User login
Using Co-Design Methods to Create a Patient-Oriented Discharge Summary
From the OpenLab, University Health Network, Toronto, Canada (Dr. Hahn-Goldberg, Dr. Okrainec, Dr. Abrams, Mr. Huynh); School of Health Policy and Management, York University, Toronto (Dr. Hahn-Goldberg); Toronto Central Local Health Integration Network (Ms. Damba); Centre for Addiction and Mental Health, Toronto (Ms. Solomon); and the Department of Medicine, University Health Network, Toronto (Dr. Okrainec, Dr. Abrams).
Abstract
- Objective: To describe the co-design process we under-took to create a patient-oriented discharge summary (PODS) with patients, caregivers, and providers.
- Method: Descriptive report.
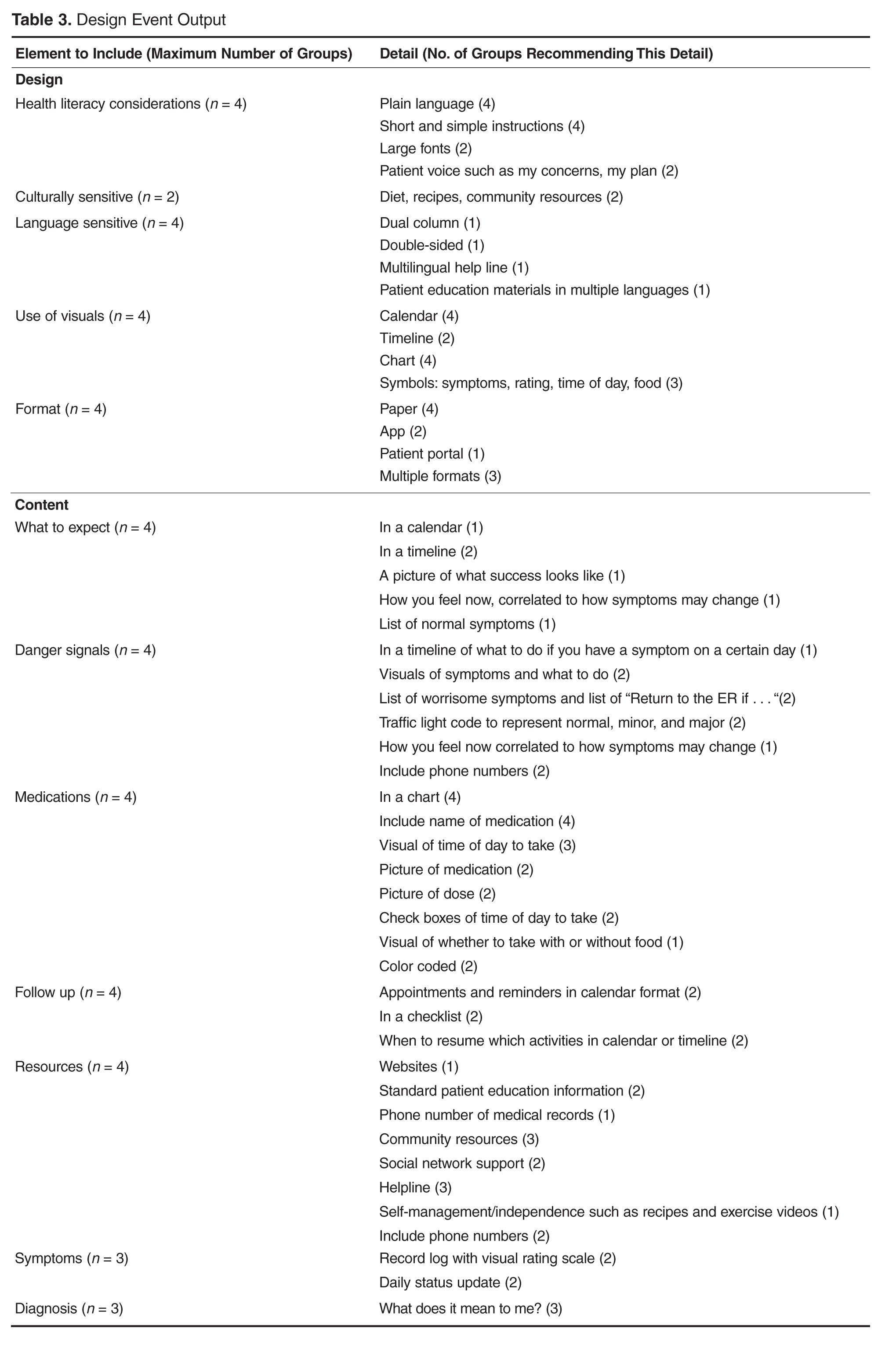
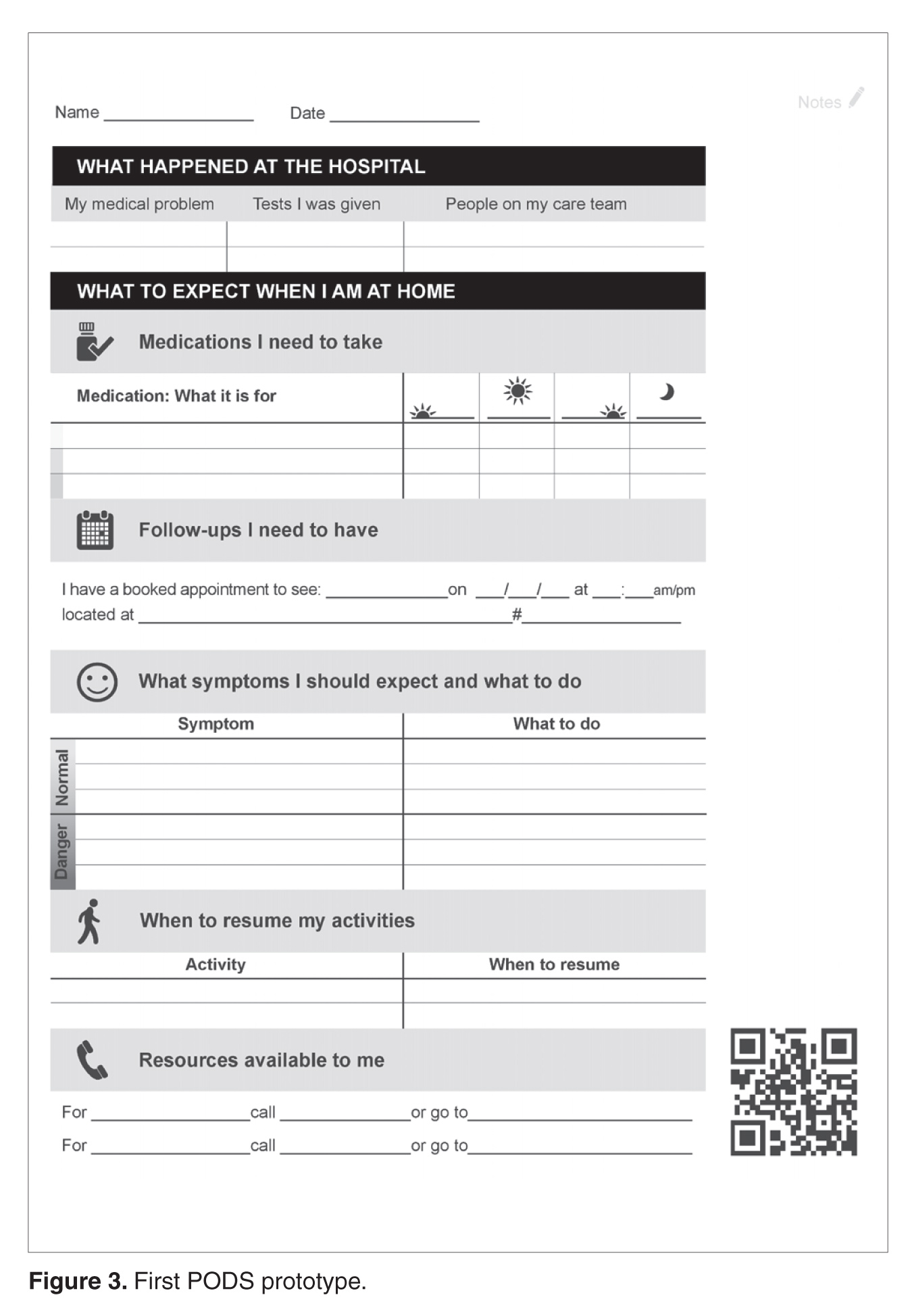
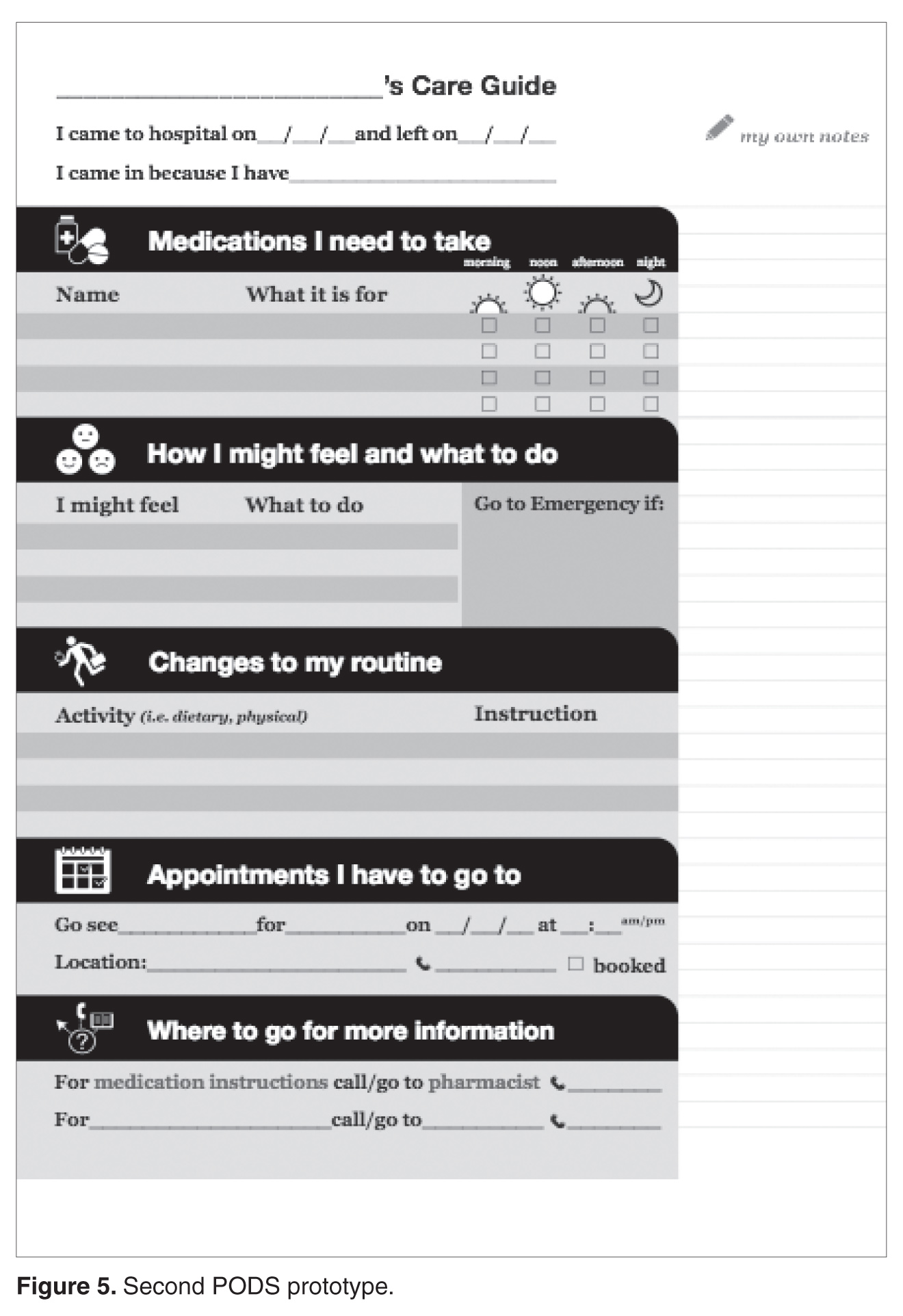
- Results: We designed and produced a prototype PODS, based on best practices in information design, graphic design, and patient education. Through a co-design process, patients, health care providers, designers and system planners worked together to establish what content needed to be included, as well as how it would be organized and presented. From an initial prototype, we then refined the PODS through an iterative participatory design process involving patients, including those from hard-to-reach groups such as patients with language barriers and/or low health literacy and patients with a primary psychiatric diagnosis.
- Conclusion: Co-design events and targeted focus groups are very useful for engaging patients and caregivers in the design and development of solutions aimed at improving their experience of care. It is important to include all users, especially those who are harder to reach, such as patients with language barriers and mental health conditions. Engaging health care providers is essential to ensure feasibility of those solutions.
Traditional discharge summaries are written primarily for the patient’s primary care provider and are not designed as tools to support communication between the clinician and patient regarding instructions for patients to follow at home post discharge. A more patient-centered version of the discharge summary is needed to complement the traditional format.
To enhance our patients’ care experience in the post-discharge period, we set out to co-design a patient-oriented discharge summary (PODS) with patients, caregivers, and providers. The main objective of this project was to develop a prototype PODS that not only addressed critical information that patients felt was the most important to know following discharge, but also provided this information in the most comprehensible format at hospitals within the Toronto area. The project focused on reformatting patient-care instructions for patients discharged from inpatient medical wards as these instructions presented the best opportunity for improvement.
This project drew on work done in countries such as India, South Africa, and Pakistan, where challenges with general and health literacy have led to the introduction of simplified discharge forms and medication instructions that place a greater emphasis on visual communication to improve information comprehension. For example, the use of pictograms in patient materials has been shown to increase patient understanding of and compliance with care instructions in these countries [1–3].
We have provided an overview of the PODS project elsewhere [4]. In this article, we describe the co-design process we undertook with patients, health care providers, and designers in creating a PODS.
Design Methods
We used several methods to design and develop the PODS and to engage multiple stakeholders in the design process. Among these methods were innovative techniques for understanding the patient experience of discharge, such as cultural probes [5], where patients were given journals and cameras to document their time at home after discharge, as described by Hahn-Goldberg et al [4]. Other key methods for determining the design of the PODS included:
Patient education consultation. A patient education representative with training and expertise in designing materials for patients with low health literacy was added to the team advisory committee to act as a consultant at all stages of the study. This helped to ensure that we would be following best practices in design for our target population.
Review of literature. We reviewed the literature pertaining to design for patients with low health literacy and language barriers, including the resources available through the patient education department at the University Health Network.
Review of Toronto Central Local Health Integration Network (TCLHIN) hospitals’ tools: current discharge summaries, components they included and how they were formatted.
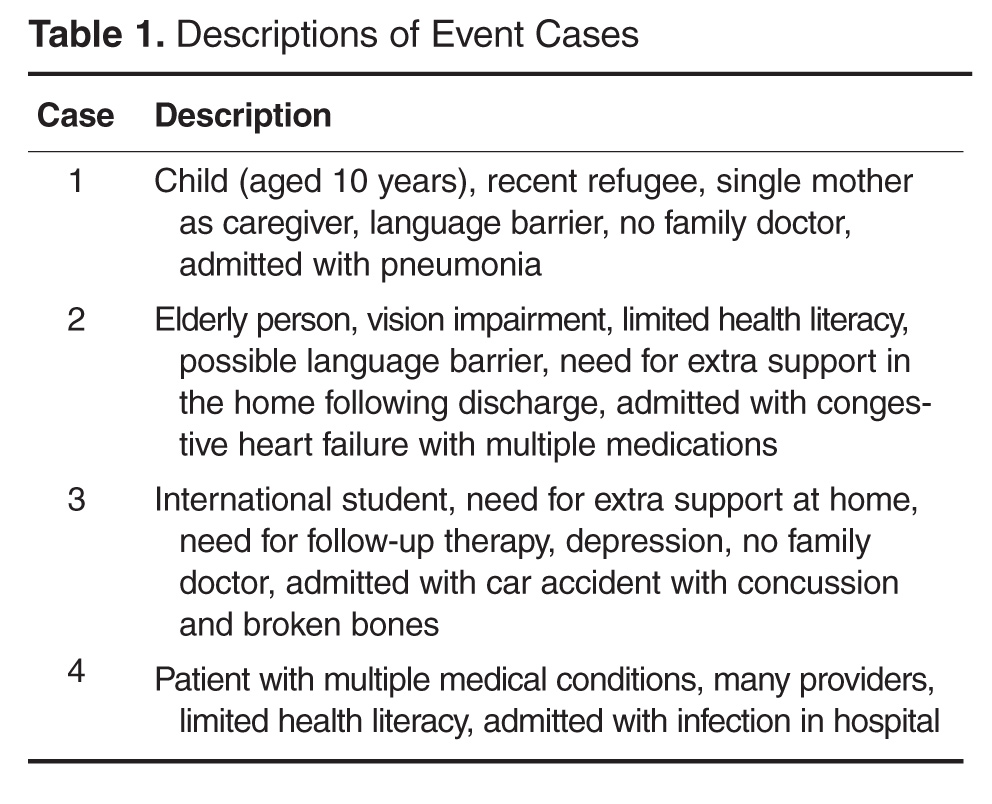
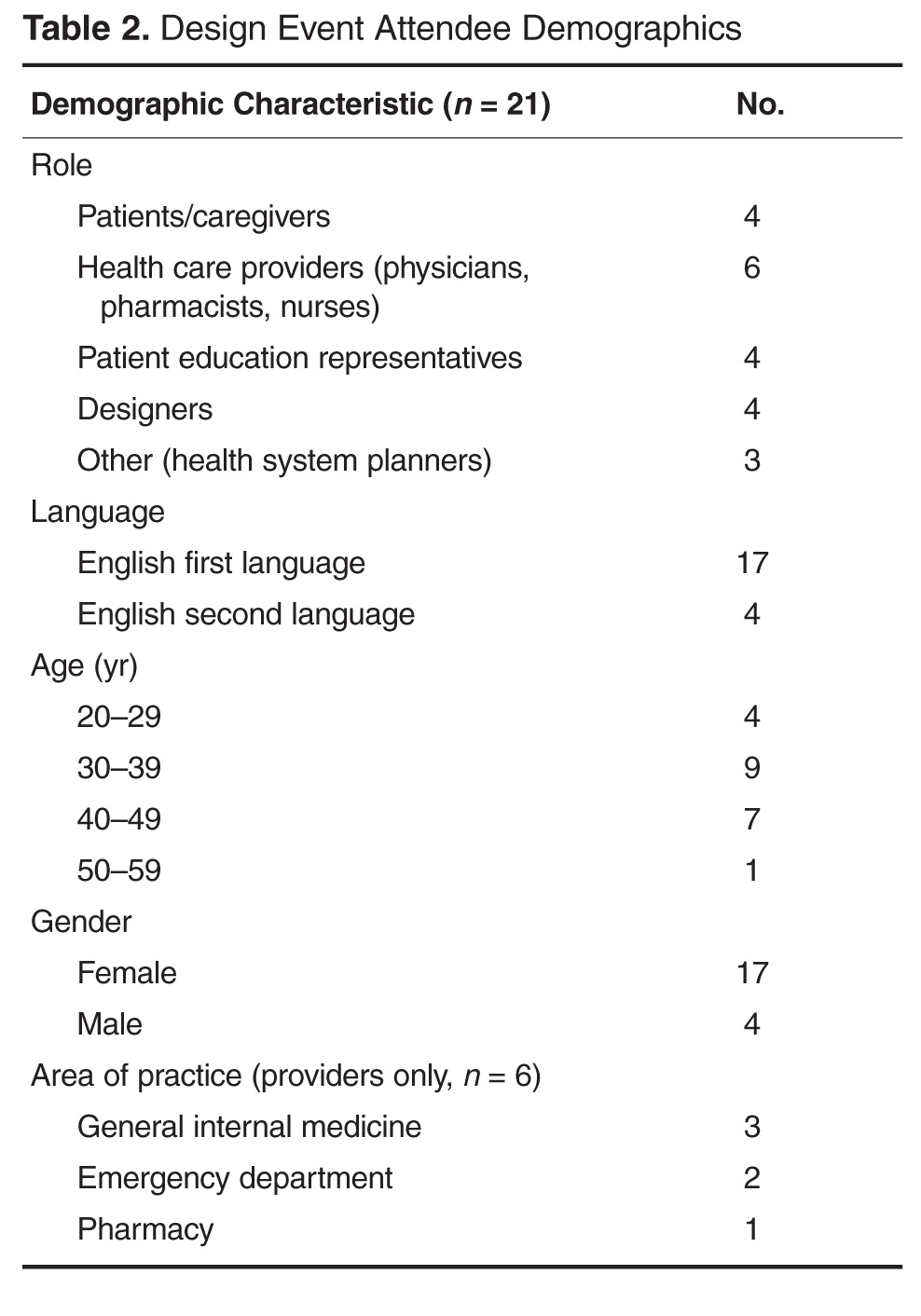
Co-design event. We held an interprofessional design event where teams of patients, health care providers, and designers worked together to create draft PODS for 4 hypothetical patient cases.
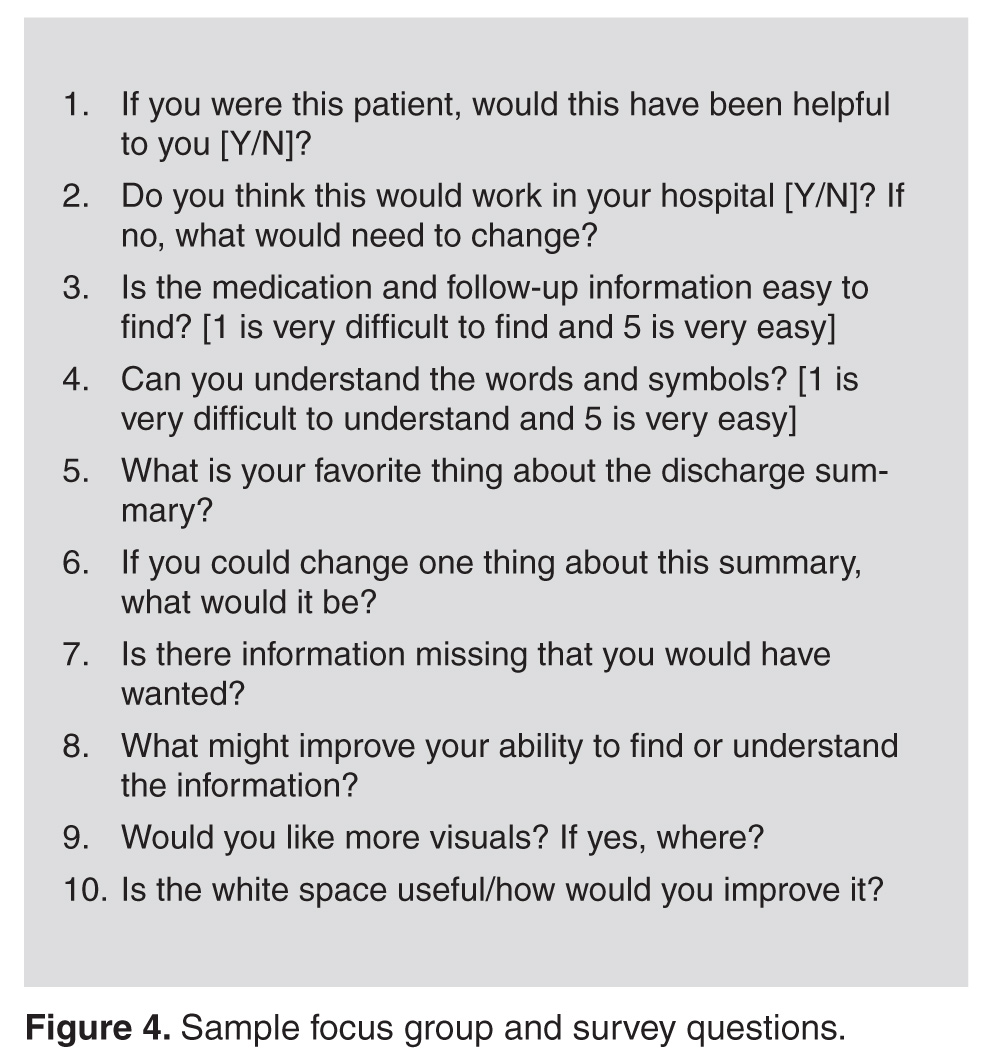
Focus groups and surveys. We used feedback from focus groups and surveys to revise and improve the first PODS prototype.
Insights from the Literature
Studies have shown that multiple interventions tend to increase adherence, that self-management should be encouraged, and that modes of communication other than verbal must be used [6]. Visual cues, such as pictures or symbols, are useful to help with recall of medications and instructions for people with language barriers or limited health literacy [7]. Simplified written instructions and larger fonts have been found to be effective in patients with language barriers or limited health literacy, as have use of illustrated medication schedules [8]. Other guidelines include using short words and sentences, writing directly to the reader, listing important points in list format, and using left justification so there is even spacing between words.
The literature is consistent with our findings from speaking with patient education representatives and patients. Patients and caregivers noted that the PODS should be written in plain language, use large fonts, include illustrations of care and medication schedules, and include headings that are meaningful to the patient. Patients also expressed the desire for charts and lists that they could use while completing their follow-up care plan.
“My mom made me a chart of when to drink water and how much (patient).”
“We were given a sheet to record all feedings (caregiver).”
“We can provide a list of patient meds in a grid format with days of the week and times of day. We use our judgement to give this to patients. It is not standard practice (pharmacist).”
“A discharge form in ‘plain English’ should be standardized (patient).”
The Co-design Event
Solutions resulting from the design event ranged from more traditional discharge summaries that were enhanced with multiple languages and images to make things clear for patients, to solutions including interactive patient portals. There were solutions that came with stickers to color-code your medications, areas for patients to write notes, and checklists for them to keep track of all their follow-up plans. 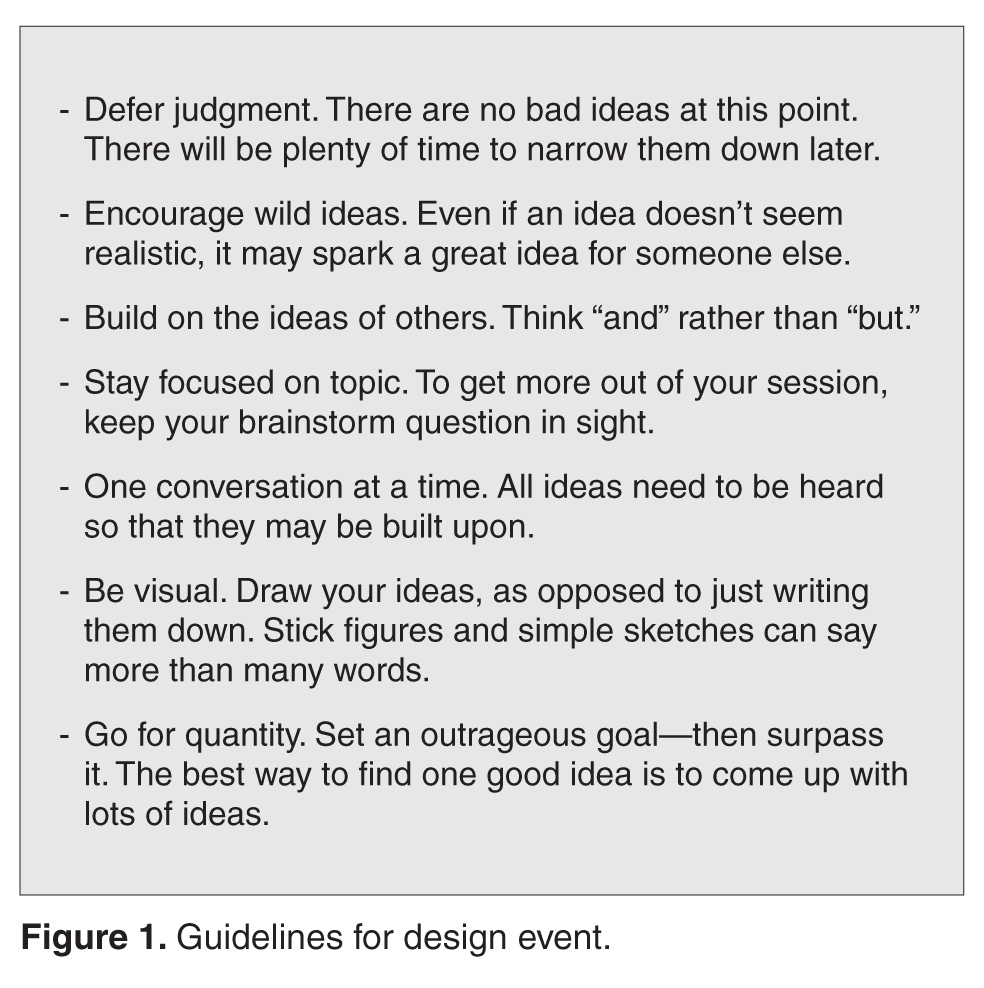
Refining the Design Using Focus Groups and Surveys
The ideas and concepts generated during the design event were analyzed by the interdisciplinary advisory team at OpenLab. In addition, several team sessions were held with health care 
This is a great piece. You guys are doing an awesome job. This would have saved me so much anxiety and fear of doing something wrong when I was discharged. I didn’t want to bother my doctors and went on a hope and prayer. Even my home care people weren’t always sure of what to do. Again this would be a great step forward in easing patients’ fears, especially senior citizens. GREAT WORK. THANKS FOR CARING.
Discussion
Innovative methods such as co-design events and targeted focus groups are very useful for 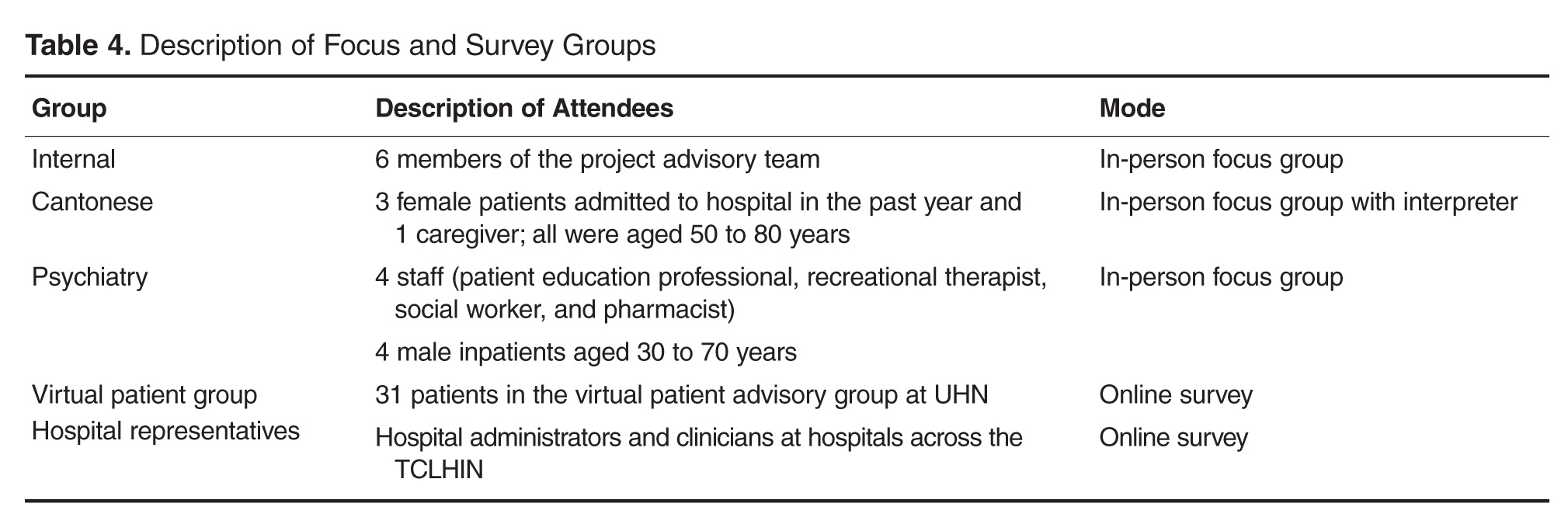

Future Plans
The PODS template has now been adapted and implemented in several hospitals in Toronto, Canada, using a supported early adopter process [10]. Future plans are to test the impact of the PODS on patient experience and health outcomes using a randomized controlled trial. Also, for now, we have focused on a paper version of PODS, but with the increasing prevalence of electronic health records and consumer-oriented health care apps, future consideration for a digital and mobile version of PODS is warranted.
Conclusion
Patients need to be prepared for discharge so that they can engage in supported self-management once they return home. 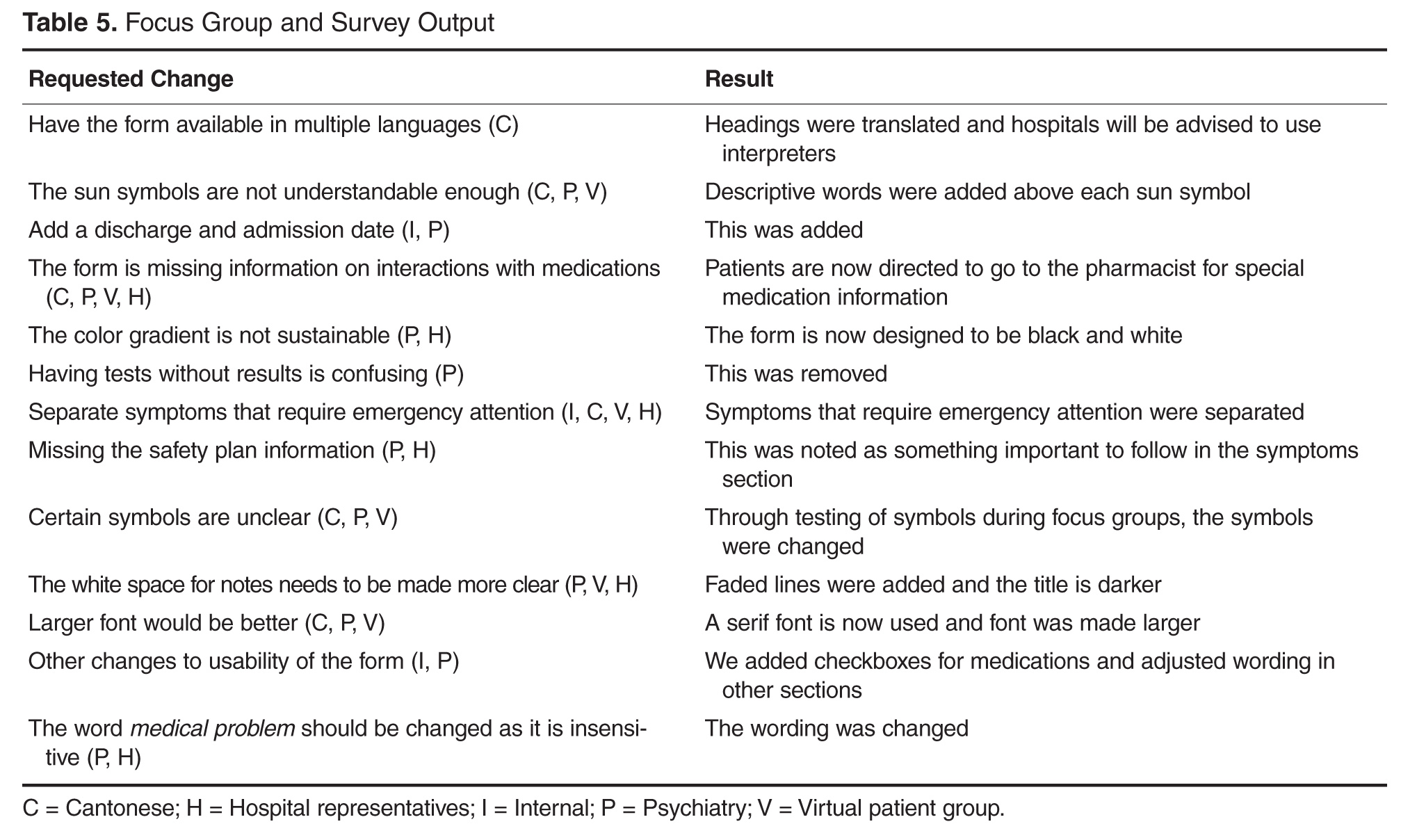
Corresponding author: Shoshana Hahn-Goldberg, PhD, 294 Mullen Dr., Thornhill, ON L4J 2P2.
Funding/support: The PODS project has been funded by the Toronto Central Local Health Integration Network.
Financial disclosures: None.
1. Rajesh R, Vidyasagar S, Varma M, Sharma S. Design And evaluation of pictograms for communicating information about adverse drug reactions to antiretroviral therapy in Indian human immunodeficiency virus positive patients. J Pharm Biomed Sci 2012;16:1–11.
2. Dowse R, Ehlers MS. The evaluation of pharmaceutical pictograms in a low-literate South African population. Patient Educ Couns 2001;45:87–99.
3. Clayton M, Syed F, Rashid A, Fayyaz U. Improving illiterate patients’ understanding and adherence to discharge medications. BMJ Qual Improv Rep 2012;1:u496.w167.
4. Hahn-Goldberg S, Okrainec K, Huynh T, et al. Co-creating patient-oriented instructions with patients, caregivers, and providers. J Hosp Med 2015;10:804–7.
5. Gaver B, Dunne T, Pacenti E. Design: cultural probes. Interactions 1999;6:21–9.
6. Sheridan SL, Halpern DJ, Viera AJ, et al. Interventions for individuals with low health literacy: a systematic review. J Health Commun 2011;16 Suppl 3:30–54.
7. Schillinger D, Machtinger EL, Wang F, et al. Language, literacy, and communication regarding medications in an anticoagulation clinic: A comparison of verbal vs. visual assessment. J Health Commun 2006;11:651–4.
8. Chugh A, Williams MV, Grigsby J, Coleman EA. Better transitions: Improving comprehension of discharge instructions. Front Health Serv Manage 2009;25:11–32.
9. IDEO. Design thinking for educators toolkit. 2nd ed. New York: IDEObooks; 2013.
10. Hahn-Goldberg S, Okrainec K, Damba C, et al. Implementing patient oriented discharge summaries (PODS): A multi-site pilot across early adopter hospitals. Healthc Q 2016;19:42–8.
From the OpenLab, University Health Network, Toronto, Canada (Dr. Hahn-Goldberg, Dr. Okrainec, Dr. Abrams, Mr. Huynh); School of Health Policy and Management, York University, Toronto (Dr. Hahn-Goldberg); Toronto Central Local Health Integration Network (Ms. Damba); Centre for Addiction and Mental Health, Toronto (Ms. Solomon); and the Department of Medicine, University Health Network, Toronto (Dr. Okrainec, Dr. Abrams).
Abstract
- Objective: To describe the co-design process we under-took to create a patient-oriented discharge summary (PODS) with patients, caregivers, and providers.
- Method: Descriptive report.
- Results: We designed and produced a prototype PODS, based on best practices in information design, graphic design, and patient education. Through a co-design process, patients, health care providers, designers and system planners worked together to establish what content needed to be included, as well as how it would be organized and presented. From an initial prototype, we then refined the PODS through an iterative participatory design process involving patients, including those from hard-to-reach groups such as patients with language barriers and/or low health literacy and patients with a primary psychiatric diagnosis.
- Conclusion: Co-design events and targeted focus groups are very useful for engaging patients and caregivers in the design and development of solutions aimed at improving their experience of care. It is important to include all users, especially those who are harder to reach, such as patients with language barriers and mental health conditions. Engaging health care providers is essential to ensure feasibility of those solutions.
Traditional discharge summaries are written primarily for the patient’s primary care provider and are not designed as tools to support communication between the clinician and patient regarding instructions for patients to follow at home post discharge. A more patient-centered version of the discharge summary is needed to complement the traditional format.
To enhance our patients’ care experience in the post-discharge period, we set out to co-design a patient-oriented discharge summary (PODS) with patients, caregivers, and providers. The main objective of this project was to develop a prototype PODS that not only addressed critical information that patients felt was the most important to know following discharge, but also provided this information in the most comprehensible format at hospitals within the Toronto area. The project focused on reformatting patient-care instructions for patients discharged from inpatient medical wards as these instructions presented the best opportunity for improvement.
This project drew on work done in countries such as India, South Africa, and Pakistan, where challenges with general and health literacy have led to the introduction of simplified discharge forms and medication instructions that place a greater emphasis on visual communication to improve information comprehension. For example, the use of pictograms in patient materials has been shown to increase patient understanding of and compliance with care instructions in these countries [1–3].
We have provided an overview of the PODS project elsewhere [4]. In this article, we describe the co-design process we undertook with patients, health care providers, and designers in creating a PODS.
Design Methods
We used several methods to design and develop the PODS and to engage multiple stakeholders in the design process. Among these methods were innovative techniques for understanding the patient experience of discharge, such as cultural probes [5], where patients were given journals and cameras to document their time at home after discharge, as described by Hahn-Goldberg et al [4]. Other key methods for determining the design of the PODS included:
Patient education consultation. A patient education representative with training and expertise in designing materials for patients with low health literacy was added to the team advisory committee to act as a consultant at all stages of the study. This helped to ensure that we would be following best practices in design for our target population.
Review of literature. We reviewed the literature pertaining to design for patients with low health literacy and language barriers, including the resources available through the patient education department at the University Health Network.
Review of Toronto Central Local Health Integration Network (TCLHIN) hospitals’ tools: current discharge summaries, components they included and how they were formatted.
Co-design event. We held an interprofessional design event where teams of patients, health care providers, and designers worked together to create draft PODS for 4 hypothetical patient cases.
Focus groups and surveys. We used feedback from focus groups and surveys to revise and improve the first PODS prototype.
Insights from the Literature
Studies have shown that multiple interventions tend to increase adherence, that self-management should be encouraged, and that modes of communication other than verbal must be used [6]. Visual cues, such as pictures or symbols, are useful to help with recall of medications and instructions for people with language barriers or limited health literacy [7]. Simplified written instructions and larger fonts have been found to be effective in patients with language barriers or limited health literacy, as have use of illustrated medication schedules [8]. Other guidelines include using short words and sentences, writing directly to the reader, listing important points in list format, and using left justification so there is even spacing between words.
The literature is consistent with our findings from speaking with patient education representatives and patients. Patients and caregivers noted that the PODS should be written in plain language, use large fonts, include illustrations of care and medication schedules, and include headings that are meaningful to the patient. Patients also expressed the desire for charts and lists that they could use while completing their follow-up care plan.
“My mom made me a chart of when to drink water and how much (patient).”
“We were given a sheet to record all feedings (caregiver).”
“We can provide a list of patient meds in a grid format with days of the week and times of day. We use our judgement to give this to patients. It is not standard practice (pharmacist).”
“A discharge form in ‘plain English’ should be standardized (patient).”
The Co-design Event
Solutions resulting from the design event ranged from more traditional discharge summaries that were enhanced with multiple languages and images to make things clear for patients, to solutions including interactive patient portals. There were solutions that came with stickers to color-code your medications, areas for patients to write notes, and checklists for them to keep track of all their follow-up plans.
Refining the Design Using Focus Groups and Surveys
The ideas and concepts generated during the design event were analyzed by the interdisciplinary advisory team at OpenLab. In addition, several team sessions were held with health care
This is a great piece. You guys are doing an awesome job. This would have saved me so much anxiety and fear of doing something wrong when I was discharged. I didn’t want to bother my doctors and went on a hope and prayer. Even my home care people weren’t always sure of what to do. Again this would be a great step forward in easing patients’ fears, especially senior citizens. GREAT WORK. THANKS FOR CARING.
Discussion
Innovative methods such as co-design events and targeted focus groups are very useful for
Future Plans
The PODS template has now been adapted and implemented in several hospitals in Toronto, Canada, using a supported early adopter process [10]. Future plans are to test the impact of the PODS on patient experience and health outcomes using a randomized controlled trial. Also, for now, we have focused on a paper version of PODS, but with the increasing prevalence of electronic health records and consumer-oriented health care apps, future consideration for a digital and mobile version of PODS is warranted.
Conclusion
Patients need to be prepared for discharge so that they can engage in supported self-management once they return home.
Corresponding author: Shoshana Hahn-Goldberg, PhD, 294 Mullen Dr., Thornhill, ON L4J 2P2.
Funding/support: The PODS project has been funded by the Toronto Central Local Health Integration Network.
Financial disclosures: None.
From the OpenLab, University Health Network, Toronto, Canada (Dr. Hahn-Goldberg, Dr. Okrainec, Dr. Abrams, Mr. Huynh); School of Health Policy and Management, York University, Toronto (Dr. Hahn-Goldberg); Toronto Central Local Health Integration Network (Ms. Damba); Centre for Addiction and Mental Health, Toronto (Ms. Solomon); and the Department of Medicine, University Health Network, Toronto (Dr. Okrainec, Dr. Abrams).
Abstract
- Objective: To describe the co-design process we under-took to create a patient-oriented discharge summary (PODS) with patients, caregivers, and providers.
- Method: Descriptive report.
- Results: We designed and produced a prototype PODS, based on best practices in information design, graphic design, and patient education. Through a co-design process, patients, health care providers, designers and system planners worked together to establish what content needed to be included, as well as how it would be organized and presented. From an initial prototype, we then refined the PODS through an iterative participatory design process involving patients, including those from hard-to-reach groups such as patients with language barriers and/or low health literacy and patients with a primary psychiatric diagnosis.
- Conclusion: Co-design events and targeted focus groups are very useful for engaging patients and caregivers in the design and development of solutions aimed at improving their experience of care. It is important to include all users, especially those who are harder to reach, such as patients with language barriers and mental health conditions. Engaging health care providers is essential to ensure feasibility of those solutions.
Traditional discharge summaries are written primarily for the patient’s primary care provider and are not designed as tools to support communication between the clinician and patient regarding instructions for patients to follow at home post discharge. A more patient-centered version of the discharge summary is needed to complement the traditional format.
To enhance our patients’ care experience in the post-discharge period, we set out to co-design a patient-oriented discharge summary (PODS) with patients, caregivers, and providers. The main objective of this project was to develop a prototype PODS that not only addressed critical information that patients felt was the most important to know following discharge, but also provided this information in the most comprehensible format at hospitals within the Toronto area. The project focused on reformatting patient-care instructions for patients discharged from inpatient medical wards as these instructions presented the best opportunity for improvement.
This project drew on work done in countries such as India, South Africa, and Pakistan, where challenges with general and health literacy have led to the introduction of simplified discharge forms and medication instructions that place a greater emphasis on visual communication to improve information comprehension. For example, the use of pictograms in patient materials has been shown to increase patient understanding of and compliance with care instructions in these countries [1–3].
We have provided an overview of the PODS project elsewhere [4]. In this article, we describe the co-design process we undertook with patients, health care providers, and designers in creating a PODS.
Design Methods
We used several methods to design and develop the PODS and to engage multiple stakeholders in the design process. Among these methods were innovative techniques for understanding the patient experience of discharge, such as cultural probes [5], where patients were given journals and cameras to document their time at home after discharge, as described by Hahn-Goldberg et al [4]. Other key methods for determining the design of the PODS included:
Patient education consultation. A patient education representative with training and expertise in designing materials for patients with low health literacy was added to the team advisory committee to act as a consultant at all stages of the study. This helped to ensure that we would be following best practices in design for our target population.
Review of literature. We reviewed the literature pertaining to design for patients with low health literacy and language barriers, including the resources available through the patient education department at the University Health Network.
Review of Toronto Central Local Health Integration Network (TCLHIN) hospitals’ tools: current discharge summaries, components they included and how they were formatted.
Co-design event. We held an interprofessional design event where teams of patients, health care providers, and designers worked together to create draft PODS for 4 hypothetical patient cases.
Focus groups and surveys. We used feedback from focus groups and surveys to revise and improve the first PODS prototype.
Insights from the Literature
Studies have shown that multiple interventions tend to increase adherence, that self-management should be encouraged, and that modes of communication other than verbal must be used [6]. Visual cues, such as pictures or symbols, are useful to help with recall of medications and instructions for people with language barriers or limited health literacy [7]. Simplified written instructions and larger fonts have been found to be effective in patients with language barriers or limited health literacy, as have use of illustrated medication schedules [8]. Other guidelines include using short words and sentences, writing directly to the reader, listing important points in list format, and using left justification so there is even spacing between words.
The literature is consistent with our findings from speaking with patient education representatives and patients. Patients and caregivers noted that the PODS should be written in plain language, use large fonts, include illustrations of care and medication schedules, and include headings that are meaningful to the patient. Patients also expressed the desire for charts and lists that they could use while completing their follow-up care plan.
“My mom made me a chart of when to drink water and how much (patient).”
“We were given a sheet to record all feedings (caregiver).”
“We can provide a list of patient meds in a grid format with days of the week and times of day. We use our judgement to give this to patients. It is not standard practice (pharmacist).”
“A discharge form in ‘plain English’ should be standardized (patient).”
The Co-design Event
Solutions resulting from the design event ranged from more traditional discharge summaries that were enhanced with multiple languages and images to make things clear for patients, to solutions including interactive patient portals. There were solutions that came with stickers to color-code your medications, areas for patients to write notes, and checklists for them to keep track of all their follow-up plans.
Refining the Design Using Focus Groups and Surveys
The ideas and concepts generated during the design event were analyzed by the interdisciplinary advisory team at OpenLab. In addition, several team sessions were held with health care
This is a great piece. You guys are doing an awesome job. This would have saved me so much anxiety and fear of doing something wrong when I was discharged. I didn’t want to bother my doctors and went on a hope and prayer. Even my home care people weren’t always sure of what to do. Again this would be a great step forward in easing patients’ fears, especially senior citizens. GREAT WORK. THANKS FOR CARING.
Discussion
Innovative methods such as co-design events and targeted focus groups are very useful for
Future Plans
The PODS template has now been adapted and implemented in several hospitals in Toronto, Canada, using a supported early adopter process [10]. Future plans are to test the impact of the PODS on patient experience and health outcomes using a randomized controlled trial. Also, for now, we have focused on a paper version of PODS, but with the increasing prevalence of electronic health records and consumer-oriented health care apps, future consideration for a digital and mobile version of PODS is warranted.
Conclusion
Patients need to be prepared for discharge so that they can engage in supported self-management once they return home.
Corresponding author: Shoshana Hahn-Goldberg, PhD, 294 Mullen Dr., Thornhill, ON L4J 2P2.
Funding/support: The PODS project has been funded by the Toronto Central Local Health Integration Network.
Financial disclosures: None.
1. Rajesh R, Vidyasagar S, Varma M, Sharma S. Design And evaluation of pictograms for communicating information about adverse drug reactions to antiretroviral therapy in Indian human immunodeficiency virus positive patients. J Pharm Biomed Sci 2012;16:1–11.
2. Dowse R, Ehlers MS. The evaluation of pharmaceutical pictograms in a low-literate South African population. Patient Educ Couns 2001;45:87–99.
3. Clayton M, Syed F, Rashid A, Fayyaz U. Improving illiterate patients’ understanding and adherence to discharge medications. BMJ Qual Improv Rep 2012;1:u496.w167.
4. Hahn-Goldberg S, Okrainec K, Huynh T, et al. Co-creating patient-oriented instructions with patients, caregivers, and providers. J Hosp Med 2015;10:804–7.
5. Gaver B, Dunne T, Pacenti E. Design: cultural probes. Interactions 1999;6:21–9.
6. Sheridan SL, Halpern DJ, Viera AJ, et al. Interventions for individuals with low health literacy: a systematic review. J Health Commun 2011;16 Suppl 3:30–54.
7. Schillinger D, Machtinger EL, Wang F, et al. Language, literacy, and communication regarding medications in an anticoagulation clinic: A comparison of verbal vs. visual assessment. J Health Commun 2006;11:651–4.
8. Chugh A, Williams MV, Grigsby J, Coleman EA. Better transitions: Improving comprehension of discharge instructions. Front Health Serv Manage 2009;25:11–32.
9. IDEO. Design thinking for educators toolkit. 2nd ed. New York: IDEObooks; 2013.
10. Hahn-Goldberg S, Okrainec K, Damba C, et al. Implementing patient oriented discharge summaries (PODS): A multi-site pilot across early adopter hospitals. Healthc Q 2016;19:42–8.
1. Rajesh R, Vidyasagar S, Varma M, Sharma S. Design And evaluation of pictograms for communicating information about adverse drug reactions to antiretroviral therapy in Indian human immunodeficiency virus positive patients. J Pharm Biomed Sci 2012;16:1–11.
2. Dowse R, Ehlers MS. The evaluation of pharmaceutical pictograms in a low-literate South African population. Patient Educ Couns 2001;45:87–99.
3. Clayton M, Syed F, Rashid A, Fayyaz U. Improving illiterate patients’ understanding and adherence to discharge medications. BMJ Qual Improv Rep 2012;1:u496.w167.
4. Hahn-Goldberg S, Okrainec K, Huynh T, et al. Co-creating patient-oriented instructions with patients, caregivers, and providers. J Hosp Med 2015;10:804–7.
5. Gaver B, Dunne T, Pacenti E. Design: cultural probes. Interactions 1999;6:21–9.
6. Sheridan SL, Halpern DJ, Viera AJ, et al. Interventions for individuals with low health literacy: a systematic review. J Health Commun 2011;16 Suppl 3:30–54.
7. Schillinger D, Machtinger EL, Wang F, et al. Language, literacy, and communication regarding medications in an anticoagulation clinic: A comparison of verbal vs. visual assessment. J Health Commun 2006;11:651–4.
8. Chugh A, Williams MV, Grigsby J, Coleman EA. Better transitions: Improving comprehension of discharge instructions. Front Health Serv Manage 2009;25:11–32.
9. IDEO. Design thinking for educators toolkit. 2nd ed. New York: IDEObooks; 2013.
10. Hahn-Goldberg S, Okrainec K, Damba C, et al. Implementing patient oriented discharge summaries (PODS): A multi-site pilot across early adopter hospitals. Healthc Q 2016;19:42–8.
Feds Raise Buprenorphine Patient Loads
Qualified physicians soon will be allowed to provide medication-assisted treatment (MAT) with buprenorphine to nearly triple the number of patients under a new rule by the Substance Abuse and Mental Health Services Administration (SAMHSA).
The rule, announced by the Health & Human Services department on July 6, allows qualified practitioners to prescribe buprenorphine to up to 275 patients, up from the previous limit of 100. Raising the cap will mean treatment of 10,000-70,000 more patients within the first year, according to HHS. The rule takes effect Aug. 5.

In addition, HHS plans to eliminate pain management questions from the payment scoring calculation of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. The removal aims to relieve pressure on clinicians to overprescribe opioids since scores on the HCAHPS survey are tied to Medicare payments to hospitals. Hospitals would continue to use the questions to survey patients about their inpatient pain management experience, but the questions would not affect the level of payment that hospitals receive, HHS Secretary Sylvia M. Burwell said during a press conference. The changes are part of a number of steps announced by HHS to build on the agency’s Opioid Initiative.
“Together, these announcements will help us take additional steps forward,” Ms. Burwell said. “They increase access to help more people receive the evidence-based treatment they need. They help providers safely prescribe while helping their patients manage chronic pain, and they fill in the gaps of our understanding of this epidemic and how best to fight it.”
The agency also released a report on ongoing, federally funded opioid misuse and pain treatment research. The report is designed to help stakeholders and external funders of research in avoiding unnecessary duplication of research currently underway, according to HHS. The agency plans to launch more than a dozen new scientific studies on opioid misuse and pain treatment in the near future, Ms. Burwell said.
Another new rule mandates that Indian Health Service (IHS) clinicians and pharmacists check their state Prescription Drug Monitoring Program database prior to prescribing or dispensing any opioid for more than 7 days. The new policy is effective immediately for IHS clinicians authorized to prescribe opioids.
Amid the new steps, Secretary Burwell and others called on Congress to approve the President Obama’s proposed $1.1 billion in new funding to further address prescription opioid abuse and heroin use. Legislators are meeting July 6 to weigh final legislation aimed at the opioid epidemic, but have thus far, not fully supported the president’s proposed funding. In a July 5 letter, Democrats vowed to oppose the bill unless it included more money to treat addicted patients.
“If you want treatment for an opioid use disorder, you should be able to access it when you need it,” Michael Botticelli, director of National Drug Control Policy said during the press conference. “There is still time for Congress to do what’s right.”
Qualified physicians soon will be allowed to provide medication-assisted treatment (MAT) with buprenorphine to nearly triple the number of patients under a new rule by the Substance Abuse and Mental Health Services Administration (SAMHSA).
The rule, announced by the Health & Human Services department on July 6, allows qualified practitioners to prescribe buprenorphine to up to 275 patients, up from the previous limit of 100. Raising the cap will mean treatment of 10,000-70,000 more patients within the first year, according to HHS. The rule takes effect Aug. 5.
In addition, HHS plans to eliminate pain management questions from the payment scoring calculation of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. The removal aims to relieve pressure on clinicians to overprescribe opioids since scores on the HCAHPS survey are tied to Medicare payments to hospitals. Hospitals would continue to use the questions to survey patients about their inpatient pain management experience, but the questions would not affect the level of payment that hospitals receive, HHS Secretary Sylvia M. Burwell said during a press conference. The changes are part of a number of steps announced by HHS to build on the agency’s Opioid Initiative.
“Together, these announcements will help us take additional steps forward,” Ms. Burwell said. “They increase access to help more people receive the evidence-based treatment they need. They help providers safely prescribe while helping their patients manage chronic pain, and they fill in the gaps of our understanding of this epidemic and how best to fight it.”
The agency also released a report on ongoing, federally funded opioid misuse and pain treatment research. The report is designed to help stakeholders and external funders of research in avoiding unnecessary duplication of research currently underway, according to HHS. The agency plans to launch more than a dozen new scientific studies on opioid misuse and pain treatment in the near future, Ms. Burwell said.
Another new rule mandates that Indian Health Service (IHS) clinicians and pharmacists check their state Prescription Drug Monitoring Program database prior to prescribing or dispensing any opioid for more than 7 days. The new policy is effective immediately for IHS clinicians authorized to prescribe opioids.
Amid the new steps, Secretary Burwell and others called on Congress to approve the President Obama’s proposed $1.1 billion in new funding to further address prescription opioid abuse and heroin use. Legislators are meeting July 6 to weigh final legislation aimed at the opioid epidemic, but have thus far, not fully supported the president’s proposed funding. In a July 5 letter, Democrats vowed to oppose the bill unless it included more money to treat addicted patients.
“If you want treatment for an opioid use disorder, you should be able to access it when you need it,” Michael Botticelli, director of National Drug Control Policy said during the press conference. “There is still time for Congress to do what’s right.”
Qualified physicians soon will be allowed to provide medication-assisted treatment (MAT) with buprenorphine to nearly triple the number of patients under a new rule by the Substance Abuse and Mental Health Services Administration (SAMHSA).
The rule, announced by the Health & Human Services department on July 6, allows qualified practitioners to prescribe buprenorphine to up to 275 patients, up from the previous limit of 100. Raising the cap will mean treatment of 10,000-70,000 more patients within the first year, according to HHS. The rule takes effect Aug. 5.
In addition, HHS plans to eliminate pain management questions from the payment scoring calculation of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. The removal aims to relieve pressure on clinicians to overprescribe opioids since scores on the HCAHPS survey are tied to Medicare payments to hospitals. Hospitals would continue to use the questions to survey patients about their inpatient pain management experience, but the questions would not affect the level of payment that hospitals receive, HHS Secretary Sylvia M. Burwell said during a press conference. The changes are part of a number of steps announced by HHS to build on the agency’s Opioid Initiative.
“Together, these announcements will help us take additional steps forward,” Ms. Burwell said. “They increase access to help more people receive the evidence-based treatment they need. They help providers safely prescribe while helping their patients manage chronic pain, and they fill in the gaps of our understanding of this epidemic and how best to fight it.”
The agency also released a report on ongoing, federally funded opioid misuse and pain treatment research. The report is designed to help stakeholders and external funders of research in avoiding unnecessary duplication of research currently underway, according to HHS. The agency plans to launch more than a dozen new scientific studies on opioid misuse and pain treatment in the near future, Ms. Burwell said.
Another new rule mandates that Indian Health Service (IHS) clinicians and pharmacists check their state Prescription Drug Monitoring Program database prior to prescribing or dispensing any opioid for more than 7 days. The new policy is effective immediately for IHS clinicians authorized to prescribe opioids.
Amid the new steps, Secretary Burwell and others called on Congress to approve the President Obama’s proposed $1.1 billion in new funding to further address prescription opioid abuse and heroin use. Legislators are meeting July 6 to weigh final legislation aimed at the opioid epidemic, but have thus far, not fully supported the president’s proposed funding. In a July 5 letter, Democrats vowed to oppose the bill unless it included more money to treat addicted patients.
“If you want treatment for an opioid use disorder, you should be able to access it when you need it,” Michael Botticelli, director of National Drug Control Policy said during the press conference. “There is still time for Congress to do what’s right.”

Feds raise buprenorphine patient loads
Qualified physicians soon will be allowed to provide medication-assisted treatment (MAT) with buprenorphine to nearly triple the number of patients under a new rule by the Substance Abuse and Mental Health Services Administration (SAMHSA).
The rule, announced by the Health & Human Services department on July 6, allows qualified practitioners to prescribe buprenorphine to up to 275 patients, up from the previous limit of 100. Raising the cap will mean treatment of 10,000-70,000 more patients within the first year, according to HHS. The rule takes effect Aug. 5.

In addition, HHS plans to eliminate pain management questions from the payment scoring calculation of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. The removal aims to relieve pressure on clinicians to overprescribe opioids since scores on the HCAHPS survey are tied to Medicare payments to hospitals. Hospitals would continue to use the questions to survey patients about their inpatient pain management experience, but the questions would not affect the level of payment that hospitals receive, HHS Secretary Sylvia M. Burwell said during a press conference. The changes are part of a number of steps announced by HHS to build on the agency’s Opioid Initiative.
“Together, these announcements will help us take additional steps forward,” Ms. Burwell said. “They increase access to help more people receive the evidence-based treatment they need. They help providers safely prescribe while helping their patients manage chronic pain, and they fill in the gaps of our understanding of this epidemic and how best to fight it.”
The agency also released a report on ongoing, federally funded opioid misuse and pain treatment research. The report is designed to help stakeholders and external funders of research in avoiding unnecessary duplication of research currently underway, according to HHS. The agency plans to launch more than a dozen new scientific studies on opioid misuse and pain treatment in the near future, Ms. Burwell said.
Another new rule mandates that Indian Health Service (IHS) clinicians and pharmacists check their state Prescription Drug Monitoring Program database prior to prescribing or dispensing any opioid for more than 7 days. The new policy is effective immediately for IHS clinicians authorized to prescribe opioids.
Amid the new steps, Secretary Burwell and others called on Congress to approve the President Obama’s proposed $1.1 billion in new funding to further address prescription opioid abuse and heroin use. Legislators are meeting July 6 to weigh final legislation aimed at the opioid epidemic, but have thus far, not fully supported the president’s proposed funding. In a July 5 letter, Democrats vowed to oppose the bill unless it included more money to treat addicted patients.
“If you want treatment for an opioid use disorder, you should be able to access it when you need it,” Michael Botticelli, director of National Drug Control Policy said during the press conference. “There is still time for Congress to do what’s right.”
On Twitter @legal_med
Qualified physicians soon will be allowed to provide medication-assisted treatment (MAT) with buprenorphine to nearly triple the number of patients under a new rule by the Substance Abuse and Mental Health Services Administration (SAMHSA).
The rule, announced by the Health & Human Services department on July 6, allows qualified practitioners to prescribe buprenorphine to up to 275 patients, up from the previous limit of 100. Raising the cap will mean treatment of 10,000-70,000 more patients within the first year, according to HHS. The rule takes effect Aug. 5.
In addition, HHS plans to eliminate pain management questions from the payment scoring calculation of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. The removal aims to relieve pressure on clinicians to overprescribe opioids since scores on the HCAHPS survey are tied to Medicare payments to hospitals. Hospitals would continue to use the questions to survey patients about their inpatient pain management experience, but the questions would not affect the level of payment that hospitals receive, HHS Secretary Sylvia M. Burwell said during a press conference. The changes are part of a number of steps announced by HHS to build on the agency’s Opioid Initiative.
“Together, these announcements will help us take additional steps forward,” Ms. Burwell said. “They increase access to help more people receive the evidence-based treatment they need. They help providers safely prescribe while helping their patients manage chronic pain, and they fill in the gaps of our understanding of this epidemic and how best to fight it.”
The agency also released a report on ongoing, federally funded opioid misuse and pain treatment research. The report is designed to help stakeholders and external funders of research in avoiding unnecessary duplication of research currently underway, according to HHS. The agency plans to launch more than a dozen new scientific studies on opioid misuse and pain treatment in the near future, Ms. Burwell said.
Another new rule mandates that Indian Health Service (IHS) clinicians and pharmacists check their state Prescription Drug Monitoring Program database prior to prescribing or dispensing any opioid for more than 7 days. The new policy is effective immediately for IHS clinicians authorized to prescribe opioids.
Amid the new steps, Secretary Burwell and others called on Congress to approve the President Obama’s proposed $1.1 billion in new funding to further address prescription opioid abuse and heroin use. Legislators are meeting July 6 to weigh final legislation aimed at the opioid epidemic, but have thus far, not fully supported the president’s proposed funding. In a July 5 letter, Democrats vowed to oppose the bill unless it included more money to treat addicted patients.
“If you want treatment for an opioid use disorder, you should be able to access it when you need it,” Michael Botticelli, director of National Drug Control Policy said during the press conference. “There is still time for Congress to do what’s right.”
On Twitter @legal_med
Qualified physicians soon will be allowed to provide medication-assisted treatment (MAT) with buprenorphine to nearly triple the number of patients under a new rule by the Substance Abuse and Mental Health Services Administration (SAMHSA).
The rule, announced by the Health & Human Services department on July 6, allows qualified practitioners to prescribe buprenorphine to up to 275 patients, up from the previous limit of 100. Raising the cap will mean treatment of 10,000-70,000 more patients within the first year, according to HHS. The rule takes effect Aug. 5.
In addition, HHS plans to eliminate pain management questions from the payment scoring calculation of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. The removal aims to relieve pressure on clinicians to overprescribe opioids since scores on the HCAHPS survey are tied to Medicare payments to hospitals. Hospitals would continue to use the questions to survey patients about their inpatient pain management experience, but the questions would not affect the level of payment that hospitals receive, HHS Secretary Sylvia M. Burwell said during a press conference. The changes are part of a number of steps announced by HHS to build on the agency’s Opioid Initiative.
“Together, these announcements will help us take additional steps forward,” Ms. Burwell said. “They increase access to help more people receive the evidence-based treatment they need. They help providers safely prescribe while helping their patients manage chronic pain, and they fill in the gaps of our understanding of this epidemic and how best to fight it.”
The agency also released a report on ongoing, federally funded opioid misuse and pain treatment research. The report is designed to help stakeholders and external funders of research in avoiding unnecessary duplication of research currently underway, according to HHS. The agency plans to launch more than a dozen new scientific studies on opioid misuse and pain treatment in the near future, Ms. Burwell said.
Another new rule mandates that Indian Health Service (IHS) clinicians and pharmacists check their state Prescription Drug Monitoring Program database prior to prescribing or dispensing any opioid for more than 7 days. The new policy is effective immediately for IHS clinicians authorized to prescribe opioids.
Amid the new steps, Secretary Burwell and others called on Congress to approve the President Obama’s proposed $1.1 billion in new funding to further address prescription opioid abuse and heroin use. Legislators are meeting July 6 to weigh final legislation aimed at the opioid epidemic, but have thus far, not fully supported the president’s proposed funding. In a July 5 letter, Democrats vowed to oppose the bill unless it included more money to treat addicted patients.
“If you want treatment for an opioid use disorder, you should be able to access it when you need it,” Michael Botticelli, director of National Drug Control Policy said during the press conference. “There is still time for Congress to do what’s right.”
On Twitter @legal_med

Medical Therapy for Osteoporosis and Approaches to Improving Adherence
From the Division of Endocrinology, Diabetes, and Metabolism, University of Alabama at Birmingham, Birmingham, Alabama.
Abstract
- Objective: To review the treatment of osteoporosis, challenges to treatment adherence, and factors associated with improved adherence.
- Methods: Review of the literature.
- Results: With the growing aging population, there is an increased number of people at risk of osteoporosis and fracture. Several medications are available that reduce the risk of fracture. However, adherence to osteoporosis medications is suboptimal. Factors related to nonadherence include dosing frequency, real side effects, and concern about potential side effects. Interventions that may improve adherence include clinician and patient education, less frequent and less complex dosing regimens, medication reminders, and adherence counseling.
- Conclusions: Improving adherence to osteoporosis medications is a complex and challenging issue. Considering and implementing strategies to improve adherence tailored to patient preferences may enhance long-term outcomes for patients with osteoporosis.
Osteoporosis is a chronic but asymptomatic disease that is characterized by an increased fragility of bones and increased risk of fractures. Hip and vertebral fractures are associated with the greatest morbidity and mortality. The prevalence of osteoporosis is estimated to be 10.3% in the US, with approximately 10.2 million adults over the age of 50 having osteoporosis based on 2010 census data and results from the National Health and Nutrition Examination Survey (NHANES) [1].
Several drugs are currently available for the treatment of osteoporosis, but adherence to treatment is low. Understanding the factors associated with low adherence and actions that can be taken to improve adherence to treatment is important given the large number of individuals with osteoporosis and the need to reduce the burden caused by fragility fracture. In this article, we review the treatment of osteoporosis, challenges to treatment adherence, and factors associated with improved adherence.
Nonprescription Medications
Calcium
There have been several published studies over the last decade evaluating calcium supplementation and its efficacy in reducing fractures. Although these studies showed that calcium reduces bone turnover by 20% and slowed postmenopausal bone loss by one third [2,3], none of these studies or a recent systematic review [4] showed any degree of fracture risk reduction with calcium supplements alone.
Although some calcium intake may be good, too much calcium has the potential to cause harm, including an increased risk of nephrolithiasis and constipation/bloating. An analysis of the Women’s Health Initiative (WHI) study reported a 17% increase in renal calculi in women who received calcium and vitamin D supplements [5]. Another recently published meta-analysis showed a 43% increase in gastrointestinal complaints in patients who were taking calcium supplements [6]. The potential for increased cardiovascular risk with calcium supplements is controversial [7]. The WHI study did not show an increased occurrence of cardiovascular events among those taking calcium supplements [8]. In a different population, men who consumed more than 1000 mg per day of supplemental calcium had higher all-cause and cardiovascular disease-specific mortality [9]. Large, well-conducted randomized controlled trials will be needed to further elucidate the question of calcium supplementation and risk of cardiovascular disease.
Vitamin D
Deficiency of vitamin D is common with one study finding more than 90% of older adults deficient in vitamin D [10]. Vitamin D is essential for proper calcium metabolism and deficiency is known to induce secondary hyperparathyroidism. Studies in mouse models have also shown that normal vitamin D receptors in enterocytes are essential for normal bone mineralization [11,12]. A systematic Cochrane database review showed that vitamin D3 supplementation decreased mortality in elderly people living independently or in institutional care [13]. Vitamin D was administered for a weighted mean of 4.4 years. Vitamin D2, alfacalcidol, and calcitriol had no statistically significant beneficial effects on mortality. Vitamin D3 combined with calcium was associated with an increased risk of nephrolithiasis during a follow-up period of 1.25 to 7 years (relative risk [RR] 1.17, 95% confidence interval (CI) 1.02–1.34) [13]. The inconsistencies of published reports looking at benefits of vitamin D supplementation may be due in part to variability in compliance with taking the supplements and baseline vitamin D levels.
Two randomized controlled trials have shown that low vitamin D appears to be an independent predictor of fall risk, and vitamin D supplementation has been found to reduce this risk of falls, through improved musculo-skeletal function [14–16]. Thus, vitamin D may play a role in fracture risk reduction beyond direct bone effects.
Prescription Osteoporosis Treatments
Bisphosphonates
Bisphosphonates are the most commonly prescribed medication for osteoporosis. The efficacy of bisphosphonates to reduce fractures is well established. There are oral bisphosphonates, which can be dosed daily, weekly, or monthly, and intravenous bisphosphonates, which can be given every 3 months or annually. Side effects with this class of medications include gastrointestinal effects with the oral options in up to 20% to 30% of users [17]. With intravenous bisphosphonates, the greatest risk is an acute phase response, which can occur in up to 42% of patients [18]. The risk of an acute phase reaction is much lower with doses beyond the first dose and lower if patients have ever previously taken an oral bisphosphonate and/or receive acetaminophen prior to the infusion. Other potential side effects with all bisphosphonates include osteonecrosis of jaw (ONJ) and atypical subtrochanteric fractures. Post marketing studies have indicated that the incidence of ONJ is less than 2 per 100,000 patient-years among those taking bisphosphonates [19,20]. A number of database analyses have shown that ONJ-like lesions can also occur in older individuals with osteoporosis who have never been exposed to bisphosphonates [21]. A case series of an osteoporotic population showed that ONJ-like lesions are lower grade than those typically seen in cancer patients who usually are exposed to higher doses of bisphosphonates [22]. A study of Swedish older men and women reported that long-term use of bisphosphonates (4 years or more) was associated with an increased incidence of atypical fractures. The RR for women was 126.0 (95% CI, 55.1–288.1) after 4 years of bisphosphonates [23]. A U.S. health care database analysis reported that 90% of those with atypical fractures were bisphosphonate users, almost half were Asian (49%), and use beyond 6 years showed the greatest risk [24].
Non-Bisphosphonate Medications
Other osteoporosis medications include denosumab, raloxifene, estrogen, and teriparatide (calcitonin will not be discussed here). Newer options currently under study, including cathepsin K inhibitors and anti-sclerostin therapies, are not available in the United States.
Denosumab is a monoclonal antibody that interferes with the receptor activator of nuclear kappa B ligand (RANK-L), which is the principal stimulus for osteoclastogenesis. Denosumab is administered once every 6 months subcutaneously. Phase III trials of denosumab demonstrated a 68% reduction in vertebral fractures and 40% and 20% reduction in fractures at hip and non-vertebral sites, respectively [25]. Similar to bisphosphonates, other risks include atypical femoral fractures and ONJ. In addition, hypocalcemia, including severe, symptomatic hypocalcemia, has been reported at rates higher than initially reported in the original clinical trials [26]. Hypocalcemia can be severe, especially in patients who are deficient in vitamin D [10,27].
Estrogen is effective in reducing the risk of vertebral fractures. Selective estrogen receptor modulators (SERMs) have both estrogen agonist and antagonist effects. The SERM, raloxifene, has been used in osteoporosis for its antiresorptive effects through the estrogen receptor [28,29]. A newer SERM, bazedoxifene, has been studied in combination with conjugated estrogen and has been reported to improve bone mineral density and other symptoms of menopause, like vasomotor symptoms and vulvo-vaginal atrophy, but its efficacy in reducing fracture risk has not been demonstrated [30,31].
Teriparatide is an anabolic agent that works by stimulating osteoblastic bone formation which results in an increase in bone density and reduction in both vertebral and non-vertebral fracture risk. In women with postmenopausal osteoporosis, it is typically reserved for those with very low bone mineral density (BMD) or those who continue to have fractures despite a bisphosphonate [32]. Barriers to use of teriparatide include high cost, the need for daily injections, and approved use for a total of two years in a lifetime. There is also a theoretical risk of osteosarcoma shown in animal studies but human cases have not been reported when used for postmenopausal osteoporosis. Published studies have shown that combination zolendronate and teriparatide have additive benefits to spine and hip BMD [33]. Another study reported that the combination of denosumab and teriparatide resulted in additive effects, ie, an increase in lumbar, hip, and femoral neck BMD [34]. These combinations have not been studied in populations large enough or for long enough duration to evaluate fracture risk reduction.
Adherence to Osteoporosis Medications
Treatment of osteoporosis reduces risk of fracture, but the benefit of osteoporosis medications is dependent on adherence. Adherence is associated with improved clinical outcomes [35,36] as well as reduced costs and utilization [37,38]; however, adherence to osteoporosis medications is poor. In a meta-analysis of 24 observational studies conducted in large populations, overall adherence for all osteoporosis therapies ranged from approximately 40% to 70% [39]. A recent retrospective claims database analysis in the U.S. reported a 60% noncompliance rate among the 57,913 postmenopausal women prescribed bisphosphonates over 1 year [40]. Another administrative database analysis from a managed care population compared the 3 oral bisphosphonates (risedronate, ibandronate, and alendronate) and found a mean medication possession ratio (MPR) between 0.57–0.58 at 12 months, which dropped to 0.47–0.50 after 24 months and 0.44–0.47 after 36 months [41]. In an observational study of 3200 older women in the U.K. low adherence was self-reported in 8.5%, and 21.6% self-discontinued treatment within 2 years [42]. In a study of Medicare Advantage prescription drug plan members, a small but significant increase in adherence was seen after osteo-porosis treatment change but overall adherence remained low (51% MPR in the change cohort and vs. 44% in the no-change cohort at 24 months, P < 0.01) [43].
Some patients restart osteoporosis therapy after a prolonged lapse in medication use. In one study, re-initiation rates for bisphosphonate therapy among persons who discontinued were as high as 30% within 6 months and 50% within 2 years [44]. Predictors of treatment re-initiation included younger age, female sex, history of fracture, recent hip fracture, nursing home discharge, and BMD testing [44].
Factors that Impact Adherence
Understanding which patients are most likely to be compliant with medications can aid physicians when monitoring osteoporosis treatment responses. In a retro-spective claims analysis, older age was found to be a predictor of compliance: women 65 years and older were more likely to be compliant than younger patients (P = 0.012) [45]. Among women receiving denosumab, improved adherence was found among women with a family history of a parent with a hip fracture, and lower adherence was seen in those with higher age, decreased mobility, and further distance from the clinic where the medication was provided [46].
Major reasons for nonadherence include a fear of potential side effects, occurrence of real side effects, the complicated dosing regimens, and perceived lack of benefit from the medications due to the asymptomatic nature of osteoporosis. In the above noted observational study from the U.K., more than half of the nonadherent patients attributed their nonadherence to side effects (53.9%), with a smaller proportion reporting fear of potential side effects (20.5%) or trouble with the dosing regimen (8.0%)[42].
Patients may also be unwilling to continue to take an osteoporosis medication if a fracture develops while on it and if they are not otherwise provided evidence that the medication is working. In a study by Costa Paiva et al, an understanding and knowledge to osteoporosis was a prerequisite to adherence and the strongest predictor of knowledge was higher education level [47]. Factors that impaired adherence were lower socioeconomic status and presence of comorbidities [47]. In a phenomenological qualitative study, trust in a health care provider was the most common reason for patients’ decision to accept an osteoporosis medication, emphasizing the importance of physician-patient communication [48].
Interventions to Enhance Adherence
Current methods of improving adherence for chronic health problems are mostly complex and not very effective [49]. In a systematic review of interventions to improve medication adherence, only 37 out of 81 studies reported improved adherence in the treatment of chronic diseases, and multifaceted treatments were more likely to succeed [49]. Improving adherence to osteoporosis medications is a complex issue, and a number of interventions evaluated in systematic reviews have shown limited efficacy [50,51]. Simplification of dosing regimens have been found to have a significant impact in chronic disease management [52,53] as well as in some studies of osteoporosis medications.
Simplification of Dosing
Among women prescribed daily vs. weekly bisphosphonates, those on the weekly regimen had significantly higher compliance [54]. However, rates were suboptimal in both groups and more than 50% of women discontinued at 1 year [54]. In addition, in a meta-analysis of osteoporosis medication adherence, a nearly two-fold higher odds of discontinuation with daily vs. weekly bisphosphonates was seen (odds ratio 1.90, 95% CI 1.81–2.00) [55]. Likewise, in a retrospective study in Spain, nearly 85% of those started on a daily bisphosphonate stopped within a year [56], while discontinuation was significantly lower in those prescribed a weekly or monthly bisphosphonate or daily teriparatide; however, discontinuation was still nearly 50% in these groups [56].
Once monthly dosing may be preferred by some patients as there is less time involved in thinking about the disease being treated and a perception of lower likelihood of side effects. In one study, postmenopausal women who had previously stopped oral bisphosphonates due to GI side effects had high adherence rates after self-selecting either monthly oral or quarterly intravenous ibandronate therapy [57]. However, not all studies show significant differences in adherence between weekly and monthly preparations [58–60].
The newer parenteral treatment options that can be given every 6 months or once yearly have the potential to significantly improve adherence. Once a year parenteral administration of a bisphosphonate was preferred over once-weekly oral administration, according to a 1-year study in patients with low bone density previously treated with alendronate [61]. A recent study that looked at persistence with an infusion of zolendronic acid in Taiwanese patients for 48 months found that 85% of patients received at least 2 infusions [62]. In patients treated with denosumab in 4 European countries, adherence and persistence at 12 months were consistently > 80% [46]. Persistence in this study was defined as receiving the subsequent injection within 6 months ± 8 weeks of the previous injection; adherence was defined as receiving 2 consecutive injections within 6 months ± 4 weeks of each other [46].
In a study by Cramer et al, increased adherence and persistence was seen with weekly alendronate compared daily alendronate at the end of 12 months [54]. Similar results were seen in a large longitudinal cohort study of weekly vs. daily bisphosphonates but less than 50% of patients were adherent with the weekly regimen [63]. When once monthly preparations of bisphosphonates became available, studies continued to support a patient preference for less frequently dosed bisphosphonates, with the majority of patients preferring monthly over weekly dosed medications [64–66].
The availability of quarterly ibandronate and yearly zoledronic acid infusions have further simplified dosing. In large, randomized, multicenter studies, patients consistently expressed a preference for yearly infusions over a weekly oral medication [61,67]. Adherence and persistence to osteoporosis medications was also greater in women receiving intravenous ibandronate compared to those receiving oral alendronate [68,69]. However, a study by Curtis et al showed low persistence with intravenous bisphosphonates in a Medicare population [70]. A possible reason for the lower adherence in this population was postulated to include the provision of the infusions at an outpatient center rather than a physician office. Automated nursing reminders with either phone calls or emails have the potential to mitigate the problem of persistence with this less frequent regimen [71,72]. In a review of patient preferences, less frequent dosing of medications was a common desire, but further generalizability were limited, emphasizing the need to individualize treatment [73].
Patient-Provider Communication
Individualizing treatment with better patient-provider communication and identification of potential barriers may increase compliance [74]. In one study, increasing patient participation in determining the treatment option was associated with improved patient adherence [57]. A systematic review of literature on interventions to improve adherence found that periodic follow-up interaction between patients and their health professionals also improved adherence [50]. Positive reinforcement via physician-patient discussion of either bone turnover markers or bone mineral density test results has also been found to improve long-term adherence with osteoporosis medications [71,75].
Better perceived physician knowledge may help with patient adherence. A study by Pickney et al reported that the patient confidence in their health care providers has influence on improved adherence, and patients were more likely to comply when the medications were prescribed by a specialist rather than a general practitioner [76].
Education, Reminders, Phone-Based
Improving patient knowledge of osteoporosis, especially with education using visual aids, may help with improving adherence [47]. In a randomized controlled trial at a single health management organization, an interactive voice response phone call plus a letter 1 week later increased the rate of obtaining a prescribed oral bisphosphonate in the intervention group (48.8% vs. 30.5% control; OR 2.3, 95% CI 1.34–3.94) when adjusted for age, sex, prior BMD, and fracture [77]. Use of an encounter decision aid also improved knowledge of osteoporosis medication options and led to a doubling of medication prescription attainment. However, adherence at 6 months was not improved [78].
Pill reminders in the form of text messages, paging systems on medication devices, and alarm beeps have been studied in patients with chronic diseases, and these technologies could be utilized for osteoporosis treatment [79–81]. A study of smart phone applications showed that many apps help with adherence, especially in noncompliant patients [82]. The researchers reported that of apps studied, MyMedSchedule, MyMeds, and RxmindMe were among the most highly rated due to their ease of use and enhanced functions. Solomon et all studied the effectiveness of a telephone-based counseling program using motivational interviewing in a large randomized study. They found no significant improvement in adherence to an osteoporosis regimen with the telephonic motivational interview compared to mailed educational materials (control group) (P = 0.07) [83]. In a 12-month multicenter, prospective randomized study, Bianchi et al examined the effectiveness of an intervention of reminders or reminders plus phone calls and meetings at the referral center in postmenopausal women initiating an oral osteoporosis prescription. No significant difference was seen in adherence at 12 months compared to standard care [84]. Adherence among the entire cohort, however, was very high [84]
Pharmacist-Based
The role of pharmacists in the treatment of chronic diseases, including osteoporosis, has been studied and shown to be cost-effective. In a study by van Boven et al, an algorithm was designed to detect patients with nonadherence and then tailor an intervention that consisted of structured counseling and active monitoring by pharmacists in initial and continuous phases [85]. This effort-intensive intervention resulted in reduced discontinuation of bisphosphonates after 12 months (reduction from 31.7% to 16.2% at 12 months) [85]. Despite the effort required, findings from the study support overall cost-effectiveness of this intervention [85]. A randomized controlled study by Lai et al showed that pharmacists can play a role in improving medication adherence through counseling patients on the importance of adherence, side effects, and goals of therapy [86]. The same authors also showed that involvement of a clinical pharmacist in the care of patients helped to further improve patient knowledge of medications and osteoporosis treatments, resolve medication-related concerns, and improve overall quality of life [87]. Such pharmacist-led interventions would require pharmacists to understand their role and the potential for drug holidays in the course of osteoporosis treatments and not mislabel patients as nonadherent when in fact purposefully holding osteoporosis medications [88].
Conclusion
Osteoporosis is a growing problem with increasing numbers of patients at risk for osteoporosis and related fractures. Currently available osteoporosis medications have shown clear benefit in reducing fracture risk; however, adherence to these therapies is required to obtain benefit. Unfortunately, osteoporosis medications have several limitations to full compliance, particularly the oral treatment options, including known possible side effects acutely and chronically, potential/feared side effects, irregular dosing intervals, complicated dosing instructions, and absence of an immediate recognizable benefit/effect. Improving adherence is complex [89] and tailoring to individual patients is of importance. Successful techniques for improving adherence may include a focus on physician-patient communication, use of the less frequently dosed medications, various medication reminders, use of available technology, and use of pharmacists for patient counseling and monitoring. Recognition of this common problem by clinicians is of utmost importance.
Corresponding author: Amy H. Warriner, MD, The University of Alabama at Birmingham, Division of Endocrinology, Diabetes and Metabolism, 702 Faculty Office Tower, 510 20th Street South, Birmingham, AL 35294, [email protected].
Financial disclosures: None.
1. Wright NC, Looker AC, Saag KG, et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res. 2014;29(11):2520–6.
2. Reid IR, Mason B, Horne A, et al. Randomized controlled trial of calcium in healthy older women. Am J Med. 2006;119(9):777–85.
3. Reid IR, Ames R, Mason B, et al. Randomized controlled trial of calcium supplementation in healthy, nonosteoporotic, older men. Arch Intern Med. 2008;168(20):2276–82.
4. Murad MH, Drake MT, Mullan RJ, et al. Clinical review. Comparative effectiveness of drug treatments to prevent fragility fractures: a systematic review and network meta-analysis. J Clin Endocrinol Metab. 2012;97(6):1871–80.
5. Jackson RD, LaCroix AZ, Gass M, et al. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006;354(7):669–83.
6. Lewis JR, Zhu K, Prince RL. Adverse events from calcium supplementation: relationship to errors in myocardial infarction self-reporting in randomized controlled trials of calcium supplementation. J Bone Miner Res. 2012;27(3):719–22.
7. Challoumas D, Stavrou A, Pericleous A, Dimitrakakis G. Effects of combined vitamin D--calcium supplements on the cardiovascular system: should we be cautious? Atherosclerosis. 2015;238(2):388–98.
8. Hsia J, Heiss G, Ren H, et al. Calcium/vitamin D supplementation and cardiovascular events. Circulation. 2007;115(7):846–54.
9. Yang B, Campbell PT, Gapstur SM, et al. Calcium intake and mortality from all causes, cancer, and cardiovascular disease: the Cancer Prevention Study II Nutrition Cohort. Am J Clin Nutr. 2016;103(3):886–94.
10. Reid IR. Efficacy, effectiveness and side effects of medications used to prevent fractures. J Intern Med. 2015;277(6):690–706.
11. Xue Y, Fleet JC. Intestinal vitamin D receptor is required for normal calcium and bone metabolism in mice. Gastroenterology. 2009;136(4):1317-27, e1–2.
12. Lieben L, Masuyama R, Torrekens S, et al. Normocalcemia is maintained in mice under conditions of calcium malabsorption by vitamin D-induced inhibition of bone mineralization. J Clin Invest. 2012;122(5):1803–15.
13. Bjelakovic G, Gluud LL, Nikolova D, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2014;1:CD007470.
14. Flicker L, Mead K, MacInnis RJ, et al. Serum vitamin D and falls in older women in residential care in Australia. J Am Geriatr Soc. 2003;51(11):1533–8.
15. Bischoff-Ferrari HA, Orav EJ, Dawson-Hughes B. Effect of cholecalciferol plus calcium on falling in ambulatory older men and women: a 3-year randomized controlled trial. Arch Intern Med. 2006;166(4):424–30.
16. Flicker L, MacInnis RJ, Stein MS, et al. Should older people in residential care receive vitamin D to prevent falls? Results of a randomized trial. J Am Geriatr Soc. 2005;53(11):1881–8.
17. Biswas PN, Wilton LV, Shakir SA. Pharmacovigilance study of alendronate in England. Osteoporos Int. 2003;14(6):507–14.
18. Reid IR, Gamble GD, Mesenbrink P, et al. Characterization of and risk factors for the acute-phase response after zoledronic acid. J Clin Endocrinol Metab. 2010;95(9):4380–7.
19. Grbic JT, Landesberg R, Lin SQ, et al. Incidence of osteonecrosis of the jaw in women with postmenopausal osteoporosis in the health outcomes and reduced incidence with zoledronic acid once yearly pivotal fracture trial. J Am Dent Assoc. 2008;139(1):32–40.
20. Grbic JT, Black DM, Lyles KW, et al. The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc. 2010;141(11):1365–70.
21. Lin TC, Yang CY, Kao Yang YH, Lin SJ. Incidence and risk of osteonecrosis of the jaw among the Taiwan osteoporosis population. Osteoporos Int. 2014;25(5):1503–11.
22. Assael LA. Oral bisphosphonates as a cause of bisphosphonate-related osteonecrosis of the jaws: clinical findings, assessment of risks, and preventive strategies. J Oral Maxillofac Surg. 2009;67(5 Suppl):35–43.
23. Schilcher J, Koeppen V, Aspenberg P, Michaelsson K. Risk of atypical femoral fracture during and after bisphosphonate use. N Engl J Med. 2014;371(10):974–6.
24. Dell RM, Adams AL, Greene DF, et al. Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res. 2012;27(12):2544–50.
25. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–65.
26. Yerram P, Kansagra S, Abdelghany O. Incidence of hypocalcemia in patients receiving denosumab for prevention of skeletal-related events in bone metastasis. J Oncol Pharm Pract. 2016.
27. Reid IR. Short-term and long-term effects of osteoporosis therapies. Nat Rev Endocrinol. 2015;11(7):418–28.
28. Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA. 1999;282(7):637–45.
29. Reid IR, Eastell R, Fogelman I, et al. A comparison of the effects of raloxifene and conjugated equine estrogen on bone and lipids in healthy postmenopausal women. Arch Intern Med. 2004;164(8):871–9.
30. Sharifi M, Lewiecki EM. Conjugated estrogens combined with bazedoxifene: the first approved tissue selective estrogen complex therapy. Expert Rev Clin Pharmacol. 2014;7(3):281–91.
31. Mirkin S, Ryan KA, Chandran AB, Komm BS. Bazedoxifene/conjugated estrogens for managing the burden of estrogen deficiency symptoms. Maturitas. 2014;77(1):24–31.
32. Warriner AH, Saag KG. Prevention and treatment of bone changes associated with exposure to glucocorticoids. Curr Osteoporos Rep. 2013;11(4):341–7.
33. Cosman F, Eriksen EF, Recknor C, et al. Effects of intravenous zoledronic acid plus subcutaneous teriparatide [rhPTH(1-34)] in postmenopausal osteoporosis. J Bone Miner Res. 2011;26(3):503–11.
34. Leder BZ, Tsai JN, Uihlein AV, et al. Two years of Denosumab and teriparatide administration in postmenopausal women with osteoporosis (The DATA Extension Study): a randomized controlled trial. J Clin Endocrinol Metab. 2014;99(5):1694–700.
35. Imaz I, Zegarra P, Gonzalez-Enriquez J, et al. Poor bisphosphonate adherence for treatment of osteoporosis increases fracture risk: systematic review and meta-analysis. Osteoporos Int. 2010;21(11):1943–51.
36. Curtis JR, Westfall AO, Cheng H, et al. Benefit of adherence with bisphosphonates depends on age and fracture type: results from an analysis of 101,038 new bisphosphonate users. J Bone Miner Res. 2008;23(9):1435–41.
37. Strom O, Borgstrom F, Kanis JA, Jonsson B. Incorporating adherence into health economic modelling of osteoporosis. Osteoporos Int. 2009;20(1):23–34.
38. Sunyecz JA, Mucha L, Baser O, et al. Impact of compliance and persistence with bisphosphonate therapy on health care costs and utilization. Osteoporos Int. 2008;19(10):1421–9.
39. Halpern R, Becker L, Iqbal SU, et al. The association of adherence to osteoporosis therapies with fracture, all-cause medical costs, and all-cause hospitalizations: a retrospective claims analysis of female health plan enrollees with osteoporosis. J Manag Care Pharm. 2011;17(1):25–39.
40. Modi A, Siris ES, Tang J, Sen S. Cost and consequences of noncompliance with osteoporosis treatment among women initiating therapy. Curr Med Res Opin. 2015;31(4):757–65.
41. Martin KE, Yu J, Campbell HE, et al. Analysis of the comparative effectiveness of 3 oral bisphosphonates in a large managed care organization: adherence, fracture rates, and all-cause cost. J Manag Care Pharm. 2011;17(8):596–609.
42. Clark EM, Gould VC, Tobias JH, Horne R. Natural history, reasons for, and impact of low/non-adherence to medications for osteoporosis in a cohort of community-dwelling older women already established on medication: a 2-year follow-up study. Osteoporos Int. 2016;27(2):579–90.
43. Ward MA, Xu Y, Viswanathan HN, et al. Association between osteoporosis treatment change and adherence, incident fracture, and total healthcare costs in a Medicare Advantage Prescription Drug plan. Osteoporos Int. 2013;24(4):1195–206.
44. Brookhart MA, Avorn J, Katz JN, et al. Gaps in treatment among users of osteoporosis medications: the dynamics of noncompliance. Am J Med. 2007;120(3):251–6.
45. Eisenberg DF, Placzek H, Gu T, et al. Cost and consequences of noncompliance to oral bisphosphonate treatment. J Manag Care Spec Pharm. 2015;21(1):56–65.
46. Hadji P, Papaioannou N, Gielen E, et al. Persistence, adherence, and medication-taking behavior in women with postmenopausal osteoporosis receiving denosumab in routine practice in Germany, Austria, Greece, and Belgium: 12-month results from a European non-interventional study. Osteoporos Int. 2015;26(10):2479–89.
47. Costa-Paiva L, Gomes DC, Morais SS, et al. Knowledge about osteoporosis in postmenopausal women undergoing antiresorptive treatment. Maturitas. 2011;69(1):81–5.
48. Sale JE, Gignac MA, Hawker G, et al. Decision to take osteoporosis medication in patients who have had a fracture and are ‘high’ risk for future fracture: a qualitative study. BMC Musculoskelet Disord. 2011;12:92.
49. Haynes RB, Yao X, Degani A, et al. Interventions to enhance medication adherence. Cochrane Database Syst Rev. 2005(4):CD000011.
50. Gleeson T, Iversen MD, Avorn J, et al. Interventions to improve adherence and persistence with osteoporosis medications: a systematic literature review. Osteoporos Int. 2009; 20(12):2127–34.
51. Hiligsmann M, Salas M, Hughes DA, et al. Interventions to improve osteoporosis medication adherence and persistence: a systematic review and literature appraisal by the ISPOR Medication Adherence & Persistence Special Interest Group. Osteoporos Int. 2013;24(12):2907–18.
52. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–310.
53. Richter A, Anton SF, Koch P, Dennett SL. The impact of reducing dose frequency on health outcomes. Clin Ther. 2003;25(8):2307–35; discussion 6.
54. Cramer JA, Amonkar MM, Hebborn A, Altman R. Compliance and persistence with bisphosphonate dosing regimens among women with postmenopausal osteoporosis. Curr Med Res Opin. 2005;21(9):1453–60.
55. Iglay K, Cao X, Mavros P, et al. Systematic Literature Review and Meta-analysis of Medication Adherence With Once-weekly Versus Once-daily Therapy. Clin Ther. 2015;37(8):1813–21 e1.
56. Carbonell-Abella C, Pages-Castella A, Javaid MK, et al. Early (1-year) Discontinuation of Different Anti-osteoporosis Medications Compared: A Population-Based Cohort Study. Calcif Tissue Int. 2015;97(6):535–41.
57. Lewiecki EM, Babbitt AM, Piziak VK, et al. Adherence to and gastrointestinal tolerability of monthly oral or quarterly intravenous ibandronate therapy in women with previous intolerance to oral bisphosphonates: a 12-month, open-label, prospective evaluation. Clin Ther. 2008;30(4):605–21.
58. Payer J, Killinger Z, Sulkova I, Celec P. Preferences of patients receiving bisphosphonates--how to influence the therapeutic adherence. Biomed Pharmacother. 2008;62(2):122–4.
59. Weycker D, Macarios D, Edelsberg J, Oster G. Compliance with drug therapy for postmenopausal osteoporosis. Osteoporos Int. 2006;17(11):1645–52.
60. Kastelan D, Lozo P, Stamenkovic D, et al. Preference for weekly and monthly bisphosphonates among patients with postmenopausal osteoporosis: results from the Croatian PROMO Study. Clin Rheumatol. 2009;28(3):321–6.
61. McClung M, Recker R, Miller P, et al. Intravenous zoledronic acid 5 mg in the treatment of postmenopausal women with low bone density previously treated with alendronate. Bone. 2007;41(1):122–8.
62. Hsieh PC. Effectiveness and safety of zoledronic acid in the treatment of osteoporosis. Orthopedics. 2016:1–8.
63. Recker RR, Gallagher R, MacCosbe PE. Effect of dosing frequency on bisphosphonate medication adherence in a large longitudinal cohort of women. Mayo Clin Proc. 2005;80(7):856–61.
64. Emkey R, Koltun W, Beusterien K, et al. Patient preference for once-monthly ibandronate versus once-weekly alendronate in a randomized, open-label, cross-over trial: the Boniva Alendronate Trial in Osteoporosis (BALTO). Curr Med Res Opin. 2005;21(12):1895–903.
65. Hadji P, Minne H, Pfeifer M, et al. Treatment preference for monthly oral ibandronate and weekly oral alendronate in women with postmenopausal osteoporosis: A randomized, crossover study (BALTO II). Joint Bone Spine. 2008;75(3):303–10.
66. Ryzner KL, Burkiewicz JS, Griffin BL, Komperda KE. Survey of bisphosphonate regimen preferences in an urban community health center. Consult Pharm. 2010;25(10):671–5.
67. Saag K, Lindsay R, Kriegman A, et al. A single zoledronic acid infusion reduces bone resorption markers more rapidly than weekly oral alendronate in postmenopausal women with low bone mineral density. Bone. 2007;40(5):1238–43.
68. Hadji P, Felsenberg D, Amling M, et al. The non-interventional BonViva Intravenous Versus Alendronate (VIVA) study: real-world adherence and persistence to medication, efficacy, and safety, in patients with postmenopausal osteoporosis. Osteoporos Int. 2014;25(1):339–47.
69. Ziller V, Kostev K, Kyvernitakis I, et al. Persistence and compliance of medications used in the treatment of osteoporosis--analysis using a large scale, representative, longitudinal German database. Int J Clin Pharmacol Ther. 2012;50(5):315–22.
70. Curtis JR, Yun H, Matthews R, et al. Adherence with intravenous zoledronate and intravenous ibandronate in the United States Medicare population. Arthritis Care Res (Hoboken). 2012;64(7):1054–60.
71. Clowes JA, Peel NF, Eastell R. The impact of monitoring on adherence and persistence with antiresorptive treatment for postmenopausal osteoporosis: a randomized controlled trial. J Clin Endocrinol Metab. 2004;89(3):1117–23.
72. Cooper A, Drake J, Brankin E; PERSIST Investigators. Treatment persistence with once-monthly ibandronate and patient support vs. once-weekly alendronate: results from the PERSIST study. Int J Clin Pract. 2006;60(8):896–905.
73. Hiligsmann M, Bours SP, Boonen A. A review of patient preferences for osteoporosis drug treatment. Curr Rheumatol Rep. 2015;17(9):61.
74. Bond WS, Hussar DA. Detection methods and strategies for improving medication compliance. Am J Hosp Pharm. 1991;48(9):1978–88.
75. Delmas PD, Vrijens B, Eastell R, et al. Effect of monitoring bone turnover markers on persistence with risedronate treatment of postmenopausal osteoporosis. J Clin Endocrinol Metab. 2007;92(4):1296–304.
76. Pickney CS, Arnason JA. Correlation between patient recall of bone densitometry results and subsequent treatment adherence. Osteoporos Int. 2005;16(9):1156–60.
77. Cizmic AD, Heilmann RM, Milchak JL, et al. Impact of interactive voice response technology on primary adherence to bisphosphonate therapy: a randomized controlled trial. Osteoporos Int. 2015;26(8):2131–6.
78. LeBlanc A, Wang AT, Wyatt K, et al. Encounter Decision Aid vs. Clinical Decision Support or Usual Care to Support Patient-Centered Treatment Decisions in Osteoporosis: The Osteoporosis Choice Randomized Trial II. PLoS One. 2015;10(5):e0128063.
79. Tao D, Xie L, Wang T, Wang T. A meta-analysis of the use of electronic reminders for patient adherence to medication in chronic disease care. J Telemed Telecare. 2015;21(1):3–13.
80. Vervloet M, van Dijk L, Santen-Reestman J, et al. SMS reminders improve adherence to oral medication in type 2 diabetes patients who are real time electronically monitored. Int J Med Inform. 2012;81(9):594–604.
81. Vervloet M, Linn AJ, van Weert JC, et al. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. J Am Med Inform Assoc. 2012;19(5):696–704.
82. Dayer L, Heldenbrand S, Anderson P, et al. Smartphone medication adherence apps: potential benefits to patients and providers. J Am Pharm Assoc (2003). 2013;53(2):172–81.
83. Solomon DH, Iversen MD, Avorn J, et al. Osteoporosis telephonic intervention to improve medication regimen adherence: a large, pragmatic, randomized controlled trial. Arch Intern Med. 2012;172(6):477–83.
84. Bianchi ML, Duca P, Vai S, et al. Improving adherence to and persistence with oral therapy of osteoporosis. Osteoporos Int. 2015;26(5):1629–38.
85. van Boven JF, Stuurman-Bieze AG, Hiddink EG, et al. Medication monitoring and optimization: a targeted pharmacist program for effective and cost-effective improvement of chronic therapy adherence. J Manag Care Spec Pharm. 2014;20(8):786–92.
86. Lai PS, Chua SS, Chan SP. Pharmaceutical care issues encountered by post-menopausal osteoporotic women prescribed bisphosphonates. J Clin Pharm Ther. 2012;37(5):536–43.
87. Lai PS, Chua SS, Chan SP. Impact of pharmaceutical care on knowledge, quality of life and satisfaction of postmenopausal women with osteoporosis. Int J Clin Pharm. 2013;35(4):629–37.
88. Murphy-Menezes M. Role of the pharmacist in medication therapy management services in patients with osteoporosis. Clin Ther. 2015;37(7):1573–86.
89. Salter C, McDaid L, Bhattacharya D, et al. Abandoned acid? Understanding adherence to bisphosphonate medications for the prevention of osteoporosis among older women: a qualitative longitudinal study. PLoS One. 2014;9(1):e83552.
From the Division of Endocrinology, Diabetes, and Metabolism, University of Alabama at Birmingham, Birmingham, Alabama.
Abstract
- Objective: To review the treatment of osteoporosis, challenges to treatment adherence, and factors associated with improved adherence.
- Methods: Review of the literature.
- Results: With the growing aging population, there is an increased number of people at risk of osteoporosis and fracture. Several medications are available that reduce the risk of fracture. However, adherence to osteoporosis medications is suboptimal. Factors related to nonadherence include dosing frequency, real side effects, and concern about potential side effects. Interventions that may improve adherence include clinician and patient education, less frequent and less complex dosing regimens, medication reminders, and adherence counseling.
- Conclusions: Improving adherence to osteoporosis medications is a complex and challenging issue. Considering and implementing strategies to improve adherence tailored to patient preferences may enhance long-term outcomes for patients with osteoporosis.
Osteoporosis is a chronic but asymptomatic disease that is characterized by an increased fragility of bones and increased risk of fractures. Hip and vertebral fractures are associated with the greatest morbidity and mortality. The prevalence of osteoporosis is estimated to be 10.3% in the US, with approximately 10.2 million adults over the age of 50 having osteoporosis based on 2010 census data and results from the National Health and Nutrition Examination Survey (NHANES) [1].
Several drugs are currently available for the treatment of osteoporosis, but adherence to treatment is low. Understanding the factors associated with low adherence and actions that can be taken to improve adherence to treatment is important given the large number of individuals with osteoporosis and the need to reduce the burden caused by fragility fracture. In this article, we review the treatment of osteoporosis, challenges to treatment adherence, and factors associated with improved adherence.
Nonprescription Medications
Calcium
There have been several published studies over the last decade evaluating calcium supplementation and its efficacy in reducing fractures. Although these studies showed that calcium reduces bone turnover by 20% and slowed postmenopausal bone loss by one third [2,3], none of these studies or a recent systematic review [4] showed any degree of fracture risk reduction with calcium supplements alone.
Although some calcium intake may be good, too much calcium has the potential to cause harm, including an increased risk of nephrolithiasis and constipation/bloating. An analysis of the Women’s Health Initiative (WHI) study reported a 17% increase in renal calculi in women who received calcium and vitamin D supplements [5]. Another recently published meta-analysis showed a 43% increase in gastrointestinal complaints in patients who were taking calcium supplements [6]. The potential for increased cardiovascular risk with calcium supplements is controversial [7]. The WHI study did not show an increased occurrence of cardiovascular events among those taking calcium supplements [8]. In a different population, men who consumed more than 1000 mg per day of supplemental calcium had higher all-cause and cardiovascular disease-specific mortality [9]. Large, well-conducted randomized controlled trials will be needed to further elucidate the question of calcium supplementation and risk of cardiovascular disease.
Vitamin D
Deficiency of vitamin D is common with one study finding more than 90% of older adults deficient in vitamin D [10]. Vitamin D is essential for proper calcium metabolism and deficiency is known to induce secondary hyperparathyroidism. Studies in mouse models have also shown that normal vitamin D receptors in enterocytes are essential for normal bone mineralization [11,12]. A systematic Cochrane database review showed that vitamin D3 supplementation decreased mortality in elderly people living independently or in institutional care [13]. Vitamin D was administered for a weighted mean of 4.4 years. Vitamin D2, alfacalcidol, and calcitriol had no statistically significant beneficial effects on mortality. Vitamin D3 combined with calcium was associated with an increased risk of nephrolithiasis during a follow-up period of 1.25 to 7 years (relative risk [RR] 1.17, 95% confidence interval (CI) 1.02–1.34) [13]. The inconsistencies of published reports looking at benefits of vitamin D supplementation may be due in part to variability in compliance with taking the supplements and baseline vitamin D levels.
Two randomized controlled trials have shown that low vitamin D appears to be an independent predictor of fall risk, and vitamin D supplementation has been found to reduce this risk of falls, through improved musculo-skeletal function [14–16]. Thus, vitamin D may play a role in fracture risk reduction beyond direct bone effects.
Prescription Osteoporosis Treatments
Bisphosphonates
Bisphosphonates are the most commonly prescribed medication for osteoporosis. The efficacy of bisphosphonates to reduce fractures is well established. There are oral bisphosphonates, which can be dosed daily, weekly, or monthly, and intravenous bisphosphonates, which can be given every 3 months or annually. Side effects with this class of medications include gastrointestinal effects with the oral options in up to 20% to 30% of users [17]. With intravenous bisphosphonates, the greatest risk is an acute phase response, which can occur in up to 42% of patients [18]. The risk of an acute phase reaction is much lower with doses beyond the first dose and lower if patients have ever previously taken an oral bisphosphonate and/or receive acetaminophen prior to the infusion. Other potential side effects with all bisphosphonates include osteonecrosis of jaw (ONJ) and atypical subtrochanteric fractures. Post marketing studies have indicated that the incidence of ONJ is less than 2 per 100,000 patient-years among those taking bisphosphonates [19,20]. A number of database analyses have shown that ONJ-like lesions can also occur in older individuals with osteoporosis who have never been exposed to bisphosphonates [21]. A case series of an osteoporotic population showed that ONJ-like lesions are lower grade than those typically seen in cancer patients who usually are exposed to higher doses of bisphosphonates [22]. A study of Swedish older men and women reported that long-term use of bisphosphonates (4 years or more) was associated with an increased incidence of atypical fractures. The RR for women was 126.0 (95% CI, 55.1–288.1) after 4 years of bisphosphonates [23]. A U.S. health care database analysis reported that 90% of those with atypical fractures were bisphosphonate users, almost half were Asian (49%), and use beyond 6 years showed the greatest risk [24].
Non-Bisphosphonate Medications
Other osteoporosis medications include denosumab, raloxifene, estrogen, and teriparatide (calcitonin will not be discussed here). Newer options currently under study, including cathepsin K inhibitors and anti-sclerostin therapies, are not available in the United States.
Denosumab is a monoclonal antibody that interferes with the receptor activator of nuclear kappa B ligand (RANK-L), which is the principal stimulus for osteoclastogenesis. Denosumab is administered once every 6 months subcutaneously. Phase III trials of denosumab demonstrated a 68% reduction in vertebral fractures and 40% and 20% reduction in fractures at hip and non-vertebral sites, respectively [25]. Similar to bisphosphonates, other risks include atypical femoral fractures and ONJ. In addition, hypocalcemia, including severe, symptomatic hypocalcemia, has been reported at rates higher than initially reported in the original clinical trials [26]. Hypocalcemia can be severe, especially in patients who are deficient in vitamin D [10,27].
Estrogen is effective in reducing the risk of vertebral fractures. Selective estrogen receptor modulators (SERMs) have both estrogen agonist and antagonist effects. The SERM, raloxifene, has been used in osteoporosis for its antiresorptive effects through the estrogen receptor [28,29]. A newer SERM, bazedoxifene, has been studied in combination with conjugated estrogen and has been reported to improve bone mineral density and other symptoms of menopause, like vasomotor symptoms and vulvo-vaginal atrophy, but its efficacy in reducing fracture risk has not been demonstrated [30,31].
Teriparatide is an anabolic agent that works by stimulating osteoblastic bone formation which results in an increase in bone density and reduction in both vertebral and non-vertebral fracture risk. In women with postmenopausal osteoporosis, it is typically reserved for those with very low bone mineral density (BMD) or those who continue to have fractures despite a bisphosphonate [32]. Barriers to use of teriparatide include high cost, the need for daily injections, and approved use for a total of two years in a lifetime. There is also a theoretical risk of osteosarcoma shown in animal studies but human cases have not been reported when used for postmenopausal osteoporosis. Published studies have shown that combination zolendronate and teriparatide have additive benefits to spine and hip BMD [33]. Another study reported that the combination of denosumab and teriparatide resulted in additive effects, ie, an increase in lumbar, hip, and femoral neck BMD [34]. These combinations have not been studied in populations large enough or for long enough duration to evaluate fracture risk reduction.
Adherence to Osteoporosis Medications
Treatment of osteoporosis reduces risk of fracture, but the benefit of osteoporosis medications is dependent on adherence. Adherence is associated with improved clinical outcomes [35,36] as well as reduced costs and utilization [37,38]; however, adherence to osteoporosis medications is poor. In a meta-analysis of 24 observational studies conducted in large populations, overall adherence for all osteoporosis therapies ranged from approximately 40% to 70% [39]. A recent retrospective claims database analysis in the U.S. reported a 60% noncompliance rate among the 57,913 postmenopausal women prescribed bisphosphonates over 1 year [40]. Another administrative database analysis from a managed care population compared the 3 oral bisphosphonates (risedronate, ibandronate, and alendronate) and found a mean medication possession ratio (MPR) between 0.57–0.58 at 12 months, which dropped to 0.47–0.50 after 24 months and 0.44–0.47 after 36 months [41]. In an observational study of 3200 older women in the U.K. low adherence was self-reported in 8.5%, and 21.6% self-discontinued treatment within 2 years [42]. In a study of Medicare Advantage prescription drug plan members, a small but significant increase in adherence was seen after osteo-porosis treatment change but overall adherence remained low (51% MPR in the change cohort and vs. 44% in the no-change cohort at 24 months, P < 0.01) [43].
Some patients restart osteoporosis therapy after a prolonged lapse in medication use. In one study, re-initiation rates for bisphosphonate therapy among persons who discontinued were as high as 30% within 6 months and 50% within 2 years [44]. Predictors of treatment re-initiation included younger age, female sex, history of fracture, recent hip fracture, nursing home discharge, and BMD testing [44].
Factors that Impact Adherence
Understanding which patients are most likely to be compliant with medications can aid physicians when monitoring osteoporosis treatment responses. In a retro-spective claims analysis, older age was found to be a predictor of compliance: women 65 years and older were more likely to be compliant than younger patients (P = 0.012) [45]. Among women receiving denosumab, improved adherence was found among women with a family history of a parent with a hip fracture, and lower adherence was seen in those with higher age, decreased mobility, and further distance from the clinic where the medication was provided [46].
Major reasons for nonadherence include a fear of potential side effects, occurrence of real side effects, the complicated dosing regimens, and perceived lack of benefit from the medications due to the asymptomatic nature of osteoporosis. In the above noted observational study from the U.K., more than half of the nonadherent patients attributed their nonadherence to side effects (53.9%), with a smaller proportion reporting fear of potential side effects (20.5%) or trouble with the dosing regimen (8.0%)[42].
Patients may also be unwilling to continue to take an osteoporosis medication if a fracture develops while on it and if they are not otherwise provided evidence that the medication is working. In a study by Costa Paiva et al, an understanding and knowledge to osteoporosis was a prerequisite to adherence and the strongest predictor of knowledge was higher education level [47]. Factors that impaired adherence were lower socioeconomic status and presence of comorbidities [47]. In a phenomenological qualitative study, trust in a health care provider was the most common reason for patients’ decision to accept an osteoporosis medication, emphasizing the importance of physician-patient communication [48].
Interventions to Enhance Adherence
Current methods of improving adherence for chronic health problems are mostly complex and not very effective [49]. In a systematic review of interventions to improve medication adherence, only 37 out of 81 studies reported improved adherence in the treatment of chronic diseases, and multifaceted treatments were more likely to succeed [49]. Improving adherence to osteoporosis medications is a complex issue, and a number of interventions evaluated in systematic reviews have shown limited efficacy [50,51]. Simplification of dosing regimens have been found to have a significant impact in chronic disease management [52,53] as well as in some studies of osteoporosis medications.
Simplification of Dosing
Among women prescribed daily vs. weekly bisphosphonates, those on the weekly regimen had significantly higher compliance [54]. However, rates were suboptimal in both groups and more than 50% of women discontinued at 1 year [54]. In addition, in a meta-analysis of osteoporosis medication adherence, a nearly two-fold higher odds of discontinuation with daily vs. weekly bisphosphonates was seen (odds ratio 1.90, 95% CI 1.81–2.00) [55]. Likewise, in a retrospective study in Spain, nearly 85% of those started on a daily bisphosphonate stopped within a year [56], while discontinuation was significantly lower in those prescribed a weekly or monthly bisphosphonate or daily teriparatide; however, discontinuation was still nearly 50% in these groups [56].
Once monthly dosing may be preferred by some patients as there is less time involved in thinking about the disease being treated and a perception of lower likelihood of side effects. In one study, postmenopausal women who had previously stopped oral bisphosphonates due to GI side effects had high adherence rates after self-selecting either monthly oral or quarterly intravenous ibandronate therapy [57]. However, not all studies show significant differences in adherence between weekly and monthly preparations [58–60].
The newer parenteral treatment options that can be given every 6 months or once yearly have the potential to significantly improve adherence. Once a year parenteral administration of a bisphosphonate was preferred over once-weekly oral administration, according to a 1-year study in patients with low bone density previously treated with alendronate [61]. A recent study that looked at persistence with an infusion of zolendronic acid in Taiwanese patients for 48 months found that 85% of patients received at least 2 infusions [62]. In patients treated with denosumab in 4 European countries, adherence and persistence at 12 months were consistently > 80% [46]. Persistence in this study was defined as receiving the subsequent injection within 6 months ± 8 weeks of the previous injection; adherence was defined as receiving 2 consecutive injections within 6 months ± 4 weeks of each other [46].
In a study by Cramer et al, increased adherence and persistence was seen with weekly alendronate compared daily alendronate at the end of 12 months [54]. Similar results were seen in a large longitudinal cohort study of weekly vs. daily bisphosphonates but less than 50% of patients were adherent with the weekly regimen [63]. When once monthly preparations of bisphosphonates became available, studies continued to support a patient preference for less frequently dosed bisphosphonates, with the majority of patients preferring monthly over weekly dosed medications [64–66].
The availability of quarterly ibandronate and yearly zoledronic acid infusions have further simplified dosing. In large, randomized, multicenter studies, patients consistently expressed a preference for yearly infusions over a weekly oral medication [61,67]. Adherence and persistence to osteoporosis medications was also greater in women receiving intravenous ibandronate compared to those receiving oral alendronate [68,69]. However, a study by Curtis et al showed low persistence with intravenous bisphosphonates in a Medicare population [70]. A possible reason for the lower adherence in this population was postulated to include the provision of the infusions at an outpatient center rather than a physician office. Automated nursing reminders with either phone calls or emails have the potential to mitigate the problem of persistence with this less frequent regimen [71,72]. In a review of patient preferences, less frequent dosing of medications was a common desire, but further generalizability were limited, emphasizing the need to individualize treatment [73].
Patient-Provider Communication
Individualizing treatment with better patient-provider communication and identification of potential barriers may increase compliance [74]. In one study, increasing patient participation in determining the treatment option was associated with improved patient adherence [57]. A systematic review of literature on interventions to improve adherence found that periodic follow-up interaction between patients and their health professionals also improved adherence [50]. Positive reinforcement via physician-patient discussion of either bone turnover markers or bone mineral density test results has also been found to improve long-term adherence with osteoporosis medications [71,75].
Better perceived physician knowledge may help with patient adherence. A study by Pickney et al reported that the patient confidence in their health care providers has influence on improved adherence, and patients were more likely to comply when the medications were prescribed by a specialist rather than a general practitioner [76].
Education, Reminders, Phone-Based
Improving patient knowledge of osteoporosis, especially with education using visual aids, may help with improving adherence [47]. In a randomized controlled trial at a single health management organization, an interactive voice response phone call plus a letter 1 week later increased the rate of obtaining a prescribed oral bisphosphonate in the intervention group (48.8% vs. 30.5% control; OR 2.3, 95% CI 1.34–3.94) when adjusted for age, sex, prior BMD, and fracture [77]. Use of an encounter decision aid also improved knowledge of osteoporosis medication options and led to a doubling of medication prescription attainment. However, adherence at 6 months was not improved [78].
Pill reminders in the form of text messages, paging systems on medication devices, and alarm beeps have been studied in patients with chronic diseases, and these technologies could be utilized for osteoporosis treatment [79–81]. A study of smart phone applications showed that many apps help with adherence, especially in noncompliant patients [82]. The researchers reported that of apps studied, MyMedSchedule, MyMeds, and RxmindMe were among the most highly rated due to their ease of use and enhanced functions. Solomon et all studied the effectiveness of a telephone-based counseling program using motivational interviewing in a large randomized study. They found no significant improvement in adherence to an osteoporosis regimen with the telephonic motivational interview compared to mailed educational materials (control group) (P = 0.07) [83]. In a 12-month multicenter, prospective randomized study, Bianchi et al examined the effectiveness of an intervention of reminders or reminders plus phone calls and meetings at the referral center in postmenopausal women initiating an oral osteoporosis prescription. No significant difference was seen in adherence at 12 months compared to standard care [84]. Adherence among the entire cohort, however, was very high [84]
Pharmacist-Based
The role of pharmacists in the treatment of chronic diseases, including osteoporosis, has been studied and shown to be cost-effective. In a study by van Boven et al, an algorithm was designed to detect patients with nonadherence and then tailor an intervention that consisted of structured counseling and active monitoring by pharmacists in initial and continuous phases [85]. This effort-intensive intervention resulted in reduced discontinuation of bisphosphonates after 12 months (reduction from 31.7% to 16.2% at 12 months) [85]. Despite the effort required, findings from the study support overall cost-effectiveness of this intervention [85]. A randomized controlled study by Lai et al showed that pharmacists can play a role in improving medication adherence through counseling patients on the importance of adherence, side effects, and goals of therapy [86]. The same authors also showed that involvement of a clinical pharmacist in the care of patients helped to further improve patient knowledge of medications and osteoporosis treatments, resolve medication-related concerns, and improve overall quality of life [87]. Such pharmacist-led interventions would require pharmacists to understand their role and the potential for drug holidays in the course of osteoporosis treatments and not mislabel patients as nonadherent when in fact purposefully holding osteoporosis medications [88].
Conclusion
Osteoporosis is a growing problem with increasing numbers of patients at risk for osteoporosis and related fractures. Currently available osteoporosis medications have shown clear benefit in reducing fracture risk; however, adherence to these therapies is required to obtain benefit. Unfortunately, osteoporosis medications have several limitations to full compliance, particularly the oral treatment options, including known possible side effects acutely and chronically, potential/feared side effects, irregular dosing intervals, complicated dosing instructions, and absence of an immediate recognizable benefit/effect. Improving adherence is complex [89] and tailoring to individual patients is of importance. Successful techniques for improving adherence may include a focus on physician-patient communication, use of the less frequently dosed medications, various medication reminders, use of available technology, and use of pharmacists for patient counseling and monitoring. Recognition of this common problem by clinicians is of utmost importance.
Corresponding author: Amy H. Warriner, MD, The University of Alabama at Birmingham, Division of Endocrinology, Diabetes and Metabolism, 702 Faculty Office Tower, 510 20th Street South, Birmingham, AL 35294, [email protected].
Financial disclosures: None.
From the Division of Endocrinology, Diabetes, and Metabolism, University of Alabama at Birmingham, Birmingham, Alabama.
Abstract
- Objective: To review the treatment of osteoporosis, challenges to treatment adherence, and factors associated with improved adherence.
- Methods: Review of the literature.
- Results: With the growing aging population, there is an increased number of people at risk of osteoporosis and fracture. Several medications are available that reduce the risk of fracture. However, adherence to osteoporosis medications is suboptimal. Factors related to nonadherence include dosing frequency, real side effects, and concern about potential side effects. Interventions that may improve adherence include clinician and patient education, less frequent and less complex dosing regimens, medication reminders, and adherence counseling.
- Conclusions: Improving adherence to osteoporosis medications is a complex and challenging issue. Considering and implementing strategies to improve adherence tailored to patient preferences may enhance long-term outcomes for patients with osteoporosis.
Osteoporosis is a chronic but asymptomatic disease that is characterized by an increased fragility of bones and increased risk of fractures. Hip and vertebral fractures are associated with the greatest morbidity and mortality. The prevalence of osteoporosis is estimated to be 10.3% in the US, with approximately 10.2 million adults over the age of 50 having osteoporosis based on 2010 census data and results from the National Health and Nutrition Examination Survey (NHANES) [1].
Several drugs are currently available for the treatment of osteoporosis, but adherence to treatment is low. Understanding the factors associated with low adherence and actions that can be taken to improve adherence to treatment is important given the large number of individuals with osteoporosis and the need to reduce the burden caused by fragility fracture. In this article, we review the treatment of osteoporosis, challenges to treatment adherence, and factors associated with improved adherence.
Nonprescription Medications
Calcium
There have been several published studies over the last decade evaluating calcium supplementation and its efficacy in reducing fractures. Although these studies showed that calcium reduces bone turnover by 20% and slowed postmenopausal bone loss by one third [2,3], none of these studies or a recent systematic review [4] showed any degree of fracture risk reduction with calcium supplements alone.
Although some calcium intake may be good, too much calcium has the potential to cause harm, including an increased risk of nephrolithiasis and constipation/bloating. An analysis of the Women’s Health Initiative (WHI) study reported a 17% increase in renal calculi in women who received calcium and vitamin D supplements [5]. Another recently published meta-analysis showed a 43% increase in gastrointestinal complaints in patients who were taking calcium supplements [6]. The potential for increased cardiovascular risk with calcium supplements is controversial [7]. The WHI study did not show an increased occurrence of cardiovascular events among those taking calcium supplements [8]. In a different population, men who consumed more than 1000 mg per day of supplemental calcium had higher all-cause and cardiovascular disease-specific mortality [9]. Large, well-conducted randomized controlled trials will be needed to further elucidate the question of calcium supplementation and risk of cardiovascular disease.
Vitamin D
Deficiency of vitamin D is common with one study finding more than 90% of older adults deficient in vitamin D [10]. Vitamin D is essential for proper calcium metabolism and deficiency is known to induce secondary hyperparathyroidism. Studies in mouse models have also shown that normal vitamin D receptors in enterocytes are essential for normal bone mineralization [11,12]. A systematic Cochrane database review showed that vitamin D3 supplementation decreased mortality in elderly people living independently or in institutional care [13]. Vitamin D was administered for a weighted mean of 4.4 years. Vitamin D2, alfacalcidol, and calcitriol had no statistically significant beneficial effects on mortality. Vitamin D3 combined with calcium was associated with an increased risk of nephrolithiasis during a follow-up period of 1.25 to 7 years (relative risk [RR] 1.17, 95% confidence interval (CI) 1.02–1.34) [13]. The inconsistencies of published reports looking at benefits of vitamin D supplementation may be due in part to variability in compliance with taking the supplements and baseline vitamin D levels.
Two randomized controlled trials have shown that low vitamin D appears to be an independent predictor of fall risk, and vitamin D supplementation has been found to reduce this risk of falls, through improved musculo-skeletal function [14–16]. Thus, vitamin D may play a role in fracture risk reduction beyond direct bone effects.
Prescription Osteoporosis Treatments
Bisphosphonates
Bisphosphonates are the most commonly prescribed medication for osteoporosis. The efficacy of bisphosphonates to reduce fractures is well established. There are oral bisphosphonates, which can be dosed daily, weekly, or monthly, and intravenous bisphosphonates, which can be given every 3 months or annually. Side effects with this class of medications include gastrointestinal effects with the oral options in up to 20% to 30% of users [17]. With intravenous bisphosphonates, the greatest risk is an acute phase response, which can occur in up to 42% of patients [18]. The risk of an acute phase reaction is much lower with doses beyond the first dose and lower if patients have ever previously taken an oral bisphosphonate and/or receive acetaminophen prior to the infusion. Other potential side effects with all bisphosphonates include osteonecrosis of jaw (ONJ) and atypical subtrochanteric fractures. Post marketing studies have indicated that the incidence of ONJ is less than 2 per 100,000 patient-years among those taking bisphosphonates [19,20]. A number of database analyses have shown that ONJ-like lesions can also occur in older individuals with osteoporosis who have never been exposed to bisphosphonates [21]. A case series of an osteoporotic population showed that ONJ-like lesions are lower grade than those typically seen in cancer patients who usually are exposed to higher doses of bisphosphonates [22]. A study of Swedish older men and women reported that long-term use of bisphosphonates (4 years or more) was associated with an increased incidence of atypical fractures. The RR for women was 126.0 (95% CI, 55.1–288.1) after 4 years of bisphosphonates [23]. A U.S. health care database analysis reported that 90% of those with atypical fractures were bisphosphonate users, almost half were Asian (49%), and use beyond 6 years showed the greatest risk [24].
Non-Bisphosphonate Medications
Other osteoporosis medications include denosumab, raloxifene, estrogen, and teriparatide (calcitonin will not be discussed here). Newer options currently under study, including cathepsin K inhibitors and anti-sclerostin therapies, are not available in the United States.
Denosumab is a monoclonal antibody that interferes with the receptor activator of nuclear kappa B ligand (RANK-L), which is the principal stimulus for osteoclastogenesis. Denosumab is administered once every 6 months subcutaneously. Phase III trials of denosumab demonstrated a 68% reduction in vertebral fractures and 40% and 20% reduction in fractures at hip and non-vertebral sites, respectively [25]. Similar to bisphosphonates, other risks include atypical femoral fractures and ONJ. In addition, hypocalcemia, including severe, symptomatic hypocalcemia, has been reported at rates higher than initially reported in the original clinical trials [26]. Hypocalcemia can be severe, especially in patients who are deficient in vitamin D [10,27].
Estrogen is effective in reducing the risk of vertebral fractures. Selective estrogen receptor modulators (SERMs) have both estrogen agonist and antagonist effects. The SERM, raloxifene, has been used in osteoporosis for its antiresorptive effects through the estrogen receptor [28,29]. A newer SERM, bazedoxifene, has been studied in combination with conjugated estrogen and has been reported to improve bone mineral density and other symptoms of menopause, like vasomotor symptoms and vulvo-vaginal atrophy, but its efficacy in reducing fracture risk has not been demonstrated [30,31].
Teriparatide is an anabolic agent that works by stimulating osteoblastic bone formation which results in an increase in bone density and reduction in both vertebral and non-vertebral fracture risk. In women with postmenopausal osteoporosis, it is typically reserved for those with very low bone mineral density (BMD) or those who continue to have fractures despite a bisphosphonate [32]. Barriers to use of teriparatide include high cost, the need for daily injections, and approved use for a total of two years in a lifetime. There is also a theoretical risk of osteosarcoma shown in animal studies but human cases have not been reported when used for postmenopausal osteoporosis. Published studies have shown that combination zolendronate and teriparatide have additive benefits to spine and hip BMD [33]. Another study reported that the combination of denosumab and teriparatide resulted in additive effects, ie, an increase in lumbar, hip, and femoral neck BMD [34]. These combinations have not been studied in populations large enough or for long enough duration to evaluate fracture risk reduction.
Adherence to Osteoporosis Medications
Treatment of osteoporosis reduces risk of fracture, but the benefit of osteoporosis medications is dependent on adherence. Adherence is associated with improved clinical outcomes [35,36] as well as reduced costs and utilization [37,38]; however, adherence to osteoporosis medications is poor. In a meta-analysis of 24 observational studies conducted in large populations, overall adherence for all osteoporosis therapies ranged from approximately 40% to 70% [39]. A recent retrospective claims database analysis in the U.S. reported a 60% noncompliance rate among the 57,913 postmenopausal women prescribed bisphosphonates over 1 year [40]. Another administrative database analysis from a managed care population compared the 3 oral bisphosphonates (risedronate, ibandronate, and alendronate) and found a mean medication possession ratio (MPR) between 0.57–0.58 at 12 months, which dropped to 0.47–0.50 after 24 months and 0.44–0.47 after 36 months [41]. In an observational study of 3200 older women in the U.K. low adherence was self-reported in 8.5%, and 21.6% self-discontinued treatment within 2 years [42]. In a study of Medicare Advantage prescription drug plan members, a small but significant increase in adherence was seen after osteo-porosis treatment change but overall adherence remained low (51% MPR in the change cohort and vs. 44% in the no-change cohort at 24 months, P < 0.01) [43].
Some patients restart osteoporosis therapy after a prolonged lapse in medication use. In one study, re-initiation rates for bisphosphonate therapy among persons who discontinued were as high as 30% within 6 months and 50% within 2 years [44]. Predictors of treatment re-initiation included younger age, female sex, history of fracture, recent hip fracture, nursing home discharge, and BMD testing [44].
Factors that Impact Adherence
Understanding which patients are most likely to be compliant with medications can aid physicians when monitoring osteoporosis treatment responses. In a retro-spective claims analysis, older age was found to be a predictor of compliance: women 65 years and older were more likely to be compliant than younger patients (P = 0.012) [45]. Among women receiving denosumab, improved adherence was found among women with a family history of a parent with a hip fracture, and lower adherence was seen in those with higher age, decreased mobility, and further distance from the clinic where the medication was provided [46].
Major reasons for nonadherence include a fear of potential side effects, occurrence of real side effects, the complicated dosing regimens, and perceived lack of benefit from the medications due to the asymptomatic nature of osteoporosis. In the above noted observational study from the U.K., more than half of the nonadherent patients attributed their nonadherence to side effects (53.9%), with a smaller proportion reporting fear of potential side effects (20.5%) or trouble with the dosing regimen (8.0%)[42].
Patients may also be unwilling to continue to take an osteoporosis medication if a fracture develops while on it and if they are not otherwise provided evidence that the medication is working. In a study by Costa Paiva et al, an understanding and knowledge to osteoporosis was a prerequisite to adherence and the strongest predictor of knowledge was higher education level [47]. Factors that impaired adherence were lower socioeconomic status and presence of comorbidities [47]. In a phenomenological qualitative study, trust in a health care provider was the most common reason for patients’ decision to accept an osteoporosis medication, emphasizing the importance of physician-patient communication [48].
Interventions to Enhance Adherence
Current methods of improving adherence for chronic health problems are mostly complex and not very effective [49]. In a systematic review of interventions to improve medication adherence, only 37 out of 81 studies reported improved adherence in the treatment of chronic diseases, and multifaceted treatments were more likely to succeed [49]. Improving adherence to osteoporosis medications is a complex issue, and a number of interventions evaluated in systematic reviews have shown limited efficacy [50,51]. Simplification of dosing regimens have been found to have a significant impact in chronic disease management [52,53] as well as in some studies of osteoporosis medications.
Simplification of Dosing
Among women prescribed daily vs. weekly bisphosphonates, those on the weekly regimen had significantly higher compliance [54]. However, rates were suboptimal in both groups and more than 50% of women discontinued at 1 year [54]. In addition, in a meta-analysis of osteoporosis medication adherence, a nearly two-fold higher odds of discontinuation with daily vs. weekly bisphosphonates was seen (odds ratio 1.90, 95% CI 1.81–2.00) [55]. Likewise, in a retrospective study in Spain, nearly 85% of those started on a daily bisphosphonate stopped within a year [56], while discontinuation was significantly lower in those prescribed a weekly or monthly bisphosphonate or daily teriparatide; however, discontinuation was still nearly 50% in these groups [56].
Once monthly dosing may be preferred by some patients as there is less time involved in thinking about the disease being treated and a perception of lower likelihood of side effects. In one study, postmenopausal women who had previously stopped oral bisphosphonates due to GI side effects had high adherence rates after self-selecting either monthly oral or quarterly intravenous ibandronate therapy [57]. However, not all studies show significant differences in adherence between weekly and monthly preparations [58–60].
The newer parenteral treatment options that can be given every 6 months or once yearly have the potential to significantly improve adherence. Once a year parenteral administration of a bisphosphonate was preferred over once-weekly oral administration, according to a 1-year study in patients with low bone density previously treated with alendronate [61]. A recent study that looked at persistence with an infusion of zolendronic acid in Taiwanese patients for 48 months found that 85% of patients received at least 2 infusions [62]. In patients treated with denosumab in 4 European countries, adherence and persistence at 12 months were consistently > 80% [46]. Persistence in this study was defined as receiving the subsequent injection within 6 months ± 8 weeks of the previous injection; adherence was defined as receiving 2 consecutive injections within 6 months ± 4 weeks of each other [46].
In a study by Cramer et al, increased adherence and persistence was seen with weekly alendronate compared daily alendronate at the end of 12 months [54]. Similar results were seen in a large longitudinal cohort study of weekly vs. daily bisphosphonates but less than 50% of patients were adherent with the weekly regimen [63]. When once monthly preparations of bisphosphonates became available, studies continued to support a patient preference for less frequently dosed bisphosphonates, with the majority of patients preferring monthly over weekly dosed medications [64–66].
The availability of quarterly ibandronate and yearly zoledronic acid infusions have further simplified dosing. In large, randomized, multicenter studies, patients consistently expressed a preference for yearly infusions over a weekly oral medication [61,67]. Adherence and persistence to osteoporosis medications was also greater in women receiving intravenous ibandronate compared to those receiving oral alendronate [68,69]. However, a study by Curtis et al showed low persistence with intravenous bisphosphonates in a Medicare population [70]. A possible reason for the lower adherence in this population was postulated to include the provision of the infusions at an outpatient center rather than a physician office. Automated nursing reminders with either phone calls or emails have the potential to mitigate the problem of persistence with this less frequent regimen [71,72]. In a review of patient preferences, less frequent dosing of medications was a common desire, but further generalizability were limited, emphasizing the need to individualize treatment [73].
Patient-Provider Communication
Individualizing treatment with better patient-provider communication and identification of potential barriers may increase compliance [74]. In one study, increasing patient participation in determining the treatment option was associated with improved patient adherence [57]. A systematic review of literature on interventions to improve adherence found that periodic follow-up interaction between patients and their health professionals also improved adherence [50]. Positive reinforcement via physician-patient discussion of either bone turnover markers or bone mineral density test results has also been found to improve long-term adherence with osteoporosis medications [71,75].
Better perceived physician knowledge may help with patient adherence. A study by Pickney et al reported that the patient confidence in their health care providers has influence on improved adherence, and patients were more likely to comply when the medications were prescribed by a specialist rather than a general practitioner [76].
Education, Reminders, Phone-Based
Improving patient knowledge of osteoporosis, especially with education using visual aids, may help with improving adherence [47]. In a randomized controlled trial at a single health management organization, an interactive voice response phone call plus a letter 1 week later increased the rate of obtaining a prescribed oral bisphosphonate in the intervention group (48.8% vs. 30.5% control; OR 2.3, 95% CI 1.34–3.94) when adjusted for age, sex, prior BMD, and fracture [77]. Use of an encounter decision aid also improved knowledge of osteoporosis medication options and led to a doubling of medication prescription attainment. However, adherence at 6 months was not improved [78].
Pill reminders in the form of text messages, paging systems on medication devices, and alarm beeps have been studied in patients with chronic diseases, and these technologies could be utilized for osteoporosis treatment [79–81]. A study of smart phone applications showed that many apps help with adherence, especially in noncompliant patients [82]. The researchers reported that of apps studied, MyMedSchedule, MyMeds, and RxmindMe were among the most highly rated due to their ease of use and enhanced functions. Solomon et all studied the effectiveness of a telephone-based counseling program using motivational interviewing in a large randomized study. They found no significant improvement in adherence to an osteoporosis regimen with the telephonic motivational interview compared to mailed educational materials (control group) (P = 0.07) [83]. In a 12-month multicenter, prospective randomized study, Bianchi et al examined the effectiveness of an intervention of reminders or reminders plus phone calls and meetings at the referral center in postmenopausal women initiating an oral osteoporosis prescription. No significant difference was seen in adherence at 12 months compared to standard care [84]. Adherence among the entire cohort, however, was very high [84]
Pharmacist-Based
The role of pharmacists in the treatment of chronic diseases, including osteoporosis, has been studied and shown to be cost-effective. In a study by van Boven et al, an algorithm was designed to detect patients with nonadherence and then tailor an intervention that consisted of structured counseling and active monitoring by pharmacists in initial and continuous phases [85]. This effort-intensive intervention resulted in reduced discontinuation of bisphosphonates after 12 months (reduction from 31.7% to 16.2% at 12 months) [85]. Despite the effort required, findings from the study support overall cost-effectiveness of this intervention [85]. A randomized controlled study by Lai et al showed that pharmacists can play a role in improving medication adherence through counseling patients on the importance of adherence, side effects, and goals of therapy [86]. The same authors also showed that involvement of a clinical pharmacist in the care of patients helped to further improve patient knowledge of medications and osteoporosis treatments, resolve medication-related concerns, and improve overall quality of life [87]. Such pharmacist-led interventions would require pharmacists to understand their role and the potential for drug holidays in the course of osteoporosis treatments and not mislabel patients as nonadherent when in fact purposefully holding osteoporosis medications [88].
Conclusion
Osteoporosis is a growing problem with increasing numbers of patients at risk for osteoporosis and related fractures. Currently available osteoporosis medications have shown clear benefit in reducing fracture risk; however, adherence to these therapies is required to obtain benefit. Unfortunately, osteoporosis medications have several limitations to full compliance, particularly the oral treatment options, including known possible side effects acutely and chronically, potential/feared side effects, irregular dosing intervals, complicated dosing instructions, and absence of an immediate recognizable benefit/effect. Improving adherence is complex [89] and tailoring to individual patients is of importance. Successful techniques for improving adherence may include a focus on physician-patient communication, use of the less frequently dosed medications, various medication reminders, use of available technology, and use of pharmacists for patient counseling and monitoring. Recognition of this common problem by clinicians is of utmost importance.
Corresponding author: Amy H. Warriner, MD, The University of Alabama at Birmingham, Division of Endocrinology, Diabetes and Metabolism, 702 Faculty Office Tower, 510 20th Street South, Birmingham, AL 35294, [email protected].
Financial disclosures: None.
1. Wright NC, Looker AC, Saag KG, et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res. 2014;29(11):2520–6.
2. Reid IR, Mason B, Horne A, et al. Randomized controlled trial of calcium in healthy older women. Am J Med. 2006;119(9):777–85.
3. Reid IR, Ames R, Mason B, et al. Randomized controlled trial of calcium supplementation in healthy, nonosteoporotic, older men. Arch Intern Med. 2008;168(20):2276–82.
4. Murad MH, Drake MT, Mullan RJ, et al. Clinical review. Comparative effectiveness of drug treatments to prevent fragility fractures: a systematic review and network meta-analysis. J Clin Endocrinol Metab. 2012;97(6):1871–80.
5. Jackson RD, LaCroix AZ, Gass M, et al. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006;354(7):669–83.
6. Lewis JR, Zhu K, Prince RL. Adverse events from calcium supplementation: relationship to errors in myocardial infarction self-reporting in randomized controlled trials of calcium supplementation. J Bone Miner Res. 2012;27(3):719–22.
7. Challoumas D, Stavrou A, Pericleous A, Dimitrakakis G. Effects of combined vitamin D--calcium supplements on the cardiovascular system: should we be cautious? Atherosclerosis. 2015;238(2):388–98.
8. Hsia J, Heiss G, Ren H, et al. Calcium/vitamin D supplementation and cardiovascular events. Circulation. 2007;115(7):846–54.
9. Yang B, Campbell PT, Gapstur SM, et al. Calcium intake and mortality from all causes, cancer, and cardiovascular disease: the Cancer Prevention Study II Nutrition Cohort. Am J Clin Nutr. 2016;103(3):886–94.
10. Reid IR. Efficacy, effectiveness and side effects of medications used to prevent fractures. J Intern Med. 2015;277(6):690–706.
11. Xue Y, Fleet JC. Intestinal vitamin D receptor is required for normal calcium and bone metabolism in mice. Gastroenterology. 2009;136(4):1317-27, e1–2.
12. Lieben L, Masuyama R, Torrekens S, et al. Normocalcemia is maintained in mice under conditions of calcium malabsorption by vitamin D-induced inhibition of bone mineralization. J Clin Invest. 2012;122(5):1803–15.
13. Bjelakovic G, Gluud LL, Nikolova D, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2014;1:CD007470.
14. Flicker L, Mead K, MacInnis RJ, et al. Serum vitamin D and falls in older women in residential care in Australia. J Am Geriatr Soc. 2003;51(11):1533–8.
15. Bischoff-Ferrari HA, Orav EJ, Dawson-Hughes B. Effect of cholecalciferol plus calcium on falling in ambulatory older men and women: a 3-year randomized controlled trial. Arch Intern Med. 2006;166(4):424–30.
16. Flicker L, MacInnis RJ, Stein MS, et al. Should older people in residential care receive vitamin D to prevent falls? Results of a randomized trial. J Am Geriatr Soc. 2005;53(11):1881–8.
17. Biswas PN, Wilton LV, Shakir SA. Pharmacovigilance study of alendronate in England. Osteoporos Int. 2003;14(6):507–14.
18. Reid IR, Gamble GD, Mesenbrink P, et al. Characterization of and risk factors for the acute-phase response after zoledronic acid. J Clin Endocrinol Metab. 2010;95(9):4380–7.
19. Grbic JT, Landesberg R, Lin SQ, et al. Incidence of osteonecrosis of the jaw in women with postmenopausal osteoporosis in the health outcomes and reduced incidence with zoledronic acid once yearly pivotal fracture trial. J Am Dent Assoc. 2008;139(1):32–40.
20. Grbic JT, Black DM, Lyles KW, et al. The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc. 2010;141(11):1365–70.
21. Lin TC, Yang CY, Kao Yang YH, Lin SJ. Incidence and risk of osteonecrosis of the jaw among the Taiwan osteoporosis population. Osteoporos Int. 2014;25(5):1503–11.
22. Assael LA. Oral bisphosphonates as a cause of bisphosphonate-related osteonecrosis of the jaws: clinical findings, assessment of risks, and preventive strategies. J Oral Maxillofac Surg. 2009;67(5 Suppl):35–43.
23. Schilcher J, Koeppen V, Aspenberg P, Michaelsson K. Risk of atypical femoral fracture during and after bisphosphonate use. N Engl J Med. 2014;371(10):974–6.
24. Dell RM, Adams AL, Greene DF, et al. Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res. 2012;27(12):2544–50.
25. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–65.
26. Yerram P, Kansagra S, Abdelghany O. Incidence of hypocalcemia in patients receiving denosumab for prevention of skeletal-related events in bone metastasis. J Oncol Pharm Pract. 2016.
27. Reid IR. Short-term and long-term effects of osteoporosis therapies. Nat Rev Endocrinol. 2015;11(7):418–28.
28. Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA. 1999;282(7):637–45.
29. Reid IR, Eastell R, Fogelman I, et al. A comparison of the effects of raloxifene and conjugated equine estrogen on bone and lipids in healthy postmenopausal women. Arch Intern Med. 2004;164(8):871–9.
30. Sharifi M, Lewiecki EM. Conjugated estrogens combined with bazedoxifene: the first approved tissue selective estrogen complex therapy. Expert Rev Clin Pharmacol. 2014;7(3):281–91.
31. Mirkin S, Ryan KA, Chandran AB, Komm BS. Bazedoxifene/conjugated estrogens for managing the burden of estrogen deficiency symptoms. Maturitas. 2014;77(1):24–31.
32. Warriner AH, Saag KG. Prevention and treatment of bone changes associated with exposure to glucocorticoids. Curr Osteoporos Rep. 2013;11(4):341–7.
33. Cosman F, Eriksen EF, Recknor C, et al. Effects of intravenous zoledronic acid plus subcutaneous teriparatide [rhPTH(1-34)] in postmenopausal osteoporosis. J Bone Miner Res. 2011;26(3):503–11.
34. Leder BZ, Tsai JN, Uihlein AV, et al. Two years of Denosumab and teriparatide administration in postmenopausal women with osteoporosis (The DATA Extension Study): a randomized controlled trial. J Clin Endocrinol Metab. 2014;99(5):1694–700.
35. Imaz I, Zegarra P, Gonzalez-Enriquez J, et al. Poor bisphosphonate adherence for treatment of osteoporosis increases fracture risk: systematic review and meta-analysis. Osteoporos Int. 2010;21(11):1943–51.
36. Curtis JR, Westfall AO, Cheng H, et al. Benefit of adherence with bisphosphonates depends on age and fracture type: results from an analysis of 101,038 new bisphosphonate users. J Bone Miner Res. 2008;23(9):1435–41.
37. Strom O, Borgstrom F, Kanis JA, Jonsson B. Incorporating adherence into health economic modelling of osteoporosis. Osteoporos Int. 2009;20(1):23–34.
38. Sunyecz JA, Mucha L, Baser O, et al. Impact of compliance and persistence with bisphosphonate therapy on health care costs and utilization. Osteoporos Int. 2008;19(10):1421–9.
39. Halpern R, Becker L, Iqbal SU, et al. The association of adherence to osteoporosis therapies with fracture, all-cause medical costs, and all-cause hospitalizations: a retrospective claims analysis of female health plan enrollees with osteoporosis. J Manag Care Pharm. 2011;17(1):25–39.
40. Modi A, Siris ES, Tang J, Sen S. Cost and consequences of noncompliance with osteoporosis treatment among women initiating therapy. Curr Med Res Opin. 2015;31(4):757–65.
41. Martin KE, Yu J, Campbell HE, et al. Analysis of the comparative effectiveness of 3 oral bisphosphonates in a large managed care organization: adherence, fracture rates, and all-cause cost. J Manag Care Pharm. 2011;17(8):596–609.
42. Clark EM, Gould VC, Tobias JH, Horne R. Natural history, reasons for, and impact of low/non-adherence to medications for osteoporosis in a cohort of community-dwelling older women already established on medication: a 2-year follow-up study. Osteoporos Int. 2016;27(2):579–90.
43. Ward MA, Xu Y, Viswanathan HN, et al. Association between osteoporosis treatment change and adherence, incident fracture, and total healthcare costs in a Medicare Advantage Prescription Drug plan. Osteoporos Int. 2013;24(4):1195–206.
44. Brookhart MA, Avorn J, Katz JN, et al. Gaps in treatment among users of osteoporosis medications: the dynamics of noncompliance. Am J Med. 2007;120(3):251–6.
45. Eisenberg DF, Placzek H, Gu T, et al. Cost and consequences of noncompliance to oral bisphosphonate treatment. J Manag Care Spec Pharm. 2015;21(1):56–65.
46. Hadji P, Papaioannou N, Gielen E, et al. Persistence, adherence, and medication-taking behavior in women with postmenopausal osteoporosis receiving denosumab in routine practice in Germany, Austria, Greece, and Belgium: 12-month results from a European non-interventional study. Osteoporos Int. 2015;26(10):2479–89.
47. Costa-Paiva L, Gomes DC, Morais SS, et al. Knowledge about osteoporosis in postmenopausal women undergoing antiresorptive treatment. Maturitas. 2011;69(1):81–5.
48. Sale JE, Gignac MA, Hawker G, et al. Decision to take osteoporosis medication in patients who have had a fracture and are ‘high’ risk for future fracture: a qualitative study. BMC Musculoskelet Disord. 2011;12:92.
49. Haynes RB, Yao X, Degani A, et al. Interventions to enhance medication adherence. Cochrane Database Syst Rev. 2005(4):CD000011.
50. Gleeson T, Iversen MD, Avorn J, et al. Interventions to improve adherence and persistence with osteoporosis medications: a systematic literature review. Osteoporos Int. 2009; 20(12):2127–34.
51. Hiligsmann M, Salas M, Hughes DA, et al. Interventions to improve osteoporosis medication adherence and persistence: a systematic review and literature appraisal by the ISPOR Medication Adherence & Persistence Special Interest Group. Osteoporos Int. 2013;24(12):2907–18.
52. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–310.
53. Richter A, Anton SF, Koch P, Dennett SL. The impact of reducing dose frequency on health outcomes. Clin Ther. 2003;25(8):2307–35; discussion 6.
54. Cramer JA, Amonkar MM, Hebborn A, Altman R. Compliance and persistence with bisphosphonate dosing regimens among women with postmenopausal osteoporosis. Curr Med Res Opin. 2005;21(9):1453–60.
55. Iglay K, Cao X, Mavros P, et al. Systematic Literature Review and Meta-analysis of Medication Adherence With Once-weekly Versus Once-daily Therapy. Clin Ther. 2015;37(8):1813–21 e1.
56. Carbonell-Abella C, Pages-Castella A, Javaid MK, et al. Early (1-year) Discontinuation of Different Anti-osteoporosis Medications Compared: A Population-Based Cohort Study. Calcif Tissue Int. 2015;97(6):535–41.
57. Lewiecki EM, Babbitt AM, Piziak VK, et al. Adherence to and gastrointestinal tolerability of monthly oral or quarterly intravenous ibandronate therapy in women with previous intolerance to oral bisphosphonates: a 12-month, open-label, prospective evaluation. Clin Ther. 2008;30(4):605–21.
58. Payer J, Killinger Z, Sulkova I, Celec P. Preferences of patients receiving bisphosphonates--how to influence the therapeutic adherence. Biomed Pharmacother. 2008;62(2):122–4.
59. Weycker D, Macarios D, Edelsberg J, Oster G. Compliance with drug therapy for postmenopausal osteoporosis. Osteoporos Int. 2006;17(11):1645–52.
60. Kastelan D, Lozo P, Stamenkovic D, et al. Preference for weekly and monthly bisphosphonates among patients with postmenopausal osteoporosis: results from the Croatian PROMO Study. Clin Rheumatol. 2009;28(3):321–6.
61. McClung M, Recker R, Miller P, et al. Intravenous zoledronic acid 5 mg in the treatment of postmenopausal women with low bone density previously treated with alendronate. Bone. 2007;41(1):122–8.
62. Hsieh PC. Effectiveness and safety of zoledronic acid in the treatment of osteoporosis. Orthopedics. 2016:1–8.
63. Recker RR, Gallagher R, MacCosbe PE. Effect of dosing frequency on bisphosphonate medication adherence in a large longitudinal cohort of women. Mayo Clin Proc. 2005;80(7):856–61.
64. Emkey R, Koltun W, Beusterien K, et al. Patient preference for once-monthly ibandronate versus once-weekly alendronate in a randomized, open-label, cross-over trial: the Boniva Alendronate Trial in Osteoporosis (BALTO). Curr Med Res Opin. 2005;21(12):1895–903.
65. Hadji P, Minne H, Pfeifer M, et al. Treatment preference for monthly oral ibandronate and weekly oral alendronate in women with postmenopausal osteoporosis: A randomized, crossover study (BALTO II). Joint Bone Spine. 2008;75(3):303–10.
66. Ryzner KL, Burkiewicz JS, Griffin BL, Komperda KE. Survey of bisphosphonate regimen preferences in an urban community health center. Consult Pharm. 2010;25(10):671–5.
67. Saag K, Lindsay R, Kriegman A, et al. A single zoledronic acid infusion reduces bone resorption markers more rapidly than weekly oral alendronate in postmenopausal women with low bone mineral density. Bone. 2007;40(5):1238–43.
68. Hadji P, Felsenberg D, Amling M, et al. The non-interventional BonViva Intravenous Versus Alendronate (VIVA) study: real-world adherence and persistence to medication, efficacy, and safety, in patients with postmenopausal osteoporosis. Osteoporos Int. 2014;25(1):339–47.
69. Ziller V, Kostev K, Kyvernitakis I, et al. Persistence and compliance of medications used in the treatment of osteoporosis--analysis using a large scale, representative, longitudinal German database. Int J Clin Pharmacol Ther. 2012;50(5):315–22.
70. Curtis JR, Yun H, Matthews R, et al. Adherence with intravenous zoledronate and intravenous ibandronate in the United States Medicare population. Arthritis Care Res (Hoboken). 2012;64(7):1054–60.
71. Clowes JA, Peel NF, Eastell R. The impact of monitoring on adherence and persistence with antiresorptive treatment for postmenopausal osteoporosis: a randomized controlled trial. J Clin Endocrinol Metab. 2004;89(3):1117–23.
72. Cooper A, Drake J, Brankin E; PERSIST Investigators. Treatment persistence with once-monthly ibandronate and patient support vs. once-weekly alendronate: results from the PERSIST study. Int J Clin Pract. 2006;60(8):896–905.
73. Hiligsmann M, Bours SP, Boonen A. A review of patient preferences for osteoporosis drug treatment. Curr Rheumatol Rep. 2015;17(9):61.
74. Bond WS, Hussar DA. Detection methods and strategies for improving medication compliance. Am J Hosp Pharm. 1991;48(9):1978–88.
75. Delmas PD, Vrijens B, Eastell R, et al. Effect of monitoring bone turnover markers on persistence with risedronate treatment of postmenopausal osteoporosis. J Clin Endocrinol Metab. 2007;92(4):1296–304.
76. Pickney CS, Arnason JA. Correlation between patient recall of bone densitometry results and subsequent treatment adherence. Osteoporos Int. 2005;16(9):1156–60.
77. Cizmic AD, Heilmann RM, Milchak JL, et al. Impact of interactive voice response technology on primary adherence to bisphosphonate therapy: a randomized controlled trial. Osteoporos Int. 2015;26(8):2131–6.
78. LeBlanc A, Wang AT, Wyatt K, et al. Encounter Decision Aid vs. Clinical Decision Support or Usual Care to Support Patient-Centered Treatment Decisions in Osteoporosis: The Osteoporosis Choice Randomized Trial II. PLoS One. 2015;10(5):e0128063.
79. Tao D, Xie L, Wang T, Wang T. A meta-analysis of the use of electronic reminders for patient adherence to medication in chronic disease care. J Telemed Telecare. 2015;21(1):3–13.
80. Vervloet M, van Dijk L, Santen-Reestman J, et al. SMS reminders improve adherence to oral medication in type 2 diabetes patients who are real time electronically monitored. Int J Med Inform. 2012;81(9):594–604.
81. Vervloet M, Linn AJ, van Weert JC, et al. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. J Am Med Inform Assoc. 2012;19(5):696–704.
82. Dayer L, Heldenbrand S, Anderson P, et al. Smartphone medication adherence apps: potential benefits to patients and providers. J Am Pharm Assoc (2003). 2013;53(2):172–81.
83. Solomon DH, Iversen MD, Avorn J, et al. Osteoporosis telephonic intervention to improve medication regimen adherence: a large, pragmatic, randomized controlled trial. Arch Intern Med. 2012;172(6):477–83.
84. Bianchi ML, Duca P, Vai S, et al. Improving adherence to and persistence with oral therapy of osteoporosis. Osteoporos Int. 2015;26(5):1629–38.
85. van Boven JF, Stuurman-Bieze AG, Hiddink EG, et al. Medication monitoring and optimization: a targeted pharmacist program for effective and cost-effective improvement of chronic therapy adherence. J Manag Care Spec Pharm. 2014;20(8):786–92.
86. Lai PS, Chua SS, Chan SP. Pharmaceutical care issues encountered by post-menopausal osteoporotic women prescribed bisphosphonates. J Clin Pharm Ther. 2012;37(5):536–43.
87. Lai PS, Chua SS, Chan SP. Impact of pharmaceutical care on knowledge, quality of life and satisfaction of postmenopausal women with osteoporosis. Int J Clin Pharm. 2013;35(4):629–37.
88. Murphy-Menezes M. Role of the pharmacist in medication therapy management services in patients with osteoporosis. Clin Ther. 2015;37(7):1573–86.
89. Salter C, McDaid L, Bhattacharya D, et al. Abandoned acid? Understanding adherence to bisphosphonate medications for the prevention of osteoporosis among older women: a qualitative longitudinal study. PLoS One. 2014;9(1):e83552.
1. Wright NC, Looker AC, Saag KG, et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res. 2014;29(11):2520–6.
2. Reid IR, Mason B, Horne A, et al. Randomized controlled trial of calcium in healthy older women. Am J Med. 2006;119(9):777–85.
3. Reid IR, Ames R, Mason B, et al. Randomized controlled trial of calcium supplementation in healthy, nonosteoporotic, older men. Arch Intern Med. 2008;168(20):2276–82.
4. Murad MH, Drake MT, Mullan RJ, et al. Clinical review. Comparative effectiveness of drug treatments to prevent fragility fractures: a systematic review and network meta-analysis. J Clin Endocrinol Metab. 2012;97(6):1871–80.
5. Jackson RD, LaCroix AZ, Gass M, et al. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006;354(7):669–83.
6. Lewis JR, Zhu K, Prince RL. Adverse events from calcium supplementation: relationship to errors in myocardial infarction self-reporting in randomized controlled trials of calcium supplementation. J Bone Miner Res. 2012;27(3):719–22.
7. Challoumas D, Stavrou A, Pericleous A, Dimitrakakis G. Effects of combined vitamin D--calcium supplements on the cardiovascular system: should we be cautious? Atherosclerosis. 2015;238(2):388–98.
8. Hsia J, Heiss G, Ren H, et al. Calcium/vitamin D supplementation and cardiovascular events. Circulation. 2007;115(7):846–54.
9. Yang B, Campbell PT, Gapstur SM, et al. Calcium intake and mortality from all causes, cancer, and cardiovascular disease: the Cancer Prevention Study II Nutrition Cohort. Am J Clin Nutr. 2016;103(3):886–94.
10. Reid IR. Efficacy, effectiveness and side effects of medications used to prevent fractures. J Intern Med. 2015;277(6):690–706.
11. Xue Y, Fleet JC. Intestinal vitamin D receptor is required for normal calcium and bone metabolism in mice. Gastroenterology. 2009;136(4):1317-27, e1–2.
12. Lieben L, Masuyama R, Torrekens S, et al. Normocalcemia is maintained in mice under conditions of calcium malabsorption by vitamin D-induced inhibition of bone mineralization. J Clin Invest. 2012;122(5):1803–15.
13. Bjelakovic G, Gluud LL, Nikolova D, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2014;1:CD007470.
14. Flicker L, Mead K, MacInnis RJ, et al. Serum vitamin D and falls in older women in residential care in Australia. J Am Geriatr Soc. 2003;51(11):1533–8.
15. Bischoff-Ferrari HA, Orav EJ, Dawson-Hughes B. Effect of cholecalciferol plus calcium on falling in ambulatory older men and women: a 3-year randomized controlled trial. Arch Intern Med. 2006;166(4):424–30.
16. Flicker L, MacInnis RJ, Stein MS, et al. Should older people in residential care receive vitamin D to prevent falls? Results of a randomized trial. J Am Geriatr Soc. 2005;53(11):1881–8.
17. Biswas PN, Wilton LV, Shakir SA. Pharmacovigilance study of alendronate in England. Osteoporos Int. 2003;14(6):507–14.
18. Reid IR, Gamble GD, Mesenbrink P, et al. Characterization of and risk factors for the acute-phase response after zoledronic acid. J Clin Endocrinol Metab. 2010;95(9):4380–7.
19. Grbic JT, Landesberg R, Lin SQ, et al. Incidence of osteonecrosis of the jaw in women with postmenopausal osteoporosis in the health outcomes and reduced incidence with zoledronic acid once yearly pivotal fracture trial. J Am Dent Assoc. 2008;139(1):32–40.
20. Grbic JT, Black DM, Lyles KW, et al. The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc. 2010;141(11):1365–70.
21. Lin TC, Yang CY, Kao Yang YH, Lin SJ. Incidence and risk of osteonecrosis of the jaw among the Taiwan osteoporosis population. Osteoporos Int. 2014;25(5):1503–11.
22. Assael LA. Oral bisphosphonates as a cause of bisphosphonate-related osteonecrosis of the jaws: clinical findings, assessment of risks, and preventive strategies. J Oral Maxillofac Surg. 2009;67(5 Suppl):35–43.
23. Schilcher J, Koeppen V, Aspenberg P, Michaelsson K. Risk of atypical femoral fracture during and after bisphosphonate use. N Engl J Med. 2014;371(10):974–6.
24. Dell RM, Adams AL, Greene DF, et al. Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res. 2012;27(12):2544–50.
25. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–65.
26. Yerram P, Kansagra S, Abdelghany O. Incidence of hypocalcemia in patients receiving denosumab for prevention of skeletal-related events in bone metastasis. J Oncol Pharm Pract. 2016.
27. Reid IR. Short-term and long-term effects of osteoporosis therapies. Nat Rev Endocrinol. 2015;11(7):418–28.
28. Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA. 1999;282(7):637–45.
29. Reid IR, Eastell R, Fogelman I, et al. A comparison of the effects of raloxifene and conjugated equine estrogen on bone and lipids in healthy postmenopausal women. Arch Intern Med. 2004;164(8):871–9.
30. Sharifi M, Lewiecki EM. Conjugated estrogens combined with bazedoxifene: the first approved tissue selective estrogen complex therapy. Expert Rev Clin Pharmacol. 2014;7(3):281–91.
31. Mirkin S, Ryan KA, Chandran AB, Komm BS. Bazedoxifene/conjugated estrogens for managing the burden of estrogen deficiency symptoms. Maturitas. 2014;77(1):24–31.
32. Warriner AH, Saag KG. Prevention and treatment of bone changes associated with exposure to glucocorticoids. Curr Osteoporos Rep. 2013;11(4):341–7.
33. Cosman F, Eriksen EF, Recknor C, et al. Effects of intravenous zoledronic acid plus subcutaneous teriparatide [rhPTH(1-34)] in postmenopausal osteoporosis. J Bone Miner Res. 2011;26(3):503–11.
34. Leder BZ, Tsai JN, Uihlein AV, et al. Two years of Denosumab and teriparatide administration in postmenopausal women with osteoporosis (The DATA Extension Study): a randomized controlled trial. J Clin Endocrinol Metab. 2014;99(5):1694–700.
35. Imaz I, Zegarra P, Gonzalez-Enriquez J, et al. Poor bisphosphonate adherence for treatment of osteoporosis increases fracture risk: systematic review and meta-analysis. Osteoporos Int. 2010;21(11):1943–51.
36. Curtis JR, Westfall AO, Cheng H, et al. Benefit of adherence with bisphosphonates depends on age and fracture type: results from an analysis of 101,038 new bisphosphonate users. J Bone Miner Res. 2008;23(9):1435–41.
37. Strom O, Borgstrom F, Kanis JA, Jonsson B. Incorporating adherence into health economic modelling of osteoporosis. Osteoporos Int. 2009;20(1):23–34.
38. Sunyecz JA, Mucha L, Baser O, et al. Impact of compliance and persistence with bisphosphonate therapy on health care costs and utilization. Osteoporos Int. 2008;19(10):1421–9.
39. Halpern R, Becker L, Iqbal SU, et al. The association of adherence to osteoporosis therapies with fracture, all-cause medical costs, and all-cause hospitalizations: a retrospective claims analysis of female health plan enrollees with osteoporosis. J Manag Care Pharm. 2011;17(1):25–39.
40. Modi A, Siris ES, Tang J, Sen S. Cost and consequences of noncompliance with osteoporosis treatment among women initiating therapy. Curr Med Res Opin. 2015;31(4):757–65.
41. Martin KE, Yu J, Campbell HE, et al. Analysis of the comparative effectiveness of 3 oral bisphosphonates in a large managed care organization: adherence, fracture rates, and all-cause cost. J Manag Care Pharm. 2011;17(8):596–609.
42. Clark EM, Gould VC, Tobias JH, Horne R. Natural history, reasons for, and impact of low/non-adherence to medications for osteoporosis in a cohort of community-dwelling older women already established on medication: a 2-year follow-up study. Osteoporos Int. 2016;27(2):579–90.
43. Ward MA, Xu Y, Viswanathan HN, et al. Association between osteoporosis treatment change and adherence, incident fracture, and total healthcare costs in a Medicare Advantage Prescription Drug plan. Osteoporos Int. 2013;24(4):1195–206.
44. Brookhart MA, Avorn J, Katz JN, et al. Gaps in treatment among users of osteoporosis medications: the dynamics of noncompliance. Am J Med. 2007;120(3):251–6.
45. Eisenberg DF, Placzek H, Gu T, et al. Cost and consequences of noncompliance to oral bisphosphonate treatment. J Manag Care Spec Pharm. 2015;21(1):56–65.
46. Hadji P, Papaioannou N, Gielen E, et al. Persistence, adherence, and medication-taking behavior in women with postmenopausal osteoporosis receiving denosumab in routine practice in Germany, Austria, Greece, and Belgium: 12-month results from a European non-interventional study. Osteoporos Int. 2015;26(10):2479–89.
47. Costa-Paiva L, Gomes DC, Morais SS, et al. Knowledge about osteoporosis in postmenopausal women undergoing antiresorptive treatment. Maturitas. 2011;69(1):81–5.
48. Sale JE, Gignac MA, Hawker G, et al. Decision to take osteoporosis medication in patients who have had a fracture and are ‘high’ risk for future fracture: a qualitative study. BMC Musculoskelet Disord. 2011;12:92.
49. Haynes RB, Yao X, Degani A, et al. Interventions to enhance medication adherence. Cochrane Database Syst Rev. 2005(4):CD000011.
50. Gleeson T, Iversen MD, Avorn J, et al. Interventions to improve adherence and persistence with osteoporosis medications: a systematic literature review. Osteoporos Int. 2009; 20(12):2127–34.
51. Hiligsmann M, Salas M, Hughes DA, et al. Interventions to improve osteoporosis medication adherence and persistence: a systematic review and literature appraisal by the ISPOR Medication Adherence & Persistence Special Interest Group. Osteoporos Int. 2013;24(12):2907–18.
52. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–310.
53. Richter A, Anton SF, Koch P, Dennett SL. The impact of reducing dose frequency on health outcomes. Clin Ther. 2003;25(8):2307–35; discussion 6.
54. Cramer JA, Amonkar MM, Hebborn A, Altman R. Compliance and persistence with bisphosphonate dosing regimens among women with postmenopausal osteoporosis. Curr Med Res Opin. 2005;21(9):1453–60.
55. Iglay K, Cao X, Mavros P, et al. Systematic Literature Review and Meta-analysis of Medication Adherence With Once-weekly Versus Once-daily Therapy. Clin Ther. 2015;37(8):1813–21 e1.
56. Carbonell-Abella C, Pages-Castella A, Javaid MK, et al. Early (1-year) Discontinuation of Different Anti-osteoporosis Medications Compared: A Population-Based Cohort Study. Calcif Tissue Int. 2015;97(6):535–41.
57. Lewiecki EM, Babbitt AM, Piziak VK, et al. Adherence to and gastrointestinal tolerability of monthly oral or quarterly intravenous ibandronate therapy in women with previous intolerance to oral bisphosphonates: a 12-month, open-label, prospective evaluation. Clin Ther. 2008;30(4):605–21.
58. Payer J, Killinger Z, Sulkova I, Celec P. Preferences of patients receiving bisphosphonates--how to influence the therapeutic adherence. Biomed Pharmacother. 2008;62(2):122–4.
59. Weycker D, Macarios D, Edelsberg J, Oster G. Compliance with drug therapy for postmenopausal osteoporosis. Osteoporos Int. 2006;17(11):1645–52.
60. Kastelan D, Lozo P, Stamenkovic D, et al. Preference for weekly and monthly bisphosphonates among patients with postmenopausal osteoporosis: results from the Croatian PROMO Study. Clin Rheumatol. 2009;28(3):321–6.
61. McClung M, Recker R, Miller P, et al. Intravenous zoledronic acid 5 mg in the treatment of postmenopausal women with low bone density previously treated with alendronate. Bone. 2007;41(1):122–8.
62. Hsieh PC. Effectiveness and safety of zoledronic acid in the treatment of osteoporosis. Orthopedics. 2016:1–8.
63. Recker RR, Gallagher R, MacCosbe PE. Effect of dosing frequency on bisphosphonate medication adherence in a large longitudinal cohort of women. Mayo Clin Proc. 2005;80(7):856–61.
64. Emkey R, Koltun W, Beusterien K, et al. Patient preference for once-monthly ibandronate versus once-weekly alendronate in a randomized, open-label, cross-over trial: the Boniva Alendronate Trial in Osteoporosis (BALTO). Curr Med Res Opin. 2005;21(12):1895–903.
65. Hadji P, Minne H, Pfeifer M, et al. Treatment preference for monthly oral ibandronate and weekly oral alendronate in women with postmenopausal osteoporosis: A randomized, crossover study (BALTO II). Joint Bone Spine. 2008;75(3):303–10.
66. Ryzner KL, Burkiewicz JS, Griffin BL, Komperda KE. Survey of bisphosphonate regimen preferences in an urban community health center. Consult Pharm. 2010;25(10):671–5.
67. Saag K, Lindsay R, Kriegman A, et al. A single zoledronic acid infusion reduces bone resorption markers more rapidly than weekly oral alendronate in postmenopausal women with low bone mineral density. Bone. 2007;40(5):1238–43.
68. Hadji P, Felsenberg D, Amling M, et al. The non-interventional BonViva Intravenous Versus Alendronate (VIVA) study: real-world adherence and persistence to medication, efficacy, and safety, in patients with postmenopausal osteoporosis. Osteoporos Int. 2014;25(1):339–47.
69. Ziller V, Kostev K, Kyvernitakis I, et al. Persistence and compliance of medications used in the treatment of osteoporosis--analysis using a large scale, representative, longitudinal German database. Int J Clin Pharmacol Ther. 2012;50(5):315–22.
70. Curtis JR, Yun H, Matthews R, et al. Adherence with intravenous zoledronate and intravenous ibandronate in the United States Medicare population. Arthritis Care Res (Hoboken). 2012;64(7):1054–60.
71. Clowes JA, Peel NF, Eastell R. The impact of monitoring on adherence and persistence with antiresorptive treatment for postmenopausal osteoporosis: a randomized controlled trial. J Clin Endocrinol Metab. 2004;89(3):1117–23.
72. Cooper A, Drake J, Brankin E; PERSIST Investigators. Treatment persistence with once-monthly ibandronate and patient support vs. once-weekly alendronate: results from the PERSIST study. Int J Clin Pract. 2006;60(8):896–905.
73. Hiligsmann M, Bours SP, Boonen A. A review of patient preferences for osteoporosis drug treatment. Curr Rheumatol Rep. 2015;17(9):61.
74. Bond WS, Hussar DA. Detection methods and strategies for improving medication compliance. Am J Hosp Pharm. 1991;48(9):1978–88.
75. Delmas PD, Vrijens B, Eastell R, et al. Effect of monitoring bone turnover markers on persistence with risedronate treatment of postmenopausal osteoporosis. J Clin Endocrinol Metab. 2007;92(4):1296–304.
76. Pickney CS, Arnason JA. Correlation between patient recall of bone densitometry results and subsequent treatment adherence. Osteoporos Int. 2005;16(9):1156–60.
77. Cizmic AD, Heilmann RM, Milchak JL, et al. Impact of interactive voice response technology on primary adherence to bisphosphonate therapy: a randomized controlled trial. Osteoporos Int. 2015;26(8):2131–6.
78. LeBlanc A, Wang AT, Wyatt K, et al. Encounter Decision Aid vs. Clinical Decision Support or Usual Care to Support Patient-Centered Treatment Decisions in Osteoporosis: The Osteoporosis Choice Randomized Trial II. PLoS One. 2015;10(5):e0128063.
79. Tao D, Xie L, Wang T, Wang T. A meta-analysis of the use of electronic reminders for patient adherence to medication in chronic disease care. J Telemed Telecare. 2015;21(1):3–13.
80. Vervloet M, van Dijk L, Santen-Reestman J, et al. SMS reminders improve adherence to oral medication in type 2 diabetes patients who are real time electronically monitored. Int J Med Inform. 2012;81(9):594–604.
81. Vervloet M, Linn AJ, van Weert JC, et al. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. J Am Med Inform Assoc. 2012;19(5):696–704.
82. Dayer L, Heldenbrand S, Anderson P, et al. Smartphone medication adherence apps: potential benefits to patients and providers. J Am Pharm Assoc (2003). 2013;53(2):172–81.
83. Solomon DH, Iversen MD, Avorn J, et al. Osteoporosis telephonic intervention to improve medication regimen adherence: a large, pragmatic, randomized controlled trial. Arch Intern Med. 2012;172(6):477–83.
84. Bianchi ML, Duca P, Vai S, et al. Improving adherence to and persistence with oral therapy of osteoporosis. Osteoporos Int. 2015;26(5):1629–38.
85. van Boven JF, Stuurman-Bieze AG, Hiddink EG, et al. Medication monitoring and optimization: a targeted pharmacist program for effective and cost-effective improvement of chronic therapy adherence. J Manag Care Spec Pharm. 2014;20(8):786–92.
86. Lai PS, Chua SS, Chan SP. Pharmaceutical care issues encountered by post-menopausal osteoporotic women prescribed bisphosphonates. J Clin Pharm Ther. 2012;37(5):536–43.
87. Lai PS, Chua SS, Chan SP. Impact of pharmaceutical care on knowledge, quality of life and satisfaction of postmenopausal women with osteoporosis. Int J Clin Pharm. 2013;35(4):629–37.
88. Murphy-Menezes M. Role of the pharmacist in medication therapy management services in patients with osteoporosis. Clin Ther. 2015;37(7):1573–86.
89. Salter C, McDaid L, Bhattacharya D, et al. Abandoned acid? Understanding adherence to bisphosphonate medications for the prevention of osteoporosis among older women: a qualitative longitudinal study. PLoS One. 2014;9(1):e83552.
Insomnia severity more pronounced in older Hispanics
Insomnia is a more pronounced problem than expected among Hispanics over age 50, according to results of a study by Christopher N. Kaufmann, PhD, and his coauthors.
Dr. Kaufmann and his colleagues studied 22,252 participants of white, Non-Hispanic black, Hispanic, or other race/ethnicity. Participant data came from a nationally representative survey from 2002 to 2010, in which patients rated the severity of four insomnia symptoms. All participants were adults older than 50 years.
Insomnia severity scores increased 0.19 points over time after the investigators controlled for sex, race/ethnicity, education, and baseline age (95% CI, 0.14-0.24; t = 7.52; design df = 56; P less than .001). After adjustment for accumulated health conditions and body mass index, this trend decreased, Dr. Kaufmann and his colleagues added. However, the increasing trajectory of insomnia severity was “significantly more pronounced” among Hispanics, compared with non-Hispanic whites, after adjustment for accumulated health conditions, body mass index, and number of depressive symptoms, the investigators said in the report.
Although health conditions can result in greater insomnia severity with age, “further research is needed to determine the reasons for a different insomnia trajectory among Hispanics,” the authors concluded.
Read the full article in the American Journal of Geriatric Psychiatry.
Insomnia is a more pronounced problem than expected among Hispanics over age 50, according to results of a study by Christopher N. Kaufmann, PhD, and his coauthors.
Dr. Kaufmann and his colleagues studied 22,252 participants of white, Non-Hispanic black, Hispanic, or other race/ethnicity. Participant data came from a nationally representative survey from 2002 to 2010, in which patients rated the severity of four insomnia symptoms. All participants were adults older than 50 years.
Insomnia severity scores increased 0.19 points over time after the investigators controlled for sex, race/ethnicity, education, and baseline age (95% CI, 0.14-0.24; t = 7.52; design df = 56; P less than .001). After adjustment for accumulated health conditions and body mass index, this trend decreased, Dr. Kaufmann and his colleagues added. However, the increasing trajectory of insomnia severity was “significantly more pronounced” among Hispanics, compared with non-Hispanic whites, after adjustment for accumulated health conditions, body mass index, and number of depressive symptoms, the investigators said in the report.
Although health conditions can result in greater insomnia severity with age, “further research is needed to determine the reasons for a different insomnia trajectory among Hispanics,” the authors concluded.
Read the full article in the American Journal of Geriatric Psychiatry.
Insomnia is a more pronounced problem than expected among Hispanics over age 50, according to results of a study by Christopher N. Kaufmann, PhD, and his coauthors.
Dr. Kaufmann and his colleagues studied 22,252 participants of white, Non-Hispanic black, Hispanic, or other race/ethnicity. Participant data came from a nationally representative survey from 2002 to 2010, in which patients rated the severity of four insomnia symptoms. All participants were adults older than 50 years.
Insomnia severity scores increased 0.19 points over time after the investigators controlled for sex, race/ethnicity, education, and baseline age (95% CI, 0.14-0.24; t = 7.52; design df = 56; P less than .001). After adjustment for accumulated health conditions and body mass index, this trend decreased, Dr. Kaufmann and his colleagues added. However, the increasing trajectory of insomnia severity was “significantly more pronounced” among Hispanics, compared with non-Hispanic whites, after adjustment for accumulated health conditions, body mass index, and number of depressive symptoms, the investigators said in the report.
Although health conditions can result in greater insomnia severity with age, “further research is needed to determine the reasons for a different insomnia trajectory among Hispanics,” the authors concluded.
Read the full article in the American Journal of Geriatric Psychiatry.
FROM THE AMERICAN JOURNAL OF GERIATRIC PSYCHIATRY
Cochrane review: Endometrial scratching may promote implantation
HELSINKI, FINLAND – Scratching the endometrium to create a “favorable inflammation” may improve the likelihood of embryo implantation in subfertile women trying to conceive either naturally or by intrauterine insemination, according to a Cochrane review.
The “injury” caused by the process, which is known as endometrial scratching, has been reported to increase the probability of pregnancy in women undergoing in vitro fertilization, especially those with recurrent implantation failure. The inflammatory response to the injury, which is performed by pipelle biopsy or a similar device, is thought to make the endometrium more receptive to implantation.
In the current meta-analysis and systematic review of eight trials comprising 1,180 women, endometrial scratching appeared to approximately double the chance of clinical pregnancy and live birth/ongoing pregnancy (relative risk, 1.92 and 2.26, respectively), compared with either no procedure or a placebo procedure, lead author Sarah Lensen reported in a poster at the annual meeting of the European Society of Human Reproduction and Embryology.
The difference between the groups was statistically significant.
The evidence suggests that endometrial scratching would increase the normal chance of a live birth or ongoing pregnancy over a set period of time from 9% to between 14% and 28%, explained Ms. Lensen, a PhD candidate at the University of Auckland, New Zealand.
No evidence was seen that endometrial scratching has any effect on miscarriage, ectopic pregnancy, or multiple pregnancy.
Pain during the procedure was reported in one of the eight studies, in which the average pain score was 6 out of 10.
Endometrial scratching is a simple and inexpensive procedure that can be conducted without analgesia during a short clinic visit, although the internal examination that is required can be associated with pain and discomfort, Ms. Lensen said.
For the review, she and her colleagues looked at randomized controlled trials evaluating endometrial scratching in women planning to have intrauterine insemination or attempting to conceive spontaneously (with or without ovulation induction), compared with either no intervention, mock intervention, or endometrial scratching performed at a different time or to a greater or lesser degree.
The researchers acknowledged that the quality of the evidence is quite low, with a risk of bias associated with most of the included trials. For this reason, the results should be viewed with caution, they said.
“High quality randomized controlled trials which recruit sufficient numbers of women are needed to confirm to refute these findings,” they wrote.
Ms. Lensen reported having no financial disclosures.
HELSINKI, FINLAND – Scratching the endometrium to create a “favorable inflammation” may improve the likelihood of embryo implantation in subfertile women trying to conceive either naturally or by intrauterine insemination, according to a Cochrane review.
The “injury” caused by the process, which is known as endometrial scratching, has been reported to increase the probability of pregnancy in women undergoing in vitro fertilization, especially those with recurrent implantation failure. The inflammatory response to the injury, which is performed by pipelle biopsy or a similar device, is thought to make the endometrium more receptive to implantation.
In the current meta-analysis and systematic review of eight trials comprising 1,180 women, endometrial scratching appeared to approximately double the chance of clinical pregnancy and live birth/ongoing pregnancy (relative risk, 1.92 and 2.26, respectively), compared with either no procedure or a placebo procedure, lead author Sarah Lensen reported in a poster at the annual meeting of the European Society of Human Reproduction and Embryology.
The difference between the groups was statistically significant.
The evidence suggests that endometrial scratching would increase the normal chance of a live birth or ongoing pregnancy over a set period of time from 9% to between 14% and 28%, explained Ms. Lensen, a PhD candidate at the University of Auckland, New Zealand.
No evidence was seen that endometrial scratching has any effect on miscarriage, ectopic pregnancy, or multiple pregnancy.
Pain during the procedure was reported in one of the eight studies, in which the average pain score was 6 out of 10.
Endometrial scratching is a simple and inexpensive procedure that can be conducted without analgesia during a short clinic visit, although the internal examination that is required can be associated with pain and discomfort, Ms. Lensen said.
For the review, she and her colleagues looked at randomized controlled trials evaluating endometrial scratching in women planning to have intrauterine insemination or attempting to conceive spontaneously (with or without ovulation induction), compared with either no intervention, mock intervention, or endometrial scratching performed at a different time or to a greater or lesser degree.
The researchers acknowledged that the quality of the evidence is quite low, with a risk of bias associated with most of the included trials. For this reason, the results should be viewed with caution, they said.
“High quality randomized controlled trials which recruit sufficient numbers of women are needed to confirm to refute these findings,” they wrote.
Ms. Lensen reported having no financial disclosures.
HELSINKI, FINLAND – Scratching the endometrium to create a “favorable inflammation” may improve the likelihood of embryo implantation in subfertile women trying to conceive either naturally or by intrauterine insemination, according to a Cochrane review.
The “injury” caused by the process, which is known as endometrial scratching, has been reported to increase the probability of pregnancy in women undergoing in vitro fertilization, especially those with recurrent implantation failure. The inflammatory response to the injury, which is performed by pipelle biopsy or a similar device, is thought to make the endometrium more receptive to implantation.
In the current meta-analysis and systematic review of eight trials comprising 1,180 women, endometrial scratching appeared to approximately double the chance of clinical pregnancy and live birth/ongoing pregnancy (relative risk, 1.92 and 2.26, respectively), compared with either no procedure or a placebo procedure, lead author Sarah Lensen reported in a poster at the annual meeting of the European Society of Human Reproduction and Embryology.
The difference between the groups was statistically significant.
The evidence suggests that endometrial scratching would increase the normal chance of a live birth or ongoing pregnancy over a set period of time from 9% to between 14% and 28%, explained Ms. Lensen, a PhD candidate at the University of Auckland, New Zealand.
No evidence was seen that endometrial scratching has any effect on miscarriage, ectopic pregnancy, or multiple pregnancy.
Pain during the procedure was reported in one of the eight studies, in which the average pain score was 6 out of 10.
Endometrial scratching is a simple and inexpensive procedure that can be conducted without analgesia during a short clinic visit, although the internal examination that is required can be associated with pain and discomfort, Ms. Lensen said.
For the review, she and her colleagues looked at randomized controlled trials evaluating endometrial scratching in women planning to have intrauterine insemination or attempting to conceive spontaneously (with or without ovulation induction), compared with either no intervention, mock intervention, or endometrial scratching performed at a different time or to a greater or lesser degree.
The researchers acknowledged that the quality of the evidence is quite low, with a risk of bias associated with most of the included trials. For this reason, the results should be viewed with caution, they said.
“High quality randomized controlled trials which recruit sufficient numbers of women are needed to confirm to refute these findings,” they wrote.
Ms. Lensen reported having no financial disclosures.
AT ESHRE 2016
Key clinical point: Endometrial scratching may improve the likelihood of embryo implantation in subfertile women.
Major finding: Endometrial scratching would increase the normal chance of a live birth or ongoing pregnancy over a set period of time from 9% to between 14% and 28%.
Data source: A meta-analysis and systematic review of eight randomized controlled studies.
Disclosures: Dr. Lensen reported having no financial disclosures.
Persistent Fatty Liver Increases Risk of Carotid Atherosclerosis
NEW YORK - Patients with persistent nonalcoholic fatty liver disease (NAFLD) face a significantly elevated risk of carotid atherosclerosis, according to a new study of Korean men.
"The most interesting finding of our research is that regression of fatty liver is associated with reduced risk of subclinical carotid atherosclerosis compared to persistent fatty liver," said Dr. Geum-Youn Gwak from Sungkyunkwan University School of Medicine in Seoul.
"So, if somebody has fatty liver at one point, he or she should try hard to resolve fatty liver. Otherwise, it is highly likely that he or she would get cardiovascular disease one day," Dr. Gwak told Reuters Health by email.
NAFLD is associated with metabolic syndrome, diabetes, and cardiovascular disease morbidity and mortality, and several studies have shown that fatty liver is associated with markers of subclinical atherosclerosis.
Dr. Gwak's team conducted a retrospective longitudinal study of 8,020 men to assess the independent association of NAFLD with the development of subclinical carotid atherosclerosis identified by ultrasound, as defined by the development of an abnormally increased carotid intima-media thickness (CIMT) or of carotid plaque.
At baseline, 39.7% of the men had NAFLD, and 17.6% of these showed regression of NAFLD during follow-up. Nearly a quarter of men (23.1%) without NAFLD at baseline had developed it by the end of follow-up, which lasted a median of 3.3 years.
The three-year cumulative incidence of subclinical carotid atherosclerosis was 14.3%, the researchers report in Gastroenterology, online June 6.
The risk of developing carotid atherosclerosis was 23% higher among men with persistent NAFLD than among those without the condition (p<0.001). This association persisted after adjusting for smoking, alcohol use, body mass index, and weight change but disappeared after adjustment for metabolic variables.
This suggests that metabolic factors mediate the association between NAFLD and the development of carotid atherosclerosis, the researchers note.
Men whose NAFLD regressed had an 18% lower risk of carotid atherosclerosis, compared with men who had persistent NAFLD (p<0.013).
Other factors associated with the development of carotid atherosclerosis included higher baseline NAFLD fibrosis score and baseline or persistent elevations of alanine aminotransferase (ALT) or gamma-glutamyltransferase (GGT).
"Once fatty liver is successfully resolved, the cardiovascular disease risk becomes similar to those without fatty liver at baseline," Dr. Gwak concluded. "That's the key message that physicians should deliver to their fatty liver patients."
SOURCE: http://bit.ly/28ODruY
Gastroenterology 2016.
NEW YORK - Patients with persistent nonalcoholic fatty liver disease (NAFLD) face a significantly elevated risk of carotid atherosclerosis, according to a new study of Korean men.
"The most interesting finding of our research is that regression of fatty liver is associated with reduced risk of subclinical carotid atherosclerosis compared to persistent fatty liver," said Dr. Geum-Youn Gwak from Sungkyunkwan University School of Medicine in Seoul.
"So, if somebody has fatty liver at one point, he or she should try hard to resolve fatty liver. Otherwise, it is highly likely that he or she would get cardiovascular disease one day," Dr. Gwak told Reuters Health by email.
NAFLD is associated with metabolic syndrome, diabetes, and cardiovascular disease morbidity and mortality, and several studies have shown that fatty liver is associated with markers of subclinical atherosclerosis.
Dr. Gwak's team conducted a retrospective longitudinal study of 8,020 men to assess the independent association of NAFLD with the development of subclinical carotid atherosclerosis identified by ultrasound, as defined by the development of an abnormally increased carotid intima-media thickness (CIMT) or of carotid plaque.
At baseline, 39.7% of the men had NAFLD, and 17.6% of these showed regression of NAFLD during follow-up. Nearly a quarter of men (23.1%) without NAFLD at baseline had developed it by the end of follow-up, which lasted a median of 3.3 years.
The three-year cumulative incidence of subclinical carotid atherosclerosis was 14.3%, the researchers report in Gastroenterology, online June 6.
The risk of developing carotid atherosclerosis was 23% higher among men with persistent NAFLD than among those without the condition (p<0.001). This association persisted after adjusting for smoking, alcohol use, body mass index, and weight change but disappeared after adjustment for metabolic variables.
This suggests that metabolic factors mediate the association between NAFLD and the development of carotid atherosclerosis, the researchers note.
Men whose NAFLD regressed had an 18% lower risk of carotid atherosclerosis, compared with men who had persistent NAFLD (p<0.013).
Other factors associated with the development of carotid atherosclerosis included higher baseline NAFLD fibrosis score and baseline or persistent elevations of alanine aminotransferase (ALT) or gamma-glutamyltransferase (GGT).
"Once fatty liver is successfully resolved, the cardiovascular disease risk becomes similar to those without fatty liver at baseline," Dr. Gwak concluded. "That's the key message that physicians should deliver to their fatty liver patients."
SOURCE: http://bit.ly/28ODruY
Gastroenterology 2016.
NEW YORK - Patients with persistent nonalcoholic fatty liver disease (NAFLD) face a significantly elevated risk of carotid atherosclerosis, according to a new study of Korean men.
"The most interesting finding of our research is that regression of fatty liver is associated with reduced risk of subclinical carotid atherosclerosis compared to persistent fatty liver," said Dr. Geum-Youn Gwak from Sungkyunkwan University School of Medicine in Seoul.
"So, if somebody has fatty liver at one point, he or she should try hard to resolve fatty liver. Otherwise, it is highly likely that he or she would get cardiovascular disease one day," Dr. Gwak told Reuters Health by email.
NAFLD is associated with metabolic syndrome, diabetes, and cardiovascular disease morbidity and mortality, and several studies have shown that fatty liver is associated with markers of subclinical atherosclerosis.
Dr. Gwak's team conducted a retrospective longitudinal study of 8,020 men to assess the independent association of NAFLD with the development of subclinical carotid atherosclerosis identified by ultrasound, as defined by the development of an abnormally increased carotid intima-media thickness (CIMT) or of carotid plaque.
At baseline, 39.7% of the men had NAFLD, and 17.6% of these showed regression of NAFLD during follow-up. Nearly a quarter of men (23.1%) without NAFLD at baseline had developed it by the end of follow-up, which lasted a median of 3.3 years.
The three-year cumulative incidence of subclinical carotid atherosclerosis was 14.3%, the researchers report in Gastroenterology, online June 6.
The risk of developing carotid atherosclerosis was 23% higher among men with persistent NAFLD than among those without the condition (p<0.001). This association persisted after adjusting for smoking, alcohol use, body mass index, and weight change but disappeared after adjustment for metabolic variables.
This suggests that metabolic factors mediate the association between NAFLD and the development of carotid atherosclerosis, the researchers note.
Men whose NAFLD regressed had an 18% lower risk of carotid atherosclerosis, compared with men who had persistent NAFLD (p<0.013).
Other factors associated with the development of carotid atherosclerosis included higher baseline NAFLD fibrosis score and baseline or persistent elevations of alanine aminotransferase (ALT) or gamma-glutamyltransferase (GGT).
"Once fatty liver is successfully resolved, the cardiovascular disease risk becomes similar to those without fatty liver at baseline," Dr. Gwak concluded. "That's the key message that physicians should deliver to their fatty liver patients."
SOURCE: http://bit.ly/28ODruY
Gastroenterology 2016.
Cosmetic Corner: Dermatologists Weigh in on OTC Acne Treatments
To improve patient care and outcomes, leading dermatologists offered their recommendations on OTC acne treatments. Consideration must be given to:
- Acne Care Gel
LovelySkin
“I particularly love this product in combination with azelaic acid for pregnant patients.”—Linda Fromm, MD, Rapid City, South Dakota
- Cleardin Acne Spot Gel
Isdin
“This product is great for spot treatments. It can be used alone or in combination with other acne products.”—Gary Goldenberg, MD, New York, New York
- Effaclar Duo
La Roche-Posay Laboratoire Dermatologique
“This is a great product with highly bioavailable benzoyl peroxide.”—Gary Goldenberg, MD, New York, New York
- Glytone Acne Treatment Spray
Pierre Fabre Dermo-Cosmetique USA
“For breakouts on the body, particularly for my male patients because it is quick and easy to use.”—Linda Fromm, MD, Rapid City, South Dakota
- Micronized BPO Cleanser 5%
BrandMDskincare
“For breakouts on the body, particularly for my male patients because it is quick and easy to use.”— Linda Fromm, MD, Rapid City, South Dakota
- Neutrogena Clear Pore Cleanser/Mask
Johnson & Johnson Consumer Inc
“This product has benzoyl peroxide, which is a known acne fighter. It can be used as a mask, which I recommend once a week.”—Anthony M. Rossi, MD, New York, New York
- Neutrogena On-the-Spot Acne Treatment
Johnson & Johnson Consumer Inc
“This product is best used for spot treating acne lesions. It is formulated as benzoyl peroxide 2.5%, which is the equivalent low yet effective concentration found in many prescription acne creams.”— Cherise M. Levi, DO, New York, New York
- PanOxyl 4% Acne Creamy Wash
Stiefel, a GSK company
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Self-tanners and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on OTC acne treatments. Consideration must be given to:
- Acne Care Gel
LovelySkin
“I particularly love this product in combination with azelaic acid for pregnant patients.”—Linda Fromm, MD, Rapid City, South Dakota
- Cleardin Acne Spot Gel
Isdin
“This product is great for spot treatments. It can be used alone or in combination with other acne products.”—Gary Goldenberg, MD, New York, New York
- Effaclar Duo
La Roche-Posay Laboratoire Dermatologique
“This is a great product with highly bioavailable benzoyl peroxide.”—Gary Goldenberg, MD, New York, New York
- Glytone Acne Treatment Spray
Pierre Fabre Dermo-Cosmetique USA
“For breakouts on the body, particularly for my male patients because it is quick and easy to use.”—Linda Fromm, MD, Rapid City, South Dakota
- Micronized BPO Cleanser 5%
BrandMDskincare
“For breakouts on the body, particularly for my male patients because it is quick and easy to use.”— Linda Fromm, MD, Rapid City, South Dakota
- Neutrogena Clear Pore Cleanser/Mask
Johnson & Johnson Consumer Inc
“This product has benzoyl peroxide, which is a known acne fighter. It can be used as a mask, which I recommend once a week.”—Anthony M. Rossi, MD, New York, New York
- Neutrogena On-the-Spot Acne Treatment
Johnson & Johnson Consumer Inc
“This product is best used for spot treating acne lesions. It is formulated as benzoyl peroxide 2.5%, which is the equivalent low yet effective concentration found in many prescription acne creams.”— Cherise M. Levi, DO, New York, New York
- PanOxyl 4% Acne Creamy Wash
Stiefel, a GSK company
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Self-tanners and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on OTC acne treatments. Consideration must be given to:
- Acne Care Gel
LovelySkin
“I particularly love this product in combination with azelaic acid for pregnant patients.”—Linda Fromm, MD, Rapid City, South Dakota
- Cleardin Acne Spot Gel
Isdin
“This product is great for spot treatments. It can be used alone or in combination with other acne products.”—Gary Goldenberg, MD, New York, New York
- Effaclar Duo
La Roche-Posay Laboratoire Dermatologique
“This is a great product with highly bioavailable benzoyl peroxide.”—Gary Goldenberg, MD, New York, New York
- Glytone Acne Treatment Spray
Pierre Fabre Dermo-Cosmetique USA
“For breakouts on the body, particularly for my male patients because it is quick and easy to use.”—Linda Fromm, MD, Rapid City, South Dakota
- Micronized BPO Cleanser 5%
BrandMDskincare
“For breakouts on the body, particularly for my male patients because it is quick and easy to use.”— Linda Fromm, MD, Rapid City, South Dakota
- Neutrogena Clear Pore Cleanser/Mask
Johnson & Johnson Consumer Inc
“This product has benzoyl peroxide, which is a known acne fighter. It can be used as a mask, which I recommend once a week.”—Anthony M. Rossi, MD, New York, New York
- Neutrogena On-the-Spot Acne Treatment
Johnson & Johnson Consumer Inc
“This product is best used for spot treating acne lesions. It is formulated as benzoyl peroxide 2.5%, which is the equivalent low yet effective concentration found in many prescription acne creams.”— Cherise M. Levi, DO, New York, New York
- PanOxyl 4% Acne Creamy Wash
Stiefel, a GSK company
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Self-tanners and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Subclinical Joint Disease
We are aware of the clinical importance of diagnosing psoriatic arthritis (PsA) as early as possible to initiate appropriate therapy. Because psoriasis precedes PsA in the majority of cases, it is incumbent on clinicians to seek any evidence of joint involvement at each clinical encounter.
In a study published online on February 25 in Annals of the Rheumatic Diseases. Faustini et al reported that patients with psoriasis but without PsA experience structural joint changes at the entheses. Therefore, evidence for structural joint alterations may already exist at the time of apparently exclusive skin involvement in psoriatic disease.
In the analysis, 85 participants without arthritis, including 55 with psoriasis and 30 healthy controls, received high-field magnetic resonance imaging (MRI) of the hand. These scans were scored for synovitis, osteitis, tenosynovitis, and periarticular inflammation. Participants with psoriasis also received complete clinical investigation as well as high-resolution peripheral quantitative computed tomography for detecting erosions and enthesiophytes. All participants were followed for at least 1 year to evaluate for the development of PsA.
Magnetic resonance imaging evaluation showed that 47% (26/55) of participants with psoriasis possessed at least 1 inflammatory lesion. Synovitis was the most prevalent inflammatory lesion (38% [21/55]), while osteitis (11% [6/55]), tenosynovitis (4% [2/55]), and periarticular inflammation (4% [2/55]) were less frequent.
The incidence of enthesiophytes and bone erosions did not differ between patients with psoriasis, with or without inflammatory changes on MRI. The risk for developing PsA was as high as 60% in those with subclinical synovitis and symptoms related to arthralgia. However, the risk was only 13% if the patients had normal MRIs and did not report arthralgia. Faustini et al concluded that the prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Specifically, arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
What’s the issue?
These findings are critical, as they indicate the nature of the potential genesis of PsA in many patients. If the data are confirmed in future investigations, it may change the way we evaluate or treat early PsA. How will these findings affect your workup for early PsA?
We are aware of the clinical importance of diagnosing psoriatic arthritis (PsA) as early as possible to initiate appropriate therapy. Because psoriasis precedes PsA in the majority of cases, it is incumbent on clinicians to seek any evidence of joint involvement at each clinical encounter.
In a study published online on February 25 in Annals of the Rheumatic Diseases. Faustini et al reported that patients with psoriasis but without PsA experience structural joint changes at the entheses. Therefore, evidence for structural joint alterations may already exist at the time of apparently exclusive skin involvement in psoriatic disease.
In the analysis, 85 participants without arthritis, including 55 with psoriasis and 30 healthy controls, received high-field magnetic resonance imaging (MRI) of the hand. These scans were scored for synovitis, osteitis, tenosynovitis, and periarticular inflammation. Participants with psoriasis also received complete clinical investigation as well as high-resolution peripheral quantitative computed tomography for detecting erosions and enthesiophytes. All participants were followed for at least 1 year to evaluate for the development of PsA.
Magnetic resonance imaging evaluation showed that 47% (26/55) of participants with psoriasis possessed at least 1 inflammatory lesion. Synovitis was the most prevalent inflammatory lesion (38% [21/55]), while osteitis (11% [6/55]), tenosynovitis (4% [2/55]), and periarticular inflammation (4% [2/55]) were less frequent.
The incidence of enthesiophytes and bone erosions did not differ between patients with psoriasis, with or without inflammatory changes on MRI. The risk for developing PsA was as high as 60% in those with subclinical synovitis and symptoms related to arthralgia. However, the risk was only 13% if the patients had normal MRIs and did not report arthralgia. Faustini et al concluded that the prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Specifically, arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
What’s the issue?
These findings are critical, as they indicate the nature of the potential genesis of PsA in many patients. If the data are confirmed in future investigations, it may change the way we evaluate or treat early PsA. How will these findings affect your workup for early PsA?
We are aware of the clinical importance of diagnosing psoriatic arthritis (PsA) as early as possible to initiate appropriate therapy. Because psoriasis precedes PsA in the majority of cases, it is incumbent on clinicians to seek any evidence of joint involvement at each clinical encounter.
In a study published online on February 25 in Annals of the Rheumatic Diseases. Faustini et al reported that patients with psoriasis but without PsA experience structural joint changes at the entheses. Therefore, evidence for structural joint alterations may already exist at the time of apparently exclusive skin involvement in psoriatic disease.
In the analysis, 85 participants without arthritis, including 55 with psoriasis and 30 healthy controls, received high-field magnetic resonance imaging (MRI) of the hand. These scans were scored for synovitis, osteitis, tenosynovitis, and periarticular inflammation. Participants with psoriasis also received complete clinical investigation as well as high-resolution peripheral quantitative computed tomography for detecting erosions and enthesiophytes. All participants were followed for at least 1 year to evaluate for the development of PsA.
Magnetic resonance imaging evaluation showed that 47% (26/55) of participants with psoriasis possessed at least 1 inflammatory lesion. Synovitis was the most prevalent inflammatory lesion (38% [21/55]), while osteitis (11% [6/55]), tenosynovitis (4% [2/55]), and periarticular inflammation (4% [2/55]) were less frequent.
The incidence of enthesiophytes and bone erosions did not differ between patients with psoriasis, with or without inflammatory changes on MRI. The risk for developing PsA was as high as 60% in those with subclinical synovitis and symptoms related to arthralgia. However, the risk was only 13% if the patients had normal MRIs and did not report arthralgia. Faustini et al concluded that the prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Specifically, arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
What’s the issue?
These findings are critical, as they indicate the nature of the potential genesis of PsA in many patients. If the data are confirmed in future investigations, it may change the way we evaluate or treat early PsA. How will these findings affect your workup for early PsA?

The importance of ‘delivery factors’ and ‘patient factors’ in the therapeutic alliance
The therapeutic alliance (interchangeably, the therapeutic relationship) is a subjective measure of the relationship between a clinician and a patient. It is an indicator of clinical trustworthiness: what a patient is referring to when she (he) expresses trust in her provider. The therapeutic alliance also is known as the working alliance, the therapeutic bond, and the helping alliance,1 and it is an important factor in patient satisfaction ratings—the gauging parameter through which clinicians and institutions measure the quality of care they provide.2
A therapeutic alliance is essential to the delivery of psychiatric care. Itself, it can be a healing factor3 and has been linked to patients’ adherence to treatment and continuation of care.4 For example, psychiatric patients who perceive the therapeutic alliance more positively have:
- a better long-term health outcome after discharge
- a significantly better psychological quality of life5
- a better follow-up record of outpatient care after inpatient discharge4,6
- better adherence to prescribed treatment7
- a reduced likelihood of relapse and readmission.6
Patient satisfaction is an indirect measure of the therapeutic alliance; many variables of the therapeutic relationship can affect that satisfaction. In this article, we call those variables patient factors and delivery factors; our aim, using the example of 2 hypothetical cases, is to highlight their importance in patients’ perception of the therapeutic alliance they have with providers.
CASE Paranoid delusions lead to termination of care
Mr. D, age 21, unmarried, unemployed, and with no medical or psychiatric history, is transferred from the medical floor to the inpatient psychiatric unit after coming to the hospital’s emergency room (ER) with a report of chest pain. Workup on the medical floor was negative for a serious cardiac event.
On questioning, Mr. D tells the team that his chest pain is caused by National Security Agency (NSA) satellites “locking” onto his heart and causing veins in his heart to “pop.”
Mr. D agrees to be transferred to the psychiatric unit. Once there, however, he refuses to take the psychotropic medications that have been prescribed or to comply with the balance of the treatment protocol. He is adamant about the influence of NSA satellites, and requests daily imaging to locate evidence of the path of the satellite tracking device that he claims is inside his body.
The treatment team repeatedly refuses to comply with Mr. D’s demand for imaging. He becomes angry and says that he does not think he is getting proper care because the nature of his problem is medical, not psychiatric.
Mr. D repeatedly asserts that he will not take any of the psychotropic medications that have been prescribed for him and will not attend follow-up appointments with the psychiatry team because he does not need treatment. He accuses the treatment team of conspiring with the NSA and causing his chest pain.
Mr. D asks to be discharged.
Patient factors: Unmodifiable and static
As Mr. D’s case exemplifies, patient factors are a set of elements, intrinsic to a given patient, that affect that patient’s perceptions independent of the quality of the care delivered. Included among patient factors are personal sociodemographic and psychopathological characteristics. These patient factors influence the therapeutic relationship in many ways.
Sociodemographics. It has been reported that patients of minority heritage and those who are male, young, and unmarried tend to be less satisfied with medical treatment in general and with psychiatric inpatient treatment in particular.8,9 Females and older patients, on the other hand, are more likely to be satisfied with the perceived delivery of care and the therapeutic alliance.8-10
Psychopathology affects patients’ perception of the delivery of care and the therapeutic alliance. Patients who are highly distressed psychologically and those who suffer chronic psychiatric illness, for example, tend to perceive themselves as having benefitted less from treatment than healthier counterparts.9,11 Such patients also tend to see their therapeutic outcome in a much less favorable light.11,12 Patients with borderline personality disorder and antisocial personality disorder12-14 and those hospitalized involuntarily8 tend to (1) be less satisfied with their therapeutic outcome and (2) see the therapeutic alliance less favorably compared with those who do not have these psychopathologies.
CASE Denied a blanket, she feels like a 'burden'
Ms. X, age 34, married and a homemaker, has a history of bipolar I disorder. She brings herself to the ER complaining of depression and suicidal ideation.
After Ms. X is seen by the psychiatry consult service in the ER, she reports that she feels frustrated and angry and thinks that the hospital’s physicians do not really want to help her. She states that she felt that the ER staff “dismissed” her, in part because she spent 4 hours in the ER waiting room before she was given a bed.
Ms. X says that, once she was placed in a room, she felt that the nursing staff and medical assistants ignored her because they did not give her the extra blanket she requested. She said she was cold as a result, while she waited to see the psychiatrist and the ER physician.
Ms. X states that she came to the ER seeking help because she felt depressed and thought that no one cared about her. Coming to the hospital made her feel worse, after all, she said, because there she has been treated like she is a burden, much like she is treated at home.
Delivery factors: Amenable to change
These mutable elements of the therapeutic alliance are dependent on the quality of the care, as they were in Ms. X’s case; they can be changed. Included among delivery factors is the quality of the relationship between provider and patient—that is, how the psychiatrist and the nursing staff relate to the patient.
Perceptions are key. Delivery factors rank as one of the most important elements that influence the patient’s perception of the therapeutic alliance.15,16 Given the objectives of psychiatric treatment—to relieve psychiatric symptoms, improve patient functioning, and alleviate psychological distress—it is no wonder that delivery factors play an important role in the perception of the therapeutic alliance: The quality of the provider−patient relationship is the axis around which treatment takes place. This relationship constantly ranks high on surveys of what is important to patients15—especially in an inpatient psychiatric setting.
Attitudes are modifiable. From the treating psychiatrist to nursing and ancillary staffs, all team members need to express attitudes and behaviors that reflect positively on the patient.17 Behaviors such as involving the patient fully in therapeutic decision-making; exuding an attitude of caring, equanimity, empathy, sincerity, and respect; and listening to the patient’s concerns can go a long way to improving the therapeutic relationship. Displaying such attitudes and behaviors also help improve the larger vision of psychiatric intervention: to bring about positive therapeutic changes.
Summing up
Ratings of the therapeutic alliance are the currency of patient satisfaction. The value of this therapeutic currency is affected by delivery factors, which are adjustable, and patient factors, which are not. Taken together, however, both types of factors are the foundation of patient satisfaction and the therapeutic alliance.
1. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Clin Psychol. 2000;68(3):438-450.
2. Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(suppl 6):38-56.
3. Priebe S, McCabe R. The therapeutic relationship in psychiatric settings. Acta Psychiatrica Scandinavica Suppl. 2006;113(429):69-72.
4. Bowersox NW, Bohnert AS, Ganoczy D, et al. Inpatient psychiatric care experience and its relationship to posthospitalization treatment participation. Psychiatr Serv. 2013;64(6):554-562.
5. Zendjidjian XY, Baumstarck K, Auquier P, et al. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Preference Adherence. 2014;8:575-583.
6. Druss BG, Rosenheck RA, Stolar M. Patient satisfaction and administrative measures as indicators of the quality of mental health care. Psychiatr Serv. 1999;50(8):1053-1058.
7. Sapra M, Weiden PJ, Schooler NR, et al. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199-206.
8. Rosenheck R, Wilson NJ, Meterko M. Influence of patient and hospital factors on consumer satisfaction with inpatient mental health treatment. Psychiatr Serv. 1997;48(12):1553-1561.
9. Hoff RA, Rosenheck RA, Meterko M, et al. Mental illness as a predictor of satisfaction with inpatient care at Veterans Affairs hospitals. Psychiatr Serv. 1999;50(5):680-685.
10. Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803-809.
11. Greenley JR, Young TB, Schoenherr RA. Psychological distress and patient satisfaction. Med Care. 1982;20(4):373-385.
12. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived coercion. Acta Psychiatr Scand. 1994;90(5):379-384.
13. Köhler S, Unger T, Hoffmann S, et al. Patient satisfaction with inpatient psychiatric treatment and its relation to treatment outcome in unipolar depression and schizophrenia. Int J Psychiatry Clin Pract. 2015;19(2):119-123.
14. Holcomb WR, Parker JC, Leong GB, et al. Customer satisfaction and self-reported treatment outcomes among psychiatric inpatients. Psychiatr Serv. 1998;49(7):929-934.
15. Hansson L, Björkman T, Berglund I. What is important in psychiatric inpatient care? Quality of care from the patient’s perspective. Qual Assur Health Care. 1993;5(1):41-48.
16. Remnik Y, Melamed Y, Swartz M, et al. Patients’ satisfaction with psychiatric inpatient care. Isr J Psychiatry Relat Sci. 2003;41(3):208-212.
17. Norcross JC, ed. Psychotherapy relationships that work: therapist contributions and responsiveness to patients. New York, NY: Oxford University Press; 2002.
The therapeutic alliance (interchangeably, the therapeutic relationship) is a subjective measure of the relationship between a clinician and a patient. It is an indicator of clinical trustworthiness: what a patient is referring to when she (he) expresses trust in her provider. The therapeutic alliance also is known as the working alliance, the therapeutic bond, and the helping alliance,1 and it is an important factor in patient satisfaction ratings—the gauging parameter through which clinicians and institutions measure the quality of care they provide.2
A therapeutic alliance is essential to the delivery of psychiatric care. Itself, it can be a healing factor3 and has been linked to patients’ adherence to treatment and continuation of care.4 For example, psychiatric patients who perceive the therapeutic alliance more positively have:
- a better long-term health outcome after discharge
- a significantly better psychological quality of life5
- a better follow-up record of outpatient care after inpatient discharge4,6
- better adherence to prescribed treatment7
- a reduced likelihood of relapse and readmission.6
Patient satisfaction is an indirect measure of the therapeutic alliance; many variables of the therapeutic relationship can affect that satisfaction. In this article, we call those variables patient factors and delivery factors; our aim, using the example of 2 hypothetical cases, is to highlight their importance in patients’ perception of the therapeutic alliance they have with providers.
CASE Paranoid delusions lead to termination of care
Mr. D, age 21, unmarried, unemployed, and with no medical or psychiatric history, is transferred from the medical floor to the inpatient psychiatric unit after coming to the hospital’s emergency room (ER) with a report of chest pain. Workup on the medical floor was negative for a serious cardiac event.
On questioning, Mr. D tells the team that his chest pain is caused by National Security Agency (NSA) satellites “locking” onto his heart and causing veins in his heart to “pop.”
Mr. D agrees to be transferred to the psychiatric unit. Once there, however, he refuses to take the psychotropic medications that have been prescribed or to comply with the balance of the treatment protocol. He is adamant about the influence of NSA satellites, and requests daily imaging to locate evidence of the path of the satellite tracking device that he claims is inside his body.
The treatment team repeatedly refuses to comply with Mr. D’s demand for imaging. He becomes angry and says that he does not think he is getting proper care because the nature of his problem is medical, not psychiatric.
Mr. D repeatedly asserts that he will not take any of the psychotropic medications that have been prescribed for him and will not attend follow-up appointments with the psychiatry team because he does not need treatment. He accuses the treatment team of conspiring with the NSA and causing his chest pain.
Mr. D asks to be discharged.
Patient factors: Unmodifiable and static
As Mr. D’s case exemplifies, patient factors are a set of elements, intrinsic to a given patient, that affect that patient’s perceptions independent of the quality of the care delivered. Included among patient factors are personal sociodemographic and psychopathological characteristics. These patient factors influence the therapeutic relationship in many ways.
Sociodemographics. It has been reported that patients of minority heritage and those who are male, young, and unmarried tend to be less satisfied with medical treatment in general and with psychiatric inpatient treatment in particular.8,9 Females and older patients, on the other hand, are more likely to be satisfied with the perceived delivery of care and the therapeutic alliance.8-10
Psychopathology affects patients’ perception of the delivery of care and the therapeutic alliance. Patients who are highly distressed psychologically and those who suffer chronic psychiatric illness, for example, tend to perceive themselves as having benefitted less from treatment than healthier counterparts.9,11 Such patients also tend to see their therapeutic outcome in a much less favorable light.11,12 Patients with borderline personality disorder and antisocial personality disorder12-14 and those hospitalized involuntarily8 tend to (1) be less satisfied with their therapeutic outcome and (2) see the therapeutic alliance less favorably compared with those who do not have these psychopathologies.
CASE Denied a blanket, she feels like a 'burden'
Ms. X, age 34, married and a homemaker, has a history of bipolar I disorder. She brings herself to the ER complaining of depression and suicidal ideation.
After Ms. X is seen by the psychiatry consult service in the ER, she reports that she feels frustrated and angry and thinks that the hospital’s physicians do not really want to help her. She states that she felt that the ER staff “dismissed” her, in part because she spent 4 hours in the ER waiting room before she was given a bed.
Ms. X says that, once she was placed in a room, she felt that the nursing staff and medical assistants ignored her because they did not give her the extra blanket she requested. She said she was cold as a result, while she waited to see the psychiatrist and the ER physician.
Ms. X states that she came to the ER seeking help because she felt depressed and thought that no one cared about her. Coming to the hospital made her feel worse, after all, she said, because there she has been treated like she is a burden, much like she is treated at home.
Delivery factors: Amenable to change
These mutable elements of the therapeutic alliance are dependent on the quality of the care, as they were in Ms. X’s case; they can be changed. Included among delivery factors is the quality of the relationship between provider and patient—that is, how the psychiatrist and the nursing staff relate to the patient.
Perceptions are key. Delivery factors rank as one of the most important elements that influence the patient’s perception of the therapeutic alliance.15,16 Given the objectives of psychiatric treatment—to relieve psychiatric symptoms, improve patient functioning, and alleviate psychological distress—it is no wonder that delivery factors play an important role in the perception of the therapeutic alliance: The quality of the provider−patient relationship is the axis around which treatment takes place. This relationship constantly ranks high on surveys of what is important to patients15—especially in an inpatient psychiatric setting.
Attitudes are modifiable. From the treating psychiatrist to nursing and ancillary staffs, all team members need to express attitudes and behaviors that reflect positively on the patient.17 Behaviors such as involving the patient fully in therapeutic decision-making; exuding an attitude of caring, equanimity, empathy, sincerity, and respect; and listening to the patient’s concerns can go a long way to improving the therapeutic relationship. Displaying such attitudes and behaviors also help improve the larger vision of psychiatric intervention: to bring about positive therapeutic changes.
Summing up
Ratings of the therapeutic alliance are the currency of patient satisfaction. The value of this therapeutic currency is affected by delivery factors, which are adjustable, and patient factors, which are not. Taken together, however, both types of factors are the foundation of patient satisfaction and the therapeutic alliance.
The therapeutic alliance (interchangeably, the therapeutic relationship) is a subjective measure of the relationship between a clinician and a patient. It is an indicator of clinical trustworthiness: what a patient is referring to when she (he) expresses trust in her provider. The therapeutic alliance also is known as the working alliance, the therapeutic bond, and the helping alliance,1 and it is an important factor in patient satisfaction ratings—the gauging parameter through which clinicians and institutions measure the quality of care they provide.2
A therapeutic alliance is essential to the delivery of psychiatric care. Itself, it can be a healing factor3 and has been linked to patients’ adherence to treatment and continuation of care.4 For example, psychiatric patients who perceive the therapeutic alliance more positively have:
- a better long-term health outcome after discharge
- a significantly better psychological quality of life5
- a better follow-up record of outpatient care after inpatient discharge4,6
- better adherence to prescribed treatment7
- a reduced likelihood of relapse and readmission.6
Patient satisfaction is an indirect measure of the therapeutic alliance; many variables of the therapeutic relationship can affect that satisfaction. In this article, we call those variables patient factors and delivery factors; our aim, using the example of 2 hypothetical cases, is to highlight their importance in patients’ perception of the therapeutic alliance they have with providers.
CASE Paranoid delusions lead to termination of care
Mr. D, age 21, unmarried, unemployed, and with no medical or psychiatric history, is transferred from the medical floor to the inpatient psychiatric unit after coming to the hospital’s emergency room (ER) with a report of chest pain. Workup on the medical floor was negative for a serious cardiac event.
On questioning, Mr. D tells the team that his chest pain is caused by National Security Agency (NSA) satellites “locking” onto his heart and causing veins in his heart to “pop.”
Mr. D agrees to be transferred to the psychiatric unit. Once there, however, he refuses to take the psychotropic medications that have been prescribed or to comply with the balance of the treatment protocol. He is adamant about the influence of NSA satellites, and requests daily imaging to locate evidence of the path of the satellite tracking device that he claims is inside his body.
The treatment team repeatedly refuses to comply with Mr. D’s demand for imaging. He becomes angry and says that he does not think he is getting proper care because the nature of his problem is medical, not psychiatric.
Mr. D repeatedly asserts that he will not take any of the psychotropic medications that have been prescribed for him and will not attend follow-up appointments with the psychiatry team because he does not need treatment. He accuses the treatment team of conspiring with the NSA and causing his chest pain.
Mr. D asks to be discharged.
Patient factors: Unmodifiable and static
As Mr. D’s case exemplifies, patient factors are a set of elements, intrinsic to a given patient, that affect that patient’s perceptions independent of the quality of the care delivered. Included among patient factors are personal sociodemographic and psychopathological characteristics. These patient factors influence the therapeutic relationship in many ways.
Sociodemographics. It has been reported that patients of minority heritage and those who are male, young, and unmarried tend to be less satisfied with medical treatment in general and with psychiatric inpatient treatment in particular.8,9 Females and older patients, on the other hand, are more likely to be satisfied with the perceived delivery of care and the therapeutic alliance.8-10
Psychopathology affects patients’ perception of the delivery of care and the therapeutic alliance. Patients who are highly distressed psychologically and those who suffer chronic psychiatric illness, for example, tend to perceive themselves as having benefitted less from treatment than healthier counterparts.9,11 Such patients also tend to see their therapeutic outcome in a much less favorable light.11,12 Patients with borderline personality disorder and antisocial personality disorder12-14 and those hospitalized involuntarily8 tend to (1) be less satisfied with their therapeutic outcome and (2) see the therapeutic alliance less favorably compared with those who do not have these psychopathologies.
CASE Denied a blanket, she feels like a 'burden'
Ms. X, age 34, married and a homemaker, has a history of bipolar I disorder. She brings herself to the ER complaining of depression and suicidal ideation.
After Ms. X is seen by the psychiatry consult service in the ER, she reports that she feels frustrated and angry and thinks that the hospital’s physicians do not really want to help her. She states that she felt that the ER staff “dismissed” her, in part because she spent 4 hours in the ER waiting room before she was given a bed.
Ms. X says that, once she was placed in a room, she felt that the nursing staff and medical assistants ignored her because they did not give her the extra blanket she requested. She said she was cold as a result, while she waited to see the psychiatrist and the ER physician.
Ms. X states that she came to the ER seeking help because she felt depressed and thought that no one cared about her. Coming to the hospital made her feel worse, after all, she said, because there she has been treated like she is a burden, much like she is treated at home.
Delivery factors: Amenable to change
These mutable elements of the therapeutic alliance are dependent on the quality of the care, as they were in Ms. X’s case; they can be changed. Included among delivery factors is the quality of the relationship between provider and patient—that is, how the psychiatrist and the nursing staff relate to the patient.
Perceptions are key. Delivery factors rank as one of the most important elements that influence the patient’s perception of the therapeutic alliance.15,16 Given the objectives of psychiatric treatment—to relieve psychiatric symptoms, improve patient functioning, and alleviate psychological distress—it is no wonder that delivery factors play an important role in the perception of the therapeutic alliance: The quality of the provider−patient relationship is the axis around which treatment takes place. This relationship constantly ranks high on surveys of what is important to patients15—especially in an inpatient psychiatric setting.
Attitudes are modifiable. From the treating psychiatrist to nursing and ancillary staffs, all team members need to express attitudes and behaviors that reflect positively on the patient.17 Behaviors such as involving the patient fully in therapeutic decision-making; exuding an attitude of caring, equanimity, empathy, sincerity, and respect; and listening to the patient’s concerns can go a long way to improving the therapeutic relationship. Displaying such attitudes and behaviors also help improve the larger vision of psychiatric intervention: to bring about positive therapeutic changes.
Summing up
Ratings of the therapeutic alliance are the currency of patient satisfaction. The value of this therapeutic currency is affected by delivery factors, which are adjustable, and patient factors, which are not. Taken together, however, both types of factors are the foundation of patient satisfaction and the therapeutic alliance.
1. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Clin Psychol. 2000;68(3):438-450.
2. Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(suppl 6):38-56.
3. Priebe S, McCabe R. The therapeutic relationship in psychiatric settings. Acta Psychiatrica Scandinavica Suppl. 2006;113(429):69-72.
4. Bowersox NW, Bohnert AS, Ganoczy D, et al. Inpatient psychiatric care experience and its relationship to posthospitalization treatment participation. Psychiatr Serv. 2013;64(6):554-562.
5. Zendjidjian XY, Baumstarck K, Auquier P, et al. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Preference Adherence. 2014;8:575-583.
6. Druss BG, Rosenheck RA, Stolar M. Patient satisfaction and administrative measures as indicators of the quality of mental health care. Psychiatr Serv. 1999;50(8):1053-1058.
7. Sapra M, Weiden PJ, Schooler NR, et al. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199-206.
8. Rosenheck R, Wilson NJ, Meterko M. Influence of patient and hospital factors on consumer satisfaction with inpatient mental health treatment. Psychiatr Serv. 1997;48(12):1553-1561.
9. Hoff RA, Rosenheck RA, Meterko M, et al. Mental illness as a predictor of satisfaction with inpatient care at Veterans Affairs hospitals. Psychiatr Serv. 1999;50(5):680-685.
10. Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803-809.
11. Greenley JR, Young TB, Schoenherr RA. Psychological distress and patient satisfaction. Med Care. 1982;20(4):373-385.
12. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived coercion. Acta Psychiatr Scand. 1994;90(5):379-384.
13. Köhler S, Unger T, Hoffmann S, et al. Patient satisfaction with inpatient psychiatric treatment and its relation to treatment outcome in unipolar depression and schizophrenia. Int J Psychiatry Clin Pract. 2015;19(2):119-123.
14. Holcomb WR, Parker JC, Leong GB, et al. Customer satisfaction and self-reported treatment outcomes among psychiatric inpatients. Psychiatr Serv. 1998;49(7):929-934.
15. Hansson L, Björkman T, Berglund I. What is important in psychiatric inpatient care? Quality of care from the patient’s perspective. Qual Assur Health Care. 1993;5(1):41-48.
16. Remnik Y, Melamed Y, Swartz M, et al. Patients’ satisfaction with psychiatric inpatient care. Isr J Psychiatry Relat Sci. 2003;41(3):208-212.
17. Norcross JC, ed. Psychotherapy relationships that work: therapist contributions and responsiveness to patients. New York, NY: Oxford University Press; 2002.
1. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Clin Psychol. 2000;68(3):438-450.
2. Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(suppl 6):38-56.
3. Priebe S, McCabe R. The therapeutic relationship in psychiatric settings. Acta Psychiatrica Scandinavica Suppl. 2006;113(429):69-72.
4. Bowersox NW, Bohnert AS, Ganoczy D, et al. Inpatient psychiatric care experience and its relationship to posthospitalization treatment participation. Psychiatr Serv. 2013;64(6):554-562.
5. Zendjidjian XY, Baumstarck K, Auquier P, et al. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Preference Adherence. 2014;8:575-583.
6. Druss BG, Rosenheck RA, Stolar M. Patient satisfaction and administrative measures as indicators of the quality of mental health care. Psychiatr Serv. 1999;50(8):1053-1058.
7. Sapra M, Weiden PJ, Schooler NR, et al. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199-206.
8. Rosenheck R, Wilson NJ, Meterko M. Influence of patient and hospital factors on consumer satisfaction with inpatient mental health treatment. Psychiatr Serv. 1997;48(12):1553-1561.
9. Hoff RA, Rosenheck RA, Meterko M, et al. Mental illness as a predictor of satisfaction with inpatient care at Veterans Affairs hospitals. Psychiatr Serv. 1999;50(5):680-685.
10. Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803-809.
11. Greenley JR, Young TB, Schoenherr RA. Psychological distress and patient satisfaction. Med Care. 1982;20(4):373-385.
12. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived coercion. Acta Psychiatr Scand. 1994;90(5):379-384.
13. Köhler S, Unger T, Hoffmann S, et al. Patient satisfaction with inpatient psychiatric treatment and its relation to treatment outcome in unipolar depression and schizophrenia. Int J Psychiatry Clin Pract. 2015;19(2):119-123.
14. Holcomb WR, Parker JC, Leong GB, et al. Customer satisfaction and self-reported treatment outcomes among psychiatric inpatients. Psychiatr Serv. 1998;49(7):929-934.
15. Hansson L, Björkman T, Berglund I. What is important in psychiatric inpatient care? Quality of care from the patient’s perspective. Qual Assur Health Care. 1993;5(1):41-48.
16. Remnik Y, Melamed Y, Swartz M, et al. Patients’ satisfaction with psychiatric inpatient care. Isr J Psychiatry Relat Sci. 2003;41(3):208-212.
17. Norcross JC, ed. Psychotherapy relationships that work: therapist contributions and responsiveness to patients. New York, NY: Oxford University Press; 2002.
