intensive care unit room. The helplessness she felt wasn’t just as a sister, but as a healthcare provider.
“As a nurse, we love to fix things,” Ms. Rynders said. “But when my sister was sick, I couldn’t do anything to fix her. The doctors didn’t even know what was going on.”
When Ms. Rynders’ sister woke from the coma, she couldn’t speak. The only comfort Ms. Rynders could provide was her presence and the ability to put a smile on her sister’s face. So, Ms. Rynders did what came naturally ...
She danced.
In that tiny hospital room, she blasted her sister’s favorite song — “Party in the U.S.A.” by Miley Cyrus — and danced around the room, doing anything she could to make her sister laugh.
And this patient who could not form words found her voice.
“She’d holler so deeply, it almost sounded like she was crying,” Ms. Rynders remembered. “The depths of her grief and the depths of her joy coming out simultaneously. It was really amazing and so healing for both of us.”
Do You Know How Powerful Dancing Really Is?
Ms. Rynders is far from the only healthcare professional who’s discovered the healing power of dance. In recent years, doctors and nurses across the country, from Los Angeles, California, to Atlanta, Georgia; from TikTok’s “Dancing Nurse,” Cindy Jones, to Max Chiu, Nebraska’s breakdancing oncologist, have demonstrated that finding new ways to move your body isn’t just good advice for patients but could be exactly what healthcare providers need to stay mentally and physically healthy.
It comes at a time when the field faces a “mental health crisis,” according to a 2023 report from the Centers for Disease Control and Prevention. Medscape Physician Burnout & Depression Report 2024 found current rates of 49% for burnout and 20% for depression.
And medical professionals are often hesitant about seeking help. Nearly 40% of physicians reported reluctance to seek out mental health treatment over fears of professional repercussions, according to 2024 recommendations by the Mayo Clinic.
The solution? It just might be dancing.
There’s ample evidence. A 2024 study from the University of Sydney, Australia, found that dancing offers more psychological and cognitive benefits — helping with everything from depression to motivation to emotional well-being — than any other type of exercise.
Another study, published in February by
Structured dance, where you learn specific movements, can offer a huge boost to mental health, according to a 2024 University of Sydney study. But so does unchoreographed dancing, where you’re basically just letting your limbs do their own thing. A 2021 study, published in Complementary Therapies in Clinical Practice, found that 95% of dancers who just moved their bodies, regardless of how it looked to the outside world, still had huge benefits with depression, anxiety, and trauma.
How to Turn a Mastectomy Into a Dance Party
Deborah Cohan, MD, 55, an obstetrician at Zuckerberg San Francisco General Hospital and Trauma Center, San Francisco, California, discovered firsthand the power of dance back in 2013. After finding a lump in her breast during a self-exam, Dr. Cohan feared the worst. Days later, her radiologist confirmed she had invasive ductal carcinoma.
“It was a complete shock,” Dr. Cohan remembered. “I took care of myself. I ate right. I had no obvious risk factors. I did work the night shift, and there’s actually an increased risk for breast cancer among ob.gyn. workers who do night shift work. But still, it took me completely by surprise. My kids were 5 and 8 at the time, and I was terrified that they’d grow up without a mom.”
So, Dr. Cohan turned to the only thing that gave her comfort — dance class. Dancing had been an escape for Dr. Cohan since she took her first ballet class at age 3. So, she skipped work and went to her weekly Soul Motion dance class, where she found herself doing the exact opposite of escaping. She embraced her fears.
“I visualized death as a dance partner,” Dr. Cohan said. “I felt a freedom come over my body. It didn’t make sense to me at the time, but it was almost joyful. Not that I was accepting death or anticipating death, but just that I acknowledged its presence. There’s so much pressure among people with cancer to be positive. [But] that’s something that needs to come from within a person, not from outside. Nobody can dictate how someone should be feeling. And as I danced, I was genuinely feeling joy even as I recognized my own fears and didn’t turn away from them. I was experiencing all the emotions at once. It was such a relief to realize this wasn’t all going to be about sadness.”
The experience was so healing for Dr. Cohan that she decided to see if she could bring those same feelings into her bilateral mastectomy. When meeting with her surgical team, Dr. Cohan made an unorthodox request: Could her pre-op include a dance party?
“I asked the anesthesiologist in the pre-op appointment if I could dance, and he said yes,” she remembered, laughing. “And then I checked with the surgeon, and he said yes. And then I asked the perioperative nurse, and he said yes, ‘but only if you don’t make me dance, too’. So somehow it all came together.”
Dr. Cohan decided on the Beyoncé song “Get Me Bodied,” which she says resonated with her because “it’s all about being in your body and being your full self. I was like, that is exactly how I want to show up in the operating room.” The moment the music kicked in and Dr. Cohan broke into dance, all of her stress melted away.
“Even though I’d been given permission to dance, I never expected anybody else to join in,” Dr. Cohan said. But that’s exactly what they did. A friend took a video, which shows Dr. Cohan in a hospital gown and bouffant cap, dancing alongside her surgical and anesthesia teams, all of whom are dressed in scrubs, at Mount Zion Hospital in San Francisco, California.
“It’s weird to say, especially about a mastectomy,” Dr. Cohan said, “but it was one of the most joyful moments of my life.”
The video’s been viewed 8.4 million times and is so inspirational — we dare you to watch it and not want to jump out of your chair to dance — that soon others were following Dr. Cohan’s lead.
- Sixteen-year-old Amari Hall danced to celebrate her successful heart transplant.
- Ana-Alecia Ayala, a 32-year-old uterine cancer survivor, danced along to “Juju on That Beat” to make chemotherapy more tolerable.
- Doreta Norris, a patient with breast cancer, chose “Gangnam Style” to serenade her into surgery.
Bringing Dance to Other Medical Pros
Ms. Rynders realized the true power of dance years before her sister’s illness, when her mother died of cancer. “I’ve always considered myself to be very resilient as a human, but I couldn’t bounce back after my mom died,” she said. “I was nursing full time in the emergency room, and I was sad all the time. And then one day I realized, you know what brings me joy? It’s always been dance.”
She went back to school to get her Master of Fine Arts in Dance from the University of Colorado at Boulder, which she believes helped her heal. “I was actually able to grieve instead of just pretending I was okay,” she said.
Inspired by these experiences, Ms. Rynders founded The Clinic in 2017, a company that provides dance workshops for healthcare professionals struggling with burnout and secondary traumatic stress.
“I see these nurses running down hospital hallways, covered in blood from patients whose lives are literally hanging on a thread,” she said. “They’re dealing with so much stress and grief and hardship. And then to see them with us, playing and laughing — those deep belly laughs that you haven’t done since you were a kid, the deep laughing that comes from deep in your soul. It can be transformational, for them and for you.”
Ms. Rynders remembers one especially healing workshop in which the participants pretended to be astronauts in deep space, using zero gravity to inform their movements. After the exercise, a veteran hospital nurse took Ms. Rynders aside to thank her, mentioning that she was still dealing with grief for her late son, who had died from suicide years earlier.
“She had a lot of guilt around it,” Ms. Rynders remembered. “And she said to me, ‘When I went to space, I felt closer to him.’ It was just this silly little game, but it gave her this lightness that she hadn’t felt in years. She was able to be free and laugh and play and feel close to her son again.”
Good Medicine
Dr. Cohan, who today is cancer free, said her experience made her completely rethink her relationship with patients. She has danced with more than a few of them, though she’s careful never to force it on them. “I never want to project my idea of joy onto others,” she said. “But more than anything, it’s changed my thinking on what it means to take ownership as a patient.”
The one thing Dr. Cohan never wanted as a patient, and the thing she never wants for her own patients, is the loss of agency. “When I danced, I didn’t feel like I was just handing over my body and begrudgingly accepting what was about to happen to me,” she said. “I was taking ownership around my decision, and I felt connected, really connected, to my surgical team.”
As a patient, Dr. Cohan experienced what she calls the “regimented” atmosphere of medicine. “You’re told where to go, what to do, and you have no control over any of it,” recalled Dr. Cohan, who’s now semiretired and runs retreats for women with breast cancer. “But by bringing in dance, it felt really radical that my healthcare team was doing my thing, not the other way around.”
(Re)Learning to Move More Consciously
Healthcare providers need these moments of escape just as much as patients living with disease. The difference is, as Ms. Rynders points out, those in the medical field aren’t always as aware of their emotional distress. “I think if you ask a nurse, ‘How can I help you? What do you need?’ They’re usually like, ‘I don’t know. I don’t even know what I need,’ ” Ms. Rynders said. “Even if they did know what they needed, I think it’s hard to ask for it and even harder to receive it.”
At Ms. Rynders’ workshops, not everybody is comfortable dancing, of course. So, new participants are always given the option just to witness, to be in the room and watch what happens. “But I also really encourage people to take advantage of this opportunity to do something different and disrupt the way we live on a daily basis,” Ms. Rynders said. “Let your brain try something new and be courageous. We’ve only had a few people who sat on the sidelines the whole time.”
It’s not always just about feelings, Dr. Cohan added, but physical relaxation. “Sometimes it’s just about remembering how to move consciously. When I was having surgery, I didn’t just dance to relax myself. I wanted my entire surgical team to be relaxed.”
For Ms. Rynders, every time she dances with her patients, or with fellow healthcare workers, she’s reminded of her sister and the comfort she was able to give her when no amount of medicine would make things better.
“We don’t always need to be fixed by things,” she said. “Sometimes we just need to be present with one another and be with each other. And sometimes, the best way to do that is by dancing till the tears roll down your cheeks.”
A version of this article appeared on Medscape.com.
In 2012, Tara Rynders’ sister was diagnosed with acute disseminated encephalomyelitis. For Ms. Rynders, a registered nurse in Denver, Colorado, the news was devastating.
“She was this beautiful 26-year-old woman, strong and healthy, and within 12 hours, she went into a coma and couldn’t move or speak,” Ms. Rynders remembered. She flew to her sister in Reno, Nevada, and moved into her intensive care unit room. The helplessness she felt wasn’t just as a sister, but as a healthcare provider.
“As a nurse, we love to fix things,” Ms. Rynders said. “But when my sister was sick, I couldn’t do anything to fix her. The doctors didn’t even know what was going on.”
When Ms. Rynders’ sister woke from the coma, she couldn’t speak. The only comfort Ms. Rynders could provide was her presence and the ability to put a smile on her sister’s face. So, Ms. Rynders did what came naturally ...
She danced.
In that tiny hospital room, she blasted her sister’s favorite song — “Party in the U.S.A.” by Miley Cyrus — and danced around the room, doing anything she could to make her sister laugh.
And this patient who could not form words found her voice.
“She’d holler so deeply, it almost sounded like she was crying,” Ms. Rynders remembered. “The depths of her grief and the depths of her joy coming out simultaneously. It was really amazing and so healing for both of us.”
Do You Know How Powerful Dancing Really Is?
Ms. Rynders is far from the only healthcare professional who’s discovered the healing power of dance. In recent years, doctors and nurses across the country, from Los Angeles, California, to Atlanta, Georgia; from TikTok’s “Dancing Nurse,” Cindy Jones, to Max Chiu, Nebraska’s breakdancing oncologist, have demonstrated that finding new ways to move your body isn’t just good advice for patients but could be exactly what healthcare providers need to stay mentally and physically healthy.
It comes at a time when the field faces a “mental health crisis,” according to a 2023 report from the Centers for Disease Control and Prevention. Medscape Physician Burnout & Depression Report 2024 found current rates of 49% for burnout and 20% for depression.
And medical professionals are often hesitant about seeking help. Nearly 40% of physicians reported reluctance to seek out mental health treatment over fears of professional repercussions, according to 2024 recommendations by the Mayo Clinic.
The solution? It just might be dancing.
There’s ample evidence. A 2024 study from the University of Sydney, Australia, found that dancing offers more psychological and cognitive benefits — helping with everything from depression to motivation to emotional well-being — than any other type of exercise.
Another study, published in February by
Structured dance, where you learn specific movements, can offer a huge boost to mental health, according to a 2024 University of Sydney study. But so does unchoreographed dancing, where you’re basically just letting your limbs do their own thing. A 2021 study, published in Complementary Therapies in Clinical Practice, found that 95% of dancers who just moved their bodies, regardless of how it looked to the outside world, still had huge benefits with depression, anxiety, and trauma.
How to Turn a Mastectomy Into a Dance Party
Deborah Cohan, MD, 55, an obstetrician at Zuckerberg San Francisco General Hospital and Trauma Center, San Francisco, California, discovered firsthand the power of dance back in 2013. After finding a lump in her breast during a self-exam, Dr. Cohan feared the worst. Days later, her radiologist confirmed she had invasive ductal carcinoma.
“It was a complete shock,” Dr. Cohan remembered. “I took care of myself. I ate right. I had no obvious risk factors. I did work the night shift, and there’s actually an increased risk for breast cancer among ob.gyn. workers who do night shift work. But still, it took me completely by surprise. My kids were 5 and 8 at the time, and I was terrified that they’d grow up without a mom.”
So, Dr. Cohan turned to the only thing that gave her comfort — dance class. Dancing had been an escape for Dr. Cohan since she took her first ballet class at age 3. So, she skipped work and went to her weekly Soul Motion dance class, where she found herself doing the exact opposite of escaping. She embraced her fears.
“I visualized death as a dance partner,” Dr. Cohan said. “I felt a freedom come over my body. It didn’t make sense to me at the time, but it was almost joyful. Not that I was accepting death or anticipating death, but just that I acknowledged its presence. There’s so much pressure among people with cancer to be positive. [But] that’s something that needs to come from within a person, not from outside. Nobody can dictate how someone should be feeling. And as I danced, I was genuinely feeling joy even as I recognized my own fears and didn’t turn away from them. I was experiencing all the emotions at once. It was such a relief to realize this wasn’t all going to be about sadness.”
The experience was so healing for Dr. Cohan that she decided to see if she could bring those same feelings into her bilateral mastectomy. When meeting with her surgical team, Dr. Cohan made an unorthodox request: Could her pre-op include a dance party?
“I asked the anesthesiologist in the pre-op appointment if I could dance, and he said yes,” she remembered, laughing. “And then I checked with the surgeon, and he said yes. And then I asked the perioperative nurse, and he said yes, ‘but only if you don’t make me dance, too’. So somehow it all came together.”
Dr. Cohan decided on the Beyoncé song “Get Me Bodied,” which she says resonated with her because “it’s all about being in your body and being your full self. I was like, that is exactly how I want to show up in the operating room.” The moment the music kicked in and Dr. Cohan broke into dance, all of her stress melted away.
“Even though I’d been given permission to dance, I never expected anybody else to join in,” Dr. Cohan said. But that’s exactly what they did. A friend took a video, which shows Dr. Cohan in a hospital gown and bouffant cap, dancing alongside her surgical and anesthesia teams, all of whom are dressed in scrubs, at Mount Zion Hospital in San Francisco, California.
“It’s weird to say, especially about a mastectomy,” Dr. Cohan said, “but it was one of the most joyful moments of my life.”
The video’s been viewed 8.4 million times and is so inspirational — we dare you to watch it and not want to jump out of your chair to dance — that soon others were following Dr. Cohan’s lead.
- Sixteen-year-old Amari Hall danced to celebrate her successful heart transplant.
- Ana-Alecia Ayala, a 32-year-old uterine cancer survivor, danced along to “Juju on That Beat” to make chemotherapy more tolerable.
- Doreta Norris, a patient with breast cancer, chose “Gangnam Style” to serenade her into surgery.
Bringing Dance to Other Medical Pros
Ms. Rynders realized the true power of dance years before her sister’s illness, when her mother died of cancer. “I’ve always considered myself to be very resilient as a human, but I couldn’t bounce back after my mom died,” she said. “I was nursing full time in the emergency room, and I was sad all the time. And then one day I realized, you know what brings me joy? It’s always been dance.”
She went back to school to get her Master of Fine Arts in Dance from the University of Colorado at Boulder, which she believes helped her heal. “I was actually able to grieve instead of just pretending I was okay,” she said.
Inspired by these experiences, Ms. Rynders founded The Clinic in 2017, a company that provides dance workshops for healthcare professionals struggling with burnout and secondary traumatic stress.
“I see these nurses running down hospital hallways, covered in blood from patients whose lives are literally hanging on a thread,” she said. “They’re dealing with so much stress and grief and hardship. And then to see them with us, playing and laughing — those deep belly laughs that you haven’t done since you were a kid, the deep laughing that comes from deep in your soul. It can be transformational, for them and for you.”
Ms. Rynders remembers one especially healing workshop in which the participants pretended to be astronauts in deep space, using zero gravity to inform their movements. After the exercise, a veteran hospital nurse took Ms. Rynders aside to thank her, mentioning that she was still dealing with grief for her late son, who had died from suicide years earlier.
“She had a lot of guilt around it,” Ms. Rynders remembered. “And she said to me, ‘When I went to space, I felt closer to him.’ It was just this silly little game, but it gave her this lightness that she hadn’t felt in years. She was able to be free and laugh and play and feel close to her son again.”
Good Medicine
Dr. Cohan, who today is cancer free, said her experience made her completely rethink her relationship with patients. She has danced with more than a few of them, though she’s careful never to force it on them. “I never want to project my idea of joy onto others,” she said. “But more than anything, it’s changed my thinking on what it means to take ownership as a patient.”
The one thing Dr. Cohan never wanted as a patient, and the thing she never wants for her own patients, is the loss of agency. “When I danced, I didn’t feel like I was just handing over my body and begrudgingly accepting what was about to happen to me,” she said. “I was taking ownership around my decision, and I felt connected, really connected, to my surgical team.”
As a patient, Dr. Cohan experienced what she calls the “regimented” atmosphere of medicine. “You’re told where to go, what to do, and you have no control over any of it,” recalled Dr. Cohan, who’s now semiretired and runs retreats for women with breast cancer. “But by bringing in dance, it felt really radical that my healthcare team was doing my thing, not the other way around.”
(Re)Learning to Move More Consciously
Healthcare providers need these moments of escape just as much as patients living with disease. The difference is, as Ms. Rynders points out, those in the medical field aren’t always as aware of their emotional distress. “I think if you ask a nurse, ‘How can I help you? What do you need?’ They’re usually like, ‘I don’t know. I don’t even know what I need,’ ” Ms. Rynders said. “Even if they did know what they needed, I think it’s hard to ask for it and even harder to receive it.”
At Ms. Rynders’ workshops, not everybody is comfortable dancing, of course. So, new participants are always given the option just to witness, to be in the room and watch what happens. “But I also really encourage people to take advantage of this opportunity to do something different and disrupt the way we live on a daily basis,” Ms. Rynders said. “Let your brain try something new and be courageous. We’ve only had a few people who sat on the sidelines the whole time.”
It’s not always just about feelings, Dr. Cohan added, but physical relaxation. “Sometimes it’s just about remembering how to move consciously. When I was having surgery, I didn’t just dance to relax myself. I wanted my entire surgical team to be relaxed.”
For Ms. Rynders, every time she dances with her patients, or with fellow healthcare workers, she’s reminded of her sister and the comfort she was able to give her when no amount of medicine would make things better.
“We don’t always need to be fixed by things,” she said. “Sometimes we just need to be present with one another and be with each other. And sometimes, the best way to do that is by dancing till the tears roll down your cheeks.”
A version of this article appeared on Medscape.com.
Modified Sleep Apnea Index Score Associated With CV Risk
Use of a modified sleep apnea index can identify cardiovascular risk factors in adults with moderate to severe obstructive sleep apnea (OSA), according to results from a new study presented at the American Academy of Otolaryngology–Head and Neck Surgery 2024 Annual Meeting.
, said Jennifer A. Goldfarb, MHS, a medical student at Thomas Jefferson University, Philadelphia, Pennsylvania, who presented the findings.
OSA has an association with many negative cardiovascular comorbidities; however, “the AHI provides only a single metric and does not provide a holistic assessment of the individual patient’s disease severity,” said senior author Colin T. Huntley, MD, also of Thomas Jefferson University.
“OSA is very complex, and having a robust system to assess the disease may be a better predictor of overall severity,” he told this news organization.
Previous research has shown a correlation between mSASI and mean arterial pressure and serum C-reactive protein in OSA patients, but the connection with cardiovascular risk factors has not been well studied, Ms. Goldfarb noted.
In the retrospective cohort study, Ms. Goldfarb and colleagues looked at mSASI scores from 260 CPAP-intolerant patients with OSA who underwent upper airway stimulation, maxillomandibular advancement, or expansion sphincter pharyngoplasty at a single sleep surgery clinic between 2014 and 2021. The mSASI uses a score of 1-3, with 3 as the highest level of OSA severity.
Cardiovascular risk factors were assessed at the patient’s initial evaluation by the sleep surgery team. They included coronary artery disease, type 2 diabetes, atrial fibrillation, congestive heart failure, hypertension, and cerebrovascular accident.
A total of 142 patients (55%) had an mSASI of 1; 91 (35%) had an mSASI of 2; and 27 (10%) had an mSASI of 3. At least one cardiovascular risk factor was present in 58%, 68%, and 63% of these groups, respectively (P = .3).
Stratifying participants by mSASI scores, the researchers found that patients with an mSASI of 2 or 3 were significantly more likely than those with an mSASI of 1 to have more cardiovascular risk factors on initial presentation, and were significantly more likely to be diagnosed with hypertension (P = .02 for both).
Using the AHI, however, patients with moderate to severe OSA (AHI > 15) had a similar number of cardiovascular risk factors as those with mild OSA (P > .05).
“A higher mSASI score, which represents worse disease, was associated with a higher Framingham risk score, which supported our hypothesis; however, the AHI was not found to be associated with an increased Framingham score,” Dr. Huntley told this news organization.
Takeaways and Next Steps
These results suggest that the AHI, while a good metric, might not be the best tool for assessment of overall disease severity, given the complexity of OSA, the impact of the disease on patient quality of life, and the risk for downstream cardiovascular disease, said Dr. Huntley.
The findings were limited by the retrospective design and use of data from a single center.
Population-level data are needed to identify variables that may be meaningful to create a future tool that provides the best picture of the individual patient’s disease, he added. Additional prospective data are also needed to assess the impact of the scoring system on long-term treatment outcomes.
“The current study is especially interesting as we are just beginning to understand the factors that predict cardiovascular risk for patients with obstructive sleep apnea,” Megan Durr, MD, of the University of California, San Francisco, said in an interview.
“For a long time, we primarily looked at the AHI and/or oxygen levels during sleep as risk factors, and we haven’t looked as much at other factors.” said Dr. Durr, who served as a moderator for the session in which the study was presented.
The current findings provide a more comprehensive look at cardiovascular risk; the inclusion of patient anatomy and symptoms add to the knowledge of this topic, and will lead to further work in this area, she added.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Huntley disclosed receiving research support from Nyxoah and Inspire, and serving as a consultant for Nyxoah, Inspire, and Avivomed.
Dr. Durr had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Use of a modified sleep apnea index can identify cardiovascular risk factors in adults with moderate to severe obstructive sleep apnea (OSA), according to results from a new study presented at the American Academy of Otolaryngology–Head and Neck Surgery 2024 Annual Meeting.
, said Jennifer A. Goldfarb, MHS, a medical student at Thomas Jefferson University, Philadelphia, Pennsylvania, who presented the findings.
OSA has an association with many negative cardiovascular comorbidities; however, “the AHI provides only a single metric and does not provide a holistic assessment of the individual patient’s disease severity,” said senior author Colin T. Huntley, MD, also of Thomas Jefferson University.
“OSA is very complex, and having a robust system to assess the disease may be a better predictor of overall severity,” he told this news organization.
Previous research has shown a correlation between mSASI and mean arterial pressure and serum C-reactive protein in OSA patients, but the connection with cardiovascular risk factors has not been well studied, Ms. Goldfarb noted.
In the retrospective cohort study, Ms. Goldfarb and colleagues looked at mSASI scores from 260 CPAP-intolerant patients with OSA who underwent upper airway stimulation, maxillomandibular advancement, or expansion sphincter pharyngoplasty at a single sleep surgery clinic between 2014 and 2021. The mSASI uses a score of 1-3, with 3 as the highest level of OSA severity.
Cardiovascular risk factors were assessed at the patient’s initial evaluation by the sleep surgery team. They included coronary artery disease, type 2 diabetes, atrial fibrillation, congestive heart failure, hypertension, and cerebrovascular accident.
A total of 142 patients (55%) had an mSASI of 1; 91 (35%) had an mSASI of 2; and 27 (10%) had an mSASI of 3. At least one cardiovascular risk factor was present in 58%, 68%, and 63% of these groups, respectively (P = .3).
Stratifying participants by mSASI scores, the researchers found that patients with an mSASI of 2 or 3 were significantly more likely than those with an mSASI of 1 to have more cardiovascular risk factors on initial presentation, and were significantly more likely to be diagnosed with hypertension (P = .02 for both).
Using the AHI, however, patients with moderate to severe OSA (AHI > 15) had a similar number of cardiovascular risk factors as those with mild OSA (P > .05).
“A higher mSASI score, which represents worse disease, was associated with a higher Framingham risk score, which supported our hypothesis; however, the AHI was not found to be associated with an increased Framingham score,” Dr. Huntley told this news organization.
Takeaways and Next Steps
These results suggest that the AHI, while a good metric, might not be the best tool for assessment of overall disease severity, given the complexity of OSA, the impact of the disease on patient quality of life, and the risk for downstream cardiovascular disease, said Dr. Huntley.
The findings were limited by the retrospective design and use of data from a single center.
Population-level data are needed to identify variables that may be meaningful to create a future tool that provides the best picture of the individual patient’s disease, he added. Additional prospective data are also needed to assess the impact of the scoring system on long-term treatment outcomes.
“The current study is especially interesting as we are just beginning to understand the factors that predict cardiovascular risk for patients with obstructive sleep apnea,” Megan Durr, MD, of the University of California, San Francisco, said in an interview.
“For a long time, we primarily looked at the AHI and/or oxygen levels during sleep as risk factors, and we haven’t looked as much at other factors.” said Dr. Durr, who served as a moderator for the session in which the study was presented.
The current findings provide a more comprehensive look at cardiovascular risk; the inclusion of patient anatomy and symptoms add to the knowledge of this topic, and will lead to further work in this area, she added.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Huntley disclosed receiving research support from Nyxoah and Inspire, and serving as a consultant for Nyxoah, Inspire, and Avivomed.
Dr. Durr had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Use of a modified sleep apnea index can identify cardiovascular risk factors in adults with moderate to severe obstructive sleep apnea (OSA), according to results from a new study presented at the American Academy of Otolaryngology–Head and Neck Surgery 2024 Annual Meeting.
, said Jennifer A. Goldfarb, MHS, a medical student at Thomas Jefferson University, Philadelphia, Pennsylvania, who presented the findings.
OSA has an association with many negative cardiovascular comorbidities; however, “the AHI provides only a single metric and does not provide a holistic assessment of the individual patient’s disease severity,” said senior author Colin T. Huntley, MD, also of Thomas Jefferson University.
“OSA is very complex, and having a robust system to assess the disease may be a better predictor of overall severity,” he told this news organization.
Previous research has shown a correlation between mSASI and mean arterial pressure and serum C-reactive protein in OSA patients, but the connection with cardiovascular risk factors has not been well studied, Ms. Goldfarb noted.
In the retrospective cohort study, Ms. Goldfarb and colleagues looked at mSASI scores from 260 CPAP-intolerant patients with OSA who underwent upper airway stimulation, maxillomandibular advancement, or expansion sphincter pharyngoplasty at a single sleep surgery clinic between 2014 and 2021. The mSASI uses a score of 1-3, with 3 as the highest level of OSA severity.
Cardiovascular risk factors were assessed at the patient’s initial evaluation by the sleep surgery team. They included coronary artery disease, type 2 diabetes, atrial fibrillation, congestive heart failure, hypertension, and cerebrovascular accident.
A total of 142 patients (55%) had an mSASI of 1; 91 (35%) had an mSASI of 2; and 27 (10%) had an mSASI of 3. At least one cardiovascular risk factor was present in 58%, 68%, and 63% of these groups, respectively (P = .3).
Stratifying participants by mSASI scores, the researchers found that patients with an mSASI of 2 or 3 were significantly more likely than those with an mSASI of 1 to have more cardiovascular risk factors on initial presentation, and were significantly more likely to be diagnosed with hypertension (P = .02 for both).
Using the AHI, however, patients with moderate to severe OSA (AHI > 15) had a similar number of cardiovascular risk factors as those with mild OSA (P > .05).
“A higher mSASI score, which represents worse disease, was associated with a higher Framingham risk score, which supported our hypothesis; however, the AHI was not found to be associated with an increased Framingham score,” Dr. Huntley told this news organization.
Takeaways and Next Steps
These results suggest that the AHI, while a good metric, might not be the best tool for assessment of overall disease severity, given the complexity of OSA, the impact of the disease on patient quality of life, and the risk for downstream cardiovascular disease, said Dr. Huntley.
The findings were limited by the retrospective design and use of data from a single center.
Population-level data are needed to identify variables that may be meaningful to create a future tool that provides the best picture of the individual patient’s disease, he added. Additional prospective data are also needed to assess the impact of the scoring system on long-term treatment outcomes.
“The current study is especially interesting as we are just beginning to understand the factors that predict cardiovascular risk for patients with obstructive sleep apnea,” Megan Durr, MD, of the University of California, San Francisco, said in an interview.
“For a long time, we primarily looked at the AHI and/or oxygen levels during sleep as risk factors, and we haven’t looked as much at other factors.” said Dr. Durr, who served as a moderator for the session in which the study was presented.
The current findings provide a more comprehensive look at cardiovascular risk; the inclusion of patient anatomy and symptoms add to the knowledge of this topic, and will lead to further work in this area, she added.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Huntley disclosed receiving research support from Nyxoah and Inspire, and serving as a consultant for Nyxoah, Inspire, and Avivomed.
Dr. Durr had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
FROM AAO-HNS 2024
Three Tips to Avoid Common Diagnostic Errors in Primary Care
Common complaints of abdominal pain, fever, shortness of breath, or rash can signal more serious disease that should be referred to specialty care or might be related to benign conditions.
Combine the vague nature of many patients’ descriptions and the pressure of short visits, and clinicians have a recipe for all manner of diagnostic error.
An estimated 5% of US adults who seek outpatient care each year experience a diagnostic error. Most Americans will eventually have this experience, according to a 2015 report from the National Academy of Medicine.
The most frequently missed diagnoses in primary care involve conditions such as pneumonia, decompensated heart failure, acute renal failure, cancer, urinary tract infection, and pyelonephritis.
“It’s not one or two or three types of diagnosis that are missed: We miss a lot of things, especially in primary care,” said Hardeep Singh, MD, MPH, a patient safety researcher at the Michael E. DeBakey VA Medical Center and the Baylor College of Medicine in Houston, Texas.
One of the most serious errors is to miss cancer, with failing to follow‐up on abnormal tests ranking consistently as one of the leading causes of malpractice claims. But most diagnostic errors do not lead to lawsuits, although they often result in missed and delayed opportunities for patients to get needed care.
In interviews with this news organization, experts who have studied the root causes of diagnostic error suggested primary care clinicians focus on several practices to avoid mistakes: Ask questions with humility and curiosity, use checklists, and brainstorm with patients the potential root cause of symptoms.
Humility and Curiosity
Clinicians should remain aware of the potential for errors and reach out for assistance when needed, keeping an open mind that common symptoms may, in rare cases, signal serious illness, Dr. Singh said.
Dr. Singh recommends continual review with what he calls “byte-sized” learning through digital tools such as the Human Diagnosis app and podcasts and webinars offered by Clinical Problem Solvers.
Continuing education activities such as classes for Maintenance of Certification (MOC) can help keep physicians up to date and alert for cases where seemingly common symptoms may turn out to be something serious, said Richard M. Wardrop, III, MD, PhD, an internal medicine physician at the Cleveland Clinic in Ohio, and chair of the internal medicine board at the American Board of Internal Medicine.
“I’ve been in practice for 20 years. I’m double board certified in peds and medicine, and I regularly teach students and residents and mentor other physicians, but the further I go in my career and in practice, the more humble I become,” Dr. Wardrop told this news organization.
He said he recently spent a few hours on MOC for pediatrics and found the review was helpful in his practice in medicine.
“If I find myself taking care of a patient in a newborn nursery anytime soon, I’m going to understand the new hyperbilirubinemia guidelines,” Dr. Wardrop said. “That takes time and energy, but when I was done with the questions for this quarter, I felt good about myself.”
Checking It Twice
Clinicians should incorporate checklists into daily practice. Reviewing these with patients can not only help rule out an illness but also serve as a nonconfrontational method to inquire about issues patients may find uncomfortable, said John Ely, MD, MSPH, professor emeritus of family medicine at the University of Iowa Carver College of Medicine in Iowa City.
Clinicians could benefit from the approach used in aviation, where checklists are a required and routine part of a pilot’s job, Dr. Ely said.
Although clinicians may assume patients expect them to work from memory and knowledge without this aide, many will see using a checklist as a sign of providing thorough care, he said.
Checklists can also open a pathway for discussions about potentially difficult or touchy issues in short visits. For example, a patient might feel defensive if a clinician asks about depression during a visit for abdominal pain. But incorporating a question in a checklist allows for a different framing of the question.
“A clinician could say ‘I didn’t say you were depressed because of your abdominal pain, I brought it up because it’s on the list,’” Dr. Ely said. The checklist is “a very easy way to bring up those things.”
Dr. Ely said he has cared for a few patients who sought help for abdominal pain that turned out to be linked to sexual abuse in their past. Dr. Ely used a checklist with these patients to review possible causes for their illness. He recalled one of these patients who had suffered sexual abuse and had depression, neither of which was readily apparent.
“There was nothing about her affect that appeared to be depressed, and she had seen multiple physicians unable to make a diagnosis,” Dr. Ely said. “She had worked up for multiple other diseases and this had never come up before.”
Cooperation
“Coproduction” is how Kathryn McDonald, PhD, describes an ideal path to getting an accurate diagnosis. The intent is for clinicians to enlist patients in helping them in finding the root cause of symptoms.
“It’s bringing the patient into knowing that they are in a partnership to coproduce, knowing that there is a process going on,” said Dr. McDonald, who is codirector of the Armstrong Institute Center for Diagnostic Excellence at Johns Hopkins University in Baltimore, Maryland.
In many cases, patients seek reassurance for ruling out a suspected condition, which the physician can sometimes provide. In others, clinicians may not be able to offer a concrete diagnosis.
“There are times when uncertainty is more pervasive and I will ask patients, ‘Let’s brainstorm this together,’” Dr. Wardrop said.
A version of this article appeared on Medscape.com.
Common complaints of abdominal pain, fever, shortness of breath, or rash can signal more serious disease that should be referred to specialty care or might be related to benign conditions.
Combine the vague nature of many patients’ descriptions and the pressure of short visits, and clinicians have a recipe for all manner of diagnostic error.
An estimated 5% of US adults who seek outpatient care each year experience a diagnostic error. Most Americans will eventually have this experience, according to a 2015 report from the National Academy of Medicine.
The most frequently missed diagnoses in primary care involve conditions such as pneumonia, decompensated heart failure, acute renal failure, cancer, urinary tract infection, and pyelonephritis.
“It’s not one or two or three types of diagnosis that are missed: We miss a lot of things, especially in primary care,” said Hardeep Singh, MD, MPH, a patient safety researcher at the Michael E. DeBakey VA Medical Center and the Baylor College of Medicine in Houston, Texas.
One of the most serious errors is to miss cancer, with failing to follow‐up on abnormal tests ranking consistently as one of the leading causes of malpractice claims. But most diagnostic errors do not lead to lawsuits, although they often result in missed and delayed opportunities for patients to get needed care.
In interviews with this news organization, experts who have studied the root causes of diagnostic error suggested primary care clinicians focus on several practices to avoid mistakes: Ask questions with humility and curiosity, use checklists, and brainstorm with patients the potential root cause of symptoms.
Humility and Curiosity
Clinicians should remain aware of the potential for errors and reach out for assistance when needed, keeping an open mind that common symptoms may, in rare cases, signal serious illness, Dr. Singh said.
Dr. Singh recommends continual review with what he calls “byte-sized” learning through digital tools such as the Human Diagnosis app and podcasts and webinars offered by Clinical Problem Solvers.
Continuing education activities such as classes for Maintenance of Certification (MOC) can help keep physicians up to date and alert for cases where seemingly common symptoms may turn out to be something serious, said Richard M. Wardrop, III, MD, PhD, an internal medicine physician at the Cleveland Clinic in Ohio, and chair of the internal medicine board at the American Board of Internal Medicine.
“I’ve been in practice for 20 years. I’m double board certified in peds and medicine, and I regularly teach students and residents and mentor other physicians, but the further I go in my career and in practice, the more humble I become,” Dr. Wardrop told this news organization.
He said he recently spent a few hours on MOC for pediatrics and found the review was helpful in his practice in medicine.
“If I find myself taking care of a patient in a newborn nursery anytime soon, I’m going to understand the new hyperbilirubinemia guidelines,” Dr. Wardrop said. “That takes time and energy, but when I was done with the questions for this quarter, I felt good about myself.”
Checking It Twice
Clinicians should incorporate checklists into daily practice. Reviewing these with patients can not only help rule out an illness but also serve as a nonconfrontational method to inquire about issues patients may find uncomfortable, said John Ely, MD, MSPH, professor emeritus of family medicine at the University of Iowa Carver College of Medicine in Iowa City.
Clinicians could benefit from the approach used in aviation, where checklists are a required and routine part of a pilot’s job, Dr. Ely said.
Although clinicians may assume patients expect them to work from memory and knowledge without this aide, many will see using a checklist as a sign of providing thorough care, he said.
Checklists can also open a pathway for discussions about potentially difficult or touchy issues in short visits. For example, a patient might feel defensive if a clinician asks about depression during a visit for abdominal pain. But incorporating a question in a checklist allows for a different framing of the question.
“A clinician could say ‘I didn’t say you were depressed because of your abdominal pain, I brought it up because it’s on the list,’” Dr. Ely said. The checklist is “a very easy way to bring up those things.”
Dr. Ely said he has cared for a few patients who sought help for abdominal pain that turned out to be linked to sexual abuse in their past. Dr. Ely used a checklist with these patients to review possible causes for their illness. He recalled one of these patients who had suffered sexual abuse and had depression, neither of which was readily apparent.
“There was nothing about her affect that appeared to be depressed, and she had seen multiple physicians unable to make a diagnosis,” Dr. Ely said. “She had worked up for multiple other diseases and this had never come up before.”
Cooperation
“Coproduction” is how Kathryn McDonald, PhD, describes an ideal path to getting an accurate diagnosis. The intent is for clinicians to enlist patients in helping them in finding the root cause of symptoms.
“It’s bringing the patient into knowing that they are in a partnership to coproduce, knowing that there is a process going on,” said Dr. McDonald, who is codirector of the Armstrong Institute Center for Diagnostic Excellence at Johns Hopkins University in Baltimore, Maryland.
In many cases, patients seek reassurance for ruling out a suspected condition, which the physician can sometimes provide. In others, clinicians may not be able to offer a concrete diagnosis.
“There are times when uncertainty is more pervasive and I will ask patients, ‘Let’s brainstorm this together,’” Dr. Wardrop said.
A version of this article appeared on Medscape.com.
Common complaints of abdominal pain, fever, shortness of breath, or rash can signal more serious disease that should be referred to specialty care or might be related to benign conditions.
Combine the vague nature of many patients’ descriptions and the pressure of short visits, and clinicians have a recipe for all manner of diagnostic error.
An estimated 5% of US adults who seek outpatient care each year experience a diagnostic error. Most Americans will eventually have this experience, according to a 2015 report from the National Academy of Medicine.
The most frequently missed diagnoses in primary care involve conditions such as pneumonia, decompensated heart failure, acute renal failure, cancer, urinary tract infection, and pyelonephritis.
“It’s not one or two or three types of diagnosis that are missed: We miss a lot of things, especially in primary care,” said Hardeep Singh, MD, MPH, a patient safety researcher at the Michael E. DeBakey VA Medical Center and the Baylor College of Medicine in Houston, Texas.
One of the most serious errors is to miss cancer, with failing to follow‐up on abnormal tests ranking consistently as one of the leading causes of malpractice claims. But most diagnostic errors do not lead to lawsuits, although they often result in missed and delayed opportunities for patients to get needed care.
In interviews with this news organization, experts who have studied the root causes of diagnostic error suggested primary care clinicians focus on several practices to avoid mistakes: Ask questions with humility and curiosity, use checklists, and brainstorm with patients the potential root cause of symptoms.
Humility and Curiosity
Clinicians should remain aware of the potential for errors and reach out for assistance when needed, keeping an open mind that common symptoms may, in rare cases, signal serious illness, Dr. Singh said.
Dr. Singh recommends continual review with what he calls “byte-sized” learning through digital tools such as the Human Diagnosis app and podcasts and webinars offered by Clinical Problem Solvers.
Continuing education activities such as classes for Maintenance of Certification (MOC) can help keep physicians up to date and alert for cases where seemingly common symptoms may turn out to be something serious, said Richard M. Wardrop, III, MD, PhD, an internal medicine physician at the Cleveland Clinic in Ohio, and chair of the internal medicine board at the American Board of Internal Medicine.
“I’ve been in practice for 20 years. I’m double board certified in peds and medicine, and I regularly teach students and residents and mentor other physicians, but the further I go in my career and in practice, the more humble I become,” Dr. Wardrop told this news organization.
He said he recently spent a few hours on MOC for pediatrics and found the review was helpful in his practice in medicine.
“If I find myself taking care of a patient in a newborn nursery anytime soon, I’m going to understand the new hyperbilirubinemia guidelines,” Dr. Wardrop said. “That takes time and energy, but when I was done with the questions for this quarter, I felt good about myself.”
Checking It Twice
Clinicians should incorporate checklists into daily practice. Reviewing these with patients can not only help rule out an illness but also serve as a nonconfrontational method to inquire about issues patients may find uncomfortable, said John Ely, MD, MSPH, professor emeritus of family medicine at the University of Iowa Carver College of Medicine in Iowa City.
Clinicians could benefit from the approach used in aviation, where checklists are a required and routine part of a pilot’s job, Dr. Ely said.
Although clinicians may assume patients expect them to work from memory and knowledge without this aide, many will see using a checklist as a sign of providing thorough care, he said.
Checklists can also open a pathway for discussions about potentially difficult or touchy issues in short visits. For example, a patient might feel defensive if a clinician asks about depression during a visit for abdominal pain. But incorporating a question in a checklist allows for a different framing of the question.
“A clinician could say ‘I didn’t say you were depressed because of your abdominal pain, I brought it up because it’s on the list,’” Dr. Ely said. The checklist is “a very easy way to bring up those things.”
Dr. Ely said he has cared for a few patients who sought help for abdominal pain that turned out to be linked to sexual abuse in their past. Dr. Ely used a checklist with these patients to review possible causes for their illness. He recalled one of these patients who had suffered sexual abuse and had depression, neither of which was readily apparent.
“There was nothing about her affect that appeared to be depressed, and she had seen multiple physicians unable to make a diagnosis,” Dr. Ely said. “She had worked up for multiple other diseases and this had never come up before.”
Cooperation
“Coproduction” is how Kathryn McDonald, PhD, describes an ideal path to getting an accurate diagnosis. The intent is for clinicians to enlist patients in helping them in finding the root cause of symptoms.
“It’s bringing the patient into knowing that they are in a partnership to coproduce, knowing that there is a process going on,” said Dr. McDonald, who is codirector of the Armstrong Institute Center for Diagnostic Excellence at Johns Hopkins University in Baltimore, Maryland.
In many cases, patients seek reassurance for ruling out a suspected condition, which the physician can sometimes provide. In others, clinicians may not be able to offer a concrete diagnosis.
“There are times when uncertainty is more pervasive and I will ask patients, ‘Let’s brainstorm this together,’” Dr. Wardrop said.
A version of this article appeared on Medscape.com.
Heightened Amygdala Activity Tied to Postpartum Depression
MILAN, ITALY — Pregnant women with heightened amygdala activity have a reduced capacity to regulate emotions and report more symptoms of depression than those with lower activity in this brain region, a new imaging study suggested.
If validated, these findings could pave the way for identifying women at higher risk for postpartum depression, said lead researcher Franziska Weinmar, MSc, from the University of Tübingen in Germany.
The study was presented at the 37th European College of Neuropsychopharmacology Congress.
Differences in Brain Activity
During pregnancy and the peripartum period, rising hormone levels create a “psychoneuroendocrinological window of vulnerability” for mental health in which 80% of women can develop transitory “baby blues,” and about one in seven develop more serious postpartum depression, Ms. Weinmar told this news organization.
The study included 47 women — 15 pregnant women and 32 nonpregnant controls. The nonpregnant women had normal menstrual cycles; 16 were in the early follicular phase with low estradiol levels (231.7 pmol/L), and 16 had high estradiol levels (516.6 pmol/L) after administration of estradiol.
To examine brain activity, participants were asked to view negative emotional images while undergoing functional MRI. They were then asked to use cognitive reappraisal to regulate their emotional response to the images.
The findings showed that both pregnant and nonpregnant women were equally successful at emotional regulation, but this process involved different brain activity in pregnant vs their nonpregnant counterpart.
All women had increased left middle frontal gyrus activity when regulating their emotions, but there was a difference in the amygdala between the pregnancy group and controls, Ms. Weinmar noted.
This suggests that pregnant women may have to exert more neural effort in emotional regulation, she said. “And pregnant women with higher amygdala activity were less able to regulate their emotions successfully compared to those with less amygdala activity.”
Linear regression analyses were performed to assess the relation of brain activity during down-regulation, regulation success, and self-reported depression scores, and this showed that higher amygdala activity was also associated with higher depression scores.
“We need to be cautious in interpreting this,” said Ms. Weinmar. “This is a small sample, and we are the first to undertake this work.”
Nonetheless, she said that if the findings are confirmed by larger studies, pregnant women could be assessed “in the waiting room” using existing questionnaires that evaluate emotional regulation.
If a woman has difficulties with emotion regulation, “there are adaptive strategies, like cognitive reappraisal that a counseling psychotherapist can help with,” said Ms. Weinmar.
“I could also imagine group sessions, for example, or online courses,” she said, adding that obstetricians could also be trained to identify these women.
Commenting on the findings in a press release, Susana Carmona, PhD, from Gregorio Marañón Hospital in Madrid, Spain, said research like this is crucial for gaining insight into one of the most intense physiological processes a human can undergo: pregnancy. It’s remarkable how much remains unknown.
“Recently, the FDA [Food and Drug Administration] approved the first treatment for postpartum depression. However, we still have a long way to go in characterizing what happens in the brain during pregnancy, identifying biomarkers that can indicate the risk of developing perinatal mental disorders, and designing strategies to prevent mother and infant suffering during the delicate and critical peripartum period,” Dr. Carmona added.
The study was supported by the Center for Integrative Neuroscience in Tübingen, Germany, and the International Research Training Group “Women’s Mental Health Across the Reproductive Years” (IRTG 2804). Ms. Weinmar and Dr. Carmona reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN, ITALY — Pregnant women with heightened amygdala activity have a reduced capacity to regulate emotions and report more symptoms of depression than those with lower activity in this brain region, a new imaging study suggested.
If validated, these findings could pave the way for identifying women at higher risk for postpartum depression, said lead researcher Franziska Weinmar, MSc, from the University of Tübingen in Germany.
The study was presented at the 37th European College of Neuropsychopharmacology Congress.
Differences in Brain Activity
During pregnancy and the peripartum period, rising hormone levels create a “psychoneuroendocrinological window of vulnerability” for mental health in which 80% of women can develop transitory “baby blues,” and about one in seven develop more serious postpartum depression, Ms. Weinmar told this news organization.
The study included 47 women — 15 pregnant women and 32 nonpregnant controls. The nonpregnant women had normal menstrual cycles; 16 were in the early follicular phase with low estradiol levels (231.7 pmol/L), and 16 had high estradiol levels (516.6 pmol/L) after administration of estradiol.
To examine brain activity, participants were asked to view negative emotional images while undergoing functional MRI. They were then asked to use cognitive reappraisal to regulate their emotional response to the images.
The findings showed that both pregnant and nonpregnant women were equally successful at emotional regulation, but this process involved different brain activity in pregnant vs their nonpregnant counterpart.
All women had increased left middle frontal gyrus activity when regulating their emotions, but there was a difference in the amygdala between the pregnancy group and controls, Ms. Weinmar noted.
This suggests that pregnant women may have to exert more neural effort in emotional regulation, she said. “And pregnant women with higher amygdala activity were less able to regulate their emotions successfully compared to those with less amygdala activity.”
Linear regression analyses were performed to assess the relation of brain activity during down-regulation, regulation success, and self-reported depression scores, and this showed that higher amygdala activity was also associated with higher depression scores.
“We need to be cautious in interpreting this,” said Ms. Weinmar. “This is a small sample, and we are the first to undertake this work.”
Nonetheless, she said that if the findings are confirmed by larger studies, pregnant women could be assessed “in the waiting room” using existing questionnaires that evaluate emotional regulation.
If a woman has difficulties with emotion regulation, “there are adaptive strategies, like cognitive reappraisal that a counseling psychotherapist can help with,” said Ms. Weinmar.
“I could also imagine group sessions, for example, or online courses,” she said, adding that obstetricians could also be trained to identify these women.
Commenting on the findings in a press release, Susana Carmona, PhD, from Gregorio Marañón Hospital in Madrid, Spain, said research like this is crucial for gaining insight into one of the most intense physiological processes a human can undergo: pregnancy. It’s remarkable how much remains unknown.
“Recently, the FDA [Food and Drug Administration] approved the first treatment for postpartum depression. However, we still have a long way to go in characterizing what happens in the brain during pregnancy, identifying biomarkers that can indicate the risk of developing perinatal mental disorders, and designing strategies to prevent mother and infant suffering during the delicate and critical peripartum period,” Dr. Carmona added.
The study was supported by the Center for Integrative Neuroscience in Tübingen, Germany, and the International Research Training Group “Women’s Mental Health Across the Reproductive Years” (IRTG 2804). Ms. Weinmar and Dr. Carmona reported no relevant disclosures.
A version of this article appeared on Medscape.com.
MILAN, ITALY — Pregnant women with heightened amygdala activity have a reduced capacity to regulate emotions and report more symptoms of depression than those with lower activity in this brain region, a new imaging study suggested.
If validated, these findings could pave the way for identifying women at higher risk for postpartum depression, said lead researcher Franziska Weinmar, MSc, from the University of Tübingen in Germany.
The study was presented at the 37th European College of Neuropsychopharmacology Congress.
Differences in Brain Activity
During pregnancy and the peripartum period, rising hormone levels create a “psychoneuroendocrinological window of vulnerability” for mental health in which 80% of women can develop transitory “baby blues,” and about one in seven develop more serious postpartum depression, Ms. Weinmar told this news organization.
The study included 47 women — 15 pregnant women and 32 nonpregnant controls. The nonpregnant women had normal menstrual cycles; 16 were in the early follicular phase with low estradiol levels (231.7 pmol/L), and 16 had high estradiol levels (516.6 pmol/L) after administration of estradiol.
To examine brain activity, participants were asked to view negative emotional images while undergoing functional MRI. They were then asked to use cognitive reappraisal to regulate their emotional response to the images.
The findings showed that both pregnant and nonpregnant women were equally successful at emotional regulation, but this process involved different brain activity in pregnant vs their nonpregnant counterpart.
All women had increased left middle frontal gyrus activity when regulating their emotions, but there was a difference in the amygdala between the pregnancy group and controls, Ms. Weinmar noted.
This suggests that pregnant women may have to exert more neural effort in emotional regulation, she said. “And pregnant women with higher amygdala activity were less able to regulate their emotions successfully compared to those with less amygdala activity.”
Linear regression analyses were performed to assess the relation of brain activity during down-regulation, regulation success, and self-reported depression scores, and this showed that higher amygdala activity was also associated with higher depression scores.
“We need to be cautious in interpreting this,” said Ms. Weinmar. “This is a small sample, and we are the first to undertake this work.”
Nonetheless, she said that if the findings are confirmed by larger studies, pregnant women could be assessed “in the waiting room” using existing questionnaires that evaluate emotional regulation.
If a woman has difficulties with emotion regulation, “there are adaptive strategies, like cognitive reappraisal that a counseling psychotherapist can help with,” said Ms. Weinmar.
“I could also imagine group sessions, for example, or online courses,” she said, adding that obstetricians could also be trained to identify these women.
Commenting on the findings in a press release, Susana Carmona, PhD, from Gregorio Marañón Hospital in Madrid, Spain, said research like this is crucial for gaining insight into one of the most intense physiological processes a human can undergo: pregnancy. It’s remarkable how much remains unknown.
“Recently, the FDA [Food and Drug Administration] approved the first treatment for postpartum depression. However, we still have a long way to go in characterizing what happens in the brain during pregnancy, identifying biomarkers that can indicate the risk of developing perinatal mental disorders, and designing strategies to prevent mother and infant suffering during the delicate and critical peripartum period,” Dr. Carmona added.
The study was supported by the Center for Integrative Neuroscience in Tübingen, Germany, and the International Research Training Group “Women’s Mental Health Across the Reproductive Years” (IRTG 2804). Ms. Weinmar and Dr. Carmona reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ECNP 2024
Purpuric Lesions on the Leg
THE DIAGNOSIS: Dengue Hemorrhagic Fever
The retiform purpura observed in our patient was suggestive of a vasculitic, thrombotic, or embolic etiology. Dengue IgM serologic testing performed based on her extensive travel history and recent return from a dengue-endemic area was positive, indicating acute infection. A clinical diagnosis of dengue hemorrhagic fever (DHF) was made based on the hemorrhagic appearance of the lesion. Histopathology revealed leukocytoclastic vasculitis (Figure). Anti–double-stranded DNA, antideoxyribonuclease, C3 and C4, CH50 (total hemolytic complement), antineutrophil cytoplasmic antibodies, HIV, and hepatitis B virus tests were normal. Direct immunofluorescence was negative.
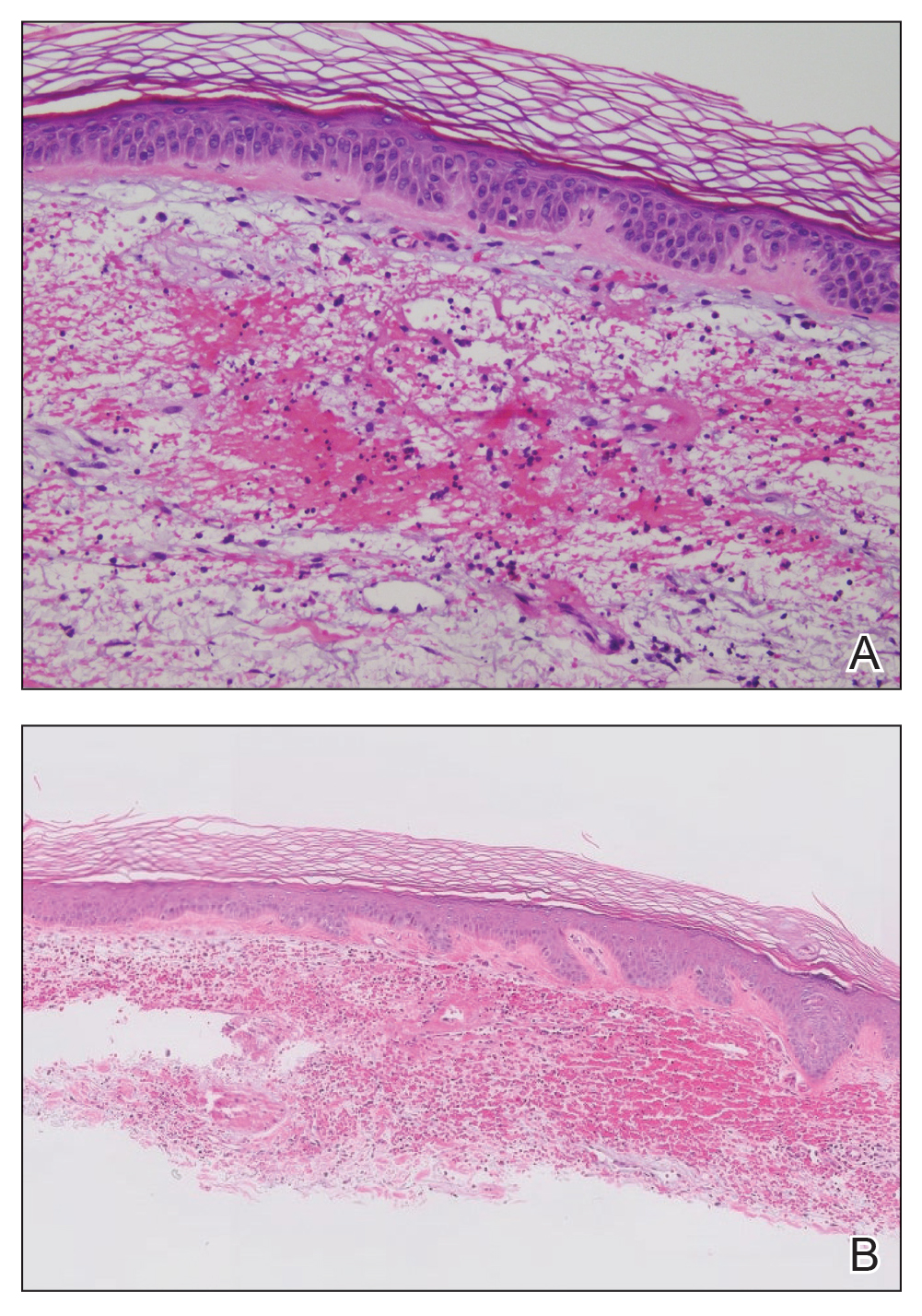
Dengue virus is a single-stranded RNA virus transmitted by Aedes aegypti and Aedes albopictus mosquitoes and is one of the most prevalent arthropod-borne viruses affecting humans today.1,2 Infection with the dengue virus generally is seen in travelers visiting tropical regions of Africa, Mexico, South America, South and Central Asia, Southeast Asia, and the Caribbean.1 The Table shows the global distribution of dengue serotypes from 2000 to 2014.3,4 There are 4 serotypes of the dengue virus: DENV-1 to DENV-4. Infection with 1 strain elicits longlasting immunity to that strain, but subsequent infection with another strain can result in severe DHF due to antibody cross-reaction.1
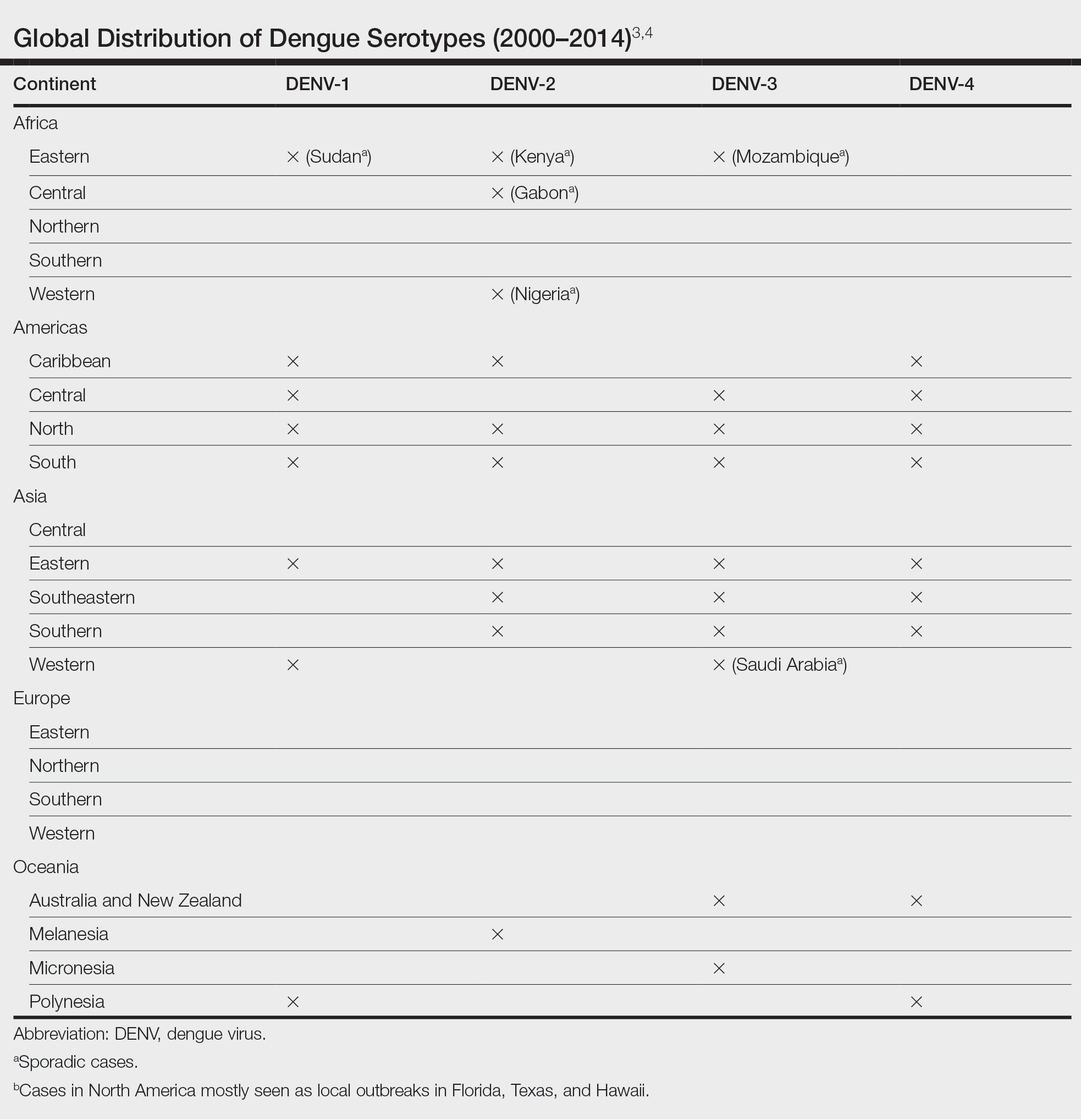
Dengue virus infection ranges from mildly symptomatic to a spectrum of increasingly severe conditions that comprise dengue fever (DF) and DHF, as well as dengue shock syndrome and brain stem hemorrhage, which may be fatal.2,5 Dengue fever manifests as severe myalgia, fever, headache (usually retro-orbital), arthralgia, erythema, and rubelliform exanthema.6 The frequency of skin eruptions in patients with DF varies with the virus strain and outbreaks.7 The lesions initially develop with the onset of fever and manifest as flushing or erythematous mottling of the face, neck, and chest areas.1,7 The morbilliform eruption develops 2 to 6 days after the onset of the fever, beginning on the trunk and spreading to the face and extremities.1,7 The rash may become confluent with characteristic sparing of small round areas of normal skin described as white islands in a sea of red.2 Verrucous papules on the ears also have been described and may resemble those seen in Cowden syndrome. In patients with prior infection with a different strain of the virus, hemorrhagic lesions may develop, including characteristic retiform purpura, a positive tourniquet test, and the appearance of petechiae on the lower legs. Pruritus and desquamation, especially on the palms and soles, may follow the termination of the eruption.7
The differential diagnosis of DF includes measles, rubella, enteroviruses, and influenza. Chikungunya and West Nile viruses in Asia and Africa and the O’nyong-nyong virus in Africa are also arboviruses that cause a clinical picture similar to DF but not DHF. Other diagnostic considerations include phases of scarlet fever, typhoid, malaria, leptospirosis, hepatitis A, and trypanosomal and rickettsial diseases.7 The differential diagnosis of DHF includes antineutrophil cytoplasmic antibody–associated vasculitis, rheumatoid vasculitis, and bacterial septic vasculitis.
Acute clinical diagnosis of DF can be challenging because of the nonspecific symptoms that can be seen in almost every infectious disease. Clinical presentation assessment should be confirmed with laboratory testing.6 Dengue virus infection usually is confirmed by the identification of viral genomic RNA, antigens, or the antibodies it elicits. Enzyme-linked immunosorbent assay–based serologic tests are cost-effective and easy to perform.5 IgM antibodies usually show cross-reactivity with platelets, but the antibody levels are not positively correlated with the severity of DF.8 Primary infection with the dengue virus is characterized by the elevation of specific IgM levels that usually occurs 3 to 5 days after symptom onset and persists during the postfebrile stage (up to 30 to 60 days). In secondary infections, the IgM levels usually rise more slowly and reach a lower level than in primary infections.9 For both primary and secondary infections, testing IgM levels after the febrile stage may be helpful with the laboratory diagnosis.
Currently, there is no antiviral drug available for dengue. Treatment of dengue infection is symptomatic and supportive.2
Dengue hemorrhagic fever is indicated by a rising hematocrit (≥20%) and a falling platelet count (>100,000/mm3) accompanying clinical signs of hemorrhage. Treatment includes intravenous fluid replacement and careful clinical monitoring of hematocrit levels, platelet count, vitals, urine output, and other signs of shock.5 For patients with a history of dengue infection, travel to areas with other serotypes is not recommended.
If any travel to a high-risk area is planned, countryspecific travel recommendations and warnings should be reviewed from the Centers for Disease Control and Prevention’s website (https://wwwnc.cdc.gov/travel/notices/level1/dengue-global). Use of an Environmental Protection Agency–registered insect repellent to avoid mosquito bites and acetaminophen for managing symptoms is advised. During travel, staying in places with window and door screens and using a bed net during sleep are suggested. Long-sleeved shirts and long pants also are preferred. Travelers should see a health care provider if they have symptoms of dengue.10
African tick bite fever (ATBF) is caused by Rickettsia africae transmitted by Amblyomma ticks. Skin findings in ATBF include erythematous, firm, tender papules with central eschars consistent with the feeding patterns of ticks.11 Histopathology of ATBF usually includes fibrinoid necrosis of vessels in the dermis with a perivascular inflammatory infiltrate and coagulation necrosis of the surrounding dermis consistent with eschar formation.12 The lack of an eschar weighs against this diagnosis.
African trypanosomiasis (also known as sleeping sickness) is caused by protozoa transmitted by the tsetse fly. A chancrelike, circumscribed, rubbery, indurated red or violaceous nodule measuring 2 to 5 cm in diameter often develops as the earliest cutaneous sign of the disease.13 Nonspecific histopathologic findings, such as infiltration of lymphocytes and macrophages and proliferation of endothelial cells and fibroblasts, may be observed.14 Extravascular parasites have been noted in skin biopsies.15 In later stages, skin lesions called trypanids may be observed as macular, papular, annular, targetoid, purpuric, and erythematous lesions, and histopathologic findings consistent with vasculitis also may be seen.13
Chikungunya virus infection is an acute-onset, mosquito-borne viral disease. Skin manifestations may start with nonspecific, generalized, morbilliform, maculopapular rashes coinciding with fever, which also may be seen initially with DHF. Skin hyperpigmentation, mostly centrofacial and involving the nose (chik sign); purpuric and ecchymotic lesions over the trunk and flexors of limbs in adults, often surmounted by subepidermal bullae and lesions resembling toxic epidermal necrolysis; and nonhealing ulcers in the genital and groin areas are common skin manifestations of chikungunya infection.16 Intraepithelial splitting with acantholysis and perivascular lymphohistiocytic infiltration may be observed in the histopathology of blistering lesions, which are not consistent with DHF.17
Zika virus infection is caused by an arbovirus within the Flaviviridae family, which also includes the dengue virus. Initial mucocutaneous findings of the Zika virus include nonspecific diffuse maculopapular eruptions. The eruption generally spares the palms and soles; however, various manifestations including involvement of the palms and soles have been reported.18 The morbilliform eruption begins on the face and extends to the trunk and extremities. Mild hemorrhagic manifestations, including petechiae and bleeding gums, may be observed. Distinguishing between dengue and Zika virus infection relies on the severity of symptoms and laboratory tests, including polymerase chain reaction or IgM antibody testing.19 The other conditions listed do not produce hemorrhagic fever.
- Pincus LB, Grossman ME, Fox LP. The exanthem of dengue fever: clinical features of two US tourists traveling abroad. J Am Acad Dermatol. 2008;58:308-316. doi:10.1016/j.jaad.2007.08.042
- Radakovic-Fijan S, Graninger W, Müller C, et al. Dengue hemorrhagic fever in a British travel guide. J Am Acad Dermatol. 2002;46:430-433. doi:10.1067/mjd.2002.111904
- Yamashita A, Sakamoto T, Sekizuka T, et al. DGV: dengue genographic viewer. Front Microbiol. 2016;7:875. doi:10.3389/fmicb.2016.00875
- Centers for Disease and Prevention. Dengue in the US states and territories. Updated October 7, 2020. Accessed September 30, 2024. https://www.cdc.gov/dengue/data-research/facts-stats/?CDC_AAref_Val=https://www.cdc.gov/dengue/areaswithrisk/in-the-us.html
- Khetarpal N, Khanna I. Dengue fever: causes, complications, and vaccine strategies. J Immunol Res. 2016;2016:6803098. doi:10.1155/2016/6803098
- Muller DA, Depelsenaire AC, Young PR. Clinical and laboratory diagnosis of dengue virus infection. J Infect Dis. 2017;215(suppl 2):S89-S95. doi:10.1093/infdis/jiw649
- Waterman SH, Gubler DJ. Dengue fever. Clin Dermatol. 1989;7:117-122. doi:10.1016/0738-081x(89)90034-5
- Lin CF, Lei HY, Liu CC, et al. Generation of IgM anti-platelet autoantibody in dengue patients. J Med Virol. 2001;63:143-149. doi:10.1002/1096- 9071(20000201)63:2<143::AID-JMV1009>3.0.CO;2-L
- Tripathi NK, Shrivastava A, Dash PK, et al. Detection of dengue virus. Methods Mol Biol. 2011;665:51-64. doi:10.1007/978-1-60761-817-1_4
- Centers for Disease Control and Prevention. Plan for travel. Accessed September 30, 2024. https://wwwnc.cdc.gov/travel
- Mack I, Ritz N. African tick-bite fever. N Engl J Med. 2019;380:960. doi:10.1056/NEJMicm1810093
- Lepidi H, Fournier PE, Raoult D. Histologic features and immunodetection of African tick-bite fever eschar. Emerg Infect Dis. 2006;12:1332- 1337. doi:10.3201/eid1209.051540
- McGovern TW, Williams W, Fitzpatrick JE, et al. Cutaneous manifestations of African trypanosomiasis. Arch Dermatol. 1995;131:1178-1182.
- Kristensson K, Bentivoglio M. Pathology of African trypanosomiasis. In: Dumas M, Bouteille B, Buguet A, eds. Progress in Human African Trypanosomiasis, Sleeping Sickness. Springer; 1999:157-181.
- Capewell P, Cren-Travaillé C, Marchesi F, et al. The skin is a significant but overlooked anatomical reservoir for vector-borne African trypanosomes. Elife. 2016;5:e17716. doi:10.7554/eLife.17716
- Singal A. Chikungunya and skin: current perspective. Indian Dermatol Online J. 2017;8:307-309. doi:10.4103/idoj.IDOJ_93_17
- Robin S, Ramful D, Zettor J, et al. Severe bullous skin lesions associated with chikungunya virus infection in small infants. Eur J Pediatr. 2009;169:67-72. doi:10.1007/s00431-009-0986-0
- Hussain A, Ali F, Latiwesh OB, et al. A comprehensive review of the manifestations and pathogenesis of Zika virus in neonates and adults. Cureus. 2018;10:E3290. doi:10.7759/cureus.3290
- Farahnik B, Beroukhim K, Blattner CM, et al. Cutaneous manifestations of the Zika virus. J Am Acad Dermatol. 2016;74:1286-1287. doi:10.1016/j.jaad.2016.02.1232
THE DIAGNOSIS: Dengue Hemorrhagic Fever
The retiform purpura observed in our patient was suggestive of a vasculitic, thrombotic, or embolic etiology. Dengue IgM serologic testing performed based on her extensive travel history and recent return from a dengue-endemic area was positive, indicating acute infection. A clinical diagnosis of dengue hemorrhagic fever (DHF) was made based on the hemorrhagic appearance of the lesion. Histopathology revealed leukocytoclastic vasculitis (Figure). Anti–double-stranded DNA, antideoxyribonuclease, C3 and C4, CH50 (total hemolytic complement), antineutrophil cytoplasmic antibodies, HIV, and hepatitis B virus tests were normal. Direct immunofluorescence was negative.
Dengue virus is a single-stranded RNA virus transmitted by Aedes aegypti and Aedes albopictus mosquitoes and is one of the most prevalent arthropod-borne viruses affecting humans today.1,2 Infection with the dengue virus generally is seen in travelers visiting tropical regions of Africa, Mexico, South America, South and Central Asia, Southeast Asia, and the Caribbean.1 The Table shows the global distribution of dengue serotypes from 2000 to 2014.3,4 There are 4 serotypes of the dengue virus: DENV-1 to DENV-4. Infection with 1 strain elicits longlasting immunity to that strain, but subsequent infection with another strain can result in severe DHF due to antibody cross-reaction.1
Dengue virus infection ranges from mildly symptomatic to a spectrum of increasingly severe conditions that comprise dengue fever (DF) and DHF, as well as dengue shock syndrome and brain stem hemorrhage, which may be fatal.2,5 Dengue fever manifests as severe myalgia, fever, headache (usually retro-orbital), arthralgia, erythema, and rubelliform exanthema.6 The frequency of skin eruptions in patients with DF varies with the virus strain and outbreaks.7 The lesions initially develop with the onset of fever and manifest as flushing or erythematous mottling of the face, neck, and chest areas.1,7 The morbilliform eruption develops 2 to 6 days after the onset of the fever, beginning on the trunk and spreading to the face and extremities.1,7 The rash may become confluent with characteristic sparing of small round areas of normal skin described as white islands in a sea of red.2 Verrucous papules on the ears also have been described and may resemble those seen in Cowden syndrome. In patients with prior infection with a different strain of the virus, hemorrhagic lesions may develop, including characteristic retiform purpura, a positive tourniquet test, and the appearance of petechiae on the lower legs. Pruritus and desquamation, especially on the palms and soles, may follow the termination of the eruption.7
The differential diagnosis of DF includes measles, rubella, enteroviruses, and influenza. Chikungunya and West Nile viruses in Asia and Africa and the O’nyong-nyong virus in Africa are also arboviruses that cause a clinical picture similar to DF but not DHF. Other diagnostic considerations include phases of scarlet fever, typhoid, malaria, leptospirosis, hepatitis A, and trypanosomal and rickettsial diseases.7 The differential diagnosis of DHF includes antineutrophil cytoplasmic antibody–associated vasculitis, rheumatoid vasculitis, and bacterial septic vasculitis.
Acute clinical diagnosis of DF can be challenging because of the nonspecific symptoms that can be seen in almost every infectious disease. Clinical presentation assessment should be confirmed with laboratory testing.6 Dengue virus infection usually is confirmed by the identification of viral genomic RNA, antigens, or the antibodies it elicits. Enzyme-linked immunosorbent assay–based serologic tests are cost-effective and easy to perform.5 IgM antibodies usually show cross-reactivity with platelets, but the antibody levels are not positively correlated with the severity of DF.8 Primary infection with the dengue virus is characterized by the elevation of specific IgM levels that usually occurs 3 to 5 days after symptom onset and persists during the postfebrile stage (up to 30 to 60 days). In secondary infections, the IgM levels usually rise more slowly and reach a lower level than in primary infections.9 For both primary and secondary infections, testing IgM levels after the febrile stage may be helpful with the laboratory diagnosis.
Currently, there is no antiviral drug available for dengue. Treatment of dengue infection is symptomatic and supportive.2
Dengue hemorrhagic fever is indicated by a rising hematocrit (≥20%) and a falling platelet count (>100,000/mm3) accompanying clinical signs of hemorrhage. Treatment includes intravenous fluid replacement and careful clinical monitoring of hematocrit levels, platelet count, vitals, urine output, and other signs of shock.5 For patients with a history of dengue infection, travel to areas with other serotypes is not recommended.
If any travel to a high-risk area is planned, countryspecific travel recommendations and warnings should be reviewed from the Centers for Disease Control and Prevention’s website (https://wwwnc.cdc.gov/travel/notices/level1/dengue-global). Use of an Environmental Protection Agency–registered insect repellent to avoid mosquito bites and acetaminophen for managing symptoms is advised. During travel, staying in places with window and door screens and using a bed net during sleep are suggested. Long-sleeved shirts and long pants also are preferred. Travelers should see a health care provider if they have symptoms of dengue.10
African tick bite fever (ATBF) is caused by Rickettsia africae transmitted by Amblyomma ticks. Skin findings in ATBF include erythematous, firm, tender papules with central eschars consistent with the feeding patterns of ticks.11 Histopathology of ATBF usually includes fibrinoid necrosis of vessels in the dermis with a perivascular inflammatory infiltrate and coagulation necrosis of the surrounding dermis consistent with eschar formation.12 The lack of an eschar weighs against this diagnosis.
African trypanosomiasis (also known as sleeping sickness) is caused by protozoa transmitted by the tsetse fly. A chancrelike, circumscribed, rubbery, indurated red or violaceous nodule measuring 2 to 5 cm in diameter often develops as the earliest cutaneous sign of the disease.13 Nonspecific histopathologic findings, such as infiltration of lymphocytes and macrophages and proliferation of endothelial cells and fibroblasts, may be observed.14 Extravascular parasites have been noted in skin biopsies.15 In later stages, skin lesions called trypanids may be observed as macular, papular, annular, targetoid, purpuric, and erythematous lesions, and histopathologic findings consistent with vasculitis also may be seen.13
Chikungunya virus infection is an acute-onset, mosquito-borne viral disease. Skin manifestations may start with nonspecific, generalized, morbilliform, maculopapular rashes coinciding with fever, which also may be seen initially with DHF. Skin hyperpigmentation, mostly centrofacial and involving the nose (chik sign); purpuric and ecchymotic lesions over the trunk and flexors of limbs in adults, often surmounted by subepidermal bullae and lesions resembling toxic epidermal necrolysis; and nonhealing ulcers in the genital and groin areas are common skin manifestations of chikungunya infection.16 Intraepithelial splitting with acantholysis and perivascular lymphohistiocytic infiltration may be observed in the histopathology of blistering lesions, which are not consistent with DHF.17
Zika virus infection is caused by an arbovirus within the Flaviviridae family, which also includes the dengue virus. Initial mucocutaneous findings of the Zika virus include nonspecific diffuse maculopapular eruptions. The eruption generally spares the palms and soles; however, various manifestations including involvement of the palms and soles have been reported.18 The morbilliform eruption begins on the face and extends to the trunk and extremities. Mild hemorrhagic manifestations, including petechiae and bleeding gums, may be observed. Distinguishing between dengue and Zika virus infection relies on the severity of symptoms and laboratory tests, including polymerase chain reaction or IgM antibody testing.19 The other conditions listed do not produce hemorrhagic fever.
THE DIAGNOSIS: Dengue Hemorrhagic Fever
The retiform purpura observed in our patient was suggestive of a vasculitic, thrombotic, or embolic etiology. Dengue IgM serologic testing performed based on her extensive travel history and recent return from a dengue-endemic area was positive, indicating acute infection. A clinical diagnosis of dengue hemorrhagic fever (DHF) was made based on the hemorrhagic appearance of the lesion. Histopathology revealed leukocytoclastic vasculitis (Figure). Anti–double-stranded DNA, antideoxyribonuclease, C3 and C4, CH50 (total hemolytic complement), antineutrophil cytoplasmic antibodies, HIV, and hepatitis B virus tests were normal. Direct immunofluorescence was negative.
Dengue virus is a single-stranded RNA virus transmitted by Aedes aegypti and Aedes albopictus mosquitoes and is one of the most prevalent arthropod-borne viruses affecting humans today.1,2 Infection with the dengue virus generally is seen in travelers visiting tropical regions of Africa, Mexico, South America, South and Central Asia, Southeast Asia, and the Caribbean.1 The Table shows the global distribution of dengue serotypes from 2000 to 2014.3,4 There are 4 serotypes of the dengue virus: DENV-1 to DENV-4. Infection with 1 strain elicits longlasting immunity to that strain, but subsequent infection with another strain can result in severe DHF due to antibody cross-reaction.1
Dengue virus infection ranges from mildly symptomatic to a spectrum of increasingly severe conditions that comprise dengue fever (DF) and DHF, as well as dengue shock syndrome and brain stem hemorrhage, which may be fatal.2,5 Dengue fever manifests as severe myalgia, fever, headache (usually retro-orbital), arthralgia, erythema, and rubelliform exanthema.6 The frequency of skin eruptions in patients with DF varies with the virus strain and outbreaks.7 The lesions initially develop with the onset of fever and manifest as flushing or erythematous mottling of the face, neck, and chest areas.1,7 The morbilliform eruption develops 2 to 6 days after the onset of the fever, beginning on the trunk and spreading to the face and extremities.1,7 The rash may become confluent with characteristic sparing of small round areas of normal skin described as white islands in a sea of red.2 Verrucous papules on the ears also have been described and may resemble those seen in Cowden syndrome. In patients with prior infection with a different strain of the virus, hemorrhagic lesions may develop, including characteristic retiform purpura, a positive tourniquet test, and the appearance of petechiae on the lower legs. Pruritus and desquamation, especially on the palms and soles, may follow the termination of the eruption.7
The differential diagnosis of DF includes measles, rubella, enteroviruses, and influenza. Chikungunya and West Nile viruses in Asia and Africa and the O’nyong-nyong virus in Africa are also arboviruses that cause a clinical picture similar to DF but not DHF. Other diagnostic considerations include phases of scarlet fever, typhoid, malaria, leptospirosis, hepatitis A, and trypanosomal and rickettsial diseases.7 The differential diagnosis of DHF includes antineutrophil cytoplasmic antibody–associated vasculitis, rheumatoid vasculitis, and bacterial septic vasculitis.
Acute clinical diagnosis of DF can be challenging because of the nonspecific symptoms that can be seen in almost every infectious disease. Clinical presentation assessment should be confirmed with laboratory testing.6 Dengue virus infection usually is confirmed by the identification of viral genomic RNA, antigens, or the antibodies it elicits. Enzyme-linked immunosorbent assay–based serologic tests are cost-effective and easy to perform.5 IgM antibodies usually show cross-reactivity with platelets, but the antibody levels are not positively correlated with the severity of DF.8 Primary infection with the dengue virus is characterized by the elevation of specific IgM levels that usually occurs 3 to 5 days after symptom onset and persists during the postfebrile stage (up to 30 to 60 days). In secondary infections, the IgM levels usually rise more slowly and reach a lower level than in primary infections.9 For both primary and secondary infections, testing IgM levels after the febrile stage may be helpful with the laboratory diagnosis.
Currently, there is no antiviral drug available for dengue. Treatment of dengue infection is symptomatic and supportive.2
Dengue hemorrhagic fever is indicated by a rising hematocrit (≥20%) and a falling platelet count (>100,000/mm3) accompanying clinical signs of hemorrhage. Treatment includes intravenous fluid replacement and careful clinical monitoring of hematocrit levels, platelet count, vitals, urine output, and other signs of shock.5 For patients with a history of dengue infection, travel to areas with other serotypes is not recommended.
If any travel to a high-risk area is planned, countryspecific travel recommendations and warnings should be reviewed from the Centers for Disease Control and Prevention’s website (https://wwwnc.cdc.gov/travel/notices/level1/dengue-global). Use of an Environmental Protection Agency–registered insect repellent to avoid mosquito bites and acetaminophen for managing symptoms is advised. During travel, staying in places with window and door screens and using a bed net during sleep are suggested. Long-sleeved shirts and long pants also are preferred. Travelers should see a health care provider if they have symptoms of dengue.10
African tick bite fever (ATBF) is caused by Rickettsia africae transmitted by Amblyomma ticks. Skin findings in ATBF include erythematous, firm, tender papules with central eschars consistent with the feeding patterns of ticks.11 Histopathology of ATBF usually includes fibrinoid necrosis of vessels in the dermis with a perivascular inflammatory infiltrate and coagulation necrosis of the surrounding dermis consistent with eschar formation.12 The lack of an eschar weighs against this diagnosis.
African trypanosomiasis (also known as sleeping sickness) is caused by protozoa transmitted by the tsetse fly. A chancrelike, circumscribed, rubbery, indurated red or violaceous nodule measuring 2 to 5 cm in diameter often develops as the earliest cutaneous sign of the disease.13 Nonspecific histopathologic findings, such as infiltration of lymphocytes and macrophages and proliferation of endothelial cells and fibroblasts, may be observed.14 Extravascular parasites have been noted in skin biopsies.15 In later stages, skin lesions called trypanids may be observed as macular, papular, annular, targetoid, purpuric, and erythematous lesions, and histopathologic findings consistent with vasculitis also may be seen.13
Chikungunya virus infection is an acute-onset, mosquito-borne viral disease. Skin manifestations may start with nonspecific, generalized, morbilliform, maculopapular rashes coinciding with fever, which also may be seen initially with DHF. Skin hyperpigmentation, mostly centrofacial and involving the nose (chik sign); purpuric and ecchymotic lesions over the trunk and flexors of limbs in adults, often surmounted by subepidermal bullae and lesions resembling toxic epidermal necrolysis; and nonhealing ulcers in the genital and groin areas are common skin manifestations of chikungunya infection.16 Intraepithelial splitting with acantholysis and perivascular lymphohistiocytic infiltration may be observed in the histopathology of blistering lesions, which are not consistent with DHF.17
Zika virus infection is caused by an arbovirus within the Flaviviridae family, which also includes the dengue virus. Initial mucocutaneous findings of the Zika virus include nonspecific diffuse maculopapular eruptions. The eruption generally spares the palms and soles; however, various manifestations including involvement of the palms and soles have been reported.18 The morbilliform eruption begins on the face and extends to the trunk and extremities. Mild hemorrhagic manifestations, including petechiae and bleeding gums, may be observed. Distinguishing between dengue and Zika virus infection relies on the severity of symptoms and laboratory tests, including polymerase chain reaction or IgM antibody testing.19 The other conditions listed do not produce hemorrhagic fever.
- Pincus LB, Grossman ME, Fox LP. The exanthem of dengue fever: clinical features of two US tourists traveling abroad. J Am Acad Dermatol. 2008;58:308-316. doi:10.1016/j.jaad.2007.08.042
- Radakovic-Fijan S, Graninger W, Müller C, et al. Dengue hemorrhagic fever in a British travel guide. J Am Acad Dermatol. 2002;46:430-433. doi:10.1067/mjd.2002.111904
- Yamashita A, Sakamoto T, Sekizuka T, et al. DGV: dengue genographic viewer. Front Microbiol. 2016;7:875. doi:10.3389/fmicb.2016.00875
- Centers for Disease and Prevention. Dengue in the US states and territories. Updated October 7, 2020. Accessed September 30, 2024. https://www.cdc.gov/dengue/data-research/facts-stats/?CDC_AAref_Val=https://www.cdc.gov/dengue/areaswithrisk/in-the-us.html
- Khetarpal N, Khanna I. Dengue fever: causes, complications, and vaccine strategies. J Immunol Res. 2016;2016:6803098. doi:10.1155/2016/6803098
- Muller DA, Depelsenaire AC, Young PR. Clinical and laboratory diagnosis of dengue virus infection. J Infect Dis. 2017;215(suppl 2):S89-S95. doi:10.1093/infdis/jiw649
- Waterman SH, Gubler DJ. Dengue fever. Clin Dermatol. 1989;7:117-122. doi:10.1016/0738-081x(89)90034-5
- Lin CF, Lei HY, Liu CC, et al. Generation of IgM anti-platelet autoantibody in dengue patients. J Med Virol. 2001;63:143-149. doi:10.1002/1096- 9071(20000201)63:2<143::AID-JMV1009>3.0.CO;2-L
- Tripathi NK, Shrivastava A, Dash PK, et al. Detection of dengue virus. Methods Mol Biol. 2011;665:51-64. doi:10.1007/978-1-60761-817-1_4
- Centers for Disease Control and Prevention. Plan for travel. Accessed September 30, 2024. https://wwwnc.cdc.gov/travel
- Mack I, Ritz N. African tick-bite fever. N Engl J Med. 2019;380:960. doi:10.1056/NEJMicm1810093
- Lepidi H, Fournier PE, Raoult D. Histologic features and immunodetection of African tick-bite fever eschar. Emerg Infect Dis. 2006;12:1332- 1337. doi:10.3201/eid1209.051540
- McGovern TW, Williams W, Fitzpatrick JE, et al. Cutaneous manifestations of African trypanosomiasis. Arch Dermatol. 1995;131:1178-1182.
- Kristensson K, Bentivoglio M. Pathology of African trypanosomiasis. In: Dumas M, Bouteille B, Buguet A, eds. Progress in Human African Trypanosomiasis, Sleeping Sickness. Springer; 1999:157-181.
- Capewell P, Cren-Travaillé C, Marchesi F, et al. The skin is a significant but overlooked anatomical reservoir for vector-borne African trypanosomes. Elife. 2016;5:e17716. doi:10.7554/eLife.17716
- Singal A. Chikungunya and skin: current perspective. Indian Dermatol Online J. 2017;8:307-309. doi:10.4103/idoj.IDOJ_93_17
- Robin S, Ramful D, Zettor J, et al. Severe bullous skin lesions associated with chikungunya virus infection in small infants. Eur J Pediatr. 2009;169:67-72. doi:10.1007/s00431-009-0986-0
- Hussain A, Ali F, Latiwesh OB, et al. A comprehensive review of the manifestations and pathogenesis of Zika virus in neonates and adults. Cureus. 2018;10:E3290. doi:10.7759/cureus.3290
- Farahnik B, Beroukhim K, Blattner CM, et al. Cutaneous manifestations of the Zika virus. J Am Acad Dermatol. 2016;74:1286-1287. doi:10.1016/j.jaad.2016.02.1232
- Pincus LB, Grossman ME, Fox LP. The exanthem of dengue fever: clinical features of two US tourists traveling abroad. J Am Acad Dermatol. 2008;58:308-316. doi:10.1016/j.jaad.2007.08.042
- Radakovic-Fijan S, Graninger W, Müller C, et al. Dengue hemorrhagic fever in a British travel guide. J Am Acad Dermatol. 2002;46:430-433. doi:10.1067/mjd.2002.111904
- Yamashita A, Sakamoto T, Sekizuka T, et al. DGV: dengue genographic viewer. Front Microbiol. 2016;7:875. doi:10.3389/fmicb.2016.00875
- Centers for Disease and Prevention. Dengue in the US states and territories. Updated October 7, 2020. Accessed September 30, 2024. https://www.cdc.gov/dengue/data-research/facts-stats/?CDC_AAref_Val=https://www.cdc.gov/dengue/areaswithrisk/in-the-us.html
- Khetarpal N, Khanna I. Dengue fever: causes, complications, and vaccine strategies. J Immunol Res. 2016;2016:6803098. doi:10.1155/2016/6803098
- Muller DA, Depelsenaire AC, Young PR. Clinical and laboratory diagnosis of dengue virus infection. J Infect Dis. 2017;215(suppl 2):S89-S95. doi:10.1093/infdis/jiw649
- Waterman SH, Gubler DJ. Dengue fever. Clin Dermatol. 1989;7:117-122. doi:10.1016/0738-081x(89)90034-5
- Lin CF, Lei HY, Liu CC, et al. Generation of IgM anti-platelet autoantibody in dengue patients. J Med Virol. 2001;63:143-149. doi:10.1002/1096- 9071(20000201)63:2<143::AID-JMV1009>3.0.CO;2-L
- Tripathi NK, Shrivastava A, Dash PK, et al. Detection of dengue virus. Methods Mol Biol. 2011;665:51-64. doi:10.1007/978-1-60761-817-1_4
- Centers for Disease Control and Prevention. Plan for travel. Accessed September 30, 2024. https://wwwnc.cdc.gov/travel
- Mack I, Ritz N. African tick-bite fever. N Engl J Med. 2019;380:960. doi:10.1056/NEJMicm1810093
- Lepidi H, Fournier PE, Raoult D. Histologic features and immunodetection of African tick-bite fever eschar. Emerg Infect Dis. 2006;12:1332- 1337. doi:10.3201/eid1209.051540
- McGovern TW, Williams W, Fitzpatrick JE, et al. Cutaneous manifestations of African trypanosomiasis. Arch Dermatol. 1995;131:1178-1182.
- Kristensson K, Bentivoglio M. Pathology of African trypanosomiasis. In: Dumas M, Bouteille B, Buguet A, eds. Progress in Human African Trypanosomiasis, Sleeping Sickness. Springer; 1999:157-181.
- Capewell P, Cren-Travaillé C, Marchesi F, et al. The skin is a significant but overlooked anatomical reservoir for vector-borne African trypanosomes. Elife. 2016;5:e17716. doi:10.7554/eLife.17716
- Singal A. Chikungunya and skin: current perspective. Indian Dermatol Online J. 2017;8:307-309. doi:10.4103/idoj.IDOJ_93_17
- Robin S, Ramful D, Zettor J, et al. Severe bullous skin lesions associated with chikungunya virus infection in small infants. Eur J Pediatr. 2009;169:67-72. doi:10.1007/s00431-009-0986-0
- Hussain A, Ali F, Latiwesh OB, et al. A comprehensive review of the manifestations and pathogenesis of Zika virus in neonates and adults. Cureus. 2018;10:E3290. doi:10.7759/cureus.3290
- Farahnik B, Beroukhim K, Blattner CM, et al. Cutaneous manifestations of the Zika virus. J Am Acad Dermatol. 2016;74:1286-1287. doi:10.1016/j.jaad.2016.02.1232
A 74-year-old woman who frequently traveled abroad presented to the dermatology department with retiform purpura of the lower leg along with gastrointestinal cramps, fatigue, and myalgia. The patient reported that the symptoms had started 10 days after returning from a recent trip to Africa.


Following the Light
Percutaneous endoscopic gastrostomy (PEG) was first introduced in the early 1980s by surgeons Michael Gauderer and Jeffrey Ponsky as a less-invasive alternative to surgical gastrostomy via open laparotomy. The concept was born after the pair observed that the light from an endoscope in an infant undergoing endoscopy caused the abdominal wall to glow in the darkened operating room.
In fact, PEG was among the first procedures that defined minimally invasive surgery, a concept that has now revolutionized the surgical field. Since that time, PEG has evolved as a preferred method for patients needing long-term nutritional support for various indications. By 2001, approximately 216,000 PEGs were placed annually in the United States. While the volume of PEG procedures has declined in recent years at some institutions as practice patterns have shifted toward interventional radiology–placed gastrostomy tubes, evaluation of patients for PEG insertion, removal, or management of PEG complications remains a core area of gastroenterology practice.

Among the most important roles of the gastroenterologist in considering potential PEG candidates is to determine whether an appropriate indication exists, a decision that requires a detailed understanding of a patient’s overall clinical condition, goals of care, values, and preferences. a common GI consultation that deserves thoughtful consideration and demands effective communication among members of the multidisciplinary team and with patients.
Also in our October issue, we highlight a recently published large multicohort study from Gastroenterology elucidating clinical, serologic, and genetic factors associated with extraintestinal manifestations in IBD. We also review key updates to colonoscopy quality indicators, including modifications to existing indicators such as ADR and the addition of two new “priority indicators” — rate of inadequate bowel prep and sessile serrated lesion detection rate.
In this month’s Member Spotlight, Dr. Stephanie Pointer of Digestive & Liver Health Specialists in Nashville, Tennessee, shares the many ways in which she has given back to her community through music and mentoring while leading a thriving GI practice. We hope you enjoy this, and all the coverage included in our October issue.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Percutaneous endoscopic gastrostomy (PEG) was first introduced in the early 1980s by surgeons Michael Gauderer and Jeffrey Ponsky as a less-invasive alternative to surgical gastrostomy via open laparotomy. The concept was born after the pair observed that the light from an endoscope in an infant undergoing endoscopy caused the abdominal wall to glow in the darkened operating room.
In fact, PEG was among the first procedures that defined minimally invasive surgery, a concept that has now revolutionized the surgical field. Since that time, PEG has evolved as a preferred method for patients needing long-term nutritional support for various indications. By 2001, approximately 216,000 PEGs were placed annually in the United States. While the volume of PEG procedures has declined in recent years at some institutions as practice patterns have shifted toward interventional radiology–placed gastrostomy tubes, evaluation of patients for PEG insertion, removal, or management of PEG complications remains a core area of gastroenterology practice.
Among the most important roles of the gastroenterologist in considering potential PEG candidates is to determine whether an appropriate indication exists, a decision that requires a detailed understanding of a patient’s overall clinical condition, goals of care, values, and preferences. a common GI consultation that deserves thoughtful consideration and demands effective communication among members of the multidisciplinary team and with patients.
Also in our October issue, we highlight a recently published large multicohort study from Gastroenterology elucidating clinical, serologic, and genetic factors associated with extraintestinal manifestations in IBD. We also review key updates to colonoscopy quality indicators, including modifications to existing indicators such as ADR and the addition of two new “priority indicators” — rate of inadequate bowel prep and sessile serrated lesion detection rate.
In this month’s Member Spotlight, Dr. Stephanie Pointer of Digestive & Liver Health Specialists in Nashville, Tennessee, shares the many ways in which she has given back to her community through music and mentoring while leading a thriving GI practice. We hope you enjoy this, and all the coverage included in our October issue.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Percutaneous endoscopic gastrostomy (PEG) was first introduced in the early 1980s by surgeons Michael Gauderer and Jeffrey Ponsky as a less-invasive alternative to surgical gastrostomy via open laparotomy. The concept was born after the pair observed that the light from an endoscope in an infant undergoing endoscopy caused the abdominal wall to glow in the darkened operating room.
In fact, PEG was among the first procedures that defined minimally invasive surgery, a concept that has now revolutionized the surgical field. Since that time, PEG has evolved as a preferred method for patients needing long-term nutritional support for various indications. By 2001, approximately 216,000 PEGs were placed annually in the United States. While the volume of PEG procedures has declined in recent years at some institutions as practice patterns have shifted toward interventional radiology–placed gastrostomy tubes, evaluation of patients for PEG insertion, removal, or management of PEG complications remains a core area of gastroenterology practice.
Among the most important roles of the gastroenterologist in considering potential PEG candidates is to determine whether an appropriate indication exists, a decision that requires a detailed understanding of a patient’s overall clinical condition, goals of care, values, and preferences. a common GI consultation that deserves thoughtful consideration and demands effective communication among members of the multidisciplinary team and with patients.
Also in our October issue, we highlight a recently published large multicohort study from Gastroenterology elucidating clinical, serologic, and genetic factors associated with extraintestinal manifestations in IBD. We also review key updates to colonoscopy quality indicators, including modifications to existing indicators such as ADR and the addition of two new “priority indicators” — rate of inadequate bowel prep and sessile serrated lesion detection rate.
In this month’s Member Spotlight, Dr. Stephanie Pointer of Digestive & Liver Health Specialists in Nashville, Tennessee, shares the many ways in which she has given back to her community through music and mentoring while leading a thriving GI practice. We hope you enjoy this, and all the coverage included in our October issue.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Pfizer’s Withdrawal of SCD Drug Raises Questions
The National Alliance of Sickle Cell Centers issued a statement urging patients not to stop voxelotor abruptly. Instead, they should work out plans with their physicians and medical teams for weaning plans.
“Don’t lose faith. This a step backward, but we will stay on the path to better outcomes for everyone,” said the alliance in a statement to patients and clinicians.
On September 25, Pfizer said it would withdraw all lots of voxelotor in all markets where it is approved. The New York–based drugmaker also said it was discontinuing all active voxelotor clinical trials and expanded access programs worldwide. The cause was data that suggested “an imbalance in vaso-occlusive crises and fatal events which require further assessment.”
Pfizer told this news organization in an email exchange that it is focused on analyzing the data and will share updates in the future about presenting or publishing on this issue.
The withdrawal came amid increased scrutiny of the drug by the European Medicines Agency (EMA). The EMA in July began a review of voxelotor after data from a clinical trial showed that a higher number of deaths occurred with the drug than with placebo and another trial showed the total number of deaths was higher than anticipated.
On September 26, the EMA’s human medicines committee recommended suspending the marketing authorization of voxelotor, citing new safety data that emerged during the review. The drug had received marketing authorization for the European Union in 2022, the agency said.
The US Food and Drug Administration (FDA), which first cleared voxelotor for sale in 2019, also said it has been conducting a safety review of the drug. The agency continues to examine post-marketing clinical trial data for voxelotor, the real-world registry studies, and data from the FDA Adverse Event Reporting System. At the conclusion of this review, the FDA will communicate any additional findings, if necessary, the agency said.
The FDA said it appeared that more deaths and a higher rate of vaso-occlusive crisis occurred in patients taking voxelotor vs placebo in post-marketing clinical trials.
“Pfizer also observed a higher rate of vaso-occlusive crisis in patients with sickle cell disease receiving Oxbryta in two real-world registry studies,” the FDA said. “Based on the totality of clinical data, Pfizer has determined the benefit of Oxbryta does not outweigh the risk.”
Gene Therapy, Tried-and-True Hydroxyurea (HU)
As a field, SCD has drawn more interest in recent years, with significant gains made lately in cutting-edge projects.
The FDA in December approved two gene-editing treatments for patients aged 12 years or older. These are considered “milestone treatments” for a debilitating and potentially life-threatening blood disorder that affects about 100,000 people in the United States. Exagamglogene autotemcel (Casgevy, Vertex Pharmaceuticals and CRISPR Therapeutics) is the first to use the gene-editing tool CRISPR. And lovotibeglogene autotemcel (Lyfgenia, bluebird bio) uses a different gene-editing tool called a lentiviral vector.
These advances have been covered widely by the news media but are not expected to be widely available, with the cost of these extensive treatments estimated around $2-$3 million per patient.
“Gene therapy is amazing in that it can offer a cure, but it’s very expensive and not all patients are suitable for it. Some have so much existing organ damage that it’s not an option for them,” said John Wood, MD, PhD, director of cardiovascular MRI at Children’s Hospital Los Angeles, Los Angeles, who does research on SCD.
“So it really is a great treatment for a very few people,” he said in an interview.
The mainstay of treatment for SCD remains a drug that Lydia Pecker, MD, a pediatric hematologist at Johns Hopkins University in Baltimore, describes as the “first, oldest, and best”: HU.
The FDA approved this in 1998 for use in SCD. It reduces the frequency of painful crises and acute chest syndrome and other complications of SCD that otherwise could be serious or even lethal, Pecker said.
“Older doctors can tell you that what they experienced with sickle cell disease in the hospitals has been completely transformed because of the high uptake of the drug,” she said, adding that it made a “profound” change. “We just don’t have data for any other agent that’s quite like that.”
Voxelotor had been a good second drug to add for some patients, in addition to HU and blood transfusions, Dr. Pecker noted. It was a first-line drug for those for whom transfusion and HU were not options, which constitutes a relatively small number of patients, she said.
“So we have, in the last 5 years, felt more hopeful because we had something else to offer,” she said.
Alexis A. Thompson, MD, MPH, chief of the Division of Hematology at Children’s Hospital of Philadelphia in Pennsylvania, said in an interview that her organization also had patients who appeared to benefit from voxelotor, some of whom had been participants in clinical trials.
Dr. Thompson, who has been a top researcher involved in the study of gene therapy, urged the need for companies to keep seeking to expand the options for people with SCD, even after the setback with voxelotor.
“I hope that there’s an appreciation for the need for continued investment in this very serious condition, for which there are insufficient options for treatments,” Dr. Thompson said. “So ongoing investment is really needed if we expect to make progress.”
Dr. Pecker disclosed ties with Novartis, Afimmune, the American Society of Hematology, and the National Institutes of Health. Thompson reported relationships with bluebird bio, Beam, Editas, Novartis, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
The National Alliance of Sickle Cell Centers issued a statement urging patients not to stop voxelotor abruptly. Instead, they should work out plans with their physicians and medical teams for weaning plans.
“Don’t lose faith. This a step backward, but we will stay on the path to better outcomes for everyone,” said the alliance in a statement to patients and clinicians.
On September 25, Pfizer said it would withdraw all lots of voxelotor in all markets where it is approved. The New York–based drugmaker also said it was discontinuing all active voxelotor clinical trials and expanded access programs worldwide. The cause was data that suggested “an imbalance in vaso-occlusive crises and fatal events which require further assessment.”
Pfizer told this news organization in an email exchange that it is focused on analyzing the data and will share updates in the future about presenting or publishing on this issue.
The withdrawal came amid increased scrutiny of the drug by the European Medicines Agency (EMA). The EMA in July began a review of voxelotor after data from a clinical trial showed that a higher number of deaths occurred with the drug than with placebo and another trial showed the total number of deaths was higher than anticipated.
On September 26, the EMA’s human medicines committee recommended suspending the marketing authorization of voxelotor, citing new safety data that emerged during the review. The drug had received marketing authorization for the European Union in 2022, the agency said.
The US Food and Drug Administration (FDA), which first cleared voxelotor for sale in 2019, also said it has been conducting a safety review of the drug. The agency continues to examine post-marketing clinical trial data for voxelotor, the real-world registry studies, and data from the FDA Adverse Event Reporting System. At the conclusion of this review, the FDA will communicate any additional findings, if necessary, the agency said.
The FDA said it appeared that more deaths and a higher rate of vaso-occlusive crisis occurred in patients taking voxelotor vs placebo in post-marketing clinical trials.
“Pfizer also observed a higher rate of vaso-occlusive crisis in patients with sickle cell disease receiving Oxbryta in two real-world registry studies,” the FDA said. “Based on the totality of clinical data, Pfizer has determined the benefit of Oxbryta does not outweigh the risk.”
Gene Therapy, Tried-and-True Hydroxyurea (HU)
As a field, SCD has drawn more interest in recent years, with significant gains made lately in cutting-edge projects.
The FDA in December approved two gene-editing treatments for patients aged 12 years or older. These are considered “milestone treatments” for a debilitating and potentially life-threatening blood disorder that affects about 100,000 people in the United States. Exagamglogene autotemcel (Casgevy, Vertex Pharmaceuticals and CRISPR Therapeutics) is the first to use the gene-editing tool CRISPR. And lovotibeglogene autotemcel (Lyfgenia, bluebird bio) uses a different gene-editing tool called a lentiviral vector.
These advances have been covered widely by the news media but are not expected to be widely available, with the cost of these extensive treatments estimated around $2-$3 million per patient.
“Gene therapy is amazing in that it can offer a cure, but it’s very expensive and not all patients are suitable for it. Some have so much existing organ damage that it’s not an option for them,” said John Wood, MD, PhD, director of cardiovascular MRI at Children’s Hospital Los Angeles, Los Angeles, who does research on SCD.
“So it really is a great treatment for a very few people,” he said in an interview.
The mainstay of treatment for SCD remains a drug that Lydia Pecker, MD, a pediatric hematologist at Johns Hopkins University in Baltimore, describes as the “first, oldest, and best”: HU.
The FDA approved this in 1998 for use in SCD. It reduces the frequency of painful crises and acute chest syndrome and other complications of SCD that otherwise could be serious or even lethal, Pecker said.
“Older doctors can tell you that what they experienced with sickle cell disease in the hospitals has been completely transformed because of the high uptake of the drug,” she said, adding that it made a “profound” change. “We just don’t have data for any other agent that’s quite like that.”
Voxelotor had been a good second drug to add for some patients, in addition to HU and blood transfusions, Dr. Pecker noted. It was a first-line drug for those for whom transfusion and HU were not options, which constitutes a relatively small number of patients, she said.
“So we have, in the last 5 years, felt more hopeful because we had something else to offer,” she said.
Alexis A. Thompson, MD, MPH, chief of the Division of Hematology at Children’s Hospital of Philadelphia in Pennsylvania, said in an interview that her organization also had patients who appeared to benefit from voxelotor, some of whom had been participants in clinical trials.
Dr. Thompson, who has been a top researcher involved in the study of gene therapy, urged the need for companies to keep seeking to expand the options for people with SCD, even after the setback with voxelotor.
“I hope that there’s an appreciation for the need for continued investment in this very serious condition, for which there are insufficient options for treatments,” Dr. Thompson said. “So ongoing investment is really needed if we expect to make progress.”
Dr. Pecker disclosed ties with Novartis, Afimmune, the American Society of Hematology, and the National Institutes of Health. Thompson reported relationships with bluebird bio, Beam, Editas, Novartis, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
The National Alliance of Sickle Cell Centers issued a statement urging patients not to stop voxelotor abruptly. Instead, they should work out plans with their physicians and medical teams for weaning plans.
“Don’t lose faith. This a step backward, but we will stay on the path to better outcomes for everyone,” said the alliance in a statement to patients and clinicians.
On September 25, Pfizer said it would withdraw all lots of voxelotor in all markets where it is approved. The New York–based drugmaker also said it was discontinuing all active voxelotor clinical trials and expanded access programs worldwide. The cause was data that suggested “an imbalance in vaso-occlusive crises and fatal events which require further assessment.”
Pfizer told this news organization in an email exchange that it is focused on analyzing the data and will share updates in the future about presenting or publishing on this issue.
The withdrawal came amid increased scrutiny of the drug by the European Medicines Agency (EMA). The EMA in July began a review of voxelotor after data from a clinical trial showed that a higher number of deaths occurred with the drug than with placebo and another trial showed the total number of deaths was higher than anticipated.
On September 26, the EMA’s human medicines committee recommended suspending the marketing authorization of voxelotor, citing new safety data that emerged during the review. The drug had received marketing authorization for the European Union in 2022, the agency said.
The US Food and Drug Administration (FDA), which first cleared voxelotor for sale in 2019, also said it has been conducting a safety review of the drug. The agency continues to examine post-marketing clinical trial data for voxelotor, the real-world registry studies, and data from the FDA Adverse Event Reporting System. At the conclusion of this review, the FDA will communicate any additional findings, if necessary, the agency said.
The FDA said it appeared that more deaths and a higher rate of vaso-occlusive crisis occurred in patients taking voxelotor vs placebo in post-marketing clinical trials.
“Pfizer also observed a higher rate of vaso-occlusive crisis in patients with sickle cell disease receiving Oxbryta in two real-world registry studies,” the FDA said. “Based on the totality of clinical data, Pfizer has determined the benefit of Oxbryta does not outweigh the risk.”
Gene Therapy, Tried-and-True Hydroxyurea (HU)
As a field, SCD has drawn more interest in recent years, with significant gains made lately in cutting-edge projects.
The FDA in December approved two gene-editing treatments for patients aged 12 years or older. These are considered “milestone treatments” for a debilitating and potentially life-threatening blood disorder that affects about 100,000 people in the United States. Exagamglogene autotemcel (Casgevy, Vertex Pharmaceuticals and CRISPR Therapeutics) is the first to use the gene-editing tool CRISPR. And lovotibeglogene autotemcel (Lyfgenia, bluebird bio) uses a different gene-editing tool called a lentiviral vector.
These advances have been covered widely by the news media but are not expected to be widely available, with the cost of these extensive treatments estimated around $2-$3 million per patient.
“Gene therapy is amazing in that it can offer a cure, but it’s very expensive and not all patients are suitable for it. Some have so much existing organ damage that it’s not an option for them,” said John Wood, MD, PhD, director of cardiovascular MRI at Children’s Hospital Los Angeles, Los Angeles, who does research on SCD.
“So it really is a great treatment for a very few people,” he said in an interview.
The mainstay of treatment for SCD remains a drug that Lydia Pecker, MD, a pediatric hematologist at Johns Hopkins University in Baltimore, describes as the “first, oldest, and best”: HU.
The FDA approved this in 1998 for use in SCD. It reduces the frequency of painful crises and acute chest syndrome and other complications of SCD that otherwise could be serious or even lethal, Pecker said.
“Older doctors can tell you that what they experienced with sickle cell disease in the hospitals has been completely transformed because of the high uptake of the drug,” she said, adding that it made a “profound” change. “We just don’t have data for any other agent that’s quite like that.”
Voxelotor had been a good second drug to add for some patients, in addition to HU and blood transfusions, Dr. Pecker noted. It was a first-line drug for those for whom transfusion and HU were not options, which constitutes a relatively small number of patients, she said.
“So we have, in the last 5 years, felt more hopeful because we had something else to offer,” she said.
Alexis A. Thompson, MD, MPH, chief of the Division of Hematology at Children’s Hospital of Philadelphia in Pennsylvania, said in an interview that her organization also had patients who appeared to benefit from voxelotor, some of whom had been participants in clinical trials.
Dr. Thompson, who has been a top researcher involved in the study of gene therapy, urged the need for companies to keep seeking to expand the options for people with SCD, even after the setback with voxelotor.
“I hope that there’s an appreciation for the need for continued investment in this very serious condition, for which there are insufficient options for treatments,” Dr. Thompson said. “So ongoing investment is really needed if we expect to make progress.”
Dr. Pecker disclosed ties with Novartis, Afimmune, the American Society of Hematology, and the National Institutes of Health. Thompson reported relationships with bluebird bio, Beam, Editas, Novartis, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
Popular Weight Loss Drugs Now for Patients With Cancer?
Demand for new weight loss drugs has surged over the past few years.
Led by the antiobesity drugs semaglutide (Wegovy) and tirzepatide (Zepbound), these popular medications — more commonly known as glucagon-like peptide 1 (GLP-1) agonists — have become game changers for shedding excess pounds.
Aside from obesity indications, both drugs have been approved to treat type 2 diabetes under different brand names and have a growing list of other potential benefits, such as reducing inflammation and depression.
While there’s limited data to support the use of GLP-1 agonists for weight loss in cancer, some oncologists have begun carefully integrating the antiobesity agents into care and studying their effects in this patient population.
The reason: Research suggests that obesity can reduce the effectiveness of cancer therapies, especially in patients with breast cancer, and can increase the risk for treatment-related side effects.
The idea is that managing patients’ weight will improve their cancer outcomes, explained Lajos Pusztai, MD, PhD, a breast cancer specialist and professor of medicine at Yale School of Medicine in New Haven, Connecticut.
Although Dr. Pusztai and his oncology peers at Yale don’t yet use GPL-1 agonists, Neil Iyengar, MD, and colleagues have begun doing so to help some patients with breast cancer manage their weight. Dr. Iyengar estimates that a few hundred — almost 40% — of his patients are on the antiobesity drugs.
“For a patient who has really tried to reduce their weight and who is in the obese range, that’s where I think the use of these medications can be considered,” said Dr. Iyengar, a breast cancer oncologist at Memorial Sloan Kettering Cancer Center in New York City.
Why GLP-1s in Cancer?
GLP-1 is a hormone that the small intestine releases after eating. GLP-1 agonists work by mimicking GLP-1 to trigger the release of insulin and reduce the production of glucagon — two processes that help regulate blood sugar.
These agents, such as Wegovy (or Ozempic when prescribed for diabetes), also slow gastric emptying and can make people feel fuller longer.
Zebound (or Mounjaro for type 2 diabetes) is considered a dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, which may enhance its weight loss benefits.
In practice, however, these drugs can increase nausea and vomiting from chemotherapy, so Dr. Iyengar typically has patients use them afterwards, during maintenance treatment.
Oncologists don’t prescribe the drugs themselves but instead refer patients to endocrinologists or weight management centers that then write the prescriptions. Taking these drugs involves weekly subcutaneous injections patients can administer themselves.
Endocrinologist Emily Gallagher, MD, PhD, of Mount Sinai Hospital in New York City, estimates she has prescribed the antiobesity drugs to a few hundred patients with cancer and, like Dr. Iyengar, uses the drugs during maintenance treatment with hormone therapy for breast cancer. She also has used these agents in patients with prostate and endometrial cancers and has found the drugs can help counter steroid weight gain in multiple myeloma.
But, to date, the evidence for using GPL-1 agonists in cancer remains limited and the practice has not yet become widespread.
Research largely comes down to a few small retrospective studies in patients with breast cancer receiving aromatase inhibitors. Although no safety issues have emerged so far, these initial reports suggest that the drugs lead to significantly less weight loss in patients with cancer compared to the general population.
Dr. Iyengar led one recent study, presented at the 2024 annual meeting of the American Society of Clinical Oncology, in which he and his team assessed outcomes in 75 women with breast cancer who received a GLP-1 agonist. Almost 80% of patients had diabetes, and 60% received hormone therapy, most commonly an aromatase inhibitor. Patients’ median body mass index (BMI) at baseline was 34 kg/m2 (range, 23-50 kg/m2).
From baseline, patients lost 6.2 kg, on average, or about 5% of their total body weight, 12 months after initiating GLP-1 therapy.
In contrast, phase 3 trials show much higher mean weight loss — about two times — in patients without cancer.
Another recent study also reported modest weight loss results in patients with breast cancer undergoing endocrine therapy. The researchers reported that, at 12 months, Wegovy led to 4.34% reduction in BMI, compared with a 14% change reported in the general population. Zebound, however, was associated with a 2.31% BMI increase overall — though some patients did experience a decrease — compared with a 15% reduction in the general population.
“These findings indicate a substantially reduced weight loss efficacy in breast cancer patients on endocrine therapy compared to the general population,” the authors concluded.
It’s unclear why the drugs appear to not work as well in patients with cancer. It’s possible that hormone therapy or metabolic changes interfere with their effectiveness, given that some cancer therapies lead to weight gain. Steroids and hormone therapies, for instance, often increase appetite, and some treatments can slow patients’ metabolism or lead to fatigue, which can make it harder to exercise.
Patients with cancer may need a higher dose of GLP-1 agonists to achieve similar weight loss to the general population, Dr. Iyengar noted.
However, Dr. Gallagher said, in her own experience, she hasn’t found the drugs to be less effective in patients with cancer, especially the newer agents, like Wegovy and Zepbound.
As for safety, Wegovy and Zepbound both carry a black box warning for thyroid C-cell tumors, including medullary thyroid carcinoma. (Recent research, however, has found that GLP-1 agonists do not increase thyroid cancer risk).
These antiobesity agents are also contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients who have multiple endocrine neoplasia syndrome type 2, which is associated with medullary thyroid carcinoma.
Dr. Gallagher hasn’t seen any secondary tumors — thyroid or otherwise — in her patients with cancer, but she follows the labeling contraindications. Dr. Iyengar also noted that more recent and larger data sets have shown no impact on this risk, which may not actually exist, he said
Dr. Gallagher remains cautious about using GPL-1 agonists in patients who have had bariatric surgery because these agents can compound the slower gastric emptying and intestinal transit from surgery, potentially leading to gastrointestinal obstructions.
Looking ahead, GPL-1 manufacturers are interested in adding cancer indications to the drug labeling. Both Dr. Iyengar and Dr. Gallagher said their institutions are in talks with companies to participate in large, multicenter, global phase 3 trials.
Dr. Iyengar welcomes the efforts, not only to test the effectiveness of GPL-1 agonists in oncology but also to “nail down” their safety in cancer.
“I don’t think that there’s mechanistically anything that’s particularly worrisome,” and current observations suggest that these drugs are likely to be safe, Dr. Iyengar said. Even so, “GLP-1 agonists do a lot of things that we don’t fully understand yet.”
The bigger challenge, Dr. Iyengar noted, is that companies will have to show a sizable benefit to using these drugs in patients with cancer to get the Food and Drug Administration’s approval. And to move the needle on cancer-specific outcomes, these antiobesity drugs will need to demonstrate significant, durable weight loss in patients with cancer.
But if these drugs can do that, “I think it’s going to be one of the biggest advances in medicine and oncology given the obesity and cancer epidemic,” Dr. Iyengar said.
Dr. Iyengar has adviser and/or researcher ties with companies that make or are developing GPL-1 agonists, including AstraZeneca, Novartis, Gilead, and Pfizer. Dr. Gallagher is a consultant for Novartis, Flare Therapeutics, Reactive Biosciences, and Seagen.
A version of this article first appeared on Medscape.com.
Demand for new weight loss drugs has surged over the past few years.
Led by the antiobesity drugs semaglutide (Wegovy) and tirzepatide (Zepbound), these popular medications — more commonly known as glucagon-like peptide 1 (GLP-1) agonists — have become game changers for shedding excess pounds.
Aside from obesity indications, both drugs have been approved to treat type 2 diabetes under different brand names and have a growing list of other potential benefits, such as reducing inflammation and depression.
While there’s limited data to support the use of GLP-1 agonists for weight loss in cancer, some oncologists have begun carefully integrating the antiobesity agents into care and studying their effects in this patient population.
The reason: Research suggests that obesity can reduce the effectiveness of cancer therapies, especially in patients with breast cancer, and can increase the risk for treatment-related side effects.
The idea is that managing patients’ weight will improve their cancer outcomes, explained Lajos Pusztai, MD, PhD, a breast cancer specialist and professor of medicine at Yale School of Medicine in New Haven, Connecticut.
Although Dr. Pusztai and his oncology peers at Yale don’t yet use GPL-1 agonists, Neil Iyengar, MD, and colleagues have begun doing so to help some patients with breast cancer manage their weight. Dr. Iyengar estimates that a few hundred — almost 40% — of his patients are on the antiobesity drugs.
“For a patient who has really tried to reduce their weight and who is in the obese range, that’s where I think the use of these medications can be considered,” said Dr. Iyengar, a breast cancer oncologist at Memorial Sloan Kettering Cancer Center in New York City.
Why GLP-1s in Cancer?
GLP-1 is a hormone that the small intestine releases after eating. GLP-1 agonists work by mimicking GLP-1 to trigger the release of insulin and reduce the production of glucagon — two processes that help regulate blood sugar.
These agents, such as Wegovy (or Ozempic when prescribed for diabetes), also slow gastric emptying and can make people feel fuller longer.
Zebound (or Mounjaro for type 2 diabetes) is considered a dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, which may enhance its weight loss benefits.
In practice, however, these drugs can increase nausea and vomiting from chemotherapy, so Dr. Iyengar typically has patients use them afterwards, during maintenance treatment.
Oncologists don’t prescribe the drugs themselves but instead refer patients to endocrinologists or weight management centers that then write the prescriptions. Taking these drugs involves weekly subcutaneous injections patients can administer themselves.
Endocrinologist Emily Gallagher, MD, PhD, of Mount Sinai Hospital in New York City, estimates she has prescribed the antiobesity drugs to a few hundred patients with cancer and, like Dr. Iyengar, uses the drugs during maintenance treatment with hormone therapy for breast cancer. She also has used these agents in patients with prostate and endometrial cancers and has found the drugs can help counter steroid weight gain in multiple myeloma.
But, to date, the evidence for using GPL-1 agonists in cancer remains limited and the practice has not yet become widespread.
Research largely comes down to a few small retrospective studies in patients with breast cancer receiving aromatase inhibitors. Although no safety issues have emerged so far, these initial reports suggest that the drugs lead to significantly less weight loss in patients with cancer compared to the general population.
Dr. Iyengar led one recent study, presented at the 2024 annual meeting of the American Society of Clinical Oncology, in which he and his team assessed outcomes in 75 women with breast cancer who received a GLP-1 agonist. Almost 80% of patients had diabetes, and 60% received hormone therapy, most commonly an aromatase inhibitor. Patients’ median body mass index (BMI) at baseline was 34 kg/m2 (range, 23-50 kg/m2).
From baseline, patients lost 6.2 kg, on average, or about 5% of their total body weight, 12 months after initiating GLP-1 therapy.
In contrast, phase 3 trials show much higher mean weight loss — about two times — in patients without cancer.
Another recent study also reported modest weight loss results in patients with breast cancer undergoing endocrine therapy. The researchers reported that, at 12 months, Wegovy led to 4.34% reduction in BMI, compared with a 14% change reported in the general population. Zebound, however, was associated with a 2.31% BMI increase overall — though some patients did experience a decrease — compared with a 15% reduction in the general population.
“These findings indicate a substantially reduced weight loss efficacy in breast cancer patients on endocrine therapy compared to the general population,” the authors concluded.
It’s unclear why the drugs appear to not work as well in patients with cancer. It’s possible that hormone therapy or metabolic changes interfere with their effectiveness, given that some cancer therapies lead to weight gain. Steroids and hormone therapies, for instance, often increase appetite, and some treatments can slow patients’ metabolism or lead to fatigue, which can make it harder to exercise.
Patients with cancer may need a higher dose of GLP-1 agonists to achieve similar weight loss to the general population, Dr. Iyengar noted.
However, Dr. Gallagher said, in her own experience, she hasn’t found the drugs to be less effective in patients with cancer, especially the newer agents, like Wegovy and Zepbound.
As for safety, Wegovy and Zepbound both carry a black box warning for thyroid C-cell tumors, including medullary thyroid carcinoma. (Recent research, however, has found that GLP-1 agonists do not increase thyroid cancer risk).
These antiobesity agents are also contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients who have multiple endocrine neoplasia syndrome type 2, which is associated with medullary thyroid carcinoma.
Dr. Gallagher hasn’t seen any secondary tumors — thyroid or otherwise — in her patients with cancer, but she follows the labeling contraindications. Dr. Iyengar also noted that more recent and larger data sets have shown no impact on this risk, which may not actually exist, he said
Dr. Gallagher remains cautious about using GPL-1 agonists in patients who have had bariatric surgery because these agents can compound the slower gastric emptying and intestinal transit from surgery, potentially leading to gastrointestinal obstructions.
Looking ahead, GPL-1 manufacturers are interested in adding cancer indications to the drug labeling. Both Dr. Iyengar and Dr. Gallagher said their institutions are in talks with companies to participate in large, multicenter, global phase 3 trials.
Dr. Iyengar welcomes the efforts, not only to test the effectiveness of GPL-1 agonists in oncology but also to “nail down” their safety in cancer.
“I don’t think that there’s mechanistically anything that’s particularly worrisome,” and current observations suggest that these drugs are likely to be safe, Dr. Iyengar said. Even so, “GLP-1 agonists do a lot of things that we don’t fully understand yet.”
The bigger challenge, Dr. Iyengar noted, is that companies will have to show a sizable benefit to using these drugs in patients with cancer to get the Food and Drug Administration’s approval. And to move the needle on cancer-specific outcomes, these antiobesity drugs will need to demonstrate significant, durable weight loss in patients with cancer.
But if these drugs can do that, “I think it’s going to be one of the biggest advances in medicine and oncology given the obesity and cancer epidemic,” Dr. Iyengar said.
Dr. Iyengar has adviser and/or researcher ties with companies that make or are developing GPL-1 agonists, including AstraZeneca, Novartis, Gilead, and Pfizer. Dr. Gallagher is a consultant for Novartis, Flare Therapeutics, Reactive Biosciences, and Seagen.
A version of this article first appeared on Medscape.com.
Demand for new weight loss drugs has surged over the past few years.
Led by the antiobesity drugs semaglutide (Wegovy) and tirzepatide (Zepbound), these popular medications — more commonly known as glucagon-like peptide 1 (GLP-1) agonists — have become game changers for shedding excess pounds.
Aside from obesity indications, both drugs have been approved to treat type 2 diabetes under different brand names and have a growing list of other potential benefits, such as reducing inflammation and depression.
While there’s limited data to support the use of GLP-1 agonists for weight loss in cancer, some oncologists have begun carefully integrating the antiobesity agents into care and studying their effects in this patient population.
The reason: Research suggests that obesity can reduce the effectiveness of cancer therapies, especially in patients with breast cancer, and can increase the risk for treatment-related side effects.
The idea is that managing patients’ weight will improve their cancer outcomes, explained Lajos Pusztai, MD, PhD, a breast cancer specialist and professor of medicine at Yale School of Medicine in New Haven, Connecticut.
Although Dr. Pusztai and his oncology peers at Yale don’t yet use GPL-1 agonists, Neil Iyengar, MD, and colleagues have begun doing so to help some patients with breast cancer manage their weight. Dr. Iyengar estimates that a few hundred — almost 40% — of his patients are on the antiobesity drugs.
“For a patient who has really tried to reduce their weight and who is in the obese range, that’s where I think the use of these medications can be considered,” said Dr. Iyengar, a breast cancer oncologist at Memorial Sloan Kettering Cancer Center in New York City.
Why GLP-1s in Cancer?
GLP-1 is a hormone that the small intestine releases after eating. GLP-1 agonists work by mimicking GLP-1 to trigger the release of insulin and reduce the production of glucagon — two processes that help regulate blood sugar.
These agents, such as Wegovy (or Ozempic when prescribed for diabetes), also slow gastric emptying and can make people feel fuller longer.
Zebound (or Mounjaro for type 2 diabetes) is considered a dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, which may enhance its weight loss benefits.
In practice, however, these drugs can increase nausea and vomiting from chemotherapy, so Dr. Iyengar typically has patients use them afterwards, during maintenance treatment.
Oncologists don’t prescribe the drugs themselves but instead refer patients to endocrinologists or weight management centers that then write the prescriptions. Taking these drugs involves weekly subcutaneous injections patients can administer themselves.
Endocrinologist Emily Gallagher, MD, PhD, of Mount Sinai Hospital in New York City, estimates she has prescribed the antiobesity drugs to a few hundred patients with cancer and, like Dr. Iyengar, uses the drugs during maintenance treatment with hormone therapy for breast cancer. She also has used these agents in patients with prostate and endometrial cancers and has found the drugs can help counter steroid weight gain in multiple myeloma.
But, to date, the evidence for using GPL-1 agonists in cancer remains limited and the practice has not yet become widespread.
Research largely comes down to a few small retrospective studies in patients with breast cancer receiving aromatase inhibitors. Although no safety issues have emerged so far, these initial reports suggest that the drugs lead to significantly less weight loss in patients with cancer compared to the general population.
Dr. Iyengar led one recent study, presented at the 2024 annual meeting of the American Society of Clinical Oncology, in which he and his team assessed outcomes in 75 women with breast cancer who received a GLP-1 agonist. Almost 80% of patients had diabetes, and 60% received hormone therapy, most commonly an aromatase inhibitor. Patients’ median body mass index (BMI) at baseline was 34 kg/m2 (range, 23-50 kg/m2).
From baseline, patients lost 6.2 kg, on average, or about 5% of their total body weight, 12 months after initiating GLP-1 therapy.
In contrast, phase 3 trials show much higher mean weight loss — about two times — in patients without cancer.
Another recent study also reported modest weight loss results in patients with breast cancer undergoing endocrine therapy. The researchers reported that, at 12 months, Wegovy led to 4.34% reduction in BMI, compared with a 14% change reported in the general population. Zebound, however, was associated with a 2.31% BMI increase overall — though some patients did experience a decrease — compared with a 15% reduction in the general population.
“These findings indicate a substantially reduced weight loss efficacy in breast cancer patients on endocrine therapy compared to the general population,” the authors concluded.
It’s unclear why the drugs appear to not work as well in patients with cancer. It’s possible that hormone therapy or metabolic changes interfere with their effectiveness, given that some cancer therapies lead to weight gain. Steroids and hormone therapies, for instance, often increase appetite, and some treatments can slow patients’ metabolism or lead to fatigue, which can make it harder to exercise.
Patients with cancer may need a higher dose of GLP-1 agonists to achieve similar weight loss to the general population, Dr. Iyengar noted.
However, Dr. Gallagher said, in her own experience, she hasn’t found the drugs to be less effective in patients with cancer, especially the newer agents, like Wegovy and Zepbound.
As for safety, Wegovy and Zepbound both carry a black box warning for thyroid C-cell tumors, including medullary thyroid carcinoma. (Recent research, however, has found that GLP-1 agonists do not increase thyroid cancer risk).
These antiobesity agents are also contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients who have multiple endocrine neoplasia syndrome type 2, which is associated with medullary thyroid carcinoma.
Dr. Gallagher hasn’t seen any secondary tumors — thyroid or otherwise — in her patients with cancer, but she follows the labeling contraindications. Dr. Iyengar also noted that more recent and larger data sets have shown no impact on this risk, which may not actually exist, he said
Dr. Gallagher remains cautious about using GPL-1 agonists in patients who have had bariatric surgery because these agents can compound the slower gastric emptying and intestinal transit from surgery, potentially leading to gastrointestinal obstructions.
Looking ahead, GPL-1 manufacturers are interested in adding cancer indications to the drug labeling. Both Dr. Iyengar and Dr. Gallagher said their institutions are in talks with companies to participate in large, multicenter, global phase 3 trials.
Dr. Iyengar welcomes the efforts, not only to test the effectiveness of GPL-1 agonists in oncology but also to “nail down” their safety in cancer.
“I don’t think that there’s mechanistically anything that’s particularly worrisome,” and current observations suggest that these drugs are likely to be safe, Dr. Iyengar said. Even so, “GLP-1 agonists do a lot of things that we don’t fully understand yet.”
The bigger challenge, Dr. Iyengar noted, is that companies will have to show a sizable benefit to using these drugs in patients with cancer to get the Food and Drug Administration’s approval. And to move the needle on cancer-specific outcomes, these antiobesity drugs will need to demonstrate significant, durable weight loss in patients with cancer.
But if these drugs can do that, “I think it’s going to be one of the biggest advances in medicine and oncology given the obesity and cancer epidemic,” Dr. Iyengar said.
Dr. Iyengar has adviser and/or researcher ties with companies that make or are developing GPL-1 agonists, including AstraZeneca, Novartis, Gilead, and Pfizer. Dr. Gallagher is a consultant for Novartis, Flare Therapeutics, Reactive Biosciences, and Seagen.
A version of this article first appeared on Medscape.com.