User login
Researchers probe ‘systematic error’ in gun injury data
These coding inaccuracies could distort our understanding of gun violence in the United States and make it seem like accidental shootings are more common than they really are, researchers reported in JAMA Network Open.
“The systematic error in intent classification is not widely known or acknowledged by researchers in this field,” Philip J. Cook, PhD, of Duke University, Durham, N.C., and Susan T. Parker, of the University of Michigan, Ann Arbor, wrote in an invited commentary about the new findings. “The bulk of all shootings, nonfatal and fatal together, are assaults, which is to say the result of one person intentionally shooting another. An accurate statistical portrait thus suggests that gun violence is predominantly a crime problem.”
In 2020, 79% of all homicides and 53% of all suicides involved firearms, the CDC reported. Gun violence is now the leading cause of death for children in the United States, government data show.
For the new study, Matthew Miller, MD, ScD, of Northeastern University and the Harvard Injury Control Research Center in Boston, and his colleagues examined how International Classification of Diseases (ICD) codes may misclassify the intent behind gunshot injuries.
Dr. Miller’s group looked at 1,227 incidents between 2008 and 2019 at three major trauma centers – Brigham and Women’s Hospital and Massachusetts General Hospital, both in Boston, and Harborview Medical Center in Seattle.
Of those shootings, 837 (68.2%) involved assaults, 168 (13.5%) were unintentional, 124 (9.9%) were deliberate self-harm, and 43 (3.4%) were instances of legal intervention, based on the researchers’ review of medical records.
ICD codes at discharge, however, labeled 581 cases (47.4%) as assaults and 432 (35.2%) as unintentional.
The researchers found that 234 of the 837 assaults (28%) and 9 of the 43 legal interventions (20.9%) were miscoded as unintentional. This problem occurred even when the “medical narrative explicitly indicated that the shooting was an act of interpersonal violence,” such as a drive-by shooting or an act of domestic violence, the researchers reported.
Hospital trauma registrars, who detail the circumstances surrounding injuries, were mostly in agreement with the researchers.
Medical coders “would likely have little trouble characterizing firearm injury intent accurately if incentives were created for them to do so,” the authors wrote.
Trends and interventions
Separately, researchers published studies showing that gun violence tends to affect various demographics differently, and that remediating abandoned houses could help reduce gun crime.
Lindsay Young, of the University of Cincinnati, and Henry Xiang, MD, PhD, director of the Center for Pediatric Trauma Research at Nationwide Children’s Hospital in Columbus, Ohio, analyzed rates of firearm deaths from 1981 to 2020.
They found that the rate of firearm-related homicide was five times higher among males than females, and the rate of suicide involving firearms was nearly seven times higher for men, they reported in PLOS ONE.
Black men were the group most affected by homicide, whereas White men were most affected by suicide, they found.
To see if fixing abandoned properties would improve health and reduce gun violence in low-income, Black neighborhoods in Philadelphia, Eugenia C. South, MD, of the University of Pennsylvania, Philadelphia, and colleagues conducted a randomized trial.
They randomly assigned abandoned properties in some areas to undergo full remediation (installing working windows and doors, cleaning trash, and weeding); trash cleanup and weeding only; or no intervention.
“Abandoned houses that were remediated showed substantial drops in nearby weapons violations (−8.43%), gun assaults (−13.12%), and to a lesser extent shootings (−6.96%),” the researchers reported.
The intervention targets effects of segregation that have resulted from “historical and ongoing government and private-sector policies” that lead to disinvestment in Black, urban communities, they wrote. Abandoned houses can be used to store firearms and for other illegal activity. They also can engender feelings of fear, neglect, and stress in communities, the researchers noted.
Dr. Miller’s study was funded by the National Collaborative on Gun Violence Research; coauthors disclosed corporate, government, and university grants. The full list of disclosures can be found with the original article. Editorialists Dr. Cook and Dr. Parker report no relevant financial relationships. Dr. South’s study was funded by the National Institutes of Health. Dr. South and some coauthors disclosed government grants.
A version of this article first appeared on Medscape.com.
These coding inaccuracies could distort our understanding of gun violence in the United States and make it seem like accidental shootings are more common than they really are, researchers reported in JAMA Network Open.
“The systematic error in intent classification is not widely known or acknowledged by researchers in this field,” Philip J. Cook, PhD, of Duke University, Durham, N.C., and Susan T. Parker, of the University of Michigan, Ann Arbor, wrote in an invited commentary about the new findings. “The bulk of all shootings, nonfatal and fatal together, are assaults, which is to say the result of one person intentionally shooting another. An accurate statistical portrait thus suggests that gun violence is predominantly a crime problem.”
In 2020, 79% of all homicides and 53% of all suicides involved firearms, the CDC reported. Gun violence is now the leading cause of death for children in the United States, government data show.
For the new study, Matthew Miller, MD, ScD, of Northeastern University and the Harvard Injury Control Research Center in Boston, and his colleagues examined how International Classification of Diseases (ICD) codes may misclassify the intent behind gunshot injuries.
Dr. Miller’s group looked at 1,227 incidents between 2008 and 2019 at three major trauma centers – Brigham and Women’s Hospital and Massachusetts General Hospital, both in Boston, and Harborview Medical Center in Seattle.
Of those shootings, 837 (68.2%) involved assaults, 168 (13.5%) were unintentional, 124 (9.9%) were deliberate self-harm, and 43 (3.4%) were instances of legal intervention, based on the researchers’ review of medical records.
ICD codes at discharge, however, labeled 581 cases (47.4%) as assaults and 432 (35.2%) as unintentional.
The researchers found that 234 of the 837 assaults (28%) and 9 of the 43 legal interventions (20.9%) were miscoded as unintentional. This problem occurred even when the “medical narrative explicitly indicated that the shooting was an act of interpersonal violence,” such as a drive-by shooting or an act of domestic violence, the researchers reported.
Hospital trauma registrars, who detail the circumstances surrounding injuries, were mostly in agreement with the researchers.
Medical coders “would likely have little trouble characterizing firearm injury intent accurately if incentives were created for them to do so,” the authors wrote.
Trends and interventions
Separately, researchers published studies showing that gun violence tends to affect various demographics differently, and that remediating abandoned houses could help reduce gun crime.
Lindsay Young, of the University of Cincinnati, and Henry Xiang, MD, PhD, director of the Center for Pediatric Trauma Research at Nationwide Children’s Hospital in Columbus, Ohio, analyzed rates of firearm deaths from 1981 to 2020.
They found that the rate of firearm-related homicide was five times higher among males than females, and the rate of suicide involving firearms was nearly seven times higher for men, they reported in PLOS ONE.
Black men were the group most affected by homicide, whereas White men were most affected by suicide, they found.
To see if fixing abandoned properties would improve health and reduce gun violence in low-income, Black neighborhoods in Philadelphia, Eugenia C. South, MD, of the University of Pennsylvania, Philadelphia, and colleagues conducted a randomized trial.
They randomly assigned abandoned properties in some areas to undergo full remediation (installing working windows and doors, cleaning trash, and weeding); trash cleanup and weeding only; or no intervention.
“Abandoned houses that were remediated showed substantial drops in nearby weapons violations (−8.43%), gun assaults (−13.12%), and to a lesser extent shootings (−6.96%),” the researchers reported.
The intervention targets effects of segregation that have resulted from “historical and ongoing government and private-sector policies” that lead to disinvestment in Black, urban communities, they wrote. Abandoned houses can be used to store firearms and for other illegal activity. They also can engender feelings of fear, neglect, and stress in communities, the researchers noted.
Dr. Miller’s study was funded by the National Collaborative on Gun Violence Research; coauthors disclosed corporate, government, and university grants. The full list of disclosures can be found with the original article. Editorialists Dr. Cook and Dr. Parker report no relevant financial relationships. Dr. South’s study was funded by the National Institutes of Health. Dr. South and some coauthors disclosed government grants.
A version of this article first appeared on Medscape.com.
These coding inaccuracies could distort our understanding of gun violence in the United States and make it seem like accidental shootings are more common than they really are, researchers reported in JAMA Network Open.
“The systematic error in intent classification is not widely known or acknowledged by researchers in this field,” Philip J. Cook, PhD, of Duke University, Durham, N.C., and Susan T. Parker, of the University of Michigan, Ann Arbor, wrote in an invited commentary about the new findings. “The bulk of all shootings, nonfatal and fatal together, are assaults, which is to say the result of one person intentionally shooting another. An accurate statistical portrait thus suggests that gun violence is predominantly a crime problem.”
In 2020, 79% of all homicides and 53% of all suicides involved firearms, the CDC reported. Gun violence is now the leading cause of death for children in the United States, government data show.
For the new study, Matthew Miller, MD, ScD, of Northeastern University and the Harvard Injury Control Research Center in Boston, and his colleagues examined how International Classification of Diseases (ICD) codes may misclassify the intent behind gunshot injuries.
Dr. Miller’s group looked at 1,227 incidents between 2008 and 2019 at three major trauma centers – Brigham and Women’s Hospital and Massachusetts General Hospital, both in Boston, and Harborview Medical Center in Seattle.
Of those shootings, 837 (68.2%) involved assaults, 168 (13.5%) were unintentional, 124 (9.9%) were deliberate self-harm, and 43 (3.4%) were instances of legal intervention, based on the researchers’ review of medical records.
ICD codes at discharge, however, labeled 581 cases (47.4%) as assaults and 432 (35.2%) as unintentional.
The researchers found that 234 of the 837 assaults (28%) and 9 of the 43 legal interventions (20.9%) were miscoded as unintentional. This problem occurred even when the “medical narrative explicitly indicated that the shooting was an act of interpersonal violence,” such as a drive-by shooting or an act of domestic violence, the researchers reported.
Hospital trauma registrars, who detail the circumstances surrounding injuries, were mostly in agreement with the researchers.
Medical coders “would likely have little trouble characterizing firearm injury intent accurately if incentives were created for them to do so,” the authors wrote.
Trends and interventions
Separately, researchers published studies showing that gun violence tends to affect various demographics differently, and that remediating abandoned houses could help reduce gun crime.
Lindsay Young, of the University of Cincinnati, and Henry Xiang, MD, PhD, director of the Center for Pediatric Trauma Research at Nationwide Children’s Hospital in Columbus, Ohio, analyzed rates of firearm deaths from 1981 to 2020.
They found that the rate of firearm-related homicide was five times higher among males than females, and the rate of suicide involving firearms was nearly seven times higher for men, they reported in PLOS ONE.
Black men were the group most affected by homicide, whereas White men were most affected by suicide, they found.
To see if fixing abandoned properties would improve health and reduce gun violence in low-income, Black neighborhoods in Philadelphia, Eugenia C. South, MD, of the University of Pennsylvania, Philadelphia, and colleagues conducted a randomized trial.
They randomly assigned abandoned properties in some areas to undergo full remediation (installing working windows and doors, cleaning trash, and weeding); trash cleanup and weeding only; or no intervention.
“Abandoned houses that were remediated showed substantial drops in nearby weapons violations (−8.43%), gun assaults (−13.12%), and to a lesser extent shootings (−6.96%),” the researchers reported.
The intervention targets effects of segregation that have resulted from “historical and ongoing government and private-sector policies” that lead to disinvestment in Black, urban communities, they wrote. Abandoned houses can be used to store firearms and for other illegal activity. They also can engender feelings of fear, neglect, and stress in communities, the researchers noted.
Dr. Miller’s study was funded by the National Collaborative on Gun Violence Research; coauthors disclosed corporate, government, and university grants. The full list of disclosures can be found with the original article. Editorialists Dr. Cook and Dr. Parker report no relevant financial relationships. Dr. South’s study was funded by the National Institutes of Health. Dr. South and some coauthors disclosed government grants.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
COVID booster shot poll: People ‘don’t think they need one’
Now, a new poll shows why so few people are willing to roll up their sleeves again.
The most common reasons people give for not getting the latest booster shot is that they “don’t think they need one” (44%) and they “don’t think the benefits are worth it” (37%), according to poll results from the Kaiser Family Foundation.
The data comes amid announcements by the Centers for Disease Control and Prevention that boosters reduced COVID-19 hospitalizations by up to 57% for U.S. adults and by up to 84% for people age 65 and older. Those figures are just the latest in a mountain of research reporting the public health benefits of COVID-19 vaccines.
Despite all of the statistical data, health officials’ recent vaccination campaigns have proven far from compelling.
So far, just 15% of people age 12 and older have gotten the latest booster, and 36% of people age 65 and older have gotten it, the CDC’s vaccination trackershows.
Since the start of the pandemic, 1.1 million people in the U.S. have died from COVID-19, with the number of deaths currently rising by 400 per day, The New York Times COVID tracker shows.
Many experts continue to note the need for everyone to get booster shots regularly, but some advocate that perhaps a change in strategy is in order.
“What the administration should do is push for vaccinating people in high-risk groups, including those who are older, those who are immunocompromised and those who have comorbidities,” Paul Offitt, MD, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, told CNN.
Federal regulators have announced they will meet Jan. 26 with a panel of vaccine advisors to examine the current recommended vaccination schedule as well as look at the effectiveness and composition of current vaccines and boosters, with an eye toward the make-up of next-generation shots.
Vaccines are the “best available protection” against hospitalization and death caused by COVID-19, said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, in a statement announcing the planned meeting.
“Since the initial authorizations of these vaccines, we have learned that protection wanes over time, especially as the virus rapidly mutates and new variants and subvariants emerge,” he said. “Therefore, it’s important to continue discussions about the optimal composition of COVID-19 vaccines for primary and booster vaccination, as well as the optimal interval for booster vaccination.”
A version of this article first appeared on WebMD.com.
Now, a new poll shows why so few people are willing to roll up their sleeves again.
The most common reasons people give for not getting the latest booster shot is that they “don’t think they need one” (44%) and they “don’t think the benefits are worth it” (37%), according to poll results from the Kaiser Family Foundation.
The data comes amid announcements by the Centers for Disease Control and Prevention that boosters reduced COVID-19 hospitalizations by up to 57% for U.S. adults and by up to 84% for people age 65 and older. Those figures are just the latest in a mountain of research reporting the public health benefits of COVID-19 vaccines.
Despite all of the statistical data, health officials’ recent vaccination campaigns have proven far from compelling.
So far, just 15% of people age 12 and older have gotten the latest booster, and 36% of people age 65 and older have gotten it, the CDC’s vaccination trackershows.
Since the start of the pandemic, 1.1 million people in the U.S. have died from COVID-19, with the number of deaths currently rising by 400 per day, The New York Times COVID tracker shows.
Many experts continue to note the need for everyone to get booster shots regularly, but some advocate that perhaps a change in strategy is in order.
“What the administration should do is push for vaccinating people in high-risk groups, including those who are older, those who are immunocompromised and those who have comorbidities,” Paul Offitt, MD, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, told CNN.
Federal regulators have announced they will meet Jan. 26 with a panel of vaccine advisors to examine the current recommended vaccination schedule as well as look at the effectiveness and composition of current vaccines and boosters, with an eye toward the make-up of next-generation shots.
Vaccines are the “best available protection” against hospitalization and death caused by COVID-19, said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, in a statement announcing the planned meeting.
“Since the initial authorizations of these vaccines, we have learned that protection wanes over time, especially as the virus rapidly mutates and new variants and subvariants emerge,” he said. “Therefore, it’s important to continue discussions about the optimal composition of COVID-19 vaccines for primary and booster vaccination, as well as the optimal interval for booster vaccination.”
A version of this article first appeared on WebMD.com.
Now, a new poll shows why so few people are willing to roll up their sleeves again.
The most common reasons people give for not getting the latest booster shot is that they “don’t think they need one” (44%) and they “don’t think the benefits are worth it” (37%), according to poll results from the Kaiser Family Foundation.
The data comes amid announcements by the Centers for Disease Control and Prevention that boosters reduced COVID-19 hospitalizations by up to 57% for U.S. adults and by up to 84% for people age 65 and older. Those figures are just the latest in a mountain of research reporting the public health benefits of COVID-19 vaccines.
Despite all of the statistical data, health officials’ recent vaccination campaigns have proven far from compelling.
So far, just 15% of people age 12 and older have gotten the latest booster, and 36% of people age 65 and older have gotten it, the CDC’s vaccination trackershows.
Since the start of the pandemic, 1.1 million people in the U.S. have died from COVID-19, with the number of deaths currently rising by 400 per day, The New York Times COVID tracker shows.
Many experts continue to note the need for everyone to get booster shots regularly, but some advocate that perhaps a change in strategy is in order.
“What the administration should do is push for vaccinating people in high-risk groups, including those who are older, those who are immunocompromised and those who have comorbidities,” Paul Offitt, MD, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, told CNN.
Federal regulators have announced they will meet Jan. 26 with a panel of vaccine advisors to examine the current recommended vaccination schedule as well as look at the effectiveness and composition of current vaccines and boosters, with an eye toward the make-up of next-generation shots.
Vaccines are the “best available protection” against hospitalization and death caused by COVID-19, said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, in a statement announcing the planned meeting.
“Since the initial authorizations of these vaccines, we have learned that protection wanes over time, especially as the virus rapidly mutates and new variants and subvariants emerge,” he said. “Therefore, it’s important to continue discussions about the optimal composition of COVID-19 vaccines for primary and booster vaccination, as well as the optimal interval for booster vaccination.”
A version of this article first appeared on WebMD.com.
Hospitals with more diverse and uninsured patients more likely to provide delayed fracture care
Regardless of individual patient-level characteristics such as race, ethnicity, or insurance status, these patients were more likely to miss the recommended 24-hour benchmark for surgery.
“Institutions that treat a less diverse patient population appeared to be more resilient to the mix of insurance status in their patient population and were more likely to meet time-to-surgery benchmarks, regardless of patient insurance status or population-based insurance mix,” write study author Ida Leah Gitajn, MD, an orthopedic trauma surgeon at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and colleagues.
“While it is unsurprising that increased delays were associated with underfunded institutions, the association between institutional-level racial disparity and surgical delays implies structural health systems bias,” the authors wrote.
The study was published online in JAMA Network Open.
Site performance varied
Racial inequalities in health care utilization and outcomes have been documented in many medical specialties, including orthopedic trauma, the study authors write. However, previous studies evaluating racial disparities in fracture care have been limited to patient-level associations rather than hospital-level factors.
The investigators conducted a secondary analysis of prospectively collected multicenter data for 2,565 patients with hip and femur fractures enrolled in two randomized trials at 23 sites in the United States and Canada. The researchers assessed whether disparities in meeting 24-hour time-to-surgery benchmarks exist at the patient level or at the institutional level, evaluating the association of race, ethnicity, and insurance status.
The cohort study used data from the Program of Randomized Trials to Evaluate Preoperative Antiseptic Skin Solutions in Orthopaedic Trauma (PREP-IT), which enrolled patients from 2018-2021 and followed them for 1 year. All patients with hip and femur fractures enrolled in the PREP-IT program were included in the analysis, which was conducted from April to September of this year.
The cohort included 2,565 patients with an average age of about 65 years. About 82% of patients were White, 13.4% were Black, 3.2% were Asian, and 1.1% were classified as another race or ethnicity. Among the study population, 32.5% of participants were employed, and 92.2% had health insurance. Nearly 40% had a femur fracture with an average injury severity score of 10.4.
Overall, 596 patients (23.2%) didn’t meet the 24-hour time-to-operating-room benchmark. Patients who didn’t meet the 24-hour surgical window were more likely to be older, women, and have a femur fracture. They were less likely to be employed.
The 23 sites had variability in meeting the 24-hour benchmark, race and ethnicity distribution, and population-based health insurance. Institutions met benchmarks at frequencies ranging from 45.2% (for 196 of 433 procedures) to 97.4% (37 of 38 procedures). Minority race and ethnicity distribution ranged from 0% (in 99 procedures) to 58.2% (in 53 of 91 procedures). The proportion of uninsured patients ranged from 0% (in 64 procedures) to 34.2% (in 13 of 38 procedures).
At the patient level, there was no association between missing the 24-hour benchmark and race or ethnicity, and there was no independent association between hospital population racial composition and surgical delay. In an analysis that controlled for patient-level characteristics, there was no association between missing the 24-hour benchmark and patient-level insurance status.
There was an independent association, however, between the hospital population insurance coverage and hospital population racial composition as an interaction term, suggesting a moderating effect (P = .03), the study authors write.
At low rates of uninsured patients, the probability of missing the 24-hour benchmark was 12.5%-14.6% when racial composition varied from 0%-50% minority patients. In contrast, at higher rates of uninsured patients, the risk of missing the 24-hour window was higher among more diverse populations. For instance, at 30% uninsured, the risk of missing the benchmark was 0.5% when the racial composition was low and 17.6% at 50% minority patients.
Additional studies are needed to understand the findings and how health system programs or structures play a role, the authors write. For instance, well-funded health systems that care for a higher proportion of insured patients likely have quality improvement programs and other support structures, such as operating room access, that ensure appropriate time-to-surgery benchmarks for time-sensitive fractures, they say.
Addressing inequalities
Troy Amen, MD, MBA, an orthopedic surgery resident at the Hospital for Special Surgery, New York, said, “Despite these disparities being reported and well documented in recent years, unfortunately, not enough has been done to address them or understand their fundamental root causes.”
Dr. Amen, who wasn’t involved with this study, has researched racial and ethnic disparities in hip fracture surgery care across the United States. He and his colleagues found disparities in delayed time-to-surgery, particularly for Black patients.
“We live in a country and society where we want and strive for equality of care for patients regardless of race, ethnicity, gender, sexual orientation, or background,” he said. “We have a moral imperative to address these disparities as health care providers, not only among ourselves, but also in conjunction with lawmakers, hospital administrators, and health policy specialists.”
Uma Srikumaran, MD, an associate professor of orthopedic surgery at Johns Hopkins University, Baltimore, wasn’t involved with this study but has researched racial disparities in the timing of radiographic assessment and surgical treatment of hip fractures.
“Though we understand that racial disparities are pervasive in health care, we have a great deal left to understand about the extent of those disparities and all the various factors that contribute to them,” Dr. Srikumaran told this news organization.
Dr. Srikumaran and colleagues have found that Black patients had longer wait times for evaluation and surgery than White patients.
“We all want to get to the solutions, but those can be difficult to execute without an intricate understanding of the problem,” he said. “We should encourage this type of research all throughout health care in general but also very locally, as solutions are not likely to be one-size-fits-all.”
Dr. Srikumaran pointed to the need to measure the problem in specific pathologies, populations, geographies, hospital types, and other factors.
“Studying the trends of this issue will help us determine whether our national or local initiatives are making a difference and which interventions are most effective for a particular hospital, geographic location, or particular pathology,” he said. “Accordingly, if a particular hospital or health system isn’t looking at differences in the delivery of care by race, they are missing an opportunity to ensure equity and raise overall quality.”
The study was supported by funding from the Patient Centered Outcomes Research Institute. Dr. Gitajn reported receiving personal fees for consulting and teaching work from Stryker outside the submitted work. Dr. Amen and Dr. Srikumaran reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Regardless of individual patient-level characteristics such as race, ethnicity, or insurance status, these patients were more likely to miss the recommended 24-hour benchmark for surgery.
“Institutions that treat a less diverse patient population appeared to be more resilient to the mix of insurance status in their patient population and were more likely to meet time-to-surgery benchmarks, regardless of patient insurance status or population-based insurance mix,” write study author Ida Leah Gitajn, MD, an orthopedic trauma surgeon at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and colleagues.
“While it is unsurprising that increased delays were associated with underfunded institutions, the association between institutional-level racial disparity and surgical delays implies structural health systems bias,” the authors wrote.
The study was published online in JAMA Network Open.
Site performance varied
Racial inequalities in health care utilization and outcomes have been documented in many medical specialties, including orthopedic trauma, the study authors write. However, previous studies evaluating racial disparities in fracture care have been limited to patient-level associations rather than hospital-level factors.
The investigators conducted a secondary analysis of prospectively collected multicenter data for 2,565 patients with hip and femur fractures enrolled in two randomized trials at 23 sites in the United States and Canada. The researchers assessed whether disparities in meeting 24-hour time-to-surgery benchmarks exist at the patient level or at the institutional level, evaluating the association of race, ethnicity, and insurance status.
The cohort study used data from the Program of Randomized Trials to Evaluate Preoperative Antiseptic Skin Solutions in Orthopaedic Trauma (PREP-IT), which enrolled patients from 2018-2021 and followed them for 1 year. All patients with hip and femur fractures enrolled in the PREP-IT program were included in the analysis, which was conducted from April to September of this year.
The cohort included 2,565 patients with an average age of about 65 years. About 82% of patients were White, 13.4% were Black, 3.2% were Asian, and 1.1% were classified as another race or ethnicity. Among the study population, 32.5% of participants were employed, and 92.2% had health insurance. Nearly 40% had a femur fracture with an average injury severity score of 10.4.
Overall, 596 patients (23.2%) didn’t meet the 24-hour time-to-operating-room benchmark. Patients who didn’t meet the 24-hour surgical window were more likely to be older, women, and have a femur fracture. They were less likely to be employed.
The 23 sites had variability in meeting the 24-hour benchmark, race and ethnicity distribution, and population-based health insurance. Institutions met benchmarks at frequencies ranging from 45.2% (for 196 of 433 procedures) to 97.4% (37 of 38 procedures). Minority race and ethnicity distribution ranged from 0% (in 99 procedures) to 58.2% (in 53 of 91 procedures). The proportion of uninsured patients ranged from 0% (in 64 procedures) to 34.2% (in 13 of 38 procedures).
At the patient level, there was no association between missing the 24-hour benchmark and race or ethnicity, and there was no independent association between hospital population racial composition and surgical delay. In an analysis that controlled for patient-level characteristics, there was no association between missing the 24-hour benchmark and patient-level insurance status.
There was an independent association, however, between the hospital population insurance coverage and hospital population racial composition as an interaction term, suggesting a moderating effect (P = .03), the study authors write.
At low rates of uninsured patients, the probability of missing the 24-hour benchmark was 12.5%-14.6% when racial composition varied from 0%-50% minority patients. In contrast, at higher rates of uninsured patients, the risk of missing the 24-hour window was higher among more diverse populations. For instance, at 30% uninsured, the risk of missing the benchmark was 0.5% when the racial composition was low and 17.6% at 50% minority patients.
Additional studies are needed to understand the findings and how health system programs or structures play a role, the authors write. For instance, well-funded health systems that care for a higher proportion of insured patients likely have quality improvement programs and other support structures, such as operating room access, that ensure appropriate time-to-surgery benchmarks for time-sensitive fractures, they say.
Addressing inequalities
Troy Amen, MD, MBA, an orthopedic surgery resident at the Hospital for Special Surgery, New York, said, “Despite these disparities being reported and well documented in recent years, unfortunately, not enough has been done to address them or understand their fundamental root causes.”
Dr. Amen, who wasn’t involved with this study, has researched racial and ethnic disparities in hip fracture surgery care across the United States. He and his colleagues found disparities in delayed time-to-surgery, particularly for Black patients.
“We live in a country and society where we want and strive for equality of care for patients regardless of race, ethnicity, gender, sexual orientation, or background,” he said. “We have a moral imperative to address these disparities as health care providers, not only among ourselves, but also in conjunction with lawmakers, hospital administrators, and health policy specialists.”
Uma Srikumaran, MD, an associate professor of orthopedic surgery at Johns Hopkins University, Baltimore, wasn’t involved with this study but has researched racial disparities in the timing of radiographic assessment and surgical treatment of hip fractures.
“Though we understand that racial disparities are pervasive in health care, we have a great deal left to understand about the extent of those disparities and all the various factors that contribute to them,” Dr. Srikumaran told this news organization.
Dr. Srikumaran and colleagues have found that Black patients had longer wait times for evaluation and surgery than White patients.
“We all want to get to the solutions, but those can be difficult to execute without an intricate understanding of the problem,” he said. “We should encourage this type of research all throughout health care in general but also very locally, as solutions are not likely to be one-size-fits-all.”
Dr. Srikumaran pointed to the need to measure the problem in specific pathologies, populations, geographies, hospital types, and other factors.
“Studying the trends of this issue will help us determine whether our national or local initiatives are making a difference and which interventions are most effective for a particular hospital, geographic location, or particular pathology,” he said. “Accordingly, if a particular hospital or health system isn’t looking at differences in the delivery of care by race, they are missing an opportunity to ensure equity and raise overall quality.”
The study was supported by funding from the Patient Centered Outcomes Research Institute. Dr. Gitajn reported receiving personal fees for consulting and teaching work from Stryker outside the submitted work. Dr. Amen and Dr. Srikumaran reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Regardless of individual patient-level characteristics such as race, ethnicity, or insurance status, these patients were more likely to miss the recommended 24-hour benchmark for surgery.
“Institutions that treat a less diverse patient population appeared to be more resilient to the mix of insurance status in their patient population and were more likely to meet time-to-surgery benchmarks, regardless of patient insurance status or population-based insurance mix,” write study author Ida Leah Gitajn, MD, an orthopedic trauma surgeon at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and colleagues.
“While it is unsurprising that increased delays were associated with underfunded institutions, the association between institutional-level racial disparity and surgical delays implies structural health systems bias,” the authors wrote.
The study was published online in JAMA Network Open.
Site performance varied
Racial inequalities in health care utilization and outcomes have been documented in many medical specialties, including orthopedic trauma, the study authors write. However, previous studies evaluating racial disparities in fracture care have been limited to patient-level associations rather than hospital-level factors.
The investigators conducted a secondary analysis of prospectively collected multicenter data for 2,565 patients with hip and femur fractures enrolled in two randomized trials at 23 sites in the United States and Canada. The researchers assessed whether disparities in meeting 24-hour time-to-surgery benchmarks exist at the patient level or at the institutional level, evaluating the association of race, ethnicity, and insurance status.
The cohort study used data from the Program of Randomized Trials to Evaluate Preoperative Antiseptic Skin Solutions in Orthopaedic Trauma (PREP-IT), which enrolled patients from 2018-2021 and followed them for 1 year. All patients with hip and femur fractures enrolled in the PREP-IT program were included in the analysis, which was conducted from April to September of this year.
The cohort included 2,565 patients with an average age of about 65 years. About 82% of patients were White, 13.4% were Black, 3.2% were Asian, and 1.1% were classified as another race or ethnicity. Among the study population, 32.5% of participants were employed, and 92.2% had health insurance. Nearly 40% had a femur fracture with an average injury severity score of 10.4.
Overall, 596 patients (23.2%) didn’t meet the 24-hour time-to-operating-room benchmark. Patients who didn’t meet the 24-hour surgical window were more likely to be older, women, and have a femur fracture. They were less likely to be employed.
The 23 sites had variability in meeting the 24-hour benchmark, race and ethnicity distribution, and population-based health insurance. Institutions met benchmarks at frequencies ranging from 45.2% (for 196 of 433 procedures) to 97.4% (37 of 38 procedures). Minority race and ethnicity distribution ranged from 0% (in 99 procedures) to 58.2% (in 53 of 91 procedures). The proportion of uninsured patients ranged from 0% (in 64 procedures) to 34.2% (in 13 of 38 procedures).
At the patient level, there was no association between missing the 24-hour benchmark and race or ethnicity, and there was no independent association between hospital population racial composition and surgical delay. In an analysis that controlled for patient-level characteristics, there was no association between missing the 24-hour benchmark and patient-level insurance status.
There was an independent association, however, between the hospital population insurance coverage and hospital population racial composition as an interaction term, suggesting a moderating effect (P = .03), the study authors write.
At low rates of uninsured patients, the probability of missing the 24-hour benchmark was 12.5%-14.6% when racial composition varied from 0%-50% minority patients. In contrast, at higher rates of uninsured patients, the risk of missing the 24-hour window was higher among more diverse populations. For instance, at 30% uninsured, the risk of missing the benchmark was 0.5% when the racial composition was low and 17.6% at 50% minority patients.
Additional studies are needed to understand the findings and how health system programs or structures play a role, the authors write. For instance, well-funded health systems that care for a higher proportion of insured patients likely have quality improvement programs and other support structures, such as operating room access, that ensure appropriate time-to-surgery benchmarks for time-sensitive fractures, they say.
Addressing inequalities
Troy Amen, MD, MBA, an orthopedic surgery resident at the Hospital for Special Surgery, New York, said, “Despite these disparities being reported and well documented in recent years, unfortunately, not enough has been done to address them or understand their fundamental root causes.”
Dr. Amen, who wasn’t involved with this study, has researched racial and ethnic disparities in hip fracture surgery care across the United States. He and his colleagues found disparities in delayed time-to-surgery, particularly for Black patients.
“We live in a country and society where we want and strive for equality of care for patients regardless of race, ethnicity, gender, sexual orientation, or background,” he said. “We have a moral imperative to address these disparities as health care providers, not only among ourselves, but also in conjunction with lawmakers, hospital administrators, and health policy specialists.”
Uma Srikumaran, MD, an associate professor of orthopedic surgery at Johns Hopkins University, Baltimore, wasn’t involved with this study but has researched racial disparities in the timing of radiographic assessment and surgical treatment of hip fractures.
“Though we understand that racial disparities are pervasive in health care, we have a great deal left to understand about the extent of those disparities and all the various factors that contribute to them,” Dr. Srikumaran told this news organization.
Dr. Srikumaran and colleagues have found that Black patients had longer wait times for evaluation and surgery than White patients.
“We all want to get to the solutions, but those can be difficult to execute without an intricate understanding of the problem,” he said. “We should encourage this type of research all throughout health care in general but also very locally, as solutions are not likely to be one-size-fits-all.”
Dr. Srikumaran pointed to the need to measure the problem in specific pathologies, populations, geographies, hospital types, and other factors.
“Studying the trends of this issue will help us determine whether our national or local initiatives are making a difference and which interventions are most effective for a particular hospital, geographic location, or particular pathology,” he said. “Accordingly, if a particular hospital or health system isn’t looking at differences in the delivery of care by race, they are missing an opportunity to ensure equity and raise overall quality.”
The study was supported by funding from the Patient Centered Outcomes Research Institute. Dr. Gitajn reported receiving personal fees for consulting and teaching work from Stryker outside the submitted work. Dr. Amen and Dr. Srikumaran reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
‘The Whale’: Is this new movie fat-phobic or fat-friendly?
“I could relate to many, many, many of the experiences and emotions that Charlie, which is Brendan Fraser’s character, was portraying,” Patricia Nece recalls after watching a preview copy of the new film “The Whale.”

Much of the movie “rang true and hit home for me as things that I, too, had experienced,” Ms. Nece, the board of directors’ chair of the Obesity Action Coalition (OAC) and a person living with obesity, shares with this news organization.
In theaters as of December 9, The Whale chronicles the experience of a 600-lb, middle-aged man named Charlie. Throughout the film, Charlie seeks to rebuild his relationship with his estranged teenage daughter. Charlie had left his daughter and family to pursue a relationship with a man, who eventually died. As he navigates the pain surrounding his partner’s death and his lack of community, Charlie turns to food for comfort.
When the movie premiered at the Venice Film Festival, Mr. Fraser received a 6-minute standing ovation. However, activists criticized the movie for casting Fraser over an actor with obesity as well as its depiction of people with obesity.
Representatives from the National Association to Advance Fat Acceptance contend that casting an actor without obesity only contributes to ongoing bias against people of size. “Medical weight stigma and other socio-political determinants of health for people of all sizes cause far more harm to fat people than body fat does. Bias endangers fat people’s health. Anti-obesity organizations, such as those consulted with for this movie, contribute to stigma rather than reducing it as they claim,” NAAFA wrote in a statement to this news organization.
And they added that though the fat suit used in the movie may be superior to previous ones, it is still not an accurate depiction: “The creators of The Whale consider its CGI-generated fat suit to be superior to tactile fat suits, but we don’t. The issue with fat suits in Hollywood is not that they aren’t realistic enough. The issue is that they are used rather than using performers who actually live in bodies like the ones being depicted. If there is a 600-pound character in a movie, there should be a 600-pound human in that role. Rather than concentrate on the hype around the fake fat body created for The Whale, we want to see Hollywood create more opportunities for fat people across the size spectrum, both in front of the camera and behind the scenes.”
Prosthetics vs. reality?
Ms. Nece says she understands the controversy surrounding the use of fat suits but believes that it was not done in poor taste.
“OAC got involved with the movie after Brendan was already chosen for the part, and we never would have gotten involved with it had the prosthetics or fat suit been used to ridicule or make fun of people with obesity, which is usually the case,” she explains.
“But we knew from the start that that was never the intent of anyone involved with The Whale. And I think that’s shown by the fact that Brendan and Darren Aronofsky, the director, reached out to people who live with obesity on a daily basis to find out and learn more about it and to educate themselves about it,” Ms. Nece continues.
In a Daily Mail article, Mr. Fraser credited his son Griffin, who is autistic and obese, with helping him understand the struggles that people with obesity face.
Rachel Goldman, PhD, a clinical psychologist in private practice in New York and a professor in the psychology department at New York University, notes that there are other considerations that played into casting. “I know there was some pushback in terms of could, a say 600-lb individual, even be able to go to be on set every day and do this kind of work, and the answer is we don’t know.”
“I’m sure Darren chose Brendan for many reasons above and beyond just his body. I think that’s very important to keep in mind that just as much as representation is very important, I think it is also about finding the right person for the right role,” adds Dr. Goldman, who served as a consultant to the film.
Fat suits, extreme weight gains all to play a role
About 42% of adults in the United States have obesity, according to the 2017-2020 National Health and Nutrition Examination Survey, but that reality is not reflected in films or television.
A study of 1018 major television characters found that 24% of men and 14% of women had either overweight or obesity – far below the national average. And when characters with obesity are portrayed, actors often wear prosthetics, like Gwyneth Paltrow in Shallow Hal or Eddie Murphy in the Nutty Professor.
But unlike Mr. Fraser, some actors gain weight quickly instead.
This practice is unhealthy, says Jaime Almandoz, MD, an associate professor at the University of Texas Southwestern Medical Center, Dallas, and a nonsurgical weight management expert. In interviews, actors have shared how they increased calorie intake by drinking two milkshakes per day, going to fast food places regularly, or, in Mark Walhberg’s case, consuming 7,000 calories per day to gain 30 pounds for his role as boxer-turned-priest in the movie Father Stu.
This method provides their bodies with excess calories they are unable to burn off. “Then the amount of sugar and fat that streams into the blood as a result creates problems both directly and indirectly as your body tries to store it. It basically ends up using overflow warehouses for fat storage, like the liver for example, so we can create a condition called fatty liver, or in the muscle and other places, and this excess sugar and fat in the bloodstream cause several factors that are both insulin resistance causing,” Dr. Almandoz explains.
Though gaining weight helps the actor understand the character’s life experience, it may also be risky.
“To have an actor deliberately put his own health at risk and gain a certain amount of weight and whatever that might entail, one – that’s not necessarily the safest thing for that actor – but two, it’s also important to highlight the authentic experience of someone who has dealt with this chronic disease as well,” says Disha Narang, MD, a quadruple-board certified endocrinologist, obesity medicine, and culinary medicine specialist at Northwestern Medicine Lake Forest Hospital, Chicago.
These extreme fluctuations in weight may create problems. “It is typically not something we recommend because there could be metabolic damages as well as health concerns when patients are trying to gain weight quickly, just as we don’t want patients to lose weight quickly,” says Kurt Hong, MD, PhD, board-certified in internal medicine and clinical nutrition at the University of Southern California, Los Angeles.
Dr. Hong notes that it may be difficult for individuals to experience sudden weight gain because the body works hard to maintain a state of homeostasis.
“Similarly, to someone trying to gain weight you overeat, initially your body will try to again, maybe enhance its metabolic efficiency to hold the body stable,” Dr. Hong adds.
Dietary choices that may contribute to insulin resistance or promote high blood sugar can contribute to inflammation and a number of other adverse health outcomes, notes Dr. Almandoz. “The things that actors need to do in order to gain this magnitude of weight and they want to do it in the most time-effective manner is often not helpful for our bodies, it can be very problematic, the same thing goes for weight loss when actors need to lose significant amounts of weight for roles,” says Dr. Almandoz.
And Dr. Hong explained that for patients trying to lose weight, they may cut calories, but the body will try to compensate by slowing down the metabolism to keep their weight the same.
‘Your own worst bully’
In “The Whale,” Charlie appears to suffer from internalized weight bias, which is common to many people living with obesity, Ms. Nece says.
“Internalized weight bias is when the person of size takes all that negativity and turns it on themselves. The easiest way to describe that is to tell you that I became my own worst bully because I started believing all the negative things people said to me about my weight,” Ms. Nece adds.
Her hope is that the film will bring attention to the harm that this bias creates, especially when it derives from other people. “There’s no telling whether it will, but what Charlie experiences in bias and stigma from others clearly happens. It’s realistic. Those of us in large bodies have experienced what he is experiencing, so some people have said the movie is fat-phobic, but I see it as I can relate to those experiences because I have them too, so they are very realistic.”
Ms. Nece notes that it is important for clinicians to understand that obesity is a multifaceted and sensitive topic. “For those medical professionals who do not already know that obesity is complex, I hope the film will begin to open their eyes to the many different facets involved in obesity and their patients with obesity, I hope it will help them empathize and show compassion to their patients with obesity,” she concludes.
A version of this article first appeared on Medscape.com.
“I could relate to many, many, many of the experiences and emotions that Charlie, which is Brendan Fraser’s character, was portraying,” Patricia Nece recalls after watching a preview copy of the new film “The Whale.”
Much of the movie “rang true and hit home for me as things that I, too, had experienced,” Ms. Nece, the board of directors’ chair of the Obesity Action Coalition (OAC) and a person living with obesity, shares with this news organization.
In theaters as of December 9, The Whale chronicles the experience of a 600-lb, middle-aged man named Charlie. Throughout the film, Charlie seeks to rebuild his relationship with his estranged teenage daughter. Charlie had left his daughter and family to pursue a relationship with a man, who eventually died. As he navigates the pain surrounding his partner’s death and his lack of community, Charlie turns to food for comfort.
When the movie premiered at the Venice Film Festival, Mr. Fraser received a 6-minute standing ovation. However, activists criticized the movie for casting Fraser over an actor with obesity as well as its depiction of people with obesity.
Representatives from the National Association to Advance Fat Acceptance contend that casting an actor without obesity only contributes to ongoing bias against people of size. “Medical weight stigma and other socio-political determinants of health for people of all sizes cause far more harm to fat people than body fat does. Bias endangers fat people’s health. Anti-obesity organizations, such as those consulted with for this movie, contribute to stigma rather than reducing it as they claim,” NAAFA wrote in a statement to this news organization.
And they added that though the fat suit used in the movie may be superior to previous ones, it is still not an accurate depiction: “The creators of The Whale consider its CGI-generated fat suit to be superior to tactile fat suits, but we don’t. The issue with fat suits in Hollywood is not that they aren’t realistic enough. The issue is that they are used rather than using performers who actually live in bodies like the ones being depicted. If there is a 600-pound character in a movie, there should be a 600-pound human in that role. Rather than concentrate on the hype around the fake fat body created for The Whale, we want to see Hollywood create more opportunities for fat people across the size spectrum, both in front of the camera and behind the scenes.”
Prosthetics vs. reality?
Ms. Nece says she understands the controversy surrounding the use of fat suits but believes that it was not done in poor taste.
“OAC got involved with the movie after Brendan was already chosen for the part, and we never would have gotten involved with it had the prosthetics or fat suit been used to ridicule or make fun of people with obesity, which is usually the case,” she explains.
“But we knew from the start that that was never the intent of anyone involved with The Whale. And I think that’s shown by the fact that Brendan and Darren Aronofsky, the director, reached out to people who live with obesity on a daily basis to find out and learn more about it and to educate themselves about it,” Ms. Nece continues.
In a Daily Mail article, Mr. Fraser credited his son Griffin, who is autistic and obese, with helping him understand the struggles that people with obesity face.
Rachel Goldman, PhD, a clinical psychologist in private practice in New York and a professor in the psychology department at New York University, notes that there are other considerations that played into casting. “I know there was some pushback in terms of could, a say 600-lb individual, even be able to go to be on set every day and do this kind of work, and the answer is we don’t know.”
“I’m sure Darren chose Brendan for many reasons above and beyond just his body. I think that’s very important to keep in mind that just as much as representation is very important, I think it is also about finding the right person for the right role,” adds Dr. Goldman, who served as a consultant to the film.
Fat suits, extreme weight gains all to play a role
About 42% of adults in the United States have obesity, according to the 2017-2020 National Health and Nutrition Examination Survey, but that reality is not reflected in films or television.
A study of 1018 major television characters found that 24% of men and 14% of women had either overweight or obesity – far below the national average. And when characters with obesity are portrayed, actors often wear prosthetics, like Gwyneth Paltrow in Shallow Hal or Eddie Murphy in the Nutty Professor.
But unlike Mr. Fraser, some actors gain weight quickly instead.
This practice is unhealthy, says Jaime Almandoz, MD, an associate professor at the University of Texas Southwestern Medical Center, Dallas, and a nonsurgical weight management expert. In interviews, actors have shared how they increased calorie intake by drinking two milkshakes per day, going to fast food places regularly, or, in Mark Walhberg’s case, consuming 7,000 calories per day to gain 30 pounds for his role as boxer-turned-priest in the movie Father Stu.
This method provides their bodies with excess calories they are unable to burn off. “Then the amount of sugar and fat that streams into the blood as a result creates problems both directly and indirectly as your body tries to store it. It basically ends up using overflow warehouses for fat storage, like the liver for example, so we can create a condition called fatty liver, or in the muscle and other places, and this excess sugar and fat in the bloodstream cause several factors that are both insulin resistance causing,” Dr. Almandoz explains.
Though gaining weight helps the actor understand the character’s life experience, it may also be risky.
“To have an actor deliberately put his own health at risk and gain a certain amount of weight and whatever that might entail, one – that’s not necessarily the safest thing for that actor – but two, it’s also important to highlight the authentic experience of someone who has dealt with this chronic disease as well,” says Disha Narang, MD, a quadruple-board certified endocrinologist, obesity medicine, and culinary medicine specialist at Northwestern Medicine Lake Forest Hospital, Chicago.
These extreme fluctuations in weight may create problems. “It is typically not something we recommend because there could be metabolic damages as well as health concerns when patients are trying to gain weight quickly, just as we don’t want patients to lose weight quickly,” says Kurt Hong, MD, PhD, board-certified in internal medicine and clinical nutrition at the University of Southern California, Los Angeles.
Dr. Hong notes that it may be difficult for individuals to experience sudden weight gain because the body works hard to maintain a state of homeostasis.
“Similarly, to someone trying to gain weight you overeat, initially your body will try to again, maybe enhance its metabolic efficiency to hold the body stable,” Dr. Hong adds.
Dietary choices that may contribute to insulin resistance or promote high blood sugar can contribute to inflammation and a number of other adverse health outcomes, notes Dr. Almandoz. “The things that actors need to do in order to gain this magnitude of weight and they want to do it in the most time-effective manner is often not helpful for our bodies, it can be very problematic, the same thing goes for weight loss when actors need to lose significant amounts of weight for roles,” says Dr. Almandoz.
And Dr. Hong explained that for patients trying to lose weight, they may cut calories, but the body will try to compensate by slowing down the metabolism to keep their weight the same.
‘Your own worst bully’
In “The Whale,” Charlie appears to suffer from internalized weight bias, which is common to many people living with obesity, Ms. Nece says.
“Internalized weight bias is when the person of size takes all that negativity and turns it on themselves. The easiest way to describe that is to tell you that I became my own worst bully because I started believing all the negative things people said to me about my weight,” Ms. Nece adds.
Her hope is that the film will bring attention to the harm that this bias creates, especially when it derives from other people. “There’s no telling whether it will, but what Charlie experiences in bias and stigma from others clearly happens. It’s realistic. Those of us in large bodies have experienced what he is experiencing, so some people have said the movie is fat-phobic, but I see it as I can relate to those experiences because I have them too, so they are very realistic.”
Ms. Nece notes that it is important for clinicians to understand that obesity is a multifaceted and sensitive topic. “For those medical professionals who do not already know that obesity is complex, I hope the film will begin to open their eyes to the many different facets involved in obesity and their patients with obesity, I hope it will help them empathize and show compassion to their patients with obesity,” she concludes.
A version of this article first appeared on Medscape.com.
“I could relate to many, many, many of the experiences and emotions that Charlie, which is Brendan Fraser’s character, was portraying,” Patricia Nece recalls after watching a preview copy of the new film “The Whale.”
Much of the movie “rang true and hit home for me as things that I, too, had experienced,” Ms. Nece, the board of directors’ chair of the Obesity Action Coalition (OAC) and a person living with obesity, shares with this news organization.
In theaters as of December 9, The Whale chronicles the experience of a 600-lb, middle-aged man named Charlie. Throughout the film, Charlie seeks to rebuild his relationship with his estranged teenage daughter. Charlie had left his daughter and family to pursue a relationship with a man, who eventually died. As he navigates the pain surrounding his partner’s death and his lack of community, Charlie turns to food for comfort.
When the movie premiered at the Venice Film Festival, Mr. Fraser received a 6-minute standing ovation. However, activists criticized the movie for casting Fraser over an actor with obesity as well as its depiction of people with obesity.
Representatives from the National Association to Advance Fat Acceptance contend that casting an actor without obesity only contributes to ongoing bias against people of size. “Medical weight stigma and other socio-political determinants of health for people of all sizes cause far more harm to fat people than body fat does. Bias endangers fat people’s health. Anti-obesity organizations, such as those consulted with for this movie, contribute to stigma rather than reducing it as they claim,” NAAFA wrote in a statement to this news organization.
And they added that though the fat suit used in the movie may be superior to previous ones, it is still not an accurate depiction: “The creators of The Whale consider its CGI-generated fat suit to be superior to tactile fat suits, but we don’t. The issue with fat suits in Hollywood is not that they aren’t realistic enough. The issue is that they are used rather than using performers who actually live in bodies like the ones being depicted. If there is a 600-pound character in a movie, there should be a 600-pound human in that role. Rather than concentrate on the hype around the fake fat body created for The Whale, we want to see Hollywood create more opportunities for fat people across the size spectrum, both in front of the camera and behind the scenes.”
Prosthetics vs. reality?
Ms. Nece says she understands the controversy surrounding the use of fat suits but believes that it was not done in poor taste.
“OAC got involved with the movie after Brendan was already chosen for the part, and we never would have gotten involved with it had the prosthetics or fat suit been used to ridicule or make fun of people with obesity, which is usually the case,” she explains.
“But we knew from the start that that was never the intent of anyone involved with The Whale. And I think that’s shown by the fact that Brendan and Darren Aronofsky, the director, reached out to people who live with obesity on a daily basis to find out and learn more about it and to educate themselves about it,” Ms. Nece continues.
In a Daily Mail article, Mr. Fraser credited his son Griffin, who is autistic and obese, with helping him understand the struggles that people with obesity face.
Rachel Goldman, PhD, a clinical psychologist in private practice in New York and a professor in the psychology department at New York University, notes that there are other considerations that played into casting. “I know there was some pushback in terms of could, a say 600-lb individual, even be able to go to be on set every day and do this kind of work, and the answer is we don’t know.”
“I’m sure Darren chose Brendan for many reasons above and beyond just his body. I think that’s very important to keep in mind that just as much as representation is very important, I think it is also about finding the right person for the right role,” adds Dr. Goldman, who served as a consultant to the film.
Fat suits, extreme weight gains all to play a role
About 42% of adults in the United States have obesity, according to the 2017-2020 National Health and Nutrition Examination Survey, but that reality is not reflected in films or television.
A study of 1018 major television characters found that 24% of men and 14% of women had either overweight or obesity – far below the national average. And when characters with obesity are portrayed, actors often wear prosthetics, like Gwyneth Paltrow in Shallow Hal or Eddie Murphy in the Nutty Professor.
But unlike Mr. Fraser, some actors gain weight quickly instead.
This practice is unhealthy, says Jaime Almandoz, MD, an associate professor at the University of Texas Southwestern Medical Center, Dallas, and a nonsurgical weight management expert. In interviews, actors have shared how they increased calorie intake by drinking two milkshakes per day, going to fast food places regularly, or, in Mark Walhberg’s case, consuming 7,000 calories per day to gain 30 pounds for his role as boxer-turned-priest in the movie Father Stu.
This method provides their bodies with excess calories they are unable to burn off. “Then the amount of sugar and fat that streams into the blood as a result creates problems both directly and indirectly as your body tries to store it. It basically ends up using overflow warehouses for fat storage, like the liver for example, so we can create a condition called fatty liver, or in the muscle and other places, and this excess sugar and fat in the bloodstream cause several factors that are both insulin resistance causing,” Dr. Almandoz explains.
Though gaining weight helps the actor understand the character’s life experience, it may also be risky.
“To have an actor deliberately put his own health at risk and gain a certain amount of weight and whatever that might entail, one – that’s not necessarily the safest thing for that actor – but two, it’s also important to highlight the authentic experience of someone who has dealt with this chronic disease as well,” says Disha Narang, MD, a quadruple-board certified endocrinologist, obesity medicine, and culinary medicine specialist at Northwestern Medicine Lake Forest Hospital, Chicago.
These extreme fluctuations in weight may create problems. “It is typically not something we recommend because there could be metabolic damages as well as health concerns when patients are trying to gain weight quickly, just as we don’t want patients to lose weight quickly,” says Kurt Hong, MD, PhD, board-certified in internal medicine and clinical nutrition at the University of Southern California, Los Angeles.
Dr. Hong notes that it may be difficult for individuals to experience sudden weight gain because the body works hard to maintain a state of homeostasis.
“Similarly, to someone trying to gain weight you overeat, initially your body will try to again, maybe enhance its metabolic efficiency to hold the body stable,” Dr. Hong adds.
Dietary choices that may contribute to insulin resistance or promote high blood sugar can contribute to inflammation and a number of other adverse health outcomes, notes Dr. Almandoz. “The things that actors need to do in order to gain this magnitude of weight and they want to do it in the most time-effective manner is often not helpful for our bodies, it can be very problematic, the same thing goes for weight loss when actors need to lose significant amounts of weight for roles,” says Dr. Almandoz.
And Dr. Hong explained that for patients trying to lose weight, they may cut calories, but the body will try to compensate by slowing down the metabolism to keep their weight the same.
‘Your own worst bully’
In “The Whale,” Charlie appears to suffer from internalized weight bias, which is common to many people living with obesity, Ms. Nece says.
“Internalized weight bias is when the person of size takes all that negativity and turns it on themselves. The easiest way to describe that is to tell you that I became my own worst bully because I started believing all the negative things people said to me about my weight,” Ms. Nece adds.
Her hope is that the film will bring attention to the harm that this bias creates, especially when it derives from other people. “There’s no telling whether it will, but what Charlie experiences in bias and stigma from others clearly happens. It’s realistic. Those of us in large bodies have experienced what he is experiencing, so some people have said the movie is fat-phobic, but I see it as I can relate to those experiences because I have them too, so they are very realistic.”
Ms. Nece notes that it is important for clinicians to understand that obesity is a multifaceted and sensitive topic. “For those medical professionals who do not already know that obesity is complex, I hope the film will begin to open their eyes to the many different facets involved in obesity and their patients with obesity, I hope it will help them empathize and show compassion to their patients with obesity,” she concludes.
A version of this article first appeared on Medscape.com.
AI versus other interventions for colonoscopy: How do they compare?
AI-based tools appear to outperform other methods intended to increase ADRs, including distal attachment devices, dye-based/virtual chromoendoscopy, water-based techniques, and balloon-assisted devices, researchers found in a systematic review and meta-analysis.
“ADR is a very important quality metric. The higher the ADR, the less likely the chance of interval cancer,” first author Muhammad Aziz, MD, co-chief gastroenterology fellow at the University of Toledo (Ohio), told this news organization. Interval cancer refers to colorectal cancer that is diagnosed within 5 years of a patient’s undergoing a negative colonoscopy.
“Numerous interventions have been attempted and researched to see the impact on ADR,” he said. “The new kid on the block – AI-assisted colonoscopy – is a game-changer. I knew that AI was impactful in improving ADR, but I didn’t know it would be the best.”
The study was published online in the Journal of Clinical Gastroenterology.
Analyzing detection rates
Current guidelines set an ADR benchmark of 25% overall, with 30% for men and 20% for women undergoing screening colonoscopy. Every 1% increase in ADR results in a 3% reduction in colorectal cancer, Dr. Aziz and his co-authors write.
Several methods can improve ADR over standard colonoscopy. Computer-aided detection and AI methods, which have emerged in recent years, alert the endoscopist of potential lesions in real time with visual signals.
No direct comparative studies had been conducted, so to make an indirect comparison, Dr. Aziz and colleagues undertook a systematic review and network meta-analysis of 94 randomized controlled trials that included 61,172 patients and 20 different study interventions.
The research team assessed the impact of AI in comparison with other endoscopic methods, using relative risk for proportional outcomes and mean difference for continuous outcomes. About 63% of the colonoscopies were for screening and surveillance, and 37% were diagnostic. The effectiveness was ranked by P-score (the probability of being the best treatment).
Overall, AI had the highest P-score (0.96), signifying the best modality of all interventions for improving ADR, the study authors write. A sensitivity analysis using the fixed effects model did not significantly alter the effect measure.
The network meta-analysis showed significantly higher ADR for AI, compared with autofluorescence imaging (relative risk, 1.33), dye-based chromoendoscopy (RR, 1.22), Endocap (RR, 1.32), Endocuff (RR, 1.19), Endocuff Vision (RR, 1.26), EndoRings (RR, 1.30), flexible spectral imaging color enhancement (RR,1.26), full-spectrum endoscopy (RR, 1.40), high-definition (HD) colonoscopy (RR, 1.41), linked color imaging (1.21), narrow-band imaging (RR, 1.33), water exchange (RR, 1.22), and water immersion (RR, 1.47).
Among 34 studies of colonoscopies for screening or surveillance only, the ADR was significantly improved for linked color imaging (RR, 1.18), I-Scan with contrast and surface enhancement (RR, 1.25), Endocuff (RR, 1.20), Endocuff Vision (RR, 1.13), and water exchange (RR, 1.24), compared with HD colonoscopy. Only one AI study was included in this analysis, because the others had significantly more patients who underwent colonoscopy for diagnostic indications. In this case, AI did not improve ADR, compared with HD colonoscopy (RR, 1.44).
In addition, a significantly improved polyp detection rate (PDR) was noted for AI, compared with autofluorescence imaging (RR, 1.28), Endocap (RR, 1.18), Endocuff Vision (RR, 1.21), EndoRings (RR, 1.30), flexible spectral imaging color enhancement (RR, 1.21), full-spectrum endoscopy (RR, 1.39), HD colonoscopy (RR, 1.34), linked color imaging (RR, 1.19), and narrow-band imaging (RR, 1.21). Again, AI had the highest P-score (RR, 0.93).
Among 17 studies of colonoscopy for screening and surveillance, only one AI study was included for PDR. A significantly higher PDR was noted for AI, compared with HD colonoscopy (RR, 1.33). None of the other interventions improved PDR over HD colonoscopy.
No AI advantage for serrated polyps
Twenty-three studies evaluated detection for serrated polyps, including three AI studies. AI did not improve the serrated polyp detection rate (SPDR), compared with other interventions. However, several modalities did improve SPDR: G-EYE, compared with full-spectrum endoscopy (RR, 3.93), linked color imaging, compared with full-spectrum endoscopy (RR, 1.88), and HD colonoscopy (RR, 1.71), and Endocuff Vision, compared with HD colonoscopy (RR, 1.36). G-EYE had the highest P-score (0.93).
AI significantly improved adenomas per colonoscopy, compared with full-spectrum endoscopy (mean difference, 0.38), HD colonoscopy (MD, 0.18), and narrow-band imaging (MD, 0.13), the authors note. However, the number of adenomas detected per colonoscopy was significantly lower for AI, compared with Endocap (-0.13). Endocap had the highest P-score (0.92).
“The strengths of this study include the wide range of endoscopic add-ons included, the number of trials included, and the granularity of some of the reporting data,” Jeremy Glissen Brown, MD, a gastroenterologist and an assistant professor of medicine at Duke University, told this news organization.
Dr. Glissen Brown, who wasn’t involved with this study, researches AI tools for polyp detection. He and colleagues have found that AI decreases adenoma miss rates and increases the number of first-pass adenomas detected per colonoscopy.
“The limitations include significant heterogeneity among many of the comparisons, as well as a high risk of bias, as it is technically difficult to achieve blinding of provider participants in the device-based RCTs [randomized controlled trials] that this analysis was based on,” he said.
Additional considerations
Dr. Aziz and colleagues note the need for additional studies of AI-based detection, particularly for screening and surveillance. For widespread adoption into clinical practice, new systems must have higher specificity, sensitivity, accuracy, and efficiency, they write.
“AI technology needs further optimization, as there is still the aspect of having a lot of false positives – lesions detected but not necessarily adenomas that can turn into cancer,” Dr. Aziz said. “This decreases the efficiency of the colonoscopy and increases the anesthesia and sedation time. In addition, different AI systems have different diagnostic yield, as it all depends on the images that were fed to the system or algorithm.”
Dr. Glissen Brown also pointed to the low number of AI-based studies involving serrated polyp lesion detection. Future research could investigate whether computer-aided detection systems (CADe) decrease miss rates and increase detection rates for sessile serrated lesions, he said.
For practical clinical purposes, Dr. Glissen Brown highlighted the potential complementary nature of the various colonoscopy tools. When used together, for instance, AI and Endocuff may increase ADRs even further and decrease the number of missed polyps through different mechanisms, he said.
“It is also important in device research to interrogate the cost versus benefit of any intervention or combination of interventions,” he said. “I think with CADe this is still something that we are figuring out. We will need to find novel ways of making these technologies affordable, especially as the debate of which clinically meaningful outcomes we examine when it comes to AI continues to evolve.”
No funding source for the study was reported. Two authors have received grant support from or have consulted for several pharmaceutical and medical device companies. Dr. Glissen Brown has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AI-based tools appear to outperform other methods intended to increase ADRs, including distal attachment devices, dye-based/virtual chromoendoscopy, water-based techniques, and balloon-assisted devices, researchers found in a systematic review and meta-analysis.
“ADR is a very important quality metric. The higher the ADR, the less likely the chance of interval cancer,” first author Muhammad Aziz, MD, co-chief gastroenterology fellow at the University of Toledo (Ohio), told this news organization. Interval cancer refers to colorectal cancer that is diagnosed within 5 years of a patient’s undergoing a negative colonoscopy.
“Numerous interventions have been attempted and researched to see the impact on ADR,” he said. “The new kid on the block – AI-assisted colonoscopy – is a game-changer. I knew that AI was impactful in improving ADR, but I didn’t know it would be the best.”
The study was published online in the Journal of Clinical Gastroenterology.
Analyzing detection rates
Current guidelines set an ADR benchmark of 25% overall, with 30% for men and 20% for women undergoing screening colonoscopy. Every 1% increase in ADR results in a 3% reduction in colorectal cancer, Dr. Aziz and his co-authors write.
Several methods can improve ADR over standard colonoscopy. Computer-aided detection and AI methods, which have emerged in recent years, alert the endoscopist of potential lesions in real time with visual signals.
No direct comparative studies had been conducted, so to make an indirect comparison, Dr. Aziz and colleagues undertook a systematic review and network meta-analysis of 94 randomized controlled trials that included 61,172 patients and 20 different study interventions.
The research team assessed the impact of AI in comparison with other endoscopic methods, using relative risk for proportional outcomes and mean difference for continuous outcomes. About 63% of the colonoscopies were for screening and surveillance, and 37% were diagnostic. The effectiveness was ranked by P-score (the probability of being the best treatment).
Overall, AI had the highest P-score (0.96), signifying the best modality of all interventions for improving ADR, the study authors write. A sensitivity analysis using the fixed effects model did not significantly alter the effect measure.
The network meta-analysis showed significantly higher ADR for AI, compared with autofluorescence imaging (relative risk, 1.33), dye-based chromoendoscopy (RR, 1.22), Endocap (RR, 1.32), Endocuff (RR, 1.19), Endocuff Vision (RR, 1.26), EndoRings (RR, 1.30), flexible spectral imaging color enhancement (RR,1.26), full-spectrum endoscopy (RR, 1.40), high-definition (HD) colonoscopy (RR, 1.41), linked color imaging (1.21), narrow-band imaging (RR, 1.33), water exchange (RR, 1.22), and water immersion (RR, 1.47).
Among 34 studies of colonoscopies for screening or surveillance only, the ADR was significantly improved for linked color imaging (RR, 1.18), I-Scan with contrast and surface enhancement (RR, 1.25), Endocuff (RR, 1.20), Endocuff Vision (RR, 1.13), and water exchange (RR, 1.24), compared with HD colonoscopy. Only one AI study was included in this analysis, because the others had significantly more patients who underwent colonoscopy for diagnostic indications. In this case, AI did not improve ADR, compared with HD colonoscopy (RR, 1.44).
In addition, a significantly improved polyp detection rate (PDR) was noted for AI, compared with autofluorescence imaging (RR, 1.28), Endocap (RR, 1.18), Endocuff Vision (RR, 1.21), EndoRings (RR, 1.30), flexible spectral imaging color enhancement (RR, 1.21), full-spectrum endoscopy (RR, 1.39), HD colonoscopy (RR, 1.34), linked color imaging (RR, 1.19), and narrow-band imaging (RR, 1.21). Again, AI had the highest P-score (RR, 0.93).
Among 17 studies of colonoscopy for screening and surveillance, only one AI study was included for PDR. A significantly higher PDR was noted for AI, compared with HD colonoscopy (RR, 1.33). None of the other interventions improved PDR over HD colonoscopy.
No AI advantage for serrated polyps
Twenty-three studies evaluated detection for serrated polyps, including three AI studies. AI did not improve the serrated polyp detection rate (SPDR), compared with other interventions. However, several modalities did improve SPDR: G-EYE, compared with full-spectrum endoscopy (RR, 3.93), linked color imaging, compared with full-spectrum endoscopy (RR, 1.88), and HD colonoscopy (RR, 1.71), and Endocuff Vision, compared with HD colonoscopy (RR, 1.36). G-EYE had the highest P-score (0.93).
AI significantly improved adenomas per colonoscopy, compared with full-spectrum endoscopy (mean difference, 0.38), HD colonoscopy (MD, 0.18), and narrow-band imaging (MD, 0.13), the authors note. However, the number of adenomas detected per colonoscopy was significantly lower for AI, compared with Endocap (-0.13). Endocap had the highest P-score (0.92).
“The strengths of this study include the wide range of endoscopic add-ons included, the number of trials included, and the granularity of some of the reporting data,” Jeremy Glissen Brown, MD, a gastroenterologist and an assistant professor of medicine at Duke University, told this news organization.
Dr. Glissen Brown, who wasn’t involved with this study, researches AI tools for polyp detection. He and colleagues have found that AI decreases adenoma miss rates and increases the number of first-pass adenomas detected per colonoscopy.
“The limitations include significant heterogeneity among many of the comparisons, as well as a high risk of bias, as it is technically difficult to achieve blinding of provider participants in the device-based RCTs [randomized controlled trials] that this analysis was based on,” he said.
Additional considerations
Dr. Aziz and colleagues note the need for additional studies of AI-based detection, particularly for screening and surveillance. For widespread adoption into clinical practice, new systems must have higher specificity, sensitivity, accuracy, and efficiency, they write.
“AI technology needs further optimization, as there is still the aspect of having a lot of false positives – lesions detected but not necessarily adenomas that can turn into cancer,” Dr. Aziz said. “This decreases the efficiency of the colonoscopy and increases the anesthesia and sedation time. In addition, different AI systems have different diagnostic yield, as it all depends on the images that were fed to the system or algorithm.”
Dr. Glissen Brown also pointed to the low number of AI-based studies involving serrated polyp lesion detection. Future research could investigate whether computer-aided detection systems (CADe) decrease miss rates and increase detection rates for sessile serrated lesions, he said.
For practical clinical purposes, Dr. Glissen Brown highlighted the potential complementary nature of the various colonoscopy tools. When used together, for instance, AI and Endocuff may increase ADRs even further and decrease the number of missed polyps through different mechanisms, he said.
“It is also important in device research to interrogate the cost versus benefit of any intervention or combination of interventions,” he said. “I think with CADe this is still something that we are figuring out. We will need to find novel ways of making these technologies affordable, especially as the debate of which clinically meaningful outcomes we examine when it comes to AI continues to evolve.”
No funding source for the study was reported. Two authors have received grant support from or have consulted for several pharmaceutical and medical device companies. Dr. Glissen Brown has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AI-based tools appear to outperform other methods intended to increase ADRs, including distal attachment devices, dye-based/virtual chromoendoscopy, water-based techniques, and balloon-assisted devices, researchers found in a systematic review and meta-analysis.
“ADR is a very important quality metric. The higher the ADR, the less likely the chance of interval cancer,” first author Muhammad Aziz, MD, co-chief gastroenterology fellow at the University of Toledo (Ohio), told this news organization. Interval cancer refers to colorectal cancer that is diagnosed within 5 years of a patient’s undergoing a negative colonoscopy.
“Numerous interventions have been attempted and researched to see the impact on ADR,” he said. “The new kid on the block – AI-assisted colonoscopy – is a game-changer. I knew that AI was impactful in improving ADR, but I didn’t know it would be the best.”
The study was published online in the Journal of Clinical Gastroenterology.
Analyzing detection rates
Current guidelines set an ADR benchmark of 25% overall, with 30% for men and 20% for women undergoing screening colonoscopy. Every 1% increase in ADR results in a 3% reduction in colorectal cancer, Dr. Aziz and his co-authors write.
Several methods can improve ADR over standard colonoscopy. Computer-aided detection and AI methods, which have emerged in recent years, alert the endoscopist of potential lesions in real time with visual signals.
No direct comparative studies had been conducted, so to make an indirect comparison, Dr. Aziz and colleagues undertook a systematic review and network meta-analysis of 94 randomized controlled trials that included 61,172 patients and 20 different study interventions.
The research team assessed the impact of AI in comparison with other endoscopic methods, using relative risk for proportional outcomes and mean difference for continuous outcomes. About 63% of the colonoscopies were for screening and surveillance, and 37% were diagnostic. The effectiveness was ranked by P-score (the probability of being the best treatment).
Overall, AI had the highest P-score (0.96), signifying the best modality of all interventions for improving ADR, the study authors write. A sensitivity analysis using the fixed effects model did not significantly alter the effect measure.
The network meta-analysis showed significantly higher ADR for AI, compared with autofluorescence imaging (relative risk, 1.33), dye-based chromoendoscopy (RR, 1.22), Endocap (RR, 1.32), Endocuff (RR, 1.19), Endocuff Vision (RR, 1.26), EndoRings (RR, 1.30), flexible spectral imaging color enhancement (RR,1.26), full-spectrum endoscopy (RR, 1.40), high-definition (HD) colonoscopy (RR, 1.41), linked color imaging (1.21), narrow-band imaging (RR, 1.33), water exchange (RR, 1.22), and water immersion (RR, 1.47).
Among 34 studies of colonoscopies for screening or surveillance only, the ADR was significantly improved for linked color imaging (RR, 1.18), I-Scan with contrast and surface enhancement (RR, 1.25), Endocuff (RR, 1.20), Endocuff Vision (RR, 1.13), and water exchange (RR, 1.24), compared with HD colonoscopy. Only one AI study was included in this analysis, because the others had significantly more patients who underwent colonoscopy for diagnostic indications. In this case, AI did not improve ADR, compared with HD colonoscopy (RR, 1.44).
In addition, a significantly improved polyp detection rate (PDR) was noted for AI, compared with autofluorescence imaging (RR, 1.28), Endocap (RR, 1.18), Endocuff Vision (RR, 1.21), EndoRings (RR, 1.30), flexible spectral imaging color enhancement (RR, 1.21), full-spectrum endoscopy (RR, 1.39), HD colonoscopy (RR, 1.34), linked color imaging (RR, 1.19), and narrow-band imaging (RR, 1.21). Again, AI had the highest P-score (RR, 0.93).
Among 17 studies of colonoscopy for screening and surveillance, only one AI study was included for PDR. A significantly higher PDR was noted for AI, compared with HD colonoscopy (RR, 1.33). None of the other interventions improved PDR over HD colonoscopy.
No AI advantage for serrated polyps
Twenty-three studies evaluated detection for serrated polyps, including three AI studies. AI did not improve the serrated polyp detection rate (SPDR), compared with other interventions. However, several modalities did improve SPDR: G-EYE, compared with full-spectrum endoscopy (RR, 3.93), linked color imaging, compared with full-spectrum endoscopy (RR, 1.88), and HD colonoscopy (RR, 1.71), and Endocuff Vision, compared with HD colonoscopy (RR, 1.36). G-EYE had the highest P-score (0.93).
AI significantly improved adenomas per colonoscopy, compared with full-spectrum endoscopy (mean difference, 0.38), HD colonoscopy (MD, 0.18), and narrow-band imaging (MD, 0.13), the authors note. However, the number of adenomas detected per colonoscopy was significantly lower for AI, compared with Endocap (-0.13). Endocap had the highest P-score (0.92).
“The strengths of this study include the wide range of endoscopic add-ons included, the number of trials included, and the granularity of some of the reporting data,” Jeremy Glissen Brown, MD, a gastroenterologist and an assistant professor of medicine at Duke University, told this news organization.
Dr. Glissen Brown, who wasn’t involved with this study, researches AI tools for polyp detection. He and colleagues have found that AI decreases adenoma miss rates and increases the number of first-pass adenomas detected per colonoscopy.
“The limitations include significant heterogeneity among many of the comparisons, as well as a high risk of bias, as it is technically difficult to achieve blinding of provider participants in the device-based RCTs [randomized controlled trials] that this analysis was based on,” he said.
Additional considerations
Dr. Aziz and colleagues note the need for additional studies of AI-based detection, particularly for screening and surveillance. For widespread adoption into clinical practice, new systems must have higher specificity, sensitivity, accuracy, and efficiency, they write.
“AI technology needs further optimization, as there is still the aspect of having a lot of false positives – lesions detected but not necessarily adenomas that can turn into cancer,” Dr. Aziz said. “This decreases the efficiency of the colonoscopy and increases the anesthesia and sedation time. In addition, different AI systems have different diagnostic yield, as it all depends on the images that were fed to the system or algorithm.”
Dr. Glissen Brown also pointed to the low number of AI-based studies involving serrated polyp lesion detection. Future research could investigate whether computer-aided detection systems (CADe) decrease miss rates and increase detection rates for sessile serrated lesions, he said.
For practical clinical purposes, Dr. Glissen Brown highlighted the potential complementary nature of the various colonoscopy tools. When used together, for instance, AI and Endocuff may increase ADRs even further and decrease the number of missed polyps through different mechanisms, he said.
“It is also important in device research to interrogate the cost versus benefit of any intervention or combination of interventions,” he said. “I think with CADe this is still something that we are figuring out. We will need to find novel ways of making these technologies affordable, especially as the debate of which clinically meaningful outcomes we examine when it comes to AI continues to evolve.”
No funding source for the study was reported. Two authors have received grant support from or have consulted for several pharmaceutical and medical device companies. Dr. Glissen Brown has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL GASTROENTEROLOGY
The 'Plaque Hypothesis': Focus on vulnerable lesions to cut events
A new strategy for the management of atherosclerotic plaque as a source of major adverse cardiac events is needed with the focus shifting from the flow-limiting coronary artery luminal lesions to the overall atherosclerotic burden, be it obstructive or nonobstructive, according to a review article.
The article, by Peter H. Stone, MD, and Peter Libby, MD, Brigham and Women’s Hospital, Boston, and William E. Boden, MD, Boston University School of Medicine, was published online in JAMA Cardiology.
The review explored new data from vascular biology, atherosclerosis imaging, natural history outcome studies, and large-scale clinical trials that support what the authors refer to as “The Plaque Hypothesis” – the idea that major adverse cardiac events such as myocardial infarction and cardiac death are triggered by destabilization of vulnerable plaque, which may be obstructive or nonobstructive.
“We need to consider embracing a new management strategy that directs our diagnostic and management focus to evaluate the entire length of the atheromatous coronary artery and broaden the target of our therapeutic intervention to include all regions of the plaque (both flow-limiting and non–flow-limiting), even those that are distant from the presumed ischemia-producing obstruction,” the authors concluded.
Dr. Stone explained to this news organization that, for several decades, the medical community has focused on plaques causing severe obstruction of coronary arteries as being responsible for major adverse cardiac events. This approach – known as the Ischemia Hypothesis – has been the accepted strategy for many years, with all guidelines advising the identification of the stenoses that cause the most obstruction for treatment with stenting.
However, the authors pointed out that a number of studies have now suggested that, while these severe obstructive stenoses cause angina, they do not seem to be responsible for the hard events of MI, acute coronary syndrome (ACS), and cardiac death.
Several studies including the COURAGE trial and BARI-2D, and the recent ISCHEMIA trial have all failed to show a reduction in these hard endpoints by intervening on these severe obstructive lesions, Dr. Stone noted.
“We present evidence for a new approach – that it is the composition and vascular biology of the atherosclerotic plaques that cause MI, ACS, and cardiac death, rather than simply how obstructive they are,” he said.
Dr. Stone pointed out that plaque seen on a coronary angiogram looks at only the lumen of the artery, but plaque is primarily based in the wall of the artery, and if that plaque is inflamed it can easily be the culprit responsible for adverse events even without encroaching into the lumen.
“Our paper describes many factors which can cause plaques to destabilize and cause an ACS. These include anatomical, biochemical, and biomechanical features that together cause plaque rupture or erosion and precipitate a clinical event. It is not sufficient to just look for obstructive plaques on a coronary angiogram,” he said. “We are barking up the wrong tree. We need to look for inflamed plaque in the whole wall of the coronary arteries.”
The authors described different factors that identify a plaque at high risk of destabilization. These include a large area of vulnerable plaque, a thin-cap atheroma, a severe inflamed core, macrocalcifications, a large plaque burden, and a physical profile that would encourage a thrombus to become trapped.
“Atherosclerotic plaques are very heterogeneous and complex structures and it is not just the mountain peaks but also the lower foothills that can precipitate a flow-limiting obstruction,” Dr. Stone noted.
“The slope of the mountain is probably very important in the ability for a thrombus to form. If the slope is gradual there isn’t a problem. But if the slope is jagged with sharp edges this can cause a thrombus to become trapped. We need to look at the entirety of plaque and all its risk features to identify the culprit areas that could cause MI or cardiac death. These are typically not the obstructive plaques we have all been fixated on for many years,” he added.
“We need to focus on plaque heterogeneity. Once plaque is old and just made up of scar tissue which is not inflamed it does not cause much [of] a problem – we can probably just leave it alone. Some of these obstructive plaques may cause some angina but many do not cause major cardiac events unless they have other high-risk features,” he said.
“Cardiac events are still caused by obstruction of blood flow but that can be an abrupt process where a thrombus attaches itself to an area of destabilized plaque. These areas of plaque were not necessarily obstructing to start with. We believe that this is the explanation behind the observation that 50% of all people who have an MI (half of which are fatal) do not have symptoms beforehand,” Dr. Stone commented.
Because these areas of destabilized plaque do not cause symptoms, he believes that vast populations of people with established cardiovascular risk factors should undergo screening. “At the moment we wait for people to experience chest pain or to have an MI – that is far too little too late.”
To identify these areas of high-risk plaques, imaging techniques looking inside the artery wall are needed such as intravascular ultrasound. However, this is an invasive procedure, and the noninvasive coronary CT angiography also gives a good picture, so it is probably the best way to begin as a wider screening modality, with more invasive screening methods then used in those found to be at risk, Dr. Stone suggested.
Plaques that are identified as likely to destabilize can be treated with percutaneous coronary intervention and stenting.
While systemic therapies are useful, those currently available are not sufficient, Dr. Stone noted. For example, there are still high levels of major cardiac events in patients treated with the PCSK9 inhibitors, which bring about very large reductions in LDL cholesterol. “These therapies are beneficial, but they are not enough on their own. So, these areas of unstable plaque would need to be treated with stenting or something similar. We believe that the intervention of stenting is good but at present it is targeted at the wrong areas,” he stated.
“Clearly what we’ve been doing – stenting only obstructive lesions – does not reduce hard clinical events. Imaging methods have improved so much in recent years that we can now identify high-risk areas of plaque. This whole field of studying the vulnerable plaque has been ongoing for many years, but it is only recently that imaging methods have become good enough to identify plaques at risk. This field is now coming of age,” he added.
The next steps are to start identifying these plaques in larger populations, more accurately characterizing those at the highest risk, and then performing randomized trials of preemptive intervention in those believed to be at highest risk, and follow up for clinical events, Dr. Stone explained.
Advances in detecting unstable plaque may also permit early evaluation of novel therapeutics and gauge the intensity of lifestyle and disease-modifying pharmacotherapy, the authors suggested.
This work was supported in part by the National Heart, Lung, and Blood Institute, the American Heart Association, the RRM Charitable Fund, the Simard Fund, and the Schaubert Family. Dr. Libby is an unpaid consultant to or involved in clinical trials with Amgen, AstraZeneca, Baim Institute, Beren Therapeutics, Esperion Therapeutics, Genentech, Kancera, Kowa Pharmaceuticals, MedImmune, Merck, Norvo Nordisk, Novartis, Pfizer, and Sanofi-Regeneron; and is a member of the scientific advisory board for Amgen, Caristo Diagnostics, Cartesian Therapeutics, CSL Behring, DalCor Pharmaceuticals, Dewpoint Therapeutics, Elucid Bioimaging, Kancera, Kowa Pharmaceuticals, Olatec Therapeutics, MedImmune, Moderna, Novartis, PlaqueTec, TenSixteen Bio, Soley Thereapeutics, and XBiotech.
A version of this article first appeared on Medscape.com.
A new strategy for the management of atherosclerotic plaque as a source of major adverse cardiac events is needed with the focus shifting from the flow-limiting coronary artery luminal lesions to the overall atherosclerotic burden, be it obstructive or nonobstructive, according to a review article.
The article, by Peter H. Stone, MD, and Peter Libby, MD, Brigham and Women’s Hospital, Boston, and William E. Boden, MD, Boston University School of Medicine, was published online in JAMA Cardiology.
The review explored new data from vascular biology, atherosclerosis imaging, natural history outcome studies, and large-scale clinical trials that support what the authors refer to as “The Plaque Hypothesis” – the idea that major adverse cardiac events such as myocardial infarction and cardiac death are triggered by destabilization of vulnerable plaque, which may be obstructive or nonobstructive.
“We need to consider embracing a new management strategy that directs our diagnostic and management focus to evaluate the entire length of the atheromatous coronary artery and broaden the target of our therapeutic intervention to include all regions of the plaque (both flow-limiting and non–flow-limiting), even those that are distant from the presumed ischemia-producing obstruction,” the authors concluded.
Dr. Stone explained to this news organization that, for several decades, the medical community has focused on plaques causing severe obstruction of coronary arteries as being responsible for major adverse cardiac events. This approach – known as the Ischemia Hypothesis – has been the accepted strategy for many years, with all guidelines advising the identification of the stenoses that cause the most obstruction for treatment with stenting.
However, the authors pointed out that a number of studies have now suggested that, while these severe obstructive stenoses cause angina, they do not seem to be responsible for the hard events of MI, acute coronary syndrome (ACS), and cardiac death.
Several studies including the COURAGE trial and BARI-2D, and the recent ISCHEMIA trial have all failed to show a reduction in these hard endpoints by intervening on these severe obstructive lesions, Dr. Stone noted.
“We present evidence for a new approach – that it is the composition and vascular biology of the atherosclerotic plaques that cause MI, ACS, and cardiac death, rather than simply how obstructive they are,” he said.
Dr. Stone pointed out that plaque seen on a coronary angiogram looks at only the lumen of the artery, but plaque is primarily based in the wall of the artery, and if that plaque is inflamed it can easily be the culprit responsible for adverse events even without encroaching into the lumen.
“Our paper describes many factors which can cause plaques to destabilize and cause an ACS. These include anatomical, biochemical, and biomechanical features that together cause plaque rupture or erosion and precipitate a clinical event. It is not sufficient to just look for obstructive plaques on a coronary angiogram,” he said. “We are barking up the wrong tree. We need to look for inflamed plaque in the whole wall of the coronary arteries.”
The authors described different factors that identify a plaque at high risk of destabilization. These include a large area of vulnerable plaque, a thin-cap atheroma, a severe inflamed core, macrocalcifications, a large plaque burden, and a physical profile that would encourage a thrombus to become trapped.
“Atherosclerotic plaques are very heterogeneous and complex structures and it is not just the mountain peaks but also the lower foothills that can precipitate a flow-limiting obstruction,” Dr. Stone noted.
“The slope of the mountain is probably very important in the ability for a thrombus to form. If the slope is gradual there isn’t a problem. But if the slope is jagged with sharp edges this can cause a thrombus to become trapped. We need to look at the entirety of plaque and all its risk features to identify the culprit areas that could cause MI or cardiac death. These are typically not the obstructive plaques we have all been fixated on for many years,” he added.
“We need to focus on plaque heterogeneity. Once plaque is old and just made up of scar tissue which is not inflamed it does not cause much [of] a problem – we can probably just leave it alone. Some of these obstructive plaques may cause some angina but many do not cause major cardiac events unless they have other high-risk features,” he said.
“Cardiac events are still caused by obstruction of blood flow but that can be an abrupt process where a thrombus attaches itself to an area of destabilized plaque. These areas of plaque were not necessarily obstructing to start with. We believe that this is the explanation behind the observation that 50% of all people who have an MI (half of which are fatal) do not have symptoms beforehand,” Dr. Stone commented.
Because these areas of destabilized plaque do not cause symptoms, he believes that vast populations of people with established cardiovascular risk factors should undergo screening. “At the moment we wait for people to experience chest pain or to have an MI – that is far too little too late.”
To identify these areas of high-risk plaques, imaging techniques looking inside the artery wall are needed such as intravascular ultrasound. However, this is an invasive procedure, and the noninvasive coronary CT angiography also gives a good picture, so it is probably the best way to begin as a wider screening modality, with more invasive screening methods then used in those found to be at risk, Dr. Stone suggested.
Plaques that are identified as likely to destabilize can be treated with percutaneous coronary intervention and stenting.
While systemic therapies are useful, those currently available are not sufficient, Dr. Stone noted. For example, there are still high levels of major cardiac events in patients treated with the PCSK9 inhibitors, which bring about very large reductions in LDL cholesterol. “These therapies are beneficial, but they are not enough on their own. So, these areas of unstable plaque would need to be treated with stenting or something similar. We believe that the intervention of stenting is good but at present it is targeted at the wrong areas,” he stated.
“Clearly what we’ve been doing – stenting only obstructive lesions – does not reduce hard clinical events. Imaging methods have improved so much in recent years that we can now identify high-risk areas of plaque. This whole field of studying the vulnerable plaque has been ongoing for many years, but it is only recently that imaging methods have become good enough to identify plaques at risk. This field is now coming of age,” he added.
The next steps are to start identifying these plaques in larger populations, more accurately characterizing those at the highest risk, and then performing randomized trials of preemptive intervention in those believed to be at highest risk, and follow up for clinical events, Dr. Stone explained.
Advances in detecting unstable plaque may also permit early evaluation of novel therapeutics and gauge the intensity of lifestyle and disease-modifying pharmacotherapy, the authors suggested.
This work was supported in part by the National Heart, Lung, and Blood Institute, the American Heart Association, the RRM Charitable Fund, the Simard Fund, and the Schaubert Family. Dr. Libby is an unpaid consultant to or involved in clinical trials with Amgen, AstraZeneca, Baim Institute, Beren Therapeutics, Esperion Therapeutics, Genentech, Kancera, Kowa Pharmaceuticals, MedImmune, Merck, Norvo Nordisk, Novartis, Pfizer, and Sanofi-Regeneron; and is a member of the scientific advisory board for Amgen, Caristo Diagnostics, Cartesian Therapeutics, CSL Behring, DalCor Pharmaceuticals, Dewpoint Therapeutics, Elucid Bioimaging, Kancera, Kowa Pharmaceuticals, Olatec Therapeutics, MedImmune, Moderna, Novartis, PlaqueTec, TenSixteen Bio, Soley Thereapeutics, and XBiotech.
A version of this article first appeared on Medscape.com.
A new strategy for the management of atherosclerotic plaque as a source of major adverse cardiac events is needed with the focus shifting from the flow-limiting coronary artery luminal lesions to the overall atherosclerotic burden, be it obstructive or nonobstructive, according to a review article.
The article, by Peter H. Stone, MD, and Peter Libby, MD, Brigham and Women’s Hospital, Boston, and William E. Boden, MD, Boston University School of Medicine, was published online in JAMA Cardiology.
The review explored new data from vascular biology, atherosclerosis imaging, natural history outcome studies, and large-scale clinical trials that support what the authors refer to as “The Plaque Hypothesis” – the idea that major adverse cardiac events such as myocardial infarction and cardiac death are triggered by destabilization of vulnerable plaque, which may be obstructive or nonobstructive.
“We need to consider embracing a new management strategy that directs our diagnostic and management focus to evaluate the entire length of the atheromatous coronary artery and broaden the target of our therapeutic intervention to include all regions of the plaque (both flow-limiting and non–flow-limiting), even those that are distant from the presumed ischemia-producing obstruction,” the authors concluded.
Dr. Stone explained to this news organization that, for several decades, the medical community has focused on plaques causing severe obstruction of coronary arteries as being responsible for major adverse cardiac events. This approach – known as the Ischemia Hypothesis – has been the accepted strategy for many years, with all guidelines advising the identification of the stenoses that cause the most obstruction for treatment with stenting.
However, the authors pointed out that a number of studies have now suggested that, while these severe obstructive stenoses cause angina, they do not seem to be responsible for the hard events of MI, acute coronary syndrome (ACS), and cardiac death.
Several studies including the COURAGE trial and BARI-2D, and the recent ISCHEMIA trial have all failed to show a reduction in these hard endpoints by intervening on these severe obstructive lesions, Dr. Stone noted.
“We present evidence for a new approach – that it is the composition and vascular biology of the atherosclerotic plaques that cause MI, ACS, and cardiac death, rather than simply how obstructive they are,” he said.
Dr. Stone pointed out that plaque seen on a coronary angiogram looks at only the lumen of the artery, but plaque is primarily based in the wall of the artery, and if that plaque is inflamed it can easily be the culprit responsible for adverse events even without encroaching into the lumen.
“Our paper describes many factors which can cause plaques to destabilize and cause an ACS. These include anatomical, biochemical, and biomechanical features that together cause plaque rupture or erosion and precipitate a clinical event. It is not sufficient to just look for obstructive plaques on a coronary angiogram,” he said. “We are barking up the wrong tree. We need to look for inflamed plaque in the whole wall of the coronary arteries.”
The authors described different factors that identify a plaque at high risk of destabilization. These include a large area of vulnerable plaque, a thin-cap atheroma, a severe inflamed core, macrocalcifications, a large plaque burden, and a physical profile that would encourage a thrombus to become trapped.
“Atherosclerotic plaques are very heterogeneous and complex structures and it is not just the mountain peaks but also the lower foothills that can precipitate a flow-limiting obstruction,” Dr. Stone noted.
“The slope of the mountain is probably very important in the ability for a thrombus to form. If the slope is gradual there isn’t a problem. But if the slope is jagged with sharp edges this can cause a thrombus to become trapped. We need to look at the entirety of plaque and all its risk features to identify the culprit areas that could cause MI or cardiac death. These are typically not the obstructive plaques we have all been fixated on for many years,” he added.
“We need to focus on plaque heterogeneity. Once plaque is old and just made up of scar tissue which is not inflamed it does not cause much [of] a problem – we can probably just leave it alone. Some of these obstructive plaques may cause some angina but many do not cause major cardiac events unless they have other high-risk features,” he said.
“Cardiac events are still caused by obstruction of blood flow but that can be an abrupt process where a thrombus attaches itself to an area of destabilized plaque. These areas of plaque were not necessarily obstructing to start with. We believe that this is the explanation behind the observation that 50% of all people who have an MI (half of which are fatal) do not have symptoms beforehand,” Dr. Stone commented.
Because these areas of destabilized plaque do not cause symptoms, he believes that vast populations of people with established cardiovascular risk factors should undergo screening. “At the moment we wait for people to experience chest pain or to have an MI – that is far too little too late.”
To identify these areas of high-risk plaques, imaging techniques looking inside the artery wall are needed such as intravascular ultrasound. However, this is an invasive procedure, and the noninvasive coronary CT angiography also gives a good picture, so it is probably the best way to begin as a wider screening modality, with more invasive screening methods then used in those found to be at risk, Dr. Stone suggested.
Plaques that are identified as likely to destabilize can be treated with percutaneous coronary intervention and stenting.
While systemic therapies are useful, those currently available are not sufficient, Dr. Stone noted. For example, there are still high levels of major cardiac events in patients treated with the PCSK9 inhibitors, which bring about very large reductions in LDL cholesterol. “These therapies are beneficial, but they are not enough on their own. So, these areas of unstable plaque would need to be treated with stenting or something similar. We believe that the intervention of stenting is good but at present it is targeted at the wrong areas,” he stated.
“Clearly what we’ve been doing – stenting only obstructive lesions – does not reduce hard clinical events. Imaging methods have improved so much in recent years that we can now identify high-risk areas of plaque. This whole field of studying the vulnerable plaque has been ongoing for many years, but it is only recently that imaging methods have become good enough to identify plaques at risk. This field is now coming of age,” he added.
The next steps are to start identifying these plaques in larger populations, more accurately characterizing those at the highest risk, and then performing randomized trials of preemptive intervention in those believed to be at highest risk, and follow up for clinical events, Dr. Stone explained.
Advances in detecting unstable plaque may also permit early evaluation of novel therapeutics and gauge the intensity of lifestyle and disease-modifying pharmacotherapy, the authors suggested.
This work was supported in part by the National Heart, Lung, and Blood Institute, the American Heart Association, the RRM Charitable Fund, the Simard Fund, and the Schaubert Family. Dr. Libby is an unpaid consultant to or involved in clinical trials with Amgen, AstraZeneca, Baim Institute, Beren Therapeutics, Esperion Therapeutics, Genentech, Kancera, Kowa Pharmaceuticals, MedImmune, Merck, Norvo Nordisk, Novartis, Pfizer, and Sanofi-Regeneron; and is a member of the scientific advisory board for Amgen, Caristo Diagnostics, Cartesian Therapeutics, CSL Behring, DalCor Pharmaceuticals, Dewpoint Therapeutics, Elucid Bioimaging, Kancera, Kowa Pharmaceuticals, Olatec Therapeutics, MedImmune, Moderna, Novartis, PlaqueTec, TenSixteen Bio, Soley Thereapeutics, and XBiotech.
A version of this article first appeared on Medscape.com.
New AHA statement on managing ACS in older adults
Age-related changes in general and cardiovascular health likely require modifications in how acute coronary syndrome (ACS) is diagnosed and managed in adults aged 75 and older, the American Heart Association says in a new scientific statement.
The statement outlines a framework to integrate geriatric risks into the management of ACS, including the diagnostic approach, pharmacotherapy, revascularization strategies, prevention of adverse events, and transition care planning.
The 31-page statement was published online in the AHA journal Circulation (2022 Dec 12. doi: 10.1161/CIR.0000000000001112). It updates a 2007 AHA statement on treatment of ACS in the elderly.
Complex patient group
Adults aged 75 and older make up roughly 30%-40% of all hospitalized patients with ACS and the majority of ACS-related deaths occur in this group, the writing group notes.

“Older patients have more pronounced anatomical changes and more severe functional impairment, and they are more likely to have additional health conditions,” writing group chair Abdulla A. Damluji, MD, PhD, director of the Inova Center of Outcomes Research in Fairfax, Va., notes in a news release.
“These include frailty, other chronic disorders (treated with multiple medications), physical dysfunction, cognitive decline and/or urinary incontinence – and these are not regularly studied in the context of ACS,” Dr. Damluji explained.
The writing group notes that the presence of one or more geriatric syndromes may substantially affect ACS clinical presentation, clinical course and prognosis, therapeutic decision-making, and response to treatment.
“It is therefore fundamental that clinicians caring for older patients with ACS be alert to the presence of geriatric syndromes and be able to integrate them into the care plan when appropriate,” they say.
They recommend a holistic, individualized, and patient-centered approach to ACS care in the elderly, taking into consideration coexisting and overlapping health issues.
Considerations for clinical care
The AHA statement offers several “considerations for clinical practice” with regard to ACS diagnosis and management in elderly adults. They include:
- ACS presentations without chest pain, such as shortness of breath, syncope, or sudden confusion, are more common in older adults.
- Many older adults have persistent elevations in cardiac troponin levels from myocardial fibrosis and kidney disease that diminish the positive predictive value of high-sensitivity cardiac troponin (hs-cTn) assays for identifying acute and chronic myocardial injury. For this reason, evaluating patterns of rise and fall is essential.
- Age-related changes in metabolism, weight, and muscle mass may require different choices in anticoagulant medications to lower bleeding risk.
- Clopidogrel (Plavix) is the preferred P2Y12 inhibitor because of a significantly lower bleeding profile than ticagrelor (Brilinta) or prasugrel (Effient). For patients with ST-segment myocardial infarction (STEMI) or complex anatomy, the use of ticagrelor is “reasonable.”
- Poor kidney function can increase the risk for contrast-induced acute kidney injury.
- Although the risks are greater, percutaneous coronary intervention or bypass surgery are beneficial in select older adults with ACS.
- Post-MI care should include cardiac rehabilitation tailored to address each patient’s circumstances and personal goals of care.
- For patients with cognitive difficulties and limited mobility, consider simplified medication plans with fewer doses per day and 90-day supplies to prevent the need for frequent refills.
- Patient care plans should be individualized, with input from a multidisciplinary team that may include cardiologists, surgeons, geriatricians, primary care clinicians, nutritionists, social workers, and family members.
- Determine a priori goals of care in older patients to help avoid an unwanted or futile intervention.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardiovascular Diseases in Older Populations Committee of the Council on Clinical Cardiology; the Council on Cardiovascular and Stroke Nursing; the Council on Cardiovascular Radiology and Intervention; and the Council on Lifestyle and Cardiometabolic Health.
A version of this article first appeared on Medscape.com.
Age-related changes in general and cardiovascular health likely require modifications in how acute coronary syndrome (ACS) is diagnosed and managed in adults aged 75 and older, the American Heart Association says in a new scientific statement.
The statement outlines a framework to integrate geriatric risks into the management of ACS, including the diagnostic approach, pharmacotherapy, revascularization strategies, prevention of adverse events, and transition care planning.
The 31-page statement was published online in the AHA journal Circulation (2022 Dec 12. doi: 10.1161/CIR.0000000000001112). It updates a 2007 AHA statement on treatment of ACS in the elderly.
Complex patient group
Adults aged 75 and older make up roughly 30%-40% of all hospitalized patients with ACS and the majority of ACS-related deaths occur in this group, the writing group notes.
“Older patients have more pronounced anatomical changes and more severe functional impairment, and they are more likely to have additional health conditions,” writing group chair Abdulla A. Damluji, MD, PhD, director of the Inova Center of Outcomes Research in Fairfax, Va., notes in a news release.
“These include frailty, other chronic disorders (treated with multiple medications), physical dysfunction, cognitive decline and/or urinary incontinence – and these are not regularly studied in the context of ACS,” Dr. Damluji explained.
The writing group notes that the presence of one or more geriatric syndromes may substantially affect ACS clinical presentation, clinical course and prognosis, therapeutic decision-making, and response to treatment.
“It is therefore fundamental that clinicians caring for older patients with ACS be alert to the presence of geriatric syndromes and be able to integrate them into the care plan when appropriate,” they say.
They recommend a holistic, individualized, and patient-centered approach to ACS care in the elderly, taking into consideration coexisting and overlapping health issues.
Considerations for clinical care
The AHA statement offers several “considerations for clinical practice” with regard to ACS diagnosis and management in elderly adults. They include:
- ACS presentations without chest pain, such as shortness of breath, syncope, or sudden confusion, are more common in older adults.
- Many older adults have persistent elevations in cardiac troponin levels from myocardial fibrosis and kidney disease that diminish the positive predictive value of high-sensitivity cardiac troponin (hs-cTn) assays for identifying acute and chronic myocardial injury. For this reason, evaluating patterns of rise and fall is essential.
- Age-related changes in metabolism, weight, and muscle mass may require different choices in anticoagulant medications to lower bleeding risk.
- Clopidogrel (Plavix) is the preferred P2Y12 inhibitor because of a significantly lower bleeding profile than ticagrelor (Brilinta) or prasugrel (Effient). For patients with ST-segment myocardial infarction (STEMI) or complex anatomy, the use of ticagrelor is “reasonable.”
- Poor kidney function can increase the risk for contrast-induced acute kidney injury.
- Although the risks are greater, percutaneous coronary intervention or bypass surgery are beneficial in select older adults with ACS.
- Post-MI care should include cardiac rehabilitation tailored to address each patient’s circumstances and personal goals of care.
- For patients with cognitive difficulties and limited mobility, consider simplified medication plans with fewer doses per day and 90-day supplies to prevent the need for frequent refills.
- Patient care plans should be individualized, with input from a multidisciplinary team that may include cardiologists, surgeons, geriatricians, primary care clinicians, nutritionists, social workers, and family members.
- Determine a priori goals of care in older patients to help avoid an unwanted or futile intervention.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardiovascular Diseases in Older Populations Committee of the Council on Clinical Cardiology; the Council on Cardiovascular and Stroke Nursing; the Council on Cardiovascular Radiology and Intervention; and the Council on Lifestyle and Cardiometabolic Health.
A version of this article first appeared on Medscape.com.
Age-related changes in general and cardiovascular health likely require modifications in how acute coronary syndrome (ACS) is diagnosed and managed in adults aged 75 and older, the American Heart Association says in a new scientific statement.
The statement outlines a framework to integrate geriatric risks into the management of ACS, including the diagnostic approach, pharmacotherapy, revascularization strategies, prevention of adverse events, and transition care planning.
The 31-page statement was published online in the AHA journal Circulation (2022 Dec 12. doi: 10.1161/CIR.0000000000001112). It updates a 2007 AHA statement on treatment of ACS in the elderly.
Complex patient group
Adults aged 75 and older make up roughly 30%-40% of all hospitalized patients with ACS and the majority of ACS-related deaths occur in this group, the writing group notes.
“Older patients have more pronounced anatomical changes and more severe functional impairment, and they are more likely to have additional health conditions,” writing group chair Abdulla A. Damluji, MD, PhD, director of the Inova Center of Outcomes Research in Fairfax, Va., notes in a news release.
“These include frailty, other chronic disorders (treated with multiple medications), physical dysfunction, cognitive decline and/or urinary incontinence – and these are not regularly studied in the context of ACS,” Dr. Damluji explained.
The writing group notes that the presence of one or more geriatric syndromes may substantially affect ACS clinical presentation, clinical course and prognosis, therapeutic decision-making, and response to treatment.
“It is therefore fundamental that clinicians caring for older patients with ACS be alert to the presence of geriatric syndromes and be able to integrate them into the care plan when appropriate,” they say.
They recommend a holistic, individualized, and patient-centered approach to ACS care in the elderly, taking into consideration coexisting and overlapping health issues.
Considerations for clinical care
The AHA statement offers several “considerations for clinical practice” with regard to ACS diagnosis and management in elderly adults. They include:
- ACS presentations without chest pain, such as shortness of breath, syncope, or sudden confusion, are more common in older adults.
- Many older adults have persistent elevations in cardiac troponin levels from myocardial fibrosis and kidney disease that diminish the positive predictive value of high-sensitivity cardiac troponin (hs-cTn) assays for identifying acute and chronic myocardial injury. For this reason, evaluating patterns of rise and fall is essential.
- Age-related changes in metabolism, weight, and muscle mass may require different choices in anticoagulant medications to lower bleeding risk.
- Clopidogrel (Plavix) is the preferred P2Y12 inhibitor because of a significantly lower bleeding profile than ticagrelor (Brilinta) or prasugrel (Effient). For patients with ST-segment myocardial infarction (STEMI) or complex anatomy, the use of ticagrelor is “reasonable.”
- Poor kidney function can increase the risk for contrast-induced acute kidney injury.
- Although the risks are greater, percutaneous coronary intervention or bypass surgery are beneficial in select older adults with ACS.
- Post-MI care should include cardiac rehabilitation tailored to address each patient’s circumstances and personal goals of care.
- For patients with cognitive difficulties and limited mobility, consider simplified medication plans with fewer doses per day and 90-day supplies to prevent the need for frequent refills.
- Patient care plans should be individualized, with input from a multidisciplinary team that may include cardiologists, surgeons, geriatricians, primary care clinicians, nutritionists, social workers, and family members.
- Determine a priori goals of care in older patients to help avoid an unwanted or futile intervention.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardiovascular Diseases in Older Populations Committee of the Council on Clinical Cardiology; the Council on Cardiovascular and Stroke Nursing; the Council on Cardiovascular Radiology and Intervention; and the Council on Lifestyle and Cardiometabolic Health.
A version of this article first appeared on Medscape.com.
Principles and Process for Reducing the Need for Insulin in Patients With Type 2 Diabetes
For people living with type 2 diabetes mellitus (T2D), exogenous insulin, whether given early or later in T2D diagnosis, can provide many pharmacologically desirable effects. But it has always been clear, and is now more widely recognized, that insulin treatments are not completely risk-free for the patient. There are now newer, non-insulin therapy options that could be used, along with certain patient lifestyle changes in diet and activity levels, that have been shown to achieve desired glucose control—without the associated risks that insulin can bring.
But is it possible to markedly reduce the need for insulin in some 90% of T2D patients and to reduce the doses in the others? Yes—if patients have sufficient beta-cell function and are willing to change their lifestyle. This mode of treatment has been slowly gaining momentum as of late in the medical community because of the benefits it ultimately provides for the patient. In my practice, I personally have done this by using an evidence-based approach that includes thinking inside a larger box. It is a 2-way street, and each should drive the other: the right drugs (in the right doses), and in the right patients.
Why avoid early insulin therapy?
Is the requirement of early insulin therapy in many or most patients a myth?
Yes. It resulted from “old logic,” which was to use insulin early to reduce glucotoxicity and lipotoxicity. The American Diabetes Association guidelines recommend that glycated hemoglobin (HbA1c) should not exceed 8.0% and consider a fasting blood glucose level >250 mg/dL as high, with a need to start insulin treatment right away; other guidelines recommend initiating insulin immediately in patients with HbA1c >9% and postprandial glucose 300 mg/dL. But this was at a time when oral agents were not as effective and took time to titrate or engender good control. We now have agents that are more effective and start working right away.
However, the main problem in early insulin treatment is the significant risk of over-insulinization—a vicious cycle of insulin-caused increased appetite, hypoglycemia-resultant increased weight gain, insulin resistance (poorer control), increased circulating insulin, etc. Moreover, weight gain and individual hypoglycemic events can cause an increase in the risk of cardiovascular (CV) events.
I believe clinicians must start as early as possible in the natural history of T2D to prevent progressive beta-cell failure. Do not believe in “first-, second-, or third-line”; in other words, do not prioritize, so there is no competition between classes. The goal I have for my patients is to provide therapies that aim for the lowest HbA1c possible without hypoglycemia, provide the greatest CV benefit, and assist in weight reduction.
My protocol, “the egregious eleven,” involves using the least number of agents in combinations that treat the greatest number of mechanisms of hyperglycemia—without the use of sulfonylureas (which cause beta-cell apoptosis, hypoglycemia, and weight gain). Fortunately, newer agents, such as glucagon-like peptide 1 receptor agonist (GLP-1 RA) and sodium-glucose cotransporter 1 (SGLT-2) inhibitors, work right away, cause weight reduction, and have side benefits of CV risk reduction—as well as preserve beta-cell function. Metformin remains a valuable agent and has its own potential side benefits, and bromocriptine-QR and pioglitazone have CV side benefits. So, there is really no need for early insulin in true T2D patients (ie, those that are non-ketosis prone and have sufficient beta-cell reserve).
Why reduce insulin in patients who are already on insulin?
Prior protocols resulted in 40%-50% of T2D patients being placed on insulin unnecessarily. As discussed, the side effects of insulin are many; they include weight gain, insulin resistance, hypoglycemia, and CV complications—all of which have been associated with a decline in quality of life.
What is your approach to reduce or eliminate insulin in those already on it (unnecessarily)?
First, I pick the right patient. Physicians should use sound clinical judgment to identify patients with likely residual beta-cell function. It is not just the “insulin-resistant patient," as 30%-50% of type 1 diabetes mellitus patients also have insulin resistance.
It needs to be a definite T2D patient: not ketosis prone, a family history T2D, no islet cell antibodies (if one has any concerns, check for them). They were often started on insulin in the emergency department with no ketosis and never received non-insulin therapy.
Patients need to be willing to commit to my strict, no-concentrated-sweets diet, to perform careful glucose monitoring, and to check their ketones. Patients should be willing to contact me if their sugar level is >250 mg/dL for 2 measurements in a row, while testing 4 times a day or using a continuous glucose-monitoring (CGM) device.
First, estimate a patient’s “current insulin need” (CIN), or the dose they might be on if they had not been subject to over-insulinization (ie, if they had not been subject to the “vicious cycle” discussed above). I do this by taking their total basal and bolus insulin dose, then reducing it by ~25% as the patient changes to a no-concentrated-sweets diet with an additional up-to-25% dose reduction if the patient has been experiencing symptomatic or asymptomatic hypoglycemia.
Next, I reduce this CIN number by ~25% upon starting a rapid-acting subcutaneous GLP-1 RA (liraglutide or oral semaglutide) and reduce the CIN another 20% as they start the SGLT-2 inhibitor. If patients come into my office on <40 U/d, I stop insulin as I start a GLP-1 RA and an SGLT-2 inhibitor and have them monitor home glucose levels to assure reasonable results as they go off the insulin and on their new therapy.
If patients come into my office on >40 U/d, they go home on a GLP-1 RA and an SGLT-2 inhibitor and ~30% of their presenting dose, apportioned between basal/bolus dosing based on when they are currently getting hypoglycemic.
The rapid initial reduction in their insulin doses, with initial adjustments in estimated insulin doses as needed based on home glucose monitoring, and rapid stabilization of glycemic levels by the effectiveness of these 2 agents give patients great motivation to keep up with the diet/program.
Then, as patients lose weight, they are told to report any glucose measurements <80 mg/dL, so that further reduction in insulin doses can be made. When patients achieve a new steady state of glycemia, weight, and GLP-1 RA and SGLT-2 inhibitor doses, you can add bromocriptine-QR, pioglitazone, and/or metformin as needed to allow for a further reduction of insulin. And, as you see the delayed effects of subsequently adding these new agents (eg, glucose <80 mg/dL), you can ultimately stop insulin when they get to <10-12 U/d. The process works very well, even in those starting on up to 300 units of insulin daily. Patients love the outcome and will greatly appreciate your care.
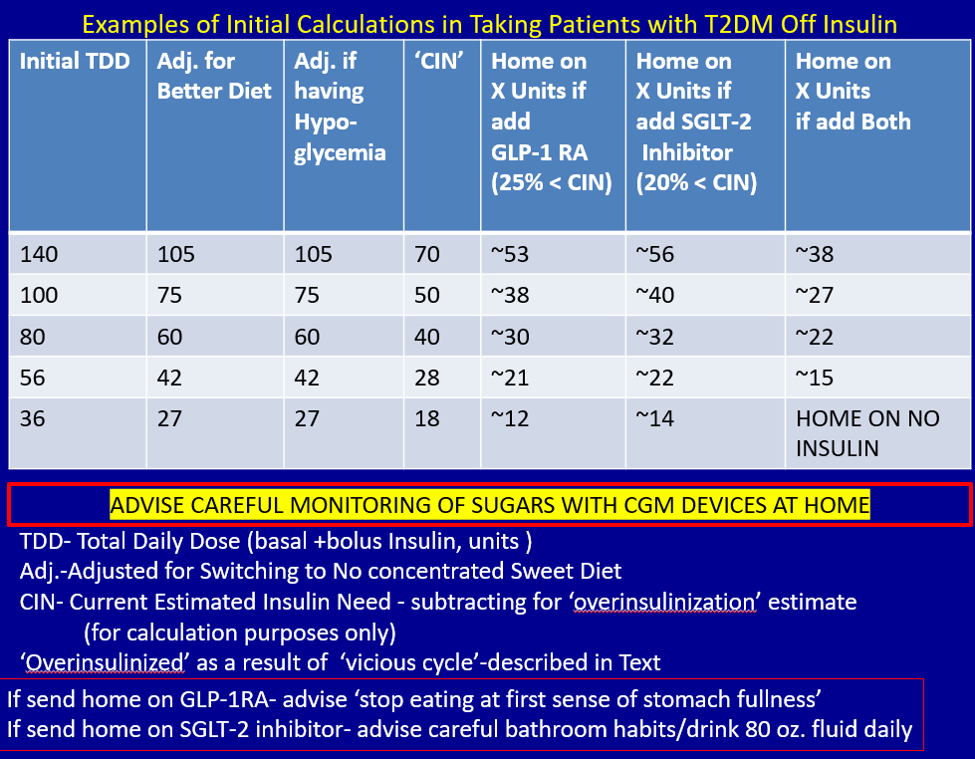
Feel free to contact Dr. Schwartz at [email protected] with any questions about his protocol or diet.
For people living with type 2 diabetes mellitus (T2D), exogenous insulin, whether given early or later in T2D diagnosis, can provide many pharmacologically desirable effects. But it has always been clear, and is now more widely recognized, that insulin treatments are not completely risk-free for the patient. There are now newer, non-insulin therapy options that could be used, along with certain patient lifestyle changes in diet and activity levels, that have been shown to achieve desired glucose control—without the associated risks that insulin can bring.
But is it possible to markedly reduce the need for insulin in some 90% of T2D patients and to reduce the doses in the others? Yes—if patients have sufficient beta-cell function and are willing to change their lifestyle. This mode of treatment has been slowly gaining momentum as of late in the medical community because of the benefits it ultimately provides for the patient. In my practice, I personally have done this by using an evidence-based approach that includes thinking inside a larger box. It is a 2-way street, and each should drive the other: the right drugs (in the right doses), and in the right patients.
Why avoid early insulin therapy?
Is the requirement of early insulin therapy in many or most patients a myth?
Yes. It resulted from “old logic,” which was to use insulin early to reduce glucotoxicity and lipotoxicity. The American Diabetes Association guidelines recommend that glycated hemoglobin (HbA1c) should not exceed 8.0% and consider a fasting blood glucose level >250 mg/dL as high, with a need to start insulin treatment right away; other guidelines recommend initiating insulin immediately in patients with HbA1c >9% and postprandial glucose 300 mg/dL. But this was at a time when oral agents were not as effective and took time to titrate or engender good control. We now have agents that are more effective and start working right away.
However, the main problem in early insulin treatment is the significant risk of over-insulinization—a vicious cycle of insulin-caused increased appetite, hypoglycemia-resultant increased weight gain, insulin resistance (poorer control), increased circulating insulin, etc. Moreover, weight gain and individual hypoglycemic events can cause an increase in the risk of cardiovascular (CV) events.
I believe clinicians must start as early as possible in the natural history of T2D to prevent progressive beta-cell failure. Do not believe in “first-, second-, or third-line”; in other words, do not prioritize, so there is no competition between classes. The goal I have for my patients is to provide therapies that aim for the lowest HbA1c possible without hypoglycemia, provide the greatest CV benefit, and assist in weight reduction.
My protocol, “the egregious eleven,” involves using the least number of agents in combinations that treat the greatest number of mechanisms of hyperglycemia—without the use of sulfonylureas (which cause beta-cell apoptosis, hypoglycemia, and weight gain). Fortunately, newer agents, such as glucagon-like peptide 1 receptor agonist (GLP-1 RA) and sodium-glucose cotransporter 1 (SGLT-2) inhibitors, work right away, cause weight reduction, and have side benefits of CV risk reduction—as well as preserve beta-cell function. Metformin remains a valuable agent and has its own potential side benefits, and bromocriptine-QR and pioglitazone have CV side benefits. So, there is really no need for early insulin in true T2D patients (ie, those that are non-ketosis prone and have sufficient beta-cell reserve).
Why reduce insulin in patients who are already on insulin?
Prior protocols resulted in 40%-50% of T2D patients being placed on insulin unnecessarily. As discussed, the side effects of insulin are many; they include weight gain, insulin resistance, hypoglycemia, and CV complications—all of which have been associated with a decline in quality of life.
What is your approach to reduce or eliminate insulin in those already on it (unnecessarily)?
First, I pick the right patient. Physicians should use sound clinical judgment to identify patients with likely residual beta-cell function. It is not just the “insulin-resistant patient," as 30%-50% of type 1 diabetes mellitus patients also have insulin resistance.
It needs to be a definite T2D patient: not ketosis prone, a family history T2D, no islet cell antibodies (if one has any concerns, check for them). They were often started on insulin in the emergency department with no ketosis and never received non-insulin therapy.
Patients need to be willing to commit to my strict, no-concentrated-sweets diet, to perform careful glucose monitoring, and to check their ketones. Patients should be willing to contact me if their sugar level is >250 mg/dL for 2 measurements in a row, while testing 4 times a day or using a continuous glucose-monitoring (CGM) device.
First, estimate a patient’s “current insulin need” (CIN), or the dose they might be on if they had not been subject to over-insulinization (ie, if they had not been subject to the “vicious cycle” discussed above). I do this by taking their total basal and bolus insulin dose, then reducing it by ~25% as the patient changes to a no-concentrated-sweets diet with an additional up-to-25% dose reduction if the patient has been experiencing symptomatic or asymptomatic hypoglycemia.
Next, I reduce this CIN number by ~25% upon starting a rapid-acting subcutaneous GLP-1 RA (liraglutide or oral semaglutide) and reduce the CIN another 20% as they start the SGLT-2 inhibitor. If patients come into my office on <40 U/d, I stop insulin as I start a GLP-1 RA and an SGLT-2 inhibitor and have them monitor home glucose levels to assure reasonable results as they go off the insulin and on their new therapy.
If patients come into my office on >40 U/d, they go home on a GLP-1 RA and an SGLT-2 inhibitor and ~30% of their presenting dose, apportioned between basal/bolus dosing based on when they are currently getting hypoglycemic.
The rapid initial reduction in their insulin doses, with initial adjustments in estimated insulin doses as needed based on home glucose monitoring, and rapid stabilization of glycemic levels by the effectiveness of these 2 agents give patients great motivation to keep up with the diet/program.
Then, as patients lose weight, they are told to report any glucose measurements <80 mg/dL, so that further reduction in insulin doses can be made. When patients achieve a new steady state of glycemia, weight, and GLP-1 RA and SGLT-2 inhibitor doses, you can add bromocriptine-QR, pioglitazone, and/or metformin as needed to allow for a further reduction of insulin. And, as you see the delayed effects of subsequently adding these new agents (eg, glucose <80 mg/dL), you can ultimately stop insulin when they get to <10-12 U/d. The process works very well, even in those starting on up to 300 units of insulin daily. Patients love the outcome and will greatly appreciate your care.
Feel free to contact Dr. Schwartz at [email protected] with any questions about his protocol or diet.
For people living with type 2 diabetes mellitus (T2D), exogenous insulin, whether given early or later in T2D diagnosis, can provide many pharmacologically desirable effects. But it has always been clear, and is now more widely recognized, that insulin treatments are not completely risk-free for the patient. There are now newer, non-insulin therapy options that could be used, along with certain patient lifestyle changes in diet and activity levels, that have been shown to achieve desired glucose control—without the associated risks that insulin can bring.
But is it possible to markedly reduce the need for insulin in some 90% of T2D patients and to reduce the doses in the others? Yes—if patients have sufficient beta-cell function and are willing to change their lifestyle. This mode of treatment has been slowly gaining momentum as of late in the medical community because of the benefits it ultimately provides for the patient. In my practice, I personally have done this by using an evidence-based approach that includes thinking inside a larger box. It is a 2-way street, and each should drive the other: the right drugs (in the right doses), and in the right patients.
Why avoid early insulin therapy?
Is the requirement of early insulin therapy in many or most patients a myth?
Yes. It resulted from “old logic,” which was to use insulin early to reduce glucotoxicity and lipotoxicity. The American Diabetes Association guidelines recommend that glycated hemoglobin (HbA1c) should not exceed 8.0% and consider a fasting blood glucose level >250 mg/dL as high, with a need to start insulin treatment right away; other guidelines recommend initiating insulin immediately in patients with HbA1c >9% and postprandial glucose 300 mg/dL. But this was at a time when oral agents were not as effective and took time to titrate or engender good control. We now have agents that are more effective and start working right away.
However, the main problem in early insulin treatment is the significant risk of over-insulinization—a vicious cycle of insulin-caused increased appetite, hypoglycemia-resultant increased weight gain, insulin resistance (poorer control), increased circulating insulin, etc. Moreover, weight gain and individual hypoglycemic events can cause an increase in the risk of cardiovascular (CV) events.
I believe clinicians must start as early as possible in the natural history of T2D to prevent progressive beta-cell failure. Do not believe in “first-, second-, or third-line”; in other words, do not prioritize, so there is no competition between classes. The goal I have for my patients is to provide therapies that aim for the lowest HbA1c possible without hypoglycemia, provide the greatest CV benefit, and assist in weight reduction.
My protocol, “the egregious eleven,” involves using the least number of agents in combinations that treat the greatest number of mechanisms of hyperglycemia—without the use of sulfonylureas (which cause beta-cell apoptosis, hypoglycemia, and weight gain). Fortunately, newer agents, such as glucagon-like peptide 1 receptor agonist (GLP-1 RA) and sodium-glucose cotransporter 1 (SGLT-2) inhibitors, work right away, cause weight reduction, and have side benefits of CV risk reduction—as well as preserve beta-cell function. Metformin remains a valuable agent and has its own potential side benefits, and bromocriptine-QR and pioglitazone have CV side benefits. So, there is really no need for early insulin in true T2D patients (ie, those that are non-ketosis prone and have sufficient beta-cell reserve).
Why reduce insulin in patients who are already on insulin?
Prior protocols resulted in 40%-50% of T2D patients being placed on insulin unnecessarily. As discussed, the side effects of insulin are many; they include weight gain, insulin resistance, hypoglycemia, and CV complications—all of which have been associated with a decline in quality of life.
What is your approach to reduce or eliminate insulin in those already on it (unnecessarily)?
First, I pick the right patient. Physicians should use sound clinical judgment to identify patients with likely residual beta-cell function. It is not just the “insulin-resistant patient," as 30%-50% of type 1 diabetes mellitus patients also have insulin resistance.
It needs to be a definite T2D patient: not ketosis prone, a family history T2D, no islet cell antibodies (if one has any concerns, check for them). They were often started on insulin in the emergency department with no ketosis and never received non-insulin therapy.
Patients need to be willing to commit to my strict, no-concentrated-sweets diet, to perform careful glucose monitoring, and to check their ketones. Patients should be willing to contact me if their sugar level is >250 mg/dL for 2 measurements in a row, while testing 4 times a day or using a continuous glucose-monitoring (CGM) device.
First, estimate a patient’s “current insulin need” (CIN), or the dose they might be on if they had not been subject to over-insulinization (ie, if they had not been subject to the “vicious cycle” discussed above). I do this by taking their total basal and bolus insulin dose, then reducing it by ~25% as the patient changes to a no-concentrated-sweets diet with an additional up-to-25% dose reduction if the patient has been experiencing symptomatic or asymptomatic hypoglycemia.
Next, I reduce this CIN number by ~25% upon starting a rapid-acting subcutaneous GLP-1 RA (liraglutide or oral semaglutide) and reduce the CIN another 20% as they start the SGLT-2 inhibitor. If patients come into my office on <40 U/d, I stop insulin as I start a GLP-1 RA and an SGLT-2 inhibitor and have them monitor home glucose levels to assure reasonable results as they go off the insulin and on their new therapy.
If patients come into my office on >40 U/d, they go home on a GLP-1 RA and an SGLT-2 inhibitor and ~30% of their presenting dose, apportioned between basal/bolus dosing based on when they are currently getting hypoglycemic.
The rapid initial reduction in their insulin doses, with initial adjustments in estimated insulin doses as needed based on home glucose monitoring, and rapid stabilization of glycemic levels by the effectiveness of these 2 agents give patients great motivation to keep up with the diet/program.
Then, as patients lose weight, they are told to report any glucose measurements <80 mg/dL, so that further reduction in insulin doses can be made. When patients achieve a new steady state of glycemia, weight, and GLP-1 RA and SGLT-2 inhibitor doses, you can add bromocriptine-QR, pioglitazone, and/or metformin as needed to allow for a further reduction of insulin. And, as you see the delayed effects of subsequently adding these new agents (eg, glucose <80 mg/dL), you can ultimately stop insulin when they get to <10-12 U/d. The process works very well, even in those starting on up to 300 units of insulin daily. Patients love the outcome and will greatly appreciate your care.
Feel free to contact Dr. Schwartz at [email protected] with any questions about his protocol or diet.
A reason for hope in the face of long COVID
In this issue, Mayo and colleagues1 summarize what we know about patients with long COVID. The report made me pause and realize that it has been 3 years since we heard the very first reports of patients infected with SARS-CoV-2, which would eventually cause the COVID-19 pandemic. I suspect that I am not alone in having been fascinated by the rapid communication of information (of variable quality and veracity) via peer-reviewed papers, pre-print servers, the media, and social media.
The early studies were largely descriptive, focusing on symptom constellations and outbreak data. Much of what we had by way of treatment was supportive and “let’s try anything”—whether reasonable or, in some cases, not. In relatively short order, though, we developed effective vaccines to help protect people from getting seriously ill, being hospitalized, and dying; we also identified targeted therapies for those who became ill.2 But variants continued—or rather, continue—to emerge, and we remain committed to meeting the demands of the day.
The Centers for Disease Control and Prevention reports that more than 98 million Americans have contracted COVID, and more than 1 million have died.3 Besides the astonishingly high total mortality, the ravages of COVID-19 include new-onset respiratory, cardiovascular, neurologic, and psychiatric illnesses.4,5 As many as half of adults hospitalized for COVID report having persistent symptoms.6
As described in this issue, what we know about long COVID appears to be following the early course of its parent illness. As was true then, we are learning about the symptoms, etiology, and best ways to manage our patients. As in the early days of the pandemic, treatment is supportive, and we await definitive therapies.
I am optimistic, though. Why? Because shortly after the first reports of COVID-19, the virus’ DNA sequence was shared online. Based on that information, diagnostic assays were developed. Within 2 years of the outbreak, we had effective vaccines and specific therapies.
Another call to action. If 5% of patients contracting COVID (a very low estimate) develop long COVID, that would translate to 4.9 million people with long COVID in the United States. That is an astounding burden of suffering that I have no doubt will motivate innovation.
Innovation is a strength of the US health care system. I believe we will rise to the next challenge that COVID-19 has put before us. We have reason to be hopeful.
1. Mayo NL, Ellenbogen RL, Mendoza MD, et al. The family physician’s role in long COVID management. J Fam Pract. 2022;71:426-431. doi: 10.12788/jfp.0517
2. Kulshreshtha A, Sizemore S, Barry HC. COVID-19 therapy: What works? What doesn’t? And what’s on the horizon? J Fam Pract. 2022;71:E3-E16. doi: 10.12788/jfp.0474
3. CDC. COVID data tracker. Accessed December 5, 2022. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
4. Taquet M, Geddes JR, Husain M, et al. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8:416-427. doi: 10.1016/s2215-0366(21) 00084-5
5. Ayoubkhani D, Khunti K, Nafilyan V, et al. Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ. 2021;372:n693. doi: 10.1136/bmj.n693
6. Writing Committee for the Comebac Study Group, Morin L, Savale L, Pham T, et al. Four-month clinical status of a cohort of patients after hospitalization for COVID-19. JAMA. 2021;325:1525-1534. doi: 10.1001/jama.2021.3331
In this issue, Mayo and colleagues1 summarize what we know about patients with long COVID. The report made me pause and realize that it has been 3 years since we heard the very first reports of patients infected with SARS-CoV-2, which would eventually cause the COVID-19 pandemic. I suspect that I am not alone in having been fascinated by the rapid communication of information (of variable quality and veracity) via peer-reviewed papers, pre-print servers, the media, and social media.
The early studies were largely descriptive, focusing on symptom constellations and outbreak data. Much of what we had by way of treatment was supportive and “let’s try anything”—whether reasonable or, in some cases, not. In relatively short order, though, we developed effective vaccines to help protect people from getting seriously ill, being hospitalized, and dying; we also identified targeted therapies for those who became ill.2 But variants continued—or rather, continue—to emerge, and we remain committed to meeting the demands of the day.
The Centers for Disease Control and Prevention reports that more than 98 million Americans have contracted COVID, and more than 1 million have died.3 Besides the astonishingly high total mortality, the ravages of COVID-19 include new-onset respiratory, cardiovascular, neurologic, and psychiatric illnesses.4,5 As many as half of adults hospitalized for COVID report having persistent symptoms.6
As described in this issue, what we know about long COVID appears to be following the early course of its parent illness. As was true then, we are learning about the symptoms, etiology, and best ways to manage our patients. As in the early days of the pandemic, treatment is supportive, and we await definitive therapies.
I am optimistic, though. Why? Because shortly after the first reports of COVID-19, the virus’ DNA sequence was shared online. Based on that information, diagnostic assays were developed. Within 2 years of the outbreak, we had effective vaccines and specific therapies.
Another call to action. If 5% of patients contracting COVID (a very low estimate) develop long COVID, that would translate to 4.9 million people with long COVID in the United States. That is an astounding burden of suffering that I have no doubt will motivate innovation.
Innovation is a strength of the US health care system. I believe we will rise to the next challenge that COVID-19 has put before us. We have reason to be hopeful.
In this issue, Mayo and colleagues1 summarize what we know about patients with long COVID. The report made me pause and realize that it has been 3 years since we heard the very first reports of patients infected with SARS-CoV-2, which would eventually cause the COVID-19 pandemic. I suspect that I am not alone in having been fascinated by the rapid communication of information (of variable quality and veracity) via peer-reviewed papers, pre-print servers, the media, and social media.
The early studies were largely descriptive, focusing on symptom constellations and outbreak data. Much of what we had by way of treatment was supportive and “let’s try anything”—whether reasonable or, in some cases, not. In relatively short order, though, we developed effective vaccines to help protect people from getting seriously ill, being hospitalized, and dying; we also identified targeted therapies for those who became ill.2 But variants continued—or rather, continue—to emerge, and we remain committed to meeting the demands of the day.
The Centers for Disease Control and Prevention reports that more than 98 million Americans have contracted COVID, and more than 1 million have died.3 Besides the astonishingly high total mortality, the ravages of COVID-19 include new-onset respiratory, cardiovascular, neurologic, and psychiatric illnesses.4,5 As many as half of adults hospitalized for COVID report having persistent symptoms.6
As described in this issue, what we know about long COVID appears to be following the early course of its parent illness. As was true then, we are learning about the symptoms, etiology, and best ways to manage our patients. As in the early days of the pandemic, treatment is supportive, and we await definitive therapies.
I am optimistic, though. Why? Because shortly after the first reports of COVID-19, the virus’ DNA sequence was shared online. Based on that information, diagnostic assays were developed. Within 2 years of the outbreak, we had effective vaccines and specific therapies.
Another call to action. If 5% of patients contracting COVID (a very low estimate) develop long COVID, that would translate to 4.9 million people with long COVID in the United States. That is an astounding burden of suffering that I have no doubt will motivate innovation.
Innovation is a strength of the US health care system. I believe we will rise to the next challenge that COVID-19 has put before us. We have reason to be hopeful.
1. Mayo NL, Ellenbogen RL, Mendoza MD, et al. The family physician’s role in long COVID management. J Fam Pract. 2022;71:426-431. doi: 10.12788/jfp.0517
2. Kulshreshtha A, Sizemore S, Barry HC. COVID-19 therapy: What works? What doesn’t? And what’s on the horizon? J Fam Pract. 2022;71:E3-E16. doi: 10.12788/jfp.0474
3. CDC. COVID data tracker. Accessed December 5, 2022. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
4. Taquet M, Geddes JR, Husain M, et al. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8:416-427. doi: 10.1016/s2215-0366(21) 00084-5
5. Ayoubkhani D, Khunti K, Nafilyan V, et al. Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ. 2021;372:n693. doi: 10.1136/bmj.n693
6. Writing Committee for the Comebac Study Group, Morin L, Savale L, Pham T, et al. Four-month clinical status of a cohort of patients after hospitalization for COVID-19. JAMA. 2021;325:1525-1534. doi: 10.1001/jama.2021.3331
1. Mayo NL, Ellenbogen RL, Mendoza MD, et al. The family physician’s role in long COVID management. J Fam Pract. 2022;71:426-431. doi: 10.12788/jfp.0517
2. Kulshreshtha A, Sizemore S, Barry HC. COVID-19 therapy: What works? What doesn’t? And what’s on the horizon? J Fam Pract. 2022;71:E3-E16. doi: 10.12788/jfp.0474
3. CDC. COVID data tracker. Accessed December 5, 2022. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
4. Taquet M, Geddes JR, Husain M, et al. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8:416-427. doi: 10.1016/s2215-0366(21) 00084-5
5. Ayoubkhani D, Khunti K, Nafilyan V, et al. Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ. 2021;372:n693. doi: 10.1136/bmj.n693
6. Writing Committee for the Comebac Study Group, Morin L, Savale L, Pham T, et al. Four-month clinical status of a cohort of patients after hospitalization for COVID-19. JAMA. 2021;325:1525-1534. doi: 10.1001/jama.2021.3331