User login
American Academy of Dermatology (AAD): Summer Academy 2015
New treatments explored for prurigo nodularis
NEW YORK – Once it reaches the plaque stage, prurigo nodularis becomes extremely difficult to control with currently available topical and systemic therapies, according to a comprehensive summary presented at the American Academy of Dermatology summer meeting.
When treatment begins at an advanced stage, “it takes years until we see a complete relief,” reported Dr. Sonja Stander of the Center for Chronic Pruritus, University Hospital Muenster (Germany). Conveying this information to the patient is “very essential” to develop realistic expectations and to enlist cooperation in the frequent treatment modifications needed to achieve maximum relief.

Prurigo nodularis is characterized by a symmetrical distribution of very itchy, hyperkeratotic, erosive nodules and papules. Scratching contributes to the “chronification” and the progression that typically takes patients from papules to nodules to plaques, according to Dr. Stander, an expert who has joined with others to create the Prurigo Nodularis League (PNL) to raise awareness about the condition.
Information on more than 600 prurigo nodularis patients has been collected in a database created by the PNL, which is designed to consolidate information on the epidemiology, pathology, and treatments for a condition that Dr. Stander said many patients describe as “agonizing” or “horrendous.” The condition has been linked to a variety of systemic and neurologic diseases, but the underlying mechanism of this condition remains poorly understood.
Until recently, commonly used first-line treatment strategies, which include PUVA, topical steroids, and the immunomodulatory agent pimecrolimus, were employed primarily on the basis of case series and expert opinion. She reported that only three randomized, controlled trials have been published relating to these approaches. All involved topical treatments.
“Do you think this is enough for treating the prurigo patient? Topical treatment? No way, but we do not have data from trials with systemic therapies,” reported Dr. Stander, who provided an algorithm that begins with topical therapies but quickly moves to second- and third-line systemic agents. Dr. Stander noted, however, that independent phase 2 trials were recently initiated with the NK1 receptor antagonists aprepitant and serlopitant, providing hope that there are “some new drugs on the horizon.”
According to Dr. Stander, European guidelines for prurigo nodularis recommend topical capsaicin and naltrexone for initial therapy. Both are used off label, but she believes both produce benefit. Other therapies supported by case studies include the neuromodulator gabapentin, the immunomodulator methotrexate, and selective serotonin receptor inhibitors. The side effects of most of these therapies, particularly drugs such as methotrexate, typically precede the benefits, according to Dr. Stander, who reiterated that patients must be warned about the slow pace of improvement.
It is hoped that the PNL database will provide enough patients to permit patterns in disease etiology to be discerned. One of the questions is where atopy, which Dr. Stander said is a prominent feature in about 50% of prurigo nodularis patients, plays a role. She explored the theory that this prurigo nodularis represents a neuropathy of the skin, citing evidence of differences in nerve fiber density in the dermal and epidermal layers of these patients when compared with individuals without this condition.
The differential diagnosis includes autoimmune diseases, such as bullous pemphigoid. In fact, Dr. Stander reported that she screens for bullous pemphigoid in every patient suspected of prurigo nodularis.
One of the peculiar features of prurigo nodularis is that there appears to be no correlation between the duration of this condition and its intensity. Rather, most patients “start with a very severe pruritus” with skin lesions exacerbated by scratching, according to Dr. Stander. She said that although it was once thought that a plaque presentation might represent a different subtype, it is now believed that this is simply an advanced stage.
Encouraging physicians who encounter prurigo nodularis to contribute cases to the database, Dr. Stander reported that “we want to raise awareness for this severe entity” through the PNL. She said the PNL website is a repository for information and invites comments to allow information to be exchanged.
Dr. Stander reported no financial relationships to disclose.
NEW YORK – Once it reaches the plaque stage, prurigo nodularis becomes extremely difficult to control with currently available topical and systemic therapies, according to a comprehensive summary presented at the American Academy of Dermatology summer meeting.
When treatment begins at an advanced stage, “it takes years until we see a complete relief,” reported Dr. Sonja Stander of the Center for Chronic Pruritus, University Hospital Muenster (Germany). Conveying this information to the patient is “very essential” to develop realistic expectations and to enlist cooperation in the frequent treatment modifications needed to achieve maximum relief.
Prurigo nodularis is characterized by a symmetrical distribution of very itchy, hyperkeratotic, erosive nodules and papules. Scratching contributes to the “chronification” and the progression that typically takes patients from papules to nodules to plaques, according to Dr. Stander, an expert who has joined with others to create the Prurigo Nodularis League (PNL) to raise awareness about the condition.
Information on more than 600 prurigo nodularis patients has been collected in a database created by the PNL, which is designed to consolidate information on the epidemiology, pathology, and treatments for a condition that Dr. Stander said many patients describe as “agonizing” or “horrendous.” The condition has been linked to a variety of systemic and neurologic diseases, but the underlying mechanism of this condition remains poorly understood.
Until recently, commonly used first-line treatment strategies, which include PUVA, topical steroids, and the immunomodulatory agent pimecrolimus, were employed primarily on the basis of case series and expert opinion. She reported that only three randomized, controlled trials have been published relating to these approaches. All involved topical treatments.
“Do you think this is enough for treating the prurigo patient? Topical treatment? No way, but we do not have data from trials with systemic therapies,” reported Dr. Stander, who provided an algorithm that begins with topical therapies but quickly moves to second- and third-line systemic agents. Dr. Stander noted, however, that independent phase 2 trials were recently initiated with the NK1 receptor antagonists aprepitant and serlopitant, providing hope that there are “some new drugs on the horizon.”
According to Dr. Stander, European guidelines for prurigo nodularis recommend topical capsaicin and naltrexone for initial therapy. Both are used off label, but she believes both produce benefit. Other therapies supported by case studies include the neuromodulator gabapentin, the immunomodulator methotrexate, and selective serotonin receptor inhibitors. The side effects of most of these therapies, particularly drugs such as methotrexate, typically precede the benefits, according to Dr. Stander, who reiterated that patients must be warned about the slow pace of improvement.
It is hoped that the PNL database will provide enough patients to permit patterns in disease etiology to be discerned. One of the questions is where atopy, which Dr. Stander said is a prominent feature in about 50% of prurigo nodularis patients, plays a role. She explored the theory that this prurigo nodularis represents a neuropathy of the skin, citing evidence of differences in nerve fiber density in the dermal and epidermal layers of these patients when compared with individuals without this condition.
The differential diagnosis includes autoimmune diseases, such as bullous pemphigoid. In fact, Dr. Stander reported that she screens for bullous pemphigoid in every patient suspected of prurigo nodularis.
One of the peculiar features of prurigo nodularis is that there appears to be no correlation between the duration of this condition and its intensity. Rather, most patients “start with a very severe pruritus” with skin lesions exacerbated by scratching, according to Dr. Stander. She said that although it was once thought that a plaque presentation might represent a different subtype, it is now believed that this is simply an advanced stage.
Encouraging physicians who encounter prurigo nodularis to contribute cases to the database, Dr. Stander reported that “we want to raise awareness for this severe entity” through the PNL. She said the PNL website is a repository for information and invites comments to allow information to be exchanged.
Dr. Stander reported no financial relationships to disclose.
NEW YORK – Once it reaches the plaque stage, prurigo nodularis becomes extremely difficult to control with currently available topical and systemic therapies, according to a comprehensive summary presented at the American Academy of Dermatology summer meeting.
When treatment begins at an advanced stage, “it takes years until we see a complete relief,” reported Dr. Sonja Stander of the Center for Chronic Pruritus, University Hospital Muenster (Germany). Conveying this information to the patient is “very essential” to develop realistic expectations and to enlist cooperation in the frequent treatment modifications needed to achieve maximum relief.
Prurigo nodularis is characterized by a symmetrical distribution of very itchy, hyperkeratotic, erosive nodules and papules. Scratching contributes to the “chronification” and the progression that typically takes patients from papules to nodules to plaques, according to Dr. Stander, an expert who has joined with others to create the Prurigo Nodularis League (PNL) to raise awareness about the condition.
Information on more than 600 prurigo nodularis patients has been collected in a database created by the PNL, which is designed to consolidate information on the epidemiology, pathology, and treatments for a condition that Dr. Stander said many patients describe as “agonizing” or “horrendous.” The condition has been linked to a variety of systemic and neurologic diseases, but the underlying mechanism of this condition remains poorly understood.
Until recently, commonly used first-line treatment strategies, which include PUVA, topical steroids, and the immunomodulatory agent pimecrolimus, were employed primarily on the basis of case series and expert opinion. She reported that only three randomized, controlled trials have been published relating to these approaches. All involved topical treatments.
“Do you think this is enough for treating the prurigo patient? Topical treatment? No way, but we do not have data from trials with systemic therapies,” reported Dr. Stander, who provided an algorithm that begins with topical therapies but quickly moves to second- and third-line systemic agents. Dr. Stander noted, however, that independent phase 2 trials were recently initiated with the NK1 receptor antagonists aprepitant and serlopitant, providing hope that there are “some new drugs on the horizon.”
According to Dr. Stander, European guidelines for prurigo nodularis recommend topical capsaicin and naltrexone for initial therapy. Both are used off label, but she believes both produce benefit. Other therapies supported by case studies include the neuromodulator gabapentin, the immunomodulator methotrexate, and selective serotonin receptor inhibitors. The side effects of most of these therapies, particularly drugs such as methotrexate, typically precede the benefits, according to Dr. Stander, who reiterated that patients must be warned about the slow pace of improvement.
It is hoped that the PNL database will provide enough patients to permit patterns in disease etiology to be discerned. One of the questions is where atopy, which Dr. Stander said is a prominent feature in about 50% of prurigo nodularis patients, plays a role. She explored the theory that this prurigo nodularis represents a neuropathy of the skin, citing evidence of differences in nerve fiber density in the dermal and epidermal layers of these patients when compared with individuals without this condition.
The differential diagnosis includes autoimmune diseases, such as bullous pemphigoid. In fact, Dr. Stander reported that she screens for bullous pemphigoid in every patient suspected of prurigo nodularis.
One of the peculiar features of prurigo nodularis is that there appears to be no correlation between the duration of this condition and its intensity. Rather, most patients “start with a very severe pruritus” with skin lesions exacerbated by scratching, according to Dr. Stander. She said that although it was once thought that a plaque presentation might represent a different subtype, it is now believed that this is simply an advanced stage.
Encouraging physicians who encounter prurigo nodularis to contribute cases to the database, Dr. Stander reported that “we want to raise awareness for this severe entity” through the PNL. She said the PNL website is a repository for information and invites comments to allow information to be exchanged.
Dr. Stander reported no financial relationships to disclose.
AT THE AAD SUMMER ACADEMY 2015

Summer AAD: Using tape to diagnose dermatologic diseases
NEW YORK – Those paying close attention to the medical literature know that common sealing and packing tapes can be used in the diagnosis of several microorganisms that infect the skin, but an expert delivering clinical pearls at the American Academy of Dermatology (AAD) summer meeting emphasized that this approach deserves both respect and wider application.

Pulling tinea versicolor off the skin by applying and removing clear tape provides a sample after staining “that is easier to see than scraping, and it provides a quick and easy diagnosis,” reported Dr. Stephen P. Stone, professor and director of clinical research, division of dermatology, Southern Illinois University, Springfield.
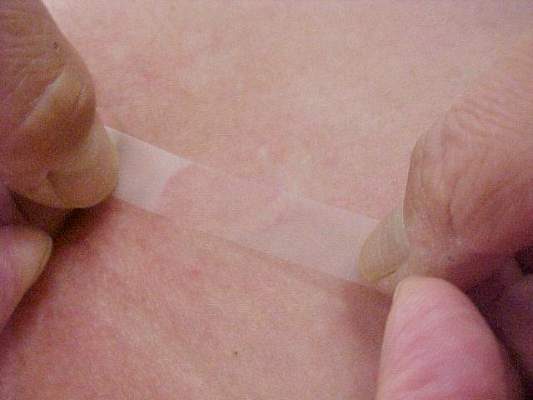
The value of a 2-inch piece of clear cellophane tape with single-sided adhesive in the diagnosis of tinea versicolor was just one of several examples of how tape can be applied for inexpensive and rapid diagnostic studies. In this case, the tape is applied to the skin to pull off scales and then placed sticky side up on a cover slide so stain can be applied. The stain, although not essential, makes the classic appearance easier to see.
“It takes no time to do this,” said Dr. Stone, who believes “ziti and macaroni” is a better characterization of tinea versicolor than the more common description of spaghetti and meatballs.
For scabies, Dr. Stone upgrades to clear packaging tape that offers greater adhesion than the basic product. He also rubs the tape on the skin to obtain a better sample. Because the packaging tape is wider, he places it across two slides with the sticky side down because there is no stain and the tape is clear so the scabies remain visible under the tape. Again, it is preferable to scraping in many situations simply because it is easier to do.

“It is wonderful with squirming babies because you are not pulling out a scalpel and trying to avoid cutting the skin,” Dr. Stone explained. When scabies are visible, he invites patients and family members to take a look at the mites under the microscope. He said this is often an effective motivator for compliance with therapy, particularly for parents of infants who are reluctant to apply topical scabies therapy effectively across large surface areas.
The tape test can often be used as a simple tool to rule out scabies in infants who have been given a diagnosis of eczema but have failed to respond to therapy. He noted that unrecognized scabies is frequently the actual underlying diagnosis in such cases.
Using tape to diagnose scabies is evidence-based practice, according to Dr. Stone. Citing a study that compared the sensitivity and specificity of dermoscopy, scraping, and tape (Arch Dermatol 2011 Apr;147[4]:468-73), Dr. Stone said that dermoscopy provided the most sensitive tool, but a tape-based diagnosis was the most specific. With tape, “you can actually see the mite, so the diagnosis is definitive,” he added.
Tape also has a role in the diagnosis of pityriasis folliculorum (Demodex), particularly in patients with resistant rosacea, according to Dr. Stone. In his experience, pityriasis folliculorum can either mimic or contribute to rosacea. In either case, effective treatment of the infection will provide a substantial reduction in the erythema that characterizes rosacea. Although he acknowledged that pityriasis folliculorum could be isolated from the face of most individuals, clinicians do not necessarily have to quantify the degree of infection to determine whether it is clinically relevant.
“If they respond to therapy, then they had too many [Demodex mites],” Dr. Stone noted.
These uses for tape for diagnosing and treating dermatologic diseases represented only some examples from a longer list, which includes the use of duct tape to treat common warts.
Dr. Stone reported financial relationships with Abbott, Acuderm, Celgene, Centocor Ortho Biotech, Johnson & Johnson, OPKO Health, Pfizer, Teva, and XOMA Corp.
To compile an authoritative index of tape applications in dermatology, Dr. Stone is interested in the experiences of others, including anecdotal experiences. Examples can be sent to him at [email protected].
NEW YORK – Those paying close attention to the medical literature know that common sealing and packing tapes can be used in the diagnosis of several microorganisms that infect the skin, but an expert delivering clinical pearls at the American Academy of Dermatology (AAD) summer meeting emphasized that this approach deserves both respect and wider application.
Pulling tinea versicolor off the skin by applying and removing clear tape provides a sample after staining “that is easier to see than scraping, and it provides a quick and easy diagnosis,” reported Dr. Stephen P. Stone, professor and director of clinical research, division of dermatology, Southern Illinois University, Springfield.
The value of a 2-inch piece of clear cellophane tape with single-sided adhesive in the diagnosis of tinea versicolor was just one of several examples of how tape can be applied for inexpensive and rapid diagnostic studies. In this case, the tape is applied to the skin to pull off scales and then placed sticky side up on a cover slide so stain can be applied. The stain, although not essential, makes the classic appearance easier to see.
“It takes no time to do this,” said Dr. Stone, who believes “ziti and macaroni” is a better characterization of tinea versicolor than the more common description of spaghetti and meatballs.
For scabies, Dr. Stone upgrades to clear packaging tape that offers greater adhesion than the basic product. He also rubs the tape on the skin to obtain a better sample. Because the packaging tape is wider, he places it across two slides with the sticky side down because there is no stain and the tape is clear so the scabies remain visible under the tape. Again, it is preferable to scraping in many situations simply because it is easier to do.
“It is wonderful with squirming babies because you are not pulling out a scalpel and trying to avoid cutting the skin,” Dr. Stone explained. When scabies are visible, he invites patients and family members to take a look at the mites under the microscope. He said this is often an effective motivator for compliance with therapy, particularly for parents of infants who are reluctant to apply topical scabies therapy effectively across large surface areas.
The tape test can often be used as a simple tool to rule out scabies in infants who have been given a diagnosis of eczema but have failed to respond to therapy. He noted that unrecognized scabies is frequently the actual underlying diagnosis in such cases.
Using tape to diagnose scabies is evidence-based practice, according to Dr. Stone. Citing a study that compared the sensitivity and specificity of dermoscopy, scraping, and tape (Arch Dermatol 2011 Apr;147[4]:468-73), Dr. Stone said that dermoscopy provided the most sensitive tool, but a tape-based diagnosis was the most specific. With tape, “you can actually see the mite, so the diagnosis is definitive,” he added.
Tape also has a role in the diagnosis of pityriasis folliculorum (Demodex), particularly in patients with resistant rosacea, according to Dr. Stone. In his experience, pityriasis folliculorum can either mimic or contribute to rosacea. In either case, effective treatment of the infection will provide a substantial reduction in the erythema that characterizes rosacea. Although he acknowledged that pityriasis folliculorum could be isolated from the face of most individuals, clinicians do not necessarily have to quantify the degree of infection to determine whether it is clinically relevant.
“If they respond to therapy, then they had too many [Demodex mites],” Dr. Stone noted.
These uses for tape for diagnosing and treating dermatologic diseases represented only some examples from a longer list, which includes the use of duct tape to treat common warts.
Dr. Stone reported financial relationships with Abbott, Acuderm, Celgene, Centocor Ortho Biotech, Johnson & Johnson, OPKO Health, Pfizer, Teva, and XOMA Corp.
To compile an authoritative index of tape applications in dermatology, Dr. Stone is interested in the experiences of others, including anecdotal experiences. Examples can be sent to him at [email protected].
NEW YORK – Those paying close attention to the medical literature know that common sealing and packing tapes can be used in the diagnosis of several microorganisms that infect the skin, but an expert delivering clinical pearls at the American Academy of Dermatology (AAD) summer meeting emphasized that this approach deserves both respect and wider application.
Pulling tinea versicolor off the skin by applying and removing clear tape provides a sample after staining “that is easier to see than scraping, and it provides a quick and easy diagnosis,” reported Dr. Stephen P. Stone, professor and director of clinical research, division of dermatology, Southern Illinois University, Springfield.
The value of a 2-inch piece of clear cellophane tape with single-sided adhesive in the diagnosis of tinea versicolor was just one of several examples of how tape can be applied for inexpensive and rapid diagnostic studies. In this case, the tape is applied to the skin to pull off scales and then placed sticky side up on a cover slide so stain can be applied. The stain, although not essential, makes the classic appearance easier to see.
“It takes no time to do this,” said Dr. Stone, who believes “ziti and macaroni” is a better characterization of tinea versicolor than the more common description of spaghetti and meatballs.
For scabies, Dr. Stone upgrades to clear packaging tape that offers greater adhesion than the basic product. He also rubs the tape on the skin to obtain a better sample. Because the packaging tape is wider, he places it across two slides with the sticky side down because there is no stain and the tape is clear so the scabies remain visible under the tape. Again, it is preferable to scraping in many situations simply because it is easier to do.
“It is wonderful with squirming babies because you are not pulling out a scalpel and trying to avoid cutting the skin,” Dr. Stone explained. When scabies are visible, he invites patients and family members to take a look at the mites under the microscope. He said this is often an effective motivator for compliance with therapy, particularly for parents of infants who are reluctant to apply topical scabies therapy effectively across large surface areas.
The tape test can often be used as a simple tool to rule out scabies in infants who have been given a diagnosis of eczema but have failed to respond to therapy. He noted that unrecognized scabies is frequently the actual underlying diagnosis in such cases.
Using tape to diagnose scabies is evidence-based practice, according to Dr. Stone. Citing a study that compared the sensitivity and specificity of dermoscopy, scraping, and tape (Arch Dermatol 2011 Apr;147[4]:468-73), Dr. Stone said that dermoscopy provided the most sensitive tool, but a tape-based diagnosis was the most specific. With tape, “you can actually see the mite, so the diagnosis is definitive,” he added.
Tape also has a role in the diagnosis of pityriasis folliculorum (Demodex), particularly in patients with resistant rosacea, according to Dr. Stone. In his experience, pityriasis folliculorum can either mimic or contribute to rosacea. In either case, effective treatment of the infection will provide a substantial reduction in the erythema that characterizes rosacea. Although he acknowledged that pityriasis folliculorum could be isolated from the face of most individuals, clinicians do not necessarily have to quantify the degree of infection to determine whether it is clinically relevant.
“If they respond to therapy, then they had too many [Demodex mites],” Dr. Stone noted.
These uses for tape for diagnosing and treating dermatologic diseases represented only some examples from a longer list, which includes the use of duct tape to treat common warts.
Dr. Stone reported financial relationships with Abbott, Acuderm, Celgene, Centocor Ortho Biotech, Johnson & Johnson, OPKO Health, Pfizer, Teva, and XOMA Corp.
To compile an authoritative index of tape applications in dermatology, Dr. Stone is interested in the experiences of others, including anecdotal experiences. Examples can be sent to him at [email protected].
EXPERT OPINION FROM THE AAD SUMMER ACADEMY 2015

Fewer moles linked with more aggressive melanoma
NEW YORK – Consistent with another recently published report but counterintuitive, patients with a high number of nevi prior to developing a melanoma have more favorable prognostic features than do those with fewer moles, according to data presented at the American Academy of Dermatology summer meeting.
Based on differences in numerous clinicopathologic features when patients with more than 50 nevi were compared with those with fewer than 50 nevi, “It is possible that there are different pathways that drive melanoma in these two patient groups, resulting in different degrees of aggressiveness,” reported Dr. Caroline Kim from the Pigmented Lesion Clinic and Cutaneous Oncology Program, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston.

In this study of 281 melanoma patients evaluated over 2 years at Dr. Kim’s clinic, those with a high nevi count (89 patients) were compared with those with a lower nevi count (192 patients). The investigators also performed comparisons on those who had dysplastic versus nondysplastic nevi. Of differences between the groups, the initial melanoma grade was the most surprising.
In the greater-than-50-nevi group, 21.6% had either stage III (18.2%) or stage IV (3.4%) disease at diagnosis vs. 40.2% in the fewer-than-50-nevi group (31.2% and 9.0% with stage III and IV disease, respectively). Conversely, melanoma was diagnosed at stage I in 71.6% in the greater-than-50-nevi group vs. only 41.8% in the fewer-than-50-nevi group.
Among patients in the fewer-than-50-nevi group, ulceration was more common (25.1% vs. 10.3%; P = .017) as was nodular subtype (11.2% vs. 2.9%; P = .035). The group with the lower nevi count also had a higher mitotic rate (3.7 vs. 2.3 count/mm2) and a greater Breslow’s depth (1.78 vs. 1.21 mm; P = .010). Although not significantly different, the proportion of females was higher in the lower nevi count group (56.2% vs. 46.4%) and more patients in this group developed a melanoma in the head or neck (21.6% vs. 15.3%).
There are several potential explanations for the differences observed in this study. One is that the process that drives a high nevi count is different than that which produces lower numbers of nevi. According to Dr. Kim, some of the pathologic features in the greater-than-50-nevi group were more consistent with BRAF mutation patterns than the fewer-than- 50-nevi group. Another is that a high nevi count drives a more robust immune response against melanoma growth. Dr. Kim cited published studies that support both theories.
However, it is also possible that high nevi count increases likelihood of dermatologic care and vigilance for early detection of melanomas. This might be supported by the fact that the age of diagnosis was significantly younger in the greater-than-50-nevi count group (40.1 vs. 50.1 years; P less than .001). However, a younger age at diagnosis could also be a product of different pathways of disease development and growth.
The greater likelihood of more aggressive melanoma in patients with a history of fewer than 50 nevi than in those with greater than 50 nevi has also been supported by another large series that was recently published (Int J Cancer. 2015 Oct 1;137[7]:1691-8.) Cited by Dr. Kim as consistent with her own findings, this study of 2,184 melanoma cases compared 5- and 10-year survival in those who had greater than 50 nevi, which represented 31.3% of this population, to those with fewer. The greater survival at 5 years in the greater-than-50-nevi group (91.2% vs. 86.4%) and 10 years (87.2% vs. 79%) remained significant after adjusting “for all known melanoma prognostic factors,” according to the authors.
Further studies evaluating differences in patterns of melanoma growth in those with fewer than 50 nevi vs. those with more are needed, according to Dr. Kim. She acknowledged that one limitation of her study was that all cases were drawn from a single center. However, there is support for an independent study, and the findings, if verified, “have major implications for public health screening and education.” In particular, she suggested that those with lower nevi counts might deserve the type of attention already being directed at those with high nevi counts “as they may be paradoxically at risk for more aggressive melanomas.”
Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.
This article was updated August 26, 2015.
NEW YORK – Consistent with another recently published report but counterintuitive, patients with a high number of nevi prior to developing a melanoma have more favorable prognostic features than do those with fewer moles, according to data presented at the American Academy of Dermatology summer meeting.
Based on differences in numerous clinicopathologic features when patients with more than 50 nevi were compared with those with fewer than 50 nevi, “It is possible that there are different pathways that drive melanoma in these two patient groups, resulting in different degrees of aggressiveness,” reported Dr. Caroline Kim from the Pigmented Lesion Clinic and Cutaneous Oncology Program, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston.
In this study of 281 melanoma patients evaluated over 2 years at Dr. Kim’s clinic, those with a high nevi count (89 patients) were compared with those with a lower nevi count (192 patients). The investigators also performed comparisons on those who had dysplastic versus nondysplastic nevi. Of differences between the groups, the initial melanoma grade was the most surprising.
In the greater-than-50-nevi group, 21.6% had either stage III (18.2%) or stage IV (3.4%) disease at diagnosis vs. 40.2% in the fewer-than-50-nevi group (31.2% and 9.0% with stage III and IV disease, respectively). Conversely, melanoma was diagnosed at stage I in 71.6% in the greater-than-50-nevi group vs. only 41.8% in the fewer-than-50-nevi group.
Among patients in the fewer-than-50-nevi group, ulceration was more common (25.1% vs. 10.3%; P = .017) as was nodular subtype (11.2% vs. 2.9%; P = .035). The group with the lower nevi count also had a higher mitotic rate (3.7 vs. 2.3 count/mm2) and a greater Breslow’s depth (1.78 vs. 1.21 mm; P = .010). Although not significantly different, the proportion of females was higher in the lower nevi count group (56.2% vs. 46.4%) and more patients in this group developed a melanoma in the head or neck (21.6% vs. 15.3%).
There are several potential explanations for the differences observed in this study. One is that the process that drives a high nevi count is different than that which produces lower numbers of nevi. According to Dr. Kim, some of the pathologic features in the greater-than-50-nevi group were more consistent with BRAF mutation patterns than the fewer-than- 50-nevi group. Another is that a high nevi count drives a more robust immune response against melanoma growth. Dr. Kim cited published studies that support both theories.
However, it is also possible that high nevi count increases likelihood of dermatologic care and vigilance for early detection of melanomas. This might be supported by the fact that the age of diagnosis was significantly younger in the greater-than-50-nevi count group (40.1 vs. 50.1 years; P less than .001). However, a younger age at diagnosis could also be a product of different pathways of disease development and growth.
The greater likelihood of more aggressive melanoma in patients with a history of fewer than 50 nevi than in those with greater than 50 nevi has also been supported by another large series that was recently published (Int J Cancer. 2015 Oct 1;137[7]:1691-8.) Cited by Dr. Kim as consistent with her own findings, this study of 2,184 melanoma cases compared 5- and 10-year survival in those who had greater than 50 nevi, which represented 31.3% of this population, to those with fewer. The greater survival at 5 years in the greater-than-50-nevi group (91.2% vs. 86.4%) and 10 years (87.2% vs. 79%) remained significant after adjusting “for all known melanoma prognostic factors,” according to the authors.
Further studies evaluating differences in patterns of melanoma growth in those with fewer than 50 nevi vs. those with more are needed, according to Dr. Kim. She acknowledged that one limitation of her study was that all cases were drawn from a single center. However, there is support for an independent study, and the findings, if verified, “have major implications for public health screening and education.” In particular, she suggested that those with lower nevi counts might deserve the type of attention already being directed at those with high nevi counts “as they may be paradoxically at risk for more aggressive melanomas.”
Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.
This article was updated August 26, 2015.
NEW YORK – Consistent with another recently published report but counterintuitive, patients with a high number of nevi prior to developing a melanoma have more favorable prognostic features than do those with fewer moles, according to data presented at the American Academy of Dermatology summer meeting.
Based on differences in numerous clinicopathologic features when patients with more than 50 nevi were compared with those with fewer than 50 nevi, “It is possible that there are different pathways that drive melanoma in these two patient groups, resulting in different degrees of aggressiveness,” reported Dr. Caroline Kim from the Pigmented Lesion Clinic and Cutaneous Oncology Program, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston.
In this study of 281 melanoma patients evaluated over 2 years at Dr. Kim’s clinic, those with a high nevi count (89 patients) were compared with those with a lower nevi count (192 patients). The investigators also performed comparisons on those who had dysplastic versus nondysplastic nevi. Of differences between the groups, the initial melanoma grade was the most surprising.
In the greater-than-50-nevi group, 21.6% had either stage III (18.2%) or stage IV (3.4%) disease at diagnosis vs. 40.2% in the fewer-than-50-nevi group (31.2% and 9.0% with stage III and IV disease, respectively). Conversely, melanoma was diagnosed at stage I in 71.6% in the greater-than-50-nevi group vs. only 41.8% in the fewer-than-50-nevi group.
Among patients in the fewer-than-50-nevi group, ulceration was more common (25.1% vs. 10.3%; P = .017) as was nodular subtype (11.2% vs. 2.9%; P = .035). The group with the lower nevi count also had a higher mitotic rate (3.7 vs. 2.3 count/mm2) and a greater Breslow’s depth (1.78 vs. 1.21 mm; P = .010). Although not significantly different, the proportion of females was higher in the lower nevi count group (56.2% vs. 46.4%) and more patients in this group developed a melanoma in the head or neck (21.6% vs. 15.3%).
There are several potential explanations for the differences observed in this study. One is that the process that drives a high nevi count is different than that which produces lower numbers of nevi. According to Dr. Kim, some of the pathologic features in the greater-than-50-nevi group were more consistent with BRAF mutation patterns than the fewer-than- 50-nevi group. Another is that a high nevi count drives a more robust immune response against melanoma growth. Dr. Kim cited published studies that support both theories.
However, it is also possible that high nevi count increases likelihood of dermatologic care and vigilance for early detection of melanomas. This might be supported by the fact that the age of diagnosis was significantly younger in the greater-than-50-nevi count group (40.1 vs. 50.1 years; P less than .001). However, a younger age at diagnosis could also be a product of different pathways of disease development and growth.
The greater likelihood of more aggressive melanoma in patients with a history of fewer than 50 nevi than in those with greater than 50 nevi has also been supported by another large series that was recently published (Int J Cancer. 2015 Oct 1;137[7]:1691-8.) Cited by Dr. Kim as consistent with her own findings, this study of 2,184 melanoma cases compared 5- and 10-year survival in those who had greater than 50 nevi, which represented 31.3% of this population, to those with fewer. The greater survival at 5 years in the greater-than-50-nevi group (91.2% vs. 86.4%) and 10 years (87.2% vs. 79%) remained significant after adjusting “for all known melanoma prognostic factors,” according to the authors.
Further studies evaluating differences in patterns of melanoma growth in those with fewer than 50 nevi vs. those with more are needed, according to Dr. Kim. She acknowledged that one limitation of her study was that all cases were drawn from a single center. However, there is support for an independent study, and the findings, if verified, “have major implications for public health screening and education.” In particular, she suggested that those with lower nevi counts might deserve the type of attention already being directed at those with high nevi counts “as they may be paradoxically at risk for more aggressive melanomas.”
Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.
This article was updated August 26, 2015.
AT THE AAD SUMMER ACADEMY 2015
Key clinical point: In patients with nevi who develop melanoma, malignancies appear to be more aggressive with a lower rather than a higher nevi count.
Major finding: Patients with fewer than 50 moles were more than twice as likely as patients with more than 50 moles to be diagnosed with stage III or IV disease.
Data source: Retrospective chart review.
Disclosures: Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.

In skin lymphoma diagnosis, pathology must match clinical presentation
NEW YORK – Both dermatologists and pathologists can make the mistake of diagnosing a long list of pseudolymphomas as lymphomas, according to Dr. Antonio Subtil, who is an associate professor of dermatology and pathology at Yale University School of Medicine, New Haven, Connecticut.
The diagnosis is not trustworthy without agreement by a team of experts, he said. Most dermatologists do not have sufficient expertise in histopathology to interpret equivocal findings. Pathologists do not typically grasp subtleties in dermatologic presentations that may also be critical to reach an accurate diagnosis regardless of histopathology.

Mycosis fungoides (MF) represents almost 60% of cutaneous T-cell lymphomas (CTCL), but only a proportion of patients with MF have a classic presentation and the extensive array of other T-cell and B-cell lesions constitute a heterogeneous profile of lesions, according to Dr. Subtil, who spoke on skin lymphoma knowledge gaps at the summer meeting of the American Academy of Dermatology (AAD). The biases of the dermatologist and the pathologist in isolation can lead to misdiagnosis, which is the reason to insist on a clear correlation between pathologic and clinical findings.
Speaking as a dermatologist, Dr. Subtil cautioned that pathologists “do not understand our terminology” and are not facile in differentiating clinical descriptions of cutaneous lesions. Speaking as a pathologist, Dr. Subtil cautioned that “I cannot trust a pathological report by itself” without understanding the clinical context.
As an example, he recounted a case of an ulcerated nodule that proved to have a lymphoid infiltrate on biopsy. When cells in the infiltrate were found to be CD30+, the likely diagnosis appeared to be an anaplastic large cell lymphoma. Only further testing revealed molluscum contagiosum, which can have a similar appearance and also feature CD30+ cells. A course of unnecessary chemotherapy was narrowly averted.
A small sample of the pseudolymphomas that can fool the clinician include lymphomatoid drug eruption, cutaneous leishmaniasis, lymphomatoid lichenoid keratosis, and reactive lymphoid hyperplasia at the site of vaccination, according to Dr. Subtil. He outlined a series of challenges that should be recognized before settling on a diagnosis.
One of the most important of these challenges is the limited specificity and sensitivity of any clinical characteristic or diagnostic study in isolation, according to Dr. Subtil. Even tissue studies with polymerase chain reaction (PCR) are associated with false positive and false negative results and, like everything else, must be evaluated in the context of the pathological and clinical findings.
Another challenge to a definitive diagnosis is the overuse of the term “atypical” by both dermatologists and pathologists. Dr. Subtil called the propensity to use this label the “atypical syndrome” and cautioned that it may sometimes be an obstacle for seeking a more definitive description of the underlying pathology. Using a team approach, which Dr. Subtil suggested might also include a hematologist and an oncologist, to reach consensus about the diagnosis substantially reduces the risk of a misdiagnosis.
NEW YORK – Both dermatologists and pathologists can make the mistake of diagnosing a long list of pseudolymphomas as lymphomas, according to Dr. Antonio Subtil, who is an associate professor of dermatology and pathology at Yale University School of Medicine, New Haven, Connecticut.
The diagnosis is not trustworthy without agreement by a team of experts, he said. Most dermatologists do not have sufficient expertise in histopathology to interpret equivocal findings. Pathologists do not typically grasp subtleties in dermatologic presentations that may also be critical to reach an accurate diagnosis regardless of histopathology.
Mycosis fungoides (MF) represents almost 60% of cutaneous T-cell lymphomas (CTCL), but only a proportion of patients with MF have a classic presentation and the extensive array of other T-cell and B-cell lesions constitute a heterogeneous profile of lesions, according to Dr. Subtil, who spoke on skin lymphoma knowledge gaps at the summer meeting of the American Academy of Dermatology (AAD). The biases of the dermatologist and the pathologist in isolation can lead to misdiagnosis, which is the reason to insist on a clear correlation between pathologic and clinical findings.
Speaking as a dermatologist, Dr. Subtil cautioned that pathologists “do not understand our terminology” and are not facile in differentiating clinical descriptions of cutaneous lesions. Speaking as a pathologist, Dr. Subtil cautioned that “I cannot trust a pathological report by itself” without understanding the clinical context.
As an example, he recounted a case of an ulcerated nodule that proved to have a lymphoid infiltrate on biopsy. When cells in the infiltrate were found to be CD30+, the likely diagnosis appeared to be an anaplastic large cell lymphoma. Only further testing revealed molluscum contagiosum, which can have a similar appearance and also feature CD30+ cells. A course of unnecessary chemotherapy was narrowly averted.
A small sample of the pseudolymphomas that can fool the clinician include lymphomatoid drug eruption, cutaneous leishmaniasis, lymphomatoid lichenoid keratosis, and reactive lymphoid hyperplasia at the site of vaccination, according to Dr. Subtil. He outlined a series of challenges that should be recognized before settling on a diagnosis.
One of the most important of these challenges is the limited specificity and sensitivity of any clinical characteristic or diagnostic study in isolation, according to Dr. Subtil. Even tissue studies with polymerase chain reaction (PCR) are associated with false positive and false negative results and, like everything else, must be evaluated in the context of the pathological and clinical findings.
Another challenge to a definitive diagnosis is the overuse of the term “atypical” by both dermatologists and pathologists. Dr. Subtil called the propensity to use this label the “atypical syndrome” and cautioned that it may sometimes be an obstacle for seeking a more definitive description of the underlying pathology. Using a team approach, which Dr. Subtil suggested might also include a hematologist and an oncologist, to reach consensus about the diagnosis substantially reduces the risk of a misdiagnosis.
NEW YORK – Both dermatologists and pathologists can make the mistake of diagnosing a long list of pseudolymphomas as lymphomas, according to Dr. Antonio Subtil, who is an associate professor of dermatology and pathology at Yale University School of Medicine, New Haven, Connecticut.
The diagnosis is not trustworthy without agreement by a team of experts, he said. Most dermatologists do not have sufficient expertise in histopathology to interpret equivocal findings. Pathologists do not typically grasp subtleties in dermatologic presentations that may also be critical to reach an accurate diagnosis regardless of histopathology.
Mycosis fungoides (MF) represents almost 60% of cutaneous T-cell lymphomas (CTCL), but only a proportion of patients with MF have a classic presentation and the extensive array of other T-cell and B-cell lesions constitute a heterogeneous profile of lesions, according to Dr. Subtil, who spoke on skin lymphoma knowledge gaps at the summer meeting of the American Academy of Dermatology (AAD). The biases of the dermatologist and the pathologist in isolation can lead to misdiagnosis, which is the reason to insist on a clear correlation between pathologic and clinical findings.
Speaking as a dermatologist, Dr. Subtil cautioned that pathologists “do not understand our terminology” and are not facile in differentiating clinical descriptions of cutaneous lesions. Speaking as a pathologist, Dr. Subtil cautioned that “I cannot trust a pathological report by itself” without understanding the clinical context.
As an example, he recounted a case of an ulcerated nodule that proved to have a lymphoid infiltrate on biopsy. When cells in the infiltrate were found to be CD30+, the likely diagnosis appeared to be an anaplastic large cell lymphoma. Only further testing revealed molluscum contagiosum, which can have a similar appearance and also feature CD30+ cells. A course of unnecessary chemotherapy was narrowly averted.
A small sample of the pseudolymphomas that can fool the clinician include lymphomatoid drug eruption, cutaneous leishmaniasis, lymphomatoid lichenoid keratosis, and reactive lymphoid hyperplasia at the site of vaccination, according to Dr. Subtil. He outlined a series of challenges that should be recognized before settling on a diagnosis.
One of the most important of these challenges is the limited specificity and sensitivity of any clinical characteristic or diagnostic study in isolation, according to Dr. Subtil. Even tissue studies with polymerase chain reaction (PCR) are associated with false positive and false negative results and, like everything else, must be evaluated in the context of the pathological and clinical findings.
Another challenge to a definitive diagnosis is the overuse of the term “atypical” by both dermatologists and pathologists. Dr. Subtil called the propensity to use this label the “atypical syndrome” and cautioned that it may sometimes be an obstacle for seeking a more definitive description of the underlying pathology. Using a team approach, which Dr. Subtil suggested might also include a hematologist and an oncologist, to reach consensus about the diagnosis substantially reduces the risk of a misdiagnosis.
EXPERT ANALYSIS AT THE SUMMER MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY

AAD adds 5 new ‘Choosing Wisely’ recommendations
NEW YORK – Five new Choosing Wisely recommendations have been issued by the American Academy of Dermatology.
The five new recommendations are:
Don’t use oral or injected corticosteroids as a long-term treatment for dermatitis.
Don’t use skin prick tests or blood tests such as the radioallergosorbet test (RAST) for the routine evaluation of eczema.
Don’t routinely use microbiologic testing in the evaluation and management of acne.
Don’t routinely use antibiotics to treat bilateral swelling and redness of the lower leg unless there is clear evidence of infection.
Don't routinely prescribe antibiotics for inflamed epidermal cysts.
The release of the list provides evidence that the AAD is “committed to serving as good stewards of limited healthcare resources,” according to AAD President Dr. Mark Lebwohl. who is also chair of the department of dermatology at Icahn School of Medicine at Mount Sinai, New York.

These diagnostic tests and treatments are often performed but are not necessarily appropriate. Some of the procedures may be reasonable in specific situations, he said, and this list “can help patients with skin, hair, and nail conditions start a conversation with their dermatologists about what tests and treatments are right for them.”
The five Choosing Wisely recommendations join the five recommendations issued in 2013 by the AAD. The Choosing Wisely campaign was launched by the American Board of Internal Medicine Foundation in 2012 and now has participation from more than 70 professional healthcare organizations.
Each of the recommendations from the AAD was issued with a background explanation. For example, it was specified that the adverse effects of long-term systemic corticosteroids make a favorable benefit-to-risk ratio unlikely in patients with chronic dermatitis. Also, determining the type of bacteria in an acne lesion has little value because it would be unlikely to change management decisions.
The five recommendations from 2103 were to avoid oral antifungal therapy for suspected nail fungus until infection has been confirmed; to refrain from further staging studies, such as sentinel lymph node biopsy, in early stage, localized melanoma; to refrain from Mohs micrographic surgery in non-melanoma skin cancer of less than 1 cm in size; to avoid oral antibiotics for atopic dermatitis in the absence of clinical evidence of infection, and to avoid topical antibiotics for infection prophylaxis for clean surgical wounds.
All 10 of the Choosing Wisely recommendations from the AAD were selected by an AAD-organized workgroup of board-certified dermatologists seeking to identify practices that are common but impose a strong potential for poor use of healthcare resources. In some cases, there is evidence that the opportunity for harm exceeds the likelihood of benefit. In others, no added value is expected from procedures that add cost.
The AAD list of 10 recommendations is part of more than 400 tests and procedures now identified in the Choosing Wisely campaign by the participating professional organizations. Importantly, this list is not just distributed to those delivering care but is expressly made available to patients to encourage them to discuss options with their physicians and to participate in determining which care is unnecessary to them.
The goal of providing patients with information that can help them participate in decisions about appropriate care is consistent with the full transparency that the AAD endorses, Dr. Lebwohl said. “We want to empower our patients to make informed healthcare decisions.”
This article was updated 8/27/15.
NEW YORK – Five new Choosing Wisely recommendations have been issued by the American Academy of Dermatology.
The five new recommendations are:
Don’t use oral or injected corticosteroids as a long-term treatment for dermatitis.
Don’t use skin prick tests or blood tests such as the radioallergosorbet test (RAST) for the routine evaluation of eczema.
Don’t routinely use microbiologic testing in the evaluation and management of acne.
Don’t routinely use antibiotics to treat bilateral swelling and redness of the lower leg unless there is clear evidence of infection.
Don't routinely prescribe antibiotics for inflamed epidermal cysts.
The release of the list provides evidence that the AAD is “committed to serving as good stewards of limited healthcare resources,” according to AAD President Dr. Mark Lebwohl. who is also chair of the department of dermatology at Icahn School of Medicine at Mount Sinai, New York.
These diagnostic tests and treatments are often performed but are not necessarily appropriate. Some of the procedures may be reasonable in specific situations, he said, and this list “can help patients with skin, hair, and nail conditions start a conversation with their dermatologists about what tests and treatments are right for them.”
The five Choosing Wisely recommendations join the five recommendations issued in 2013 by the AAD. The Choosing Wisely campaign was launched by the American Board of Internal Medicine Foundation in 2012 and now has participation from more than 70 professional healthcare organizations.
Each of the recommendations from the AAD was issued with a background explanation. For example, it was specified that the adverse effects of long-term systemic corticosteroids make a favorable benefit-to-risk ratio unlikely in patients with chronic dermatitis. Also, determining the type of bacteria in an acne lesion has little value because it would be unlikely to change management decisions.
The five recommendations from 2103 were to avoid oral antifungal therapy for suspected nail fungus until infection has been confirmed; to refrain from further staging studies, such as sentinel lymph node biopsy, in early stage, localized melanoma; to refrain from Mohs micrographic surgery in non-melanoma skin cancer of less than 1 cm in size; to avoid oral antibiotics for atopic dermatitis in the absence of clinical evidence of infection, and to avoid topical antibiotics for infection prophylaxis for clean surgical wounds.
All 10 of the Choosing Wisely recommendations from the AAD were selected by an AAD-organized workgroup of board-certified dermatologists seeking to identify practices that are common but impose a strong potential for poor use of healthcare resources. In some cases, there is evidence that the opportunity for harm exceeds the likelihood of benefit. In others, no added value is expected from procedures that add cost.
The AAD list of 10 recommendations is part of more than 400 tests and procedures now identified in the Choosing Wisely campaign by the participating professional organizations. Importantly, this list is not just distributed to those delivering care but is expressly made available to patients to encourage them to discuss options with their physicians and to participate in determining which care is unnecessary to them.
The goal of providing patients with information that can help them participate in decisions about appropriate care is consistent with the full transparency that the AAD endorses, Dr. Lebwohl said. “We want to empower our patients to make informed healthcare decisions.”
This article was updated 8/27/15.
NEW YORK – Five new Choosing Wisely recommendations have been issued by the American Academy of Dermatology.
The five new recommendations are:
Don’t use oral or injected corticosteroids as a long-term treatment for dermatitis.
Don’t use skin prick tests or blood tests such as the radioallergosorbet test (RAST) for the routine evaluation of eczema.
Don’t routinely use microbiologic testing in the evaluation and management of acne.
Don’t routinely use antibiotics to treat bilateral swelling and redness of the lower leg unless there is clear evidence of infection.
Don't routinely prescribe antibiotics for inflamed epidermal cysts.
The release of the list provides evidence that the AAD is “committed to serving as good stewards of limited healthcare resources,” according to AAD President Dr. Mark Lebwohl. who is also chair of the department of dermatology at Icahn School of Medicine at Mount Sinai, New York.
These diagnostic tests and treatments are often performed but are not necessarily appropriate. Some of the procedures may be reasonable in specific situations, he said, and this list “can help patients with skin, hair, and nail conditions start a conversation with their dermatologists about what tests and treatments are right for them.”
The five Choosing Wisely recommendations join the five recommendations issued in 2013 by the AAD. The Choosing Wisely campaign was launched by the American Board of Internal Medicine Foundation in 2012 and now has participation from more than 70 professional healthcare organizations.
Each of the recommendations from the AAD was issued with a background explanation. For example, it was specified that the adverse effects of long-term systemic corticosteroids make a favorable benefit-to-risk ratio unlikely in patients with chronic dermatitis. Also, determining the type of bacteria in an acne lesion has little value because it would be unlikely to change management decisions.
The five recommendations from 2103 were to avoid oral antifungal therapy for suspected nail fungus until infection has been confirmed; to refrain from further staging studies, such as sentinel lymph node biopsy, in early stage, localized melanoma; to refrain from Mohs micrographic surgery in non-melanoma skin cancer of less than 1 cm in size; to avoid oral antibiotics for atopic dermatitis in the absence of clinical evidence of infection, and to avoid topical antibiotics for infection prophylaxis for clean surgical wounds.
All 10 of the Choosing Wisely recommendations from the AAD were selected by an AAD-organized workgroup of board-certified dermatologists seeking to identify practices that are common but impose a strong potential for poor use of healthcare resources. In some cases, there is evidence that the opportunity for harm exceeds the likelihood of benefit. In others, no added value is expected from procedures that add cost.
The AAD list of 10 recommendations is part of more than 400 tests and procedures now identified in the Choosing Wisely campaign by the participating professional organizations. Importantly, this list is not just distributed to those delivering care but is expressly made available to patients to encourage them to discuss options with their physicians and to participate in determining which care is unnecessary to them.
The goal of providing patients with information that can help them participate in decisions about appropriate care is consistent with the full transparency that the AAD endorses, Dr. Lebwohl said. “We want to empower our patients to make informed healthcare decisions.”
This article was updated 8/27/15.
AT THE SUMMER MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY

Daylight photodynamic therapy best for disseminated actinic keratoses
NEW YORK – For treating actinic keratoses appearing over large or disseminated surface areas, daylight is often a better strategy than artificial light is for activating photodynamic therapy (PDT), according to an update on strategies at the summer meeting of the American Academy of Dermatology.
The evidence that daylight is at least as effective as artificial light for grade 1 and 2 actinic keratoses has created a “really exciting new opportunity” for those with disseminated disease, according to Dr. Emily J. Fisher, director of Mohs surgery at Mercy Health Physicians, Cincinnati, Ohio. This approach is not only a more efficient way to treat large or multiple areas of skin, but it is better tolerated, further facilitating treatment of bigger surface areas.

Moreover, for physicians not currently equipped with blue or red artificial light, daylight activation “is a great way to incorporate PDT into your practice,” Dr. Fisher added. She suggested that PDT, which has been associated with clearance rates exceeding 70% with a single treatment in many studies, appears to be at least as effective as the topical treatments that are employed more often, such as 5-fluorouracil (5-FU) or imiquimod.
When comparing efficacy across studies, “PDT seems to have a higher response than [does] our topical treatments,” but Dr. Fisher cautioned that there are no high-quality, head-to-head comparisons, so there is no definitive evidence of the superiority of one over the other.
However, in patients with multiple actinic keratoses spread over a substantial area of the skin or who have lesions in more than one anatomical site, daylight PDT is a practical approach now widely used in Europe and several other parts of the world, according to Dr. Fisher. She reported that five randomized trials have demonstrated that daylight PDT is effective.
Most aspects of daylight PDT are the same as conventional PDT, according to Dr. Fisher. The skin is first prepared by removing scales and crusts to improve penetration of the photodynamic agent, whether aminolevulinate acid (ALA) or methyl aminolevulinate (MAL). Prior to light exposure, the occlusion time with the photodynamic agent is the same 3 hours. Also, light exposure in both cases should begin within 30 minutes, which may be a consideration for those depending on daylight.
“Patients really should not go indoors or into shade for more than 5 minutes at a time,” Dr. Fisher reported. The problem is that the activity of the intracellular photosensitizing chemicals can build up without light exposure, producing pain and reducing the tolerability of the treatment.
Consensus guidelines have been published for daylight PDT in Australia (J Eur Acad Dermatol Venereol. 2012 Jun;26[6]:673-9.). According to Dr. Fisher, the guidelines recommend a light intensity of greater than 130 W/m2, which is a dose provided by sunlight within the continental United States but not at distant points from the equator, such as Alaska. The guidelines also specify that sun exposure take place with a minimum temperature of 10° C. Dr. Fisher said that activity is diminished at lower temperatures.
“After 2 hours of exposure, patients should wash off the ALA and avoid further exposure for about 48 hours,” said Dr. Fisher, who recommended chemical sunscreens on areas of the skin not being treated.
“I think that over the next few years, this is going to have a big place in patient treatment. It is more convenient and better tolerated,” Dr. Fisher reported. She said that several modifications with the potential to enhance efficacy, such as pretreatment with retinoids or employing 5-FU after PDT, are strategies that have shown promise in small studies and may prove to be helpful through expanded clinical investigation.
NEW YORK – For treating actinic keratoses appearing over large or disseminated surface areas, daylight is often a better strategy than artificial light is for activating photodynamic therapy (PDT), according to an update on strategies at the summer meeting of the American Academy of Dermatology.
The evidence that daylight is at least as effective as artificial light for grade 1 and 2 actinic keratoses has created a “really exciting new opportunity” for those with disseminated disease, according to Dr. Emily J. Fisher, director of Mohs surgery at Mercy Health Physicians, Cincinnati, Ohio. This approach is not only a more efficient way to treat large or multiple areas of skin, but it is better tolerated, further facilitating treatment of bigger surface areas.
Moreover, for physicians not currently equipped with blue or red artificial light, daylight activation “is a great way to incorporate PDT into your practice,” Dr. Fisher added. She suggested that PDT, which has been associated with clearance rates exceeding 70% with a single treatment in many studies, appears to be at least as effective as the topical treatments that are employed more often, such as 5-fluorouracil (5-FU) or imiquimod.
When comparing efficacy across studies, “PDT seems to have a higher response than [does] our topical treatments,” but Dr. Fisher cautioned that there are no high-quality, head-to-head comparisons, so there is no definitive evidence of the superiority of one over the other.
However, in patients with multiple actinic keratoses spread over a substantial area of the skin or who have lesions in more than one anatomical site, daylight PDT is a practical approach now widely used in Europe and several other parts of the world, according to Dr. Fisher. She reported that five randomized trials have demonstrated that daylight PDT is effective.
Most aspects of daylight PDT are the same as conventional PDT, according to Dr. Fisher. The skin is first prepared by removing scales and crusts to improve penetration of the photodynamic agent, whether aminolevulinate acid (ALA) or methyl aminolevulinate (MAL). Prior to light exposure, the occlusion time with the photodynamic agent is the same 3 hours. Also, light exposure in both cases should begin within 30 minutes, which may be a consideration for those depending on daylight.
“Patients really should not go indoors or into shade for more than 5 minutes at a time,” Dr. Fisher reported. The problem is that the activity of the intracellular photosensitizing chemicals can build up without light exposure, producing pain and reducing the tolerability of the treatment.
Consensus guidelines have been published for daylight PDT in Australia (J Eur Acad Dermatol Venereol. 2012 Jun;26[6]:673-9.). According to Dr. Fisher, the guidelines recommend a light intensity of greater than 130 W/m2, which is a dose provided by sunlight within the continental United States but not at distant points from the equator, such as Alaska. The guidelines also specify that sun exposure take place with a minimum temperature of 10° C. Dr. Fisher said that activity is diminished at lower temperatures.
“After 2 hours of exposure, patients should wash off the ALA and avoid further exposure for about 48 hours,” said Dr. Fisher, who recommended chemical sunscreens on areas of the skin not being treated.
“I think that over the next few years, this is going to have a big place in patient treatment. It is more convenient and better tolerated,” Dr. Fisher reported. She said that several modifications with the potential to enhance efficacy, such as pretreatment with retinoids or employing 5-FU after PDT, are strategies that have shown promise in small studies and may prove to be helpful through expanded clinical investigation.
NEW YORK – For treating actinic keratoses appearing over large or disseminated surface areas, daylight is often a better strategy than artificial light is for activating photodynamic therapy (PDT), according to an update on strategies at the summer meeting of the American Academy of Dermatology.
The evidence that daylight is at least as effective as artificial light for grade 1 and 2 actinic keratoses has created a “really exciting new opportunity” for those with disseminated disease, according to Dr. Emily J. Fisher, director of Mohs surgery at Mercy Health Physicians, Cincinnati, Ohio. This approach is not only a more efficient way to treat large or multiple areas of skin, but it is better tolerated, further facilitating treatment of bigger surface areas.
Moreover, for physicians not currently equipped with blue or red artificial light, daylight activation “is a great way to incorporate PDT into your practice,” Dr. Fisher added. She suggested that PDT, which has been associated with clearance rates exceeding 70% with a single treatment in many studies, appears to be at least as effective as the topical treatments that are employed more often, such as 5-fluorouracil (5-FU) or imiquimod.
When comparing efficacy across studies, “PDT seems to have a higher response than [does] our topical treatments,” but Dr. Fisher cautioned that there are no high-quality, head-to-head comparisons, so there is no definitive evidence of the superiority of one over the other.
However, in patients with multiple actinic keratoses spread over a substantial area of the skin or who have lesions in more than one anatomical site, daylight PDT is a practical approach now widely used in Europe and several other parts of the world, according to Dr. Fisher. She reported that five randomized trials have demonstrated that daylight PDT is effective.
Most aspects of daylight PDT are the same as conventional PDT, according to Dr. Fisher. The skin is first prepared by removing scales and crusts to improve penetration of the photodynamic agent, whether aminolevulinate acid (ALA) or methyl aminolevulinate (MAL). Prior to light exposure, the occlusion time with the photodynamic agent is the same 3 hours. Also, light exposure in both cases should begin within 30 minutes, which may be a consideration for those depending on daylight.
“Patients really should not go indoors or into shade for more than 5 minutes at a time,” Dr. Fisher reported. The problem is that the activity of the intracellular photosensitizing chemicals can build up without light exposure, producing pain and reducing the tolerability of the treatment.
Consensus guidelines have been published for daylight PDT in Australia (J Eur Acad Dermatol Venereol. 2012 Jun;26[6]:673-9.). According to Dr. Fisher, the guidelines recommend a light intensity of greater than 130 W/m2, which is a dose provided by sunlight within the continental United States but not at distant points from the equator, such as Alaska. The guidelines also specify that sun exposure take place with a minimum temperature of 10° C. Dr. Fisher said that activity is diminished at lower temperatures.
“After 2 hours of exposure, patients should wash off the ALA and avoid further exposure for about 48 hours,” said Dr. Fisher, who recommended chemical sunscreens on areas of the skin not being treated.
“I think that over the next few years, this is going to have a big place in patient treatment. It is more convenient and better tolerated,” Dr. Fisher reported. She said that several modifications with the potential to enhance efficacy, such as pretreatment with retinoids or employing 5-FU after PDT, are strategies that have shown promise in small studies and may prove to be helpful through expanded clinical investigation.
AT THE SUMMER MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: For disseminated actinic keratoses, daylight is often the best way to activate photodynamic therapy.
Major finding: As effective as artificial light in five randomized trials, daylight photodynamic therapy for actinic keratoses is better tolerated and allows treatment of larger surface areas.
Data source: Review of data from randomized trials.
Disclosures: Dr. Fisher reported having no financial disclosures.
