User login
Gastric Involvement in NSG
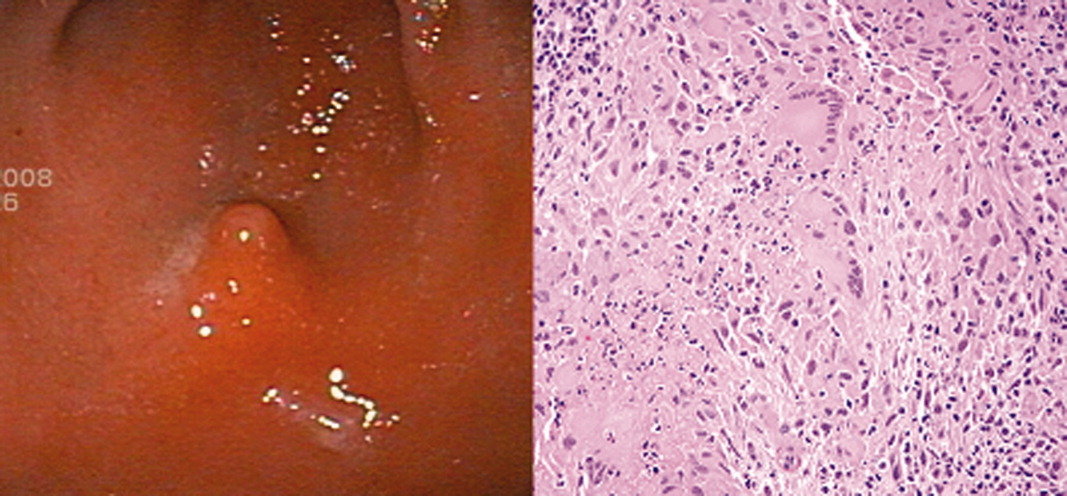
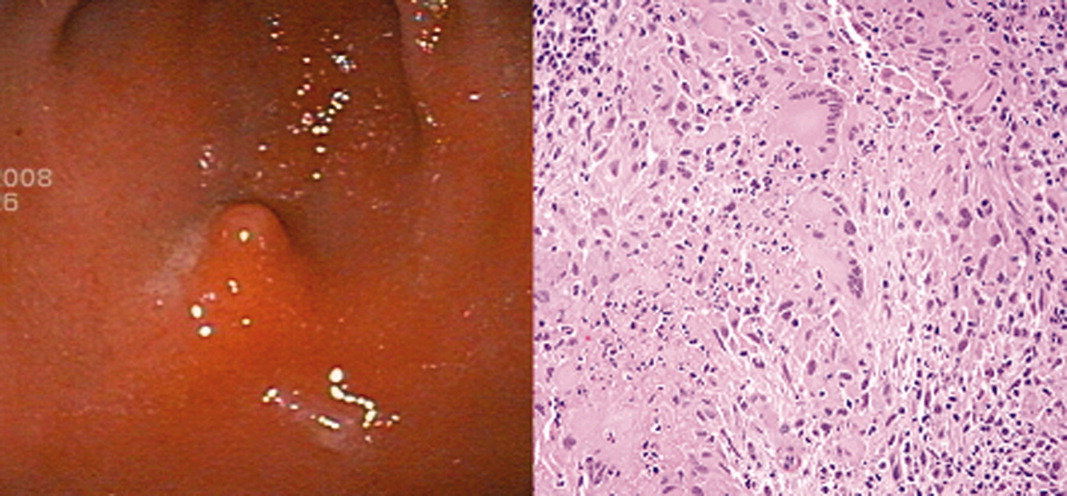
Necrotizing sarcoid granulomatosis (NSG) is an immune system disorder characterized by necrotizing granulomas, as opposed to noncaseating granulomas in classical sarcoidosis. Over the past 3 decades there have been over 120 reported cases of NSG with pulmonary and extrapulmonary involvement.1 We present a patient found to have histological evidence of necrotizing granuloma in her gastric antrum, and we believe this is the first Case Report of NSG involving the stomach.
Case Report
A 21‐year‐old African‐American female first presented to an outside hospital with fever, epigastric pain, shortness of breath, and headache. Two days later she complained of nonbloody, nonbilious vomiting, and was found to have leukocytosis (17,770 cells/m3), elevated lipase (224 U/L), elevated C‐reactive protein (14.7 mg/L), and an inflamed pancreas on computed tomography (CT). She was treated conservatively for pancreatitis and started on ampicillin/sulbactam. After 2 contrast CT scans on consecutive days, she developed acute renal failure (creatinine 2.0 mg/dL compared to baseline of 1.0 mg/dL), and was transferred to our hospital for further evaluation and management.
Upon transfer, the patient's temperature was 37.0C, pulse was 102 beats/minute, blood pressure was 141/84 mm Hg, and oxygen saturation was 94%. On examination, she was tender to palpation in her epigastrium and right upper quadrant, but the remainder of the physical exam was unremarkable. She was started on moxifloxacin and managed with intravenous (IV) fluid hydration and pain control. Within 3 days, CT showed resolving pancreatitis, magnetic resonance cholangiopancreatography (MRCP) was negative, and her creatinine began normalizing (1.3 mg/dL). Nonetheless, she continued to complain of abdominal pain, shortness of breath, and intermittent low‐grade fevers. She then also developed bilateral panuveitis requiring high‐dose steroid eye drops.
Chest x‐ray showed subtle bilateral nodular and bronchiolitic infiltrates with no evidence of enlarged hilar nodes, and subsequent bronchoscopy showed no abnormalities. Additional workup included negative blood and urine cultures, purified protein derivative (PPD), and Clostridium difficile assay; as well as negative human immunodeficiency virus (HIV), cryptococcus, Helicobacter pylori, Borellia burgdorferi, syphilis (fluorescent treponemal antibody), aspergillus, histoplasma, and rheumatological serologies. Her white blood count (20,900 cells/m3), C‐reactive protein (6.6 mg/L), and erythrocyte sedimentation rate (100 mm/hour) remained elevated.
The patient continued to complain of epigastric pain. Repeat abdominal CT scan showed large retroperitoneal and mesenteric lymph nodes, and esophagogastroduodenoscopy (EGD) showed gastritis with an antral nodule (Figure 1). Biopsy of the nodule revealed a necrotizing granuloma with mixed cellular infiltrate. Biopsy stains were negative for bacteria, borellia, treponemes, acid‐fast bacilli, and fungi. The patient was diagnosed with necrotizing sarcoid granulomatosis and started on an oral prednisone taper. She responded to steroid treatment with prompt resolution of her uveitis, shortness of breath, abdominal pain, and fevers. She was discharged following treatment, has continued to do well, and is seen regularly at the sarcoid clinic for follow‐up.
Discussion
NSG was first characterized as a distinct variation from sarcoidosis by Liebow2 in 1973, and was noted to have 3 characteristic differences: (1) histological evidence of sarcoid‐appearing granuloma and necrosis, (2) pulmonary nodules without hilar lymphadenopathy on imaging, and (3) a clinically benign course. Over the past 3 decades, there have been more than 120 cases of reported NSG involving the lungs, gastrointestinal tract, kidney, skin, and central nervous system.1 Since Liebow's2 description, newly reported NSG cases have generally been found to be consistent with the aforementioned criteria, although hilar lymphadenopathy may be particularly more common than previously thought. One review noted a range of 8% to 79% prevalence of hilar lymphadenopathy in reported NSG series.3 Therefore, while hilar lymphadenopathy still currently appears to be less common in NSG than in typical sarcoidosis, its presence should not rule out the diagnosis.
Our patient's history is consistent with Liebow's2 criteria since she had histological evidence of necrotizing granuloma and pulmonary involvement without hilar lymphadenopathy, and responded promptly to steroid treatment. To our knowledge, this is the first case of NSG reported in the stomach.
While less than 1% of sarcoid patients are reported to have gastrointestinal involvement, all of these cases have either been noncaseating granulomas (classical sarcoidosis) or were found outside the stomach.1, 4, 5 Most of the data regarding sarcoid symptomatology and treatment are derived from reports on classical sarcoidosis. In classical sarcoidosis, there is gastric antral involvement in approximately 10% of patients with systemic disease.4 These patients may present with nausea, vomiting, and weight loss, and are often effectively treated with a single dose of prednisone 30 to 40 mg followed by a maintenance dose of 10 to 15 mg daily over 6 months.5 Less data are available regarding necrotizing sarcoid presentation and treatment, especially with regard to gastrointestinal involvement.
We hope to raise awareness regarding: (1) the variation in noncaseating versus necrotizing sarcoid‐type disorders, (2) the benefit of steroid treatment once infectious etiologies are ruled out, and (3) the potential for further extrapulmonary involvement in previously unreported organ systems.
- ,,.Necrotizing sarcoid granulomatosis mimicking an intracranial neoplasm: clinicopathologic features and review of the literature.Mod Pathol.2000;13(8)909–913.
- .Pulmonary angiitis and granulomatosis.Am J Respir Dis.1973;108:1–18.
- ,,,.Pulmonary angiitis and granulomatosis: radiologic‐pathologic correlation.Radiographics.1998;18(3):687–710.
- ,,, et al.Multiple antral ulcers in gastric sarcoid.J Clin Gastroenterol.1997;24(2):97–99.
- ,,.Gastric sarcoidosis: a case report and review of the literature.South Med J.2007;100(3):301–303.
Necrotizing sarcoid granulomatosis (NSG) is an immune system disorder characterized by necrotizing granulomas, as opposed to noncaseating granulomas in classical sarcoidosis. Over the past 3 decades there have been over 120 reported cases of NSG with pulmonary and extrapulmonary involvement.1 We present a patient found to have histological evidence of necrotizing granuloma in her gastric antrum, and we believe this is the first Case Report of NSG involving the stomach.
Case Report
A 21‐year‐old African‐American female first presented to an outside hospital with fever, epigastric pain, shortness of breath, and headache. Two days later she complained of nonbloody, nonbilious vomiting, and was found to have leukocytosis (17,770 cells/m3), elevated lipase (224 U/L), elevated C‐reactive protein (14.7 mg/L), and an inflamed pancreas on computed tomography (CT). She was treated conservatively for pancreatitis and started on ampicillin/sulbactam. After 2 contrast CT scans on consecutive days, she developed acute renal failure (creatinine 2.0 mg/dL compared to baseline of 1.0 mg/dL), and was transferred to our hospital for further evaluation and management.
Upon transfer, the patient's temperature was 37.0C, pulse was 102 beats/minute, blood pressure was 141/84 mm Hg, and oxygen saturation was 94%. On examination, she was tender to palpation in her epigastrium and right upper quadrant, but the remainder of the physical exam was unremarkable. She was started on moxifloxacin and managed with intravenous (IV) fluid hydration and pain control. Within 3 days, CT showed resolving pancreatitis, magnetic resonance cholangiopancreatography (MRCP) was negative, and her creatinine began normalizing (1.3 mg/dL). Nonetheless, she continued to complain of abdominal pain, shortness of breath, and intermittent low‐grade fevers. She then also developed bilateral panuveitis requiring high‐dose steroid eye drops.
Chest x‐ray showed subtle bilateral nodular and bronchiolitic infiltrates with no evidence of enlarged hilar nodes, and subsequent bronchoscopy showed no abnormalities. Additional workup included negative blood and urine cultures, purified protein derivative (PPD), and Clostridium difficile assay; as well as negative human immunodeficiency virus (HIV), cryptococcus, Helicobacter pylori, Borellia burgdorferi, syphilis (fluorescent treponemal antibody), aspergillus, histoplasma, and rheumatological serologies. Her white blood count (20,900 cells/m3), C‐reactive protein (6.6 mg/L), and erythrocyte sedimentation rate (100 mm/hour) remained elevated.
The patient continued to complain of epigastric pain. Repeat abdominal CT scan showed large retroperitoneal and mesenteric lymph nodes, and esophagogastroduodenoscopy (EGD) showed gastritis with an antral nodule (Figure 1). Biopsy of the nodule revealed a necrotizing granuloma with mixed cellular infiltrate. Biopsy stains were negative for bacteria, borellia, treponemes, acid‐fast bacilli, and fungi. The patient was diagnosed with necrotizing sarcoid granulomatosis and started on an oral prednisone taper. She responded to steroid treatment with prompt resolution of her uveitis, shortness of breath, abdominal pain, and fevers. She was discharged following treatment, has continued to do well, and is seen regularly at the sarcoid clinic for follow‐up.
Discussion
NSG was first characterized as a distinct variation from sarcoidosis by Liebow2 in 1973, and was noted to have 3 characteristic differences: (1) histological evidence of sarcoid‐appearing granuloma and necrosis, (2) pulmonary nodules without hilar lymphadenopathy on imaging, and (3) a clinically benign course. Over the past 3 decades, there have been more than 120 cases of reported NSG involving the lungs, gastrointestinal tract, kidney, skin, and central nervous system.1 Since Liebow's2 description, newly reported NSG cases have generally been found to be consistent with the aforementioned criteria, although hilar lymphadenopathy may be particularly more common than previously thought. One review noted a range of 8% to 79% prevalence of hilar lymphadenopathy in reported NSG series.3 Therefore, while hilar lymphadenopathy still currently appears to be less common in NSG than in typical sarcoidosis, its presence should not rule out the diagnosis.
Our patient's history is consistent with Liebow's2 criteria since she had histological evidence of necrotizing granuloma and pulmonary involvement without hilar lymphadenopathy, and responded promptly to steroid treatment. To our knowledge, this is the first case of NSG reported in the stomach.
While less than 1% of sarcoid patients are reported to have gastrointestinal involvement, all of these cases have either been noncaseating granulomas (classical sarcoidosis) or were found outside the stomach.1, 4, 5 Most of the data regarding sarcoid symptomatology and treatment are derived from reports on classical sarcoidosis. In classical sarcoidosis, there is gastric antral involvement in approximately 10% of patients with systemic disease.4 These patients may present with nausea, vomiting, and weight loss, and are often effectively treated with a single dose of prednisone 30 to 40 mg followed by a maintenance dose of 10 to 15 mg daily over 6 months.5 Less data are available regarding necrotizing sarcoid presentation and treatment, especially with regard to gastrointestinal involvement.
We hope to raise awareness regarding: (1) the variation in noncaseating versus necrotizing sarcoid‐type disorders, (2) the benefit of steroid treatment once infectious etiologies are ruled out, and (3) the potential for further extrapulmonary involvement in previously unreported organ systems.
Necrotizing sarcoid granulomatosis (NSG) is an immune system disorder characterized by necrotizing granulomas, as opposed to noncaseating granulomas in classical sarcoidosis. Over the past 3 decades there have been over 120 reported cases of NSG with pulmonary and extrapulmonary involvement.1 We present a patient found to have histological evidence of necrotizing granuloma in her gastric antrum, and we believe this is the first Case Report of NSG involving the stomach.
Case Report
A 21‐year‐old African‐American female first presented to an outside hospital with fever, epigastric pain, shortness of breath, and headache. Two days later she complained of nonbloody, nonbilious vomiting, and was found to have leukocytosis (17,770 cells/m3), elevated lipase (224 U/L), elevated C‐reactive protein (14.7 mg/L), and an inflamed pancreas on computed tomography (CT). She was treated conservatively for pancreatitis and started on ampicillin/sulbactam. After 2 contrast CT scans on consecutive days, she developed acute renal failure (creatinine 2.0 mg/dL compared to baseline of 1.0 mg/dL), and was transferred to our hospital for further evaluation and management.
Upon transfer, the patient's temperature was 37.0C, pulse was 102 beats/minute, blood pressure was 141/84 mm Hg, and oxygen saturation was 94%. On examination, she was tender to palpation in her epigastrium and right upper quadrant, but the remainder of the physical exam was unremarkable. She was started on moxifloxacin and managed with intravenous (IV) fluid hydration and pain control. Within 3 days, CT showed resolving pancreatitis, magnetic resonance cholangiopancreatography (MRCP) was negative, and her creatinine began normalizing (1.3 mg/dL). Nonetheless, she continued to complain of abdominal pain, shortness of breath, and intermittent low‐grade fevers. She then also developed bilateral panuveitis requiring high‐dose steroid eye drops.
Chest x‐ray showed subtle bilateral nodular and bronchiolitic infiltrates with no evidence of enlarged hilar nodes, and subsequent bronchoscopy showed no abnormalities. Additional workup included negative blood and urine cultures, purified protein derivative (PPD), and Clostridium difficile assay; as well as negative human immunodeficiency virus (HIV), cryptococcus, Helicobacter pylori, Borellia burgdorferi, syphilis (fluorescent treponemal antibody), aspergillus, histoplasma, and rheumatological serologies. Her white blood count (20,900 cells/m3), C‐reactive protein (6.6 mg/L), and erythrocyte sedimentation rate (100 mm/hour) remained elevated.
The patient continued to complain of epigastric pain. Repeat abdominal CT scan showed large retroperitoneal and mesenteric lymph nodes, and esophagogastroduodenoscopy (EGD) showed gastritis with an antral nodule (Figure 1). Biopsy of the nodule revealed a necrotizing granuloma with mixed cellular infiltrate. Biopsy stains were negative for bacteria, borellia, treponemes, acid‐fast bacilli, and fungi. The patient was diagnosed with necrotizing sarcoid granulomatosis and started on an oral prednisone taper. She responded to steroid treatment with prompt resolution of her uveitis, shortness of breath, abdominal pain, and fevers. She was discharged following treatment, has continued to do well, and is seen regularly at the sarcoid clinic for follow‐up.
Discussion
NSG was first characterized as a distinct variation from sarcoidosis by Liebow2 in 1973, and was noted to have 3 characteristic differences: (1) histological evidence of sarcoid‐appearing granuloma and necrosis, (2) pulmonary nodules without hilar lymphadenopathy on imaging, and (3) a clinically benign course. Over the past 3 decades, there have been more than 120 cases of reported NSG involving the lungs, gastrointestinal tract, kidney, skin, and central nervous system.1 Since Liebow's2 description, newly reported NSG cases have generally been found to be consistent with the aforementioned criteria, although hilar lymphadenopathy may be particularly more common than previously thought. One review noted a range of 8% to 79% prevalence of hilar lymphadenopathy in reported NSG series.3 Therefore, while hilar lymphadenopathy still currently appears to be less common in NSG than in typical sarcoidosis, its presence should not rule out the diagnosis.
Our patient's history is consistent with Liebow's2 criteria since she had histological evidence of necrotizing granuloma and pulmonary involvement without hilar lymphadenopathy, and responded promptly to steroid treatment. To our knowledge, this is the first case of NSG reported in the stomach.
While less than 1% of sarcoid patients are reported to have gastrointestinal involvement, all of these cases have either been noncaseating granulomas (classical sarcoidosis) or were found outside the stomach.1, 4, 5 Most of the data regarding sarcoid symptomatology and treatment are derived from reports on classical sarcoidosis. In classical sarcoidosis, there is gastric antral involvement in approximately 10% of patients with systemic disease.4 These patients may present with nausea, vomiting, and weight loss, and are often effectively treated with a single dose of prednisone 30 to 40 mg followed by a maintenance dose of 10 to 15 mg daily over 6 months.5 Less data are available regarding necrotizing sarcoid presentation and treatment, especially with regard to gastrointestinal involvement.
We hope to raise awareness regarding: (1) the variation in noncaseating versus necrotizing sarcoid‐type disorders, (2) the benefit of steroid treatment once infectious etiologies are ruled out, and (3) the potential for further extrapulmonary involvement in previously unreported organ systems.
- ,,.Necrotizing sarcoid granulomatosis mimicking an intracranial neoplasm: clinicopathologic features and review of the literature.Mod Pathol.2000;13(8)909–913.
- .Pulmonary angiitis and granulomatosis.Am J Respir Dis.1973;108:1–18.
- ,,,.Pulmonary angiitis and granulomatosis: radiologic‐pathologic correlation.Radiographics.1998;18(3):687–710.
- ,,, et al.Multiple antral ulcers in gastric sarcoid.J Clin Gastroenterol.1997;24(2):97–99.
- ,,.Gastric sarcoidosis: a case report and review of the literature.South Med J.2007;100(3):301–303.
- ,,.Necrotizing sarcoid granulomatosis mimicking an intracranial neoplasm: clinicopathologic features and review of the literature.Mod Pathol.2000;13(8)909–913.
- .Pulmonary angiitis and granulomatosis.Am J Respir Dis.1973;108:1–18.
- ,,,.Pulmonary angiitis and granulomatosis: radiologic‐pathologic correlation.Radiographics.1998;18(3):687–710.
- ,,, et al.Multiple antral ulcers in gastric sarcoid.J Clin Gastroenterol.1997;24(2):97–99.
- ,,.Gastric sarcoidosis: a case report and review of the literature.South Med J.2007;100(3):301–303.
Nonphysicians in Hospital Medicine
Ford and Britting's1 editorial in this month's Journal of Hospital Medicine raises important questions concerning the use of nonphysician providers in hospital medicine. They focus primarily on the use of mid‐level providers (MLPs), namely physician‐assistants (PAs) and nurse practitioners (NPs), as a potential solution to the current physician workforce shortages in our field. While we acknowledge the challenges of meeting workforce needs, we also believe that much is unknown about the optimal use of MLPs on inpatient general medicine services and it is premature to tout MLPs as the solution to hospital medicine staffing problems. This is especially true in those hospitals where hospitalists care for complex, general medical patients with a wide variety of medical conditions, a trend that is especially common in academic medical centers.2
This article discusses the current literature, our own experiences with MLPs, and suggests some future initiatives that might help better integrate MLPs into hospital medicine.
The Literature on MLPs in Inpatient Venues
The existing literature on the use of MLPs in inpatient venues is quite limited, and a recent review, while suggesting that the existing literature does describe benefits of MLPs in the inpatient setting, also states that the overall quality of the evidence is quite poor and that many studies suffer from significant limitations, including small populations, limited patient mixes, use of selected settings, and short durations of outcome assessment.3
Ford and Britting,1 in their article, cite several studies46 as evidence that a MLP model of care either improved outcomes or provided cost benefits. Each of these studies has important limitations that are worth examining.
The study by Myers et al.4 described the use of MLPs in a chest pain unit. NPs partnered with hospitalists to care for a low‐acuity chest pain population. In addition, 5 NPs only staffed the unit during daytime weekday hours. Off‐hour and weekend staffing was accomplished through the use of resident physicians. Notably, the work suggests the service only admitted 113 low‐risk patients over 10 months. The service was staffed by 3 full‐time equivalent (FTE) NPs in addition to involving hospitalists during the day. It is not surprising, given the extremely low volume of patients coupled with a daytime‐only focus, that this service showed efficiency gains. In addition, given the service was only staffed by NPs 40 hours a week and by resident physicians on nights and weekends, the true cost of such an intervention needs to take into account the full cost of 24/7 coverage. In addition, the model of using residents to cover nonteaching patients is no longer permitted by the current Accreditation Council for Graduate Medical Education (ACGME) Internal Medicine Residency Requirements7 and thus implementation of a model such as this in 2009 would require alternative means of nighttime coverage.
The study by Nishimura et al.,5 also describing the use of MLPs in cardiovascular care, has important caveats that make full assessment of the model impossible. The model describes the implementation of a care team consisting of an attending, a fellow, and MLPs to replace a traditional teaching team of an attending, senior resident, and 2 interns. The study states that the model resulted in a lower length of stay (LOS) and lower costs per case. Importantly, the new MLP‐based team only admitted during the hours of 7 AM to 2 PM. The study does not fully describe the number of MLPs required nor does it fully describe the role of cardiovascular fellows in the model. The study does state that the cost savings offset the cost of the MLPs but it is not clear if this cost analysis took into account the cost of the fellow's daytime involvement or if it measured attending time required before and after the implementation of the new model. In addition, this model presumes the availability of other services to admit patients during afternoon and nighttime hours and so may not be generalizable to other settings.
The final study by Cowan et al.6 describes the addition of a NP, a hospitalist medical director, and daily multidisciplinary rounds to a traditional teaching service model. Importantly, the NP was not involved in the admission process nor were they the primary providers for day‐to‐day medical care but rather they focused on implementation of care protocols, multidisciplinary coordination of care and discharge planning, and postdischarge follow‐up. In addition, the NP worked only weekdays for about 40 hours a week. It is not surprising that adding multiple additional resources to existing care models might provide benefits but this does not address any issues in terms of the workforce since the care in this model required a higher total input of providers than the usual care model being studied. Cost savings from such a model may make it cost‐effective but it does not represent a workforce solution.
There have been other studies examining the use of MLPs in the inpatient setting in internal medicine. Some of these studies have suggested that MLP‐based models result in equivalent outcomes and efficiency810 to traditional teaching or nonteaching physician‐only models. There are 2 important caveats, however, that must be considered. The total resources required for such models may be quite high, especially taking into account the costs of 24/7 coverage and physician backup of the MLPs, and most importantly there is almost no literature that robustly examines ultimate clinical outcomes in these models. We do note that a recent study11 did show a lower inpatient mortality rate over a 2‐year period of time after substituting a PA‐hospitalist model for a traditional academic medicine residency model in a community hospital. Importantly, however, the new model also added 24/7 hospitalist physicians and night and weekend intensivists that were not present in the prior residency‐based model. Thus, the lower mortality rate could be attributed to the addition of hospitalists or the more robust in‐house physician coverage during off‐hours rather than the use of MLPs.
Notably, while the evidence base in internal medicine is not robust, many studies have described successful use of MLPs in non‐internal medicine inpatient settings.1214 The reasons for this success is debatable, but it may be that MLPs are more successful in settings where the care is either more protocol‐driven or where there is less diagnostic and therapeutic complexity.
Recent Experiences with MLPs in Academic Hospital Medicine
Given the paucity of data, it is clear that further research is needed on the role of MLPs in hospital medicine. While waiting for such evidence to appear, it may be worthwhile to reflect on the recent experience of 3 major medical centers. A recent article described 5 hospitalist models at major academic medical centers across the country. Two of the institutions described at the time (University of Michigan Health System, Ann Arbor, MI; and Brigham and Women's Hospital, Boston, MA) utilized MLPs as a major element of their staffing of nonresident hospitalist services while another (University of California, San Francisco [UCSF] Medical Center at Mt. Zion, San Francisco, CA) had previously used MLPs as part of its model but phased them out about 1 year prior to publication of the article.2 The model used by the Brigham and Women's Hospital was later described in more detail in a subsequent publication.8 Recently 1 of these institutions (Michigan) has chosen to phase out MLPs. At Michigan, a 4‐year experience with PAs on a general‐medicine focused hospitalist service eventually led to the conclusion that continued use of PAs was not cost‐effective. Significant barriers to success included a steep learning curve and the significant time required before PAs developed sufficient autonomy and efficiency in caring for a highly complex heterogeneous patient population. In the Michigan experience, PAs took up to 2 years to attain a significant level of autonomy and efficiency and even then some PAs still required a significant amount of physician oversight. Similar concerns at UCSF Mt. Zion led to the elimination of their MLP program as well. At Brigham and Women's, the MLP service continues but has required additional hospitalist staffing due to difficulties recruiting qualified MLPs with appropriate inpatient experience. In all cases, the models were challenged by high costs and the difficulty of developing MLPs to attain the level of autonomy and efficiency needed to justify their continued use. A key point is that in each institution, MLPs continue to play an important role in some specialty inpatient areas such as Hematology/Oncology and Bone Marrow Transplant, which is where MLPs have traditionally found their niche in inpatient Internal Medicine. These focus shops allow MLPs to develop a niche and expertise in a specialized area, where they may become more autonomous and efficient than house staff. Thus these settings may be more appropriate for MLPs than a heterogeneous general medicine inpatient setting.
Reviewing the Financial Case
In their article, Ford and Britting1 cite potential financial advantages for the use of MLPs in hospital medicine by comparing the relative salaries of MLPs to Hospitalists. What was missing in their analysis was the relative productivity of the 2 types of providers. We do have some limited data from the Society of Hospital Medicine (SHM) annual survey that looks at MLPs in hospital medicine but, again, the number of respondents for most data elements is less than 70, making generalizability difficult. Nonetheless, the data suggest that MLPs in hospital medicine average about 60% to 75% of the productivity of a physician when measured by encounters, although there is wide variability depending on the employment model (academic vs. multispecialty group).15 Importantly, the existing data do not provide any measure of how much physician input is provided to these MLPs but we suspect that in most models there is some physician time and input. If we presume that the MLPs bill independently and collect 85% of the physician fee schedule for a Medicare population, then collections would be about 50% to 65% of a typical physician. Given that median total compensation including benefits from the SHM survey was $120,000 for MLPs and $216,000 for physiciansabout a 55% ratiothis would argue for potential financial neutrality when substituting MLPs for physicians in a 2:1 ratio but only if we presume they require no physician supervision, which in our own experience is not likely in a general medicine population. In an alternative model, in which the physician sees every patient with the MLP and the physician bills, one would need to see roughly 50% more patients to achieve a financially neutral situation. In our experience at our own institutions, this level of increased productivity was not achievable. It is important to note that our figures are median compensation and benefit cost figures and local markets vary widely. We know that in major east and west coast cities MLPs may command far higher salaries while early career hospitalist physicians may be paid somewhat less than the reported medians. Recent market changes have significantly pressured MLP salaries,15, 16 further impacting the financial equation and perhaps tilting it farther against a financial benefit for MLPs. Furthermore, night coverage for MLP services should always be considered in a financial analysis and is not captured in this simple analysis.
Next Steps
Given the current shortage of physicians, we imagine that many hospitalist groups will consider the use of MLPs as a solution to the current workforce issues. However, data on how best to utilize MLPs and the true impact on both the cost and quality of such models is lacking. In addition to urging increased publication and dissemination of existing experiences with NP and PAs, we strongly suggest that groups considering starting a MLP model do so in a way which would facilitate robust analysis and comparison of the model with alternatives. We also suggest that SHM consider the following: modifying its biennial survey to better capture the nuances of MLP productivity (such as assessing the amount of physician input and supervision required); targeting MLPs so as to increase the number of respondents; and doing an additional survey to capture demographics and basic data on existing MLP models given the lack of published literature.
In addition to gathering more data on effective models, a critical gap that we have identified is the development of models for the training and development of MLPs interested in hospital medicine. It would be a mistake to believe that MLPs could function in a manner similar to residency‐trained physicians if they do not undergo similar training. NP/PA programs generally do not have a significant inpatient internal medicine focus and so newly minted graduates often lack the skills needed to succeed in hospital medicine.17 Some hospitalist programs train their MLPs on the job, but many programs cannot afford the amount of time and effort required to do this on their own. There are a small number of advanced training options for MLPs in hospital medicine18 but it is not likely such models will proliferate given the inherent opportunity costs that exist for extended training in the current competitive job market for MLPs. Instead we think that very motivated hospital medicine groups may develop training relationships with PA and NP schools in an effort to train their own. In addition, national initiatives such as the Hospital Medicine Boot Camp for NPs and PAs, which is cosponsored by SHM, the American Association of Physician Assistants (AAPA), and the American Academy of Nurse Practitioners (AANP),19 can help fill the educational needs for MLPs who are already in practice.
Conclusions
While some literature exists that suggests that MLPs can successfully be used in the inpatient internal medicine setting, it is important to note that the evidence is quite limited and cannot be generalized across all care settings and patient populations. There is an urgent need to gather more data and share our collective experiences to better inform our decision‐making before we state that MLPs are the solution to workforce shortages in hospital medicine. In addition, existing data and experience suggest that MLPs may not be a cost‐effective workforce solution for complex general medical patients who require significant physician input. We believe that redesigning the clinical training of MLPs to focus on inpatient skills may hold promise and encourage interested parties to consider developing partnerships with MLP training programs and hospital medicine groups, as a way to build a more robust and successful hospital medicine MLP workforce.
- ,.Nonphysician providers in the hospitalist model: a prescription for change and a warning about unintended side effects.J Hosp Med.2010;5:99–102.
- ,,,,.Non‐housestaff medicine services in academic medical centers: models and challenges.J Hosp Med.2008;3:247–255.
- ,,.Nurse practitioners and physician assistants in the intensive care unit: an evidence‐based review.Crit Care Med.2008;36:2888–2897.
- ,,.Improving resource utilization in a teaching hospital: development of a nonteaching service for chest pain admissions.Acad Med.2006;81:432–435.
- ,,,,,.A nonresident cardiovascular inpatient service improves residents' experiences in an academic medical center: a new model to meet the challenges of the new millennium.Acad Med.2004;79;426–431.
- .The effect of a multidisciplinary hospitalist/physician and advance practice nurse collaboration on hospital care.J Nurs Adm.2006;36:79–85.
- Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Residency Education in Internal Medicine. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/140_internal_ medicine_07012009.pdf. Accessed July2009.
- ,,, et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3:361–368.
- ,,.Resource use by physician assistant services versus teaching services.JAAPA.2002;15:33–38.
- ,,,, et al.Outcomes‐based trial of an inpatient nurse practitioner service for general medical patients.J Eval Clin Pract.2001;7:21–33.
- ,.Replacing an academic internal medicine residency program with a physician assistant‐hospitalist model: a comparative analysis study.Am J Med Qual.2009;2:132–139.
- ,,,,.Integrating midlevel practitioners into a teaching service.Am J Surg.2006;1:119–124.
- ,,, et al.Physician extenders impact trauma systems.J Trauma.2005;58(5):917–920.
- ,.Physician assistants in cardiothoracic surgery: a 30‐year experience in a university center.Ann Thorac Surg.2006;1:195–199.
- 2007–2008 Society of Hospital Medicine Bi‐Annual Survey: the Authoritative Source on the State of the Hospital Medicine Movement.Philadelphia:Society of Hospital Medicine;2008.
- American Association of Physician Assistants. Physician Assistant Income. Available at: http://www.aapa.org/images/stories/iu08incchange. pdf. Accessed July2009.
- Accreditation Review Commission on Education for the Physician Assistant. Accreditation Standards for Physician Assistant Education, 3rd ed. Available at: http://www.arcpa.org/Standards/3rdeditionwithPDchangesandregionals4.24.08a.pdf. Accessed July2009.
- Association of Postgraduate PA Programs. Postgraduate PA Program Listing by State. Available at: http://www.appap.org/index1.html. Accessed July2009.
- American Association of Physician Assistants. Adult Hospitalist Physician Assistant and Nurse Practitioner Boot Camp. Available at: http://www. aapa.org/component/content/article/23‐‐general‐/673‐adult‐hospitalist‐physician‐assistant‐and‐nurse‐practitioner‐boot‐camp. Accessed July2009.
Ford and Britting's1 editorial in this month's Journal of Hospital Medicine raises important questions concerning the use of nonphysician providers in hospital medicine. They focus primarily on the use of mid‐level providers (MLPs), namely physician‐assistants (PAs) and nurse practitioners (NPs), as a potential solution to the current physician workforce shortages in our field. While we acknowledge the challenges of meeting workforce needs, we also believe that much is unknown about the optimal use of MLPs on inpatient general medicine services and it is premature to tout MLPs as the solution to hospital medicine staffing problems. This is especially true in those hospitals where hospitalists care for complex, general medical patients with a wide variety of medical conditions, a trend that is especially common in academic medical centers.2
This article discusses the current literature, our own experiences with MLPs, and suggests some future initiatives that might help better integrate MLPs into hospital medicine.
The Literature on MLPs in Inpatient Venues
The existing literature on the use of MLPs in inpatient venues is quite limited, and a recent review, while suggesting that the existing literature does describe benefits of MLPs in the inpatient setting, also states that the overall quality of the evidence is quite poor and that many studies suffer from significant limitations, including small populations, limited patient mixes, use of selected settings, and short durations of outcome assessment.3
Ford and Britting,1 in their article, cite several studies46 as evidence that a MLP model of care either improved outcomes or provided cost benefits. Each of these studies has important limitations that are worth examining.
The study by Myers et al.4 described the use of MLPs in a chest pain unit. NPs partnered with hospitalists to care for a low‐acuity chest pain population. In addition, 5 NPs only staffed the unit during daytime weekday hours. Off‐hour and weekend staffing was accomplished through the use of resident physicians. Notably, the work suggests the service only admitted 113 low‐risk patients over 10 months. The service was staffed by 3 full‐time equivalent (FTE) NPs in addition to involving hospitalists during the day. It is not surprising, given the extremely low volume of patients coupled with a daytime‐only focus, that this service showed efficiency gains. In addition, given the service was only staffed by NPs 40 hours a week and by resident physicians on nights and weekends, the true cost of such an intervention needs to take into account the full cost of 24/7 coverage. In addition, the model of using residents to cover nonteaching patients is no longer permitted by the current Accreditation Council for Graduate Medical Education (ACGME) Internal Medicine Residency Requirements7 and thus implementation of a model such as this in 2009 would require alternative means of nighttime coverage.
The study by Nishimura et al.,5 also describing the use of MLPs in cardiovascular care, has important caveats that make full assessment of the model impossible. The model describes the implementation of a care team consisting of an attending, a fellow, and MLPs to replace a traditional teaching team of an attending, senior resident, and 2 interns. The study states that the model resulted in a lower length of stay (LOS) and lower costs per case. Importantly, the new MLP‐based team only admitted during the hours of 7 AM to 2 PM. The study does not fully describe the number of MLPs required nor does it fully describe the role of cardiovascular fellows in the model. The study does state that the cost savings offset the cost of the MLPs but it is not clear if this cost analysis took into account the cost of the fellow's daytime involvement or if it measured attending time required before and after the implementation of the new model. In addition, this model presumes the availability of other services to admit patients during afternoon and nighttime hours and so may not be generalizable to other settings.
The final study by Cowan et al.6 describes the addition of a NP, a hospitalist medical director, and daily multidisciplinary rounds to a traditional teaching service model. Importantly, the NP was not involved in the admission process nor were they the primary providers for day‐to‐day medical care but rather they focused on implementation of care protocols, multidisciplinary coordination of care and discharge planning, and postdischarge follow‐up. In addition, the NP worked only weekdays for about 40 hours a week. It is not surprising that adding multiple additional resources to existing care models might provide benefits but this does not address any issues in terms of the workforce since the care in this model required a higher total input of providers than the usual care model being studied. Cost savings from such a model may make it cost‐effective but it does not represent a workforce solution.
There have been other studies examining the use of MLPs in the inpatient setting in internal medicine. Some of these studies have suggested that MLP‐based models result in equivalent outcomes and efficiency810 to traditional teaching or nonteaching physician‐only models. There are 2 important caveats, however, that must be considered. The total resources required for such models may be quite high, especially taking into account the costs of 24/7 coverage and physician backup of the MLPs, and most importantly there is almost no literature that robustly examines ultimate clinical outcomes in these models. We do note that a recent study11 did show a lower inpatient mortality rate over a 2‐year period of time after substituting a PA‐hospitalist model for a traditional academic medicine residency model in a community hospital. Importantly, however, the new model also added 24/7 hospitalist physicians and night and weekend intensivists that were not present in the prior residency‐based model. Thus, the lower mortality rate could be attributed to the addition of hospitalists or the more robust in‐house physician coverage during off‐hours rather than the use of MLPs.
Notably, while the evidence base in internal medicine is not robust, many studies have described successful use of MLPs in non‐internal medicine inpatient settings.1214 The reasons for this success is debatable, but it may be that MLPs are more successful in settings where the care is either more protocol‐driven or where there is less diagnostic and therapeutic complexity.
Recent Experiences with MLPs in Academic Hospital Medicine
Given the paucity of data, it is clear that further research is needed on the role of MLPs in hospital medicine. While waiting for such evidence to appear, it may be worthwhile to reflect on the recent experience of 3 major medical centers. A recent article described 5 hospitalist models at major academic medical centers across the country. Two of the institutions described at the time (University of Michigan Health System, Ann Arbor, MI; and Brigham and Women's Hospital, Boston, MA) utilized MLPs as a major element of their staffing of nonresident hospitalist services while another (University of California, San Francisco [UCSF] Medical Center at Mt. Zion, San Francisco, CA) had previously used MLPs as part of its model but phased them out about 1 year prior to publication of the article.2 The model used by the Brigham and Women's Hospital was later described in more detail in a subsequent publication.8 Recently 1 of these institutions (Michigan) has chosen to phase out MLPs. At Michigan, a 4‐year experience with PAs on a general‐medicine focused hospitalist service eventually led to the conclusion that continued use of PAs was not cost‐effective. Significant barriers to success included a steep learning curve and the significant time required before PAs developed sufficient autonomy and efficiency in caring for a highly complex heterogeneous patient population. In the Michigan experience, PAs took up to 2 years to attain a significant level of autonomy and efficiency and even then some PAs still required a significant amount of physician oversight. Similar concerns at UCSF Mt. Zion led to the elimination of their MLP program as well. At Brigham and Women's, the MLP service continues but has required additional hospitalist staffing due to difficulties recruiting qualified MLPs with appropriate inpatient experience. In all cases, the models were challenged by high costs and the difficulty of developing MLPs to attain the level of autonomy and efficiency needed to justify their continued use. A key point is that in each institution, MLPs continue to play an important role in some specialty inpatient areas such as Hematology/Oncology and Bone Marrow Transplant, which is where MLPs have traditionally found their niche in inpatient Internal Medicine. These focus shops allow MLPs to develop a niche and expertise in a specialized area, where they may become more autonomous and efficient than house staff. Thus these settings may be more appropriate for MLPs than a heterogeneous general medicine inpatient setting.
Reviewing the Financial Case
In their article, Ford and Britting1 cite potential financial advantages for the use of MLPs in hospital medicine by comparing the relative salaries of MLPs to Hospitalists. What was missing in their analysis was the relative productivity of the 2 types of providers. We do have some limited data from the Society of Hospital Medicine (SHM) annual survey that looks at MLPs in hospital medicine but, again, the number of respondents for most data elements is less than 70, making generalizability difficult. Nonetheless, the data suggest that MLPs in hospital medicine average about 60% to 75% of the productivity of a physician when measured by encounters, although there is wide variability depending on the employment model (academic vs. multispecialty group).15 Importantly, the existing data do not provide any measure of how much physician input is provided to these MLPs but we suspect that in most models there is some physician time and input. If we presume that the MLPs bill independently and collect 85% of the physician fee schedule for a Medicare population, then collections would be about 50% to 65% of a typical physician. Given that median total compensation including benefits from the SHM survey was $120,000 for MLPs and $216,000 for physiciansabout a 55% ratiothis would argue for potential financial neutrality when substituting MLPs for physicians in a 2:1 ratio but only if we presume they require no physician supervision, which in our own experience is not likely in a general medicine population. In an alternative model, in which the physician sees every patient with the MLP and the physician bills, one would need to see roughly 50% more patients to achieve a financially neutral situation. In our experience at our own institutions, this level of increased productivity was not achievable. It is important to note that our figures are median compensation and benefit cost figures and local markets vary widely. We know that in major east and west coast cities MLPs may command far higher salaries while early career hospitalist physicians may be paid somewhat less than the reported medians. Recent market changes have significantly pressured MLP salaries,15, 16 further impacting the financial equation and perhaps tilting it farther against a financial benefit for MLPs. Furthermore, night coverage for MLP services should always be considered in a financial analysis and is not captured in this simple analysis.
Next Steps
Given the current shortage of physicians, we imagine that many hospitalist groups will consider the use of MLPs as a solution to the current workforce issues. However, data on how best to utilize MLPs and the true impact on both the cost and quality of such models is lacking. In addition to urging increased publication and dissemination of existing experiences with NP and PAs, we strongly suggest that groups considering starting a MLP model do so in a way which would facilitate robust analysis and comparison of the model with alternatives. We also suggest that SHM consider the following: modifying its biennial survey to better capture the nuances of MLP productivity (such as assessing the amount of physician input and supervision required); targeting MLPs so as to increase the number of respondents; and doing an additional survey to capture demographics and basic data on existing MLP models given the lack of published literature.
In addition to gathering more data on effective models, a critical gap that we have identified is the development of models for the training and development of MLPs interested in hospital medicine. It would be a mistake to believe that MLPs could function in a manner similar to residency‐trained physicians if they do not undergo similar training. NP/PA programs generally do not have a significant inpatient internal medicine focus and so newly minted graduates often lack the skills needed to succeed in hospital medicine.17 Some hospitalist programs train their MLPs on the job, but many programs cannot afford the amount of time and effort required to do this on their own. There are a small number of advanced training options for MLPs in hospital medicine18 but it is not likely such models will proliferate given the inherent opportunity costs that exist for extended training in the current competitive job market for MLPs. Instead we think that very motivated hospital medicine groups may develop training relationships with PA and NP schools in an effort to train their own. In addition, national initiatives such as the Hospital Medicine Boot Camp for NPs and PAs, which is cosponsored by SHM, the American Association of Physician Assistants (AAPA), and the American Academy of Nurse Practitioners (AANP),19 can help fill the educational needs for MLPs who are already in practice.
Conclusions
While some literature exists that suggests that MLPs can successfully be used in the inpatient internal medicine setting, it is important to note that the evidence is quite limited and cannot be generalized across all care settings and patient populations. There is an urgent need to gather more data and share our collective experiences to better inform our decision‐making before we state that MLPs are the solution to workforce shortages in hospital medicine. In addition, existing data and experience suggest that MLPs may not be a cost‐effective workforce solution for complex general medical patients who require significant physician input. We believe that redesigning the clinical training of MLPs to focus on inpatient skills may hold promise and encourage interested parties to consider developing partnerships with MLP training programs and hospital medicine groups, as a way to build a more robust and successful hospital medicine MLP workforce.
Ford and Britting's1 editorial in this month's Journal of Hospital Medicine raises important questions concerning the use of nonphysician providers in hospital medicine. They focus primarily on the use of mid‐level providers (MLPs), namely physician‐assistants (PAs) and nurse practitioners (NPs), as a potential solution to the current physician workforce shortages in our field. While we acknowledge the challenges of meeting workforce needs, we also believe that much is unknown about the optimal use of MLPs on inpatient general medicine services and it is premature to tout MLPs as the solution to hospital medicine staffing problems. This is especially true in those hospitals where hospitalists care for complex, general medical patients with a wide variety of medical conditions, a trend that is especially common in academic medical centers.2
This article discusses the current literature, our own experiences with MLPs, and suggests some future initiatives that might help better integrate MLPs into hospital medicine.
The Literature on MLPs in Inpatient Venues
The existing literature on the use of MLPs in inpatient venues is quite limited, and a recent review, while suggesting that the existing literature does describe benefits of MLPs in the inpatient setting, also states that the overall quality of the evidence is quite poor and that many studies suffer from significant limitations, including small populations, limited patient mixes, use of selected settings, and short durations of outcome assessment.3
Ford and Britting,1 in their article, cite several studies46 as evidence that a MLP model of care either improved outcomes or provided cost benefits. Each of these studies has important limitations that are worth examining.
The study by Myers et al.4 described the use of MLPs in a chest pain unit. NPs partnered with hospitalists to care for a low‐acuity chest pain population. In addition, 5 NPs only staffed the unit during daytime weekday hours. Off‐hour and weekend staffing was accomplished through the use of resident physicians. Notably, the work suggests the service only admitted 113 low‐risk patients over 10 months. The service was staffed by 3 full‐time equivalent (FTE) NPs in addition to involving hospitalists during the day. It is not surprising, given the extremely low volume of patients coupled with a daytime‐only focus, that this service showed efficiency gains. In addition, given the service was only staffed by NPs 40 hours a week and by resident physicians on nights and weekends, the true cost of such an intervention needs to take into account the full cost of 24/7 coverage. In addition, the model of using residents to cover nonteaching patients is no longer permitted by the current Accreditation Council for Graduate Medical Education (ACGME) Internal Medicine Residency Requirements7 and thus implementation of a model such as this in 2009 would require alternative means of nighttime coverage.
The study by Nishimura et al.,5 also describing the use of MLPs in cardiovascular care, has important caveats that make full assessment of the model impossible. The model describes the implementation of a care team consisting of an attending, a fellow, and MLPs to replace a traditional teaching team of an attending, senior resident, and 2 interns. The study states that the model resulted in a lower length of stay (LOS) and lower costs per case. Importantly, the new MLP‐based team only admitted during the hours of 7 AM to 2 PM. The study does not fully describe the number of MLPs required nor does it fully describe the role of cardiovascular fellows in the model. The study does state that the cost savings offset the cost of the MLPs but it is not clear if this cost analysis took into account the cost of the fellow's daytime involvement or if it measured attending time required before and after the implementation of the new model. In addition, this model presumes the availability of other services to admit patients during afternoon and nighttime hours and so may not be generalizable to other settings.
The final study by Cowan et al.6 describes the addition of a NP, a hospitalist medical director, and daily multidisciplinary rounds to a traditional teaching service model. Importantly, the NP was not involved in the admission process nor were they the primary providers for day‐to‐day medical care but rather they focused on implementation of care protocols, multidisciplinary coordination of care and discharge planning, and postdischarge follow‐up. In addition, the NP worked only weekdays for about 40 hours a week. It is not surprising that adding multiple additional resources to existing care models might provide benefits but this does not address any issues in terms of the workforce since the care in this model required a higher total input of providers than the usual care model being studied. Cost savings from such a model may make it cost‐effective but it does not represent a workforce solution.
There have been other studies examining the use of MLPs in the inpatient setting in internal medicine. Some of these studies have suggested that MLP‐based models result in equivalent outcomes and efficiency810 to traditional teaching or nonteaching physician‐only models. There are 2 important caveats, however, that must be considered. The total resources required for such models may be quite high, especially taking into account the costs of 24/7 coverage and physician backup of the MLPs, and most importantly there is almost no literature that robustly examines ultimate clinical outcomes in these models. We do note that a recent study11 did show a lower inpatient mortality rate over a 2‐year period of time after substituting a PA‐hospitalist model for a traditional academic medicine residency model in a community hospital. Importantly, however, the new model also added 24/7 hospitalist physicians and night and weekend intensivists that were not present in the prior residency‐based model. Thus, the lower mortality rate could be attributed to the addition of hospitalists or the more robust in‐house physician coverage during off‐hours rather than the use of MLPs.
Notably, while the evidence base in internal medicine is not robust, many studies have described successful use of MLPs in non‐internal medicine inpatient settings.1214 The reasons for this success is debatable, but it may be that MLPs are more successful in settings where the care is either more protocol‐driven or where there is less diagnostic and therapeutic complexity.
Recent Experiences with MLPs in Academic Hospital Medicine
Given the paucity of data, it is clear that further research is needed on the role of MLPs in hospital medicine. While waiting for such evidence to appear, it may be worthwhile to reflect on the recent experience of 3 major medical centers. A recent article described 5 hospitalist models at major academic medical centers across the country. Two of the institutions described at the time (University of Michigan Health System, Ann Arbor, MI; and Brigham and Women's Hospital, Boston, MA) utilized MLPs as a major element of their staffing of nonresident hospitalist services while another (University of California, San Francisco [UCSF] Medical Center at Mt. Zion, San Francisco, CA) had previously used MLPs as part of its model but phased them out about 1 year prior to publication of the article.2 The model used by the Brigham and Women's Hospital was later described in more detail in a subsequent publication.8 Recently 1 of these institutions (Michigan) has chosen to phase out MLPs. At Michigan, a 4‐year experience with PAs on a general‐medicine focused hospitalist service eventually led to the conclusion that continued use of PAs was not cost‐effective. Significant barriers to success included a steep learning curve and the significant time required before PAs developed sufficient autonomy and efficiency in caring for a highly complex heterogeneous patient population. In the Michigan experience, PAs took up to 2 years to attain a significant level of autonomy and efficiency and even then some PAs still required a significant amount of physician oversight. Similar concerns at UCSF Mt. Zion led to the elimination of their MLP program as well. At Brigham and Women's, the MLP service continues but has required additional hospitalist staffing due to difficulties recruiting qualified MLPs with appropriate inpatient experience. In all cases, the models were challenged by high costs and the difficulty of developing MLPs to attain the level of autonomy and efficiency needed to justify their continued use. A key point is that in each institution, MLPs continue to play an important role in some specialty inpatient areas such as Hematology/Oncology and Bone Marrow Transplant, which is where MLPs have traditionally found their niche in inpatient Internal Medicine. These focus shops allow MLPs to develop a niche and expertise in a specialized area, where they may become more autonomous and efficient than house staff. Thus these settings may be more appropriate for MLPs than a heterogeneous general medicine inpatient setting.
Reviewing the Financial Case
In their article, Ford and Britting1 cite potential financial advantages for the use of MLPs in hospital medicine by comparing the relative salaries of MLPs to Hospitalists. What was missing in their analysis was the relative productivity of the 2 types of providers. We do have some limited data from the Society of Hospital Medicine (SHM) annual survey that looks at MLPs in hospital medicine but, again, the number of respondents for most data elements is less than 70, making generalizability difficult. Nonetheless, the data suggest that MLPs in hospital medicine average about 60% to 75% of the productivity of a physician when measured by encounters, although there is wide variability depending on the employment model (academic vs. multispecialty group).15 Importantly, the existing data do not provide any measure of how much physician input is provided to these MLPs but we suspect that in most models there is some physician time and input. If we presume that the MLPs bill independently and collect 85% of the physician fee schedule for a Medicare population, then collections would be about 50% to 65% of a typical physician. Given that median total compensation including benefits from the SHM survey was $120,000 for MLPs and $216,000 for physiciansabout a 55% ratiothis would argue for potential financial neutrality when substituting MLPs for physicians in a 2:1 ratio but only if we presume they require no physician supervision, which in our own experience is not likely in a general medicine population. In an alternative model, in which the physician sees every patient with the MLP and the physician bills, one would need to see roughly 50% more patients to achieve a financially neutral situation. In our experience at our own institutions, this level of increased productivity was not achievable. It is important to note that our figures are median compensation and benefit cost figures and local markets vary widely. We know that in major east and west coast cities MLPs may command far higher salaries while early career hospitalist physicians may be paid somewhat less than the reported medians. Recent market changes have significantly pressured MLP salaries,15, 16 further impacting the financial equation and perhaps tilting it farther against a financial benefit for MLPs. Furthermore, night coverage for MLP services should always be considered in a financial analysis and is not captured in this simple analysis.
Next Steps
Given the current shortage of physicians, we imagine that many hospitalist groups will consider the use of MLPs as a solution to the current workforce issues. However, data on how best to utilize MLPs and the true impact on both the cost and quality of such models is lacking. In addition to urging increased publication and dissemination of existing experiences with NP and PAs, we strongly suggest that groups considering starting a MLP model do so in a way which would facilitate robust analysis and comparison of the model with alternatives. We also suggest that SHM consider the following: modifying its biennial survey to better capture the nuances of MLP productivity (such as assessing the amount of physician input and supervision required); targeting MLPs so as to increase the number of respondents; and doing an additional survey to capture demographics and basic data on existing MLP models given the lack of published literature.
In addition to gathering more data on effective models, a critical gap that we have identified is the development of models for the training and development of MLPs interested in hospital medicine. It would be a mistake to believe that MLPs could function in a manner similar to residency‐trained physicians if they do not undergo similar training. NP/PA programs generally do not have a significant inpatient internal medicine focus and so newly minted graduates often lack the skills needed to succeed in hospital medicine.17 Some hospitalist programs train their MLPs on the job, but many programs cannot afford the amount of time and effort required to do this on their own. There are a small number of advanced training options for MLPs in hospital medicine18 but it is not likely such models will proliferate given the inherent opportunity costs that exist for extended training in the current competitive job market for MLPs. Instead we think that very motivated hospital medicine groups may develop training relationships with PA and NP schools in an effort to train their own. In addition, national initiatives such as the Hospital Medicine Boot Camp for NPs and PAs, which is cosponsored by SHM, the American Association of Physician Assistants (AAPA), and the American Academy of Nurse Practitioners (AANP),19 can help fill the educational needs for MLPs who are already in practice.
Conclusions
While some literature exists that suggests that MLPs can successfully be used in the inpatient internal medicine setting, it is important to note that the evidence is quite limited and cannot be generalized across all care settings and patient populations. There is an urgent need to gather more data and share our collective experiences to better inform our decision‐making before we state that MLPs are the solution to workforce shortages in hospital medicine. In addition, existing data and experience suggest that MLPs may not be a cost‐effective workforce solution for complex general medical patients who require significant physician input. We believe that redesigning the clinical training of MLPs to focus on inpatient skills may hold promise and encourage interested parties to consider developing partnerships with MLP training programs and hospital medicine groups, as a way to build a more robust and successful hospital medicine MLP workforce.
- ,.Nonphysician providers in the hospitalist model: a prescription for change and a warning about unintended side effects.J Hosp Med.2010;5:99–102.
- ,,,,.Non‐housestaff medicine services in academic medical centers: models and challenges.J Hosp Med.2008;3:247–255.
- ,,.Nurse practitioners and physician assistants in the intensive care unit: an evidence‐based review.Crit Care Med.2008;36:2888–2897.
- ,,.Improving resource utilization in a teaching hospital: development of a nonteaching service for chest pain admissions.Acad Med.2006;81:432–435.
- ,,,,,.A nonresident cardiovascular inpatient service improves residents' experiences in an academic medical center: a new model to meet the challenges of the new millennium.Acad Med.2004;79;426–431.
- .The effect of a multidisciplinary hospitalist/physician and advance practice nurse collaboration on hospital care.J Nurs Adm.2006;36:79–85.
- Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Residency Education in Internal Medicine. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/140_internal_ medicine_07012009.pdf. Accessed July2009.
- ,,, et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3:361–368.
- ,,.Resource use by physician assistant services versus teaching services.JAAPA.2002;15:33–38.
- ,,,, et al.Outcomes‐based trial of an inpatient nurse practitioner service for general medical patients.J Eval Clin Pract.2001;7:21–33.
- ,.Replacing an academic internal medicine residency program with a physician assistant‐hospitalist model: a comparative analysis study.Am J Med Qual.2009;2:132–139.
- ,,,,.Integrating midlevel practitioners into a teaching service.Am J Surg.2006;1:119–124.
- ,,, et al.Physician extenders impact trauma systems.J Trauma.2005;58(5):917–920.
- ,.Physician assistants in cardiothoracic surgery: a 30‐year experience in a university center.Ann Thorac Surg.2006;1:195–199.
- 2007–2008 Society of Hospital Medicine Bi‐Annual Survey: the Authoritative Source on the State of the Hospital Medicine Movement.Philadelphia:Society of Hospital Medicine;2008.
- American Association of Physician Assistants. Physician Assistant Income. Available at: http://www.aapa.org/images/stories/iu08incchange. pdf. Accessed July2009.
- Accreditation Review Commission on Education for the Physician Assistant. Accreditation Standards for Physician Assistant Education, 3rd ed. Available at: http://www.arcpa.org/Standards/3rdeditionwithPDchangesandregionals4.24.08a.pdf. Accessed July2009.
- Association of Postgraduate PA Programs. Postgraduate PA Program Listing by State. Available at: http://www.appap.org/index1.html. Accessed July2009.
- American Association of Physician Assistants. Adult Hospitalist Physician Assistant and Nurse Practitioner Boot Camp. Available at: http://www. aapa.org/component/content/article/23‐‐general‐/673‐adult‐hospitalist‐physician‐assistant‐and‐nurse‐practitioner‐boot‐camp. Accessed July2009.
- ,.Nonphysician providers in the hospitalist model: a prescription for change and a warning about unintended side effects.J Hosp Med.2010;5:99–102.
- ,,,,.Non‐housestaff medicine services in academic medical centers: models and challenges.J Hosp Med.2008;3:247–255.
- ,,.Nurse practitioners and physician assistants in the intensive care unit: an evidence‐based review.Crit Care Med.2008;36:2888–2897.
- ,,.Improving resource utilization in a teaching hospital: development of a nonteaching service for chest pain admissions.Acad Med.2006;81:432–435.
- ,,,,,.A nonresident cardiovascular inpatient service improves residents' experiences in an academic medical center: a new model to meet the challenges of the new millennium.Acad Med.2004;79;426–431.
- .The effect of a multidisciplinary hospitalist/physician and advance practice nurse collaboration on hospital care.J Nurs Adm.2006;36:79–85.
- Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Residency Education in Internal Medicine. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/140_internal_ medicine_07012009.pdf. Accessed July2009.
- ,,, et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3:361–368.
- ,,.Resource use by physician assistant services versus teaching services.JAAPA.2002;15:33–38.
- ,,,, et al.Outcomes‐based trial of an inpatient nurse practitioner service for general medical patients.J Eval Clin Pract.2001;7:21–33.
- ,.Replacing an academic internal medicine residency program with a physician assistant‐hospitalist model: a comparative analysis study.Am J Med Qual.2009;2:132–139.
- ,,,,.Integrating midlevel practitioners into a teaching service.Am J Surg.2006;1:119–124.
- ,,, et al.Physician extenders impact trauma systems.J Trauma.2005;58(5):917–920.
- ,.Physician assistants in cardiothoracic surgery: a 30‐year experience in a university center.Ann Thorac Surg.2006;1:195–199.
- 2007–2008 Society of Hospital Medicine Bi‐Annual Survey: the Authoritative Source on the State of the Hospital Medicine Movement.Philadelphia:Society of Hospital Medicine;2008.
- American Association of Physician Assistants. Physician Assistant Income. Available at: http://www.aapa.org/images/stories/iu08incchange. pdf. Accessed July2009.
- Accreditation Review Commission on Education for the Physician Assistant. Accreditation Standards for Physician Assistant Education, 3rd ed. Available at: http://www.arcpa.org/Standards/3rdeditionwithPDchangesandregionals4.24.08a.pdf. Accessed July2009.
- Association of Postgraduate PA Programs. Postgraduate PA Program Listing by State. Available at: http://www.appap.org/index1.html. Accessed July2009.
- American Association of Physician Assistants. Adult Hospitalist Physician Assistant and Nurse Practitioner Boot Camp. Available at: http://www. aapa.org/component/content/article/23‐‐general‐/673‐adult‐hospitalist‐physician‐assistant‐and‐nurse‐practitioner‐boot‐camp. Accessed July2009.
Acute Pancreatitis with Eruptive Xanthomas
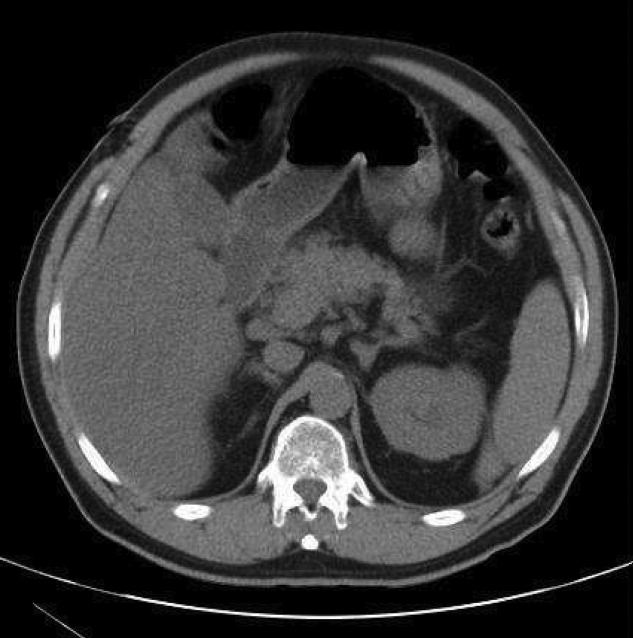
A 54‐year‐old man presented with a 1‐day history of epigastric abdominal pain. He also described 1 month of a nonpruritic but tender rash, on his right elbow, abdomen, buttocks, posterior thighs, and knees. He was obese with a past medical history remarkable for uncontrolled type 2 diabetes mellitus and hemoglobin A1C of 12.7. His abdomen was tender to palpation in the epigastric area with no rebound or guarding. Skin examination demonstrated multiple yellow waxy papules on the extensor surfaces of his arms, abdomen, thighs, knees, and buttocks, consistent with eruptive xanthomas (Figure 1). Laboratory values were significant for lipase at 852 g/L (normal, 8‐78 g/L) and triglycerides at 6200 mg/dL. An abdominal computed tomography (CT) scan without contrast demonstrated extensive inflammatory changes surrounding the head of the pancreas, consistent with acute pancreatitis (Figure 2). The diagnosis of acute pancreatitis secondary to hypertriglyceridemia was made. Dietary and pharmacologic interventions helped decrease the triglyceride level and his rash and abdominal pain were improved at outpatient follow‐up 2 weeks later.

Hypertriglyceridemia increases the risk of acute pancreatitis.1 Eruptive xanthomas can be associated with primary and secondary hypertriglyceridemia, particularly in the setting of poorly controlled diabetes.2 The risk of acute pancreatitis and eruptive xanthomas increases when the level of serum triglyceride reaches the thousands.
Rapid recognition of eruptive xanthomas can assist in identifying the etiology of acute pancreatitis.
- .Hyperlipidemic pancreatitis. [Review].Gastroenterol Clin North Am.1990;19(4):783–791.
- .Xanthomas and hyperlipidemias.J Am Acad Dermatol.1985;13(1):1–30.
A 54‐year‐old man presented with a 1‐day history of epigastric abdominal pain. He also described 1 month of a nonpruritic but tender rash, on his right elbow, abdomen, buttocks, posterior thighs, and knees. He was obese with a past medical history remarkable for uncontrolled type 2 diabetes mellitus and hemoglobin A1C of 12.7. His abdomen was tender to palpation in the epigastric area with no rebound or guarding. Skin examination demonstrated multiple yellow waxy papules on the extensor surfaces of his arms, abdomen, thighs, knees, and buttocks, consistent with eruptive xanthomas (Figure 1). Laboratory values were significant for lipase at 852 g/L (normal, 8‐78 g/L) and triglycerides at 6200 mg/dL. An abdominal computed tomography (CT) scan without contrast demonstrated extensive inflammatory changes surrounding the head of the pancreas, consistent with acute pancreatitis (Figure 2). The diagnosis of acute pancreatitis secondary to hypertriglyceridemia was made. Dietary and pharmacologic interventions helped decrease the triglyceride level and his rash and abdominal pain were improved at outpatient follow‐up 2 weeks later.
Hypertriglyceridemia increases the risk of acute pancreatitis.1 Eruptive xanthomas can be associated with primary and secondary hypertriglyceridemia, particularly in the setting of poorly controlled diabetes.2 The risk of acute pancreatitis and eruptive xanthomas increases when the level of serum triglyceride reaches the thousands.
Rapid recognition of eruptive xanthomas can assist in identifying the etiology of acute pancreatitis.
A 54‐year‐old man presented with a 1‐day history of epigastric abdominal pain. He also described 1 month of a nonpruritic but tender rash, on his right elbow, abdomen, buttocks, posterior thighs, and knees. He was obese with a past medical history remarkable for uncontrolled type 2 diabetes mellitus and hemoglobin A1C of 12.7. His abdomen was tender to palpation in the epigastric area with no rebound or guarding. Skin examination demonstrated multiple yellow waxy papules on the extensor surfaces of his arms, abdomen, thighs, knees, and buttocks, consistent with eruptive xanthomas (Figure 1). Laboratory values were significant for lipase at 852 g/L (normal, 8‐78 g/L) and triglycerides at 6200 mg/dL. An abdominal computed tomography (CT) scan without contrast demonstrated extensive inflammatory changes surrounding the head of the pancreas, consistent with acute pancreatitis (Figure 2). The diagnosis of acute pancreatitis secondary to hypertriglyceridemia was made. Dietary and pharmacologic interventions helped decrease the triglyceride level and his rash and abdominal pain were improved at outpatient follow‐up 2 weeks later.
Hypertriglyceridemia increases the risk of acute pancreatitis.1 Eruptive xanthomas can be associated with primary and secondary hypertriglyceridemia, particularly in the setting of poorly controlled diabetes.2 The risk of acute pancreatitis and eruptive xanthomas increases when the level of serum triglyceride reaches the thousands.
Rapid recognition of eruptive xanthomas can assist in identifying the etiology of acute pancreatitis.
- .Hyperlipidemic pancreatitis. [Review].Gastroenterol Clin North Am.1990;19(4):783–791.
- .Xanthomas and hyperlipidemias.J Am Acad Dermatol.1985;13(1):1–30.
- .Hyperlipidemic pancreatitis. [Review].Gastroenterol Clin North Am.1990;19(4):783–791.
- .Xanthomas and hyperlipidemias.J Am Acad Dermatol.1985;13(1):1–30.

HM Often Lends a Critical-Care Hand
Hospitalists serving as attending physicians were overwhelmingly found in ICUs in hospitals where intensivists were used mostly as elective consultations, according to a study to be published in this month’s Journal of Hospital Medicine.
The report, "Characteristics of Intensive Care Units in Michigan: Not an Open and Closed Case" (JHM. 2010;5:4-9), is a cross-sectional survey of 115 ICUs in 72 Michigan hospitals. The way critical care is delivered is an issue many hospitalists pay mind to as they often are called upon to compensate for workforce shortages even though few are board-certified in critical care. The study reported that 25% of sites used a closed model of intensive care, and that those units were larger than sites with open ICUs (P<0.05). Hospitalists serving as attendings were "strongly associated with an open ICU" (odds ratio 95%; confidence interval=12.2).
"Because our study shows that hospitalists are already providing intensive care in many areas of Michigan … the best strategy [for hospitalists] would be to work within that context,” says lead researcher Robert C. Hyzy, MD, FCCM, associate professor in the Department of Internal Medicine and director of the Critical Care Medicine Unit at the University of Michigan in Ann Arbor.
Dr. Hyzy says hospitalists will "continue to play an important role" in ICU care as long as the intensivist shortage continues, even though many don’t have the extensive training to do so. Telemedicine has been used in recent years to help address the ICU physician shortage, although the debate continues as to its effectiveness on morbidity and mortality rates. In the meantime, Dr. Hyzy reports, only 20% of the sites in his study reported all attending physicians were board-certified in critical care; 60 sites had less than 50% board-certified attending physicians.
“Hospitalists can play a role in acknowledging the limitations of individuals who are not properly trained in critical care to advocate for transfer to larger centers under explicit clinical circumstances,” Dr. Hyzy says.
As a member of the Society of Critical Care Medicine’s (SCCM) fellowship program, Dr. Hyzy also urges any hospitalists who deliver critical-care services to investigate the SCCM’s certification track and to take advantage of any training opportunities available to them.
Hospitalists serving as attending physicians were overwhelmingly found in ICUs in hospitals where intensivists were used mostly as elective consultations, according to a study to be published in this month’s Journal of Hospital Medicine.
The report, "Characteristics of Intensive Care Units in Michigan: Not an Open and Closed Case" (JHM. 2010;5:4-9), is a cross-sectional survey of 115 ICUs in 72 Michigan hospitals. The way critical care is delivered is an issue many hospitalists pay mind to as they often are called upon to compensate for workforce shortages even though few are board-certified in critical care. The study reported that 25% of sites used a closed model of intensive care, and that those units were larger than sites with open ICUs (P<0.05). Hospitalists serving as attendings were "strongly associated with an open ICU" (odds ratio 95%; confidence interval=12.2).
"Because our study shows that hospitalists are already providing intensive care in many areas of Michigan … the best strategy [for hospitalists] would be to work within that context,” says lead researcher Robert C. Hyzy, MD, FCCM, associate professor in the Department of Internal Medicine and director of the Critical Care Medicine Unit at the University of Michigan in Ann Arbor.
Dr. Hyzy says hospitalists will "continue to play an important role" in ICU care as long as the intensivist shortage continues, even though many don’t have the extensive training to do so. Telemedicine has been used in recent years to help address the ICU physician shortage, although the debate continues as to its effectiveness on morbidity and mortality rates. In the meantime, Dr. Hyzy reports, only 20% of the sites in his study reported all attending physicians were board-certified in critical care; 60 sites had less than 50% board-certified attending physicians.
“Hospitalists can play a role in acknowledging the limitations of individuals who are not properly trained in critical care to advocate for transfer to larger centers under explicit clinical circumstances,” Dr. Hyzy says.
As a member of the Society of Critical Care Medicine’s (SCCM) fellowship program, Dr. Hyzy also urges any hospitalists who deliver critical-care services to investigate the SCCM’s certification track and to take advantage of any training opportunities available to them.
Hospitalists serving as attending physicians were overwhelmingly found in ICUs in hospitals where intensivists were used mostly as elective consultations, according to a study to be published in this month’s Journal of Hospital Medicine.
The report, "Characteristics of Intensive Care Units in Michigan: Not an Open and Closed Case" (JHM. 2010;5:4-9), is a cross-sectional survey of 115 ICUs in 72 Michigan hospitals. The way critical care is delivered is an issue many hospitalists pay mind to as they often are called upon to compensate for workforce shortages even though few are board-certified in critical care. The study reported that 25% of sites used a closed model of intensive care, and that those units were larger than sites with open ICUs (P<0.05). Hospitalists serving as attendings were "strongly associated with an open ICU" (odds ratio 95%; confidence interval=12.2).
"Because our study shows that hospitalists are already providing intensive care in many areas of Michigan … the best strategy [for hospitalists] would be to work within that context,” says lead researcher Robert C. Hyzy, MD, FCCM, associate professor in the Department of Internal Medicine and director of the Critical Care Medicine Unit at the University of Michigan in Ann Arbor.
Dr. Hyzy says hospitalists will "continue to play an important role" in ICU care as long as the intensivist shortage continues, even though many don’t have the extensive training to do so. Telemedicine has been used in recent years to help address the ICU physician shortage, although the debate continues as to its effectiveness on morbidity and mortality rates. In the meantime, Dr. Hyzy reports, only 20% of the sites in his study reported all attending physicians were board-certified in critical care; 60 sites had less than 50% board-certified attending physicians.
“Hospitalists can play a role in acknowledging the limitations of individuals who are not properly trained in critical care to advocate for transfer to larger centers under explicit clinical circumstances,” Dr. Hyzy says.
As a member of the Society of Critical Care Medicine’s (SCCM) fellowship program, Dr. Hyzy also urges any hospitalists who deliver critical-care services to investigate the SCCM’s certification track and to take advantage of any training opportunities available to them.
In the Literature: Research You Need to Know
Clinical question: Are aldosterone antagonists appropriately used in heart failure patients?
Background: Aldosterone antagonists are Class 1 treatment for patients with heart failure (HF) and low left ventricular ejection fraction (LVEF), according to the latest American College of Cardiology/American Heart Association (ACC/AHA) Chronic HF Guidelines. However, acceptance of the guidelines has been slow, possibly because of contraindications and adverse effects in some patients.
Study design: Observational cohort.
Setting: Inpatients at 241 hospitals participating in an HF registry.
Synopsis: Eligible inpatients from a QI registry who were discharged home from January 2005 to December 2007 were analyzed for appropriate and inappropriate aldosterone antagonist use.
Among the 12,565 patients who met the criteria for aldosterone antagonist therapy, only 4,087 (32.5%) received the therapy at discharge. In contrast, of the 8,610 total patients with HF discharged on aldosterone antagonists, 269 (3.1%) met at least one criterion for inappropriate use, and 640 (7.4%) met at least one criteria for potentially inappropriate use.
Use of an aldosterone antagonist was more likely in certain patient groups, including those who were younger, African-American, had lower systolic blood pressure, had no history of renal insufficiency, and those with implantable cardioverter-defibrillators. The authors noted aldosterone use increased significantly during the study period.
The study was limited by the possibility that aldosterone antagonists were used for non-HF conditions and the fact that it was retrospective.
Bottom line: Aldosterone antagonists are used in less than one-third of eligible HF patients.
Citation: Albert NM, Yancy CW, Liang L, et al. Use of aldosterone antagonists in heart failure. JAMA. 2009;302(15):1658-1665.
Reviewed for TH eWire by Jill Goldenberg, MD, Alan Briones, MD, Dennis Chang, MD, Brian Markoff, MD, FHM, Erin Rule, MD, Andrew Dunn, MD, FACP, FHM, Division of General Internal Medicine, Mount Sinai School of Medicine, New York City
For more HM-related literature reviews, visit our Web site.
Clinical question: Are aldosterone antagonists appropriately used in heart failure patients?
Background: Aldosterone antagonists are Class 1 treatment for patients with heart failure (HF) and low left ventricular ejection fraction (LVEF), according to the latest American College of Cardiology/American Heart Association (ACC/AHA) Chronic HF Guidelines. However, acceptance of the guidelines has been slow, possibly because of contraindications and adverse effects in some patients.
Study design: Observational cohort.
Setting: Inpatients at 241 hospitals participating in an HF registry.
Synopsis: Eligible inpatients from a QI registry who were discharged home from January 2005 to December 2007 were analyzed for appropriate and inappropriate aldosterone antagonist use.
Among the 12,565 patients who met the criteria for aldosterone antagonist therapy, only 4,087 (32.5%) received the therapy at discharge. In contrast, of the 8,610 total patients with HF discharged on aldosterone antagonists, 269 (3.1%) met at least one criterion for inappropriate use, and 640 (7.4%) met at least one criteria for potentially inappropriate use.
Use of an aldosterone antagonist was more likely in certain patient groups, including those who were younger, African-American, had lower systolic blood pressure, had no history of renal insufficiency, and those with implantable cardioverter-defibrillators. The authors noted aldosterone use increased significantly during the study period.
The study was limited by the possibility that aldosterone antagonists were used for non-HF conditions and the fact that it was retrospective.
Bottom line: Aldosterone antagonists are used in less than one-third of eligible HF patients.
Citation: Albert NM, Yancy CW, Liang L, et al. Use of aldosterone antagonists in heart failure. JAMA. 2009;302(15):1658-1665.
Reviewed for TH eWire by Jill Goldenberg, MD, Alan Briones, MD, Dennis Chang, MD, Brian Markoff, MD, FHM, Erin Rule, MD, Andrew Dunn, MD, FACP, FHM, Division of General Internal Medicine, Mount Sinai School of Medicine, New York City
For more HM-related literature reviews, visit our Web site.
Clinical question: Are aldosterone antagonists appropriately used in heart failure patients?
Background: Aldosterone antagonists are Class 1 treatment for patients with heart failure (HF) and low left ventricular ejection fraction (LVEF), according to the latest American College of Cardiology/American Heart Association (ACC/AHA) Chronic HF Guidelines. However, acceptance of the guidelines has been slow, possibly because of contraindications and adverse effects in some patients.
Study design: Observational cohort.
Setting: Inpatients at 241 hospitals participating in an HF registry.
Synopsis: Eligible inpatients from a QI registry who were discharged home from January 2005 to December 2007 were analyzed for appropriate and inappropriate aldosterone antagonist use.
Among the 12,565 patients who met the criteria for aldosterone antagonist therapy, only 4,087 (32.5%) received the therapy at discharge. In contrast, of the 8,610 total patients with HF discharged on aldosterone antagonists, 269 (3.1%) met at least one criterion for inappropriate use, and 640 (7.4%) met at least one criteria for potentially inappropriate use.
Use of an aldosterone antagonist was more likely in certain patient groups, including those who were younger, African-American, had lower systolic blood pressure, had no history of renal insufficiency, and those with implantable cardioverter-defibrillators. The authors noted aldosterone use increased significantly during the study period.
The study was limited by the possibility that aldosterone antagonists were used for non-HF conditions and the fact that it was retrospective.
Bottom line: Aldosterone antagonists are used in less than one-third of eligible HF patients.
Citation: Albert NM, Yancy CW, Liang L, et al. Use of aldosterone antagonists in heart failure. JAMA. 2009;302(15):1658-1665.
Reviewed for TH eWire by Jill Goldenberg, MD, Alan Briones, MD, Dennis Chang, MD, Brian Markoff, MD, FHM, Erin Rule, MD, Andrew Dunn, MD, FACP, FHM, Division of General Internal Medicine, Mount Sinai School of Medicine, New York City
For more HM-related literature reviews, visit our Web site.
Case 1: Management Decisions in an Adult Comorbid Patient With Type 2 Diabetes Having Primary HyperlipidemiaCase 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
Case 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
A Case Studies Compendium supplement to Internal Medicine News. This supplement was sponsored by Daiichi Sankyo, Inc.
•Case 1 Topics
•Case 2 Topics
•Faculty/Faculty Disclosures
To view the supplement, click the image above.
Case 1 Topics
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Case 2 Topics
• Background
• Current Visit: Exam Findings
• Current Treatment Regimen
• Health History
• Laboratory Results
• Clinical Discussion
• Cardiologist Visit
• Three Months After Visiting the Cardiologist
• Add-On Therapy With Welchol for Patients With T2DM and CHD
• Treatment Goals for Alice
• Conclusions
Faculty/Faculty Disclosures
Yehuda Handelsman, MD, FACP, FACE
Medical Director
Metabolic Institute of America
Chair and Program Director
7th World Congress on InsulinResistance
Chair, International Committeefor Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web Site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb
Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Tethys,
and Xoma; he has received clinical research grant funding from Daiichi Sankyo, Inc., GlaxoSmithKline, Novo Nordisk, and Takeda; and he ison the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Peter H. Jones, MD, FACP
Co-Director, Lipid Metabolism
and Atherosclerosis Clinic
Medical Director, Weight
Management Center
The Methodist Hospital
Associate Professor of Medicine
Section of Atherosclerosis andLipid Research
Baylor College of Medicine
Houston, TX 77030
E-mail: [email protected]
Dr Jones has disclosed that he has received support in the form of consulting agreements from Abbott Laboratories, AstraZeneca Pharmaceuticals LP, Daiichi Sankyo, Inc., and Merck.
Copyright © 2010 Elsevier Inc.
A Case Studies Compendium supplement to Internal Medicine News. This supplement was sponsored by Daiichi Sankyo, Inc.
•Case 1 Topics
•Case 2 Topics
•Faculty/Faculty Disclosures
To view the supplement, click the image above.
Case 1 Topics
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Case 2 Topics
• Background
• Current Visit: Exam Findings
• Current Treatment Regimen
• Health History
• Laboratory Results
• Clinical Discussion
• Cardiologist Visit
• Three Months After Visiting the Cardiologist
• Add-On Therapy With Welchol for Patients With T2DM and CHD
• Treatment Goals for Alice
• Conclusions
Faculty/Faculty Disclosures
Yehuda Handelsman, MD, FACP, FACE
Medical Director
Metabolic Institute of America
Chair and Program Director
7th World Congress on InsulinResistance
Chair, International Committeefor Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web Site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb
Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Tethys,
and Xoma; he has received clinical research grant funding from Daiichi Sankyo, Inc., GlaxoSmithKline, Novo Nordisk, and Takeda; and he ison the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Peter H. Jones, MD, FACP
Co-Director, Lipid Metabolism
and Atherosclerosis Clinic
Medical Director, Weight
Management Center
The Methodist Hospital
Associate Professor of Medicine
Section of Atherosclerosis andLipid Research
Baylor College of Medicine
Houston, TX 77030
E-mail: [email protected]
Dr Jones has disclosed that he has received support in the form of consulting agreements from Abbott Laboratories, AstraZeneca Pharmaceuticals LP, Daiichi Sankyo, Inc., and Merck.
Copyright © 2010 Elsevier Inc.
A Case Studies Compendium supplement to Internal Medicine News. This supplement was sponsored by Daiichi Sankyo, Inc.
•Case 1 Topics
•Case 2 Topics
•Faculty/Faculty Disclosures
To view the supplement, click the image above.
Case 1 Topics
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Case 2 Topics
• Background
• Current Visit: Exam Findings
• Current Treatment Regimen
• Health History
• Laboratory Results
• Clinical Discussion
• Cardiologist Visit
• Three Months After Visiting the Cardiologist
• Add-On Therapy With Welchol for Patients With T2DM and CHD
• Treatment Goals for Alice
• Conclusions
Faculty/Faculty Disclosures
Yehuda Handelsman, MD, FACP, FACE
Medical Director
Metabolic Institute of America
Chair and Program Director
7th World Congress on InsulinResistance
Chair, International Committeefor Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web Site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb
Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Tethys,
and Xoma; he has received clinical research grant funding from Daiichi Sankyo, Inc., GlaxoSmithKline, Novo Nordisk, and Takeda; and he ison the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Peter H. Jones, MD, FACP
Co-Director, Lipid Metabolism
and Atherosclerosis Clinic
Medical Director, Weight
Management Center
The Methodist Hospital
Associate Professor of Medicine
Section of Atherosclerosis andLipid Research
Baylor College of Medicine
Houston, TX 77030
E-mail: [email protected]
Dr Jones has disclosed that he has received support in the form of consulting agreements from Abbott Laboratories, AstraZeneca Pharmaceuticals LP, Daiichi Sankyo, Inc., and Merck.
Copyright © 2010 Elsevier Inc.
Case 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
Case 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
An Approach to the Management of Type 2 Diabetes Mellitus in Patients Receiving Add-On Therapy With Colesevelam HCl
A Journal Scan supplement to Family Practice News
A Journal Scan supplement to Family Practice News
A Journal Scan supplement to Family Practice News
CASE STUDY: Management Decisions in a Comorbid Patient With Type 2 Diabetes Having Primary Hyperlipidemia
A supplement to Internal Medicine News. This supplement was sponsored by Daiichi Sankyo, Inc.
•Topics
•Faculty/Faculty Disclosures

To view the supplement, click the image above.
Topics
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Faculty
Yehuda Handelsman, MD, FACP, FACE
Medical Director, Metabolic Institute of America
Chair and Program Director, 7th World Congress on Insulin Resistance Chair, International Committee for Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Xoma, and Tethys;he has received clinical research grant funding from Takeda, Daiichi Sankyo Inc., GlaxoSmithKline, and Novo Nordisk; and he is on the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Copyright © 2010 Elsevier Inc.
A supplement to Internal Medicine News. This supplement was sponsored by Daiichi Sankyo, Inc.
•Topics
•Faculty/Faculty Disclosures
To view the supplement, click the image above.
Topics
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Faculty
Yehuda Handelsman, MD, FACP, FACE
Medical Director, Metabolic Institute of America
Chair and Program Director, 7th World Congress on Insulin Resistance Chair, International Committee for Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Xoma, and Tethys;he has received clinical research grant funding from Takeda, Daiichi Sankyo Inc., GlaxoSmithKline, and Novo Nordisk; and he is on the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Copyright © 2010 Elsevier Inc.
A supplement to Internal Medicine News. This supplement was sponsored by Daiichi Sankyo, Inc.
•Topics
•Faculty/Faculty Disclosures
To view the supplement, click the image above.
Topics
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Faculty
Yehuda Handelsman, MD, FACP, FACE
Medical Director, Metabolic Institute of America
Chair and Program Director, 7th World Congress on Insulin Resistance Chair, International Committee for Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Xoma, and Tethys;he has received clinical research grant funding from Takeda, Daiichi Sankyo Inc., GlaxoSmithKline, and Novo Nordisk; and he is on the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Copyright © 2010 Elsevier Inc.

Telemedicine on Trial
A new study questioning the efficacy of telemedicine in reducing length of stay (LOS) and improving patient care in the ICU is further proof that remote patient care only works when there is a strong support structure behind it, according to a former SHM president.
“The studies in the past have not shown that just because you have an intensivist available that you are going to get a lot of bang for the buck. You need to have a real process. … If you don’t implement something properly, you can’t expect to get results,” says Mary Jo Gorman, MD, MBA, FHM, former SHM president and CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine.
Investigators at the University of Texas Health Science Center at Houston reviewed some 4,000 patients in six ICUs at five hospitals in a large U.S. healthcare system by measuring outcomes before and after implementation of a “tele-ICU” from 2003 to 2006. No statistically significant impacts were seen in mortality rates, complications, or LOS (JAMA. 2009;302[24]:2671-2678). Conversely, an accompanying editorial in the Journal of the American Medical Association argued that “tele-ICU is a potentially valuable change in ICU care, but its complexity means that ‘tele-ICU improves care’ is not a testable hypothesis.”
The use of off-site intensivists to monitor patients has been used in recent years to address the shortage of ICU physicians. Still, the study team argues that “there are few data in the peer-reviewed literature evaluating its effect on morbidity and mortality.”
Dr. Gorman suggests that HM groups looking to partner with telemedicine providers consider the importance of:
- Following the costs and intricacies of technical implementation;
- Getting local physician buy-in;
- Creating a multidisciplinary approach that includes nurses and pharmacists; and
- Putting periodic reviews in place to measure quality metrics.
“The tool is not the problem,” Dr. Gorman adds. “It’s how do you implement the tool.”
A new study questioning the efficacy of telemedicine in reducing length of stay (LOS) and improving patient care in the ICU is further proof that remote patient care only works when there is a strong support structure behind it, according to a former SHM president.
“The studies in the past have not shown that just because you have an intensivist available that you are going to get a lot of bang for the buck. You need to have a real process. … If you don’t implement something properly, you can’t expect to get results,” says Mary Jo Gorman, MD, MBA, FHM, former SHM president and CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine.
Investigators at the University of Texas Health Science Center at Houston reviewed some 4,000 patients in six ICUs at five hospitals in a large U.S. healthcare system by measuring outcomes before and after implementation of a “tele-ICU” from 2003 to 2006. No statistically significant impacts were seen in mortality rates, complications, or LOS (JAMA. 2009;302[24]:2671-2678). Conversely, an accompanying editorial in the Journal of the American Medical Association argued that “tele-ICU is a potentially valuable change in ICU care, but its complexity means that ‘tele-ICU improves care’ is not a testable hypothesis.”
The use of off-site intensivists to monitor patients has been used in recent years to address the shortage of ICU physicians. Still, the study team argues that “there are few data in the peer-reviewed literature evaluating its effect on morbidity and mortality.”
Dr. Gorman suggests that HM groups looking to partner with telemedicine providers consider the importance of:
- Following the costs and intricacies of technical implementation;
- Getting local physician buy-in;
- Creating a multidisciplinary approach that includes nurses and pharmacists; and
- Putting periodic reviews in place to measure quality metrics.
“The tool is not the problem,” Dr. Gorman adds. “It’s how do you implement the tool.”
A new study questioning the efficacy of telemedicine in reducing length of stay (LOS) and improving patient care in the ICU is further proof that remote patient care only works when there is a strong support structure behind it, according to a former SHM president.
“The studies in the past have not shown that just because you have an intensivist available that you are going to get a lot of bang for the buck. You need to have a real process. … If you don’t implement something properly, you can’t expect to get results,” says Mary Jo Gorman, MD, MBA, FHM, former SHM president and CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine.
Investigators at the University of Texas Health Science Center at Houston reviewed some 4,000 patients in six ICUs at five hospitals in a large U.S. healthcare system by measuring outcomes before and after implementation of a “tele-ICU” from 2003 to 2006. No statistically significant impacts were seen in mortality rates, complications, or LOS (JAMA. 2009;302[24]:2671-2678). Conversely, an accompanying editorial in the Journal of the American Medical Association argued that “tele-ICU is a potentially valuable change in ICU care, but its complexity means that ‘tele-ICU improves care’ is not a testable hypothesis.”
The use of off-site intensivists to monitor patients has been used in recent years to address the shortage of ICU physicians. Still, the study team argues that “there are few data in the peer-reviewed literature evaluating its effect on morbidity and mortality.”
Dr. Gorman suggests that HM groups looking to partner with telemedicine providers consider the importance of:
- Following the costs and intricacies of technical implementation;
- Getting local physician buy-in;
- Creating a multidisciplinary approach that includes nurses and pharmacists; and
- Putting periodic reviews in place to measure quality metrics.
“The tool is not the problem,” Dr. Gorman adds. “It’s how do you implement the tool.”
In the Literature: The Latest Research You Need to Know
Clinical question: What are the efficacy and safety of a simplified “1+1” pain protocol using 1-mg IV hydromorphone followed by an optional repeat dose at patient request 15 minutes later in patients with acute pain?
Background: ED patients receive inadequate treatment of pain. Previously studied protocols utilized weight-based dosing, complex pain scales, and frequent nurse contact to assess and treat pain, making them less useful in a busy ED. A 2-mg single dose hydromorphone protocol provided pain relief, but was associated with oxygen desaturation.
Study design: Prospective interventional cohort study.
Setting: Adult, urban, academic ED with an annual census of approximately 89,000.
Synopsis: Participants included 223 ED patients ages 21 to 64 years old presenting with acute pain (<7 days duration) of sufficient severity to warrant use of IV opioids. Notable exclusion criteria included use of opioids within the past seven days, history of chronic pain, room air saturation <95%, systolic blood pressure <90 mm/Hg, or contraindication to hydromorphone; thus, findings are applicable to a limited set of ED patients presenting with acute pain. The hydromorphone protocol achieved patient expectations of pain relief (defined by decision to forgo additional opioid medication) in 77% of patients within 15 minutes and 96% of patients within one hour. 5% of patients dropped their oxygen saturations to <95%, but all increased promptly with 4L nasal cannula. Only 1% of patients dropped their respiratory rate to <12 breaths/minute and systolic blood pressure to <100 mm/Hg; none required naloxone use.
Limitations include lack of comparison group, unblinded design, and findings from a single urban center (in which participants were 60% Hispanic, 29% black, and 65% female). While there were no serious adverse events, the sample size is not large enough to identify rare events.
Bottom line: In nonelderly adult ED patients without a history of chronic pain or recent opioids, a pain protocol of 1-mg IV hydromorphone repeated in 15 minutes if needed is effective and safe, assuming typical ED monitoring for hypoxia and respiratory depression.
Citation: Chang AK, Bijur PE, Campbell CM, Murphy MK, Gallagher EJ. Safety and efficacy of rapid titration using 1mg doses of intravenous hydromorphone in emergency department patients with acute severe pain: the “1+1” protocol. Ann Emerg Med. 2009;54(2):221-225.
Reviewed for TH eWire by Bhaskar Arora, MD, Thomas Barrett, MD, MCR, FHM, Honora Englander, MD, Stephanie Halvorson, MD, Alan J. Hunter, MD, David Kagen, MD, Blake Lesselroth, MD, MBI, Portland Veterans Affairs Medical Center and Division of Hospital Medicine, Oregon Health & Science University
For more HM-related literature reviews, visit our Web site.
Clinical question: What are the efficacy and safety of a simplified “1+1” pain protocol using 1-mg IV hydromorphone followed by an optional repeat dose at patient request 15 minutes later in patients with acute pain?
Background: ED patients receive inadequate treatment of pain. Previously studied protocols utilized weight-based dosing, complex pain scales, and frequent nurse contact to assess and treat pain, making them less useful in a busy ED. A 2-mg single dose hydromorphone protocol provided pain relief, but was associated with oxygen desaturation.
Study design: Prospective interventional cohort study.
Setting: Adult, urban, academic ED with an annual census of approximately 89,000.
Synopsis: Participants included 223 ED patients ages 21 to 64 years old presenting with acute pain (<7 days duration) of sufficient severity to warrant use of IV opioids. Notable exclusion criteria included use of opioids within the past seven days, history of chronic pain, room air saturation <95%, systolic blood pressure <90 mm/Hg, or contraindication to hydromorphone; thus, findings are applicable to a limited set of ED patients presenting with acute pain. The hydromorphone protocol achieved patient expectations of pain relief (defined by decision to forgo additional opioid medication) in 77% of patients within 15 minutes and 96% of patients within one hour. 5% of patients dropped their oxygen saturations to <95%, but all increased promptly with 4L nasal cannula. Only 1% of patients dropped their respiratory rate to <12 breaths/minute and systolic blood pressure to <100 mm/Hg; none required naloxone use.
Limitations include lack of comparison group, unblinded design, and findings from a single urban center (in which participants were 60% Hispanic, 29% black, and 65% female). While there were no serious adverse events, the sample size is not large enough to identify rare events.
Bottom line: In nonelderly adult ED patients without a history of chronic pain or recent opioids, a pain protocol of 1-mg IV hydromorphone repeated in 15 minutes if needed is effective and safe, assuming typical ED monitoring for hypoxia and respiratory depression.
Citation: Chang AK, Bijur PE, Campbell CM, Murphy MK, Gallagher EJ. Safety and efficacy of rapid titration using 1mg doses of intravenous hydromorphone in emergency department patients with acute severe pain: the “1+1” protocol. Ann Emerg Med. 2009;54(2):221-225.
Reviewed for TH eWire by Bhaskar Arora, MD, Thomas Barrett, MD, MCR, FHM, Honora Englander, MD, Stephanie Halvorson, MD, Alan J. Hunter, MD, David Kagen, MD, Blake Lesselroth, MD, MBI, Portland Veterans Affairs Medical Center and Division of Hospital Medicine, Oregon Health & Science University
For more HM-related literature reviews, visit our Web site.
Clinical question: What are the efficacy and safety of a simplified “1+1” pain protocol using 1-mg IV hydromorphone followed by an optional repeat dose at patient request 15 minutes later in patients with acute pain?
Background: ED patients receive inadequate treatment of pain. Previously studied protocols utilized weight-based dosing, complex pain scales, and frequent nurse contact to assess and treat pain, making them less useful in a busy ED. A 2-mg single dose hydromorphone protocol provided pain relief, but was associated with oxygen desaturation.
Study design: Prospective interventional cohort study.
Setting: Adult, urban, academic ED with an annual census of approximately 89,000.
Synopsis: Participants included 223 ED patients ages 21 to 64 years old presenting with acute pain (<7 days duration) of sufficient severity to warrant use of IV opioids. Notable exclusion criteria included use of opioids within the past seven days, history of chronic pain, room air saturation <95%, systolic blood pressure <90 mm/Hg, or contraindication to hydromorphone; thus, findings are applicable to a limited set of ED patients presenting with acute pain. The hydromorphone protocol achieved patient expectations of pain relief (defined by decision to forgo additional opioid medication) in 77% of patients within 15 minutes and 96% of patients within one hour. 5% of patients dropped their oxygen saturations to <95%, but all increased promptly with 4L nasal cannula. Only 1% of patients dropped their respiratory rate to <12 breaths/minute and systolic blood pressure to <100 mm/Hg; none required naloxone use.
Limitations include lack of comparison group, unblinded design, and findings from a single urban center (in which participants were 60% Hispanic, 29% black, and 65% female). While there were no serious adverse events, the sample size is not large enough to identify rare events.
Bottom line: In nonelderly adult ED patients without a history of chronic pain or recent opioids, a pain protocol of 1-mg IV hydromorphone repeated in 15 minutes if needed is effective and safe, assuming typical ED monitoring for hypoxia and respiratory depression.
Citation: Chang AK, Bijur PE, Campbell CM, Murphy MK, Gallagher EJ. Safety and efficacy of rapid titration using 1mg doses of intravenous hydromorphone in emergency department patients with acute severe pain: the “1+1” protocol. Ann Emerg Med. 2009;54(2):221-225.
Reviewed for TH eWire by Bhaskar Arora, MD, Thomas Barrett, MD, MCR, FHM, Honora Englander, MD, Stephanie Halvorson, MD, Alan J. Hunter, MD, David Kagen, MD, Blake Lesselroth, MD, MBI, Portland Veterans Affairs Medical Center and Division of Hospital Medicine, Oregon Health & Science University
For more HM-related literature reviews, visit our Web site.