User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
CDC panel: No COVID-19 vaccine safety surprises
The United States is nearly 6 weeks into its historic campaign to vaccinate Americans against the virus that causes COVID-19, and so far, the two vaccines in use look remarkably low risk, according to new data presented today at a meeting of vaccine experts that advise the Centers for Disease Control and Prevention.
With 23.5 million doses of the Pfizer and Moderna vaccines now given, there have been very few serious side effects. In addition, deaths reported after people got the vaccine do not seem to be related to it.
The most common symptoms reported after vaccination were pain where people got the shot, fatigue, headache, and muscle soreness. These were more common after the second dose. In addition, about one in four people reported fever and chills after the second shot.
“On the whole, I thought it was very reassuring,” said William Schaffner, MD, an infectious disease expert with Vanderbilt University, Nashville, Tenn., who listened to the presentations.
The CDC is collecting safety information through multiple channels. These include a new smartphone-based app called V-Safe, which collects daily information from people who’ve been vaccinated; the federal Vaccine Adverse Event Reporting System, which accepts reports from anyone; and the Vaccine Safety Datalink, which is a collaboration between the CDC and nine major hospital systems. There’s also the Clinical Immunization Safety Assessment Project, a collaboration between the CDC and vaccine safety experts.
After surveying these systems, experts heading the safety committee for the CDC’s Advisory Committee on Immunization Practices said there have been few serious side effects reported.
Very rarely, severe allergic reactions – called anaphylaxis – have occurred after vaccination. There have been 50 of these cases reported after the Pfizer vaccine and 21 cases reported after the Moderna vaccine to date. Nearly all of them – 94% of the anaphylaxis cases after Pfizer vaccines and 100% of those after Moderna’s vaccine – have been in women, though it’s not clear why.
That translates to a rate of about five cases of anaphylaxis for every million doses of the Pfizer vaccine and about three for every million doses of the Moderna vaccine. Most of these occur within 15 minutes after getting a vaccine dose, with one reported as long as 20 hours after the shot.
The CDC suspects these may be related to an ingredient called polyethylene glycol (PEG). PEG is a part of the particles that slip the vaccines’ mRNA into cells with instructions to make the spike protein of the virus. Cells then express these spikes on their surfaces so the immune system can learn to recognize them and make defenses against them. PEG is a common ingredient in many drugs and occasionally triggers anaphylaxis.
Reported deaths seem unrelated to vaccines
Through Jan. 18, 196 people have died after getting a vaccine.
Most of these deaths (129) were in patients in long term care facilities. These deaths are still being investigated, but when they were compared with the number of deaths that might be expected over the same period because of natural causes, they seemed to be coincidental and not caused by the vaccine, said Tom Shimabukuro, MD, deputy director of the Immunization Safety Office at the CDC, who studied the data.
In fact, death rates were lower among vaccinated nursing home residents, compared with those who had not been vaccinated.
“These findings suggest that short-term mortality rates appear unrelated to vaccination for COVID-19,” Dr. Shimabukuro said.
This also appeared to be true for younger adults who died after their shots.
There were 28 people aged under 65 years who died after being vaccinated. Most of these deaths were heart related, according to autopsy reports. When investigators compared the number of sudden cardiac deaths expected to occur in this population naturally, they found people who were vaccinated had a lower rate than would have been expected without vaccination. This suggests that these deaths were also unrelated to the vaccine.
More vaccines on the horizon
The panel also heard an update from drug company AstraZeneca on its vaccine. It’s being used in 18 countries but has not yet been authorized in the United States.
That vaccine is currently in phase 3 of its U.S. clinical trials, and more than 26,000 people who have volunteered to get the shot had received their second dose as of Jan. 21, the company said.
The Food and Drug Administration requires at least 2 months of follow-up before it will evaluate a vaccine for an emergency-use authorization, which means the company would be ready to submit by the end of March, with a possible approval by April.
The AstraZeneca vaccine uses a more traditional method to create immunity, slipping a key part of the virus that causes COVID-19 into the shell of an adenovirus – a virus that causes cold-like symptoms – that normally infects monkeys. When the immune system sees the virus, it generates protective defenses against it.
The two-dose vaccine can be stored in a regular refrigerator for up to 6 months, which makes it easier to handle than the mRNA vaccines, which require much colder storage. Another advantage appears to be that it’s less likely to trigger severe allergic reactions. So far, there have been no cases of anaphylaxis reported after this shot.
In total, four serious side effects have been reported with the AstraZeneca vaccine, including two cases of transverse myelitis, a serious condition that causes swelling of the spinal cord, leading to pain, muscle weakness, and paralysis. One of these was in the group that got the placebo. The reports paused the trial, but it was allowed to continue after a safety review.
This vaccine also appears to be less effective than the mRNA shots. Data presented to the panel show it appears to cut the risk of developing a COVID infection that has symptoms by 62%. That’s over the 50% threshold the FDA set for approval but less than seen with the mRNA vaccines, which are more than 90% effective at preventing infections.
“Is the average person going to want to take the AstraZeneca shot? What role is this going to play in our vaccination program?” Dr. Schaffner said.
Johnson & Johnson will have enough data from its clinical trials to submit it to the FDA within the next week, the company said in a call with shareholders on Tuesday. So far, its one-dose shots looks to be about as effective as both the Pfizer and Moderna vaccines.
“It could be that we wind up with four vaccines: Three that can run very fast, and one that’s not so fast,” Dr. Schaffner said.
A version of this article first appeared on Medscape.com.
The United States is nearly 6 weeks into its historic campaign to vaccinate Americans against the virus that causes COVID-19, and so far, the two vaccines in use look remarkably low risk, according to new data presented today at a meeting of vaccine experts that advise the Centers for Disease Control and Prevention.
With 23.5 million doses of the Pfizer and Moderna vaccines now given, there have been very few serious side effects. In addition, deaths reported after people got the vaccine do not seem to be related to it.
The most common symptoms reported after vaccination were pain where people got the shot, fatigue, headache, and muscle soreness. These were more common after the second dose. In addition, about one in four people reported fever and chills after the second shot.
“On the whole, I thought it was very reassuring,” said William Schaffner, MD, an infectious disease expert with Vanderbilt University, Nashville, Tenn., who listened to the presentations.
The CDC is collecting safety information through multiple channels. These include a new smartphone-based app called V-Safe, which collects daily information from people who’ve been vaccinated; the federal Vaccine Adverse Event Reporting System, which accepts reports from anyone; and the Vaccine Safety Datalink, which is a collaboration between the CDC and nine major hospital systems. There’s also the Clinical Immunization Safety Assessment Project, a collaboration between the CDC and vaccine safety experts.
After surveying these systems, experts heading the safety committee for the CDC’s Advisory Committee on Immunization Practices said there have been few serious side effects reported.
Very rarely, severe allergic reactions – called anaphylaxis – have occurred after vaccination. There have been 50 of these cases reported after the Pfizer vaccine and 21 cases reported after the Moderna vaccine to date. Nearly all of them – 94% of the anaphylaxis cases after Pfizer vaccines and 100% of those after Moderna’s vaccine – have been in women, though it’s not clear why.
That translates to a rate of about five cases of anaphylaxis for every million doses of the Pfizer vaccine and about three for every million doses of the Moderna vaccine. Most of these occur within 15 minutes after getting a vaccine dose, with one reported as long as 20 hours after the shot.
The CDC suspects these may be related to an ingredient called polyethylene glycol (PEG). PEG is a part of the particles that slip the vaccines’ mRNA into cells with instructions to make the spike protein of the virus. Cells then express these spikes on their surfaces so the immune system can learn to recognize them and make defenses against them. PEG is a common ingredient in many drugs and occasionally triggers anaphylaxis.
Reported deaths seem unrelated to vaccines
Through Jan. 18, 196 people have died after getting a vaccine.
Most of these deaths (129) were in patients in long term care facilities. These deaths are still being investigated, but when they were compared with the number of deaths that might be expected over the same period because of natural causes, they seemed to be coincidental and not caused by the vaccine, said Tom Shimabukuro, MD, deputy director of the Immunization Safety Office at the CDC, who studied the data.
In fact, death rates were lower among vaccinated nursing home residents, compared with those who had not been vaccinated.
“These findings suggest that short-term mortality rates appear unrelated to vaccination for COVID-19,” Dr. Shimabukuro said.
This also appeared to be true for younger adults who died after their shots.
There were 28 people aged under 65 years who died after being vaccinated. Most of these deaths were heart related, according to autopsy reports. When investigators compared the number of sudden cardiac deaths expected to occur in this population naturally, they found people who were vaccinated had a lower rate than would have been expected without vaccination. This suggests that these deaths were also unrelated to the vaccine.
More vaccines on the horizon
The panel also heard an update from drug company AstraZeneca on its vaccine. It’s being used in 18 countries but has not yet been authorized in the United States.
That vaccine is currently in phase 3 of its U.S. clinical trials, and more than 26,000 people who have volunteered to get the shot had received their second dose as of Jan. 21, the company said.
The Food and Drug Administration requires at least 2 months of follow-up before it will evaluate a vaccine for an emergency-use authorization, which means the company would be ready to submit by the end of March, with a possible approval by April.
The AstraZeneca vaccine uses a more traditional method to create immunity, slipping a key part of the virus that causes COVID-19 into the shell of an adenovirus – a virus that causes cold-like symptoms – that normally infects monkeys. When the immune system sees the virus, it generates protective defenses against it.
The two-dose vaccine can be stored in a regular refrigerator for up to 6 months, which makes it easier to handle than the mRNA vaccines, which require much colder storage. Another advantage appears to be that it’s less likely to trigger severe allergic reactions. So far, there have been no cases of anaphylaxis reported after this shot.
In total, four serious side effects have been reported with the AstraZeneca vaccine, including two cases of transverse myelitis, a serious condition that causes swelling of the spinal cord, leading to pain, muscle weakness, and paralysis. One of these was in the group that got the placebo. The reports paused the trial, but it was allowed to continue after a safety review.
This vaccine also appears to be less effective than the mRNA shots. Data presented to the panel show it appears to cut the risk of developing a COVID infection that has symptoms by 62%. That’s over the 50% threshold the FDA set for approval but less than seen with the mRNA vaccines, which are more than 90% effective at preventing infections.
“Is the average person going to want to take the AstraZeneca shot? What role is this going to play in our vaccination program?” Dr. Schaffner said.
Johnson & Johnson will have enough data from its clinical trials to submit it to the FDA within the next week, the company said in a call with shareholders on Tuesday. So far, its one-dose shots looks to be about as effective as both the Pfizer and Moderna vaccines.
“It could be that we wind up with four vaccines: Three that can run very fast, and one that’s not so fast,” Dr. Schaffner said.
A version of this article first appeared on Medscape.com.
The United States is nearly 6 weeks into its historic campaign to vaccinate Americans against the virus that causes COVID-19, and so far, the two vaccines in use look remarkably low risk, according to new data presented today at a meeting of vaccine experts that advise the Centers for Disease Control and Prevention.
With 23.5 million doses of the Pfizer and Moderna vaccines now given, there have been very few serious side effects. In addition, deaths reported after people got the vaccine do not seem to be related to it.
The most common symptoms reported after vaccination were pain where people got the shot, fatigue, headache, and muscle soreness. These were more common after the second dose. In addition, about one in four people reported fever and chills after the second shot.
“On the whole, I thought it was very reassuring,” said William Schaffner, MD, an infectious disease expert with Vanderbilt University, Nashville, Tenn., who listened to the presentations.
The CDC is collecting safety information through multiple channels. These include a new smartphone-based app called V-Safe, which collects daily information from people who’ve been vaccinated; the federal Vaccine Adverse Event Reporting System, which accepts reports from anyone; and the Vaccine Safety Datalink, which is a collaboration between the CDC and nine major hospital systems. There’s also the Clinical Immunization Safety Assessment Project, a collaboration between the CDC and vaccine safety experts.
After surveying these systems, experts heading the safety committee for the CDC’s Advisory Committee on Immunization Practices said there have been few serious side effects reported.
Very rarely, severe allergic reactions – called anaphylaxis – have occurred after vaccination. There have been 50 of these cases reported after the Pfizer vaccine and 21 cases reported after the Moderna vaccine to date. Nearly all of them – 94% of the anaphylaxis cases after Pfizer vaccines and 100% of those after Moderna’s vaccine – have been in women, though it’s not clear why.
That translates to a rate of about five cases of anaphylaxis for every million doses of the Pfizer vaccine and about three for every million doses of the Moderna vaccine. Most of these occur within 15 minutes after getting a vaccine dose, with one reported as long as 20 hours after the shot.
The CDC suspects these may be related to an ingredient called polyethylene glycol (PEG). PEG is a part of the particles that slip the vaccines’ mRNA into cells with instructions to make the spike protein of the virus. Cells then express these spikes on their surfaces so the immune system can learn to recognize them and make defenses against them. PEG is a common ingredient in many drugs and occasionally triggers anaphylaxis.
Reported deaths seem unrelated to vaccines
Through Jan. 18, 196 people have died after getting a vaccine.
Most of these deaths (129) were in patients in long term care facilities. These deaths are still being investigated, but when they were compared with the number of deaths that might be expected over the same period because of natural causes, they seemed to be coincidental and not caused by the vaccine, said Tom Shimabukuro, MD, deputy director of the Immunization Safety Office at the CDC, who studied the data.
In fact, death rates were lower among vaccinated nursing home residents, compared with those who had not been vaccinated.
“These findings suggest that short-term mortality rates appear unrelated to vaccination for COVID-19,” Dr. Shimabukuro said.
This also appeared to be true for younger adults who died after their shots.
There were 28 people aged under 65 years who died after being vaccinated. Most of these deaths were heart related, according to autopsy reports. When investigators compared the number of sudden cardiac deaths expected to occur in this population naturally, they found people who were vaccinated had a lower rate than would have been expected without vaccination. This suggests that these deaths were also unrelated to the vaccine.
More vaccines on the horizon
The panel also heard an update from drug company AstraZeneca on its vaccine. It’s being used in 18 countries but has not yet been authorized in the United States.
That vaccine is currently in phase 3 of its U.S. clinical trials, and more than 26,000 people who have volunteered to get the shot had received their second dose as of Jan. 21, the company said.
The Food and Drug Administration requires at least 2 months of follow-up before it will evaluate a vaccine for an emergency-use authorization, which means the company would be ready to submit by the end of March, with a possible approval by April.
The AstraZeneca vaccine uses a more traditional method to create immunity, slipping a key part of the virus that causes COVID-19 into the shell of an adenovirus – a virus that causes cold-like symptoms – that normally infects monkeys. When the immune system sees the virus, it generates protective defenses against it.
The two-dose vaccine can be stored in a regular refrigerator for up to 6 months, which makes it easier to handle than the mRNA vaccines, which require much colder storage. Another advantage appears to be that it’s less likely to trigger severe allergic reactions. So far, there have been no cases of anaphylaxis reported after this shot.
In total, four serious side effects have been reported with the AstraZeneca vaccine, including two cases of transverse myelitis, a serious condition that causes swelling of the spinal cord, leading to pain, muscle weakness, and paralysis. One of these was in the group that got the placebo. The reports paused the trial, but it was allowed to continue after a safety review.
This vaccine also appears to be less effective than the mRNA shots. Data presented to the panel show it appears to cut the risk of developing a COVID infection that has symptoms by 62%. That’s over the 50% threshold the FDA set for approval but less than seen with the mRNA vaccines, which are more than 90% effective at preventing infections.
“Is the average person going to want to take the AstraZeneca shot? What role is this going to play in our vaccination program?” Dr. Schaffner said.
Johnson & Johnson will have enough data from its clinical trials to submit it to the FDA within the next week, the company said in a call with shareholders on Tuesday. So far, its one-dose shots looks to be about as effective as both the Pfizer and Moderna vaccines.
“It could be that we wind up with four vaccines: Three that can run very fast, and one that’s not so fast,” Dr. Schaffner said.
A version of this article first appeared on Medscape.com.
Are there COVID-19–related ‘long-haul’ skin issues?
– as a result of infection with or exposure to the SARS-CoV-2 virus, but some dermatologists question if the skin signs and symptoms are truly related.

In their commentary in the Lancet Infectious Diseases, Esther P. Freeman, MD, PhD, and colleagues who lead and participate in the American Academy of Dermatology’s international registry said their analysis “revealed a previously unreported subset of patients who experience long-haul symptoms in dermatology-dominant COVID-19.”
Some of the data was presented at the 29th European Academy of Dermatology and Venereology in late October 2020, but has since been updated with more cases.
Dermatologists who spoke with this news organization said it has not been settled that some skin manifestations – such as pernio/chilblains rashes, seen primarily in nonhospitalized patients, and described in the registry – are definitively caused by COVID. They also noted that in some cases, patients who initially test negative for COVID-19 by polymerase chain reaction (PCR) sometimes do not ever develop antibodies, which could mean they were never actually exposed to SARS-CoV-2.

“I still question whether the perniosis is directly related to infection with SARS-CoV-2 or not,” said Anthony Fernandez, MD, PhD, director of medical and inpatient dermatology and assistant professor of dermatopathology at the Cleveland Clinic. His uncertainty is driven by the lack of seroconversion and that few cases were seen over the summer in the United States – suggesting that it may still be a result of cold temperatures.
“I’m not sure there is a definitive correct answer, definitely not that everyone would agree on,” said Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Conn.
Dr. Freeman, however, believed that pernio and especially persistent lesions are caused by an immune response to COVID.
In an interview, she noted the multiple cases of patients in the registry who did seroconvert and that, while a registry is not a perfect means of getting an answer, it is good for generating questions. Taken collectively, the cases in the registry can “tell a story for further hypotheses,” said Dr. Freeman, who is director of global health dermatology at Massachusetts General Hospital and assistant professor of dermatology at Harvard University, both in Boston.
“We were noticing this signal across the world” that patients “developed these toe lesions and they never got better,” said Dr. Freeman. Generally, people who experience pernio, also described as COVID toes or “COVID fingers,” recover in 4-8 weeks. But in the registry, “we did have this subset of patients who really were experiencing these very longstanding symptoms,” she added.
Two patients with lab-confirmed COVID have had long-lasting pernio of 133 days and 150 days. “I’m caring for a cohort in Boston who have had long COVID of the skin and symptoms for over 10 months,” Dr. Freeman said.
Pernio dominates
The registry – a collaboration between the AAD and the International League of Dermatological Societies – was launched in April 2020. Any medical professional can enter case information. From April to October, 1,030 total cases and 331 laboratory-confirmed or suspected COVID-19 cases with dermatological manifestations were entered from 41 countries.
Most of the cases were just recorded at a single time point, which is an acknowledged limitation of the study.
Dr. Freeman and colleagues reached out to registry participants in June and August to get updates on COVID lab test results and sign and symptom duration. Overall, 234 total and 96 lab-confirmed COVID infections had more lengthy data about sign and symptom duration.
Pernio lasted a median of 15 days in patients with suspected disease and 12 days for those with lab-confirmed COVID, compared with a median of 7 days for morbilliform eruptions, 4 days for urticarial eruptions, and 20 days for papulosquamous eruptions – all in patients with lab-confirmed disease.
Of the 103 cases of pernio, 7 had symptoms lasting more than 60 days. Only two of those seven patients had lab-confirmed COVID. Initially, the one patient tested negative with nasopharyngeal PCR, and serum IgM and IgG. Six weeks after pernio onset, the patient – still experiencing fatigue and pernio – seroconverted to anti–SARS-CoV-2 IgM positivity.
The other long-haul patient, after a negative PCR, tested positive for SARS-CoV-2 serum IgG 1 month after pernio onset.
Robust immune response?
Dr. Freeman said these patients might have a very high interferon response initially to the virus, which makes for a mild to nonexistent disease, but could create inflammation elsewhere. “I almost view the toes as an innocent bystander of a robust immune response to SARS-CoV-2.”
Although he has not seen extended pernio or other skin manifestations in his patients, Dr. Fernandez said the interferon hypothesis is “fair,” and “the best that’s out there.” Dr. Fernandez is currently studying cutaneous manifestations of COVID-19 as a principal investigator of a trial sponsored by the Clinical and Translational Science Collaborative of Cleveland.

Dr. Ko said in an interview that she has not observed long-haul skin issues in her patients, but Yale colleagues have.
In a study, she and Yale colleagues published in September, SARS-CoV-2 spike protein was detected in perniotic lesions, but not nuclear protein or viral RNA. The test they used – immunohistochemistry – can be nonspecific, which muddied results.
She does not think there is replicating virus in the skin or the lesions. Instead, said Dr. Ko, “either there is viral spike protein that has somehow become disassociated from actively replicating virus that somehow got deposited in endothelial cells,” or the staining “was spurious,” or some other protein is cross-reacting. “And the people who are unlucky enough to have that protein in their endothelial cells can manifest this COVID-toe, COVID-finger phenomenon.”
To her, it’s an unsolved mystery. “The weird thing is, we’ve never before had this much perniosis,” Dr. Ko said.
Dr. Fernandez is not convinced yet, noting that, in Cleveland, more pernio cases were observed in March and April than in the summer. “If it is a manifestation of the infection then you also need the right environment, the cold weather for this manifestation to present,” he said. “Or, it really isn’t a direct manifestation of COVID-19 but may be more related to other factors,” such as lifestyle changes related to limitations implemented to help mitigate the spread of the disease.
“To me the jury is still out whether or not the perniotic lesions really can tell us something about a patient’s exposure and infection with SARS-CoV-2,” he said.
Dr. Freeman reported receiving a grant from the International League of Dermatological Societies and nonfinancial support from the AAD for the study. Dr. Ko reported no conflicts. Dr. Fernadnez had no disclosures.
– as a result of infection with or exposure to the SARS-CoV-2 virus, but some dermatologists question if the skin signs and symptoms are truly related.
In their commentary in the Lancet Infectious Diseases, Esther P. Freeman, MD, PhD, and colleagues who lead and participate in the American Academy of Dermatology’s international registry said their analysis “revealed a previously unreported subset of patients who experience long-haul symptoms in dermatology-dominant COVID-19.”
Some of the data was presented at the 29th European Academy of Dermatology and Venereology in late October 2020, but has since been updated with more cases.
Dermatologists who spoke with this news organization said it has not been settled that some skin manifestations – such as pernio/chilblains rashes, seen primarily in nonhospitalized patients, and described in the registry – are definitively caused by COVID. They also noted that in some cases, patients who initially test negative for COVID-19 by polymerase chain reaction (PCR) sometimes do not ever develop antibodies, which could mean they were never actually exposed to SARS-CoV-2.
“I still question whether the perniosis is directly related to infection with SARS-CoV-2 or not,” said Anthony Fernandez, MD, PhD, director of medical and inpatient dermatology and assistant professor of dermatopathology at the Cleveland Clinic. His uncertainty is driven by the lack of seroconversion and that few cases were seen over the summer in the United States – suggesting that it may still be a result of cold temperatures.
“I’m not sure there is a definitive correct answer, definitely not that everyone would agree on,” said Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Conn.
Dr. Freeman, however, believed that pernio and especially persistent lesions are caused by an immune response to COVID.
In an interview, she noted the multiple cases of patients in the registry who did seroconvert and that, while a registry is not a perfect means of getting an answer, it is good for generating questions. Taken collectively, the cases in the registry can “tell a story for further hypotheses,” said Dr. Freeman, who is director of global health dermatology at Massachusetts General Hospital and assistant professor of dermatology at Harvard University, both in Boston.
“We were noticing this signal across the world” that patients “developed these toe lesions and they never got better,” said Dr. Freeman. Generally, people who experience pernio, also described as COVID toes or “COVID fingers,” recover in 4-8 weeks. But in the registry, “we did have this subset of patients who really were experiencing these very longstanding symptoms,” she added.
Two patients with lab-confirmed COVID have had long-lasting pernio of 133 days and 150 days. “I’m caring for a cohort in Boston who have had long COVID of the skin and symptoms for over 10 months,” Dr. Freeman said.
Pernio dominates
The registry – a collaboration between the AAD and the International League of Dermatological Societies – was launched in April 2020. Any medical professional can enter case information. From April to October, 1,030 total cases and 331 laboratory-confirmed or suspected COVID-19 cases with dermatological manifestations were entered from 41 countries.
Most of the cases were just recorded at a single time point, which is an acknowledged limitation of the study.
Dr. Freeman and colleagues reached out to registry participants in June and August to get updates on COVID lab test results and sign and symptom duration. Overall, 234 total and 96 lab-confirmed COVID infections had more lengthy data about sign and symptom duration.
Pernio lasted a median of 15 days in patients with suspected disease and 12 days for those with lab-confirmed COVID, compared with a median of 7 days for morbilliform eruptions, 4 days for urticarial eruptions, and 20 days for papulosquamous eruptions – all in patients with lab-confirmed disease.
Of the 103 cases of pernio, 7 had symptoms lasting more than 60 days. Only two of those seven patients had lab-confirmed COVID. Initially, the one patient tested negative with nasopharyngeal PCR, and serum IgM and IgG. Six weeks after pernio onset, the patient – still experiencing fatigue and pernio – seroconverted to anti–SARS-CoV-2 IgM positivity.
The other long-haul patient, after a negative PCR, tested positive for SARS-CoV-2 serum IgG 1 month after pernio onset.
Robust immune response?
Dr. Freeman said these patients might have a very high interferon response initially to the virus, which makes for a mild to nonexistent disease, but could create inflammation elsewhere. “I almost view the toes as an innocent bystander of a robust immune response to SARS-CoV-2.”
Although he has not seen extended pernio or other skin manifestations in his patients, Dr. Fernandez said the interferon hypothesis is “fair,” and “the best that’s out there.” Dr. Fernandez is currently studying cutaneous manifestations of COVID-19 as a principal investigator of a trial sponsored by the Clinical and Translational Science Collaborative of Cleveland.
Dr. Ko said in an interview that she has not observed long-haul skin issues in her patients, but Yale colleagues have.
In a study, she and Yale colleagues published in September, SARS-CoV-2 spike protein was detected in perniotic lesions, but not nuclear protein or viral RNA. The test they used – immunohistochemistry – can be nonspecific, which muddied results.
She does not think there is replicating virus in the skin or the lesions. Instead, said Dr. Ko, “either there is viral spike protein that has somehow become disassociated from actively replicating virus that somehow got deposited in endothelial cells,” or the staining “was spurious,” or some other protein is cross-reacting. “And the people who are unlucky enough to have that protein in their endothelial cells can manifest this COVID-toe, COVID-finger phenomenon.”
To her, it’s an unsolved mystery. “The weird thing is, we’ve never before had this much perniosis,” Dr. Ko said.
Dr. Fernandez is not convinced yet, noting that, in Cleveland, more pernio cases were observed in March and April than in the summer. “If it is a manifestation of the infection then you also need the right environment, the cold weather for this manifestation to present,” he said. “Or, it really isn’t a direct manifestation of COVID-19 but may be more related to other factors,” such as lifestyle changes related to limitations implemented to help mitigate the spread of the disease.
“To me the jury is still out whether or not the perniotic lesions really can tell us something about a patient’s exposure and infection with SARS-CoV-2,” he said.
Dr. Freeman reported receiving a grant from the International League of Dermatological Societies and nonfinancial support from the AAD for the study. Dr. Ko reported no conflicts. Dr. Fernadnez had no disclosures.
– as a result of infection with or exposure to the SARS-CoV-2 virus, but some dermatologists question if the skin signs and symptoms are truly related.
In their commentary in the Lancet Infectious Diseases, Esther P. Freeman, MD, PhD, and colleagues who lead and participate in the American Academy of Dermatology’s international registry said their analysis “revealed a previously unreported subset of patients who experience long-haul symptoms in dermatology-dominant COVID-19.”
Some of the data was presented at the 29th European Academy of Dermatology and Venereology in late October 2020, but has since been updated with more cases.
Dermatologists who spoke with this news organization said it has not been settled that some skin manifestations – such as pernio/chilblains rashes, seen primarily in nonhospitalized patients, and described in the registry – are definitively caused by COVID. They also noted that in some cases, patients who initially test negative for COVID-19 by polymerase chain reaction (PCR) sometimes do not ever develop antibodies, which could mean they were never actually exposed to SARS-CoV-2.
“I still question whether the perniosis is directly related to infection with SARS-CoV-2 or not,” said Anthony Fernandez, MD, PhD, director of medical and inpatient dermatology and assistant professor of dermatopathology at the Cleveland Clinic. His uncertainty is driven by the lack of seroconversion and that few cases were seen over the summer in the United States – suggesting that it may still be a result of cold temperatures.
“I’m not sure there is a definitive correct answer, definitely not that everyone would agree on,” said Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Conn.
Dr. Freeman, however, believed that pernio and especially persistent lesions are caused by an immune response to COVID.
In an interview, she noted the multiple cases of patients in the registry who did seroconvert and that, while a registry is not a perfect means of getting an answer, it is good for generating questions. Taken collectively, the cases in the registry can “tell a story for further hypotheses,” said Dr. Freeman, who is director of global health dermatology at Massachusetts General Hospital and assistant professor of dermatology at Harvard University, both in Boston.
“We were noticing this signal across the world” that patients “developed these toe lesions and they never got better,” said Dr. Freeman. Generally, people who experience pernio, also described as COVID toes or “COVID fingers,” recover in 4-8 weeks. But in the registry, “we did have this subset of patients who really were experiencing these very longstanding symptoms,” she added.
Two patients with lab-confirmed COVID have had long-lasting pernio of 133 days and 150 days. “I’m caring for a cohort in Boston who have had long COVID of the skin and symptoms for over 10 months,” Dr. Freeman said.
Pernio dominates
The registry – a collaboration between the AAD and the International League of Dermatological Societies – was launched in April 2020. Any medical professional can enter case information. From April to October, 1,030 total cases and 331 laboratory-confirmed or suspected COVID-19 cases with dermatological manifestations were entered from 41 countries.
Most of the cases were just recorded at a single time point, which is an acknowledged limitation of the study.
Dr. Freeman and colleagues reached out to registry participants in June and August to get updates on COVID lab test results and sign and symptom duration. Overall, 234 total and 96 lab-confirmed COVID infections had more lengthy data about sign and symptom duration.
Pernio lasted a median of 15 days in patients with suspected disease and 12 days for those with lab-confirmed COVID, compared with a median of 7 days for morbilliform eruptions, 4 days for urticarial eruptions, and 20 days for papulosquamous eruptions – all in patients with lab-confirmed disease.
Of the 103 cases of pernio, 7 had symptoms lasting more than 60 days. Only two of those seven patients had lab-confirmed COVID. Initially, the one patient tested negative with nasopharyngeal PCR, and serum IgM and IgG. Six weeks after pernio onset, the patient – still experiencing fatigue and pernio – seroconverted to anti–SARS-CoV-2 IgM positivity.
The other long-haul patient, after a negative PCR, tested positive for SARS-CoV-2 serum IgG 1 month after pernio onset.
Robust immune response?
Dr. Freeman said these patients might have a very high interferon response initially to the virus, which makes for a mild to nonexistent disease, but could create inflammation elsewhere. “I almost view the toes as an innocent bystander of a robust immune response to SARS-CoV-2.”
Although he has not seen extended pernio or other skin manifestations in his patients, Dr. Fernandez said the interferon hypothesis is “fair,” and “the best that’s out there.” Dr. Fernandez is currently studying cutaneous manifestations of COVID-19 as a principal investigator of a trial sponsored by the Clinical and Translational Science Collaborative of Cleveland.
Dr. Ko said in an interview that she has not observed long-haul skin issues in her patients, but Yale colleagues have.
In a study, she and Yale colleagues published in September, SARS-CoV-2 spike protein was detected in perniotic lesions, but not nuclear protein or viral RNA. The test they used – immunohistochemistry – can be nonspecific, which muddied results.
She does not think there is replicating virus in the skin or the lesions. Instead, said Dr. Ko, “either there is viral spike protein that has somehow become disassociated from actively replicating virus that somehow got deposited in endothelial cells,” or the staining “was spurious,” or some other protein is cross-reacting. “And the people who are unlucky enough to have that protein in their endothelial cells can manifest this COVID-toe, COVID-finger phenomenon.”
To her, it’s an unsolved mystery. “The weird thing is, we’ve never before had this much perniosis,” Dr. Ko said.
Dr. Fernandez is not convinced yet, noting that, in Cleveland, more pernio cases were observed in March and April than in the summer. “If it is a manifestation of the infection then you also need the right environment, the cold weather for this manifestation to present,” he said. “Or, it really isn’t a direct manifestation of COVID-19 but may be more related to other factors,” such as lifestyle changes related to limitations implemented to help mitigate the spread of the disease.
“To me the jury is still out whether or not the perniotic lesions really can tell us something about a patient’s exposure and infection with SARS-CoV-2,” he said.
Dr. Freeman reported receiving a grant from the International League of Dermatological Societies and nonfinancial support from the AAD for the study. Dr. Ko reported no conflicts. Dr. Fernadnez had no disclosures.
FROM THE LANCET INFECTIOUS DISEASES
USMLE stuns again: Clinical skills test permanently ended
The Step 2 Clinical Skills (CS) test for medical school students and graduates has been permanently canceled, cosponsors of the U.S. Medical Licensing Examination (USMLE) announced in a press release this afternoon.
As previously reported by this news organization, the USMLE cosponsors, the Federation of State Medical Boards and the National Board of Medical Examiners, had announced in May that they would take the following 12-18 months to revamp the required test.
COVID-19 had forced a suspension of the all-day test, which requires test takers to have physical contact with standardized patients. It’s designed to gauge how soon-to-be doctors gather information from patients, perform physical exams, and communicate their findings to patients and colleagues.
However, the cosponsors said today, “we have no plans to bring back Step 2 CS, but we intend to take this opportunity to focus on working with our colleagues in medical education and at the state medical boards to determine innovative ways to assess clinical skills.”
David Johnson, FSMB’s chief assessment officer, said in an interview that, after months of study, “it became clear that the relaunch of a modified Step 2 CS exam would not meet our expectations to be appreciably better than the prior exam.”
Only weeks ago, NBME was hiring for the revamp
The news came as a huge surprise. Just weeks earlier, NBME was advertising for a position key to modifying the exam. The description for the position read: “This role will focus on operational planning and coordination both within the NBME and with ECFMG [Educational Commission for Foreign Medical Graduates] to effectively deliver a modified Step 2 Clinical Skills exam.”
Bryan Carmody, MD, MPH, an assistant professor at Eastern Virginia Medical School, Norfolk, noted in a Jan. 15 tweet that the position requires extensive information technology experience, “suggesting plans for a virtual test remain intact.”
Dr. Johnson said that, although the opportunities for helping lead the revamp of the test were posted until the announcement, no one had been hired for the position.
Today’s announcement stated that the USMLE still believes independent standardized tests for medical knowledge and clinical skills are important; however, it now feels clinical reasoning and communication skills will be able to be assessed in other steps.
“Computer-based case simulations in Step 3 and communication content recently bolstered in Step 1 are examples of these efforts that will continue,” the press release stated. “While not a replacement for Step 2 CS, these formats continue to contribute positively, e.g., measuring critical knowledge of medical communication.”
Critics ‘thrilled’ by test termination
Lydia Flier, MD, from the department of internal medicine at Harvard Medical School, Boston – who wrote an editorial for this news organization in August 2020 advocating that Step 2 CS be changed completely or ended entirely – said in an interview that she was “surprised and thrilled” by the announcement.
She said the cosponsors hadn’t initially appeared to agree with the growing sentiment that disruption from the pandemic had “proven the test was unnecessary and it looked like they really were going to try and keep it.”
“I’m thrilled for future generations,” she said. “It is proof of what many people have known all along, which is that the test is a no-value-add proposition that did not actually help determine people’s clinical skills.”
The test “met a breaking point” during the pandemic, she said, “from which CS could not recover.”
She noted in her editorial that the test costs $1,300 plus travel fees, as the test had been offered at only five sites. She agreed that the skills assessed by the Step 2 CS are already covered in medical school and through other Steps.
“It seems as though they could not justify it anymore. It’s the obvious right answer,” said Dr. Flier, who in 2016 cofounded #EndStep2CS, a nationwide movement demanding an end to the exam.
Another cofounder in that movement, Christopher Henderson, MD, a staff physician with Kaiser Permanente in Seattle, said in an interview that “this decision represents tremendous progress in the fight to reduce unnecessary costs in medical education, and is a win for future students. Credit goes to the many women and men who organized and voiced their desire for change.” He added that his views are his own and “do not reflect or imply the views of my organization.”
For the FSMB’s part, Dr. Johnson acknowledged that “the consideration of cost and value were two of many important factors for the Step 2 CS revitalization work.”
Dr. Johnson, Dr. Flier, and Dr. Henderson have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Step 2 Clinical Skills (CS) test for medical school students and graduates has been permanently canceled, cosponsors of the U.S. Medical Licensing Examination (USMLE) announced in a press release this afternoon.
As previously reported by this news organization, the USMLE cosponsors, the Federation of State Medical Boards and the National Board of Medical Examiners, had announced in May that they would take the following 12-18 months to revamp the required test.
COVID-19 had forced a suspension of the all-day test, which requires test takers to have physical contact with standardized patients. It’s designed to gauge how soon-to-be doctors gather information from patients, perform physical exams, and communicate their findings to patients and colleagues.
However, the cosponsors said today, “we have no plans to bring back Step 2 CS, but we intend to take this opportunity to focus on working with our colleagues in medical education and at the state medical boards to determine innovative ways to assess clinical skills.”
David Johnson, FSMB’s chief assessment officer, said in an interview that, after months of study, “it became clear that the relaunch of a modified Step 2 CS exam would not meet our expectations to be appreciably better than the prior exam.”
Only weeks ago, NBME was hiring for the revamp
The news came as a huge surprise. Just weeks earlier, NBME was advertising for a position key to modifying the exam. The description for the position read: “This role will focus on operational planning and coordination both within the NBME and with ECFMG [Educational Commission for Foreign Medical Graduates] to effectively deliver a modified Step 2 Clinical Skills exam.”
Bryan Carmody, MD, MPH, an assistant professor at Eastern Virginia Medical School, Norfolk, noted in a Jan. 15 tweet that the position requires extensive information technology experience, “suggesting plans for a virtual test remain intact.”
Dr. Johnson said that, although the opportunities for helping lead the revamp of the test were posted until the announcement, no one had been hired for the position.
Today’s announcement stated that the USMLE still believes independent standardized tests for medical knowledge and clinical skills are important; however, it now feels clinical reasoning and communication skills will be able to be assessed in other steps.
“Computer-based case simulations in Step 3 and communication content recently bolstered in Step 1 are examples of these efforts that will continue,” the press release stated. “While not a replacement for Step 2 CS, these formats continue to contribute positively, e.g., measuring critical knowledge of medical communication.”
Critics ‘thrilled’ by test termination
Lydia Flier, MD, from the department of internal medicine at Harvard Medical School, Boston – who wrote an editorial for this news organization in August 2020 advocating that Step 2 CS be changed completely or ended entirely – said in an interview that she was “surprised and thrilled” by the announcement.
She said the cosponsors hadn’t initially appeared to agree with the growing sentiment that disruption from the pandemic had “proven the test was unnecessary and it looked like they really were going to try and keep it.”
“I’m thrilled for future generations,” she said. “It is proof of what many people have known all along, which is that the test is a no-value-add proposition that did not actually help determine people’s clinical skills.”
The test “met a breaking point” during the pandemic, she said, “from which CS could not recover.”
She noted in her editorial that the test costs $1,300 plus travel fees, as the test had been offered at only five sites. She agreed that the skills assessed by the Step 2 CS are already covered in medical school and through other Steps.
“It seems as though they could not justify it anymore. It’s the obvious right answer,” said Dr. Flier, who in 2016 cofounded #EndStep2CS, a nationwide movement demanding an end to the exam.
Another cofounder in that movement, Christopher Henderson, MD, a staff physician with Kaiser Permanente in Seattle, said in an interview that “this decision represents tremendous progress in the fight to reduce unnecessary costs in medical education, and is a win for future students. Credit goes to the many women and men who organized and voiced their desire for change.” He added that his views are his own and “do not reflect or imply the views of my organization.”
For the FSMB’s part, Dr. Johnson acknowledged that “the consideration of cost and value were two of many important factors for the Step 2 CS revitalization work.”
Dr. Johnson, Dr. Flier, and Dr. Henderson have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Step 2 Clinical Skills (CS) test for medical school students and graduates has been permanently canceled, cosponsors of the U.S. Medical Licensing Examination (USMLE) announced in a press release this afternoon.
As previously reported by this news organization, the USMLE cosponsors, the Federation of State Medical Boards and the National Board of Medical Examiners, had announced in May that they would take the following 12-18 months to revamp the required test.
COVID-19 had forced a suspension of the all-day test, which requires test takers to have physical contact with standardized patients. It’s designed to gauge how soon-to-be doctors gather information from patients, perform physical exams, and communicate their findings to patients and colleagues.
However, the cosponsors said today, “we have no plans to bring back Step 2 CS, but we intend to take this opportunity to focus on working with our colleagues in medical education and at the state medical boards to determine innovative ways to assess clinical skills.”
David Johnson, FSMB’s chief assessment officer, said in an interview that, after months of study, “it became clear that the relaunch of a modified Step 2 CS exam would not meet our expectations to be appreciably better than the prior exam.”
Only weeks ago, NBME was hiring for the revamp
The news came as a huge surprise. Just weeks earlier, NBME was advertising for a position key to modifying the exam. The description for the position read: “This role will focus on operational planning and coordination both within the NBME and with ECFMG [Educational Commission for Foreign Medical Graduates] to effectively deliver a modified Step 2 Clinical Skills exam.”
Bryan Carmody, MD, MPH, an assistant professor at Eastern Virginia Medical School, Norfolk, noted in a Jan. 15 tweet that the position requires extensive information technology experience, “suggesting plans for a virtual test remain intact.”
Dr. Johnson said that, although the opportunities for helping lead the revamp of the test were posted until the announcement, no one had been hired for the position.
Today’s announcement stated that the USMLE still believes independent standardized tests for medical knowledge and clinical skills are important; however, it now feels clinical reasoning and communication skills will be able to be assessed in other steps.
“Computer-based case simulations in Step 3 and communication content recently bolstered in Step 1 are examples of these efforts that will continue,” the press release stated. “While not a replacement for Step 2 CS, these formats continue to contribute positively, e.g., measuring critical knowledge of medical communication.”
Critics ‘thrilled’ by test termination
Lydia Flier, MD, from the department of internal medicine at Harvard Medical School, Boston – who wrote an editorial for this news organization in August 2020 advocating that Step 2 CS be changed completely or ended entirely – said in an interview that she was “surprised and thrilled” by the announcement.
She said the cosponsors hadn’t initially appeared to agree with the growing sentiment that disruption from the pandemic had “proven the test was unnecessary and it looked like they really were going to try and keep it.”
“I’m thrilled for future generations,” she said. “It is proof of what many people have known all along, which is that the test is a no-value-add proposition that did not actually help determine people’s clinical skills.”
The test “met a breaking point” during the pandemic, she said, “from which CS could not recover.”
She noted in her editorial that the test costs $1,300 plus travel fees, as the test had been offered at only five sites. She agreed that the skills assessed by the Step 2 CS are already covered in medical school and through other Steps.
“It seems as though they could not justify it anymore. It’s the obvious right answer,” said Dr. Flier, who in 2016 cofounded #EndStep2CS, a nationwide movement demanding an end to the exam.
Another cofounder in that movement, Christopher Henderson, MD, a staff physician with Kaiser Permanente in Seattle, said in an interview that “this decision represents tremendous progress in the fight to reduce unnecessary costs in medical education, and is a win for future students. Credit goes to the many women and men who organized and voiced their desire for change.” He added that his views are his own and “do not reflect or imply the views of my organization.”
For the FSMB’s part, Dr. Johnson acknowledged that “the consideration of cost and value were two of many important factors for the Step 2 CS revitalization work.”
Dr. Johnson, Dr. Flier, and Dr. Henderson have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Biggest challenges practices faced from COVID last year: MGMA
according to a December 2020 report from the Medical Group Management Association.
The report was assembled from the results of weekly Stat polls by MGMA, which consists of 15,000 group practices representing more than 350,000 physicians. During the course of the year, more than 4,800 practice leaders were surveyed, but the individual polls had far fewer respondents.
The 2020 data represents snapshots from different points in the developing public health crisis. Still, much of what practices experienced earlier in the pandemic continues to apply, and it’s likely to persist this year as long as the coronavirus spreads and its toll deepens.
One top-line conclusion of the report: the economic pain felt by practices has resulted in layoffs, furloughs, and/or reduced compensation for providers and staff.
In the May 19 weekly survey, 82% of respondents said some or all of their providers’ compensation had been affected by the crisis. About 62% said every provider had been affected. Provider compensation was cut in several ways, including reduced hours and salaries, reduced or eliminated bonuses, and lower allowances for continuing medical education.
About 61% of health care leaders said in the June 26 poll that their own compensation had decreased.
In the following week’s survey, one in three managers said their organization had reduced staff compensation. Nearly all of the respondents in this category predicted the salary reductions would be temporary.
As of March 17, early in the pandemic, 40% of health care leaders said they were experiencing staff shortages. An April 21 poll found that 53% of health care leaders were taking steps to address their providers’ and staffers’ mental health.
“The mental and emotional toll on everyone continues to be a concern, as public health authorities continue to report alarming numbers of new [COVID-19] cases, hospitalizations, and deaths,” MGMA commented.
Telehealth and remote monitoring
Nearly all of the health care leaders surveyed on March 31 reported that their practices had expanded telehealth access because of COVID-19. The percentage of patient visits handled remotely had dropped substantially by the fall, according to a Harvard University/Commonwealth Fund/Phreesia survey. Still, it remains significantly higher than it was before the pandemic.
“At the end of 2020, telemedicine continues to play a vital role in everyday practice operations and long-term planning,” the MGMA report said. One indication of this, the association said, is that health care leaders are recognizing new best practices in specialty telemedicine, such as pediatrics and ob.gyn.
According to an April 28 poll, the top three coding/billing challenges for telehealth and telephone visits amid COVID-19 were inconsistent payer rules, pay parity and accuracy, and documentation of virtual visits.
While the Centers for Medicare & Medicaid Services has loosened its regulations to allow reimbursement of telehealth in all locations and at the same level as in-person visits, most of those changes will not last beyond the public health crisis without new legislation.
More health care leaders are considering the use of remote patient monitoring, MGMA said, but only 21% of practices offered such services as of Sept. 15. The report drew a connection between these plans and the current challenge of deferred care.
In the July 21 poll, 87% of health care leaders reported that safety concerns were the top reason that patients deferred care amid COVID-19. The MGMA report quoted JaeLynn Williams, CEO of Air Methods, which provides helicopter ambulance services, as saying that many people are staying home even when they face life-threatening conditions such as chest pain, drug symptoms, inflamed appendix, and gallbladder pain.
Operational issues
Overall, MGMA said, practices that have taken a financial risk have done better during the pandemic than fee-for-service practices because their monthly capitation revenue has continued unabated. In contrast, “most groups’ struggles to sustain visits and procedures meant less revenue and lower compensation,” the report said.
In the August 18 survey, one in three health care leaders reported their practices were changing their operational metrics and how often they looked at those measures because of the pandemic. “Practice managers are asking for dashboard data in weeks instead of months to measure the drop in charges and forecast the resulting change in collections,” MGMA noted. “The type of data practice managers are asking for has also changed.”
Among the new metrics that practices are interested in, according to an MGMA article, are measures that track telehealth visits, the productivity of staff working at home, and the number of ancillary services and procedures that new patients might need based on historical data.
Nearly all health care leaders surveyed on Aug. 11 said the cost of obtaining personal protective equipment had increased during 2020. MGMA said it expects this situation to worsen if the pandemic lasts through the summer of 2021.
While everyone is talking about the botched launch of the COVID-19 vaccination campaign, there were also problems with flu vaccination in 2020. In the Sept. 25 poll, 34% of health care leaders reported their practices were experiencing delays in getting the flu vaccine.
Looking ahead
Looking further ahead, the report recommended that practices make plans to boost staff morale by restoring bonuses.
In addition, MGMA suggested that physician groups reassess their space needs. “The equation is simple – fewer nonclinical staff members at your facility means you should repurpose that office space or consider finding a better fit for your new real estate needs in 2021.”
Finally, MGMA noted that the practices expanding rather than contracting their business are those increasing their value-based revenues by taking on more risk. For those groups, “growing the patient panel can help [them] seek better rates in contract negotiations.”
A version of this article first appeared on Medscape.com.
according to a December 2020 report from the Medical Group Management Association.
The report was assembled from the results of weekly Stat polls by MGMA, which consists of 15,000 group practices representing more than 350,000 physicians. During the course of the year, more than 4,800 practice leaders were surveyed, but the individual polls had far fewer respondents.
The 2020 data represents snapshots from different points in the developing public health crisis. Still, much of what practices experienced earlier in the pandemic continues to apply, and it’s likely to persist this year as long as the coronavirus spreads and its toll deepens.
One top-line conclusion of the report: the economic pain felt by practices has resulted in layoffs, furloughs, and/or reduced compensation for providers and staff.
In the May 19 weekly survey, 82% of respondents said some or all of their providers’ compensation had been affected by the crisis. About 62% said every provider had been affected. Provider compensation was cut in several ways, including reduced hours and salaries, reduced or eliminated bonuses, and lower allowances for continuing medical education.
About 61% of health care leaders said in the June 26 poll that their own compensation had decreased.
In the following week’s survey, one in three managers said their organization had reduced staff compensation. Nearly all of the respondents in this category predicted the salary reductions would be temporary.
As of March 17, early in the pandemic, 40% of health care leaders said they were experiencing staff shortages. An April 21 poll found that 53% of health care leaders were taking steps to address their providers’ and staffers’ mental health.
“The mental and emotional toll on everyone continues to be a concern, as public health authorities continue to report alarming numbers of new [COVID-19] cases, hospitalizations, and deaths,” MGMA commented.
Telehealth and remote monitoring
Nearly all of the health care leaders surveyed on March 31 reported that their practices had expanded telehealth access because of COVID-19. The percentage of patient visits handled remotely had dropped substantially by the fall, according to a Harvard University/Commonwealth Fund/Phreesia survey. Still, it remains significantly higher than it was before the pandemic.
“At the end of 2020, telemedicine continues to play a vital role in everyday practice operations and long-term planning,” the MGMA report said. One indication of this, the association said, is that health care leaders are recognizing new best practices in specialty telemedicine, such as pediatrics and ob.gyn.
According to an April 28 poll, the top three coding/billing challenges for telehealth and telephone visits amid COVID-19 were inconsistent payer rules, pay parity and accuracy, and documentation of virtual visits.
While the Centers for Medicare & Medicaid Services has loosened its regulations to allow reimbursement of telehealth in all locations and at the same level as in-person visits, most of those changes will not last beyond the public health crisis without new legislation.
More health care leaders are considering the use of remote patient monitoring, MGMA said, but only 21% of practices offered such services as of Sept. 15. The report drew a connection between these plans and the current challenge of deferred care.
In the July 21 poll, 87% of health care leaders reported that safety concerns were the top reason that patients deferred care amid COVID-19. The MGMA report quoted JaeLynn Williams, CEO of Air Methods, which provides helicopter ambulance services, as saying that many people are staying home even when they face life-threatening conditions such as chest pain, drug symptoms, inflamed appendix, and gallbladder pain.
Operational issues
Overall, MGMA said, practices that have taken a financial risk have done better during the pandemic than fee-for-service practices because their monthly capitation revenue has continued unabated. In contrast, “most groups’ struggles to sustain visits and procedures meant less revenue and lower compensation,” the report said.
In the August 18 survey, one in three health care leaders reported their practices were changing their operational metrics and how often they looked at those measures because of the pandemic. “Practice managers are asking for dashboard data in weeks instead of months to measure the drop in charges and forecast the resulting change in collections,” MGMA noted. “The type of data practice managers are asking for has also changed.”
Among the new metrics that practices are interested in, according to an MGMA article, are measures that track telehealth visits, the productivity of staff working at home, and the number of ancillary services and procedures that new patients might need based on historical data.
Nearly all health care leaders surveyed on Aug. 11 said the cost of obtaining personal protective equipment had increased during 2020. MGMA said it expects this situation to worsen if the pandemic lasts through the summer of 2021.
While everyone is talking about the botched launch of the COVID-19 vaccination campaign, there were also problems with flu vaccination in 2020. In the Sept. 25 poll, 34% of health care leaders reported their practices were experiencing delays in getting the flu vaccine.
Looking ahead
Looking further ahead, the report recommended that practices make plans to boost staff morale by restoring bonuses.
In addition, MGMA suggested that physician groups reassess their space needs. “The equation is simple – fewer nonclinical staff members at your facility means you should repurpose that office space or consider finding a better fit for your new real estate needs in 2021.”
Finally, MGMA noted that the practices expanding rather than contracting their business are those increasing their value-based revenues by taking on more risk. For those groups, “growing the patient panel can help [them] seek better rates in contract negotiations.”
A version of this article first appeared on Medscape.com.
according to a December 2020 report from the Medical Group Management Association.
The report was assembled from the results of weekly Stat polls by MGMA, which consists of 15,000 group practices representing more than 350,000 physicians. During the course of the year, more than 4,800 practice leaders were surveyed, but the individual polls had far fewer respondents.
The 2020 data represents snapshots from different points in the developing public health crisis. Still, much of what practices experienced earlier in the pandemic continues to apply, and it’s likely to persist this year as long as the coronavirus spreads and its toll deepens.
One top-line conclusion of the report: the economic pain felt by practices has resulted in layoffs, furloughs, and/or reduced compensation for providers and staff.
In the May 19 weekly survey, 82% of respondents said some or all of their providers’ compensation had been affected by the crisis. About 62% said every provider had been affected. Provider compensation was cut in several ways, including reduced hours and salaries, reduced or eliminated bonuses, and lower allowances for continuing medical education.
About 61% of health care leaders said in the June 26 poll that their own compensation had decreased.
In the following week’s survey, one in three managers said their organization had reduced staff compensation. Nearly all of the respondents in this category predicted the salary reductions would be temporary.
As of March 17, early in the pandemic, 40% of health care leaders said they were experiencing staff shortages. An April 21 poll found that 53% of health care leaders were taking steps to address their providers’ and staffers’ mental health.
“The mental and emotional toll on everyone continues to be a concern, as public health authorities continue to report alarming numbers of new [COVID-19] cases, hospitalizations, and deaths,” MGMA commented.
Telehealth and remote monitoring
Nearly all of the health care leaders surveyed on March 31 reported that their practices had expanded telehealth access because of COVID-19. The percentage of patient visits handled remotely had dropped substantially by the fall, according to a Harvard University/Commonwealth Fund/Phreesia survey. Still, it remains significantly higher than it was before the pandemic.
“At the end of 2020, telemedicine continues to play a vital role in everyday practice operations and long-term planning,” the MGMA report said. One indication of this, the association said, is that health care leaders are recognizing new best practices in specialty telemedicine, such as pediatrics and ob.gyn.
According to an April 28 poll, the top three coding/billing challenges for telehealth and telephone visits amid COVID-19 were inconsistent payer rules, pay parity and accuracy, and documentation of virtual visits.
While the Centers for Medicare & Medicaid Services has loosened its regulations to allow reimbursement of telehealth in all locations and at the same level as in-person visits, most of those changes will not last beyond the public health crisis without new legislation.
More health care leaders are considering the use of remote patient monitoring, MGMA said, but only 21% of practices offered such services as of Sept. 15. The report drew a connection between these plans and the current challenge of deferred care.
In the July 21 poll, 87% of health care leaders reported that safety concerns were the top reason that patients deferred care amid COVID-19. The MGMA report quoted JaeLynn Williams, CEO of Air Methods, which provides helicopter ambulance services, as saying that many people are staying home even when they face life-threatening conditions such as chest pain, drug symptoms, inflamed appendix, and gallbladder pain.
Operational issues
Overall, MGMA said, practices that have taken a financial risk have done better during the pandemic than fee-for-service practices because their monthly capitation revenue has continued unabated. In contrast, “most groups’ struggles to sustain visits and procedures meant less revenue and lower compensation,” the report said.
In the August 18 survey, one in three health care leaders reported their practices were changing their operational metrics and how often they looked at those measures because of the pandemic. “Practice managers are asking for dashboard data in weeks instead of months to measure the drop in charges and forecast the resulting change in collections,” MGMA noted. “The type of data practice managers are asking for has also changed.”
Among the new metrics that practices are interested in, according to an MGMA article, are measures that track telehealth visits, the productivity of staff working at home, and the number of ancillary services and procedures that new patients might need based on historical data.
Nearly all health care leaders surveyed on Aug. 11 said the cost of obtaining personal protective equipment had increased during 2020. MGMA said it expects this situation to worsen if the pandemic lasts through the summer of 2021.
While everyone is talking about the botched launch of the COVID-19 vaccination campaign, there were also problems with flu vaccination in 2020. In the Sept. 25 poll, 34% of health care leaders reported their practices were experiencing delays in getting the flu vaccine.
Looking ahead
Looking further ahead, the report recommended that practices make plans to boost staff morale by restoring bonuses.
In addition, MGMA suggested that physician groups reassess their space needs. “The equation is simple – fewer nonclinical staff members at your facility means you should repurpose that office space or consider finding a better fit for your new real estate needs in 2021.”
Finally, MGMA noted that the practices expanding rather than contracting their business are those increasing their value-based revenues by taking on more risk. For those groups, “growing the patient panel can help [them] seek better rates in contract negotiations.”
A version of this article first appeared on Medscape.com.
President Biden signs 10 new orders to help fight COVID-19
“For the past year, we couldn’t rely on the federal government to act with the urgency and focus and coordination we needed, and we have seen the tragic cost of that failure,” Mr. Biden said in remarks from the White House, unveiling his 198-page National Strategy for the COVID-19 Response and Pandemic Preparedness.
He said as many as 500,000 Americans will have died by February. “It’s going to take months for us to turn things around,” he said.
“Our national strategy is comprehensive – it’s based on science, not politics; it’s based on truth, not denial,” Mr. Biden said. He also promised to restore public trust, in part by having scientists and public health experts speak to the public. “That’s why you’ll be hearing a lot more from Dr. Fauci again, not from the president,” he said, adding that the experts will be “free from political interference.”
While the president’s executive orders can help accomplish some of the plan’s proposals, the majority will require new funding from Congress and will be included in the $1.9 trillion American Rescue package that Mr. Biden hopes legislators will approve.
Ten new orders
The 10 new pandemic-related orders Biden signed on Jan. 21 follow two he signed on his first day in office.
One establishes a COVID-19 Response Office responsible for coordinating the pandemic response across all federal departments and agencies and also reestablishes the White House Directorate on Global Health Security and Biodefense, which was disabled by the Trump administration.
The other order requires masks and physical distancing in all federal buildings, on all federal lands, and by federal employees and contractors.
Among the new orders will be directives that:
- Require individuals to also wear masks in airports and planes, and when using other modes of public transportation including trains, boats, and intercity buses, and also require international travelers to produce proof of a recent negative COVID-19 test prior to entry and to quarantine after entry.
- Federal agencies use all powers, including the Defense Production Act, to accelerate manufacturing and delivery of supplies such as N95 masks, gowns, gloves, swabs, reagents, pipette tips, rapid test kits, and nitrocellulose material for rapid antigen tests, and all equipment and material needed to accelerate manufacture, delivery, and administration of COVID-19 vaccine.
- Create a Pandemic Testing Board to expand supply and access, to promote more surge capacity, and to ensure equitable access to tests.
- Facilitate discovery, development, and trials of potential COVID-19 treatments, as well as expand access to programs that can meet the long-term health needs of those recovering from the disease.
- Facilitate more and better data sharing that will allow businesses, schools, hospitals, and individuals to make real-time decisions based on spread in their community.
- Direct the Education and Health & Human Services departments to provide schools and child-care operations guidance on how to reopen and operate safely.
- Direct the Occupational Safety and Health Administration (OSHA) to immediately release clear guidance for employers to help keep workers safe and to enforce health and safety requirements.
The plan also sets goals for vaccination – including 100 million shots in the administration’s first 100 days. President Biden had already previewed his goals for vaccination, including setting up mass vaccination sites and mobile vaccination sites. During his remarks, Mr. Biden said that he had already directed the Federal Emergency Management Agency (FEMA) to begin setting up the vaccination centers.
The administration is also going to look into improving reimbursement for giving vaccines. As a start, the HHS will ask the Centers for Medicare & Medicaid Services to consider if a higher rate “may more accurately compensate providers,” according to the Biden plan.
“But the brutal truth is it will take months before we can get the majority of Americans vaccinated,” said Mr. Biden.
As part of the goal of ensuring an equitable pandemic response, the president will sign an order that establishes a COVID-19 Health Equity Task Force. The task force is charged with providing recommendations for allocating resources and funding in communities with inequities in COVID-19 outcomes by race, ethnicity, geography, disability, and other considerations.
Finally, the administration has committed to being more transparent and sharing more information. The national plan calls for the federal government to conduct regular, expert-led, science-based public briefings and to release regular reports on the pandemic. The administration said it will launch massive science-based public information campaigns – in multiple languages – to educate Americans on masks, testing, and vaccines, and also work to counter misinformation and disinformation.
The American Academy of Family Physicians (AAFP) applauded Mr. Biden’s initiative. “If enacted, this bold legislative agenda will provide much-needed support to American families struggling during the pandemic – especially communities of color and those hardest hit by the virus,” Ada D. Stewart, MD, AAFP president, said in a statement.
Dr. Stewart also noted that family physicians “are uniquely positioned in their communities to educate patients, prioritize access, and coordinate administration of the COVID-19 vaccines,” and urged the administration to ensure that family physicians and staff be vaccinated as soon as possible, to help them “more safely provide care to their communities.”
A version of this article first appeared on Medscape.com.
“For the past year, we couldn’t rely on the federal government to act with the urgency and focus and coordination we needed, and we have seen the tragic cost of that failure,” Mr. Biden said in remarks from the White House, unveiling his 198-page National Strategy for the COVID-19 Response and Pandemic Preparedness.
He said as many as 500,000 Americans will have died by February. “It’s going to take months for us to turn things around,” he said.
“Our national strategy is comprehensive – it’s based on science, not politics; it’s based on truth, not denial,” Mr. Biden said. He also promised to restore public trust, in part by having scientists and public health experts speak to the public. “That’s why you’ll be hearing a lot more from Dr. Fauci again, not from the president,” he said, adding that the experts will be “free from political interference.”
While the president’s executive orders can help accomplish some of the plan’s proposals, the majority will require new funding from Congress and will be included in the $1.9 trillion American Rescue package that Mr. Biden hopes legislators will approve.
Ten new orders
The 10 new pandemic-related orders Biden signed on Jan. 21 follow two he signed on his first day in office.
One establishes a COVID-19 Response Office responsible for coordinating the pandemic response across all federal departments and agencies and also reestablishes the White House Directorate on Global Health Security and Biodefense, which was disabled by the Trump administration.
The other order requires masks and physical distancing in all federal buildings, on all federal lands, and by federal employees and contractors.
Among the new orders will be directives that:
- Require individuals to also wear masks in airports and planes, and when using other modes of public transportation including trains, boats, and intercity buses, and also require international travelers to produce proof of a recent negative COVID-19 test prior to entry and to quarantine after entry.
- Federal agencies use all powers, including the Defense Production Act, to accelerate manufacturing and delivery of supplies such as N95 masks, gowns, gloves, swabs, reagents, pipette tips, rapid test kits, and nitrocellulose material for rapid antigen tests, and all equipment and material needed to accelerate manufacture, delivery, and administration of COVID-19 vaccine.
- Create a Pandemic Testing Board to expand supply and access, to promote more surge capacity, and to ensure equitable access to tests.
- Facilitate discovery, development, and trials of potential COVID-19 treatments, as well as expand access to programs that can meet the long-term health needs of those recovering from the disease.
- Facilitate more and better data sharing that will allow businesses, schools, hospitals, and individuals to make real-time decisions based on spread in their community.
- Direct the Education and Health & Human Services departments to provide schools and child-care operations guidance on how to reopen and operate safely.
- Direct the Occupational Safety and Health Administration (OSHA) to immediately release clear guidance for employers to help keep workers safe and to enforce health and safety requirements.
The plan also sets goals for vaccination – including 100 million shots in the administration’s first 100 days. President Biden had already previewed his goals for vaccination, including setting up mass vaccination sites and mobile vaccination sites. During his remarks, Mr. Biden said that he had already directed the Federal Emergency Management Agency (FEMA) to begin setting up the vaccination centers.
The administration is also going to look into improving reimbursement for giving vaccines. As a start, the HHS will ask the Centers for Medicare & Medicaid Services to consider if a higher rate “may more accurately compensate providers,” according to the Biden plan.
“But the brutal truth is it will take months before we can get the majority of Americans vaccinated,” said Mr. Biden.
As part of the goal of ensuring an equitable pandemic response, the president will sign an order that establishes a COVID-19 Health Equity Task Force. The task force is charged with providing recommendations for allocating resources and funding in communities with inequities in COVID-19 outcomes by race, ethnicity, geography, disability, and other considerations.
Finally, the administration has committed to being more transparent and sharing more information. The national plan calls for the federal government to conduct regular, expert-led, science-based public briefings and to release regular reports on the pandemic. The administration said it will launch massive science-based public information campaigns – in multiple languages – to educate Americans on masks, testing, and vaccines, and also work to counter misinformation and disinformation.
The American Academy of Family Physicians (AAFP) applauded Mr. Biden’s initiative. “If enacted, this bold legislative agenda will provide much-needed support to American families struggling during the pandemic – especially communities of color and those hardest hit by the virus,” Ada D. Stewart, MD, AAFP president, said in a statement.
Dr. Stewart also noted that family physicians “are uniquely positioned in their communities to educate patients, prioritize access, and coordinate administration of the COVID-19 vaccines,” and urged the administration to ensure that family physicians and staff be vaccinated as soon as possible, to help them “more safely provide care to their communities.”
A version of this article first appeared on Medscape.com.
“For the past year, we couldn’t rely on the federal government to act with the urgency and focus and coordination we needed, and we have seen the tragic cost of that failure,” Mr. Biden said in remarks from the White House, unveiling his 198-page National Strategy for the COVID-19 Response and Pandemic Preparedness.
He said as many as 500,000 Americans will have died by February. “It’s going to take months for us to turn things around,” he said.
“Our national strategy is comprehensive – it’s based on science, not politics; it’s based on truth, not denial,” Mr. Biden said. He also promised to restore public trust, in part by having scientists and public health experts speak to the public. “That’s why you’ll be hearing a lot more from Dr. Fauci again, not from the president,” he said, adding that the experts will be “free from political interference.”
While the president’s executive orders can help accomplish some of the plan’s proposals, the majority will require new funding from Congress and will be included in the $1.9 trillion American Rescue package that Mr. Biden hopes legislators will approve.
Ten new orders
The 10 new pandemic-related orders Biden signed on Jan. 21 follow two he signed on his first day in office.
One establishes a COVID-19 Response Office responsible for coordinating the pandemic response across all federal departments and agencies and also reestablishes the White House Directorate on Global Health Security and Biodefense, which was disabled by the Trump administration.
The other order requires masks and physical distancing in all federal buildings, on all federal lands, and by federal employees and contractors.
Among the new orders will be directives that:
- Require individuals to also wear masks in airports and planes, and when using other modes of public transportation including trains, boats, and intercity buses, and also require international travelers to produce proof of a recent negative COVID-19 test prior to entry and to quarantine after entry.
- Federal agencies use all powers, including the Defense Production Act, to accelerate manufacturing and delivery of supplies such as N95 masks, gowns, gloves, swabs, reagents, pipette tips, rapid test kits, and nitrocellulose material for rapid antigen tests, and all equipment and material needed to accelerate manufacture, delivery, and administration of COVID-19 vaccine.
- Create a Pandemic Testing Board to expand supply and access, to promote more surge capacity, and to ensure equitable access to tests.
- Facilitate discovery, development, and trials of potential COVID-19 treatments, as well as expand access to programs that can meet the long-term health needs of those recovering from the disease.
- Facilitate more and better data sharing that will allow businesses, schools, hospitals, and individuals to make real-time decisions based on spread in their community.
- Direct the Education and Health & Human Services departments to provide schools and child-care operations guidance on how to reopen and operate safely.
- Direct the Occupational Safety and Health Administration (OSHA) to immediately release clear guidance for employers to help keep workers safe and to enforce health and safety requirements.
The plan also sets goals for vaccination – including 100 million shots in the administration’s first 100 days. President Biden had already previewed his goals for vaccination, including setting up mass vaccination sites and mobile vaccination sites. During his remarks, Mr. Biden said that he had already directed the Federal Emergency Management Agency (FEMA) to begin setting up the vaccination centers.
The administration is also going to look into improving reimbursement for giving vaccines. As a start, the HHS will ask the Centers for Medicare & Medicaid Services to consider if a higher rate “may more accurately compensate providers,” according to the Biden plan.
“But the brutal truth is it will take months before we can get the majority of Americans vaccinated,” said Mr. Biden.
As part of the goal of ensuring an equitable pandemic response, the president will sign an order that establishes a COVID-19 Health Equity Task Force. The task force is charged with providing recommendations for allocating resources and funding in communities with inequities in COVID-19 outcomes by race, ethnicity, geography, disability, and other considerations.
Finally, the administration has committed to being more transparent and sharing more information. The national plan calls for the federal government to conduct regular, expert-led, science-based public briefings and to release regular reports on the pandemic. The administration said it will launch massive science-based public information campaigns – in multiple languages – to educate Americans on masks, testing, and vaccines, and also work to counter misinformation and disinformation.
The American Academy of Family Physicians (AAFP) applauded Mr. Biden’s initiative. “If enacted, this bold legislative agenda will provide much-needed support to American families struggling during the pandemic – especially communities of color and those hardest hit by the virus,” Ada D. Stewart, MD, AAFP president, said in a statement.
Dr. Stewart also noted that family physicians “are uniquely positioned in their communities to educate patients, prioritize access, and coordinate administration of the COVID-19 vaccines,” and urged the administration to ensure that family physicians and staff be vaccinated as soon as possible, to help them “more safely provide care to their communities.”
A version of this article first appeared on Medscape.com.
PCPs play a small part in low-value care spending
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.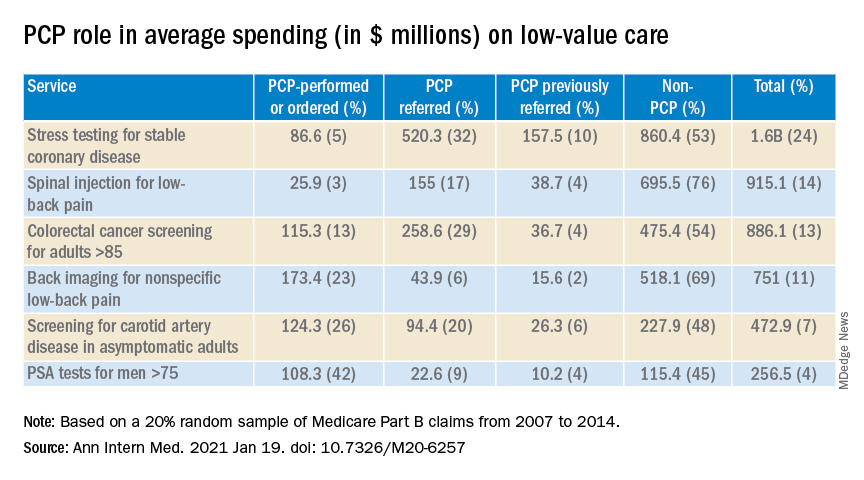
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
President Biden kicks off health agenda with COVID actions, WHO outreach
President Joe Biden kicked off his new administration Jan. 20 with an immediate focus on attempts to stop the spread of COVID-19, including closer coordination with other nations.
Mr. Biden signed 17 executive orders, memoranda, and directives addressing not only the pandemic but also economic concerns, climate change, and racial inequity.
At the top of the list of actions was what his transition team called a “100 Days Masking Challenge.” Mr. Biden issued an executive order requiring masks and physical distancing in all federal buildings, on all federal lands, and by federal employees and contractors.
The president also halted the Trump administration’s process of withdrawing from the World Health Organization. Instead, Mr. Biden named Anthony Fauci, MD, the director of the National Institute for Allergy and Infectious Diseases, as the head of a delegation to participate in the WHO executive board meeting that is being held this week.
Mr. Biden also signed an executive order creating the position of COVID-19 response coordinator, which will report directly to the president and be responsible for coordinating all elements of the COVID-19 response across government, including the production and distribution of vaccines and medical supplies.
The newly inaugurated president also intends to restore the National Security Council’s Directorate for Global Health Security and Biodefense, which will aid in the response to the pandemic, his transition team said.
The American Medical Association was among the first to commend the first-day actions.
“Defeating COVID-19 requires bold, coordinated federal leadership and strong adherence to the public health steps we know stop the spread of this virus – wearing masks, practicing physical distancing, and washing hands,” said AMA President Susan R. Bailey, MD in a news release. “We are pleased by the Biden administration’s steps today, including universal mask wearing within federal jurisdictions, providing federal leadership for COVID-19 response, and reengaging with the World Health Organization. Taking these actions on day 1 of the administration sends the right message – that our nation is laser focused on stopping the ravages of COVID-19.”
A version of this article first appeared on Medscape.com.
President Joe Biden kicked off his new administration Jan. 20 with an immediate focus on attempts to stop the spread of COVID-19, including closer coordination with other nations.
Mr. Biden signed 17 executive orders, memoranda, and directives addressing not only the pandemic but also economic concerns, climate change, and racial inequity.
At the top of the list of actions was what his transition team called a “100 Days Masking Challenge.” Mr. Biden issued an executive order requiring masks and physical distancing in all federal buildings, on all federal lands, and by federal employees and contractors.
The president also halted the Trump administration’s process of withdrawing from the World Health Organization. Instead, Mr. Biden named Anthony Fauci, MD, the director of the National Institute for Allergy and Infectious Diseases, as the head of a delegation to participate in the WHO executive board meeting that is being held this week.
Mr. Biden also signed an executive order creating the position of COVID-19 response coordinator, which will report directly to the president and be responsible for coordinating all elements of the COVID-19 response across government, including the production and distribution of vaccines and medical supplies.
The newly inaugurated president also intends to restore the National Security Council’s Directorate for Global Health Security and Biodefense, which will aid in the response to the pandemic, his transition team said.
The American Medical Association was among the first to commend the first-day actions.
“Defeating COVID-19 requires bold, coordinated federal leadership and strong adherence to the public health steps we know stop the spread of this virus – wearing masks, practicing physical distancing, and washing hands,” said AMA President Susan R. Bailey, MD in a news release. “We are pleased by the Biden administration’s steps today, including universal mask wearing within federal jurisdictions, providing federal leadership for COVID-19 response, and reengaging with the World Health Organization. Taking these actions on day 1 of the administration sends the right message – that our nation is laser focused on stopping the ravages of COVID-19.”
A version of this article first appeared on Medscape.com.
President Joe Biden kicked off his new administration Jan. 20 with an immediate focus on attempts to stop the spread of COVID-19, including closer coordination with other nations.
Mr. Biden signed 17 executive orders, memoranda, and directives addressing not only the pandemic but also economic concerns, climate change, and racial inequity.
At the top of the list of actions was what his transition team called a “100 Days Masking Challenge.” Mr. Biden issued an executive order requiring masks and physical distancing in all federal buildings, on all federal lands, and by federal employees and contractors.
The president also halted the Trump administration’s process of withdrawing from the World Health Organization. Instead, Mr. Biden named Anthony Fauci, MD, the director of the National Institute for Allergy and Infectious Diseases, as the head of a delegation to participate in the WHO executive board meeting that is being held this week.
Mr. Biden also signed an executive order creating the position of COVID-19 response coordinator, which will report directly to the president and be responsible for coordinating all elements of the COVID-19 response across government, including the production and distribution of vaccines and medical supplies.
The newly inaugurated president also intends to restore the National Security Council’s Directorate for Global Health Security and Biodefense, which will aid in the response to the pandemic, his transition team said.
The American Medical Association was among the first to commend the first-day actions.
“Defeating COVID-19 requires bold, coordinated federal leadership and strong adherence to the public health steps we know stop the spread of this virus – wearing masks, practicing physical distancing, and washing hands,” said AMA President Susan R. Bailey, MD in a news release. “We are pleased by the Biden administration’s steps today, including universal mask wearing within federal jurisdictions, providing federal leadership for COVID-19 response, and reengaging with the World Health Organization. Taking these actions on day 1 of the administration sends the right message – that our nation is laser focused on stopping the ravages of COVID-19.”
A version of this article first appeared on Medscape.com.
Von Willebrand disease guidelines address women’s bleeding concerns
New guidelines issued jointly by four major international hematology groups focus on the management of patients with von Willebrand disease (VWD), the most common bleeding disorder in the world.
The evidence-based guidelines, published in Blood Advances, were developed in collaboration by the American Society of Hematology (ASH), the International Society on Thrombosis and Haemostasis, the National Hemophilia Foundation, and the World Federation of Hemophilia. They outline key recommendations spanning the care of patients with a broad range of therapeutic needs.
“We addressed some of the questions that were most important to the community, but certainly there are a lot of areas that we couldn’t cover” said coauthor Veronica H. Flood, MD, of the Medical College of Wisconsin in Milwaukee.
The guidelines process began with a survey sent to the von Willebrand disease community, including patients, caregivers, nurses, physicians, and scientists. The respondents were asked to prioritize issues that they felt should be addressed in the guidelines.
“Interestingly, some of the issues were the same between patients and caregivers and physicians, and some were different, but there were obviously some areas that we just couldn’t cover,” she said in an interview.
One of the areas of greatest concern for respondents was bleeding in women, and many of the recommendations include specific considerations for management of gynecologic and obstetric patients, Dr. Flood said.
“We also tried to make the questions applicable to as many patients with von Willebrand disease as possible,” she added.
Some of the questions, such as recommendation 1, regarding prophylaxis, are geared toward management of patients with severe disease, while others, such as recommendations for treatment of menstrual bleeding, are more suited for patients with milder VWD.
All of the recommendations in the guidelines are “conditional” (suggested), due to very low certainty in the evidence of effects, the authors noted.
Prophylaxis
The guidelines suggest long-term prophylaxis for patients with a history of severe and frequent bleeds, with periodic assessment of the need for prophylaxis.
Desmopressin
For those patients who may benefit from the use of desmopressin, primarily those with type 1 VWD, and who have a baseline von Willebrand factor (VWF) level below 0.30 IU/mL, the panel issued a conditional recommendation for a desmopressin trial with treatment based on the patient’s results compared with not performing a trial and treating with tranexamic acid or factor concentrate. The guidelines also advise against treating with desmopressin in the absence of a trial. In a section of “good practice statements,” the guidelines indicate that using desmopressin in patients with type 2B VWD is generally contraindicated, because of the risk of thrombocytopenia as a result of increased platelet binding. In addition, desmopressin is generally contraindicated in patients with active cardiovascular disease, patients with seizure disorders, patients less than 2 years old, and patients with type 1C VWD in the setting of surgery.
Antithrombotic therapy
The guideline panelists conditionally recommend antithrombotic therapy with either antiplatelet agents or anticoagulants, with an emphasis on reassessing bleeding risk throughout the course of treatment.
An accompanying good practice statement calls for individualized assessments of risks and benefits of specific antithrombotic therapies by a multidisciplinary team including hematologists, cardiovascular specialists, and the patient.
Major surgery
This section includes a recommendation for targeting both factor VIII and VWF activity levels to a minimum of 50 IU/mL for at least 3 days after surgery, and a suggestion against using factor VIII target levels alone.
Minor surgery/invasive procedures
The panelists suggest increasing VWF activity levels to a minimum of 0.50 IU/mL with desmopressin or factor concentrate with the addition of tranexamic acid over raising VWF levels to at least 0.50 IU/mL with desmopressin or factor concentrate alone.
In addition, the panelists suggest “giving tranexamic acid alone over increasing VWF activity levels to a minimum threshold of 0.50 IU/mL with any intervention in patients with type 1 VWD with baseline VWF activity levels of 0.30 IU/mL and a mild bleeding phenotype undergoing minor mucosal procedures.”
Heavy menstrual bleeding
In women with heavy menstrual bleeding who do not plan to conceive, the panel suggests either combined hormonal therapy or levonorgestrel-releasing intrauterine system, or tranexamic acid over desmopressin.
In women who wish to conceive, the panel suggests using tranexamic acid over desmopressin.
Neuraxial anesthesia during labor
For women in labor for whom neuraxial anesthesia is considered, the guidelines suggest targeting a VWF activity level from 0.50 to 1.50 IU/mL over targeting a level above 1.50 IU/mL.
Postpartum management
“The guideline panel suggests the use of tranexamic acid over not using it in women with type 1 VWD or low VWF levels (and this may also apply to types 2 and 3 VWD) during the postpartum period,” the guidelines say.
An accompanying good practice statement says that tranexamic acid can be provided orally or intravenously. The oral dose is 25 mg/kg three times daily for 10-14 days, or longer if blood loss remains heavy.
Dr. Flood said that the guidelines were developed under the assumption that they would apply to care of patients in regions with a high or moderately high degree of clinical resources.
“We recognize that this eliminates a great deal of the globe, and our hope is that ASH and the other sponsoring organizations are going to let us revise this and do a version for lower-resourced settings,” she said.
New guidelines issued jointly by four major international hematology groups focus on the management of patients with von Willebrand disease (VWD), the most common bleeding disorder in the world.
The evidence-based guidelines, published in Blood Advances, were developed in collaboration by the American Society of Hematology (ASH), the International Society on Thrombosis and Haemostasis, the National Hemophilia Foundation, and the World Federation of Hemophilia. They outline key recommendations spanning the care of patients with a broad range of therapeutic needs.
“We addressed some of the questions that were most important to the community, but certainly there are a lot of areas that we couldn’t cover” said coauthor Veronica H. Flood, MD, of the Medical College of Wisconsin in Milwaukee.
The guidelines process began with a survey sent to the von Willebrand disease community, including patients, caregivers, nurses, physicians, and scientists. The respondents were asked to prioritize issues that they felt should be addressed in the guidelines.
“Interestingly, some of the issues were the same between patients and caregivers and physicians, and some were different, but there were obviously some areas that we just couldn’t cover,” she said in an interview.
One of the areas of greatest concern for respondents was bleeding in women, and many of the recommendations include specific considerations for management of gynecologic and obstetric patients, Dr. Flood said.
“We also tried to make the questions applicable to as many patients with von Willebrand disease as possible,” she added.
Some of the questions, such as recommendation 1, regarding prophylaxis, are geared toward management of patients with severe disease, while others, such as recommendations for treatment of menstrual bleeding, are more suited for patients with milder VWD.
All of the recommendations in the guidelines are “conditional” (suggested), due to very low certainty in the evidence of effects, the authors noted.
Prophylaxis
The guidelines suggest long-term prophylaxis for patients with a history of severe and frequent bleeds, with periodic assessment of the need for prophylaxis.
Desmopressin
For those patients who may benefit from the use of desmopressin, primarily those with type 1 VWD, and who have a baseline von Willebrand factor (VWF) level below 0.30 IU/mL, the panel issued a conditional recommendation for a desmopressin trial with treatment based on the patient’s results compared with not performing a trial and treating with tranexamic acid or factor concentrate. The guidelines also advise against treating with desmopressin in the absence of a trial. In a section of “good practice statements,” the guidelines indicate that using desmopressin in patients with type 2B VWD is generally contraindicated, because of the risk of thrombocytopenia as a result of increased platelet binding. In addition, desmopressin is generally contraindicated in patients with active cardiovascular disease, patients with seizure disorders, patients less than 2 years old, and patients with type 1C VWD in the setting of surgery.
Antithrombotic therapy
The guideline panelists conditionally recommend antithrombotic therapy with either antiplatelet agents or anticoagulants, with an emphasis on reassessing bleeding risk throughout the course of treatment.
An accompanying good practice statement calls for individualized assessments of risks and benefits of specific antithrombotic therapies by a multidisciplinary team including hematologists, cardiovascular specialists, and the patient.
Major surgery
This section includes a recommendation for targeting both factor VIII and VWF activity levels to a minimum of 50 IU/mL for at least 3 days after surgery, and a suggestion against using factor VIII target levels alone.
Minor surgery/invasive procedures
The panelists suggest increasing VWF activity levels to a minimum of 0.50 IU/mL with desmopressin or factor concentrate with the addition of tranexamic acid over raising VWF levels to at least 0.50 IU/mL with desmopressin or factor concentrate alone.
In addition, the panelists suggest “giving tranexamic acid alone over increasing VWF activity levels to a minimum threshold of 0.50 IU/mL with any intervention in patients with type 1 VWD with baseline VWF activity levels of 0.30 IU/mL and a mild bleeding phenotype undergoing minor mucosal procedures.”
Heavy menstrual bleeding
In women with heavy menstrual bleeding who do not plan to conceive, the panel suggests either combined hormonal therapy or levonorgestrel-releasing intrauterine system, or tranexamic acid over desmopressin.
In women who wish to conceive, the panel suggests using tranexamic acid over desmopressin.
Neuraxial anesthesia during labor
For women in labor for whom neuraxial anesthesia is considered, the guidelines suggest targeting a VWF activity level from 0.50 to 1.50 IU/mL over targeting a level above 1.50 IU/mL.
Postpartum management
“The guideline panel suggests the use of tranexamic acid over not using it in women with type 1 VWD or low VWF levels (and this may also apply to types 2 and 3 VWD) during the postpartum period,” the guidelines say.
An accompanying good practice statement says that tranexamic acid can be provided orally or intravenously. The oral dose is 25 mg/kg three times daily for 10-14 days, or longer if blood loss remains heavy.
Dr. Flood said that the guidelines were developed under the assumption that they would apply to care of patients in regions with a high or moderately high degree of clinical resources.
“We recognize that this eliminates a great deal of the globe, and our hope is that ASH and the other sponsoring organizations are going to let us revise this and do a version for lower-resourced settings,” she said.
New guidelines issued jointly by four major international hematology groups focus on the management of patients with von Willebrand disease (VWD), the most common bleeding disorder in the world.
The evidence-based guidelines, published in Blood Advances, were developed in collaboration by the American Society of Hematology (ASH), the International Society on Thrombosis and Haemostasis, the National Hemophilia Foundation, and the World Federation of Hemophilia. They outline key recommendations spanning the care of patients with a broad range of therapeutic needs.
“We addressed some of the questions that were most important to the community, but certainly there are a lot of areas that we couldn’t cover” said coauthor Veronica H. Flood, MD, of the Medical College of Wisconsin in Milwaukee.
The guidelines process began with a survey sent to the von Willebrand disease community, including patients, caregivers, nurses, physicians, and scientists. The respondents were asked to prioritize issues that they felt should be addressed in the guidelines.
“Interestingly, some of the issues were the same between patients and caregivers and physicians, and some were different, but there were obviously some areas that we just couldn’t cover,” she said in an interview.
One of the areas of greatest concern for respondents was bleeding in women, and many of the recommendations include specific considerations for management of gynecologic and obstetric patients, Dr. Flood said.
“We also tried to make the questions applicable to as many patients with von Willebrand disease as possible,” she added.
Some of the questions, such as recommendation 1, regarding prophylaxis, are geared toward management of patients with severe disease, while others, such as recommendations for treatment of menstrual bleeding, are more suited for patients with milder VWD.
All of the recommendations in the guidelines are “conditional” (suggested), due to very low certainty in the evidence of effects, the authors noted.
Prophylaxis
The guidelines suggest long-term prophylaxis for patients with a history of severe and frequent bleeds, with periodic assessment of the need for prophylaxis.
Desmopressin
For those patients who may benefit from the use of desmopressin, primarily those with type 1 VWD, and who have a baseline von Willebrand factor (VWF) level below 0.30 IU/mL, the panel issued a conditional recommendation for a desmopressin trial with treatment based on the patient’s results compared with not performing a trial and treating with tranexamic acid or factor concentrate. The guidelines also advise against treating with desmopressin in the absence of a trial. In a section of “good practice statements,” the guidelines indicate that using desmopressin in patients with type 2B VWD is generally contraindicated, because of the risk of thrombocytopenia as a result of increased platelet binding. In addition, desmopressin is generally contraindicated in patients with active cardiovascular disease, patients with seizure disorders, patients less than 2 years old, and patients with type 1C VWD in the setting of surgery.
Antithrombotic therapy
The guideline panelists conditionally recommend antithrombotic therapy with either antiplatelet agents or anticoagulants, with an emphasis on reassessing bleeding risk throughout the course of treatment.
An accompanying good practice statement calls for individualized assessments of risks and benefits of specific antithrombotic therapies by a multidisciplinary team including hematologists, cardiovascular specialists, and the patient.
Major surgery
This section includes a recommendation for targeting both factor VIII and VWF activity levels to a minimum of 50 IU/mL for at least 3 days after surgery, and a suggestion against using factor VIII target levels alone.
Minor surgery/invasive procedures
The panelists suggest increasing VWF activity levels to a minimum of 0.50 IU/mL with desmopressin or factor concentrate with the addition of tranexamic acid over raising VWF levels to at least 0.50 IU/mL with desmopressin or factor concentrate alone.
In addition, the panelists suggest “giving tranexamic acid alone over increasing VWF activity levels to a minimum threshold of 0.50 IU/mL with any intervention in patients with type 1 VWD with baseline VWF activity levels of 0.30 IU/mL and a mild bleeding phenotype undergoing minor mucosal procedures.”
Heavy menstrual bleeding
In women with heavy menstrual bleeding who do not plan to conceive, the panel suggests either combined hormonal therapy or levonorgestrel-releasing intrauterine system, or tranexamic acid over desmopressin.
In women who wish to conceive, the panel suggests using tranexamic acid over desmopressin.
Neuraxial anesthesia during labor
For women in labor for whom neuraxial anesthesia is considered, the guidelines suggest targeting a VWF activity level from 0.50 to 1.50 IU/mL over targeting a level above 1.50 IU/mL.
Postpartum management
“The guideline panel suggests the use of tranexamic acid over not using it in women with type 1 VWD or low VWF levels (and this may also apply to types 2 and 3 VWD) during the postpartum period,” the guidelines say.
An accompanying good practice statement says that tranexamic acid can be provided orally or intravenously. The oral dose is 25 mg/kg three times daily for 10-14 days, or longer if blood loss remains heavy.
Dr. Flood said that the guidelines were developed under the assumption that they would apply to care of patients in regions with a high or moderately high degree of clinical resources.
“We recognize that this eliminates a great deal of the globe, and our hope is that ASH and the other sponsoring organizations are going to let us revise this and do a version for lower-resourced settings,” she said.
FROM BLOOD ADVANCES
Could an osteoporosis drug reduce need for hip revision surgery?
A single injection of denosumab (Prolia, Amgen), frequently used to treat osteoporosis, may reduce the need for revision surgery in patients with symptomatic osteolysis following total hip arthroplasty, a new proof-of-concept study suggests.
Aseptic loosening is the result of wear-induced osteolysis caused by the prosthetic hip and is a major contributor to the need for revision surgery in many parts of the world.
“The only established treatment for prosthesis-related osteolysis after joint replacement is revision surgery, which carries substantially greater morbidity and mortality than primary joint replacement,” Mohit M. Mahatma, MRes, of the University of Sheffield, England, and colleagues wrote in their article, published online Jan. 11 in The Lancet Rheumatology.
As well as an increased risk of infection and other complications, revision surgery is much more costly than a first-time operation, they added.
“The results of this proof-of-concept clinical trial indicate that denosumab is effective at reducing bone resorption activity within osteolytic lesion tissue and is well tolerated within the limitations of the single dose used here,” they concluded.
Commenting on the findings, Antonia Chen, MD, associate professor of orthopedic surgery, Harvard Medical School, Boston, emphasized that further studies are needed to assess the effectiveness of this strategy to reduce the need for hip revision surgery.
Nevertheless, “osteolysis is still unfortunately a problem we do have to deal with and we do not have any other way to prevent it,” she said in an interview. “So it’s a good start ... although further studies are definitely needed,” Dr. Chen added.
In an accompanying editorial, Hannu Aro, MD, Turku University Hospital in Finland, agreed: “Without a doubt, the trial is a breakthrough, but it represents only the first step in the development of pharmacological therapy aiming to slow, prevent, or even reverse the process of wear-induced periprosthetic osteolysis.”
Small single-center study
The phase 2, single-center, randomized, controlled trial involved 22 patients who had previously undergone hip replacement surgery at Sheffield Teaching Hospitals and were scheduled for revision surgery due to symptomatic osteolysis. They were randomized to a single subcutaneous injection of denosumab at a dose of 60 mg, or placebo, on their second hospital visit.
“The primary outcome was the between-group difference in the number of osteoclasts per mm of osteolytic membrane at the osteolytic membrane-bone interface at week 8,” the authors noted.
At this time point, there were 83% fewer osteoclasts at the interface in the denosumab group compared with placebo, at a median of 0.05 per mm in the treatment group compared with 0.30 per mm in the placebo group (P = .011).
Secondary histological outcomes were also significantly improved in favor of the denosumab group compared with placebo.
Potential to prevent half of all hip revision surgeries?
Patients who received denosumab also demonstrated an acute fall in serum and urinary markers of bone resorption following administration of the drug, reaching a nadir at week 4, which was maintained until revision surgery at week 8.
In contrast, “no change in these markers was observed in the placebo group [P < .0003 for all biomarkers],” the investigators noted. Rates of adverse events were comparable in both treatment groups.
As the authors explained, osteolysis occurs following joint replacement surgery when particles of plastic wear off from the prosthesis, triggering an immune reaction that attacks the bone around the implant, causing the joint to loosen.
“It is very clear from our bone biopsies and bone imaging that the [denosumab] injection stops the bone absorbing the microplastic particles from the replacement joint and therefore could prevent the bone from being eaten away and the need for revision surgery,” senior author Mark Wilkinson, MBChB, PhD, honorary consultant orthopedic surgeon, Sheffield Teaching Hospitals, said in a press release from his institution.
“This study is a significant breakthrough as we’ve demonstrated that there is a drug, already available and successful in the treatment of osteoporosis, that has the potential to prevent up to half of all revised replacement surgeries which are caused by osteolysis,” he added.
Dr. Wilkinson and coauthors said their results justify the need for future trials targeting earlier-stage disease to further test the use of denosumab to prevent or reduce the need for revision surgery.
In 2018, aseptic loosening accounted for over half of all revision procedures, as reported to the National Joint Registry in England and Wales.
Older polyethylene prostheses are the main culprit
Commenting further on the study, Dr. Chen noted that osteolysis still plagues orthopedic surgeons because the original polyethylene prostheses were not very good. A better prosthesis developed at Massachusetts General Hospital is made up of highly crossed-link polyethylene and still wears over time but to a much lesser extent than the older polyethylene prostheses.
Metal and ceramic prostheses also can induce osteolysis, but again to a much lesser extent than the older polyethylene implants.
“Any particle can technically cause osteolysis but plastic produces the most particles,” Dr. Chen explained. Although hip revision rates in the United States are low to begin with, aseptic loosening is still one of the main reasons that patients need to undergo revision surgery, she observed.
“A lot of patients are still living with the old plastic [implants] so there is still a need for something like this,” she stressed.
However, many questions about this potential new strategy remain to be answered, including when best to initiate treatment and how to manage patients at risk for osteolysis 20-30 years after they have received their original implant.
In his editorial, Dr. Aro said that serious adverse consequences often become evident 10-20 years after patients have undergone the original hip replacement procedures, when they are potentially less physically fit than they were at the time of the operation and thus less able to withstand the rigors of a difficult revision surgery.
“In this context, the concept of nonsurgical pharmacological treatment of periprosthetic osteolysis ... brings a new hope for the ever-increasing population of patients with total hip arthroplasty to avoid revision surgery,” Dr. Aro suggested.
However, Dr. Aro cautioned that reduction of bone turnover by antiresorptive agents such as denosumab has been associated with the development of atypical femoral fractures.
The study was funded by Amgen. Dr. Wilkinson has reported receiving a grant from Amgen. Dr. Chen has reported serving as a consultant for Striker and b-One Ortho. Dr. Aro has reported receiving a grant to his institution from Amgen Finland and the Academy of Finland. He has also served as a member of an advisory scientific board for Amgen Finland.
A version of this article first appeared on Medscape.com.
A single injection of denosumab (Prolia, Amgen), frequently used to treat osteoporosis, may reduce the need for revision surgery in patients with symptomatic osteolysis following total hip arthroplasty, a new proof-of-concept study suggests.
Aseptic loosening is the result of wear-induced osteolysis caused by the prosthetic hip and is a major contributor to the need for revision surgery in many parts of the world.
“The only established treatment for prosthesis-related osteolysis after joint replacement is revision surgery, which carries substantially greater morbidity and mortality than primary joint replacement,” Mohit M. Mahatma, MRes, of the University of Sheffield, England, and colleagues wrote in their article, published online Jan. 11 in The Lancet Rheumatology.
As well as an increased risk of infection and other complications, revision surgery is much more costly than a first-time operation, they added.
“The results of this proof-of-concept clinical trial indicate that denosumab is effective at reducing bone resorption activity within osteolytic lesion tissue and is well tolerated within the limitations of the single dose used here,” they concluded.
Commenting on the findings, Antonia Chen, MD, associate professor of orthopedic surgery, Harvard Medical School, Boston, emphasized that further studies are needed to assess the effectiveness of this strategy to reduce the need for hip revision surgery.
Nevertheless, “osteolysis is still unfortunately a problem we do have to deal with and we do not have any other way to prevent it,” she said in an interview. “So it’s a good start ... although further studies are definitely needed,” Dr. Chen added.
In an accompanying editorial, Hannu Aro, MD, Turku University Hospital in Finland, agreed: “Without a doubt, the trial is a breakthrough, but it represents only the first step in the development of pharmacological therapy aiming to slow, prevent, or even reverse the process of wear-induced periprosthetic osteolysis.”
Small single-center study
The phase 2, single-center, randomized, controlled trial involved 22 patients who had previously undergone hip replacement surgery at Sheffield Teaching Hospitals and were scheduled for revision surgery due to symptomatic osteolysis. They were randomized to a single subcutaneous injection of denosumab at a dose of 60 mg, or placebo, on their second hospital visit.
“The primary outcome was the between-group difference in the number of osteoclasts per mm of osteolytic membrane at the osteolytic membrane-bone interface at week 8,” the authors noted.
At this time point, there were 83% fewer osteoclasts at the interface in the denosumab group compared with placebo, at a median of 0.05 per mm in the treatment group compared with 0.30 per mm in the placebo group (P = .011).
Secondary histological outcomes were also significantly improved in favor of the denosumab group compared with placebo.
Potential to prevent half of all hip revision surgeries?
Patients who received denosumab also demonstrated an acute fall in serum and urinary markers of bone resorption following administration of the drug, reaching a nadir at week 4, which was maintained until revision surgery at week 8.
In contrast, “no change in these markers was observed in the placebo group [P < .0003 for all biomarkers],” the investigators noted. Rates of adverse events were comparable in both treatment groups.
As the authors explained, osteolysis occurs following joint replacement surgery when particles of plastic wear off from the prosthesis, triggering an immune reaction that attacks the bone around the implant, causing the joint to loosen.
“It is very clear from our bone biopsies and bone imaging that the [denosumab] injection stops the bone absorbing the microplastic particles from the replacement joint and therefore could prevent the bone from being eaten away and the need for revision surgery,” senior author Mark Wilkinson, MBChB, PhD, honorary consultant orthopedic surgeon, Sheffield Teaching Hospitals, said in a press release from his institution.
“This study is a significant breakthrough as we’ve demonstrated that there is a drug, already available and successful in the treatment of osteoporosis, that has the potential to prevent up to half of all revised replacement surgeries which are caused by osteolysis,” he added.
Dr. Wilkinson and coauthors said their results justify the need for future trials targeting earlier-stage disease to further test the use of denosumab to prevent or reduce the need for revision surgery.
In 2018, aseptic loosening accounted for over half of all revision procedures, as reported to the National Joint Registry in England and Wales.
Older polyethylene prostheses are the main culprit
Commenting further on the study, Dr. Chen noted that osteolysis still plagues orthopedic surgeons because the original polyethylene prostheses were not very good. A better prosthesis developed at Massachusetts General Hospital is made up of highly crossed-link polyethylene and still wears over time but to a much lesser extent than the older polyethylene prostheses.
Metal and ceramic prostheses also can induce osteolysis, but again to a much lesser extent than the older polyethylene implants.
“Any particle can technically cause osteolysis but plastic produces the most particles,” Dr. Chen explained. Although hip revision rates in the United States are low to begin with, aseptic loosening is still one of the main reasons that patients need to undergo revision surgery, she observed.
“A lot of patients are still living with the old plastic [implants] so there is still a need for something like this,” she stressed.
However, many questions about this potential new strategy remain to be answered, including when best to initiate treatment and how to manage patients at risk for osteolysis 20-30 years after they have received their original implant.
In his editorial, Dr. Aro said that serious adverse consequences often become evident 10-20 years after patients have undergone the original hip replacement procedures, when they are potentially less physically fit than they were at the time of the operation and thus less able to withstand the rigors of a difficult revision surgery.
“In this context, the concept of nonsurgical pharmacological treatment of periprosthetic osteolysis ... brings a new hope for the ever-increasing population of patients with total hip arthroplasty to avoid revision surgery,” Dr. Aro suggested.
However, Dr. Aro cautioned that reduction of bone turnover by antiresorptive agents such as denosumab has been associated with the development of atypical femoral fractures.
The study was funded by Amgen. Dr. Wilkinson has reported receiving a grant from Amgen. Dr. Chen has reported serving as a consultant for Striker and b-One Ortho. Dr. Aro has reported receiving a grant to his institution from Amgen Finland and the Academy of Finland. He has also served as a member of an advisory scientific board for Amgen Finland.
A version of this article first appeared on Medscape.com.
A single injection of denosumab (Prolia, Amgen), frequently used to treat osteoporosis, may reduce the need for revision surgery in patients with symptomatic osteolysis following total hip arthroplasty, a new proof-of-concept study suggests.
Aseptic loosening is the result of wear-induced osteolysis caused by the prosthetic hip and is a major contributor to the need for revision surgery in many parts of the world.
“The only established treatment for prosthesis-related osteolysis after joint replacement is revision surgery, which carries substantially greater morbidity and mortality than primary joint replacement,” Mohit M. Mahatma, MRes, of the University of Sheffield, England, and colleagues wrote in their article, published online Jan. 11 in The Lancet Rheumatology.
As well as an increased risk of infection and other complications, revision surgery is much more costly than a first-time operation, they added.
“The results of this proof-of-concept clinical trial indicate that denosumab is effective at reducing bone resorption activity within osteolytic lesion tissue and is well tolerated within the limitations of the single dose used here,” they concluded.
Commenting on the findings, Antonia Chen, MD, associate professor of orthopedic surgery, Harvard Medical School, Boston, emphasized that further studies are needed to assess the effectiveness of this strategy to reduce the need for hip revision surgery.
Nevertheless, “osteolysis is still unfortunately a problem we do have to deal with and we do not have any other way to prevent it,” she said in an interview. “So it’s a good start ... although further studies are definitely needed,” Dr. Chen added.
In an accompanying editorial, Hannu Aro, MD, Turku University Hospital in Finland, agreed: “Without a doubt, the trial is a breakthrough, but it represents only the first step in the development of pharmacological therapy aiming to slow, prevent, or even reverse the process of wear-induced periprosthetic osteolysis.”
Small single-center study
The phase 2, single-center, randomized, controlled trial involved 22 patients who had previously undergone hip replacement surgery at Sheffield Teaching Hospitals and were scheduled for revision surgery due to symptomatic osteolysis. They were randomized to a single subcutaneous injection of denosumab at a dose of 60 mg, or placebo, on their second hospital visit.
“The primary outcome was the between-group difference in the number of osteoclasts per mm of osteolytic membrane at the osteolytic membrane-bone interface at week 8,” the authors noted.
At this time point, there were 83% fewer osteoclasts at the interface in the denosumab group compared with placebo, at a median of 0.05 per mm in the treatment group compared with 0.30 per mm in the placebo group (P = .011).
Secondary histological outcomes were also significantly improved in favor of the denosumab group compared with placebo.
Potential to prevent half of all hip revision surgeries?
Patients who received denosumab also demonstrated an acute fall in serum and urinary markers of bone resorption following administration of the drug, reaching a nadir at week 4, which was maintained until revision surgery at week 8.
In contrast, “no change in these markers was observed in the placebo group [P < .0003 for all biomarkers],” the investigators noted. Rates of adverse events were comparable in both treatment groups.
As the authors explained, osteolysis occurs following joint replacement surgery when particles of plastic wear off from the prosthesis, triggering an immune reaction that attacks the bone around the implant, causing the joint to loosen.
“It is very clear from our bone biopsies and bone imaging that the [denosumab] injection stops the bone absorbing the microplastic particles from the replacement joint and therefore could prevent the bone from being eaten away and the need for revision surgery,” senior author Mark Wilkinson, MBChB, PhD, honorary consultant orthopedic surgeon, Sheffield Teaching Hospitals, said in a press release from his institution.
“This study is a significant breakthrough as we’ve demonstrated that there is a drug, already available and successful in the treatment of osteoporosis, that has the potential to prevent up to half of all revised replacement surgeries which are caused by osteolysis,” he added.
Dr. Wilkinson and coauthors said their results justify the need for future trials targeting earlier-stage disease to further test the use of denosumab to prevent or reduce the need for revision surgery.
In 2018, aseptic loosening accounted for over half of all revision procedures, as reported to the National Joint Registry in England and Wales.
Older polyethylene prostheses are the main culprit
Commenting further on the study, Dr. Chen noted that osteolysis still plagues orthopedic surgeons because the original polyethylene prostheses were not very good. A better prosthesis developed at Massachusetts General Hospital is made up of highly crossed-link polyethylene and still wears over time but to a much lesser extent than the older polyethylene prostheses.
Metal and ceramic prostheses also can induce osteolysis, but again to a much lesser extent than the older polyethylene implants.
“Any particle can technically cause osteolysis but plastic produces the most particles,” Dr. Chen explained. Although hip revision rates in the United States are low to begin with, aseptic loosening is still one of the main reasons that patients need to undergo revision surgery, she observed.
“A lot of patients are still living with the old plastic [implants] so there is still a need for something like this,” she stressed.
However, many questions about this potential new strategy remain to be answered, including when best to initiate treatment and how to manage patients at risk for osteolysis 20-30 years after they have received their original implant.
In his editorial, Dr. Aro said that serious adverse consequences often become evident 10-20 years after patients have undergone the original hip replacement procedures, when they are potentially less physically fit than they were at the time of the operation and thus less able to withstand the rigors of a difficult revision surgery.
“In this context, the concept of nonsurgical pharmacological treatment of periprosthetic osteolysis ... brings a new hope for the ever-increasing population of patients with total hip arthroplasty to avoid revision surgery,” Dr. Aro suggested.
However, Dr. Aro cautioned that reduction of bone turnover by antiresorptive agents such as denosumab has been associated with the development of atypical femoral fractures.
The study was funded by Amgen. Dr. Wilkinson has reported receiving a grant from Amgen. Dr. Chen has reported serving as a consultant for Striker and b-One Ortho. Dr. Aro has reported receiving a grant to his institution from Amgen Finland and the Academy of Finland. He has also served as a member of an advisory scientific board for Amgen Finland.
A version of this article first appeared on Medscape.com.
FDA finalizes guidance for power morcellators in gynecologic surgery

The agency noted that physicians should conduct a thorough preoperative screening and that the devices should only be used for hysterectomies and myomectomies. Clinicians should not use the devices in cases involving uterine malignancy or suspected uterine malignancy.
In addition, clinicians should not use morcellators to remove uterine tissue containing suspected fibroids in women older than 50 years or who are postmenopausal. Nor should the devices be used for women who are “candidates for removal of tissue (en bloc) through the vagina or via a minilaparotomy incision,” the agency said.
The safety communication, which was issued on Dec. 29, 2020, updates previous guidance from February 2020. The updated recommendations are consistent with final labeling guidance for laparoscopic power morcellators, also issued by the FDA on Dec. 29.
Risk of disease spread
Prior evidence suggests that use of uncontained power morcellators in women with malignant uterine tissue can spread disease.
Even among women who do not have malignant uterine tissue, containment is important. The agency noted an association between uncontained power morcellation and the spread of benign uterine tissue, such as parasitic myomas and disseminated peritoneal leiomyomatosis, which could require additional surgeries.
In 2016, the FDA approved the PneumoLiner, a containment system for isolating uterine tissue that is not suspected of containing cancer.
“While unsuspected cancer can occur at any age, the prevalence of unsuspected cancer in women undergoing hysterectomy for fibroids increases with age such that the benefit-risk profile of using [laparoscopic power morcellators] is worse in older women when compared to younger women,” according to the new labeling guidance. “Also, the surgical technique of en bloc tissue removal eliminates the need to perform morcellation, thereby reducing the risk of iatrogenic dissemination and upstaging of an occult sarcoma. A thorough preoperative screening should be conducted; however, it is important to note that no screening procedure that can reliably detect sarcoma preoperatively has been identified.”
“The FDA will continue to review the latest data and scientific literature on laparoscopic power morcellation, including gathering real-world evidence from patients, providers and others, and encouraging innovation to better detect uterine cancer and develop containment systems for gynecologic surgery,” said Jeffrey Shuren, MD, JD, director of the FDA’s Center for Devices and Radiological Health, in a news release. “The FDA seeks to ensure women and their health care providers are fully informed when considering laparoscopic power morcellators for gynecologic surgeries.”
A version of this article first appeared on Medscape.com.
The agency noted that physicians should conduct a thorough preoperative screening and that the devices should only be used for hysterectomies and myomectomies. Clinicians should not use the devices in cases involving uterine malignancy or suspected uterine malignancy.
In addition, clinicians should not use morcellators to remove uterine tissue containing suspected fibroids in women older than 50 years or who are postmenopausal. Nor should the devices be used for women who are “candidates for removal of tissue (en bloc) through the vagina or via a minilaparotomy incision,” the agency said.
The safety communication, which was issued on Dec. 29, 2020, updates previous guidance from February 2020. The updated recommendations are consistent with final labeling guidance for laparoscopic power morcellators, also issued by the FDA on Dec. 29.
Risk of disease spread
Prior evidence suggests that use of uncontained power morcellators in women with malignant uterine tissue can spread disease.
Even among women who do not have malignant uterine tissue, containment is important. The agency noted an association between uncontained power morcellation and the spread of benign uterine tissue, such as parasitic myomas and disseminated peritoneal leiomyomatosis, which could require additional surgeries.
In 2016, the FDA approved the PneumoLiner, a containment system for isolating uterine tissue that is not suspected of containing cancer.
“While unsuspected cancer can occur at any age, the prevalence of unsuspected cancer in women undergoing hysterectomy for fibroids increases with age such that the benefit-risk profile of using [laparoscopic power morcellators] is worse in older women when compared to younger women,” according to the new labeling guidance. “Also, the surgical technique of en bloc tissue removal eliminates the need to perform morcellation, thereby reducing the risk of iatrogenic dissemination and upstaging of an occult sarcoma. A thorough preoperative screening should be conducted; however, it is important to note that no screening procedure that can reliably detect sarcoma preoperatively has been identified.”
“The FDA will continue to review the latest data and scientific literature on laparoscopic power morcellation, including gathering real-world evidence from patients, providers and others, and encouraging innovation to better detect uterine cancer and develop containment systems for gynecologic surgery,” said Jeffrey Shuren, MD, JD, director of the FDA’s Center for Devices and Radiological Health, in a news release. “The FDA seeks to ensure women and their health care providers are fully informed when considering laparoscopic power morcellators for gynecologic surgeries.”
A version of this article first appeared on Medscape.com.
The agency noted that physicians should conduct a thorough preoperative screening and that the devices should only be used for hysterectomies and myomectomies. Clinicians should not use the devices in cases involving uterine malignancy or suspected uterine malignancy.
In addition, clinicians should not use morcellators to remove uterine tissue containing suspected fibroids in women older than 50 years or who are postmenopausal. Nor should the devices be used for women who are “candidates for removal of tissue (en bloc) through the vagina or via a minilaparotomy incision,” the agency said.
The safety communication, which was issued on Dec. 29, 2020, updates previous guidance from February 2020. The updated recommendations are consistent with final labeling guidance for laparoscopic power morcellators, also issued by the FDA on Dec. 29.
Risk of disease spread
Prior evidence suggests that use of uncontained power morcellators in women with malignant uterine tissue can spread disease.
Even among women who do not have malignant uterine tissue, containment is important. The agency noted an association between uncontained power morcellation and the spread of benign uterine tissue, such as parasitic myomas and disseminated peritoneal leiomyomatosis, which could require additional surgeries.
In 2016, the FDA approved the PneumoLiner, a containment system for isolating uterine tissue that is not suspected of containing cancer.
“While unsuspected cancer can occur at any age, the prevalence of unsuspected cancer in women undergoing hysterectomy for fibroids increases with age such that the benefit-risk profile of using [laparoscopic power morcellators] is worse in older women when compared to younger women,” according to the new labeling guidance. “Also, the surgical technique of en bloc tissue removal eliminates the need to perform morcellation, thereby reducing the risk of iatrogenic dissemination and upstaging of an occult sarcoma. A thorough preoperative screening should be conducted; however, it is important to note that no screening procedure that can reliably detect sarcoma preoperatively has been identified.”
“The FDA will continue to review the latest data and scientific literature on laparoscopic power morcellation, including gathering real-world evidence from patients, providers and others, and encouraging innovation to better detect uterine cancer and develop containment systems for gynecologic surgery,” said Jeffrey Shuren, MD, JD, director of the FDA’s Center for Devices and Radiological Health, in a news release. “The FDA seeks to ensure women and their health care providers are fully informed when considering laparoscopic power morcellators for gynecologic surgeries.”
A version of this article first appeared on Medscape.com.