User login
Mid-Life Hospitalists
Look at hospitalists and you’ll find more gray hair, crow’s feet, and accumulated wisdom than you might expect. While many hospitalists are physicians fresh from residency, the average age of a hospitalist is actually 40—in part because some hospitalist are docs who have left office practices in favor of hospital work.
These docs, who we’ll call “mid-career hospitalists,” take diverse paths to this change. Some miss the adrenaline rush of acute care. Others have become weary of the flat reimbursements and high patient volumes needed to maintain office practices today. Whatever their paths, they’re an interesting lot.
The most common scenario by which mid-career hospitalists make a transition is when hospital administrators recruit their own. That’s how Robert Brannon, MD, an Ob/Gyn in private practice since 1968, became a hospitalist at Presbyterian Hospital of Dallas in July 2005. Shrinking reimbursements, the costs of running an office, having to cover night call, and a national request for proposal (RFP) by the hospital precipitated Dr. Brannon’s career move.
He and nine other Ob/Gyns submitted a proposal in response to the RFP; hospital administrators awarded the group, OB on Call, LLP, a contract to start a hospitalist service for a largely indigent population in a hospital with more than 7,000 births annually.

I had already started to phase out the office practice and was working in a Medicaid clinic and an osteoporosis clinic when the hospital decided it had to do better with its indigent patients, particularly the 80 to 90 each month who came in with no prenatal care,” says Dr. Brannon. “The medical staff knew that resident work rules precluded their work off hours, so patient needs indicated that full-time hospitalists were in order.”
Now Dr. Brannon has the camaraderie of working with other hospitalists and neonatologists, delivering many babies, but still eliminating on-call obligations when he’s off duty.
“I’m doing more significant obstetrics work, re-honing my skills, and doing high-risk deliveries,” he says. “I’m doing what I love without the administrative hassles of a private practice.”
Jeffrey Frank, MD, had an even bigger nut to crack when he switched from an office-based practice to start a hospitalist medicine service at Doctors Medical Center (DMC) in San Pablo, Calif. The 45-year-old internist graduated from medical school in 1987 and worked in a four-person medical group in the area he describes as “very industrial, with oil refineries all around and the home base of the Hells Angels.”
—Scott Oxenhandler, MD
Helping to cover hospitalized patients for five HMOs precipitated his career change. “That was a mini-hospitalist assignment, and I felt I could adapt to full-time,” says Dr. Frank.
On DMC’s medical staff for years, Dr. Frank saw the hospital go from first in market share to a distant second after entrepreneurial doctors built a newer hospital north of town. Dr. Frank’s patients were aging and the prospects for improving the office practice were poor. Then there was Dr. Frank’s 800-pound gorilla: Kaiser-Permanente, a giant with 45% market share, with plans geared to younger patients, and physician salaries that his group couldn’t match. DMC continued slowly downhill, with closure a real risk.
In 2004, with his family’s acceptance of the long hours that launching a hospitalist program would take, Dr. Frank initiated discussions with hospital administrators to become its first chief hospitalist. Rather than leaving the office practice and launching a hospitalist service simultaneously, Dr. Frank approached established vendors for help. He chose IPC for its technology infrastructure and electronic medical records, competitive salaries, and the hope of attracting more physicians, whom Dr. Frank eventually recruited locally.
He built the hospitalist patient base by admitting all patients of the two largest medical groups. His entrepreneurial spirit intrigued both IPC and the hospital’s chief financial officer by reducing the average length of stay from 5.3 to 4.0 days, which improved the bottom line. Dr. Frank’s salary then increased by 30%. He says he loves doing acute care again and sees many of his former patients because the medical group has transferred hospital work to the hospitalists.

—Jeffrey Frank, MD
“I was worried about being at the hospital all the time,” says Dr. Frank. “I’m 45 years old, but energetic because there’s lots of work. I can keep up with three of the hospitalists just out of residency. Seeing my old patients also connects me to my old practice.”
Across the country in Hollywood, Fla., Scott Oxenhandler, MD, a geriatrician, couldn’t be happier with his mid-career change from office-based doctor to hospitalist. He left a thriving practice of eight physicians he helped start in 1987 to be chief hospitalist at Hollywood Memorial Regional Hospital (Fla.). Seeing five to eight hospitalized patients every day as their primary physician, he knew the hospital’s inner workings and how to start a hospitalist program—largely for unassigned patients.
“I wanted a free hand practicing acute care medicine, good compensation and benefits, lack of paperwork hassles, and a great schedule,” says Dr. Oxenhandler.
When he started in July 2004 Dr. Oxenhandler had no problem structuring a hospital medicine service that attracted physicians with competitive salaries and schedules to accommodate individual needs. He now has 21 full- and part-time hospitalists. They mostly work 8 a.m. to 5 p.m. with an average daily census of 12 to 15 and several consults. A nocturnist admits patients from 8 p.m. to 8 a.m., and 10 doctors handle 5 p.m. to 8 p.m. short call four times per month.
Overall, the transition for the 48-year-old veteran was surprisingly easy. “I was in the hospital all the time anyway, and the way internal medicine is evolving there have to be connections between inpatient and outpatient doctors,” says Dr. Oxenhandler. As the hospitalist leader he mentors young doctors, knows how to distribute the workload, and loves to share clinical insights.
Other Paths
For a doctor who finished residency at nearly 40, “mid-career change” takes on new meaning. Ron Jacobs, MD, internist, chief medical officer, and co-founder of PrimeDoc Management Services of Asheville, N.C., was a businessman in his 20s, then studied medicine and started an office practice in 1997. That practice—with four internists, a pulmonologist, and a cardiologist—was thriving. But Dr. Jacobs was bored. He missed the hospital’s intensity, was used to visiting six or eight hospitalized patients daily, and decided that seeing 16 or 18 patients without the office practice would suit him. So he co-founded PrimeDoc, which now has 100 hospitalists practicing in 15 programs throughout the Southeast and Mid-Atlantic.
The 49-year-old doctor eases the transition for other mid-lifers, recognizing that avoiding burnout as a hospitalist requires mental and physical preparation.
“The sheer volume of rounding, whether for an [average daily census] of 18 or 13 consults a day is tough,” says Dr. Jacobs. “They’ve got to be solid internists with strong ICU skills. I like diverse teams of older and younger docs. They work well because a team of hospitalists all just out of residency can easily burn out. They need the experience and mentoring of older docs to augment their up-to-date clinical skills.”
Academia is also fertile ground for mid-career changes. A doctor with an office practice and a faculty appointment may someday close the office and return to the hospital he or she loves. (See the profile of Joseph Snitzer, MD: “Sibling Rivalry,” in The Hospitalist, Sept. 2005.) Scott Wilson, MD, of The University of Iowa Hospitals and Clinic, Rapid City, left to start a hospitalist program in 2000 for the 880-bed University Hospital and its 250-bed Veterans Affairs Hospital after many years of teaching in the medical school. Dr. Wilson was tapped to start the hospitalist program because of improvements he had made in educating physicians.

—Ron Jacobs, MD
“Our program has some unique features, particularly our interaction with residents, improving the med school curriculum, and building research into our practice,” says Dr. Wilson.
In 2004 that included a study showing that patients managed by hospitalists had shorter length of stay (LOS) and lower costs than patients managed by non-hospitalists, but had higher costs per day. (Kaboli PJ, Barnett MJ, Rosenthal GE. Associations with reduced length of stay and costs on an academic hospitalist service. Am J Manag Care. 2004 Aug;10 (8):561-568). The schedule’s tough for a non-20-something: call every fourth night, three-week blocks for six months, then six months of research.
Dr. Wilson enjoys the challenge and the $1 million hospital support the program garnered in 2005. “We meet their needs to reduce LOS and improve quality, and we keep growing our program through new tasks such as surgical co-management of orthopedics,” he says.
Recruiting Them
Hospital administrators who want to recruit mid-career physicians as hospitalists need look no further than their own backyards. The internist or family practice doctor who relishes hospital rounds but has to rush back to the office, such as Dr. Oxenhandler, is a prime candidate for hospitalist recruitment. Areas where medical groups have trouble recruiting new doctors because reimbursements are flat (e.g., San Pablo) are also fertile ground for recruiting. Entrepreneurial physicians like Drs. Brannon and Jacobs, who had already dabbled in other medical careers before becoming hospitalists, are another choice.
Doctors in each of these categories are still brimming with energy and enthusiasm for medicine and are a looking for ways to make things better for patients and themselves. They might be your next hospitalist recruit. TH
Look at hospitalists and you’ll find more gray hair, crow’s feet, and accumulated wisdom than you might expect. While many hospitalists are physicians fresh from residency, the average age of a hospitalist is actually 40—in part because some hospitalist are docs who have left office practices in favor of hospital work.
These docs, who we’ll call “mid-career hospitalists,” take diverse paths to this change. Some miss the adrenaline rush of acute care. Others have become weary of the flat reimbursements and high patient volumes needed to maintain office practices today. Whatever their paths, they’re an interesting lot.
The most common scenario by which mid-career hospitalists make a transition is when hospital administrators recruit their own. That’s how Robert Brannon, MD, an Ob/Gyn in private practice since 1968, became a hospitalist at Presbyterian Hospital of Dallas in July 2005. Shrinking reimbursements, the costs of running an office, having to cover night call, and a national request for proposal (RFP) by the hospital precipitated Dr. Brannon’s career move.
He and nine other Ob/Gyns submitted a proposal in response to the RFP; hospital administrators awarded the group, OB on Call, LLP, a contract to start a hospitalist service for a largely indigent population in a hospital with more than 7,000 births annually.
I had already started to phase out the office practice and was working in a Medicaid clinic and an osteoporosis clinic when the hospital decided it had to do better with its indigent patients, particularly the 80 to 90 each month who came in with no prenatal care,” says Dr. Brannon. “The medical staff knew that resident work rules precluded their work off hours, so patient needs indicated that full-time hospitalists were in order.”
Now Dr. Brannon has the camaraderie of working with other hospitalists and neonatologists, delivering many babies, but still eliminating on-call obligations when he’s off duty.
“I’m doing more significant obstetrics work, re-honing my skills, and doing high-risk deliveries,” he says. “I’m doing what I love without the administrative hassles of a private practice.”
Jeffrey Frank, MD, had an even bigger nut to crack when he switched from an office-based practice to start a hospitalist medicine service at Doctors Medical Center (DMC) in San Pablo, Calif. The 45-year-old internist graduated from medical school in 1987 and worked in a four-person medical group in the area he describes as “very industrial, with oil refineries all around and the home base of the Hells Angels.”
—Scott Oxenhandler, MD
Helping to cover hospitalized patients for five HMOs precipitated his career change. “That was a mini-hospitalist assignment, and I felt I could adapt to full-time,” says Dr. Frank.
On DMC’s medical staff for years, Dr. Frank saw the hospital go from first in market share to a distant second after entrepreneurial doctors built a newer hospital north of town. Dr. Frank’s patients were aging and the prospects for improving the office practice were poor. Then there was Dr. Frank’s 800-pound gorilla: Kaiser-Permanente, a giant with 45% market share, with plans geared to younger patients, and physician salaries that his group couldn’t match. DMC continued slowly downhill, with closure a real risk.
In 2004, with his family’s acceptance of the long hours that launching a hospitalist program would take, Dr. Frank initiated discussions with hospital administrators to become its first chief hospitalist. Rather than leaving the office practice and launching a hospitalist service simultaneously, Dr. Frank approached established vendors for help. He chose IPC for its technology infrastructure and electronic medical records, competitive salaries, and the hope of attracting more physicians, whom Dr. Frank eventually recruited locally.
He built the hospitalist patient base by admitting all patients of the two largest medical groups. His entrepreneurial spirit intrigued both IPC and the hospital’s chief financial officer by reducing the average length of stay from 5.3 to 4.0 days, which improved the bottom line. Dr. Frank’s salary then increased by 30%. He says he loves doing acute care again and sees many of his former patients because the medical group has transferred hospital work to the hospitalists.
—Jeffrey Frank, MD
“I was worried about being at the hospital all the time,” says Dr. Frank. “I’m 45 years old, but energetic because there’s lots of work. I can keep up with three of the hospitalists just out of residency. Seeing my old patients also connects me to my old practice.”
Across the country in Hollywood, Fla., Scott Oxenhandler, MD, a geriatrician, couldn’t be happier with his mid-career change from office-based doctor to hospitalist. He left a thriving practice of eight physicians he helped start in 1987 to be chief hospitalist at Hollywood Memorial Regional Hospital (Fla.). Seeing five to eight hospitalized patients every day as their primary physician, he knew the hospital’s inner workings and how to start a hospitalist program—largely for unassigned patients.
“I wanted a free hand practicing acute care medicine, good compensation and benefits, lack of paperwork hassles, and a great schedule,” says Dr. Oxenhandler.
When he started in July 2004 Dr. Oxenhandler had no problem structuring a hospital medicine service that attracted physicians with competitive salaries and schedules to accommodate individual needs. He now has 21 full- and part-time hospitalists. They mostly work 8 a.m. to 5 p.m. with an average daily census of 12 to 15 and several consults. A nocturnist admits patients from 8 p.m. to 8 a.m., and 10 doctors handle 5 p.m. to 8 p.m. short call four times per month.
Overall, the transition for the 48-year-old veteran was surprisingly easy. “I was in the hospital all the time anyway, and the way internal medicine is evolving there have to be connections between inpatient and outpatient doctors,” says Dr. Oxenhandler. As the hospitalist leader he mentors young doctors, knows how to distribute the workload, and loves to share clinical insights.
Other Paths
For a doctor who finished residency at nearly 40, “mid-career change” takes on new meaning. Ron Jacobs, MD, internist, chief medical officer, and co-founder of PrimeDoc Management Services of Asheville, N.C., was a businessman in his 20s, then studied medicine and started an office practice in 1997. That practice—with four internists, a pulmonologist, and a cardiologist—was thriving. But Dr. Jacobs was bored. He missed the hospital’s intensity, was used to visiting six or eight hospitalized patients daily, and decided that seeing 16 or 18 patients without the office practice would suit him. So he co-founded PrimeDoc, which now has 100 hospitalists practicing in 15 programs throughout the Southeast and Mid-Atlantic.
The 49-year-old doctor eases the transition for other mid-lifers, recognizing that avoiding burnout as a hospitalist requires mental and physical preparation.
“The sheer volume of rounding, whether for an [average daily census] of 18 or 13 consults a day is tough,” says Dr. Jacobs. “They’ve got to be solid internists with strong ICU skills. I like diverse teams of older and younger docs. They work well because a team of hospitalists all just out of residency can easily burn out. They need the experience and mentoring of older docs to augment their up-to-date clinical skills.”
Academia is also fertile ground for mid-career changes. A doctor with an office practice and a faculty appointment may someday close the office and return to the hospital he or she loves. (See the profile of Joseph Snitzer, MD: “Sibling Rivalry,” in The Hospitalist, Sept. 2005.) Scott Wilson, MD, of The University of Iowa Hospitals and Clinic, Rapid City, left to start a hospitalist program in 2000 for the 880-bed University Hospital and its 250-bed Veterans Affairs Hospital after many years of teaching in the medical school. Dr. Wilson was tapped to start the hospitalist program because of improvements he had made in educating physicians.
—Ron Jacobs, MD
“Our program has some unique features, particularly our interaction with residents, improving the med school curriculum, and building research into our practice,” says Dr. Wilson.
In 2004 that included a study showing that patients managed by hospitalists had shorter length of stay (LOS) and lower costs than patients managed by non-hospitalists, but had higher costs per day. (Kaboli PJ, Barnett MJ, Rosenthal GE. Associations with reduced length of stay and costs on an academic hospitalist service. Am J Manag Care. 2004 Aug;10 (8):561-568). The schedule’s tough for a non-20-something: call every fourth night, three-week blocks for six months, then six months of research.
Dr. Wilson enjoys the challenge and the $1 million hospital support the program garnered in 2005. “We meet their needs to reduce LOS and improve quality, and we keep growing our program through new tasks such as surgical co-management of orthopedics,” he says.
Recruiting Them
Hospital administrators who want to recruit mid-career physicians as hospitalists need look no further than their own backyards. The internist or family practice doctor who relishes hospital rounds but has to rush back to the office, such as Dr. Oxenhandler, is a prime candidate for hospitalist recruitment. Areas where medical groups have trouble recruiting new doctors because reimbursements are flat (e.g., San Pablo) are also fertile ground for recruiting. Entrepreneurial physicians like Drs. Brannon and Jacobs, who had already dabbled in other medical careers before becoming hospitalists, are another choice.
Doctors in each of these categories are still brimming with energy and enthusiasm for medicine and are a looking for ways to make things better for patients and themselves. They might be your next hospitalist recruit. TH
Look at hospitalists and you’ll find more gray hair, crow’s feet, and accumulated wisdom than you might expect. While many hospitalists are physicians fresh from residency, the average age of a hospitalist is actually 40—in part because some hospitalist are docs who have left office practices in favor of hospital work.
These docs, who we’ll call “mid-career hospitalists,” take diverse paths to this change. Some miss the adrenaline rush of acute care. Others have become weary of the flat reimbursements and high patient volumes needed to maintain office practices today. Whatever their paths, they’re an interesting lot.
The most common scenario by which mid-career hospitalists make a transition is when hospital administrators recruit their own. That’s how Robert Brannon, MD, an Ob/Gyn in private practice since 1968, became a hospitalist at Presbyterian Hospital of Dallas in July 2005. Shrinking reimbursements, the costs of running an office, having to cover night call, and a national request for proposal (RFP) by the hospital precipitated Dr. Brannon’s career move.
He and nine other Ob/Gyns submitted a proposal in response to the RFP; hospital administrators awarded the group, OB on Call, LLP, a contract to start a hospitalist service for a largely indigent population in a hospital with more than 7,000 births annually.
I had already started to phase out the office practice and was working in a Medicaid clinic and an osteoporosis clinic when the hospital decided it had to do better with its indigent patients, particularly the 80 to 90 each month who came in with no prenatal care,” says Dr. Brannon. “The medical staff knew that resident work rules precluded their work off hours, so patient needs indicated that full-time hospitalists were in order.”
Now Dr. Brannon has the camaraderie of working with other hospitalists and neonatologists, delivering many babies, but still eliminating on-call obligations when he’s off duty.
“I’m doing more significant obstetrics work, re-honing my skills, and doing high-risk deliveries,” he says. “I’m doing what I love without the administrative hassles of a private practice.”
Jeffrey Frank, MD, had an even bigger nut to crack when he switched from an office-based practice to start a hospitalist medicine service at Doctors Medical Center (DMC) in San Pablo, Calif. The 45-year-old internist graduated from medical school in 1987 and worked in a four-person medical group in the area he describes as “very industrial, with oil refineries all around and the home base of the Hells Angels.”
—Scott Oxenhandler, MD
Helping to cover hospitalized patients for five HMOs precipitated his career change. “That was a mini-hospitalist assignment, and I felt I could adapt to full-time,” says Dr. Frank.
On DMC’s medical staff for years, Dr. Frank saw the hospital go from first in market share to a distant second after entrepreneurial doctors built a newer hospital north of town. Dr. Frank’s patients were aging and the prospects for improving the office practice were poor. Then there was Dr. Frank’s 800-pound gorilla: Kaiser-Permanente, a giant with 45% market share, with plans geared to younger patients, and physician salaries that his group couldn’t match. DMC continued slowly downhill, with closure a real risk.
In 2004, with his family’s acceptance of the long hours that launching a hospitalist program would take, Dr. Frank initiated discussions with hospital administrators to become its first chief hospitalist. Rather than leaving the office practice and launching a hospitalist service simultaneously, Dr. Frank approached established vendors for help. He chose IPC for its technology infrastructure and electronic medical records, competitive salaries, and the hope of attracting more physicians, whom Dr. Frank eventually recruited locally.
He built the hospitalist patient base by admitting all patients of the two largest medical groups. His entrepreneurial spirit intrigued both IPC and the hospital’s chief financial officer by reducing the average length of stay from 5.3 to 4.0 days, which improved the bottom line. Dr. Frank’s salary then increased by 30%. He says he loves doing acute care again and sees many of his former patients because the medical group has transferred hospital work to the hospitalists.
—Jeffrey Frank, MD
“I was worried about being at the hospital all the time,” says Dr. Frank. “I’m 45 years old, but energetic because there’s lots of work. I can keep up with three of the hospitalists just out of residency. Seeing my old patients also connects me to my old practice.”
Across the country in Hollywood, Fla., Scott Oxenhandler, MD, a geriatrician, couldn’t be happier with his mid-career change from office-based doctor to hospitalist. He left a thriving practice of eight physicians he helped start in 1987 to be chief hospitalist at Hollywood Memorial Regional Hospital (Fla.). Seeing five to eight hospitalized patients every day as their primary physician, he knew the hospital’s inner workings and how to start a hospitalist program—largely for unassigned patients.
“I wanted a free hand practicing acute care medicine, good compensation and benefits, lack of paperwork hassles, and a great schedule,” says Dr. Oxenhandler.
When he started in July 2004 Dr. Oxenhandler had no problem structuring a hospital medicine service that attracted physicians with competitive salaries and schedules to accommodate individual needs. He now has 21 full- and part-time hospitalists. They mostly work 8 a.m. to 5 p.m. with an average daily census of 12 to 15 and several consults. A nocturnist admits patients from 8 p.m. to 8 a.m., and 10 doctors handle 5 p.m. to 8 p.m. short call four times per month.
Overall, the transition for the 48-year-old veteran was surprisingly easy. “I was in the hospital all the time anyway, and the way internal medicine is evolving there have to be connections between inpatient and outpatient doctors,” says Dr. Oxenhandler. As the hospitalist leader he mentors young doctors, knows how to distribute the workload, and loves to share clinical insights.
Other Paths
For a doctor who finished residency at nearly 40, “mid-career change” takes on new meaning. Ron Jacobs, MD, internist, chief medical officer, and co-founder of PrimeDoc Management Services of Asheville, N.C., was a businessman in his 20s, then studied medicine and started an office practice in 1997. That practice—with four internists, a pulmonologist, and a cardiologist—was thriving. But Dr. Jacobs was bored. He missed the hospital’s intensity, was used to visiting six or eight hospitalized patients daily, and decided that seeing 16 or 18 patients without the office practice would suit him. So he co-founded PrimeDoc, which now has 100 hospitalists practicing in 15 programs throughout the Southeast and Mid-Atlantic.
The 49-year-old doctor eases the transition for other mid-lifers, recognizing that avoiding burnout as a hospitalist requires mental and physical preparation.
“The sheer volume of rounding, whether for an [average daily census] of 18 or 13 consults a day is tough,” says Dr. Jacobs. “They’ve got to be solid internists with strong ICU skills. I like diverse teams of older and younger docs. They work well because a team of hospitalists all just out of residency can easily burn out. They need the experience and mentoring of older docs to augment their up-to-date clinical skills.”
Academia is also fertile ground for mid-career changes. A doctor with an office practice and a faculty appointment may someday close the office and return to the hospital he or she loves. (See the profile of Joseph Snitzer, MD: “Sibling Rivalry,” in The Hospitalist, Sept. 2005.) Scott Wilson, MD, of The University of Iowa Hospitals and Clinic, Rapid City, left to start a hospitalist program in 2000 for the 880-bed University Hospital and its 250-bed Veterans Affairs Hospital after many years of teaching in the medical school. Dr. Wilson was tapped to start the hospitalist program because of improvements he had made in educating physicians.
—Ron Jacobs, MD
“Our program has some unique features, particularly our interaction with residents, improving the med school curriculum, and building research into our practice,” says Dr. Wilson.
In 2004 that included a study showing that patients managed by hospitalists had shorter length of stay (LOS) and lower costs than patients managed by non-hospitalists, but had higher costs per day. (Kaboli PJ, Barnett MJ, Rosenthal GE. Associations with reduced length of stay and costs on an academic hospitalist service. Am J Manag Care. 2004 Aug;10 (8):561-568). The schedule’s tough for a non-20-something: call every fourth night, three-week blocks for six months, then six months of research.
Dr. Wilson enjoys the challenge and the $1 million hospital support the program garnered in 2005. “We meet their needs to reduce LOS and improve quality, and we keep growing our program through new tasks such as surgical co-management of orthopedics,” he says.
Recruiting Them
Hospital administrators who want to recruit mid-career physicians as hospitalists need look no further than their own backyards. The internist or family practice doctor who relishes hospital rounds but has to rush back to the office, such as Dr. Oxenhandler, is a prime candidate for hospitalist recruitment. Areas where medical groups have trouble recruiting new doctors because reimbursements are flat (e.g., San Pablo) are also fertile ground for recruiting. Entrepreneurial physicians like Drs. Brannon and Jacobs, who had already dabbled in other medical careers before becoming hospitalists, are another choice.
Doctors in each of these categories are still brimming with energy and enthusiasm for medicine and are a looking for ways to make things better for patients and themselves. They might be your next hospitalist recruit. TH
CODE PINK
Something didn’t seem quite right. The person in the hooded sweatshirt standing near the entrance looked suspicious to respiratory therapist Betty Collins as she entered the newborn nursery on the evening of Jan. 12, 2006, during her shift at Ouachita County Medical Center in Camden, Ark. Perhaps this is why she shielded her fingers as she punched in the combination to the lock on the nursery door before entering to check on a baby inside.
Leaving minutes later, her work done, Collins’ suspicions were confirmed when Nikenya Washington, 18, shoved her way into the nursery yelling, “Move out my way, I’ll shoot you b----!”
Collins and the other nurse in the unit bravely wrestled with the would-be abductor. A Code Pink was called.
It is notable that January’s Ouachita Hospital case is unique as the first reported case of physical violence during an in-hospital abduction.
This frightening episode is one example of the phenomenon of infant abduction, and according to Cathy Nahirny of the National Center for Missing and Exploited Children (NCMEC) it is the first reported case in 2006.
Infant abduction is defined as the act of kidnapping an infant less than six months of age by a non-family member. Code Pink is the almost universally adopted code word signaling that an abduction is taking place. Though infrequent by comparison to other types of kidnapping or exploitation of children, infant abduction—like many pediatric situations—is quite dramatic.
This crime is of particular concern to pediatric hospitalists because about half of these events occur within the hospital setting. It plays on the fears of expectant parents and communities, and a successful abduction can be catastrophic for a hospital’s image and reputation. Preventing infant abduction and maintaining preparedness for Code Pink situations represents an ongoing challenge for the approximately 3,500 hospitals where about 4 million American babies are born each year.

Small Number, Large Impact
According to Daniel Broughton, MD, infant abduction is a small subset of a much larger problem. As the director of the Child Abuse Program at the Mayo Clinic in Rochester, Minn., and co-author of the American Academy of Pediatrics’ Clinical Report on the pediatrician’s role in the prevention of missing children, he is an expert on the subject.
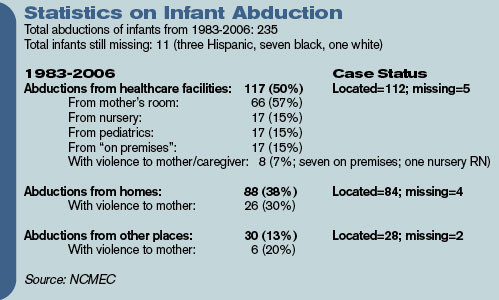
There are an estimated 1-2 million runaways and as many as 200,000 abductions by family members in the United States each year. By contrast, since 1983 when the NCMEC began to collect information on reports of infant abduction, there have been a total of 235 recorded infant kidnappings by non-family members. Nevertheless, “from the standpoint of impact both on families and the hospitals, it is huge,” says Dr. Broughton of infant abduction.
Bob Chicarello, the interim head of security at the Brigham and Women’s Hospital in Boston, agrees.
“You want to do everything possible to prevent [an infant abduction] because it could really shake an institution to its knees,” he says.
In addition, the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) considers infant abduction such a safety priority that it was made a reportable “Sentinel Event” in 1998. Of the reported 235 reported cases 117 abductions—or 50%—have occurred in the hospital setting. Most children taken from the hospital—57%—are taken from their mother’s room. Roughly 15% each are taken from the newborn nursery, other pediatric wards, or from other parts of the hospital grounds.
Among abductions occurring outside the healthcare setting, 38% of the total occurred from private homes, and the final 13% of the total in other public venues.
A Unique Crime
Infant abduction seems to be distinct from other types of kidnapping in several ways. The first unique characteristic of infant abduction is the profile of the stereotypical perpetrator. Examination of case reports shows that the vast majority of abductors are females of childbearing age. Most live in or near the city where the abduction takes place. Many are overweight, and they may have a history of depression or lying, manipulative behavior.
Additionally, the motives of these women are notably different than those of other kidnappers who are interested in sexual exploitation, money, or revenge. Instead, these women most often desire to have a child of their own. This may be to replace a child or pregnancy that was lost, or to appease a significant other who they perceive may leave them if they cannot produce a child. Notably, many of the kidnappers, later caught, have been observed to provide adequate care for the infants.
Though the timing of an infant abduction can be impulsive, many kidnappers show evidence of elaborate planning beforehand. Several women have staged fictitious pregnancies on one or more occasions. Some kidnappers have even bought baby items or furnished nurseries in anticipation of having a child. Many offenders visit the hospitals or other facilities they later target on several occasions prior to an attempted abduction. They will try to become familiar with hospital personnel often by asking probing questions about security and procedure. A common ploy is for the kidnappers to impersonate nurses, lab technicians, or other hospital personnel in an attempt to gain access to the children. Some even acquire hospital uniforms or other disguises.
They may pose as family members of other patients in order to befriend the parents of their victims. This was the case of Nikenya Washington, who actually entered the room of the would-be victim’s mother early in the evening on the night of the crime. She stated that she had walked into the wrong room and tried to strike up a conversation before leaving.
Prevention is Key
Preventing infant abduction is key, and this process starts by putting proper procedures and hardware in place at healthcare facilities.
“We use a multilayered approach,” says Chicarello. This includes prior planning, physical barriers, electronic aides, and ongoing training and education of staff and parents alike. At Brigham and Women’s, security starts in the lobby where admittance to the maternity ward is gained only after signing in and using a specific elevator. Hospital personnel wear specific nursery badges, and they obtain access to the ward by key card.
The hospital also uses various forms of technology including closed circuit TV monitors, silent “panic” buttons at the nurse’s stations, and electronic wrist/ankle bracelets for the babies.
Chicarello stresses the importance of both initial training for new personnel as well as ongoing education throughout the hospital. This includes hospital-wide awareness drives and an annual Code Pink Fair. Education for parents is incorporated into a pre-natal curriculum. A big part of ongoing training is the use of monthly unscheduled Code Pink drills.
“We try to vary the scenarios to keep the staff on their toes and to expose any weaknesses,” he says. Such scenarios might include having people pose as lab personnel or pulling the fire alarm to create a diversion. “My favorite was once when we had a pizza delivered to the nurses station.” Fortunately, this didn’t work.
Dr. Broughton echoes the notion that a multifaceted approach is important. In addition to well-defined procedures in the birthing suite, the Mayo Clinic’s plan for preventing infant abduction extends to the larger children’s hospital and even to the clinic. Having a well-defined abduction plan has other positive effects as well, notes Dr. Broughton. Such programs are useful in preventing other types of theft, in aiding infection control efforts, and in locating ambulatory children who might wander or get lost.
The process requires input from several disciplines including nursing, security, and physicians. “I think pediatricians should be completely supportive of programs that provide a safety net,” says Dr. Broughton. “[Physicians] should be the leaders in the hospital setting.” One problem he has seen is that physicians sometimes don’t want to be bothered by little details like wearing a proper ID or leaving doors properly locked. Getting physicians to say, “this is important” is an essential first step.
A Disturbing Trend
Though changes in the landscape of infant abduction are difficult to discern, a few trends are notable. Encouragingly, in-hospital abductions are a smaller fraction of the total incidence, perhaps in response to better deterrence by medical facilities. As evidence of this, there was a recent 20-month period without a single abduction from a hospital setting. More disturbingly, though, the incidence of out-of-hospital abductions and the use of violence in abductions seem on the rise. Among these about 29% have involved violence to the parents or family of the infant including eight cases of homicide.
Obviously, preventing abductions outside the hospital presents its own challenges. Nahirny cautions strongly against the publication of birth information on the local press or on Web sites. “These shouldn’t include any specifically identifying information,” she states, such as full names of parents or a home address.
Second, parents must understand the potential danger of posting signs or balloons outside the home after a birth, as these might alert a potential abductor to the presence of an infant. Finally, parents should be careful with unknown, unexpected, or recently acquainted visitors shortly after coming home from the hospital. There are several cases of abductors posing as home-health nurses, social workers, or other official personnel.
Conclusion
Even though she was able to grab the child and make it out of the room, Nikenya Washington did not make if off the hospital ward before being subdued by a security guard and other hospital personnel. Thankfully, the healthy 8-pound, 1-once baby girl was safely returned to her mother. In fact, hospital personnel in conjunction with local law enforcement and media safely recover most abducted infants thanks to orderly responses. However, the best option for all parties involved is a well-planned strategy of prevention. This includes physical barriers, electronic aides, and education of personnel and parents, as well as constant vigilance.
For those who want to get involved in preventing infant abduction, several resources are available. The NCMEC has quite a bit of information on its Web site (www.missingkids.com). There is also an excellent educational video produced by Mead Johnson Nutritionals called “Safeguard Their Tomorrows” available for viewing.
The most definitive resource for clinicians is a book entitled Guidelines for the Prevention of and Response to Infant Abduction. Currently in its eighth edition by John Rabun of the NCEMC, the book discusses the problem of infant abduction and defines its scope. There are various practical recommendations on the general, proactive, and physical measures to prevent abductions and on how to respond once an incident has occurred. There are also sections on how to advise parents and how to assess level of preparedness.
Dr. Axon is an instructor, Departments of Medicine and Pediatrics, Medical University of South Carolina Medical Center, Charleston.
Bibliography
- Ankrom LG, Lent CJ. Cradle robbers: A study of the infant abductor. The FBI Law Enforcement Bulletin. 1995;64(9):112-118.
- Hillen M. Teen held in attempt to abduct newborn. Arkansas Democrat Gazette. 16 January, 2006.
- Rabun J. For Healthcare Professionals: Guidelines for the Prevention of and Response to Infant Abduction. 8th ed. Alexandria, Virginia: National Center for Missing and Exploited Children; 2005.
Pediatric Special Section
In the Literature
By G. Ronald Nicholis, MD, Children’s Mercy Hospital, Kansas City, Mo., Gina Weddle, RN, CPNP, Section of Pediatric Hospitalists, Department of Pediatrics, Children’s Mercy Hospitals and Clinics (Kansas City, Mo.), and J. Christopher Day, MD, Section of Pediatric Hospitalists, Department of Pediatrics, Children’s Mercy Hospitals and Clinics (Kansas City, Mo.)
Computerized Physician Order Entry—Not a Finished Product
Han YY, Carcillo JA, Venkataraman ST, et al. Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2005;116(6):1506-1512.
Over the past several years attention has been increasingly focused on the inadequacy of patient safety in our practices. In response, hospitals, insurers, and practices have examined many potential changes to current systems in an effort to improve safety.
The Institute of Medicine (IOM) and the Leapfrog Group have championed computerized physician order entry (CPOE) as necessary for improving patient safety, citing the inadequacy of paper and pen for the ordering process. Research documenting that CPOE systems used in the hospital setting can decrease adverse drug events has fostered the promise and potential for CPOE to make the hospital a safer place for our patients, particularly when enhanced with decision support. Decision support can allow the physician to be alerted to errors in dose, drug-drug interaction, drug-food interaction, allergies, and the need for dosage corrections based on laboratory values at the time of ordering. Contrary to the research demonstrating improved safety, some studies have shown an increase in unique errors after implementation of CPOE.
The current study from the Departments of Critical Care Medicine and Pediatrics at Children’s Hospital of Pittsburgh calls our attention to significant issues with implementation of CPOE that have potential to inhibit the goal of improving patient safety. Citing a study by Upperman, et al. from their own institution, which noted significant improvement in adverse drug events after implementation of CPOE, the authors of the current study state, “Children’s Hospital of Pittsburgh implemented … Cerner’s commercial CPOE system in October 2002 in an effort to become one of the first children’s hospitals in the U.S. to attain 100% CPOE status.”
The study was designed to measure the effect of CPOE implementation on mortality rate for patients transferred into this pediatric tertiary care facility who required “immediate processing … and stabilization orders.” This retrospective study examined an 18-month period of mortality data: Thirteen months before the implementation of CPOE and five months after.
They discovered an unexpected increase in unadjusted mortality rate after the implementation of CPOE from 2.8% to 6.57%, (P<0.001). Mortality odds ratios were calculated, and observed mortality before CPOE implementation was consistently better than after CPOE implementation. Regression analysis with and without Pediatric Risk of Mortality comparisons were performed and CPOE, in addition to other factors, was associated with increased mortality in both analyses. How should this be interpreted?
The authors note several factors having impact on the validity of the study, specifically mentioning that “study design precludes any statements regarding cause and effect,” “[researchers] examined a unique patient population admitted through interfacility transport … (thus) findings may not be generalizable to the hospital experience as a whole,” and “[the] observation period after CPOE implementation was brief.”
Seasonal variability was also a potential confounding factor because CPOE implementation was in October and the observation period post-CPOE extended only five months—to March of the next year. However, a statistical comparison between matched five-month periods supported the association between implementation of CPOE and increased mortality in this population.
In addition, the authors discuss how their institution’s chosen implementation process for CPOE affected the work processes and pattern of care provided to these critically ill patients. Issues such as being unable to enter orders on a patient in preparation of their arrival because they were not yet enrolled in the electronic system hampered the availability of important medications at the time of arrival. Forcing all of the orders to go through their designed CPOE process in an effort to use the error prevention capabilities of the system caused potentially significant delays in the administration of life-saving medications.
The lack of functional order sets further delayed the physician’s ability to efficiently enter orders electronically. These variables may have impacted mortality rates. Further delays were evident due to the fact that a nurse had to activate orders placed by the physician, bypassing some of the efficiency of an electronic system. Similarly, the pharmacy reviewed and processed the order before the medication was available to the nurse for delivery to the patient.
These checks and balances have the potential to prevent errors in medication ordering, but if inefficient, they may not be appropriate for an intensive care setting in every circumstance. Researchers stated the new workflow took the physicians and nurses away from the patient’s bedside, potentially decreasing observation benefits for the patient. The capacity of the system to compute at times seemed “frozen” causing further delays—not necessarily an uncommon occurrence with any electronic system.
The practice of medicine is complex and work processes do not easily translate to the electronic models currently available. It is crucial that hospitalists, other specialists, all ancillary services, as well as administration be involved in the building and implementation of the systems to be used in our individual facilities. The systems and technology for effective CPOE in hospital settings—especially in pediatric settings—have yet to be developed. The implementation of CPOE for improved patient safety requires exploration given the exposed inadequacies of our current methods of practice.
Like any best practice this exploration will be continuous and require evaluation and improvement. While we must involve ourselves with the development and implementation of CPOE, we must not let the inadequacies of new systems negatively affect patient care. The dichotomy may be omnipresent: Use the system to gain protections from errors and bypass the system when its design or function interferes with good patient practice. This will require us to possess the wisdom to determine the correct path to follow in any instance.
Every day in our practice we make efforts to compensate for failures in our methods to prevent errors from affecting our patient’s care. Electronic systems do not excuse us from continued vigilance, communication, and action to protect our patients from medical errors. The authors appropriately state that “accurate evaluation of CPOE will require systems-based troubleshooting with well-funded, well-designed, multicenter studies that can adequately address these questions.”
Unfortunately, because of the proven inadequacies of the current system, CPOE, like other methodologies we use in the advancement of patient care, cannot wait for proof of perfection before being used to enhance the outcomes of our patients. Thus we need to be vigorous in our participation of the development and implementation of CPOE for our individual institutions and alert to the prevention of harm in all we do. Software companies cannot accomplish improvement in our practices without our involvement, and we cannot meet our demands for quality without good software companies.
The Link between Age and Orchiectomy Due to Testicular Torsion
Mansbach J, Forbes P, Peters C. Testicular torsion and risk factors for orchiectomy. Arch Pediatr Adolesc Med. 2005;159(12):1167-1171.
Testicular torsion is a urologic emergency that requires a four- to eight-hour window from presentation of symptoms until intervention in order to increase the potential for a viable testis. Steps to ensure a viable testis include timely presentation, rapid diagnosis, and curative intervention.
Chart review was done from a national database consisting of 984 hospitals in 22 states. The review included 436 patients ranging from one to 25 years. The incidence of torsion was 4.5 cases/100,000 male subjects with a peak at 10-19 years of age. Of the 436 subjects, 34% required orchiectomy. After all factors (race, insurance status, income, region, and hospital location) were evaluated, increased age at presentation was the only statistically significant factor associated orchiectomy. Male subjects were hesitant to seek medical attention for conditions associated with the genitals. Healthcare providers need to provide anticipatory guidance when educating males about testicular disorders. Testicular exam should be incorporated as part of every physical exam, especially if an abdominal complaint exists.
Heliox Aids Peds with Moderate to Severe Asthma
Kim K, Phrampus E, Venkataraman S, et al. Helium/oxygen-driven albuterol nebulization in the treatment of children with moderate to severe asthma exacerbations: A randomized controlled trial. Pediatrics. 2005;116(5):1127-1133.
Heliox is a 70%/30% helium/oxygen mixture. Heliox mixtures have a lower gas density than oxygen and, therefore, can increase pulmonary gas delivery. This study compared heliox versus oxygen delivery of continuous albuterol nebulization for patients with asthma treated in the emergency department.
Investigators enrolled 30 subjects between ages two and 18 with moderate to severe asthma. Severity of asthma was determined by a pulmonary index (PI) of >8. PI scores are based on respiratory rate, wheezing, accessory muscle use, inspiratory/expiratory ratio, and pulse oximetry. All children were given one 5mg albuterol treatment using traditional oxygen delivery along with oral steroids dosed at 2mg/kg. After the initial treatment and steroids if the PI score was >8 they were randomly assigned to receive continuous albuterol by heliox or traditional oxygen delivery.
The study showed that continuous albuterol delivered by heliox mixture lowered PI scores from baseline to 240 minutes into the study (P<0.001). Results also demonstrated a trend towards improved rate of discharge from the emergency department and hospital, but the study was not powered to adequately evaluate these outcomes Limitations of the study include lack of complete blinding and a small sample size. TH
Something didn’t seem quite right. The person in the hooded sweatshirt standing near the entrance looked suspicious to respiratory therapist Betty Collins as she entered the newborn nursery on the evening of Jan. 12, 2006, during her shift at Ouachita County Medical Center in Camden, Ark. Perhaps this is why she shielded her fingers as she punched in the combination to the lock on the nursery door before entering to check on a baby inside.
Leaving minutes later, her work done, Collins’ suspicions were confirmed when Nikenya Washington, 18, shoved her way into the nursery yelling, “Move out my way, I’ll shoot you b----!”
Collins and the other nurse in the unit bravely wrestled with the would-be abductor. A Code Pink was called.
It is notable that January’s Ouachita Hospital case is unique as the first reported case of physical violence during an in-hospital abduction.
This frightening episode is one example of the phenomenon of infant abduction, and according to Cathy Nahirny of the National Center for Missing and Exploited Children (NCMEC) it is the first reported case in 2006.
Infant abduction is defined as the act of kidnapping an infant less than six months of age by a non-family member. Code Pink is the almost universally adopted code word signaling that an abduction is taking place. Though infrequent by comparison to other types of kidnapping or exploitation of children, infant abduction—like many pediatric situations—is quite dramatic.
This crime is of particular concern to pediatric hospitalists because about half of these events occur within the hospital setting. It plays on the fears of expectant parents and communities, and a successful abduction can be catastrophic for a hospital’s image and reputation. Preventing infant abduction and maintaining preparedness for Code Pink situations represents an ongoing challenge for the approximately 3,500 hospitals where about 4 million American babies are born each year.
Small Number, Large Impact
According to Daniel Broughton, MD, infant abduction is a small subset of a much larger problem. As the director of the Child Abuse Program at the Mayo Clinic in Rochester, Minn., and co-author of the American Academy of Pediatrics’ Clinical Report on the pediatrician’s role in the prevention of missing children, he is an expert on the subject.
There are an estimated 1-2 million runaways and as many as 200,000 abductions by family members in the United States each year. By contrast, since 1983 when the NCMEC began to collect information on reports of infant abduction, there have been a total of 235 recorded infant kidnappings by non-family members. Nevertheless, “from the standpoint of impact both on families and the hospitals, it is huge,” says Dr. Broughton of infant abduction.
Bob Chicarello, the interim head of security at the Brigham and Women’s Hospital in Boston, agrees.
“You want to do everything possible to prevent [an infant abduction] because it could really shake an institution to its knees,” he says.
In addition, the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) considers infant abduction such a safety priority that it was made a reportable “Sentinel Event” in 1998. Of the reported 235 reported cases 117 abductions—or 50%—have occurred in the hospital setting. Most children taken from the hospital—57%—are taken from their mother’s room. Roughly 15% each are taken from the newborn nursery, other pediatric wards, or from other parts of the hospital grounds.
Among abductions occurring outside the healthcare setting, 38% of the total occurred from private homes, and the final 13% of the total in other public venues.
A Unique Crime
Infant abduction seems to be distinct from other types of kidnapping in several ways. The first unique characteristic of infant abduction is the profile of the stereotypical perpetrator. Examination of case reports shows that the vast majority of abductors are females of childbearing age. Most live in or near the city where the abduction takes place. Many are overweight, and they may have a history of depression or lying, manipulative behavior.
Additionally, the motives of these women are notably different than those of other kidnappers who are interested in sexual exploitation, money, or revenge. Instead, these women most often desire to have a child of their own. This may be to replace a child or pregnancy that was lost, or to appease a significant other who they perceive may leave them if they cannot produce a child. Notably, many of the kidnappers, later caught, have been observed to provide adequate care for the infants.
Though the timing of an infant abduction can be impulsive, many kidnappers show evidence of elaborate planning beforehand. Several women have staged fictitious pregnancies on one or more occasions. Some kidnappers have even bought baby items or furnished nurseries in anticipation of having a child. Many offenders visit the hospitals or other facilities they later target on several occasions prior to an attempted abduction. They will try to become familiar with hospital personnel often by asking probing questions about security and procedure. A common ploy is for the kidnappers to impersonate nurses, lab technicians, or other hospital personnel in an attempt to gain access to the children. Some even acquire hospital uniforms or other disguises.
They may pose as family members of other patients in order to befriend the parents of their victims. This was the case of Nikenya Washington, who actually entered the room of the would-be victim’s mother early in the evening on the night of the crime. She stated that she had walked into the wrong room and tried to strike up a conversation before leaving.
Prevention is Key
Preventing infant abduction is key, and this process starts by putting proper procedures and hardware in place at healthcare facilities.
“We use a multilayered approach,” says Chicarello. This includes prior planning, physical barriers, electronic aides, and ongoing training and education of staff and parents alike. At Brigham and Women’s, security starts in the lobby where admittance to the maternity ward is gained only after signing in and using a specific elevator. Hospital personnel wear specific nursery badges, and they obtain access to the ward by key card.
The hospital also uses various forms of technology including closed circuit TV monitors, silent “panic” buttons at the nurse’s stations, and electronic wrist/ankle bracelets for the babies.
Chicarello stresses the importance of both initial training for new personnel as well as ongoing education throughout the hospital. This includes hospital-wide awareness drives and an annual Code Pink Fair. Education for parents is incorporated into a pre-natal curriculum. A big part of ongoing training is the use of monthly unscheduled Code Pink drills.
“We try to vary the scenarios to keep the staff on their toes and to expose any weaknesses,” he says. Such scenarios might include having people pose as lab personnel or pulling the fire alarm to create a diversion. “My favorite was once when we had a pizza delivered to the nurses station.” Fortunately, this didn’t work.
Dr. Broughton echoes the notion that a multifaceted approach is important. In addition to well-defined procedures in the birthing suite, the Mayo Clinic’s plan for preventing infant abduction extends to the larger children’s hospital and even to the clinic. Having a well-defined abduction plan has other positive effects as well, notes Dr. Broughton. Such programs are useful in preventing other types of theft, in aiding infection control efforts, and in locating ambulatory children who might wander or get lost.
The process requires input from several disciplines including nursing, security, and physicians. “I think pediatricians should be completely supportive of programs that provide a safety net,” says Dr. Broughton. “[Physicians] should be the leaders in the hospital setting.” One problem he has seen is that physicians sometimes don’t want to be bothered by little details like wearing a proper ID or leaving doors properly locked. Getting physicians to say, “this is important” is an essential first step.
A Disturbing Trend
Though changes in the landscape of infant abduction are difficult to discern, a few trends are notable. Encouragingly, in-hospital abductions are a smaller fraction of the total incidence, perhaps in response to better deterrence by medical facilities. As evidence of this, there was a recent 20-month period without a single abduction from a hospital setting. More disturbingly, though, the incidence of out-of-hospital abductions and the use of violence in abductions seem on the rise. Among these about 29% have involved violence to the parents or family of the infant including eight cases of homicide.
Obviously, preventing abductions outside the hospital presents its own challenges. Nahirny cautions strongly against the publication of birth information on the local press or on Web sites. “These shouldn’t include any specifically identifying information,” she states, such as full names of parents or a home address.
Second, parents must understand the potential danger of posting signs or balloons outside the home after a birth, as these might alert a potential abductor to the presence of an infant. Finally, parents should be careful with unknown, unexpected, or recently acquainted visitors shortly after coming home from the hospital. There are several cases of abductors posing as home-health nurses, social workers, or other official personnel.
Conclusion
Even though she was able to grab the child and make it out of the room, Nikenya Washington did not make if off the hospital ward before being subdued by a security guard and other hospital personnel. Thankfully, the healthy 8-pound, 1-once baby girl was safely returned to her mother. In fact, hospital personnel in conjunction with local law enforcement and media safely recover most abducted infants thanks to orderly responses. However, the best option for all parties involved is a well-planned strategy of prevention. This includes physical barriers, electronic aides, and education of personnel and parents, as well as constant vigilance.
For those who want to get involved in preventing infant abduction, several resources are available. The NCMEC has quite a bit of information on its Web site (www.missingkids.com). There is also an excellent educational video produced by Mead Johnson Nutritionals called “Safeguard Their Tomorrows” available for viewing.
The most definitive resource for clinicians is a book entitled Guidelines for the Prevention of and Response to Infant Abduction. Currently in its eighth edition by John Rabun of the NCEMC, the book discusses the problem of infant abduction and defines its scope. There are various practical recommendations on the general, proactive, and physical measures to prevent abductions and on how to respond once an incident has occurred. There are also sections on how to advise parents and how to assess level of preparedness.
Dr. Axon is an instructor, Departments of Medicine and Pediatrics, Medical University of South Carolina Medical Center, Charleston.
Bibliography
- Ankrom LG, Lent CJ. Cradle robbers: A study of the infant abductor. The FBI Law Enforcement Bulletin. 1995;64(9):112-118.
- Hillen M. Teen held in attempt to abduct newborn. Arkansas Democrat Gazette. 16 January, 2006.
- Rabun J. For Healthcare Professionals: Guidelines for the Prevention of and Response to Infant Abduction. 8th ed. Alexandria, Virginia: National Center for Missing and Exploited Children; 2005.
Pediatric Special Section
In the Literature
By G. Ronald Nicholis, MD, Children’s Mercy Hospital, Kansas City, Mo., Gina Weddle, RN, CPNP, Section of Pediatric Hospitalists, Department of Pediatrics, Children’s Mercy Hospitals and Clinics (Kansas City, Mo.), and J. Christopher Day, MD, Section of Pediatric Hospitalists, Department of Pediatrics, Children’s Mercy Hospitals and Clinics (Kansas City, Mo.)
Computerized Physician Order Entry—Not a Finished Product
Han YY, Carcillo JA, Venkataraman ST, et al. Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2005;116(6):1506-1512.
Over the past several years attention has been increasingly focused on the inadequacy of patient safety in our practices. In response, hospitals, insurers, and practices have examined many potential changes to current systems in an effort to improve safety.
The Institute of Medicine (IOM) and the Leapfrog Group have championed computerized physician order entry (CPOE) as necessary for improving patient safety, citing the inadequacy of paper and pen for the ordering process. Research documenting that CPOE systems used in the hospital setting can decrease adverse drug events has fostered the promise and potential for CPOE to make the hospital a safer place for our patients, particularly when enhanced with decision support. Decision support can allow the physician to be alerted to errors in dose, drug-drug interaction, drug-food interaction, allergies, and the need for dosage corrections based on laboratory values at the time of ordering. Contrary to the research demonstrating improved safety, some studies have shown an increase in unique errors after implementation of CPOE.
The current study from the Departments of Critical Care Medicine and Pediatrics at Children’s Hospital of Pittsburgh calls our attention to significant issues with implementation of CPOE that have potential to inhibit the goal of improving patient safety. Citing a study by Upperman, et al. from their own institution, which noted significant improvement in adverse drug events after implementation of CPOE, the authors of the current study state, “Children’s Hospital of Pittsburgh implemented … Cerner’s commercial CPOE system in October 2002 in an effort to become one of the first children’s hospitals in the U.S. to attain 100% CPOE status.”
The study was designed to measure the effect of CPOE implementation on mortality rate for patients transferred into this pediatric tertiary care facility who required “immediate processing … and stabilization orders.” This retrospective study examined an 18-month period of mortality data: Thirteen months before the implementation of CPOE and five months after.
They discovered an unexpected increase in unadjusted mortality rate after the implementation of CPOE from 2.8% to 6.57%, (P<0.001). Mortality odds ratios were calculated, and observed mortality before CPOE implementation was consistently better than after CPOE implementation. Regression analysis with and without Pediatric Risk of Mortality comparisons were performed and CPOE, in addition to other factors, was associated with increased mortality in both analyses. How should this be interpreted?
The authors note several factors having impact on the validity of the study, specifically mentioning that “study design precludes any statements regarding cause and effect,” “[researchers] examined a unique patient population admitted through interfacility transport … (thus) findings may not be generalizable to the hospital experience as a whole,” and “[the] observation period after CPOE implementation was brief.”
Seasonal variability was also a potential confounding factor because CPOE implementation was in October and the observation period post-CPOE extended only five months—to March of the next year. However, a statistical comparison between matched five-month periods supported the association between implementation of CPOE and increased mortality in this population.
In addition, the authors discuss how their institution’s chosen implementation process for CPOE affected the work processes and pattern of care provided to these critically ill patients. Issues such as being unable to enter orders on a patient in preparation of their arrival because they were not yet enrolled in the electronic system hampered the availability of important medications at the time of arrival. Forcing all of the orders to go through their designed CPOE process in an effort to use the error prevention capabilities of the system caused potentially significant delays in the administration of life-saving medications.
The lack of functional order sets further delayed the physician’s ability to efficiently enter orders electronically. These variables may have impacted mortality rates. Further delays were evident due to the fact that a nurse had to activate orders placed by the physician, bypassing some of the efficiency of an electronic system. Similarly, the pharmacy reviewed and processed the order before the medication was available to the nurse for delivery to the patient.
These checks and balances have the potential to prevent errors in medication ordering, but if inefficient, they may not be appropriate for an intensive care setting in every circumstance. Researchers stated the new workflow took the physicians and nurses away from the patient’s bedside, potentially decreasing observation benefits for the patient. The capacity of the system to compute at times seemed “frozen” causing further delays—not necessarily an uncommon occurrence with any electronic system.
The practice of medicine is complex and work processes do not easily translate to the electronic models currently available. It is crucial that hospitalists, other specialists, all ancillary services, as well as administration be involved in the building and implementation of the systems to be used in our individual facilities. The systems and technology for effective CPOE in hospital settings—especially in pediatric settings—have yet to be developed. The implementation of CPOE for improved patient safety requires exploration given the exposed inadequacies of our current methods of practice.
Like any best practice this exploration will be continuous and require evaluation and improvement. While we must involve ourselves with the development and implementation of CPOE, we must not let the inadequacies of new systems negatively affect patient care. The dichotomy may be omnipresent: Use the system to gain protections from errors and bypass the system when its design or function interferes with good patient practice. This will require us to possess the wisdom to determine the correct path to follow in any instance.
Every day in our practice we make efforts to compensate for failures in our methods to prevent errors from affecting our patient’s care. Electronic systems do not excuse us from continued vigilance, communication, and action to protect our patients from medical errors. The authors appropriately state that “accurate evaluation of CPOE will require systems-based troubleshooting with well-funded, well-designed, multicenter studies that can adequately address these questions.”
Unfortunately, because of the proven inadequacies of the current system, CPOE, like other methodologies we use in the advancement of patient care, cannot wait for proof of perfection before being used to enhance the outcomes of our patients. Thus we need to be vigorous in our participation of the development and implementation of CPOE for our individual institutions and alert to the prevention of harm in all we do. Software companies cannot accomplish improvement in our practices without our involvement, and we cannot meet our demands for quality without good software companies.
The Link between Age and Orchiectomy Due to Testicular Torsion
Mansbach J, Forbes P, Peters C. Testicular torsion and risk factors for orchiectomy. Arch Pediatr Adolesc Med. 2005;159(12):1167-1171.
Testicular torsion is a urologic emergency that requires a four- to eight-hour window from presentation of symptoms until intervention in order to increase the potential for a viable testis. Steps to ensure a viable testis include timely presentation, rapid diagnosis, and curative intervention.
Chart review was done from a national database consisting of 984 hospitals in 22 states. The review included 436 patients ranging from one to 25 years. The incidence of torsion was 4.5 cases/100,000 male subjects with a peak at 10-19 years of age. Of the 436 subjects, 34% required orchiectomy. After all factors (race, insurance status, income, region, and hospital location) were evaluated, increased age at presentation was the only statistically significant factor associated orchiectomy. Male subjects were hesitant to seek medical attention for conditions associated with the genitals. Healthcare providers need to provide anticipatory guidance when educating males about testicular disorders. Testicular exam should be incorporated as part of every physical exam, especially if an abdominal complaint exists.
Heliox Aids Peds with Moderate to Severe Asthma
Kim K, Phrampus E, Venkataraman S, et al. Helium/oxygen-driven albuterol nebulization in the treatment of children with moderate to severe asthma exacerbations: A randomized controlled trial. Pediatrics. 2005;116(5):1127-1133.
Heliox is a 70%/30% helium/oxygen mixture. Heliox mixtures have a lower gas density than oxygen and, therefore, can increase pulmonary gas delivery. This study compared heliox versus oxygen delivery of continuous albuterol nebulization for patients with asthma treated in the emergency department.
Investigators enrolled 30 subjects between ages two and 18 with moderate to severe asthma. Severity of asthma was determined by a pulmonary index (PI) of >8. PI scores are based on respiratory rate, wheezing, accessory muscle use, inspiratory/expiratory ratio, and pulse oximetry. All children were given one 5mg albuterol treatment using traditional oxygen delivery along with oral steroids dosed at 2mg/kg. After the initial treatment and steroids if the PI score was >8 they were randomly assigned to receive continuous albuterol by heliox or traditional oxygen delivery.
The study showed that continuous albuterol delivered by heliox mixture lowered PI scores from baseline to 240 minutes into the study (P<0.001). Results also demonstrated a trend towards improved rate of discharge from the emergency department and hospital, but the study was not powered to adequately evaluate these outcomes Limitations of the study include lack of complete blinding and a small sample size. TH
Something didn’t seem quite right. The person in the hooded sweatshirt standing near the entrance looked suspicious to respiratory therapist Betty Collins as she entered the newborn nursery on the evening of Jan. 12, 2006, during her shift at Ouachita County Medical Center in Camden, Ark. Perhaps this is why she shielded her fingers as she punched in the combination to the lock on the nursery door before entering to check on a baby inside.
Leaving minutes later, her work done, Collins’ suspicions were confirmed when Nikenya Washington, 18, shoved her way into the nursery yelling, “Move out my way, I’ll shoot you b----!”
Collins and the other nurse in the unit bravely wrestled with the would-be abductor. A Code Pink was called.
It is notable that January’s Ouachita Hospital case is unique as the first reported case of physical violence during an in-hospital abduction.
This frightening episode is one example of the phenomenon of infant abduction, and according to Cathy Nahirny of the National Center for Missing and Exploited Children (NCMEC) it is the first reported case in 2006.
Infant abduction is defined as the act of kidnapping an infant less than six months of age by a non-family member. Code Pink is the almost universally adopted code word signaling that an abduction is taking place. Though infrequent by comparison to other types of kidnapping or exploitation of children, infant abduction—like many pediatric situations—is quite dramatic.
This crime is of particular concern to pediatric hospitalists because about half of these events occur within the hospital setting. It plays on the fears of expectant parents and communities, and a successful abduction can be catastrophic for a hospital’s image and reputation. Preventing infant abduction and maintaining preparedness for Code Pink situations represents an ongoing challenge for the approximately 3,500 hospitals where about 4 million American babies are born each year.
Small Number, Large Impact
According to Daniel Broughton, MD, infant abduction is a small subset of a much larger problem. As the director of the Child Abuse Program at the Mayo Clinic in Rochester, Minn., and co-author of the American Academy of Pediatrics’ Clinical Report on the pediatrician’s role in the prevention of missing children, he is an expert on the subject.
There are an estimated 1-2 million runaways and as many as 200,000 abductions by family members in the United States each year. By contrast, since 1983 when the NCMEC began to collect information on reports of infant abduction, there have been a total of 235 recorded infant kidnappings by non-family members. Nevertheless, “from the standpoint of impact both on families and the hospitals, it is huge,” says Dr. Broughton of infant abduction.
Bob Chicarello, the interim head of security at the Brigham and Women’s Hospital in Boston, agrees.
“You want to do everything possible to prevent [an infant abduction] because it could really shake an institution to its knees,” he says.
In addition, the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) considers infant abduction such a safety priority that it was made a reportable “Sentinel Event” in 1998. Of the reported 235 reported cases 117 abductions—or 50%—have occurred in the hospital setting. Most children taken from the hospital—57%—are taken from their mother’s room. Roughly 15% each are taken from the newborn nursery, other pediatric wards, or from other parts of the hospital grounds.
Among abductions occurring outside the healthcare setting, 38% of the total occurred from private homes, and the final 13% of the total in other public venues.
A Unique Crime
Infant abduction seems to be distinct from other types of kidnapping in several ways. The first unique characteristic of infant abduction is the profile of the stereotypical perpetrator. Examination of case reports shows that the vast majority of abductors are females of childbearing age. Most live in or near the city where the abduction takes place. Many are overweight, and they may have a history of depression or lying, manipulative behavior.
Additionally, the motives of these women are notably different than those of other kidnappers who are interested in sexual exploitation, money, or revenge. Instead, these women most often desire to have a child of their own. This may be to replace a child or pregnancy that was lost, or to appease a significant other who they perceive may leave them if they cannot produce a child. Notably, many of the kidnappers, later caught, have been observed to provide adequate care for the infants.
Though the timing of an infant abduction can be impulsive, many kidnappers show evidence of elaborate planning beforehand. Several women have staged fictitious pregnancies on one or more occasions. Some kidnappers have even bought baby items or furnished nurseries in anticipation of having a child. Many offenders visit the hospitals or other facilities they later target on several occasions prior to an attempted abduction. They will try to become familiar with hospital personnel often by asking probing questions about security and procedure. A common ploy is for the kidnappers to impersonate nurses, lab technicians, or other hospital personnel in an attempt to gain access to the children. Some even acquire hospital uniforms or other disguises.
They may pose as family members of other patients in order to befriend the parents of their victims. This was the case of Nikenya Washington, who actually entered the room of the would-be victim’s mother early in the evening on the night of the crime. She stated that she had walked into the wrong room and tried to strike up a conversation before leaving.
Prevention is Key
Preventing infant abduction is key, and this process starts by putting proper procedures and hardware in place at healthcare facilities.
“We use a multilayered approach,” says Chicarello. This includes prior planning, physical barriers, electronic aides, and ongoing training and education of staff and parents alike. At Brigham and Women’s, security starts in the lobby where admittance to the maternity ward is gained only after signing in and using a specific elevator. Hospital personnel wear specific nursery badges, and they obtain access to the ward by key card.
The hospital also uses various forms of technology including closed circuit TV monitors, silent “panic” buttons at the nurse’s stations, and electronic wrist/ankle bracelets for the babies.
Chicarello stresses the importance of both initial training for new personnel as well as ongoing education throughout the hospital. This includes hospital-wide awareness drives and an annual Code Pink Fair. Education for parents is incorporated into a pre-natal curriculum. A big part of ongoing training is the use of monthly unscheduled Code Pink drills.
“We try to vary the scenarios to keep the staff on their toes and to expose any weaknesses,” he says. Such scenarios might include having people pose as lab personnel or pulling the fire alarm to create a diversion. “My favorite was once when we had a pizza delivered to the nurses station.” Fortunately, this didn’t work.
Dr. Broughton echoes the notion that a multifaceted approach is important. In addition to well-defined procedures in the birthing suite, the Mayo Clinic’s plan for preventing infant abduction extends to the larger children’s hospital and even to the clinic. Having a well-defined abduction plan has other positive effects as well, notes Dr. Broughton. Such programs are useful in preventing other types of theft, in aiding infection control efforts, and in locating ambulatory children who might wander or get lost.
The process requires input from several disciplines including nursing, security, and physicians. “I think pediatricians should be completely supportive of programs that provide a safety net,” says Dr. Broughton. “[Physicians] should be the leaders in the hospital setting.” One problem he has seen is that physicians sometimes don’t want to be bothered by little details like wearing a proper ID or leaving doors properly locked. Getting physicians to say, “this is important” is an essential first step.
A Disturbing Trend
Though changes in the landscape of infant abduction are difficult to discern, a few trends are notable. Encouragingly, in-hospital abductions are a smaller fraction of the total incidence, perhaps in response to better deterrence by medical facilities. As evidence of this, there was a recent 20-month period without a single abduction from a hospital setting. More disturbingly, though, the incidence of out-of-hospital abductions and the use of violence in abductions seem on the rise. Among these about 29% have involved violence to the parents or family of the infant including eight cases of homicide.
Obviously, preventing abductions outside the hospital presents its own challenges. Nahirny cautions strongly against the publication of birth information on the local press or on Web sites. “These shouldn’t include any specifically identifying information,” she states, such as full names of parents or a home address.
Second, parents must understand the potential danger of posting signs or balloons outside the home after a birth, as these might alert a potential abductor to the presence of an infant. Finally, parents should be careful with unknown, unexpected, or recently acquainted visitors shortly after coming home from the hospital. There are several cases of abductors posing as home-health nurses, social workers, or other official personnel.
Conclusion
Even though she was able to grab the child and make it out of the room, Nikenya Washington did not make if off the hospital ward before being subdued by a security guard and other hospital personnel. Thankfully, the healthy 8-pound, 1-once baby girl was safely returned to her mother. In fact, hospital personnel in conjunction with local law enforcement and media safely recover most abducted infants thanks to orderly responses. However, the best option for all parties involved is a well-planned strategy of prevention. This includes physical barriers, electronic aides, and education of personnel and parents, as well as constant vigilance.
For those who want to get involved in preventing infant abduction, several resources are available. The NCMEC has quite a bit of information on its Web site (www.missingkids.com). There is also an excellent educational video produced by Mead Johnson Nutritionals called “Safeguard Their Tomorrows” available for viewing.
The most definitive resource for clinicians is a book entitled Guidelines for the Prevention of and Response to Infant Abduction. Currently in its eighth edition by John Rabun of the NCEMC, the book discusses the problem of infant abduction and defines its scope. There are various practical recommendations on the general, proactive, and physical measures to prevent abductions and on how to respond once an incident has occurred. There are also sections on how to advise parents and how to assess level of preparedness.
Dr. Axon is an instructor, Departments of Medicine and Pediatrics, Medical University of South Carolina Medical Center, Charleston.
Bibliography
- Ankrom LG, Lent CJ. Cradle robbers: A study of the infant abductor. The FBI Law Enforcement Bulletin. 1995;64(9):112-118.
- Hillen M. Teen held in attempt to abduct newborn. Arkansas Democrat Gazette. 16 January, 2006.
- Rabun J. For Healthcare Professionals: Guidelines for the Prevention of and Response to Infant Abduction. 8th ed. Alexandria, Virginia: National Center for Missing and Exploited Children; 2005.
Pediatric Special Section
In the Literature
By G. Ronald Nicholis, MD, Children’s Mercy Hospital, Kansas City, Mo., Gina Weddle, RN, CPNP, Section of Pediatric Hospitalists, Department of Pediatrics, Children’s Mercy Hospitals and Clinics (Kansas City, Mo.), and J. Christopher Day, MD, Section of Pediatric Hospitalists, Department of Pediatrics, Children’s Mercy Hospitals and Clinics (Kansas City, Mo.)
Computerized Physician Order Entry—Not a Finished Product
Han YY, Carcillo JA, Venkataraman ST, et al. Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2005;116(6):1506-1512.
Over the past several years attention has been increasingly focused on the inadequacy of patient safety in our practices. In response, hospitals, insurers, and practices have examined many potential changes to current systems in an effort to improve safety.
The Institute of Medicine (IOM) and the Leapfrog Group have championed computerized physician order entry (CPOE) as necessary for improving patient safety, citing the inadequacy of paper and pen for the ordering process. Research documenting that CPOE systems used in the hospital setting can decrease adverse drug events has fostered the promise and potential for CPOE to make the hospital a safer place for our patients, particularly when enhanced with decision support. Decision support can allow the physician to be alerted to errors in dose, drug-drug interaction, drug-food interaction, allergies, and the need for dosage corrections based on laboratory values at the time of ordering. Contrary to the research demonstrating improved safety, some studies have shown an increase in unique errors after implementation of CPOE.
The current study from the Departments of Critical Care Medicine and Pediatrics at Children’s Hospital of Pittsburgh calls our attention to significant issues with implementation of CPOE that have potential to inhibit the goal of improving patient safety. Citing a study by Upperman, et al. from their own institution, which noted significant improvement in adverse drug events after implementation of CPOE, the authors of the current study state, “Children’s Hospital of Pittsburgh implemented … Cerner’s commercial CPOE system in October 2002 in an effort to become one of the first children’s hospitals in the U.S. to attain 100% CPOE status.”
The study was designed to measure the effect of CPOE implementation on mortality rate for patients transferred into this pediatric tertiary care facility who required “immediate processing … and stabilization orders.” This retrospective study examined an 18-month period of mortality data: Thirteen months before the implementation of CPOE and five months after.
They discovered an unexpected increase in unadjusted mortality rate after the implementation of CPOE from 2.8% to 6.57%, (P<0.001). Mortality odds ratios were calculated, and observed mortality before CPOE implementation was consistently better than after CPOE implementation. Regression analysis with and without Pediatric Risk of Mortality comparisons were performed and CPOE, in addition to other factors, was associated with increased mortality in both analyses. How should this be interpreted?
The authors note several factors having impact on the validity of the study, specifically mentioning that “study design precludes any statements regarding cause and effect,” “[researchers] examined a unique patient population admitted through interfacility transport … (thus) findings may not be generalizable to the hospital experience as a whole,” and “[the] observation period after CPOE implementation was brief.”
Seasonal variability was also a potential confounding factor because CPOE implementation was in October and the observation period post-CPOE extended only five months—to March of the next year. However, a statistical comparison between matched five-month periods supported the association between implementation of CPOE and increased mortality in this population.
In addition, the authors discuss how their institution’s chosen implementation process for CPOE affected the work processes and pattern of care provided to these critically ill patients. Issues such as being unable to enter orders on a patient in preparation of their arrival because they were not yet enrolled in the electronic system hampered the availability of important medications at the time of arrival. Forcing all of the orders to go through their designed CPOE process in an effort to use the error prevention capabilities of the system caused potentially significant delays in the administration of life-saving medications.
The lack of functional order sets further delayed the physician’s ability to efficiently enter orders electronically. These variables may have impacted mortality rates. Further delays were evident due to the fact that a nurse had to activate orders placed by the physician, bypassing some of the efficiency of an electronic system. Similarly, the pharmacy reviewed and processed the order before the medication was available to the nurse for delivery to the patient.
These checks and balances have the potential to prevent errors in medication ordering, but if inefficient, they may not be appropriate for an intensive care setting in every circumstance. Researchers stated the new workflow took the physicians and nurses away from the patient’s bedside, potentially decreasing observation benefits for the patient. The capacity of the system to compute at times seemed “frozen” causing further delays—not necessarily an uncommon occurrence with any electronic system.
The practice of medicine is complex and work processes do not easily translate to the electronic models currently available. It is crucial that hospitalists, other specialists, all ancillary services, as well as administration be involved in the building and implementation of the systems to be used in our individual facilities. The systems and technology for effective CPOE in hospital settings—especially in pediatric settings—have yet to be developed. The implementation of CPOE for improved patient safety requires exploration given the exposed inadequacies of our current methods of practice.
Like any best practice this exploration will be continuous and require evaluation and improvement. While we must involve ourselves with the development and implementation of CPOE, we must not let the inadequacies of new systems negatively affect patient care. The dichotomy may be omnipresent: Use the system to gain protections from errors and bypass the system when its design or function interferes with good patient practice. This will require us to possess the wisdom to determine the correct path to follow in any instance.
Every day in our practice we make efforts to compensate for failures in our methods to prevent errors from affecting our patient’s care. Electronic systems do not excuse us from continued vigilance, communication, and action to protect our patients from medical errors. The authors appropriately state that “accurate evaluation of CPOE will require systems-based troubleshooting with well-funded, well-designed, multicenter studies that can adequately address these questions.”
Unfortunately, because of the proven inadequacies of the current system, CPOE, like other methodologies we use in the advancement of patient care, cannot wait for proof of perfection before being used to enhance the outcomes of our patients. Thus we need to be vigorous in our participation of the development and implementation of CPOE for our individual institutions and alert to the prevention of harm in all we do. Software companies cannot accomplish improvement in our practices without our involvement, and we cannot meet our demands for quality without good software companies.
The Link between Age and Orchiectomy Due to Testicular Torsion
Mansbach J, Forbes P, Peters C. Testicular torsion and risk factors for orchiectomy. Arch Pediatr Adolesc Med. 2005;159(12):1167-1171.
Testicular torsion is a urologic emergency that requires a four- to eight-hour window from presentation of symptoms until intervention in order to increase the potential for a viable testis. Steps to ensure a viable testis include timely presentation, rapid diagnosis, and curative intervention.
Chart review was done from a national database consisting of 984 hospitals in 22 states. The review included 436 patients ranging from one to 25 years. The incidence of torsion was 4.5 cases/100,000 male subjects with a peak at 10-19 years of age. Of the 436 subjects, 34% required orchiectomy. After all factors (race, insurance status, income, region, and hospital location) were evaluated, increased age at presentation was the only statistically significant factor associated orchiectomy. Male subjects were hesitant to seek medical attention for conditions associated with the genitals. Healthcare providers need to provide anticipatory guidance when educating males about testicular disorders. Testicular exam should be incorporated as part of every physical exam, especially if an abdominal complaint exists.
Heliox Aids Peds with Moderate to Severe Asthma
Kim K, Phrampus E, Venkataraman S, et al. Helium/oxygen-driven albuterol nebulization in the treatment of children with moderate to severe asthma exacerbations: A randomized controlled trial. Pediatrics. 2005;116(5):1127-1133.
Heliox is a 70%/30% helium/oxygen mixture. Heliox mixtures have a lower gas density than oxygen and, therefore, can increase pulmonary gas delivery. This study compared heliox versus oxygen delivery of continuous albuterol nebulization for patients with asthma treated in the emergency department.
Investigators enrolled 30 subjects between ages two and 18 with moderate to severe asthma. Severity of asthma was determined by a pulmonary index (PI) of >8. PI scores are based on respiratory rate, wheezing, accessory muscle use, inspiratory/expiratory ratio, and pulse oximetry. All children were given one 5mg albuterol treatment using traditional oxygen delivery along with oral steroids dosed at 2mg/kg. After the initial treatment and steroids if the PI score was >8 they were randomly assigned to receive continuous albuterol by heliox or traditional oxygen delivery.
The study showed that continuous albuterol delivered by heliox mixture lowered PI scores from baseline to 240 minutes into the study (P<0.001). Results also demonstrated a trend towards improved rate of discharge from the emergency department and hospital, but the study was not powered to adequately evaluate these outcomes Limitations of the study include lack of complete blinding and a small sample size. TH
Mental Health in Colonial America
Insanity in colonial America was not pretty: emotional torment, social isolation, physical pain—and these were just the treatments! In the late 1700s facilities and treatments were often crude and barbaric; however, this doesn’t mean that those who applied them were fueled by cruelty. There were often dedicated and intelligent individuals behind the torturers’ masks. How can this be? Prevailing thoughts on the etiology of mental illness and political forces played large roles in how patients were treated. An excellent example of this is the story of North America’s first public mental health hospital: the Public Hospital for Persons of Insane and Disordered Minds in Williamsburg, Va.
Prior to the opening of the mental health hospital in 1773, the prevailing goal was to minimize the trouble caused to the community by the mentally ill. The quietly insane were simply left to their own devices in the countryside. Those who committed crimes, caused a nuisance or posed a potential threat of either, though, were subject to imprisonment in the local jail.
Virginia’s Acting-Royal Governor and Chief Administrative Officer Francis Fauquier (1758-1768) struggled with the legality of imprisoning the innocent, as well as the lack of treatment for them. Publicly run hospitals specifically for the insane had been in practice for a century in France and England. Fauquier proposed a similar idea to be implemented on American soil.
The hospital was born of unruly times. In 1766, pre-Revolutionary-War America experienced growing anti-British grumblings and political unrest. Just one year prior, a 1765 British Stamp Tax had been imposed on the colonies. Mass riots and pillage ensued. Eventually the tax was repealed. Fauquier gave a speech calling for citizens’ gratitude and obedience to the British Parliament for this concession.
He also proposed the mental health hospital in this speech. Given the juxtaposition, it has been suggested that the governor was likening the violent protests against the Stamp Tax to unreasoned acts of the mentally ill. He described the insane as “persons who are so unhappy as to be deprived of their reason,” a phrase that could equally describe unruly dissenters. Taking this further, one might wonder if Fauquier hoped these protesters would be similarly contained.
What qualified as mental illness? A list of “supposed or assumed causes of insanity” for the hospital’s 754 patients in 1879 identifies 46 such causes. Many, such as excessive study, seduction, matrimony, or the fall of the confederacy, are unlikely to make the modern DSM. But some are familiar (e.g., loss of property, disappointment in love, intemperance, excessive fatigue, and ill health).
It seems the more things change, the more they stay the same: In those predisposed to depression, mania, or psychosis, psychosocial stressors often precipitated acute psychiatric decompensation. In addition, physiological factors such as substance abuse, insomnia, and delirium often played a large role as well.
The treatments of the time seem like torture today. During the hospital’s first 60 years prevailing treatments included solitary confinement, conditioned fear of doctors, powerful but minimally effective drugs, bleeding, shackles, and plunge baths. It was thought that the patients had chosen a life of insanity and needed to decide to change their ways.
Eventually, thought changed. In 1790s post-revolution France, the beginnings of the “moral management” movement took place. This was based on the idea that mental illness was rooted in emotions and that harsh treatment simply confirmed the patients’ fears, thus being ineffective and detrimental.
By the 1840s, these ideas finally spread to Williamsburg. John Minson Galt II took over the hospital in 1841 and dedicated himself to maximizing the use of respect and kindness in shaping the behavior of the mentally ill. He instituted treatments such as good nutrition and sleep, socialization, and recreational therapy. The hospital census swelled, stretching resources thin. As the Civil War brewed, support shifted to the war effort, and the hospital was forced to release many patients into the countryside.
Thus, things had come full circle. Due to the political upheaval, mental healthcare had returned to pre-Revolutionary War conditions. Despite continued interest in the “moral management” methods of treatment, the political times could not provide the support.
As is so common today, the struggle between idealism and practicality was clearly reflected in the patients’ treatments and lives. Though the pendulum did swing back, bringing better treatment for the mentally ill, we continue to seek this fine balance. TH
Reference
Zwelling SS. Quest for a cure: The public hospital in Williamsburg, Virginia, 1773-1885. Williamsburg, Va; Colonial Williamsburg Foundation: 1986.
Insanity in colonial America was not pretty: emotional torment, social isolation, physical pain—and these were just the treatments! In the late 1700s facilities and treatments were often crude and barbaric; however, this doesn’t mean that those who applied them were fueled by cruelty. There were often dedicated and intelligent individuals behind the torturers’ masks. How can this be? Prevailing thoughts on the etiology of mental illness and political forces played large roles in how patients were treated. An excellent example of this is the story of North America’s first public mental health hospital: the Public Hospital for Persons of Insane and Disordered Minds in Williamsburg, Va.
Prior to the opening of the mental health hospital in 1773, the prevailing goal was to minimize the trouble caused to the community by the mentally ill. The quietly insane were simply left to their own devices in the countryside. Those who committed crimes, caused a nuisance or posed a potential threat of either, though, were subject to imprisonment in the local jail.
Virginia’s Acting-Royal Governor and Chief Administrative Officer Francis Fauquier (1758-1768) struggled with the legality of imprisoning the innocent, as well as the lack of treatment for them. Publicly run hospitals specifically for the insane had been in practice for a century in France and England. Fauquier proposed a similar idea to be implemented on American soil.
The hospital was born of unruly times. In 1766, pre-Revolutionary-War America experienced growing anti-British grumblings and political unrest. Just one year prior, a 1765 British Stamp Tax had been imposed on the colonies. Mass riots and pillage ensued. Eventually the tax was repealed. Fauquier gave a speech calling for citizens’ gratitude and obedience to the British Parliament for this concession.
He also proposed the mental health hospital in this speech. Given the juxtaposition, it has been suggested that the governor was likening the violent protests against the Stamp Tax to unreasoned acts of the mentally ill. He described the insane as “persons who are so unhappy as to be deprived of their reason,” a phrase that could equally describe unruly dissenters. Taking this further, one might wonder if Fauquier hoped these protesters would be similarly contained.
What qualified as mental illness? A list of “supposed or assumed causes of insanity” for the hospital’s 754 patients in 1879 identifies 46 such causes. Many, such as excessive study, seduction, matrimony, or the fall of the confederacy, are unlikely to make the modern DSM. But some are familiar (e.g., loss of property, disappointment in love, intemperance, excessive fatigue, and ill health).
It seems the more things change, the more they stay the same: In those predisposed to depression, mania, or psychosis, psychosocial stressors often precipitated acute psychiatric decompensation. In addition, physiological factors such as substance abuse, insomnia, and delirium often played a large role as well.
The treatments of the time seem like torture today. During the hospital’s first 60 years prevailing treatments included solitary confinement, conditioned fear of doctors, powerful but minimally effective drugs, bleeding, shackles, and plunge baths. It was thought that the patients had chosen a life of insanity and needed to decide to change their ways.
Eventually, thought changed. In 1790s post-revolution France, the beginnings of the “moral management” movement took place. This was based on the idea that mental illness was rooted in emotions and that harsh treatment simply confirmed the patients’ fears, thus being ineffective and detrimental.
By the 1840s, these ideas finally spread to Williamsburg. John Minson Galt II took over the hospital in 1841 and dedicated himself to maximizing the use of respect and kindness in shaping the behavior of the mentally ill. He instituted treatments such as good nutrition and sleep, socialization, and recreational therapy. The hospital census swelled, stretching resources thin. As the Civil War brewed, support shifted to the war effort, and the hospital was forced to release many patients into the countryside.
Thus, things had come full circle. Due to the political upheaval, mental healthcare had returned to pre-Revolutionary War conditions. Despite continued interest in the “moral management” methods of treatment, the political times could not provide the support.
As is so common today, the struggle between idealism and practicality was clearly reflected in the patients’ treatments and lives. Though the pendulum did swing back, bringing better treatment for the mentally ill, we continue to seek this fine balance. TH
Reference
Zwelling SS. Quest for a cure: The public hospital in Williamsburg, Virginia, 1773-1885. Williamsburg, Va; Colonial Williamsburg Foundation: 1986.
Insanity in colonial America was not pretty: emotional torment, social isolation, physical pain—and these were just the treatments! In the late 1700s facilities and treatments were often crude and barbaric; however, this doesn’t mean that those who applied them were fueled by cruelty. There were often dedicated and intelligent individuals behind the torturers’ masks. How can this be? Prevailing thoughts on the etiology of mental illness and political forces played large roles in how patients were treated. An excellent example of this is the story of North America’s first public mental health hospital: the Public Hospital for Persons of Insane and Disordered Minds in Williamsburg, Va.
Prior to the opening of the mental health hospital in 1773, the prevailing goal was to minimize the trouble caused to the community by the mentally ill. The quietly insane were simply left to their own devices in the countryside. Those who committed crimes, caused a nuisance or posed a potential threat of either, though, were subject to imprisonment in the local jail.
Virginia’s Acting-Royal Governor and Chief Administrative Officer Francis Fauquier (1758-1768) struggled with the legality of imprisoning the innocent, as well as the lack of treatment for them. Publicly run hospitals specifically for the insane had been in practice for a century in France and England. Fauquier proposed a similar idea to be implemented on American soil.
The hospital was born of unruly times. In 1766, pre-Revolutionary-War America experienced growing anti-British grumblings and political unrest. Just one year prior, a 1765 British Stamp Tax had been imposed on the colonies. Mass riots and pillage ensued. Eventually the tax was repealed. Fauquier gave a speech calling for citizens’ gratitude and obedience to the British Parliament for this concession.
He also proposed the mental health hospital in this speech. Given the juxtaposition, it has been suggested that the governor was likening the violent protests against the Stamp Tax to unreasoned acts of the mentally ill. He described the insane as “persons who are so unhappy as to be deprived of their reason,” a phrase that could equally describe unruly dissenters. Taking this further, one might wonder if Fauquier hoped these protesters would be similarly contained.
What qualified as mental illness? A list of “supposed or assumed causes of insanity” for the hospital’s 754 patients in 1879 identifies 46 such causes. Many, such as excessive study, seduction, matrimony, or the fall of the confederacy, are unlikely to make the modern DSM. But some are familiar (e.g., loss of property, disappointment in love, intemperance, excessive fatigue, and ill health).
It seems the more things change, the more they stay the same: In those predisposed to depression, mania, or psychosis, psychosocial stressors often precipitated acute psychiatric decompensation. In addition, physiological factors such as substance abuse, insomnia, and delirium often played a large role as well.
The treatments of the time seem like torture today. During the hospital’s first 60 years prevailing treatments included solitary confinement, conditioned fear of doctors, powerful but minimally effective drugs, bleeding, shackles, and plunge baths. It was thought that the patients had chosen a life of insanity and needed to decide to change their ways.
Eventually, thought changed. In 1790s post-revolution France, the beginnings of the “moral management” movement took place. This was based on the idea that mental illness was rooted in emotions and that harsh treatment simply confirmed the patients’ fears, thus being ineffective and detrimental.
By the 1840s, these ideas finally spread to Williamsburg. John Minson Galt II took over the hospital in 1841 and dedicated himself to maximizing the use of respect and kindness in shaping the behavior of the mentally ill. He instituted treatments such as good nutrition and sleep, socialization, and recreational therapy. The hospital census swelled, stretching resources thin. As the Civil War brewed, support shifted to the war effort, and the hospital was forced to release many patients into the countryside.
Thus, things had come full circle. Due to the political upheaval, mental healthcare had returned to pre-Revolutionary War conditions. Despite continued interest in the “moral management” methods of treatment, the political times could not provide the support.
As is so common today, the struggle between idealism and practicality was clearly reflected in the patients’ treatments and lives. Though the pendulum did swing back, bringing better treatment for the mentally ill, we continue to seek this fine balance. TH
Reference
Zwelling SS. Quest for a cure: The public hospital in Williamsburg, Virginia, 1773-1885. Williamsburg, Va; Colonial Williamsburg Foundation: 1986.
Their Own Twist
Every facility has their own twist for what an occupational therapist might do,” says Marla Quinney, OTR/L, assistant director of Adult Inpatient Therapy Services at the University of Chicago (UC) Medical Center. Occupational therapists look at “how patients spend their days and ask, ‘What do they engage in and what do they not engage in because of the current condition?’”
The occupational therapist then helps to rehabilitate patients to baseline. “In an acute care facility,” says Quinney, “a lot of what we do is evaluation and then getting patients to the correct discharge disposition and follow-up care.”
Depending on the institution, occupational therapy offerings may involve management for range of motion, strength, coordination, and sensation; they also include therapy for activities of daily living (ADLs), such as self-care, home management, and community involvement, including vision retraining and cognitive and/or perceptual retraining as they relate to ADLs. Occupational therapists might also include management using assistive devices, and the provision of adaptive equipment. In some institutions, occupational therapy involves aspects of home evaluations, and feeding and swallowing therapy.
Working with Hospitalists: Challenges and Highlights for Occupational Therapists

Occupational therapists cite a few areas where hospitalists could provide more help to their fellow professionals in occupational therapy.
Distinction between occupational and physical therapists: To expedite care, hospitalists need to know whether to refer patients to occupational therapy or physical therapy.
“In general, a physical therapist would look at gross motor functions, which affect the patient’s ability to be mobilized from one place to another,” says Quinney. “This also includes whether or not they need assistance to do that safely, and then there’s a myriad of things they look at, including wound care, generalized weakness, and—with a general medicine patient—deconditioning, to make sure that they’re safe in their mobility. An occupational therapist looks more at ADLs, and what patients need to do in order to function in their daily lives and the safety associated with that.”
Timeliness of referrals: Quinney concedes that in the case of a patient who is deconditioned, it might be difficult to discern whether a patient requires occupational therapy or physical therapy. That is one reason why the timeliness of referral is important. If an occupational therapist receives a referral on the day the patient is scheduled for discharge, it may be too late to help them.
But referrals can also be made too soon, says Quinney, “because when the patient is in the ER being admitted, what’s needed may be something as simple as getting their fluids corrected, and once that’s done, then [occupational] therapy is no longer indicated.”
Another example of inappropriate referral timing, she says, might be in the case of a diabetic “whose blood sugars are too high or too low, and clearly, they’re not functioning at their premorbid level. But given the right intervention by the medical team, they’ll bounce back to their baseline.”
Other inappropriate referrals: A patient might also be assessed as having too high or too low a functional status to benefit from occupational therapy. For instance, “a patient might be at too low a level if they came from a nursing home for a UTI or some other complication,” says Quinney, “but their functional status is not something that a therapist would be able to impact in a short hospital stay once that medical problem is corrected.”
From what his occupational therapists tell him, Vijay Rajput, MD, FACP, senior hospitalist at Cooper University Hospital in Camden, N.J., concurs. “If the patient has been in a nursing home for 10 years and is completely custodial and bed-bound, when that patient comes to the hospital and a hospitalist has ordered an occupational therapy consult … , the occupational therapist then has to assess it, and there are no [achievable] goals of care in terms of occupational therapy, then the therapists think that is a [poor use of their] time.”

In that case, however, the family may benefit from a home visit that will provide maintenance or training.
When Quinney receives what she believes is an inappropriate referral from a hospitalist or other provider, she encourages her therapists to say that back to the hospitalist in a direct, to-the-point communication. Therapists are encouraged to say, “This is what I saw with patient X. I’m not seeing any skilled therapy needs. Is there something else I’m missing?”
“We always give [the provider] the benefit of the doubt of having done an assessment in their mind,” explains Quinney.
How consults are written: Quinney’s team has discussed whether to ask hospitalists to be specific about what they are referring for, so “we as therapists are able to affect the whole person. Because if they only give a referral for a specific task, then it makes it more limiting,” she explains. “If they write a referral for ‘functional ability’ or [one] that says ‘concerned with balance,’ that [allows us] to do some problem-solving.”
Tiffani Morales, LOTR, the occupational therapy team leader at Our Lady of Lourdes Regional Medical Center in Lafayette, La., agrees. “We’ve only had hospitalists for about a year, and the three that we have are really doing a good job, [including the way in which] they’re writing their consults,” says Morales. “They’re leaving it open and trusting us to make recommendations, and they’re going along with them.”
Because hospitalists write the chart note as “Consult,” occupational therapy “gives us leeway to make any equipment recommendations or, actually, any of the treatments that may be warranted versus having to call them back, which takes time to keep giving an order over the phone,” explains Morales.
Geography of patient assignments: The system or structure by which patients are assigned will usually differ between occupational therapists and hospitalists. For instance, at Cooper University Hospital, a 520-bed academic, tertiary hospital in Camden, N.J., where Dr. Rajput began the hospitalist program, the six occupational therapists are assigned patients on a geographical basis, according to floor in a 10-story building. But the group of 25 hospitalists, which has grown from four since 1999, is not assigned that way.
“If I am on service,” says Dr. Rajput, “my patients are assigned [perhaps as] one on the 10th floor, one on the ninth floor, [and] one on the eighth floor.”
His occupational therapists told him that if the hospitalists could be assigned to patients the way they are, it would certainly improve the communication between the two groups.
“It is much better to have a verbal communication with the hospitalist than [simply] reviewing the chart,” says Dr. Rajput.
Some hospitalist groups are looking at returning to this geographically based system. “To restructure the whole system would be very complex,” says Dr. Rajput, who is also the program director for the Internal Medicine Residency Program at UMNDNJ—Robert Wood Johnson Medical School in Camden, “but… it still makes sense [from a communication perspective], for instance, the way it does in the ICU.”
Given the difficulties and drawbacks of making that system a widespread reality, however, Plan B would be to increase and encourage contact between occupational therapists and hospitalists. At the UC Hospital, which employs 12 occupational therapists who work with the patient population that hospitalists are responsible for, “the volume of [patients in] the general medicine unit is too high for OTs to meet with hospitalists daily” explains Quinney, who has been with the UC hospitals for six years.
To breach what might be a communication gap, however, she says, “all OTs have pagers, and whenever they write their note in the chart they will leave their pager number. There is always a way for someone to get in touch with them.”
That, of course, can also be said of hospitalists. And because hospitalists respond quickly when occupational therapists page or call them, says Morales, it can help with patient satisfaction.
“The hospitalists round more quickly or at certain times; they have a routine down,” she says. “And that’s a big thing because when patients are ready to be discharged, they want it now. They don’t want to wait.” And when they can be discharged expediently, “we all look better.”
Throughput and quality care: At the UC Medical Center, as at most institutions, hospitalists are encouraged to move patients from admitting through discharge in the most timely and efficient way possible.
“Hospitalists know that [occupational] therapy is part of that important closure of getting them from one site to another,” says Quinney. But sometimes she hears a [hospitalist or resident] say, “I was just told I need to refer them to you in order to get my patient out of the hospital.”
That’s important, Quinney emphasizes, because occupational therapists want to be part of discharge planning. “But we want to be referred to appropriately so that the people who need us most can utilize us, versus going after patients that aren’t appropriate and are using our resources,” she says. “It’s not that we aren’t happy to see those patients, we truly are; it’s a matter of getting people in a timely manner so that we can really make a difference.”
Great Working Relationships
Morales thinks hospitalists have a good understanding of the services that are available from occupational therapists “because whenever we see them about a patient, if they’re not sure about something, they ask questions such as, ‘Is there anything else you can offer?’” she says. “I think they’re right on target [with us].”
Morales’ team thinks hospitalists are involved, friendly, and open. “It’s just a great work relationship,” she says, “because they’re actually seeing the patients in therapy and asking for our input; it’s very refreshing.” Most of all, she appreciates how they show respect for what the occupational therapists do. “They are listening to what we are saying and that makes a difference.”

Educational Opportunities
Because hospitalists look at the bigger picture of what is going on with patients, they generally consult occupational therapy early enough so that therapists can educate hospitalists, patients, and families at Morales’ institution. This also helps prevent patients’ further deconditioning, and helps them to arrive at a discharge disposition earlier.
Dr. Rajput, who is an associate professor of medicine at the University of Medicine and Dentistry, (Brunswick) New Jersey–Robert Wood Johnson Medical School, thinks it would benefit those involved in medical education and hospital medicine “to see that there is sufficient formal training for the residency level or hospitalist level to understand the component [of occupational therapy] and the indication for occupational therapy, and occupational therapy versus physical therapy, as practice.”
Conclusion
Hospitalists can help their occupational therapist colleagues by recognizing the distinction between occupational therapy and physical therapy, making timely and appropriate referrals, writing consults in an open-ended manner to allow occupational therapists to do “whole-person” assessments, and making sure to educate themselves and their hospitalist colleagues on the services and needs of occupational therapists. TH
Andrea Sattinger regularly writes the “Alliances” department.
Every facility has their own twist for what an occupational therapist might do,” says Marla Quinney, OTR/L, assistant director of Adult Inpatient Therapy Services at the University of Chicago (UC) Medical Center. Occupational therapists look at “how patients spend their days and ask, ‘What do they engage in and what do they not engage in because of the current condition?’”
The occupational therapist then helps to rehabilitate patients to baseline. “In an acute care facility,” says Quinney, “a lot of what we do is evaluation and then getting patients to the correct discharge disposition and follow-up care.”
Depending on the institution, occupational therapy offerings may involve management for range of motion, strength, coordination, and sensation; they also include therapy for activities of daily living (ADLs), such as self-care, home management, and community involvement, including vision retraining and cognitive and/or perceptual retraining as they relate to ADLs. Occupational therapists might also include management using assistive devices, and the provision of adaptive equipment. In some institutions, occupational therapy involves aspects of home evaluations, and feeding and swallowing therapy.
Working with Hospitalists: Challenges and Highlights for Occupational Therapists
Occupational therapists cite a few areas where hospitalists could provide more help to their fellow professionals in occupational therapy.
Distinction between occupational and physical therapists: To expedite care, hospitalists need to know whether to refer patients to occupational therapy or physical therapy.
“In general, a physical therapist would look at gross motor functions, which affect the patient’s ability to be mobilized from one place to another,” says Quinney. “This also includes whether or not they need assistance to do that safely, and then there’s a myriad of things they look at, including wound care, generalized weakness, and—with a general medicine patient—deconditioning, to make sure that they’re safe in their mobility. An occupational therapist looks more at ADLs, and what patients need to do in order to function in their daily lives and the safety associated with that.”
Timeliness of referrals: Quinney concedes that in the case of a patient who is deconditioned, it might be difficult to discern whether a patient requires occupational therapy or physical therapy. That is one reason why the timeliness of referral is important. If an occupational therapist receives a referral on the day the patient is scheduled for discharge, it may be too late to help them.
But referrals can also be made too soon, says Quinney, “because when the patient is in the ER being admitted, what’s needed may be something as simple as getting their fluids corrected, and once that’s done, then [occupational] therapy is no longer indicated.”
Another example of inappropriate referral timing, she says, might be in the case of a diabetic “whose blood sugars are too high or too low, and clearly, they’re not functioning at their premorbid level. But given the right intervention by the medical team, they’ll bounce back to their baseline.”
Other inappropriate referrals: A patient might also be assessed as having too high or too low a functional status to benefit from occupational therapy. For instance, “a patient might be at too low a level if they came from a nursing home for a UTI or some other complication,” says Quinney, “but their functional status is not something that a therapist would be able to impact in a short hospital stay once that medical problem is corrected.”
From what his occupational therapists tell him, Vijay Rajput, MD, FACP, senior hospitalist at Cooper University Hospital in Camden, N.J., concurs. “If the patient has been in a nursing home for 10 years and is completely custodial and bed-bound, when that patient comes to the hospital and a hospitalist has ordered an occupational therapy consult … , the occupational therapist then has to assess it, and there are no [achievable] goals of care in terms of occupational therapy, then the therapists think that is a [poor use of their] time.”
In that case, however, the family may benefit from a home visit that will provide maintenance or training.
When Quinney receives what she believes is an inappropriate referral from a hospitalist or other provider, she encourages her therapists to say that back to the hospitalist in a direct, to-the-point communication. Therapists are encouraged to say, “This is what I saw with patient X. I’m not seeing any skilled therapy needs. Is there something else I’m missing?”
“We always give [the provider] the benefit of the doubt of having done an assessment in their mind,” explains Quinney.
How consults are written: Quinney’s team has discussed whether to ask hospitalists to be specific about what they are referring for, so “we as therapists are able to affect the whole person. Because if they only give a referral for a specific task, then it makes it more limiting,” she explains. “If they write a referral for ‘functional ability’ or [one] that says ‘concerned with balance,’ that [allows us] to do some problem-solving.”
Tiffani Morales, LOTR, the occupational therapy team leader at Our Lady of Lourdes Regional Medical Center in Lafayette, La., agrees. “We’ve only had hospitalists for about a year, and the three that we have are really doing a good job, [including the way in which] they’re writing their consults,” says Morales. “They’re leaving it open and trusting us to make recommendations, and they’re going along with them.”
Because hospitalists write the chart note as “Consult,” occupational therapy “gives us leeway to make any equipment recommendations or, actually, any of the treatments that may be warranted versus having to call them back, which takes time to keep giving an order over the phone,” explains Morales.
Geography of patient assignments: The system or structure by which patients are assigned will usually differ between occupational therapists and hospitalists. For instance, at Cooper University Hospital, a 520-bed academic, tertiary hospital in Camden, N.J., where Dr. Rajput began the hospitalist program, the six occupational therapists are assigned patients on a geographical basis, according to floor in a 10-story building. But the group of 25 hospitalists, which has grown from four since 1999, is not assigned that way.
“If I am on service,” says Dr. Rajput, “my patients are assigned [perhaps as] one on the 10th floor, one on the ninth floor, [and] one on the eighth floor.”
His occupational therapists told him that if the hospitalists could be assigned to patients the way they are, it would certainly improve the communication between the two groups.
“It is much better to have a verbal communication with the hospitalist than [simply] reviewing the chart,” says Dr. Rajput.
Some hospitalist groups are looking at returning to this geographically based system. “To restructure the whole system would be very complex,” says Dr. Rajput, who is also the program director for the Internal Medicine Residency Program at UMNDNJ—Robert Wood Johnson Medical School in Camden, “but… it still makes sense [from a communication perspective], for instance, the way it does in the ICU.”
Given the difficulties and drawbacks of making that system a widespread reality, however, Plan B would be to increase and encourage contact between occupational therapists and hospitalists. At the UC Hospital, which employs 12 occupational therapists who work with the patient population that hospitalists are responsible for, “the volume of [patients in] the general medicine unit is too high for OTs to meet with hospitalists daily” explains Quinney, who has been with the UC hospitals for six years.
To breach what might be a communication gap, however, she says, “all OTs have pagers, and whenever they write their note in the chart they will leave their pager number. There is always a way for someone to get in touch with them.”
That, of course, can also be said of hospitalists. And because hospitalists respond quickly when occupational therapists page or call them, says Morales, it can help with patient satisfaction.
“The hospitalists round more quickly or at certain times; they have a routine down,” she says. “And that’s a big thing because when patients are ready to be discharged, they want it now. They don’t want to wait.” And when they can be discharged expediently, “we all look better.”
Throughput and quality care: At the UC Medical Center, as at most institutions, hospitalists are encouraged to move patients from admitting through discharge in the most timely and efficient way possible.
“Hospitalists know that [occupational] therapy is part of that important closure of getting them from one site to another,” says Quinney. But sometimes she hears a [hospitalist or resident] say, “I was just told I need to refer them to you in order to get my patient out of the hospital.”
That’s important, Quinney emphasizes, because occupational therapists want to be part of discharge planning. “But we want to be referred to appropriately so that the people who need us most can utilize us, versus going after patients that aren’t appropriate and are using our resources,” she says. “It’s not that we aren’t happy to see those patients, we truly are; it’s a matter of getting people in a timely manner so that we can really make a difference.”
Great Working Relationships
Morales thinks hospitalists have a good understanding of the services that are available from occupational therapists “because whenever we see them about a patient, if they’re not sure about something, they ask questions such as, ‘Is there anything else you can offer?’” she says. “I think they’re right on target [with us].”
Morales’ team thinks hospitalists are involved, friendly, and open. “It’s just a great work relationship,” she says, “because they’re actually seeing the patients in therapy and asking for our input; it’s very refreshing.” Most of all, she appreciates how they show respect for what the occupational therapists do. “They are listening to what we are saying and that makes a difference.”
Educational Opportunities
Because hospitalists look at the bigger picture of what is going on with patients, they generally consult occupational therapy early enough so that therapists can educate hospitalists, patients, and families at Morales’ institution. This also helps prevent patients’ further deconditioning, and helps them to arrive at a discharge disposition earlier.
Dr. Rajput, who is an associate professor of medicine at the University of Medicine and Dentistry, (Brunswick) New Jersey–Robert Wood Johnson Medical School, thinks it would benefit those involved in medical education and hospital medicine “to see that there is sufficient formal training for the residency level or hospitalist level to understand the component [of occupational therapy] and the indication for occupational therapy, and occupational therapy versus physical therapy, as practice.”
Conclusion
Hospitalists can help their occupational therapist colleagues by recognizing the distinction between occupational therapy and physical therapy, making timely and appropriate referrals, writing consults in an open-ended manner to allow occupational therapists to do “whole-person” assessments, and making sure to educate themselves and their hospitalist colleagues on the services and needs of occupational therapists. TH
Andrea Sattinger regularly writes the “Alliances” department.
Every facility has their own twist for what an occupational therapist might do,” says Marla Quinney, OTR/L, assistant director of Adult Inpatient Therapy Services at the University of Chicago (UC) Medical Center. Occupational therapists look at “how patients spend their days and ask, ‘What do they engage in and what do they not engage in because of the current condition?’”
The occupational therapist then helps to rehabilitate patients to baseline. “In an acute care facility,” says Quinney, “a lot of what we do is evaluation and then getting patients to the correct discharge disposition and follow-up care.”
Depending on the institution, occupational therapy offerings may involve management for range of motion, strength, coordination, and sensation; they also include therapy for activities of daily living (ADLs), such as self-care, home management, and community involvement, including vision retraining and cognitive and/or perceptual retraining as they relate to ADLs. Occupational therapists might also include management using assistive devices, and the provision of adaptive equipment. In some institutions, occupational therapy involves aspects of home evaluations, and feeding and swallowing therapy.
Working with Hospitalists: Challenges and Highlights for Occupational Therapists
Occupational therapists cite a few areas where hospitalists could provide more help to their fellow professionals in occupational therapy.
Distinction between occupational and physical therapists: To expedite care, hospitalists need to know whether to refer patients to occupational therapy or physical therapy.
“In general, a physical therapist would look at gross motor functions, which affect the patient’s ability to be mobilized from one place to another,” says Quinney. “This also includes whether or not they need assistance to do that safely, and then there’s a myriad of things they look at, including wound care, generalized weakness, and—with a general medicine patient—deconditioning, to make sure that they’re safe in their mobility. An occupational therapist looks more at ADLs, and what patients need to do in order to function in their daily lives and the safety associated with that.”
Timeliness of referrals: Quinney concedes that in the case of a patient who is deconditioned, it might be difficult to discern whether a patient requires occupational therapy or physical therapy. That is one reason why the timeliness of referral is important. If an occupational therapist receives a referral on the day the patient is scheduled for discharge, it may be too late to help them.
But referrals can also be made too soon, says Quinney, “because when the patient is in the ER being admitted, what’s needed may be something as simple as getting their fluids corrected, and once that’s done, then [occupational] therapy is no longer indicated.”
Another example of inappropriate referral timing, she says, might be in the case of a diabetic “whose blood sugars are too high or too low, and clearly, they’re not functioning at their premorbid level. But given the right intervention by the medical team, they’ll bounce back to their baseline.”
Other inappropriate referrals: A patient might also be assessed as having too high or too low a functional status to benefit from occupational therapy. For instance, “a patient might be at too low a level if they came from a nursing home for a UTI or some other complication,” says Quinney, “but their functional status is not something that a therapist would be able to impact in a short hospital stay once that medical problem is corrected.”
From what his occupational therapists tell him, Vijay Rajput, MD, FACP, senior hospitalist at Cooper University Hospital in Camden, N.J., concurs. “If the patient has been in a nursing home for 10 years and is completely custodial and bed-bound, when that patient comes to the hospital and a hospitalist has ordered an occupational therapy consult … , the occupational therapist then has to assess it, and there are no [achievable] goals of care in terms of occupational therapy, then the therapists think that is a [poor use of their] time.”
In that case, however, the family may benefit from a home visit that will provide maintenance or training.
When Quinney receives what she believes is an inappropriate referral from a hospitalist or other provider, she encourages her therapists to say that back to the hospitalist in a direct, to-the-point communication. Therapists are encouraged to say, “This is what I saw with patient X. I’m not seeing any skilled therapy needs. Is there something else I’m missing?”
“We always give [the provider] the benefit of the doubt of having done an assessment in their mind,” explains Quinney.
How consults are written: Quinney’s team has discussed whether to ask hospitalists to be specific about what they are referring for, so “we as therapists are able to affect the whole person. Because if they only give a referral for a specific task, then it makes it more limiting,” she explains. “If they write a referral for ‘functional ability’ or [one] that says ‘concerned with balance,’ that [allows us] to do some problem-solving.”
Tiffani Morales, LOTR, the occupational therapy team leader at Our Lady of Lourdes Regional Medical Center in Lafayette, La., agrees. “We’ve only had hospitalists for about a year, and the three that we have are really doing a good job, [including the way in which] they’re writing their consults,” says Morales. “They’re leaving it open and trusting us to make recommendations, and they’re going along with them.”
Because hospitalists write the chart note as “Consult,” occupational therapy “gives us leeway to make any equipment recommendations or, actually, any of the treatments that may be warranted versus having to call them back, which takes time to keep giving an order over the phone,” explains Morales.
Geography of patient assignments: The system or structure by which patients are assigned will usually differ between occupational therapists and hospitalists. For instance, at Cooper University Hospital, a 520-bed academic, tertiary hospital in Camden, N.J., where Dr. Rajput began the hospitalist program, the six occupational therapists are assigned patients on a geographical basis, according to floor in a 10-story building. But the group of 25 hospitalists, which has grown from four since 1999, is not assigned that way.
“If I am on service,” says Dr. Rajput, “my patients are assigned [perhaps as] one on the 10th floor, one on the ninth floor, [and] one on the eighth floor.”
His occupational therapists told him that if the hospitalists could be assigned to patients the way they are, it would certainly improve the communication between the two groups.
“It is much better to have a verbal communication with the hospitalist than [simply] reviewing the chart,” says Dr. Rajput.
Some hospitalist groups are looking at returning to this geographically based system. “To restructure the whole system would be very complex,” says Dr. Rajput, who is also the program director for the Internal Medicine Residency Program at UMNDNJ—Robert Wood Johnson Medical School in Camden, “but… it still makes sense [from a communication perspective], for instance, the way it does in the ICU.”
Given the difficulties and drawbacks of making that system a widespread reality, however, Plan B would be to increase and encourage contact between occupational therapists and hospitalists. At the UC Hospital, which employs 12 occupational therapists who work with the patient population that hospitalists are responsible for, “the volume of [patients in] the general medicine unit is too high for OTs to meet with hospitalists daily” explains Quinney, who has been with the UC hospitals for six years.
To breach what might be a communication gap, however, she says, “all OTs have pagers, and whenever they write their note in the chart they will leave their pager number. There is always a way for someone to get in touch with them.”
That, of course, can also be said of hospitalists. And because hospitalists respond quickly when occupational therapists page or call them, says Morales, it can help with patient satisfaction.
“The hospitalists round more quickly or at certain times; they have a routine down,” she says. “And that’s a big thing because when patients are ready to be discharged, they want it now. They don’t want to wait.” And when they can be discharged expediently, “we all look better.”
Throughput and quality care: At the UC Medical Center, as at most institutions, hospitalists are encouraged to move patients from admitting through discharge in the most timely and efficient way possible.
“Hospitalists know that [occupational] therapy is part of that important closure of getting them from one site to another,” says Quinney. But sometimes she hears a [hospitalist or resident] say, “I was just told I need to refer them to you in order to get my patient out of the hospital.”
That’s important, Quinney emphasizes, because occupational therapists want to be part of discharge planning. “But we want to be referred to appropriately so that the people who need us most can utilize us, versus going after patients that aren’t appropriate and are using our resources,” she says. “It’s not that we aren’t happy to see those patients, we truly are; it’s a matter of getting people in a timely manner so that we can really make a difference.”
Great Working Relationships
Morales thinks hospitalists have a good understanding of the services that are available from occupational therapists “because whenever we see them about a patient, if they’re not sure about something, they ask questions such as, ‘Is there anything else you can offer?’” she says. “I think they’re right on target [with us].”
Morales’ team thinks hospitalists are involved, friendly, and open. “It’s just a great work relationship,” she says, “because they’re actually seeing the patients in therapy and asking for our input; it’s very refreshing.” Most of all, she appreciates how they show respect for what the occupational therapists do. “They are listening to what we are saying and that makes a difference.”
Educational Opportunities
Because hospitalists look at the bigger picture of what is going on with patients, they generally consult occupational therapy early enough so that therapists can educate hospitalists, patients, and families at Morales’ institution. This also helps prevent patients’ further deconditioning, and helps them to arrive at a discharge disposition earlier.
Dr. Rajput, who is an associate professor of medicine at the University of Medicine and Dentistry, (Brunswick) New Jersey–Robert Wood Johnson Medical School, thinks it would benefit those involved in medical education and hospital medicine “to see that there is sufficient formal training for the residency level or hospitalist level to understand the component [of occupational therapy] and the indication for occupational therapy, and occupational therapy versus physical therapy, as practice.”
Conclusion
Hospitalists can help their occupational therapist colleagues by recognizing the distinction between occupational therapy and physical therapy, making timely and appropriate referrals, writing consults in an open-ended manner to allow occupational therapists to do “whole-person” assessments, and making sure to educate themselves and their hospitalist colleagues on the services and needs of occupational therapists. TH
Andrea Sattinger regularly writes the “Alliances” department.
Near Misses
The medical literature pertaining to patient safety is voluminous, especially since the publication of the 1999 Institute of Medicine (IOM) report estimating that between 44,000 and 98,000 Americans die from medical errors each year.1 When focusing on hospitalists and the matter of near misses, however, where the outcome of the error has been intercepted before harm can occur, the volume of published information is far more limited.2
“There are few good data about the role that hospitalists play in preventing adverse events,” says Saul Weingart, MD, PhD, vice president for patient safety at the Dana-Farber Cancer Institute, Boston, “so most accounts are anecdotal. My own sense is that hospital medicine plays a critical role in preventing and mitigating errors in the acute care setting.”
One study, conducted by two hospitalists in a 200-bed academic hospital and published in 2003 in the Journal of General Internal Medicine, distinguished near misses from adverse events.3 The investigators set out to determine the frequency, types, and consequences of errors that can be detected by hospitalists during routine clinical care, and to compare the types of errors first discovered by hospitalists to those discovered by other providers.
Sarwat Chaudhry, MD, a former hospitalist who is now a health services researcher and assistant professor of medicine at the Yale School of Medicine in New Haven, Conn., was the lead investigator in that study. “Oftentimes the errors that are ‘sexier’ and more exciting for people to talk about are the adverse events,” she says. “But I think what are perhaps more common and more informative are the near misses.”
Definitions
For purposes of Chaudhry, et al.’s study, “adverse events” were defined as adverse outcomes that resulted from errors.3 Errors that did not result in patient harm, but could have, were categorized as near misses. The umbrella definition of error fit that which was used in the IOM report; that is, “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.”1 Cases in which a bad outcome occurred (such as death or disability) without a preventable cause were not considered errors and, therefore, were not included in the data.
A more practical understanding of a near miss is apparent in the following illustration: “If pharmacy came to me and said, ‘Oh, Dr. Chaudhry, one of the physicians on your team wrote for drug X but the patient is also on drug Y and that’s a known contraindication so we don’t think this should be administered, do you agree?’ I’d say, ‘Yes, I agree.’ So the drug was never given, but it was a near miss for the way it was written if it hadn’t been picked up on.”
—Saul Weingart, MD, PhD
In fact there are two kinds of near misses. “One is where the error is intercepted by [a] pharmacy or somebody else before harm is done,” says Dr. Weingart. “The other kind is where the error reaches the patient—for instance, where he or she receives the antibiotic to which they are allergic—but no reaction takes place.”
An important element in the study was that both types of errors were identified during the course of routine, clinical care by Dr. Chaudhry and her colleague, Kolawole Olofinboba, MD. Errors first detected by other healthcare workers were also recorded. Of the 528 patients included in the study, 10.4% experienced at least one error: 6.2% a near miss and 4.2% an adverse event. Interestingly, most of the errors first detected by house staff, nurses, and laboratory technicians were adverse events, whereas most of the errors first detected by the attending hospitalists, pharmacists, and consultants were near misses. Drug errors were the most common type of error overall.
Although differences did not achieve statistical significance, Dr. Chaudhry says the data were illuminating and the hospital administration was anxious to clarify the processes of care that could be modified to make the workflow more efficient and the different pieces of each patient’s critical data more integrated.
“For instance,” she says, “at our hospital there was a lot of separation of data. … The vitals were right outside the patient’s room. The list of medications was kept in a central pharmacy location, and the medical chart with everyone’s notes was in a third location.”
After the study’s completion, the integration of data was facilitated by the adoption of an electronic medical record (EMR) and there is ongoing research at that institution concerning whether that has affected error rates.

—Sarwat Chaudhry, MD
Lessons Learned
“This was one of the first and, still I think, only studies of attending physicians reporting their own errors,” says Dr. Chaudhry, “as well as reporting the scope, type, and frequency of the errors.”
There were several lessons learned. The first is that near misses are very common—at least as common as adverse events and perhaps more frequent. The second is that the nature of near misses is similar enough to that of adverse events that they can still be informative in preventing harm to patients. The third lesson arises from the investigators’ review of the kinds of errors that were reported by the different providers. “Different types of providers are going to pick up on different kinds of errors,” says Dr. Chaudhry. “Pharmacy, of course, is going to be detecting drug errors. But nurses are going to be detecting a different kind of error than residents, and residents are detecting a different kind of error than attending physicians.”
Dr. Weingart, who was trained as an internist, says his sense is that “we often pick up errors that occur just upstream in the process of care. For instance, pharmacy finds doctor prescribing errors and nursing finds pharmacy dispensing errors.”
Drs. Chaudhry and Olofinboba discovered 17/47 (36%) of the errors on their own, and pharmacists, resident physicians, consulting physicians, nurses, and ancillary staff discovered the remaining 30/47 (64%). The hospitalists were more likely to detect therapeutic errors; house staff physicians were more likely to detect drug errors. House staff also detected procedural errors at a higher rate than did the hospitalists. Consequently, Dr. Chaudhry emphasizes, another highlight of these data shows that “engaging as many different kinds of healthcare providers in error reporting is very important to understand what’s going on.”
Documenting Errors
The two hospitalists in Dr. Chaudhry’s study underwent no formal training in error detection, and all errors identified were documented. This in itself is a remarkable aspect of this study for hospitalists to note.
“In most hospitals, the risk management department feels like breaking out a bottle of champagne to celebrate every time a physician submits an incident report,” says Dr. Weingart, “because in most hospitals physicians don’t view incident reporting as part of their responsibility. On the other hand, physicians constantly talk about the errors, near misses, and adverse events they encounter day-to-day. Unfortunately, formal incident reporting isn’t an activity that most physicians see as a part of their duty to deliver excellent care at the bedside.” By virtue of this, he says, “critical information is often lost to the system. Error experience is transmitted person-to-person but isn’t captured and analyzed.”
The good news here, however, is that by simply launching a study of this nature and capturing the data it is reasonable to expect that any hospitalist group could take it on and any hospital’s quality of care would be improved.
“There is a spectrum of practice review that is conducted by a variety of people,” says Dr. Chaudhry. “On one end of the spectrum, you have the uninvolved reviewer coming in and doing formal chart reviews … and our process was at other end of spectrum, where we were going about our daily business, the routine clinical care of patients.”
By maintaining the potential for errors at the forefront of their thinking, she says, it became the background against which they performed the constant daily review of patient data. “When I would go to the bedside in the morning,” she says, “to see the patient, talk to the patient, review the chart, look at notes, look at vitals, look at meds—that was my process for picking up on errors.”
—Saul Weingart, MD, PhD
Barriers and Opportunities
There are two major barriers to performing this kind of research in other institutions where hospitalists practice, but they are easily resolved. The first is the importance of standardizing definitions.
“We came to consensus before the study began of what things should count and what things shouldn’t count,” says Dr. Chaudhry. “Because there is a degree of subjectivity and especially when a patient experiences harm, it’s a bit easier to attribute that to an error—though not always. For instance, with a patient with asthma who ends up with fluid overload and gets intubated. Well, was that an error? … Or was that just the patient’s own asthma getting worse? How much did the fluid contribute to that?”
There is still a degree of judgment, even there, she says, “but as much as possible we wanted to come to consensus at least about our definitions, our terminology, and our categorization.”
The second barrier to performing this research is the real or perceived risk of litigation. There was a lot of concern at the beginning of her study, says Dr. Chaudhry (and again at the time of publication), regarding the aftermath of disclosing errors.
“As much as the Institute of Medicine and other accreditation and safety organizations talk about how error reporting is so important and that physicians have to be willing to come forward with their errors, there are really no formal, legal, protective mechanisms in place,” she says, adding that this was true three years ago, and she does not believe much has changed.
Consequently, when constructing the study, she reached out to the authors of other error studies and asked them how they had handled the risk of potential litigation. Most of them told her they did not think there was much risk of being sued, but disclosing errors in the literature is certainly not something an institution or individuals would be clamoring to do. If a multi-center study of this nature might be undertaken, she says, these barriers could be traversed and it would be worth it. “Because if we let that opportunity slip through our fingers, it will be taken on by nonphysicians,” she cautions, “by the external reviewers, by the accreditation organizations, by professional quality control people.”
Dr. Chaudhry’s overall recommendation to hospitalists involves the position they hold at this time. “Hospitalists are ideally poised to take a lead in promoting patient safety by becoming more involved and developing the systems for error reporting,” she says.
Dr. Weingart tells hospitalist audiences that the most important areas for detecting errors in their practice include safe prescription writing and error-proofing high-risk activities (such as hand-offs and sign-outs, and follow-up of test results). He also recommends that hospitalists play the role of responsible citizens in their institutions and be open to ways your patients can contribute by helping you detect errors in their care.4 These issues will be addressed in more detail in future articles in The Hospitalist.
Although Dr. Chaudhry is no longer practicing as a hospitalist, she believes that hospital teams working closely together in patient care have a strong advantage to identify any errors.
“As physicians, with hospital medicine expanding,” she says, “this is the opportune time to take on a leadership role, and this needs to be part of the hospitalist mission. Not everyone has to come out and report their adverse events, especially since the legal risks are still unclear. But a safe way and equally informative way to work on preventing harm is to focus on those near misses.”
Conclusion
Hospitalists who search for near misses, volunteer this information, and enroll their colleagues in doing the same contribute to reforming systems and processes that will ultimately reduce the potential for all errors. Those who pay close attention to standardized rules for prescription-writing, error-proofing high-risk activities, and their roles for institutional citizenship and encouraging patient contribution in regard to possible errors, are doing the best possible job to prevent harm to patients and the institution as a whole. TH
Andrea Sattinger will write about apology in medicine in the June issue.
References
- Kohn LT, Corrigan JM, Donaldson MS, Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
- Bleich S. Medical Errors: Five Years After the IOM Report. New York: Commonwealth Fund; July 2005: Available at: www.mihealthandsafety.org/pdfs/pub-4-commonwealth.pdf. Last accessed March 22, 2006.
- Chaudhry SI, Olofinboba KA, Krumholz HM. Detection of errors by attending physicians on a general medicine service. J Gen Intern Med. 2003 Aug;18(8):595-600.
- Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005 Sep;20(9):830-836.
The medical literature pertaining to patient safety is voluminous, especially since the publication of the 1999 Institute of Medicine (IOM) report estimating that between 44,000 and 98,000 Americans die from medical errors each year.1 When focusing on hospitalists and the matter of near misses, however, where the outcome of the error has been intercepted before harm can occur, the volume of published information is far more limited.2
“There are few good data about the role that hospitalists play in preventing adverse events,” says Saul Weingart, MD, PhD, vice president for patient safety at the Dana-Farber Cancer Institute, Boston, “so most accounts are anecdotal. My own sense is that hospital medicine plays a critical role in preventing and mitigating errors in the acute care setting.”
One study, conducted by two hospitalists in a 200-bed academic hospital and published in 2003 in the Journal of General Internal Medicine, distinguished near misses from adverse events.3 The investigators set out to determine the frequency, types, and consequences of errors that can be detected by hospitalists during routine clinical care, and to compare the types of errors first discovered by hospitalists to those discovered by other providers.
Sarwat Chaudhry, MD, a former hospitalist who is now a health services researcher and assistant professor of medicine at the Yale School of Medicine in New Haven, Conn., was the lead investigator in that study. “Oftentimes the errors that are ‘sexier’ and more exciting for people to talk about are the adverse events,” she says. “But I think what are perhaps more common and more informative are the near misses.”
Definitions
For purposes of Chaudhry, et al.’s study, “adverse events” were defined as adverse outcomes that resulted from errors.3 Errors that did not result in patient harm, but could have, were categorized as near misses. The umbrella definition of error fit that which was used in the IOM report; that is, “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.”1 Cases in which a bad outcome occurred (such as death or disability) without a preventable cause were not considered errors and, therefore, were not included in the data.
A more practical understanding of a near miss is apparent in the following illustration: “If pharmacy came to me and said, ‘Oh, Dr. Chaudhry, one of the physicians on your team wrote for drug X but the patient is also on drug Y and that’s a known contraindication so we don’t think this should be administered, do you agree?’ I’d say, ‘Yes, I agree.’ So the drug was never given, but it was a near miss for the way it was written if it hadn’t been picked up on.”
—Saul Weingart, MD, PhD
In fact there are two kinds of near misses. “One is where the error is intercepted by [a] pharmacy or somebody else before harm is done,” says Dr. Weingart. “The other kind is where the error reaches the patient—for instance, where he or she receives the antibiotic to which they are allergic—but no reaction takes place.”
An important element in the study was that both types of errors were identified during the course of routine, clinical care by Dr. Chaudhry and her colleague, Kolawole Olofinboba, MD. Errors first detected by other healthcare workers were also recorded. Of the 528 patients included in the study, 10.4% experienced at least one error: 6.2% a near miss and 4.2% an adverse event. Interestingly, most of the errors first detected by house staff, nurses, and laboratory technicians were adverse events, whereas most of the errors first detected by the attending hospitalists, pharmacists, and consultants were near misses. Drug errors were the most common type of error overall.
Although differences did not achieve statistical significance, Dr. Chaudhry says the data were illuminating and the hospital administration was anxious to clarify the processes of care that could be modified to make the workflow more efficient and the different pieces of each patient’s critical data more integrated.
“For instance,” she says, “at our hospital there was a lot of separation of data. … The vitals were right outside the patient’s room. The list of medications was kept in a central pharmacy location, and the medical chart with everyone’s notes was in a third location.”
After the study’s completion, the integration of data was facilitated by the adoption of an electronic medical record (EMR) and there is ongoing research at that institution concerning whether that has affected error rates.
—Sarwat Chaudhry, MD
Lessons Learned
“This was one of the first and, still I think, only studies of attending physicians reporting their own errors,” says Dr. Chaudhry, “as well as reporting the scope, type, and frequency of the errors.”
There were several lessons learned. The first is that near misses are very common—at least as common as adverse events and perhaps more frequent. The second is that the nature of near misses is similar enough to that of adverse events that they can still be informative in preventing harm to patients. The third lesson arises from the investigators’ review of the kinds of errors that were reported by the different providers. “Different types of providers are going to pick up on different kinds of errors,” says Dr. Chaudhry. “Pharmacy, of course, is going to be detecting drug errors. But nurses are going to be detecting a different kind of error than residents, and residents are detecting a different kind of error than attending physicians.”
Dr. Weingart, who was trained as an internist, says his sense is that “we often pick up errors that occur just upstream in the process of care. For instance, pharmacy finds doctor prescribing errors and nursing finds pharmacy dispensing errors.”
Drs. Chaudhry and Olofinboba discovered 17/47 (36%) of the errors on their own, and pharmacists, resident physicians, consulting physicians, nurses, and ancillary staff discovered the remaining 30/47 (64%). The hospitalists were more likely to detect therapeutic errors; house staff physicians were more likely to detect drug errors. House staff also detected procedural errors at a higher rate than did the hospitalists. Consequently, Dr. Chaudhry emphasizes, another highlight of these data shows that “engaging as many different kinds of healthcare providers in error reporting is very important to understand what’s going on.”
Documenting Errors
The two hospitalists in Dr. Chaudhry’s study underwent no formal training in error detection, and all errors identified were documented. This in itself is a remarkable aspect of this study for hospitalists to note.
“In most hospitals, the risk management department feels like breaking out a bottle of champagne to celebrate every time a physician submits an incident report,” says Dr. Weingart, “because in most hospitals physicians don’t view incident reporting as part of their responsibility. On the other hand, physicians constantly talk about the errors, near misses, and adverse events they encounter day-to-day. Unfortunately, formal incident reporting isn’t an activity that most physicians see as a part of their duty to deliver excellent care at the bedside.” By virtue of this, he says, “critical information is often lost to the system. Error experience is transmitted person-to-person but isn’t captured and analyzed.”
The good news here, however, is that by simply launching a study of this nature and capturing the data it is reasonable to expect that any hospitalist group could take it on and any hospital’s quality of care would be improved.
“There is a spectrum of practice review that is conducted by a variety of people,” says Dr. Chaudhry. “On one end of the spectrum, you have the uninvolved reviewer coming in and doing formal chart reviews … and our process was at other end of spectrum, where we were going about our daily business, the routine clinical care of patients.”
By maintaining the potential for errors at the forefront of their thinking, she says, it became the background against which they performed the constant daily review of patient data. “When I would go to the bedside in the morning,” she says, “to see the patient, talk to the patient, review the chart, look at notes, look at vitals, look at meds—that was my process for picking up on errors.”
—Saul Weingart, MD, PhD
Barriers and Opportunities
There are two major barriers to performing this kind of research in other institutions where hospitalists practice, but they are easily resolved. The first is the importance of standardizing definitions.
“We came to consensus before the study began of what things should count and what things shouldn’t count,” says Dr. Chaudhry. “Because there is a degree of subjectivity and especially when a patient experiences harm, it’s a bit easier to attribute that to an error—though not always. For instance, with a patient with asthma who ends up with fluid overload and gets intubated. Well, was that an error? … Or was that just the patient’s own asthma getting worse? How much did the fluid contribute to that?”
There is still a degree of judgment, even there, she says, “but as much as possible we wanted to come to consensus at least about our definitions, our terminology, and our categorization.”
The second barrier to performing this research is the real or perceived risk of litigation. There was a lot of concern at the beginning of her study, says Dr. Chaudhry (and again at the time of publication), regarding the aftermath of disclosing errors.
“As much as the Institute of Medicine and other accreditation and safety organizations talk about how error reporting is so important and that physicians have to be willing to come forward with their errors, there are really no formal, legal, protective mechanisms in place,” she says, adding that this was true three years ago, and she does not believe much has changed.
Consequently, when constructing the study, she reached out to the authors of other error studies and asked them how they had handled the risk of potential litigation. Most of them told her they did not think there was much risk of being sued, but disclosing errors in the literature is certainly not something an institution or individuals would be clamoring to do. If a multi-center study of this nature might be undertaken, she says, these barriers could be traversed and it would be worth it. “Because if we let that opportunity slip through our fingers, it will be taken on by nonphysicians,” she cautions, “by the external reviewers, by the accreditation organizations, by professional quality control people.”
Dr. Chaudhry’s overall recommendation to hospitalists involves the position they hold at this time. “Hospitalists are ideally poised to take a lead in promoting patient safety by becoming more involved and developing the systems for error reporting,” she says.
Dr. Weingart tells hospitalist audiences that the most important areas for detecting errors in their practice include safe prescription writing and error-proofing high-risk activities (such as hand-offs and sign-outs, and follow-up of test results). He also recommends that hospitalists play the role of responsible citizens in their institutions and be open to ways your patients can contribute by helping you detect errors in their care.4 These issues will be addressed in more detail in future articles in The Hospitalist.
Although Dr. Chaudhry is no longer practicing as a hospitalist, she believes that hospital teams working closely together in patient care have a strong advantage to identify any errors.
“As physicians, with hospital medicine expanding,” she says, “this is the opportune time to take on a leadership role, and this needs to be part of the hospitalist mission. Not everyone has to come out and report their adverse events, especially since the legal risks are still unclear. But a safe way and equally informative way to work on preventing harm is to focus on those near misses.”
Conclusion
Hospitalists who search for near misses, volunteer this information, and enroll their colleagues in doing the same contribute to reforming systems and processes that will ultimately reduce the potential for all errors. Those who pay close attention to standardized rules for prescription-writing, error-proofing high-risk activities, and their roles for institutional citizenship and encouraging patient contribution in regard to possible errors, are doing the best possible job to prevent harm to patients and the institution as a whole. TH
Andrea Sattinger will write about apology in medicine in the June issue.
References
- Kohn LT, Corrigan JM, Donaldson MS, Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
- Bleich S. Medical Errors: Five Years After the IOM Report. New York: Commonwealth Fund; July 2005: Available at: www.mihealthandsafety.org/pdfs/pub-4-commonwealth.pdf. Last accessed March 22, 2006.
- Chaudhry SI, Olofinboba KA, Krumholz HM. Detection of errors by attending physicians on a general medicine service. J Gen Intern Med. 2003 Aug;18(8):595-600.
- Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005 Sep;20(9):830-836.
The medical literature pertaining to patient safety is voluminous, especially since the publication of the 1999 Institute of Medicine (IOM) report estimating that between 44,000 and 98,000 Americans die from medical errors each year.1 When focusing on hospitalists and the matter of near misses, however, where the outcome of the error has been intercepted before harm can occur, the volume of published information is far more limited.2
“There are few good data about the role that hospitalists play in preventing adverse events,” says Saul Weingart, MD, PhD, vice president for patient safety at the Dana-Farber Cancer Institute, Boston, “so most accounts are anecdotal. My own sense is that hospital medicine plays a critical role in preventing and mitigating errors in the acute care setting.”
One study, conducted by two hospitalists in a 200-bed academic hospital and published in 2003 in the Journal of General Internal Medicine, distinguished near misses from adverse events.3 The investigators set out to determine the frequency, types, and consequences of errors that can be detected by hospitalists during routine clinical care, and to compare the types of errors first discovered by hospitalists to those discovered by other providers.
Sarwat Chaudhry, MD, a former hospitalist who is now a health services researcher and assistant professor of medicine at the Yale School of Medicine in New Haven, Conn., was the lead investigator in that study. “Oftentimes the errors that are ‘sexier’ and more exciting for people to talk about are the adverse events,” she says. “But I think what are perhaps more common and more informative are the near misses.”
Definitions
For purposes of Chaudhry, et al.’s study, “adverse events” were defined as adverse outcomes that resulted from errors.3 Errors that did not result in patient harm, but could have, were categorized as near misses. The umbrella definition of error fit that which was used in the IOM report; that is, “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.”1 Cases in which a bad outcome occurred (such as death or disability) without a preventable cause were not considered errors and, therefore, were not included in the data.
A more practical understanding of a near miss is apparent in the following illustration: “If pharmacy came to me and said, ‘Oh, Dr. Chaudhry, one of the physicians on your team wrote for drug X but the patient is also on drug Y and that’s a known contraindication so we don’t think this should be administered, do you agree?’ I’d say, ‘Yes, I agree.’ So the drug was never given, but it was a near miss for the way it was written if it hadn’t been picked up on.”
—Saul Weingart, MD, PhD
In fact there are two kinds of near misses. “One is where the error is intercepted by [a] pharmacy or somebody else before harm is done,” says Dr. Weingart. “The other kind is where the error reaches the patient—for instance, where he or she receives the antibiotic to which they are allergic—but no reaction takes place.”
An important element in the study was that both types of errors were identified during the course of routine, clinical care by Dr. Chaudhry and her colleague, Kolawole Olofinboba, MD. Errors first detected by other healthcare workers were also recorded. Of the 528 patients included in the study, 10.4% experienced at least one error: 6.2% a near miss and 4.2% an adverse event. Interestingly, most of the errors first detected by house staff, nurses, and laboratory technicians were adverse events, whereas most of the errors first detected by the attending hospitalists, pharmacists, and consultants were near misses. Drug errors were the most common type of error overall.
Although differences did not achieve statistical significance, Dr. Chaudhry says the data were illuminating and the hospital administration was anxious to clarify the processes of care that could be modified to make the workflow more efficient and the different pieces of each patient’s critical data more integrated.
“For instance,” she says, “at our hospital there was a lot of separation of data. … The vitals were right outside the patient’s room. The list of medications was kept in a central pharmacy location, and the medical chart with everyone’s notes was in a third location.”
After the study’s completion, the integration of data was facilitated by the adoption of an electronic medical record (EMR) and there is ongoing research at that institution concerning whether that has affected error rates.
—Sarwat Chaudhry, MD
Lessons Learned
“This was one of the first and, still I think, only studies of attending physicians reporting their own errors,” says Dr. Chaudhry, “as well as reporting the scope, type, and frequency of the errors.”
There were several lessons learned. The first is that near misses are very common—at least as common as adverse events and perhaps more frequent. The second is that the nature of near misses is similar enough to that of adverse events that they can still be informative in preventing harm to patients. The third lesson arises from the investigators’ review of the kinds of errors that were reported by the different providers. “Different types of providers are going to pick up on different kinds of errors,” says Dr. Chaudhry. “Pharmacy, of course, is going to be detecting drug errors. But nurses are going to be detecting a different kind of error than residents, and residents are detecting a different kind of error than attending physicians.”
Dr. Weingart, who was trained as an internist, says his sense is that “we often pick up errors that occur just upstream in the process of care. For instance, pharmacy finds doctor prescribing errors and nursing finds pharmacy dispensing errors.”
Drs. Chaudhry and Olofinboba discovered 17/47 (36%) of the errors on their own, and pharmacists, resident physicians, consulting physicians, nurses, and ancillary staff discovered the remaining 30/47 (64%). The hospitalists were more likely to detect therapeutic errors; house staff physicians were more likely to detect drug errors. House staff also detected procedural errors at a higher rate than did the hospitalists. Consequently, Dr. Chaudhry emphasizes, another highlight of these data shows that “engaging as many different kinds of healthcare providers in error reporting is very important to understand what’s going on.”
Documenting Errors
The two hospitalists in Dr. Chaudhry’s study underwent no formal training in error detection, and all errors identified were documented. This in itself is a remarkable aspect of this study for hospitalists to note.
“In most hospitals, the risk management department feels like breaking out a bottle of champagne to celebrate every time a physician submits an incident report,” says Dr. Weingart, “because in most hospitals physicians don’t view incident reporting as part of their responsibility. On the other hand, physicians constantly talk about the errors, near misses, and adverse events they encounter day-to-day. Unfortunately, formal incident reporting isn’t an activity that most physicians see as a part of their duty to deliver excellent care at the bedside.” By virtue of this, he says, “critical information is often lost to the system. Error experience is transmitted person-to-person but isn’t captured and analyzed.”
The good news here, however, is that by simply launching a study of this nature and capturing the data it is reasonable to expect that any hospitalist group could take it on and any hospital’s quality of care would be improved.
“There is a spectrum of practice review that is conducted by a variety of people,” says Dr. Chaudhry. “On one end of the spectrum, you have the uninvolved reviewer coming in and doing formal chart reviews … and our process was at other end of spectrum, where we were going about our daily business, the routine clinical care of patients.”
By maintaining the potential for errors at the forefront of their thinking, she says, it became the background against which they performed the constant daily review of patient data. “When I would go to the bedside in the morning,” she says, “to see the patient, talk to the patient, review the chart, look at notes, look at vitals, look at meds—that was my process for picking up on errors.”
—Saul Weingart, MD, PhD
Barriers and Opportunities
There are two major barriers to performing this kind of research in other institutions where hospitalists practice, but they are easily resolved. The first is the importance of standardizing definitions.
“We came to consensus before the study began of what things should count and what things shouldn’t count,” says Dr. Chaudhry. “Because there is a degree of subjectivity and especially when a patient experiences harm, it’s a bit easier to attribute that to an error—though not always. For instance, with a patient with asthma who ends up with fluid overload and gets intubated. Well, was that an error? … Or was that just the patient’s own asthma getting worse? How much did the fluid contribute to that?”
There is still a degree of judgment, even there, she says, “but as much as possible we wanted to come to consensus at least about our definitions, our terminology, and our categorization.”
The second barrier to performing this research is the real or perceived risk of litigation. There was a lot of concern at the beginning of her study, says Dr. Chaudhry (and again at the time of publication), regarding the aftermath of disclosing errors.
“As much as the Institute of Medicine and other accreditation and safety organizations talk about how error reporting is so important and that physicians have to be willing to come forward with their errors, there are really no formal, legal, protective mechanisms in place,” she says, adding that this was true three years ago, and she does not believe much has changed.
Consequently, when constructing the study, she reached out to the authors of other error studies and asked them how they had handled the risk of potential litigation. Most of them told her they did not think there was much risk of being sued, but disclosing errors in the literature is certainly not something an institution or individuals would be clamoring to do. If a multi-center study of this nature might be undertaken, she says, these barriers could be traversed and it would be worth it. “Because if we let that opportunity slip through our fingers, it will be taken on by nonphysicians,” she cautions, “by the external reviewers, by the accreditation organizations, by professional quality control people.”
Dr. Chaudhry’s overall recommendation to hospitalists involves the position they hold at this time. “Hospitalists are ideally poised to take a lead in promoting patient safety by becoming more involved and developing the systems for error reporting,” she says.
Dr. Weingart tells hospitalist audiences that the most important areas for detecting errors in their practice include safe prescription writing and error-proofing high-risk activities (such as hand-offs and sign-outs, and follow-up of test results). He also recommends that hospitalists play the role of responsible citizens in their institutions and be open to ways your patients can contribute by helping you detect errors in their care.4 These issues will be addressed in more detail in future articles in The Hospitalist.
Although Dr. Chaudhry is no longer practicing as a hospitalist, she believes that hospital teams working closely together in patient care have a strong advantage to identify any errors.
“As physicians, with hospital medicine expanding,” she says, “this is the opportune time to take on a leadership role, and this needs to be part of the hospitalist mission. Not everyone has to come out and report their adverse events, especially since the legal risks are still unclear. But a safe way and equally informative way to work on preventing harm is to focus on those near misses.”
Conclusion
Hospitalists who search for near misses, volunteer this information, and enroll their colleagues in doing the same contribute to reforming systems and processes that will ultimately reduce the potential for all errors. Those who pay close attention to standardized rules for prescription-writing, error-proofing high-risk activities, and their roles for institutional citizenship and encouraging patient contribution in regard to possible errors, are doing the best possible job to prevent harm to patients and the institution as a whole. TH
Andrea Sattinger will write about apology in medicine in the June issue.
References
- Kohn LT, Corrigan JM, Donaldson MS, Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
- Bleich S. Medical Errors: Five Years After the IOM Report. New York: Commonwealth Fund; July 2005: Available at: www.mihealthandsafety.org/pdfs/pub-4-commonwealth.pdf. Last accessed March 22, 2006.
- Chaudhry SI, Olofinboba KA, Krumholz HM. Detection of errors by attending physicians on a general medicine service. J Gen Intern Med. 2003 Aug;18(8):595-600.
- Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005 Sep;20(9):830-836.
The New Orleans Nocturnalist
Editors’ note: We originally conceived this article with the authors just before Hurricanes Katrina and Rita devastated the Gulf Coast last year. Once the hurricanes hit, we decided to “bump” this article in favor of running coverage of the hurricanes and their effects on hospitals in the Gulf Coast area.
The Ochsner Clinic Foundation rests on the eastern bank of an acute flexure in the Mississippi river similar to its twin just downstream, which lurches around a crescent forming the historic and infamous French Vieux Carré, or Old Quarter. From a perch on the hospital’s 11th floor I often start my evening by taking in the full scope of the river’s powerful swirling eddies and copious flotsam churning past in the westerly sun. The view has become a familiar sight to me over the past several years as our hospital’s primary night shift internist.
Though my comrades jokingly refer to me as Ochsner’s “nocturnist,” an assignment surprisingly relished by few, the position has proven mutually beneficial in serving a vital role for the hospital and our group, while accommodating my own crepuscular nature and lifestyle.
Our night position—officially known as IHC (or in-house call)—was conceived from several requisites desired by both administration and physicians. Ochsner Clinic Foundation is steeped in academic history, and the nights have traditionally been dominated by semi-autonomously operating residents. During the past five years, practice changes in the local area afforded Ochsner unprecedented growth, requiring constant accommodation and development of our hospitalist group. Many of these changes were accelerated by the devastation wrought by Hurricane Katrina. With a nod to quality over quantity, we decided against expanding the teaching program in favor of developing several non-resident-based hospital services.
These unique and burgeoning parallel systems of care quickly presented many challenges for those staff clinicians stationed at home when problems arose during the evening. The original expectation was that the residents would have no direct involvement in the care of this subset of patients to avoid overburdening a system already operating near capacity. Subsequent intradepartmental disputation ensued over how to provide our patients with personal on-site care through the wee hours while arresting the surge of hectoring beeps that inevitably start after midnight. The exigency of solving this problem grew as our physicians’ slumber waned and patient admissions soared over the following months.
Our group’s consensus that a full-time night staff physician was needed soon emerged as the best potential remedy for our predicament. As no person wanted to be commandeered for the job, volunteers were sought for a trial run with the very reasonable hours of 4 p.m. to midnight, Monday through Friday. Hardly ever retiring to bed before the witching hour, I accepted the first week of our nascent, early evening shift.
The Rise of the Nocturnist
The expectations were simple. I was to independently admit “bounce-backs:” observation level patients, hip fracture service patients, and overflow admissions from a frequently dropsical emergency department. This specious solution proved very successful but ultimately served to highlight the overall need for a hospitalist to remain in-house for the duration of the evening and early morning hours.
The subsequent creation of a newly expanded, more permanent role for our IHC was proffered for consideration. This vision of moving to 24-hour staff coverage on site met with universal acceptance from the physicians, nursing staff, residents, and administration. The lone problem remained of finding physicians willing to dedicate themselves to working primarily at night.
Rather than rotating doctors weekly, we hoped to maintain some consistency by having certain physicians dedicated to staffing nights. From this graveyard shift arose true nocturnists, as in my case, working evenings nearly 75% of the time. Implementation of a weekend nocturnist to cover Saturday and Sunday is being developed as the need for coverage increases and the success of the current system continues.
Rapid Growth
These expanded changes to the system soon proved fortuitous. Within one year after the inception of IHC, admissions to the medicine services had consistently swollen to between 20 and 30 patients each night—a record for even the busiest periods in the history of the institution. The surge of patients being admitted through our emergency department to medicine proved to be an enduring change, which progressed unabated until Katrina struck. By necessity, the number of “unresidented” services quickly grew to accommodate our patients’ needs and concerns.
In addition, residency-review guidelines governing capitation of resident admissions were also carefully maintained to provide a consistent teaching environment for the house staff. Though stalling momentarily after Katrina struck, medical admissions have continued to climb seemingly without limit. The capacity of our six inpatient medical services with residents is now matched by an equal number of services managed privately by attending physicians alone.
Post-Katrina, the responsibilities of our three primary “nocturnists” have grown in tandem with the increasing number of patients on the wards to now cover the sub-acute nursing facility patients, geriatric nursing home patients, and acute preoperative clearances throughout the night. The lion’s share of time is still spent assisting and facilitating the admissions process for our patients through the emergency department.
In the past several years the role of the night hospitalist has become an integral part of our emergency department. In effect, most of the night is now spent in the emergency department providing consults, triage help, and early assistance with the care of patients ultimately bound for medicine admission. Besides the pragmatic benefits of expedited care, new interpersonal bonds of understanding and empathy have been forged between the two departments. I now count most of the emergency department staff, from physicians to nurses and secretaries, as personal friends and colleagues. The beleaguered admitting process has gradually transformed into a more cooperative, harmonious transfer of patient care between trusting teams.
Tracking Patients
With so many patients now spilling over the next day to various teams, one of the most vital functions of the IHC staff is to provide complete and accurate information about each patient assigned to the accepting teams the following day. This has required cooperation from both emergency staff in writing temporary floor orders, proper information flow between the on-call resident, night float resident and IHC staff, and proper notification of direct admissions arriving on the floor of patients accepted from the on call medicine staff during the day.
Currently each patient is simultaneously tracked by name, clinic number, and diagnosis by both the IHC staff and the overnight resident. The lists are frequently compared for accuracy, and in the morning an individual e-mail notification is sent to every physician on service for the day of every admission, distribution, and diagnosis by the IHC staff. As a second line of defense against error, the resident places an individual phone call to each physician receiving an overnight admission to reiterate any clinical problems.
As a department we have crafted fixed schedules of admission for the following morning so each day a physician knows whether to expect patients on the service or not. These numbers are forwarded to admissions for that day in order to keep each of the services as numerically equitable as possible. These careful tracking mechanisms, expectations of good communication between our physicians, and months of trial and error have proven invaluable during the months of highest volume when essentially every patient admitted overnight must be redistributed to various teams in the morning.
In addition to securing safe transition of the patient between teams and ensuring proper medical care, each patient is greeted in his or her room in the emergency department by the IHC staff, who take a moment to explain the admission process, the future plan of care, and who will assume the patient’s case in the morning. This has continuously provided an early opportunity to establish bonds of trust with each patient and assuage any lingering questions the patient may have after evaluation by the resident physician. Many of our patients are now displaced, frightened, and homeless. The value of providing face-to-face, 24-hour attending level care for our patients cannot be overstated.
Conclusion
Auguring the future of medical practice in New Orleans since hurricanes Katrina and Rita ravaged the city has proved difficult if not impossible. The degree of change during the past six months has shown that flexibility and adaptability are mainstays of the ability to practice good medicine. Without doubt, New Orleans will return more lively, more resilient, and wiser for all of our losses over the past year. TH
Dr. Blalock is based at the Department of Hospital-Based Internal Medicine, Ochsner Clinic Foundation, New Orleans. Special thanks to Steven B. Deitelzweig, MD, Doris Lin, MD, and Srinivas Vuppala, MD, for their assistance with this article.
Editors’ note: We originally conceived this article with the authors just before Hurricanes Katrina and Rita devastated the Gulf Coast last year. Once the hurricanes hit, we decided to “bump” this article in favor of running coverage of the hurricanes and their effects on hospitals in the Gulf Coast area.
The Ochsner Clinic Foundation rests on the eastern bank of an acute flexure in the Mississippi river similar to its twin just downstream, which lurches around a crescent forming the historic and infamous French Vieux Carré, or Old Quarter. From a perch on the hospital’s 11th floor I often start my evening by taking in the full scope of the river’s powerful swirling eddies and copious flotsam churning past in the westerly sun. The view has become a familiar sight to me over the past several years as our hospital’s primary night shift internist.
Though my comrades jokingly refer to me as Ochsner’s “nocturnist,” an assignment surprisingly relished by few, the position has proven mutually beneficial in serving a vital role for the hospital and our group, while accommodating my own crepuscular nature and lifestyle.
Our night position—officially known as IHC (or in-house call)—was conceived from several requisites desired by both administration and physicians. Ochsner Clinic Foundation is steeped in academic history, and the nights have traditionally been dominated by semi-autonomously operating residents. During the past five years, practice changes in the local area afforded Ochsner unprecedented growth, requiring constant accommodation and development of our hospitalist group. Many of these changes were accelerated by the devastation wrought by Hurricane Katrina. With a nod to quality over quantity, we decided against expanding the teaching program in favor of developing several non-resident-based hospital services.
These unique and burgeoning parallel systems of care quickly presented many challenges for those staff clinicians stationed at home when problems arose during the evening. The original expectation was that the residents would have no direct involvement in the care of this subset of patients to avoid overburdening a system already operating near capacity. Subsequent intradepartmental disputation ensued over how to provide our patients with personal on-site care through the wee hours while arresting the surge of hectoring beeps that inevitably start after midnight. The exigency of solving this problem grew as our physicians’ slumber waned and patient admissions soared over the following months.
Our group’s consensus that a full-time night staff physician was needed soon emerged as the best potential remedy for our predicament. As no person wanted to be commandeered for the job, volunteers were sought for a trial run with the very reasonable hours of 4 p.m. to midnight, Monday through Friday. Hardly ever retiring to bed before the witching hour, I accepted the first week of our nascent, early evening shift.
The Rise of the Nocturnist
The expectations were simple. I was to independently admit “bounce-backs:” observation level patients, hip fracture service patients, and overflow admissions from a frequently dropsical emergency department. This specious solution proved very successful but ultimately served to highlight the overall need for a hospitalist to remain in-house for the duration of the evening and early morning hours.
The subsequent creation of a newly expanded, more permanent role for our IHC was proffered for consideration. This vision of moving to 24-hour staff coverage on site met with universal acceptance from the physicians, nursing staff, residents, and administration. The lone problem remained of finding physicians willing to dedicate themselves to working primarily at night.
Rather than rotating doctors weekly, we hoped to maintain some consistency by having certain physicians dedicated to staffing nights. From this graveyard shift arose true nocturnists, as in my case, working evenings nearly 75% of the time. Implementation of a weekend nocturnist to cover Saturday and Sunday is being developed as the need for coverage increases and the success of the current system continues.
Rapid Growth
These expanded changes to the system soon proved fortuitous. Within one year after the inception of IHC, admissions to the medicine services had consistently swollen to between 20 and 30 patients each night—a record for even the busiest periods in the history of the institution. The surge of patients being admitted through our emergency department to medicine proved to be an enduring change, which progressed unabated until Katrina struck. By necessity, the number of “unresidented” services quickly grew to accommodate our patients’ needs and concerns.
In addition, residency-review guidelines governing capitation of resident admissions were also carefully maintained to provide a consistent teaching environment for the house staff. Though stalling momentarily after Katrina struck, medical admissions have continued to climb seemingly without limit. The capacity of our six inpatient medical services with residents is now matched by an equal number of services managed privately by attending physicians alone.
Post-Katrina, the responsibilities of our three primary “nocturnists” have grown in tandem with the increasing number of patients on the wards to now cover the sub-acute nursing facility patients, geriatric nursing home patients, and acute preoperative clearances throughout the night. The lion’s share of time is still spent assisting and facilitating the admissions process for our patients through the emergency department.
In the past several years the role of the night hospitalist has become an integral part of our emergency department. In effect, most of the night is now spent in the emergency department providing consults, triage help, and early assistance with the care of patients ultimately bound for medicine admission. Besides the pragmatic benefits of expedited care, new interpersonal bonds of understanding and empathy have been forged between the two departments. I now count most of the emergency department staff, from physicians to nurses and secretaries, as personal friends and colleagues. The beleaguered admitting process has gradually transformed into a more cooperative, harmonious transfer of patient care between trusting teams.
Tracking Patients
With so many patients now spilling over the next day to various teams, one of the most vital functions of the IHC staff is to provide complete and accurate information about each patient assigned to the accepting teams the following day. This has required cooperation from both emergency staff in writing temporary floor orders, proper information flow between the on-call resident, night float resident and IHC staff, and proper notification of direct admissions arriving on the floor of patients accepted from the on call medicine staff during the day.
Currently each patient is simultaneously tracked by name, clinic number, and diagnosis by both the IHC staff and the overnight resident. The lists are frequently compared for accuracy, and in the morning an individual e-mail notification is sent to every physician on service for the day of every admission, distribution, and diagnosis by the IHC staff. As a second line of defense against error, the resident places an individual phone call to each physician receiving an overnight admission to reiterate any clinical problems.
As a department we have crafted fixed schedules of admission for the following morning so each day a physician knows whether to expect patients on the service or not. These numbers are forwarded to admissions for that day in order to keep each of the services as numerically equitable as possible. These careful tracking mechanisms, expectations of good communication between our physicians, and months of trial and error have proven invaluable during the months of highest volume when essentially every patient admitted overnight must be redistributed to various teams in the morning.
In addition to securing safe transition of the patient between teams and ensuring proper medical care, each patient is greeted in his or her room in the emergency department by the IHC staff, who take a moment to explain the admission process, the future plan of care, and who will assume the patient’s case in the morning. This has continuously provided an early opportunity to establish bonds of trust with each patient and assuage any lingering questions the patient may have after evaluation by the resident physician. Many of our patients are now displaced, frightened, and homeless. The value of providing face-to-face, 24-hour attending level care for our patients cannot be overstated.
Conclusion
Auguring the future of medical practice in New Orleans since hurricanes Katrina and Rita ravaged the city has proved difficult if not impossible. The degree of change during the past six months has shown that flexibility and adaptability are mainstays of the ability to practice good medicine. Without doubt, New Orleans will return more lively, more resilient, and wiser for all of our losses over the past year. TH
Dr. Blalock is based at the Department of Hospital-Based Internal Medicine, Ochsner Clinic Foundation, New Orleans. Special thanks to Steven B. Deitelzweig, MD, Doris Lin, MD, and Srinivas Vuppala, MD, for their assistance with this article.
Editors’ note: We originally conceived this article with the authors just before Hurricanes Katrina and Rita devastated the Gulf Coast last year. Once the hurricanes hit, we decided to “bump” this article in favor of running coverage of the hurricanes and their effects on hospitals in the Gulf Coast area.
The Ochsner Clinic Foundation rests on the eastern bank of an acute flexure in the Mississippi river similar to its twin just downstream, which lurches around a crescent forming the historic and infamous French Vieux Carré, or Old Quarter. From a perch on the hospital’s 11th floor I often start my evening by taking in the full scope of the river’s powerful swirling eddies and copious flotsam churning past in the westerly sun. The view has become a familiar sight to me over the past several years as our hospital’s primary night shift internist.
Though my comrades jokingly refer to me as Ochsner’s “nocturnist,” an assignment surprisingly relished by few, the position has proven mutually beneficial in serving a vital role for the hospital and our group, while accommodating my own crepuscular nature and lifestyle.
Our night position—officially known as IHC (or in-house call)—was conceived from several requisites desired by both administration and physicians. Ochsner Clinic Foundation is steeped in academic history, and the nights have traditionally been dominated by semi-autonomously operating residents. During the past five years, practice changes in the local area afforded Ochsner unprecedented growth, requiring constant accommodation and development of our hospitalist group. Many of these changes were accelerated by the devastation wrought by Hurricane Katrina. With a nod to quality over quantity, we decided against expanding the teaching program in favor of developing several non-resident-based hospital services.
These unique and burgeoning parallel systems of care quickly presented many challenges for those staff clinicians stationed at home when problems arose during the evening. The original expectation was that the residents would have no direct involvement in the care of this subset of patients to avoid overburdening a system already operating near capacity. Subsequent intradepartmental disputation ensued over how to provide our patients with personal on-site care through the wee hours while arresting the surge of hectoring beeps that inevitably start after midnight. The exigency of solving this problem grew as our physicians’ slumber waned and patient admissions soared over the following months.
Our group’s consensus that a full-time night staff physician was needed soon emerged as the best potential remedy for our predicament. As no person wanted to be commandeered for the job, volunteers were sought for a trial run with the very reasonable hours of 4 p.m. to midnight, Monday through Friday. Hardly ever retiring to bed before the witching hour, I accepted the first week of our nascent, early evening shift.
The Rise of the Nocturnist
The expectations were simple. I was to independently admit “bounce-backs:” observation level patients, hip fracture service patients, and overflow admissions from a frequently dropsical emergency department. This specious solution proved very successful but ultimately served to highlight the overall need for a hospitalist to remain in-house for the duration of the evening and early morning hours.
The subsequent creation of a newly expanded, more permanent role for our IHC was proffered for consideration. This vision of moving to 24-hour staff coverage on site met with universal acceptance from the physicians, nursing staff, residents, and administration. The lone problem remained of finding physicians willing to dedicate themselves to working primarily at night.
Rather than rotating doctors weekly, we hoped to maintain some consistency by having certain physicians dedicated to staffing nights. From this graveyard shift arose true nocturnists, as in my case, working evenings nearly 75% of the time. Implementation of a weekend nocturnist to cover Saturday and Sunday is being developed as the need for coverage increases and the success of the current system continues.
Rapid Growth
These expanded changes to the system soon proved fortuitous. Within one year after the inception of IHC, admissions to the medicine services had consistently swollen to between 20 and 30 patients each night—a record for even the busiest periods in the history of the institution. The surge of patients being admitted through our emergency department to medicine proved to be an enduring change, which progressed unabated until Katrina struck. By necessity, the number of “unresidented” services quickly grew to accommodate our patients’ needs and concerns.
In addition, residency-review guidelines governing capitation of resident admissions were also carefully maintained to provide a consistent teaching environment for the house staff. Though stalling momentarily after Katrina struck, medical admissions have continued to climb seemingly without limit. The capacity of our six inpatient medical services with residents is now matched by an equal number of services managed privately by attending physicians alone.
Post-Katrina, the responsibilities of our three primary “nocturnists” have grown in tandem with the increasing number of patients on the wards to now cover the sub-acute nursing facility patients, geriatric nursing home patients, and acute preoperative clearances throughout the night. The lion’s share of time is still spent assisting and facilitating the admissions process for our patients through the emergency department.
In the past several years the role of the night hospitalist has become an integral part of our emergency department. In effect, most of the night is now spent in the emergency department providing consults, triage help, and early assistance with the care of patients ultimately bound for medicine admission. Besides the pragmatic benefits of expedited care, new interpersonal bonds of understanding and empathy have been forged between the two departments. I now count most of the emergency department staff, from physicians to nurses and secretaries, as personal friends and colleagues. The beleaguered admitting process has gradually transformed into a more cooperative, harmonious transfer of patient care between trusting teams.
Tracking Patients
With so many patients now spilling over the next day to various teams, one of the most vital functions of the IHC staff is to provide complete and accurate information about each patient assigned to the accepting teams the following day. This has required cooperation from both emergency staff in writing temporary floor orders, proper information flow between the on-call resident, night float resident and IHC staff, and proper notification of direct admissions arriving on the floor of patients accepted from the on call medicine staff during the day.
Currently each patient is simultaneously tracked by name, clinic number, and diagnosis by both the IHC staff and the overnight resident. The lists are frequently compared for accuracy, and in the morning an individual e-mail notification is sent to every physician on service for the day of every admission, distribution, and diagnosis by the IHC staff. As a second line of defense against error, the resident places an individual phone call to each physician receiving an overnight admission to reiterate any clinical problems.
As a department we have crafted fixed schedules of admission for the following morning so each day a physician knows whether to expect patients on the service or not. These numbers are forwarded to admissions for that day in order to keep each of the services as numerically equitable as possible. These careful tracking mechanisms, expectations of good communication between our physicians, and months of trial and error have proven invaluable during the months of highest volume when essentially every patient admitted overnight must be redistributed to various teams in the morning.
In addition to securing safe transition of the patient between teams and ensuring proper medical care, each patient is greeted in his or her room in the emergency department by the IHC staff, who take a moment to explain the admission process, the future plan of care, and who will assume the patient’s case in the morning. This has continuously provided an early opportunity to establish bonds of trust with each patient and assuage any lingering questions the patient may have after evaluation by the resident physician. Many of our patients are now displaced, frightened, and homeless. The value of providing face-to-face, 24-hour attending level care for our patients cannot be overstated.
Conclusion
Auguring the future of medical practice in New Orleans since hurricanes Katrina and Rita ravaged the city has proved difficult if not impossible. The degree of change during the past six months has shown that flexibility and adaptability are mainstays of the ability to practice good medicine. Without doubt, New Orleans will return more lively, more resilient, and wiser for all of our losses over the past year. TH
Dr. Blalock is based at the Department of Hospital-Based Internal Medicine, Ochsner Clinic Foundation, New Orleans. Special thanks to Steven B. Deitelzweig, MD, Doris Lin, MD, and Srinivas Vuppala, MD, for their assistance with this article.
Skin Dilemma
A75-year-old previously healthy woman presented with one-month history of extensive necrotic coalescing erythematous weeping vesicles and bullae. A skin biopsy was performed. (See right and right bottom for images.)
Based on the skin biopsy and clinical presentation, the most likely diagnosis is:
- Pemphigoid;
- Pemphigus vulgaris;
- Staphylococcus scalded skin syndrome;
- Porphyria cutanea tarda; or
- Darier’s disease.

Discussion
The correct answer is B: pemphigus vulgaris. The skin biopsy demonstrates an intra-epidermal split along the basal layer of keratinocytes. The basal cells along the basement membrane zone demonstrate tombstoning consistent with pemphigus vulgaris. Clinically, she has erythematous superficial erosions with slight re-epithelialization.
Pemphigoid is another blistering disorder that often affects the elderly and classically presents with tense bulla that demonstrate an infra-basilar split on histology. Staphylococcus scalded skin syndrome may present similarly, but histology shows acantholysis in the superficial epidermis. Porphyria cutanea tarda often is on the hands, arms, and other sun-exposed areas, and biopsy reveals dermal papillae protruding up toward the bulla (festooning). Darier’s disease is autosomal dominant and presents with greasy hyperkeratotic papules that show acantholysis and dyskeratosis on histology, with occasional suprabasal clefting.
Pemphigus vulgaris is an autoimmune process that often affects those in middle age. It usually first involves the mucous membranes and then progresses to the skin, where intraepidermal bullae form. These bullae are flaccid and easily rupture, often easily extending beyond their original dimensions with only slight perturbation. Because of their fragility patients may not present with any intact bullae and instead only have painful erosions, as in this case.
The disease is mediated by circulating immunoglobulin G (IgG), which binds to the cell surface of keratinocytes, breaking up intercellular connections and resulting in acantholysis and bulla formation. The process is diagnosed with the shown histology and with direct in vivo immunofluorescence, which demonstrates a “chicken-wire” pattern around keratinocytes. Paraneoplastic pemphigus and pemphigus foliaceous are the other two types of pemphigus, and a work up for underlying malignancy is indicated to rule out the former. Opportunistic infections are common and can lead to exacerbation of the disease, so culture and antimicrobial therapy often play an important role in recovery.
Pemphigus can often be controlled with adequate immunosuppression. High-dose systemic steroids are the first-line treatment. Other immunosuppressive medications, such as dapsone, azathioprine, and mycophenolate mofetil, are used for maintenance therapy during and after the patient has recovered from a flare-up. Intravenous immunoglobulin (IVIG) and plasmapheresis therapy has also showed promising results.1,2
This case was complicated by superinfection with both methicillin-resistant staphylococcus aureus (MRSA) and herpes simplex virus. One course of IVIG produced no benefit. The patient then underwent intensive inpatient wet-dressing therapy with topical steroids and antimicrobial treatment. She was placed on high-dose prednisone and began to recover, without new lesion development and with re-epithelialization. First mycophenolate mofetil followed by azathioprine were started, to which the patient responded well. TH
References
- Bystryn JC, Rudolph JL. IVIG treatment of pemphigus: how it works and how to use it. J Investig Dermatol. 2005 Dec;125(6):1093-1098.
- Stanley JR. Therapy of pemphigus vulgaris. Arch Dermatol. 1999 Jan;135(1):76-78.
A75-year-old previously healthy woman presented with one-month history of extensive necrotic coalescing erythematous weeping vesicles and bullae. A skin biopsy was performed. (See right and right bottom for images.)
Based on the skin biopsy and clinical presentation, the most likely diagnosis is:
- Pemphigoid;
- Pemphigus vulgaris;
- Staphylococcus scalded skin syndrome;
- Porphyria cutanea tarda; or
- Darier’s disease.
Discussion
The correct answer is B: pemphigus vulgaris. The skin biopsy demonstrates an intra-epidermal split along the basal layer of keratinocytes. The basal cells along the basement membrane zone demonstrate tombstoning consistent with pemphigus vulgaris. Clinically, she has erythematous superficial erosions with slight re-epithelialization.
Pemphigoid is another blistering disorder that often affects the elderly and classically presents with tense bulla that demonstrate an infra-basilar split on histology. Staphylococcus scalded skin syndrome may present similarly, but histology shows acantholysis in the superficial epidermis. Porphyria cutanea tarda often is on the hands, arms, and other sun-exposed areas, and biopsy reveals dermal papillae protruding up toward the bulla (festooning). Darier’s disease is autosomal dominant and presents with greasy hyperkeratotic papules that show acantholysis and dyskeratosis on histology, with occasional suprabasal clefting.
Pemphigus vulgaris is an autoimmune process that often affects those in middle age. It usually first involves the mucous membranes and then progresses to the skin, where intraepidermal bullae form. These bullae are flaccid and easily rupture, often easily extending beyond their original dimensions with only slight perturbation. Because of their fragility patients may not present with any intact bullae and instead only have painful erosions, as in this case.
The disease is mediated by circulating immunoglobulin G (IgG), which binds to the cell surface of keratinocytes, breaking up intercellular connections and resulting in acantholysis and bulla formation. The process is diagnosed with the shown histology and with direct in vivo immunofluorescence, which demonstrates a “chicken-wire” pattern around keratinocytes. Paraneoplastic pemphigus and pemphigus foliaceous are the other two types of pemphigus, and a work up for underlying malignancy is indicated to rule out the former. Opportunistic infections are common and can lead to exacerbation of the disease, so culture and antimicrobial therapy often play an important role in recovery.
Pemphigus can often be controlled with adequate immunosuppression. High-dose systemic steroids are the first-line treatment. Other immunosuppressive medications, such as dapsone, azathioprine, and mycophenolate mofetil, are used for maintenance therapy during and after the patient has recovered from a flare-up. Intravenous immunoglobulin (IVIG) and plasmapheresis therapy has also showed promising results.1,2
This case was complicated by superinfection with both methicillin-resistant staphylococcus aureus (MRSA) and herpes simplex virus. One course of IVIG produced no benefit. The patient then underwent intensive inpatient wet-dressing therapy with topical steroids and antimicrobial treatment. She was placed on high-dose prednisone and began to recover, without new lesion development and with re-epithelialization. First mycophenolate mofetil followed by azathioprine were started, to which the patient responded well. TH
References
- Bystryn JC, Rudolph JL. IVIG treatment of pemphigus: how it works and how to use it. J Investig Dermatol. 2005 Dec;125(6):1093-1098.
- Stanley JR. Therapy of pemphigus vulgaris. Arch Dermatol. 1999 Jan;135(1):76-78.
A75-year-old previously healthy woman presented with one-month history of extensive necrotic coalescing erythematous weeping vesicles and bullae. A skin biopsy was performed. (See right and right bottom for images.)
Based on the skin biopsy and clinical presentation, the most likely diagnosis is:
- Pemphigoid;
- Pemphigus vulgaris;
- Staphylococcus scalded skin syndrome;
- Porphyria cutanea tarda; or
- Darier’s disease.
Discussion
The correct answer is B: pemphigus vulgaris. The skin biopsy demonstrates an intra-epidermal split along the basal layer of keratinocytes. The basal cells along the basement membrane zone demonstrate tombstoning consistent with pemphigus vulgaris. Clinically, she has erythematous superficial erosions with slight re-epithelialization.
Pemphigoid is another blistering disorder that often affects the elderly and classically presents with tense bulla that demonstrate an infra-basilar split on histology. Staphylococcus scalded skin syndrome may present similarly, but histology shows acantholysis in the superficial epidermis. Porphyria cutanea tarda often is on the hands, arms, and other sun-exposed areas, and biopsy reveals dermal papillae protruding up toward the bulla (festooning). Darier’s disease is autosomal dominant and presents with greasy hyperkeratotic papules that show acantholysis and dyskeratosis on histology, with occasional suprabasal clefting.
Pemphigus vulgaris is an autoimmune process that often affects those in middle age. It usually first involves the mucous membranes and then progresses to the skin, where intraepidermal bullae form. These bullae are flaccid and easily rupture, often easily extending beyond their original dimensions with only slight perturbation. Because of their fragility patients may not present with any intact bullae and instead only have painful erosions, as in this case.
The disease is mediated by circulating immunoglobulin G (IgG), which binds to the cell surface of keratinocytes, breaking up intercellular connections and resulting in acantholysis and bulla formation. The process is diagnosed with the shown histology and with direct in vivo immunofluorescence, which demonstrates a “chicken-wire” pattern around keratinocytes. Paraneoplastic pemphigus and pemphigus foliaceous are the other two types of pemphigus, and a work up for underlying malignancy is indicated to rule out the former. Opportunistic infections are common and can lead to exacerbation of the disease, so culture and antimicrobial therapy often play an important role in recovery.
Pemphigus can often be controlled with adequate immunosuppression. High-dose systemic steroids are the first-line treatment. Other immunosuppressive medications, such as dapsone, azathioprine, and mycophenolate mofetil, are used for maintenance therapy during and after the patient has recovered from a flare-up. Intravenous immunoglobulin (IVIG) and plasmapheresis therapy has also showed promising results.1,2
This case was complicated by superinfection with both methicillin-resistant staphylococcus aureus (MRSA) and herpes simplex virus. One course of IVIG produced no benefit. The patient then underwent intensive inpatient wet-dressing therapy with topical steroids and antimicrobial treatment. She was placed on high-dose prednisone and began to recover, without new lesion development and with re-epithelialization. First mycophenolate mofetil followed by azathioprine were started, to which the patient responded well. TH
References
- Bystryn JC, Rudolph JL. IVIG treatment of pemphigus: how it works and how to use it. J Investig Dermatol. 2005 Dec;125(6):1093-1098.
- Stanley JR. Therapy of pemphigus vulgaris. Arch Dermatol. 1999 Jan;135(1):76-78.
An Analysis of Clinical Reasoning Errors
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. Mar;2003:25(2);177-181.
Many hospitalists are involved in processes to reduce errors in the hospital. Given the dozens of clinical decisions hospitalists make each day, errors in clinical reasoning are worth exploring. However, few physicians are familiar with the terminology and classes of clinical reasoning errors as described in the literature.
This article outlines two models of clinical reasoning and explains common biases that distort clinical reasoning. Although the examples used to illustrate these errors draw from primary care internal medicine, they are easily recognizable.
Biases are defined as inaccurate beliefs that affect decision-making.
When generating a differential diagnosis, the bias of availability (aka recall bias) involves a clinician being influenced by what is easily recalled, creating a false sense of prevalence. This is especially common with less experienced clinicians, residents, and medical students.
The bias of representativeness (aka judging by similarity) involves the physician choosing a diagnosis based solely on signs and symptoms, while neglecting the prevalence of competing diagnoses.
The bias of confirmation involves the clinician using additional testing to confirm a suspected diagnosis, but failing to test competing hypotheses.
The bias of anchoring and adjustment involves the clinician inadequately adjusting the differential in light of new data.
The bias of bounded rationality (aka search satisfying) involves the clinician stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Outcome bias involves judging a clinical decision retrospectively based on the outcome, rather than on logic and evidence supporting the original decision.
Omission bias involves placing undue emphasis on avoiding the adverse effect of a therapy, leading to under-utilization of a beneficial treatment.
Most of the work in clinical reasoning errors is published in the cognitive psychology and education literature, which most hospitalists do not regularly read. By becoming familiar with the concepts and terminology, hospitalists can more readily engage in discussions of clinical reasoning errors and how to avoid them. TH
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. Mar;2003:25(2);177-181.
Many hospitalists are involved in processes to reduce errors in the hospital. Given the dozens of clinical decisions hospitalists make each day, errors in clinical reasoning are worth exploring. However, few physicians are familiar with the terminology and classes of clinical reasoning errors as described in the literature.
This article outlines two models of clinical reasoning and explains common biases that distort clinical reasoning. Although the examples used to illustrate these errors draw from primary care internal medicine, they are easily recognizable.
Biases are defined as inaccurate beliefs that affect decision-making.
When generating a differential diagnosis, the bias of availability (aka recall bias) involves a clinician being influenced by what is easily recalled, creating a false sense of prevalence. This is especially common with less experienced clinicians, residents, and medical students.
The bias of representativeness (aka judging by similarity) involves the physician choosing a diagnosis based solely on signs and symptoms, while neglecting the prevalence of competing diagnoses.
The bias of confirmation involves the clinician using additional testing to confirm a suspected diagnosis, but failing to test competing hypotheses.
The bias of anchoring and adjustment involves the clinician inadequately adjusting the differential in light of new data.
The bias of bounded rationality (aka search satisfying) involves the clinician stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Outcome bias involves judging a clinical decision retrospectively based on the outcome, rather than on logic and evidence supporting the original decision.
Omission bias involves placing undue emphasis on avoiding the adverse effect of a therapy, leading to under-utilization of a beneficial treatment.
Most of the work in clinical reasoning errors is published in the cognitive psychology and education literature, which most hospitalists do not regularly read. By becoming familiar with the concepts and terminology, hospitalists can more readily engage in discussions of clinical reasoning errors and how to avoid them. TH
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. Mar;2003:25(2);177-181.
Many hospitalists are involved in processes to reduce errors in the hospital. Given the dozens of clinical decisions hospitalists make each day, errors in clinical reasoning are worth exploring. However, few physicians are familiar with the terminology and classes of clinical reasoning errors as described in the literature.
This article outlines two models of clinical reasoning and explains common biases that distort clinical reasoning. Although the examples used to illustrate these errors draw from primary care internal medicine, they are easily recognizable.
Biases are defined as inaccurate beliefs that affect decision-making.
When generating a differential diagnosis, the bias of availability (aka recall bias) involves a clinician being influenced by what is easily recalled, creating a false sense of prevalence. This is especially common with less experienced clinicians, residents, and medical students.
The bias of representativeness (aka judging by similarity) involves the physician choosing a diagnosis based solely on signs and symptoms, while neglecting the prevalence of competing diagnoses.
The bias of confirmation involves the clinician using additional testing to confirm a suspected diagnosis, but failing to test competing hypotheses.
The bias of anchoring and adjustment involves the clinician inadequately adjusting the differential in light of new data.
The bias of bounded rationality (aka search satisfying) involves the clinician stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Outcome bias involves judging a clinical decision retrospectively based on the outcome, rather than on logic and evidence supporting the original decision.
Omission bias involves placing undue emphasis on avoiding the adverse effect of a therapy, leading to under-utilization of a beneficial treatment.
Most of the work in clinical reasoning errors is published in the cognitive psychology and education literature, which most hospitalists do not regularly read. By becoming familiar with the concepts and terminology, hospitalists can more readily engage in discussions of clinical reasoning errors and how to avoid them. TH
To Be or Not To Be a Fellow
In the past decade numerous trends and influences have caused organized trauma surgery to re-examine our role in the care of all acutely ill surgical patients and the training of future general surgeons who will care for these patients.1 In this article we’ll briefly review the influences that brought us to this point, the issues we feel need to be addressed, and the solution that trauma surgery has proposed. In many ways, we believe these trends parallel the influences that led to the development of the hospitalists and, thus, call for a surgical equivalent.
Surgical Trends
The development of laparoscopic surgery has had profound influence on surgical practice. Cholecystectomies and appendectomies are generally 23-hour admissions. Even bariatric surgery is now little more than outpatient surgery, with the average length of stay at two days. Along with laparoscopy, breast surgery is now one of the fastest growing surgical subspecialties.
Many surgeons have tailored their practices to a largely outpatient base. There has been an explosion of free-standing surgery centers with a large shift of this low acuity patient population away from hospitals. This follows an overall shift in medicine to ambulatory practice, which is now projected to increase by 24% over the next five to 10 years. Thus, fewer and fewer surgeons have large inpatient practices. There is growing concern about the reluctance of many surgeons to deal with complex, high acuity patients. The obvious exceptions are transplant and trauma surgeons.
In the past decade profound changes in trauma care have also affected the practices of surgeons and the career choices of surgical residents.2 Following the peak of gun-related violence in the early 1990s, there has been a steady and significant decline in penetrating trauma with a concomitant decrease in operations. Slow but steady improvement in motor vehicle passive safety devices has also decreased the incidence of serious injury to the torso following car crashes.
When a solid organ (liver, spleen, kidney) injury does occur after car crash, fall, or assault, the management has largely shifted away from exploratory laparotomy to non-operative management. This has been made possible by improved imaging techniques, careful monitoring in the ICU and judicious use of interventional radiologic techniques of embolization and percutaneous drainage. Currently, some 60% to 80% of liver and spleen injuries are treated with observation or interventional techniques. Although most surgical residents enjoy the challenges of both trauma surgery and critical care, the decline in operative opportunities has limited the appeal of trauma/critical care as a career choice.2
Many trauma surgeons feel there is a convergence of these two issues—a group of patients that may be underserved and an opportunity to enhance the training and desirability of caring for acutely ill surgical patients.3-5 Either through years of experience or formal training, the vast majority of trauma surgeons are highly experienced in evaluating, operating upon, and providing post-operative care for critically ill and injured patients. In fact, the majority of surgical critical care fellowships are based at level 1 trauma centers and are run primarily by trauma surgeons. Thus, trauma surgeons are ideally situated to address these issues.

—Rohit Uppal, MD, MBA
A New Specialty
In 2001 Ron V. Maier, MD, then president of the American Association for the Surgery of Trauma (AAST), commissioned a committee to address these issues and develop an action plan. With broad representation from numerous surgical societies, the committee met several times to consider various training and practice models as potential solutions. After much discussion, the group proposed a model based upon trauma surgery, emergency general surgery, and critical care. This process is outlined in a white paper authored by the committee in 2005.
Basically, the committee recommends the evolution of trauma surgery into a new specialty based on broad training in elective and emergency general surgery, trauma, and critical care surgery. Specific steps to accomplish this goal were outlined by the committee and considerable progress has already been made. After much debate regarding the name, including the consideration of “surgical hospitalists,” the AAST elected to support the name “acute care surgeon.” In fact, this model is how many of us trauma surgeons practice; we take trauma and emergency general surgery call and provide critical care services for these patients.
What was missing from the paradigm was a formal incorporation of emergency general surgery into the training of trauma/surgical critical care fellows and analysis of the benefits of such programs. While this practice paradigm has long been the model at many urban safety net hospitals in cities such as Atlanta, Dallas, Denver, Los Angeles, and Seattle, the practice of many trauma surgeons is often restrained at university hospitals and most level II trauma centers.
Strong Results
The trauma program at University of Pennsylvania, Pittsburgh, under the leadership of C. William Schwab, MD, the current president of the AAST, has taken the lead in documenting the value of incorporating emergency surgery into trauma/surgical critical care training. The addition of emergency general surgery into a trauma/surgical critical care fellowship increases operative experience and fellow satisfaction.3-6 Emergency general surgery now accounts for 57% of operations performed by their faculty. This helps maintain their operative experience despite a decline in operative trauma volume. Finally, with a careful analysis of performance improvement data, there is no compromise in trauma patient outcomes despite the increased patient load.4-5 This experience has been replicated at other trauma centers and strongly suggests that incorporating emergency general surgery into trauma training increases attractiveness to trainees and maintains high standards of patient care. The question is whether it meets an unfilled need.
Recent experience at Vanderbilt Medical Center suggests that the formal incorporation of emergency general surgery into a service has benefits for patients and the hospital.6 The service brings in more referrals from the surrounding community and increases trauma surgeon operative cases. The elective general surgeons also experience an increase in operations and admissions after removing the disruption of emergency admissions. The hospital benefits by the addition of new patients that frequently require operations and intensive care.
In a recent supplement to the The Hospitalist Larry Wellikson, MD, notes that hospitalists add value by (among other things):
- Providing measurable quality improvement;
- Creating seamless continuity from inpatient to outpatient care, from emergency department to floor, and from ICU to floor;
- Doing things other physicians had given up, such as indigent care and hospital committee functions;
- Creating healthcare teams to improve the working environment; and
- Taking care of acutely ill, complex hospitalized patients.7
We believe that trauma surgeons, or acute care surgeons, exemplify these values. We have provided these services to surgical patients for the past 25 years. Trauma surgeons have been leaders in quality improvement, as demonstrated by the American College of Surgeons Committee on Trauma verification program.
We take care of whoever comes through the door, regardless of acuity, time of day (or night), or payer status. We have always provided comprehensive care for our patients—from involvement in prehospital care and planning, through the emergency department, operating room, ICU, and even post-discharge rehabilitation. This requires an effective healthcare team and a truly multidisciplinary approach with other physicians (orthopedics, neurosurgery, anesthesia), nurses, and others, including respiratory, occupational, and physical therapy.
Conclusion
We see a synergy between hospitalist and acute-care surgeons. Both groups have stepped forward to fill a void in patient care. The redefining of trauma surgery as acute care surgery and the development of dedicated training programs will no doubt benefit current and future surgeons, but our patients will benefit the most. TH
Dr. Spain is professor of surgery and chief of Trauma, Emergency and Critical Care Surgery, Stanford University (California). He is also chairman of the Critical Care Committee, American Association for the Surgery of Trauma. Dr. Jurkovich is professor of surgery at the University of Washington, chief of Trauma and Emergency Surgical Services at Harborview Medical Center, and chairman of the Acute Care Surgeon Committee, American Association for the Surgery of Trauma.
References
- Committee to Develop the Reorganized Specialty of Trauma, Surgical Critical Care, and Emergency Surgery. Acute care surgery: trauma, critical care, and emergency surgery. J Trauma. 2005;58:614-616.
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212-217.
- Pryor JP, Reilly PM, Schwab CW, et al. Integrating emergency general surgery with a trauma service: impact on the care of injured patients. J Trauma. 2004 Sep;57(3):467-471.
- Reilly PM, Schwab CW, Haut ER, et al. Training in trauma surgery: quantitative and qualitative aspects of a new paradigm for fellowship. Ann Surg. 2003 Oct;238(4):596-603.
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004 Jul;199(1):96-101.
- Austin MT, Diaz JJ Jr, Feurer ID, et al. Creating an emergency general surgery service enhances the productivity of trauma surgeons, general surgeons and the hospital. J Trauma. 2005 May;58(5):906-910.
- Wellikson L. Hospitals recognize and reward value. The Hospitalist. 2005;9:3-5.
In the past decade numerous trends and influences have caused organized trauma surgery to re-examine our role in the care of all acutely ill surgical patients and the training of future general surgeons who will care for these patients.1 In this article we’ll briefly review the influences that brought us to this point, the issues we feel need to be addressed, and the solution that trauma surgery has proposed. In many ways, we believe these trends parallel the influences that led to the development of the hospitalists and, thus, call for a surgical equivalent.
Surgical Trends
The development of laparoscopic surgery has had profound influence on surgical practice. Cholecystectomies and appendectomies are generally 23-hour admissions. Even bariatric surgery is now little more than outpatient surgery, with the average length of stay at two days. Along with laparoscopy, breast surgery is now one of the fastest growing surgical subspecialties.
Many surgeons have tailored their practices to a largely outpatient base. There has been an explosion of free-standing surgery centers with a large shift of this low acuity patient population away from hospitals. This follows an overall shift in medicine to ambulatory practice, which is now projected to increase by 24% over the next five to 10 years. Thus, fewer and fewer surgeons have large inpatient practices. There is growing concern about the reluctance of many surgeons to deal with complex, high acuity patients. The obvious exceptions are transplant and trauma surgeons.
In the past decade profound changes in trauma care have also affected the practices of surgeons and the career choices of surgical residents.2 Following the peak of gun-related violence in the early 1990s, there has been a steady and significant decline in penetrating trauma with a concomitant decrease in operations. Slow but steady improvement in motor vehicle passive safety devices has also decreased the incidence of serious injury to the torso following car crashes.
When a solid organ (liver, spleen, kidney) injury does occur after car crash, fall, or assault, the management has largely shifted away from exploratory laparotomy to non-operative management. This has been made possible by improved imaging techniques, careful monitoring in the ICU and judicious use of interventional radiologic techniques of embolization and percutaneous drainage. Currently, some 60% to 80% of liver and spleen injuries are treated with observation or interventional techniques. Although most surgical residents enjoy the challenges of both trauma surgery and critical care, the decline in operative opportunities has limited the appeal of trauma/critical care as a career choice.2
Many trauma surgeons feel there is a convergence of these two issues—a group of patients that may be underserved and an opportunity to enhance the training and desirability of caring for acutely ill surgical patients.3-5 Either through years of experience or formal training, the vast majority of trauma surgeons are highly experienced in evaluating, operating upon, and providing post-operative care for critically ill and injured patients. In fact, the majority of surgical critical care fellowships are based at level 1 trauma centers and are run primarily by trauma surgeons. Thus, trauma surgeons are ideally situated to address these issues.
—Rohit Uppal, MD, MBA
A New Specialty
In 2001 Ron V. Maier, MD, then president of the American Association for the Surgery of Trauma (AAST), commissioned a committee to address these issues and develop an action plan. With broad representation from numerous surgical societies, the committee met several times to consider various training and practice models as potential solutions. After much discussion, the group proposed a model based upon trauma surgery, emergency general surgery, and critical care. This process is outlined in a white paper authored by the committee in 2005.
Basically, the committee recommends the evolution of trauma surgery into a new specialty based on broad training in elective and emergency general surgery, trauma, and critical care surgery. Specific steps to accomplish this goal were outlined by the committee and considerable progress has already been made. After much debate regarding the name, including the consideration of “surgical hospitalists,” the AAST elected to support the name “acute care surgeon.” In fact, this model is how many of us trauma surgeons practice; we take trauma and emergency general surgery call and provide critical care services for these patients.
What was missing from the paradigm was a formal incorporation of emergency general surgery into the training of trauma/surgical critical care fellows and analysis of the benefits of such programs. While this practice paradigm has long been the model at many urban safety net hospitals in cities such as Atlanta, Dallas, Denver, Los Angeles, and Seattle, the practice of many trauma surgeons is often restrained at university hospitals and most level II trauma centers.
Strong Results
The trauma program at University of Pennsylvania, Pittsburgh, under the leadership of C. William Schwab, MD, the current president of the AAST, has taken the lead in documenting the value of incorporating emergency surgery into trauma/surgical critical care training. The addition of emergency general surgery into a trauma/surgical critical care fellowship increases operative experience and fellow satisfaction.3-6 Emergency general surgery now accounts for 57% of operations performed by their faculty. This helps maintain their operative experience despite a decline in operative trauma volume. Finally, with a careful analysis of performance improvement data, there is no compromise in trauma patient outcomes despite the increased patient load.4-5 This experience has been replicated at other trauma centers and strongly suggests that incorporating emergency general surgery into trauma training increases attractiveness to trainees and maintains high standards of patient care. The question is whether it meets an unfilled need.
Recent experience at Vanderbilt Medical Center suggests that the formal incorporation of emergency general surgery into a service has benefits for patients and the hospital.6 The service brings in more referrals from the surrounding community and increases trauma surgeon operative cases. The elective general surgeons also experience an increase in operations and admissions after removing the disruption of emergency admissions. The hospital benefits by the addition of new patients that frequently require operations and intensive care.
In a recent supplement to the The Hospitalist Larry Wellikson, MD, notes that hospitalists add value by (among other things):
- Providing measurable quality improvement;
- Creating seamless continuity from inpatient to outpatient care, from emergency department to floor, and from ICU to floor;
- Doing things other physicians had given up, such as indigent care and hospital committee functions;
- Creating healthcare teams to improve the working environment; and
- Taking care of acutely ill, complex hospitalized patients.7
We believe that trauma surgeons, or acute care surgeons, exemplify these values. We have provided these services to surgical patients for the past 25 years. Trauma surgeons have been leaders in quality improvement, as demonstrated by the American College of Surgeons Committee on Trauma verification program.
We take care of whoever comes through the door, regardless of acuity, time of day (or night), or payer status. We have always provided comprehensive care for our patients—from involvement in prehospital care and planning, through the emergency department, operating room, ICU, and even post-discharge rehabilitation. This requires an effective healthcare team and a truly multidisciplinary approach with other physicians (orthopedics, neurosurgery, anesthesia), nurses, and others, including respiratory, occupational, and physical therapy.
Conclusion
We see a synergy between hospitalist and acute-care surgeons. Both groups have stepped forward to fill a void in patient care. The redefining of trauma surgery as acute care surgery and the development of dedicated training programs will no doubt benefit current and future surgeons, but our patients will benefit the most. TH
Dr. Spain is professor of surgery and chief of Trauma, Emergency and Critical Care Surgery, Stanford University (California). He is also chairman of the Critical Care Committee, American Association for the Surgery of Trauma. Dr. Jurkovich is professor of surgery at the University of Washington, chief of Trauma and Emergency Surgical Services at Harborview Medical Center, and chairman of the Acute Care Surgeon Committee, American Association for the Surgery of Trauma.
References
- Committee to Develop the Reorganized Specialty of Trauma, Surgical Critical Care, and Emergency Surgery. Acute care surgery: trauma, critical care, and emergency surgery. J Trauma. 2005;58:614-616.
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212-217.
- Pryor JP, Reilly PM, Schwab CW, et al. Integrating emergency general surgery with a trauma service: impact on the care of injured patients. J Trauma. 2004 Sep;57(3):467-471.
- Reilly PM, Schwab CW, Haut ER, et al. Training in trauma surgery: quantitative and qualitative aspects of a new paradigm for fellowship. Ann Surg. 2003 Oct;238(4):596-603.
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004 Jul;199(1):96-101.
- Austin MT, Diaz JJ Jr, Feurer ID, et al. Creating an emergency general surgery service enhances the productivity of trauma surgeons, general surgeons and the hospital. J Trauma. 2005 May;58(5):906-910.
- Wellikson L. Hospitals recognize and reward value. The Hospitalist. 2005;9:3-5.
In the past decade numerous trends and influences have caused organized trauma surgery to re-examine our role in the care of all acutely ill surgical patients and the training of future general surgeons who will care for these patients.1 In this article we’ll briefly review the influences that brought us to this point, the issues we feel need to be addressed, and the solution that trauma surgery has proposed. In many ways, we believe these trends parallel the influences that led to the development of the hospitalists and, thus, call for a surgical equivalent.
Surgical Trends
The development of laparoscopic surgery has had profound influence on surgical practice. Cholecystectomies and appendectomies are generally 23-hour admissions. Even bariatric surgery is now little more than outpatient surgery, with the average length of stay at two days. Along with laparoscopy, breast surgery is now one of the fastest growing surgical subspecialties.
Many surgeons have tailored their practices to a largely outpatient base. There has been an explosion of free-standing surgery centers with a large shift of this low acuity patient population away from hospitals. This follows an overall shift in medicine to ambulatory practice, which is now projected to increase by 24% over the next five to 10 years. Thus, fewer and fewer surgeons have large inpatient practices. There is growing concern about the reluctance of many surgeons to deal with complex, high acuity patients. The obvious exceptions are transplant and trauma surgeons.
In the past decade profound changes in trauma care have also affected the practices of surgeons and the career choices of surgical residents.2 Following the peak of gun-related violence in the early 1990s, there has been a steady and significant decline in penetrating trauma with a concomitant decrease in operations. Slow but steady improvement in motor vehicle passive safety devices has also decreased the incidence of serious injury to the torso following car crashes.
When a solid organ (liver, spleen, kidney) injury does occur after car crash, fall, or assault, the management has largely shifted away from exploratory laparotomy to non-operative management. This has been made possible by improved imaging techniques, careful monitoring in the ICU and judicious use of interventional radiologic techniques of embolization and percutaneous drainage. Currently, some 60% to 80% of liver and spleen injuries are treated with observation or interventional techniques. Although most surgical residents enjoy the challenges of both trauma surgery and critical care, the decline in operative opportunities has limited the appeal of trauma/critical care as a career choice.2
Many trauma surgeons feel there is a convergence of these two issues—a group of patients that may be underserved and an opportunity to enhance the training and desirability of caring for acutely ill surgical patients.3-5 Either through years of experience or formal training, the vast majority of trauma surgeons are highly experienced in evaluating, operating upon, and providing post-operative care for critically ill and injured patients. In fact, the majority of surgical critical care fellowships are based at level 1 trauma centers and are run primarily by trauma surgeons. Thus, trauma surgeons are ideally situated to address these issues.
—Rohit Uppal, MD, MBA
A New Specialty
In 2001 Ron V. Maier, MD, then president of the American Association for the Surgery of Trauma (AAST), commissioned a committee to address these issues and develop an action plan. With broad representation from numerous surgical societies, the committee met several times to consider various training and practice models as potential solutions. After much discussion, the group proposed a model based upon trauma surgery, emergency general surgery, and critical care. This process is outlined in a white paper authored by the committee in 2005.
Basically, the committee recommends the evolution of trauma surgery into a new specialty based on broad training in elective and emergency general surgery, trauma, and critical care surgery. Specific steps to accomplish this goal were outlined by the committee and considerable progress has already been made. After much debate regarding the name, including the consideration of “surgical hospitalists,” the AAST elected to support the name “acute care surgeon.” In fact, this model is how many of us trauma surgeons practice; we take trauma and emergency general surgery call and provide critical care services for these patients.
What was missing from the paradigm was a formal incorporation of emergency general surgery into the training of trauma/surgical critical care fellows and analysis of the benefits of such programs. While this practice paradigm has long been the model at many urban safety net hospitals in cities such as Atlanta, Dallas, Denver, Los Angeles, and Seattle, the practice of many trauma surgeons is often restrained at university hospitals and most level II trauma centers.
Strong Results
The trauma program at University of Pennsylvania, Pittsburgh, under the leadership of C. William Schwab, MD, the current president of the AAST, has taken the lead in documenting the value of incorporating emergency surgery into trauma/surgical critical care training. The addition of emergency general surgery into a trauma/surgical critical care fellowship increases operative experience and fellow satisfaction.3-6 Emergency general surgery now accounts for 57% of operations performed by their faculty. This helps maintain their operative experience despite a decline in operative trauma volume. Finally, with a careful analysis of performance improvement data, there is no compromise in trauma patient outcomes despite the increased patient load.4-5 This experience has been replicated at other trauma centers and strongly suggests that incorporating emergency general surgery into trauma training increases attractiveness to trainees and maintains high standards of patient care. The question is whether it meets an unfilled need.
Recent experience at Vanderbilt Medical Center suggests that the formal incorporation of emergency general surgery into a service has benefits for patients and the hospital.6 The service brings in more referrals from the surrounding community and increases trauma surgeon operative cases. The elective general surgeons also experience an increase in operations and admissions after removing the disruption of emergency admissions. The hospital benefits by the addition of new patients that frequently require operations and intensive care.
In a recent supplement to the The Hospitalist Larry Wellikson, MD, notes that hospitalists add value by (among other things):
- Providing measurable quality improvement;
- Creating seamless continuity from inpatient to outpatient care, from emergency department to floor, and from ICU to floor;
- Doing things other physicians had given up, such as indigent care and hospital committee functions;
- Creating healthcare teams to improve the working environment; and
- Taking care of acutely ill, complex hospitalized patients.7
We believe that trauma surgeons, or acute care surgeons, exemplify these values. We have provided these services to surgical patients for the past 25 years. Trauma surgeons have been leaders in quality improvement, as demonstrated by the American College of Surgeons Committee on Trauma verification program.
We take care of whoever comes through the door, regardless of acuity, time of day (or night), or payer status. We have always provided comprehensive care for our patients—from involvement in prehospital care and planning, through the emergency department, operating room, ICU, and even post-discharge rehabilitation. This requires an effective healthcare team and a truly multidisciplinary approach with other physicians (orthopedics, neurosurgery, anesthesia), nurses, and others, including respiratory, occupational, and physical therapy.
Conclusion
We see a synergy between hospitalist and acute-care surgeons. Both groups have stepped forward to fill a void in patient care. The redefining of trauma surgery as acute care surgery and the development of dedicated training programs will no doubt benefit current and future surgeons, but our patients will benefit the most. TH
Dr. Spain is professor of surgery and chief of Trauma, Emergency and Critical Care Surgery, Stanford University (California). He is also chairman of the Critical Care Committee, American Association for the Surgery of Trauma. Dr. Jurkovich is professor of surgery at the University of Washington, chief of Trauma and Emergency Surgical Services at Harborview Medical Center, and chairman of the Acute Care Surgeon Committee, American Association for the Surgery of Trauma.
References
- Committee to Develop the Reorganized Specialty of Trauma, Surgical Critical Care, and Emergency Surgery. Acute care surgery: trauma, critical care, and emergency surgery. J Trauma. 2005;58:614-616.
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212-217.
- Pryor JP, Reilly PM, Schwab CW, et al. Integrating emergency general surgery with a trauma service: impact on the care of injured patients. J Trauma. 2004 Sep;57(3):467-471.
- Reilly PM, Schwab CW, Haut ER, et al. Training in trauma surgery: quantitative and qualitative aspects of a new paradigm for fellowship. Ann Surg. 2003 Oct;238(4):596-603.
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004 Jul;199(1):96-101.
- Austin MT, Diaz JJ Jr, Feurer ID, et al. Creating an emergency general surgery service enhances the productivity of trauma surgeons, general surgeons and the hospital. J Trauma. 2005 May;58(5):906-910.
- Wellikson L. Hospitals recognize and reward value. The Hospitalist. 2005;9:3-5.
The Acute Care Surgeon
In the past decade numerous trends and influences have caused organized trauma surgery to re-examine our role in the care of all acutely ill surgical patients and the training of future general surgeons who will care for these patients.1 In this article we’ll briefly review the influences that brought us to this point, the issues we feel need to be addressed, and the solution that trauma surgery has proposed. In many ways, we believe these trends parallel the influences that led to the development of the hospitalists and, thus, call for a surgical equivalent.
Surgical Trends
The development of laparoscopic surgery has had profound influence on surgical practice. Cholecystectomies and appendectomies are generally 23-hour admissions. Even bariatric surgery is now little more than outpatient surgery, with the average length of stay at two days. Along with laparoscopy, breast surgery is now one of the fastest growing surgical subspecialties.
Many surgeons have tailored their practices to a largely outpatient base. There has been an explosion of free-standing surgery centers with a large shift of this low acuity patient population away from hospitals. This follows an overall shift in medicine to ambulatory practice, which is now projected to increase by 24% over the next five to 10 years. Thus, fewer and fewer surgeons have large inpatient practices. There is growing concern about the reluctance of many surgeons to deal with complex, high acuity patients. The obvious exceptions are transplant and trauma surgeons.
In the past decade profound changes in trauma care have also affected the practices of surgeons and the career choices of surgical residents.2 Following the peak of gun-related violence in the early 1990s, there has been a steady and significant decline in penetrating trauma with a concomitant decrease in operations. Slow but steady improvement in motor vehicle passive safety devices has also decreased the incidence of serious injury to the torso following car crashes.
When a solid organ (liver, spleen, kidney) injury does occur after car crash, fall, or assault, the management has largely shifted away from exploratory laparotomy to non-operative management. This has been made possible by improved imaging techniques, careful monitoring in the ICU and judicious use of interventional radiologic techniques of embolization and percutaneous drainage. Currently, some 60% to 80% of liver and spleen injuries are treated with observation or interventional techniques. Although most surgical residents enjoy the challenges of both trauma surgery and critical care, the decline in operative opportunities has limited the appeal of trauma/critical care as a career choice.2
Many trauma surgeons feel there is a convergence of these two issues—a group of patients that may be underserved and an opportunity to enhance the training and desirability of caring for acutely ill surgical patients.3-5 Either through years of experience or formal training, the vast majority of trauma surgeons are highly experienced in evaluating, operating upon, and providing post-operative care for critically ill and injured patients. In fact, the majority of surgical critical care fellowships are based at level 1 trauma centers and are run primarily by trauma surgeons. Thus, trauma surgeons are ideally situated to address these issues.
—Rohit Uppal, MD, MBA
A New Specialty
In 2001 Ron V. Maier, MD, then president of the American Association for the Surgery of Trauma (AAST), commissioned a committee to address these issues and develop an action plan. With broad representation from numerous surgical societies, the committee met several times to consider various training and practice models as potential solutions. After much discussion, the group proposed a model based upon trauma surgery, emergency general surgery, and critical care. This process is outlined in a white paper authored by the committee in 2005.
Basically, the committee recommends the evolution of trauma surgery into a new specialty based on broad training in elective and emergency general surgery, trauma, and critical care surgery. Specific steps to accomplish this goal were outlined by the committee and considerable progress has already been made. After much debate regarding the name, including the consideration of “surgical hospitalists,” the AAST elected to support the name “acute care surgeon.” In fact, this model is how many of us trauma surgeons practice; we take trauma and emergency general surgery call and provide critical care services for these patients.
What was missing from the paradigm was a formal incorporation of emergency general surgery into the training of trauma/surgical critical care fellows and analysis of the benefits of such programs. While this practice paradigm has long been the model at many urban safety net hospitals in cities such as Atlanta, Dallas, Denver, Los Angeles, and Seattle, the practice of many trauma surgeons is often restrained at university hospitals and most level II trauma centers.
Strong Results
The trauma program at University of Pennsylvania, Pittsburgh, under the leadership of C. William Schwab, MD, the current president of the AAST, has taken the lead in documenting the value of incorporating emergency surgery into trauma/surgical critical care training. The addition of emergency general surgery into a trauma/surgical critical care fellowship increases operative experience and fellow satisfaction.3-6 Emergency general surgery now accounts for 57% of operations performed by their faculty. This helps maintain their operative experience despite a decline in operative trauma volume. Finally, with a careful analysis of performance improvement data, there is no compromise in trauma patient outcomes despite the increased patient load.4-5 This experience has been replicated at other trauma centers and strongly suggests that incorporating emergency general surgery into trauma training increases attractiveness to trainees and maintains high standards of patient care. The question is whether it meets an unfilled need.
Recent experience at Vanderbilt Medical Center suggests that the formal incorporation of emergency general surgery into a service has benefits for patients and the hospital.6 The service brings in more referrals from the surrounding community and increases trauma surgeon operative cases. The elective general surgeons also experience an increase in operations and admissions after removing the disruption of emergency admissions. The hospital benefits by the addition of new patients that frequently require operations and intensive care.
In a recent supplement to the The Hospitalist Larry Wellikson, MD, notes that hospitalists add value by (among other things):
- Providing measurable quality improvement;
- Creating seamless continuity from inpatient to outpatient care, from emergency department to floor, and from ICU to floor;
- Doing things other physicians had given up, such as indigent care and hospital committee functions;
- Creating healthcare teams to improve the working environment; and
- Taking care of acutely ill, complex hospitalized patients.7
We believe that trauma surgeons, or acute care surgeons, exemplify these values. We have provided these services to surgical patients for the past 25 years. Trauma surgeons have been leaders in quality improvement, as demonstrated by the American College of Surgeons Committee on Trauma verification program.
We take care of whoever comes through the door, regardless of acuity, time of day (or night), or payer status. We have always provided comprehensive care for our patients—from involvement in prehospital care and planning, through the emergency department, operating room, ICU, and even post-discharge rehabilitation. This requires an effective healthcare team and a truly multidisciplinary approach with other physicians (orthopedics, neurosurgery, anesthesia), nurses, and others, including respiratory, occupational, and physical therapy.


Conclusion
We see a synergy between hospitalist and acute-care surgeons. Both groups have stepped forward to fill a void in patient care. The redefining of trauma surgery as acute care surgery and the development of dedicated training programs will no doubt benefit current and future surgeons, but our patients will benefit the most. TH
Dr. Spain is professor of surgery and chief of Trauma, Emergency and Critical Care Surgery, Stanford University (California). He is also chairman of the Critical Care Committee, American Association for the Surgery of Trauma. Dr. Jurkovich is professor of surgery at the University of Washington, chief of Trauma and Emergency Surgical Services at Harborview Medical Center, and chairman of the Acute Care Surgeon Committee, American Association for the Surgery of Trauma.
References
- Committee to Develop the Reorganized Specialty of Trauma, Surgical Critical Care, and Emergency Surgery. Acute care surgery: trauma, critical care, and emergency surgery. J Trauma. 2005;58:614-616.
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212-217.
- Pryor JP, Reilly PM, Schwab CW, et al. Integrating emergency general surgery with a trauma service: impact on the care of injured patients. J Trauma. 2004 Sep;57(3):467-471.
- Reilly PM, Schwab CW, Haut ER, et al. Training in trauma surgery: quantitative and qualitative aspects of a new paradigm for fellowship. Ann Surg. 2003 Oct;238(4):596-603.
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004 Jul;199(1):96-101.
- Austin MT, Diaz JJ Jr, Feurer ID, et al. Creating an emergency general surgery service enhances the productivity of trauma surgeons, general surgeons and the hospital. J Trauma. 2005 May;58(5):906-910.
- Wellikson L. Hospitals recognize and reward value. The Hospitalist. 2005;9:3-5.
In the past decade numerous trends and influences have caused organized trauma surgery to re-examine our role in the care of all acutely ill surgical patients and the training of future general surgeons who will care for these patients.1 In this article we’ll briefly review the influences that brought us to this point, the issues we feel need to be addressed, and the solution that trauma surgery has proposed. In many ways, we believe these trends parallel the influences that led to the development of the hospitalists and, thus, call for a surgical equivalent.
Surgical Trends
The development of laparoscopic surgery has had profound influence on surgical practice. Cholecystectomies and appendectomies are generally 23-hour admissions. Even bariatric surgery is now little more than outpatient surgery, with the average length of stay at two days. Along with laparoscopy, breast surgery is now one of the fastest growing surgical subspecialties.
Many surgeons have tailored their practices to a largely outpatient base. There has been an explosion of free-standing surgery centers with a large shift of this low acuity patient population away from hospitals. This follows an overall shift in medicine to ambulatory practice, which is now projected to increase by 24% over the next five to 10 years. Thus, fewer and fewer surgeons have large inpatient practices. There is growing concern about the reluctance of many surgeons to deal with complex, high acuity patients. The obvious exceptions are transplant and trauma surgeons.
In the past decade profound changes in trauma care have also affected the practices of surgeons and the career choices of surgical residents.2 Following the peak of gun-related violence in the early 1990s, there has been a steady and significant decline in penetrating trauma with a concomitant decrease in operations. Slow but steady improvement in motor vehicle passive safety devices has also decreased the incidence of serious injury to the torso following car crashes.
When a solid organ (liver, spleen, kidney) injury does occur after car crash, fall, or assault, the management has largely shifted away from exploratory laparotomy to non-operative management. This has been made possible by improved imaging techniques, careful monitoring in the ICU and judicious use of interventional radiologic techniques of embolization and percutaneous drainage. Currently, some 60% to 80% of liver and spleen injuries are treated with observation or interventional techniques. Although most surgical residents enjoy the challenges of both trauma surgery and critical care, the decline in operative opportunities has limited the appeal of trauma/critical care as a career choice.2
Many trauma surgeons feel there is a convergence of these two issues—a group of patients that may be underserved and an opportunity to enhance the training and desirability of caring for acutely ill surgical patients.3-5 Either through years of experience or formal training, the vast majority of trauma surgeons are highly experienced in evaluating, operating upon, and providing post-operative care for critically ill and injured patients. In fact, the majority of surgical critical care fellowships are based at level 1 trauma centers and are run primarily by trauma surgeons. Thus, trauma surgeons are ideally situated to address these issues.
—Rohit Uppal, MD, MBA
A New Specialty
In 2001 Ron V. Maier, MD, then president of the American Association for the Surgery of Trauma (AAST), commissioned a committee to address these issues and develop an action plan. With broad representation from numerous surgical societies, the committee met several times to consider various training and practice models as potential solutions. After much discussion, the group proposed a model based upon trauma surgery, emergency general surgery, and critical care. This process is outlined in a white paper authored by the committee in 2005.
Basically, the committee recommends the evolution of trauma surgery into a new specialty based on broad training in elective and emergency general surgery, trauma, and critical care surgery. Specific steps to accomplish this goal were outlined by the committee and considerable progress has already been made. After much debate regarding the name, including the consideration of “surgical hospitalists,” the AAST elected to support the name “acute care surgeon.” In fact, this model is how many of us trauma surgeons practice; we take trauma and emergency general surgery call and provide critical care services for these patients.
What was missing from the paradigm was a formal incorporation of emergency general surgery into the training of trauma/surgical critical care fellows and analysis of the benefits of such programs. While this practice paradigm has long been the model at many urban safety net hospitals in cities such as Atlanta, Dallas, Denver, Los Angeles, and Seattle, the practice of many trauma surgeons is often restrained at university hospitals and most level II trauma centers.
Strong Results
The trauma program at University of Pennsylvania, Pittsburgh, under the leadership of C. William Schwab, MD, the current president of the AAST, has taken the lead in documenting the value of incorporating emergency surgery into trauma/surgical critical care training. The addition of emergency general surgery into a trauma/surgical critical care fellowship increases operative experience and fellow satisfaction.3-6 Emergency general surgery now accounts for 57% of operations performed by their faculty. This helps maintain their operative experience despite a decline in operative trauma volume. Finally, with a careful analysis of performance improvement data, there is no compromise in trauma patient outcomes despite the increased patient load.4-5 This experience has been replicated at other trauma centers and strongly suggests that incorporating emergency general surgery into trauma training increases attractiveness to trainees and maintains high standards of patient care. The question is whether it meets an unfilled need.
Recent experience at Vanderbilt Medical Center suggests that the formal incorporation of emergency general surgery into a service has benefits for patients and the hospital.6 The service brings in more referrals from the surrounding community and increases trauma surgeon operative cases. The elective general surgeons also experience an increase in operations and admissions after removing the disruption of emergency admissions. The hospital benefits by the addition of new patients that frequently require operations and intensive care.
In a recent supplement to the The Hospitalist Larry Wellikson, MD, notes that hospitalists add value by (among other things):
- Providing measurable quality improvement;
- Creating seamless continuity from inpatient to outpatient care, from emergency department to floor, and from ICU to floor;
- Doing things other physicians had given up, such as indigent care and hospital committee functions;
- Creating healthcare teams to improve the working environment; and
- Taking care of acutely ill, complex hospitalized patients.7
We believe that trauma surgeons, or acute care surgeons, exemplify these values. We have provided these services to surgical patients for the past 25 years. Trauma surgeons have been leaders in quality improvement, as demonstrated by the American College of Surgeons Committee on Trauma verification program.
We take care of whoever comes through the door, regardless of acuity, time of day (or night), or payer status. We have always provided comprehensive care for our patients—from involvement in prehospital care and planning, through the emergency department, operating room, ICU, and even post-discharge rehabilitation. This requires an effective healthcare team and a truly multidisciplinary approach with other physicians (orthopedics, neurosurgery, anesthesia), nurses, and others, including respiratory, occupational, and physical therapy.
Conclusion
We see a synergy between hospitalist and acute-care surgeons. Both groups have stepped forward to fill a void in patient care. The redefining of trauma surgery as acute care surgery and the development of dedicated training programs will no doubt benefit current and future surgeons, but our patients will benefit the most. TH
Dr. Spain is professor of surgery and chief of Trauma, Emergency and Critical Care Surgery, Stanford University (California). He is also chairman of the Critical Care Committee, American Association for the Surgery of Trauma. Dr. Jurkovich is professor of surgery at the University of Washington, chief of Trauma and Emergency Surgical Services at Harborview Medical Center, and chairman of the Acute Care Surgeon Committee, American Association for the Surgery of Trauma.
References
- Committee to Develop the Reorganized Specialty of Trauma, Surgical Critical Care, and Emergency Surgery. Acute care surgery: trauma, critical care, and emergency surgery. J Trauma. 2005;58:614-616.
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212-217.
- Pryor JP, Reilly PM, Schwab CW, et al. Integrating emergency general surgery with a trauma service: impact on the care of injured patients. J Trauma. 2004 Sep;57(3):467-471.
- Reilly PM, Schwab CW, Haut ER, et al. Training in trauma surgery: quantitative and qualitative aspects of a new paradigm for fellowship. Ann Surg. 2003 Oct;238(4):596-603.
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004 Jul;199(1):96-101.
- Austin MT, Diaz JJ Jr, Feurer ID, et al. Creating an emergency general surgery service enhances the productivity of trauma surgeons, general surgeons and the hospital. J Trauma. 2005 May;58(5):906-910.
- Wellikson L. Hospitals recognize and reward value. The Hospitalist. 2005;9:3-5.
In the past decade numerous trends and influences have caused organized trauma surgery to re-examine our role in the care of all acutely ill surgical patients and the training of future general surgeons who will care for these patients.1 In this article we’ll briefly review the influences that brought us to this point, the issues we feel need to be addressed, and the solution that trauma surgery has proposed. In many ways, we believe these trends parallel the influences that led to the development of the hospitalists and, thus, call for a surgical equivalent.
Surgical Trends
The development of laparoscopic surgery has had profound influence on surgical practice. Cholecystectomies and appendectomies are generally 23-hour admissions. Even bariatric surgery is now little more than outpatient surgery, with the average length of stay at two days. Along with laparoscopy, breast surgery is now one of the fastest growing surgical subspecialties.
Many surgeons have tailored their practices to a largely outpatient base. There has been an explosion of free-standing surgery centers with a large shift of this low acuity patient population away from hospitals. This follows an overall shift in medicine to ambulatory practice, which is now projected to increase by 24% over the next five to 10 years. Thus, fewer and fewer surgeons have large inpatient practices. There is growing concern about the reluctance of many surgeons to deal with complex, high acuity patients. The obvious exceptions are transplant and trauma surgeons.
In the past decade profound changes in trauma care have also affected the practices of surgeons and the career choices of surgical residents.2 Following the peak of gun-related violence in the early 1990s, there has been a steady and significant decline in penetrating trauma with a concomitant decrease in operations. Slow but steady improvement in motor vehicle passive safety devices has also decreased the incidence of serious injury to the torso following car crashes.
When a solid organ (liver, spleen, kidney) injury does occur after car crash, fall, or assault, the management has largely shifted away from exploratory laparotomy to non-operative management. This has been made possible by improved imaging techniques, careful monitoring in the ICU and judicious use of interventional radiologic techniques of embolization and percutaneous drainage. Currently, some 60% to 80% of liver and spleen injuries are treated with observation or interventional techniques. Although most surgical residents enjoy the challenges of both trauma surgery and critical care, the decline in operative opportunities has limited the appeal of trauma/critical care as a career choice.2
Many trauma surgeons feel there is a convergence of these two issues—a group of patients that may be underserved and an opportunity to enhance the training and desirability of caring for acutely ill surgical patients.3-5 Either through years of experience or formal training, the vast majority of trauma surgeons are highly experienced in evaluating, operating upon, and providing post-operative care for critically ill and injured patients. In fact, the majority of surgical critical care fellowships are based at level 1 trauma centers and are run primarily by trauma surgeons. Thus, trauma surgeons are ideally situated to address these issues.
—Rohit Uppal, MD, MBA
A New Specialty
In 2001 Ron V. Maier, MD, then president of the American Association for the Surgery of Trauma (AAST), commissioned a committee to address these issues and develop an action plan. With broad representation from numerous surgical societies, the committee met several times to consider various training and practice models as potential solutions. After much discussion, the group proposed a model based upon trauma surgery, emergency general surgery, and critical care. This process is outlined in a white paper authored by the committee in 2005.
Basically, the committee recommends the evolution of trauma surgery into a new specialty based on broad training in elective and emergency general surgery, trauma, and critical care surgery. Specific steps to accomplish this goal were outlined by the committee and considerable progress has already been made. After much debate regarding the name, including the consideration of “surgical hospitalists,” the AAST elected to support the name “acute care surgeon.” In fact, this model is how many of us trauma surgeons practice; we take trauma and emergency general surgery call and provide critical care services for these patients.
What was missing from the paradigm was a formal incorporation of emergency general surgery into the training of trauma/surgical critical care fellows and analysis of the benefits of such programs. While this practice paradigm has long been the model at many urban safety net hospitals in cities such as Atlanta, Dallas, Denver, Los Angeles, and Seattle, the practice of many trauma surgeons is often restrained at university hospitals and most level II trauma centers.
Strong Results
The trauma program at University of Pennsylvania, Pittsburgh, under the leadership of C. William Schwab, MD, the current president of the AAST, has taken the lead in documenting the value of incorporating emergency surgery into trauma/surgical critical care training. The addition of emergency general surgery into a trauma/surgical critical care fellowship increases operative experience and fellow satisfaction.3-6 Emergency general surgery now accounts for 57% of operations performed by their faculty. This helps maintain their operative experience despite a decline in operative trauma volume. Finally, with a careful analysis of performance improvement data, there is no compromise in trauma patient outcomes despite the increased patient load.4-5 This experience has been replicated at other trauma centers and strongly suggests that incorporating emergency general surgery into trauma training increases attractiveness to trainees and maintains high standards of patient care. The question is whether it meets an unfilled need.
Recent experience at Vanderbilt Medical Center suggests that the formal incorporation of emergency general surgery into a service has benefits for patients and the hospital.6 The service brings in more referrals from the surrounding community and increases trauma surgeon operative cases. The elective general surgeons also experience an increase in operations and admissions after removing the disruption of emergency admissions. The hospital benefits by the addition of new patients that frequently require operations and intensive care.
In a recent supplement to the The Hospitalist Larry Wellikson, MD, notes that hospitalists add value by (among other things):
- Providing measurable quality improvement;
- Creating seamless continuity from inpatient to outpatient care, from emergency department to floor, and from ICU to floor;
- Doing things other physicians had given up, such as indigent care and hospital committee functions;
- Creating healthcare teams to improve the working environment; and
- Taking care of acutely ill, complex hospitalized patients.7
We believe that trauma surgeons, or acute care surgeons, exemplify these values. We have provided these services to surgical patients for the past 25 years. Trauma surgeons have been leaders in quality improvement, as demonstrated by the American College of Surgeons Committee on Trauma verification program.
We take care of whoever comes through the door, regardless of acuity, time of day (or night), or payer status. We have always provided comprehensive care for our patients—from involvement in prehospital care and planning, through the emergency department, operating room, ICU, and even post-discharge rehabilitation. This requires an effective healthcare team and a truly multidisciplinary approach with other physicians (orthopedics, neurosurgery, anesthesia), nurses, and others, including respiratory, occupational, and physical therapy.
Conclusion
We see a synergy between hospitalist and acute-care surgeons. Both groups have stepped forward to fill a void in patient care. The redefining of trauma surgery as acute care surgery and the development of dedicated training programs will no doubt benefit current and future surgeons, but our patients will benefit the most. TH
Dr. Spain is professor of surgery and chief of Trauma, Emergency and Critical Care Surgery, Stanford University (California). He is also chairman of the Critical Care Committee, American Association for the Surgery of Trauma. Dr. Jurkovich is professor of surgery at the University of Washington, chief of Trauma and Emergency Surgical Services at Harborview Medical Center, and chairman of the Acute Care Surgeon Committee, American Association for the Surgery of Trauma.
References
- Committee to Develop the Reorganized Specialty of Trauma, Surgical Critical Care, and Emergency Surgery. Acute care surgery: trauma, critical care, and emergency surgery. J Trauma. 2005;58:614-616.
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212-217.
- Pryor JP, Reilly PM, Schwab CW, et al. Integrating emergency general surgery with a trauma service: impact on the care of injured patients. J Trauma. 2004 Sep;57(3):467-471.
- Reilly PM, Schwab CW, Haut ER, et al. Training in trauma surgery: quantitative and qualitative aspects of a new paradigm for fellowship. Ann Surg. 2003 Oct;238(4):596-603.
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004 Jul;199(1):96-101.
- Austin MT, Diaz JJ Jr, Feurer ID, et al. Creating an emergency general surgery service enhances the productivity of trauma surgeons, general surgeons and the hospital. J Trauma. 2005 May;58(5):906-910.
- Wellikson L. Hospitals recognize and reward value. The Hospitalist. 2005;9:3-5.