User login
Musical instruments can throw skin out of tune
Violin and viola players can pay a price for the music they create: Many suffer from skin irritation and inflammation where the instruments touch their necks and upper bodies.

“These skin conditions are disfiguring, and they also carry so much psychological burden. Not only are these patients under constant pressure to perform at their maximum at all times, it really is troublesome when there is a barrier between you and performing art that you absolutely love,” lead author Henry Lim, an osteopathic medical student at the University of North Texas Health Science Center at Fort Worth, said in an interview.

The results of the literature review were presented in a poster at the Inaugural Symposium for Inflammatory Skin Disease.
Mr. Lim, who has a special interest in skin, said his own musical experience inspired the research. “Throughout my experience as a violinist, I faced many dermatologic issues because of my violin, and it affected my performance,” he said. “As time went on, I recognized that many other stringed instrumentalists were dealing with similar issues but chose to live with it because it came with the territory.”
One physician told Mr. Lim that he needed to quit in order to permanently treat his skin problems. He didn’t accept this answer and instead launched the literature review with colleagues Marshall Hall, MPH, also an osteopathic medical student with an interest in dermatology, and Sajid Surve, DO, codirector of the UNT Texas Center for Performing Arts Health.
Mr. Lim and colleagues evaluated 23 articles, which included case studies and literature reviews, about dermatitis in violinists, violists, cellists, bassists, guitarists and harpists. “Stringed instrumentalists are the highest at-risk population compared to performers who play other types of instruments,” Mr. Lim said.
The poster he presented at the meeting largely focuses on fiddler’s neck, which he defined as “simply dermatitis related to friction and allergic irritation from playing violin or viola.” Many people, he noted, are allergic to nickel, and the bracket that secures the violin’s chin rest “most often contains nickel. Even a very small concentration of nickel can cause massive reactions, and we found that the C string of a viola – the thickest, lowest-sounding string – contains a nickel concentration of up to 37%.”
Gold-coated strings are an alternative option, he said, but they’re more expensive.
Stringed instrumentalists may also be allergic to rosin applied to “bow hairs,” which is the hair – typically from horses – that is used to string bows, also described in the poster. “We found that there is an overall common allergy to the main ingredient called colophony,” Mr. Lim said. The legendary violin maker Antonio Stradivari “was rumored to have used colophony and another irritating ingredient called propolis in the wood varnish of his instruments. Because he was such a great influence on the art of violin crafting, his technique is still used in the modern era, which may be another contributing factor to the allergic reactions seen in stringed instrumentalists.”
(In the poster, the authors refer to one of the articles in the review, which described a violin maker allergic to colophony and propolis, who was treated with cetirizine, mild corticosteroids, and avoidance.)
What should dermatologists know about skin conditions in these musicians? Mr. Hall, one of the coauthors of the report, suggested they invite the patients to play their instruments during a visit. “The musicians may not understand that they are doing certain things with their movements, but looking from a clinical lens, we are able to see how their biomechanics and posture [are] contributing to their dermatitis,” he said.
Dr. Surve, the other coauthor, also suggested speaking to the patient’s teacher, coach, or mentor. “Keeping that person in the loop regarding what you are seeing and recommending will go a long way towards helping your patient,” he said. “If the teacher doesn’t understand or agree with what you’re trying to accomplish, they may try to undermine your plan of care. But if they are on board, they become a valuable tool for facilitating and reinforcing it.”
As for treatments, avoidance of the instruments is the most effective, but is simply not feasible for many musicians. “Certain interventions like creating a barrier between the musician and the instrument can reduce the risk of contact dermatitis without compromising the quality [of playing] as much,” Mr. Hall said. The poster reported that a handkerchief was used for this purpose in one case attributed to nickel sulfate in a 16-year-old .
Purchasing more expensive instrument materials to prevent reactions is another option, he said, and players can also purchase stands. But musicians may be resistant to any treatment that changes how the instruments sound or forces them to adjust the way they do things, he cautioned.
No funding for the study or author disclosures were reported.
Violin and viola players can pay a price for the music they create: Many suffer from skin irritation and inflammation where the instruments touch their necks and upper bodies.
“These skin conditions are disfiguring, and they also carry so much psychological burden. Not only are these patients under constant pressure to perform at their maximum at all times, it really is troublesome when there is a barrier between you and performing art that you absolutely love,” lead author Henry Lim, an osteopathic medical student at the University of North Texas Health Science Center at Fort Worth, said in an interview.
The results of the literature review were presented in a poster at the Inaugural Symposium for Inflammatory Skin Disease.
Mr. Lim, who has a special interest in skin, said his own musical experience inspired the research. “Throughout my experience as a violinist, I faced many dermatologic issues because of my violin, and it affected my performance,” he said. “As time went on, I recognized that many other stringed instrumentalists were dealing with similar issues but chose to live with it because it came with the territory.”
One physician told Mr. Lim that he needed to quit in order to permanently treat his skin problems. He didn’t accept this answer and instead launched the literature review with colleagues Marshall Hall, MPH, also an osteopathic medical student with an interest in dermatology, and Sajid Surve, DO, codirector of the UNT Texas Center for Performing Arts Health.
Mr. Lim and colleagues evaluated 23 articles, which included case studies and literature reviews, about dermatitis in violinists, violists, cellists, bassists, guitarists and harpists. “Stringed instrumentalists are the highest at-risk population compared to performers who play other types of instruments,” Mr. Lim said.
The poster he presented at the meeting largely focuses on fiddler’s neck, which he defined as “simply dermatitis related to friction and allergic irritation from playing violin or viola.” Many people, he noted, are allergic to nickel, and the bracket that secures the violin’s chin rest “most often contains nickel. Even a very small concentration of nickel can cause massive reactions, and we found that the C string of a viola – the thickest, lowest-sounding string – contains a nickel concentration of up to 37%.”
Gold-coated strings are an alternative option, he said, but they’re more expensive.
Stringed instrumentalists may also be allergic to rosin applied to “bow hairs,” which is the hair – typically from horses – that is used to string bows, also described in the poster. “We found that there is an overall common allergy to the main ingredient called colophony,” Mr. Lim said. The legendary violin maker Antonio Stradivari “was rumored to have used colophony and another irritating ingredient called propolis in the wood varnish of his instruments. Because he was such a great influence on the art of violin crafting, his technique is still used in the modern era, which may be another contributing factor to the allergic reactions seen in stringed instrumentalists.”
(In the poster, the authors refer to one of the articles in the review, which described a violin maker allergic to colophony and propolis, who was treated with cetirizine, mild corticosteroids, and avoidance.)
What should dermatologists know about skin conditions in these musicians? Mr. Hall, one of the coauthors of the report, suggested they invite the patients to play their instruments during a visit. “The musicians may not understand that they are doing certain things with their movements, but looking from a clinical lens, we are able to see how their biomechanics and posture [are] contributing to their dermatitis,” he said.
Dr. Surve, the other coauthor, also suggested speaking to the patient’s teacher, coach, or mentor. “Keeping that person in the loop regarding what you are seeing and recommending will go a long way towards helping your patient,” he said. “If the teacher doesn’t understand or agree with what you’re trying to accomplish, they may try to undermine your plan of care. But if they are on board, they become a valuable tool for facilitating and reinforcing it.”
As for treatments, avoidance of the instruments is the most effective, but is simply not feasible for many musicians. “Certain interventions like creating a barrier between the musician and the instrument can reduce the risk of contact dermatitis without compromising the quality [of playing] as much,” Mr. Hall said. The poster reported that a handkerchief was used for this purpose in one case attributed to nickel sulfate in a 16-year-old .
Purchasing more expensive instrument materials to prevent reactions is another option, he said, and players can also purchase stands. But musicians may be resistant to any treatment that changes how the instruments sound or forces them to adjust the way they do things, he cautioned.
No funding for the study or author disclosures were reported.
Violin and viola players can pay a price for the music they create: Many suffer from skin irritation and inflammation where the instruments touch their necks and upper bodies.
“These skin conditions are disfiguring, and they also carry so much psychological burden. Not only are these patients under constant pressure to perform at their maximum at all times, it really is troublesome when there is a barrier between you and performing art that you absolutely love,” lead author Henry Lim, an osteopathic medical student at the University of North Texas Health Science Center at Fort Worth, said in an interview.
The results of the literature review were presented in a poster at the Inaugural Symposium for Inflammatory Skin Disease.
Mr. Lim, who has a special interest in skin, said his own musical experience inspired the research. “Throughout my experience as a violinist, I faced many dermatologic issues because of my violin, and it affected my performance,” he said. “As time went on, I recognized that many other stringed instrumentalists were dealing with similar issues but chose to live with it because it came with the territory.”
One physician told Mr. Lim that he needed to quit in order to permanently treat his skin problems. He didn’t accept this answer and instead launched the literature review with colleagues Marshall Hall, MPH, also an osteopathic medical student with an interest in dermatology, and Sajid Surve, DO, codirector of the UNT Texas Center for Performing Arts Health.
Mr. Lim and colleagues evaluated 23 articles, which included case studies and literature reviews, about dermatitis in violinists, violists, cellists, bassists, guitarists and harpists. “Stringed instrumentalists are the highest at-risk population compared to performers who play other types of instruments,” Mr. Lim said.
The poster he presented at the meeting largely focuses on fiddler’s neck, which he defined as “simply dermatitis related to friction and allergic irritation from playing violin or viola.” Many people, he noted, are allergic to nickel, and the bracket that secures the violin’s chin rest “most often contains nickel. Even a very small concentration of nickel can cause massive reactions, and we found that the C string of a viola – the thickest, lowest-sounding string – contains a nickel concentration of up to 37%.”
Gold-coated strings are an alternative option, he said, but they’re more expensive.
Stringed instrumentalists may also be allergic to rosin applied to “bow hairs,” which is the hair – typically from horses – that is used to string bows, also described in the poster. “We found that there is an overall common allergy to the main ingredient called colophony,” Mr. Lim said. The legendary violin maker Antonio Stradivari “was rumored to have used colophony and another irritating ingredient called propolis in the wood varnish of his instruments. Because he was such a great influence on the art of violin crafting, his technique is still used in the modern era, which may be another contributing factor to the allergic reactions seen in stringed instrumentalists.”
(In the poster, the authors refer to one of the articles in the review, which described a violin maker allergic to colophony and propolis, who was treated with cetirizine, mild corticosteroids, and avoidance.)
What should dermatologists know about skin conditions in these musicians? Mr. Hall, one of the coauthors of the report, suggested they invite the patients to play their instruments during a visit. “The musicians may not understand that they are doing certain things with their movements, but looking from a clinical lens, we are able to see how their biomechanics and posture [are] contributing to their dermatitis,” he said.
Dr. Surve, the other coauthor, also suggested speaking to the patient’s teacher, coach, or mentor. “Keeping that person in the loop regarding what you are seeing and recommending will go a long way towards helping your patient,” he said. “If the teacher doesn’t understand or agree with what you’re trying to accomplish, they may try to undermine your plan of care. But if they are on board, they become a valuable tool for facilitating and reinforcing it.”
As for treatments, avoidance of the instruments is the most effective, but is simply not feasible for many musicians. “Certain interventions like creating a barrier between the musician and the instrument can reduce the risk of contact dermatitis without compromising the quality [of playing] as much,” Mr. Hall said. The poster reported that a handkerchief was used for this purpose in one case attributed to nickel sulfate in a 16-year-old .
Purchasing more expensive instrument materials to prevent reactions is another option, he said, and players can also purchase stands. But musicians may be resistant to any treatment that changes how the instruments sound or forces them to adjust the way they do things, he cautioned.
No funding for the study or author disclosures were reported.
FROM SISD 2021
3 cases of hormone therapy optimized to match the patient problem
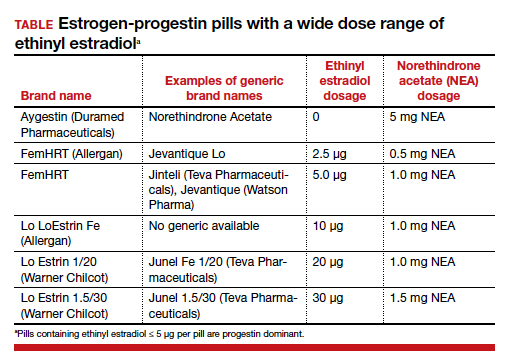
There are dozens of medications containing combinations of estrogen and progestin. I am often confused by the bewildering proliferation of generic brand names used to describe the same estrogen-progestin (E-P) regimen. For example, the combination medication containing ethinyl estradiol 20 µg plus norethindrone acetate (NEA) 1 mg is available under at least 5 different names: Lo Estrin 1/20 (Warner Chilcot), Junel 1/20 (Teva Pharmaceuticals), Microgestin Fe 1/20 (Mayne Pharma), Gildess 1/20 (Qualitest Pharmaceuticals), and Larin 1/20 (Novast Laboratories). To reduce the confusion, it is often useful to select a single preferred estrogen and progestin and use the dose combinations that are available to treat a wide range of gynecology problems (TABLE). In this editorial I focus on using various dose combinations of ethinyl estradiol and NEA to treat 3 common gynecologic problems.
CASE 1 Polycystic ovary syndrome
A 19-year-old woman reports 4 spontaneous menses in the past year and bothersome facial hair and acne. Her total testosterone concentration is at the upper limit of normal (0.46 ng/mL) and her sex hormone binding globulin (SHBG) concentration is at the lower limit of normal (35 nM). For treatment of the patient’s menstrual disorder, what is an optimal E-P combination?
Prioritize the use of an estrogen-dominant medication
Based on the Rotterdam criteria this woman has polycystic ovary syndrome (PCOS).1 In women with PCOS, luteinizing hormone (LH) secretion is increased, stimulating excessive ovarian production of testosterone.2 In addition, many women with PCOS have decreased hepatic secretion of SHBG, a binding protein that prevents testosterone from entering cells, resulting in excessive bioavailable testosterone.3 The Endocrine Society recommends that women with PCOS who have menstrual dysfunction or hirsutism be treated initially with a combination E-P hormone medication.1 Combination E-P medications suppress pituitary secretion of LH, thereby reducing ovarian production of testosterone, and ethinyl estradiol increases hepatic secretion of SHBG, reducing bioavailable testosterone. These two goals are best accomplished with an oral E-P hormone medication containing ethinyl estradiol doses of 20 µg to 30 µg per pill. An E-P hormone medication containing pills with an ethinyl estradiol dose ≤ 10 µg-daily may stimulate less hepatic production of SHBG than a pill with an ethinyl estradiol dose of 20 µg or 30 µg daily.4,5 In addition, E-P pills containing levonorgestrel suppress SHBG hormone secretion compared with E-P pills with other progestins.6 Therefore, levonorgestrel-containing E-P pills should not be prioritized for use in women with PCOS because the estrogen-induced increase in SHBG will be blunted by levonorgestrel.
CASE 2 Moderate to severe pelvic pain caused by endometriosis
A 25-year-old woman (G0) with severe dysmenorrhea had a laparoscopy showing endometriosis lesions in the cul-de-sac and a peritoneal window near the left uterosacral ligament. Biopsy showed endometriosis. Postoperatively, the patient was treated with an E-P pill containing 30 µg ethinyl estradiol and 0.15 mg desogestrel per pill using a continuous-dosing protocol. During the year following the laparoscopy, her pelvic pain symptoms gradually increased until they became severe, preventing her from performing daily activities on multiple days per month. She was prescribed elagolix but her insurance did not approve the treatment. What alternative treatment would you prescribe?
Continue to: Use progestin-dominant pills to treat pelvic pain...
Use progestin-dominant pills to treat pelvic pain
Cellular activity in endometriosis lesions is stimulated by estradiol and inhibited by a high concentration of androgenic progestins or androgens. This simplified endocrine paradigm explains the effectiveness of hormonal treatments that suppress ovarian estradiol production, including leuprolide, elagolix, medroxyprogesterone acetate, and NEA. For the woman in the above case, I would advocate for elagolix treatment but, following the insurance denial of the prescription, an alternative treatment for moderate or severe pelvic pain caused by endometriosis would be a progestin-dominant hormone medication (for example, NEA 5 mg daily). Norethindrone acetate 5 mg daily may be associated with bothersome adverse effects including weight gain (16% of patients; mean weight gain, 3.1 kg), acne (10%), mood lability (9%), hot flashes (8%), depression (6%), scalp hair loss (4%), headache (4%), nausea (3%), and deepening of the voice (1%).7
I sometimes see women with moderate to severe pelvic pain caused by endometriosis being treated with norethindrone 0.35 mg daily. This dose of norethindrone is suboptimal for pain treatment because it does not reliably suppress ovarian production of estradiol. In addition, the cells in endometriosis lesions are often resistant to the effects of progesterone, requiring higher dosages to produce secretory or decidual changes. In most situations, I recommend against the use of norethindrone 0.35 mg daily for the treatment of pelvic pain caused by endometriosis.
Patients commonly ask if NEA 5 mg daily has contraceptive efficacy. Although it is not approved at this dosage by the US Food and Drug Administration as a contraceptive,8 norethindrone 0.35 mg daily is approved as a progestin-only contraceptive.9 Norethindrone acetate is rapidly and completely deacetylated to norethindrone and the disposition of oral NEA is indistinguishable from that of norethindrone (which is the FDA-approved dosage mentioned above). Since norethindrone 0.35 mg daily is approved as a contraceptive, it is highly likely that NEA 5 mg daily has contraceptive efficacy, especially if there is good adherence with the daily medication.
CASE 3 Perimenopausal AUB
A 45-year-old woman reports varying menstrual cycle lengths from 24 to 60 days with very heavy menses in some cycles. Pelvic ultrasonography shows no abnormality. Endometrial biopsy shows a proliferative endometrium. Her serum progesterone level, obtained 1 week before the onset of menses, is < 3 ng/mL. She has no past history of heavy menses, easy bruising, excessive bleeding with procedures, or a family history of bleeding problems. She also reports occasional hot flashes that wake her from sleep.
Use an estrogen step-down regimen to manage postmenopause transition
This patient is likely in the perimenopause transition, and the abnormal uterine bleeding (AUB) is caused, in part, by oligo- or anovulation. Perimenopausal women with AUB may have cycles characterized by above normal ovarian estradiol production and below normal progesterone production, or frank anovulation.10 Elevated ovarian estrogen and low progesterone production sets the stage for heavy bleeding in the perimenopause, regardless of the presence of uterine pathology such as fibroids.
For perimenopausal women, one option for treatment of AUB due to anovulation is to prescribe an estrogen step-down regimen. For the 45-year-old woman in this case, initiating treatment with an E-P pill containing ethinyl estradiol 10 µg and NEA 1 mg will likely control the AUB and her occasional hot flash.11 As the woman ages, the ethinyl estradiol dose can be decreased to pills containing 5 µg and then 2.5 µg, covering the transition into postmenopause. Once the woman is in the postmenopause, treatment with transdermal estradiol and oral micronized progesterone is an option to treat menopausal vasomotor symptoms.
Optimize estrogen and progestin treatment for your patients
Many gynecologic problems are effectively treated by estrogen and/or progestin steroids. The dose of estrogen and progestin should be tailored to the specific problem. For PCOS, the estrogen dose selected should be sufficient to safely stimulate hepatic SHBG production. For endometriosis, if a GnRH antagonist is not available to the patient, a high-dose progestin, such as NEA 5 mg, may be an effective treatment. During the perimenopause transition in a woman with AUB, a treatment plan using a sequential E-P step-down program might control symptoms and help smoothly glide the patient into the postmenopause. ●
- Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98:4565-4592. doi: 10.1210/jc.2013-2350.
- Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. 2016;37:467-520. doi: 10.1210/er.2015-1104.
- Zhu JL, Chen Z, Feng WJ, et al. Sex hormone-binding globulin and polycystic ovary syndrome. Clin Chim Acta. 2019;499:142-148. doi: 10.1016/j.cca.2019.09.010.
- Oner G, Muderris II. A prospective randomized trial comparing low-dose ethinyl estradiol and drospirenone 24/4 combined oral contraceptive vs. ethinyl estradiol and drospirenone 21/7 combined oral contraceptive in the treatment of hirsutism. Contraception. 2011;84:508-511. doi: 10.1016/j.contraception.2011.03.002.
- Boyd RA, Zegarac EA, Posvar EL, et al. Minimal androgenic activity of a new oral contraceptive containing norethindrone acetate and graduated doses of ethinyl estradiol. Contraception. 2001;63:71-76. doi: 10.1016/s0010-7824(01)00179-2.
- Thorneycroft IH, Stanczyk FZ, Bradshaw KD, et al. Effect of low-dose oral contraceptives on androgenic markers and acne. Contraception. 1999;60:255-262. doi: 10.1016/s0010-7824(99)00093-1.
- Kaser DJ, Missmer SA, Berry KF, et al. Use of norethindrone acetate alone for postoperative suppression of endometriosis symptoms. J Pediatr Adolesc Gynecol. 2012;25:105-108. doi: 10.1016/j.jpag.2011.09.013.
- Aygestin [package insert]. Pomona, NY: Duramed Pharmaceuticals; 2007.
- Camila [package insert]. Greenville, NC; Mayne Pharma; 2018.
- Santoro N, Brown JR, Adel T, et al. Characterization of reproductive hormonal dynamics in the perimenopause. J Clin Endocrinol Metab. 1996;81:1495-1501. doi: 10.1210/jcem.81.4.8636357.
- Speroff L, Symons J, Kempfert N, et al; FemHrt Study Investigators. The effect of varying low-dose combinations of norethindrone acetate and ethinyl estradiol (Femhrt) on the frequency and intensity of vasomotor symptoms. Menopause. 2000;7:383-390. doi: 10.1097/00042192-200011000-00003.

Robert L. Barbieri, MD
Chair Emeritus, Department of Obstetrics and Gynecology
Interim Chief, Obstetrics
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Chair Emeritus, Department of Obstetrics and Gynecology
Interim Chief, Obstetrics
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Chair Emeritus, Department of Obstetrics and Gynecology
Interim Chief, Obstetrics
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
Dr. Barbieri reports no financial relationships relevant to this article.
There are dozens of medications containing combinations of estrogen and progestin. I am often confused by the bewildering proliferation of generic brand names used to describe the same estrogen-progestin (E-P) regimen. For example, the combination medication containing ethinyl estradiol 20 µg plus norethindrone acetate (NEA) 1 mg is available under at least 5 different names: Lo Estrin 1/20 (Warner Chilcot), Junel 1/20 (Teva Pharmaceuticals), Microgestin Fe 1/20 (Mayne Pharma), Gildess 1/20 (Qualitest Pharmaceuticals), and Larin 1/20 (Novast Laboratories). To reduce the confusion, it is often useful to select a single preferred estrogen and progestin and use the dose combinations that are available to treat a wide range of gynecology problems (TABLE). In this editorial I focus on using various dose combinations of ethinyl estradiol and NEA to treat 3 common gynecologic problems.
CASE 1 Polycystic ovary syndrome
A 19-year-old woman reports 4 spontaneous menses in the past year and bothersome facial hair and acne. Her total testosterone concentration is at the upper limit of normal (0.46 ng/mL) and her sex hormone binding globulin (SHBG) concentration is at the lower limit of normal (35 nM). For treatment of the patient’s menstrual disorder, what is an optimal E-P combination?
Prioritize the use of an estrogen-dominant medication
Based on the Rotterdam criteria this woman has polycystic ovary syndrome (PCOS).1 In women with PCOS, luteinizing hormone (LH) secretion is increased, stimulating excessive ovarian production of testosterone.2 In addition, many women with PCOS have decreased hepatic secretion of SHBG, a binding protein that prevents testosterone from entering cells, resulting in excessive bioavailable testosterone.3 The Endocrine Society recommends that women with PCOS who have menstrual dysfunction or hirsutism be treated initially with a combination E-P hormone medication.1 Combination E-P medications suppress pituitary secretion of LH, thereby reducing ovarian production of testosterone, and ethinyl estradiol increases hepatic secretion of SHBG, reducing bioavailable testosterone. These two goals are best accomplished with an oral E-P hormone medication containing ethinyl estradiol doses of 20 µg to 30 µg per pill. An E-P hormone medication containing pills with an ethinyl estradiol dose ≤ 10 µg-daily may stimulate less hepatic production of SHBG than a pill with an ethinyl estradiol dose of 20 µg or 30 µg daily.4,5 In addition, E-P pills containing levonorgestrel suppress SHBG hormone secretion compared with E-P pills with other progestins.6 Therefore, levonorgestrel-containing E-P pills should not be prioritized for use in women with PCOS because the estrogen-induced increase in SHBG will be blunted by levonorgestrel.
CASE 2 Moderate to severe pelvic pain caused by endometriosis
A 25-year-old woman (G0) with severe dysmenorrhea had a laparoscopy showing endometriosis lesions in the cul-de-sac and a peritoneal window near the left uterosacral ligament. Biopsy showed endometriosis. Postoperatively, the patient was treated with an E-P pill containing 30 µg ethinyl estradiol and 0.15 mg desogestrel per pill using a continuous-dosing protocol. During the year following the laparoscopy, her pelvic pain symptoms gradually increased until they became severe, preventing her from performing daily activities on multiple days per month. She was prescribed elagolix but her insurance did not approve the treatment. What alternative treatment would you prescribe?
Continue to: Use progestin-dominant pills to treat pelvic pain...
Use progestin-dominant pills to treat pelvic pain
Cellular activity in endometriosis lesions is stimulated by estradiol and inhibited by a high concentration of androgenic progestins or androgens. This simplified endocrine paradigm explains the effectiveness of hormonal treatments that suppress ovarian estradiol production, including leuprolide, elagolix, medroxyprogesterone acetate, and NEA. For the woman in the above case, I would advocate for elagolix treatment but, following the insurance denial of the prescription, an alternative treatment for moderate or severe pelvic pain caused by endometriosis would be a progestin-dominant hormone medication (for example, NEA 5 mg daily). Norethindrone acetate 5 mg daily may be associated with bothersome adverse effects including weight gain (16% of patients; mean weight gain, 3.1 kg), acne (10%), mood lability (9%), hot flashes (8%), depression (6%), scalp hair loss (4%), headache (4%), nausea (3%), and deepening of the voice (1%).7
I sometimes see women with moderate to severe pelvic pain caused by endometriosis being treated with norethindrone 0.35 mg daily. This dose of norethindrone is suboptimal for pain treatment because it does not reliably suppress ovarian production of estradiol. In addition, the cells in endometriosis lesions are often resistant to the effects of progesterone, requiring higher dosages to produce secretory or decidual changes. In most situations, I recommend against the use of norethindrone 0.35 mg daily for the treatment of pelvic pain caused by endometriosis.
Patients commonly ask if NEA 5 mg daily has contraceptive efficacy. Although it is not approved at this dosage by the US Food and Drug Administration as a contraceptive,8 norethindrone 0.35 mg daily is approved as a progestin-only contraceptive.9 Norethindrone acetate is rapidly and completely deacetylated to norethindrone and the disposition of oral NEA is indistinguishable from that of norethindrone (which is the FDA-approved dosage mentioned above). Since norethindrone 0.35 mg daily is approved as a contraceptive, it is highly likely that NEA 5 mg daily has contraceptive efficacy, especially if there is good adherence with the daily medication.
CASE 3 Perimenopausal AUB
A 45-year-old woman reports varying menstrual cycle lengths from 24 to 60 days with very heavy menses in some cycles. Pelvic ultrasonography shows no abnormality. Endometrial biopsy shows a proliferative endometrium. Her serum progesterone level, obtained 1 week before the onset of menses, is < 3 ng/mL. She has no past history of heavy menses, easy bruising, excessive bleeding with procedures, or a family history of bleeding problems. She also reports occasional hot flashes that wake her from sleep.
Use an estrogen step-down regimen to manage postmenopause transition
This patient is likely in the perimenopause transition, and the abnormal uterine bleeding (AUB) is caused, in part, by oligo- or anovulation. Perimenopausal women with AUB may have cycles characterized by above normal ovarian estradiol production and below normal progesterone production, or frank anovulation.10 Elevated ovarian estrogen and low progesterone production sets the stage for heavy bleeding in the perimenopause, regardless of the presence of uterine pathology such as fibroids.
For perimenopausal women, one option for treatment of AUB due to anovulation is to prescribe an estrogen step-down regimen. For the 45-year-old woman in this case, initiating treatment with an E-P pill containing ethinyl estradiol 10 µg and NEA 1 mg will likely control the AUB and her occasional hot flash.11 As the woman ages, the ethinyl estradiol dose can be decreased to pills containing 5 µg and then 2.5 µg, covering the transition into postmenopause. Once the woman is in the postmenopause, treatment with transdermal estradiol and oral micronized progesterone is an option to treat menopausal vasomotor symptoms.
Optimize estrogen and progestin treatment for your patients
Many gynecologic problems are effectively treated by estrogen and/or progestin steroids. The dose of estrogen and progestin should be tailored to the specific problem. For PCOS, the estrogen dose selected should be sufficient to safely stimulate hepatic SHBG production. For endometriosis, if a GnRH antagonist is not available to the patient, a high-dose progestin, such as NEA 5 mg, may be an effective treatment. During the perimenopause transition in a woman with AUB, a treatment plan using a sequential E-P step-down program might control symptoms and help smoothly glide the patient into the postmenopause. ●
There are dozens of medications containing combinations of estrogen and progestin. I am often confused by the bewildering proliferation of generic brand names used to describe the same estrogen-progestin (E-P) regimen. For example, the combination medication containing ethinyl estradiol 20 µg plus norethindrone acetate (NEA) 1 mg is available under at least 5 different names: Lo Estrin 1/20 (Warner Chilcot), Junel 1/20 (Teva Pharmaceuticals), Microgestin Fe 1/20 (Mayne Pharma), Gildess 1/20 (Qualitest Pharmaceuticals), and Larin 1/20 (Novast Laboratories). To reduce the confusion, it is often useful to select a single preferred estrogen and progestin and use the dose combinations that are available to treat a wide range of gynecology problems (TABLE). In this editorial I focus on using various dose combinations of ethinyl estradiol and NEA to treat 3 common gynecologic problems.
CASE 1 Polycystic ovary syndrome
A 19-year-old woman reports 4 spontaneous menses in the past year and bothersome facial hair and acne. Her total testosterone concentration is at the upper limit of normal (0.46 ng/mL) and her sex hormone binding globulin (SHBG) concentration is at the lower limit of normal (35 nM). For treatment of the patient’s menstrual disorder, what is an optimal E-P combination?
Prioritize the use of an estrogen-dominant medication
Based on the Rotterdam criteria this woman has polycystic ovary syndrome (PCOS).1 In women with PCOS, luteinizing hormone (LH) secretion is increased, stimulating excessive ovarian production of testosterone.2 In addition, many women with PCOS have decreased hepatic secretion of SHBG, a binding protein that prevents testosterone from entering cells, resulting in excessive bioavailable testosterone.3 The Endocrine Society recommends that women with PCOS who have menstrual dysfunction or hirsutism be treated initially with a combination E-P hormone medication.1 Combination E-P medications suppress pituitary secretion of LH, thereby reducing ovarian production of testosterone, and ethinyl estradiol increases hepatic secretion of SHBG, reducing bioavailable testosterone. These two goals are best accomplished with an oral E-P hormone medication containing ethinyl estradiol doses of 20 µg to 30 µg per pill. An E-P hormone medication containing pills with an ethinyl estradiol dose ≤ 10 µg-daily may stimulate less hepatic production of SHBG than a pill with an ethinyl estradiol dose of 20 µg or 30 µg daily.4,5 In addition, E-P pills containing levonorgestrel suppress SHBG hormone secretion compared with E-P pills with other progestins.6 Therefore, levonorgestrel-containing E-P pills should not be prioritized for use in women with PCOS because the estrogen-induced increase in SHBG will be blunted by levonorgestrel.
CASE 2 Moderate to severe pelvic pain caused by endometriosis
A 25-year-old woman (G0) with severe dysmenorrhea had a laparoscopy showing endometriosis lesions in the cul-de-sac and a peritoneal window near the left uterosacral ligament. Biopsy showed endometriosis. Postoperatively, the patient was treated with an E-P pill containing 30 µg ethinyl estradiol and 0.15 mg desogestrel per pill using a continuous-dosing protocol. During the year following the laparoscopy, her pelvic pain symptoms gradually increased until they became severe, preventing her from performing daily activities on multiple days per month. She was prescribed elagolix but her insurance did not approve the treatment. What alternative treatment would you prescribe?
Continue to: Use progestin-dominant pills to treat pelvic pain...
Use progestin-dominant pills to treat pelvic pain
Cellular activity in endometriosis lesions is stimulated by estradiol and inhibited by a high concentration of androgenic progestins or androgens. This simplified endocrine paradigm explains the effectiveness of hormonal treatments that suppress ovarian estradiol production, including leuprolide, elagolix, medroxyprogesterone acetate, and NEA. For the woman in the above case, I would advocate for elagolix treatment but, following the insurance denial of the prescription, an alternative treatment for moderate or severe pelvic pain caused by endometriosis would be a progestin-dominant hormone medication (for example, NEA 5 mg daily). Norethindrone acetate 5 mg daily may be associated with bothersome adverse effects including weight gain (16% of patients; mean weight gain, 3.1 kg), acne (10%), mood lability (9%), hot flashes (8%), depression (6%), scalp hair loss (4%), headache (4%), nausea (3%), and deepening of the voice (1%).7
I sometimes see women with moderate to severe pelvic pain caused by endometriosis being treated with norethindrone 0.35 mg daily. This dose of norethindrone is suboptimal for pain treatment because it does not reliably suppress ovarian production of estradiol. In addition, the cells in endometriosis lesions are often resistant to the effects of progesterone, requiring higher dosages to produce secretory or decidual changes. In most situations, I recommend against the use of norethindrone 0.35 mg daily for the treatment of pelvic pain caused by endometriosis.
Patients commonly ask if NEA 5 mg daily has contraceptive efficacy. Although it is not approved at this dosage by the US Food and Drug Administration as a contraceptive,8 norethindrone 0.35 mg daily is approved as a progestin-only contraceptive.9 Norethindrone acetate is rapidly and completely deacetylated to norethindrone and the disposition of oral NEA is indistinguishable from that of norethindrone (which is the FDA-approved dosage mentioned above). Since norethindrone 0.35 mg daily is approved as a contraceptive, it is highly likely that NEA 5 mg daily has contraceptive efficacy, especially if there is good adherence with the daily medication.
CASE 3 Perimenopausal AUB
A 45-year-old woman reports varying menstrual cycle lengths from 24 to 60 days with very heavy menses in some cycles. Pelvic ultrasonography shows no abnormality. Endometrial biopsy shows a proliferative endometrium. Her serum progesterone level, obtained 1 week before the onset of menses, is < 3 ng/mL. She has no past history of heavy menses, easy bruising, excessive bleeding with procedures, or a family history of bleeding problems. She also reports occasional hot flashes that wake her from sleep.
Use an estrogen step-down regimen to manage postmenopause transition
This patient is likely in the perimenopause transition, and the abnormal uterine bleeding (AUB) is caused, in part, by oligo- or anovulation. Perimenopausal women with AUB may have cycles characterized by above normal ovarian estradiol production and below normal progesterone production, or frank anovulation.10 Elevated ovarian estrogen and low progesterone production sets the stage for heavy bleeding in the perimenopause, regardless of the presence of uterine pathology such as fibroids.
For perimenopausal women, one option for treatment of AUB due to anovulation is to prescribe an estrogen step-down regimen. For the 45-year-old woman in this case, initiating treatment with an E-P pill containing ethinyl estradiol 10 µg and NEA 1 mg will likely control the AUB and her occasional hot flash.11 As the woman ages, the ethinyl estradiol dose can be decreased to pills containing 5 µg and then 2.5 µg, covering the transition into postmenopause. Once the woman is in the postmenopause, treatment with transdermal estradiol and oral micronized progesterone is an option to treat menopausal vasomotor symptoms.
Optimize estrogen and progestin treatment for your patients
Many gynecologic problems are effectively treated by estrogen and/or progestin steroids. The dose of estrogen and progestin should be tailored to the specific problem. For PCOS, the estrogen dose selected should be sufficient to safely stimulate hepatic SHBG production. For endometriosis, if a GnRH antagonist is not available to the patient, a high-dose progestin, such as NEA 5 mg, may be an effective treatment. During the perimenopause transition in a woman with AUB, a treatment plan using a sequential E-P step-down program might control symptoms and help smoothly glide the patient into the postmenopause. ●
- Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98:4565-4592. doi: 10.1210/jc.2013-2350.
- Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. 2016;37:467-520. doi: 10.1210/er.2015-1104.
- Zhu JL, Chen Z, Feng WJ, et al. Sex hormone-binding globulin and polycystic ovary syndrome. Clin Chim Acta. 2019;499:142-148. doi: 10.1016/j.cca.2019.09.010.
- Oner G, Muderris II. A prospective randomized trial comparing low-dose ethinyl estradiol and drospirenone 24/4 combined oral contraceptive vs. ethinyl estradiol and drospirenone 21/7 combined oral contraceptive in the treatment of hirsutism. Contraception. 2011;84:508-511. doi: 10.1016/j.contraception.2011.03.002.
- Boyd RA, Zegarac EA, Posvar EL, et al. Minimal androgenic activity of a new oral contraceptive containing norethindrone acetate and graduated doses of ethinyl estradiol. Contraception. 2001;63:71-76. doi: 10.1016/s0010-7824(01)00179-2.
- Thorneycroft IH, Stanczyk FZ, Bradshaw KD, et al. Effect of low-dose oral contraceptives on androgenic markers and acne. Contraception. 1999;60:255-262. doi: 10.1016/s0010-7824(99)00093-1.
- Kaser DJ, Missmer SA, Berry KF, et al. Use of norethindrone acetate alone for postoperative suppression of endometriosis symptoms. J Pediatr Adolesc Gynecol. 2012;25:105-108. doi: 10.1016/j.jpag.2011.09.013.
- Aygestin [package insert]. Pomona, NY: Duramed Pharmaceuticals; 2007.
- Camila [package insert]. Greenville, NC; Mayne Pharma; 2018.
- Santoro N, Brown JR, Adel T, et al. Characterization of reproductive hormonal dynamics in the perimenopause. J Clin Endocrinol Metab. 1996;81:1495-1501. doi: 10.1210/jcem.81.4.8636357.
- Speroff L, Symons J, Kempfert N, et al; FemHrt Study Investigators. The effect of varying low-dose combinations of norethindrone acetate and ethinyl estradiol (Femhrt) on the frequency and intensity of vasomotor symptoms. Menopause. 2000;7:383-390. doi: 10.1097/00042192-200011000-00003.
- Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98:4565-4592. doi: 10.1210/jc.2013-2350.
- Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. 2016;37:467-520. doi: 10.1210/er.2015-1104.
- Zhu JL, Chen Z, Feng WJ, et al. Sex hormone-binding globulin and polycystic ovary syndrome. Clin Chim Acta. 2019;499:142-148. doi: 10.1016/j.cca.2019.09.010.
- Oner G, Muderris II. A prospective randomized trial comparing low-dose ethinyl estradiol and drospirenone 24/4 combined oral contraceptive vs. ethinyl estradiol and drospirenone 21/7 combined oral contraceptive in the treatment of hirsutism. Contraception. 2011;84:508-511. doi: 10.1016/j.contraception.2011.03.002.
- Boyd RA, Zegarac EA, Posvar EL, et al. Minimal androgenic activity of a new oral contraceptive containing norethindrone acetate and graduated doses of ethinyl estradiol. Contraception. 2001;63:71-76. doi: 10.1016/s0010-7824(01)00179-2.
- Thorneycroft IH, Stanczyk FZ, Bradshaw KD, et al. Effect of low-dose oral contraceptives on androgenic markers and acne. Contraception. 1999;60:255-262. doi: 10.1016/s0010-7824(99)00093-1.
- Kaser DJ, Missmer SA, Berry KF, et al. Use of norethindrone acetate alone for postoperative suppression of endometriosis symptoms. J Pediatr Adolesc Gynecol. 2012;25:105-108. doi: 10.1016/j.jpag.2011.09.013.
- Aygestin [package insert]. Pomona, NY: Duramed Pharmaceuticals; 2007.
- Camila [package insert]. Greenville, NC; Mayne Pharma; 2018.
- Santoro N, Brown JR, Adel T, et al. Characterization of reproductive hormonal dynamics in the perimenopause. J Clin Endocrinol Metab. 1996;81:1495-1501. doi: 10.1210/jcem.81.4.8636357.
- Speroff L, Symons J, Kempfert N, et al; FemHrt Study Investigators. The effect of varying low-dose combinations of norethindrone acetate and ethinyl estradiol (Femhrt) on the frequency and intensity of vasomotor symptoms. Menopause. 2000;7:383-390. doi: 10.1097/00042192-200011000-00003.

Focus on cancer risk
Hereditary cancer risk assessment is the key to identifying patients and families who are at increased risk for developing cancer. The knowledge generated by cancer risk assessment impacts clinical decisions that obstetricians and gynecologists and their patients make every day. Previvors—patients predisposed to developing cancer, because of their family history or a pathogenic gene variant, who have not had cancer—benefit from counseling, heightened surveillance, and medical and surgical options.
For the last 25 years, this field has been growing dramatically, and although the scientific advances are present, only 15.3% of patients with a personal history of breast or ovarian cancer who meet hereditary cancer testing criteria have been tested.1 As many as 1 in 4 women who present for a gynecologic examination may have a personal history or a family history that qualifies them for genetic testing.2
Cancer risk app considerations
The ability to leverage mobile device applications can provide clinicians and patients with a useful screening tool to identify women who are at increased cancer risk. Only a handful of apps are available today and most are geared to patients. Such apps explore the different testing modalities, including genetic testing, as well as treatment options. When evaluating the best app for patients, using the ACOG-recommended rubric shown on page 35, the qualities to keep in mind and that should score 4 out of 4 include design, authority, usefulness, and accuracy.
A few apps provide reminders for appointments, such as mammograms, magnetic resonance imaging, or breast self-exams, and allow patients to track treatment plans. To date, no app addresses prevention and treatment opportunities that are specific to patients who have a hereditary predisposition. At least one app lists hereditary cancer testing guidelines. Many more apps are geared toward individuals with cancer rather than toward previvors.
As ObGyns, we have an opportunity to educate and identify women and, subsequently, better counsel women identified as at increased risk for developing cancer. We can utilize medical apps to efficiently incorporate this screening into clinical practice. ●
- Childers P, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- DeFrancesco M, Waldman RN, Pearlstone MM, et al. Hereditary cancer risk assessment and genetic testing in a community practice setting. Obstet Gynecol. 2018;132:1121-1129.

Richard Waldman, MD
Dr. Waldman is Past President of the American College of Obstetricians and Gynecologists, Past President of Associates for Women’s Medicine, and Immediate Past Chairman, Department of Obstetrics and Gynecology, St. Joseph’s Hospital, Syracuse, New York.
The author reports no financial relationships relevant to this article.
Richard Waldman, MD
Dr. Waldman is Past President of the American College of Obstetricians and Gynecologists, Past President of Associates for Women’s Medicine, and Immediate Past Chairman, Department of Obstetrics and Gynecology, St. Joseph’s Hospital, Syracuse, New York.
The author reports no financial relationships relevant to this article.
Richard Waldman, MD
Dr. Waldman is Past President of the American College of Obstetricians and Gynecologists, Past President of Associates for Women’s Medicine, and Immediate Past Chairman, Department of Obstetrics and Gynecology, St. Joseph’s Hospital, Syracuse, New York.
The author reports no financial relationships relevant to this article.
Hereditary cancer risk assessment is the key to identifying patients and families who are at increased risk for developing cancer. The knowledge generated by cancer risk assessment impacts clinical decisions that obstetricians and gynecologists and their patients make every day. Previvors—patients predisposed to developing cancer, because of their family history or a pathogenic gene variant, who have not had cancer—benefit from counseling, heightened surveillance, and medical and surgical options.
For the last 25 years, this field has been growing dramatically, and although the scientific advances are present, only 15.3% of patients with a personal history of breast or ovarian cancer who meet hereditary cancer testing criteria have been tested.1 As many as 1 in 4 women who present for a gynecologic examination may have a personal history or a family history that qualifies them for genetic testing.2
Cancer risk app considerations
The ability to leverage mobile device applications can provide clinicians and patients with a useful screening tool to identify women who are at increased cancer risk. Only a handful of apps are available today and most are geared to patients. Such apps explore the different testing modalities, including genetic testing, as well as treatment options. When evaluating the best app for patients, using the ACOG-recommended rubric shown on page 35, the qualities to keep in mind and that should score 4 out of 4 include design, authority, usefulness, and accuracy.
A few apps provide reminders for appointments, such as mammograms, magnetic resonance imaging, or breast self-exams, and allow patients to track treatment plans. To date, no app addresses prevention and treatment opportunities that are specific to patients who have a hereditary predisposition. At least one app lists hereditary cancer testing guidelines. Many more apps are geared toward individuals with cancer rather than toward previvors.
As ObGyns, we have an opportunity to educate and identify women and, subsequently, better counsel women identified as at increased risk for developing cancer. We can utilize medical apps to efficiently incorporate this screening into clinical practice. ●
Hereditary cancer risk assessment is the key to identifying patients and families who are at increased risk for developing cancer. The knowledge generated by cancer risk assessment impacts clinical decisions that obstetricians and gynecologists and their patients make every day. Previvors—patients predisposed to developing cancer, because of their family history or a pathogenic gene variant, who have not had cancer—benefit from counseling, heightened surveillance, and medical and surgical options.
For the last 25 years, this field has been growing dramatically, and although the scientific advances are present, only 15.3% of patients with a personal history of breast or ovarian cancer who meet hereditary cancer testing criteria have been tested.1 As many as 1 in 4 women who present for a gynecologic examination may have a personal history or a family history that qualifies them for genetic testing.2
Cancer risk app considerations
The ability to leverage mobile device applications can provide clinicians and patients with a useful screening tool to identify women who are at increased cancer risk. Only a handful of apps are available today and most are geared to patients. Such apps explore the different testing modalities, including genetic testing, as well as treatment options. When evaluating the best app for patients, using the ACOG-recommended rubric shown on page 35, the qualities to keep in mind and that should score 4 out of 4 include design, authority, usefulness, and accuracy.
A few apps provide reminders for appointments, such as mammograms, magnetic resonance imaging, or breast self-exams, and allow patients to track treatment plans. To date, no app addresses prevention and treatment opportunities that are specific to patients who have a hereditary predisposition. At least one app lists hereditary cancer testing guidelines. Many more apps are geared toward individuals with cancer rather than toward previvors.
As ObGyns, we have an opportunity to educate and identify women and, subsequently, better counsel women identified as at increased risk for developing cancer. We can utilize medical apps to efficiently incorporate this screening into clinical practice. ●
- Childers P, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- DeFrancesco M, Waldman RN, Pearlstone MM, et al. Hereditary cancer risk assessment and genetic testing in a community practice setting. Obstet Gynecol. 2018;132:1121-1129.
- Childers P, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- DeFrancesco M, Waldman RN, Pearlstone MM, et al. Hereditary cancer risk assessment and genetic testing in a community practice setting. Obstet Gynecol. 2018;132:1121-1129.
Mobile apps in ObGyn practice: Tools for enhancing women’s preventive health care
Evolutionary changes in ObGyn
Preventive medicine guidelines have evolved to reflect enhanced cervical cancer screening tests, longer-acting contraceptive options, and better data on the lack of utility of the annual pelvic exam that has changed the focus of the annual visit for both physicians and patients.1 These changes allow us to pivot and leverage the trust we build with our patients to make meaningful impacts in preventing chronic disease, improving prepregnancy health, reducing maternal mortality and morbidity, and improving the quality and longevity of our patients’ lives. New guidelines, coupled with the knowledge of the leading causes of morbidity for women, provide the chance to incorporate areas of screening and intervention that, while we are capable of addressing, we traditionally have not done so for various reasons.
The ACOG Presidential Task Force identified 5 areas of preventive health that significantly influence the long-term morbidity of women: obesity, cardiovascular disease, preconception counseling, diabetes, and cancer risk. ObGyns are uniquely positioned to identify and initiate the conversation and subsequently manage, treat, and address these critical health areas. To make this daunting task more manageable, the Task Force not only published webinars to address the clinical knowledge pertaining to these areas of health but also specifically looked at how to use technology to aid obstetrician-gynecologists in addressing them with patients.
Making use of technology in clinical practice
Technology is emerging as an influential player in health care. Major corporations, such as Amazon, Google, Apple, and Facebook, are making headlines in health care as they consider strategies (moves) to revolutionize technology and, in turn, patient visits like we have never seen before. Examples include incorporating artificial intelligence in a patient’s care and allowing better access for primary care.
The changes that we will see over the next 10 years, influenced by industry, will be more than those seen in our lifetime. To prepare for these changes, we need to incorporate technology into our daily practice. This encompasses much more than just the electronic medical record. Consequently, the Task Force intentionally looked at mobile medical apps to aid physicians in addressing the 5 specific areas of preventive health identified.
While a small step compared with what is to come, apps are a great resource to leverage in making this transition. However, with hundreds of thousands of medical apps available in app stores and the constant updates and iterations of each, it would be impossible to recommend any single app. There is much value in having a framework to use to efficiently measure the benefit of an app that you or your patient comes across in clinical practice. The objective of this series was to provide clinicians with an effective tool to evaluate a medical app that could be used, for example, when addressing obesity or optimizing prepregnancy health.
Continue to: The recommended rubric for evaluating apps...
The recommended rubric for evaluating apps
To evaluate mobile drug information apps, the Task Force members recommend a user-friendly, convenient rubric developed by the American Society of Health-System Pharmacists (ASHP) (see page 35). The rubric can help obstetrician-gynecologists evaluate and compare the value of various medical apps that specifically address obesity, diabetes mellitus, cardiovascular disease, improving maternal morbidity with enhanced preconception counseling, and cancer risk assessment.
The authors of this Task Force series have attempted to highlight the key features of an app as it pertains to a particular area of focus. It is important to keep in mind the primary user and the goal when choosing or recommending an app for practice or for patient use. The ASHP’s rubric is a tool meant to aid clinicians in evaluating medical apps, but it is ultimately the user’s decision to determine if the deficiencies of an app should deter its use. Although all the criteria are relevant and important, as medical experts it is incumbent on us to pay careful attention to the accuracy, authority, objectivity, timeliness, and security of any app we consider incorporating into clinical practice.
While integrating the use of medical apps into clinical practice will be novel for some, for others, junior Fellows in particular, it has become part of their practice and education. Dr. Eva Hoffmann, Chief Resident in the NYU Langone Health System, offers this perspective: “As medical trainees we use mobile apps to enhance our patient interaction and guide high-quality, continuous care. In today’s modern technological world, apps help keep us up to date with the ever-changing guidelines in pregnancy and routine gynecologic care as well as communicate directly and discreetly with a patient whenever the need arises. The most significant apps provide guidance on abnormal Pap results, indicated deliveries prior to 39 weeks, and the ability to respond to obstetrical emergencies. They also allow for quick society-endorsed references in seconds. Apps have changed the way that we practice by providing evidence-based medicine literally at our fingertips—in a shareable and communicable way—making the practice of medicine even more efficient and effective.”
Opportunity to reaffirm expertise
Dr. Chalas’ initiative was meant to shed light on the opportunity obstetrician-gynecologists have to reassert themselves as women’s health experts, to consider redefining their practice by incorporating new preventive guidelines, and to leverage medical apps for achieving better health outcomes for women across their lifetime. We hope that by opening a dialogue about how ubiquitous medical apps are (for both physicians and patients) in today’s health arena, how many apps are inaccurate and/or misused, and how a simple rubric can be used to assess an app’s value, you are inspired and feel more comfortable to incorporate medical apps into your practice.
Health care will continually undergo advancements, and as a specialty we must evolve to address women’s needs. Obstetrician-gynecologists are well suited to contribute significantly to the well-being of women and mothers. We can leverage technology-based apps to help us redefine our roles and priorities at the patient’s annual visit. We can reaffirm ourselves as the leading women’s health care physicians.
An additional resource
To enhance your understanding of apps and how to evaluate them, Dr. Katherine Chen’s App Review series in
In appreciation
The members of this Task Force want to thank the Editorial Board and staff of
- Women’s Preventive Services Initiative website. Recommendations for well-woman care: a well-woman chart. https:// www.womenspreventivehealth.org/wellwomanchart/. Accessed June 11, 2021.
- Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125:1478-1483.

Hartaj K. Powell, MD, MPH
Dr. Powell is OB Hospitalist, Ascension Saint Agnes Hospital, Baltimore, Maryland.

Matthew Wells, MD, MBA
Dr. Wells is Attending Physician, Women and Children’s Services, NYU Langone Health Hospital, and Unified Women’s Healthcare, Mineola, New York

Eva Hoffmann, MD
Dr. Hoffmann is Resident Physician, Department of Obstetrics and Gynecology, NYU Langone Hospital–Long Island, Long Island School of Medicine, Mineola, New York.
The authors report no financial relationships relevant to this article.
Hartaj K. Powell, MD, MPH
Dr. Powell is OB Hospitalist, Ascension Saint Agnes Hospital, Baltimore, Maryland.
Matthew Wells, MD, MBA
Dr. Wells is Attending Physician, Women and Children’s Services, NYU Langone Health Hospital, and Unified Women’s Healthcare, Mineola, New York
Eva Hoffmann, MD
Dr. Hoffmann is Resident Physician, Department of Obstetrics and Gynecology, NYU Langone Hospital–Long Island, Long Island School of Medicine, Mineola, New York.
The authors report no financial relationships relevant to this article.
Hartaj K. Powell, MD, MPH
Dr. Powell is OB Hospitalist, Ascension Saint Agnes Hospital, Baltimore, Maryland.
Matthew Wells, MD, MBA
Dr. Wells is Attending Physician, Women and Children’s Services, NYU Langone Health Hospital, and Unified Women’s Healthcare, Mineola, New York
Eva Hoffmann, MD
Dr. Hoffmann is Resident Physician, Department of Obstetrics and Gynecology, NYU Langone Hospital–Long Island, Long Island School of Medicine, Mineola, New York.
The authors report no financial relationships relevant to this article.
Evolutionary changes in ObGyn
Preventive medicine guidelines have evolved to reflect enhanced cervical cancer screening tests, longer-acting contraceptive options, and better data on the lack of utility of the annual pelvic exam that has changed the focus of the annual visit for both physicians and patients.1 These changes allow us to pivot and leverage the trust we build with our patients to make meaningful impacts in preventing chronic disease, improving prepregnancy health, reducing maternal mortality and morbidity, and improving the quality and longevity of our patients’ lives. New guidelines, coupled with the knowledge of the leading causes of morbidity for women, provide the chance to incorporate areas of screening and intervention that, while we are capable of addressing, we traditionally have not done so for various reasons.
The ACOG Presidential Task Force identified 5 areas of preventive health that significantly influence the long-term morbidity of women: obesity, cardiovascular disease, preconception counseling, diabetes, and cancer risk. ObGyns are uniquely positioned to identify and initiate the conversation and subsequently manage, treat, and address these critical health areas. To make this daunting task more manageable, the Task Force not only published webinars to address the clinical knowledge pertaining to these areas of health but also specifically looked at how to use technology to aid obstetrician-gynecologists in addressing them with patients.
Making use of technology in clinical practice
Technology is emerging as an influential player in health care. Major corporations, such as Amazon, Google, Apple, and Facebook, are making headlines in health care as they consider strategies (moves) to revolutionize technology and, in turn, patient visits like we have never seen before. Examples include incorporating artificial intelligence in a patient’s care and allowing better access for primary care.
The changes that we will see over the next 10 years, influenced by industry, will be more than those seen in our lifetime. To prepare for these changes, we need to incorporate technology into our daily practice. This encompasses much more than just the electronic medical record. Consequently, the Task Force intentionally looked at mobile medical apps to aid physicians in addressing the 5 specific areas of preventive health identified.
While a small step compared with what is to come, apps are a great resource to leverage in making this transition. However, with hundreds of thousands of medical apps available in app stores and the constant updates and iterations of each, it would be impossible to recommend any single app. There is much value in having a framework to use to efficiently measure the benefit of an app that you or your patient comes across in clinical practice. The objective of this series was to provide clinicians with an effective tool to evaluate a medical app that could be used, for example, when addressing obesity or optimizing prepregnancy health.
Continue to: The recommended rubric for evaluating apps...
The recommended rubric for evaluating apps
To evaluate mobile drug information apps, the Task Force members recommend a user-friendly, convenient rubric developed by the American Society of Health-System Pharmacists (ASHP) (see page 35). The rubric can help obstetrician-gynecologists evaluate and compare the value of various medical apps that specifically address obesity, diabetes mellitus, cardiovascular disease, improving maternal morbidity with enhanced preconception counseling, and cancer risk assessment.
The authors of this Task Force series have attempted to highlight the key features of an app as it pertains to a particular area of focus. It is important to keep in mind the primary user and the goal when choosing or recommending an app for practice or for patient use. The ASHP’s rubric is a tool meant to aid clinicians in evaluating medical apps, but it is ultimately the user’s decision to determine if the deficiencies of an app should deter its use. Although all the criteria are relevant and important, as medical experts it is incumbent on us to pay careful attention to the accuracy, authority, objectivity, timeliness, and security of any app we consider incorporating into clinical practice.
While integrating the use of medical apps into clinical practice will be novel for some, for others, junior Fellows in particular, it has become part of their practice and education. Dr. Eva Hoffmann, Chief Resident in the NYU Langone Health System, offers this perspective: “As medical trainees we use mobile apps to enhance our patient interaction and guide high-quality, continuous care. In today’s modern technological world, apps help keep us up to date with the ever-changing guidelines in pregnancy and routine gynecologic care as well as communicate directly and discreetly with a patient whenever the need arises. The most significant apps provide guidance on abnormal Pap results, indicated deliveries prior to 39 weeks, and the ability to respond to obstetrical emergencies. They also allow for quick society-endorsed references in seconds. Apps have changed the way that we practice by providing evidence-based medicine literally at our fingertips—in a shareable and communicable way—making the practice of medicine even more efficient and effective.”
Opportunity to reaffirm expertise
Dr. Chalas’ initiative was meant to shed light on the opportunity obstetrician-gynecologists have to reassert themselves as women’s health experts, to consider redefining their practice by incorporating new preventive guidelines, and to leverage medical apps for achieving better health outcomes for women across their lifetime. We hope that by opening a dialogue about how ubiquitous medical apps are (for both physicians and patients) in today’s health arena, how many apps are inaccurate and/or misused, and how a simple rubric can be used to assess an app’s value, you are inspired and feel more comfortable to incorporate medical apps into your practice.
Health care will continually undergo advancements, and as a specialty we must evolve to address women’s needs. Obstetrician-gynecologists are well suited to contribute significantly to the well-being of women and mothers. We can leverage technology-based apps to help us redefine our roles and priorities at the patient’s annual visit. We can reaffirm ourselves as the leading women’s health care physicians.
An additional resource
To enhance your understanding of apps and how to evaluate them, Dr. Katherine Chen’s App Review series in
In appreciation
The members of this Task Force want to thank the Editorial Board and staff of
Evolutionary changes in ObGyn
Preventive medicine guidelines have evolved to reflect enhanced cervical cancer screening tests, longer-acting contraceptive options, and better data on the lack of utility of the annual pelvic exam that has changed the focus of the annual visit for both physicians and patients.1 These changes allow us to pivot and leverage the trust we build with our patients to make meaningful impacts in preventing chronic disease, improving prepregnancy health, reducing maternal mortality and morbidity, and improving the quality and longevity of our patients’ lives. New guidelines, coupled with the knowledge of the leading causes of morbidity for women, provide the chance to incorporate areas of screening and intervention that, while we are capable of addressing, we traditionally have not done so for various reasons.
The ACOG Presidential Task Force identified 5 areas of preventive health that significantly influence the long-term morbidity of women: obesity, cardiovascular disease, preconception counseling, diabetes, and cancer risk. ObGyns are uniquely positioned to identify and initiate the conversation and subsequently manage, treat, and address these critical health areas. To make this daunting task more manageable, the Task Force not only published webinars to address the clinical knowledge pertaining to these areas of health but also specifically looked at how to use technology to aid obstetrician-gynecologists in addressing them with patients.
Making use of technology in clinical practice
Technology is emerging as an influential player in health care. Major corporations, such as Amazon, Google, Apple, and Facebook, are making headlines in health care as they consider strategies (moves) to revolutionize technology and, in turn, patient visits like we have never seen before. Examples include incorporating artificial intelligence in a patient’s care and allowing better access for primary care.
The changes that we will see over the next 10 years, influenced by industry, will be more than those seen in our lifetime. To prepare for these changes, we need to incorporate technology into our daily practice. This encompasses much more than just the electronic medical record. Consequently, the Task Force intentionally looked at mobile medical apps to aid physicians in addressing the 5 specific areas of preventive health identified.
While a small step compared with what is to come, apps are a great resource to leverage in making this transition. However, with hundreds of thousands of medical apps available in app stores and the constant updates and iterations of each, it would be impossible to recommend any single app. There is much value in having a framework to use to efficiently measure the benefit of an app that you or your patient comes across in clinical practice. The objective of this series was to provide clinicians with an effective tool to evaluate a medical app that could be used, for example, when addressing obesity or optimizing prepregnancy health.
Continue to: The recommended rubric for evaluating apps...
The recommended rubric for evaluating apps
To evaluate mobile drug information apps, the Task Force members recommend a user-friendly, convenient rubric developed by the American Society of Health-System Pharmacists (ASHP) (see page 35). The rubric can help obstetrician-gynecologists evaluate and compare the value of various medical apps that specifically address obesity, diabetes mellitus, cardiovascular disease, improving maternal morbidity with enhanced preconception counseling, and cancer risk assessment.
The authors of this Task Force series have attempted to highlight the key features of an app as it pertains to a particular area of focus. It is important to keep in mind the primary user and the goal when choosing or recommending an app for practice or for patient use. The ASHP’s rubric is a tool meant to aid clinicians in evaluating medical apps, but it is ultimately the user’s decision to determine if the deficiencies of an app should deter its use. Although all the criteria are relevant and important, as medical experts it is incumbent on us to pay careful attention to the accuracy, authority, objectivity, timeliness, and security of any app we consider incorporating into clinical practice.
While integrating the use of medical apps into clinical practice will be novel for some, for others, junior Fellows in particular, it has become part of their practice and education. Dr. Eva Hoffmann, Chief Resident in the NYU Langone Health System, offers this perspective: “As medical trainees we use mobile apps to enhance our patient interaction and guide high-quality, continuous care. In today’s modern technological world, apps help keep us up to date with the ever-changing guidelines in pregnancy and routine gynecologic care as well as communicate directly and discreetly with a patient whenever the need arises. The most significant apps provide guidance on abnormal Pap results, indicated deliveries prior to 39 weeks, and the ability to respond to obstetrical emergencies. They also allow for quick society-endorsed references in seconds. Apps have changed the way that we practice by providing evidence-based medicine literally at our fingertips—in a shareable and communicable way—making the practice of medicine even more efficient and effective.”
Opportunity to reaffirm expertise
Dr. Chalas’ initiative was meant to shed light on the opportunity obstetrician-gynecologists have to reassert themselves as women’s health experts, to consider redefining their practice by incorporating new preventive guidelines, and to leverage medical apps for achieving better health outcomes for women across their lifetime. We hope that by opening a dialogue about how ubiquitous medical apps are (for both physicians and patients) in today’s health arena, how many apps are inaccurate and/or misused, and how a simple rubric can be used to assess an app’s value, you are inspired and feel more comfortable to incorporate medical apps into your practice.
Health care will continually undergo advancements, and as a specialty we must evolve to address women’s needs. Obstetrician-gynecologists are well suited to contribute significantly to the well-being of women and mothers. We can leverage technology-based apps to help us redefine our roles and priorities at the patient’s annual visit. We can reaffirm ourselves as the leading women’s health care physicians.
An additional resource
To enhance your understanding of apps and how to evaluate them, Dr. Katherine Chen’s App Review series in
In appreciation
The members of this Task Force want to thank the Editorial Board and staff of
- Women’s Preventive Services Initiative website. Recommendations for well-woman care: a well-woman chart. https:// www.womenspreventivehealth.org/wellwomanchart/. Accessed June 11, 2021.
- Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125:1478-1483.
- Women’s Preventive Services Initiative website. Recommendations for well-woman care: a well-woman chart. https:// www.womenspreventivehealth.org/wellwomanchart/. Accessed June 11, 2021.
- Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125:1478-1483.
Texas doctor accused of vaccine theft faces grand jury
Hasan Gokal, MD, was fired from his job and charged with theft by a public servant. A judge dismissed the theft charge in January 2021, saying there was no probable cause, but prosecutors took the accusation to the Harris County Grand Jury, which on June 30 decided no prosecution was warranted, the Associated Press reported.
“I came as a practicing ER doctor into public health and as an ER doctor, I err on the side of life and that’s how I chose to make my decision,” Dr. Gokal told the Associated Press. “It was the right thing to do and it meant saving more lives.”
Dr. Gokal, 48, was supervising a COVID-19 vaccination clinic Dec. 29, 2020, in Humble, Tex., when the clinic closed for the day with an open vial containing nine doses of Moderna vaccine, the New York Times reported.
Since the vaccine would expire in 6 hours, Dr. Gokal scrambled to find people with medical conditions who needed vaccinating, he said. He gave the last dose to his wife, who has a lung condition, pulmonary sarcoidosis.
Dr. Gokal said he contacted his supervisor before acting and provided documentation the next day. He was fired for breaking protocol and then charged with theft.
“He abused his position to place his friends and family in line in front of people who had gone through the lawful process to be there,” Harris County District Attorney Kim Ogg said in a January statement. “What he did was illegal and he’ll be held accountable under the law.”
The AP reported that on June 30 the DA’s office issued a statement saying: “We respect the decision of the grand jury in this and every case. Evidence, not public opinion, is the guiding principle of our work.”
The AP said numerous doctors voiced support for Dr. Gokal and that the Texas Medical Board dismissed an investigation against him.
Dr. Gokal told the AP he’d still like to work in public health. Since being fired by the health department, he’s worked part time in the emergency departments at two Houston hospitals.
A version of this article first appeared on WebMD.com.
Hasan Gokal, MD, was fired from his job and charged with theft by a public servant. A judge dismissed the theft charge in January 2021, saying there was no probable cause, but prosecutors took the accusation to the Harris County Grand Jury, which on June 30 decided no prosecution was warranted, the Associated Press reported.
“I came as a practicing ER doctor into public health and as an ER doctor, I err on the side of life and that’s how I chose to make my decision,” Dr. Gokal told the Associated Press. “It was the right thing to do and it meant saving more lives.”
Dr. Gokal, 48, was supervising a COVID-19 vaccination clinic Dec. 29, 2020, in Humble, Tex., when the clinic closed for the day with an open vial containing nine doses of Moderna vaccine, the New York Times reported.
Since the vaccine would expire in 6 hours, Dr. Gokal scrambled to find people with medical conditions who needed vaccinating, he said. He gave the last dose to his wife, who has a lung condition, pulmonary sarcoidosis.
Dr. Gokal said he contacted his supervisor before acting and provided documentation the next day. He was fired for breaking protocol and then charged with theft.
“He abused his position to place his friends and family in line in front of people who had gone through the lawful process to be there,” Harris County District Attorney Kim Ogg said in a January statement. “What he did was illegal and he’ll be held accountable under the law.”
The AP reported that on June 30 the DA’s office issued a statement saying: “We respect the decision of the grand jury in this and every case. Evidence, not public opinion, is the guiding principle of our work.”
The AP said numerous doctors voiced support for Dr. Gokal and that the Texas Medical Board dismissed an investigation against him.
Dr. Gokal told the AP he’d still like to work in public health. Since being fired by the health department, he’s worked part time in the emergency departments at two Houston hospitals.
A version of this article first appeared on WebMD.com.
Hasan Gokal, MD, was fired from his job and charged with theft by a public servant. A judge dismissed the theft charge in January 2021, saying there was no probable cause, but prosecutors took the accusation to the Harris County Grand Jury, which on June 30 decided no prosecution was warranted, the Associated Press reported.
“I came as a practicing ER doctor into public health and as an ER doctor, I err on the side of life and that’s how I chose to make my decision,” Dr. Gokal told the Associated Press. “It was the right thing to do and it meant saving more lives.”
Dr. Gokal, 48, was supervising a COVID-19 vaccination clinic Dec. 29, 2020, in Humble, Tex., when the clinic closed for the day with an open vial containing nine doses of Moderna vaccine, the New York Times reported.
Since the vaccine would expire in 6 hours, Dr. Gokal scrambled to find people with medical conditions who needed vaccinating, he said. He gave the last dose to his wife, who has a lung condition, pulmonary sarcoidosis.
Dr. Gokal said he contacted his supervisor before acting and provided documentation the next day. He was fired for breaking protocol and then charged with theft.
“He abused his position to place his friends and family in line in front of people who had gone through the lawful process to be there,” Harris County District Attorney Kim Ogg said in a January statement. “What he did was illegal and he’ll be held accountable under the law.”
The AP reported that on June 30 the DA’s office issued a statement saying: “We respect the decision of the grand jury in this and every case. Evidence, not public opinion, is the guiding principle of our work.”
The AP said numerous doctors voiced support for Dr. Gokal and that the Texas Medical Board dismissed an investigation against him.
Dr. Gokal told the AP he’d still like to work in public health. Since being fired by the health department, he’s worked part time in the emergency departments at two Houston hospitals.
A version of this article first appeared on WebMD.com.
Researchers follow development of axial SpA in first-degree relatives of patients
Healthy first-degree relatives of individuals with HLA-B27–positive axial spondyloarthritis who also were HLA-B27 positive were at increased risk for developing the disease themselves within 1 year, based on data from an ongoing prospective cohort study that involved 202 first-degree relatives.
Axial spondyloarthritis (axSpA) generally arises between ages 18 and 40 years, but diagnosis can be delayed, in part because of the lack of biomarkers and nonspecific symptoms, wrote Henriëtte M.Y. de Jong, MD, PhD, of the University of Amsterdam, and colleagues.
Individuals who carry the HLA-B27 gene are predisposed to axSpA, and their first-degree relatives (FDRs) are at increased risk as well, the researchers said. Therefore, “studying [FDRs] could help to identify clinical signs, imaging abnormalities, and biomarkers that are predictive of development of axSpA,” they said.
In a study published in Arthritis Care & Research, the investigators reviewed data from patients in the Pre-SpA cohort, a 5-year prospective study of healthy-seeming FDRs of patients with HLA-B27–positive axSpA. The researchers previously reported that up to one-third of 51 FDRs had clinical features associated with SpA at baseline, despite the lack of a diagnosis.
The current study included an additional 151 FDRs who had answered yearly questions about back pain and undergone a yearly physical exam and plain radiographs and MRI imaging at baseline.
Overall, 65% reported back pain at baseline and 19% met criteria for inflammatory back pain, with a median visual analog score (VAS) for back pain of 22. No active arthritis was noted, but 5 FDRs reported a past arthritis diagnosis, 48 reported arthralgia, and 16 had at least one tender joint on physical exam. Eight FDRs had past diagnoses of enthesitis, and one had a history of dactylitis.
In assessing disease activity, the researchers found an elevated C-reactive protein (CRP) level in 24 FDRs and 11 had an elevated erythrocyte sedimentation rate (ESR).
On MRI of the sacroiliac joint at baseline, 10% of the FDRs had SPARCC (Spondyloarthritis Research Consortium of Canada) scores of 2 or higher, 4% had scores of 5 or higher, and 4% had deep lesions.
A total of 123 FDRs had complete data at a 1-year follow-up visit.
“All features were equally distributed between HLA-B27–positive and –negative FDRs,” the researchers noted. However, at the end of the 1-year follow-up period, seven (6%) of the FDRs were clinically diagnosed with axSpA, and six of them were HLA-B27 positive. Disease activity measures had increased at 1 year in all seven patients with newly diagnosed axSpA.
The study findings were limited by several factors, including the possible channeling of FDRs with current complaints of back pain into the study and the inability to confirm details of family and medical history, the researchers noted. However, the VAS back pain scores reported by the FDRs suggest that this pain was not a fixture in daily life, they wrote.
The results confirm the prevalent subclinical signs of SpA in healthy FDRs of patients with axSpA who were positive and negative for HLA-B27, but also confirm that clinical progression occurred primarily in the HLA-B27–positive patients in conjunction with inflammatory back pain, the researchers said.
“Further follow-up of the Pre-SpA cohort will give more robust insight into the characteristics of FDRs that progress towards clinical SpA, thereby hopefully enabling the characterization of high-risk FDRs,” they concluded.
The Pre-SpA cohort is supported by the Dutch Arthritis Society. Lead author Dr. de Jong had no financial conflicts to disclose. One coauthor is employed by UCB, and several others disclosed relationships with AbbVie, Eli Lilly, Janssen, Novartis, Pfizer, and UCB.
Healthy first-degree relatives of individuals with HLA-B27–positive axial spondyloarthritis who also were HLA-B27 positive were at increased risk for developing the disease themselves within 1 year, based on data from an ongoing prospective cohort study that involved 202 first-degree relatives.
Axial spondyloarthritis (axSpA) generally arises between ages 18 and 40 years, but diagnosis can be delayed, in part because of the lack of biomarkers and nonspecific symptoms, wrote Henriëtte M.Y. de Jong, MD, PhD, of the University of Amsterdam, and colleagues.
Individuals who carry the HLA-B27 gene are predisposed to axSpA, and their first-degree relatives (FDRs) are at increased risk as well, the researchers said. Therefore, “studying [FDRs] could help to identify clinical signs, imaging abnormalities, and biomarkers that are predictive of development of axSpA,” they said.
In a study published in Arthritis Care & Research, the investigators reviewed data from patients in the Pre-SpA cohort, a 5-year prospective study of healthy-seeming FDRs of patients with HLA-B27–positive axSpA. The researchers previously reported that up to one-third of 51 FDRs had clinical features associated with SpA at baseline, despite the lack of a diagnosis.
The current study included an additional 151 FDRs who had answered yearly questions about back pain and undergone a yearly physical exam and plain radiographs and MRI imaging at baseline.
Overall, 65% reported back pain at baseline and 19% met criteria for inflammatory back pain, with a median visual analog score (VAS) for back pain of 22. No active arthritis was noted, but 5 FDRs reported a past arthritis diagnosis, 48 reported arthralgia, and 16 had at least one tender joint on physical exam. Eight FDRs had past diagnoses of enthesitis, and one had a history of dactylitis.
In assessing disease activity, the researchers found an elevated C-reactive protein (CRP) level in 24 FDRs and 11 had an elevated erythrocyte sedimentation rate (ESR).
On MRI of the sacroiliac joint at baseline, 10% of the FDRs had SPARCC (Spondyloarthritis Research Consortium of Canada) scores of 2 or higher, 4% had scores of 5 or higher, and 4% had deep lesions.
A total of 123 FDRs had complete data at a 1-year follow-up visit.
“All features were equally distributed between HLA-B27–positive and –negative FDRs,” the researchers noted. However, at the end of the 1-year follow-up period, seven (6%) of the FDRs were clinically diagnosed with axSpA, and six of them were HLA-B27 positive. Disease activity measures had increased at 1 year in all seven patients with newly diagnosed axSpA.
The study findings were limited by several factors, including the possible channeling of FDRs with current complaints of back pain into the study and the inability to confirm details of family and medical history, the researchers noted. However, the VAS back pain scores reported by the FDRs suggest that this pain was not a fixture in daily life, they wrote.
The results confirm the prevalent subclinical signs of SpA in healthy FDRs of patients with axSpA who were positive and negative for HLA-B27, but also confirm that clinical progression occurred primarily in the HLA-B27–positive patients in conjunction with inflammatory back pain, the researchers said.
“Further follow-up of the Pre-SpA cohort will give more robust insight into the characteristics of FDRs that progress towards clinical SpA, thereby hopefully enabling the characterization of high-risk FDRs,” they concluded.
The Pre-SpA cohort is supported by the Dutch Arthritis Society. Lead author Dr. de Jong had no financial conflicts to disclose. One coauthor is employed by UCB, and several others disclosed relationships with AbbVie, Eli Lilly, Janssen, Novartis, Pfizer, and UCB.
Healthy first-degree relatives of individuals with HLA-B27–positive axial spondyloarthritis who also were HLA-B27 positive were at increased risk for developing the disease themselves within 1 year, based on data from an ongoing prospective cohort study that involved 202 first-degree relatives.
Axial spondyloarthritis (axSpA) generally arises between ages 18 and 40 years, but diagnosis can be delayed, in part because of the lack of biomarkers and nonspecific symptoms, wrote Henriëtte M.Y. de Jong, MD, PhD, of the University of Amsterdam, and colleagues.
Individuals who carry the HLA-B27 gene are predisposed to axSpA, and their first-degree relatives (FDRs) are at increased risk as well, the researchers said. Therefore, “studying [FDRs] could help to identify clinical signs, imaging abnormalities, and biomarkers that are predictive of development of axSpA,” they said.
In a study published in Arthritis Care & Research, the investigators reviewed data from patients in the Pre-SpA cohort, a 5-year prospective study of healthy-seeming FDRs of patients with HLA-B27–positive axSpA. The researchers previously reported that up to one-third of 51 FDRs had clinical features associated with SpA at baseline, despite the lack of a diagnosis.
The current study included an additional 151 FDRs who had answered yearly questions about back pain and undergone a yearly physical exam and plain radiographs and MRI imaging at baseline.
Overall, 65% reported back pain at baseline and 19% met criteria for inflammatory back pain, with a median visual analog score (VAS) for back pain of 22. No active arthritis was noted, but 5 FDRs reported a past arthritis diagnosis, 48 reported arthralgia, and 16 had at least one tender joint on physical exam. Eight FDRs had past diagnoses of enthesitis, and one had a history of dactylitis.
In assessing disease activity, the researchers found an elevated C-reactive protein (CRP) level in 24 FDRs and 11 had an elevated erythrocyte sedimentation rate (ESR).
On MRI of the sacroiliac joint at baseline, 10% of the FDRs had SPARCC (Spondyloarthritis Research Consortium of Canada) scores of 2 or higher, 4% had scores of 5 or higher, and 4% had deep lesions.
A total of 123 FDRs had complete data at a 1-year follow-up visit.
“All features were equally distributed between HLA-B27–positive and –negative FDRs,” the researchers noted. However, at the end of the 1-year follow-up period, seven (6%) of the FDRs were clinically diagnosed with axSpA, and six of them were HLA-B27 positive. Disease activity measures had increased at 1 year in all seven patients with newly diagnosed axSpA.
The study findings were limited by several factors, including the possible channeling of FDRs with current complaints of back pain into the study and the inability to confirm details of family and medical history, the researchers noted. However, the VAS back pain scores reported by the FDRs suggest that this pain was not a fixture in daily life, they wrote.
The results confirm the prevalent subclinical signs of SpA in healthy FDRs of patients with axSpA who were positive and negative for HLA-B27, but also confirm that clinical progression occurred primarily in the HLA-B27–positive patients in conjunction with inflammatory back pain, the researchers said.
“Further follow-up of the Pre-SpA cohort will give more robust insight into the characteristics of FDRs that progress towards clinical SpA, thereby hopefully enabling the characterization of high-risk FDRs,” they concluded.
The Pre-SpA cohort is supported by the Dutch Arthritis Society. Lead author Dr. de Jong had no financial conflicts to disclose. One coauthor is employed by UCB, and several others disclosed relationships with AbbVie, Eli Lilly, Janssen, Novartis, Pfizer, and UCB.
FROM ARTHRITIS CARE & RESEARCH
Bleeding events tied to higher mortality in patients with factor V inhibition
Coagulation factor V (FV) inhibitor is a rare disease with a mortality rate of nearly 15%. Increased mortality was significantly associated with the incidence of major bleeding, according to a review of PubMed case reports published in Thrombosis Update.
FV autoantibodies are most often detected in patients in the postoperative state, in those who have received a blood transfusion, in patients treated with antibiotics, and in those with immune diseases, according to the online report by Hideo Wada, MD, PhD, of the Mie Prefectural General Medical Center, Yokkaichi, Japan, and colleagues. These patients who acquired immune FV inhibitor (AIFVD) vary widely in symptoms from asymptomatic to mild or severe hemorrhagic manifestations, with some reports of thrombotic complications, the authors added.
Their review assessed the PubMed literature from Jan. 1, 1968, to July 31, 2020, and found 212 case reports on acquired FV deficiency. Of these, 150 cases with confirmed FV inhibitor positivity were included. The 150 reported cases of FV inhibitor were primarily from the United States (n = 48) and Japan (n = 43). The median patient age was 68.0 years, and the female to male ratio of patients was 0.47, according to the authors. The largest associated percentage of underlying conditions were postoperative state (25.3%), idiopathic (18.7%), infection (12.7%) and malignant neoplasms and autoimmune disease, at 7.3% each.
Major bleeds
A total of 73 cases were positive for major bleeding (48.7%) and 30 cases were negative (20.0%), while the rest were undetermined (31.3%). The FV activity was ≤ 28% in all patients with FV inhibitor.
The overall mortality rate was 14.6%, with half of the nonsurvivors dying of major bleeding. The mortality rate was more than twofold higher in the group with major bleeding (23.3% mortality) compared to the group without major bleeding (10.0%), yielding an odds ratio of 2.73 of death because of a major bleed. The most frequent types of fatal bleeding were intracranial bleeding and gastrointestinal bleeding. Of the 20 deaths reported in 135 patients with data, the causes of death were major bleeding (12 patients), infection (6 patients) and thrombosis (2 patients). Remission was observed in three of the nonsurvivors, indicating that even after remission, patients with FV inhibitor might still be susceptible to infection or thrombosis, according to the authors.
“[Major bleeding] should be treated aggressively; however, the best treatment is not clear and even patients in remission should be followed closely due to the risk of death from infection or thrombosis,” the authors concluded.
They reported having no conflicts of interest.
Coagulation factor V (FV) inhibitor is a rare disease with a mortality rate of nearly 15%. Increased mortality was significantly associated with the incidence of major bleeding, according to a review of PubMed case reports published in Thrombosis Update.
FV autoantibodies are most often detected in patients in the postoperative state, in those who have received a blood transfusion, in patients treated with antibiotics, and in those with immune diseases, according to the online report by Hideo Wada, MD, PhD, of the Mie Prefectural General Medical Center, Yokkaichi, Japan, and colleagues. These patients who acquired immune FV inhibitor (AIFVD) vary widely in symptoms from asymptomatic to mild or severe hemorrhagic manifestations, with some reports of thrombotic complications, the authors added.
Their review assessed the PubMed literature from Jan. 1, 1968, to July 31, 2020, and found 212 case reports on acquired FV deficiency. Of these, 150 cases with confirmed FV inhibitor positivity were included. The 150 reported cases of FV inhibitor were primarily from the United States (n = 48) and Japan (n = 43). The median patient age was 68.0 years, and the female to male ratio of patients was 0.47, according to the authors. The largest associated percentage of underlying conditions were postoperative state (25.3%), idiopathic (18.7%), infection (12.7%) and malignant neoplasms and autoimmune disease, at 7.3% each.
Major bleeds
A total of 73 cases were positive for major bleeding (48.7%) and 30 cases were negative (20.0%), while the rest were undetermined (31.3%). The FV activity was ≤ 28% in all patients with FV inhibitor.
The overall mortality rate was 14.6%, with half of the nonsurvivors dying of major bleeding. The mortality rate was more than twofold higher in the group with major bleeding (23.3% mortality) compared to the group without major bleeding (10.0%), yielding an odds ratio of 2.73 of death because of a major bleed. The most frequent types of fatal bleeding were intracranial bleeding and gastrointestinal bleeding. Of the 20 deaths reported in 135 patients with data, the causes of death were major bleeding (12 patients), infection (6 patients) and thrombosis (2 patients). Remission was observed in three of the nonsurvivors, indicating that even after remission, patients with FV inhibitor might still be susceptible to infection or thrombosis, according to the authors.
“[Major bleeding] should be treated aggressively; however, the best treatment is not clear and even patients in remission should be followed closely due to the risk of death from infection or thrombosis,” the authors concluded.
They reported having no conflicts of interest.
Coagulation factor V (FV) inhibitor is a rare disease with a mortality rate of nearly 15%. Increased mortality was significantly associated with the incidence of major bleeding, according to a review of PubMed case reports published in Thrombosis Update.
FV autoantibodies are most often detected in patients in the postoperative state, in those who have received a blood transfusion, in patients treated with antibiotics, and in those with immune diseases, according to the online report by Hideo Wada, MD, PhD, of the Mie Prefectural General Medical Center, Yokkaichi, Japan, and colleagues. These patients who acquired immune FV inhibitor (AIFVD) vary widely in symptoms from asymptomatic to mild or severe hemorrhagic manifestations, with some reports of thrombotic complications, the authors added.
Their review assessed the PubMed literature from Jan. 1, 1968, to July 31, 2020, and found 212 case reports on acquired FV deficiency. Of these, 150 cases with confirmed FV inhibitor positivity were included. The 150 reported cases of FV inhibitor were primarily from the United States (n = 48) and Japan (n = 43). The median patient age was 68.0 years, and the female to male ratio of patients was 0.47, according to the authors. The largest associated percentage of underlying conditions were postoperative state (25.3%), idiopathic (18.7%), infection (12.7%) and malignant neoplasms and autoimmune disease, at 7.3% each.
Major bleeds
A total of 73 cases were positive for major bleeding (48.7%) and 30 cases were negative (20.0%), while the rest were undetermined (31.3%). The FV activity was ≤ 28% in all patients with FV inhibitor.
The overall mortality rate was 14.6%, with half of the nonsurvivors dying of major bleeding. The mortality rate was more than twofold higher in the group with major bleeding (23.3% mortality) compared to the group without major bleeding (10.0%), yielding an odds ratio of 2.73 of death because of a major bleed. The most frequent types of fatal bleeding were intracranial bleeding and gastrointestinal bleeding. Of the 20 deaths reported in 135 patients with data, the causes of death were major bleeding (12 patients), infection (6 patients) and thrombosis (2 patients). Remission was observed in three of the nonsurvivors, indicating that even after remission, patients with FV inhibitor might still be susceptible to infection or thrombosis, according to the authors.
“[Major bleeding] should be treated aggressively; however, the best treatment is not clear and even patients in remission should be followed closely due to the risk of death from infection or thrombosis,” the authors concluded.
They reported having no conflicts of interest.
FROM THROMBOSIS UPDATE
Britney Spears and her 13-year conservatorship: An abuse of involuntary care?
The public has watched the ongoing drama unfold in the media for the past 13 years. In 2008, pop star Britney Spears was placed on conservatorship – a court process that gave decision-making powers over her personal, legal, and financial decisions to another person.
On June 23, 2021, Ms. Spears announced in open court that she is traumatized by being conserved and wants her rights back, but we know little about what behaviors left her family and a judge to determine that she was not capable of managing her own affairs, and why this would remain the case for so many years.
Adam Nelson, MD, practices psychiatry in Marin County, Calif. He explained in an interview that there are different types of conservatorships. “Probate conservatorship is the traditional path for conservatorship of person, estate, and/or finances based on evidence of incapacity due to any medical condition. This is the type of conservatorship that Britney Spears has had and which she is now contesting.”
Ms. Spears was placed on conservatorship after two involuntary hospitalizations for psychiatric illness and/or substance abuse. Her father, Jamie Spears, was appointed by the court to be her conservator.
In a New York Times article, reporters Liz Day, Samantha Stark, and Joe Coscarelli recently wrote: “But now, confidential court records obtained by the New York Times reveal that Ms. Spears, 39, expressed serious opposition to the conservatorship earlier and more often than had previously been known, and said that it restricted everything from whom she dated to the color of her kitchen cabinets.” The article goes on to say: “The newly obtained court records show that Ms. Spears questioned [her father’s] fitness for the role. As early as 2014, in a hearing closed to the public, Ms. Spears’s court-appointed lawyer, Samuel D. Ingham III, said she wanted to explore removing her father as conservator, citing his drinking, among other objections on a ‘shopping list’ of grievances.
“As the fight drags on, the bills are piling up – and, in a quirk of the conservatorship system, Ms. Spears has to pay for lawyers on both sides, including those arguing against her wishes in court. A recent $890,000 bill from one set of Mr. Spears’s lawyers, covering about 4 months of work, included media strategizing for defending the conservatorship.”
The case heated up at the June 23 hearing, when Ms. Spears had a telephone hearing with Los Angeles probate Judge Brenda Penney. The call was transcribed and published in Variety. The purpose of the hearing was for Ms. Spears to request an expedited release from her conservatorship without a psychiatric evaluation.
Ms. Spears began her 23-minute testimony to the judge by discussing her work and how she felt compelled to perform. “My management said, if I don’t do this tour, I will have to find an attorney, and by contract my own management could sue me if I didn’t follow through with the tour. ... So out of fear, I went ahead and I did the tour.”
She then discussed concerns by her manager that she was not complying with her medication regimen.
“Three days later, after I said no to Vegas,” Ms. Spears continued, “my therapist sat me down in a room and said he had a million phone calls about how I was not cooperating in rehearsals, and I haven’t been taking my medication. All this was false. He immediately, the next day, put me on lithium out of nowhere. He took me off my normal meds I’ve been on for 5 years. ... There were six different nurses in my home and they wouldn’t let me get in my car to go anywhere for a month.”
She spoke about entering rehab at the insistence of the conservatorship, and relayed her distress about this experience. She talked poignantly about her frustration of feeling she was not being heard by the court the last time she spoke and about the financial conflicts of interest created by her conservatorship. Ms. Spears, who has appeared on national television, recorded albums, and gone on performance tours during this period, has a net worth estimated at $60 million.
“It’s been a long time since I’ve owned my money. And it’s my wish and my dream for all of this to end without being tested,” she told the judge. “Again, it makes no sense whatsoever for the state of California to sit back and literally watch me with their own two eyes, make a living for so many people, and pay so many people trucks and buses on the road with me and be told, I’m not good enough. But I’m great at what I do. And I allow these people to control what I do, ma’am. And it’s enough. It makes no sense at all.”
Finally, Ms. Spears expressed a heart-wrenching desire to have another child and she asserted that the conservatorship will not allow her to see a doctor to have her IUD removed. She talked about being required to go to therapy three times a week and contended that she is traumatized by all that has transpired.
Ms. Spears has not filed the necessary paperwork to have her conservatorship ended. In an interview with Vice, attorney Scott Rahn noted that the process to end conservatorship can be a lengthy and difficult path. To do so, she might first need to petition the court to be allowed to hire her own attorney. If uncontested, the conservatorship could possibly be ended within months, but otherwise this could entail a lengthy trial over the course of years. While ending conservatorship may entail discovery, depositions, and hearings over years, a scathing story in the New Yorker detailed how Ms. Spears was placed into this conservatorship in a matter of days, without being present to give her own testimony. In the usual circumstances, California law requires that the person being conserved must be given 5 days’ notice before a conservatorship takes place, but Ms. Spears was deemed to be at risk of substantial harm and the judge allowed for an immediate conservatorship. The article notes that even axe murderers are allowed to hire lawyers, while those placed in conservatorships are not.
Reasoning behind such actions
Often, people are appointed guardians, conservators, or payees because of concerns that their psychiatric or substance use disorders, dementia, or impaired intellectual states lead them to poor decisions that endanger their financial stability. Usually the money they may lose is from a government disability benefit, an inheritance, or former accrued wealth. In this unusual celebrity case, Britney Spears has been conserved while she maintained a rigorous work schedule and actively earned the money she is being protected from spending.

Dr. Nelson talked about how people come to be conserved. “The law regarding conservatorship is a state law, but conservatorships in California are done at the county level, and the counties don’t have a vested interest in protecting people from themselves unless a third party or a family member comes forward. I imagine there is another side to this story, I have never seen it used like this for someone who is working. Questions remain about why this conservatorship has gone on for 13 years.”
Dr. Nelson believes that the current California laws leave room for abuse. “If the children of a wealthy parent observes the parent spending their inheritance in a way they don’t approve of, they can claim the parent is impaired and needs to be conserved. Usually it doesn’t work, but it’s possible there are times when the courts are swayed.”
Why does it matter and why should psychiatrists be concerned? The issue of involuntary treatment is a contentious one, and the stakeholders on all sides are vocal when it comes to our country’s sickest and most vulnerable individuals. Any story with a whiff of abuse, or of someone who is not severely impaired being denied basic civil rights – including the right to refuse treatment – dilutes and stains the efforts of those who are trying to protect people who suffer from chronic psychotic disorders. And when society reaches further to say that an individual is not entitled to make their own basic life decisions, this further stigmatizes those with psychiatric illnesses. And people with both mental illnesses and substance use disorders often get better, so why would conservatorships be permanent?
Does our society want the courts to protect people from their own poor judgment? Should there be judges at every casino entrance? Where are the conservators for those who live in the streets? Again, this is a half-told story, one where the potential for abuse of the conserved remains a high risk, and the long-term message about involuntary care is one of taking a way a person’s rights unnecessarily.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. She has no disclosures.
The public has watched the ongoing drama unfold in the media for the past 13 years. In 2008, pop star Britney Spears was placed on conservatorship – a court process that gave decision-making powers over her personal, legal, and financial decisions to another person.
On June 23, 2021, Ms. Spears announced in open court that she is traumatized by being conserved and wants her rights back, but we know little about what behaviors left her family and a judge to determine that she was not capable of managing her own affairs, and why this would remain the case for so many years.
Adam Nelson, MD, practices psychiatry in Marin County, Calif. He explained in an interview that there are different types of conservatorships. “Probate conservatorship is the traditional path for conservatorship of person, estate, and/or finances based on evidence of incapacity due to any medical condition. This is the type of conservatorship that Britney Spears has had and which she is now contesting.”
Ms. Spears was placed on conservatorship after two involuntary hospitalizations for psychiatric illness and/or substance abuse. Her father, Jamie Spears, was appointed by the court to be her conservator.
In a New York Times article, reporters Liz Day, Samantha Stark, and Joe Coscarelli recently wrote: “But now, confidential court records obtained by the New York Times reveal that Ms. Spears, 39, expressed serious opposition to the conservatorship earlier and more often than had previously been known, and said that it restricted everything from whom she dated to the color of her kitchen cabinets.” The article goes on to say: “The newly obtained court records show that Ms. Spears questioned [her father’s] fitness for the role. As early as 2014, in a hearing closed to the public, Ms. Spears’s court-appointed lawyer, Samuel D. Ingham III, said she wanted to explore removing her father as conservator, citing his drinking, among other objections on a ‘shopping list’ of grievances.
“As the fight drags on, the bills are piling up – and, in a quirk of the conservatorship system, Ms. Spears has to pay for lawyers on both sides, including those arguing against her wishes in court. A recent $890,000 bill from one set of Mr. Spears’s lawyers, covering about 4 months of work, included media strategizing for defending the conservatorship.”
The case heated up at the June 23 hearing, when Ms. Spears had a telephone hearing with Los Angeles probate Judge Brenda Penney. The call was transcribed and published in Variety. The purpose of the hearing was for Ms. Spears to request an expedited release from her conservatorship without a psychiatric evaluation.
Ms. Spears began her 23-minute testimony to the judge by discussing her work and how she felt compelled to perform. “My management said, if I don’t do this tour, I will have to find an attorney, and by contract my own management could sue me if I didn’t follow through with the tour. ... So out of fear, I went ahead and I did the tour.”
She then discussed concerns by her manager that she was not complying with her medication regimen.
“Three days later, after I said no to Vegas,” Ms. Spears continued, “my therapist sat me down in a room and said he had a million phone calls about how I was not cooperating in rehearsals, and I haven’t been taking my medication. All this was false. He immediately, the next day, put me on lithium out of nowhere. He took me off my normal meds I’ve been on for 5 years. ... There were six different nurses in my home and they wouldn’t let me get in my car to go anywhere for a month.”
She spoke about entering rehab at the insistence of the conservatorship, and relayed her distress about this experience. She talked poignantly about her frustration of feeling she was not being heard by the court the last time she spoke and about the financial conflicts of interest created by her conservatorship. Ms. Spears, who has appeared on national television, recorded albums, and gone on performance tours during this period, has a net worth estimated at $60 million.
“It’s been a long time since I’ve owned my money. And it’s my wish and my dream for all of this to end without being tested,” she told the judge. “Again, it makes no sense whatsoever for the state of California to sit back and literally watch me with their own two eyes, make a living for so many people, and pay so many people trucks and buses on the road with me and be told, I’m not good enough. But I’m great at what I do. And I allow these people to control what I do, ma’am. And it’s enough. It makes no sense at all.”
Finally, Ms. Spears expressed a heart-wrenching desire to have another child and she asserted that the conservatorship will not allow her to see a doctor to have her IUD removed. She talked about being required to go to therapy three times a week and contended that she is traumatized by all that has transpired.
Ms. Spears has not filed the necessary paperwork to have her conservatorship ended. In an interview with Vice, attorney Scott Rahn noted that the process to end conservatorship can be a lengthy and difficult path. To do so, she might first need to petition the court to be allowed to hire her own attorney. If uncontested, the conservatorship could possibly be ended within months, but otherwise this could entail a lengthy trial over the course of years. While ending conservatorship may entail discovery, depositions, and hearings over years, a scathing story in the New Yorker detailed how Ms. Spears was placed into this conservatorship in a matter of days, without being present to give her own testimony. In the usual circumstances, California law requires that the person being conserved must be given 5 days’ notice before a conservatorship takes place, but Ms. Spears was deemed to be at risk of substantial harm and the judge allowed for an immediate conservatorship. The article notes that even axe murderers are allowed to hire lawyers, while those placed in conservatorships are not.
Reasoning behind such actions
Often, people are appointed guardians, conservators, or payees because of concerns that their psychiatric or substance use disorders, dementia, or impaired intellectual states lead them to poor decisions that endanger their financial stability. Usually the money they may lose is from a government disability benefit, an inheritance, or former accrued wealth. In this unusual celebrity case, Britney Spears has been conserved while she maintained a rigorous work schedule and actively earned the money she is being protected from spending.
Dr. Nelson talked about how people come to be conserved. “The law regarding conservatorship is a state law, but conservatorships in California are done at the county level, and the counties don’t have a vested interest in protecting people from themselves unless a third party or a family member comes forward. I imagine there is another side to this story, I have never seen it used like this for someone who is working. Questions remain about why this conservatorship has gone on for 13 years.”
Dr. Nelson believes that the current California laws leave room for abuse. “If the children of a wealthy parent observes the parent spending their inheritance in a way they don’t approve of, they can claim the parent is impaired and needs to be conserved. Usually it doesn’t work, but it’s possible there are times when the courts are swayed.”
Why does it matter and why should psychiatrists be concerned? The issue of involuntary treatment is a contentious one, and the stakeholders on all sides are vocal when it comes to our country’s sickest and most vulnerable individuals. Any story with a whiff of abuse, or of someone who is not severely impaired being denied basic civil rights – including the right to refuse treatment – dilutes and stains the efforts of those who are trying to protect people who suffer from chronic psychotic disorders. And when society reaches further to say that an individual is not entitled to make their own basic life decisions, this further stigmatizes those with psychiatric illnesses. And people with both mental illnesses and substance use disorders often get better, so why would conservatorships be permanent?
Does our society want the courts to protect people from their own poor judgment? Should there be judges at every casino entrance? Where are the conservators for those who live in the streets? Again, this is a half-told story, one where the potential for abuse of the conserved remains a high risk, and the long-term message about involuntary care is one of taking a way a person’s rights unnecessarily.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. She has no disclosures.
The public has watched the ongoing drama unfold in the media for the past 13 years. In 2008, pop star Britney Spears was placed on conservatorship – a court process that gave decision-making powers over her personal, legal, and financial decisions to another person.
On June 23, 2021, Ms. Spears announced in open court that she is traumatized by being conserved and wants her rights back, but we know little about what behaviors left her family and a judge to determine that she was not capable of managing her own affairs, and why this would remain the case for so many years.
Adam Nelson, MD, practices psychiatry in Marin County, Calif. He explained in an interview that there are different types of conservatorships. “Probate conservatorship is the traditional path for conservatorship of person, estate, and/or finances based on evidence of incapacity due to any medical condition. This is the type of conservatorship that Britney Spears has had and which she is now contesting.”
Ms. Spears was placed on conservatorship after two involuntary hospitalizations for psychiatric illness and/or substance abuse. Her father, Jamie Spears, was appointed by the court to be her conservator.
In a New York Times article, reporters Liz Day, Samantha Stark, and Joe Coscarelli recently wrote: “But now, confidential court records obtained by the New York Times reveal that Ms. Spears, 39, expressed serious opposition to the conservatorship earlier and more often than had previously been known, and said that it restricted everything from whom she dated to the color of her kitchen cabinets.” The article goes on to say: “The newly obtained court records show that Ms. Spears questioned [her father’s] fitness for the role. As early as 2014, in a hearing closed to the public, Ms. Spears’s court-appointed lawyer, Samuel D. Ingham III, said she wanted to explore removing her father as conservator, citing his drinking, among other objections on a ‘shopping list’ of grievances.
“As the fight drags on, the bills are piling up – and, in a quirk of the conservatorship system, Ms. Spears has to pay for lawyers on both sides, including those arguing against her wishes in court. A recent $890,000 bill from one set of Mr. Spears’s lawyers, covering about 4 months of work, included media strategizing for defending the conservatorship.”
The case heated up at the June 23 hearing, when Ms. Spears had a telephone hearing with Los Angeles probate Judge Brenda Penney. The call was transcribed and published in Variety. The purpose of the hearing was for Ms. Spears to request an expedited release from her conservatorship without a psychiatric evaluation.
Ms. Spears began her 23-minute testimony to the judge by discussing her work and how she felt compelled to perform. “My management said, if I don’t do this tour, I will have to find an attorney, and by contract my own management could sue me if I didn’t follow through with the tour. ... So out of fear, I went ahead and I did the tour.”
She then discussed concerns by her manager that she was not complying with her medication regimen.
“Three days later, after I said no to Vegas,” Ms. Spears continued, “my therapist sat me down in a room and said he had a million phone calls about how I was not cooperating in rehearsals, and I haven’t been taking my medication. All this was false. He immediately, the next day, put me on lithium out of nowhere. He took me off my normal meds I’ve been on for 5 years. ... There were six different nurses in my home and they wouldn’t let me get in my car to go anywhere for a month.”
She spoke about entering rehab at the insistence of the conservatorship, and relayed her distress about this experience. She talked poignantly about her frustration of feeling she was not being heard by the court the last time she spoke and about the financial conflicts of interest created by her conservatorship. Ms. Spears, who has appeared on national television, recorded albums, and gone on performance tours during this period, has a net worth estimated at $60 million.
“It’s been a long time since I’ve owned my money. And it’s my wish and my dream for all of this to end without being tested,” she told the judge. “Again, it makes no sense whatsoever for the state of California to sit back and literally watch me with their own two eyes, make a living for so many people, and pay so many people trucks and buses on the road with me and be told, I’m not good enough. But I’m great at what I do. And I allow these people to control what I do, ma’am. And it’s enough. It makes no sense at all.”
Finally, Ms. Spears expressed a heart-wrenching desire to have another child and she asserted that the conservatorship will not allow her to see a doctor to have her IUD removed. She talked about being required to go to therapy three times a week and contended that she is traumatized by all that has transpired.
Ms. Spears has not filed the necessary paperwork to have her conservatorship ended. In an interview with Vice, attorney Scott Rahn noted that the process to end conservatorship can be a lengthy and difficult path. To do so, she might first need to petition the court to be allowed to hire her own attorney. If uncontested, the conservatorship could possibly be ended within months, but otherwise this could entail a lengthy trial over the course of years. While ending conservatorship may entail discovery, depositions, and hearings over years, a scathing story in the New Yorker detailed how Ms. Spears was placed into this conservatorship in a matter of days, without being present to give her own testimony. In the usual circumstances, California law requires that the person being conserved must be given 5 days’ notice before a conservatorship takes place, but Ms. Spears was deemed to be at risk of substantial harm and the judge allowed for an immediate conservatorship. The article notes that even axe murderers are allowed to hire lawyers, while those placed in conservatorships are not.
Reasoning behind such actions
Often, people are appointed guardians, conservators, or payees because of concerns that their psychiatric or substance use disorders, dementia, or impaired intellectual states lead them to poor decisions that endanger their financial stability. Usually the money they may lose is from a government disability benefit, an inheritance, or former accrued wealth. In this unusual celebrity case, Britney Spears has been conserved while she maintained a rigorous work schedule and actively earned the money she is being protected from spending.
Dr. Nelson talked about how people come to be conserved. “The law regarding conservatorship is a state law, but conservatorships in California are done at the county level, and the counties don’t have a vested interest in protecting people from themselves unless a third party or a family member comes forward. I imagine there is another side to this story, I have never seen it used like this for someone who is working. Questions remain about why this conservatorship has gone on for 13 years.”
Dr. Nelson believes that the current California laws leave room for abuse. “If the children of a wealthy parent observes the parent spending their inheritance in a way they don’t approve of, they can claim the parent is impaired and needs to be conserved. Usually it doesn’t work, but it’s possible there are times when the courts are swayed.”
Why does it matter and why should psychiatrists be concerned? The issue of involuntary treatment is a contentious one, and the stakeholders on all sides are vocal when it comes to our country’s sickest and most vulnerable individuals. Any story with a whiff of abuse, or of someone who is not severely impaired being denied basic civil rights – including the right to refuse treatment – dilutes and stains the efforts of those who are trying to protect people who suffer from chronic psychotic disorders. And when society reaches further to say that an individual is not entitled to make their own basic life decisions, this further stigmatizes those with psychiatric illnesses. And people with both mental illnesses and substance use disorders often get better, so why would conservatorships be permanent?
Does our society want the courts to protect people from their own poor judgment? Should there be judges at every casino entrance? Where are the conservators for those who live in the streets? Again, this is a half-told story, one where the potential for abuse of the conserved remains a high risk, and the long-term message about involuntary care is one of taking a way a person’s rights unnecessarily.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. She has no disclosures.
When can your hypochondria help patients?
Hypochondria has been useful to my patients. I mean my own hypochondria. It may not take one to know one, but we hypochondriacs understand each other.

Hypochondriacs worry that we are sick, worry that our fears are foolish and that we will be mocked for worrying about nothing, and worry even more that this time, we finally worried about something after all. Reassurance leaves us sheepish, then elated. Elation soon fades, and a new worry appears. Worry, rinse, repeat. . Some folks are just needy. Soothing the needs of the needy can feel like trying to drain the seven seas with a teaspoon. Those who work with people must either find ways to cope with the spectrum of neediness, or find another kind of work to do.
Some patient needs call for diagnosis and treatment. Other needs go beyond the strictly medical. Beyond knowing whether they are ill, patients have questions like, “Will this get worse?” “Will I be ashamed to go out in public?” “Can I visit my grandchildren, or will my daughter-in-law throw me out as contagious?” “Is this the beginning of the end?” or, worst of all, “Am I losing my hair?”
The list of possible patient needs is long, though not endless. Lining them up one after the other can make them sound melodramatic, even silly. (Other people’s worries often sound silly; your own never do.) Can a small growth or slight itch really cause existential agitation? Anyone who deals with complaints like these knows that the answer is yes.
Hypochondriacs with medical degrees cannot reassure themselves, but we can bring useful experience to help other members of the worry club. Doing so means paying attention not just to what doctors worry about but what patients do.
Sometimes a patient is terrified, the doctor not at all. Gentle sympathy may be enough. But the reverse can also be true: The doctor is concerned, but the patient thinks there is no problem. Sometimes I am worried enough to ask a patient to call or email an update. Patients who have already stopped worrying may not bother to answer the phone or shoot back an email. Failure to respond may mean they are fine, or in intensive care. Silence is hard to interpret.
Skin doctors have one advantageous disadvantage: Few tests help us beyond a skin scraping, the odd blood test, or a biopsy. Otherwise, most of the time all we can do is look, and perhaps apply “tincture of time,” watching the clinical course. We cannot send patients for the complex and expensive tests our colleagues use “just to be sure,” because we have no such tests to send them for.
Practice and experience help us recognize needs and worries that patients might not express. For instance, a man may show up with pimples on his back. His concerns seem intense. “What worries you?” we ask. The patient whispers, “It couldn’t be ... shingles, could it?” No, it couldn’t be shingles, because it is bilateral and for many other reasons.
The question is not whether he has shingles but why he thinks he does. Maybe his aunt suggested it. Or an article told him to watch out for it. Or his pharmacy is promoting zoster vaccination by showing huge, full-color photos of shingles cases worthy of horror movies. (Shingles the 13th!) Because he wants to visit his grandkids and his daughter is in her fourth month of pregnancy. In other words, along with the fear of cancer, fear of shingles is just out there. There are other such public concerns. Over time, we come to recognize them.
Anyone can worry, but anxiety paralyzes some to such an extent that referral to a mental health professional seems reasonable. The problem with advising it is that patients who somaticize may take exception to suggestions, however delicately put, that make us sound dismissive, locating their concern “all in the head.” Over the years, my attempts to make such referrals have met with limited success.
Dealing with needs – and neediness – can take up more of a doctor’s day than making specific diagnoses and prescribing helpful treatments. Besides, addressing needs and neediness demands skills not always stressed at school.
Practice at noting neediness makes you better at it, but no doctor nails the true wellsprings of worry all the time. We hypochondriacs can be devilishly inventive.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His latest book, “Doctoring from the Outside In,” was recently published. Write to him at [email protected].
Hypochondria has been useful to my patients. I mean my own hypochondria. It may not take one to know one, but we hypochondriacs understand each other.
Hypochondriacs worry that we are sick, worry that our fears are foolish and that we will be mocked for worrying about nothing, and worry even more that this time, we finally worried about something after all. Reassurance leaves us sheepish, then elated. Elation soon fades, and a new worry appears. Worry, rinse, repeat. . Some folks are just needy. Soothing the needs of the needy can feel like trying to drain the seven seas with a teaspoon. Those who work with people must either find ways to cope with the spectrum of neediness, or find another kind of work to do.
Some patient needs call for diagnosis and treatment. Other needs go beyond the strictly medical. Beyond knowing whether they are ill, patients have questions like, “Will this get worse?” “Will I be ashamed to go out in public?” “Can I visit my grandchildren, or will my daughter-in-law throw me out as contagious?” “Is this the beginning of the end?” or, worst of all, “Am I losing my hair?”
The list of possible patient needs is long, though not endless. Lining them up one after the other can make them sound melodramatic, even silly. (Other people’s worries often sound silly; your own never do.) Can a small growth or slight itch really cause existential agitation? Anyone who deals with complaints like these knows that the answer is yes.
Hypochondriacs with medical degrees cannot reassure themselves, but we can bring useful experience to help other members of the worry club. Doing so means paying attention not just to what doctors worry about but what patients do.
Sometimes a patient is terrified, the doctor not at all. Gentle sympathy may be enough. But the reverse can also be true: The doctor is concerned, but the patient thinks there is no problem. Sometimes I am worried enough to ask a patient to call or email an update. Patients who have already stopped worrying may not bother to answer the phone or shoot back an email. Failure to respond may mean they are fine, or in intensive care. Silence is hard to interpret.
Skin doctors have one advantageous disadvantage: Few tests help us beyond a skin scraping, the odd blood test, or a biopsy. Otherwise, most of the time all we can do is look, and perhaps apply “tincture of time,” watching the clinical course. We cannot send patients for the complex and expensive tests our colleagues use “just to be sure,” because we have no such tests to send them for.
Practice and experience help us recognize needs and worries that patients might not express. For instance, a man may show up with pimples on his back. His concerns seem intense. “What worries you?” we ask. The patient whispers, “It couldn’t be ... shingles, could it?” No, it couldn’t be shingles, because it is bilateral and for many other reasons.
The question is not whether he has shingles but why he thinks he does. Maybe his aunt suggested it. Or an article told him to watch out for it. Or his pharmacy is promoting zoster vaccination by showing huge, full-color photos of shingles cases worthy of horror movies. (Shingles the 13th!) Because he wants to visit his grandkids and his daughter is in her fourth month of pregnancy. In other words, along with the fear of cancer, fear of shingles is just out there. There are other such public concerns. Over time, we come to recognize them.
Anyone can worry, but anxiety paralyzes some to such an extent that referral to a mental health professional seems reasonable. The problem with advising it is that patients who somaticize may take exception to suggestions, however delicately put, that make us sound dismissive, locating their concern “all in the head.” Over the years, my attempts to make such referrals have met with limited success.
Dealing with needs – and neediness – can take up more of a doctor’s day than making specific diagnoses and prescribing helpful treatments. Besides, addressing needs and neediness demands skills not always stressed at school.
Practice at noting neediness makes you better at it, but no doctor nails the true wellsprings of worry all the time. We hypochondriacs can be devilishly inventive.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His latest book, “Doctoring from the Outside In,” was recently published. Write to him at [email protected].
Hypochondria has been useful to my patients. I mean my own hypochondria. It may not take one to know one, but we hypochondriacs understand each other.
Hypochondriacs worry that we are sick, worry that our fears are foolish and that we will be mocked for worrying about nothing, and worry even more that this time, we finally worried about something after all. Reassurance leaves us sheepish, then elated. Elation soon fades, and a new worry appears. Worry, rinse, repeat. . Some folks are just needy. Soothing the needs of the needy can feel like trying to drain the seven seas with a teaspoon. Those who work with people must either find ways to cope with the spectrum of neediness, or find another kind of work to do.
Some patient needs call for diagnosis and treatment. Other needs go beyond the strictly medical. Beyond knowing whether they are ill, patients have questions like, “Will this get worse?” “Will I be ashamed to go out in public?” “Can I visit my grandchildren, or will my daughter-in-law throw me out as contagious?” “Is this the beginning of the end?” or, worst of all, “Am I losing my hair?”
The list of possible patient needs is long, though not endless. Lining them up one after the other can make them sound melodramatic, even silly. (Other people’s worries often sound silly; your own never do.) Can a small growth or slight itch really cause existential agitation? Anyone who deals with complaints like these knows that the answer is yes.
Hypochondriacs with medical degrees cannot reassure themselves, but we can bring useful experience to help other members of the worry club. Doing so means paying attention not just to what doctors worry about but what patients do.
Sometimes a patient is terrified, the doctor not at all. Gentle sympathy may be enough. But the reverse can also be true: The doctor is concerned, but the patient thinks there is no problem. Sometimes I am worried enough to ask a patient to call or email an update. Patients who have already stopped worrying may not bother to answer the phone or shoot back an email. Failure to respond may mean they are fine, or in intensive care. Silence is hard to interpret.
Skin doctors have one advantageous disadvantage: Few tests help us beyond a skin scraping, the odd blood test, or a biopsy. Otherwise, most of the time all we can do is look, and perhaps apply “tincture of time,” watching the clinical course. We cannot send patients for the complex and expensive tests our colleagues use “just to be sure,” because we have no such tests to send them for.
Practice and experience help us recognize needs and worries that patients might not express. For instance, a man may show up with pimples on his back. His concerns seem intense. “What worries you?” we ask. The patient whispers, “It couldn’t be ... shingles, could it?” No, it couldn’t be shingles, because it is bilateral and for many other reasons.
The question is not whether he has shingles but why he thinks he does. Maybe his aunt suggested it. Or an article told him to watch out for it. Or his pharmacy is promoting zoster vaccination by showing huge, full-color photos of shingles cases worthy of horror movies. (Shingles the 13th!) Because he wants to visit his grandkids and his daughter is in her fourth month of pregnancy. In other words, along with the fear of cancer, fear of shingles is just out there. There are other such public concerns. Over time, we come to recognize them.
Anyone can worry, but anxiety paralyzes some to such an extent that referral to a mental health professional seems reasonable. The problem with advising it is that patients who somaticize may take exception to suggestions, however delicately put, that make us sound dismissive, locating their concern “all in the head.” Over the years, my attempts to make such referrals have met with limited success.
Dealing with needs – and neediness – can take up more of a doctor’s day than making specific diagnoses and prescribing helpful treatments. Besides, addressing needs and neediness demands skills not always stressed at school.
Practice at noting neediness makes you better at it, but no doctor nails the true wellsprings of worry all the time. We hypochondriacs can be devilishly inventive.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His latest book, “Doctoring from the Outside In,” was recently published. Write to him at [email protected].
What’s my number? Do I really need $10 million to retire from my medical practice?
“What’s my number?” When I hear this from my financial planning clients, I know they mean: In my 20-year career, this “magic number” is by far the most common thing physicians want to know.

If you look online, articles may recommend having a portfolio valued at $2 million, $5 million, and not uncommonly $10 million or more to retire. Really? $10 million? You might be thinking that surely not everyone needs that amount. Luckily, that’s true.
There’s no magic number your portfolio should be – just your number.
It’s human nature to want a simple, clear target to shoot for. But unfortunately, there’s no generic answer when it comes to saving for retirement. Even after a comprehensive hour-long review of a client’s financial plan – including insurance, investments, estate planning, and other items – the most honest answer I can give is: “It depends.” Not satisfying, I know. But there are still too many holes to fill.
By far the most important factor in getting beyond “it depends” is having an accurate estimate of annual retirement expenses. I have clients who live comfortably on $50,000 a year in retirement and others who need $250,000 or more. Knowing how much you need – your personal number – depends on the individual’s unique dream for retirement and calculating what that dream will cost.
Form a guesstimate based on savings and anticipated expenses
The total portfolio value needed to sustain an annual expense of $50,000 a year in retirement spending versus the portfolio size needed for $250,000 or more, blows apart the fiction of a universal “magic number.” It’s just not that simple. While it’s hard to gauge exactly what you will need, the right information can lead to a logical guesstimate about what size portfolio will provide you with financial independence.
In the end, it’s up to you to determine your desired retirement lifestyle. Then, the only way to get there is to calculate how much it will cost and save up for it by following a well-informed financial plan. This plan will be based on strategy that shifts from the middle to the later stages of your medical career and into retirement.
Let’s see how it works.
Early to mid-career: Focus on building up retirement savings
We ultimately want to save enough to meet our retirement expenses. But figuring out how much to save when you’re in your 40s and 50s is difficult. A mid-career physician likely has significant family- and child-related expenses. When we become empty-nesters, those expenses will decline. In retirement they may disappear entirely, but new expenses may arise.
With large variations in expenses at different life stages, it’s hard to calculate exactly how much you will need to save. Early on, the most sensible thing is putting aside a “reasonable” percentage of gross income for retirement savings.
What is a ‘reasonable’ savings goal for retirement?
As is often the case with high-income earners, many of our clients don’t have a budget or a clear picture of their current expenses and spending habits. That’s alright as long as they are building up a reasonable nest egg for the future – which begs the question of what is reasonable.
For mid-career docs, a reasonable goal to aim for is putting aside 20% of gross income for retirement. What you spend the rest of your money on is less important than how much you’re saving.
This is quite different from how you’ll handle expenses during retirement, when you no longer have a steady stream of income; rather, you have a pot of money that needs to last you another 20, 30, or even 40 years. At that point, thinking about specific expenses becomes more important (more on this topic later). That said, if you’re a mid-career doctor who is not meeting this 20% savings goal, it’s time to make a plan that will free up cash for retirement savings and investments.
Later-career docs: Calculate your spending level in retirement
Financial success means having a portfolio that can support your retirement dreams – with the confidence that your money will last and you won’t need to watch every dollar you spend. As you near retirement, your focus will shift away from accumulating savings to calculating the annual expenses you will have to meet in retirement.
A good place to start is figuring out which expenses will be necessary and which will be more flexible. To do this, separate your anticipated spending into these two categories:
- Fixed expenses: You can confidently forecast your “must-have” fixed expenses – such as property taxes, property/casualty insurance, health care costs, utilities, and groceries – because they remain steady from month to month.
- Discretionary expenses: These “like-to-have” expenses vary from month to month. This makes them harder to predict but easier to control. They might include dining out, travel, and charitable contributions.
As a retiree, understanding your fixed and discretionary expenses can help you prepare for a bear market, when the stock market can decline by 20% or more. Your portfolio won’t consist entirely of stocks, so it shouldn’t drop to that degree. Still, it will decline significantly. You may need to cut back on spending for a year or 2 to allow your portfolio to recover, particularly if the portfolio declines early in retirement.
Are you ready for retirement?
During the long bull market preceding the great recession of 2007 and 2009, many physicians retired –only to return to their practices when their portfolio values plummeted. In the exuberance of the moment, many failed to heed the warnings of many economists and got caught flat-footed.
Right now it’s a bull market, but we’re seeing concerning signs, such as an out-of-control housing market and rumblings about inflation and rising consumer costs. Sound familiar? If you hope to retire soon, take the time to objectively look around the corner so you can plan appropriately – whether your goal is to retire completely, stay in practice part-time, or even take on a new opportunity.
In an “it-depends” world, don’t be lured by a fictitious magic number, no matter what comes up when you Google: “When can I retire?” Instead, save early, imagine your dream retirement, and calculate expenses later to see what’s possible.
Dr. Greenwald is a graduate of the Albert Einstein College of Medicine, New York. Dr. Greenwald completed his internal medicine residency at the University of Minnesota, Minneapolis. He practiced internal medicine in the Twin Cities for 11 years before making the transition to financial planning for physicians, beginning in 1998.
A version of this article first appeared on Medscape.com.
“What’s my number?” When I hear this from my financial planning clients, I know they mean: In my 20-year career, this “magic number” is by far the most common thing physicians want to know.
If you look online, articles may recommend having a portfolio valued at $2 million, $5 million, and not uncommonly $10 million or more to retire. Really? $10 million? You might be thinking that surely not everyone needs that amount. Luckily, that’s true.
There’s no magic number your portfolio should be – just your number.
It’s human nature to want a simple, clear target to shoot for. But unfortunately, there’s no generic answer when it comes to saving for retirement. Even after a comprehensive hour-long review of a client’s financial plan – including insurance, investments, estate planning, and other items – the most honest answer I can give is: “It depends.” Not satisfying, I know. But there are still too many holes to fill.
By far the most important factor in getting beyond “it depends” is having an accurate estimate of annual retirement expenses. I have clients who live comfortably on $50,000 a year in retirement and others who need $250,000 or more. Knowing how much you need – your personal number – depends on the individual’s unique dream for retirement and calculating what that dream will cost.
Form a guesstimate based on savings and anticipated expenses
The total portfolio value needed to sustain an annual expense of $50,000 a year in retirement spending versus the portfolio size needed for $250,000 or more, blows apart the fiction of a universal “magic number.” It’s just not that simple. While it’s hard to gauge exactly what you will need, the right information can lead to a logical guesstimate about what size portfolio will provide you with financial independence.
In the end, it’s up to you to determine your desired retirement lifestyle. Then, the only way to get there is to calculate how much it will cost and save up for it by following a well-informed financial plan. This plan will be based on strategy that shifts from the middle to the later stages of your medical career and into retirement.
Let’s see how it works.
Early to mid-career: Focus on building up retirement savings
We ultimately want to save enough to meet our retirement expenses. But figuring out how much to save when you’re in your 40s and 50s is difficult. A mid-career physician likely has significant family- and child-related expenses. When we become empty-nesters, those expenses will decline. In retirement they may disappear entirely, but new expenses may arise.
With large variations in expenses at different life stages, it’s hard to calculate exactly how much you will need to save. Early on, the most sensible thing is putting aside a “reasonable” percentage of gross income for retirement savings.
What is a ‘reasonable’ savings goal for retirement?
As is often the case with high-income earners, many of our clients don’t have a budget or a clear picture of their current expenses and spending habits. That’s alright as long as they are building up a reasonable nest egg for the future – which begs the question of what is reasonable.
For mid-career docs, a reasonable goal to aim for is putting aside 20% of gross income for retirement. What you spend the rest of your money on is less important than how much you’re saving.
This is quite different from how you’ll handle expenses during retirement, when you no longer have a steady stream of income; rather, you have a pot of money that needs to last you another 20, 30, or even 40 years. At that point, thinking about specific expenses becomes more important (more on this topic later). That said, if you’re a mid-career doctor who is not meeting this 20% savings goal, it’s time to make a plan that will free up cash for retirement savings and investments.
Later-career docs: Calculate your spending level in retirement
Financial success means having a portfolio that can support your retirement dreams – with the confidence that your money will last and you won’t need to watch every dollar you spend. As you near retirement, your focus will shift away from accumulating savings to calculating the annual expenses you will have to meet in retirement.
A good place to start is figuring out which expenses will be necessary and which will be more flexible. To do this, separate your anticipated spending into these two categories:
- Fixed expenses: You can confidently forecast your “must-have” fixed expenses – such as property taxes, property/casualty insurance, health care costs, utilities, and groceries – because they remain steady from month to month.
- Discretionary expenses: These “like-to-have” expenses vary from month to month. This makes them harder to predict but easier to control. They might include dining out, travel, and charitable contributions.
As a retiree, understanding your fixed and discretionary expenses can help you prepare for a bear market, when the stock market can decline by 20% or more. Your portfolio won’t consist entirely of stocks, so it shouldn’t drop to that degree. Still, it will decline significantly. You may need to cut back on spending for a year or 2 to allow your portfolio to recover, particularly if the portfolio declines early in retirement.
Are you ready for retirement?
During the long bull market preceding the great recession of 2007 and 2009, many physicians retired –only to return to their practices when their portfolio values plummeted. In the exuberance of the moment, many failed to heed the warnings of many economists and got caught flat-footed.
Right now it’s a bull market, but we’re seeing concerning signs, such as an out-of-control housing market and rumblings about inflation and rising consumer costs. Sound familiar? If you hope to retire soon, take the time to objectively look around the corner so you can plan appropriately – whether your goal is to retire completely, stay in practice part-time, or even take on a new opportunity.
In an “it-depends” world, don’t be lured by a fictitious magic number, no matter what comes up when you Google: “When can I retire?” Instead, save early, imagine your dream retirement, and calculate expenses later to see what’s possible.
Dr. Greenwald is a graduate of the Albert Einstein College of Medicine, New York. Dr. Greenwald completed his internal medicine residency at the University of Minnesota, Minneapolis. He practiced internal medicine in the Twin Cities for 11 years before making the transition to financial planning for physicians, beginning in 1998.
A version of this article first appeared on Medscape.com.
“What’s my number?” When I hear this from my financial planning clients, I know they mean: In my 20-year career, this “magic number” is by far the most common thing physicians want to know.
If you look online, articles may recommend having a portfolio valued at $2 million, $5 million, and not uncommonly $10 million or more to retire. Really? $10 million? You might be thinking that surely not everyone needs that amount. Luckily, that’s true.
There’s no magic number your portfolio should be – just your number.
It’s human nature to want a simple, clear target to shoot for. But unfortunately, there’s no generic answer when it comes to saving for retirement. Even after a comprehensive hour-long review of a client’s financial plan – including insurance, investments, estate planning, and other items – the most honest answer I can give is: “It depends.” Not satisfying, I know. But there are still too many holes to fill.
By far the most important factor in getting beyond “it depends” is having an accurate estimate of annual retirement expenses. I have clients who live comfortably on $50,000 a year in retirement and others who need $250,000 or more. Knowing how much you need – your personal number – depends on the individual’s unique dream for retirement and calculating what that dream will cost.
Form a guesstimate based on savings and anticipated expenses
The total portfolio value needed to sustain an annual expense of $50,000 a year in retirement spending versus the portfolio size needed for $250,000 or more, blows apart the fiction of a universal “magic number.” It’s just not that simple. While it’s hard to gauge exactly what you will need, the right information can lead to a logical guesstimate about what size portfolio will provide you with financial independence.
In the end, it’s up to you to determine your desired retirement lifestyle. Then, the only way to get there is to calculate how much it will cost and save up for it by following a well-informed financial plan. This plan will be based on strategy that shifts from the middle to the later stages of your medical career and into retirement.
Let’s see how it works.
Early to mid-career: Focus on building up retirement savings
We ultimately want to save enough to meet our retirement expenses. But figuring out how much to save when you’re in your 40s and 50s is difficult. A mid-career physician likely has significant family- and child-related expenses. When we become empty-nesters, those expenses will decline. In retirement they may disappear entirely, but new expenses may arise.
With large variations in expenses at different life stages, it’s hard to calculate exactly how much you will need to save. Early on, the most sensible thing is putting aside a “reasonable” percentage of gross income for retirement savings.
What is a ‘reasonable’ savings goal for retirement?
As is often the case with high-income earners, many of our clients don’t have a budget or a clear picture of their current expenses and spending habits. That’s alright as long as they are building up a reasonable nest egg for the future – which begs the question of what is reasonable.
For mid-career docs, a reasonable goal to aim for is putting aside 20% of gross income for retirement. What you spend the rest of your money on is less important than how much you’re saving.
This is quite different from how you’ll handle expenses during retirement, when you no longer have a steady stream of income; rather, you have a pot of money that needs to last you another 20, 30, or even 40 years. At that point, thinking about specific expenses becomes more important (more on this topic later). That said, if you’re a mid-career doctor who is not meeting this 20% savings goal, it’s time to make a plan that will free up cash for retirement savings and investments.
Later-career docs: Calculate your spending level in retirement
Financial success means having a portfolio that can support your retirement dreams – with the confidence that your money will last and you won’t need to watch every dollar you spend. As you near retirement, your focus will shift away from accumulating savings to calculating the annual expenses you will have to meet in retirement.
A good place to start is figuring out which expenses will be necessary and which will be more flexible. To do this, separate your anticipated spending into these two categories:
- Fixed expenses: You can confidently forecast your “must-have” fixed expenses – such as property taxes, property/casualty insurance, health care costs, utilities, and groceries – because they remain steady from month to month.
- Discretionary expenses: These “like-to-have” expenses vary from month to month. This makes them harder to predict but easier to control. They might include dining out, travel, and charitable contributions.
As a retiree, understanding your fixed and discretionary expenses can help you prepare for a bear market, when the stock market can decline by 20% or more. Your portfolio won’t consist entirely of stocks, so it shouldn’t drop to that degree. Still, it will decline significantly. You may need to cut back on spending for a year or 2 to allow your portfolio to recover, particularly if the portfolio declines early in retirement.
Are you ready for retirement?
During the long bull market preceding the great recession of 2007 and 2009, many physicians retired –only to return to their practices when their portfolio values plummeted. In the exuberance of the moment, many failed to heed the warnings of many economists and got caught flat-footed.
Right now it’s a bull market, but we’re seeing concerning signs, such as an out-of-control housing market and rumblings about inflation and rising consumer costs. Sound familiar? If you hope to retire soon, take the time to objectively look around the corner so you can plan appropriately – whether your goal is to retire completely, stay in practice part-time, or even take on a new opportunity.
In an “it-depends” world, don’t be lured by a fictitious magic number, no matter what comes up when you Google: “When can I retire?” Instead, save early, imagine your dream retirement, and calculate expenses later to see what’s possible.
Dr. Greenwald is a graduate of the Albert Einstein College of Medicine, New York. Dr. Greenwald completed his internal medicine residency at the University of Minnesota, Minneapolis. He practiced internal medicine in the Twin Cities for 11 years before making the transition to financial planning for physicians, beginning in 1998.
A version of this article first appeared on Medscape.com.