User login
For MD-IQ use only
Docs misdiagnose aneurysm and patient dies; must pay $29M; more
and untreated, according to a story posted on Boston.com, among other news sites.
On the morning of Jan. 13, 2018, Joseph Brown awoke with shortness of breath and upper abdominal pain, which eventually spread to his chest and back. Taken to Salem Hospital’s emergency department, Mr. Brown was seen by Steven D. Browell, MD, an emergency medicine specialist.
Dr. Browell ordered tests that ruled out both a heart attack and a pulmonary embolism. He called for a blood test, which indicated that the patient’s white blood count was elevated. Suspecting an infection, Dr. Browell ordered that Mr. Brown be admitted to the hospital.
Accepting Mr. Brown’s admission was William D. Kenyon, MD, a hospitalist, who also examined the patient and concurred with Dr. Browell’s probable diagnosis. The patient was then sent to the medical floor.
There he underwent additional testing, including a chest x-ray, which proved negative except for one finding: a “mild hazy interstitial opacity that could represent a small airway inflammation or developing/early pneumonia.” Because Mr. Brown had reported that he had punctured his foot several days earlier, he also underwent a foot x-ray, which showed a possible foreign body. It was thought that might be the source of his infection.
Neither Dr. Browell nor Dr. Kenyon had completely ruled out a possible aortic aneurysm and dissection. Mr. Brown’s symptoms, after all, were in some ways suggestive of those conditions. Then again, he was very young – only 43 at the time – and his pain, while severe, didn’t correspond to the “searing” pain that, at trial, Dr. Kenyon described as typical of an aneurysm and dissection. As the hospitalist testified at trial, Mr. Brown had “a constellation of nonspecific symptoms” and an “unusual presentation of a rare condition,” typically seen in patients aged 65 and older.
Given these factors – and the results of Mr. Brown’s tests, lab studies, and physical exam – Dr. Kenyon didn’t think that the case warranted a CT scan to rule out an aortic aneurysm or aortic dissection.
By early the next morning, though, Mr. Brown’s shortness of breath and pain had intensified significantly. The on-duty doctor ordered a CT scan, which showed “a massive aneurysm at the beginning of [the patient’s] aorta and a dissection extending through most of his aorta.”
Mr. Brown was flown to Boston to undergo emergency surgery. En route to the helicopter, his aorta ruptured, stopping his heart and causing his death.
During the 8-day trial, each side introduced expert witnesses. Speaking for the plaintiffs, experts in cardiothoracic surgery and emergency medicine testified that the treating physicians were negligent in failing to order a CT scan on Jan. 13. Had they done so, the patient would have almost certainly undergone surgery earlier, which would have prevented his death.
Experts for the defense saw things differently. They testified that, given the evidence, it was reasonable and appropriate for Dr. Browell and Dr. Kenyon to have treated their patient for an infection rather than an aneurysm or dissection.
The jury found the defense’s arguments unconvincing, however. After deliberating 3 hours, it awarded the plaintiffs $20,000,000, to be paid out over time largely to Mr. Brown’s two daughters, who were aged 12 and 18 when he died. Including interest, the total award is close to $29 million.
In a statement following the verdict, lead plaintiff’s attorney Robert M. Higgins, of Lubin & Meyer, Boston, said the takeaway from the case was: “If you just treat people based on what the likelihood is, statistically, you’re going to miss a lot of life-threatening conditions. And that’s what happened in this case.”
Urologists typically prevail in BPH suits
Malpractice claims following surgery for benign prostatic hyperplasia (BPH) tend to be limited in scope and are typically resolved in favor of the surgeon-defendant, as a study in The Cureus Journal of Medical Science makes clear.
The study – conducted by a team of researchers that included Joao G. Porto, MD, of the Desai Sethi Urology Institute, University of Miami – investigated whether such surgeries pose a significant malpractice risk for urologists.
With information gleaned from two well-known legal databases, the team used a variety of key terms to identify BPH-related claims from January 2000 to December 2021.
Within this universe of claims, researchers identified several significant trends:
- Among BPH-related procedures, transurethral resection of the prostate was the most frequently identified (37%);
- Among the most-often cited reasons cited for a claim, allegations of inadequate postoperative care were the most common (33%);
- Of possible postsurgical complications, those that led to the greatest number of suits were urinary incontinence (23%), erectile dysfunction (13%), and urinary retention (13%); and,
- Not unexpectedly, the specialist most frequently named in a suit was a urologist (57%).
Interestingly, in all but two of the claims, the verdict favored the doctor-defendant. In the two cases in which the plaintiff prevailed, each involved unexpected and serious postsurgical complications.
A version of this article originally appeared on Medscape.com.
and untreated, according to a story posted on Boston.com, among other news sites.
On the morning of Jan. 13, 2018, Joseph Brown awoke with shortness of breath and upper abdominal pain, which eventually spread to his chest and back. Taken to Salem Hospital’s emergency department, Mr. Brown was seen by Steven D. Browell, MD, an emergency medicine specialist.
Dr. Browell ordered tests that ruled out both a heart attack and a pulmonary embolism. He called for a blood test, which indicated that the patient’s white blood count was elevated. Suspecting an infection, Dr. Browell ordered that Mr. Brown be admitted to the hospital.
Accepting Mr. Brown’s admission was William D. Kenyon, MD, a hospitalist, who also examined the patient and concurred with Dr. Browell’s probable diagnosis. The patient was then sent to the medical floor.
There he underwent additional testing, including a chest x-ray, which proved negative except for one finding: a “mild hazy interstitial opacity that could represent a small airway inflammation or developing/early pneumonia.” Because Mr. Brown had reported that he had punctured his foot several days earlier, he also underwent a foot x-ray, which showed a possible foreign body. It was thought that might be the source of his infection.
Neither Dr. Browell nor Dr. Kenyon had completely ruled out a possible aortic aneurysm and dissection. Mr. Brown’s symptoms, after all, were in some ways suggestive of those conditions. Then again, he was very young – only 43 at the time – and his pain, while severe, didn’t correspond to the “searing” pain that, at trial, Dr. Kenyon described as typical of an aneurysm and dissection. As the hospitalist testified at trial, Mr. Brown had “a constellation of nonspecific symptoms” and an “unusual presentation of a rare condition,” typically seen in patients aged 65 and older.
Given these factors – and the results of Mr. Brown’s tests, lab studies, and physical exam – Dr. Kenyon didn’t think that the case warranted a CT scan to rule out an aortic aneurysm or aortic dissection.
By early the next morning, though, Mr. Brown’s shortness of breath and pain had intensified significantly. The on-duty doctor ordered a CT scan, which showed “a massive aneurysm at the beginning of [the patient’s] aorta and a dissection extending through most of his aorta.”
Mr. Brown was flown to Boston to undergo emergency surgery. En route to the helicopter, his aorta ruptured, stopping his heart and causing his death.
During the 8-day trial, each side introduced expert witnesses. Speaking for the plaintiffs, experts in cardiothoracic surgery and emergency medicine testified that the treating physicians were negligent in failing to order a CT scan on Jan. 13. Had they done so, the patient would have almost certainly undergone surgery earlier, which would have prevented his death.
Experts for the defense saw things differently. They testified that, given the evidence, it was reasonable and appropriate for Dr. Browell and Dr. Kenyon to have treated their patient for an infection rather than an aneurysm or dissection.
The jury found the defense’s arguments unconvincing, however. After deliberating 3 hours, it awarded the plaintiffs $20,000,000, to be paid out over time largely to Mr. Brown’s two daughters, who were aged 12 and 18 when he died. Including interest, the total award is close to $29 million.
In a statement following the verdict, lead plaintiff’s attorney Robert M. Higgins, of Lubin & Meyer, Boston, said the takeaway from the case was: “If you just treat people based on what the likelihood is, statistically, you’re going to miss a lot of life-threatening conditions. And that’s what happened in this case.”
Urologists typically prevail in BPH suits
Malpractice claims following surgery for benign prostatic hyperplasia (BPH) tend to be limited in scope and are typically resolved in favor of the surgeon-defendant, as a study in The Cureus Journal of Medical Science makes clear.
The study – conducted by a team of researchers that included Joao G. Porto, MD, of the Desai Sethi Urology Institute, University of Miami – investigated whether such surgeries pose a significant malpractice risk for urologists.
With information gleaned from two well-known legal databases, the team used a variety of key terms to identify BPH-related claims from January 2000 to December 2021.
Within this universe of claims, researchers identified several significant trends:
- Among BPH-related procedures, transurethral resection of the prostate was the most frequently identified (37%);
- Among the most-often cited reasons cited for a claim, allegations of inadequate postoperative care were the most common (33%);
- Of possible postsurgical complications, those that led to the greatest number of suits were urinary incontinence (23%), erectile dysfunction (13%), and urinary retention (13%); and,
- Not unexpectedly, the specialist most frequently named in a suit was a urologist (57%).
Interestingly, in all but two of the claims, the verdict favored the doctor-defendant. In the two cases in which the plaintiff prevailed, each involved unexpected and serious postsurgical complications.
A version of this article originally appeared on Medscape.com.
and untreated, according to a story posted on Boston.com, among other news sites.
On the morning of Jan. 13, 2018, Joseph Brown awoke with shortness of breath and upper abdominal pain, which eventually spread to his chest and back. Taken to Salem Hospital’s emergency department, Mr. Brown was seen by Steven D. Browell, MD, an emergency medicine specialist.
Dr. Browell ordered tests that ruled out both a heart attack and a pulmonary embolism. He called for a blood test, which indicated that the patient’s white blood count was elevated. Suspecting an infection, Dr. Browell ordered that Mr. Brown be admitted to the hospital.
Accepting Mr. Brown’s admission was William D. Kenyon, MD, a hospitalist, who also examined the patient and concurred with Dr. Browell’s probable diagnosis. The patient was then sent to the medical floor.
There he underwent additional testing, including a chest x-ray, which proved negative except for one finding: a “mild hazy interstitial opacity that could represent a small airway inflammation or developing/early pneumonia.” Because Mr. Brown had reported that he had punctured his foot several days earlier, he also underwent a foot x-ray, which showed a possible foreign body. It was thought that might be the source of his infection.
Neither Dr. Browell nor Dr. Kenyon had completely ruled out a possible aortic aneurysm and dissection. Mr. Brown’s symptoms, after all, were in some ways suggestive of those conditions. Then again, he was very young – only 43 at the time – and his pain, while severe, didn’t correspond to the “searing” pain that, at trial, Dr. Kenyon described as typical of an aneurysm and dissection. As the hospitalist testified at trial, Mr. Brown had “a constellation of nonspecific symptoms” and an “unusual presentation of a rare condition,” typically seen in patients aged 65 and older.
Given these factors – and the results of Mr. Brown’s tests, lab studies, and physical exam – Dr. Kenyon didn’t think that the case warranted a CT scan to rule out an aortic aneurysm or aortic dissection.
By early the next morning, though, Mr. Brown’s shortness of breath and pain had intensified significantly. The on-duty doctor ordered a CT scan, which showed “a massive aneurysm at the beginning of [the patient’s] aorta and a dissection extending through most of his aorta.”
Mr. Brown was flown to Boston to undergo emergency surgery. En route to the helicopter, his aorta ruptured, stopping his heart and causing his death.
During the 8-day trial, each side introduced expert witnesses. Speaking for the plaintiffs, experts in cardiothoracic surgery and emergency medicine testified that the treating physicians were negligent in failing to order a CT scan on Jan. 13. Had they done so, the patient would have almost certainly undergone surgery earlier, which would have prevented his death.
Experts for the defense saw things differently. They testified that, given the evidence, it was reasonable and appropriate for Dr. Browell and Dr. Kenyon to have treated their patient for an infection rather than an aneurysm or dissection.
The jury found the defense’s arguments unconvincing, however. After deliberating 3 hours, it awarded the plaintiffs $20,000,000, to be paid out over time largely to Mr. Brown’s two daughters, who were aged 12 and 18 when he died. Including interest, the total award is close to $29 million.
In a statement following the verdict, lead plaintiff’s attorney Robert M. Higgins, of Lubin & Meyer, Boston, said the takeaway from the case was: “If you just treat people based on what the likelihood is, statistically, you’re going to miss a lot of life-threatening conditions. And that’s what happened in this case.”
Urologists typically prevail in BPH suits
Malpractice claims following surgery for benign prostatic hyperplasia (BPH) tend to be limited in scope and are typically resolved in favor of the surgeon-defendant, as a study in The Cureus Journal of Medical Science makes clear.
The study – conducted by a team of researchers that included Joao G. Porto, MD, of the Desai Sethi Urology Institute, University of Miami – investigated whether such surgeries pose a significant malpractice risk for urologists.
With information gleaned from two well-known legal databases, the team used a variety of key terms to identify BPH-related claims from January 2000 to December 2021.
Within this universe of claims, researchers identified several significant trends:
- Among BPH-related procedures, transurethral resection of the prostate was the most frequently identified (37%);
- Among the most-often cited reasons cited for a claim, allegations of inadequate postoperative care were the most common (33%);
- Of possible postsurgical complications, those that led to the greatest number of suits were urinary incontinence (23%), erectile dysfunction (13%), and urinary retention (13%); and,
- Not unexpectedly, the specialist most frequently named in a suit was a urologist (57%).
Interestingly, in all but two of the claims, the verdict favored the doctor-defendant. In the two cases in which the plaintiff prevailed, each involved unexpected and serious postsurgical complications.
A version of this article originally appeared on Medscape.com.
ChatGPT in medicine: The good, the bad, and the unknown
CHICAGO – , so like them or not, physicians might as well figure out how to optimize their role in medicine and health care. That’s the takeaway from a three-expert panel session about the technology held at the annual Digestive Disease Week® (DDW).
The chatbot can help doctors to a certain extent by suggesting differential diagnoses, assisting with clinical note-taking, and producing rapid and easy-to-understand patient communication and educational materials, they noted. However, it can also make mistakes. And, unlike a medical trainee who might give a clinical answer and express some doubt, ChatGPT (Open AI/Microsoft) clearly states its findings as fact, even when it’s wrong.
Known as “hallucinating,” this problem of AI inaccuracy was displayed at the packed DDW session.
When asked when Leonardo da Vinci painted the Mona Lisa, for example, ChatGPT replied 1815. That’s off by about 300 years; the masterpiece was created sometime between 1503 and 1519. Asked for a fact about George Washington, ChatGPT said he invented the cotton gin. Also not true. (Eli Whitney patented the cotton gin.)
In an example more suited for gastroenterologists at DDW, ChatGPT correctly stated that Barrett esophagus can lead to adenocarcinoma of the esophagus in some cases. However, the technology also said that the condition could lead to prostate cancer.
So, if someone asked ChatGPT for a list of possible risks for Barrett’s esophagus, it would include prostate cancer. A person without medical knowledge “could take it at face value that it causes prostate cancer,” said panelist Sravanthi Parasa, MD, a gastroenterologist at Swedish Medical Center, Seattle.
“That is a lot of misinformation that is going to come our way,” she added at the session, which was sponsored by the American Society for Gastrointestinal Endoscopy.
The potential for inaccuracy is a downside to ChatGPT, agreed panelist Prateek Sharma, MD, a gastroenterologist at the University of Kansas Medical Center in Kansas City, Kansas.
“There is no quality control. You have to double check its answers,” said Dr. Sharma, who is president-elect of ASGE.
ChatGPT is not going to replace physicians in general or gastroenterologists doing endoscopies, said Ian Gralnek, MD, chief of the Institute of Gastroenterology and Hepatology at Emek Medical Center in Afula, Israel.
Even though the tool could play a role in medicine, “we need to be very careful as a society going forward ... and see where things are going,” Dr. Gralnek said.
How you ask makes a difference
Future iterations of ChatGPT are likely to produce fewer hallucinations, the experts said. In the meantime, users can lower the risk by paying attention to how they’re wording their queries, a practice known as “prompt engineering.”
It’s best to ask a question that has a firm answer to it. If you ask a vague question, you’ll likely get a vague answer, Dr. Sharma said.
ChatGPT is a large language model (LLM). GPT stands for “generative pretrained transformer” – specialized algorithms that find long-range patterns in sequences of data. LLMs can predict the next word in a sentence.
“That’s why this is also called generative AI,” Dr. Sharma said. “For example, if you put in ‘Where are we?’, it will predict for you that perhaps the next word is ‘going?’ ”
The current public version is ChatGPT 3.5, which was trained on open-source online information up until early 2022. It can gather information from open-access scientific journals and medical society guidelines, as well as from Twitter, Reddit, and other social media. It does not have access to private information, like electronic health records.
The use of ChatGPT has exploded in the past 6 months, Dr. Sharma said.
“ChatGPT has been the most-searched website or platform ever in history since it was launched in December of 2022,” he said.
What’s in it for doctors?
Although not specifically trained for health care–related tasks, the panelists noted that ChatGPT does have potential as a virtual medical assistant, chatbot, clinical decision-support tool, source of medical education, natural language processor for documentation, or medical note-taker.
ChatGPT can help physicians write a letter of support to a patient who, for example, was just diagnosed with stage IV colon cancer. It can do that in only 15 seconds, whereas it would take us much longer, Dr. Sharma said.
ChatGPT is the “next frontier” for generating patient education materials, Dr. Parasa said. It can help time-constrained health care providers, as long as the information is accurate.
ChatGPT 4.0, now available by subscription, can do “almost real-time note-taking during patient encounters,” she added.
Another reason to be familiar with the technology: “Many of your patients are using it, even if you don’t know about it,” Dr. Sharma said.
Questions abound
A conference attendee asked the panel what to do when a patient comes in with ChatGPT medical advice that does not align with official guidelines.
Dr. Gralnek said that he would explain to patients that medical information based on guidelines are not “black and white.” The panel likened it to how patients come to an appointment now armed with information from the Internet, which is not always correct, that must then be countered by doctors. The same would likely happen with ChatGPT.
Another attendee asked whether ChatGPT eventually will work in accordance with electronic health record systems.
“Open AI and Microsoft are already working with Epic,” Dr. Parasa said.
A question arose about the reading level of information provided by ChatGPT. Dr. Parasa noted that it’s not standard. However, a person can prompt ChatGPT to provide an answer either at an eighth-grade reading level or for a well-trained physician.
Dr. Sharma offered a final warning: The technology learns over time.
“It knows what your habits are. It will learn what you’re doing,” Dr. Sharma said. “Everything else on your browsers that are open, it’s learning from that also. So be careful what websites you visit before you go to ChatGPT.”
Dr. Sharma is a stock shareholder in Microsoft. Dr. Parasa and Dr. Gralneck reported no relevant financial relationships.
DDW is sponsored by the American Association for the Study of Liver Diseases, the American Gastroenterological Association, the American Society for Gastrointestinal Endoscopy, and The Society for Surgery of the Alimentary Tract.
A version of this article originally appeared on Medscape.com.
CHICAGO – , so like them or not, physicians might as well figure out how to optimize their role in medicine and health care. That’s the takeaway from a three-expert panel session about the technology held at the annual Digestive Disease Week® (DDW).
The chatbot can help doctors to a certain extent by suggesting differential diagnoses, assisting with clinical note-taking, and producing rapid and easy-to-understand patient communication and educational materials, they noted. However, it can also make mistakes. And, unlike a medical trainee who might give a clinical answer and express some doubt, ChatGPT (Open AI/Microsoft) clearly states its findings as fact, even when it’s wrong.
Known as “hallucinating,” this problem of AI inaccuracy was displayed at the packed DDW session.
When asked when Leonardo da Vinci painted the Mona Lisa, for example, ChatGPT replied 1815. That’s off by about 300 years; the masterpiece was created sometime between 1503 and 1519. Asked for a fact about George Washington, ChatGPT said he invented the cotton gin. Also not true. (Eli Whitney patented the cotton gin.)
In an example more suited for gastroenterologists at DDW, ChatGPT correctly stated that Barrett esophagus can lead to adenocarcinoma of the esophagus in some cases. However, the technology also said that the condition could lead to prostate cancer.
So, if someone asked ChatGPT for a list of possible risks for Barrett’s esophagus, it would include prostate cancer. A person without medical knowledge “could take it at face value that it causes prostate cancer,” said panelist Sravanthi Parasa, MD, a gastroenterologist at Swedish Medical Center, Seattle.
“That is a lot of misinformation that is going to come our way,” she added at the session, which was sponsored by the American Society for Gastrointestinal Endoscopy.
The potential for inaccuracy is a downside to ChatGPT, agreed panelist Prateek Sharma, MD, a gastroenterologist at the University of Kansas Medical Center in Kansas City, Kansas.
“There is no quality control. You have to double check its answers,” said Dr. Sharma, who is president-elect of ASGE.
ChatGPT is not going to replace physicians in general or gastroenterologists doing endoscopies, said Ian Gralnek, MD, chief of the Institute of Gastroenterology and Hepatology at Emek Medical Center in Afula, Israel.
Even though the tool could play a role in medicine, “we need to be very careful as a society going forward ... and see where things are going,” Dr. Gralnek said.
How you ask makes a difference
Future iterations of ChatGPT are likely to produce fewer hallucinations, the experts said. In the meantime, users can lower the risk by paying attention to how they’re wording their queries, a practice known as “prompt engineering.”
It’s best to ask a question that has a firm answer to it. If you ask a vague question, you’ll likely get a vague answer, Dr. Sharma said.
ChatGPT is a large language model (LLM). GPT stands for “generative pretrained transformer” – specialized algorithms that find long-range patterns in sequences of data. LLMs can predict the next word in a sentence.
“That’s why this is also called generative AI,” Dr. Sharma said. “For example, if you put in ‘Where are we?’, it will predict for you that perhaps the next word is ‘going?’ ”
The current public version is ChatGPT 3.5, which was trained on open-source online information up until early 2022. It can gather information from open-access scientific journals and medical society guidelines, as well as from Twitter, Reddit, and other social media. It does not have access to private information, like electronic health records.
The use of ChatGPT has exploded in the past 6 months, Dr. Sharma said.
“ChatGPT has been the most-searched website or platform ever in history since it was launched in December of 2022,” he said.
What’s in it for doctors?
Although not specifically trained for health care–related tasks, the panelists noted that ChatGPT does have potential as a virtual medical assistant, chatbot, clinical decision-support tool, source of medical education, natural language processor for documentation, or medical note-taker.
ChatGPT can help physicians write a letter of support to a patient who, for example, was just diagnosed with stage IV colon cancer. It can do that in only 15 seconds, whereas it would take us much longer, Dr. Sharma said.
ChatGPT is the “next frontier” for generating patient education materials, Dr. Parasa said. It can help time-constrained health care providers, as long as the information is accurate.
ChatGPT 4.0, now available by subscription, can do “almost real-time note-taking during patient encounters,” she added.
Another reason to be familiar with the technology: “Many of your patients are using it, even if you don’t know about it,” Dr. Sharma said.
Questions abound
A conference attendee asked the panel what to do when a patient comes in with ChatGPT medical advice that does not align with official guidelines.
Dr. Gralnek said that he would explain to patients that medical information based on guidelines are not “black and white.” The panel likened it to how patients come to an appointment now armed with information from the Internet, which is not always correct, that must then be countered by doctors. The same would likely happen with ChatGPT.
Another attendee asked whether ChatGPT eventually will work in accordance with electronic health record systems.
“Open AI and Microsoft are already working with Epic,” Dr. Parasa said.
A question arose about the reading level of information provided by ChatGPT. Dr. Parasa noted that it’s not standard. However, a person can prompt ChatGPT to provide an answer either at an eighth-grade reading level or for a well-trained physician.
Dr. Sharma offered a final warning: The technology learns over time.
“It knows what your habits are. It will learn what you’re doing,” Dr. Sharma said. “Everything else on your browsers that are open, it’s learning from that also. So be careful what websites you visit before you go to ChatGPT.”
Dr. Sharma is a stock shareholder in Microsoft. Dr. Parasa and Dr. Gralneck reported no relevant financial relationships.
DDW is sponsored by the American Association for the Study of Liver Diseases, the American Gastroenterological Association, the American Society for Gastrointestinal Endoscopy, and The Society for Surgery of the Alimentary Tract.
A version of this article originally appeared on Medscape.com.
CHICAGO – , so like them or not, physicians might as well figure out how to optimize their role in medicine and health care. That’s the takeaway from a three-expert panel session about the technology held at the annual Digestive Disease Week® (DDW).
The chatbot can help doctors to a certain extent by suggesting differential diagnoses, assisting with clinical note-taking, and producing rapid and easy-to-understand patient communication and educational materials, they noted. However, it can also make mistakes. And, unlike a medical trainee who might give a clinical answer and express some doubt, ChatGPT (Open AI/Microsoft) clearly states its findings as fact, even when it’s wrong.
Known as “hallucinating,” this problem of AI inaccuracy was displayed at the packed DDW session.
When asked when Leonardo da Vinci painted the Mona Lisa, for example, ChatGPT replied 1815. That’s off by about 300 years; the masterpiece was created sometime between 1503 and 1519. Asked for a fact about George Washington, ChatGPT said he invented the cotton gin. Also not true. (Eli Whitney patented the cotton gin.)
In an example more suited for gastroenterologists at DDW, ChatGPT correctly stated that Barrett esophagus can lead to adenocarcinoma of the esophagus in some cases. However, the technology also said that the condition could lead to prostate cancer.
So, if someone asked ChatGPT for a list of possible risks for Barrett’s esophagus, it would include prostate cancer. A person without medical knowledge “could take it at face value that it causes prostate cancer,” said panelist Sravanthi Parasa, MD, a gastroenterologist at Swedish Medical Center, Seattle.
“That is a lot of misinformation that is going to come our way,” she added at the session, which was sponsored by the American Society for Gastrointestinal Endoscopy.
The potential for inaccuracy is a downside to ChatGPT, agreed panelist Prateek Sharma, MD, a gastroenterologist at the University of Kansas Medical Center in Kansas City, Kansas.
“There is no quality control. You have to double check its answers,” said Dr. Sharma, who is president-elect of ASGE.
ChatGPT is not going to replace physicians in general or gastroenterologists doing endoscopies, said Ian Gralnek, MD, chief of the Institute of Gastroenterology and Hepatology at Emek Medical Center in Afula, Israel.
Even though the tool could play a role in medicine, “we need to be very careful as a society going forward ... and see where things are going,” Dr. Gralnek said.
How you ask makes a difference
Future iterations of ChatGPT are likely to produce fewer hallucinations, the experts said. In the meantime, users can lower the risk by paying attention to how they’re wording their queries, a practice known as “prompt engineering.”
It’s best to ask a question that has a firm answer to it. If you ask a vague question, you’ll likely get a vague answer, Dr. Sharma said.
ChatGPT is a large language model (LLM). GPT stands for “generative pretrained transformer” – specialized algorithms that find long-range patterns in sequences of data. LLMs can predict the next word in a sentence.
“That’s why this is also called generative AI,” Dr. Sharma said. “For example, if you put in ‘Where are we?’, it will predict for you that perhaps the next word is ‘going?’ ”
The current public version is ChatGPT 3.5, which was trained on open-source online information up until early 2022. It can gather information from open-access scientific journals and medical society guidelines, as well as from Twitter, Reddit, and other social media. It does not have access to private information, like electronic health records.
The use of ChatGPT has exploded in the past 6 months, Dr. Sharma said.
“ChatGPT has been the most-searched website or platform ever in history since it was launched in December of 2022,” he said.
What’s in it for doctors?
Although not specifically trained for health care–related tasks, the panelists noted that ChatGPT does have potential as a virtual medical assistant, chatbot, clinical decision-support tool, source of medical education, natural language processor for documentation, or medical note-taker.
ChatGPT can help physicians write a letter of support to a patient who, for example, was just diagnosed with stage IV colon cancer. It can do that in only 15 seconds, whereas it would take us much longer, Dr. Sharma said.
ChatGPT is the “next frontier” for generating patient education materials, Dr. Parasa said. It can help time-constrained health care providers, as long as the information is accurate.
ChatGPT 4.0, now available by subscription, can do “almost real-time note-taking during patient encounters,” she added.
Another reason to be familiar with the technology: “Many of your patients are using it, even if you don’t know about it,” Dr. Sharma said.
Questions abound
A conference attendee asked the panel what to do when a patient comes in with ChatGPT medical advice that does not align with official guidelines.
Dr. Gralnek said that he would explain to patients that medical information based on guidelines are not “black and white.” The panel likened it to how patients come to an appointment now armed with information from the Internet, which is not always correct, that must then be countered by doctors. The same would likely happen with ChatGPT.
Another attendee asked whether ChatGPT eventually will work in accordance with electronic health record systems.
“Open AI and Microsoft are already working with Epic,” Dr. Parasa said.
A question arose about the reading level of information provided by ChatGPT. Dr. Parasa noted that it’s not standard. However, a person can prompt ChatGPT to provide an answer either at an eighth-grade reading level or for a well-trained physician.
Dr. Sharma offered a final warning: The technology learns over time.
“It knows what your habits are. It will learn what you’re doing,” Dr. Sharma said. “Everything else on your browsers that are open, it’s learning from that also. So be careful what websites you visit before you go to ChatGPT.”
Dr. Sharma is a stock shareholder in Microsoft. Dr. Parasa and Dr. Gralneck reported no relevant financial relationships.
DDW is sponsored by the American Association for the Study of Liver Diseases, the American Gastroenterological Association, the American Society for Gastrointestinal Endoscopy, and The Society for Surgery of the Alimentary Tract.
A version of this article originally appeared on Medscape.com.
AT DDW 2023
A 63-year-old male presented for evaluation of worsening genital lesions and associated swelling
.1 Clinically, ENV presents as verrucous, hyperkeratotic, cobblestone-like patches, plaques, and nodules with associated nonpitting edema of the affected body area.1 Secondary bacterial infections are common and often worsen the clinical course. The etiology of ENV involves chronic lymphatic obstruction and venous insufficiency, with additional risk factors including obesity, chronic lymphedema, bacterial infection, surgery or trauma, neoplasia, radiation, congestive heart failure, or scleroderma.2,3 While most commonly presenting on the lower extremities, cases have been reported involving the abdomen, sacrum, ears, buttocks, and penoscrotal area.1,2

Regardless of location, the pathogenesis of ENV remains the same. Chronic lymphatic obstruction results in accumulation and lymphostasis of protein-rich dermal fluid, which subsequently precipitates fibroblast proliferation and activation, suppression of the local immune response and development of recurrent lymphangitis, chronic inflammation, and potential secondary bacterial infection.2,4
There is no standard of care for the treatment and management of ENV and recurrence is common. Interventions often involve those used for chronic lymphedema – including leg elevation, compression stockings or devices, skin hygiene, and lymphatic pumping.2,3 Medical management with topical and oral retinoids has been reported, as well as emphasis on weight loss and infection control.1,4 Surgical intervention is often reserved for refractory cases that fail to respond to more conservative management, or severe presentations resulting in extensive functional and aesthetic impairment. Less commonly reported treatment modalities include lymphaticovenular anastomosis and ablative carbon dioxide laser use, although this latter intervention demonstrated minimal improvement in this patient.5,6
Penoscrotal ENV is a rare form of ENV affecting the genital region of males, often resulting in significant disfigurement, functional impairment, and psychosocial distress. Penoscrotal elephantiasis can be idiopathic, due to filarial infections, scleroinflammatory stricture of the urethra, Chlamydia trachomatis infection, and lymphostasis secondary to chronic inflammatory conditions such as streptococcal infections, radiotherapy, surgery, chronic venous stasis, or Kaposi sarcoma.7
In addition, hidradenitis suppurativa (HS) has been documented multiple times in the literature in association with the development of ENV, detailing lymphatic scarring secondary to chronic inguinal HS as the main pathogenic factor.8,9
Surgery is the mainstay of treatment for penoscrotal ENV, which not only improves functionality and cosmesis, but also aids in prevention of rare malignant sequelae, such as lymphangiosarcoma.10 Such interventions can involve lymphangioplasty to aid in lymphatic drainage or excision of the mass and subcutaneous tissue with full-thickness skin grafting for reconstruction.7 Collaboration between urology, plastic surgery, and dermatology is often essential to obtain adequate care with satisfactory outcomes and minimal recurrence for patients with this uncommon condition.
This case and photo were submitted by Marlee Hill, a medical student at the University of Oklahoma, Oklahoma City; and Michael Franzetti, MD, and Jeffrey McBride, MD, department of dermatology, University of Oklahoma Health Sciences Center. The column was edited by Donna Bilu Martin, MD.
Dr. Donna Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to d[email protected].
References
1. Hadian Y et al. Dermatol Online J. 2019 Dec 15;25(12):13030/qt6rn1s8ff.
2. Judge N and Kilic A. J Dermatol Case Rep. 2016 Nov 13;10(2):32-4.
3. Dean SM et al. J Am Acad Dermatol. 2011 Jun;64(6):1104-10.
4. Sisto K and Khachemoune A. Am J Clin Dermatol. 2008;9(3):141-6.
5. Motegi S et al. Dermatology. 2007;215(2):147-51.
6. Robinson CG et al. J Cutan Med Surg. 2018;22(6):611-3.
7. Koualla S et al. Ann Chir Plast Esthet. 2023 Apr 10;S0294-1260(23)00035-3.
8. Lelonek E et al. Acta Derm Venereol. 2021 Feb 11;101(2):adv00389.
9. Good LM et al. J Am Acad Dermatol. 2011 May;64(5):993-4.
10. Cerri A et al. Eur J Dermatol. 1998 Oct-Nov;8(7):511-4.
.1 Clinically, ENV presents as verrucous, hyperkeratotic, cobblestone-like patches, plaques, and nodules with associated nonpitting edema of the affected body area.1 Secondary bacterial infections are common and often worsen the clinical course. The etiology of ENV involves chronic lymphatic obstruction and venous insufficiency, with additional risk factors including obesity, chronic lymphedema, bacterial infection, surgery or trauma, neoplasia, radiation, congestive heart failure, or scleroderma.2,3 While most commonly presenting on the lower extremities, cases have been reported involving the abdomen, sacrum, ears, buttocks, and penoscrotal area.1,2
Regardless of location, the pathogenesis of ENV remains the same. Chronic lymphatic obstruction results in accumulation and lymphostasis of protein-rich dermal fluid, which subsequently precipitates fibroblast proliferation and activation, suppression of the local immune response and development of recurrent lymphangitis, chronic inflammation, and potential secondary bacterial infection.2,4
There is no standard of care for the treatment and management of ENV and recurrence is common. Interventions often involve those used for chronic lymphedema – including leg elevation, compression stockings or devices, skin hygiene, and lymphatic pumping.2,3 Medical management with topical and oral retinoids has been reported, as well as emphasis on weight loss and infection control.1,4 Surgical intervention is often reserved for refractory cases that fail to respond to more conservative management, or severe presentations resulting in extensive functional and aesthetic impairment. Less commonly reported treatment modalities include lymphaticovenular anastomosis and ablative carbon dioxide laser use, although this latter intervention demonstrated minimal improvement in this patient.5,6
Penoscrotal ENV is a rare form of ENV affecting the genital region of males, often resulting in significant disfigurement, functional impairment, and psychosocial distress. Penoscrotal elephantiasis can be idiopathic, due to filarial infections, scleroinflammatory stricture of the urethra, Chlamydia trachomatis infection, and lymphostasis secondary to chronic inflammatory conditions such as streptococcal infections, radiotherapy, surgery, chronic venous stasis, or Kaposi sarcoma.7
In addition, hidradenitis suppurativa (HS) has been documented multiple times in the literature in association with the development of ENV, detailing lymphatic scarring secondary to chronic inguinal HS as the main pathogenic factor.8,9
Surgery is the mainstay of treatment for penoscrotal ENV, which not only improves functionality and cosmesis, but also aids in prevention of rare malignant sequelae, such as lymphangiosarcoma.10 Such interventions can involve lymphangioplasty to aid in lymphatic drainage or excision of the mass and subcutaneous tissue with full-thickness skin grafting for reconstruction.7 Collaboration between urology, plastic surgery, and dermatology is often essential to obtain adequate care with satisfactory outcomes and minimal recurrence for patients with this uncommon condition.
This case and photo were submitted by Marlee Hill, a medical student at the University of Oklahoma, Oklahoma City; and Michael Franzetti, MD, and Jeffrey McBride, MD, department of dermatology, University of Oklahoma Health Sciences Center. The column was edited by Donna Bilu Martin, MD.
Dr. Donna Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to d[email protected].
References
1. Hadian Y et al. Dermatol Online J. 2019 Dec 15;25(12):13030/qt6rn1s8ff.
2. Judge N and Kilic A. J Dermatol Case Rep. 2016 Nov 13;10(2):32-4.
3. Dean SM et al. J Am Acad Dermatol. 2011 Jun;64(6):1104-10.
4. Sisto K and Khachemoune A. Am J Clin Dermatol. 2008;9(3):141-6.
5. Motegi S et al. Dermatology. 2007;215(2):147-51.
6. Robinson CG et al. J Cutan Med Surg. 2018;22(6):611-3.
7. Koualla S et al. Ann Chir Plast Esthet. 2023 Apr 10;S0294-1260(23)00035-3.
8. Lelonek E et al. Acta Derm Venereol. 2021 Feb 11;101(2):adv00389.
9. Good LM et al. J Am Acad Dermatol. 2011 May;64(5):993-4.
10. Cerri A et al. Eur J Dermatol. 1998 Oct-Nov;8(7):511-4.
.1 Clinically, ENV presents as verrucous, hyperkeratotic, cobblestone-like patches, plaques, and nodules with associated nonpitting edema of the affected body area.1 Secondary bacterial infections are common and often worsen the clinical course. The etiology of ENV involves chronic lymphatic obstruction and venous insufficiency, with additional risk factors including obesity, chronic lymphedema, bacterial infection, surgery or trauma, neoplasia, radiation, congestive heart failure, or scleroderma.2,3 While most commonly presenting on the lower extremities, cases have been reported involving the abdomen, sacrum, ears, buttocks, and penoscrotal area.1,2
Regardless of location, the pathogenesis of ENV remains the same. Chronic lymphatic obstruction results in accumulation and lymphostasis of protein-rich dermal fluid, which subsequently precipitates fibroblast proliferation and activation, suppression of the local immune response and development of recurrent lymphangitis, chronic inflammation, and potential secondary bacterial infection.2,4
There is no standard of care for the treatment and management of ENV and recurrence is common. Interventions often involve those used for chronic lymphedema – including leg elevation, compression stockings or devices, skin hygiene, and lymphatic pumping.2,3 Medical management with topical and oral retinoids has been reported, as well as emphasis on weight loss and infection control.1,4 Surgical intervention is often reserved for refractory cases that fail to respond to more conservative management, or severe presentations resulting in extensive functional and aesthetic impairment. Less commonly reported treatment modalities include lymphaticovenular anastomosis and ablative carbon dioxide laser use, although this latter intervention demonstrated minimal improvement in this patient.5,6
Penoscrotal ENV is a rare form of ENV affecting the genital region of males, often resulting in significant disfigurement, functional impairment, and psychosocial distress. Penoscrotal elephantiasis can be idiopathic, due to filarial infections, scleroinflammatory stricture of the urethra, Chlamydia trachomatis infection, and lymphostasis secondary to chronic inflammatory conditions such as streptococcal infections, radiotherapy, surgery, chronic venous stasis, or Kaposi sarcoma.7
In addition, hidradenitis suppurativa (HS) has been documented multiple times in the literature in association with the development of ENV, detailing lymphatic scarring secondary to chronic inguinal HS as the main pathogenic factor.8,9
Surgery is the mainstay of treatment for penoscrotal ENV, which not only improves functionality and cosmesis, but also aids in prevention of rare malignant sequelae, such as lymphangiosarcoma.10 Such interventions can involve lymphangioplasty to aid in lymphatic drainage or excision of the mass and subcutaneous tissue with full-thickness skin grafting for reconstruction.7 Collaboration between urology, plastic surgery, and dermatology is often essential to obtain adequate care with satisfactory outcomes and minimal recurrence for patients with this uncommon condition.
This case and photo were submitted by Marlee Hill, a medical student at the University of Oklahoma, Oklahoma City; and Michael Franzetti, MD, and Jeffrey McBride, MD, department of dermatology, University of Oklahoma Health Sciences Center. The column was edited by Donna Bilu Martin, MD.
Dr. Donna Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to d[email protected].
References
1. Hadian Y et al. Dermatol Online J. 2019 Dec 15;25(12):13030/qt6rn1s8ff.
2. Judge N and Kilic A. J Dermatol Case Rep. 2016 Nov 13;10(2):32-4.
3. Dean SM et al. J Am Acad Dermatol. 2011 Jun;64(6):1104-10.
4. Sisto K and Khachemoune A. Am J Clin Dermatol. 2008;9(3):141-6.
5. Motegi S et al. Dermatology. 2007;215(2):147-51.
6. Robinson CG et al. J Cutan Med Surg. 2018;22(6):611-3.
7. Koualla S et al. Ann Chir Plast Esthet. 2023 Apr 10;S0294-1260(23)00035-3.
8. Lelonek E et al. Acta Derm Venereol. 2021 Feb 11;101(2):adv00389.
9. Good LM et al. J Am Acad Dermatol. 2011 May;64(5):993-4.
10. Cerri A et al. Eur J Dermatol. 1998 Oct-Nov;8(7):511-4.

PV: Novel rusfertide shows ‘impressive’ efficacy
“The results are surprisingly positive,” said senior author Ronald Hoffman, MD, of the Icahn School of Medicine at Mount Sinai, New York, in discussing the late-breaking research at a press briefing during the European Hematology Association Hybrid Congress 2023.
“Importantly, the study met all of its efficacy endpoints, including the proportion of responders, absence of phlebotomy eligibility, and hematocrit control,” Dr. Hoffman said.
PV, a relatively common clonal myeloproliferative neoplasm, is characterized by uncontrolled erythrocytosis, or excessive production of red blood cells, increasing the risk for serious complications such as thromboembolic and cardiovascular events – the most common causes of morbidity and mortality in this blood cancer.
To treat PV, the maintenance of hematocrit levels at below 45% is critical. However, the current standard of care, therapeutic phlebotomy, with or without cytoreductive agents, falls short in maintaining those lower levels in the majority of patients, Dr. Hoffman explained.
To improve responses, rusfertide was developed as a novel, synthetic form of hepcidin, a peptide hormone that is produced by the liver and functions to maintain iron homeostasis and control the formation of red blood cells.
“This is somewhat of a paradigm shift,” said Dr. Hoffman in the press briefing. “We’re trying to use a hormone made by the liver to control excessive red blood cell production from polycythemia vera.”
For the phase 2 REVIVE study evaluating rusfertide in PV, the authors enrolled 53 patients with PV who had a high phlebotomy burden while receiving the current standard of care. The study’s criteria called for patients to have received at least three therapeutic phlebotomies in the 28 weeks prior to enrollment, with or without concurrent cytoreductive agents.
During a first part of the study, patients received subcutaneous rusfertide once weekly over 28 weeks, during which period the dose was adjusted individually to achieve control of HCT levels below 45%.
The second part was a withdrawal phase extending from weeks 29 to 41, in which patients were randomized in a blinded fashion to either continue on rusfertide (n = 26) or receive a placebo (n = 27).
The patients had a median age of 58; they were 71.7% male, and 54.7% had previously been treated with therapeutic phlebotomy alone while 45.3% received therapeutic phlebotomy plus cytoreductive agents.
Patients were considered to be responders if they met three criteria, including having HCT control without phlebotomy eligibility, no therapeutic phlebotomy, and having completed 12 weeks of treatment.
At the end of the second phase, 69.2% of patients receiving rusfertide were responders versus just 18.5% in the placebo group (P = .0003).
Notably, the improvement with rusfertide was observed among those receiving therapeutic phlebotomy alone, as well as with cytoreductive agents (both P = .02).
Compared with placebo, rusfertide provided significant improvement in measures including the maintenance of response, the absence of the need for therapeutic phlebotomy, and persistent HCT control (P < .0001 for all).
Whereas the phlebotomy-free rate with rusfertide during the dose-finding weeks of 1-17 was 76.9% and in weeks 17-29, 87.3%, the rate increased in part 2 of the study to 92.3%.
Additional symptom benefits reported with rusfertide at week 29 versus baseline in part 1 of the study included significant improvements in concentration (P = .0018), itching (P = .0054), fatigue (P = .0074), and inactivity (P = .0005).
In terms of safety, rusfertide was generally well tolerated, with 83% of treatment-emergent adverse events (TEAEs) being grade 1-2, while 17% were grade 3, and none were grade 4 or 5.
The most common TEAEs consisted of injection-site reactions, which were localized, and grade 1-2 in severity. The incidence of reactions decreased with ongoing treatment. There were only two discontinuations resulting from TEAEs.
Among a total of 70 patients who were enrolled, 52 (74.3%) have continued to receive rusfertide for at least 1 year, 32 (45.7%) for at least 1.5 years, and 10 (14.3%) for at least 2 years, indicating the long-term tolerability of rusfertide.
Further commenting, first author Marina Kremyanskaya, MD, PhD, an assistant professor of medicine, hematology, and medical oncology at the Icahn School of Medicine at Mount Sinai, added that a key benefit is rusfertide’s tolerability with combination therapies, which is important in enabling the avoidance of phlebotomies.
“Many patients on cytoreductive therapies still require phlebotomies, and they can’t tolerate a dose increase, either due to cytopenias or other adverse reactions,” she said in an interview. “So adding rusfertide allows for better control of their hematocrits on a lower dose of their respective cytoreductive drug.”
“The combination treatment thus allows for elimination of phlebotomy requirements and potentially improves their symptoms,” Dr. Kremyanskaya said, adding that “using a lower dose of cytoreductive drug such as interferon or hydroxyurea could offer a symptomatic relief to patients as well.”
Overall, she agreed that the responses are remarkably positive.
“I think this is what is so impressive about this agent – basically everybody responds,” Dr. Kremyanskaya said. “When we first started treating patients, we were so impressed, as none of the other drugs we use to treat PV, or any other hematologic malignancy, come anywhere close to this response rate.”
In commenting on the study, Claire Harrison, MD, a professor of myeloproliferative neoplasms and deputy medical director of research at Guy’s and St Thomas’ NHS Foundation Trust in London, agreed that “these data show a strong signal for effectiveness of this therapy in controlling red cell proliferation in PV without inducing iron deficiency and adding to the symptom burden of patients.”
The alternative of phlebotomy “is painful and consumes patient time and hospital resources,” she said in an interview.
Dr. Harrison noted that an earlier signal suggested squamous cell cancer might be of potential concern, but the signal “has not re-emerged [suggesting] this does indeed seem to be a safe and extremely effective therapy.”
Further commenting on the study during the press briefing, Konstanze Döhner, MD, of the University of Ulm (Germany) added that “this is exciting data.”
“For a long time, we had no therapeutic options for PV, and now the field is rapidly developing,” she said.
In ongoing research, rusfertide is currently being studied in the phase 3, placebo-controlled VERIFY randomized trial.
The study was sponsored by Protagonist Therapeutics. Dr. Hoffman reports being on the advisory board for Protagonist Therapeutics, and Dr. Kremyanskaya is a consultant for Protagonist Therapeutics. Dr. Harrison had no disclosures to report.
“The results are surprisingly positive,” said senior author Ronald Hoffman, MD, of the Icahn School of Medicine at Mount Sinai, New York, in discussing the late-breaking research at a press briefing during the European Hematology Association Hybrid Congress 2023.
“Importantly, the study met all of its efficacy endpoints, including the proportion of responders, absence of phlebotomy eligibility, and hematocrit control,” Dr. Hoffman said.
PV, a relatively common clonal myeloproliferative neoplasm, is characterized by uncontrolled erythrocytosis, or excessive production of red blood cells, increasing the risk for serious complications such as thromboembolic and cardiovascular events – the most common causes of morbidity and mortality in this blood cancer.
To treat PV, the maintenance of hematocrit levels at below 45% is critical. However, the current standard of care, therapeutic phlebotomy, with or without cytoreductive agents, falls short in maintaining those lower levels in the majority of patients, Dr. Hoffman explained.
To improve responses, rusfertide was developed as a novel, synthetic form of hepcidin, a peptide hormone that is produced by the liver and functions to maintain iron homeostasis and control the formation of red blood cells.
“This is somewhat of a paradigm shift,” said Dr. Hoffman in the press briefing. “We’re trying to use a hormone made by the liver to control excessive red blood cell production from polycythemia vera.”
For the phase 2 REVIVE study evaluating rusfertide in PV, the authors enrolled 53 patients with PV who had a high phlebotomy burden while receiving the current standard of care. The study’s criteria called for patients to have received at least three therapeutic phlebotomies in the 28 weeks prior to enrollment, with or without concurrent cytoreductive agents.
During a first part of the study, patients received subcutaneous rusfertide once weekly over 28 weeks, during which period the dose was adjusted individually to achieve control of HCT levels below 45%.
The second part was a withdrawal phase extending from weeks 29 to 41, in which patients were randomized in a blinded fashion to either continue on rusfertide (n = 26) or receive a placebo (n = 27).
The patients had a median age of 58; they were 71.7% male, and 54.7% had previously been treated with therapeutic phlebotomy alone while 45.3% received therapeutic phlebotomy plus cytoreductive agents.
Patients were considered to be responders if they met three criteria, including having HCT control without phlebotomy eligibility, no therapeutic phlebotomy, and having completed 12 weeks of treatment.
At the end of the second phase, 69.2% of patients receiving rusfertide were responders versus just 18.5% in the placebo group (P = .0003).
Notably, the improvement with rusfertide was observed among those receiving therapeutic phlebotomy alone, as well as with cytoreductive agents (both P = .02).
Compared with placebo, rusfertide provided significant improvement in measures including the maintenance of response, the absence of the need for therapeutic phlebotomy, and persistent HCT control (P < .0001 for all).
Whereas the phlebotomy-free rate with rusfertide during the dose-finding weeks of 1-17 was 76.9% and in weeks 17-29, 87.3%, the rate increased in part 2 of the study to 92.3%.
Additional symptom benefits reported with rusfertide at week 29 versus baseline in part 1 of the study included significant improvements in concentration (P = .0018), itching (P = .0054), fatigue (P = .0074), and inactivity (P = .0005).
In terms of safety, rusfertide was generally well tolerated, with 83% of treatment-emergent adverse events (TEAEs) being grade 1-2, while 17% were grade 3, and none were grade 4 or 5.
The most common TEAEs consisted of injection-site reactions, which were localized, and grade 1-2 in severity. The incidence of reactions decreased with ongoing treatment. There were only two discontinuations resulting from TEAEs.
Among a total of 70 patients who were enrolled, 52 (74.3%) have continued to receive rusfertide for at least 1 year, 32 (45.7%) for at least 1.5 years, and 10 (14.3%) for at least 2 years, indicating the long-term tolerability of rusfertide.
Further commenting, first author Marina Kremyanskaya, MD, PhD, an assistant professor of medicine, hematology, and medical oncology at the Icahn School of Medicine at Mount Sinai, added that a key benefit is rusfertide’s tolerability with combination therapies, which is important in enabling the avoidance of phlebotomies.
“Many patients on cytoreductive therapies still require phlebotomies, and they can’t tolerate a dose increase, either due to cytopenias or other adverse reactions,” she said in an interview. “So adding rusfertide allows for better control of their hematocrits on a lower dose of their respective cytoreductive drug.”
“The combination treatment thus allows for elimination of phlebotomy requirements and potentially improves their symptoms,” Dr. Kremyanskaya said, adding that “using a lower dose of cytoreductive drug such as interferon or hydroxyurea could offer a symptomatic relief to patients as well.”
Overall, she agreed that the responses are remarkably positive.
“I think this is what is so impressive about this agent – basically everybody responds,” Dr. Kremyanskaya said. “When we first started treating patients, we were so impressed, as none of the other drugs we use to treat PV, or any other hematologic malignancy, come anywhere close to this response rate.”
In commenting on the study, Claire Harrison, MD, a professor of myeloproliferative neoplasms and deputy medical director of research at Guy’s and St Thomas’ NHS Foundation Trust in London, agreed that “these data show a strong signal for effectiveness of this therapy in controlling red cell proliferation in PV without inducing iron deficiency and adding to the symptom burden of patients.”
The alternative of phlebotomy “is painful and consumes patient time and hospital resources,” she said in an interview.
Dr. Harrison noted that an earlier signal suggested squamous cell cancer might be of potential concern, but the signal “has not re-emerged [suggesting] this does indeed seem to be a safe and extremely effective therapy.”
Further commenting on the study during the press briefing, Konstanze Döhner, MD, of the University of Ulm (Germany) added that “this is exciting data.”
“For a long time, we had no therapeutic options for PV, and now the field is rapidly developing,” she said.
In ongoing research, rusfertide is currently being studied in the phase 3, placebo-controlled VERIFY randomized trial.
The study was sponsored by Protagonist Therapeutics. Dr. Hoffman reports being on the advisory board for Protagonist Therapeutics, and Dr. Kremyanskaya is a consultant for Protagonist Therapeutics. Dr. Harrison had no disclosures to report.
“The results are surprisingly positive,” said senior author Ronald Hoffman, MD, of the Icahn School of Medicine at Mount Sinai, New York, in discussing the late-breaking research at a press briefing during the European Hematology Association Hybrid Congress 2023.
“Importantly, the study met all of its efficacy endpoints, including the proportion of responders, absence of phlebotomy eligibility, and hematocrit control,” Dr. Hoffman said.
PV, a relatively common clonal myeloproliferative neoplasm, is characterized by uncontrolled erythrocytosis, or excessive production of red blood cells, increasing the risk for serious complications such as thromboembolic and cardiovascular events – the most common causes of morbidity and mortality in this blood cancer.
To treat PV, the maintenance of hematocrit levels at below 45% is critical. However, the current standard of care, therapeutic phlebotomy, with or without cytoreductive agents, falls short in maintaining those lower levels in the majority of patients, Dr. Hoffman explained.
To improve responses, rusfertide was developed as a novel, synthetic form of hepcidin, a peptide hormone that is produced by the liver and functions to maintain iron homeostasis and control the formation of red blood cells.
“This is somewhat of a paradigm shift,” said Dr. Hoffman in the press briefing. “We’re trying to use a hormone made by the liver to control excessive red blood cell production from polycythemia vera.”
For the phase 2 REVIVE study evaluating rusfertide in PV, the authors enrolled 53 patients with PV who had a high phlebotomy burden while receiving the current standard of care. The study’s criteria called for patients to have received at least three therapeutic phlebotomies in the 28 weeks prior to enrollment, with or without concurrent cytoreductive agents.
During a first part of the study, patients received subcutaneous rusfertide once weekly over 28 weeks, during which period the dose was adjusted individually to achieve control of HCT levels below 45%.
The second part was a withdrawal phase extending from weeks 29 to 41, in which patients were randomized in a blinded fashion to either continue on rusfertide (n = 26) or receive a placebo (n = 27).
The patients had a median age of 58; they were 71.7% male, and 54.7% had previously been treated with therapeutic phlebotomy alone while 45.3% received therapeutic phlebotomy plus cytoreductive agents.
Patients were considered to be responders if they met three criteria, including having HCT control without phlebotomy eligibility, no therapeutic phlebotomy, and having completed 12 weeks of treatment.
At the end of the second phase, 69.2% of patients receiving rusfertide were responders versus just 18.5% in the placebo group (P = .0003).
Notably, the improvement with rusfertide was observed among those receiving therapeutic phlebotomy alone, as well as with cytoreductive agents (both P = .02).
Compared with placebo, rusfertide provided significant improvement in measures including the maintenance of response, the absence of the need for therapeutic phlebotomy, and persistent HCT control (P < .0001 for all).
Whereas the phlebotomy-free rate with rusfertide during the dose-finding weeks of 1-17 was 76.9% and in weeks 17-29, 87.3%, the rate increased in part 2 of the study to 92.3%.
Additional symptom benefits reported with rusfertide at week 29 versus baseline in part 1 of the study included significant improvements in concentration (P = .0018), itching (P = .0054), fatigue (P = .0074), and inactivity (P = .0005).
In terms of safety, rusfertide was generally well tolerated, with 83% of treatment-emergent adverse events (TEAEs) being grade 1-2, while 17% were grade 3, and none were grade 4 or 5.
The most common TEAEs consisted of injection-site reactions, which were localized, and grade 1-2 in severity. The incidence of reactions decreased with ongoing treatment. There were only two discontinuations resulting from TEAEs.
Among a total of 70 patients who were enrolled, 52 (74.3%) have continued to receive rusfertide for at least 1 year, 32 (45.7%) for at least 1.5 years, and 10 (14.3%) for at least 2 years, indicating the long-term tolerability of rusfertide.
Further commenting, first author Marina Kremyanskaya, MD, PhD, an assistant professor of medicine, hematology, and medical oncology at the Icahn School of Medicine at Mount Sinai, added that a key benefit is rusfertide’s tolerability with combination therapies, which is important in enabling the avoidance of phlebotomies.
“Many patients on cytoreductive therapies still require phlebotomies, and they can’t tolerate a dose increase, either due to cytopenias or other adverse reactions,” she said in an interview. “So adding rusfertide allows for better control of their hematocrits on a lower dose of their respective cytoreductive drug.”
“The combination treatment thus allows for elimination of phlebotomy requirements and potentially improves their symptoms,” Dr. Kremyanskaya said, adding that “using a lower dose of cytoreductive drug such as interferon or hydroxyurea could offer a symptomatic relief to patients as well.”
Overall, she agreed that the responses are remarkably positive.
“I think this is what is so impressive about this agent – basically everybody responds,” Dr. Kremyanskaya said. “When we first started treating patients, we were so impressed, as none of the other drugs we use to treat PV, or any other hematologic malignancy, come anywhere close to this response rate.”
In commenting on the study, Claire Harrison, MD, a professor of myeloproliferative neoplasms and deputy medical director of research at Guy’s and St Thomas’ NHS Foundation Trust in London, agreed that “these data show a strong signal for effectiveness of this therapy in controlling red cell proliferation in PV without inducing iron deficiency and adding to the symptom burden of patients.”
The alternative of phlebotomy “is painful and consumes patient time and hospital resources,” she said in an interview.
Dr. Harrison noted that an earlier signal suggested squamous cell cancer might be of potential concern, but the signal “has not re-emerged [suggesting] this does indeed seem to be a safe and extremely effective therapy.”
Further commenting on the study during the press briefing, Konstanze Döhner, MD, of the University of Ulm (Germany) added that “this is exciting data.”
“For a long time, we had no therapeutic options for PV, and now the field is rapidly developing,” she said.
In ongoing research, rusfertide is currently being studied in the phase 3, placebo-controlled VERIFY randomized trial.
The study was sponsored by Protagonist Therapeutics. Dr. Hoffman reports being on the advisory board for Protagonist Therapeutics, and Dr. Kremyanskaya is a consultant for Protagonist Therapeutics. Dr. Harrison had no disclosures to report.
FROM EHA 2023
FDA warns of tattoo ink tied to dangerous infections
The Food and Drug Administration draft guidance released recently on possible contamination of tattoo ink was not concerning Whitney Donohue, 34, owner of Forget Me Not Tattoo in Billings, Mont.
“I get our ink directly through the manufacturer – not at a store or through Amazon or eBay,” she said. “You never know if it’s going to be repackaged.”
Tattoo artists themselves, she said, regulate the quality of ink they use.
Still, the threat is real, said Bruce Brod, MD, a clinical professor of dermatology at the University of Pennsylvania Health System. “I’ve seen several different infections from tattooing, and they are from organisms that tend to contaminate things in damp, liquid-type environments.”
, dermatologists said.
“Tattooing involves puncturing the epidermis about 100 times per second with needles and depositing ink 1.5 to 2 millimeters below the surface of the skin, deep into the dermis,” the guidance states. “Contaminated tattoo ink can cause infections and serious injuries. Because these inks are injected, pathogens or other harmful substances in these inks can travel from the injection site through the blood and lymphatic systems to other parts of the body.”
The guidance comes as body art continues to get more popular. According to a 2019 poll, 30% of Americans had at least one tattoo – up from 21% in 2012. Forty percent of people 18-34 and 36% of those ages 35-54 had at least one tattoo. And though they are commonplace, tattoos come with medical risks that should be known beforehand, doctors said.
Commonly reported symptoms of tattoo ink–associated infections include rashes, blisters, painful nodules, and severe abscesses. One of the most common bacteria found in contaminated tattoo ink is nontuberculous mycobacteria, which is related to the bacteria that causes tuberculosis and can be found in soil and water.
The guidance lists several unsanitary manufacturing conditions that may lead to ink contamination, including:
- Preparing or packing of tattoo inks in facilities that are hard to sanitize, such as carpeted areas
- Ink or ink components left uncovered, especially near open air ducts
- Unsanitary mixing of tattoo inks, including with unclean utensils or containers
- Lack of appropriate attire by staff, failure to use hairnets, lab coats, aprons, gowns, masks, or gloves
“Infections will often spread along the drainage channels in the skin and create squiggly, uneven lines of big red, lumpy nodules,” Dr. Brod said.
Between 2003 and 2023, there were 18 recalls of tattoo inks that were contaminated with various microorganisms, according to the FDA. In May 2019, the FDA issued a safety alert advising consumers, tattoo artists, and retailers to avoid using or selling certain tattoo inks contaminated with microorganisms.
Reputable ink manufacturers use a process called gamma radiation, which refers to electromagnetic radiation of high frequencies to kill microorganisms in the ink and its packaging.
Most of the trustworthy, high-quality ink manufacturers are well-known among tattoo artists, Ms. Donohue said.
While she has seen customers with sensitive skin have allergic reactions, she has not seen someone come back with an infection in her 9 years working in the tattoo industry.
Because tattoo ink is considered a cosmetic product, there is not much regulatory oversight involved, which means the sterility and quality of ingredients vary, said Teo Soleymani, MD, an assistant clinical professor of dermatology and dermatological surgery at the UCLA David Geffen School of Medicine.
“Cosmeceuticals aren’t regulated by the FDA like prescription medication,” he said. “What we’ve seen many times is inadvertent contamination during the application process or contamination while the inks are being made.”
In years past, unclean needles spreading hepatitis and HIV were more of a concern, but those rates have dropped significantly, Dr. Soleymani said.
The infections that have increased are from rare bacteria that exist in stagnant water. And they are injected into a part of the body that allows them to evade the immune system, he said: shallow enough that there aren’t many associated blood vessels, but not still below the layer of skin that gets sloughed off every 28 days.
Sometimes, antibiotics alone won’t cut it, and the tattoo will require surgical removal.
“The aesthetic you were going for has to be not only removed, but you’re left with a surgical scar,” Dr. Soleymani said. “Tattoos can be beautiful, but they can come with unwanted visitors that can cause months of misery.”
A version of this article first appeared on WebMD.com.
The Food and Drug Administration draft guidance released recently on possible contamination of tattoo ink was not concerning Whitney Donohue, 34, owner of Forget Me Not Tattoo in Billings, Mont.
“I get our ink directly through the manufacturer – not at a store or through Amazon or eBay,” she said. “You never know if it’s going to be repackaged.”
Tattoo artists themselves, she said, regulate the quality of ink they use.
Still, the threat is real, said Bruce Brod, MD, a clinical professor of dermatology at the University of Pennsylvania Health System. “I’ve seen several different infections from tattooing, and they are from organisms that tend to contaminate things in damp, liquid-type environments.”
, dermatologists said.
“Tattooing involves puncturing the epidermis about 100 times per second with needles and depositing ink 1.5 to 2 millimeters below the surface of the skin, deep into the dermis,” the guidance states. “Contaminated tattoo ink can cause infections and serious injuries. Because these inks are injected, pathogens or other harmful substances in these inks can travel from the injection site through the blood and lymphatic systems to other parts of the body.”
The guidance comes as body art continues to get more popular. According to a 2019 poll, 30% of Americans had at least one tattoo – up from 21% in 2012. Forty percent of people 18-34 and 36% of those ages 35-54 had at least one tattoo. And though they are commonplace, tattoos come with medical risks that should be known beforehand, doctors said.
Commonly reported symptoms of tattoo ink–associated infections include rashes, blisters, painful nodules, and severe abscesses. One of the most common bacteria found in contaminated tattoo ink is nontuberculous mycobacteria, which is related to the bacteria that causes tuberculosis and can be found in soil and water.
The guidance lists several unsanitary manufacturing conditions that may lead to ink contamination, including:
- Preparing or packing of tattoo inks in facilities that are hard to sanitize, such as carpeted areas
- Ink or ink components left uncovered, especially near open air ducts
- Unsanitary mixing of tattoo inks, including with unclean utensils or containers
- Lack of appropriate attire by staff, failure to use hairnets, lab coats, aprons, gowns, masks, or gloves
“Infections will often spread along the drainage channels in the skin and create squiggly, uneven lines of big red, lumpy nodules,” Dr. Brod said.
Between 2003 and 2023, there were 18 recalls of tattoo inks that were contaminated with various microorganisms, according to the FDA. In May 2019, the FDA issued a safety alert advising consumers, tattoo artists, and retailers to avoid using or selling certain tattoo inks contaminated with microorganisms.
Reputable ink manufacturers use a process called gamma radiation, which refers to electromagnetic radiation of high frequencies to kill microorganisms in the ink and its packaging.
Most of the trustworthy, high-quality ink manufacturers are well-known among tattoo artists, Ms. Donohue said.
While she has seen customers with sensitive skin have allergic reactions, she has not seen someone come back with an infection in her 9 years working in the tattoo industry.
Because tattoo ink is considered a cosmetic product, there is not much regulatory oversight involved, which means the sterility and quality of ingredients vary, said Teo Soleymani, MD, an assistant clinical professor of dermatology and dermatological surgery at the UCLA David Geffen School of Medicine.
“Cosmeceuticals aren’t regulated by the FDA like prescription medication,” he said. “What we’ve seen many times is inadvertent contamination during the application process or contamination while the inks are being made.”
In years past, unclean needles spreading hepatitis and HIV were more of a concern, but those rates have dropped significantly, Dr. Soleymani said.
The infections that have increased are from rare bacteria that exist in stagnant water. And they are injected into a part of the body that allows them to evade the immune system, he said: shallow enough that there aren’t many associated blood vessels, but not still below the layer of skin that gets sloughed off every 28 days.
Sometimes, antibiotics alone won’t cut it, and the tattoo will require surgical removal.
“The aesthetic you were going for has to be not only removed, but you’re left with a surgical scar,” Dr. Soleymani said. “Tattoos can be beautiful, but they can come with unwanted visitors that can cause months of misery.”
A version of this article first appeared on WebMD.com.
The Food and Drug Administration draft guidance released recently on possible contamination of tattoo ink was not concerning Whitney Donohue, 34, owner of Forget Me Not Tattoo in Billings, Mont.
“I get our ink directly through the manufacturer – not at a store or through Amazon or eBay,” she said. “You never know if it’s going to be repackaged.”
Tattoo artists themselves, she said, regulate the quality of ink they use.
Still, the threat is real, said Bruce Brod, MD, a clinical professor of dermatology at the University of Pennsylvania Health System. “I’ve seen several different infections from tattooing, and they are from organisms that tend to contaminate things in damp, liquid-type environments.”
, dermatologists said.
“Tattooing involves puncturing the epidermis about 100 times per second with needles and depositing ink 1.5 to 2 millimeters below the surface of the skin, deep into the dermis,” the guidance states. “Contaminated tattoo ink can cause infections and serious injuries. Because these inks are injected, pathogens or other harmful substances in these inks can travel from the injection site through the blood and lymphatic systems to other parts of the body.”
The guidance comes as body art continues to get more popular. According to a 2019 poll, 30% of Americans had at least one tattoo – up from 21% in 2012. Forty percent of people 18-34 and 36% of those ages 35-54 had at least one tattoo. And though they are commonplace, tattoos come with medical risks that should be known beforehand, doctors said.
Commonly reported symptoms of tattoo ink–associated infections include rashes, blisters, painful nodules, and severe abscesses. One of the most common bacteria found in contaminated tattoo ink is nontuberculous mycobacteria, which is related to the bacteria that causes tuberculosis and can be found in soil and water.
The guidance lists several unsanitary manufacturing conditions that may lead to ink contamination, including:
- Preparing or packing of tattoo inks in facilities that are hard to sanitize, such as carpeted areas
- Ink or ink components left uncovered, especially near open air ducts
- Unsanitary mixing of tattoo inks, including with unclean utensils or containers
- Lack of appropriate attire by staff, failure to use hairnets, lab coats, aprons, gowns, masks, or gloves
“Infections will often spread along the drainage channels in the skin and create squiggly, uneven lines of big red, lumpy nodules,” Dr. Brod said.
Between 2003 and 2023, there were 18 recalls of tattoo inks that were contaminated with various microorganisms, according to the FDA. In May 2019, the FDA issued a safety alert advising consumers, tattoo artists, and retailers to avoid using or selling certain tattoo inks contaminated with microorganisms.
Reputable ink manufacturers use a process called gamma radiation, which refers to electromagnetic radiation of high frequencies to kill microorganisms in the ink and its packaging.
Most of the trustworthy, high-quality ink manufacturers are well-known among tattoo artists, Ms. Donohue said.
While she has seen customers with sensitive skin have allergic reactions, she has not seen someone come back with an infection in her 9 years working in the tattoo industry.
Because tattoo ink is considered a cosmetic product, there is not much regulatory oversight involved, which means the sterility and quality of ingredients vary, said Teo Soleymani, MD, an assistant clinical professor of dermatology and dermatological surgery at the UCLA David Geffen School of Medicine.
“Cosmeceuticals aren’t regulated by the FDA like prescription medication,” he said. “What we’ve seen many times is inadvertent contamination during the application process or contamination while the inks are being made.”
In years past, unclean needles spreading hepatitis and HIV were more of a concern, but those rates have dropped significantly, Dr. Soleymani said.
The infections that have increased are from rare bacteria that exist in stagnant water. And they are injected into a part of the body that allows them to evade the immune system, he said: shallow enough that there aren’t many associated blood vessels, but not still below the layer of skin that gets sloughed off every 28 days.
Sometimes, antibiotics alone won’t cut it, and the tattoo will require surgical removal.
“The aesthetic you were going for has to be not only removed, but you’re left with a surgical scar,” Dr. Soleymani said. “Tattoos can be beautiful, but they can come with unwanted visitors that can cause months of misery.”
A version of this article first appeared on WebMD.com.
PCOS associated with shorter lifespan
CHICAGO –
In the study, involving nearly 10,000 women with PCOS and matched controls from Finland, women with PCOS died on average a year earlier than their age-matched counterparts, primarily from diseases of the circulatory system, cancer, and diabetes.
PCOS is the most common endocrine disorder of reproductive-age women, of whom about 50%-70% also have obesity.
“I think we need to acknowledge that this is a health burden and not just a reproductive problem. In many cases we deal with the reproductive problem, and then these women are left alone. … So I think the message is we need to look beyond the reproductive outcomes, which are … really good. We can manage that,” said Terhi T. Piltonen, MD, PhD, during a press briefing held June 15 at the annual meeting of the Endocrine Society.
“I think the difficult part is [managing] the lifelong health for these women and supporting them to achieve the best health they can get. We need a multidisciplinary effort and to put more resources into the research,” added Dr. Piltonen, professor in the departments of ob.gyn. and reproductive endocrinology at the University of Oulu, Finland.
Indeed, Punith Kempegowda, MD, PhD, of the University of Birmingham (England) observed: “In our medical schools in the U.K., over 5 years, students get 45 minutes [of education] on PCOS, and they’re expected to learn about it.”
And over the last 20 years, funding for research into the condition has totaled less than a half percent of overall medical funding. “And we’re talking about 10% of all women. …We need to acknowledge it and educate people more. We need more published studies to understand more about it,” he noted.
Asked to comment, Greg Dodell, MD, owner and president of Central Park Endocrinology, New York, said: “PCOS is about a lot more than fertility, and that may not be the goal or on the mind of a woman at the time they start having symptoms of PCOS or get the diagnosis.”
“PCOS is largely a metabolic condition rooted in insulin resistance, and therefore, the potential clinical outcomes, including mortality, are important to recognize.”
Dr. Dodell, who has a special interest in PCOS, advised that, for women with the condition, “focus on reducing insulin resistance with health-promoting behaviors and medications as needed. Data demonstrate that improving fitness, irrespective of a change in weight, can improve metabolic markers.” And, he advised that these women be routinely screened for mental health issues.
He also noted, “PCOS occurs across the size spectrum, but those patients in larger bodies may face weight stigma which has negative health consequences. These patients may avoid going to doctors for routine health screenings, so it is an important issue to continue to address.”
Women with PCOS lose a year of life
The new data come from 9,839 women with PCOS and 70,705 age- and region-matched controls from the Finnish Care Register for Health Care. The group with PCOS had been diagnosed at a mean age of 27 years.
The mean follow-up time was 13.1 years in both groups, during which 1,003 controls and 177 women with PCOS died. The mean age at death was 51.4 years for the PCOS group versus 52.6 years for the control women, a significant difference (P < .001).
Causes of death that were significantly higher among the women with PCOS versus controls after adjustments were cancer (hazard ratio, 1.39), and diseases of the circulatory system (1.68).
In more specific subcategories, after adjustment for education, the women with PCOS had increased mortality from nonischemic diseases, such as hypertensive heart disease, pulmonary embolism, etc. (HR, 2.06), and diabetes (HR, 2.85).
One study limitation was the inability to adjust for body mass index, Dr. Piltonen noted.
Dr. Piltonen, Dr. Kempegowda, and Dr. Dodell have no disclosures.
CHICAGO –
In the study, involving nearly 10,000 women with PCOS and matched controls from Finland, women with PCOS died on average a year earlier than their age-matched counterparts, primarily from diseases of the circulatory system, cancer, and diabetes.
PCOS is the most common endocrine disorder of reproductive-age women, of whom about 50%-70% also have obesity.
“I think we need to acknowledge that this is a health burden and not just a reproductive problem. In many cases we deal with the reproductive problem, and then these women are left alone. … So I think the message is we need to look beyond the reproductive outcomes, which are … really good. We can manage that,” said Terhi T. Piltonen, MD, PhD, during a press briefing held June 15 at the annual meeting of the Endocrine Society.
“I think the difficult part is [managing] the lifelong health for these women and supporting them to achieve the best health they can get. We need a multidisciplinary effort and to put more resources into the research,” added Dr. Piltonen, professor in the departments of ob.gyn. and reproductive endocrinology at the University of Oulu, Finland.
Indeed, Punith Kempegowda, MD, PhD, of the University of Birmingham (England) observed: “In our medical schools in the U.K., over 5 years, students get 45 minutes [of education] on PCOS, and they’re expected to learn about it.”
And over the last 20 years, funding for research into the condition has totaled less than a half percent of overall medical funding. “And we’re talking about 10% of all women. …We need to acknowledge it and educate people more. We need more published studies to understand more about it,” he noted.
Asked to comment, Greg Dodell, MD, owner and president of Central Park Endocrinology, New York, said: “PCOS is about a lot more than fertility, and that may not be the goal or on the mind of a woman at the time they start having symptoms of PCOS or get the diagnosis.”
“PCOS is largely a metabolic condition rooted in insulin resistance, and therefore, the potential clinical outcomes, including mortality, are important to recognize.”
Dr. Dodell, who has a special interest in PCOS, advised that, for women with the condition, “focus on reducing insulin resistance with health-promoting behaviors and medications as needed. Data demonstrate that improving fitness, irrespective of a change in weight, can improve metabolic markers.” And, he advised that these women be routinely screened for mental health issues.
He also noted, “PCOS occurs across the size spectrum, but those patients in larger bodies may face weight stigma which has negative health consequences. These patients may avoid going to doctors for routine health screenings, so it is an important issue to continue to address.”
Women with PCOS lose a year of life
The new data come from 9,839 women with PCOS and 70,705 age- and region-matched controls from the Finnish Care Register for Health Care. The group with PCOS had been diagnosed at a mean age of 27 years.
The mean follow-up time was 13.1 years in both groups, during which 1,003 controls and 177 women with PCOS died. The mean age at death was 51.4 years for the PCOS group versus 52.6 years for the control women, a significant difference (P < .001).
Causes of death that were significantly higher among the women with PCOS versus controls after adjustments were cancer (hazard ratio, 1.39), and diseases of the circulatory system (1.68).
In more specific subcategories, after adjustment for education, the women with PCOS had increased mortality from nonischemic diseases, such as hypertensive heart disease, pulmonary embolism, etc. (HR, 2.06), and diabetes (HR, 2.85).
One study limitation was the inability to adjust for body mass index, Dr. Piltonen noted.
Dr. Piltonen, Dr. Kempegowda, and Dr. Dodell have no disclosures.
CHICAGO –
In the study, involving nearly 10,000 women with PCOS and matched controls from Finland, women with PCOS died on average a year earlier than their age-matched counterparts, primarily from diseases of the circulatory system, cancer, and diabetes.
PCOS is the most common endocrine disorder of reproductive-age women, of whom about 50%-70% also have obesity.
“I think we need to acknowledge that this is a health burden and not just a reproductive problem. In many cases we deal with the reproductive problem, and then these women are left alone. … So I think the message is we need to look beyond the reproductive outcomes, which are … really good. We can manage that,” said Terhi T. Piltonen, MD, PhD, during a press briefing held June 15 at the annual meeting of the Endocrine Society.
“I think the difficult part is [managing] the lifelong health for these women and supporting them to achieve the best health they can get. We need a multidisciplinary effort and to put more resources into the research,” added Dr. Piltonen, professor in the departments of ob.gyn. and reproductive endocrinology at the University of Oulu, Finland.
Indeed, Punith Kempegowda, MD, PhD, of the University of Birmingham (England) observed: “In our medical schools in the U.K., over 5 years, students get 45 minutes [of education] on PCOS, and they’re expected to learn about it.”
And over the last 20 years, funding for research into the condition has totaled less than a half percent of overall medical funding. “And we’re talking about 10% of all women. …We need to acknowledge it and educate people more. We need more published studies to understand more about it,” he noted.
Asked to comment, Greg Dodell, MD, owner and president of Central Park Endocrinology, New York, said: “PCOS is about a lot more than fertility, and that may not be the goal or on the mind of a woman at the time they start having symptoms of PCOS or get the diagnosis.”
“PCOS is largely a metabolic condition rooted in insulin resistance, and therefore, the potential clinical outcomes, including mortality, are important to recognize.”
Dr. Dodell, who has a special interest in PCOS, advised that, for women with the condition, “focus on reducing insulin resistance with health-promoting behaviors and medications as needed. Data demonstrate that improving fitness, irrespective of a change in weight, can improve metabolic markers.” And, he advised that these women be routinely screened for mental health issues.
He also noted, “PCOS occurs across the size spectrum, but those patients in larger bodies may face weight stigma which has negative health consequences. These patients may avoid going to doctors for routine health screenings, so it is an important issue to continue to address.”
Women with PCOS lose a year of life
The new data come from 9,839 women with PCOS and 70,705 age- and region-matched controls from the Finnish Care Register for Health Care. The group with PCOS had been diagnosed at a mean age of 27 years.
The mean follow-up time was 13.1 years in both groups, during which 1,003 controls and 177 women with PCOS died. The mean age at death was 51.4 years for the PCOS group versus 52.6 years for the control women, a significant difference (P < .001).
Causes of death that were significantly higher among the women with PCOS versus controls after adjustments were cancer (hazard ratio, 1.39), and diseases of the circulatory system (1.68).
In more specific subcategories, after adjustment for education, the women with PCOS had increased mortality from nonischemic diseases, such as hypertensive heart disease, pulmonary embolism, etc. (HR, 2.06), and diabetes (HR, 2.85).
One study limitation was the inability to adjust for body mass index, Dr. Piltonen noted.
Dr. Piltonen, Dr. Kempegowda, and Dr. Dodell have no disclosures.
AT ENDO 2023
Cancer drug shortages spur worry, rationing, and tough choices
CHICAGO – Oncologist Denise Yardley, MD, isn’t used to expressing uncertainty when she tells patients about what’s in store for them in terms of drug treatment. But things are dramatically different now amid a severe national shortage of carboplatin and cisplatin, two common and crucial cancer drugs.
“There’s a regimen I’m thinking about,” Dr. Yardley told a new patient recently, “but we’ll have to wait until you finish your staging evaluation to see whether I can deliver this. Another regimen that’s a little more toxic is my second choice.” And, she added, the alternative chemotherapy treatment – anthracycline instead of carboplatin – requires a longer treatment period.
This ambiguity is hardly ideal, said Dr. Yardley, of Tennessee Oncology and Sarah Cannon Research Institute in Nashville. “It’s another factor in being overwhelmed in a first-time visit and wanting to know the details about what your treatment is going to look like. You’re not walking out knowing exactly what you’re going to take or the exact timing so you can start mapping out your calendar and work schedule.”
This kind of scenario is becoming all too familiar this spring, according to oncologists who gathered at the annual meeting of the American Society of Clinical Oncology (ASCO). In interviews, these physicians said the limited supply of multiple cancer drugs – including the chemotherapies carboplatin and cisplatin – is having an unprecedented negative effect since their use is so widespread in cancer care.
“Every patient could get impacted. That’s why we need to address this sooner rather than later,” said oncologist Aditya Baria, MBBS, MPH, director of the Breast Cancer Research Program at Massachusetts General Hospital, Boston.
Shortages of cancer drugs are not unusual. Three-quarters of oncology pharmacists at 68 organizations surveyed from 2019 to 2020 said shortages prompted treatment delays, reduced doses, or alternative regimens. But the current shortages are having a much wider impact.
The National Comprehensive Cancer Network recently reported that 93% of 27 member institutions surveyed in late May are short on carboplatin, and 70% have reported a shortage of cisplatin. Plus, 20% of 19 centers said they weren’t able to continue carboplatin regimens for all patients.
The drugs are mainstays of multiple types of treatment for a long list of cancer types including lung, breast, gynecologic, and many others.
Several scenarios are possible when the drugs are in short supply, said Dr. Yardley, who noted that the shortage is more severe than any she’s seen in her medical career of more than 3 decades. Patients may need to be switched to regimens with more side effects, even when they’re in the middle of a treatment, she said. Or patients might have to go longer between treatments.
In some cases, Dr. Yardley said, the shortage is forcing patients to go without an important component of a larger combination therapy regimen. “The Keynote 522 neoadjuvant regimen for triple-negative breast cancer has carboplatin given with Taxol [paclitaxel] and Keytruda [pembrolizumab]. We are just deleting the carboplatin.”
She added that carboplatin is part of the following so-called TCHP regimen for HER2+ early-stage breast cancer: Taxotere (docetaxel), carboplatin, Herceptin (trastuzumab), and Perjeta (pertuzumab).
“You can delete [carboplatin] or consider substituting cyclophosphamide for carboplatin,” she said. But she cautioned the Keynote 522 and TCHP regimens haven’t been tested without carboplatin in curative-intent trials.
At Duke University in Durham, N.C., doses of carboplatin for many patients are being lowered by a third to the level that’s commonly used for older and frail patients, said oncologist Arif Kamal, MD, MBA, MHS, who works at the academic center and is the chief patient officer at the American Cancer Society.
“We don’t know if [the lower doses will negatively affect cancer patients’ outcomes]. What’s amazing is how many patients [are understanding about having to take smaller amounts of the chemotherapy],” he said.
Medical organizations are offering guidance. The Society of Gynecologic Oncology, for example, in late April recommended that oncologists increase intervals between chemotherapy treatments when appropriate, round down vial sizes to ensure “efficient use,” and eliminate or minimize use of cisplatin and carboplatin in certain platinum-resistant cancers.
In early June, ASCO published guidance regarding alternatives to cisplatin, carboplatin, and 5-fluorouracil, which is also in short supply, in gastrointestinal cancer. As the guidance notes, some alternatives are more untested or more toxic than ideal treatments.
In addition, ASCO has a webpage devoted to news and resources about shortages of cancer drugs. It offers drug availability updates, general guidance, and breast cancer guidance. ASCO also offers ethical guidance about handling drug shortages.
Patients in clinical trials and those who hope to join them are especially vulnerable to the drug shortage, oncologists interviewed for this story said. Cisplatin and carboplatin are the backbones of many clinical trials, Dr. Yardley said. “When you can’t supply a drug in one of the [trial] arms, that puts the whole trial on pause.”
Even clinics that have managed to find adequate supplies of the drugs are planning for when they run out.
“Our institution and other institutions are trying to come up with a rationing protocol, deciding which patients are going to get access, and which ones have reasonable alternatives,” radiation oncologist Corey Speers MD, PhD, of University Hospitals Seidman Cancer Center and Case Western Reserve University, Cleveland, said in an interview. “In some settings, there really isn’t an effective alternative. Or the alternatives are tens of thousands of dollars more expensive.”
Oncologists also noted that cisplatin and carboplatin aren’t the only cancer drugs in short supply.
“Methotrexate is critically low, and 5FU [fluorouracil] is critically low,” Dr. Yardley said, referring to drugs that each treat several types of cancer. According to the May NCNN survey, 67% of respondents reported low supplies of methotrexate, and 26% said they were low on 5FU.
“Viscous lidocaine is a component of many supportive care mouth rinses for the stomatitis caused by our drugs but is not available at all,” Dr. Yardley said.
She added that there are also low supplies of fludarabine, which is used to treat chronic lymphocytic lymphom; clofarabine, which is used to treat acute lymphoblastic leukemia; and rasburicase, which is used to treat high levels of uric acid in patients on chemotherapy.
Dr. Speers said his institution is facing a shortage of capecitabine, which is used to treat several types of cancer.
“Numerous trials have demonstrated the improved, safety, efficacy, and convenience of oral capecitabine. With the shortage we’re having to use infusional 5FU, which not only is less convenient but also ends up being more costly and requires infusion room space or continuous infusion pumps. This impacts our ability to treat cancer patients,” he said. “Our capacity is becoming more limited to accommodate these added patients, and we have to use infusional formulations of a drug that previously was readily available via an oral formulation. Patients and caregivers now have to come to the cancer center for appointments and infusions that previously weren’t needed as they could take an oral pill.”
Dr. Speers added that his institution is rationing methotrexate. “We are now prioritizing patients being treated with curative intent and adjusting protocols to use the lowest allowable doses to conserve supply,” he said.
The roots of the platinum chemotherapy drug shortage link back to the India-based Intas Pharmaceuticals company, a major manufacturer of cisplatin and carboplatin. According to Kellyann Zuzulo, spokeperson for Accord Healthcare, an Instas U.S. subsidiary, a facility inspection in December 2022 prompted a decision to temporarily stop making the drugs. The inspection identified multiple problems.
“Intas and Accord are working with the FDA on a plan to return to manufacturing,” Ms. Zuzulo said in an interview. “This will allow for continued production of products that will be prioritized based on medical necessity. A date has not yet been confirmed in which the facility will return to manufacturing for cisplatin, carboplatin or any other products.”
Ms. Zuzulo said the company is not a health care provider and cannot offer advice to patients about alternatives.
Other companies that make cisplatin and carboplatin have also reported shortages. In interviews, representatives for Fresenius Kabi and Pfizer said the companies have limited supplies because of increased demand – not because of manufacturing problems.
On June 12, the American Society of Health-System Pharmacists (ASHP) reported that carboplatin remains in short supply, with all five companies that sell the drug listed as having limited or back-ordered supplies. Cisplatin is also in short supply, the organization reported in a June 9 update, although some is available.
In a June 12 update on methotrexate, ASHP said manufacturing delays at Accord have caused a shortage, and other companies are running low due to increased demand.
As for the future, Congress and the Biden administration, according to a report by Bloomberg, are trying to figure out what to do regarding shortages of cheap generic drugs such as cisplatin and carboplatin. The FDA is exploring a partnership with a Chinese drugmaker to make cisplatin, NBC News reported.
However, fixes will be challenging, according to former FDA commissioner and Pfizer board member, Scott Gottlieb, MD.
“This generic business, particularly for these complex drugs, these complex formulations, is not a healthy business right now. Yet it’s a vital business from a public standpoint,” he told CBS News.
In an interview, Dr. Kamal said that there is even talk about boosting the prices of cheap generic drugs “to ensure that there’s enough incentive for multiple manufacturers to be involved.”
Dr. Kamal said he is crossing his fingers that cutting chemotherapy doses at his clinic doesn’t result in worse outcomes for his patients.
“Right now, I think dropping someone by 25% or 30% is okay. And for some patients, particularly in a curative setting, we try to keep them at as much as 100% as possible. But there’s just a lot of unknowns,” he said.
CHICAGO – Oncologist Denise Yardley, MD, isn’t used to expressing uncertainty when she tells patients about what’s in store for them in terms of drug treatment. But things are dramatically different now amid a severe national shortage of carboplatin and cisplatin, two common and crucial cancer drugs.
“There’s a regimen I’m thinking about,” Dr. Yardley told a new patient recently, “but we’ll have to wait until you finish your staging evaluation to see whether I can deliver this. Another regimen that’s a little more toxic is my second choice.” And, she added, the alternative chemotherapy treatment – anthracycline instead of carboplatin – requires a longer treatment period.
This ambiguity is hardly ideal, said Dr. Yardley, of Tennessee Oncology and Sarah Cannon Research Institute in Nashville. “It’s another factor in being overwhelmed in a first-time visit and wanting to know the details about what your treatment is going to look like. You’re not walking out knowing exactly what you’re going to take or the exact timing so you can start mapping out your calendar and work schedule.”
This kind of scenario is becoming all too familiar this spring, according to oncologists who gathered at the annual meeting of the American Society of Clinical Oncology (ASCO). In interviews, these physicians said the limited supply of multiple cancer drugs – including the chemotherapies carboplatin and cisplatin – is having an unprecedented negative effect since their use is so widespread in cancer care.
“Every patient could get impacted. That’s why we need to address this sooner rather than later,” said oncologist Aditya Baria, MBBS, MPH, director of the Breast Cancer Research Program at Massachusetts General Hospital, Boston.
Shortages of cancer drugs are not unusual. Three-quarters of oncology pharmacists at 68 organizations surveyed from 2019 to 2020 said shortages prompted treatment delays, reduced doses, or alternative regimens. But the current shortages are having a much wider impact.
The National Comprehensive Cancer Network recently reported that 93% of 27 member institutions surveyed in late May are short on carboplatin, and 70% have reported a shortage of cisplatin. Plus, 20% of 19 centers said they weren’t able to continue carboplatin regimens for all patients.
The drugs are mainstays of multiple types of treatment for a long list of cancer types including lung, breast, gynecologic, and many others.
Several scenarios are possible when the drugs are in short supply, said Dr. Yardley, who noted that the shortage is more severe than any she’s seen in her medical career of more than 3 decades. Patients may need to be switched to regimens with more side effects, even when they’re in the middle of a treatment, she said. Or patients might have to go longer between treatments.
In some cases, Dr. Yardley said, the shortage is forcing patients to go without an important component of a larger combination therapy regimen. “The Keynote 522 neoadjuvant regimen for triple-negative breast cancer has carboplatin given with Taxol [paclitaxel] and Keytruda [pembrolizumab]. We are just deleting the carboplatin.”
She added that carboplatin is part of the following so-called TCHP regimen for HER2+ early-stage breast cancer: Taxotere (docetaxel), carboplatin, Herceptin (trastuzumab), and Perjeta (pertuzumab).
“You can delete [carboplatin] or consider substituting cyclophosphamide for carboplatin,” she said. But she cautioned the Keynote 522 and TCHP regimens haven’t been tested without carboplatin in curative-intent trials.
At Duke University in Durham, N.C., doses of carboplatin for many patients are being lowered by a third to the level that’s commonly used for older and frail patients, said oncologist Arif Kamal, MD, MBA, MHS, who works at the academic center and is the chief patient officer at the American Cancer Society.
“We don’t know if [the lower doses will negatively affect cancer patients’ outcomes]. What’s amazing is how many patients [are understanding about having to take smaller amounts of the chemotherapy],” he said.
Medical organizations are offering guidance. The Society of Gynecologic Oncology, for example, in late April recommended that oncologists increase intervals between chemotherapy treatments when appropriate, round down vial sizes to ensure “efficient use,” and eliminate or minimize use of cisplatin and carboplatin in certain platinum-resistant cancers.
In early June, ASCO published guidance regarding alternatives to cisplatin, carboplatin, and 5-fluorouracil, which is also in short supply, in gastrointestinal cancer. As the guidance notes, some alternatives are more untested or more toxic than ideal treatments.
In addition, ASCO has a webpage devoted to news and resources about shortages of cancer drugs. It offers drug availability updates, general guidance, and breast cancer guidance. ASCO also offers ethical guidance about handling drug shortages.
Patients in clinical trials and those who hope to join them are especially vulnerable to the drug shortage, oncologists interviewed for this story said. Cisplatin and carboplatin are the backbones of many clinical trials, Dr. Yardley said. “When you can’t supply a drug in one of the [trial] arms, that puts the whole trial on pause.”
Even clinics that have managed to find adequate supplies of the drugs are planning for when they run out.
“Our institution and other institutions are trying to come up with a rationing protocol, deciding which patients are going to get access, and which ones have reasonable alternatives,” radiation oncologist Corey Speers MD, PhD, of University Hospitals Seidman Cancer Center and Case Western Reserve University, Cleveland, said in an interview. “In some settings, there really isn’t an effective alternative. Or the alternatives are tens of thousands of dollars more expensive.”
Oncologists also noted that cisplatin and carboplatin aren’t the only cancer drugs in short supply.
“Methotrexate is critically low, and 5FU [fluorouracil] is critically low,” Dr. Yardley said, referring to drugs that each treat several types of cancer. According to the May NCNN survey, 67% of respondents reported low supplies of methotrexate, and 26% said they were low on 5FU.
“Viscous lidocaine is a component of many supportive care mouth rinses for the stomatitis caused by our drugs but is not available at all,” Dr. Yardley said.
She added that there are also low supplies of fludarabine, which is used to treat chronic lymphocytic lymphom; clofarabine, which is used to treat acute lymphoblastic leukemia; and rasburicase, which is used to treat high levels of uric acid in patients on chemotherapy.
Dr. Speers said his institution is facing a shortage of capecitabine, which is used to treat several types of cancer.
“Numerous trials have demonstrated the improved, safety, efficacy, and convenience of oral capecitabine. With the shortage we’re having to use infusional 5FU, which not only is less convenient but also ends up being more costly and requires infusion room space or continuous infusion pumps. This impacts our ability to treat cancer patients,” he said. “Our capacity is becoming more limited to accommodate these added patients, and we have to use infusional formulations of a drug that previously was readily available via an oral formulation. Patients and caregivers now have to come to the cancer center for appointments and infusions that previously weren’t needed as they could take an oral pill.”
Dr. Speers added that his institution is rationing methotrexate. “We are now prioritizing patients being treated with curative intent and adjusting protocols to use the lowest allowable doses to conserve supply,” he said.
The roots of the platinum chemotherapy drug shortage link back to the India-based Intas Pharmaceuticals company, a major manufacturer of cisplatin and carboplatin. According to Kellyann Zuzulo, spokeperson for Accord Healthcare, an Instas U.S. subsidiary, a facility inspection in December 2022 prompted a decision to temporarily stop making the drugs. The inspection identified multiple problems.
“Intas and Accord are working with the FDA on a plan to return to manufacturing,” Ms. Zuzulo said in an interview. “This will allow for continued production of products that will be prioritized based on medical necessity. A date has not yet been confirmed in which the facility will return to manufacturing for cisplatin, carboplatin or any other products.”
Ms. Zuzulo said the company is not a health care provider and cannot offer advice to patients about alternatives.
Other companies that make cisplatin and carboplatin have also reported shortages. In interviews, representatives for Fresenius Kabi and Pfizer said the companies have limited supplies because of increased demand – not because of manufacturing problems.
On June 12, the American Society of Health-System Pharmacists (ASHP) reported that carboplatin remains in short supply, with all five companies that sell the drug listed as having limited or back-ordered supplies. Cisplatin is also in short supply, the organization reported in a June 9 update, although some is available.
In a June 12 update on methotrexate, ASHP said manufacturing delays at Accord have caused a shortage, and other companies are running low due to increased demand.
As for the future, Congress and the Biden administration, according to a report by Bloomberg, are trying to figure out what to do regarding shortages of cheap generic drugs such as cisplatin and carboplatin. The FDA is exploring a partnership with a Chinese drugmaker to make cisplatin, NBC News reported.
However, fixes will be challenging, according to former FDA commissioner and Pfizer board member, Scott Gottlieb, MD.
“This generic business, particularly for these complex drugs, these complex formulations, is not a healthy business right now. Yet it’s a vital business from a public standpoint,” he told CBS News.
In an interview, Dr. Kamal said that there is even talk about boosting the prices of cheap generic drugs “to ensure that there’s enough incentive for multiple manufacturers to be involved.”
Dr. Kamal said he is crossing his fingers that cutting chemotherapy doses at his clinic doesn’t result in worse outcomes for his patients.
“Right now, I think dropping someone by 25% or 30% is okay. And for some patients, particularly in a curative setting, we try to keep them at as much as 100% as possible. But there’s just a lot of unknowns,” he said.
CHICAGO – Oncologist Denise Yardley, MD, isn’t used to expressing uncertainty when she tells patients about what’s in store for them in terms of drug treatment. But things are dramatically different now amid a severe national shortage of carboplatin and cisplatin, two common and crucial cancer drugs.
“There’s a regimen I’m thinking about,” Dr. Yardley told a new patient recently, “but we’ll have to wait until you finish your staging evaluation to see whether I can deliver this. Another regimen that’s a little more toxic is my second choice.” And, she added, the alternative chemotherapy treatment – anthracycline instead of carboplatin – requires a longer treatment period.
This ambiguity is hardly ideal, said Dr. Yardley, of Tennessee Oncology and Sarah Cannon Research Institute in Nashville. “It’s another factor in being overwhelmed in a first-time visit and wanting to know the details about what your treatment is going to look like. You’re not walking out knowing exactly what you’re going to take or the exact timing so you can start mapping out your calendar and work schedule.”
This kind of scenario is becoming all too familiar this spring, according to oncologists who gathered at the annual meeting of the American Society of Clinical Oncology (ASCO). In interviews, these physicians said the limited supply of multiple cancer drugs – including the chemotherapies carboplatin and cisplatin – is having an unprecedented negative effect since their use is so widespread in cancer care.
“Every patient could get impacted. That’s why we need to address this sooner rather than later,” said oncologist Aditya Baria, MBBS, MPH, director of the Breast Cancer Research Program at Massachusetts General Hospital, Boston.
Shortages of cancer drugs are not unusual. Three-quarters of oncology pharmacists at 68 organizations surveyed from 2019 to 2020 said shortages prompted treatment delays, reduced doses, or alternative regimens. But the current shortages are having a much wider impact.
The National Comprehensive Cancer Network recently reported that 93% of 27 member institutions surveyed in late May are short on carboplatin, and 70% have reported a shortage of cisplatin. Plus, 20% of 19 centers said they weren’t able to continue carboplatin regimens for all patients.
The drugs are mainstays of multiple types of treatment for a long list of cancer types including lung, breast, gynecologic, and many others.
Several scenarios are possible when the drugs are in short supply, said Dr. Yardley, who noted that the shortage is more severe than any she’s seen in her medical career of more than 3 decades. Patients may need to be switched to regimens with more side effects, even when they’re in the middle of a treatment, she said. Or patients might have to go longer between treatments.
In some cases, Dr. Yardley said, the shortage is forcing patients to go without an important component of a larger combination therapy regimen. “The Keynote 522 neoadjuvant regimen for triple-negative breast cancer has carboplatin given with Taxol [paclitaxel] and Keytruda [pembrolizumab]. We are just deleting the carboplatin.”
She added that carboplatin is part of the following so-called TCHP regimen for HER2+ early-stage breast cancer: Taxotere (docetaxel), carboplatin, Herceptin (trastuzumab), and Perjeta (pertuzumab).
“You can delete [carboplatin] or consider substituting cyclophosphamide for carboplatin,” she said. But she cautioned the Keynote 522 and TCHP regimens haven’t been tested without carboplatin in curative-intent trials.
At Duke University in Durham, N.C., doses of carboplatin for many patients are being lowered by a third to the level that’s commonly used for older and frail patients, said oncologist Arif Kamal, MD, MBA, MHS, who works at the academic center and is the chief patient officer at the American Cancer Society.
“We don’t know if [the lower doses will negatively affect cancer patients’ outcomes]. What’s amazing is how many patients [are understanding about having to take smaller amounts of the chemotherapy],” he said.
Medical organizations are offering guidance. The Society of Gynecologic Oncology, for example, in late April recommended that oncologists increase intervals between chemotherapy treatments when appropriate, round down vial sizes to ensure “efficient use,” and eliminate or minimize use of cisplatin and carboplatin in certain platinum-resistant cancers.
In early June, ASCO published guidance regarding alternatives to cisplatin, carboplatin, and 5-fluorouracil, which is also in short supply, in gastrointestinal cancer. As the guidance notes, some alternatives are more untested or more toxic than ideal treatments.
In addition, ASCO has a webpage devoted to news and resources about shortages of cancer drugs. It offers drug availability updates, general guidance, and breast cancer guidance. ASCO also offers ethical guidance about handling drug shortages.
Patients in clinical trials and those who hope to join them are especially vulnerable to the drug shortage, oncologists interviewed for this story said. Cisplatin and carboplatin are the backbones of many clinical trials, Dr. Yardley said. “When you can’t supply a drug in one of the [trial] arms, that puts the whole trial on pause.”
Even clinics that have managed to find adequate supplies of the drugs are planning for when they run out.
“Our institution and other institutions are trying to come up with a rationing protocol, deciding which patients are going to get access, and which ones have reasonable alternatives,” radiation oncologist Corey Speers MD, PhD, of University Hospitals Seidman Cancer Center and Case Western Reserve University, Cleveland, said in an interview. “In some settings, there really isn’t an effective alternative. Or the alternatives are tens of thousands of dollars more expensive.”
Oncologists also noted that cisplatin and carboplatin aren’t the only cancer drugs in short supply.
“Methotrexate is critically low, and 5FU [fluorouracil] is critically low,” Dr. Yardley said, referring to drugs that each treat several types of cancer. According to the May NCNN survey, 67% of respondents reported low supplies of methotrexate, and 26% said they were low on 5FU.
“Viscous lidocaine is a component of many supportive care mouth rinses for the stomatitis caused by our drugs but is not available at all,” Dr. Yardley said.
She added that there are also low supplies of fludarabine, which is used to treat chronic lymphocytic lymphom; clofarabine, which is used to treat acute lymphoblastic leukemia; and rasburicase, which is used to treat high levels of uric acid in patients on chemotherapy.
Dr. Speers said his institution is facing a shortage of capecitabine, which is used to treat several types of cancer.
“Numerous trials have demonstrated the improved, safety, efficacy, and convenience of oral capecitabine. With the shortage we’re having to use infusional 5FU, which not only is less convenient but also ends up being more costly and requires infusion room space or continuous infusion pumps. This impacts our ability to treat cancer patients,” he said. “Our capacity is becoming more limited to accommodate these added patients, and we have to use infusional formulations of a drug that previously was readily available via an oral formulation. Patients and caregivers now have to come to the cancer center for appointments and infusions that previously weren’t needed as they could take an oral pill.”
Dr. Speers added that his institution is rationing methotrexate. “We are now prioritizing patients being treated with curative intent and adjusting protocols to use the lowest allowable doses to conserve supply,” he said.
The roots of the platinum chemotherapy drug shortage link back to the India-based Intas Pharmaceuticals company, a major manufacturer of cisplatin and carboplatin. According to Kellyann Zuzulo, spokeperson for Accord Healthcare, an Instas U.S. subsidiary, a facility inspection in December 2022 prompted a decision to temporarily stop making the drugs. The inspection identified multiple problems.
“Intas and Accord are working with the FDA on a plan to return to manufacturing,” Ms. Zuzulo said in an interview. “This will allow for continued production of products that will be prioritized based on medical necessity. A date has not yet been confirmed in which the facility will return to manufacturing for cisplatin, carboplatin or any other products.”
Ms. Zuzulo said the company is not a health care provider and cannot offer advice to patients about alternatives.
Other companies that make cisplatin and carboplatin have also reported shortages. In interviews, representatives for Fresenius Kabi and Pfizer said the companies have limited supplies because of increased demand – not because of manufacturing problems.
On June 12, the American Society of Health-System Pharmacists (ASHP) reported that carboplatin remains in short supply, with all five companies that sell the drug listed as having limited or back-ordered supplies. Cisplatin is also in short supply, the organization reported in a June 9 update, although some is available.
In a June 12 update on methotrexate, ASHP said manufacturing delays at Accord have caused a shortage, and other companies are running low due to increased demand.
As for the future, Congress and the Biden administration, according to a report by Bloomberg, are trying to figure out what to do regarding shortages of cheap generic drugs such as cisplatin and carboplatin. The FDA is exploring a partnership with a Chinese drugmaker to make cisplatin, NBC News reported.
However, fixes will be challenging, according to former FDA commissioner and Pfizer board member, Scott Gottlieb, MD.
“This generic business, particularly for these complex drugs, these complex formulations, is not a healthy business right now. Yet it’s a vital business from a public standpoint,” he told CBS News.
In an interview, Dr. Kamal said that there is even talk about boosting the prices of cheap generic drugs “to ensure that there’s enough incentive for multiple manufacturers to be involved.”
Dr. Kamal said he is crossing his fingers that cutting chemotherapy doses at his clinic doesn’t result in worse outcomes for his patients.
“Right now, I think dropping someone by 25% or 30% is okay. And for some patients, particularly in a curative setting, we try to keep them at as much as 100% as possible. But there’s just a lot of unknowns,” he said.
AT ASCO 2023
10 ways in which ObGyn care can be more environmentally sustainable
Climate change has been called the biggest health threat of the 21st century.1 The health care sector is a huge contributor to global carbon emissions, accounting for almost double the emissions of global aviation. While other industries and countries are implementing mitigation measures to decrease their emissions, health care is currently on track to double its carbon emissions by 2050, even though it should be carbon neutral by that time to comply with the Paris Climate Agreement.2 There have been some national efforts to curb health care emissions, including the creation of the Office of Climate Change and Health Equity in 2021 and the passage of the Inflation Reduction Act in 2022.3 These are top-down, administrative approaches, and to be successful we will also need clinicians to understand and address this problem.
The negative impacts of heat, air pollution, and exposure to toxic substances on human health have been well documented in multiple regions across multiple specialties.4-7 The United States makes up 27% of the global health care carbon footprint—more emissions than the entire United Kingdom as a country—despite having only 4% of the world’s population.2 Culture and incentives for an overabundance of single-use supplies, not evidence for patient safety, have led to this uniquely American problem. It is evident that our health care industry is an excellent place to implement mitigation measures for carbon emissions that contribute to climate change and can improve health outcomes.
In this article, we recommend 10 practices that can decrease our carbon footprint in ObGyn. We focus on the classic motto of “Reduce, Reuse, Recycle,” while adding “Remove” and “Reimagine” to classify the ways in which we can reduce emissions while not compromising our care to patients.
Reduce
1. Minimize opened materials and single-use devices in the OR and labor and delivery
Health care is a unique setting where a culture of infection prevention and efficiency has led low-cost, single-use supplies to dominate over reusable items. While single-use items can have inexpensive purchasing costs compared to reusable items, the environmental costs required for the production and disposal of the former are often much greater. In operating rooms (ORs) and labor and delivery (LD) units, single-use items are omnipresent. Over the past decade, researchers and clinicians have started to take a closer look at these items and their carbon footprint. One group evaluated hysterectomy through a waste audit and found that the vast majority of waste from all of the cases was Spunbond Meltblown Spunbond, or SMS; plastic materialthat comprises gowns; blue wraps; and drapes; followed by hard plastic material that comprises trays and packaging.8 Moreover, production and manufacturing processes contributed to 95% of the environmental impacts of these items.8
In an effort to be time efficient, OR staff will open sterile surgical packs and individual peel-pack items prior to surgery to minimize having to find items during surgery. However, this creates an inordinate amount of waste. One group of neurosurgeons who evaluated their opened but unused supplies found that 85% of their unused items were individually opened items, leading to a waste of $2.9 million per year.9 Minor procedures like dilation and curettage, cystoscopy, and hysteroscopy do not need such a large sterile field, as these procedures are also safe to perform in the office. Hand surgeons have been quick to lead in this space, particularly with minor procedures such as carpal tunnel release. One division was able to eliminate 2.8 tons of waste and save $13,000 in a 2-year period by reducing the sterile field.10 ObGyns can work with OR and LD staff to create custom packs that minimize unused or underutilized items, helping to reduce both the carbon footprint and health care spending.
Bottom line: ObGyns can help foster a culture of having supplies available but not opened until needed during a case.
Continue to: 2. Decrease regulated medical waste...
2. Decrease regulated medical waste
Health care is unique from other fields in that there are multiple waste streams to consider. Infectious waste and items saturated in blood or capable of causing infection must be placed into regulated medical waste (RMW), or more commonly, red biohazard bags. RMW is autoclaved or incinerated prior to disposal in a landfill. This process is more financially and environmentally costly than general municipal waste (GMW). This process also requires more transport—1 study revealed that GMW traveled 20 km to a landfill for disposal, compared with the 50 km that RMW traveled for sterilized-prior-to-landfill disposal.11
Unfortunately, the vast majority of items placed in RMW are incorrectly triaged and should instead be disposed in GMW.12,13 One study performed in an emergency department revealed that 85% of waste was incorrectly placed in the RMW.12
Bottom line: ObGyns can avoid placing items in RMW that may not qualify and advocate for institution policy changes to remove RMW from places such as waiting rooms, at the patient bedside, or next to scrub sinks.
3. Reduce energy use
ORs and LD units use a lot of energy, and numerous studies have demonstrated that the heating, ventilation, and air conditioning (HVAC) system plays a large role in emissions.8,11 This can easily be fixed by “HVAC setbacks” and powering down rooms when not in use. One institution powered down ORs when not in use and reduced 234 metric tons of CO2 emissions and saved $33,000 per year.14 Transitioning to light-emitting diode (LED) lights reduced energy usage at 1 institution by almost 50%.15 Finally, computers in clinical offices, examination rooms, and administrative offices can be powered down at the end of the day. One study found that in 1 radiology department, 29 computers left on overnight and on weekends emitted 17.7 tons of CO2 emissions in 1 year.16
Bottom line: We as ObGyns can advocate for how energy can be saved outside of surgical cases, including powering down ORs and LD units, transitioning to LED lighting, and powering down workstations.
Reuse
4. Choose reusable equipment
In ObGyn practice, the most commonly used tool is the speculum. Given its omnipresence, the speculum is a great place to start to decrease our carbon footprint. Two studies have evaluated the environmental impact of reusable versus single-use disposable specula, and both demonstrated that the stainless-steel versions have less global warming potential than the acrylic varieties.17,18 Donahue and colleagues17 demonstrated that it only took 2 to 3 pelvic examinations for the cost of stainless-steel specula to break even, even when sterilized in a half-filled autoclave tray. Rodriquez, et al18 revealed that, compared with an acrylic model, the stainless-steel specula had fewer negative impacts in terms of global warming, acidification, respiratory effects, smog, and fossil fuel depletion.18
Bottom line: Strongly consider using stainless-steel specula to reduce costs and carbon emissions.
In addition to specula, ObGyns can choose reusable equipment in the OR. For example, surgeons can use stainless-steel trocars instead of disposable trocars.19 In vaginal cases, Breisky-Navratil retractors can be used instead of disposable self-retaining retractors. Plastic basins that often are included in sterile supply packs can be replaced with stainless-steel basins, which could have profound positive effects on the carbon footprint of gynecologic surgery.8 One study of ObGyns demonstrated that 95% of physicians supported waste-reduction efforts, and 66% supported utilizing reusable surgical tools instead of disposable tools.20
Bottom line: As surgeons, ObGyns have influence over what they want to use in the OR, and they can petition for reusable options over disposable options.
5. Launder the sterile blue towels
Sterile blue towels, which are made of cotton, have the largest environmental footprint compared with other disposable materials, such as plastics, and contribute greatly to toxicity in human health.8,11 Although these towels cannot be laundered and sterilized again for use in a sterile surgical field, they can be laundered and repurposed, including by environmental services to clean hospital rooms. Blue towels should be able to be laundered no matter how saturated in body fluids they are.
Bottom line: ObGyns should strive to always launder the blue towels and educate trainees and other staff in the OR to do the same.
Recycle
6. Recycle and reprocess materials and devices
While recycling is immensely important, it requires a large amount of energy to break down a material to its raw components for manufacturing. It likely reduces our carbon footprint from OR procedures by only 5%.8 However, recycling is still a good way to divert appropriate materials from landfill, saving costs and emissions at the end of a material’s life. One example is sterile blue wrap, which is a petroleum product with a recycling number of 6 and a filtration rating of N99. Blue wrap can be recycled into plastic pellets, or it can be recreated into other hospital supplies, such as gowns.
Bottom line: ObGyns can petition their hospitals to work with suppliers and waste-processing companies who have recycling programs built into their supply chains.
By contrast, reprocessing can have a much larger impact on carbon emissions. Complex items, such as advanced energy devices that can be reprocessed, result in a greater reduction in carbon emissions due to the reuse of their complex materials and manufacturing when compared with such devices that cannot be reprocessed. Recycling and reprocessing programs are already in place for several devices (TABLE). Authors of a systematic review showed that there is no evidence to support the use of single-use supplies and instruments over reprocessed items when considering instrument function, ease of use, patient safety, transmission of infection, or long-term patient outcomes.21
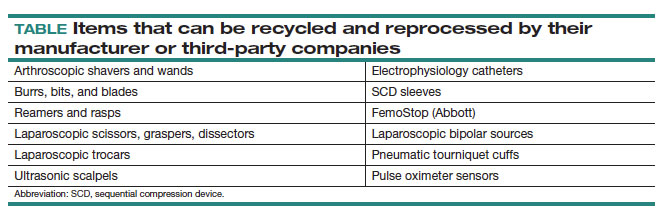
Bottom line: ObGyns can choose to use reprocessed items in ORs instead of single-use devices and educate staff on the safety of these items.
Continue to: Remove...
Remove
7. Remove desflurane and other volatile gases from formularies
Volatile anesthetic gases, such as desflurane, isoflurane, and nitrous oxide, are themselves potent greenhouse gases, comprising a large portion of the carbon emissions that come from the OR.22 Desflurane was developed to have a rapid onset for induction and quick recovery; however, studies have shown no clinical benefit over other gases.23 Furthermore, the costs and greenhouse gas potential are substantial. Desflurane costs 2 to 3 times more and has more than 20 times the global warming potential of the other volatile gases (FIGURE).8 Using 1 hour of desflurane is equivalent to driving 378 miles in a gas-powered vehicle, while the use of isoflurane and sevoflurane create equivalents of only 15 and 8 miles, respectively.23
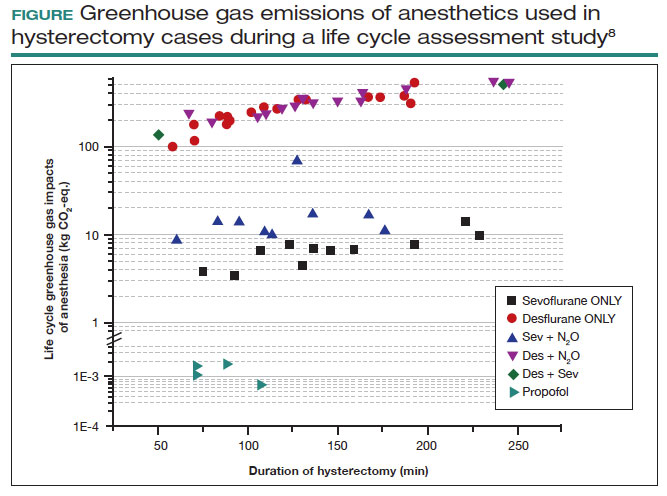
Nitrous oxide is another powerful greenhouse gas that is a direct ozone depletor and can stay in the atmosphere for 114 years.22 Nitrous oxide has limited clinical use in hospitals, but it is often stored in central hospital piping. Most of the impact of nitrous oxide comes through leaks in a poor system design rather than patient delivery. One estimate reveals that more than 13 million liters of nitrous oxide are lost annually from leaks in European hospitals.22 The American Society of Anesthesiologists recommends decommissioning central piping of nitrous oxide in favor of cylinders at the point of care.24
Literature on enhanced recovery after surgery in gynecology promotes the use of propofol over volatile gases for our patients because of the high rate of postoperative nausea and vomiting seen with gases.25 Volatile gases should be a last-choice anesthetic for our patients.
Bottom line: It is critical that ObGyns work with colleagues in anesthesia to develop climate- and patient-friendly protocols for procedures.
8. Remove endocrine-disrupting chemicals from clinical supplies
Endocrine-disrupting chemicals (EDCs) are a type of chemical that alter the hormonal systems of humans, which can result in adverse health effects. Multiple studies and reviews have tied EDCs to reproductive abnormalities, such as the effects of bisphenol A (BPA) on estradiol levels, antral follicle counts, oocyte quality, and implantation rates; phthalates on fibroid burden; triclosan on embryo quality; parabens on live birth rates; and perfluoroalkylsubstances (PFAS or “forever substances”) on hypertensive disorders of pregnancy.5,26,27
What might be most shocking is that these EDCs are incorporated into medical supplies and pharmaceuticals. For example, BPA is known to line dialysis and ointment tubes, parabens are used for their antimicrobial properties in ultrasound gel and hep-locks, and phthalates are found in up to 40% of medical-use plastics and controlled-release medications. Authors of an observational study found that 74% of patients admitted to an LD unit were exposed to EDCs. In a neonatal intensive care unit (NICU), most of the supplies contained an EDC, and urinary BPA levels were elevated in neonates admitted to a NICU, raising concerns about long-term health risks.5
Bottom line: Physicians and health care institutions have an obligation to petition industry partners and suppliers to remove EDCs from their supply chains.
Reimagine
9. Educate
The field of health care sustainability remains in its infancy, but from 2007 to 2019, publications on climate change and health in academia increased by a factor of 8.29 Additionally, through waste audits, quality-improvement projects, and life cycle analyses (analytical tools to evaluate product or process emissions from materials extraction to disposal), we have gained insight into the scope of the problem, with evidence showing that our practices are largely derived from culture. It is time to provide formal education on health care sustainability to medical trainees, staff, and clinicians alike, who desire to see this topic reflected in their formal curricula.30 Start talking about it!
Bottom line: Commentaries, webinars, formal didactics sessions, in-services, and hospital workgroups to introduce this topic are a good way to teach others about the carbon footprint of our care and solutions to minimize it.
10. Engage in advocacy
Physicians have an ethical duty to advocate for change at the local, regional, and national levels if we want to see a better future for our patients, their children, and even ourselves. We should reimagine this work as an important public health initiative.31 Surveys of physicians, including ObGyns, reveal a concern about the sustainability of health care and a commitment to addressing this issue.20 ObGyns are on the frontlines of delivering care every day, so we are poised to implement changes that can impact our patients, especially when we can lead and petition hospital or local committees.20,28,32 There is much to be done, but every voice counts and can make impactful changes at every level. ●
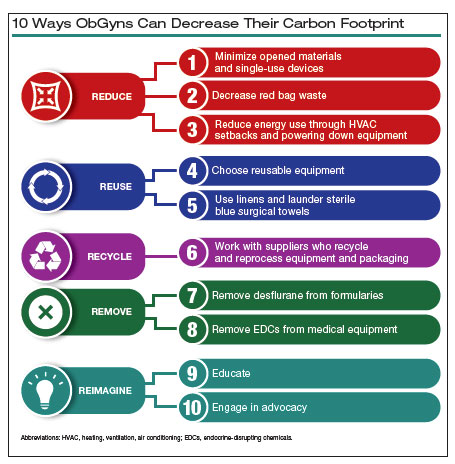
- Costello A, Abbas M, Allen et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. Lancet. 2009;373:1693-1733.
- Health care climate footprint report. Health Care Without Harm website. https://www.noharm.org/ClimateFootprintReport. Accessed May 12, 2023.
- Balbus JM, McCannon CJ, Mataka A, et al. After COP26—putting health and equity at the center of the climate movement. N Engl J Med. 2022;386:1295-1297.
- Bekkar B, Pacheco S, Basu R, et al. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: a systematic review. JAMA Netw Open. 2020;3:e208243.
- Genco M, Anderson-Shaw L, Sargis RM. Unwitting accomplices: endocrine disruptors confounding clinical care. J Clin Endocrinol Metab. 2020;105:e3822-e3827.
- Al-Kindi SG, Sarode A, Zullo M, et al. Ambient air pollution and mortality after cardiac transplantation. J Am Coll Cardiol. 2019;74:30263035.
- Ghosh R, Gauderman WJ, Minor H, et al. Air pollution, weight loss and metabolic benefits of bariatric surgery: a potential model for study of metabolic effects of environmental exposures. Pediatr Obes. 2018;13:312-320.
- Thiel CL, Eckelman M, Guido R, et al. Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United States. Environ Sci Technol. 2015;49:1779-1786.
- Zygourakis CC, Yoon S, Valencia V, et al. Operating room waste: disposable supply utilization in neurosurgical procedures. J Neurosurg. 2017;126:620-625.
- van Demark RE, Smith VJS, Fiegen A. Lean and green hand surgery. J Hand Surg. 2018;43:179-181.
- Campion N, Thiel CL, DeBlois J, et al. Life cycle assessment perspectives on delivering an infant in the US. Sci Total Environ. 2012;425:191198.
- Hsu S, Thiel CL, Mello MJ, Slutzman JE. Dumpster diving in the emergency department. West J Emerg Med. 2020;21:1211-1217.
- Mcgain F, Story D, Hendel S. An audit of intensive care unit recyclable waste. Anaesthesia. 2009;64:1299-1302.
- Wormer BA, Augenstein VA, Carpenter CL, et al. The green operating room: simple changes to reduce cost and our carbon footprint. Am Surg. 2013;79:666-671.
- Kagoma Y, Stall N, Rubinstein E, et al. People, planet and profits: the case for greening operating rooms. Can Med Assoc J. 2012;184:19051911.
- McCarthy CJ, Gerstenmaier JF, O’ Neill AC, et al. “EcoRadiology”— pulling the plug on wasted energy in the radiology department. Acad Radiol. 2014;21:1563-1566.
- Donahue LM, Hilton S, Bell SG, et al. A comparative carbon footprint analysis of disposable and reusable vaginal specula. Am J Obstet Gynecol. 2020;223:225.e1-225.e7.
- Rodriguez Morris MI, Hicks A. Life cycle assessment of stainless-steel reusable speculums versus disposable acrylic speculums in a university clinic setting: a case study. Environ Res Commun. 2022;4:025002.
- MacNeill AJ, Lillywhite R, Brown CJ. The impact of surgery on global climate: a carbon footprinting study of operating theatres in three health systems. Lancet Planet Health. 2017;1:e381-e388.
- Thiel C, Duncan P, Woods N. Attitude of US obstetricians and gynaecologists to global warming and medical waste. J Health Serv Res Policy. 2017;22:162-167.
- Siu J, Hill AG, MacCormick AD. Systematic review of reusable versus disposable laparoscopic instruments: costs and safety. ANZ J Surg. 2017;87:28-33.
- Ryan SM, Nielsen CJ. Global warming potential of inhaled anesthetics: application to clinical use. Anesth Analg. 2010;111:92-98.
- Meyer MJ. Desflurane should des-appear: global and financial rationale. Anesth Analg. 2020;131:1317-1322.
- Rollins MD, Arendt KW, Carvalho B, et al. ASA Committee on Obstetric Anesthesia Working Group. Nitrous oxide. American Society of Anesthesiologists website. Accessed May 12, 2023. https://www .asahq.org/about-asa/governance-and-committees/asa-committees /committee-on-obstetric-anesthesia/nitrous-oxide.
- Kalogera E, Dowdy SC. Enhanced recovery pathway in gynecologic surgery: improving outcomes through evidence-based medicine. Obstet Gynecol Clin North Am. 2016;43:551-573.
- Zota AR, Geller RJ, Calafat AM, et al. Phthalates exposure and uterine fibroid burden among women undergoing surgical treatment for fibroids: a preliminary study. Fertil Steril. 2019;111:112-121.
- Bommartio PA, Ferguson KK, Meeker JD, et al. Maternal levels of perfluoroalkyl substances (PFAS) during early pregnancy in relation to preeclampsia subtypes and biomarkers of preeclampsia risk. Environ Health Perspect. 2021;129:107004.
- Azouz S, Boyll P, Swanson M, et al. Managing barriers to recycling in the operating room. Am J Surg. 2019;217:634-638.
- Watts N, Amann M, Arnell N, et al. The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises. Lancet. 2021;397:129-170.
- Ryan EC, Dubrow R, Sherman JD. Medical, nursing, and physician assistant student knowledge and attitudes toward climate change, pollution, and resource conservation in health care. BMC Med Educ. 2020;20:200.
- Giudice LC, Llamas-Clark EF, DeNicola Net al; FIGO Committee on Climate Change and Toxic Environmental Exposures. Climate change, women’s health, and the role of obstetricians and gynecologists in leadership. Int J Gynaecol Obstet. 2021;155:345-356.
- Yates EF, Bowder AN, Roa L, et al. Empowering surgeons, anesthesiologists, and obstetricians to incorporate environmental sustainability in the operating room. Ann Surg. 2021;273:1108-1114.
Climate change has been called the biggest health threat of the 21st century.1 The health care sector is a huge contributor to global carbon emissions, accounting for almost double the emissions of global aviation. While other industries and countries are implementing mitigation measures to decrease their emissions, health care is currently on track to double its carbon emissions by 2050, even though it should be carbon neutral by that time to comply with the Paris Climate Agreement.2 There have been some national efforts to curb health care emissions, including the creation of the Office of Climate Change and Health Equity in 2021 and the passage of the Inflation Reduction Act in 2022.3 These are top-down, administrative approaches, and to be successful we will also need clinicians to understand and address this problem.
The negative impacts of heat, air pollution, and exposure to toxic substances on human health have been well documented in multiple regions across multiple specialties.4-7 The United States makes up 27% of the global health care carbon footprint—more emissions than the entire United Kingdom as a country—despite having only 4% of the world’s population.2 Culture and incentives for an overabundance of single-use supplies, not evidence for patient safety, have led to this uniquely American problem. It is evident that our health care industry is an excellent place to implement mitigation measures for carbon emissions that contribute to climate change and can improve health outcomes.
In this article, we recommend 10 practices that can decrease our carbon footprint in ObGyn. We focus on the classic motto of “Reduce, Reuse, Recycle,” while adding “Remove” and “Reimagine” to classify the ways in which we can reduce emissions while not compromising our care to patients.
Reduce
1. Minimize opened materials and single-use devices in the OR and labor and delivery
Health care is a unique setting where a culture of infection prevention and efficiency has led low-cost, single-use supplies to dominate over reusable items. While single-use items can have inexpensive purchasing costs compared to reusable items, the environmental costs required for the production and disposal of the former are often much greater. In operating rooms (ORs) and labor and delivery (LD) units, single-use items are omnipresent. Over the past decade, researchers and clinicians have started to take a closer look at these items and their carbon footprint. One group evaluated hysterectomy through a waste audit and found that the vast majority of waste from all of the cases was Spunbond Meltblown Spunbond, or SMS; plastic materialthat comprises gowns; blue wraps; and drapes; followed by hard plastic material that comprises trays and packaging.8 Moreover, production and manufacturing processes contributed to 95% of the environmental impacts of these items.8
In an effort to be time efficient, OR staff will open sterile surgical packs and individual peel-pack items prior to surgery to minimize having to find items during surgery. However, this creates an inordinate amount of waste. One group of neurosurgeons who evaluated their opened but unused supplies found that 85% of their unused items were individually opened items, leading to a waste of $2.9 million per year.9 Minor procedures like dilation and curettage, cystoscopy, and hysteroscopy do not need such a large sterile field, as these procedures are also safe to perform in the office. Hand surgeons have been quick to lead in this space, particularly with minor procedures such as carpal tunnel release. One division was able to eliminate 2.8 tons of waste and save $13,000 in a 2-year period by reducing the sterile field.10 ObGyns can work with OR and LD staff to create custom packs that minimize unused or underutilized items, helping to reduce both the carbon footprint and health care spending.
Bottom line: ObGyns can help foster a culture of having supplies available but not opened until needed during a case.
Continue to: 2. Decrease regulated medical waste...
2. Decrease regulated medical waste
Health care is unique from other fields in that there are multiple waste streams to consider. Infectious waste and items saturated in blood or capable of causing infection must be placed into regulated medical waste (RMW), or more commonly, red biohazard bags. RMW is autoclaved or incinerated prior to disposal in a landfill. This process is more financially and environmentally costly than general municipal waste (GMW). This process also requires more transport—1 study revealed that GMW traveled 20 km to a landfill for disposal, compared with the 50 km that RMW traveled for sterilized-prior-to-landfill disposal.11
Unfortunately, the vast majority of items placed in RMW are incorrectly triaged and should instead be disposed in GMW.12,13 One study performed in an emergency department revealed that 85% of waste was incorrectly placed in the RMW.12
Bottom line: ObGyns can avoid placing items in RMW that may not qualify and advocate for institution policy changes to remove RMW from places such as waiting rooms, at the patient bedside, or next to scrub sinks.
3. Reduce energy use
ORs and LD units use a lot of energy, and numerous studies have demonstrated that the heating, ventilation, and air conditioning (HVAC) system plays a large role in emissions.8,11 This can easily be fixed by “HVAC setbacks” and powering down rooms when not in use. One institution powered down ORs when not in use and reduced 234 metric tons of CO2 emissions and saved $33,000 per year.14 Transitioning to light-emitting diode (LED) lights reduced energy usage at 1 institution by almost 50%.15 Finally, computers in clinical offices, examination rooms, and administrative offices can be powered down at the end of the day. One study found that in 1 radiology department, 29 computers left on overnight and on weekends emitted 17.7 tons of CO2 emissions in 1 year.16
Bottom line: We as ObGyns can advocate for how energy can be saved outside of surgical cases, including powering down ORs and LD units, transitioning to LED lighting, and powering down workstations.
Reuse
4. Choose reusable equipment
In ObGyn practice, the most commonly used tool is the speculum. Given its omnipresence, the speculum is a great place to start to decrease our carbon footprint. Two studies have evaluated the environmental impact of reusable versus single-use disposable specula, and both demonstrated that the stainless-steel versions have less global warming potential than the acrylic varieties.17,18 Donahue and colleagues17 demonstrated that it only took 2 to 3 pelvic examinations for the cost of stainless-steel specula to break even, even when sterilized in a half-filled autoclave tray. Rodriquez, et al18 revealed that, compared with an acrylic model, the stainless-steel specula had fewer negative impacts in terms of global warming, acidification, respiratory effects, smog, and fossil fuel depletion.18
Bottom line: Strongly consider using stainless-steel specula to reduce costs and carbon emissions.
In addition to specula, ObGyns can choose reusable equipment in the OR. For example, surgeons can use stainless-steel trocars instead of disposable trocars.19 In vaginal cases, Breisky-Navratil retractors can be used instead of disposable self-retaining retractors. Plastic basins that often are included in sterile supply packs can be replaced with stainless-steel basins, which could have profound positive effects on the carbon footprint of gynecologic surgery.8 One study of ObGyns demonstrated that 95% of physicians supported waste-reduction efforts, and 66% supported utilizing reusable surgical tools instead of disposable tools.20
Bottom line: As surgeons, ObGyns have influence over what they want to use in the OR, and they can petition for reusable options over disposable options.
5. Launder the sterile blue towels
Sterile blue towels, which are made of cotton, have the largest environmental footprint compared with other disposable materials, such as plastics, and contribute greatly to toxicity in human health.8,11 Although these towels cannot be laundered and sterilized again for use in a sterile surgical field, they can be laundered and repurposed, including by environmental services to clean hospital rooms. Blue towels should be able to be laundered no matter how saturated in body fluids they are.
Bottom line: ObGyns should strive to always launder the blue towels and educate trainees and other staff in the OR to do the same.
Recycle
6. Recycle and reprocess materials and devices
While recycling is immensely important, it requires a large amount of energy to break down a material to its raw components for manufacturing. It likely reduces our carbon footprint from OR procedures by only 5%.8 However, recycling is still a good way to divert appropriate materials from landfill, saving costs and emissions at the end of a material’s life. One example is sterile blue wrap, which is a petroleum product with a recycling number of 6 and a filtration rating of N99. Blue wrap can be recycled into plastic pellets, or it can be recreated into other hospital supplies, such as gowns.
Bottom line: ObGyns can petition their hospitals to work with suppliers and waste-processing companies who have recycling programs built into their supply chains.
By contrast, reprocessing can have a much larger impact on carbon emissions. Complex items, such as advanced energy devices that can be reprocessed, result in a greater reduction in carbon emissions due to the reuse of their complex materials and manufacturing when compared with such devices that cannot be reprocessed. Recycling and reprocessing programs are already in place for several devices (TABLE). Authors of a systematic review showed that there is no evidence to support the use of single-use supplies and instruments over reprocessed items when considering instrument function, ease of use, patient safety, transmission of infection, or long-term patient outcomes.21
Bottom line: ObGyns can choose to use reprocessed items in ORs instead of single-use devices and educate staff on the safety of these items.
Continue to: Remove...
Remove
7. Remove desflurane and other volatile gases from formularies
Volatile anesthetic gases, such as desflurane, isoflurane, and nitrous oxide, are themselves potent greenhouse gases, comprising a large portion of the carbon emissions that come from the OR.22 Desflurane was developed to have a rapid onset for induction and quick recovery; however, studies have shown no clinical benefit over other gases.23 Furthermore, the costs and greenhouse gas potential are substantial. Desflurane costs 2 to 3 times more and has more than 20 times the global warming potential of the other volatile gases (FIGURE).8 Using 1 hour of desflurane is equivalent to driving 378 miles in a gas-powered vehicle, while the use of isoflurane and sevoflurane create equivalents of only 15 and 8 miles, respectively.23
Nitrous oxide is another powerful greenhouse gas that is a direct ozone depletor and can stay in the atmosphere for 114 years.22 Nitrous oxide has limited clinical use in hospitals, but it is often stored in central hospital piping. Most of the impact of nitrous oxide comes through leaks in a poor system design rather than patient delivery. One estimate reveals that more than 13 million liters of nitrous oxide are lost annually from leaks in European hospitals.22 The American Society of Anesthesiologists recommends decommissioning central piping of nitrous oxide in favor of cylinders at the point of care.24
Literature on enhanced recovery after surgery in gynecology promotes the use of propofol over volatile gases for our patients because of the high rate of postoperative nausea and vomiting seen with gases.25 Volatile gases should be a last-choice anesthetic for our patients.
Bottom line: It is critical that ObGyns work with colleagues in anesthesia to develop climate- and patient-friendly protocols for procedures.
8. Remove endocrine-disrupting chemicals from clinical supplies
Endocrine-disrupting chemicals (EDCs) are a type of chemical that alter the hormonal systems of humans, which can result in adverse health effects. Multiple studies and reviews have tied EDCs to reproductive abnormalities, such as the effects of bisphenol A (BPA) on estradiol levels, antral follicle counts, oocyte quality, and implantation rates; phthalates on fibroid burden; triclosan on embryo quality; parabens on live birth rates; and perfluoroalkylsubstances (PFAS or “forever substances”) on hypertensive disorders of pregnancy.5,26,27
What might be most shocking is that these EDCs are incorporated into medical supplies and pharmaceuticals. For example, BPA is known to line dialysis and ointment tubes, parabens are used for their antimicrobial properties in ultrasound gel and hep-locks, and phthalates are found in up to 40% of medical-use plastics and controlled-release medications. Authors of an observational study found that 74% of patients admitted to an LD unit were exposed to EDCs. In a neonatal intensive care unit (NICU), most of the supplies contained an EDC, and urinary BPA levels were elevated in neonates admitted to a NICU, raising concerns about long-term health risks.5
Bottom line: Physicians and health care institutions have an obligation to petition industry partners and suppliers to remove EDCs from their supply chains.
Reimagine
9. Educate
The field of health care sustainability remains in its infancy, but from 2007 to 2019, publications on climate change and health in academia increased by a factor of 8.29 Additionally, through waste audits, quality-improvement projects, and life cycle analyses (analytical tools to evaluate product or process emissions from materials extraction to disposal), we have gained insight into the scope of the problem, with evidence showing that our practices are largely derived from culture. It is time to provide formal education on health care sustainability to medical trainees, staff, and clinicians alike, who desire to see this topic reflected in their formal curricula.30 Start talking about it!
Bottom line: Commentaries, webinars, formal didactics sessions, in-services, and hospital workgroups to introduce this topic are a good way to teach others about the carbon footprint of our care and solutions to minimize it.
10. Engage in advocacy
Physicians have an ethical duty to advocate for change at the local, regional, and national levels if we want to see a better future for our patients, their children, and even ourselves. We should reimagine this work as an important public health initiative.31 Surveys of physicians, including ObGyns, reveal a concern about the sustainability of health care and a commitment to addressing this issue.20 ObGyns are on the frontlines of delivering care every day, so we are poised to implement changes that can impact our patients, especially when we can lead and petition hospital or local committees.20,28,32 There is much to be done, but every voice counts and can make impactful changes at every level. ●
Climate change has been called the biggest health threat of the 21st century.1 The health care sector is a huge contributor to global carbon emissions, accounting for almost double the emissions of global aviation. While other industries and countries are implementing mitigation measures to decrease their emissions, health care is currently on track to double its carbon emissions by 2050, even though it should be carbon neutral by that time to comply with the Paris Climate Agreement.2 There have been some national efforts to curb health care emissions, including the creation of the Office of Climate Change and Health Equity in 2021 and the passage of the Inflation Reduction Act in 2022.3 These are top-down, administrative approaches, and to be successful we will also need clinicians to understand and address this problem.
The negative impacts of heat, air pollution, and exposure to toxic substances on human health have been well documented in multiple regions across multiple specialties.4-7 The United States makes up 27% of the global health care carbon footprint—more emissions than the entire United Kingdom as a country—despite having only 4% of the world’s population.2 Culture and incentives for an overabundance of single-use supplies, not evidence for patient safety, have led to this uniquely American problem. It is evident that our health care industry is an excellent place to implement mitigation measures for carbon emissions that contribute to climate change and can improve health outcomes.
In this article, we recommend 10 practices that can decrease our carbon footprint in ObGyn. We focus on the classic motto of “Reduce, Reuse, Recycle,” while adding “Remove” and “Reimagine” to classify the ways in which we can reduce emissions while not compromising our care to patients.
Reduce
1. Minimize opened materials and single-use devices in the OR and labor and delivery
Health care is a unique setting where a culture of infection prevention and efficiency has led low-cost, single-use supplies to dominate over reusable items. While single-use items can have inexpensive purchasing costs compared to reusable items, the environmental costs required for the production and disposal of the former are often much greater. In operating rooms (ORs) and labor and delivery (LD) units, single-use items are omnipresent. Over the past decade, researchers and clinicians have started to take a closer look at these items and their carbon footprint. One group evaluated hysterectomy through a waste audit and found that the vast majority of waste from all of the cases was Spunbond Meltblown Spunbond, or SMS; plastic materialthat comprises gowns; blue wraps; and drapes; followed by hard plastic material that comprises trays and packaging.8 Moreover, production and manufacturing processes contributed to 95% of the environmental impacts of these items.8
In an effort to be time efficient, OR staff will open sterile surgical packs and individual peel-pack items prior to surgery to minimize having to find items during surgery. However, this creates an inordinate amount of waste. One group of neurosurgeons who evaluated their opened but unused supplies found that 85% of their unused items were individually opened items, leading to a waste of $2.9 million per year.9 Minor procedures like dilation and curettage, cystoscopy, and hysteroscopy do not need such a large sterile field, as these procedures are also safe to perform in the office. Hand surgeons have been quick to lead in this space, particularly with minor procedures such as carpal tunnel release. One division was able to eliminate 2.8 tons of waste and save $13,000 in a 2-year period by reducing the sterile field.10 ObGyns can work with OR and LD staff to create custom packs that minimize unused or underutilized items, helping to reduce both the carbon footprint and health care spending.
Bottom line: ObGyns can help foster a culture of having supplies available but not opened until needed during a case.
Continue to: 2. Decrease regulated medical waste...
2. Decrease regulated medical waste
Health care is unique from other fields in that there are multiple waste streams to consider. Infectious waste and items saturated in blood or capable of causing infection must be placed into regulated medical waste (RMW), or more commonly, red biohazard bags. RMW is autoclaved or incinerated prior to disposal in a landfill. This process is more financially and environmentally costly than general municipal waste (GMW). This process also requires more transport—1 study revealed that GMW traveled 20 km to a landfill for disposal, compared with the 50 km that RMW traveled for sterilized-prior-to-landfill disposal.11
Unfortunately, the vast majority of items placed in RMW are incorrectly triaged and should instead be disposed in GMW.12,13 One study performed in an emergency department revealed that 85% of waste was incorrectly placed in the RMW.12
Bottom line: ObGyns can avoid placing items in RMW that may not qualify and advocate for institution policy changes to remove RMW from places such as waiting rooms, at the patient bedside, or next to scrub sinks.
3. Reduce energy use
ORs and LD units use a lot of energy, and numerous studies have demonstrated that the heating, ventilation, and air conditioning (HVAC) system plays a large role in emissions.8,11 This can easily be fixed by “HVAC setbacks” and powering down rooms when not in use. One institution powered down ORs when not in use and reduced 234 metric tons of CO2 emissions and saved $33,000 per year.14 Transitioning to light-emitting diode (LED) lights reduced energy usage at 1 institution by almost 50%.15 Finally, computers in clinical offices, examination rooms, and administrative offices can be powered down at the end of the day. One study found that in 1 radiology department, 29 computers left on overnight and on weekends emitted 17.7 tons of CO2 emissions in 1 year.16
Bottom line: We as ObGyns can advocate for how energy can be saved outside of surgical cases, including powering down ORs and LD units, transitioning to LED lighting, and powering down workstations.
Reuse
4. Choose reusable equipment
In ObGyn practice, the most commonly used tool is the speculum. Given its omnipresence, the speculum is a great place to start to decrease our carbon footprint. Two studies have evaluated the environmental impact of reusable versus single-use disposable specula, and both demonstrated that the stainless-steel versions have less global warming potential than the acrylic varieties.17,18 Donahue and colleagues17 demonstrated that it only took 2 to 3 pelvic examinations for the cost of stainless-steel specula to break even, even when sterilized in a half-filled autoclave tray. Rodriquez, et al18 revealed that, compared with an acrylic model, the stainless-steel specula had fewer negative impacts in terms of global warming, acidification, respiratory effects, smog, and fossil fuel depletion.18
Bottom line: Strongly consider using stainless-steel specula to reduce costs and carbon emissions.
In addition to specula, ObGyns can choose reusable equipment in the OR. For example, surgeons can use stainless-steel trocars instead of disposable trocars.19 In vaginal cases, Breisky-Navratil retractors can be used instead of disposable self-retaining retractors. Plastic basins that often are included in sterile supply packs can be replaced with stainless-steel basins, which could have profound positive effects on the carbon footprint of gynecologic surgery.8 One study of ObGyns demonstrated that 95% of physicians supported waste-reduction efforts, and 66% supported utilizing reusable surgical tools instead of disposable tools.20
Bottom line: As surgeons, ObGyns have influence over what they want to use in the OR, and they can petition for reusable options over disposable options.
5. Launder the sterile blue towels
Sterile blue towels, which are made of cotton, have the largest environmental footprint compared with other disposable materials, such as plastics, and contribute greatly to toxicity in human health.8,11 Although these towels cannot be laundered and sterilized again for use in a sterile surgical field, they can be laundered and repurposed, including by environmental services to clean hospital rooms. Blue towels should be able to be laundered no matter how saturated in body fluids they are.
Bottom line: ObGyns should strive to always launder the blue towels and educate trainees and other staff in the OR to do the same.
Recycle
6. Recycle and reprocess materials and devices
While recycling is immensely important, it requires a large amount of energy to break down a material to its raw components for manufacturing. It likely reduces our carbon footprint from OR procedures by only 5%.8 However, recycling is still a good way to divert appropriate materials from landfill, saving costs and emissions at the end of a material’s life. One example is sterile blue wrap, which is a petroleum product with a recycling number of 6 and a filtration rating of N99. Blue wrap can be recycled into plastic pellets, or it can be recreated into other hospital supplies, such as gowns.
Bottom line: ObGyns can petition their hospitals to work with suppliers and waste-processing companies who have recycling programs built into their supply chains.
By contrast, reprocessing can have a much larger impact on carbon emissions. Complex items, such as advanced energy devices that can be reprocessed, result in a greater reduction in carbon emissions due to the reuse of their complex materials and manufacturing when compared with such devices that cannot be reprocessed. Recycling and reprocessing programs are already in place for several devices (TABLE). Authors of a systematic review showed that there is no evidence to support the use of single-use supplies and instruments over reprocessed items when considering instrument function, ease of use, patient safety, transmission of infection, or long-term patient outcomes.21
Bottom line: ObGyns can choose to use reprocessed items in ORs instead of single-use devices and educate staff on the safety of these items.
Continue to: Remove...
Remove
7. Remove desflurane and other volatile gases from formularies
Volatile anesthetic gases, such as desflurane, isoflurane, and nitrous oxide, are themselves potent greenhouse gases, comprising a large portion of the carbon emissions that come from the OR.22 Desflurane was developed to have a rapid onset for induction and quick recovery; however, studies have shown no clinical benefit over other gases.23 Furthermore, the costs and greenhouse gas potential are substantial. Desflurane costs 2 to 3 times more and has more than 20 times the global warming potential of the other volatile gases (FIGURE).8 Using 1 hour of desflurane is equivalent to driving 378 miles in a gas-powered vehicle, while the use of isoflurane and sevoflurane create equivalents of only 15 and 8 miles, respectively.23
Nitrous oxide is another powerful greenhouse gas that is a direct ozone depletor and can stay in the atmosphere for 114 years.22 Nitrous oxide has limited clinical use in hospitals, but it is often stored in central hospital piping. Most of the impact of nitrous oxide comes through leaks in a poor system design rather than patient delivery. One estimate reveals that more than 13 million liters of nitrous oxide are lost annually from leaks in European hospitals.22 The American Society of Anesthesiologists recommends decommissioning central piping of nitrous oxide in favor of cylinders at the point of care.24
Literature on enhanced recovery after surgery in gynecology promotes the use of propofol over volatile gases for our patients because of the high rate of postoperative nausea and vomiting seen with gases.25 Volatile gases should be a last-choice anesthetic for our patients.
Bottom line: It is critical that ObGyns work with colleagues in anesthesia to develop climate- and patient-friendly protocols for procedures.
8. Remove endocrine-disrupting chemicals from clinical supplies
Endocrine-disrupting chemicals (EDCs) are a type of chemical that alter the hormonal systems of humans, which can result in adverse health effects. Multiple studies and reviews have tied EDCs to reproductive abnormalities, such as the effects of bisphenol A (BPA) on estradiol levels, antral follicle counts, oocyte quality, and implantation rates; phthalates on fibroid burden; triclosan on embryo quality; parabens on live birth rates; and perfluoroalkylsubstances (PFAS or “forever substances”) on hypertensive disorders of pregnancy.5,26,27
What might be most shocking is that these EDCs are incorporated into medical supplies and pharmaceuticals. For example, BPA is known to line dialysis and ointment tubes, parabens are used for their antimicrobial properties in ultrasound gel and hep-locks, and phthalates are found in up to 40% of medical-use plastics and controlled-release medications. Authors of an observational study found that 74% of patients admitted to an LD unit were exposed to EDCs. In a neonatal intensive care unit (NICU), most of the supplies contained an EDC, and urinary BPA levels were elevated in neonates admitted to a NICU, raising concerns about long-term health risks.5
Bottom line: Physicians and health care institutions have an obligation to petition industry partners and suppliers to remove EDCs from their supply chains.
Reimagine
9. Educate
The field of health care sustainability remains in its infancy, but from 2007 to 2019, publications on climate change and health in academia increased by a factor of 8.29 Additionally, through waste audits, quality-improvement projects, and life cycle analyses (analytical tools to evaluate product or process emissions from materials extraction to disposal), we have gained insight into the scope of the problem, with evidence showing that our practices are largely derived from culture. It is time to provide formal education on health care sustainability to medical trainees, staff, and clinicians alike, who desire to see this topic reflected in their formal curricula.30 Start talking about it!
Bottom line: Commentaries, webinars, formal didactics sessions, in-services, and hospital workgroups to introduce this topic are a good way to teach others about the carbon footprint of our care and solutions to minimize it.
10. Engage in advocacy
Physicians have an ethical duty to advocate for change at the local, regional, and national levels if we want to see a better future for our patients, their children, and even ourselves. We should reimagine this work as an important public health initiative.31 Surveys of physicians, including ObGyns, reveal a concern about the sustainability of health care and a commitment to addressing this issue.20 ObGyns are on the frontlines of delivering care every day, so we are poised to implement changes that can impact our patients, especially when we can lead and petition hospital or local committees.20,28,32 There is much to be done, but every voice counts and can make impactful changes at every level. ●
- Costello A, Abbas M, Allen et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. Lancet. 2009;373:1693-1733.
- Health care climate footprint report. Health Care Without Harm website. https://www.noharm.org/ClimateFootprintReport. Accessed May 12, 2023.
- Balbus JM, McCannon CJ, Mataka A, et al. After COP26—putting health and equity at the center of the climate movement. N Engl J Med. 2022;386:1295-1297.
- Bekkar B, Pacheco S, Basu R, et al. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: a systematic review. JAMA Netw Open. 2020;3:e208243.
- Genco M, Anderson-Shaw L, Sargis RM. Unwitting accomplices: endocrine disruptors confounding clinical care. J Clin Endocrinol Metab. 2020;105:e3822-e3827.
- Al-Kindi SG, Sarode A, Zullo M, et al. Ambient air pollution and mortality after cardiac transplantation. J Am Coll Cardiol. 2019;74:30263035.
- Ghosh R, Gauderman WJ, Minor H, et al. Air pollution, weight loss and metabolic benefits of bariatric surgery: a potential model for study of metabolic effects of environmental exposures. Pediatr Obes. 2018;13:312-320.
- Thiel CL, Eckelman M, Guido R, et al. Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United States. Environ Sci Technol. 2015;49:1779-1786.
- Zygourakis CC, Yoon S, Valencia V, et al. Operating room waste: disposable supply utilization in neurosurgical procedures. J Neurosurg. 2017;126:620-625.
- van Demark RE, Smith VJS, Fiegen A. Lean and green hand surgery. J Hand Surg. 2018;43:179-181.
- Campion N, Thiel CL, DeBlois J, et al. Life cycle assessment perspectives on delivering an infant in the US. Sci Total Environ. 2012;425:191198.
- Hsu S, Thiel CL, Mello MJ, Slutzman JE. Dumpster diving in the emergency department. West J Emerg Med. 2020;21:1211-1217.
- Mcgain F, Story D, Hendel S. An audit of intensive care unit recyclable waste. Anaesthesia. 2009;64:1299-1302.
- Wormer BA, Augenstein VA, Carpenter CL, et al. The green operating room: simple changes to reduce cost and our carbon footprint. Am Surg. 2013;79:666-671.
- Kagoma Y, Stall N, Rubinstein E, et al. People, planet and profits: the case for greening operating rooms. Can Med Assoc J. 2012;184:19051911.
- McCarthy CJ, Gerstenmaier JF, O’ Neill AC, et al. “EcoRadiology”— pulling the plug on wasted energy in the radiology department. Acad Radiol. 2014;21:1563-1566.
- Donahue LM, Hilton S, Bell SG, et al. A comparative carbon footprint analysis of disposable and reusable vaginal specula. Am J Obstet Gynecol. 2020;223:225.e1-225.e7.
- Rodriguez Morris MI, Hicks A. Life cycle assessment of stainless-steel reusable speculums versus disposable acrylic speculums in a university clinic setting: a case study. Environ Res Commun. 2022;4:025002.
- MacNeill AJ, Lillywhite R, Brown CJ. The impact of surgery on global climate: a carbon footprinting study of operating theatres in three health systems. Lancet Planet Health. 2017;1:e381-e388.
- Thiel C, Duncan P, Woods N. Attitude of US obstetricians and gynaecologists to global warming and medical waste. J Health Serv Res Policy. 2017;22:162-167.
- Siu J, Hill AG, MacCormick AD. Systematic review of reusable versus disposable laparoscopic instruments: costs and safety. ANZ J Surg. 2017;87:28-33.
- Ryan SM, Nielsen CJ. Global warming potential of inhaled anesthetics: application to clinical use. Anesth Analg. 2010;111:92-98.
- Meyer MJ. Desflurane should des-appear: global and financial rationale. Anesth Analg. 2020;131:1317-1322.
- Rollins MD, Arendt KW, Carvalho B, et al. ASA Committee on Obstetric Anesthesia Working Group. Nitrous oxide. American Society of Anesthesiologists website. Accessed May 12, 2023. https://www .asahq.org/about-asa/governance-and-committees/asa-committees /committee-on-obstetric-anesthesia/nitrous-oxide.
- Kalogera E, Dowdy SC. Enhanced recovery pathway in gynecologic surgery: improving outcomes through evidence-based medicine. Obstet Gynecol Clin North Am. 2016;43:551-573.
- Zota AR, Geller RJ, Calafat AM, et al. Phthalates exposure and uterine fibroid burden among women undergoing surgical treatment for fibroids: a preliminary study. Fertil Steril. 2019;111:112-121.
- Bommartio PA, Ferguson KK, Meeker JD, et al. Maternal levels of perfluoroalkyl substances (PFAS) during early pregnancy in relation to preeclampsia subtypes and biomarkers of preeclampsia risk. Environ Health Perspect. 2021;129:107004.
- Azouz S, Boyll P, Swanson M, et al. Managing barriers to recycling in the operating room. Am J Surg. 2019;217:634-638.
- Watts N, Amann M, Arnell N, et al. The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises. Lancet. 2021;397:129-170.
- Ryan EC, Dubrow R, Sherman JD. Medical, nursing, and physician assistant student knowledge and attitudes toward climate change, pollution, and resource conservation in health care. BMC Med Educ. 2020;20:200.
- Giudice LC, Llamas-Clark EF, DeNicola Net al; FIGO Committee on Climate Change and Toxic Environmental Exposures. Climate change, women’s health, and the role of obstetricians and gynecologists in leadership. Int J Gynaecol Obstet. 2021;155:345-356.
- Yates EF, Bowder AN, Roa L, et al. Empowering surgeons, anesthesiologists, and obstetricians to incorporate environmental sustainability in the operating room. Ann Surg. 2021;273:1108-1114.
- Costello A, Abbas M, Allen et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. Lancet. 2009;373:1693-1733.
- Health care climate footprint report. Health Care Without Harm website. https://www.noharm.org/ClimateFootprintReport. Accessed May 12, 2023.
- Balbus JM, McCannon CJ, Mataka A, et al. After COP26—putting health and equity at the center of the climate movement. N Engl J Med. 2022;386:1295-1297.
- Bekkar B, Pacheco S, Basu R, et al. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: a systematic review. JAMA Netw Open. 2020;3:e208243.
- Genco M, Anderson-Shaw L, Sargis RM. Unwitting accomplices: endocrine disruptors confounding clinical care. J Clin Endocrinol Metab. 2020;105:e3822-e3827.
- Al-Kindi SG, Sarode A, Zullo M, et al. Ambient air pollution and mortality after cardiac transplantation. J Am Coll Cardiol. 2019;74:30263035.
- Ghosh R, Gauderman WJ, Minor H, et al. Air pollution, weight loss and metabolic benefits of bariatric surgery: a potential model for study of metabolic effects of environmental exposures. Pediatr Obes. 2018;13:312-320.
- Thiel CL, Eckelman M, Guido R, et al. Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United States. Environ Sci Technol. 2015;49:1779-1786.
- Zygourakis CC, Yoon S, Valencia V, et al. Operating room waste: disposable supply utilization in neurosurgical procedures. J Neurosurg. 2017;126:620-625.
- van Demark RE, Smith VJS, Fiegen A. Lean and green hand surgery. J Hand Surg. 2018;43:179-181.
- Campion N, Thiel CL, DeBlois J, et al. Life cycle assessment perspectives on delivering an infant in the US. Sci Total Environ. 2012;425:191198.
- Hsu S, Thiel CL, Mello MJ, Slutzman JE. Dumpster diving in the emergency department. West J Emerg Med. 2020;21:1211-1217.
- Mcgain F, Story D, Hendel S. An audit of intensive care unit recyclable waste. Anaesthesia. 2009;64:1299-1302.
- Wormer BA, Augenstein VA, Carpenter CL, et al. The green operating room: simple changes to reduce cost and our carbon footprint. Am Surg. 2013;79:666-671.
- Kagoma Y, Stall N, Rubinstein E, et al. People, planet and profits: the case for greening operating rooms. Can Med Assoc J. 2012;184:19051911.
- McCarthy CJ, Gerstenmaier JF, O’ Neill AC, et al. “EcoRadiology”— pulling the plug on wasted energy in the radiology department. Acad Radiol. 2014;21:1563-1566.
- Donahue LM, Hilton S, Bell SG, et al. A comparative carbon footprint analysis of disposable and reusable vaginal specula. Am J Obstet Gynecol. 2020;223:225.e1-225.e7.
- Rodriguez Morris MI, Hicks A. Life cycle assessment of stainless-steel reusable speculums versus disposable acrylic speculums in a university clinic setting: a case study. Environ Res Commun. 2022;4:025002.
- MacNeill AJ, Lillywhite R, Brown CJ. The impact of surgery on global climate: a carbon footprinting study of operating theatres in three health systems. Lancet Planet Health. 2017;1:e381-e388.
- Thiel C, Duncan P, Woods N. Attitude of US obstetricians and gynaecologists to global warming and medical waste. J Health Serv Res Policy. 2017;22:162-167.
- Siu J, Hill AG, MacCormick AD. Systematic review of reusable versus disposable laparoscopic instruments: costs and safety. ANZ J Surg. 2017;87:28-33.
- Ryan SM, Nielsen CJ. Global warming potential of inhaled anesthetics: application to clinical use. Anesth Analg. 2010;111:92-98.
- Meyer MJ. Desflurane should des-appear: global and financial rationale. Anesth Analg. 2020;131:1317-1322.
- Rollins MD, Arendt KW, Carvalho B, et al. ASA Committee on Obstetric Anesthesia Working Group. Nitrous oxide. American Society of Anesthesiologists website. Accessed May 12, 2023. https://www .asahq.org/about-asa/governance-and-committees/asa-committees /committee-on-obstetric-anesthesia/nitrous-oxide.
- Kalogera E, Dowdy SC. Enhanced recovery pathway in gynecologic surgery: improving outcomes through evidence-based medicine. Obstet Gynecol Clin North Am. 2016;43:551-573.
- Zota AR, Geller RJ, Calafat AM, et al. Phthalates exposure and uterine fibroid burden among women undergoing surgical treatment for fibroids: a preliminary study. Fertil Steril. 2019;111:112-121.
- Bommartio PA, Ferguson KK, Meeker JD, et al. Maternal levels of perfluoroalkyl substances (PFAS) during early pregnancy in relation to preeclampsia subtypes and biomarkers of preeclampsia risk. Environ Health Perspect. 2021;129:107004.
- Azouz S, Boyll P, Swanson M, et al. Managing barriers to recycling in the operating room. Am J Surg. 2019;217:634-638.
- Watts N, Amann M, Arnell N, et al. The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises. Lancet. 2021;397:129-170.
- Ryan EC, Dubrow R, Sherman JD. Medical, nursing, and physician assistant student knowledge and attitudes toward climate change, pollution, and resource conservation in health care. BMC Med Educ. 2020;20:200.
- Giudice LC, Llamas-Clark EF, DeNicola Net al; FIGO Committee on Climate Change and Toxic Environmental Exposures. Climate change, women’s health, and the role of obstetricians and gynecologists in leadership. Int J Gynaecol Obstet. 2021;155:345-356.
- Yates EF, Bowder AN, Roa L, et al. Empowering surgeons, anesthesiologists, and obstetricians to incorporate environmental sustainability in the operating room. Ann Surg. 2021;273:1108-1114.
ACS officer provides ASCO highlights: Targeting hidden cancer, AI in oncology
And it didn’t just sparkle because of the sequined Taylor Swift fans clogging the nearby streets during the meeting.
Arif Kamal, MD, MBA, MHS, who is also an oncologist at Duke University, Durham, N.C., said he was impressed by a pair of landmark studies released at the meeting that show hidden cancer can be targeted with “really remarkable outcomes.” He also highlighted sessions that examined the role of artificial intelligence (AI) in oncology, during an interview.
Below are lightly edited excerpts from a conversation with Dr. Kamal:
Question: What are some of most groundbreaking studies released at ASCO?
Answer: One is an interim analysis of the NATALEE trial, which involved patients with early-stage hormone receptor-positive, HER2-negative (HR+/HER2–) breast tumors. This phase 3 randomized trial compared maintenance therapy with the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor ribociclib (Kisqali) plus endocrine therapy with an aromatase inhibitor to endocrine therapy alone in patients with node-positive or node-negative and stage II or III HR+/HER– breast cancer.
For a long time, the standard care in these patients has been to use endocrine therapy alone. This is the first big trial to show that upstream usage of additional therapy in early stages is also beneficial for disease-free survival. The 3-year invasive disease-free survival rate was 90.4% in the rebociclib-endocrine therapy group vs. 87.1% for patients who received only endocrine therapy (P = .0014).
Q: How do these findings add to current knowledge?
A: Typically, we let people get metastatic disease before we use CDK4/6 inhibitors. These findings show that systemic treatment beyond endocrine therapy will be helpful in cases where you’ve got smaller disease that has not spread yet.
Even in patients with node-negative breast cancer, micrometastatic disease is clearly there, because the medication killed the negative lymph nodes.
Q: What else struck you as especially important research?
A: The NATALEE findings match what we saw in another study – the ADAURA trial, which looked at adjuvant osimertinib in non–small-cell lung cancer patients with EGFR-mutated, stage IB to IIIA disease – cancer that has not spread to the lymph nodes.
This is another example where you have a treatment being used in earlier-stage disease that’s showing really remarkable outcomes. The study found that 5-year overall survival was 88% in an osimertinib group vs. 78% in a placebo group (P < .001). This is a disease where, in stage IB, we wouldn’t even necessarily give these patients treatment at all, other than surgical resection of the tumor and maybe give them a little bit of chemotherapy.
Even in these smaller, early tumors, osimertinib makes a difference.
Q: As a whole, what are these studies telling us about cancer cells that can’t be easily detected?
A: To find a disease-free survival benefit with adding ribociclib in a stage II, stage III setting, particularly in node-negative disease, is remarkable because it says that the cells in hiding are bad actors, and they are going to cause trouble. The study shows that medications can find these cells and reverse that risk of bad outcomes.
If you think about the paradigm of cancer, that’s pretty remarkable because the ADAURA trial does the same thing: You do surgery for [early-stage] lung cancers that have not spread to the lymph nodes and you figure, “Well, I’ve got it all, right? The margins are real big, healthy, clean.” And yet, people still have recurrences, and you ask the same question: “Can any medicine find those few cells, the hundreds of cells that are still left somewhere in hiding?” And the answer is again, yes. It’s changing the paradigm of our understanding of minimal residual disease.
That’s why there’s so much interest in liquid biopsies. Let’s say that after treatment we don’t see any cancer radiologically, but there’s a signal from a liquid biopsy [detecting residual cancer]. These two trials demonstrate that there’s something we can do about it.
Q: There were quite a few studies about artificial intelligence released at ASCO. Where do we stand on that front?
A: We’re just at the beginning of people thinking about the use of generative AI for clinical decision support, clinical trial matching, and pathology review. But AI, at least for now, still has the issue of making up things that aren’t true. That’s not something patients are going to be okay with.
Q: How can AI be helpful to medical providers considering its limitations?
A: AI is going to be very good at the data-to-information transition. You’ll start seeing people use AI to start clinical notes for them and to match patients to the best clinical trials for them. But fundamentally, the clinician’s role will continue to be to check facts and offer wisdom.
Q: Will AI threaten the careers of oncologists?
A: The body of knowledge about oncology is growing exponentially, and no one can actually keep up. There’s so much data that’s out there that needs to be turned into usable information amid a shortage of oncologists. At the same time, the prevalence of cancer is going up, even though mortality is going down.
Synthesis of data is what oncologists are waiting for from AI. They’ll welcome it as opposed to being worried. That’s the sentiment I heard from my colleagues.
Dr. Kamal has no disclosures.
And it didn’t just sparkle because of the sequined Taylor Swift fans clogging the nearby streets during the meeting.
Arif Kamal, MD, MBA, MHS, who is also an oncologist at Duke University, Durham, N.C., said he was impressed by a pair of landmark studies released at the meeting that show hidden cancer can be targeted with “really remarkable outcomes.” He also highlighted sessions that examined the role of artificial intelligence (AI) in oncology, during an interview.
Below are lightly edited excerpts from a conversation with Dr. Kamal:
Question: What are some of most groundbreaking studies released at ASCO?
Answer: One is an interim analysis of the NATALEE trial, which involved patients with early-stage hormone receptor-positive, HER2-negative (HR+/HER2–) breast tumors. This phase 3 randomized trial compared maintenance therapy with the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor ribociclib (Kisqali) plus endocrine therapy with an aromatase inhibitor to endocrine therapy alone in patients with node-positive or node-negative and stage II or III HR+/HER– breast cancer.
For a long time, the standard care in these patients has been to use endocrine therapy alone. This is the first big trial to show that upstream usage of additional therapy in early stages is also beneficial for disease-free survival. The 3-year invasive disease-free survival rate was 90.4% in the rebociclib-endocrine therapy group vs. 87.1% for patients who received only endocrine therapy (P = .0014).
Q: How do these findings add to current knowledge?
A: Typically, we let people get metastatic disease before we use CDK4/6 inhibitors. These findings show that systemic treatment beyond endocrine therapy will be helpful in cases where you’ve got smaller disease that has not spread yet.
Even in patients with node-negative breast cancer, micrometastatic disease is clearly there, because the medication killed the negative lymph nodes.
Q: What else struck you as especially important research?
A: The NATALEE findings match what we saw in another study – the ADAURA trial, which looked at adjuvant osimertinib in non–small-cell lung cancer patients with EGFR-mutated, stage IB to IIIA disease – cancer that has not spread to the lymph nodes.
This is another example where you have a treatment being used in earlier-stage disease that’s showing really remarkable outcomes. The study found that 5-year overall survival was 88% in an osimertinib group vs. 78% in a placebo group (P < .001). This is a disease where, in stage IB, we wouldn’t even necessarily give these patients treatment at all, other than surgical resection of the tumor and maybe give them a little bit of chemotherapy.
Even in these smaller, early tumors, osimertinib makes a difference.
Q: As a whole, what are these studies telling us about cancer cells that can’t be easily detected?
A: To find a disease-free survival benefit with adding ribociclib in a stage II, stage III setting, particularly in node-negative disease, is remarkable because it says that the cells in hiding are bad actors, and they are going to cause trouble. The study shows that medications can find these cells and reverse that risk of bad outcomes.
If you think about the paradigm of cancer, that’s pretty remarkable because the ADAURA trial does the same thing: You do surgery for [early-stage] lung cancers that have not spread to the lymph nodes and you figure, “Well, I’ve got it all, right? The margins are real big, healthy, clean.” And yet, people still have recurrences, and you ask the same question: “Can any medicine find those few cells, the hundreds of cells that are still left somewhere in hiding?” And the answer is again, yes. It’s changing the paradigm of our understanding of minimal residual disease.
That’s why there’s so much interest in liquid biopsies. Let’s say that after treatment we don’t see any cancer radiologically, but there’s a signal from a liquid biopsy [detecting residual cancer]. These two trials demonstrate that there’s something we can do about it.
Q: There were quite a few studies about artificial intelligence released at ASCO. Where do we stand on that front?
A: We’re just at the beginning of people thinking about the use of generative AI for clinical decision support, clinical trial matching, and pathology review. But AI, at least for now, still has the issue of making up things that aren’t true. That’s not something patients are going to be okay with.
Q: How can AI be helpful to medical providers considering its limitations?
A: AI is going to be very good at the data-to-information transition. You’ll start seeing people use AI to start clinical notes for them and to match patients to the best clinical trials for them. But fundamentally, the clinician’s role will continue to be to check facts and offer wisdom.
Q: Will AI threaten the careers of oncologists?
A: The body of knowledge about oncology is growing exponentially, and no one can actually keep up. There’s so much data that’s out there that needs to be turned into usable information amid a shortage of oncologists. At the same time, the prevalence of cancer is going up, even though mortality is going down.
Synthesis of data is what oncologists are waiting for from AI. They’ll welcome it as opposed to being worried. That’s the sentiment I heard from my colleagues.
Dr. Kamal has no disclosures.
And it didn’t just sparkle because of the sequined Taylor Swift fans clogging the nearby streets during the meeting.
Arif Kamal, MD, MBA, MHS, who is also an oncologist at Duke University, Durham, N.C., said he was impressed by a pair of landmark studies released at the meeting that show hidden cancer can be targeted with “really remarkable outcomes.” He also highlighted sessions that examined the role of artificial intelligence (AI) in oncology, during an interview.
Below are lightly edited excerpts from a conversation with Dr. Kamal:
Question: What are some of most groundbreaking studies released at ASCO?
Answer: One is an interim analysis of the NATALEE trial, which involved patients with early-stage hormone receptor-positive, HER2-negative (HR+/HER2–) breast tumors. This phase 3 randomized trial compared maintenance therapy with the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor ribociclib (Kisqali) plus endocrine therapy with an aromatase inhibitor to endocrine therapy alone in patients with node-positive or node-negative and stage II or III HR+/HER– breast cancer.
For a long time, the standard care in these patients has been to use endocrine therapy alone. This is the first big trial to show that upstream usage of additional therapy in early stages is also beneficial for disease-free survival. The 3-year invasive disease-free survival rate was 90.4% in the rebociclib-endocrine therapy group vs. 87.1% for patients who received only endocrine therapy (P = .0014).
Q: How do these findings add to current knowledge?
A: Typically, we let people get metastatic disease before we use CDK4/6 inhibitors. These findings show that systemic treatment beyond endocrine therapy will be helpful in cases where you’ve got smaller disease that has not spread yet.
Even in patients with node-negative breast cancer, micrometastatic disease is clearly there, because the medication killed the negative lymph nodes.
Q: What else struck you as especially important research?
A: The NATALEE findings match what we saw in another study – the ADAURA trial, which looked at adjuvant osimertinib in non–small-cell lung cancer patients with EGFR-mutated, stage IB to IIIA disease – cancer that has not spread to the lymph nodes.
This is another example where you have a treatment being used in earlier-stage disease that’s showing really remarkable outcomes. The study found that 5-year overall survival was 88% in an osimertinib group vs. 78% in a placebo group (P < .001). This is a disease where, in stage IB, we wouldn’t even necessarily give these patients treatment at all, other than surgical resection of the tumor and maybe give them a little bit of chemotherapy.
Even in these smaller, early tumors, osimertinib makes a difference.
Q: As a whole, what are these studies telling us about cancer cells that can’t be easily detected?
A: To find a disease-free survival benefit with adding ribociclib in a stage II, stage III setting, particularly in node-negative disease, is remarkable because it says that the cells in hiding are bad actors, and they are going to cause trouble. The study shows that medications can find these cells and reverse that risk of bad outcomes.
If you think about the paradigm of cancer, that’s pretty remarkable because the ADAURA trial does the same thing: You do surgery for [early-stage] lung cancers that have not spread to the lymph nodes and you figure, “Well, I’ve got it all, right? The margins are real big, healthy, clean.” And yet, people still have recurrences, and you ask the same question: “Can any medicine find those few cells, the hundreds of cells that are still left somewhere in hiding?” And the answer is again, yes. It’s changing the paradigm of our understanding of minimal residual disease.
That’s why there’s so much interest in liquid biopsies. Let’s say that after treatment we don’t see any cancer radiologically, but there’s a signal from a liquid biopsy [detecting residual cancer]. These two trials demonstrate that there’s something we can do about it.
Q: There were quite a few studies about artificial intelligence released at ASCO. Where do we stand on that front?
A: We’re just at the beginning of people thinking about the use of generative AI for clinical decision support, clinical trial matching, and pathology review. But AI, at least for now, still has the issue of making up things that aren’t true. That’s not something patients are going to be okay with.
Q: How can AI be helpful to medical providers considering its limitations?
A: AI is going to be very good at the data-to-information transition. You’ll start seeing people use AI to start clinical notes for them and to match patients to the best clinical trials for them. But fundamentally, the clinician’s role will continue to be to check facts and offer wisdom.
Q: Will AI threaten the careers of oncologists?
A: The body of knowledge about oncology is growing exponentially, and no one can actually keep up. There’s so much data that’s out there that needs to be turned into usable information amid a shortage of oncologists. At the same time, the prevalence of cancer is going up, even though mortality is going down.
Synthesis of data is what oncologists are waiting for from AI. They’ll welcome it as opposed to being worried. That’s the sentiment I heard from my colleagues.
Dr. Kamal has no disclosures.
AT ASCO 2023
‘New standard of care’ for capecitabine hand-foot syndrome
researchers reported in a study that has been hailed by experts as “practice changing.”
Hand-foot syndrome causes painful, bleeding blisters and ulcers on the palms and soles. It often leads to dose reductions and sometimes even discontinuations, both of which limit the effectiveness of capecitabine, a standard oral chemotherapy drug widely used for colorectal and breast cancers.
In a new study presented at the annual meeting of the American Society of Clinical Oncology, Indian researchers reported that a cheap, safe, and widely available over-the-counter nonsteroidal anti-inflammatory gel containing 1% diclofenac reduced the incidence of hand-foot syndrome by 75% among patients with cancer being treated with capecitabine.
Up until now, the oral anti-inflammatory celecoxib (Celebrex) was the only agent proven to prevent the problem, but it’s rarely used because of the risk for strokes, gastric bleeding, and other issues, none of which are a concern with topical diclofenac, which osteoarthritis patients have used safely for years.
The Indian trial, dubbed D-Torch, establishes “1% topical diclofenac gel as the new standard of care to prevent capecitabine-associated hand-foot syndrome,” said investigator and study presenter Atul Batra, MD, a medical oncologist at the All India Institute of Medical Sciences, New Delhi.
Dr. Batra told ASCO Daily News that there is no need for a second trial. “We don’t feel there’s a need to replicate these results” in a larger study “because this was adequately powered, and the results speak for themselves. There’s no confusion about these results. Diclofenac is clearly effective.”
Dr. Batra also commented that his clinic now uses topical diclofenac routinely during capecitabine treatment and that he hopes oncology practices elsewhere will do the same.
Diclofenac gel is sold under the brand name Voltaren and is also available as a generic; in the United States, a 150-gram tube costs about $18 at Walmart.
‘The most practice-changing study’ at ASCO 2023
Audience members at ASCO’s annual meeting immediately saw the importance of the study.
Tarah Ballinger, MD, a breast cancer specialist at Indiana University, Indianapolis, said on Twitter that “this might be the most practice changing study I heard at ASCO23.” Topical diclofenac is “widely available, affordable, [and] addresses [a] major” quality of life issue.
The study discussant at the meeting, gastrointestinal cancer specialist Pallavi Kumar, MD, of the University of Pennsylvania, Philadelphia, concurred: “For me as a GI oncologist, topical diclofenac for prevention of HFS for patients on capecitabine is practice changing,” she said.
The takeaway is “that topical diclofenac significantly reduces the incidence of grade 2 or higher HFS in patients receiving capecitabine.” The results are “very impressive,” Dr. Kumar said.
Study details
The idea for the new study came after Batra and colleagues realized that celecoxib, a COX-2 enzyme inhibitor, helps prevent capecitabine hand-foot syndrome (HFS) by blocking a key process that leads to it, the up-regulation of COX-2 and subsequent release of proinflammatory prostaglandins.
They turned to diclofenac gel hoping to get the same effect but more safely; diclofenac is also a COX-2 blocker, and its topical formulation has a strong safety record.
To test the approach, the team randomly assigned 130 patients to topical diclofenac and 133 to placebo – the gel vehicle without the medication – while they were being treated with capecitabine for 12 weeks; 56% were being treated for breast cancer and the rest for gastrointestinal cancers.
Subjects rubbed one fingertip’s worth of gel – about half a gram – on each palm and the back of each hand twice a day. The dose was about 4 grams/day, which is well below maximal dosages for osteoarthritis (up to 32 g/day over all affected joints). Adherence to treatment was about 95% in both arms.
By the end of 12 weeks, the incidence of grade 2 or higher HFS was 3.8% in the diclofenac arm (5 patients) versus 15% (n = 20) with placebo (P = .003), a 75% risk reduction.
The incidence of any grade HFS was 6.1% in the treatment group versus 18.1% with placebo (P = .003).
Hand-foot syndrome led to dose reductions of capecitabine in 13.5% of placebo but only 3.8% of those in the diclofenac group (P = .002).
The findings held regardless of whether patients were being treated for breast or GI cancer or if they were men or women.
Other capecitabine-induced adverse events, including diarrhea, mucositis, and myelosuppression, were not significantly different between the groups.
The treatment arms were well balanced, with a median age of 47 years in both groups and women making up about 70% of each. About 40% of subjects in each group were on capecitabine monotherapy with the rest on combination treatments. The mean dose of capecitabine was just over 1,880 mg/m2 in both groups.
At the meeting, Dr. Batra was asked if topical diclofenac would also work for another common problem in oncology: hand-food syndrome occurring as a side-effect with VEGF–tyrosine kinase inhibitors. He didn’t think so because it probably has a different cause than capecitabine HFS, one not strongly related to COX-2 up-regulation.
The study was partly funded by the Indian Supportive Care of Cancer Association. The investigators reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers reported in a study that has been hailed by experts as “practice changing.”
Hand-foot syndrome causes painful, bleeding blisters and ulcers on the palms and soles. It often leads to dose reductions and sometimes even discontinuations, both of which limit the effectiveness of capecitabine, a standard oral chemotherapy drug widely used for colorectal and breast cancers.
In a new study presented at the annual meeting of the American Society of Clinical Oncology, Indian researchers reported that a cheap, safe, and widely available over-the-counter nonsteroidal anti-inflammatory gel containing 1% diclofenac reduced the incidence of hand-foot syndrome by 75% among patients with cancer being treated with capecitabine.
Up until now, the oral anti-inflammatory celecoxib (Celebrex) was the only agent proven to prevent the problem, but it’s rarely used because of the risk for strokes, gastric bleeding, and other issues, none of which are a concern with topical diclofenac, which osteoarthritis patients have used safely for years.
The Indian trial, dubbed D-Torch, establishes “1% topical diclofenac gel as the new standard of care to prevent capecitabine-associated hand-foot syndrome,” said investigator and study presenter Atul Batra, MD, a medical oncologist at the All India Institute of Medical Sciences, New Delhi.
Dr. Batra told ASCO Daily News that there is no need for a second trial. “We don’t feel there’s a need to replicate these results” in a larger study “because this was adequately powered, and the results speak for themselves. There’s no confusion about these results. Diclofenac is clearly effective.”
Dr. Batra also commented that his clinic now uses topical diclofenac routinely during capecitabine treatment and that he hopes oncology practices elsewhere will do the same.
Diclofenac gel is sold under the brand name Voltaren and is also available as a generic; in the United States, a 150-gram tube costs about $18 at Walmart.
‘The most practice-changing study’ at ASCO 2023
Audience members at ASCO’s annual meeting immediately saw the importance of the study.
Tarah Ballinger, MD, a breast cancer specialist at Indiana University, Indianapolis, said on Twitter that “this might be the most practice changing study I heard at ASCO23.” Topical diclofenac is “widely available, affordable, [and] addresses [a] major” quality of life issue.
The study discussant at the meeting, gastrointestinal cancer specialist Pallavi Kumar, MD, of the University of Pennsylvania, Philadelphia, concurred: “For me as a GI oncologist, topical diclofenac for prevention of HFS for patients on capecitabine is practice changing,” she said.
The takeaway is “that topical diclofenac significantly reduces the incidence of grade 2 or higher HFS in patients receiving capecitabine.” The results are “very impressive,” Dr. Kumar said.
Study details
The idea for the new study came after Batra and colleagues realized that celecoxib, a COX-2 enzyme inhibitor, helps prevent capecitabine hand-foot syndrome (HFS) by blocking a key process that leads to it, the up-regulation of COX-2 and subsequent release of proinflammatory prostaglandins.
They turned to diclofenac gel hoping to get the same effect but more safely; diclofenac is also a COX-2 blocker, and its topical formulation has a strong safety record.
To test the approach, the team randomly assigned 130 patients to topical diclofenac and 133 to placebo – the gel vehicle without the medication – while they were being treated with capecitabine for 12 weeks; 56% were being treated for breast cancer and the rest for gastrointestinal cancers.
Subjects rubbed one fingertip’s worth of gel – about half a gram – on each palm and the back of each hand twice a day. The dose was about 4 grams/day, which is well below maximal dosages for osteoarthritis (up to 32 g/day over all affected joints). Adherence to treatment was about 95% in both arms.
By the end of 12 weeks, the incidence of grade 2 or higher HFS was 3.8% in the diclofenac arm (5 patients) versus 15% (n = 20) with placebo (P = .003), a 75% risk reduction.
The incidence of any grade HFS was 6.1% in the treatment group versus 18.1% with placebo (P = .003).
Hand-foot syndrome led to dose reductions of capecitabine in 13.5% of placebo but only 3.8% of those in the diclofenac group (P = .002).
The findings held regardless of whether patients were being treated for breast or GI cancer or if they were men or women.
Other capecitabine-induced adverse events, including diarrhea, mucositis, and myelosuppression, were not significantly different between the groups.
The treatment arms were well balanced, with a median age of 47 years in both groups and women making up about 70% of each. About 40% of subjects in each group were on capecitabine monotherapy with the rest on combination treatments. The mean dose of capecitabine was just over 1,880 mg/m2 in both groups.
At the meeting, Dr. Batra was asked if topical diclofenac would also work for another common problem in oncology: hand-food syndrome occurring as a side-effect with VEGF–tyrosine kinase inhibitors. He didn’t think so because it probably has a different cause than capecitabine HFS, one not strongly related to COX-2 up-regulation.
The study was partly funded by the Indian Supportive Care of Cancer Association. The investigators reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers reported in a study that has been hailed by experts as “practice changing.”
Hand-foot syndrome causes painful, bleeding blisters and ulcers on the palms and soles. It often leads to dose reductions and sometimes even discontinuations, both of which limit the effectiveness of capecitabine, a standard oral chemotherapy drug widely used for colorectal and breast cancers.
In a new study presented at the annual meeting of the American Society of Clinical Oncology, Indian researchers reported that a cheap, safe, and widely available over-the-counter nonsteroidal anti-inflammatory gel containing 1% diclofenac reduced the incidence of hand-foot syndrome by 75% among patients with cancer being treated with capecitabine.
Up until now, the oral anti-inflammatory celecoxib (Celebrex) was the only agent proven to prevent the problem, but it’s rarely used because of the risk for strokes, gastric bleeding, and other issues, none of which are a concern with topical diclofenac, which osteoarthritis patients have used safely for years.
The Indian trial, dubbed D-Torch, establishes “1% topical diclofenac gel as the new standard of care to prevent capecitabine-associated hand-foot syndrome,” said investigator and study presenter Atul Batra, MD, a medical oncologist at the All India Institute of Medical Sciences, New Delhi.
Dr. Batra told ASCO Daily News that there is no need for a second trial. “We don’t feel there’s a need to replicate these results” in a larger study “because this was adequately powered, and the results speak for themselves. There’s no confusion about these results. Diclofenac is clearly effective.”
Dr. Batra also commented that his clinic now uses topical diclofenac routinely during capecitabine treatment and that he hopes oncology practices elsewhere will do the same.
Diclofenac gel is sold under the brand name Voltaren and is also available as a generic; in the United States, a 150-gram tube costs about $18 at Walmart.
‘The most practice-changing study’ at ASCO 2023
Audience members at ASCO’s annual meeting immediately saw the importance of the study.
Tarah Ballinger, MD, a breast cancer specialist at Indiana University, Indianapolis, said on Twitter that “this might be the most practice changing study I heard at ASCO23.” Topical diclofenac is “widely available, affordable, [and] addresses [a] major” quality of life issue.
The study discussant at the meeting, gastrointestinal cancer specialist Pallavi Kumar, MD, of the University of Pennsylvania, Philadelphia, concurred: “For me as a GI oncologist, topical diclofenac for prevention of HFS for patients on capecitabine is practice changing,” she said.
The takeaway is “that topical diclofenac significantly reduces the incidence of grade 2 or higher HFS in patients receiving capecitabine.” The results are “very impressive,” Dr. Kumar said.
Study details
The idea for the new study came after Batra and colleagues realized that celecoxib, a COX-2 enzyme inhibitor, helps prevent capecitabine hand-foot syndrome (HFS) by blocking a key process that leads to it, the up-regulation of COX-2 and subsequent release of proinflammatory prostaglandins.
They turned to diclofenac gel hoping to get the same effect but more safely; diclofenac is also a COX-2 blocker, and its topical formulation has a strong safety record.
To test the approach, the team randomly assigned 130 patients to topical diclofenac and 133 to placebo – the gel vehicle without the medication – while they were being treated with capecitabine for 12 weeks; 56% were being treated for breast cancer and the rest for gastrointestinal cancers.
Subjects rubbed one fingertip’s worth of gel – about half a gram – on each palm and the back of each hand twice a day. The dose was about 4 grams/day, which is well below maximal dosages for osteoarthritis (up to 32 g/day over all affected joints). Adherence to treatment was about 95% in both arms.
By the end of 12 weeks, the incidence of grade 2 or higher HFS was 3.8% in the diclofenac arm (5 patients) versus 15% (n = 20) with placebo (P = .003), a 75% risk reduction.
The incidence of any grade HFS was 6.1% in the treatment group versus 18.1% with placebo (P = .003).
Hand-foot syndrome led to dose reductions of capecitabine in 13.5% of placebo but only 3.8% of those in the diclofenac group (P = .002).
The findings held regardless of whether patients were being treated for breast or GI cancer or if they were men or women.
Other capecitabine-induced adverse events, including diarrhea, mucositis, and myelosuppression, were not significantly different between the groups.
The treatment arms were well balanced, with a median age of 47 years in both groups and women making up about 70% of each. About 40% of subjects in each group were on capecitabine monotherapy with the rest on combination treatments. The mean dose of capecitabine was just over 1,880 mg/m2 in both groups.
At the meeting, Dr. Batra was asked if topical diclofenac would also work for another common problem in oncology: hand-food syndrome occurring as a side-effect with VEGF–tyrosine kinase inhibitors. He didn’t think so because it probably has a different cause than capecitabine HFS, one not strongly related to COX-2 up-regulation.
The study was partly funded by the Indian Supportive Care of Cancer Association. The investigators reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ASCO 2023